Embed Size (px)
Citation preview

UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
CENTRO DE CIÊNCIAS DA SAÚDE
CURSO DE GRADUAÇÃO EM FARMÁCIA
JÚLIA SCARLET BATISTA OLIVEIRA
INIBIDORES DE BOMBA DE PRÓTONS E INTERAÇÕESMEDICAMENTOSAS EM FARMÁCIAS COMUNITÁRIAS: UMA
ABORDAGEM POR ANÁLISE DE REDE
NATAL/RN
2021

JÚLIA SCARLET BATISTA OLIVEIRA
INIBIDORES DE BOMBA DE PRÓTONS E INTERAÇÕESMEDICAMENTOSAS EM FARMÁCIAS COMUNITÁRIAS: UMA
ABORDAGEM POR ANÁLISE DE REDE
NATAL/RN
2021

Universidade Federal do Rio Grande do Norte - UFRNSistema de Bibliotecas - SISBI
Catalogação de Publicação na Fonte. UFRN - Biblioteca Setorial do Centro Ciências da Saúde - CCS
Oliveira, Julia Scarlet Batista.Inibidores de bomba de prótons e interações
medicamentosas em farmácias comunitárias: umaabordagem por análise de redes / Julia Scarlet Batista
Oliveira. - 2021.30f.: il.
Trabalho de Conclusão de Curso - TCC (Graduação emFarmácia) - Universidade Federal do Rio Grande doNorte. Centro de Ciências da Saúde, Departamento de
Farmácia. Natal, RN, 2021.Orientador: Rand Randall Martins.
1. Interações medicamentosas - TCC. 2. Ambulatório- TCC. 3. Automedicação - TCC. I. Martins, Rand
Randall. II. Título.
RN/UF/BS-CCS CDU615.015.2
Elaborado por ANA CRISTINA DA SILVA LOPES - CRB-15/263

JÚLIA SCARLET BATISTA OLIVEIRA
INIBIDORES DE BOMBA DE PRÓTONS E INTERAÇÕESMEDICAMENTOSAS EM FARMÁCIAS COMUNITÁRIAS: UMA
ABORDAGEM POR ANÁLISE DE REDE
Aprovado em:____de____de_____
_____________________________________
Profº. Drº. Rand Randall Martins. Orientador – UFRN
_____________________________________
Profº. Drº. Fernando Henrique Andrade Nogueira. Examinador – UFRN
_____________________________________
Dr. Miguel Adelino da Silva Filho . Examinador – EBSERH /HUAB

TÍTULO: Inibidores de bomba de prótons e interações medicamentosas em
farmácias comunitárias: Uma abordagem por análise de redes
Autores:
Júlia Scarlet Batista Oliveira1
Lorena Maria Lima de Araújo 2
*Rand Randall Martins1
Author affiliations:
1. Departamento de Farmácia, Universidade Federal do Rio Grande doNorte, Natal, RN, Brasil.
2. Programa de Pós Graduação em Ciências Farmacêuticas, UniversidadeFederal do Rio Grande do Norte, Natal, RN, Brasil.
Address of the corresponding author:
* Faculdade de Farmácia, Centro de Ciências da Saúde, Universidade Federal
do Rio Grande do Norte UFRN, Av. General Gustavo Cordeiro de Farias.
Petrópolis, Natal-RN 59012-570, Brazil. Phone: +55 84 3342 9824; Fax +55 84
3342 9833. E-mail: [email protected]
4

RESUMO
Introdução: Interações medicamentosas são comuns entre usuários de
farmácia comunitária e IBPs são potentes inibidores das enzimas da CYP450.
Objetivo: Identificar a prevalência, fatores associados e os medicamentos mais
implicados com interações medicamentosas via análise de rede em usuários de
farmácias comunitárias sob uso de IBPs. Método: Estudo observacional
transversal executado entre março de 2018 e março de 2019 em 22 farmácias
comunitárias. Estudo aprovado pelo comitê de Ética e Pesquisa institucional.
Foram avaliados 194 clientes com predomínio de mulheres (63,2%) e maiores
de 18 anos (55,0 ± 17,7 anos) que adquiriram pelo menos um IBP. Para
avaliação dos fatores associados à ocorrência de interações, utilizou-se o
modelo multivariado por regressão logística (p<0,05). Para a análise de redes,
utilizou-se o software Gephi 9.01 para avaliação das interações via centralidade
de intermediação. Resultado: Identificou-se uma prevalência de 16,4% de IM,
sobretudo em pacientes com maior idade (OR=1,05 – 4,47; IC95% 1,03 – 1,07;
P>0.01) e do sexo feminino (OR 2,27; IC95% 1,15 – 4,47; P>0,02). A análise
de rede identificou IMs envolvendo omeprazol e o pantoprazol como mais
relevantes e relacionadas a prescrição de levotiroxina, clopidogrel e cilostazol.
Conclusão: IM entre usuários de IBP são frequentes aumentando com a idade
e entre mulheres. A análise de redes mostrou que as interações mais
relevantes com IBPs associam-se à levotiroxina, cilostazol e clopidogrel.
Palavras-chave: Interações medicamentosas; ambulatório; automedicação.
5

INTRODUÇÃO
Os inibidores de bomba de prótons (IBP) estão entre os medicamentos
mais utilizados pela população (1) e são comumente prescritos associados a
medicamentos de uso contínuo (2). O próprio IBP, recomendado normalmente
por poucas semanas (3), vem sendo cada vez mais utilizados por longos
períodos (4,5) por usuários de farmácia comunitária (3).
É importante enfatizar que é comum a presença de interações
medicamentosas em receitas de usuários de farmácia comunitária (6,8). Isso se
torna preocupante em relação aos inibidores de bomba de prótons, pois os
mesmos são potentes inibidores competitivos de enzimas da família CYP450,
principalmente a CYP2C19, ocasionando riscos de interações graves (9,11).
Essas interações medicamentosas podem envolver múltiplos
medicamentos em uma mesma prescrição. Nestes casos, técnicas que
identifiquem padrões complexos em dados sobre saúde permitem uma análise
eficaz, uma das abordagens para isso é a análise de rede (12,14). Até onde
sabemos, inexistem estudos que analisem o perfil de interações associadas aos
IBPs utilizando as ferramentas de análise de redes.
Este estudo objetiva identificar a prevalência e fatores associados à
ocorrência de interações medicamentosas em usuários de farmácias
comunitárias em Natal-RN sob uso de IBPs, além de identificar os
medicamentos mais significativos nas interações via análise de rede.
.
METODOLOGIA
Desenho do estudo
Trata-se de um estudo observacional, transversal, com coleta
prospectiva de dados, de indivíduos maiores de 18 anos que adquiriram
inibidores de bomba de prótons para consumo próprio na população de clientes
de farmácias comunitárias privadas da rede Pague Menos, no município de
6

