Embed Size (px)
Citation preview
UNIVERSIDADE FEDERAL DO RIO DE JANEIRO
Centro de Ciência da Saúde
Faculdade de Odontologia
Departamento de Odontopediatria e Ortodontia
Rio de Janeiro 2014
EFEITO PREVENTIVO E TERAPÊUTICO DE CÁRIE DE
NANOCOMPOSTOS DE CICLODEXTRINAS E TIF4: ESTUDO IN
VITRO
THIAGO ISIDRO VIEIRA
UNIVERSIDADE FEDERAL DO RIO DE JANEIRO
Centro de Ciência da Saúde
Faculdade de Odontologia
Departamento de Odontopediatria e Ortodontia
Rio de Janeiro 2014
THIAGO ISIDRO VIEIRA
EFEITO PREVENTIVO E TERAPÊUTICO DE CÁRIE DE
NANOCOMPOSTOS DE CICLODEXTRINAS E TIF4: ESTUDO IN
VITRO
Dissertação de Mestrado apresentada ao Programa
de Pós-graduação em Odontologia (Área de Concentração:
Odontopediatria) da Faculdade de Odontologia da
Universidade Federal do Rio de Janeiro como parte dos
requisitos para obtenção do título de Mestre em Odontologia
(Área de Concentração: Odontopediatria).
Orientadoras: Profa Dra. Lucianne Cople Maia de Faria Profa Dra. Ana Maria Gondim Valença
FICHA CATALOGRÁFICA
Vieira, Thiago Isidro.
Efeito preventivo e terapêutico de cárie de nanocompostos de
ciclodextrinas e TiF4: estudo in vitro. / Thiago Isidro Vieira – Rio de
Janeiro: Faculdade de Odontologia, 2014.
Orientadoras: Lucianne Cople Maia e Ana Maria Gondim Valença
Dissertação (mestrado) - UFRJ, FO, Programa de Pós-graduação em
Odontologia, Odontopediatria, 2014.
Referências bibliográficas: f..
1. - Epidemiologia. 2. - Complicações. 3. - Anormalidades. 4. Saliva -
microbiologia. 5. Higiene bucal. 6. Estudos de casos e controles. 7.
Criança. 8. Adolescente. 9. Odontopediatria - Tese. I. Maia, Lucianne
Cople. II. Valença, Ana Maria Gondim. III. Universidade Federal do Rio
de Janeiro, FO, Programa de Pós-graduação em Odontologia,
Odontopediatria.
“Não haverá borboletas se a vida não passar por longas e silenciosas metamorfoses”.
Rubem Alves
DEDICATÓRIA
Aos meus queridos pais, Renato e Maria José, por me apoiarem em todas as
minhas decisões com muita lucidez e carinho. Gostaria de deixar registrado aqui
meu eterno agradecimento por me proporcionar um lar acolhedor, com muito amor e
sensibilidade e que me impulsionou para mais essa conquista. Tenho uma gratidão
imensa pela vida por ter me presenteado com a presença de vocês. Pais tão
zelosos, atenciosos e incentivadores. Vocês são o alicerce da minha vida. Eu amo
vocês. Obrigado por tudo.
A minha amada irmã, Thaiza, que não importa quão longe eu fique de casa,
sempre compreendeu a minha ausência e me deu apoio. Um exemplo de amiga e
companheira. Eu amo você para sempre.
AGRADECIMENTOS ESPECIAIS
À minha orientadora, Profª. Drª. Lucianne Cople Maia, por acreditar na
pesquisa e em seu poder transformador do conhecimento e por ter acreditado em
mim. Aprendi muito com suas sugestões, críticas e exemplo. Agradeço o cuidado
especial em todas as orientações que recebi durante esse trabalho de dissertação.
Você é incentivadora! Muito obrigado.
À minha orientadora, Profª. Drª. Ana Maria Gondim Valença, pelas sábias
orientações desde a iniciação científica durante a graduação de Odontologia. É um
privilégio participar do seu grupo de pesquisa e ter sido seu orientando. Sempre
atenciosa e um exemplo inspirador. Você é motivadora!
Muito obrigado.

AGRADECIMENTOS
À minha amada família Renato, Maria José e Thaiza. Reforço aqui meu
eterno agradecimento. Vocês são os melhores sempre e para sempre.
À doutoranda Adílis Kalina Alexandria que foi essencial para a realização
deste trabalho. Sempre prestativa e muito cuidadosa nas orientações, dicas e
sugestões. Gostaria de registrar aqui meu agradecimento pela sua criteriosa
atenção no tratamento estatístico dos resultados. E a Camila Nassur por ter me
possibilitado a realização de parte desse trabalho.
À minha querida turma, Adrielle, Clarissa, Lívia e Marina por todos os
momentos nesses dois anos. Amizade que levarei comigo e fez parte da minha
história. Cada uma, à sua maneira, contribuiu para essa turma ser para mim uma
turma bastante especial. As adversidades por qual passamos nos manteve mais
forte. Obrigado pelo companheirismo e pelas experiências que vivemos juntos.
Às amigas do Mestrado, Elaine, Helena, Nashalie, Queila e Tacíria que
tornaram a rotina diária menos árdua. As dicas, experiências de sucesso
compartilhadas e uma palavra de acalanto no momento oportuno. Uma turma que
deixou saudades.
Aos colegas também do Mestrado, Aline Letieri, Andrea Laudares,
Fernanda Mafei, Káiron e Paula Moraes que são sempre atenciosos e prestativos.
Muito obrigado.
À Tatiana Kelly por ser uma entusiasta da pesquisa, criteriosa e agregadora.
Muito bonito enxergar em você essa dedicação e essa colaboração em ajudar.
Obrigado por me socorrer em momentos cruciais.
Aos professores Dr. Rogerio Gleiser e Dra Ivete Pomarico Ribeiro de
Souza, por todo conhecimento transmitido durante as aulas. Sempre com dicas
pertinentes e sugestões. Foram aulas semanais com intensa arguição que valeram à
pena. Recompensador perceber como melhoramos após essas dicas. Exemplos
inspiradores.
À professora Dra Gloria Fernanda Castro que conduz a Clínica de Pacientes
Especiais com um olhar sensível e acolhedor. Foi um prazer realizar supervisão
dessa clínica.
À professora Laura Guimarães Primo que conduz a clínica do segundo ano
do Mestrado. Sempre atenta e com ótimas dicas de isolamento absoluto! Senso de
humor apurado. Muito obrigado.
Aos professores do Programa de Pós-Graduação em Odontopediatria
(FO/UFRJ)
Dr. Thomaz Chianca, Dra. Aline de Almeida Neves, Dra. Andréa
Gonçalves Antonio, Dra. Luciana Pomarico, e Dr. Marcelo de Castro Costa,
pelas orientações, apoio e transmissão do conhecimento. Muito obrigado.
Aos professores João Farinhas, Nena Requejo, Carla Martins, Vanessa
Moraes e Marta Fornasari pelo conhecimento transmitido, palavras de apoio e
compreensão.
Ao professor Lúcio Mendes Cabral, da Faculdade de Farmácia, da
Universidade Federal do Rio de Janeiro e a doutoranda Lilian Henriques Amaral
também da Faculdade de Farmácia, pelo preparo das soluções fluoretadas testadas
nesse trabalho, orientações metodológicas e paciência para dirimir minhas dúvidas.
Aos amigos do doutorado, Marcello Rotter, Marlus Cajazeira, Michelle
Ammari, Michele Lenzi, Andrea Pintor, Thaís Soares, Cláudia Tavares, pelo
convívio fraterno e pelas experiências compartilhadas.
À todos os funcionários da Disciplina de Odontopediatria (FO/UFRJ), João
Carlos Monteiro, Zezé, Robson, Luiza, Rose, Isabel, Patrícia, Mere, Andréa e
Kátia Seixas, agradeço pela atenção, carinho e zelo.
Ao Gustavo Roque, por toda atenção que recebi quando cheguei ao Rio de
Janeiro.
Aos professores Dra Lívia Maria Andaló Tenuta, Dr Jaime Cury e o técnico
Waldomiro Vieira Filho do Laboratório de Bioquímica Oral da Faculdade de
Odontologia de Piracicaba – UNICAMP pelo auxílio nas análises de flúor.
À CAPES pela concessão de bolsa que permitiu a realização desse estudo. E
a FAPERJ e CNPq pelo incentivo nesse trabalho.
À todos os pacientes da Disciplina de Odontopediatria (FO/UFRJ) que
contribuíram para a minha formação, aos responsáveis desses pacientes pela
credibilidade confiada. Muito obrigado.
RESUMO
VIEIRA, Thiago Isidro. EFEITO PREVENTIVO E TERAPÊUTICO DE CÁRIE DE NANOCOMPOSTOS DE CICLODEXTRINAS E TIF4: ESTUDO IN VITRO. Rio de Janeiro, 2014 Dissertação (Mestrado em Odontologia – Área de concentração: Odontopediatria) – Faculdade de Odontologia, Universidade Federal do Rio de Janeiro, Rio de Janeiro, 2014.
Os objetivos do presente trabalho in vitro foram analisar se as inclusões de TiF4 a hidroxipropil-β-CD (HP-β-CD) ou gama-ciclodextrina (γ-CD) nos diferentes tempos de agitação/complexação (12 ou 72 horas) inibem a desmineralização do esmalte hígido (estudo 1) e investigar se a inclusão do tetrafluoreto de titânio (TiF4) à beta ciclodextrina (β-CD) com 72 horas de agitação remineraliza o esmalte previamente desmineralizado (estudo 2). Para o estudo 1, noventa e seis blocos foram selecionados pela microdureza superficial e aleatoriamente alocados nos seguintes grupos (n=12 cada): G1: Água Mili-Q, G2: HP-β-CD 1%, G3: γ-CD 1%, G4: TiF4 1%, G5: HP-β-CD associada ao TiF4 1% com 12 horas de agitação, G6: γ-CD associada ao TiF4 1% com 12 horas de agitação, G7: HP-β-CD associada ao TiF4 1% com 72 horas de complexação e G8: γ-CD associada ao TiF4 1% com 72 horas de complexação. Para o estudo 2, quarenta e oito blocos (previamente desmineralizados) foram alocados em 4 grupos (n=12 cada) da seguinte maneira: controle (água Mili-Q), solução β-CD 1%, solução TiF4 1% e TiF4:β-CD. Todas as soluções foram aplicadas uma única vez na superfície do esmalte com o microbrush por um minuto e submetidos a ciclagem de pH (37º C) por 8 dias mais 24 horas na solução remineralizante. A variável resposta para o estudo 1 foi o percentual de perda de microdureza superficial (%PMS). Para o estudo 2, foram %PMS e microdureza transversal (MT).. Em ambos estudos, os blocos foram avaliados pela microscopia eletrônica de varredura e pela espectrometria de energia dispersiva de raios-X (EDX). Os achados foram avaliados pelo ANOVA e Tukey (p-valor < 0,05). Para o primeiro objetivo, G1 não diferiu estatisticamente de G2 e G3 (p>0.05). G5 produziu menor %PMS comparado a G1 (p<0,01), G2 (p<0,01), G3 (p<0,01), G7 (p=0,03) e G8 (p=0,01), sem diferença estatística para o G4 e G6. Eles não diferiram de nenhum dos grupos, mas foram inferiores a G5. Para o segundo objetivo, na superfície, todos os grupos foram capazes de promover a remineralização do esmalte sem diferença estatística entre eles (p>0,05). Na MT, nenhum grupo diferiu do controle, mas TiF4:β-CD foi estatisticamente superior (p=0,03) comparado ao TiF4. Os blocos tratados com TiF4 e TiF4:CD apresentaram camada de TiO2 e na avaliação do EDX o titânio foi detectado nos grupos de TiF4 e TiF4:CD apenas na superfície. Conclui-se que a solução de HP-β-CD: TiF4 com 12 horas de complexação demonstrou significativa habilidade em reduzir a desmineralização superficial do esmalte hígido e a solução de TiF4:β-CD com 72 horas de agitação foi superior a solução do TiF4 em remineralizar a subsuperfície do esmalte.
Palavras Chave: Cárie dentária, Esmalte dentário, Flúor, Remineralização dentária.
ABSTRACT
VIEIRA, Thiago Isidro. PREVENTIVE AND THERAPEUTIC EFFECT OF CARIES OF NANOCOMPLEXES FORMED OF CYCLODEXTRINS AND TIF4: IN VITRO STUDY. Rio de Janeiro, 2014 Dissertação (Mestrado em Odontologia – Área de concentração: Odontopediatria) – Faculdade de Odontologia, Universidade Federal do Rio de Janeiro, Rio de Janeiro, 2014.
The aims of the present in vitro study were to evaluate if the titanium tetrafluoride (TiF4) inclusions to hydroxypropyl-β-CD (HP-β-CD) and gamma-cyclodextrin (γ-CD) with different periods of stirring (12 or 72 hours) reduce demineralization of sound enamel (study 1) and to assess if the inclusion of titanium tetrafluoride (TiF4) to beta-cyclodextrin (β-CD) with 72 hours of stirring remineralize previously demineralized enamel blocks (study 2). For study 1, ninety six blocks were selected by surface microhardness and randomly allocated in the following groups (n=12 each) G1: Mili-Q water, G2: 1% HP-β-CD, G3: 1% γ-CD, G4: 1% TiF4, G5: HP-β-CD associated with 1% TiF4 at 12 hours of complexation, G6: γ-CD associated with 1% TiF4 at 12 hours of complexation, G7: HP-β-CD connected to 1% TiF4 at 72 hours of complexation and G8: γ-CD connected to 1% TiF4 at 72 hours of complexation. For study 2, forty eight enamel blocks (previously demineralized) were allocated in 4 groups (n=12 each) as follows: control (Mili-Q water), solution of 1% β-CD, solution of 1% TiF4 and solution TiF4:β-CD. All solutions were applied once over enamel surface with a microbrush for one minute and the submitted to pH-cycling regimen (37º C) for 8 days plus 24 hours on remineralizing solution. For study 1, the response variable was percentage of surface microhardness change (%SMC). For study 2, %SMC and cross-sectional microhardness (CSMH) were assessed. The enamel blocks were evaluated by scanning electron microscopy and energy dispersive spectrometry (EDX) for both studies. Findings were tested using ANOVA and Tukey (p-value < 0.05). For the first aim, G1 did not differ statistically from G2 and G3 (p>0.05). G5 produced less %SMC when compared to G1 (p<0.01), G2 (p<0.01), G3 (p<0.01), G7 (p=0.03) and G8 (p=0.01), although no statistical difference was observed compared to G4 and G6. G4 and G6 were not different from any of the groups, but were inferior to G5. For the second aim, all groups were able to promote rehardening of enamel surface without statistical difference between them (p> 0.05). In cross-sectional microhardness, no group differed from the control, but TiF4:β-CD was statistically superior (p = 0.03) compared to TiF4. The slabs treated with TiF4 and TiF4:CD groups showed TiO2 glaze-layer and the EDX evaluation identified titanium in TiF4 and TiF4:CD groups only on the surface.In conclusion, the solution containing the inclusion complex of HP-β-CD: TiF4 at 12 hours of complexation period demonstrated significant ability to reduce the surface demineralization of sound enamel and the solution containing TiF4 and β-cyclodextrin inclusion complex was superior than the TiF4 solution itself on rehardening enamel subsurface and.
Key words: Dental caries, Enamel, Fluoride, Tooth remineralization.
LISTA DE TABELAS
Artigo 1
Table 1 Mean values at baseline of pH, mV, total fluoride (ppm) and total soluble
fluoride (ppm) from the tested solutions. .................................................................. 48
Table 2 Mean values of surface microhardness from bovine enamel blocks before
and after pH-cycling and percentage of surface microhardness change of all groups.
................................................................................................................................. 49
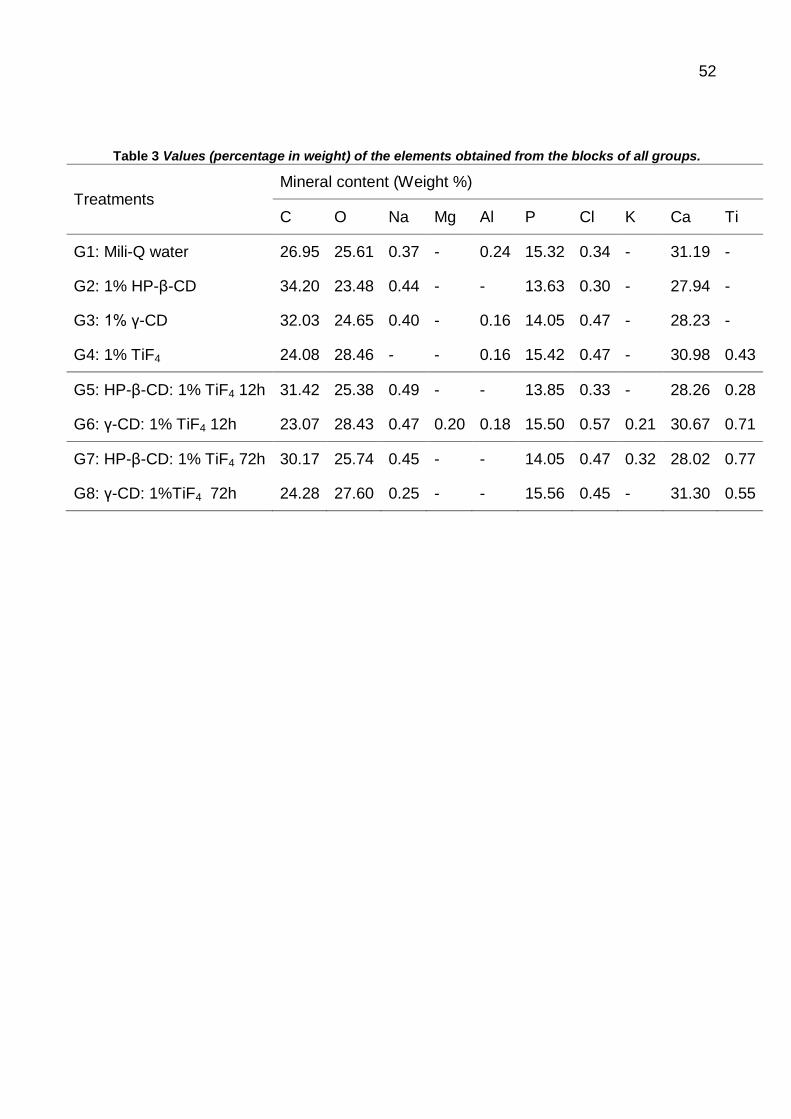
Table 3 Values (percentage in weight) of the elements obtained from the blocks of all
groups. ..................................................................................................................... 52
Artigo 2
LISTA DE TABELAS
Table 1. Values (mean and standard deviation) of surface microhardness (SMH)
analysis of enamel blocks before and after pH-cycling, percentage of enamel surface
change according to the treatments. ........................................................................ 69
Table 2: Values (mean) of cross-sectional microhardness (CMSH) analysis of enamel
blocks according to the treatments and depths and ΔZ. ........................................... 69
LISTA DE FIGURAS
Artigo 1
Figure 1 SEM surface images of enamel blocks after the pH-cycling regimen at
1000x on the left and EDX analysis on the right. A) G1: arrow indicates
demineralization areas. B) G2: arrow indicates demineralization areas. C) G3: arrow
indicates demineralization areas. D) G4: arrow indicates the TiO2 glaze-layer. On the
right, titanium was detected in the surface ............................................................... 50
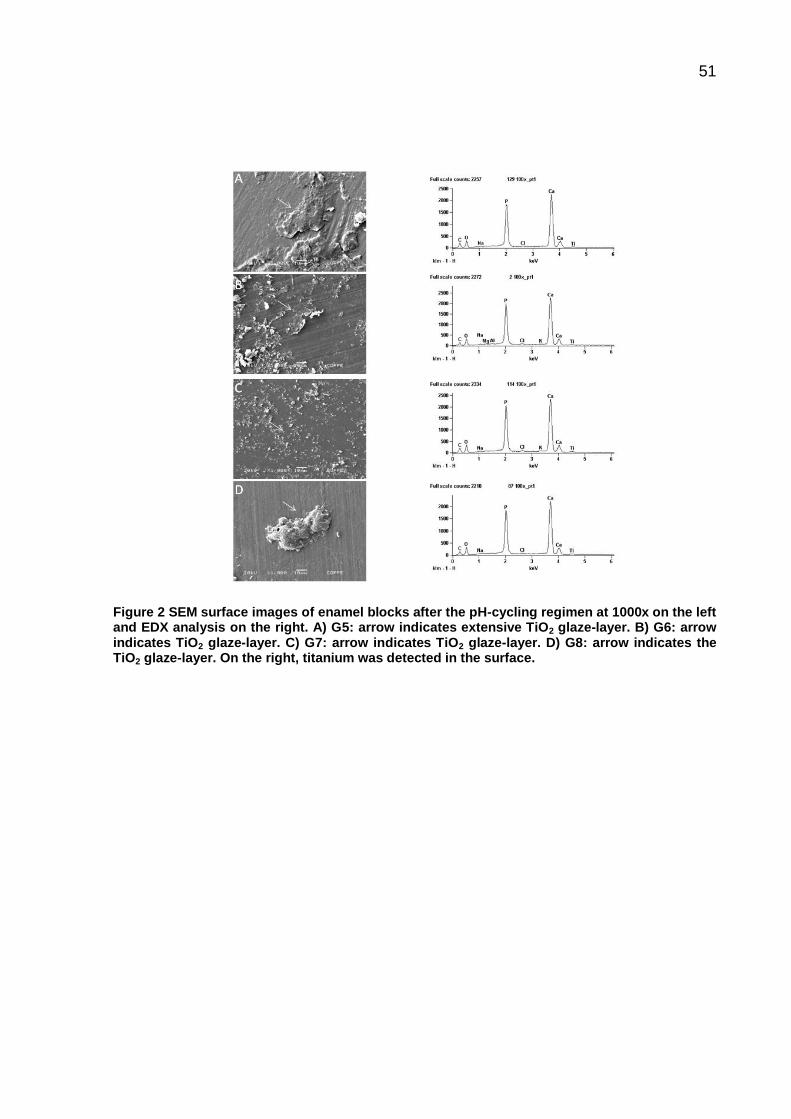
Figure 2 SEM surface images of enamel blocks after the pH-cycling regimen at
1000x on the left and EDX analysis on the right. A) G5: arrow indicates extensive
TiO2 glaze-layer. B) G6: arrow indicates TiO2 glaze-layer. C) G7: arrow indicates TiO2
glaze-layer. D) G8: arrow indicates the TiO2 glaze-layer. On the right, titanium was
detected in the surface. ............................................................................................ 51
Artigo 2
Figure 1: Values (mean) of cross-sectional microhardness versus depth for enamel
blocks previously demineralized. ΔZ values were obtained from the 50 µm depth. .. 70
Figure 2: SEM surface images of the enamel blocks after the pH-cycling regimen at
1000x on the left and EDX analysis on the right. First image: Group treated with Mili-
Q water. Second image: Group treated with 1% β-CD. Third image: Group treated
with 1% TiF4. Fourth image: Group treated with TiF4:β-CD. TiO2 glaze-layer was
observed in the third and fourth image. On the right, titanium was detected in the
surface of the block from TiF4 and TiF4:β-CD. .......................................................... 71
Figure 3: SEM subsurface images of the enamel blocks after the pH-cycling regimen
at 1000x on the left and EDX analysis on the right. First image: Group treated with
Mili-Q water. Second image: Group treated with 1% β-CD. Third image: Group
treated with 1% TiF4. Fourth image: Group treated with TiF4:β-CD. Titanium was not
detected in the subsurface of the block from TiF4 and TiF4:β-CD. ............................ 72
LISTA DE ABREVIATURAS
%GMS Porcentagem de ganho de microdureza superficial
%PMS Porcentagem de perda de microdureza superficial
CD Ciclodextrina
CDV Calorimetria diferencial de varredura
cm Centímetro
CPOD Índice de dentes cariados, perdidos e obturados
dimetil- β-CD Dimetil beta ciclodextrina
DPRX Difração de pó por raios-X
FAP Fluorapatita
g Grama
HAP Hidroxiapatita
HP-β-CD Hidroxipropril beta ciclodextrina
IVTR Espectroscopia de infravermelho transformada de Fourier
KBr Brometo de potássio
kV Quilovoltagem
L Litro
M Concentração molar
mA Miliampere

