Embed Size (px)
Citation preview

MARISTELA PINHEIRO FREIRE
Aquisição de bactéria gram-negativa
multidroga resistente antes do transplante
de fígado : o impacto no desfecho
Tese apresentada à Faculdade de Medicina da
Universidade de São Paulo para obtenção do título
de Doutora em Ciências
Programa de Doenças Infecciosas e Parasitárias
Orientador: Prof. Dr. Edson Abdala
São Paulo
2017

Dados Internacionais de Catalogação na Publicação (CIP)
Preparada pela Biblioteca da
Faculdade de Medicina da Universidade de São Paulo
reprodução autorizada pelo autor
Freire, Maristela Pinheiro
Aquisição de bactéria gram-negativa multidroga resistente antes do transplante
de fígado: o impacto no desfecho / Maristela Pinheiro Freire -- São Paulo, 2017.
Tese (doutorado)--Faculdade de Medicina da Universidade de São Paulo.
Programa de Doenças Infecciosas e Parasitárias.
Orientador: Edson Abdala.
Descritores: 1.Transplante de fígado 2.Bactéria multi-droga resistente
3.Fator de risco 4.Mortalidade 5.Bacilo Gram-negative 6.Resistência a
carbapênico
USP/FM/DBD-244/17

MARISTELA PINHEIRO FREIRE
Multidrug-resistant gram-negative bacteria
acquired before liver transplantation : the
impact on the outcome
Thesis presented at the Faculdade de Medicina da
Universidade de São Paulo for acquisition of the
title of Philosophiae Doctor (PhD)
Infectious Diseases Program
Advisor: Prof. Dr. Edson Abdala
São Paulo
2017
This thesis is in accordance with the following rules, validity at the moment of
the publication.
References: adapted from International Committee of Medical Journals Editors
(Vancouver).
Universidade de São Paulo. Faculdade de Medicina. Divisão de Biblioteca e
Documentação. Guia de apresentação de dissertações, teses e monografias.
Authors: Anneliese Carneiro da Cunha, Maria Julia de A. L. Freddi, Maria F.
Crestana, Marinalva de Souza Aragão, Suely Campos Cardoso, Valéria
Vilhena. 3a edition. São Paulo: Divisão de Biblioteca e Documentação: 2011.
Abbreviations of periodic titles are in accordance with List of Journals Indexed
in Index Medicus.

TABLES OF CONTENTS
Abbreviations and Acronyms List
Figures List
Tables List
Resumo
Abstract
1 INTRODUCTION ................................................................................................................ 1
2 OBJECTIVES..................................................................................................................... 11
2.1 Primary objective ................................................................................. 11
2.2 Secondary objectives ......................................................................... 11
3 METHOD ............................................................................................................................. 12
3.1 Study Design ....................................................................................... 12
3.2 Participants .......................................................................................... 12
3.3 Prophylaxis .......................................................................................... 13
3.4 Immunosuppression ............................................................................ 14
3.5 Microbiology ........................................................................................ 14
3.5.1 Surveillance Culture .................................................................. 14
3.5.2 Processing of surveillance culture samples .............................. 15
3.5.3 Culture for diagnosis of infection ............................................ 17
3.5.4 Molecular typing – Pulsed Field Electrophoresis ................... 18
3.6 Definitions ............................................................................................ 21
3.6.1 Multidrug-resistant bacteria definition ........................................ 21
3.6.2 Diagnostic Criteria for bacterial colonization .......................... 22
3.6.3 Criteria for diagnosis of healthcare-associated infection ....... 22
3.6.4 Definition of acquisition of Multidrug-resistant bacteria ......... 23
3.6.5 Criteria for diagnosis of acute cellular rejection ..................... 24
3.6.6 Criteria for severity of liver failure: .......................................... 24
3.7 Statistical treatment ............................................................................ 25
3.7.1 Performance of surveillance culture: ......................................... 25
3.7.2 Outcome variables ................................................................... 25
3.7.3 Variables analyzed .................................................................. 26
3.7.4 Statistical analysis ................................................................... 28

4 RESULTS............................................................................................................................ 30
4.1 Characterization of the population ....................................................... 30
4.2 Surveillance cultures ............................................................................ 34
4.3 Identification of KPC-producing Enterobacteriaceae ........................... 36
4.4 Analysis of risk factors for Multidrug-resistant Gram-negative bacteria acquisition after liver transplantation ...................................... 37
4.4.1 Analysis of risk factors for carbapenem-resistant K.
pneumoniae acquisition after liver transplantation .................... 39
4.4.2 Analysis of risk factors analysis of carbapenem-resistant A.
baumannii acquisition after liver transplantation ........................ 41
4.4.3 Analysis of risk factors analysis of carbapenem-resistant P.
aeruginosa acquisition after liver transplantation ...................... 44
4.5 Healthcare-associated infections (HAI) after liver transplantation ....... 46
4.5.1 Surgical site infections .............................................................. 48
4.5.2 Bloodstream Infections after Liver Transplantation ................... 50
4.5.3 Lower respiratory tract infection after liver transplantation ........ 51
4.5.4 Other types of infection after liver transplantation ..................... 52
4.6 Analysis of risk factors for healthcare-associated infection by MDR GNB after liver transplantation ............................................................. 53
4.6.1 Analysis of risk factors analysis of healthcare-associated
infection by carbapenem-resistant K. pneumoniae after liver
transplantation ........................................................................... 56
4.6.2 Analysis of risk factors for healthcare-associated infection by
carbapenem-resistant A. baumannii after liver transplantation . 58
4.6.3 Analysis of risk factors for healthcare-associated infection by
carbapenem-resistant P. aeruginosa after liver
transplantation ........................................................................... 60
4.7 Evaluation of strains clonality through PFGE ...................................... 62
4.8 Survival analysis .................................................................................. 66
5 DISCUSSION..................................................................................................................... 69
6 BIBLIOGRAPHY ............................................................................................................... 84
7 APPENDIX

Abbreviations and Acronyms List
SOT – Solid organ transplantation
CMV – Cytomegalovirus
EBV – Epstein-Barr virus
HAI – Healthcare-associated infection
MDR – Multidrug-resistant bacteria
LT – Liver Transplantation
MRSA – Methicillin-resistant Staphylococcus aureus
MELD – Model for End-Stage Liver Disease
VRE – Vancomycin-resistant enterococci
GNB – Gram-negative bacilli
ESBL – Extended spectrum beta-lactamase
CRE – Carbapenem-resistant Enterobacteriaceae
CRPA – Carbapenem-resistant Pseudomonas aeruginosa
CRKP – Carbapenem-resistant Klebsiella pneumoniae
CVC – Central venous catheter
BHI – Brain Heart Infusion
CLSI – Clinical Laboratory Standards Institute
PFGE – Pulsed-field Gel Electrophoresis

SSI-OE – Organ-space Surgical Site Infection
SSI-I – Incisional surgical site infection
BSI – Bloodstream infection
UTI – Urinary tract infection
RR – Relative risk
CI – Confidence interval
OR – Odds Ratio

Figures List
Figure 1 – Distribution of PFGE pulsotype of carbapenem-resistant A.
baumannii strains from November 2009 to November 2011 ......... 62
Figure 2 – Dendogram of carbapenem-resistant A. baumannii strains from
eight patients who acquired CRAB before LT and developed
infection by CRAB after LT ............................................................ 63
Figure 3 – Distribution of PFGE cluster of carbapenem-resistant blaKPC-
positive K. pneumoniae strains from January 2010 to November
2011 .............................................................................................. 64
Figure 4 – Dendogram of carbapenem-resistant K. pneumoniae isolated
from Liver transplant patients from November 2009 to
November 2011 ............................................................................. 65
Figure 5 – 60-day survival curve adjusted according to LT surgery duration
and post-LT dialysis, categorized by type of microorganism
isolated from HAI after LT.............................................................. 68

Tables List
Table 1 – Baseline diseases of 195 patients submitted to liver
transplantation ............................................................................. 31
Table 2 – Demographic and clinical characteristics of 195 patients
submitted to liver transplantation ................................................. 32
Table 3 – Sites, microorganisms and sensitivity profile of 50 infections
identified in up to ten days before liver transplantation ................. 33
Table 4 – Positivity rate of surveillance culture by site of harvest from the
different Multidrug-resistant Gram-negative bacteria in 180
patients submitted to liver transplantation ................................... 35
Table 5 – Performance of surveillance culture of different MDR GNB in
180 patients submitted to liver transplantation ............................ 35
Table 6 – Distribution of blaKPC gene positivity rate among strains of
carbapenem-resistant Enterobacteriaceae isolated from
surveillance culture...................................................................... 36
Table 7 – Univariate analysis of risk factors for acquisition of MDR GNB
after LT in 105 patients – categorical variables ........................... 37
Table 8 – Univariate analysis for risk factors for acquisition of MDR GNB
after LT in 105 patients – continuous variables ........................... 38
Table 9 – Multivariate analysis of risk factors for acquisition of MDR
GNB after LT in 105 patients ....................................................... 38
Table 10 – Univariate analysis of risk factors for acquisition of
carbapenem-resistant K. pneumoniae after LT in 172 patients –
categorical variables.................................................................... 39
Table 11 – Univariate analysis of risk factors for acquisition of
carbapenem-resistant K. pneumoniae after LT in 172 patients
– continuous variables ................................................................. 40
Table 12 – Multivariate analysis of risk factors for acquisition of
carbapenem-resistant K. pneumoniae after LT in 172 patients....... 40
Table 13 – Univariate analysis of risk factors for acquisition of
carbapenem-resistant A. baumannii after LT in 171 patients –
categorical variables.................................................................... 42
Table 14 – Univariate analysis of risk factors for acquisition of
carbapenem-resistant A. baumannii after LT in 171 patients –
continuous variables.................................................................... 43

Table 15 – Multivariate analysis of risk factors for acquisition of
carbapenem-resistant A. baumannii after LT in 171 patients ...... 43
Table 16 – Univariate analysis of risk factors for acquisition of
carbapenem-resistant P. aeruginosa after LT in 190 patients –
categorical variables.................................................................... 44
Table 17 – Univariate analysis of risk factors for acquisition of
carbapenem-resistant P. aeruginosa after LT in 190 patients –
continuous variables.................................................................... 45
Table 18 – Multivariate analysis of risk factors for acquisition of
carbapenem-resistant P. aeruginosa after LT in 190 patients ....... 45
Table 19 – Distribution of the sites of 201 healthcare-associated infections
after liver transplantation ............................................................. 46
Table 20 – Distribution of microorganism isolated from 201 healthcare-
associated infections after liver transplantation ........................... 47
Table 21 – Microorganisms isolated from post-transplant organ space
surgical site infections, percentage of bacteremia and
resistance profile. ........................................................................ 49
Table 22 – Microorganisms isolated from post-transplant bloodstream
infections and resistance profile .................................................. 50
Table 23 – Microorganisms isolated from lower respiratory tract infection,
secondary bacteremia and resistance profile. ............................. 51
Table 24 – Microorganisms isolated from post-transplant urinary tract
infections and resistance profile. ................................................. 52
Table 25 – Microorganisms isolated from soft tissue infections and
resistance profile ......................................................................... 53
Table 26 – Univariate analysis of risk factors for healthcare-associated
infection by MDR GNB after liver transplantation in 195
patients – categorical variables ................................................... 54
Table 27 – Univariate analysis of risk factors for healthcare-associated
infection by MDR GNB after liver transplantation in 195
patients – continuous variables ................................................... 55
Table 28 – Multivariate analysis of risk factors for healthcare-associated
infection by MDR GNB after LT in 195 patients ........................... 55
Table 29 – Univariate analysis of risk factors for healthcare-associated
infection by carbapenem-resistant K. pneumoniae after liver
transplantation in 194 patients – categorical variables ................ 56

Table 30 – Univariate analysis of risk factors for healthcare-associated
infection by carbapenem-resistant K. pneumoniae after LT in
194 patients – continuous variables ............................................ 57
Table 31 – Multivariate analysis of risk factors for healthcare-associated
infection by carbapenem-resistant K. pneumoniae after liver
transplantation in 194 patients .................................................... 57
Table 32 – Univariate analysis of risk factors for healthcare-associated
infection by carbapenem-resistant A. baumannii after liver
transplantation in 193 patients – categorical variables ................ 58
Table 33 – Univariate analysis of risk factors for healthcare-associated
infection by carbapenem-resistant A. baumannii after liver
transplantation in 193 patients – continuous variables ................ 59
Table 34 – Multivariate analysis of risk factors for healthcare-associated
infection by carbapenem-resistant A. baumannii after liver
transplantation in 193 patients – categorical variables ................... 59
Table 35 – Univariate analysis of risk factors for healthcare-associated
infection by carbapenem-resistant P. aeruginosa after liver
transplantation in 195 patients – categorical variables ................ 60
Table 36 – Univariate analysis of risk factors for healthcare-associated
infection by carbapenem-resistant P. aeruginosa after liver
transplantation in 195 patients – continuous variables ................ 61
Table 37 – Multivariate analysis of risk factors for healthcare-associated
infection by carbapenem-resistant P. aeruginosa after liver
transplantation in 195 patients – categorical variables ................ 61
Table 38 – Univariate analysis of risk factors for death in the 60 first days
after liver transplantation, among 195 patients – categorical
variables ...................................................................................... 66
Table 39 – Univariate analysis of risk factors for death in the 60 first days
after liver transplantation, among 195 patients – continuous
variables ...................................................................................... 67
Table 40 – Multivariate analysis of risk factor for death in the 60 first days
after liver transplantation, among 195 patients ............................ 67

RESUMO
Freire MP. Aquisição de bactéria gram-negativa multidroga resistente antes do transplante de fígado: o impacto no desfecho [Tese]. São Paulo: Faculdade de Medicina, Universidade de São Paulo; 2017.
As infecções em pacientes submetidos a transplantes de órgãos sólidos são importante causa de morbidade, além de serem definidoras da sobrevida desta população. A maioria das infecções que ocorre nos dois primeiros meses pós-transplante é relacionada à assistência à saúde (IRAS). O objetivo deste trabalho é identificar fatores de risco para IRAS por bactérias Gram-negativas (BGN) multi-droga resistentes (MDR) em pacientes submetidos a transplante de fígado (TF), nos dois primeiros meses após o transplante. Os objetivos secundários são: identificar fatores de risco para aquisição por MDR GNB em pacientes submetidos a TF, e determinar o impacto das IRAS por MDR GNB na sobrevida desses pacientes. Foram avaliados os TF consecutivos realizados em pacientes adultos no Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HCFMUSP) no período de novembro de 2009 a novembro de 2011. A vigilância microbiológica foi realizada no dia do TF, e semanalmente até a alta hospitalar ou 60 dias após o transplante. Os sítios de coleta f o r a m swab de orofaringe ou secreção traqueal, swab retal e swab axilar. Foram pesquisadas as seguintes bactérias: A. baumannii. P. aeruginosa e Enterobactérias resistentes a carbapenêmico, e K. pneumoniae e E. coli produtoras de betalactamase de espectro estendido (ESBL). Posteriormente, as amostras clínicas foram comparadas com as cepas da mesma espécie isoladas em culturas de vigilância por tipagem molecular. A análise de fatores de risco foi realizada por tipo de infecção e espécie de bactéria. Na análise estatística utilizou-se o teste qui-quadrado ou teste exato de Fisher para variáveis dicotômicas, e teste de Mann-Whitney para variáveis ordenáveis. A análise multivariada foi realizada por regressão logística. A análise de sobrevida foi realizada por regressão de Cox. O nível de significância de P considerado foi 0,05. Foram realizados, no período, 229 transplantes em 202 pacientes, e analisados 214 transplantes em 195 pacientes. O motivo de indicação do transplante mais frequente foi cirrose pelo vírus C, 33%. Foram identificados no período do estudo 110 pacientes (56,4%) com IRAS pós-TF, e um total de 201 infecções. Em 76,3% dos pacientes com IRAS (84/110) foi isolado MDR GNB em alguma amostra clínica relacionada à infecção. Os dois principais sítios de infecção foram infecção de sitio cirúrgico (32%) e infecção primária de corrente sanguínea (27%). Os dois microrganismos mais frequentemente isolados das IRAS foram A. baumannii e K. pneumoniae, e a proporção de infecções por cepas resistentes a carbapênemico foi, respectivamente, 100% e 48,9%. Os fatores de risco para infecções por MDR GNB pós-TF foram: retransplante precoce, volume de concentrados de hemácias transfundidos no intra-operatório da cirurgia do TF, colonização por MDR GNB no pré-transplante, tempo prolongado de internação em UTI e tempo prolongado de

isquemia fria. Cento e cinco pacientes adquiriram algum MDR GNB nos 60 dias pós-TF, e o único fator de risco detectado para aquisição de MDR GMB no pós-TF foi tempo prolongado de sonda vesical de demora. A análise de clonalidade demonstrou que as cepas de MDR identificadas pré-TF eram fortemente relacionadas às cepas isoladas das infecções no pós-TF para A. baumannii e K. pneumoniae resistente a carbapenêmico. As infecções por MDR GNB apresentaram uma tendência a aumentar o risco de óbito nos 60 primeiros dias pós-TF, mas esta.
Descritores: transplante de fígado; bactéria multi-droga resistente; fator de risco, mortalidade; bacilo Gram-negativo; resistência a carbapenêmico

ABSTRACT
Freire MP. Multidrug-resistant Gram-negative bacteria acquired before liver transplantation: the impact on the outcome [Thesis]. São Paulo: "Faculdade de Medicina, Universidade de São Paulo"; 2017. Bacterial infections among patients submitted to liver transplantation (LT) are an important cause of morbidity and have huge impact on patients' survival. The majority of infections in the first two months after LT are related to healthcare assistance. The aim of this study has been to identify risk factors for healthcare-associated infections (HAI) caused by multidrug-resistant Gram-negative bacteria (MDR GNB) in liver transplant patients in the first two months after LT. The secondary aims have been to identify risk factors for acquisition of MDR BGN among liver transplant patients and analyze the survival rate during the first two months after LT. We analyzed consecutive liver transplantations performed at Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HCFMUSP) from November 2009 to November 2011. Surveillance cultures were performed on a weekly basis, starting on the day of the LT until the hospital discharge or 60 days after the LT. We collected surveillance cultures through swab from oropharynx (or tracheal secretion), axillary and inguinal rectal sites. We surveyed the following bacteria: carbapenem-resistant A. baumanni, P. aeruginosa, Enterobacteriaceae, ESBL-producing K. pneumoniae, and E. coli. The strains isolated from surveillance culture were compared to strains isolated from clinical cultures through PFGE. The risk factor analysis was performed for each type of MDR bacterium for risk of colonization and infection. The statistical analysis was carried out for dichotomous variables using chi-square tests or Fisher's exact tests when appropriate; Mann-Whitney tests were used for continuous variable and step-wise logistic regression was used for multivariate analysis. The survival rate analysis was performed using Cox regression. The significant value of P was 0.05. During the study period, 229 liver transplantations were performed in 202 patients and we analyzed 214 LT performed in 195 patients. The main baseline disease that warranted LT was virus C cirrhosis, 33%. 110 (56.4%) patients developed healthcare-associated infections after the LT and a total of 201 infections were identified; 84 (76.3%) patients had MDR GNB isolated from clinical cultures related to HAI. Surgical wounds (31%) and primary bloodstream (27%) were the most prevalent infection sites. The risk factors for HAI by MDR GNB after the LT were: re-transplantation, volume of blood units transfused during the LT surgery, colonization by MDR GNB before the LT, prolonged time of ICU stay, and prolonged time of cold ischemia. 105 patients acquired MDR GNB during the first 60 days after the LT; the only risk factor identified was the prolonged use of urinary drain. The clonal analysis showed that strains isolated in the period before the LT were closely related to strains isolated from clinical culture after the LT for carbapenem-resistant A. baumannii e K. pneumoniae. The infections by MDR GNB have been shown to increase the risk of death in the first 60 days after LT. Descriptors: liver transplantation, multidrug-resistant bacteria, risk factor, mortality, Gram-negative bacillus, carbapenem resistance

1 INTRODUCTION
Infections in patients undergoing solid organ transplant (SOT) are an
important cause of morbidity and have a decisive role in survival of this
population. Those infections may be didactically divided into three periods,
in which the incidence of different pathogens varies according to the state of
immunosuppression and environmental exposures: (1)
1. First or early period - comprises the first thirty days after the
transplantation, when most infections occur. Risk factors are mainly
related to the surgical procedure and the postoperative hospital stay.
The most common agents are bacteria commonly related to
healthcare-associated infection (HAI) and fungi that cause HAI,
especially Candida species. Herpes simplex virus infections may
already occur at this stage.
2. Second period - extends from the second to the sixth month post-
transplantation, and the infections are in general related to the
immunosuppression state. In this period there can occur opportunistic
infections caused by cytomegalovirus (CMV), Pneumocystis jiroveci
pneumonia and infections by Aspergillus species. Besides that, latent
infections such as tuberculosis can be reactivated.