Natal-RN. Foram excluídos os sujeitos que apresentaram incapacidade
evidente para responder o questionário (portadores de distúrbios auditivos,
cognitivos e da fala). Para que a amostra representasse aproximadamente a
densidade populacional de cada zona do município, o número de usuários
incluídos no estudo foi proporcional ao número de residentes por região e o
número de entrevistados em cada farmácia foi proporcional ao número de
residentes abrangido por cada farmácia. Os dados foram coletados, entre
março de 2018 a março de 2019.
Este estudo foi aprovado pelo Comitê de Ética e Pesquisa da UFRN,
conforme determinações da Resolução CNS nº 466/12 do Conselho Nacional
de Saúde, com parecer nº 2.446.211 e CAAE: 80257417.0.0000.5292. Todos
os indivíduos que aceitaram participar da pesquisa assinaram o termo de
consentimento livre e esclarecido (TCLE).
Coleta de dados
Os indivíduos que adquiriram inibidores de bomba de prótons foram
abordados sobre o interesse em participar da pesquisa. Após apresentação
sobre o estudo e informação sobre os direitos do sujeito de pesquisa foi
assinado o TCLE e aplicada a entrevista. O questionário utilizado foi elaborado
em 3 blocos, o primeiro se refere a dados para caracterização da amostra
(idade, sexo, renda, escolaridade, tabagismo, consumo de álcool, peso e
altura), o segundo às doenças autorreferidas e os medicamentos empregados
e o terceiro ao IBP adquirido (princípio ativo, dose, ocorrência de
automedicação, forma de utilização, tempo de uso e motivação para primeiro
uso). Os usuários foram questionados quanto ao motivo de uso e
conhecimento acerca de outras indicações e potenciais riscos do uso
prolongado. O questionário foi previamente testado em um piloto, para avaliar a
adequação do mesmo na obtenção das informações desejadas.
Foram identificadas as interações medicamentosas potenciais (IMP)
caracterizadas como uma situação clínica em que um fármaco pode modificar a
ação de outro fármaco que foi administrado simultaneamente ou
sucessivamente (14). As interações medicamentosas apresentam quatro níveis
de severidade, no nível maior as interações podem ser fatais e ou exigir
7

intervenção médica para minimizar ou prevenir efeitos adversos sérios, no caso
do nível moderado as interações podem resultar em exacerbação da condição
do paciente e exigir uma alteração na terapia e quando as interações
apresentam um efeito clínico limitado é classificada como de nível menor (15).
Análise Estatística
O tamanho da amostra foi calculado em 359 participantes. Este número
assegura, com uma confiança de 95%, um erro máximo das estimativas de ± 7
pontos percentuais. A análise das informações coletadas foi realizada mediante
processo sistematizado em base estatística de dados pelo programa Stata
versão 15 (Stata Corporation, College Station, TX, USA) envolvendo a
aplicação de estatística descritiva. Os dados foram apresentados em média e
desvio padrão ou frequências relativas e absolutas quando pertinente. Para a
identificação dos fatores associados à ocorrência de IMP envolvendo IBPs foi
utilizada análise univariada por regressão logística. As variáveis com valor de
p>0,10 foram excluídas e um modelo multivariado por regressão logística foi
empregado (p<0,05).
As redes potenciais de IMP foram analisadas usando Gephi, um
programa de software de análise de rede de código aberto que permite
visualização e análise quantitativa de mapas de rede e é receptivo a plugins
desenvolvidos pelo usuário que ampliam sua funcionalidade. Para produzir
mapas de rede entre os pares de IMP, os dados foram importados diretamente
para o Gephi onde as conexões (nós) representam os medicamentos e as
linhas, as interações entre eles. A visualização final das redes de IMP para este
trabalho foi realizada usando o algoritmo de layout Yifan Hu (16) para
apresentar clusters intuitivos, com nós dimensionados pela centralidade de
intermediação. Versões simplificadas das redes foram obtidas por filtragem.
Toda a rede foi exportada para visualização na web usando o plug-in
exportador Sigmajs do Gephi.
RESULTADOS
8

De acordo com a Tabela 01, entre os pacientes analisados, é obtida uma
média de idade entre 55,0 ± 17,7 anos e há predominância do sexo feminino
63,2%. No tópico relacionado a doenças autorreferidas, destacam-se os
problemas cardiovasculares, com maior número de casos relatados (45,1%).
Na Tabela 02, percebe-se uma prevalência de 16,4% de interações e há
um indicativo de predominância dos fármacos anti hipertensivos (35,0%),
seguido pelos antidiabéticos (11,9%) e os agentes modificadores de lipídios
(11,4%). Entre os IBPs mais consumidos, está o pantoprazol com 43%, o
omeprazol com 29,9% e o esomeprazol com 14,2%. Destaca-se que 41,2%
dos entrevistados relataram o uso contínuo de inibidores há mais de 3 anos.
Por fim, na Tabela 03, em relação a análise multivariada, a maior idade
(OR=1,05 – 4,47; IC95% 1,03 – 1,07; P>0.01) e o sexo feminino (OR 2,27;
IC95% 1,15 – 4,47; P>0,02) foram identificados como fatores de risco para
maior ocorrência de interações medicamentosas potenciais com IBPs.
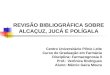
Na análise de redes (Figura 01), o omeprazol e o pantoprazol são os
IBPs que apresentam influência na estrutura, destacando-se pela sua maior
centralidade. Logo, a prescrição destes IBPs implica em maior risco de IMP,
sobretudo com a levotiroxina e, em menor frequência, com o clopidogrel e
cilostazol. O esomeprazol apresentou o mesmo padrão de conexões, contudo,
tem menor centralidade na estrutura.
DISCUSSÃO
Através de um estudo prospectivo de base populacional, identificamos
que 16,4% dos usuários de farmácia comunitária apresentam alguma interação
medicamentosa potencial relacionada a IBPs, sobretudo em indivíduos de
maior idade e do sexo feminino. O padrão das interações via análise de rede
destacou o pantoprazol, omeprazol e esomeprazol como os IBPs mais
relevantes, sobretudo interagindo potencialmente com levotiroxina e
antiagregantes plaquetários. Interação medicamentosa é um tema bastante
explorado na literatura em vários cenários de prática profissional. Contudo,
geralmente, estes trabalhos apontam a frequência das interações, mas não
9