mg Miligrama
min Minuto
mL Mililitro
mM Milimolar
mmol Milimol
MSF Microdureza superficial final
MSI Microdureza superficial inicial
MT Microdureza transversal
NaF Fluoreto de sódio
ºC Grau Celsius
pH Potencial hidrogeniônico
ppm Partes por milhão
s Segundo
TiF4 Tetrafluoreto de titânio
TiO2 Dióxido de titânio
β-CD Beta ciclodextrina
γ-CD Gama ciclodextrina
μm Micrômetro

LISTA DE SÍMBOLOS
> maior que
< menor que
= igual
± mais ou menos
% porcentagem
Δ delta
Ɵ teta
α alfa
β beta
ϒ gama
SUMÁRIO
1 INTRODUÇÃO ...................................................................................................... 18
2 OBJETIVOS .......................................................................................................... 23
2.1 Objetivo Geral................................................................................................. 23
2.2 Objetivos Específicos ..................................................................................... 23
3 DELINEAMENTO DA PESQUISA ........................................................................ 24
3.1 Desenho do estudo......................................................................................... 24
3.2 Delineamento geral do estudo ........................................................................ 24
3.2.1 Prevenção da desmineralização do esmalte hígido.................................. 24
3.3 Preparo dos complexos de ciclodextrina......................................................... 25
3.4 Preparo e caracterização dos complexos de união ......................................... 26
3.7 Microdureza superficial inicial para pré-seleção dos blocos que compuseram a
amostra ................................................................................................................ 28
3.8 Tratamento e ciclagem de pH ......................................................................... 28
3.9 Análise final da microdureza superficial e transversal ..................................... 29
3.10 Análise estatística ......................................................................................... 30
4 DESENVOLVIMENTO DA PESQUISA ................................................................ 32
Artigo 1 EFFECT OF NEW CYCLODEXTRINS AND TIF4 NANOCOMPLEXES ON
ENAMEL DEMINERALIZATION ........................................................................... 33
Artigo 2 Effect Of Tif4 And Β -Cyclodextrin Inclusion Complex On Demineralized
Enamel Rehardening ............................................................................................ 53
5. DISCUSSÃO ........................................................................................................ 73
6. CONCLUSÕES .................................................................................................... 78
REFERÊNCIAS BIBLIOGRÁFICAS ......................................................................... 79
18
1 INTRODUÇÃO
No ano de 2010, realizou-se um inquérito epidemiológico nacional no qual se
investigou, dentre outros agravos, a experiência de cárie dentária em pré-escolares,
escolares, adolescentes, adultos e idosos. Nesse levantamento, pode-se constatar
um índice ceod de 2,43 para crianças aos 5 anos de idade e um índice CPOD de
2,07, 4,25, 16,75 e 27,53, respectivamente, para a idade de 12 anos e as faixas
etárias de 15 a 19, 35 a 44 e 65 a 74 (BRASIL, 2011). Com base nesse estudo, pode
se observar uma diminuição expressiva da doença cárie na idade de 12 anos no
país. Tal efeito foi alcançado, devido dentre outros fatores, ao uso preventivo de
compostos fluoretados (NARVAI et al., 2006).
Um dos principais propósitos da fluorterapia consiste em transformar a
hidroxiapatita (HAP) em fluorapatita (FAP), em outras palavras, gerando uma
camada com menos solubilidade na superfície do esmalte (FRAGA et al., 2010).
Quando o dente é exposto a uma solução que contenha flúor em concentração de
até 100 ppm, há a conversão de HAP em FAP. Todavia, quando ocorre uma
exposição com solução fluoretadas com concentrações de flúor superiores a 100
ppm, observa-se a dissolução do esmalte e formação de fluoreto de cálcio, que
consiste em reservatórios constantes de disponibilidade de flúor para a formação da
FAP, mesmo após o uso do da solução fluoretada (LEACH, 1959).
Tão logo o fluoreto de cálcio seja formado, ocorre a deposição de íons cálcio
e fósforo da saliva sobre o próprio fluoreto de cálcio, gerando dessa maneira uma
camada protetora, diminuindo a sua degradação no ambiente oral (SAXEGAARA;
LAGERLÖF; ROLLA, 1988). À medida que os desafios cariogênicos acontecem na
cavidade bucal, essa camada é solubilizada e assim, dessa maneira, também
ocorrerá solubilização do fluoreto de cálcio liberando íons flúor que atuarão nos
processos de desmineralização e remineralização do esmalte dentário.
19
Convém lembrar que após aplicação de altas concentrações de flúor, uma
porção desse íon penetra no interior do esmalte seja pelos poros intercristalinos
(TARBET; FOSDICK, 1971) ou no cristal de apatita (GRON, 1977) enquanto que
outra porção desse íon permanece livremente mantida apenas por forças
eletrostáticas (MELLBERG; RIPA, 1983).
Existem alguns métodos de uso de fluoretos consagrados na literatura tais
como: água fluoretada em programas voltados para a comunidade, uso individual de
dentifrícios e bochechos e uso profissional de vernizes, solução, mousses e géis.
A água de abastecimento público fluoretada é indubitavelmente um meio de
sucesso para liberação de flúor a níveis populacionais. Dentre os métodos
individuais, os dentifrícios fluoretados são os mais importantes, pois conciliam a
remoção mecânica do biofilme dentário acrescido do flúor. É comprovado na
literatura que soluções para bochecho fluoretadas apresentam efeito inibitório sobre
a cárie dentária, tanto no uso semanal a uma concentração de 0,2% de NaF (900
ppm de flúor) quanto no uso diário de 0,05% de NaF ( 225 ppm de flúor) (MARINHO
et al., 2004). Já para o uso profissional, destacam-se os géis, mousses, soluções e
vernizes com altas concentrações de flúor (de 9000 a 12300 ppm de flúor para os
géis e mousses e 22500 ppm para os vernizes) (TENUTA; CURY, 2010).
O fluoreto de sódio foi um dos primeiros agentes fluoretados a ser adotado
nas aplicações tópicas profissionais de flúor para o controle da cárie dentária. Duas
concentrações foram propostas para a solução de fluoreto de sódio: 1% e 2% e para
o fluoreto estanhoso, as concentrações propostas foram a 8% e a 10% (HOROWITZ;
HEIFETZ, 1969)
Após a aplicação profissional do tetrafluoreto de titânio (TiF4) observa-se a
formação de uma camada ácido-resistente de TiO2, há um aumento na incorporação
de fluoreto e incorporação do titânio no cristal de hidroxiapatita (GU et al., 1996). A
essa cobertura de TiO2 é atribuída seu efeito anticariogênico pois atua impedindo a
perda de minerais do dente (EXTERKATE; TEN CATE, 2007).
20
Associada à expansão da fluoretação das águas de abastecimento público e
a mudança de enfoque nos programas de Odontologia em saúde pública em todas
as regiões do país, a fluorterapia é conhecida como um dos principais fatores na
redução da ocorrência de cárie (NARVAI et al., 2006). Dentre os principais produtos
fluoretados de uso profissional, o tetrafluoreto de titânio (TiF4) tem sido bastante
empregado em estudos laboratoriais e in situ como um recurso minimamente
invasivo no controle da doença. Apesar de promissor, o TiF4 apresenta certa
limitação que é a sua instabilidade química. Para tornar esse composto mais estável
pode se utilizar os complexos de inclusão (NASSUR et al., 2013)
Sendo assim, uma das áreas de grande interesse da biotecnologia é o
processo que envolve a complexação molecular, pois possibilita a seleção,
separação, solubilização e estabilização de várias biomoléculas (SINGH; SHARMA;
BANERJEE, 2002). As ciclodextrinas (CDs) são agentes que desempenham muito
bem essas funções devido, entre outros fatores, a sua conformação em cadeia,
contribuindo para a dissolução em meio aquoso de compostos de baixa solubilidade
(BRITTO; NASCIMENTO JÚNIOR; SANTOS, 2004) e conferindo estabilidade ao
TiF4.
As CDs são oligossacarídeos cíclicos constituídos de moléculas de D-glicose
unidas por intermédio de ligações glicosídicas do tipo α(1 – 4) e são obtidas a partir
da degradação do amido pela atuação da enzima glicosiltransferase. As principais
CDs são as seguintes: α, β e γ-ciclodextrinas (VALLE, 2004).
Elas são organizadas estruturalmente na forma tronco-cônica com as
extremidades apresentando sítios hidrofílicos devido à presença de grupos hidroxilas
e o interior da cavidade em questão apresenta átomos de hidrogênio e pontes de
oxigênio glicosídicas, atribuindo a elas também um caráter altamente hidrofóbico
(BUDAL, 2003; CALDERINI, 2006). Por serem bons solubilizantes, as CDs estão
sendo alvo de diversas pesquisas e em distintas áreas (VENTURINI et al., 2008)
com a finalidade de se alcançar melhoria terapêutica e estabilidade química de
certos compostos.

