Embed Size (px)
Citation preview

ALESSANDRA NARCISO GARCIA
EFEITOS DAS INTERVENÇÕES BACK SCHOOL E MCKENZIE EM
PACIENTES COM DOR LOMBAR CRÔNICA NÃO ESPECÍFICA: UM
ESTUDO CONTROLADO ALEATORIZADO
UNIVERSIDADE CIDADE DE SÃO PAULO
SÃO PAULO
2012
ALESSANDRA NARCISO GARCIA
EFEITOS DAS INTERVENÇÕES BACK SCHOOL E MCKENZIE EM
PACIENTES COM DOR LOMBAR CRÔNICA NÃO ESPECÍFICA: UM
ESTUDO CONTROLADO ALEATORIZADO
Defesa apresentada ao Programa de Mestrado em Fisioterapia da Universidade Cidade de São Paulo, como requisito para obtenção do título de Mestre, sob orientação do Prof. Dr. Leonardo Oliveira Pena Costa e co-orientação da Prof.a
Dr.aLucíola da Cunha Menezes Costa
UNIVERSIDADE CIDADE DE SÃO PAULO
SÃO PAULO
2012
Banca Examinadora
Prof. Dr. Leonardo Oliveira Pena Costa ___________________________
Universidade Cidade de São Paulo
Prof. Dra. Sandra Regina Alouche___________________________
Universidade Cidade de São Paulo
Prof. Luciana Andrade Carneiro Machado_____________________________
Universidade Federal de Minas Gerais

DEDICATÓRIA
Dedico esta dissertação aos meus pais, Isidro da Silva Garcia e Lucimara Narciso
Garcia, que tanto me incentivaram e apoiaram durante minha trajetória de vida.
Deixaram muitas vezes seus interesses de lado para que eu pudesse ter a chance de
estudar, investiram no meu conhecimento para que hoje eu pudesse ver um sonho
concretizado na minha vida. São verdadeiros referenciais eternos para mim de
dedicação, esforço, caráter e perseverança!
AGRADECIMENTOS
Agradeço primeiramente a Deus por ter me concedido vida, saúde e motivação durante
esse tempo de estudo no mestrado e à minha família pela paciência e incentivo.
Serei sempre muito agradecida ao meu orientador Professor Dr. Leonardo Oliveira Pena
Costa por ter me dado a oportunidade e a honra de ser orientada por ele durante meu
mestrado. Sua orientação e convivência me permitiram não somente descobrir o gosto
pela pesquisa, como também enxergar o quanto aprendi e cresci durante esse período.
Agradeço por tudo que me ensinou sempre com tanta paciência, competência e
disposição, pelos momentos de conversa, palavras de motivação e apoio. Será sempre
um exemplo para mim de pesquisador, professor e pessoa!
Agradeço também à minha co-orientadora Lucíola da Cunha Menezes Costa, que além
de ter sido uma professora incrível, foi também uma amiga muito querida. Agradeço
pelas considerações sempre muito pertinentes e na hora certa, que me fizeram aprender
ainda mais durante meu mestrado. Posso dizer que sua participação abrilhantou ainda
mais a orientação que recebi.
À minha professora de graduação e amiga Francine Lopes Barreto Gondo por ter
acreditado em meu potencial, me incentivado em cada etapa de minha formação, pelos
conselhos, conversas e apoio para que eu fizesse o mestrado. Será sempre um
referencial na minha vida.
À avaliadora do estudo e grande amiga Tatiane Mota da Silva por ter abraçado com
carinho e dedicação o desafio da função de avaliadora do estudo e pelo trabalho que
realizou com tanta excelência. Foi um prazer trabalhar ao seu lado.

Aos meus amigos do grupo de estudos de dor lombar agradeço pelas opiniões, sugestões
e críticas que auxiliaram muito no desenvolvimento e concretização deste trabalho.
Aos meus professores do Programa de Mestrado em Fisioterapia por terem contribuído
na minha formação, conhecimento e aprendizado.
Sou muito grata também a todos os pacientes que consentiram em participar desse
estudo, pois sem eles não teria sido possível concluir esse mestrado. À equipe de
funcionários da Clínica de Fisioterapia da Universidade Cidade de São Paulo agradeço
pelo espaço concedido para atendimento dos pacientes do estudo durante esse período.
À Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), pelo apoio e
financiamento do estudo.

SUMÁRIO
Páginas
Sumário..........................................................................................................................vii
Prefácio............................................................................................................................ix
Resumo............................................................................................................................xi
Abstract.........................................................................................................................xiii
Capítulo 1: Contextualização.........................................................................................1
1.1 Epidemiologia da dor lombar..........................................................................2
1.2 Diagnóstico da dor lombar...............................................................................4
1.3 Prognóstico da dor lombar...............................................................................6
1.4 Intervenções para o tratamento da dor lombar.................................................7
1.5 Método Back School........................................................................................9
1.6 Método McKenzie..........................................................................................10
1.7 Justificativa....................................................................................................12
1.8 Objetivos da dissertação................................................................................12
1.9 Referências.....................................................................................................13
Capítulo 2: Effectiveness of Back School and McKenzie techniques in patients with
chronic non specific low back pain: a protocol of a randomised controlled trial....20
Abstract................................................................................................................21
Background..........................................................................................................21
Methods/Design...................................................................................................22
Approval and registration of the study................................................................22
Eligibility criteria................................................................................................22
Procedures..........................................................................................................23
Randomisation procedures...................................................................................23
Outcomes.............................................................................................................23
Interventions........................................................................................................24
Statistical analysis.............................................................................................26
Discussion............................................................................................................26
References............................................................................................................26
Apêndice 1: Apostila de avaliação do estudo......................................................28
Capítulo 3: Effectiveness of Back School versus McKenzie exercises in patients
with chronic non-specific low back pain: a randomised controlled trial.................55
Abstract................................................................................................................57
Background..........................................................................................................59
Methods...............................................................................................................61
Results..................................................................................................................70
Discussion............................................................................................................75
Conclusion...........................................................................................................79
References............................................................................................................80
Appendices...........................................................................................................87
Apêndice 2: Efeitos de duas intervenções fisioterapêuticas em pacientes com dor
lombar crônica não específica: viabilidade de um estudo controlado
aleatorizado..........................................................................................................92
Capítulo 4: Considerações Finais...............................................................................101
4.1 Resultados encontrados................................................................................102
4.2 Implicações clínicas.....................................................................................103
4.3 Recomendações para futuros estudos..........................................................104
4.4 Referências...................................................................................................105
Anexo 1: Instruções para os autores - Physical Therapy..........................................106
Anexo 2: Aprovação do Comitê de Ética e Pesquisa e Registro do estudo.............111
PREFÁCIO
Essa dissertação de mestrado aborda tópicos relacionados à dor lombar; especificamente
sobre os efeitos de duas intervenções terapêuticas: Back School e McKenzie, no
tratamento dessa condição, para os desfechos intensidade de dor, desempenho
funcional, qualidade de vida e amplitude de movimento de flexão de tronco. É
constituída por quatro capítulos, sendo que cada um deles possui sua própria lista de
referências bibliográficas. O Programa de Mestrado em Fisioterapia da Universidade
Cidade de São Paulo (UNICID) permite a inclusão de artigos publicados, aceitos ou
submetidos para publicação em seu formato de publicação ou submissão no corpo do
exemplar da dissertação.
O capítulo 1 apresenta uma contextualização de tópicos relevantes a respeito da dor
lombar, como definição, prevalência, custos, classificação, prognóstico e principais
intervenções utilizadas para tratar essa condição. Nesse mesmo capítulo estão
apresentados os métodos Back School e McKenzie e os objetivos da dissertação. O
capítulo 2 consiste no projeto de pesquisa do estudo controlado aleatorizado que
apresenta em maiores detalhes os métodos desse estudo. Este capítulo está apresentado
no formato de artigo no periódico BMC Musculoskeletal Disorders, em que o referido
projeto foi publicado. No apêndice 1 está anexada a apostila de avaliação utilizada no
estudo.
O capítulo 3 tem como objetivo apresentar os resultados do estudo controlado
aleatorizado. Este capítulo está formatado nas normas da revista Physical Therapy na
qual o artigo está em processo de revisão (a versão apresentada corresponde a uma
versão que já passou por uma rodada de revisões nesse periódico). No apêndice 2 está
anexado o artigo sobre a viabilidade do estudo controlado aleatorizado, desenvolvido no

início da pesquisa com o intuito de verificar como estava o andamento do estudo. Esse
artigo foi publicado na Revista Brasileira de Fisioterapia. O Capítulo 4 apresenta as
considerações finais da dissertação, bem como as implicações dos resultados para a
prática clínica e para a pesquisa e sugestões de estudos futuros sobre o tópico.
Uma cópia das “instruções para os autores” da revista Physical Therapy está
apresentada como anexo. O estudo controlado aleatorizado dessa dissertação foi
aprovado pelo Comitê de Ética em Pesquisa da Universidade Cidade de São Paulo
(13469394) e registrado previamente ao início do estudo no Australian New Zealand
Clinical Trials Registry (ACTRN12610000435088).
RESUMO
Contextualização: A dor lombar crônica não-específica é um importante problema de
saúde e de ordem socioeconômica responsável por um alto índice de absenteísmo no
trabalho, redução do desempenho funcional e alterações emocionais. Atualmente, sabe-
se que uma das melhores opções para o tratamento de pacientes com essa condição é a
prática de programas de exercício, combinados com programas de educação. Os
métodos Back School e McKenzie são intervenções populares que incluem uma
combinação de exercícios e orientações no tratamento de pacientes com dor lombar
crônica não específica.
Objetivo: Comparar os efeitos das intervenções Back School e McKenzie em pacientes
com dor lombar crônica não específica nos desfechos: intensidade de dor, desempenho
funcional, qualidade de vida e amplitude de movimento de flexão de tronco.
Desenho do estudo: Estudo controlado aleatorizado com dois braços, avaliador cego,
registrado prospectivamente.
Local: Este estudo foi conduzido na clínica de Fisioterapia da Universidade Cidade de
São Paulo.
Pacientes: 148 pacientes com dor lombar crônica não específica.
Intervenções: Programa de quatro semanas de tratamento (uma vez por semana) com
os métodos Back School (realizado em grupo) ou McKenzie (abordagem individual). Os
participantes foram orientados a fazer exercícios em casa diariamente.
Desfechos: Os desfechos clínicos foram obtidos com 1, 3 e 6 meses após a
aleatorização. Os desfechos primários foram intensidade de dor (medida pela Escala
Numérica de Dor que varia de 0-10 pontos) e desempenho funcional (medido pelo

questionário de Incapacidade Roland Morris 0-24 questões) 1 mês após a aleatorização.
Os desfechos secundários foram intensidade de dor e desempenho funcional com 3 e 6
meses após a aleatorização; qualidade de vida (medida pelo questionário de qualidade
de vida da Organização Mundial de Saúde versão curta com 1, 3 e 6 meses após a
aleatorização e amplitude de movimento de flexão de tronco (medida pelo inclinômetro)
com 1 mês após a aleatorização. Os dados foram coletados por um avaliador cego.
Resultados: Os pacientes alocados no grupo McKenzie obtiveram melhores resultados
para o desfecho desempenho funcional após o tratamento; (média da diferença de 2,37
pontos; IC a 95% 0,76 a 3,99), mas não para a dor (média da diferença de 0,66 pontos;
IC a 95% -0,29 a 1,62). Não foram encontradas diferenças entre os grupos para os
demais desfechos.
Conclusão: Esse estudo fornece evidência de alta qualidade que os programas de
tratamento Back School e McKenzie produziram redução dos níveis de dor e melhora do
desempenho funcional em pacientes com dor lombar crônica não específica. O método
McKenzie foi discretamente mais efetivo do que o método Back School para o
desempenho funcional, mas não para a dor imediatamente após o tratamento em
pacientes com dor lombar crônica.
ABSTRACT
Background: Chronic non-specific low back pain is an important health and
socioeconomic problem, which is associated with work absenteeism, disability and
emotional changes. One of the best options in the treatment of patients with chronic low
back pain are exercise programs combined with education. The Back School and
McKenzie methods are popular active treatment approaches that include both exercises
and education for patients with chronic non-specific low back pain.
Objectives: To compare the effectiveness of Back School and McKenzie methods in
the treatment of patients with chronic non-specific low back pain for pain intensity,
disability, quality of life and trunk flexion range of motion.
Design: Prospectively registered, two-arm, randomised controlled trial with a blinded
assessor.
Setting: This study was conducted in the outpatient physical therapy clinic of the
Universidade Cidade de São Paulo in Brazil.
Patients: The participants were 148 patients with chronic non-specific low back pain.
Interventions: A four-week treatment program (one session/week) based upon the
Back School (delivered in group) or McKenzie (delivered individually) principles. The
participants were also instructed to perform a daily set of home exercises.
Measurements: Clinical outcomes were obtained at follow up appointments at 1, 3 and
6 months after randomisation. Primary outcomes were pain intensity (measured by the
0-10 Pain Numerical Rating Scale) and disability (measured by the 24-item Roland
Morris Disability Questionnaire) 1 month after randomisation. Secondary outcomes
were pain intensity and disability at 3 and 6 months after randomisation; quality of life
(measured by World Health Organization Quality of Life Bref Questionnaire) at 1, 3
and 6 months after randomisation and trunk flexion range of motion (measured by an
inclinometer) at 1 month after randomisation. The data were collected by a blinded
assessor.
Results: Patients allocated to the McKenzie group had greater improvements in
disability at one month (mean effect 2.37 points; 95% CI 0.76 to 3.99) but not in pain
intensity (mean effect 0.66 points; 95% CI -0.29 to 1.62). No between-group differences
were observed for all other outcomes.
Conclusion: Our study provides high-quality evidence that a treatment program based
on the Back School and McKenzie methods produced small reduction in pain intensity
and disability in patients with chronic non specific low back pain. The McKenzie
method was slightly more effective than Back School for disability, but not for pain
intensity immediately after treatment in patients with chronic low back pain.

Capítulo 1
Contextualização

1.1 Epidemiologia da dor lombar
A dor lombar pode ser definida como dor ou desconforto entre as margens costais e pregas
glúteas inferiores, com ou sem irradiação para os membros inferiores1. A dor lombar é um
sintoma que representa um importante problema de saúde, tanto para os pacientes, que
muitas vezes não sabem como lidar com essa condição; quanto para os profissionais de
saúde e para a sociedade, por ser um sintoma associado a um alto índice de absenteísmo no
trabalho, utilização mais frequente dos serviços de saúde e dos benefícios por afastamento
do trabalho2. Esta condição de saúde também está frequentemente associada a alterações
emocionais3 e possíveis limitações de movimento da coluna4, sendo hoje um dos
problemas mais comuns de saúde no mundo5.
A dor lombar é uma condição extremamente prevalente5. Estima-se que com o
envelhecimento, o número de pessoas que sofrem de dor lombar aumente ao longo dos
anos5. A prevalência pontual de dor lombar corresponde a 18,3%, a prevalência nos
últimos 30 dias a 30,8%, nos últimos 12 meses corresponde a 38% e a prevalência em
algum momento da vida equivale a 38,9%5. Outros dados indicam que a dor lombar é mais
prevalente em mulheres5, 6 e em indivíduos com idades entre 40 e 80 anos5. No Brasil, a
Pesquisa Nacional por Amostra de Domicílios (PNAD) apontou a dor lombar como a
segunda condição de saúde mais prevalente, atrás apenas da hipertensão arterial sistêmica7.
A dor lombar corresponde não somente a um problema de saúde, como também de ordem
socioeconômica, estando associada a altos custos para o seu tratamento8. Estimativas
apontam que em países europeus os custos diretos e indiretos variam de 2 a 4 bilhões de
Euros anuais8. Outros dados mostram que os custos diretos9 (que incluem serviços
médicos, emergenciais, ambulatoriais e hospitalares, medicamentos e exames de
diagnóstico) e indiretos9 (absenteísmo, licença por doença, aposentadoria precoce e
comprometimento do desempenho funcional e ocupacional) estão estimados em mais de
100 bilhões de dólares por ano9. Uma revisão sistemática10 apontou que as intervenções
relativas à dor lombar que mais impõem custos diretos para a sociedade são fisioterapia e
internações hospitalares (17%), seguidas por gastos com medicamentos (13%), cuidados
primários de saúde (13%), serviços ambulatoriais (8%), exames de imagem (7%), médicos
especialistas (7%), cirurgia (5%), quiropraxia (5%) e outros serviços (5%). Na dor lombar
crônica, as maiores despesas tem sido destinadas aos cuidados primários dessa condição11.
Para o custo indireto as maiores despesas foram com licença para afastamento do trabalho
e aposentadoria precoce10. Apesar do custo direto ser mais facilmente mensurável, os
maiores custos identificados foram com os indiretos10, que representam aproximadamente
90% dos custos totais com dor lombar8. Finalmente, há evidências10 que mostram que o
aumento nos custos com o tratamento da dor lombar parece ser proporcional ao tempo de
comprometimento do desempenho funcional, ou seja, maior no cuidado de pacientes
crônicos.
Uma revisão sistemática12 que buscou verificar o custo benefício da abordagem clínica
primária da dor lombar, mostrou que essa abordagem isoladamente não parece ser a opção
com melhor custo benefício para o tratamento de pacientes com dor lombar. No entanto,
essa revisão mostrou que a adição de programas de exercício, reabilitação física e
orientações no cuidado de pacientes com dor lombar resulta em melhora do custo benefício
da abordagem clínica desses pacientes12. Isso significa que os profissionais da saúde que
fizerem essa primeira abordagem dos pacientes com dor lombar, têm maior probabilidade
de obter uma melhor resposta com um menor custo para o tratamento desses pacientes, se
os encaminharem também para serviços secundários de saúde, como por exemplo, para
serviços de fisioterapia12.

1.2 Diagnóstico e classificação da dor lombar
Elaborar o diagnóstico de pacientes com dor lombar é uma das decisões mais complexas e
importante na prática profissional, visto que possibilita verificar a presença de doenças
sérias13, predizer o prognóstico e direcionar o tratamento dos pacientes2. Essa decisão se
baseia na avaliação clínica (história clínica e exame físico), devendo esta, ser clara e
conduzida a partir de um processo lógico2.
A forma mais comum e aceita de classificar pacientes com dor lombar é por meio da
duração dos sintomas8. Pacientes com dor lombar aguda são aqueles em que os sintomas
estiverem presentes por até 6 semanas; subaguda de 6 a 12 semanas e crônica igual ou
superior a 12 semanas8. Outras formas de classificação se baseiam no tipo e localização
dos sintomas2, para a partir desse processo, subdividir os pacientes em grupos homogêneos
e facilitar/aprimorar a intervenção clínica14. Seguindo essa linha de pensamento, alguns
autores propuseram sistemas de classificação para a dor lombar14.
Waddell2, por exemplo, propôs uma triagem diagnóstica baseada na avaliação clínica e
resposta sintomática (local da dor, sintomas neurológicos e deformidades) para classificar
os pacientes em três grupos: 1) dor lombar não específica (dor mecânica de origem
musculoesquelética); 2) compressão de raiz nervosa (prolapso do disco intervertebral,
estenose espinal ou aderência cicatricial por cirurgia); e 3) doenças graves de coluna
(tumores, infecções, fraturas e doenças inflamatórias). A maior parte dos pacientes (95%)
se enquadra no primeiro grupo, cerca de 5% no grupo de compressão de raiz nervosa e
menos de 1% no grupo de doenças graves de coluna2.
Como a maior parte das dores lombares não tem causa específica, a triagem diagnóstica
desse grupo é direcionada por critérios de exclusão2. Por exemplo, num primeiro momento
da anamnese busca-se identificar indicativos de doenças graves de coluna13, 15, como perda
de peso inexplicável, história prévia de tumor ou de traumas2, 16. Os exames de imagem
nesse caso podem ser úteis para pacientes que apresentem fatores de risco para doenças
graves de coluna2. Caso o paciente apresente sinais e sintomas sugestivos de doenças
graves de coluna, busca-se entender melhor sua condição por meio de exames específicos.
É importante ressaltar que somente uma pequena proporção de pacientes deveria, num
primeiro momento, ser submetida a exames de maior complexidade17.
Num segundo momento, questiona-se o local e o comportamento da dor e realiza-se um
exame neurológico para identificar se existe algum comprometimento de raiz nervosa2.
Pacientes com dor lombar bem delimitada no trajeto do nervo para somente um dos
membros inferiores, podendo atingir até os dedos do pé, são suspeitos de apresentarem dor
por irritação ou compressão de raiz nervosa2. Se o paciente apresentar sinais como
hiposensibilidade, hiporreflexia e fraqueza muscular, sua dor é considerada como dor por
compressão de raiz nervosa2. Alguns testes provocativos como teste de Laségue e de
extensão da perna reta auxiliam no diagnóstico desse grupo. Os pacientes que não se
encaixarem nos grupos citados acima, são então classificados no grupo de dor lombar não
específica2. Pacientes com dor lombar não específica geralmente apresentam dor mal
localizada que se modifica de acordo com o movimento que a pessoa realiza durante o dia2.
Há algumas outras formas de classificação não tão generalistas que apresentam um
raciocínio semelhante ao de Waddell (baseado na história clínica e comportamento dos
sinais e sintomas clínicos), mas que visam a classificação dos pacientes em subgrupos que
tendem a responder melhor ou pior a uma intervenção específica18, 19. Delitto et al18 por
exemplo, propuseram um sistema que visa identificar subgrupos de pacientes que tinham
maior predisposição de responder às intervenções: exercícios com direção específica,
manipulação, estabilização e tração18. Já Robin McKenzie20 propôs um sistema de
classificação baseado não só na história clínica do paciente como também na resposta

sintomática e mecânica durante os movimentos de coluna. Por meio desse método os
distúrbios relacionados à coluna podem ser classificados em 3 subgrupos (ou síndromes):
1) síndrome do desarranjo, 2) síndrome de disfunção ou 3) síndrome postural19, 21.
Como visto, a dor lombar pode ser classificada de várias maneiras, sendo que a maior parte
dos sistemas de classificação existentes enfatizam as características biomédicas em
detrimento das biopsicossoais14. Nessa dissertação optamos em utilizar a classificação de
duração dos sintomas a fim de incluir pacientes crônicos (com dor há pelo menos 12
semanas ou mais)1 e a classificação de Waddell2 para incluir pacientes com dor lombar não
específica. A partir desse ponto do texto, todas as vezes em que estiver escrito o termo dor
lombar crônica, pede-se que o leitor entenda como dor lombar crônica não específica,
apenas para fins de padronização dos termos.
Classificar pacientes com dor lombar quanto à duração dos sintomas e tipo dos mesmos,
além de facilitar a construção do raciocínio e a tomada de decisão clínica, também auxilia a
evitar gastos desnecessários com exames complementares,minimizar a preocupação e
ansiedade dos pacientes com a sua própria condição e predizer com boa acurácia o
prognóstico dos mesmos2.
1.3 Prognóstico da dor lombar
O prognóstico da dor lombar está diretamente relacionado ao tempo de duração dos
sintomas. Pacientes com dor lombar crônica apresentam um prognóstico menos favorável
do que pacientes com dor lombar aguda22, 23. Uma revisão sistemática com meta análise24
mostrou que tanto os pacientes com dor lombar aguda quanto persistente (subaguda e
crônica) tendem a apresentar melhoras rápidas na dor e desempenho funcional nas seis
primeiras semanas após o início dos sintomas, porém após um ano do início dos sintomas

