Embed Size (px)
Citation preview


Conflito de Interesse
De acordo com a resolução do Conselho Federal de Medicina nº 1595/2000 e Resolução da Diretoria Colegiada da ANVISA nº 96/2008, eu declaro que:
• Pesquisa Clínica – Como investigador: Novartis
• Apresentações científicas – Como palestrante: Novartis, Amgen, Roche, Alexion, Janssen, Pfizer
• Atividades de Consultoria – Como membro de Advisory Boards: Novartis, Abbvie, Roche, Alexion, Janssen, Pfizer
Declaro não ter ações em bolsa de valores das empresas supracitadas.
Meus pré-requisitos para participar destas atividades são o intercâmbio científico, a autonomia do pensamento científico, independência de opinião e liberdade de expressão, aspectos estes respeitados pela Takeda.

Inibidor de complemento na HPN:
passado, presente e futuro
Phillip Scheinberg
Hospital A Beneficência Portuguesa
São Paulo

THE COMPLEMENT CASCADE REGULATION IN PNH
C3b
C3
+C3b
C5
convertase
Classical
pathway
Lectin
pathway
Alternative
pathway
Physiological
C3 tick-over
CD55 CD55
Amplification
loop
PNH RBCs
C3b

THE COMPLEMENT CASCADE REGULATION IN PNH
C3b
C3
+ C5b
C5
C3b
C5
convertase
PNH RBCs
Classical
pathway
Lectin
pathway
Alternative
pathway
C6MAC
Physiological
C3 tick-over
C7 C8 C9
CD55 CD55 CD59
Amplification
loop
C3b

THE COMPLEMENT CASCADE REGULATION IN PNH
C3b
C3
+ C5b
C5
C3b
C5
convertase
PNH RBCs
Classical
pathway
Lectin
pathway
Alternative
pathway
C6MAC
Physiological
C3 tick-over
C7 C8 C9
CD55 CD55 CD59
Amplification
loop
C3b MAC

THE COMPLEMENT CASCADE REGULATION IN PNH
C3b
C3
+ C5b
C5
C3b
C5
convertase
PNH RBCs
Classical
pathway
Lectin
pathway
Alternative
pathway
C6MAC
Physiological
C3 tick-over
C7 C8 C9
CD55 CD55 CD59
Amplification
loop
C3b
MAC-mediated intravascular hemolysis

THE COMPLEMENT CASCADE REGULATION IN PNH
C3b
C3
+
C5
C3b
C5
convertase
Classical
pathway
Lectin
pathway
Alternative
pathway
Physiological
C3 tick-over
C5b
C6MACC7 C8 C9
CD55 CD55
Amplification
loop
Eculizumab
Risitano et al, Blood 2009
MAC-mediated intravascular hemolysisPNH RBCs
C3b

EFFECT OF ECULIZUMAB ON HEMOLYSISLactate dehydrogenase (LDH) and transfusion independency
Time, Weeks
Lacta
te D
eh
yd
rog
en
ase (
U/L
)
0
500
1000
1500
2000
2500
3000
0 10 20 30 40 50
TRIUMPH – Placebo/extension
TRIUMPH – SOLIRIS/extension
SHEPHERD – SOLIRIS
Study Week
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Pa
tien
ts A
vo
idin
g T
ran
sfu
sio
n (
%)
0
10
20
30
40
50
60
70
80
90
100
P < 0.000001
Eculizumab
Placebo
51%
0%
44% reduction in
PRBC units
transfused

0
2
4
6
8
10
12
14
16
Pre-Eculizumab Treatment Eculizumab Treatment
Th
rom
bo
sis
Ev
en
t R
ate
(TE
pe
r 1
00
pt-
ye
ars
)
92% reduction in event rate with eculizumab
(n=195) (n=195)
39 events 3 events
P = 0.0001
Hillmen et al.,
Blood 2007
Normalized by
time of
observation
(pre and post)

Long-term effect of eculizumab treatment in PNHA retrospective comparison (Loschi et al, AJH 2016)
PNH patients with indication to
eculizumab (clinically meaningful
hemolysis and/or thrombosis)
– Eculizumab: n=123 (>2005)
– Non-eculizumab: n=191

