Embed Size (px)
Citation preview

Seraacute o paracetamol eficaz na eliminaccedilatildeo
da dor apoacutes extracccedilatildeo do terceiro molar
inferior
ANAacuteLISE DA ANALGESIA DO PARACETAMOL COMPARADA Agrave DE
NSAIDrsquoS
SERAacute O PARACETAMOL EFICAZ NA ELIMINACcedilAtildeO DA DOR
APOacuteS EXTRACCcedilAtildeO DO TERCEIRO MOLAR INFERIOR1
Anaacutelise da analgesia do paracetamol comparada agrave de NSAIDrsquos
Catarina Cardoso
Ivo Cavalheiro
Nuno Pinto
Sara Mendes
FACULDADE DE MEDICINA DENTAacuteRIA DA UNIVERSIDADE DE LISBOA
Mestrado Integrado em Medicina Dentaacuteria
Biologia Oral I
2ordm Ano ndash 1ordm Semestre
23 de Dezembro de 2011
1 Este trabalho estaacute escrito segundo as regras do Acordo Ortograacutefico de 1945
RESUMO
Objectivos Investigar a eficaacutecia e os efeitos secundaacuterios do paracetamol
(1000mg) na eliminaccedilatildeo da dor dentaacuteria poacutes-operatoacuteria resultante da extracccedilatildeo de
terceiros molares inferiores comparaacute-la agrave eficaacutecia relativa dos vaacuterios NSAIDrsquos e a
combinaccedilotildees com outros faacutermacos
Materiais e meacutetodos A pesquisa foi realizada em bases de dados secundaacuterias
(Cochrane Database of Systematic Reviews Evidentista CEBD EBD e Lilacs) assim
como em bases de dados primaacuterias (Medline atraveacutes dos motores de busca PubMed e
NICE) entre 7 e 19 de Novembro Os artigos encontrados foram avaliados numa fase
inicial (com base nos seus tiacutetulos e abstracts) para averiguar a sua relevacircncia de acordo
com o seguinte sistema de classificaccedilatildeo adequado provavelmente adequado
inadequado
Resultados Foi encontrado um total de 161 registos incluindo revisotildees
sistemaacuteticas e ensaios cliacutenicos aleatorizados dos quais apenas 31 foram classificados
pelo seu tiacutetulo e abstract como Adequados ou Provavelmente Adequados A anaacutelise
mais aprofundada dos abstracts juntamente com uma leitura transversal dos artigos
resultou em 8 publicaccedilotildees que preenchiam definitivamente os criteacuterios de inclusatildeo e
foram por isso avaliadas com recurso agraves fichas CASP
Conclusotildees Atraveacutes dos estudos analisados conclui-se que o paracetamol eacute uma
analgeacutesico seguro e eficaz dado que apresenta um benefiacutecio estatisticamente
significativo quando comparado a placebo No entanto exibe menor eficaacutecia quando
comparado a outros NSAIDrsquos nomeadamente ibuprofeno e a combinaccedilotildees dos mesmos
(paracetamol+NSAID) Apesar dos melhores resultados alguns NSAIDrsquos manifestam
efeitos secundaacuterios de alta severidade por oposiccedilatildeo aos do paracetamol Revela-se
assim necessaacuterio o desenvolvimento de estudos que investiguem de melhor forma os
efeitos adversos destes faacutermacos e o mecanismo de acccedilatildeo do paracetamol e incluam
outros dados - como custo financeiro e disponibilidade no mercado
Palavras-Chave Paracetamol NSAIDrsquos terceiro molar inferior extracccedilatildeo
dentaacuteria dor poacutes-operatoacuteria aliacutevio da dor Escala Visual Analoacutegica
ABSTRACT
Aims To investigate the efficacy and side effects of paracetamol (1000mg) on
the lower third molar extraction post-operative pain relief to compare it to other
NSAIDrsquos efficacy as well as the combination of both
Methods Searches were conducted in secondary databases (Cochrane Database
of Systematic Reviews Evidentista CEBD EBD and Lilacs) as well as in primary
databases (Medline atraveacutes dos motores de busca PubMed e NICE) between 7 and
November 19 The encountered articles were initially evaluated based on their titles and
abstracts in order to assess their relevance This was done according to a classification
system ldquoadequaterdquo ldquoprobably adequaterdquo ldquoinadequaterdquo
Results A total of 161 records were found including systematic reviews and
randomized clinical trials only 31 were classified as ldquoadequaterdquo or ldquoprobably
adequaterdquo After a more thorough analysis of each abstract in addition to further
reading of the papers only 8 articles fulfilled the inclusion criteria Thus they were
evaluated according to the CASP critical appraisal sheets
Conclusions Paracetamol is a safe and effective analgesic which presents a
statistical significant advantage when compared to a placebo However paracetamol
shows less efficacy when compared to other NSAIDrsquos such as ibuprofen The
combination of paracetamol + other NSAID also shows to be more effective displaying
the additive effect of this compound Although NSAIDrsquos show the best pain relief
scores some can cause severe side effects as opposed to paracetamol Further studies
are needed in order to better investigate the adverse effects of these drugs as well as the
mechanism of action of paracetamol which still remains unclear Other data such as
financial cost and market availability should be approached in future studies
Keywords Paracetamol NSAIDrsquos lower third molar tooth extraction post-operative
pain pain relief Visual Analogic Scale
5
IacuteNDICE
PERGUNTA FORMULADA PELO PACIENTE 6
QUESTAtildeO PICO 6
OBJECTIVOS 6
INTRODUCcedilAtildeO 7
PESQUISA 12
Criteacuterios de Selecccedilatildeo 12
Tipos de Estudos escolhidos participantes intervenccedilatildeo e de mediccedilatildeo 12
Avaliaccedilatildeo dos Estudos 13
Estrateacutegias de Pesquisa 12
Cochrane Database for Systematic Reviews helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 13
Evidence-Based Dentistry (EBD) helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 14
National Institute of Health and Clinical Excellence (NICE) helliphelliphelliphelliphelliphellip 14
Literatura Latino-Americana e do Caribe em Ciecircncias da Sauacutede (LILACS) 14
PubMed 15
AVALIACcedilAtildeO CRIacuteTICA 17
Revisotildees Sistemaacuteticas 17
Ensaios Cliacutenicos Aleatorizados 28
DISCUSSAtildeO 52
RESPOSTA DADA AO PACIENTE 55
REFEREcircNCIAS BIBLIOGRAacuteFICAS 56
ANEXOS 61
Anexo A ndash Tabela de Artigos Excluiacutedos 61
Anexo B ndash Artigos Incluiacutedos em formato integral 62
6
PERGUNTA FORMULADA PELO PACIENTE
Apoacutes uma exodontia de um terceiro molar inferior ldquoDoutor natildeo me vai passar
mais nada aleacutem do paracetamol para as dores Eacute eficaz Natildeo vou ter doresrdquo
QUESTAtildeO PICO
Com base na questatildeo apresentada pelo paciente eacute possiacutevel identificar
Populaccedilatildeo ndash Pacientes adultos com pelo menos um terceiro molar inferior
Intervenccedilatildeo ndash administraccedilatildeo poacutes-operatoacuteria de paracetamol (1000g) aquando
duma exodontia do terceiro molar inferior
Comparaccedilatildeo ndash outros analgeacutesicos e NSAIDrsquos (Non-Steroidal Anti-
Inflammatory Drugs) convencionais
Outcome ndash Eliminaccedilatildeo ou atenuaccedilatildeo da dor medida atraveacutes da escala visual
analoacutegica de dor
Em pacientes adultos apoacutes exodontia do 3ordm molar inferior a administraccedilatildeo
de paracetamol eacute mais eficaz na terapecircutica analgeacutesica comparativamente a outros
analgeacutesicos e anti-inflamatoacuterios natildeo esteroacuteides convencionais utilizando uma
escala visual analoacutegica de dor
OBJECTIVOS
Primaacuterios
Investigar a eficaacutecia do paracetamol (1000mg) na eliminaccedilatildeo da dor dentaacuteria
poacutes-operatoacuteria e comparaacute-la com outros NSAIDrsquos comparando os efeitos secundaacuterios
associados a cada faacutermaco
Secundaacuterios
Aferir a eficaacutecia relativa dos vaacuterios NSAIDrsquos bem como combinaccedilotildees de
paracetamol com outros compostos
7
INTRODUCcedilAtildeO
EXODONTIA DE TERCEIROS MOLARES INFERIORES
A extracccedilatildeo de terceiros molares eacute um procedimento ciruacutergico no campo da
sauacutede oral amplamente praticado e difundido A dor poacutes-operatoacuteria desta intervenccedilatildeo
tornou-se o modelo mais frequentemente usado em ensaios sobre dor aguda por ser um
procedimento comum com dor moderada a severa e com um nuacutemero suficiente de
pacientes para se realizar um estudo de forma relativamente faacutecil (1 2)
Os motivos que conduzem agrave exodontia de terceiros molares devem ser
considerados cuidadosamente natildeo soacute na sua dimensatildeo cliacutenica como no encontro dos
interesses do paciente econoacutemicos e outros Algumas situaccedilotildees constituem uma razatildeo
largamente aceite para a extracccedilatildeo sendo descritas em normas de orientaccedilatildeo cliacutenica
Natildeo se pode excluir poreacutem uma selecccedilatildeo e procura cuidadosa por parte do cliacutenico da
melhor evidecircncia cientiacutefica
Segundo as normas de orientaccedilatildeo cliacutenica NICE a extracccedilatildeo de sisos impactados
deve ser limitada a pacientes que evidenciam patologia como caacuteries irrestauraacuteveis
patologias pulpares ou periapicais natildeo trataacuteveis abcesso e osteomielite reabsorccedilatildeo
internaexterna do dente ou dentes adjacentes fractura dentaacuteria quistos tumores e
outros (3) Terceiros molares impactados mas livres de patologia natildeo devem ser
extraiacutedos pois natildeo haacute evidecircncia de que sugira que traria benefiacutecios para os pacientes
Iria tambeacutem sujeitar pacientes saudaacuteveis aos riscos que acompanha este tipo de
procedimento e os efeitos poacutes-operatoacuterios do mesmo Existe controveacutersia em redor
deste assunto e sobre se existe algum benefiacutecio na extraccedilatildeo profilaacutetica ldquoNo evidence
was found to support or refute routine prophylactic removal of asymptomatic impacted
wisdom teeth in adults There is some reliable evidence that suggests that the
prophylactic removal of asymptomatic impacted wisdom teeth in adolescents neither
reduces nor prevents late incisor crowdingrdquo (4) A extracccedilatildeo de um dente natildeo impactado
deve ser executada quando a natildeo extracccedilatildeo do mesmo eacute ou potencialmente viraacute a
constituir uma situaccedilatildeo patoloacutegica Este procedimento ciruacutergico conduz a um niacutevel
significante de dor poacutes-operatoacuteria sendo esta mais severa nas primeiras doze horas apoacutes
o procedimento com o pico de intensidade nas 6-8 horas poacutes-operatoacuterias (5)
8
ETIOLOGIA DA DOR
Os tecidos lesados ou traumatizados na sequecircncia da remoccedilatildeo do terceiro molar
conduzem agrave libertaccedilatildeo de mediadores bioquiacutemicos (celulares e soluacuteveis) A inflamaccedilatildeo
aguda surge como resposta ao stress tecidual e passa por um aumento da irrigaccedilatildeo
sanguiacutenea - vasodilataccedilatildeo e aumento de permeabilidade vascular Pode-se enfatizar os
papeacuteis das histamina e a bradiquinina (recruta NO) como mediadores soluacuteveis
importantes na vasodilataccedilatildeo
Os prostanoacuteides ndash moleacuteculas envolvidas nos processos de inflamaccedilatildeo- satildeo
ecosanoacuteides ou seja derivados de precursores de aacutecidos gordos e sintetizados via
cascata do aacutecido araquidoacutenico (6 p 503 7 p 800 8) em condiccedilotildees fisioloacutegicas tecircm
um papel preponderante na citoprotecccedilatildeo da mucosa gaacutestrica hemostase e
hemodinacircmica renal A este grupo pertencem as prostaglandinas prostaciclinas
tromboxanos e leucotrienos Enquanto que as prostaglandinas satildeo sintetizadas a partir
do aacutecido araquidoacutenico por acccedilatildeo de enzimas como as ciclo-oxigenases (COX) os
leucotrienos resultam da acccedilatildeo da lipoxigenase Havendo stress tecidual a membrana
celular eacute danificada conduzindo agrave actividade da enzima fosfolipase Esta ao iniciar a
lipoacutelise possibilita a obtenccedilatildeo do percursor dos prostanoacuteides o aacutecido araquidoacutenico Por
um lado os produtos da acccedilatildeo da lipoxigenase podem estar envolvidos na formaccedilatildeo do
edema por outro os produtos da ciclo-oxigenase nomeadamente prostaglandinas estatildeo
envolvidos no processo de dor e pirexia
A ciclo-oxigenase possui 2 isoenzimas COX-1 e COX-2 (7 p 800)
A COX-1 eacute constitutiva da maioria dos tecidos humanos mas com especial
relevacircncia para mediar a integridade da mucosa gaacutestrica endoteacutelio vascular rins e
plaquetas
A COX-2 eacute expressa apoacutes lesatildeo e aquando a libertaccedilatildeo de mediadores como a
Interleucina-1 o Factor de Activaccedilatildeo de Plaquetas (PAF) ou endotoxinas
lipopolissacaacuterido (LPS) (9) Contribui para o processo inflamatoacuterio e hiperalgesia pois
ao formar prostaglandinas sensibiliza as terminaccedilotildees nervosas locais livres
nociceptivas
PARACETAMOL
O paracetamol eacute uma das drogas mais importantes usadas no tratamento da dor
aguda moderada a severa quando natildeo eacute necessaacuterio um efeito anti-inflamatoacuterio (10)
Classificado como analgeacutesico actua no sistema nervoso pela activaccedilatildeo indirecta de
9
receptores canabinoacuteides (11) embora este mecanismo ainda natildeo esteja totalmente
esclarecido (12) secundariamente inibe a COX-1 e COX-2 e por consequente a
siacutentese das prostaglandinas Como antipireacutetico age no centro hipotalacircmico que regula a
temperatura produzindo vasodilataccedilatildeo perifeacuterica e aumento do fluxo sanguiacuteneo
diminuindo a temperatura pela sudorese e perda de calor pela pele
O paracetamol eacute usualmente administrado oralmente (10) Apresenta uma meia-
vida de 2-3 horas Apesar de ser comparaacutevel agrave aspirina como analgeacutesico e antipireacutetico
eficaz o paracetamol difere no facto de natildeo possuir propriedades anti-inflamatoacuterias
(10) Difere dos analgeacutesicos opioacuteides porque natildeo provoca euforia nem altera o estado
de humor do doente Da mesma forma que os (NSAIDrsquos) natildeo causa problemas de
dependecircncia toleracircncia e siacutendrome de abstinecircncia Eacute muito utilizado e seguro com a
dosagem recomendada de 4g por dia mas nem sempre oferece um aliacutevio adequado da
dor aguda por si soacute (13)
NSAIDrsquoS
Os NSAIDrsquos satildeo dos agentes terapecircuticos mais utilizados no mundo inteiro
inclui-se neste grupo o ibuprofeno importante no tratamento da dor aguda e croacutenica
(14) Dos inibidores selectivos da COX-2 mais recentes nomeadamente rofecoxib
valdecoxib e celecoxib apenas este uacuteltimo foi comercializado nos EUA devido aos
restantes terem sido associados a eventos tromboacuteticos cardiovasculares (15 pp 277-
281) Apresentam trecircs acccedilotildees principais que resultam da inibiccedilatildeo da COX-2 e da
consequente reduccedilatildeo da siacutentese de prostanoacuteides
Acccedilatildeo anti-inflamatoacuteria a modificaccedilatildeo da resposta inflamatoacuteria ocorre pela
reduccedilatildeo do nordm de prostaglandinas vasodilatadoras (PGE2 prostaciclina)
associada a menor vasodilataccedilatildeo e indirectamente a menos edema No entanto a
acumulaccedilatildeo de ceacutelulas inflamatoacuterias natildeo eacute diminuiacuteda
Efeito analgeacutesico a reduccedilatildeo da siacutentese de prostaglandinas diminui a
sensibilizaccedilatildeo das terminaccedilotildees nervosas nociceptivas a mediadores da
inflamaccedilatildeo (como bradicinina e 5-hidroxitriptamina) provoca tambeacutem a reduccedilatildeo
da vasodilataccedilatildeo e desse modo o aliacutevio da cefaleia
10
Efeito antipireacutetico deve-se em parte agrave diminuiccedilatildeo da prostaglandina
mediadora a interleucina-1 responsaacutevel pela estimulaccedilatildeo do hipotaacutelamo e
consequente aumento de temperatura ndash febre (10 pp 1056-1061)
Eacute de referir ainda que todos os NSAIDrsquos agrave excepccedilatildeo dos inibidores selectivos da
COX-2 e salicilatos natildeo-acetilados tecircm um efeito inibitoacuterio na agregaccedilatildeo de plaquetas
(15 pp 277-281)
Os efeitos secundaacuterios resultam em grande parte da inibiccedilatildeo da COX-1 Entre
os mais frequentes encontram-se Dispepsia naacuteuseas e voacutemitos associados a lesotildees
gaacutestricas provocadas pela anulaccedilatildeo do efeito protector da prostaglandina sobre a mucosa
gaacutestrica Insuficiecircncia renal Reacccedilotildees cutacircneas Distuacuterbios hepaacuteticos Riscos
cardiovasculares e outros (10)
ESCALAS DE MEDICcedilAtildeO DE DOR - ESCALA VISUAL ANALOacuteGICA
A dor sendo um fenoacutemeno subjectivo compreende um grande conjunto de
componentes - componentes fisioloacutegicos cognitivos sensoriais comportamentais entre
outros Avaliar a dor utilizando uma medida que abranja todas as suas facetas e seja
fidedigna tem-se demonstrado impossiacutevelldquoUm instrumento ideal para a mensuraccedilatildeo da
dor deveria ter propriedades de uma escala de razatildeo fornecer informaccedilatildeo imediata
sobre a fidedignidade do desempenho dos pacientes ser relativamente livre de vieacuteses
ser simples de utilizar com pacientes () demonstrar utilidade tanto para a dor
experimental quanto para a dor cliacutenica permitindo comparaccedilotildees confiaacuteveis entre ambos
os tipos de dorrdquo(16)
A Escala Visual Analoacutegica (VAS) consiste numa mediccedilatildeo da dor em mm (0-
100mm) em que agrave extremidade 0 corresponde ldquonenhuma dorrdquo e agrave extremidade
antagoacutenica ldquopior dor possiacutevelrdquo Eacute uma forma simples eficaz - dentro das limitaccedilotildees - e
faacutecil de reproduzir ldquoou seja pode ser compreendida em distintas situaccedilotildees onde haacute
diferenccedilas culturais ou de linguagem do avaliador cliacutenico ou examinadorrdquo(16)
Para responder agrave questatildeo colocada pelo paciente eacute necessaacuterio a procura da
melhor evidecircncia cientiacutefica integrando-a com o proacuteprio interesse do paciente e a
expertise do cliacutenico Estes objectivos da Medicina Dentaacuteria Baseada na Evidecircncia satildeo
em parte consequecircncia de uma actualizaccedilatildeo constante de praacuteticas cliacutenicas consequentes
de novas evidecircncias cientiacuteficas e com a noccedilatildeo de que nenhum tratamento eacute completo
11
sem que ldquoas expectativas exigecircncias e direitos legiacutetimos dos pacientes sejam integrados
nos processos de decisatildeo cliacutenica sendo tal facto reconhecidamente essencial para a
melhoria da qualidade de vidardquo(17)
12
PESQUISA
CRITEacuteRIOS DE SELECCcedilAtildeO
Tipos de Estudos Escolhidos
Para este trabalho foram escolhidos apenas ensaios cliacutenicos aleatorizados cegos
(preferencialmente duplamente cegos) controlados ou natildeo por placebo e revisotildees
sistemaacuteticas
Tipos de participantes
Indiviacuteduos com idade superior a 15 anos
Sujeitos a cirurgia para extracccedilatildeo unilateral ou bilateral do 3ordm molar inferior
Que natildeo estivessem a tomar qualquer outro tipo de medicaccedilatildeo com efeitos
idecircnticos ou semelhantes aos faacutermacos em estudo
Sem patologias orais que provoquem dor moderada a forte ou outras patologias
que afectem a percepccedilatildeo da dor
Tipos de intervenccedilatildeo
Administraccedilatildeo apenas por via oral de
Paracetamol (1000mg) vs placebo
Paracetamol (1000mg) vs outro(s) NSAIDrsquos
Paracetamol ( 1000mg) vs outro(s) NSAIDrsquos vs placebo
Paracetamol (1000mg) + outro(s) NSAIDrsquos
ou Paracetamol (1000mg) + outro(s) NSAIDrsquos vs placebo
Estudos com outros tipos de intervenccedilatildeo natildeo foram incluiacutedos Os estudos que
apenas incluiacuteram o paracetamol sob a forma de proacute-farmaco foram excluiacutedos
Mediccedilatildeo de Resultados
A mediccedilatildeo de resultados foi obtida atraveacutes da escala visual analoacutegica (VAS ndash
visual analogic scale)
13
Avaliaccedilatildeo dos Estudos
Todos os estudos foram avaliados segundo fichas CASP (Critical Appraisal
Skills Programme) Estas consistem num conjunto de questotildees que permitem avaliar um
artigo cientiacutefico no seu todo para em uacuteltima anaacutelise aferir a sua aplicabilidade validade
e fiabilidade (18) Estas fichas existem para vaacuterios tipos de estudo as CASP utilizadas
neste trabalho foram as referentes a revisotildees sistemaacuteticas e ensaios cliacutenicos
aleatorizados
ESTRATEacuteGIAS DE PESQUISA
Apoacutes cada pesquisa os artigos encontrados foram avaliados numa fase inicial
com base nos seus tiacutetulos e abstracts para averiguar a sua relevacircncia A seguinte escala
foi utilizada adequado possivelmente adequado inadequado Toda a pesquisa foi
efectuada entre 7 e 19 de Novembro de 2011
Primeiramente foram consultadas bases de dados secundaacuterias apoacutes pesquisa
nestas fontes seguiram-se bases de dados primaacuterias
Cochrane Database for Systematic Reviews
Na pesquisa avanccedilada desta base de dados secundaacuteria foi introduzida a seguinte
combinaccedilatildeo de termos utilizando conectores boleanos e seleccionando as opccedilotildees
ldquosearch all textrdquo e ldquoCochrane Database of Systematic Reviewsrdquo
paracetamol AND third molar removal AND pain relief AND analgesicrdquo
Foram encontrados 14 resultados (3 protocolos e 11 revisotildees sistemaacuteticas) dos
quais uma revisatildeo foi categorizada como ldquoadequadardquo
Paracetamol for pain relief after surgical removal of lower wisdom teeth Weil
Hooper (19) Esta revisatildeo foi novamente encontrada na base de dados EBD bem
como na NICE e no PubMed
E outra classificada como ldquopossivelmente adequadardquo mas posteriormente
excluiacuteda (20)
14
Evidence-Based Dentistry (EBD)
Nesta base de dados foi introduzida a combinaccedilatildeo de termos
ldquoParacetamol OR acetaminophen AND third molar AND painrdquo utilizando os
filtros ldquoBritish Dental Journalrdquo e ldquoEvidence-Based Dentistryrdquo
Foram encontrados 28 resultados dos quais uma revisatildeo foi classificada como
ldquoadequadardquo
Relative efficacy of oral analgesics after third molar extraction ndash a 2011 update
Derry Wiffen (21)
E ainda dois artigos classificados como ldquopossivelmente adequadordquo
An investigation into the comparative efficacy of soluble aspirin and solid
paracetamol in postoperative pain after third molar surgery Seymour
Hawkesford (22)
Relative efficacy of oral analgesics after third molar extraction Barden
Edwards (23)
National Institute of Health and Clinical Excellence (NICE)
Nesta base de dados foi introduzida a seguinte combinaccedilatildeo de termos
ldquoParacetamol and third molar removal and pain and analgesicrdquo
Dos 28 resultados obtidos 1 foi previamente encontrado e classificado (19)
Dos restantes 27 artigos nenhum foi classificado como adequado ou possivelmente
adequado
LILACS
Nesta base de dados primaacuteria foi introduzida a seguinte combinaccedilatildeo de termos
ldquoParacetamol terceiro molar dorrdquo
Dos 3 resultados obtidos um foi classificado como possivelmente adequado mas
posteriormente excluiacutedo (24)
15
PUBMED
Nesta base de dados primaacuteria foram efectuadas duas pesquisas com termos
diferentes Apenas foram utilizados termos MeSH foram utilizados conectores
boleanos em ambas as pesquisas
Pesquisa 1
Search ((((Acetaminophen[Mesh]) AND Anti-Inflammatory Agents[Mesh])
AND Molar Third[Mesh]) AND Tooth Extraction[Mesh]) AND Pain
Postoperative[Mesh]
Limits only items with abstracts Humans Clinical Trial Meta-Analysis
Randomized Controlled Trial Review Comparative Study Controlled Clinical
Trial English Spanish Portuguese
Foram obtidos 32 resultados dos quais 5 artigos foram classificados como
ldquoadequadosrdquo
Combining paracetamol with a selective cyclooxygenase-2 inhibitor for acute
pain relief after third molar surgery a randomized double-blind placebo-
controlled study Haglund and von Bultzingslowen (25)
Dos restantes quatro artigos um (22) era repetido e os outros trecircs (26-28) foram
posteriormente excluiacutedos
Quatro foram considerados ldquopossivelmente adequadosrdquo dos quais trecircs (29-31)
foram posteriormente excluiacutedos O artigo remanescente foi
Analgesic efficacy of lysine clonixinate paracetamol and dipyrone in lower
third molar extraction a randomized controlled trial (32)
Pesquisa 2
Search (((Acetaminophen[Mesh]) AND Analgesics[Mesh]) AND Molar
Third[Mesh]) AND Tooth Extraction[Mesh]
Limits only items with abstracts Humans Clinical Trial Meta-Analysis
Randomized Controlled Trial Review English
16
Obtiveram-se 56 resultados em que sete foram seleccionados como sendo
ldquoadequadosrdquo
Combined acetaminophen and ibuprofen for pain relief after oral surgery in
adults a randomized controlled trial Merry Gibbs (13)
Destes artigos seis (19 22 23 25 28 32) eram repetidos
Oito artigos foram classificados como ldquopossivelmente adequadosrdquo
Onset of analgesia with sodium ibuprofen ibuprofen acid incorporating poloxamer
and acetaminophen--a single-dose double-blind placebo-controlled study in
patients with post-operative dental pain Daniels Reader (33)
Dos oito artigos cinco foram repetidos (26 27 29-31) dois (34 35) foi
posteriormente excluiacutedo
No anexo A encontra-se uma tabela de artigos excluiacutedos cujas razotildees satildeo
discriminadas
Eacute de notar que este tipo de estrateacutegia de pesquisa traz associada grande
quantidade de resultados irrelevantes superior agrave de artigos de interesse mas facilita a
aquisiccedilatildeo de todos os artigos importantes colocando em primeiro plano a sensibilidade
e natildeo a especificidade (36) A utilizaccedilatildeo de conectores boleanos e de filtros especiacuteficos
foi uma forma de minimizar o nuacutemero de resultados natildeo relacionados (17) preservando
os de interesse
17
AVALIACcedilAtildeO CRIacuteTICA
REVISOtildeES SISTEMAacuteTICAS
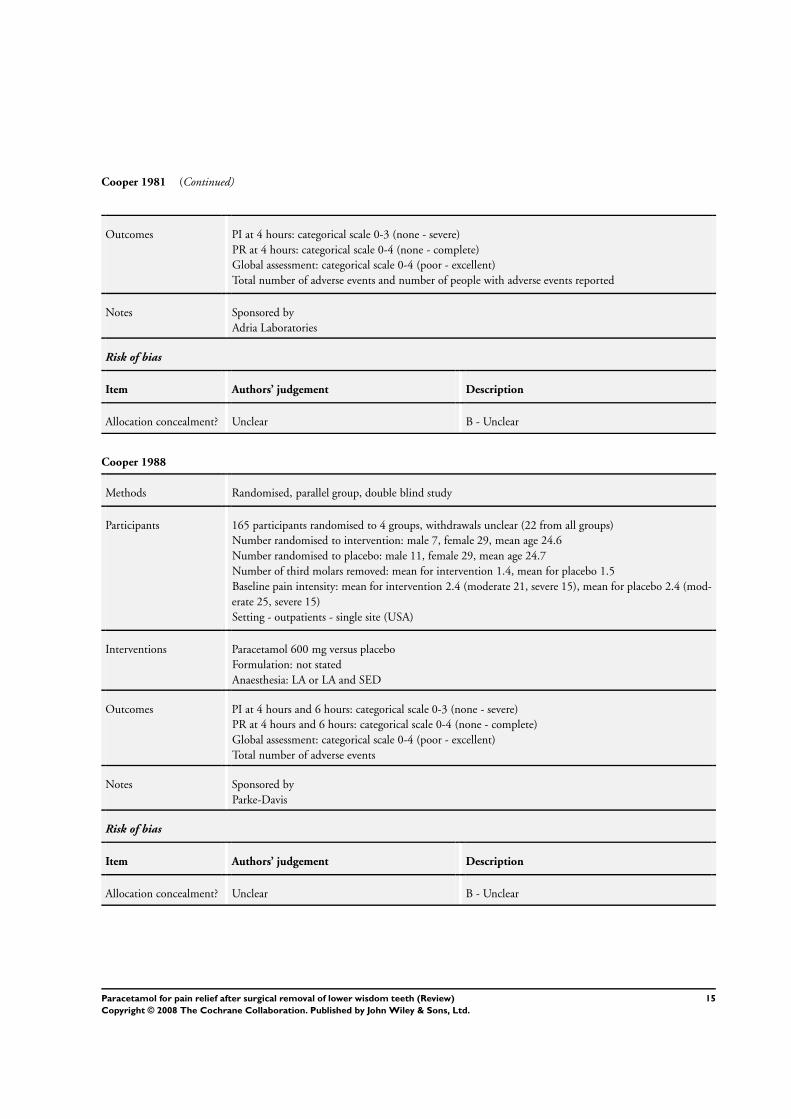
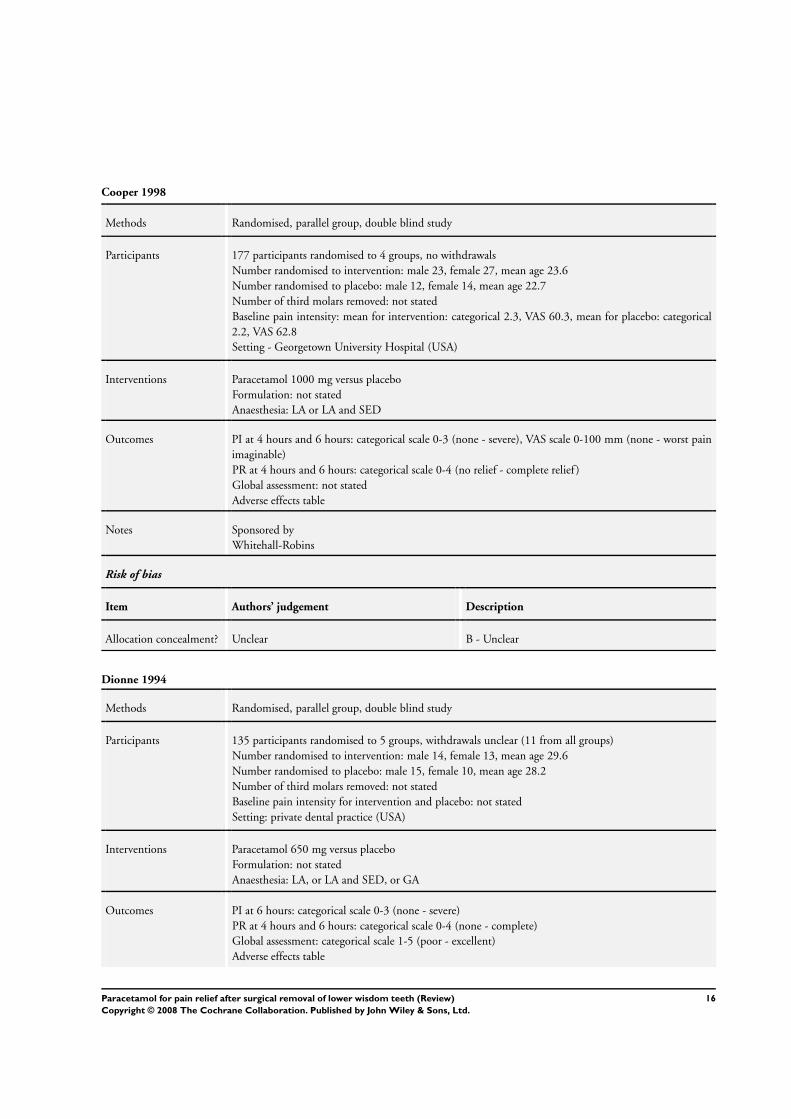
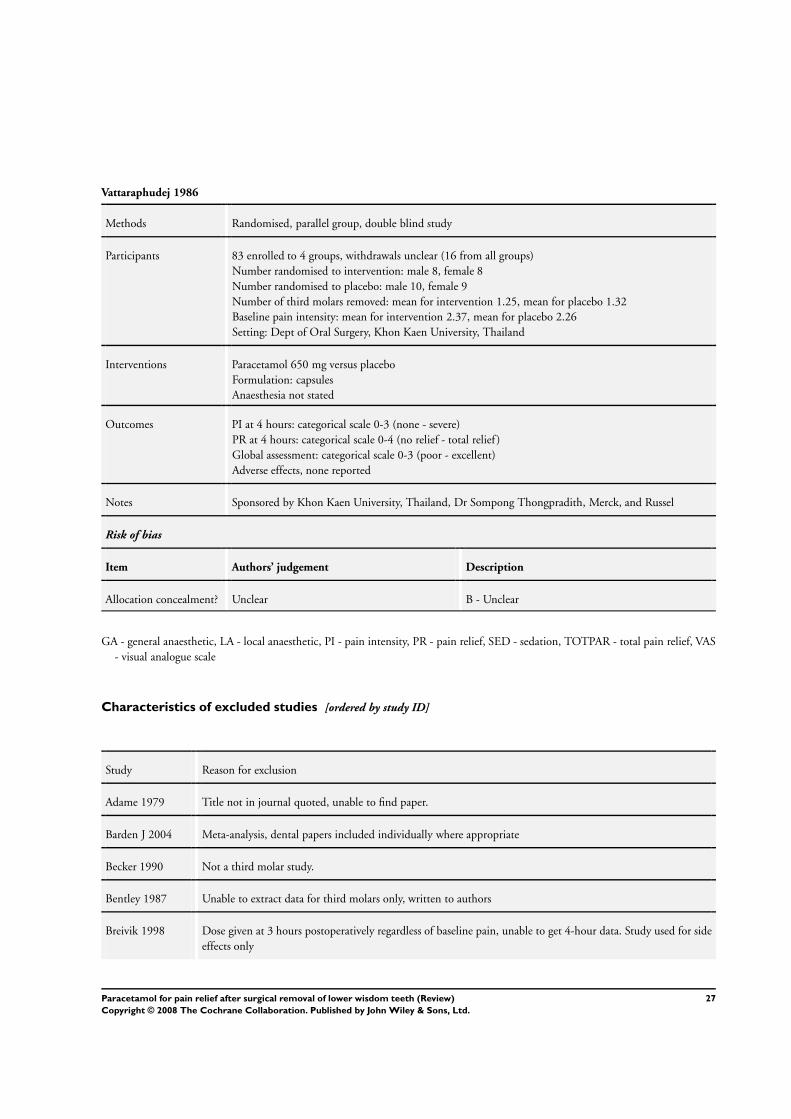
Paracetamol for pain relief after surgical removal of lower
wisdom teeth Weil Hooper (19)
1 Did the review ask a clearly-focused question
Sim A populaccedilatildeo em estudo compreende pacientes de qualquer estado de sauacutede
que necessitem de uma exodontia do terceiro molar inferior e que apresentam uma
intensidade de dor basal moderada a forte Foram excluiacutedos pacientes que estivessem a
tomar outro analgeacutesico A intervenccedilatildeo foi baseada em dois aspectos ndash eficaacutecia e efeitos
secundaacuterios
A terapecircutica usada para avaliar a eficaacutecia consistiu na administraccedilatildeo de uma
dose uacutenica de paracetamol por via oral independentemente da formulaccedilatildeo ou do
momento em que o faacutermaco foi tomado
Em relaccedilatildeo aos efeitos secundaacuterios foram incluiacutedos estudos natildeo soacute de dose
uacutenica como tambeacutem de doses muacuteltiplas de acetaminofeno consideraram-se estudos em
que este composto foi tomado ateacute 7 dias apoacutes a primeira toma Para este trabalho apenas
seratildeo considerados os resultados com base na administraccedilatildeo poacutes-operatoacuteria do
paracetamol
Os resultados ndash intensidade da dor e aliacutevio da dor ndash foram medidos usando as
escalas visual analoacutegica categoacuterica verbal numeacuterica verbal global subjectiva de
avaliaccedilatildeo de eficaacutecia e outras categoacutericas Os outcomes derivados do aliacutevio da dor
contabilizados foram total pain relief (TOTPAR) e summed pain intensity difference
(SPID) durante 4 e 6 horas Foram ainda contabilizados os efeitos secundaacuterios
2 Did the review include the right type of study
Os uacutenicos estudos incluiacutedos foram ensaios cliacutenicos aleatorizados duplamente
cegos que comparam o paracetamol a um placebo bem como dosagens diferentes
avaliando efeitos agraves 4 e 6 horas Este tipo de estudo eacute adequado pois implica um baixo
risco de vieacutes
18
3 Did the reviewers try to identify all relevant studies
Sim Os autores utilizaram estudos de todos os idiomas recorrendo agrave sua
traduccedilatildeo quando necessaacuterio Foram consultadas bases de dados bibliograacuteficas
electroacutenicas The Cochrane Oral Health Grouprsquos Trials Register The Cochrane Central
Register of Controlled Trials The Cochrane Pain Palliative and Supportive Care
Grouprsquos Trials Register MEDLINE EMBASE e Current Controlled Trials Register
Tambeacutem foram realizadas pesquisas manuais em revistas como parte do Cochrane Oral
Health Grouprsquos ongoing journal handsearching programme A pesquisa visou estudos
publicados entre 1966 e 25 de Agosto de 2006
Foram enviadas cartas a autores de ensaios cliacutenicos aleatorizados com vista a
obter estudos natildeo publicados bem como a empresas farmacecircuticas fabricantes de
analgeacutesicos
Os autores deste estudo consultaram ainda referecircncias bibliograacuteficas de papers
reviews e referecircncias pessoais
4 Did the reviewers asses the quality of the included studies
Sim Foi utilizada uma estrateacutegia clara e bem definida para a determinaccedilatildeo dos
estudos a incluir Este processo foi realizado independentemente por dois autores da
revisatildeo ndash natildeo cegos ndash baseando-se em dois criteacuterios centrais atribuiccedilatildeo oculta do
faacutermaco e a existecircncia de um follow-up completo Para estes criteacuterios foi utilizado um
sistema de pontuaccedilatildeo Desta forma a cada estudo foi-lhe atribuiacuteda uma pontuaccedilatildeo
formando-se dois grupos
Baixo risco de vieacutes
Moderado ou alto risco de vieacutes
5 If the results of the studies have been combined was it reasonable to do so
Sim os resultados foram apresentados de forma combinada e loacutegica Em
primeiro lugar foram apresentadas tabelas uma para cada artigoestudo incluiacutedo em
que se encontravam discriminados os meacutetodos participantes intervenccedilotildees resultados e
outras notas Os resultados dos diferentes estudos foram agrupados em 2 outcomes
tendo cada outcome 2 divisotildees
Outcome 1 ndash TOTPAR agraves 4h
A ndash Dosagem de paracetamol ateacute 1000mg vs placebo
B ndash Dosagem de paracetamol igual ou superior a 1000mg vs placebo
19
Outcome 2 ndash TOTPAR agraves 6h
A ndash Dosagem de paracetamol ateacute 1000mg vs placebo
B ndash Dosagem de paracetamol igual ou superior a 1000mg vs placebo
Todos estes grupos foram analisados e comparados segundos 2 paracircmetros
Comparaccedilatildeo 1- Medidas de aliacutevio da dor
Comparaccedilatildeo 2- Medidas de intensidade da dor
Tendo em conta todas estas variaacuteveis foram realizadas meta-anaacutelises por
subgrupo (pp 29-40) utilizando graacuteficos forest plot
Anaacutelise 11 ndash Comparaccedilatildeo 1 de A vs B ndash Outcome 1
Anaacutelise 12 ndash Comparaccedilatildeo 1 de A vs B ndash Outcome 2
Anaacutelise 21 ndash Comparaccedilatildeo 2 de A vs B ndash Outcome 1
Anaacutelise 22 ndash Comparaccedilatildeo 2 de A vs B ndash Outcome 2
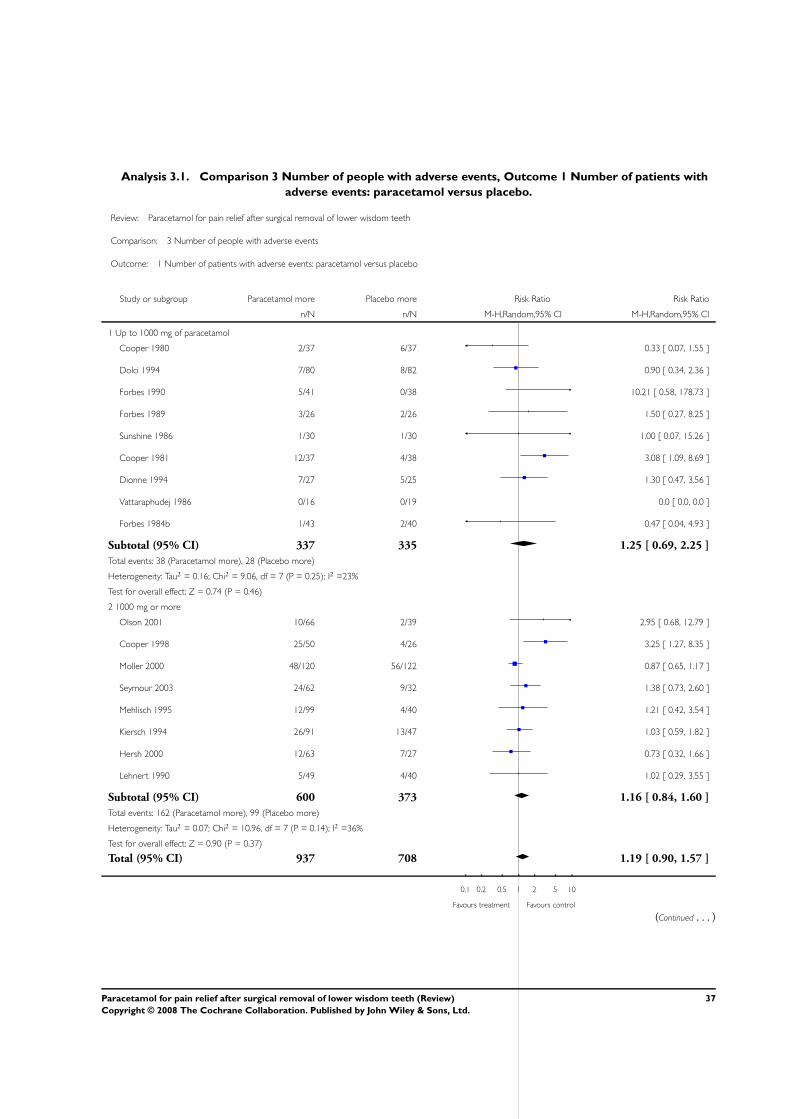
Anaacutelise 3 ndash Comparaccedilatildeo do nuacutemero de efeitos adversos de paracetamol vs
placebo comparando ainda as duas dosagens diferentes
Valores de heterogeneidade (representados por I2) proacuteximos de 25 indicam
baixa discrepacircncia 50 satildeo indicadores de heterogeneidade moderada e valores
proacuteximos de 75 satildeo sinal de alta heterogeneidade entre os estudos (37)
Olhando para os valores de I2 dois possuem alta heterogeneidade um moderada
e dois baixa Nos grupos que apresentam uma discrepacircncia estatiacutestica significativa dos
resultados a aglutinaccedilatildeo dos mesmos natildeo foi muito bem sucedida Nestes grupos ainda
que a heterogeneidade seja elevada a apresentaccedilatildeo dos resultados de cada estudo foram
correcta e individualmente apresentados Aleacutem deste aspecto os diferentes meacutetodos ndash
dosagem e tempo - foram agrupados exactamente para que as formas de intervenccedilatildeo e
meacutetodos com o menor risco de vieacutes
Tabela 1 ndash Valores de heterogeneidade (I2) de cada anaacutelise
Total de I2
()
Anaacutelise 11 Anaacutelise 12 Anaacutelise 21 Anaacutelise 22 Anaacutelise 3
76 81 66 29 28
Natildeo foram discutidas as variaccedilotildees nos resultados
20
6 How are the results presented and what is the main result
A meta-anaacutelise por subgrupos foi realizada com recurso agrave medida de eficaacutecia de
intervenccedilatildeo Risco Relativo (RR) Analisando o graacutefico forest plot os ldquoquadradosrdquo a azul
representam o RR e o poliacutegono (semelhante a um losango) sumariza todas as
informaccedilotildees (provenientes dos vaacuterios estudos) sobre o efeito do paracetamol (38)
ldquoQuando o IC natildeo ultrapassa a linha de nulidade pode-se afirmar que o resultado eacute
estatisticamente significativo Estudos maiores possuem IC mais estreitos ou seja
resultados mais precisos e maior contribuiccedilatildeo para a meta-anaacutelise que tambeacutem eacute repre-
sentada graficamente (quanto maior a aacuterea do quadrado maior o peso) e valor
percentualrdquo (39) A significacircncia aumenta com a distacircncia do poliacutegono da linha de natildeo
efeito
Independentemente do tempo (4 ou 6h) dosagens ateacute 1000mg de paracetamol
apresentam uma pequena discrepacircncia nos resultados sendo que o paracetamol eacute
ligeiramente mais eficaz que o placebo Doses iguais ou superiores a 1000mg de
paracetamol traduzem-se num maior aliacutevio da dor poacutes-operatoacuteria (poliacutegono afastado da
linha de natildeo-efeito)
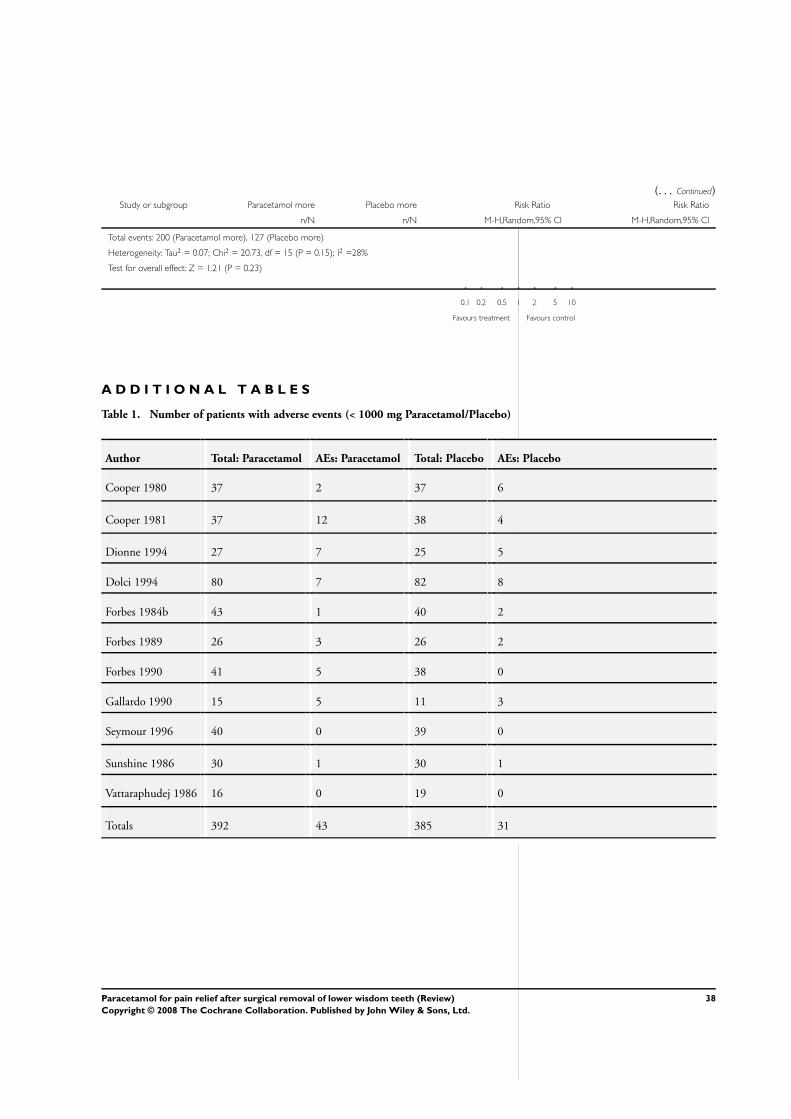
Em relaccedilatildeo agrave anaacutelise 3 ateacute doses de 1 g de paracetamol nuacutemero de casos de
efeitos adversos eacute muito semelhante entre placebo e a substacircncia activa Para
concentraccedilotildees superiores a 1000 mg o nuacutemero de efeiros adversos eacute superior para
paracetamol Eacute possiacutevel concluir que natildeo haacute uma diferenccedila notoacuteria no nuacutemero de casos
de efeitos adversos O poliacutegono cruza sempre a linha de natildeo efeito
O paracetamol eacute consideravelmente mais eficaz que o placebo no aliacutevio de 50
da dor principalmente em doses iguais ou superiores a 1000mg Natildeo haacute diferenccedila
significativa em relaccedilatildeo aos efeitos adversos
7 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em consideraccedilatildeo que o
poliacutegono natildeo intersecta a linha de natildeo efeito os resultados satildeo precisos (anaacutelise 1 a 2)
Na anaacutelise 3 mesmo com um IC 95 o poliacutegono cruza a linha de natildeo efeito logo natildeo eacute
possiacutevel tirar conclusotildees semelhantes em relaccedilatildeo aos limites inferior e superior do IC
Eacute de notar que a elaboraccedilatildeo de uma meta-anaacutelise contribui para a robustez dos
resultados daiacute provenientes combinar os resultados de cada estudo individual numa
meta-anaacutelise aumenta o poder estatiacutestico gerando resultados mais precisos (40)
21
8 Can the results be applied to the local population
Sim A extracccedilatildeo de terceiros molares inferiores eacute uma praacutetica cliacutenica comum
em Portugal O paracetamol eacute um analgeacutesico largamente comercializado e administrado
(sendo natildeo sujeito a receita meacutedica) pelo que era possiacutevel reproduzir esta forma de
tratamento
No entanto os estudos incluiacutedos na revisatildeo referem-se a uma dose uacutenica que
embora reproduziacutevel na populaccedilatildeo local seria necessaacuteria uma modificaccedilatildeo do
paradigma cultural em relaccedilatildeo agrave toma de medicamentos
9 Were all important outcomes considered
Natildeo A revisatildeo considera a eficaacutecia do paracetamol vs placebo no aliacutevio da dor
e simultaneamente a ocorrecircncia de efeitos secundaacuterios Satildeo abordados directamente
dois aspectos ndash o da praacutetica cliacutenica e o da investigaccedilatildeo Ambos satildeo relativos ao
profissional de sauacutede e implicitamente ao proacuteprio indiviacuteduo e aos familiares (ao serem
referidas as doses periacuteodos entre tomas e combinaccedilotildees com outros NSAIDrsquos mais
eficazes e simultaneamente seguras)
Poreacutem nada eacute referido em relaccedilatildeo a novas poliacuteticas de sauacutede nomeadamente na
implementaccedilatildeo de uma dose uacutenica culminando numa mudanccedila dos haacutebitos de sauacutede da
comunidade Tambeacutem natildeo foram abordados aspectos econoacutemicos tal como um balanccedilo
entre benefiacutecios e encargos de sauacutede que justifique a utilizaccedilatildeo deste faacutermaco como
tratamento preferencial
10 Should policy or practice change as a result of the evidence contained in this
review
Natildeo Esta revisatildeo demonstra que comparativamente a um placebo o paracetamol
eacute mais eficaz principalmente em doses elevadas e que natildeo haacute diferenccedila estatiacutestica
significativa no nuacutemero de efeitos secundaacuterios Poreacutem natildeo eacute possiacutevel tirar conclusotildees
sobre a dor depois do periacuteodo considerado de 6h Desta forma implementar uma dose
uacutenica de paracetamol a 1000mg seria imprudente sem previamente realizar estudos
complementares sobre a evoluccedilatildeo da dor apoacutes as 6h bem como comparar este faacutermaco
com outros compostos que possam ser igualmente eficazes por um raacutecio custo-benefiacutecio
melhor ou vice-versa
22
Relative efficacy of oral analgesics after third molar extraction
Barden Edwards (23)
Relative efficacy of oral analgesics after third molar extraction -
a 2011 update Derry Wiffen (21)
A avaliaccedilatildeo feita e disposta abaixo contemplou tanto a revisatildeo sistemaacutetica que
remonta a 2004 como a sua actualizaccedilatildeo de 2011 Uma vez estando inter-relacionados
consideraacutemos pertinente juntar as apreciaccedilotildees destas revisotildees porque caso contraacuterio
perder-se-ia o contexto de ambas
1 Did the review ask a clearly-focused question
Sim A populaccedilatildeo em estudo comporta pacientes com mais de 15 anos de idade
com uma intensidade de dor basal poacutes-operatoacuteria de moderada a severa apoacutes extracccedilatildeo
de um terceiro molar
A intervenccedilatildeo consistiu no tratamento da dor poacutes-operatoacuteria de intensidade
moderada a severa com doses uacutenicas de analgeacutesicos orais ou placebo sendo que os
analgeacutesicos orais corresponderam a um total de 15 combinaccedilotildees diferentes de faacutermacos
e respectivas dosagens
Os resultados foram obtidos atraveacutes da mediccedilatildeo do aliacutevio total da dor
(TOTPAR) ou da diferenccedila de intensidade da dor (SPID) utilizando uma escala
standard de 5 niacuteveis de aliacutevio da dor uma escala standard de 4 niacuteveis de aliacutevio da dor
ou uma escala visual analoacutegica (VAS) Os efeitos secundaacuterios foram tambeacutem relatados
comparando a proporccedilatildeo de pacientes que apresentaram efeitos generalizados e que
apresentaram efeitos particulares
Actualizaccedilatildeo de 2011
A intervenccedilatildeo consistiu tambeacutem no tratamento da dor poacutes-operatoacuteria de
intensidade moderada a severa com doses uacutenicas de analgeacutesicos orais ou placebo no
entanto os analgeacutesicos utilizados foram diferentes A revisatildeo de 2004 incluiu rofecoxib
and valdecoxib nenhum dos quais se encontra disponiacutevel no mercado Em vez disso
foram utilizadas combinaccedilotildees de ibuprofeno com paracetamol formulaccedilotildees diferentes
de ibuprofeno e diclofenac e etoricoxib
23
2 Did the review include the right type of study
Sim Os estudos que foram incluiacutedos nesta revisatildeo correspondem a ensaios
cliacutenicos aleatorizados duplamente cegos que comparam a eficaacutecia dos diferentes
analgeacutesicos e com placebo na terapecircutica da dor aguda poacutes-operatoacuteria Os grupos
formados possuiacuteam grupos com um miacutenimo de 10 pessoas Em todos os estudos foram
seguidas as guidelines QUORUM e utilizados criteacuterios de inclusatildeo para a dor poacutes-
operatoacuteria em que os resultados satildeo avaliados durante um periacuteodo de 4 a 6 horas apoacutes
medicaccedilatildeo
3 Did the reviewers try to identify all relevant studies
Sim Os autores da revisatildeo tentaram identificar todos os estudos relevantes
pesquisando nas bases de dados electroacutenicas Cochrane Library Biological Abstracts
MEDLINE PubMed e Oxford Pain Relief Para aleacutem disso consultaram a bibliografia
dos artigos de revisatildeo incluiacutedos de modo a encontrar informaccedilatildeo adicional e possiacuteveis
estudos natildeo publicados os quais apresentam na sua maioria datas de pesquisa que
remontam a 2002 No entanto eacute de mencionar que natildeo contactaram os autores e os
fabricantes para recolha de dados nem procuraram estudos com idiomas diferentes do
inglecircs
Actualizaccedilatildeo de 2011
Com o passar dos anos os artigos inseridos na revisatildeo foram actualizados de
forma a incluir outros analgeacutesicos e obter ensaios cliacutenicos adicionais e relevantes Desta
forma a actualizaccedilatildeo da revisatildeo sistemaacutetica de 2004 incluiu 35 revisotildees da Cochrane
com 38 anaacutelises realizadas em diferentes analgeacutesicos de dose uacutenica para determinar a
sua eficaacutecia na dor poacutes-operatoacuteria
4 Did the reviewers assess the quality of the included studies
Sim A qualidade dos estudos incluiacutedos foi avaliada vaacuterios autores
independentes e natildeo cegos (pelo facto de estes conhecerem a literatura existente)
utilizando uma escala de qualidade numerada de 1 a 5 e baseada em 3 criteacuterios
distribuiccedilatildeo aleatorizada dos pacientes se os pacientes e os examinadores se
encontravam cegos se houve remoccedilotildees ou desistecircncias durante o estudo A
classificaccedilatildeo maacutexima de um estudo incluiacutedo foi de 5 e a miacutenima foi de 2
24
Os ensaios cliacutenicos que apresentam uma classificaccedilatildeo igual ou superior a 3
(baixo risco de vieacutes) demonstraram menores efeitos secundaacuterios que os ensaios cliacutenicos
que apresentam uma classificaccedilatildeo igual ou inferior a 2 (alto risco de vieacutes)
5 If the results of the studies have been combined was it reasonable to do so
Sim Os resultados dos diferentes estudos foram apresentados sob a forma de
tabelas nomeadamente a eficaacutecia dos vaacuterios analgeacutesicos e a ocorrecircncia de efeitos
secundaacuterios foram dispostas em tabelas Aqui eram resumidos os resultados o tipo de
intervenccedilatildeo e respectivo nuacutemero total de pacientes e nordm de estudos realizados
Esta revisatildeo sistemaacutetica natildeo incluiu a realizaccedilatildeo de testes heterogeacuteneos nem a
avaliaccedilatildeo do risco de vieacutes das publicaccedilotildees atraveacutes de forest plots dado que na opiniatildeo
dos autores estas abordagens mostraram-se pouco adequados para este tipo de estudos
No entanto a homogeneidade foi avaliada atraveacutes de um modo visual
A resposta a esta questatildeo eacute claramente afirmativa porque a elevada semelhanccedila
das caracteriacutesticas dos diferentes estudos (meacutetodos utilizados tipo de intervenccedilatildeo e
mediccedilatildeo dos resultados) tornou por um lado inadequada a realizaccedilatildeo uma meta-anaacutelise
para avaliar a heterogeneidade mas por outro adequada a realizaccedilatildeo de uma avaliaccedilatildeo
visual da homogeneidade dos mesmos
6 How are the results presented and what is the main result
Os resultados foram medidos atraveacutes da proporccedilatildeo de pacientes do grupo de
tratamento vs placebo que atingiram pelo menos 50 de maxTOTPAR ou seja aliacutevio
de dor A qual foi utilizada para determinar o benefiacutecio relativo e o NNT bem como o
risco relativo dos diferentes estudos incluiacutedos
Atraveacutes da anaacutelise das tabelas eacute possiacutevel tirar 3 conclusotildees principais
1 A proporccedilatildeo de pacientes que atingiram pelo menos 50 de aliacutevio de dor eacute maior
no grupo de tratamento que no grupo placebo agrave excepccedilatildeo do estudo que utilizou
dihidrocodeiacutena 30mg em que as diferenccedilas natildeo foram estatisticamente relevantes
2 Por comparaccedilatildeo ao paracetamol (independentemente das diferentes dosagens) os
anti-inflamatoacuterios natildeo-esteroacuteides inibidores da COX-2 apresentam um maior
benefiacutecio relativo e necessitam do menor nordm de pacientes tratados para atingirem o
objectivo de 50 de aliacutevio de dor
25
3 O paracetamol apresenta um maior risco relativo na medida em que insurgem mais
efeitos secundaacuterios nos estudos em que foi administrado por oposiccedilatildeo aos
NSAIDrsquos
Os anti-inflamatoacuterios natildeo-esteroacuteides inibidores da COX-2 satildeo mais eficazes no
tratamento da dor basal poacutes-operatoacuteria moderada a intensa que o paracetamol
Actualizaccedilatildeo de 2011
Os resultados foram obtidos da mesma forma que na versatildeo de 2004 sendo que
um novo outcome foi considerado ndash tempo meacutedio necessaacuterio para que os pacientes
necessitem de re-medicaccedilatildeo aproximadamente 8 horas Agrave semelhanccedila do que aconteceu
na revisatildeo anterior os dados sobre a dihidrocodeiacutena natildeo foram conclusivos devido agrave
pouca informaccedilatildeo disponiacutevel nos estudos
7 How precise are these results
Os resultados satildeo precisos uma vez que utilizam um intervalo de confianccedila de
95 Eacute de ressalvar que os valores de NNT ou NNH apenas eram calculados quando o
riscobenefiacutecio relativo satildeo significativos isto eacute quando natildeo incluem o valor de 1 No
limite superior do intervalo de confianccedila a intervenccedilatildeo realizada seria a mesma No
entanto dado que o NNH natildeo foi calculado eacute possiacutevel concluir que o risco relativo natildeo
era significativo pelo que permanece uma incerteza se no limite inferior do intervalo de
confianccedila a intervenccedilatildeo realizada seria a mesma
8 Can the results be applied to the local population
Sim Os resultados da revisatildeo sistemaacutetica podem ser aplicados agrave nossa
populaccedilatildeo local porque os criteacuterios de inclusatildeo utilizados correspondem na sua
maioria a mecanismos fisioloacutegicos caracteriacutesticos do ser humano Para aleacutem disso as
teacutecnicas utilizadas satildeo simples e de faacutecil reproduccedilatildeo na medida em que os faacutermacos
utilizados nos ensaios cliacutenicos estatildeo agrave disposiccedilatildeo dos interessados e os meacutetodos
terapecircuticos baacutesicos
No entanto os estudos incluiacutedos nesta revisatildeo incluiacuteram um tratamento com
uma dose uacutenica de analgeacutesico oral que embora reprodutiacutevel difere do paradigma actual
da nossa populaccedilatildeo (em que haacute a tendecircncia para a auto-medicaccedilatildeo e de recorrer a
diferentes faacutermacos)
26
9 Were all important outcomes considered
Natildeo Os resultados enfatizam a eficaacutecia de vaacuterios analgeacutesicos no aliacutevio de 50
dor em comparaccedilatildeo com placebo Eacute focada ainda o benefiacutecio relativo (95 IC) e o NNT
da mesma problemaacutetica Aleacutem deste conjunto de dados satildeo considerados o nuacutemero de
pacientes com efeitos secundaacuterios risco relativo (95 IC) culminando no caacutelculo do
NNH
Contudo natildeo eacute especificado o tipo de efeitos secundaacuterios que podem ser
desencadeados pela toma dos diferentes analgeacutesicos nem aspectos diferenciadores em
analgeacutesicos com eficaacutecia e benefiacutecios idecircnticos (por exemplo custo econoacutemico) Isto
constituiria uma mais-valia para uma escolha mais consciente do analgeacutesico tanto pelos
profissionais como pelos pacientes (individual) e beneficiaria tambeacutem o Sistema
Nacional de Sauacutede (comunidade em geral)
Actualizaccedilatildeo de 2011
Um dos outcomes considerados semelhante ao que foi abordado na revisatildeo de
2004 foi a percentagem de pacientes com dor moderada (30- 60 mm VAS) ou dor
severa (mais de 60 mm) que obtiveram 50 de aliacutevio de dor Contudo foi adicionado
um novo outcome relevante o tempo necessaacuterio para que metade dos pacientes requeriu
re-medicaccedilatildeo
10 Should policy or practice change as a result of the evidence contained in this
review
Natildeo Os resultados desta revisatildeo evidenciam a eficaacutecia dos analgeacutesicos
comparativamente a um placebo nomeadamente que o ibuprofeno e o paracetamol
possuem maior maior o benefiacutecioefeito analgeacutesico quanto maior forem as dosagens
Poreacutem natildeo eacute evidecircncia suficiente para mudar o paradigma de tratamento pois ldquoWhat
these comparisons do not do is to tell dentists what to prescriberdquo Satildeo sim uma
importante ferramenta para a tomada de decisotildees que devem ser adaptadas a cada
paciente tendo presente que 80 dos analgeacutesicos prescritos possuem elevados iacutendices
de eficaacutecia e seguranccedila Em adiccedilatildeo nem todos os analgeacutesicos nesta revisatildeo estatildeo
disponiacuteveis no mercado para serem receitados pelos meacutedicos-dentistas
Conclui-se que para que esta revisatildeo fosse pilar basilar nas prescriccedilotildees de
analgeacutesicos teriam de ser apresentadas evidecircncias de benefiacuteciocusto dos analgeacutesicos
27
com melhores resultados (aspecto econoacutemico e detalhe dos efeitos adversos) Todavia a
informaccedilatildeo presente na mesma sobre a eficaacutecia e efeitos secundaacuterios assim como toda a
bibliografia jaacute existente sobre este assunto eacute uacutetil e deve ser utilizada para tomar inicio agrave
criaccedilatildeo de um formulaacuterio em medicina dentaacuteria
Actualizaccedilatildeo de 2011
Os resultados obtidos da mesma forma que na revisatildeo anterior natildeo foram
suficientemente relevantes para que as poliacuteticas de sauacutede mudassem No entanto a
quantidade de informaccedilatildeo disponiacutevel sobre analgeacutesicos de dose uacutenica para aliacutevio da dor
poacutes-operatoacuteria eacute grande e bastante acessiacutevel Podem assim servir como boas
ferramentas para a formulaccedilatildeo de poliacuteticas e prescriccedilotildees farmacecircuticas para a populaccedilatildeo
quando existirem dados cliacutenicos mais conclusivos
28
AVALIACcedilAtildeO CRIacuteTICA
ENSAIOS CLIacuteNICOS ALEATORIZADOS
Combining paracetamol with a selective cyclooxygenase-2
inhibitor for acute pain relief after third molar surgery a
randomized double-blind placebo-controlled study Haglund and
von Bultzingslowen (25)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo compreende indiviacuteduos saudaacuteveis com idade superior a 18
anos peso entre 50 e 120 kg e com necessidade de extrair terceiros molares inferiores
com remoccedilatildeo oacutessea Foram excluiacutedos pacientes intolerantes ao aacutecido acetilsaliciacutelico
paracetamol eou NSAIDrsquos que estivessem a tomar outro tipo de medicaccedilatildeo (excepto
contraceptivos) graacutevidas ou em periacuteodo de amamentaccedilatildeo problemas com drogas ou
aacutelcool Apenas pacientes que reportaram dor moderada a intensa apoacutes a cirurgia foram
incluiacutedos
Existiram quatro grupos de intervenccedilatildeo
Grupo A rofecoxib 50mg + paracetamol 1g dose uacutenica 155 plusmn 37 minutos apoacutes
cirurgia
Grupo B rofecoxib 50mg dose uacutenica 170 plusmn 45 minutos apoacutes cirurgia
Grupo C paracetamol 1g dose uacutenica 184 plusmn 53 minutos apoacutes cirurgia
Grupo D placebo dose uacutenica 161 plusmn 30 minutos apoacutes cirurgia
Os resultados prenderam-se com a intensidade da dor medida atraveacutes da escala
visual analoacutegica (VAS) de 30 em 30 minutos desde a ingestatildeo do faacutermaco durante 8
horas Atraveacutes destas avaliaccedilotildees da dor foi possiacutevel obter valores de
aliacutevio total da dor TOTPAR
soma da diferenccedila de intensidade da dor SPID nas primeiras trecircs horas
soma da diferenccedila de intensidade da dor SPID ateacute agraves 8 horas
Foram obtidos resultados referentes a uma avaliaccedilatildeo global do tratamento feita
4h e 8h apoacutes a toma do faacutermaco O uso de rescue medication foi tomado em conta bem
como o tempo ateacute agrave sua necessidade Foram ainda avaliados eventuais efeitos
secundaacuterios
29
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim A atribuiccedilatildeo de cada tratamento foi cega para todos os pacientes
investigadores e pessoal envolvido Foi levada a cabo a aleatorizaccedilatildeo pela empresa
farmacecircutica responsaacutevel pela produccedilatildeo das caacutepsulas administradas
Natildeo existindo entraves de teor eacutetico ou de disponibilidade de recursos um
ensaio cliacutenico aleatorizado eacute a escolha mais pertinente quando eacute necessaacuterio comparar
dois ou mais tipos de tratamento O facto de existir um grupo de controlo minimiza o
risco de vieacutes
3 Were participants appropriately allocated to intervention and control groups
A colocaccedilatildeo dos pacientes em cada um dos quarto grupos de tratamento foi
concretizada atraveacutes de tabelas de aleatorizaccedilatildeo
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim Sendo um ensaio cliacutenico duplamente cego tanto o staff investigadores e
pacientes estiveram cegos durante todo o estudo Todas as caacutepsulas eram idecircnticas
sendo que cada embalagem selada continha sempre 6 caacutepsulas Desta forma eacute possiacutevel
garantir que o paciente estaacute cego Sendo cada embalagem feita e selada pela empresa
farmacecircutica eacute igualmente possiacutevel inferir que os investigadores tambeacutem se
encontravam cegos Apenas o investigador principal acedeu aos coacutedigos para fazer os
caacutelculos finais
5 Were all of the participants who entered the trial accounted for at its
conclusion
Os grupos de intervenccedilatildeo foram atribuiacutedos de forma aleatoacuteria e cega os
resultados foram analisados de acordo com o grupo a que inicialmente tinham sido
associados
Inicialmente o desenho do estudo previa 120 participantes
Grupo A n = 40
Grupo B n = 40
Grupo C n = 20
30
Grupo D n = 20 (controlo)
No entanto no final do estudo foram apurados resultados de 107 indiviacuteduos Isto
deve-se a
Apoacutes a cirurgia alguns pacientes (n = 8) natildeo sentiram dor moderada a forte
no entanto quiseram mesmo assim participar sendo os seus resultados
subtraiacutedos aos caacutelculos
Alguns pacientes (n = 5) foram excluiacutedos sendo que um foi drop-out e os
restantes natildeo entregaram ou preencheram os questionaacuterios pedidos
No final a distribuiccedilatildeo de indiviacuteduos por grupos era a seguinte
Grupo A n = 34
Grupo B n = 36
Grupo C n = 20
Grupo D n = 17
Embora se verifique uma ligeira alteraccedilatildeo natildeo eacute motivo relevante de vieacutes
6 Were the participants in all groups followed up and data collected in the same
way
Sim Todos os pacientes tiveram acesso aos mesmos questionaacuterios entregues
pelo investigador Em caso de duacutevida ateacute ao final da duraccedilatildeo do estudo (8 horas) o
paciente podia telefonar ao investigador com quaisquer duacutevidas que surgissem Poreacutem
o paciente era responsaacutevel pelo iniacutecio do estudo ao administrar a si mesmo o faacutermaco
em casa no momento em que o fizesse devia telefonar ao investigador para este ter
conhecimento do iniacutecio do estudo Se o paciente natildeo contactasse o investigador ateacute 3
horas apoacutes a cirurgia o investigador contactaria o paciente Os valores maacuteximo e
miacutenimo de tempo entre a cirurgia e iniacutecio do estudo de foram 118 e 237 minutos a este
facto eacute inerente um risco de vieacutes pois nem todos os pacientes estavam na mesma
condiccedilatildeo quando iniciaram o tratamento podendo reflectir-se nos resultados
7 Did the study have enough participants to minimise the play of chance
Sim Os caacutelculos foram efectuados assumindo que existiria uma diferenccedila na
SPID entre grupos A e B de 20 Foram utilizados testes natildeo-parameacutetricos (Mann-
Whitney U-test) sendo definido que pelo menos 22 pacientes deveriam ser incluiacutedos em
cada um destes grupos
31
8 How are the results presented and what is the main result
Os caacutelculos estatiacutesticos necessaacuterios para a elaboraccedilatildeo dos resultados foram
efectuados no programa Statistical Package for Social Sciences (SPSS) v 12 As
significacircncias entre grupos de tratamento em relaccedilatildeo agraves respostas agrave VAS foram
testadas com t-test de variaacutevel independente em todas as avaliaccedilotildees de dor A mesma
estrateacutegia foi aplicada para a SPID agraves 3 e 8 horas A TOTPAR foi baseada na
assumpccedilatildeo que os resultados satildeo parte de uma escala de intervalos O mesmo teste foi
utilizado para a diferenccedila entre grupos relativamente ao uso de rescue medication Os
testes dos dados provenientes de escalas categoacutericas (PAR e a avaliaccedilatildeo global) foram
realizados atraveacutes de testes natildeo-parameacutetricos (Mann-Whitney U-test)
Intensidade da dor Os resultados favorecem o grupo A ateacute 15h apoacutes o iniacutecio do
tratamento A partir das 2h o grupo A natildeo tem uma eficaacutecia estatisticamente maior que
o grupo B Ambos os grupos tecircm melhores resultados globais que o grupo C O Grupo
D (placebo) eacute notoriamente menos eficaz que todos os outros grupos
Aliacutevio da dor (PAR) Os resultados meacutedios desta afericcedilatildeo satildeo semelhantes aos da
intensidade da dor
TOTPAR Natildeo houve uma diferenccedila significativa entre o grupo A e o grupo B
Ambos foram significativamente melhores que o C todos os grupos de tratamento
activo tiveram melhores resultados que o grupo D (placebo)
SPID Embora o grupo A mostre a maior SPID meacutedia (05 ndash 3h) natildeo foi
estatisticamente diferente do grupo B o grupo C tambeacutem natildeo foi estatisticamente
diferente do grupo B A SPID meacutedia total foi estatisticamente semelhante entre os
grupos A e B mas superior agrave do grupo C O grupo D (placebo) teve resultados
inferiores aos dos restantes grupos
Uso de rescue medication Embora tenha existido um nuacutemero notoriamente
superior de casos entre os grupos A e B comparativamente ao C e ao D esta diferenccedila
natildeo eacute relevante estatisticamente devido ao baixo nuacutemero de pacientes que recorreram a
esta medicaccedilatildeo
Avaliaccedilatildeo global tanto agraves 4 como agraves 8h os grupos A e B receberam avaliaccedilotildees
semelhantes tendo as melhores classificaccedilotildees e sendo significativamente superiores agraves
do grupo C Todos foram melhores que o D (placebo) Agraves 8h as percentagens de
pacientes que avaliaram o tratamento como bom ou excelente foram
Grupo A 90
32
Grupo B 83
Grupo C 42
9 How precise are these results
No artigo natildeo satildeo mencionados intervalos de confianccedila No entanto nos graacuteficos
referentes agrave intensidade da dor eacute possiacutevel ver as barras correspondentes ao intervalo de
confianccedila Existem sempre que necessaacuterio valores de p associados aos resultados
10 Were all important outcomes considered so the results can be applied
Sim A extracccedilatildeo de terceiros molares em Portugal eacute uma praacutetica cliacutenica comum
pelo que o estudo pode ser facilmente reproduzido desde que haja acesso agrave medicaccedilatildeo
utilizada e que esta esteja em formato idecircntico (para garantir que natildeo existe vieacutes)
Poreacutem o facto de ser utilizada uma dose uacutenica poderaacute natildeo ir de encontro com o padratildeo
actual sendo necessaacuteria uma sensibilizaccedilatildeo do paciente diferente para este meacutetodo
Um facto importante foi referido na discussatildeo deste artigo posteriormente agrave
recolha de dados do mesmo surgiram preocupaccedilotildees seacuterias sobre efeitos nocivos
cardiovasculares em tratamentos de longa duraccedilatildeo com rofecoxib embora estes efeito
secundaacuterios tendam a estar relacionados com as doses e natildeo apenas com a selectividade
COX-2 (8 25) Esta informaccedilatildeo eacute altamente relevante de todos os pontos de vista do
paciente e famiacutelia do profissional de sauacutede e oacutergatildeos legislativos
Tendo em conta este facto seriam necessaacuterios estudos adicionais para aferir o
risco de seguir um tratamento como o visado neste ensaio cliacutenico
33
Combined acetaminophen and ibuprofen for pain relief after oral
surgery in adults a randomized controlled trial (13)
1 Did the study ask a clearly-focused question
Sim Foram incluiacutedos pacientes sujeitos a extracccedilatildeo de pelo menos um terceiro
molar inferior Foram excluiacutedos pacientes com idade inferior a 16 anos peso inferior a
50 kg que tivessem tomado NSAIDrsquos (excepto aspirina a 150mg) ou paracetamol 24h
antes da cirurgia entre outros(inserir referencia para a pagina pois sao muitos)
Existiram 3 grupos de intervenccedilatildeo
Grupo A 500mg paracetamol + 150mg ibuprofeno
Grupo B 500mg paracetamol
Grupo C 150mg ibuprofeno
Todos os grupos de intervenccedilatildeo tomaram 2 comprimidos imediatamente antes da
cirurgia e depois 4 comprimidos diariamente (de 6 em 6 horas) durante 48h
Os resultados passaram pela intensidade da dor medida atraveacutes da VAS (mm)
em trecircs momentos distintos antes de tomar qualquer medicaccedilatildeo do estudo
imediatamente apoacutes a cirurgia e de 2 em 2 horas ateacute terminar o periacuteodo de 48 horas A
medida utilizada foi a area under the curve (AUC) dividida pelo tempo resultando em
AUCh Este caacutelculo foi efectuado para encontrar valores ldquomeacutediosrdquo pois houve ligeiras
diferenccedilas no momento da afericcedilatildeo dos valores da VAS Mediu-se tambeacutem o consumo
de rescue medication ao longo das 48 horas
Foram ainda utilizadas escalas categoacutericas de avaliaccedilatildeo global da dor e da
naacuteusea realizadas no final do estudo bem como uma escala VAS para medir os
distuacuterbios no sono apoacutes cada noite
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim A atribuiccedilatildeo de cada tratamento foi cega para todos os pacientes
investigadores e pessoal envolvido O responsaacutevel pela aleatorizaccedilatildeo do estudo foi o
estatiacutestico do estudo O estatiacutestico foi a uacutenica pessoa com acesso agraves informaccedilotildees da
atribuiccedilatildeo de tratamento aos pacientes
34
3 Were participants appropriately allocated to intervention and control groups
A colocaccedilatildeo de pacientes em cada um dos trecircs grupos de tratamento foi
aleatorizada A sequecircncia de aleatorizaccedilatildeo foi gerada por computador pelo estatiacutestico
do estudo Foi utilizada uma proporccedilatildeo de 111 para os trecircs grupos de tratamento isto
foi conseguido atraveacutes de permutaccedilatildeo de blocos com estratificaccedilatildeo para o tipo de
anestesia (local ou geral) e centro de estudo A utilizaccedilatildeo da aleatorizaccedilatildeo por
permutaccedilatildeo de blocos assegura uma distribuiccedilatildeo equilibrada por grupos de tratamento
quando o nuacutemero de indiviacuteduos eacute menor que mil (inserir referencia do artigo de
aleatorizajao MJA)
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim Este ensaio cliacutenico foi duplamente cego Como tal cada tipo de tratamento
consistia em comprimidos idecircnticos colocados num pacote selado as instruccedilotildees sobre
dosagens eram tambeacutem iguais garantindo que o estudo permanecia cego aos
investigadores staff e pacientes prevenindo a existecircncia de vieacuteses
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim O estudo previa um nuacutemero miacutenimo de 120 indiviacuteduos 40 em cada grupo
de tratamento Dos 135 pacientes que concordaram participar apoacutes serem abordados
pelo meacutedico apenas 122 foram incluiacutedos no estudo (os 13 que foram excluiacutedos natildeo
entregaram o diaacuterio de tratamento que lhes foi pedido)
Grupo A n = 40
Grupo B n = 43
Grupo C n = 39
Todos os 122 pacientes incluiacutedos foram seguidos ateacute ao final do estudo
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os pacientes foram abordados primariamente por um cirurgiatildeo e
seguidamente por uma enfermeira responsaacutevel pelo seguimento dos pacientes ao longo
do estudo O seguimento de cada paciente foi realizado de igual forma no hospital e fora
35
dele onde o contacto era estabelecido por telefone de forma a facilitar a recolha de
informaccedilatildeo levada a cabo por meio da entrega de diaacuterios
Em relaccedilatildeo agrave recolha dos dados relativos agrave dor poacutes-operatoacuteria experienciada os
intervalos de tempo utilizados foram semelhantes (imediatamente antes da
administraccedilatildeo da primeira dose logo apoacutes a cirurgia e de 2 em 2 horas durante um
periacuteodo de 48 horas) e a monitorizaccedilatildeo dos pacientes feita utilizando as mesmas
guidelines
7 Did the study have enough participants to minimise the play of chance
Sim Os investigadores do estudo realizaram a power calculation Estimaram
que eram necessaacuterios 120 participantes distribuiacutedos equitativamente pelos 3 grupos O
power foi de 80 na detecccedilatildeo de diferenccedilas entre os grupos de 9 mm (SD de 14mm)
para mediccedilotildees relativas agrave altura de repouso e os de 13mm (SD de 21mm) e para
mediccedilotildees relativas agrave altura de actividade
Dos 135 pacientes incluiacutedos no estudo 13 natildeo devolveram os seus diaacuterios pelo
que ficaram disponiacuteveis 122 participantes a enquadrar a populaccedilatildeo de tratamento (ITT
population) para anaacutelise dos criteacuterios de comparaccedilatildeo primaacuterios (primary endpoints)
Como o criteacuterio de possuir participantes necessaacuterios foi preenchido os
resultados da comparaccedilatildeo do objectivo primaacuterio deste estudo (mediccedilatildeo da intensidade
meacutedia de dor ao longo do estudo) tecircm uma elevada importacircncia cliacutenica Esta
importacircncia eacute equiparaacutevel aos resultados de estudos publicados anteriormente
8 How are the results presented and what is the main result
Os resultados foram apresentados sob a forma de mediccedilotildees nomeadamente as
principais diferenccedilas (mean differences) entre o paracetamolacetaminofeno ibuprofeno
e combinaccedilatildeo dos dois comparando a eficaacutecia farmacocineacutetica e efeitos secundaacuterios
respectivos a cada um Agraves quais estaacute associada uma taxa de erro de 5 (SEM) ou seja
intervalo de confianccedila de 95 (CI) e um valor de P lt001
Foi realizada a mediccedilatildeo da time-adjusted AUC (AUCh) da VAS que
juntamente com a classificaccedilatildeo global de dor revelou-se substancial e
significativamente menor no grupo que utilizou a combinaccedilatildeo do que nos outros dois
grupos (tanto no periacuteodo de repouso como no periacuteodo de actividade)
Apesar de alguns criteacuterios de comparaccedilatildeo secundaacuterios (secondary endpoints) o
uso de medicaccedilatildeo de resgate apoiarem o uso da combinaccedilatildeo do faacutermaco natildeo possuem
36
relevacircncia estatiacutestica Aleacutem disso o tipo de anestesia utilizada na cirurgia e o nordm de
dentes extraiacutedos os paracircmetros farmacocineacuteticos e a ocorrecircncia dos efeitos secundaacuterios
natildeo mostraram diferenccedilas significativas entre os 3 grupos de estudo
Os pacientes medicados com a combinaccedilatildeo de paracetamol e ibuprofeno
experienciaram menos dor poacutes-operatoacuteria durante as 48 horas que os pacientes que
usaram os medicamentos isolados
9 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em conta que foi preacute-
definido um valor para P de 005 de forma determinar se os valores obtidos possuem
relevacircncia estatiacutestica ou natildeo os resultados satildeo precisos
Isto mostra que para que a combinaccedilatildeo dos dois medicamentos possa ser
considerada sem incerteza mais adequada que outros meacutetodos de medicaccedilatildeo seriam
necessaacuterios resultados expliacutecitos e com elevada relevacircncia estatiacutestica
10 Were all important outcomes considered so the results can be applied
Sim O estudo realizado tal como acontece em todos os outros apresenta os
seus pontos fortes e fracos No entanto a pluralidade de criteacuterios utilizados na
comparaccedilatildeo dos vaacuterios grupos de estudo permitiu uma boa percepccedilatildeo da relaccedilatildeo
custobenefiacutecio aqui presente Apesar de certos paracircmetros como a utilizaccedilatildeo de
placebo recrutamento de crianccedilas e avaliaccedilatildeo significativa dos efeitos secundaacuterios natildeo
terem sido explorados estes natildeo apresentam grande peso no que respeita agrave validaccedilatildeo dos
resultados em si Isto acontece pois a bibliografia existente e a praacutetica cliacutenica jaacute nos
permitem deduzir e extrapolar conclusotildees em relaccedilatildeo agravequeles paracircmetros
Deste modo a questatildeo-chave recai sobre o facto de a combinaccedilatildeo de
paracetamol com ibuprofeno ser mais vantajosa e eficaz que a toma de apenas um deles
Caso estes resultados sejam confirmados por estudos de outras entidades a jaacute muito
utilizada combinaccedilatildeo paracetamol+ibuprofeno poderaacute mesmo tornar-se procedimento
padratildeo na terapecircutica da dor aguda moderada (em pacientes sem contra-indicaccedilatildeo para
NSAIDrsquos)
37
Analgesic efficacy of lysine clonixinate paracetamol and
dipyrone in lower third molar extraction a randomized
controlled trial (32)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo em estudo comporta 90 pacientes entre os 18 e 26 anos de
idade com uma indicaccedilatildeo cliacutenica para extracccedilatildeo de um 3ordm molar inferior impactado
(com classe I e II)
A intervenccedilatildeo consistiu no tratamento da dor apoacutes extracccedilatildeo do 3ordm molar atraveacutes
da medicaccedilatildeo com um dos 3 analgeacutesicos em estudo utilizando 8 comprimidos do
respectivo analgeacutesico a serem tomados 1 hora preacute-cirurgia e a cada 6 horas poacutes-cirurgia
durante um periacuteodo de 24 horas
Os resultados foram obtidos atraveacutes da mediccedilatildeo da intensidade da dor utilizando
a escala visual analoacutegica (VAS) mesmo antes da cirurgia e seguidamente 1 2 4 6 8
12 e 24 horas apoacutes a cirurgia Aleacutem disso para cada uma destas mediccedilotildees os pacientes
tinham de relatar o niacutevel de dor em que se encontravam (percepccedilatildeo da dor) atraveacutes de
uma escala decimal com os seguintes criteacuterios
0 cm Sem dor
01- 3 cm Dor ligeira
31-7 cm Dor moderada
71-10 cm Dor intensa
A presenccedila ou ausecircncia de efeitos secundaacuterios foi tambeacutem uma das
preocupaccedilotildees deste estudo e algo avaliado nos resultados Dado que havia a
possibilidade de ocorrecircncia de agranulocitose anemia anafilaxia e complicaccedilotildees
gastrointestinais
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo em questatildeo consiste num ensaio cliacutenico aleatorizado Esta
abordagem foi a mais adequada para a questatildeo colocada uma vez que o objectivo final
eacute comparar a eficaacutecia da lisina clonixinato com o paracetamol e com a dipirona na
analgesia da dor poacutes-operatoacuteria Para obter informaccedilotildees mais completas respeitantes agrave
seguranccedila e eficaacutecia dos faacutermacos comparados eacute necessaacuterio o recrutamento e
aleatorizaccedilatildeo de um determinado nuacutemero de pacientes Eacute necessaacuterio tambeacutem medicaacute-
38
los medir e avaliar os resultados de forma imparcial e objectiva Desta forma eacute mais
provaacutevel chegar a uma conclusatildeo fidedigna e vaacutelida tanto interna como externamente
Pelas razotildees acima enumeradas a realizaccedilatildeo de um ensaio cliacutenico aleatorizado
foi a melhor abordagem a seguir
3 Were participants appropriately allocated to intervention and control groups
Sim Os pacientes foram divididos pelos diferentes grupos de estudo de uma
forma aleatoacuteria utilizando um meacutetodo relativamente simples Os analgeacutesicos foram
repartidos em recipientes brancos opacos e idecircnticos numerados de 1 a 90 Cada
recipiente continha 8 comprimidos de um dos 3 faacutermacos em comparaccedilatildeo (dipirona
500mg paracetamol 750mg lisina clonixinato 125 mg) Por sua vez foi pedido aos
pacientes para retirarem o recipiente agrave sua escolha e ao acaso os quais desconheciam o
seu conteuacutedo
Dos 90 pacientes recrutados de iniacutecio 26 desistiram pelo que os restantes 64
pacientes foram distribuiacutedos por 3 grupos correspondentes a diferentes analgeacutesicos
orais lisina clonixinato composto por 20 indiviacuteduos (8 masculinos 12 femininos)
Paracetamol composto por 23 indiviacuteduos (9M 14F) Dipirona composto por 21
indiviacuteduos (6M 15F)
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Natildeo eacute possiacutevel dizer Os pacientes deste estudo estavam lsquocegosrsquo quanto ao grupo
de estudo em que iriam ser colocados O processo de distribuiccedilatildeo dos indiviacuteduos foi
feito de uma forma aleatoacuteria atraveacutes de um meacutetodo bastante simples de escolha de
recipiente
Quanto aos funcionaacuterios e revisores deste estudo o mesmo pode natildeo ter
acontecido pois nenhuma informaccedilatildeo sobre este aspecto eacute mencionada no artigo
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim No estudo realizado os participantes foram distribuiacutedos por 3 grupos um
de estudo ou intervenccedilatildeo onde foi administrado lisina clonixinato e dois de controlo
onde se administrou paracetamol num e dipirona noutro Natildeo houve redistribuiccedilatildeo dos
39
participantes isto eacute cada participante foi tratado uacutenica e exclusivamente com o faacutermaco
correspondente ao seu grupo
Houve um seguimento dos pacientes durante um periacuteodo de 24 horas de modo a
avaliar a eficaacutecia de cada analgeacutesico na eliminaccedilatildeo da dor poacutes-operatoacuteria de forma
indirecta (quanto maior o aliacutevio de dor ao longo do periacuteodo de estudo maior a eficaacutecia
do respectivo analgeacutesico) Tendo isso em conta os resultados e anaacutelise dos dados foram
realizados em cada grupo e depois comparados com os outros grupos
Os investigadores do estudo poderiam ter formado um grupo placebo e
comparado os seus resultados com os restantes grupos Assim averiguar-se-ia a eficaacutecia
de cada um dos analgeacutesicos e natildeo apenas a eficaacutecia relativa a outros faacutermacos
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os participantes dos diferentes grupos foram seguidos da mesma maneira e
os dados recolhidos de igual forma Os resultados foram avaliados nos mesmos
intervalos de tempo ou seja antes da cirurgia e 1 2 4 6 8 12 e 24 horas apoacutes a
mesma Os pacientes receberam o mesmo tempo de atenccedilatildeo - 24 horas de seguimento e
os dados foram recolhidos utilizando os mesmos paracircmetros a escala visual analoacutegica
para determinar o aliacutevio de dor e a escala decimal para a percepccedilatildeo de dor dos pacientes
e questionaacuterios individuais
Para aleacutem do jaacute referido os investigadores tiveram em atenccedilatildeo a forma como a
cirurgia foi realizada diminuindo o risco de vieacutes
Intervieram 2 cirurgiotildees calibrados entre si na niacutevel da teacutecnica minimizando a
ocorrecircncia de abordagens ciruacutergicas diferentes
o periacuteodo de duraccedilatildeo foi controlado e por isso natildeo influenciou o comportamento
da dor no estudo (meacutedia de 339 minutos com SD plusmn98 min)
Estas cirurgias satildeo bastantes conhecidas e muitas vezes satildeo procedimentos
standard permitindo uma selecccedilatildeo muito mais facilitada e raacutepida de casos cliacutenicos a
incluir no estudo e diminuindo o nuacutemero de eventos de difiacutecil controlo que poderiam
levar a vieacutes dos resultados
7 Did the study have enough participants to minimise the play of chance
Natildeo eacute possiacutevel dizer Dos 90 pacientes inicialmente recrutados para o estudo 26
deles desistiram Os investigadores natildeo referiram o impacto deste nuacutemero de drop-outs
40
na extrapolaccedilatildeo de conclusotildees a partir dos resultados obtidos Igualmente natildeo foram
mencionados quaisquer caacutelculos que determinassem o nuacutemero necessaacuterio de indiviacuteduos
para o estudo ter validade
8 How are the results presented and what is the main result
Os resultados obtidos no estudo foram categorizados por droga e analisados de
acordo com o desenvolvimento da dor poacutes-operatoacuteria Seguidamente foram
apresentados atraveacutes de mediccedilotildees descritivas da variaccedilatildeo da dor as quais utilizaram
paracircmetros como miacutenimo maacuteximo mean median e desvio-padratildeo (SD)
Por sua vez a anaacutelise dos dados foi feita com os testes de Kruskal-Wallis e de
Friedman onde os resultados satildeo considerados estatisticamente relevantes se
culminarem num valor de lsquoprsquo igual ou inferior a 005 (95 IC) e apresentada utilizando
os mesmos paracircmetros de miacutenimo maacuteximo e SD
O valor de P encontra-se claramente acima do valor de referencia preacute-definido
pelo que os resultados natildeo apresentam relevacircncia estatiacutestica suficiente para aferir que
possuem um melhor outcome que o paracetamol
A lisina clonixinato assim como a dipirona e o paracetamol eacute eficiente no
controlo da dor resultante da extracccedilatildeo de um 3ordmmolar inferior pelo que natildeo apresenta
nenhuma diferenccedila significativa dos outros analgeacutesicos mencionados
9 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em conta que os valores de
P obtidos apoacutes anaacutelise dos resultados se encontrarem abaixo de 001 eacute possiacutevel auferir
que os resultados deste estudo satildeo bastante precisos
10 Were all important outcomes considered so the results can be applied
Natildeo Os efeitos gerados pela lisina clonoxinato no tratamento da dor derivada de
extracccedilatildeo do 3ordm molar natildeo foram estatisticamente relevantes quando comparados aos do
paracetamol e dipiridona Apesar de as condiccedilotildees pelas quais o estudo foi realizado
serem reprodutiacuteveis na nossa populaccedilatildeo local (tipo de pessoas localizaccedilatildeo e
reprodutibilidade do tratamento) nada eacute referido em relaccedilatildeo a novas poliacuteticas de sauacutede
nomeadamente na implementaccedilatildeo de uma dose uacutenica culminando numa mudanccedila dos
haacutebitos de sauacutede da comunidade Tambeacutem natildeo foram abordados aspectos econoacutemicos
41
tal como um balanccedilo entre benefiacutecios e encargos de sauacutede que justifique a utilizaccedilatildeo
deste faacutermaco como tratamento preferencial
42
Onset of analgesia with sodium ibuprofen ibuprofen acidin
corporating poloxamer and acetaminophenmdasha single-dose
double-blind placebo-controlled study in patients with post-
operative dental pain Daniels Reader (33)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo em estudo refere-se a pacientes com idade entre os 16 e os 40
anos apresentando uma intensidade de dor basal poacutes-operatoacuteria moderada a severa O
diagnoacutestico para a extracccedilatildeo poderia ser um dos seguintes pelo menos um 3ordm molar
mandibular indicado para remoccedilatildeo (grau de impactaccedilatildeo superior a 4) ou dois terceiros
molares ipsilaretais com pontuaccedilatildeo de impactaccedilatildeo conjunta natildeo superir a 6
A intervenccedilatildeo traduz-se no tratamento da dor poacutes-ciruacutergica com doses uacutenicas de
diferentes faacutermacos Inicialmente cada participante tem a mesma probabilidade de ser
colocado num dos 4 grupos
A ibuprofeno de soacutedio 2x256 mg (ibuprofeno de soacutedio di-hidratado equivalente a
400 mg de ibuprofeno aacutecido + placebos de ibuprofeno poloxamo e
acetaminofeno
B ibuprofenopoloxacircmero (400mg de Ibuprofeno e 120mg de poloxacircmero
surfactante 407) + placebos de ibuprofeno de soacutedio e paracetamol
C 1000mg acetaminofeno + placebos equivalentes
D placebo para as 3 formas de substacircncias activas
O endpoint primaacuterio consistiu no tempo necessaacuterio para um aliacutevio da dor
perceptiacutevel pelos pacientes Foram considerados inuacutemeros endpoints secundaacuterios (foi
utilizada uma escala categoacuterica e VAS para os endpoints 2 3 e 4)
1 Caacutelculo da AUC e SPRID (0 a 6 horas poacutes-tratamento) e tempo necessaacuterio para
um aliacutevio significativo da dor
2 Aliacutevio total da dor (TOTPAR) SPID e SPRID
3 Aliacutevio da dor e intensidade da mesma em termos individuais (5 minutos - 6
horas)
4 PID ao longo do periacuteodo de estudo e o momento em que este foigt ou igual a 1
5 Instante em que os pacientes recorreram a medicaccedilatildeo de recurso
6 Tempo e proporccedilatildeo de pacientes que sentiram 50 aliacutevio da dor
43
7 Abstracccedilatildeo agrave dor (1 e 6 horas) e percepccedilatildeo da interferecircncia causada pela dor nas
actividades quotidianas (escala de Ranvier)
8 Avaliaccedilatildeo qualitativa da medicaccedilatildeo tomada pelos dos participantes
Os efeitos adversos foram obtidos atraveacutes da procura de informaccedilatildeo em
documentaccedilatildeo e relacionados (ou natildeo) com a medicaccedilatildeo do estudo pelo investigador
Foi efectuada uma mediccedilatildeo de sinais vitais 6 horas apoacutes a toma e na visita follow-up na
qual tambeacutem foi realizado um exame fiacutesico
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo em questatildeo eacute descrito como um ensaio cliacutenico duplamente cego e
controlado com placebo Eacute o tipo de estudo indicado para comparar diferentes formas de
tratamento atraveacutes da divisatildeo dos pacientes por grupos Eacute necessaacuterio ter em
consideraccedilatildeo o aspecto eacutetico de tais tratamentos pois ldquoexposing patients to an
intervention believed to be inferior to current treatment is often thought unethicalrdquo (41)
Para garantir a eacutetica dos tratamentos incluiacutedos o estudo foi conduzido de acordo com a
Declaraccedilatildeo de Helsiacutenquia como referido na Directiva da EU de 200120EC e
concordante com a Conferecircncia Internacional de Harmonizaccedilatildeo (ICH) e a GCP (boa
praacutetica cliacutenica)
3 Were participants appropriately allocated to intervention and control groups
Sim Os indiviacuteduos foram divididos aleatoriamente para serem inseridos num
dos 4 grupos de tratamento numa proporccedilatildeo 1111 O meacutetodo de aleatorizaccedilatildeo foi
gerado pelo computador atraveacutes de um randomization Schedule
Para equilibrar a alocaccedilatildeo dos pacientes realizou-se uma estratificaccedilatildeo por sexo
e por intensidade da dor basal O protocolo do estudo foi revisto e aprovado pela
Quorum Review Inc o que leva a querer que a subdivisatildeo foi realmente rigorosa
Os grupos encontram-se equilibrados tanto em nuacutemero como noutras variaacuteveis
particularmente geacutenero intensidade dor basal e idade Deste modo diferenccedilas
reportadas nos resultados natildeo satildeo consequecircncia da heterogeneidade dentro dos grupos
de tratamento
44
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
A aleatorizaccedilatildeo dos participantes foi gerada pelo computador O protocolo do
estudo foi posteriormente revisto como anteriormente referido Agrave partida tanto o
investigador e pacientes natildeo interferiram no processo
Foram usados comprimidos para o ibuprofeno de soacutedio ibuprofenopoloxamero
e caacutepsulas para o paracetamol tanto para as formas activas como placebo
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim Os 322 participantes incluiacutedos de 614 inicialmente recrutados 318
completaram o estudo e 321 foram incluiacutedos na populaccedilatildeo ITT (intended do treat)
No grupo ibuprofeno de soacutedio todos os 80 participantes concluiacuteram a anaacutelise
No grupo B dos 80 inicialmente alocados 76 completaram a anaacutelise Um foi
excluiacutedo perdeu-se o follow-up de outro e os restantes natildeo concluiacuteram por
outros motivos
Dos 81 do grupo do paracetamol um natildeo foi incluiacutedo no ITT (falhou em
providenciar os dados da intensidade da dor basal diaacuteria)
No grupo placebo todos os pacientes concluiacuteram o estudo
Os resultados de cada paciente foram analisados agrave luz do grupo de tratamento
em que estes foram colocados
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os participantes permaneceram nos centros de investigaccedilatildeo cliacutenica apoacutes a
toma durante 8-15h Durante as 6 horas apoacutes o tratamento a eficaacutecia foi medida em
intervalos preacute-determinados Para avaliar a existecircncia de efeitos secundaacuterios foi
realizada uma mediccedilatildeo de sinais vitais conduzido um follow-up poacutes-operativo (5 a 12
dias poacutes-cirurgia) e repetida a avaliaccedilatildeo de efeitos adversos Pode-se considerar anaacutelogo
o acompanhamento entre os vaacuterios pacientes poacutes-cirurgia e medicaccedilatildeo pois constituiu
um seguimento proacuteximo maioritariamente presencial e rigoroso
45
7 Did the study have enough participants to minimise the play of chance
Foram usados dados de estudos preacutevios os quais continham informaccedilatildeo acerca
de AUC e PRID Com estes dados foi determinado que um nuacutemero de 80 pacientes por
grupo providenciaria um power de 90 em detectar diferenccedilas entre os grupos de
tratamento com um niacutevel de significacircncia de 0025 Natildeo foi possiacutevel calcular um power
ldquoformalrdquo para o aliacutevio de dor significativo No entanto a resposta eacute afirmativa para a
questatildeo CASP uma vez que foram realizados esforccedilos para que o nuacutemero das amostras
fosse significativo e correcto
8 How are the results presented and what is the main result
Os resultados satildeo apresentados em termos de percentagens e diferenccedilas meacutedias
(mean differences) alguns com recurso a curvas de Kaplan-Meier (survival curves) Os
efeitos secundaacuterios satildeo apresentados sob a forma de tabela com a percentagem de
pacientes dentro de cada grupo que sofreram os efeitos descritos na mesma
Os grupos A e B exibem resultados substancialmente melhores no que diz
respeito aos seguintes pontos
AUC e SPID satildeo significativamente menores A com 963 e B com 90 face a
C com 675 e D com 25 O tempo para atingir aliacutevio da dor
SPRID Esta eacute semelhante entre os grupos A B e C ateacute aos 45 minutos A partir
deste periacuteodo o ibuprofeno possui uma eficaacutecia superior ao paracetamol
Abstracccedilatildeo agrave dor e percepccedilatildeo da interferecircncia causada pela dor nas actividades
quotidianas (escala de Ranvier)
Utilizaccedilatildeo da medicaccedilatildeo de recurso A com 325 e B com 225 face a C com
438 e D em que a maioria dos pacientes usou a mesma
Avaliaccedilatildeo dos medicamentos por parte dos pacientes (resposta ldquoboardquo ldquomuito
boardquo ou ldquoexcelenterdquo)
No que se refere aos efeitos secundaacuterios 118 da populaccedilatildeo do estudo sofreu
mais efeitos sendo que a maior percentagem ocorreu no grupo do C
Quando comparado com acetaminofeno o ibuprofeno de soacutedio e
Ibuprofenopoloxamero possui uma eficaacutecia analgeacutesica significativamente superior
46
9 How precise are these results
Nos endpoints primaacuterios as diferenccedilas entre as duas formulaccedilotildees de ibuprofeno e
paracetamol foram avaliadas tendo por base o teste de Wilcoxon rank-sum O hazard
ratio e respectivo IC de 975 foram calculados para as comparaccedilotildees entre os
compostos Os endpoints secundaacuterios que agregavam vaacuterios periacuteodos de tempo foram
calculados atraveacutes da AUC Diferenccedilas entre tratamentos foram avaliadas utilizando
valores de α de 005 o intervalo de confianccedila de 95 (CI) foi calculado por meio dos
paracircmetros do modelo adequado
Eacute introduzido o valor de P que na sua generalidade possui valores reduzidos e
menores que 0005 Considerando a homogeneidade dos grupos o caacutelculo do nuacutemero da
amostra com elevado power e os valores de P podemos concluir que no contexto os
resultados satildeo precisos (42)
10 Were all important outcomes considered so the results can be applied
Eacute plausiacutevel que a populaccedilatildeo utilizada no estudo fosse semelhante num estudo
anaacutelogo Tanto o local como o proacuteprio tratamento poderiam ser reproduzidos visto que
os compostos em questatildeo satildeo largamente comercializados
Os resultados satildeo importantes para uma escolha mais consciente por parte dos
indiviacuteduos entre tomar paracetamol ou ibuprofeno apoacutes uma cirurgia de um 3ordm molar Eacute
afirmado na discussatildeo deste estudo que o ibuprofeno possui menores efeitos adversos
gastrointestinais que outros NSAIDrsquos Tendo isso em conta pode conduzir a uma
escolha deste composto no tratamento da dor poacutes ciruacutergica por parte dos profissionais
ldquothese findings support a recommendation for this agent as an analgesic of choice for
the treatment of post-operative dental painrdquo A preocupaccedilatildeo pela comunidade em geral
estaacute impliacutecita neste aspecto se possuir menores efeitos secundaacuterios e benefiacutecio superior
eacute melhor para a populaccedilatildeo em geral O custo financeiro destes medicamentos natildeo se
traduz num ponto diferenciador visto que em Portugal existem geneacutericos de ambos
Eacute uma boa base de comparaccedilatildeo entre o paracetamol e ibuprofeno em muitos
aspectos Na procura da melhor evidecircncia e no sentido de a aplicar eacute importante
completar este estudo com outros que nomeadamente se foquem nos efeitos
secundaacuterios
47
An investigation into the comparative efficacy of soluble aspirin
and solid paracetamol in postoperative pain after third molar
surgery Seymour Hawkesford (22)
1 Did the study ask a clearly-focused question
Sim O estudo em questatildeo trata-se de um ensaio cliacutenico aleatorizado duplamente
cego e controlado por placebo O seu objectivo central eacute comparar a eficaacutecia da aspirina
soluacutevel agrave do paracetamol soacutelido em pacientes com dor poacutes-operatoacuteria apoacutes extracccedilatildeo do
3ordm molar Foi utilizado um grupo placebo como controlo negativo
Soacute foram incluiacutedos pacientes que necessitavam da extracccedilatildeo do 3ordm molar
saudaacuteveis segundo categoria 1 da American Society of Anaesthesiologists (ASA I) ou agrave
discriccedilatildeo do cirurgiatildeo oral categoria 2 Soacute foram abrangidos pacientes que atingiram o
limiar de dor necessaacuterio ou que requeriram analgeacutesicos ateacute 90 minutos apoacutes a cirurgia
Cada paciente incluiacutedo no estudo foi colocado num dos trecircs grupos de
tratamento
Grupo 1 Aspirina soluacutevel 900mg dose uacutenica
Grupo 2 paracetamol soacutelido 1000mg dose uacutenica
Grupo 3 placebo dose uacutenica
Foi utilizado o meacutetodo de double-dummy ndash assim cada grupo recebeu o seu tipo
de tratamento e um placebo do tratamento alternativo No caso do grupo 3 os pacientes
receberam placebos para os dois tipos de tratamento
Os outcomes passaram pela
Comparaccedilatildeo de medidas de intensidade da dor atraveacutes da escala VAS (mm)
entre os grupos de tratamento aos 10 15 20 e 30 minutos apoacutes a dosagem
inicial
Comparaccedilatildeo da AUC240 com recurso a anaacutelise de co-variacircncia usando o
centro do estudo geacutenero baseline pain intensity duraccedilatildeo da cirurgia e
nuacutemero de molares removidos como co-variaacuteveis
Necessidade de recurso a rescue medication
Impressatildeo geral dos pacientes e enfermeiros sobre a medicaccedilatildeo atraveacutes de
uma regressatildeo binomial logiacutestica (em que um resultado positivo se refere a
uma avaliaccedilatildeo ldquomuito boardquo ou ldquoboardquo)
As comparaccedilotildees feitas foram aspirina vs paracetamol e aspirina vs placebo
48
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo apresentado eacute um RCT por vaacuterias razotildees sendo a mais relevante a
aleatorizaccedilatildeo dos grupos de tratamento em que os pacientes incluiacutedos foram
distribuiacutedos com a mesma probabilidade e aleatoriamente para cada grupo de estudo Os
grupos de tratamento tecircm tamanhos semelhantes e satildeo homogeacuteneos e os pacientes
foram seguidos de forma semelhante - as uacutenicas diferenccedilas residem no tratamento
oferecido
A utilizaccedilatildeo deste tipo de estudo foi loacutegica Um ensaio cliacutenico aleatorizado eacute
ideal para comparar efeitos de determinadas intervenccedilotildees e consequentemente ideal
para comparar eficaacutecia entre medicamentos
3 Were participants appropriately allocated to intervention and control groups
Foi realizada uma alocaccedilatildeo aleatoacuteria dos pacientes incluiacutedos assim como uma
aleatorizaccedilatildeo por blocos de cinco para assegurar equiliacutebrio entre grupos de tratamento
ldquoA key advantage of blocked randomization is that treatment groups will be equal in
size and will tend to be uniformly distributed by key outcome-related characteristicsrdquo
(43)
Foi ainda efectuada uma aleatorizaccedilatildeo estratificada por geacutenero de modo a
equilibrar nos trecircs grupos o nuacutemero de mulheres e homens e aumentar a credibilidade
das comparaccedilotildees entre os mesmos (proporccedilatildeo MF 21)
Tabela 2 ndash Dados demograacuteficos dos pacientes do estudo
Variaacutevel Aspirina soluacutevel
900mg
Paracetamol soacutelido
1000 mg
Placebo
Nuacutemero de pacientes 59 62 32
Raacutecio geacutenero MF 1940 1943 1121
Todos os pacientes incluiacutedos receberam anestesia de acordo com a praacutetica
cliacutenica a extracccedilatildeo dos molares impactados foi realizada seguindo a teacutecnica standard
Estes factores contribuem para a semelhanccedila da forma de tratamento dos 3 grupos Com
estes aspectos em comum a todos os pacientes incluiacutedos em adiccedilatildeo agrave homogeneidade
dos grupos nos seus aspectos demograacuteficos diferenccedilas encontradas nos resultados satildeo
consequecircncias de outros factores
49
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim A administraccedilatildeo uacutenica tem a vantagem de natildeo requerer monitorizaccedilatildeo de
um processo ldquodelicadordquo por parte do paciente De facto todo o estudo eacute realizado num
periacuteodo de 4 horas apoacutes a cirurgia e com ajuda de enfermeiros Olhando do ponto de
vista do paciente pode-se consideraacute-lo cego
Se os meacutetodos foram realmente aleatoacuterios o investigador eacute tambeacutem considerado
cego e pode-se afirmar que foram feitos esforccedilos necessaacuterios para o alcanccedilar Tanto a
aspirina soluacutevel como o placebo foram oferecidos sob a forma de uma bebida cor-de-
laranja o paracetamol com substacircncia activa e placebo oferecidos como comprimidos
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim Inicialmente todos os pacientes tinham a mesma probabilidade de serem
incluiacutedos num dos trecircs grupos A distribuiccedilatildeo sendo aleatoacuteria natildeo soacute coloca um
paciente num determinado grupo de tratamento como impossibilita que o mesmo venha
a pertencer a outro O seguimento foi realizado de igual forma para todos os grupos e
intimamente controlado Os resultados foram apresentados separadamente para cada
grupo Dos 167 pacientes foram medicados 153 Dos 14 pacientes natildeo tratados 10 natildeo
desenvolveram dor suficiente para serem incluiacutedos 1 obteve uma reacccedilatildeo adversa agrave
anestesia e 1 natildeo seguiu o protocolo
O grupo da aspirina soluacutevel apresentou melhores resultados que o grupo do
paracetamol e do placebo na medida em que os pacientes reportaram menos dor
apresentou menor intensidade de dor (aos 10 e 30 minutes em comparaccedilatildeo ao
paracetamol e apenas 30 minutos face ao placebo) e os valores de dor global medidos
pela AUC240 foram significativamente menores
6 Were the participants in all groups followed up and data collected in the same
way
Sim A intensidade da dor foi medida frequentemente ao longo de 4 horas
(segundo a VAS) e os pacientes foram informados da possibilidade de tomar medicaccedilatildeo
adicional se necessaacuterio A avaliaccedilatildeo sobre o tratamento dos enfermeiros e dos proacuteprios
pacientes foi tida em consideraccedilatildeo para os resultados
50
Aleacutem disso ao longo do periacuteodo de investigaccedilatildeo a enfermeira do estudo ficou
responsaacutevel por monitorizar os pacientes e registar a ocorrecircncia de quaisquer eventos
adversos Deste modo eacute muito provaacutevel que todos os pacientes tenham recebido o
mesmo niacutevel de atenccedilatildeo
7 Did the study have enough participants to minimise the play of chance
Natildeo eacute possiacutevel dizer No estudo natildeo eacute referida a utilizaccedilatildeo de power calculations
ou outros meacutetodos para determinar o tamanho da amostra Apenas se pode concluir que
o grupo de controlo negativo tem um menor nuacutemero de pacientes consequecircncia de
desistecircncias ou pelo simples facto de agrave partida se conhecerem os resultados
8 How are the results presented and what is the main result
A intensidade da dor foi medida numa escala VAS aos 10 15 20 e 30 minutos
apoacutes a administraccedilatildeo Foi possiacutevel tirar vaacuterias conclusotildees a partir da observaccedilatildeo dos
resultados
A aspirina demonstrou ser significativamente mais eficaz que o paracetamol ou
placebo embora ateacute aos 15 minutos natildeo seja uma diferenccedila muito expressiva
Relativamente agrave AUC240 experiecircncia global da dor no periacuteodo de 4 horas da
investigaccedilatildeo esta foi significativamente menor para o grupo 1
Natildeo existiu diferenccedila significativa entre os grupos no que diz respeito agrave rescue
medication utilizada No entanto o tempo para a administraccedilatildeo da mesma foi
superior no grupo 1 e 2 em relaccedilatildeo ao grupo placebo
Em relaccedilatildeo agrave impressatildeo global natildeo haacute discrepacircncias consideraacuteveis entre grupo 1
e 2 no que diz respeito agrave percentagem de outcomes positivos (58 e 53
respectivamente) O grupo 3 apresentou apenas 31 de outcomes positivos
A tabela com a percentagem de pacientes que desenvolveram efeitos adversos
para cada grupo mostra que 41 dos pacientes apresentaram efeitos secundaacuterios
nos grupos com tratamento activo no entanto muitos destes estavam
relacionados com o procedimento ciruacutergico
A aspirina soluacutevel 900mg providencia uma analgesia mais significante e raacutepida
que o paracetamol 1000mg no periacuteodo imediato apoacutes a cirurgia do 3ordm molar embora natildeo
seja muito expressiva a percepccedilatildeo desta diferenccedila por parte dos pacientes e enfermeiros
51
9 How precise are these results
Os resultados satildeo precisos e apresentados atraveacutes de um intervalo de confianccedila
de 95 satildeo tambeacutem apresentados valores de p
Os valores de p satildeo menores que 005 excepto aos 10 e 15 minutos
Para a intensidade da dor ao longo dos 30 minutos e AUC240 da comparaccedilatildeo
aspirina vs placebo a intervenccedilatildeo utilizada seria a mesma tanto no limite superior
como no inferior excepto aos 10 e 15 minutos Na comparaccedilatildeo aspirina soluacutevel vs
paracetamol soacutelido a decisatildeo seria a mesma independentemente dos limites do intervalo
apenas para os minutos 10 20 e 30
O mesmo aconteceria para a medicaccedilatildeo de recurso (outcome C) e a avaliaccedilatildeo do
tratamento por parte dos pacientes e enfermeiros (outcome D)
Pelo intervalo de confianccedila estar presente e pelo facto de os valores de p serem
bastante reduzidos os resultados satildeo precisos ao ponto de ajudarem a suportar uma
decisatildeo
10 Were all important outcomes considered so the results can be applied
Sim Os pacientes incluiacutedos no estudo o local e o tratamento visados no mesmo
poderiam ser extrapulados e aplicados noutro ambiente O seguimento dos pacientes
durante 4 horas e com ajuda de enfermeiros natildeo se apresenta como muito viaacutevel mas
ainda assim eacute exequiacutevel e seguro
O estudo avalia dados importantes para os profissionais de sauacutede ao afirmar que
a dose (900mg) e a forma (soluacutevel) em que a aspirina eacute tomada conduz a um poder
analgeacutesico superior que o paracetamol No entanto em termos individuais e de poliacuteticas
de sauacutede os efeitos secundaacuterios consequentes da medicaccedilatildeo (excluindo os que se
relacionassem com a cirurgia) deveriam ser completados com estudos suplementares
Segundo este ensaio cliacutenico a incidecircncia de efeitos secundaacuterios natildeo eacute muito
dissemelhante entre aspirina soluacutevel e paracetamol soacutelido nas doses maacuteximas
recomendadas e nestas circunstacircncias a aspirina tem maior poder analgeacutesico Por este
prisma a praacutetica cliacutenica poderia passar pela prescriccedilatildeo de aspirina soluacutevel 900mg para
aliacutevio dor poacutes-operatoacuteria da extracccedilatildeo do terceiro molar Poreacutem eacute necessaacuterio ter em
conta que visa somente a dor nas primeiras quatro horas poacutes-operatoacuterias sendo
importante investigar alternativas eficazes que sejam mais duradouras ou a eficaacutecia e
efeitos secundaacuterios de repetir este tratamento apoacutes as quatro horas iniciais
52
DISCUSSAtildeO
A partir da anaacutelise feita das revisotildees sistemaacuteticas de Weil (19) e de Barden (23)
conclui-se que o paracetamol eacute uma analgeacutesico seguro e eficaz no tratamento da dor
relativa agrave exodontia de terceiros molares pois apresenta um benefiacutecio estatisticamente
significativo quando comparado a placebo Ambas consideram que os melhores valores
de aliacutevio de dor e da diminuiccedilatildeo da intensidade da mesma satildeo alcanccedilados agraves 4 e 6 horas
apoacutes ingestatildeo do faacutermaco
Com base na primeira revisatildeo acima referida o paracetamol exibe uma dose
uacutenica oacuteptima de 1000mg e um periacuteodo de medicaccedilatildeo apropriado de 8 em 8 horas A
maioria dos artigos incluiacutedos apresenta um risco de vieacutes moderado causado
principalmente pela falta de informaccedilatildeo sobre o mecanismo de alocaccedilatildeo de pacientes
podendo levar a uma descredibilidade dos resultados (36)
Na revisatildeo de Barden (23) a comparaccedilatildeo entre os diferentes NSAIDrsquos
demonstrou que este tipo de faacutermacos e particularmente os inibidores da COX-2
exibem os melhores valores de NNT Atraveacutes de uma comparaccedilatildeo indirecta entre
ibuprofeno vs paracetamol os vaacuterios estudos mostraram que o ibuprofeno apresenta
melhores resultados na analgesia da dor poacutes-operatoacuteria (44)
Os estudos de Seymour (22) de Haglund (25) e de Daniels (33) comparam
diferentes compostos activos a um placebo onde o paracetamol estaacute sempre presente
Todos comprovam que enquanto analgeacutesico apresenta uma eficaacutecia largamente
significativa em termos de aliacutevio da dor (usando a escala VAS) Pelo menos 50 dos
indiviacuteduos incluiacutedos que receberam este faacutermaco avaliaram globalmente o tratamento de
forma positiva Poreacutem todos os artigos que
1 Comparam este composto a outro nomeadamente NSAIDrsquos mostram que estes
tecircm uma eficaacutecia significativamente superior agrave do paracetamol tanto em relaccedilatildeo
a valores mais baixos na escala VAS como subjectivamente na avaliaccedilatildeo global
Cerca de 80 dos indiviacuteduos que tomaram NSAIDrsquos classificaram o tratamento
positivamente (agrave excepccedilatildeo dos estudos (32) e (22)) Reportam ainda os efeitos
adversos mais comuns como tonturas naacuteuseas cefaleia e sonolecircncia que
embora de gravidade reduzida tecircm uma incidecircncia superior no paracetamol que
na aspirina e ibuprofeno
53
2 Combinam o paracetamol com NSAIDrsquos provam o efeito aditivo daquele bem
como o facto de estas combinaccedilotildees serem mais eficazes que qualquer um dos
faacutermacos em separado (Merry (13) e Haglund (25))
De acordo com os estudos analisados os NSAIDrsquos aparentam ser uma escolha
preferencial face ao paracetamol porque apresentam uma maior eficaacutecia no aliacutevio da dor
apoacutes extracccedilatildeo de terceiros molares embora disponham de propriedades anti-
inflamatoacuterias notoacuterias (e pertinentes no sucesso do tratamento poacutes-operatoacuterio)
O mecanismo de acccedilatildeo do paracetamol necessita de investigaccedilatildeo adicional que
permita uma melhor compreensatildeo e que traga novas respostas na praacutetica cliacutenica Como
aspecto positivo eacute de acrescentar que natildeo existem diferenccedilas estatisticamente
significantes entre o paracetamol e placebo no que diz respeito a efeitos secundaacuterios
(baixo grau de severidade) podendo ser considerado um composto seguro
A revisatildeo de Barden (23) indica que os resultados da eficaacutecia dos NSAIDrsquos
podem atrair os cliacutenicos a aumentar a sua prescriccedilatildeo sem terem em atenccedilatildeo a sua
relaccedilatildeo com o aumento dos efeitos adversos Isto eacute uma situaccedilatildeo insustentaacutevel na
medida em que nas uacuteltimas duas deacutecadas alguns destes medicamentos foram retirados
do mercado devido a eventos adversos graves posteriormente descobertos Um exemplo
eacute o caso do rofecoxib e valdecoxib que produziram acidentes cardiovasculares seacuterios
provavelmente consequentes da dosagem e natildeo da sua selectividade para a COX-2
(25))
Os efeitos adversos satildeo um motivo de peso para que os pacientes deixem de
tomar determinada substacircncia ou sejam incapazes de tolerar uma dose eficaz da mesma
Informaccedilotildees complementares que englobassem este aspecto seriam ideais e exequiacuteveis
se os autores de ensaios cliacutenicos lhes dessem maior relevo (45)
Outros dados - como custo financeiro e disponibilidade no mercado - poderiam
ser um auxiacutelio na selecccedilatildeo entre paracetamol e outros medicamentos Eacute de ressalvar
que em Portugal os geneacutericos vieram a baixar os preccedilos de analgeacutesicos e NSAIDrsquos
Medicamentos agrave base de ibuprofeno satildeo dos mais dispendiosos (46)
Os NSAIDrsquos tecircm um problema adicional relacionado com a hemostase ndash inibir a
produccedilatildeo de tromboxano A2 e consequentemente aumentar o risco de hemorragia
prolongada (11) No entanto estes efeitos secundaacuterios estatildeo directamente relacionados
com a dosagem pelo que apenas eacute relevante considerar este aspecto em paciente com
problemas de coagulaccedilatildeo
54
Conclui-se que embora a toma de paracetamol seja um procedimento seguro e
eficaz existem no mercado compostos com igual seguranccedila e eficaacutecia superior Apesar
de os inibidores da COX-2 serem os compostos mais eficazes abarcam os efeitos
secundaacuterios mais graves pelo que a realizaccedilatildeo de estudos adicionais eacute imperativo no
sentido de colmatar esta falha
55
RESPOSTA AO PACIENTE
ldquoTendo em conta a evidecircncia cientiacutefica disponiacutevel sobre este assunto e
considerando que natildeo tem problemas gaacutestricos ou de coagulaccedilatildeo sanguiacutenea recomendo
que tome 1g de paracetamol de 8 em 8 horas pois eacute bastante eficaz no aliacutevio da dor
Poreacutem existem outras opccedilotildees como por exemplo combinar o paracetamol a 200mg de
ibuprofeno pode ainda apenas tomar o paracetamol e se sentir necessidade recorrer ao
ibuprofeno 400mg no maacuteximo trecircs vezes ao dia
Tanto o paracetamol como o ibuprofeno tecircm poucos efeitos secundaacuterios e os
mais frequentes satildeo de baixo grau de gravidade Embora existam outros medicamentos
mais eficazes na eliminaccedilatildeo da dor estes tecircm efeitos secundaacuterios mais graves que natildeo
justificam a sua utilizaccedilatildeo
56
REFEREcircNCIAS BIBLIOGRAacuteFICAS
1 Barden J Edwards JE McQuay HJ Andrew Moore R Pain and analgesic
response after third molar extraction and other postsurgical pain Pain 2004107(1-
2)86-90 Epub 20040113
2 Cooper SA Desjardins PJ The value of the dental impaction pain model in drug
development Methods in molecular biology (Clifton NJ) 2010617175-90 Epub
20100326
3 NICE Guidance on the Extraction of Wisdom Teeth2000 13 December 2011
Available from httppublicationsniceorgukguidance-on-the-extraction-of-wisdom-
teeth-ta1clinical-need-and-practice
4 Mettes Dirk TG Nienhuijs Marloes MEL van der Sanden Wil JM Verdonschot
Emiel H Plasschaert A Interventions for treating asymptomatic impacted wisdom teeth
in adolescents and adults Cochrane Database of Systematic Reviews [Internet] 2005
(2) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD003879frameht
ml
5 Seymour RA Use of analgesics in postoperative dental pain a review Journal
of the Royal Society of Medicine 198477(11)949-54 Epub 19841101
6 Berg JM Tymoczko JL Stryer L Biochemistry 5 ed W H Freeman 2002
1050 p
7 Nelson DL Cox MM Lehninger Principles of Biochemistry 5 ed W H
Freeman 2005 1119 p
8 Sciulli MG Capone ML Tacconelli S Patrignani P The future of traditional
nonsteroidal antiinflammatory drugs and cyclooxygenase-2 inhibitors in the treatment
of inflammation and pain Pharmacological reports PR 200557 Suppl66-85 Epub
20060118
9 Devlin TD Devlins Textbook of Biochemistry 6 ed Hoboken NJ Wiley
2006 1208 p
10 Katzung BG Basical and Clinical Pharmacology 10 ed McGraw-Hill 2006
11 Naclerio-Homem Mg Fau - Deboni MCZ Deboni Mc Fau - Rapoport A
Rapoport A Fau - Chin VKL Chin VK Effects of ketoprofen and diclofenac potassium
on blood coagulation tests after removal of third molars (1936-7163 (Electronic))
57
12 Toms L McQuay H Derry S Moore R Single dose oral paracetamol
(acetaminophen) for post-operative pain in adults Cochrane Database of Systematic
Reviews 2008(4)
13 Merry AF Gibbs RD Edwards J Ting GS Frampton C Davies E et al
Combined acetaminophen and ibuprofen for pain relief after oral surgery in adults a
randomized controlled trial British journal of anaesthesia 2010104(1)80-8 Epub
20091217
14 Derry C Derry S Moore R McQuay H Single Dose Oral Ibuprofen for Acute
Post-Operative Pain in Adults Cochrane Database of Systematic Reviews 2009(3)
15 Rang HP Dale MM Ritter JM Moore PK Farmacologia 5 ed Elsevier 2003
Elsevier p
16 Scopel E Alencar M Cruz RM Medidas de avaliaccedilatildeo da dor efdeportes
2007(105)
17 Mata AD Marques D Silveira J Marques J Medicina Dentaacuteria Baseada na
Evidecircncia Novas Opccedilotildees para Velhas Praacuteticas Rev Port Estomatol Cir Maxilofac
200849(1)31-7
18 CASP UK [13 Dezembro 2011] Available from httpwwwcasp-
uknetabout-caspabout-casp
19 Weil K Hooper L Afzal Z Esposito M Worthington Helen V van Wijk A et
al Paracetamol for pain relief after surgical removal of lower wisdom teeth Cochrane
Database of Systematic Reviews [Internet] 2007 (3) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD004487frameht
ml
20 Toms L Derry S Moore RA McQuay Henry J Single dose oral paracetamol
(acetaminophen) with codeine for postoperative pain in adults Cochrane Database of
Systematic Reviews [Internet] 2009 (1) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD001547frameht
ml
21 Derry S Wiffen PJ Moore RA Relative efficacy of oral analgesics after third
molar extraction - a 2011 update Br Dent J 2011211(9)419-20
22 Seymour RA Hawkesford JE Sykes J Stillings M Hill CM An investigation
into the comparative efficacy of soluble aspirin and solid paracetamol in postoperative
pain after third molar surgery Br Dent J 2003194(3)153-7
58
