-
8/3/2019 9789241596657_eng anemia
1/51
-
8/3/2019 9789241596657_eng anemia
2/51
-
8/3/2019 9789241596657_eng anemia
3/51
Worldwide
prevalence of anaemia19932005who Gb db
ai
Editors
Bruno de Benoist
w h ogizi
G, siz
Erin McLean
w h ogizi
G, siz
Ines Egli
Ii si nii,
eth Zi, siz
Mary Cogswellc di c pi
a, Ggi
-
8/3/2019 9789241596657_eng anemia
4/51
World Health Organization 2008
All rights reserved. Publications o the World Health
Organization can be obtained rom WHO Press, World Health
Organization, 20 Avenue Appia,1211 Geneva 27, Switzerland (tel.:
+41 22 791 3264; ax: +41 22 791 4857; e-mail: [email protected]).
Requests or permission to reproduce ortranslate WHO publications
whether or sale or or noncommercial distribution should be
addressed to WHO Press, at the above address (ax: +41
22 791 4806; e-mail: [email protected]).The designations
employed and the presentation o the material in this publication do
not imply the expression o any opinion whatsoever on the part othe
World Health Organization concerning the legal status o any
country, territory, city or area or o its authorities, or
concerning the delimitation o itsrontiers or boundaries. Dotted
lines on maps represent approximate border lines or which there may
not yet be ull agreement.
The mention o specic companies or o certain manuacturers
products does not imply that they are endorsed or recommended by
the World HealthOrganization in preerence to others o a similar
nature that are not mentioned. Errors and omissions excepted, the
names o proprietary products aredistinguished by initial capital
letters.
All reasonable precautions have been taken by the World Health
Organization to veriy the inormation contained in this publication.
However, thepublished material is being distributed without
warranty o any kind, either expressed or implied. The
responsibility or the interpretation and use o thematerial lies
with the reader. In no event shall the World Health Organization be
liable or damages arising rom its use.
The named authors alone are responsible or the views expressed
in this publication.
Cover photographs by Virot Pierre, Armando Waak, Carlos
Gaggero
Designed by minimum graphicsPrinted in Spain
WHO Library Cataloguing-in-Publication Data
Worldwide prevalence o anaemia 19932005 : WHO global database on
anaemia / Edited by Bruno de Benoist,Erin McLean, Ines Egli and
Mary Cogswell.
1.Anemia prevention and control. 2.Anemia epidemiology.
3.Prevalence. I.World Health Organization.
ISBN 978 92 4 159665 7 (NLM classication: WH 155)
-
8/3/2019 9789241596657_eng anemia
5/51
Contents
Preace v Acknowledgements Abbreviations
1. Introduction 1
1.1 Anaemia: a public health problem 1
1.1.1 Etiology 11.1.2 Health consequences 11.1.3 Assessing
anaemia 1
1.2 Control o anaemia 11.2.1 Correcting anaemia 1
2. Methods 3
2.1 Data sources The WHO Global Database on Anaemia 32.2
Selection o survey data 3
2.2.1 Administrative level 32.2.2 Population groups 4
2.3 Dening anaemia 4
2.3.1 Haemoglobin threshold 42.3.2 Estimated anaemia prevalence
or countries with no survey data 52.3.3 Uncertainty o estimates
52.3.4 Combining national estimates 52.3.5 Global anaemia
prevalence 52.3.6 Classication o anaemia as a problem o public
health signicance 6
2.4 Population coverage, proportion o population, and the number
o individuals with anaemia 62.4.1 Population coverage 62.4.2
Proportion o population and the number o individuals aected 6
3. Results and Discussion 7
3.1 Results 7
3.1.1. Population coverage 73.1.2 Proportion o population and
number o individuals with anaemia 73.1.3 Classication o countries
by degree o public health signicance o anaemia 8
3.2 Discussion 83.2.1 Population coverage 83.2.2 Strengths o
estimates 83.2.3 Limitations o estimates 83.2.4 Proportion o
population and the number o individuals with anaemia 123.2.5
Classication o countries by degree o public health signicance o
anaemia, based on
haemoglobin concentration 123.2.6 Comparison to previous
estimates 12
3.3 Conclusion 12
References 14
iiicontents
-
8/3/2019 9789241596657_eng anemia
6/51
Annexes
Annex 1 WHO Member States grouped by WHO and UN regions 15Table
A1.1 WHO Member States grouped by WHO regions 15Table A1.2 WHO
Member States grouped by UN regions and subregions 16
Annex 2 Results by UN region 18Table A2.1 Population coverage by
anaemia prevalence surveys (national or subnational)
conducted between 1993 and 2005 by UN region 18Table A2.2
Anaemia prevalence by UN region 18
Annex 3 National estimates o anaemia 20Table A3.1 Country
estimates o anaemia prevalence in preschool-age children 20Table
A3.2 Country estimates o anaemia prevalence in pregnant women
25Table A3.3 Country estimates o anaemia prevalence in non-pregnant
women o reproductive age 30Table A3.4 Country reerences 35
Tables
Table 2.1 Haemoglobin thresholds used to dene anaemia 4Table 2.2
Prediction equations used to generate anaemia estimates or
countries without survey data 5Table 2.3 Classication o anaemia as
a problem o public health signicance 6
Table 3.1 Population coverage (%) by anaemia prevalence surveys
(national or subnational) conductedbetween 1993 and 2005 7
Table 3.2 Global anaemia prevalence and number o individuals
aected 7Table 3.3 Anaemia prevalence and number o individuals
aected in preschool-age children, non-pregnant
women and pregnant women in each WHO region 8Table 3.4 Number o
countries categorized by public health signicance o anaemia 8
Figures
Figure 3.1 Anaemia as a public health problem by country(a)
Preschool-age children 9(b) Pregnant women 10(c) Non-pregnant women
o reproductive age 11
worldwIde prevalence o anaemIa 19932005iv
-
8/3/2019 9789241596657_eng anemia
7/51
Preface
Anaemia is a public health problem that aects populationsin both
rich and poor countries. Although the primarycause is iron
deciency, it is seldom present in isolation.More requently it
coexists with a number o other causes,such as malaria, parasitic
inection, nutritional deciencies,
and haemoglobinopathies.Given the importance o this pathology in
the world, nu-
merous countries conduct interventions to reduce
anaemia;particularly in the groups most susceptible to its
devastat-ing eects: pregnant women and young children. In orderto
assess the impact o these interventions, the adequacyo the
strategies implemented, and the progress made inthe ght against
anaemia, inormation on anaemia preva-lence must be collected. This
is the primary objective o theWHO Global Database on Anaemia.
However, estimateso anaemia prevalence by themselves are only useul
i they
are associated with a picture o the various causal actorsthat
contribute to the development o anaemia in specicsettings. Indeed
these actors are multiple and complex, andit is critical to collect
accurate inormation about them toprovide the basis or developing
the best interventions oranaemia control.
In the last three decades, there have been various at-tempts to
produce estimates o the prevalence o anaemiaat dierent levels
including at the global level, but untilthe present time, there has
never been a systematic reviewo all o the data collected and
published with the objec-tive o deriving regional and global
estimates. The WHO
Global Database on Anaemia has lled this gap: data rom93
countries, representing as much as 76% o the popula-tion in the
case o preschool-age children, were analysedand used to develop
statistical models to generate nationalprevalence estimates or
countries with no data within thetime rame specied.
It is surprising that given the public health importanceo
anaemia, there are numerous countries lacking nationalprevalence
data. Moreover, most survey data are relatedto the three population
groups: preschool-age children,pregnant women, and non-pregnant
women o reproduc-
tive age, which is why the report ocuses on these groups.
The data available or school-age children, men, and theelderly
were not sucient to generate regional or country-level estimates or
these groups, and thereore only globalestimates or these groups are
presented.
In addition, despite the act that iron deciency is con-
sidered to be the primary cause o anaemia, there are ewdata on
the prevalence o this deciency. The likely reasonis that iron
assessment is dicult because the available in-dicators o iron
status do not provide sucient inormationalone and must be used in
combination to obtain reliableinormation on the existence o iron
deciency. Further-more, there is no real consensus on the best
combination oindicators to use. Another reason is that the role o
actorsother than iron deciency in the development o anaemiahas been
underestimated by public health ocials, becauseor a long time
anaemia has been conused with iron de-
ciency anaemia, and this has infuenced the development
ostrategies and programmes designed to control anaemia.In this
report, the prevalence o anaemia is presented by
country and by WHO regions. Because these prevalencedata may be
used to identiy programme needs by otherUnited Nations agencies, we
have presented the estimatesclassied by United Nations regions in
the annexes. In ad-dition, one chapter is dedicated to the criteria
used to iden-tiy, revise, and select the surveys, and the
methodologydeveloped to generate national, regional, and global
esti-mates.
A lesson learned rom producing this report is that in
order or the database to reach its ull potentia l, data shouldbe
collected on other vulnerable population groups such asthe elderly
and school-age children, and surveys should bemore inclusive and
collect inormation on iron status andother causes o anaemia.
This report is written or public health ocials, nutri-tionists,
and researchers. We hope that readers nd it useuland eel ree to
share any comments with us.
Bruno de Benoist
Coordinator, Micronutrient Unit
World Health Organization
vpreace
-
8/3/2019 9789241596657_eng anemia
8/51
Acknowledgements
WHO wishes to thank the numerous individuals, insti-tutions,
governments, non-governmental, and internationalorganizations or
providing data or the database. Withoutcontinual international
collaboration in keeping the data-base up-to-date, this compilation
on the global situation
and trends in anaemia prevalence would not have been pos-sible.
Special thanks are due to ministries o health o theWHO Member
States, WHO regional oces, and WHOcountry oces.
worldwIde prevalence o anaemIa 19932005vi
The WHO Global Database on Anaemia was developed bythe
Micronutrient team in the Department o Nutrition orHealth and
Development with the nancial support o theCenters or Disease
Control and Prevention.
The estimates or the database were produced by Erin
McLean, Mary Cogswell, Ines Egli, and Daniel Wojdyla with
contributions rom Trudy Wijnhoven, LaurenceGrummer-Strawn, and
Bradley Woodru, under the co-ordination o Bruno de Benoist. Grace
Rob and Ann-BethMoller assisted in data management.
