-
8/14/2019 17 COM TRADU++O
1/8
Recruitment Maneuvers for Acute Lung InjuryA Systematic
Review
Eddy Fan1,2, M. Elizabeth Wilcox1, Roy G. Brower2, Thomas E.
Stewart1, Sangeeta Mehta1, Stephen E. Lapinsky1,Maureen O. Meade3,
and Niall D. Ferguson1
1Interdepartmental Division of Critical Care Medicine,
University of Toronto, Toronto, Ontario, Canada; 2Division of
Pulmonary and Critical Care
Medicine, Johns Hopkins University, Baltimore, Maryland; and
3Departments of Clinical Epidemiology and Biostatistics, and
Medicine, McMaster
University, Hamilton, Ontario, Canada
Rationale: There are conflicting data regarding the safety
and
efficacy of recruitment maneuvers(RMs) in patients with acute
lung
injury (ALI).
Objectives: To summarize the physiologic effects and adverse
events
in adult patients with ALI receiving RMs.
Methods: Systematicreview of case series,observational
studies,and
randomized clinical trials with pooling of study-level data.
Measurements and Main Results: Forty studies (1,185 patients)
met
inclusion criteria. Oxygenation (31 studies; 636 patients) was
signif-
icantly increasedafteranRM (PaO2:106versus193mmHg,P50.001;
andPaO2/FIO2 ratio:139versus251mmHg, P,0.001).There were no
persistent, clinically significant changes in hemodynamic
parame-
ters after an RM. Ventilatory parameters (32 studies; 548
patients)
were notsignificantly alteredby an RM,except forhigher
PEEPpost-
RM (11 versus 16 cm H2O; P 5 0.02). Hypotension (12%) and
desaturation (9%) were the most common adverse events (31
studies; 985 patients). Serious adverse events (e.g.,
barotrauma
[1%]and arrhythmias [1%]) were infrequent. Only 10 (1%)
patients
had their RMs terminated prematurely due to adverse events.
Conclusions: Adult patients with ALI receiving RMs
experienced
a significant increase in oxygenation, with few serious
adverse
events. Transient hypotension and desaturation during RMs is
common but is self-limited without serious short-term
sequelae.
Given the uncertain benefitof transient
oxygenationimprovements
in patients with ALIand thelack of information on their
influence on
clinicaloutcomes,the routine useof RMscannot be recommended
or
discouraged at this time. RMs should be considered for use on
an
individualized basis in patients with ALI who have
life-threatening
hypoxemia.
Keywords: artificial respiration; adult respiratory distress
syndrome;respiratory physiology; systematic review
Acute lung injury (ALI) is characterized by the acute onset
ofhypoxemia (PaO
2/FIO
2
-
8/14/2019 17 COM TRADU++O
2/8
such as barotrauma (e.g., pneumothorax), arrhythmias,
andbacterial translocation, may occur (15, 19, 20). Due to the
con-flicting results regarding the efficacy and safety of RMs in
ALI,we undertook this systematic review to synthesize knowledgefrom
published studies. Specifically, we intended to summarizethe
physiologic effects (i.e., changes in respiratory variables)and
adverse events (during and after RMs) in adult patientswith ALI
receiving RMs.
MATERIALS AND METHODS
Data Sources and Searches
We searched Medline (May 1950 to Week 3, 2008), AMED (1985 toMay
2008), CENTRAL (second quarter 2008), EMBASE (1980 toWeek 22,
2008), CINAHL (May 1985 to Week 5, 2008), andHEALTHSTAR (1975 to
April 2008) using a sensitive search strategy(21) combining Medical
Subject Headings and keywords where appro-priate (see the online
supplement for details). We examined biblio-graphies of all
selected articles and all relevant review articles and handsearched
abstracts from recent (20032007) major conferences (Amer-ican
Thoracic Society, European Society of Intensive Care Medicine,and
Society of Critical Care Medicine) for additional relevant
studies.
Study Selection and Data AbstractionWe selected studies meeting
the following inclusion criteria: (1)randomized clinical trial or
controlled observational study or clinicalcase series (study
design), (2) exclusively adult patients at least 18 yearsof age
(study population), and (3) undergoing a recruitment
maneuverlasting less than 30 minutes and that may be repeated. No
languagerestrictions were used. We specified that recruitment
maneuvers betransient (,30 minutes) to exclude studies that used a
fixed ventilationstrategy (e.g., high versus low PEEP) for
recruitment. We excludedclinical studies that met the selection
criteria but did not report onphysiologic or adverse effects.
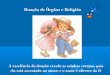
Figure 1 summarizes the study selection process. Two
reviewers(EF and NDF) independently assessed the eligibility of
each study andresolved disagreements by consensus. We used the
kappa statistic tomeasure agreement in these assessments between
the two reviewershe.
Data from included studies were abstracted in duplicate (EF,
MEW, RGB, TES, SM, SEL, and NDF) using customized,
pilot-testedforms. The reviewers abstracted the data on description
of the cohort,study design and methods, physiologic and ventilatory
variables,adverse events, and patient survival. Reported aggregated
physiologicand ventilatory variables were abstracted from studies
at a minimum oftwo time points: pre-RM (i.e., at baseline or before
the start of RM)and post-RM (i.e., the first reported values after
RM).
Statistical Analysis
Descriptive statistics from individual studies were reported
usingproportions and mean 6 SD unless otherwise stated. We
pooledavailable data using an n-weighted mean 6 SD based on study
size.We compared proportions using Fishers exact test.