Introduction 2
3. Third or late post-transplantation period - after six months of
transplantation, the majority of the patients are prone to lower levels
of immunosuppression. At this stage, infections are usually the
same as those acquired in the community by the immunocompetent
population. There are, however, some exceptions, such as those
patients who develop late acute rejection or chronic rejection or
other situations requiring an increase in immunosuppression, which
increases the risk of opportunistic infections. Development of
chronic infections such as hepatitis B and C and lymphoproliferative
diseases associated with Epstein-Barr virus (EBV) can also occur.
Currently, some late opportunistic infections such as CMV infection
can occur in this period if prophylaxis has been given earlier.
The risk of opportunistic infections is much more dependent on the
area under the curve of immunosuppression over time than on the dose of
immunosuppressant drug. Thus, in the early period the majority of infections
are not caused by opportunistic pathogens but are mainly related to patient
care and the surgical procedure, i.e., HAI. (2) (1)
Most infections in patients undergoing SOT occurred in the early
period. In 95% of the cases, the causative agent is a bacterium, and it is
estimated that about 60% of the infections are caused by multidrug-resistant
bacteria (MDR). (1) (3)
In this first period, patients undergoing liver transplantation (LT) are
particularly susceptible to HAI compared to patients who have been

Introduction 3
submitted to other SOT. There are certainly many factors that can contribute
to this fact: the complexity of the procedure, prolonged hospital and
intensive care stay, immunosuppression caused by baseline diseases,
frequency of renal failure, malnutrition and hepatic failure by itself. It is
expected that up to 68% of the patients will develop some kind of infection
during the first months after LT compared with 47% of kidney transplant and
54% of lung transplant recipients. (1) (2) (4)
Among bacterial infections after LT, those caused by Gram-positive
bacteria have been described as the most frequent ones in many studies.
The most commonly isolated agent was S. aureus, with an average incidence
of 25% and a high proportion of infections caused by methicillin-resistant
strains(MRSA). (5) (6) The prevalence of MRSA varies from 1.3% to 22.7% in
the post-LT period. (7) Among the patients undergoing LT at the Hospital das
Clínicas of the University of São Paulo Medical School (HCFMUSP), MRSA
have also been identified as the most frequent pathogens in the period from
2000 to 2005, accounting for 16% of the infections in the first month post-
transplant, with 94% of methicillin resistance. (8) Risk factors for MRSA
infection after LT are well established, and among them, the most important
is the previous colonization, both pre- and post-LT. (9) (10) It is estimated that
pre-transplant colonization increases the risk of infection by MRSA in the
post-transplant period in more than five times. (7) Another risk factor identified
in some studies has been the degree of hepatic impairment, measured by
MELD (Model for End-Stage Liver Disease) or prothrombin time test. (10)
Screening all patients, decolonization of carriers, and maintenance of straight

Introduction 4
contact precautions measures for hospitalized, colonized patients have been
shown to reduce the incidence of MRSA infections. Singh et al have shown a
drop from 40% to 4% in the rate of MRSA infection with the implementation of
this bundle of measures. (11)
Enterococcus spp. is a gram-positive bacterium with an increasing
prevalence among patients submitted to LT, the incidence ranging from 1 to
16%, and vancomycin resistance in up to 40% depending on the
epidemiological resistance profile of the transplant center. The prevalence
of vancomycin-resistant Enterococcus (VRE) post-transplantation is on
average 11.9%, ranging from 6.8% to 18.2%. (7) In our service this agent
was identified in 11% of cases of the infections in the first month after LT,
and vancomycin resistance was detected in 42% of the cases. (12) The
predisposing factors to Enterococcus spp. infections are the prior use of
antibiotics, biliary-digestive anastomosis and surgical complications related
to the biliary tree. (12) (13) (14). Colonization by VRE significantly increases the
risk of infection by this pathogen, and it is estimated that the probability of
VRE-colonized LT patients developing a VRE infection in the post-LT period
is five times higher than that of non-colonized patients. (14)
The prevalence of infections caused by Gram-negative bacilli (GNB)
has been increasing in recent years. Singh et al have identified an increase in
Gram-negative bacteremia cases, justified in part by the better management
of fungal and viral infections surveillance. At our center, Gram-negative
infections accounted for 47% of HAI in the first month post-LT. (15) (8) (16) Other
studies have also pointed to GNB as the predominant causative pathogen

Introduction 5
among post-LT bacteremic infections. Currently, Gram-negative infections
may account for up to 65% of post-LT bacterial infections. (17)
In addition to the increase in the prevalence, certain species with
reduced susceptibility to many classes of antimicrobial agents are on the
increase in this group of bacteria. (18) (19) (20) Singh et al have found that 54% of
the Gram-negative isolates in post-LT infections are classified as MDR, and
that there has been an increase in extended-spectrum beta-lactamase-
producing (ESBL) strains over time. The one-year mortality rate was
significantly higher for patients with infections caused by MDR bacteria. (21)
High morbidity and mortality rates of Gram-negative HAI can be
associated with this frequent multidrug resistance profile, which increases
the probability of errors in empiric treatment, and reduces the range of
options available for effective antimicrobial therapy. (6)
Pseudomonas aeruginosa is often isolated after LT and is a frequent
etiologic agent of pneumonia. (6) (17) Some reports claim that patients submitted
to LT are three times more susceptible to developing P. aeruginosa
bacteremia than other SOT patients. (22) Among patients submitted to LT at
HCFMUSP, P. aeruginosa was the fourth most prevalent HAI-causing
Gram-negative bacillus, but remained the most common etiologic agent of
pneumonia. (8)
Although P. aeruginosa is frequently associated with pneumonia,
some studies have reported that this bacterium is also commonly isolated
from intra-abdominal infections, and biliary intercurrences after LT are risk

Introduction 6
factors for infection by that etiologic agent. (23) (24) Other risk factors
described are: the intensive care unit (ICU) stay, re-transplantation and
bloodstream infection (BSI) associated with health assistance. (25)
Solid Organ Transplantations were previously described as risk factors
for infection by carbapenem-resistant P. aeruginosa (CRPA). (26) Other risk
factors often identified for HAI by CRPA in the general population are:
prolonged hospital stay and antibiotic use, common situations found in Liver
transplant patients. (27) (28) A Brazilian study has identified this microorganism
as the most frequent MDR bacteria in LT. (29) The resistance of P. aeruginosa
to carbapenem in LT recipients is described in the literature as ranging from
30 to 83%. (21) (30) A cohort study of 49 cases of P. aeruginosa bacteremia in
SOT patients identified the following factors associated with CRPA:
re-transplantation, septic shock, nosocomial acquisition. (31)
Infections by Acinetobacter baumannii in LT recipients range widely in
their incidence depending on the institution. Torre-Cisneros et al identified A.
baumannii in 7.6% of BSI. (5) Among the patients submitted to LT at
HCFMUSP, A. baumannii was the second most common Gram-negative
agent causative of HAI in the first post-LT period, corresponding to 12% of
the isolated microorganisms. (8) In that population, the A. baumannii was the
most frequent pathogen isolated from surgical site infections, and 94% of
the strains were resistant to carbapenem. (32)
The lung is the most common site of infection by this agent in SOT
patients. However, particularly in LT patients, intra-abdominal infections are
the predominant site in most series. (33) (34) (35)

Introduction 7
Previously documented risk factors for HAI by A. baumannii in
the general population are: disease severity, surgical procedures,
immunosuppressive drug use, previous antibiotic use and ICU stay. (36)
Those characteristics are usually identified in patients undergoing LT, and
so we expect that in services with a high prevalence of A. baumannii
infections, the LT population is an important group that develops HAI
caused by this agent. Specific risk factors for A. baumannii infection in
patients submitted to SOT described in the literature are: high pre-LT MELD
score, prior use of carbapenem, use of central venous catheters and
dialysis. Those studies, however, were not subjected to a multivariate
analysis to identify risk factors due to the small number of cases. (33) (37)
Klebsiella pneumoniae is the second most frequently identified Gram-
negative after LT in the literature, and the most frequent microorganism
identified at HCFMUSP. (8) Wade and colleagues, in a study of 284 liver
transplant patients identified infections by these microorganisms as a risk
for increased length of hospital stay. (38) Liver transplant recipients are
particularly susceptible to infections by Enterobacteriaceae. (30) In an
outbreak of ESBL-producing Escherichia coli (E. coli), 67% of the patients
were from an LT ward. (39) The intestine is the most frequent site of
colonization by Enterobacteriaceae and Liver transplant patients have an
increased risk of bacterial translocation due to frequent complications of
biliary tract and Roux-en-Y hepatojejunostomy anastomosis. Besides that,
LT patients are often exposed to antimicrobials, which increase the risk of
infections caused by ESBL-producing strains.

Introduction 8
Zhou et al identified 55 Enterobacteriaceae infections after LT. 32.4%
of them were ESBL-producing Enterobacter cloacae strains and 24% of
them were ESBL-producing AmpC. (40)
Infections caused by ESBL-producing Enterobacteriaceae are highly
prevalent among SOT recipients, approximately 10 to 50%. The mean
incidence is highly variable, and unlike other MDR bacterial infections,
infections by ESBL-producing Enterobacteriaceae are also described in
later periods after transplantation. (6) (41) (42) The single factor identified as a
risk of infection by ESBL-producing Enterobacteriaceae in transplant
patients is the need for post-transplant hemodialysis. (6)
Currently, Enterobacteriaceae resistance to carbapenem (CRE) is
being increasingly reported with a high worldwide prevalence of these
agents. (43) (44) This resistance can occur due to several mechanisms: AmpC
hyper-expression or class A ESBL (either TEM or SHV) associated with
changes in the membrane (permeability of the outer membrane or hyper-
regulation of efflux bombs), or the production of enzymes that hydrolyze
carbapenem (carbapenemases). The carbapenemases identified in
Enterobacteriaceae can be categorized as metallo-β-lactamases, extended-
spectrum β-lactamase oxicilinases or carbapenemases inhibited by
clavulanic acid. (19) Carbapenemases inhibited by clavulanic acid belong to
Ambler’s Class A, among which KPC are the most frequent enzymes. (19)
The mortality rate associated with CRE infections ranges between 28%
and 68%. The introduction of effective therapy usually suffers greater delay,
with a consequent more prolonged hospital stay after diagnosis. (44) (45) (46)

Introduction 9
For KPC-producing K. pneumoniae (KPKPC), there are reports of an
increased risk of death by up to four times, and the risk factors associated
with higher mortality rates are high Acute Physiology and Chronic Health
Evaluation II (APACHE II) score, inadequate initial antibiotic therapy, age,
and septic shock at diagnosis of infection. (44) (47) (48) (46) (49) (50) (51)
The risk factors identified for CRE infections are an increased number
of invasive procedures, immunosuppression, use of cephalosporins,
carbapenems, anti-pseudomonas penicillin and fluoroquinolone, high APACHE
II score, mechanical ventilation, length of hospital stay, patient’s severity rating,
ICU stay, transplant of hematopoietic stem cells and SOT. (48) (47) (52) (53) (54)
Although patients submitted to SOT are at a higher risk for CRE
infections, there is scarce data in the literature on this specific population.
A KPKPC outbreak report in a hospital in São Paulo city described the
evolution of 10 SOT recipients: four kidney transplants, four LT and two
heart transplants, with an associated mortality rate of 50%. (55)
The incidence of KPKPC in patients undergoing LT varies from zero
to 25% of the bacterial infections in the first year post transplant.
Bloodstream infections and intra-abdominal infections are the two most
common types of infection. These infections have a significant impact on
the patient’s survival, and an associated mortality rate that ranges from 42%
to 71%. (55) (56) (57) (58)
In the Liver Transplant Service of the HCFMUSP, the carbapenem-
resistant K. pneumoniae infections were more frequent in intra-abdominal

Introduction 10
sites, mainly surgical site infections (SSI) with a high incidence of
bacteremia, in 46% of the cases. Mortality rate was 27%, and the risk
factors identified for carbapenem-resistant K. pneumoniae (CRKP)
infection were previous colonization and the need for dialysis. In the
literature the risk factors identified for infection by CRKP in LT recipients
are: mechanical ventilation for more than 48 hours, recurrent hepatitis C
virus infection, dialysis, high MELD score, Roux-en-Y biliary anastomosis,
biliary fistula, and colonization by CRKP. (59) (60)
Apparently, infections caused by MDR-GNB in patients undergoing
LT are strongly influenced by the frequency and sensitivity profile of the
microorganisms found not only in the transplant facilities, but also in all the
other hospital areas. Therefore, considering the growing incidence of MDR-
GNB, it seems essential that the analysis of risk factors for MDR-GNB
infections include active screening of colonization. The role and impact of
colonization as a risk for infection by these agents are not yet definitely
established in the literature. A better understanding of the epidemiology of
infections by MDR-GNB can contribute to the development of more effective
control strategies, as well as the most appropriate management of patients
with suspected infection by these agents.

11
2 OBJECTIVES
2.1 Primary objective
The primary objective was to analyze the impact of MDR-GNB
acquisition prior to LT on the incidence of healthcare-associated infections
by MDR-GNB in the first two months after LT.
2.2 Secondary objectives
To identify risk factors for healthcare-associated infection by
MDR-GNB in the first two months after LT.
To identify risk factors for MDR-GNB acquisition in the first two
months after LT.
To identify risk factors for acquisition and infection by the following
species of MDR-GNB (carbapenem-resistant P. aeruginosa, A.
baumannii, and Enterobacteriaceae) in the first two months after LT.
To analyze the impact of MDR-GNB infection in the 60-day
mortality rate after LT.

12
3 METHOD
3.1 Study Design
This was a prospective cohort study without intervention.
3.2 Participants
We evaluated consecutive liver transplants performed in LT patients
at HCFMUSP from October 2009 to October 2011. The exclusion criterion
was death in up to 48 hours after LT.
The liver transplantation service of HCFMUSP has been in activity
since 1988. During the study period an average of 100 transplants a year
were performed.
Data collection was prospective, using the following sources: the
patient's medical record, the records of the LT infectious diseases team,
infection control service database and the record of post-LT follow-up.
If the patient were discharged in less than two months after the liver
transplantation, the monitoring was conducted in an LT outpatient care setting.

Method 13
The HAI data and incidence of MDR bacteria were monitored monthly
by the hospital’s infection control service and surveillance cultures for CRE,
VRE and carbapenem-resistant Acinetobacter baumannii (CRAB) were
collected at admission and on a weekly basis for all patients in the liver
transplant ward and ICU.
3.3 Prophylaxis
The surgical prophylaxis used during the study period consisted of
a 48-hour administration of ampicillin plus cefotaxime. In the case of
patients undergoing LT during the treatment of infections, we used the
therapeutic antibiotic for prophylaxis provided its spectrum was similar to or
wider than that of the scheme used for surgical prophylaxis. For
prophylaxis in LT recipients whose donors were under infection treatment,
we used the same antimicrobial as the one received by the donor, or a
similar one, provided its spectrum was similar to or wider than that of the
scheme used for surgical prophylaxis.
Antifungal prophylaxis was performed for all patients with fulminant
hepatitis, dialysis indication, re-transplantation or treatment for acute cellular
rejection. Patients with indication for antifungal prophylaxis received
amphotericin B for 7 days.

Method 14
3.4 Immunosuppression
The standard immunosuppression regimen was performed with
tacrolimus associated with corticosteroids. The initial dose of tacrolimus was
0.3 mg/kg/day given every 12 hours (approximately 1 mg PO bid) for the first
days post-transplant and was adjusted to achieve a blood concentration of 8-
12 in the first three months. The induction immunosuppression was performed
with 1g of methylprednisolone administrated during the anhepatic phase.
3.5 Microbiology
3.5.1 Surveillance Culture
Cultures for identification of colonization by CRE, ESBL-producing
Enterobacteriaceae, CRPA and CRAB were performed immediately before
transplantation and weekly after LT while the patient was hospitalized. If the
patient happened to be re-hospitalized within two months after LT, the collection
of cultures was again performed at readmission and on a weekly base.
The materials for surveillance cultures were collected by oropharyngeal
swab or tracheal aspirates (if the patient was on mechanical ventilation),
and by axillary and inguinal-rectal swab.

Method 15
The transport of the material was carried out in dry sterile bottles in
the case of tracheal aspirates, or culture transport swab (Mueller Hinton) for
oropharyngeal, axillary and inguinal-rectal samples.
The first surveillance culture (SC) was collected on the transplantation
day. SC samples were collected twice a week, on Mondays and Thursdays,
so that the second week SC was collected in an interval that varied from six
to nine days from the first collection. The main researcher performed all the
SC collections.
3.5.2 Processing of surveillance culture samples
The SC were processed at HCFMUSP’s bacteriology and clinical
research laboratory (LIM 54).
Surveillance cultures were plated on selective media containing either
imipenem (1ml of Brain Heart Infusion broth (BHI) with a 10-µg-imipenem
disk) or ceftriaxone (1,8ml of BHI with a 30-µg-Ceftriaxone disk).
For identification, the isolated bacterial colonies were subjected to
optical microscopy and biochemical tests. The identification of the colonies
was carried out after the analysis of bacterial growth in different culture
media, observing its characteristics of size, edge, elevation, color, density,
consistency and hemolysis on blood agar media.

Method 16
The Enterobacteriaceae were identified by IAL medium (modified
Rugai) and oxidase and citrate utilization tests. (61) Nonfermenting Gram-
negative bacilli were identified through biochemical tests.
Several colonies were used in identification and subsequently
subjected to sensitivity tests for confirmation of their phenotype.
Suspected colonies were characterized by a commercial microorganism
identification kit (API 20E; BioMérieux).
Disk-diffusion test (Kirby-Bauer method)
a) Preparation of the bacterial suspension and its inoculation on plates
A bacterial suspension at a scale of 0.5 McFarland (~ 1.5 x 108 CFU /
ml) was prepared by spectrophotometry, with the optical density of 0.08-0.1
at 625nm. A cotton swab was used to inoculate a homogeneous bacterial
suspension on a Petri dish containing Mueller-Hinton agar (diameter
150mm). The procedures followed in this step were performed according to
standardized rules for the document M2-A7. (62)
b) Application of the disks and incubation of the plates
After a period of 15 minutes, the antibiotic disks were applied to the
plates. The samples were incubated at 35°C for 16 to 20 hours in the
ambient atmosphere. The antibiotic discs were chosen according to the
bacteria identified, following the recommendations of the Clinical Laboratory
Standards Institute (CLSI). (63)

Method 17
c) Reading of the plates
The diameters (mm) of the inhibition halos were measured with the
aid of a ruler and compared to the cutoff points proposed by CLSI. (63) The
isolates were then characterized as either sensitive or resistant.
Confirmation of carbapenem sensitivity for P. aeruginosa and A.
baumannii was checked using the disk-diffusion method (Kirby-Bauer method)
and (mm) the inhibition zone diameters were measured with the aid of a ruler
and compared to the cutoffs standardized by the CLSI (64). We used the E-test
for confirmation of strains with MIC ≥2 mg / ml for carbapenem.
The detection of ESBL was carried out using the disk-diffusion
method, Ceftazidime and Cefotaxime for screening, followed by a
combination of Disc Test (with or without the addition of clavulanic acid),
and E-test strips when necessary (Ceftazidime and Cefotaxime with or
without clavulanic acid).
3.5.3 Culture for diagnosis of infection
Cultures for diagnosis of infection were performed as part of the health
assistance routine and collected according to indication after evaluation by
the LT infectious diseases team.
The identification and sensitivity tests of the isolated microorganisms
were performed using the CLSI methodology described above. (64)
Method 18
The identification and initial susceptibility testing of microorganisms were
performed by automated method (Vitek - BioMérieux Marcy l'Etoile, France).
The cultures of clinical samples were initially processed at
HCFMUSP’s Microbiology Laboratory of the Central Laboratory Division,
and then forwarded to the LIM 54 for further investigation.
Cultures of interest for this project that were sent to the LIM 54 were
isolated from ESBL-producing Klebsiella pneumoniae, ESBL-producing E.
coli, cephalosporin-resistant Enterobacter spp., CRPA, CRAB and CRE.
The sources of interest were surgical sites (wound secretion or ascites fluid),
pneumonia (tracheal aspirate or bronchoalveolar lavage) and bloodstream
(blood culture).
All carbapenem-resistant Enterobacteriaceae strains isolated via
surveillance or clinical culture were submitted to polymerase chain reaction
(PCR) for the blaKPC.
3.5.4 Molecular typing – Pulsed Field Electrophoresis
The tests for molecular typing were performed at the LIM 54.
Microorganims phenotypically identified as CRKP, CRAB and CRPA were
analyzed by pulsed-field gel electrophoresis (PFGE).

Method 19
3.5.4.1 Protocol for molecular characterization by pulsed-field
gel electrophoresis (PFGE)
Molecular analysis was performed by electrophoresis of pulsed-field
gels, according to the protocols described by Ridley and Kaufmann. (65) (66)
Preparation of the bacterial suspension
Bacteria were subcultured on 5% sheep-blood agar medium and
incubated for 18-24 hours at 35 ° C 2°C. Three to five colonies were
transferred into tubes containing 3 ml of broth and incubated at 35 ° C 2 ° C,
overnight. They were transferred into a previously weighed microtube, and
extracted about 2 ml of the broth bacterial growth. The micro centrifuge tubes
were centrifuged for 20 minutes at 11,000 rpm. The supernatant was discarded
and the sediment was washed three times using 1 ml of sterile saline solution.
After the last wash, the supernatant was discarded and the microtube was
weighed on an analytical balance. The bacterial mass was calculated and then
an appropriate volume of 25 mm EDTA pH 8.0 solution was added to give the
bacterial suspension a resulting concentration of 100g/L.
Preparation of agarose blocks
DNA blocks were obtained by mixing 225 L of TEN buffer solution
(100 mM of Tris, pH 7.5; 100 mM of EDTA; 150 mM of NaCl) plus 25 L of
the bacterial suspension with 250 L of agarose 2% in 0.5X TBE buffer
(0.089 M of Tris, 0.089 M of boric acid, 0.002 M of EDTA). This mixture was
poured into specific molds and chilled at 4 ºC for 30 minutes.

Method 20
Bacterial DNA extraction step
The agarose blocks were removed from the molds and incubated in
EC 2ml of buffer (6 mM of Tris, pH7.5; 1 M of NaCl; 0.01 M of EDTA, 0.5%
Sarkosyl, 0.2% deoxycholate) for 5 hours at 37°C under gentle agitation.
After that time period, the buffer was removed and CHEF TE-buffer (2 mL)
(0.1 M of Tris, pH 7.5; 0.1 M of EDTA) was added. The latter buffer was
washed and then the blocks were treated with a solution with a final
concentration of proteinase K (Invitrogen Life Technologies, Carlsbad, USA)
at 1.0 mg / mL in ES buffer ( 0.4M of EDTA, pH9,3, 1.0% Sarkosyl),
overnight at 50°C. After this incubation period, the blocks were then washed
five times with 2 mL of CHEF-TE buffer at intervals of one hour under gentle
agitation. After the last wash, the blocks were stored at 4ºC.
Restriction enzyme step
Before performing the enzymatic treatment, agarose blocks were
washed five times with DNS buffer (0.1 M of Tris pH 8.0, 5 mM magnesium
chloride) with one-hour intervals between washes. For each species of
bacteria isolated a specific restriction enzyme was used.
Gel preparation
The treated wafers were dipped in agarose gel at 1% (TBE 0.5X).
Electrophoresis was performed using CHEF-DRII system (Bio-Rad,
Richmond, USA).
The patterns of electric current variation (time switch) were
established according to the microorganism studied. In the case of K.

Method 21
pneumoniae, race conditions were 5 to 30 seconds (initial and final switch
time), 6 V / cm (electric current) and 23 hours of run time. After the
electrophoresis, the gel was stained with ethidium bromide solution (1µg/ml)
for 40 minutes, bleached in distilled water for 40 minutes and photographed.
Image analysis
The PFGE images were processed and analyzed by Bioumerics
software version 7.1 (Applied Maths, Sint-Martens-Latem, Belgium). The
images were normalized using standard molecular markers and then the
band patterns were compared. The genetic similarity analysis was
performed using the Dice coefficient with a band position tolerance of 1.25%
and 0.5% optimization. Isolates were separated by similarity and grouped by
pair by the arithmetic mean method. Only the biggest bands of 45.5 kb were
included in the analysis.
3.6 Definitions
3.6.1 Multidrug-resistant bacteria definition
Multidrug-resistant bacterium was defined considering the following
resistance profiles:
• Carbapenem-resistant P. aeruginosa
• Carbapenem-resistant A. baumannii

Method 22
• ESBL-producing E. coli and K. pneumoniae
• Carbapenem-resistant Enterobacteriaceae
• Methicillin-resistant S. aureus
• Vancomycin-resistant Enterococcus
3.6.2 Diagnostic criteria for bacterial colonization
Colonization was defined as proliferation of microorganisms detected
on the patient’s surface or internally, without necessarily resulting in
detectable immune response, cellular damage or clinical symptoms.
The criteria used to define the patient only colonized by a MDR GNB
was the isolation of the agent in one or more clinical specimen samples or
surveillance cultures, and the exclusion of any active infection by this agent
at the time of collection.
3.6.3 Criteria for diagnosis of healthcare-associated infection
The diagnoses of bacterial and fungal infectious diseases were
performed through medical history, physical examination findings and
laboratory data, based on the criteria defined by the Centers for Disease
Control and Prevention (CDC / NHSN). (67)

Method 23
Post-LT healthcare-associated infections were those that occurred at
least 24 hours after the LT procedure. The cases of superficial fungal
infections and esophageal candidiasis were excluded.
The surgical site infections were categorized as superficial incisional,
when infection affected the skin and subcutaneous tissue; deep incisional,
when infection affected fascial or muscle layers; and organ space infection
when the infection involved any part of the anatomy other than the incision
that was opened or manipulated during the surgical procedure. (67)
The primary BSI was positive if patients had a recognized pathogen
isolated in one or more blood samples and this microorganism was not
associated with infection at another site. The BSI were defined as
associated with central venous catheter (CVC) if the patient had been in use
of the CVC for more than 2 days before the diagnosis of infection,
considering the 1st day the day of the implant. Infections with a single agent
in blood culture but with criteria for infection of other sites were defined as
secondary BSI. (67)
3.6.4 Definition of acquisition of multidrug-resistant bacteria
The acquisition of MDR GNB was characterized in the case of
patients who had not had either colonization or infection caused by a certain
agent in over two years, and the MDR GNB was isolated through clinical
culture or SC. during the two-month follow-up period after LT.