avaliam a fundo o perfil intricado que estas várias interações podem apresentar
em determinado grupo de pacientes. Nesse sentido, as interações
medicamentosas podem ser caracterizadas de forma mais eficiente utilizando
análise de redes. Esta abordagem computacional permite processar um grande
volume de dados em busca de padrões complexos, abrangendo desde a
estrutura de proteínas ao desenvolvimento de novos medicamentos e seus
mecanismos de interação (12-14).
Até onde sabemos, inexistem estudos que objetivem caracterizar
interações medicamentosas a partir da abordagem por análise de redes. Em
uma pesquisa de mestrado, da Universidade de Coimbra, os IBPs representam
13,09% das interações (8). Ao analisar interações com medicamentos
específicos, numa pesquisa sobre as estatinas, os IBPs correspondem a 11,1%
(6) e em outra com medicamentos antidiabéticos, representam 12,4% do total
de interações (7). Em outra pesquisa, brasileira, feita em Salvador, os
inibidores de bomba de prótons destacam-se entre os 10 medicamentos que
mais apresentam interações, abrangendo cerca de 3% (17).
Nossos dados apontam para a maior idade e o sexo feminino como
fatores relacionados ao maior risco de IMP com IBPs. Estas duas
características associam-se fortemente a maior uso de medicamentos, fator
determinante para ocorrência de interações medicamentosas. A polifarmácia é
mais comum em pacientes idosos (18), sendo o omeprazol um dos
medicamentos mais prescritos para este segmento (4). Confirmando nossos
dados, o sexo feminino é predominante quanto ao uso de medicamentos e
possui uma média maior de medicamentos por pessoa (1, 4, 18, 19). Inclusive
quanto ao uso de inibidores de bomba de prótons, há uma maior prevalência
de prescrição de omeprazol em pacientes do sexo feminino (4, 20).
Dentre as interações encontradas neste estudo, os medicamentos que
apresentaram maior relevância foram o clopidogrel, cilostazol e a levotiroxina.
Os IBPs promovem diminuição significativa na absorção da levotiroxina (21,
22). Apesar de limitado, um estudo com 10 pacientes indicou elevação nos
valores de TSH por consequência desta interação (23). Já a interação entre os
IBPs e o clopidogrel é baseada na inibição competitiva da enzima CYP2C19
10

(10, 24). O clopidogrel depende da metabolização hepática para gerar seu
metabólito ativo, logo, a ação de inibição metabólica do omeprazol diminui sua
eficácia terapêutica (25). Um estudo envolvendo 13636 idosos, identificou
maior risco de infarto recorrente do miocárdio em indivíduos com uso de IBPs
concomitantemente à terapêutica antiplaquetária com clopidogrel (26).
Os principais metabólitos do cilostazol, OPC- 13015 e OPC-13213,
responsáveis por cerca de 50% da sua ação farmacológica, são gerados
principalmente pela CYP3A4 e CYP2C19 e os inibidores de bomba de prótons
são inibidores dessas enzimas (27). A partir da avaliação farmacocinética de 20
indivíduos saudáveis, observou-se um aumento de 50% na Cmax de cilostazol
em indivíduos que receberam 100 mg em dose única associado a 40 mg de
omeprazol (28).
Este estudo apresentou algumas limitações. Foi restrito a uma única
cidade, realizado apenas em uma área urbana e em uma única rede de
farmácias. O número de pacientes que recusaram participar da pesquisa não
foi sistematicamente coletado. Não tivemos acesso ao histórico clínico para
confirmação do diagnóstico autorreferido ou quando havia relato de
medicamento prescrito sem a presença da prescrição, logo a possibilidade de
vias de memória sendo essas informações autorrelatadas.
Devido às informações encontradas neste estudo, o conhecimento sobre
as potenciais interações medicamentosas relacionadas aos IBPs, quais
medicamentos mais implicados e quais são os fatores associados, em
farmácias comunitárias, apresenta-se relevante. Desse modo, auxiliam os
profissionais de saúde, sobretudo o farmacêutico, para que possam orientar
sobre a terapia medicamentosa mais eficaz e segura para o paciente.
.
CONCLUSÃO
Entre os usuários de inibidores de bomba de prótons, que adquiriram o
medicamento em farmácias comunitárias, 16,04% deles apresentam alguma
interação medicamentosa potencial. Essas interações são mais recorrentes em
11

mulheres e em pessoas com mais idade. O estudo de análise de redes mostrou
que as interações mais relevantes com IBPs (omeprazol, pantoprazol e
esomeprazol) associam-se a levotiroxina, cilostazol e clopidogrel.
REFERÊNCIAS BIBLIOGRÁFICAS
1. Moreira T de A, Alvares-Teodoro J, Barbosa MM, Júnior AAG,
Acurcio F de A. Use of medicines by adults in primary care: Survey on
health services in Minas Gerais, Brazil. Rev Bras Epidemiol. 2020
2. Salgado AL, Palma AL do R, Ramos L de P, Miranda PE, Oliveira
FG, Cortelli AFD, et al. Uso indiscriminado de inibidores da bomba de
prótons em receituários de medicamentos de uso contínuo. Brazilian J
Heal Rev. 2019;2(6):5883–97.
3. Carranza Caricol F. Seguridad del omeprazol: ¿es adecuada la
duración de los tratamientos? Farm Comunitarios. 2015;7(1):5–9.
4. Costa MP, Damascena RS. Perfil de Usuários de Omeprazol e
Considerações Sobre Seu Uso Racional: Uma Revisão Bibliográfica /
Profile of Omeprazol Users and Considerations About Their Rational Use:
A Bibliographic Review. ID line Rev Psicol. 2020;14(50):1185–96.
5. Syafhan NF, Augustine M, Ramadhani U, Hersunaryati Y.
Proton-pump inhibitor use and potential drug interactions in outpatients.
Int J Appl Pharm. 2018;10(Special Issue 1):358–63.
6. Samardzic I, Benkovic I, Vrca VB. Incidence of statin-drug
interactions in Croatian community pharmacy. Pharmazie.
2017;72(3):187–91.
7. Samardzic I, Bacic-Vrca V. Incidence of potential drug-drug
interactions with antidiabetic drugs. Pharmazie. 2015;70(6):410–5.
8. Nunes AIJM, Fortuna AC. Análise e avaliação de interações
farmacológicas identificadas em prescrições médicas dispensadas numa
12