23 Barden J Edwards JE McQuay HJ Wiffen PJ Moore RA Relative efficacy of
oral analgesics after third molar extraction Br Dent J 2004197(7)407-11
24 Saska S Scartezini GR Souza RFd Hochuli-Vieira E Pereira Filho VA
Gabrielli MAC Cloridrato de tramadolparacetamol no controle da dor poacutes-operatoacuteria
em cirurgias de terceiros molares inclusos
Tramadolacetaminophen in the control of postoperative pain for impacted third molar
surgery Rev cir traumatol buco-maxilo-fac 20099(4)
25 Haglund B von Bultzingslowen I Combining paracetamol with a selective
cyclooxygenase-2 inhibitor for acute pain relief after third molar surgery a randomized
double-blind placebo-controlled study European journal of oral sciences
2006114(4)293-301 Epub 20060817
26 Kubitzek F Ziegler G Gold MS Liu JM Ionescu E Analgesic efficacy of low-
dose diclofenac versus paracetamol and placebo in postoperative dental pain Journal of
orofacial pain 200317(3)237-44 Epub 20031003
27 Bjornsson GA Haanaes HR Skoglund LA A randomized double-blind
crossover trial of paracetamol 1000 mg four times daily vs ibuprofen 600 mg effect on
swelling and other postoperative events after third molar surgery British journal of
clinical pharmacology 200355(4)405-12 Epub 20030419
28 Macleod AG Ashford B Voltz M Williams B Cramond T Gorta L et al
Paracetamol versus paracetamol-codeine in the treatment of post-operative dental pain
a randomized double-blind prospective trial Australian dental journal
200247(2)147-51 Epub 20020726
29 Bjornsson GA Haanaes HR Skoglund LA Ketoprofen 75 mg qid versus
acetaminophen 1000 mg qid for 3 days on swelling pain and other postoperative events
after third-molar surgery Journal of clinical pharmacology 200343(3)305-14 Epub
20030318
30 Chopra D Rehan HS Mehra P Kakkar AK A randomized double-blind
placebo-controlled study comparing the efficacy and safety of paracetamol
serratiopeptidase ibuprofen and betamethasone using the dental impaction pain model
International journal of oral and maxillofacial surgery 200938(4)350-5 Epub
20090127
31 Dolci G Ripari M Pacifici L Umile A Evaluation of piroxicam-beta-
cyclodextrin piroxicam paracetamol and placebo in post-operative oral surgery pain
59
International journal of clinical pharmacology research 199414(5-6)185-91 Epub
19940101
32 Noronha VR Gurgel GD Alves LC Noman-Ferreira LC Mendonca LL Aguiar
EG et al Analgesic efficacy of lysine clonixinate paracetamol and dipyrone in lower
third molar extraction a randomized controlled trial Medicina oral patologia oral y
cirugia bucal 200914(8)e411-5 Epub 20090506
33 Daniels S Reader S Berry P Goulder M Onset of analgesia with sodium
ibuprofen ibuprofen acid incorporating poloxamer and acetaminophen--a single-dose
double-blind placebo-controlled study in patients with post-operative dental pain
European journal of clinical pharmacology 200965(4)343-53 Epub 20090303
34 Medve RA Wang J Karim R Tramadol and acetaminophen tablets for dental
pain Anesthesia progress 200148(3)79-81 Epub 20011129
35 Bjornsson GA Haanaes HR Skoglund LA Naproxen 500 mg bid versus
acetaminophen 1000 mg qid effect on swelling and other acute postoperative events
after bilateral third molar surgery Journal of clinical pharmacology 200343(8)849-58
Epub 20030905
36 Marques JF Marques D Silveira J Mata AD Revisotildees Sistemaacuteticas o que satildeo
e para que servem Rev Port Estomatol Cir Maxilofac 200849(3)171-8
37 Rodrigues CL Ziegelmann PK Meta-anaacuteliseum guia praacutetico HCPA
201030(4)436-47
38 Alderson P Absence of evidence is not evidence of absence Bmj
2004328(7438)476-7
39 Berwanger O Suzumura EA Buehler AM Oliveira JB Como Avaliar
Criticamente Revisotildees Sistemaacuteticas e Meta-anaacutelises Revista Brasileira de Terapia
Intensiva 200719(4)475-80
40 Noordzij M Zoccali C Dekker FW Jager KJ Adding up the evidence
systematic reviews and meta-analyses Nephron Clinical practice 2011119(4)c310-6
Epub 20111203
41 Sibbald B Roland M Understanding controlled trials Why are randomised
controlled trials important Bmj 1998316(7126)201
42 Primer on Statistical Significance and P Values Effective Clinical Practice
20014(4)183-4
43 Efird J Blocked randomization with randomly selected block sizes International
journal of environmental research and public health 20118(1)15-20 Epub 20110215
60
44 Cooper S Schachtel B Goldman E Gelb S Cohn P Ibuprofen and
acetaminophen in the relief of acute pain a randomized double blind placebo
controlled study The Journal of Clinical Pharmacology 198929(11)1026-30
45 Edwards JE McQuay HJ Moore RA Collins SL Reporting of Adverse Effects
in Clinical Trials Should Be Improved Lessons from Acute Postoperative Pain Journal
of pain and symptom management 199918(6)427-37
46 Faacutermaco mais vendido versus mais barato Deco Proteste [updated Julho
200919 Dezembro 2011] Available from httpwwwdecoprotesteptservicos-de-
saudefarmaco-mais-vendido-versus-mais-barato-s568081htm
61
ANEXOS
ANEXO A ndash TABELA DE CARACTERIacuteSTICAS DE ARTIGOS EXCLUIacuteDOS
Artigo Fonte Classificaccedilatildeo
inicial Motivo de Exclusatildeo
Toms Derry (20) Cochrane
Library
Possivelmente
Adequado
Natildeo eacute um estudo sobre
extracccedilatildeo de terceiros molares
Saska Scartezini
(24) LILACS
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (27) PubMed Adequado
Estudo natildeo se foca na dor poacutes-
operatoacuteria
Kubitzek Ziegler
(26) PubMed Adequado Artigo natildeo disponiacutevel
Macleod
Ashford (28) PubMed Adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (29) PubMed
Possivelmente
adequado Artigo natildeo disponiacutevel
Chopra Rehan
(30) PubMed
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Dolci Ripari (31) PubMed Possivelmente
adequado Artigo natildeo disponiacutevel
Medve Wang
(34) PubMed
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (35) PubMed
Possivelmente
adequado Artigo natildeo disponiacutevel
62
ANEXO B ndash ARTIGOS INCLUIacuteDOS EM FORMATO
INTEGRALi
i Nota os seguintes artigos estatildeo paginados fora do contexto deste trabalho de acordo com a sua
paginaccedilatildeo original
Paracetamol for pain relief after surgical removal of lower
wisdom teeth (Review)
Weil K Hooper L Afzal Z Esposito M Worthington HV van Wijk A Coulthard P
This is a reprint of a Cochrane review prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2008 Issue 4
httpwwwthecochranelibrarycom
Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
T A B L E O F C O N T E N T S
1HEADER
1ABSTRACT
2PLAIN LANGUAGE SUMMARY
2BACKGROUND
3OBJECTIVES
3METHODS
5RESULTS
8DISCUSSION
9AUTHORSrsquo CONCLUSIONS
9ACKNOWLEDGEMENTS
10REFERENCES
13CHARACTERISTICS OF STUDIES
30DATA AND ANALYSES
Analysis 11 Comparison 1 50 pain relief using pain relief measures Outcome 1 Paracetamol versus placebo number of
people with at least 50 pain relief at 4 hours 31
Analysis 12 Comparison 1 50 pain relief using pain relief measures Outcome 2 Paracetamol versus placebo number of
people with at least 50 pain relief at 6 hours 33
Analysis 21 Comparison 2 50 pain relief using pain intensity measures Outcome 1 Paracetamol versus placebo number
of people with at least 50 pain relief at 4 hours 34
Analysis 22 Comparison 2 50 pain relief using pain intensity measures Outcome 2 Paracetamol versus placebo number
of people with at least 50 pain relief at 6 hours 35
Analysis 31 Comparison 3 Number of people with adverse events Outcome 1 Number of patients with adverse events
paracetamol versus placebo 37
38ADDITIONAL TABLES
42APPENDICES
43WHATrsquoS NEW
43HISTORY
43CONTRIBUTIONS OF AUTHORS
43DECLARATIONS OF INTEREST
44SOURCES OF SUPPORT
44INDEX TERMS
iParacetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
[Intervention Review]
Paracetamol for pain relief after surgical removal of lowerwisdom teeth
Kiaran Weil1 Lee Hooper2 Zahid Afzal3 Marco Esposito1 Helen V Worthington4 Arjen van Wijk5 Paul Coulthard1
1Department of Oral and Maxillofacial Surgery School of Dentistry The University of Manchester Manchester UK 2School of
Medicine Health Policy amp Practice University of East Anglia Norwich UK 3Oral and Maxillofacial Surgery City Hospital Birming-
ham UK 4Cochrane Oral Health Group MANDEC School of Dentistry The University of Manchester Manchester UK 5Social
Dentistry and Behavioural Sciences ACTA Amsterdam Netherlands
Contact address Kiaran Weil Department of Oral and Maxillofacial Surgery School of Dentistry The University of Manchester
Higher Cambridge Street Manchester M15 6FH UK kiaran_weilhotmailcom
Editorial group Cochrane Oral Health Group
Publication status and date Edited (no change to conclusions) published in Issue 4 2008
Review content assessed as up-to-date 21 May 2007
Citation Weil K Hooper L Afzal Z Esposito M Worthington HV van Wijk A Coulthard P Paracetamol for pain relief af-
ter surgical removal of lower wisdom teeth Cochrane Database of Systematic Reviews 2007 Issue 3 Art No CD004487 DOI
10100214651858CD004487pub2
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Paracetamol has been commonly used for the relief of postoperative pain following oral surgery In this review we investigated the
optimal dose of paracetamol and the optimal time for drug administration to provide pain relief taking into account the side effects
of different doses of the drug This will inform dentists and their patients of the best strategy for pain relief after the surgical removal
of wisdom teeth
Objectives
To assess the beneficial and harmful effects of paracetamol for pain relief after surgical removal of lower wisdom teeth compared to
placebo at different doses and administered postoperatively
Search strategy
We searched the Cochrane Oral Health Grouprsquos Trials Register the Cochrane Pain Palliative and Supportive Care Grouprsquos Trials Register
CENTRAL MEDLINE EMBASE and the Current Controlled Trials Register Handsearching included several dental journals We
checked the bibliographies of relevant clinical trials and review articles for studies outside the handsearched journals We wrote to
authors of the identified randomised controlled trials (RCTs) to manufacturers of analgesic pharmaceuticals we searched personal
references in an attempt to identify unpublished or ongoing RCTs No language restriction was applied The last electronic search was
conducted on 24th August 2006
Selection criteria
Randomised parallel group placebo controlled double blind clinical trials of paracetamol for acute pain following third molar surgery
Data collection and analysis
All trials identified were scanned independently and in duplicate by two review authors any disagreements were resolved by discussion
or if necessary a third review author was consulted The proportion of patients with at least 50 pain relief was calculated for both
paracetamol and placebo The number of patients experiencing adverse events andor the total number of adverse events reported were
analysed
1Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Main results
Twenty-one trials met the inclusion criteria A total of 2048 patients were initially enrolled in the trials (1148 received paracetamol
and 892 the placebo) and of these 1968 (96) were included in the meta-analysis (1133 received paracetamol and 835 the placebo)
Paracetamol provided a statistically significant benefit when compared with placebo for pain relief and pain intensity at both 4 and 6
hours Most studies were found to have moderate risk of bias with poorly reported allocation concealment being the main problem
Risk ratio values for pain relief at 4 hours 285 (95 confidence interval (CI) 189 to 429) and at 6 hours 332 (95 CI 188 to 587)
A statistically significant benefit was also found between up to 1000 mg and 1000 mg doses the higher the dose giving greater benefit
for each measure at both time points There was no statistically significant difference between the number of patients who reported
adverse events overall this being 19 in the paracetamol group and 16 in the placebo group
Authorsrsquo conclusions
Paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom teeth
P L A I N L A N G U A G E S U M M A R Y
Paracetamol for pain relief after surgical removal of lower wisdom teeth
The surgical removal of wisdom teeth (third molars) is the most commonly performed surgical procedure undertaken in oral surgery
practice Postoperative complications may include swelling bruising and limited mouth opening but patients are most often concerned
about postoperative pain which may be severe Paracetamol is effective in relieving pain with a low incidence of adverse effects It is one
of the most commonly used analgesics and is widely available without prescription around the world In this review we investigated the
optimal dose of paracetamol and the optimal time for drug administration to provide pain relief after the surgical removal of wisdom
teeth The side effects of different doses of the drug were also explored
Twenty-one trials (with over 2000 participants) were included Paracetamol provided a statistically significant benefit when compared
with placebo for pain relief at both 4 and 6 hours after taking the drug It is most effective at 1000 mg dose and can be taken at six
hourly intervals without compromising safety There was no statistically significant difference between the number of patients who
reported adverse events overall this being 19 in the paracetamol group and 16 in the placebo group It should be noted that most
of the studies were found to have some limitations mainly due to poor reporting of information However the review concludes that
paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom teeth
B A C K G R O U N D
The surgical removal of wisdom teeth is the most commonly per-
formed surgical procedure undertaken in oral surgery practice
Postoperative complications may include swelling bruising and
limited mouth opening but patients are most often concerned
about postoperative pain which may be severe The pain ex-
perienced after oral surgery is a validated and widely used pain
model for the clinical evaluation of analgesic efficacy (Cooper
1976) Tissue damage produced during surgery releases chemicals
that initiate inflammatory pain by activating and sensitising nerve
fibre receptors (Loeser 1999) Chemicals include bradykinin
prostaglandins serotonin and histamine (Dray 1997)
Paracetamol (acetaminophen) is a nonopioid analgesic possessing
antipyretic activity and is effective in relieving pain with a low in-
cidence of adverse effects (Moore 1998) It is one of the most com-
monly used analgesics and is widely available without prescription
around the world Paracetamol is often grouped with the nons-
teroidal anti-inflammatory drug (NSAID) family however it is
considered only to have relatively weak anti-inflammatory activity
(Rang 2003) NSAIDs are assumed largely to produce their anal-
gesia as a result of the inhibition of prostaglandin production by
the enzyme cyclo-oxygenase (Malmberg 1992) The mechanism
of action has not been fully understood Among several theories
it has been suggested that paracetamol is a selective inhibitor of
the newly described COX-3 enzyme a cyclo-oxygenase-1 variant
in the central nervous system This inhibition could represent a
primary central mechanism by which paracetamol decreases pain
and possibly fever (Chandrasekharan 2002) Major evidence has
2Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
been accumulated showing that paracetamol inhibits cyclo-oxy-
genase by reducing the higher oxidative state of the cyclo-oxyge-
nase enzyme by reducing oxygen radical co-substrates (Aronoff
2006) Paracetamol has been shown to be an effective analgesic in
the control of postoperative dental pain in a number of clinical
trials (Bentley 1987 Kiersch 1994 Mehlisch 1990) Pain inten-
sity following third molar surgery has been suggested to reach its
maximum between 3 to 5 hours following surgery (Fisher 1988
Seymour 1985) and therefore this pain model is used to test the
efficacy of a single analgesic dose
A recent systematic review (Barden J 2004) has looked at the ef-
ficacy and safety of paracetamol for postoperative pain manage-
ment and has included the findings of studies involving a wide
variety of types of surgery such as gynaecology surgery abdomi-
nal surgery orthopaedic surgery amongst others including the re-
moval of wisdom teeth There is some debate as to whether dental
pain is different from other pain It has been suggested that the
effect of some analgesics including tramadol were worse for dental
pain than for other types of postsurgical pain (Moore 1997)
In this review we investigated the optimal dose of paracetamol and
the optimal time for drug administration to provide pain relief
taking into account the side effects of different doses of the drug
This will inform dentists and their patients of the best strategy for
best pain relief after the surgical removal of wisdom teeth
O B J E C T I V E S
To assess the beneficial and harmful effects of paracetamol for
pain relief after surgical removal of lower wisdom teeth compared
to placebo at different doses and administered preoperatively or
postoperatively
Primary
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between paracetamol and placebo for pain
relief in patients requiring surgical removal of a lower wisdom
tooth or teeth against the alternative hypothesis of a difference
Secondary
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between different doses of paracetamol for
pain relief in patients requiring surgical removal of a lower
wisdom tooth or teeth against the alternative hypothesis of a
difference
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between different times of administration of
paracetamol for pain relief in patients requiring surgical removal
of a lower wisdom tooth or teeth against the alternative
hypothesis of a difference
M E T H O D S
Criteria for considering studies for this review
Types of studies
All randomised controlled double blind clinical trials
Types of participants
Patients of all health states who required the surgical removal of
a lower wisdom tooth and who had at least had a baseline pain
intensity of moderate to severe pain Patients who also required
removal of an additional tooth or teeth were included Surgery
was undertaken under local anaesthesia intravenous sedation or
general anaesthesia Patients taking concurrent analgesia were ex-
cluded
Types of interventions
Efficacy
bull Paracetamol given as a single dose by mouth in any dose
and in any formulation (for example immediate or slow release)
regardless of when the single dose was given (for example
preoperatively or postoperatively)
Side effects
In order to investigate side effects more thoroughly we included
both single and multiple dose studies
bull Paracetamol given up to 7 days by mouth in any dose and
in any formulation (for example immediate or slow release)
regardless of when the first dose was given (for example
preoperatively or postoperatively)
Types of outcome measures
bull Pain intensity (visual analogue scale (VAS) categorical
verbal rating verbal numerical scale global subjective efficacy
ratings and other categorical rating scales)
bull Pain relief (VAS categorical verbal rating verbal numerical
scale global subjective efficacy ratings and other categorical
rating scales) and derived pain relief outcomes extracted will be
3Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
total pain relief (TOTPAR) summed pain intensity difference
(SPID) over 4 and 6 hours
bull Side effects (for example hepatic and renal) (binary)
Search methods for identification of studies
To identify studies for inclusion or consideration in this review a
detailed search strategy was developed for each database searched
These were based on the search strategy developed for MEDLINE
but revised appropriately for each database The search strategy
combined a sensitive search strategy for randomised controlled
trials (RCTs) revised from phases 1 and 2 of the Cochrane Sensi-
tive Search Strategy for RCTs (as published in Appendix 5b in the
Cochrane Handbook for Systematic Reviews of Interventions 426
(updated September 2006)) The subject search used a combina-
tion of controlled vocabulary and free text terms based on the
search strategy for searching CENTRAL (see Appendix 1)
Databases to be searched
The Cochrane Oral Health Grouprsquos Trials Register (to 24th August
2006)
The Cochrane Central Register of Controlled Trials (CENTRAL)
(The Cochrane Library 2006 Issue 3)
The Cochrane Pain Palliative and Supportive Care Grouprsquos Trials
Register (to 24th August 2006)
MEDLINE (1966 to 24th August 2006)
EMBASE (1980 to 25th August 2006)
Current Controlled Trials Register (wwwcontrolled-trialscom)
(to 24th August 2006)
The bibliographies of papers and review articles were checked for
studies outside the handsearched journals Personal references were
also searched
Language
There were no language restrictions and where necessary transla-
tion into the English language of relevant studies was conducted
Unpublished studies
Authors of RCTs identified were written to in order to obtain
further information about the trial and to attempt to identify
unpublished or ongoing studies We also wrote to manufacturers
of analgesic pharmaceuticals
Handsearching
Several journals relevant to this review were handsearched as part
of the Cochrane Oral Health Grouprsquos ongoing journal hand-
searching programme The list of the dental journals hand-
searched by The Cochrane Collaboration can be found at http
wwwohgcochraneorg
Data collection and analysis
The titles and abstracts (when available) of all reports identified
were scanned independently and in duplicate by two review au-
thors For studies appearing to meet the inclusion criteria or for
which there were insufficient data in the title and abstract to make
a clear decision the full report was obtained and assessed indepen-
dently and in duplicate by two review authors to establish whether
the studies met the inclusion criteria or not Disagreements were
resolved by discussion Where resolution was not possible a third
review author was consulted All studies meeting the inclusion
criteria then underwent quality assessment and data extracted
Studies rejected at this or subsequent stages were recorded in the
Characteristics of excluded studies table and reasons for exclusion
were recorded
Quality assessment
The quality assessment of the included trials was undertaken inde-
pendently and in duplicate by two review authors based on what
is written in the articles
Only double blind trials were included in the review so blinding
was not included in the quality assessment
Two main quality criteria were examined
(1) Allocation concealment recorded as
(A) Adequate -2 points
(B) Unclear - 1 point
(C) Inadequate - 0 points
(2) Completeness of follow up (is there a clear explanation for
withdrawals and drop outs in each treatment group) assessed as
(A) Yes - 1 point
(B) No - 0 points
The agreement for the quality criteria between assessors was de-
termined by Kappa statistics
After taking into account the additional information provided by
the authors of the trials studies were grouped into the following
categories
(A) Low risk of bias - 3 points (plausible bias unlikely to seriously
alter the results) if all criteria were met
(B) Moderate or high risk of bias - 0 to 2 points Moderate risk
of bias - plausible bias that raises some doubt about the results if
one or more criteria are partly met (for example when authors
responded that they had made some attempts to conceal the al-
location of patients to give an explanation for withdrawals but
these attempts were not judged to be ideal these criteria were cat-
egorised as rsquopartlyrsquo) High risk of bias - plausible bias that seriously
weakens confidence in the results if one or more criteria were not
met as described in the Cochrane Handbook for Systematic Reviews
of Interventions 426
We also reported whether the authors of included trials have con-
ducted a sample size calculation
4Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data extraction
Data were extracted by two review authors independently and
in duplicate using specially designed data extraction forms Any
disagreement was discussed and a third review author consulted
where necessary Authors were contacted for clarification of miss-
ing information Data were excluded until further clarification was
available if agreement could not be reached
For each trial the following data were recorded
bull Year of publication country of origin setting and source of
study funding
bull Details of the participants including demographic
characteristics and criteria for inclusion
bull Details on the study design (parallel group or cross-over
design)
bull Details on the type of intervention
bull Details of the outcomes reported including method of
assessment and time intervals
Data synthesis
From the mean total pain relief (TOTPAR) or summed pain in-
tensity difference (SPID) pain indices reported we computed a
dichotomous outcome variable for the number of patients with
at least 50 pain relief according to the methods outlined in a
Cochrane review (Collins 1999) For each of the three objectives
we examined the appropriateness of different continuous outcome
measurements and these were meta-analysed and reported in the
final review
For dichotomous outcomes the estimate of an intervention was
expressed as risk ratios together with 95 confidence intervals
For continuous outcomes mean differences and 95 confidence
intervals were used to summarise the data for each trial
Clinical heterogeneity was assessed by examining the types of par-
ticipants interventions and outcomes in each study Meta-analyses
were conducted only with studies of similar comparisons report-
ing the same outcome measures Risk ratios were used to combine
dichotomous data and mean differences for continuous data us-
ing random-effects models The significance of any discrepancies
in the estimates of the treatment effects from the different trials
was assessed by means of Cochranrsquos test for heterogeneity and any
heterogeneity investigated
Where both visual analogue scale (VAS) and categorical scales were
used to measure pain intensity or pain relief or both the categorical
data were used in the meta-analysis as this was the most frequently
used scale
Subgroup analyses
Subgroup analyses were planned for studies
bull Where patients underwent surgery with local anaesthesia
alone local anaesthesia and intravenous sedation general
anaesthesia alone and general anaesthesia with local anaesthetic
bull Where different types of formulation of paracetamol were
used for instance immediate release versus slow release
bull Where different doses of paracetamol were used (1000 mg
or more and less than 1000 mg)
bull Where time of administration of paracetamol differs
preoperative versus postoperative
bull Where TOTPAR was calculated using pain relief measures
and pain intensity measures
The difference between studies comparing up to 1000 mg doses
with studies comparing 1000 mg or more was examined by per-
forming random-effects metaregression analyses in Stata version
90 (Stata Corporation USA) using the program Metareg
The results of the metaregressions for comparing the two dose
levels up to 1000 mg and 1000 mg or more are presented in
Additional Table 1
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
See Characteristics of included studies and Characteristics of
excluded studies tables
Characteristics of the trial setting and investigators
Of the 67 eligible trials 46 were excluded as shown in the ex-
cluded studies section Of the 21 included studies one was con-
ducted in Denmark (Moller 2000) two in Germany (Kubitzek
2003 Lehnert 1990) one in Italy (Dolci 1994) one in Nor-
way (Skoglund 1991) two in Puerto Rico (Olson 2001 Sunshine
1986) one in Thailand (Vattaraphudej 1986) two in the United
Kingdom (Seymour 1996 Seymour 2003) and 11 in the United
States of America (Cooper 1980 Cooper 1981 Cooper 1988
Cooper 1998 Dionne 1994 Forbes 1984b Forbes 1989 Forbes
1990 Hersh 2000 Kiersch 1994 Mehlisch 1995) Six trials
were conducted at university clinics (Cooper 1998 Hersh 2000
Moller 2000 Olson 2001 Sunshine 1986 Vattaraphudej 1986)
five at private practices (Dionne 1994 Forbes 1984b Forbes
1989 Forbes 1990 Kubitzek 2003) seven did not state a set-
ting (Cooper 1981 Dolci 1994 Kiersch 1994 Mehlisch 1995
Seymour 1996 Seymour 2003 Skoglund 1991) One reported a
single site (Cooper 1988) two reported two sites (Forbes 1989
Seymour 2003) and six specifically stated outpatients (Cooper
1980 Cooper 1988 Forbes 1989 Forbes 1990 Hersh 2000
5Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Lehnert 1990) Seventeen trials were sponsored by industry
(Cooper 1981 Cooper 1988 Cooper 1998 Dionne 1994 Forbes
1984b Forbes 1989 Forbes 1990 Hersh 2000 Kiersch 1994
Kubitzek 2003 Lehnert 1990 Mehlisch 1995 Moller 2000
Olson 2001 Seymour 2003 Skoglund 1991 Sunshine 1986)
one by a university grant (Vattaraphudej 1986) and it was unclear
as whether the remaining three trials (Cooper 1980 Dolci 1994
Seymour 1996) were sponsored but it is likely that they were from
correspondence with some of the authors
Characteristics of interventions
All included interventions were randomised parallel group and
double blind Eleven trials used doses of paracetamol of less than
1000 mg (Cooper 1980 Cooper 1981 Cooper 1988 Dionne
1994 Dolci 1994 Forbes 1984b Forbes 1989 Forbes 1990
Seymour 1996 Sunshine 1986 Vattaraphudej 1986) Eleven tri-
als used doses of 1000 mg (Cooper 1998 Hersh 2000 Kiersch
1994 Kubitzek 2003 Lehnert 1990 Mehlisch 1995 Moller
2000 Olson 2001 Seymour 1996 Seymour 2003 Skoglund
1991) One study (Seymour 1996) used both doses Seven tri-
als used paracetamol in tablet form (Dolci 1994 Forbes 1989
Kubitzek 2003 Mehlisch 1995 Moller 2000 Seymour 2003
Skoglund 1991) Seven trials used capsules (Forbes 1984b Forbes
1989 Forbes 1990 Kiersch 1994 Lehnert 1990 Sunshine 1986
Vattaraphudej 1986) Two trials used caplets (Hersh 2000 Olson
2001) and one trial used effervescent tablets (Moller 2000) Five
trials did not state what formulation was used (Cooper 1980
Cooper 1981 Cooper 1988 Cooper 1998 Dionne 1994) All
trials used placebos in the same formulation as the intervention
Characteristics of outcome measures
For all trials it was possible to calculate the number of patients
with at least 50 total pain relief (TOTPAR) at either 4 hours
6 hours or both Pain intensity was measured in all but one trial
(Kubitzek 2003) pain relief was measured in all but two trials
(Kubitzek 2003 Seymour 2003) Kubitzek 2003 gave a figure for
TOTPAR at six hours and Seymour 2003 measured pain intensity
only Fifteen trials measured pain intensity at 4 hours using a 4-
point categorical scale of 0 to 3 where 0 was no pain at all and 3
was severe pain Five trials measured pain intensity using a visual
analogue scale (VAS) of 0 to 100 mm where 0 was no pain and
100 was the worst pain imaginable Twelve trials measured pain
intensity at 6 hours using a 4-point categorical scale where 0 was
no pain and 3 was severe pain and three trials measured pain
intensity at 6 hours using a VAS of 0 to 100 mm where 0 was no
pain and 100 mm was the worst pain imaginable Sixteen trials
measured pain relief at 4 hours using a 5-point categorical scale
of 0 to 4 where 0 was none and 4 was complete pain relief two
trials measured pain relief at 4 hours using a VAS of 0 to 100 mm
in one trial 0 was none and 100 was complete relief and in the
other trial 0 was complete relief and 100 was no relief (these data
were reversed for statistical purposes) Twelve trials measured pain
relief at 6 hours using a 5-point categorical scale of 0 to 4 where
0 was none and 4 was complete pain relief two trials measured
pain relief at 6 hours using a VAS of 0 to 100 mm in one trial 0
was none and 100 was complete relief and in the other trial 0 was
complete relief and 100 was no relief (these data were reversed for
statistical purposes)
Adverse events and global assessments were recorded in most of
the trials Nineteen trials reported the number of patients with
side effects eight for doses of 1000 mg or more and 15 for doses
of less than 1000 mg Fifteen trials reported the number of adverse
events seven for doses of 1000 mg or more and eight for doses
of less than 1000 mg Fourteen trials recorded global assessment
using a 5-point categorical scale of either 0 to 4 or 1 to 5 where
0 or 1 was poor and 4 or 5 was excellent and four trials used a
4-point categorical scale of 0 to 3 where 0 was poor and 3 was
excellent
Risk of bias in included studies
Details of the quality assessment are presented in Additional Table
2 Seven out of the 21 studies reported adequate concealed al-
location for the remaining studies it was unclear Over half of
the studies (1121) gave clear explanation of withdrawals or drop
outs Taking these two factors into account only three trials were
assessed as being at low risk of bias
Effects of interventions
Comparison 1 Paracetamol versus placebo using
pain relief measurements
(Comparison 1 Outcome 11 amp Comparison 1 Outcome 12)
(Analysis 11 Analysis 12)
There are 16 studies providing pain relief measurements for com-
paring paracetamol versus placebo at 4 hours 11 at doses up to
1000 mg and 5 at doses of 1000 mg Overall there was a highly
statistically significant benefit with the paracetamol with risk ratio
(RR) values for achieving 50 pain relief for all doses of parac-
etamol for 4 hours RR 285 (95 confidence interval (CI) 189
to 429) Chi2 = 6294 degrees of freedom (df ) = 15 P lt 0001
I2 = 76 number needed to treat (to benefit) (NNT) 4 (95
CI 3 to 4) The statistically significant benefit was apparent for
both subgroups with RR for up to 1000 mg 196 (95 CI 134
to 286) Chi2 = 2644 df = 9 P = 0002 I2 = 660 NNT 4
(95 CI 3 to 5) and RR for 1000 mg 456 (95 CI 286 to
727) Chi2 = 544 df = 5 P = 036 I2 = 82 NNT 3 (95
CI 3 to 4) Although both had a statistically significant benefit
6Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
over placebo there was a statistically significant difference between
the two subgroups with an enhanced benefit for the higher doses
(metaregression P lt 0001 Additional Table 3) This subgroup
analysis explained some of the heterogeneity in the overall com-
parison however there is still some unexplained heterogeneity be-
tween the trials in the up to 1000 mg dose comparison
There are 13 studies providing pain relief measurements for com-
paring paracetamol versus placebo at 6 hours 6 doses up to 1000
mg paracetamol and 7 doses of 1000 mg paracetamol Overall
there was a highly statistically significant benefit with the parac-
etamol with RR values for 50 pain relief at 6 hours RR 332
(95 CI 188 to 587) Chi2 = 6335 df = 12 P lt 000001 I2 = 811 NNT 3 (95 CI 3 to 4) The statistically significant
benefit was apparent in both subgroups with RR for up to 1000
mg 189 (95 CI 098 to 367) Chi2 = 1445 df = 5 P = 001
I2 = 654 NNT 6 (95 CI 4 to 10) and RR for 1000 mg
421 (95 CI 297 to 598) Chi2 = 509 df = 6 P = 053 I2 =
0 NNT 3 (95 CI 2 to 3) Although both had a statistically
significant benefit over placebo there was a statistically significant
difference between the two subgroups with an enhanced benefit
for the higher doses (metaregression P lt 0001 Additional Table
3) This subgroup analysis explained some of the heterogeneity in
the overall comparison however there is still some unexplained
heterogeneity between the trials in the up to 1000 mg dose com-
parison
Comparison 2 Paracetamol versus placebo using
pain intensity difference measurements
(Comparison 2 Outcome 21 amp Comparison 2 Outcome 22)
(Analysis 21 Analysis 22)
There are 18 studies providing pain intensity measurements for
comparing paracetamol versus placebo at 4 hours 10 at doses up
to 1000 mg and 8 at doses of 1000 mg Overall there was a highly
statistically significant benefit with paracetamol with RR values
for 50 pain relief at 4 hours RR 487 (95 CI 283 to 837)
Chi2 = 4973 df = 17 P lt 00001 I2 = 658 NNT 3 (95 CI
3 to 5) The statistically significant benefit was apparent in both
subgroups with RR up to 1000 mg 433 (95 CI 219 to 858)
Chi2 = 2622 df = 9 P = 0002 I2 = 657 NNT 3 (95 CI
3 to 4) and RR for 1000 mg 646 (95 CI 234 to 1785) Chi2 = 2347 df = 7 P = 0001 I2 = 702 NNT 4 (95 CI 3
to 5) Both had a statistically significant benefit over placebo but
there was no statistically significant difference between the two
subgroups (metaregression P = 067 Additional Table 3)
There are 14 studies providing pain intensity measurements for
comparing paracetamol versus placebo at 6 hours 6 at doses up
to 1000 mg and 8 at doses of 1000 mg Overall there was a highly
statistically significant benefit with paracetamol with RR values
for 50 pain relief RR 341 (95 CI 234 to 497) Chi2 = 1823
df = 13 P = 015 I2 = 287 NNT 4 (95 CI 3 to 4) The
statistically significant benefit was apparent in both groups with
RR up to 1000 mg 267 (95 CI 146 to 490) Chi2 = 705 df
= 5 P = 022 I2 = 291 NNT 5 (95 CI 3 to 7) and RR for
1000 mg 396 (95 CI 252 to 623) Chi2 = 863 df = 7 P =
028 I2 = 189 NNT 3 (95 CI 3 to 4) Both had a statisti-
cally significant benefit over placebo but there was no statistically
significant difference between the two subgroups (metaregression
P = 015 Additional Table 3)
Comparison 3 Number of patients with adverse
events for paracetamol versus placebo
(Comparison 3 Outcome 31) (Analysis 31)
There are 17 studies that reported the number of patients with
adverse events for paracetamol versus placebo 9 studies used less
than 1000 mg and 8 studies used 1000 mg There was no statisti-
cally significant difference in any group For all doses of paraceta-
mol the RR for an adverse event RR 119 (95 CI 090 to 157)
Chi2 = 2073 df = 15 P = 015 I2 = 276 number needed to
treat to harm (NNTH) 33 (95 CI 143 to infinity) For doses of
less than 1000 mg RR 125 (95 CI 069 to 225) Chi2 = 906
df = 7 P = 025 I2 = 228 NNTH 33 (95 CI 143 to infinity)
For 1000 mg paracetamol RR 116 (95 CI 084 to 160) Chi2
= 1096 df = 7 P = 014 I2 = 362 NNTH 33 (95 CI 125
to infinity)
Subgroup analyses
Where patients underwent surgery with local anaesthesia
alone local anaesthesia and intravenous sedation general
anaesthesia alone and general anaesthesia with local
anaesthetic
When the data were reviewed it was not possible to do a meta-anal-
ysis Of the 21 included studies 7 did not state what anaesthesia
was used 7 used combinations of anaesthesia but were unclear in
reporting which patients received which anaesthesia 4 used local
anaesthetic only and 3 used general anaesthetic only
Where different types of formulation of paracetamol were
used (immediate release versus slow release)
Most included studies did not report on the formulation other
than to say whether it was tablets capsules or caplets Only one
7Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
paper indicated that their study used effervescent tablets (Moller
2000) and their results showed that effervescent tablets gave a faster
onset of pain relief Median value for time to onset of analgesia
was 20 minutes in the effervescent group and 45 minutes in the
tablet group and time to meaningful pain relief was 45 minutes
in the effervescent group and 1 hour in the tablet group However
at the end of a 4-hour period pain relief was better in the tablet
group (44) than the effervescent group (37)
Where different doses of paracetamol were used (1000 mg
or more and less than 1000 mg)
This meta-analysis was conducted 11 studies used doses of 1000
mg or more and 11 studies used doses of less than 1000 mg
(Seymour 1996 used both doses)
NNT for lt 1000 mg of paracetamol is 4 (95 CI 3 to 5) at
4 hours and 6 (95 CI 4 to 10) at 6 hours (using pain relief
measurements)
NNT for lt 1000 mg of paracetamol is 3 (95 CI 3 to 4) at 4 hours
and 5 (95 CI 3 to 7) at 6 hours (using intesity measurements)
NNT for 1000 mg of paracetamol is 3 (95 CI 3 to 4) at 4 hours
and 3 (95 CI 2 to 3) at 6 hours (using pain relief measurements)
NNT for 1000 mg of paracetamol is 4 (95 CI 3 to 5) at 4 hours
and 3 (95 CI 3 to 4) at 6 hours (using intensity measurements)
Where time of administration of paracetamol differs
preoperative versus postoperative
No included study used a preoperative dose as the patients did
not reach moderate or severe pain before the intervention
Where total pain relief (TOTPAR) was calculated using pain
relief measures and pain intensity measures
This meta-analysis was undertaken where the relevant data were
available 16 studies had pain relief data and 17 studies had pain
intensity data
NNT using pain relief scales for lt 1000 mg of paracetamol is 4
(95 CI 3 to 5) at 4 hours and 6 (95 CI 4 to 10) at 6 hours
NNT using pain intensity scales for lt 1000 mg of paracetamol is
3 (95 CI 3 to 4) at 4 hours and 5 (95 CI 3 to 7) at 6 hours
NNT using pain relief scales for 1000 mg of paracetamol is 3 (95
CI 3 to 4) at 4 hours and 3 (95 CI 2 to 3) at 6 hours
NNT using pain intensity scales for 1000 mg of paracetamol is 4
(95 CI 3 to 5) at 4 hours and 3 (95 CI 3 to 4) at 6 hours
D I S C U S S I O N
The results show paracetamol to be an effective analgesia for use
following third molar surgery The number needed to treat (to
benefit) (NNTs) and number needed to treat to harm (NNTHs)
support the use of 1000 mg as an optimal dose It is effective over
both 4 and 6 hours In considering the use of pain relief or pain
intensity difference as a measure of efficacy it was of interest that
metaregression showed that pain relief scales showed a statistically
significant difference for increased dose and pain intensity did
not It is acknowledged that this review only considered single
dose studies when considering efficacy multidosed studies may be
considered when updating the review The NNTs and NNTHs
found in this review are similar to those recorded by a systematic
review (Barden J 2004) where they investigated paracetamol for
pain involving various types of surgery This would confirm yet
again the value of the third molar pain model showing that dental
pain is comparable with pain from other sources The implemen-
tation of NICE (National Institute for Health and Clinical Excel-
lence) Guidelines for removal of third molars has led to a decrease
in the performance of this surgery which may have an adverse
effect on the number of trials able to use the third molar model
In the United States of America such guidelines have not yet been
adopted It is of interest that in striving to provide evidence based
treatment the opportunity for research using the third molar pain
model may be adversely affected
The data available for adverse events show that NNTH for lt 1000
mg of paracetamol is 33 (143 to infinity) for 1000 mg of parac-
etamol is 33 (125 to infinity) and for all doses 33 (143 to infin-
ity) suggesting it is an extremely safe drug Only one severe ad-
verse event was recorded by any researchers and that was a severe
headache (Olson 2001) two other participants stopped taking
paracetamol because of vomiting However there was a high degree
of inconsistency across the trials in the way that adverse events were
recorded raising the concern that only adverse events considered
by the researchers to be attributable to paracetamol were recorded
with some trials recording many AEs and some reporting none
The diverse way in which adverse events were recorded led to there
being over 20 categories of adverse events The main categories
are shown in Additional Table 4 Of interest are adverse events
where placebo scored more highly than paracetamol which could
suggest that paracetamol may possibly have a beneficial effect eg
dry socket but this would require further investigation As all pa-
tients had surgery and various combinations of local anaesthesia
general anaesthesia and sedation making it difficult to ascertain
which effects are directly related to the intervention However the
results strongly support the use of paracetamol in doses up to 1000
mg as a safe effective analgesia
8Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
The efficacy of paracetamol decreases with times and the recom-
mended interval between doses is 8 hours which would suggest
there may be some benefit in a slow release formulation None of
the studies in this trial used a slow release formulation but a trial
(Coulthard 2001) compared sustained release and standard release
formulations of paracetamol and found that the sustained release
was statistically significantly more effective at 6 and 8 hours with
no loss of efficacy at 4 hours Safety for both formulations was
comparable making sustained release paracetamol a safe and ef-
fective choice
The methodology used in the included trials was generally good
This resulted in a large number of participants being included
in this meta-analysis while using only double blind randomised
trials The included trials gave a strong consistent result Many
of the trials were done by researchers with extensive experience
in the field of pain research whose methods have been refined
with experience A large proportion of the trials were done in the
United States and were mostly funded by pharmaceutical com-
panies This seems to be reflected in the methodology However
quality assessment showed there were only three trials with a low
risk of bias and 18 with moderatehigh risk This was mainly the
result of unreported allocation concealment methods In speaking
to some of the authors it is highly likely that the allocation con-
cealment was good in all the trials but that the details were not
well reported Most trials were sponsored by pharmaceutical com-
panies who supplied paracetamol and placebo in identical appear-
ance The reporting of withdrawals and drop outs was sporadic
and even when numbers were cited it was not always clear to which
treatment group the participant had been originally allocated
Mean global assessments (Additional Table 5 Table 6 Table 7
Table 8) all showed higher scores for paracetamol than placebo
It is of interest that despite achieving 50 pain relief participants
did not record 50 on a global assessment scale This again raises
the question of the value of the instruments used to measure the
efficacy of an intervention None of the trials relied on global
assessments as their only measure of efficacy but this information
could be of value to other researchers It raises interesting questions
concerning patientrsquos expectations and the difficulties associated
with quantifying such a subjective experience
A lot of valuable information was gathered incidental to the main
findings in most of the trials So though the topic was concerned
with the use of paracetamol for pain information collected in
many of the trials shed valuable light on subjects such as side effects
measuring instruments and methodology Further appraisal of
the multidisciplinary approach to research a broader view of data
collection and a more accurate reporting of data already collected
could be extremely valuable in the future It would allow research
to be more widely used in various meta-analyses Data from areas
seemingly unrelated to the original null hypothesis eg comparison
of pain relief and pain intensity as a measuring tool adverse event
reporting the significance of global assessments etc could be more
readily available If the third molar trial population does decrease
it would be advantageous to collect as much data as possible from
any trial being undertaken
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
Paracetamol (acetaminophen) is an effective drug to use for post-
operative pain following oral surgery and the reporting of adverse
events shows it to be a safe drug (number needed to treat (to ben-
efit) (NNT) is 3 for 1000 mg of paracetamol at 6 hours number
needed to treat to harm (NNTH) 33) It is most effective at 1000
mg dose and can be taken at six hourly intervals without compro-
mising safety It could be considered more readily by dentist and
patients both as a first choice analgesic or to be taken alternately
with doses of other analgesics such as nonsteroidal anti-inflamma-
tory drugs (NSAIDS)
Implications for research
There is a large body of research in this area and further research
other than as a comparison seems unnecessary However in one
trial (Moller 2000) it was found that an effervescent formulation
appeared to have a faster onset of pain relief which would be
beneficial to patients who are looking for a rapid onset of relief
It may be helpful to undertake some research to confirm these
findings The use of pain relief and pain intensity difference as a
measure of pain relief may be another area for further investigation
It is valuable to have NNTNNTH as a baseline for comparison
with other analgesics Maximizing the third molar pain model
population by multidisciplinary research is another area of interest
highlighted by this review
A C K N O W L E D G E M E N T S
We wish to thank Sylvia Bickley (Cochrane Oral Health Group)
for her assistance with literature searching and Luisa Fernandez
Mauleffinch (Cochrane Oral Health Group) for her help with the
preparation of this review We would also like to thank the follow-
ing referees who reviewed this work at various stages Barry El-
liott Cole Mike Hill Kimito Yamashiro and Lasse Skoglund We
are grateful to Stephen Cooper Donald Mehlisch Philip Moller
Alberto Umile for providing information on their trials and to
Prisana Pripatnanont for translation and information
9Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Cooper 1980 published data only
Cooper SA Precheur H Rauch D Rosenheck A Ladov M
Engel J Evaluation of oxycodone and acetaminophen in
treatment of postoperative dental pain Oral Surgery Oral
Medicine and Oral Pathology 198050(6)496ndash501
Cooper 1981 published data only
Cooper SA Breen JF Giuliani RL The relative efficacy of
indoprofen with opiod-analgesic combinations Journal of
Oral Surgery 198139(1)21ndash5
Cooper 1988 published data only
Cooper SA Firestein A Cohn P Double-blind comparison
of meclofenamate sodium with acetaminophen
acetaminophen with codeine and placebo for relief of
postsurgical dental pain The Journal of Clinical Dentistry
19881(2)31ndash4
Cooper 1998 published data only
Cooper SA Reynolds DC Reynolds B Hersh EV Analgesic
efficacy and safety of (R)- ketoprofen in postoperative dental
pain Journal of Clinical Pharmacology 199838(2 Suppl)
11Sndash18S
Dionne 1994 published data only
Dionne RA Snyder J Hargreaves KM Analgesic efficacy
of flurbiprofen in comparison with acetaminophen
acetaminophen plus codeine and placebo after impacted
third molar removal Journal of Oral and Maxillofacial
Surgery 199452(9)919ndash24
Dolci 1994 published data only
Dolci G Ripari M Pacifici L Umile A Evaluation of
piroxicam-beta-cyclodextrin piroxicam paracetamol and
placebo in post-operative oral surgery pain International
Journal of Clinical Pharmacology Research 199414(5-6)
185ndash91
Forbes 1984b published data only
Forbes JA Barkaszi BA Ragland RN Hankle JJ
Analgesic effect of acetaminophen phenyltoloxamine
and their combination in postoperative oral surgery pain
Pharmacotherapy 19844(4)221ndash6
Forbes 1989 published data only
Forbes JA Butterworth GA Burchfield WH Yorio
CC Selinger LR Rosenmertz SK et alEvaluation of
flurbiprofen acetaminophen an acetaminophen-codeine
combination and placebo in postoperative oral surgery
pain Pharmacotherapy 19899(5)322ndash30
Forbes 1990 published data only
Forbes JA Kehm CJ Grodin CD Beaver WT Evaluation
of ketorolac ibuprofen acetaminophen and an
acetaminophen-codeine combination in postoperative
oral surgery pain Pharmacotherapy 199010(6(Pt 2)))
94Sndash105S
Hersh 2000 published data only
Hersh EV Levin LM Cooper SA Doyle G Waksman J
Wedell D et alIbuprofen liquigel for oral surgery pain
Clinical Therapeutics 200022(11)1306ndash18
Kiersch 1994 published data only
Kiersch TA Halladay SC Hormel PC A single-
dose double-blind comparison of naproxen sodium
acetaminophen and placebo in postoperative dental pain
Clinical Therapeutics 199416(3)394ndash404
Kubitzek 2003 published data only
Kubitzek F Ziegler G Gold MS Liu JM Ionescu E
Analgesic efficacy of low-dose diclofenac versus paracetamol
and placebo in postoperative dental pain Journal of
Orofacial Pain 200317(3)237ndash44
Lehnert 1990 published data only
Lehnert S Reuther J Wahl G Barthel K [The efficacy of
paracetamol (Tylenol) and acetyl salicylic acid (Aspirin)
in treating postoperative pain] Deutsche Zahnarztliche
Zeitschrift 199045(1)23ndash6
Mehlisch 1995 published data only
Mehlisch DR Jasper RD Brown P Korn SH McCarroll K
Murakami AA Comparative study of ibuprofen lysine and
acetaminophen in patients with postoperative dental pain
Clinical Therapeutics 199517(5)852ndash60
Moller 2000 published data only
Moller PL Norholt SE Ganry HE Insuasty JH Vincent
FG Skoglund LA et alTime of onset of analgesia and
analgesic efficacy of effervescent acetaminophen 1000
mg compared to tablet acetominophen 1000 mg in
postoperative dental pain a single-dose double-blind
randomized placebo-controlled study Journal of Clinical
Pharmacology 200040(4)370ndash8
Olson 2001 published data only
Olson NZ Otero AM Marrero I Tirado S Cooper S
Doyle G et alOnset of analgesia for liquigel ibuprofen
400 mg acetaminophen 1000 mg ketoprofen 25 mg
and placebo in the treatment of postoperative dental pain
Journal of Clinical Pharmacology 200141(11)1238ndash47
Seymour 1996 published data only
Seymour RA Kelly PJ Hawkesford JE The efficacy
of ketoprofen and paracetamol (acetaminopen) in
postoperative pain after third molar surgery British Journal
of Clinical Pharmacology 199641(6)581ndash5
Seymour 2003 published data only
Seymour RA Hawkesford JE Sykes J Stillings M Hill
CM An investigation into the comparative efficacy of
soluble aspirin and solid paracetamol in postoperative pain
after third molar surgery British Dental Journal 2003194
(3)153ndash7
Skoglund 1991 published data only
Skoglund LA Skjelbred P Fyllingen G Analgesic efficacy
of acetaminophen 1000 mg acetaminophen 2000 mg and
the combination of acetaminophen 1000 mg and codeine
10Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
phosphate 60 mg versus placebo in acute postoperative
pain Pharmacotherapy 199111(5)364ndash9
Sunshine 1986 published data only
Sunshine A Marrero I Olson N McCormick N Laska
EM Comparative study of flurbiprofen zomepirac sodium
acetaminophen plus codeine and acetaminophen for the
relief of postsurgical dental pain The American Journal of
Medicine 198680(3A)50ndash4
Vattaraphudej 1986 published data only
Vattaraphudej T Thongnoppakao P Koukongviriyapan V
[Comparison of the efficacy of analgesics in pain after oral
surgery] The Journal of the Dental Association of Thailand
198636(6)198ndash206
References to studies excluded from this review
Adame 1979 published data only
Adame C et alPostoperative development of inflammation
after extraction of impacted third molar as a model
for clinical assessment of anti-inflammatory drugs I
Preliminary report Boletin de Estudios Medicos y Biologicos
197930(8)308ndash9
Barden J 2004 published data only
Barden J Edwards J Moore A McQuay H Single dose
oral paracetamol (acetaminophen) for postoperative pain
Cochrane Database of Systematic Reviews 2004 Issue 1
[DOI DOI 10100214651858CD004602]
Becker 1990 published data only
Becker J Beckmann J Bertelt C Gundert-Remy U
Rohmel J Ohlendorf D [Double blind biometric study on
postoperative effects of analgesics] Deutsche Zahnarztliche
Zeitschrift 199045(1)36ndash8
Bentley 1987 published data only
Bentley KC Head TW The additive analgesic efficacy of
acetaminophen 1000 mg and codeine 60 mg in dental
pain Clinical Pharmacology and Therapeutics 198742(6)
634ndash40
Breivik 1998 published data only
Breivik EK Bjornsson GA Variation in surgical trauma and
baseline pain intensity effects on assay sensitivity of an
analgesic trial European Journal of Oral Sciences 1998106
(4)844ndash52
Cooper 1986 published data only
Cooper SA Erlichman MC Mardirossian G Double-
blind comparison of an acetaminophen-codeine-caffeine
combination in oral surgery pain Anesthesia Progress 1986
33(3)139ndash42
Cooper 1989 published data only
Cooper SA Schachtel BP Goldman E Gelb S Cohn P
Ibuprofen and acetaminophen in the relief of acute pain
a randomized double-blind placebo-controlled study
Journal of Clinical Pharmacology 198929(11)1026ndash30
Cooper 1991 published data only
Cooper SA Kupperman A The analgesic efficacy of
flurbiprofen compared to acetaminophen with codeine The
Journal of Clinical Dentistry 19912(3)70ndash4
Dionne 1983 (1) published data only
Dionne RA Campbell RA Cooper SA Hall DL
Buckingham B Suppression of postoperative pain by
preoperative administration of ibuprofen in comparison to
placebo acetaminophen and acetaminophen plus codeine
Journal of Clinical Pharmacology 198323(1)37ndash43
Dionne 1983 (2) published data only
Dionne RA Sisk AL Fox PC Wirdzek PR Gracely
RH Dubner R Suppression of postoperative pain by
preoperative adminsitration of flurbiprofen in comparison
to acetominophen and oxycodone plus acetominophen
Current Therapeutic Research 198334(1)15ndash29
Dionne 1986 published data only
Dionne RA Suppression of dental pain by the preoperative
administration of flurbiprofen The American Journal of
Medicine 198680(3A)41ndash9
Dolci 1993 published data only
Dolci G Ripari M Pacifici L Umile A [Analgesic efficacy
and the tolerance for piroxicam-beta-cyclodextrin compared
to piroxicam paracetamol and placebo in the treatment of
postextraction dental pain] Minerva Stomatologica 199342
(5)235ndash41
Edwards 2002 published data only
Edwards JE McQuay HJ Moore RA Combination
analgesic efficacy individual patient data meta-analysis
of single-dose oral tramadol plus acetaminophen in
acute postoperative pain Journal of Pain and Symptom
Management 200223(2)121ndash30
Forbes 1982 published data only
Forbes JA Beaver WT White EH White RW Neilson GB
Shackleford RW Diflunisal A new oral analgesic with an
unusually long duration of action JAMA 1982248(17)
2139ndash42
Forbes 1984a published data only
Forbes JA Kolodny AL Chachich BM Beaver WT
Nalbuphine acetaminophen and their combination in
postoperative pain Clinical Pharamacology and Therapeutics
198435(6)843ndash51
Gallardo 1990 published data only
Gallardo F Rossi E Analgesic efficacy of flurbiprofen as
compared to acetaminophen and placebo after periodontal
surgery Journal of Periodontology 199061(4)224ndash7
Gustafsson 1983 published data only
Gustafsson I Nystrom E Quiding H Effect of preoperative
paracetamol on pain after oral surgery European Journal of
Clinical Pharmacology 198324(1)63ndash5
Haanaes 1986 published data only
Haanaes HR Benterud UJ Skoglund LA RF 46-790 versus
paracetamol effect on post-operative pain International
Journal of Clinical Pharmacology Therapy and Toxicology
198624(11)598ndash601
Irvine 1982 published data only
Irvine GH Lutterloch MJ Bowerman JE Comparison
of diflunisal and paracetamol in the management of pain
11Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
following wisdom teeth removal British Dental Journal
1982152(1)18ndash20
Laska 1983 published data only
Laska EM Sunshine A Zighelboim I Roure C Marrero
I Wanderling J et alEffect of caffeine on acetaminophen
analgesia Clinical Pharmacology and Therapeutics 198333
(4)498ndash509
Lecointre 1991 published data only
Lecointre C [Efficacy and tolerance of tiaprofenic acid
for extraction complications Results of a randomized
double-blind study tiaprofenic acid versus paracetamol]
LrsquoInformation Dentaire 199173(35)3063ndash6
Liashek 1987 published data only
Liashek P Jr Desjardins PJ Triplett RG Effect of
pretreatment with acetaminophen-propoxyphene for oral
surgery pain Journal of Oral and Maxillofacial Surgery 1987
45(2)99ndash103
Macleod 2002 published data only
Macleod AG Ashford B Voltz M Williams B Cramond T
Gorta L et alParacetamol versus paracetamol-codeine in
the treatment of post-operative dental pain a randomized
double-blind prospective trial Australian Dental Journal
200247(2)147ndash51
Medve 2001 published data only
Medve RA Wang J Karim R Tramadol and acetaminophen
tablets for dental pain Anesthesia Progress 200148(3)
79ndash81
Mehlisch 1984 published data only
Mehlisch DR Frakes LA A controlled comparative
evaluation of acetaminophen and aspirin in the treatment of
postoperative pain Clinical Therapeutics 19847(1)89ndash97
Mehlisch 1990 published data only
Mehlisch DR Sollecito WA Helfrick JF Leibold DG
Markowitz R Schow CE Jr et alMulticenter clinical
trial of ibuprofen and acetaminophen in the treatment of
postoperative dental pain Journal of the American Dental
Association 1990121(2)257ndash63
Moore 1986 published data only
Moore PA Werther JR Seldin EB Stevens CM Analgesic
regimens for third molar surgery pharmacologic and
behavioral considerations Journal of the American Dental
Association 1986113(5)739ndash44
Nystrom 1988 published data only
Nystrom E Gustafsson I Quiding H The pain intensity
at analgesic intake and the efficacy of diflunisal in single
doses and effervescent acetaminophen in single and repeated
doses Pharmacotherapy 19888(3)201ndash9
Petersen 1983 published data only
Petersen JK A double-blind cross-over study of the analgesic
and anti-inflammatory effects of dexamethasone and
paracetamol following surgical removal of lower impacted
third molars International Journal of Oral Surgery 198312
(4)266
Quiding 1981 published data only
Quiding H Oksala E Happonen RP Lehtimaki K Ojala
T The visual analog scale in multiple-dose evaluations of
analgesics The Journal of Clinical Pharmacology 198121
(10)424ndash9
Quiding 1982 (1) published data only
Quiding H Oikarinen V Huitfeldt B Koskimo M
Leikomaa H Nyman C An analgesic study with repeated
doses of phenazone phenazone plus dextropropoxyphene
and paracetamol using a visual analogue scale International
Journal of Oral Surgery 198211(5)304ndash9
Quiding 1982 (2) published data only
Quiding H Persson G Ahlstrom U Bangens S Hellem S
Johansson G et alParacetamol plus supplementary doses
of codeine an analgesic study of repeated doses European
Journal of Clinical Pharmacology 198223(4)315ndash9
Quiding 1984 published data only
Quiding H Oikarinen V Sane J Sjoblad AM Analgesic
efficacy after single and repeated doses of codeine and
acetaminophen Journal of Clinical Pharmacology 198424
(1)27ndash34
Ragot 1991 published data only
Ragot JP [Comparison of analgesic activity of mefenamic
acid and paracetamol in treatment of pain after extraction
of impacted lower 3d molar] LrsquoInformation Dentaire 1991
73(21)1659ndash64
Reijntjes 1987 published data only
Reijntjes RJ Boering G Wesseling H van Rijn LG
Suprofen versus paracetamol after oral surgery International
Journal of Oral and Maxillofacial Surgery 198716(1)45ndash9
Rodrigo 1987 published data only
Rodrigo MR Rosenquist JB Cheung LK Paracetamol
and diflunisal for pain relief following third molar surgery
in Hong Kong Chinese International Journal of Oral and
Maxillofacial Surgery 198716(5)566ndash71
Rodrigo 1989 published data only
Rodrigo C Chau M Rosenquist J A comparison of
paracetamol and diflunisal for pain control following
3rd molar surgery International Journal of Oral and
Maxillofacial Surgery 198918(3)130ndash2
Rosen 1985 published data only
Rosen M Absi EG Webster JA Suprofen compared to
dextropropoxyphene hydrochloride and paracetamol
(Cosalgesic) after extraction of wisdom teeth under general
anaesthesia Anaesthesia 198540(7)639ndash41
Sakata 1989 published data only
Sakata LA Rocha B et alEffects of benzydamine after
surgical removal of impacted teeth [Efeitos da benzidamina
apoacutes a extraccedilaumlo de dentes inclusos] Revista da Associacao
Paulista de Cirurgioes Dentistas 198943(4)167ndash70
Selcuk 1996 published data only
Selcuk E Gomel M Bellibas SE Kose T Tuglular I
Comparison of the analgesic effects of diflunisal and
paracetamol in the treatment of postoperative dental pain
12Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
International Journal of Clinical Pharmacology Research
199616(2-3)57ndash65
Seymour 1981 published data only
Seymour RA Rawlins MD Pharmacokinetics of parenteral
paracetamol and its analgesic effects in post-operative dental
pain European Journal of Clinical Pharmacology 198120
(3)215ndash8
Seymour 1983 published data only
Seymour RA Analgesic efficacy and plasma concentration
of three analgesics in pain after lower third molar removal
SAAD Digest 19835(7)172ndash88
Skjelbred 1979 published data only
Skjelbred P Lokken P Paracetamol versus placebo effects
on post-operative course European Journal of Clinical
Pharmacology 197915(1)27ndash33
Strom 1990 published data only
Strom C Forsberg O Quiding H Engevall S Larsson
O Analgesic efficacy of acetaminophen sustained release
Journal of Clinical Pharmacology 199030(7)654ndash9
Van Aken 2004 published data only
Van Aken H Thys L Veekman L Buerkle H Assessing
analgesia in single and repeated administrations of
propacetamol for postoperative pain comparison with
morphine after dental surgery Anesthesia and Analgesia
200498(1)159ndash65
Winter 1983 published data only
Winter L Appleby F Ciccone PE Pigeon JG A double-
blind comparative evaluation of acetaminophen caffeine
and the combination of acetaminophen and caffeine in
outpatients with postoperative oral surgery pain Current
Therapeutic Research 198333(1)115ndash22
Additional references
Aronoff 2006
Aronoff DM Oates JA Boutaud O New insights into
the mechanism of action of acetaminophen Its clinical
pharmacologic characteristics reflect its inhibition of the
two prostaglandin H2 synthases Clinical Pharmacology and
Therapeutics 200679(1)9ndash19
Chandrasekharan 2002
Chandrasekharan NV Dai H Roos KL Evanson NK
Tomsik J Elton TS et alCOX-3 a cyclooxygenase-1 variant
inhibited by acetaminophen and other analgesicantipyretic
drugs cloning structure and expression Proceedings of the
National Academy of Sciences of the United States of America
200299(21)13926ndash31
Collins 1999
Collins SL Moore RA McQuay HJ Wiffen PJ Edwards JE
Single dose oral ibuprofen and diclofenac for postoperative
pain Cochrane Database of Systematic Reviews 1999
Issue 1 [DOI Art No CD001548 DOI 101002
14651858CD001548]
Cooper 1976
Cooper SA Beaver WT A model to evaluate mild analgesics
in oral surgery outpatients Clinical Pharmacology and
Therapeutics 197620(2)241ndash50
Coulthard 2001
Coulthard P Hill CM Frame JW Barry H Ridge BD
Bacon TH Pain control with paracetamol from a sustained
release formulation and a standard release formulation after
third molar surgery a randomised controlled trial British
Dental Journal 2001191(6)319ndash24
Dray 1997
Dray A Kinins and their receptors in hyperalgesia
Canadian Journal of Physiology and Pharmacology 199775
(6)704ndash12
Fisher 1988
Fisher SE Frame JW Rout PG McEntegart DJ Factors
affecting the onset and severity of pain following the surgical
removal of unilateral impacted mandibular third molar
teeth British Dental Journal 1988164(11)351ndash4
Loeser 1999
Loeser JD Melzack R Pain an overview Lancet 1999353
(9164)1607ndash9
Malmberg 1992
Malmberg AB Yaksh TL Antinociceptive effects of spinal
non-steroidal anti-inflammatory agents on the formalin
test in the rat Journal of Pharmacology and Experimental
Therapeutics 1992263136ndash46
Moore 1997
Moore RA McQuay HJ Single-patient data meta-analysis
of 3453 postoperative patients oral tramadol versus
placebo codeine and combination analgesics Pain 199769
(3)287ndash94
Moore 1998
Moore A Collins S Carroll D McQuay H Edwards
J Single dose paracetamol (acetaminophen) with and
without codeine for postoperative pain Cochrane Database
of Systematic Reviews 1998 Issue 4 [DOI Art No
CD001547 DOI 10100214651858CD001547]
Rang 2003
Rang HP Dale MM Ritter JM Moore PK Anti-
inflammatory and immunosuppresant drugs Pharmacology
5th Edition Churchill Livingstone 2003244ndash61
Seymour 1985
Seymour RA Meechan JG Blair GS An investigation into
post-operative pain after third molar surgery under local
analgesia The British Journal of Oral and Maxillofacial
Surgery 198523(6)410ndash8lowast Indicates the major publication for the study
13Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Cooper 1980
Methods Randomised parallel group double blind study
Participants 298 participants randomised to 6 groups withdrawals unclear (51 from all groups)
Number randomised to intervention male 13 female 24 mean age 225
Number randomised to placebo male 11 female 27 mean age 235
Number of third molars removed mean for intervention and placebo 19
Baseline pain intensity mean for intervention 241 (moderate 22 severe 15) mean for placebo 242
(moderate 22 severe 16)
Setting - outpatients (USA)
Interventions Paracetamol 500 mg versus placebo
Formulation not stated
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse events table
Notes Sponsored unclear
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Cooper 1981
Methods Randomised parallel group double blind study
Participants 248 participants randomised to 5 groups withdrawals unclear (48 from all groups)
Number randomised to intervention male 15 female 22 mean age 222
Number randomised to placebo male 13 female 24 mean age 237
Number of third molars removed not stated
Baseline pain intensity mean for intervention 22 (moderate 29 severe 9) mean for placebo 23 (moderate
26 severe 11)
Setting not stated (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation not stated
Anaesthesia LA or GA
14Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Cooper 1981 (Continued)
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Total number of adverse events and number of people with adverse events reported
Notes Sponsored by
Adria Laboratories
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Cooper 1988
Methods Randomised parallel group double blind study
Participants 165 participants randomised to 4 groups withdrawals unclear (22 from all groups)
Number randomised to intervention male 7 female 29 mean age 246
Number randomised to placebo male 11 female 29 mean age 247
Number of third molars removed mean for intervention 14 mean for placebo 15
Baseline pain intensity mean for intervention 24 (moderate 21 severe 15) mean for placebo 24 (mod-
erate 25 severe 15)
Setting - outpatients - single site (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Total number of adverse events
Notes Sponsored by
Parke-Davis
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
15Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Cooper 1998
Methods Randomised parallel group double blind study
Participants 177 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 23 female 27 mean age 236
Number randomised to placebo male 12 female 14 mean age 227
Number of third molars removed not stated
Baseline pain intensity mean for intervention categorical 23 VAS 603 mean for placebo categorical
22 VAS 628
Setting - Georgetown University Hospital (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe) VAS scale 0-100 mm (none - worst pain
imaginable)
PR at 4 hours and 6 hours categorical scale 0-4 (no relief - complete relief )
Global assessment not stated
Adverse effects table
Notes Sponsored by
Whitehall-Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Dionne 1994
Methods Randomised parallel group double blind study
Participants 135 participants randomised to 5 groups withdrawals unclear (11 from all groups)
Number randomised to intervention male 14 female 13 mean age 296
Number randomised to placebo male 15 female 10 mean age 282
Number of third molars removed not stated
Baseline pain intensity for intervention and placebo not stated
Setting private dental practice (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED or GA
Outcomes PI at 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 1-5 (poor - excellent)
Adverse effects table
16Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Dionne 1994 (Continued)
Notes Sponsored by
Upjohn
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Dolci 1994
Methods Randomised parallel group double blind study
Participants 338 participants enrolled in 4 groups withdrawals unclear (40 from all groups)
Number randomised to intervention male 28 female 44 mean age 279 age range 18-49
Number randomised to placebo male 28 female 48 mean age 272 age range 18-45
Number of third molars removed not stated
Baseline pain intensity range for intervention and placebo given together as average 214 (208 - 219)
Setting not stated (Italy)
Interventions Paracetamol 500 mg versus placebo
Formulation tablets
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (negative - very good)
Adverse effects table
Notes Sponsored - unclear
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Forbes 1984b
Methods Randomised parallel group double blind study
Participants 191 participants randomised to 4 groups withdrawals unclear (43 from all groups 164 used in reporting
of adverse events)
Number randomised to intervention male 19 female 20 mean age 2195
Number of third molars removed mean 244
Number randomised to placebo male 21 female 15 mean age 15-32
Number of third molars removed mean 278
17Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Forbes 1984b (Continued)
Baseline pain intensity mean for intervention 246 (moderate 21 severe 18) mean for placebo 247
(moderate 19 severe 17)
Setting private dental practice (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse effects reported as total number of adverse events and number of patients with adverse events
Notes Sponsored by McNeil Consumer Products
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Forbes 1989
Methods Randomised parallel group double blind study
Participants 107 participants randomised to 5 groups withdrawals unclear (19 from all groups 98 participants used
in reporting of adverse events)
Number randomised to intervention male 9 female 13 mean age 2059 age range 17-31
Number randomised to placebo male 12 female 11 mean age 2374 age range 16-39
Number of third molars removed mean for intervention 259 mean for placebo 209
Baseline pain intensity mean for intervention 245 mean for placebo 239
Setting - 2 sites private dental practice outpatients (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation - 1 tablet amp 1 capsule
Anaesthesia LA and GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects reported by number of patients with adverse events
Notes Sponsored by
Boots Company Ltd GH Besselaar Associates
Risk of bias
Item Authorsrsquo judgement Description
18Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Forbes 1989 (Continued)
Allocation concealment Unclear B - Unclear
Forbes 1990
Methods Randomised parallel group double blind study
Participants 206 participants randomised to 6 groups
Number randomised to intervention male 20 female 16 (5 withdrawals) mean age 225 age range 16-
46
Number randomised to placebo male 18 female 16 (4 withdrawals) mean age 2365 age range 16-45
Number of third molars removed mean for intervention 258 mean for placebo 235
Baseline pain intensity mean for intervention 239 (moderate 22 severe 14) mean for placebo 232
(moderate 23 severe 11)
Setting - private dental practice outpatients (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation capsules
Anaesthesia LA and GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects table
Notes Sponsored by
Syntex Research
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Hersh 2000
Methods Randomised parallel group double blind study
Participants 210 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 20 female 43 mean age 233
Number of third molars removedpatient (11) (26) (35) (451)
Number randomised to placebo male 9 female 8 mean age 237
Number of wisdom teeth removed per patient (11) (25) (33) (418)
Baseline pain intensity mean for intervention 23 (moderate 47 severe 16) mean for placebo 22 (mod-
erate 22 severe 5)
Setting - University of Pennsylvania School of Dental Medicine - outpatients (USA)
19Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hersh 2000 (Continued)
Interventions Paracetamol 1000 mg versus placebo
Formulation caplets
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical 0-3 (none - severe)
PR at 4 hours and 6 hours categorical 0-4 (no relief - complete relief )
Global assessment categorical 0-4 (poor - excellent)
Adverse effects by total number of adverse events and number of patients with adverse events
Notes Sponsored by
Whitehall-Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Kiersch 1994
Methods Randomised parallel group double blind study
Participants 232 participants enrolled in 3 groups
Number randomised to intervention 91 withdrawals 4 (2 before and 2 after randomisation) male 72
female 17 mean age 231 age range 15-39
Number of third molars removedpatient (10) (20) (331) (454)
Number randomised to placebo 47 withdrawals 2 male 35 female 10 mean age 247 age range 15-39
Number of third molars removedpatient (10) (20) (319) (426)
Baseline pain intensity mean for intervention and placebo categorical 212 VAS 5835
Setting not stated (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation capsules
Anaesthesia not stated
Outcomes PI at 4 hours and 6 hours categorical 0-3 (none - severe)
PR at 4 hours and 6 hours categorical 0-4 (none - complete) VAS 0-100 mm (no pain - worst pain I can
imagine)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects reported by total number of adverse events and by number of patients with adverse events
Notes Sponsored by
Syntex Research
Risk of bias
Item Authorsrsquo judgement Description
20Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Kiersch 1994 (Continued)
Allocation concealment Unclear B - Unclear
Kubitzek 2003
Methods Randomised parallel group double blind study
Participants 245 participants randomised to 3 groups no withdrawals
Number randomised to intervention 78
Number randomised to placebo 84 malefemale 40 male over both groups
Number of third molars removed 1 or 2 for each patient
Baseline pain intensity moderate to severe 65-76 in both groups
Setting dental practice (Germany)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia LA
Outcomes PI not stated
PR given as TOTPAR at 6 hours
Global assessment categorical 1-5 (poor - excellent)
Adverse effects not stated
Notes Sponsored by
Novartis Consumer Health
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Lehnert 1990
Methods Randomised parallel group double blind study
Participants 150 participants randomised to 3 groups 50 to each
Number randomised to intervention 1 withdrawal male 23 female 26 mean age 253 age range 17-52
Number randomised to placebo 2 withdrawals male 24 female 18 mean age 251 age range 18-53
Number of hird molars removed not stated
Baseline pain intensity mean for intervention 255 (moderate 22 severe 27) mean for placebo 25
(moderate 21 severe 21)
Setting outpatients (Germany)
Interventions Paracetamol 1000 mg versus placebo
Formulation capsules
Anaesthesia not stated
21Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Lehnert 1990 (Continued)
Outcomes PI at 6 hours categorical scale 0-3 (no pain - severe)
PR at 6 hours categorical scale 0-3 (none - complete)
Global assessment categorical scale 0-3 (poor - excellent)
Adverse effects by number of patients
Notes Sponsored by GH Besselar Associates
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Mehlisch 1995
Methods Randomised parallel group double blind study
Participants 240 participants randomised to 3 groups 1 withdrawal from the acetaminophen group
Number randomised to intervention (1 withdrawal) male 30 female 71 mean age 253 age range 15-
60
Number of third molars removedpatient (10 295 33 43)
Number randomised to placebo male 19 female 21 mean age 242 age range 15-48
Number of third molars removedpatient (10 239 30 41)
Baseline pain intensity mean for intervention 221 (moderate 80 severe 21) mean for placebo 220
(moderate 32 severe 8)
Setting not stated (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation 2 tablets
Anaesthesia not stated
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse events reported by number of patients
Notes Sponsored by
Biomedical Research Group and Merck Research Laboratories
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
22Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Moller 2000
Methods Randomised parallel group double blind study
Participants 242 participants randomised to 4 groups no withdrawals
Number randomised to Intervention A male 27 female 33 mean age 245
Number randomised to Intervention B male 26 female 34 mean age 262
Number randomised to Placebo A male 21 female 41 mean age 250
Number randomised to Placebo B male 24 female 36 mean age 246
Number of third molars removed per patient in both groups 1
Mean baseline intensity Intervention A categorical 200 (moderate 60) VAS 494
Mean baseline intensity Intervention B categorical 200 (moderate 60) VAS 473
Mean baseline intensity Placebo A categorical 200 (moderate 61 severe 1) VAS 505
Mean baseline intensity Placebo B categorical 200 (moderate 61) VAS 476
Setting Department of Oral and Maxillofacial Surgery Royal Dental College Aarhus (Denmark)
Interventions Intervention A Paracetamol 1000 mg versus Placebo A
Formulation effervescent tablets
Intervention B Paracetamol 1000 mg versus Placebo B
Formulation tablets
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe) VAS scale 0-100 mm (no pain - worst possible pain)
PR at 4 hours categorical 0-4 (none - complete)
Global assessment categorical 0-3 (poor - excellent)
Adverse effects reported as total number of adverse events and number of patients with adverse events
Notes Sponsored by
Bristol Myers Squibb
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Olson 2001
Methods Randomised parallel group double blind study
Participants 239 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 22 female 44 mean age 222
Number randomised to placebo male 11 female 28 mean age 239
Number of third molars removedpatient intervention - (11) (264) (31) (40) placebo - (11) (2
38) (30) (40)
Baseline pain intensity mean for intervention 286 (moderate 9 severe 57) mean for placebo 29 (moderate
4 severe 35)
Setting University of Puerto Rico School of Dentistry (Puerto Rico)
23Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Olson 2001 (Continued)
Interventions Paracetamol 1000 mg versus placebo
Formulation caplets
Anaesthesia LA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete relief )
Global assessment categorical scale 0-4 (poor - excellent)
Adverse effects table
Notes Sponsored by
Whitehall Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Seymour 1996
Methods Randomised parallel group double blind study
Participants 206 participants randomised to 5 groups
Number randomised to intervention A 1 withdrawal male 12 female 28 mean age 238
Number randomised to intervention B 1 withdrawal male 12 female 28 mean age 277 1 withdrawal
Number randomised to placebo 2 withdrawals male 15 female 24 mean age 246
Number of third molars removedpatient not stated
Baseline pain intensity mean for intervention A VAS 549 mean for intervention B VAS 542 mean
for placebo VAS 565
Setting not stated (UK)
Interventions Intervention A paracetamol 500 mg versus placebo
Intervention B paracetamol 1000 mg versus placebo
Formulation not stated
Anaesthesia GA
Outcomes PI at 6 hours VAS scale 0-100 mm (no pain - unbearable pain)
Global assessment categorical 0 -3 (very good - very poor)
but categories 1 amp 2 and 4 amp 5 not reported separately so unable to include data in tables
Adverse effects - none reported by any participants in any group
Notes Sponsored - unclear
Risk of bias
Item Authorsrsquo judgement Description
24Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Seymour 1996 (Continued)
Allocation concealment Unclear B - Unclear
Seymour 2003
Methods Randomised parallel group double blind study
Participants 167 randomised to 3 groups withdrawals unclear (14 from all groups)
Number randomised to intervention male 19 female 43 mean age 250
Number randomised to placebo male 11 female 21 mean age 251
Number of third molars removedpatient intervention - (12) (214) (312) (434) placebo - (13)
(25) (39) (415)
Baseline pain intensity mean for intervention 506 mean for placebo 541
Setting not clear (2 sites Cardiff and Hexham UK)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia GA
Outcomes PI at 4 hours VAS scale 0-100 mm (none - worst pain imaginable)
PR not stated
Global assessment categorical scale 1-5 (very poor - very good)
Adverse effects table
Notes Sponsored by
Reckitt Benckiser Healthcare
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Skoglund 1991
Methods Randomised parallel group double blind study
Participants 147 participants randomised to 4 groups withdrawals unclear (8 from all groups)
Number randomised to intervention male 16 female 16 mean age 247
Number randomised to placebo male 16 female 17 mean age 244
Number of third molars removed not stated
Baseline pain intensity mean for intervention approx 55 mean for placebo approx 45
Setting not stated (Norway)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia LA
25Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Skoglund 1991 (Continued)
Outcomes PI at 4 hours and 6 hours VAS scale 0-100 mm (none - pain cannot be worse)
PR at 4 hours and 6 hours VAS scale 0-100 mm (complete relief - no relief ) reversed for statistical analysis
Global assessment not stated
Adverse effects table
Notes Sponsored by
Apothekernes Laboratorium
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Sunshine 1986
Methods Randomised parallel group double blind study
Participants 182 participants randomised to 6 groups no withdrawals (only patients with moderate to severe pain
were randomised)
Number randomised to intervention male 6 female 24 mean age 219
Number randomised to placebo male 14 female 16 mean age 23
Number of third molars removed not stated
Baseline pain intensity mean for intervention 200 mean for placebo 200
Setting University of Puerto Rico School of Dentistry Clinic
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia LA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none 0 - complete 100)
Global assessment categorical 0-3 (poor - excellent)
Overall improvement 1-7 (very much worse - very much better)
Adverse effects reported by number of patients with adverse events
Notes Sponsored by
Upjohn
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
26Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Vattaraphudej 1986
Methods Randomised parallel group double blind study
Participants 83 enrolled to 4 groups withdrawals unclear (16 from all groups)
Number randomised to intervention male 8 female 8
Number randomised to placebo male 10 female 9
Number of third molars removed mean for intervention 125 mean for placebo 132
Baseline pain intensity mean for intervention 237 mean for placebo 226
Setting Dept of Oral Surgery Khon Kaen University Thailand
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (no relief - total relief )
Global assessment categorical scale 0-3 (poor - excellent)
Adverse effects none reported
Notes Sponsored by Khon Kaen University Thailand Dr Sompong Thongpradith Merck and Russel
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
GA - general anaesthetic LA - local anaesthetic PI - pain intensity PR - pain relief SED - sedation TOTPAR - total pain relief VAS
- visual analogue scale
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Adame 1979 Title not in journal quoted unable to find paper
Barden J 2004 Meta-analysis dental papers included individually where appropriate
Becker 1990 Not a third molar study
Bentley 1987 Unable to extract data for third molars only written to authors
Breivik 1998 Dose given at 3 hours postoperatively regardless of baseline pain unable to get 4-hour data Study used for side
effects only
27Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Cooper 1986 Unable to extract third molar data written to authors
Cooper 1989 Unable to extract third molar data written to authors
Cooper 1991 Unclear if third molars only written to authors
Dionne 1983 (1) Not single dose administered preoperatively
Dionne 1983 (2) Not placebo controlled not single dose administered preoperatively
Dionne 1986 Not placebo controlled
Dolci 1993 The data for the participants in this study are duplicated in Dolci 1994
Edwards 2002 This was a meta-analysis Need to identify source of data to clarify whether third molar studies and exclude
duplication Written to authors
Forbes 1982 Unable to extract third molar data written to authors
Forbes 1984a Not third molar study
Gallardo 1990 Not third molar study (periodontal surgery)
Gustafsson 1983 Patients given either paracetamol preoperatively and placebo postoperatively or vice versa unable to extract
relevant data
Haanaes 1986 Not placebo controlled Study used for side effects only
Irvine 1982 Not placebo controlled
Laska 1983 Not placebo controlled
Lecointre 1991 Not placebo controlled
Liashek 1987 Multiple doses unable to extract single dose data
Macleod 2002 Not placebo controlled
Medve 2001 Only 8-hour SPID and TOTPAR available need 4-hour andor 6-hour to include in review written to authors
Mehlisch 1984 Unable to extract third molar data written to authors
Mehlisch 1990 Unable to extract third molar data
Moore 1986 Multiple doses given unable to extract single dose data
Nystrom 1988 Not placebo controlled
28Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Petersen 1983 Unable to locate complete article
Quiding 1981 Not placebo controlled
Quiding 1982 (1) Not placebo controlled
Quiding 1982 (2) Not placebo controlled
Quiding 1984 No placebo used
Ragot 1991 Not placebo controlled
Reijntjes 1987 Not placebo controlled
Rodrigo 1987 Mixed parallel and cross-over trial multiple doses unable to extract relevant data
Rodrigo 1989 Not placebo controlled
Rosen 1985 Not placebo controlled multiple doses used unable to extract single dose data
Sakata 1989 Unable to obtain study
Selcuk 1996 Not placebo controlled
Seymour 1981 Cross-over trial baseline pain not stated unable to extract relevant data
Seymour 1983 Acetaminophen administered intravenously
Skjelbred 1979 Multiple doses unable to extract single dose data
Strom 1990 Not placebo controlled
Van Aken 2004 Propacetamol administered intravenously
Winter 1983 Unable to extract third molar data written to authors
SPID - summed pain intensity difference TOTPAR - total pain relief
29Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
Comparison 1 50 pain relief using pain relief measures
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Paracetamol versus placebo
number of people with at least
50 pain relief at 4 hours
16 1498 Risk Ratio (M-H Random 95 CI) 285 [189 429]
11 Up to 1000 mg of
paracetamol
10 710 Risk Ratio (M-H Random 95 CI) 196 [134 286]
12 1000 mg or more 6 788 Risk Ratio (M-H Random 95 CI) 456 [286 727]
2 Paracetamol versus placebo
number of people with at least
50 pain relief at 6 hours
13 1155 Risk Ratio (M-H Random 95 CI) 332 [188 587]
21 Up to 1000 mg of
paracetamol
6 378 Risk Ratio (M-H Random 95 CI) 189 [098 367]
22 1000 mg or more 7 777 Risk Ratio (M-H Random 95 CI) 421 [297 598]
Comparison 2 50 pain relief using pain intensity measures
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Paracetamol versus placebo
number of people with at least
50 pain relief at 4 hours
17 1658 Risk Ratio (M-H Random 95 CI) 487 [283 837]
11 Up to 1000 mg of
paracetamol
10 737 Risk Ratio (M-H Random 95 CI) 433 [219 858]
12 1000 mg or more 8 921 Risk Ratio (M-H Random 95 CI) 646 [234 1785]
2 Paracetamol versus placebo
number of people with at least
50 pain relief at 6 hours
13 1184 Risk Ratio (M-H Random 95 CI) 341 [234 497]
21 Up to 1000 mg of
paracetamol
6 403 Risk Ratio (M-H Random 95 CI) 267 [146 490]
22 1000 mg or more 8 781 Risk Ratio (M-H Random 95 CI) 396 [252 623]
30Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Comparison 3 Number of people with adverse events
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Number of patients with adverse
events paracetamol versus
placebo
17 1645 Risk Ratio (M-H Random 95 CI) 119 [090 157]
11 Up to 1000 mg of
paracetamol
9 672 Risk Ratio (M-H Random 95 CI) 125 [069 225]
12 1000 mg or more 8 973 Risk Ratio (M-H Random 95 CI) 116 [084 160]
Analysis 11 Comparison 1 50 pain relief using pain relief measures Outcome 1 Paracetamol versus
placebo number of people with at least 50 pain relief at 4 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 1 50 pain relief using pain relief measures
Outcome 1 Paracetamol versus placebo number of people with at least 50 pain relief at 4 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Dolci 1994 5472 2576 100 228 [ 161 323 ]
Cooper 1980 1137 1138 82 103 [ 051 207 ]
Forbes 1990 936 134 30 850 [ 114 6357 ]
Forbes 1989 522 023 17 1148 [ 067 19607 ]
Cooper 1988 1636 1240 87 148 [ 081 269 ]
Cooper 1981 2137 637 77 350 [ 160 767 ]
Forbes 1984b 1339 136 30 1200 [ 165 8716 ]
Vattaraphudej 1986 716 219 47 416 [ 100 1726 ]
Sunshine 1986 1830 1530 95 120 [ 076 190 ]
Dionne 1994 2527 1725 102 136 [ 102 182 ]
Subtotal (95 CI) 352 358 667 196 [ 134 286 ]
Total events 179 (Paracetamol better) 90 (Placebo better)
Heterogeneity Tau2 = 018 Chi2 = 2644 df = 9 (P = 0002) I2 =66
Test for overall effect Z = 349 (P = 000048)
2 1000 mg or more
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
31Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Mehlisch 1995 40101 240 49 792 [ 201 3124 ]
Cooper 1998 1850 326 59 312 [ 101 963 ]
Olson 2001 4266 539 74 496 [ 215 1148 ]
Moller 2000 27120 0122 18 5591 [ 345 90627 ]
Hersh 2000 4063 527 75 343 [ 152 773 ]
Kiersch 1994 2589 345 58 421 [ 134 1321 ]
Subtotal (95 CI) 489 299 333 456 [ 286 727 ]
Total events 192 (Paracetamol better) 18 (Placebo better)
Heterogeneity Tau2 = 003 Chi2 = 544 df = 5 (P = 036) I2 =8
Test for overall effect Z = 637 (P lt 000001)
Total (95 CI) 841 657 1000 285 [ 189 429 ]
Total events 371 (Paracetamol better) 108 (Placebo better)
Heterogeneity Tau2 = 040 Chi2 = 6294 df = 15 (Plt000001) I2 =76
Test for overall effect Z = 503 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
32Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 12 Comparison 1 50 pain relief using pain relief measures Outcome 2 Paracetamol versus
placebo number of people with at least 50 pain relief at 6 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 1 50 pain relief using pain relief measures
Outcome 2 Paracetamol versus placebo number of people with at least 50 pain relief at 6 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Forbes 1989 322 023 29 730 [ 040 13375 ]
Cooper 1988 1236 940 99 148 [ 071 310 ]
Forbes 1990 736 034 30 1419 [ 084 23928 ]
Dionne 1994 2427 1825 115 123 [ 093 163 ]
Forbes 1984b 1039 036 31 1943 [ 118 31995 ]
Sunshine 1986 1530 1030 104 150 [ 081 279 ]
Subtotal (95 CI) 190 188 407 189 [ 098 367 ]
Total events 71 (Paracetamol better) 37 (Placebo better)
Heterogeneity Tau2 = 032 Chi2 = 1445 df = 5 (P = 001) I2 =65
Test for overall effect Z = 189 (P = 0058)
2 1000 mg or more
Kubitzek 2003 4569 773 99 680 [ 329 1404 ]
Mehlisch 1995 35101 140 49 1386 [ 196 9779 ]
Kiersch 1994 2089 345 79 337 [ 106 1075 ]
Olson 2001 4166 539 94 485 [ 209 1122 ]
Hersh 2000 3563 527 95 300 [ 132 682 ]
Lehnert 1990 2349 640 96 313 [ 141 693 ]
Cooper 1998 1750 326 81 295 [ 095 914 ]
Subtotal (95 CI) 487 290 593 421 [ 297 598 ]
Total events 216 (Paracetamol better) 30 (Placebo better)
Heterogeneity Tau2 = 00 Chi2 = 509 df = 6 (P = 053) I2 =00
Test for overall effect Z = 806 (P lt 000001)
Total (95 CI) 677 478 1000 332 [ 188 587 ]
Total events 287 (Paracetamol better) 67 (Placebo better)
Heterogeneity Tau2 = 072 Chi2 = 6335 df = 12 (Plt000001) I2 =81
Test for overall effect Z = 412 (P = 0000038)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
33Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 21 Comparison 2 50 pain relief using pain intensity measures Outcome 1 Paracetamol versus
placebo number of people with at least 50 pain relief at 4 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 2 50 pain relief using pain intensity measures
Outcome 1 Paracetamol versus placebo number of people with at least 50 pain relief at 4 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Dolci 1994 4972 576 86 1034 [ 437 2449 ]
Seymour 1996 1940 1039 96 185 [ 099 346 ]
Cooper 1980 737 438 74 180 [ 057 563 ]
Forbes 1990 1036 034 28 1986 [ 121 32639 ]
Forbes 1989 622 023 28 1357 [ 081 22736 ]
Cooper 1988 1236 840 90 167 [ 077 361 ]
Sunshine 1986 1830 630 90 300 [ 138 650 ]
Forbes 1984b 1339 036 28 2498 [ 154 40542 ]
Vattaraphudej 1986 616 119 44 713 [ 095 5317 ]
Cooper 1981 1537 037 28 3100 [ 192 49971 ]
Subtotal (95 CI) 365 372 592 433 [ 219 858 ]
Total events 155 (Paracetamol better) 34 (Placebo better)
Heterogeneity Tau2 = 063 Chi2 = 2622 df = 9 (P = 0002) I2 =66
Test for overall effect Z = 421 (P = 0000026)
2 1000 mg or more
Cooper 1998 1350 026 28 1429 [ 088 23130 ]
Mehlisch 1995 41101 340 75 541 [ 178 1648 ]
Hersh 2000 3663 127 46 1543 [ 223 10685 ]
Skoglund 1991 1632 033 28 3400 [ 213 54391 ]
Seymour 2003 1262 432 78 155 [ 054 442 ]
Seymour 1996 2040 1039 96 195 [ 105 362 ]
Kiersch 1994 989 045 28 971 [ 058 16317 ]
Moller 2000 28120 0122 28 5794 [ 358 93840 ]
Subtotal (95 CI) 557 364 408 646 [ 234 1785 ]
Total events 175 (Paracetamol better) 18 (Placebo better)
Heterogeneity Tau2 = 124 Chi2 = 2347 df = 7 (P = 0001) I2 =70
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
34Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Test for overall effect Z = 360 (P = 000032)
Total (95 CI) 922 736 1000 487 [ 283 837 ]
Total events 330 (Paracetamol better) 52 (Placebo better)
Heterogeneity Tau2 = 070 Chi2 = 4973 df = 17 (P = 000005) I2 =66
Test for overall effect Z = 571 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
Analysis 22 Comparison 2 50 pain relief using pain intensity measures Outcome 2 Paracetamol versus
placebo number of people with at least 50 pain relief at 6 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 2 50 pain relief using pain intensity measures
Outcome 2 Paracetamol versus placebo number of people with at least 50 pain relief at 6 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Seymour 1996 1840 939 152 195 [ 100 380 ]
Forbes 1989 422 023 16 939 [ 054 16485 ]
Cooper 1988 936 640 105 167 [ 066 422 ]
Forbes 1990 836 032 17 1516 [ 091 25267 ]
Forbes 1984b 1139 036 17 2128 [ 130 34843 ]
Sunshine 1986 1430 530 111 280 [ 115 680 ]
Subtotal (95 CI) 203 200 418 267 [ 146 490 ]
Total events 64 (Paracetamol better) 20 (Placebo better)
Heterogeneity Tau2 = 015 Chi2 = 705 df = 5 (P = 022) I2 =29
Test for overall effect Z = 318 (P = 00015)
2 1000 mg or more
Hersh 2000 3163 127 33 1329 [ 191 9242 ]
Mehlisch 1995 39101 340 82 515 [ 169 1571 ]
Olson 2001 4266 739 146 355 [ 177 711 ]
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
35Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Seymour 1996 2140 939 157 228 [ 119 433 ]
Cooper 1998 1250 026 17 1324 [ 081 21504 ]
Kiersch 1994 489 045 16 460 [ 025 8361 ]
Lehnert 1990 2449 542 114 411 [ 172 983 ]
Skoglund 1991 1432 033 17 2988 [ 186 48076 ]
Subtotal (95 CI) 490 291 582 396 [ 252 623 ]
Total events 187 (Paracetamol better) 25 (Placebo better)
Heterogeneity Tau2 = 008 Chi2 = 863 df = 7 (P = 028) I2 =19
Test for overall effect Z = 597 (P lt 000001)
Total (95 CI) 693 491 1000 341 [ 234 497 ]
Total events 251 (Paracetamol better) 45 (Placebo better)
Heterogeneity Tau2 = 013 Chi2 = 1823 df = 13 (P = 015) I2 =29
Test for overall effect Z = 637 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
36Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 31 Comparison 3 Number of people with adverse events Outcome 1 Number of patients with
adverse events paracetamol versus placebo
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 3 Number of people with adverse events
Outcome 1 Number of patients with adverse events paracetamol versus placebo
Study or subgroup Paracetamol more Placebo more Risk Ratio Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Cooper 1980 237 637 033 [ 007 155 ]
Dolci 1994 780 882 090 [ 034 236 ]
Forbes 1990 541 038 1021 [ 058 17873 ]
Forbes 1989 326 226 150 [ 027 825 ]
Sunshine 1986 130 130 100 [ 007 1526 ]
Cooper 1981 1237 438 308 [ 109 869 ]
Dionne 1994 727 525 130 [ 047 356 ]
Vattaraphudej 1986 016 019 00 [ 00 00 ]
Forbes 1984b 143 240 047 [ 004 493 ]
Subtotal (95 CI) 337 335 125 [ 069 225 ]
Total events 38 (Paracetamol more) 28 (Placebo more)
Heterogeneity Tau2 = 016 Chi2 = 906 df = 7 (P = 025) I2 =23
Test for overall effect Z = 074 (P = 046)
2 1000 mg or more
Olson 2001 1066 239 295 [ 068 1279 ]
Cooper 1998 2550 426 325 [ 127 835 ]
Moller 2000 48120 56122 087 [ 065 117 ]
Seymour 2003 2462 932 138 [ 073 260 ]
Mehlisch 1995 1299 440 121 [ 042 354 ]
Kiersch 1994 2691 1347 103 [ 059 182 ]
Hersh 2000 1263 727 073 [ 032 166 ]
Lehnert 1990 549 440 102 [ 029 355 ]
Subtotal (95 CI) 600 373 116 [ 084 160 ]
Total events 162 (Paracetamol more) 99 (Placebo more)
Heterogeneity Tau2 = 007 Chi2 = 1096 df = 7 (P = 014) I2 =36
Test for overall effect Z = 090 (P = 037)
Total (95 CI) 937 708 119 [ 090 157 ]
01 02 05 1 2 5 10
Favours treatment Favours control
(Continued )
37Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol more Placebo more Risk Ratio Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Total events 200 (Paracetamol more) 127 (Placebo more)
Heterogeneity Tau2 = 007 Chi2 = 2073 df = 15 (P = 015) I2 =28
Test for overall effect Z = 121 (P = 023)
01 02 05 1 2 5 10
Favours treatment Favours control
A D D I T I O N A L T A B L E S
Table 1 Number of patients with adverse events (lt 1000 mg ParacetamolPlacebo)
Author Total Paracetamol AEs Paracetamol Total Placebo AEs Placebo
Cooper 1980 37 2 37 6
Cooper 1981 37 12 38 4
Dionne 1994 27 7 25 5
Dolci 1994 80 7 82 8
Forbes 1984b 43 1 40 2
Forbes 1989 26 3 26 2
Forbes 1990 41 5 38 0
Gallardo 1990 15 5 11 3
Seymour 1996 40 0 39 0
Sunshine 1986 30 1 30 1
Vattaraphudej 1986 16 0 19 0
Totals 392 43 385 31
38Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Quality assessment
Author Allocation concealment Follow up Total (Max-3)
Cooper 1980 1 0 1
Cooper 1981 1 0 1
Cooper 1988 1 0 1
Cooper 1998 1 1 2
Dionne 1994 1 0 1
Dolci 1994 1 0 1
Forbes 1984b 2 0 2
Forbes 1989 1 0 1
Forbes 1990 2 0 2
Hersh 2000 1 1 2
Kiersch 1994 1 1 2
Kubitzek 2003 1 1 2
Lehnert 1990 1 1 2
Mehlisch 1995 2 1 3
Moller 2000 1 1 2
Olson 2001 2 1 3
Seymour 1996 1 1 2
Seymour 2003 2 0 2
Skoglund 1991 2 0 2
Sunshine 1986 2 1 3
Vattaraphudej 1986 1 1 2
39Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Random-effects metaregression lt 1000 mg vs 1000 mg Paracetamol vs Placebo
Outcome Number of studies Slope estimate 95 CI Slope interpretation P value
50 pain relief at 4
hours (using pain re-
lief )
16 094 (036 to 152) more pain relief for
higher doses
0001
50 pain relife at 6
hours (using pain re-
lief )
13 114 (071 to 156) more pain relief for
higher doses
lt0001
50 pain relief at
4 hours (using pain
intensity)
16 023 (-084 to 130) more pain relief for
higher doses
067
50 pain relief at
6 hours (using pain
intensity)
14 043 (-015 to 101) more pain relief for
higher doses
015
Table 4 List of adverse events
Adverse events Paracetamol Placebo
Nausea 21 11
Vomiting 11 3
Nausea andor vomiting stomach cramps
abdominal pain
3 3
Headache 47 31
Drowsiness sleepiness somnolence 36 13
Dizziness fainting syncope 9 4
Bleeding 11 7
Chills flushes fever flu-like symptoms 5 0
Paraesthesia 4 2
Jawache 1 0
Swelling 1 6
Cellulitis 1 0
40Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 List of adverse events (Continued)
Dry socket 11 12
Surgical complications 6 13
CNS 5 6
GI 12 2
Body as a whole 8 3
Respiratory 2 0
Psychiatric 0 1
Other hiccups hearingvestibular miosis 5 1
Table 5 Global assessment - 5-point scale(lt 1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Cooper 1980 37 089 38 089
Cooper 1981 37 192 37 062
Cooper 1988 36 238 40 205
Dionne 1994 27 240 25 200
Dolci 1994 72 210 76 217
Forbes 1984 39 126 36 028
Mean 248 183 252 144
Table 6 Global assessment - 4-point scale (lt 1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Forbes 1989 26 100 26 030
Forbes 1990 41 147 38 056
Sunshine 1986 30 120 30 093
Vattaraphudej 1986 16 16 19 116
41Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 6 Global assessment - 4-point scale (lt 1000 mg Paracetamol) (Continued)
Mean 113 131 113 070
Table 7 Global assessment - 5-point scale (1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Kiersch 1994 91 130 47 060
Kubitzek 2003 78 198 84 145
Mehlisch 1995 101 157 40 045
Olson 2001 66 281 39 193
Seymour 2003 62 250 32 214
Mean 398 194 242 129
Table 8 Global assessment - 4-point scale (1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Hersh 2000 63 229 27 085
Moller 2000 120 188 122 154
Mean 183 202 149 141
A P P E N D I C E S
Appendix 1 CENTRAL search strategy
1 MOLAR THIRD single term (MeSH)
2 (wisdom next tooth)
3 (wisdom next teeth)
4 (third near molar)
5 (1 or 2 or 3 or 4)
6 TOOTH EXTRACTION single term (MeSH)
7 (extract near tooth)
8 (extract near teeth)
9 (extract near (third next molar))
10 (extract near (third near molar))
42Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
11 (remov near tooth)
12 (remov near teeth)
13 (surgical near remov)
14 (surgery near remov)
15 (surgical near extract)
16 (surgery near extract)
17 (6 or 7 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16)
18 (5 and 17)
W H A T rsquo S N E W
Last assessed as up-to-date 21 May 2007
Date Event Description
31 July 2008 Amended Converted to new review format
H I S T O R Y
Protocol first published Issue 4 2003
Review first published Issue 3 2007
C O N T R I B U T I O N S O F A U T H O R S
Conceiving designing and co-ordinating the review (Kiaran Weil (KW) Paul Coulthard (PC))
Developing search strategy and undertaking searches (Zahid Afzal (ZA) Arjen van Wijk (AJW) KW)
Screening search results and retrieved papers against inclusion criteria (ZA KW) Marco Esposito (ME) Lee Hooper (LH) PC)
Appraising quality (KW ZA)
Extracting data from papers (KW LH Helen Worthington (HW))
Writing to authors for additional information (KW)
Data management for the review and entering data into RevMan (KW)
Analysis and interpretation of data (KW LH HW)
Writing the review (KW)
Providing general advice on the review (ME LH PC HW)
Performing previous work that was the foundation of current study (PC)
43Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D E C L A R A T I O N S O F I N T E R E S T
None known
S O U R C E S O F S U P P O R T
Internal sources
bull The University of Manchester UK
bull The University of Amsterdam Netherlands
External sources
bull No sources of support supplied
I N D E X T E R M S
Medical Subject Headings (MeSH)
Acetaminophen [adverse effects lowasttherapeutic use] Analgesics Non-Narcotic [adverse effects lowasttherapeutic use] Molar Third [lowastsurgery]
Outcome Assessment (Health Care) Pain Postoperative [lowastdrug therapy] Pain Measurement Randomized Controlled Trials as Topic
Tooth Extraction [lowastadverse effects]
MeSH check words
Humans
44Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 407
Relative efficacy of oral analgesics after thirdmolar extractionJ Barden1 J E Edwards2 H J McQuay3 P J Wiffen4 and R A Moore5
Objectives To compare the relative efficacy of analgesics after thirdmolar extraction from systematic reviews of randomised double blindstudiesData sources Dental trials from systematic reviews of randomiseddouble-blind studies of analgesics in acute painData selection Number of patients with moderate or severe painachieving at least half pain relief over 4 to 6 hours after a single oraldose of analgesicData extraction Independently by two reviewersData synthesis Use of dichotomous information from active andplacebo treatments first to calculate the statistical significance usingrelative risk and then to evaluate the clinical relevance using numberneeded to treat (NNT) Non-steroidal anti-inflammatory drugs (NSAIDs)and cyclo-oxygenase-2 (COX-2) inhibitors had the lowest (best) NNTsfor the outcome of at least half pain relief over 4-6 hours comparedwith placebo With the best performing analgesics 50-70 patients out of100 had good pain relief compared with about 10 out of 100 withplacebo Only paracetamol 600650 mg plus codeine 60 mg wasassociated with any significant increase in any patient experiencing anadverse eventConclusions NSAIDs and COX-2 inhibitors have the lowest (best) NNTsThey may also have fewer adverse effects after third molar surgerythough conclusive evidence is lacking At least 80 of analgesicprescribing by UK dentists is in line with the best available evidence onefficacy and safety
Acute pain has been studied in single dose designs first pro-posed by Beecher and colleagues12 and formalised by Houdeand Wallenstein3 The problem with single trials is that whilethey can demonstrate statistical superiority of analgesic overplacebo variation because of random chance means that if
1Research Associate 2Senior Research Associate 3Professor of Pain Relief 4PrescribingAdvisor 5Research Director Pain Research and Nuffield Department of AnaestheticsUniversity of Oxford Oxford Radcliffe Hospital The Churchill Headington Oxford OX3 7LJ UKCorrespondence to Dr R A MooreE-mail andrewmoorepruoxacuk
Refereed paperReceived 150403 Accepted 121103doi101038sjbdj4811721copy British Dental Journal 2004 197 407ndash411
small they provide a poor estimate of the size of the analgesiceffect4 Combining results from clinically homogeneous trials ina meta-analysis gives an accurate estimate of the extent of theanalgesic effect when sufficient numbers of patients have beenrandomised45
Clinical trials in acute pain normally last 4 to 6 hours becausethat is the duration of effect of most analgesics whether injectedor as tablets and whether simple analgesics NSAIDs or opioidsMeta-analysis in acute pain has concentrated on the use of thearea under the total pain relief versus time curve (TOTPAR)dichotomized into those patients who do or do not achieve atleast half pain relief (at least 50 maximum TOTPAR)6 Thismeasure is the one most frequently reported and it avoids theproblem of reporting continuous pain data as the mean of ahighly skewed distribution7 It has the benefit of being intuitivelymeaningful to patients and professionals as well as being meas-urable
Meta-analyses in acute pain usually combine studies from avariety of pain models and relative efficacy of analgesics inthese studies has been examined6 A majority of studies were inthird molar extraction but any postoperative pain condition islikely to be included In the largest dataset that of aspirin8
pain model (dental or other surgery) made no difference to theNNT
Dentists ask rightly about relative efficacy in dental painThe number of prescription items issued by dentists in Englandwas remarkably consistent between 1998 and 2001 (Table 1)with ibuprofen dihydrocodeine and paracetamol being mostfrequently prescribed This review set out to examine single-dose oral analgesics after third molar extraction from a numberof updated systematic reviews both for the analgesics common-ly prescribed in England and for those for which comparableevidence exists including the newer cyclo-oxygenase-2 selec-tive inhibitors like rofecoxib celecoxib and valdecoxib