Method 24
3.6.5 Criteria for diagnosis of acute cellular rejection
Acute cellular rejection was defined as graft inflammation caused by
genetic mismatch between donor and recipient, affecting primarily
interlobular bile duct and vascular endothelium, including portal vein,
hepatic venules and occasionally hepatic artery and its branches. (68)
The diagnosis of rejection was histologically determined. The criterion
used was based on biopsy findings of at least two of the following:
predominantly mononuclear portal infiltrate with lymphocytes in blast phase,
neutrophils and frequent eosinophils and inflammation/injury of the bile
ducts; subendothelial inflammation of the portal vein or hepatic venule
terminals. (68) The classification used the Banff criteria. (68)
3.6.6 Criteria for severity of liver failure
MELD was used as a prognostic index for the assessment of liver
failure. The MELD was calculated immediately before the LT. The MELD is
a score that was initially used for patients with cirrhosis undergoing
transjugular intrahepatic portosystemic shunt, and then validated to assess
survival in patients with end-stage liver disease. The formula for the
calculation uses the total bilirubin levels, serum creatinine and International
Normalized Ratio (INR). (69)

Method 25
3.7 Statistical treatment
3.7.1 Performance of surveillance culture
For each SC collection site, the positivity rate was calculated as
follows: total number of positive SC tests for a given MDR GNB at a specific
collection site divided by the total number of positive SC tests for that MDR
GNB. For all patients, cultures were reviewed from three months before LT
to three months after LT.
The sensitivity rates was calculated following the formula: number of
patients with a positive SC test for a specific MDR GNB divided by the total
number of patients with a specific MDR GNB isolated in a clinical or
Surveillance Culture test.
3.7.2 Outcome variables
The outcome variables analyzed were:
• HAI by MDR in the first 60 days after LT;
• HAI by CRPA in the first 60 days after LT;
• HAI by CRAB in the first 60 days after LT;
• HAI by CRKP in the first 60 days after LT;
• Acquisition of MDR GNB in the first 60 days after LT;
Method 26
• Acquisition of CRPA in the first 60 days after LT;
• Acquisition of CRAB in the first 60 days after LT;
• Acquisition of CRKP in the first 60 days after LT;
• Death in the first 60 days after LT.
3.7.3 Variables analyzed
The receptor-related independent variables were:
• Continuous: Length of pre-transplant hospital stay in days, age in
years, pre-transplant functional MELD score, duration of central
venous catheter use in days, duration of urinary catheter use in
days, duration of mechanical ventilation use in days, duration of
intra-abdominal drain use in days, days of parenteral nutrition, use
of antimicrobial in the three months from pre-LT to the outcome or
60 days after LT for non-cases.
• Categorical: acute cellular rejection, use of Pulse corticosteroid
therapy for treatment of rejection, infection within 10 days from
previous LT, post-transplant bacterial infection, acquisition of MDR
GNB after the transplant, acquisition of MDR GNB before LT, post-
transplant fungal infection, use of therapeutic antibiotics in the
three months prior to the LT, performing surgical procedures after
LT, re-transplantation less than two months from the first transplant,
performing of hemodialysis, type of immunosuppression used after

Method 27
transplantation - defined as standard scheme, the use of two
immunosuppressant drugs (tacrolimus and corticosteroids),
fulminant hepatitis as indication of LT, the occurrence of CMV
infection, biliary complications, and American Society
Anesthesiology score (ASA).
• The variables related to transplant were:
• Continuous: duration of transplant surgery in minutes, cold and
total ischemia time in minutes, numbers of blood cell units
transfused during the LT.
• Categorical: Senior Surgeon (main surgeon who performed the
transplant with over eight years’ experience), type of antibiotic
prophylaxis used in LT (standard prophylaxis was defined as
ampicillin and cefotaxime for elective surgery and clindamycin,
cefotaxime and amphotericin B for fulminant hepatitis), type of
biliary anastomosis (defined as standard choledocho-
choledochostomy).
Patients who had MDR GNB identified before LT were excluded from
the analysis of risk of acquiring MDR GNB. Patients who underwent LT
while under treatment for MDR GNB infection were excluded from the
analysis of risk factor for post-LT MDR GNB infection.

Method 28
Variables related to exposure time
For patients with positive outcome, we considered the exposure time
up to the outcome. For patients with a negative outcome, we considered the
total exposure time during the first 60 days after LT. For each outcome the
exposure time was calculated separately.
The variables were ordered after the initial analysis, and all of them
were converted into categorical. The cutoff point adopted was the median of
the variable of the cases considered, except in cases of surgical time and cold
ischemia time, where the cutoff was the 75th percentile of the total samples.
For the multivariate analysis, the choice between the continuous and
categorical variable of the same information was that with the less value of P.
3.7.4 Statistical analysis
Univariate analysis was performed using the chi-square test or
Fisher's exact test for categorical variables when indicated, and the Mann-
Whitney test for continuous variables, considering a significance level of P
= .05. For the multivariate analysis we used stepwise logistic regression.
Variables that reached a significance level of less than or equal to 0.2 in the
univariate analysis were included in the model, following the ascending
order of the P value. Variables were sustained in the model if they reached
a P <0.05 or reduced the log-likelihood ratio by -2. The mortality rate analysis
and survival plots were performed using Cox regression. The following

Method 29
variables were treated as time-depended variables: age, post-LT dialysis,
acute cellular rejection, HAI, HAI by MDR and CMV infection.
The inclusion criterion in the mortality rate multivariate analysis was P
value lower or equal to 0.2 in the univariate analysis. The inclusion of
mortality in the multivariate analysis model was also by Stepwise. The
statistical software used for performing the analysis was SPSS 17.0.

30
4 RESULTS
4.1 Characterization of the population
During the study period, 229 transplants were performed in 202
patients. Seven patients were excluded due to death in less than 48 hours.
A total of 214 LT in 195 patients were evaluated.
The most common baseline disease that motivated LT was cirrhosis
due to hepatitis C virus, in 33% of the cases. (Table 1)
Demographic and clinical characteristics of the 195 patients
evaluated are shown in Table 2.

Results 31
Table 1 – Baseline diseases of 195 patients submitted to liver transplantation
Baseline diseases N Proportion
Cirrhosis due to hepatitis C virus 51 26%
Alcoholic cirrhosis 26 13%
Cryptogenic cirrhosis 21 11%
Fulminant hepatitis 16 8%
Alcoholic and hepatitis C virus cirrhosis 13 7%
Cirrhosis due to hepatitis B virus 13 6%
Autoimmune hepatitis 6 3%
Primary biliary cirrhosis 5 3%
Hemochromatosis 5 3%
Budd-Chiari syndrome 4 2%
Non-alcoholic steatohepatitis 4 2%
Familial paramyloidosis 4 2%
Primary sclerosing cholangitis 3 2%
Ductopenic diseases 3 2%
Wilson diseases 3 2%
Biliary atresia 2 1%
Cholestatic syndrome 2 1%
Alfa-1-antitrypsin deficiency 2 1%
Schistosomiasis 2 1%
Intra-hepatic lithiasis 1 1%
Caroli’s disease 1 1%
Graft dysfunction 1 1%
Glycogenosis type ii 1 1%
Cirrhosis due to C and B virus 1 1%
Hemangioendothelioma 1 1%
Thrombosis of hepatic artery 1 1%
Alcoholic and hepatitis B virus cirrhosis 1 1%
Alagille syndrome 1 1%
Secondary biliary cirrhosis 1 1%

Results 32
Table 2 – Demographic and clinical characteristics of 195 patients submitted to liver
transplantation
Characteristic Proportion (N) Median (min-max)
Gender (Female) 35% (69) -
Live donor 12% (25) -
Age (years) - 49 (16-73)
Length of hospital stay (days) - 32 (3-146)
Hepatocellular carcinoma 31% (61) -
Early re-transplantation 13% (26) -
Liver-kidney transplant 6% (12) -
Reoperation after LT 32% (62) -
Length of hospital stay before LT (days) - 6 (0-67)
ASA score >3 54% (97) -
Surgery duration (minutes) - 488 (210-1330)
Choledocho-choledochostomy 94%(184) -
MELD score - 23 (6-53)
Total ischemia time (minutes) - 428 (65-960)
Cold ischemia time (minutes) - 397 (20-910)
Nº of blood units transfused in LT procedure - 2 (0-15)
Serum creatinine on the day of LT (mg/dl) - 1,1 (0.51-6.79)
Post-LT dialysis 58% (110) -
Immunosuppression therapy with 3 drugs 45% (87) -
Cytomegalovirus infection 23% (44) -
Bacterial infection 10 days before LT 25% (49) -
Acute rejection treatment * 24% (43) -
Length of stay in ICU (days) - 16 (1-74)
Colonization or infection by Vancomycin-resistant Enterococcus spp. 47% (92)
*Standard treatment rejection was done with pulsed methylprednisolone therapy
LT – liver transplantation; ASA – American society of anesthesiology; MELD – model for end-stage liver disease, ICU-
intensive care unit.
Forty-nine (25%) patients were diagnosed with bacterial infection 10
days before LT. Table 3 describes the agents and sites of infection of those
infections. One patient had two different infections in less than 10 days
before transplantation. The average number of days between infection and

Results 33
the transplant was four days. Thirty patients (15.4%) had a diagnosis of
infection within 48 hours before the transplantation.
Table 3 – Sites, microorganisms and sensitivity profile of 50 infections identified in up
to ten days before liver transplantation
Site of infection N (%) Nº Infections
with causative
agent identified
Microorganism Nº
N MDR
(%)
Bacteremia
Intra-abdominal infection 21 (43%) 18 (86%) K. pneumoniae 6 3 (50%)* 3 (50%)
Enterococcus spp. 7 4 (57%) 3 (43%)
E. cloacae 4 0 2 (50%)
E. coli 3 1 (33%)** 2 (67%)
S. aureus 3 3 (100%) 2 (67%)
C. tropicalis 3 0 2 (67%)
Streptococcus spp. 2 0 1 (50%)
P. aeruginosa 2 0 1 (50%)
Gram-negative bacillus
1 0 0
P. mirabilis 1 0 0
A. baumannii 1 1 (100%) 1 (100%)
C. freundii 1 0% 0
Bloodstream Infection 20 (41%) 20 (100%) S .aureus 4 3 (75%) 4 (100%)
Enterococcus spp. 3 0% 3 (100%)
A. baumannii 3 3 (100%) 3 (100%)
K. pneumoniae 3 2 (67%)*** 3 (100%)
E. coli 2 0 2 (100%)
SCN 2 0 2 (100%)
C. albicans 2 0 2 (100%)
E. cloacae 2 0 2 (100%)
C. glabrata 1 0 1 (100%)
E. aerogenes 1 0 1 (100%)
Pneumonia/Bronchitis 4 (8%) 4 (100%) K. pneumoniae 1 1 (100%)*** 0
A. baumannii 1 1 (100%) 1 (100%)
E. aerogenes 1 1 (100%) 1 (100%)
Urinary tract infection 4 (8%) 4 (100%) P. mirabilis 1 0% 0%
S. aureus 1 1 (100%) 0%
E. coli 1 0% 0%
E. faecalis 1 1 (100%) 0%
Soft tissues 1 (2%) Zero
* 1 strain resistant to carbapenem and 2 ESBL- producing strains
**resistant to carbapenem
***ESBL producer
CNS – Coagulase-negative Staphylococcus ; MDR – Multidrug-resistant bacteria

Results 34
4.2 Surveillance cultures
A total of 4110 samples of SC were collected from three sites
(inguinal-rectal, oropharyngeal and axillary). Fifteen patients had no
samples collected by the protocol, but were not excluded because all had
had at least one SC performed for Enterobacteriaceae and CRAB during
hospital stay, which was processed in the routine microbiology laboratory.
On average, patients had SC samples every three weeks, the period
ranging between one and 14 weeks.
The site with the highest SC positivity rate for all MDR GNB was
inguinal-rectal, followed by the oropharynx. (Table 4)
The MDR-GNB SC with the lowest positivity rate was CRAB, with 19%
of patients with CRAB having negative SC; among patients with SC and
positive clinical cultures, the positivity rate of SC was higher for
carbapenem-resistant Enterobacteriaceae and lower for ESBL-producing
Enterobacteriaceae. (Table 5)

Results 35
Table 4 – Positivity rate of surveillance culture by site of harvest from the different
Multidrug-resistant Gram-negative bacteria in 180 patients submitted to liver
transplantation
MDR GNB Total number of patients
with MDR GNB
Sensitivity rate of
inguinal-rectal site
Sensitivity rate of
oropharyngeal site
Sensitivity rate of
axillary site
non-identification rate if SC was collected only from rectal site
Carbapenem resistant A. baumannii
105 53.3% 47.6% 27.6% 35.3%
Carbapenem resistant P. aeruginosa
30 80.8% 57.7% 26.9% 30.7%
Carbapenem resistant K. pneumoniae
79 92.4% 53.0% 34.8% 7.6%
Others carbapenem resistant Enterobacteriaceae
38 80.6% 52.8% 41.7% 19.4%
Enterobacteriaceae ESBL-producing
78 84.0% 36.0% 17.3% 16.0%
MDR GNB – Multidrug-resistant Gram-negative bacteria; SC – surveillance culture; ESBL – extended spectrum
betalactamases.
Table 5 – Performance of surveillance culture of different MDR GNB in 180 patients
submitted to liver transplantation
MDR GNB Total number of patients with MDR
GNB
Total number of patients
with positive SC
Positivity rate of SC among patients with positive MDR GNB clinical
culture
Proportion of patients in whom SC was the first
positive culture for MDR GNB
Carbapenem-resistant A. baumannii
105 85 (81.0%) 54 (74.0%) 59 (56.2%)
Carbapenem-resistant P. aeruginosa
30 26 (86.7%) 7 (66.7%) 26 (86.7%)
Carbapenem-resistant K. pneumoniae
79 73 (92.4%) 20 (76.9%) 70 (88.6%)
Other carbapenem-resistantt Enterobacteriaceae
38 36 (94.7%) 6 (85.7%) 5 (71.4%)
ESBL-producing Enterobacteriaceae
78 68 (87.2%) 11 (52.3%) 68 (87.2%)
MDR GNB – Multidrug-resistant Gram-negative bacteria; SC – surveillance culture; ESBL – extended spectrum
betalactamases.

Results 36
4.3 Identification of KPC-producing Enterobacteriaceae
Carbapenem-Resistant Klebsiella Pneumoniae (CRKP) was identified
in 146 samples of SC isolated from 57 patients. The blaKPC gene was
positive in 19 (33.3%) of the patients tested. The positivity of the KPC gene
among patients with CRKP identified in the 1st, 2nd, 3rd and from the 4th
week was respectively 34.8% (8/23), 26.7% (4/15), 26.7% (4/15) and 75.0%
(3/4). A tendency to increase the proportion of strains with blaKPC among
CRKP during the study period (Table 6) was observed.
Other non-K. pneumoniae CRE were identified in SC from 42 patients.
The search blaKPC gene was positive in 7 (16.7%) of the tested patients. The
distribution of positive blaKPC strains was uniform during the study period.
(Table 6)
Among clinical samples, blaKPC gene was isolated in nine patients
with positive culture by CRKP. Among patients with clinical cultures for other
carbapenem-resistant Enterobacteriaceae species, blaKPC gene was not
identified in any sample.
Table 6 – Distribution of blaKPC gene positivity rate among strains of carbapenem-
resistant Enterobacteriaceae isolated from surveillance culture
2º sem 2009
1º sem 2010
2º sem 2010
1º sem 2011
2º sem 2011
P
K. pneumoniae 0% (0/8) 20.8% (11/53) 18.2% (2/11)
20.0% (2/10)
100% (4/4)
0.02
Other Enterobacteriaceae 0% (0/5) 45.5% (5/11) 6.3% (1/16) 9.1%(1/11) 0% (0/0) 0.28
E. cloacae 0% (0/1) 50.0% (1/2) 0% (0/5) 33% (1/3)
E. aerogenes 0% (0/3) 0% (0/4) 0% (0/6) 0% (0/4)
Enterobacter spp 0% (0/1) 75.0% (3/4) 0% (0/4) 0% (0/4)
E. coli 100% (1/1) 100% (1/1)

Results 37
4.4 Analysis of risk factors for multidrug-resistant Gram-
negative bacteria acquisition after liver transplantation
Among 195 patients included in this study, 90 of them had some MDR
GNB identified in the pre-LT period, therefore the risk factor analysis for MDR
GNB acquisition after LT was performed in 105 patients. (Tables 7, 8 and 9)
After LT, 42 of the 105 (40.0%) patients acquired at least one MDR GNB.
Table 7 – Univariate analysis of risk factors for acquisition of MDR GNB after LT in 105
patients – categorical variables
Variable Patients with MDR GNB after LT (N=63)
N (%)
Patients without
MDR GNB after LT (N=42)
N (%)
P RR (CI95%)
Pre-LT characteristics
Bacterial infection before LT 13 (20.6%) 5 (11.9%) 0.25 1.11 (0.94-1.31)
Gender (F) 30 (69.8%) 13 (30.3%) 0.09 0.65 (0.39-1.09)
Hepatocellular carcinoma 15 (23.8%) 18 (42.9%) 0.04 0.75 (0.56-1.01)
Fulminant hepatitis 9 (14.3%) 1 (2.4%) 0.05 1.14 (1.02-1.27)
ASA score - - 0.79 -
LT surgical procedure characteristics
Combined liver-kidney transplant 4 (6.3%) 2 (4.2%) 1.00 1.02 (0.93-1.12)
Living-donor transplant 9 (14.3%) 9 (21.4%) 0.34 0.92 (0.76-1.11)
Senior surgeon 32 (50.8%) 21 (50.0%) 0.94 1.02 (0.69-1.51)
Duct-to-duct biliary anastomosis 60 (95.2%) 39 (92.9%) 0.68 1.50 (0.32-7.08)
Post-LT Evolution
Standard immunosuppressant therapy 29 (46.0%) 26 (61.9%) 0.11 0.71 (0.45-1.11)
Re-transplantation 10 (15.9%) 2 (4.8%) 0.12 1.13 (1.00-1.28)
Re-operation 11 (17.5%) 5 (11.9%) 0.58 1.07 (0.91-1.25)
CMV infection 3 (4.8%) 4 (9.5%) 0.43 0.95 (0.85-1.06)
Vancomycin-resistant Enterococcus colonization 30 (47.6%) 7 (16.7%) 0.01 1.59 (1.21-2.09)
Acute cellular rejection 9 (14.3%) 5 (11.9%) 0.78 1.03 (0.89-1.19)
Post-LT dialysis 28 (44.4%) 12 (28.6%) 0.10 1.29 (0.96-1.72)
MDR GNB – Multidrug-resistant Gram-negative bacteria; LT – liver transplantation; CMV - cytomegalovirus

Results 38
Table 8 – Univariate analysis for risk factors for acquisition of MDR GNB after LT in
105 patients – continuous variables
Variable
Patients with MDR GNB after LT
(N=63)
Median (min-max)
Patient without MDR GNB after LT
(N=42)
Median (min-max)
P
Pre-LT characteristics
Pre-LT length of hospital stay (days) 1 (0-22) 1 (0-46) 0.42
Age (years) 49 (16-70) 53 (21-73) 0.31
MELD score 23 (6-53) 17 (6-34) 0.03
Pre-LT serum creatinine (mg/dl)
ASA score
1.15 (0.10-10.54) 0.94 (0.41-6.49) 0.2
LT surgical procedure characteristics
Cold ischemia time (minutes) 400 (20-960) 389 (62-754) 0.42
Total ischemia time (minutes) 428 (81-910) 415 (100-730) 0.40
Duration of LT surgery (minutes) 460 (245-920) 492 (275-1330) 0.72
Units of blood transfused during LT surgery 2 (0-10) 0 (0-9) 0.02
Post-LT Evolution
Carbapenem use (days) 0 (0-32) 0 (0-30) 0.08
Quinolone use (days) 0 (0-4) 0 (0-0) 0.30
Polymyxin use (days) 0 (0-8) 0 (0-4) 0.12
Cephalosporin use (days) 2 (0-20) 2 (0-7) 0.67
Piperacillin/Tazobactan use (days) 0 (0-12) 0 (0-21) 0.98
Penicillin use (in days) 1 (0-9) 2 (0-6) 0.61
Length of dialysis after LT (days) 0 (0-24) 0 (0-50) 0.06
Length of central venous catheter (days) 6 (0-31) 4 (1-50) 0.02
Length of mechanical ventilator (days) 1 (0-17) 0 (0-9) 0.05
Length of urinary catheter (days) 6 (0-19) 4 (1-13) 0.01
Length of abdominal drain (days) 7 (0-23) 6 (0-21) 0.78
Length of ICU stay (days) 7(1-25) 4 (2-14) 0.007
MDR GNB – Multidrug-resistant Gram-negative bacteria; LT – liver transplantation; MELD – model of end-stage liver
disease, ICU – intensive care unit; ASA - American Society of Anesthesiologists (ASA) Physical Status classification.
Table 9 – Multivariate analysis of risk factors for acquisition of MDR GNB after LT in
105 patients
Variable P OR CI95%
Fulminant hepatitis 0.11 5.74 0.67-49.28
Length of urinary catheter (days) 0.02 1.16 1.03-1.32

Results 39
4.4.1 Analysis of risk factors for carbapenem-resistant K. pneumoniae
acquisition after liver transplantation
CRKP acquisition was identified in 25 patients before LT, therefore
those patients were excluded from this analysis. A total of 54 patients
acquired CRKP after LT. The analysis of risk factors for CRKP acquisition is
shown in tables 10, 11 and 12.
Table 10 – Univariate analysis of risk factors for acquisition of carbapenem-resistant K.
pneumoniae after LT in 172 patients – categorical variables
Variable Patients with carbapenem-resistant K.
pneumoniae after LT (N=54)
N (%)
Patients without
carbapenem-resistant K. pneumoniae
after LT (N=118)
N(%)
P RR (CI95%)
Pre-LT characteristics
Bacterial infection before LT 15 (27.8%) 33 (28.4%) 0.93 0.97 (0.80-1.19)
Gender (F) 34 (61.5%) 76 (66.1%) 0.57 0.88 (0.58-1.35)
Hepatocellular carcinoma 14 (25.9%) 38 (32.8%) 0.29 0.89 (0.73-1.09)
Fulminant hepatitis 4 (7.4%) 12 (10.3%) 0.78 0.97 (0.88-1.08)
ASA score - - 0.54 -
LT surgical procedure characteristics
Combined liver-kidney transplant 3 (5.6%) 6 (5.2%) >0.99 1.01 (0.93-1.09)
Living-donor transplant 7 (13.0%) 16 (13.8%) 0.99 1.00 (0.89-1.14)
Senior surgeon 22 (40.7%) 61 (52.6%) 0.26 0.84 (0.62-1.13)
Duct-to-duct biliary anastomosis 51 (94.4%) 110 (94.8%) 1.00 0.88 (0.23-3.39)
Post-LT evolution
Standard immunosuppressant therapy 24 (44.4%) 64 (55.2%) 0.19 0.76 (0.56-1.89)
Reoperation 16 (30.2%) 24 (20.7%) 0.12 1.16 (0.94-1.43)
Re-transplantation 5 (9.4%) 11 (9.5%) 0.78 0.98 (0.88-1.08)
Dialysis 32 (59.3%) 52 (44.8%) 0.08 1.65 (1.06-2.58)
Vancomycin-resistant Enterococcus
colonization 28 (53.8%) 53 (44.9%) 0.28 1.19 (0.85-1.67)
Acute cellular rejection 6 (11.1%) 23 (19.8%) 0.20 0.91 (0.80-1.04)
CMV infection 5 (9.3%) 15 (13.0%) 0.48 0.97 (0.86-1.08)
LT – liver transplantation; ASA - American Society of Anesthesiologists (ASA) Physical Status classification; CMV -
cytomegalovirus

Results 40
Table 11 – Univariate analysis of risk factors for acquisition of carbapenem-resistant K.
pneumoniae after LT in 172 patients – continuous variables
Variable Patients with carbapenem-resistant K.
pneumoniae after LT (N=52)
Patients without carbapenem-resistant K.
pneumoniae after LT (N=118)
P
Pre-LT characteristics
Age (years) 51 (17-70) 53 (16-73) 0.35
Length of hospital stay before LT (days) 1 (0-46) 1 (0-56) 0.69
Meld score 23 (6-53) 21 (6-52) 0.78
Pre-LT serum creatinine (mg/dl) 1.20 (0.51-6.57) 1.09 (0.40-10.54) 0.49
LT surgical procedure characteristics
Cold ischemia time (minutes) 440 (47-695) 384 (20-960) 0.07
Total ischemia time (minutes) 462 (81-740) 413 (65-910) 0.07
Duration of LT surgery (minutes) 435 (245-910) 488 (210-1330) 0.03
Units of blood transfused during LT surgery 2 (0-10) 2 (0-15) 0.72
Post-LT evolution
Quinolone use (days) Zero 0 (0-6) 0.20
Piperacillin/Tazobactan use (days) 0 (0-21) 0 (0-33) 0.61
Cephalosporin use (days) 2 (0-20) 2 (0-21) 0.14
Penicillin use (days) 2 (0-9) 1 (0-21) 0.83
Polymyxin use (days) 0 (0-26) 0 (0-69) 0.47
Carbapenem use (days) 0 (0-40) 1 (0-64) 0.42
Length of mechanical ventilator (days) 1 (0-60) 1 (0-78) 0.68
Length of abdominal drain (days) 8 (0-26) 7 (0-49) 0.43
Length of central venous catheter (days) 9 (2-73) 6 (1-96) 0.20
Length of urinary catheter (days) 9 (0-66) 6 (1-89) 0.26
Length of dialysis after LT (days) 4 (0-58) 0 (0-91) 0.17
Length of ICU stay (days) 9 (1-72) 6 (1-71) 0.27
LT – liver transplantation; MELD – model for end-stage liver disease, CMV – cytomegalovirus
Table 12 – Multivariate analysis of risk factors for acquisition of carbapenem-resistant
K. pneumoniae after LT in 172 patients
Variable P OR CI (95%)
Dialysis after LT 0.02 2.33 1.17-4.64

Results 41
4.4.2 Analysis of risk factors analysis of carbapenem-resistant A. baumannii
acquisition after liver transplantation
CRAB was identified in 24 (12.3%) patients before LT. Among those,
four developed infection in the pre-LT period: two primary BSIs, one
pneumonia and one cholangitis. Two patients were submitted to LT with
active infection by CRAB.
The risk factors analysis for post-LT acquisition of CRAB was
performed on 171 patients.
Among the patients with CRAB, seven presented strains with reduced
MIC for polymyxin.
Tables 13, 14 and 15 show the risk factor analysis for CRAB
acquisition after LT.