-
8/3/2019 9789241596657_eng anemia
9/51
viiaBBrevIatIons
Abbreviations
CDC Centers or Disease Control and PreventionHb HaemoglobinHDI
Human Development Index: a composite indicator o wealth, lie
expectancy and education developed by
the United Nations Development Programme.IDA Iron deciency
anaemia
NHANES National Health and Nutrition Examination SurveyNPW
Non-pregnant women (15.0049.99 yrs)PreSAC Preschool-age children
(0.004.99 yrs)PW Pregnant womenSD Standard deviationUN United
NationsVMNIS Vitamin and mineral nutrition inormation system WHO
World Health OrganizationCRP C-reactive protein
-
8/3/2019 9789241596657_eng anemia
10/51
-
8/3/2019 9789241596657_eng anemia
11/51
1
1. Introduction
1.1 Anaemia: a public health problem
Anaemia is a global public health problem aecting bothdeveloping
and developed countries with major conse-quences or human health as
well as social and economicdevelopment. It occurs at all stages o
the lie cycle, but
is more prevalent in pregnant women and young children.In 2002,
iron deciency anaemia (IDA) was considered tobe among the most
important contributing actors to theglobal burden o disease
(1).
1.1.1 Etiology
Anaemia is the result o a wide variety o causes that can
beisolated, but more oten coexist. Globally, the most signi-cant
contributor to the onset o anaemia is iron deciencyso that IDA and
anaemia are oten used synonymously, andthe prevalence o anaemia has
oten been used as a proxyor IDA. It is generally assumed that 50% o
the cases oanaemia are due to iron deciency (2), but the
proportionmay vary among population groups and in dierent
areasaccording to the local conditions. The main risk actors orIDA
include a low intake o iron, poor absorption o ironrom diets high
in phytate or phenolic compounds, and pe-riod o lie when iron
requirements are especially high (i.e.growth and pregnancy).
Among the other causes o anaemia, heavy blood loss asa result o
menstruation, or parasite inections such as hook-worms, ascaris,
and schistosomiasis can lower blood haemo-globin (Hb)
concentrations. Acute and chronic inections,
including malaria, cancer, tuberculosis, and HIV can alsolower
blood Hb concentrations. The presence o other micro-nutrient
deciencies, including vitamins A and B12, olate,ribofavin, and
copper can increase the risk o anaemia. Fur-thermore, the impact o
haemoglobinopathies on anaemiaprevalence needs to be considered
within some populations.
1.1.2 Health consequences
Anaemia is an indicator o both poor nutrition and poorhealth.
The most dramatic health eects o anaemia, i.e.,increased risk o
maternal and child mortality due to severeanaemia, have been well
documented (35). In addition,
1. IntroductIon
the negative consequences o IDA on cognitive and physi-cal
development o children, and on physical perormance particularly
work productivity in adults are o majorconcern (2).
1.1.3 Assessing anaemiaHb concentration is the most reliable
indicator o anae-mia at the population level, as opposed to
clinical meas-ures which are subjective and thereore have more room
orerror. Measuring Hb concentration is relatively easy
andinexpensive, and this measurement is requently used as aproxy
indicator o iron deciency. However, anaemia canbe caused by actors
other than iron deciency. In addition,in populations where the
prevalence o inherited haemo-globinopathies is high, the mean level
o Hb concentrationmay be lowered. This underlines that the etiology
o anae-
mia should be interpreted with caution i the only indicatorused
is Hb concentration. The main objective or assess-ing anaemia is to
inorm decision-makers on the type omeasures to be taken to prevent
and control anaemia. Thisimplies that in addition to the
measurement o Hb concen-tration, the causes o anaemia need to be
identied consid-ering that they may vary according to the
population.
1.2 Control of anaemia
1.2.1 Correcting anaemia
Given the multiactorial nature o this disease, correctinganaemia
oten requires an integrated approach. In order
to eectively combat it, the contributing actors must beidentied
and addressed. In settings where iron deciencyis the most requent
cause, additional iron intake is usuallyprovided through iron
supplements to vulnerable groups;in particular pregnant women and
young children. Food-based approaches to increase iron intake
through oodortication and dietary diversication are important,
sus-tainable strategies or preventing IDA in the general
pop-ulation. In settings where iron deciency is not the onlycause o
anaemia, approaches that combine iron interven-tions with other
measures are needed.
Strategies should include addressing other causes o
-
8/3/2019 9789241596657_eng anemia
12/51
worldwIde prevalence o anaemIa 199320052
anaemia (6,7),1.2 and should be built into the primaryhealth
care system and existing programmes. These strat-egies should be
tailored to local conditions, taking intoaccount the specic
etiology and prevalence o anaemia ina given setting and population
group.
1 http://www.who.int/malaria/docs/TreatmentGuidelines2006.pd2
http://www.who.int/wormcontrol/documents/en/Controlling%20
Helminths.pd
-
8/3/2019 9789241596657_eng anemia
13/51
3
2. Methods
2.1 Data sources The WHO Global Databaseon Anaemia
The estimates presented are based on data rom the WHOGlobal
Database on Anaemia; a part o the Vitamin andMineral Nutrition
Inormation System (VMNIS), main-
tained at WHO.Data are collected rom the scientic literature
and
through collaborators, including WHO regional andcountry oces,
United Nations organizations, ministrieso health, research and
academic institutions, and non-governmental organizations. MEDLINE
and WHO re-gional databases were searched systematically, and
manualsearches were conducted to nd articles published in
non-indexed medical and proessional journals. For inclusion inthe
database, Hb must be measured in capillary, venous,or cord blood
using quantitative photometric methods or
automated cell counters. In addition, anaemia prevalence ormean
Hb concentrations have to be reported. Surveys wereexcluded i they
measured only clinical signs o anaemia orhaematocrit. Data are
included in the database i they arerepresentative o any
administrative level within a country,including nationally
representative data and surveys repre-sentative o a region, the rst
administrative level bound-ary, second administrative level
boundary or local surveys.As o December 31, 2005, 696 surveys were
available in thedatabase; the majority o these in women or
preschool-agechildren.
2.2 Selection of survey dataThe time rame or the current
estimates is 19932005 andsurvey data or WHOs 1921 Member States
were extractedrom the database. Data on anaemia were selected or
each
country using two variables: the administrative level or which
the survey was representative, and the populationgroup
surveyed.
2.2.1 Administrative level
Surveys were selected based on the administrative levelthey
represented. Surveys were classied as national whenthey were based
on a nationally representative sample. Sub-national surveys were
also available in the database andwere classied according to the
population that they rep-resented as regional (multiple states),
state (representativeo the rst administrative level boundary),
district (repre-sentative o the second administrative level
boundary), orlocal surveys.
Data rom the most recent national survey was used inpreerence to
subnational surveys. For one country, where
an area had been let out o a national survey because osecurity
concerns, available data rom the missing regionwas pooled with the
national data and weighted by the gen-eral population estimate or
that area to provide a nationalestimate or that country. This
proportion was determinedby using the most recent census data rom
the country. Itwo national surveys were conducted in the same year,
sur-vey results were pooled into a single summary measure
andweighted by the survey sample size.
In the absence o national data, surveys representative oat least
the rst administrative level boundary were used itwo or more
surveys at this level were available or the pop-
ulation group and country concerned within the accept-able time
rame. Results were pooled into a single summarymeasure, weighted by
the total general population or thatregion or state, and based on
the most recent and availablecensus data between 1993 and 2005.
Local- and district-level surveys were not used in these estimates
since theyhave the potential or more bias.
Surveys with prevalence data based on a sample size oless than
100 subjects were excluded in most cases. Thiswas done because with
a sample size o 100 and a con-dence level o 95%, the error around
an estimate o anae-
mia prevalence o 50% would be +/-10 percentage points. Asmaller
sample size would have an even larger error. How-
1 On 3 June 2006, the Permanent Representative o the Republic o
Serbiato the United Nations and other International Organizations
in Genevainormed the Acting Director-General o the WHO that the
member-ship o the state union Serbia and Montenegro in the United
Nations,including all organs and the organizations o the United
Nations sys-tem, is continued by the Republic o Serbia on the basis
o Article 60 othe Constitutional Charter o Serbia and Montenegro,
activated by theDeclaration o Independence adopted by the National
Assembly o Mon-tenegro on 3 June 2006. Estimates used or reerred to
in this documentcover a period o time preceding that
communication.
2. methods
-
8/3/2019 9789241596657_eng anemia
14/51
worldwide prevalence of anaemia 199320054
ever, a ew exceptions were made. National surveys with
ewer than 100 subjects but more than 50 subjects were
only accepted where the results were being extrapolated to
ewer than 500,000 people; or to pregnant women, since
the numbers in this group are requently small, especially in
populations with a lower rate o reproduction.
2.2.2 Population groups
Population groups are as ollows: preschool-age children
(04.99 yrs), school-age children (5.0014.99 yrs), preg-
nant women (no age range defned), non-pregnant women
(15.0049.99 yrs), men (15.0059.99 yrs), and elderly (both
sexes >60 yrs). Wherever possible, children below 0.5 yrs
were excluded rom the estimate or preschool-age children
since the cut-o or anaemia is not defned in this age group.
However, the estimate was applied to the entire popula-
tion o children less than 5 yrs o age. Occasionally, in the
non-pregnant women group, pregnant women could not beexcluded
because all women were included in the fgure pro-
vided in the country report; but pregnant women were oten
a small proportion o the group and their exclusion would
not be expected to change the fgure signifcantly. I a sur-
vey reported results by physiological status, lactating
women
were combined with non-pregnant non-lactating women to
provide the estimate or non-pregnant women.
Data disaggregated by age closest to the defned age
range or the population groups were used. I the age range
overlapped two population groups, the survey was placed
with the group with the greatest overlap in age. When theage
range was unavailable, the mean age o the sample was
used to classiy the data. I this was unavailable or i the
age
range equally spanned two population groups, the popula-
tion-specifc Hb concentration threshold was used to clas-
siy the data. I data represented less than 20% o the age
range o a population group, the survey was excluded.