Continuousvariables were compared using the Wilcoxon signed
rank-sum test.We performed sensitivity analyses for all outcomes
restricted to: (1)prospective studies, (2) studies that reported
physiologic and/orventilatory data 30 minutes or less post-RM (to
capture transienteffects related to RMs), and (3) studies using
sustained inflation (e.g.,continuous positive airway pressure
[CPAP] 3040 cm H2O for 3040seconds) (RM type). We also performed
three a priori subgroupanalyses: (1) studies with a pre-to-postRM
PEEP difference 5 cmH2O or less versus greater than 5 cm H2O, (2)
baseline PaO
2/FIO
2ratio
less than 150 mm Hg (lower) versus 150 mm Hg or greater
(higher),and (3) baseline respiratory system compliance less than
30 mL/cmH2O (lower) versus 30 mL/cm H2O or greater (higher). All
analyseswere performed using Microsoft Excel 2004 (Microsoft
Corporation,Redmond, WA) and Stata 10.0 statistical software (Stata
Corporation,College Station, TX). A nominal Pvalue less than 0.05
was used todetermine statistical significance. Due to the
heterogeneity in study
populations, interventions, and reported outcomes, a
quantitativemeta-analysis of effect sizes was not performed.
RESULTS
Study Search and Selection
The initial search generated 248 citations, of which 91
wereduplicate reports from multiple databases. Iterative review
oftitles, abstracts, and full-length articles yielded 40 unique
stu-dies, which are included in this review (Figure 1). These
studieshad a mean sample size of 30 (range, 8366) and included a
totalof 1,185 patients. Agreement on study selection was
nearperfect, with a kappa statistic of 0.90 (22).
Study Characteristics
Of the 40 studies, 32 were prospective studies (1417, 2252),four
were randomized controlled trials (15, 20, 53, 54), and fourwere
retrospective cohort studies (5558). Seventeen studies(43%)
enrolled consecutive eligible and consenting patients,and 17 (43%)
did not report on patient enrollment procedures.In the majority of
studies (78%), RMs were conducted specif-ically for experimental
purposes (i.e., designed with the explicitpurpose of examining
outcomes after the use of RMs), ascompared with those conducted in
the context of usual clinicalcare (Tables 1 and 2). Sustained
inflation was the most common(45%) type of RM used.
Figure 1. Literature review schematic illustrating the number of
articles
identified at each stage of the review process for potential
inclusion in
the systematic review. Iterative review of titles, abstracts,
and full-length articles yielded 40 unique studies, which are
included in thisreview.
Fan, Wilcox, Brower, et al.: Recruitment Maneuvers in ALI
1157
-
8/14/2019 17 COM TRADU++O
3/8
The baseline characteristics of the study patients are
pre-sented in Table 3. Across studies, patients had a mean age
of526 9.5 years, with mean APACHE II score 21 6 3.3 and meanLung
Injury Score of 3.0 6 0.26. Patients were ventilated atbaseline,
with a mean plateau pressure 28 6 4.8 cm H2O, meanVTof 7.0 6 1.2
mL/kg body weight (as reported by each study),and mean PEEP of 12 6
2.1 cm H2O. The etiologic risk factorfor ALI was reported in 36
studies (786 patients); 43% of thesepatients developed ALI from a
direct pulmonary insult. Co-interventions were reported in 16
studies (327 patients), withprone positioning used most frequently
(22%).
Physiologic and Ventilatory Variables
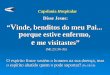
Thirty-one studies reported on the acute physiologic effects
ofan RM in 636 patients (Table 4). Oxygenation was
significantlyincreased after an RM (PaO
2: 106 versus 193 mm Hg; P5 0.001
and PaO2/FIO
2ratio: 139 versus 251 mm Hg; P, 0.001) (Figure
2). Few studies reported oxygenation beyond a 3- to
6-hourpost-RM (30, 36, 43, 46, 54), with many studies reporting a
rapiddecline in oxygenation gains, some within 15 to 20 minutes
ofthe RM (14, 25, 26, 30, 34, 36, 42, 46, 52, 53). Heart rate
(104versus 105 beats per minute; P 5 0.04), pH (7.34 versus 7.30;P5
0.04), and central venous pressure (CVP) (13 versus 16 mmHg; P5
0.009) were statistically significantly higher post-RM,although the
clinical significance of these changes is question-able. Other
hemodynamic parameters, including mean arterial
pressure, pulmonary capillary wedge pressure, cardiac
output/index, and mixed venous oxygen saturation, were not
signifi-cantly changed after an RM. Ventilatory parameters
werereported in 32 studies (548 patients) and were not
significantlyaltered by an RM, except for higher PEEP post-RM (11
versus 16cm H2O; P5 0.02).Respiratorysystem compliance was
marginallyhigher after an RM (34 versus 35 mL/cm H2O;P5 0.03).
Adverse Events and Mortality
Thirty-one studies evaluated adverse events (985 patients).
Themajority of these events occurred during an RM, with
hypo-tension (12%) and desaturation (8%) being the most
commoncomplications (Table 5). Serious adverse events, such as
baro-trauma (1%) and arrhythmias (1%), were infrequent. Only 10(1%)
patients were reported to have had RMs terminatedprematurely due to
adverse events. Seventeen studies (287patients) reported no adverse
events from RMs. Overall mortal-ity was reported in 20 studies (409
patients) and was 38%.
Sensitivity Analyses
Sensitivity analyses restricted to prospective studies (32
studies)yielded results similar to the main analysis, with
significantlyincreased oxygenation (PaO
2: 105 versus 190 mm Hg; P, 0.001
and PaO2
/FIO2
ratio: 142 versus 224 mm Hg; P , 0.001) andmodest changes in
heart rate (104 versus 105 beats per minute;P 5 0.04), pH (7.33
versus 7.30; P 5 0.04), CVP (13 versus16 mm Hg; P50.009), and
respiratory system compliance (34versus 35 mL/cm H2O;P5 0.03).
Hypotension (11 versus 19%;P,0.001) and desaturation (7 versus 18%;
P, 0.001) duringRMs were reported less frequently. There were no
significantdifferences in barotrauma rates between prospective and
retro-spective studies.
Studies have reported data on physiologic and
ventilatoryparameters at varying times after an RM (range, 3120
minutes).In sensitivity analyses restricted to studies that
reported data30 minutes or less post-RM (25 studies), there
continued to besignificant increases in oxygenation (PaO
2: 106 versus 214 mm Hg;
P5 0.005 and PaO2/FIO
2ratio: 138 versus 254 mm Hg;P, 0.001),
with modest increases in CVP (13 versus 16 mm Hg; P5 0.01)and
PEEP (11 versus 17 cm H2O; P 5 0.01). There were nosignificant
differences in the rates of any adverse events betweengroups with
data 30 minutes or less post-RM versus more than30 minutes
post-RM.