Hematological response
Hgb ≥1136.6%
8 ≤ Hgb < 1143.9%
≤50%12.2%
>50%7.3%
THE CLINICAL RESPONSE TO ECULIZUMAB
• Normal or almost-normal LDH level in all patients
• Persistent reticulocytosis in almost all patients
n= 41
Risitano et al, Blood 2009


Hemolysis
Cytopenia
Aplastic Anemia
PNH
Bone Marrow Failure and PNH
Normal
Aplastic

Hemoglobinuria}
–8731––38119AST
29171687697––7842624LDH
3310933332-310Urine
2101312111091-80Days
Eculizumab Eculizumab
“BREAKTHROUGH” hemolysis during eculizumab treatmentPharmakokinetic breakthrough
… but in patient’s chart it has been written “possible pharmakodinamic breakthrough”!?

Polymorphisms of C5 at Arg 885
– Single heterozygous missence (p.Arg885His) mutation (generating a
new ApaLI restriction site) found in 11 out 11 Japanese PNH patients
lacking any response to eculizumab (n=345; 3,3%)
– also found in healthy Japanese population (allelic frequence 3,5%)
The mutation affected the
binding to eculizumab
– A similar mutation (p.Arg885Cys)
was found in a non-responder
from Argentina (Asian ancestry)
Genetics of response to eculizumab in PNH: C5Rare C5 mutation may result in resistance (Nishimura et al, NEJM 2014)

Ricklin et al,
Blood 2015

Unmet clinical needs in anti-complement therapy
1. Rare intrinsic (genetic) resistance
2. Suboptimal hematological benefit
• Underlying bone marrow failure
• Breakthrough (pharmacokinetic and
pharmacodynamics)
• C3-mediated extravascular hemolysis
3. Patient perspective: i.v. therapy, bi-monthly infusion,
(hospitalization)
4. Limited access (worldwide) and costs


Classical pathway Lectin pathway Alternative pathway
C1q
C1rC1s
C2 C4
C4b2a
C3
MBL
MASPs
C3bBbC3(H2O)Bb
C3
hydrolysis
fB fI
P
(tick-over)
Immune
complexes Bacterial LPS
and membranes
C4b2aC3b C3bBbC3b
C6
MAC
C7
C8
C9
C3 convertases
C5 convertases
Lytic complex
C3b
C3a
C5 C5b
C5a
Novel anti-C5 agents:
• Other mAbs: ALXN1210,
SKY59, REGN3918, LFG316,
Mubodina (Adienne)
• Small peptides (e.g.,
RA101348)
• Coversin
• Aptamers
• siRNAs
Amplification
loop

Chugai-RocheRO7112689 / SKY59 / RO/CH7092230 / RG6107
▪ Humanized anti-C5 “recycling” mAb. Based on Chugai’s Sequential Monoclonal
Antibody Recycling Technology – Immunoglobulin (SMART-Ig) platformDescription
▪ Phase 1/2 global PNH study (naïve and switch patients) underwayPhase
▪ IV and SC initially weekly (regimen may be modified based on data from Part 2 of
the study)
Dosing &
RoA
▪ Chugai is conducting a 3 part adaptive phase 1 /2 trial in NHV followed by PNH
patients in 9 disclosed countries. Trial includes IV and SC (@170mg/ml
concentration) and use of placebo comparator
– Part 1: Phase 1 SAD in healthy adult males
– Part 2: Naïve transfusion dependent PNH patients and patients with C5
polymorphism
– Part 3: Stable PNH patients adequately controlled on eculizumab
– Per Eudra website, the trial represents first in human administration
▪ Trial endpoints include:
– Safety (% patients with dose limiting events, AEs, SAEs, terminal complement
activity, ADAs);
– Clinical efficacy measures (LDH, free Hgb, FACIT-fatigue, HRQoL, # PRBC
transfusions etc);
– PK / PD (Cmax, Tmax, AUC, T1/2, bioavailability, C5 levels, etc.)
▪ n: between 39-74 (different public sites describe different patient numbers)
Ongoing
clinical
development
NCT03157635; EudraCT 2016-002128-10