2.3 Defning anaemia
2.3.1 Haemoglobin threshold
Normal Hb distributions vary with age, sex, and physiolog-
ical status, e.g., during pregnancy (8). WHO Hb thresh-
olds were used to classiy individuals living at sea level
asanaemic (Table 2.1) (2). Statistical and physiological evi-
dence indicate that Hb distributions vary with smoking (9)
and altitude (10), and thereore the prevalence o anaemia
corrected or these actors was used when provided by the
survey. No other corrections were accepted.
Some surveys did not present data using the WHO Hb
thresholds to defne anaemia. When this occurred, preva-
lence was estimated by assuming that the Hb concentration
was normally distributed within the population and esti-
mating anaemia prevalence by using one o the ollowing
methods in order o preerence:
1. The mean and standard deviation (SD) o the Hb con-
centration were used to estimate the proportion o in-
dividuals alling below the appropriate Hb cut-o or
the population group (n=20 surveys). The correlation
between the estimated and predicted prevalence o anae-
mia was determined using surveys rom the database
where a mean, an SD, and a prevalence or the WHO
age- and sex-specifc cut-o were provided. The relation-
ship was plotted (n=508 surveys), and or most surveys,
the two fgures were extremely close (r20.95, p
-
8/3/2019 9789241596657_eng anemia
15/51
52. methods
one non-WHO cut-o or anaemia where two should havebeen used; or
2) using two non-WHO cut-os. In the rstcase, the prevalence was
adjusted or the WHO cut-o thatapplied to the group in the majority.
In the second case,the prevalence was adjusted by assuming that the
cut-oapplied to the group in the majority had been used or
theentire group.
Data provided or separate groups requently had to becombined,
such as data or women by physiological statusor any other
population group disaggregated by age. Prev-alence estimates were
combined and weighted by samplesize, and where this inormation was
unavailable or oneo the groups, it was assumed to have the average
numbero subjects o the other groups. I sample size inormationwas
missing rom all data pooled, equal weight was givento each
survey.
2.3.2 Estimated anaemia prevalence or countries withno survey
data
Some countries did not have any survey data that met thecriteria
or the estimates. Thereore, a regression model wasdeveloped using
countries with anaemia prevalence dataand the 2002 United Nations
Human Development Index(HDI) (11) which is a composite indicator o
a lie expect-ancy index, an education index, and a wealth index
(12) and health indicators rom the World Health StatisticsDatabase
(13), so that anaemia prevalence could be pre-dicted or the
countries without data.
Separate prediction equations or each population groupwere based
on countries with anaemia prevalence data orthat group. Seventeen
countries did not have an HDI, andso HDI was estimated using two o
the components and aproxy indicator or education (average years o
schoolingin adults) (1416). HDI and estimated HDI were used
topredict the prevalence o anaemia using a multiple regres-sion
model.
Anaemia prevalence was estimated by using the predic-tion
equations (Table 2.2) in countries where only explana-tory
variables were known. For one country, none o thecovariates were
available and thereore, a country-level esti-mate was not
generated.
2.3.3 Uncertainty o estimates
For estimates based on survey data, each estimate was
con-sidered to be representative o the entire country whetherrom a
national or subnational sample, and the variance wascalculated in
the logit scale using the sample size. A designeect o 2 was applied
since most surveys utilized clustersampling. From the prevalence,
the variance and the de-sign eect, a 95% condence interval was
generated in logitscale and then transormed to the original scale
(17,18).
For regression-based estimates, a point estimate and95%
prediction interval were computed by using the logit
transormations in the regression models (19) and
thenback-transorming them to the original scale (20).
2.3.4 Combining national estimates
Country estimates were combined to provide estimates atthe
global level as well as by WHO region or women andpreschool-age
children by pooling the data and weightingit by the population that
each estimate represented. Ninety-ve percent condence intervals
were constructed using theestimated variance o the weighted
average. For one coun-try without data, no proxy indicators were
available and so
no country estimate was generated, but the UN
subregionalestimate had to be applied to that country to make
regionaland global estimates.
2.3.5 Global anaemia prevalence
The global prevalence o anaemia was calculated by com-bining the
estimates or all population groups, which cov-ered the entire
population except or one segment (women
Table 2.2 Prediction equations used to generate anaemia
estimates or countries without survey data
Population Number of Equation R2 p-value
group countries for model
p-g 82 = 3.5979-4.9093*hdIb-0.0657*e 0.0003*e 0.550
-
8/3/2019 9789241596657_eng anemia
16/51
-
8/3/2019 9789241596657_eng anemia
17/51
7
3. Results and Discussion
3.1 Results
3.1.1 Population coverage
Almost the entire population was covered by survey data
or regression-based estimates, since all countries except
or one had an estimate. The proportion o the population
covered by survey data was high or preschool-age children(76.1%)
and pregnant (69.0%) and non-pregnant women
(73.5%), but lower or school-age children (33.0%), men
(40.2%), and the elderly (39.1%) (Table 3.1). By WHO
region, the coverage was highest in the Western Pacifc and
lowest in Europe. Based on this population coverage, it was
decided that there were insufcient data in school-age chil-
dren, men, and the elderly to generate regional estimates.
Table 3.1 Population coverage (%) by anaemia prevalence surveys
(national or subnational) conducted between1993 and 2005
WHO region PreSACa PW NPW SAC Men Elderly All
a (46)b 74.6 (26) 65.8 (22) 61.4 (23) 13.2 (8) 21.9 (11) 0.0 (0)
40.7
as (35) 76.7 (16) 53.8 (15) 56.2 (13) 47.1 (9) 34.3 (2) 47.6 (1)
58.0
Sth-est as (11) 85.1 (9) 85.6 (8) 85.4 (10) 13.6 (3) 4.1 (2) 5.2
(1) 14.9
e (52) 26.5 (12) 8.3 (4) 28.0 (12) 9.3 (3) 14.1 (3) 8.0 (2)
22.9
est mt (21) 67.4 (11) 58.7 (7) 73.5 (11) 15.5 (6) 27.5 (6) 3.2
(3) 84.3
wst pf (27) 90.4 (10) 90.2 (8) 96.9 (13) 83.1 (7) 96.2 (10) 93.3
(6) 13.8
Global (192) 76.1 (84) 69.0 (64) 73.5 (82) 33.0 (36) 40.2 (34)
39.1 (13) 48.8
pt gs: pSac, sh-g h (0.004.99 ys); pw, gt ( g g f); npw, -gt
(15.0049.99 ys), Sac, sh-g
h (5.0014.99 ys), m (15.0059.99 ys), ey (60.00 ys).b
nb ts h gg. Tt b ts th t, fg s v a s h ty y b ty v by s t gs, bt
ts hv t 6 -
t gs ts hv t 5059 ys g.
Table 3.2 Global anaemia prevalence and number of individuals
affected
Population group Prevalence of anaemia Population affected
Percent 95% CI Number (million) 95% CI
psh-g h 47.4 45.749.1 293 283303
Sh-g h 25.4 19.930.9 305 238371
pgt 41.8 39.943.8 56 5459
n-gt 30.2 28.731.6 468 446491
m 12.7 8.616.9 260 175345
ey 23.9 18.329.4 164 126202
Total population 24.8 22.926.7 1620 15001740
3.1.2 Proportion of population and number of
individuals with anaemia
Globally, anaemia aects 1.62 billion people (95% CI:
1.501.74 billion), which corresponds to 24.8% o the pop-
ulation (95% CI: 22.926.7%) (Table 3.2). The highest
prevalence is in preschool-age children (47.4%, 95%
CI:45.749.1), and the lowest prevalence is in men (12.7%,
95% CI: 8.616.9%). However, the population group with
the greatest number o individuals aected is non-pregnant
women (468.4 million, 95% CI: 446.2490.6).
WHO regional estimates generated or preschool-age
children and pregnant and non-pregnant women indi-
cate that the highest proportion o individuals aected
are in Arica (47.567.6%), while the greatest number a-
3. reSulTS and diScuSSion
-
8/3/2019 9789241596657_eng anemia
18/51
worldwIde prevalence o anaemIa 199320058
ected are in South-East Asia where 315 million (95% CI:291340)
individuals in these three population groups areaected (Table
3.3).
3.1.3 Classifcation o countries by degree o public
health signifcance o anaemia
There are almost no countries where anaemia is not at least
a mild public health problem in all three o the populationgroups
or which country-level estimates were generated(Table 3.4). For
pregnant women, over 80% o the coun-tries have a moderate or severe
public health problem.
The level o the public health problem across countries
isillustrated by maps or preschool-age children and pregnantand
non-pregnant women in Figure 3.1.
3.2 Discussion
3.2.1 Population coverage
The population covered by survey data is high or the
threepopulation groups considered to be the most
vulnerable;preschool-age children, pregnant women, and
non-pregnantwomen o childbearing age. A greater number o
countrieshave undertaken surveys to assess anaemia in
non-pregnant
women than in pregnant women. However, since some othe surveys
conducted in pregnant women are rom coun-tries with a large
population, the proportion o the globalpopulation covered by these
surveys is similar between thetwo population groups.
3.2.2 Strengths o estimates
These estimates are based on a high proportion o nation-ally
representative survey data. For the three most vulner-able
population groups, preschool-age children, pregnantwomen, and
non-pregnant women, nationally representative
data covered more than two thirds o the population in eachgroup.
This eliminates the bias that comes rom local data, which may
greatly over- or under-represent the nationalsituation.
Regression-based estimates were used or countries with-out data,
and these estimates explained a large amount othe variation in
anaemia prevalence among countries withsurvey data (3258%).