Results 42
Table 13 – Univariate analysis of risk factors for acquisition of carbapenem-resistant A.
baumannii after LT in 171 patients – categorical variables
Variable Patients with carbapenem-resistant A.
baumannii after LT (N=81)
N (%)
Patients without
carbapenem-resistant A. baumannii
after LT (N=90)
N (%)
P RR (CI95%)
Pre-LT characteristics
Bacterial infection before LT 24 (30.0) 22 (24.2) 0.39 1.08 (0.91-1.32)
Gender (F) 50 (62.5) 61 (67.0) 0.53 0.89 (0.59-1.34)
Hepatocellular carcinoma 17 (21.3) 36 (39.6) 0.01 0.77 (0.63-0.94)
Fulminant hepatitis 11 (13.8) 2 (2.2) 0.004 1.15 (1.04-1.26)
ASA score - - 0.67
LT surgical procedure characteristics
Combined liver-kidney transplant 11 (13.8) 13 (14.3) 0.92 0.99 (0.88-1.12)
Living-donor transplant 4 (5.0) 5 (5.5) >0.99 0.99 (0.93-1.07)
Senior surgeon 45 (56.3) 42 (46.2) 0.19 1.23 (0.87-1.65)
Duct-to-duct biliary anastomosis 77 (96.3) 86 (94.5) 0.73 0.98 (0.92-1.05)
Post-LT evolution
Standard immunosuppressant therapy 39 (48.8) 52 (57.1) 0.27 0.84 (0.61-1.15
Reoperation 17 (20.9) 19 (21.3) 0.95 1.05 (0.86-1.17)
Retransplantation 13 (16.3) 1 (1.1) <0.001 1.19 (1.08-1.31)
Dialysis 47 (58.0) 34 (37.4) 0.005 1.52 (1.13-2.05)
Vancomycin-resistant Enterococcus colonization
9 (11.1) 17 (18.7) 0.18 0.92 (0.81-1.04)
Acute cellular rejection 44 (55.0) 30 (33.3) 0.004 2.44 (1.31 5.55)-
CMV infection 6 (7.4) 14 (15.4) 0.11 0.92 (0.82-1.02)
LT – liver transplantation; ASA - American Society of Anesthesiologists (ASA) Physical Status classification; CMV -
cytomegalovirus

Results 43
Table 14 – Univariate analysis of risk factors for acquisition of carbapenem-resistant A.
baumannii after LT in 171 patients – continuous variables
Variable
Patients with carbapenem-resistant A.
baumannii after LT (N=81)
Median (max-min)
Patients without carbapenem-resistant A.
baumannii after LT (N=90)
Median (max-min)
P
Pre-LT characteristics
Pre-LT length of hospital stay (days) 1.0 (0-42) 1.0 (1.0-46.0) 0.24
Age (years) 50.0(16-70) 53.5 (18.0-73.0) 0.29
MELD score 26.0(6-51) 19.0 (6.0-5.0) 0.02
Pre-LT serum creatinine (mg/dl) 1.05 (0.51-8.43) 0.84 (0.55-6.57) 0.26
LT surgical procedure characteristics
Cold ischemic time (minutes) 445.0 (20-910) 390.0 (28-754) 0.27
Total ischemic time (minutes) 461.0 (70-960) 420 (65-768) 0.23
Duration of LT surgery (minutes) 465.0 (210-920) 465.0 (245-1330) 0.48
Units of blood transfused during LT surgery 2.0 (0-15) 0.5 (0-9) 0.006
Post-LT Evolution
Carbapenem use (days) 2.5 (0-32) 0.0 (0-68) <0.001
Quinolone use (days) 0.0 (0-5) 0.0 (0-0) >0.99
Polymyxin use (days) 0.0 (0-15) 0.0 (0-26) <0.001
Cephalosporin use (days) 2.00 (0-13) 0.0 (0-20) 0.98
Piperacillin/Tazobactan use (days) 0.0 (0-16) 0.0 (0-33) 0.005
Penicillin use (days) 1.00 (0-6) 2.0 (0-16) 0.21
Length of dialysis after LT (days) 2.00 (0-58) .0.0 (0-52) 0.006
Length of central venous catheter (days) 8.0 (1.0-68.0) 4.0 (1.0-54.0) 0.01
Length of mechanical ventilator (days) 2.00 (0-25) 0.0 (0-29) 0.007
Length of urinary catheter (days) 7.0 (1.0-28.0) 5.0 (1.0-47.0) 0.08
Length of abdominal drain (days) 7.0 (0.0-83.0) 6.0 (0.0-49.0) 0.35
Length of ICU stay (days) 7.0 (1.0-28.0) 5.0 (2.0-44.0) 0.02
LT – liver transplantation; ICU – intensive care unit; MELD – model for end-stage liver disease
Table 15 – Multivariate analysis of risk factors for acquisition of carbapenem-resistant
A. baumannii after LT in 171 patients
Variable P OR CI (95%)
Hepatocellular carcinoma 0.05 0.46 0.22-0.98
Units of blood transfused during LT surgery 0.06 1.17 0.99-1.37
Re-transplantation 0.01 10.09 1.22-83.10
Previous use of carbapenem 0.001 3.31 1.66-6.60
Previous use of piperacillin / tazobactam 0.02 2.19 1.11-4.32

Results 44
4.4.3 Analysis of risk factors analysis of carbapenem-resistant P.
aeruginosa acquisition after liver transplantation
CRPA was identified in a total of 30 LT recipients. In five patients
CRPA was identified before LT, and those patients were excluded from risk
factors analysis for CRPA acquisition after LT. (Table 16, 17 and 18) No
infections by CRPA were identified in the pre-LT period.
Table 16 – Univariate analysis of risk factors for acquisition of carbapenem-resistant P.
aeruginosa after LT in 190 patients – categorical variables
Variable Patient with carbapenem-resistant P. aeruginosa
(N=25)
N (%)
Patient without
carbapenem-resistant P. aeruginosa
(N=165)
N (%)
P RR (CI95%)
Pre-LT characteristics
Bacterial infection before LT 8 (32.0%) 52 (31.5%) 0.96 1.01 (0.76-1.34)
Gender (F) 12 (48%) 109 (66.1%) 0.08 0.65 (0.42-1.01)
Hepatocellular carcinoma 5 (20%) 52 (31.5%) 0.24 0.86 (0.69-1.07)
Fulminant hepatitis 4 (16%) 14 (8.5%) 0.27 1.09 (0.91-1.30)
ASA score - - 0.11 -
LT surgical procedure characteristics
Combined liver-kidney transplant 2 (8%) 23 (13.9%) 0.54 0.94 (0.82-1.07)
Living-donor transplant 2 (8%) 10 (6.1%) 0.66 1.02 (0.90-1.15)
Senior surgeon 11 (44%) 86 (52.1%) 0.45 0.86 (0.58-1.25)
Duct-to-duct biliary anastomosis 23 (92%) 156 (94.5%) 0.61 0.68 (0.16-2.98)
Post-LT Evolution
Standard immunosuppressant therapy 12 (48%) 75 (45.5%) 0.81 1.05 (0.70-1.57)
Re-transplantation 12 (48%) 45 (27.4%) 0.04 1.40 (0.95-2.06)
Re-operation 6 (24%) 19 (11.7%) 0.09 1.16 (0.93-1.46)
CMV infection 6 (24%) 32 (19.6%) 0.61 1.06 (0.84-1.34)
Vancomycin-resistant Enterococcus colonization 17 (68%) 72 (43.6%) 0.02 1.76 (0.98-3.17)
Acute cellular rejection 6 (24%) 38 (23.2%) 0.93 1.01 (0.80-1.28)
Post-LT dialysis 20 (80%) 90 (54.5%) 0.02 2.27 (1.02-5.07)
LT – liver transplantation; ASA - American Society of Anesthesiologists (ASA) Physical Status classification; CMV -
cytomegalovirus

Results 45
Table 17 – Univariate analysis of risk factors for acquisition of carbapenem-resistant P.
aeruginosa after LT in 190 patients – continuous variables
Variable Patient with carbapenem-resistant P.
aeruginosa after LT (N=25)
Median (min-max)
Patient without carbapenem-resistant P.
aeruginosa after LT (N=165)
Median (max-min)
P
Pre-LT characteristics
Pre-LT length of hospital stay (days) 6 (0-31) 1 (0-67) 0.02
Age (years) 55 (25-70) 53 (16-73) 0.64
MELD score 25 (6-45) 22 (6-53) 0.08
Pre-LT serum creatinine (mg/dl) 1.59 (0.5-4.7) 1.15 (0.4-10.5) 0.59
LT surgical procedure characteristics
Cold ischemic time (minutes) 460 (65-713) 390 (20-960) 0.02
Total ischemic time (minutes) 502 (105-758) 420 (65-910) 0.004
Duration of LT surgery (minutes) 475 (210-910) 460 (245-1330) 0.80
Units of blood transfused during LT surgery 3.0 (0-15) 2.0 (0-12) 0.009
Post-LT evolution
Piperacillin / tazobactam use (days) 0 (0-16) 0 (0-33) 0.27
Carbapenem use (days) 12 (0-45) 4 (0-87) 0.30
Polymyxin use (days) 0 (0-52) 0 (0-78) 0.17
Cephalosporin use (days) 2 (0-13) 2 (0-21) 0.68
Penicillin use (days) 1 (0-5) 1 (0-21) 0.23
Length of dialysis after LT (days) 6 (0-36) 2 (0-78) 0.04
Length of central venous catheter (days) 17 (2-68) 7 (1-85) 0.01
Length of mechanical ventilator (days) 5 (0-44) 1 (0-67) 0.01
Length of urinary catheter (days) 11 (2-72) 7 (0-90) 0.05
Length of abdominal drain (days) 9 (2-28) 7 (0-81) 0.12
Length of ICU stay (days) 14 (0-75) 7 (1-63) 0.02
LT – liver transplantation; ICU – intensive care unit; MELD – model for end-stage liver disease
Table 18 – Multivariate analysis of risk factors for acquisition of carbapenem-resistant
P. aeruginosa after LT in 190 patients
Variable P OR CI 95%
Length of dialysis (days) 0,12 0,97 0,94-1,01
Units of blood transfused during liver transplantation surgery 0,02 1,20 1,03-1,39
Length of intensive care unit stay (days) 0,02 1,04 1,01-1,07
Cold ischemic time (minutes) 0,07 1,01 1,00-1,01

Results 46
4.5 Healthcare-associated infections (HAI) after liver
transplantation
During the study period we identified 201 HAI in 110 (56.4%) patients
after LT.
The two most frequent sites of infection were the surgical site and BSI
(Table 19), and the two most frequent agents were A. baumannii e
K. pneumoniae. (Table 20).
Table 19 – Distribution of the sites of 201 healthcare-associated infections after liver
transplantation
Site of infection N %
Organ space surgical site 56 28%
Catheter related bloodstream 44 22%
Pneumonia 35 17%
Gastroenteritis 13 6%
Urinary tract infection 13 6%
Primary bloodstream 10 5%
Incisional surgical site 8 4%
Soft tissues 8 4%
Intra-abdominal 6 3%
Bronchitis 3 1%
Insertion catheter site 3 1%
Genital tract 1 0%
Total 201 100%

Results 47
Table 20 – Distribution of microorganism isolated from 201 healthcare-associated
infections after liver transplantation
Agent N Bacteremia (%) Multidrug-resistance N(%)
A. baumannii 56 36 (64.3%) 56 (100%)
K. pneumoniae 47 26 (55.3%) 40 (85.1%)*
E. faecium 29 15 (51.7%) 29 (100%)
P. aeruginosa 17 9 (52.9%) 13 (76.4%)
E. coli 13 7 (53.8%) 7 (53.8%)**
E. cloacae 9 4 (44.4%) 2 (22.2%)
E. aerogenes 9 4 (44.4%) 3 (33.3%)
Coagulase- negative Staphylococcous 9 5 (55.6%) 0
E. faecalis 7 3 (42.9%) 1 (14.3%)
S. aureus 6 3 (50.0%) 5 (83.3%)
M. morgannii 5 3 (60.0%) 0
C. albicans 5 1 (20.0%) -
C. glabrata 4 1 (25.0%) -
C. krusei 3 2 (66.7%) -
C. parapsilosis 2 1 (50.0%) -
P. mirabilis 2 1 (50.0%) 1 (50.0%)***
C. freundii 2 1 (50.0%) 0
A. faecalis 1 1 (100.0%) -
B. ovalus 1 1 (100.0%) -
Gram-negative bacilus 1 1 (100.0%) -
C. dubliensis 1 1 (100.0%) -
Enterococcus sp 1 1 (100.0%) 0
S. marcencens 1 1 (100.0%) 0
C. davisae 1 0 0
Aspergillus spp. 1 0 -
S. bovis 1 1 (100.0%) 0
P. stuartii 1 1 (100.0%) 0
C. pelliculosa 1 1 (100.0%) -
S. viridans 1 0 0
Total 237 132 (55.7%) 125 (52.7%)
*among the resistant isolates, 57.5% (23) were carbapenem-resistant and 42.5% (17) ESBL-producing;** ESBL-
producing; 1 strain resistant to carbapenem; *** ESBL-producing

Results 48
4.5.1 Surgical site infections
Surgical site infection corresponded to 31.8% of the HAI after LT, and
87.5% of those were classified as organ-space (OESI). In one case of
combined kidney-liver transplant, the infection was identified in the renal
graft. The time period between LT and OESI was on average 13 days, and
the median time period from LT to OESI was 10 days. In 24 (43.0%) cases
of OESI more than one agent was identified.
Among bacteria that caused OESI, 38 (77.6%) were GNB and 29
(76.3%) were classified as MDR. Two cases had no etiological agent
identified (3.6%). (Table 21)

Results 49
Table 21 – Microorganisms isolated from post-transplant organ space surgical site
infections, percentage of bacteremia and resistance profile.
Agent N Secondary bacteremia N(%)
Multidrug-resistance N(%)
A. baumannii 18 15 (83.3%) 18 (100%)
K. pneumoniae 16 9 (56%) 14 (88%)*
E. faecium 15 6 (40%) 15 (100%)
E. cloacae 6 3 (50%) 2 (33%)
E. aerogenes 5 2 (40%) 2(40%)
E. coli 4 2 (50%) 2 (50%)**
M. morgannii 4 2 (50%) 0%
P. aeruginosa 4 3 (75%) 3 (75%)
C. glabrata 3 1 (33%) -
S. aureus 3 2 (67%) 2 (67%)
S. Coagulase-negative 3 1 (33%) 0%
C. krusei 2 2 (100%) -
E. faecalis 2 0% 0%
A. faecalis 1 1 (100%) -
B. ovalus 1 1 (100%) -
Gram-negative bacillus 1 1 (100%) -
C. albicans 1 1 (100%) -
C. dubliensis 1 1 (100%) -
C. parapsilosis 1 0% -
Enterococcus sp 1 1 (100%) 0%
S. marcencens 1 1 (100%) 0%
Total Geral 94 55 (59%) -
* Among resistant isolates, 78.6% (11) were carbapenem-resistant and 21.4% (3) ESBL-producing; ** ESBL-producing
SCN – coagulase-negative Staphylococcus ; BSI – bloodstream infection
In the case of incisional surgical site infections (ISSI), an etiological
agent was identified in only half of them. No case of secondary bacteremia
was observed. The identified agents were: two coagulase-negative
Staphylococcus, one susceptible E. faecalis, one VRE and one CRAB.

Results 50
4.5.2 Bloodstream Infections after liver transplantation
Among BSI, 44 (68.7%) were classified as catheter-related BSI and
10 (18.5%) were classified as primary BSI.
In eight (15.0%) BSI more than one agent was identified. Among
isolated microorganisms, 44 (68.8%) were GNB. The most common Gram-
positive bacterium was Enterococcus in 12 (60.0%) cases. Among BSI
bacterial infections, 69% were classified as MDR, and among infections
caused by K. pneumoniae, 31.3% (5) were resistant to carbapenem. (Table 22)
Table 22 – Microorganisms isolated from post-transplant bloodstream infections and
resistance profile
Agent N Multidrug-resistance N(%)
K. pneumoniae* 16 11 (69%)
A. baumannii 14 15 (100%)
E. faecium 9 9 (100%)
E. coli** 5 3 (60%)
P. aeruginosa 4 2 (50%)
E. faecalis 3 1 (33%)
S. epidermidis 2 0%
S. haemolyticus 2 0%
C. freundii 1 0%
C. parapsilosis 1 -
C. pelliculosa 1 -
E. aerogenes 1 0%
E. cloacae 1 0%
P. mirabilis*** 1 1 (100%)
P. stuartii 1 0%
S. aureus 1 1 (100%)
S. bovis 1 0%
Total 64 -
*four strain were carbapenem-resistant and seven ESBL-producing ; ** one strain was carbapenem-resistant and two
ESBL-producing; ***ESBL-producing
The average between LT and BSI diagnosis was 28 days, and the
median was 19 days.

Results 51
4.5.3 Lower respiratory tract infection after liver transplantation
During the study period 35 pneumonia cases were identified, in one
case the causative agent was not identified, and in 13 (37.1%) cases more
than one microorganism was identified. Three cases of tracheobronchitis
were identified in the study period and none presented secondary
bacteremia. In one case, C. glabrata was implicated as the etiological agent
of empyema, this microorganism was isolated from pleural liquid with no
evidence of intra-abdominal infection. (Tabela 23)
Table 23 – Microorganisms isolated from lower respiratory tract infection, secondary
bacteremia and resistance profile.
Agent N Secondary bacteremia Multidrug-resistance N(%)
A. baumannii 20 6 (30.0%) 20 (100%)
P. aeruginosa 7 2 (29%) 7 (100%)
K. pneumoniae* 6 1 (17%) 6 (100%)
E. cloacae 2 0% 0%
E. aerogenes 2 1 (50.0%) 1 (50%)
C. glabrata 1 0% -
E. coli** 1 0% 1 (100%)
E. faecalis 1 0% 0%
C. davisae 1 0% 0%
M. morgannii 1 1 (100%) 0%
Aspergillus spp. 1 0% -
S. aureus 2 0% 2 (100%)
S. viridans 1 0% 0%
Total 47 11 (23%) -
* three strains ESBL producing and three strains resistant to carbapenem; **ESBL producing; BSI-bloodstream infection
Twenty-four cases of pneumonia (68.6%) and two (66.7%) cases of
tracheitis were associated to ventilator use.
The average length of time between LT and pneumonia was 18 days,
and the median of this interval was 15 days.

Results 52
4.5.4 Other types of infection after liver transplantation
The urinary tract infection (UTI) was the fourth most frequent infection.
No case of secondary bacteremia was identified. (Table 9) Among bacterial
infections, 86% of the agents were considered MDR. The mean time
between LT and UTI was 17 days. In two infection cases more than one
agent was identified. Four (30.8%) UTI cases were related to urinary
catheter use.
Table 24 – Microorganisms isolated from post-transplant urinary tract infections and
resistance profile.
Agent N Multidrug-resistant N(%)
K. pneumoniae* 5 5 (100%)
C. albicans 3 -
E. faecium 3 3 (100%)
A. baumannii 1 1 (100%)
C. freundii 1 0%
C. krusei 1 -
E. coli 1 0%
P. aeruginosa 1 1 (100%)
Total 16 -
*four strains were resistant to carbapenem and one was ESBL-producing
One patient had balanoposthitis by CRKP.
During the study period 13 Clostridium difficile strains were identified,
the average time between LT and Clostridium gastroenteritis was 15 days
and the median was 10 days.

Results 53
We identified eight soft tissue infections and the causative agent was
identified in only 38%; there were two cases of polymicrobial infection and
one case of secondary bacteremia by CRAB. (Table 10) 57% percent of
bacterial agents were classified as MDR.
Table 25 – Microorganisms isolated from soft tissue infections and resistance profile
Agent N Multidrug-resistant N(%)
E. coli* 2 1 (50%)
A. baumannii 1 1 (100%)
C. albicans 1 -
E. aerogenes 1 0%
E. faecium 1 1 (100%)
K. pneumoniae * 1 1 (100%)
P. aeruginosa 1 0%
Total 8 4 (50,0%)
*ESBL – producing
4.6 Analysis of risk factors for healthcare-associated
infection by MDR GNB after liver transplantation
HAI were identified in 110 (56.4%) patients after LT. Among the
patients who developed HAI, 84 (76.3%) had an MDR GNB isolated from a
clinical culture related to that infection. The analysis of risk factors for
developing HAI by MDR GNB after LT is described in Tables 26, 27, 28.
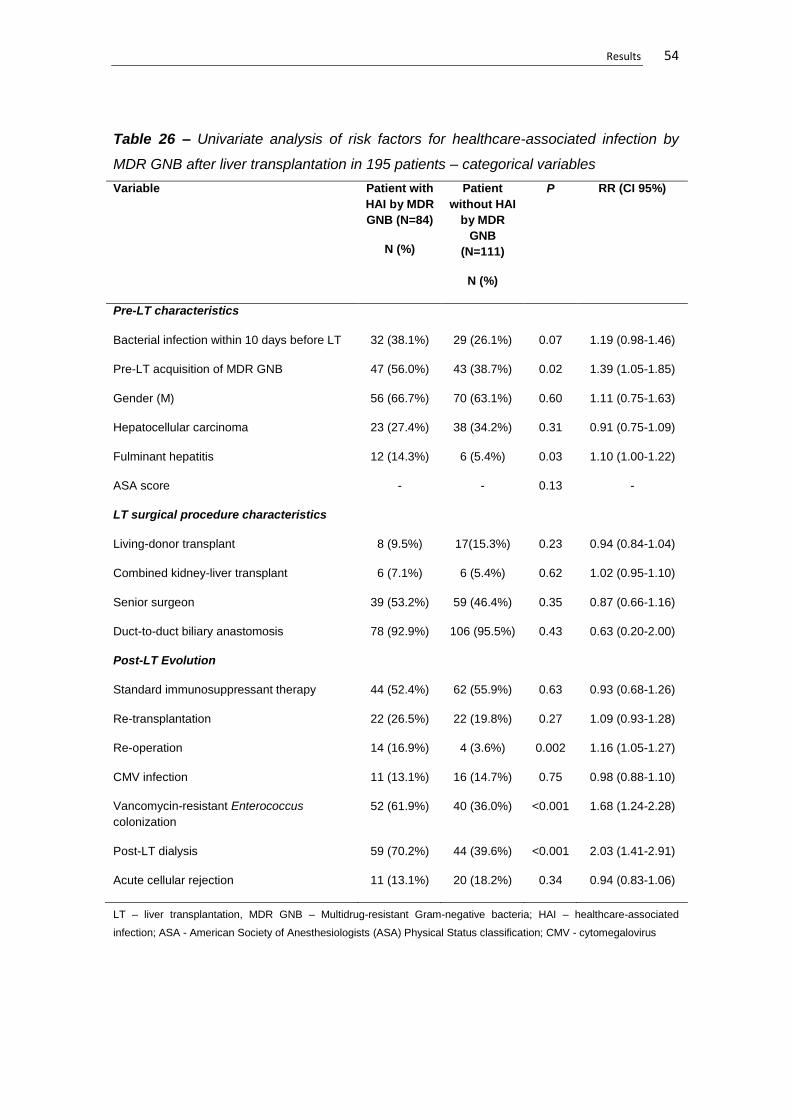
Results 54
Table 26 – Univariate analysis of risk factors for healthcare-associated infection by
MDR GNB after liver transplantation in 195 patients – categorical variables
Variable Patient with
HAI by MDR
GNB (N=84)
N (%)
Patient
without HAI
by MDR
GNB
(N=111)
N (%)
P RR (CI 95%)
Pre-LT characteristics
Bacterial infection within 10 days before LT 32 (38.1%) 29 (26.1%) 0.07 1.19 (0.98-1.46)
Pre-LT acquisition of MDR GNB 47 (56.0%) 43 (38.7%) 0.02 1.39 (1.05-1.85)
Gender (M) 56 (66.7%) 70 (63.1%) 0.60 1.11 (0.75-1.63)
Hepatocellular carcinoma 23 (27.4%) 38 (34.2%) 0.31 0.91 (0.75-1.09)
Fulminant hepatitis 12 (14.3%) 6 (5.4%) 0.03 1.10 (1.00-1.22)
ASA score - - 0.13 -
LT surgical procedure characteristics
Living-donor transplant 8 (9.5%) 17(15.3%) 0.23 0.94 (0.84-1.04)
Combined kidney-liver transplant 6 (7.1%) 6 (5.4%) 0.62 1.02 (0.95-1.10)
Senior surgeon 39 (53.2%) 59 (46.4%) 0.35 0.87 (0.66-1.16)
Duct-to-duct biliary anastomosis 78 (92.9%) 106 (95.5%) 0.43 0.63 (0.20-2.00)
Post-LT Evolution
Standard immunosuppressant therapy 44 (52.4%) 62 (55.9%) 0.63 0.93 (0.68-1.26)
Re-transplantation 22 (26.5%) 22 (19.8%) 0.27 1.09 (0.93-1.28)
Re-operation 14 (16.9%) 4 (3.6%) 0.002 1.16 (1.05-1.27)
CMV infection 11 (13.1%) 16 (14.7%) 0.75 0.98 (0.88-1.10)
Vancomycin-resistant Enterococcus
colonization
52 (61.9%) 40 (36.0%) <0.001 1.68 (1.24-2.28)
Post-LT dialysis 59 (70.2%) 44 (39.6%) <0.001 2.03 (1.41-2.91)
Acute cellular rejection 11 (13.1%) 20 (18.2%) 0.34 0.94 (0.83-1.06)
LT – liver transplantation, MDR GNB – Multidrug-resistant Gram-negative bacteria; HAI – healthcare-associated
infection; ASA - American Society of Anesthesiologists (ASA) Physical Status classification; CMV - cytomegalovirus

