Embed Size (px)
Citation preview
15/12/2012
1
João Flávio Nogueira, MD Fortaleza, Brasil
• Discutir a anatomia básica da laringe
• Entender seu funcionamento e principais doenças

15/12/2012
2
• Evitar aspiração de líquidos/comida nos pulmões
• Proteger via aérea de conteúdo abdominal
– Refluxo
– Vômitos
– Pressão intra-abdominal
• Fonação
The original use of the larynx was to keep us alive through breakfast. Its main function
is stop solids and liquids from entering the trachea and choking us to death. Its
secondary functions are to bear down, phonation and speech. The larynx of humans
and great apes in infancy is higher in the neck so that they can breathe and suckle at the
same time. In humans it descends before the age of two.

15/12/2012
3

15/12/2012
4
• Hyaline cartilage
• Largest
• Encloses the larynx anteriorly and laterally
• Two alae
• Ossification

15/12/2012
5
Hyaline cartilage
Directly below the thyroid cartilage
Stongest
Shape: Signet ring
Lamina – flat portion
Only complete annular support of the larynx
Articulates w/ Inferior cornu of the thyroid cartilage
• Fibroelastic cartilage
• Leaf-shaped structure
• Petiole – small narrow portion of the glottis
15/12/2012
6
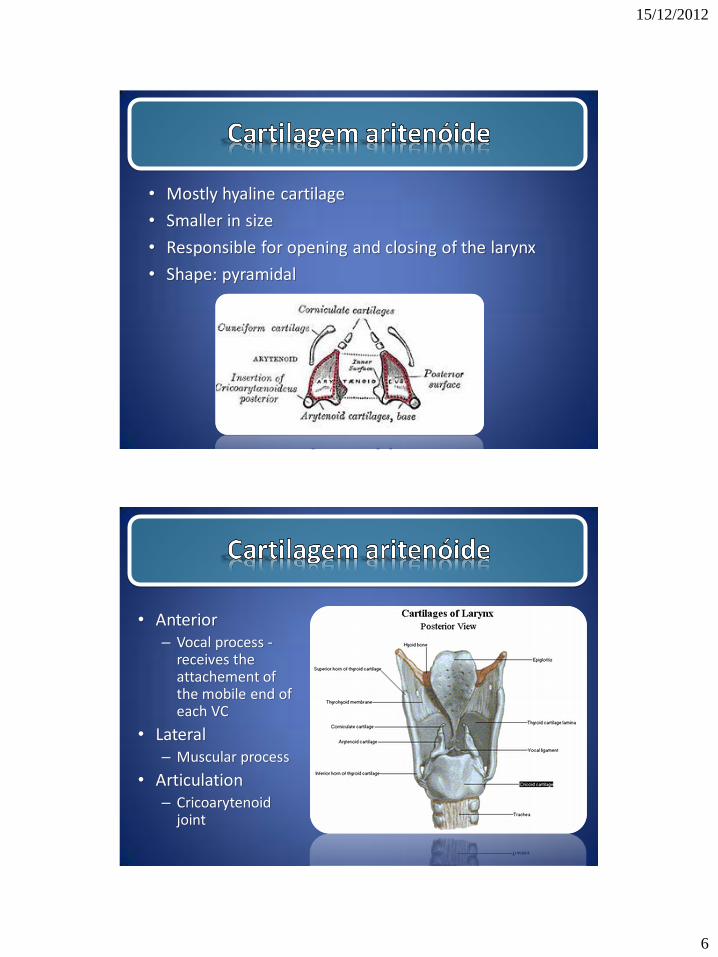
• Mostly hyaline cartilage
• Smaller in size
• Responsible for opening and closing of the larynx
• Shape: pyramidal
• Anterior – Vocal process -
receives the attachement of the mobile end of each VC
• Lateral – Muscular process
• Articulation – Cricoarytenoid
joint