3.2.3 Limitations o estimates
There were ewer surveys that collected data in
school-agechildren, men, and the elderly, and in some cases there
were
no data or an entire region. Thus, country- or regional-
Table 3.3 Anaemia prevalence and number o individuals aected in
preschool-age children, pregnant women,and non-pregnant women in
each WHO region
WHO region Preschool-age childrena Pregnant women Non-pregnant
women
Prevalence # affected Prevalence # affected Prevalence #
affected(%) (millions) (%) (millions) (%) (millions)
ai 67.6 83.5 57.1 17.2 47.5 69.9
(64.371.0)b (79.487.6) (52.861.3) (15.918.5) (43.451.6)
(63.975.9)
ai 29.3 23.1 24.1 3.9 17.8 39.0
(26.831.9) (21.125.1) (17.330.8) (2.85.0) (12.922.7)
(28.349.7)
s-e 65.5 115.3 48.2 18.1 45.7 182.0
ai (61.070.0) (107.3123.2) (43.952.5) (16.419.7) (41.949.4)
(166.9197.1)
e 21.7 11.1 25.1 2.6 19.0 40.8
(15.428.0) (7.914.4) (18.631.6) (2.03.3) (14.723.3)
(31.550.1)
e 46.7 0.8 44.2 7.1 32.4 39.8
mi (42.251.2) (0.41.1) (38.250.3) (6.18.0) (29.235.6)
(35.843.8)
w 23.1 27.4 30.7 7.6 21.5 97.0
pif (21.924.4) (25.928.9) (28.832.7) (7.18.1) (20.822.2)
(94.0100.0)
Global 47.4 293.1 41.8 56.4 30.2 468.4
(45.749.1) (282.8303.5) (39.943.8) (53.859.1) (28.731.6)
(446.2490.6)
pi bg: p-g i (0.004.99 y); pg ( g g f); n-g (15.0049.99 y).b 95%
cf I.
Table 3.4 Number o countries categorized by publichealth
signifcance o anaemia
Public Preschool-age Pregnant Non-pregnanthealth childrenb women
womenproblema nb i nb i nb i
n 2 0 1
mi 40 33 59
m 81 91 78
s 69 68 54
t i bi b i giz :
-
8/3/2019 9789241596657_eng anemia
19/51
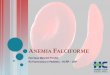
Figure 3.1a Anaemia as a public health problem by country:
Preschool-age children
Category of public health
significance (anaemia prevalence)
Normal (40.0%)
No data
3.resultsanddIscussIon
9
-
8/3/2019 9789241596657_eng anemia
20/51
Figure 3.1b Anaemia as a public health problem by country:
Pregnant women
Category of public health
significance (anaemia prevalence)
Normal (40.0%)
No data
worldwIdepreval
enceofanaemIa19932005
10
-
8/3/2019 9789241596657_eng anemia
21/51
Figure 3.1c Anaemia as a public health problem by country:
Non-pregnant women o reproductive age
Category of public health
significance (anaemia prevalence)
Normal (40.0%)
No data
3.resultsanddIscussIon
11
-
8/3/2019 9789241596657_eng anemia
22/51
worldwIde prevalence o anaemIa 1993200512
level estimates or these population groups were not pre-sented.
Even the global estimates should be interpretedwith caution since
they are based primarily on regression-based estimates or these
population groups.
Furthermore, the estimates generated or women (5059yrs) were not
based on any data rom this population groupsince it is not
routinely collected. It is why this estimate wasused or the global
gure only and not as an estimate orthis group o women.
These estimates were based on a number o assumptions.All surveys
were treated equally, although in act their qual-ity varied
greatly. For example, some surveys used samplingproportionate to
the population distribution within thecountry, while others did
not, and in some national sur-veys, specic areas had to be let out
due to security or ac-cessibility issues. Furthermore or some
population groups(e.g., children 0.54.99 yrs), the population
sampled cov-
ered only a portion o the desired age range (e.g., children11.99
yrs). For the purpose o our analysis, these surveyswere considered
equal to those that covered the entire agerange. However, an
estimate rom children in only the low-er or higher end o the range
would signicantly impactthe prevalence estimate, since children
below two years oage are much more likely to be anaemic than those
abovethis age.
While there were only three countries or which sub-national data
were used to generate prevalence estimates inpreschool-age
children, these data may result in an over- or
under-estimation o anaemia prevalence or those coun-tries.In
some cases, anaemia prevalence was calculated us-
ing Hb concentration and assuming that it was
distributednormally. This may have lead to a slight
over-estimationo anaemia prevalence, since Hb distributions tend to
benegatively skewed in populations with a high prevalence
odeciency.
The estimates or pregnant women did not account orthe trimester
o pregnancy since this inormation is notroutinely reported in
publications. Prevalence would beexpected to vary by trimester, and
thus the estimates or
pregnant women may have been biased i there was not aneven
distribution o women at various stages o pregnancy.Furthermore, we
do not have prevalence gures or thethird trimester when anaemia is
most likely to aect therisk o maternal mortality.
3.2.4 Proportion o population and the number o
individuals with anaemia
One in our people is aected by anaemia, and pregnantwomen and
preschool-age children are at the greatest risk.The WHO regions o
Arica and South-East Asia have
the highest risk, where about two thirds o preschool-agechildren
and hal o all women are aected. In numbers,
the main burden is concentrated in South-East Asia, whereabout
40% o anaemic preschool-age children and non-pregnant women, and
about 30% o pregnant women re-side.
3.2.5 Classifcation o countries by degree o public
health signifcance o anaemia, based on
haemoglobin concentration
Anaemia is a public health problem or pregnant womenin all o
WHOs Member States. Given the consequenceso anaemia during
pregnancy, this problem urgently needsto be addressed. The
situation is similar in preschool-agechildren and non-pregnant
women or whom only one ortwo countries do not have an anaemia
public health prob-lem. For women and young children, the majority
o WHOMember States (132 to 159, depending on the populationgroup)
have a moderate-to-severe public health problem
with anaemia; meaning that over 20% o the populationgroup in
these countries is aected. This should draw theattention o the
public health authorities on the need tore-evaluate current
strategies to control anaemia by mak-ing sure that the various
actors contributing to anaemiahave been identied and addressed
properly through an in-tegrated approach.
3.2.6 Comparison to previous estimates
It is a challenge to assess global progress in the control
oanaemia, since the methodology used or these estimates
is so dierent rom those used in previous estimates. Pre-vious
global estimates made by DeMaeyer in 1985 indi-cated that
approximately 30% o the worlds populationwas anaemic (23). These
estimates seem to be based on anextrapolation o the prevalence in
preschool-age children,school-age children, women, and men. These
estimates,which excluded China where 20% o the global
populationresides, indicated that 43% o preschool-age children,
35%o all women, and 51% o pregnant women were anaemic.Current
estimates, excluding China, are 52%, 34%, and44%, respectively.
Variations in the methods employed,and a larger proportion o
nationally representative data,
are more likely to account or the dierences between
theseestimates than a change in anaemia prevalence.
In 1992, WHO estimates or the year 1988 indicatedthat 37%, 51%,
and 35% o all women and pregnant andnon-pregnant women were anaemic
(24). These estimatesincluded subnational data or China. The
current estimateswhich use nationally representative data or China
(31%,42%, and 30%) may or may not be lower, since the
meth-odologies used are substantially dierent.
3.3 Conclusion
The data available or these estimates are the most
repre-sentative data to date, and we can consider that these
esti-
-
8/3/2019 9789241596657_eng anemia
23/51
133. results and dIscussIon
mates are the most accurate refection o the global
anaemiaprevalence published so ar. However, countries withoutsurvey
data should be encouraged to collect data, since re-gression-based
estimates are good at the regional and globallevel, but may not be
the most accurate refection o thesituation or an individual
country.
The generation o these estimates and the maintenanceo the
anaemia database provide a reliable tool to trackthe global
progress towards the elimination o anaemiaand the eectiveness o the
current strategies or anaemiacontrol. However, since inormation on
causal actors is
not routinely collected, the database does not provide
in-ormation on the ability o the strategies to address theseactors.
Hopeully, these estimates will encourage countriesto plan surveys
which assess the prevalence o actors thatcontribute to anaemia not
only iron deciency, but alsoinectious diseases and other
micronutrient deciencies.The understanding o how these actors vary
by geography,level o development, and other social and economic
actorswill make it easier to design interventions that are more
e-ective and integrative in addressing multiple contributingactors
at the same time.
-
8/3/2019 9789241596657_eng anemia
24/51
References
1. World Health Organization. The World Health Report 2002:
Reducing risks, promoting healthy lie. Geneva,World Health
Organization, 2002.
2. Iron deciency anaemia: assessment, prevention, and con-trol.
A guide or programme managers. Geneva, WorldHealth Organization,
2001 (WHO/NHD/01.3).
3. Macgregor M. Maternal anaemia as a actor in prema-turity and
perinatal mortality. Scottish Medical Journal,1963, 8:134.
4. Scholl TO, Hediger ML. Anemia and iron-deciencyanemia:
compilation o data on pregnancy outcome.
American Journal o Clinical Nutrition , 1994, 59:492S500S.
5. Bothwell T, Charlton R, eds. Iron deciency in
women.Washington DC, Nutrition Foundation, 1981.
6. Guidelines or the treatment o malaria. Geneva, RollBack
Malaria Department, World Health Organiza-tion, 2006
(WHO/HTM/MAL/2006.1108).
7. Crompton DWT et al., eds. Controlling disease due tohelminth
inections. Geneva, World Health Organiza-tion, 2003.
8. Koller O. The clinical signicance o hemodilutionduring
pregnancy. Obstetrical and Gynecological Survey,1982,
37:649652.
9. Nordenberg D, Yip R, Binkin NJ. The eect o ciga-rette smoking
on hemoglobin levels and anemia screen-ing.Journal o the American
Medical Association, 1990,264:15561559.
10. Hurtado A., Merino C, Delgado E. Infuence o anox-emia on
haematopoietic activities. Archives o Internal
Medicine, 1945, 75:284323.
11. Human Development Report 2002, Deepening democ-racy in a
ragmented world. New York, United NationsDevelopment Programme,
2002.
12. Human Development Indicators. In: Cait Murphy BR-L, ed.
Human Development Report 2004. New York,United Nations Development
Programme, 2004: 139250.
13. World Health Organization. World Health Statistics2005.
Geneva, World Health Organization, 2005.
14. Mathers CD, Loncar D. Projections o global mortalityand
burden o disease rom 2002 to 2030. PLoS Medi-cine, 2006,
3:e442.