21
Várias pesquisas têm sido elaboradas para avaliar o impacto de formulações
que apresentem a ciclodextrina no complexo de inclusão. Isso se deve, dentre
outros aspectos, à capacidade da mesma em criar complexos de inclusão com um
grande número de moléculas. Vale salientar, entretanto, que nem todas as
moléculas (fármacos) podem formar complexos estáveis. Substâncias altamente
solúveis, geralmente, não conseguem ser incluídas (CAL; CENTKOWSKA, 2008).
Resultados favoráveis à complexação foram encontrados quando se analisou
o ácido benzóico com a β-CD (AREE; CHAICHIT, 2003); o coumestrol encapsulado
pela β-CD e hidroxipropil-β-CD obteve a sua solubilidade aumentada em 80%
(CANNAVÀ et al., 2008); a dimetil-β-CD foi capaz de melhorar a solubilidade da
isoquercitrina (WANG et al., 2009); o trimetoprim (agente antibacteriano) quando em
presença da β-CD aleatoriamente metilada demonstrou um aumento significativo da
solubilidade (KUBOTA, 2010); a estabilidade do ácido clorogênico foi aprimorada
quando complexado com a β-CD (ZHAO et al., 2010).
Outros resultados positivos também foram obtidos com a utilização de
ciclodextrinas. As taxas de dissolução do naproxeno e flurbiprofeno
(antiinflamatórios) no complexo de inclusão com a γ-CD foram as mesmas, sendo
assim, úteis para terapias de recombinação (HIGASHI et al., 2010). Em oftalmologia,
foi possível controlar a taxa de liberação da dexametasona quando associada a γ-
CD ou hidroxipropil- γ-CD, sendo promissora na liberação do fármaco para a
esclerótica (JANSOOK et al., 2010). Aumento da taxa de dissolução do edaravone
(medicamento removedor de radicais livres) e diminuição da sua degradação
quando associado a hidroxipropil-β-CD (ZENG et al., 2011).
22
Já se conhece a inibição da desmineralização de blocos de esmalte bovino
quando tratados com solução contendo o complexo de inclusão β-CD com o TiF4
(NASSUR et al., 2013). Porém, o potencial de inibição da desmineralização das
outras ciclodextrinas (hidroxipropilβ- e γ-) e efeito remineralizador do complexo de
inclusão β-CD com o TiF4 sobre o esmalte bovino previamente desmineralizado
associadas a essa molécula ainda não foram investigadas. Sendo então, alvo no
momento da presente pesquisa.
Considerando o exposto, a presente pesquisa tem por objetivo avaliar o efeito
preventivo e terapêutico de cárie de novas inclusões de CD à solução de TiF4 com
vistas a contribuir com o estudo das ciclodextrinas (hidroxipropilβ-, β- e γ-)
associadas ao TiF4.
23
2 OBJETIVOS
2.1 Objetivo Geral
Avaliar in vitro o efeito preventivo e remineralizador para lesões de cárie de
novas inclusões de ciclodextrinas à solução de TiF4.
2.2 Objetivos Específicos
Investigar se a inclusões hidroxipropilβ-CD/TiF4 e γ-CD/TiF4 inibem a
desmineralização do esmalte hígido, submetido a alto desafio cariogênico;
Analisar se β-CD/TiF4 com 72 horas de complexação remineraliza o esmalte
desmineralizado.

24
3 DELINEAMENTO DA PESQUISA
3.1 Desenho do estudo
O presente trabalho foi composto por dois estudos. O primeiro objetivou
analisar se a inclusão de hidroxipropilβ-CD e γ-CD à solução de TiF4 inibe a
desmineralização do esmalte hígido submetido a condições in vitro que simulem alto
desafio cariogênico e o segundo objetivou avaliar se a inclusão da β-CD à solução
de TiF4 remineraliza o esmalte desmineralizado.
O estudo foi realizado no Laboratório Multidisciplinar de Odontologia do
Departamento de Odontopediatria e Ortodontia da Faculdade de Odontologia da
Universidade Federal do Rio de Janeiro (FO/UFRJ), em parceria com o Laboratório
de Tecnologia Industrial Farmacêutica - Faculdade de Farmácia da Universidade
Federal do Rio de Janeiro.
3.2 Delineamento geral do estudo
3.2.1 Prevenção da desmineralização do esmalte hígido
Esse trabalho (artigo 1) contou com 8 grupos contendo 12 blocos de esmalte
bovino hígidos cada. Os blocos foram aleatoriamente escolhidos para avaliação das
seguintes condições experimentais: 1) água destilada e deionizada (controle
negativo), 2) solução de 1% de hidroxipropilβ-CD, 3) solução de 1% de γ-CD, 4)
solução contendo 1% de TiF4 (controle positivo), 5) solução com associação de
hidroxipropilβ-CD/TiF4 com 12 horas de agitação, 6) solução com associação de γ-
CD/TiF4 com 12 horas de agitação, 7) solução com associação de hidroxipropilβ-
CD/TiF4 com 72 horas de agitação e 8) solução com associação de γ-CD/TiF4 com
72 horas de agitação.
Os desfechos estudados foram: a concentração de flúor total, concentração
de flúor solúvel total, pH das soluções testadas, percentual de perda da microdureza
superficial do esmalte, modificações da camada externa do esmalte pela
microscopia eletrônica de varredura e análise do conteúdo mineral.

25
3.2.2 Remineralização do esmalte desmineralizado
Esse trabalho (artigo 2) consistiu em um experimento in vitro e contou com 4
grupos contendo cada um 12 blocos de esmalte bovino previamente
desmineralizados. Os blocos foram aleatoriamente escolhidos para avaliação das
seguintes condições experimentais: 1) água destilada e deionizada (controle
negativo), 2) solução de 1% de β-CD, 3) solução contendo 1% de TiF4 (controle
positivo) e 4) solução com associação de β-CD à solução de TiF4 com 72 horas de
agitação.
Os desfechos estudados foram: o percentual de ganho da microdureza
superficial do esmalte, a microdureza transversal do esmalte, modificações da
superfície e subsuperfície do esmalte pela microscopia eletrônica de varredura e
análise do conteúdo mineral.
3.3 Preparo dos complexos de ciclodextrina
Para o artigo 1, seguindo o método de solução, as proporções adequadas de
TiF4 (0,1974g) e HP-β-CD (2,0112g) ou γ-CD (2,0064g) foram misturados em 20 ml
de água destilada com um agitador magnético durante 12 horas e 72 horas. As
amostras permaneceram congeladas em nitrogênio líquido e liofilizadas. O tamanho
de partícula foi também calibrado com uma peneira de malha 40. Calculou-se o
rendimento de inclusão por espectroscopia ultravioleta.
26
Para o artigo 2, adotou-se os métodos de empastamento e de solução. O
método de empastamento consiste em misturar em um gral de porcelana com o
auxílio de um pistilo, as proporções molares de 1:1, 1:2, 1:3 e 1:4 de β-CD e TiF4.
Foi adicionada a essa mistura uma solução de etanol/água 70/30 v/v até a formação
de uma pasta e homogeneizou-se por 30 minutos. A pasta foi então seca e ajustou-
se a granulometria em malha 40. O método de solução no qual proporções
adequadas de TiF4 e β-CD foram misturados em 20 ml de água destilada em um
agitador magnético por 72 horas (NASSUR et al., 2013).
3.4 Preparo e caracterização dos complexos de união
Caracterizou-se esses nanossistemas por difração de pó por raios-X (DPRX),
espectroscopia de infravermelho transformada de Fourier (IVTF) e calorimetria
diferencial de varredura (CDV). Padrões de difração de raios-X de nanosistemas,
misturas físicas e substâncias puras foram gravadas com um difratômetro Rigaku
Miniflex BD11197 (Rigaku, Shibuya-ku, Tóquio, Japão), utilizando CuK radiação,
com uma corrente de 30 mA, voltagem de 40 kV e uma 2Ɵ ângulo entre 2° e 20°.
Coletou-se espectros de IVTF por um IR Prestige-21 Shimadzu A210045 (Shimadzu,
Nakagyo-ku, Kyoto, Japão), utilizando 2% de espectrômetro pastilhas de KBr e um
comprimento de onda número compreendido entre 4000 e 400 cm-1. As análises de
CDV foram realizadas com uma máquina CDV 882E Mettler-Toledo usando panelas
de alumínio hermeticamente seladas sob um fluxo de nitrogênio de 28 mL min-1 e
uma taxa de aquecimento de 10°C min-1 (NASSUR et al., 2013).
27
3.5 Determinação do flúor e pH
As análises foram realizadas em duplicata. Nesse estudo, curvas de
calibração foram efetuadas com soluções de padrões de flúor de 0,062 a 8 ppm de
flúor. Um eletrodo específico de flúor e potenciômetro foram utilizados (CONDE;
REBELO; CURY, 2003). A determinação do pH foi efetuada em um eletrodo
específico previamente calibrado em pH 4,00 e 7,00.
3.6 Preparo dos blocos de esmalte bovino
Os blocos de esmalte (4 mm x 4 mm) foram preparados a partir de incisivos
bovinos, esterilizados e armazenados em solução de formaldeído a 2% (pH 7,0). Os
blocos foram embutidos em dispositivos de acrílico (tarugos), lixados e polidos. A
dentina foi lixada com lixa de granulação 600, na velocidade 1 em uma lixadeira
politriz modelo PLF (Fortel®) durante 30 segundos e a superfície do esmalte do
mesmo modo foi lixada com lixa de granulação 600, na velocidade 1 da lixadeira
politriz modelo PLF(Fortel®) por 30 segundos com a finalidade de se obter uma
‘janela’ de esmalte exposto planificado.
Logo em seguida, os blocos foram sonicados em água milli-Q por 8 minutos
para remover possíveis fragmentos de esmalte. Uma vez atingida essa etapa, os
mesmos foram lixados na lixa de granulação 1200 durante 30 segundos na
velocidade 1 de uma lixadeira politriz modelo PLF (Fortel®) com o objetivo de conferir
polimento aos blocos.
28
3.7 Microdureza superficial inicial para pré-seleção dos blocos que
compuseram a amostra
A microdureza foi aferida pelo microdurômetro (Buehler, MICROMET 5104,
679-MIT4-00335, Japan) com um endentador Knoop com carga de 50g por 5s.
Efetuou-se cinco endentações com espaços de 100µm entre cada registro no centro
da superfície do esmalte.
Inicialmente, realizou-se a microdureza de todos os blocos de esmalte com a
finalidade de pré-seleção para compor a amostra. Após a obtenção de todos os
valores correspondentes de cada bloco, calculou-se a média±10%, ou seja, foram
selecionados para o estudo aqueles blocos que apresentaram uma microdureza
compreendida entre 10% a mais ou a menos em torno da média, de modo a se
alcançar uma homogeneidade dos blocos.
3.8 Tratamento e ciclagem de pH
As soluções foram previamente codificadas de maneira a não permitir ao
pesquisador sua identificação sendo aplicada uma única vez na superfície dos
blocos por intermédio de um microbrush durante 1 minuto. Logo em seguida, os
mesmos foram lavados com água destilada e deionizada e secos com papel
absorvente. Uma vez cumprida essa etapa, foi iniciada a ciclagem de pH.
Para o artigo 1, o regime aconteceu da seguinte maneira: durante 8 dias, os
blocos permaneceram a uma temperatura de 37°C por 4 horas na solução
desmineralizante e 20 horas em solução remineralizante. Para o artigo 2, o regime
ocorreu da seguinte maneira: durante 8 dias, os blocos permaneceram a uma
temperatura de 37°C por 2 horas na solução desmineralizante e 22 horas em
solução remineralizante. (QUEIROZ et al., 2008).
29
A solução desmineralizante utilizada continha 0,05 M de tampão de acetato
em pH 5,0, 1,28 mM de cálcio, 0,74 mM de fósforo, 0,03 mg de flúor/mL. A solução
remineralizante apresentou 1,5 mmol/L de cálcio, 0,9 mmol/L de fósforo, 150 mmol/L
de cloreto de potássio, 0,05 mg de flúor/mL em 0,1 mol/L de solução tampão Tris
com um pH 7,0. No quarto dia do regime de ciclagem de pH, as soluções
supracitadas foram trocadas por soluções frescas de mesmo caráter. Após o oitavo
dia do ciclo, os blocos permaneceram na solução remineralizante por 24 horas
adicionais antes de se iniciar as análises (QUEIROZ et al., 2008).
3.9 Análise final da microdureza superficial e transversal
Para análise da microdureza superficial (artigos 1 e 2), depois dos
tratamentos e da ciclagem de pH, a referida microdureza foi novamente mensurada
realizando 5 endentações espaçadas 100µm daquelas realizadas no baseline
(TENUTA et al., 2003). A porcentagem da perda de microdureza superficial de
esmalte foi obtida mediante o uso da equação a seguir:
%PMS = MSI – MSF/MSI x 100
A sigla %PMS na equação acima significa percentual de perda de
microdureza superficial, MSI representa a microdureza superficial inicial dos blocos
de esmalte antes do início da ciclagem de pH e MSF significa microdureza
superficial final que representa o valor de dureza obtido após a ciclagem de pH.
Para avaliação da porcentagem de ganho da microdureza superficial, adotou-
se a seguinte equação:
%GMS= MS após desmineralizado – MS após ciclagem / MS após
desmineralizado x 100
30
A sigla %GMS na equação acima significa percentual de ganho de
microdureza superficial, MS após desmineralizado representa a microdureza
superficial inicial dos blocos de esmalte após serem submetidos a solução
desmineralizante e antes do início da ciclagem de pH e MS após ciclagem significa
microdureza superficial final que representa o valor de dureza obtido após a
ciclagem de pH.
Para avaliação da microdureza transversal (artigo 2), os blocos foram
seccionados longitudinalmente na porção central do corpo-de-prova e para tal,
utilizou-se uma cortadeira (ISOMET Low Speed machine, Buehler Ltd., Lake Bluff,
IL, USA) acoplada a um disco diamantado (Buehler Ltd., Lake Bluff, IL, USA). Uma
das metades de cada bloco foi acoplada ao tarugo de acrílico e lixadas nas lixas de
granulações de 600 e 1200 e a avaliação foi efetuada através do microdurômetro
(Buehler) com um endentador Knoop com carga de 25g por 10 segundos. A outra
metade foi avaliada descritivamente pela microscopia eletrônica de varredura e o
conteúdo mineral foi analisado pela espectroscopia de dispersão de raios-x.
Duas seqüências de endentações (distantes 100µm entre si) foram realizadas
em 10µm, 20µm, 30µm, 40µm, 50µm, 60µm, 70µm, 80µm, 90µm, 100µm, 120µm,
140µm, 160µm, 180µm e 200µm de profundidade (NASSUR et al., 2013). Os
tratamentos foram comparados para cada profundidade e pela área de perda
mineral.
3.10 Análise estatística
Os dados quantitativos de microdureza superficial e transversal foram
avaliados quanto à normalidade por meio do teste de Shapiro-Wilk. Para a
microdureza superficial e transversal, utilizou-se os teste de ANOVA e Tukey (p-valor
< 0,05).

31
Para o cálculo da perda de microdureza superficial, empregou-se o ANOVA 1-
way seguido do teste de Tukey post hoc; para o cálculo da microdureza transversal,
calculou-se a área da curva ΔZ e ANOVA 1-way seguido do teste de Tukey post hoc
(p-valor <0,05).
32
4 DESENVOLVIMENTO DA PESQUISA
Artigo 1: EFFECT OF NEW CYCLODEXTRINS AND TIF4
NANOCOMPLEXES ON ENAMEL DEMINERALIZATION
Artigo 2: EFFECT OF TIF4 AND β-CYCLODEXTRIN INCLUSION COMPLEX
ON DEMINERALIZED ENAMEL REHARDENING
33
Artigo 1 EFFECT OF NEW CYCLODEXTRINS AND TIF4
NANOCOMPLEXES ON ENAMEL DEMINERALIZATION
Thiago Isidro VIEIRA 1
Adílis Kalina ALEXANDRIA 2
Lilian Henriques AMARAL 3
Lúcio Mendes CABRAL 4
Ana Maria Gondim VALENÇA 5
Lucianne Cople MAIA 6
1 DDS, Master student, Department of Pediatric Dentistry and Orthodontics, School of
Dentistry, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil
2 DDS, Doctor student, Department of Pediatric Dentistry and Orthodontics, School of
Dentistry, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil
3 DDS, Doctor student, School of Pharmacy, Universidade Federal do Rio de Janeiro, Rio
de Janeiro, RJ, Brazil
4 DDS, MSD, PhD, Full Professor, School of Pharmacy, Universidade Federal do Rio de
Janeiro, Rio de Janeiro, RJ, Brazil
5 DDS, MSD, PhD, Adjunct Professor, Department of Clinic and Social Dentistry, School of
Dentistry, Universidade Federal da Paraíba, Paraíba, Brazil.
6 DDS, MSD, PhD, Full Professor, Department of Pediatric Dentistry and Orthodontics,
School of Dentistry, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil

34
Correspondence Author - Lucianne Cople Maia
Caixa Postal: 68066 – Cidade Universitária - CCS
CEP: 21941-971 - Rio de Janeiro – RJ– Brazil
E-mail: [email protected]
Fax/phone: +5521 39382098
35
ABSTRACT
The aim of this study was to assess the effect of new nanocomplexes formed of hydroxypropyl-β-cyclodextrin (HP-β-CD) or γ-cyclodextrin (γ-CD) and 1% titanium tetrafluoride (TiF4) with distinct complexation periods (12 or 72 hours) on demineralization of bovine enamel in vitro. Bovine sound enamel blocks (n = 96) were selected by surface microhardness and allocated to each group (n = 12): G1: Mili-Q water, G2: 1% HP-β-CD, G3: 1% γ-CD, G4: 1% TiF4, G5: HP-β-CD associated with 1% TiF4 after 12 hours of complexation, G6: γ-CD associated with 1% TiF4 after 12 hours of complexation, G7: HP-β-CD associated with 1% TiF4 after 72 hours of complexation and G8: γ-CD associated with 1% TiF4 after 72 hours of complexation. The solutions were applied once with a microbrush for 1 minute. The groups were submitted to a pH-cycling regimen (37º C) for 8 days. The outcome variable was the percentage of surface microhardness change (%SMC). Scanning electron micrographs and energy dispersive spectrometry (EDX) was also obtained. Findings were tested using ANOVA and Tukey tests (p-value < 0.05) regarding %SMC. G1 did not differ statistically from G2 and G3 (p>0.05). G5 produced less %SMC when compared to G1 (p=0.00), G2 (p=0.00), G3 (p=0.00), G7 (p=0.03) and G8 (p=0.01), although no statistical difference was observed compared to G4 and G6. G4 and G6 were not different from any of the groups (p> 0.05), but were inferior to G5 (p> 0.05). The enamel treated with TiF4 and TiF4:CD groups showed TiO2 glaze-layer and the EDX evaluation identified titanium in TiF4 and TiF4:CD groups. The solution containing the inclusion complex of HP-β-CD: TiF4 with 12 hours of complexation period demonstrated a significant ability to reduce surface demineralization of sound enamel under an artificial cariogenic challenge.
Keywords: Dental caries, Titanium tetrafluoride, Cyclodextrins, Tooth
demineralization, Enamel.
36
INTRODUCTION
Dental caries is still a worldwide public health problem, regardless of being
preventable and reversible at early stages by topical application of fluoride and
change in dietary habits and oral hygiene [1]. It has already been shown that the
complete substitution of hydroxyapatite by fluorapatite does not result on prevention
of enamel demineralization [2]. An effective inhibition of enamel dissolution is rather
achieved by the fluoride available on the oral environment than intrinsic fluoride
content of dental enamel [3,4]. For this reason, frequent application of topical fluoride
should be emphasized in order to provide a constant source of fluoride on the oral
environment that will influence on de- and remineralization kinetics of dental hard
tissues [5].
Titanium tetrafluoride (TiF4) is one of the agents adopted in the control of
dental caries. Studies indicate that a single application of this product is enough to
decrease enamel dissolution [6-11]. However, its instability and acidic pH limited its
potential clinical use. To overcome the problems caused by acidic pH of TiF4 and to
improve the stability of this agent, research has focused on developing new fluoride
delivery systems such as cyclodextrin complexes [6], however there are no studies
involving hydroxypropyl-β-cyclodextrin or γ-cyclodextrin associated with TiF4 on
reducing enamel demineralization.
Thus, the aim of this study was to assess the effect of new nanocomplexes
formed of hydroxypropyl-β-cyclodextrin (HP-β-CD) or gamma-cyclodextrin (γ-CD)
and 1% titanium tetrafluoride with distinct complexation periods (12 or 72 hours) on
demineralization of bovine enamel in vitro.