15/12/2012
7
• Fibroelastic
• Cartilages of Santorini
• Small cartilages above the arytenoid and in the aryepiglottic folds
• Firboelastic cartilages
• Cartilages of Wrisberg
• Elongated pieces of small yellow elastic cartilage in the aryepiglottic folds
15/12/2012
8

15/12/2012
9

15/12/2012
10
15/12/2012
11
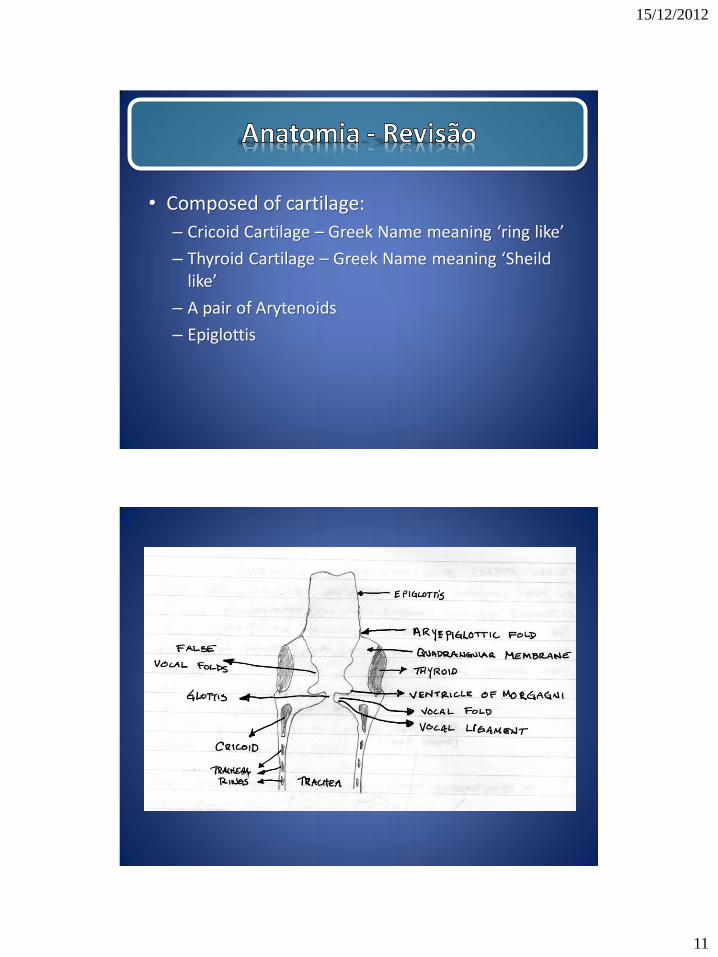
• Composed of cartilage:
– Cricoid Cartilage – Greek Name meaning ‘ring like’
– Thyroid Cartilage – Greek Name meaning ‘Sheild like’
– A pair of Arytenoids
– Epiglottis

15/12/2012
12
Laryngeal Anatomy anatomy.uams.edu/anatomyhtml/atlas_html/rsa3p2.html
1. Hyoid bone
2. Thyroid cartilage
3. Cricoid cartilage
4. Tracheal cartilages
www.bartleby.com/107/illus952.html

15/12/2012
13
www.ling.yale.edu:16080/ling120/Larynx/Larynx_side.gif
Larynx
Cricoid
anatomy.uams.edu/.../atlas_html/rsa3p6.html
1. Anterior arch
2. Posterior
lamina
3. Articular facet

15/12/2012
14
Thyroid Cartilage
/www.yorku.ca/earmstro/journey/images/thyroid.gif
ARYTENOIDS
homepages.wmich.edu/~gunderwo/intro_voice.htm

15/12/2012
15
1. Thyroid prominence
2. Cricothyroid ligament
3. Arytenoid cartilage
4. Corniculate cartilage
5. Vocal ligament
6. Vestibular fold
7. Cricoid cartilage
8. Articular facet for inferior
cornu of thyroid cartilage
anatomy.uams.edu/anatomyhtml/graphics/rsa3p8.gif
1. Epiglottis
2. Arytenoid cartilage
3. Corniculate cartilage
4. Aryepiglottic fold
anatomy.uams.edu/anatomyhtml/graphics/rsa3p10.gif