15. World Health Organization. The World Health Report2000:
Health systems: improving perormance. Geneva,World Health
Organization, 2000.
16. World Health Organization. The World Health Report:2004:
Changing History. Geneva, World Health Or-ganization, 2004.
17. Wackerly D, Mendenhall W, Scheaer RL. Math-ematical
Statistics with Applications, 6th edition. PacicGrove, CA, Duxbury
Press, 2001.
18. Lohr SL. Sampling: Design and Analysis, 1st edition.Pacic
Grove, CA, Duxbury Press, 1998.
19. Neter J et al.Applied Linear Statistical Models, 4th
edi-tion. New York, McGraw-Hill/Irwin, 1996.
20. Allison PD. Logistic Regression using the SAS System.
In-dianapolis, IN, WA (Wiley-SAS), 2001.
21. Whelan EA et al. Menstrual and reproductive charac-teristics
and age at natural menopause.American Jour-nal o Epidemiology,
1990, 131:625632.
22. United Nations PD. World Population Prospects the2004
revision . New York, 2005.
23. DeMaeyer E, Adiels-Tegman M. The prevalence oanaemia in the
world. World Health Statistics Quarterly,
1985, 38:302316.24. World Health Organization. The Prevalence o
Anae-mia in Women: A Tabulation o Available Inormation.1992
(WHO/MCH/MSM/92.2).
worldwIde prevalence o anaemIa 1993200514
-
8/3/2019 9789241596657_eng anemia
25/51
Annex 1
WHO Member States groupedby WHO region as of 2005
Table A1.1 WHO Member States grouped by WHO region
AfricaAlgeria
Angola
BeninBotswana
Burkina Faso
Burundi
Cameroon
Cape Verde
Central African Republic
Chad
Comoros
Congo
Cte dIvoire
Democratic Republic of
the CongoEquatorial Guinea
Eritrea
Ethiopia
Gabon
Gambia
Ghana
Guinea
Guinea-Bissau
Kenya
Lesotho
LiberiaMadagascar
Malawi
Mali
Mauritania
Mauritius
Mozambique
Namibia
Niger
Nigeria
Rwanda
Sao Tome and Principe
Senegal
Seychelles
Sierra Leone
South Africa
Swaziland
Togo
Uganda
United Republic of
Tanzania
Zambia
Zimbabwe
AmericasAntigua and Barbuda
Argentina
Bahamas
Barbados
BelizeBolivia
Brazil
Canada
Chile
Colombia
Costa Rica
Cuba
Dominica
Dominican Republic
Ecuador
El SalvadorGrenada
Guatemala
Guyana
Haiti
Honduras
Jamaica
Mexico
Nicaragua
Panama
Paraguay
Peru
Saint Kitts and NevisSaint Lucia
Saint Vincent and the
Grenadines
Suriname
Trinidad and Tobago
United States of America
Uruguay
Venezuela (Bolivarian
Republic of )
South-East AsiaBangladesh
Bhutan
Democratic Peoples
Republic of Korea
India
IndonesiaMaldives
Myanmar
Nepal
Sri Lanka
Thailand
Timor-Leste
Europe
Albania
Andorra
ArmeniaAustria
Azerbaijan
Belarus
Belgium
Bosnia and Herzegovina
Bulgaria
Croatia
Cyprus
Czech Republic
Denmark
Estonia
Finland
France
Georgia
Germany
Greece
Hungary
Iceland
Ireland
Israel
ItalyKazakhstan
Kyrgyzstan
Latvia
Lithuania
Luxembourg
Malta
Monaco
Netherlands
Norway
Poland
PortugalRepublic of Moldova
Romania
Russian Federation
San Marino
Serbia and Montenegro1
1 On 3 June 2006, the Permanent Representative of the Republic
of Serbiato the United Nations and other International
Organizations in Genevainformed the Acting Director-General of the
WHO that the mem-bership of the state union Serbia and Montenegro
in the United Na-tions, including all organs and the organizations
of the United Nationssystem, is continued by the Republic of Serbia
on the basis of Article60 of the Constitutional Charter of Serbia
and Montenegro, activated
by the Declaration of Independence adopted by the National
Assemblyof Montenegro on 3 June 2006. Estimates used or referred to
in thisdocument cover a period of time preceding that
communication.
Annex 1 15
-
8/3/2019 9789241596657_eng anemia
26/51
Slovakia
Slovenia
Spain
Sweden
Switzerland
Tajikistan
The former Yugoslav
Republic of Macedonia
Turkey
Turkmenistan
Ukraine
United Kingdom of Great
Britain and Northern
Ireland
Uzbekistan
Eastern Mediterranean
Afghanistan
Bahrain
Djibouti
Egypt
Iran (Islamic Republic of )
Iraq
Jordan
Kuwait
Lebanon
Libyan Arab Jamahiriya
Morocco
Oman
Pakistan
Qatar
Saudi Arabia
Somalia
Sudan
Syrian Arab Republic
Tunisia
United Arab Emirates
Yemen
Western Pacifc
Australia
Brunei Darussalam
Cambodia
China
Cook Islands
Fiji
Japan
Kiribati
Lao Peoples Democratic
Republic
Malaysia
Marshall Islands
Micronesia (Federated
States of)
Mongolia
Nauru
New Zealand
Niue
Palau
Papua New Guinea
Philippines
Republic of Korea
Samoa
Singapore
Solomon Islands
Tonga
Tuvalu
Vanuatu
Viet Nam
Table A1.2 WHO Member States grouped by UN region and
subregion1
Gabon
Sao Tome and Principe
Northern Africa
Algeria
Egypt
Libyan Arab Jamahiriya
MoroccoSudan
Tunisia
Southern Africa
Botswana
Lesotho
Namibia
South Africa
Swaziland
Western Africa
Benin
Burkina Faso
Cape Verde
Cte dIvoire
Gambia
Ghana
Guinea
Guinea-Bissau
Liberia
Mali
Mauritania
Niger
Nigeria
Senegal
Sierra Leone
Togo
Asia
Central AsiaKazakstan
Kyrgyzstan
Tajikistan
Turkmenistan
Uzbekistan
Eastern Asia
China
Democratic Peoples
Republic of Korea
JapanMongolia
Republic of Korea
Southern Asia
Afghanistan
Bangladesh
Bhutan
India
Iran (Islamic Republic of )
Maldives
Nepal
Pakistan
Sri Lanka
South-eastern Asia
Brunei Darussalam
Lao Peoples Democratic
Republic
MalaysiaMyanmar
Philippines
Singapore
Thailand
Timor-Leste
Viet Nam
Western Asia
Armenia
Azerbaijan
BahrainCyprus
Georgia
Iraq
Israel
Jordan
Kuwait
Lebanon
Oman
Arica
Eastern Africa
Burundi
Comoros
Djibouti
Eritrea
Ethiopia
KenyaMadagascar
Malawi
Mauritius
Mozambique
Rwanda
Seychelles
Somalia
Uganda
United Republic of
Tanzania
ZambiaZimbabwe
Middle Africa
Angola
Cameroon
Central African Republic
Chad
Congo
Democratic Republic of
The Congo
Equatorial Guinea
1 http://unstats.un.org/unsd/methods/m49/m49regin.htm
worldwide prevAlence of AnAemiA 1993200516
-
8/3/2019 9789241596657_eng anemia
27/51
Annex 1
Qatar
Saudi Arabia
Syrian Arab Republic
Turkey
United Arab Emirates
Yemen
Europe
Eastern Europe
Belarus
Bulgaria
Czech Republic
Hungary
Poland
Republic of Moldova
Romania
Russian Federation
SlovakiaUkraine
Northern Europe
Denmark
Estonia
Finland
Iceland
Ireland
Latvia
Lithuania
NorwaySweden
United Kingdom of Great
Britain and Northern
Ireland
Southern Europe
Albania
Andorra
Bosnia and Herzegovina
Croatia
Greece
Italy
Malta
Portugal
San Marino
Serbia and Montenegro
Slovenia
Spain
The former Yugoslav
Republic of Macedonia
Western Europe
AustriaBelgium
France
Germany
Luxembourg
Monaco
Netherlands
Switzerland
Americas
Latin America and
the Caribbean
Caribbean
Antigua and Barbuda
Bahamas
Barbados
Cuba
Dominica
Dominican Republic
Grenada
Haiti
Jamaica
Saint Kitts and Nevis
Saint Lucia
Saint Vincent and the
Grenadines
Trinidad and Tobago
Central America
Belize
Costa Rica
El Salvador
Guatemala
HondurasMexico
Nicaragua
Panama
South America
Argentina
Bolivia
Brazil
Chile
Colombia
EcuadorGuyana
Paraguay
Peru
Suriname
Uruguay
Venezuela (Bolivarian
Republic of )
Northern America
Canada
United States of America
Oceania
Australia-New Zealand
Australia
New Zealand
Melanesia
Fiji
Papua New Guinea
Solomon Islands
Vanuatu
Micronesia
Kiribati
Marshall Islands
Micronesia (Federated
States of)
Nauru
Palau
Polynesia
Cook IslandsNiue
Samoa
Tonga
Tuvalu
17
-
8/3/2019 9789241596657_eng anemia
28/51
annex 2
Results by UN region
Table A2.1 Population coverage (%) by anaemia prevalence surveys
(national or subnational) conducted between
1993 and 2005, by UN region
UN region PreSACa PW NPW SAC Men Elderly All
ai (53)b 76.7 (30) 65.3 (25) 63.6 (26) 18.6 (10) 32.0 (14) 1.8
(1) 40.7
ai (47) 82.1 (30) 80.9 (21) 88.8 (34) 37.0 (11) 47.6 (13) 54.1
(7) 58.0
e (41) 19.2 (5) 0.9 (1) 23.9 (5) 12.9 (3) 15.9 (2) 8.7 (2) 14.9l
a cibb (33) 70.5 (15) 38.4 (14) 37.5 (12) 28.9 (8) 0.1 (1) 0.0 (0)
22.9
n ai (2) 92.4 (1) 92.8 (1) 89.9 (1) 91.3 (1) 89.9 (1) 89.6 (1)
84.3
oi (16) 5.1 (3) 4.7 (2) 16.5 (4) 15.1 (3) 15.6 (3) 15.1 (2)
13.8
Global (192) 76.1 (84) 69.0 (64) 73.5 (82) 33.0 (36) 40.2 (34)
39.1 (13) 48.8
pi g: psac, -g i (0.004.99 y); pw, g ( g g f); npw, -g
(15.0049.99 y), sac, -g
i (5.0014.99 y), m (15.0059.99 y), ey (60.00 y).b nb i i gig. t
b i i . n fg i i a i y y b i y by i g, b i
6 i g i 5059 y g.