When restricted to studies using sustained inflation (18studies)
as compared with other RM types (e.g., sigh/highVT), only the
change in the PaO
2/FIO
2ratio remained significant
(149 versus 235; P5 0.005). Point estimates for other
variableswere similar to those in the main analysis, but the
findings werenot statistically significant. There were no
significant differencesin the rates of any adverse events during
RMs between sus-tained inflation versus other RM type groups.
Subgroup AnalysesPatients with a pre- to post-RM PEEP difference
5 cm H2O orless still had a significant increase in oxygenation
(PaO
2: 102
versus 125 mm Hg; P5 0.02 and PaO2/FIO
2ratio: 145 versus 210
mm Hg;P5 0.04), with a modest change in respiratory
systemcompliance (35 versus 38 mL/cm H2O;P5 0.04). There were
nosignificant differences in the rates of any adverse events
duringRMs in the groups with pre- to post-RM PEEP difference 5
cmH2O or less versus greater than 5 cm H2O.
Oxygenation improved after RMs irrespective of baselinePaO
2/FIO
2ratio: lower group (PaO
2/FIO
2ratio ,150 mm Hg)
(PaO2: 84 versus 181 mm Hg; P 5 0.02 and PaO
2/FIO
2ratio:
128 versus 245 mm Hg; P5 0.002) and higher group (PaO2/FIO
2
TABLE 1. STUDY CHARACTERISTICS
Characteristic Studies (n 5 40)
Study years, range 19992007
No. patients receiving RMs
Total 1,185
Per study, mean (SD) 30 (56)
Number of centers
Total 98
Mean (SD) 2.5 (5.4)
Study duration, h
Total 387Mean (SD) 11 (29)
Study design/purpose,*n (%)
Randomized controlled trial 4 (10)
Clinical 1 (25)
Experimental 3 (75)
Prospective cohort study 32 (80)
Clinical 5 (16)
Experimental 27 (84)
Retrospective cohort study 4 (10)
Clinical 3 (75)
Experimental 1 (25)
Type of RM used, n (%)
Sustained inflation 18 (45)
High pressure-controlled ventilation 9 (23)
Incremental positive end-ex pi ratory press ure 8 (20)
High VT/sigh 4 (10)
Other 1 (2)
RM performed with FIO2 5 1.0, n (%)
Yes 11 (28)
No 13 (32)
Sometimes 0 (0)
Not reported 16 (40)
RM performed on paralysis,n (%)
Yes 22 (55)
No 6 (15)
Sometimes 2 (5)
Not reported 10 (25)
Definition of abbreviation: RM 5 recruitment maneuver.
* Percentage reported for study design is proportion of all
studies (n 5 37);
percentage reported for study purpose is proportion of preceding
study design.
1158 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
VOL 178 2008
-
8/14/2019 17 COM TRADU++O
4/8
ratio>
150 mm Hg) (PaO2: 153 versus 236 mm Hg;
P50.03 andPaO
2/FIO
2ratio: 180 versus 229 mm Hg; P5 0.04). CVP was also
significantly higher post-RM in the lower PaO2/FIO
2ratio sub-
group (13 versus 15 mm Hg; P5 0.02).In the subgroup of patients
with lower baseline respiratory
system compliance (,30 mL/cm H2O), there were no
significantdifferences in any physiologic or ventilatory parameters
after anRM. However, patients with higher baseline respiratory
systemcompliance (>30 mL/cm H2O) had a significantly higher
PaO
2/
FIO2
ratio after an RM (130 versus 180 mm Hg;P5 0.02). Therewere no
significant differences in any adverse events duringRMs in either
subgroup (pre- versus post-RM).
DISCUSSION
In this systematic review of nearly 1,200 adult patients
withALI, the use of RMs was associated with significant,
albeittransient, increases in oxygenation (as measured by PaO
2and
PaO2/FIO
2ratio). There were no clinically significant changes in
short-term hemodynamic or ventilatory variables, except for
asmall increase in CVP post-RM. Hypotension and desaturationwere
the most common adverse events during RMs, but therewere few
serious short-term adverse events (e.g., barotraumasor
arrhythmias), and an extremely small number of RMs wereterminated
early due to adverse events. Overall mortality wassimilar to
previous observational studies of patients with ALI. Ingeneral,
these findings (oxygenation, adverse events) were robustacross our
sensitivity and subgroup analyses.
Improvements in oxygenation after an RM have beendemonstrated in
many studies (14, 23, 27, 28, 31, 32, 34, 35,37, 39, 40, 42, 44,
47, 48, 5053, 55). However, many studiesreport a rapid decline in
these oxygenation gains over thesubsequent 24 hours, some within 15
to 20 minutes of the RM(14, 26, 27, 31, 35, 37, 43, 47, 52, 53).