37
MATERIALS AND METHODS
Preparation and characterization of nanocomplexes formed of cyclodextrins
and TiF4
According to the solution method, appropriate portions of TiF4 (0.1974 g) and
HP-β-CD (2.0112 g) or γ-CD (2.0064 g) were mixed in 20 mL of distilled water using
a magnetic stirrer for 12 or 72 hours. The specimens were frozen in liquid nitrogen
and lyophilized. The particle size was also calibrated with a 40 mesh sieve. The
inclusion yield was calculated by UV spectroscopy. These nanosystems were
characterized by X-ray powder diffraction (XRPD), Fourier transform infrared
spectroscopy (FTIR) and differential scanning calorimetry (DSC) [6].
Fluoride and pH determination
The analyses were performed in duplicate. In this study, calibration curves
were obtained using a standard fluoride solution containing 0.062 to 8 ppm F. A
specific F electrode and an ion analyzer were used. Total fluoride and total soluble
fluoride were determined. The first represents total soluble plus insoluble fluoride and
the second indicates free ionic fluoride [12]. The pH was measured in a specific pH
electrode previously calibrated to pH 4.00 and 7.00.
Preparation of bovine enamel blocks
The enamel blocks (4 mm x 4 mm) were prepared from bovine incisors,
sterilized by storage in a 2% formaldehyde (pH 7.0) solution. The blocks were
embedded in acrylic devices, ground flat and polished. The grinding process was
carried out as follows: enamel and dentin were ground flat with 600 grit Al2O3 paper
in a semi-automatic polisher (model PLF, Fortel®) for 30 seconds in order to obtain a
'window' of flattened exposed enamel.
Shortly thereafter, the blocks were sonicated in Mili-Q water for 8 minutes to
remove any loose fragments of enamel. Once reached this stage, they were ground
38
flat with 1200 grit Al2O3 paper for 30 seconds in a semi-automatic polisher (model
PLF, Fortel®).
Ninety-six blocks were selected by surface microhardness (341±10%KHN)
and randomly allocated to each group/treatment each containing 12 speciments: G1:
Mili-Q water, G2: 1% HP-β-CD, G3: 1% γ-CD, G4: 1% TiF4, G5: HP-β-CD
associated with 1% TiF4 after 12 hours of complexation, G6: γ-CD associated with
1% TiF4 after 12 hours of complexation, G7: HP-β-CD associated with 1% TiF4 after
72 hours of complexation and G8: γ-CD associated with 1% TiF4 after 72 hours of
complexation.
Treatmznt and pH-cycling regimen
The solutions were applied once on the surface of the blocks with the aid of a
microbrush for 1 minute. The operator was blinded regarding each of the used
solutions. Shortly thereafter, the blocks were washed with distilled and deionized
water and dried with soft absorbent paper. After that, the pH-cycling was initiated.
The regimen took place as follows: during 8 days, the blocks remained at 37
°C for 4 hours in the demineralizing solution and 20 hours in remineralizing solution
[13]. The demineralizing solution consisted of 0.05 M acetate buffer with pH 5.0, 1.28
mM calcium, 0.74 mM phosphorus, 0.03 mg / mL fluorine. The remineralizing solution
consisted of 1.5 mmol / L calcium, 0.9 mmol / L of phosphorus, 150 mmol / L
potassium chloride, 0.05 mg of fluorine / ml in 0.1 mol / L Tris buffer at pH 7.0. On the
fourth day of pH cycling, the solutions mentioned above were replaced with similar
fresh solutions. After the eighth day of the cycle, the blocks remained in
remineralizing solution for an additional 24 hours before starting the analysis [13].
Surface microhardness determination
The microhardness was measured by microhardness tester (Buehler,
MICROMET 5104, 679-MIT4-00335, Japan) with a Knoop indenter with a load of 50g
for 5s. Five indentations, each spaced by 100 μm were performed in each block.
Initially, it was determined the surface microhardness of all enamel blocks with the

39
purpose of pre-selection for the sample. After obtaining all the corresponding values
of each block, it was calculated the mean ± 10%, in others words, it was selected to
work those blocks that present a hardness between 10% more or less around the
mean, so to achieve homogeneity of the blocks.
Surface microhardness analysiss after treatment and pH cycling was
performed by making 5 indentations spaced by 100μm, far from those already carried
out at baseline. The percentage of enamel microhardness loss was obtained by
using the following equation: %SMC= (SM before – SM after) x 100 / SM before.
Scanning electron microscopy (SEM) and energy dispersive X-ray
spectrometry (EDX) assessment
Enamel blocks were mounted on aluminium stubs and evaluated using an
environmental scanning electron microscope (JEOL-JSM; 6460LV, Tokyo, Japan).
The topography of the enamel surfaces was analyzed in secondary electrons at 20
kV voltage, low vacuum mode (45 Pa) to obtain images with a 1000x magnification.
Assessment of mineral content was carried out using EDX with link and
automatic image analyzer system Kontron to identify chemical elements and its
percentage in weight.
Data analysis
The outcome variable was percentage of surface microhardness change
(%SMC). The micrographs observed by SEM and EDX analysis were evaluated
descriptively. Data were assessed for normality using the Shapiro-Wilk test. The
surface microhardness was used evaluated by the ANOVA and Tukey's test. To
calculate the loss of microhardness, it was used the one-way followed by Tukey post
hoc test ANOVA. The level of significance was set at 0.05%.

40
RESULTS
The mean baseline values of pH, total fluoride (ppm) and total soluble fluoride
(ppm) from all the experimental and control groups are presented in Table 1.
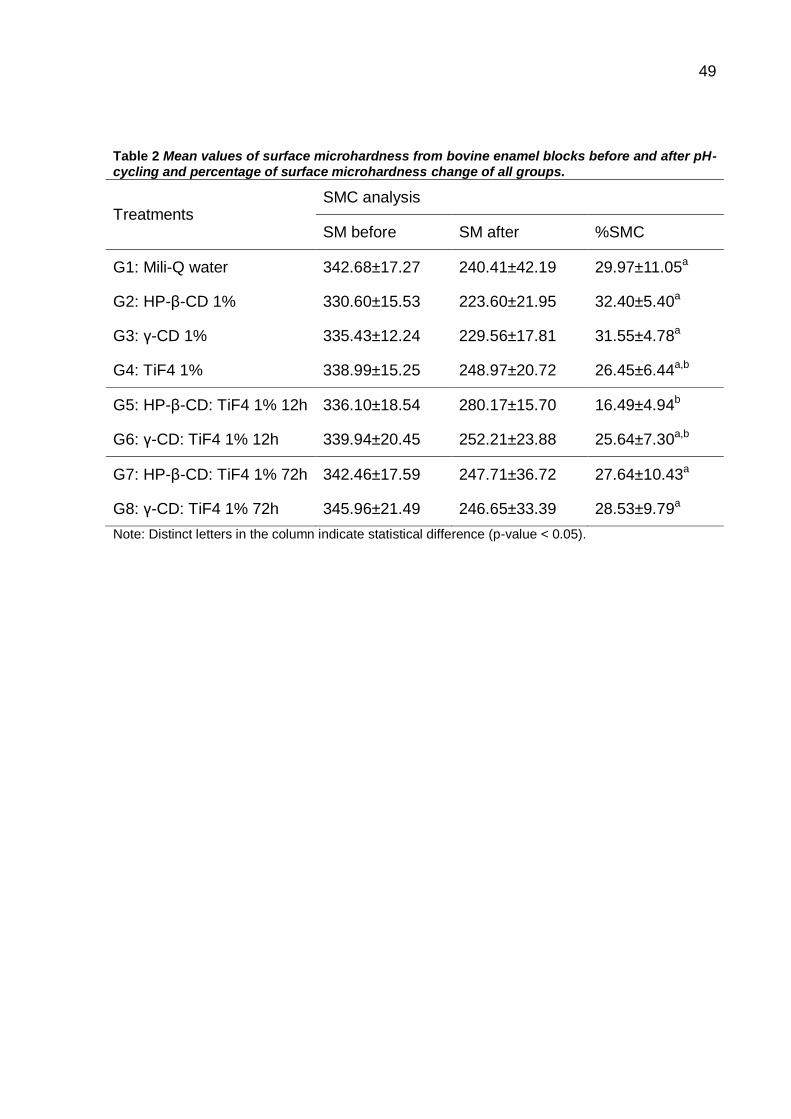
Regarding the percentage of surface microhardness change (%SMC), G1 did
not differ statistically from G2 and G3 (p>0.05). G5 produced less %SMC when
compared to G1 (p=0.00), G2 (p=0.00), G3 (p=0.00), G7 (p=0.03) and G8 (p=0.01),
although no statistical difference was observed compared to G4 and G6. These data
are shown in Table 2.
SEM images indicated the formation of TiO2 glaze-layer on the surface of the
slabs treated with TiF4 and TiF4:CD (Figure 1 and 2). On the surface of the blocks
treated with Mili-Q water, HP-β-CD and γ-CD a clear area of demineralization was
observed. EDX assessment showed the presence of titanium on the surface of the
blocks treated with TiF4 and TiF4:CD, as can be visualized on Table 3.
DISCUSSION
Cyclodextrins are cyclic oligosaccharides composed of dextrose units joined
by a α-1,4 linkage. Cyclodextrins with seven and eight dextrose units have been
named β-CD and γ-CD. CH2CH(OH)CH3 plus β-CD result hydroxypropyl-β-CD. The
inclusion complexes formed between certain drugs and CDs may show extremely
different properties from those of the parent drug or CD itself. Inclusion complexes
thus, may increase solubility and dissolution rate of the compound, modify local
irritation, decrease volatility and increase the stability of drugs [14].
Several studies have been developed to evaluate the impact of formulations
that contain cyclodextrins as inclusion complexes [15-24]. This is due, among other
things, the ability to create some inclusion complexes with a large number of
molecules. It is noteworthy, however, that not all molecules (drugs) can form stable
complexes. There are some limitations as for instance, highly soluble substances;
these generally may not be included [25]. For these reasons, cyclodextrins have
been selected as TiF4 carriers in the present study.

41
A study was conducted in order to improve the stability of aqueous TiF4
solutions with β-CD measured by pH and reduction microhardness in a period of 90
days. Maintenance of fluoride concentration was observed throughout the study and
the pH was increased since baseline until the period of ninety days [6]. Taking into
account these considerations, the present study was designed to evaluate two
different cyclodextrins carriers in two different complexation periods in order to
explore the effect of these nanocomplexes on bovine enamel demineralization.
Although previous research [6] reported a decrease in pH of a TiF4 solution,
after using β-CD, in the present study, the pH values of the nanocomplexes formed
of HP-β-CD or γ-CD and 1% TiF4 were slightly higher compared to TiF4. It proves that
these nanocomplexes employed here were not successful to decrease pH which is
the main negative aspect of TiF4. One can speculate that the method employed in the
first study (kneading method) and the molar ratio used 1:4 used could explain this
difference. Even with this inconvenience, the nanocomplexes of the present study
were able to reduce the loss of enamel surface microhardness.
The nanocomplexes prepared from HP-β-CD containing 1% TiF4 constitute a
very powerful source in dental field research. Despite in vitro conditions and bovine
enamel substratum, the results demonstrated here highlight the ability of the
nanocomplex formed of HP-β-CD: TiF4 with 12 hours of stirring to decrease enamel
softening under adverse conditions (pH-cycling), acting in the prevention of dental
caries.
42
The amount of fluoride released by solutions containing the inclusion
complexes was evaluated in Table 1. Despite all the solutions containing fluoride
show an expected fluoride averaged concentration of 6135 ppm, none of the
products tested here achieved that concentration, however HP-β-CD: 1% TiF4 with
12 hours of stirring was able to control the loss of enamel microhardness. This
particularly solution could affect the enamel surface through other ways, preventing
enamel softening which was not observed in the others groups/treatments. It is highly
probable that a slow release of fluoride is occurring in this solution in order to obtain
a constant concentration of fluoride available for interaction with dental hard tissue,
decreasing enamel demineralization. This explains its performance different from
other groups/treatments as can be visualized on Table 2.
Previous studies demonstrated that solutions containing TiF4 decrease surface
microhardness loss [6-7]. Although the present results corroborate with these
previous studies there is a superiority of TiF4 when it is complexed in the form of HP-
β-CD: 1% TiF4 with 12 hours of stirring.
Study analyzed the effect of TiF solutions on enamel de- and remineralization
in vitro in a pH-cycling model. It was observed that the enamel blocks treated with TiF
presented complete inhibition of calcium loss. These authors also assessed the
permanence of protection for 14 days and they concluded that 80% inhibition of
demineralization was achieved in the slabs treated with TiF [26]. Despite the present
study adopted TiF4 and measurements by microhardness, the results here displayed
also demonstrate decrease in mineral content loss by enamel blocks treated with HP-
β-CD: 1% TiF4 with 12 hours of stirring.
Still referring to the control of the surface microhardness loss, another aspect
to be emphasized is the formation of a TiO2 layer on the surface of the enamel
treated with TiF4, in the complexed form or not. The results obtained in the present
study are attributed the presence of this layer on the surface of bovine enamel blocks
hindering the decalcification. The protective ability of TiF4 is owed to the formation of
an acid-resistant surface layer composed of TiO2 [5]. After professional topical

43
application, this coating is formed by the link between titanium and oxygen of the
phosphate group and acts like diffusion barrier. The specific property found in that
glaze-layer consists of titanium incorporation into the hydroxyapatite lattice and an
increased fluoride uptake. This barrier may block the transport of calcium and
phosphate, preventing the enamel underneath from demineralization [26]. As can be
visualized in the Figure 1 and 2, the acid-resistant barrier of TiO2 was observed on
the surface of the blocks treated with TiF4 and TiF4:CD, especially in HP-β-CD: 1%
TiF4 after 12 hours of complexation. Titanium was detected in the slabs treated with
TiF4 and TiF4:CD as Table 3 displays. One can speculate that TiO2 glaze-layer plus
slow release of fluoride from HP-β-CD: 1% TiF4 with 12 hours of complexation group
hinder the enamel dissolution. On the other hand, the enamel blocks from Mili-Q
water, HP-β-CD and γ-CD groups exhibited areas of demineralization as can be
visualized in Figure 1 and these features are in agreement by high %SMC, according
to Table 2. This result was expected since cyclodextrins solely and water do not
present any effect on inhibiting enamel dissolution.
This is the first study which evaluated the potential of HP-β-CD or γ-CD and
1% TiF4 on reducing bovine enamel dissolution under cariogenic challenge in vitro.
Future studies should be carried out to evaluate its performance in in situ conditions,
to assess the cytotoxicity of these solutions against cells from oral mucosa and to
observe if the fluoride delivery from the solutions with cyclodextrins employed here
demonstrate the same performance throughout time apart from baseline.