Table A2.2 Anaemia prevalence and number o individuals aected in
preschool-age children, pregnant women,
and non-pregnant women in each UN region
UN regiona Preschool-age childrenb Pregnant women Non-pregnant
women
Prevalence # affected Prevalence # affected Prevalence #
affected(%) (millions) (%) (millions) (%) (millions)
ai 64.6 93.2 55.8 19.3 44.4 82.9
(61.767.5) (89.197.4) (51.959.6) (18.020.7) (40.947.8)
(76.589.4)
ai 47.7 170.0 41.6 31.7 33.0 318.3
(45.250.3) (161.0178.9) (39.044.2) (29.733.6) (31.334.7)
(302.0334.6)
e 16.7 6.1 18.7 1.4 15.2 26.6
(10.523.0) (3.88.4) (12.325.1) (0.91.8) (10.519.9)
(18.434.9)
lac 39.5 22.3 31.1 3.6 23.5 33.0
(36.043.0) (20.324.3) (21.840.4) (2.54.7) (15.931.0)
(22.443.6)
na 3.4 0.8 6.1 0.3 7.6 6.0
(2.04.9) (0.41.1) (3.48.8) (0.20.4) (5.99.4) (4.67.3)
oi 28.0 0.7 30.4 0.2 20.2 1.5
(15.840.2) (0.41.0) (17.043.9) (0.10.2) (9.530.9) (0.72.4)
Global 47.4 293.1 41.8 56.4 30.2 468.4
(45.749.1) (282.8303.5) (39.943.8) (53.859.1) (28.731.6)
(446.2490.6)
un gi: ai, ai, e, li ai cibb (lac), n ai (na), oi.b pi g: psac,
-g i (0.004.99 y); pw, g ( g g f); npw, -g (15.0049.99 y). 95% cf
I.
18 worldwIde prevalence o anaemIa 19932005
-
8/3/2019 9789241596657_eng anemia
29/51
-
8/3/2019 9789241596657_eng anemia
30/51
-
8/3/2019 9789241596657_eng anemia
31/51
-
8/3/2019 9789241596657_eng anemia
32/51
-
8/3/2019 9789241596657_eng anemia
33/51
-
8/3/2019 9789241596657_eng anemia
34/51
-
8/3/2019 9789241596657_eng anemia
35/51
-
8/3/2019 9789241596657_eng anemia
36/51
-
8/3/2019 9789241596657_eng anemia
37/51
-
8/3/2019 9789241596657_eng anemia
38/51
-
8/3/2019 9789241596657_eng anemia
39/51
-
8/3/2019 9789241596657_eng anemia
40/51
-
8/3/2019 9789241596657_eng anemia
41/51
-
8/3/2019 9789241596657_eng anemia
42/51
-
8/3/2019 9789241596657_eng anemia
43/51
-
8/3/2019 9789241596657_eng anemia
44/51
-
8/3/2019 9789241596657_eng anemia
45/51
35annex 3
A3.4 Country references
Aghanistan
Ministry o Public Health o the Islamic Republic o Agha-nistan et
al. Summary Report o the National Nutrition Sur-vey, Aghanistan,
2004. Ministry o Public Health o theIslamic Republic o Aghanistan,
2005. Re 5173.
Angola
Ministry o Health et al. Assessing vitamin A and iron de- ciency
anaemia, nutritional anaemia among children aged060 months in the
Republic o Angola [technical report].Ministry o Health, 2000. Re
2839.
Antigua and Barbuda
Micronutrient Working Group. Iron and vitamin A statusin ve
Caribbean countries. Cajanus, 2002, 35 (1): 434.Re 3758.
Armenia
National Statistical Service et al.Armenia Demographic andHealth
Survey 2000. Calverton, MD, National StatisticalService, 2001. Re
3208.
Azerbaijan
Serbanescu F et al., eds. Reproductive health survey Azerbai-
jan, 2001. Atlanta, Centers or Disease Control and Pre-vention,
2003. Re 4682.
Bahrain
Al-Dallal ZS et al. Impact o the national four ortication
program on the prevalence o iron deciency and anemiaamong women at
reproductive age in the Kingdom o Bahrain.Kingdom o Bahrain,
Ministry o Health, Public HealthDirectorate, Nutrition Section,
2003. Re 5391.
Bangladesh
Helen Keller International et al. Anemia: a severe publichealth
problem in pre-school children and pregnant womenin rural
Bangladesh. HKI-Nutrition Surveillance ProjectBulletin, 2002. Re
3256.
Belize
Ministry o Health et al. Study o iron deciency anaemiaamong
pregnant women in Belize. Belmopan, Ministry oHealth, 1996.
(BZ-NUT/F/003). Re 1062.
Benin
Institut National de la Statistique et de lAnalyse cono-mique et
al. Enqute Dmographique et de Sant au Bnin,2001. Calverton, MD,
Institut National de la Statistique etde lAnalyse conomique et ORC
Macro, 2002. Re 3461.
Bhutan
Royal Government o Bhutan Ministry o Health andEducation.Anemia
among men, women and children in Bhu-tan: How big is the problem?
Bhutan, Ministry o Healthand Education, 2003. Re 5150.
Bolivia
Gutirrez Sardn M et al. Bolivia Encuesta Nacional de De-mograa y
Salud 2003 [Bolivia National Demographic andHealth Survey 2003]. La
Paz, Ministerio de Salud y Depor-tes, Instituto Nacional de
Estadstica, 2004. Re 5095.
Botswana
Ministry o Health Botswana et al. Micronutrient malnu-trition in
Botswana. A national survey to assess the status o iodine, iron,
and vitamin A. Gaborone, Ministry o Health,1996. Re 2805.
Brazil
Governo de Sergipe et al. III Pesquisa de sade materno-in- antil
e nutrio do estado de Sergipe. Pesmise 98. Brasilia,Governo de
Sergipe, Secretaria de Estado da Sade, 2001.Re 614.
Torres MAA et al. Anemia em crianas menores de doisanos
atendidas nas unidades bsicas de sade no Estado deSo Paulo, Brasil
[Anemia in children under 2 years in basichealth care units in the
State o So Paulo, Brazil]. Revistade Sade Pblica, 1994, 28 (4):
290294. Re 2375.
Osrio MM et al. Prevalence o anemia in children 659months old in
the state o Pernambuco, Brazil. Revista Pa-namericana de Salud
Pblica, 2001, 10 (21): 101107. Re
2843.
Brunei Darussalam
Ministry o Health. National Nutritional Status Survey,1997.
Negara, Ministry o Health, 1997. Re 3334.
Nutritional status o children under ve years old and pre- gnant
women in Brunei Darussalam. A collaborative studybetween Institute
o Medical Research, Ministry o Health,
Malaysia, Ministry o Health, Brunei Darussalam, Ministryo
Health, Lao PDR,19951996. Negara, Brunei Darussa-lam, 1996. Re
3328.
Burkina Faso
Institut National de la Statistique et de la Dmographie[Burkina
Faso] et al. Burkina Faso Enqute Dmographiqueet de Sant 2003
[Burkina Faso Demographic and HealthSurvey 2003]. Calverton, MD,
ORC Macro, 2004. Re4948.
Burundi
Kimboka S. Burundi National Anaemia Survey. Bujumbura,Burundi,
Ministere de la Sante Publique, 2004. Re5782.
-
8/3/2019 9789241596657_eng anemia
46/51
worldwIde prevalence o anaemIa 1993200536
Cambodia
Ministry o Health et al. Cambodia Demographic and HealthSurvey
2000. Phnom Penh, Ministry o Health, 2001. Re
3206.
Cameroon
Institut National de la Statistique et al. Enqute Dmogra-phique
et de Sant: Cameroon 2004. [Demographic HealthSurvey: Cameroon
2004]. Calverton, MD, ORC Macro,2005. Re 5214.
Central Arican Republic
Ministere Delegue a lEconomie au Plan et a la Coopera-tion
Internationale et al. Enqute nationale sur lavitaminose
A, la carence en er et la consommation du sel iode. Republi-que
Centraricaine, 2000. Re 1722.
ChileMinisterio de Salud. Resultados 1: Encuesta de Salud,
Chile2003. Santiago, Departmento de Epidemiologa, Ministe-rio de
Salud, 2003. Re 5783.
China
Chinese Center or Disease Control and Prevention. Theprevalence
o anemia in China, 2002, by age and gender. Bei- jing, Chinese
Center or Disease Control and Prevention,2005. Re 5287.
Costa Rica
Ministerio de Salud. Encuesta Nacional de Nutricin: 2 Fasc-culo
Micronutrientes [National nutrition survey: Part 2
micro-nutrients]. San Jos, Ministerio de Salud, 1996. Re 1634.
Cunningham L et al. Prevalencia de anemia, deciencia dehierro y
olatos en nios menores de siete aos: Costa Rica,1996 [Prevalence o
anemia, iron and olate deciency inchildren smaller than seven
years: Costa Rica, 1996]. Ar-chivos Latinoamericanos de Nutricin,
2001, 51 (1): 3743.Re 3555.
Rodriguez S et al. Prevalencia de las anemias nutricionalesde
mujeres en edad rtil, Costa Rica: encuesta nacional denutricin,
1996 [Prevalence o nutritional anemia in womeno reproductive age,
Costa Rica: national nutrition survey,1996]. Archivos
Latinoamericanos de Nutricin, 2001, 51(1): 1924. Re 3556.