Animal models suggestthat the type of RM used (e.g., sustained
inflation versus highpressure-controlled ventilation) may also
influence the durabil-ity of RM-induced oxygenation (18). In
addition, the applica-tion of higher levels of PEEP after an RM may
affect thesustainability of the effect (17, 41). Few studies
included in oursystematic review reported oxygenation beyond 6
hours, mak-ing it difficult to confirm these results. The
importance of thesetransient effects is questionable because there
are conflictingdata from observational studies regarding the
association be-
tween oxygenation and mortality in ALI (59). Furthermore,despite
having reduced oxygenation on Day 1 (as comparedwith the control
group), patients randomized to low VTventilation in the ARDS
Network study ultimately deriveda survival advantage from this
intervention (7). However, theARDS Network study used a ventilation
strategy in the controlgroup that resulted in sustained higher
tidal volumes andincreased airway pressures, as opposed to the
transient natureof the RMs being studied in this review. Improving
oxygenationis unlikely to be inherently harmful; rather, it seems
likely that itis the manner in which this is achieved that is
important.Whether improvements in oxygenation with RMs are
associatedwith reduced VILI and improved clinically important
outcomes
TABLE 2. RANDOMIZED CONTROLLED TRIALS OF RECRUITMENT
MANEUVERS
Trial n Type of RM Used Frequency of RM Main Outcome Measures
Adverse Events
ARDSNet (15) 57 Sustained inflation (CPAP
3540 cm H2O for 30 s)
Every other day (alternating
with sham RMs)
Greater increase in SpO2with RM vs. sham RM
(1.7% 6 0.2% vs. 0.6%
6 0.3%; P, 0.01);
changes in FIO2/PEEP
requirements were not
significantly different up
to 8 h from RM or sham RM
Greater decrease in SBP
with RM vs. sham RM
(29.4 6 1.1 vs. 23.1 6
1.1 mm Hg; P, 0.01);
three RMs terminated
early due to transient
hypotension or desaturation;
new barotraumas after
one RM and one sham RMMe ade ( 54) 28 Sustain ed i nflation
(CPAP
3540 cm H2O for 2040 s)
Twice daily No net effect on oxygenation
or pulmonary mechanics
after first or subsequent RMs
Ventilator dysynchrony
(five patients),
barotraumas requiring
intervention (four
patients), appeared
uncomfortable (two
patients), transient
hypotension (two patients)
Oczenski (53) 30 Sustained inflation (CPAP
50 cm H2O for 30 s)
Once Significant increase in
P/F ratio at 3 min post-RM
(139 6 46 vs. 246 6
111 mm Hg, P, 0.001)
with return to baseline
values by 30 min; no
significant differences in
P/F ratio between RM and
control group at baseline
and after 30 min
No change in any
hemodynamic variables
at 3 min post-RM compared
with baseline values; no
significant differences
between groups in any
hemodynamic
variables detected
at 30 min compared
with baseline values
Stewart (20) 366 Sustained inflation (CPAP
40 cm H2O for 40 s)
Up to four times daily None reported 81 (22%) patients
with complications from
151 (11%) RMs: hypotension
(61 [5%]), desaturation
(58 [4%]), tachycardia/
bradycardia (24 [2%]),
new air leak (4 [0.3%]),
new arrhythmia (4 [0.3%])
Definition of abbreviations: CPAP 5 continuous positive airway
pressure; P/F ratio5 ratio of partial pressure of arterial oxygen
to fraction of inspired oxygen; PEEP5
positive end-expiratory pressure; RM 5 recruitment maneuver.
Fan, Wilcox, Brower, et al.: Recruitment Maneuvers in ALI
1159
-
8/14/2019 17 COM TRADU++O
5/8
remains to be determined, although a few studies have showna
survival advantage with a lung protective ventilation
strategyincorporating RMs (6, 8). In the interim, RMs may also
benefitthe minority of patients with ALI who develop
life-threateningrefractory hypoxemia.
Given the uncertain importance of transient oxygenationbenefits
derived from RMs, any important risks would be criticalin
decision-making around their use in patients with ALI.Adverse
events (e.g., hypotension and desaturation) were mostcommon during
the performance of RMs and were generallytransient and
self-limited, given the small proportion of patients(1%) that had
RMs terminated early due to adverse events.Serious complications
(e.g., barotrauma, arrhythmia) were un-common. Though difficult to
quantify, it is possible that evena transient increase in
transpulmonary pressure during an RM
may lead to enhanced VILI due to overdistention of
relativelyhealthy lung units. Furthermore, given that most
patientsrequire increased sedation and/or paralysis during the use
ofRMs, there is a potential for indirect adverse effects on
long-term outcomes (e.g., neurocognitive and neuromuscular
func-tion) (60). Although our results suggest that RMs are
generallywell tolerated, the risks and sequelae of RMs may
differsubstantially from patient to patient because even
transientevents may be detrimental in severely ill patients.
Because increased PEEP alone can lead to direct increasesin
oxygenation, we conducted a subgroup analysis with studiesthat had
a pre- to post-RM PEEP change of 5 cm H2O or less(versus .5 c m
H2O) in an attempt to isolate RM-specific
effects. RMs led to improved oxygenation in both
subgroups,although the changes were not statistically significant
in the pre-to post-RM PEEP change greater than 5 cm H2O group,
likelydue to the small number of studies (and patients) in
thatsubgroup. The level of post-RM PEEP may be critical
instabilizing and maintaining alveoli opened by the precedingRM;
failure to maintain inflation of recruited alveoli post-RMmay
potentiate VILI further through cyclic recruitment-dere-cruitment
and may explain the lack of a durable oxygenation
response seen in many studies (14, 26, 27, 31, 35, 37, 39, 43,
47,52, 53). Studies using a decremental PEEP trial to identify
anoptimal level of post-RM PEEP have maintained significant
Figure 2. Oxygenation (PaO2/FIO
2ratio) pre- and postrecruitment
maneuver by study (20 studies). The relationship between
oxygenation(P/F ratio) after the application of a recruitment
maneuver (RM) (post-
RM) with baseline (pre-RM) oxygenation in each individual study
is
presented. Oxygenation was significantly increased after an RM
(PaO2/
FIO2
ratio: 139 versus 251 mm Hg;P,0.001).
TABLE 3. BASELINE CHARACTERISTICS*
Characteristic
Age, yr 52 (9.5)
Female,n 8 (6.4)
Severity of illness (APACHE II Score) 21 (3.3)
Severity of ALI
Lung injury score 3.0 (0.26)
PaO2/FIO2 ratio, mm Hg 142 (39)
Respiratory system compliance, mL/cm H2O 34 (5.5)
ALI risk factor
Pulmonary,n (%) 336 (43)Pneumonia 212 (27)
Aspiration 64 (8)
Other 60 (8)
Extrapulmonary,n (%) 450 (57)
Sepsis 170 (22)
Pancreatitis 25 (3)
Trauma 113 (14)
Burns 5 (1)
Transfusion-related acute lung injury 5 (1)
Other 132 (16)
Ventilatory parameters
Peak inspiratory pressure, cm H2O 29 (3.7)
Plateau pressure, cm H2O 28 (4.8)
Positive end-expiratory pressure, cm H2O 12 (2.1)
VT, mL 508 (58)
VT, mL/kg 7.0 (1.2)
Respiratory rate, breaths per minute 19 (4.5)_VE, L/min 9.9
(2.2)
Co-interventions, no. (%)
Prone positioning 82 (22)
High-frequency oscillatory ventilation 0 (0)
Inhaled nitric oxide 19 (5)
High-dose corticosteroids 0 (0)
None 9 (2)
Definition of abbreviations: ALI 5 acute lung injury; APACHE 5
Acute Physiol-
ogy and Chronic Health Evaluation; FRM 5 recruitment
maneuver.