Farmácia Comunitária. Coimbra. Dissertação [Mestrado em Ciências
Farmacêuticas] - Universidade de Coimbra; 2015.
9. Kamiya C, Inui N, Hakamata A, Miyakawa S, Tanaka S, Uchida S,
et al. Effect of co-administered inducer or inhibitor on omeprazole
pharmacokinetics based on CYP2C19 genotype. J Pharmacol Sci
[Internet]. 2019;139(4):361–6. Available from:
https://doi.org/10.1016/j.jphs.2019.03.001
10. Cunha N, Machado AP. Proton pump inhibitors and the risk of
severe adverse events – A cardiovascular bombshell? Rev Port Cardiol
[Internet]. 2018;37(10):859–63. Available from:
https://doi.org/10.1016/j.repc.2017.10.012
11. Forgerini M, Mieli S, Mastroianni P de C. Safety assessment of
omeprazole use: A review. Sao Paulo Med J. 2018;136(6):557–70.
12. Ferdousi R, Safdari R, Omidi Y. Computational prediction of
drug-drug interactions based on drugs functional similarities. J Biomed
Inform [Internet]. 2017;70:54–64. Available from:
http://dx.doi.org/10.1016/j.jbi.2017.04.021
13. Ding Y, Tang J, Guo F. Identification of drug-target interactions via
multiple information integration. Inf Sci (Ny) [Internet].
2017;418–419:546–60. Available from:
http://dx.doi.org/10.1016/j.ins.2017.08.045
14. Sahu SK, Anand A. Drug-drug interaction extraction from
biomedical texts using long short-term memory network. J Biomed Inform
[Internet]. 2018;86(August):15–24. Available from:
https://doi.org/10.1016/j.jbi.2018.08.005.
15. Micromedex.Truven Health Analytics.2017. Disponível em:
http://www-micromedexsolutionscom.ez18.periodicos.capes.gov.br/micro
medex2/librarian. Acesso em: 15 de agosto de 2019.
16. Yifan H. “Efficient, high-quality force-directed graph drawing”. The
13

Mathematica Journal, 10, v. 1, 2006. Acesso em: 21/10/2019.
17. Leão DFL, de Moura CS, de Medeiros DS. Avaliação de
interações medicamentosas potenciais em prescrições da atenção
primária de Vitória da Conquista (BA), Brasil. Cienc e Saude Coletiva.
2014;19(1):311–8.
18. Pereira KG, Peres MA, Iop D, Boing AC, Boing AF, Aziz M, et al.
Polifarmácia em idosos: Um estudo de base populacional. Rev Bras
Epidemiol. 2017;20(2):335–44.
19. Cristina E, Muniz S, Goulart FC, Lazarini CA, José M, Marin S.
Análise do uso de medicamentos por idosos usuários de plano de saúde
suplementar. 1981;
20. Hipólito P, Rocha BS da, Oliveira FJAQ de. Perfil de usuários com
prescrição de omeprazol em uma Unidade Básica de Saúde do Sul do
Brasil: considerações sobre seu uso racional. Rev Bras Med Família e
Comunidade. 2016;11(38):1–10.
21. Azran C, Porat D, Fine-Shamir N, Hanhan N, Dahan A. Oral
levothyroxine therapy postbariatric surgery: Biopharmaceutical aspects
and clinical effects. Surg Obes Relat Dis [Internet]. 2019;15(2):333–41.
Available from: https://doi.org/10.1016/j.soard.2019.01.001
22. Dahan A, Miller JM, Amidon GL. Prediction of Solubility and
Permeability Class Membership: Provisional BCS Classification of the
World’s Top Oral Drugs. The AAPS Journal [Internet]. 2009 Dec 04 [cited
2020 Oct 9];Pharmacokinetics, Biopharmaceutics and Bioequivalence:
History and Perspectives:740-746. DOI 10.1208/s12248-009-9144-x.
Available from: PudMed
23. Skelin M, Lucijanić T, Amidžić Klarić D, Rešić A, Bakula M,
Liberati-Čizmek AM, et al. Factors Affecting Gastrointestinal Absorption of
Levothyroxine: A Review. Clin Ther. 2017;39(2):378–403.
24. Batchelor R, Kumar R, Gilmartin-Thomas JFM, Hopper I, Kemp
14

W, Liew D. Systematic review with meta-analysis: risk of adverse
cardiovascular events with proton pump inhibitors independent of
clopidogrel. Aliment Pharmacol Ther. 2018;48(8):780–96.
25. Tangamornsuksan W, Thiansupornpong P, Morasuk T, Lohitnavy
O, Lohitnavy M. A pharmacokinetic model of drug-drug interaction
between clopidogrel and omeprazole at CYP2C19 in humans. Proc Annu
Int Conf IEEE Eng Med Biol Soc EMBS. 2017;2704–7.
26. Gaglia MA. Proton Pump Inhibitors and Clopidogrel. Antiplatelet
Ther Cardiovasc Dis. 2014;180(7):300–5.
27. Hiratsuka M, Hinai Y, Sasaki T, Konno Y, Imagawa K, Ishikawa M,
et al. Characterization of human cytochrome P450 enzymes involved in
the metabolism of cilostazol. Drug Metab Dispos. 2007;35(10):1730–2.
28. Suri A, Bramer SL. Effect of omeprazole on the metabolism of
cilostazol. Clin Pharmacokinet. 1999;37(SUPPL. 2):53–9.
15