RA pharmaRA 101495
Company website; Company IPO prospectus;
NCT03030183; NCT03078582; Eudra CT 2016-003522-16
▪ Synthetic 15-amino acid macrocyclic peptide C5 inhibitor
▪ Binds to C5 at a site that also blocks C6 binding to C5b, preventing MAC
formation even if C5 cleaves
Description
▪ 2 Phase 2 open label studies underway
▪ Testing daily SC - loading dose 0.3mg/kg; 0.1mg/kg/d (week 1); opportunity to
up-titrate maintenance dose to up to 0.3mg/kg/d in weeks 2-12 using a 40mg/ml
solution
Dosing &
RoA
▪ RA Pharma is conducting two Phase 2 studies:
– Study 1 (ex-US): Cohort A Naïve PNH subjects with LDH≥2xULN; Cohort B
PNH patients on eculizumab therapy for at least 6 months prior to screening
– Study 2 (US only): Patients with inadequate response to eculizumab defined
as having received eculizumab for at least 6 months plus a documented LDH
level ≥ 1.5 x ULN and/or the presence of a known C5 mutation conferring
resistance to eculizumab
▪ Trial endpoints include:
– Change from baseline in LDH (primary endpoint), total bilirubin, total
hemoglobin, free hemoglobin, haptoglobin, reticulocytes, and hemoglobinuria
▪ n: 20 patients in study 1 (Cohort A ~12; Cohort B~8); 8 patients in Study 2
Ongoing
clinical
development
Phase

ALNYLAMALN-CC5
Company website and statements;
NCT02352493
▪ GalNAc-siRNA conjugate interfering with production of C5 protein; targets
hepatocytes via the Asialoglycoprotein Receptor
▪ Recruits RNA-Induced Silencing Complex (RISC) for catalytic (as opposed to
stoichiometric) mRNA silencing
Description
▪ PNH patients from Phase 1b (Part C) open label study are still being followed
▪ Subcutaneous administration
▪ Alnylam’s prior statements suggest quarterly 600mg ‘CC5 + 300 or 600mg Q4W
eculizumab in PNH
Dosing &
RoA
▪ 3 part Phase 1 study active – all subjects enrolled:
– Part A: Single ascending dose in healthy subjects
– Part B: Multiple ascending dose in healthy subjects
– Part C (Phase 1b): 6 PNH patients recruited. Data presented at EHA and
ASH 2016. Company statements suggest these patients continue to be
followed
▪ Part C endpoints include:
– Primary – Safety and tolerability
– Secondary – PK, C5, LDH, complement activity
▪ n: 6 PNH patients, 3 naïve to eculizumab therapy, 2 patients previously stable
on 900mg Q2W eculizumab, 1 patient previously on 1200mg Q2W eculizumab
Ongoing
clinical
development
Phase

AKARICoversin
Company website and statements;
ASH 2014 & EHA 2017
▪ Small (16 kDa) protein of the lipocalin family with anti-complement activity
isolated from the tick of Ornithodoros moubata
▪ Binds to human C5 and prevents its cleavage by C5 convertases
▪ In vitro effect in preventing hemolysis of PNH erythrocytes, but:
– Inhibition doesn’t seem complete
– No expected effect on C3 decoration
▪ Immunogenicity (evolutionary distant protein)?
Description
▪ Phase I in HV
▪ Phase I/II in PNH (untreated)
▪ Subcutaneous administration, dailyDosing &
RoA
▪ Phase II in PNH
– N=5 screened (4 on treatment)
– 60 mg loading dose followed by 23.5 mg BID, then QID
– PD: CH50 fully inhibited
– Hematological response, with LDH reduction (< 2x ULN)
– One patient with R885 H/C C5 polymorphism
▪ Phase III in PNH announced (poor responders and/or untreated)
Ongoing
clinical
development
Phase

ALEXIONALXN1210
ALXN1210 Innovative Engineering Immediate, complete, sustained
reduction of free C5 activity ≥99% – High affinity Anti-C5 monoclonal
antibody
– Derived from eculizumab through
targeted engineering designed to:
Enhance Fc receptor recycling
Increase half-life
Maintain favorable safety and
tolerability profile
Clinical development– Phase I and Phase II completed
– Two phase III trials in PNH
ongoing
PNH 301: untreated patients
PNH 302: patients on ecu, with
stable response