15/12/2012
16
The thyroid rests superiorly on the cricoid and attaches posterior-laterally at the cricoid’s inferior articulator facets. This attachment (the cricothyroid joint)
hinges the cricoid and thyroid allowing their anterior sides to adduct, changing
vocal fold length.
people.umass.edu/jkingstn/ling414/figure%202.19%20arytenoid%20movement%20f05.jpg

15/12/2012
17
Composition of the Larynx (Con’t)
• Composed of Muscle:
–Extrinsic Laryngeal Muscles
–Intrinsic Laryngeal Muscles
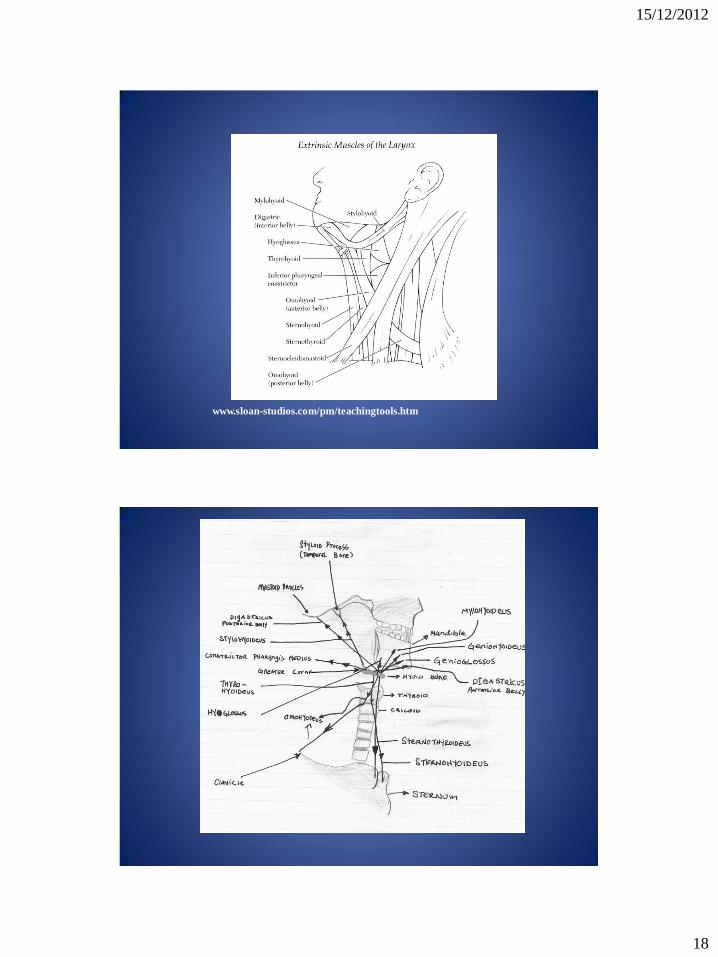
Extrinsic Muscle
TWO Groups of Extrinsic Muscles:
• Suprahyoids – Attach to points above the Hyoid (Jaw, Skull and Tongue) when they contract they raise or elevate the Larynx eg Swallowing
• Infrahyoids – Attach to points below the Hyoid (one connects to the thyroid, however the others connect to the sternum and the scapula) when they contract they lower or depress the Larynx
15/12/2012
18
www.sloan-studios.com/pm/teachingtools.htm
15/12/2012
19
Intrinsic Muscles
• Adductors – vocal folds are together
• Abductors – vocal folds apart
• Tensors - Stiffen
• Relaxors - Relax
Adductors
• Lateral Cricoarytenoids
• Interarytenoids
–Transverse Arytenoids
–Oblique Arytenoids

15/12/2012
20
Adductors artemis.austincollege.edu/acad/music/wcrannell/vocalped/images/larynx1.gif
Adductors artemis.austincollege.edu/acad/music/wcrannell/vocalped/images/larynx1.gif