os pacientes com dor lombar aguda tendem a apresentar níveis muito baixos de dor e
comprometimento do desempenho funcional, ao contrário dos pacientes com dor lombar
persistente que ainda apresentam níveis moderados de dor e comprometimento do
desempenho funcional após esse mesmo tempo. Além disso, aproximadamente 60% dos
pacientes com dor lombar crônica não se consideram recuperados num período de um ano
após o início dos sintomas24. O prognóstico de dor lombar crônica parece ser menos
favorável para pessoas que consideram seu prognóstico ruim, para os pacientes que
apresentam baixo nível educacional e para os pacientes que já tiveram licença de trabalho
por dor lombar previamente, além de altos índices de dor e incapacidade no início dos
sintomas23.
Em suma, a maior parte dos pacientes que apresentam dor lombar aguda, independente de
receberem ou não um tratamento específico, tendem a apresentar melhora da dor e
desempenho funcional a curto prazo25, ao contrário dos pacientes crônicos que em sua
grande maioria tornam-se frequentadores dos serviços de saúde na procura por
intervenções que auxiliem na redução da dor e no desempenho de suas atividades diárias e
profissionais.
1.4 Intervenções para o tratamento da dor lombar
A literatura apresenta várias possibilidades para o tratamento da dor lombar, que
diferenciam-se entre si, dependendo da duração dos sintomas e da classificação dessa
condição1. No caso da dor lombar aguda não específica, que possui um prognóstico mais
favorável25, recomenda-se pelas Diretrizes Européias para Conduta de Pacientes com Dor
Lombar Aguda26: orientar o paciente a manter-se ativo na medida do possível, tanto nas
suas atividades diárias em casa, quanto em atividades de trabalho e lazer; uso de
analgésicos e relaxantes musculares, manipulação ou mobilização vertebral e programas de
tratamento multidisciplinar.
Com relação à dor lombar crônica não específica, as Diretrizes Européias para Conduta de
Pacientes com Dor Lombar Crônica1 recomendam: terapia cognitivo comportamental,
associada a tratamento multidisciplinar; intervenção educacional; manipulação e
antiinflamatórios, e em casos mais graves recomenda-se o uso de opióides, antidepressivos
e relaxantes musculares1. Além dessas recomendações, na maioria das diretrizes de prática
clínica, a terapia com exercícios supervisionados também tem se mostrado eficaz na
redução da dor e melhora do desempenho funcional, no tratamento de pacientes com dor
lombar crônica não específica1, 27, 28.
A terapia com exercícios apresenta também uma boa relação de custo benefício no
tratamento de pacientes com dor lombar crônica29. Os métodos Back School (realizado em
grupo) e McKenzie (abordagem individual) são opções populares de terapia ativa, que
utilizam exercícios específicos para o tratamento da dor lombar, além de informações
teóricas que visam à educação do paciente, para que o mesmo seja capaz de entender
melhor sua condição e aprender como modificar sua conduta frente à dor lombar30-32.
1.5 Método Back School
O método Back School foi descrito pela primeira vez em 1969 na Suécia pela fisioterapeuta
Mariane Zachrisson Forssel, com o propósito de tratar pacientes com dor na coluna e
prevenir os episódios recorrentes de dor33. Originalmente o programa incluía grupos de 6 a
8 pessoas que apresentassem dor em qualquer parte da coluna, independente do tempo de
duração34. Era composto por 4 sessões de aproximadamente 45 minutos, que contavam
com a presença de um componente teórico e um componente prático33. O componente
teórico era constituído por noções de anatomia e biomecânica da coluna; epidemiologia;
fisiopatologia das desordens mais frequentes da coluna; postura ideal e postura de repouso;
ergonomia e explicações das modalidades mais comuns de tratamento33, 34. O componente
prático era constituído de exercícios que tinham como objetivo melhorar a mobilidade,
flexibilidade e força33.
Alguns anos após a sua criação, sistemas de saúde de países como Canadá, Estados Unidos
e Brasil implantaram o método, porém com algumas modificações/adaptações,
relacionadas ao público alvo, número de pacientes no grupo, duração do programa e de
cada sessão e sequência do conteúdo do método33, 34. Por exemplo, no Canadá o programa
se destinava ao tratamento de 10 a 15 pacientes com dor lombar crônica, com duração de
90 minutos por sessão34. Já nos Estados Unidos manteve-se a mesma duração das sessões,
porém só eram incluídos até 4 pacientes que apresentassem dor lombar com ou sem
irradiação para membros inferiores34. No Brasil, diversos programas foram implantados,
sendo que a maioria deles se destinou a pacientes crônicos34. As principais diferenças entre
eles foram com relação ao tempo de tratamento e duração das sessões34.
Uma revisão sistemática recente sobre o método Back School33 no tratamento de pacientes
com dor lombar não específica encontrou um total de dezenove estudos, sendo seis
considerados estudos de alta qualidade. Um total de seis estudos avaliou a efetividade
desse método em comparação com outros tratamentos conservadores para dor lombar
crônica. Porém, esses estudos35-40 apresentam baixos escores de qualidade metodológica e
descrição estatística mensurados pela escala PEDro41 (isto é, abaixo de 5 pontos numa
escala de 11 pontos). A escala PEDro avalia a qualidade metodológica de estudos
controlados aleatorizados por meio de critérios pré definidos e seu escore pode variar de 0
a 10 pontos41. Quanto maior o escore significa que melhor a qualidade metodológica do
estudo41. As principais limitações metodológicas identificadas nesses estudos foram a

alocação não ter sido secreta, não cegamento dos avaliadores e ausência da análise por
intenção de tratamento. Essas limitações metodológicas tendem a superestimar os efeitos
de intervenções, portanto os resultados desses estudos devem ser interpretados com
cautela42. Alguns estudos mostraram resultados a favor do método Back School quando
comparado a grupo controle37 e programa de fortalecimento de membros superiores e
inferiores39 e quando utilizado como intervenção adicional a tratamentos como programas
de exercícios43, medicamentos44 e agentes eletrofísicos43 para intensidade da dor37, 43,
desempenho funcional39, 43, qualidade de vida39, 43, 44 e recorrência de dor43.
1.6 Método McKenzie
Em 1981, na Nova Zelândia, Robin McKenzie propôs um sistema de classificação e
tratamento individualizado para a dor lombar nomeado “Diagnóstico e Terapia Mecânica”
ou simplesmente método McKenzie19, 30. O método McKenzie é constituído por três etapas:
avaliação, tratamento e profilaxia20, 21. A avaliação possibilita que por meio de movimentos
repetidos e posições sustentadas, pacientes com dor lombar sejam classificados em três
síndromes: 1) síndrome do desarranjo; 2) síndrome de disfunção; e 3) síndrome postural 21.
O tratamento da dor lombar pelo método McKenzie é definido a partir do resultado da
avaliação. No caso da síndrome do desarranjo as estratégias de carga são aplicadas para
reduzir, abolir e/ou centralizar os sintomas21. No caso da síndrome de disfunção o
movimento escolhido é aquele que produz a dor do paciente no final da amplitude do
movimento, pois esse movimento visa remodelar as estruturas afetadas21. Pacientes com
diagnostico de síndrome postural são orientados quanto à correção da postura21.
A profilaxia consiste em educar e estimular o paciente a fim de que ele exerça o auto-
cuidado21, 45. A maior parte dos estudos sobre o método McKenzie recrutou populações

heterogêneas (ex: pacientes com dor aguda, subaguda e crônica46-53). Os estudos que
recrutaram somente pacientes com dor lombar crônica54-59, apresentam escores de menores
ou iguais a 5 na escala PEDro. Alguns estudos que compararam o método McKenzie com
programas de fortalecimento de tronco56 e estabilização54 não encontraram diferença entre
os grupos. Outro estudos encontraram resultados a favor do método McKenzie quando
comparado a treino de resistência muscular58, método de Williams55 e exercícios não
supervisionados na melhora da dor57.
1.7 Justificativa
Atualmente, sabe-se que uma das melhores opções para o tratamento de pacientes com dor
lombar crônica não específica é a prática de programas de exercício, combinados com
programas de educação. No entanto, há forte evidência na literatura60 de que um programa
de exercício não é superior a outro para pacientes com dor lombar crônica. Os métodos
Back School e McKenzie (combinação de exercícios e orientações) utilizados na prática
clínica possuem ainda evidência científica questionável, devido ao alto risco de viés dos
estudos19, 33 com pacientes crônicos. Além disso, até o momento somente um estudo61 se
propôs a comparar essas duas intervenções, porém em pacientes com dor lombar aguda e
nenhum estudo se propôs a comparar os efeitos dessas duas intervenções em pacientes com
dor lombar crônica não específica. Sendo assim, estudos controlados aleatorizados de alta
qualidade metodológica são necessários para verificar os efeitos desses métodos em
pacientes com dor lombar crônica.
1.8 Objetivos da dissertação
Objetivo geral: Comparar os efeitos das intervenções Back School (abordagem em grupo)
e McKenzie (abordagem individual) em pacientes com dor lombar crônica não específica.

Objetivo específico: Comparar os efeitos das intervenções Back School e McKenzie em
pacientes com dor lombar crônica não específica nos desfechos intensidade de dor,
desempenho funcional, qualidade de vida e amplitude de movimento de flexão de tronco.
1.9 Referências
1. Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, et
al. Chapter 4. European guidelines for the management of chronic nonspecific low back
pain. Eur Spine J. 2006; 15 (2): 192-300.
2. Waddell G. The Back Pain Revolution. Second ed: Churchill Livingstone; 2004.
3. Morone NE, Karp JF, Lynch CS, Bost JE, El Khoudary SR, Weiner DK. Impact of
chronic musculoskeletal pathology on older adults: a study of differences between knee
OA and low back pain. Pain Med. 2009; 10 (4): 693-701.
4. Briganó JU, Macedo CSG. Análise da mobilidade lombar e influência da terapia
manual e cinesioterapia na lombalgia. Ciênc Biol e da Saúde. 2005; 26 (2): 75-82.
5. Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, et al. A systematic
review of the global prevalence of low back pain. Arthritis Rheum. 2012; 64 (6): 2028-37.
6. O'Sullivan PB, Beales DJ, Smith AJ, Straker LM. Low back pain in 17 year olds
has substantial impact and represents an important public health disorder: a cross-sectional
study. BMC Public Health. 2012; 12 (1): 100.
7. Instituto Brasileiro de Geografia e Estatística. Pesquisa por Amostra de Domicílios.
Um panorama da saúde no Brasil: acesso e utilização dos serviços, condições de saúde e
fatores de risco e proteção à saúde. 2008.
8. Tulder MV. Chapter 1. European guidelines Eur Spine J. 2006; 15 (2): 134-35.
9. Indrakanti SS, Weber MH, Takemoto SK, Hu SS, Polly D, Berven SH. Value-based
care in the management of spinal disorders: a systematic review of cost-utility analysis.
Clin Orthop Relat Res. 2011; 470 (4): 1106-23.
10. Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of
illness studies in the United States and internationally. Spine J. 2008; 8 (1): 8-20.
11. Hong J, Reed C, Novick D, Happich M. Costs Associated With Treatment of
Chronic Low Back Pain: An Analysis of the UK General Practice Research Database.
Spine (Phila Pa 1976). 2012.
12. Lin CW, Haas M, Maher CG, Machado LA, van Tulder MW. Cost-effectiveness of
general practice care for low back pain: a systematic review. Eur Spine J. 2011; 20 (7):
1012-23.
13. Ross MD, Boissonnault WG. Red flags: to screen or not to screen? J Orthop Sports
Phys Ther. 2010; 40 (11): 682-4.
14. Apeldoorn AT, Ostelo RW, van Helvoirt H, Fritz JM, de Vet HC, van Tulder MW.
The cost-effectiveness of a treatment-based classification system for low back pain: design
of a randomised controlled trial and economic evaluation. BMC Musculoskelet Disord.
2010; 11: 58.
15. Ferguson F, Holdsworth L, Rafferty D. Low back pain and physiotherapy use of red
flags: the evidence from Scotland. Physiotherapy. 2010; 96 (4): 282-8.
16. Casazza BA. Diagnosis and treatment of acute low back pain. Am Fam Physician.
2012; 85 (4): 343-50.
17. Chou R, Qaseem A, Owens DK, Shekelle P. Diagnostic imaging for low back pain:
advice for high-value health care from the American College of Physicians. Ann Intern
Med. 2011; 154 (3): 181-9.
18. Delitto A, Erhard RE, Bowling RW. A treatment-based classification approach to
low back syndrome: identifying and staging patients for conservative treatment. Phys Ther.
1995; 75 (6): 470-85; discussion 85-9.
19. Machado LA, de Souza MS, Ferreira PH, Ferreira ML. The McKenzie method for
low back pain: a systematic review of the literature with a meta-analysis approach. Spine
(Phila Pa 1976). 2006; 31 (9): 254-62.
20. Mckenzie R, May S. The Lumbar Spine Mechanical Diagnosis & Therapy Vol I.
Second ed. New Zealand: Spinal Publications; 2003.
21. Mckenzie R, May S. The Lumbar Spine Mechanical Diagnosis & Therapy Vol II.
Second ed. New Zealand Spinal Publications; 2003.
22. Henschke N, Maher CG, Refshauge KM, Herbert RD, Cumming RG, Bleasel J, et
al. Prognosis in patients with recent onset low back pain in Australian primary care:
inception cohort study. BMJ. 2008; 337 (7662): 154-7.
23. Costa Lda C, Maher CG, McAuley JH, Hancock MJ, Herbert RD, Refshauge KM,
et al. Prognosis for patients with chronic low back pain: inception cohort study. BMJ.
2009; 339: 3829.
24. Menezes Costa Lda C, Maher CG, Hancock MJ, McAuley JH, Herbert RD, Costa
LO. The prognosis of acute and persistent low-back pain: a meta-analysis. CMAJ. 2012;
184 (11): E613-24.
25. Pengel LHM, Herbert RD, Maher CG, Refshauge KM. Acute low back pain:
systematic review of its prognosis. BMJ. 2003; 327: 323-5.
26. Koes Bart W, Tulder MV, Lin CWC, Macedo LG, McAuley J, Maher C. An
updated overview of clinical guidelines for the management of non-specific low back pain
in primary care. Eur Spine J. 2010; 19 (12): 2075-94.
27. Costa LO, Maher CG, Latimer J, Hodges PW, Herbert RD, Refshauge KM, et al.
Motor control exercise for chronic low back pain: a randomized placebo-controlled trial.
Phys Ther. 2009; 89 (12): 1275-86.
28. Van Middelkoop M, Rubinstein SM, Verhagen AP, Ostelo RW, Koes BW, van
Tulder MW. Exercise therapy for chronic nonspecific low-back pain. Best Pract Res Clin
Rheumatol. 2010; 24 (2): 193-204.
29. Lin CW, Haas M, Maher CG, Machado LA, van Tulder MW. Cost-effectiveness of
guideline-endorsed treatments for low back pain: a systematic review. Eur Spine J. 20 (7):
1024-38.
30. Clare HA, Adams R, Maher CG. A systematic review of efficacy of McKenzie
therapy for spinal pain. Aust J Physiother. 2004; 50 (4): 209-16.
31. Engers A, Jellema P, Wensing M, Windt VD, Grol R, Tulder MW. Educación del
paciente individual para el dolor lumbar. La Biblioteca Cochrane Plus. 2008; (2).
32. Heymans MW, van Tulder MW, Esmail R, Bombardier C, Koes BW. Back schools
for acute and subacute non-specific low-back pain. Cochrane Database of Syst Rev. 2004.
33. Martijn H, Van Tukder MW, Rosmin E, Claire B, Bart WK. Back schools for non-
specific low-back pain. Cochrane Database Syst Rev. 2012; 3 (1): CD006555.
34. Andrade SC, Araujo AG, Vilar MJ. Back school for patients with non-specific
chronic low-back pain: benefits from the association of an exercise program with patient's
education. Acta Reumatol Port. 2008; 33 (4): 443-50.
35. Donchin M, Woolf O, Kaplan L, Floman Y. Secondary prevention of low-back
pain. A clinical trial. Spine (Phila Pa 1976). 1990; 15 (12): 1317-20.
36. Harkapaa K, Jarvikoski A, Mellin G, Hurri H. A controlled study on the outcome of
inpatient and outpatient treatment of low back pain. Part I. Pain, disability, compliance,
and reported treatment benefits three months after treatment. Scand J Rehabil Med. 1989;
21 (2): 81-9.
37. Hurri H. The Swedish back school in chronic low back pain. Part I. Benefits. Scand
J Rehabil Med. 1989; 21 (1): 33-40.
38. Klaber Moffett JA, Chase SM, Portek I, Ennis JR. A controlled, prospective study
to evaluate the effectiveness of a back school in the relief of chronic low back pain. Spine
(Phila Pa 1976). 1986; 11 (2): 120-2.
39. Penttinen J, Nevala-Puranen N, Airaksinen O, Jaaskelainen M, Sintonen H, Takala
J. Randomized controlled trial of back school with and without peer support. J Occup
Rehabil. 2002; 12 (1): 21-9.
40. Postacchini F, Facchini M, Palieri P. Efficacy of various forms of conservative
treatment in low back pain. A comparative study. Neuro-Orthopedics. 1988; 6: 28-35.
41. Shiwa SR, Costa LPC, Moser ADL, Aguiar IC, Oliveira LVF. PEDro: the
physiotherapy evidence database. Fisioter mov. 2011; 24 (3): 523-33.
42. Herbert R, Jamtvedt G, Mead J, Hageb KB. Practical Evidence-Based
Physiotherapy: Elsevier; 2005.
43. Sahin N, Albayrak I, Durmus B, Ugurlu H. Effectiveness of back school for
treatment of pain and functional disability in patients with chronic low back pain: a
randomized controlled trial. J Rehabil Med. 2011; 43 (3): 224-9.
44. Tavafian SS, Jamshidi AR, Montazeri A. A randomized study of back school in
women with chronic low back pain: quality of life at three, six, and twelve months follow-
up. Spine (Phila Pa 1976). 2008; 33 (15): 1617-21.
45. May S, Donelson R. Evidence-informed management of chronic low back pain
with the McKenzie method. Spine J. 2008; 8 (1): 134-41.
46. Buswell J. Low back pain: a comparison of two treatment programmes. NZJP.
1982; 10 (2): 13-7.
47. Cherkin DC, Deyo RA, Battie M, Street J, Barlow W. A comparison of physical
therapy, chiropractic manipulation, and provision of an educational booklet for the
treatment of patients with low back pain. N Engl J Med. 1998; 339 (15): 1021-9.
48. Kilpikoski S, Alen M, Paatelma M, Simonen R, Heinonen A, Videman T. Outcome
comparison among working adults with centralizing low back pain: secondary analysis of a
randomized controlled trial with 1-year follow-up. Adv Physiother. 2009; 11 (4): 210-7.
49. Long A, Donelson R, Fung T. Does it matter which exercise? A randomized control
trial of exercise for low back pain. Spine (Phila Pa 1976). 2004; 29 (23): 2593-602.
50. Paatelma M, Kilpikoski S, Simonen R, Heinonen A, Alen M, Videman T.
Orthopaedic manual therapy, McKenzie method or advice only for low back pain in
working adults: a randomized controlled trial with one year follow-up. J Rehabil Med.
2008; 40 (10): 858-63.
51. Petersen T, Kryger P, Ekdahl C, Olsen S, Jacobsen S. The effect of McKenzie
therapy as compared with that of intensive strengthening training for the treatment of
patients with subacute or chronic low back pain: A randomized controlled trial. Spine
(Phila Pa 1976). 2002; 27 (16): 1702-9.
52. Petersen T, Larsen K, Nordsteen J, Olsen S, Fournier G, Jacobsen S. The McKenzie
method compared with manipulation when used adjunctive to information and advice in
low back pain patients presenting with centralization or peripheralization: a randomized
controlled trial. Spine (Phila Pa 1976). 36 (24): 1999-2010.
53. Schenk RJ, Jozefczyk C, Kopf A. A randomized trial comparing interventions in
patients with lumbar posterior derangement. JMMT. 2003; 11 (2): 95-102.
54. Miller ER, Schenk RJ, Karnes JL, Rousselle JG. A comparison of the McKenzie
approach to a specific spine stabilization program for chronic low back pain. JMMT 2005;
13 (2): 103-12.
55. Nwuga G, V. N. Relative therapeutic efficacy of the Williams and McKenzie
protocols in back pain management. Physiother Pract. 1985; 1 (2): 99-105.
56. Petersen T, Larsen K, Jacobsen S. One-year follow-up comparison of the
effectiveness of McKenzie treatment and strengthening training for patients with chronic
low back pain: outcome and prognostic factors. Spine (Phila Pa 1976). 2007; 32 (26):
2948-56.
57. Sakai Y, Matsuyama Y, Nakamura H, Katayama Y, Imagama S, Ito Z, et al. The
effect of muscle relaxant on the paraspinal muscle blood flow: a randomized controlled
trial in patients with chronic low back pain. Spine (Phila Pa 1976). 2008; 33 (6): 581-7.
58. Udermann BE, Mayer JM, Donelson RG, Graves JE, Murray SR. Combining
Lumbar Extension Training with McKenzie Therapy: Effects on Pain, Disability, and
Psychosocial Functioning in Chronic Low Back Pain Patients. Gunders Luth Med J. 2004;
3 (2): 7-12.
59. Elnaggar IM, Nordin M, Sheikhzadeh A, Parnianpour M, Kahanovitz N. Effects of
spinal flexion and extension exercises on low-back pain and spinal mobility in chronic
mechanical low-back pain patients. Spine (Phila Pa 1976). 1991; 16 (8): 967-72.
60. Hayden J, van Tulder MW, Malmivaara A, Koes BW. Exercise therapy for
treatment of non-specific low back pain. Cochrane Database Syst Rev. 2012; 2 (9):
CD000335.
61. Stankovic R, Johnell O. Conservative treatment of acute low-back pain. A
prospective randomized trial: McKenzie method of treatment versus patient education in
"mini back school". Spine (Phila Pa 1976). 1990; 15 (2): 120-3.

Capítulo 2
Effectiveness of Back School and McKenzie techniques in patients with
chronic non specific low back pain:
a protocol of a randomised controlled trial

Apêndice 1
Apostila de Avaliação do Estudo

Nome:___________________________________________Data:____/____/______ Trial:________
Paciente está interessado em participar do estudo? Sim ���� Não ����
Critérios de inclusão e de exclusão
Critérios de inclusão
Todas as questões devem ser respondidas SIM para determinar a entrada do paciente no estudo
Sim Não
� � Dor lombar há pelo menos 3 meses
� � Idade entre 18 e 80 anos
Critérios de exclusão
Todas as questões devem ser respondidas NÃO para determinar a entrada do paciente no estudo
Sim Não
� � Contra indicações ao exercício
� � Gravidez
� � Patologias graves de coluna
� � Condições radiculares da coluna
� � Patologias cardiorrespiratórias
Comentários (Se o sujeito for inelegível, por favor, registrar abaixo o motivo): ________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________

Nome:___________________________________________Data:____/____/______ Trial:________
COMITÊ DE ÉTICA EM PESQUISA DA UNIVERSIDADE CIDADE DE SÃO PAULO (UNICID)
TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO
As informações que seguem estão sendo fornecidas para a sua participação voluntária nesta pesquisa cujo título é “Efeitos dos métodos Back School e McKenzie no tratamento de pacientes com dor lombar crônica não específica: estudo controlado randomizado.”
Objetivos do estudo: Comparar os efeitos das técnicas Back School e McKenzie em pacientes com dor lombar crônica não específica nos desfechos: intensidade de dor, dempenho funcional, qualidade de vida e amplitude de movimento de flexão de tronco. Segue abaixo o planejamento da pesquisa:
1ª etapa: decisória para sua participação na pesquisa
Preenchimento da ficha de avaliação, que conterá informações como: dados pessoais, história do quadro da dor, características da dor e critérios de elegibilidade que determinarão sua participação ou não nessa pesquisa (apresentar dor lombar há 3 meses ou mais, não estar grávida, não apresentar doença grave de coluna e restrição médica para a realização de exercício físico, não ser portador de doenças cardiorrespiratórias).
--------------------------------------------------------------------------------------------------------------------------------------
2ª etapa: avaliação
-Avaliação da dor na coluna – Escala Numérica de Dor;
-Avaliação do quanto essa dor interfere na realização de suas atividades diárias – Questionário de Incapacidade Roland Morris;
-Avaliação da qualidade de vida – Questionário de qualidade de vida da Organização Mundial de Saúde - versão curta;
-Avaliação da amplitude de movimento de flexão de tronco - Flexímetro.
--------------------------------------------------------------------------------------------------------------------------------------
3ª etapa: após a avaliação, será sorteado um número que determinará com qual técnica você será atendido: Back School um método de tratamento em grupo que utiliza conteúdos teóricos e práticos para redução da dor lombar ou McKenzie, um método individualizado de exercícios para a dor lombar. Ambos os tratamentos serão realizados por um mesmo terapeuta na clínica de Fisioterapia da Universidade Cidade de São Paulo, com duração de 4 semanas. Você receberá um atendimento por semana de aproximadamente 45 minutos.
--------------------------------------------------------------------------------------------------------------------------------------
4ª etapa: após o término da 4ª sessão de tratamento você será avaliado novamente da mesma forma descrita na 2ª etapa.
--------------------------------------------------------------------------------------------------------------------------------------
5ª etapa: após 3 e 6 meses da avaliação o pesquisador entrará em contato com você via telefone para saber como está a intensidade da dor lombar, função da coluna e qualidade de vida.
O presente estudo é orientado pelo Prof. Leonardo Oliveira Pena Costa e realizado pela fisioterapeuta mestranda pela Universidade Cidade de São Paulo, Alessandra Narciso Garcia (011) 7282-8289.
Os pesquisadores garantem que não há riscos de qualquer natureza para os participantes. Você também tem a garantia de que, em qualquer etapa do estudo, terá acesso aos pesquisadores responsáveis para esclarecimento de eventuais dúvidas. Se desejar, é garantida a liberdade da retirada de consentimento a qualquer momento e de deixar de participar do estudo. As informações obtidas serão analisadas em conjunto com as dos demais participantes, não sendo divulgada a identificação dos mesmos. Não há despesas pessoais para o participante em qualquer fase do estudo. Também não há compensação financeira relacionada à sua participação. Os pesquisadores se comprometem a utilizar os dados coletados somente para esta pesquisa.
Acredito ter sido suficientemente informado a respeito das informações que li ou que foram lidas para mim, descrevendo o estudo. Ficaram claros para mim quais são os propósitos do estudo, seus desconfortos e riscos, as garantias de confidencialidade e de esclarecimentos. Concordo voluntariamente em participar desta pesquisa e poderei retirar o meu consentimento a qualquer momento, antes ou durante a mesma, sem penalidades ou prejuízo.
Eu,_____________________________________________________,RG:________________________, do sexo ____________,nascido em ____/____/________,local:_______________________ residente à ____________________________________________________na cidade de _________________________________, declaro ter sido informado e estar devidamente esclarecido sobre os objetivos deste estudo sobre as técnicas e procedimentos e que estarei sendo submetido e sobre os riscos e desconfortos que poderão ocorrer. Recebi garantias de total de sigilo e de obter novos esclarecimentos sempre que desejar. Sei que minha participação esta isenta de
despesas e que tenho direito a tratamento hospitalar (ou outro), se necessário. Assim, concordo em participar voluntariamente deste estudo e sei que posso retirar meu consentimento a qualquer momento, sem nenhum prejuízo ou perda de qualquer beneficio (caso o sujeito de pesquisa esteja matriculado na Instituição onde a pesquisa está sendo realizada).
Data: ___/___/2011
___________________________
Assinatura do sujeito da pesquisa
ou representante legal
COMITÊ DE ÉTICA EM PESQUISA
Pesquisador responsável / orientador
Eu, Leonardo Oliveira Pena Costa
Responsável pela pesquisa “Efeitos dos métodos Back School e McKenzie no tratamento de pacientes com dor lombar crônica não específica: estudo controlado randomizado”, declaro que obtive espontaneamente o consentimento deste sujeito de pesquisa (ou de seu representante legal) para realizar este estudo.
Data:___/___/2011
___________________
Assinatura Pesquisador
DADOS DO PACIENTE
Informações gerais
Duração da dor lombar:_______(Meses) Idade________ Data de nascimento:_____/_____/______
Gênero ( ) Masculino ( ) Feminino Estado civil: ( ) solteiro ( ) casado ( ) divorciado ( )________
Peso (em quilos):___________ Altura (em metros):___________
Alfabetizado: ( ) Não ( ) Sim Escolaridade: ( ) fundamental ( ) médio ( ) superior
Profissão: _______________________ Lazer:_________________________
Você utiliza algum medicamento para a dor lombar? Sim � Não �
Qual?________________________
Você teve algum episódio de dor lombar recentemente? Sim � Não �
Quando?______________________
Você pratica alguma atividade física? Sim � Não �
Se sim, qual______________Há quanto tempo___________ Feqüência/Duração_______________
Fumante? Sim � Não �
Como ficou sabendo do programa de tratamento?________________________________________
Dados para contato
Por favor, escreva abaixo seus dados para contato:
Tel residencial:______________Tel celular:______________ Tel comercial:_____________
Email:__________________________________________________
Endereço: Rua/Av______________________________________ nº______Complemento:______
Bairro:______________Cidade:______________ CEP:__________________
Contato de um parente ou amigo
Para nos ajudar e entrar em contato com você caso você se mude de casa, por favor escreva os
dados de contato de um parente ou amigo seu que não more com você mas saiba para onde você
vai mudar:
Nome do parente/amigo:___________________________________________
O que essa pessoa é sua:__________________________________________
Tel residencial:______________Tel celular:______________ Tel comercial:_____________
E-mail:__________________________________________________
Caracterização da dor e do quadro clínico do paciente
Posturas / Estresses:______________________________________________________________
Freqüência da dor: ( ) dói o tempo todo ( ) dói somente uma parte do dia
Quando? ____________________Sintomas atuais______________________________________
Pontuação NRS_______________(com base nos últimos 7 dias):
Presentes desde__________ ( ) Melhorando ( ) Estável ( ) Piorando
HMA: Começou como resultado de____________________________________________________ ________________________________________________________________________________ou sem razão aparente ( )
Sintomas no início ( ) costas ( ) coxa ( ) perna
Sintoma constantes ( ) costas ( ) coxa ( ) perna
Sintomas intermitentes ( ) costas ( ) coxa ( ) perna
Pior ( ) curvando ( ) sentado ( ) levantando ( ) em pé ( ) andando ( ) deitado ( ) manhã
( ) durante o dia ( ) final do dia ( ) parado ( ) movimentando ( ) outros___________
Melhor ( ) curvando ( ) sentado ( ) levantando ( ) em pé ( ) andando ( ) deitado ( ) manhã
( ) durante o dia ( ) final do dia ( ) parado ( ) movimentando ( ) outros___________
Distúrbio do sono: ( ) sim não ( )
Posição de dormir: ( ) prono ( ) supino ( ) lado D ( ) lado E
Colchão: ( ) firme ( ) duro ( ) macio
Episódios anteriores: ( ) 0 ( ) 1-5 ( ) 6-10 ( ) 11+ Ano do 1º episódio___________________
História Pregressa:________________________________________________________________
Tratamentos anteriores:_____________________________________________________________
PERGUNTAS ESPECÍFICAS
Tossir / espirrar / esforço ( ) positivo ( ) negativo Bexiga: ( ) normal ( ) normal_____________
Modo de andar: ( ) normal anormal ( ) Saúde geral: ( ) boa ( ) regular ( ) ruim
Imagens: ( ) sim ( ) não __________________________________________________________________
Cirurgia recente ou de grande porte: ( ) sim ( ) não __________________________________________________________________
Perda inexplicada de peso ( ) sim ( ) não
Dor durante a noite: ( ) sim ( ) não Acidentes: ( ) sim ( ) não
Outros:__________________________________________________________________________
POSTURA
Sentada: ( ) boa ( ) regular ( ) ruim Em pé: ( ) boa ( ) regular ( ) ruim
Lordose: ( ) reduzida ( ) acentuada ( ) normal Desvio lateral: ( ) dir ( ) esq ( ) simétrico
Correção da postura ( ) melhor ( ) pior ( ) nenhum efeito_______________________________
Outras observações:_______________________________________________________________