METHODSIn all the systematic reviews QUORUM guidelines were fol-lowed9 In the reviews studies for inclusion were soughtthrough searching the Cochrane Library Biological AbstractsMEDLINE PubMed and the Oxford Pain Relief database10 Ref-erence lists and review articles were examined for possible addi-tional references Most had search dates in 2002
This paper reviews the available high quality information on analgesics commonlyprescribed by dentists including COX-2 selective inhibitors
Problems related to chance effects are avoided by combining multiple trials in a meta-analysis
There is good evidence of efficacy for most commonly-prescribed analgesics Standard doses of NSAIDs and COX-2 inhibitors provide the best analgesia and lowest
rate of adverse events
I N B R I E F
RESEARCH
07p407-411qxd 10092004 1518 Page 407
RESEARCH
408 BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004
References for the reviews are as followsAspirin Edwards et al 19998 additional searching in
2002 found no new studiesCelecoxib An unpublished review being submitted as a
Cochrane ReviewDiclofenac An updated version of a Cochrane review11
Dihydrocodeine A Cochrane review12
Ibuprofen An updated version of a Cochrane review11
Paracetamol An updated version of a Cochrane review13
Paracetamol An updated version of a Cochrane review13
plus codeineRofecoxib An updated version of a systematic review14
Valdecoxib A systematic review in preparation
Criteria for inclusion for postoperative dental pain werestudy in third molar extraction full journal publication (exceptvaldecoxib which included information from a poster) ran-domised controlled trials which included single dose treatmentgroups of oral analgesic and placebo double blind designbaseline postoperative pain of moderate to severe intensitypatients over 15 years of age at least 10 patients per group andthe pain outcome measures of total pain relief (TOTPAR) orsummed pain intensity difference (SPID) over 4-6 hours or suf-ficient data to allow their calculation Pain measures allowedfor the calculation of TOTPAR or SPID were a standard fivepoint pain relief scale (none slight moderate good complete)a standard four point pain intensity scale (none mild moder-ate severe) or a standard visual analogue scale (VAS) for pain
relief or pain intensity For adverse events the primary out-come sought was the proportion of patients experiencing anyadverse event with secondary outcomes of patients experienc-ing particular adverse events Although adverse events areoften reported inconsistently in acute pain trials15 the outcomeof any patient experiencing any adverse event was the mostconsistently reported
Each report which could possibly be described as a randomisedcontrolled trial was read independently by several authors andscored using a commonly-used three item 1-5 score qualityscale16 Consensus was then achieved The maximum score of anincluded study was 5 and the minimum score was 2 Authors werenot blinded because they already knew the literature This scoringsystem takes account of randomisation blinding and withdrawalsand drop outs Trials that score 3 or more (less biased) have beenshown repeatedly to have lower treatment effects than those scor-ing 2 or less1718
For each trial mean TOTPAR SPID VAS-TOTPAR or VAS-SPIDvalues for each treatment group were converted to maxTOTPARby division into the calculated maximum value19 The proportionof patients in each treatment group who achieved at least 50maxTOTPAR was calculated using valid equations20-22 The num-ber of patients randomised was taken as the basis for calculationsto produce an intention to treat analysis The number of patientswith at least 50 maxTOTPAR was then used to calculate relativebenefit and NNT for analgesic versus placebo The same methodswere used for adverse events where the number needed to harm(NNH) was calculated
Table 1 Numbers of prescription items issued by dentists and dispensed in EnglandAnalgesic 1998 1999 2000 2001
Ibuprofen 400 mg 107200 110400 109000 103900
Dihydrocodeine 30 mg 53700 50300 49100 46700
Ibuprofen 600 mg 34200 39700 40800 42600
Ibuprofen 200 mg 36300 34600 32000 30600
Paracetamol 500 mg 11100 12800 15400 17200
Paracetamol 500 mg soluble 800 1000 900 900
Pethidine 50 mg 1100 900 700 700
Aspirin 300 mg 200 200 200 200
Source DOH statistics division 2002 calendar year January to December
Dihydrocodeine 30 mgParacetamol 300 mg + codeine 30 mg
Paracetamol 600650 mgAspirin 600650 mg
Paracetamol 9751000 mgCelecoxib 200 mg
Paracetamol 600650 mg + codeine 60 mgIbuprofen 200 mgDiclofenac 50 mgRofecoxib 50 mgIbuprofen 400 mgValdecoxib 20 mgDiclofenac 100 mgValdecoxib 40 mgIbuprofen 600 mg
0 10 20 30 40 50 60 70 80 90 10095 confidence interval of the percent ofpatients achieving at least 50 pain relief
Fig 1 The 95confidence interval ofthe proportion ofpatients with at leasthalf pain relief over 4-6hours compared withplacebo in third molarextraction trials
07p407-411qxd 10092004 1519 Page 408
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 409
of patients had at least half pain relief with active treatment in onesmall trial in dental pain (Table 2)
The adverse event outcome of a patient experiencing anyadverse event is shown in Table 3 from 10113 patients in 107 tri-als Of the 15 drug and dose combinations only paracetamol600650 mg plus codeine 60 mg could be statistically distin-guished from placebo in 10 trials and 824 patients The NNH was53 (41 to 74) indicating that five patients had to be treated withparacetamol 600650 mg plus codeine 60 mg for one of them tohave an adverse event that would not have occurred with placeboFor all other drugs and doses there was no difference betweenanalgesic and placebo
DISCUSSIONSystematic review and meta-analysis both depend on two interde-pendent criteria for them to make sense the quality of the compo-nent individual studies and the total size of the sample availablefor analysis
We know that if trials are of poor reporting quality1718 or notrandomised30 or not blind or both31 then the tendency is to over-estimate the benefits of treatment The reviews included here alldemanded that trials should be both randomised and double-blindas a minimum requirement for inclusion
We also know that even if trials are done well small samplesize can lead to an incorrect answer just because of the randomplay of chance4 For these studies we also know just how muchinformation is needed to be 95 confident of an NNT to withplusmn05 units4 With an NNT of 23 it is 400 patients in the compari-son with an NNT of 29 it is 1000 patients and with an NNT of42 it is many more than with 1000 At NNTs of 4 or more evenwith 1000 patients fewer than 75 of trials will be within plusmn05of the overall NNT
The analgesics for which these two criteria were metunequivocally were valdecoxib (combining 20 mg and 40 mg)rofecoxib 50 mg ibuprofen 400 mg diclofenac 50 mg and prob-ably ibuprofen 200 mg For paracetamol the numbers were bor-derline and for diclofenac 100 mg too small to make any safejudgement There is good evidence of good efficacy for the anal-gesics most commonly prescribed by dentists with the excep-tion of dihydrocodeine where there was little evidence in totaland no convincing evidence of efficacy
Relative benefit and relative risk estimates were calculated with95 confidence intervals using a fixed effects model23 Hetero-geneity tests were not used as they have previously been shown tobe unhelpful2425 though homogeneity was examined visually26
Publication bias was not assessed using funnel plots as these testshave been shown to be unhelpful2728 The number needed to treator harm (NNT and NNH) with confidence intervals was calculatedby the method of Cook and Sackett29 from the sum of all eventsand patients for treatment and placebo
Relative benefit or risk was considered to be statistically signifi-cant when the 95 confidence interval did not include 1 NNT val-ues were only calculated when the relative risk or benefit was sta-tistically significant and are reported with the 95 confidenceinterval Calculations were performed using Microsoft Excel 2001on a Power Macintosh G4
RESULTSTable 2 shows the main results from 14150 patients in 155 trials of15 drug and dose combinations against placebo in third molarextractions Of those 15 drug and dose combinations only dihy-drocodeine 30 mg could not be statistically distinguished fromplacebo because there were no trials with any useful informationin third molar extraction Figure 1 shows the proportion ofpatients achieving at least 50 pain relief with treatment Thesmallest sample for any comparison was 136 patients for celecoxib200 mg Only five of the 14 comparisons had more than 1000patients and seven had fewer than 500 patients In all systematicreviews the majority of trials had quality scores of 3 or more
The lowest (best) NNTs were for NSAIDs and COX-2 inhibitorsat standard or high doses For these NNTs could be as low as about2 (meaning that two patients had to be treated with NSAID orCOXIB for one of them to have an outcome of at least half painrelief that would not have occurred with placebo) Valdecoxib 20mg and 40 mg rofecoxib 50 mg ibuprofen 400 mg and diclofenac50 mg and 100 mg all had NNTs below 24 For all of them about60-70 of patients had at least half pain relief with active treat-ment compared with about 10 with placebo
Paracetamol 9751000 mg aspirin 600650 mg and paraceta-mol 600650 mg had NNTs of between 4 and 5 Fewer than 40 ofpatients with paracetamol at these doses had at least half painrelief with active treatment With dihydrocodeine 30 mg only 16
Table 2 Efficacy of analgesics after third molar extraction from systematic reviews of randomised double blind trials
Number () of patientswith at least 50 pain relief
Drug and dose Treatment Placebo Relative benefit Number needed to treat Total patients Total trials(95 CI) (95 CI)
Valdecoxib 40 mg 204279 (73) 19194 (10) 73 (48 to 112) 16 (14 to 17) 473 4
Diclofenac 100 mg 71102 (70) 8102 (8) 89 (45 to 175) 16 (14 to 19) 204 2
Valdecoxib 20 mg 69101 (68) 8103 (8) 88 (45 to 173) 17 (14 to 20) 204 2
Diclofenac 50 mg 112189 (59) 21178 (12) 49 (33 to 75) 21 (18 to 26) 367 5
Rofecoxib 50 mg 318557 (57) 23262 (9) 66 (44 to 99) 21 (19 to 23) 819 6
Ibuprofen 400 mg 10351835 (56) 1861567 (12) 47 (40 to 54) 22 (21 to 24) 3402 37
Ibuprofen 200 mg 323695 (46) 47499 (9) 46 (35 to 61) 27 (24 to 31) 1194 14
Ibuprofen 600 mg 90114 (79) 3889 (43) 19 (15 to 25) 28 (20 to 43) 203 3
Celecoxib 200 mg 3991 (43) 445 (9) 48 (18 to 127) 29 (21 to 48) 136 1
Paracetamol 9751000 mg 226616 (37) 40422 (9) 38 (28 to 52) 37 (31 to 47) 1038 10
Paracetamol 600650 mg + codeine 60 mg 217532 (48) 64380 (19) 25 (19 to 31) 42 (34 to 55) 911 12
Paracetamol 600650 mg 224630 (36) 76635 (12) 29 (23 to 37) 42 (36 to 52) 1265 10
Aspirin 600650 mg 6271788 (36) 2551847 (15) 25 (22 to 29) 47 (42 to 54) 3635 46
Paracetamol 300 mg + codeine 30 mg 48175 (29) 11124 (9) 33 (18 to 62) 54 (37 to 97) 299 3
Dihydrocodeine 30 mg 849 (16) 250 (4) 41 (09 to 18) not calc 99 1
Shaded areas are those analgesics used by dentists in the UK
07p407-411qxd 10092004 1519 Page 409
RESEARCH
410 BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004
With the information available standard doses of NSAIDs andCOX-2 inhibitors provided the best analgesia (Fig 2) NNTs of 2and below are indicative of very effective medicines32 The indirectcomparisons that allow us to arrive at this conclusion are only sus-tainable because the trials have the same design use patients withthe same entry criterion (moderate or severe pain intensity) withstandard measurements made in the same way over the same peri-od of time and with the same output from each trial and oneknown to be legitimate The validity of the indirect comparisonsare buttressed by the dose response of two doses of ibuprofen (400mg was better than 200 mg) and two doses of paracetamol(9751000 mg was better than 600650 mg) where there were cred-ible amounts of information A systematic review of ibuprofenversus paracetamol in dental studies also concluded that ibuprofenwas superior concordant with the indirect comparison33
The adverse event information we have tells us only aboutpatients experiencing any adverse event With the amount ofinformation available it appears that only higher doses ofcodeine with paracetamol resulted in a significantly higher ratefor this outcome than placebo In Table 3 the rate at which thisadverse event occurred with placebo varied greatly between 2
and 52 This variation will be due partly to small sizes4 butalso because we know that methods of collecting adverse eventdata impact significantly on the reported incidence and becausemethods used varied15
Information about specific adverse events is even more difficultto obtain and very large data sets are required to produce infor-mation about for instance gastric irritation with aspirin use8 Ofinterest to dentists might be the rate of alveolitis or dry socket Thisis reported in some of the newer COXIB studies but not in olderstudies There is just too little information to make a judgement
What these comparisons do not do is to tell dentists what toprescribe They and the products of other systematic reviewsshould not be used as rules but rather as evidence-based toolsto help make better policy decisions and decisions about indi-vidual patients Present prescribing practice (Table 1) showsthat for the most part effective and safe analgesics are beingused in 80 of prescriptions The exception is prescribing dihy-drocodeine 30 mg (20 of prescriptions) for which we lack sin-gle dose evidence of efficacy in dental surgery and which couldnot be distinguished from placebo in other conditions againwith little data6
Paracetamol 300 + codeine 30 mgAspirin 600650 mg
Paracteamol 600650 mgParacetamol 600650 + codeine 60 mg
Paracetamol 9751000 mgCelecoxib 200 mgIbuprofen 200 mgDiclofenac 50 mgIbuprofen 400 mgRofecoxib 50 mg
Valdecoxib 20 mgValdecoxib 40 mgDiclofenac 100 mg
1 2 3 4 5 6 7 8 9 1095 confidence interval of the NNT
Fig 2 The 95confidence interval ofthe number needed totreat (NNT) for at leasthalf pain relief over 4-6hours compared withplacebo in third molarextraction trials
Table 3 Patients experiencing any adverse event with analgesics after third molar extraction from systematic reviews of randomised double blind trials
Number () of patientsharmed with
Drug and dose Treatment Placebo Relative risk Number needed to harm Total patients Total trials(95 CI) (95 CI)
Valdecoxib 40 mg 63180 (35) 76144 (53) 06 (05 to 08) not calc 324 3
Diclofenac 100 mg 252 (4) 252 (4) 10 (12 to 68) not calc 104 1
Valdecoxib 20 mg 36100 (36) 55103 (53) 07 (05 to 09) not calc 203 2
Diclofenac 50 mg 15222 (7) 12210 (6) 12 (06 to 24) not calc 432 4
Rofecoxib 50 mg 105314 (33) 48122 (39) 09 (07 to 11) not calc 436 3
Ibuprofen 400 mg 120972 (13) 91805 (12) 11 (08 to 14) not calc 1777 19
Ibuprofen 200 mg 84554 (15) 69372 (19) 08 (06 to 10) not calc 926 10
Ibuprofen 600 mg no data
Celecoxib 200 mg no data
Paracetamol 9751000 mg 175836 (24) 103464 (20) 11 (09 to 13) not calc 1300 9
Paracetamol 600650 mg + codeine 60 mg 156490 (25) 43333 (14) 18 (13 to 25) 53 (41 to 74) 824 10
Paracetamol 600650 mg 32228 (14) 20229 (9) 16 (09 to 27) not calc 457 7
Aspirin 600650 mg 1551320 (12) 1681422 (12) 10 (08 to 12) not calc 3031 36
Paracetamol 300 mg + codeine 30 mg 29175 (15) 20124 (16) 09 (06 to 16) not calc 299 3
Dihydrocodeine 30 mg 149 (2) 150 (2) 10 (01 to 17) not calc 99 1
Shaded areas are those analgesics used by dentists in the UK
07p407-411qxd 10092004 1520 Page 410
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 411
Not all the analgesics in this review are presently available forprescribing by dentists at least in the UK The information on effi-cacy on harm and on the amount of information available shouldbe useful in any initiative to develop a prescribing formulary indentistry especially as we have growing confidence in the value ofindirect comparisons34
COMPETING INTERESTSRAM has been a consultant for MSD RAM amp HJM have consulted for variouspharmaceutical companies RAM HJM amp JE have received lecture fees frompharmaceutical companies related to analgesics and other healthcareinterventions All authors have received research support from charitiesgovernment and industry sources at various times but no such support wasreceived for this work No author has any direct stock holding in anypharmaceutical company
AUTHORS CONTRIBUTIONSJB was involved with searching data extraction quality scoring analysis andwriting JE was involved with searching data extraction quality scoring andwriting HJM was involved in analysis and writing RAM was involved in dataextraction quality scoring analysis and writing PW was involved with theoriginal concept with researching prescribing data and writing
The work was supported by Pain Research Funds and the Oxford Pain Relief TrustThe authors would like to thank Frances Fairman of the Cochrane Pain Palliativeand Supportive Care systematic review group for bringing this issue to ourattention The Department of Health Statistics Division provided data onprescribing by dentists
1 Beecher H K Keats A S Mosteller F The effectiveness of oral analgesics (morphinecodeine acetylsalicylic acid) and the problem of placebo lsquoreactorsrsquo and lsquononreactorsrsquo J Pharmacol 1953 109 93-400
2 Beecher H K The measurement of pain Pharmacol Rev 1957 9 59-2103 Houde R W Wallenstein S L Beaver W T Clinical measurement of pain In G De
Stevens (ed) Analgetics pp75-122 New York and London Academic Press 1965 4 Moore R A Gavaghan D Tramegraver M R Collins S L McQuay H J Size is everything mdash
large amounts of information are needed to overcome random effects in estimatingdirection and magnitude of treatment effects Pain 98 78 209-216
5 Ioannidis J P A Lau J Evolution of treatment effects over time Empirical insight fromrecursive cumulative metaanalyses PNAS 2001 98 831-836
6 McQuay H J Moore R A An evidence-based resource for pain relief Oxford OxfordUniversity Press 1998
7 McQuay H J Carroll D Moore R A Variation in the placebo effect in randomisedcontrolled trials of analgesics all is as blind as it seems Pain 1996 64 331-335
8 Edwards J E Oldman A Smith L Wiffen P J Carroll D McQuay H J Moore R A Oralaspirin in postoperative pain a quantitative systematic review Pain 1999 81 289-297
9 Moher D Cook D J Eastwood S Olkin I Rennie D Stroup D F Improving the quality ofreports of meta-analyses of randomised controlled the QUOROM statement Lancet1999 354 1896-1900
10 Jadad A R Carroll D Moore A McQuay H Developing a database of published reportsof randomised clinical trials in pain research Pain 1996 66 239-46
11 Collins S L Moore R A McQuay H J Wiffen P J Edward J S Single dose oral ibuprofenand diclofenac for postoperative pain In The Cochrane Library Issue 4 2000 OxfordUpdate Software
12 Edwards J E McQuay H J Moore R A Single-dose dihydrocodeine for acute
postoperative pain In The Cochrane Library Issue 4 2000 Oxford Update Software13 Moore R A Collins S L Carroll D McQuay H J Edwards J Single dose paracetamol
(acetaminophen) with and without codeine for postoperative pain In The CochraneLibrary Issue 4 2000 Oxford Update Software
14 Barden J Edwards J E McQuay H J Moore R A Rofecoxib in acute postoperative painquantitative systematic review BMC Anesthesiol 2002 2 4httpwwwbiomedcentralcom1471-225324
15 Edwards J E McQuay H J Moore R A Collins S L Reporting of adverse effects inclinical trials should be improved Lessons from acute postoperative pain J PainSympt Manage 1999 18 427-437
16 Jadad A R Moore R A Carroll D et al Assessing the quality of reports of randomizedclinical trials is blinding necessary Control Clin Trials 1996 17 1-12
17 Khan K S Daya S Jadad A R The importance of quality of primary studies inproducing unbiased systematic reviews Arch Intern Med 1996 156 661-666
18 Moher D Pham B Jones A et al Does quality of reports of randomised trials affectestimates of intervention efficacy reported in meta-analyses Lancet 1998 352609-613
19 Cooper S A Single-dose analgesic studies the upside and downside of assaysensitivity In Max M B Portenoy R K and Laska E M (eds) The design of analgesicclinical trials (Advances in Pain Research and Therapy Vol 18) pp117-124 New YorkRaven Press 1991
20 Moore A McQuay H Gavaghan D Deriving dichotomous outcome measures fromcontinuous data in randomised controlled trials of analgesics Pain 1996 66 229-237
21 Moore A McQuay H Gavaghan D Deriving dichotomous outcome measures fromcontinuous data in randomised controlled trials of analgesics Verification fromindependent data Pain 1997 69 127-130
22 Moore A Moore O McQuay H Gavaghan D Deriving dichotomous outcome measuresfrom continuous data in randomised controlled trials of analgesics Use of painintensity and visual analogue scales Pain 1997 69 311-315
23 Morris J A Gardner M J Calculating confidence intervals for relative risk odds ratiosand standardised ratios and rates In Gardner M J and Altman D G(eds) Statistics withconfidence mdash confidence intervals and statistical guidelines pp50-63 LondonBritish Medical Journal 1995
24 Gavaghan D J Moore R A McQuay H J An evaluation of homogeneity tests in meta-analyses in pain using simulations of individual patient data Pain 2000 85 415-424
25 Higgins J Thompson S Deeks J Altman D Statistical heterogeneity in systematicreviews of clinical trials a critical appraisal of guidelines and practice J Health SurvRes Policy 2002 7 51-61
26 LAbbeacute K A Detsky A S ORourke K Meta-analysis in clinical research Ann Intern Med1987 107 224-233
27 Sterne J A Gavaghan D Egger M Publication and related bias in meta-analysispower of statistical tests and prevalence in the literature J Clin Epidemiol 2000 531119-1129
28 Tang J-L Liu J L Y Misleading funnel plot for detection of bias in meta-analysis J ClinEpidemiol 2000 53 477-484
29 Cook R J Sackett D L The number needed to treat a clinically useful measure oftreatment effect Br Med J 1995 310 452-454
30 Carroll D Tramegraver M McQuay H Nye B Moore A Randomization is important instudies with pain outcomes systematic review of transcutaneous electrical nervestimulation in acute postoperative pain Br J Anaesth 1996 77 798-803
31 Schulz K F Chalmers I Hayes R J Altman D G Empirical evidence of bias dimensionsof methodological quality associated with estimates of treatment effects incontrolled trials J Am Med Assoc1995 273 408-412
32 McQuay H J Moore R A Using numerical results from systematic reviews in clinicalpractice Ann Intern Med 1997 126 712-720
33 M Hyllested Jones S Pedersen J L Kehlet H Comparative effect of paracetamolNSAIDs or their combination in postoperative pain management a qualitative reviewBr J Anaesth 2002 88 199-214
34 F Song Altman D G Glenny A M Deeks J J Validity of indirect comparison forestimating efficacy of competing interventions empirical evidence from publishedmeta-analyses Br Med J 2003 326 472-476
07p407-411qxd 10092004 1520 Page 411
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
Relative efficacy of oral analgesics after third molar extraction ndash a 2011 updateS Derry1 P J Wiffen2 and R A Moore3
and reporting and were all of high meth-odological quality the relative efficacy of different analgesics is justifiable when established against the common comparator of placebo3 Moreover the methods have been extensively examined and validated using individual patient data analyses45
Several approaches can be used to pre-sent results The percentage of patients who benefit with treatment is one approach obviously the higher the number
In 2004 the British Dental Journal carried a review examining analgesic efficacy meas-ured after third molar extractions1 predom-inantly derived from Cochrane reviews of single dose analgesics in established mod-erate or severe pain In the intervening years the reviews on which it was based have been extended to other analgesics and updated to include relevant additional clinical trials performed in the past decade
The culmination of this work has been the publication by the Cochrane Collaboration of an overview of these updated systematic reviews2 The overview included 35 sepa-rate Cochrane Reviews with 38 analyses of single dose oral analgesics tested in acute postoperative pain models with results from about 45000 participants studied in approximately 350 individual studies About 29000 patients contributed data to trials in dental pain
Each individual review reported results for dental studies where data were avail-able overwhelmingly in the third molar extraction pain model Because all of the reviews used identical methods outcomes
This article provides a summary of the efficacy and relative efficacy of 38 different drugs or drug combinations tested in standard postoperative pain trials It will help clinicians and patients make informed choices about analgesia based on pain relief duration of action and adverse events which can then be put into context for the individual patient depending on local availability This article highlights the fact that no single drug is effective in all patients ndash even the best drugs fail to provide good levels of pain relief in at least 30 These patients should try a different analgesic
the better Another way is to look at the number needed to treat (NNT) for one patient to benefit this is the treatment-specific effect and can be expressed as 100(active - placebo) The ideal NNT is 1 where everyone gets better with treatment and no one does with placebo lower numbers are better In dental tri-als where about 10 of patients benefit with placebo the best possible NNT is 100100 - 10 = 11
13Pain Research and Nuffield Division of Anaesthet-ics Department of Clinical Neurosciences University of Oxford The Churchill Hospital Oxford OX3 7LJ 2UK Cochrane Centre Summertown Pavilion 18-24 Middle Way Oxford OX2 7LG Correspondence to R Andrew Moore Email andrewmoorepruoxacuk
Refereed Paper Accepted 12 September 2011 DOI 101038sjbdj2011905 copyBritish Dental Journal 2011 211 419-420
bull Summarises the known evidence on efficacy of oral analgesics in dental pain
bull Describes shorter term pain relief and time needed before remedication
bull Provides an evidential context for making decisions about individual patients or practice guidelines
I N B R I E F
PRA
CTICE
Table 1 Efficacy results in dental pain studies for a range of commonly used analgesics
Drug and dose (mg)Number of
Percent with at least 50 maxi-mum pain relief NNT
Median time to remedication (hr)
Trials Patients Active Placebo
Aspirin 600650 mg 45 3581 36 14 45 (40 to 52) 30
Aspirin 1000 mg 4 436 35 11 42 (32 to 60) no data
Celecoxib 400 mg 4 620 34 3 25 (22 to 29) 84
Diclofenac 50 mg (Na and K) 9 1119 56 19 27 (24 to 31) 43
Diclofenac 50 mg K 5 622 65 16 21 (19 to 24) no data
Etoriocoxib 120 mg 4 500 71 9 16 (15 to 18) gt24
Ibuprofen 400 mg 49 5428 55 12 23 (22 to 24) 56
Ibuprofen 400 mg soluble 9 959 66 10 18 (17 to 20) no data
Ibuprofen 200 mg + paracetamol 500 mg 2 280 74 10 16 (14 to 18) gt8
Naproxen 500550 mg 5 402 61 7 18 (16 to 21) 89
Paracetamol 1000 mg 19 2157 41 10 32 (29 to 36) 39
Note that data for remedication time were not generally available for dental studies separately and the values reported apply to all postoperative conditions though predominantly third molar extraction
BRITISH DENTAL JOURNAL VOLUME 211 NO 9 NOV 12 2011 419
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
PRACTICE
This brief report describes the main results of interest to dentists using results from the Cochrane overview and from a recent analysis of a combination of ibu-profen and paracetamol5
RESULTSTable 1 reports data for aspirin celecoxib diclofenac etoricoxib ibuprofen ibu-profen plus paracetamol naproxen and paracetamol Widely differing amounts of information were available for individual drugs from as few as 402 patients for nap-roxen 500550 mg and as many as 5428 for ibuprofen 400 mg
One outcome reported is the percentage of patients with initially moderate pain (30-60 mm on a 100 mm VAS) or severe pain (more than 60 mm) who obtained at least 50 of the maximum possible pain relief over a 4-6 hour period after taking the tab-lets This is a high test of efficacy achieved by only about 10 of patients who received no active treatment (placebo) but achieved by 34-74 of those who did get the active drug Ibuprofen 200 mg plus paracetamol 500 mg and etoricoxib 120 mg achieved
response rates above 70 paracetamol 1000 mg achieved only a 41 response rate
Several products had an NNT of about 2 or below the combination of ibupro-fen 200 mg plus paracetamol 500 mg etoricoxib 120 mg ibuprofen 400 mg in a soluble form naproxen 500550 mg and 50 mg of the potassium salt of diclofenac (the sodium salt being much less effective in this assay Fig 1)
A new outcome that some will con-sider relevant is the time required for half the patients to need more analgesia the time to remedication Longer duration is another indicator of greater effect and for a number of analgesics median remedica-tion times are beyond eight hours
DISCUSSIONThe 2004 review included evidence for rofecoxib and valdecoxib neither of which is available today New relevant informa-tion includes data on the ibuprofen plus paracetamol combination different ibu-profen and diclofenac formulations and etoricoxib all of which are among the most efficacious analgesics after third
molar surgery Greater efficacy and longer duration of action tended to go together
For one analgesic relevant to dentistry the evidence is largely silent For dihydrocodeine 30 mg (still commonly used by dentists) only 136 patients were found in trials in dental pain with only 24 obtaining at least 50 maximum pain relief compared with 7 with placebo The resultant NNT was 6 far worse than available for drugs in Table 1 and far worse than ibuprofen 400 mg in the only direct comparison6 The Cochrane overview concluded that the results for dihy-drocodeine were not robust because of the smallness of the data set available and that unpublished results from just 46 patients in zero effect trials would be needed to make any result clinically irrelevant
CONCLUSIONThe amount of evidence available on single dose studies of analgesics in dental pain is large and readily available These results are tools to help formulate policy and pre-scribing for individuals and populations
1 Barden J Edwards J E McQuay H J Wiffen P J Moore R A Relative efficacy of oral analgesics after third molar extraction Br Dent J 2004 197 407ndash411
2 Moore R A Derry S McQuay H J Wiffen P J Single dose oral analgesics for acute postoperative pain in adults Cochrane Database Syst Rev 2011 9 CD008659
3 Song F Altman D G Glenny A M Deeks J J Validity of indirect comparison for estimating efficacy of competing interventions empirical evidence from published meta-analyses BMJ 2003 326 472
4 Moore R A Edwards J E McQuay H J Acute pain individual patient meta-analysis shows the impact of different ways of analysing and presenting results Pain 2005 116 322ndash331
5 Moore R A Straube S Paine J Derry S McQuay H J Minimum efficacy criteria for comparisons between treatments using individual patient meta-analysis of acute pain trials examples of etoricoxib paracetamol ibuprofen and ibuprofenparacetamol combinations after third molar extraction Pain 2011b 152 982ndash989
6 Moore R A Edwards J Derry S McQuay H J Single dose oral dihydrocodeine for acute postop-erative pain Cochrane Database Syst Rev 2000 2 CD002760
Ibuprofen 200mg + paracetamol 500 mg
Ibuprofen 400 mg
Aspirin 600650 mg
Aspirin 1000 mg
Paracetamol 1000
Naproxen 500550
Diclofenac 50 mg (Na and K)
Celecoxib 400 mg
Diclofenac 50 mg K
Ibuprofen 400 mg soluble
Etoriocoxib 120 mg
1 2 3 4 5 6
NNT for at least 50 maximum pain relief (95 CI)
Fig 1 NNTs in dental pain studies for a range of commonly used analgesics
420 BRITISH DENTAL JOURNAL VOLUME 211 NO 9 NOV 12 2011
Combining paracetamol with a selectivecyclooxygenase-2 inhibitor for acutepain relief after third molar surgerya randomized double-blindplacebo-controlled study
Birgitta Haglund12 Inger vonBltzingslccedilwen1
1Public Dental Health Service KarlstadVrmland Sweden 2Department of ClinicalPharmacology Sahlgrenska Academy atGccedilteborg University Sweden
Traditional non-steroidal anti-inflammatory drugs(NSAIDs) [ie non-selective cyclooxygenase (COX)inhibitors such as ibuprofen and diclofenac] have beenwidely used in outpatients for acute pain relief followingoral surgery Their anti-inflammatory and analgesicproperties together with well-established tolerabilitymake them an initial choice for the management of mostforms of mild to moderate pain in outpatients (1 2)However these drugs have well-documented adverseeffects such as gastrointestinal intolerability Further-more they need to be administered several times a dayMore effective and practical pain relief regimes withfewer side-effects are needed for moderate to severe painafter oral surgeryNSAIDs act by inhibiting COX enzymes which are
responsible for the production of prostaglandin fromarachidonic acid This acid emerges from the breakdownof phospholipids in the cell walls of damaged tissue (3)Prostaglandin elicits a number of biological effects someof which contribute to the inflammatory process leading
to pain Multiple COX enzymes have been identifiedCOX-1 is mainly expressed under physiological condi-tions throughout the body for example by platelets (4)and COX-2 is related to inflammation and pain (4ndash6)although COX-1 and COX-2 also have overlappingproperties (7) Improved knowledge on more selectiveCOX enzymes led to the development of specific COX-2inhibitors such as rofecoxib (8) and celecoxib withanalgesic anti-inflammatory and gastroprotective prop-erties Of these drugs rofecoxib has been shown to bemore effective than celecoxib (9ndash11)Rofecoxib has the same analgesic effect as ibuprofen
but with the benefit of a longer duration (9 10 12) It hasa long half-life which makes it suitable for once-dailydosing (12) compared with traditional NSAIDs thatneed to be taken several times per day Rofecoxib hasalso been suggested to be more effective than paracet-amol combined with codeine (13 14) The COX-2inhibitor rofecoxib may be an interesting choice for acutepain relief after oral surgery
Haglund B von Bulzingslowen I Combining paracetamol with a selective cyclooxyge-nase-2 inhibitor for acute pain relief after third molar surgery a randomized double-blind placebo-controlled study Eur J Oral Sci 2006 114 293ndash301 2006 The AuthorsJournal compilation 2006 Eur J Oral Sci
Severe pain after third molar surgery is often encountered and more effective treatmentregimes are warranted The objective of this study was to evaluate if the combinationof paracetamol and rofecoxib a selective cyclooxygenase-2 (COX-2) inhibitorimproves analgesic effects following third molar surgery compared with rofecoxibalone Paracetamol alone was also evaluated Altogether 120 patients with moderate tosevere pain after third molar surgery were given a single postoperative dose of one ofthe following treatments rofecoxib + paracetamol rofecoxib alone paracetamolalone or placebo Patients assessed level of pain and pain relief every 30 min for 8 hafter surgery and made a global evaluation of the medication 4 and 8 h after surgeryParacetamol and rofecoxib combined improved the analgesic effect compared withrofecoxib alone for the first 15 h Rofecoxib alone and the combination of paracet-amol and rofecoxib had a significantly better analgesic effect than paracetamol alonefrom 3 h onwards The early onset of pain relief for the combination of paracetamoland rofecoxib compared with rofecoxib alone could be of great importance whentreating acute pain after third molar surgery After data collection for this studyrofecoxib was withdrawn from the market as a result of reported fatal cardiovascularevents Whether this is relevant for short-term use is unknown but it has to be con-sidered before rofecoxib may be used for pain relief following third molar surgery
Birgitta Haglund Folktandvrden TingvallaBox 577 SE-651 13 Karlstad Sweden
Telefax +46ndash54ndash137435E-mail birgittahaglundlivse
Key words COX-2 inhibitor pain relief para-cetamol randomized trial third molar surgery
Accepted for publication April 2006
Eur J Oral Sci 2006 114 293ndash301Printed in Singapore All rights reserved
2006 The AuthorsJournal compilation 2006 Eur J Oral Sci
European Journal ofOral Sciences
Combining drugs that cause analgesia through differ-ent mechanisms may give additive analgesic effects (15)and lead to dose-sparing effects and improved safety(16) The analgesic mechanism of COX inhibition ispredominantly peripheral Research on paracetamol hasnot been able to delineate a clear mechanism of actionbut it is suggested to lie predominantly in the centralnervous system (17) Some studies indicate that combi-ning a traditional NSAID and paracetamol after oralsurgery may enhance the analgesic effect compared withsingle drug regimes (18 19)The theory of the analgesic effect of traditional
NSAIDs being caused by COX-2 inhibition leads to thethought that an additive effect should be present alsowhen combining rofecoxib and paracetamol The aim ofthis study was therefore to explore in a third molarsurgery pain model (20) if there is an additive analgesiceffect when combining the COX-2 selective inhibitorrofecoxib with paracetamol compared with rofecoxibalone for acute pain relief We also compared the anal-gesic efficiency of rofecoxib and paracetamol becausethis to our knowledge has not been reported followingthird molar surgery
Material and methods
Study design
This study was designed as a multicenter randomizeddouble-blind placebo-controlled study with a single dose ofrofecoxib 50 mg and paracetamol 1 g combined vs rofec-oxib 50 mg alone vs paracetamol 1 g alone vs placebogiven postoperatively to patients stating moderate to severepain after surgical removal of one or two lower third molarsPatients were asked to give written informed consent toparticipate after being told about the procedures A total of120 patients were randomized into four different treatmentgroups as follows 40 patients receiving the combination ofrofecoxib 50 mg and paracetamol 1 g 40 patients receivingrofecoxib 50 mg alone 20 patients receiving paracetamol 1 galone and 20 patients receiving placebo The patientsrsquoevaluations of the treatments were obtained by using aquestionnaire which the patients filled in at home during an8-h study period following intake of the study medicationThe trial was approved by the Regional Ethical Committeeof Medical Research in Orebro Sweden and the MedicalProducts Agency in Uppsala Sweden
Patients
Consecutive patients visiting four general dental practicesand in need of mandibular third molar surgery in accordancewith the National Institutes of Health (NIH) guidelines (21)were screened for enrollment Only patients with thirdmolars needing bone removal were included Other inclusioncriteria were age gt18 yr weight gt50 kg butlt120 kg andan appointment before noon for surgery This was necessaryin order for the patients to have time to fill in the ques-tionnaire for 8 h after intake of the study medication beforebedtime Exclusion criteria were as follows intolerance toacetylsalicylic acid (ASA) paracetamol andor NSAIDsany ongoing medication (except contraceptives) pregnancylactation inadequate contraception alcohol or drug abusePatients with evidence of previous or present cardiovascular
respiratory diabetic hepatic gastric renal neurological orneoplastic diseases were also excluded as were those withongoing pericoronitis or other local oral infections involvingpain Patients with an intake of any analgesics 6 h precedingsurgery was also excluded All patients who met the studycriteria and reported moderate to severe pain after the sur-gery were included in the study
Surgery
The surgery was performed by one of four dentists speciallytrained in dento-alveolar surgery using local anesthesia(lidocaine 20 mg ml)1 plus epinephrine 125 lg ml)1) Theremoval of bone was carried out with a burr under thecooling of saline
Masking randomization and rescue medication
The study medications were masked by being encapsula-ted in identical capsules The capsules contained 50 mg ofrofecoxib 200 mg of paracetamol or placebo All patientswere given a sealed container containing six capsules(Table 1) so that the patients in the different treatmentgroups received the correct amount of medication and stillthe same number of capsules The capsules were manu-factured by Apoteket Production amp Laboratories (APLStockholm Sweden) Randomization of the patients intothe four treatment groups was performed for the group intotal by Apoteket using randomization tables All studypersonnel and participating patients were blinded totreatment assignment for the duration of the study Themain investigator broke the codes for the final calcula-tionsIbuprofen 400 mg was used as a rescue medication in case
patients needed additional analgesia at any time during the8-h study period The rescue medication was kept in aseparate container If patients felt that rescue medicationwas needed they were instructed to wait 90 min if possibleafter intake of their study medication to allow for the studydrug to take effect
Intake of study medication and information about thequestionnaire
After surgery the patients were given their two containerswith study and rescue medications respectively together
Table 1
Distribution of the drug capsules with the different substances percontainer in each study group
Study groups
Rofecoxib50 mg +
paracetamol 1 gRofecoxib50 mg
Paracetamol1 g Placebo
Rofecoxib50 mg
1 1 0 0
Paracetamol200 mg
5 0 5 0
Placebo 0 5 1 6Total no ofcapsules ineach container
6 6 6 6
294 Haglund amp Bultzingslowen
with the questionnaire Routine postoperative informationwas given The patients were instructed to go home and takeno medication before calling the investigator when theyregained full sensibility in the lower lip following the dis-appearance of the local anesthesia If the patient had notcalled the investigatorrsquos mobile phone within 3 h after theend of surgery the investigator called the patientAt the telephone contact the patients were asked to state
their level of pain in the questionnaire using a 3-point scalefrom mild to moderate to severe pain If patients statedmoderate or severe pain they were asked to break the seal ofthe container with their study medication and take all sixcapsules Detailed instructions were provided on how to fill inthe questionnaire To ascertain that patients adhered to theprotocol information was given to contact the investigatorwith any questions regarding medication or other issuesconcerning the studyduring the 8-h postoperative periodThestudy period started at the time of intake of the study medi-cation If patients stated mild pain they were asked if theycould tolerate waiting before taking any medication In suchcases a second telephone contact was made If patients stillstatedmild pain they were asked if it was possible for them toreturn their sealed container with the study medicationPatients who did so were replaced with another patient
Efficacy assessments
The outcome measures of the trial were pain intensity painrelief (PAR) global evaluation score (patientsrsquo overallassessment of the medication) derived summary measuresuse of rescue medication and side-effects experienced allrecorded by the patients in their questionnaire After intakeof the study medication pain intensity and PAR wasassessed by the patient every 30 min for 8 h and the globalevaluation score was measured at 4 and 8 h The startingpoint for each patient was the time for intake of studymedication The final measurement point was the end of theobservation period (ie 8 h later) or the time of intake ofrescue medication If rescue medication was used patientswere asked to assess pain intensity and pain relief and give aglobal evaluation score at the time of intake These scoreswere then used for the rest of the observation period inaccordance with a study by Laska et al (22)Pain intensity was evaluated by the patients using a
horizontal visual analog scale (VAS) of 10 cm marked nopain at 0 and worst possible pain at 10 PAR was meas-ured on a 5-point scale as follows 0 no pain relief 1 somepain relief 2 medium pain relief 3 good pain relief and 4total pain relief Global evaluation score was measured on a4-point scale as follows 0 poor 1 fair 2 good and 3excellent Patients using rescue medication recorded the timeof intake A question about any side-effects experienced wasanswered by yes or no at the end of the study period Ifyes the patients estimated adverse events on a 3-point scale(1 slight 2 moderate 3 severe) and reported what kind ofside-effect was experienced
Analysis
The analgesic effect of the drugs measured every 30 min bypain intensity (VAS) and PAR scores was comparedSummary measures were calculated by the use of the fol-lowing total pain relief (TOTPAR the sum of all PARscores for the whole study period of 05ndash8 h) pain intensitydifference (PID pain intensity at the start minus painintensity at any given observation point) sum of PID for the
05ndash3-h period (SPID05)3 h) and sum of PID for the total05ndash8-h period (SPIDtotal) PID values were not analyzedseparately but used for the calculation of SPIDThe use of rescue medication was compared between the
treatment groups by calculating the percentage of patientsin each group who used rescue Also the mean timebetween intake of the study medication and intake of therescue medication in the different groups was analyzedSide-effects in the treatment groups were compared interms of percentage of patients in each group whoexperienced such problems Median global evaluationscores between the different groups were analyzed as wellas the percentage of patients in each group using the dif-ferent scores
Statistics
The sample size calculations were carried out assuming adifference in SPID outcome between groups using thecombination of rofecoxib + paracetamol and rofecoxibalone amounting to 20 (18) with a power of at least 80and a standard deviation (SD) of 15 using non-para-metric statistics (MannndashWhitney U-test) This calculationestimated that a minimum of 22 patients should be includedin each groupStandard descriptive statistics and tests were used and the
calculations were performed in Statistical Package for SocialSciences (spss) version 12 The principle of last observationcarried forward was used Significances between groupsregarding VAS scores were tested with an independent-samples t-test at each time point for all possible compari-sons as we considered VAS to be a continuous scale inaccordance with Max et al (23) The same applies for thetesting of SPID up to 3 and 8 h The analysis of TOTPARwas based on an assumption that the scores are consideredinterval scaled (23) and significance testing was carried outwith an independent samples t-test The same test was usedfor testing differences between study groups regarding theuse of rescue medication Hypothesis testing of valuesmeasured with categorical ordinal scales (ie PAR andglobal evaluation) was performed with a non-parametrictest (MannndashWhitney U-test) P-values of lt005 were con-sidered statistically significant
Results
Altogether 126 consecutive patients who fulfilled theinclusion criteria gave written informed consent to par-ticipate in the study The majority of the patients whowere asked to participate agreed to do so Patients whodeclined to participate usually did not have a before-noon appointment for the surgery Out of the 126patients six were excluded as they stated their pain asmild at the telephone contacts and were able to returntheir sealed study medication A total of 120 patientsparticipated by taking the randomized study medicationSome patients (n frac14 8) who did not fulfill the criterion ofmoderate to severe pain but nevertheless wanted toparticipate took their study medication but wereexcluded from the calculations Of these patients ahigher proportion was men (75) compared with thestudied population Some patients (n frac14 5) were excludedfor other reasons one patient randomized to the
COX-2 inhibitor and paracetamol after oral surgery 295
rofecoxib group took her rescue medication after only30 min as a result of severe pain and withdrew from thestudy one did not manage to fill in the questionnaireand three did not return their questionnaires althoughthey were repeatedly reminded to do so Final outcomedata were calculated on the following cohort of 107 pa-tients rofecoxib + paracetamol (n frac14 34) rofecoxibalone (n frac1436) paracetamol alone (n frac14 20) and placebo(n frac14 17)The principal investigator and one of the dentists
performed the majority of the operations 43 and 55respectively in total 98 out of 120 The remaining 22operations were performed by the two other dentists oneoperating on 10 and the other on 12 patients as theirstock of patients fulfilling the inclusion criteria wassmaller The principal investigator was in contact withand gave instructions to the 98 patients The 22remaining patients received their instructions from oneof the other two dentists performing the operationsThere were no differences between groups regarding
baseline characteristics and the number of molarsremoved (Tables 2 and 3) In total 56 of the partici-pants were men The mean age of the patients was 27 yr(range 18ndash54) and the mean weight was 73 kg (range 50ndash120) Mean total duration of the surgery was 14 min Intotal 91 patients (85) had one mandibular molar
removed during the operation and 16 (18) had anadditional maxillary molar removed The remaining 16patients (15) had two mandibular molars removed atthe same session (Table 3) There was no difference inpain intensity (VAS) at the start between patients whohad one or two molars removed At the time of intake ofthe study medication 83 of all patients included in theanalysis reported moderate pain and 17 reportedsevere pain There were no major differences in painreported among patients operated on by the differentdentists
Analgesic effect
Pain intensity (VAS) ndash The analgesic effect over the 8-hstudy period recorded by patients using the VAS isshown in Fig 1 Separate curves with confidence inter-vals for study groups are presented in Fig 2 Patientsused the scale from 0 up to 95There was a significant difference in mean VAS score
between the combination group and the rofecoxibgroup at 30 min 1 h and 15 h in favor of thecombination (P lt 005) At 2 h and subsequentlyparacetamol did not show any statistically significantadditive effect when combined with rofecoxib com-pared with rofecoxib aloneWhen comparing rofecoxib and paracetamol after
30 min paracetamol was significantly better regardingeffect on pain intensity (P lt 005) Paracetamol tendedto have a better analgesic effect than rofecoxib (althoughthis was not statistically significant) for another hourafter the starting point From 3 h until the end of thestudy period rofecoxib was significantly better thanparacetamol (P lt 005)Compared with placebo the combination treatment
as well as the single drug treatments resulted in signifi-cantly lower pain intensity scores at all observationpoints except for rofecoxib at 30 min
Pain relief (PAR) ndash The median PAR scores (Fig 3)showed a pattern similar to the mean pain intensityassessment The combination treatment was significantly
Table 2
Baseline characteristics for each study group
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Gender malefemale 1915 2016 128 98Age (yr) 25 (19ndash35) 26 (18ndash41) 29 (19ndash52) 28 (19ndash54)Weight (kg) 73 plusmn 9 70 plusmn 13 79 plusmn 17 72 plusmn 13Volume of local anesthetic (ml) 54 plusmn 2 58 plusmn 1 56 plusmn 1 56 plusmn 1Length of surgery (min) 13 plusmn 7 15 plusmn 8 13 plusmn 7 15 plusmn 6Time from end of surgery tointake of study medication (min)
155 plusmn 37 170 plusmn 45 184 plusmn 53 161 plusmn 30
Pain intensity (VAS) at the start 51 plusmn 18 54 plusmn 16 51 plusmn 18 46 plusmn 15
Mean (range)Mean plusmn SDVAS visual analog scale
Table 3
Number of mandibular and maxillar third molars removed in eachstudy group
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
1 mandibular 24 24 15 122 mandibulars 5 6 3 21 mandibular+ 1 maxillar
5 6 2 3
296 Haglund amp Bultzingslowen
better than rofecoxib alone at 30 min (P lt 005) and at1 h (P lt 001) For the rest of the observation periodthere was no significant difference
Between rofecoxib and paracetamol there was a sig-nificant difference in median PAR score in favor ofparacetamol at 30 min and at 1 h (P lt 005) after drug
Placebo
01234567
0 1 2 3 4 5 6 7 8
Paracetamol 1g
01234567
0 1 2 3 4 5 6 7 8
Rofecoxib 50 mg
01234567
0 1 2 3 4 5 6 7 8
Rofecoxib 50 mg+paracetamol 1 g
01234567
0 1 2 3 4 5 6 7 8
Fig 2 Mean pain intensity recorded on a visual analog scale (VAS) and confidence intervals in study groups during the studyperiod of 8 h
0
1
2
3
4
5
6
0 05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
AV
s S
cr
oe
placebo
paracetamol 1g
rofecoxib 50mg
rofecoxib 50mg +paracetamol 1g
Hours from intake of study medication
Fig 1 Mean pain intensity in study groups recorded on a 10-cm visual analog scale (VAS) at each observation point For signifi-cance tests see the Results
0
05
1
15
2
25
3
35
Pai
n r
elie
f sc
ore
placebo
rofecoxib 50mg
rofecoxib 50mg +
05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
paracetamol 1g
paracetamol 1g
Hours from intake of study medication
Fig 3 Median pain relief (PAR) score in study groups at each observation point Pain relief was assessed using the following scale0 no pain relief 1 some pain relief 2 medium pain relief 3 good pain relief and 4 total pain relief For significance tests see theResults
COX-2 inhibitor and paracetamol after oral surgery 297
intake There was instead a significant difference in favorof rofecoxib from 25 h (P lt 005) and from 3 h(P lt 001) to the end of the observation period Only atthe observation time-points of 15- and 2-h was there nosignificant difference between the two drugs regardingmedian PAR scoresThe combination treatment and the single treatments
were significantly better than placebo throughout thewhole observation period of 8 h
Total pain relief (TOTPAR) ndash There was no significantdifference in mean TOTPAR between the combinationtreatment group and the rofecoxib-alone group (Table 4)However rofecoxib gave significantly better TOTPARthan paracetamol (P lt 005) All the active treatmentgroups gave better TOTPAR than placebo (P lt 0001)
Sum of pain intensity differences (SPID) ndash The combi-nation group had the highest mean SPID05)3 h scorehowever this was not statistically different from rofecoxibalone (Table 4)No significant difference in SPID0)3 h wasseen between rofecoxib and paracetamol All active treat-ments were significantly better than placebo (P lt 0001)
The mean PID over the whole observation period (iemean SPIDtotal) shows that the combination group didnot differ from the rofecoxib group (Table 4) Therofecoxib group was significantly better than paracet-amol alone (P lt 005) All active treatments weresignificantly better than placebo (P lt 0001)
Use of rescue medication ndash The use of rescue medicationmeasured as the cumulative percentage of patients ineach study group needing analgesic rescue at any timeduring the 8-h observation period is shown in Fig 4There was no significant difference regarding the totalpercentage of patients using rescue when comparing thecombination group with the rofecoxib group (Table 4)Figure 4 indicates a major difference between the rofec-oxib and paracetamol groups This difference is how-ever not significant (P frac14 0055) owing to few patientsneeding rescue medication Both the combination groupand the rofecoxib group used significantly less rescuethan the placebo group (P lt 0001) Paracetamol failedto show a significant difference to placebo regardingpercentage of patients using rescue medication (P frac140066)
Table 4
Summary of efficiency measures
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Mean TOTPAR05ndash8 h (SE)
452 (20) 409 (27) 287 (44) 91 (27)
Mean SPID05ndash3 h (SE)
182 (19) 151 (18) 111 (34) )32 (23)
Mean SPIDtotal (SE)
526 (59) 515 (60) 208 (96) )101 (57)
Percentage of patients using rescue medication (SE) 88 (49) 167 (63) 400 (112) 706 (114)Mean time (min) to use of rescue medication (SE) 234 (42) 270 (58) 228 (48) 127 (16)Median global evaluation score (0ndash4) at 4 h 2 2 1 0Median global evaluation score (0ndash4) at 8 h 3 2 1 0
P lt 005 vs placebo P lt 001 vs placebo P lt 0001 vs placeboP lt 005 vs paracetamol P lt 001 vs paracetamol P lt 0001 vs paracetamolSE standard error SPID sum of pain intensity differences TOTPAR total pain relief
0
10
20
30
40
50
60
70
80
05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
Hours from intake of study medication
Cum
ula
itve
perc
enat
geof
paite
nst
taki
gnre
scue
me
idca
tion placebo
paracetamol 1g
rofecoxib 50mg
rofecoxib 50mg +paracetamol 1g
Fig 4 Cumulative percentage of patients in each group using rescue medication during the study period of 8 h For significance testssee the Results
298 Haglund amp Bultzingslowen
There was no statistically significant difference in themean time from intake of study medication to intake ofrescue medication in the different active treatmentgroups However for all active treatments the time wassignificantly longer than for placebo (Table 4)
Side-effects
The majority of all patients 738 reported no adverseevents while 187 experienced side-effects Another75 did not answer this question The majority (789)of the patients with side-effects reported that these wereonly slight while 211 reported moderate side-effectsNo patients reported any severe side-effects No pro-nounced difference was seen between the groupsregarding side-effects The types of side-effects experi-enced are listed in Table 5
Global evaluation
Patientsrsquo median global evaluation scores of their studymedications are shown in Table 4 After 4 h thecombination treatment and rofecoxib alone receivedsimilar evaluations Both groups were significantlybetter than paracetamol (P lt 0001 P lt 001) at thistime All active treatments were significantly betterthan placeboAt 8 h the combination group had the highest score
but the difference from the rofecoxib group was verysmall and not significant (Table 4) Both groups weresignificantly better than paracetamol alone (P lt 0001P lt 001) at 8 h All treatment groups were significantlybetter than placeboThe global evaluation scores are further specified in
Table 6 After 8 h 90 of the patients in the combina-tion group rated their medication as good or excellentFor the rofecoxib group the corresponding value was83 Of the patients treated with paracetamol 42rated their medication as good or excellent after 8 h
Discussion
In this study we showed that for the acute inflammatorypain following third molar surgery there was an additive
analgesic effect when combining rofecoxib with paracet-amol as compared with rofecoxib alone for the first 15 hafter intake After this time point the combination ofrofecoxib and paracetamol gave similar pain relief to thatof the rofecoxib group Paracetamol alone was also moreeffective for the first 15 h while rofecoxib was signifi-cantly better thanparacetamol from3 honwards The factthat rofecoxib and paracetamol were more effective thanplacebo shows that the method used was sensitive enoughto distinguish between different substancesAfter the clinical part of this study was carried out
serious concerns regarding cardiovascular effects of long-term treatment with rofecoxib were raised following re-ports of an increased incidence of myocardial infarctionand stroke among patients treated with rofecoxib in aplacebo-controlled study (24) After a highly significant19-fold increase in the incidence of thrombo-embolicserious adverse events was shown in yet another study(25) rofecoxib was withdrawn from the market Theside-effects of rofecoxib became progressively greaterafter 1 yr of treatment which suggests that the cardio-vascular risk is dose-dependent and not only associatedwith COX-2 selectivity (6) The need for acute pain reliefafter third molar surgery is short and the surgery ismainly performed in otherwise healthy young peopleamong whom the risk for serious cardiovascular events issmall It cannot be ruled out that future further devel-oped selective COX-2 inhibitors may be useful intreating acute pain after third molar surgery in this groupof patients with the advantage of only one dose a dayand minimizing the risk for gastrointestinal symptomsRofecoxib and paracetamol differ in onset time and
patients treated with rofecoxib reach meaningful painrelief after 15 h (8) compared with 05 h for paracet-amol This corresponds well with the results obtained inour study The group treated with paracetamol reportedtheir lowest VAS score by 1 h whereas at this time pointthe rofecoxib group still reported a high VAS scoreThereafter the medium VAS score for the paracetamolgroup increased while patients treated with rofecoxibcontinued to receive good pain relief until the end of theobservation period From these results it is reasonable toassume that the combination grouprsquos significantly betteranalgesic effect between 05 and 1 h compared with
Table 5
Side-effects as stated in patientsrsquo own words
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Fatigue 4 2 3 2Headache 1 2 ndash 2Fever ndash ndash ndash 1Dizziness 1 ndash 2 ndashStomach pains 1 ndash 1 ndashSickness ndash 1 ndash ndashShivers 1 2 ndash ndashPerspirations ndash 1 ndash ndash
Table 6
Percentage of patients in each study group stating their overallexperience of the study medication at 4 and 8 h
Study groups
Rofecoxib+
paracet-amol
(n frac14 34)Rofecoxib(n frac14 36)
Paracet-amol
(n frac14 20)Placebo(n frac14 17)
4 h 8 h 4 h 8 h 4 h 8 h 4 h 8 h
Poor 0 0 7 6 30 32 75 76Fair 6 10 7 11 40 26 18 18Good 47 32 43 36 15 26 7 6Excellent 47 58 43 47 15 16 0 0
COX-2 inhibitor and paracetamol after oral surgery 299
rofecoxib alone was a result of the earlier onset of theeffect of paracetamol The mean VAS scores for thecombination group and the paracetamol group corres-ponds totally at the 30-min observation pointThe peak pain after third molar surgery has been
shown to occur 4ndash6 h postoperatively (26) which coin-cides well with the time for the additive effect of para-cetamol to take effect in our study This supports the useof the combination treatment of rofecoxib and paracet-amol after third molar surgery to gain an early onsetparticularly if pain relief medication is started postop-eratively as it is of great clinical importance to have anearly onset of pain relief when treating acute pain Iftreatment starts pre-operatively the addition of para-cetamol is likely to have less clinical relevance This issupported by a study in which patients were givenrofecoxib and paracetamol before Ear Nose and Throat(ENT) surgery (27) The addition of paracetamol in thatsetting failed to improve the analgesic effects of rofec-oxibRofecoxib and paracetamol also differ in duration
The effect of paracetamol 1 g lasts up to 6 h and the drughas to be administered four times daily while rofecoxib50 mg has an analgesic effect up to 24 h (12) The presentstudy was a single-dose comparison In a normal clinicalsetting another 1 g of paracetamol would probably beprescribed after 6 h which would give another period ofadditive effectThe disparity in effect between rofecoxib and para-
cetamol in the present study from 3 h onwards is inaccordance with the findings of two studies on post-operative pain relief after otolaryngologic surgerycomparing rofecoxib and paracetamol given pre-operatively (11 28) A study regarding inflammatorypain in patients with knee osteoarthritis also showedrofecoxib to be superior to paracetamol (29) The resultof our study from 3 h after baseline and onwards thusconfirms the findings of these studies in a third molarpain modelOur study did not show the same additive effect of
combining rofecoxib and paracetamol as in a study byBreivik et al in which they combined diclofenac andparacetamol (18) These authors demonstrated anadditive effect of paracetamol over the whole studyperiod of 8 h Their study also showed less use of rescuemedication in the combination group compared with thepatients treated with diclofenac alone something alsofound in a study by Matthews et al (19) It would seemreasonable to assume that the additive effect of para-cetamol in our study would be the same as in these twostudies as rofecoxib and ibuprofen have been shown tohave the same analgesic effect following third molarsurgery (9 10 12) and the effects of ibuprofen anddiclofenac are similar (30ndash32) It cannot be ruled out thatthere is a difference in additive effect of paracetamolwhen combining it with rofecoxib compared withdiclofenac This theory is in accordance with the result ofa study by Pickering et al on pain relief after tonsil-lectomy in children in which rofecoxib combined withparacetamol did not significantly alter the need for earlyanalgesia as did ibuprofen combined with paracetamol
(33) Further studies may clarify differences between thetwo drugsIn conclusion the present study indicates that there is
an early additive effect up to 2 h when combiningparacetamol with rofecoxib postoperatively as comparedwith rofecoxib alone which coincides with peak painintensity after the removal of third molars Rofecoxibhad a significantly better analgesic effect than paracet-amol from 3 h onwards Our results indicate that para-cetamol does not enhance the analgesic effect ofrofecoxib over a longer period of time As rofecoxib hasbeen shown to have serious cardiovascular side-effectsfuture studies are needed to determine any serious side-effect during short-term treatment
Acknowledgements ndash This study was supported by grants fromLIV The Country Council of Varmland which made it inde-pendent from all manufacturers of the studied drugs There areno conflicts of interest by any of the authors with any drugcompany We thank Dr Carl-Mauritz Bratt DDS Dr PeterTroberg DDS and Dr Tobias Block DDS for performingsome of the surgery
References1 Cooper SA Five studies on ibuprofen for postsurgical dental
pain Am J Med 1984 77 70ndash772 Dionne RA Campbell RA Cooper SA Hall DL Buck-
ingham B Suppression of postoperative pain by preoperativeadministration of ibuprofen in comparison to placebo acet-aminophen and acetaminophen plus codeine J Clin Pharmacol1983 23 37ndash43
3 Vane JR Inhibition of prostaglandin synthesis as a mechanismof action for the aspirinlike drugs Nature 1971 231 232ndash235
4 Meade EA Smith WL De Witt DL Differential inhibition ofprostaglandin endoperoxide synthase (cyclo-oxygenase) iso-zymes by aspirin and other non-steroidal anti-inflammatorydrugs J Biol Chem 1993 268 6610ndash6614
5 Smith TJ Cyclooxygenase as the principal targets for action ofNSAIDs Rheum Dis Clin North Am 1998 24 501ndash523
6 Sciulli MG Capone ML Tacconelli S Patrignani P Thefuture of traditional nonsteroidal anti-inflammatory drugs andcyclooxygenase-2 inhibitors in the treatment of inflammationand pain Pharmacol Rep 2005 57 66ndash85
7 Spink M Bann S Glickman R Clinical implications of cyclo-oxygenase-2 inhibitors for acute dental pain managementbenefits and risks J Am Dent Assoc 2005 136 1439ndash1448
8 Ehrich EW Dallob A De Lepeleire I Van Hecken ARiendeau D Yuan W Porras A Wittreich J Seibold JRDe Shepper P Mellisch DR Gertz BJ Characterization ofrofecoxib as a cyclooxygenase-2 isoform inhibitor and demon-stration of analgesia in the dental pain model Clin Pharm Ther1999 65 336ndash347
9 Malmstrom K Fricke J Kotey P Kress B Morrisson B Acomparison of rofecoxib versus celecoxib in treating pain afterdental surgery a singlecenter randomized double-blind pla-cebo- and active-comparator-controlled parallel group single-dose study using the dental impaction pain model Clin Ther2002 24 1549ndash1560
10 Malmstrom K Daniels S Kotey P Seidenberg B Desjar-
dins PJ Comparison of rofecoxib and celecoxib two cyclo-oxygenase-2-inhibitors in postoperative dental pain Arandomized placebo- and active-comparator-controlled clinicaltrail Clin Ther 1999 21 1653ndash1663
11 Watcha MF Issioui T Klein KW White PF Costs andeffectiveness of rofecoxib celecoxib and acetaminophen forpreventing pain after ambulatory otolaryngologic surgeryAnesth Analg 2003 96 987ndash994
300 Haglund amp Bultzingslowen
12 Morrisson BW Christensen S Yuan W Brown J Amlani
S Seidenberg B Analgesic efficacy of the cyclooxygenase-2-specific inhibitor rofecoxib in post-dental surgery pain arandomized controlled trial Clin Ther 1999 21 943ndash953
13 Chang DJ Fricke JR Bird RS Bohidar NR Dobbins TWGeba GP Rofecoxib versus codeineacetaminophen in post-operative dental pain a double-blind randomized placebo-and active comparator-controlled clinical trial Clin Ther 200123 1446ndash1455
14 Chang DJ Desjardins PJ Bird SR Black P Chen EPetruschke RA Geba GP Comparison of rofecoxib and amultidose oxycodoneacetaminophen regimen for the treatmentof acute pain following oral surgery a randomized controlledtrial Curr Med Res Opin 2004 20 939ndash949
15 Berenbaum MC What is synergy Pharmacol Rev 1989 4193ndash141
16 Altman RD A rationale for combining acetaminophen andNSAIDs for mild to moderate pain Clin Exp Rheumatol 200422 110ndash117
17 Bjorkman R Hallman KM Hedner J Hedner T Henning
M Acetaminophen blocks spinal hyperalgesia induced byNMDA and substance P Pain 1994 57 259ndash264
18 Breivik EK Barkvoll P Skovlund E Combining diclofenacwith acetaminophen or acetaminophen-codeine after oral sur-gery a randomized double-blind single-dose study ClinPharmacol Ther 1999 66 625ndash635
19 Matthews RW Scully CM Levers BG The efficacy ofdiclofenac sodium (Voltarol) with and without paracetamol inthe control of post-surgical dental pain Br Dent J 1984 157357ndash359
20 Norholt SE Treatment of acute pain following removal ofmandibular third molars use of the dental pain model inpharmacological research and development of a comparableanimal model Int J Oral Maxillofac Surg 1998 27 1ndash41
21 NIH Consensus Development Conference For Removal OfThird Molars J Oral Surg 1980 38 235ndash236
22 Laska EM Siegel C Sunshine A Onset and durationmeasurement and analysis In Max MB Portenoy RKLaska EM eds Advances in pain research and therapy NewYork Raven Press 1991 691ndash698
23 Max MB Laska EM Single-dose analgesic comparisons InMax MB Portenoy RK Laska EM eds Advances in painresearch and therapy New York Raven Press 1991 55ndash97
24 Bombardier C Laine L Reicin A Shapiro D Burgos-Vargas R Davis B Day R Ferraz MB Hawkey CJHochbergMC Kvien TK Schitzer TJ Comparison of uppergastrointestinal toxicity of rofecoxib and naproxen in patientswith rheumatoid arthritis N Engl J Med 2005 343 1520ndash1528
25 Bresalier RS Sandler RS QuanH Bolognese JA Oxenius
B Horgan K Lines C Riddell R Morton D Lanas AKonstam MA Baron JA Cardiovascular events associatedwith rofecoxib in a colorectal adenoma chemoprevention trialN Engl J Med 2005 17 1092ndash1102
26 Szmyd L Shannon ILMohnac AM Control of postoperativesequelae in impacted third molar surgery J Oral Ther Phar-macol 1965 1 491ndash496
27 Issioui T Klein KW White PF Hu J Skrivanek GDAnalgesic efficacy of rofecoxib alone or in combination withacetaminophen in the ambulatory setting Anesthesiology 200195 A35
28 Issioui T KleinKWhite PWatchaM SkrivanekG JonesSHu J BradleyM Caleb I Cost-efficacy of rofecoxib versusacetaminophen for preventing pain after ambulatory surgeryAnesthesiology 2002 97 931ndash937
29 Geba GP Weaver AL Polis AB Dixon ME Schnitzer TJEfficacy of rofecoxib celecoxib and acetaminophen in osteo-arthritis of the knee a randomized trial JAMA 2002 287 64ndash71
30 Joshi A Parara E Macfarlane TV A double-blind rand-omised controlled clinical trial of the effect of preoperativeibuprofen diclofenac paracetamol with codeine and placebotablets for relief of postoperative pain after removal of impac-ted third molars Br J Oral Maxillofac Surg 2004 42 299ndash306
31 Bakshi R Frenkel G Dietlein G Meurer-Witt B Schn-eider B Sinterhauf U A placebo-controlled comparativeevaluation of diclofenac dispersible versus ibuprofen in post-operative pain after third molar surgery J Clin Pharmacol 199434 225ndash230
32 Ahlstrom U Bakshi R Nilsson P Wahlander L Theanalgesic efficacy of diclofenac dispersible and ibuprofen inpostoperative pain after dental extraction Eur J Clin Pharma-col 1993 44 587ndash588
33 Pickering AE Bridge HS Nolan J Stoddart A Double-blind placebo-controlled analgesic study of ibuprofen orrofecoxib in combination with paracetamol for tonsillectomy inchildren Br J Anaesth 2002 88 72ndash77
COX-2 inhibitor and paracetamol after oral surgery 301
Combined acetaminophen and ibuprofen for pain relief after oralsurgery in adults a randomized controlled trial
A F Merry1 2 R D Gibbs3 J Edwards4 G S Ting3 C Frampton5 E Davies1 2
and B J Anderson1
1Department of Anaesthesiology University of Auckland Private Bag 92019 Auckland New Zealand2Department of Anaesthesia Auckland City Hospital Auckland New Zealand 3Oral Health Unit Greenlane
Clinical Centre 214 Greenlane West Epsom Auckland New Zealand 4Oral and Maxillofacial Service Quay
Park Medical Centre 68 Beach Road Auckland Central Auckland New Zealand 5Department of Medicine
Christchurch School of Medicine and Health Sciences University of Otago New Zealand
Corresponding author E-mail amerryaucklandacnz
Background Acetaminophen is often used with a non-steriodal anti-inflammatory drug for
acute pain Hitherto these drugs have had to be given separately typically at different time
intervals Maxigesicw tablets combine acetaminophen and ibuprofen in clinically appropriate
doses to simplify administration and dosage regimen We compared this combination with each
of the constituent drugs for the relief of pain after extraction of third molar teeth
Methods Adults (more than 16 yr) having one or more wisdom teeth removed under general
or local anaesthesia were instructed to take two tablets before operation then two tablets
every 6 h for up to 48 h of (i) a combination of acetaminophen 500 mg and ibuprofen 150 mg
per tablet (Maxigesicw) (ii) acetaminophen 500 mg per tablet alone or (iii) ibuprofen 150 mg
per tablet alone The primary outcome measure was the area under the curve (AUC) of the
100 mm visual analogue scale pain measurements taken for up to 48 h after surgery divided by
time at rest and on activity Pharmacokinetic data were collected in a subset of patients
Results The mean (SEM) time-corrected AUC on rest and activity respectively were combi-
nation group 223 (32) and 284 (34) acetaminophen group 330 (31) and 404 (33) and ibu-
profen group 348 (32) and 402 (34) P001 for each of the four comparisons of combination
vs constituent drug There was no pharmacokinetic interaction between acetaminophen and
ibuprofen administered together
Conclusions Maxigesicw tablets provide superior pain relief after oral surgery to acetamino-
phen or ibuprofen alone
Br J Anaesth 2010 104 80ndash8
Keywords anaesthesia dental analgesia postoperative analgesics non-opioid acetaminophen
analgesics non-opioid ibuprofen non-steroidal anti-inflammatory drugs
Accepted for publication October 16 2009
The relief of pain has been described as a universal human
right but is not always easily achieved1 Opioid analgesics
are effective but have troublesome and potentially danger-
ous side-effects and their potential for abuse may lead to
regulatory and logistical difficulties Non-steroidal anti-
inflammatory drugs (NSAIDs) have fewer regulatory
restrictions but they too have important adverse effects
which are more likely at higher dose or with longer
courses2 Acetaminophen is widely used and is very safe
at the recommended dose of 4 g per day3 but does not
always provide adequate pain relief on its own Combining
analgesics offers the possibility of increasing effectiveness
without increasing dose (and therefore risk)4 5 NSAIDs
are often combined with acetaminophen particularly for
treating postoperative pain6 ndash 10
Prescribing acetaminophen and ibuprofen together is
common in clinical practice6 8 9 11 ndash 13 Ibuprofen has the
advantage of a well-established safety record (particularly
at doses below 15 g per day in adults)14 and in many
countries (including the UK) it is available without
The Author [2010] Published by Oxford University Press on behalf of the British Journal of Anaesthesia
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (httpcreativecommonsorglicensesby-nc25uk)
which permits unrestricted non-commercial use distribution and reproduction in any medium provided the original work is properly cited
British Journal of Anaesthesia 104 (1) 80ndash8 (2010)
doi101093bjaaep338
prescription Typically acetaminophen is given in a dose
regimen of 1 g 6 hourly whereas ibuprofen is given in a
dose of 400 mg 8 hourly3 Compliance with the prescribed
dosing regimen is important for achieving the desired
result with any drug and is often poor with asynchronous
dosing15 A single formulation with a simplified regimen
would probably be appreciated by patients and might
improve compliance
Maxigesicw is a new formulation of acetaminophen 500
mg and ibuprofen 150 mg Taking two tablets 6 hourly
provides the appropriate daily dose of both drugs relatively
simply We have investigated the hypothesis that in adult
patients undergoing a common surgical procedure (extrac-
tion of third molar teeth) this formulation provides
superior analgesia to either of its components alone
Methods
With ethics committee approval we recruited and fol-
lowed up patients between March 2005 and February
2008 Trial registration ANZCTRORGAU (identifier
ACTRN12606000291583)
Setting
This study was conducted at a publicly funded teaching
hospital and a private day-surgical clinic in metropolitan
New Zealand
Participants
We included adults undergoing extraction of at least one
lower wisdom tooth with or without one or more upper
wisdom teeth by one of three participating surgeons We
excluded patients if they were under 16 yr old weighed
50 kg had taken any NSAID (other than aspirin in a
dose of 150 mg daily or less) within 24 h of the operation
had taken acetaminophen or acetaminophen containing
medicines within 12 h of the operation were taking an
angiotensin-converting enzyme inhibitor warfarin steroid
(other than interoperative dexamethasone) or any immu-
nosuppressive drug were intolerant to any NSAID or acet-
aminophen were suffering from a severe local infection
had a history of peptic ulceration asthma or severe hae-
mopoetic renal or hepatic disease were participating in
the investigation of another experimental agent or if the
clinician believed for any other reason that participation in
the study might not be in their best interests
Randomization and blinding
Tablets of identical appearance packaging and dosage
instructions were provided in each of the following formu-
lations (i) acetaminophen 500 mgthornibuprofen 150 mg per
tablet (Maxigesicw Sigma Laboratories Nashik India which
was MHRA approved for manufacturing pharmaceuticals
under GMP) (ii) acetaminophen 500 mg per tablet or
(iii) ibuprofen 150 mg per tablet
Patients were first approached by the surgeon and then
by the study nurse They were given written and verbal
information about the study and invited to participate If
they consented patients were then randomized into one of
the three study groups in a sequential order to receive one
of these formulations in blinded packs The randomization
sequence was computer generated by the study statistician
as a 111 allocation ratio to the three treatments in a
sequence of permuted blocks with stratification for anaes-
thetic type (local or general) and study centre
Stratification by anaesthetic type ensured a balance
between treatments in terms of the number of teeth
extracted as most patients having more than two teeth
extracted have a general anaesthetic Only the statistician
had access to the schedule of patient numbers by drug
allocation Participants and investigators were blinded and
the randomization code was not broken until the final data-
base had been checked and locked
Intervention
Participants were asked to take two tablets of the study
medication before operation (as close as possible to the
start of surgery) and then 4 times a day (as close as poss-
ible to 6 hourly) for up to 48 h after surgery All partici-
pants were given bupivacaine local anaesthetic blocks by
the surgeons For those participants undergoing general
anaesthesia this was induced with propofol and main-
tained with isoflurane and nitrous oxide in oxygen
Monitoring was in accordance with the guidelines of the
Australian and New Zealand College of Anaesthetists16
All extractions were carried out by one of three surgeons
each using his normal technique
If participants required additional postoperative pain
relief while in hospital a rescue dose of fentanyl 10 mg
was given iv as required After discharge to home
codeine was provided (again as rescue medication) in 30
mg tablets one to two to be taken as needed up to
4 hourly
Outcomes
Participants were asked to rate their pain on 100 mm visual
analogue scales (VAS) printed one per double page in a
booklet that they took home Ratings were requested at
baseline (immediately before administration of the first
dose of study medication) after operation (once the partici-
pants were sufficiently awake to respond) and 1ndash2 hourly
thereafter while awake for 48 h The study nurse main-
tained contact with participants by telephone to facilitate
compliance with data collection and the return of diaries
The primary outcome measure was the area under the
curve (AUC) of these VAS ratings divided by time at rest
and on activity The AUC was divided by the period of
the completed assessments to adjust for the fact that some
Combined acetaminophen and ibuprofen for analgesia
81
patients recorded pain for shorter periods than others This
calculation in effect produces a measure of average pain
intensity over the study period
Secondary efficacy outcome measures were a categorical
global pain rating by the participants taken at the end of the
study period rescue analgesia consumption over the study
period a categorical global rating of nausea by the partici-
pants taken at the end of study period the number of epi-
sodes of vomiting over the study period and a rating of
sleep disturbance on a 100 mm VAS assessed after each
night during the study period In addition participants were
asked to rate their experiences of participating in the study
Sample size estimation
We obtained blood samples from the 38 participants
undergoing general anaesthesia in order to have evaluable
pharmacokinetic data for at least 30 patients The first
sample was obtained 30 min after the first dose of study
medication the second sample at the end of anaesthesia
and additional one or two samples after operation in hospi-
tal The plasma concentration of acetaminophen and ibu-
profen were measured by the sponsor and used to form
individual timendashconcentration profiles The analytical
method used an HPLC-DAD (Diode Array Detector) assay
for the simultaneous determination of acetaminophen and
ibuprofen in plasma Precision and accuracy for acetami-
nophen and ibuprofen assay were validated over the con-
centration range 05ndash50 mg ml21 for both drugs The
intra- and inter-batch precision of the assays at low
medium and high concentrations of acetaminophen and
ibuprofen varied from theoretical values by 15 The
lower limit of quantification for each drug was 05 mg
ml21 The sponsor monitored all data collected during the
study and queries and corrections were made when any
inaccuracies or inconsistencies were identified
Sample size estimation
We estimated that 120 participants (40 per group) in the
intention-to-treat (ITT) population would provide 80
power to detect differences between the groups of 9 (SD
14) mm in our primary endpoint for resting assessments
and 13 (SD 21) for measures during activity10 17 with a
one-sided type I error rate of 5 These differences equate
to 25 Differences of this magnitude were considered
clinically important and comparable with differences
typical of previous published studies10
Statistical methods
The data were analysed using SPSS version 150 (SPSS
Inc Chicago IL USA) Efficacy analyses were conducted
on an ITT basis with the additional provision that
there were at least three VAS measurements over at
least 12 h available to calculate the primary endpoint All
participants who were randomized into the study were
included in the safety evaluations As the first dose of
study medication was taken before operation while under
the supervision of the surgeon all randomized patients
took at least a single dose of study medication A last
observation carried forward approach was used for those
subjects who left the study prematurely for non-AUC
based variables
We compared the primary endpoint between the combi-
nation group and each of the acetaminophen and ibuprofen
arms at rest and on activity using a general linear model
(GLM) which included terms for treatment the centre and
anaesthetic stratum Additionally to confirm the consist-
ency of the treatment effects across strata the stratum
treatment interaction terms were tested and included in
the final model The analysis was also checked with
number of teeth extracted as an additional factor
Continuous secondary efficacy endpoints were tested for
significance using the same models as used for the
primary endpoint
A one-tailed P005 was pre-specified to indicate stat-
istical significance We required a statistically significant
result favouring the combination from each of the two
planned comparisons with the constituents to define super-
iority for either rest or on activity measures We used one-
tailed tests as there seemed no theoretical or empirical
basis for expecting that combining these analgesics could
result in a reduction in efficacy and because the require-
ment for each of two comparisons to be significant at
P005 is stringent Secondary categorical efficacy end-
points were compared between the groups using x2 tests
and MannndashWhitney U-tests as appropriate
We used non-linear mixed effect models (NONMEM
VI Globomax LLC Hanover MD USA) to estimate
population pharmacokinetics with a Compaq Digital
Fortran Version 66A compiler on an Intel Celeron 333
MHz CPU (Intel Corp Santa Clara CA USA) under MS
Windows XP (Microsoft Corp Seattle WA USA) This
model allows assessment of inter-individual variability
covariance between pharmacokinetic parameters and
residual error We judged the quality of fit of the pharma-
cokinetic model to data using the NONMEM objective
function examination of plots of observed vs predicted
concentrations and visual predictive checks
Results
After initial screening 189 patients were approached 135
agreed to participate One to four teeth were extracted
with local anaesthetic alone in 69 patients and with local
anaesthetic in combination with general anaesthesia in 66
Thirteen patients did not return their patient diaries so
122 patients were included in the evaluable ITT popu-
lation for the analysis of the primary endpoints (Fig 1)
The treatment groups were adequately matched in baseline
patient and clinical characteristics (Table 1) Of those in
Merry et al
82
the combination group 600 had three or four teeth
extracted compared with 436 for ibuprofen and 535
for acetaminophen
Efficacy
The time-adjusted AUCs were substantially and signifi-
cantly lower at rest and on activity in the combination
group than in either of the other two treatment groups
(Table 2 Figs 2 and 3) with all four P001 The consist-
ency of the treatment effects across strata was confirmed
from the GLM with P-values for the treatment stratum
interaction of 0955 and 0984 for time-adjusted AUCs at
rest and on activity respectively The type of anaesthetic
(local vs general) and number of teeth extracted did not
change the outcome of either analysis
Although all four secondary endpoints favour the com-
bination treatment (Table 3) only the global pain rating
reached statistical significance More participants experi-
enced lsquonilrsquo or lsquomildrsquo pain with the combination (684)
than with either other group this difference was significant
for acetaminophen (375 Pfrac140008) but not for ibupro-
fen (543 Pfrac140263) The use of any rescue medication
also favoured the combination treatment (Table 4) but this
did not reach statistical significance
Pharmacokinetics
There were no significant differences between the combi-
nation group and either constituent group in any of the
estimated pharmacokinetic parameters (Table 5) The
visual predictive plots of individual concentration showed
that 90 of the observations were within the 90 pre-
diction intervals
Twelve participants were given both acetaminophen and
ibuprofen For calculation of the pharmacokinetic vari-
ables a scaling factor was applied to clearance and
volume of distribution in turn for those participants receiv-
ing the combination of acetaminophen and ibuprofen This
scaling factor had no impact on either acetaminophen or
ibuprofen pharmacokinetic parameters indicating that
there was no pharmacokinetic interaction between acetami-
nophen and ibuprofen when administered together
(P005)
Clearance (CLF) and volume of distribution (VF) par-
ameters observed in the study are consistent with those
reported previously (acetaminophen CLFfrac14126ndash210
litre h21 70 kg21 VFfrac14483ndash710 litre 70 kg21 ibupro-
fen CLFfrac1429ndash59 litre h21 70 kg21 VFfrac1464ndash235 litre
70 kg21)18 ndash 20
Adverse effects
The frequency of adverse effects was consistent with the
known effects of the constituent drugs and there were no
Screened(n =189)
Randomized(n =135)
Acetaminophentreatmentgroup(n =47)
Ibuprofentreatment group(n =44)
Combinationtreatment group(n =44)
Patient diariesnot returned(n =4)
Patient diariesnot returned(n =5)
Patient diariesnot returned(n =4)
Included in theanalysis(n =43)
Included in theanalysis(n =39)
Included in theanalysis(n =40)
Fig 1 Flow of participants through trial Not randomized (nfrac1454) (i)
declined to participate (nfrac1415) (ii) did not meet inclusion criteria
(nfrac1414) (iii) other reasons (nfrac1425) other reasons the surgery was
cancelled or rescheduled patient could not be contacted patient was
given the wrong date of the surgery
Table 1 Patient characteristic and baseline information (SD)
Acetaminophen (n547) Ibuprofen (n544) Combination (n544)
Age [mean (range)] (yr) 235 (160ndash404) 237 (168ndash389) 250 (183ndash404)
Weight [mean (SD)] (kg) 713 (156) 808 (201) 711 (135)
Ethnicity [n ()]
Asian 4 (85) 1 (23) 2 (45)
Black 1 (21) 0 (00) 1 (23)
Caucasian 33 (702) 31 (705) 34 (773)
Maori 4 (85) 4 (91) 4 (91)
Pacific Islander 4 (85) 5 (114) 2 (45)
Other 1 (21) 3 (68) 1 (23)
Male [n ()] 13 (277) 21 (477) 13 (295)
Shift workers [n ()] 10 (213) 5 (114) 3 (68)
Preoperative pain scores at rest [mean (SD)] (mm) 19 (51) 21 (52) 26 (68)
Preoperative pain scores on activity [mean (SD)] (mm) 41 (133) 27 (83) 29 (66)
Sleep disturbance for night before surgery as VAS [mean (SD)] (mm) 647 (229) 691 (260) 715 (241)
Combined acetaminophen and ibuprofen for analgesia
83
definitive indications that the adverse event profile is
changed when the two drugs are combined (Table 6)
however the numbers were too small to make meaningful
comparisons between the groups Two participants experi-
enced postoperative bleeding (attributed to surgical
causes) which resolved without readmission to hospital
No gastrointestinal bleeding was reported during the study
Most adverse events were evaluated as mild (574) or
moderate (352) and on review were considered not
related (175) or unlikely to be related (667) to study
medication
General
The majority of participants rated the experience of taking
part in the study as very positive (31) or positive (47)
0
10
20
30
40
50
60
70
80
90
100
ActivityRest
Acetaminophen alone
Ibuprofen alone
Combination
AU
Ch
(m
m)
Fig 2 Mean (thorn95 CI) mm of time-adjusted AUC (AUCtime) for VAS
at rest and on activity by treatment group
Table 2 Mean (SEM 95 CI) of time-adjusted AUC of visual analogue pain
scores at rest and on activity by treatment group The differences between
combination and each constituent were significant at rest (vs acetaminophen
Pfrac140007 and vs ibuprofen Pfrac140003) and on activity (vs acetaminophen
Pfrac140006 and vs ibuprofen Pfrac140007)
Acetaminophen
(n543)
Ibuprofen (n539) Combination
(n540)
At rest 330 (31 279ndash381) 348 (32 294ndash402) 223 (32 170ndash277)
On
activity
404 (33 350ndash458) 402 (34 346ndash459) 284 (34 228ndash341)
0
1020
30
40
5060
70
8090
100A
B
0 4 8 12 16 20 24 28 32 36 40 44 48
0 4 8 12 16 20 24 28 32 36 40 44 48
Hours post-surgery
VA
S s
core
(m
m)
0
10
2030
40
50
60
7080
90
100
Hours post-surgery
VA
S s
core
(m
m)
Acetaminophen aloneIbuprofen aloneCombination
Fig 3 Mean (SE) mm VAS out of 100 at rest (A) and on activity (B)
Table 3 Secondary efficacy endpoints by treatment group The only
significant difference was between the global pain ratings for combination and
acetaminophen (Pfrac140008 MannndashWhitney U-test)
Acetaminophen Ibuprofen Combination
Global pain rating [n ()]
Nil 3 (75) 4 (114) 4 (105)
Mild 12 (300) 15 (429) 22 (579)
Moderate 22 (550) 14 (400) 12 (316)
Severe 3 (75) 2 (57) 0 (00)
Global nausea rating [n ()]
Nil 26 (650) 25 (714) 30 (790)
Mild 10 (250) 8 (229) 7 (184)
Moderate 3 (75) 2 (57) 1 (26)
Severe 1 (25) 0 (00) 0 (00)
Vomiting episodes (n) 5 (in 3 subjects) 0 0
Sleep disturbance night
1 vs baseline VAS
[mean (SD)] (mm)
2219 (292) 2174 (229) 2166 (247)
Sleep disturbance night
2 vs baseline VAS
[mean (SD)] (mm)
2137 (329) 296 (258) 285 (201)
Table 4 Rescue analgesia by group n () none of these differences were
significant
Rescue analgesic Acetaminophen Ibuprofen Combination
Fentanyl in hospital 5 (116) 9 (237) 6 (154)
Codeine in the first 24 h 21 (4770) 16 (4320) 13 (3250)
Codeine in the second 24 h 22 (5370) 14 (4240) 16 (4210)
Any rescue medication over 48 h 25 (625) 18 (5810) 21 (568)
Table 5 Mean (SD) pharmacokinetic parameters (individual Bayesian
estimates used for descriptive statistics) for a one-compartment first-order
absorption first-order elimination model none of the differences for
combination formulations was significant CLF clearance VF volume of
distribution Tabs absorption half-time Cmax maximum concentration Tmax
time to achieve Cmax
Acetaminophen
alone (n515)
Acetaminophen
in combination(n512)
Ibuprofen
alone(n511)
Ibuprofen in
combination(n512)
CLF (litre
h21)
141 (26) 142 (18) 39 (17) 38 (13)
VF (litre) 557 (194) 482 (183) 106 (21) 98 (15)
Tabs (h) 042 (076) 016 (010) 058 (078) 085 (085)
Tmax (h) 109 (112) 064 (031) 116 (090) 144 (093)
Cmax (mg
litre21)
158 (65) 192 (64) 208 (83) 191 (78)
Merry et al
84
and 19 rated the experience as neutral Four participants
(3) found the experience negative and none rated it as
very negative The ratings were not significantly different
between the study groups
Discussion
We found that patients using the combination of acetami-
nophen and ibuprofen experienced less pain during the
first 48 h after oral surgery than those using the same
daily dosage of either agent alone and we think the differ-
ence was clinically relevant There was no evidence of any
pharmacokinetic interaction between acetaminophen and
ibuprofen Patients receiving ibuprofen alone reported the
lowest frequency of adverse events but the numbers are
too small for meaningful comparisons between the groups
and we saw no cause for concern in any group
Our data are consistent with previous evidence showing
that a combination of ibuprofen and acetaminophen pro-
vides better analgesia than acetaminophen alone8 9 13 21
Note however that two of these studies were in children9 13
so data in adults are relatively limited On the other hand
there are many studies supporting the more general point
that the addition of various NSAIDs improves the pain
relief obtainable from acetaminophen alone More impor-
tantly our data add convincingly to the sparse evidence
supporting the more controversial proposition that this
combination is superior to ibuprofen alone12 In a smaller
study in an orthopaedic pain model (which was positive
for the combination in comparison with acetaminophen)
Dahl and colleagues8 showed no such benefit whereas
Viitanen and colleagues13 (in a paediatric tonsillectomy
study) showed an advantage for the combination only in
the period after discharge from hospital The similarity in
efficacy between ibuprofen and acetaminophen on their
own seen in our study contrasts with the findings of
superior pain relief from ibuprofen after dental surgery by
Cooper and colleagues22 but theirs was a single-dose
study
Limitations and strengths of the study
Our results are limited to adults and to the doses and
model of pain studied We think our conclusions are likely
to apply to other age groups and other types of pain but
this will require confirmation We have not explored the
optimal dosage of the combination drug but the dosage
used is consistent with current clinical practice The
inclusion of patients who underwent both general and
local anaesthesia implies that our findings are likely to
apply in either case It is not possible to draw firm con-
clusions on the safety of any drug from a study of only 40
participants per group but acetaminophen and ibuprofen
are well established widely used and considered very safe
in appropriate doses3 23 There is no theoretical reason
Table 6 Adverse events and their relationship with study medication as evaluated by the investigators Postoperative pain was noted as a complication in 2 0
and 1 patient in the acetaminophen ibuprofen and combination groups respectively Some individuals experienced more than one adverse event
Relationship System organ class Acetaminophen Ibuprofen Combination Total
Not related Gastrointestinal disorders (numbness of tongue) 1 0 0 1
General disorders and administration site conditions (swollen arm infusion site
phlebitis)
0 0 2 2
Infections and infestations (dry socket alveolitis of jaw) 1 0 1 2
Injury poisoning and procedural complications (bruising of arm postoperative
pain)
0 0 2 2
Musculoskeletal and connective tissue disorders ( jaw stiffness) 0 0 1 1
Skin and sc tissue disorders (swelling face) 1 1 0 2
Subtotal 3 1 6 10
Unlikely related Blood and lymphatic system disorders (swollen glands) 1 0 0 1
Ear and labyrinth disorders (pain in ear tinnitus) 2 0 0 2
Gastrointestinal disorders (vomiting nausea stomach cramps dry lips) 6 1 2 9
Injury poisoning and procedural complications (postoperative bleeding) 0 0 1 1
Musculoskeletal and connective tissue disorders ( jaw stiffness aches and pains in
legs jaw pain)
2 0 1 3
Nervous system disorders (headache felt faint sleepy balance difficulty light
headiness dizziness drowsiness lethargic)
6 4 4 14
Psychiatric disorders (disorientation) 0 1 0 1
Respiratory thoracic and mediastinal disorders (sore throat pharyngeal ulceration
hypoventilation coughing)
1 1 2 4
Investigations (body temperature increased) 0 0 1 1
Skin and sc tissue disorders (rash redness of external ear swelling face) 0 1 1 2
Subtotal 18 8 12 38
Possibly related Gastrointestinal disorders (stomach cramps abdominal pain constipation stomach
ache vomiting)
3 0 2 5
General disorders and administration site conditions (fever) 1 0 0 1
Injury poisoning and procedural complications (postoperative bleeding) 0 0 1 1
Nervous system disorders (sleepy headache) 1 0 1 2
Subtotal 5 0 4 9
Total 26 9 22 57
Combined acetaminophen and ibuprofen for analgesia
85
and no empirical suggestion from our data to suggest that
the combination would be any less safe than the constitu-
ent drugs on their own Our safety data are observational
rather than based on prospective laboratory investigations
but we followed up participants for adverse events for 3
weeks and it seems unlikely that clinically important
harm would have been missed
Pain after oral surgery can persist for several days10 but
we considered 48 h to be a clinically relevant period and
a longer period of study is likely to have resulted in poorer
compliance with data collection
It could be asked whether a more typical (albeit
complex) regimen for ibuprofen alone might have pro-
vided better analgesia than seen with the 4 hourly
approach used here but this seems unlikely particularly
given that our clinical efficacy data were supported by esti-
mates of population pharmacokinetics We had planned to
correlate drug plasma concentration with pain scores but
the drug plasma concentration results were too sparse and
there were too many confounding variables (such as ethni-
city comparators and rescue analgesia) for this to be
undertaken We did demonstrate a lack of interaction
between the constituent drugs when used in combination
and provided evidence that equivalent and predicted blood
concentrations were achieved (the observations of timendash
concentration profile decreased within 90 of prediction
limits for both acetaminophen and ibuprofen) Furthermore
pharmacokinetic parameter estimates observed in the current
study are very similar to those previously reported18 ndash20
The evaluations used in the efficacy analysis have
established construct validity and are appropriate for
parametric analysis24 25
In designing analgesic studies it is an advantage to
minimize the exposure of participants to inadequate
analgesia while controlling for various sources of bias
Some designs incorporate a placebo group but the efficacy
of both ibuprofen26 and acetaminophen27 in comparison
with placebo are well established by previous research
and we would argue that the use of a placebo in this situ-
ation is unnecessary and perhaps even unethical28 There
would be little value in another lsquome toorsquo analgesic unless
it had clear advantages over established agents Therefore
the question of interest lies in the comparisons between
the new agent (Maxigesicw) and the reference standard of
care and in this case we have actually shown superiority to
both of two possible reference standardsmdashacetaminophen
alone and ibuprofen alone One classic approach to analgesic
studies involves treating established acute pain This has the
alleged advantage that pain relief can be assessed (eg by
using AUC to estimate total pain relief or TOTPAR29 30 or
by calculating a pain reduction index per tablet)31 Our
design in contrast follows the widely accepted clinical prac-
tice of anticipating and treating pain before it occurs which
in our unit at least has long been considered best practice
Furthermore rescue medication was readily available and
those requiring it were evenly distributed between the
groups It is notable that most patients did require rescue
medication suggesting that pain after oral surgery can some-
times be severe enough that even the combination of ibupro-
fen and acetaminophen requires supplementation (and it
might be asked whether it would be a good idea for codeine
for example to be added to the combined formulation)
Nevertheless we think it important that the vast majority of
the participants in all groups reported pain scores that were
reasonably low and that all received analgesic regimens
accepted in contemporary practice The predominantly posi-
tive evaluation by participants of their experience in taking
part in the study provides empirical reassurance on this point
(and also other aspects of the conduct of the study)
The treatment of pain is central to medical practice in
hospitals and in primary care If these results are con-
firmed in other settings the already widely used combi-
nation of acetaminophen and ibuprofen may become the
standard of care for the initial management of moderate
acute pain at least for those patients who do not have
contra-indications to NSAIDs Even using the drugs indi-
vidually the dosage regimen studied here is simpler than
that currently recommended and may well improve com-
pliance with and therefore success with this combination
Providing both drugs in one tablet simplifies this regimen
even further and our data confirm that the specific formu-
lation studied here is effective and that there is no inter-
action between its constituent drugs
Conclusions
Doctors treating pain after oral surgery in hospital and at
home and probably pain in many other situations should
consider using acetaminophen and ibuprofen together four
times a day provided there are no contraindications to
either drug and taking into account the known risks of
NSAIDs The combination formulation studied here sim-
plifies this regimen
Funding
This work was supported by AFT Pharmaceuticals Ltd
assisted by New Zealand Trade and Enterprise
Development Grants
Appendix
Declaration of interest
The Department of Anaesthesiology of the University of
Auckland has received payment from AFT
Pharmaceuticals for conducting this study but none of the
investigators has received payment in their personal
capacity
Merry et al
86
Contributors
AFM BJA CF and Hartley Atkinson designed the
study with input from RDG and JE Hartley Atkinson
obtained funding RDG GST and JE performed the
surgery and contributed to patient recruitment and to the
care of patients during their participation in the study
ED was the study coordinator and was responsible for
patient recruitment and follow-up data collection quality
control and many other logistic aspects of the study The
statistical analysis of clinical data was undertaken by CF
and of the pharmacokinetic data by BJA AFM took
primary responsibility for the manuscript with assistance
from Jennifer Zhang All authors edited and commented
on the manuscript AFM is the guarantor
Chief Executive Officer AFT Pharmaceuticals
Clinical TrialRegulatory Assistant AFT Pharmaceuticals
Ethics approval
This study was approved by the Northern X Regional Ethics
Committee 650 Great South Road Penrose Auckland New
Zealand
Ethics Committee Approval Number AKX0410298
Health Authorities (MEDSAFE) Approval Number
TT50-7316 (458)
Role of the sponsor
The sponsor (AFT Pharmaceuticals Ltd) participated in
the study design and protocol development and provided
logistical support during the trial Monitoring of the
study was performed by the sponsor who also main-
tained the trial database Statistical analyses were
independently performed by the biostatistician and the
results cross-checked by sponsors and investigators The
sponsor assisted with the preparation of the manuscript
and was permitted to review it and to make suggestions
but responsibility for the content of this paper lay with
the academic authors and the style and emphasis is that
of the principle investigator The academic authors had
the explicit right to access all data and publish these
results
Provenance and peer review
This paper was not commissioned informal external peer
review has been obtained before submission to the Journal
Additional contributions
We thank Ms Jenny Rous Pharmacy Manager from the
Mercy Hospital Pharmacy for study drug management
Dr Ralph Richardson Program Manager from Institute of
Environment Science amp Research Limited Wellington in
New Zealand for the plasma sample assays Sally Merry
for proofreading and editing on the manuscript the anaes-
thetists Judy Bent Jack Hill Joanna Rose Joanne Paver
Andrew Warmington and Lisa Chapman at Greenlane
Clinical Centre Kerry Gunn Chris Chambers and
Jonathan Cross at Quay Park Clinic for facilitating the
administration of the study protocol and contributing
substantially to the clinical care of the patients and the
participants for their participation
References1 Cousins MJ Brennan F Carr DB Pain relief a universal human
right Pain 2004 112 1ndash42 Merry A Power I Perioperative NSAIDs towards greater safety
Pain Rev 1995 2 268ndash913 MARTINDALE The Extra Pharmacopoeia London The Royal
Pharmaceutical Society of Great Britain 19964 Mehlisch DR The efficacy of combination analgesic therapy in
relieving dental pain J Am Dent Assoc 2002 133 861ndash71
5 Desmeules J Rollason V Piguet V Dayer P Clinical pharmacologyand rationale of analgesic combinations Eur J Anaesthesiol Suppl2003 20 7ndash11
6 Altman RD A rationale for combining acetaminophen andNSAIDs for mild-to-moderate pain Clin Exp Rheumatol 2004 22
110ndash77 Hyllested M Jones S Pedersen JL Kehlet H Comparative effect
of paracetamol NSAIDs or their combination in postoperativepain management a qualitative review Br J Anaesth 2002 88
199ndash2148 Dahl V Dybvik T Steen T Aune AK Rosenlund EK Raeligder JC
Ibuprofen vs acetaminophen vs ibuprofen and acetaminophenafter arthroscopically assisted anterior cruciate ligament recon-struction Eur J Anaesthesiol 2004 21 471ndash5
9 Gazal G Mackie IC A comparison of paracetamol ibuprofen ortheir combination for pain relief following extractions in childrenunder general anaesthesia a randomized controlled trial Int JPaediatr Dent 2007 17 169ndash77
10 Merry AF Swinburn PF Middleton NG Edwards JL Calder MV
Tenoxicam and paracetamolndashcodeine combination after oralsurgery a prospective randomized double-blind placebo-controlled study Br J Anaesth 1998 81 875ndash80
11 Mitchell A van Zanten SV Inglis K Porter G A randomized con-trolled trial comparing acetaminophen plus ibuprofen versus acet-
aminophen plus codeine plus caffeine after outpatient generalsurgery J Am Coll Surg 2008 206 472ndash9
12 Menhinick KA Gutmann JL Regan JD Taylor SE Buschang PHThe efficacy of pain control following nonsurgical root canal
treatment using ibuprofen or a combination of ibuprofen andacetaminophen in a randomized double-blind placebo-controlledstudy Int Endod J 2004 37 531ndash41
13 Viitanen H Tuominen N Vaaraniemi H Nikanne E Annila PAnalgesic efficacy of rectal acetaminophen and ibuprofen alone
or in combination for paediatric day-case adenoidectomy Br JAnaesth 2003 91 363ndash7
14 Henry D McGettigan P Epidemiology overview of gastrointestinaland renal toxicity of NSAIDs Int J Clin Pract 2003 Suppl (135)43ndash9
15 TGA Medicines Evaluation Committee 2003 Review of non-prescription analgesics Multiple Strength of Oral LiquidsAustralia Therapeutic Goods Administration 2003
Combined acetaminophen and ibuprofen for analgesia
87
16 Australian and New Zealand College of Anaesthetists Monitoringduring anaesthesia (Review P18) Melbourne The College 2008
17 Merry AF Sidebotham DA Middleton NG Calder MV WebsterCS Tenoxicam 20 mg or 40 mg after thoracotomy a prospective
randomized double-blind placebo-controlled study AnaesthIntensive Care 2002 30 160ndash6
18 Davies NM Clinical pharmacokinetics of ibuprofen The first 30years Clin Pharmacokinet 1998 34 101ndash54
19 Prescott LF Pharmacokinetics of paracetamol Paracetamol(Acetaminophen) A Critical Bibliographic Review New York Taylor ampFrancis Inc 2001 205ndash15
20 Rainsford KD The pharmacokinetics of ibuprofen in humans andanimals Ibuprofen A Critical Bibliographic Review London Taylor amp
Francis 1999 92ndash521 Ianiro S Jeansonne B McNeal S Eleazer P The effect of pre-
