Embed Size (px)
Citation preview

Sistema de classificação de fabricação e seus impactos nas
alterações pós-registro
APS Manufacturing Classification System Working Group
Kendal Pitt, GlaxoSmithKline Michael Leane, BMS Gavin Reynolds, AZ
1
Novas fronteiras farmacêuticas nas ciências, tecnologia, regulamentação
e sistema da qualidade, Brasilia. 22 de junho 2015

Manufacturing classification system and its impact on post-registration changes
APS Manufacturing Classification System Working Group
2
New frontiers in manufacturing technology, regulatory sciences and
pharmaceutical quality system, Brasilia June 22nd 2015
Kendal Pitt, GlaxoSmithKline Michael Leane, BMS Gavin Reynolds, AZ

Biopharmaceutics Classification System (BCS)
I High Permeability
High Solubility
II High Permeability
Low Solubility
III Low Permeability
High Solubility
IV Low Permeability
Low Solubility
High
Low
Permeability
• BCS is a scientific framework for classifying drugs based on their solubility and permeability. When combined with the in vitro dissolution characteristics of the drug product, the BCS takes into account: solubility, intestinal permeability, (and dissolution rate), all of which govern the rate and extent of oral drug absorption from IR solid oral-dosage forms.
Amidon GL, Pharm. Res., 12 (3), 1995. - Guidance for industry, Waiver of In Vivo Bioavailability and Bioequivalence Studies for Immediate Release Solid Oral Dosage Forms Based on a Biopharmaceutics Classification System. August 2000, CDER/FDA.

MCS: Why have one?
• Borrowing from BCS, use properties of particles to form a new classification to aid drug product manufacturing.
• Defines the “right particles” and “best process”. • Assist in particle engineering to provide targets for API
properties. • Aid development and subsequent transfer to manufacturing. • Provide a common understanding of risk. • Fits with QbD principles. Potential of obtaining regulatory relief
by demonstrating that the properties of the ingoing API and excipients are within established ranges for the process.

‘Difficult’ API

“Good” API

APS Joint Focus Group Meeting
BCS to MCS: From the particle to drug product: Predictions
from Material Science through to manufacturing
May 13th and 14th 2013, East Midlands Conference Centre, University of Nottingham, UK.
• Mat Sci and PEFDM focus groups
MCS: Initial discussions
. .
• Class I Direct compression. • Class II: Dry Granulation, • Class III: Wet Granulation, • Class IV: Other Technologies.
• Assumes there is a preference for simpler
manufacturing routes. • Builds on prior knowledge e.g. Hancock’s direct
compression criteria could form the foundation of MCS Class I.
• Ultimate aim of prediction from previous experience.
MCS Based on Processing Route

MCS Based on Processing Route

Direct compression

Dry Granulation

Wet granulation

White Paper
• Industry and academic collaboration • International contributions • Feedback questionnaire rolled out http://informahealthcare.com/doi/abs/10.3109/10837450.2014.954728