NEUROLÓGICO
Déficit motor:___________________________________________________
Déficit sensorial:_________________________________________________
Reflexos:______________________________________________________
Sinais da dura:__________________________________________________
PERDA DE MOVIMENTO Gde Mod Min Sem Dor
Flexão
Extensão
Deslocamento lateral D
Deslocamento lateral E
MOVIMENTOS DO TESTE: descreva os efeitos na dor atual – durante: produz, abole, aumenta, diminui, NE. Centralizando, periferilizando. Após: melhor, pior, não melhor, não pior, NE, centralizado, periferilizando.
Sintomas Sintomas Resposta Motora
durante o teste após teste
ADM ADM
NE
Sintomas pré teste em pé
FEP
FEP Rep
EEP
EEP Rep
Sintomas pré teste deitado
FD
FD Rep
ED
ED Rep
Se necessário, sintomas
pré teste
DLEP D
DLEP D Rep
DLEP E
DLEP E Rep
TESTES ESTÁTICOS
Sentar relaxado____________________________Sentar ereto_____________________________
Em pé relaxado__________________________Em pé ereto_______________________________
Deitado em prono em extensão__________________Sentar alongado_______________________
Outros testes_____________________________________________________________________
CLASSIFICAÇÃO PROVISÓRIA
( ) Desarranjo ( ) Disfunção ( ) Postural ( ) Outra______________________________
Subclassificação__________________________________________________________________
PRINCÍPIO DE TRATAMENTO
Educação:_______________________________Equipamento indicado______________________
Terapia mecânica_________________________________________________________________
Princípio de Extensão__________ Princípio Lateral__________ Princípio de flexão_____________
Outro___________________________________________________________________________
AMPLITUDE DE MOVIMENTO ARTICULAR DE FLEXÃO DE TRONCO_____________________________
Roland Morris Disability Questionnaire
Quando suas costas doem você pode achar difícil fazer coisas que normalmente fazia. Esta lista contém frases de pessoas descrevendo a si mesmas quando sentem dor nas costas. Você pode achar entre estas frases que você lê algumas que descrevem você hoje. À medida que você lê estas frases, pense em você hoje. Marque a sentença que descreve você hoje. Se a frase não descreve o que você sente, ignore-a e leia a seguinte. Lembre-se, só marque a frase se você tiver certeza que ela descreve você hoje.
1 Sim ( ) Não ( ) Fico em casa a maior parte do tempo por causa de minhas costas.
2 Sim ( ) Não ( ) Mudo de posição frequentemente tentando deixar minhas costas confortáveis.
3 Sim ( ) Não ( ) Ando mais devagar que o habitual por causa de minhas costas.
4 Sim ( ) Não ( ) Por causa de minhas costas eu não estou fazendo nenhum dos trabalhos que geralmente faço em casa.
5 Sim ( ) Não ( ) Por causa de minhas costas, eu uso um corrimão para subir escadas.
6 Sim ( ) Não ( ) Por causa de minhas costas, eu me deito para descansar frequentemente.
7 Sim ( ) Não ( ) Por causa de minhas costas, eu tenho que me apoiar em alguma coisa para me levantar de uma cadeira normal.
8 Sim ( ) Não ( ) Por causa de minhas costas, tento conseguir com que outras pessoas façam coisas por mim.
9 Sim ( ) Não ( ) Eu me visto mais lentamente que o habitual por causa de minhas costas.
10 Sim ( ) Não ( ) Eu fico de pé somente por períodos curtos de tempo, por causa de minhas costas.
11 Sim ( ) Não ( ) Por causa de minhas costas, eu evito me abaixar ou me ajoelhar.
12 Sim ( ) Não ( ) Encontro dificuldades em me levantar de uma cadeira por causa de minhas costas.
13 Sim ( ) Não ( ) As minhas costas doem quase o tempo todo.
14 Sim ( ) Não ( ) Tenho dificuldade em me virar na cama por causa de minhas costas.
15 Sim ( ) Não ( ) Meu apetite não é bom por causa de dores em minhas costas.
16 Sim ( ) Não ( ) Tenho problemas para colocar minhas meias (ou meia calça), por causa das dores em minhas costas.
17 Sim ( ) Não ( ) Caminho apenas curta distâncias por causa de dores em minhas
costas.
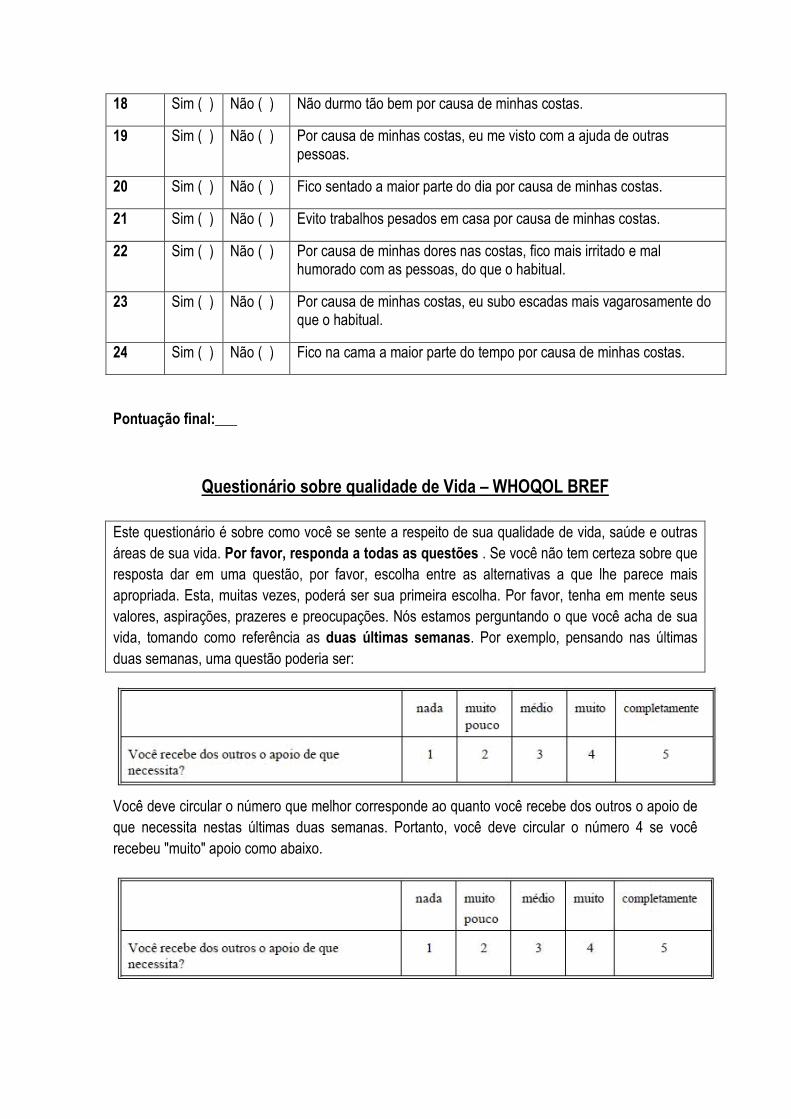
18 Sim ( ) Não ( ) Não durmo tão bem por causa de minhas costas.
19 Sim ( ) Não ( ) Por causa de minhas costas, eu me visto com a ajuda de outras pessoas.
20 Sim ( ) Não ( ) Fico sentado a maior parte do dia por causa de minhas costas.
21 Sim ( ) Não ( ) Evito trabalhos pesados em casa por causa de minhas costas.
22 Sim ( ) Não ( ) Por causa de minhas dores nas costas, fico mais irritado e mal humorado com as pessoas, do que o habitual.
23 Sim ( ) Não ( ) Por causa de minhas costas, eu subo escadas mais vagarosamente do que o habitual.
24 Sim ( ) Não ( ) Fico na cama a maior parte do tempo por causa de minhas costas.
Pontuação final:___
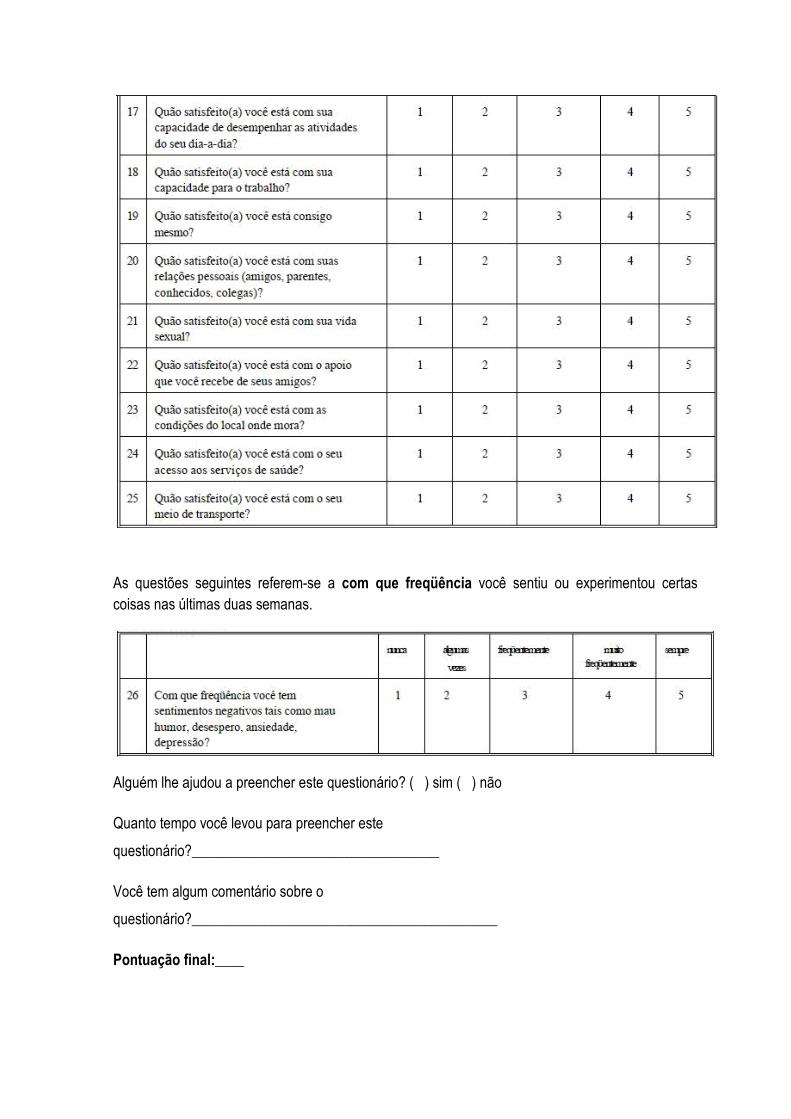
Questionário sobre qualidade de Vida – WHOQOL BREF
Este questionário é sobre como você se sente a respeito de sua qualidade de vida, saúde e outras áreas de sua vida. Por favor, responda a todas as questões . Se você não tem certeza sobre que resposta dar em uma questão, por favor, escolha entre as alternativas a que lhe parece mais apropriada. Esta, muitas vezes, poderá ser sua primeira escolha. Por favor, tenha em mente seus valores, aspirações, prazeres e preocupações. Nós estamos perguntando o que você acha de sua vida, tomando como referência as duas últimas semanas. Por exemplo, pensando nas últimas duas semanas, uma questão poderia ser:
Você deve circular o número que melhor corresponde ao quanto você recebe dos outros o apoio de que necessita nestas últimas duas semanas. Portanto, você deve circular o número 4 se você recebeu "muito" apoio como abaixo.

Você deve circular o número 1 se você não recebeu "nada" de apoio.
--------------------------------------------------------------------------------------------------------------------------------------------------
Por favor, leia cada questão, veja o que você acha e circule no número e lhe parece a melhor resposta.
As questões seguintes são sobre o quanto você tem sentido algumas coisas nas últimas duas semanas.
As questões seguintes perguntam sobre quão completamente você tem sentido ou é capaz de fazer certas coisas nestas últimas duas semanas.
As questões seguintes perguntam sobre quão bem ou satisfeito você se sentiu a respeito de vários aspectos e sua vida nas últimas duas semanas.

As questões seguintes referem-se a com que freqüência você sentiu ou experimentou certas coisas nas últimas duas semanas.
Alguém lhe ajudou a preencher este questionário? ( ) sim ( ) não
Quanto tempo você levou para preencher este
questionário?__________________________________
Você tem algum comentário sobre o
questionário?__________________________________________
Pontuação final:____
AVALIAÇÃO
APÓS 4 SEMANAS
Perguntas:
1. Durante esse período do estudo você considera que sua dor lombar está completamente
recuperada?
Sim ���� Não ����
2. Durante esse período do estudo você apresentou algum sintoma diferente ou piora do
quadro inicial?
Sim ���� Não ����
3. Durante esse período do estudo, você procurou algum outro tipo de tratamento?
Sim ���� Não ����
Qual?_____________________________
PS: Confirmar os dados de contato do paciente.
Por favor, classifique sua dor de 0 a 10 sendo 0 sem dor nenhuma e 10 a pior dor possível com base nos últimos 7 dias:
Pontuação NRS_______________
Amplitude de movimento articular de flexão de tronco__________________
Roland Morris Disability Questionnaire
Quando suas costas doem você pode achar difícil fazer coisas que normalmente fazia. Esta lista contém frases de pessoas descrevendo a si mesmas quando sentem dor nas costas. Você pode achar entre estas frases que você lê algumas que descrevem você hoje. À medida que você lê estas frases, pense em você hoje. Marque a sentença que descreve você hoje. Se a frase não descreve o que você sente, ignore-a e leia a seguinte. Lembre-se, só marque a frase se você tiver certeza que ela descreve você hoje.
1 Sim ( ) Não ( ) Fico em casa a maior parte do tempo por causa de minhas costas.
2 Sim ( ) Não ( ) Mudo de posição frequentemente tentando deixar minhas costas confortáveis.
3 Sim ( ) Não ( ) Ando mais devagar que o habitual por causa de minhas costas.
4 Sim ( ) Não ( ) Por causa de minhas costas eu não estou fazendo nenhum dos trabalhos que geralmente faço em casa.
5 Sim ( ) Não ( ) Por causa de minhas costas, eu uso um corrimão para subir escadas.
6 Sim ( ) Não ( ) Por causa de minhas costas, eu me deito para descansar frequentemente.
7 Sim ( ) Não ( ) Por causa de minhas costas, eu tenho que me apoiar em alguma coisa para me levantar de uma cadeira normal.
8 Sim ( ) Não ( ) Por causa de minhas costas, tento conseguir com que outras pessoas façam coisas por mim.
9 Sim ( ) Não ( ) Eu me visto mais lentamente que o habitual por causa de minhas costas.
10 Sim ( ) Não ( ) Eu fico de pé somente por períodos curtos de tempo, por causa de minhas costas.
11 Sim ( ) Não ( ) Por causa de minhas costas, eu evito me abaixar ou me ajoelhar.
12 Sim ( ) Não ( ) Encontro dificuldades em me levantar de uma cadeira por causa de minhas costas.
13 Sim ( ) Não ( ) As minhas costas doem quase o tempo todo.
14 Sim ( ) Não ( ) Tenho dificuldade em me virar na cama por causa de minhas costas.
15 Sim ( ) Não ( ) Meu apetite não é bom por causa de dores em minhas costas.
16 Sim ( ) Não ( ) Tenho problemas para colocar minhas meias (ou meia calça), por causa das dores em minhas costas.
17 Sim ( ) Não ( ) Caminho apenas curta distâncias por causa de dores em minhas
costas.
18 Sim ( ) Não ( ) Não durmo tão bem por causa de minhas costas.
19 Sim ( ) Não ( ) Por causa de minhas costas, eu me visto com a ajuda de outras pessoas.
20 Sim ( ) Não ( ) Fico sentado a maior parte do dia por causa de minhas costas.
21 Sim ( ) Não ( ) Evito trabalhos pesados em casa por causa de minhas costas.
22 Sim ( ) Não ( ) Por causa de minhas dores nas costas, fico mais irritado e mal humorado com as pessoas, do que o habitual.
23 Sim ( ) Não ( ) Por causa de minhas costas, eu subo escadas mais vagarosamente do que o habitual.
24 Sim ( ) Não ( ) Fico na cama a maior parte do tempo por causa de minhas costas.
Pontuação final:___
Questionário sobre qualidade de Vida – WHOQOL BREF
Este questionário é sobre como você se sente a respeito de sua qualidade de vida, saúde e outras áreas de sua vida. Por favor, responda a todas as questões . Se você não tem certeza sobre que resposta dar em uma questão, por favor, escolha entre as alternativas a que lhe parece mais apropriada. Esta, muitas vezes, poderá ser sua primeira escolha. Por favor, tenha em mente seus valores, aspirações, prazeres e preocupações. Nós estamos perguntando o que você acha de sua vida, tomando como referência as duas últimas semanas. Por exemplo, pensando nas últimas duas semanas, uma questão poderia ser:
Você deve circular o número que melhor corresponde ao quanto você recebe dos outros o apoio de que necessita nestas últimas duas semanas. Portanto, você deve circular o número 4 se você recebeu "muito" apoio como abaixo.

Você deve circular o número 1 se você não recebeu "nada" de apoio.
--------------------------------------------------------------------------------------------------------------------------------------------------
Por favor, leia cada questão, veja o que você acha e circule no número e lhe parece a melhor resposta.
As questões seguintes são sobre o quanto você tem sentido algumas coisas nas últimas duas semanas.
As questões seguintes perguntam sobre quão completamente você tem sentido ou é capaz de fazer certas coisas nestas últimas duas semanas.
As questões seguintes perguntam sobre quão bem ou satisfeito você se sentiu a respeito de vários aspectos e sua vida nas últimas duas semanas.
As questões seguintes referem-se a com que freqüência você sentiu ou experimentou certas coisas nas últimas duas semanas.
Alguém lhe ajudou a preencher este questionário? ( ) sim ( ) não
Quanto tempo você levou para preencher este
questionário?__________________________________
Você tem algum comentário sobre o
questionário?__________________________________________
Pontuação final:____
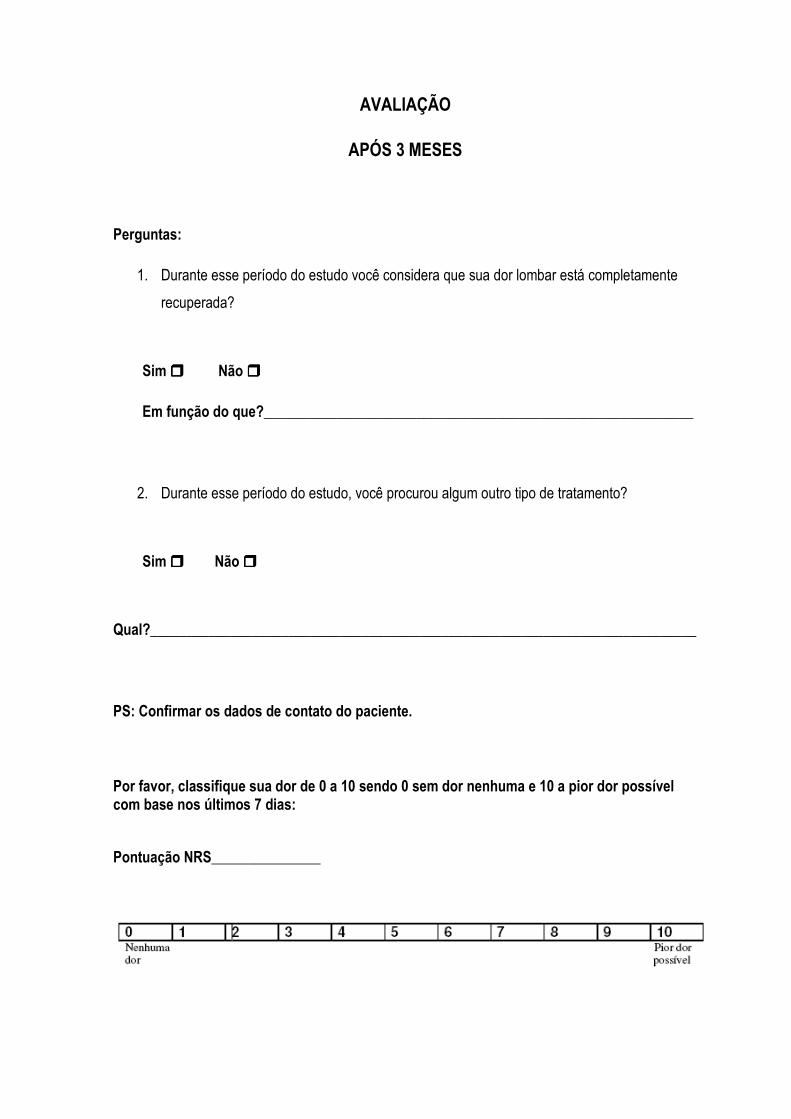
AVALIAÇÃO
APÓS 3 MESES
Perguntas:
1. Durante esse período do estudo você considera que sua dor lombar está completamente
recuperada?
Sim ���� Não ����
Em função do que?___________________________________________________________
2. Durante esse período do estudo, você procurou algum outro tipo de tratamento?
Sim ���� Não ����
Qual?___________________________________________________________________________
PS: Confirmar os dados de contato do paciente.
Por favor, classifique sua dor de 0 a 10 sendo 0 sem dor nenhuma e 10 a pior dor possível com base nos últimos 7 dias:
Pontuação NRS_______________