44
CONCLUSION
This study showed that TiF4 was capable of forming an inclusion complex with
HP-β-CD or γ-CD in molar ratio of 1:1 and HP-β-CD: 1% TiF4 with 12 hours of stirring
was significantly able to reduce the surface demineralization of sound enamel under
cariogenic challenge.
ACKNOWLEDGEMENTS
This study was supported by FAPERJ and CNPq
45
REFERENCES
[1] Bönecker M, Tenuta LMA, Pucca Júnior GA, Costa PB, Pitts N. A social
movement to reduce caries prevalence in the world. Braz. Oral Res. 2013 (27): 5-6.
[2] Ogaard B, Rolla G, Ruben J, Dijkman T, Arends J. Microradiographic study of
demineralization of shark enamel in a human caries model. Scand. J. Dent. Res.
1988 (96): 209-11.
[3] Wahengbam P, Tikku AP, Lee WB. Role of titanium tetrafluoride (TiF4) in
conservative dentistry: a systematic review. J. Conserv. Dent. 2011 (14):98-102.
[4] Ogaard B, Rolla G, Dukman T, Ruben J, Arends J. Effects of fluoride mouth
rinsing on caries lesion development in shark enamel and in-situ caries model study.
Scand. J. Dent. Res. 1991 (99): 372-7.
[5] Wiegand A, Magalhães, A. C.; Attin, T. Is titanium tetrafluoride (TiF4) effective to
prevent carious and erosive lesions? A review of the literature. Oral Health Prev.
Dent. 2010 (8): 159-164.
[6] Nassur C, Alexandria AK, Pomarico L, Sousa VP, Cabral LM, Maia LC.
Characterization of a new TiF4 and β-cyclodextrin inclusion complex and its in vitro
evaluation on inhibiting enamel demineralization. Arch Oral Biol. 2013 (58): 239-47.
[7] Comar LP, Wiegand A, Moron BM, Rios D, Buzalaf MAR, Buchalla W, Magalhães
AC. In situ effect of sodium fluoride or titanium tetrafluoride varnish and solution on
carious demineralization of enamel. Eur. J. Oral Sci. 2012 (120): 342-8.
[8] Magalhães AC, Comar LP, Rios D, Delbem ACB, Buzalaf MAR. Effect of 4%
titanium tetrafluoride (TiF4) varnish on demineralisation and remineralisation of
bovine enamel in vitro. J. Dent. 2008 (36): 158-162.
[9] Castro RAL, Chevitarese O, Souza IPR. Action of titanium tetrafluoride on
occlusal human enamel in situ. Fluoride 2003 (36): 252-262.
46
[10] Tezel H, Ergücü Z, Önal B. Effects of topical fluoride agents on artificial enamel
lesion formation in vitro. Quintessence int. 2002 (33): 347-52.
[11] Reed AJ, Bibby BG. Preliminary report on effect of topical applications of
titanium tetrafluoride on dental caries. J. Dent. Res. 1976 (55): 357-8.
[12] Conde NCO, Rebelo MAB, Cury JA. Evaluation of the fluoride stability of
dentifrices sold in Manaus, AM, Brazil. Pesqui. Odontol. Bras. 2003 (17): 247-53.
[13] Queiroz CS, Hara AT, Paes Leme AF, Cury JA. pH-cycling models to evaluate
the effect of low fluoride dentifrice on enamel de- and remineralization. Braz. Dent.
J. 2008 (19): 21-27.
[14] Rajewski RA, Stella VJ. Pharmaceutical applications of cyclodextrins. 2. In vivo
drug delivery. J. Pharma. Sci. 1996 (85): 1142-1169.
[15] Aree T, Chaichit N. Crystal structure of β-cyclodextrin – benzoic acid inclusion
complex. Carbohydrate Res. 2003 (338): 439-446.
[16] Cannavà C, Crupi V, Ficarra P, Guardo M, Majolino D, Stancanelli R, Venuti V.
Physicochemical characterization of coumestrol/β-cyclodextrins inclusion complexes
by UV–vis and FTIR-ATR spectroscopies. Vibrational Spectroscopy 2008 (48):
172-178.
[17] Wang Y, Qiao X, Li W, Zhou Y, Jiao Y, Yang C, Dong C, Inoue Y, Shuang S.
Study on the complexation of isoquercitrin with β-cyclodextrin and its derivatives by
spectroscopy. Anal. Chim. Acta 2009 (650): 124-130.
[18] Zhao M, Wang H, Yang B, Tao H. Identification of cyclodextrin inclusion complex
of chlorogenic acid and its antimicrobial activity. Food Chem. 2010 (120): 1138-
1142.
[19] Higashi K, Ideura S, Waraya H, Limwikrant W, Moribe K, Yamamoto K.
Simultaneous dissolution of naproxen and flurbiprofen from a novel ternary gamma-
cyclodextrin complex. Chem. Pharma. Bulletin (Tokyo) 2010 (58): 769-772.
47
[20] Jansook P, Ritthidej GC, Ueda H, Stefánsson E, Loftsson T. yCD/HPyCD
mixtures as solubilizer: solid-state characterization and sample dexamethasone eye
drop suspension. J. Pharma. Pharma. Sci. 2010 (13): 336-350.
[21] Zeng J, Ren Y, Zhou C, Yu S, Chen H. Preparation and physicochemical
characteristics of the complex of edaravone with hydroxypropyl-β-cyclodextrin.
Carbohydrate Polymers 2011 (83): 1101-1105.
[22] Choi SG, Lee SE, Kang BS, Ng CL, Davaa E, Park JS. Thermosensitive and
mucoadhesive sol-gel composites of paclitaxel/dimethyl-β-cyclodextrin for buccal
delivery. Plos one 2014 (9): 1-7.
[23] Vermet G, Degoutin S, Chai F, Maton M, Bria M, Danel C, Hildebrand HF,
Blanchemain N, Martel B. Visceral mesh modified with cyclodextrin for the local
sustained delivery of ropivacaine. Int. J. Pharm. 2014 (467): 149-159.
[24] Gaurav C, Goutam R, Rohan KN, Sweta KT, Abhay CS, Amit GK. (Copper-
curcumin) β-cyclodextrin vaginal gel: delivering a novel metal-herbal approach for the
development of topical contraception prophylaxis. Eur. J. Pharm. Sci., 2014 In
press.
[25] Cal C, Centkowska K. Use of cyclodextrins in topical formulations: practical
aspects. Eur. J. Pharm. Biopharm. 2008 (68): 467-78.
[26] Exterkate RAM, ten Cate JM. Effects of a new titanium fluoride derivate on
enamel de- and remineralization. Eur. J. Oral Sci. 2007 (115): 143-157.

48
Table 1 Mean values at baseline of pH, mV, total fluoride (ppm) and total soluble fluoride (ppm) from the tested solutions.
Treatments
Fluoride mensuration
pH mV Total fluoride (ppm)
mV
Total soluble fluoride (ppm)
G1: Mili-Q water 5.80 211.35 0.0200 - -
G2: 1% HP-β-CD 7.13 - - - -
G3: 1% γ-CD 4.74 - - - -
G4: 1% TiF4 1.64 68.30 5459.5 65.90 5991.9
G5: HP-β-CD: 1% TiF4 12h 1.84 80.65 3366.6 79.90 3466.7
G6: γ-CD: 1% TiF4 12h 1.72 75.55 4109.5 75.30 4149.5
G7: HP-β-CD: 1% TiF4 72h 1.83 81.15 3301.8 80.45 3392.9
G8: γ-CD: 1%TiF4 72h 1.72 74.80 4234.0 74.25 4323.4
49
Table 2 Mean values of surface microhardness from bovine enamel blocks before and after pH-
cycling and percentage of surface microhardness change of all groups.
Treatments SMC analysis
SM before SM after %SMC
G1: Mili-Q water 342.68±17.27 240.41±42.19 29.97±11.05a
G2: HP-β-CD 1% 330.60±15.53 223.60±21.95 32.40±5.40a
G3: γ-CD 1% 335.43±12.24 229.56±17.81 31.55±4.78a
G4: TiF4 1% 338.99±15.25 248.97±20.72 26.45±6.44a,b
G5: HP-β-CD: TiF4 1% 12h 336.10±18.54 280.17±15.70 16.49±4.94b
G6: γ-CD: TiF4 1% 12h 339.94±20.45 252.21±23.88 25.64±7.30a,b
G7: HP-β-CD: TiF4 1% 72h 342.46±17.59 247.71±36.72 27.64±10.43a
G8: γ-CD: TiF4 1% 72h 345.96±21.49 246.65±33.39 28.53±9.79a
Note: Distinct letters in the column indicate statistical difference (p-value < 0.05).

50
Figure 1 SEM surface images of enamel blocks after the pH-cycling regimen at 1000x on the left and EDX analysis on the right. A) G1: arrow indicates demineralization areas. B) G2: arrow indicates demineralization areas. C) G3: arrow indicates demineralization areas. D) G4: arrow indicates the TiO2 glaze-layer. On the right, titanium was detected in the surface
51
Figure 2 SEM surface images of enamel blocks after the pH-cycling regimen at 1000x on the left and EDX analysis on the right. A) G5: arrow indicates extensive TiO2 glaze-layer. B) G6: arrow indicates TiO2 glaze-layer. C) G7: arrow indicates TiO2 glaze-layer. D) G8: arrow indicates the TiO2 glaze-layer. On the right, titanium was detected in the surface.
52
Table 3 Values (percentage in weight) of the elements obtained from the blocks of all groups.
Treatments Mineral content (Weight %)
C O Na Mg Al P Cl K Ca Ti
G1: Mili-Q water 26.95 25.61 0.37 - 0.24 15.32 0.34 - 31.19 -
G2: 1% HP-β-CD 34.20 23.48 0.44 - - 13.63 0.30 - 27.94 -
G3: 1% γ-CD 32.03 24.65 0.40 - 0.16 14.05 0.47 - 28.23 -
G4: 1% TiF4 24.08 28.46 - - 0.16 15.42 0.47 - 30.98 0.43
G5: HP-β-CD: 1% TiF4 12h 31.42 25.38 0.49 - - 13.85 0.33 - 28.26 0.28
G6: γ-CD: 1% TiF4 12h 23.07 28.43 0.47 0.20 0.18 15.50 0.57 0.21 30.67 0.71
G7: HP-β-CD: 1% TiF4 72h 30.17 25.74 0.45 - - 14.05 0.47 0.32 28.02 0.77
G8: γ-CD: 1%TiF4 72h 24.28 27.60 0.25 - - 15.56 0.45 - 31.30 0.55
53
Artigo 2 Effect Of Tif4 And Β -Cyclodextrin Inclusion Complex On
Demineralized Enamel Rehardening
Thiago Isidro VIEIRA 1
Camila NASSUR1
Adílis Kalina ALEXANDRIA 2
Luciana POMARICO 2
Valeria Pereira de SOUSA 3
Lúcio Mendes CABRAL 3
Ana Maria Gondim VALENÇA 4
Lucianne Cople MAIA 5
1 DDS, Master student, Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil
2Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
3School of Pharmacy, Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
4DDS, MSD, PhD, Adjunct Professor, Department of Clinic and Social Dentistry, School of Dentistry, Universidade Federal da Paraíba, Paraíba, Brazil.
5 DDS, MSD, PhD, Full Professor, Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil

54
Correspondence Author - Lucianne Cople Maia
Caixa Postal: 68066 – Cidade Universitária - CCS
CEP: 21941-971 - Rio de Janeiro – RJ –Brazil
E-mail: [email protected]
Fax/phone: +5521 25622098

55
ABSTRACT
The frequent low level of fluoride from topical applications is crucial for the caries lesion repair. Titanium tetrafluoride (TiF4) is a topical agent used in the control of dental caries. The solution is however, very acidic and highly instable. To minimize this effect, inclusion complexes formed of TiF4 and cyclodextrins can be used. This study evaluated the in vitro potential of a TiF4 and β-cyclodextrin inclusion complex on the remineralization of artificially demineralized enamel blocks. Forty-eight bovine enamel blocks selected by microhardness, were randomly assigned to four groups (n = 12): control (distilled and deionized water), solution of 1% β-CD, solution of 1% TiF4 and a TiF4:β-CD solution. The blocks were submitted to a pH cycling regimen for 8 days. After that, samples were evaluated by SMH, %SMR, cross-sectional microhardness (CSMH), scanning electron microscope (SEM) and energy dispersive spectrometry (EDX). Data were assessed for normality and analyzed using ANOVA and Tukey tests (p-value < 0.05). On the surface, all groups were able to promote rehardening of enamel with no statistical difference between them (p> 0.05). In cross-sectional microhardness, no group differed from the control, but TiF4:β-CD was statistically superior (p = 0.03) compared to TiF4. SEM photomicrographs revealed the titanium dioxide coating on slabs treated with TiF4 and TiF4:β-CD. EDX assessment demonstrated the presence of titanium on the surface of slabs treated with TiF4 and TiF4:β-CD. The solution containing TiF4 and β-cyclodextrin inclusion complex was superior than the TiF4 solution itself on the rehardening enamel subsurface
Keywords: Titanium tetrafluoride, β-Cyclodextrin, Enamel remineralization,
Fluoride, Dental caries

56
INTRODUCTION
The use of fluoride is known as a major factor in reducing the occurrence of
caries [1]. Among the main products, titanium tetrafluoride (TiF4) has been widely
employed for minimally invasive treatment of this disease. Despite the positive effects
of TiF4 on improving the rehardening of previous artificial carious lesions [2], it has
never found a broad application in the clinical field. On the other hand, the literature
indicates that remineralization is also inhibited by TiF4 [3]. The very low pH of the
pure solution (pH 1.0) is one of the major disadvantages of the TiF4 [4, 5]. Although
promising, the high instability of the solution represents a limitation for clinical use
and to obtain its therapeutic improvement, inclusion complexes should be adopted
[6].
Molecular complexation is an area of great interest in biotechnology because it
enables the selection, separation, solubilization and stabilization of various
biomolecules [7]. For the purpose of improving the stability of certain chemical
compounds, cyclodextrins (CDs) have been the subject of many studies in different
areas [8]. βCD is the most useful carrier due to its effectiveness and low price [9]. It is
structurally organized in the truncated cone form with the ends showing hydrophilic
sites due to the presence of hydroxyl groups, while the cavity presents hydrogen
atoms and glycosidic oxygen bridges assigning a highly hydrophobic character [10].
Owing to the paucity of in vitro studies analyzing the effect of TiF4 in
association with βCD on enamel remineralization, the present study was designed as
a laboratory assay. Thus, the aim of this study was to evaluate the in vitro effect of
TiF4 and β-cyclodextrin inclusion complex on the remineralization of artificially
demineralized enamel blocks.
57
MATERIALS AND METHODS
Preparation of cyclodextrin complexes
The inclusion complexes of TiF4:β-cyclodextrin (TiF4: β-CD) were prepared by
kneading, solubilization and freeze drying at molar ratios of 1:4. Physical mixtures
were prepared by mixing β-CD and TiF4 in a mortar at the same molar ratios in a
mortar for 5 min. An ethanol:water (70:30; v/v) solution was added and mixed for 30
min to obtain a homogeneous paste which was dried under reduced pressure. The
granulometry was adjusted using a 40 mesh sieve [6].
Regarding the solution method, appropriate proportions of TiF4 and β-CD were
blended in 20 mL of distilled water with a magnetic stirrer for 72 hours. The samples
remained frozen in liquid nitrogen and were lyophilized. The particle size was
calibrated with a 40 mesh sieve. The inclusion yield was calculated by UV
spectroscopy.
Preparation of enamel blocks
Forty-eight bovine sound enamel blocks (4 x 4 x 3 mm) stored in 2%
formaldehyde solutions were included in acrylic devices and polished with 600 and
1200 grit silicon carbide paper, followed by 3 and 1 µm diamond abrasive slurry
(Buehler Ltd., Lake Bluff, Illinois, USA). The selection of the slabs was based on the
baseline surface microhardness (SMH) (mean 321.35 ± 32.13 kg/mm2). SMH was
measured using a microhardness tester (HVS-1000, Time Group Inc., Beijing, China)
with a Knoop diamond under a 50 g load for 5 s, by making 5 indentations spaced
100µm [11] from each other at the center of the enamel surface.
58
Demineralization of the enamel blocks
As previously mentioned, forty-eight enamel blocks were submitted to a
demineralizing solution at a ratio of 2 mL/mm of enamel area for 16 h and after that,
the mineral loss was evaluated. After 16 h of this demineralization regimen, enamel
blocks presented measurable caries-like subsurface lesions without surface erosion,
allowing the evaluation of mineral loss or gain by surface microhardness [12]. The
slabs with a known surface microhardness (SMH) (sound enamel) were subjected to
the demineralizing solution for 16 h and after that, the SMH was again measured
(demineralized enamel).
Experimental design on enamel rehardening
This study assessed the remineralizing ability of a new inclusion complex
(TiF4:β-CD) on previous demineralized bovine enamel blocks. Four groups with 12
predemineralized bovine enamel blocks each were randomly chosen to evaluate the
following 4 treatment groups: control (distilled deionized water), a solution containing
1% β-CD, a solution carrying 1% TiF4 and the experimental formulation containing
TiF4:β-CD.
The outcome variables investigated were: percentage of surface
microhardness recovery (%SMR) and cross-sectional microhardness (CSMH).
Alterations on the surface and subsurface as visualized by SEM and mineral content
by energy X-ray spectrometry (EDX) analysis were qualitatively assessed.
Treatment and rehardening pH-cycling
The solutions were blindly applied only once on the surface of the blocks with
a microbrush® and left for 1 min. After this, the blocks were rinsed with deionized and
distilled water and dried with soft paper. Posteriorly, the rehardening regimen started.