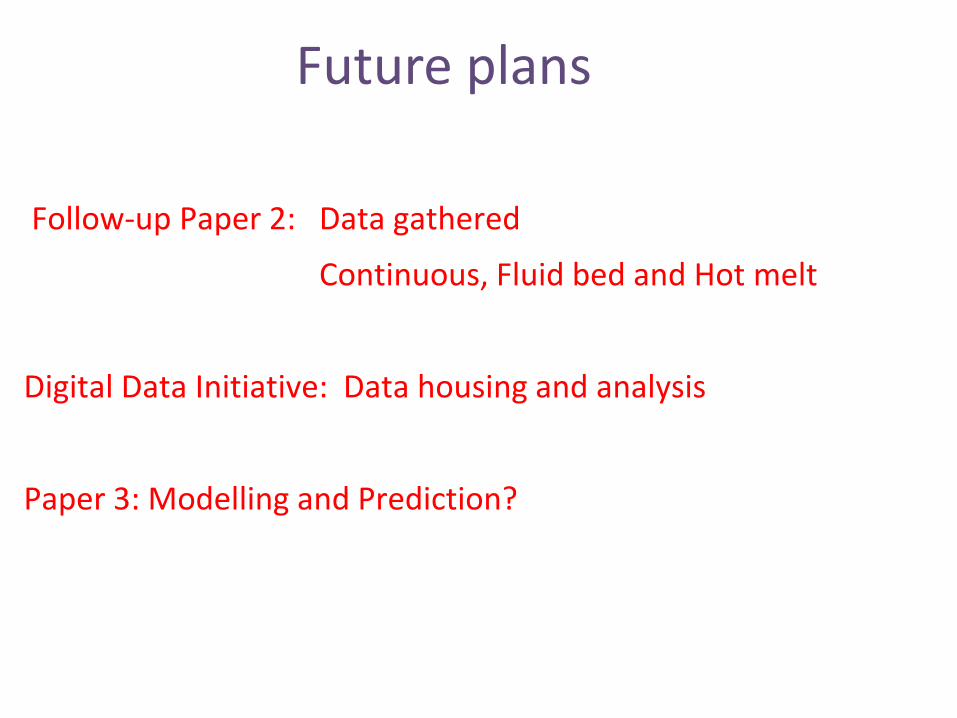
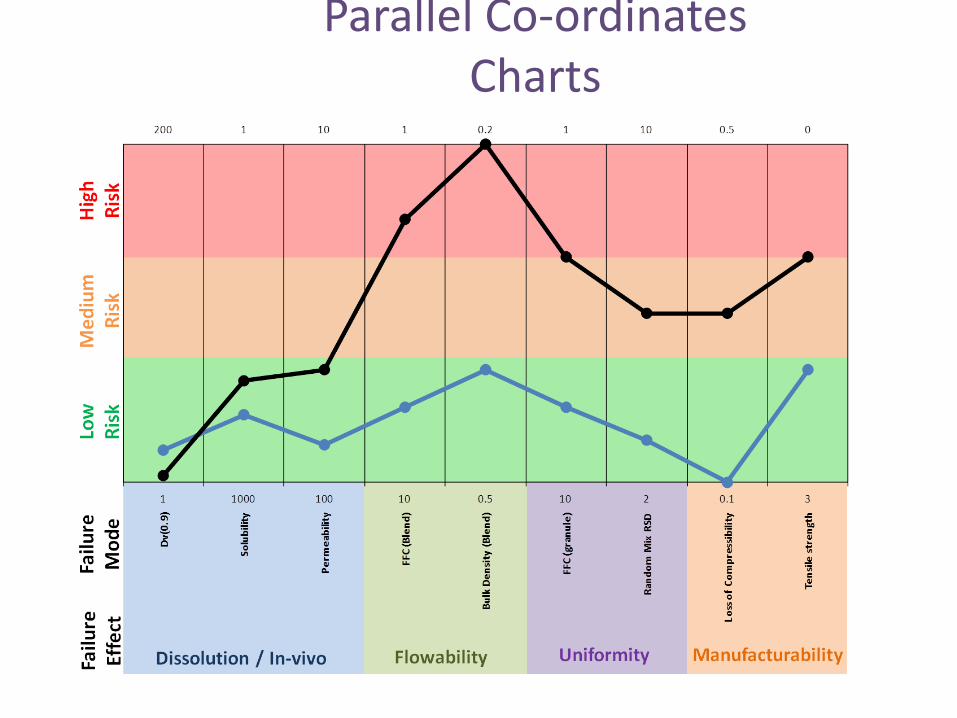
Parallel Co-ordinates Charts

Visualisation: Radar Charts Example representation; Best is nearest the bulls eye!
Capping and in-filling No issues
Powder flow, variable density and dissolution Capping in film coater

Abstract in Paper: next steps
“ This paper is intended to stimulate contribution from a broad range of stakeholders to develop the MCS concept further and apply it to practice. In particular, opinions are sought on what API properties are important when selecting or modifying materials to enable an efficient and robust pharmaceutical manufacturing process.”
16

AAPS 2014 + Webinar (San Diego) Global input
IFPAC 2015 (Washington DC) 25-28 Jan 2015: Regulatory Input
SSPC meeting 14 April15: Particle formation
ANVISA, Brasilia, 22nd -23rd June 2015 Sistema de classificação de fabricação e seus impactos nas alterações pós-registro
UK Pharm Sci 2015 (Nottingham UK): EU input
FIP 2015 (Dusseldorf) 28 Sept -3rd Oct 2015 Summary
Events for Input

Survey Questions • What next steps do you think the MCS
working group should take: – Pre-competitive sharing of API properties – Setting up boundaries for DC, RC, WG, OT – Identifying surrogate materials to represent
the different zones – Using modelling tools to link API properties to
manufacturing performance – Others?