Roland Morris Disability Questionnaire
Quando suas costas doem você pode achar difícil fazer coisas que normalmente fazia. Esta lista contém frases de pessoas descrevendo a si mesmas quando sentem dor nas costas. Você pode achar entre estas frases que você lê algumas que descrevem você hoje. À medida que você lê estas frases, pense em você hoje. Marque a sentença que descreve você hoje. Se a frase não descreve o que você sente, ignore-a e leia a seguinte. Lembre-se, só marque a frase se você tiver certeza que ela descreve você hoje.
1 Sim ( ) Não ( ) Fico em casa a maior parte do tempo por causa de minhas costas.
2 Sim ( ) Não ( ) Mudo de posição frequentemente tentando deixar minhas costas confortáveis.
3 Sim ( ) Não ( ) Ando mais devagar que o habitual por causa de minhas costas.
4 Sim ( ) Não ( ) Por causa de minhas costas eu não estou fazendo nenhum dos trabalhos que geralmente faço em casa.
5 Sim ( ) Não ( ) Por causa de minhas costas, eu uso um corrimão para subir escadas.
6 Sim ( ) Não ( ) Por causa de minhas costas, eu me deito para descansar frequentemente.
7 Sim ( ) Não ( ) Por causa de minhas costas, eu tenho que me apoiar em alguma coisa para me levantar de uma cadeira normal.
8 Sim ( ) Não ( ) Por causa de minhas costas, tento conseguir com que outras pessoas façam coisas por mim.
9 Sim ( ) Não ( ) Eu me visto mais lentamente que o habitual por causa de minhas costas.
10 Sim ( ) Não ( ) Eu fico de pé somente por períodos curtos de tempo, por causa de minhas costas.
11 Sim ( ) Não ( ) Por causa de minhas costas, eu evito me abaixar ou me ajoelhar.
12 Sim ( ) Não ( ) Encontro dificuldades em me levantar de uma cadeira por causa de minhas costas.
13 Sim ( ) Não ( ) As minhas costas doem quase o tempo todo.
14 Sim ( ) Não ( ) Tenho dificuldade em me virar na cama por causa de minhas costas.
15 Sim ( ) Não ( ) Meu apetite não é bom por causa de dores em minhas costas.
16 Sim ( ) Não ( ) Tenho problemas para colocar minhas meias (ou meia calça), por causa das dores em minhas costas.
17 Sim ( ) Não ( ) Caminho apenas curta distâncias por causa de dores em minhas costas.
18 Sim ( ) Não ( ) Não durmo tão bem por causa de minhas costas.
19 Sim ( ) Não ( ) Por causa de minhas costas, eu me visto com a ajuda de outras pessoas.
20 Sim ( ) Não ( ) Fico sentado a maior parte do dia por causa de minhas costas.
21 Sim ( ) Não ( ) Evito trabalhos pesados em casa por causa de minhas costas.
22 Sim ( ) Não ( ) Por causa de minhas dores nas costas, fico mais irritado e mal humorado com as pessoas, do que o habitual.
23 Sim ( ) Não ( ) Por causa de minhas costas, eu subo escadas mais vagarosamente do que o habitual.
24 Sim ( ) Não ( ) Fico na cama a maior parte do tempo por causa de minhas costas.
Pontuação final:___
Questionário sobre qualidade de Vida – WHOQOL BREF
Este questionário é sobre como você se sente a respeito de sua qualidade de vida, saúde e outras áreas de sua vida. Por favor, responda a todas as questões . Se você não tem certeza sobre que resposta dar em uma questão, por favor, escolha entre as alternativas a que lhe parece mais apropriada. Esta, muitas vezes, poderá ser sua primeira escolha. Por favor, tenha em mente seus valores, aspirações, prazeres e preocupações. Nós estamos perguntando o que você acha de sua vida, tomando como referência as duas últimas semanas. Por exemplo, pensando nas últimas duas semanas, uma questão poderia ser:
Você deve circular o número que melhor corresponde ao quanto você recebe dos outros o apoio de que necessita nestas últimas duas semanas. Portanto, você deve circular o número 4 se você recebeu "muito" apoio como abaixo.
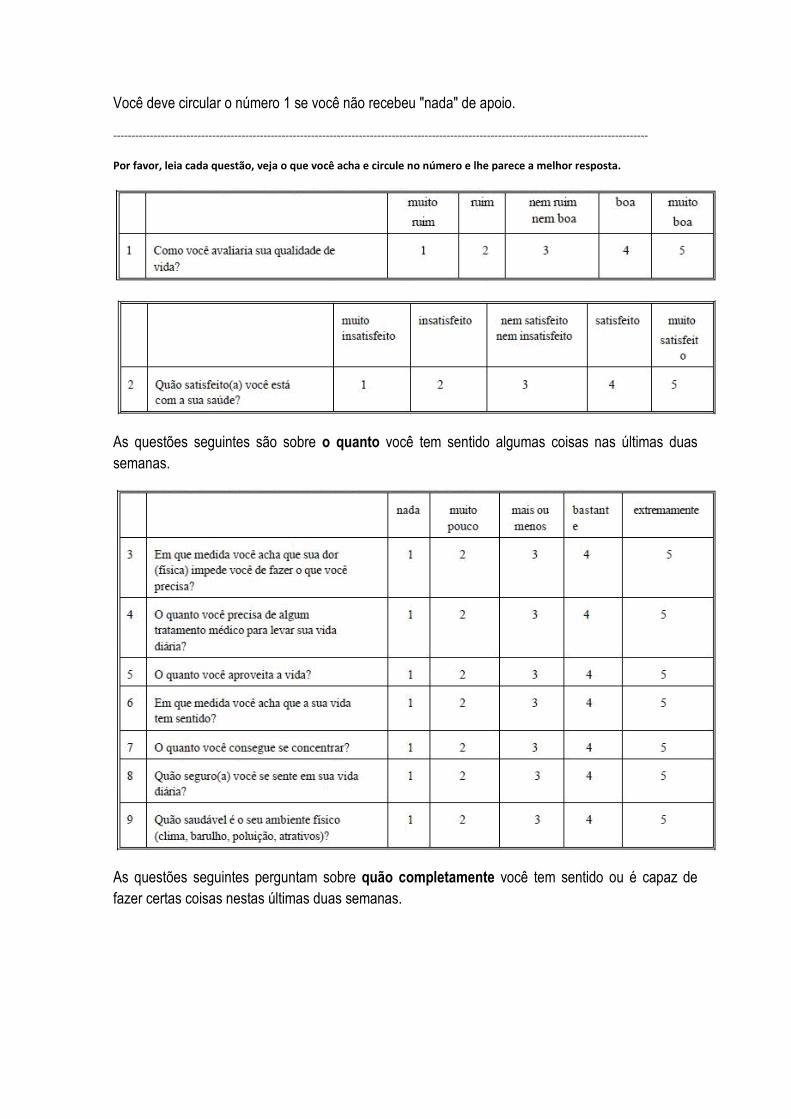
Você deve circular o número 1 se você não recebeu "nada" de apoio.
--------------------------------------------------------------------------------------------------------------------------------------------------
Por favor, leia cada questão, veja o que você acha e circule no número e lhe parece a melhor resposta.
As questões seguintes são sobre o quanto você tem sentido algumas coisas nas últimas duas semanas.
As questões seguintes perguntam sobre quão completamente você tem sentido ou é capaz de fazer certas coisas nestas últimas duas semanas.
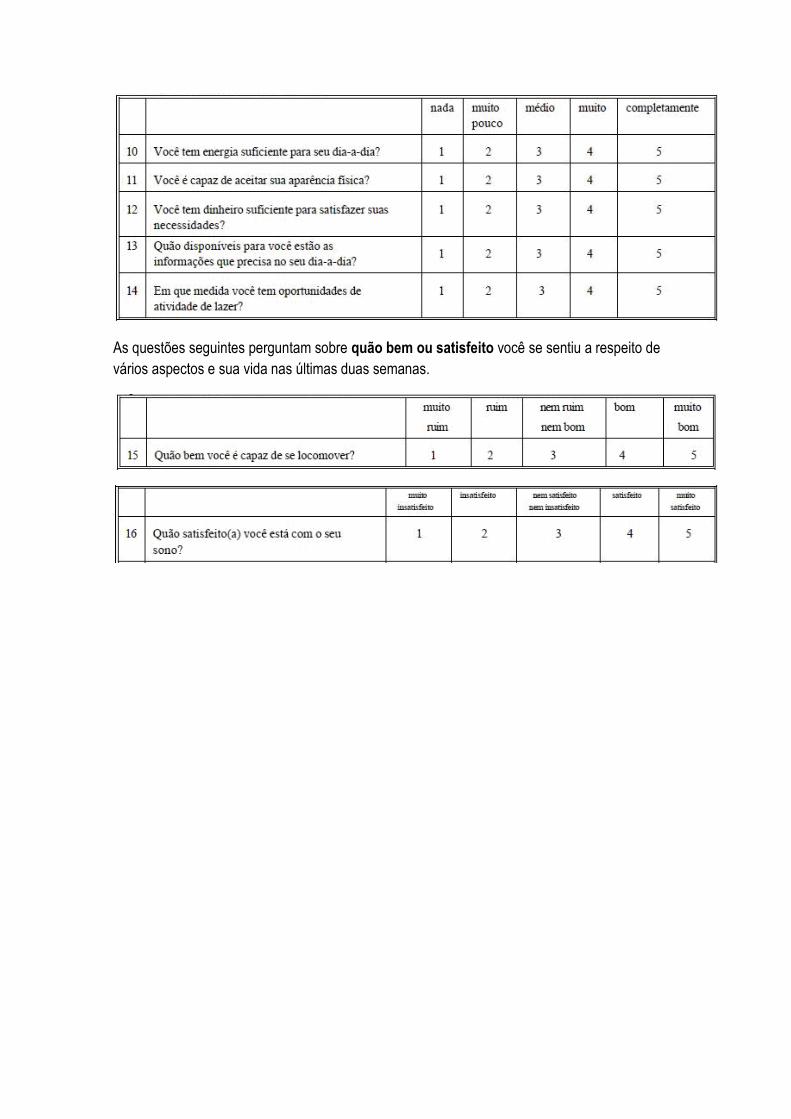
As questões seguintes perguntam sobre quão bem ou satisfeito você se sentiu a respeito de vários aspectos e sua vida nas últimas duas semanas.

As questões seguintes referem-se a com que freqüência você sentiu ou experimentou certas coisas nas últimas duas semanas.
Alguém lhe ajudou a preencher este questionário? ( ) sim ( ) não
Quanto tempo você levou para preencher este
questionário?__________________________________
Você tem algum comentário sobre o
questionário?__________________________________________
Pontuação final:____
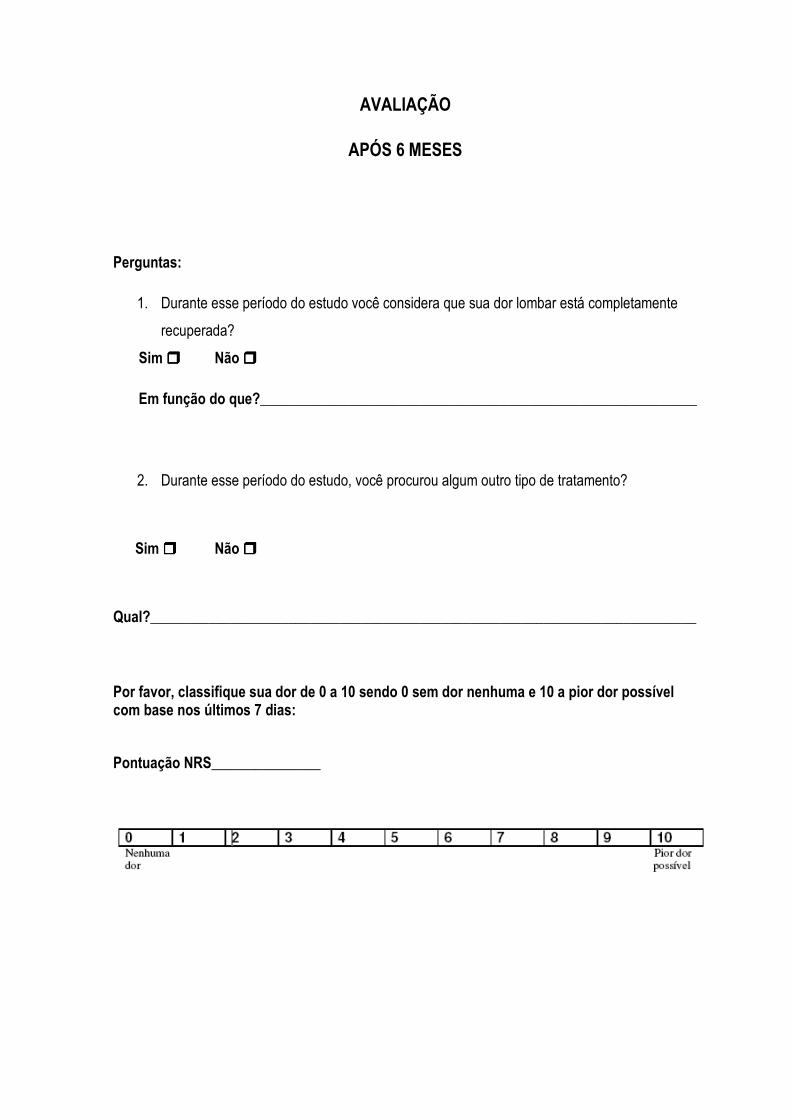
AVALIAÇÃO
APÓS 6 MESES
Perguntas:
1. Durante esse período do estudo você considera que sua dor lombar está completamente
recuperada?
Sim ���� Não ����
Em função do que?____________________________________________________________
2. Durante esse período do estudo, você procurou algum outro tipo de tratamento?
Sim ���� Não ����
Qual?___________________________________________________________________________
Por favor, classifique sua dor de 0 a 10 sendo 0 sem dor nenhuma e 10 a pior dor possível com base nos últimos 7 dias:
Pontuação NRS_______________
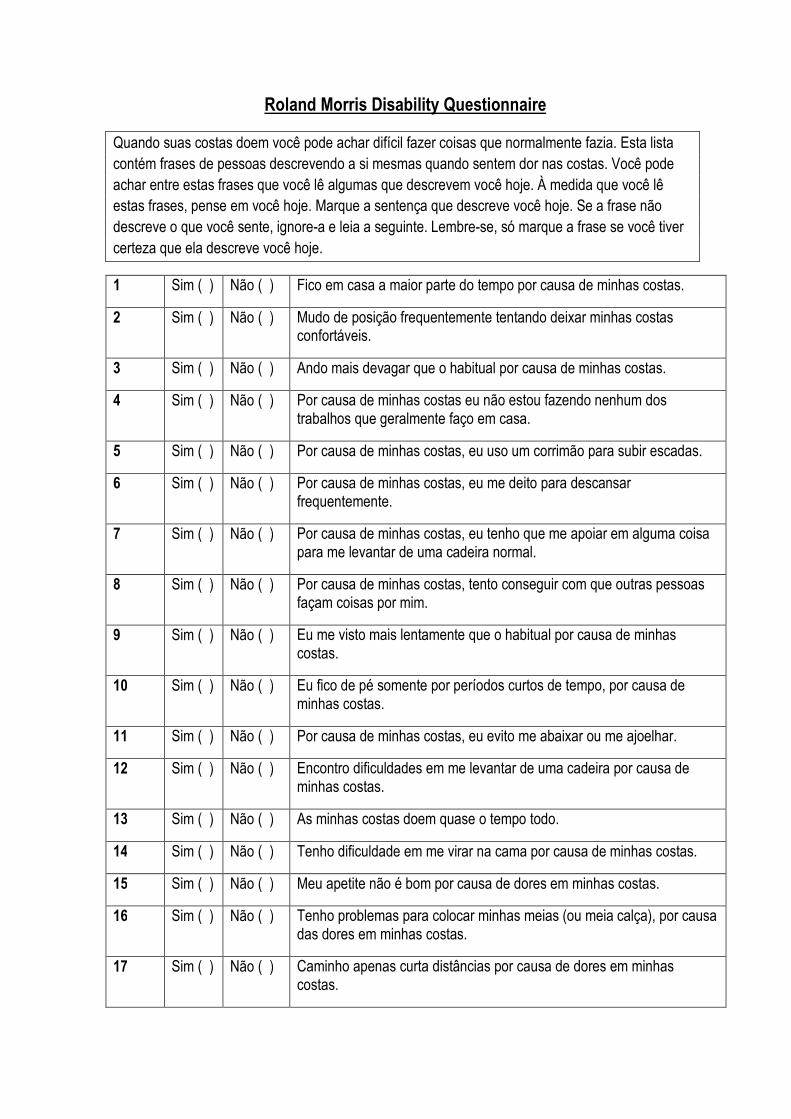
Roland Morris Disability Questionnaire
Quando suas costas doem você pode achar difícil fazer coisas que normalmente fazia. Esta lista contém frases de pessoas descrevendo a si mesmas quando sentem dor nas costas. Você pode achar entre estas frases que você lê algumas que descrevem você hoje. À medida que você lê estas frases, pense em você hoje. Marque a sentença que descreve você hoje. Se a frase não descreve o que você sente, ignore-a e leia a seguinte. Lembre-se, só marque a frase se você tiver certeza que ela descreve você hoje.
1 Sim ( ) Não ( ) Fico em casa a maior parte do tempo por causa de minhas costas.
2 Sim ( ) Não ( ) Mudo de posição frequentemente tentando deixar minhas costas confortáveis.
3 Sim ( ) Não ( ) Ando mais devagar que o habitual por causa de minhas costas.
4 Sim ( ) Não ( ) Por causa de minhas costas eu não estou fazendo nenhum dos trabalhos que geralmente faço em casa.
5 Sim ( ) Não ( ) Por causa de minhas costas, eu uso um corrimão para subir escadas.
6 Sim ( ) Não ( ) Por causa de minhas costas, eu me deito para descansar frequentemente.
7 Sim ( ) Não ( ) Por causa de minhas costas, eu tenho que me apoiar em alguma coisa para me levantar de uma cadeira normal.
8 Sim ( ) Não ( ) Por causa de minhas costas, tento conseguir com que outras pessoas façam coisas por mim.
9 Sim ( ) Não ( ) Eu me visto mais lentamente que o habitual por causa de minhas costas.
10 Sim ( ) Não ( ) Eu fico de pé somente por períodos curtos de tempo, por causa de minhas costas.
11 Sim ( ) Não ( ) Por causa de minhas costas, eu evito me abaixar ou me ajoelhar.
12 Sim ( ) Não ( ) Encontro dificuldades em me levantar de uma cadeira por causa de minhas costas.
13 Sim ( ) Não ( ) As minhas costas doem quase o tempo todo.
14 Sim ( ) Não ( ) Tenho dificuldade em me virar na cama por causa de minhas costas.
15 Sim ( ) Não ( ) Meu apetite não é bom por causa de dores em minhas costas.
16 Sim ( ) Não ( ) Tenho problemas para colocar minhas meias (ou meia calça), por causa das dores em minhas costas.
17 Sim ( ) Não ( ) Caminho apenas curta distâncias por causa de dores em minhas costas.
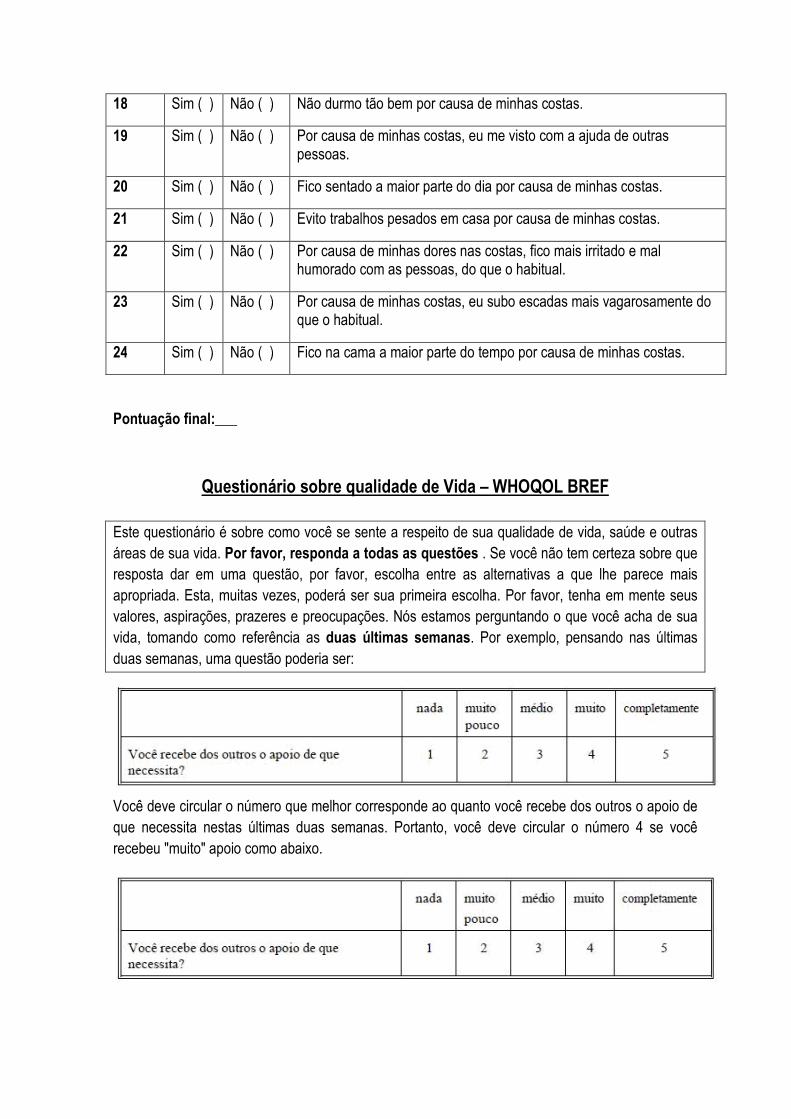
18 Sim ( ) Não ( ) Não durmo tão bem por causa de minhas costas.
19 Sim ( ) Não ( ) Por causa de minhas costas, eu me visto com a ajuda de outras pessoas.
20 Sim ( ) Não ( ) Fico sentado a maior parte do dia por causa de minhas costas.
21 Sim ( ) Não ( ) Evito trabalhos pesados em casa por causa de minhas costas.
22 Sim ( ) Não ( ) Por causa de minhas dores nas costas, fico mais irritado e mal humorado com as pessoas, do que o habitual.
23 Sim ( ) Não ( ) Por causa de minhas costas, eu subo escadas mais vagarosamente do que o habitual.
24 Sim ( ) Não ( ) Fico na cama a maior parte do tempo por causa de minhas costas.
Pontuação final:___
Questionário sobre qualidade de Vida – WHOQOL BREF
Este questionário é sobre como você se sente a respeito de sua qualidade de vida, saúde e outras áreas de sua vida. Por favor, responda a todas as questões . Se você não tem certeza sobre que resposta dar em uma questão, por favor, escolha entre as alternativas a que lhe parece mais apropriada. Esta, muitas vezes, poderá ser sua primeira escolha. Por favor, tenha em mente seus valores, aspirações, prazeres e preocupações. Nós estamos perguntando o que você acha de sua vida, tomando como referência as duas últimas semanas. Por exemplo, pensando nas últimas duas semanas, uma questão poderia ser:
Você deve circular o número que melhor corresponde ao quanto você recebe dos outros o apoio de que necessita nestas últimas duas semanas. Portanto, você deve circular o número 4 se você recebeu "muito" apoio como abaixo.
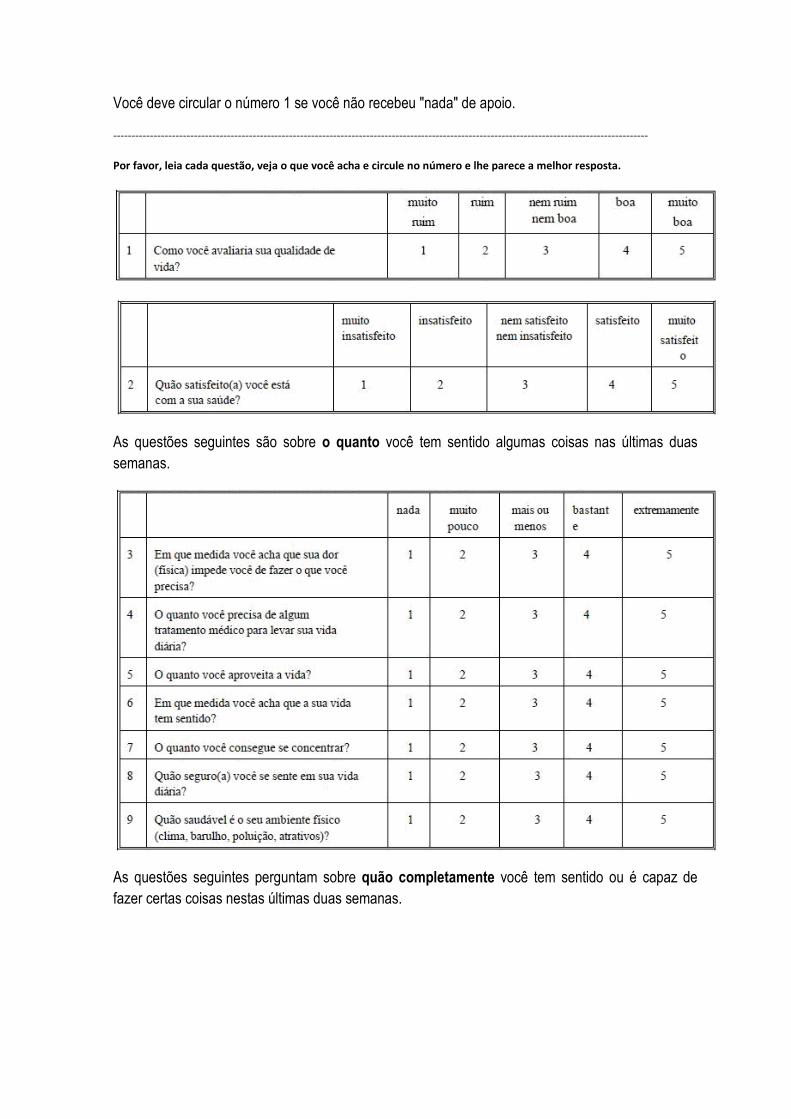
Você deve circular o número 1 se você não recebeu "nada" de apoio.
--------------------------------------------------------------------------------------------------------------------------------------------------
Por favor, leia cada questão, veja o que você acha e circule no número e lhe parece a melhor resposta.
As questões seguintes são sobre o quanto você tem sentido algumas coisas nas últimas duas semanas.
As questões seguintes perguntam sobre quão completamente você tem sentido ou é capaz de fazer certas coisas nestas últimas duas semanas.