* All values are mean (SD) unless otherwise indicated. ALI risk
factors were reported in 37 studies (786 patients).
Co-interventions were reported in 17 studies (378 patients).
TABLE 4. PHYSIOLOGIC AND VENTILATORY VARIABLES*
Variable Pre-RM Post-RM Pvalue
Hemodynamics
Mean arterial blood pressure, mm Hg 83 (5.4) 84 (5.2) 0.53
Heart rate, beats per mi nute 104 (12.5) 105 (12.5) 0.04
Central venous press ure, mm Hg 13 (3.6) 16 (5.0) 0.009
Pulmonary capillary wedge pressure,
mm Hg
14 (1.2) 14 (0.8) 0.85
Q, L/min 8.6 (2.0) 8.6 (2.0) 0.58
Cardiac index, L/min/m2 4.4 (1.0) 4.1 (1.0) 0.19
Mi xed ve nous oxyge n saturat ion, % 70 (10) 77 (11)
0.07Arterial blood gas
pH 7.34 (0.08) 7.30 (0.15) 0.04
PaO2, mm Hg 106 (51.3) 193 (133) 0.001
PaCO2, mm Hg 46 (6.8) 48 (13.8) 0.87
Arterial oxygen saturation, % 92 (3.7) 95 (2.1) 0.17
Ventilatory settings
Peak inspiratory pressure, cm H2O 31 (2.8) 34 (4.7) 0.07
Plateau pressure, cm H2O 27 (3.8) 31 (6.4) 0.53
Mean airway pressure, cm H2O 18 (1.7) 22 (5.2) 0.12
Positive end-expiratory pressure, cm H2O 11 (3.1) 16 (5.9)
0.02
VT, mL 506 (57) 470 (251) 0.56
VT, mL/kg 8.1 (2.6) 6.6 (4.2) 0.84
FIO2, % 81 (18) 72 (23) 0.09
Respiratory mechanics
Respiratory system compliance,
mL/cm H2O
34 (4.5) 35 (8.1) 0.03
PaO2/FIO2 Ratio, mm Hg 139 (31.3) 251 (117.0) ,0.001
* All values are n-weighted mean (SD) unless otherwise
indicated. Physiologic variables were reported in 31 studies (636
patients) Ventilatory variables were reported in 32 studies (548
patients)
1160 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
VOL 178 2008
-
8/14/2019 17 COM TRADU++O
6/8
oxygenation benefits for at least 4 to 6 hours (41, 46). It
remainsunclear whether prolonged benefits in oxygenation,
perhapsusing different RM techniques, have an impact on
importantclinical outcomes in patients with ALI. Finally, it is
impossiblewithin the confines of this systematic review to isolate
RM- andPEEP-independent effects on oxygenation, which would
re-quire an experimental design (i.e., a controlled clinical
trial).However, we believe that this analysis is hypothesis
generatingfor testing in future studies.
Our study provides conflicting data on the oxygenationbenefit
from RMs based on baseline ALI severity. Patients
with a lower baseline PaO2/F
IO2 ratio experienced a significantoxygenation improvement,
whereas those with lower baseline
respiratory system compliance did not. The lack of
oxygenationbenefit in patients with lower baseline respiratory
system com-pliance may be consistent with a subgroup of patients
with ALIwho are not easily recruitable and in whom the risks of
RMsmay outweigh the potential benefits. Although hypotension
hasbeen reported to be more common in patients with poor chestwall
compliance and limited RM-induced oxygenation benefit(61), we did
not observe any difference in hypotension in asimilar subgroup of
patients in our study with low baselinerespiratory system
compliance. In contrast, Gattinoni andcolleagues demonstrated that
patients with ALI who had lowerbaseline ALI disease severity
(respiratory system compliance 496 16 mL/cm H2O; PaO
2/FIO
2ratio 220 6 70 mm Hg) had a lower
potential for recruitment due to fewer targets available
(i.e.,diseased, atelectatic lung units) for recruitment (13).
Patientsincluded in our systematic review had more severe ALI
atbaseline (as measured by baseline respiratory system compli-ance
and PaO
2/FiO
2ratio), which may explain these divergent
results.Our study has other potential limitations. First,
because the
studies were heterogeneous in design, type of RM used,
andoutcomes measured and reported, we could not performa
quantitative meta-analysis with true effect sizes (i.e.,
relativerisk or odds ratio). Furthermore, too few randomized
controlledtrials of RMs have been conducted to allow a summary of
theeffects of RMs as compared with placebo (or sham) in
patients
with ALI. However, the results of our analysis are similar to
thefew randomized controlled trials that have been reported (15,20,
53, 54). Second, most studies did not directly measurealveolar
recruitment, making it difficult to attribute our findingsof
improved oxygenation to successful RMs alone. Changes inoxygenation
alone may not directly reflect recruitment becauseoxygenation may
be influenced by other factors affected byRMs, such as cardiac
output. However, cardiac output (orindex) did not change
significantly after an RM in studies thatreported these parameters.