15/12/2012
21
137.222.110.150/calnet/H+N/image/deep%20muscles%20of%20larynx-lateral%20view.jpg
Abductors • Posterior Cricoarytenoids

15/12/2012
22
Vocal Folds
• Muscle
–External Thyroarytenoids – inserts into the
muscular process on the Arytenoids and the Thyroid notch (shorten and adduct)
–Internal Thyroarytenoids – inserts into the
vocal process on the Arytenoids and the Thyroid Notch (shortens and stiffens), act antagonistically to the Cricothyroids
• Membrane
137.222.110.150/calnet/H+N/image/deep%20muscles%20of%20larynx-lateral%20view.jpg

15/12/2012
23
Membranes
• False Vocal Folds – Ventricular folds
• Laryngeal Ventricle
• Conus Elasticus (interconnects the thyroid, cricoid and arytenoids
cartilages)
• Lamina propria (mucosal cover of the vocalis muscle) – can vibrate independently of the vocalis muscle
• Vocal Ligament – the thread like collagenous fibers of the deep layer of the lamina propria
Relaxors and Tensors
• External Thyroarytenoid – Relaxor, shortens and adducts
• Internal Thyroarytenoid – Tensor, shortens and stiffens
• Cricothyroid Muscles – Tensor, lengthens and stiffens
Pitch is determined by Relaxors and Tensors

15/12/2012
24
www.kolumbus.fi/msts/larynx/larynx.htm
Fundamental Frequency
Phonation is made up of a fundamental
frequency or Fo (the number of times the folds
open and close per second-CPS) and harmonic
multiples of the Fo (two times the Fo, three
times, four times etc.) that fall in intensity
(volume) in an inverse relationship as the
harmonics rise in frequency or as the pitch
rises the volume falls.

15/12/2012
25
Fundamental Frequency
10
9
8
7
6
5
4
3
2
1
100 200 300 400 500 600 700 800 900 1000
INTENSITY
(VOLUME)
FREQUENCY
(PITCH)
Pitch
• Fundamental frequency (average: baby 500Hz, children 250-400Hz
men 125Hz women 200Hz) is primarily affected by applying more or less longitudinal tension to the VF using:
• Cricothyroids
• Tension in the vocalis muscle
OR • Adjustments in vertical tension – depressing or elevating the
Larynx via suprahyiod and infrahyoid muscles

15/12/2012
26
Vocal Fold Tension, Elasticity and Movement
• Thicker or thinner
• Shorter or longer
• Open or close
• Intermediate positions
• Stiff or elastic
Movement:
Bronx Cheer or Raspberry– “the sound is that or air escaping in rapid bursts, not the sound of the lips moving” – Borden and Harris. Aerodynamic forces acting on the elastic body of the lips
ADMET – Aero Dynamic Myo-Elastic Theory
Glottal vibration is the result or refers to interaction between aero-dynamic forces and vocal fold muscular action.
• Sub-Glottal Pressure
• Bernoulli Effect – set vocal folds into vibration due to the elasticity of the folds (elastic recoil – the force which restores any elastic body back to its resting place)
• Muscular Force – Muscles act to bring the folds together so they can vibrate, and muscles regulate their thickness and tension to alter fundamental frequency. Folds are FULLY or PARTIALLY ADDUCTED for phonation

15/12/2012
27
Bernoulli Effect
• An increase in velocity results in a drop in the pressure exerted by the molecules of moving gas or liquid, the pressure drops being perpendicular the direction of the flow
Schematic showing the Bernoulli Effect. The arrows indicate movement of pressure. As the air
moves through a narrowing, inside pressure drops and outside pressure increases pulling the sides
inward.