As questões seguintes perguntam sobre quão bem ou satisfeito você se sentiu a respeito de vários aspectos e sua vida nas últimas duas semanas.
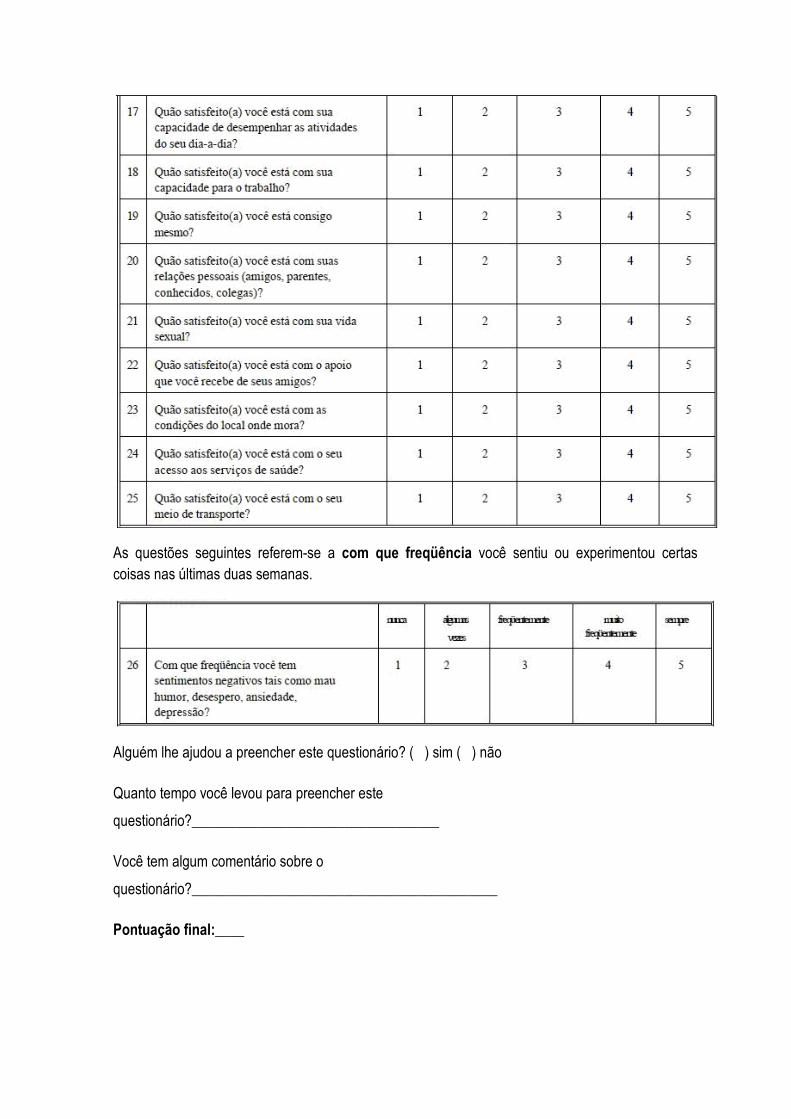
As questões seguintes referem-se a com que freqüência você sentiu ou experimentou certas coisas nas últimas duas semanas.
Alguém lhe ajudou a preencher este questionário? ( ) sim ( ) não
Quanto tempo você levou para preencher este
questionário?__________________________________
Você tem algum comentário sobre o
questionário?__________________________________________
Pontuação final:____

Capítulo 3
Effectiveness of Back School versus McKenzie exercises in patients with
chronic non-specific low back pain: a randomised controlled trial
Effectiveness of Back School versus McKenzie exercises in patients with chronic non-
specific low back pain: a randomised controlled trial
Alessandra Narciso Garcia1, Lucíola da Cunha Menezes Costa1, Tatiane Mota da Silva1, Francine Lopes
Barreto Gondo3, Fábio Navarro Cyrillo2, Renata Alqualo Costa2, Leonardo Oliveira Pena Costa1,3, *
1Masters in Physical Therapy, Universidade Cidade de São Paulo, São Paulo, SP, Brazil; 2Physical Therapy
Department, Universidade Cidade de São Paulo , São Paulo, SP, Brazil; 3Musculoskeletal Division, The
George Institute for Global Health, Sydney, NSW, Australia.
*Corresponding author: Leonardo Costa, Rua Cesário Galeno 448, Tatuapé, São Paulo, SP, Brazil. Postcode
03071-100; Phone: +55 (11) 2178 1564; Email: [email protected].
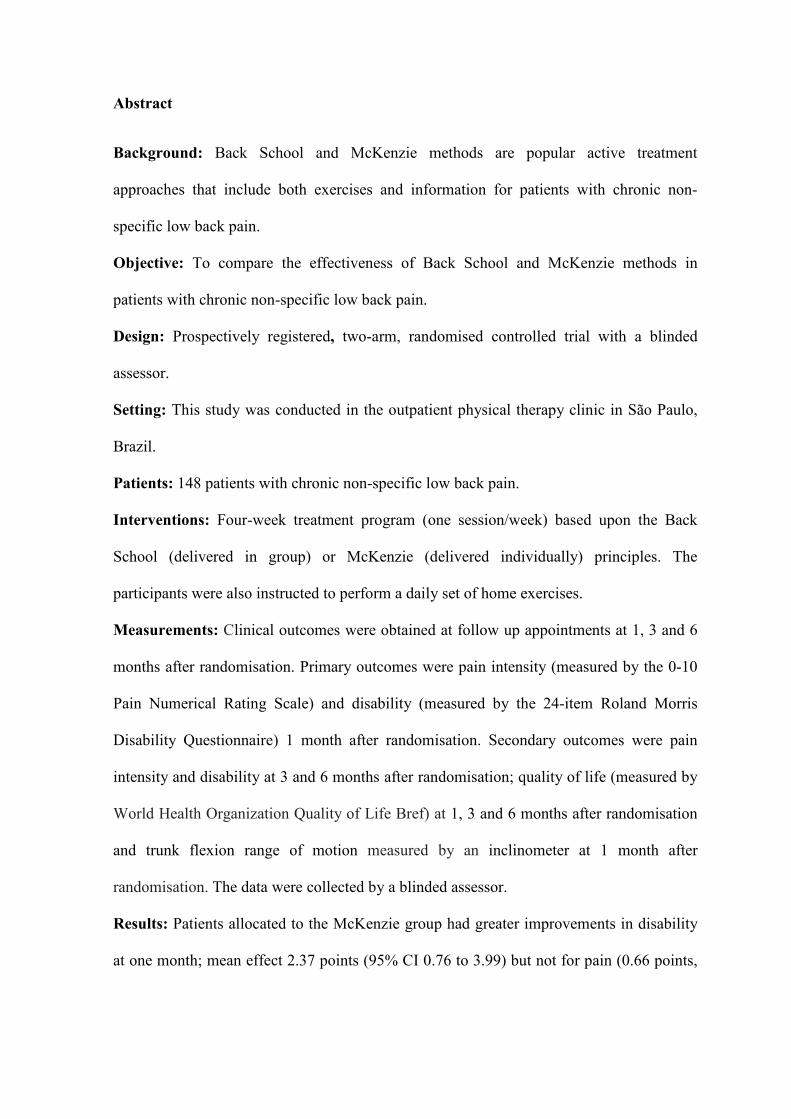
Abstract
Background: Back School and McKenzie methods are popular active treatment
approaches that include both exercises and information for patients with chronic non-
specific low back pain.
Objective: To compare the effectiveness of Back School and McKenzie methods in
patients with chronic non-specific low back pain.
Design: Prospectively registered, two-arm, randomised controlled trial with a blinded
assessor.
Setting: This study was conducted in the outpatient physical therapy clinic in São Paulo,
Brazil.
Patients: 148 patients with chronic non-specific low back pain.
Interventions: Four-week treatment program (one session/week) based upon the Back
School (delivered in group) or McKenzie (delivered individually) principles. The
participants were also instructed to perform a daily set of home exercises.
Measurements: Clinical outcomes were obtained at follow up appointments at 1, 3 and 6
months after randomisation. Primary outcomes were pain intensity (measured by the 0-10
Pain Numerical Rating Scale) and disability (measured by the 24-item Roland Morris
Disability Questionnaire) 1 month after randomisation. Secondary outcomes were pain
intensity and disability at 3 and 6 months after randomisation; quality of life (measured by
World Health Organization Quality of Life Bref) at 1, 3 and 6 months after randomisation
and trunk flexion range of motion measured by an inclinometer at 1 month after
randomisation. The data were collected by a blinded assessor.
Results: Patients allocated to the McKenzie group had greater improvements in disability
at one month; mean effect 2.37 points (95% CI 0.76 to 3.99) but not for pain (0.66 points,
95% CI -0.29 to 1.62). No between-group differences were observed for all secondary
outcomes.
Limitations: It was not possible to monitor the home exercises program. Therapists and
patients were not blinded.
Conclusions: The McKenzie method (a more resource intensive intervention) was slightly
more effective than Back School for disability, but not for pain intensity immediately after
treatment in patients with chronic low back pain.
Trial registration: ACTRN12610000435088
Funding: This study was funded by the Fundação de Amparo à Pesquisa do Estado de São
Paulo (FAPESP), Brazil.

Background
Chronic non-specific low back pain (i.e. low back pain of at least 12 weeks duration and
without a specific cause)1, 2 is one of the most common health conditions worldwide3.
Chronic low back pain is highly associated with disability1, emotional changes2 and work
absenteeism1. Given that chronic low back pain is very prevalent4, the costs associated
with this condition are very high5. Approximately 60% of patients with chronic low back
pain did not consider themselves recovered in a period of one year from the onset of
symptoms, with moderate levels of pain and disability persisting over time6, 7. Therefore,
many of these patients become frequent users of healthcare services in order to find
treatments to minimize the severity of their symptoms.
Supervised exercise therapy1, 8 associated with an educational component9 has been
considered as one of the most effective interventions in reducing pain and disability in
patients with chronic non-specific low back pain1, 8, 9. The effects of exercise therapy tends
to remain for at least six months after treatment10 when compared to usual care9.
Furthermore, there is evidence that exercises may also reduce the number of recurrent
episodes of low back pain11. Back School (a group-based treatment approach) and
McKenzie (an individually-based treatment approach) methods are good active therapy
options that include both exercises and education for the treatment of patients with chronic
low back pain12, 13.
The Back School method was developed in 1969 in Sweden by Mariane Zachrisson
Forssel, with the goal of managing the patient’s current episode and preventing recurrent
episodes13 of low back pain. The program is composed of four sessions lasting
approximately 45 minutes with each session organized by theoretical components and
including exercises that aim to improve mobility, flexibility and strength13. The McKenzie
method (which is also known as “Diagnostic and Mechanical Therapy”) was proposed by
Robin McKenzie in 198114. This method has three basic components: 1) evaluation (that is
conducted using sustained postures and repeated movements where the symptoms in the
lower back and lower limbs are classified into three syndromes: derangement, dysfunction
and postural syndromes); 2) intervention exercises (that are based upon the direction of
preference of patients) and 3) prevention (that is an educational component aimed to
encourage patients to use simple self-management strategies to control their symptoms)14,
15.
The evidence on the effectiveness of these methods in patients with chronic non-specific
low back pain is still conflicting due to the high risk of bias among the studies12, 13. A
recent systematic review on the Back School method for patients with non-specific low
back pain13 found a total of nineteen randomised controlled trials with only six trials
classified as of high quality. A total of six studies evaluated the effectiveness of this
method compared with other conservative treatments for chronic low back pain, but these
trials16-21 have some methodological limitations such no concealed allocation, unblinded
assessors and absence of intention to treat analysis. These trials have shown a greater
effectiveness of Back School method when compared with a control group17, a global
strengthening program19 and when used as an additional intervention to treatments such as
exercise programs22, medication23 and electro physical agents22 in patients with chronic
low back pain for different outcomes, such as pain intensity17, 22, disability19, 22, quality of
life19, 22, 23 and recurrent pain22.
Regarding the McKenzie method, most studies recruited mixed populations (i.e. patients
with acute, sub-acute and chronic low back pain)24-40. Among the studies which recruited
only chronic low back pain patients41-45, the methodological quality of them was moderate
to low. Different active control groups were used in these trials, such as trunk

strengthening43 and stabilization programs41 and no statistical between-group differences
were identified. Other studies with lower methodological quality identified that the
McKenzie method was better than other interventions, such as resistance exercise
training45, the Williams method42 and no supervised exercise44.
Therefore, high quality randomised controlled trials are still needed for a better
understanding of the effects of these two popular interventions. Moreover, no study has
directly compared the effectiveness of these two methods for patients with chronic low
back pain. Therefore, the objective of this randomised controlled trial was to compare the
effectiveness of the Back School and McKenzie methods in patients with chronic non-
specific low back pain for the outcomes of pain intensity, disability, quality of life and
range of motion.
Methods
Design Overview
Prospectively registered, two-arm, randomised controlled trial with a blinded assessor. All
methodological steps of this study are described in detail in the published protocol46.
Setting and Participants
This study was conducted in the outpatient physical therapy clinic of the Universidade
Cidade de São Paulo, Brazil, between July 2010 and July 2012. To be eligible patients
seeking care had to have non-specific low back pain with duration of at least three months
and be aged between 18 and 80 years. Patients with any contraindication to physical
exercise based on the recommendations of the guidelines of the American College of
Sports Medicine47; serious spinal pathology (for example tumors, fractures and
inflammatory diseases); previous spinal surgery; nerve root compromise; cardio respiratory
illnesses and pregnancy were excluded.
Randomisation and interventions
A simple randomisation sequence was computer-generated using Microsoft Excel Program
by one of the investigators of the study who was not directly involved with the assessments
and treatment of patients. The allocation was concealed by using consecutive numbered,
sealed and opaque envelopes. Eligible patients were allocated to the treatment groups
(Back School or McKenzie) by a physical therapist who opened the next available
numbered envelope prior to the first treatment session. Participants from both groups
received 4 one-hour sessions over 4 weeks, once a week. All patients received the
exercises under the supervision of the physical therapist. At the end of each treatment
session, these patients were asked to perform the same exercises at home once a day (3 sets
of 10 repetitions that could be performed on the same day or in different times of day
depending on the patient’s availability). Although patients were instructed to do the home
exercises, we have not monitored the home exercise dose. The number of sessions was
chosen following the recommendations from the original Back School manual method13.
Since there is no consensus regarding the optimal number of sessions for the McKenzie
method, the same treatment duration was chosen. The care provider, who treated the
patients in both groups, was a fully certified McKenzie therapist (certified by the
McKenzie Institute of Brazil) and has received extensively Back School training during her
undergraduate training program. Our outcome assessor received two months of McKenzie
training from our McKenzie certified therapist. Table 1 presents a summarized description
of the treatments that were provided in this study. Patients from both groups received
information in order to maintain lordosis while sitting, included patients with no direction

preference for extension, without exacerbating their symptoms. Patients from the
McKenzie group with a direction preference for extension were also instructed to use a
back roll while sitting as recommended by the "Treat your own back" book48.
Table 1. Summarized description of McKenzie and Back School treatment programs
McKenzie Method Back School Method
1st
week -Presentation of the method, including history and general information about the McKenzie method; -Completion of the exercises after initial evaluation and indication of movement direction preference: flexion, extension, or lateral shift of the spine; -Education component: basic information about low back pain and spinal anatomy; mechanical pain; how and why to do exercises; and types of responses that can occur in response to the exercise program; -Guidance on completing the exercises at home.
-Presentation of the method, including history and general information about the Back School method; -Anatomy and biomechanics of the spine; -Low back pain epidemiology; -Muscle function and their influence on the spine; -Pathophysiology of the main disorders that adversely affect the spine; -Theoretical presentation of commonly used treatment modalities.
2nd
week -Progression of the exercises defined after 1st session and progression in line with the responses of each patient; -Educational component: basic information about the most likely causes of low back pain, emphasizing posture when seated for a prolonged time; practice on finding the correct seated position and maintenance of lumbar lordosis while seated; -Guidance on continuing the exercises at home.
-Variation of the mechanical forces in different movements of the back; -Theoretical presentation of relaxation posture; -Guidance on position when seated or standing; -Instruction on breathing exercises, kinesthetic training, stretching of the lower back, quadriceps, and hamstrings; -Guidance on completing exercises at home once a day.
3rd
week -Progression of the exercises defined after 2nd session and progression towards other position in line with the responses of the patient; -Educational component: basic information about the most likely causes of low back pain, emphasizing work on bending
-Observation of the exercises that were performed at home; -Instruction on exercises for abdominal muscular strength; -Orientation about joint protection during daily activities; -Guidance on how to perform the exercises at home once a day.