59
The pH-cycling regimen occurred in 8 days, and the blocks were kept at 37°C
for 2 h in the demineralizing solution and for 22 h in the remineralizing solution. The
demineralizing solution contained 0.05M acetate buffer pH 5.0, 1.28 mM Ca, 0.74
mM P and 0.03 µg F/mL. The remineralizing solution contained 1.5 mmol/L Ca, 0.9
mmol/L P, 150 mmol/L KCl, and 0.05 µg F/mL in 0.1 mol/L Tris buffer, pH 7.0. The
proportion of de- and remineralizating solutions per area of block was 6.25 mL/mm2
and 3.12 mL/mm2, respectively. The solutions were replaced by fresh ones on the 4th
day. Then, in the 8th of the cycle, the blocks remained in the remineralizing solution
for an additional 24 h until analysis [12].
Microhardness evaluation
Enamel SMH was measured again by making 5 indentations spaced 100 µm
[11] from the baseline ones. The percentage of surface microhardness recovery
(%SMR) for the predemineralized specimens was calculated using the following
equation: %SMR = demineralized SMH – SMH after pH-cycling / demineralized SMH
x 100.
Cross-sectional microhardness analysis
The slabs were longitudinally sectioned at the middle of the fragment with a
cutting machine (Isomet, Buehler, Lake Bluff, IL, USA) coupled to a diamond disk,
resulting in two halves. One half was included in the stub and the cut surfaces were
exposed and polished with 600 and 1200 grit silicon carbide paper. The cross-
sectional microhardness (CSMH) evaluation was performed by a microhardness
tester (Buehler, MICROMET 5104, 679-MIT4-00335, Japan) with a Knoop diamond
and a 25 g static load that was applied for 10 s.
Two lines of 15 indentations were made at from 10 to 100 µm depth
indentations at 10 µm intervals and from 100 to 200 µm depth at 20 µm intervals
were made from the outer enamel surface, 100 µm apart from each other [6].
60
Scanning electron microscopy (SEM) analysis
The blocks were mounted on aluminium stubs and visualized using a
scanning electron microscopy (JEOL-JSM, 6460LV, Tokyo, Japan). The topography
of the sectioned surfaces and the enamel surfaces were analyzed in backscattered
electrons at 20 kV voltage, low vacuum mode (45 Pa) to achieve images at 1000x
magnification. The area to be examined was the central part of the sample on the
surface and on the cross-sectional half.
Energy dispersive X-ray spectrometry (EDX) analysis
The mineral content assessment from the enamel surface and from the cross-
sectional side was performed using EDX with link and automatic image analyzer
system Kontron. This part of the study was carried out to identify the chemical
elements in the inner enamel after the experimental protocol. Potassium, Silicon,
Chlorine, Phosphorus, Aluminium, Magnesium, Sodium, Carbon, Calcium, Oxygen
and Titanium were analyzed [6].
Statistical analysis
SPSS 17.0 was used for the statistical analysis. The p-value < 0.05 was
considered significant. The Shapiro-Wilk test was employed to verify the normal
distribuition. The Student´s paired t-test was performed to compare the surface
microhardness before and after pH-cycling of all groups with a p-value of 0.05.
ANOVA 1-way followed by Tukey´s post hoc test was applied to analyze the
%SMR differences among treatments. For analyses of CSMH, the area under curve
(ΔZ) was calculated, the differences among treatments were analyzed by ANOVA 1-
way and Tukey´s post hoc test.
61
RESULTS
Surface and cross-sectional microhardness
On the surface, all groups were able to promote rehardening of enamel. Table
1 shows that the inclusion complex of TiF4:β-CD revealed a higher percentage of
surface microhardness recovery with value of 5.72%. Even though, this finding was
not statistically different (p-value > 0.05) from the other treatments.
As showed on Table 2, as the enamel depth increases, the mean cross-
sectional microhardness values of TiF4:βCD become higher than the other
treatments. TiF4:βCD was able to increase enamel transverse microhardness when
compared to TiF4 group (Table 2 and Figure 1).
SEM and EDX evaluation
The enamel surface images showed the formation of an acid-resistant titanium
dioxide coating on the slabs treated with TiF4 and TiF4:βCD, as can be seen at Figure
2.The cross-sectional images were similar among the groups, according to Figure 3.
The chemical analysis (EDX) revealed the presence of titanium in all slabs treated
with TiF4 and TiF4:βCD at the enamel surface, in accordance with Figure 2. The
presence of titanium was not evident at the subsurface of the blocks treated with TiF4
and TiF4:βCD at the enamel surface, as shown in Table 3.
DISCUSSION
TiF4 is a topical fluoride agent which leaves, after its application on the enamel
surface a rich-titanium glaze/coating. To this resistant coating, an anticariogenic
effect in enamel is observed in studies dealing with de- and remineralization. This
layer offers a diffusion barrier and retains fluoride, leading to slow release to the tooth
and its environment [13]. Since 1967, it is known that TiF4 suffers rapid hydrolysis [4]
and in face of this data, huge effort has been made to create new compounds to
establish and potencialize its clinical use [6].
62
The effects of βCD on the chemical stability of TiF4 have been already
examined in the literature [6]. A remineralizing ph-cycling regimen was chosen
because its potential on penetrating the demineralized enamel was not studied yet.
This is the first study that analyzed the effect of TiF4 associated to βCD incorporated
into solution on a remineralization study design.
This study aimed to analyze the in vitro potential of TiF4 and βCD inclusion
complex on remineralizing predemineralized bovine enamel. As described in Table 1,
the inclusion complex tested here was capable of rehardening the enamel surface
after pH-cycling (p<0.05). However, this surface rehardening effect did not differ from
the other groups (p>0.05). Despite of this, the results demonstrated the effectiveness
of the TiF4:βCD inclusion complex on enhancing the mineral content at enamel
subsurface, when compared to solution of TiF4 (p<0.05), as visualized in Table 2 and
Figure 1.
According to Figure 1 and Table 2, the TiF4:β-CD inclusion complex solution
was capable of remineralizing the predemineralized enamel subsurface up to a 50
µm depth, as mentioned previously. Nevertheless, an in situ study evaluating the
effect of sodium fluoride and TiF4 varnish and solution on carious demineralization of
enamel demonstrated that TiF4 was able to rehard only the enamel surface [14]. One
can hypothesize that the in situ conditions performed in the study (presence of
biofilm) did not allow the penetration of the titanium at the enamel subsurface.
The group TiF4 solution showed a 14 ± 7 mean value for %SMR [14] while in
our study, the mean value for TiF4 was 4.118 which was not different (p-value > 0.05)
from others treatments (control, βCD and TiF4:βCD). It is noteworthy that despite the
fact that no statistical was found among the treatments, the mean value for TiF4:βCD
was higher than for the others groups (%SMR 5.72).
Some researchers corroborate with our results regarding the enhancement of
subsurface hardness. When conducting an in vitro study on demineralization and
remineralization of bovine enamel by 4% TiF4 varnish, it was observed that a 4% TiF4
varnish significantly enhanced the mineral content compared to the others treatments
63
(Duraphat® and Duofluorid®) up to a 30 µm enamel depth [2]. Similar to those
reported in the present study, the inclusion complex tested here was able to improve
the mineral content up to 50 µm depth, according to Figure 1. A difference
concerning these two studies refers to the adopted concentration which was 1% and
the solution of a nanoinclusion complex of TiF4:βCD instead of a TiF4 varnish. It is
important to point out that this study [2] and the present paper adopted a single
application of TiF4 over the enamel blocks.
Regarding the improvement of enamel surface hardness, TiF4 induced higher
remineralization of previous carious enamel with 27 ± 4 mean value of %SMR [2].
However, in the present study, the increase in percentage of surface microhardness
recovery when TiF4 was associated to βCD (from 4.12 to 5.72) was not significantly
different from the others groups (p-value > 0.05).
The SEM observation of the predemineralized enamel blocks showed the
formation of the acid-resistant titanium dioxide coating changing the resistance to
acid attack of this surface [15-17] as observed in Figure 2. From this coating one may
speculate that titanium could penetrate the enamel layer, resulting in an increased
mineral hardness. However, in spite of the presence of elements such as oxygen,
chlorine, potassium, carbon phosphorus and sodium, being available in the surface
and subsurface enamel, according to Figure 2 and Figure 3, the presence of titanium,
on TiF4 and TiF4:βCD groups, was only observed in the enamel surface. Although the
depth of titanium penetration could not be observed at the subsurface cross-sectional
slabs using EDX analysis method, one can conclude that the titanium released from
TiF4:βCD induced the rehardening of enamel subsurface. We can suppose that a
small amount of this compound was able to be incorporated into the enamel favoring
its mineral content. Other possibility that can explain the absence of titanium in inner
enamel is that its penetration seems to be greater in sound enamel than in
predemineralized enamel [5, 18]. This difference could be related to a higher quantity
of water, carbonate and oxygen, improving the reactivity between titanium and the
oxygen available in dental structure [6].

64
It is well known that fluoride uptake is higher among decalcified enamel when
compared to sound enamel [19] due to the porosity present in the decayed enamel
[20]. However, titanium penetration occurred more deeply into sound enamel
compared to artificially demineralized enamel [18]. This can be explained by the
decrease in water and carbonate in the carious enamel, which decreases the
titanium connection with oxygen on dental structure. It is reasonable to suggest that
titanium applied into the predemineralized enamel blocks surface used in this study
has contributed to enhance the microhardness of inner enamel (referring to Table 2)
by modifying the underlying enamel but this amount of titanium was not enough to be
detected in the EDX analysis.
The cavity of the cyclodextrin molecule is lipophilic (lined with skeletal carbons
and ethereal oxygens of the glucose residues) resulting in a microenviroment into
which suitably sized drug molecules may enter and be included bestowing a useful
property of these excipients such as retarding or accelerating degradation. The
cyclodextrin molecule shields the drug molecule from attack by various reactive
molecules. In other words, the CD can insulate a labile compound from a potentially
corrosive environment reducing drug hydrolysis, oxidation, steric rearrangement,
racemization, polymerization and enzymatic decomposition [21].
From all natural CDs, βCD is the most accessible, lowest-priced and generally
the most effective [9]. The advantages of the βCD employed here have already been
enlightened such as an increase in the pH of the TiF4 nanosystems in solution,
allowing professional use and thermal stability [6]. Further studies are necessary to
assess the rehardening effect of other inclusion complexes.
Several studies are limited to the potential of TiF4 on reducing
demineralization of dental hard tissue [22-24, 6]. The fact that remineralization is
inhibited by TiF [5] was explained by that manuscript. It was assessed the effect of a
new TiF on enamel remineralization. It was observed that the group treated with TiF
derivative resulted in strongly reduced calcium loss but calcium uptake was also
inhibited [5]. This finding highlights that this compound may not be capable of
65
improving lesion repair.
In this laboratory study, TiF4:βCD inclusion complex was effective in
rehardening artificially predemineralized bovine enamel blocks. The in vitro results
obtained here suggest that TiF4 associated to βCD possesses a desirable property as
a topical agent for remineralizing caries incipient lesions. On the other hand, TiF4
seems to be more advantageous on protecting from demineralization as lesion
arrestment seemed to be the maximum result [5, 6] because it provides a long-lasting
fluoride delivery and leaves large amounts of titanium on the surface glaze layer [17].
The solution containing TiF4 and β-cyclodextrin inclusion complex was superior to the
TiF4 solution itself on remineralizing enamel subsurface.
ACKNOWLEDGEMENTS
This study was supported by FAPERJ and CNPq.
66
REFERENCES
[1] Narvai, P.C.; Frazão, P.; Roncalli, A.G.; Antunes, J.L.F. Cárie dentária no Brasil:
declínio, polarização, iniqüidade e exclusão social. Rev. Pan. Salud Públ., 2006,
19(6), 385-393.
[2] Magalhães, A.C.; Comar, L.P.; Rios, D.; Delbem, A.C.B.; Buzalaf, M.A.R. Effect of
a 4% titanium tetrafluoride (TiF4) varnish on demineralisation and remineralisation of
bovine enamel in vitro. J. Dent., 2008, 36(2), 158- 162.
[3] Castro, R.A.L.; Chevitarese, O.; De Souza, I.P.R. Action of titanium tetrafluoride
on occlusal human enamel in situ. Fluoride, 2003, 36, 252-262.
[4] Buslaev, A.; Dyer, D.S.; Ragsdale, R. O. Hydrolysis of titanium tetrafluoride. Inorg.
Chem., 1967, 6(12), 2208-2212.
[5] Exterkate, R.A.M.; Ten Cate, J.M. Effects of a new titanium fluoride derivate on
enamel de- and remineralization. Eur. J. Oral Sci., 2007, 115(2), 143-157.
[6] Nassur, C.; Alexandria, A.K.; Pomarico, L.; Sousa, V.P.; Cabral, L.M.; Maia, L.C.
Characterization of a new TiF4 and β-cyclodextrin inclusion complex and its in vitro
evaluation on inhibiting enamel demineralization. Arch. Oral Biol., 2013, 58(3), 239-
247.
[7] Singh, M.; Sharma, R.; Banerjee, V.C. Biotechnological applications of
cyclodextrins. Biotechnol. Adv., 2002, 20(5-6), 341–359.
[8] Venturini, C.G.; Nicolini, J.; Machado, C.; Machado, V.G. Propriedades e
aplicações recentes das ciclodextrinas. Quím. Nova, 2008, 31(2), 360-368.
[9] Valle, E.M.M.D. Cyclodextrins and their uses: a review. Process Biochem., 2004,
39(9), 1033-1046.
67
[10] Britto, M.A.F.O.; Nascimento Júnior, C.S.; Santos, H.F. Análise estrutural de
ciclodextrinas: um estudo comparativo entre métodos teóricos clássicos e quânticos.
Quím. Nova, 2004, 27(6), 882-888.
[11] Tenuta, L.M.A.; Lima, J.E.; Cardoso, C.L.; Tabchoury, C.P.; Cury, J.A. Effect of
plaque accumulation and salivary factors on enamel demineralization and plaque
composition in situ. Pesq. Odontol. Bras., 2003, 17(4), 326-331.
[12] Queiroz, C.S.; Hara, A.T.; Paes Leme, A.F.; Cury, J.A. pH-cycling models to
evaluate the effect of low fluoride dentifrice on enamel de- and remineralization.
Braz. Dent. J., 2008, 19(1), 21-27.
[13] Tveit, A.; Klinge, B.; Tötdal, B.; Selvig, K.A. Long-term retention of TiF4 and
SnF2 after topical application to dentin in dogs. Scand. J. Dent. Res., 1988, 96,
p.536-540.
[14] Comar, L.P.; Wiegand, A.; Moron, B.M.; Rios, D.; Buzalaf, M.A.R.; Buchalia, W.;
Magalhães, A.C. In situ effect of sodium fluoride or titanium tetrafluoride varnish and
solution on carious demineralization of enamel. Eur. J. Oral Sci., 2012, 120(4), 342-
348.
[15] Wei, S.H.; Soboroff, D.M.; Wefel, J.S. Effects of titanium tetrafluoride on human
enamel. J. Dent. Res., 1976, 55(3), 426-431.
[16] Gu, Z.; Soremark, R. Influence of tooth surface conditions on enamel fluoride
uptake after topical application of TiF4 in vitro. Acta Odontol. Scand., 1996, 54(5),
279-281.
[17] Wefel, J.S.; Harless, J.D. The effect of topical fluoride agents on fluoride uptake
and surface morphology. J. Dent. Res., 1981, 60(11), 1842-1848.
[18] Chevitarese, A.B.; Chevitarese, O.; Chevitarese, L.M.; Dutra, P.B. Titanium
penetration in human enamel after TiF4 application. J. Clin. Pediatr. Dent., 2004,
28(3), 253-256.

68
[19] Ögaard, B.; Rölla, G., Helgeland, K. Fluoride retention in sound and
demineralized enamel in vivo after treatment with a fluoride varnish (Duraphat).
Scand. J. Dent. Res., 1984, 92, 190-197.
[20] Arends, J.; Christoffersen, J. The nature of early caries lesions in enamel. J.
Dent. Res., 1986, 65, 2-11.
[21] Loftsson, T.; Brewster, M.E. Pharmaceutical applications of cyclodextrins. I. Drug
solubilization and stabilization. J. Pharm. Sci., 1996, 85(10), 1017-1025.
[22] Reed, A.J.; Bibby, B.G. Preliminary report on effect of topical applications of
titanium tetrafluoride on dental caries. J. Dent. Res., 1976, 357-358.
[23] Büyükyilmaz, T.; Tangugsorn, V.; Ogaard, B.; Arends, J.; Ruben, J.; Rolla, G.
The effect of titanium tetrafluoride (TiF4) application around orthodontic brackets. Am
J Orthod Dentofacial Orthop ., 1994, 105, 293-296.
[24] Tezel, H.; Ergücü, Z.; Önal, B. Effects of topical fluoride agents on artificial
enamel lesion formation in vitro. Quintessence Int., 2002, 33(5), 347-352.