Blanco A et al. Anemias nutricionales en mujeres lactantesde
Costa Rica [Nutritional anemia in nursing women inCosta
Rica].Archivos Latinoamericanos de Nutricin, 2003,53 (1): 2834. Re
4524.
Democratic Peoples Republic o Korea
UNICEF et al. The Multiple Indicator Cluster Survey in
theDemocratic Peoples Republic o Korea, 1998. Pyongyang,United
Nations Childrens Fund, 1998. Re 3090.
Central Bureau o Statistics et al. DPRK 2004 Nutrition
assessment report o survey results. The Democratic
PeoplesRepublic o Korea, Central Bureau o Statistics, Institute
oChild Nutrition, 2005. Re 5068.
Democratic Republic o Congo
Ministre du Sant, Programme National de NutritionPRONANUT.
Enquete sur la prevalence de lanemie enRpublique Dmographique du
Congo. Rpublique D-mocratique du Congo, Programme National de
NutritionPRONANUT, 2005. Re 5764.
Dominica
Micronutrient Working Group. Iron and vitamin A statusin ve
Caribbean countries. Cajanus, 2002, 35 (1):434. Re
3758.
Egypt
El-Zanaty F et al. Egypt Demographic and Health
Survey.Calverton, MD, Ministry o Health and Population,
Egypt,National Population Council and ORC Macro, 2001. Re1940.
El Salvador
Salvadoran Demographic Association (ADS) et al. EncuestaNacional
de Salud Familiar FESAL-98. [National FamilyHealth Survey
FESAL-98]. San Salvador, Salvadoran De-mographic Association, 2000.
Re 3107.
Salvadoran Demographic Association (ADS) et al. EncuestaNacional
de Salud Familiar FESAL 20022003: Inorme -nal. San Salvador, 2004.
Re 5171.
Fiji
Saito S. 1993 national nutrition survey. Suva, National Foodand
Nutrition Committee, 1995. Re 2699.
France
Galn P et al. Determining actors in the iron status oadult women
in the SU.VI.MAX study. European Journal oClinical Nutrition, 1998,
52 (6): 383388. Re 2392.
Gambia
Bah A et al. Nationwide survey on the prevalence o vitaminA and
iron deciency in women and children in the Gambia.Banjul, National
Nutrition Agency, 2001. Re 2806.
-
8/3/2019 9789241596657_eng anemia
47/51
37annex 3
Ghana
Ghana Statistical Service (GSS) et al. Ghana Demographicand
Health Survey 2003. Calverton, MD, ORC Macro,2004. Re 4943.
Guatemala
Ministerio de Salud Publica y Asistencia Social et al.
Gua-temala, Encuesta Nacional de Salud Materno Inantil
2002.Guatemala, Ministerio de Salud Publica y Asistencia So-cial,
2003. Re 4586.
Guinea
Ministre de la Sant Publique. Enqute nationale sur lan-mie
erriprive en Guine. Rapport Final: rsum. Guinee,2001. Re 2780.
Guyana
Ministry o Health [Guyana] et al. Executive summary
micro-nutrient study report Guyana. An assessment o the vitaminA,
E, beta-carotene, iron and iodine status in the
population.Georgetown, Ministry o Health, 1997. Re 3094.
Haiti
Republique dHaiti et al. Enqute Mortalit, Morbidit etUtilisation
des Services EMMUS-III Hati 2000. Republi-que dHaiti, 2001. Re
3264.
Honduras
Ministerio de Salud Pblica et al. Encuesta Nacional de Mi-
cronutrientes Honduras, 1996. Tegucigalpa, Secretaria deSalud,
Ministerio de Salud Pblica, 1997. Re 3095.
Secretara de Salud et al. Encuesta Nacional de Salud Mascu-lina
ENSM-2001. Tegucigalpa, Secretara de Salud, 2002.Re 3096.
India
International Institute or Population Sciences et al. Na-tional
Family Health Survey (NFHS-2), 19981999: India.Mumbai,
International Institute or Population Sciences,2000. Re 2972.
International Institute or Population Sciences et al. Na-tional
Family Health Survey (NFHS-2), India, 19981999,Northeastern States:
Arunachal Pradesh, Manipur, Megha-laya, Mizoram, Nagaland and
Tripura. Mumbai, Interna-tional Institute or Population Sciences,
2002. Re 3780.
Iran (Islamic Republic o)
Ministry o Health and Medical Education et al. Multi-centre
study on iron deciency anemia among 15 to 49 year oldwomen in the
Islamic Republic o Iran . Islamic Republic oIran, Nutrition
Department, Ministry o Health and Me-
dical Education, 1995. Re 3015.
Jamaica
WHO Pan American Health Organization et al.Micronu-trient study
report: an assessment o the vitamin A, E, beta-carotene, and iron
status in Jamaica. Kingston, WHO, PanAmerican Health Organization,
Caribbean Food and Nu-trition Institute, 1998 (PAHO/CFNI/98.J1). Re
3093.
Micronutrient Working Group. Assessment o the iron sup-
plementation programme or pregnant women in Jamaica.Cajanus, 2002,
35 (1): 3549. Re 3759.
Japan
National Institute o Health and Nutrition. National Nu-trition
Survey o Japan in 2001 and 2002. Japan, NationalInstitute o Health
and Nutrition, 2002. Re 5177.
Jordan
Department o Statistics et al. Jordan Population and Fa-
mily Health Survey 2002. Calverton, MD, Department oStatistics
Jordan, ORC Macro, 2003. Re 3389.
Ministry o Health Jordan et al. National baseline survey oniron
deciency anemia and vitamin A deciency. Amman,Ministry o Health,
2002. Re 4382.
Kazakhstan
Academy o Preventive Medicine Kazakhstan et al. Ka-zakhstan
Demographic and Health Survey 1999. Calverton,MD, Academy o
Preventive Medicine and Macro Interna-tional Inc, 1999. Re
2675.
Kenya
Mwaniki DL et al. Anaemia and status o iron, vitamin Aand zinc
in Kenya. The 1999 National Survey. Nairobi, Mi-nistry o Health,
2002. Re 3442.
Kuwait
Jackson RT et al. Gender and age dierences in anemiaprevalence
during the liecycle in Kuwait. Ecology o Foodand Nutrition, 2004,
43 (12):6175. Re 4375.
Kyrgyzstan
Research Institute o Obstetrics and Pediatrics et al.
KyrgyzRepublic Demographic and Health Survey, 1997. Calverton,MD,
Research Institute o Obstetrics and Pediatrics, Mi-nistry o Health
o the Kyrgyz Republic and Macro Inter-national Inc, 1998. Re
2295.
Lao Peoples Democratic Republic
Ministry o Health, Lao Peoples Democratic Republic. Re-port on
national health survey: health status o the People o LAO PDR.
Vientiane, Ministry o Health, 2001. Re 770.
-
8/3/2019 9789241596657_eng anemia
48/51
worldwIde prevalence o anaemIa 1993200538
Lebanon
Hwalla N et al. Prevalence and selected determinant o
irondeciency anemia in women and under ve children in Leba-non.
Beirut, 1998. Re 3221.
Lesotho
Ministry o Health and Social Welare et al. Lesotho De-mographic
and Health Survey 2004. Calverton, MD, ORCMacro, 2005. Re 5356.
Liberia
Mulder-Sibanda M et al. National Micronutrient Survey. Anational
prevalence study on vitamin A deciency, iron de-
ciency anemia, iodine deciency. Monrovia, Ministry oHealth and
Social Welare, Family Health Division, Uni-ted Nations Childrens
Fund, 1999. Re 1242.
MadagascarInstitut National de la Statistique et al. Enqute
Dmogra-phique et de Sant de Madagascar 20032004. Calverton,MD, ORC
Macro, 2005. Re 5190.
Malaysia
Ministry o Health Malaysia. Family Health. Sub SystemHealth
Management Inormation System, 2004. Malaysia,Ministry o Health,
2005. Re 5795.
Malawi
National Statistical Oce et al. Malawi Demographic and
Health Survey 2004. Calverton, MD, ORC Macro, 2005.Re 5201.
Maldives
Ministry o Health and Welare et al. Nutritional status andchild
eeding practices o Maldivian children Report o theNational
Nutrition Survey. Mal, 1994. Re 831.
Minister o Health, Republic o Maldives.Multiple Indica-tor
Cluster Survey (MICS 2), Maldives. Mal, Ministry oHealth, 2001. Re
2987.
MaliCellule de Planication et de Statistique du Ministre dela
Sant et al. Enqute Dmographique et de Sant au Mali
2001. Calverton, MD, ORC Macro, 2002. Re 3446.
Mauritius
Ministry o Health Mauritius.A survey o nutrition in Mau-ritius
and Rodrigues (1995). Port Louis, Ministry o Health,1995. Re
395.
Mexico
Instituto Nacional de Salud Publica. Encuesta Nacional de
Nutricin 1999. Mexico City, Instituto Nacional de SaludPublica,
1999. Re 2997.
Micronesia (Federated States o)
Auerbach SB.Maternal-Child Health Survey: Pohnpei, Fe-derated
States o Micronesia, 1993 [summary table]. Palikir,Pohnpei, US
Public Health Service/Department o HealthServices [Federated States
o Micronesia], 1999. Re 4942.
Socorro P et al. Results o vitamin A, anemia and blood
leadsurvey among 24 year old children and reproductive-agedwomen in
Yap proper and Kosrae State, Federated States o
Micronesia. Atlanta, Centers or Disease Control and Pre-vention,
2000. Re 2548.
Mongolia
Enkhbat S. Third National Nutrition Survey 2004 [perso-nal
communication]. Mongolia, Ministry o Health, 2004.Re 5247.
Morocco
Ministre de la Sant Maroc. Enqute nationale sur la ca-rence en
er lutilisation du sel iod et la supplmentation parla vitamine A,
2000. Morocco, 2000. Re 3469.
Mozambique
Ministrio da Sade et al. Inqurito nacional seovre a de-cincia de
vitamina A, prevalncia de anemia e malria emcrianas dos 659 meses e
respectivas mes. Maputo, InstitutoNacional de Sade, 2003. Re
589.