Survey

What kind of things could we find out from this data?
• What processes are being used to manufacture currently approved products?
• How important are company and geographical factors in choosing processes?
• Have preferences changed over time? e.g. has there been a move away from wet granulation to dry granulation over time?
• How many products are made by non-traditional processes?
• Can we plot drug loadings / therapeutic area vs process choice?
20

EMA review; initial observations
21

Example Results
Therapeutic area
Commercial name
Active Ingredient
Dose Dosage form Route of
administration
Strength
Manufacturing process of Final Medicinal
Product
Manufacturer responsible for batch release
Marketing Authorization
Holder
Classification
Date of Approved/ Submited
Breast Neoplasms
Colonic Neoplasms Colorectal Neoplasms
Stomach Neoplasms
Ecansya (previously
Capecitabine Krka)
capecitabine
625 - 1250
mg/m2
body surface
area
tablet, film-coated
oral use 150 mg, 300 mg, and 500
mg
GW = Wet granulation (GW), sieving, mixing, granulation, drying,
sizing and lubrication prior to compression to
tablets and film coating.
Accord Healthcare Ltd., United Kingdom;
Pharmacare Premium Ltd.,
Malta; KRKA, d.d., Novo mesto,
Slovenia
Krka, d.d., Novo mesto,
Slovenia Generic
20/04/2012
Prostatic Neoplasms
Xofigo radium Ra223
dichloride
50 kBq/kg body
weight
solution for injection
intravenous use
1000 kBq/mL
SS = Dilution and mixing (to obtain target
radioactivity concentration), filling
and sterilization by autoclaving (SS).
Bayer, Norway Bayer Pharma AG, Germany
Reference 13/11/201
3
Carcinoma, Non-Small-Cell
Lung Xalkori crizotinib
200 - 250 mg
capsule, hard oral use 200 and 250
mg Process not specified.
Pfizer Manufacturing
Deutschland GmbH, Germany
Pfizer Ltd., United
Kingdom Reference
23/10/2012
Prostatic Neoplasms
Firmagon degarelix 80 and 240 mg
powder and solvent for solution for
injection
subcutaneous use
80 and 120 mg powder and solvent for solution for injection
AP = Sterile filtration of the formulated bulk,
aseptic filling and freeze-drying under aseptic process (AP).
Ferring GmbH, Germany
Ferring Pharmaceuticals A/S, Denmark
Reference 17/02/200
9
Cancer Area
Table 1. Examples of data collected from EMA documents of products approved for use in Cancer area in the EEA.

Example Results Cancer Area
Graph 2. Types of tablets approved for human use in Cancer Area in EEA.
74%
20%
6% tablets, film-coated
tablets
tablets,dispersible/tablet,buccal
43%
23%
17%
8% 9%
wet granulation
direct compression
dry granulation
Granulation process notspecified
Entire process notspecified
Graph 3. Manufacturing procedures applied in the production of tablets approved for human use in Cancer area in EEA.
Total of 35 products.
Total of 35 products.