operative acetaminophen or a combination of acetaminophen andibuprofen on the success of inferior alveolar nerve block forteeth with irreversible pulpitis J Endod 2007 33 11ndash4
22 Cooper SA Schachtel BP Goldman E Gelb S Cohn P Ibuprofenand acetaminophen in the relief of acute pain a randomizeddouble-blind placebo-controlled study J Clin Pharmacol 1989 291026ndash30
23 AHFS Drug Information Bethesda MD American Society of
Health-System Pharmacist 2007
24 Coll AM Ameen JRM Mead D Postoperative pain assessmenttools in day surgery literature review J Adv Nurs 2004 46 124ndash33
25 Philip BK Parametric statistics for evaluation of the visual ana-logue scale Anesth Analg 1990 71 710
26 Schou S Nielsen H Nattestad A et al Analgesic dosendashresponserelationship of ibuprofen 50 100 200 and 400 mg after surgicalremoval of third molars a single-dose randomized placebo-controlled and double-blind study of 304 patients J Clin
Pharmacol 1998 38 447ndash5427 Barden J Edwards J Moore A McQuay H Single dose oral para-
cetamol (acetaminophen) for postoperative pain CochraneDatabase Syst Rev (Online) 2004
28 Anderson B Cranswick N The placebo (I shall please)mdashis it so
pleasing in children Paediatr Anaesth 2005 15 809ndash1329 Australian and New Zealand College of Anaesthetists and Faculty
of Pain Medicine Acute Pain Management Scientific EvidenceAustralian Government National Health and Medical ResearchCouncil 2005
30 Moore RA Edwards JE McQuay HJ Acute pain individualpatient meta-analysis shows the impact of different ways of ana-lysing and presenting results Pain 2005 116 322ndash31
31 Quiding H Oksala E Happonen RP Lehtimaki K Ojala T Thevisual analog scale in multiple-dose evaluations of analgesics J Clin
Pharmacol 1981 21 424ndash9
Merry et al
88
e411
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Journal section Oral Medicine and PathologyPublication Types Research
Analgesic efficacy of Lysine Clonixinate paracetamol and dipyrone in lower third molar extraction A randomized controlled trial
Vladimir-Reimar-Augusto-de Souza Noronha 1 Gladson-de Souza Gurgel 1 Luiz-Ceacutesar-Fonseca Alves 2 Luiz-Claacuteudio Noman-Ferreira 2 Lisette-Lobato Mendonccedila 2 Evandro-Guimaratildees de Aguiar 2 Evandro-Neves Abdo 2
1 Student in Oral and Maxillofacial Surgery and Traummatology Dental School Federal University of Minas Gerais Belo Hori-zonte Brazil2 Senior Lectures of Department of Surgery Pathology and Clinic Dental School Federal University of Minas Gerais Belo Horizonte Brazil
Correspondence Faculdade de Odontologia Universidade Federal de Minas GeraisAv Antonio Carlos 6627Belo Horizonte ndash Minas Gerais - BrasilCEP 31270-901evandroabdogmailcom
Received 18082008Accepted 20032009
Noronha VRA Gurgel GS Alves LCF Noman-Ferreira LC Mendonccedila LL Aguiar EG Abdo EN Analgesic efficacy of lysine clonixinate para-cetamol and dipyrone in lower third molar extraction A randomized con-trolled trial Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 httpwwwmedicinaoralcommedoralfree01v14i8medoralv14i8p412pdf
AbstractObjective The purpose of this study is to compare the analgesic effect of lysine clonixinate paracetamol and dipyrone after lower third molar extraction Material and Methods The sample consisted of 90 individuals with clinical indication for inferior third molars extraction The mean age of the sample was 223 years (DPplusmn25) The individuals received the medication in uni-dentified bottles along with the intake instructions The postoperative pain parameters were measured according to Visual Analogical Scale (VAS) and the data was evaluated using the Kruskal-Wallis Test and Friedman Test with the latter used to test different time intervals for each one of the drugsResults The final sample consisted of 64 individuals including 23 males (459) and 41 females (641) The mean age of the entire sample was 223 years (plusmn25) The average length of the procedures was 339 minutes (plusmn98) The distribution of mean values for this variable showed little variance for the different drugs (p=007) Conclusion Lysine Clonixinate did not show any substantial impact on the postoperative pain control when com-pared to other drugs
Key words Lysine Clonixinate paracetamol dipyrone postoperative pain impacted third molar
Article Number 2409 httpwwwmedicinaoralcomcopy Medicina Oral S L CIF B 96689336 - pISSN 1698-4447 - eISSN 1698-6946eMail medicinamedicinaoralcom Indexed in
-SCI EXPANDED-JOURNAL CITATION REPORTS-Index Medicus MEDLINE PubMed -EMBASE Excerpta Medica-SCOPUS-Indice Meacutedico Espantildeol
e412
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Introduction Surgical extraction of third molars is a very usual clini-cal procedure for controlling problems caused by im-pacted tooth and usually is followed by postoperative pain (1) As a result several studies have been published comparing the drugs used to control postoperative pain after surgical removal of third molars (1-4)Lysine Clonixinate is an analgesic that inhibits prostag-landin synthesis A study comparing Lysine Clonixi-nate with Paracetamol on the oral postoperative pain did not find any significantly difference between them (5) In animals Lysine Clonixinate showed a life span of 3 hours and it is recognized as a non-steroid anti-in-flammatory with the shortest life span when compared to other drugs of its category (6)It bonds to plasma proteins in up to 96-98 and its me-tabolism takes place in the liver four different inactive metabolites being derived Seventy-four percent of its excretion is renal and 25 fecal (7) It holds an ex-cellent bio-tolerance and low incidence of collateral ef-fect in the treatment of painful syndrome such as renal neurogenic muscular and tooth pain (89) and migraine (7) The Visual Analogical Scale (VAS) is considered the best and easiest instrument to measure this type of pain The parameters used by VAS determine the intensity of pain as following no pain mild pain moderate pain and severe pain (10-12) The postoperative pain in dentistry should be controlled even before the surgical procedure itself For that many studies suggest the prescription of anti-inflammatory drugs steroids or not or analgesic drugs with some level of anti-inflammatory properties (1314)Paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom tooth (1516) and dipyrone is similar to other analgesics frequently used in the treatment of moderate to severe postoperative pain (17)Although the drugs under test are safe it is possible the occurrence of adverse effect The estimated ex-cess mortality due to community-acquired agranu-locytosis aplastic anemia anaphylaxis and serious upperrsquogastrointestinal complications was 20 per 100 million for paracetamol 25 per 100 million for dipy-rone (18)Regarding the Paracetamol and Dipyrone large use in Brazil Spain and other countries as well (1719) we decided to use them in order to compare the Lysine Clo-nixinate clinic performance The adverse effects due to the use of Lysine Clonixinate could be nausea vomit-ing allergic reactions vertigo and insomnia (9)
Material and MethodsThe sample of 90 individual consisted of all patients under treatment in that semester at the clinic of Oral
Surgery and Oral Traumatology from Federal Univer-sity of Minas Gerais The following conditions were ob-served in order to select the cases (I) individuals with clinical indication for the removal impacted mandibular third molar in Class I or II positioning A or B accord-ing to Pell et al (20) regardless gender race or social class (II) surgeries that would not extend more than 60 minutes (III) age between 18 and 26 years old (IV) absence of allergies to the drugs under test (V) absence of systemic conditions All surgeries were carried out under local anesthesia-Lidocaine 2 with Felipressine 12500 - Novocoreg (SSWhite Artigos Dentais LTDA Rio de Janeiro Brazil)The patients were informed about the purpose of the research project and were asked to give their written consent The research was approved by the local Ethical CommitteeThe drugs tested were bottled in identical opaque white recipient numbered from 1 to 90 Each recipient con-tained eight tablets of either one of the drugs under test (Dipyrone 500mg Paracetamol 750mg Lysine Clonixi-nate 125 mg) The patients themselves chose the recipi-ent at random and they were unaware of its contentEach patient was told to take one tablet from the given recipient one hour before the surgery and another tablet was taken after the surgery in 6 hours intervals after first dose during 24 hours If the pain persisted the pa-tient was given the liberty to take any other drug and the dentist should be informed The assessment of pain was performed according to VAS Pain was measured just after the surgical proce-dure and 1246812 and 24 hours after the operation For each one of the above options they had also to in-form the level of pain according to a decimal scale The criteria used by the authors to assess patientrsquos pain level were 0 cm no pain 01-3 cm light pain 31-7 cm mo-derate pain 71-10 cm intense pain (9) The descriptive analyses are presented in percentages with mean minimum (min) maximum (max) and standard deviation (SD) Kruskal-Wallis and Friedman tests were used and results were considered statistically significant when value of p was less or equal to 005 at least 95 of the confidence
ResultsThe drop-out in the experiment was of twenty-six cases and therefore the sample was reduced to sixty-four The Lysine Clonixinate group was comprised of 20 in-dividuals (8 males and 12 females) The Paracetamol Group was comprised of 23 individuals (9 males and 14 females) and Dipyrone Group was comprised of 21 individuals (6 males and 15 females) The mean age of the entire sample was 223 years (plusmn25) The length of the procedures was in average 339 min-utes (plusmn98) (Table 1) (Table 2) and (Fig 1) depict each
e413
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Interval drugdescriptive measurement
Pmin max median mean SD
Right after Lysine clonixinate 000 100 000 020 040 09370
Paracetamol 000 300 000 030 070
Dipyrone 000 100 000 010 040
1 hour afterLysine clonixinate 000 200 100 070 060 08130
Paracetamol 000 300 100 060 070
Dipyrone 000 200 100 070 070
2 hours afterLysine clonixinate 000 200 100 080 070 09310
Paracetamol 000 300 100 080 090
Dipyrone 000 300 100 080 080
4 hours afterLysine clonixinate 000 200 100 090 070 08760
Paracetamol 000 200 100 080 070
Dipyrone 000 300 100 100 100
6 horus afterLysine clonixinate 000 200 100 060 060 05330
Paracetamol 000 300 100 080 090
Dipyrone 000 300 000 060 080
8 hours afterLysine clonixinate 000 200 050 060 060 03110
Paracetamol 000 200 000 060 080
Dipyrone 000 300 000 040 080
12 hours afterLysine clonixinate 000 200 000 040 060 05930
Paracetamol 000 200 000 055 070
Dipyrone 000 300 000 040 090
24 hours afterLysine clonixinate 000 200 000 030 060 05820
Paracetamol 000 200 000 040 070
Dipyrone 000 300 000 030 070
Fig 1 Distribution of the scale of pain according to the different time interval for each of the drugs tested
Table 1 Distribution of the variable pain according to VAS in different time period for the tree drugs tested
P refers to Kruskal-Wallis test
e414
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
one of the VAS parameters distributed according to drugs tested No adverse effect was observed with the drugs tested
DiscussionSixty-four individuals underwent surgical removal of their inferior third molars among them 23 (359) were male and 41 (641) female As reported before by Morin et al (21) the variable gender did not play any important role in the distribution of the variable pain after surgery The mean age was 223 years (SDplusmn25 years) and the sample was quite homogeneous in that aspect which is an advantage for the categorization of pain related to age Age can influence the pain control because third molar surgical extraction in older individuals can be-come troublesome due the cortical bone thickness and bone resilience loss (1) Chiapasco et al (1) reported a decrease in morbidity and postoperative complication of third molars in young patients Olmedo-Gaya et al (14) attributed an increase of pain in older patients due to the more bone density and narrower periodontal liga-ment
The patients underwent all the surgical procedures by 2 surgeons with calibration of the techniques avoiding therefore different approaches The surgeries length was controlled and therefore did not influence the be-havior of pain in this study- 339 min (SDplusmn98 min) Regarding this the authors believe there is no bias con-cerning the time-period of surgery on the results here presentedThe surgery of third molar is a well known procedure It allows a standardization of case selection reducing therefore the number of uncontrolled events that may lead to biasQuestionnaire and VAS were used to obtain the data The data bank was categorized by drug and analyzed according to the development of the postoperative con-dition as presented in (Table 1)The results in this study show no statistically significant difference between the drugs under test for controlling postoperative pain Martiacute et al (5) found similar results comparing Paracetamol and Lysine ClonixinateThe high number of patients without any pain in the postoperative period can be related to the local anesthe-sia The number of patients without pain in the postop-
DescriptionDrug Interval min Max median mean SD p
Lisyne clonixinate
Right after 00 10 00 02 04
lt 0001
1 hour after 00 20 10 07 062 hours after 00 20 10 08 074 hours after 00 20 10 09 076 hours after 00 20 10 06 068 hours after 00 20 05 06 0612 hours after 00 20 00 04 0624 hours after 00 20 00 03 06
Paracetamol
Right after 00 30 00 03 07
lt 0001
1 hour after 00 30 10 06 072 hours after 00 30 10 08 094 hours after 00 20 10 08 076 hours after 00 30 10 08 098 hours after 00 20 00 06 0812 hours after 00 20 00 05 0724 hours after 00 20 00 04 07
Dipyrone
Right after 00 10 00 01 04
lt 0001
1 hour after 00 20 10 07 072 hours after 00 30 10 08 084 hours after 00 30 10 10 106 hours after 00 30 00 06 088 hours after 00 30 00 04 0812 hours after 00 30 00 04 0924 hours after 00 30 00 03 07
Table 2 Distribution of pain perception in the different time intervals after surgery according to VAS
P refers to Friedman test
e415
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
erative period decreases with the passing of time Four hours after the surgery this percentage was the smallest and it increases slightly on the 6th and 8th hour after surgery reaching its peak with 24 hours The results presented here are similar to those of Olme-do-Gaya et al (14) who found out that the postoperative pain reaches its higher intensity during the first 8 hours after the surgery The moderate postoperative pain is re-ported when the production of pain mediator increases and also when the effect of local anesthesia is fading away After the 8th hour and during the subsequently days the pain decreases progressivelyThe results of this study show that the Lysine Clonixi-nate as well as Dipyrone and Paracetamol are efficient in controlling the postoperative pain in the surgery of inferior impacted third molars Lysine Clonixinate pos-sesses an analgesic activity similar to that of Dipyrone and Paracetamol and did not show any substantial im-pact on the control of postoperative pain when com-pared to those drugs
References1 Chiapasco M De Cicco L Marrone G Side effects and complica-tions associated with third molar surgery Oral Surg Oral Med Oral Pathol 199376412-20 2 Laureano Filho JR Maurette PE Allais M Cotinho M Fernandes C Clinical comparative study of the effectiveness of two dosages of Dexamethasone to control postoperative swelling trismus and pain after the surgical extraction of mandibular impacted third molars Med Oral Patol Oral Cir Bucal 200813E129-32 3 Loacutepez-Carriches C Martiacutenez-Gonzaacutelez JM Donado-Rodriacuteguez M Analgesic efficacy of diclofenac versus methylprednisolone in the control of postoperative pain after surgical removal of lower third molars Med Oral Patol Oral Cir Bucal 200510432-9 4 Esteller-Martiacutenez V Paredes-Garciacutea J Valmaseda-Castelloacuten E Berini-Ayteacutes L Gay-Escoda C Analgesic efficacy of diclofenac sodium versus ibuprofen following surgical extraction of impacted lower third molars Med Oral Patol Oral Cir Bucal 20049448-53 444-8 5 Martiacute ML De los Santos AR Di Girolamo G Gil M Manero EO Fraga C Lysine clonixinate in minor dental surgery double-blind randomized parallel study versus paracetamol Int J Tissue React 199315207-13 6 Gonzaacutelez-Martin G Cattan C Zuntildeiga S Pharmacokinetics of lysine clonixinate in children in postoperative care Int J Clin Phar-macol Ther 199634396-9 7 Krymchantowski AV Peixoto P Higashi R Silva A Jr Schutz V Lysine clonixinate vs naproxen sodium for the acute treatment of mi-graine a double-blind randomized crossover study MedGenMed 2005769 8 Ortiacute E Coirini H Pico JC Site-specific effects of the nonsteroidal anti-inflammatory drug lysine clonixinate on rat brain opioid recep-tors Pharmacology 199958190-9 9 Krymchantowski AV Barbosa JS Cheim C Alves LA Oral lysine clonixinate in the acute treatment of migraine a double-blind place-bo-controlled study Arq Neuropsiquiatr 20015946-9 10 Kremer E Atkinson JH Ignelzi RJ Measurement of pain patient preference does not confound pain measurement Pain 198110241-8 11 Price DD McGrath PA Rafii A Buckingham B The validation of visual analogue scales as ratio scale measures for chronic and ex-perimental pain Pain 19831745-56 12 Collins SL Moore RA McQuay HJ The visual analogue
pain intensity scale what is moderate pain in millimetres Pain 19977295-7 13 Seymour RA Walton JG Pain control after third molar surgery Int J Oral Surg 198413457-85 14 Olmedo-Gaya MV Vallecillo-Capilla M Galvez-Mateos R Rela-tion of patient and surgical variables to postoperative pain and inflam-mation in the extraction of third molars Med Oral 20027360-9 15 Weil K Hooper L Afzal Z Esposito M Worthington HV Van Wijk AJ et al Paracetamol for pain relief after surgical removal of lower wisdom teeth Cochrane Database Syst Rev 20073CD004487 16 Moore A Collins S Carroll D McQuay H Paracetamol with and without codeine in acute pain a quantitative systematic review Pain 199770193-201 17 Edwards JE Meseguer F Faura CC Moore RA McQuay HJ Single-dose dipyrone for acute postoperative pain Cochrane Data-base Syst Rev 20013CD003227 18 Andrade SE Martinez C Walker AM Comparative safety evalu-ation of non-narcotic analgesics J Clin Epidemiol 1998511357-65 19 Lorenzetti BB Ferreira SH Mode of analgesic action of dipy-rone direct antagonism of inflammatory hyperalgesia Eur J Phar-macol 1985114375-81 20 Pell GJ Gregory BT Impacted mandibular third molars clas-sification and modified techniques for removal Dent Digest 193339330-821 Morin C Lund JP Villarroel T Clokie CM Feine JS Differences between the sexes in post-surgical pain Pain 20008579-85
CLINICAL TRIAL
Onset of analgesia with sodium ibuprofen ibuprofen acidincorporating poloxamer and acetaminophenmdasha single-dosedouble-blind placebo-controlled study in patientswith post-operative dental pain
Stephen Daniels amp Sandie Reader amp Phillip Berry amp
Michael Goulder
Received 24 September 2008 Accepted 6 January 2009 Published online 28 February 2009 Springer-Verlag 2009
AbstractObjective To compare the onset of action and efficacy ofsodium ibuprofen (ibuprofen sodium dihydrate) and ibu-profen acid incorporating poloxamer (ibuprofenpoloxamer)with that of acetaminophen and placebo in patients withpost-operative dental painMethods A double-blind randomised placebo-controlledactive comparator two-centre study assessing the analgesicefficacy of sodium ibuprofen (512 mg equivalent to400 mg ibuprofen acid) ibuprofenpoloxamer (containing400 mg ibuprofen acid and 120 mg poloxamer 407)acetaminophen (1000 mg) and placebo in patients withmoderate-to-severe pain after third molar extraction (n=322) Onset of action was assessed using the two-stopwatchtechnique and pain intensity and relief were measuredusing validated traditional descriptor scales
Results Significantly more patients achieved confirmedperceptible pain relief and meaningful pain relief withsodium ibuprofen (963 Plt00001) and ibuprofenpoloxamer (900 P=00005) than with acetaminophen(675) The onset of action of both ibuprofen formula-tions was comparable with that of acetaminophen up to45 min post-dose a marked divergence in onset times infavour of the ibuprofen formulations occurred from45 min onward Mean values for the area under the painrelief and pain intensity differences curve (0ndash6 h) weresignificantly greater for sodium ibuprofen (346) andibuprofen acid (349) than for acetaminophen (225) (Plt0001) Other pain relief and pain intensity endpointsfavoured both ibuprofen formulations over acetamino-phen Distractibility from pain (6 h) was significantlygreater with the ibuprofen formulations than with acet-aminophen (P=0008 for sodium ibuprofen P=003 foribuprofenpoloxamer) In patients receiving ibuprofenpain interfered less with daily activities (at 1 and 6 h)than in those receiving acetaminophen (Ple0015) Bothibuprofen formulations had significantly better meanglobal assessment scores than acetaminophen (Plt0001)Tolerability profiles of the ibuprofen formulations werecomparable with that of acetaminophenConclusions Compared with acetaminophen sodiumibuprofen was associated with significantly greateranalgesic efficacy pain relief in a greater proportion ofpatients and greater patient satisfaction
Keywords Acetaminophen Dental pain
Ibuprofenpoloxamer Impacted teeth Post-operative pain
Sodium ibuprofen
Eur J Clin Pharmacol (2009) 65343ndash353DOI 101007s00228-009-0614-y
S DanielsPremier Research Group Clinical Research Center3200 Red RiverAustin TX 78705 USA
S Reader P Berry ()Reckitt Benckiser Healthcare UKDansom LaneHull HU8 7DS UKe-mail phillipberryreckittbenckisercom
M GoulderWorldwide Clinical Trials UK Ltd Isaac Newton CentreNottingham Science and Technology ParkNottingham NG7 2RH UK
Introduction
Ibuprofen [2-(4-isobutylphenyl) propionic acid] is awidely used non-steroidal anti-inflammatory drug(NSAID) currently licensed and marketed worldwide Itexhibits anti-inflammatory analgesic and antipyreticeffects in humans by working as a potent inhibitor of thecyclooxygenase enzyme system and is used to treat painresulting from a wide variety of ailments There is anextensive amount of published literature describing theefficacy of ibuprofen [1ndash7]
Patients with acute pain require rapid relief from over-the-counter (OTC) analgesics Rapidly absorbed ibuprofenformulations have been developed [8] and it was antici-pated that this rapid absorption would result in early onsetof analgesia This placebo-controlled double-blind rando-mised single-dose study was conducted to measure thetime to onset and degree of analgesia from two investiga-tional ibuprofen formulations The first investigationalibuprofen formulation contains the sodium salt of the drugibuprofen sodium dihydrate (sodium ibuprofen) Theformulation used in this study contains 256 mg of theibuprofen sodium salt equivalent to 200 mg ibuprofen acidIt is well documented that ibuprofen salts such asibuprofen sodium lysine and arginate are more rapidlyabsorbed than formulations of free ibuprofen acid [9] andseveral studies have shown that faster absorbed formula-tions lead to faster onset of analgesia [10ndash12] The saltdissolves rapidly in the gastrointestinal tract leading tofaster absorption Pharmacokinetic analyses show that thetime to peak plasma concentration (Tmax) with ibuprofensodium dihydrate is achieved in approximately 30ndash40 min[8] in contrast to the 1ndash2 h reported for standard ibuprofentablets [13 14] The second investigational ibuprofenformulation contains ibuprofen acid plus the surfactantpoloxamer 407 [from the poloxamer family of polymericnon-ionic surface active agents (ibuprofenpoloxamer)]mdashtoincrease the rate of dissolution of the tablet and enable morerapid absorption relative to standard ibuprofen formula-tions Acetaminophen another widely used OTC analgesicand antipyretic indicated for the same mild-to-moderatepain conditions as ibuprofen was included in the study as areference
The dental pain model was used because it is the mostappropriate model to investigate onset of analgesic actionIt is an established post-surgical pain model that involvesextraction of impacted third molars (wisdom teeth) arelatively consistent surgical technique that predictablyproduces moderate-to-severe pain The model is widelyaccepted and has a proven record of assay sensitivity (ieseparating active drugs from each other as well as fromplacebo) [11 12 15ndash18] The model is sensitive enough todemonstrate a correlation between plasma levels of ibupro-
fen and onset of analgesia with faster absorbed formula-tions such as ibuprofen arginate having a faster clinicalresponse time than standard ibuprofen [11 12 19] Theresults from dental pain studies have been widely extrap-olated to other general pain conditions including mostcommon OTC conditions
Onset of analgesic action was assessed using the two-stopwatch technique [11 12 19] and pain intensity andpain relief at each of the assessment timepoints wereassessed using traditional descriptor scales Exploratoryanalyses were conducted to give additional informationabout the rate of onset of action of the medications and tocompare the extent of relief provided by each of the activeformulations
Both ibuprofen formulations were given at a doseequivalent to 400 mg ibuprofen acid The acetaminophenproduct included in the study was Tylenol Extra Strength(1000 mg) a commercially available product The brandedprinting was removed from the Tylenol caplets to enable amatched placebo to be produced The doses of both drugsare the maximum licensed OTC doses in the USA and mostother countries and they have well-established safety andefficacy profiles
The primary objective of the study was to determine thetime to onset of analgesia following dosing with sodiumibuprofen tablets (2times256 mg ibuprofen sodium dihydrate)and ibuprofen acid tablets incorporating poloxamer (2times200 mg ibuprofen plus 60 mg poloxamer 407) hereafterreferred to as ibuprofenpoloxamer in patients with post-operative dental pain The secondary objective was tocompare the efficacy of the two ibuprofen formulationswith that of 1000 mg acetaminophen and placebo in termsof onset peak and duration of analgesic action
The study was conducted in accordance with theDeclaration of Helsinki [20] as referenced in EU Directive200120EC [21] and complies with International Confer-ence on Harmonisation (ICH) Good Clinical Practice(GCP) and applicable regulatory requirements
Methods
Study design
This study was a randomised double-blind placebo-controlled single-dose parallel-group study using thedental pain model It was conducted in two clinical researchcentres (Austin Texas and San Marcos Texas)
Patients andor their legal guardians provided informedconsent before the conduct of study-related proceduresPatients were screened within the 28 days before surgeryOn the day of surgery patients underwent surgical removalof one partially or full bone impacted mandibular third
344 Eur J Clin Pharmacol (2009) 65343ndash353
molar or two ipsilateral third molars with a total impactionscore of 4 5 or 6
Degree of impaction Points
Erupted 0Soft tissue 1Partial bone 2Complete (full) bone 3Unusual impaction (horizontalinverted or posterior-anterior) 4
Surgery was performed under local anaesthetic (approx-imately 100 mg lidocaine 2 with 110000 epinephrine)with conscious sedation (35 lmin 50 nitrous oxide for15 min) using standard surgical techniques Followingsurgery patients who fulfilled the inclusion criteria regard-ing baseline pain intensity were randomly allocated to oneof four treatment groups (sodium ibuprofen ibuprofenpoloxamer acetaminophen or placebo) in a 1111 ratioaccording to a computer-generated randomisation schedulethat stratified patients by sex and baseline pain intensityAfter dosing patients remained in the centre for 8ndash15 hOnset of action and efficacy assessments were recorded atpre-determined intervals during the 6 h post-dose A post-operative follow-up was conducted 5ndash12 days after surgery
The study protocol and its amendments together with thepatient information and consent documents were reviewedand approved by Quorum Review Inc (Seattle WA)
Patients
Patients were recruited from the Premier Research GroupClinical Research Centers database via advertising andpractitioner referral Eligible patients were males andfemales 16ndash40 years of age with a primary diagnosis of
amp at least one mandibular third molar (with full bonyimpaction and an impaction score of ge4 on a 5-pointscale) indicated for removal
amp two ipsilateral third molars with a combined totalimpaction score no greater than 6
In either case patients were required to have moderate orsevere baseline pain intensity as assessed using a 4-pointcategorical pain intensity scale and confirmed with a visualanalogue scale (VAS) score of ge50 mm but le85 mm (where0=no pain and 100 mm=worst pain)
The main exclusion criteria were history of significantdisease that rendered the patient unsuitable for inclusionsignificant ongoing painful conditions other than thatassociated with third molar surgery any ongoing conditionthat may have interfered with the absorption distributionmetabolism or excretion of study medications history ofallergy gastrointestinal complaints (including ulcers heart-burn dyspepsia and indigestion) migraine headaches
within the last year psychotic illness or drug abuse useof concomitant medication that may have confoundedassessments of pain relief (eg psychotropic drugs anti-depressants or sedative-hypnotics) pregnancylactationingestion of any analgesic or anti-inflammatory drug frommidnight of the night before surgery
Sample size determination
For the primary endpoint data were available for the time toperceptible relief from three studies using ibuprofen arginate[11 12 19] These data suggested that the time to perceptiblerelief would be 9 to 14 min for the two test formulationsassuming a similar onset of action to that of ibuprofen arginateSince it was assumed that the majority of placebo patientswould not achieve meaningful relief it was planned that thetime to confirmed perceptible relief for these patients would becensored at 4 h Although the spread of observations was notprovided for the arginate formulation it was assumed conser-vatively that the standard deviation (SD) for time to confirmedperceptible relief would be 1 h (based on the possible rangebeing 0ndash4 h and covering plusmn 2 SD) Hence this study was highlypowered (gt99) to detect such a large difference for the time toconfirmed perceptible relief using the Wilcoxon test
For the area under the curve (AUC) (pain relief intensitydifference [PRID] from 0 to 6 h) data were available fromtwo previous studies which compared ibuprofen lysine [22]and liquigel [23] ibuprofen with acetaminophen In the formerstudy PRID to 6 h was not provided but the sum of painintensity differences (SPID) to 6 h was given This gave adifference of 251 between ibuprofen lysine and acetamino-phen The within-group SD for acetaminophen was 447Using these data it was calculated that with 80 patients pergroup this study would have a 90 power to detect adifference between the ibuprofen formulations and acetamin-ophen at a significance level of 0025 If the data from theliquigel paper were used for sum of the measures of pain reliefand pain intensity difference (SPRID) to 6 h a slightly higherpower would be achieved It was not possible to performformal power calculations for the second endpoint in the closedtest procedure namely time to meaningful relief
Study and concomitant treatments
Following surgery eligible patients received a single oraldose (four tablets and two caplets) of one of the followingfour study treatments
amp sodium ibuprofen 2times256 mg ibuprofen sodium dihy-drate tablets (each tablet equivalent to 200 mg ibupro-fen acid) plus two matched placebo for ibuprofenpoloxamer tablets plus two matched placebo for 500 mgacetaminophen caplets
Eur J Clin Pharmacol (2009) 65343ndash353 345
amp ibuprofenpoloxamer 2times200 mg ibuprofen acid tabletseach tablet incorporating 60 mg of the surfactantpoloxamer 407 plus two matched placebo for sodiumibuprofen tablets plus two matched placebo for 500 mgacetaminophen caplets
amp acetaminophen 2times500 mg acetaminophen (TylenolExtra Strength) caplets plus two matched placebo forsodium ibuprofen tablets plus two matched placebo foribuprofenpoloxamer tablets
amp placebo two matched placebo for sodium ibuprofentablets plus two matched placebo for ibuprofenpolox-amer tablets plus two matched placebo for 500 mgacetaminophen caplets
Patients were encouraged to wait at least 90 min afterreceiving the study treatment before consuming rescuemedication although rescue medication was available atany time after dosing If rescue medication was neededwithin the first 4 h of dosing an intra-muscular injection ofketorolac tromethamine (60 mg) was administered Ifrescue medication was needed later than 4 h after studydrug administration acetaminophen 500 mghydrocodone5 mg or ketorolac tromethamine was given A prescriptionfor acetaminophen 500 mghydrocodone 5 mg was provid-ed to patients for home use at the time of discharge
The use of intravenous oral or inhaled (nitrous)sedation during surgery was prohibited Analgesic andanti-inflammatory drugs (except for the permitted rescuemedications antibiotics and anaesthetics) were not per-mitted during the 6-h post-dose assessment periodPenicillins macrolide antibiotics clindamycin and topicaltetracycline gelfoam were permitted the use of selectiveserotonin-reuptake inhibitors (SSRIs) and selective nor-epinephrine-reuptake inhibitors (SNRIs) was also accept-able in patients who had maintained a stable dose for atleast 4 weeks prior to the first visit Caffeine-containingfoods and drinks were to be discontinued from midnightprior to surgery until the end of the 6-h post-doseassessment period Ice packs were not allowed for thefirst 3 h after dosing
Efficacy endpoints
Patients were queried at pre-determined intervals by thestudy staff and all pain assessments were recorded by thepatient in their diary
Pain intensity (categorical and VAS)
Pain intensity (PI) was assessed at the following timesbaseline (0 h) and at 5 10 15 20 25 30 35 40 45 60 90120 180 240 300 and 360 min after dosing The PI wasmeasured on a categorical scale in response to the question
ldquoWhat is your pain level at this timerdquo with patient responsechoices of none=0 mild=1 moderate=2 and severe=3 Inaddition patients were also asked to draw a single vertical lineto indicate their current level of PI on the 100-mm VASPatients were randomised to treatment when they rated theirbaseline PI as moderate or severe and the score on the VASwas ge50 mm but le85 mm
Pain relief and pain half-gone
Pain relief (PR) was assessed at the same times as PI (withthe exception of 0 h) in response to the question ldquoHowmuch relief have you had from your starting painrdquo withpatient response choices of none=0 a little=1 some=2 alot=3 and complete=4 In addition patients were alsoasked ldquoIs your starting pain at least half gonerdquo withpatient responses as no=0 or yes=1
Perceptible and meaningful PR
Two stopwatches were started at the time of dosing Eachpatient was instructed ldquoStop the first stopwatch when you firstfeel any pain relief whatsoever This does not mean you feelcompletely better although you might but when you first feelany relief in the pain you have nowrdquo The patient wasinstructed ldquoStop the second stopwatch when the pain relief ismeaningful to yourdquo If the patient did not press thestopwatches within the first 4 h of the treatment period or ifrescue medication was required the patients were no longerrequired to use the stopwatches
Distractibility from pain
Distractibility from pain was assessed at baseline and at 60and 360 min after dosing in response to the question ldquoHoweasy is it for you to distract yourself from your painrdquoPatients responded using a 100-mm VAS scale where 0 =very easy and 100 = impossible
Rainier scale
Patients completed the Rainier scale at baseline and at 60and 360 min after dosing This assessed perceivedfunctional impairment of activities of daily living (ieeating driving sleeping reading working and speaking)Patients rated the perceived pain interference with eachactivity on a scale of 1 to 10 where 1 = would not interfereat all and 10 = would completely interfere
Rescue medication
The time of rescue medication was recorded Patientstaking rescue medication completed all pain intensity and
346 Eur J Clin Pharmacol (2009) 65343ndash353
pain relief assessments immediately before rescue medica-tion and continued to record their pain assessmentsthroughout the 6-h assessment period
Global evaluation
At the end of 6 h or at the time of rescue medication patientswere asked ldquoHow effective do you think the study medicationis as a treatment for painrdquo Response choices were 1 =excellent 2 = very good 3 = good 4 = fair or 5 = poor
The primary efficacy endpoint was the time to firstconfirmed perceptible pain relief There were two keysecondary endpoints (1) the AUC for SPRID from 0 to 6 hand (2) the time to meaningful pain relief
Other secondary endpoints included (1) total pain relief(TOTPAR) SPID (categorical and VAS) SPRID from 0 to4 h (2) TOTPAR SPID (categorical and VAS) from 0 to6 h (3) individual pain relief and pain intensity (categoricaland VAS) readings at each timepoint from 5 min to 6 h (4)peak pain relief and pain intensity difference (PID)(categorical and VAS) throughout the 6-h evaluation period(5) first time at which PID was ge1 (6) time to first use ofrescue medication (7) time to and proportion of patientswith pain half-gone (8) distractibility from pain at baselineand at 1 and 6 h post-dose and perceived pain interferencewith daily activities (Rainier scale) at 1 and 6 h post-dose(9) patientrsquos overall assessment of the medication
Safety assessments
Adverse events (AEs) were assessed by non-directedquestioning recorded in the source documentation andthen assessed by the Investigator with respect to severityand relationship to study medication Vital signs (bloodpressure heart rate and oral temperature) were assessed atscreening baseline (pre-dose) at 6 h post-dose and at thefollow-up visit A physical examination was also conductedat screening and at the follow-up visit 5ndash12 days aftersurgery
Statistical analyses
All calculations and figures were produced using SAS ver91 or S-PLUS 62 (SAS Institute Cary NC) The analysisof the primary endpoints was performed via a closed testprocedure The actual protocol-defined primary endpointwas the time to first confirmed perceptible pain reliefPairwise differences between the two ibuprofen formula-tions and placebo were assessed at a significance level of25 so the overall alpha-level of 5 was maintained Forthe primary endpoint pairwise differences between the twoibuprofen formulations and placebo were assessed using theWilcoxon rank-sum test A sensitivity analysis was also
performed where differences between the ibuprofen for-mulations and placebo were assessed using a Cox regres-sion analysis with treatment group study site gender andbaseline pain intensity (categorical) included in the modelThe hazard ratio and associated 975 confidence intervals(CIs) were calculated for the pairwise comparisons
It was planned that if either of the primary pairwisecomparisons were significant at the 25 level the keysecondary endpoints (SPRID 0ndash6 h and time to meaningfulpain relief) were to be assessed for that formulation under aclosed-test procedure Each endpoint was assessed in theorder specified and only if the previous assessments for thatformulation were significant were the subsequent end-points assessed in a confirmatory sense Once the endpointwas not significant then all subsequent assessments wereconsidered exploratory
Endpoints aggregated over several time points werecalculated using AUC as per the secondary endpointDifferences between the treatments were assessed at atwo-sided alpha of 005 A 95 CI for the pairwisedifferences between the treatments was calculated fromthe parameter estimates of the fitted model The pairwisecomparisons of interest were between each of the ibuprofenformulations and placebo and between each of theibuprofen formulations and acetaminophen For the time-to-event parameters such as time to first (unconfirmed)perceptible pain relief differences between the treatmentgroups were assessed as per the primary endpoint
Differences between each of the two ibuprofen formu-lations and acetaminophen in the key secondary endpointsand in the majority of the other secondary endpoints wereanalysed by analysis of covariance (ANCOVA) includingtreatment group study site gender and baseline painintensity (categorical scale) as factors
All assessments completed after the patient had takenrescue medication were considered to be missing For bothpain relief and pain intensity differences missing valuesbetween two available assessments were linearly interpo-lated Missing readings that could not be interpolated werereplaced with the baseline pain intensity or zero relief
All enrolled patients who received a dose of studymedication were included in the safety population All AEswere listed and tabulated by treatment severity relationshipto therapy and body system according to the MedicalDictionary for Regulatory Activities (MedDRA) Version81
Results
Between June and October 2005 a total of 322 patients(mean age 213 years) were randomised to receive studytreatment Of the 322 randomised patients 318 (988)
Eur J Clin Pharmacol (2009) 65343ndash353 347
completed the study The trial profile including the totalnumber of patients withdrawn and analysed is illustrated inFig 1 A total of 321 patients all of whom were balancedacross treatment groups with respect to baseline demo-graphics pain intensity and clinical characteristics (Table 1)were included in the intent-to-treat (ITT) population
Primary efficacy endpoint
Significantly more patients reported confirmed perceptiblepain relief with sodium ibuprofen (963) and ibuprofenpoloxamer (900) than with acetaminophen (675) (Plt00001 and P=00005 respectively) In the placebo grouponly 259 patients reported confirmed perceptible painrelief KaplanndashMeier median times to confirmed perceptiblepain relief were 170 min for sodium ibuprofen 185 minfor ibuprofenpoloxamer and 201 min for acetaminophen(Fig 2) Median time could not be estimated for placebo asfewer than 50 of patients assigned to this groupexperienced confirmed perceptible pain relief Comparisonsof pairwise differences between the two ibuprofen formu-lations and placebo using Wilcoxon rank-sum tests and Coxregression analysis were highly significant (Plt0001 forboth analyses)
Key secondary efficacy endpoints
Mean SPRID (0ndash6 h) values were 346 349 225 and073 for the sodium ibuprofen ibuprofenpoloxamer
acetaminophen and placebo groups respectively Pair-wise comparisons of ibuprofen and acetaminophen werehighly significant in favour of both ibuprofen formula-tions (Plt0001)
Significantly more patients reported meaningful painrelief with sodium ibuprofen (963) or ibuprofenpolox-amer (900) than with acetaminophen (675) (Plt00001and P=00005 respectively) (Fig 3) Of the patientsreceiving placebo 259 reported meaningful pain reliefThe KaplanndashMeier median times to meaningful relief were451 min (sodium ibuprofen) 447 min (ibuprofenpolox-amer) and 541 min (acetaminophen) Neither of the twoWilcoxon rank-sum comparisons between the ibuprofenformulations and acetaminophen were statistically signifi-cant whereas pairwise comparisons obtained via Coxregression analysis were statistically significantly different(P le 0002) The KaplanndashMeier survival curves were similarfor the ibuprofen and acetaminophen groups up to 45 minbut the degree of separation from 45 min onward wasmarked with more patients achieving meaningful painrelief with ibuprofen
Sitendashtreatment interactions
In general site was a statistically significant factor subjectsfrom the SanMarcos site had less favourable outcomes For theprimary efficacy endpoint and for the key secondary efficacyendpoints of SPRID (0ndash6 h) and time to meaningful pain reliefsite was statistically significantly For all three measures the
Withdrawn from ITT (failure toprovide baseline diary data) 1Withdrawn from ITT (failure toprovide baseline diary data) 1Withdrawn from ITT (failure toprovide baseline diary data) 1
IBUPROFENPOLOXAMER
Total screened 614
Total randomised 322
Excluded prior to surgery (n=240)
Excluded prior to dosing (n=52)
Failure to meet inclusion criteria (n=292)
Allocated to intervention 80
ACETAMINOPHEN
Allocated to intervention 81
PLACEBO
Allocated to intervention 81
Completed 80 Completed 81 Completed 81
Total analysed (ITTa) 80 Total analysed (ITTa) 80 Total analysed (ITTa) 81
Completed 76
Withdrew consent 1Lost to follow-up 1Other reasons 2
Withdrawn 0 Withdrawn 0 Withdrawn 0
Total analysed (ITTa) 80
SODIUM IBUPROFEN
Not included in ITT (failure to provide baseline diary data) 1
Allocated to intervention 80
Fig 1 Flow diagram illustrat-ing patient inclusion and exclu-sion throughout the study ITTIntent to treat aThe ITT popula-tion consisted of all patientswho were randomised whocompleted the baseline efficacyassessments and who had atleast one post-baseline assess-ment (primary efficacy set)
348 Eur J Clin Pharmacol (2009) 65343ndash353
interaction between site and treatment was formally investigat-ed In all cases the interaction term was not statisticallysignificant implying that treatment group responses wereconsistent between the sites
Exploratory secondary efficacy endpoints
Pain relief andor reduction in pain intensity
All summary endpoints related to pain relief andor PIDwere significantly more favourable for the two ibuprofenformulations than for acetaminophen or placebo (Plt0001for both ibuprofen formulations vs acetaminophen orplacebo in all comparisons)
A summary of pain relief scores at specified time pointsfrom 5 min to 6 h is displayed in Fig 4 The superiority of
the two ibuprofen formulations over acetaminophen canclearly be seen from 45 min post-dose onward A summaryof PID (categorical) scores at specified time points from5 min to 6 h is displayed in Fig 5 The superiority of thetwo ibuprofen formulations over acetaminophen can beclearly seen from 60 min post-dose onward
Individual PR and PID
The pain relief and PID (categorical and VAS) scores showthat sodium ibuprofen provided more effective pain reliefthan placebo at 15 min [P=0021 (PR) P=004 (PIDcategorical) P=0036 (PID VAS)] Similarly ibuprofenpoloxamer provided more effective relief than placebo at25 min [P=0002 (PR) P=0002 (PID categorical)] and at20 min [P=0008 (PID VAS)]
Timepoint (mins)
a
ttain
ing
conf
irmed
per
cept
ible
rel
ief
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 2 KaplanndashMeier curves for time to first confirmed perceptiblepain relief
Timepoint (mins)
a
ttain
ing
mea
ning
ful r
elie
f
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 3 KaplanndashMeier curves for time to meaningful pain relief
Table 1 Patient demographics and clinical characteristics at baseline (ITT population)
Baseline patient characteristics Treatment group
Sodium ibuprofen(n=80)
Ibuprofenpoloxamer(n=80)
Acetaminophen(n=80)
Placebo(n=81)
Total(n=321)
Age (years) mean (SD) 214 (388) 214 (360) 212 (443) 211 (408) 213 (399)Sex n ()Male 31 (388) 31 (388) 30 (375) 31 (383) 123 (383)Female 49 (613) 49 (613) 50 (625) 50 (617) 198 (617)
Baseline pain intensity (categorical) n ()Moderate 61 (763) 60 (750) 60 (750) 62 (765) 243 (757)Severe 19 (238) 20 (250) 20 (250) 19 (235) 78 (243)
Baseline pain intensity (VAS) mean (SD)Mean (SD) 6816 (874) 6881 (949) 6703 (932) 6737 (1003) 6784 (939)Range 51ndash85 50ndash89 52ndash84 50ndash85 50ndash89
ITT intent-to-treat SD standard deviation VAS visual analogue scaleTreatment definitions sodium ibuprofen=2times256 mg ibuprofen sodium dihydrate tablets (each tablet equivalent to 200 mg ibuprofen acid)ibuprofenpoloxamer=2times200 mg ibuprofen acid tablets acetaminophen=2times500 mg acetaminophen caplets
Eur J Clin Pharmacol (2009) 65343ndash353 349
First time to PID ge 1
There were no significant differences between the activetreatment groups in the proportion of the time to reportingof PID ge 1
Time to first use of rescue medication
Rescue medication was required by significantly fewerpatients in the sodium ibuprofen group (325) and theibuprofenpoloxamer group (225) than in the acetamin-ophen (438) group Owing to the relatively smallproportion of patients reporting the use of rescue medica-tion KaplanndashMeier median times to first use of rescuemedication could not be calculated The pairwise compar-isons between the two ibuprofen formulations and acet-aminophen were both statistically significant using theWilcoxon rank-sum test with P=0019 and P=0001 forsodium ibuprofen and the ibuprofenpoloxamer formula-tion respectively (Fig 6) The vast majority of patientsrandomised to placebo took rescue medication (827)
Time to and proportion of patients with pain half-gone
The proportion of patients reporting pain half-gone were938 888 75 and 370 for sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo re-spectively The median time to pain half-gone wassimilar for all three active treatment groupsmdash350 min(sodium ibuprofen) 375 min (ibuprofenpoloxamer) and450 min (acetaminophen) The Wilcoxon rank-sumcomparisons between the ibuprofen formulations andacetaminophen were not statistically significant (P=007and P=018 for sodium ibuprofen and ibuprofenpolox-amer respectively) but the two equivalent comparisonswere statistically significant when the Cox regression wasused (P=0013 and P=002 for sodium ibuprofen andibuprofenpoloxamer respectively) This may be explainedin terms of a greater proportion of patients randomised toeither of the ibuprofen formulations reporting the endpointscompared with acetaminophen However as for time tomeaningful relief the separation in onset times in favour ofibuprofen was only apparent from 45 min post-doseonward
Distractibility from pain (VAS)
At 1-h post-dose the mean values for the distractibilityfrom pain (VAS) scores were 290 321 381 and657 mm for sodium ibuprofen ibuprofenpoloxameracetaminophen and placebo respectively Both ibuprofenformations had lower (more favourable) scores thanplacebo (Plt0001) and sodium ibuprofen versus acetamin-ophen was statistically significant (P=0010) whereas theibuprofenpoloxamer versus acetaminophen comparisonswere non-significant (P=0083)
At 6 h post-dose both ibuprofen formulations hadmore favourable distractibility from pain scores thanacetaminophen (P=0008 and P=003 sodium ibuprofen
Timepoint (minutes)
Mea
n pa
in in
tens
ity d
iffer
ence
s
00
05
10
15
0 15 35 60 90 120 180 240 300 360
Sodium ibuprofen IbuprofenpoloxamerAcetaminophenPlacebo
Fig 5 Mean pain intensity difference (categorical) at each timepoint
Timepoint (mins)
ta
ken
resc
ue m
edic
atio
n
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 6 KaplanndashMeier curves for time to first use of rescue medication
Fig 4 Mean pain relief at each timepoint
350 Eur J Clin Pharmacol (2009) 65343ndash353
and ibuprofenpoloxamer respectively) The vast majorityof patients randomised to placebo took rescue medicationso only 14 patients provided valid data within this grouphence this analysis was not performed for the placebogroup
Pain interference with daily activities (Rainier scale)
At 1-h post-dose the mean values on the Rainier scale were188 223 268 and 432 for the sodium ibuprofen ibuprofenpoloxamer acetaminophen and placebo groups respectivelyThe scores were statistically significantly lower for bothibuprofen formulations than for placebo (Plt0001) andacetaminophen [P=0001 (sodium ibuprofen) and P=0015(ibuprofenpoloxamer)] At 6-h post-dose the mean valueswere 151 171 224 and 163 for the sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo groupsrespectively Both ibuprofen formulations maintained signif-icantly lower (more favourable) values on the Rainier scalethan acetaminophen (P=0004 and P=0011 for sodiumibuprofen and ibuprofenpoloxamer) Placebo treatment wasnot analysed for this comparison as only 14 patients in thisgroup provided valid data
Patientrsquos overall assessment of medication as a treatmentfor pain
Significantly more patients in the sodium ibuprofen (813)and ibuprofenpoloxamer (848) groups rated the studymedication as good very good or excellent than in the groupsthat received acetaminophen (538) or placebo (173)Furthermore the mean global assessment scores weresignificantly lower (more favourable) for both ibuprofenformulationsmdash240 (sodium ibuprofen) and 244 (ibuprofenpoloxamer)mdashthan for acetaminophen or for placebo (341 and446 respectively Plt0001)
Safety findings
A total of 118 of all patients had AEs that were consideredby the investigators to be possibly related to study medicationno events were classified as definitely or probably related tostudy treatment Adverse events were experienced by 300238 309 and 296 of patients receiving sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo respec-tively The majority of AEs (73) were mild-to-moderate inseverity and the most frequently reported AEs includednausea headache vomiting and dizziness Adverse eventsoccurring in at least 5 of all patients in any treatment groupare summarised in Table 2 Severe AEs (including vomitingnausea dizziness abdominal pain and headache) occurred atrates of 63 (sodium ibuprofen) 25 (ibuprofenpolox-amer) 123 (acetaminophen) and 99 (placebo) therewere no deaths or withdrawals attributable to AEs during thestudy period There were no significant differences betweenstudy medications in terms of tolerability
Discussion
This placebo-controlled study demonstrated excellent assaysensitivity for every measure of efficacy with bothibuprofen formulations and acetaminophen showing clini-cally and statistically significant analgesia that was superiorto placebo Furthermore the overall analgesic efficacy(duration and total effect) of both ibuprofen formulationswas shown to be superior to acetaminophen
Data from this study showed statistically significant differ-ences between both the ibuprofen test formulations andplacebo for the primary endpoint ie the time to firstconfirmed perceptible pain relief In addition a significantlygreater proportion of patients receiving ibuprofen experiencedconfirmed perceptible pain relief than those receiving acet-
Table 2 Adverse events occurring in gt5 of patients in any treatment group
Sodium ibuprofen (n=80) Ibuprofenpoloxamer (n=80) Acetaminophen (n=81) Placebo (n=81)
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Any AE 43 24 (300) 27 19 (238) 41 25 (309) 39 24 (296)GastrointestinalNausea 10 9 (113) 5 5 (63) 8 8 (99) 14 14 (173)Vomiting 2 2 (25) 1 1 (13) 6 6 (74) 8 8 (99)Nervous systemDizziness 4 4 (50) 0 0 (00) 6 5 (62) 5 5 (62)Headache 11 11 (138) 5 4 (50) 4 4 (49) 3 3 (37)
AE Adverse eventTreatment definitions sodium ibuprofen=2times256 mg ibuprofen sodium dihydrate tablets (each tablet equivalent to 200 mg ibuprofen acid)ibuprofenpoloxamer=2times200 mg ibuprofenpoloxamer tablets acetaminophen=2times500 mg acetaminophen capletsa Percentages based on total number of patients per treatment group
Eur J Clin Pharmacol (2009) 65343ndash353 351
aminophen The median time to meaningful pain relief was45 min for both ibuprofen formulations and 54 min foracetaminophen Although a much greater proportion ofpatients reported relief on the two ibuprofen formulationsthe divergence in onset times was only apparent from 45 minpost-dose onward ie there was a much higher proportion ofresponders from 45 min onward for the ibuprofen treatmentsthan for acetaminophen Because of this late divergence theWilcoxon rank-sum test was not sensitive enough to detectsignificant differences whereas the Cox proportional hazardsregression analysis showed significant differences in favour ofibuprofen over acetaminophen In terms of SPRID over 6 hboth ibuprofen test formulations were significantly moreefficacious than acetaminophen
Previous studies using the post-operative dental painmodel have demonstrated that treatment with a differentibuprofen salt formulation ibuprofen arginate (l-argininesalt of ibuprofen) resulted in faster onset times to analgesiaand greater overall efficacy than treatment with conven-tional (standard) ibuprofen [11 12 19] The pharmacoki-netic profile of the ibuprofen sodium formulation used inthis study has been shown to be similar to that of ibuprofenarginate with peak plasma concentrations achieved atapproximately 30ndash40 min compared with 1ndash2 h forstandard ibuprofen [8 13 14] Therefore it was anticipatedthat the rapid absorption associated with sodium ibuprofenwould result in early onset of analgesia similar to thatobserved for ibuprofen arginate This study was notintended nor was it sufficiently powered to compare thetwo ibuprofen formulations
When comparing the median time to meaningful painrelief data from this study with previous studies bothibuprofen test formulations in this study were found to be atthe upper end of the range for ibuprofen arginate andibuprofen lysine data (range 24ndash42 min) [11 12 19 22]ie 451 min (sodium ibuprofen) and 447 min (ibuprofenpoloxamer) In the earlier studies where ibuprofen arginatewas compared with conventional ibuprofen the mediantime to meaningful pain relief obtained for ibuprofenarginate was approximately half that of the conventionalibuprofen [11 12 19] A recent bioavailability study hasalso shown that the Tmax for sodium ibuprofen was lessthan half that of standard ibuprofen (ie 35 min vs 90 minrespectively) [8] Therefore it was not unexpected thatsodium ibuprofen had a fast onset of analgesic effect in thisstudy that was in a similar order of magnitude as thosepreviously reported for faster absorbed formulations
The analyses of secondary endpoints related to degreeof pain relief andor reduction in pain intensity (TOT-PAR SPRID SPID peak PID and peak PR) consistentlyfavoured both ibuprofen formulations over acetamino-phen Only in terms of time to PID of at least 1 werethere no statistically significant differences observed
compared with acetaminophen Measures of analgesicdurationmdashthe proportion of patients taking rescue med-ication and the time to rescue medicationmdashshowed thatthose in the acetaminophen group received rescuemedication sooner than those in either of the twoibuprofen groups This suggests that both ibuprofenformulations had a longer duration of action thanacetaminophen which is in keeping with that previouslyreported for ibuprofen lysine [22] and ibuprofen liquigel[23] In terms of pain relief and PID the timepoint at whicha significant difference was first observed between either ofthe ibuprofen formulations and placebo was 15 min(sodium ibuprofen) a significant difference between eitherof the ibuprofen formulations and acetaminophen was firstobserved at 45 min (sodium ibuprofen) In comparison withpreviously published data studies with ibuprofen arginateand ibuprofen lysine demonstrated significant differences inpain relief and PID between ibuprofen and placebo at 10ndash15 min [11 12 19 23] Furthermore significant differ-ences between ibuprofen lysine and acetaminophen wereobserved at 15 min much sooner than the 45 min observedin our study [22] These differences could be explained bythe different formulations of ibuprofen the fact that adifferent brand of acetaminophen was used in each of therespective studies or the inherent variability associated witha small sample size
Patients in both ibuprofen groups were able to distractthemselves from their pain at 1 and 6 h after dosingsignificantly more easily than those in the placebo andacetaminophen groups (6 h only) Patients in both ibupro-fen groups also reported that pain would interfere with theirdaily activities significantly less than patients in theacetaminophen group Patients in the two ibuprofen groupsrated the study medication as good very good or excellentmore frequently than those in the acetaminophen andplacebo groups
Ibuprofen is a well-tolerated NSAID at low doses [24]However even at prescribed doses ibuprofen is associatedwith the least risk of gastrointestinal complications com-pared with other NSAIDs [25ndash27] No new safety concernswere raised by the current study treatment with singledoses of sodium ibuprofen and ibuprofenpoloxamer werewell tolerated with AE profiles comparable to that ofacetaminophen The most frequently reported AEs consid-ered to be related to study treatment (ie nausea headachevomiting and dizziness) are not unexpected in patientsrecovering from dental surgery
In conclusion these results suggest that compared withacetaminophen both the sodium ibuprofen and ibuprofenacid incorporating poloxamer formulations are more effi-cacious in providing rapid and sustained analgesia and areassociated with pain relief in a greater proportion ofpatients undergoing surgical removal of impacted third
352 Eur J Clin Pharmacol (2009) 65343ndash353
molars Together with the favourable safety profile ofibuprofen these findings support a recommendation forthis agent as an analgesic of choice for the treatment ofpost-operative dental pain
Acknowledgements The authors would like to acknowledgeFranklin S Bonasso DDS and R Dean Jasper DDS (Central OralSurgery Group) Barbara Hernandez MA CCRC Michael Goulder(Worldwide Clinical Trials UK Ltd) for statistical support andVandana Sahajpal PhD and Quyen Chu PhD (Sudler amp HennesseyLondon) for medical writing support
Conflict of interest This study was funded by Reckitt BenckiserGroup plc Stephen Daniels (Premier Research Group ClinicalResearch Centers USA) is the Co-ordinating Investigator SandieReader and Phillip Berry are employees of Reckitt Benckiser Group plc
References
1 Sweetman SC (ed) (2002) Ibuprofen In Martindale the completedrug reference 33rd edn Pharmaceutical Press London
2 Mehlisch DR Sollecito WA Helfrick JF et al (1990) Multicenterclinical trial of ibuprofen and acetaminophen in the treatment ofpostoperative dental pain J Am Dent Assoc 121257ndash263
3 Roy S (1983) A double-blind comparison of propionic acidderivative (ibuprofen) and a fenamate (mefanamic acid) in thetreatment of dysmenorrhoea Obstet Gynecol 61628ndash632
4 Moran M (1991) Double-blind comparison of diclofenac potassi-um ibuprofen and placebo in the treatment of ankle sprain J IntMed Res 19121ndash130
5 Goswick CB (1983) Ibuprofen versus propoxyphene hydrochlo-ride and placebo in acute musculoskeletal trauma Curr Ther ResClin Exp 34685ndash692
6 Schachtel BP Thoden WR (1988) Onset of action of ibuprofenin the treatment of muscle-contraction headache Headache28471ndash474
7 Pearce I Frank GJ Pearce JMS (1983) Ibuprofen compared withacetaminophen in migraine Practitioner 227465ndash467
8 Dewland P Reader S Berry P (2008) Bioavailability of ibuprofenfollowing oral administration of standard ibuprofen sodiumibuprofen or ibuprofen acid incorporating poloxamer in healthyvolunteers Eur J Clin Pharmacol (submitted)
9 Geisslinger G Menzel S Wissel K Brune K (1993) Single dosepharmacokinetics of different formulations of ibuprofen andaspirin Drug Invest 5238ndash242
10 Schleier P Prochnau A Schmidt-Westhausen AM et al (2007)Ibuprofen sodium dihydrate an ibuprofen formulation withimproved absorption characteristics provides faster and great-er pain relief than ibuprofen acid Int J Clin Pharmacol Ther4589ndash97
11 Black P Max MB Desjardins P et al (2002) A randomizeddouble-blind placebo-controlled comparison of the analgesic
efficacy onset of action and tolerability of ibuprofen arginateand ibuprofen in postoperative dental pain Clin Ther241072ndash1089
12 Desjardins P Black P Papageorge M et al (2002) Ibuprofenarginate provides effective relief from postoperative dental painwith a more rapid onset of action than ibuprofen Eur J ClinPharmacol 58387ndash394
13 Albert KS Gernaat CM (1984) Pharmacokinetics of ibuprofenAm J Med 7740ndash46
14 Davies NM (1998) Clinical pharmacokinetics of ibuprofen Thefirst 30 years Clin Pharmacokinet 34101ndash114
15 Cooper SA Precheur H Rauch D et al (1984) The analgesicefficacy of ibuprofen compared to acetaminophen with codeine(abstract) Clin Pharmacol Ther 35232
16 Mehlisch D Frakes L (1984) A controlled comparative evaluationof acetaminophen and aspirin in the treatment of post-operativepain Clin Ther Exerpta Med 789ndash97
17 Mehlisch D Markenson J Schnitzer T (1999) The efficacy ofnonsteroidal anti-inflammatory drugs for acute pain CancerControl 65ndash9
18 Daniels SE Desjardins PJ Talwalker S et al (2002) The analgesicefficacy of valdecoxib vs oxycodoneacetaminophen after oralsurgery J Am Dental Assoc 133611ndash621
19 Mehlisch DR Ardia A Pallotta T (2002) A controlled compar-ative study of ibuprofen arginate versus conventional ibuprofen inthe treatment of postoperative dental pain J Clin Pharmacol42904ndash911
20 World Medical Association (1964) Declaration of HelsinkiEthical principles for medical research involving human patientsAdopted by the 18th WMA General Assembly 1964 and amendedby the 29th 35th 41st and 48th WMA General Assemblies
21 European Parliament and Council of 4 April 2001 (2001)Directive 200120EC of the approximation of the laws regu-lations and administrative provisions of the Member Statesrelating to the implementation of good clinical practice in theconduct of clinical trials on medicinal products for human useOfficial Journal of the European Communities Brussels
22 Mehlisch DR Jasper RD Brown P et al (1995) Comparativestudy of ibuprofen lysine and acetaminophen in patients withpostoperative dental pain Clin Ther 17852ndash860
23 Olson NZ Otero AM Marrero I et al (2001) Onset of analgesiafor liquigel ibuprofen 400 mg acetaminophen 1000 mg ketopro-fen 25 mg and placebo in the treatment of postoperative dentalpain J Clin Pharmacol 411238ndash1247
24 Sachs C (2005) Oral analgesics for acute nonspecific pain AmFam Physician 71913ndash918
25 Doyle G Furey S Berlin R et al (1999) Gastrointestinal safetyand tolerance of ibuprofen at maximum over-the-counter doseAliment Pharmacol Ther 13897ndash906
26 Henry D Lim LL Garcia Rodriguez LA et al (1996) Variability inrisk of gastrointestinal complications with individual non-steroidalanti-inflammatory drugs results of collaborative met-analysis BrMed J 3121563ndash1566
27 Henry D McGettigan P (2003) Epidemiology overview ofgastrointestinal and renal toxicity of NSAIDs Int J Clin Pract13543ndash49
Eur J Clin Pharmacol (2009) 65343ndash353 353
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 153
RESEARCH
An investigation into the comparative efficacyof soluble aspirin and solid paracetamol inpostoperative pain after third molar surgeryR A Seymour1 J E Hawkesford2 J Sykes3 M Stillings4 and C M Hill5
Objective To compare the efficacy of soluble aspirin 900 mg andparacetamol 1000 mg in patients with postoperative pain after thirdmolar surgeryDesign A randomised placebo controlled double-blind studySetting Day stay units of Oral and Maxillofacial Surgery at CardiffDental Hospital and Hexham General Hospital NorthumberlandSubjects and methods One hundred and sixty-seven (104 female)patients who required the removal of their impacted third molars undergeneral anaesthesiaIntervention In the early postoperative period patients were medicatedwith either a single dose of soluble aspirin 900 mg solid paracetamol1000 mg or placebo Main outcome measures Pain intensity was measured on 100 mmvisual analogue scales at 0 5 10 15 20 30 45 60 90 120 and 240minutes after dosing Other efficacy variables evaluated included time torescue medication and an overall assessment of the study medicationefficacy by the patient on completion of the studyResults One hundred and sixty-seven patients consented to take part inthe study but only 153 were medicated Of the 14 patients not treated10 failed to develop sufficient pain to enter the study two withdrewconsent one had an adverse reaction to the general anaesthetic and onewas a protocol violator Over the four hour investigation period patientstreated with soluble aspirin reported significantly less pain whencompared with those treated with paracetamol (mean difference inAUC0-240 = -2001 95 CI ndash3893 to ndash109 p=0038) and placebo (meandifference in AUC0-240 = -3470 95 CI ndash5719 to ndash1221 p=0003)
1Head of Department Professor of Restorative Dentistry Department of RestorativeDentistry Dental School University of Newcastle Newcastle upon Tyne 2Consultant Oraland Maxillofacial Surgeon Department of Oral and Maxillofacial Surgery NewcastleGeneral Hospital Newcastle upon Tyne 3Clinical Statistician Reckitt Benckiser Healthcare(UK) Hull 4Head of Global Professional Relations Reckitt Benckiser Healthcare (UK) Hull5Consultant Oral and Maxillofacial Surgeon Department of Oral Surgery Dental SchoolUniversity of Wales College of Medicine Cardiff Correspondence to Professor R A Seymour Department of Restorative Dentistry DentalSchool University of Newcastle upon Tyne Framlington Place Newcastle upon TyneEngland NE2 4BWE-mail R A Seymournclacuk
Refereed paperReceived 080302 Accepted 060902copy British Dental Journal 2003 194 153ndash157
Similarly at 20 and 30 minutes after dosing patients in the solubleaspirin group were reporting significantly less pain than those in theparacetamol treatment group (mean difference in pain intensity at 20minutes ndash79 95 CI ndash153 to ndash06 p=0035 at 30 minutes ndash106 95CI ndash186 to ndash26 p=0010) There were no significant differences betweentreatment groups with respect to the number of patients requiringrescue medication however the time to dosing was significantly longerfor those taking soluble aspirin when compared with placebo (hazardratio 234 95 CI 141 to 388 plt0001) Conclusion The findings from this study showed that soluble aspirin900 mg provides significant and more rapid analgesia than paracetamol1000 mg in the early postoperative period after third molar surgery
INTRODUCTIONBoth aspirin (acetylsalicylic acid) and paracetamol (acetamino-phen) are widely available analgesics The drugs are used exten-sively in dentistry either self-prescribed by the patient or recom-mended by the dental surgeon Despite such use there have beenfew comparative studies on these analgesics and the studies pub-lished seem to suggest that the drugs are equi-analgesic1 Morerecent evidence suggests that many factors appear to influence theefficacy of aspirin in postoperative dental pain These include for-mulation dose and plasma concentration of acetylsalicylate2-5
The latter appears to be determined by plasma aspirin esteraseactivity By contrast there is limited information on the efficacy ofparacetamol in postoperative dental pain
Historically there have been many studies comparing the effi-cacy of a whole range of analgesics which have used aspirin as thestandard treatment (positive control) In such studies the formula-tion chosen has invariably been a solid format of the drug This hasled to the impression that aspirin is relatively weak and slow act-ing Previous studies34 have shown that soluble aspirin provides agreater onset of action and is overall more effective than solidaspirin However up to the present time there has been no studycomparing the efficacy of soluble aspirin with solid paracetamolThe present study was designed to investigate whether the superi-ority of soluble aspirin over solid aspirin would be reproducedwhen compared with solid paracetamol The doses chosen for each
This study has shown the benefits of soluble aspirin (900 mg) over solid paracetamol (1000 mg)in the control of postoperative pain after third molar extractions
The aspirin preparation provided an earlier onset of pain relief when compared with paracetamol Most patients in the study did require additional analgesia in the early postoperative period
but the time to remedication was significantly longer in soluble aspirin group whencompared with the placebo
Adverse events due to the medication were few and showed no differences between treatmentgroups
Soluble aspirin 900 mg appears to be a more useful analgesic than paracetamol in the controlof postoperative pain after third molar surgery
I N B R I E F
RESEARCH
154 BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003
preparation used in this study is the maximum recommendedwhen purchased as over the counter (OTC) medications
Removal of impacted third molars remains a common dentalsurgical procedure that results in a significant level of postopera-tive pain6 Pain is usually of short duration and reaches its maxi-mum intensity in the early postoperative period7 It is during thistime period that analgesics are frequently prescribed The nature ofthe pain and its duration make the third molar pain model usefulfor evaluation of analgesic efficacy
The overall aim of the present study was to directly compare theefficacy of soluble aspirin with that of solid paracetamol tablets inpatients with postoperative pain after third molar surgery A place-bo group was also used to act as a negative control Within thisoverall remit the primary aim of the study was to compare theonset of efficacy between the two preparations
MATERIAL AND METHODSAdult patients who required the removal of at least one impactedlower third molar were invited to participate in the study Patientswere enrolled from two centres (Cardiff and Hexham) Informedwritten consent was obtained from each patient prior to theirentry into the study which had received ethical approval from theappropriate local Health Authority Ethical Committees Patientsenrolled into the study were fit and healthy and complied with thecriteria of the American Society of Anaesthesiologists categoryone or at the discretion of the dental surgeon category two Allpatients attended a screening clinic prior to their participation inthe study The pre-screening was held up to a maximum of threeweeks before surgery Patients were asked to abstain from takingany analgesics for 24 hours prior to their third molar extractions
Patients underwent the removal of their impacted third molarsunder general anaesthesia The anaesthetic regimen was accord-ing to routine clinical practice at the dental centre and includedinduction with intravenous propofol Muscle relaxation wasachieved with vecuronium atracurium pancurium mivacuriumor suxamethonium Anaesthesia was maintained with nitrousoxide oxygen and either isoflurane enflurane or sevofluranePerioperative analgesia was provided by fentanyl or alfentanyl
Impacted third molars were removed following a standard tech-nique Bone removal was carried out with a drill under saline sprayThe operating time (from first incision to completion of last suture)was recorded for each patient On completion of the surgical proce-dure time was allowed for the patients to recover fully from theeffects of the anaesthetic They were then returned to the wardwhere they were monitored by the study nurse and their pain inten-sity assessed on 100 mm visual analogue scales (VAS) The bound-aries of the scale were marked lsquono painrsquo and lsquoworst pain imaginablersquoWhen patientsrsquo pain intensity reached a level in excess of 30 mm onthe VAS they were randomised to study medication Patients whosepain intensity did not reach the required level or who did notrequest analgesia within 1frac12 hours post-operatively were with-drawn from the study Each eligible patient was randomly allocatedto one of the following treatment groups soluble aspirin (Disprinreg)900 mg solid paracetamol tablets BP 1000 mg or placebo In order
to double-blind the study a double-dummy technique was usedEach patient assigned to receive active soluble aspirin or activesolid paracetamol also received a placebo for the alternative treat-ment and placebo patients received a placebo for both formula-tions Soluble aspirin and the aspirin placebo were presented as anorange drink Paracetamol active and placebo were given as tabletsPatients were randomised to treatment groups in the ratio of 2aspirin2 paracetamol1 placebo The randomisation was stratifiedfor gender A randomisation block size of five was used to ensurebalance between the treatment groups
Pain assessmentThe following measures were used to evaluate efficacya) Pain intensity measures were recorded immediately pre-dose (0
minutes) and at 5 10 15 20 30 45 60 90 120 and 240 minutesafter dosing Onset of analgesia was primarily assessed by painintensity measures at 10 15 20 and 30 minutes
b)Pain intensity over the four hour investigation period The serial VAS measures of the four hour investigation periodwere compiled into a graph of pain (mm) versus time (minutes)The area under the graph (AUC) was calculated using the trape-zoidal method and denoted as AUC240 Such a measure gives anoverall assessment of each patientrsquos pain experience throughoutthe four hour investigation period8
c) Use of rescue medicationIn the event of poor pain control patients were allowed access toalternative analgesia (ibuprofen 400 mg) Patients were encour-aged not to request re-medication in the first hour post-dosingin order to give the study medication time to work For thosetaking additional analgesics the time was recorded and theirlast pre-rescue medication intensity score was extrapolated overthe remaining time points9
d)Overall evaluation At the end of the four hour investigation period (or prior to tak-ing rescue medication) the study nurses and the patients wereasked to provide an overall evaluation of the efficacy of thestudy medication The categories were lsquovery goodrsquo lsquogoodrsquo lsquosatis-factoryrsquo lsquopoorrsquo and lsquovery poorrsquo
Throughout the investigation period a study nurse was respon-sible for monitoring the patients and recording any adverse events
Statistical methodsA previous study in postoperative pain after removal of impactedthird molars4 suggested that mean VAS differences between solu-ble aspirin and placebo and soluble aspirin and solid paracetamolof 26 mm and 14 mm respectively might be anticipated at 20 min-utes post treatment Using a randomisation of 2 soluble aspirin 2paracetamol 1 placebo a total sample size of 150 patients had atleast 80 power to detect this difference
The VAS pain intensity measurements at 10 15 20 and 30minutes after dosing and AUC240 were compared between treat-ment groups using an analysis of covariance using centre gen-der baseline pain intensity operation duration and number of
Table 1 Demographic details of patients who were medicated for the study Where appropriate results are expressed as mean (SD)Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo
Number of patients 59 62 32Gender ratio MF 1940 1943 1121Age (years) 256 (56) 250 (53) 251 (47)Weight (kg) 702 (16) 719 (145) 743 (149)Mean operating time (mins) 173 (101) 165 (101) 130 (130)Number of molars removed 1 3 (5) 2 (3) 3 (9)[ patients ()] 2 15 (25) 14 (23) 5 (16)
3 11 (19) 12 (19) 9 (28)4 30 (51) 34 (55) 15 (47)
Mean baseline pain score on 100 mm VAS 574 (176) 506 (142) 541 (144)
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 155
in Hexham and the remainder in Cardiff Of the 14 patients nottreated 10 failed to develop sufficient pain to enter the studytwo withdrew consent one had an adverse reaction to the anaes-thesia and one was a protocol violator Demographic details ofthe patients are shown in Table 1 The three groups were bal-anced for demographic variables
The primary aim of the study was to compare the rate of onset ofanalgesia and the 20-minute time was considered to be appropriatefor such an assessment Pain scores as recorded on the VAS at eachtime point are illustrated in Figure 1 and Tables 2a and 2b VASscores decreased in all treatment groups during the first 15 minutespost dosing (Figure 1) At 20 minutes post dosing patients in the sol-
molars removed as covariates Use of rescue medication and thestudy nursesrsquo and patientsrsquo overall impression of their medicationwere analysed using binomial logistic regression with a lsquopositiversquooutcome defined as a response of lsquovery goodrsquo or lsquogoodrsquo Time toadministration of rescue medication was compared betweentreatment groups using Coxrsquos proportional hazard model Com-parisons were performed for soluble aspirin versus solid paraceta-mol and soluble aspirin versus placebo
RESULTSOne hundred and sixty seven patients consented to take part inthe study and 153 were medicated Of these 29 were medicated
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 30 45 60 90 120 240
Time (mins)
Pain
(mm
)
Soluble AspirinParacetamolPlacebo
Figure 1 Graph to show mean pain scores (mm) versus time (mins) for patients after treatment with placebo solid paracetamol 1000 mg and solubleaspirin 900 mg
Table 2a Summary of efficacy parameters recorded during the investigation period pain scoresBetween treatment comparisons
Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Mean difference (95 CI) p-value Mean difference (95 CI) p-value
Pain score (in mm) 10 mins after dosing 412 (28) 482 (29) 474 (33) -61 (-133 to 10) 0092 -70 (-130 to ndash09) 0024Pain score (in mm) 15 mins after dosing 407 (32) 458 (33) 445 (38) -39 (-120 to 43) 0350 -51 (-120 to 18) 0143Pain score (in mm) 20 mins after dosing 402 (34) 481 (35) 500 (40) -98 (-186 to ndash11) 0028 -79 (-153 to ndash06) 0035Pain score (in mm) 30 mins after dosing 356 (37) 462 (38) 476 (44) -120 (-216 to ndash25) 0014 -106 (-186 to ndash26) 0010Overall pain - AUC240(mmmins) 8001 (871) 10002 (898) 11471 (1035) -3470 (-5719 to ndash1221) 0003 -2001 (-3893 to ndash109) 0038
data presented are adjusted (least squares) mean (standard error of the mean)
Table 2b Summary of efficacy parameters recorded during the investigation period use of escape medicationBetween treatment comparisons
Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds (hazard) ratio (95 CI) p-value Odds (hazard) ratio (95 CI) p-value
Number of patients 48 (81) 46 (74) 29 (91) 0172 (0020 to 1052) 0078 1485 (0455 to 5197) 0518taking escape analgesics
Time (minutes) to 115 (63 - 165) 94 (47 - ++) 64 (42 ndash 117) 234 (141 to 388) lt0001 130 (084 to 203) 0236remedication
data presented are median (Inter Quartile Range)++ Upper quartile cannot be estimated
RESEARCH
156 BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003
uble aspirin group reported significantly less pain than those treatedwith solid paracetamol (p=0035) or placebo (p=0028) Similarlypain intensity was significantly less at 10 and 30 minutes post dos-ing for patients treated with soluble aspirin when compared withsolid paracetamol (p=0024 and 0010 respectively) Pain intensitywas also significantly less for patients treated with soluble aspirinwhen compared with placebo at 30 minutes post dosing (p=0014)but was not significant at 10 minutes post-dosing (p=0092) By con-trast to these findings at 15 minutes after dosing pain scores werenot significantly different between soluble aspirin and placebo(p=0350) or between soluble aspirin and solid paracetamol(p=0143) Overall pain scores as assessed by the AUC240 were sig-nificantly lower in the soluble aspirin group when compared withsolid paracetamol (p=0038) and placebo (p=0003) There was nosignificant centre difference for any of the pain intensity variables
The use of rescue medication and time to requesting such med-ication is also shown in Table 2b There was no significant differ-ence between soluble aspirin and solid paracetamol or placebowith respect to the number of patients requiring rescue medicationduring the four hour investigation period (pgt005) However thetime to administration of rescue medication was significantlylonger for those patients taking soluble aspirin when comparedwith placebo (plt0001) There was no significant difference in timeto rescue medication between the soluble aspirin treated patientsand those treated with solid paracetamol (p=0236) The time toadministration of rescue medication did show a significant centreeffect with those patients enrolled in Cardiff requiring rescueanalgesia at an earlier time point than those in Hexham (plt0001)
The study nursesrsquo and patientsrsquo overall assessment of the effica-cy of the medication is shown in Tables 3a and 3b There was nosignificant difference between soluble aspirin and solid paraceta-mol (p=0285) with respect to the percentage of lsquopositiversquo outcomesassessed by the patients however soluble aspirin was favoured incomparison with placebo (p=0010) Results were similar for thestudy nursesrsquo assessment (p=0387 p=0024)
Adverse events were reported by 41 of patients with a higheroverall incidence in the active treatment groups (Table 4) Many ofthese events were related to the procedure The most commonadverse events were in the central and peripheral nervous system(primarily dizziness) and the gastro-intestinal system (primarilynausea) The incidence of dizziness was similar in the soluble
aspirin and placebo groups (14 and 13 respectively) and wasgreater than in the solid paracetamol group (6) The incidence ofnausea was comparable in the soluble aspirin and solid paraceta-mol groups (15 and 16 respectively) and was greater than thatin the placebo group (6) Gingival bleeding (the only adverseevent recorded under lsquohaemostasisrsquo) had a slightly lower incidencein the soluble aspirin group (8) than in the solid paracetamolgroup (13) and was only slightly higher than that reported in theplacebo group (3) This finding is contrary to any expectationsthat aspirin might exacerbate post-operative bleeding
DISCUSSIONThe present study has shown that soluble aspirin 900 mg is an effec-tive analgesic in the control of postoperative pain after the removalof impacted third molars confirming the evidence from previousstudies34 In addition soluble aspirin provided better pain controlthan solid paracetamol 1000 mg This superior efficacy is reflectedin the overall pain score (Table 2a and Figure 1) and also in the painscores reported during the first 30 minutes post dosing The datasuggest that soluble aspirin is providing a more rapid reduction inpain in the early postoperative period when compared with solidparacetamol If the pain scores are examined in terms of percentagereduction when compared with baseline the results show that solu-ble aspirin is twice as effective as solid paracetamol (at 20 and 30minutes the percentage reduction for soluble aspirin is 310 and406 respectively whilst the figures for solid paracetamol are142 and 204) From the perspective of patient management arapid reduction in pain is an important requisite of any analgesicformulation10 The exception to this pattern is the pain scores at 15minutes post dosing At this time point pain intensity scores aftersoluble aspirin are not significantly different from either placebo orsolid paracetamol mdash the reason for this finding is unclear
Previous comparative efficacy studies between aspirin andparacetamol in postoperative dental pain have revealed somewhatequivocal results11112 The consensus view1 is that both aspirin andparacetamol are both equi-analgesic and equipotent The studiesuse a solid tablet formulation of aspirin at a dose of 650 mg Studiesusing similar methodology have shown that the efficacy of aspirinin postoperative dental pain is related to dose and formulation34
The use of a soluble formulation and the 900 mg dose may explainthe superior efficacy of aspirin in this study
Table 3b Distribution of scores from study nursesrsquo global assessment of the medication (number ())Score Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds Ratio (95 CI) p-value Odds Ratio (95 CI) p-value
Positive outcome 32 (54) 32 (52) 10 (31) 2974 (1179 to 7951) 0024 1403 (0655 to 3054) 0387Very good 15 (25) 11 (18) 3 (9)Good 17 (29) 21 (34) 7 (22)Satisfactory 17 (29) 14 (23) 12 (38)Poor 8 (14) 14 (23) 7 (22)Very poor 2 (3) 2 (3) 3 (9)Total 59 62 32
positive outcome = response of lsquovery goodrsquo or lsquogoodrsquo
Table 3a Distribution of scores from patientsrsquo global assessment of the medication (number ())Score Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds Ratio (95 CI) p-value Odds Ratio (95 CI) p-value
Positive outcome 34 (58) 33 (53) 10 (31) 3591 (1402 to 9828) 0010 1530 (0706 to 3380) 0285Very good 15 (25) 12 (19) 3 (9)Good 19 (32) 21 (34) 7 (22)Satisfactory 15 (25) 12 (19) 10 (31)Poor 8 (14) 15 (24) 9 (28)Very poor 2 (3) 2 (3) 3 (9)Total 59 62 32
positive outcome = response of lsquovery goodrsquo or lsquogoodrsquo
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 157
The primary aim of this investigation was to compare both anal-gesics with respect to onset of action Early time points were chosenfor this comparison as they represent a suitable period from dosingwhen patients would expect to experience meaningful pain reliefSoluble aspirin was significantly superior to both placebo and solidparacetamol at both 20 and 30 minutes post dosing and there wereindications of superiority as early as at 10 minutes In part this maybe due to the rapid absorption of soluble aspirin and the subsequentpeak concentrations of acetylsalicylate (Tmax) that occurs at thesetime points It has been previously shown that plasma concentra-tions of acetylsalicylate are also important determinants of aspirinrsquosefficacy in postoperative dental pain2 By contrast the absorption ofsolid paracetamol tablets is slow with a Tmax of 60 minutes13 Thusdifferences in pharmacokinetics may account for the differences inonset of analgesia observed in the present study
It is now well established that aspirin exerts both analgesic andanti-inflammatory action by inhibiting prostaglandin synthesis14
Aspirin irreversibly inhibits both cyclo-oxygenase 1 and 2 (Cox-1and Cox-2) by acetylating serine 530 thus preventing the bindingof arachidonic acid to the active sites of the enzyme The pharma-codynamics of paracetamol are uncertain and by comparison withaspirin the drug exhibits weak anti-inflammatory action This lackof a pronounced anti-inflammatory effect may also explain theweaker efficacy of this drug in postoperative dental pain
We can conclude from this study that a single dose of solubleaspirin 900 mg provides significant and more rapid analgesia thansolid paracetamol 1000 mg in the early postoperative period afterthird molar surgery This study confirms the value of soluble aspirinin the management of pain after dental surgical procedures
The authors are grateful to Reckitt Benckiser Healthcare for their support inthis study
1 Cooper S A Comparative analgesic efficacies of aspirin and acetaminophen ArchIntern Med 1981 141 282-285
2 Seymour R A Williams F M Ward A Rawlins M D Aspirin metabolism and efficacyin postoperative dental pain Br J Clin Pharmacol 1984 17 697-701
3 Seymour R A Williams F M Luyk N M et al Comparative efficacy of soluble aspirinand aspirin tablets in postoperative dental pain Eur J Clin Pharmacol 1986 30495-498
4 Holland I S Seymour R A Ward-Booth R P Ord R A Lim K L Hoare R C Anevaluation of different doses of soluble aspirin and aspirin tablets in postoperativedental pain Br J Clin Pharmacol 1988 26 463-468
5 Seymour R A Weldon M Kelly P Nicholson E Hawkesford J E An evaluation ofbuffered aspirin and aspirin tablets in postoperative pain after third molar surgeryBr J Clin Pharmacol 1992 33 395-399
6 Seymour R A Blair G S Wyatt F A Post-operative dental pain and analgesicefficacy Part I Br J Oral Surg 1983 21 290-297
7 Seymour R A Meechan J G Blair G S An investigation into post-operative painafter third molar surgery under local analgesia Br J Oral Maxillofac Surg 1985 23410-418
8 Matthews J N Altman D G Campbell M J Royston P Analysis of serialmeasurements in medical research Br Med J 1990 300 230-235
9 Lasagna L Analgesic methodology a brief history and commentary J ClinPharmacol 1980 20 373-376
10 Meechan J G Seymour R A The use of third molar surgery in clinicalpharmacology Br J Oral Maxillofac Surg 1993 31 360-365
11 Skjelbred P Album B Lokken P Acetylsalicylic acid vs paracetamol effects onpost-operative course Eur J Clin Pharmacol 1977 12 257-264
12 Mehlisch D R Frakes L A A controlled comparative evaluation of acetaminophenand aspirin in the treatment of postoperative pain Clin Ther 1984 7 89-97
13 Muir N Nichols J D Stillings M R Sykes J Comparative bioavailability of aspirinand paracetamol following single dose administration of soluble and plain tabletsCurr Med Res Opin 1997 13 491-500
14 Vane J Botting R Inflammation and the mechanism of action of anti-inflammatory drugs Faseb J 1987 1 89-96
Table 4 Incidence and distribution of adverse events for each treatment groupPercentage of patients reporting events (number of events)
Body system Soluble aspirin (n=59) Solid paracetamol (n=62) Placebo (n=32) Total (n=153)
CNS 20 (14) 8 (5) 19 (6) 15 (25)GI 17 (12) 16 (12) 6 (2) 14 (26)Body as a whole 7 (4) 13 (8) 6 (3) 9 (15)Haemostasis 8 (7) 13 (8) 3 (1) 9 (16)Respiratory 7 (4) 3 (2) 0 (0) 4 (6)Psychiatric 2 (1) 0 (0) 3 (1) 1 (2)Hearingvestibular 0 (0) 2 (1) 0 (0) 1 (1)Skinappendages 2 (1) 0 (0) 0 (0) 1 (1)Vision 2 (1) 0 (0) 0 (0) 1 (1)Total 51 (44) 39 (36) 28 (13) 41 (93)

SERAacute O PARACETAMOL EFICAZ NA ELIMINACcedilAtildeO DA DOR
APOacuteS EXTRACCcedilAtildeO DO TERCEIRO MOLAR INFERIOR1
Anaacutelise da analgesia do paracetamol comparada agrave de NSAIDrsquos
Catarina Cardoso
Ivo Cavalheiro
Nuno Pinto
Sara Mendes
FACULDADE DE MEDICINA DENTAacuteRIA DA UNIVERSIDADE DE LISBOA
Mestrado Integrado em Medicina Dentaacuteria
Biologia Oral I
2ordm Ano ndash 1ordm Semestre
23 de Dezembro de 2011
1 Este trabalho estaacute escrito segundo as regras do Acordo Ortograacutefico de 1945
RESUMO
Objectivos Investigar a eficaacutecia e os efeitos secundaacuterios do paracetamol
(1000mg) na eliminaccedilatildeo da dor dentaacuteria poacutes-operatoacuteria resultante da extracccedilatildeo de
terceiros molares inferiores comparaacute-la agrave eficaacutecia relativa dos vaacuterios NSAIDrsquos e a
combinaccedilotildees com outros faacutermacos
Materiais e meacutetodos A pesquisa foi realizada em bases de dados secundaacuterias
(Cochrane Database of Systematic Reviews Evidentista CEBD EBD e Lilacs) assim
como em bases de dados primaacuterias (Medline atraveacutes dos motores de busca PubMed e
NICE) entre 7 e 19 de Novembro Os artigos encontrados foram avaliados numa fase
inicial (com base nos seus tiacutetulos e abstracts) para averiguar a sua relevacircncia de acordo
com o seguinte sistema de classificaccedilatildeo adequado provavelmente adequado
inadequado
Resultados Foi encontrado um total de 161 registos incluindo revisotildees
sistemaacuteticas e ensaios cliacutenicos aleatorizados dos quais apenas 31 foram classificados
pelo seu tiacutetulo e abstract como Adequados ou Provavelmente Adequados A anaacutelise
mais aprofundada dos abstracts juntamente com uma leitura transversal dos artigos
resultou em 8 publicaccedilotildees que preenchiam definitivamente os criteacuterios de inclusatildeo e
foram por isso avaliadas com recurso agraves fichas CASP
Conclusotildees Atraveacutes dos estudos analisados conclui-se que o paracetamol eacute uma
analgeacutesico seguro e eficaz dado que apresenta um benefiacutecio estatisticamente
significativo quando comparado a placebo No entanto exibe menor eficaacutecia quando
comparado a outros NSAIDrsquos nomeadamente ibuprofeno e a combinaccedilotildees dos mesmos
(paracetamol+NSAID) Apesar dos melhores resultados alguns NSAIDrsquos manifestam
efeitos secundaacuterios de alta severidade por oposiccedilatildeo aos do paracetamol Revela-se
assim necessaacuterio o desenvolvimento de estudos que investiguem de melhor forma os
efeitos adversos destes faacutermacos e o mecanismo de acccedilatildeo do paracetamol e incluam
outros dados - como custo financeiro e disponibilidade no mercado
Palavras-Chave Paracetamol NSAIDrsquos terceiro molar inferior extracccedilatildeo
dentaacuteria dor poacutes-operatoacuteria aliacutevio da dor Escala Visual Analoacutegica
ABSTRACT
Aims To investigate the efficacy and side effects of paracetamol (1000mg) on
the lower third molar extraction post-operative pain relief to compare it to other
NSAIDrsquos efficacy as well as the combination of both
Methods Searches were conducted in secondary databases (Cochrane Database
of Systematic Reviews Evidentista CEBD EBD and Lilacs) as well as in primary
databases (Medline atraveacutes dos motores de busca PubMed e NICE) between 7 and
November 19 The encountered articles were initially evaluated based on their titles and
abstracts in order to assess their relevance This was done according to a classification
system ldquoadequaterdquo ldquoprobably adequaterdquo ldquoinadequaterdquo
Results A total of 161 records were found including systematic reviews and
randomized clinical trials only 31 were classified as ldquoadequaterdquo or ldquoprobably
adequaterdquo After a more thorough analysis of each abstract in addition to further
reading of the papers only 8 articles fulfilled the inclusion criteria Thus they were
evaluated according to the CASP critical appraisal sheets
Conclusions Paracetamol is a safe and effective analgesic which presents a
statistical significant advantage when compared to a placebo However paracetamol
shows less efficacy when compared to other NSAIDrsquos such as ibuprofen The
combination of paracetamol + other NSAID also shows to be more effective displaying
the additive effect of this compound Although NSAIDrsquos show the best pain relief
scores some can cause severe side effects as opposed to paracetamol Further studies
are needed in order to better investigate the adverse effects of these drugs as well as the
mechanism of action of paracetamol which still remains unclear Other data such as
financial cost and market availability should be approached in future studies
Keywords Paracetamol NSAIDrsquos lower third molar tooth extraction post-operative
pain pain relief Visual Analogic Scale
5
IacuteNDICE
PERGUNTA FORMULADA PELO PACIENTE 6
QUESTAtildeO PICO 6
OBJECTIVOS 6
INTRODUCcedilAtildeO 7
PESQUISA 12
Criteacuterios de Selecccedilatildeo 12
Tipos de Estudos escolhidos participantes intervenccedilatildeo e de mediccedilatildeo 12
Avaliaccedilatildeo dos Estudos 13
Estrateacutegias de Pesquisa 12
Cochrane Database for Systematic Reviews helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 13
Evidence-Based Dentistry (EBD) helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 14
National Institute of Health and Clinical Excellence (NICE) helliphelliphelliphelliphelliphellip 14
Literatura Latino-Americana e do Caribe em Ciecircncias da Sauacutede (LILACS) 14
PubMed 15
AVALIACcedilAtildeO CRIacuteTICA 17
Revisotildees Sistemaacuteticas 17
Ensaios Cliacutenicos Aleatorizados 28
DISCUSSAtildeO 52
RESPOSTA DADA AO PACIENTE 55
REFEREcircNCIAS BIBLIOGRAacuteFICAS 56
ANEXOS 61
Anexo A ndash Tabela de Artigos Excluiacutedos 61
Anexo B ndash Artigos Incluiacutedos em formato integral 62
6
PERGUNTA FORMULADA PELO PACIENTE
Apoacutes uma exodontia de um terceiro molar inferior ldquoDoutor natildeo me vai passar
mais nada aleacutem do paracetamol para as dores Eacute eficaz Natildeo vou ter doresrdquo
QUESTAtildeO PICO
Com base na questatildeo apresentada pelo paciente eacute possiacutevel identificar
Populaccedilatildeo ndash Pacientes adultos com pelo menos um terceiro molar inferior
Intervenccedilatildeo ndash administraccedilatildeo poacutes-operatoacuteria de paracetamol (1000g) aquando
duma exodontia do terceiro molar inferior
Comparaccedilatildeo ndash outros analgeacutesicos e NSAIDrsquos (Non-Steroidal Anti-
Inflammatory Drugs) convencionais
Outcome ndash Eliminaccedilatildeo ou atenuaccedilatildeo da dor medida atraveacutes da escala visual
analoacutegica de dor
Em pacientes adultos apoacutes exodontia do 3ordm molar inferior a administraccedilatildeo
de paracetamol eacute mais eficaz na terapecircutica analgeacutesica comparativamente a outros
analgeacutesicos e anti-inflamatoacuterios natildeo esteroacuteides convencionais utilizando uma
escala visual analoacutegica de dor
OBJECTIVOS
Primaacuterios
Investigar a eficaacutecia do paracetamol (1000mg) na eliminaccedilatildeo da dor dentaacuteria
poacutes-operatoacuteria e comparaacute-la com outros NSAIDrsquos comparando os efeitos secundaacuterios
associados a cada faacutermaco
Secundaacuterios
Aferir a eficaacutecia relativa dos vaacuterios NSAIDrsquos bem como combinaccedilotildees de
paracetamol com outros compostos
7
INTRODUCcedilAtildeO
EXODONTIA DE TERCEIROS MOLARES INFERIORES
A extracccedilatildeo de terceiros molares eacute um procedimento ciruacutergico no campo da
sauacutede oral amplamente praticado e difundido A dor poacutes-operatoacuteria desta intervenccedilatildeo
tornou-se o modelo mais frequentemente usado em ensaios sobre dor aguda por ser um
procedimento comum com dor moderada a severa e com um nuacutemero suficiente de
pacientes para se realizar um estudo de forma relativamente faacutecil (1 2)
Os motivos que conduzem agrave exodontia de terceiros molares devem ser
considerados cuidadosamente natildeo soacute na sua dimensatildeo cliacutenica como no encontro dos
interesses do paciente econoacutemicos e outros Algumas situaccedilotildees constituem uma razatildeo
largamente aceite para a extracccedilatildeo sendo descritas em normas de orientaccedilatildeo cliacutenica
Natildeo se pode excluir poreacutem uma selecccedilatildeo e procura cuidadosa por parte do cliacutenico da
melhor evidecircncia cientiacutefica
Segundo as normas de orientaccedilatildeo cliacutenica NICE a extracccedilatildeo de sisos impactados
deve ser limitada a pacientes que evidenciam patologia como caacuteries irrestauraacuteveis
patologias pulpares ou periapicais natildeo trataacuteveis abcesso e osteomielite reabsorccedilatildeo
internaexterna do dente ou dentes adjacentes fractura dentaacuteria quistos tumores e
outros (3) Terceiros molares impactados mas livres de patologia natildeo devem ser
extraiacutedos pois natildeo haacute evidecircncia de que sugira que traria benefiacutecios para os pacientes
Iria tambeacutem sujeitar pacientes saudaacuteveis aos riscos que acompanha este tipo de
procedimento e os efeitos poacutes-operatoacuterios do mesmo Existe controveacutersia em redor
deste assunto e sobre se existe algum benefiacutecio na extraccedilatildeo profilaacutetica ldquoNo evidence
was found to support or refute routine prophylactic removal of asymptomatic impacted
wisdom teeth in adults There is some reliable evidence that suggests that the
prophylactic removal of asymptomatic impacted wisdom teeth in adolescents neither
reduces nor prevents late incisor crowdingrdquo (4) A extracccedilatildeo de um dente natildeo impactado
deve ser executada quando a natildeo extracccedilatildeo do mesmo eacute ou potencialmente viraacute a
constituir uma situaccedilatildeo patoloacutegica Este procedimento ciruacutergico conduz a um niacutevel
significante de dor poacutes-operatoacuteria sendo esta mais severa nas primeiras doze horas apoacutes
o procedimento com o pico de intensidade nas 6-8 horas poacutes-operatoacuterias (5)
8
ETIOLOGIA DA DOR
Os tecidos lesados ou traumatizados na sequecircncia da remoccedilatildeo do terceiro molar
conduzem agrave libertaccedilatildeo de mediadores bioquiacutemicos (celulares e soluacuteveis) A inflamaccedilatildeo
aguda surge como resposta ao stress tecidual e passa por um aumento da irrigaccedilatildeo
sanguiacutenea - vasodilataccedilatildeo e aumento de permeabilidade vascular Pode-se enfatizar os
papeacuteis das histamina e a bradiquinina (recruta NO) como mediadores soluacuteveis
importantes na vasodilataccedilatildeo
Os prostanoacuteides ndash moleacuteculas envolvidas nos processos de inflamaccedilatildeo- satildeo
ecosanoacuteides ou seja derivados de precursores de aacutecidos gordos e sintetizados via
cascata do aacutecido araquidoacutenico (6 p 503 7 p 800 8) em condiccedilotildees fisioloacutegicas tecircm
um papel preponderante na citoprotecccedilatildeo da mucosa gaacutestrica hemostase e
hemodinacircmica renal A este grupo pertencem as prostaglandinas prostaciclinas
tromboxanos e leucotrienos Enquanto que as prostaglandinas satildeo sintetizadas a partir
do aacutecido araquidoacutenico por acccedilatildeo de enzimas como as ciclo-oxigenases (COX) os
leucotrienos resultam da acccedilatildeo da lipoxigenase Havendo stress tecidual a membrana
celular eacute danificada conduzindo agrave actividade da enzima fosfolipase Esta ao iniciar a
lipoacutelise possibilita a obtenccedilatildeo do percursor dos prostanoacuteides o aacutecido araquidoacutenico Por
um lado os produtos da acccedilatildeo da lipoxigenase podem estar envolvidos na formaccedilatildeo do
edema por outro os produtos da ciclo-oxigenase nomeadamente prostaglandinas estatildeo
envolvidos no processo de dor e pirexia
A ciclo-oxigenase possui 2 isoenzimas COX-1 e COX-2 (7 p 800)
A COX-1 eacute constitutiva da maioria dos tecidos humanos mas com especial
relevacircncia para mediar a integridade da mucosa gaacutestrica endoteacutelio vascular rins e
plaquetas
A COX-2 eacute expressa apoacutes lesatildeo e aquando a libertaccedilatildeo de mediadores como a
Interleucina-1 o Factor de Activaccedilatildeo de Plaquetas (PAF) ou endotoxinas
lipopolissacaacuterido (LPS) (9) Contribui para o processo inflamatoacuterio e hiperalgesia pois
ao formar prostaglandinas sensibiliza as terminaccedilotildees nervosas locais livres
nociceptivas
PARACETAMOL
O paracetamol eacute uma das drogas mais importantes usadas no tratamento da dor
aguda moderada a severa quando natildeo eacute necessaacuterio um efeito anti-inflamatoacuterio (10)
Classificado como analgeacutesico actua no sistema nervoso pela activaccedilatildeo indirecta de
9
receptores canabinoacuteides (11) embora este mecanismo ainda natildeo esteja totalmente
esclarecido (12) secundariamente inibe a COX-1 e COX-2 e por consequente a
siacutentese das prostaglandinas Como antipireacutetico age no centro hipotalacircmico que regula a
temperatura produzindo vasodilataccedilatildeo perifeacuterica e aumento do fluxo sanguiacuteneo
diminuindo a temperatura pela sudorese e perda de calor pela pele
O paracetamol eacute usualmente administrado oralmente (10) Apresenta uma meia-
vida de 2-3 horas Apesar de ser comparaacutevel agrave aspirina como analgeacutesico e antipireacutetico
eficaz o paracetamol difere no facto de natildeo possuir propriedades anti-inflamatoacuterias
(10) Difere dos analgeacutesicos opioacuteides porque natildeo provoca euforia nem altera o estado
de humor do doente Da mesma forma que os (NSAIDrsquos) natildeo causa problemas de
dependecircncia toleracircncia e siacutendrome de abstinecircncia Eacute muito utilizado e seguro com a
dosagem recomendada de 4g por dia mas nem sempre oferece um aliacutevio adequado da
dor aguda por si soacute (13)
NSAIDrsquoS
Os NSAIDrsquos satildeo dos agentes terapecircuticos mais utilizados no mundo inteiro
inclui-se neste grupo o ibuprofeno importante no tratamento da dor aguda e croacutenica
(14) Dos inibidores selectivos da COX-2 mais recentes nomeadamente rofecoxib
valdecoxib e celecoxib apenas este uacuteltimo foi comercializado nos EUA devido aos
restantes terem sido associados a eventos tromboacuteticos cardiovasculares (15 pp 277-
281) Apresentam trecircs acccedilotildees principais que resultam da inibiccedilatildeo da COX-2 e da
consequente reduccedilatildeo da siacutentese de prostanoacuteides
Acccedilatildeo anti-inflamatoacuteria a modificaccedilatildeo da resposta inflamatoacuteria ocorre pela
reduccedilatildeo do nordm de prostaglandinas vasodilatadoras (PGE2 prostaciclina)
associada a menor vasodilataccedilatildeo e indirectamente a menos edema No entanto a
acumulaccedilatildeo de ceacutelulas inflamatoacuterias natildeo eacute diminuiacuteda
Efeito analgeacutesico a reduccedilatildeo da siacutentese de prostaglandinas diminui a
sensibilizaccedilatildeo das terminaccedilotildees nervosas nociceptivas a mediadores da
inflamaccedilatildeo (como bradicinina e 5-hidroxitriptamina) provoca tambeacutem a reduccedilatildeo
da vasodilataccedilatildeo e desse modo o aliacutevio da cefaleia
10
Efeito antipireacutetico deve-se em parte agrave diminuiccedilatildeo da prostaglandina
mediadora a interleucina-1 responsaacutevel pela estimulaccedilatildeo do hipotaacutelamo e
consequente aumento de temperatura ndash febre (10 pp 1056-1061)
Eacute de referir ainda que todos os NSAIDrsquos agrave excepccedilatildeo dos inibidores selectivos da
COX-2 e salicilatos natildeo-acetilados tecircm um efeito inibitoacuterio na agregaccedilatildeo de plaquetas
(15 pp 277-281)
Os efeitos secundaacuterios resultam em grande parte da inibiccedilatildeo da COX-1 Entre
os mais frequentes encontram-se Dispepsia naacuteuseas e voacutemitos associados a lesotildees
gaacutestricas provocadas pela anulaccedilatildeo do efeito protector da prostaglandina sobre a mucosa
gaacutestrica Insuficiecircncia renal Reacccedilotildees cutacircneas Distuacuterbios hepaacuteticos Riscos
cardiovasculares e outros (10)
ESCALAS DE MEDICcedilAtildeO DE DOR - ESCALA VISUAL ANALOacuteGICA
A dor sendo um fenoacutemeno subjectivo compreende um grande conjunto de
componentes - componentes fisioloacutegicos cognitivos sensoriais comportamentais entre
outros Avaliar a dor utilizando uma medida que abranja todas as suas facetas e seja
fidedigna tem-se demonstrado impossiacutevelldquoUm instrumento ideal para a mensuraccedilatildeo da
dor deveria ter propriedades de uma escala de razatildeo fornecer informaccedilatildeo imediata
sobre a fidedignidade do desempenho dos pacientes ser relativamente livre de vieacuteses
ser simples de utilizar com pacientes () demonstrar utilidade tanto para a dor
experimental quanto para a dor cliacutenica permitindo comparaccedilotildees confiaacuteveis entre ambos
os tipos de dorrdquo(16)
A Escala Visual Analoacutegica (VAS) consiste numa mediccedilatildeo da dor em mm (0-
100mm) em que agrave extremidade 0 corresponde ldquonenhuma dorrdquo e agrave extremidade
antagoacutenica ldquopior dor possiacutevelrdquo Eacute uma forma simples eficaz - dentro das limitaccedilotildees - e
faacutecil de reproduzir ldquoou seja pode ser compreendida em distintas situaccedilotildees onde haacute
diferenccedilas culturais ou de linguagem do avaliador cliacutenico ou examinadorrdquo(16)
Para responder agrave questatildeo colocada pelo paciente eacute necessaacuterio a procura da
melhor evidecircncia cientiacutefica integrando-a com o proacuteprio interesse do paciente e a
expertise do cliacutenico Estes objectivos da Medicina Dentaacuteria Baseada na Evidecircncia satildeo
em parte consequecircncia de uma actualizaccedilatildeo constante de praacuteticas cliacutenicas consequentes
de novas evidecircncias cientiacuteficas e com a noccedilatildeo de que nenhum tratamento eacute completo
11