ALXN1210 Phase 3 PNH Switch Study:Trial Design (Ravulizumab)
15aALXN1210 dosage: loading dose = 2400 mg for patients weighing ≥ 40 to < 60 kg, 2700 mg for patients weighing ≥ 60 to < 100 kg, 3000 mg for patients weighing ≥ 100 kg; maintenance dose=3000 mg for
patients weighing ≥ 40 to < 60 kg, 3300 mg for patients weighing ≥ 60 to < 100 kg, 3600 mg for patients weighing ≥ 100 kg. bSoliris maintenance dose=900 mg.
NCT03056040. Clinical Trial.gov website. https://clinicaltrials.gov/ct2/show/NCT03056040
Provided April 26, 2018, as part of an oral presentation and is qualified by such, contains forward-looking statements, actual results may vary materially; Alexion disclaims any duty to update.
Randomized treatment period
26 weeks
Primary Objective: Assess non-inferiority of ALXN1210 compared to Soliris® in patients with PNH who are clinically stable after having
been treated with Soliris® for at least the past 6 months
Primary Endpoint: Hemolysis as directly measured by percentage change in LDH levels from Baseline to Day 183.
Patients who meet eligibility criteria
and on Soliris® for≥ 6 months
N=195
Stratification Randomization
1:1 Soliris® maintenance doseb
Day 1 and every 2 weeks
ALXN1210maintenance dosea
Day 197 and every 8 weeks
ALXN1210loading dosea
Day 183
15 17 19 21 23 25
ALXN1210 loading dosea Day 1
3
Continue ALXN1210 maintenance doseEvery 8 weeks
aALXN1210 maintenance dosea
Day 15 and every 8 weeks
19 26
5 7 9 11 13
11
3
Q8W
Q8W
Screening up
to 4 weeks
Extension period
2 years


Normalização de LDH
Blood 133: 530, 2019




The perfect complement inhibitor for PNH
1. As safe as first-generation inhibitors (eculizumab)
2. Similar control of intravascular hemolysis, as
compared with eculizumab
3. Possible effect on C3-mediated extravascular
hemolysis
4. Effective in rare genotypes?
5. Possibly better in terms of patients compliance
(administration route, frequency): no hospitalization?
6. Cost: a cheap treatment for everybody, worldwide

Classical pathway Lectin pathway Alternative pathway
C1q
C1rC1s
C2 C4
C4b2a
C3
MBL
MASPs
C3bBbC3(H2O)Bb
C3
hydrolysis
fB fI
P
(tick-over)
Immune
complexes Bacterial LPS
and membranes
C4b2aC3b C3bBbC3b
C6
MAC
C7
C8
C9
C3 convertases
C5 convertases
Lytic complex
C3b
C3a
C5 C5b
C5a
Proximal complement
inhibitors (alternative pathway-
specific):
• Factor B (fB) inhibitors
• Factor D (fD) inhibitors
• Properdin (P) inhibitors
• Factor H (fH)-based protein
(e.g., TT30)
• Complement Receptor 1
(CR1)-based proteins**: may also modulate other
complement pathways
Amplification
loop

Classical pathway Lectin pathway Alternative pathway
C1q
C1rC1s
C2 C4
C4b2a
C3
MBL
MASPs
C3bBbC3(H2O)Bb
C3
hydrolysis
fB fI
P
(tick-over)
Immune
complexes Bacterial LPS
and membranes
C4b2aC3b C3bBbC3b
C6
MAC
C7
C8
C9
C3 convertases
C5 convertases
Lytic complex
C3b
C3a
C5 C5b
C5a
Broad C3 inhibitors:
• Compstatin and derivativesAmplification
loop

COMPSTATINA Peptide Drug to Block Complement at the C3 Level
Qu et al., 2012, Immunobiology
4V9H3,000 nM
4(1MeW)10 nM
Cp400.5 nM
1996 2006 2012
AMD [Phase II]POT-4 [Potentia/Alcon]
AMD, PNH, Sepsis,Hemodialysis, …
C3b
C5
C5aMAC
C4
C2
FD
FB
C3a C3b C3d
C1 MBL Fic P
Compsta n
iC3b
C3
P1:1 (molar) binding