positions; standing up; relaxing after vigorous activity; remaining in standing position for prolonged periods; lying down; and resting, coughing and sneezing. -Guidance on continuing the exercises at home.
4th
week -Progression of the exercises defined after 3rd session and progression towards other positions in line with the responses of the patient; -Educational component, review of the most important points since the first week.
-Practical application of all the exercises and learned techniques.
McKenzie group
The McKenzie method is a classification-based treatment system which involves a
comprehensive clinical examination of posture and range of motion of the spine, associated
with the assessment of patient’s symptomatic responses49. This method is based on
exercises (sustained postures or repeated movements) and also includes an educational
component and postural training49, 50.
Patients allocated to the McKenzie group received theoretical information regarding the
care of the spine and performed specific exercises (appendix 1) according to the direction
of preference of movement identify by a relief of pain, centralization of the pain (pain
referred in a peripheral location from the spine is progressively abolished) or abolishment
of pain. The direction of preference can be flexion, extension or lateral shift of the spine50.
During the baseline assessment the assessor identified the directional preference (for all
patients) and informed the treatment therapist before the randomisation. Although the
assessor evaluated and diagnosed each of the patients, the final decision about the patient´s
McKenzie diagnosis and treatment was taken by the therapist. In the case of patients with
dysfunction syndrome, the selected movement for treatment was the one that produced
consistently pain at the end range of motion, with reduction or elimination of symptoms
after returning from this movement14. This movement was performed to stretch shortened
tissues. Patients with postural syndrome were treated by correcting sitting postures, since
these patients have pain in a relaxed sitting posture for a long time14.
The directional preference could be modified during the treatment sessions if needed and
the therapist could progress the level of the exercises tailoring the treatment to each of the
patients. The progression of the exercises of McKenzie method was based on the concept
of "progression of forces"14 and the use of "alternative forces"14. This decision of using
self-overpressure and/or manual mobilization was based upon symptomatic and
mechanical responses of each of the patients. Another progression strategy used was
"patient movement in a greater range of motion with extra pressure applied by the
therapist". In the cases of major posterior derangement syndrome, acute lumbar kyphosis
and/or upper limb functional limitation we prescribed static positions (i.e. sustained
extension) as their treatments. All possibilities of progression of exercises were used on an
individual level following the McKenzie method principles.
Back School group
The Back School method is based on a program of exercises that aim to improve mobility,
flexibility and strength51. New exercises were prescribed and progressed on every
treatment session. This program also has an education component based upon advice
which includes basic components of anatomy and biomechanics of the spine, ideal posture
and rest postures, ergonomics and most common types of treatment13, 52. Patients allocated
to this group received theoretical and practical information (appendix 2) during the
treatment sessions. The first session was conducted individually, and the three remaining
sessions were conducted in groups. The reason for this was to avoid that patients allocated
to this group wait for a long period of time for composing a new treatment group.
Therefore these patients could start to receive treatment immediately after randomisation.
The protocol of advice and exercises of this method was developed based upon the original
manual13 and by another manual specifically written for patients with chronic low back
pain52.
Outcomes and Follow up
Prior to the randomisation, patients were evaluated by an assessor who was blinded to
treatment allocation. During the baseline assessment, patients received information about
the study and signed a consent form to participate in the study. Patients were questioned
about their symptoms and were also submitted to a clinical neurological examination to
rule out possible nerve root compromise2.
The primary outcomes were pain intensity (measured by the 0-10 Pain Numerical Rating
Scale - NRS)53 and disability (measured by the 0-24 Roland Morris Disability
Questionnaire - RMDQ)54, 55 at 1 month after randomisation. The secondary outcomes
were trunk flexion range of motion (measured by an inclinometer)56 at 1 month, pain
intensity and disability at 3 and 6 months and quality of life (measured by the World
Health Organization Quality of Life Bref - Whoqol)57 at 1 month, 3 months and 6 months
after randomisation. We measured trunk flexion range of motion only at baseline and
immediately after treatment to avoid potential loss to follow up at 3 and 6 months after
randomisation. The remaining measures were collected at all time points. Most follow ups
were collected over the phone. We also observed and recorded patients’ adverse effects in
every treatment sessions by asking two questions: 1) “Since you started receiving this
treatment, did you experience any different symptom?”, and 2) “Since you started
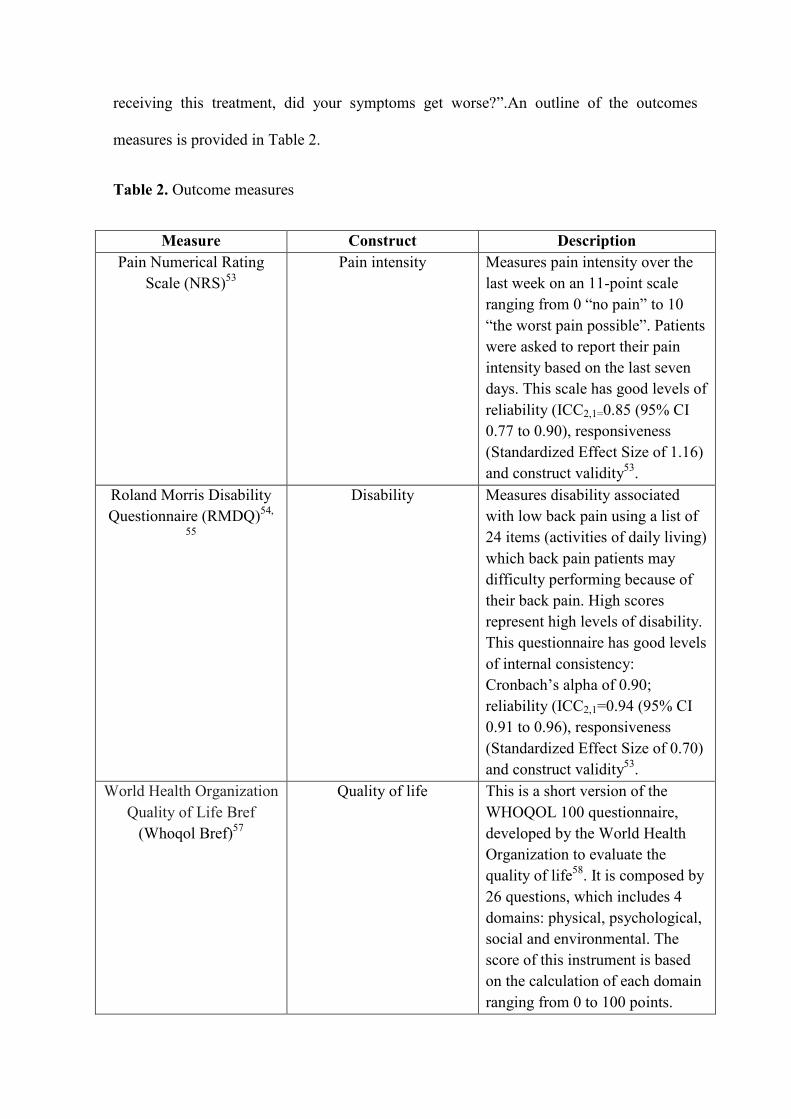
receiving this treatment, did your symptoms get worse?”.An outline of the outcomes
measures is provided in Table 2.
Table 2. Outcome measures
Measure Construct Description Pain Numerical Rating
Scale (NRS)53 Pain intensity Measures pain intensity over the
last week on an 11-point scale ranging from 0 “no pain” to 10 “the worst pain possible”. Patients were asked to report their pain intensity based on the last seven days. This scale has good levels of reliability (ICC2,1=0.85 (95% CI 0.77 to 0.90), responsiveness (Standardized Effect Size of 1.16) and construct validity53.
Roland Morris Disability Questionnaire (RMDQ)54,
55
Disability Measures disability associated with low back pain using a list of 24 items (activities of daily living) which back pain patients may difficulty performing because of their back pain. High scores represent high levels of disability. This questionnaire has good levels of internal consistency: Cronbach’s alpha of 0.90; reliability (ICC2,1=0.94 (95% CI 0.91 to 0.96), responsiveness (Standardized Effect Size of 0.70) and construct validity53.
World Health Organization Quality of Life Bref
(Whoqol Bref)57
Quality of life This is a short version of the WHOQOL 100 questionnaire, developed by the World Health Organization to evaluate the quality of life58. It is composed by 26 questions, which includes 4 domains: physical, psychological, social and environmental. The score of this instrument is based on the calculation of each domain ranging from 0 to 100 points.
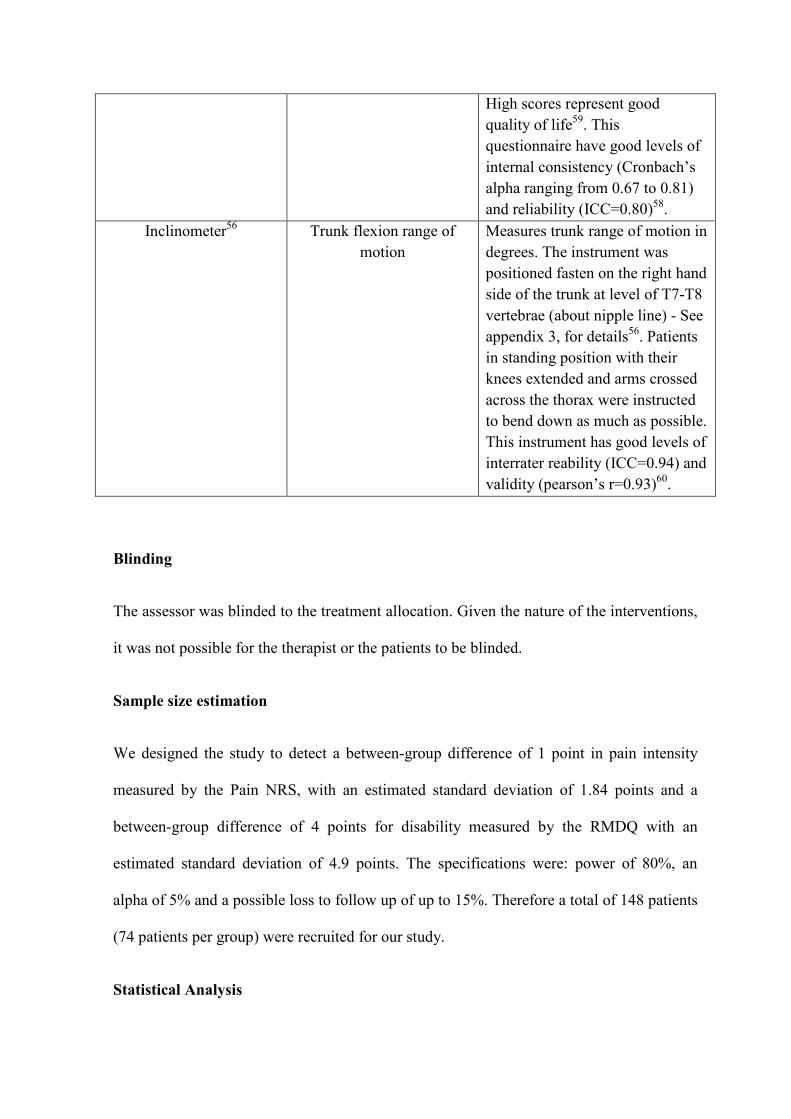
High scores represent good quality of life59. This questionnaire have good levels of internal consistency (Cronbach’s alpha ranging from 0.67 to 0.81) and reliability (ICC=0.80)58.
Inclinometer56
Trunk flexion range of motion
Measures trunk range of motion in degrees. The instrument was positioned fasten on the right hand side of the trunk at level of T7-T8 vertebrae (about nipple line) - See appendix 3, for details56. Patients in standing position with their knees extended and arms crossed across the thorax were instructed to bend down as much as possible. This instrument has good levels of interrater reability (ICC=0.94) and validity (pearson’s r=0.93)60.
Blinding
The assessor was blinded to the treatment allocation. Given the nature of the interventions,
it was not possible for the therapist or the patients to be blinded.
Sample size estimation
We designed the study to detect a between-group difference of 1 point in pain intensity
measured by the Pain NRS, with an estimated standard deviation of 1.84 points and a
between-group difference of 4 points for disability measured by the RMDQ with an
estimated standard deviation of 4.9 points. The specifications were: power of 80%, an
alpha of 5% and a possible loss to follow up of up to 15%. Therefore a total of 148 patients
(74 patients per group) were recruited for our study.
Statistical Analysis
The statistical analysis was conducted on an intention to treat basis, i.e. the subjects were
analyzed in the groups they were allocated to. Data normality was tested through visual
inspection of histograms and all outcomes had normal distribution. The characteristics of
the participants were calculated through descriptive statistical tests. The between-group
differences and their respective 95% confidence intervals were calculated using linear
mixed models. This statistical technique deals with the dependency of baseline measures
(i.e. the effects of treatment were adjusted for baseline estimates only). We also estimated
the number needed to treat for the primary outcomes by dichotomizing patients who have
reached the minimum clinical important difference of 20% (i.e. at least 2 points in Pain
Intensity and 5 points in Disability) compared to those who have not reached minimum
clinical important difference. The estimates used in our sample size calculation were lower
than the ones suggested as the minimum clinical important difference in order to increase
the precision of the effects of the interventions. A higher between-group difference to be
detected would dramatically reduce our sample size and this has been one of the major
limitations on previous trials. We used SPSS 19 for Windows for all analyses.
Ethics approval and clinical trial registration
This study was approved by the Research Ethics Committee of the Universidade Cidade de
São Paulo-UNICID (number PP 1349394 - CAAE 0073.0.186.000-11) and registered prior
to the recruitment of the first patient with the Australian and New Zealand Clinical Trials
Registry (http://www.anzctr.org.au/ACTRN12610000435088.aspx) - Registration number
ACTRN12610000435088. The study protocol for the study was previously published46.
There were no deviations from the registered protocol.
Results
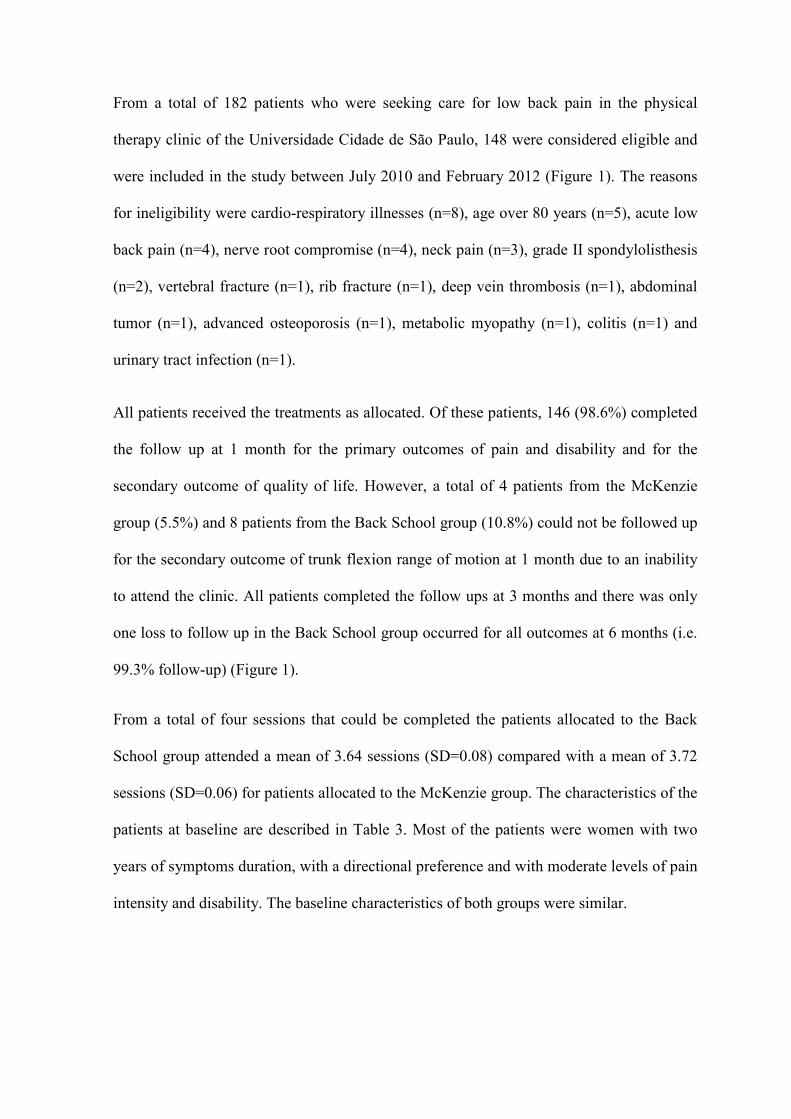
From a total of 182 patients who were seeking care for low back pain in the physical
therapy clinic of the Universidade Cidade de São Paulo, 148 were considered eligible and
were included in the study between July 2010 and February 2012 (Figure 1). The reasons
for ineligibility were cardio-respiratory illnesses (n=8), age over 80 years (n=5), acute low
back pain (n=4), nerve root compromise (n=4), neck pain (n=3), grade II spondylolisthesis
(n=2), vertebral fracture (n=1), rib fracture (n=1), deep vein thrombosis (n=1), abdominal
tumor (n=1), advanced osteoporosis (n=1), metabolic myopathy (n=1), colitis (n=1) and
urinary tract infection (n=1).
All patients received the treatments as allocated. Of these patients, 146 (98.6%) completed
the follow up at 1 month for the primary outcomes of pain and disability and for the
secondary outcome of quality of life. However, a total of 4 patients from the McKenzie
group (5.5%) and 8 patients from the Back School group (10.8%) could not be followed up
for the secondary outcome of trunk flexion range of motion at 1 month due to an inability
to attend the clinic. All patients completed the follow ups at 3 months and there was only
one loss to follow up in the Back School group occurred for all outcomes at 6 months (i.e.
99.3% follow-up) (Figure 1).
From a total of four sessions that could be completed the patients allocated to the Back
School group attended a mean of 3.64 sessions (SD=0.08) compared with a mean of 3.72
sessions (SD=0.06) for patients allocated to the McKenzie group. The characteristics of the
patients at baseline are described in Table 3. Most of the patients were women with two
years of symptoms duration, with a directional preference and with moderate levels of pain
intensity and disability. The baseline characteristics of both groups were similar.
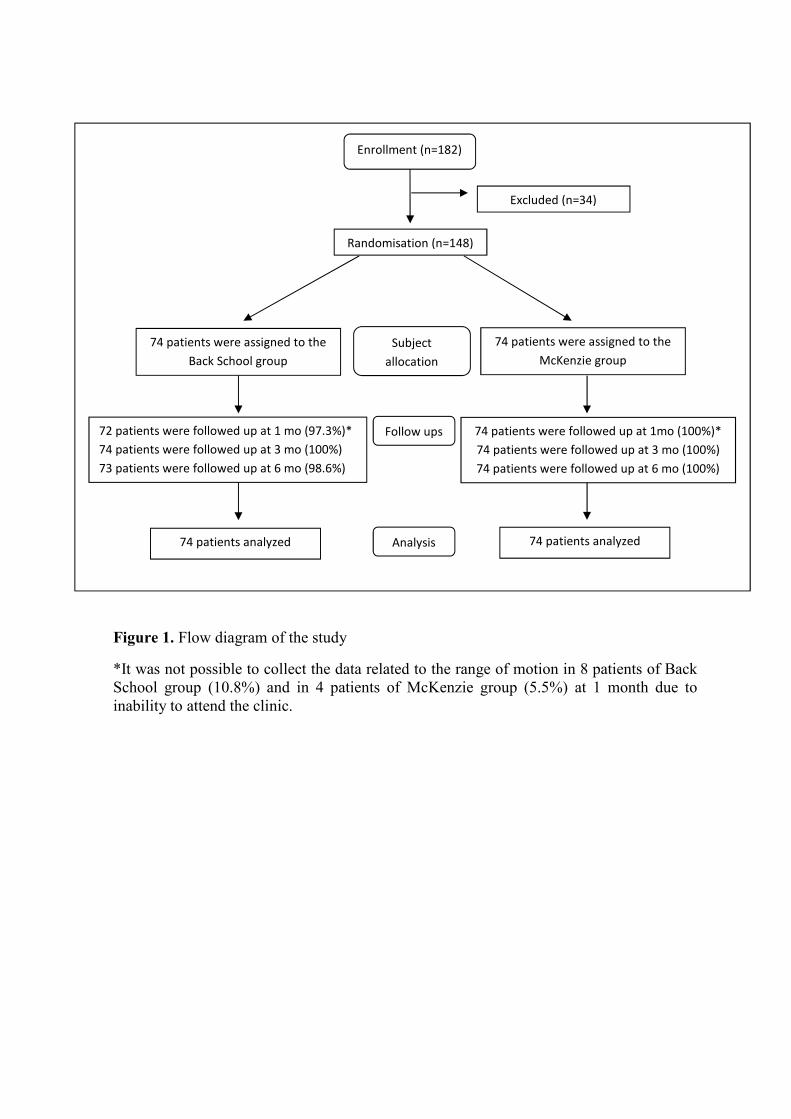
Figure 1. Flow diagram of the study
*It was not possible to collect the data related to the range of motion in 8 patients of Back School group (10.8%) and in 4 patients of McKenzie group (5.5%) at 1 month due to inability to attend the clinic.
Enrollment (n=182)
Subject
allocation
Randomisation (n=148)
74 patients were assigned to the
Back School group
Follow ups 72 patients were followed up at 1 mo (97.3%)*
74 patients were followed up at 3 mo (100%)
73 patients were followed up at 6 mo (98.6%)
Analysis 74 patients analyzed
74 patients were assigned to the
McKenzie group
74 patients analyzed
Excluded (n=34)
74 patients were followed up at 1mo (100%)*
74 patients were followed up at 3 mo (100%)
74 patients were followed up at 6 mo (100%)

Table 3. Demographic and clinical characteristics of the participants at baseline (n=148)
Variables Back School McKenzie Gender
Female 51 (68.90) 58 (78.40) Male 23 (31.10) 16 (21.60)
Age (years) 54.16 (1.57) 53.70 (1.53) Duration of symptoms (months)* 24 (83) 21 (28) Weight (kilograms) 73.73 (1.59) 71.70 (1.59) Height (meters) 1.64 (0.01) 1.61 (0.01) Marital status
Single 12 (16.20) 17 (23) Married 45 (60.80) 41 (55.40) Divorced 5 (6.80) 5 (6.80) Widow 11 (14.90) 9 (12.20) Other 1 (1.40) 2 (2.70)
Education status Elementary degree 27 (36.50) 28 (37.80) High school 33 (44.60) 33 (44.60) University 14 (18.90) 12 (16.20) Illiterate 0 (0) 1 (1.40)
Use of medication 54 (74) 54 (73) Physically active 27 (36.50) 20 (27) Smoker 5 (7.10) 8 (11.10) Recent low back pain episode 47 (63.50) 46 (62.20) Pain intensity (0-10) 6.41 (0.29) 6.77 (0.24) Disability (0-24) 11.08 (0.68) 11.32 (0.57) Quality of life (0-100) Physical Domain Psychological Domain Social Domain Environmental Domain
51.48 (1.98) 60.11 (1.85) 63.51 (2.20) 54.74 (1.87)
51.64 (1.68) 62.88 (1.82) 63.62 (2.12) 55.40 (1.58)
Trunk flexion range of motion (degrees) Mechanical diagnostic Posterior Derangement Syndrome Anterior Derangement Syndrome Dysfunction Syndrome Postural Syndrome Other Directional Preference
78.93 (2.63)
63 (85.1) 5 (6.8) 2 (2.7) 2 (2.7) 2 (2.7)
68 (91.9)
79.28 (2.07)
63 (85.1) 2 (2.7) 6 (8.1) 2 (2.7) 1 (1.4)
65 (87.8)
Categorical variables are expressed as number (%), continuous variables are expressed as mean (SD) *Duration of symptoms is expressed as median (interquartile range).
One patient from the Back School group reported an adverse effect (temporary
exacerbation of pain) in the 3rd session, but this symptom had ceased by the fourth week.
No other adverse event was observed. All patients allocated to the Back School group got
all the exercises. However it was necessary to make some adjustments whenever needed
(for example using a lower range of motion during kinesthetic training exercise and
abdominal exercises). Even with these adjustments, the patients got a similar amount of
exercise. We observed a reduction in pain intensity and disability after treatment (1 month)
in both groups (Table 4). Patients allocated to the McKenzie group had greater
improvements in disability (treatment effect 2.37 points, 95% CI 0.76 to 3.99) after
treatment (at 1 month follow up). There was no statistically significant between-group
difference for pain with a treatment effect of 0.66 points (95% CI -0.29 to 1.62). For the
secondary outcomes we observed a between-group difference only for the physical domain
of quality of life after 3 months by a mean of -4.67 points (95% CI -9.26 to -0.07) in favor
to the McKenzie group. A total of 42 patients allocated to the Back School group and 43
patients allocated to the McKenzie Group met the minimum clinical important difference
for pain intensity (i.e. improved at least 2 points on the Pain Numerical Rating Scale). A
total of 22 patients allocated to the Back School group and 39 patients allocated to the
McKenzie Group met the minimum clinical important difference for disability (i.e.
improved at least 5 points on the Roland Morris Disability Scale. The numbers needed to
treat were 72 (95% CI -7 to 6) and 4 (95% CI 3 to 14) for pain intensity and disability,
respectively in favor of the McKenzie Group.
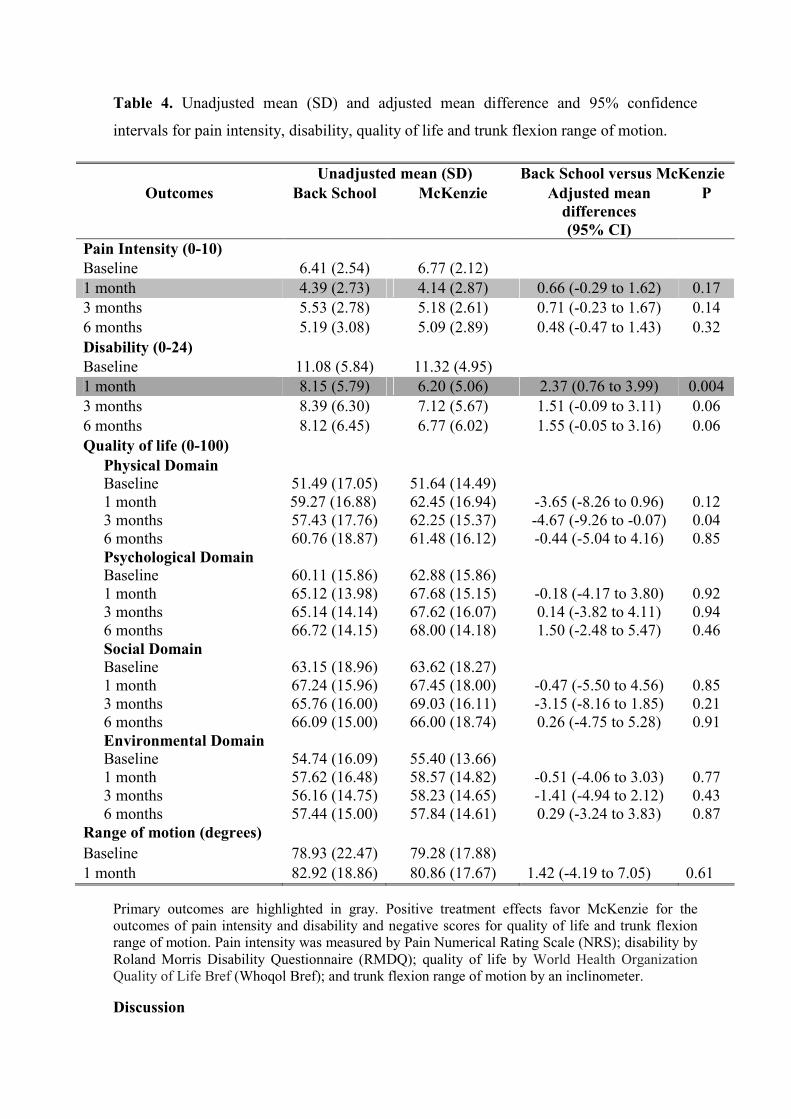
Table 4. Unadjusted mean (SD) and adjusted mean difference and 95% confidence
intervals for pain intensity, disability, quality of life and trunk flexion range of motion.
Unadjusted mean (SD) Back School versus McKenzie Outcomes Back School McKenzie Adjusted mean
differences (95% CI)
P
Pain Intensity (0-10) Baseline 6.41 (2.54) 6.77 (2.12) 1 month 4.39 (2.73) 4.14 (2.87) 0.66 (-0.29 to 1.62) 0.17 3 months 5.53 (2.78) 5.18 (2.61) 0.71 (-0.23 to 1.67) 0.14 6 months 5.19 (3.08) 5.09 (2.89) 0.48 (-0.47 to 1.43) 0.32 Disability (0-24) Baseline 11.08 (5.84) 11.32 (4.95) 1 month 8.15 (5.79) 6.20 (5.06) 2.37 (0.76 to 3.99) 0.004 3 months 8.39 (6.30) 7.12 (5.67) 1.51 (-0.09 to 3.11) 0.06 6 months 8.12 (6.45) 6.77 (6.02) 1.55 (-0.05 to 3.16) 0.06 Quality of life (0-100)
Physical Domain Baseline 1 month 3 months 6 months
51.49 (17.05) 59.27 (16.88) 57.43 (17.76) 60.76 (18.87)
51.64 (14.49) 62.45 (16.94) 62.25 (15.37) 61.48 (16.12)
-3.65 (-8.26 to 0.96) -4.67 (-9.26 to -0.07) -0.44 (-5.04 to 4.16)
0.12 0.04 0.85
Psychological Domain Baseline 1 month 3 months 6 months
60.11 (15.86) 65.12 (13.98) 65.14 (14.14) 66.72 (14.15)
62.88 (15.86) 67.68 (15.15) 67.62 (16.07) 68.00 (14.18)
-0.18 (-4.17 to 3.80) 0.14 (-3.82 to 4.11) 1.50 (-2.48 to 5.47)
0.92 0.94 0.46
Social Domain Baseline 1 month 3 months 6 months
63.15 (18.96) 67.24 (15.96) 65.76 (16.00) 66.09 (15.00)
63.62 (18.27) 67.45 (18.00) 69.03 (16.11) 66.00 (18.74)
-0.47 (-5.50 to 4.56) -3.15 (-8.16 to 1.85) 0.26 (-4.75 to 5.28)
0.85 0.21 0.91
Environmental Domain Baseline 1 month 3 months 6 months
54.74 (16.09) 57.62 (16.48) 56.16 (14.75) 57.44 (15.00)
55.40 (13.66) 58.57 (14.82) 58.23 (14.65) 57.84 (14.61)
-0.51 (-4.06 to 3.03) -1.41 (-4.94 to 2.12) 0.29 (-3.24 to 3.83)
0.77 0.43 0.87
Range of motion (degrees) Baseline 78.93 (22.47) 79.28 (17.88) 1 month 82.92 (18.86) 80.86 (17.67) 1.42 (-4.19 to 7.05) 0.61
Primary outcomes are highlighted in gray. Positive treatment effects favor McKenzie for the outcomes of pain intensity and disability and negative scores for quality of life and trunk flexion range of motion. Pain intensity was measured by Pain Numerical Rating Scale (NRS); disability by Roland Morris Disability Questionnaire (RMDQ); quality of life by World Health Organization Quality of Life Bref (Whoqol Bref); and trunk flexion range of motion by an inclinometer.
Discussion
Statement of principal findings
The objective of this randomised controlled trial was to compare the effectiveness of the
Back School and McKenzie methods in patients with chronic non-specific low back pain.
At 1 month follow up we observed a reduction in both pain intensity and disability in both
groups. Most of the improvements in outcomes observed at short term follow up were
maintained at 3 and 6 months after randomisation for both primary and secondary
outcomes. Patients allocated to the McKenzie group had greater improvements in
disability, but not pain intensity, at 1 month follow up compared to patients allocated to the
Back School group.
Meaning of the study: possible explanation and implication for clinicians and
policymakers
This study provided only precise estimates of treatment effects. A minimal clinically
important difference can be defined as 20% improvement for both pain61 and disability62.
We considered that the magnitude of the difference of disability found in this study is
small (i.e 2.37 points on a 0-24 point scale)62 and possibly of doubtful clinically
importance. From this perspective, clinicians should inform their patients about these
treatment options in order to define which method will be used, taking into account the
potential costs of each of the interventions as well as patient preferences.
Strengths and weaknesses in relation to other studies
Although the dose used for the McKenzie group in our trial (i.e. four treatment sessions)
can be considered as low for some McKenzie therapists, our aim was to keep the dosage of
both treatments similar to avoid attention control bias. We fully reviewed all previous trials
about the McKenzie method for chronic low back pain patients. We found two trials that
used similar dosage than our study44, 45. These trials found a statistically significant
difference in favor to the McKenzie exercises compared to non-supervised exercise
program44 and muscular resistance exercises45. Interestingly, trials that used a higher
dosage41, 43 (i.e. 6 sessions41 and 15 sessions43) and have also prescribed home exercises,
actually found no advantage for the McKenzie group compared to stabilization exercises41
and trunk strengthening exercises43. It might be a good idea for future studies to compare
different doses of McKenzie exercises on this population.
For the Back School method there is no evidence in reducing pain and disability during
short and mid-term follow up compared with myofascial therapy and advice13. Other
studies have shown a greater effectiveness of Back School method when compared with a
non-treatment control group17 and global strengthening program19 and when used as an
additional intervention to treatments such as exercise programs22, medication23 and electro
physical agents22 in patients with chronic back pain for pain intensity22, disability22, quality
of life19, 22, 23 and recurrent pain22.
Our study also aimed to assess the quality of life of patients, which is one of the outcomes
recommended in the literature63 for evaluating patients with low back pain and found that
the McKenzie method was superior only in the physical domain of quality of life after 3
months than Back School method. Although the result was statistically significant, the
effect size was very small (4.67 points (95% CI -9.26 to -0.07) on a 0-100 point scale).
Only one study45 proposed to assess the quality of life of patients treated with the
McKenzie method. The authors found positive results in favor of the McKenzie method,
but this finding should be interpreted with caution due to the low quality of the study. For
the Back School method there is evidence that patients treated with this method improved
in quality of life in general health64, 65, physical and mental66 when compared to those
patients who received only medical assistance/medical visits. Although patients from both
groups their levels of pain and disability reduced, there were no improvements in range of
motion. This finding is consistent with a recent systematic review67 which found a weak
evidence to support the relationship between the changes found in clinical outcomes of
pain and disability and in outcomes related to mobility, muscle strength and endurance
after practice therapeutic exercises67.
Strengths and weaknesses of the study
Our study has good levels of internal and external validity and so can guide therapists and
patients considering treatment options for back pain. The trial includes a number of
features to minimize bias. The trial was prospectively registered and followed a published
protocol46. We used true randomisation, concealed allocation, blinded assessment, an
intention to treat analysis and achieved excellent follow-up. The treatments were
conducted by a single therapist who was properly trained to perform the interventions and
there was an excellent treatment adherence.
Some limitations of our study were to not monitor the home exercise program and not
blinding both therapist and patients to the treatment allocation. Although we believe that
the therapist had similar levels of skills in delivering both interventions, this can be
considered as a limitation of the study one well-trained therapist for each treatment group
would be ideal. We have not included a non-treatment or placebo control group in our
study, which can also be considered as a limitation. The rationale for not including a non-
treatment group in our study is based upon the most recent Cochrane review that
investigated the effect of exercise therapy in patients with chronic low back pain68. This
review concluded that exercise therapy (regardless the type of exercise) is at least 10 points
(on a 0-100 point scale) more effective than a non-treatment group. To our knowledge,
there is no randomised controlled trial of McKenzie exercise compared to placebo or non-