Tabela 1 – Caracterização da população (n = 359)
Características ValoresIdade em anos (m, dp) 55.0 17.7Sexo feminino (n, %) 227 63.2Renda em SM (n, %)
0 -5 252 71.06-10. 53 14.9> 10 50 14.1
Escolaridade (n, %)Não alfabetizado 15 4.2Médio 50 13.8Fundamental 147 41.0Superior 147 41.0
Tabagista (n, %) 17 4.8Usuário de álcool (n, %) 46 12.8Doenças autorreferidas (n, %)
Doenças cardiovasculares 162 45.1Sem comorbidades 117 32.6Doenças ósseas 22 6.1Doenças reumáticas 7 2.0Doença renal 5 1.4Doenças musculoesqueléticas 4 1.1Hepatopatias 1 0.3
Legenda: média e desvio padrão (m, dp), frequência absoluta e relativa (n, %)
16

Tabela 2 – Perfil de prescrição de medicamentos em usuários de IBPs
Características ValoresMedicamentos por classe ATC, exceto IBPs (n, %)
Antihipertensivos 247 35.0Antidiabéticos 84 11.9Hipolipemiantes 80 11.4Suplementos e vitaminas 43 6.1Antidepressivos 37 5.3Hormônio tiroidiano 36 5.1Anticoagulantes 27 3.8Sedativos e hipnóticos 26 3.7Anti-inflamatórios 21 3.0Outros 103 14.6Total 704 100.0
Pacientes em uso de IBPs (n, %)Pantoprazol 154 43.0Omeprazol 107 29.9Esomeprazol 51 14.2Dexlansoprazol 35 9.8Lanzoprazol 10 2.8Rabeprazol 1 0.3
Uso contínuo de IBPs superior a 3 anos (n, %) 148 41.2
Prevalência de IMP (n, %) 59 16.4
Legenda: frequência absoluta e relativa (n, %)
17

Tabela 3 - Modelo multivariado de regressão logística para os fatores
relacionados a IMP em usuários de IBPs
CaracterísticaUnivariada
pMultivariada
pOR 95%CI OR 95%CI
Idade em anos 1.051 1.031 1.071 >0.001 1.050 1.030 1.070 >0.001
Sexo feminino 2.326 1.205 4.491 0.012 2.270 1.152 4.475 0.018
Renda superior a 6 SM 1.608 0.895 2.889 0.112
Escolaridade superior 1.073 0.609 1.888 0.808
Tabagista 1.094 0.304 3.934 0.890
Usuário de álcool 0.447 0.154 1.297 0.139
Doenças autorreferidas
Doenças cardiovasculares 3.370 1.849 6.141 >0.001
Doenças ósseas 3.204 1.279 8.027 0.013
Doenças reumáticas 2.070 0.392 10.933 0.391
IBPs por mais de 3 anos (n, %) 1.596 0.911 2.795 0.102
Legenda: Razão de chances (OR), valor de p (p), intervalo de confiança de 95% (IC95%).
18

Figura 01 – Análise de rede dos pares de interações potenciais com IBP em
usuários de farmácia comunitárias.
19

Brazilian Journal of Pharmaceutical Sciences (BJPS)Scope and politics
The Brazilian Journal of Pharmaceutical Sciences(BJPS) is a peer-reviewed electronic journal publishedquarterly by the School of Pharmaceutical Sciences of theUniversity of São Paulo.
The purpose of the Brazilian Journal ofPharmaceutical Sciences is to publish manuscripts thatsignificantly contribute to knowledge in all areas ofPharmaceutical Sciences, including Medicines and Drugs,Pharmaceutical and Health Care, Food and ExperimentalNutrition, Clinical Chemistry, Toxicology, MedicinalChemistry, Pharmaceutical Technology, Biotechnologyamong others.The following papers will not be accepted for publication:
● Studies on human subjects not approved by anaccredited Ethics Committee or without writteninformed consent from the subject or legalguardian.
● Studies on animals not approved by an accreditedEthics and Animal Care Committee.
● Manuscripts describing plant extract activity thatdo not identify quali and quantitative markers ofthe extract.
●
Preparation of the manuscripts
Manuscripts that do not agree to the Instructions will be refused prior topeer review.Manuscripts must be submitted in English.
Submission of a manuscript to BJPS implies that the data have not beenpublished previously and will not be submitted for publication elsewherewhile the manuscript is under review.
Co-authors should be individuals who have contributed substantially tothe content of the paper.Manuscripts in accordance to the “Preparing your manuscript section”will be submitted for peer review to at least two independent,anonymous referees indicated by the Associated Editors. Based on peerreview, the Associate Editors will suggest manuscript acceptance or notto the Editor-in-Chief, who is responsible for the final decision.
In the case revision is suggested, the authors are asked to resubmit themanuscript incorporating the suggestions and recommendations of thereferees within 15 calendar days. If the revised version is not receivedwithin the time specified from the date of notice, the manuscript processwill be canceled. All revisions must be accompanied with a letterdetailing the changes made to the original document and answering allthe reviewer comments, on a point-by-point basis. All alterations mustbe identified in the revised manuscript.
Manuscripts must have their copyright assigned to the BJPS beforesubmitting to the Journal.The dates of receipt and acceptance will be published for each article.
20

Authors are expected to return reviewed manuscripts to the Journalwithin 15 calendar days, and to return galley proofs of acceptedmanuscripts within 72 hours. The total number of "late" days will beadded to the submission date at the time of publication.
Authors are required to suggest 4 potential reviewers with information ofinstitutional and e-mail address. At least 2 of the potential reviewerssuggested should be from a different country to the correspondingauthors. The Editors reserve the right to indicate these or otherreviewers for manuscript evaluation.
Manuscript categoriesThe authors should state in the cover letter that the manuscript isintended to be Full-length Original Paper, Short Communication, ReviewArticle, Mini-review article, Concepts and Comments and Book Reviews.The Journal will also publish Thematic or Congress AbstractsSupplements under invitation by the Editors or previous approval of theEditorial Board.BJPS will publish the following type of articles:
Full-length Original PaperEach manuscript should clearly state its objective or hypothesis; theexperimental design and methods used; the essential features of anyinterventions; the main outcome measures; the main results of thestudy; and a discussion placing the results in the context of publishedliterature.The manuscript should contain:
● abstract of no more than 250 words● no more than 6 key words● a running title to be used as a page heading, which should not
exceed 60 letters and spaces● manuscript main body divided into separate sections
(Introduction, Material and Methods, Results and Discussion).● no more than 40 references (without exceptions)● Supplementary data can be submitted as Suppmentary
information session.
Short CommunicationA short communication is a report on a single subject, which shouldbe concise but definitive. The scope of this section is intended to be wideand to encompass methodology and experimental data on subjects ofinterest to the readers of the Journal.The manuscript should contain:
● abstract of no more than 250 words● no more than 6 key words● a running title to be used as a page heading, which should not
exceed 60 letters and spaces● manuscript main body divided into separate sections
(Introduction, Material and Methods, Results and Discussion),without a separate section for conclusions
● no more than 20 references (without exceptions)● no more than three illustrations (figures and/or tables)
Review ArticleA review article should provide a synthetic and critical analysis of a
21