Results 55
Table 27 – Univariate analysis of risk factors for healthcare-associated infection by
MDR GNB after liver transplantation in 195 patients – continuous variables
Variable Patient with HAIs by MDR GNB (N=84)
Median (min-max)
Patient without HAIs by MDR GNB (N=111)
Median (min-max)
P
Pre-LT characteristics
Pre-LT length of hospital stay (in days) 2 (0-46) 1 (0-67) 0.004
Age (years) 52 (16-70) 53 (16-73) 0.93
MELD score 24 (6-52) 19 (6-53) 0.002
Pre-LT serum creatinine (mg/dl) 1.58 (0.40-6.79) 1.07 (0.41-10.54) 0.11
LT surgical procedure characteristics
Cold ischemia time (minutes) 441 (47-960) 365 (65-730) 0.002
Total ischemia time (minutes) 466 (81-910) 405 (65-730) 0.002
Duration of LT surgery (minutes) 470 (210-850) 450 (245-1330) 0.56
Units of blood transfused during LT surgery 3 (0-15) 1 (0-9) <0.001
Post-LT Evolution
Carbapenem use (days) 6 (0-40) 0 (0-42) 0.001
Polymyxin use (days) 0 (0-21) 0 (0-31) 0.003
Cephalosporin use (days) 2 (0-15) 2 (0-21) 0.11
Duration of piperacilin / tazobactam use (days) 1 (0-21) 0 (0-33) 0.18
Duration of penicillin use (days) 1 (0-12) 2 (0-21) 0.23
Duration of dialysis after LT (days) 5 (0-50) 0 (0-45) <0.001
Duration of use of central venous catheter (days) 10 (1-50) 5 (1-67) <0.001
Duration of use of mechanical ventilator (days) 4 (0-30) 0 (0-10) <0.001
Duration of use of urinary catheter (days) 9 (0-35) 5 (0-35) <0.001
Duration of use of abdominal drain (days) 7 (0-60) 7 (0-34) 0.78
Duration of ICU stay (days) 10 (1-42) 5 (1-52) <0.001
LT – liver transplantation; MELD – model for end-stage liver disease, HAI – Healthcare-associated infection; MDR GNB
– Multidrug-resistant Gram-negative bacilli; ICU – intensive care unit
Table 28 – Multivariate analysis of risk factors for healthcare-associated infection by
MDR GNB after LT in 195 patients
Variable P OR CI 95%
Bacterial infection within 10 days before LT 0,33 0,68 0,31-1,48
Re-transplantation 0,04 3,85 1,06-14,03
Number of blood units transfused in LT surgery 0,005 1,25 1,07-1,46
Acquisition of MDR GNB before LT 0,05 1,98 0,99-3,93
Length of ICU stay (days) 0,04 1,05 1,02-1,11
Cold ischemia time (minutes) 0,06 1,02 1,01-1,04
LT – liver transplantation; MDR GNB – Multidrug-resistant Gram-negative bacilli; ICU – intensive care unit

Results 56
4.6.1 Analysis of risk factors analysis of healthcare-associated infection
by carbapenem-resistant K. pneumoniae after liver transplantation
A total of 23 patients developed HAI by CRKP after LT. One patient
was submitted to LT while under treatment for a CRKP active infection and
was excluded from the risk factors analysis. The risk factors analysis for
CRKP after LT is described in Tables 29, 30 e 31.
Table 29 – Univariate analysis of risk factors for healthcare-associated infection by
carbapenem-resistant K. pneumoniae after liver transplantation in 194 patients –
categorical variables
Variable Patients with HAIs by
carbapenem-resistant K. pneumoniae
after LT (N=23)
N (%)
Patients without HAIs
by carbapenem-resistant K. pneumoniae
after LT (N=171)
N (%)
P RR (CI95%)
Pre-LT characteristics
Bacterial infection within 10 days before LT 10 (43.5%) 51 (29.7%) 0.18 1.25 (0.86-1.80)
Pre-LT acquisition of CRKP 7 (30.4%) 18 (10.5%) 0.007 1.29 (0.98-1.70)
Gender (M) 16 (69.6%) 110 (64.0%) 0.60 1.18 (0.62-2.27)
Hepatocellular carcinoma 8 (34.8%) 53 (30.8%) 0.70 1.06 (0.77-1.45)
Fulminant hepatitis 1 (4.3%) 17 (9.9%) 0.70 0.94 (0.85-1.04)
ASA score - - 0.38 -
LT surgical procedure characteristics
Living-donor transplant 4 (17.4%) 21 (12.2%) 0.51 1.06 (0.87-1.29)
Combined kidney-liver transplant 2 (8.7%) 10 (5.8%) 0.64 1.03 (0.90-1.18)
Senior surgeon 14 (60.9%) 84 (48.8%) 0.28 1.31 (0.77-2.22)
Duct-to-duct biliary anastomosis 20 (87.0%) 164 (95.3%) 0.10 0.36 (0.10-1.25)
Post-LT Evolution
Standard immunosuppressant therapy 14 (60.9%) 91 (53.2%) 0.49 1.20 (0.70-2.04)
Re-operation 7 (31.8%) 37 (21.5%) 0.28 1.15 (0.86-1.55)
Re-transplantation 2 (9.1%) 16 (9.4%) 1.00 1.00 (0.87-1.15)
Post-LT dialysis 16 (69.6%) 87 (50.6%) 0.09 1.62 (0.86-3.07)
Acute cellular rejection 2 (8.7%) 29 (17.0%) 0.54 0.91 (0.79-1.05)
Colonization by vancomycin-resistant Enterococcus 10 (43.5%) 82 (47.7%) 0.71 0.93 (0.63-1.36)
CMV infection 4 (17.4%) 23 (13.5%) 0.54 1.05 (0.86-1.27)
LT – liver transplantation; HAI – healthcare-associated infection; CRKP – carbapenem-resistant K. pneumoniae; ASA -
American Society of Anesthesiologists (ASA) Physical Status classification; CMV – cytomegalovirus

Results 57
Table 30 – Univariate analysis of risk factors for healthcare-associated infection by
carbapenem-resistant K. pneumoniae after LT in 194 patients – continuous variables
Variable Patients with HAIs by carbapenem-
resistant K. pneumoniae after LT
(N=23)
Patients without HAIs by carbapenem-
resistant K. pneumoniae after LT
(N=171)
P
Pre-LT characteristics
Age (years) 50.0 (18.0-70.0) 53.0 (16.0-73.0) 0.81
Duration of hospital stay before LT (days) 1.0 (0.0-46.0) 1.0 (0.0-67.0) 0.15
MELD score 23.0 (7.0-52.0) 22.0 (6.0-53.0) 0.86
Serum creatinine at LT (mg/dl) 1.77 (0.57-4.26) 1.09 (0.40-10.54) 0.28
LT surgical procedure characteristics
Duration of cold ischemia (minutes) 480.0 (81.0-758.0) 435.0 (65.0-960.0) 0.08
Duration of total ischemia (minutes) 445.0 (47.0-713.0) 385.0 (20.0-910.0) 0.04
Duration of LT surgery (minutes) 460.0 (250.0-850.0) 470.0 (210.0-1330.0) 0.61
Units of blood transfused during LT surgery 3.0 (0.0-12.0) 2.0 (0.0-15.0) 0.67
Post-LT Evolution
Duration of use of quinolone (days) 0.0 (0.0-4.0) 0.0 (0.0-6.0) 0.45
Duration of use of piperacilin / tazobactam (days) 2.0 (0.0-22.0) 0.0 (0.0-33.0) 0.28
Duration of use of cephalosporins (days) 1.0 (0.0-15.0) 2.0 (0.0-21.0) 0.48
Duration of use of penicillin (days) 1.0 (0.0-9.0) 1.0 (0.0-21.0) 0.25
Duration of use of polymyxin (days) 12.0 (0.0-86.0) 0.0 (0.0-77.0) 0.002
Duration of use of carbapenem (days) 20.0 (0.0-39.0) 4.0 (0.0-72.0) 0.003
Duration of use of ventilator (days) 5.0 (0.0-101.0) 1.0 (0.0-107.0) 0.06
Duration of use of abdominal drain (days) 9.0 (0.0-39.0) 7.0 (0.0-83.0) 0.49
Duration of use of central venous catheter (days) 25.0 (2.0-98.0) 8.0 (0.0-102) 0.02
Duration of use of urinary catheter (days) 15.0 (2.0-86.0) 7.0 (0.0-110.0) 0.003
Duration of use of dialysis after LT (days) 21.0 (0-91.0) 3.0 (0.0-101.0) 0.009
Duration of ICU stay (days) 18.0 (1.0-98.0) 7.0 (0.0-110.0) 0.008
LT – liver transplantation; HAI – healthcare-associated infection; MELD - model for end-stage liver disease; ICU –
intensive care unit
Table 31 – Multivariate analysis of risk factors for healthcare-associated infection by
carbapenem-resistant K. pneumoniae after liver transplantation in 194 patients
Variable P OR CI (95%)
Pre-LT acquisition of CRKP 0.003 4.70 1.72-12.85
Carbapenem use (days) 0.09 1.02 1.00-1.05
LT – liver transplantation; CRKP – carbapenem-resistant K. pneumoniae

Results 58
4.6.2 Analysis of risk factors for healthcare-associated infection by
carbapenem-resistant A. baumannii after liver transplantation
Fifty-six cases of HAI by CRAB were identified during the study period.
Two patients had active infection by CRAB at the moment of LT and were
excluded from the risk factors analysis of infection after LT. The analysis of risk
for developing HAI by CRAB after LT is shown in Tables 32, 33 and 34.
Table 32 – Univariate analysis of risk factors for healthcare-associated infection by
carbapenem-resistant A. baumannii after liver transplantation in 193 patients –
categorical variables
Variable Patients with HAI by
carbapenem-resistant A. baumannii
after LT (N=56)
N (%)
Patients without HAI
by carbapenem-resistant A. baumannii
after LT (N=137)
N( %)
P RR (CI95%)
Pre-LT characteristics
Bacterial infection within 10 days before LT 22 (40.0) 37 (26.8) 0.07 1.22 (0.95-2.30)
Pre-LT acquisition of CRAB 11 (19.6) 11 (8.0) 0.09 1.48 (0.95-2.30)
Gender (M) 37 (67.3) 88 (63.8) 0.65 1.11 (0.74-1.80)
Hepatocellular carcinoma 14 (25.5) 47 (34.3) 0.25 0.89 (0.72-1.05)
Fulminant hepatitis 9 (16.4) 8 (5.8) 0.02 1.13 (1.01-1.30)
ASA score - - 0.63 -
LT surgical procedure characteristics
Living-donor transplant 5 (9.1) 20 (14.5) 0.31 0.94 (0.84-1.04)
Combined kidney-liver transplant 3 (5.5) 8 (5.8) >0.99 0.99 (0.92-1.07)
Senior surgeon 26 (47.3) 72 (52.2) 0.54 0.91 (0.70-1.29)
Duct-to-duct biliary anastomosis 54 (98.2) 130 (94.3) 0.24 3.19 (0.43-26.00)
Post-LT Evolution
Standard immunosuppressant therapy 25 (45.5) 81 (58.7) 0.10 0.76 (0.55-1.04)
Re-operation 16 (29.1) 35 (25.4) 0.60 1.05 (0.86-1.25)
Re-transplantation 11 (20.0) 10 (7.2) 0.01 1.16 (1.00-1.32)
Post-LT dialysis 41 (74.5) 62 (44.9) <0.001 2.16 (1.37-3.42)
Acute cellular rejection 9 (16.4) 25 (18.2) 0.77 0.98 (0.85-1.11)
Colonization by vancomycin-resistant Enterococcus 35 (63.6) 55 (39.9) 0.003 1.65 (1.14-2.41)
CMV infection 6 (10.9) 26 (19.0) 0.18 0.91 (0.80-1.02)
LT – liver transplantation; HAI – healthcare-associated infection; ASA - American Society of Anesthesiologists (ASA)
Physical Status classification; CRAB – carbapenem-resistant A. baumannii; CMV - cytomegalovirus

Results 59
Table 33 – Univariate analysis of risk factors for healthcare-associated infection by
carbapenem-resistant A. baumannii after liver transplantation in 193 patients –
continuous variables
Variable
Patients with HAI by carbapenem-
resistant A. baumannii after LT
(N=56)
Median (max-min)
Patients without HAI by carbapenem-
resistant A. baumannii after LT
(N=137)
Median (max-min)
P
Pre-LT characteristics
Pre-LT length of hospital stay (days) 2.0 (0.0-42.0) 1.0 (0.0-56.0) 0.19
Age (years) 52.0 (16-70) 53.0 (16.0-73.0) 0.78
MELD score 27.0 (6-52) 21.0 (6.0-53.0) 0.002
Pre-LT serum creatinine (mg/dl) 1.59 (0.40-6.79) 1.07 (0.41-10.54) 0.22
LT surgical procedure characteristics
Duration of cold ischemia (minutes) 441.0 (50-910) 375.0 (20.0-754.0) 0.01
Duration of total ischemia (minutes) 467.5 (95-960) 410.0 (65-798) 0.006
Duration of LT surgery (minutes) 467.5 (210.0-829.0) 460.0 (245.0-1330.0) 0.78
Units of blood transfused during LT surgery 2.0 (0.0-15.0) 1.0 (0.0-9.0) 0.004
Post-LT Evolution
Duration of use of carbapenem (days) 6.0 (0.0-40.0) 0.0 (0-72) 0.07
Duration of use of quinolone (days) 0.0 (0-0) 0.0 (0-6) 0.94
Duration of use of polymyxin (days) 0.0 (0-21) 0.0 (0-26) 0.18
Duration of use of cephalosporin (days) 2.0 (0-15) 2.0 (0-21) 0.25
Duration of use of piperacilin / tazobactam (days) 1.0 (0-19) 0.0 (0-33) 0.25
Duration of use of penicillin use (days) 0.0 (0-9) 2.0 (0-21) 0.003
Duration of dialysis after LT (days) 7.0 (0-90) 0.0 (0-78) 0.001
Duration of use of central venous catheter (days) 10.0 (1.0-49.0) 6.0 (1.0-91.0) 0.008
Duration of use of ventilator (days) 4.0 (0-30) 0.0 (0-29) <0.001
Duration of use of urinary catheter (days) 7.5 (3.0-35.0) 6.5 (3.0-56.0) 0.09
Duration of use of abdominal drain (days) 7.0 (1.0-35.0) 7.0 (0.0-49.0) 0.99
Duration of ICU stay in days 9.5 (1.0-42.0) 6.0 (2.0-44.0) 0.01
LT – liver transplantation; HAI – healthcare-associated infection; ICU – intensive care unit; MELD – model for end-stage
liver disease
Table 34 – Multivariate analysis of risk factors for healthcare-associated infection by
carbapenem-resistant A. baumannii after liver transplantation in 193 patients –
categorical variables
Variable P OR CI (95%)
Fulminant hepatitis 0.02 3.41 1.19-9.77
Pre-LT acquisition of CRAB 0.06 2.57 0.94-7.05
Cold ischemia time (minutes) 0.01 1.03 1.01-1.06
Post-LT dialysis 0.003 3.08 1.46-6.49
Carbapenem use (days) 0.25 0.98 0.96-1.01
CRAB – carbapenem-resistant A. baumannii; LT – liver transplantation;

Results 60
4.6.3 Analysis of risk factors for healthcare-associated infection by
carbapenem-resistant P. aeruginosa after liver transplantation
No patient had an infection by CRPA before LT, and 12 developed
infection by this agent after LT. The analysis of risk factors associated to
CRPA HAI after LT is demonstrated in Tables 35, 36 and 37.
Table 35 – Univariate analysis of risk factors for healthcare-associated infection by
carbapenem-resistant P. aeruginosa after liver transplantation in 195 patients –
categorical variables
Variable Patients with HAIs by
carbapenem-resistant P. aeruginosa
after LT (N=12)
N (%)
Patients without HAIs
by carbapenem-
resistant
P. aeruginosa after LT (N=183)
N (%)
P RR (CI95%)
Pre-LT characteristics
Bacterial infection within 10 days before LT 5 (41.7) 56 (30.6) 0.42 1.19 (0.73-1.94)
Pre-LT acquisition of CRPA 2 (16.7) 3 (1.6) 0.03 1.18 (0.92-1.52)
Gender (M) 9 (75.0) 117 (63.9) 0.55 1.44 (0.53-3.92)
Hepatocellular carcinoma 2 (16.7) 59 (32.2) 0.35 0.81 (0.62-1.07)
Fulminant hepatitis 0 18 (9.8) 0.61 0.90 (0.86-0.95)
ASA score - - 0.84 -
LT surgical procedure characteristics
Living-donor transplant 0 25 (13.7%) 0.37 0.86 (0.82-0.92)
Combined kidney-liver transplant 1 (8.3) 11 (6.0) 0.54 1.03 (0.86-1.22)
Senior surgeon 4 (33.3) 94 (51.4) 0.25 0.73 (0.48-1.12)
Duct-to-duct biliary anastomosis 11 (91.7) 173 (94.5) 0.51 0.66 (0.09-4.71)
Post-LT Evolution
Standard immunosuppressant therapy 5 (41.7) 101 (55.2) 0.36 0.77 (0.46-1.27)
Re-operation 5 (41.7) 54 (29.5) 0.52 1.21 (0.74-1.97)
Re-transplantation 3 (25.0) 23 (12.6) 0.20 1.17 (0.84-1.62)
Post-LT dialysis 12 (100) 101 (55.2) 0.001 -
Acute cellular rejection 3 (25.0) 44 (24.2) >0.99 1.01 (0.72-1.42)
Colonization by vancomycin-resistant Enterococcus 9 (75.0) 83 (45.3) 0.07 2.19 (0.81-5.88)
CMV infection 4 (33.3) 38 (21.0) 0.30 1.19 (0.79-1.78)
LT – liver transplantation; CRPA – carbapenem-resistant P. aeruginosa; ASA - American Society of Anesthesiologists
(ASA) Physical Status classification; CMV - cytomegalovirus

Results 61
Table 36 – Univariate analysis of risk factors for healthcare-associated infection by
carbapenem-resistant P. aeruginosa after liver transplantation in 195 patients –
continuous variables
Variable Patients with HAIs by
carbapenem-resistant P.
aeruginosa after LT (N=12)
Median (min-max)
Patients without HAIs by
carbapenem- resistant P.
aeruginosa after LT (N=183)
Median (min-max)
P
Pre-LT characteristics
Pre-LT length of hospital stay (days) 9.5 (0-31) 1.0 (0-67) 0.004
Age (years) 58.0 (25-70) 53.0 (16-73) 0.12
MELD score 23.5 (16-44) 22.0 (6-53) 0.17
Serum creatinine at LT (mg/dl) 2.14 (0.82-3.99) 1.12 (0.40-10.54) 0.08
LT surgical procedure characteristics
Duration of cold ischemia (minutes) 450.5 (335-713) 385.0 (20-910) 0.02
Duration of total ischemia time (minutes) 525 (380-758) 435.0 (65-960) 0.009
Duration of LT surgery (minutes) 457.5 (277-660) 460.0 (210-1330) 0.79
Units of blood transfused during LT surgery 3.5 (0-15) 2.0 (0-12) 0.01
Post-LT Evolution
Duration of use of piperacilin/tazobactam (days) 0.0 (0-6) 0.0 (0-33) 0.09
Duration of use of carbapenem (days) 29 (12-71) 4.0 (0-87) <0.001
Duration of use of polymyxin (days) 11.5 (3-80) 0.0 (0-81) <0.001
Duration of use of cephalosporin (days) 2.0 (0-9) 2.0 (0-21) 0.71
Duration of use of penicillin (days) 0.0 (0-6) 1.0 (0-21) 0.05
Duration of dialysis after LT (days) 27.0 (6-45) 3.0 (0-74) <0.001
Duration of use of of central venous catheter (days) 35 (8-67) 8.0 (1-92) <0.001
Duration of mechanical ventilation (days) 20.5 (3-44) 1.0 (0-78) <0.001
Duration of use of urinary catheter (days) 18.0 (5-71) 7.0 (0-98) <0.001
Duration of use of abdominal drain (days) 12.0 (2-37) 7.0 (0-83) 0.05
Duration of ICU stay (days) 28.5 (13-83) 7.0 (1-75) <0.001
LT – liver transplantation; HAI – healthcare-associated infection; MELD – model for end-stage liver disease, ICU –
intensive care unit
Table 37 – Multivariate analysis of risk factors for healthcare-associated infection by
carbapenem-resistant P. aeruginosa after liver transplantation in 195 patients –
categorical variables
Variável P OR CI95%
Units of blood transfused in LT surgery 0.06 1.22 0.99-1.52
Length of ICU stay (days) <0.001 1.08 1.04-1.12
CRPA acquisition before LT 0.007 34.02 2.59-416.14
Total ischemia time (minutes) 0.08 1.005 1.00-1.01
LT – liver transplantation; CRPA – carbapenem-resistant P. aeruginosa; ICU – intensive care unit

Results 62
4.7 Evaluation of strains clonality through PFGE
We analyzed the genetic similarity between CRAB and CRKP strains
through PFGE.
Eighty-five strains of CRAB from 51 (62.2%) patients were analyzed.
Seven pulsotypes were identified during the study period: pulsotype A 5 (9.6%);
pulsotype B 34 (65.4%); pulsotype C 3 (5.8%); pulsotype D 5 (9.6%); pulsotype
E 3 (5.8%); pulsotype F 1 (1.9%); pulsotype G 1 (1.9%). In one patient, two
different pulsotypes were identified. Pulsotype B was the most prevalent and
had a homogeneous distribution during the study period. (Figure 1)
Figure 1 – Distribution of PFGE pulsotype of carbapenem-resistant A. baumannii
strains from November 2009 to November 2011
Eleven patients acquired CRAB before LT and developed infection by
this agent after LT. The paired analysis of isolates before LT and from
infection after LT was possible in 8 patients. Among those eight paired
0
5
10
15
20
25
4º trim2009
1º trim2010
2º trim2010
3º trim2010
4º trim2010
1º trim2011
2º trim2011
3º trim2011
4º trim2011
g
f
e
d
c
b
a

Results 63
isolates, five pulsotypes were identified, and in seven patients the strain
isolated after and before LT belonged to the same cluster (Figure 2)
Figure 2 – Dendogram of carbapenem-resistant A. baumannii strains from eight
patients who acquired CRAB before LT and developed infection by CRAB after LT
Twenty-six strains from 18 (75.0%) blaKPC-positive-CRKP patients
were analyzed,16 from SC and 10 from clinical cultures. Seven clusters and
nine PFGE pulsotypes were identified: cluster A 11 (42.3%); cluster B 7
(26.9%); cluster E 4 (15.4%); cluster F 1 (3.8%); cluster O 1 (3.8%); cluster
S 1 (3.8%); cluster X 1 (3.8%). Cluster A was the most prevalent one in
2010 and cluster E was more common in 2011. (Figure 3) In three blaKPC-
positive-CRKP patients it was possible to analyze the paired cultures
(before and after LT), and all strains belonged to cluster A.