15/12/2012
28
Glottal Cycle
• Vertical Phase Difference – vocal folds open at the bottom first. As top part opens bottom part closes. Wave like motion
www.phon.ox.ac.uk/~jcoleman/phonation.htm
15/12/2012
29
Chest (Modal Register)
• Low fundamental frequency
• Vocalis muscle activity
• Folds are thick and short
• Low stiffness
Falsetto Register
• Longer and thinner folds
• Stiff folds
• Small amplitude of vibration
• Incomplete closure of the folds
• Shutter like appearance – Vibrate more like strings

15/12/2012
30
Vocal Onset
• How we bring the folds together:
– Attack
– Breathy
– Vocal Fry
– Partial adduction – Whispering or falsetto register
(Note: Folds come together FULLY but without force for Modal register)
Pitch
• Lies in the stiffness of the folds resulting from lengthening and contraction of the thyroarytenoids, especially the vocalis portion

15/12/2012
31
• Tabaco – Cigarros de enrolar
– Marijuana
• Álcool • Refluxo GE
• HPV
Tumores de laringe
Fatores de risco
AG.QUIMICOS
POLUIÇÃO GENÉTICA?
TABACO
ALCOOL
CA
LARINGE

15/12/2012
32
Anatomia – subdivisão
Source: AJCC Cancer Staging Manual, 6th Ed (2002)
• Ca mais comum de cabeça e pescoço (excluindo pele)
• Homens = 4 : 1
• > 90% carcinoma epidermóide • Variações de prevalência ao redor do mundo
Incidência por local
Supraglótico 40%
Glótico 59%
Subglótico 1%
Tumores de laringe
Epidemiologia
American Cancer Society: Cancer Facts and Figures 2008. Atlanta, Ga: American Cancer Society, 2008.

15/12/2012
33
Cancer supraglótico
• Predominância de lesões em epiglote, falsas pregas vocais e prega ariepiglótica
• Extensão para valéculas, base da lingua, seio piriformee tireóide
• “silencioso”; dor de garganta, disfagia, otalgia reflexa, tu no pescoço
Cancer glótico
• Mais comum: 59-65%
• ROUQUIDÃO, estridor ou dispnéia
15/12/2012
34
Cancer subglótico
• Raro (1%)
• Estridor, dispnéia
• Sinais e sintomas
– ROUQUIDÃO, disfagia, hemoptíase, dispnéia, aspiração
– Dor de garganta
– Otalgia reflexa (ramo do N. Vago = sugere estágio avançado)
– CA Glótico = ROUQUIDÃO = diagnóstico precoce
– CA Supraglótico = diagnóstico tardio
• Tu volumosos ao diagnóstico
• Provável comprometimento de linfonódios regionais
• Emagrecimento
Tumores de laringe
Quadro clínico