relevant area and should not be merely a chronological description ofthe literature. A review article by investigators who have madesubstantial contributions to a specific area of Pharmaceutical Scienceswill be published by invitation of the Editors. However, an outline of areview article may be submitted to the Editors without priorconsultation. If it is judged appropriate for the Journal, the author(s) willbe invited to prepare the article for peer review. The manuscript shouldcontain:
● abstract of no more than 250 words● no more than 6 key words● a running title to be used as a page heading, which should not
exceed 60 letters and spaces● manuscript main body divided into sections with appropriate titles
and subtitles● no more than 90 references (without exceptions)
Mini-review ArticleA mini-review is focused on a restricted part of a subject normallycovered in a review article. The structure of the mini-review follows thesame rules as the review.
Concepts and CommentsThe Concepts and Comments section provides a platform for readers topresent ideas, theories and views.
The manuscript should contain:
● abstract of no more than 250 words● no more than 6 key words● a running title to be used as a page heading, which should not
exceed 60 letters and spaces● manuscript main body divided into sections with appropriate titles
and subtitles● no more than 40 references (without exceptions)
Book ReviewsWritten by experts indicated by the Editors or written by the authors.
Preparing your manuscript
Cover LetterIt is important that you include a cover letter with your manuscript.Take the time to consider why this manuscript is suitable for publicationin the Brazilian Journal of Pharmaceutical Sciences. Why will your paperinspire other members of your field, and how will it drive researchforward? Please explain this in your cover letter.The cover letter should also contain the following information:
● Title of article.● Name(s) of all author(s).● Information of Corresponding Author (name, full address,
telephone number and e-mail).
Authorship requirementsOnly people who directly contributed to the intellectual content of thepaper should be listed as authors. All manuscripts must be, submitted,
22

only, by electronic way. The confirmation of submission is sent by emailfor all the authors, for their agreement.Authors should meet all of the following criteria, thereby taking publicresponsibility for the content of the paper:
● Conceived, planned and carried out the experiments presented inthe manuscript or interpreted the data, or both.
● Wrote the paper, or reviewed successive versions.● Approved the final version.● Holding positions of administrative leadership, contributing
patients, and collecting and assembling data, however importantto the research, are not by themselves criteria for authorship.Any person who has made substantial, direct contribution to thework but cannot be considered an author should be cited in theAcknowledgment section, with permission and a description ofhis/her specific contribution to the research.
Text format
● The text of a manuscript can only be accepted as a MicrosoftWord file created with MS Word as a "doc", "docx" or "rtf"document.
● Manuscripts should be sent in 30-36 lines, 1,5 spaced,● Each page should contain the page number in the upper
right-hand corner starting with the title page as page 1.● Report all measurements in Système International, SI
(http://physics.nist.gov/cuu/Units) and standard units whereapplicable
● Names of plants, animals and chemicals should be mentionedaccording to International Rules available.
● Names of drugs can follow the International rules (DCI) orcurrent Brazilian rules (DCB)
● Trademarks may be mentioned only once in the text (betweenparenthesis and initial in capital letter)
● Do not use abbreviations in the title and limit their use in theabstract and text.
● The length of the manuscript and the number of tables andfigures must be kept to a minimum.
● Ensure that all references are cited in the text.● Generic names must be used for all drugs. Instruments may be
referred to by proprietary name; the name and country of themanufacturer should be given in parenthesis.
Organization of the ManuscriptMost articles published in BJPS will be organized into the followingsections:Title, Authors, Abstract, Key words, Running Title, Author forCorrespondence and email addressIntroductionMaterial and MethodsResults and DiscussionAcknowledgmentsReferencesTables with a descriptive title and footnote legendsFigures with a descriptive title, descriptive legends and uniformity informat
23

Continuous page numbers are required for all pages including figures.There are no specific length restrictions for the overall manuscript orindividual sections. However, we urge authors to present and discusstheir findings concisely. We recognize that some articles will not be bestpresented in our research article format. If you have a manuscript thatwould benefit from a different format, please contact the editors todiscuss this further.
Title Page
Title - The title should be as short and informative as possible, shouldnot contain non-standard acronyms or abbreviations, and should notexceed two printed lines.
Examples:Freeze-drying of ampicillin solid lipid nanoparticles using mannitol ascryoprotectantA fully validated microbiological assay for daptomycin injection andcomparison to HPLC methodPharmacokinetics, safety and tolerability of L-3-n-butylphthalide tabletafter single and multiple oral administrations in healthy Chinesevolunteers.
Authors and AffiliationsFull name (matched with superscript numbers identifying affiliation).Institution(s) (Department, Faculty, University, City, State, Country) ofeach author (in English).
Examples:Hongmei Xia1 * , Yongfeng Cheng2 , Yinxiang Xu3 ,Zhiqing Cheng1 1College of Pharmacy, Anhui University of Chinese Medicine, Hefei,People's Republic of China.2School of Life Science, University of Science and Technology of China,Hefei, People's Republic of China.3Zhaoke (Hefei) Pharmaceutical Co. Ltd., Hefei, People's Republic ofChina.
AbstractSince abstracts are published separately by Information Services, theyshould contain sufficient hard data to be appreciated by the reader. Theabstract should not exceed 250 words and should be prepared in asingle paragraph.The abstract should briefly and clearly present the objective,experimental approach, new results as quantitative data if possible, andconclusions. It should mention the techniques used without going intomethodological detail and mention the most important results.Abbreviations should be kept to a minimum and should be defined inboth the Abstract and text. Please do not include any reference citationsin the abstract. If the use of a reference is unavoidable, the full citationshould be given within the abstract.
Key WordsA list of key words or indexing terms (no more than 6) should beincluded avoiding generic terms.
24