Results 64
Figure 3 – Distribution of PFGE cluster of carbapenem-resistant blaKPC-positive
K. pneumoniae strains from January 2010 to November 2011
Among blaKPC-negative-CRKP strains, the analysis of genetic
similarity was performed in 36 strains from 29 (52.7%) patients. Among the
36 strains analyzed, 24 were isolated from SC and 12 from clinical cultures.
Nineteen PFGE clusters were identified: cluster C 8 (22.2%); cluster D 5
(13.9%); cluster F 1 (2.8%); cluster G 2 (5.6%); cluster H 2 (5.6%); cluster I
2 (5.6%); cluster J 3 (8.3%); cluster K 2 (5.6%); cluster L 1 (2.8%); cluster M
1 (2.8%); cluster N 1 (2.8%); cluster P 1 (2.8%); cluster Q 1 (2.8%); cluster
R 1 (2.8%); cluster T 1 (2.8%); cluster U 1 (2.8%); cluster W 1 (2.8%);
cluster Y 1 (2.8%); cluster Z 1 (2.8%). Paired isolates (before and after LT)
were analyzed in two patients, and in those two cases the strains belonged
to the same PFGE cluster. (Figure 4)
0
1
2
3
4
5
6
7
8
1º trim2010
2º trim2010
3º trim2010
4º trim2010
1º trim2011
2º trim2011
3º trim2011
4º trim2011
X
S
O
F
E
B
A

Results 65
Figure 4 – Dendogram of carbapenem-resistant K. pneumoniae isolated from Liver
transplant patients from November 2009 to November 2011
82.8
79.0
75.3
94.8
97.4
88.5
92.3
88.2
96.6
90.9
85.1
80.0
82.8
78.7
77.6
74.5
83.3
72.3
96.3
92.1
89.3
88.0
71.5
69.4
69.0
68.1
96.6
86.3
78.6
70.4
65.9
57.5
PFGE
10
0
95
90
85
80
75
70
65
60
PFGE
paciente nº LIM
18
18
12
123
118
55
60
32
33
34
44
33
55
59
34
119
68
81
62
72
81
62
180
79
167
47
56
100
21
25
29
31
39
90
131
132
115
86
115
28
94
9
9
67
11
11
50
66
76
175
183
183
183
188
147
147
146
152
3
143
160
160
Amostra
colonização pós
cultura clinica
cultura clinica
colonização pré
colonização pós
cultura clinica
cultura clinica
colonização pós
colonização pré
colonização pré
colonização pré
cultura clinica
colonização pós
colonização pós
cultura clinica
cultura clinica
cultura clinica
cultura clinica
colonização pré
colonização pós
colonização pós
cultura clinica
colonização pós
colonização pós
cultura clinica
colonização pós
colonização pós
colonização pós
colonização pós
colonização pós
colonização pré
colonização pré
colonização pós
colonização pós
colonização pós
colonização pós
colonização pré
cultura clinica
cultura clinica
colonização pré
colonização pós
cultura clinica
colonização pós
cultura clinica
colonização pré B
cultura clinica
cultura clinica
colonização pós
colonização pré
colonização pós
cultura clinica
cultura clinica
colonização pós
colonização pós
colonização pós
cultura clinica
colonização pós
colonização pós
colonização pós
cultura clinica
colonização pós
cultura clinica
KPC
neg
neg
neg
neg
neg
pos
pos
pos
pos
pos
pos
pos
pos
pos
pos
pos
pos
pos
pos
pos
pos
pos
pos
neg
pos
neg
neg
neg
neg
neg
neg
neg
neg
pos
neg
neg
neg
neg
neg
neg
pos
neg
neg
neg
neg
neg
neg
neg
neg
pos
pos
pos
pos
pos
neg
neg
neg
neg
neg
neg
neg
neg
Pulsotype
I1
I1
L
M
N
A1
A1
A1
A1
A1
A1
A1
A1
A1
A1
A2
B1
B1
B1
B1
B1
B1
B2
F1
F2
C1
C2
C3
C3
C3
C3
C3
C3
O
P
Q
J1
J1
J1
R
S
D1
D1
D2
D3
D3
T
U
W
X
E1
E1
E1
E1
K1
K2
G1
G1
Y
Z
H1
H1

Results 66
4.8 Survival analysis
During the study period, 67 (34.4%) patients evolved to death in the
first 60-days after LT. The risk factors for 60-day mortality after LT are
described in Tables 38, 39 and 40.
Table 38 – Univariate analysis of risk factors for death in the 60 first days after liver
transplantation, among 195 patients – categorical variables
Variable Patients who did not
survive within 60-days of LT (N=67) N (%)
Patients who survived
within 60-days of LT (N=128)
N (%)
P HR (IC95%)
Pre-LT characteristics
Bacterial infection within 10 days before LT 23 (34.3) 37 (29.1) 0.42 1.23 (0.75-2.04)
Gender (M) 46 (68.7) 79 (62.2) 0.33 0.76 (0.46-1.30)
Hepatocellular carcinoma 20 (29.9) 41 (32.3) 0.82 0.94 (0.56-1.59)
Fulminant hepatitis 11 (16.4) 7 (5.5) 0.02 2.21 (1.16-4.22)
ASA score - - 0.05 1.54 (1.01-2.36)
Acquisition of MDR GNB before LT 35 (52.2) 54 (42.5) 0.23 1.34 (0.83-2.17)
Acquisition of carbapenem-resistant GNB before LT 26 (38.8) 32 (25.2) 0.04 1.66 (1.02-2.72)
Acquisition of CRAB before LT 12 (17.9) 11 (8.7) 0.03 1.99 (1.06-3.71)
Acquisition of CRKP before LT 12 (17.9) 12 (9.4) 0.06 1.82 (0.97-3.40)
LT surgical procedure characteristics
Living-donor LT 7 (10.4) 18 (14.2) 0.43 0.73 (0.33-1.59)
Kidney-liver combined transplant 5 (7.5) 6 (4.7) 0.29 1.64 (0.66-4.07)
Senior surgeon 35 (52.2) 63 (49.6) 0.73 1.09 (0.67-1.76)
Duct-to-duct anastomosis 63 (94.0) 121 (95.3) 0.81 1.13 (0.41-3.11)
Post-LT Evolution
Standard immunosuppressant therapy 26 (38.8) 62 (48.8) 0.14 0.69 (0.42-1.13)
Reoperation 28 (41.8) 33 (26.0) 0.09 1.52 (0.94-2.48)
Re-transplantation 18 (26.9) 8 (6.3) <0.001 0.34 (0.20-0.59)
Post-LT dialysis 61 (91.0) 51 (40.2) <0.001 10.0 (4.32-23.15)
Acute cellular rejection 20 (30.3) 27 (21.6) 0.33 1.30 (0.77-2.19)
Colonization by vancomycin-resistant Enterococcus 32 (47.8) 59 (46.5) 0.95 0.99 (0.61-1.59)
Healthcare-associated infection after LT 50 (74.6) 59 (46.5) 0.001 2.53 (1.46-4.38)
HAI by MDR bacteria after LT 45 (67.2) 42 (33.1) <0.001 2.82 (1.69-4.70)
HAI by carbapenem-resistant GNB after LT 42 (62.7) 33 (26.0) <0.001 3.12 (1.90-5.13)
HAI by CRAB after LT 32 (47.8) 24 (18.9) <0.001 2.63 (1.62-4.25)
HAI by CRKP after LT 13 (19.4) 11 (8.7) 0.06 1.78 (0.97-3.27)
Surgical site infection 26 (38.8) 27 (21.3) 0.04 1.67 (1.02-2.73)
Pneumonia 19 (28.4) 14 (11.0) 0.003 2.24 (1.31-3.81)
Bloodstream infection 20 (29.9) 28 (22.0) 0.33 1.30 (0.77-2.20)
CMV infection 9 (13.4) 35 (27.6) 0.02 0.43 (0.22-0.88)
LT – liver transplantation; MDR – Multidrug-resistant; GNB – Gram-negative bacilli; ASA - American Society of
Anesthesiologists (ASA) Physical Status classification; HAI – healthcare-associated infection; CMV - cytomegalovirus

Results 67
Table 39 – Univariate analysis of risk factors for death in the 60 first days after liver
transplantation, among 195 patients – continuous variables
Variable Patients who not survival in
60-days after LT (N=67)
Median (min-max)
Patients who survival in 60-days after LT
(N=128)
Median (min-max)
P HR (CI95%)
Pre-LT characteristics
length of Pre-LT hospital stay (days) 2.0 (0-56) 1.0 (0-46) 0.16 1.02 (0.99-1.04)
Age (years) 55.0 (16-70) 52.0 (16-73) 0.10 1.02 (1.00-1.04)
MELD score 27.0 (6-52) 21.0 (6-53) 0.004 1.03 (1.01-1.05)
Serum creatinine at LT (mg/dl) 1.56 (0.40-6.79) 1.04 (0.44-10.54) 0.03 1.15 (1.01-1.31)
LT surgical procedure characteristics
Duration of cold ischemia (minutes) 415 (20-910) 390.0 (20-740) 0.07 1.001 (1.000-1.003)
Duration of total ischemia (minutes) 460 (84-960) 420.0 (65-754) 0.05 1.002 (1.000-1.003)
Duration of LT surgery (minutes) 490.0 (250-1330) 445.0 (210-915) 0.03 1.002 (1.000-1.003)
Units of blood transfused during LT surgery 2.0 (0-15) 1.0 (0-10) 0.006 1.11 (1.03-1.20)
LT – liver transplantation, MELD – model for end-stage liver disease
Table 40 – Multivariate analysis of risk factor for death in the 60 first days after liver
transplantation, among 195 patients
Variable P HR CI 95%
Post-LT dialysis <0.001 7.91 3.33-18.94
Duration of LT surgery (minutes) 0.05 1.002 1.001-1.003
HAI by carbapenem-resistant Gram-negative bacilli 0.06 1.65 0.98-2.76
LT – liver transplantation; HAI – healthcare associated infection;

Results 68
The 60-day survival curve is shown in Figure 5.
Figure 5 – 60-day survival curve adjusted according to LT surgery duration and post-LT
dialysis, categorized by type of microorganism isolated from HAI after LT.
The P value was calculated based on group without HAI; HAI by
CRAB - <0.001; HAI by CRE – 0.06; HAI by more than one carbapenem-
resistant GNB – 0.002; HAI by non-MDR agent – 0.13.

69
5 DISCUSSION
This study was performed in a scenario of high prevalence of MDR
GNB, especially CRAB and CRKP. Although CRKP was very frequent among
LT patients in the present study, the incidence of blaKPC-producing strains
was 14.9%, which is a moderate incidence when compared to other studies
in liver transplant patients. (70) (71) Having said that, we were able to observe a
significant increase in the prevalence of blaKPC-producing-CRKP strains
during the period of this study, which was not observed for the other CRE.
The dissemination of blaKPC-producing-CRKP strains is a phenomenon
described worldwide (72) (73), therefore this epidemiological find was probably a
reflection of the general occurrence in our hospital and our city.
The incidence of CRE after liver transplantation ranges widely among
transplant centers, from 3 to 23%, and recent reports have described higher
rates of colonization and infection by CRE. (60) (71) (59) The SC for CRKP
showed a high performance, with a good sensitivity and negative predictive
value (NPV). The SC positivity rate for CRKP was highest (nearly 93%) for
samples collected from the inguinal-rectal area, a finding that is in
agreement with those of previous reports (70) (74). An important aspect
described in this study is the difference in SC sensitivity rate when CRKP is
compared with the other CRE. In the literature the sensitivity rate of CRE

Discussion 70
SC ranges between 87.5 and 100%, similar to the rate found in the present
study. (74) (70) However, the SC sensitivity rate for the other CRE in our study
was substantially lower. The comparison of SC performance between the
species of CRE is scarce in literature (74) (75) and the most plausible
explanation for this difference observed in the sensitivity rate between
CRKP and other CRE is the lowest incidence of the latter.
At our facility, CRAB was the most common MDR GNB colonization
pathogen and in early post-LT infections. Other authors have shown that
CRAB is the MDR GNB that most often colonizes LT recipients before and
after transplant. (32) Although the prevalence of CRAB colonization was quite
high in our patient sample, there are, to our knowledge, no comparative
data in literature regarding the prevalence of CRAB colonization in the
context of active, weekly surveillance after LT.
This high prevalence of MDR GNB may influence the overall rate of SC
sensitivity, which was found to be higher than that from other reports in
literature, especially for non-fermenting GNB. The sensitivity of SC for CRAB
described in literature ranges between 55 and 72%, compared to 80.6% in
the present study; (76) (77) (78) Another possible reason for the impressive
results obtained in this study is that immunocompromised patients have
higher loads of MDR microorganisms colonizing the sites sampled.
For CRAB, the perineum-rectal site proved to be the site with the best
SC positivity rate, followed by oropharynges. (77) (79) Other studies have
found that the oropharynx site had a better positivity rate than the rectal site
for CRAB isolation, however neither of these studies collected swabs from

Discussion 71
groin and rectal sites at the same time. (78) One study that analyzed different
anatomic sites of skin for CRAB found that the groin site and the perirectal
site had better sensitivity when compared to the perirectal site alone, which
allows us to infer that the groin is an important region of CRAB colonization
and therefore carrying out simultaneous SC of this region and the rectal site
may enhance the chances of identifying colonized patients. (76) On the other
hand, according to previous findings in literature and confirmed by data in
the present study, the use of only one site implicates in an important loss of
SC sensitivity for CRAB. (77)
Another important MDR GNB related to HAI in LT recipients is CRPA.
The prevalence of this agent in our service was lower when compared to
other MDR GNB. Also, when compared to other MDR GNB in this study,
CRPA had a lower proportion of colonized patients who developed infection.
Other study that evaluated living-donor LT found that the rate of pre-LT
carriers that developed infection in post-LT period was 13%; (24) In another
population this rate is described as 19.0% in HSCT recipients and 38.5% in
ICU patients. (80) (81) The SC site with the best positivity rate for CRPA was
the perineum-rectal site. Other studies that analyzed the CRAP SC positivity
rate for different sites reported that the best site was the rectal site; however
the positivity rate for this site ranged between 47% and 54%, compared to
84% in the present study. (82) (77) Among patients with CRPA isolated in
clinical cultures, 76.9% had positive SC; this finding has been described
before in HCST patients, in whom only 53.8% of the patients with CRPA
infection had CRPA detected in SC. (81) Therefore SC for CRPA seems to

Discussion 72
be an inefficient tool for direct empirical therapy, especially in the
immunocompromised population.
Our study found a low rate of infection by ESBL-producing
Enterobacteriaceae, the proportion rate of colonized patients who developed
infection was 16.3% for ESBL-producing K. pneumoniae and 16.7% for the
other ESBL-producing Enterobacteriaceae. One study that screened recipients
for ESBL-producing Enterobacteriaceae in the pre-LT period found that 48%
of LT recipients with positive SC developed infection. (83) In HSCT patients
this proportion was even higher, 61%. (84) One possible explanation for our
findings is that ESBL-producing Enterobacteriaceae are less virulent than CRE,
and so patients who were colonized by those two types of Enterobacteriaceae
had a higher probability of developing infection by CRE (85). Based on this
reasoning, we could infer that the same is applicable for CRBA and ESBL-
producing Enterobacteriaceae, since CRBA has been described as an
impressively virulent bacterium in LT recipients. (86) (35). The sensitivity of SC
for ESBL-producing Enterobacteriaceae was quite low, particularly for K.
pneumoniae. The site with the best positivity rate was the perineum-rectal
site, however if this had been the only site surveyed, more than 15% of K.
pneumoniae ESBL carriers would have been left out. Previous reports of
sensitivity for ESBL-producing Enterobacteriaceae SC range largely between
48.8 and 100%, and in most studies the only site surveyed was the rectal site,
therefore it was not possible to establish whether or not SC for ESBL-
producing Enterobacteriaceae is a good strategy for identifying the
asymptomatic carriers (87) (88) (76)

Discussion 73
Therefore this study confirms that SC was a sensitive tool in detecting
LT recipients colonized by carbapenem-resistant GNB. The SC for non-
fermenting GNB should include more than one body site. Moreover, the
active surveillance should be considered in transplant services with
moderate and high incidence of MDR GNB once the proportion of colonized
patients who developed infection is impressively high.
In the present study the only risk factor identified for acquisition
of MDR GNB was the duration of use of urinary drain counted in days.
The group of patients who acquired MDR GNB was very heterogeneous,
with different GNB species and different resistance profiles, and this may
be the major reason for the fact that few acquisition risk factors were
identified. The use of invasive devices is often described as a risk factor for
MDR bacteria acquisition in the general population and also among LT
recipients. (89) (36) (28) (72) Besides that, the use of a urinary drain is an indirect
marker of renal function impairment and also a marker of patients with less
independence in self-care activities.
In the present study, post-LT CRAB acquisition was also dependent
on the degree to which hepatic function was impaired. Patients submitted to
re-transplantation usually recover hepatic function more slowly and more
often develop post-operative complications such as biliary leaks and
thrombosis. (90) In contrast, patients submitted to LT for treatment of
hepatocellular carcinoma typically present with more preserved hepatic
function before LT, lower MELD score at LT, and fewer postoperative
complications. (91)

Discussion 74
Another major finding of the present study was that the use of broad-
spectrum antibiotics, such as carbapenem and piperacillin-tazobactam,
increased the risk for CRAB acquisition. Antibiotic use is frequently related
to the emergence of MDR bacteria and has previously been correlated with
CRAB colonization in immunocompetent individuals. (92) (93) In addition, the
use of such antibiotics before or after SOT has been associated with a
greater risk for MDR GNB infection in the recipients. (37) (18) (89)
Dialysis was found to be a risk factor for CRKP acquisition after LT in
this study. Renal failure is a well-known risk for infection after LT. (94)
Patients under dialysis usually need a central venous catheter, are more
frequently submitted to kidney-liver transplant and have a longer duration of
stay in ICU, all conditions associated with an increased risk for MDR
bacteria acquisition. (18) (89)
CRPA was, in this cohort study, the MDR GNB with the lowest
incidence. The risk factors associated to CRPA acquisition were length of
ICU stay and number of blood units transfused in LT surgery. These two
conditions may be related to an increased risk of acquiring MDR bacteria in
general in the hospital and not specifically in the LT unit. (27) (28) Patients in
ICU clearly have an increased risk of acquiring MDR bacteria, as they
usually have more invasive devices, more severe conditions and need
surgical procedures more frequently. Volume of intra-operative blood
transfusion was an indirect marker of a more complex procedure and was
previously associated to increase risk of infection after LT. (32) (95) Besides
that, transfusion itself plays an immunosuppressive role.

Discussion 75
A liver transplant surgery is a complex and prolonged procedure,
therefore surgical site infection is the most common infection reported in the
early post-LT period. (2) In the present study SSI were identified in 32% of
the patients. The majority of these infections were classified as organ-space
and more than half had secondary bacteremia associated. The data in
literature are very similar to our findings, with a reported incidence of SSI up
to 37%, the proportion of intra-abdominal commitment ranges between 67%
and 79% and bacteremia was reported in 10-46% of the cases. (96) (95) (97)
The most impressive data of our study about the epidemiology of post-
LT infection was the high incidence of GNB with a high percentage of MDR
strains. Liver transplant recipients have been described as a group of risk for
MDR bacterial infection. (98) (89) (6)The postoperative care is associated to
frequent manipulation, use of invasive devices, prolonged length of ICU stay
and frequent renal replacement therapy; also these patients receive a high
amount of broad-spectrum antibiotic in pre-transplant and early post-transplant
period. All these factors increase the risk for MDR bacteria acquisition.
As infections in early post-LT period are in their majority HAI,
the microbial agent profile is closely related to the overall epidemiology of
the institution where transplantation occurs. (2) The most recent studies
report a tendency of an increase in MDR GNB as agents of post-LT early
infections. (98) (89) Bert et al in a cohort study of 704 LT recipients reported
that the most frequent agents of BSI in the first year after LT were
Enterobacteriaceae species. (30) Shi et all in a cohort study of 475 LT
recipients described that 32% developed bacteremia due to GNB in the first

Discussion 76
six months after LT, and 56.3% of those GNB isolated were categorized as
MDR; the most frequent MDR GNB was CRAB. (18) In contrast a Spanish
study that analyzed all bacteremia cases occurring in hospitalized SOT
recipients during a five-year period, found that CRPA was the most frequent
MDR bacteria in LT recipients. (6)
The CRPA is a common agent related to HAI after LT; the most
common site of CRPA infection is pneumonia, CRPA being isolated in up to
18% of this type of infection. (31) (99) (24) (100) CRPA can be the causative agent
in 9% of BSI. (6) (89) In this cohort study CRPA infection was identified in 6.2%
of patients after LT, and the most common site was also pneumonia and was
the agent isolated in 18.4% of the infections in the lower respiratory tract.
Risk factors identified in the present study associated to MDR GNB
infection were: prolonged ICU stay, large amount of blood transfusion during
LT surgery, re-transplantation and colonization by MDR GNB prior to LT.
The amount of blood transfusion during LT surgery and re-
transplantation were two variables associated with graft complication. It was
expected that variables associated with an increased risk for SSI would be
identified in the risk factor analysis for MDR GNB infection, once SSI
represented a great number of infections in our cohort study and as
described in literature infections by MDR bacteria were more commonly
isolated from graft infection than from SSI. (71) (35) (89)
As discussed for CRAB acquisition, re-transplantation is associated
to slower recovery of hepatic function and more frequent postoperative

Discussion 77
complications such as biliary leaks and thrombosis, which also increases
the risk for post-LT infection. (90) A Spanish cohort study of 276 episodes of
bacteremia in SOT recipients described that patients with prior
transplantation had an increased risk for current bacteremia by MDR
bacteria. (6) A study designed to identify risk for SSI after LT also found that
re-transplantation was associated with higher number of SSI. (96)
Amount of blood transfused during LT surgery, as discussed earlier,
is a marker of complication during this procedure. In literature patients who
received more blood during transplant surgery had an increased risk
of developing SSI; this finding was described in LT but also in other types
of SOT. (101)
Patients in ICU have an increased risk for developing infection, due to
the severity of the patient and the degree of invasiveness they are
submitted to. In other populations ICU stay was frequently associated with
risk for MDR GNB infection, such CRKP and CRAB. (85) (28) One study that
evaluated bacteremia by P. aeruginosa in transplant patients identified that
previous ICU stay was a risk for bacteremia by CRPA in non-lung transplant
recipients. (31)
The incidence of post-LT CRE infection also varies among transplant
centers, ranging from 3% to 23%, and recent studies have reported higher
rates of CRE colonization and infection. (71) (60) (59) At our facility, the
incidence of CRE infection is high, as evidenced by the number of colonized
patients in the present study, as well as by the progressive increase in the
proportion of KPC-producing strains over the study period.