Because shunt from airless lungregions is a major cause of arterial
hypoxemia in ALI (1), RM-induced recruitment is likely the cause of
the transient oxygen-ation improvements. Furthermore, our results
were robust inthe subgroup of patients with a pre- to post-RM
PEEPdifference of 5 cm H2O or less. Third, given the
previousfindings of transient RM-induced oxygenation effects,
ourinclusion of a wide range of reported data at the post-RM
timepoint may not accurately reflect the true effect of
RMs.However, by including data up to 120 minutes post-RM, thiswould
have biased our results toward finding no significantdifference in
oxygenation pre- to post-RM. In addition, ourresults were robust in
a sensitivity analysis restricted to datareported less than 30
minutes post-RM. Finally, the results fromour subgroup analyses
based on baseline ALI severity may
differ depending on the thresholds chosen for PaO2/FIO2 ratioand
respiratory system compliance. Both thresholds werechosen to
balance clinical and practical considerations; for thelatter, this
allowed enough patients to be included in eachsubgroup to make a
meaningful comparison.
In conclusion, adult patients with ALI receiving RMsexperienced
a significant increase in short-term oxygenation,with few serious
short-term adverse events. Transient hypoten-sion and desaturation
during RMs is common, although likelyself-limited without serious
sequelae. The risks of RMs mayoutweigh the potential benefits in
patients with ALI who havelow baseline respiratory system
compliance, although thesefindings require confirmation in future
studies. Given the un-certain benefit of transient oxygenation
improvements in patients
with ALI and the lack of information on their clinical
outcomeeffects, the routine use of RMs cannot be recommended
ordiscouraged at this time. RMs should be considered on
anindividualized basis in patients with ALI with
life-threateningrefractory hypoxemia.
Conflict of Interest Statement: None of the authors has a
financial relationshipwith a commercial entity that has an interest
in the subject of this manuscript.
References
1. Ware LB, Matthay MA. The acute respiratory distress
syndrome.
N Engl J Med 2000;342:13341349.2. Rubenfeld GD, Herridge MS.
Epidemiology and outcomes of acute lung
injury.Chest2007;131:554562.3. Rubenfeld GD, Caldwell MS,
Peabody E, Weaver J, Martin DP, Neff M,
Stern EJ, Hudson LD. Incidence and outcomes of acute lung
injury. NEngl J Med 2005;353:16851693.
4. Esteban A, Anzueto A, Frutos F, Alia I, Brochard L, Stewart
TE,
Benito S, Epstein SK, Apezteguia C, Nightingale P, et al.
Character-istics and outcomes in adult patients receiving
mechanical ventilation:a 28-day international study. JAMA
2002;287:345355.
5. Fan E, Needham DM, Stewart TE. Ventilatory management of
acute
lung injury and acute respiratory distress
syndrome.JAMA2005;294:28892896.
6. Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino
GP,
Lorenzi-Filho G, Kairalla RA, Deheinzelin D, Munoz C, Oliveira
R,et al. Effect of a protective-ventilation strategy on mortality
in theacute respiratory distress syndrome. N Engl J Med
1998;338:347354.
TABLE 5. ADVERSE EVENTS AND MORTALITY
Adverse Event or Outcome Pre-RM During RM Post-RM
Cardiovascular,* no. (%)
Cardiac arrest 0 0 0
Arrhythmia 0 8 (1) 0
Myocardial ischemia/infarction 0 0 0
Hypertension 0 0 0
Hypotension 0 114 (12) 0
Other cardiovascular 0 24 (2) 0
Respiratory,* no. (%)
Desaturation 1 (0) 82 (8) 0Barotrauma 0 9 (1) 9 (1)
Refractory respiratory acidosis 0 0 0
Other respiratory 0 5 (1) 0
Other (noncardiovascular, nonrespiratory),*n (%) 0 4 (1) 0
Studies with no adverse events,
n (no. of patients)
17 (287)
Studies that did not report adverse events,
n (no. of patients)
9 (201)
RMs terminated due to adverse events, n (%) 10 (1)
Mortality, n(%) 157 (38)
Studies that did not report mortality,
n (no. of patients)
20 (736)
Definition of abbreviations: ICU 5 intensive care unit; RM 5
recruitment
maneuver.
* Adverse events were reported in 31 studies (985 patients).
Mortality was reported in 20 studies (409 patients).
Fan, Wilcox, Brower, et al.: Recruitment Maneuvers in ALI
1161
-
8/14/2019 17 COM TRADU++O
7/8
7. The Acute Respiratory Distress Syndrome Network. Ventilation
with
lower tidal volumes as compared with traditional tidal volumes
foracute lung injury and the acute respiratory distress syndrome. N
Engl
J Med 2000;342:13011308.8. Villar J, Kacmarek RM, Perez-Mendez
L, Aguirre-Jaime A. A high
positive end-expiratory pressure, low tidal volume ventilatory
strategyimproves outcome in persistent acute respiratory distress
syndrome:a randomized, controlled trial. Crit Care Med
2006;34:13111318.
9. Lapinsky SE, Mehta S. Bench-to-bedside review: recruitment
and
recruiting maneuvers. Crit Care 2005;9:6065.10. Trembley LN,
Slutsky AS. Ventilator-induced lung injury: from the
bench to the bedside. Intensive Care Med 2006;32:2433.11.
Gattinoni L, Pesenti A. The concept of baby lung.Intensive Care
Med
2005;31:776784.12. Dreyfuss D, Saumon G. Ventilator-induced lung
injury: lessons from
experimental studies. Am J Respir Crit Care Med
1998;157:294323.13. Lapinsky SE, Aubin M, Mehta S, Boiteau P,
Slutsky A. Safety and
efficacy of a sustained inflation for alveolar recruitment in
adults withrespiratory failure. Intensive Care Med
1999;25:12971301.
14. Pelosi P, Cadringher P, Bottino N, Panigada M, Carrieri F,
Riva E,
Lissoni A, Gattinoni L. Sigh in acute respiratory distress
syndrome.Am J Respir Crit Care Med1999;159:872880.
15. The ARDS Clinical Trials Network. Effects of recruitment
maneuvers in
patients with acute lung injury and acute respiratory distress
syn-drome ventilated with high positive end-expiratory
pressure.Crit CareMed 2003;31:25922597.
16. Pelosi P, DOnofrio D, Chiumello D, Paolo S, Chiara G,
Capelozzi VL,
Barbas CS, Chiaranda M, Gattinoni L. Pulmonary and
extrapulmo-
nary acute respiratory distress syndrome are different. Eur
Respir JSuppl2003;42:48S56S.