sem que ldquoas expectativas exigecircncias e direitos legiacutetimos dos pacientes sejam integrados
nos processos de decisatildeo cliacutenica sendo tal facto reconhecidamente essencial para a
melhoria da qualidade de vidardquo(17)
12
PESQUISA
CRITEacuteRIOS DE SELECCcedilAtildeO
Tipos de Estudos Escolhidos
Para este trabalho foram escolhidos apenas ensaios cliacutenicos aleatorizados cegos
(preferencialmente duplamente cegos) controlados ou natildeo por placebo e revisotildees
sistemaacuteticas
Tipos de participantes
Indiviacuteduos com idade superior a 15 anos
Sujeitos a cirurgia para extracccedilatildeo unilateral ou bilateral do 3ordm molar inferior
Que natildeo estivessem a tomar qualquer outro tipo de medicaccedilatildeo com efeitos
idecircnticos ou semelhantes aos faacutermacos em estudo
Sem patologias orais que provoquem dor moderada a forte ou outras patologias
que afectem a percepccedilatildeo da dor
Tipos de intervenccedilatildeo
Administraccedilatildeo apenas por via oral de
Paracetamol (1000mg) vs placebo
Paracetamol (1000mg) vs outro(s) NSAIDrsquos
Paracetamol ( 1000mg) vs outro(s) NSAIDrsquos vs placebo
Paracetamol (1000mg) + outro(s) NSAIDrsquos
ou Paracetamol (1000mg) + outro(s) NSAIDrsquos vs placebo
Estudos com outros tipos de intervenccedilatildeo natildeo foram incluiacutedos Os estudos que
apenas incluiacuteram o paracetamol sob a forma de proacute-farmaco foram excluiacutedos
Mediccedilatildeo de Resultados
A mediccedilatildeo de resultados foi obtida atraveacutes da escala visual analoacutegica (VAS ndash
visual analogic scale)
13
Avaliaccedilatildeo dos Estudos
Todos os estudos foram avaliados segundo fichas CASP (Critical Appraisal
Skills Programme) Estas consistem num conjunto de questotildees que permitem avaliar um
artigo cientiacutefico no seu todo para em uacuteltima anaacutelise aferir a sua aplicabilidade validade
e fiabilidade (18) Estas fichas existem para vaacuterios tipos de estudo as CASP utilizadas
neste trabalho foram as referentes a revisotildees sistemaacuteticas e ensaios cliacutenicos
aleatorizados
ESTRATEacuteGIAS DE PESQUISA
Apoacutes cada pesquisa os artigos encontrados foram avaliados numa fase inicial
com base nos seus tiacutetulos e abstracts para averiguar a sua relevacircncia A seguinte escala
foi utilizada adequado possivelmente adequado inadequado Toda a pesquisa foi
efectuada entre 7 e 19 de Novembro de 2011
Primeiramente foram consultadas bases de dados secundaacuterias apoacutes pesquisa
nestas fontes seguiram-se bases de dados primaacuterias
Cochrane Database for Systematic Reviews
Na pesquisa avanccedilada desta base de dados secundaacuteria foi introduzida a seguinte
combinaccedilatildeo de termos utilizando conectores boleanos e seleccionando as opccedilotildees
ldquosearch all textrdquo e ldquoCochrane Database of Systematic Reviewsrdquo
paracetamol AND third molar removal AND pain relief AND analgesicrdquo
Foram encontrados 14 resultados (3 protocolos e 11 revisotildees sistemaacuteticas) dos
quais uma revisatildeo foi categorizada como ldquoadequadardquo
Paracetamol for pain relief after surgical removal of lower wisdom teeth Weil
Hooper (19) Esta revisatildeo foi novamente encontrada na base de dados EBD bem
como na NICE e no PubMed
E outra classificada como ldquopossivelmente adequadardquo mas posteriormente
excluiacuteda (20)
14
Evidence-Based Dentistry (EBD)
Nesta base de dados foi introduzida a combinaccedilatildeo de termos
ldquoParacetamol OR acetaminophen AND third molar AND painrdquo utilizando os
filtros ldquoBritish Dental Journalrdquo e ldquoEvidence-Based Dentistryrdquo
Foram encontrados 28 resultados dos quais uma revisatildeo foi classificada como
ldquoadequadardquo
Relative efficacy of oral analgesics after third molar extraction ndash a 2011 update
Derry Wiffen (21)
E ainda dois artigos classificados como ldquopossivelmente adequadordquo
An investigation into the comparative efficacy of soluble aspirin and solid
paracetamol in postoperative pain after third molar surgery Seymour
Hawkesford (22)
Relative efficacy of oral analgesics after third molar extraction Barden
Edwards (23)
National Institute of Health and Clinical Excellence (NICE)
Nesta base de dados foi introduzida a seguinte combinaccedilatildeo de termos
ldquoParacetamol and third molar removal and pain and analgesicrdquo
Dos 28 resultados obtidos 1 foi previamente encontrado e classificado (19)
Dos restantes 27 artigos nenhum foi classificado como adequado ou possivelmente
adequado
LILACS
Nesta base de dados primaacuteria foi introduzida a seguinte combinaccedilatildeo de termos
ldquoParacetamol terceiro molar dorrdquo
Dos 3 resultados obtidos um foi classificado como possivelmente adequado mas
posteriormente excluiacutedo (24)
15
PUBMED
Nesta base de dados primaacuteria foram efectuadas duas pesquisas com termos
diferentes Apenas foram utilizados termos MeSH foram utilizados conectores
boleanos em ambas as pesquisas
Pesquisa 1
Search ((((Acetaminophen[Mesh]) AND Anti-Inflammatory Agents[Mesh])
AND Molar Third[Mesh]) AND Tooth Extraction[Mesh]) AND Pain
Postoperative[Mesh]
Limits only items with abstracts Humans Clinical Trial Meta-Analysis
Randomized Controlled Trial Review Comparative Study Controlled Clinical
Trial English Spanish Portuguese
Foram obtidos 32 resultados dos quais 5 artigos foram classificados como
ldquoadequadosrdquo
Combining paracetamol with a selective cyclooxygenase-2 inhibitor for acute
pain relief after third molar surgery a randomized double-blind placebo-
controlled study Haglund and von Bultzingslowen (25)
Dos restantes quatro artigos um (22) era repetido e os outros trecircs (26-28) foram
posteriormente excluiacutedos
Quatro foram considerados ldquopossivelmente adequadosrdquo dos quais trecircs (29-31)
foram posteriormente excluiacutedos O artigo remanescente foi
Analgesic efficacy of lysine clonixinate paracetamol and dipyrone in lower
third molar extraction a randomized controlled trial (32)
Pesquisa 2
Search (((Acetaminophen[Mesh]) AND Analgesics[Mesh]) AND Molar
Third[Mesh]) AND Tooth Extraction[Mesh]
Limits only items with abstracts Humans Clinical Trial Meta-Analysis
Randomized Controlled Trial Review English
16
Obtiveram-se 56 resultados em que sete foram seleccionados como sendo
ldquoadequadosrdquo
Combined acetaminophen and ibuprofen for pain relief after oral surgery in
adults a randomized controlled trial Merry Gibbs (13)
Destes artigos seis (19 22 23 25 28 32) eram repetidos
Oito artigos foram classificados como ldquopossivelmente adequadosrdquo
Onset of analgesia with sodium ibuprofen ibuprofen acid incorporating poloxamer
and acetaminophen--a single-dose double-blind placebo-controlled study in
patients with post-operative dental pain Daniels Reader (33)
Dos oito artigos cinco foram repetidos (26 27 29-31) dois (34 35) foi
posteriormente excluiacutedo
No anexo A encontra-se uma tabela de artigos excluiacutedos cujas razotildees satildeo
discriminadas
Eacute de notar que este tipo de estrateacutegia de pesquisa traz associada grande
quantidade de resultados irrelevantes superior agrave de artigos de interesse mas facilita a
aquisiccedilatildeo de todos os artigos importantes colocando em primeiro plano a sensibilidade
e natildeo a especificidade (36) A utilizaccedilatildeo de conectores boleanos e de filtros especiacuteficos
foi uma forma de minimizar o nuacutemero de resultados natildeo relacionados (17) preservando
os de interesse
17
AVALIACcedilAtildeO CRIacuteTICA
REVISOtildeES SISTEMAacuteTICAS
Paracetamol for pain relief after surgical removal of lower
wisdom teeth Weil Hooper (19)
1 Did the review ask a clearly-focused question
Sim A populaccedilatildeo em estudo compreende pacientes de qualquer estado de sauacutede
que necessitem de uma exodontia do terceiro molar inferior e que apresentam uma
intensidade de dor basal moderada a forte Foram excluiacutedos pacientes que estivessem a
tomar outro analgeacutesico A intervenccedilatildeo foi baseada em dois aspectos ndash eficaacutecia e efeitos
secundaacuterios
A terapecircutica usada para avaliar a eficaacutecia consistiu na administraccedilatildeo de uma
dose uacutenica de paracetamol por via oral independentemente da formulaccedilatildeo ou do
momento em que o faacutermaco foi tomado
Em relaccedilatildeo aos efeitos secundaacuterios foram incluiacutedos estudos natildeo soacute de dose
uacutenica como tambeacutem de doses muacuteltiplas de acetaminofeno consideraram-se estudos em
que este composto foi tomado ateacute 7 dias apoacutes a primeira toma Para este trabalho apenas
seratildeo considerados os resultados com base na administraccedilatildeo poacutes-operatoacuteria do
paracetamol
Os resultados ndash intensidade da dor e aliacutevio da dor ndash foram medidos usando as
escalas visual analoacutegica categoacuterica verbal numeacuterica verbal global subjectiva de
avaliaccedilatildeo de eficaacutecia e outras categoacutericas Os outcomes derivados do aliacutevio da dor
contabilizados foram total pain relief (TOTPAR) e summed pain intensity difference
(SPID) durante 4 e 6 horas Foram ainda contabilizados os efeitos secundaacuterios
2 Did the review include the right type of study
Os uacutenicos estudos incluiacutedos foram ensaios cliacutenicos aleatorizados duplamente
cegos que comparam o paracetamol a um placebo bem como dosagens diferentes
avaliando efeitos agraves 4 e 6 horas Este tipo de estudo eacute adequado pois implica um baixo
risco de vieacutes
18
3 Did the reviewers try to identify all relevant studies
Sim Os autores utilizaram estudos de todos os idiomas recorrendo agrave sua
traduccedilatildeo quando necessaacuterio Foram consultadas bases de dados bibliograacuteficas
electroacutenicas The Cochrane Oral Health Grouprsquos Trials Register The Cochrane Central
Register of Controlled Trials The Cochrane Pain Palliative and Supportive Care
Grouprsquos Trials Register MEDLINE EMBASE e Current Controlled Trials Register
Tambeacutem foram realizadas pesquisas manuais em revistas como parte do Cochrane Oral
Health Grouprsquos ongoing journal handsearching programme A pesquisa visou estudos
publicados entre 1966 e 25 de Agosto de 2006
Foram enviadas cartas a autores de ensaios cliacutenicos aleatorizados com vista a
obter estudos natildeo publicados bem como a empresas farmacecircuticas fabricantes de
analgeacutesicos
Os autores deste estudo consultaram ainda referecircncias bibliograacuteficas de papers
reviews e referecircncias pessoais
4 Did the reviewers asses the quality of the included studies
Sim Foi utilizada uma estrateacutegia clara e bem definida para a determinaccedilatildeo dos
estudos a incluir Este processo foi realizado independentemente por dois autores da
revisatildeo ndash natildeo cegos ndash baseando-se em dois criteacuterios centrais atribuiccedilatildeo oculta do
faacutermaco e a existecircncia de um follow-up completo Para estes criteacuterios foi utilizado um
sistema de pontuaccedilatildeo Desta forma a cada estudo foi-lhe atribuiacuteda uma pontuaccedilatildeo
formando-se dois grupos
Baixo risco de vieacutes
Moderado ou alto risco de vieacutes
5 If the results of the studies have been combined was it reasonable to do so
Sim os resultados foram apresentados de forma combinada e loacutegica Em
primeiro lugar foram apresentadas tabelas uma para cada artigoestudo incluiacutedo em
que se encontravam discriminados os meacutetodos participantes intervenccedilotildees resultados e
outras notas Os resultados dos diferentes estudos foram agrupados em 2 outcomes
tendo cada outcome 2 divisotildees
Outcome 1 ndash TOTPAR agraves 4h
A ndash Dosagem de paracetamol ateacute 1000mg vs placebo
B ndash Dosagem de paracetamol igual ou superior a 1000mg vs placebo
19
Outcome 2 ndash TOTPAR agraves 6h
A ndash Dosagem de paracetamol ateacute 1000mg vs placebo
B ndash Dosagem de paracetamol igual ou superior a 1000mg vs placebo
Todos estes grupos foram analisados e comparados segundos 2 paracircmetros
Comparaccedilatildeo 1- Medidas de aliacutevio da dor
Comparaccedilatildeo 2- Medidas de intensidade da dor
Tendo em conta todas estas variaacuteveis foram realizadas meta-anaacutelises por
subgrupo (pp 29-40) utilizando graacuteficos forest plot
Anaacutelise 11 ndash Comparaccedilatildeo 1 de A vs B ndash Outcome 1
Anaacutelise 12 ndash Comparaccedilatildeo 1 de A vs B ndash Outcome 2
Anaacutelise 21 ndash Comparaccedilatildeo 2 de A vs B ndash Outcome 1
Anaacutelise 22 ndash Comparaccedilatildeo 2 de A vs B ndash Outcome 2
Anaacutelise 3 ndash Comparaccedilatildeo do nuacutemero de efeitos adversos de paracetamol vs
placebo comparando ainda as duas dosagens diferentes
Valores de heterogeneidade (representados por I2) proacuteximos de 25 indicam
baixa discrepacircncia 50 satildeo indicadores de heterogeneidade moderada e valores
proacuteximos de 75 satildeo sinal de alta heterogeneidade entre os estudos (37)
Olhando para os valores de I2 dois possuem alta heterogeneidade um moderada
e dois baixa Nos grupos que apresentam uma discrepacircncia estatiacutestica significativa dos
resultados a aglutinaccedilatildeo dos mesmos natildeo foi muito bem sucedida Nestes grupos ainda
que a heterogeneidade seja elevada a apresentaccedilatildeo dos resultados de cada estudo foram
correcta e individualmente apresentados Aleacutem deste aspecto os diferentes meacutetodos ndash
dosagem e tempo - foram agrupados exactamente para que as formas de intervenccedilatildeo e
meacutetodos com o menor risco de vieacutes
Tabela 1 ndash Valores de heterogeneidade (I2) de cada anaacutelise
Total de I2
()
Anaacutelise 11 Anaacutelise 12 Anaacutelise 21 Anaacutelise 22 Anaacutelise 3
76 81 66 29 28
Natildeo foram discutidas as variaccedilotildees nos resultados
20
6 How are the results presented and what is the main result
A meta-anaacutelise por subgrupos foi realizada com recurso agrave medida de eficaacutecia de
intervenccedilatildeo Risco Relativo (RR) Analisando o graacutefico forest plot os ldquoquadradosrdquo a azul
representam o RR e o poliacutegono (semelhante a um losango) sumariza todas as
informaccedilotildees (provenientes dos vaacuterios estudos) sobre o efeito do paracetamol (38)
ldquoQuando o IC natildeo ultrapassa a linha de nulidade pode-se afirmar que o resultado eacute
estatisticamente significativo Estudos maiores possuem IC mais estreitos ou seja
resultados mais precisos e maior contribuiccedilatildeo para a meta-anaacutelise que tambeacutem eacute repre-
sentada graficamente (quanto maior a aacuterea do quadrado maior o peso) e valor
percentualrdquo (39) A significacircncia aumenta com a distacircncia do poliacutegono da linha de natildeo
efeito
Independentemente do tempo (4 ou 6h) dosagens ateacute 1000mg de paracetamol
apresentam uma pequena discrepacircncia nos resultados sendo que o paracetamol eacute
ligeiramente mais eficaz que o placebo Doses iguais ou superiores a 1000mg de
paracetamol traduzem-se num maior aliacutevio da dor poacutes-operatoacuteria (poliacutegono afastado da
linha de natildeo-efeito)
Em relaccedilatildeo agrave anaacutelise 3 ateacute doses de 1 g de paracetamol nuacutemero de casos de
efeitos adversos eacute muito semelhante entre placebo e a substacircncia activa Para
concentraccedilotildees superiores a 1000 mg o nuacutemero de efeiros adversos eacute superior para
paracetamol Eacute possiacutevel concluir que natildeo haacute uma diferenccedila notoacuteria no nuacutemero de casos
de efeitos adversos O poliacutegono cruza sempre a linha de natildeo efeito
O paracetamol eacute consideravelmente mais eficaz que o placebo no aliacutevio de 50
da dor principalmente em doses iguais ou superiores a 1000mg Natildeo haacute diferenccedila
significativa em relaccedilatildeo aos efeitos adversos
7 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em consideraccedilatildeo que o
poliacutegono natildeo intersecta a linha de natildeo efeito os resultados satildeo precisos (anaacutelise 1 a 2)
Na anaacutelise 3 mesmo com um IC 95 o poliacutegono cruza a linha de natildeo efeito logo natildeo eacute
possiacutevel tirar conclusotildees semelhantes em relaccedilatildeo aos limites inferior e superior do IC
Eacute de notar que a elaboraccedilatildeo de uma meta-anaacutelise contribui para a robustez dos
resultados daiacute provenientes combinar os resultados de cada estudo individual numa
meta-anaacutelise aumenta o poder estatiacutestico gerando resultados mais precisos (40)
21
8 Can the results be applied to the local population
Sim A extracccedilatildeo de terceiros molares inferiores eacute uma praacutetica cliacutenica comum
em Portugal O paracetamol eacute um analgeacutesico largamente comercializado e administrado
(sendo natildeo sujeito a receita meacutedica) pelo que era possiacutevel reproduzir esta forma de
tratamento
No entanto os estudos incluiacutedos na revisatildeo referem-se a uma dose uacutenica que
embora reproduziacutevel na populaccedilatildeo local seria necessaacuteria uma modificaccedilatildeo do
paradigma cultural em relaccedilatildeo agrave toma de medicamentos
9 Were all important outcomes considered
Natildeo A revisatildeo considera a eficaacutecia do paracetamol vs placebo no aliacutevio da dor
e simultaneamente a ocorrecircncia de efeitos secundaacuterios Satildeo abordados directamente
dois aspectos ndash o da praacutetica cliacutenica e o da investigaccedilatildeo Ambos satildeo relativos ao
profissional de sauacutede e implicitamente ao proacuteprio indiviacuteduo e aos familiares (ao serem
referidas as doses periacuteodos entre tomas e combinaccedilotildees com outros NSAIDrsquos mais
eficazes e simultaneamente seguras)
Poreacutem nada eacute referido em relaccedilatildeo a novas poliacuteticas de sauacutede nomeadamente na
implementaccedilatildeo de uma dose uacutenica culminando numa mudanccedila dos haacutebitos de sauacutede da
comunidade Tambeacutem natildeo foram abordados aspectos econoacutemicos tal como um balanccedilo
entre benefiacutecios e encargos de sauacutede que justifique a utilizaccedilatildeo deste faacutermaco como
tratamento preferencial
10 Should policy or practice change as a result of the evidence contained in this
review
Natildeo Esta revisatildeo demonstra que comparativamente a um placebo o paracetamol
eacute mais eficaz principalmente em doses elevadas e que natildeo haacute diferenccedila estatiacutestica
significativa no nuacutemero de efeitos secundaacuterios Poreacutem natildeo eacute possiacutevel tirar conclusotildees
sobre a dor depois do periacuteodo considerado de 6h Desta forma implementar uma dose
uacutenica de paracetamol a 1000mg seria imprudente sem previamente realizar estudos
complementares sobre a evoluccedilatildeo da dor apoacutes as 6h bem como comparar este faacutermaco
com outros compostos que possam ser igualmente eficazes por um raacutecio custo-benefiacutecio
melhor ou vice-versa
22
Relative efficacy of oral analgesics after third molar extraction
Barden Edwards (23)
Relative efficacy of oral analgesics after third molar extraction -
a 2011 update Derry Wiffen (21)
A avaliaccedilatildeo feita e disposta abaixo contemplou tanto a revisatildeo sistemaacutetica que
remonta a 2004 como a sua actualizaccedilatildeo de 2011 Uma vez estando inter-relacionados
consideraacutemos pertinente juntar as apreciaccedilotildees destas revisotildees porque caso contraacuterio
perder-se-ia o contexto de ambas
1 Did the review ask a clearly-focused question
Sim A populaccedilatildeo em estudo comporta pacientes com mais de 15 anos de idade
com uma intensidade de dor basal poacutes-operatoacuteria de moderada a severa apoacutes extracccedilatildeo
de um terceiro molar
A intervenccedilatildeo consistiu no tratamento da dor poacutes-operatoacuteria de intensidade
moderada a severa com doses uacutenicas de analgeacutesicos orais ou placebo sendo que os
analgeacutesicos orais corresponderam a um total de 15 combinaccedilotildees diferentes de faacutermacos
e respectivas dosagens
Os resultados foram obtidos atraveacutes da mediccedilatildeo do aliacutevio total da dor
(TOTPAR) ou da diferenccedila de intensidade da dor (SPID) utilizando uma escala
standard de 5 niacuteveis de aliacutevio da dor uma escala standard de 4 niacuteveis de aliacutevio da dor
ou uma escala visual analoacutegica (VAS) Os efeitos secundaacuterios foram tambeacutem relatados
comparando a proporccedilatildeo de pacientes que apresentaram efeitos generalizados e que
apresentaram efeitos particulares
Actualizaccedilatildeo de 2011
A intervenccedilatildeo consistiu tambeacutem no tratamento da dor poacutes-operatoacuteria de
intensidade moderada a severa com doses uacutenicas de analgeacutesicos orais ou placebo no
entanto os analgeacutesicos utilizados foram diferentes A revisatildeo de 2004 incluiu rofecoxib
and valdecoxib nenhum dos quais se encontra disponiacutevel no mercado Em vez disso
foram utilizadas combinaccedilotildees de ibuprofeno com paracetamol formulaccedilotildees diferentes
de ibuprofeno e diclofenac e etoricoxib
23
2 Did the review include the right type of study
Sim Os estudos que foram incluiacutedos nesta revisatildeo correspondem a ensaios
cliacutenicos aleatorizados duplamente cegos que comparam a eficaacutecia dos diferentes
analgeacutesicos e com placebo na terapecircutica da dor aguda poacutes-operatoacuteria Os grupos
formados possuiacuteam grupos com um miacutenimo de 10 pessoas Em todos os estudos foram
seguidas as guidelines QUORUM e utilizados criteacuterios de inclusatildeo para a dor poacutes-
operatoacuteria em que os resultados satildeo avaliados durante um periacuteodo de 4 a 6 horas apoacutes
medicaccedilatildeo
3 Did the reviewers try to identify all relevant studies
Sim Os autores da revisatildeo tentaram identificar todos os estudos relevantes
pesquisando nas bases de dados electroacutenicas Cochrane Library Biological Abstracts
MEDLINE PubMed e Oxford Pain Relief Para aleacutem disso consultaram a bibliografia
dos artigos de revisatildeo incluiacutedos de modo a encontrar informaccedilatildeo adicional e possiacuteveis
estudos natildeo publicados os quais apresentam na sua maioria datas de pesquisa que
remontam a 2002 No entanto eacute de mencionar que natildeo contactaram os autores e os
fabricantes para recolha de dados nem procuraram estudos com idiomas diferentes do
inglecircs
Actualizaccedilatildeo de 2011
Com o passar dos anos os artigos inseridos na revisatildeo foram actualizados de
forma a incluir outros analgeacutesicos e obter ensaios cliacutenicos adicionais e relevantes Desta
forma a actualizaccedilatildeo da revisatildeo sistemaacutetica de 2004 incluiu 35 revisotildees da Cochrane
com 38 anaacutelises realizadas em diferentes analgeacutesicos de dose uacutenica para determinar a
sua eficaacutecia na dor poacutes-operatoacuteria
4 Did the reviewers assess the quality of the included studies
Sim A qualidade dos estudos incluiacutedos foi avaliada vaacuterios autores
independentes e natildeo cegos (pelo facto de estes conhecerem a literatura existente)
utilizando uma escala de qualidade numerada de 1 a 5 e baseada em 3 criteacuterios
distribuiccedilatildeo aleatorizada dos pacientes se os pacientes e os examinadores se
encontravam cegos se houve remoccedilotildees ou desistecircncias durante o estudo A
classificaccedilatildeo maacutexima de um estudo incluiacutedo foi de 5 e a miacutenima foi de 2
24
Os ensaios cliacutenicos que apresentam uma classificaccedilatildeo igual ou superior a 3
(baixo risco de vieacutes) demonstraram menores efeitos secundaacuterios que os ensaios cliacutenicos
que apresentam uma classificaccedilatildeo igual ou inferior a 2 (alto risco de vieacutes)
5 If the results of the studies have been combined was it reasonable to do so
Sim Os resultados dos diferentes estudos foram apresentados sob a forma de
tabelas nomeadamente a eficaacutecia dos vaacuterios analgeacutesicos e a ocorrecircncia de efeitos
secundaacuterios foram dispostas em tabelas Aqui eram resumidos os resultados o tipo de
intervenccedilatildeo e respectivo nuacutemero total de pacientes e nordm de estudos realizados
Esta revisatildeo sistemaacutetica natildeo incluiu a realizaccedilatildeo de testes heterogeacuteneos nem a
avaliaccedilatildeo do risco de vieacutes das publicaccedilotildees atraveacutes de forest plots dado que na opiniatildeo
dos autores estas abordagens mostraram-se pouco adequados para este tipo de estudos
No entanto a homogeneidade foi avaliada atraveacutes de um modo visual
A resposta a esta questatildeo eacute claramente afirmativa porque a elevada semelhanccedila
das caracteriacutesticas dos diferentes estudos (meacutetodos utilizados tipo de intervenccedilatildeo e
mediccedilatildeo dos resultados) tornou por um lado inadequada a realizaccedilatildeo uma meta-anaacutelise
para avaliar a heterogeneidade mas por outro adequada a realizaccedilatildeo de uma avaliaccedilatildeo
visual da homogeneidade dos mesmos
6 How are the results presented and what is the main result
Os resultados foram medidos atraveacutes da proporccedilatildeo de pacientes do grupo de
tratamento vs placebo que atingiram pelo menos 50 de maxTOTPAR ou seja aliacutevio
de dor A qual foi utilizada para determinar o benefiacutecio relativo e o NNT bem como o
risco relativo dos diferentes estudos incluiacutedos
Atraveacutes da anaacutelise das tabelas eacute possiacutevel tirar 3 conclusotildees principais
1 A proporccedilatildeo de pacientes que atingiram pelo menos 50 de aliacutevio de dor eacute maior
no grupo de tratamento que no grupo placebo agrave excepccedilatildeo do estudo que utilizou
dihidrocodeiacutena 30mg em que as diferenccedilas natildeo foram estatisticamente relevantes
2 Por comparaccedilatildeo ao paracetamol (independentemente das diferentes dosagens) os
anti-inflamatoacuterios natildeo-esteroacuteides inibidores da COX-2 apresentam um maior
benefiacutecio relativo e necessitam do menor nordm de pacientes tratados para atingirem o
objectivo de 50 de aliacutevio de dor
25
3 O paracetamol apresenta um maior risco relativo na medida em que insurgem mais
efeitos secundaacuterios nos estudos em que foi administrado por oposiccedilatildeo aos
NSAIDrsquos
Os anti-inflamatoacuterios natildeo-esteroacuteides inibidores da COX-2 satildeo mais eficazes no
tratamento da dor basal poacutes-operatoacuteria moderada a intensa que o paracetamol
Actualizaccedilatildeo de 2011
Os resultados foram obtidos da mesma forma que na versatildeo de 2004 sendo que
um novo outcome foi considerado ndash tempo meacutedio necessaacuterio para que os pacientes
necessitem de re-medicaccedilatildeo aproximadamente 8 horas Agrave semelhanccedila do que aconteceu
na revisatildeo anterior os dados sobre a dihidrocodeiacutena natildeo foram conclusivos devido agrave
pouca informaccedilatildeo disponiacutevel nos estudos
7 How precise are these results
Os resultados satildeo precisos uma vez que utilizam um intervalo de confianccedila de
95 Eacute de ressalvar que os valores de NNT ou NNH apenas eram calculados quando o
riscobenefiacutecio relativo satildeo significativos isto eacute quando natildeo incluem o valor de 1 No
limite superior do intervalo de confianccedila a intervenccedilatildeo realizada seria a mesma No
entanto dado que o NNH natildeo foi calculado eacute possiacutevel concluir que o risco relativo natildeo
era significativo pelo que permanece uma incerteza se no limite inferior do intervalo de
confianccedila a intervenccedilatildeo realizada seria a mesma
8 Can the results be applied to the local population
Sim Os resultados da revisatildeo sistemaacutetica podem ser aplicados agrave nossa
populaccedilatildeo local porque os criteacuterios de inclusatildeo utilizados correspondem na sua
maioria a mecanismos fisioloacutegicos caracteriacutesticos do ser humano Para aleacutem disso as
teacutecnicas utilizadas satildeo simples e de faacutecil reproduccedilatildeo na medida em que os faacutermacos
utilizados nos ensaios cliacutenicos estatildeo agrave disposiccedilatildeo dos interessados e os meacutetodos
terapecircuticos baacutesicos
No entanto os estudos incluiacutedos nesta revisatildeo incluiacuteram um tratamento com
uma dose uacutenica de analgeacutesico oral que embora reprodutiacutevel difere do paradigma actual
da nossa populaccedilatildeo (em que haacute a tendecircncia para a auto-medicaccedilatildeo e de recorrer a
diferentes faacutermacos)
26
9 Were all important outcomes considered
Natildeo Os resultados enfatizam a eficaacutecia de vaacuterios analgeacutesicos no aliacutevio de 50
dor em comparaccedilatildeo com placebo Eacute focada ainda o benefiacutecio relativo (95 IC) e o NNT
da mesma problemaacutetica Aleacutem deste conjunto de dados satildeo considerados o nuacutemero de
pacientes com efeitos secundaacuterios risco relativo (95 IC) culminando no caacutelculo do
NNH
Contudo natildeo eacute especificado o tipo de efeitos secundaacuterios que podem ser
desencadeados pela toma dos diferentes analgeacutesicos nem aspectos diferenciadores em
analgeacutesicos com eficaacutecia e benefiacutecios idecircnticos (por exemplo custo econoacutemico) Isto
constituiria uma mais-valia para uma escolha mais consciente do analgeacutesico tanto pelos
profissionais como pelos pacientes (individual) e beneficiaria tambeacutem o Sistema
Nacional de Sauacutede (comunidade em geral)
Actualizaccedilatildeo de 2011
Um dos outcomes considerados semelhante ao que foi abordado na revisatildeo de
2004 foi a percentagem de pacientes com dor moderada (30- 60 mm VAS) ou dor
severa (mais de 60 mm) que obtiveram 50 de aliacutevio de dor Contudo foi adicionado
um novo outcome relevante o tempo necessaacuterio para que metade dos pacientes requeriu
re-medicaccedilatildeo
10 Should policy or practice change as a result of the evidence contained in this
review
Natildeo Os resultados desta revisatildeo evidenciam a eficaacutecia dos analgeacutesicos
comparativamente a um placebo nomeadamente que o ibuprofeno e o paracetamol
possuem maior maior o benefiacutecioefeito analgeacutesico quanto maior forem as dosagens
Poreacutem natildeo eacute evidecircncia suficiente para mudar o paradigma de tratamento pois ldquoWhat
these comparisons do not do is to tell dentists what to prescriberdquo Satildeo sim uma
importante ferramenta para a tomada de decisotildees que devem ser adaptadas a cada
paciente tendo presente que 80 dos analgeacutesicos prescritos possuem elevados iacutendices
de eficaacutecia e seguranccedila Em adiccedilatildeo nem todos os analgeacutesicos nesta revisatildeo estatildeo
disponiacuteveis no mercado para serem receitados pelos meacutedicos-dentistas
Conclui-se que para que esta revisatildeo fosse pilar basilar nas prescriccedilotildees de
analgeacutesicos teriam de ser apresentadas evidecircncias de benefiacuteciocusto dos analgeacutesicos
27
com melhores resultados (aspecto econoacutemico e detalhe dos efeitos adversos) Todavia a
informaccedilatildeo presente na mesma sobre a eficaacutecia e efeitos secundaacuterios assim como toda a
bibliografia jaacute existente sobre este assunto eacute uacutetil e deve ser utilizada para tomar inicio agrave
criaccedilatildeo de um formulaacuterio em medicina dentaacuteria
Actualizaccedilatildeo de 2011
Os resultados obtidos da mesma forma que na revisatildeo anterior natildeo foram
suficientemente relevantes para que as poliacuteticas de sauacutede mudassem No entanto a
quantidade de informaccedilatildeo disponiacutevel sobre analgeacutesicos de dose uacutenica para aliacutevio da dor
poacutes-operatoacuteria eacute grande e bastante acessiacutevel Podem assim servir como boas
ferramentas para a formulaccedilatildeo de poliacuteticas e prescriccedilotildees farmacecircuticas para a populaccedilatildeo
quando existirem dados cliacutenicos mais conclusivos
28
AVALIACcedilAtildeO CRIacuteTICA
ENSAIOS CLIacuteNICOS ALEATORIZADOS
Combining paracetamol with a selective cyclooxygenase-2
inhibitor for acute pain relief after third molar surgery a
randomized double-blind placebo-controlled study Haglund and
von Bultzingslowen (25)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo compreende indiviacuteduos saudaacuteveis com idade superior a 18
anos peso entre 50 e 120 kg e com necessidade de extrair terceiros molares inferiores
com remoccedilatildeo oacutessea Foram excluiacutedos pacientes intolerantes ao aacutecido acetilsaliciacutelico
paracetamol eou NSAIDrsquos que estivessem a tomar outro tipo de medicaccedilatildeo (excepto
contraceptivos) graacutevidas ou em periacuteodo de amamentaccedilatildeo problemas com drogas ou
aacutelcool Apenas pacientes que reportaram dor moderada a intensa apoacutes a cirurgia foram
incluiacutedos
Existiram quatro grupos de intervenccedilatildeo
Grupo A rofecoxib 50mg + paracetamol 1g dose uacutenica 155 plusmn 37 minutos apoacutes
cirurgia
Grupo B rofecoxib 50mg dose uacutenica 170 plusmn 45 minutos apoacutes cirurgia
Grupo C paracetamol 1g dose uacutenica 184 plusmn 53 minutos apoacutes cirurgia
Grupo D placebo dose uacutenica 161 plusmn 30 minutos apoacutes cirurgia
Os resultados prenderam-se com a intensidade da dor medida atraveacutes da escala
visual analoacutegica (VAS) de 30 em 30 minutos desde a ingestatildeo do faacutermaco durante 8
horas Atraveacutes destas avaliaccedilotildees da dor foi possiacutevel obter valores de
aliacutevio total da dor TOTPAR
soma da diferenccedila de intensidade da dor SPID nas primeiras trecircs horas
soma da diferenccedila de intensidade da dor SPID ateacute agraves 8 horas
Foram obtidos resultados referentes a uma avaliaccedilatildeo global do tratamento feita
4h e 8h apoacutes a toma do faacutermaco O uso de rescue medication foi tomado em conta bem
como o tempo ateacute agrave sua necessidade Foram ainda avaliados eventuais efeitos
secundaacuterios
29
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim A atribuiccedilatildeo de cada tratamento foi cega para todos os pacientes
investigadores e pessoal envolvido Foi levada a cabo a aleatorizaccedilatildeo pela empresa
farmacecircutica responsaacutevel pela produccedilatildeo das caacutepsulas administradas
Natildeo existindo entraves de teor eacutetico ou de disponibilidade de recursos um
ensaio cliacutenico aleatorizado eacute a escolha mais pertinente quando eacute necessaacuterio comparar
dois ou mais tipos de tratamento O facto de existir um grupo de controlo minimiza o
risco de vieacutes
3 Were participants appropriately allocated to intervention and control groups
A colocaccedilatildeo dos pacientes em cada um dos quarto grupos de tratamento foi
concretizada atraveacutes de tabelas de aleatorizaccedilatildeo
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim Sendo um ensaio cliacutenico duplamente cego tanto o staff investigadores e
pacientes estiveram cegos durante todo o estudo Todas as caacutepsulas eram idecircnticas
sendo que cada embalagem selada continha sempre 6 caacutepsulas Desta forma eacute possiacutevel
garantir que o paciente estaacute cego Sendo cada embalagem feita e selada pela empresa
farmacecircutica eacute igualmente possiacutevel inferir que os investigadores tambeacutem se
encontravam cegos Apenas o investigador principal acedeu aos coacutedigos para fazer os
caacutelculos finais
5 Were all of the participants who entered the trial accounted for at its
conclusion
Os grupos de intervenccedilatildeo foram atribuiacutedos de forma aleatoacuteria e cega os
resultados foram analisados de acordo com o grupo a que inicialmente tinham sido
associados
Inicialmente o desenho do estudo previa 120 participantes
Grupo A n = 40
Grupo B n = 40
Grupo C n = 20
30
Grupo D n = 20 (controlo)
No entanto no final do estudo foram apurados resultados de 107 indiviacuteduos Isto
deve-se a
Apoacutes a cirurgia alguns pacientes (n = 8) natildeo sentiram dor moderada a forte
no entanto quiseram mesmo assim participar sendo os seus resultados
subtraiacutedos aos caacutelculos
Alguns pacientes (n = 5) foram excluiacutedos sendo que um foi drop-out e os
restantes natildeo entregaram ou preencheram os questionaacuterios pedidos
No final a distribuiccedilatildeo de indiviacuteduos por grupos era a seguinte
Grupo A n = 34
Grupo B n = 36
Grupo C n = 20
Grupo D n = 17
Embora se verifique uma ligeira alteraccedilatildeo natildeo eacute motivo relevante de vieacutes
6 Were the participants in all groups followed up and data collected in the same
way
Sim Todos os pacientes tiveram acesso aos mesmos questionaacuterios entregues
pelo investigador Em caso de duacutevida ateacute ao final da duraccedilatildeo do estudo (8 horas) o
paciente podia telefonar ao investigador com quaisquer duacutevidas que surgissem Poreacutem
o paciente era responsaacutevel pelo iniacutecio do estudo ao administrar a si mesmo o faacutermaco
em casa no momento em que o fizesse devia telefonar ao investigador para este ter
conhecimento do iniacutecio do estudo Se o paciente natildeo contactasse o investigador ateacute 3
horas apoacutes a cirurgia o investigador contactaria o paciente Os valores maacuteximo e
miacutenimo de tempo entre a cirurgia e iniacutecio do estudo de foram 118 e 237 minutos a este
facto eacute inerente um risco de vieacutes pois nem todos os pacientes estavam na mesma
condiccedilatildeo quando iniciaram o tratamento podendo reflectir-se nos resultados
7 Did the study have enough participants to minimise the play of chance
Sim Os caacutelculos foram efectuados assumindo que existiria uma diferenccedila na
SPID entre grupos A e B de 20 Foram utilizados testes natildeo-parameacutetricos (Mann-
Whitney U-test) sendo definido que pelo menos 22 pacientes deveriam ser incluiacutedos em
cada um destes grupos
31
8 How are the results presented and what is the main result
Os caacutelculos estatiacutesticos necessaacuterios para a elaboraccedilatildeo dos resultados foram
efectuados no programa Statistical Package for Social Sciences (SPSS) v 12 As
significacircncias entre grupos de tratamento em relaccedilatildeo agraves respostas agrave VAS foram
testadas com t-test de variaacutevel independente em todas as avaliaccedilotildees de dor A mesma
estrateacutegia foi aplicada para a SPID agraves 3 e 8 horas A TOTPAR foi baseada na
assumpccedilatildeo que os resultados satildeo parte de uma escala de intervalos O mesmo teste foi
utilizado para a diferenccedila entre grupos relativamente ao uso de rescue medication Os
testes dos dados provenientes de escalas categoacutericas (PAR e a avaliaccedilatildeo global) foram
realizados atraveacutes de testes natildeo-parameacutetricos (Mann-Whitney U-test)
Intensidade da dor Os resultados favorecem o grupo A ateacute 15h apoacutes o iniacutecio do
tratamento A partir das 2h o grupo A natildeo tem uma eficaacutecia estatisticamente maior que
o grupo B Ambos os grupos tecircm melhores resultados globais que o grupo C O Grupo
D (placebo) eacute notoriamente menos eficaz que todos os outros grupos
Aliacutevio da dor (PAR) Os resultados meacutedios desta afericcedilatildeo satildeo semelhantes aos da
intensidade da dor
TOTPAR Natildeo houve uma diferenccedila significativa entre o grupo A e o grupo B
Ambos foram significativamente melhores que o C todos os grupos de tratamento
activo tiveram melhores resultados que o grupo D (placebo)
SPID Embora o grupo A mostre a maior SPID meacutedia (05 ndash 3h) natildeo foi
estatisticamente diferente do grupo B o grupo C tambeacutem natildeo foi estatisticamente
diferente do grupo B A SPID meacutedia total foi estatisticamente semelhante entre os
grupos A e B mas superior agrave do grupo C O grupo D (placebo) teve resultados
inferiores aos dos restantes grupos
Uso de rescue medication Embora tenha existido um nuacutemero notoriamente
superior de casos entre os grupos A e B comparativamente ao C e ao D esta diferenccedila
natildeo eacute relevante estatisticamente devido ao baixo nuacutemero de pacientes que recorreram a
esta medicaccedilatildeo
Avaliaccedilatildeo global tanto agraves 4 como agraves 8h os grupos A e B receberam avaliaccedilotildees
semelhantes tendo as melhores classificaccedilotildees e sendo significativamente superiores agraves
do grupo C Todos foram melhores que o D (placebo) Agraves 8h as percentagens de
pacientes que avaliaram o tratamento como bom ou excelente foram
Grupo A 90
32
Grupo B 83
Grupo C 42
9 How precise are these results
No artigo natildeo satildeo mencionados intervalos de confianccedila No entanto nos graacuteficos
referentes agrave intensidade da dor eacute possiacutevel ver as barras correspondentes ao intervalo de
confianccedila Existem sempre que necessaacuterio valores de p associados aos resultados
10 Were all important outcomes considered so the results can be applied
Sim A extracccedilatildeo de terceiros molares em Portugal eacute uma praacutetica cliacutenica comum
pelo que o estudo pode ser facilmente reproduzido desde que haja acesso agrave medicaccedilatildeo
utilizada e que esta esteja em formato idecircntico (para garantir que natildeo existe vieacutes)
Poreacutem o facto de ser utilizada uma dose uacutenica poderaacute natildeo ir de encontro com o padratildeo
actual sendo necessaacuteria uma sensibilizaccedilatildeo do paciente diferente para este meacutetodo
Um facto importante foi referido na discussatildeo deste artigo posteriormente agrave
recolha de dados do mesmo surgiram preocupaccedilotildees seacuterias sobre efeitos nocivos
cardiovasculares em tratamentos de longa duraccedilatildeo com rofecoxib embora estes efeito
secundaacuterios tendam a estar relacionados com as doses e natildeo apenas com a selectividade
COX-2 (8 25) Esta informaccedilatildeo eacute altamente relevante de todos os pontos de vista do
paciente e famiacutelia do profissional de sauacutede e oacutergatildeos legislativos
Tendo em conta este facto seriam necessaacuterios estudos adicionais para aferir o
risco de seguir um tratamento como o visado neste ensaio cliacutenico
33
Combined acetaminophen and ibuprofen for pain relief after oral
surgery in adults a randomized controlled trial (13)
1 Did the study ask a clearly-focused question
Sim Foram incluiacutedos pacientes sujeitos a extracccedilatildeo de pelo menos um terceiro
molar inferior Foram excluiacutedos pacientes com idade inferior a 16 anos peso inferior a
50 kg que tivessem tomado NSAIDrsquos (excepto aspirina a 150mg) ou paracetamol 24h
antes da cirurgia entre outros(inserir referencia para a pagina pois sao muitos)
Existiram 3 grupos de intervenccedilatildeo
Grupo A 500mg paracetamol + 150mg ibuprofeno
Grupo B 500mg paracetamol
Grupo C 150mg ibuprofeno
Todos os grupos de intervenccedilatildeo tomaram 2 comprimidos imediatamente antes da
cirurgia e depois 4 comprimidos diariamente (de 6 em 6 horas) durante 48h
Os resultados passaram pela intensidade da dor medida atraveacutes da VAS (mm)
em trecircs momentos distintos antes de tomar qualquer medicaccedilatildeo do estudo
imediatamente apoacutes a cirurgia e de 2 em 2 horas ateacute terminar o periacuteodo de 48 horas A
medida utilizada foi a area under the curve (AUC) dividida pelo tempo resultando em
AUCh Este caacutelculo foi efectuado para encontrar valores ldquomeacutediosrdquo pois houve ligeiras
diferenccedilas no momento da afericcedilatildeo dos valores da VAS Mediu-se tambeacutem o consumo
de rescue medication ao longo das 48 horas
Foram ainda utilizadas escalas categoacutericas de avaliaccedilatildeo global da dor e da
naacuteusea realizadas no final do estudo bem como uma escala VAS para medir os
distuacuterbios no sono apoacutes cada noite
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim A atribuiccedilatildeo de cada tratamento foi cega para todos os pacientes
investigadores e pessoal envolvido O responsaacutevel pela aleatorizaccedilatildeo do estudo foi o
estatiacutestico do estudo O estatiacutestico foi a uacutenica pessoa com acesso agraves informaccedilotildees da
atribuiccedilatildeo de tratamento aos pacientes
34
3 Were participants appropriately allocated to intervention and control groups
A colocaccedilatildeo de pacientes em cada um dos trecircs grupos de tratamento foi
aleatorizada A sequecircncia de aleatorizaccedilatildeo foi gerada por computador pelo estatiacutestico
do estudo Foi utilizada uma proporccedilatildeo de 111 para os trecircs grupos de tratamento isto
foi conseguido atraveacutes de permutaccedilatildeo de blocos com estratificaccedilatildeo para o tipo de
anestesia (local ou geral) e centro de estudo A utilizaccedilatildeo da aleatorizaccedilatildeo por
permutaccedilatildeo de blocos assegura uma distribuiccedilatildeo equilibrada por grupos de tratamento
quando o nuacutemero de indiviacuteduos eacute menor que mil (inserir referencia do artigo de
aleatorizajao MJA)
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim Este ensaio cliacutenico foi duplamente cego Como tal cada tipo de tratamento
consistia em comprimidos idecircnticos colocados num pacote selado as instruccedilotildees sobre
dosagens eram tambeacutem iguais garantindo que o estudo permanecia cego aos
investigadores staff e pacientes prevenindo a existecircncia de vieacuteses
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim O estudo previa um nuacutemero miacutenimo de 120 indiviacuteduos 40 em cada grupo
de tratamento Dos 135 pacientes que concordaram participar apoacutes serem abordados
pelo meacutedico apenas 122 foram incluiacutedos no estudo (os 13 que foram excluiacutedos natildeo
entregaram o diaacuterio de tratamento que lhes foi pedido)
Grupo A n = 40
Grupo B n = 43
Grupo C n = 39
Todos os 122 pacientes incluiacutedos foram seguidos ateacute ao final do estudo
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os pacientes foram abordados primariamente por um cirurgiatildeo e
seguidamente por uma enfermeira responsaacutevel pelo seguimento dos pacientes ao longo
do estudo O seguimento de cada paciente foi realizado de igual forma no hospital e fora
35
dele onde o contacto era estabelecido por telefone de forma a facilitar a recolha de
informaccedilatildeo levada a cabo por meio da entrega de diaacuterios
Em relaccedilatildeo agrave recolha dos dados relativos agrave dor poacutes-operatoacuteria experienciada os
intervalos de tempo utilizados foram semelhantes (imediatamente antes da
administraccedilatildeo da primeira dose logo apoacutes a cirurgia e de 2 em 2 horas durante um
periacuteodo de 48 horas) e a monitorizaccedilatildeo dos pacientes feita utilizando as mesmas
guidelines
7 Did the study have enough participants to minimise the play of chance
Sim Os investigadores do estudo realizaram a power calculation Estimaram
que eram necessaacuterios 120 participantes distribuiacutedos equitativamente pelos 3 grupos O
power foi de 80 na detecccedilatildeo de diferenccedilas entre os grupos de 9 mm (SD de 14mm)
para mediccedilotildees relativas agrave altura de repouso e os de 13mm (SD de 21mm) e para
mediccedilotildees relativas agrave altura de actividade
Dos 135 pacientes incluiacutedos no estudo 13 natildeo devolveram os seus diaacuterios pelo
que ficaram disponiacuteveis 122 participantes a enquadrar a populaccedilatildeo de tratamento (ITT
population) para anaacutelise dos criteacuterios de comparaccedilatildeo primaacuterios (primary endpoints)
Como o criteacuterio de possuir participantes necessaacuterios foi preenchido os
resultados da comparaccedilatildeo do objectivo primaacuterio deste estudo (mediccedilatildeo da intensidade
meacutedia de dor ao longo do estudo) tecircm uma elevada importacircncia cliacutenica Esta
importacircncia eacute equiparaacutevel aos resultados de estudos publicados anteriormente
8 How are the results presented and what is the main result
Os resultados foram apresentados sob a forma de mediccedilotildees nomeadamente as
principais diferenccedilas (mean differences) entre o paracetamolacetaminofeno ibuprofeno
e combinaccedilatildeo dos dois comparando a eficaacutecia farmacocineacutetica e efeitos secundaacuterios
respectivos a cada um Agraves quais estaacute associada uma taxa de erro de 5 (SEM) ou seja
intervalo de confianccedila de 95 (CI) e um valor de P lt001
Foi realizada a mediccedilatildeo da time-adjusted AUC (AUCh) da VAS que
juntamente com a classificaccedilatildeo global de dor revelou-se substancial e
significativamente menor no grupo que utilizou a combinaccedilatildeo do que nos outros dois
grupos (tanto no periacuteodo de repouso como no periacuteodo de actividade)
Apesar de alguns criteacuterios de comparaccedilatildeo secundaacuterios (secondary endpoints) o
uso de medicaccedilatildeo de resgate apoiarem o uso da combinaccedilatildeo do faacutermaco natildeo possuem
36
relevacircncia estatiacutestica Aleacutem disso o tipo de anestesia utilizada na cirurgia e o nordm de
dentes extraiacutedos os paracircmetros farmacocineacuteticos e a ocorrecircncia dos efeitos secundaacuterios
natildeo mostraram diferenccedilas significativas entre os 3 grupos de estudo
Os pacientes medicados com a combinaccedilatildeo de paracetamol e ibuprofeno
experienciaram menos dor poacutes-operatoacuteria durante as 48 horas que os pacientes que
usaram os medicamentos isolados
9 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em conta que foi preacute-
definido um valor para P de 005 de forma determinar se os valores obtidos possuem
relevacircncia estatiacutestica ou natildeo os resultados satildeo precisos
Isto mostra que para que a combinaccedilatildeo dos dois medicamentos possa ser
considerada sem incerteza mais adequada que outros meacutetodos de medicaccedilatildeo seriam
necessaacuterios resultados expliacutecitos e com elevada relevacircncia estatiacutestica
10 Were all important outcomes considered so the results can be applied
Sim O estudo realizado tal como acontece em todos os outros apresenta os
seus pontos fortes e fracos No entanto a pluralidade de criteacuterios utilizados na
comparaccedilatildeo dos vaacuterios grupos de estudo permitiu uma boa percepccedilatildeo da relaccedilatildeo
custobenefiacutecio aqui presente Apesar de certos paracircmetros como a utilizaccedilatildeo de
placebo recrutamento de crianccedilas e avaliaccedilatildeo significativa dos efeitos secundaacuterios natildeo
terem sido explorados estes natildeo apresentam grande peso no que respeita agrave validaccedilatildeo dos
resultados em si Isto acontece pois a bibliografia existente e a praacutetica cliacutenica jaacute nos
permitem deduzir e extrapolar conclusotildees em relaccedilatildeo agravequeles paracircmetros
Deste modo a questatildeo-chave recai sobre o facto de a combinaccedilatildeo de
paracetamol com ibuprofeno ser mais vantajosa e eficaz que a toma de apenas um deles
Caso estes resultados sejam confirmados por estudos de outras entidades a jaacute muito
utilizada combinaccedilatildeo paracetamol+ibuprofeno poderaacute mesmo tornar-se procedimento
padratildeo na terapecircutica da dor aguda moderada (em pacientes sem contra-indicaccedilatildeo para
NSAIDrsquos)
37
Analgesic efficacy of lysine clonixinate paracetamol and
dipyrone in lower third molar extraction a randomized
controlled trial (32)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo em estudo comporta 90 pacientes entre os 18 e 26 anos de
idade com uma indicaccedilatildeo cliacutenica para extracccedilatildeo de um 3ordm molar inferior impactado
(com classe I e II)
A intervenccedilatildeo consistiu no tratamento da dor apoacutes extracccedilatildeo do 3ordm molar atraveacutes
da medicaccedilatildeo com um dos 3 analgeacutesicos em estudo utilizando 8 comprimidos do
respectivo analgeacutesico a serem tomados 1 hora preacute-cirurgia e a cada 6 horas poacutes-cirurgia
durante um periacuteodo de 24 horas
Os resultados foram obtidos atraveacutes da mediccedilatildeo da intensidade da dor utilizando
a escala visual analoacutegica (VAS) mesmo antes da cirurgia e seguidamente 1 2 4 6 8
12 e 24 horas apoacutes a cirurgia Aleacutem disso para cada uma destas mediccedilotildees os pacientes
tinham de relatar o niacutevel de dor em que se encontravam (percepccedilatildeo da dor) atraveacutes de
uma escala decimal com os seguintes criteacuterios
0 cm Sem dor
01- 3 cm Dor ligeira
31-7 cm Dor moderada
71-10 cm Dor intensa
A presenccedila ou ausecircncia de efeitos secundaacuterios foi tambeacutem uma das
preocupaccedilotildees deste estudo e algo avaliado nos resultados Dado que havia a
possibilidade de ocorrecircncia de agranulocitose anemia anafilaxia e complicaccedilotildees
gastrointestinais
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo em questatildeo consiste num ensaio cliacutenico aleatorizado Esta
abordagem foi a mais adequada para a questatildeo colocada uma vez que o objectivo final
eacute comparar a eficaacutecia da lisina clonixinato com o paracetamol e com a dipirona na
analgesia da dor poacutes-operatoacuteria Para obter informaccedilotildees mais completas respeitantes agrave
seguranccedila e eficaacutecia dos faacutermacos comparados eacute necessaacuterio o recrutamento e
aleatorizaccedilatildeo de um determinado nuacutemero de pacientes Eacute necessaacuterio tambeacutem medicaacute-
38
los medir e avaliar os resultados de forma imparcial e objectiva Desta forma eacute mais
provaacutevel chegar a uma conclusatildeo fidedigna e vaacutelida tanto interna como externamente
Pelas razotildees acima enumeradas a realizaccedilatildeo de um ensaio cliacutenico aleatorizado
foi a melhor abordagem a seguir
3 Were participants appropriately allocated to intervention and control groups
Sim Os pacientes foram divididos pelos diferentes grupos de estudo de uma
forma aleatoacuteria utilizando um meacutetodo relativamente simples Os analgeacutesicos foram
repartidos em recipientes brancos opacos e idecircnticos numerados de 1 a 90 Cada
recipiente continha 8 comprimidos de um dos 3 faacutermacos em comparaccedilatildeo (dipirona
500mg paracetamol 750mg lisina clonixinato 125 mg) Por sua vez foi pedido aos
pacientes para retirarem o recipiente agrave sua escolha e ao acaso os quais desconheciam o
seu conteuacutedo
Dos 90 pacientes recrutados de iniacutecio 26 desistiram pelo que os restantes 64
pacientes foram distribuiacutedos por 3 grupos correspondentes a diferentes analgeacutesicos
orais lisina clonixinato composto por 20 indiviacuteduos (8 masculinos 12 femininos)
Paracetamol composto por 23 indiviacuteduos (9M 14F) Dipirona composto por 21
indiviacuteduos (6M 15F)
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Natildeo eacute possiacutevel dizer Os pacientes deste estudo estavam lsquocegosrsquo quanto ao grupo
de estudo em que iriam ser colocados O processo de distribuiccedilatildeo dos indiviacuteduos foi
feito de uma forma aleatoacuteria atraveacutes de um meacutetodo bastante simples de escolha de
recipiente
Quanto aos funcionaacuterios e revisores deste estudo o mesmo pode natildeo ter
acontecido pois nenhuma informaccedilatildeo sobre este aspecto eacute mencionada no artigo
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim No estudo realizado os participantes foram distribuiacutedos por 3 grupos um
de estudo ou intervenccedilatildeo onde foi administrado lisina clonixinato e dois de controlo
onde se administrou paracetamol num e dipirona noutro Natildeo houve redistribuiccedilatildeo dos
39
participantes isto eacute cada participante foi tratado uacutenica e exclusivamente com o faacutermaco
correspondente ao seu grupo
Houve um seguimento dos pacientes durante um periacuteodo de 24 horas de modo a
avaliar a eficaacutecia de cada analgeacutesico na eliminaccedilatildeo da dor poacutes-operatoacuteria de forma
indirecta (quanto maior o aliacutevio de dor ao longo do periacuteodo de estudo maior a eficaacutecia
do respectivo analgeacutesico) Tendo isso em conta os resultados e anaacutelise dos dados foram
realizados em cada grupo e depois comparados com os outros grupos
Os investigadores do estudo poderiam ter formado um grupo placebo e
comparado os seus resultados com os restantes grupos Assim averiguar-se-ia a eficaacutecia
de cada um dos analgeacutesicos e natildeo apenas a eficaacutecia relativa a outros faacutermacos
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os participantes dos diferentes grupos foram seguidos da mesma maneira e
os dados recolhidos de igual forma Os resultados foram avaliados nos mesmos
intervalos de tempo ou seja antes da cirurgia e 1 2 4 6 8 12 e 24 horas apoacutes a
mesma Os pacientes receberam o mesmo tempo de atenccedilatildeo - 24 horas de seguimento e
os dados foram recolhidos utilizando os mesmos paracircmetros a escala visual analoacutegica
para determinar o aliacutevio de dor e a escala decimal para a percepccedilatildeo de dor dos pacientes
e questionaacuterios individuais
Para aleacutem do jaacute referido os investigadores tiveram em atenccedilatildeo a forma como a
cirurgia foi realizada diminuindo o risco de vieacutes
Intervieram 2 cirurgiotildees calibrados entre si na niacutevel da teacutecnica minimizando a
ocorrecircncia de abordagens ciruacutergicas diferentes
o periacuteodo de duraccedilatildeo foi controlado e por isso natildeo influenciou o comportamento
da dor no estudo (meacutedia de 339 minutos com SD plusmn98 min)
Estas cirurgias satildeo bastantes conhecidas e muitas vezes satildeo procedimentos
standard permitindo uma selecccedilatildeo muito mais facilitada e raacutepida de casos cliacutenicos a
incluir no estudo e diminuindo o nuacutemero de eventos de difiacutecil controlo que poderiam
levar a vieacutes dos resultados
7 Did the study have enough participants to minimise the play of chance
Natildeo eacute possiacutevel dizer Dos 90 pacientes inicialmente recrutados para o estudo 26
deles desistiram Os investigadores natildeo referiram o impacto deste nuacutemero de drop-outs
40
na extrapolaccedilatildeo de conclusotildees a partir dos resultados obtidos Igualmente natildeo foram
mencionados quaisquer caacutelculos que determinassem o nuacutemero necessaacuterio de indiviacuteduos
para o estudo ter validade
8 How are the results presented and what is the main result
Os resultados obtidos no estudo foram categorizados por droga e analisados de
acordo com o desenvolvimento da dor poacutes-operatoacuteria Seguidamente foram
apresentados atraveacutes de mediccedilotildees descritivas da variaccedilatildeo da dor as quais utilizaram
paracircmetros como miacutenimo maacuteximo mean median e desvio-padratildeo (SD)
Por sua vez a anaacutelise dos dados foi feita com os testes de Kruskal-Wallis e de
Friedman onde os resultados satildeo considerados estatisticamente relevantes se
culminarem num valor de lsquoprsquo igual ou inferior a 005 (95 IC) e apresentada utilizando
os mesmos paracircmetros de miacutenimo maacuteximo e SD
O valor de P encontra-se claramente acima do valor de referencia preacute-definido
pelo que os resultados natildeo apresentam relevacircncia estatiacutestica suficiente para aferir que
possuem um melhor outcome que o paracetamol
A lisina clonixinato assim como a dipirona e o paracetamol eacute eficiente no
controlo da dor resultante da extracccedilatildeo de um 3ordmmolar inferior pelo que natildeo apresenta
nenhuma diferenccedila significativa dos outros analgeacutesicos mencionados
9 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em conta que os valores de
P obtidos apoacutes anaacutelise dos resultados se encontrarem abaixo de 001 eacute possiacutevel auferir
que os resultados deste estudo satildeo bastante precisos
10 Were all important outcomes considered so the results can be applied
Natildeo Os efeitos gerados pela lisina clonoxinato no tratamento da dor derivada de
extracccedilatildeo do 3ordm molar natildeo foram estatisticamente relevantes quando comparados aos do
paracetamol e dipiridona Apesar de as condiccedilotildees pelas quais o estudo foi realizado
serem reprodutiacuteveis na nossa populaccedilatildeo local (tipo de pessoas localizaccedilatildeo e
reprodutibilidade do tratamento) nada eacute referido em relaccedilatildeo a novas poliacuteticas de sauacutede
nomeadamente na implementaccedilatildeo de uma dose uacutenica culminando numa mudanccedila dos
haacutebitos de sauacutede da comunidade Tambeacutem natildeo foram abordados aspectos econoacutemicos
41
tal como um balanccedilo entre benefiacutecios e encargos de sauacutede que justifique a utilizaccedilatildeo
deste faacutermaco como tratamento preferencial
42
Onset of analgesia with sodium ibuprofen ibuprofen acidin
corporating poloxamer and acetaminophenmdasha single-dose
double-blind placebo-controlled study in patients with post-
operative dental pain Daniels Reader (33)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo em estudo refere-se a pacientes com idade entre os 16 e os 40
anos apresentando uma intensidade de dor basal poacutes-operatoacuteria moderada a severa O
diagnoacutestico para a extracccedilatildeo poderia ser um dos seguintes pelo menos um 3ordm molar
mandibular indicado para remoccedilatildeo (grau de impactaccedilatildeo superior a 4) ou dois terceiros
molares ipsilaretais com pontuaccedilatildeo de impactaccedilatildeo conjunta natildeo superir a 6
A intervenccedilatildeo traduz-se no tratamento da dor poacutes-ciruacutergica com doses uacutenicas de
diferentes faacutermacos Inicialmente cada participante tem a mesma probabilidade de ser
colocado num dos 4 grupos
A ibuprofeno de soacutedio 2x256 mg (ibuprofeno de soacutedio di-hidratado equivalente a
400 mg de ibuprofeno aacutecido + placebos de ibuprofeno poloxamo e
acetaminofeno
B ibuprofenopoloxacircmero (400mg de Ibuprofeno e 120mg de poloxacircmero
surfactante 407) + placebos de ibuprofeno de soacutedio e paracetamol
C 1000mg acetaminofeno + placebos equivalentes
D placebo para as 3 formas de substacircncias activas
O endpoint primaacuterio consistiu no tempo necessaacuterio para um aliacutevio da dor
perceptiacutevel pelos pacientes Foram considerados inuacutemeros endpoints secundaacuterios (foi
utilizada uma escala categoacuterica e VAS para os endpoints 2 3 e 4)
1 Caacutelculo da AUC e SPRID (0 a 6 horas poacutes-tratamento) e tempo necessaacuterio para
um aliacutevio significativo da dor
2 Aliacutevio total da dor (TOTPAR) SPID e SPRID
3 Aliacutevio da dor e intensidade da mesma em termos individuais (5 minutos - 6
horas)
4 PID ao longo do periacuteodo de estudo e o momento em que este foigt ou igual a 1
5 Instante em que os pacientes recorreram a medicaccedilatildeo de recurso
6 Tempo e proporccedilatildeo de pacientes que sentiram 50 aliacutevio da dor
43
7 Abstracccedilatildeo agrave dor (1 e 6 horas) e percepccedilatildeo da interferecircncia causada pela dor nas
actividades quotidianas (escala de Ranvier)
8 Avaliaccedilatildeo qualitativa da medicaccedilatildeo tomada pelos dos participantes
Os efeitos adversos foram obtidos atraveacutes da procura de informaccedilatildeo em
documentaccedilatildeo e relacionados (ou natildeo) com a medicaccedilatildeo do estudo pelo investigador
Foi efectuada uma mediccedilatildeo de sinais vitais 6 horas apoacutes a toma e na visita follow-up na
qual tambeacutem foi realizado um exame fiacutesico
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo em questatildeo eacute descrito como um ensaio cliacutenico duplamente cego e
controlado com placebo Eacute o tipo de estudo indicado para comparar diferentes formas de
tratamento atraveacutes da divisatildeo dos pacientes por grupos Eacute necessaacuterio ter em
consideraccedilatildeo o aspecto eacutetico de tais tratamentos pois ldquoexposing patients to an
intervention believed to be inferior to current treatment is often thought unethicalrdquo (41)
Para garantir a eacutetica dos tratamentos incluiacutedos o estudo foi conduzido de acordo com a
Declaraccedilatildeo de Helsiacutenquia como referido na Directiva da EU de 200120EC e
concordante com a Conferecircncia Internacional de Harmonizaccedilatildeo (ICH) e a GCP (boa
praacutetica cliacutenica)
3 Were participants appropriately allocated to intervention and control groups
Sim Os indiviacuteduos foram divididos aleatoriamente para serem inseridos num
dos 4 grupos de tratamento numa proporccedilatildeo 1111 O meacutetodo de aleatorizaccedilatildeo foi
gerado pelo computador atraveacutes de um randomization Schedule
Para equilibrar a alocaccedilatildeo dos pacientes realizou-se uma estratificaccedilatildeo por sexo
e por intensidade da dor basal O protocolo do estudo foi revisto e aprovado pela
Quorum Review Inc o que leva a querer que a subdivisatildeo foi realmente rigorosa
Os grupos encontram-se equilibrados tanto em nuacutemero como noutras variaacuteveis
particularmente geacutenero intensidade dor basal e idade Deste modo diferenccedilas
reportadas nos resultados natildeo satildeo consequecircncia da heterogeneidade dentro dos grupos
de tratamento
44
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
A aleatorizaccedilatildeo dos participantes foi gerada pelo computador O protocolo do
estudo foi posteriormente revisto como anteriormente referido Agrave partida tanto o
investigador e pacientes natildeo interferiram no processo
Foram usados comprimidos para o ibuprofeno de soacutedio ibuprofenopoloxamero
e caacutepsulas para o paracetamol tanto para as formas activas como placebo
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim Os 322 participantes incluiacutedos de 614 inicialmente recrutados 318
completaram o estudo e 321 foram incluiacutedos na populaccedilatildeo ITT (intended do treat)
No grupo ibuprofeno de soacutedio todos os 80 participantes concluiacuteram a anaacutelise
No grupo B dos 80 inicialmente alocados 76 completaram a anaacutelise Um foi
excluiacutedo perdeu-se o follow-up de outro e os restantes natildeo concluiacuteram por
outros motivos
Dos 81 do grupo do paracetamol um natildeo foi incluiacutedo no ITT (falhou em
providenciar os dados da intensidade da dor basal diaacuteria)
No grupo placebo todos os pacientes concluiacuteram o estudo
Os resultados de cada paciente foram analisados agrave luz do grupo de tratamento
em que estes foram colocados
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os participantes permaneceram nos centros de investigaccedilatildeo cliacutenica apoacutes a
toma durante 8-15h Durante as 6 horas apoacutes o tratamento a eficaacutecia foi medida em
intervalos preacute-determinados Para avaliar a existecircncia de efeitos secundaacuterios foi
realizada uma mediccedilatildeo de sinais vitais conduzido um follow-up poacutes-operativo (5 a 12
dias poacutes-cirurgia) e repetida a avaliaccedilatildeo de efeitos adversos Pode-se considerar anaacutelogo
o acompanhamento entre os vaacuterios pacientes poacutes-cirurgia e medicaccedilatildeo pois constituiu
um seguimento proacuteximo maioritariamente presencial e rigoroso
45
7 Did the study have enough participants to minimise the play of chance
Foram usados dados de estudos preacutevios os quais continham informaccedilatildeo acerca
de AUC e PRID Com estes dados foi determinado que um nuacutemero de 80 pacientes por
grupo providenciaria um power de 90 em detectar diferenccedilas entre os grupos de
tratamento com um niacutevel de significacircncia de 0025 Natildeo foi possiacutevel calcular um power
ldquoformalrdquo para o aliacutevio de dor significativo No entanto a resposta eacute afirmativa para a
questatildeo CASP uma vez que foram realizados esforccedilos para que o nuacutemero das amostras
fosse significativo e correcto
8 How are the results presented and what is the main result
Os resultados satildeo apresentados em termos de percentagens e diferenccedilas meacutedias
(mean differences) alguns com recurso a curvas de Kaplan-Meier (survival curves) Os
efeitos secundaacuterios satildeo apresentados sob a forma de tabela com a percentagem de
pacientes dentro de cada grupo que sofreram os efeitos descritos na mesma
Os grupos A e B exibem resultados substancialmente melhores no que diz
respeito aos seguintes pontos
AUC e SPID satildeo significativamente menores A com 963 e B com 90 face a
C com 675 e D com 25 O tempo para atingir aliacutevio da dor
SPRID Esta eacute semelhante entre os grupos A B e C ateacute aos 45 minutos A partir
deste periacuteodo o ibuprofeno possui uma eficaacutecia superior ao paracetamol
Abstracccedilatildeo agrave dor e percepccedilatildeo da interferecircncia causada pela dor nas actividades
quotidianas (escala de Ranvier)
Utilizaccedilatildeo da medicaccedilatildeo de recurso A com 325 e B com 225 face a C com
438 e D em que a maioria dos pacientes usou a mesma
Avaliaccedilatildeo dos medicamentos por parte dos pacientes (resposta ldquoboardquo ldquomuito
boardquo ou ldquoexcelenterdquo)
No que se refere aos efeitos secundaacuterios 118 da populaccedilatildeo do estudo sofreu
mais efeitos sendo que a maior percentagem ocorreu no grupo do C
Quando comparado com acetaminofeno o ibuprofeno de soacutedio e
Ibuprofenopoloxamero possui uma eficaacutecia analgeacutesica significativamente superior
46
9 How precise are these results
Nos endpoints primaacuterios as diferenccedilas entre as duas formulaccedilotildees de ibuprofeno e
paracetamol foram avaliadas tendo por base o teste de Wilcoxon rank-sum O hazard
ratio e respectivo IC de 975 foram calculados para as comparaccedilotildees entre os
compostos Os endpoints secundaacuterios que agregavam vaacuterios periacuteodos de tempo foram
calculados atraveacutes da AUC Diferenccedilas entre tratamentos foram avaliadas utilizando
valores de α de 005 o intervalo de confianccedila de 95 (CI) foi calculado por meio dos
paracircmetros do modelo adequado
Eacute introduzido o valor de P que na sua generalidade possui valores reduzidos e
menores que 0005 Considerando a homogeneidade dos grupos o caacutelculo do nuacutemero da
amostra com elevado power e os valores de P podemos concluir que no contexto os
resultados satildeo precisos (42)
10 Were all important outcomes considered so the results can be applied
Eacute plausiacutevel que a populaccedilatildeo utilizada no estudo fosse semelhante num estudo
anaacutelogo Tanto o local como o proacuteprio tratamento poderiam ser reproduzidos visto que
os compostos em questatildeo satildeo largamente comercializados
Os resultados satildeo importantes para uma escolha mais consciente por parte dos
indiviacuteduos entre tomar paracetamol ou ibuprofeno apoacutes uma cirurgia de um 3ordm molar Eacute
afirmado na discussatildeo deste estudo que o ibuprofeno possui menores efeitos adversos
gastrointestinais que outros NSAIDrsquos Tendo isso em conta pode conduzir a uma
escolha deste composto no tratamento da dor poacutes ciruacutergica por parte dos profissionais
ldquothese findings support a recommendation for this agent as an analgesic of choice for
the treatment of post-operative dental painrdquo A preocupaccedilatildeo pela comunidade em geral
estaacute impliacutecita neste aspecto se possuir menores efeitos secundaacuterios e benefiacutecio superior
eacute melhor para a populaccedilatildeo em geral O custo financeiro destes medicamentos natildeo se
traduz num ponto diferenciador visto que em Portugal existem geneacutericos de ambos
Eacute uma boa base de comparaccedilatildeo entre o paracetamol e ibuprofeno em muitos
aspectos Na procura da melhor evidecircncia e no sentido de a aplicar eacute importante
completar este estudo com outros que nomeadamente se foquem nos efeitos
secundaacuterios
47
An investigation into the comparative efficacy of soluble aspirin
and solid paracetamol in postoperative pain after third molar
surgery Seymour Hawkesford (22)
1 Did the study ask a clearly-focused question
Sim O estudo em questatildeo trata-se de um ensaio cliacutenico aleatorizado duplamente
cego e controlado por placebo O seu objectivo central eacute comparar a eficaacutecia da aspirina
soluacutevel agrave do paracetamol soacutelido em pacientes com dor poacutes-operatoacuteria apoacutes extracccedilatildeo do
3ordm molar Foi utilizado um grupo placebo como controlo negativo
Soacute foram incluiacutedos pacientes que necessitavam da extracccedilatildeo do 3ordm molar
saudaacuteveis segundo categoria 1 da American Society of Anaesthesiologists (ASA I) ou agrave
discriccedilatildeo do cirurgiatildeo oral categoria 2 Soacute foram abrangidos pacientes que atingiram o
limiar de dor necessaacuterio ou que requeriram analgeacutesicos ateacute 90 minutos apoacutes a cirurgia
Cada paciente incluiacutedo no estudo foi colocado num dos trecircs grupos de
tratamento
Grupo 1 Aspirina soluacutevel 900mg dose uacutenica
Grupo 2 paracetamol soacutelido 1000mg dose uacutenica
Grupo 3 placebo dose uacutenica
Foi utilizado o meacutetodo de double-dummy ndash assim cada grupo recebeu o seu tipo
de tratamento e um placebo do tratamento alternativo No caso do grupo 3 os pacientes
receberam placebos para os dois tipos de tratamento
Os outcomes passaram pela
Comparaccedilatildeo de medidas de intensidade da dor atraveacutes da escala VAS (mm)
entre os grupos de tratamento aos 10 15 20 e 30 minutos apoacutes a dosagem
inicial
Comparaccedilatildeo da AUC240 com recurso a anaacutelise de co-variacircncia usando o
centro do estudo geacutenero baseline pain intensity duraccedilatildeo da cirurgia e
nuacutemero de molares removidos como co-variaacuteveis
Necessidade de recurso a rescue medication
Impressatildeo geral dos pacientes e enfermeiros sobre a medicaccedilatildeo atraveacutes de
uma regressatildeo binomial logiacutestica (em que um resultado positivo se refere a
uma avaliaccedilatildeo ldquomuito boardquo ou ldquoboardquo)
As comparaccedilotildees feitas foram aspirina vs paracetamol e aspirina vs placebo
48
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo apresentado eacute um RCT por vaacuterias razotildees sendo a mais relevante a
aleatorizaccedilatildeo dos grupos de tratamento em que os pacientes incluiacutedos foram
distribuiacutedos com a mesma probabilidade e aleatoriamente para cada grupo de estudo Os
grupos de tratamento tecircm tamanhos semelhantes e satildeo homogeacuteneos e os pacientes
foram seguidos de forma semelhante - as uacutenicas diferenccedilas residem no tratamento
oferecido
A utilizaccedilatildeo deste tipo de estudo foi loacutegica Um ensaio cliacutenico aleatorizado eacute
ideal para comparar efeitos de determinadas intervenccedilotildees e consequentemente ideal
para comparar eficaacutecia entre medicamentos
3 Were participants appropriately allocated to intervention and control groups
Foi realizada uma alocaccedilatildeo aleatoacuteria dos pacientes incluiacutedos assim como uma
aleatorizaccedilatildeo por blocos de cinco para assegurar equiliacutebrio entre grupos de tratamento
ldquoA key advantage of blocked randomization is that treatment groups will be equal in
size and will tend to be uniformly distributed by key outcome-related characteristicsrdquo
(43)
Foi ainda efectuada uma aleatorizaccedilatildeo estratificada por geacutenero de modo a
equilibrar nos trecircs grupos o nuacutemero de mulheres e homens e aumentar a credibilidade
das comparaccedilotildees entre os mesmos (proporccedilatildeo MF 21)
Tabela 2 ndash Dados demograacuteficos dos pacientes do estudo
Variaacutevel Aspirina soluacutevel
900mg
Paracetamol soacutelido
1000 mg
Placebo
Nuacutemero de pacientes 59 62 32
Raacutecio geacutenero MF 1940 1943 1121
Todos os pacientes incluiacutedos receberam anestesia de acordo com a praacutetica
cliacutenica a extracccedilatildeo dos molares impactados foi realizada seguindo a teacutecnica standard
Estes factores contribuem para a semelhanccedila da forma de tratamento dos 3 grupos Com
estes aspectos em comum a todos os pacientes incluiacutedos em adiccedilatildeo agrave homogeneidade
dos grupos nos seus aspectos demograacuteficos diferenccedilas encontradas nos resultados satildeo
consequecircncias de outros factores
49
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim A administraccedilatildeo uacutenica tem a vantagem de natildeo requerer monitorizaccedilatildeo de
um processo ldquodelicadordquo por parte do paciente De facto todo o estudo eacute realizado num
periacuteodo de 4 horas apoacutes a cirurgia e com ajuda de enfermeiros Olhando do ponto de
vista do paciente pode-se consideraacute-lo cego
Se os meacutetodos foram realmente aleatoacuterios o investigador eacute tambeacutem considerado
cego e pode-se afirmar que foram feitos esforccedilos necessaacuterios para o alcanccedilar Tanto a
aspirina soluacutevel como o placebo foram oferecidos sob a forma de uma bebida cor-de-
laranja o paracetamol com substacircncia activa e placebo oferecidos como comprimidos
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim Inicialmente todos os pacientes tinham a mesma probabilidade de serem
incluiacutedos num dos trecircs grupos A distribuiccedilatildeo sendo aleatoacuteria natildeo soacute coloca um
paciente num determinado grupo de tratamento como impossibilita que o mesmo venha
a pertencer a outro O seguimento foi realizado de igual forma para todos os grupos e
intimamente controlado Os resultados foram apresentados separadamente para cada
grupo Dos 167 pacientes foram medicados 153 Dos 14 pacientes natildeo tratados 10 natildeo
desenvolveram dor suficiente para serem incluiacutedos 1 obteve uma reacccedilatildeo adversa agrave
anestesia e 1 natildeo seguiu o protocolo
O grupo da aspirina soluacutevel apresentou melhores resultados que o grupo do
paracetamol e do placebo na medida em que os pacientes reportaram menos dor
apresentou menor intensidade de dor (aos 10 e 30 minutes em comparaccedilatildeo ao
paracetamol e apenas 30 minutos face ao placebo) e os valores de dor global medidos
pela AUC240 foram significativamente menores
6 Were the participants in all groups followed up and data collected in the same
way
Sim A intensidade da dor foi medida frequentemente ao longo de 4 horas
(segundo a VAS) e os pacientes foram informados da possibilidade de tomar medicaccedilatildeo
adicional se necessaacuterio A avaliaccedilatildeo sobre o tratamento dos enfermeiros e dos proacuteprios
pacientes foi tida em consideraccedilatildeo para os resultados
50
Aleacutem disso ao longo do periacuteodo de investigaccedilatildeo a enfermeira do estudo ficou
responsaacutevel por monitorizar os pacientes e registar a ocorrecircncia de quaisquer eventos
adversos Deste modo eacute muito provaacutevel que todos os pacientes tenham recebido o
mesmo niacutevel de atenccedilatildeo
7 Did the study have enough participants to minimise the play of chance
Natildeo eacute possiacutevel dizer No estudo natildeo eacute referida a utilizaccedilatildeo de power calculations
ou outros meacutetodos para determinar o tamanho da amostra Apenas se pode concluir que
o grupo de controlo negativo tem um menor nuacutemero de pacientes consequecircncia de
desistecircncias ou pelo simples facto de agrave partida se conhecerem os resultados
8 How are the results presented and what is the main result
A intensidade da dor foi medida numa escala VAS aos 10 15 20 e 30 minutos
apoacutes a administraccedilatildeo Foi possiacutevel tirar vaacuterias conclusotildees a partir da observaccedilatildeo dos
resultados
A aspirina demonstrou ser significativamente mais eficaz que o paracetamol ou
placebo embora ateacute aos 15 minutos natildeo seja uma diferenccedila muito expressiva
Relativamente agrave AUC240 experiecircncia global da dor no periacuteodo de 4 horas da
investigaccedilatildeo esta foi significativamente menor para o grupo 1
Natildeo existiu diferenccedila significativa entre os grupos no que diz respeito agrave rescue
medication utilizada No entanto o tempo para a administraccedilatildeo da mesma foi
superior no grupo 1 e 2 em relaccedilatildeo ao grupo placebo
Em relaccedilatildeo agrave impressatildeo global natildeo haacute discrepacircncias consideraacuteveis entre grupo 1
e 2 no que diz respeito agrave percentagem de outcomes positivos (58 e 53
respectivamente) O grupo 3 apresentou apenas 31 de outcomes positivos
A tabela com a percentagem de pacientes que desenvolveram efeitos adversos
para cada grupo mostra que 41 dos pacientes apresentaram efeitos secundaacuterios
nos grupos com tratamento activo no entanto muitos destes estavam
relacionados com o procedimento ciruacutergico
A aspirina soluacutevel 900mg providencia uma analgesia mais significante e raacutepida
que o paracetamol 1000mg no periacuteodo imediato apoacutes a cirurgia do 3ordm molar embora natildeo
seja muito expressiva a percepccedilatildeo desta diferenccedila por parte dos pacientes e enfermeiros
51
9 How precise are these results
Os resultados satildeo precisos e apresentados atraveacutes de um intervalo de confianccedila
de 95 satildeo tambeacutem apresentados valores de p
Os valores de p satildeo menores que 005 excepto aos 10 e 15 minutos
Para a intensidade da dor ao longo dos 30 minutos e AUC240 da comparaccedilatildeo
aspirina vs placebo a intervenccedilatildeo utilizada seria a mesma tanto no limite superior
como no inferior excepto aos 10 e 15 minutos Na comparaccedilatildeo aspirina soluacutevel vs
paracetamol soacutelido a decisatildeo seria a mesma independentemente dos limites do intervalo
apenas para os minutos 10 20 e 30
O mesmo aconteceria para a medicaccedilatildeo de recurso (outcome C) e a avaliaccedilatildeo do
tratamento por parte dos pacientes e enfermeiros (outcome D)
Pelo intervalo de confianccedila estar presente e pelo facto de os valores de p serem
bastante reduzidos os resultados satildeo precisos ao ponto de ajudarem a suportar uma
decisatildeo
10 Were all important outcomes considered so the results can be applied
Sim Os pacientes incluiacutedos no estudo o local e o tratamento visados no mesmo
poderiam ser extrapulados e aplicados noutro ambiente O seguimento dos pacientes
durante 4 horas e com ajuda de enfermeiros natildeo se apresenta como muito viaacutevel mas
ainda assim eacute exequiacutevel e seguro
O estudo avalia dados importantes para os profissionais de sauacutede ao afirmar que
a dose (900mg) e a forma (soluacutevel) em que a aspirina eacute tomada conduz a um poder
analgeacutesico superior que o paracetamol No entanto em termos individuais e de poliacuteticas
de sauacutede os efeitos secundaacuterios consequentes da medicaccedilatildeo (excluindo os que se
relacionassem com a cirurgia) deveriam ser completados com estudos suplementares
Segundo este ensaio cliacutenico a incidecircncia de efeitos secundaacuterios natildeo eacute muito
dissemelhante entre aspirina soluacutevel e paracetamol soacutelido nas doses maacuteximas
recomendadas e nestas circunstacircncias a aspirina tem maior poder analgeacutesico Por este
prisma a praacutetica cliacutenica poderia passar pela prescriccedilatildeo de aspirina soluacutevel 900mg para
aliacutevio dor poacutes-operatoacuteria da extracccedilatildeo do terceiro molar Poreacutem eacute necessaacuterio ter em
conta que visa somente a dor nas primeiras quatro horas poacutes-operatoacuterias sendo
importante investigar alternativas eficazes que sejam mais duradouras ou a eficaacutecia e
efeitos secundaacuterios de repetir este tratamento apoacutes as quatro horas iniciais
52
DISCUSSAtildeO
A partir da anaacutelise feita das revisotildees sistemaacuteticas de Weil (19) e de Barden (23)
conclui-se que o paracetamol eacute uma analgeacutesico seguro e eficaz no tratamento da dor
relativa agrave exodontia de terceiros molares pois apresenta um benefiacutecio estatisticamente
significativo quando comparado a placebo Ambas consideram que os melhores valores
de aliacutevio de dor e da diminuiccedilatildeo da intensidade da mesma satildeo alcanccedilados agraves 4 e 6 horas
apoacutes ingestatildeo do faacutermaco
Com base na primeira revisatildeo acima referida o paracetamol exibe uma dose
uacutenica oacuteptima de 1000mg e um periacuteodo de medicaccedilatildeo apropriado de 8 em 8 horas A
maioria dos artigos incluiacutedos apresenta um risco de vieacutes moderado causado
principalmente pela falta de informaccedilatildeo sobre o mecanismo de alocaccedilatildeo de pacientes
podendo levar a uma descredibilidade dos resultados (36)
Na revisatildeo de Barden (23) a comparaccedilatildeo entre os diferentes NSAIDrsquos
demonstrou que este tipo de faacutermacos e particularmente os inibidores da COX-2
exibem os melhores valores de NNT Atraveacutes de uma comparaccedilatildeo indirecta entre
ibuprofeno vs paracetamol os vaacuterios estudos mostraram que o ibuprofeno apresenta
melhores resultados na analgesia da dor poacutes-operatoacuteria (44)
Os estudos de Seymour (22) de Haglund (25) e de Daniels (33) comparam
diferentes compostos activos a um placebo onde o paracetamol estaacute sempre presente
Todos comprovam que enquanto analgeacutesico apresenta uma eficaacutecia largamente
significativa em termos de aliacutevio da dor (usando a escala VAS) Pelo menos 50 dos
indiviacuteduos incluiacutedos que receberam este faacutermaco avaliaram globalmente o tratamento de
forma positiva Poreacutem todos os artigos que
1 Comparam este composto a outro nomeadamente NSAIDrsquos mostram que estes
tecircm uma eficaacutecia significativamente superior agrave do paracetamol tanto em relaccedilatildeo
a valores mais baixos na escala VAS como subjectivamente na avaliaccedilatildeo global
Cerca de 80 dos indiviacuteduos que tomaram NSAIDrsquos classificaram o tratamento
positivamente (agrave excepccedilatildeo dos estudos (32) e (22)) Reportam ainda os efeitos
adversos mais comuns como tonturas naacuteuseas cefaleia e sonolecircncia que
embora de gravidade reduzida tecircm uma incidecircncia superior no paracetamol que
na aspirina e ibuprofeno
53
2 Combinam o paracetamol com NSAIDrsquos provam o efeito aditivo daquele bem
como o facto de estas combinaccedilotildees serem mais eficazes que qualquer um dos
faacutermacos em separado (Merry (13) e Haglund (25))
De acordo com os estudos analisados os NSAIDrsquos aparentam ser uma escolha
preferencial face ao paracetamol porque apresentam uma maior eficaacutecia no aliacutevio da dor
apoacutes extracccedilatildeo de terceiros molares embora disponham de propriedades anti-
inflamatoacuterias notoacuterias (e pertinentes no sucesso do tratamento poacutes-operatoacuterio)
O mecanismo de acccedilatildeo do paracetamol necessita de investigaccedilatildeo adicional que
permita uma melhor compreensatildeo e que traga novas respostas na praacutetica cliacutenica Como
aspecto positivo eacute de acrescentar que natildeo existem diferenccedilas estatisticamente
significantes entre o paracetamol e placebo no que diz respeito a efeitos secundaacuterios
(baixo grau de severidade) podendo ser considerado um composto seguro
A revisatildeo de Barden (23) indica que os resultados da eficaacutecia dos NSAIDrsquos
podem atrair os cliacutenicos a aumentar a sua prescriccedilatildeo sem terem em atenccedilatildeo a sua
relaccedilatildeo com o aumento dos efeitos adversos Isto eacute uma situaccedilatildeo insustentaacutevel na
medida em que nas uacuteltimas duas deacutecadas alguns destes medicamentos foram retirados
do mercado devido a eventos adversos graves posteriormente descobertos Um exemplo
eacute o caso do rofecoxib e valdecoxib que produziram acidentes cardiovasculares seacuterios
provavelmente consequentes da dosagem e natildeo da sua selectividade para a COX-2
(25))
Os efeitos adversos satildeo um motivo de peso para que os pacientes deixem de
tomar determinada substacircncia ou sejam incapazes de tolerar uma dose eficaz da mesma
Informaccedilotildees complementares que englobassem este aspecto seriam ideais e exequiacuteveis
se os autores de ensaios cliacutenicos lhes dessem maior relevo (45)
Outros dados - como custo financeiro e disponibilidade no mercado - poderiam
ser um auxiacutelio na selecccedilatildeo entre paracetamol e outros medicamentos Eacute de ressalvar
que em Portugal os geneacutericos vieram a baixar os preccedilos de analgeacutesicos e NSAIDrsquos
Medicamentos agrave base de ibuprofeno satildeo dos mais dispendiosos (46)
Os NSAIDrsquos tecircm um problema adicional relacionado com a hemostase ndash inibir a
produccedilatildeo de tromboxano A2 e consequentemente aumentar o risco de hemorragia
prolongada (11) No entanto estes efeitos secundaacuterios estatildeo directamente relacionados
com a dosagem pelo que apenas eacute relevante considerar este aspecto em paciente com
problemas de coagulaccedilatildeo
54
Conclui-se que embora a toma de paracetamol seja um procedimento seguro e
eficaz existem no mercado compostos com igual seguranccedila e eficaacutecia superior Apesar
de os inibidores da COX-2 serem os compostos mais eficazes abarcam os efeitos
secundaacuterios mais graves pelo que a realizaccedilatildeo de estudos adicionais eacute imperativo no
sentido de colmatar esta falha
55
RESPOSTA AO PACIENTE
ldquoTendo em conta a evidecircncia cientiacutefica disponiacutevel sobre este assunto e
considerando que natildeo tem problemas gaacutestricos ou de coagulaccedilatildeo sanguiacutenea recomendo
que tome 1g de paracetamol de 8 em 8 horas pois eacute bastante eficaz no aliacutevio da dor
Poreacutem existem outras opccedilotildees como por exemplo combinar o paracetamol a 200mg de
ibuprofeno pode ainda apenas tomar o paracetamol e se sentir necessidade recorrer ao
ibuprofeno 400mg no maacuteximo trecircs vezes ao dia
Tanto o paracetamol como o ibuprofeno tecircm poucos efeitos secundaacuterios e os
mais frequentes satildeo de baixo grau de gravidade Embora existam outros medicamentos
mais eficazes na eliminaccedilatildeo da dor estes tecircm efeitos secundaacuterios mais graves que natildeo
justificam a sua utilizaccedilatildeo
56
REFEREcircNCIAS BIBLIOGRAacuteFICAS
1 Barden J Edwards JE McQuay HJ Andrew Moore R Pain and analgesic
response after third molar extraction and other postsurgical pain Pain 2004107(1-
2)86-90 Epub 20040113
2 Cooper SA Desjardins PJ The value of the dental impaction pain model in drug
development Methods in molecular biology (Clifton NJ) 2010617175-90 Epub
20100326
3 NICE Guidance on the Extraction of Wisdom Teeth2000 13 December 2011
Available from httppublicationsniceorgukguidance-on-the-extraction-of-wisdom-
teeth-ta1clinical-need-and-practice
4 Mettes Dirk TG Nienhuijs Marloes MEL van der Sanden Wil JM Verdonschot
Emiel H Plasschaert A Interventions for treating asymptomatic impacted wisdom teeth
in adolescents and adults Cochrane Database of Systematic Reviews [Internet] 2005
(2) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD003879frameht
ml
5 Seymour RA Use of analgesics in postoperative dental pain a review Journal
of the Royal Society of Medicine 198477(11)949-54 Epub 19841101
6 Berg JM Tymoczko JL Stryer L Biochemistry 5 ed W H Freeman 2002
1050 p
7 Nelson DL Cox MM Lehninger Principles of Biochemistry 5 ed W H
Freeman 2005 1119 p
8 Sciulli MG Capone ML Tacconelli S Patrignani P The future of traditional
nonsteroidal antiinflammatory drugs and cyclooxygenase-2 inhibitors in the treatment
of inflammation and pain Pharmacological reports PR 200557 Suppl66-85 Epub
20060118
9 Devlin TD Devlins Textbook of Biochemistry 6 ed Hoboken NJ Wiley
2006 1208 p
10 Katzung BG Basical and Clinical Pharmacology 10 ed McGraw-Hill 2006
11 Naclerio-Homem Mg Fau - Deboni MCZ Deboni Mc Fau - Rapoport A
Rapoport A Fau - Chin VKL Chin VK Effects of ketoprofen and diclofenac potassium
on blood coagulation tests after removal of third molars (1936-7163 (Electronic))
57
12 Toms L McQuay H Derry S Moore R Single dose oral paracetamol
(acetaminophen) for post-operative pain in adults Cochrane Database of Systematic
Reviews 2008(4)
13 Merry AF Gibbs RD Edwards J Ting GS Frampton C Davies E et al
Combined acetaminophen and ibuprofen for pain relief after oral surgery in adults a
randomized controlled trial British journal of anaesthesia 2010104(1)80-8 Epub
20091217
14 Derry C Derry S Moore R McQuay H Single Dose Oral Ibuprofen for Acute
Post-Operative Pain in Adults Cochrane Database of Systematic Reviews 2009(3)
15 Rang HP Dale MM Ritter JM Moore PK Farmacologia 5 ed Elsevier 2003
Elsevier p
16 Scopel E Alencar M Cruz RM Medidas de avaliaccedilatildeo da dor efdeportes
2007(105)
17 Mata AD Marques D Silveira J Marques J Medicina Dentaacuteria Baseada na
Evidecircncia Novas Opccedilotildees para Velhas Praacuteticas Rev Port Estomatol Cir Maxilofac
200849(1)31-7
18 CASP UK [13 Dezembro 2011] Available from httpwwwcasp-
uknetabout-caspabout-casp
19 Weil K Hooper L Afzal Z Esposito M Worthington Helen V van Wijk A et
al Paracetamol for pain relief after surgical removal of lower wisdom teeth Cochrane
Database of Systematic Reviews [Internet] 2007 (3) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD004487frameht
ml
20 Toms L Derry S Moore RA McQuay Henry J Single dose oral paracetamol
(acetaminophen) with codeine for postoperative pain in adults Cochrane Database of
Systematic Reviews [Internet] 2009 (1) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD001547frameht
ml
21 Derry S Wiffen PJ Moore RA Relative efficacy of oral analgesics after third
molar extraction - a 2011 update Br Dent J 2011211(9)419-20
22 Seymour RA Hawkesford JE Sykes J Stillings M Hill CM An investigation
into the comparative efficacy of soluble aspirin and solid paracetamol in postoperative
pain after third molar surgery Br Dent J 2003194(3)153-7
58
23 Barden J Edwards JE McQuay HJ Wiffen PJ Moore RA Relative efficacy of
oral analgesics after third molar extraction Br Dent J 2004197(7)407-11
24 Saska S Scartezini GR Souza RFd Hochuli-Vieira E Pereira Filho VA
Gabrielli MAC Cloridrato de tramadolparacetamol no controle da dor poacutes-operatoacuteria
em cirurgias de terceiros molares inclusos
Tramadolacetaminophen in the control of postoperative pain for impacted third molar
surgery Rev cir traumatol buco-maxilo-fac 20099(4)
25 Haglund B von Bultzingslowen I Combining paracetamol with a selective
cyclooxygenase-2 inhibitor for acute pain relief after third molar surgery a randomized
double-blind placebo-controlled study European journal of oral sciences
2006114(4)293-301 Epub 20060817
26 Kubitzek F Ziegler G Gold MS Liu JM Ionescu E Analgesic efficacy of low-
dose diclofenac versus paracetamol and placebo in postoperative dental pain Journal of
orofacial pain 200317(3)237-44 Epub 20031003
27 Bjornsson GA Haanaes HR Skoglund LA A randomized double-blind
crossover trial of paracetamol 1000 mg four times daily vs ibuprofen 600 mg effect on
swelling and other postoperative events after third molar surgery British journal of
clinical pharmacology 200355(4)405-12 Epub 20030419
28 Macleod AG Ashford B Voltz M Williams B Cramond T Gorta L et al
Paracetamol versus paracetamol-codeine in the treatment of post-operative dental pain
a randomized double-blind prospective trial Australian dental journal
200247(2)147-51 Epub 20020726
29 Bjornsson GA Haanaes HR Skoglund LA Ketoprofen 75 mg qid versus
acetaminophen 1000 mg qid for 3 days on swelling pain and other postoperative events
after third-molar surgery Journal of clinical pharmacology 200343(3)305-14 Epub
20030318
30 Chopra D Rehan HS Mehra P Kakkar AK A randomized double-blind
placebo-controlled study comparing the efficacy and safety of paracetamol
serratiopeptidase ibuprofen and betamethasone using the dental impaction pain model
International journal of oral and maxillofacial surgery 200938(4)350-5 Epub
20090127
31 Dolci G Ripari M Pacifici L Umile A Evaluation of piroxicam-beta-
cyclodextrin piroxicam paracetamol and placebo in post-operative oral surgery pain
59
International journal of clinical pharmacology research 199414(5-6)185-91 Epub
19940101
32 Noronha VR Gurgel GD Alves LC Noman-Ferreira LC Mendonca LL Aguiar
EG et al Analgesic efficacy of lysine clonixinate paracetamol and dipyrone in lower
third molar extraction a randomized controlled trial Medicina oral patologia oral y
cirugia bucal 200914(8)e411-5 Epub 20090506
33 Daniels S Reader S Berry P Goulder M Onset of analgesia with sodium
ibuprofen ibuprofen acid incorporating poloxamer and acetaminophen--a single-dose
double-blind placebo-controlled study in patients with post-operative dental pain
European journal of clinical pharmacology 200965(4)343-53 Epub 20090303
34 Medve RA Wang J Karim R Tramadol and acetaminophen tablets for dental
pain Anesthesia progress 200148(3)79-81 Epub 20011129
35 Bjornsson GA Haanaes HR Skoglund LA Naproxen 500 mg bid versus
acetaminophen 1000 mg qid effect on swelling and other acute postoperative events
after bilateral third molar surgery Journal of clinical pharmacology 200343(8)849-58
Epub 20030905
36 Marques JF Marques D Silveira J Mata AD Revisotildees Sistemaacuteticas o que satildeo
e para que servem Rev Port Estomatol Cir Maxilofac 200849(3)171-8
37 Rodrigues CL Ziegelmann PK Meta-anaacuteliseum guia praacutetico HCPA
201030(4)436-47
38 Alderson P Absence of evidence is not evidence of absence Bmj
2004328(7438)476-7
39 Berwanger O Suzumura EA Buehler AM Oliveira JB Como Avaliar
Criticamente Revisotildees Sistemaacuteticas e Meta-anaacutelises Revista Brasileira de Terapia
Intensiva 200719(4)475-80
40 Noordzij M Zoccali C Dekker FW Jager KJ Adding up the evidence
systematic reviews and meta-analyses Nephron Clinical practice 2011119(4)c310-6
Epub 20111203
41 Sibbald B Roland M Understanding controlled trials Why are randomised
controlled trials important Bmj 1998316(7126)201
42 Primer on Statistical Significance and P Values Effective Clinical Practice
20014(4)183-4
43 Efird J Blocked randomization with randomly selected block sizes International
journal of environmental research and public health 20118(1)15-20 Epub 20110215
60
44 Cooper S Schachtel B Goldman E Gelb S Cohn P Ibuprofen and
acetaminophen in the relief of acute pain a randomized double blind placebo
controlled study The Journal of Clinical Pharmacology 198929(11)1026-30
45 Edwards JE McQuay HJ Moore RA Collins SL Reporting of Adverse Effects
in Clinical Trials Should Be Improved Lessons from Acute Postoperative Pain Journal
of pain and symptom management 199918(6)427-37
46 Faacutermaco mais vendido versus mais barato Deco Proteste [updated Julho
200919 Dezembro 2011] Available from httpwwwdecoprotesteptservicos-de-
saudefarmaco-mais-vendido-versus-mais-barato-s568081htm
61
ANEXOS
ANEXO A ndash TABELA DE CARACTERIacuteSTICAS DE ARTIGOS EXCLUIacuteDOS
Artigo Fonte Classificaccedilatildeo
inicial Motivo de Exclusatildeo
Toms Derry (20) Cochrane
Library
Possivelmente
Adequado
Natildeo eacute um estudo sobre
extracccedilatildeo de terceiros molares
Saska Scartezini
(24) LILACS
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (27) PubMed Adequado
Estudo natildeo se foca na dor poacutes-
operatoacuteria
Kubitzek Ziegler
(26) PubMed Adequado Artigo natildeo disponiacutevel
Macleod
Ashford (28) PubMed Adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (29) PubMed
Possivelmente
adequado Artigo natildeo disponiacutevel
Chopra Rehan
(30) PubMed
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Dolci Ripari (31) PubMed Possivelmente
adequado Artigo natildeo disponiacutevel
Medve Wang
(34) PubMed
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (35) PubMed
Possivelmente
adequado Artigo natildeo disponiacutevel
62
ANEXO B ndash ARTIGOS INCLUIacuteDOS EM FORMATO
INTEGRALi
i Nota os seguintes artigos estatildeo paginados fora do contexto deste trabalho de acordo com a sua
paginaccedilatildeo original
Paracetamol for pain relief after surgical removal of lower
wisdom teeth (Review)
Weil K Hooper L Afzal Z Esposito M Worthington HV van Wijk A Coulthard P
This is a reprint of a Cochrane review prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2008 Issue 4
httpwwwthecochranelibrarycom
Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
T A B L E O F C O N T E N T S
1HEADER
1ABSTRACT
2PLAIN LANGUAGE SUMMARY
2BACKGROUND
3OBJECTIVES
3METHODS
5RESULTS
8DISCUSSION
9AUTHORSrsquo CONCLUSIONS
9ACKNOWLEDGEMENTS
10REFERENCES
13CHARACTERISTICS OF STUDIES
30DATA AND ANALYSES
Analysis 11 Comparison 1 50 pain relief using pain relief measures Outcome 1 Paracetamol versus placebo number of
people with at least 50 pain relief at 4 hours 31
Analysis 12 Comparison 1 50 pain relief using pain relief measures Outcome 2 Paracetamol versus placebo number of
people with at least 50 pain relief at 6 hours 33
Analysis 21 Comparison 2 50 pain relief using pain intensity measures Outcome 1 Paracetamol versus placebo number
of people with at least 50 pain relief at 4 hours 34
Analysis 22 Comparison 2 50 pain relief using pain intensity measures Outcome 2 Paracetamol versus placebo number
of people with at least 50 pain relief at 6 hours 35
Analysis 31 Comparison 3 Number of people with adverse events Outcome 1 Number of patients with adverse events
paracetamol versus placebo 37
38ADDITIONAL TABLES
42APPENDICES
43WHATrsquoS NEW
43HISTORY
43CONTRIBUTIONS OF AUTHORS
43DECLARATIONS OF INTEREST
44SOURCES OF SUPPORT
44INDEX TERMS
iParacetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
[Intervention Review]
Paracetamol for pain relief after surgical removal of lowerwisdom teeth
Kiaran Weil1 Lee Hooper2 Zahid Afzal3 Marco Esposito1 Helen V Worthington4 Arjen van Wijk5 Paul Coulthard1
1Department of Oral and Maxillofacial Surgery School of Dentistry The University of Manchester Manchester UK 2School of
Medicine Health Policy amp Practice University of East Anglia Norwich UK 3Oral and Maxillofacial Surgery City Hospital Birming-
ham UK 4Cochrane Oral Health Group MANDEC School of Dentistry The University of Manchester Manchester UK 5Social
Dentistry and Behavioural Sciences ACTA Amsterdam Netherlands
Contact address Kiaran Weil Department of Oral and Maxillofacial Surgery School of Dentistry The University of Manchester
Higher Cambridge Street Manchester M15 6FH UK kiaran_weilhotmailcom
Editorial group Cochrane Oral Health Group
Publication status and date Edited (no change to conclusions) published in Issue 4 2008
Review content assessed as up-to-date 21 May 2007
Citation Weil K Hooper L Afzal Z Esposito M Worthington HV van Wijk A Coulthard P Paracetamol for pain relief af-
ter surgical removal of lower wisdom teeth Cochrane Database of Systematic Reviews 2007 Issue 3 Art No CD004487 DOI
10100214651858CD004487pub2
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Paracetamol has been commonly used for the relief of postoperative pain following oral surgery In this review we investigated the
optimal dose of paracetamol and the optimal time for drug administration to provide pain relief taking into account the side effects
of different doses of the drug This will inform dentists and their patients of the best strategy for pain relief after the surgical removal
of wisdom teeth
Objectives
To assess the beneficial and harmful effects of paracetamol for pain relief after surgical removal of lower wisdom teeth compared to
placebo at different doses and administered postoperatively
Search strategy
We searched the Cochrane Oral Health Grouprsquos Trials Register the Cochrane Pain Palliative and Supportive Care Grouprsquos Trials Register
CENTRAL MEDLINE EMBASE and the Current Controlled Trials Register Handsearching included several dental journals We
checked the bibliographies of relevant clinical trials and review articles for studies outside the handsearched journals We wrote to
authors of the identified randomised controlled trials (RCTs) to manufacturers of analgesic pharmaceuticals we searched personal
references in an attempt to identify unpublished or ongoing RCTs No language restriction was applied The last electronic search was
conducted on 24th August 2006
Selection criteria
Randomised parallel group placebo controlled double blind clinical trials of paracetamol for acute pain following third molar surgery
Data collection and analysis
All trials identified were scanned independently and in duplicate by two review authors any disagreements were resolved by discussion
or if necessary a third review author was consulted The proportion of patients with at least 50 pain relief was calculated for both
paracetamol and placebo The number of patients experiencing adverse events andor the total number of adverse events reported were
analysed
1Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Main results
Twenty-one trials met the inclusion criteria A total of 2048 patients were initially enrolled in the trials (1148 received paracetamol
and 892 the placebo) and of these 1968 (96) were included in the meta-analysis (1133 received paracetamol and 835 the placebo)
Paracetamol provided a statistically significant benefit when compared with placebo for pain relief and pain intensity at both 4 and 6
hours Most studies were found to have moderate risk of bias with poorly reported allocation concealment being the main problem
Risk ratio values for pain relief at 4 hours 285 (95 confidence interval (CI) 189 to 429) and at 6 hours 332 (95 CI 188 to 587)
A statistically significant benefit was also found between up to 1000 mg and 1000 mg doses the higher the dose giving greater benefit
for each measure at both time points There was no statistically significant difference between the number of patients who reported
adverse events overall this being 19 in the paracetamol group and 16 in the placebo group
Authorsrsquo conclusions
Paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom teeth
P L A I N L A N G U A G E S U M M A R Y
Paracetamol for pain relief after surgical removal of lower wisdom teeth
The surgical removal of wisdom teeth (third molars) is the most commonly performed surgical procedure undertaken in oral surgery
practice Postoperative complications may include swelling bruising and limited mouth opening but patients are most often concerned
about postoperative pain which may be severe Paracetamol is effective in relieving pain with a low incidence of adverse effects It is one
of the most commonly used analgesics and is widely available without prescription around the world In this review we investigated the
optimal dose of paracetamol and the optimal time for drug administration to provide pain relief after the surgical removal of wisdom
teeth The side effects of different doses of the drug were also explored
Twenty-one trials (with over 2000 participants) were included Paracetamol provided a statistically significant benefit when compared
with placebo for pain relief at both 4 and 6 hours after taking the drug It is most effective at 1000 mg dose and can be taken at six
hourly intervals without compromising safety There was no statistically significant difference between the number of patients who
reported adverse events overall this being 19 in the paracetamol group and 16 in the placebo group It should be noted that most
of the studies were found to have some limitations mainly due to poor reporting of information However the review concludes that
paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom teeth
B A C K G R O U N D
The surgical removal of wisdom teeth is the most commonly per-
formed surgical procedure undertaken in oral surgery practice
Postoperative complications may include swelling bruising and
limited mouth opening but patients are most often concerned
about postoperative pain which may be severe The pain ex-
perienced after oral surgery is a validated and widely used pain
model for the clinical evaluation of analgesic efficacy (Cooper
1976) Tissue damage produced during surgery releases chemicals
that initiate inflammatory pain by activating and sensitising nerve
fibre receptors (Loeser 1999) Chemicals include bradykinin
prostaglandins serotonin and histamine (Dray 1997)
Paracetamol (acetaminophen) is a nonopioid analgesic possessing
antipyretic activity and is effective in relieving pain with a low in-
cidence of adverse effects (Moore 1998) It is one of the most com-
monly used analgesics and is widely available without prescription
around the world Paracetamol is often grouped with the nons-
teroidal anti-inflammatory drug (NSAID) family however it is
considered only to have relatively weak anti-inflammatory activity
(Rang 2003) NSAIDs are assumed largely to produce their anal-
gesia as a result of the inhibition of prostaglandin production by
the enzyme cyclo-oxygenase (Malmberg 1992) The mechanism
of action has not been fully understood Among several theories
it has been suggested that paracetamol is a selective inhibitor of
the newly described COX-3 enzyme a cyclo-oxygenase-1 variant
in the central nervous system This inhibition could represent a
primary central mechanism by which paracetamol decreases pain
and possibly fever (Chandrasekharan 2002) Major evidence has
2Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
been accumulated showing that paracetamol inhibits cyclo-oxy-
genase by reducing the higher oxidative state of the cyclo-oxyge-
nase enzyme by reducing oxygen radical co-substrates (Aronoff
2006) Paracetamol has been shown to be an effective analgesic in
the control of postoperative dental pain in a number of clinical
trials (Bentley 1987 Kiersch 1994 Mehlisch 1990) Pain inten-
sity following third molar surgery has been suggested to reach its
maximum between 3 to 5 hours following surgery (Fisher 1988
Seymour 1985) and therefore this pain model is used to test the
efficacy of a single analgesic dose
A recent systematic review (Barden J 2004) has looked at the ef-
ficacy and safety of paracetamol for postoperative pain manage-
ment and has included the findings of studies involving a wide
variety of types of surgery such as gynaecology surgery abdomi-
nal surgery orthopaedic surgery amongst others including the re-
moval of wisdom teeth There is some debate as to whether dental
pain is different from other pain It has been suggested that the
effect of some analgesics including tramadol were worse for dental
pain than for other types of postsurgical pain (Moore 1997)
In this review we investigated the optimal dose of paracetamol and
the optimal time for drug administration to provide pain relief
taking into account the side effects of different doses of the drug
This will inform dentists and their patients of the best strategy for
best pain relief after the surgical removal of wisdom teeth
O B J E C T I V E S
To assess the beneficial and harmful effects of paracetamol for
pain relief after surgical removal of lower wisdom teeth compared
to placebo at different doses and administered preoperatively or
postoperatively
Primary
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between paracetamol and placebo for pain
relief in patients requiring surgical removal of a lower wisdom
tooth or teeth against the alternative hypothesis of a difference
Secondary
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between different doses of paracetamol for
pain relief in patients requiring surgical removal of a lower
wisdom tooth or teeth against the alternative hypothesis of a
difference
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between different times of administration of
paracetamol for pain relief in patients requiring surgical removal
of a lower wisdom tooth or teeth against the alternative
hypothesis of a difference
M E T H O D S
Criteria for considering studies for this review
Types of studies
All randomised controlled double blind clinical trials
Types of participants
Patients of all health states who required the surgical removal of
a lower wisdom tooth and who had at least had a baseline pain
intensity of moderate to severe pain Patients who also required
removal of an additional tooth or teeth were included Surgery