15/12/2012
35
Tu de laringe Quadro clínico
• Exame físico – Exame completo de cabeça e pescoço
• Palpação de linfonódios; restrição do crepitar laringeo
– Qualidade da voz
• Soprosa = paralisia de prega vocal
• Abafada = lesão supraglótica
– Laringoscopia
• Indireta com espelho de laringe
• Videolaringoscopia
• Notar: bordos, cor, vibração, mobilidade da prega vocal, e lesões.
Tumores de laringe Diagnóstico diferencial
• Laringite crônica
• Doenças granulomatosas (TB, sarcoidose)
• Papilomatose juvenil
• Linfoma
Rotina
1) Videoendoscopia
2) Exames de imagem
3) Biópsia e histologia
15/12/2012
36
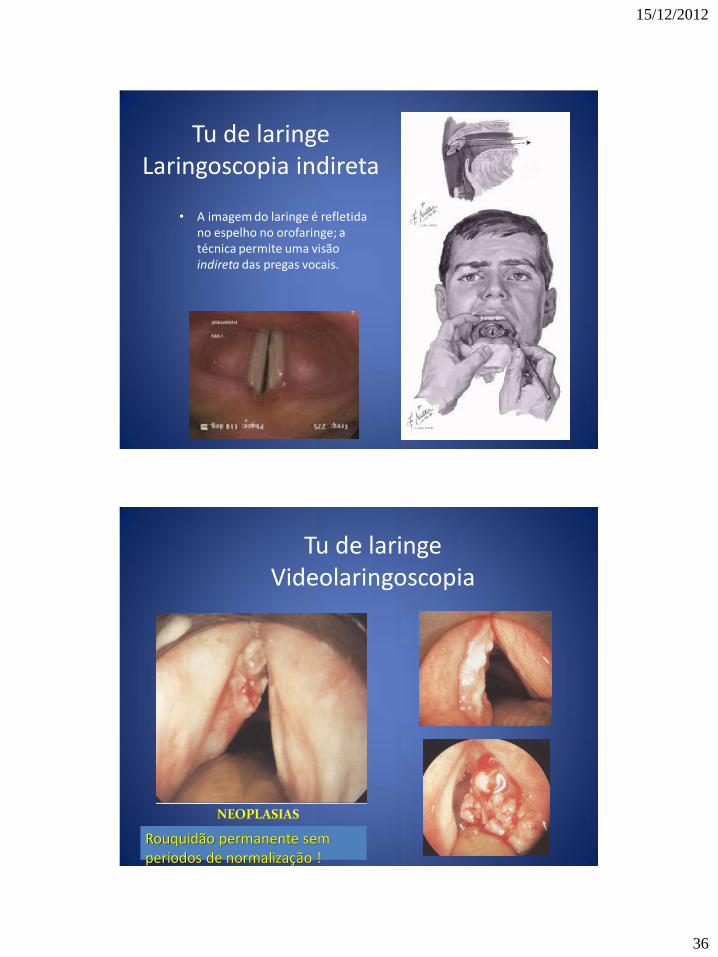
Tu de laringe Laringoscopia indireta
• A imagem do laringe é refletida no espelho no orofaringe; a técnica permite uma visão indireta das pregas vocais.
Tu de laringe Videolaringoscopia
NEOPLASIAS
Rouquidão permanente sem períodos de normalização !

15/12/2012
37
Tu de laringe Imagem
• CT ou MRI – Avaliar estruturas adjacentes: espaço pré-epiglótico ou paraepiglótico
– Erosão da cartilagem tireoidea
– Linfonódios cervicais comprometidos
Tu de laringe Biópsia e histologia
• Microlaringoscopia direta com biópsia
• Histologia:
–CARCINOMA EPIDERMÓIDE (>90%)
• Histo normal hiperplasia displasia ca in situ ca invasivo
• Tabaco + alcool

15/12/2012
38
Tu de laringe Biópsia e histologia
• Histologia (outros tumores):
– Glândula salivares
• Carcinoma adenocístico
• Carcinoma mucoepidermóide
– Sarcomas (condrosarcoma)
– Diversos: linfoma, metastáses
• Supraglottis – Tis: CA in-situ
– T1: limited to subsite of supraglots w/normal cord mobility
– T2: invade mucosa of > 1 subsite of supraglottis, glottis, or outside of supraglottis w/out fixation of the larynx
– T3: limited to larynx w/vocal cord fixation and/or invades postcricoid area, pre-epiglottic tissues, paraglottic space, and/or minor thyroid cartilage erosion
– T4a: invades thyroid cartilage and/or tissues beyond larynx
– T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures
• Glottis – Tis: CA in-situ
– T1: limited to cord;
T1a: one cord; T1b: two cords
– T2: extends to supraglottis,
and/or subglottis, and/or
w/impaired cord mobility
– T3: limited to larynx w/vocal cord
fixation and/or invades
paraglottic space, and/or minor
thyroid cartilage erosion
– T4a: invades thyroid cartilage
and/or tissues beyond larynx
– T4b: invades prevertebral
space, encases carotid artery, or
invades mediastinal structures
• Subglottis – Tis: CA in-situ
– T1: limited to subglottis
– T2: extends to vocal cord with normal or impaired mobility
– T3: limited to larynx w/vocal cord fixation
– T4a: invades cricoid or thyroid cartilage, and/or invades tissues beyond the larynx
– T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures
Tu laringe – estadiamento (TNM)
Source: AJCC Cancer Staging Manual, 6th Ed (2002)