Effect of compstatin analogs on hemolysis of PNH RBCsDose-dependent inhibition
PNH RBC hemolysis:Cp40 (AMY-101) and PEG-Cp40 (AMY-105)
0
10
20
30
40
50
60
70
80
90
100
0,1 1 10 100
Concentration (uM)
% o
f ly
sis
ob
serv
ed
in
aN
HS
CP30
AMY-101
AMY-105
Risitano et al, Blood 2014
C3-FITC
Erythrocytes in
acidified serum
+ Cp40 10 uM
CD
59
-PE
CD
59
-PE
Erythrocytes in
acidified serum
+ PEG-Cp40 10 uM
Both Cp40 and its PEGylated derivative completely
abolish hemolysis of PNH erythrocytes in vitro
Cp40 and PEG-Cp40 completely prevent C3 fragment
deposition on PNH RBCs incubated in aNHS

Other compstatin analogs (Apellis Pharmaceuticals)
• APL-1 and APL-2: PEGylated derivatives of the first-generation
compstatin (POT-4)
• In vitro, efficacy comparable to that of novel derivatives
• Complete inhibition of lysis
• Complete prevention of C3 deposition
• Clinical translation ongoing (with APL-2):
• Phase I in healthy volunteers
• Phase Ib in PNH patients already on eculizumab

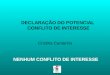
PADDOCK (interim): APL-2 shows potential to reach normal LDH levels
as monotherapy in treatment in naïve PNH patients – 270 mg/day
0
2600
2400
2200
2000
1800
1600
1400
1200
1000
800
600
400
20019 18 19 17 15 15 15 14 12 11
1 15 29 43 57 71 85 99 113 127 141 155 169
LD
H(U
/L)
Day
• Reductions in LDH were rapid following initiation of APL-2 therapy, with 95% of
subjects achieving an LDH in the normal range by day 29
• Reductions in LDH have been sustained and durable, with mean
LDH maintained within the normal range at all timepoints beyond day
29
Decrease in LDH
normal
• All 19 subjects responded rapidly after initiating APL-2 therapy, and by day
29 mean baseline Hb increased from 8.0 g/dL to 10.8 g/dL
• Increases in Hb were sustained and durable as represented by a mean Hb of
12.2 g/dL at day 85
5
7
9
11
13
15
17
19
1 15 29 43 57 71 85 99 113 127 141 155 169
Day
Hem
og
lob
in(g
/dL
)
Increase in Hemoglobin
normal
19 18 19 17 15 15 15 14 12 11n n
Interim data as reported Dec 2, 2018
38



PHAROAH: APL-2 add-on to Soliris® - all four patients
successfully transitioned to APL-2 monotherapy
Eculizumab
Monotherapyi
APL-2 +
Eculizumabii
APL-2
Monotherapyiii
Hemoglobin (g/dL) * 8.9 11.9 11.4
Annual Transfusions (avg.) 6.0 0 0
LDH (ULN) * 1.0x 0.8x 0.9x
Reticulocytes (ULN)* 2.7x 1.2x 0.8x
Patient Years (Total) NA 5.9 Years 1.9 Years
Multiple of Eculizumab Label Dose
(900mg x 2wk.)1.6x 1.0x -
*Average last available reading for all four patients on each dosing regimen(i) last reading during eculizumab monotherapy prior to co-treatment with APL-2
(ii) last reading during co-treatment and prior to APL-2 monotherapy
(iii) last reading while on APL-2 monotherapy
Interim data as reported Sept 4, 2018
41

Other compstatin analogs (Apellis Pharmaceuticals)
Plans for Phase III just announced (different indications)

Second generation complement inhibitors for PNHTake home messages
1. Alternative anti-C5 agents (or terminal complement inhibitors) may
result in limited benefit Possible improvement of treatment compliance: administration route and
intervals (reduced/abolished hospitalization?)
Reduced costs?
Likely no clinical benefit over eculizumab (except for C5 mutations)
2. Second-generation inhibitors must target early complement activation C3-mediated extravascular hemolysis is the main unmet clinical need in
PNH
i. C3 inhibitors: compstatin
Optimal strategy for PNH, due to deranged regulation along all the three
pathways
Initial data in PNH very encouraging (mostly add-on therapy)
Subcutaneous availability, but need of s.c. INFUSIONS
ii. Alternative pathway inhibitors: anti-FB and anti-FD
Preliminary data in PNH (anti-FD only) very promising (add-on therapy)
Orally available
short half-life; risk concerning “missing doses”