treatment group for chronic low back pain. Given that our randomisation was successful
(i.e. our baseline estimates were very similar), we can conclude that confounders such as
regression to the mean, placebo effects and natural history are very likely to occur
similarly in both groups. Therefore the difference observed in the primary outcome of
disability, although small, is real and probably above these confounding effects. It would
be interesting to compare these interventions with a placebo group in the future in order to
provide more precise estimates of the effect of these popular physical therapy
interventions.
Unanswered questions and future research
We observed that patient outcomes improved following both treatments which is consistent
with the results reported in the literature that demonstrate the effectiveness of the
combination of exercise programs and education in the treatment of patients with chronic
non-specific low back pain1. Although our study does not include an economic analysis, it
is likely that when treatment outcomes are similar, a group treatment such as Back School
will be more cost-effective than an individualized intervention such as the McKenzie
method. Another consideration in treatment planning would be patient preferences for each
treatment as it may be that some patients prefer individual treatment and vice versa. Given
the similar treatment outcomes with both treatments we would suggest future studies
evaluating the cost effectiveness and patient preferences for the McKenzie and Back
School methods as important to help clinicians make informed treatment choices in this
area.
Another important point that should be taken into consideration while interpreting our trial
results is that maybe individual characteristics of patients would predict a better response
to one of the interventions (i.e. subgroups)69. There are many treatment-based
classifications available in order to better identify patients who would possibly respond
better to different interventions70. However, these treatment-based classifications and
clinical prediction rules are in development stages and clinicians cannot yet precisely
match the “right patient” to the “right treatment”71. In the case of patients who experience
the centralization phenomenon usually tend to respond better to the McKenzie
intervention15, 72 but our study was not powered enough to permit this type of subgroup
analysis. We suggest for future studies aiming to test the McKenzie method that it would
be interesting to consider the centralization phenomenon as an eligibility criteria.
Conclusion
Patients allocated to the McKenzie group experienced greater improvements in disability,
but not in pain intensity, after treatment compared to patients allocated to the Back School
group, but the magnitude of this effect was small and possibly of doubtful clinically
importance.
Acknowledgements
This study was funded by the Fundação de Amparo à Pesquisa do Estado de São Paulo
(FAPESP). Ms Garcia had her master scholarship supported by FAPESP.
Registration / Protocol
This study design was approved by the Ethics Committee in Research of UNICID (number
134699394) and was also prospectively registered with the Australian and New Zealand
Clinical Trials Registry (ACTRN12610000435088). The research protocol was published
elsewhere46.
References
1. Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, et al. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006; 15 (2): 192-300.
2. Waddell G. The Back Pain Revolution. Second ed: Churchill Livingstone; 2004.
3. Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012; 64 (6): 2028-37.
4. Walker BF. The prevalence of low back pain: a systematic review of the literature from 1966 to 1998. J Spinal Disord. 2000; 13 (3): 205-17.
5. Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008; 8 (1): 8-20.
6. Costa Lda C, Maher CG, McAuley JH, Hancock MJ, Herbert RD, Refshauge KM, et al. Prognosis for patients with chronic low back pain: inception cohort study. BMJ. 2009; 339: 3829.
7. Menezes Costa Lda C, Maher CG, Hancock MJ, McAuley JH, Herbert RD, Costa LO. The prognosis of acute and persistent low-back pain: a meta-analysis. CMAJ. 2012; 184 (11): E613-24.
8. Tulder MV. Chapter 1. European guidelines Eur Spine J. 2006; 15 (2): 134-35.
9. van Middelkoop M, Rubinstein SM, Kuijpers T, Verhagen AP, Ostelo R, Koes BW, et al. A systematic review on the effectiveness of physical and rehabilitation interventions for chronic non-specific low back pain. Eur Spine J. 2011; 20 (1): 19-39.
10. Smith C, Grimmer-Somers K. The treatment effect of exercise programmes for chronic low back pain. J Eval Clin Pract. 2010; 16 (3): 484-91.
11. Choi BK, Verbeek JH, Tam WW, Jiang JY. Exercises for prevention of recurrences of low-back pain. Cochrane Database Syst Rev. 2012; 1 (1): CD006555.
12. Machado LA, de Souza MS, Ferreira PH, Ferreira ML. The McKenzie method for low back pain: a systematic review of the literature with a meta-analysis approach. Spine (Phila Pa 1976). 2006; 31 (9): 254-62.
13. Martijn H, Van Tukder MW, Rosmin E, Claire B, Bart WK. Back schools for non-specific low-back pain. Cochrane Database Syst Rev. 2012; 3 (1): CD006555.
14. Mckenzie R, May S. The Lumbar Spine Mechanical Diagnosis & Therapy Vol II. Second ed. New Zealand Spinal Publications; 2003.
15. Mckenzie R, May S. The Lumbar Spine Mechanical Diagnosis & Therapy Vol I. Second ed. New Zealand: Spinal Publications; 2003.
16. Klaber Moffett JA, Chase SM, Portek I, Ennis JR. A controlled, prospective study to evaluate the effectiveness of a back school in the relief of chronic low back pain. Spine (Phila Pa 1976). 1986; 11 (2): 120-2.
17. Hurri H. The Swedish back school in chronic low back pain. Part I. Benefits. Scand J Rehabil Med. 1989; 21 (1): 33-40.
18. Donchin M, Woolf O, Kaplan L, Floman Y. Secondary prevention of low-back pain. A clinical trial. Spine (Phila Pa 1976). 1990; 15 (12): 1317-20.
19. Penttinen J, Nevala-Puranen N, Airaksinen O, Jaaskelainen M, Sintonen H, Takala J. Randomized controlled trial of back school with and without peer support. J Occup Rehabil. 2002; 12 (1): 21-9.
20. Postacchini F, Facchini M, Palieri P. Efficacy of various forms of conservative treatment in low back pain. A comparative study. Neuro-Orthopedics. 1988; 6: 28-35.
21. Harkapaa K, Jarvikoski A, Mellin G, Hurri H. A controlled study on the outcome of inpatient and outpatient treatment of low back pain. Part I. Pain, disability, compliance, and reported treatment benefits three months after treatment. Scand J Rehabil Med. 1989; 21 (2): 81-9.
22. Sahin N, Albayrak I, Durmus B, Ugurlu H. Effectiveness of back school for treatment of pain and functional disability in patients with chronic low back pain: a randomized controlled trial. J Rehabil Med. 2011; 43 (3): 224-9.
23. Tavafian SS, Jamshidi AR, Montazeri A. A randomized study of back school in women with chronic low back pain: quality of life at three, six, and twelve months follow-up. Spine (Phila Pa 1976). 2008; 33 (15): 1617-21.
24. Long A, Donelson R, Fung T. Does it matter which exercise? A randomized control trial of exercise for low back pain. Spine (Phila Pa 1976). 2004; 29 (23): 2593-602.

25. Buswell J. Low back pain: a comparison of two treatment programmes. NZJP. 1982; 10 (2): 13-7.
26. Cherkin DC, Deyo RA, Battie M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med. 1998; 339 (15): 1021-9.
27. Kilpikoski S, Alen M, Paatelma M, Simonen R, Heinonen A, Videman T. Outcome comparison among working adults with centralizing low back pain: secondary analysis of a randomized controlled trial with 1-year follow-up. Adv Physiother. 2009; 11 (4): 210-7.
28. Paatelma M, Kilpikoski S, Simonen R, Heinonen A, Alen M, Videman T. Orthopaedic manual therapy, McKenzie method or advice only for low back pain in working adults: a randomized controlled trial with one year follow-up. J Rehabil Med. 2008; 40 (10): 858-63.
29. Petersen T, Kryger P, Ekdahl C, Olsen S, Jacobsen S. The effect of McKenzie therapy as compared with that of intensive strengthening training for the treatment of patients with subacute or chronic low back pain: A randomized controlled trial. Spine (Phila Pa 1976). 2002; 27 (16): 1702-9.
30. Petersen T, Larsen K, Nordsteen J, Olsen S, Fournier G, Jacobsen S. The McKenzie method compared with manipulation when used adjunctive to information and advice in low back pain patients presenting with centralization or peripheralization: a randomized controlled trial. Spine (Phila Pa 1976). 36 (24): 1999-2010.
31. Schenk RJ, Jozefczyk C, Kopf A. A randomized trial comparing interventions in patients with lumbar posterior derangement. JMMT. 2003; 11 (2): 95-102.
32. Gillan MG, Ross JC, McLean IP, Porter RW. The natural history of trunk list, its associated disability and the influence of McKenzie management. Eur Spine J. 1998; 7 (6): 480-83.
33. Dettori JR, Bullock SH, Sutlive TG, Franklin RJ, Patience T. The effects of spinal flexion and extension exercises and their associated postures in patients with acute low back pain. Spine (Phila Pa 1976). 1995; 20 (21): 2303-12.
34. Malmivaara A, Hakkinen U, Aro T, Heinrichs ML, Koskenniemi L, Kuosma E, et al. The treatment of acute low back pain--bed rest, exercises, or ordinary activity? N Engl J Med. 1995; 332 (6): 351-5.
35. Stankovic R, Johnell O. Conservative treatment of acute low-back pain. A prospective randomized trial: McKenzie method of treatment versus patient education in "mini back school". Spine (Phila Pa 1976). 1990; 15 (2): 120-3.
36. Erhard RE, Delitto A, Cibulka MT. Relative effectiveness of an extension program and a combined program of manipulation and flexion and extension exercises in patients with acute low back syndrome. Phys Ther. 1994; 74 (12): 1093-100.
37. Delitto A, Cibulka MT, Erhard RE, Bowling RW, Tenhula JA. Evidence for use of an extension-mobilization category in acute low back syndrome: a prescriptive validation pilot study. Phys Ther. 1993; 73 (4): 216-22.
38. Underwood MR, Morgan J. The use of a back class teaching extension exercises in the treatment of acute low back pain in primary care. Fam Pract. 1998; 15 (1): 9-15.
39. Browder DA, Childs JD, Cleland JA, Fritz JM. Effectiveness of an extension-oriented treatment approach in a subgroup of subjects with low back pain: a randomized clinical trial. Phys Ther. 2007; 87 (12): 1608-18.
40. Brennan GP, Fritz JM, Hunter SJ, Thackeray A, Delitto A, Erhard RE. Identifying subgroups of patients with acute/subacute "nonspecific" low back pain: results of a randomized clinical trial. Spine (Phila Pa 1976). 2006; 31 (6): 623-31.
41. Miller ER, Schenk RJ, Karnes JL, Rousselle JG. A comparison of the McKenzie approach to a specific spine stabilization program for chronic low back pain. JMMT 2005; 13 (2): 103-12.
42. Nwuga G, V. N. Relative therapeutic efficacy of the Williams and McKenzie protocols in back pain management. Physiother Pract. 1985; 1 (2): 99-105.
43. Petersen T, Larsen K, Jacobsen S. One-year follow-up comparison of the effectiveness of McKenzie treatment and strengthening training for patients with chronic low back pain: outcome and prognostic factors. Spine (Phila Pa 1976). 2007; 32 (26): 2948-56.
44. Sakai Y, Matsuyama Y, Nakamura H, Katayama Y, Imagama S, Ito Z, et al. The effect of muscle relaxant on the paraspinal muscle blood flow: a randomized controlled trial in patients with chronic low back pain. Spine (Phila Pa 1976). 2008; 33 (6): 581-7.
45. Udermann BE, Mayer JM, Donelson RG, Graves JE, Murray SR. Combining Lumbar Extension Training with McKenzie Therapy: Effects on Pain, Disability, and Psychosocial Functioning in Chronic Low Back Pain Patients. Gunders Luth Med J. 2004; 3 (2): 7-12.
46. Garcia AN, Gondo FL, Costa RA, Cyrillo FN, Silva TM, Costa LC, et al. Effectiveness of the back school and mckenzie techniques in patients with chronic non-specific low back pain: a protocol of a randomised controlled trial. BMC Musculoskelet Disord. 2011; 12: 179.
47. Kenney W. ACMS: ACSM's Guidelines for exercise testing and prescription: Baltimore; 1995.
48. Mckenzie R. Trate você mesmo a sua coluna. RJ: TTMT; 1998.
49. Machado LA, Maher CG, Herbert RD, Clare H, McAuley JH. The effectiveness of the McKenzie method in addition to first-line care for acute low back pain: a randomized controlled trial. BMC Med. 2010; 8: 10.
50. Machado L, VanTulder MW, Lin CWC, Clare H, Hayden JA. The Mckenzie method for chronic non specific low back pain: study protocol. Cochrane Database of Systematic Rev. 2012: 1-16.
51. Andrade SC, Araújo AGR, Vilar MJP. Back School: Historical revision and its applcation in chronic low back pain. Rev Bras Reumatol. 2005; 45 (4): 224-8.
52. Andrade SC, Araujo AG, Vilar MJ. Back school for patients with non-specific chronic low-back pain: benefits from the association of an exercise program with patient's education. Acta Reumatol Port. 2008; 33 (4): 443-50.
53. Costa LO, Maher CG, Latimer J, Ferreira PH, Ferreira ML, Pozzi GC, et al. Clinimetric testing of three self-report outcome measures for low back pain patients in Brazil: which one is the best? Spine (Phila Pa 1976). 2008; 33 (22): 2459-63.
54. Costa LO, Maher CG, Latimer J, Ferreira PH, Pozzi GC, Ribeiro RN. Psychometric characteristics of the Brazilian-Portuguese versions of the Functional Rating Index and the Roland Morris Disability Questionnaire. Spine (Phila Pa 1976). 2007; 32 (17): 1902-7.
55. Nusbaum L, Natour J, Ferraz MB, Goldenberg J. Translation, adaptation and validation of the Roland-Morris questionnaire--Brazil Roland-Morris. Braz J Med Biol Res. 2001; 34 (2): 203-10.
56. Pesquisa ICd. ICP software solution pack. 2008.
57. Fleck MP, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. [Application of the Portuguese version of the abbreviated instrument of quality life WHOQOL-bref]. Rev Saúde Pública. 2000; 34 (2): 178-83.
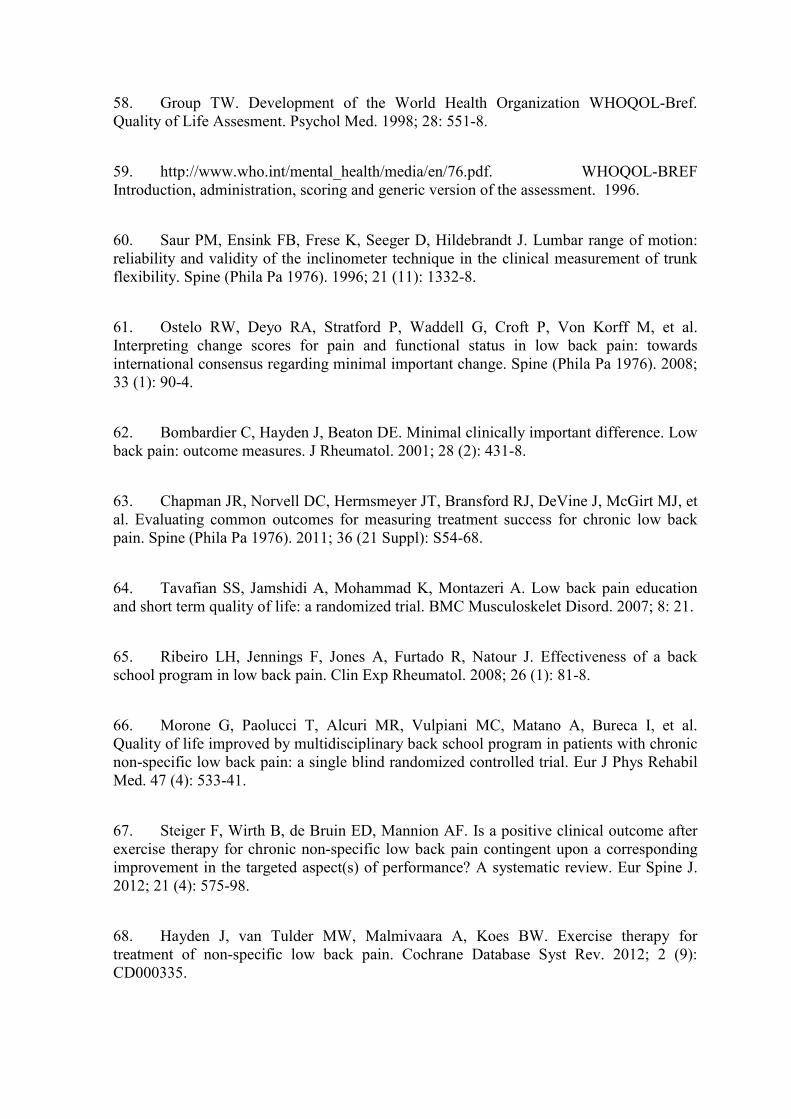
58. Group TW. Development of the World Health Organization WHOQOL-Bref. Quality of Life Assesment. Psychol Med. 1998; 28: 551-8.
59. http://www.who.int/mental_health/media/en/76.pdf. WHOQOL-BREF Introduction, administration, scoring and generic version of the assessment. 1996.
60. Saur PM, Ensink FB, Frese K, Seeger D, Hildebrandt J. Lumbar range of motion: reliability and validity of the inclinometer technique in the clinical measurement of trunk flexibility. Spine (Phila Pa 1976). 1996; 21 (11): 1332-8.
61. Ostelo RW, Deyo RA, Stratford P, Waddell G, Croft P, Von Korff M, et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine (Phila Pa 1976). 2008; 33 (1): 90-4.
62. Bombardier C, Hayden J, Beaton DE. Minimal clinically important difference. Low back pain: outcome measures. J Rheumatol. 2001; 28 (2): 431-8.
63. Chapman JR, Norvell DC, Hermsmeyer JT, Bransford RJ, DeVine J, McGirt MJ, et al. Evaluating common outcomes for measuring treatment success for chronic low back pain. Spine (Phila Pa 1976). 2011; 36 (21 Suppl): S54-68.
64. Tavafian SS, Jamshidi A, Mohammad K, Montazeri A. Low back pain education and short term quality of life: a randomized trial. BMC Musculoskelet Disord. 2007; 8: 21.
65. Ribeiro LH, Jennings F, Jones A, Furtado R, Natour J. Effectiveness of a back school program in low back pain. Clin Exp Rheumatol. 2008; 26 (1): 81-8.
66. Morone G, Paolucci T, Alcuri MR, Vulpiani MC, Matano A, Bureca I, et al. Quality of life improved by multidisciplinary back school program in patients with chronic non-specific low back pain: a single blind randomized controlled trial. Eur J Phys Rehabil Med. 47 (4): 533-41.
67. Steiger F, Wirth B, de Bruin ED, Mannion AF. Is a positive clinical outcome after exercise therapy for chronic non-specific low back pain contingent upon a corresponding improvement in the targeted aspect(s) of performance? A systematic review. Eur Spine J. 2012; 21 (4): 575-98.
68. Hayden J, van Tulder MW, Malmivaara A, Koes BW. Exercise therapy for treatment of non-specific low back pain. Cochrane Database Syst Rev. 2012; 2 (9): CD000335.
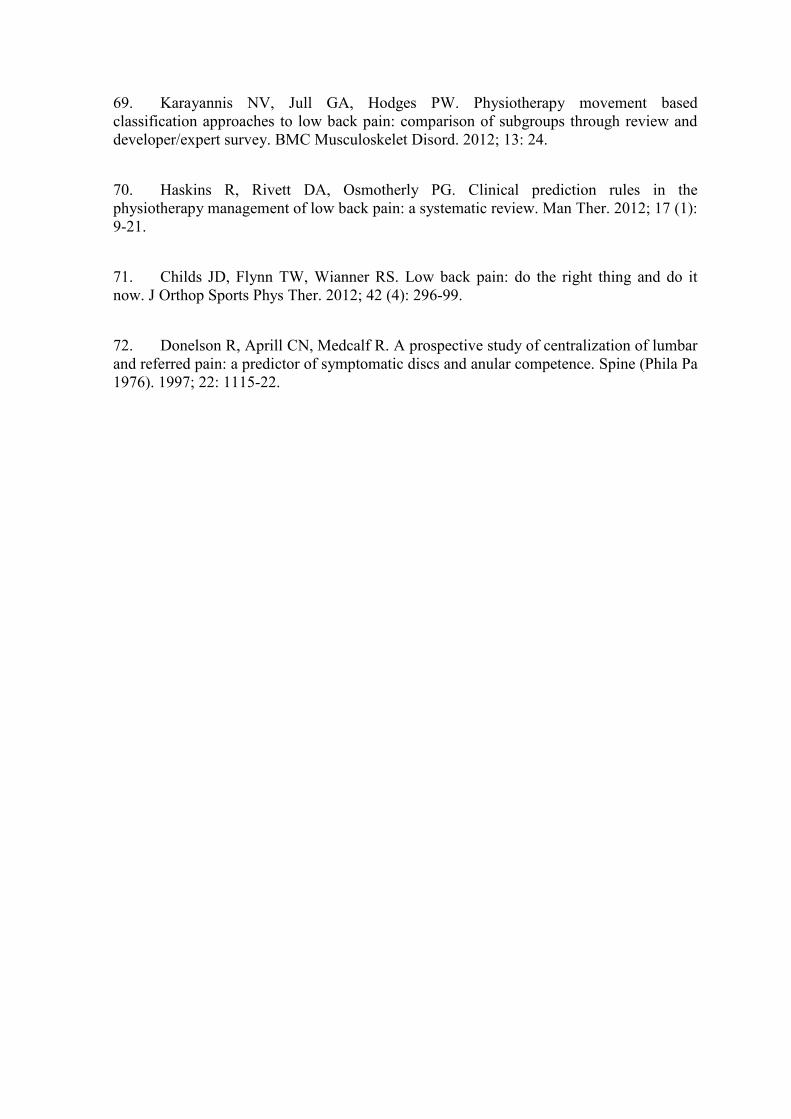
69. Karayannis NV, Jull GA, Hodges PW. Physiotherapy movement based classification approaches to low back pain: comparison of subgroups through review and developer/expert survey. BMC Musculoskelet Disord. 2012; 13: 24.
70. Haskins R, Rivett DA, Osmotherly PG. Clinical prediction rules in the physiotherapy management of low back pain: a systematic review. Man Ther. 2012; 17 (1): 9-21.
71. Childs JD, Flynn TW, Wianner RS. Low back pain: do the right thing and do it now. J Orthop Sports Phys Ther. 2012; 42 (4): 296-99.
72. Donelson R, Aprill CN, Medcalf R. A prospective study of centralization of lumbar and referred pain: a predictor of symptomatic discs and anular competence. Spine (Phila Pa 1976). 1997; 22: 1115-22.
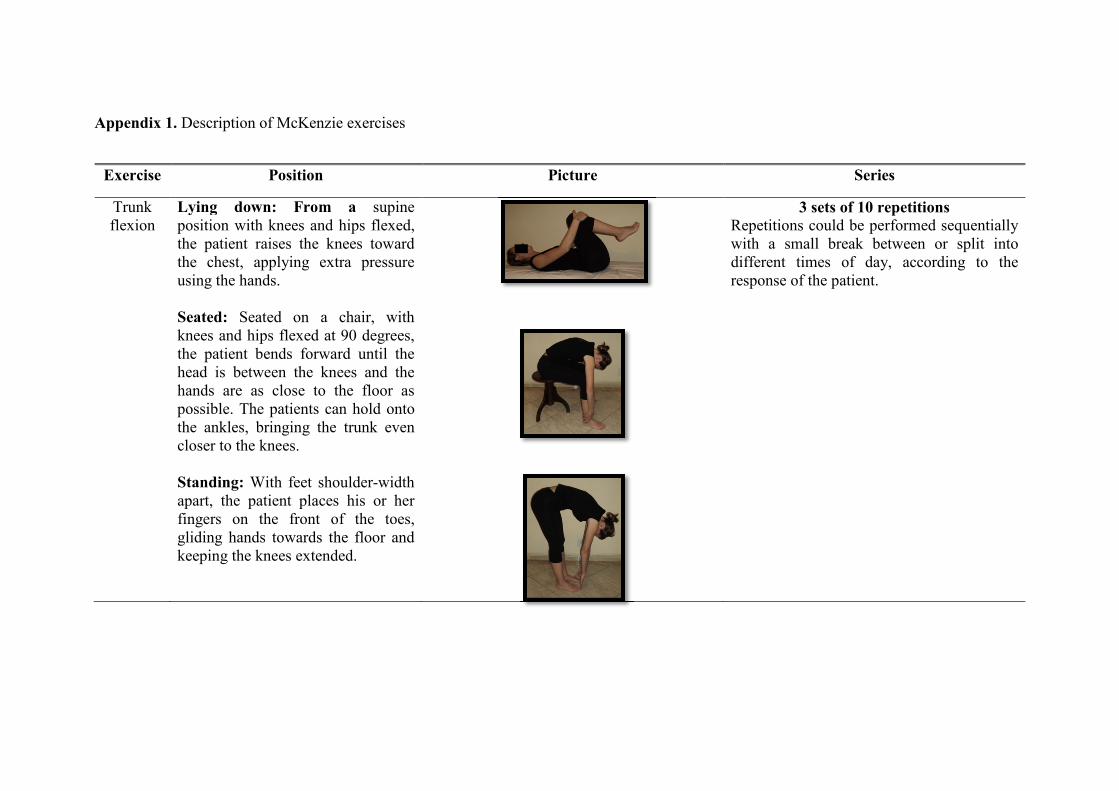
Appendix 1. Description of McKenzie exercises
Exercise Position Picture Series
Trunk flexion
Lying down: From a supine position with knees and hips flexed, the patient raises the knees toward the chest, applying extra pressure using the hands. Seated: Seated on a chair, with knees and hips flexed at 90 degrees, the patient bends forward until the head is between the knees and the hands are as close to the floor as possible. The patients can hold onto the ankles, bringing the trunk even closer to the knees. Standing: With feet shoulder-width apart, the patient places his or her fingers on the front of the toes, gliding hands towards the floor and keeping the knees extended.
3 sets of 10 repetitions Repetitions could be performed sequentially with a small break between or split into different times of day, according to the response of the patient.
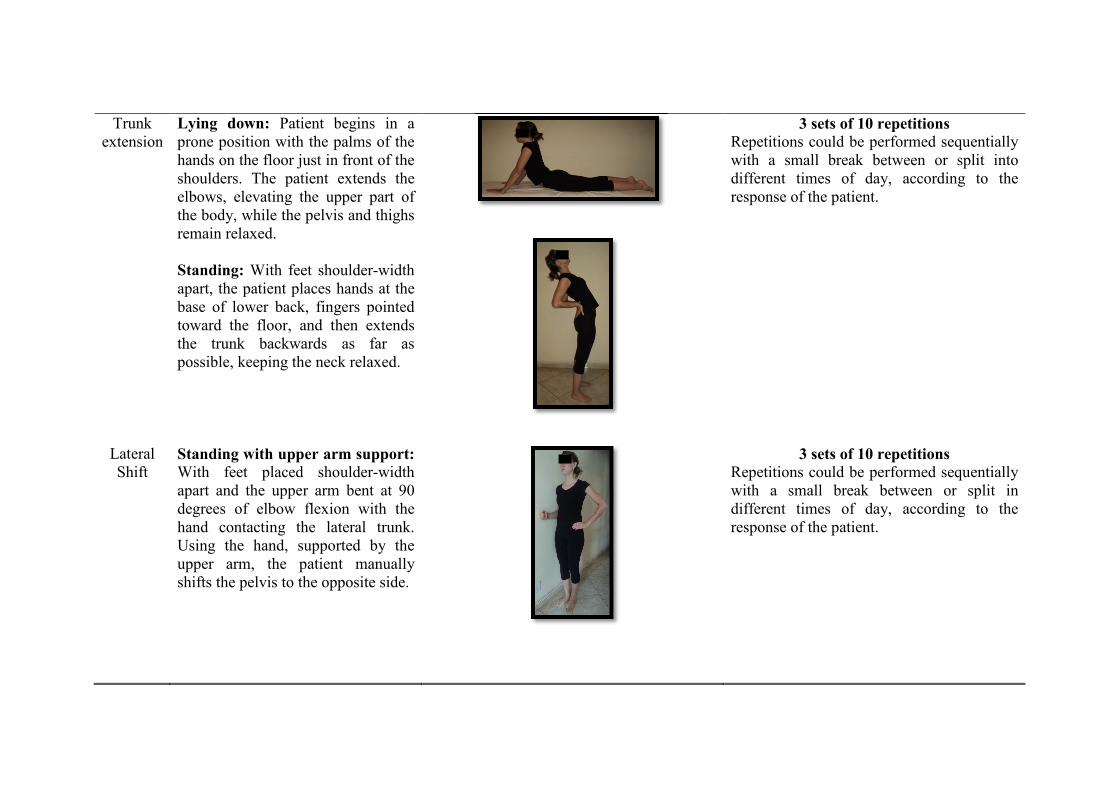
Trunk extension
Lying down: Patient begins in a prone position with the palms of the hands on the floor just in front of the shoulders. The patient extends the elbows, elevating the upper part of the body, while the pelvis and thighs remain relaxed. Standing: With feet shoulder-width apart, the patient places hands at the base of lower back, fingers pointed toward the floor, and then extends the trunk backwards as far as possible, keeping the neck relaxed.
3 sets of 10 repetitions Repetitions could be performed sequentially with a small break between or split into different times of day, according to the response of the patient.
Lateral Shift
Standing with upper arm support: With feet placed shoulder-width apart and the upper arm bent at 90 degrees of elbow flexion with the hand contacting the lateral trunk. Using the hand, supported by the upper arm, the patient manually shifts the pelvis to the opposite side.
3 sets of 10 repetitions Repetitions could be performed sequentially with a small break between or split in different times of day, according to the response of the patient.
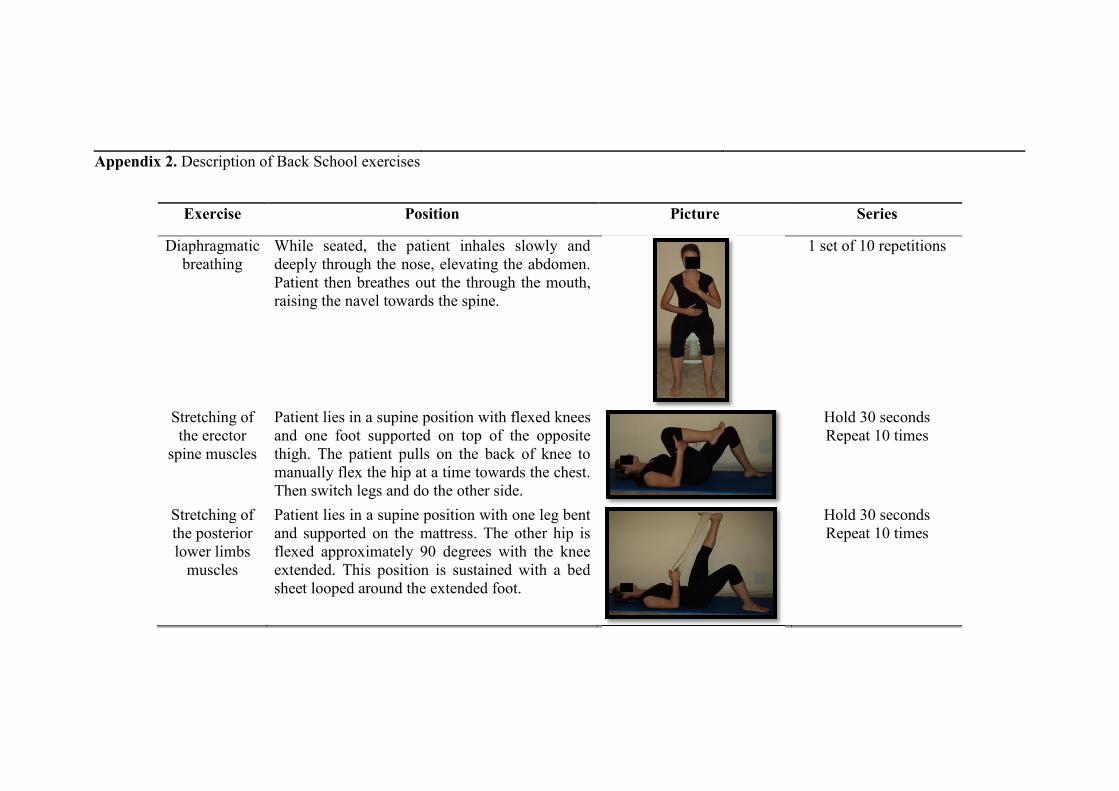
Appendix 2. Description of Back School exercises
Exercise Position Picture Series
Diaphragmatic breathing
While seated, the patient inhales slowly and deeply through the nose, elevating the abdomen. Patient then breathes out the through the mouth, raising the navel towards the spine.
1 set of 10 repetitions
Stretching of the erector
spine muscles
Patient lies in a supine position with flexed knees and one foot supported on top of the opposite thigh. The patient pulls on the back of knee to manually flex the hip at a time towards the chest. Then switch legs and do the other side.
Hold 30 seconds Repeat 10 times
Stretching of the posterior lower limbs
muscles
Patient lies in a supine position with one leg bent and supported on the mattress. The other hip is flexed approximately 90 degrees with the knee extended. This position is sustained with a bed sheet looped around the extended foot.
Hold 30 seconds Repeat 10 times