69
Table 1. Values (mean and standard deviation) of surface microhardness (SMH) analysis of enamel blocks before and after pH-cycling, percentage of enamel surface change according to the treatments.
Treatments SMH sound SMH demineralized
SMH treated
Difference between treated and demineralized
%SMR
Control 321.61±13.14 30.69±6.49 43.33±29.67 12.64 4.29a
βCD 323.87±12.66 29.44±3.88 41.88±12.15 12.43 4.19a
TiF4 320.77±14.24 28.40±4.25 40.52±13.92 12.12 4.12a
TiF4: βCD 325.11±10.27 30.88±4.54 47.85±31.11 16.97 5.72a
Note: there was no statistical difference between the groups (p-value > 0.05). Control group = Mili-Q water.
Table 2: Values (mean) of cross-sectional microhardness (CMSH) analysis of enamel blocks according to the treatments and depths and ΔZ.
Depth Treatments
Control βCD TiF4 TiF4: βCD
10µm 19.91±3.53 19.00±3.53 18.74±9.03 26.50±14.84
20µm 67.77±26.11 51.58±2.12 49.27±56.84 105.34±108.51
30µm 180.70±89.34 113.17±63.11 106.77±93.28 223.01±68.55
40µm 215.58±81.83 202.81±46.14 207.76±110.52 252.27±60.40
50µm 252.50±58.77 253.32±111.40 278.25±58.76 271.88±55.40
ΔZ 1194.19a,b 1328.97a,b 1433.54b 896.12a
Note: Means followed by distinct letters are statistically different (p-value < 0.05). μm: micrometres.
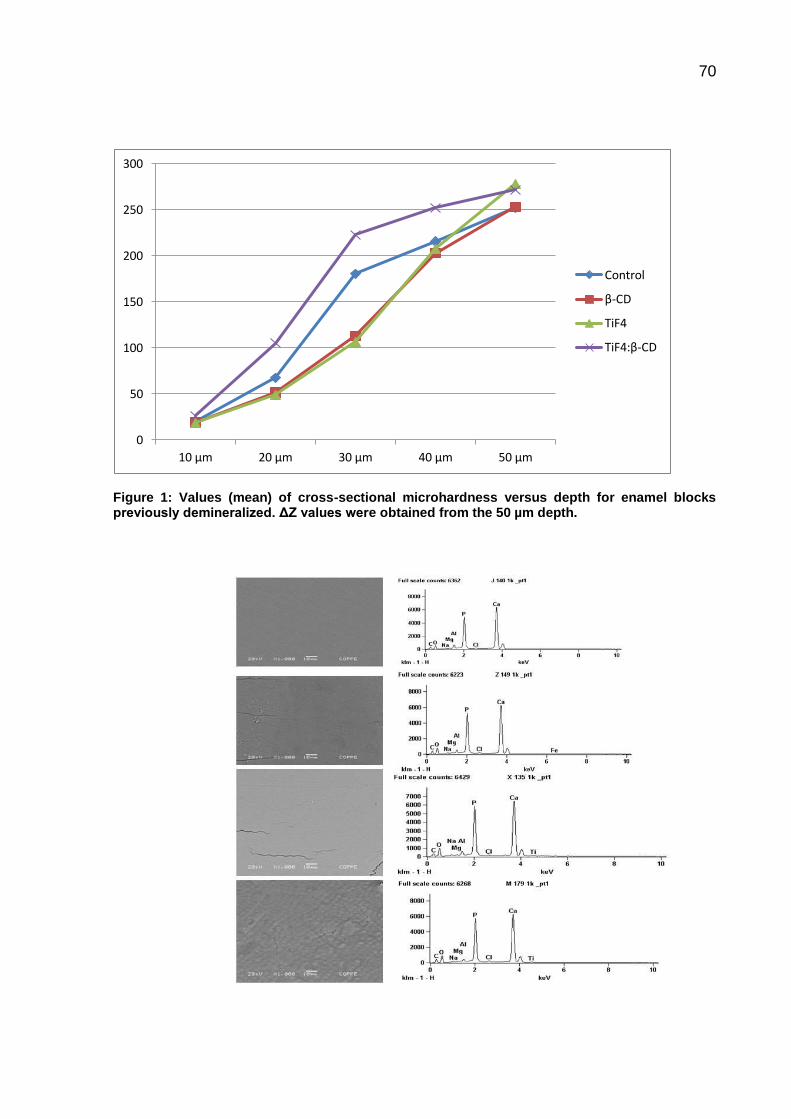
70
Figure 1: Values (mean) of cross-sectional microhardness versus depth for enamel blocks previously demineralized. ΔZ values were obtained from the 50 µm depth.
0
50
100
150
200
250
300
10 µm 20 µm 30 µm 40 µm 50 µm
Control
β-CD
TiF4
TiF4:β-CD
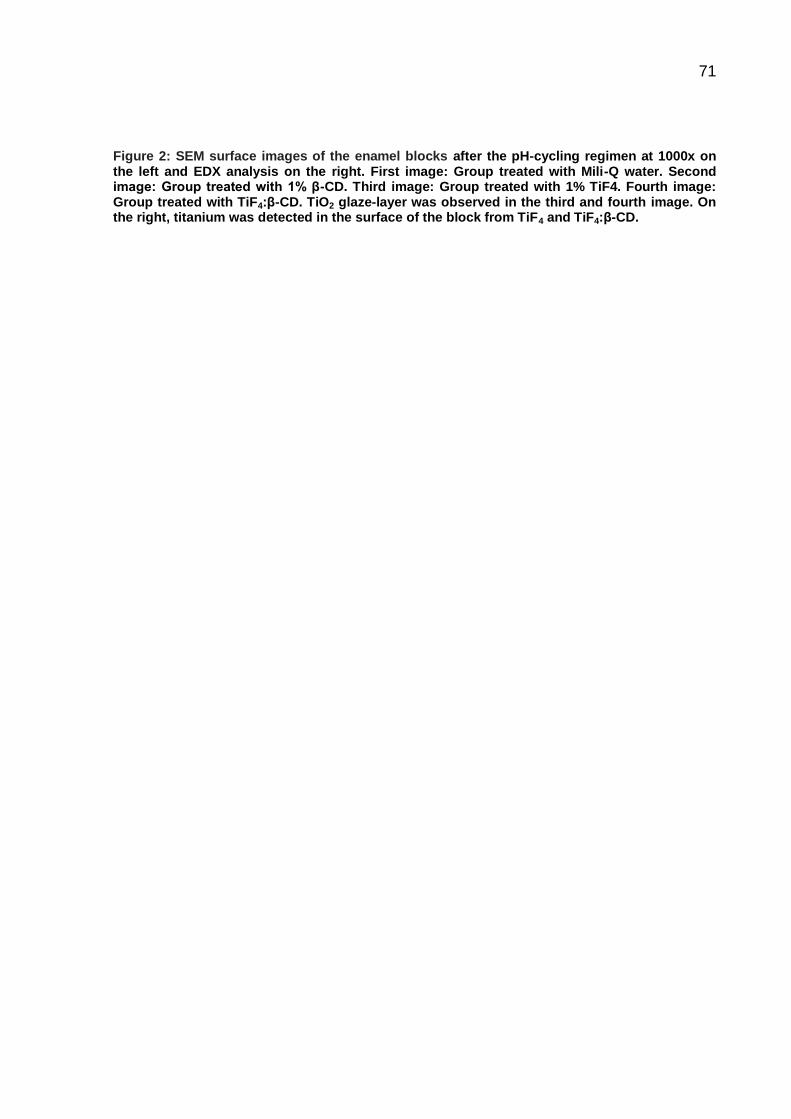
71
Figure 2: SEM surface images of the enamel blocks after the pH-cycling regimen at 1000x on the left and EDX analysis on the right. First image: Group treated with Mili-Q water. Second image: Group treated with 1% β-CD. Third image: Group treated with 1% TiF4. Fourth image: Group treated with TiF4:β-CD. TiO2 glaze-layer was observed in the third and fourth image. On the right, titanium was detected in the surface of the block from TiF4 and TiF4:β-CD.
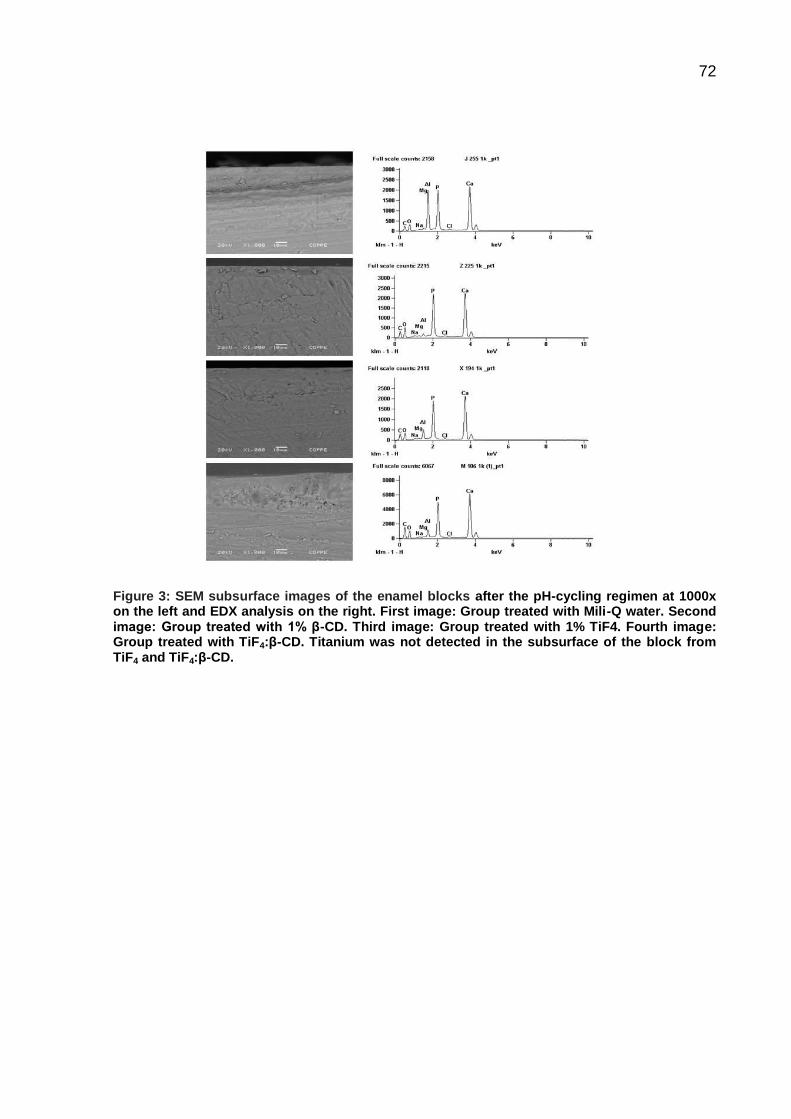
72
Figure 3: SEM subsurface images of the enamel blocks after the pH-cycling regimen at 1000x on the left and EDX analysis on the right. First image: Group treated with Mili-Q water. Second image: Group treated with 1% β-CD. Third image: Group treated with 1% TiF4. Fourth image: Group treated with TiF4:β-CD. Titanium was not detected in the subsurface of the block from TiF4 and TiF4:β-CD.
73
5. DISCUSSÃO
Este trabalho avaliou o potencial in vitro de soluções contendo complexos de
ciclodextrinas com o TiF4 na desmineralização do esmalte. As ciclodextrinas têm
sido extensivamente utilizadas para aprimoramento de diversas moléculas (AREE;
CHAICHIT, 2003; CANNAVÀ et al., 2008; WANG et al., 2009; ZHAO et al., 2010;
HIGASHI et al., 2010; JANSOOK et al., 2010; ZENG et al., 2011; CHOI et al., 2014;
VERMET et al., 2014; GAURAV et al., 2014) . Todavia, não há na literatura
pertinente a esta temática estudo que avalie a inclusão do TiF4 a HP-β-CD ou γ-CD
na cinética des- e remineralização dos tecidos dentários duros. Assim, o presente
trabalho foi o primeiro a investigar o efeito dessas soluções na desmineralização do
esmalte bovino in vitro. Vale ressaltar que um estudo prévio analisou o efeito da
inclusão do TiF4 a β-CD na desmineralização do esmalte bovino in vitro (NASSUR et
al., 2013). E a partir dos resultados promissores obtidos neste estudo, optou-se pela
seleção de outras ciclodextrinas (HP-β-CD e γ-CD) com distintos tempos de
complexação/agitação (12 e 72 horas) para investigar se tais carreadores se
comportariam de maneira análoga ao já encontrado no estudo.
Após a aplicação de uma única camada de solução de TiF4 1% por um minuto
prontamente se observa a formação de uma cobertura ácido-resistente de TiO2
(NASSUR et al., 2013). A essa cobertura, que atua como uma barreira, tem sido
atribuída seu efeito anticariogênico e antierosivo (MAGALHÃES et al., 2008;
WAHENGBAM et al., 2011; COMAR et al., 2012). Conforme anteriormente apontado
nos artigos 1 e 2, essa camada se forma diante da ligação química do titânio com o
oxigênio do grupo fosfato da hidroxiapatita (BUYUKYILMAZ et al., 1997). Esse efeito
anticariogênico deve-se a cobertura de TiO2, a um aumento na incorporação de
fluoreto e incorporação do titânio no cristal de hidroxiapatita (GU et al., 1996).
74
Observa-se no artigo 1 que os blocos de esmalte bovino foram avaliados
quanto ao percentual de perda de microdureza superficial. Futuros estudos devem
ser realizados para averiguar a microdureza interna desses blocos a fim de constatar
se as soluções as quais esses blocos foram tratados preveniram a desmineralização
na subsuperfície do esmalte e, do mesmo modo, analisar por meio da
espectrometria de energia dispersiva de raios- X (EDX) a presença ou não do titânio
na subsuperfície do esmalte.
É controverso na literatura o efeito remineralizador do TiF4. O TiF4, conforme
anteriormente exposto, forma uma camada ácido-resistente sobre a superfície do
esmalte após aplicação tópica e assim, essa cobertura atuaria inibindo o transporte
de cálcio e fosfato para o interior da lesão. Por esta razão, autores apontam que o
uso do TiF4 funcionaria mais para paralisar a lesão cariosa do que para remineralizá-
la na subsuperfície, uma vez que o acesso do cálcio e fosfato estaria impedido
(EXTERKATE, TEN CATE, 2007). Supõe-se que a própria ciclagem de pH adotada
no estudo produziu uma superfície mais permeável permitindo assim a penetração
da camada de TiO2 para a subsuperfície, o que explicaria o aumento da dureza até a
camada de 30 µm (MAGALHÃES et al., 2008).
Apesar de ser um tema que gera controvérsia, optou-se por avaliar no artigo 2
o efeito da β-CD associada ao TiF4 na remineralização do esmalte previamente
desmineralizado in vitro com a finalidade de se constatar se, quando complexado
com a β-CD, ele se comportaria de maneira semelhante aos dados relatados na
literatura.
75
Embora algumas soluções testadas no artigo 1 apresentaram um potencial de
inibição da desmineralização superficial do esmalte como a solução de HP-β-CD:
TiF4 com 12 horas de agitação, é necessário avaliar em pesquisas futuras a
liberação de flúor dessa solução e compará-la com o TiF4 isolado com o propósito de
se investigar se essa associação presente nesse grupo possibilitou uma
manutenção da concentração do flúor, bem como a alteração do pH no decorrer do
tempo. Já as soluções empregadas no artigo 2 já foram avaliadas quanto a
concentração de flúor ao longo do tempo de 90 dias e pH (NASSUR et al., 2013).
Vários métodos têm sido propostos para se estudar as lesões cariosas
geradas em estudos in vitro, e dentre eles, pode-se destacar a microscopia de luz
polarizada (TODD et al., 1999; SANTOS et al., 2009), microdureza (MAGALHÃES et
al., 2008; NASSUR et al., 2013) e microrradiografia transversal (EXTERKATE; TEN
CATE, 2007; COMAR et al., 2012). A microscopia de luz polarizada baseia-se na
interpretação da birrefrigência do esmalte desmineralizado. Essa característica de
birrefrigência é oriunda do conteúdo mineral (que gera uma birrefrigência intrínseca
com um sinal negativo) e do volume não mineralizado (produz uma birrefrigência
com um sinal positivo). A imagem obtida é a resultante do somatório desses dois
tipos de birrefrigência. A birrefrigência gerada pelo volume desmineralizado (cariado)
representa a propriedade óptica alterada pelo meio de imersão e é interpretada por
uma equação formulada para materiais heterogêneos em que se avalia o índice de
refração e o volume (SOUSA et al., 2006).