Running titleThis short title, to be used as a page heading, should not exceed 60letters and spaces.
Corresponding authorOne of the authors should be designated as the corresponding author. Itis the corresponding author´s responsibility to ensure that the authorlist is accurate and complete. If the article has been submitted on behalfof a consortium, all consortium members and affiliations should be listedin the Acknowledgments section. Provide the name and email address ofthe author to whom correspondence should be sent identified with anasterisk.
Introduction The Introduction should put the focus of the manuscript into a broadercontext and reflects the present state-of-art of the subject. This shouldstate briefly and clearly the objectives of the investigation with referenceto previous works. Extensive review of the literature should be avoidedand substituted for references of recent review publications.
Material and MethodsThese should be described in sufficient detail that the work can bereproduced. Well-established procedures and techniques require only acitation of the original source, except when they are substantiallymodified. Reports of experimental studies on humans and animals mustcertify that the research received prior approval by the appropriateinstitutional review Ethics Committee.
Results and Discussion: Results must be presented clearly andconcisely and in logical order. This section should provide results of all ofexperiments required to support the conclusions of the paper. Whenpossible, use figures or tables to present data rather than text. Largedatasets, including raw data, should be submitted as supplementaryfiles; these are published online linked to the article. Discussion shouldinterpret the results and assess their significance in relation to existingknowledge. Speculation not warranted by actual data should be avoided.The Discussion should spell out the major conclusions andinterpretations of the work including some explanation of thesignificance of these conclusions.
Acknowledgments When appropriate, briefly acknowledge technical assistance, advice andcontributions from colleagues. People who contributed to the work butdo not fit the criteria for authors should be listed in theAcknowledgments section, along with their contributions. Donations ofanimals, cells, or reagents should also be acknowledged. You must alsoensure that anyone named in the Acknowledgments agrees to being sonamed. Financial support for the research and fellowships should beacknowledged in this section (agency and grant number).
FiguresFigures must be submitted in high-resolution version (600 dpi).
Preparing figure files for submissionBJPS encourages authors to use figures where this will increase theclarity of an article. The use of color figures in articles is free of charge.The following guidelines must be observed when preparing figures.Failure to do so is likely to delay acceptance and publication of thearticle.
25

● Each figure of a manuscript should be submitted as a single file.● Figures should be numbered in the order they are first mentioned
in the text, and uploaded in this order.● Figure titles and legends should be provided in the main
manuscript as a List of Figures, not in the graphic file.● The aim of the figure legend should be to describe the key
messages of the figure, but the figure should also be discussed inthe text.
● An enlarged version of the figure and its full legend will often beviewed in a separate window online, and it should be possible fora reader to understand the figure without moving back and forthbetween this window and the relevant parts of the text.
● The legend itself should be succinct, while still explaining allsymbols and abbreviations. Avoid lengthy descriptions ofmethods. Statistical information should be given as well as thestatistical tests used.
● Arrows or letters should be used in the figure and explained inthe legend to identify important structures.
● Figures with multiple panels should use capital letters A, B, C,etc. to identify the panels.
● Each figure should be closely cropped to minimize the amount ofwhite space surrounding the illustration. Cropping figuresimproves accuracy when placing the figure in combination withother elements, when the accepted manuscript is prepared forpublication.
● Individual figure files should not exceed 5 MB. If a suitableformat is chosen, this file size is adequate for extremely highquality figures.
Please note that it is the responsibility of the author(s) to obtainpermission from the copyright holder to reproduce figures (or tables)that have previously been published elsewhere. In order for all figures tobe open-access, authors must have permission from the rights holder ifthey wish to include images that have been published elsewhere innon-open-access journals. Permission should be indicated in the figurelegend, and the original source included in the reference list;
Supported file type
The following file format can be accepted: TIFF (suitable for images) orJPEG with 600 dpi, and Word file for the manuscript.
Tables
● Tables must be submitted in Word (.doc) or Excel (.xls), not asan image.
● Tables must be numbered consecutively with Roman numerals inthe text.
● Tables must have a concise and descriptive title.● All explanatory information should be given in a footnote below
the table. Footnotes should be used to explain abbreviations andprovide statistical information, including statistical tests used.
● All abbreviations must be defined in this footnote, even if theyare explained in the text.
● Tables must be understandable without referring to the text.● Tables occupying more than one printed page should be avoided,
if possible.
26

● Vertical and diagonal lines should not be used in tables; instead,indentation and vertical or horizontal space should be used togroup data.
ReferencesReferences should be prepared and listed according to Vancouverstandard reference style. Entries should be arranged in alphabeticalorder by author at the end of the paper. All authors’ names should begiven. Accuracy and completeness of reference data is the responsibilityof the authors.Only published references should be included in the reference list.Meeting abstracts, conference talks, or papers that have been submittedbut not yet accepted should not be cited. Limited citation of unpublishedwork should be included in the body of the text only. All personalcommunications should be supported by a letter from the relevantauthors.References should be cited in the text by the authors’ names, with onlythe first letter in capital letter followed by the year of publication. Formore than three authors, the first has to be cited followed by theexpression et al. (in italic). Small letters close to the year mustdifferentiate references of the same authors and year of publication.Examples:(Fujisawa, Atsumi, Kadoma, 1989)(Aviral et al., 2009)(Dodu, Rotari, Vazques, 2012)(Liu et al., 2011a)(Liu et al., 2011b)
Please use the following style for the reference list:
Published Papers. First 6 authors followed by et al., Title, Journal(abbreviation in italic), Year, Volume, Complete Pages.Abe T, Fukushima N, Brune K, Boehm C, Sato N, Matsubayashi H, et al.Genome-Wide allelotypes of familial pancreatic adenocarcinomas andfamilial and sporadic intraductal papillary muninous neoplasms. ClinCancer Res. 2007;13(20):6019-25.Ali A, Iqbal F, Taj A, Iqbal Z, Amin MJ, Iqbal QZ. Prevalence ofmicrovascular complications in newly diagnosed patients with Type 2diabetes. Pak J Med Sci. 2013,29(4): 899-902.Calvo A, Gimenez MJ. Ex Vivo Serum Activity (Killing Rates) AfterGemifloxacin 320 mg Versus Trovafloxacin 200 mg Single Doses AgainstCiprofloxacin-Susceptible and -Resistant Streptococcus pneumoniae. IntJ Antimicr Ag. 2007;20:144-6.Lammers AE, Hislop AA, Flynn Y, Haworth SG. The 6-minute walk test:normal values for children of 4-11 years of age. Arch DisChild. 2008;93:464-468.Zhang Q, Malik P, Pandey D, Gupta S, Jagnandan D, Belin de CE, et al.Paradoxical activation of endothelial nitric oxide synthase by NADPHoxidase. Arterioscler Thromb Vasc Biol. 2008;28:1627-1633.
Article accepted for publication but not yet published. First 6 authorsfollowed by et al., Title, Journal (abbreviation in italic), Year of expectedpublication, (in press) at the end of the citation. Janiszewski M, Lopes LR, Carmo AO, Pedro MA, Brandes RP, SantosCXC, et al. Regulation of NAD(P)H oxidase by associated proteindisulfide isomerase in vascular smooth muscle cells. J Biol Chem. 2005(in press).
27