Examples of information in public domain Sources: EPAR, NIH, Dictionnaire Vidal
24
. Drug Therapy Area Tradename Dose (mg) BCS Drug Load (%) Drug Product Process Launch date Company MCSRanitidine Ulcers 150 3 >50 DC 1981 GSKZidovudine HIV 300 1 >50 Wet granulated 1986 GSKAbacavir HIV 300 3 60 Direct Compression 1998 GSKFosamprenavir HIV 700 2 60 Wet granulated 2004 GSKRetigabine Epilepsy 50 to 400 1 63 Common Granulation 2010 GSKDolutegravir HIV 50 2 17 Wet Granulation 2012 GSKDaclatasvir HCV Dalkinza 30, 60 Dry Granulation 2014 BMSEfavirenz HIV Sustiva 600 Wet granulation 2002 BMSAripiprazole Anti-psychoticAbilify 5, 10, 20, 30 Fluid bed Wet Granula 2005 BMSEfavirenz/emtricHIV Atripla 600+200+300 Bilayer: Wet granulatio 2007 BMS/GileadEntecavir HCV Baraclude 0.5, 1 Wet granulation 2006 BMSWarfarin CV CoumadinHydroxyurea DroxiaApixaban CV Eliquis 2.5, 5 Roller compaction 2012 BMSATV/Cobi HIV EvotazMetformin Diabetes GlucophageMegestrol Megace 20, 40Clopidrogrel CV Plavix 75, 300Pravastatin CV PravacholAtazanavir HIV Reyataz 100, 150, 200 Low shear wet granula 2005 BMSDasatinib Anti-cancer Sprycel 20, 50, 70 25% Wet granulation 2006 BMSDidanosine HIV Videx 200 BMSStavudine HIV Zerit 5, 10, 20, 40 Dry granulation (sluggi 2005 BMSMitotane Anti-cancer Lysodren 500gefitinib Oncology (NSCIressa 250 2 >50 Wet Granulation 2009 AZdapagliflozen Diabetes Forxiga 5/10 3 low Roller Compaction 2012 BMS/AZvandetanib Oncology (MTCcaprelsa 100, 300 2 ~40 Wet Granulation 2012 AZ

Data interrogation:
25
Dose (mg)BCS Drug Load (%) Launch date Process MCS Mod150 3 >50 1981 DC YES300 1 >50 1986 WG NO300 3 60 1998 DC YES
50 to 400 1 63 2010 WG NO50 2 17 2012 WG NO

Table 2: Properties of an Ideal Direct-Compression Material Would this be applicable to Continuous Manufacture?
26
Property Value Target Value Particle Size and Shape D 4,3 (mean volume diameter) > 80µm
D 10 (10th percentile diameter) D 90 (90th percentile diameter)
Aspect Ratio
> 30µm ≤ 1000 µm
< 1.5 Blend Uniformity Blend Potency <2% relative standard deviation
Powder Flow Effective angle of internal friction
< 41°
Powder density True 1.0 - 2.5 g/mL Bulk > 0.5 g/mL
Tableting performance Dwell time sensitivity Low Precompression force Low Compression stress
(at ~ 0.85 solid fraction) 20 - 125 MPa
Compact mechanical properties Tensile strength > 1.0 MPa (at ~ 0.85 solid fraction) Brittle fracture index < 0.2
Indentation hardness 75 - 250 MPa
Adapted from McCormick 200534 from a talk given by BC Hancock “Identifying candidates for direct compression using material-sparing formulation tools” presented at AAPS November 2004

MCS: Applying DC to Continuous
27
.
Table 2 Properties of an Ideal direct-compression materialOriginal Source A Source B Source C
D50 >80micrond10 >30micronD90 <100micron
Blend RSD <2%
Internal Friction <41degree ? ? ? ?True Density 1-2.5g/mlBulk Density >0.5g/ml
Dwell time sensitivity LowPre Compression force LowPressure at 0.85 SF 20-125
TS at 0.85SF >1MPaBFI <0.2 ? ? ? ?Indent Hardness 75-250 MPa ? ? ? ?Flow Function >10 ?Continuous Processing ?
Follow-up Paper 2: Data gathered
Continuous, Fluid bed and Hot melt
Digital Data Initiative: Data housing and analysis
Paper 3: Modelling and Prediction?
Future plans

The MCS as part of a Regulatory System? .
Resolve
Identify differences
Discuss impact of differences
Framework for assessment
29 .
Parallel Co-ordinates Charts

Acknowledgements
• APS • Michael Leane (BMS) • Gavin Reynolds (AZ) • Members of the MCS working group
• Federal University of Rio de Janeiro (Faculty of Pharmacy):
Prof. Dr. Bianca Aloise Maneira Corrêa Santos Prof.Dr. Flávia Almada do Carmo

Comments / Questions
Obrigado !