76
A microdureza pode ser definida como a resistência de um determinado
material (nesse caso, esmalte bovino) à deformação. Alguns autores indicam que os
valores de dureza medidos pela penetração do endentador (Knoop) refletem apenas
a resiliência do esmalte bovino (KIELBASSA et al., 1999). Outros, todavia, afirmam
que os valores de microdureza do esmalte bovino expressos em KHN medem a
integridade estrutural da lesão cariosa, em outras palavras, é uma medida
combinada do grau de mineralização e espessura da camada superficial, distribuição
mineral e extensão de mineralização da subsuperfície. Empregou-se essa análise no
presente estudo, pois a microdureza pode ser utilizada em pesquisas em que se
avaliem condições que simulem a cárie dentária (LIPPERT; LYNCH, 2014).
Em relação ao tipo de substrato, o esmalte bovino adotado no presente
estudo apresenta as seguintes características em comparação com o esmalte
humano: é mais poroso, apresenta mais carbonato e menos fluoreto (GANTT et al.,
1984; FEATHERSTONE; MELLBERG, 1981; MELLBERG; LOERTSCHER, 1974).
Tais aspectos podem não refletir o real efeito das soluções testadas nos artigos 1 e
2 sobre o esmalte humano, todavia, elegeu-se esse substrato, pois eles apresentam
uma facilidade de obtenção bem como uma área extensa para análise (4 x 4 mm).
No tocante aos tempos de agitação/complexação entre as ciclodextrinas (HP-
β-CD e γ-CD) e o TiF4, empregou-se no artigo 1 os tempos de 12 e 72 horas.
Selecionaram-se esses dois tempos de complexação já que é conhecido na
literatura o potencial de inibição da desmineralização do esmalte bovino tratado com
TiF4 associado a β-CD com 72 horas de agitação (NASSUR et al., 2013). Partiu-se
da hipótese de que as novas ciclodextrinas avaliadas apresentariam efeito na
redução da desmineralização dos blocos de esmalte bovino com um tempo de
complexação de 12 horas. Essa hipótese foi confirmada de acordo com os
resultados obtidos no artigo 1.
77
No que se refere ao tempo de aplicação das soluções fluoretadas sobre a
superfície dos blocos de esmalte, optou-se por 1 minuto. Esse item metodológico
empregado nos artigos 1 e 2 está de acordo com o que a literatura indica para
estudos laboratoriais (CHEVITARESE et al., 2004; MAGALHÃES et al., 2008;
NASSUR et al., 2013).
Os resultados obtidos no presente trabalho são promissores para uma
aplicação clínica. Entretanto, estudos de citotoxicidade devem ser conduzidos para
avaliar se as soluções de β-CD:TiF4 com 72 horas de complexação e HP-β-CD:TiF4
com 12 horas de agitação apresentam algum efeito nocivo contra células da mucosa
bucal. Trabalhos com metodologia ‘in situ’ na qual se simula condições orais ideais
também devem ser realizados com a finalidade de se investigar se o desempenho
obtido no laboratório será reproduzido no modelo ‘in situ’.
Por fim, todas as análises foram realizadas por um único pesquisador
treinado, estando ele ‘cego’ para o tipo de tratamento recebido em cada bloco
durante todas as diferentes fases do estudo. O cegamento foi estabelecido também
para a única pesquisadora que efetuou a aplicação sobre os blocos das soluções
testadas nos artigos 1 e 2 com a finalidade de reduzir interferências durante a
execução desta etapa. Esse rigor metodológico foi adotado e conduzido com o
intuito de eliminar vieses de execução e de detecção durante, respectivamente, a
realização da intervenção (aplicação das soluções) e a obtenção e análise dos
resultados, aumentando, dessa maneira, a confiabilidade dos achados obtidos no
presente trabalho.
78
6. CONCLUSÕES
Com base na análise dos resultados obtidos, é lícito concluir que:
A solução de hidroxipropil-β-ciclodextrina associada ao TiF4 a 1% com 12
horas de complexação foi capaz de reduzir a desmineralização da superfície
do esmalte hígido sob alto desafio cariogênico;
A solução de β-ciclodextrina associada ao TiF4 a 1% com 72 horas de
complexação foi superior a solução do TiF4 a 1% na remineralização da
subsuperfície do esmalte desmineralizado.

79
REFERÊNCIAS BIBLIOGRÁFICAS
AREE, T.; CHAICHIT, N. Crystal structure of β-cyclodextrin – benzoic acid inclusion complex. Carbohydrate Res., v. 338, n. 5, p. 439-446. Fev. 2003.
BÖNECKER, M.; TENUTA, L. M. A.; PUCCA JÚNIOR, G. A.; COSTA, P. B.; PITTS, N. A social movement to reduce caries prevalence in the world. Braz. Oral Res., v. 27, n. 1, p. 5-6. Jan-Fev. 2013.
BRASIL. Ministério da Saúde. Projeto SBBrasil 2010: Pesquisa Nacional de Saúde Bucal – Resultados Principais. Brasília: Ministério da Saúde; 2011.
BRITTO, M. A. F. O.; NASCIMENTO JÚNIOR, C. S.; SANTOS, H. F. Análise estrutural de ciclodextrinas: um estudo comparativo entre métodos teóricos clássicos e quânticos. Química Nova, São Paulo, v. 27, n. 6, p. 882-888, nov./dez. 2004.
BUDAL, R, M. Estudos de formação de complexos de inclusão em ciclodextrinas. Santa Catarina, 2003. Tese de Doutorado. Instituto de Química. Universidade Federal de Santa Catarina.
BUYUKYILMAZ, T.; OGAARD, B.; ROLLA, G. The resistance of titanium tetrafluoride-treated human enamel to strong hydrochloric acid. Eur. J. Oral Sci., v. 105, n. 5, p. 473-7. Out. 1997.
CAL, C.; CENTKOWSKA, K. Use of cyclodextrins in topical formulations: practical aspects. Eur. J. Pharm. Biopharm., v. 68, n. 3, p. 467-78. Mar. 2008.
CALDERINI, A. Encapsulação e caracterização físico-química do fármaco vasodilatador minoxidil em ciclodextrinas. Campinas, 2006. Dissertação de mestrado. Instituto de Química, UNICAMP.
CANNAVÀ, C.; CRUPI, V.; FICARRA, P. GUARDO, M.; MAJOLINO, D.; STANCANELLI, R.; VENUTI, V. Physicochemical characterization of coumestrol/β-cyclodextrins inclusion complexes by UV–vis and FTIR-ATR spectroscopies. Vibrational Spectroscopy, v. 48, p. 172-178. 2008.
CASTRO, R. A. L.; CHEVITARESE, O.; SOUZA, I. P. R. Action of titanium tetrafluoride on occlusal human enamel in situ. Fluoride, v. 36, n. 4., p. 252-262. 2003.
CHEVITARESE, A. B.; CHEVITARESE, O.; CHEVITARESE, L. M.; DUTRA, P. B. Titanium penetration in human enamel after TiF4 application. J. Clin. Pediatr. Dent., v. 28, n. 3, p. 253-6. 2004.
CHOI, S. G.; LEE, S. E.; KANG, B. S.; NG, C. L.; DAVAA, E.; PARK, J. S. Thermosensitive and mucoadhesive sol-gel composites of paclitaxel/dimethyl-β-cyclodextrin for buccal delivery. Plos one, v. 9, n. 10, p. 1-7. Out. 2014.

80
COMAR, L. P.; WIEGAND, A.; MORON, B. M.; RIOS, D.; BUZALAF, M. A. R.; BUCHALLA, W.; MAGALHÃES, A. C. In situ effect of sodium fluoride or titanium tetrafluoride varnish and solution on carious demineralization of enamel. Eur. J. Oral Sci., v. 120, n. 4, p. 342-8. Ago. 2012.
CONDE, N. C. O.; REBELO, M. A. B.; CURY, J. A. Evaluation of the fluoride stability of dentifrices sold in Manaus, AM, Brazil. Pesqui. Odontol. Bras., v. 17, n. 3, p. 247-53. Jul-Set. 2003.
EXTERKATE, R. A. M.; TEN CATE, J. M. Effects of a new titanium fluoride derivate on enamel de- and remineralization. Eur. J. Oral Sci., v. 115, n. 2, p. 143-157, abr. 2007.
FEATHERSTONE, J. D.; MELLBERG, J. R. Relatives rates of progress of artificial carious lesions in bovine, ovine and human enamel. Caries Res., v. 15, n. 1, p. 109-14. 1981.
FRAGA, C. P. T.; BÖNECKER, M. J. S.; CHEDID, S. J.; GUEDES-PINTO, A. C. Flúor – uso externo. In.: GUEDES-PINTO, A. C. Odontopediatria. São Paulo: Santos, 2010. cap.26, p. 469-502.
GANTT, D. G.; SILVERSTONE, L. M.; FEATHERSTONE, J. D. B.; HICKS, M. J. Structural comparison of sound and demineralized human and bovine enamel. J. Dent. Res., v. 63, p. 273, 1984.
GAURAV, C.; GOUTAM, R.; ROHAN, K. N.; SWETA, K. T.; ABHAY, C. S.; AMIT, G. K. (Copper-curcumin) β-cyclodextrin vaginal gel: delivering a novel metal-herbal approach for the development of topical contraception prophylaxis. Eur. J. Pharm. Sci., 2014 In press.
GRON, P. Chemistry of topical fluorides. Caries Research, Basel, v. 11, n. 1, p. 172-204, 1977.
GU, Z.; LI, J.; SÖREMARK, R. Influence of tooth surface conditions on enamel fluoride uptake after topical application of TiF4 in vitro. Acta Odontol. Scand., v. 54, n. 5, p. 279-81. Out. 1996.
HIGASHI, K.; IDEURA, S.; WARAYA, H.; LIMWIKRANT, W.; MORIBE, K.; YAMAMOTO, K. Simultaneous dissolution of naproxen and flurbiprofen from a novel ternary gamma-cyclodextrin complex. Chem. Pharma. Bulletin (Tokyo), v. 58, n. 8, p. 769-772. Maio. 2010.
HOROWITZ, H. S.; HEIFETZ, S. B. Evaluation of topical applications of stannous fluoride to teeth of children born and reared in a fluoridated community: final report. ASDC Journal of Dentistry for children, v. 36, n. 5, p. 355-61, set-out. 1969
81
JANSOOK, P.; RITTHIDEJ, G. C.; UEDA, H.; STEFÁNSSON, E.; LOFTSSON, T. yCD/HPyCD mixtures as solubilizer: solid-state characterization and sample dexamethasone eye drop suspension. J. Pharma. Pharma. Sci., v. 13, n. 3, p. 336-350, 2010.
KIELBASSA, A. M.; WRBAS, K. TH.; SCHULTE-MÖNTING, J.; HELLWIG, E. Correlation of transversal microradiography and microhardness on in situ-induced demineralization in irradiated and nonirradiated human dental enamel. Ach. Oral Biol., v. 44, n. 3, p. 243-51. Mar. 1999.
KUBOTA, D. Estudo físico-químico do complexo de inclusão do fármaco trimetoprim com a β ciclodextrina aleatoriamente metilada. 2010. 83p. Dissertação (Mestrado em Química) – Programa de Pós-Graduação em Química, Pró-Reitoria de Pós-Graduação e Pesquisa, Universidade Federal de Sergipe, 2010.
LEACH, S. A. Reactions of fluoride with powdered enamel and dentin. British Dental Journal, v. 106, p. 133-142, 1959.
LIPPERT, F.; LYNCH, R. J. M. Comparison of Knoop and Vickers surface microhardness and transverse microradiography for the study of early caries lesion formation in human and bovine enamel. Arch. Oral Biol., v. 59, n. 7, p. 704-10. Jul. 2014.
MAGALHÃES, A. C.; COMAR, L. P.; RIOS, D.; DELBEM, A. C. B.; BUZALAF, M. A. R. Effect of 4% titanium tetrafluoride (TiF4) varnish on demineralization and remineralisation of bovine enamel in vitro. J. Dent., v. 36, n. 2, p. 158-162. Fev. 2008.
MARINHO, V. C.; HIGGINS, J. P.; LOGAN, S. Combinations of topical fluoride (toothpastes, mouthrinses, gels, varnishes) versus single single topical fluoride for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2004; (1): CD002781.
MELLBERG, J. R.; LOERTSCHER, K. L. Comparison of in vitro fluoride uptake by human and bovine enamel from acidulated phosphate-fluoride solutions. J. Dent. Res., v. 53, n. 1, p. 64-7. Jan-Fev. 1974.
MELLBERG, J. R.; RIPA, L. W. Fluoride in preventive Dentistry theory and clinical applications. Chicago: Quintessence, p. 290, 1983.
NARVAI, P. C.; FRAZÃO, P.; RONCALLI, A. G.; ANTUNES, J. L. F. Cárie dentária no Brasil: declínio, polarização, iniqüidade e exclusão social. Revista Panamericana de Salud Pública, Washington, v. 19, n. 6, p. 385-393, jun. 2006.
NASSUR, C.; ALEXANDRIA, A. K.; POMARICO, L.; SOUSA, V. P.; CABRAL, L. M.; MAIA, L. C. Characterization of a new TiF4 and β-cyclodextrin inclusion complex

82
and its in vitro evaluation on inhibiting enamel demineralization. Arch Oral Biol., v. 58, n. 3, p. 239-47. Mar. 2013.
OGAARD, B.; ROLLA, G.; DUKMAN, T.; RUBEN, J.; ARENDS, J. Effects of fluoride mouth rinsing on caries lesion development in shark enamel and in-situ caries model study. Scand. J. Dent. Res., v. 99, n. 5, p. 372-7. Out. 1991.
OGAARD, B.; ROLLA, G.; RUBEN, J.; DIJKMAN, T.; ARENDS, J. Microradiographic study of demineralization of shark enamel in a human caries model. Scand. J. Dent. Res., v. 96, n. 3, p. 209-11. Jun. 1988.
QUEIROZ, C. S.; HARA, A. T.; PAES LEME, A. F.; CURY, J. A. pH-cycling models to evaluate the effect of low fluoride dentifrice on enamel de- and remineralization. Braz. Dent. J., v. 19, n. 1, p. 21-27. 2008.
RAJEWSKI, R. A.; STELLA, V. J. Pharmaceutical applications of cyclodextrins. 2. In vivo drug delivery. J. Pharma. Sci., v. 85, n. 11, p. 1142-1169. Nov. 1996.
REED, A. J.; BIBBY, B. G. Preliminary report on effect of topical applications of titanium tetrafluoride on dental caries. J. Dent. Res., v. 55, n. 3, p. 357-8. Maio-Jun. 1976.
SANTOS, L. M.; REIS, J. I. L.; MEDEIROS, M. P.; RAMOS, S. M.; ARAÚJO, J. M. In vitro evaluation of fluoride products in the development of carious lesions in deciduous teeth. Braz. Oral Res., 23, n. 3, p. 296-301. Jul-Set. 2009.
SAXEGAARA, E.; LAGERLÖF, F.; ROLLA, G. Dissolution of calcium fluoride in human saliva. Acta Odontologica Scandinavica, v. 46, n. 6, p.355-359, dez. 1988.
SINGH, M.; SHARMA, R.; BANERJEE, V. C. Biotechnological applications of cyclodextrins. Biotechnology Advances, v. 20, n. 5-6, p. 341–359, dez. 2002.
SOUSA, F. B.; VIANNA, S. S.; SANTOS-MAGALHÃES, N. S. A new approach for improving the birefringence analysis of dental enamel content using polarizing microscopy. J. Microsc., v. 221, n. 2, p. 79-83. Fev. 2006.
TARBET, W. J.; FOSDICK, L. S. Permeability of human dental enamel of acriflavine and potassium fluoride. Archives of Oral Biology, v. 16, n. 8, p. 951-961, ago. 1971.
TENUTA, L. M. A.; CURY, J. A. Fluoride: its role in dentistry. Braz. Oral Res., São Paulo, v. 24, n. 1, p. 9-17, 2010.
TEZEL, H.; ERGÜCÜ, Z.; ÖNAL, B. Effects of topical fluoride agents on artificial enamel lesion formation in vitro. Quintessence int., v. 33, n. 5, 347-52. Maio. 2002.

83
TODD, M. A.; STALEY, R. N.; KANELLIS, M. J.; DONLY, K. J.; WEFEL, J. S. Effect of a fluoride varnish on demineralization adjacent to orthodontic brackets. Am. J. Orthod. Dentofacial Orthop., v. 116, n. 2, p. 159-67. Ago. 1999.
VALLE, E. M. M. D. Cyclodextrins and their uses: a review. Process Biochemistry, v. 39, n. 9, p. 1033-1046, maio. 2004.
VENTURINI, C. G.; NICOLINI, J.; MACHADO, C.; MACHADO, V. G. Propriedades e aplicações recentes das ciclodextrinas. Química Nova, São Paulo, v. 31, n. 2, p. 360-368, 2008.
VERMET, G.; DEGOUTIN, S.; CHAI, F.; MATON, M.; BRIA, M.; DANEL, C.; HILDEBRAND, H. F.; BLANCHEMAIN, N.; MARTEL, B. Visceral mesh modified with cyclodextrin for the local sustained delivery of ropivacaine. Int. J. Pharm., v. 467. n. 1-2, p. 149-159. Set. 2014.
WAHENGBAM, P.; TIKKU A. P.; LEE, W. B. Role of titanium tetrafluoride (TiF4) in conservative dentistry: a systematic review. J. Conserv. Dent., v. 14, n. 2, p. 98-102. Abr. 2011.
WANG, Y.; QIAO, X.; LI, W.; ZHOU, Y.; JIAO, Y.; YANG, C.; DONG, C.; INOUE, Y.; SHUANG, S. Study on the complexation of isoquercitrin with β-cyclodextrin and its derivatives by spectroscopy. Analytica Chimica Acta, v. 650, n. 1, p. 124-130. Set. 2009.
WIEGAND, A.; MAGALHÃES, A. C.; ATTIN, T. Is titanium tetrafluoride (TiF4) effective to prevent carious and erosive lesions? A review of the literature. Oral Health Prev. Dent.; v. 8, n. 2, p. 159-164. 2010.
ZENG, J.; REN, Y.; ZHOU, C.; YU, S.; CHEN, H. Preparation and physicochemical characteristics of the complex of edaravone with hydroxypropyl-β-cyclodextrin. Carbohydrate Polymers, v. 83, n. 3, p. 1101-1105. Jan. 2011.
ZHAO, M.; WANG, H.; YANG, B.; TAO, H. Identification of cyclodextrin inclusion complex of chlorogenic acid and its antimicrobial activity. Food Chem., v. 120, p. 1138-1142. 2010.