Discussion 78
An interesting aspect described in this study is that despite the fact
that the rate of colonized patients who developed infection in a relatively
short period of follow-up was high (27.3%), this proportion is lower than was
described in other reports of LT recipients, which ranges between 39.0%
and 88.9%. (70) (59) One possible explanation for that finding is that blaKPC-
producing CRKP are described as more virulent than the strains that harbor
other types of carbapenem resistance mechanisms and in this cohort the
majority of CRE were blaKPC negative. (85)
There have been few studies analyzing the risk of CRE acquisition
and infection in Liver transplant patients in a context of weekly screening.
Giannella et al. analyzed 237 LT recipients who were screened weekly for
CRE starting at LT and they identified CRE acquisition at any time (pre- or
post-LT) as the variable most strongly correlated with post-LT CRE infection.
(59) In our study, pre-LT acquisition was also the only risk factor identified for
developing CRE infection.
The reported prevalence of post-transplant CRAB infection among
LT recipients varies widely across facilities, ranging between 2.8% and
16.8%. (6) (18) (102) In the present study, the prevalence of CRAB infection was
high, 27.7%. In our analysis, we identified other factors associated with an
increased risk of post-LT CRAB infection: post-LT need for dialysis,
prolonged cold ischemia time, and LT performed due to fulminant hepatitis.
Cold ischemia time longer than 400 minutes has previously been identified
as a risk factor for SSI after LT, (32) and in the present study a prolonged
total ischemia time was associated with an increased risk for infection by

Discussion 79
CRPA. In general, it can be assumed that longer ischemia time is
associated with slower post-LT recovery of the systemic inflammatory
response, as well as, indirectly, longer ICU stays, increased use of invasive
devices, and delayed recovery of renal function. (103) (104)
The need for dialysis after LT is a well-known risk factor for early
postoperative bacterial infections. (94) Patients requiring dialysis are more
often subjected to the use of invasive devices and are more often admitted
into ICU, thus having a higher incidence of bacterial infection. (89) (18) Renal
failure itself plays an immunosuppressive role and can be an indirect marker
of graft malfunction. Acute kidney injury can also be seen in LT recipients
with severe preoperative hepatic impairment. Gouvêa et al. reported that
hemodialysis after SOT is more common among recipients who develop
infection with CRAB than among those who develop infection with
carbapenem-susceptible A. baumannii. (37)
Patients undergoing LT due to fulminant hepatitis typically show high
MELD scores at the time of transplantation, and such patients also often
have longer ICU stays and need dialysis before LT. (32) A high MELD score
at LT has been associated with a greater risk of bacterial infection,
specifically post-LT bacteremia caused by Enterobacteriaceae. (105) In a
univariate analysis, Hsieh et al. demonstrated that a high MELD score is a
risk factor for A. baumannii infection after LT. (33)
This study has demonstrated that the acquisition of MDR GNB in pre-
LT can increase the risk for developing infection by these agents in post-LT
period. This was also true when specific MDR GNB were separately

Discussion 80
analyzed, namely CRKP, CRAB and CRPA. One possible explanation for
this finding is that pre-LT MDR GNB acquisition could be a marker of poorer
clinical conditions, which would increase the risk of developing post-LT
complications. Another possibility is that the standard antibiotic prophylaxis
might have been less effective in the patients colonized by MDR GNB.
There is little knowledge regarding outcomes in SOT recipients
colonized by MDR GNB before transplant, and the impact of modifying the
surgical prophylaxis has not been established. (99) (101) In the present study,
modifying the surgical prophylaxis did not prevent the occurrence of post-LT
GNB MDR infection. However, because of the small number of cases in
which the prophylaxis was adjusted, it was not possible to draw a conclusion
about the efficacy of that measure. At our facility, surgical prophylaxis is not
systematically modified on the basis of colonization of the recipient by MDR
bacteria, but rather only on the basis of preoperative infection. It is therefore
likely that the patients in whom the surgical prophylaxis was modified were
those who were the sickest. In addition, the total number of patients
recognized as colonized before LT was too small to demonstrate the benefit
of this strategy.
In addition, the PFGE analysis showed that most of the patients
developed post-LT infection from the same strain that they harbored in the
pre-LT period. That was also true for the patients who harbored strains
other than the predominant clone. The impact that pre-LT colonization by
MDR GNB has on infectious outcomes after LT has not been well defined.
Kim et al. reported that, in a small number of LT recipients, colonization by

Discussion 81
A. baumannii, identified in sputum on the day of LT, was associated with the
risk of A. baumannii-associated pneumonia in the post-transplant period. (99)
In another study, involving 475 LT recipients, microbiologically proven pre-
LT infection was found to be a risk factor for post-LT death from MDR GNB
infection. (18)
In one study, surveillance samples were collected to culture for
extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae
before LT (19). The authors also found that pre-LT acquisition substantially
increased the risk of infection in the post-LT period; 48% of the patients
colonized in the pre-LT period developed infection with ESBL-producing
Enterobacteriaceae after LT, compared with 6.7% of the patients not
colonized (19).
One study in living-donor liver transplant analyzed the impact of pre-LT
colonization by CRPA in risk of infection after LT by this agent. This study did
not find any correlation, however there was no active screening for detection
of CRPA colonization in any time during pre and post LT period. (24)
We performed an analysis for 60-day mortality risk factors in order to
investigate the role of MDR GNB infection in LT recipient surveillance. The
infection by carbapenem-resistant GNB showed a considerable trend
toward significance as risk for 60-day mortality.
In our study infection by carbapenem-resistant GNB after LT was
related to increased 60-day mortality after LT. Although the p-value showed
a trend toward significance, this finding has a high biological plausibility.
Discussion 82
Other studies that analyzed infection by MDR GNB in LT recipients usually
found a high associated mortality. (70) (71) (35) (3) In the survival analysis,
infection by CRGNB infection had the best fitness in the final model
compared to other MDR GNB infections. In spite of that, in survival plot it is
possible to observe that CRAB had the highest mortality rate when
compared to patients with other MDR GNB infections.
Post-SOT infection with A. baumannii is associated with high mortality,
reportedly as high as 80.0%, and carbapenem resistance appears to increase
the risk of death significantly. In literature, the mortality associated with CRE
infection in LT recipients’ ranges between 41% and 72%. (59) (70) (56) (71) (106)
Because SOT recipients infected with MDR bacteria are more likely to
receive initial antibiotic therapy that is inappropriate, to have longer ICU stay,
and to require mechanical ventilation, mortality rates are higher among such
patients than among SOT recipients infected with bacteria that are drug-
susceptible and among those without infection. (6) (102) (98)
Other risk factors identified in our 60-day risk factor analysis were
to have performed dialysis after LT and prolonged LT surgical time.
Renal impairment was consistently associated to a lower survival in post-LT.
A national wide study in Finland that included 631 LT recipients found that
glomerular filtration rate is inversely proportional to patient survival. (107)
Another large population based cohort study from Taiwan that included
2938 patients submitted to LT described that dialysis increase the mortality
rate in up to 100%. (108)
Discussion 83
Surgical time length is a very good marker for surgery complexity.
Longer surgical times were associated to increased mortality once they
have a worse systemic inflammatory response syndrome, increase in the
risk of infection, and are more associated to technical surgeries
complication as bleeding and biliary lesions. (109) (110)
In conclusion, we found that patients who acquired MDR GNB prior to
LT were at a greater risk for post-LT MDR GNB infection, which has a
negative impact on recipient’s survival. We also found that the risk of MDR
GNB infection was higher among patients submitted to re-transplantation,
patients who received large amount of blood units during LT surgery and
had a prolonged ICU stay. Patients who were colonized by MDR GNB when
they underwent LT should be carefully evaluated for the best moment for LT,
and measures for minimizing that risk, such as adjusting the antibiotic
prophylaxis or decolonization treatment, should be investigated and
implemented.

84
6 BIBLIOGRAPHY
1. JA, Fishman. Infections in immunocompromised hosts and organ transplant
recipients: essentials. Liver Transpl. 2011, Vols. Suppl 3:S34-7.
2. Patel G, Huprikar S. Infectious complications after orthotopic liver transplantation.
Semin Respir Crit Care Med. 2012, Vols. 33(1):111-24.
3. Cervera C, van Delden C, Gavaldà J, Welte T, Akova M, Carratalà J and Hosts,
ESCMID Study Group for Infections in Compromised. Multidrug-resistant bacteria in
solid organ transplant recipients. Clin Microbiol Infect. 2014, Vols. Suppl 7:49-73.
4. Razonable RR, Findlay JY, O'Riordan A, Burroughs SG, Ghobrial RM, Agarwal B,
Davenport A, Gropper M. Critical care issues in patients after liver transplantation.
Liver Transpl. 2011, Vols. 17(5):511-27.
5. Torre-Cisneros J, Herrero C, Cañas E, Reguera JM, De La Mata M, Gómez-Bravo
MA. High mortality related with Staphylococcus aureus bacteremia after liver
transplantation. Eur J Clin Microbiol Infect Dis. 2002, Vols. 21(5):385-8.
6. Bodro M, Sabé N, Tubau F, Lladó L, Baliellas C, Roca J, Cruzado JM, Carratalà J.
Risk factors and outcomes of bacteremia caused by drug-resistant ESKAPE
pathogens in solid-organ transplant recipients. Transplantation. 2013, Vols.
15;96(9):843-9.
7. Ziakas PD, Pliakos EE, Zervou FN et al. MRSA and VRE Colonization in Solid
Organ Transplantation: A Meta-Analysis of Published Studies. Am J Transpl. 2014,
Vols. 14: 1887–1894.
8. MP, Freire. Tese (Mestrado) – Faculdade de Medicina, Universidade de São
Paulo. Infecções hospitalares em pacientes submetidos a transplante de fígado:
fatores de risco relacionados ao doador. São Paulo : s.n., 2007.
9. Bert F, Bellier C, Lassel L, et al. Risk factors for Staphylococcus aureus infection in
liver transplant recipients. Liver Transplant. 2005, Vols. 11: 1093–1099.
10. Desai D, Desai N, Nightingale P, Elliott T, Neuberger J. Carriage of methicillin-
resistant Staphylococcus aureus is associated with an increased risk of infection
after liver transplantation. Liver Transplant. 2003, Vols. 9: 754–759.

Bibliography 85
11. Singh N, Squier C, Wannstedt C, Keyes L, Wagener MM, Cacciarelli TV. Impact of
an aggressive infection control strategy on endemic Staphylococcus aureus
infection in liver transplant recipients. Infect Control Hosp Epidemiol. 2006, Vols.
27: 122–126.
12. Freire MP, Bonazzi P, Boszczowski I, et al. Risk factors for colonization/infection
for vancomycin-resistant enterococcus in cohort of liver transplantation recipients
with surveillance cultures. Liver Transplant . 2009, Vol. 15: S230.
13. Bucheli E, Kralidis G, Boggian K, et al. Impact of enterococcal colonization and
infection in solid organ transplantation recipients from the Swiss Transplant Cohort
Study. Transplant Infect Dis. 2014, Vols. 16: 26–36.
14. Russell DL, Flood A, Zaroda TE, et al. Outcomes of colonization with MRSA and
VRE among liver transplant candidates and recipients. Am J Transplant. 2008,
Vols. 8: 1737–1743.
15. Singh N, Wagener MM, Obman A, Cacciarelli TV, de Vera ME, Gayowski T.
Bacteremias in liver transplant recipients: shift toward gram-negative bacteria as
predominant pathogens. Liver Transpl. 2004, Vols. 10(7):844-9.
16. Oriol I, Sabé N, Melilli E, Lladó L, González-Costello J, Soldevila L, Carratalà L.
Factors influencing mortality in solid organ transplant recipients with bloodstream
infection. Clin Microbiol Infect. 2015, Vols. 21 (12):1104e9-14.
17. Mrzljak A, Peric Z, Kovacevic V, Gustin D, Vrhovac R, Andrasevic AT. Rising
problem of multidrug-resistant gram-negative bacteria causing bloodstream
infections after liver transplantation: how should we handle the issue? Liver
Transpl. 2010, Vols. 16(10):1217-9.
18. Shi SH, Kong HS, Xu J, Zhang WJ, Jia CK, Wang WL, Shen Y, Zhang M, Zheng SS.
Multidrug resistant gram-negative bacilli as predominant bacteremic pathogens in
liver transplant recipients. Transpl Infect Dis. 2009, Vols. 11(5):405-12.
19. Jacoby GA, Munoz-Price LS. The new b-lactamases. N Engl J Med. 2005, Vols.
352:380-391.
20. Pitout JD, Laupland KB. Extended-spectrum b-lactamase–producing
Enterobacteriaceae: an emerging public-health concern. Lancet Infect Dis . 2008,
Vols. 8:159-166.
21. Singh N, Gayowski T, Rihs JD, Wagener MM, Marino IR. Evolving trends in multiple
antibiotic resistant bacteria in liver transplant recipients: a longitudinal study of
antimicrobial susceptibility patterns. Liver Transpl Surg. 2001, Vols. 7:22-6.
22. Kotloff RM, Ahya VN, Crawford SW et al. Pulmonary complications of solid organ
and hemathopoietic stem cell transplantation. Am J Resp Crit Care Med. 2004,
Vols. 170: 21-48.

Bibliography 86
23. Korvick JA, Marsh JW, Starzl TE, Yu VL. Pseudomonas aeruginosa bacteremia in
patients undergoing liver transplantation: an emerging problem. Surgery. 1991,
Vols. 109:62-8.
24. Hashimoto M, Sugawara Y, Tamura S, Kaneko J, Matsui Y, Kokudo N, Makuuchi
M. Pseudomonas aeruginosa infection after living-donor liver transplantation in
adults. Transpl Infect Dis. 2009, Vols. 11(1):11-9.
25. Johnson LE1, D'Agata EM, Paterson DL, Clarke L, Qureshi ZA, Potoski BA, Peleg
AY. Pseudomonas aeruginosa bacteremia over a 10-year period: multidrug
resistance and outcomes in transplant recipients. Transpl Infect Dis. 2009, Vols.
11(3):227-34.
26. Troillet N, Samore MH, Carmeli Y. Imipenem-resistant Pseudomonas aeruginosa:
risk factors and antibiotic susceptibility patterns. Clin Infect Dis . 1997, Vols.
25:1094-8.
27. Fortaleza CM, Freire MP, Filho Dde C, de Carvalho Ramos M. Risk factors for
recovery of imipenem- or ceftazidime-resistant pseudomonas aeruginosa among
patients admitted to a teaching hospital in Brazil. Infect Control Hosp Epidemiol. .
2006, Vols. 27(9):901-6.
28. Falagas ME, Kopterides P. Risk factors for the isolation of multi-drug-resistant
Acinetobacter baumannii and Pseudomonas aeruginosa: a systematic review of
the literature. J Hosp Infect. 2006, Vols. 64:7-15.
29. Gouvêa EF1, Branco RC, Monteiro RC, Halpern M, Ribeiro-Filho J, Silveira VG,
Tavares GC, Rodrigues MS, Coelho HS, Basto ST, Santoro-Lopes G. Outcome of
infections caused by multiple drug-resistant bacteria in liver transplant recipients.
Transplant Proc. . 2004, Vols. 36(4):958-60.
30. Bert F, Larroque B, Paugam-Burtz C, Janny S, Durand F, Dondero F, Valla DC,
Belghiti J, Moreau R, Nicolas-Chanoine MH. Microbial epidemiology and outcome
of bloodstream infections in liver transplant recipients: an analysis of 259 episodes.
Liver Transpl. 2010, Vols. 16(3):393-401.
31. Bodro M, Sabé N, Tubau F, Lladó L, Baliellas C, González-Costello J, Cruzado
JM, Carratalà J. Extensively drug-resistant Pseudomonas aeruginosa bacteremia
in solid organ transplant recipients. Transplantation. 2015, Vols. 99(3):616-22.
32. Freire MP, Soares Oshiro IC, Bonazzi PR, Guimarães T, Ramos Figueira ER,
Bacchella T, Costa SF, Carneiro D'Albuquerque LA, Abdala E. Surgical site
infections in liver transplant recipients in the model for end-stage liver disease era:
an analysis of the epidemiology, risk factors, and outcomes. Liver Transpl. 2013,
Vols. 19(9):1011-9.

Bibliography 87
33. Hsieh CE, Chen YL, Lin PY, Lin KH, Lin HC et al. Liver transplantation in patients
infected with gram-negative bacteria: non-Acinetobacter baumannii and
Acinetobacter baumannii. Transplant Proc. 2013, Vols. 45(1):225-30.
34. Shields RK, Clancy CJ, Gillis LM, Kwak EJ, Silveira FP et al. Epidemiology, clinical
characteristics and outcomes of extensively drug-resistant Acinetobacter
baumannii infections among solid organ transplant recipients. PLoS One. 2012,
Vol. 7(12):e52349.
35. Kim YJ, Yoon JH, Kim SI, Hong KW, Kim JI et al. High mortality associated with
Acinetobacter species infection in liver transplant patients. Transplant Proc. 2011,
Vols. 43(6):2397-9.
36. DL, Paterson. The Epidemiological Profile of Infections with Multidrug-Resistant
Pseudomonas aeruginosa and Acinetobacter Species. Clin Infect Dis. 2006, Vols.
S43-S48.
37. Gouvêa EF, Martins IS, Halpern M, Ferreira AL, Basto ST et al. The influence of
carbapenem resistance on mortality in solid organ transplant recipients with
Acinetobacter baumannii infection. BMC Infect Dis. 2012, Vol. 12:351.
38. Wade J, Rolando N, Williams R. The significance of aerobic gram-negative bacilli
in clinical specimens following orthotopic liver transplantation. Liver Transpl Surg.
1998, Vols. 4:51-7.
39. Patterson DL, Muder RR et al. Outbreak of infection with E.coli ESBL harboring
extended spectrum beta-lactamase(ESBL) in a liver transplant unit:could
norfloxacin administration to carriers contribute to control? Clin Infect Dis. 2001,
Vols. 33:126-8.
40. Zhou JD, Guo JJ, Zhang Q et al. Drug resistance of infectious pathogens after liver
transplantation. Hepatobiliary Pancreat Dis Int. 2005, Vols. 5:190-4.
41. Aguiar EB, Maciel LC, Halpern M, de Lemos AS, Ferreira AL, Basto ST,
Gonçalves RT, de Gouvêa EF, Santoro-Lopes G. Outcome of bacteremia caused
by extended-spectrum β-lactamase-producing Enterobacteriaceae after solid
organ transplantation. Transplant Proc. 2014, Vols. 46(6):1753-6.
42. Winters HA, Parbhoo RK, Schafer JJ, Goff DA. Extended-spectrum beta-
lactamase-producing bacterial infections in adult solid organ transplant recipients.
Ann Pharmacother. 2011, Vols. 45(3):309-16.
43. Bradford PA, Bratu S, Urban C, Visalli M, Mariano N, Landman D, Rahal JJ,
Brooks S, Cebular S, Quale J. Emergence of carbapenem-resistant Klebsiella
species possessing the class A carbapenem-hydrolyzing KPC-2 and inhibitor-
resistant TEM-30 beta-lactamases in New York City. Clin Infect Dis. 2004, Vols.
39(1):55-60.

Bibliography 88
44. Gasink LB, Edelstein PH, Lautenbach E, Synnestvedt M, Fishman NO. Risk
factors and clinical impacto f Klebsiella pneumonia carbapenemase-producing K.
pneumoniae. Infect Control Hosp Epidemiol. 2009, Vols. 30:1180-5.
45. Mouloudi E, Protonotariou E, Zagorianou A et al. Bloodstream Infections Caused
by Metallo–b-Lactamase/Klebsiella pneumoniae Carbapenemase–Producing K.
pneumoniae among Intensive Care Unit Patients in Greece: Risk Factors for
Infection and Impact of Type of Resistance on Outcomes. Infect Control Hosp
Epidemiol. 2010, Vols. 31(12):1250-6.
46. Marchaim D, Navon-Venezia S, Schwaber MJ, Carmeli Y. Isolation of imipenem-
resistant Enterobacter species: Emergence of KPC-2 carbapenemase, molecular
characterization, epidemiology and outcome. Antimicrob Agents Chemother. 2008,
Vols. 52:1413-8.
47. Schwaber Mj, Lidji SK, Navon-venezia, Schwartz D, Leavitt A, Carmeli Y.
Predictors of Carbapenem-resistant Klebsiella pneumoniae acquisition among
hospitalized adults and effect of acquisition on mortality. Antimicrobial Agents
Chemotherapy. 2008, Vol. 52:102.
48. Patel G, Huprikar S, Factor SH, Jenkins SG, Calfee DP. Outcomes of
carbapenem-resistant Klebsiella pneumoniae infection and the impact of
antimicrobial and adjunctive therapies. Infect Control Hosp Epidemiol. 2008, Vols.
29:1099-1106.
49. Tumbarello M, Viale P, Viscoli C, Trecarichi EM,Tumietto F et al. Predictors of
Mortality in Bloodstream Infections Caused by Klebsiella pneumoniae
Carbapenemase–Producing K. pneumoniae: Importance of Combination Therapy.
Clin Infect Dis. 2012, Vols. 55(7):943–50.
50. Zarkotou O, Pournaras S, Tselioti P, Dragoumanos V, Pitiriga V et al. Predictors of
mortality in patients with bloodstream infections caused by KPC-producing
Klebsiella pneumoniae and impact of appropriate antimicrobial treatment. Clin
Microbiol Infect. 2011, Vols. 17: 1798–1803.
51. Souli M, Galani I, Antoniadou A, Papadomichelakis E, Poulakou G, Panagea T,
Vourli S, Zerva L, Armaganidis A, Kanellakopoulou K, Giamarellou H. An outbreak
of infection due to b-lactamase Klebsiella pneumoniae carbapenemase 2-
producing in greek university hospital: molecular characterization, epidemiology
and outcomes. Clin Infect Dis. 2010, Vols. 50:364-73.
52. Orsi GB, Bencardino A, Vena A, Carattoli A, Venditti C, Falcone M, Giordano A,
Venditti M. Patient risk factors for outer membrane permeability and KPC-
producing carbapenem-resistant Klebsiella pneumoniae isolation: results of a
double case–control study. Infection. 2013, Vols. 41(1):61-7.

Bibliography 89
53. Gyung Y, Choi SH, Choo EJ, Chung JW, Jeong JY, Kim NJ, Woo JH, Ryu J, Kim
YS. Risk factors for the acquisition of carbapenem-resistant Klebsiella pneumonia
among hospitalized patients. Microbial Drug Resistance . 2005, Vols. 11:165-8.
54. Mlynarczyk G, Kosykowska E, de Walthoffen SW, Szymanek-Majchrzak K,
Sawicka-Grzelak A et al. A threat of the Klebsiella pneumoniae carbapenemase-
producing strains among transplant recipients. Transplant Proc. 2011, Vols.
43(8):3135-6.
55. Bergamasco MD, Barroso Barbosa M, de Oliveira Garcia D, Cipullo R, Moreira JC,
Baia C, Barbosa V, Abboud CS. Infection with Klebsiella pneumoniae
carbapenemase (KPC)-producing K. pneumoniae in solid organ transplantation.
Transpl Infect Dis. 2012, Vols. 14(2):198-205.
56. Kalpoe JS, Sonnenberg E, Factor SH, del Rio Martin J, Schiano T, Patel G,
Huprikar S. Mortality associated with carbapenem-resistant Klebsiella pneumoniae
infections in liver transplant recipients. Liver Transpl. 2012, Vols. 18(4):468-74.
57. Mathers AJ, Cox HL, Bonatti H, Kitchel B, Brassinga AK, Wispelwey B, Sawyer
RG, Pruett TL, Hazen KC, Patel JB, Sifri CD. Fatal cross infection by carbapenem-
resistant Klebsiella in two liver transplant recipients. Transpl Infect Dis. 2009, Vols.
11(3):257-65.
58. Nguyen M, Eschenauer GA, Bryan M, O'Neil K, Furuya EY, Della-Latta P, Kubin
CJ. Carbapenem-resistant Klebsiella pneumoniae bacteremia: factors correlated
with clinical and microbiologic outcomes. Diagn Microbiol Infect Dis. 2010, Vols.
67(2):180-4.
59. Giannella M, Bartoletti M, Morelli MC, Tedeschi S, Cristini F, Tumietto F,
Pasqualini E, Danese I, Campoli C, Lauria ND, Faenza S, Ercolani G, Lewis R,
Pinna AD, Viale P. Risk factors for infection with carbapenem-resistant Klebsiella
pneumoniae after liver transplantation: the importance of pre- and posttransplant
colonization. Am J Transplant. 2015, Vol. Am J Transplant.
60. Pereira MR, Scully BF, Pouch SM, Uhlemann AC, Goudie S, Emond JE et al. Risk
Factors and Outcomes of Carbapenem-Resistant Klebsiella pneumoniae Infections
in Liver Transplant Recipients. Liver Transpl. 2015, Vol. [Epub ahead of print].
61. Murray, PR, Baron, EJ, Jorgensen, JH, Pfaller, MA, Yolken,RH. Manual of clinical
microbiology. Washington DC : ASM, 2003 8ed.
62. Standards, National Committee for Clinical Laboratory. Performance standards for
antimicrobial disk susceptibility tests; approved standard. NCCLS Document M2-
A7. Wayne, Pa, USA : s.n., 2002, seventh edition.
63. Institute., Clinical and Laboratory Standards. Performance standards for
antimicrobial susceptibility testing. Supplement M100-S18. Wayne, PA : s.n., 2008.