was undertaken under local anaesthesia intravenous sedation or
general anaesthesia Patients taking concurrent analgesia were ex-
cluded
Types of interventions
Efficacy
bull Paracetamol given as a single dose by mouth in any dose
and in any formulation (for example immediate or slow release)
regardless of when the single dose was given (for example
preoperatively or postoperatively)
Side effects
In order to investigate side effects more thoroughly we included
both single and multiple dose studies
bull Paracetamol given up to 7 days by mouth in any dose and
in any formulation (for example immediate or slow release)
regardless of when the first dose was given (for example
preoperatively or postoperatively)
Types of outcome measures
bull Pain intensity (visual analogue scale (VAS) categorical
verbal rating verbal numerical scale global subjective efficacy
ratings and other categorical rating scales)
bull Pain relief (VAS categorical verbal rating verbal numerical
scale global subjective efficacy ratings and other categorical
rating scales) and derived pain relief outcomes extracted will be
3Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
total pain relief (TOTPAR) summed pain intensity difference
(SPID) over 4 and 6 hours
bull Side effects (for example hepatic and renal) (binary)
Search methods for identification of studies
To identify studies for inclusion or consideration in this review a
detailed search strategy was developed for each database searched
These were based on the search strategy developed for MEDLINE
but revised appropriately for each database The search strategy
combined a sensitive search strategy for randomised controlled
trials (RCTs) revised from phases 1 and 2 of the Cochrane Sensi-
tive Search Strategy for RCTs (as published in Appendix 5b in the
Cochrane Handbook for Systematic Reviews of Interventions 426
(updated September 2006)) The subject search used a combina-
tion of controlled vocabulary and free text terms based on the
search strategy for searching CENTRAL (see Appendix 1)
Databases to be searched
The Cochrane Oral Health Grouprsquos Trials Register (to 24th August
2006)
The Cochrane Central Register of Controlled Trials (CENTRAL)
(The Cochrane Library 2006 Issue 3)
The Cochrane Pain Palliative and Supportive Care Grouprsquos Trials
Register (to 24th August 2006)
MEDLINE (1966 to 24th August 2006)
EMBASE (1980 to 25th August 2006)
Current Controlled Trials Register (wwwcontrolled-trialscom)
(to 24th August 2006)
The bibliographies of papers and review articles were checked for
studies outside the handsearched journals Personal references were
also searched
Language
There were no language restrictions and where necessary transla-
tion into the English language of relevant studies was conducted
Unpublished studies
Authors of RCTs identified were written to in order to obtain
further information about the trial and to attempt to identify
unpublished or ongoing studies We also wrote to manufacturers
of analgesic pharmaceuticals
Handsearching
Several journals relevant to this review were handsearched as part
of the Cochrane Oral Health Grouprsquos ongoing journal hand-
searching programme The list of the dental journals hand-
searched by The Cochrane Collaboration can be found at http
wwwohgcochraneorg
Data collection and analysis
The titles and abstracts (when available) of all reports identified
were scanned independently and in duplicate by two review au-
thors For studies appearing to meet the inclusion criteria or for
which there were insufficient data in the title and abstract to make
a clear decision the full report was obtained and assessed indepen-
dently and in duplicate by two review authors to establish whether
the studies met the inclusion criteria or not Disagreements were
resolved by discussion Where resolution was not possible a third
review author was consulted All studies meeting the inclusion
criteria then underwent quality assessment and data extracted
Studies rejected at this or subsequent stages were recorded in the
Characteristics of excluded studies table and reasons for exclusion
were recorded
Quality assessment
The quality assessment of the included trials was undertaken inde-
pendently and in duplicate by two review authors based on what
is written in the articles
Only double blind trials were included in the review so blinding
was not included in the quality assessment
Two main quality criteria were examined
(1) Allocation concealment recorded as
(A) Adequate -2 points
(B) Unclear - 1 point
(C) Inadequate - 0 points
(2) Completeness of follow up (is there a clear explanation for
withdrawals and drop outs in each treatment group) assessed as
(A) Yes - 1 point
(B) No - 0 points
The agreement for the quality criteria between assessors was de-
termined by Kappa statistics
After taking into account the additional information provided by
the authors of the trials studies were grouped into the following
categories
(A) Low risk of bias - 3 points (plausible bias unlikely to seriously
alter the results) if all criteria were met
(B) Moderate or high risk of bias - 0 to 2 points Moderate risk
of bias - plausible bias that raises some doubt about the results if
one or more criteria are partly met (for example when authors
responded that they had made some attempts to conceal the al-
location of patients to give an explanation for withdrawals but
these attempts were not judged to be ideal these criteria were cat-
egorised as rsquopartlyrsquo) High risk of bias - plausible bias that seriously
weakens confidence in the results if one or more criteria were not
met as described in the Cochrane Handbook for Systematic Reviews
of Interventions 426
We also reported whether the authors of included trials have con-
ducted a sample size calculation
4Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data extraction
Data were extracted by two review authors independently and
in duplicate using specially designed data extraction forms Any
disagreement was discussed and a third review author consulted
where necessary Authors were contacted for clarification of miss-
ing information Data were excluded until further clarification was
available if agreement could not be reached
For each trial the following data were recorded
bull Year of publication country of origin setting and source of
study funding
bull Details of the participants including demographic
characteristics and criteria for inclusion
bull Details on the study design (parallel group or cross-over
design)
bull Details on the type of intervention
bull Details of the outcomes reported including method of
assessment and time intervals
Data synthesis
From the mean total pain relief (TOTPAR) or summed pain in-
tensity difference (SPID) pain indices reported we computed a
dichotomous outcome variable for the number of patients with
at least 50 pain relief according to the methods outlined in a
Cochrane review (Collins 1999) For each of the three objectives
we examined the appropriateness of different continuous outcome
measurements and these were meta-analysed and reported in the
final review
For dichotomous outcomes the estimate of an intervention was
expressed as risk ratios together with 95 confidence intervals
For continuous outcomes mean differences and 95 confidence
intervals were used to summarise the data for each trial
Clinical heterogeneity was assessed by examining the types of par-
ticipants interventions and outcomes in each study Meta-analyses
were conducted only with studies of similar comparisons report-
ing the same outcome measures Risk ratios were used to combine
dichotomous data and mean differences for continuous data us-
ing random-effects models The significance of any discrepancies
in the estimates of the treatment effects from the different trials
was assessed by means of Cochranrsquos test for heterogeneity and any
heterogeneity investigated
Where both visual analogue scale (VAS) and categorical scales were
used to measure pain intensity or pain relief or both the categorical
data were used in the meta-analysis as this was the most frequently
used scale
Subgroup analyses
Subgroup analyses were planned for studies
bull Where patients underwent surgery with local anaesthesia
alone local anaesthesia and intravenous sedation general
anaesthesia alone and general anaesthesia with local anaesthetic
bull Where different types of formulation of paracetamol were
used for instance immediate release versus slow release
bull Where different doses of paracetamol were used (1000 mg
or more and less than 1000 mg)
bull Where time of administration of paracetamol differs
preoperative versus postoperative
bull Where TOTPAR was calculated using pain relief measures
and pain intensity measures
The difference between studies comparing up to 1000 mg doses
with studies comparing 1000 mg or more was examined by per-
forming random-effects metaregression analyses in Stata version
90 (Stata Corporation USA) using the program Metareg
The results of the metaregressions for comparing the two dose
levels up to 1000 mg and 1000 mg or more are presented in
Additional Table 1
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
See Characteristics of included studies and Characteristics of
excluded studies tables
Characteristics of the trial setting and investigators
Of the 67 eligible trials 46 were excluded as shown in the ex-
cluded studies section Of the 21 included studies one was con-
ducted in Denmark (Moller 2000) two in Germany (Kubitzek
2003 Lehnert 1990) one in Italy (Dolci 1994) one in Nor-
way (Skoglund 1991) two in Puerto Rico (Olson 2001 Sunshine
1986) one in Thailand (Vattaraphudej 1986) two in the United
Kingdom (Seymour 1996 Seymour 2003) and 11 in the United
States of America (Cooper 1980 Cooper 1981 Cooper 1988
Cooper 1998 Dionne 1994 Forbes 1984b Forbes 1989 Forbes
1990 Hersh 2000 Kiersch 1994 Mehlisch 1995) Six trials
were conducted at university clinics (Cooper 1998 Hersh 2000
Moller 2000 Olson 2001 Sunshine 1986 Vattaraphudej 1986)
five at private practices (Dionne 1994 Forbes 1984b Forbes
1989 Forbes 1990 Kubitzek 2003) seven did not state a set-
ting (Cooper 1981 Dolci 1994 Kiersch 1994 Mehlisch 1995
Seymour 1996 Seymour 2003 Skoglund 1991) One reported a
single site (Cooper 1988) two reported two sites (Forbes 1989
Seymour 2003) and six specifically stated outpatients (Cooper
1980 Cooper 1988 Forbes 1989 Forbes 1990 Hersh 2000
5Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Lehnert 1990) Seventeen trials were sponsored by industry
(Cooper 1981 Cooper 1988 Cooper 1998 Dionne 1994 Forbes
1984b Forbes 1989 Forbes 1990 Hersh 2000 Kiersch 1994
Kubitzek 2003 Lehnert 1990 Mehlisch 1995 Moller 2000
Olson 2001 Seymour 2003 Skoglund 1991 Sunshine 1986)
one by a university grant (Vattaraphudej 1986) and it was unclear
as whether the remaining three trials (Cooper 1980 Dolci 1994
Seymour 1996) were sponsored but it is likely that they were from
correspondence with some of the authors
Characteristics of interventions
All included interventions were randomised parallel group and
double blind Eleven trials used doses of paracetamol of less than
1000 mg (Cooper 1980 Cooper 1981 Cooper 1988 Dionne
1994 Dolci 1994 Forbes 1984b Forbes 1989 Forbes 1990
Seymour 1996 Sunshine 1986 Vattaraphudej 1986) Eleven tri-
als used doses of 1000 mg (Cooper 1998 Hersh 2000 Kiersch
1994 Kubitzek 2003 Lehnert 1990 Mehlisch 1995 Moller
2000 Olson 2001 Seymour 1996 Seymour 2003 Skoglund
1991) One study (Seymour 1996) used both doses Seven tri-
als used paracetamol in tablet form (Dolci 1994 Forbes 1989
Kubitzek 2003 Mehlisch 1995 Moller 2000 Seymour 2003
Skoglund 1991) Seven trials used capsules (Forbes 1984b Forbes
1989 Forbes 1990 Kiersch 1994 Lehnert 1990 Sunshine 1986
Vattaraphudej 1986) Two trials used caplets (Hersh 2000 Olson
2001) and one trial used effervescent tablets (Moller 2000) Five
trials did not state what formulation was used (Cooper 1980
Cooper 1981 Cooper 1988 Cooper 1998 Dionne 1994) All
trials used placebos in the same formulation as the intervention
Characteristics of outcome measures
For all trials it was possible to calculate the number of patients
with at least 50 total pain relief (TOTPAR) at either 4 hours
6 hours or both Pain intensity was measured in all but one trial
(Kubitzek 2003) pain relief was measured in all but two trials
(Kubitzek 2003 Seymour 2003) Kubitzek 2003 gave a figure for
TOTPAR at six hours and Seymour 2003 measured pain intensity
only Fifteen trials measured pain intensity at 4 hours using a 4-
point categorical scale of 0 to 3 where 0 was no pain at all and 3
was severe pain Five trials measured pain intensity using a visual
analogue scale (VAS) of 0 to 100 mm where 0 was no pain and
100 was the worst pain imaginable Twelve trials measured pain
intensity at 6 hours using a 4-point categorical scale where 0 was
no pain and 3 was severe pain and three trials measured pain
intensity at 6 hours using a VAS of 0 to 100 mm where 0 was no
pain and 100 mm was the worst pain imaginable Sixteen trials
measured pain relief at 4 hours using a 5-point categorical scale
of 0 to 4 where 0 was none and 4 was complete pain relief two
trials measured pain relief at 4 hours using a VAS of 0 to 100 mm
in one trial 0 was none and 100 was complete relief and in the
other trial 0 was complete relief and 100 was no relief (these data
were reversed for statistical purposes) Twelve trials measured pain
relief at 6 hours using a 5-point categorical scale of 0 to 4 where
0 was none and 4 was complete pain relief two trials measured
pain relief at 6 hours using a VAS of 0 to 100 mm in one trial 0
was none and 100 was complete relief and in the other trial 0 was
complete relief and 100 was no relief (these data were reversed for
statistical purposes)
Adverse events and global assessments were recorded in most of
the trials Nineteen trials reported the number of patients with
side effects eight for doses of 1000 mg or more and 15 for doses
of less than 1000 mg Fifteen trials reported the number of adverse
events seven for doses of 1000 mg or more and eight for doses
of less than 1000 mg Fourteen trials recorded global assessment
using a 5-point categorical scale of either 0 to 4 or 1 to 5 where
0 or 1 was poor and 4 or 5 was excellent and four trials used a
4-point categorical scale of 0 to 3 where 0 was poor and 3 was
excellent
Risk of bias in included studies
Details of the quality assessment are presented in Additional Table
2 Seven out of the 21 studies reported adequate concealed al-
location for the remaining studies it was unclear Over half of
the studies (1121) gave clear explanation of withdrawals or drop
outs Taking these two factors into account only three trials were
assessed as being at low risk of bias
Effects of interventions
Comparison 1 Paracetamol versus placebo using
pain relief measurements
(Comparison 1 Outcome 11 amp Comparison 1 Outcome 12)
(Analysis 11 Analysis 12)
There are 16 studies providing pain relief measurements for com-
paring paracetamol versus placebo at 4 hours 11 at doses up to
1000 mg and 5 at doses of 1000 mg Overall there was a highly
statistically significant benefit with the paracetamol with risk ratio
(RR) values for achieving 50 pain relief for all doses of parac-
etamol for 4 hours RR 285 (95 confidence interval (CI) 189
to 429) Chi2 = 6294 degrees of freedom (df ) = 15 P lt 0001
I2 = 76 number needed to treat (to benefit) (NNT) 4 (95
CI 3 to 4) The statistically significant benefit was apparent for
both subgroups with RR for up to 1000 mg 196 (95 CI 134
to 286) Chi2 = 2644 df = 9 P = 0002 I2 = 660 NNT 4
(95 CI 3 to 5) and RR for 1000 mg 456 (95 CI 286 to
727) Chi2 = 544 df = 5 P = 036 I2 = 82 NNT 3 (95
CI 3 to 4) Although both had a statistically significant benefit
6Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
over placebo there was a statistically significant difference between
the two subgroups with an enhanced benefit for the higher doses
(metaregression P lt 0001 Additional Table 3) This subgroup
analysis explained some of the heterogeneity in the overall com-
parison however there is still some unexplained heterogeneity be-
tween the trials in the up to 1000 mg dose comparison
There are 13 studies providing pain relief measurements for com-
paring paracetamol versus placebo at 6 hours 6 doses up to 1000
mg paracetamol and 7 doses of 1000 mg paracetamol Overall
there was a highly statistically significant benefit with the parac-
etamol with RR values for 50 pain relief at 6 hours RR 332
(95 CI 188 to 587) Chi2 = 6335 df = 12 P lt 000001 I2 = 811 NNT 3 (95 CI 3 to 4) The statistically significant
benefit was apparent in both subgroups with RR for up to 1000
mg 189 (95 CI 098 to 367) Chi2 = 1445 df = 5 P = 001
I2 = 654 NNT 6 (95 CI 4 to 10) and RR for 1000 mg
421 (95 CI 297 to 598) Chi2 = 509 df = 6 P = 053 I2 =
0 NNT 3 (95 CI 2 to 3) Although both had a statistically
significant benefit over placebo there was a statistically significant
difference between the two subgroups with an enhanced benefit
for the higher doses (metaregression P lt 0001 Additional Table
3) This subgroup analysis explained some of the heterogeneity in
the overall comparison however there is still some unexplained
heterogeneity between the trials in the up to 1000 mg dose com-
parison
Comparison 2 Paracetamol versus placebo using
pain intensity difference measurements
(Comparison 2 Outcome 21 amp Comparison 2 Outcome 22)
(Analysis 21 Analysis 22)
There are 18 studies providing pain intensity measurements for
comparing paracetamol versus placebo at 4 hours 10 at doses up
to 1000 mg and 8 at doses of 1000 mg Overall there was a highly
statistically significant benefit with paracetamol with RR values
for 50 pain relief at 4 hours RR 487 (95 CI 283 to 837)
Chi2 = 4973 df = 17 P lt 00001 I2 = 658 NNT 3 (95 CI
3 to 5) The statistically significant benefit was apparent in both
subgroups with RR up to 1000 mg 433 (95 CI 219 to 858)
Chi2 = 2622 df = 9 P = 0002 I2 = 657 NNT 3 (95 CI
3 to 4) and RR for 1000 mg 646 (95 CI 234 to 1785) Chi2 = 2347 df = 7 P = 0001 I2 = 702 NNT 4 (95 CI 3
to 5) Both had a statistically significant benefit over placebo but
there was no statistically significant difference between the two
subgroups (metaregression P = 067 Additional Table 3)
There are 14 studies providing pain intensity measurements for
comparing paracetamol versus placebo at 6 hours 6 at doses up
to 1000 mg and 8 at doses of 1000 mg Overall there was a highly
statistically significant benefit with paracetamol with RR values
for 50 pain relief RR 341 (95 CI 234 to 497) Chi2 = 1823
df = 13 P = 015 I2 = 287 NNT 4 (95 CI 3 to 4) The
statistically significant benefit was apparent in both groups with
RR up to 1000 mg 267 (95 CI 146 to 490) Chi2 = 705 df
= 5 P = 022 I2 = 291 NNT 5 (95 CI 3 to 7) and RR for
1000 mg 396 (95 CI 252 to 623) Chi2 = 863 df = 7 P =
028 I2 = 189 NNT 3 (95 CI 3 to 4) Both had a statisti-
cally significant benefit over placebo but there was no statistically
significant difference between the two subgroups (metaregression
P = 015 Additional Table 3)
Comparison 3 Number of patients with adverse
events for paracetamol versus placebo
(Comparison 3 Outcome 31) (Analysis 31)
There are 17 studies that reported the number of patients with
adverse events for paracetamol versus placebo 9 studies used less
than 1000 mg and 8 studies used 1000 mg There was no statisti-
cally significant difference in any group For all doses of paraceta-
mol the RR for an adverse event RR 119 (95 CI 090 to 157)
Chi2 = 2073 df = 15 P = 015 I2 = 276 number needed to
treat to harm (NNTH) 33 (95 CI 143 to infinity) For doses of
less than 1000 mg RR 125 (95 CI 069 to 225) Chi2 = 906
df = 7 P = 025 I2 = 228 NNTH 33 (95 CI 143 to infinity)
For 1000 mg paracetamol RR 116 (95 CI 084 to 160) Chi2
= 1096 df = 7 P = 014 I2 = 362 NNTH 33 (95 CI 125
to infinity)
Subgroup analyses
Where patients underwent surgery with local anaesthesia
alone local anaesthesia and intravenous sedation general
anaesthesia alone and general anaesthesia with local
anaesthetic
When the data were reviewed it was not possible to do a meta-anal-
ysis Of the 21 included studies 7 did not state what anaesthesia
was used 7 used combinations of anaesthesia but were unclear in
reporting which patients received which anaesthesia 4 used local
anaesthetic only and 3 used general anaesthetic only
Where different types of formulation of paracetamol were
used (immediate release versus slow release)
Most included studies did not report on the formulation other
than to say whether it was tablets capsules or caplets Only one
7Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
paper indicated that their study used effervescent tablets (Moller
2000) and their results showed that effervescent tablets gave a faster
onset of pain relief Median value for time to onset of analgesia
was 20 minutes in the effervescent group and 45 minutes in the
tablet group and time to meaningful pain relief was 45 minutes
in the effervescent group and 1 hour in the tablet group However
at the end of a 4-hour period pain relief was better in the tablet
group (44) than the effervescent group (37)
Where different doses of paracetamol were used (1000 mg
or more and less than 1000 mg)
This meta-analysis was conducted 11 studies used doses of 1000
mg or more and 11 studies used doses of less than 1000 mg
(Seymour 1996 used both doses)
NNT for lt 1000 mg of paracetamol is 4 (95 CI 3 to 5) at
4 hours and 6 (95 CI 4 to 10) at 6 hours (using pain relief
measurements)
NNT for lt 1000 mg of paracetamol is 3 (95 CI 3 to 4) at 4 hours
and 5 (95 CI 3 to 7) at 6 hours (using intesity measurements)
NNT for 1000 mg of paracetamol is 3 (95 CI 3 to 4) at 4 hours
and 3 (95 CI 2 to 3) at 6 hours (using pain relief measurements)
NNT for 1000 mg of paracetamol is 4 (95 CI 3 to 5) at 4 hours
and 3 (95 CI 3 to 4) at 6 hours (using intensity measurements)
Where time of administration of paracetamol differs
preoperative versus postoperative
No included study used a preoperative dose as the patients did
not reach moderate or severe pain before the intervention
Where total pain relief (TOTPAR) was calculated using pain
relief measures and pain intensity measures
This meta-analysis was undertaken where the relevant data were
available 16 studies had pain relief data and 17 studies had pain
intensity data
NNT using pain relief scales for lt 1000 mg of paracetamol is 4
(95 CI 3 to 5) at 4 hours and 6 (95 CI 4 to 10) at 6 hours
NNT using pain intensity scales for lt 1000 mg of paracetamol is
3 (95 CI 3 to 4) at 4 hours and 5 (95 CI 3 to 7) at 6 hours
NNT using pain relief scales for 1000 mg of paracetamol is 3 (95
CI 3 to 4) at 4 hours and 3 (95 CI 2 to 3) at 6 hours
NNT using pain intensity scales for 1000 mg of paracetamol is 4
(95 CI 3 to 5) at 4 hours and 3 (95 CI 3 to 4) at 6 hours
D I S C U S S I O N
The results show paracetamol to be an effective analgesia for use
following third molar surgery The number needed to treat (to
benefit) (NNTs) and number needed to treat to harm (NNTHs)
support the use of 1000 mg as an optimal dose It is effective over
both 4 and 6 hours In considering the use of pain relief or pain
intensity difference as a measure of efficacy it was of interest that
metaregression showed that pain relief scales showed a statistically
significant difference for increased dose and pain intensity did
not It is acknowledged that this review only considered single
dose studies when considering efficacy multidosed studies may be
considered when updating the review The NNTs and NNTHs
found in this review are similar to those recorded by a systematic
review (Barden J 2004) where they investigated paracetamol for
pain involving various types of surgery This would confirm yet
again the value of the third molar pain model showing that dental
pain is comparable with pain from other sources The implemen-
tation of NICE (National Institute for Health and Clinical Excel-
lence) Guidelines for removal of third molars has led to a decrease
in the performance of this surgery which may have an adverse
effect on the number of trials able to use the third molar model
In the United States of America such guidelines have not yet been
adopted It is of interest that in striving to provide evidence based
treatment the opportunity for research using the third molar pain
model may be adversely affected
The data available for adverse events show that NNTH for lt 1000
mg of paracetamol is 33 (143 to infinity) for 1000 mg of parac-
etamol is 33 (125 to infinity) and for all doses 33 (143 to infin-
ity) suggesting it is an extremely safe drug Only one severe ad-
verse event was recorded by any researchers and that was a severe
headache (Olson 2001) two other participants stopped taking
paracetamol because of vomiting However there was a high degree
of inconsistency across the trials in the way that adverse events were
recorded raising the concern that only adverse events considered
by the researchers to be attributable to paracetamol were recorded
with some trials recording many AEs and some reporting none
The diverse way in which adverse events were recorded led to there
being over 20 categories of adverse events The main categories
are shown in Additional Table 4 Of interest are adverse events
where placebo scored more highly than paracetamol which could
suggest that paracetamol may possibly have a beneficial effect eg
dry socket but this would require further investigation As all pa-
tients had surgery and various combinations of local anaesthesia
general anaesthesia and sedation making it difficult to ascertain
which effects are directly related to the intervention However the
results strongly support the use of paracetamol in doses up to 1000
mg as a safe effective analgesia
8Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
The efficacy of paracetamol decreases with times and the recom-
mended interval between doses is 8 hours which would suggest
there may be some benefit in a slow release formulation None of
the studies in this trial used a slow release formulation but a trial
(Coulthard 2001) compared sustained release and standard release
formulations of paracetamol and found that the sustained release
was statistically significantly more effective at 6 and 8 hours with
no loss of efficacy at 4 hours Safety for both formulations was
comparable making sustained release paracetamol a safe and ef-
fective choice
The methodology used in the included trials was generally good
This resulted in a large number of participants being included
in this meta-analysis while using only double blind randomised
trials The included trials gave a strong consistent result Many
of the trials were done by researchers with extensive experience
in the field of pain research whose methods have been refined
with experience A large proportion of the trials were done in the
United States and were mostly funded by pharmaceutical com-
panies This seems to be reflected in the methodology However
quality assessment showed there were only three trials with a low
risk of bias and 18 with moderatehigh risk This was mainly the
result of unreported allocation concealment methods In speaking
to some of the authors it is highly likely that the allocation con-
cealment was good in all the trials but that the details were not
well reported Most trials were sponsored by pharmaceutical com-
panies who supplied paracetamol and placebo in identical appear-
ance The reporting of withdrawals and drop outs was sporadic
and even when numbers were cited it was not always clear to which
treatment group the participant had been originally allocated
Mean global assessments (Additional Table 5 Table 6 Table 7
Table 8) all showed higher scores for paracetamol than placebo
It is of interest that despite achieving 50 pain relief participants
did not record 50 on a global assessment scale This again raises
the question of the value of the instruments used to measure the
efficacy of an intervention None of the trials relied on global
assessments as their only measure of efficacy but this information
could be of value to other researchers It raises interesting questions
concerning patientrsquos expectations and the difficulties associated
with quantifying such a subjective experience
A lot of valuable information was gathered incidental to the main
findings in most of the trials So though the topic was concerned
with the use of paracetamol for pain information collected in
many of the trials shed valuable light on subjects such as side effects
measuring instruments and methodology Further appraisal of
the multidisciplinary approach to research a broader view of data
collection and a more accurate reporting of data already collected
could be extremely valuable in the future It would allow research
to be more widely used in various meta-analyses Data from areas
seemingly unrelated to the original null hypothesis eg comparison
of pain relief and pain intensity as a measuring tool adverse event
reporting the significance of global assessments etc could be more
readily available If the third molar trial population does decrease
it would be advantageous to collect as much data as possible from
any trial being undertaken
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
Paracetamol (acetaminophen) is an effective drug to use for post-
operative pain following oral surgery and the reporting of adverse
events shows it to be a safe drug (number needed to treat (to ben-
efit) (NNT) is 3 for 1000 mg of paracetamol at 6 hours number
needed to treat to harm (NNTH) 33) It is most effective at 1000
mg dose and can be taken at six hourly intervals without compro-
mising safety It could be considered more readily by dentist and
patients both as a first choice analgesic or to be taken alternately
with doses of other analgesics such as nonsteroidal anti-inflamma-
tory drugs (NSAIDS)
Implications for research
There is a large body of research in this area and further research
other than as a comparison seems unnecessary However in one
trial (Moller 2000) it was found that an effervescent formulation
appeared to have a faster onset of pain relief which would be
beneficial to patients who are looking for a rapid onset of relief
It may be helpful to undertake some research to confirm these
findings The use of pain relief and pain intensity difference as a
measure of pain relief may be another area for further investigation
It is valuable to have NNTNNTH as a baseline for comparison
with other analgesics Maximizing the third molar pain model
population by multidisciplinary research is another area of interest
highlighted by this review
A C K N O W L E D G E M E N T S
We wish to thank Sylvia Bickley (Cochrane Oral Health Group)
for her assistance with literature searching and Luisa Fernandez
Mauleffinch (Cochrane Oral Health Group) for her help with the
preparation of this review We would also like to thank the follow-
ing referees who reviewed this work at various stages Barry El-
liott Cole Mike Hill Kimito Yamashiro and Lasse Skoglund We
are grateful to Stephen Cooper Donald Mehlisch Philip Moller
Alberto Umile for providing information on their trials and to
Prisana Pripatnanont for translation and information
9Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Cooper 1980 published data only
Cooper SA Precheur H Rauch D Rosenheck A Ladov M
Engel J Evaluation of oxycodone and acetaminophen in
treatment of postoperative dental pain Oral Surgery Oral
Medicine and Oral Pathology 198050(6)496ndash501
Cooper 1981 published data only
Cooper SA Breen JF Giuliani RL The relative efficacy of
indoprofen with opiod-analgesic combinations Journal of
Oral Surgery 198139(1)21ndash5
Cooper 1988 published data only
Cooper SA Firestein A Cohn P Double-blind comparison
of meclofenamate sodium with acetaminophen
acetaminophen with codeine and placebo for relief of
postsurgical dental pain The Journal of Clinical Dentistry
19881(2)31ndash4
Cooper 1998 published data only
Cooper SA Reynolds DC Reynolds B Hersh EV Analgesic
efficacy and safety of (R)- ketoprofen in postoperative dental
pain Journal of Clinical Pharmacology 199838(2 Suppl)
11Sndash18S
Dionne 1994 published data only
Dionne RA Snyder J Hargreaves KM Analgesic efficacy
of flurbiprofen in comparison with acetaminophen
acetaminophen plus codeine and placebo after impacted
third molar removal Journal of Oral and Maxillofacial
Surgery 199452(9)919ndash24
Dolci 1994 published data only
Dolci G Ripari M Pacifici L Umile A Evaluation of
piroxicam-beta-cyclodextrin piroxicam paracetamol and
placebo in post-operative oral surgery pain International
Journal of Clinical Pharmacology Research 199414(5-6)
185ndash91
Forbes 1984b published data only
Forbes JA Barkaszi BA Ragland RN Hankle JJ
Analgesic effect of acetaminophen phenyltoloxamine
and their combination in postoperative oral surgery pain
Pharmacotherapy 19844(4)221ndash6
Forbes 1989 published data only
Forbes JA Butterworth GA Burchfield WH Yorio
CC Selinger LR Rosenmertz SK et alEvaluation of
flurbiprofen acetaminophen an acetaminophen-codeine
combination and placebo in postoperative oral surgery
pain Pharmacotherapy 19899(5)322ndash30
Forbes 1990 published data only
Forbes JA Kehm CJ Grodin CD Beaver WT Evaluation
of ketorolac ibuprofen acetaminophen and an
acetaminophen-codeine combination in postoperative
oral surgery pain Pharmacotherapy 199010(6(Pt 2)))
94Sndash105S
Hersh 2000 published data only
Hersh EV Levin LM Cooper SA Doyle G Waksman J
Wedell D et alIbuprofen liquigel for oral surgery pain
Clinical Therapeutics 200022(11)1306ndash18
Kiersch 1994 published data only
Kiersch TA Halladay SC Hormel PC A single-
dose double-blind comparison of naproxen sodium
acetaminophen and placebo in postoperative dental pain
Clinical Therapeutics 199416(3)394ndash404
Kubitzek 2003 published data only
Kubitzek F Ziegler G Gold MS Liu JM Ionescu E
Analgesic efficacy of low-dose diclofenac versus paracetamol
and placebo in postoperative dental pain Journal of
Orofacial Pain 200317(3)237ndash44
Lehnert 1990 published data only
Lehnert S Reuther J Wahl G Barthel K [The efficacy of
paracetamol (Tylenol) and acetyl salicylic acid (Aspirin)
in treating postoperative pain] Deutsche Zahnarztliche
Zeitschrift 199045(1)23ndash6
Mehlisch 1995 published data only
Mehlisch DR Jasper RD Brown P Korn SH McCarroll K
Murakami AA Comparative study of ibuprofen lysine and
acetaminophen in patients with postoperative dental pain
Clinical Therapeutics 199517(5)852ndash60
Moller 2000 published data only
Moller PL Norholt SE Ganry HE Insuasty JH Vincent
FG Skoglund LA et alTime of onset of analgesia and
analgesic efficacy of effervescent acetaminophen 1000
mg compared to tablet acetominophen 1000 mg in
postoperative dental pain a single-dose double-blind
randomized placebo-controlled study Journal of Clinical
Pharmacology 200040(4)370ndash8
Olson 2001 published data only
Olson NZ Otero AM Marrero I Tirado S Cooper S
Doyle G et alOnset of analgesia for liquigel ibuprofen
400 mg acetaminophen 1000 mg ketoprofen 25 mg
and placebo in the treatment of postoperative dental pain
Journal of Clinical Pharmacology 200141(11)1238ndash47
Seymour 1996 published data only
Seymour RA Kelly PJ Hawkesford JE The efficacy
of ketoprofen and paracetamol (acetaminopen) in
postoperative pain after third molar surgery British Journal
of Clinical Pharmacology 199641(6)581ndash5
Seymour 2003 published data only
Seymour RA Hawkesford JE Sykes J Stillings M Hill
CM An investigation into the comparative efficacy of
soluble aspirin and solid paracetamol in postoperative pain
after third molar surgery British Dental Journal 2003194
(3)153ndash7
Skoglund 1991 published data only
Skoglund LA Skjelbred P Fyllingen G Analgesic efficacy
of acetaminophen 1000 mg acetaminophen 2000 mg and
the combination of acetaminophen 1000 mg and codeine
10Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
phosphate 60 mg versus placebo in acute postoperative
pain Pharmacotherapy 199111(5)364ndash9
Sunshine 1986 published data only
Sunshine A Marrero I Olson N McCormick N Laska
EM Comparative study of flurbiprofen zomepirac sodium
acetaminophen plus codeine and acetaminophen for the
relief of postsurgical dental pain The American Journal of
Medicine 198680(3A)50ndash4
Vattaraphudej 1986 published data only
Vattaraphudej T Thongnoppakao P Koukongviriyapan V
[Comparison of the efficacy of analgesics in pain after oral
surgery] The Journal of the Dental Association of Thailand
198636(6)198ndash206
References to studies excluded from this review
Adame 1979 published data only
Adame C et alPostoperative development of inflammation
after extraction of impacted third molar as a model
for clinical assessment of anti-inflammatory drugs I
Preliminary report Boletin de Estudios Medicos y Biologicos
197930(8)308ndash9
Barden J 2004 published data only
Barden J Edwards J Moore A McQuay H Single dose
oral paracetamol (acetaminophen) for postoperative pain
Cochrane Database of Systematic Reviews 2004 Issue 1
[DOI DOI 10100214651858CD004602]
Becker 1990 published data only
Becker J Beckmann J Bertelt C Gundert-Remy U
Rohmel J Ohlendorf D [Double blind biometric study on
postoperative effects of analgesics] Deutsche Zahnarztliche
Zeitschrift 199045(1)36ndash8
Bentley 1987 published data only
Bentley KC Head TW The additive analgesic efficacy of
acetaminophen 1000 mg and codeine 60 mg in dental
pain Clinical Pharmacology and Therapeutics 198742(6)
634ndash40
Breivik 1998 published data only
Breivik EK Bjornsson GA Variation in surgical trauma and
baseline pain intensity effects on assay sensitivity of an
analgesic trial European Journal of Oral Sciences 1998106
(4)844ndash52
Cooper 1986 published data only
Cooper SA Erlichman MC Mardirossian G Double-
blind comparison of an acetaminophen-codeine-caffeine
combination in oral surgery pain Anesthesia Progress 1986
33(3)139ndash42
Cooper 1989 published data only
Cooper SA Schachtel BP Goldman E Gelb S Cohn P
Ibuprofen and acetaminophen in the relief of acute pain
a randomized double-blind placebo-controlled study
Journal of Clinical Pharmacology 198929(11)1026ndash30
Cooper 1991 published data only
Cooper SA Kupperman A The analgesic efficacy of
flurbiprofen compared to acetaminophen with codeine The
Journal of Clinical Dentistry 19912(3)70ndash4
Dionne 1983 (1) published data only
Dionne RA Campbell RA Cooper SA Hall DL
Buckingham B Suppression of postoperative pain by
preoperative administration of ibuprofen in comparison to
placebo acetaminophen and acetaminophen plus codeine
Journal of Clinical Pharmacology 198323(1)37ndash43
Dionne 1983 (2) published data only
Dionne RA Sisk AL Fox PC Wirdzek PR Gracely
RH Dubner R Suppression of postoperative pain by
preoperative adminsitration of flurbiprofen in comparison
to acetominophen and oxycodone plus acetominophen
Current Therapeutic Research 198334(1)15ndash29
Dionne 1986 published data only
Dionne RA Suppression of dental pain by the preoperative
administration of flurbiprofen The American Journal of
Medicine 198680(3A)41ndash9
Dolci 1993 published data only
Dolci G Ripari M Pacifici L Umile A [Analgesic efficacy
and the tolerance for piroxicam-beta-cyclodextrin compared
to piroxicam paracetamol and placebo in the treatment of
postextraction dental pain] Minerva Stomatologica 199342
(5)235ndash41
Edwards 2002 published data only
Edwards JE McQuay HJ Moore RA Combination
analgesic efficacy individual patient data meta-analysis
of single-dose oral tramadol plus acetaminophen in
acute postoperative pain Journal of Pain and Symptom
Management 200223(2)121ndash30
Forbes 1982 published data only
Forbes JA Beaver WT White EH White RW Neilson GB
Shackleford RW Diflunisal A new oral analgesic with an
unusually long duration of action JAMA 1982248(17)
2139ndash42
Forbes 1984a published data only
Forbes JA Kolodny AL Chachich BM Beaver WT
Nalbuphine acetaminophen and their combination in
postoperative pain Clinical Pharamacology and Therapeutics
198435(6)843ndash51
Gallardo 1990 published data only
Gallardo F Rossi E Analgesic efficacy of flurbiprofen as
compared to acetaminophen and placebo after periodontal
surgery Journal of Periodontology 199061(4)224ndash7
Gustafsson 1983 published data only
Gustafsson I Nystrom E Quiding H Effect of preoperative
paracetamol on pain after oral surgery European Journal of
Clinical Pharmacology 198324(1)63ndash5
Haanaes 1986 published data only
Haanaes HR Benterud UJ Skoglund LA RF 46-790 versus
paracetamol effect on post-operative pain International
Journal of Clinical Pharmacology Therapy and Toxicology
198624(11)598ndash601
Irvine 1982 published data only
Irvine GH Lutterloch MJ Bowerman JE Comparison
of diflunisal and paracetamol in the management of pain
11Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
following wisdom teeth removal British Dental Journal
1982152(1)18ndash20
Laska 1983 published data only
Laska EM Sunshine A Zighelboim I Roure C Marrero
I Wanderling J et alEffect of caffeine on acetaminophen
analgesia Clinical Pharmacology and Therapeutics 198333
(4)498ndash509
Lecointre 1991 published data only
Lecointre C [Efficacy and tolerance of tiaprofenic acid
for extraction complications Results of a randomized
double-blind study tiaprofenic acid versus paracetamol]
LrsquoInformation Dentaire 199173(35)3063ndash6
Liashek 1987 published data only
Liashek P Jr Desjardins PJ Triplett RG Effect of
pretreatment with acetaminophen-propoxyphene for oral
surgery pain Journal of Oral and Maxillofacial Surgery 1987
45(2)99ndash103
Macleod 2002 published data only
Macleod AG Ashford B Voltz M Williams B Cramond T
Gorta L et alParacetamol versus paracetamol-codeine in
the treatment of post-operative dental pain a randomized
double-blind prospective trial Australian Dental Journal
200247(2)147ndash51
Medve 2001 published data only
Medve RA Wang J Karim R Tramadol and acetaminophen
tablets for dental pain Anesthesia Progress 200148(3)
79ndash81
Mehlisch 1984 published data only
Mehlisch DR Frakes LA A controlled comparative
evaluation of acetaminophen and aspirin in the treatment of
postoperative pain Clinical Therapeutics 19847(1)89ndash97
Mehlisch 1990 published data only
Mehlisch DR Sollecito WA Helfrick JF Leibold DG
Markowitz R Schow CE Jr et alMulticenter clinical
trial of ibuprofen and acetaminophen in the treatment of
postoperative dental pain Journal of the American Dental
Association 1990121(2)257ndash63
Moore 1986 published data only
Moore PA Werther JR Seldin EB Stevens CM Analgesic
regimens for third molar surgery pharmacologic and
behavioral considerations Journal of the American Dental
Association 1986113(5)739ndash44
Nystrom 1988 published data only
Nystrom E Gustafsson I Quiding H The pain intensity
at analgesic intake and the efficacy of diflunisal in single
doses and effervescent acetaminophen in single and repeated
doses Pharmacotherapy 19888(3)201ndash9
Petersen 1983 published data only
Petersen JK A double-blind cross-over study of the analgesic
and anti-inflammatory effects of dexamethasone and
paracetamol following surgical removal of lower impacted
third molars International Journal of Oral Surgery 198312
(4)266
Quiding 1981 published data only
Quiding H Oksala E Happonen RP Lehtimaki K Ojala
T The visual analog scale in multiple-dose evaluations of
analgesics The Journal of Clinical Pharmacology 198121
(10)424ndash9
Quiding 1982 (1) published data only
Quiding H Oikarinen V Huitfeldt B Koskimo M
Leikomaa H Nyman C An analgesic study with repeated
doses of phenazone phenazone plus dextropropoxyphene
and paracetamol using a visual analogue scale International
Journal of Oral Surgery 198211(5)304ndash9
Quiding 1982 (2) published data only
Quiding H Persson G Ahlstrom U Bangens S Hellem S
Johansson G et alParacetamol plus supplementary doses
of codeine an analgesic study of repeated doses European
Journal of Clinical Pharmacology 198223(4)315ndash9
Quiding 1984 published data only
Quiding H Oikarinen V Sane J Sjoblad AM Analgesic
efficacy after single and repeated doses of codeine and
acetaminophen Journal of Clinical Pharmacology 198424
(1)27ndash34
Ragot 1991 published data only
Ragot JP [Comparison of analgesic activity of mefenamic
acid and paracetamol in treatment of pain after extraction
of impacted lower 3d molar] LrsquoInformation Dentaire 1991
73(21)1659ndash64
Reijntjes 1987 published data only
Reijntjes RJ Boering G Wesseling H van Rijn LG
Suprofen versus paracetamol after oral surgery International
Journal of Oral and Maxillofacial Surgery 198716(1)45ndash9
Rodrigo 1987 published data only
Rodrigo MR Rosenquist JB Cheung LK Paracetamol
and diflunisal for pain relief following third molar surgery
in Hong Kong Chinese International Journal of Oral and
Maxillofacial Surgery 198716(5)566ndash71
Rodrigo 1989 published data only
Rodrigo C Chau M Rosenquist J A comparison of
paracetamol and diflunisal for pain control following
3rd molar surgery International Journal of Oral and
Maxillofacial Surgery 198918(3)130ndash2
Rosen 1985 published data only
Rosen M Absi EG Webster JA Suprofen compared to
dextropropoxyphene hydrochloride and paracetamol
(Cosalgesic) after extraction of wisdom teeth under general
anaesthesia Anaesthesia 198540(7)639ndash41
Sakata 1989 published data only
Sakata LA Rocha B et alEffects of benzydamine after
surgical removal of impacted teeth [Efeitos da benzidamina
apoacutes a extraccedilaumlo de dentes inclusos] Revista da Associacao
Paulista de Cirurgioes Dentistas 198943(4)167ndash70
Selcuk 1996 published data only
Selcuk E Gomel M Bellibas SE Kose T Tuglular I
Comparison of the analgesic effects of diflunisal and
paracetamol in the treatment of postoperative dental pain
12Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
International Journal of Clinical Pharmacology Research
199616(2-3)57ndash65
Seymour 1981 published data only
Seymour RA Rawlins MD Pharmacokinetics of parenteral
paracetamol and its analgesic effects in post-operative dental
pain European Journal of Clinical Pharmacology 198120
(3)215ndash8
Seymour 1983 published data only
Seymour RA Analgesic efficacy and plasma concentration
of three analgesics in pain after lower third molar removal
SAAD Digest 19835(7)172ndash88
Skjelbred 1979 published data only
Skjelbred P Lokken P Paracetamol versus placebo effects
on post-operative course European Journal of Clinical
Pharmacology 197915(1)27ndash33
Strom 1990 published data only
Strom C Forsberg O Quiding H Engevall S Larsson
O Analgesic efficacy of acetaminophen sustained release
Journal of Clinical Pharmacology 199030(7)654ndash9
Van Aken 2004 published data only
Van Aken H Thys L Veekman L Buerkle H Assessing
analgesia in single and repeated administrations of
propacetamol for postoperative pain comparison with
morphine after dental surgery Anesthesia and Analgesia
200498(1)159ndash65
Winter 1983 published data only
Winter L Appleby F Ciccone PE Pigeon JG A double-
blind comparative evaluation of acetaminophen caffeine
and the combination of acetaminophen and caffeine in
outpatients with postoperative oral surgery pain Current
Therapeutic Research 198333(1)115ndash22
Additional references
Aronoff 2006
Aronoff DM Oates JA Boutaud O New insights into
the mechanism of action of acetaminophen Its clinical
pharmacologic characteristics reflect its inhibition of the
two prostaglandin H2 synthases Clinical Pharmacology and
Therapeutics 200679(1)9ndash19
Chandrasekharan 2002
Chandrasekharan NV Dai H Roos KL Evanson NK
Tomsik J Elton TS et alCOX-3 a cyclooxygenase-1 variant
inhibited by acetaminophen and other analgesicantipyretic
drugs cloning structure and expression Proceedings of the
National Academy of Sciences of the United States of America
200299(21)13926ndash31
Collins 1999
Collins SL Moore RA McQuay HJ Wiffen PJ Edwards JE
Single dose oral ibuprofen and diclofenac for postoperative
pain Cochrane Database of Systematic Reviews 1999
Issue 1 [DOI Art No CD001548 DOI 101002
14651858CD001548]
Cooper 1976
Cooper SA Beaver WT A model to evaluate mild analgesics
in oral surgery outpatients Clinical Pharmacology and
Therapeutics 197620(2)241ndash50
Coulthard 2001
Coulthard P Hill CM Frame JW Barry H Ridge BD
Bacon TH Pain control with paracetamol from a sustained
release formulation and a standard release formulation after
third molar surgery a randomised controlled trial British
Dental Journal 2001191(6)319ndash24
Dray 1997
Dray A Kinins and their receptors in hyperalgesia
Canadian Journal of Physiology and Pharmacology 199775
(6)704ndash12
Fisher 1988
Fisher SE Frame JW Rout PG McEntegart DJ Factors
affecting the onset and severity of pain following the surgical
removal of unilateral impacted mandibular third molar
teeth British Dental Journal 1988164(11)351ndash4
Loeser 1999
Loeser JD Melzack R Pain an overview Lancet 1999353
(9164)1607ndash9
Malmberg 1992
Malmberg AB Yaksh TL Antinociceptive effects of spinal
non-steroidal anti-inflammatory agents on the formalin
test in the rat Journal of Pharmacology and Experimental
Therapeutics 1992263136ndash46
Moore 1997
Moore RA McQuay HJ Single-patient data meta-analysis
of 3453 postoperative patients oral tramadol versus
placebo codeine and combination analgesics Pain 199769
(3)287ndash94
Moore 1998
Moore A Collins S Carroll D McQuay H Edwards
J Single dose paracetamol (acetaminophen) with and
without codeine for postoperative pain Cochrane Database
of Systematic Reviews 1998 Issue 4 [DOI Art No
CD001547 DOI 10100214651858CD001547]
Rang 2003
Rang HP Dale MM Ritter JM Moore PK Anti-
inflammatory and immunosuppresant drugs Pharmacology
5th Edition Churchill Livingstone 2003244ndash61
Seymour 1985
Seymour RA Meechan JG Blair GS An investigation into
post-operative pain after third molar surgery under local
analgesia The British Journal of Oral and Maxillofacial
Surgery 198523(6)410ndash8lowast Indicates the major publication for the study
13Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Cooper 1980
Methods Randomised parallel group double blind study
Participants 298 participants randomised to 6 groups withdrawals unclear (51 from all groups)
Number randomised to intervention male 13 female 24 mean age 225
Number randomised to placebo male 11 female 27 mean age 235
Number of third molars removed mean for intervention and placebo 19
Baseline pain intensity mean for intervention 241 (moderate 22 severe 15) mean for placebo 242
(moderate 22 severe 16)
Setting - outpatients (USA)
Interventions Paracetamol 500 mg versus placebo
Formulation not stated
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse events table
Notes Sponsored unclear
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Cooper 1981
Methods Randomised parallel group double blind study
Participants 248 participants randomised to 5 groups withdrawals unclear (48 from all groups)
Number randomised to intervention male 15 female 22 mean age 222
Number randomised to placebo male 13 female 24 mean age 237
Number of third molars removed not stated
Baseline pain intensity mean for intervention 22 (moderate 29 severe 9) mean for placebo 23 (moderate
26 severe 11)
Setting not stated (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation not stated
Anaesthesia LA or GA
14Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Cooper 1981 (Continued)
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Total number of adverse events and number of people with adverse events reported
Notes Sponsored by
Adria Laboratories
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Cooper 1988
Methods Randomised parallel group double blind study
Participants 165 participants randomised to 4 groups withdrawals unclear (22 from all groups)
Number randomised to intervention male 7 female 29 mean age 246
Number randomised to placebo male 11 female 29 mean age 247
Number of third molars removed mean for intervention 14 mean for placebo 15
Baseline pain intensity mean for intervention 24 (moderate 21 severe 15) mean for placebo 24 (mod-
erate 25 severe 15)
Setting - outpatients - single site (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Total number of adverse events
Notes Sponsored by
Parke-Davis
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
15Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Cooper 1998
Methods Randomised parallel group double blind study
Participants 177 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 23 female 27 mean age 236
Number randomised to placebo male 12 female 14 mean age 227
Number of third molars removed not stated
Baseline pain intensity mean for intervention categorical 23 VAS 603 mean for placebo categorical
22 VAS 628
Setting - Georgetown University Hospital (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe) VAS scale 0-100 mm (none - worst pain
imaginable)
PR at 4 hours and 6 hours categorical scale 0-4 (no relief - complete relief )
Global assessment not stated
Adverse effects table
Notes Sponsored by
Whitehall-Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Dionne 1994
Methods Randomised parallel group double blind study
Participants 135 participants randomised to 5 groups withdrawals unclear (11 from all groups)
Number randomised to intervention male 14 female 13 mean age 296
Number randomised to placebo male 15 female 10 mean age 282
Number of third molars removed not stated
Baseline pain intensity for intervention and placebo not stated
Setting private dental practice (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED or GA
Outcomes PI at 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 1-5 (poor - excellent)
Adverse effects table
16Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Dionne 1994 (Continued)
Notes Sponsored by
Upjohn
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Dolci 1994
Methods Randomised parallel group double blind study
Participants 338 participants enrolled in 4 groups withdrawals unclear (40 from all groups)
Number randomised to intervention male 28 female 44 mean age 279 age range 18-49
Number randomised to placebo male 28 female 48 mean age 272 age range 18-45
Number of third molars removed not stated
Baseline pain intensity range for intervention and placebo given together as average 214 (208 - 219)
Setting not stated (Italy)
Interventions Paracetamol 500 mg versus placebo
Formulation tablets
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (negative - very good)
Adverse effects table
Notes Sponsored - unclear
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Forbes 1984b
Methods Randomised parallel group double blind study
Participants 191 participants randomised to 4 groups withdrawals unclear (43 from all groups 164 used in reporting
of adverse events)
Number randomised to intervention male 19 female 20 mean age 2195
Number of third molars removed mean 244
Number randomised to placebo male 21 female 15 mean age 15-32
Number of third molars removed mean 278
17Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Forbes 1984b (Continued)
Baseline pain intensity mean for intervention 246 (moderate 21 severe 18) mean for placebo 247
(moderate 19 severe 17)
Setting private dental practice (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse effects reported as total number of adverse events and number of patients with adverse events
Notes Sponsored by McNeil Consumer Products
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Forbes 1989
Methods Randomised parallel group double blind study
Participants 107 participants randomised to 5 groups withdrawals unclear (19 from all groups 98 participants used
in reporting of adverse events)
Number randomised to intervention male 9 female 13 mean age 2059 age range 17-31
Number randomised to placebo male 12 female 11 mean age 2374 age range 16-39
Number of third molars removed mean for intervention 259 mean for placebo 209
Baseline pain intensity mean for intervention 245 mean for placebo 239
Setting - 2 sites private dental practice outpatients (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation - 1 tablet amp 1 capsule
Anaesthesia LA and GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects reported by number of patients with adverse events
Notes Sponsored by
Boots Company Ltd GH Besselaar Associates
Risk of bias
Item Authorsrsquo judgement Description
18Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Forbes 1989 (Continued)
Allocation concealment Unclear B - Unclear
Forbes 1990
Methods Randomised parallel group double blind study
Participants 206 participants randomised to 6 groups
Number randomised to intervention male 20 female 16 (5 withdrawals) mean age 225 age range 16-
46
Number randomised to placebo male 18 female 16 (4 withdrawals) mean age 2365 age range 16-45
Number of third molars removed mean for intervention 258 mean for placebo 235
Baseline pain intensity mean for intervention 239 (moderate 22 severe 14) mean for placebo 232
(moderate 23 severe 11)
Setting - private dental practice outpatients (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation capsules
Anaesthesia LA and GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects table
Notes Sponsored by
Syntex Research
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Hersh 2000
Methods Randomised parallel group double blind study
Participants 210 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 20 female 43 mean age 233
Number of third molars removedpatient (11) (26) (35) (451)
Number randomised to placebo male 9 female 8 mean age 237
Number of wisdom teeth removed per patient (11) (25) (33) (418)
Baseline pain intensity mean for intervention 23 (moderate 47 severe 16) mean for placebo 22 (mod-
erate 22 severe 5)
Setting - University of Pennsylvania School of Dental Medicine - outpatients (USA)
19Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hersh 2000 (Continued)
Interventions Paracetamol 1000 mg versus placebo
Formulation caplets
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical 0-3 (none - severe)
PR at 4 hours and 6 hours categorical 0-4 (no relief - complete relief )
Global assessment categorical 0-4 (poor - excellent)
Adverse effects by total number of adverse events and number of patients with adverse events
Notes Sponsored by
Whitehall-Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Kiersch 1994
Methods Randomised parallel group double blind study
Participants 232 participants enrolled in 3 groups
Number randomised to intervention 91 withdrawals 4 (2 before and 2 after randomisation) male 72
female 17 mean age 231 age range 15-39
Number of third molars removedpatient (10) (20) (331) (454)
Number randomised to placebo 47 withdrawals 2 male 35 female 10 mean age 247 age range 15-39
Number of third molars removedpatient (10) (20) (319) (426)
Baseline pain intensity mean for intervention and placebo categorical 212 VAS 5835
Setting not stated (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation capsules
Anaesthesia not stated
Outcomes PI at 4 hours and 6 hours categorical 0-3 (none - severe)
PR at 4 hours and 6 hours categorical 0-4 (none - complete) VAS 0-100 mm (no pain - worst pain I can
imagine)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects reported by total number of adverse events and by number of patients with adverse events
Notes Sponsored by
Syntex Research
Risk of bias
Item Authorsrsquo judgement Description
20Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Kiersch 1994 (Continued)
Allocation concealment Unclear B - Unclear
Kubitzek 2003
Methods Randomised parallel group double blind study
Participants 245 participants randomised to 3 groups no withdrawals
Number randomised to intervention 78
Number randomised to placebo 84 malefemale 40 male over both groups
Number of third molars removed 1 or 2 for each patient
Baseline pain intensity moderate to severe 65-76 in both groups
Setting dental practice (Germany)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia LA
Outcomes PI not stated
PR given as TOTPAR at 6 hours
Global assessment categorical 1-5 (poor - excellent)
Adverse effects not stated
Notes Sponsored by
Novartis Consumer Health
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Lehnert 1990
Methods Randomised parallel group double blind study
Participants 150 participants randomised to 3 groups 50 to each
Number randomised to intervention 1 withdrawal male 23 female 26 mean age 253 age range 17-52
Number randomised to placebo 2 withdrawals male 24 female 18 mean age 251 age range 18-53
Number of hird molars removed not stated
Baseline pain intensity mean for intervention 255 (moderate 22 severe 27) mean for placebo 25
(moderate 21 severe 21)
Setting outpatients (Germany)
Interventions Paracetamol 1000 mg versus placebo
Formulation capsules
Anaesthesia not stated
21Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Lehnert 1990 (Continued)
Outcomes PI at 6 hours categorical scale 0-3 (no pain - severe)
PR at 6 hours categorical scale 0-3 (none - complete)
Global assessment categorical scale 0-3 (poor - excellent)
Adverse effects by number of patients
Notes Sponsored by GH Besselar Associates
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Mehlisch 1995
Methods Randomised parallel group double blind study
Participants 240 participants randomised to 3 groups 1 withdrawal from the acetaminophen group
Number randomised to intervention (1 withdrawal) male 30 female 71 mean age 253 age range 15-
60
Number of third molars removedpatient (10 295 33 43)
Number randomised to placebo male 19 female 21 mean age 242 age range 15-48
Number of third molars removedpatient (10 239 30 41)
Baseline pain intensity mean for intervention 221 (moderate 80 severe 21) mean for placebo 220
(moderate 32 severe 8)
Setting not stated (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation 2 tablets
Anaesthesia not stated
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse events reported by number of patients
Notes Sponsored by
Biomedical Research Group and Merck Research Laboratories
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
22Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Moller 2000
Methods Randomised parallel group double blind study
Participants 242 participants randomised to 4 groups no withdrawals
Number randomised to Intervention A male 27 female 33 mean age 245
Number randomised to Intervention B male 26 female 34 mean age 262
Number randomised to Placebo A male 21 female 41 mean age 250
Number randomised to Placebo B male 24 female 36 mean age 246
Number of third molars removed per patient in both groups 1
Mean baseline intensity Intervention A categorical 200 (moderate 60) VAS 494
Mean baseline intensity Intervention B categorical 200 (moderate 60) VAS 473
Mean baseline intensity Placebo A categorical 200 (moderate 61 severe 1) VAS 505
Mean baseline intensity Placebo B categorical 200 (moderate 61) VAS 476
Setting Department of Oral and Maxillofacial Surgery Royal Dental College Aarhus (Denmark)
Interventions Intervention A Paracetamol 1000 mg versus Placebo A
Formulation effervescent tablets
Intervention B Paracetamol 1000 mg versus Placebo B
Formulation tablets
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe) VAS scale 0-100 mm (no pain - worst possible pain)
PR at 4 hours categorical 0-4 (none - complete)
Global assessment categorical 0-3 (poor - excellent)
Adverse effects reported as total number of adverse events and number of patients with adverse events
Notes Sponsored by
Bristol Myers Squibb
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Olson 2001
Methods Randomised parallel group double blind study
Participants 239 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 22 female 44 mean age 222
Number randomised to placebo male 11 female 28 mean age 239
Number of third molars removedpatient intervention - (11) (264) (31) (40) placebo - (11) (2
38) (30) (40)
Baseline pain intensity mean for intervention 286 (moderate 9 severe 57) mean for placebo 29 (moderate
4 severe 35)
Setting University of Puerto Rico School of Dentistry (Puerto Rico)
23Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Olson 2001 (Continued)
Interventions Paracetamol 1000 mg versus placebo
Formulation caplets
Anaesthesia LA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete relief )
Global assessment categorical scale 0-4 (poor - excellent)
Adverse effects table
Notes Sponsored by
Whitehall Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Seymour 1996
Methods Randomised parallel group double blind study
Participants 206 participants randomised to 5 groups
Number randomised to intervention A 1 withdrawal male 12 female 28 mean age 238
Number randomised to intervention B 1 withdrawal male 12 female 28 mean age 277 1 withdrawal
Number randomised to placebo 2 withdrawals male 15 female 24 mean age 246
Number of third molars removedpatient not stated
Baseline pain intensity mean for intervention A VAS 549 mean for intervention B VAS 542 mean
for placebo VAS 565
Setting not stated (UK)
Interventions Intervention A paracetamol 500 mg versus placebo
Intervention B paracetamol 1000 mg versus placebo
Formulation not stated
Anaesthesia GA
Outcomes PI at 6 hours VAS scale 0-100 mm (no pain - unbearable pain)
Global assessment categorical 0 -3 (very good - very poor)
but categories 1 amp 2 and 4 amp 5 not reported separately so unable to include data in tables
Adverse effects - none reported by any participants in any group
Notes Sponsored - unclear
Risk of bias
Item Authorsrsquo judgement Description
24Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Seymour 1996 (Continued)
Allocation concealment Unclear B - Unclear
Seymour 2003
Methods Randomised parallel group double blind study
Participants 167 randomised to 3 groups withdrawals unclear (14 from all groups)
Number randomised to intervention male 19 female 43 mean age 250
Number randomised to placebo male 11 female 21 mean age 251
Number of third molars removedpatient intervention - (12) (214) (312) (434) placebo - (13)
(25) (39) (415)
Baseline pain intensity mean for intervention 506 mean for placebo 541
Setting not clear (2 sites Cardiff and Hexham UK)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia GA
Outcomes PI at 4 hours VAS scale 0-100 mm (none - worst pain imaginable)
PR not stated
Global assessment categorical scale 1-5 (very poor - very good)
Adverse effects table
Notes Sponsored by
Reckitt Benckiser Healthcare
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Skoglund 1991
Methods Randomised parallel group double blind study
Participants 147 participants randomised to 4 groups withdrawals unclear (8 from all groups)
Number randomised to intervention male 16 female 16 mean age 247
Number randomised to placebo male 16 female 17 mean age 244
Number of third molars removed not stated
Baseline pain intensity mean for intervention approx 55 mean for placebo approx 45
Setting not stated (Norway)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia LA
25Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Skoglund 1991 (Continued)
Outcomes PI at 4 hours and 6 hours VAS scale 0-100 mm (none - pain cannot be worse)
PR at 4 hours and 6 hours VAS scale 0-100 mm (complete relief - no relief ) reversed for statistical analysis
Global assessment not stated
Adverse effects table
Notes Sponsored by
Apothekernes Laboratorium
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Sunshine 1986
Methods Randomised parallel group double blind study
Participants 182 participants randomised to 6 groups no withdrawals (only patients with moderate to severe pain
were randomised)
Number randomised to intervention male 6 female 24 mean age 219
Number randomised to placebo male 14 female 16 mean age 23
Number of third molars removed not stated
Baseline pain intensity mean for intervention 200 mean for placebo 200
Setting University of Puerto Rico School of Dentistry Clinic
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia LA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none 0 - complete 100)
Global assessment categorical 0-3 (poor - excellent)
Overall improvement 1-7 (very much worse - very much better)
Adverse effects reported by number of patients with adverse events
Notes Sponsored by
Upjohn
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
26Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Vattaraphudej 1986
Methods Randomised parallel group double blind study
Participants 83 enrolled to 4 groups withdrawals unclear (16 from all groups)
Number randomised to intervention male 8 female 8
Number randomised to placebo male 10 female 9
Number of third molars removed mean for intervention 125 mean for placebo 132
Baseline pain intensity mean for intervention 237 mean for placebo 226
Setting Dept of Oral Surgery Khon Kaen University Thailand
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (no relief - total relief )
Global assessment categorical scale 0-3 (poor - excellent)
Adverse effects none reported
Notes Sponsored by Khon Kaen University Thailand Dr Sompong Thongpradith Merck and Russel
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
GA - general anaesthetic LA - local anaesthetic PI - pain intensity PR - pain relief SED - sedation TOTPAR - total pain relief VAS
- visual analogue scale
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Adame 1979 Title not in journal quoted unable to find paper
Barden J 2004 Meta-analysis dental papers included individually where appropriate
Becker 1990 Not a third molar study
Bentley 1987 Unable to extract data for third molars only written to authors
Breivik 1998 Dose given at 3 hours postoperatively regardless of baseline pain unable to get 4-hour data Study used for side
effects only
27Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Cooper 1986 Unable to extract third molar data written to authors
Cooper 1989 Unable to extract third molar data written to authors
Cooper 1991 Unclear if third molars only written to authors
Dionne 1983 (1) Not single dose administered preoperatively
Dionne 1983 (2) Not placebo controlled not single dose administered preoperatively
Dionne 1986 Not placebo controlled
Dolci 1993 The data for the participants in this study are duplicated in Dolci 1994
Edwards 2002 This was a meta-analysis Need to identify source of data to clarify whether third molar studies and exclude
duplication Written to authors
Forbes 1982 Unable to extract third molar data written to authors
Forbes 1984a Not third molar study
Gallardo 1990 Not third molar study (periodontal surgery)
Gustafsson 1983 Patients given either paracetamol preoperatively and placebo postoperatively or vice versa unable to extract
relevant data
Haanaes 1986 Not placebo controlled Study used for side effects only
Irvine 1982 Not placebo controlled
Laska 1983 Not placebo controlled
Lecointre 1991 Not placebo controlled
Liashek 1987 Multiple doses unable to extract single dose data
Macleod 2002 Not placebo controlled
Medve 2001 Only 8-hour SPID and TOTPAR available need 4-hour andor 6-hour to include in review written to authors
Mehlisch 1984 Unable to extract third molar data written to authors
Mehlisch 1990 Unable to extract third molar data
Moore 1986 Multiple doses given unable to extract single dose data
Nystrom 1988 Not placebo controlled
28Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Petersen 1983 Unable to locate complete article
Quiding 1981 Not placebo controlled
Quiding 1982 (1) Not placebo controlled
Quiding 1982 (2) Not placebo controlled
Quiding 1984 No placebo used
Ragot 1991 Not placebo controlled
Reijntjes 1987 Not placebo controlled
Rodrigo 1987 Mixed parallel and cross-over trial multiple doses unable to extract relevant data
Rodrigo 1989 Not placebo controlled
Rosen 1985 Not placebo controlled multiple doses used unable to extract single dose data
Sakata 1989 Unable to obtain study
Selcuk 1996 Not placebo controlled
Seymour 1981 Cross-over trial baseline pain not stated unable to extract relevant data
Seymour 1983 Acetaminophen administered intravenously
Skjelbred 1979 Multiple doses unable to extract single dose data
Strom 1990 Not placebo controlled
Van Aken 2004 Propacetamol administered intravenously
Winter 1983 Unable to extract third molar data written to authors
SPID - summed pain intensity difference TOTPAR - total pain relief
29Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
Comparison 1 50 pain relief using pain relief measures
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Paracetamol versus placebo
number of people with at least
50 pain relief at 4 hours
16 1498 Risk Ratio (M-H Random 95 CI) 285 [189 429]
11 Up to 1000 mg of
paracetamol
10 710 Risk Ratio (M-H Random 95 CI) 196 [134 286]
12 1000 mg or more 6 788 Risk Ratio (M-H Random 95 CI) 456 [286 727]
2 Paracetamol versus placebo
number of people with at least
50 pain relief at 6 hours
13 1155 Risk Ratio (M-H Random 95 CI) 332 [188 587]
21 Up to 1000 mg of
paracetamol
6 378 Risk Ratio (M-H Random 95 CI) 189 [098 367]
22 1000 mg or more 7 777 Risk Ratio (M-H Random 95 CI) 421 [297 598]
Comparison 2 50 pain relief using pain intensity measures
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Paracetamol versus placebo
number of people with at least
50 pain relief at 4 hours
17 1658 Risk Ratio (M-H Random 95 CI) 487 [283 837]
11 Up to 1000 mg of
paracetamol
10 737 Risk Ratio (M-H Random 95 CI) 433 [219 858]
12 1000 mg or more 8 921 Risk Ratio (M-H Random 95 CI) 646 [234 1785]
2 Paracetamol versus placebo
number of people with at least
50 pain relief at 6 hours
13 1184 Risk Ratio (M-H Random 95 CI) 341 [234 497]
21 Up to 1000 mg of
paracetamol
6 403 Risk Ratio (M-H Random 95 CI) 267 [146 490]
22 1000 mg or more 8 781 Risk Ratio (M-H Random 95 CI) 396 [252 623]
30Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Comparison 3 Number of people with adverse events
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Number of patients with adverse
events paracetamol versus
placebo
17 1645 Risk Ratio (M-H Random 95 CI) 119 [090 157]
11 Up to 1000 mg of
paracetamol
9 672 Risk Ratio (M-H Random 95 CI) 125 [069 225]
12 1000 mg or more 8 973 Risk Ratio (M-H Random 95 CI) 116 [084 160]
Analysis 11 Comparison 1 50 pain relief using pain relief measures Outcome 1 Paracetamol versus
placebo number of people with at least 50 pain relief at 4 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 1 50 pain relief using pain relief measures
Outcome 1 Paracetamol versus placebo number of people with at least 50 pain relief at 4 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Dolci 1994 5472 2576 100 228 [ 161 323 ]
Cooper 1980 1137 1138 82 103 [ 051 207 ]
Forbes 1990 936 134 30 850 [ 114 6357 ]
Forbes 1989 522 023 17 1148 [ 067 19607 ]
Cooper 1988 1636 1240 87 148 [ 081 269 ]
Cooper 1981 2137 637 77 350 [ 160 767 ]
Forbes 1984b 1339 136 30 1200 [ 165 8716 ]
Vattaraphudej 1986 716 219 47 416 [ 100 1726 ]
Sunshine 1986 1830 1530 95 120 [ 076 190 ]
Dionne 1994 2527 1725 102 136 [ 102 182 ]
Subtotal (95 CI) 352 358 667 196 [ 134 286 ]
Total events 179 (Paracetamol better) 90 (Placebo better)
Heterogeneity Tau2 = 018 Chi2 = 2644 df = 9 (P = 0002) I2 =66
Test for overall effect Z = 349 (P = 000048)
2 1000 mg or more
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
31Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Mehlisch 1995 40101 240 49 792 [ 201 3124 ]
Cooper 1998 1850 326 59 312 [ 101 963 ]
Olson 2001 4266 539 74 496 [ 215 1148 ]
Moller 2000 27120 0122 18 5591 [ 345 90627 ]
Hersh 2000 4063 527 75 343 [ 152 773 ]
Kiersch 1994 2589 345 58 421 [ 134 1321 ]
Subtotal (95 CI) 489 299 333 456 [ 286 727 ]
Total events 192 (Paracetamol better) 18 (Placebo better)
Heterogeneity Tau2 = 003 Chi2 = 544 df = 5 (P = 036) I2 =8
Test for overall effect Z = 637 (P lt 000001)
Total (95 CI) 841 657 1000 285 [ 189 429 ]
Total events 371 (Paracetamol better) 108 (Placebo better)
Heterogeneity Tau2 = 040 Chi2 = 6294 df = 15 (Plt000001) I2 =76
Test for overall effect Z = 503 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
32Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 12 Comparison 1 50 pain relief using pain relief measures Outcome 2 Paracetamol versus
placebo number of people with at least 50 pain relief at 6 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 1 50 pain relief using pain relief measures
Outcome 2 Paracetamol versus placebo number of people with at least 50 pain relief at 6 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Forbes 1989 322 023 29 730 [ 040 13375 ]
Cooper 1988 1236 940 99 148 [ 071 310 ]
Forbes 1990 736 034 30 1419 [ 084 23928 ]
Dionne 1994 2427 1825 115 123 [ 093 163 ]
Forbes 1984b 1039 036 31 1943 [ 118 31995 ]
Sunshine 1986 1530 1030 104 150 [ 081 279 ]
Subtotal (95 CI) 190 188 407 189 [ 098 367 ]
Total events 71 (Paracetamol better) 37 (Placebo better)
Heterogeneity Tau2 = 032 Chi2 = 1445 df = 5 (P = 001) I2 =65
Test for overall effect Z = 189 (P = 0058)
2 1000 mg or more
Kubitzek 2003 4569 773 99 680 [ 329 1404 ]
Mehlisch 1995 35101 140 49 1386 [ 196 9779 ]
Kiersch 1994 2089 345 79 337 [ 106 1075 ]
Olson 2001 4166 539 94 485 [ 209 1122 ]
Hersh 2000 3563 527 95 300 [ 132 682 ]
Lehnert 1990 2349 640 96 313 [ 141 693 ]
Cooper 1998 1750 326 81 295 [ 095 914 ]
Subtotal (95 CI) 487 290 593 421 [ 297 598 ]
Total events 216 (Paracetamol better) 30 (Placebo better)
Heterogeneity Tau2 = 00 Chi2 = 509 df = 6 (P = 053) I2 =00
Test for overall effect Z = 806 (P lt 000001)
Total (95 CI) 677 478 1000 332 [ 188 587 ]
Total events 287 (Paracetamol better) 67 (Placebo better)
Heterogeneity Tau2 = 072 Chi2 = 6335 df = 12 (Plt000001) I2 =81
Test for overall effect Z = 412 (P = 0000038)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
33Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 21 Comparison 2 50 pain relief using pain intensity measures Outcome 1 Paracetamol versus
placebo number of people with at least 50 pain relief at 4 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 2 50 pain relief using pain intensity measures
Outcome 1 Paracetamol versus placebo number of people with at least 50 pain relief at 4 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Dolci 1994 4972 576 86 1034 [ 437 2449 ]
Seymour 1996 1940 1039 96 185 [ 099 346 ]
Cooper 1980 737 438 74 180 [ 057 563 ]
Forbes 1990 1036 034 28 1986 [ 121 32639 ]
Forbes 1989 622 023 28 1357 [ 081 22736 ]
Cooper 1988 1236 840 90 167 [ 077 361 ]
Sunshine 1986 1830 630 90 300 [ 138 650 ]
Forbes 1984b 1339 036 28 2498 [ 154 40542 ]
Vattaraphudej 1986 616 119 44 713 [ 095 5317 ]
Cooper 1981 1537 037 28 3100 [ 192 49971 ]
Subtotal (95 CI) 365 372 592 433 [ 219 858 ]
Total events 155 (Paracetamol better) 34 (Placebo better)
Heterogeneity Tau2 = 063 Chi2 = 2622 df = 9 (P = 0002) I2 =66
Test for overall effect Z = 421 (P = 0000026)
2 1000 mg or more
Cooper 1998 1350 026 28 1429 [ 088 23130 ]
Mehlisch 1995 41101 340 75 541 [ 178 1648 ]
Hersh 2000 3663 127 46 1543 [ 223 10685 ]
Skoglund 1991 1632 033 28 3400 [ 213 54391 ]
Seymour 2003 1262 432 78 155 [ 054 442 ]
Seymour 1996 2040 1039 96 195 [ 105 362 ]
Kiersch 1994 989 045 28 971 [ 058 16317 ]
Moller 2000 28120 0122 28 5794 [ 358 93840 ]
Subtotal (95 CI) 557 364 408 646 [ 234 1785 ]
Total events 175 (Paracetamol better) 18 (Placebo better)
Heterogeneity Tau2 = 124 Chi2 = 2347 df = 7 (P = 0001) I2 =70
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
34Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Test for overall effect Z = 360 (P = 000032)
Total (95 CI) 922 736 1000 487 [ 283 837 ]
Total events 330 (Paracetamol better) 52 (Placebo better)
Heterogeneity Tau2 = 070 Chi2 = 4973 df = 17 (P = 000005) I2 =66
Test for overall effect Z = 571 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
Analysis 22 Comparison 2 50 pain relief using pain intensity measures Outcome 2 Paracetamol versus
placebo number of people with at least 50 pain relief at 6 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 2 50 pain relief using pain intensity measures
Outcome 2 Paracetamol versus placebo number of people with at least 50 pain relief at 6 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Seymour 1996 1840 939 152 195 [ 100 380 ]
Forbes 1989 422 023 16 939 [ 054 16485 ]
Cooper 1988 936 640 105 167 [ 066 422 ]
Forbes 1990 836 032 17 1516 [ 091 25267 ]
Forbes 1984b 1139 036 17 2128 [ 130 34843 ]
Sunshine 1986 1430 530 111 280 [ 115 680 ]
Subtotal (95 CI) 203 200 418 267 [ 146 490 ]
Total events 64 (Paracetamol better) 20 (Placebo better)
Heterogeneity Tau2 = 015 Chi2 = 705 df = 5 (P = 022) I2 =29
Test for overall effect Z = 318 (P = 00015)
2 1000 mg or more
Hersh 2000 3163 127 33 1329 [ 191 9242 ]
Mehlisch 1995 39101 340 82 515 [ 169 1571 ]
Olson 2001 4266 739 146 355 [ 177 711 ]
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
35Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Seymour 1996 2140 939 157 228 [ 119 433 ]
Cooper 1998 1250 026 17 1324 [ 081 21504 ]
Kiersch 1994 489 045 16 460 [ 025 8361 ]
Lehnert 1990 2449 542 114 411 [ 172 983 ]
Skoglund 1991 1432 033 17 2988 [ 186 48076 ]
Subtotal (95 CI) 490 291 582 396 [ 252 623 ]
Total events 187 (Paracetamol better) 25 (Placebo better)
Heterogeneity Tau2 = 008 Chi2 = 863 df = 7 (P = 028) I2 =19
Test for overall effect Z = 597 (P lt 000001)
Total (95 CI) 693 491 1000 341 [ 234 497 ]
Total events 251 (Paracetamol better) 45 (Placebo better)
Heterogeneity Tau2 = 013 Chi2 = 1823 df = 13 (P = 015) I2 =29
Test for overall effect Z = 637 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
36Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 31 Comparison 3 Number of people with adverse events Outcome 1 Number of patients with
adverse events paracetamol versus placebo
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 3 Number of people with adverse events
Outcome 1 Number of patients with adverse events paracetamol versus placebo
Study or subgroup Paracetamol more Placebo more Risk Ratio Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Cooper 1980 237 637 033 [ 007 155 ]
Dolci 1994 780 882 090 [ 034 236 ]
Forbes 1990 541 038 1021 [ 058 17873 ]
Forbes 1989 326 226 150 [ 027 825 ]
Sunshine 1986 130 130 100 [ 007 1526 ]
Cooper 1981 1237 438 308 [ 109 869 ]
Dionne 1994 727 525 130 [ 047 356 ]
Vattaraphudej 1986 016 019 00 [ 00 00 ]
Forbes 1984b 143 240 047 [ 004 493 ]
Subtotal (95 CI) 337 335 125 [ 069 225 ]
Total events 38 (Paracetamol more) 28 (Placebo more)
Heterogeneity Tau2 = 016 Chi2 = 906 df = 7 (P = 025) I2 =23
Test for overall effect Z = 074 (P = 046)
2 1000 mg or more
Olson 2001 1066 239 295 [ 068 1279 ]
Cooper 1998 2550 426 325 [ 127 835 ]
Moller 2000 48120 56122 087 [ 065 117 ]
Seymour 2003 2462 932 138 [ 073 260 ]
Mehlisch 1995 1299 440 121 [ 042 354 ]
Kiersch 1994 2691 1347 103 [ 059 182 ]
Hersh 2000 1263 727 073 [ 032 166 ]
Lehnert 1990 549 440 102 [ 029 355 ]
Subtotal (95 CI) 600 373 116 [ 084 160 ]
Total events 162 (Paracetamol more) 99 (Placebo more)
Heterogeneity Tau2 = 007 Chi2 = 1096 df = 7 (P = 014) I2 =36
Test for overall effect Z = 090 (P = 037)
Total (95 CI) 937 708 119 [ 090 157 ]
01 02 05 1 2 5 10
Favours treatment Favours control
(Continued )
37Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol more Placebo more Risk Ratio Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Total events 200 (Paracetamol more) 127 (Placebo more)
Heterogeneity Tau2 = 007 Chi2 = 2073 df = 15 (P = 015) I2 =28
Test for overall effect Z = 121 (P = 023)
01 02 05 1 2 5 10
Favours treatment Favours control
A D D I T I O N A L T A B L E S
Table 1 Number of patients with adverse events (lt 1000 mg ParacetamolPlacebo)
Author Total Paracetamol AEs Paracetamol Total Placebo AEs Placebo
Cooper 1980 37 2 37 6
Cooper 1981 37 12 38 4
Dionne 1994 27 7 25 5
Dolci 1994 80 7 82 8
Forbes 1984b 43 1 40 2
Forbes 1989 26 3 26 2
Forbes 1990 41 5 38 0
Gallardo 1990 15 5 11 3
Seymour 1996 40 0 39 0
Sunshine 1986 30 1 30 1
Vattaraphudej 1986 16 0 19 0
Totals 392 43 385 31
38Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Quality assessment
Author Allocation concealment Follow up Total (Max-3)
Cooper 1980 1 0 1
Cooper 1981 1 0 1
Cooper 1988 1 0 1
Cooper 1998 1 1 2
Dionne 1994 1 0 1
Dolci 1994 1 0 1
Forbes 1984b 2 0 2
Forbes 1989 1 0 1
Forbes 1990 2 0 2
Hersh 2000 1 1 2
Kiersch 1994 1 1 2
Kubitzek 2003 1 1 2
Lehnert 1990 1 1 2
Mehlisch 1995 2 1 3
Moller 2000 1 1 2
Olson 2001 2 1 3
Seymour 1996 1 1 2
Seymour 2003 2 0 2
Skoglund 1991 2 0 2
Sunshine 1986 2 1 3
Vattaraphudej 1986 1 1 2
39Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Random-effects metaregression lt 1000 mg vs 1000 mg Paracetamol vs Placebo
Outcome Number of studies Slope estimate 95 CI Slope interpretation P value
50 pain relief at 4
hours (using pain re-
lief )
16 094 (036 to 152) more pain relief for
higher doses
0001
50 pain relife at 6
hours (using pain re-
lief )
13 114 (071 to 156) more pain relief for
higher doses
lt0001
50 pain relief at
4 hours (using pain
intensity)
16 023 (-084 to 130) more pain relief for
higher doses
067
50 pain relief at
6 hours (using pain
intensity)
14 043 (-015 to 101) more pain relief for
higher doses
015
Table 4 List of adverse events
Adverse events Paracetamol Placebo
Nausea 21 11
Vomiting 11 3
Nausea andor vomiting stomach cramps
abdominal pain
3 3
Headache 47 31
Drowsiness sleepiness somnolence 36 13
Dizziness fainting syncope 9 4
Bleeding 11 7
Chills flushes fever flu-like symptoms 5 0
Paraesthesia 4 2
Jawache 1 0
Swelling 1 6
Cellulitis 1 0
40Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 List of adverse events (Continued)
Dry socket 11 12
Surgical complications 6 13
CNS 5 6
GI 12 2
Body as a whole 8 3
Respiratory 2 0
Psychiatric 0 1
Other hiccups hearingvestibular miosis 5 1
Table 5 Global assessment - 5-point scale(lt 1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Cooper 1980 37 089 38 089
Cooper 1981 37 192 37 062
Cooper 1988 36 238 40 205
Dionne 1994 27 240 25 200
Dolci 1994 72 210 76 217
Forbes 1984 39 126 36 028
Mean 248 183 252 144
Table 6 Global assessment - 4-point scale (lt 1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Forbes 1989 26 100 26 030
Forbes 1990 41 147 38 056
Sunshine 1986 30 120 30 093
Vattaraphudej 1986 16 16 19 116
41Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 6 Global assessment - 4-point scale (lt 1000 mg Paracetamol) (Continued)
Mean 113 131 113 070
Table 7 Global assessment - 5-point scale (1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Kiersch 1994 91 130 47 060
Kubitzek 2003 78 198 84 145
Mehlisch 1995 101 157 40 045
Olson 2001 66 281 39 193
Seymour 2003 62 250 32 214
Mean 398 194 242 129
Table 8 Global assessment - 4-point scale (1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Hersh 2000 63 229 27 085
Moller 2000 120 188 122 154
Mean 183 202 149 141
A P P E N D I C E S
Appendix 1 CENTRAL search strategy
1 MOLAR THIRD single term (MeSH)
2 (wisdom next tooth)
3 (wisdom next teeth)
4 (third near molar)
5 (1 or 2 or 3 or 4)
6 TOOTH EXTRACTION single term (MeSH)
7 (extract near tooth)
8 (extract near teeth)
9 (extract near (third next molar))
10 (extract near (third near molar))
42Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
11 (remov near tooth)
12 (remov near teeth)
13 (surgical near remov)
14 (surgery near remov)
15 (surgical near extract)
16 (surgery near extract)
17 (6 or 7 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16)
18 (5 and 17)
W H A T rsquo S N E W
Last assessed as up-to-date 21 May 2007
Date Event Description
31 July 2008 Amended Converted to new review format
H I S T O R Y
Protocol first published Issue 4 2003
Review first published Issue 3 2007
C O N T R I B U T I O N S O F A U T H O R S
Conceiving designing and co-ordinating the review (Kiaran Weil (KW) Paul Coulthard (PC))
Developing search strategy and undertaking searches (Zahid Afzal (ZA) Arjen van Wijk (AJW) KW)
Screening search results and retrieved papers against inclusion criteria (ZA KW) Marco Esposito (ME) Lee Hooper (LH) PC)
Appraising quality (KW ZA)
Extracting data from papers (KW LH Helen Worthington (HW))
Writing to authors for additional information (KW)
Data management for the review and entering data into RevMan (KW)
Analysis and interpretation of data (KW LH HW)
Writing the review (KW)
Providing general advice on the review (ME LH PC HW)
Performing previous work that was the foundation of current study (PC)
43Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D E C L A R A T I O N S O F I N T E R E S T
None known
S O U R C E S O F S U P P O R T
Internal sources
bull The University of Manchester UK
bull The University of Amsterdam Netherlands
External sources
bull No sources of support supplied
I N D E X T E R M S
Medical Subject Headings (MeSH)
Acetaminophen [adverse effects lowasttherapeutic use] Analgesics Non-Narcotic [adverse effects lowasttherapeutic use] Molar Third [lowastsurgery]
Outcome Assessment (Health Care) Pain Postoperative [lowastdrug therapy] Pain Measurement Randomized Controlled Trials as Topic
Tooth Extraction [lowastadverse effects]
MeSH check words
Humans
44Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 407
Relative efficacy of oral analgesics after thirdmolar extractionJ Barden1 J E Edwards2 H J McQuay3 P J Wiffen4 and R A Moore5
Objectives To compare the relative efficacy of analgesics after thirdmolar extraction from systematic reviews of randomised double blindstudiesData sources Dental trials from systematic reviews of randomiseddouble-blind studies of analgesics in acute painData selection Number of patients with moderate or severe painachieving at least half pain relief over 4 to 6 hours after a single oraldose of analgesicData extraction Independently by two reviewersData synthesis Use of dichotomous information from active andplacebo treatments first to calculate the statistical significance usingrelative risk and then to evaluate the clinical relevance using numberneeded to treat (NNT) Non-steroidal anti-inflammatory drugs (NSAIDs)and cyclo-oxygenase-2 (COX-2) inhibitors had the lowest (best) NNTsfor the outcome of at least half pain relief over 4-6 hours comparedwith placebo With the best performing analgesics 50-70 patients out of100 had good pain relief compared with about 10 out of 100 withplacebo Only paracetamol 600650 mg plus codeine 60 mg wasassociated with any significant increase in any patient experiencing anadverse eventConclusions NSAIDs and COX-2 inhibitors have the lowest (best) NNTsThey may also have fewer adverse effects after third molar surgerythough conclusive evidence is lacking At least 80 of analgesicprescribing by UK dentists is in line with the best available evidence onefficacy and safety
Acute pain has been studied in single dose designs first pro-posed by Beecher and colleagues12 and formalised by Houdeand Wallenstein3 The problem with single trials is that whilethey can demonstrate statistical superiority of analgesic overplacebo variation because of random chance means that if
1Research Associate 2Senior Research Associate 3Professor of Pain Relief 4PrescribingAdvisor 5Research Director Pain Research and Nuffield Department of AnaestheticsUniversity of Oxford Oxford Radcliffe Hospital The Churchill Headington Oxford OX3 7LJ UKCorrespondence to Dr R A MooreE-mail andrewmoorepruoxacuk
Refereed paperReceived 150403 Accepted 121103doi101038sjbdj4811721copy British Dental Journal 2004 197 407ndash411
small they provide a poor estimate of the size of the analgesiceffect4 Combining results from clinically homogeneous trials ina meta-analysis gives an accurate estimate of the extent of theanalgesic effect when sufficient numbers of patients have beenrandomised45
Clinical trials in acute pain normally last 4 to 6 hours becausethat is the duration of effect of most analgesics whether injectedor as tablets and whether simple analgesics NSAIDs or opioidsMeta-analysis in acute pain has concentrated on the use of thearea under the total pain relief versus time curve (TOTPAR)dichotomized into those patients who do or do not achieve atleast half pain relief (at least 50 maximum TOTPAR)6 Thismeasure is the one most frequently reported and it avoids theproblem of reporting continuous pain data as the mean of ahighly skewed distribution7 It has the benefit of being intuitivelymeaningful to patients and professionals as well as being meas-urable
Meta-analyses in acute pain usually combine studies from avariety of pain models and relative efficacy of analgesics inthese studies has been examined6 A majority of studies were inthird molar extraction but any postoperative pain condition islikely to be included In the largest dataset that of aspirin8
pain model (dental or other surgery) made no difference to theNNT
Dentists ask rightly about relative efficacy in dental painThe number of prescription items issued by dentists in Englandwas remarkably consistent between 1998 and 2001 (Table 1)with ibuprofen dihydrocodeine and paracetamol being mostfrequently prescribed This review set out to examine single-dose oral analgesics after third molar extraction from a numberof updated systematic reviews both for the analgesics common-ly prescribed in England and for those for which comparableevidence exists including the newer cyclo-oxygenase-2 selec-tive inhibitors like rofecoxib celecoxib and valdecoxib
METHODSIn all the systematic reviews QUORUM guidelines were fol-lowed9 In the reviews studies for inclusion were soughtthrough searching the Cochrane Library Biological AbstractsMEDLINE PubMed and the Oxford Pain Relief database10 Ref-erence lists and review articles were examined for possible addi-tional references Most had search dates in 2002
This paper reviews the available high quality information on analgesics commonlyprescribed by dentists including COX-2 selective inhibitors
Problems related to chance effects are avoided by combining multiple trials in a meta-analysis
There is good evidence of efficacy for most commonly-prescribed analgesics Standard doses of NSAIDs and COX-2 inhibitors provide the best analgesia and lowest
rate of adverse events
I N B R I E F
RESEARCH
07p407-411qxd 10092004 1518 Page 407
RESEARCH
408 BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004
References for the reviews are as followsAspirin Edwards et al 19998 additional searching in
2002 found no new studiesCelecoxib An unpublished review being submitted as a
Cochrane ReviewDiclofenac An updated version of a Cochrane review11
Dihydrocodeine A Cochrane review12
Ibuprofen An updated version of a Cochrane review11
Paracetamol An updated version of a Cochrane review13
Paracetamol An updated version of a Cochrane review13
plus codeineRofecoxib An updated version of a systematic review14
Valdecoxib A systematic review in preparation
Criteria for inclusion for postoperative dental pain werestudy in third molar extraction full journal publication (exceptvaldecoxib which included information from a poster) ran-domised controlled trials which included single dose treatmentgroups of oral analgesic and placebo double blind designbaseline postoperative pain of moderate to severe intensitypatients over 15 years of age at least 10 patients per group andthe pain outcome measures of total pain relief (TOTPAR) orsummed pain intensity difference (SPID) over 4-6 hours or suf-ficient data to allow their calculation Pain measures allowedfor the calculation of TOTPAR or SPID were a standard fivepoint pain relief scale (none slight moderate good complete)a standard four point pain intensity scale (none mild moder-ate severe) or a standard visual analogue scale (VAS) for pain
relief or pain intensity For adverse events the primary out-come sought was the proportion of patients experiencing anyadverse event with secondary outcomes of patients experienc-ing particular adverse events Although adverse events areoften reported inconsistently in acute pain trials15 the outcomeof any patient experiencing any adverse event was the mostconsistently reported
Each report which could possibly be described as a randomisedcontrolled trial was read independently by several authors andscored using a commonly-used three item 1-5 score qualityscale16 Consensus was then achieved The maximum score of anincluded study was 5 and the minimum score was 2 Authors werenot blinded because they already knew the literature This scoringsystem takes account of randomisation blinding and withdrawalsand drop outs Trials that score 3 or more (less biased) have beenshown repeatedly to have lower treatment effects than those scor-ing 2 or less1718
For each trial mean TOTPAR SPID VAS-TOTPAR or VAS-SPIDvalues for each treatment group were converted to maxTOTPARby division into the calculated maximum value19 The proportionof patients in each treatment group who achieved at least 50maxTOTPAR was calculated using valid equations20-22 The num-ber of patients randomised was taken as the basis for calculationsto produce an intention to treat analysis The number of patientswith at least 50 maxTOTPAR was then used to calculate relativebenefit and NNT for analgesic versus placebo The same methodswere used for adverse events where the number needed to harm(NNH) was calculated
Table 1 Numbers of prescription items issued by dentists and dispensed in EnglandAnalgesic 1998 1999 2000 2001
Ibuprofen 400 mg 107200 110400 109000 103900
Dihydrocodeine 30 mg 53700 50300 49100 46700
Ibuprofen 600 mg 34200 39700 40800 42600
Ibuprofen 200 mg 36300 34600 32000 30600
Paracetamol 500 mg 11100 12800 15400 17200
Paracetamol 500 mg soluble 800 1000 900 900
Pethidine 50 mg 1100 900 700 700
Aspirin 300 mg 200 200 200 200
Source DOH statistics division 2002 calendar year January to December
Dihydrocodeine 30 mgParacetamol 300 mg + codeine 30 mg
Paracetamol 600650 mgAspirin 600650 mg
Paracetamol 9751000 mgCelecoxib 200 mg
Paracetamol 600650 mg + codeine 60 mgIbuprofen 200 mgDiclofenac 50 mgRofecoxib 50 mgIbuprofen 400 mgValdecoxib 20 mgDiclofenac 100 mgValdecoxib 40 mgIbuprofen 600 mg
0 10 20 30 40 50 60 70 80 90 10095 confidence interval of the percent ofpatients achieving at least 50 pain relief
Fig 1 The 95confidence interval ofthe proportion ofpatients with at leasthalf pain relief over 4-6hours compared withplacebo in third molarextraction trials
07p407-411qxd 10092004 1519 Page 408
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 409
of patients had at least half pain relief with active treatment in onesmall trial in dental pain (Table 2)
The adverse event outcome of a patient experiencing anyadverse event is shown in Table 3 from 10113 patients in 107 tri-als Of the 15 drug and dose combinations only paracetamol600650 mg plus codeine 60 mg could be statistically distin-guished from placebo in 10 trials and 824 patients The NNH was53 (41 to 74) indicating that five patients had to be treated withparacetamol 600650 mg plus codeine 60 mg for one of them tohave an adverse event that would not have occurred with placeboFor all other drugs and doses there was no difference betweenanalgesic and placebo
DISCUSSIONSystematic review and meta-analysis both depend on two interde-pendent criteria for them to make sense the quality of the compo-nent individual studies and the total size of the sample availablefor analysis
We know that if trials are of poor reporting quality1718 or notrandomised30 or not blind or both31 then the tendency is to over-estimate the benefits of treatment The reviews included here alldemanded that trials should be both randomised and double-blindas a minimum requirement for inclusion
We also know that even if trials are done well small samplesize can lead to an incorrect answer just because of the randomplay of chance4 For these studies we also know just how muchinformation is needed to be 95 confident of an NNT to withplusmn05 units4 With an NNT of 23 it is 400 patients in the compari-son with an NNT of 29 it is 1000 patients and with an NNT of42 it is many more than with 1000 At NNTs of 4 or more evenwith 1000 patients fewer than 75 of trials will be within plusmn05of the overall NNT
The analgesics for which these two criteria were metunequivocally were valdecoxib (combining 20 mg and 40 mg)rofecoxib 50 mg ibuprofen 400 mg diclofenac 50 mg and prob-ably ibuprofen 200 mg For paracetamol the numbers were bor-derline and for diclofenac 100 mg too small to make any safejudgement There is good evidence of good efficacy for the anal-gesics most commonly prescribed by dentists with the excep-tion of dihydrocodeine where there was little evidence in totaland no convincing evidence of efficacy
Relative benefit and relative risk estimates were calculated with95 confidence intervals using a fixed effects model23 Hetero-geneity tests were not used as they have previously been shown tobe unhelpful2425 though homogeneity was examined visually26
Publication bias was not assessed using funnel plots as these testshave been shown to be unhelpful2728 The number needed to treator harm (NNT and NNH) with confidence intervals was calculatedby the method of Cook and Sackett29 from the sum of all eventsand patients for treatment and placebo
Relative benefit or risk was considered to be statistically signifi-cant when the 95 confidence interval did not include 1 NNT val-ues were only calculated when the relative risk or benefit was sta-tistically significant and are reported with the 95 confidenceinterval Calculations were performed using Microsoft Excel 2001on a Power Macintosh G4
RESULTSTable 2 shows the main results from 14150 patients in 155 trials of15 drug and dose combinations against placebo in third molarextractions Of those 15 drug and dose combinations only dihy-drocodeine 30 mg could not be statistically distinguished fromplacebo because there were no trials with any useful informationin third molar extraction Figure 1 shows the proportion ofpatients achieving at least 50 pain relief with treatment Thesmallest sample for any comparison was 136 patients for celecoxib200 mg Only five of the 14 comparisons had more than 1000patients and seven had fewer than 500 patients In all systematicreviews the majority of trials had quality scores of 3 or more
The lowest (best) NNTs were for NSAIDs and COX-2 inhibitorsat standard or high doses For these NNTs could be as low as about2 (meaning that two patients had to be treated with NSAID orCOXIB for one of them to have an outcome of at least half painrelief that would not have occurred with placebo) Valdecoxib 20mg and 40 mg rofecoxib 50 mg ibuprofen 400 mg and diclofenac50 mg and 100 mg all had NNTs below 24 For all of them about60-70 of patients had at least half pain relief with active treat-ment compared with about 10 with placebo
Paracetamol 9751000 mg aspirin 600650 mg and paraceta-mol 600650 mg had NNTs of between 4 and 5 Fewer than 40 ofpatients with paracetamol at these doses had at least half painrelief with active treatment With dihydrocodeine 30 mg only 16
Table 2 Efficacy of analgesics after third molar extraction from systematic reviews of randomised double blind trials
Number () of patientswith at least 50 pain relief
Drug and dose Treatment Placebo Relative benefit Number needed to treat Total patients Total trials(95 CI) (95 CI)
Valdecoxib 40 mg 204279 (73) 19194 (10) 73 (48 to 112) 16 (14 to 17) 473 4
Diclofenac 100 mg 71102 (70) 8102 (8) 89 (45 to 175) 16 (14 to 19) 204 2
Valdecoxib 20 mg 69101 (68) 8103 (8) 88 (45 to 173) 17 (14 to 20) 204 2
Diclofenac 50 mg 112189 (59) 21178 (12) 49 (33 to 75) 21 (18 to 26) 367 5
Rofecoxib 50 mg 318557 (57) 23262 (9) 66 (44 to 99) 21 (19 to 23) 819 6
Ibuprofen 400 mg 10351835 (56) 1861567 (12) 47 (40 to 54) 22 (21 to 24) 3402 37
Ibuprofen 200 mg 323695 (46) 47499 (9) 46 (35 to 61) 27 (24 to 31) 1194 14
Ibuprofen 600 mg 90114 (79) 3889 (43) 19 (15 to 25) 28 (20 to 43) 203 3
Celecoxib 200 mg 3991 (43) 445 (9) 48 (18 to 127) 29 (21 to 48) 136 1
Paracetamol 9751000 mg 226616 (37) 40422 (9) 38 (28 to 52) 37 (31 to 47) 1038 10
Paracetamol 600650 mg + codeine 60 mg 217532 (48) 64380 (19) 25 (19 to 31) 42 (34 to 55) 911 12
Paracetamol 600650 mg 224630 (36) 76635 (12) 29 (23 to 37) 42 (36 to 52) 1265 10
Aspirin 600650 mg 6271788 (36) 2551847 (15) 25 (22 to 29) 47 (42 to 54) 3635 46
Paracetamol 300 mg + codeine 30 mg 48175 (29) 11124 (9) 33 (18 to 62) 54 (37 to 97) 299 3
Dihydrocodeine 30 mg 849 (16) 250 (4) 41 (09 to 18) not calc 99 1
Shaded areas are those analgesics used by dentists in the UK
07p407-411qxd 10092004 1519 Page 409
RESEARCH
410 BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004
With the information available standard doses of NSAIDs andCOX-2 inhibitors provided the best analgesia (Fig 2) NNTs of 2and below are indicative of very effective medicines32 The indirectcomparisons that allow us to arrive at this conclusion are only sus-tainable because the trials have the same design use patients withthe same entry criterion (moderate or severe pain intensity) withstandard measurements made in the same way over the same peri-od of time and with the same output from each trial and oneknown to be legitimate The validity of the indirect comparisonsare buttressed by the dose response of two doses of ibuprofen (400mg was better than 200 mg) and two doses of paracetamol(9751000 mg was better than 600650 mg) where there were cred-ible amounts of information A systematic review of ibuprofenversus paracetamol in dental studies also concluded that ibuprofenwas superior concordant with the indirect comparison33
The adverse event information we have tells us only aboutpatients experiencing any adverse event With the amount ofinformation available it appears that only higher doses ofcodeine with paracetamol resulted in a significantly higher ratefor this outcome than placebo In Table 3 the rate at which thisadverse event occurred with placebo varied greatly between 2
and 52 This variation will be due partly to small sizes4 butalso because we know that methods of collecting adverse eventdata impact significantly on the reported incidence and becausemethods used varied15
Information about specific adverse events is even more difficultto obtain and very large data sets are required to produce infor-mation about for instance gastric irritation with aspirin use8 Ofinterest to dentists might be the rate of alveolitis or dry socket Thisis reported in some of the newer COXIB studies but not in olderstudies There is just too little information to make a judgement
What these comparisons do not do is to tell dentists what toprescribe They and the products of other systematic reviewsshould not be used as rules but rather as evidence-based toolsto help make better policy decisions and decisions about indi-vidual patients Present prescribing practice (Table 1) showsthat for the most part effective and safe analgesics are beingused in 80 of prescriptions The exception is prescribing dihy-drocodeine 30 mg (20 of prescriptions) for which we lack sin-gle dose evidence of efficacy in dental surgery and which couldnot be distinguished from placebo in other conditions againwith little data6
Paracetamol 300 + codeine 30 mgAspirin 600650 mg
Paracteamol 600650 mgParacetamol 600650 + codeine 60 mg
Paracetamol 9751000 mgCelecoxib 200 mgIbuprofen 200 mgDiclofenac 50 mgIbuprofen 400 mgRofecoxib 50 mg
Valdecoxib 20 mgValdecoxib 40 mgDiclofenac 100 mg
1 2 3 4 5 6 7 8 9 1095 confidence interval of the NNT
Fig 2 The 95confidence interval ofthe number needed totreat (NNT) for at leasthalf pain relief over 4-6hours compared withplacebo in third molarextraction trials
Table 3 Patients experiencing any adverse event with analgesics after third molar extraction from systematic reviews of randomised double blind trials
Number () of patientsharmed with
Drug and dose Treatment Placebo Relative risk Number needed to harm Total patients Total trials(95 CI) (95 CI)
Valdecoxib 40 mg 63180 (35) 76144 (53) 06 (05 to 08) not calc 324 3
Diclofenac 100 mg 252 (4) 252 (4) 10 (12 to 68) not calc 104 1
Valdecoxib 20 mg 36100 (36) 55103 (53) 07 (05 to 09) not calc 203 2
Diclofenac 50 mg 15222 (7) 12210 (6) 12 (06 to 24) not calc 432 4
Rofecoxib 50 mg 105314 (33) 48122 (39) 09 (07 to 11) not calc 436 3
Ibuprofen 400 mg 120972 (13) 91805 (12) 11 (08 to 14) not calc 1777 19
Ibuprofen 200 mg 84554 (15) 69372 (19) 08 (06 to 10) not calc 926 10
Ibuprofen 600 mg no data
Celecoxib 200 mg no data
Paracetamol 9751000 mg 175836 (24) 103464 (20) 11 (09 to 13) not calc 1300 9
Paracetamol 600650 mg + codeine 60 mg 156490 (25) 43333 (14) 18 (13 to 25) 53 (41 to 74) 824 10
Paracetamol 600650 mg 32228 (14) 20229 (9) 16 (09 to 27) not calc 457 7
Aspirin 600650 mg 1551320 (12) 1681422 (12) 10 (08 to 12) not calc 3031 36
Paracetamol 300 mg + codeine 30 mg 29175 (15) 20124 (16) 09 (06 to 16) not calc 299 3
Dihydrocodeine 30 mg 149 (2) 150 (2) 10 (01 to 17) not calc 99 1
Shaded areas are those analgesics used by dentists in the UK
07p407-411qxd 10092004 1520 Page 410
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 411
Not all the analgesics in this review are presently available forprescribing by dentists at least in the UK The information on effi-cacy on harm and on the amount of information available shouldbe useful in any initiative to develop a prescribing formulary indentistry especially as we have growing confidence in the value ofindirect comparisons34
COMPETING INTERESTSRAM has been a consultant for MSD RAM amp HJM have consulted for variouspharmaceutical companies RAM HJM amp JE have received lecture fees frompharmaceutical companies related to analgesics and other healthcareinterventions All authors have received research support from charitiesgovernment and industry sources at various times but no such support wasreceived for this work No author has any direct stock holding in anypharmaceutical company
AUTHORS CONTRIBUTIONSJB was involved with searching data extraction quality scoring analysis andwriting JE was involved with searching data extraction quality scoring andwriting HJM was involved in analysis and writing RAM was involved in dataextraction quality scoring analysis and writing PW was involved with theoriginal concept with researching prescribing data and writing
The work was supported by Pain Research Funds and the Oxford Pain Relief TrustThe authors would like to thank Frances Fairman of the Cochrane Pain Palliativeand Supportive Care systematic review group for bringing this issue to ourattention The Department of Health Statistics Division provided data onprescribing by dentists
1 Beecher H K Keats A S Mosteller F The effectiveness of oral analgesics (morphinecodeine acetylsalicylic acid) and the problem of placebo lsquoreactorsrsquo and lsquononreactorsrsquo J Pharmacol 1953 109 93-400
2 Beecher H K The measurement of pain Pharmacol Rev 1957 9 59-2103 Houde R W Wallenstein S L Beaver W T Clinical measurement of pain In G De
Stevens (ed) Analgetics pp75-122 New York and London Academic Press 1965 4 Moore R A Gavaghan D Tramegraver M R Collins S L McQuay H J Size is everything mdash
large amounts of information are needed to overcome random effects in estimatingdirection and magnitude of treatment effects Pain 98 78 209-216
5 Ioannidis J P A Lau J Evolution of treatment effects over time Empirical insight fromrecursive cumulative metaanalyses PNAS 2001 98 831-836
6 McQuay H J Moore R A An evidence-based resource for pain relief Oxford OxfordUniversity Press 1998
7 McQuay H J Carroll D Moore R A Variation in the placebo effect in randomisedcontrolled trials of analgesics all is as blind as it seems Pain 1996 64 331-335