15/12/2012
39
• Subglottis – Tis: CA in-situ
– T1: limited to subglottis
– T2: extends to vocal cord with normal or impaired mobility
– T3: limited to larynx w/vocal cord fixation
– T4a: invades cricoid or thyroid cartilage, and/or invades tissues beyond the larynx
– T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures
Estadiamento
• Nodes – N0: no regional node mets
– N1: single ipsilateral node, ≤ 3 cm
– N2a: single ipsilateral node, > 3 cm, ≤ 6 cm
– N2b: multiple ipsilateral nodes, ≤ 6 cm
– N2c: bilateral or contralateral nodes, ≤ 6 cm
– N3: node > 6 cm
• Mets – Mx: unknown
– M0: no distant mets
– M1: distant mets
Source: AJCC Cancer Staging Manual, 6th Ed (2002)
Tu de laringe Drenagem de linfonódios
Tu
subglótico
Tu supraglótico

15/12/2012
40
Estadiamento agrupado
Estágio 0 Tis N0 M0
I T1 N0 M0
II T2 N0 M0
III T3 N0 M0
T1-3 N1 M0
IVA T4a N0-1 M0
T1-4a N2 M0
IVB T4b any N M0
any T N3 M0
Stage IVC any T any N M1
Inicial
Avançado
• Cirurgia – Microlaringocirurgia
– Hemilaringectomia fronto-lateral (vertical)
– Hemilaringectomia supraglótica (horizontal)
– Laringectomia total
• Radiaterapia
• Quimioterapia
Tu de laringe
Tratamento – Opções:
A considerar
1) Local e tipo do tumor
2) Invasão adjacente
3) Metástases

15/12/2012
41
• Alternativas possíveis:
– Microcirurgia com laser (transoral)
– Hemilaringectomias
– Radioterapia
• Resultados similares entre cirurgia x radioterapia
• Recomendação atual: radioterapia inicial e cirurgia reservada para recorrências locais (??)
Tu de laringe
Tratamento – Estágios I/II
Mendenhall WM et al., Cancer. 2004 May 1;100(9)
5-anos sobrevida:
Estágio I = 90%
Estágio II= 70%
• Disgeusia (=dor de garganta)
• Mucosite
• Dermatites
• Xerostomia
• Fibrose superficial
• Fistulas
• Hipotireoidismo
Complicações da radioterapia

15/12/2012
42
Tu de laringe Tratamento – Estágios III/IV
1) Quimioterapia
2) Radioterapia x Laringectomia total
3) Laringectomia total ou Radioterapia posop
Department of Veterans Affairs Laryngeal Cancer Study Group, N Engl J Med 1991;324:1685-90.
Treatment – Advanced Stage (III/IV) – RTOG 91-11 Study
Concurrent
chemoXRT
Induction chemo
XRT
XRT alone
2 yrs 5 yrs 2 yrs 5 yrs 2 yrs 5 yrs
Dz Free
SurvivalA
61% 36% 52% 38% 44% 27%
Overall
SurvivalB
74% 54% 76% 55% 75% 56%
Distant
metsC
8% 12% 9% 15% 16% 22%
AChemo therapy significant decreased in dz free survival
compared to XRT
alone (P =0.02 compared w/induction, P = 0.06 compared
w/conccurent Tx) BNo significant difference CDifference only significant comparing concurrent
chemoXRT vs XRT alone.
Forastiere AA et al, N Engl J Med 2003;349:2091-8.

15/12/2012
43
Tu de laringe Reabilitação posop
Métodos:
A) Escrita
B) Fala esofageana
C) Eletrolaringe
D) Valvula traqueo-esofágica
Eletrolaringe

15/12/2012
44
Válvula traqueo-esofágica
Vida sem laringe ?

15/12/2012
45
Dúvidas?





