Internet Communication. Ensure that URLs are active and available.Provide DOI, if available.
Brasil. Ministério da Saúde, Secretaria de Vigilância em Saúde.Leishmaniose visceralgrave: normas e condutas [Internet]. Brasília (DF): Ministério da Saúde,2006. [citado2008 Jan 7]. 60 p. (Série A. Normas e Manuais Técnicos). Disponívelem:http://dtr2001.saude.gov.br/editora/produtos/livros/pdf/06_0072_M.pdf
CAPES Statistics. [citad 2006 Mar 16]. Available from:http://www.capes.gov.br/capes/portal.
Developmental toxicology. [citad 2015 Apr 10]. Available from:http://www.devtox.org/nomenclature/organ.php.
Book, Whole. Authors, Book title, Edition, City, Publisher, Year.Hewitt W. Microbiological assay for pharmaceutical analysis: a rationalapproach. Boca Raton: CRC Press; 2003.Jenkins PF. Making sense of the chest x-ray: a hands-on guide. NewYork: Oxford University Press; 2005. 194 p.Milech A, et al., Oliveira JEP, Vencio S, organizadores. Diretrizes daSociedade Brasileira de Diabetes. São Paulo: A.C. Farmacêutica;2016.
Book, Chapter. Authors, Chapter Title, Editors, Book title, Edition, City,Publisher, Year, Pages of citation.Beizer JL, Timiras ML. Pharmacology and drug management in theelderly. In: Timiras PS, editor. Physiological basis of aging andgeriatrics. 2nd ed. Boca Raton: CRC Press; 1994. p. 279-84.Rojko JL, Hardy WD Jr. Feline leukemia virus and other retroviruses. In:Sherding RG, editor. The cat: diseases and clinical management. NewYork: Churchill Livingstone; 1989. p. 229-332.
Report
World Health Organization. WHO. Department of Mental Health andSubstance Abuse. Mental health atlas 2005. Geneva: World HealthOrganization; 2005. 409 p.
World Health Organization. WHO. Working to overcome the globalimpact of neglected tropical diseases, First WHO report on neglectedtropical diseases. Geneva, Switzerland: WHO Press; 2010.
Thesis and Dissertations
Joselevitch C. Visão no ultravioleta em Carassius auratus (Ostariophysi,Cypriformes, Cyprinidae): estudo eletrofisiológico do sistema cone -células horizontais. [Master's dissertation]. São Paulo: Instituto dePsicologia, USP; 1999.
Marcolongo R. Dissolução de medicamentos: fundamentos, aplicações,aspectos regulatórios e perspectivas na área farmacêutica.[dissertação]. São Paulo: Universidade de São Paulo, Faculdade deCiências Farmacêuticas; 2003.
LawsAgência Nacional de Vigilância Sanitária (Brasil). Resolução nº. 259, de
28

20 de setembro de 2002. Regulamento Técnico para Rotulagem deAlimentos Embalados. Diário Oficial da União 23 set 2002; Seção 1.
Conference, Symposium Proceedings. Cite papers only frompublished proceedings.
Hejzlar RM, Diogo PA. The use of water quality modelling for optimizingoperation of a drinking water reservoir. In: Proceedings of theInternational Conference Fluid Mechanics and Hydrology. 1999 Jun23-26; Prague. Prague: Institute of Hydrodynamics AS CR; 1999. p475-482.
Proceedings of the 10th annual meeting of the Canadian Society forPharmaceuticalSciences. J Pharm Pharm Sci. 2007 Dec 3;10(4):1s-186s.
Audiovisual MaterialPhysician's Desk Reference (PDR). Release 2003.1AX. [CD-ROM].Montvale: Thomson PDR; 2003.
Computer ProgramDean AG, Dean JA, Coulombier D, Brendel KA, Smith DC, Burton AH, etal. Epi info, version 6.04: a word processing database and statisticsprogram for public health on IBM-compatiblemicrocomputers. [Computer program]. Atlanta: Centers of DiseaseControl and Prevention; 1998.
PatentLarsen CE, Trip R, Johnson CR. Methods for procedures related to theelectrophysiology of the heart. Patent No. 5.529.067. NovosteCorporation; 1995.
"Unpublished results" and "Personal communication". Referenceshould appear in the text with the individual name(s) and initials and notin the reference list. (Santos CS, da-Silva GB, Martins LT, unpublishedresults).It is assumed that the author has obtained permission from the sourcewhen "personal communication" is cited.
Submitting manuscripts
Submission should be sent electronically through the ScholarOnesystem (mc04.manuscriptcentral.com/bjps-scielo).
If you need further assistance, please contact the Journal Staff([email protected]).
There is no charges for article’s submissions, evaluations andpublication.
Additional informations:Brazilian Journal of Pharmaceutical SciencesDivisão de Biblioteca e Documentação do Conjunto dasQuímicas/USPServiço de Publicações e CirculaçãoAv. Prof. Lineu Prestes, 95005508-000 - São Paulo - SP - BrasilTel: +55 11 3091.2314E-mail: [email protected]
29

30