17. Gattinoni L, Caironi P, Cressoni M, Chiumello D, Ranieri VM,
Quintel
M, Russo S, Patroniti N, Cornejo R, Bugedo G. Lung recruitment
inpatients with acute respiratory distress syndrome. N Engl J Med
2006;354:17751786.
18. Lim SC, Adams AB, Simonson DA, Dries DJ, Broccard AF,
Hotchkiss
JR, Marini JJ. Intercomparison of recruitment maneuver efficacy
inthree models of acute lung injury. Crit Care Med
2003;32:23712377.
19. Cakar N, Akinci O, Tugrul S, Ozcan PE, Esen F, Eraksoy H,
Cagatay A,
Telci L, Nahum A. Recruitment maneuver: does it promote
bacterialtranslocation?Crit Care Med2002;30:21032106.
20. Stewart TE, Cooper J, Laufer B, Lapinsky SE, Langevin S,
Granton JT,
Muscedere J, Ward M, Woolfe C, Lesur O. Complications of
re-cruitment maneuvers in a multicenter trial of lung protective
venti-lation in ALI/ARDS. Am J Respir Crit Care Med
2007;175:A943.
21. Higgins JPT, Green S, editors. Cochrane handbook for
systematicreviews of interventions 5.0.0 [updated February 2008;
accessed July27, 2008]. Available from:
http://www.cochrane-handbook.org/.
22. Landis JR, Koch GG. The measurement of observer agreement
for
categorical data. Biometrics1977;33:159174.23. Bugedo G, Bruhn
A, Hernandez G, Rojas G, Varela C, Tapia JC,
Castillo L. Lung computed tomography during a lung
recruitmentmaneuver in patients with acute lung injury. Intensive
Care Med2003;29:218225.
24. Claesson J, Lehtipalo S, Winso O. Do lung recruitment
maneuvers
decrease gastric mucosal perfusion? Intensive Care Med
2003;29:13141321.
25. Ferguson ND, Chiche J-D, Kacmarek RM, Hallett DC, Mehta S,
Findlay
GP, Granton JT, Slutsky AS, Stewart TE. Combining
high-frequencyoscillatory ventilation and recruitment maneuvers in
adults with earlyacute respiratory distress syndrome: The Treatment
with Oscillationand an Open Lung Strategy (TOOLS) Trial pilot
study. Crit Care
Med 2005;33:479486.26. Foti G, Cereda M, Sparacino ME, De Marchi
L, Villa F, Pesenti A. Effects
of periodic lung recruitment maneuvers on gas exchange and
respira-tory mechanics in mechanically ventilated acute respiratory
distresssyndrome (ARDS) patients. Intensive Care Med
2000;26:501507.
27. Grasso S, Mascia L, Del Turco M, Malacarne P, Giunta F,
Brochard L,
Slutsky AS, Marco Ranieri V. Effects of recruiting maneuvers
inpatients with acute respiratory distress syndrome ventilated
withprotective ventilatory strategy. Anesthesiology
2002;96:795802.
28. Johannigman JA, Miller SL, Davis BR, Davis K Jr, Campbell
RS,
Branson RD. Influence of low tidal volumes on gas exchange in
acuterespiratory distress syndrome and the role of recruitment
maneuvers.
J Trauma2003;54:320325.29. Lim C-M, Jung H, Koh Y, Lee JS, Shim
TS, Lee SD, Kim WS, Kim DS,
Kim WD. Effect of alveolar recruitment maneuver in early
acute
respiratory distress syndrome according to antiderecruitment
strat-egy, etiological category of diffuse lung injury, and body
position ofpatient.Crit Care Med 2003;31:411418.
30. Lim C-M, Koh Y, Park W, Chin JY, Shim TS, Lee SD, Kim WS,
Kim
DS, Kim WD. Mechanistic scheme and effect of extended sigh asa
recruitment maneuver in patients with acute respiratory
distresssyndrome: a preliminary study. Crit Care Med
2001;29:12551260.
31. Oczenski W, Hormann C, Keller C, Lorenzi N, Kepka A, Schwarz
S,
Fitzgerald RD. Recruitment maneuvers during prone positioning
inpatients with acute respiratory distress syndrome.Crit Care
Med2005;33:5461.
32. Park KJ, Lee YJ, Oh YJ, Lee KS, Sheen SS, Hwang SC. Combined
effectsof inhaled nitric oxide and a recruitment maneuver in
patients withacute respiratory distress syndrome. Yonsei Med J
2003;44:219226.
33. Patroniti N, Fot G, Cortinovis B, Maggioni E, Bigatello LM,
Cereda M,
Pesenti A. Sigh improves gas exchange and lung volume in
patientswth acute respiratory distress syndrome undergoing pressure
supportventilation.Anesthesiology 2002;96:788794.
34. Pelosi P, Bottino N, Chiumello D, Caironi P, Panigada M,
Gamberoni C,
Colombo G, Bigatello LM, Gattinoni L. Sign in supine and
proneposition during acute respiratory distress syndrome. Am J
Respir CritCare Med 2003;167:521527.
35. Povoa P, Almeida E, Fernandes A, Mealha R, Moreira P, Sabino
H.
Evaluation of a recruitment maneuver with positive
inspiratorypressure and high PEEP in patients with severe ARDS.
Acta Anaes-thesiol Scand 2004;48:287293.
36. Richard J-C, Maggiore SM, Jonson B, Mancebo J, Lemaire F,
Brochard
L. Influence of tidal volume on alveolar recruitment. Am J
Respir Crit
Care Med 2001;163:16091613.37. Schreiter D, Reske A, Scheibner
L, Glien C, Katscher S, Josten C. The
open lung concept: a clinical trial in severe chest
trauma.Chuirg2002;73:353359.
38. Takeuchi M, Imanaka H, Tachibana K, Ogino H, Ando M,
Nishimura
M. Recruitment maneuver and high positive end-expiratory
pressureimprove hypoxemia in patients after pulmonary
thromboendarterec-tomy for chronic pulmonary throboembolism. Crit
Care Med2005;33:20102014.