Stretching of the anterior hip muscle
Patient lies down in the lateral decubitus position. The hip should be in a neutral position with knees flexed. The patient passively extends the hips. The contra lateral limb is flexed at 90 degrees, with the internal side of the knee supported by the mattress.
Hold 30 seconds Repeat 10 times
Kinaesthetic training
In a standing position, the patient moves the pelvis in a front–back pelvic inclination in a comfortable range.
1 set of 10 repetitions
Strengthening of the
abdominal muscles
a) Patient lays in a supine position with knees bent and both feet supported on the mattress. Arms are placed at the sides. The patient raises the head and flexes the trunk while exhaling, maintaining alignment of the cervical spine.
b) Patient lies in a supine position with head supported on the mattress. Patient extends one leg at a 45-degree angle and flexes the hip, with the other leg held in triple flexion with the hands. Patient alternates legs, with leg extension performed while exhaling, maintaining contraction of the transverse abdominis, paravertebral, and pelvic floor muscles.
a)1 set of 10 repetitions
b)1 set of 10 repetitions for each limb
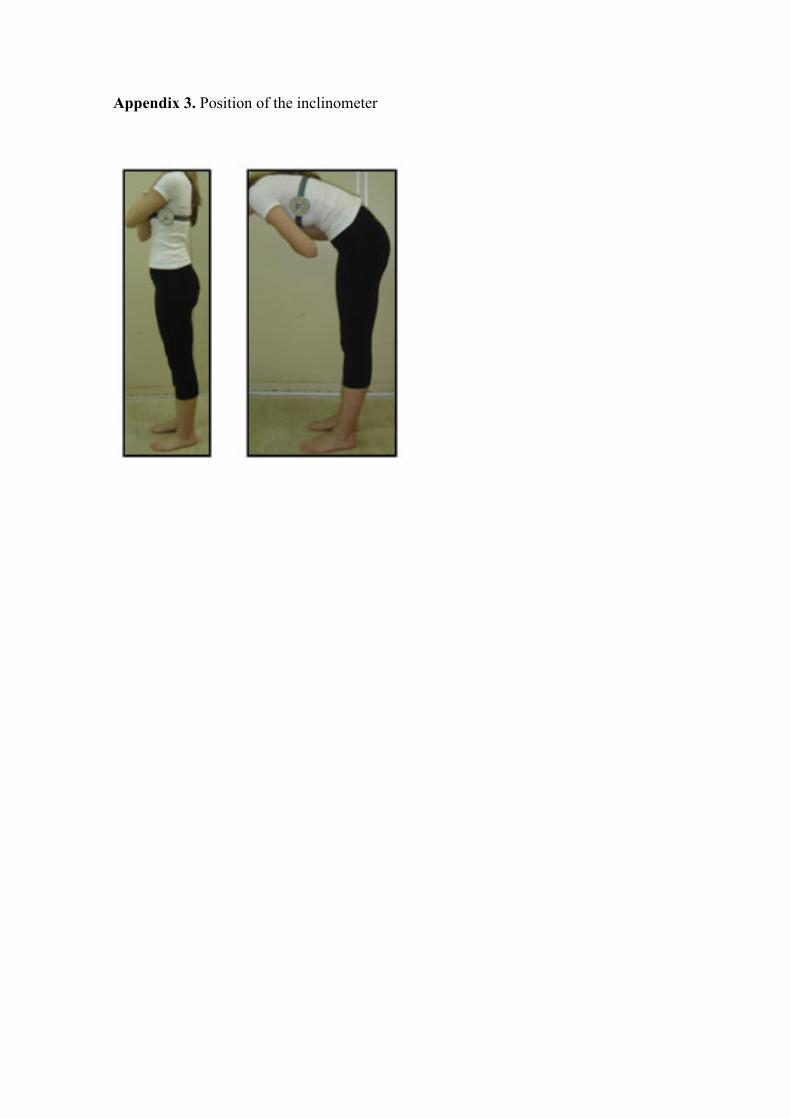
Appendix 3. Position of the inclinometer
Apêndice 2
Efeitos de duas intervenções fisioterapêuticas em pacientes com dor
lombar crônica não específica: viabilidade de um estudo controlado
aleatorizado

Capítulo 4
Considerações Finais
4.1 Resultados encontrados
O objetivo dessa dissertação de mestrado foi comparar os efeitos das intervenções Back
School e McKenzie em pacientes com dor lombar crônica não específica para os desfechos
intensidade de dor, desempenho funcional, qualidade de vida e amplitude de movimento de
flexão de tronco. Após as 4 semanas de tratamento, nós observamos que ambos os grupos
apresentaram melhora da dor e do desempenho funcional e que a maior parte desses efeitos
observados a curto prazo, se mantiveram após 3 e 6 meses da randomização tanto para os
desfechos primários quanto para os secundários. Os pacientes do grupo McKenzie
apresentaram melhores resultados para o desempenho funcional após as 4 semanas de
tratamento quando comparados com os pacientes do grupo Back School. No entanto, a
magnitude da diferença encontrada pode ser considerada pequena (ex: 2,37 pontos numa
escala de 0-24 pontos)1 e possivelmente duvidosa quanto ao efeito clinicamente
importante. Para todos os demais desfechos não foram encontradas diferenças entre os
grupos. As informações referentes aos resultados do estudo estão reportadas no capítulo 3
da dissertação.
Uma possível explicação para o resultado encontrado a favor do método McKenzie para o
desempenho funcional, é que esse método, além de ser uma intervenção individualizada e
que, portanto permite que o paciente tenha um espaço maior para expor suas dificuldades e
esclarecer suas dúvidas, possui como um dos focos do seu tratamento, o componente
educacional2. Esse componente preconiza que o paciente adquira uma posição mais ativa
no tratamento, que o torne o mais independente possível no cuidado com sua saúde; crie
estratégias de controle da dor e realize sem ajuda de outras pessoas e sem medo os
movimentos requeridos durante suas atividades diárias2. Os pacientes no nosso estudo que
foram tratados pelo método McKenzie, receberam orientações advindas do próprio livro do
método confeccionado para pacientes3. Poderíamos atribuir essa melhora do desempenho
funcional à maior confiança que os pacientes adquiriram durante o tratamento, para
realizarem suas atividades de forma independente.
4.2 Implicações clínicas
A partir dos resultados encontrados nesse estudo, foi possível concluir (com exceção do
desempenho funcional), que não houve diferença estatisticamente significante e
clinicamente importante entre os grupos para todos os demais desfechos analisados.
Clinicamente, isso significa que pelo fato dos dois métodos apresentarem resultados
semelhantes, caberá aos clínicos com formação e conhecimento nesses métodos
informarem seus pacientes sobre esses dados e discutirem com os mesmos, para que seja
definido qual método será utilizado durante o tratamento, levando em consideração os
potenciais custos de cada uma das intervenções assim como as preferências dos pacientes.
Apesar do nosso estudo não ter mensurado os custos para cada método, entendemos que
um método como o Back School que propõe que as sessões sejam realizadas em grupo,
tende a ser mais barato do que uma intervenção individualizada como o método McKenzie.
Desta forma acreditamos que o método Back School, que permite abranger um número
maior de pessoas no tratamento, poderia ser oferecido pelo governo para as pessoas que
estão nas filas de espera de postos de saúde, ambulatórios e hospitais aguardando por
tratamento, com a segurança de que teriam resultados tão positivos quanto de um método
individualizado.
4.3 Recomendações para futuros estudos
Um ponto importante que deve ser levado em consideração ao interpretar os resultados dos
nosso estudo, é que talvez as características individuais dos pacientes podem ter predizido
uma melhor resposta a uma das intervenções (ex: subgrupos)4. Existem vários métodos de
classificação disponíveis que visam identificar os pacientes que possivelmente respondem
melhor a diferentes intervenções5. No entanto, esses métodos de classificação e regras de
predição clínica estão em fase de desenvolvimento e os clínicos ainda não podem
recomendar precisamente qual seria o “paciente adequado” para o “tratamento adequado”6.
No caso dos pacientes que apresentam o fenômeno de centralização dos sintomas, sabe-se
que geralmente tendem a responder melhor ao tratamento com o método McKenzie7, 8.
Porém nosso estudo não tem poder estatístico suficiente que permita uma análise de
subgrupos. Para estudos futuros com o método McKenzie acreditamos que seria
interessante considerar o fenômeno de centralização como um critério de elegibilidade.
Outra sugestão para estudos futuros é que sejam conduzidos estudos controlados
aleatorizados de boa qualidade metodológica com pacientes crônicos que considerem a
análise de custo efetividade dos métodos McKenzie e Back School, principalmente para o
método Back School que engloba um número maior de pessoas no tratamento, a fim de
trazer informações que podem vir a auxiliar na redução de custos com o tratamento da dor
lombar.
4.4 Referências
1. Bombardier C, Hayden J, Beaton DE. Minimal clinically important difference. Low
back pain: outcome measures. J Rheumatol. 2001; 28 (2): 431-8.
2. Mckenzie R, May S. The Lumbar Spine Mechanical Diagnosis & Therapy Vol II.
edition S, editor. New Zealand Spinal Publications; 2003.
3. Mckenzie R. Trate você mesmo a sua coluna. RJ: TTMT; 1998.
4. Karayannis NV, Jull GA, Hodges PW. Physiotherapy movement based
classification approaches to low back pain: comparison of subgroups through review and
developer/expert survey. BMC Musculoskelet Disord. 2012; 13: 24.
5. Haskins R, Rivett DA, Osmotherly PG. Clinical prediction rules in the
physiotherapy management of low back pain: a systematic review. Man Ther. 2012; 17 (1):
9-21.
6. Childs JD, Flynn TW, Wianner RS. Low back pain: do the right thing and do it
now. J Orthop Sports Phys Ther. 2012; 42 (4): 296-99.
7. Donelson R, Aprill CN, Medcalf R. A prospective study of centralization of lumbar
and referred pain: a predictor of symptomatic discs and anular competence. Spine (Phila Pa
1976). 1997; 22: 1115-22.
8. Mckenzie R, May S. The Lumbar Spine Mechanical Diagnosis & Therapy Vol I.
edition S, editor. New Zealand: Spinal Publications; 2003.

Anexo 1
Instruções para os autores - Physical Therapy
Anexo 1 - Instruções para os autores - Physical Therapy
Formatting
PTJ endorses the Uniform Requirements for Manuscripts Submitted to Biomedical Journals put forth by the International Committee of Medical Journal Editors (ICMJE). PTJ follows the American Medical Association [AMA] Manual of Style, 10th ed, published by Williams & Wilkins (Baltimore, Md). PTJ promotes "people-first" language. That is, patients and subjects should not be referred to by disability or condition (eg, use "patients who have had a stroke" or "patients with stroke," rather than "stroke patients" or "stroke survivors").
All manuscripts must be formatted double-spaced, with pages AND lines numbered. Please use 12-point font. Submit both a masked copy and an unmasked copy. In the masked version, please remove author names and any affiliations within the article.
Sections, in order of appearance: (1) Title page, (2) Abstract, (3) Body of article, (4) Acknowledgments, (5) References, (6) Tables, (7) Figure legends, (8) Figures, (9) Video legends, (10) Appendixes.
Title. Titles should not be vague and should reflect measured variables. For instance, instead of using "physical therapy" to refer to intervention, state specific interventions (eg, "strengthening exercises"). For randomized trials, add the subtitle "A Randomized, Controlled Trial" to the full title of your manuscript. Titles (including subtitles) should be no longer than 150 characters (including punctuation and spaces).
Abstract. Word limit: 275 words. Structure: Background, Objective, Design, Setting, Patients, Intervention, Measurements, Results, Limitations, Conclusions (see Haynes).
Body of Manuscript. Word limit: 4,500 words (excluding abstract and references). Please provide the manuscript word count on the abstract page of your manuscript. Sections: Introduction, Methods, Results, and Discussion. Use the following Methods section subheadings: Design Overview; Setting and Participants; Randomization and Interventions; Outcomes and Follow-up; Statistical Analysis; Role of the Funding Source. The Discussion section ideally should contain no more than 5 paragraphs and should address:
- statement of principal findings - strengths and weaknesses of the study - strengths and weaknesses in relation to other studies, discussing important
differences in results - meaning of the study: possible explanations and implications for clinicians and
policymakers - unanswered questions and future research

Acknowledgments. Acknowledgments should be formal and as brief as possible and limited to recognizing individuals who have made specific and important contributions to the work being reported.
References. 75 or fewer. References should be listed in the order of appearance in the manuscript, by numerical superscripts that appear consecutively in the text. If you use End Notes, please use version 6.0 or higher.
Tables. Tables should be formatted in Word, numbered consecutively, and placed together.
In tables that describe characteristics of 2 or more groups:
Report averages with standard deviations when data are normally distributed. Report median (minimum, maximum) or median (25th, 75th percentile [interquartile
range, or IQR]) when data are not normally distributed.
There should be no more than 6 tables and figures (total). Additional tables and figures can be posted online only.
For more information, see "Tips for Figures and Tables."
Figures. For peer-review purposes, figures can be attached to the manuscript after the figure legends; however, figures also should be submitted as separate, high-res graphic files in tif, jpg, eps, or pdf format, with the resolution set at a minimum of 300 dpi. The separate image files will help PTJ staff to produce the sharpest images both in print and online. Rule of thumb: the larger the figure (eg, 8.5" × 11"), the better. If electronic formats are not available to you, figures must be submitted as 5" × 7" camera-ready glossies and mailed to the Editorial Office. Figures should be numbered consecutively. For helpful guidelines on submitting figures online, visit Cadmus Journal Services. Lettering should be large, sharp, and clear, and abbreviations used within figures should agree with Journal style. Color photographs are encouraged, in sharp focus and with good contrast.
There should be no more than 6 tables and figures (total). Additional tables and figures can be posted online only.
Appendixes. Appendixes should be numbered consecutively and placed at the very end of the manuscript. Use appendixes to provide essential material not suitable for figures, tables, or text.
Online-Only Materials. PTJ hosts a variety of supplemental data that cannot be published in print or that exceeds allowed word, table, or figure counts. Supplemental files can include tables, figures, appendixes, video clips, PowerPoint files, or Excel spreadsheets.
If a manuscript contains tables or figures that exceed PTJ's maximum, the review team may recommend that some of them appear online only as a PDF. These tables and figures would have the same format and style as those in the final published article.
To help the reader, PTJ recommends that Research Report and Case Report authors submit study protocols, treatment manuals, detailed descriptions of evaluation and intervention procedures, treatment progression algorithms, etc. These can be submitted as online-only tables, figures, appendixes, or video clips. They are reviewed by the editors and Editorial Board and should be submitted at the same time that the manuscript is submitted. The videos can be of patients, procedures, interventions, or any other relevant part of the study or case. (See Video Central for recent examples.)
Video Requirements. PTJ's preferred format for video clips is MPEG (Moving Picture Experts Group). Because of sophisticated compression techniques, MPEG files are much smaller than other formats for the same quality. These files also are compatible with both Windows Media Player (PC) and QuickTime (Mac). Other acceptable formats include: .mov (QuickTime Movie), .wmv (Windows Media Video), .mp4, and .avi (Audio Video Interleave).
If the manuscript is accepted for publication, PTJ staff will convert the video file to MPEG format and it will accompany the final print version of the article online.
File size: To minimize the time it takes for video files to download, the file size of the video should be as small as possible but large enought to still preserve clarity and sharpnesss. Minimum dimensions: 320 pixels wide by 240 pixels deep. Maximum length: 5 minutes
Where applicable, include a citation to each video in the manuscript text and include the title (10-15 words maximum) and a legend for the video in the manuscript after the figure captions.
If patients are in the video, either they should not be identifiable or they must give written permission to use the video.
If you have questions about videos, please contact the Online Editor.
Measurements. Please use the International System of Units. (English units may be given in parentheses.)
Equipment manufacturers. For all equipment and products mentioned in the text, place the model name/number and the manufacturer and location (city and state) in parentheses in the text.
In the "Data Analysis" section, specify the statistical software—version, manufacturer, and manufacturer's location—that was used for analyses.
Explanatory footnotes. For any explanatory footnotes, use consecutive symbols (*, †, ‡, §, ||, #, **, ††, ‡‡, §§, ||||, ##).
Statistics
Requirements for addressing clinical relevance. In reporting statistical results, P values alone are insufficient. PTJ authors are required report the magnitude and/or precision of
statistical estimates (eg, 95% CI) to enhance data interpretation and clarify which results potentially have an impact on clinical practice.
Percentages. Report percentages to one decimal place (ie, xx.x %).
Standard deviations. Use "mean (SD)" rather than "mean ± SD" notation. Report confidence intervals (CI) rather than standard errors.
P values. Report exact P values to 2 decimal places, except when P≤.001 and in that case P ≤.001 is sufficient. P values alone are insufficient and must be accompanied with appropriate magnitude and precision estimate.
Photograph and Video Release—Patient Permission
Authors must obtain and submit written permission to publish photographs or post video clips in which patients are recognizable. This statement must be signed by the patient, parent, or guardian.
Reprinted Materials
Authors must obtain and submit written permission from the original sources, in the name of APTA, to publish in their article illustrations, photographs, figures, or tables taken from those sources.
Related Articles
If other articles using the same data set or otherwise related to this manuscript have been published or are under review by other journals, submit a masked copy of the article(s) along with your manuscript.
Raw Data
PTJ works to maintain the highest levels of integrity and accountability. The Editors therefore reserve the right to ask researchers to provide the raw data for their studies during review or at any time up to 5 years after publication in PTJ. This would likely happen only in rare instances, when credibility of the research is brought into serious question.

Anexo 2
Aprovação do Comitê de Ética e Pesquisa e Registro do estudo

Anexo 2 - Aprovação do Comitê de Ética e Pesquisa e Registro do estudo





