8 Edwards J E Oldman A Smith L Wiffen P J Carroll D McQuay H J Moore R A Oralaspirin in postoperative pain a quantitative systematic review Pain 1999 81 289-297
9 Moher D Cook D J Eastwood S Olkin I Rennie D Stroup D F Improving the quality ofreports of meta-analyses of randomised controlled the QUOROM statement Lancet1999 354 1896-1900
10 Jadad A R Carroll D Moore A McQuay H Developing a database of published reportsof randomised clinical trials in pain research Pain 1996 66 239-46
11 Collins S L Moore R A McQuay H J Wiffen P J Edward J S Single dose oral ibuprofenand diclofenac for postoperative pain In The Cochrane Library Issue 4 2000 OxfordUpdate Software
12 Edwards J E McQuay H J Moore R A Single-dose dihydrocodeine for acute
postoperative pain In The Cochrane Library Issue 4 2000 Oxford Update Software13 Moore R A Collins S L Carroll D McQuay H J Edwards J Single dose paracetamol
(acetaminophen) with and without codeine for postoperative pain In The CochraneLibrary Issue 4 2000 Oxford Update Software
14 Barden J Edwards J E McQuay H J Moore R A Rofecoxib in acute postoperative painquantitative systematic review BMC Anesthesiol 2002 2 4httpwwwbiomedcentralcom1471-225324
15 Edwards J E McQuay H J Moore R A Collins S L Reporting of adverse effects inclinical trials should be improved Lessons from acute postoperative pain J PainSympt Manage 1999 18 427-437
16 Jadad A R Moore R A Carroll D et al Assessing the quality of reports of randomizedclinical trials is blinding necessary Control Clin Trials 1996 17 1-12
17 Khan K S Daya S Jadad A R The importance of quality of primary studies inproducing unbiased systematic reviews Arch Intern Med 1996 156 661-666
18 Moher D Pham B Jones A et al Does quality of reports of randomised trials affectestimates of intervention efficacy reported in meta-analyses Lancet 1998 352609-613
19 Cooper S A Single-dose analgesic studies the upside and downside of assaysensitivity In Max M B Portenoy R K and Laska E M (eds) The design of analgesicclinical trials (Advances in Pain Research and Therapy Vol 18) pp117-124 New YorkRaven Press 1991
20 Moore A McQuay H Gavaghan D Deriving dichotomous outcome measures fromcontinuous data in randomised controlled trials of analgesics Pain 1996 66 229-237
21 Moore A McQuay H Gavaghan D Deriving dichotomous outcome measures fromcontinuous data in randomised controlled trials of analgesics Verification fromindependent data Pain 1997 69 127-130
22 Moore A Moore O McQuay H Gavaghan D Deriving dichotomous outcome measuresfrom continuous data in randomised controlled trials of analgesics Use of painintensity and visual analogue scales Pain 1997 69 311-315
23 Morris J A Gardner M J Calculating confidence intervals for relative risk odds ratiosand standardised ratios and rates In Gardner M J and Altman D G(eds) Statistics withconfidence mdash confidence intervals and statistical guidelines pp50-63 LondonBritish Medical Journal 1995
24 Gavaghan D J Moore R A McQuay H J An evaluation of homogeneity tests in meta-analyses in pain using simulations of individual patient data Pain 2000 85 415-424
25 Higgins J Thompson S Deeks J Altman D Statistical heterogeneity in systematicreviews of clinical trials a critical appraisal of guidelines and practice J Health SurvRes Policy 2002 7 51-61
26 LAbbeacute K A Detsky A S ORourke K Meta-analysis in clinical research Ann Intern Med1987 107 224-233
27 Sterne J A Gavaghan D Egger M Publication and related bias in meta-analysispower of statistical tests and prevalence in the literature J Clin Epidemiol 2000 531119-1129
28 Tang J-L Liu J L Y Misleading funnel plot for detection of bias in meta-analysis J ClinEpidemiol 2000 53 477-484
29 Cook R J Sackett D L The number needed to treat a clinically useful measure oftreatment effect Br Med J 1995 310 452-454
30 Carroll D Tramegraver M McQuay H Nye B Moore A Randomization is important instudies with pain outcomes systematic review of transcutaneous electrical nervestimulation in acute postoperative pain Br J Anaesth 1996 77 798-803
31 Schulz K F Chalmers I Hayes R J Altman D G Empirical evidence of bias dimensionsof methodological quality associated with estimates of treatment effects incontrolled trials J Am Med Assoc1995 273 408-412
32 McQuay H J Moore R A Using numerical results from systematic reviews in clinicalpractice Ann Intern Med 1997 126 712-720
33 M Hyllested Jones S Pedersen J L Kehlet H Comparative effect of paracetamolNSAIDs or their combination in postoperative pain management a qualitative reviewBr J Anaesth 2002 88 199-214
34 F Song Altman D G Glenny A M Deeks J J Validity of indirect comparison forestimating efficacy of competing interventions empirical evidence from publishedmeta-analyses Br Med J 2003 326 472-476
07p407-411qxd 10092004 1520 Page 411
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
Relative efficacy of oral analgesics after third molar extraction ndash a 2011 updateS Derry1 P J Wiffen2 and R A Moore3
and reporting and were all of high meth-odological quality the relative efficacy of different analgesics is justifiable when established against the common comparator of placebo3 Moreover the methods have been extensively examined and validated using individual patient data analyses45
Several approaches can be used to pre-sent results The percentage of patients who benefit with treatment is one approach obviously the higher the number
In 2004 the British Dental Journal carried a review examining analgesic efficacy meas-ured after third molar extractions1 predom-inantly derived from Cochrane reviews of single dose analgesics in established mod-erate or severe pain In the intervening years the reviews on which it was based have been extended to other analgesics and updated to include relevant additional clinical trials performed in the past decade
The culmination of this work has been the publication by the Cochrane Collaboration of an overview of these updated systematic reviews2 The overview included 35 sepa-rate Cochrane Reviews with 38 analyses of single dose oral analgesics tested in acute postoperative pain models with results from about 45000 participants studied in approximately 350 individual studies About 29000 patients contributed data to trials in dental pain
Each individual review reported results for dental studies where data were avail-able overwhelmingly in the third molar extraction pain model Because all of the reviews used identical methods outcomes
This article provides a summary of the efficacy and relative efficacy of 38 different drugs or drug combinations tested in standard postoperative pain trials It will help clinicians and patients make informed choices about analgesia based on pain relief duration of action and adverse events which can then be put into context for the individual patient depending on local availability This article highlights the fact that no single drug is effective in all patients ndash even the best drugs fail to provide good levels of pain relief in at least 30 These patients should try a different analgesic
the better Another way is to look at the number needed to treat (NNT) for one patient to benefit this is the treatment-specific effect and can be expressed as 100(active - placebo) The ideal NNT is 1 where everyone gets better with treatment and no one does with placebo lower numbers are better In dental tri-als where about 10 of patients benefit with placebo the best possible NNT is 100100 - 10 = 11
13Pain Research and Nuffield Division of Anaesthet-ics Department of Clinical Neurosciences University of Oxford The Churchill Hospital Oxford OX3 7LJ 2UK Cochrane Centre Summertown Pavilion 18-24 Middle Way Oxford OX2 7LG Correspondence to R Andrew Moore Email andrewmoorepruoxacuk
Refereed Paper Accepted 12 September 2011 DOI 101038sjbdj2011905 copyBritish Dental Journal 2011 211 419-420
bull Summarises the known evidence on efficacy of oral analgesics in dental pain
bull Describes shorter term pain relief and time needed before remedication
bull Provides an evidential context for making decisions about individual patients or practice guidelines
I N B R I E F
PRA
CTICE
Table 1 Efficacy results in dental pain studies for a range of commonly used analgesics
Drug and dose (mg)Number of
Percent with at least 50 maxi-mum pain relief NNT
Median time to remedication (hr)
Trials Patients Active Placebo
Aspirin 600650 mg 45 3581 36 14 45 (40 to 52) 30
Aspirin 1000 mg 4 436 35 11 42 (32 to 60) no data
Celecoxib 400 mg 4 620 34 3 25 (22 to 29) 84
Diclofenac 50 mg (Na and K) 9 1119 56 19 27 (24 to 31) 43
Diclofenac 50 mg K 5 622 65 16 21 (19 to 24) no data
Etoriocoxib 120 mg 4 500 71 9 16 (15 to 18) gt24
Ibuprofen 400 mg 49 5428 55 12 23 (22 to 24) 56
Ibuprofen 400 mg soluble 9 959 66 10 18 (17 to 20) no data
Ibuprofen 200 mg + paracetamol 500 mg 2 280 74 10 16 (14 to 18) gt8
Naproxen 500550 mg 5 402 61 7 18 (16 to 21) 89
Paracetamol 1000 mg 19 2157 41 10 32 (29 to 36) 39
Note that data for remedication time were not generally available for dental studies separately and the values reported apply to all postoperative conditions though predominantly third molar extraction
BRITISH DENTAL JOURNAL VOLUME 211 NO 9 NOV 12 2011 419
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
PRACTICE
This brief report describes the main results of interest to dentists using results from the Cochrane overview and from a recent analysis of a combination of ibu-profen and paracetamol5
RESULTSTable 1 reports data for aspirin celecoxib diclofenac etoricoxib ibuprofen ibu-profen plus paracetamol naproxen and paracetamol Widely differing amounts of information were available for individual drugs from as few as 402 patients for nap-roxen 500550 mg and as many as 5428 for ibuprofen 400 mg
One outcome reported is the percentage of patients with initially moderate pain (30-60 mm on a 100 mm VAS) or severe pain (more than 60 mm) who obtained at least 50 of the maximum possible pain relief over a 4-6 hour period after taking the tab-lets This is a high test of efficacy achieved by only about 10 of patients who received no active treatment (placebo) but achieved by 34-74 of those who did get the active drug Ibuprofen 200 mg plus paracetamol 500 mg and etoricoxib 120 mg achieved
response rates above 70 paracetamol 1000 mg achieved only a 41 response rate
Several products had an NNT of about 2 or below the combination of ibupro-fen 200 mg plus paracetamol 500 mg etoricoxib 120 mg ibuprofen 400 mg in a soluble form naproxen 500550 mg and 50 mg of the potassium salt of diclofenac (the sodium salt being much less effective in this assay Fig 1)
A new outcome that some will con-sider relevant is the time required for half the patients to need more analgesia the time to remedication Longer duration is another indicator of greater effect and for a number of analgesics median remedica-tion times are beyond eight hours
DISCUSSIONThe 2004 review included evidence for rofecoxib and valdecoxib neither of which is available today New relevant informa-tion includes data on the ibuprofen plus paracetamol combination different ibu-profen and diclofenac formulations and etoricoxib all of which are among the most efficacious analgesics after third
molar surgery Greater efficacy and longer duration of action tended to go together
For one analgesic relevant to dentistry the evidence is largely silent For dihydrocodeine 30 mg (still commonly used by dentists) only 136 patients were found in trials in dental pain with only 24 obtaining at least 50 maximum pain relief compared with 7 with placebo The resultant NNT was 6 far worse than available for drugs in Table 1 and far worse than ibuprofen 400 mg in the only direct comparison6 The Cochrane overview concluded that the results for dihy-drocodeine were not robust because of the smallness of the data set available and that unpublished results from just 46 patients in zero effect trials would be needed to make any result clinically irrelevant
CONCLUSIONThe amount of evidence available on single dose studies of analgesics in dental pain is large and readily available These results are tools to help formulate policy and pre-scribing for individuals and populations
1 Barden J Edwards J E McQuay H J Wiffen P J Moore R A Relative efficacy of oral analgesics after third molar extraction Br Dent J 2004 197 407ndash411
2 Moore R A Derry S McQuay H J Wiffen P J Single dose oral analgesics for acute postoperative pain in adults Cochrane Database Syst Rev 2011 9 CD008659
3 Song F Altman D G Glenny A M Deeks J J Validity of indirect comparison for estimating efficacy of competing interventions empirical evidence from published meta-analyses BMJ 2003 326 472
4 Moore R A Edwards J E McQuay H J Acute pain individual patient meta-analysis shows the impact of different ways of analysing and presenting results Pain 2005 116 322ndash331
5 Moore R A Straube S Paine J Derry S McQuay H J Minimum efficacy criteria for comparisons between treatments using individual patient meta-analysis of acute pain trials examples of etoricoxib paracetamol ibuprofen and ibuprofenparacetamol combinations after third molar extraction Pain 2011b 152 982ndash989
6 Moore R A Edwards J Derry S McQuay H J Single dose oral dihydrocodeine for acute postop-erative pain Cochrane Database Syst Rev 2000 2 CD002760
Ibuprofen 200mg + paracetamol 500 mg
Ibuprofen 400 mg
Aspirin 600650 mg
Aspirin 1000 mg
Paracetamol 1000
Naproxen 500550
Diclofenac 50 mg (Na and K)
Celecoxib 400 mg
Diclofenac 50 mg K
Ibuprofen 400 mg soluble
Etoriocoxib 120 mg
1 2 3 4 5 6
NNT for at least 50 maximum pain relief (95 CI)
Fig 1 NNTs in dental pain studies for a range of commonly used analgesics
420 BRITISH DENTAL JOURNAL VOLUME 211 NO 9 NOV 12 2011
Combining paracetamol with a selectivecyclooxygenase-2 inhibitor for acutepain relief after third molar surgerya randomized double-blindplacebo-controlled study
Birgitta Haglund12 Inger vonBltzingslccedilwen1
1Public Dental Health Service KarlstadVrmland Sweden 2Department of ClinicalPharmacology Sahlgrenska Academy atGccedilteborg University Sweden
Traditional non-steroidal anti-inflammatory drugs(NSAIDs) [ie non-selective cyclooxygenase (COX)inhibitors such as ibuprofen and diclofenac] have beenwidely used in outpatients for acute pain relief followingoral surgery Their anti-inflammatory and analgesicproperties together with well-established tolerabilitymake them an initial choice for the management of mostforms of mild to moderate pain in outpatients (1 2)However these drugs have well-documented adverseeffects such as gastrointestinal intolerability Further-more they need to be administered several times a dayMore effective and practical pain relief regimes withfewer side-effects are needed for moderate to severe painafter oral surgeryNSAIDs act by inhibiting COX enzymes which are
responsible for the production of prostaglandin fromarachidonic acid This acid emerges from the breakdownof phospholipids in the cell walls of damaged tissue (3)Prostaglandin elicits a number of biological effects someof which contribute to the inflammatory process leading
to pain Multiple COX enzymes have been identifiedCOX-1 is mainly expressed under physiological condi-tions throughout the body for example by platelets (4)and COX-2 is related to inflammation and pain (4ndash6)although COX-1 and COX-2 also have overlappingproperties (7) Improved knowledge on more selectiveCOX enzymes led to the development of specific COX-2inhibitors such as rofecoxib (8) and celecoxib withanalgesic anti-inflammatory and gastroprotective prop-erties Of these drugs rofecoxib has been shown to bemore effective than celecoxib (9ndash11)Rofecoxib has the same analgesic effect as ibuprofen
but with the benefit of a longer duration (9 10 12) It hasa long half-life which makes it suitable for once-dailydosing (12) compared with traditional NSAIDs thatneed to be taken several times per day Rofecoxib hasalso been suggested to be more effective than paracet-amol combined with codeine (13 14) The COX-2inhibitor rofecoxib may be an interesting choice for acutepain relief after oral surgery
Haglund B von Bulzingslowen I Combining paracetamol with a selective cyclooxyge-nase-2 inhibitor for acute pain relief after third molar surgery a randomized double-blind placebo-controlled study Eur J Oral Sci 2006 114 293ndash301 2006 The AuthorsJournal compilation 2006 Eur J Oral Sci
Severe pain after third molar surgery is often encountered and more effective treatmentregimes are warranted The objective of this study was to evaluate if the combinationof paracetamol and rofecoxib a selective cyclooxygenase-2 (COX-2) inhibitorimproves analgesic effects following third molar surgery compared with rofecoxibalone Paracetamol alone was also evaluated Altogether 120 patients with moderate tosevere pain after third molar surgery were given a single postoperative dose of one ofthe following treatments rofecoxib + paracetamol rofecoxib alone paracetamolalone or placebo Patients assessed level of pain and pain relief every 30 min for 8 hafter surgery and made a global evaluation of the medication 4 and 8 h after surgeryParacetamol and rofecoxib combined improved the analgesic effect compared withrofecoxib alone for the first 15 h Rofecoxib alone and the combination of paracet-amol and rofecoxib had a significantly better analgesic effect than paracetamol alonefrom 3 h onwards The early onset of pain relief for the combination of paracetamoland rofecoxib compared with rofecoxib alone could be of great importance whentreating acute pain after third molar surgery After data collection for this studyrofecoxib was withdrawn from the market as a result of reported fatal cardiovascularevents Whether this is relevant for short-term use is unknown but it has to be con-sidered before rofecoxib may be used for pain relief following third molar surgery
Birgitta Haglund Folktandvrden TingvallaBox 577 SE-651 13 Karlstad Sweden
Telefax +46ndash54ndash137435E-mail birgittahaglundlivse
Key words COX-2 inhibitor pain relief para-cetamol randomized trial third molar surgery
Accepted for publication April 2006
Eur J Oral Sci 2006 114 293ndash301Printed in Singapore All rights reserved
2006 The AuthorsJournal compilation 2006 Eur J Oral Sci
European Journal ofOral Sciences
Combining drugs that cause analgesia through differ-ent mechanisms may give additive analgesic effects (15)and lead to dose-sparing effects and improved safety(16) The analgesic mechanism of COX inhibition ispredominantly peripheral Research on paracetamol hasnot been able to delineate a clear mechanism of actionbut it is suggested to lie predominantly in the centralnervous system (17) Some studies indicate that combi-ning a traditional NSAID and paracetamol after oralsurgery may enhance the analgesic effect compared withsingle drug regimes (18 19)The theory of the analgesic effect of traditional
NSAIDs being caused by COX-2 inhibition leads to thethought that an additive effect should be present alsowhen combining rofecoxib and paracetamol The aim ofthis study was therefore to explore in a third molarsurgery pain model (20) if there is an additive analgesiceffect when combining the COX-2 selective inhibitorrofecoxib with paracetamol compared with rofecoxibalone for acute pain relief We also compared the anal-gesic efficiency of rofecoxib and paracetamol becausethis to our knowledge has not been reported followingthird molar surgery
Material and methods
Study design
This study was designed as a multicenter randomizeddouble-blind placebo-controlled study with a single dose ofrofecoxib 50 mg and paracetamol 1 g combined vs rofec-oxib 50 mg alone vs paracetamol 1 g alone vs placebogiven postoperatively to patients stating moderate to severepain after surgical removal of one or two lower third molarsPatients were asked to give written informed consent toparticipate after being told about the procedures A total of120 patients were randomized into four different treatmentgroups as follows 40 patients receiving the combination ofrofecoxib 50 mg and paracetamol 1 g 40 patients receivingrofecoxib 50 mg alone 20 patients receiving paracetamol 1 galone and 20 patients receiving placebo The patientsrsquoevaluations of the treatments were obtained by using aquestionnaire which the patients filled in at home during an8-h study period following intake of the study medicationThe trial was approved by the Regional Ethical Committeeof Medical Research in Orebro Sweden and the MedicalProducts Agency in Uppsala Sweden
Patients
Consecutive patients visiting four general dental practicesand in need of mandibular third molar surgery in accordancewith the National Institutes of Health (NIH) guidelines (21)were screened for enrollment Only patients with thirdmolars needing bone removal were included Other inclusioncriteria were age gt18 yr weight gt50 kg butlt120 kg andan appointment before noon for surgery This was necessaryin order for the patients to have time to fill in the ques-tionnaire for 8 h after intake of the study medication beforebedtime Exclusion criteria were as follows intolerance toacetylsalicylic acid (ASA) paracetamol andor NSAIDsany ongoing medication (except contraceptives) pregnancylactation inadequate contraception alcohol or drug abusePatients with evidence of previous or present cardiovascular
respiratory diabetic hepatic gastric renal neurological orneoplastic diseases were also excluded as were those withongoing pericoronitis or other local oral infections involvingpain Patients with an intake of any analgesics 6 h precedingsurgery was also excluded All patients who met the studycriteria and reported moderate to severe pain after the sur-gery were included in the study
Surgery
The surgery was performed by one of four dentists speciallytrained in dento-alveolar surgery using local anesthesia(lidocaine 20 mg ml)1 plus epinephrine 125 lg ml)1) Theremoval of bone was carried out with a burr under thecooling of saline
Masking randomization and rescue medication
The study medications were masked by being encapsula-ted in identical capsules The capsules contained 50 mg ofrofecoxib 200 mg of paracetamol or placebo All patientswere given a sealed container containing six capsules(Table 1) so that the patients in the different treatmentgroups received the correct amount of medication and stillthe same number of capsules The capsules were manu-factured by Apoteket Production amp Laboratories (APLStockholm Sweden) Randomization of the patients intothe four treatment groups was performed for the group intotal by Apoteket using randomization tables All studypersonnel and participating patients were blinded totreatment assignment for the duration of the study Themain investigator broke the codes for the final calcula-tionsIbuprofen 400 mg was used as a rescue medication in case
patients needed additional analgesia at any time during the8-h study period The rescue medication was kept in aseparate container If patients felt that rescue medicationwas needed they were instructed to wait 90 min if possibleafter intake of their study medication to allow for the studydrug to take effect
Intake of study medication and information about thequestionnaire
After surgery the patients were given their two containerswith study and rescue medications respectively together
Table 1
Distribution of the drug capsules with the different substances percontainer in each study group
Study groups
Rofecoxib50 mg +
paracetamol 1 gRofecoxib50 mg
Paracetamol1 g Placebo
Rofecoxib50 mg
1 1 0 0
Paracetamol200 mg
5 0 5 0
Placebo 0 5 1 6Total no ofcapsules ineach container
6 6 6 6
294 Haglund amp Bultzingslowen
with the questionnaire Routine postoperative informationwas given The patients were instructed to go home and takeno medication before calling the investigator when theyregained full sensibility in the lower lip following the dis-appearance of the local anesthesia If the patient had notcalled the investigatorrsquos mobile phone within 3 h after theend of surgery the investigator called the patientAt the telephone contact the patients were asked to state
their level of pain in the questionnaire using a 3-point scalefrom mild to moderate to severe pain If patients statedmoderate or severe pain they were asked to break the seal ofthe container with their study medication and take all sixcapsules Detailed instructions were provided on how to fill inthe questionnaire To ascertain that patients adhered to theprotocol information was given to contact the investigatorwith any questions regarding medication or other issuesconcerning the studyduring the 8-h postoperative periodThestudy period started at the time of intake of the study medi-cation If patients stated mild pain they were asked if theycould tolerate waiting before taking any medication In suchcases a second telephone contact was made If patients stillstatedmild pain they were asked if it was possible for them toreturn their sealed container with the study medicationPatients who did so were replaced with another patient
Efficacy assessments
The outcome measures of the trial were pain intensity painrelief (PAR) global evaluation score (patientsrsquo overallassessment of the medication) derived summary measuresuse of rescue medication and side-effects experienced allrecorded by the patients in their questionnaire After intakeof the study medication pain intensity and PAR wasassessed by the patient every 30 min for 8 h and the globalevaluation score was measured at 4 and 8 h The startingpoint for each patient was the time for intake of studymedication The final measurement point was the end of theobservation period (ie 8 h later) or the time of intake ofrescue medication If rescue medication was used patientswere asked to assess pain intensity and pain relief and give aglobal evaluation score at the time of intake These scoreswere then used for the rest of the observation period inaccordance with a study by Laska et al (22)Pain intensity was evaluated by the patients using a
horizontal visual analog scale (VAS) of 10 cm marked nopain at 0 and worst possible pain at 10 PAR was meas-ured on a 5-point scale as follows 0 no pain relief 1 somepain relief 2 medium pain relief 3 good pain relief and 4total pain relief Global evaluation score was measured on a4-point scale as follows 0 poor 1 fair 2 good and 3excellent Patients using rescue medication recorded the timeof intake A question about any side-effects experienced wasanswered by yes or no at the end of the study period Ifyes the patients estimated adverse events on a 3-point scale(1 slight 2 moderate 3 severe) and reported what kind ofside-effect was experienced
Analysis
The analgesic effect of the drugs measured every 30 min bypain intensity (VAS) and PAR scores was comparedSummary measures were calculated by the use of the fol-lowing total pain relief (TOTPAR the sum of all PARscores for the whole study period of 05ndash8 h) pain intensitydifference (PID pain intensity at the start minus painintensity at any given observation point) sum of PID for the
05ndash3-h period (SPID05)3 h) and sum of PID for the total05ndash8-h period (SPIDtotal) PID values were not analyzedseparately but used for the calculation of SPIDThe use of rescue medication was compared between the
treatment groups by calculating the percentage of patientsin each group who used rescue Also the mean timebetween intake of the study medication and intake of therescue medication in the different groups was analyzedSide-effects in the treatment groups were compared interms of percentage of patients in each group whoexperienced such problems Median global evaluationscores between the different groups were analyzed as wellas the percentage of patients in each group using the dif-ferent scores
Statistics
The sample size calculations were carried out assuming adifference in SPID outcome between groups using thecombination of rofecoxib + paracetamol and rofecoxibalone amounting to 20 (18) with a power of at least 80and a standard deviation (SD) of 15 using non-para-metric statistics (MannndashWhitney U-test) This calculationestimated that a minimum of 22 patients should be includedin each groupStandard descriptive statistics and tests were used and the
calculations were performed in Statistical Package for SocialSciences (spss) version 12 The principle of last observationcarried forward was used Significances between groupsregarding VAS scores were tested with an independent-samples t-test at each time point for all possible compari-sons as we considered VAS to be a continuous scale inaccordance with Max et al (23) The same applies for thetesting of SPID up to 3 and 8 h The analysis of TOTPARwas based on an assumption that the scores are consideredinterval scaled (23) and significance testing was carried outwith an independent samples t-test The same test was usedfor testing differences between study groups regarding theuse of rescue medication Hypothesis testing of valuesmeasured with categorical ordinal scales (ie PAR andglobal evaluation) was performed with a non-parametrictest (MannndashWhitney U-test) P-values of lt005 were con-sidered statistically significant
Results
Altogether 126 consecutive patients who fulfilled theinclusion criteria gave written informed consent to par-ticipate in the study The majority of the patients whowere asked to participate agreed to do so Patients whodeclined to participate usually did not have a before-noon appointment for the surgery Out of the 126patients six were excluded as they stated their pain asmild at the telephone contacts and were able to returntheir sealed study medication A total of 120 patientsparticipated by taking the randomized study medicationSome patients (n frac14 8) who did not fulfill the criterion ofmoderate to severe pain but nevertheless wanted toparticipate took their study medication but wereexcluded from the calculations Of these patients ahigher proportion was men (75) compared with thestudied population Some patients (n frac14 5) were excludedfor other reasons one patient randomized to the
COX-2 inhibitor and paracetamol after oral surgery 295
rofecoxib group took her rescue medication after only30 min as a result of severe pain and withdrew from thestudy one did not manage to fill in the questionnaireand three did not return their questionnaires althoughthey were repeatedly reminded to do so Final outcomedata were calculated on the following cohort of 107 pa-tients rofecoxib + paracetamol (n frac14 34) rofecoxibalone (n frac1436) paracetamol alone (n frac14 20) and placebo(n frac14 17)The principal investigator and one of the dentists
performed the majority of the operations 43 and 55respectively in total 98 out of 120 The remaining 22operations were performed by the two other dentists oneoperating on 10 and the other on 12 patients as theirstock of patients fulfilling the inclusion criteria wassmaller The principal investigator was in contact withand gave instructions to the 98 patients The 22remaining patients received their instructions from oneof the other two dentists performing the operationsThere were no differences between groups regarding
baseline characteristics and the number of molarsremoved (Tables 2 and 3) In total 56 of the partici-pants were men The mean age of the patients was 27 yr(range 18ndash54) and the mean weight was 73 kg (range 50ndash120) Mean total duration of the surgery was 14 min Intotal 91 patients (85) had one mandibular molar
removed during the operation and 16 (18) had anadditional maxillary molar removed The remaining 16patients (15) had two mandibular molars removed atthe same session (Table 3) There was no difference inpain intensity (VAS) at the start between patients whohad one or two molars removed At the time of intake ofthe study medication 83 of all patients included in theanalysis reported moderate pain and 17 reportedsevere pain There were no major differences in painreported among patients operated on by the differentdentists
Analgesic effect
Pain intensity (VAS) ndash The analgesic effect over the 8-hstudy period recorded by patients using the VAS isshown in Fig 1 Separate curves with confidence inter-vals for study groups are presented in Fig 2 Patientsused the scale from 0 up to 95There was a significant difference in mean VAS score
between the combination group and the rofecoxibgroup at 30 min 1 h and 15 h in favor of thecombination (P lt 005) At 2 h and subsequentlyparacetamol did not show any statistically significantadditive effect when combined with rofecoxib com-pared with rofecoxib aloneWhen comparing rofecoxib and paracetamol after
30 min paracetamol was significantly better regardingeffect on pain intensity (P lt 005) Paracetamol tendedto have a better analgesic effect than rofecoxib (althoughthis was not statistically significant) for another hourafter the starting point From 3 h until the end of thestudy period rofecoxib was significantly better thanparacetamol (P lt 005)Compared with placebo the combination treatment
as well as the single drug treatments resulted in signifi-cantly lower pain intensity scores at all observationpoints except for rofecoxib at 30 min
Pain relief (PAR) ndash The median PAR scores (Fig 3)showed a pattern similar to the mean pain intensityassessment The combination treatment was significantly
Table 2
Baseline characteristics for each study group
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Gender malefemale 1915 2016 128 98Age (yr) 25 (19ndash35) 26 (18ndash41) 29 (19ndash52) 28 (19ndash54)Weight (kg) 73 plusmn 9 70 plusmn 13 79 plusmn 17 72 plusmn 13Volume of local anesthetic (ml) 54 plusmn 2 58 plusmn 1 56 plusmn 1 56 plusmn 1Length of surgery (min) 13 plusmn 7 15 plusmn 8 13 plusmn 7 15 plusmn 6Time from end of surgery tointake of study medication (min)
155 plusmn 37 170 plusmn 45 184 plusmn 53 161 plusmn 30
Pain intensity (VAS) at the start 51 plusmn 18 54 plusmn 16 51 plusmn 18 46 plusmn 15
Mean (range)Mean plusmn SDVAS visual analog scale
Table 3
Number of mandibular and maxillar third molars removed in eachstudy group
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
1 mandibular 24 24 15 122 mandibulars 5 6 3 21 mandibular+ 1 maxillar
5 6 2 3
296 Haglund amp Bultzingslowen
better than rofecoxib alone at 30 min (P lt 005) and at1 h (P lt 001) For the rest of the observation periodthere was no significant difference
Between rofecoxib and paracetamol there was a sig-nificant difference in median PAR score in favor ofparacetamol at 30 min and at 1 h (P lt 005) after drug
Placebo
01234567
0 1 2 3 4 5 6 7 8
Paracetamol 1g
01234567
0 1 2 3 4 5 6 7 8
Rofecoxib 50 mg
01234567
0 1 2 3 4 5 6 7 8
Rofecoxib 50 mg+paracetamol 1 g
01234567
0 1 2 3 4 5 6 7 8
Fig 2 Mean pain intensity recorded on a visual analog scale (VAS) and confidence intervals in study groups during the studyperiod of 8 h
0
1
2
3
4
5
6
0 05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
AV
s S
cr
oe
placebo
paracetamol 1g
rofecoxib 50mg
rofecoxib 50mg +paracetamol 1g
Hours from intake of study medication
Fig 1 Mean pain intensity in study groups recorded on a 10-cm visual analog scale (VAS) at each observation point For signifi-cance tests see the Results
0
05
1
15
2
25
3
35
Pai
n r
elie
f sc
ore
placebo
rofecoxib 50mg
rofecoxib 50mg +
05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
paracetamol 1g
paracetamol 1g
Hours from intake of study medication
Fig 3 Median pain relief (PAR) score in study groups at each observation point Pain relief was assessed using the following scale0 no pain relief 1 some pain relief 2 medium pain relief 3 good pain relief and 4 total pain relief For significance tests see theResults
COX-2 inhibitor and paracetamol after oral surgery 297
intake There was instead a significant difference in favorof rofecoxib from 25 h (P lt 005) and from 3 h(P lt 001) to the end of the observation period Only atthe observation time-points of 15- and 2-h was there nosignificant difference between the two drugs regardingmedian PAR scoresThe combination treatment and the single treatments
were significantly better than placebo throughout thewhole observation period of 8 h
Total pain relief (TOTPAR) ndash There was no significantdifference in mean TOTPAR between the combinationtreatment group and the rofecoxib-alone group (Table 4)However rofecoxib gave significantly better TOTPARthan paracetamol (P lt 005) All the active treatmentgroups gave better TOTPAR than placebo (P lt 0001)
Sum of pain intensity differences (SPID) ndash The combi-nation group had the highest mean SPID05)3 h scorehowever this was not statistically different from rofecoxibalone (Table 4)No significant difference in SPID0)3 h wasseen between rofecoxib and paracetamol All active treat-ments were significantly better than placebo (P lt 0001)
The mean PID over the whole observation period (iemean SPIDtotal) shows that the combination group didnot differ from the rofecoxib group (Table 4) Therofecoxib group was significantly better than paracet-amol alone (P lt 005) All active treatments weresignificantly better than placebo (P lt 0001)
Use of rescue medication ndash The use of rescue medicationmeasured as the cumulative percentage of patients ineach study group needing analgesic rescue at any timeduring the 8-h observation period is shown in Fig 4There was no significant difference regarding the totalpercentage of patients using rescue when comparing thecombination group with the rofecoxib group (Table 4)Figure 4 indicates a major difference between the rofec-oxib and paracetamol groups This difference is how-ever not significant (P frac14 0055) owing to few patientsneeding rescue medication Both the combination groupand the rofecoxib group used significantly less rescuethan the placebo group (P lt 0001) Paracetamol failedto show a significant difference to placebo regardingpercentage of patients using rescue medication (P frac140066)
Table 4
Summary of efficiency measures
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Mean TOTPAR05ndash8 h (SE)
452 (20) 409 (27) 287 (44) 91 (27)
Mean SPID05ndash3 h (SE)
182 (19) 151 (18) 111 (34) )32 (23)
Mean SPIDtotal (SE)
526 (59) 515 (60) 208 (96) )101 (57)
Percentage of patients using rescue medication (SE) 88 (49) 167 (63) 400 (112) 706 (114)Mean time (min) to use of rescue medication (SE) 234 (42) 270 (58) 228 (48) 127 (16)Median global evaluation score (0ndash4) at 4 h 2 2 1 0Median global evaluation score (0ndash4) at 8 h 3 2 1 0
P lt 005 vs placebo P lt 001 vs placebo P lt 0001 vs placeboP lt 005 vs paracetamol P lt 001 vs paracetamol P lt 0001 vs paracetamolSE standard error SPID sum of pain intensity differences TOTPAR total pain relief
0
10
20
30
40
50
60
70
80
05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
Hours from intake of study medication
Cum
ula
itve
perc
enat
geof
paite
nst
taki
gnre
scue
me
idca
tion placebo
paracetamol 1g
rofecoxib 50mg
rofecoxib 50mg +paracetamol 1g
Fig 4 Cumulative percentage of patients in each group using rescue medication during the study period of 8 h For significance testssee the Results
298 Haglund amp Bultzingslowen
There was no statistically significant difference in themean time from intake of study medication to intake ofrescue medication in the different active treatmentgroups However for all active treatments the time wassignificantly longer than for placebo (Table 4)
Side-effects
The majority of all patients 738 reported no adverseevents while 187 experienced side-effects Another75 did not answer this question The majority (789)of the patients with side-effects reported that these wereonly slight while 211 reported moderate side-effectsNo patients reported any severe side-effects No pro-nounced difference was seen between the groupsregarding side-effects The types of side-effects experi-enced are listed in Table 5
Global evaluation
Patientsrsquo median global evaluation scores of their studymedications are shown in Table 4 After 4 h thecombination treatment and rofecoxib alone receivedsimilar evaluations Both groups were significantlybetter than paracetamol (P lt 0001 P lt 001) at thistime All active treatments were significantly betterthan placeboAt 8 h the combination group had the highest score
but the difference from the rofecoxib group was verysmall and not significant (Table 4) Both groups weresignificantly better than paracetamol alone (P lt 0001P lt 001) at 8 h All treatment groups were significantlybetter than placeboThe global evaluation scores are further specified in
Table 6 After 8 h 90 of the patients in the combina-tion group rated their medication as good or excellentFor the rofecoxib group the corresponding value was83 Of the patients treated with paracetamol 42rated their medication as good or excellent after 8 h
Discussion
In this study we showed that for the acute inflammatorypain following third molar surgery there was an additive
analgesic effect when combining rofecoxib with paracet-amol as compared with rofecoxib alone for the first 15 hafter intake After this time point the combination ofrofecoxib and paracetamol gave similar pain relief to thatof the rofecoxib group Paracetamol alone was also moreeffective for the first 15 h while rofecoxib was signifi-cantly better thanparacetamol from3 honwards The factthat rofecoxib and paracetamol were more effective thanplacebo shows that the method used was sensitive enoughto distinguish between different substancesAfter the clinical part of this study was carried out
serious concerns regarding cardiovascular effects of long-term treatment with rofecoxib were raised following re-ports of an increased incidence of myocardial infarctionand stroke among patients treated with rofecoxib in aplacebo-controlled study (24) After a highly significant19-fold increase in the incidence of thrombo-embolicserious adverse events was shown in yet another study(25) rofecoxib was withdrawn from the market Theside-effects of rofecoxib became progressively greaterafter 1 yr of treatment which suggests that the cardio-vascular risk is dose-dependent and not only associatedwith COX-2 selectivity (6) The need for acute pain reliefafter third molar surgery is short and the surgery ismainly performed in otherwise healthy young peopleamong whom the risk for serious cardiovascular events issmall It cannot be ruled out that future further devel-oped selective COX-2 inhibitors may be useful intreating acute pain after third molar surgery in this groupof patients with the advantage of only one dose a dayand minimizing the risk for gastrointestinal symptomsRofecoxib and paracetamol differ in onset time and
patients treated with rofecoxib reach meaningful painrelief after 15 h (8) compared with 05 h for paracet-amol This corresponds well with the results obtained inour study The group treated with paracetamol reportedtheir lowest VAS score by 1 h whereas at this time pointthe rofecoxib group still reported a high VAS scoreThereafter the medium VAS score for the paracetamolgroup increased while patients treated with rofecoxibcontinued to receive good pain relief until the end of theobservation period From these results it is reasonable toassume that the combination grouprsquos significantly betteranalgesic effect between 05 and 1 h compared with
Table 5
Side-effects as stated in patientsrsquo own words
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Fatigue 4 2 3 2Headache 1 2 ndash 2Fever ndash ndash ndash 1Dizziness 1 ndash 2 ndashStomach pains 1 ndash 1 ndashSickness ndash 1 ndash ndashShivers 1 2 ndash ndashPerspirations ndash 1 ndash ndash
Table 6
Percentage of patients in each study group stating their overallexperience of the study medication at 4 and 8 h
Study groups
Rofecoxib+
paracet-amol
(n frac14 34)Rofecoxib(n frac14 36)
Paracet-amol
(n frac14 20)Placebo(n frac14 17)
4 h 8 h 4 h 8 h 4 h 8 h 4 h 8 h
Poor 0 0 7 6 30 32 75 76Fair 6 10 7 11 40 26 18 18Good 47 32 43 36 15 26 7 6Excellent 47 58 43 47 15 16 0 0
COX-2 inhibitor and paracetamol after oral surgery 299
rofecoxib alone was a result of the earlier onset of theeffect of paracetamol The mean VAS scores for thecombination group and the paracetamol group corres-ponds totally at the 30-min observation pointThe peak pain after third molar surgery has been
shown to occur 4ndash6 h postoperatively (26) which coin-cides well with the time for the additive effect of para-cetamol to take effect in our study This supports the useof the combination treatment of rofecoxib and paracet-amol after third molar surgery to gain an early onsetparticularly if pain relief medication is started postop-eratively as it is of great clinical importance to have anearly onset of pain relief when treating acute pain Iftreatment starts pre-operatively the addition of para-cetamol is likely to have less clinical relevance This issupported by a study in which patients were givenrofecoxib and paracetamol before Ear Nose and Throat(ENT) surgery (27) The addition of paracetamol in thatsetting failed to improve the analgesic effects of rofec-oxibRofecoxib and paracetamol also differ in duration
The effect of paracetamol 1 g lasts up to 6 h and the drughas to be administered four times daily while rofecoxib50 mg has an analgesic effect up to 24 h (12) The presentstudy was a single-dose comparison In a normal clinicalsetting another 1 g of paracetamol would probably beprescribed after 6 h which would give another period ofadditive effectThe disparity in effect between rofecoxib and para-
cetamol in the present study from 3 h onwards is inaccordance with the findings of two studies on post-operative pain relief after otolaryngologic surgerycomparing rofecoxib and paracetamol given pre-operatively (11 28) A study regarding inflammatorypain in patients with knee osteoarthritis also showedrofecoxib to be superior to paracetamol (29) The resultof our study from 3 h after baseline and onwards thusconfirms the findings of these studies in a third molarpain modelOur study did not show the same additive effect of
combining rofecoxib and paracetamol as in a study byBreivik et al in which they combined diclofenac andparacetamol (18) These authors demonstrated anadditive effect of paracetamol over the whole studyperiod of 8 h Their study also showed less use of rescuemedication in the combination group compared with thepatients treated with diclofenac alone something alsofound in a study by Matthews et al (19) It would seemreasonable to assume that the additive effect of para-cetamol in our study would be the same as in these twostudies as rofecoxib and ibuprofen have been shown tohave the same analgesic effect following third molarsurgery (9 10 12) and the effects of ibuprofen anddiclofenac are similar (30ndash32) It cannot be ruled out thatthere is a difference in additive effect of paracetamolwhen combining it with rofecoxib compared withdiclofenac This theory is in accordance with the result ofa study by Pickering et al on pain relief after tonsil-lectomy in children in which rofecoxib combined withparacetamol did not significantly alter the need for earlyanalgesia as did ibuprofen combined with paracetamol
(33) Further studies may clarify differences between thetwo drugsIn conclusion the present study indicates that there is
an early additive effect up to 2 h when combiningparacetamol with rofecoxib postoperatively as comparedwith rofecoxib alone which coincides with peak painintensity after the removal of third molars Rofecoxibhad a significantly better analgesic effect than paracet-amol from 3 h onwards Our results indicate that para-cetamol does not enhance the analgesic effect ofrofecoxib over a longer period of time As rofecoxib hasbeen shown to have serious cardiovascular side-effectsfuture studies are needed to determine any serious side-effect during short-term treatment
Acknowledgements ndash This study was supported by grants fromLIV The Country Council of Varmland which made it inde-pendent from all manufacturers of the studied drugs There areno conflicts of interest by any of the authors with any drugcompany We thank Dr Carl-Mauritz Bratt DDS Dr PeterTroberg DDS and Dr Tobias Block DDS for performingsome of the surgery
References1 Cooper SA Five studies on ibuprofen for postsurgical dental
pain Am J Med 1984 77 70ndash772 Dionne RA Campbell RA Cooper SA Hall DL Buck-
ingham B Suppression of postoperative pain by preoperativeadministration of ibuprofen in comparison to placebo acet-aminophen and acetaminophen plus codeine J Clin Pharmacol1983 23 37ndash43
3 Vane JR Inhibition of prostaglandin synthesis as a mechanismof action for the aspirinlike drugs Nature 1971 231 232ndash235
4 Meade EA Smith WL De Witt DL Differential inhibition ofprostaglandin endoperoxide synthase (cyclo-oxygenase) iso-zymes by aspirin and other non-steroidal anti-inflammatorydrugs J Biol Chem 1993 268 6610ndash6614
5 Smith TJ Cyclooxygenase as the principal targets for action ofNSAIDs Rheum Dis Clin North Am 1998 24 501ndash523
6 Sciulli MG Capone ML Tacconelli S Patrignani P Thefuture of traditional nonsteroidal anti-inflammatory drugs andcyclooxygenase-2 inhibitors in the treatment of inflammationand pain Pharmacol Rep 2005 57 66ndash85
7 Spink M Bann S Glickman R Clinical implications of cyclo-oxygenase-2 inhibitors for acute dental pain managementbenefits and risks J Am Dent Assoc 2005 136 1439ndash1448
8 Ehrich EW Dallob A De Lepeleire I Van Hecken ARiendeau D Yuan W Porras A Wittreich J Seibold JRDe Shepper P Mellisch DR Gertz BJ Characterization ofrofecoxib as a cyclooxygenase-2 isoform inhibitor and demon-stration of analgesia in the dental pain model Clin Pharm Ther1999 65 336ndash347
9 Malmstrom K Fricke J Kotey P Kress B Morrisson B Acomparison of rofecoxib versus celecoxib in treating pain afterdental surgery a singlecenter randomized double-blind pla-cebo- and active-comparator-controlled parallel group single-dose study using the dental impaction pain model Clin Ther2002 24 1549ndash1560
10 Malmstrom K Daniels S Kotey P Seidenberg B Desjar-
dins PJ Comparison of rofecoxib and celecoxib two cyclo-oxygenase-2-inhibitors in postoperative dental pain Arandomized placebo- and active-comparator-controlled clinicaltrail Clin Ther 1999 21 1653ndash1663
11 Watcha MF Issioui T Klein KW White PF Costs andeffectiveness of rofecoxib celecoxib and acetaminophen forpreventing pain after ambulatory otolaryngologic surgeryAnesth Analg 2003 96 987ndash994
300 Haglund amp Bultzingslowen
12 Morrisson BW Christensen S Yuan W Brown J Amlani
S Seidenberg B Analgesic efficacy of the cyclooxygenase-2-specific inhibitor rofecoxib in post-dental surgery pain arandomized controlled trial Clin Ther 1999 21 943ndash953
13 Chang DJ Fricke JR Bird RS Bohidar NR Dobbins TWGeba GP Rofecoxib versus codeineacetaminophen in post-operative dental pain a double-blind randomized placebo-and active comparator-controlled clinical trial Clin Ther 200123 1446ndash1455
14 Chang DJ Desjardins PJ Bird SR Black P Chen EPetruschke RA Geba GP Comparison of rofecoxib and amultidose oxycodoneacetaminophen regimen for the treatmentof acute pain following oral surgery a randomized controlledtrial Curr Med Res Opin 2004 20 939ndash949
15 Berenbaum MC What is synergy Pharmacol Rev 1989 4193ndash141
16 Altman RD A rationale for combining acetaminophen andNSAIDs for mild to moderate pain Clin Exp Rheumatol 200422 110ndash117
17 Bjorkman R Hallman KM Hedner J Hedner T Henning
M Acetaminophen blocks spinal hyperalgesia induced byNMDA and substance P Pain 1994 57 259ndash264
18 Breivik EK Barkvoll P Skovlund E Combining diclofenacwith acetaminophen or acetaminophen-codeine after oral sur-gery a randomized double-blind single-dose study ClinPharmacol Ther 1999 66 625ndash635
19 Matthews RW Scully CM Levers BG The efficacy ofdiclofenac sodium (Voltarol) with and without paracetamol inthe control of post-surgical dental pain Br Dent J 1984 157357ndash359
20 Norholt SE Treatment of acute pain following removal ofmandibular third molars use of the dental pain model inpharmacological research and development of a comparableanimal model Int J Oral Maxillofac Surg 1998 27 1ndash41
21 NIH Consensus Development Conference For Removal OfThird Molars J Oral Surg 1980 38 235ndash236
22 Laska EM Siegel C Sunshine A Onset and durationmeasurement and analysis In Max MB Portenoy RKLaska EM eds Advances in pain research and therapy NewYork Raven Press 1991 691ndash698
23 Max MB Laska EM Single-dose analgesic comparisons InMax MB Portenoy RK Laska EM eds Advances in painresearch and therapy New York Raven Press 1991 55ndash97
24 Bombardier C Laine L Reicin A Shapiro D Burgos-Vargas R Davis B Day R Ferraz MB Hawkey CJHochbergMC Kvien TK Schitzer TJ Comparison of uppergastrointestinal toxicity of rofecoxib and naproxen in patientswith rheumatoid arthritis N Engl J Med 2005 343 1520ndash1528
25 Bresalier RS Sandler RS QuanH Bolognese JA Oxenius
B Horgan K Lines C Riddell R Morton D Lanas AKonstam MA Baron JA Cardiovascular events associatedwith rofecoxib in a colorectal adenoma chemoprevention trialN Engl J Med 2005 17 1092ndash1102
26 Szmyd L Shannon ILMohnac AM Control of postoperativesequelae in impacted third molar surgery J Oral Ther Phar-macol 1965 1 491ndash496
27 Issioui T Klein KW White PF Hu J Skrivanek GDAnalgesic efficacy of rofecoxib alone or in combination withacetaminophen in the ambulatory setting Anesthesiology 200195 A35
28 Issioui T KleinKWhite PWatchaM SkrivanekG JonesSHu J BradleyM Caleb I Cost-efficacy of rofecoxib versusacetaminophen for preventing pain after ambulatory surgeryAnesthesiology 2002 97 931ndash937
29 Geba GP Weaver AL Polis AB Dixon ME Schnitzer TJEfficacy of rofecoxib celecoxib and acetaminophen in osteo-arthritis of the knee a randomized trial JAMA 2002 287 64ndash71
30 Joshi A Parara E Macfarlane TV A double-blind rand-omised controlled clinical trial of the effect of preoperativeibuprofen diclofenac paracetamol with codeine and placebotablets for relief of postoperative pain after removal of impac-ted third molars Br J Oral Maxillofac Surg 2004 42 299ndash306
31 Bakshi R Frenkel G Dietlein G Meurer-Witt B Schn-eider B Sinterhauf U A placebo-controlled comparativeevaluation of diclofenac dispersible versus ibuprofen in post-operative pain after third molar surgery J Clin Pharmacol 199434 225ndash230
32 Ahlstrom U Bakshi R Nilsson P Wahlander L Theanalgesic efficacy of diclofenac dispersible and ibuprofen inpostoperative pain after dental extraction Eur J Clin Pharma-col 1993 44 587ndash588
33 Pickering AE Bridge HS Nolan J Stoddart A Double-blind placebo-controlled analgesic study of ibuprofen orrofecoxib in combination with paracetamol for tonsillectomy inchildren Br J Anaesth 2002 88 72ndash77
COX-2 inhibitor and paracetamol after oral surgery 301
Combined acetaminophen and ibuprofen for pain relief after oralsurgery in adults a randomized controlled trial
A F Merry1 2 R D Gibbs3 J Edwards4 G S Ting3 C Frampton5 E Davies1 2
and B J Anderson1
1Department of Anaesthesiology University of Auckland Private Bag 92019 Auckland New Zealand2Department of Anaesthesia Auckland City Hospital Auckland New Zealand 3Oral Health Unit Greenlane
Clinical Centre 214 Greenlane West Epsom Auckland New Zealand 4Oral and Maxillofacial Service Quay
Park Medical Centre 68 Beach Road Auckland Central Auckland New Zealand 5Department of Medicine
Christchurch School of Medicine and Health Sciences University of Otago New Zealand
Corresponding author E-mail amerryaucklandacnz
Background Acetaminophen is often used with a non-steriodal anti-inflammatory drug for
acute pain Hitherto these drugs have had to be given separately typically at different time
intervals Maxigesicw tablets combine acetaminophen and ibuprofen in clinically appropriate
doses to simplify administration and dosage regimen We compared this combination with each
of the constituent drugs for the relief of pain after extraction of third molar teeth
Methods Adults (more than 16 yr) having one or more wisdom teeth removed under general
or local anaesthesia were instructed to take two tablets before operation then two tablets
every 6 h for up to 48 h of (i) a combination of acetaminophen 500 mg and ibuprofen 150 mg
per tablet (Maxigesicw) (ii) acetaminophen 500 mg per tablet alone or (iii) ibuprofen 150 mg
per tablet alone The primary outcome measure was the area under the curve (AUC) of the
100 mm visual analogue scale pain measurements taken for up to 48 h after surgery divided by
time at rest and on activity Pharmacokinetic data were collected in a subset of patients
Results The mean (SEM) time-corrected AUC on rest and activity respectively were combi-
nation group 223 (32) and 284 (34) acetaminophen group 330 (31) and 404 (33) and ibu-
profen group 348 (32) and 402 (34) P001 for each of the four comparisons of combination
vs constituent drug There was no pharmacokinetic interaction between acetaminophen and
ibuprofen administered together
Conclusions Maxigesicw tablets provide superior pain relief after oral surgery to acetamino-
phen or ibuprofen alone
Br J Anaesth 2010 104 80ndash8
Keywords anaesthesia dental analgesia postoperative analgesics non-opioid acetaminophen
analgesics non-opioid ibuprofen non-steroidal anti-inflammatory drugs
Accepted for publication October 16 2009
The relief of pain has been described as a universal human
right but is not always easily achieved1 Opioid analgesics
are effective but have troublesome and potentially danger-
ous side-effects and their potential for abuse may lead to
regulatory and logistical difficulties Non-steroidal anti-
inflammatory drugs (NSAIDs) have fewer regulatory
restrictions but they too have important adverse effects
which are more likely at higher dose or with longer
courses2 Acetaminophen is widely used and is very safe
at the recommended dose of 4 g per day3 but does not
always provide adequate pain relief on its own Combining
analgesics offers the possibility of increasing effectiveness
without increasing dose (and therefore risk)4 5 NSAIDs
are often combined with acetaminophen particularly for
treating postoperative pain6 ndash 10
Prescribing acetaminophen and ibuprofen together is
common in clinical practice6 8 9 11 ndash 13 Ibuprofen has the
advantage of a well-established safety record (particularly
at doses below 15 g per day in adults)14 and in many
countries (including the UK) it is available without
The Author [2010] Published by Oxford University Press on behalf of the British Journal of Anaesthesia
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (httpcreativecommonsorglicensesby-nc25uk)
which permits unrestricted non-commercial use distribution and reproduction in any medium provided the original work is properly cited
British Journal of Anaesthesia 104 (1) 80ndash8 (2010)
doi101093bjaaep338
prescription Typically acetaminophen is given in a dose
regimen of 1 g 6 hourly whereas ibuprofen is given in a
dose of 400 mg 8 hourly3 Compliance with the prescribed
dosing regimen is important for achieving the desired
result with any drug and is often poor with asynchronous
dosing15 A single formulation with a simplified regimen
would probably be appreciated by patients and might
improve compliance
Maxigesicw is a new formulation of acetaminophen 500
mg and ibuprofen 150 mg Taking two tablets 6 hourly
provides the appropriate daily dose of both drugs relatively
simply We have investigated the hypothesis that in adult
patients undergoing a common surgical procedure (extrac-
tion of third molar teeth) this formulation provides
superior analgesia to either of its components alone
Methods
With ethics committee approval we recruited and fol-
lowed up patients between March 2005 and February
2008 Trial registration ANZCTRORGAU (identifier
ACTRN12606000291583)
Setting
This study was conducted at a publicly funded teaching
hospital and a private day-surgical clinic in metropolitan
New Zealand
Participants
We included adults undergoing extraction of at least one
lower wisdom tooth with or without one or more upper
wisdom teeth by one of three participating surgeons We
excluded patients if they were under 16 yr old weighed
50 kg had taken any NSAID (other than aspirin in a
dose of 150 mg daily or less) within 24 h of the operation
had taken acetaminophen or acetaminophen containing
medicines within 12 h of the operation were taking an
angiotensin-converting enzyme inhibitor warfarin steroid
(other than interoperative dexamethasone) or any immu-
nosuppressive drug were intolerant to any NSAID or acet-
aminophen were suffering from a severe local infection
had a history of peptic ulceration asthma or severe hae-
mopoetic renal or hepatic disease were participating in
the investigation of another experimental agent or if the
clinician believed for any other reason that participation in
the study might not be in their best interests
Randomization and blinding
Tablets of identical appearance packaging and dosage
instructions were provided in each of the following formu-
lations (i) acetaminophen 500 mgthornibuprofen 150 mg per
tablet (Maxigesicw Sigma Laboratories Nashik India which
was MHRA approved for manufacturing pharmaceuticals
under GMP) (ii) acetaminophen 500 mg per tablet or
(iii) ibuprofen 150 mg per tablet
Patients were first approached by the surgeon and then
by the study nurse They were given written and verbal
information about the study and invited to participate If
they consented patients were then randomized into one of
the three study groups in a sequential order to receive one
of these formulations in blinded packs The randomization
sequence was computer generated by the study statistician
as a 111 allocation ratio to the three treatments in a
sequence of permuted blocks with stratification for anaes-
thetic type (local or general) and study centre
Stratification by anaesthetic type ensured a balance
between treatments in terms of the number of teeth
extracted as most patients having more than two teeth
extracted have a general anaesthetic Only the statistician
had access to the schedule of patient numbers by drug
allocation Participants and investigators were blinded and
the randomization code was not broken until the final data-
base had been checked and locked
Intervention
Participants were asked to take two tablets of the study
medication before operation (as close as possible to the
start of surgery) and then 4 times a day (as close as poss-
ible to 6 hourly) for up to 48 h after surgery All partici-
pants were given bupivacaine local anaesthetic blocks by
the surgeons For those participants undergoing general
anaesthesia this was induced with propofol and main-
tained with isoflurane and nitrous oxide in oxygen
Monitoring was in accordance with the guidelines of the
Australian and New Zealand College of Anaesthetists16
All extractions were carried out by one of three surgeons
each using his normal technique
If participants required additional postoperative pain
relief while in hospital a rescue dose of fentanyl 10 mg
was given iv as required After discharge to home
codeine was provided (again as rescue medication) in 30
mg tablets one to two to be taken as needed up to
4 hourly
Outcomes
Participants were asked to rate their pain on 100 mm visual
analogue scales (VAS) printed one per double page in a
booklet that they took home Ratings were requested at
baseline (immediately before administration of the first
dose of study medication) after operation (once the partici-
pants were sufficiently awake to respond) and 1ndash2 hourly
thereafter while awake for 48 h The study nurse main-
tained contact with participants by telephone to facilitate
compliance with data collection and the return of diaries
The primary outcome measure was the area under the
curve (AUC) of these VAS ratings divided by time at rest
and on activity The AUC was divided by the period of
the completed assessments to adjust for the fact that some
Combined acetaminophen and ibuprofen for analgesia
81
patients recorded pain for shorter periods than others This
calculation in effect produces a measure of average pain
intensity over the study period
Secondary efficacy outcome measures were a categorical
global pain rating by the participants taken at the end of the
study period rescue analgesia consumption over the study
period a categorical global rating of nausea by the partici-
pants taken at the end of study period the number of epi-
sodes of vomiting over the study period and a rating of
sleep disturbance on a 100 mm VAS assessed after each
night during the study period In addition participants were
asked to rate their experiences of participating in the study
Sample size estimation
We obtained blood samples from the 38 participants
undergoing general anaesthesia in order to have evaluable
pharmacokinetic data for at least 30 patients The first
sample was obtained 30 min after the first dose of study
medication the second sample at the end of anaesthesia
and additional one or two samples after operation in hospi-
tal The plasma concentration of acetaminophen and ibu-
profen were measured by the sponsor and used to form
individual timendashconcentration profiles The analytical
method used an HPLC-DAD (Diode Array Detector) assay
for the simultaneous determination of acetaminophen and
ibuprofen in plasma Precision and accuracy for acetami-
nophen and ibuprofen assay were validated over the con-
centration range 05ndash50 mg ml21 for both drugs The
intra- and inter-batch precision of the assays at low
medium and high concentrations of acetaminophen and
ibuprofen varied from theoretical values by 15 The
lower limit of quantification for each drug was 05 mg
ml21 The sponsor monitored all data collected during the
study and queries and corrections were made when any
inaccuracies or inconsistencies were identified
Sample size estimation
We estimated that 120 participants (40 per group) in the
intention-to-treat (ITT) population would provide 80
power to detect differences between the groups of 9 (SD
14) mm in our primary endpoint for resting assessments
and 13 (SD 21) for measures during activity10 17 with a
one-sided type I error rate of 5 These differences equate
to 25 Differences of this magnitude were considered
clinically important and comparable with differences
typical of previous published studies10
Statistical methods
The data were analysed using SPSS version 150 (SPSS
Inc Chicago IL USA) Efficacy analyses were conducted
on an ITT basis with the additional provision that
there were at least three VAS measurements over at
least 12 h available to calculate the primary endpoint All
participants who were randomized into the study were
included in the safety evaluations As the first dose of
study medication was taken before operation while under
the supervision of the surgeon all randomized patients
took at least a single dose of study medication A last
observation carried forward approach was used for those
subjects who left the study prematurely for non-AUC
based variables
We compared the primary endpoint between the combi-
nation group and each of the acetaminophen and ibuprofen
arms at rest and on activity using a general linear model
(GLM) which included terms for treatment the centre and
anaesthetic stratum Additionally to confirm the consist-
ency of the treatment effects across strata the stratum
treatment interaction terms were tested and included in
the final model The analysis was also checked with
number of teeth extracted as an additional factor
Continuous secondary efficacy endpoints were tested for
significance using the same models as used for the
primary endpoint
A one-tailed P005 was pre-specified to indicate stat-
istical significance We required a statistically significant
result favouring the combination from each of the two
planned comparisons with the constituents to define super-
iority for either rest or on activity measures We used one-
tailed tests as there seemed no theoretical or empirical
basis for expecting that combining these analgesics could
result in a reduction in efficacy and because the require-
ment for each of two comparisons to be significant at
P005 is stringent Secondary categorical efficacy end-
points were compared between the groups using x2 tests
and MannndashWhitney U-tests as appropriate
We used non-linear mixed effect models (NONMEM
VI Globomax LLC Hanover MD USA) to estimate
population pharmacokinetics with a Compaq Digital
Fortran Version 66A compiler on an Intel Celeron 333
MHz CPU (Intel Corp Santa Clara CA USA) under MS
Windows XP (Microsoft Corp Seattle WA USA) This
model allows assessment of inter-individual variability
covariance between pharmacokinetic parameters and
residual error We judged the quality of fit of the pharma-
cokinetic model to data using the NONMEM objective
function examination of plots of observed vs predicted
concentrations and visual predictive checks
Results
After initial screening 189 patients were approached 135
agreed to participate One to four teeth were extracted
with local anaesthetic alone in 69 patients and with local
anaesthetic in combination with general anaesthesia in 66
Thirteen patients did not return their patient diaries so
122 patients were included in the evaluable ITT popu-
lation for the analysis of the primary endpoints (Fig 1)
The treatment groups were adequately matched in baseline
patient and clinical characteristics (Table 1) Of those in
Merry et al
82
the combination group 600 had three or four teeth
extracted compared with 436 for ibuprofen and 535
for acetaminophen
Efficacy
The time-adjusted AUCs were substantially and signifi-
cantly lower at rest and on activity in the combination
group than in either of the other two treatment groups
(Table 2 Figs 2 and 3) with all four P001 The consist-
ency of the treatment effects across strata was confirmed
from the GLM with P-values for the treatment stratum
interaction of 0955 and 0984 for time-adjusted AUCs at
rest and on activity respectively The type of anaesthetic
(local vs general) and number of teeth extracted did not
change the outcome of either analysis
Although all four secondary endpoints favour the com-
bination treatment (Table 3) only the global pain rating
reached statistical significance More participants experi-
enced lsquonilrsquo or lsquomildrsquo pain with the combination (684)
than with either other group this difference was significant
for acetaminophen (375 Pfrac140008) but not for ibupro-
fen (543 Pfrac140263) The use of any rescue medication
also favoured the combination treatment (Table 4) but this
did not reach statistical significance
Pharmacokinetics
There were no significant differences between the combi-
nation group and either constituent group in any of the
estimated pharmacokinetic parameters (Table 5) The
visual predictive plots of individual concentration showed
that 90 of the observations were within the 90 pre-
diction intervals
Twelve participants were given both acetaminophen and
ibuprofen For calculation of the pharmacokinetic vari-
ables a scaling factor was applied to clearance and
volume of distribution in turn for those participants receiv-
ing the combination of acetaminophen and ibuprofen This
scaling factor had no impact on either acetaminophen or
ibuprofen pharmacokinetic parameters indicating that
there was no pharmacokinetic interaction between acetami-
nophen and ibuprofen when administered together
(P005)
Clearance (CLF) and volume of distribution (VF) par-
ameters observed in the study are consistent with those
reported previously (acetaminophen CLFfrac14126ndash210
litre h21 70 kg21 VFfrac14483ndash710 litre 70 kg21 ibupro-
fen CLFfrac1429ndash59 litre h21 70 kg21 VFfrac1464ndash235 litre
70 kg21)18 ndash 20
Adverse effects
The frequency of adverse effects was consistent with the
known effects of the constituent drugs and there were no
Screened(n =189)
Randomized(n =135)
Acetaminophentreatmentgroup(n =47)
Ibuprofentreatment group(n =44)
Combinationtreatment group(n =44)
Patient diariesnot returned(n =4)
Patient diariesnot returned(n =5)
Patient diariesnot returned(n =4)
Included in theanalysis(n =43)
Included in theanalysis(n =39)
Included in theanalysis(n =40)
Fig 1 Flow of participants through trial Not randomized (nfrac1454) (i)
declined to participate (nfrac1415) (ii) did not meet inclusion criteria
(nfrac1414) (iii) other reasons (nfrac1425) other reasons the surgery was
cancelled or rescheduled patient could not be contacted patient was
given the wrong date of the surgery
Table 1 Patient characteristic and baseline information (SD)
Acetaminophen (n547) Ibuprofen (n544) Combination (n544)
Age [mean (range)] (yr) 235 (160ndash404) 237 (168ndash389) 250 (183ndash404)
Weight [mean (SD)] (kg) 713 (156) 808 (201) 711 (135)
Ethnicity [n ()]
Asian 4 (85) 1 (23) 2 (45)
Black 1 (21) 0 (00) 1 (23)
Caucasian 33 (702) 31 (705) 34 (773)
Maori 4 (85) 4 (91) 4 (91)
Pacific Islander 4 (85) 5 (114) 2 (45)
Other 1 (21) 3 (68) 1 (23)
Male [n ()] 13 (277) 21 (477) 13 (295)
Shift workers [n ()] 10 (213) 5 (114) 3 (68)
Preoperative pain scores at rest [mean (SD)] (mm) 19 (51) 21 (52) 26 (68)
Preoperative pain scores on activity [mean (SD)] (mm) 41 (133) 27 (83) 29 (66)
Sleep disturbance for night before surgery as VAS [mean (SD)] (mm) 647 (229) 691 (260) 715 (241)
Combined acetaminophen and ibuprofen for analgesia
83
definitive indications that the adverse event profile is
changed when the two drugs are combined (Table 6)
however the numbers were too small to make meaningful
comparisons between the groups Two participants experi-
enced postoperative bleeding (attributed to surgical
causes) which resolved without readmission to hospital
No gastrointestinal bleeding was reported during the study
Most adverse events were evaluated as mild (574) or
moderate (352) and on review were considered not
related (175) or unlikely to be related (667) to study
medication
General
The majority of participants rated the experience of taking
part in the study as very positive (31) or positive (47)
0
10
20
30
40
50
60
70
80
90
100
ActivityRest
Acetaminophen alone
Ibuprofen alone
Combination
AU
Ch
(m
m)
Fig 2 Mean (thorn95 CI) mm of time-adjusted AUC (AUCtime) for VAS
at rest and on activity by treatment group
Table 2 Mean (SEM 95 CI) of time-adjusted AUC of visual analogue pain
scores at rest and on activity by treatment group The differences between
combination and each constituent were significant at rest (vs acetaminophen
Pfrac140007 and vs ibuprofen Pfrac140003) and on activity (vs acetaminophen
Pfrac140006 and vs ibuprofen Pfrac140007)
Acetaminophen
(n543)
Ibuprofen (n539) Combination
(n540)
At rest 330 (31 279ndash381) 348 (32 294ndash402) 223 (32 170ndash277)
On
activity
404 (33 350ndash458) 402 (34 346ndash459) 284 (34 228ndash341)
0
1020
30
40
5060
70
8090
100A
B
0 4 8 12 16 20 24 28 32 36 40 44 48
0 4 8 12 16 20 24 28 32 36 40 44 48
Hours post-surgery
VA
S s
core
(m
m)
0
10
2030
40
50
60
7080
90
100
Hours post-surgery
VA
S s
core
(m
m)
Acetaminophen aloneIbuprofen aloneCombination
Fig 3 Mean (SE) mm VAS out of 100 at rest (A) and on activity (B)
Table 3 Secondary efficacy endpoints by treatment group The only
significant difference was between the global pain ratings for combination and
acetaminophen (Pfrac140008 MannndashWhitney U-test)
Acetaminophen Ibuprofen Combination
Global pain rating [n ()]
Nil 3 (75) 4 (114) 4 (105)
Mild 12 (300) 15 (429) 22 (579)
Moderate 22 (550) 14 (400) 12 (316)
Severe 3 (75) 2 (57) 0 (00)
Global nausea rating [n ()]
Nil 26 (650) 25 (714) 30 (790)
Mild 10 (250) 8 (229) 7 (184)
Moderate 3 (75) 2 (57) 1 (26)
Severe 1 (25) 0 (00) 0 (00)
Vomiting episodes (n) 5 (in 3 subjects) 0 0
Sleep disturbance night
1 vs baseline VAS
[mean (SD)] (mm)
2219 (292) 2174 (229) 2166 (247)
Sleep disturbance night
2 vs baseline VAS
[mean (SD)] (mm)
2137 (329) 296 (258) 285 (201)
Table 4 Rescue analgesia by group n () none of these differences were
significant
Rescue analgesic Acetaminophen Ibuprofen Combination
Fentanyl in hospital 5 (116) 9 (237) 6 (154)
Codeine in the first 24 h 21 (4770) 16 (4320) 13 (3250)
Codeine in the second 24 h 22 (5370) 14 (4240) 16 (4210)
Any rescue medication over 48 h 25 (625) 18 (5810) 21 (568)
Table 5 Mean (SD) pharmacokinetic parameters (individual Bayesian
estimates used for descriptive statistics) for a one-compartment first-order
absorption first-order elimination model none of the differences for
combination formulations was significant CLF clearance VF volume of
distribution Tabs absorption half-time Cmax maximum concentration Tmax
time to achieve Cmax
Acetaminophen
alone (n515)
Acetaminophen
in combination(n512)
Ibuprofen
alone(n511)
Ibuprofen in
combination(n512)
CLF (litre
h21)
141 (26) 142 (18) 39 (17) 38 (13)
VF (litre) 557 (194) 482 (183) 106 (21) 98 (15)
Tabs (h) 042 (076) 016 (010) 058 (078) 085 (085)
Tmax (h) 109 (112) 064 (031) 116 (090) 144 (093)
Cmax (mg
litre21)
158 (65) 192 (64) 208 (83) 191 (78)
Merry et al
84
and 19 rated the experience as neutral Four participants
(3) found the experience negative and none rated it as
very negative The ratings were not significantly different
between the study groups
Discussion
We found that patients using the combination of acetami-
nophen and ibuprofen experienced less pain during the
first 48 h after oral surgery than those using the same
daily dosage of either agent alone and we think the differ-
ence was clinically relevant There was no evidence of any
pharmacokinetic interaction between acetaminophen and
ibuprofen Patients receiving ibuprofen alone reported the
lowest frequency of adverse events but the numbers are
too small for meaningful comparisons between the groups
and we saw no cause for concern in any group
Our data are consistent with previous evidence showing
that a combination of ibuprofen and acetaminophen pro-
vides better analgesia than acetaminophen alone8 9 13 21
Note however that two of these studies were in children9 13
so data in adults are relatively limited On the other hand
there are many studies supporting the more general point
that the addition of various NSAIDs improves the pain
relief obtainable from acetaminophen alone More impor-
tantly our data add convincingly to the sparse evidence
supporting the more controversial proposition that this
combination is superior to ibuprofen alone12 In a smaller
study in an orthopaedic pain model (which was positive
for the combination in comparison with acetaminophen)
Dahl and colleagues8 showed no such benefit whereas
Viitanen and colleagues13 (in a paediatric tonsillectomy
study) showed an advantage for the combination only in
the period after discharge from hospital The similarity in
efficacy between ibuprofen and acetaminophen on their
own seen in our study contrasts with the findings of
superior pain relief from ibuprofen after dental surgery by
Cooper and colleagues22 but theirs was a single-dose
study
Limitations and strengths of the study
Our results are limited to adults and to the doses and
model of pain studied We think our conclusions are likely
to apply to other age groups and other types of pain but
this will require confirmation We have not explored the
optimal dosage of the combination drug but the dosage
used is consistent with current clinical practice The
inclusion of patients who underwent both general and
local anaesthesia implies that our findings are likely to
apply in either case It is not possible to draw firm con-
clusions on the safety of any drug from a study of only 40
participants per group but acetaminophen and ibuprofen
are well established widely used and considered very safe
in appropriate doses3 23 There is no theoretical reason
Table 6 Adverse events and their relationship with study medication as evaluated by the investigators Postoperative pain was noted as a complication in 2 0
and 1 patient in the acetaminophen ibuprofen and combination groups respectively Some individuals experienced more than one adverse event
Relationship System organ class Acetaminophen Ibuprofen Combination Total
Not related Gastrointestinal disorders (numbness of tongue) 1 0 0 1
General disorders and administration site conditions (swollen arm infusion site
phlebitis)
0 0 2 2
Infections and infestations (dry socket alveolitis of jaw) 1 0 1 2
Injury poisoning and procedural complications (bruising of arm postoperative
pain)
0 0 2 2
Musculoskeletal and connective tissue disorders ( jaw stiffness) 0 0 1 1
Skin and sc tissue disorders (swelling face) 1 1 0 2
Subtotal 3 1 6 10
Unlikely related Blood and lymphatic system disorders (swollen glands) 1 0 0 1
Ear and labyrinth disorders (pain in ear tinnitus) 2 0 0 2
Gastrointestinal disorders (vomiting nausea stomach cramps dry lips) 6 1 2 9
Injury poisoning and procedural complications (postoperative bleeding) 0 0 1 1
Musculoskeletal and connective tissue disorders ( jaw stiffness aches and pains in
legs jaw pain)
2 0 1 3
Nervous system disorders (headache felt faint sleepy balance difficulty light
headiness dizziness drowsiness lethargic)
6 4 4 14
Psychiatric disorders (disorientation) 0 1 0 1
Respiratory thoracic and mediastinal disorders (sore throat pharyngeal ulceration
hypoventilation coughing)
1 1 2 4
Investigations (body temperature increased) 0 0 1 1
Skin and sc tissue disorders (rash redness of external ear swelling face) 0 1 1 2
Subtotal 18 8 12 38
Possibly related Gastrointestinal disorders (stomach cramps abdominal pain constipation stomach
ache vomiting)
3 0 2 5
General disorders and administration site conditions (fever) 1 0 0 1
Injury poisoning and procedural complications (postoperative bleeding) 0 0 1 1
Nervous system disorders (sleepy headache) 1 0 1 2
Subtotal 5 0 4 9
Total 26 9 22 57
Combined acetaminophen and ibuprofen for analgesia
85
and no empirical suggestion from our data to suggest that
the combination would be any less safe than the constitu-
ent drugs on their own Our safety data are observational
rather than based on prospective laboratory investigations
but we followed up participants for adverse events for 3
weeks and it seems unlikely that clinically important
harm would have been missed
Pain after oral surgery can persist for several days10 but
we considered 48 h to be a clinically relevant period and
a longer period of study is likely to have resulted in poorer
compliance with data collection
It could be asked whether a more typical (albeit
complex) regimen for ibuprofen alone might have pro-
vided better analgesia than seen with the 4 hourly
approach used here but this seems unlikely particularly
given that our clinical efficacy data were supported by esti-
mates of population pharmacokinetics We had planned to
correlate drug plasma concentration with pain scores but
the drug plasma concentration results were too sparse and
there were too many confounding variables (such as ethni-
city comparators and rescue analgesia) for this to be
undertaken We did demonstrate a lack of interaction
between the constituent drugs when used in combination
and provided evidence that equivalent and predicted blood
concentrations were achieved (the observations of timendash
concentration profile decreased within 90 of prediction
limits for both acetaminophen and ibuprofen) Furthermore
pharmacokinetic parameter estimates observed in the current
study are very similar to those previously reported18 ndash20
The evaluations used in the efficacy analysis have
established construct validity and are appropriate for
parametric analysis24 25
In designing analgesic studies it is an advantage to
minimize the exposure of participants to inadequate
analgesia while controlling for various sources of bias
Some designs incorporate a placebo group but the efficacy
of both ibuprofen26 and acetaminophen27 in comparison
with placebo are well established by previous research
and we would argue that the use of a placebo in this situ-
ation is unnecessary and perhaps even unethical28 There
would be little value in another lsquome toorsquo analgesic unless
it had clear advantages over established agents Therefore
the question of interest lies in the comparisons between
the new agent (Maxigesicw) and the reference standard of
care and in this case we have actually shown superiority to
both of two possible reference standardsmdashacetaminophen
alone and ibuprofen alone One classic approach to analgesic
studies involves treating established acute pain This has the
alleged advantage that pain relief can be assessed (eg by
using AUC to estimate total pain relief or TOTPAR29 30 or
by calculating a pain reduction index per tablet)31 Our
design in contrast follows the widely accepted clinical prac-
tice of anticipating and treating pain before it occurs which
in our unit at least has long been considered best practice
Furthermore rescue medication was readily available and
those requiring it were evenly distributed between the
groups It is notable that most patients did require rescue
medication suggesting that pain after oral surgery can some-
times be severe enough that even the combination of ibupro-
fen and acetaminophen requires supplementation (and it
might be asked whether it would be a good idea for codeine
for example to be added to the combined formulation)
Nevertheless we think it important that the vast majority of
the participants in all groups reported pain scores that were
reasonably low and that all received analgesic regimens
accepted in contemporary practice The predominantly posi-
tive evaluation by participants of their experience in taking
part in the study provides empirical reassurance on this point
(and also other aspects of the conduct of the study)
The treatment of pain is central to medical practice in
hospitals and in primary care If these results are con-
firmed in other settings the already widely used combi-
nation of acetaminophen and ibuprofen may become the
standard of care for the initial management of moderate
acute pain at least for those patients who do not have
contra-indications to NSAIDs Even using the drugs indi-
vidually the dosage regimen studied here is simpler than
that currently recommended and may well improve com-
pliance with and therefore success with this combination
Providing both drugs in one tablet simplifies this regimen
even further and our data confirm that the specific formu-
lation studied here is effective and that there is no inter-
action between its constituent drugs
Conclusions
Doctors treating pain after oral surgery in hospital and at
home and probably pain in many other situations should
consider using acetaminophen and ibuprofen together four
times a day provided there are no contraindications to
either drug and taking into account the known risks of
NSAIDs The combination formulation studied here sim-
plifies this regimen
Funding
This work was supported by AFT Pharmaceuticals Ltd
assisted by New Zealand Trade and Enterprise
Development Grants
Appendix
Declaration of interest
The Department of Anaesthesiology of the University of
Auckland has received payment from AFT
Pharmaceuticals for conducting this study but none of the
investigators has received payment in their personal
capacity
Merry et al
86
Contributors
AFM BJA CF and Hartley Atkinson designed the
study with input from RDG and JE Hartley Atkinson
obtained funding RDG GST and JE performed the
surgery and contributed to patient recruitment and to the
care of patients during their participation in the study
ED was the study coordinator and was responsible for
patient recruitment and follow-up data collection quality
control and many other logistic aspects of the study The
statistical analysis of clinical data was undertaken by CF
and of the pharmacokinetic data by BJA AFM took
primary responsibility for the manuscript with assistance
from Jennifer Zhang All authors edited and commented
on the manuscript AFM is the guarantor
Chief Executive Officer AFT Pharmaceuticals
Clinical TrialRegulatory Assistant AFT Pharmaceuticals
Ethics approval
This study was approved by the Northern X Regional Ethics
Committee 650 Great South Road Penrose Auckland New
Zealand
Ethics Committee Approval Number AKX0410298
Health Authorities (MEDSAFE) Approval Number
TT50-7316 (458)
Role of the sponsor
The sponsor (AFT Pharmaceuticals Ltd) participated in
the study design and protocol development and provided
logistical support during the trial Monitoring of the
study was performed by the sponsor who also main-
tained the trial database Statistical analyses were
independently performed by the biostatistician and the
results cross-checked by sponsors and investigators The
sponsor assisted with the preparation of the manuscript
and was permitted to review it and to make suggestions
but responsibility for the content of this paper lay with
the academic authors and the style and emphasis is that
of the principle investigator The academic authors had
the explicit right to access all data and publish these
results
Provenance and peer review
This paper was not commissioned informal external peer
review has been obtained before submission to the Journal
Additional contributions
We thank Ms Jenny Rous Pharmacy Manager from the
Mercy Hospital Pharmacy for study drug management
Dr Ralph Richardson Program Manager from Institute of
Environment Science amp Research Limited Wellington in
New Zealand for the plasma sample assays Sally Merry
for proofreading and editing on the manuscript the anaes-
thetists Judy Bent Jack Hill Joanna Rose Joanne Paver
Andrew Warmington and Lisa Chapman at Greenlane
Clinical Centre Kerry Gunn Chris Chambers and
Jonathan Cross at Quay Park Clinic for facilitating the
administration of the study protocol and contributing
substantially to the clinical care of the patients and the
participants for their participation
References1 Cousins MJ Brennan F Carr DB Pain relief a universal human
right Pain 2004 112 1ndash42 Merry A Power I Perioperative NSAIDs towards greater safety
Pain Rev 1995 2 268ndash913 MARTINDALE The Extra Pharmacopoeia London The Royal
Pharmaceutical Society of Great Britain 19964 Mehlisch DR The efficacy of combination analgesic therapy in
relieving dental pain J Am Dent Assoc 2002 133 861ndash71
5 Desmeules J Rollason V Piguet V Dayer P Clinical pharmacologyand rationale of analgesic combinations Eur J Anaesthesiol Suppl2003 20 7ndash11
6 Altman RD A rationale for combining acetaminophen andNSAIDs for mild-to-moderate pain Clin Exp Rheumatol 2004 22
110ndash77 Hyllested M Jones S Pedersen JL Kehlet H Comparative effect
of paracetamol NSAIDs or their combination in postoperativepain management a qualitative review Br J Anaesth 2002 88
199ndash2148 Dahl V Dybvik T Steen T Aune AK Rosenlund EK Raeligder JC
Ibuprofen vs acetaminophen vs ibuprofen and acetaminophenafter arthroscopically assisted anterior cruciate ligament recon-struction Eur J Anaesthesiol 2004 21 471ndash5
9 Gazal G Mackie IC A comparison of paracetamol ibuprofen ortheir combination for pain relief following extractions in childrenunder general anaesthesia a randomized controlled trial Int JPaediatr Dent 2007 17 169ndash77
10 Merry AF Swinburn PF Middleton NG Edwards JL Calder MV
Tenoxicam and paracetamolndashcodeine combination after oralsurgery a prospective randomized double-blind placebo-controlled study Br J Anaesth 1998 81 875ndash80
11 Mitchell A van Zanten SV Inglis K Porter G A randomized con-trolled trial comparing acetaminophen plus ibuprofen versus acet-
aminophen plus codeine plus caffeine after outpatient generalsurgery J Am Coll Surg 2008 206 472ndash9
12 Menhinick KA Gutmann JL Regan JD Taylor SE Buschang PHThe efficacy of pain control following nonsurgical root canal
treatment using ibuprofen or a combination of ibuprofen andacetaminophen in a randomized double-blind placebo-controlledstudy Int Endod J 2004 37 531ndash41
13 Viitanen H Tuominen N Vaaraniemi H Nikanne E Annila PAnalgesic efficacy of rectal acetaminophen and ibuprofen alone
or in combination for paediatric day-case adenoidectomy Br JAnaesth 2003 91 363ndash7
14 Henry D McGettigan P Epidemiology overview of gastrointestinaland renal toxicity of NSAIDs Int J Clin Pract 2003 Suppl (135)43ndash9
15 TGA Medicines Evaluation Committee 2003 Review of non-prescription analgesics Multiple Strength of Oral LiquidsAustralia Therapeutic Goods Administration 2003
Combined acetaminophen and ibuprofen for analgesia
87
16 Australian and New Zealand College of Anaesthetists Monitoringduring anaesthesia (Review P18) Melbourne The College 2008
17 Merry AF Sidebotham DA Middleton NG Calder MV WebsterCS Tenoxicam 20 mg or 40 mg after thoracotomy a prospective
randomized double-blind placebo-controlled study AnaesthIntensive Care 2002 30 160ndash6
18 Davies NM Clinical pharmacokinetics of ibuprofen The first 30years Clin Pharmacokinet 1998 34 101ndash54
19 Prescott LF Pharmacokinetics of paracetamol Paracetamol(Acetaminophen) A Critical Bibliographic Review New York Taylor ampFrancis Inc 2001 205ndash15
20 Rainsford KD The pharmacokinetics of ibuprofen in humans andanimals Ibuprofen A Critical Bibliographic Review London Taylor amp
Francis 1999 92ndash521 Ianiro S Jeansonne B McNeal S Eleazer P The effect of pre-
operative acetaminophen or a combination of acetaminophen andibuprofen on the success of inferior alveolar nerve block forteeth with irreversible pulpitis J Endod 2007 33 11ndash4
22 Cooper SA Schachtel BP Goldman E Gelb S Cohn P Ibuprofenand acetaminophen in the relief of acute pain a randomizeddouble-blind placebo-controlled study J Clin Pharmacol 1989 291026ndash30
23 AHFS Drug Information Bethesda MD American Society of
Health-System Pharmacist 2007
24 Coll AM Ameen JRM Mead D Postoperative pain assessmenttools in day surgery literature review J Adv Nurs 2004 46 124ndash33
25 Philip BK Parametric statistics for evaluation of the visual ana-logue scale Anesth Analg 1990 71 710
26 Schou S Nielsen H Nattestad A et al Analgesic dosendashresponserelationship of ibuprofen 50 100 200 and 400 mg after surgicalremoval of third molars a single-dose randomized placebo-controlled and double-blind study of 304 patients J Clin
Pharmacol 1998 38 447ndash5427 Barden J Edwards J Moore A McQuay H Single dose oral para-
cetamol (acetaminophen) for postoperative pain CochraneDatabase Syst Rev (Online) 2004
28 Anderson B Cranswick N The placebo (I shall please)mdashis it so
pleasing in children Paediatr Anaesth 2005 15 809ndash1329 Australian and New Zealand College of Anaesthetists and Faculty
of Pain Medicine Acute Pain Management Scientific EvidenceAustralian Government National Health and Medical ResearchCouncil 2005
30 Moore RA Edwards JE McQuay HJ Acute pain individualpatient meta-analysis shows the impact of different ways of ana-lysing and presenting results Pain 2005 116 322ndash31
31 Quiding H Oksala E Happonen RP Lehtimaki K Ojala T Thevisual analog scale in multiple-dose evaluations of analgesics J Clin
Pharmacol 1981 21 424ndash9
Merry et al
88
e411
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Journal section Oral Medicine and PathologyPublication Types Research
Analgesic efficacy of Lysine Clonixinate paracetamol and dipyrone in lower third molar extraction A randomized controlled trial
Vladimir-Reimar-Augusto-de Souza Noronha 1 Gladson-de Souza Gurgel 1 Luiz-Ceacutesar-Fonseca Alves 2 Luiz-Claacuteudio Noman-Ferreira 2 Lisette-Lobato Mendonccedila 2 Evandro-Guimaratildees de Aguiar 2 Evandro-Neves Abdo 2
1 Student in Oral and Maxillofacial Surgery and Traummatology Dental School Federal University of Minas Gerais Belo Hori-zonte Brazil2 Senior Lectures of Department of Surgery Pathology and Clinic Dental School Federal University of Minas Gerais Belo Horizonte Brazil
Correspondence Faculdade de Odontologia Universidade Federal de Minas GeraisAv Antonio Carlos 6627Belo Horizonte ndash Minas Gerais - BrasilCEP 31270-901evandroabdogmailcom
Received 18082008Accepted 20032009
Noronha VRA Gurgel GS Alves LCF Noman-Ferreira LC Mendonccedila LL Aguiar EG Abdo EN Analgesic efficacy of lysine clonixinate para-cetamol and dipyrone in lower third molar extraction A randomized con-trolled trial Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 httpwwwmedicinaoralcommedoralfree01v14i8medoralv14i8p412pdf
AbstractObjective The purpose of this study is to compare the analgesic effect of lysine clonixinate paracetamol and dipyrone after lower third molar extraction Material and Methods The sample consisted of 90 individuals with clinical indication for inferior third molars extraction The mean age of the sample was 223 years (DPplusmn25) The individuals received the medication in uni-dentified bottles along with the intake instructions The postoperative pain parameters were measured according to Visual Analogical Scale (VAS) and the data was evaluated using the Kruskal-Wallis Test and Friedman Test with the latter used to test different time intervals for each one of the drugsResults The final sample consisted of 64 individuals including 23 males (459) and 41 females (641) The mean age of the entire sample was 223 years (plusmn25) The average length of the procedures was 339 minutes (plusmn98) The distribution of mean values for this variable showed little variance for the different drugs (p=007) Conclusion Lysine Clonixinate did not show any substantial impact on the postoperative pain control when com-pared to other drugs
Key words Lysine Clonixinate paracetamol dipyrone postoperative pain impacted third molar
Article Number 2409 httpwwwmedicinaoralcomcopy Medicina Oral S L CIF B 96689336 - pISSN 1698-4447 - eISSN 1698-6946eMail medicinamedicinaoralcom Indexed in
-SCI EXPANDED-JOURNAL CITATION REPORTS-Index Medicus MEDLINE PubMed -EMBASE Excerpta Medica-SCOPUS-Indice Meacutedico Espantildeol
e412
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Introduction Surgical extraction of third molars is a very usual clini-cal procedure for controlling problems caused by im-pacted tooth and usually is followed by postoperative pain (1) As a result several studies have been published comparing the drugs used to control postoperative pain after surgical removal of third molars (1-4)Lysine Clonixinate is an analgesic that inhibits prostag-landin synthesis A study comparing Lysine Clonixi-nate with Paracetamol on the oral postoperative pain did not find any significantly difference between them (5) In animals Lysine Clonixinate showed a life span of 3 hours and it is recognized as a non-steroid anti-in-flammatory with the shortest life span when compared to other drugs of its category (6)It bonds to plasma proteins in up to 96-98 and its me-tabolism takes place in the liver four different inactive metabolites being derived Seventy-four percent of its excretion is renal and 25 fecal (7) It holds an ex-cellent bio-tolerance and low incidence of collateral ef-fect in the treatment of painful syndrome such as renal neurogenic muscular and tooth pain (89) and migraine (7) The Visual Analogical Scale (VAS) is considered the best and easiest instrument to measure this type of pain The parameters used by VAS determine the intensity of pain as following no pain mild pain moderate pain and severe pain (10-12) The postoperative pain in dentistry should be controlled even before the surgical procedure itself For that many studies suggest the prescription of anti-inflammatory drugs steroids or not or analgesic drugs with some level of anti-inflammatory properties (1314)Paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom tooth (1516) and dipyrone is similar to other analgesics frequently used in the treatment of moderate to severe postoperative pain (17)Although the drugs under test are safe it is possible the occurrence of adverse effect The estimated ex-cess mortality due to community-acquired agranu-locytosis aplastic anemia anaphylaxis and serious upperrsquogastrointestinal complications was 20 per 100 million for paracetamol 25 per 100 million for dipy-rone (18)Regarding the Paracetamol and Dipyrone large use in Brazil Spain and other countries as well (1719) we decided to use them in order to compare the Lysine Clo-nixinate clinic performance The adverse effects due to the use of Lysine Clonixinate could be nausea vomit-ing allergic reactions vertigo and insomnia (9)
Material and MethodsThe sample of 90 individual consisted of all patients under treatment in that semester at the clinic of Oral
Surgery and Oral Traumatology from Federal Univer-sity of Minas Gerais The following conditions were ob-served in order to select the cases (I) individuals with clinical indication for the removal impacted mandibular third molar in Class I or II positioning A or B accord-ing to Pell et al (20) regardless gender race or social class (II) surgeries that would not extend more than 60 minutes (III) age between 18 and 26 years old (IV) absence of allergies to the drugs under test (V) absence of systemic conditions All surgeries were carried out under local anesthesia-Lidocaine 2 with Felipressine 12500 - Novocoreg (SSWhite Artigos Dentais LTDA Rio de Janeiro Brazil)The patients were informed about the purpose of the research project and were asked to give their written consent The research was approved by the local Ethical CommitteeThe drugs tested were bottled in identical opaque white recipient numbered from 1 to 90 Each recipient con-tained eight tablets of either one of the drugs under test (Dipyrone 500mg Paracetamol 750mg Lysine Clonixi-nate 125 mg) The patients themselves chose the recipi-ent at random and they were unaware of its contentEach patient was told to take one tablet from the given recipient one hour before the surgery and another tablet was taken after the surgery in 6 hours intervals after first dose during 24 hours If the pain persisted the pa-tient was given the liberty to take any other drug and the dentist should be informed The assessment of pain was performed according to VAS Pain was measured just after the surgical proce-dure and 1246812 and 24 hours after the operation For each one of the above options they had also to in-form the level of pain according to a decimal scale The criteria used by the authors to assess patientrsquos pain level were 0 cm no pain 01-3 cm light pain 31-7 cm mo-derate pain 71-10 cm intense pain (9) The descriptive analyses are presented in percentages with mean minimum (min) maximum (max) and standard deviation (SD) Kruskal-Wallis and Friedman tests were used and results were considered statistically significant when value of p was less or equal to 005 at least 95 of the confidence
ResultsThe drop-out in the experiment was of twenty-six cases and therefore the sample was reduced to sixty-four The Lysine Clonixinate group was comprised of 20 in-dividuals (8 males and 12 females) The Paracetamol Group was comprised of 23 individuals (9 males and 14 females) and Dipyrone Group was comprised of 21 individuals (6 males and 15 females) The mean age of the entire sample was 223 years (plusmn25) The length of the procedures was in average 339 min-utes (plusmn98) (Table 1) (Table 2) and (Fig 1) depict each
e413
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Interval drugdescriptive measurement
Pmin max median mean SD
Right after Lysine clonixinate 000 100 000 020 040 09370
Paracetamol 000 300 000 030 070
Dipyrone 000 100 000 010 040
1 hour afterLysine clonixinate 000 200 100 070 060 08130
Paracetamol 000 300 100 060 070
Dipyrone 000 200 100 070 070
2 hours afterLysine clonixinate 000 200 100 080 070 09310
Paracetamol 000 300 100 080 090
Dipyrone 000 300 100 080 080
4 hours afterLysine clonixinate 000 200 100 090 070 08760
Paracetamol 000 200 100 080 070
Dipyrone 000 300 100 100 100
6 horus afterLysine clonixinate 000 200 100 060 060 05330
Paracetamol 000 300 100 080 090
Dipyrone 000 300 000 060 080
8 hours afterLysine clonixinate 000 200 050 060 060 03110
Paracetamol 000 200 000 060 080
Dipyrone 000 300 000 040 080
12 hours afterLysine clonixinate 000 200 000 040 060 05930
Paracetamol 000 200 000 055 070
Dipyrone 000 300 000 040 090
24 hours afterLysine clonixinate 000 200 000 030 060 05820
Paracetamol 000 200 000 040 070
Dipyrone 000 300 000 030 070
Fig 1 Distribution of the scale of pain according to the different time interval for each of the drugs tested
Table 1 Distribution of the variable pain according to VAS in different time period for the tree drugs tested
P refers to Kruskal-Wallis test
e414
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
one of the VAS parameters distributed according to drugs tested No adverse effect was observed with the drugs tested
DiscussionSixty-four individuals underwent surgical removal of their inferior third molars among them 23 (359) were male and 41 (641) female As reported before by Morin et al (21) the variable gender did not play any important role in the distribution of the variable pain after surgery The mean age was 223 years (SDplusmn25 years) and the sample was quite homogeneous in that aspect which is an advantage for the categorization of pain related to age Age can influence the pain control because third molar surgical extraction in older individuals can be-come troublesome due the cortical bone thickness and bone resilience loss (1) Chiapasco et al (1) reported a decrease in morbidity and postoperative complication of third molars in young patients Olmedo-Gaya et al (14) attributed an increase of pain in older patients due to the more bone density and narrower periodontal liga-ment
The patients underwent all the surgical procedures by 2 surgeons with calibration of the techniques avoiding therefore different approaches The surgeries length was controlled and therefore did not influence the be-havior of pain in this study- 339 min (SDplusmn98 min) Regarding this the authors believe there is no bias con-cerning the time-period of surgery on the results here presentedThe surgery of third molar is a well known procedure It allows a standardization of case selection reducing therefore the number of uncontrolled events that may lead to biasQuestionnaire and VAS were used to obtain the data The data bank was categorized by drug and analyzed according to the development of the postoperative con-dition as presented in (Table 1)The results in this study show no statistically significant difference between the drugs under test for controlling postoperative pain Martiacute et al (5) found similar results comparing Paracetamol and Lysine ClonixinateThe high number of patients without any pain in the postoperative period can be related to the local anesthe-sia The number of patients without pain in the postop-
DescriptionDrug Interval min Max median mean SD p
Lisyne clonixinate
Right after 00 10 00 02 04
lt 0001
1 hour after 00 20 10 07 062 hours after 00 20 10 08 074 hours after 00 20 10 09 076 hours after 00 20 10 06 068 hours after 00 20 05 06 0612 hours after 00 20 00 04 0624 hours after 00 20 00 03 06
Paracetamol
Right after 00 30 00 03 07
lt 0001
1 hour after 00 30 10 06 072 hours after 00 30 10 08 094 hours after 00 20 10 08 076 hours after 00 30 10 08 098 hours after 00 20 00 06 0812 hours after 00 20 00 05 0724 hours after 00 20 00 04 07
Dipyrone
Right after 00 10 00 01 04
lt 0001
1 hour after 00 20 10 07 072 hours after 00 30 10 08 084 hours after 00 30 10 10 106 hours after 00 30 00 06 088 hours after 00 30 00 04 0812 hours after 00 30 00 04 0924 hours after 00 30 00 03 07
Table 2 Distribution of pain perception in the different time intervals after surgery according to VAS
P refers to Friedman test
e415
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
erative period decreases with the passing of time Four hours after the surgery this percentage was the smallest and it increases slightly on the 6th and 8th hour after surgery reaching its peak with 24 hours The results presented here are similar to those of Olme-do-Gaya et al (14) who found out that the postoperative pain reaches its higher intensity during the first 8 hours after the surgery The moderate postoperative pain is re-ported when the production of pain mediator increases and also when the effect of local anesthesia is fading away After the 8th hour and during the subsequently days the pain decreases progressivelyThe results of this study show that the Lysine Clonixi-nate as well as Dipyrone and Paracetamol are efficient in controlling the postoperative pain in the surgery of inferior impacted third molars Lysine Clonixinate pos-sesses an analgesic activity similar to that of Dipyrone and Paracetamol and did not show any substantial im-pact on the control of postoperative pain when com-pared to those drugs
References1 Chiapasco M De Cicco L Marrone G Side effects and complica-tions associated with third molar surgery Oral Surg Oral Med Oral Pathol 199376412-20 2 Laureano Filho JR Maurette PE Allais M Cotinho M Fernandes C Clinical comparative study of the effectiveness of two dosages of Dexamethasone to control postoperative swelling trismus and pain after the surgical extraction of mandibular impacted third molars Med Oral Patol Oral Cir Bucal 200813E129-32 3 Loacutepez-Carriches C Martiacutenez-Gonzaacutelez JM Donado-Rodriacuteguez M Analgesic efficacy of diclofenac versus methylprednisolone in the control of postoperative pain after surgical removal of lower third molars Med Oral Patol Oral Cir Bucal 200510432-9 4 Esteller-Martiacutenez V Paredes-Garciacutea J Valmaseda-Castelloacuten E Berini-Ayteacutes L Gay-Escoda C Analgesic efficacy of diclofenac sodium versus ibuprofen following surgical extraction of impacted lower third molars Med Oral Patol Oral Cir Bucal 20049448-53 444-8 5 Martiacute ML De los Santos AR Di Girolamo G Gil M Manero EO Fraga C Lysine clonixinate in minor dental surgery double-blind randomized parallel study versus paracetamol Int J Tissue React 199315207-13 6 Gonzaacutelez-Martin G Cattan C Zuntildeiga S Pharmacokinetics of lysine clonixinate in children in postoperative care Int J Clin Phar-macol Ther 199634396-9 7 Krymchantowski AV Peixoto P Higashi R Silva A Jr Schutz V Lysine clonixinate vs naproxen sodium for the acute treatment of mi-graine a double-blind randomized crossover study MedGenMed 2005769 8 Ortiacute E Coirini H Pico JC Site-specific effects of the nonsteroidal anti-inflammatory drug lysine clonixinate on rat brain opioid recep-tors Pharmacology 199958190-9 9 Krymchantowski AV Barbosa JS Cheim C Alves LA Oral lysine clonixinate in the acute treatment of migraine a double-blind place-bo-controlled study Arq Neuropsiquiatr 20015946-9 10 Kremer E Atkinson JH Ignelzi RJ Measurement of pain patient preference does not confound pain measurement Pain 198110241-8 11 Price DD McGrath PA Rafii A Buckingham B The validation of visual analogue scales as ratio scale measures for chronic and ex-perimental pain Pain 19831745-56 12 Collins SL Moore RA McQuay HJ The visual analogue