Myanmar
National Nutrition Center et al.A study on hemoglobin statusand
ood practices o Myanmar women. Myanmar, NationalNutrition Center,
Department o Health, 2001. Re 5246.
Nepal
Ministry o Health Nepal et al. Nepal Micronutrient StatusSurvey
1998. Kathmandu, Ministry o Health, 1999. Re1083.
New Zealand
Russell D et al. NZ Food: NZ People: key results o the
1997National Nutrition Survey. New Zealand, Ministry o
Health, 1999. Re 3192.
Nicaragua
Ministerio de Salud. Encuesta nacional de micronutrien-tes (ENM
2000) [National survey o micronutrients (ENM
2000)]. Managua, Ministerio de Salud, 2002. Re 3109.
Ministerio de Salud. Sistema integrado de vigilancia de
inter-venciones nutricionales (SIVIN): primer inorme de
progreso
20022003 [Integrated system o monitoring nutrition
inter-ventions (SIVIN): rst progress report 20022003]. Mana-gua,
Ministerio de Salud, 2004. Re 4466.
-
8/3/2019 9789241596657_eng anemia
49/51
39annex 3
Nigeria
Federal Ministry o Health and Social Services et al. Nige-ria
National Micronutrient Survey, 1993. Nigeria, FederalMinistry o
Health and Social Services, 1996. Re 50.
Oman
Al-Riyami A et al. National Health Survey, 2000. Volume II
Reproductive Health Study. Ministry o Health the Sulta-nate o Oman,
2000. Re 4218.
Al-Riyami A et al. Genetic Blood Disorders Survey in
theSultanate o Oman. Journal o Tropical Pediatrics, 2003, 49(Suppl
1): i120. Re 5204.
Pakistan
Pakistan Institute o Development Economics et al. Natio-nal
Nutrition Survey 20012002. Islamabad, Governmento Pakistan,
Planning Commission, 2003. Re 4640.
Panama
Ministerio de Salud, et al. Encuesta nacional de vitamina Ay
anemia por deciencia de hierro [National survey o vitaminA and iron
deciency anemia]. Panama City, Ministerio deSalud, 2000. Re
3097.
Peru
Ministerio de Salud Publica et al. Monitoreo nacional
deindicadores nutricionales 2004. Lima, Ministerio de SaludPublica,
Instituto Nacional de Salud, 2004. Re 5359.
Philippines
Food and Nutrition Research Institute, Philippines. TheSixth
National Survey 2003 [personal communication].Manila, 2003. Re
5242.
Qatar
Amine EK. Nutritional assessment in Qatar; 1995 Oct 20Nov 3
[assignment report]. Qatar, WHO Regional Oceor the Eastern
Mediterranean, 1995. Re 820.
Republic o Korea
WHO Regional Oce or the Eastern Mediterranean.1995 National
Nutrition Survey Report. Republic o Korea,Ministry o Health and
Welare, 1997. Re 3327.
Korean Ministry o Health and Welare. National Healthand
Nutrition Survey, 2001. Seoul, Korean Ministry oHealth and Welare,
2005. Re 5249.
Romania
Alred Rusescu Institute or Mother and Child Protec-tion.
Nutritional status o pregnant women, children under5 years and
school children aged 67 years. Alred Rusescu
Institute or Mother and Child Protection, 2005. Re 164.
Rwanda
Ministre de la Sant et al. National Nutrition Survey o Wo-men
and Children in Rwanda in 1996 [nal report]. Kigali,Ministre de la
Sant, 1997. Re 2558.
Samoa
Mackerras D et al. Samoa national nutritional survey 1999,part
1: anaemia survey [technical report]. Apia, Departmento Health,
2002. Re 3226.
Serbia and Montenegro1
Petrovic O et al. Multiple Indicator Cluster Survey II.
Thereport or the Federal Republic o Yugoslavia. Belgrade,UNICEF,
2000. Re 2441.
Singapore
Department o Nutrition et al. National Nutrition Survey
1998. Singapore, Ministry o Health, 2001. Re 760.
South Arica
South Arican Vitamin A Consultation Group (SAVACG).Children aged
6 to 71 months in South Arica, 1994: theiranthropometric, vitamin
A, iron and immunisation coveragestatus. Johannesburg, South Arican
Vitamin A Consulta-tive Group, 1995. Re 48.
Sri Lanka
Piyasena C et al. Assessment o anaemia status in Sri Lanka2001
[survey report]. Colombo, Ministry o Health, Nutri-
tion and Welare, Department o Health Services, MedicalResearch
Institute, 2003. Re 4972.
Sudan
Federal Ministry o Health et al. Comprehensive NutritionSurvey.
Khartoum, Federal Ministry o Health, NationalNutrition Department,
1997. Re 1443.
Elnour A et al. Endemic goiter with iodine suciency: apossible
role or the consumption o pearl millet in the etio-logy o endemic
goiter.American Journal o Clinical Nutri-tion, 2000, 71 (1): 5966.
Re 1553.
1 On 3 June 2006, the Permanent Representative o the Republic o
Ser-bia to the United Nations and other International Organizations
inGeneva inormed the Acting Director-General o the W HO that
themembership o the state union Serbia and Montenegro in the
UnitedNations, including all organs and the organizations o the
United Na-tions system, is continued by the Republic o Serbia on
the basis o Article 60 o the Constitutional Charter o Serbia and
Montenegro,activated by the Declaration o Independence adopted by
the NationalAssembly o Montenegro on 3 June 2006. Estimates used or
reerred
to in this document cover a period o time preceding that
communica-tion.
-
8/3/2019 9789241596657_eng anemia
50/51
worldwIde prevalence o anaemIa 1993200540
Switzerland
Hess SY et al. A national survey o iron and olate status
inpregnant women in Switzerland. International Journal orVitamin
and Nutrition Research, 2001, 71 (5): 268273. Re
3402.
Tajikistan
Branca F et al. Micro-nutrient status survey in Tajikistan.Rome,
National Institute or Research on Food and Nutri-tion, Kazakh
Academy o Nutrition, 2004. Re 4182.
Thailand
Ministry o Public Health et al. The Fourth National Nutri-tion
Survey o Thailand 1995. Bangkok, Ministry o PublicHealth,
Department o Health, 1998. Re 3961.
The ormer Yugoslav Republic o Macedonia
Branca F et al. Multiple indicator cluster survey in
FYRMacedonia with micronutrient component. Rome, NationalInstitute
o Nutrition, 2000. Re 1609.
Timor-Leste
Ministry o Health Timor-Leste et al. Timor Leste 2003Demographic
and Health Survey. Newcastle, Australia, Mi-nistry o
Health/University o Newcastle, 2003. Re 5050.
Tunisia
Ministre de la Sant Publique et al. Rapport national:valuation
de l tat nutritionnel de la population tunisienne
[National report: evaluation o the nutritional status o
theTunisian population]. Tunis, Ministre de la Sant Publi-que,
1996. Re 2485.
Turkmenistan
Gurbansoltan Eje Clinical Research Center or Maternaland Child
Health et al. Turkmenistan Demographic andHealth Survey 2000.
Calverton, MD, ORC Macro, 2001.Re 3209.
Uganda
Uganda Bureau o Statistics (UBOS) et al. Uganda Demo- graphic
and Health Survey 20002001. Calverton, MD,ORC Macro, 2001. Re
3207.
Ukraine
Academy o Medical Science o Ukraine et al. Report o theNational
Micronutrient Survey Ukraine. Ukraine, Academyo Medical Science o
Ukraine, 2004. Re 5172.
United Kingdom o Great Britain and Northern Ireland
Gregory JR et al. National Diet and Nutrition Survey: chil-dren
aged 1 to 4 years. Volume 1: report o the diet and
nutrition survey. London, Her Majestys Stationery Oce,1995. Re
3279.
Ruston D et al. The National Diet & Nutrition Survey:adults
aged 19 to 64 years. Volume 4: nutritional status (an-thropometry
and blood analytes), blood pressure and physicalactivity. London,
Her Majestys Stationery Oce, 2004.Re 4154.
United Republic o Tanzania
National Bureau o Statistics (NBS) Tanzania et al. Tan-zania
Demographic and Health Survey 200405. Dar esSalaam, National Bureau
o Statistics, ORC Macro. 2005.Re 5221.
United States o America
Centers or Disease Control and Prevention. NationalHealth and
Nutrition Examination Survey 19992000,
20012002[personal communication], 2002. Re 4738.
Uzbekistan
Institute o Obstetrics and Gynecology et al.
UzbekistanDemographic and Health Survey, 1996. Calverton,
MD,Institute o Obstetrics and Gynecology, Macro Internatio-nal Inc,
1997. Re 2293.
Analytical and Inormation Center et al. Uzbekistan
HealthExamination Survey 2002. Calverton, MD, Analytical
andInormation Center, State Department o Statistics, ORCMacro,
2004. Re 4950.
Vanuatu
Harvey P et al. Report o the second national nutrition
survey1996. Port Vila, Department o Health, 1998. Re 3196.
Viet Nam
Khoi HH et al. Report on Vietnam National anemia Sur-vey, 2000.
Hanoi, National Institute o Nutrition, 2001.Re 3408.
Zambia
Luo C et al. National baseline survey on prevalence and
aetio-logy o anaemia in Zambia: a random cluster community sur-vey
involving children, women and men. Lusaka, National
Food and Nutrition Commission, 1999. Re 2477.Micronutrient
Operational Strategies and Technologies(MOST) et al. Report o the
national survey to evaluatethe impact o vitamin A interventions in
Zambia, July andNovember 2003. Zambia, Micronutrient Operational
Stra-tegies and Technologies, United States Agency or
Inter-national Development (USAID) Micronutrient Program,2003. Re
5098.
Zimbabwe
Ministry o Health and Child Welare, Nutrition Unit.
Zimbabwe National Micronutrient Survey: 1999. Harare,Ministry o
Health and Child Welare, 2001. Re 2641.
-
8/3/2019 9789241596657_eng anemia
51/51
WHO Global Database on Anaemia
www.who.int/vmnis
For further information about the WHO Global Database on
Anaemia,
or if you would like to provide information, please contact:
[email protected]
ISBN 978 92 4 159665 7