39. Villagra A, Ochagavia A, Vatua S, Murias G, Del Mar
Fernandez M,
Lopez Aguilar J, Fernandez R, Blanch L. Recruitment
maneuversduring lung protective ventilation in acute respiratory
distress syn-drome.Am J Respir Crit Care Med 2002;165:165170.
40. Wauer VH, Groll G, Krausch D, Lehmann C, Kox WJ. Clinical
experi-
ences with the open lung concept.Anaesthesiol
Reanim2003;28:844.41. Borges JB, Okamoto VN, Matos GF, Caramez MP,
Arantes PR, Barros
F, Souza CE, Victorino JA, Kacmarek RM, Barbas CS, et al.
Re-versibility of lung collapse and hypoxemia in early acute
respiratorydistress syndrome. Am J Respir Crit Care Med
2006;174:268278.
42. Galiatsou E, Kostanti E, Svarna E, Kitsakos A, Koulouras V,
Efremidis
SC, Nakos G. Prone position augments recruitment and
preventsalveolar overinflation in acute lung injury.Am J Respir
Crit Care Med2006;174:187197.
43. Lapinsky SE, Aubin M, Mehta S, Boiteau P, Slutsky AS. Safety
and
efficacy of a sustained inflation for alveolar recruitment in
adults withrespiratory failure. Intensive Care Med
1999;25:12971301.
44. Puls A, Pollok-Kopp B, Wrigge H, Quintel M, Neumann P.
Effects of
a single-lung recruitment maneuver on the systemic release
ofinflammatory mediators. Intensive Care Med 2006;32:10801085.
45. Antonaglia V, Pascotto S, De Simoni L, Zin WA. Effects of a
sigh on the
respiratory mechanical properties in ALI patients. J Clin
MonitComput2006;20:243249.
46. Girgis K, Hamed H, Khater Y, Kacmarek RM. A decremental
PEEP
trial identifies the PEEP level that maintains oxygenation after
lungrecruitment.Respir Care 2006;51:11321139.
47. Li M-Q, Zhang Z, Li S-M, Shi ZX, Xu JY, Lu F, Li L, Wang
HM.
Comparative study on recruitment maneuvers in acute
respiratorydistress syndrome with pulmonary and extrapulmonary
origin. ChinCrit Care Med 2006;18:355358.
48. Yi H-M, Cai C-J, Lu M-Q, Wang GS, Yi SH, Yang Y, Xu C, Li H,
Chen
GH. The treatment strategy of early ALI after liver
transplantation.Chin J Surg 2006;44:889893.
49. Constantin J-M, Cayot-Constantin S, Roszyk L, Futier E,
Saphin V,
Dastugue B, Bazin JE, Rouby JJ. Response to recruitment
maneuverinfluences net alveolar fluid clearance in acute
respiratory distresssyndrome.Anesthesiology 2007;106:944951.
50. Tugrul S, Akinci O, Ozcan PE, Ince S, Esen F, Telci L, Akpir
K, Cakar
N. Effects of sustained inflation and postinflation positive
end-
1162 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
VOL 178 2008
-
8/14/2019 17 COM TRADU++O
8/8
expiratory pressure in acute respiratory distress syndrome:
focusingon pulmonary and extrapulmonary factors. Crit Care Med
2003;31:738744.
51. Toth I, Leiner T, Mikor A, Szakmany T, Bogar L, Molnar Z.
Hemody-namic and respiratory changes during lung recruitment and
descend-ing optimal positive end-expiratory pressure titration in
patients withacute respiratory distress syndrome. Crit Care
Med2007;35:787793.
52. Talmor D, Sarge T, Legedza A, ODonnell CR, Ritz R, Loring
SH,Malhotra A. Cytokine release following recruitment
maneuvers.Chest2007;132:14341439.
53. Oczenski W, Hormann C, Keller C, Lorenzi N, Kepka A, Schwarz
S,
Fitzgerald RD. Recruitment maneuvers after a positive
end-expira-tory pressure trial do not induce sustained effects in
early adultrespiratory distress syndrome. Anesthesiology
2004;101:620625.
54. Meade MO, Guyatt GH, Cook DJ, Lapinsky SE, Hand L, Griffith
L,Stewart TE. Physiologic randomized pilot study of a lung
recruitmentmaneuver in acute lung injury. Am J Respir Crit Care Med
2002;165:A683.
55. Richards G, White H, Hopley M. Rapid reduction of
oxygenation indexby employment of a recruitment technique in
patients with severeARDS.J Intensive Care Med2001;16:193199.
56. Schreiter D, Reske A, Stichert B, Seiwerts M, Bohm SH,
Kloeppel R,Josten C. Alveolar recruitment in combination with
sufficient pos-itive end-expiratory pressure increases oxygenation
and lung aera-tion in patients with severe chest trauma. Crit Care
Med 2004;32:968975.
57. Suh GY, Kwon OJ, Yoon JW, Park SJ, Ham HS, Kang SJ, Koh
WH,Chung MP, Kim HJ. A practical protocol for titrating optimalPEEP
in acute lung injury: recruitment maneuver and PEEP decre-ment.J
Korean Med Sci 2003;18:349354.
58. Yang Z-J, Zhang X-Y, Fan H-R, Jiang X, Wang QX, Shen JF,
Chen L.The analysis of 252 episodes of recruitment maneuvers
during
mechanical ventilation in surgery intensive care unit. Chin Crit
CareMed2007;19:539541.59. WareLB.Prognostic determinantsof acute
respiratorydistresssyndrome in
adults: impact on clinical trial design. Crit Care Med
2005;33:S217S222.60. Desai SV, Boucher K, Fan E, Needham D.
Long-term outcomes after
acute lung injury. Contemporary Crit Care 2006;4:110.61. Rothen
HU, Sporre B, Engberg G, Wegenius G, Hogman M,
Hedenstierna G. Influence of gas composition on recurrence
ofatelectasis after a reexpansion maneuver during general
anesthesia.
Anesthesiology1995;82:832842.
Fan, Wilcox, Brower, et al.: Recruitment Maneuvers in ALI
1163