Bibliography 90
64. Institute, Clinical and Laboratory Standards. Performance standards for
antimicrobial susceptibility testing. CLSI document M100-S22. twenty-second
informational supplement, Wayne, PA: CLSI, 2012, 2012.
65. Kaufmann, M.E. Pulsed-Field Gel Electrophoresis. [book auth.] Johnson AP
Woodford N. Molecular Bacteriology: Protocols and Clinical Applications.1st ed.
Ed. New Jersey: : Humana Press.15: 33-50, 1998.
66. Ridley, A.M. Genomic Fingerprinting by Application of REP-PCR. [book auth.]
Johnson AP Woodford N. Molecular Bacteriology: Protocols and Clinical
Applications. New Jersey: : Ed. Humana Press. Cap.15. p.103-15, 1998.
67. CDC/NHSN Surveillance Definitions for Specific Types of Infections. NHSN/CDC.
[Online] 04 2015. [Cited: junho 05, 2015.]
http://www.cdc.gov/nhsn/PDFs/pscManual/17pscNosInfDef_current.pdf.
68. An International Panel. Update of the International Banff Schema for Liver Allograft
Rejection: Working recommendations for the histopathologic staging and reporting
of chronic rejection. Hepatology. 2000, Vols. 31:792-799.
69. Kamath OS, Wiesner RH, Malinchoc M, et al. A Model Predict Survival in Patients
With End-Stage Liver Disease. Hepatology. 2001, Vols. 33:464-70.
70. Lübbert C, Rodloff AC, Laudi S, Simon P, Busch T, Mössner J, Bartels M, Kaisers
UX. Lessons learned from excess mortality associated with Klebsiella pneumoniae
carbapenemase 2-producing K. pneumoniae in liver transplant recipients. Liver
Transpl. 2014, Vols. ;20(6):736-8.
71. Satlin MJ, Jenkins SG, Walsh TJ. The global challenge of carbapenem-resistant
Enterobacteriaceae in transplant recipients and patients with hematologic
malignancies. Clin Infect Dis. 2014, Vols. 58(9):1274-83.
72. Nordmann P, Cuzon G, Naas T. The real threat of Klebsiella pneumonia
carbapenemase-producing bacteria. Lancet Infect Dis. 2009, Vols. 9:228-36.
73. Munoz-Price LS, Poirel L, Bonomo RA, Schwaber MJ, Daikos GL, Cormican M et
al. Clinical epidemiology of the global expansion of Klebsiella pneumoniae
carbapenemases. Lancet Infect Dis. 2013, Vols. 13(9):785-96.
74. Schechner V, Straus-Robinson K, Schwartz D, Pfeffer I, Tarabeia J, Moskovich R,
Chmelnitsky I, Schwaber MJ, Carmeli Y, Navon-Venezia S. Evaluation of PCR-
based testing for surveillance of KPC-producing carbapenem-resistant members of
the Enterobacteriaceae family. J Clin Microbiol. 2008, Vols. 47(10):3261-5.
75. Adler A, Navon-Venezia S, Moran-Gilad J, Marcos E, Schwartz D, Carmeli Y.
Laboratory and Clinical Evaluation of Screening Agar Plates for Detection of
Carbapenem-Resistant Enterobacteriaceae from Surveillance Rectal Swabs. J Clin
Microbiol. 2011, Vols. 49 (6): 2239-42.

Bibliography 91
76. Weintrob AC, Roediger MP, Barber M, Summers A, Fieberg AM, Dunn J, Seldon
V, Leach F, Huang XZ, Nikolich MP, Wortmann GW. Natural history of colonization
with gram-negative multidrug-resistant organisms among hospitalized patients.
Infect Control Hosp Epidemiol. 2010, Vols. 31(4):330-7.
77. Dalben MF, Oliveira MS, Garcia CP, Lobo RD, Costa SF, Toscano CM, Levin AS.
Swab cultures across three different body sites among carriers of carbapenem-
resistant P. aeruginosa and Acinetobacter species: a poor surveillance strategy. J
Hosp Infect. 2010, Vols. 74(4):395-6.
78. Marchaim D, Navon-Venezia S, Schwartz D, Tarabeia J, Fefer I, Schwaber MJ,
Carmeli Y. Surveillance cultures and duration of carriage of multidrug-resistant
Acinetobacter baumannii. J Clin Microbiol. 2007, Vols. 45(5):1551-5.
79. Latibeaudiere R, Rosa R, Laowansiri P, Arheart K, Namias N, Munoz-Price LS.
Surveillance cultures growing carbapenem-Resistant Acinetobacter baumannii
predict the development of clinical infections: a retrospective cohort study. Clin
Infect Dis. 2015, Vols. 60(3):415-22.
80. Gómez-Zorrilla S, Camoez M, Tubau F, Cañizares R, Periche E, Dominguez MA,
Ariza J, Peña C. Prospective observational study of prior rectal colonization status
as a predictor for subsequent development of Pseudomonas aeruginosa clinical
infections. Antimicrob Agents Chemother. 2015, Vols. 59(9):5213-9.
81. Nesher L, Rolston KV, Shah DP, Tarrand JT, Mulanovich V, Ariza-Heredia EJ,
Chemaly RF. Fecal colonization and infection with Pseudomonas aeruginosa in
recipients of allogeneic hematopoietic stem cell transplantation. Transpl Infect Dis.
2015, Vols. 17(1):33-8.
82. Araoka H, Kimura M, Abe M, Takahashi N, Yoneyama A. Appropriate sampling
sites for the surveillance of multidrug-resistant Pseudomonas aeruginosa
colonization. Jpn J Infect Dis. 2014, Vols. 67(2):118-9.
83. Bert F, Larroque B, Dondero F, Durand F, Paugam-Burtz C, Belghiti J, Moreau R,
Nicolas-Chanoine MH. Risk factors associated with preoperative fecal carriage of
extended-spectrum β-lactamase-producing Enterobacteriaceae in liver transplant
recipients. Transpl Infect Dis. 2014, Vols. 16(1):84-9.
84. Liss BJ, Vehreschild JJ, Cornely OA, Hallek M, Fätkenheuer G, Wisplinghoff H,
Seifert H, Vehreschild MJ. Intestinal colonisation and blood stream infections due
to vancomycin-resistant enterococci (VRE) and extended-spectrum beta-
lactamase-producing Enterobacteriaceae (ESBLE) in patients with haematological
and oncological malignancies. Infection. 2012, Vols. 40(6):613-9.
85. Bogan C, Kaye KS, Chopra T, Hayakawa K, Pogue JM, Lephart PR, Bheemreddy
S, Lazarovitch T, Zaidenstein R, Perez F, Bonomo RA, Marchaim D. Outcomes of
carbapenem-resistant Enterobacteriaceae isolation: matched analysis. Am J Infect
Control. 2014, Vols. 42(6):612-20.
Bibliography 92
86. Reddy P, Zembower TR, Ison MG, Baker TA, Stosor V. Carbapenem-resistant
Acinetobacter baumannii infections after organ transplantation. Transpl Infect Dis.
2010, Vols. 12(1):87-93.
87. Lowe CF, Katz K, McGeer AJ, Muller MP and Group., Toronto ESBL Working.
Efficacy of admission screening for extended-spectrum beta-lactamase producing
Enterobacteriaceae. PLoS One. 2013, Vol. 26;8(4):e62678.
88. Reddy P, Malczynski M, Obias A, Reiner S, Jin N, Huang J, Noskin GA, Zembower
T. Screening for Extended-Spectrum b-Lactamase–Producing Enterobacteriaceae
among High-Risk Patients and Rates of Subsequent Bacteremia. Clin Infect Dis.
2007, Vols. 45(7):846-52.
89. Zhong L, Men TY, Li H, Peng ZH, Gu Y, Ding X, Xing TH, Fan JW. Multidrug-
resistant gram-negative bacterial infections after liver transplantation - spectrum
and risk factors. J Infect. 2012, Vols. 64(3):299-310.
90. Immordino G, Bottino G, De Negri A, Diviacco P, Moraglia E et al. Predictability
and survival in liver replantransplantation: monocentric experience. Transplant
Proc. 2014, Vols. 46 (7): 2290-2.
91. Morise Z, Kawabe N, Tomishige H, Nagata H, Kawase J et al. Recent advances in
the surgical treatment of hepatocellular carcinoma. World J Gastroenterol. 2014,
Vols. 20(39):14381-14392.
92. Giamarellou H, Antoniadou A, Kanellakopoulou K. Acinetobacter baumannii: a
universal threat to public health? Int J Antimicrob Agents. 2008, Vols. 32(2), 106-
119.
93. Playford EG, Craig JC, Iredell JR. Carbapenem-resistant Acinetobacter baumannii
in intensive care unit patients: risk factors for acquisition, infection and their
consequences. J Hosp Infect. 2007, Vols. 65(3), 204-11.
94. Singh N, Gayowski T, Wagener MM. Posttransplantation dialysis-associated
infections: morbidity and impact on outcome in liver transplant recipients. Liver
Transpl. 2001, Vols. 7(2), 100-5.
95. Shah H, Hellinger WC, Heckman MG, Diehl N, Shalev JA et al. Surgical site
infections after liver retransplantation: incidence and risk factors. Liver Transpl.
2014, Vols. 20(8):930-6.
96. Hellinger WC, Crook JE, Heckman MG, Diehl NN, Shalev JA et al. Surgical site
infection after liver transplantation: risk factors and association with graft loss or
death. Transplantation. 2009, Vols. 87(9):1387-93.
97. SI, Kim. Bacterial infection after liver transplantation. World J Gastroenterol. 2014,
Vols. 20(20):6211-20.

Bibliography 93
98. van Duin D, van Delden C and Practice, AST Infectious Diseases Community of
Practice. Multidrug-resistant gram-negative bacteria infections in solid organ
transplantation. Am J Transplant. 2013, Vols. Suppl 4:31-41.
99. Kim YJ, Kim SI, Jun YH, Choi JY, Yoon SK et al. Clinical significance of
surveillance culture in liver transplant recipients. Transplant Proc. 2014, Vols.
46(3):828-31.
100. Su H, Ye Q, Wan Q, Zhou J. Predictors of Mortality in Abdominal Organ
Transplant Recipients with Pseudomonas aeruginosa Infections. Ann Transplant.
2016, Vols. 21:86-93.
101. Freire MP, Antonopoulos IM, Piovesan AC, Moura ML, de Paula FJ et al.
Amikacin Prophylaxis and Risk Factors for Surgical Site Infection After Kidney
Transplantation. Transplantation. 2015, Vols. 99(3):521-7.
102. Ye QF, Zhao J, Wan QQ, Qiao BB, Zhou JD. Frequency and clinical outcomes of
ESKAPE bacteremia in solid organ transplantation and the risk factors for
mortality. Transpl Infect Dis. 2014, Vols. 16(5):767-74.
103. Martin EF, Huang J, Xiang Q, Klein JP, Bajaj J, Saeian K. Recipient survival and
graft survival are not diminished by simultaneous liver-kidney transplantation: an
analysisof the united network for sharing database. Liver Transpl. 2012, Vols.
18(8), 914-29.
104. Paugam-Burtz C, Kavafyan J, Merckx P, Dahmani S, Sommacale D et al.
Postreperfusion syndrome during liver transplantation for cirrhosis outcome and
predictors. Liver Transpl. 2009, Vols. 15(5), 522-9.
105. Bellier C, Bert F, Durand F, Retout S, Belghiti J, Mentré F, Fantin B. Risk factors
for Enterobacteriaceae bacteremia after liver transplantation. Transpl Int. 2008,
Vols. 21(8):755-63.
106. Clancy CJ, Chen L, Shields RK, Zhao Y, Cheng S, Chavda KD, Hao B, Hong JH,
Doi Y, Kwak EJ, Silveira FP, Abdel-Massih R, Bogdanovich T, Humar A, Perlin DS,
Kreiswirth BN, Hong Nguyen M. Epidemiology and molecular characterization of
bacteremia due to carbapenem-resistant Klebsiella pneumoniae in transplant
recipients. Am J Transplant. 2013, Vols. 13(10):2619-33.
107. Åberg F, Nordin A, Toivonen L, Isoniemi H. Early Predictors of Long-term
Outcomes of HCV-negative Liver Transplant Recipients Having Survived the First
Postoperative Year. Transplantation. 2016, Vols. 100(2):382-90.
108. Chen HP, Tsai YF, Lin JR, Liu FC, Yu HP. Recipient Age and Mortality Risk after
Liver Transplantation: A Population-Based Cohort Study. PLoS One. 2016, Vol.
11(3):e0152324.

Bibliography 94
109. Gastaca M, Matarranz A, Martinez L, Valdivieso A, Ruiz P et al. Risk factors for
biliary complications after orthotopic liver transplantation with T-tube: a single-
center cohort of 743 transplants. Transplant Proc. 2014, Vols. 46(9):3097-9.
110. Viehman JA, Clancy CJ, Clarke L, Shields RK, Silveira FP, Kwak EJ et al.
Surgical Site Infections After Liver Transplantation: Emergence of Multidrug-
Resistant Bacteria and Implications for Prophylaxis and Treatment Strategies.
Transplantation. 2016, Vols. 100(10):2107-14.

7 APPENDIX
Manuscripts derived from this thesis published in index medical
journals:
A. Surveillance culture for multidrug-resistant gram-negative bacteria: Performance in liver transplant recipients. Freire MP, Villela Soares Oshiro IC, Bonazzi PR, Pierrotti LC, de Oliveira LM, Machado AS, Van Der Heijdenn IM, Rossi F, Costa SF, Carneiro D'Albuquerque LA, Abdala E. Am J Infect Control. 2017 Mar 1;45(3):e40-e44. doi: 10.1016/j.ajic.2016.12.010.
B. Carbapenem-Resistant Enterobacteriaceae Acquired Before Liver Transplantation: Impact on Recipient Outcomes. Freire MP, Oshiro IC, Pierrotti LC, Bonazzi PR, de Oliveira LM, Song AT, Camargo CH, van der Heijden IM, Rossi F, Costa SF, DʼAlbuquerque LA, Abdala E. Transplantation. 2017 Apr;101(4):811-820. doi: 10.1097/TP.0000000000001620
C. Carbapenem-resistant Acinetobacter baumannii acquired before liver transplantation: Impact on recipient outcomes. Freire MP, Pierrotti LC, Oshiro IC, Bonazzi PR, Oliveira LM, Machado AS, Van Der Heijden IM, Rossi F, Costa SF, D'Albuquerque LA, Abdala E. Liver Transpl. 2016 May;22(5):615-26. doi: 10.1002/lt.24389
D. Polymyxin use as a risk factor for colonization or infection with polymyxin-resistant Acinetobacter baumannii after liver transplantation. Freire MP, Van Der Heijden IM, do Prado GV, Cavalcante LS, Boszczowski I, Bonazzi PR, Rossi F, Guimarães T, D'Albuquerque LA, Costa SF, Abdala E. Transpl Infect Dis. 2014 Jun;16(3):369-78. doi: 10.1111/tid.12210. Epub 2014 Apr 12.

Appendix
Appendix A

Appendix
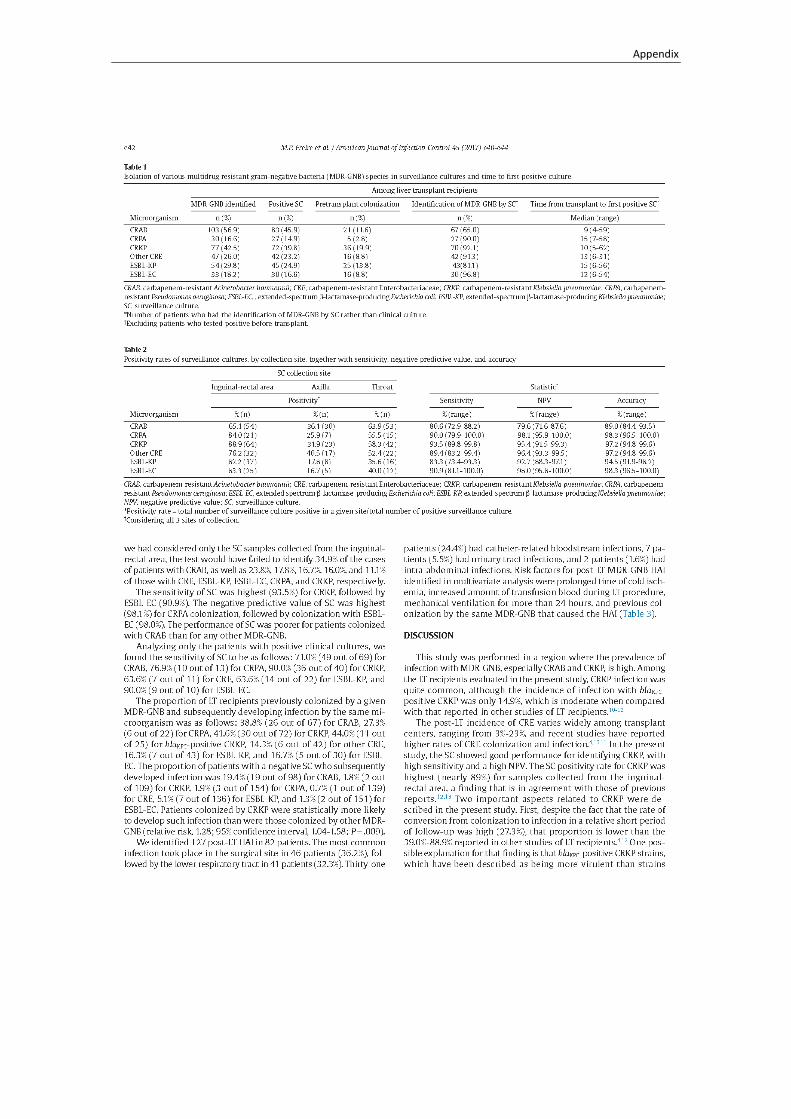
Appendix
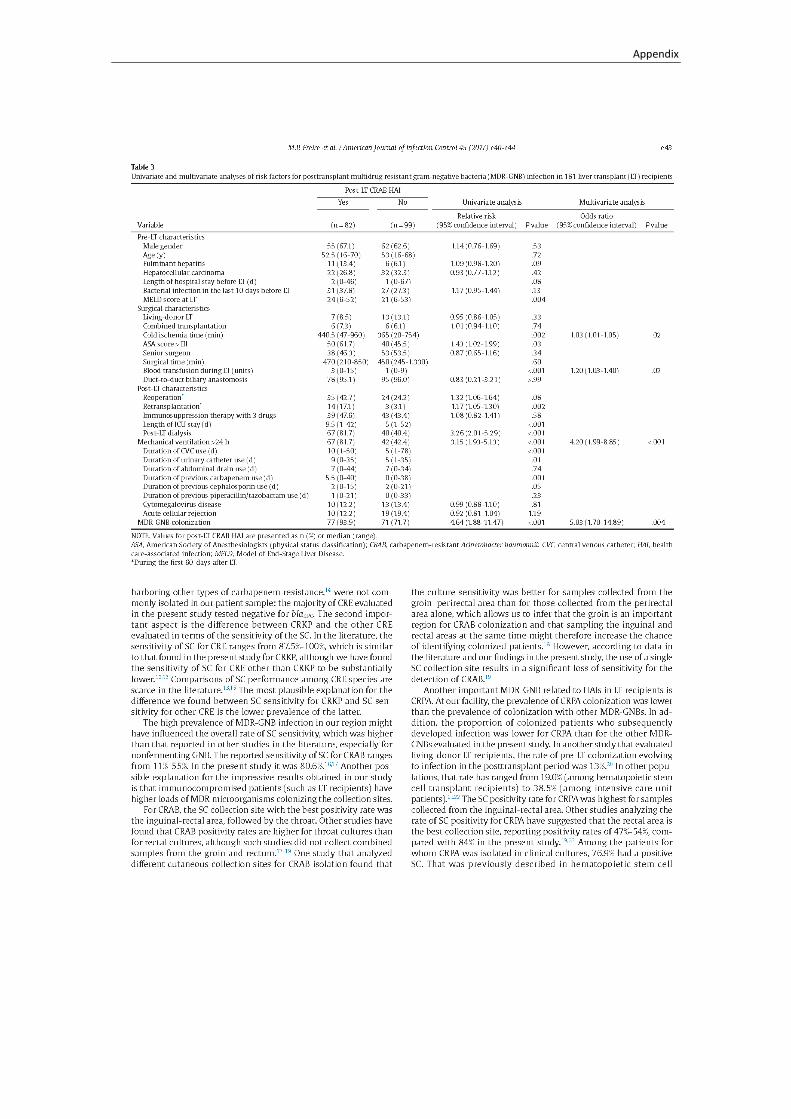
Appendix

Appendix

Appendix
Appendix B

Appendix

Appendix

Appendix
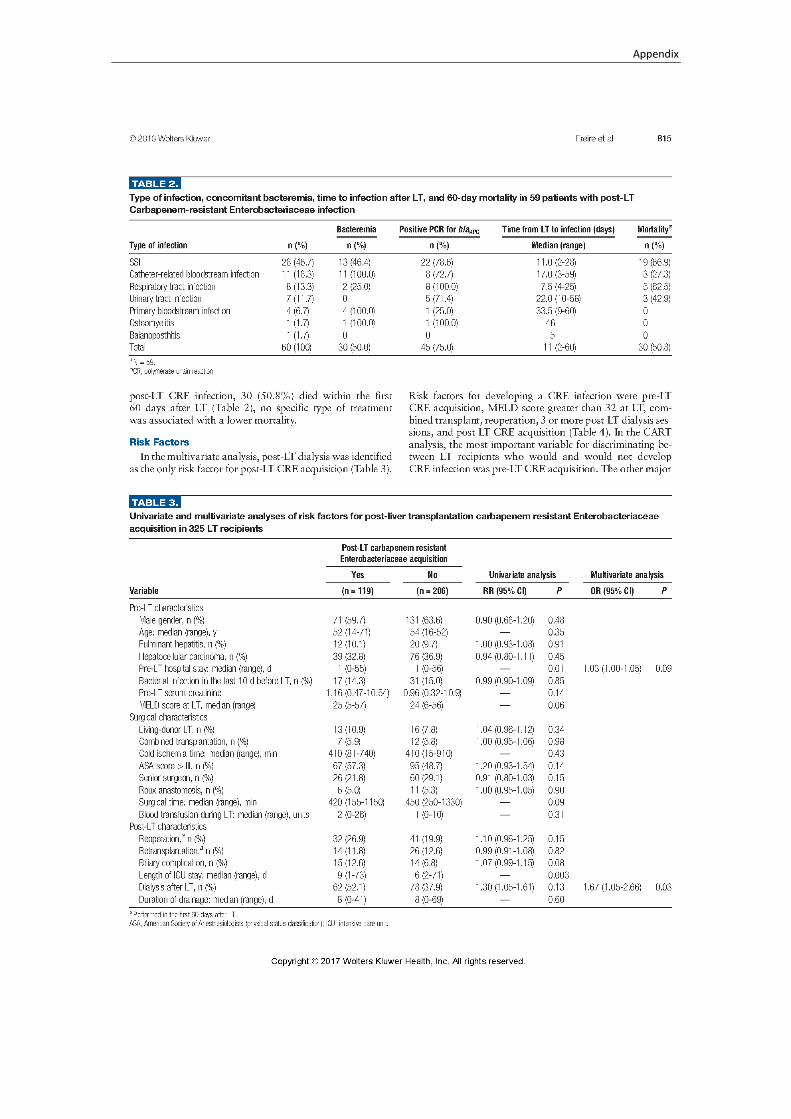
Appendix

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix
Appendix C

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix
Appendix D

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix

Appendix





