pain intensity scale what is moderate pain in millimetres Pain 19977295-7 13 Seymour RA Walton JG Pain control after third molar surgery Int J Oral Surg 198413457-85 14 Olmedo-Gaya MV Vallecillo-Capilla M Galvez-Mateos R Rela-tion of patient and surgical variables to postoperative pain and inflam-mation in the extraction of third molars Med Oral 20027360-9 15 Weil K Hooper L Afzal Z Esposito M Worthington HV Van Wijk AJ et al Paracetamol for pain relief after surgical removal of lower wisdom teeth Cochrane Database Syst Rev 20073CD004487 16 Moore A Collins S Carroll D McQuay H Paracetamol with and without codeine in acute pain a quantitative systematic review Pain 199770193-201 17 Edwards JE Meseguer F Faura CC Moore RA McQuay HJ Single-dose dipyrone for acute postoperative pain Cochrane Data-base Syst Rev 20013CD003227 18 Andrade SE Martinez C Walker AM Comparative safety evalu-ation of non-narcotic analgesics J Clin Epidemiol 1998511357-65 19 Lorenzetti BB Ferreira SH Mode of analgesic action of dipy-rone direct antagonism of inflammatory hyperalgesia Eur J Phar-macol 1985114375-81 20 Pell GJ Gregory BT Impacted mandibular third molars clas-sification and modified techniques for removal Dent Digest 193339330-821 Morin C Lund JP Villarroel T Clokie CM Feine JS Differences between the sexes in post-surgical pain Pain 20008579-85
CLINICAL TRIAL
Onset of analgesia with sodium ibuprofen ibuprofen acidincorporating poloxamer and acetaminophenmdasha single-dosedouble-blind placebo-controlled study in patientswith post-operative dental pain
Stephen Daniels amp Sandie Reader amp Phillip Berry amp
Michael Goulder
Received 24 September 2008 Accepted 6 January 2009 Published online 28 February 2009 Springer-Verlag 2009
AbstractObjective To compare the onset of action and efficacy ofsodium ibuprofen (ibuprofen sodium dihydrate) and ibu-profen acid incorporating poloxamer (ibuprofenpoloxamer)with that of acetaminophen and placebo in patients withpost-operative dental painMethods A double-blind randomised placebo-controlledactive comparator two-centre study assessing the analgesicefficacy of sodium ibuprofen (512 mg equivalent to400 mg ibuprofen acid) ibuprofenpoloxamer (containing400 mg ibuprofen acid and 120 mg poloxamer 407)acetaminophen (1000 mg) and placebo in patients withmoderate-to-severe pain after third molar extraction (n=322) Onset of action was assessed using the two-stopwatchtechnique and pain intensity and relief were measuredusing validated traditional descriptor scales
Results Significantly more patients achieved confirmedperceptible pain relief and meaningful pain relief withsodium ibuprofen (963 Plt00001) and ibuprofenpoloxamer (900 P=00005) than with acetaminophen(675) The onset of action of both ibuprofen formula-tions was comparable with that of acetaminophen up to45 min post-dose a marked divergence in onset times infavour of the ibuprofen formulations occurred from45 min onward Mean values for the area under the painrelief and pain intensity differences curve (0ndash6 h) weresignificantly greater for sodium ibuprofen (346) andibuprofen acid (349) than for acetaminophen (225) (Plt0001) Other pain relief and pain intensity endpointsfavoured both ibuprofen formulations over acetamino-phen Distractibility from pain (6 h) was significantlygreater with the ibuprofen formulations than with acet-aminophen (P=0008 for sodium ibuprofen P=003 foribuprofenpoloxamer) In patients receiving ibuprofenpain interfered less with daily activities (at 1 and 6 h)than in those receiving acetaminophen (Ple0015) Bothibuprofen formulations had significantly better meanglobal assessment scores than acetaminophen (Plt0001)Tolerability profiles of the ibuprofen formulations werecomparable with that of acetaminophenConclusions Compared with acetaminophen sodiumibuprofen was associated with significantly greateranalgesic efficacy pain relief in a greater proportion ofpatients and greater patient satisfaction
Keywords Acetaminophen Dental pain
Ibuprofenpoloxamer Impacted teeth Post-operative pain
Sodium ibuprofen
Eur J Clin Pharmacol (2009) 65343ndash353DOI 101007s00228-009-0614-y
S DanielsPremier Research Group Clinical Research Center3200 Red RiverAustin TX 78705 USA
S Reader P Berry ()Reckitt Benckiser Healthcare UKDansom LaneHull HU8 7DS UKe-mail phillipberryreckittbenckisercom
M GoulderWorldwide Clinical Trials UK Ltd Isaac Newton CentreNottingham Science and Technology ParkNottingham NG7 2RH UK
Introduction
Ibuprofen [2-(4-isobutylphenyl) propionic acid] is awidely used non-steroidal anti-inflammatory drug(NSAID) currently licensed and marketed worldwide Itexhibits anti-inflammatory analgesic and antipyreticeffects in humans by working as a potent inhibitor of thecyclooxygenase enzyme system and is used to treat painresulting from a wide variety of ailments There is anextensive amount of published literature describing theefficacy of ibuprofen [1ndash7]
Patients with acute pain require rapid relief from over-the-counter (OTC) analgesics Rapidly absorbed ibuprofenformulations have been developed [8] and it was antici-pated that this rapid absorption would result in early onsetof analgesia This placebo-controlled double-blind rando-mised single-dose study was conducted to measure thetime to onset and degree of analgesia from two investiga-tional ibuprofen formulations The first investigationalibuprofen formulation contains the sodium salt of the drugibuprofen sodium dihydrate (sodium ibuprofen) Theformulation used in this study contains 256 mg of theibuprofen sodium salt equivalent to 200 mg ibuprofen acidIt is well documented that ibuprofen salts such asibuprofen sodium lysine and arginate are more rapidlyabsorbed than formulations of free ibuprofen acid [9] andseveral studies have shown that faster absorbed formula-tions lead to faster onset of analgesia [10ndash12] The saltdissolves rapidly in the gastrointestinal tract leading tofaster absorption Pharmacokinetic analyses show that thetime to peak plasma concentration (Tmax) with ibuprofensodium dihydrate is achieved in approximately 30ndash40 min[8] in contrast to the 1ndash2 h reported for standard ibuprofentablets [13 14] The second investigational ibuprofenformulation contains ibuprofen acid plus the surfactantpoloxamer 407 [from the poloxamer family of polymericnon-ionic surface active agents (ibuprofenpoloxamer)]mdashtoincrease the rate of dissolution of the tablet and enable morerapid absorption relative to standard ibuprofen formula-tions Acetaminophen another widely used OTC analgesicand antipyretic indicated for the same mild-to-moderatepain conditions as ibuprofen was included in the study as areference
The dental pain model was used because it is the mostappropriate model to investigate onset of analgesic actionIt is an established post-surgical pain model that involvesextraction of impacted third molars (wisdom teeth) arelatively consistent surgical technique that predictablyproduces moderate-to-severe pain The model is widelyaccepted and has a proven record of assay sensitivity (ieseparating active drugs from each other as well as fromplacebo) [11 12 15ndash18] The model is sensitive enough todemonstrate a correlation between plasma levels of ibupro-
fen and onset of analgesia with faster absorbed formula-tions such as ibuprofen arginate having a faster clinicalresponse time than standard ibuprofen [11 12 19] Theresults from dental pain studies have been widely extrap-olated to other general pain conditions including mostcommon OTC conditions
Onset of analgesic action was assessed using the two-stopwatch technique [11 12 19] and pain intensity andpain relief at each of the assessment timepoints wereassessed using traditional descriptor scales Exploratoryanalyses were conducted to give additional informationabout the rate of onset of action of the medications and tocompare the extent of relief provided by each of the activeformulations
Both ibuprofen formulations were given at a doseequivalent to 400 mg ibuprofen acid The acetaminophenproduct included in the study was Tylenol Extra Strength(1000 mg) a commercially available product The brandedprinting was removed from the Tylenol caplets to enable amatched placebo to be produced The doses of both drugsare the maximum licensed OTC doses in the USA and mostother countries and they have well-established safety andefficacy profiles
The primary objective of the study was to determine thetime to onset of analgesia following dosing with sodiumibuprofen tablets (2times256 mg ibuprofen sodium dihydrate)and ibuprofen acid tablets incorporating poloxamer (2times200 mg ibuprofen plus 60 mg poloxamer 407) hereafterreferred to as ibuprofenpoloxamer in patients with post-operative dental pain The secondary objective was tocompare the efficacy of the two ibuprofen formulationswith that of 1000 mg acetaminophen and placebo in termsof onset peak and duration of analgesic action
The study was conducted in accordance with theDeclaration of Helsinki [20] as referenced in EU Directive200120EC [21] and complies with International Confer-ence on Harmonisation (ICH) Good Clinical Practice(GCP) and applicable regulatory requirements
Methods
Study design
This study was a randomised double-blind placebo-controlled single-dose parallel-group study using thedental pain model It was conducted in two clinical researchcentres (Austin Texas and San Marcos Texas)
Patients andor their legal guardians provided informedconsent before the conduct of study-related proceduresPatients were screened within the 28 days before surgeryOn the day of surgery patients underwent surgical removalof one partially or full bone impacted mandibular third
344 Eur J Clin Pharmacol (2009) 65343ndash353
molar or two ipsilateral third molars with a total impactionscore of 4 5 or 6
Degree of impaction Points
Erupted 0Soft tissue 1Partial bone 2Complete (full) bone 3Unusual impaction (horizontalinverted or posterior-anterior) 4
Surgery was performed under local anaesthetic (approx-imately 100 mg lidocaine 2 with 110000 epinephrine)with conscious sedation (35 lmin 50 nitrous oxide for15 min) using standard surgical techniques Followingsurgery patients who fulfilled the inclusion criteria regard-ing baseline pain intensity were randomly allocated to oneof four treatment groups (sodium ibuprofen ibuprofenpoloxamer acetaminophen or placebo) in a 1111 ratioaccording to a computer-generated randomisation schedulethat stratified patients by sex and baseline pain intensityAfter dosing patients remained in the centre for 8ndash15 hOnset of action and efficacy assessments were recorded atpre-determined intervals during the 6 h post-dose A post-operative follow-up was conducted 5ndash12 days after surgery
The study protocol and its amendments together with thepatient information and consent documents were reviewedand approved by Quorum Review Inc (Seattle WA)
Patients
Patients were recruited from the Premier Research GroupClinical Research Centers database via advertising andpractitioner referral Eligible patients were males andfemales 16ndash40 years of age with a primary diagnosis of
amp at least one mandibular third molar (with full bonyimpaction and an impaction score of ge4 on a 5-pointscale) indicated for removal
amp two ipsilateral third molars with a combined totalimpaction score no greater than 6
In either case patients were required to have moderate orsevere baseline pain intensity as assessed using a 4-pointcategorical pain intensity scale and confirmed with a visualanalogue scale (VAS) score of ge50 mm but le85 mm (where0=no pain and 100 mm=worst pain)
The main exclusion criteria were history of significantdisease that rendered the patient unsuitable for inclusionsignificant ongoing painful conditions other than thatassociated with third molar surgery any ongoing conditionthat may have interfered with the absorption distributionmetabolism or excretion of study medications history ofallergy gastrointestinal complaints (including ulcers heart-burn dyspepsia and indigestion) migraine headaches
within the last year psychotic illness or drug abuse useof concomitant medication that may have confoundedassessments of pain relief (eg psychotropic drugs anti-depressants or sedative-hypnotics) pregnancylactationingestion of any analgesic or anti-inflammatory drug frommidnight of the night before surgery
Sample size determination
For the primary endpoint data were available for the time toperceptible relief from three studies using ibuprofen arginate[11 12 19] These data suggested that the time to perceptiblerelief would be 9 to 14 min for the two test formulationsassuming a similar onset of action to that of ibuprofen arginateSince it was assumed that the majority of placebo patientswould not achieve meaningful relief it was planned that thetime to confirmed perceptible relief for these patients would becensored at 4 h Although the spread of observations was notprovided for the arginate formulation it was assumed conser-vatively that the standard deviation (SD) for time to confirmedperceptible relief would be 1 h (based on the possible rangebeing 0ndash4 h and covering plusmn 2 SD) Hence this study was highlypowered (gt99) to detect such a large difference for the time toconfirmed perceptible relief using the Wilcoxon test
For the area under the curve (AUC) (pain relief intensitydifference [PRID] from 0 to 6 h) data were available fromtwo previous studies which compared ibuprofen lysine [22]and liquigel [23] ibuprofen with acetaminophen In the formerstudy PRID to 6 h was not provided but the sum of painintensity differences (SPID) to 6 h was given This gave adifference of 251 between ibuprofen lysine and acetamino-phen The within-group SD for acetaminophen was 447Using these data it was calculated that with 80 patients pergroup this study would have a 90 power to detect adifference between the ibuprofen formulations and acetamin-ophen at a significance level of 0025 If the data from theliquigel paper were used for sum of the measures of pain reliefand pain intensity difference (SPRID) to 6 h a slightly higherpower would be achieved It was not possible to performformal power calculations for the second endpoint in the closedtest procedure namely time to meaningful relief
Study and concomitant treatments
Following surgery eligible patients received a single oraldose (four tablets and two caplets) of one of the followingfour study treatments
amp sodium ibuprofen 2times256 mg ibuprofen sodium dihy-drate tablets (each tablet equivalent to 200 mg ibupro-fen acid) plus two matched placebo for ibuprofenpoloxamer tablets plus two matched placebo for 500 mgacetaminophen caplets
Eur J Clin Pharmacol (2009) 65343ndash353 345
amp ibuprofenpoloxamer 2times200 mg ibuprofen acid tabletseach tablet incorporating 60 mg of the surfactantpoloxamer 407 plus two matched placebo for sodiumibuprofen tablets plus two matched placebo for 500 mgacetaminophen caplets
amp acetaminophen 2times500 mg acetaminophen (TylenolExtra Strength) caplets plus two matched placebo forsodium ibuprofen tablets plus two matched placebo foribuprofenpoloxamer tablets
amp placebo two matched placebo for sodium ibuprofentablets plus two matched placebo for ibuprofenpolox-amer tablets plus two matched placebo for 500 mgacetaminophen caplets
Patients were encouraged to wait at least 90 min afterreceiving the study treatment before consuming rescuemedication although rescue medication was available atany time after dosing If rescue medication was neededwithin the first 4 h of dosing an intra-muscular injection ofketorolac tromethamine (60 mg) was administered Ifrescue medication was needed later than 4 h after studydrug administration acetaminophen 500 mghydrocodone5 mg or ketorolac tromethamine was given A prescriptionfor acetaminophen 500 mghydrocodone 5 mg was provid-ed to patients for home use at the time of discharge
The use of intravenous oral or inhaled (nitrous)sedation during surgery was prohibited Analgesic andanti-inflammatory drugs (except for the permitted rescuemedications antibiotics and anaesthetics) were not per-mitted during the 6-h post-dose assessment periodPenicillins macrolide antibiotics clindamycin and topicaltetracycline gelfoam were permitted the use of selectiveserotonin-reuptake inhibitors (SSRIs) and selective nor-epinephrine-reuptake inhibitors (SNRIs) was also accept-able in patients who had maintained a stable dose for atleast 4 weeks prior to the first visit Caffeine-containingfoods and drinks were to be discontinued from midnightprior to surgery until the end of the 6-h post-doseassessment period Ice packs were not allowed for thefirst 3 h after dosing
Efficacy endpoints
Patients were queried at pre-determined intervals by thestudy staff and all pain assessments were recorded by thepatient in their diary
Pain intensity (categorical and VAS)
Pain intensity (PI) was assessed at the following timesbaseline (0 h) and at 5 10 15 20 25 30 35 40 45 60 90120 180 240 300 and 360 min after dosing The PI wasmeasured on a categorical scale in response to the question
ldquoWhat is your pain level at this timerdquo with patient responsechoices of none=0 mild=1 moderate=2 and severe=3 Inaddition patients were also asked to draw a single vertical lineto indicate their current level of PI on the 100-mm VASPatients were randomised to treatment when they rated theirbaseline PI as moderate or severe and the score on the VASwas ge50 mm but le85 mm
Pain relief and pain half-gone
Pain relief (PR) was assessed at the same times as PI (withthe exception of 0 h) in response to the question ldquoHowmuch relief have you had from your starting painrdquo withpatient response choices of none=0 a little=1 some=2 alot=3 and complete=4 In addition patients were alsoasked ldquoIs your starting pain at least half gonerdquo withpatient responses as no=0 or yes=1
Perceptible and meaningful PR
Two stopwatches were started at the time of dosing Eachpatient was instructed ldquoStop the first stopwatch when you firstfeel any pain relief whatsoever This does not mean you feelcompletely better although you might but when you first feelany relief in the pain you have nowrdquo The patient wasinstructed ldquoStop the second stopwatch when the pain relief ismeaningful to yourdquo If the patient did not press thestopwatches within the first 4 h of the treatment period or ifrescue medication was required the patients were no longerrequired to use the stopwatches
Distractibility from pain
Distractibility from pain was assessed at baseline and at 60and 360 min after dosing in response to the question ldquoHoweasy is it for you to distract yourself from your painrdquoPatients responded using a 100-mm VAS scale where 0 =very easy and 100 = impossible
Rainier scale
Patients completed the Rainier scale at baseline and at 60and 360 min after dosing This assessed perceivedfunctional impairment of activities of daily living (ieeating driving sleeping reading working and speaking)Patients rated the perceived pain interference with eachactivity on a scale of 1 to 10 where 1 = would not interfereat all and 10 = would completely interfere
Rescue medication
The time of rescue medication was recorded Patientstaking rescue medication completed all pain intensity and
346 Eur J Clin Pharmacol (2009) 65343ndash353
pain relief assessments immediately before rescue medica-tion and continued to record their pain assessmentsthroughout the 6-h assessment period
Global evaluation
At the end of 6 h or at the time of rescue medication patientswere asked ldquoHow effective do you think the study medicationis as a treatment for painrdquo Response choices were 1 =excellent 2 = very good 3 = good 4 = fair or 5 = poor
The primary efficacy endpoint was the time to firstconfirmed perceptible pain relief There were two keysecondary endpoints (1) the AUC for SPRID from 0 to 6 hand (2) the time to meaningful pain relief
Other secondary endpoints included (1) total pain relief(TOTPAR) SPID (categorical and VAS) SPRID from 0 to4 h (2) TOTPAR SPID (categorical and VAS) from 0 to6 h (3) individual pain relief and pain intensity (categoricaland VAS) readings at each timepoint from 5 min to 6 h (4)peak pain relief and pain intensity difference (PID)(categorical and VAS) throughout the 6-h evaluation period(5) first time at which PID was ge1 (6) time to first use ofrescue medication (7) time to and proportion of patientswith pain half-gone (8) distractibility from pain at baselineand at 1 and 6 h post-dose and perceived pain interferencewith daily activities (Rainier scale) at 1 and 6 h post-dose(9) patientrsquos overall assessment of the medication
Safety assessments
Adverse events (AEs) were assessed by non-directedquestioning recorded in the source documentation andthen assessed by the Investigator with respect to severityand relationship to study medication Vital signs (bloodpressure heart rate and oral temperature) were assessed atscreening baseline (pre-dose) at 6 h post-dose and at thefollow-up visit A physical examination was also conductedat screening and at the follow-up visit 5ndash12 days aftersurgery
Statistical analyses
All calculations and figures were produced using SAS ver91 or S-PLUS 62 (SAS Institute Cary NC) The analysisof the primary endpoints was performed via a closed testprocedure The actual protocol-defined primary endpointwas the time to first confirmed perceptible pain reliefPairwise differences between the two ibuprofen formula-tions and placebo were assessed at a significance level of25 so the overall alpha-level of 5 was maintained Forthe primary endpoint pairwise differences between the twoibuprofen formulations and placebo were assessed using theWilcoxon rank-sum test A sensitivity analysis was also
performed where differences between the ibuprofen for-mulations and placebo were assessed using a Cox regres-sion analysis with treatment group study site gender andbaseline pain intensity (categorical) included in the modelThe hazard ratio and associated 975 confidence intervals(CIs) were calculated for the pairwise comparisons
It was planned that if either of the primary pairwisecomparisons were significant at the 25 level the keysecondary endpoints (SPRID 0ndash6 h and time to meaningfulpain relief) were to be assessed for that formulation under aclosed-test procedure Each endpoint was assessed in theorder specified and only if the previous assessments for thatformulation were significant were the subsequent end-points assessed in a confirmatory sense Once the endpointwas not significant then all subsequent assessments wereconsidered exploratory
Endpoints aggregated over several time points werecalculated using AUC as per the secondary endpointDifferences between the treatments were assessed at atwo-sided alpha of 005 A 95 CI for the pairwisedifferences between the treatments was calculated fromthe parameter estimates of the fitted model The pairwisecomparisons of interest were between each of the ibuprofenformulations and placebo and between each of theibuprofen formulations and acetaminophen For the time-to-event parameters such as time to first (unconfirmed)perceptible pain relief differences between the treatmentgroups were assessed as per the primary endpoint
Differences between each of the two ibuprofen formu-lations and acetaminophen in the key secondary endpointsand in the majority of the other secondary endpoints wereanalysed by analysis of covariance (ANCOVA) includingtreatment group study site gender and baseline painintensity (categorical scale) as factors
All assessments completed after the patient had takenrescue medication were considered to be missing For bothpain relief and pain intensity differences missing valuesbetween two available assessments were linearly interpo-lated Missing readings that could not be interpolated werereplaced with the baseline pain intensity or zero relief
All enrolled patients who received a dose of studymedication were included in the safety population All AEswere listed and tabulated by treatment severity relationshipto therapy and body system according to the MedicalDictionary for Regulatory Activities (MedDRA) Version81
Results
Between June and October 2005 a total of 322 patients(mean age 213 years) were randomised to receive studytreatment Of the 322 randomised patients 318 (988)
Eur J Clin Pharmacol (2009) 65343ndash353 347
completed the study The trial profile including the totalnumber of patients withdrawn and analysed is illustrated inFig 1 A total of 321 patients all of whom were balancedacross treatment groups with respect to baseline demo-graphics pain intensity and clinical characteristics (Table 1)were included in the intent-to-treat (ITT) population
Primary efficacy endpoint
Significantly more patients reported confirmed perceptiblepain relief with sodium ibuprofen (963) and ibuprofenpoloxamer (900) than with acetaminophen (675) (Plt00001 and P=00005 respectively) In the placebo grouponly 259 patients reported confirmed perceptible painrelief KaplanndashMeier median times to confirmed perceptiblepain relief were 170 min for sodium ibuprofen 185 minfor ibuprofenpoloxamer and 201 min for acetaminophen(Fig 2) Median time could not be estimated for placebo asfewer than 50 of patients assigned to this groupexperienced confirmed perceptible pain relief Comparisonsof pairwise differences between the two ibuprofen formu-lations and placebo using Wilcoxon rank-sum tests and Coxregression analysis were highly significant (Plt0001 forboth analyses)
Key secondary efficacy endpoints
Mean SPRID (0ndash6 h) values were 346 349 225 and073 for the sodium ibuprofen ibuprofenpoloxamer
acetaminophen and placebo groups respectively Pair-wise comparisons of ibuprofen and acetaminophen werehighly significant in favour of both ibuprofen formula-tions (Plt0001)
Significantly more patients reported meaningful painrelief with sodium ibuprofen (963) or ibuprofenpolox-amer (900) than with acetaminophen (675) (Plt00001and P=00005 respectively) (Fig 3) Of the patientsreceiving placebo 259 reported meaningful pain reliefThe KaplanndashMeier median times to meaningful relief were451 min (sodium ibuprofen) 447 min (ibuprofenpolox-amer) and 541 min (acetaminophen) Neither of the twoWilcoxon rank-sum comparisons between the ibuprofenformulations and acetaminophen were statistically signifi-cant whereas pairwise comparisons obtained via Coxregression analysis were statistically significantly different(P le 0002) The KaplanndashMeier survival curves were similarfor the ibuprofen and acetaminophen groups up to 45 minbut the degree of separation from 45 min onward wasmarked with more patients achieving meaningful painrelief with ibuprofen
Sitendashtreatment interactions
In general site was a statistically significant factor subjectsfrom the SanMarcos site had less favourable outcomes For theprimary efficacy endpoint and for the key secondary efficacyendpoints of SPRID (0ndash6 h) and time to meaningful pain reliefsite was statistically significantly For all three measures the
Withdrawn from ITT (failure toprovide baseline diary data) 1Withdrawn from ITT (failure toprovide baseline diary data) 1Withdrawn from ITT (failure toprovide baseline diary data) 1
IBUPROFENPOLOXAMER
Total screened 614
Total randomised 322
Excluded prior to surgery (n=240)
Excluded prior to dosing (n=52)
Failure to meet inclusion criteria (n=292)
Allocated to intervention 80
ACETAMINOPHEN
Allocated to intervention 81
PLACEBO
Allocated to intervention 81
Completed 80 Completed 81 Completed 81
Total analysed (ITTa) 80 Total analysed (ITTa) 80 Total analysed (ITTa) 81
Completed 76
Withdrew consent 1Lost to follow-up 1Other reasons 2
Withdrawn 0 Withdrawn 0 Withdrawn 0
Total analysed (ITTa) 80
SODIUM IBUPROFEN
Not included in ITT (failure to provide baseline diary data) 1
Allocated to intervention 80
Fig 1 Flow diagram illustrat-ing patient inclusion and exclu-sion throughout the study ITTIntent to treat aThe ITT popula-tion consisted of all patientswho were randomised whocompleted the baseline efficacyassessments and who had atleast one post-baseline assess-ment (primary efficacy set)
348 Eur J Clin Pharmacol (2009) 65343ndash353
interaction between site and treatment was formally investigat-ed In all cases the interaction term was not statisticallysignificant implying that treatment group responses wereconsistent between the sites
Exploratory secondary efficacy endpoints
Pain relief andor reduction in pain intensity
All summary endpoints related to pain relief andor PIDwere significantly more favourable for the two ibuprofenformulations than for acetaminophen or placebo (Plt0001for both ibuprofen formulations vs acetaminophen orplacebo in all comparisons)
A summary of pain relief scores at specified time pointsfrom 5 min to 6 h is displayed in Fig 4 The superiority of
the two ibuprofen formulations over acetaminophen canclearly be seen from 45 min post-dose onward A summaryof PID (categorical) scores at specified time points from5 min to 6 h is displayed in Fig 5 The superiority of thetwo ibuprofen formulations over acetaminophen can beclearly seen from 60 min post-dose onward
Individual PR and PID
The pain relief and PID (categorical and VAS) scores showthat sodium ibuprofen provided more effective pain reliefthan placebo at 15 min [P=0021 (PR) P=004 (PIDcategorical) P=0036 (PID VAS)] Similarly ibuprofenpoloxamer provided more effective relief than placebo at25 min [P=0002 (PR) P=0002 (PID categorical)] and at20 min [P=0008 (PID VAS)]
Timepoint (mins)
a
ttain
ing
conf
irmed
per
cept
ible
rel
ief
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 2 KaplanndashMeier curves for time to first confirmed perceptiblepain relief
Timepoint (mins)
a
ttain
ing
mea
ning
ful r
elie
f
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 3 KaplanndashMeier curves for time to meaningful pain relief
Table 1 Patient demographics and clinical characteristics at baseline (ITT population)
Baseline patient characteristics Treatment group
Sodium ibuprofen(n=80)
Ibuprofenpoloxamer(n=80)
Acetaminophen(n=80)
Placebo(n=81)
Total(n=321)
Age (years) mean (SD) 214 (388) 214 (360) 212 (443) 211 (408) 213 (399)Sex n ()Male 31 (388) 31 (388) 30 (375) 31 (383) 123 (383)Female 49 (613) 49 (613) 50 (625) 50 (617) 198 (617)
Baseline pain intensity (categorical) n ()Moderate 61 (763) 60 (750) 60 (750) 62 (765) 243 (757)Severe 19 (238) 20 (250) 20 (250) 19 (235) 78 (243)
Baseline pain intensity (VAS) mean (SD)Mean (SD) 6816 (874) 6881 (949) 6703 (932) 6737 (1003) 6784 (939)Range 51ndash85 50ndash89 52ndash84 50ndash85 50ndash89
ITT intent-to-treat SD standard deviation VAS visual analogue scaleTreatment definitions sodium ibuprofen=2times256 mg ibuprofen sodium dihydrate tablets (each tablet equivalent to 200 mg ibuprofen acid)ibuprofenpoloxamer=2times200 mg ibuprofen acid tablets acetaminophen=2times500 mg acetaminophen caplets
Eur J Clin Pharmacol (2009) 65343ndash353 349
First time to PID ge 1
There were no significant differences between the activetreatment groups in the proportion of the time to reportingof PID ge 1
Time to first use of rescue medication
Rescue medication was required by significantly fewerpatients in the sodium ibuprofen group (325) and theibuprofenpoloxamer group (225) than in the acetamin-ophen (438) group Owing to the relatively smallproportion of patients reporting the use of rescue medica-tion KaplanndashMeier median times to first use of rescuemedication could not be calculated The pairwise compar-isons between the two ibuprofen formulations and acet-aminophen were both statistically significant using theWilcoxon rank-sum test with P=0019 and P=0001 forsodium ibuprofen and the ibuprofenpoloxamer formula-tion respectively (Fig 6) The vast majority of patientsrandomised to placebo took rescue medication (827)
Time to and proportion of patients with pain half-gone
The proportion of patients reporting pain half-gone were938 888 75 and 370 for sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo re-spectively The median time to pain half-gone wassimilar for all three active treatment groupsmdash350 min(sodium ibuprofen) 375 min (ibuprofenpoloxamer) and450 min (acetaminophen) The Wilcoxon rank-sumcomparisons between the ibuprofen formulations andacetaminophen were not statistically significant (P=007and P=018 for sodium ibuprofen and ibuprofenpolox-amer respectively) but the two equivalent comparisonswere statistically significant when the Cox regression wasused (P=0013 and P=002 for sodium ibuprofen andibuprofenpoloxamer respectively) This may be explainedin terms of a greater proportion of patients randomised toeither of the ibuprofen formulations reporting the endpointscompared with acetaminophen However as for time tomeaningful relief the separation in onset times in favour ofibuprofen was only apparent from 45 min post-doseonward
Distractibility from pain (VAS)
At 1-h post-dose the mean values for the distractibilityfrom pain (VAS) scores were 290 321 381 and657 mm for sodium ibuprofen ibuprofenpoloxameracetaminophen and placebo respectively Both ibuprofenformations had lower (more favourable) scores thanplacebo (Plt0001) and sodium ibuprofen versus acetamin-ophen was statistically significant (P=0010) whereas theibuprofenpoloxamer versus acetaminophen comparisonswere non-significant (P=0083)
At 6 h post-dose both ibuprofen formulations hadmore favourable distractibility from pain scores thanacetaminophen (P=0008 and P=003 sodium ibuprofen
Timepoint (minutes)
Mea
n pa
in in
tens
ity d
iffer
ence
s
00
05
10
15
0 15 35 60 90 120 180 240 300 360
Sodium ibuprofen IbuprofenpoloxamerAcetaminophenPlacebo
Fig 5 Mean pain intensity difference (categorical) at each timepoint
Timepoint (mins)
ta
ken
resc
ue m
edic
atio
n
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 6 KaplanndashMeier curves for time to first use of rescue medication
Fig 4 Mean pain relief at each timepoint
350 Eur J Clin Pharmacol (2009) 65343ndash353
and ibuprofenpoloxamer respectively) The vast majorityof patients randomised to placebo took rescue medicationso only 14 patients provided valid data within this grouphence this analysis was not performed for the placebogroup
Pain interference with daily activities (Rainier scale)
At 1-h post-dose the mean values on the Rainier scale were188 223 268 and 432 for the sodium ibuprofen ibuprofenpoloxamer acetaminophen and placebo groups respectivelyThe scores were statistically significantly lower for bothibuprofen formulations than for placebo (Plt0001) andacetaminophen [P=0001 (sodium ibuprofen) and P=0015(ibuprofenpoloxamer)] At 6-h post-dose the mean valueswere 151 171 224 and 163 for the sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo groupsrespectively Both ibuprofen formulations maintained signif-icantly lower (more favourable) values on the Rainier scalethan acetaminophen (P=0004 and P=0011 for sodiumibuprofen and ibuprofenpoloxamer) Placebo treatment wasnot analysed for this comparison as only 14 patients in thisgroup provided valid data
Patientrsquos overall assessment of medication as a treatmentfor pain
Significantly more patients in the sodium ibuprofen (813)and ibuprofenpoloxamer (848) groups rated the studymedication as good very good or excellent than in the groupsthat received acetaminophen (538) or placebo (173)Furthermore the mean global assessment scores weresignificantly lower (more favourable) for both ibuprofenformulationsmdash240 (sodium ibuprofen) and 244 (ibuprofenpoloxamer)mdashthan for acetaminophen or for placebo (341 and446 respectively Plt0001)
Safety findings
A total of 118 of all patients had AEs that were consideredby the investigators to be possibly related to study medicationno events were classified as definitely or probably related tostudy treatment Adverse events were experienced by 300238 309 and 296 of patients receiving sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo respec-tively The majority of AEs (73) were mild-to-moderate inseverity and the most frequently reported AEs includednausea headache vomiting and dizziness Adverse eventsoccurring in at least 5 of all patients in any treatment groupare summarised in Table 2 Severe AEs (including vomitingnausea dizziness abdominal pain and headache) occurred atrates of 63 (sodium ibuprofen) 25 (ibuprofenpolox-amer) 123 (acetaminophen) and 99 (placebo) therewere no deaths or withdrawals attributable to AEs during thestudy period There were no significant differences betweenstudy medications in terms of tolerability
Discussion
This placebo-controlled study demonstrated excellent assaysensitivity for every measure of efficacy with bothibuprofen formulations and acetaminophen showing clini-cally and statistically significant analgesia that was superiorto placebo Furthermore the overall analgesic efficacy(duration and total effect) of both ibuprofen formulationswas shown to be superior to acetaminophen
Data from this study showed statistically significant differ-ences between both the ibuprofen test formulations andplacebo for the primary endpoint ie the time to firstconfirmed perceptible pain relief In addition a significantlygreater proportion of patients receiving ibuprofen experiencedconfirmed perceptible pain relief than those receiving acet-
Table 2 Adverse events occurring in gt5 of patients in any treatment group
Sodium ibuprofen (n=80) Ibuprofenpoloxamer (n=80) Acetaminophen (n=81) Placebo (n=81)
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Any AE 43 24 (300) 27 19 (238) 41 25 (309) 39 24 (296)GastrointestinalNausea 10 9 (113) 5 5 (63) 8 8 (99) 14 14 (173)Vomiting 2 2 (25) 1 1 (13) 6 6 (74) 8 8 (99)Nervous systemDizziness 4 4 (50) 0 0 (00) 6 5 (62) 5 5 (62)Headache 11 11 (138) 5 4 (50) 4 4 (49) 3 3 (37)
AE Adverse eventTreatment definitions sodium ibuprofen=2times256 mg ibuprofen sodium dihydrate tablets (each tablet equivalent to 200 mg ibuprofen acid)ibuprofenpoloxamer=2times200 mg ibuprofenpoloxamer tablets acetaminophen=2times500 mg acetaminophen capletsa Percentages based on total number of patients per treatment group
Eur J Clin Pharmacol (2009) 65343ndash353 351
aminophen The median time to meaningful pain relief was45 min for both ibuprofen formulations and 54 min foracetaminophen Although a much greater proportion ofpatients reported relief on the two ibuprofen formulationsthe divergence in onset times was only apparent from 45 minpost-dose onward ie there was a much higher proportion ofresponders from 45 min onward for the ibuprofen treatmentsthan for acetaminophen Because of this late divergence theWilcoxon rank-sum test was not sensitive enough to detectsignificant differences whereas the Cox proportional hazardsregression analysis showed significant differences in favour ofibuprofen over acetaminophen In terms of SPRID over 6 hboth ibuprofen test formulations were significantly moreefficacious than acetaminophen
Previous studies using the post-operative dental painmodel have demonstrated that treatment with a differentibuprofen salt formulation ibuprofen arginate (l-argininesalt of ibuprofen) resulted in faster onset times to analgesiaand greater overall efficacy than treatment with conven-tional (standard) ibuprofen [11 12 19] The pharmacoki-netic profile of the ibuprofen sodium formulation used inthis study has been shown to be similar to that of ibuprofenarginate with peak plasma concentrations achieved atapproximately 30ndash40 min compared with 1ndash2 h forstandard ibuprofen [8 13 14] Therefore it was anticipatedthat the rapid absorption associated with sodium ibuprofenwould result in early onset of analgesia similar to thatobserved for ibuprofen arginate This study was notintended nor was it sufficiently powered to compare thetwo ibuprofen formulations
When comparing the median time to meaningful painrelief data from this study with previous studies bothibuprofen test formulations in this study were found to be atthe upper end of the range for ibuprofen arginate andibuprofen lysine data (range 24ndash42 min) [11 12 19 22]ie 451 min (sodium ibuprofen) and 447 min (ibuprofenpoloxamer) In the earlier studies where ibuprofen arginatewas compared with conventional ibuprofen the mediantime to meaningful pain relief obtained for ibuprofenarginate was approximately half that of the conventionalibuprofen [11 12 19] A recent bioavailability study hasalso shown that the Tmax for sodium ibuprofen was lessthan half that of standard ibuprofen (ie 35 min vs 90 minrespectively) [8] Therefore it was not unexpected thatsodium ibuprofen had a fast onset of analgesic effect in thisstudy that was in a similar order of magnitude as thosepreviously reported for faster absorbed formulations
The analyses of secondary endpoints related to degreeof pain relief andor reduction in pain intensity (TOT-PAR SPRID SPID peak PID and peak PR) consistentlyfavoured both ibuprofen formulations over acetamino-phen Only in terms of time to PID of at least 1 werethere no statistically significant differences observed
compared with acetaminophen Measures of analgesicdurationmdashthe proportion of patients taking rescue med-ication and the time to rescue medicationmdashshowed thatthose in the acetaminophen group received rescuemedication sooner than those in either of the twoibuprofen groups This suggests that both ibuprofenformulations had a longer duration of action thanacetaminophen which is in keeping with that previouslyreported for ibuprofen lysine [22] and ibuprofen liquigel[23] In terms of pain relief and PID the timepoint at whicha significant difference was first observed between either ofthe ibuprofen formulations and placebo was 15 min(sodium ibuprofen) a significant difference between eitherof the ibuprofen formulations and acetaminophen was firstobserved at 45 min (sodium ibuprofen) In comparison withpreviously published data studies with ibuprofen arginateand ibuprofen lysine demonstrated significant differences inpain relief and PID between ibuprofen and placebo at 10ndash15 min [11 12 19 23] Furthermore significant differ-ences between ibuprofen lysine and acetaminophen wereobserved at 15 min much sooner than the 45 min observedin our study [22] These differences could be explained bythe different formulations of ibuprofen the fact that adifferent brand of acetaminophen was used in each of therespective studies or the inherent variability associated witha small sample size
Patients in both ibuprofen groups were able to distractthemselves from their pain at 1 and 6 h after dosingsignificantly more easily than those in the placebo andacetaminophen groups (6 h only) Patients in both ibupro-fen groups also reported that pain would interfere with theirdaily activities significantly less than patients in theacetaminophen group Patients in the two ibuprofen groupsrated the study medication as good very good or excellentmore frequently than those in the acetaminophen andplacebo groups
Ibuprofen is a well-tolerated NSAID at low doses [24]However even at prescribed doses ibuprofen is associatedwith the least risk of gastrointestinal complications com-pared with other NSAIDs [25ndash27] No new safety concernswere raised by the current study treatment with singledoses of sodium ibuprofen and ibuprofenpoloxamer werewell tolerated with AE profiles comparable to that ofacetaminophen The most frequently reported AEs consid-ered to be related to study treatment (ie nausea headachevomiting and dizziness) are not unexpected in patientsrecovering from dental surgery
In conclusion these results suggest that compared withacetaminophen both the sodium ibuprofen and ibuprofenacid incorporating poloxamer formulations are more effi-cacious in providing rapid and sustained analgesia and areassociated with pain relief in a greater proportion ofpatients undergoing surgical removal of impacted third
352 Eur J Clin Pharmacol (2009) 65343ndash353
molars Together with the favourable safety profile ofibuprofen these findings support a recommendation forthis agent as an analgesic of choice for the treatment ofpost-operative dental pain
Acknowledgements The authors would like to acknowledgeFranklin S Bonasso DDS and R Dean Jasper DDS (Central OralSurgery Group) Barbara Hernandez MA CCRC Michael Goulder(Worldwide Clinical Trials UK Ltd) for statistical support andVandana Sahajpal PhD and Quyen Chu PhD (Sudler amp HennesseyLondon) for medical writing support
Conflict of interest This study was funded by Reckitt BenckiserGroup plc Stephen Daniels (Premier Research Group ClinicalResearch Centers USA) is the Co-ordinating Investigator SandieReader and Phillip Berry are employees of Reckitt Benckiser Group plc
References
1 Sweetman SC (ed) (2002) Ibuprofen In Martindale the completedrug reference 33rd edn Pharmaceutical Press London
2 Mehlisch DR Sollecito WA Helfrick JF et al (1990) Multicenterclinical trial of ibuprofen and acetaminophen in the treatment ofpostoperative dental pain J Am Dent Assoc 121257ndash263
3 Roy S (1983) A double-blind comparison of propionic acidderivative (ibuprofen) and a fenamate (mefanamic acid) in thetreatment of dysmenorrhoea Obstet Gynecol 61628ndash632
4 Moran M (1991) Double-blind comparison of diclofenac potassi-um ibuprofen and placebo in the treatment of ankle sprain J IntMed Res 19121ndash130
5 Goswick CB (1983) Ibuprofen versus propoxyphene hydrochlo-ride and placebo in acute musculoskeletal trauma Curr Ther ResClin Exp 34685ndash692
6 Schachtel BP Thoden WR (1988) Onset of action of ibuprofenin the treatment of muscle-contraction headache Headache28471ndash474
7 Pearce I Frank GJ Pearce JMS (1983) Ibuprofen compared withacetaminophen in migraine Practitioner 227465ndash467
8 Dewland P Reader S Berry P (2008) Bioavailability of ibuprofenfollowing oral administration of standard ibuprofen sodiumibuprofen or ibuprofen acid incorporating poloxamer in healthyvolunteers Eur J Clin Pharmacol (submitted)
9 Geisslinger G Menzel S Wissel K Brune K (1993) Single dosepharmacokinetics of different formulations of ibuprofen andaspirin Drug Invest 5238ndash242
10 Schleier P Prochnau A Schmidt-Westhausen AM et al (2007)Ibuprofen sodium dihydrate an ibuprofen formulation withimproved absorption characteristics provides faster and great-er pain relief than ibuprofen acid Int J Clin Pharmacol Ther4589ndash97
11 Black P Max MB Desjardins P et al (2002) A randomizeddouble-blind placebo-controlled comparison of the analgesic
efficacy onset of action and tolerability of ibuprofen arginateand ibuprofen in postoperative dental pain Clin Ther241072ndash1089
12 Desjardins P Black P Papageorge M et al (2002) Ibuprofenarginate provides effective relief from postoperative dental painwith a more rapid onset of action than ibuprofen Eur J ClinPharmacol 58387ndash394
13 Albert KS Gernaat CM (1984) Pharmacokinetics of ibuprofenAm J Med 7740ndash46
14 Davies NM (1998) Clinical pharmacokinetics of ibuprofen Thefirst 30 years Clin Pharmacokinet 34101ndash114
15 Cooper SA Precheur H Rauch D et al (1984) The analgesicefficacy of ibuprofen compared to acetaminophen with codeine(abstract) Clin Pharmacol Ther 35232
16 Mehlisch D Frakes L (1984) A controlled comparative evaluationof acetaminophen and aspirin in the treatment of post-operativepain Clin Ther Exerpta Med 789ndash97
17 Mehlisch D Markenson J Schnitzer T (1999) The efficacy ofnonsteroidal anti-inflammatory drugs for acute pain CancerControl 65ndash9
18 Daniels SE Desjardins PJ Talwalker S et al (2002) The analgesicefficacy of valdecoxib vs oxycodoneacetaminophen after oralsurgery J Am Dental Assoc 133611ndash621
19 Mehlisch DR Ardia A Pallotta T (2002) A controlled compar-ative study of ibuprofen arginate versus conventional ibuprofen inthe treatment of postoperative dental pain J Clin Pharmacol42904ndash911
20 World Medical Association (1964) Declaration of HelsinkiEthical principles for medical research involving human patientsAdopted by the 18th WMA General Assembly 1964 and amendedby the 29th 35th 41st and 48th WMA General Assemblies
21 European Parliament and Council of 4 April 2001 (2001)Directive 200120EC of the approximation of the laws regu-lations and administrative provisions of the Member Statesrelating to the implementation of good clinical practice in theconduct of clinical trials on medicinal products for human useOfficial Journal of the European Communities Brussels
22 Mehlisch DR Jasper RD Brown P et al (1995) Comparativestudy of ibuprofen lysine and acetaminophen in patients withpostoperative dental pain Clin Ther 17852ndash860
23 Olson NZ Otero AM Marrero I et al (2001) Onset of analgesiafor liquigel ibuprofen 400 mg acetaminophen 1000 mg ketopro-fen 25 mg and placebo in the treatment of postoperative dentalpain J Clin Pharmacol 411238ndash1247
24 Sachs C (2005) Oral analgesics for acute nonspecific pain AmFam Physician 71913ndash918
25 Doyle G Furey S Berlin R et al (1999) Gastrointestinal safetyand tolerance of ibuprofen at maximum over-the-counter doseAliment Pharmacol Ther 13897ndash906
26 Henry D Lim LL Garcia Rodriguez LA et al (1996) Variability inrisk of gastrointestinal complications with individual non-steroidalanti-inflammatory drugs results of collaborative met-analysis BrMed J 3121563ndash1566
27 Henry D McGettigan P (2003) Epidemiology overview ofgastrointestinal and renal toxicity of NSAIDs Int J Clin Pract13543ndash49
Eur J Clin Pharmacol (2009) 65343ndash353 353
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 153
RESEARCH
An investigation into the comparative efficacyof soluble aspirin and solid paracetamol inpostoperative pain after third molar surgeryR A Seymour1 J E Hawkesford2 J Sykes3 M Stillings4 and C M Hill5
Objective To compare the efficacy of soluble aspirin 900 mg andparacetamol 1000 mg in patients with postoperative pain after thirdmolar surgeryDesign A randomised placebo controlled double-blind studySetting Day stay units of Oral and Maxillofacial Surgery at CardiffDental Hospital and Hexham General Hospital NorthumberlandSubjects and methods One hundred and sixty-seven (104 female)patients who required the removal of their impacted third molars undergeneral anaesthesiaIntervention In the early postoperative period patients were medicatedwith either a single dose of soluble aspirin 900 mg solid paracetamol1000 mg or placebo Main outcome measures Pain intensity was measured on 100 mmvisual analogue scales at 0 5 10 15 20 30 45 60 90 120 and 240minutes after dosing Other efficacy variables evaluated included time torescue medication and an overall assessment of the study medicationefficacy by the patient on completion of the studyResults One hundred and sixty-seven patients consented to take part inthe study but only 153 were medicated Of the 14 patients not treated10 failed to develop sufficient pain to enter the study two withdrewconsent one had an adverse reaction to the general anaesthetic and onewas a protocol violator Over the four hour investigation period patientstreated with soluble aspirin reported significantly less pain whencompared with those treated with paracetamol (mean difference inAUC0-240 = -2001 95 CI ndash3893 to ndash109 p=0038) and placebo (meandifference in AUC0-240 = -3470 95 CI ndash5719 to ndash1221 p=0003)
1Head of Department Professor of Restorative Dentistry Department of RestorativeDentistry Dental School University of Newcastle Newcastle upon Tyne 2Consultant Oraland Maxillofacial Surgeon Department of Oral and Maxillofacial Surgery NewcastleGeneral Hospital Newcastle upon Tyne 3Clinical Statistician Reckitt Benckiser Healthcare(UK) Hull 4Head of Global Professional Relations Reckitt Benckiser Healthcare (UK) Hull5Consultant Oral and Maxillofacial Surgeon Department of Oral Surgery Dental SchoolUniversity of Wales College of Medicine Cardiff Correspondence to Professor R A Seymour Department of Restorative Dentistry DentalSchool University of Newcastle upon Tyne Framlington Place Newcastle upon TyneEngland NE2 4BWE-mail R A Seymournclacuk
Refereed paperReceived 080302 Accepted 060902copy British Dental Journal 2003 194 153ndash157
Similarly at 20 and 30 minutes after dosing patients in the solubleaspirin group were reporting significantly less pain than those in theparacetamol treatment group (mean difference in pain intensity at 20minutes ndash79 95 CI ndash153 to ndash06 p=0035 at 30 minutes ndash106 95CI ndash186 to ndash26 p=0010) There were no significant differences betweentreatment groups with respect to the number of patients requiringrescue medication however the time to dosing was significantly longerfor those taking soluble aspirin when compared with placebo (hazardratio 234 95 CI 141 to 388 plt0001) Conclusion The findings from this study showed that soluble aspirin900 mg provides significant and more rapid analgesia than paracetamol1000 mg in the early postoperative period after third molar surgery
INTRODUCTIONBoth aspirin (acetylsalicylic acid) and paracetamol (acetamino-phen) are widely available analgesics The drugs are used exten-sively in dentistry either self-prescribed by the patient or recom-mended by the dental surgeon Despite such use there have beenfew comparative studies on these analgesics and the studies pub-lished seem to suggest that the drugs are equi-analgesic1 Morerecent evidence suggests that many factors appear to influence theefficacy of aspirin in postoperative dental pain These include for-mulation dose and plasma concentration of acetylsalicylate2-5
The latter appears to be determined by plasma aspirin esteraseactivity By contrast there is limited information on the efficacy ofparacetamol in postoperative dental pain
Historically there have been many studies comparing the effi-cacy of a whole range of analgesics which have used aspirin as thestandard treatment (positive control) In such studies the formula-tion chosen has invariably been a solid format of the drug This hasled to the impression that aspirin is relatively weak and slow act-ing Previous studies34 have shown that soluble aspirin provides agreater onset of action and is overall more effective than solidaspirin However up to the present time there has been no studycomparing the efficacy of soluble aspirin with solid paracetamolThe present study was designed to investigate whether the superi-ority of soluble aspirin over solid aspirin would be reproducedwhen compared with solid paracetamol The doses chosen for each
This study has shown the benefits of soluble aspirin (900 mg) over solid paracetamol (1000 mg)in the control of postoperative pain after third molar extractions
The aspirin preparation provided an earlier onset of pain relief when compared with paracetamol Most patients in the study did require additional analgesia in the early postoperative period
but the time to remedication was significantly longer in soluble aspirin group whencompared with the placebo
Adverse events due to the medication were few and showed no differences between treatmentgroups
Soluble aspirin 900 mg appears to be a more useful analgesic than paracetamol in the controlof postoperative pain after third molar surgery
I N B R I E F
RESEARCH
154 BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003
preparation used in this study is the maximum recommendedwhen purchased as over the counter (OTC) medications
Removal of impacted third molars remains a common dentalsurgical procedure that results in a significant level of postopera-tive pain6 Pain is usually of short duration and reaches its maxi-mum intensity in the early postoperative period7 It is during thistime period that analgesics are frequently prescribed The nature ofthe pain and its duration make the third molar pain model usefulfor evaluation of analgesic efficacy
The overall aim of the present study was to directly compare theefficacy of soluble aspirin with that of solid paracetamol tablets inpatients with postoperative pain after third molar surgery A place-bo group was also used to act as a negative control Within thisoverall remit the primary aim of the study was to compare theonset of efficacy between the two preparations
MATERIAL AND METHODSAdult patients who required the removal of at least one impactedlower third molar were invited to participate in the study Patientswere enrolled from two centres (Cardiff and Hexham) Informedwritten consent was obtained from each patient prior to theirentry into the study which had received ethical approval from theappropriate local Health Authority Ethical Committees Patientsenrolled into the study were fit and healthy and complied with thecriteria of the American Society of Anaesthesiologists categoryone or at the discretion of the dental surgeon category two Allpatients attended a screening clinic prior to their participation inthe study The pre-screening was held up to a maximum of threeweeks before surgery Patients were asked to abstain from takingany analgesics for 24 hours prior to their third molar extractions
Patients underwent the removal of their impacted third molarsunder general anaesthesia The anaesthetic regimen was accord-ing to routine clinical practice at the dental centre and includedinduction with intravenous propofol Muscle relaxation wasachieved with vecuronium atracurium pancurium mivacuriumor suxamethonium Anaesthesia was maintained with nitrousoxide oxygen and either isoflurane enflurane or sevofluranePerioperative analgesia was provided by fentanyl or alfentanyl
Impacted third molars were removed following a standard tech-nique Bone removal was carried out with a drill under saline sprayThe operating time (from first incision to completion of last suture)was recorded for each patient On completion of the surgical proce-dure time was allowed for the patients to recover fully from theeffects of the anaesthetic They were then returned to the wardwhere they were monitored by the study nurse and their pain inten-sity assessed on 100 mm visual analogue scales (VAS) The bound-aries of the scale were marked lsquono painrsquo and lsquoworst pain imaginablersquoWhen patientsrsquo pain intensity reached a level in excess of 30 mm onthe VAS they were randomised to study medication Patients whosepain intensity did not reach the required level or who did notrequest analgesia within 1frac12 hours post-operatively were with-drawn from the study Each eligible patient was randomly allocatedto one of the following treatment groups soluble aspirin (Disprinreg)900 mg solid paracetamol tablets BP 1000 mg or placebo In order
to double-blind the study a double-dummy technique was usedEach patient assigned to receive active soluble aspirin or activesolid paracetamol also received a placebo for the alternative treat-ment and placebo patients received a placebo for both formula-tions Soluble aspirin and the aspirin placebo were presented as anorange drink Paracetamol active and placebo were given as tabletsPatients were randomised to treatment groups in the ratio of 2aspirin2 paracetamol1 placebo The randomisation was stratifiedfor gender A randomisation block size of five was used to ensurebalance between the treatment groups
Pain assessmentThe following measures were used to evaluate efficacya) Pain intensity measures were recorded immediately pre-dose (0
minutes) and at 5 10 15 20 30 45 60 90 120 and 240 minutesafter dosing Onset of analgesia was primarily assessed by painintensity measures at 10 15 20 and 30 minutes
b)Pain intensity over the four hour investigation period The serial VAS measures of the four hour investigation periodwere compiled into a graph of pain (mm) versus time (minutes)The area under the graph (AUC) was calculated using the trape-zoidal method and denoted as AUC240 Such a measure gives anoverall assessment of each patientrsquos pain experience throughoutthe four hour investigation period8
c) Use of rescue medicationIn the event of poor pain control patients were allowed access toalternative analgesia (ibuprofen 400 mg) Patients were encour-aged not to request re-medication in the first hour post-dosingin order to give the study medication time to work For thosetaking additional analgesics the time was recorded and theirlast pre-rescue medication intensity score was extrapolated overthe remaining time points9
d)Overall evaluation At the end of the four hour investigation period (or prior to tak-ing rescue medication) the study nurses and the patients wereasked to provide an overall evaluation of the efficacy of thestudy medication The categories were lsquovery goodrsquo lsquogoodrsquo lsquosatis-factoryrsquo lsquopoorrsquo and lsquovery poorrsquo
Throughout the investigation period a study nurse was respon-sible for monitoring the patients and recording any adverse events
Statistical methodsA previous study in postoperative pain after removal of impactedthird molars4 suggested that mean VAS differences between solu-ble aspirin and placebo and soluble aspirin and solid paracetamolof 26 mm and 14 mm respectively might be anticipated at 20 min-utes post treatment Using a randomisation of 2 soluble aspirin 2paracetamol 1 placebo a total sample size of 150 patients had atleast 80 power to detect this difference
The VAS pain intensity measurements at 10 15 20 and 30minutes after dosing and AUC240 were compared between treat-ment groups using an analysis of covariance using centre gen-der baseline pain intensity operation duration and number of
Table 1 Demographic details of patients who were medicated for the study Where appropriate results are expressed as mean (SD)Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo
Number of patients 59 62 32Gender ratio MF 1940 1943 1121Age (years) 256 (56) 250 (53) 251 (47)Weight (kg) 702 (16) 719 (145) 743 (149)Mean operating time (mins) 173 (101) 165 (101) 130 (130)Number of molars removed 1 3 (5) 2 (3) 3 (9)[ patients ()] 2 15 (25) 14 (23) 5 (16)
3 11 (19) 12 (19) 9 (28)4 30 (51) 34 (55) 15 (47)
Mean baseline pain score on 100 mm VAS 574 (176) 506 (142) 541 (144)
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 155
in Hexham and the remainder in Cardiff Of the 14 patients nottreated 10 failed to develop sufficient pain to enter the studytwo withdrew consent one had an adverse reaction to the anaes-thesia and one was a protocol violator Demographic details ofthe patients are shown in Table 1 The three groups were bal-anced for demographic variables
The primary aim of the study was to compare the rate of onset ofanalgesia and the 20-minute time was considered to be appropriatefor such an assessment Pain scores as recorded on the VAS at eachtime point are illustrated in Figure 1 and Tables 2a and 2b VASscores decreased in all treatment groups during the first 15 minutespost dosing (Figure 1) At 20 minutes post dosing patients in the sol-
molars removed as covariates Use of rescue medication and thestudy nursesrsquo and patientsrsquo overall impression of their medicationwere analysed using binomial logistic regression with a lsquopositiversquooutcome defined as a response of lsquovery goodrsquo or lsquogoodrsquo Time toadministration of rescue medication was compared betweentreatment groups using Coxrsquos proportional hazard model Com-parisons were performed for soluble aspirin versus solid paraceta-mol and soluble aspirin versus placebo
RESULTSOne hundred and sixty seven patients consented to take part inthe study and 153 were medicated Of these 29 were medicated
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 30 45 60 90 120 240
Time (mins)
Pain
(mm
)
Soluble AspirinParacetamolPlacebo
Figure 1 Graph to show mean pain scores (mm) versus time (mins) for patients after treatment with placebo solid paracetamol 1000 mg and solubleaspirin 900 mg
Table 2a Summary of efficacy parameters recorded during the investigation period pain scoresBetween treatment comparisons
Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Mean difference (95 CI) p-value Mean difference (95 CI) p-value
Pain score (in mm) 10 mins after dosing 412 (28) 482 (29) 474 (33) -61 (-133 to 10) 0092 -70 (-130 to ndash09) 0024Pain score (in mm) 15 mins after dosing 407 (32) 458 (33) 445 (38) -39 (-120 to 43) 0350 -51 (-120 to 18) 0143Pain score (in mm) 20 mins after dosing 402 (34) 481 (35) 500 (40) -98 (-186 to ndash11) 0028 -79 (-153 to ndash06) 0035Pain score (in mm) 30 mins after dosing 356 (37) 462 (38) 476 (44) -120 (-216 to ndash25) 0014 -106 (-186 to ndash26) 0010Overall pain - AUC240(mmmins) 8001 (871) 10002 (898) 11471 (1035) -3470 (-5719 to ndash1221) 0003 -2001 (-3893 to ndash109) 0038
data presented are adjusted (least squares) mean (standard error of the mean)
Table 2b Summary of efficacy parameters recorded during the investigation period use of escape medicationBetween treatment comparisons
Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds (hazard) ratio (95 CI) p-value Odds (hazard) ratio (95 CI) p-value
Number of patients 48 (81) 46 (74) 29 (91) 0172 (0020 to 1052) 0078 1485 (0455 to 5197) 0518taking escape analgesics
Time (minutes) to 115 (63 - 165) 94 (47 - ++) 64 (42 ndash 117) 234 (141 to 388) lt0001 130 (084 to 203) 0236remedication
data presented are median (Inter Quartile Range)++ Upper quartile cannot be estimated
RESEARCH
156 BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003
uble aspirin group reported significantly less pain than those treatedwith solid paracetamol (p=0035) or placebo (p=0028) Similarlypain intensity was significantly less at 10 and 30 minutes post dos-ing for patients treated with soluble aspirin when compared withsolid paracetamol (p=0024 and 0010 respectively) Pain intensitywas also significantly less for patients treated with soluble aspirinwhen compared with placebo at 30 minutes post dosing (p=0014)but was not significant at 10 minutes post-dosing (p=0092) By con-trast to these findings at 15 minutes after dosing pain scores werenot significantly different between soluble aspirin and placebo(p=0350) or between soluble aspirin and solid paracetamol(p=0143) Overall pain scores as assessed by the AUC240 were sig-nificantly lower in the soluble aspirin group when compared withsolid paracetamol (p=0038) and placebo (p=0003) There was nosignificant centre difference for any of the pain intensity variables
The use of rescue medication and time to requesting such med-ication is also shown in Table 2b There was no significant differ-ence between soluble aspirin and solid paracetamol or placebowith respect to the number of patients requiring rescue medicationduring the four hour investigation period (pgt005) However thetime to administration of rescue medication was significantlylonger for those patients taking soluble aspirin when comparedwith placebo (plt0001) There was no significant difference in timeto rescue medication between the soluble aspirin treated patientsand those treated with solid paracetamol (p=0236) The time toadministration of rescue medication did show a significant centreeffect with those patients enrolled in Cardiff requiring rescueanalgesia at an earlier time point than those in Hexham (plt0001)
The study nursesrsquo and patientsrsquo overall assessment of the effica-cy of the medication is shown in Tables 3a and 3b There was nosignificant difference between soluble aspirin and solid paraceta-mol (p=0285) with respect to the percentage of lsquopositiversquo outcomesassessed by the patients however soluble aspirin was favoured incomparison with placebo (p=0010) Results were similar for thestudy nursesrsquo assessment (p=0387 p=0024)
Adverse events were reported by 41 of patients with a higheroverall incidence in the active treatment groups (Table 4) Many ofthese events were related to the procedure The most commonadverse events were in the central and peripheral nervous system(primarily dizziness) and the gastro-intestinal system (primarilynausea) The incidence of dizziness was similar in the soluble
aspirin and placebo groups (14 and 13 respectively) and wasgreater than in the solid paracetamol group (6) The incidence ofnausea was comparable in the soluble aspirin and solid paraceta-mol groups (15 and 16 respectively) and was greater than thatin the placebo group (6) Gingival bleeding (the only adverseevent recorded under lsquohaemostasisrsquo) had a slightly lower incidencein the soluble aspirin group (8) than in the solid paracetamolgroup (13) and was only slightly higher than that reported in theplacebo group (3) This finding is contrary to any expectationsthat aspirin might exacerbate post-operative bleeding
DISCUSSIONThe present study has shown that soluble aspirin 900 mg is an effec-tive analgesic in the control of postoperative pain after the removalof impacted third molars confirming the evidence from previousstudies34 In addition soluble aspirin provided better pain controlthan solid paracetamol 1000 mg This superior efficacy is reflectedin the overall pain score (Table 2a and Figure 1) and also in the painscores reported during the first 30 minutes post dosing The datasuggest that soluble aspirin is providing a more rapid reduction inpain in the early postoperative period when compared with solidparacetamol If the pain scores are examined in terms of percentagereduction when compared with baseline the results show that solu-ble aspirin is twice as effective as solid paracetamol (at 20 and 30minutes the percentage reduction for soluble aspirin is 310 and406 respectively whilst the figures for solid paracetamol are142 and 204) From the perspective of patient management arapid reduction in pain is an important requisite of any analgesicformulation10 The exception to this pattern is the pain scores at 15minutes post dosing At this time point pain intensity scores aftersoluble aspirin are not significantly different from either placebo orsolid paracetamol mdash the reason for this finding is unclear
Previous comparative efficacy studies between aspirin andparacetamol in postoperative dental pain have revealed somewhatequivocal results11112 The consensus view1 is that both aspirin andparacetamol are both equi-analgesic and equipotent The studiesuse a solid tablet formulation of aspirin at a dose of 650 mg Studiesusing similar methodology have shown that the efficacy of aspirinin postoperative dental pain is related to dose and formulation34
The use of a soluble formulation and the 900 mg dose may explainthe superior efficacy of aspirin in this study
Table 3b Distribution of scores from study nursesrsquo global assessment of the medication (number ())Score Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds Ratio (95 CI) p-value Odds Ratio (95 CI) p-value
Positive outcome 32 (54) 32 (52) 10 (31) 2974 (1179 to 7951) 0024 1403 (0655 to 3054) 0387Very good 15 (25) 11 (18) 3 (9)Good 17 (29) 21 (34) 7 (22)Satisfactory 17 (29) 14 (23) 12 (38)Poor 8 (14) 14 (23) 7 (22)Very poor 2 (3) 2 (3) 3 (9)Total 59 62 32
positive outcome = response of lsquovery goodrsquo or lsquogoodrsquo
Table 3a Distribution of scores from patientsrsquo global assessment of the medication (number ())Score Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds Ratio (95 CI) p-value Odds Ratio (95 CI) p-value
Positive outcome 34 (58) 33 (53) 10 (31) 3591 (1402 to 9828) 0010 1530 (0706 to 3380) 0285Very good 15 (25) 12 (19) 3 (9)Good 19 (32) 21 (34) 7 (22)Satisfactory 15 (25) 12 (19) 10 (31)Poor 8 (14) 15 (24) 9 (28)Very poor 2 (3) 2 (3) 3 (9)Total 59 62 32
positive outcome = response of lsquovery goodrsquo or lsquogoodrsquo
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 157
The primary aim of this investigation was to compare both anal-gesics with respect to onset of action Early time points were chosenfor this comparison as they represent a suitable period from dosingwhen patients would expect to experience meaningful pain reliefSoluble aspirin was significantly superior to both placebo and solidparacetamol at both 20 and 30 minutes post dosing and there wereindications of superiority as early as at 10 minutes In part this maybe due to the rapid absorption of soluble aspirin and the subsequentpeak concentrations of acetylsalicylate (Tmax) that occurs at thesetime points It has been previously shown that plasma concentra-tions of acetylsalicylate are also important determinants of aspirinrsquosefficacy in postoperative dental pain2 By contrast the absorption ofsolid paracetamol tablets is slow with a Tmax of 60 minutes13 Thusdifferences in pharmacokinetics may account for the differences inonset of analgesia observed in the present study
It is now well established that aspirin exerts both analgesic andanti-inflammatory action by inhibiting prostaglandin synthesis14
Aspirin irreversibly inhibits both cyclo-oxygenase 1 and 2 (Cox-1and Cox-2) by acetylating serine 530 thus preventing the bindingof arachidonic acid to the active sites of the enzyme The pharma-codynamics of paracetamol are uncertain and by comparison withaspirin the drug exhibits weak anti-inflammatory action This lackof a pronounced anti-inflammatory effect may also explain theweaker efficacy of this drug in postoperative dental pain
We can conclude from this study that a single dose of solubleaspirin 900 mg provides significant and more rapid analgesia thansolid paracetamol 1000 mg in the early postoperative period afterthird molar surgery This study confirms the value of soluble aspirinin the management of pain after dental surgical procedures
The authors are grateful to Reckitt Benckiser Healthcare for their support inthis study
1 Cooper S A Comparative analgesic efficacies of aspirin and acetaminophen ArchIntern Med 1981 141 282-285
2 Seymour R A Williams F M Ward A Rawlins M D Aspirin metabolism and efficacyin postoperative dental pain Br J Clin Pharmacol 1984 17 697-701
3 Seymour R A Williams F M Luyk N M et al Comparative efficacy of soluble aspirinand aspirin tablets in postoperative dental pain Eur J Clin Pharmacol 1986 30495-498
4 Holland I S Seymour R A Ward-Booth R P Ord R A Lim K L Hoare R C Anevaluation of different doses of soluble aspirin and aspirin tablets in postoperativedental pain Br J Clin Pharmacol 1988 26 463-468
5 Seymour R A Weldon M Kelly P Nicholson E Hawkesford J E An evaluation ofbuffered aspirin and aspirin tablets in postoperative pain after third molar surgeryBr J Clin Pharmacol 1992 33 395-399
6 Seymour R A Blair G S Wyatt F A Post-operative dental pain and analgesicefficacy Part I Br J Oral Surg 1983 21 290-297
7 Seymour R A Meechan J G Blair G S An investigation into post-operative painafter third molar surgery under local analgesia Br J Oral Maxillofac Surg 1985 23410-418
8 Matthews J N Altman D G Campbell M J Royston P Analysis of serialmeasurements in medical research Br Med J 1990 300 230-235
9 Lasagna L Analgesic methodology a brief history and commentary J ClinPharmacol 1980 20 373-376
10 Meechan J G Seymour R A The use of third molar surgery in clinicalpharmacology Br J Oral Maxillofac Surg 1993 31 360-365
11 Skjelbred P Album B Lokken P Acetylsalicylic acid vs paracetamol effects onpost-operative course Eur J Clin Pharmacol 1977 12 257-264
12 Mehlisch D R Frakes L A A controlled comparative evaluation of acetaminophenand aspirin in the treatment of postoperative pain Clin Ther 1984 7 89-97
13 Muir N Nichols J D Stillings M R Sykes J Comparative bioavailability of aspirinand paracetamol following single dose administration of soluble and plain tabletsCurr Med Res Opin 1997 13 491-500
14 Vane J Botting R Inflammation and the mechanism of action of anti-inflammatory drugs Faseb J 1987 1 89-96
Table 4 Incidence and distribution of adverse events for each treatment groupPercentage of patients reporting events (number of events)
Body system Soluble aspirin (n=59) Solid paracetamol (n=62) Placebo (n=32) Total (n=153)
CNS 20 (14) 8 (5) 19 (6) 15 (25)GI 17 (12) 16 (12) 6 (2) 14 (26)Body as a whole 7 (4) 13 (8) 6 (3) 9 (15)Haemostasis 8 (7) 13 (8) 3 (1) 9 (16)Respiratory 7 (4) 3 (2) 0 (0) 4 (6)Psychiatric 2 (1) 0 (0) 3 (1) 1 (2)Hearingvestibular 0 (0) 2 (1) 0 (0) 1 (1)Skinappendages 2 (1) 0 (0) 0 (0) 1 (1)Vision 2 (1) 0 (0) 0 (0) 1 (1)Total 51 (44) 39 (36) 28 (13) 41 (93)
RESUMO
Objectivos Investigar a eficaacutecia e os efeitos secundaacuterios do paracetamol
(1000mg) na eliminaccedilatildeo da dor dentaacuteria poacutes-operatoacuteria resultante da extracccedilatildeo de
terceiros molares inferiores comparaacute-la agrave eficaacutecia relativa dos vaacuterios NSAIDrsquos e a
combinaccedilotildees com outros faacutermacos
Materiais e meacutetodos A pesquisa foi realizada em bases de dados secundaacuterias
(Cochrane Database of Systematic Reviews Evidentista CEBD EBD e Lilacs) assim
como em bases de dados primaacuterias (Medline atraveacutes dos motores de busca PubMed e
NICE) entre 7 e 19 de Novembro Os artigos encontrados foram avaliados numa fase
inicial (com base nos seus tiacutetulos e abstracts) para averiguar a sua relevacircncia de acordo
com o seguinte sistema de classificaccedilatildeo adequado provavelmente adequado
inadequado
Resultados Foi encontrado um total de 161 registos incluindo revisotildees
sistemaacuteticas e ensaios cliacutenicos aleatorizados dos quais apenas 31 foram classificados
pelo seu tiacutetulo e abstract como Adequados ou Provavelmente Adequados A anaacutelise
mais aprofundada dos abstracts juntamente com uma leitura transversal dos artigos
resultou em 8 publicaccedilotildees que preenchiam definitivamente os criteacuterios de inclusatildeo e
foram por isso avaliadas com recurso agraves fichas CASP
Conclusotildees Atraveacutes dos estudos analisados conclui-se que o paracetamol eacute uma
analgeacutesico seguro e eficaz dado que apresenta um benefiacutecio estatisticamente
significativo quando comparado a placebo No entanto exibe menor eficaacutecia quando
comparado a outros NSAIDrsquos nomeadamente ibuprofeno e a combinaccedilotildees dos mesmos
(paracetamol+NSAID) Apesar dos melhores resultados alguns NSAIDrsquos manifestam
efeitos secundaacuterios de alta severidade por oposiccedilatildeo aos do paracetamol Revela-se
assim necessaacuterio o desenvolvimento de estudos que investiguem de melhor forma os
efeitos adversos destes faacutermacos e o mecanismo de acccedilatildeo do paracetamol e incluam
outros dados - como custo financeiro e disponibilidade no mercado
Palavras-Chave Paracetamol NSAIDrsquos terceiro molar inferior extracccedilatildeo
dentaacuteria dor poacutes-operatoacuteria aliacutevio da dor Escala Visual Analoacutegica
ABSTRACT
Aims To investigate the efficacy and side effects of paracetamol (1000mg) on
the lower third molar extraction post-operative pain relief to compare it to other
NSAIDrsquos efficacy as well as the combination of both
Methods Searches were conducted in secondary databases (Cochrane Database
of Systematic Reviews Evidentista CEBD EBD and Lilacs) as well as in primary
databases (Medline atraveacutes dos motores de busca PubMed e NICE) between 7 and
November 19 The encountered articles were initially evaluated based on their titles and
abstracts in order to assess their relevance This was done according to a classification
system ldquoadequaterdquo ldquoprobably adequaterdquo ldquoinadequaterdquo
Results A total of 161 records were found including systematic reviews and
randomized clinical trials only 31 were classified as ldquoadequaterdquo or ldquoprobably
adequaterdquo After a more thorough analysis of each abstract in addition to further
reading of the papers only 8 articles fulfilled the inclusion criteria Thus they were
evaluated according to the CASP critical appraisal sheets
Conclusions Paracetamol is a safe and effective analgesic which presents a
statistical significant advantage when compared to a placebo However paracetamol
shows less efficacy when compared to other NSAIDrsquos such as ibuprofen The
combination of paracetamol + other NSAID also shows to be more effective displaying
the additive effect of this compound Although NSAIDrsquos show the best pain relief
scores some can cause severe side effects as opposed to paracetamol Further studies
are needed in order to better investigate the adverse effects of these drugs as well as the
mechanism of action of paracetamol which still remains unclear Other data such as
financial cost and market availability should be approached in future studies
Keywords Paracetamol NSAIDrsquos lower third molar tooth extraction post-operative
pain pain relief Visual Analogic Scale
5
IacuteNDICE
PERGUNTA FORMULADA PELO PACIENTE 6
QUESTAtildeO PICO 6
OBJECTIVOS 6
INTRODUCcedilAtildeO 7
PESQUISA 12
Criteacuterios de Selecccedilatildeo 12
Tipos de Estudos escolhidos participantes intervenccedilatildeo e de mediccedilatildeo 12
Avaliaccedilatildeo dos Estudos 13
Estrateacutegias de Pesquisa 12
Cochrane Database for Systematic Reviews helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 13
Evidence-Based Dentistry (EBD) helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 14
National Institute of Health and Clinical Excellence (NICE) helliphelliphelliphelliphelliphellip 14
Literatura Latino-Americana e do Caribe em Ciecircncias da Sauacutede (LILACS) 14
PubMed 15
AVALIACcedilAtildeO CRIacuteTICA 17
Revisotildees Sistemaacuteticas 17
Ensaios Cliacutenicos Aleatorizados 28
DISCUSSAtildeO 52
RESPOSTA DADA AO PACIENTE 55
REFEREcircNCIAS BIBLIOGRAacuteFICAS 56
ANEXOS 61
Anexo A ndash Tabela de Artigos Excluiacutedos 61
Anexo B ndash Artigos Incluiacutedos em formato integral 62
6
PERGUNTA FORMULADA PELO PACIENTE
Apoacutes uma exodontia de um terceiro molar inferior ldquoDoutor natildeo me vai passar
mais nada aleacutem do paracetamol para as dores Eacute eficaz Natildeo vou ter doresrdquo
QUESTAtildeO PICO
Com base na questatildeo apresentada pelo paciente eacute possiacutevel identificar
Populaccedilatildeo ndash Pacientes adultos com pelo menos um terceiro molar inferior
Intervenccedilatildeo ndash administraccedilatildeo poacutes-operatoacuteria de paracetamol (1000g) aquando
duma exodontia do terceiro molar inferior
Comparaccedilatildeo ndash outros analgeacutesicos e NSAIDrsquos (Non-Steroidal Anti-
Inflammatory Drugs) convencionais
Outcome ndash Eliminaccedilatildeo ou atenuaccedilatildeo da dor medida atraveacutes da escala visual
analoacutegica de dor
Em pacientes adultos apoacutes exodontia do 3ordm molar inferior a administraccedilatildeo
de paracetamol eacute mais eficaz na terapecircutica analgeacutesica comparativamente a outros
analgeacutesicos e anti-inflamatoacuterios natildeo esteroacuteides convencionais utilizando uma
escala visual analoacutegica de dor
OBJECTIVOS
Primaacuterios
Investigar a eficaacutecia do paracetamol (1000mg) na eliminaccedilatildeo da dor dentaacuteria
poacutes-operatoacuteria e comparaacute-la com outros NSAIDrsquos comparando os efeitos secundaacuterios
associados a cada faacutermaco
Secundaacuterios
Aferir a eficaacutecia relativa dos vaacuterios NSAIDrsquos bem como combinaccedilotildees de
paracetamol com outros compostos
7
INTRODUCcedilAtildeO
EXODONTIA DE TERCEIROS MOLARES INFERIORES
A extracccedilatildeo de terceiros molares eacute um procedimento ciruacutergico no campo da
sauacutede oral amplamente praticado e difundido A dor poacutes-operatoacuteria desta intervenccedilatildeo
tornou-se o modelo mais frequentemente usado em ensaios sobre dor aguda por ser um
procedimento comum com dor moderada a severa e com um nuacutemero suficiente de
pacientes para se realizar um estudo de forma relativamente faacutecil (1 2)
Os motivos que conduzem agrave exodontia de terceiros molares devem ser
considerados cuidadosamente natildeo soacute na sua dimensatildeo cliacutenica como no encontro dos
interesses do paciente econoacutemicos e outros Algumas situaccedilotildees constituem uma razatildeo
largamente aceite para a extracccedilatildeo sendo descritas em normas de orientaccedilatildeo cliacutenica
Natildeo se pode excluir poreacutem uma selecccedilatildeo e procura cuidadosa por parte do cliacutenico da
melhor evidecircncia cientiacutefica
Segundo as normas de orientaccedilatildeo cliacutenica NICE a extracccedilatildeo de sisos impactados
deve ser limitada a pacientes que evidenciam patologia como caacuteries irrestauraacuteveis
patologias pulpares ou periapicais natildeo trataacuteveis abcesso e osteomielite reabsorccedilatildeo
internaexterna do dente ou dentes adjacentes fractura dentaacuteria quistos tumores e
outros (3) Terceiros molares impactados mas livres de patologia natildeo devem ser
extraiacutedos pois natildeo haacute evidecircncia de que sugira que traria benefiacutecios para os pacientes
Iria tambeacutem sujeitar pacientes saudaacuteveis aos riscos que acompanha este tipo de
procedimento e os efeitos poacutes-operatoacuterios do mesmo Existe controveacutersia em redor
deste assunto e sobre se existe algum benefiacutecio na extraccedilatildeo profilaacutetica ldquoNo evidence
was found to support or refute routine prophylactic removal of asymptomatic impacted
wisdom teeth in adults There is some reliable evidence that suggests that the
prophylactic removal of asymptomatic impacted wisdom teeth in adolescents neither
reduces nor prevents late incisor crowdingrdquo (4) A extracccedilatildeo de um dente natildeo impactado
deve ser executada quando a natildeo extracccedilatildeo do mesmo eacute ou potencialmente viraacute a
constituir uma situaccedilatildeo patoloacutegica Este procedimento ciruacutergico conduz a um niacutevel
significante de dor poacutes-operatoacuteria sendo esta mais severa nas primeiras doze horas apoacutes
o procedimento com o pico de intensidade nas 6-8 horas poacutes-operatoacuterias (5)
8
ETIOLOGIA DA DOR
Os tecidos lesados ou traumatizados na sequecircncia da remoccedilatildeo do terceiro molar
conduzem agrave libertaccedilatildeo de mediadores bioquiacutemicos (celulares e soluacuteveis) A inflamaccedilatildeo
aguda surge como resposta ao stress tecidual e passa por um aumento da irrigaccedilatildeo
sanguiacutenea - vasodilataccedilatildeo e aumento de permeabilidade vascular Pode-se enfatizar os
papeacuteis das histamina e a bradiquinina (recruta NO) como mediadores soluacuteveis
importantes na vasodilataccedilatildeo
Os prostanoacuteides ndash moleacuteculas envolvidas nos processos de inflamaccedilatildeo- satildeo
ecosanoacuteides ou seja derivados de precursores de aacutecidos gordos e sintetizados via
cascata do aacutecido araquidoacutenico (6 p 503 7 p 800 8) em condiccedilotildees fisioloacutegicas tecircm
um papel preponderante na citoprotecccedilatildeo da mucosa gaacutestrica hemostase e
hemodinacircmica renal A este grupo pertencem as prostaglandinas prostaciclinas
tromboxanos e leucotrienos Enquanto que as prostaglandinas satildeo sintetizadas a partir
do aacutecido araquidoacutenico por acccedilatildeo de enzimas como as ciclo-oxigenases (COX) os
leucotrienos resultam da acccedilatildeo da lipoxigenase Havendo stress tecidual a membrana
celular eacute danificada conduzindo agrave actividade da enzima fosfolipase Esta ao iniciar a
lipoacutelise possibilita a obtenccedilatildeo do percursor dos prostanoacuteides o aacutecido araquidoacutenico Por
um lado os produtos da acccedilatildeo da lipoxigenase podem estar envolvidos na formaccedilatildeo do
edema por outro os produtos da ciclo-oxigenase nomeadamente prostaglandinas estatildeo
envolvidos no processo de dor e pirexia
A ciclo-oxigenase possui 2 isoenzimas COX-1 e COX-2 (7 p 800)
A COX-1 eacute constitutiva da maioria dos tecidos humanos mas com especial
relevacircncia para mediar a integridade da mucosa gaacutestrica endoteacutelio vascular rins e
plaquetas
A COX-2 eacute expressa apoacutes lesatildeo e aquando a libertaccedilatildeo de mediadores como a
Interleucina-1 o Factor de Activaccedilatildeo de Plaquetas (PAF) ou endotoxinas
lipopolissacaacuterido (LPS) (9) Contribui para o processo inflamatoacuterio e hiperalgesia pois
ao formar prostaglandinas sensibiliza as terminaccedilotildees nervosas locais livres
nociceptivas
PARACETAMOL
O paracetamol eacute uma das drogas mais importantes usadas no tratamento da dor
aguda moderada a severa quando natildeo eacute necessaacuterio um efeito anti-inflamatoacuterio (10)
Classificado como analgeacutesico actua no sistema nervoso pela activaccedilatildeo indirecta de
9
receptores canabinoacuteides (11) embora este mecanismo ainda natildeo esteja totalmente
esclarecido (12) secundariamente inibe a COX-1 e COX-2 e por consequente a
siacutentese das prostaglandinas Como antipireacutetico age no centro hipotalacircmico que regula a
temperatura produzindo vasodilataccedilatildeo perifeacuterica e aumento do fluxo sanguiacuteneo
diminuindo a temperatura pela sudorese e perda de calor pela pele
O paracetamol eacute usualmente administrado oralmente (10) Apresenta uma meia-
vida de 2-3 horas Apesar de ser comparaacutevel agrave aspirina como analgeacutesico e antipireacutetico
eficaz o paracetamol difere no facto de natildeo possuir propriedades anti-inflamatoacuterias
(10) Difere dos analgeacutesicos opioacuteides porque natildeo provoca euforia nem altera o estado
de humor do doente Da mesma forma que os (NSAIDrsquos) natildeo causa problemas de
dependecircncia toleracircncia e siacutendrome de abstinecircncia Eacute muito utilizado e seguro com a
dosagem recomendada de 4g por dia mas nem sempre oferece um aliacutevio adequado da
dor aguda por si soacute (13)
NSAIDrsquoS
Os NSAIDrsquos satildeo dos agentes terapecircuticos mais utilizados no mundo inteiro
inclui-se neste grupo o ibuprofeno importante no tratamento da dor aguda e croacutenica
(14) Dos inibidores selectivos da COX-2 mais recentes nomeadamente rofecoxib
valdecoxib e celecoxib apenas este uacuteltimo foi comercializado nos EUA devido aos
restantes terem sido associados a eventos tromboacuteticos cardiovasculares (15 pp 277-
281) Apresentam trecircs acccedilotildees principais que resultam da inibiccedilatildeo da COX-2 e da
consequente reduccedilatildeo da siacutentese de prostanoacuteides
Acccedilatildeo anti-inflamatoacuteria a modificaccedilatildeo da resposta inflamatoacuteria ocorre pela
reduccedilatildeo do nordm de prostaglandinas vasodilatadoras (PGE2 prostaciclina)
associada a menor vasodilataccedilatildeo e indirectamente a menos edema No entanto a
acumulaccedilatildeo de ceacutelulas inflamatoacuterias natildeo eacute diminuiacuteda
Efeito analgeacutesico a reduccedilatildeo da siacutentese de prostaglandinas diminui a
sensibilizaccedilatildeo das terminaccedilotildees nervosas nociceptivas a mediadores da
inflamaccedilatildeo (como bradicinina e 5-hidroxitriptamina) provoca tambeacutem a reduccedilatildeo
da vasodilataccedilatildeo e desse modo o aliacutevio da cefaleia
10
Efeito antipireacutetico deve-se em parte agrave diminuiccedilatildeo da prostaglandina
mediadora a interleucina-1 responsaacutevel pela estimulaccedilatildeo do hipotaacutelamo e
consequente aumento de temperatura ndash febre (10 pp 1056-1061)
Eacute de referir ainda que todos os NSAIDrsquos agrave excepccedilatildeo dos inibidores selectivos da
COX-2 e salicilatos natildeo-acetilados tecircm um efeito inibitoacuterio na agregaccedilatildeo de plaquetas
(15 pp 277-281)
Os efeitos secundaacuterios resultam em grande parte da inibiccedilatildeo da COX-1 Entre
os mais frequentes encontram-se Dispepsia naacuteuseas e voacutemitos associados a lesotildees
gaacutestricas provocadas pela anulaccedilatildeo do efeito protector da prostaglandina sobre a mucosa
gaacutestrica Insuficiecircncia renal Reacccedilotildees cutacircneas Distuacuterbios hepaacuteticos Riscos
cardiovasculares e outros (10)
ESCALAS DE MEDICcedilAtildeO DE DOR - ESCALA VISUAL ANALOacuteGICA
A dor sendo um fenoacutemeno subjectivo compreende um grande conjunto de
componentes - componentes fisioloacutegicos cognitivos sensoriais comportamentais entre
outros Avaliar a dor utilizando uma medida que abranja todas as suas facetas e seja
fidedigna tem-se demonstrado impossiacutevelldquoUm instrumento ideal para a mensuraccedilatildeo da
dor deveria ter propriedades de uma escala de razatildeo fornecer informaccedilatildeo imediata
sobre a fidedignidade do desempenho dos pacientes ser relativamente livre de vieacuteses
ser simples de utilizar com pacientes () demonstrar utilidade tanto para a dor
experimental quanto para a dor cliacutenica permitindo comparaccedilotildees confiaacuteveis entre ambos
os tipos de dorrdquo(16)
A Escala Visual Analoacutegica (VAS) consiste numa mediccedilatildeo da dor em mm (0-
100mm) em que agrave extremidade 0 corresponde ldquonenhuma dorrdquo e agrave extremidade
antagoacutenica ldquopior dor possiacutevelrdquo Eacute uma forma simples eficaz - dentro das limitaccedilotildees - e
faacutecil de reproduzir ldquoou seja pode ser compreendida em distintas situaccedilotildees onde haacute
diferenccedilas culturais ou de linguagem do avaliador cliacutenico ou examinadorrdquo(16)
Para responder agrave questatildeo colocada pelo paciente eacute necessaacuterio a procura da
melhor evidecircncia cientiacutefica integrando-a com o proacuteprio interesse do paciente e a
expertise do cliacutenico Estes objectivos da Medicina Dentaacuteria Baseada na Evidecircncia satildeo
em parte consequecircncia de uma actualizaccedilatildeo constante de praacuteticas cliacutenicas consequentes
de novas evidecircncias cientiacuteficas e com a noccedilatildeo de que nenhum tratamento eacute completo
11
sem que ldquoas expectativas exigecircncias e direitos legiacutetimos dos pacientes sejam integrados
nos processos de decisatildeo cliacutenica sendo tal facto reconhecidamente essencial para a
melhoria da qualidade de vidardquo(17)
12
PESQUISA
CRITEacuteRIOS DE SELECCcedilAtildeO
Tipos de Estudos Escolhidos
Para este trabalho foram escolhidos apenas ensaios cliacutenicos aleatorizados cegos
(preferencialmente duplamente cegos) controlados ou natildeo por placebo e revisotildees
sistemaacuteticas
Tipos de participantes
Indiviacuteduos com idade superior a 15 anos
Sujeitos a cirurgia para extracccedilatildeo unilateral ou bilateral do 3ordm molar inferior
Que natildeo estivessem a tomar qualquer outro tipo de medicaccedilatildeo com efeitos
idecircnticos ou semelhantes aos faacutermacos em estudo
Sem patologias orais que provoquem dor moderada a forte ou outras patologias
que afectem a percepccedilatildeo da dor
Tipos de intervenccedilatildeo
Administraccedilatildeo apenas por via oral de
Paracetamol (1000mg) vs placebo
Paracetamol (1000mg) vs outro(s) NSAIDrsquos
Paracetamol ( 1000mg) vs outro(s) NSAIDrsquos vs placebo
Paracetamol (1000mg) + outro(s) NSAIDrsquos
ou Paracetamol (1000mg) + outro(s) NSAIDrsquos vs placebo
Estudos com outros tipos de intervenccedilatildeo natildeo foram incluiacutedos Os estudos que
apenas incluiacuteram o paracetamol sob a forma de proacute-farmaco foram excluiacutedos
Mediccedilatildeo de Resultados
A mediccedilatildeo de resultados foi obtida atraveacutes da escala visual analoacutegica (VAS ndash
visual analogic scale)
13
Avaliaccedilatildeo dos Estudos
Todos os estudos foram avaliados segundo fichas CASP (Critical Appraisal
Skills Programme) Estas consistem num conjunto de questotildees que permitem avaliar um
artigo cientiacutefico no seu todo para em uacuteltima anaacutelise aferir a sua aplicabilidade validade
e fiabilidade (18) Estas fichas existem para vaacuterios tipos de estudo as CASP utilizadas
neste trabalho foram as referentes a revisotildees sistemaacuteticas e ensaios cliacutenicos
aleatorizados
ESTRATEacuteGIAS DE PESQUISA
Apoacutes cada pesquisa os artigos encontrados foram avaliados numa fase inicial
com base nos seus tiacutetulos e abstracts para averiguar a sua relevacircncia A seguinte escala
foi utilizada adequado possivelmente adequado inadequado Toda a pesquisa foi
efectuada entre 7 e 19 de Novembro de 2011
Primeiramente foram consultadas bases de dados secundaacuterias apoacutes pesquisa
nestas fontes seguiram-se bases de dados primaacuterias
Cochrane Database for Systematic Reviews
Na pesquisa avanccedilada desta base de dados secundaacuteria foi introduzida a seguinte
combinaccedilatildeo de termos utilizando conectores boleanos e seleccionando as opccedilotildees
ldquosearch all textrdquo e ldquoCochrane Database of Systematic Reviewsrdquo
paracetamol AND third molar removal AND pain relief AND analgesicrdquo
Foram encontrados 14 resultados (3 protocolos e 11 revisotildees sistemaacuteticas) dos
quais uma revisatildeo foi categorizada como ldquoadequadardquo
Paracetamol for pain relief after surgical removal of lower wisdom teeth Weil
Hooper (19) Esta revisatildeo foi novamente encontrada na base de dados EBD bem
como na NICE e no PubMed
E outra classificada como ldquopossivelmente adequadardquo mas posteriormente
excluiacuteda (20)
14
Evidence-Based Dentistry (EBD)
Nesta base de dados foi introduzida a combinaccedilatildeo de termos
ldquoParacetamol OR acetaminophen AND third molar AND painrdquo utilizando os
filtros ldquoBritish Dental Journalrdquo e ldquoEvidence-Based Dentistryrdquo
Foram encontrados 28 resultados dos quais uma revisatildeo foi classificada como
ldquoadequadardquo
Relative efficacy of oral analgesics after third molar extraction ndash a 2011 update
Derry Wiffen (21)
E ainda dois artigos classificados como ldquopossivelmente adequadordquo
An investigation into the comparative efficacy of soluble aspirin and solid
paracetamol in postoperative pain after third molar surgery Seymour
Hawkesford (22)
Relative efficacy of oral analgesics after third molar extraction Barden
Edwards (23)
National Institute of Health and Clinical Excellence (NICE)
Nesta base de dados foi introduzida a seguinte combinaccedilatildeo de termos
ldquoParacetamol and third molar removal and pain and analgesicrdquo
Dos 28 resultados obtidos 1 foi previamente encontrado e classificado (19)
Dos restantes 27 artigos nenhum foi classificado como adequado ou possivelmente
adequado
LILACS
Nesta base de dados primaacuteria foi introduzida a seguinte combinaccedilatildeo de termos
ldquoParacetamol terceiro molar dorrdquo
Dos 3 resultados obtidos um foi classificado como possivelmente adequado mas
posteriormente excluiacutedo (24)
15
PUBMED
Nesta base de dados primaacuteria foram efectuadas duas pesquisas com termos
diferentes Apenas foram utilizados termos MeSH foram utilizados conectores
boleanos em ambas as pesquisas
Pesquisa 1
Search ((((Acetaminophen[Mesh]) AND Anti-Inflammatory Agents[Mesh])
AND Molar Third[Mesh]) AND Tooth Extraction[Mesh]) AND Pain
Postoperative[Mesh]
Limits only items with abstracts Humans Clinical Trial Meta-Analysis
Randomized Controlled Trial Review Comparative Study Controlled Clinical
Trial English Spanish Portuguese
Foram obtidos 32 resultados dos quais 5 artigos foram classificados como
ldquoadequadosrdquo
Combining paracetamol with a selective cyclooxygenase-2 inhibitor for acute
pain relief after third molar surgery a randomized double-blind placebo-
controlled study Haglund and von Bultzingslowen (25)
Dos restantes quatro artigos um (22) era repetido e os outros trecircs (26-28) foram
posteriormente excluiacutedos
Quatro foram considerados ldquopossivelmente adequadosrdquo dos quais trecircs (29-31)
foram posteriormente excluiacutedos O artigo remanescente foi
Analgesic efficacy of lysine clonixinate paracetamol and dipyrone in lower
third molar extraction a randomized controlled trial (32)
Pesquisa 2
Search (((Acetaminophen[Mesh]) AND Analgesics[Mesh]) AND Molar
Third[Mesh]) AND Tooth Extraction[Mesh]
Limits only items with abstracts Humans Clinical Trial Meta-Analysis
Randomized Controlled Trial Review English
16
Obtiveram-se 56 resultados em que sete foram seleccionados como sendo
ldquoadequadosrdquo
Combined acetaminophen and ibuprofen for pain relief after oral surgery in
adults a randomized controlled trial Merry Gibbs (13)
Destes artigos seis (19 22 23 25 28 32) eram repetidos
Oito artigos foram classificados como ldquopossivelmente adequadosrdquo
Onset of analgesia with sodium ibuprofen ibuprofen acid incorporating poloxamer
and acetaminophen--a single-dose double-blind placebo-controlled study in
patients with post-operative dental pain Daniels Reader (33)
Dos oito artigos cinco foram repetidos (26 27 29-31) dois (34 35) foi
posteriormente excluiacutedo
No anexo A encontra-se uma tabela de artigos excluiacutedos cujas razotildees satildeo
discriminadas
Eacute de notar que este tipo de estrateacutegia de pesquisa traz associada grande
quantidade de resultados irrelevantes superior agrave de artigos de interesse mas facilita a
aquisiccedilatildeo de todos os artigos importantes colocando em primeiro plano a sensibilidade
e natildeo a especificidade (36) A utilizaccedilatildeo de conectores boleanos e de filtros especiacuteficos
foi uma forma de minimizar o nuacutemero de resultados natildeo relacionados (17) preservando
os de interesse
17
AVALIACcedilAtildeO CRIacuteTICA
REVISOtildeES SISTEMAacuteTICAS
Paracetamol for pain relief after surgical removal of lower
wisdom teeth Weil Hooper (19)
1 Did the review ask a clearly-focused question
Sim A populaccedilatildeo em estudo compreende pacientes de qualquer estado de sauacutede
que necessitem de uma exodontia do terceiro molar inferior e que apresentam uma
intensidade de dor basal moderada a forte Foram excluiacutedos pacientes que estivessem a
tomar outro analgeacutesico A intervenccedilatildeo foi baseada em dois aspectos ndash eficaacutecia e efeitos
secundaacuterios
A terapecircutica usada para avaliar a eficaacutecia consistiu na administraccedilatildeo de uma
dose uacutenica de paracetamol por via oral independentemente da formulaccedilatildeo ou do
momento em que o faacutermaco foi tomado
Em relaccedilatildeo aos efeitos secundaacuterios foram incluiacutedos estudos natildeo soacute de dose
uacutenica como tambeacutem de doses muacuteltiplas de acetaminofeno consideraram-se estudos em
que este composto foi tomado ateacute 7 dias apoacutes a primeira toma Para este trabalho apenas
seratildeo considerados os resultados com base na administraccedilatildeo poacutes-operatoacuteria do
paracetamol
Os resultados ndash intensidade da dor e aliacutevio da dor ndash foram medidos usando as
escalas visual analoacutegica categoacuterica verbal numeacuterica verbal global subjectiva de
avaliaccedilatildeo de eficaacutecia e outras categoacutericas Os outcomes derivados do aliacutevio da dor
contabilizados foram total pain relief (TOTPAR) e summed pain intensity difference
(SPID) durante 4 e 6 horas Foram ainda contabilizados os efeitos secundaacuterios
2 Did the review include the right type of study
Os uacutenicos estudos incluiacutedos foram ensaios cliacutenicos aleatorizados duplamente
cegos que comparam o paracetamol a um placebo bem como dosagens diferentes
avaliando efeitos agraves 4 e 6 horas Este tipo de estudo eacute adequado pois implica um baixo
risco de vieacutes
18
3 Did the reviewers try to identify all relevant studies
Sim Os autores utilizaram estudos de todos os idiomas recorrendo agrave sua
traduccedilatildeo quando necessaacuterio Foram consultadas bases de dados bibliograacuteficas
electroacutenicas The Cochrane Oral Health Grouprsquos Trials Register The Cochrane Central
Register of Controlled Trials The Cochrane Pain Palliative and Supportive Care
Grouprsquos Trials Register MEDLINE EMBASE e Current Controlled Trials Register
Tambeacutem foram realizadas pesquisas manuais em revistas como parte do Cochrane Oral
Health Grouprsquos ongoing journal handsearching programme A pesquisa visou estudos
publicados entre 1966 e 25 de Agosto de 2006
Foram enviadas cartas a autores de ensaios cliacutenicos aleatorizados com vista a
obter estudos natildeo publicados bem como a empresas farmacecircuticas fabricantes de
analgeacutesicos
Os autores deste estudo consultaram ainda referecircncias bibliograacuteficas de papers
reviews e referecircncias pessoais
4 Did the reviewers asses the quality of the included studies
Sim Foi utilizada uma estrateacutegia clara e bem definida para a determinaccedilatildeo dos
estudos a incluir Este processo foi realizado independentemente por dois autores da
revisatildeo ndash natildeo cegos ndash baseando-se em dois criteacuterios centrais atribuiccedilatildeo oculta do
faacutermaco e a existecircncia de um follow-up completo Para estes criteacuterios foi utilizado um
sistema de pontuaccedilatildeo Desta forma a cada estudo foi-lhe atribuiacuteda uma pontuaccedilatildeo
formando-se dois grupos
Baixo risco de vieacutes
Moderado ou alto risco de vieacutes
5 If the results of the studies have been combined was it reasonable to do so
Sim os resultados foram apresentados de forma combinada e loacutegica Em
primeiro lugar foram apresentadas tabelas uma para cada artigoestudo incluiacutedo em
que se encontravam discriminados os meacutetodos participantes intervenccedilotildees resultados e
outras notas Os resultados dos diferentes estudos foram agrupados em 2 outcomes
tendo cada outcome 2 divisotildees
Outcome 1 ndash TOTPAR agraves 4h
A ndash Dosagem de paracetamol ateacute 1000mg vs placebo
B ndash Dosagem de paracetamol igual ou superior a 1000mg vs placebo
19
Outcome 2 ndash TOTPAR agraves 6h
A ndash Dosagem de paracetamol ateacute 1000mg vs placebo
B ndash Dosagem de paracetamol igual ou superior a 1000mg vs placebo
Todos estes grupos foram analisados e comparados segundos 2 paracircmetros
Comparaccedilatildeo 1- Medidas de aliacutevio da dor
Comparaccedilatildeo 2- Medidas de intensidade da dor
Tendo em conta todas estas variaacuteveis foram realizadas meta-anaacutelises por
subgrupo (pp 29-40) utilizando graacuteficos forest plot
Anaacutelise 11 ndash Comparaccedilatildeo 1 de A vs B ndash Outcome 1
Anaacutelise 12 ndash Comparaccedilatildeo 1 de A vs B ndash Outcome 2
Anaacutelise 21 ndash Comparaccedilatildeo 2 de A vs B ndash Outcome 1
Anaacutelise 22 ndash Comparaccedilatildeo 2 de A vs B ndash Outcome 2
Anaacutelise 3 ndash Comparaccedilatildeo do nuacutemero de efeitos adversos de paracetamol vs
placebo comparando ainda as duas dosagens diferentes
Valores de heterogeneidade (representados por I2) proacuteximos de 25 indicam
baixa discrepacircncia 50 satildeo indicadores de heterogeneidade moderada e valores
proacuteximos de 75 satildeo sinal de alta heterogeneidade entre os estudos (37)
Olhando para os valores de I2 dois possuem alta heterogeneidade um moderada
e dois baixa Nos grupos que apresentam uma discrepacircncia estatiacutestica significativa dos
resultados a aglutinaccedilatildeo dos mesmos natildeo foi muito bem sucedida Nestes grupos ainda
que a heterogeneidade seja elevada a apresentaccedilatildeo dos resultados de cada estudo foram
correcta e individualmente apresentados Aleacutem deste aspecto os diferentes meacutetodos ndash
dosagem e tempo - foram agrupados exactamente para que as formas de intervenccedilatildeo e
meacutetodos com o menor risco de vieacutes
Tabela 1 ndash Valores de heterogeneidade (I2) de cada anaacutelise
Total de I2
()
Anaacutelise 11 Anaacutelise 12 Anaacutelise 21 Anaacutelise 22 Anaacutelise 3
76 81 66 29 28
Natildeo foram discutidas as variaccedilotildees nos resultados
20
6 How are the results presented and what is the main result
A meta-anaacutelise por subgrupos foi realizada com recurso agrave medida de eficaacutecia de
intervenccedilatildeo Risco Relativo (RR) Analisando o graacutefico forest plot os ldquoquadradosrdquo a azul
representam o RR e o poliacutegono (semelhante a um losango) sumariza todas as
informaccedilotildees (provenientes dos vaacuterios estudos) sobre o efeito do paracetamol (38)
ldquoQuando o IC natildeo ultrapassa a linha de nulidade pode-se afirmar que o resultado eacute
estatisticamente significativo Estudos maiores possuem IC mais estreitos ou seja
resultados mais precisos e maior contribuiccedilatildeo para a meta-anaacutelise que tambeacutem eacute repre-
sentada graficamente (quanto maior a aacuterea do quadrado maior o peso) e valor
percentualrdquo (39) A significacircncia aumenta com a distacircncia do poliacutegono da linha de natildeo
efeito
Independentemente do tempo (4 ou 6h) dosagens ateacute 1000mg de paracetamol
apresentam uma pequena discrepacircncia nos resultados sendo que o paracetamol eacute
ligeiramente mais eficaz que o placebo Doses iguais ou superiores a 1000mg de
paracetamol traduzem-se num maior aliacutevio da dor poacutes-operatoacuteria (poliacutegono afastado da
linha de natildeo-efeito)
Em relaccedilatildeo agrave anaacutelise 3 ateacute doses de 1 g de paracetamol nuacutemero de casos de
efeitos adversos eacute muito semelhante entre placebo e a substacircncia activa Para
concentraccedilotildees superiores a 1000 mg o nuacutemero de efeiros adversos eacute superior para
paracetamol Eacute possiacutevel concluir que natildeo haacute uma diferenccedila notoacuteria no nuacutemero de casos
de efeitos adversos O poliacutegono cruza sempre a linha de natildeo efeito
O paracetamol eacute consideravelmente mais eficaz que o placebo no aliacutevio de 50
da dor principalmente em doses iguais ou superiores a 1000mg Natildeo haacute diferenccedila
significativa em relaccedilatildeo aos efeitos adversos
7 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em consideraccedilatildeo que o
poliacutegono natildeo intersecta a linha de natildeo efeito os resultados satildeo precisos (anaacutelise 1 a 2)
Na anaacutelise 3 mesmo com um IC 95 o poliacutegono cruza a linha de natildeo efeito logo natildeo eacute
possiacutevel tirar conclusotildees semelhantes em relaccedilatildeo aos limites inferior e superior do IC
Eacute de notar que a elaboraccedilatildeo de uma meta-anaacutelise contribui para a robustez dos
resultados daiacute provenientes combinar os resultados de cada estudo individual numa
meta-anaacutelise aumenta o poder estatiacutestico gerando resultados mais precisos (40)
21
8 Can the results be applied to the local population
Sim A extracccedilatildeo de terceiros molares inferiores eacute uma praacutetica cliacutenica comum
em Portugal O paracetamol eacute um analgeacutesico largamente comercializado e administrado
(sendo natildeo sujeito a receita meacutedica) pelo que era possiacutevel reproduzir esta forma de
tratamento
No entanto os estudos incluiacutedos na revisatildeo referem-se a uma dose uacutenica que
embora reproduziacutevel na populaccedilatildeo local seria necessaacuteria uma modificaccedilatildeo do
paradigma cultural em relaccedilatildeo agrave toma de medicamentos
9 Were all important outcomes considered
Natildeo A revisatildeo considera a eficaacutecia do paracetamol vs placebo no aliacutevio da dor
e simultaneamente a ocorrecircncia de efeitos secundaacuterios Satildeo abordados directamente
dois aspectos ndash o da praacutetica cliacutenica e o da investigaccedilatildeo Ambos satildeo relativos ao
profissional de sauacutede e implicitamente ao proacuteprio indiviacuteduo e aos familiares (ao serem
referidas as doses periacuteodos entre tomas e combinaccedilotildees com outros NSAIDrsquos mais
eficazes e simultaneamente seguras)
Poreacutem nada eacute referido em relaccedilatildeo a novas poliacuteticas de sauacutede nomeadamente na
implementaccedilatildeo de uma dose uacutenica culminando numa mudanccedila dos haacutebitos de sauacutede da
comunidade Tambeacutem natildeo foram abordados aspectos econoacutemicos tal como um balanccedilo
entre benefiacutecios e encargos de sauacutede que justifique a utilizaccedilatildeo deste faacutermaco como
tratamento preferencial
10 Should policy or practice change as a result of the evidence contained in this
review
Natildeo Esta revisatildeo demonstra que comparativamente a um placebo o paracetamol
eacute mais eficaz principalmente em doses elevadas e que natildeo haacute diferenccedila estatiacutestica
significativa no nuacutemero de efeitos secundaacuterios Poreacutem natildeo eacute possiacutevel tirar conclusotildees
sobre a dor depois do periacuteodo considerado de 6h Desta forma implementar uma dose
uacutenica de paracetamol a 1000mg seria imprudente sem previamente realizar estudos
complementares sobre a evoluccedilatildeo da dor apoacutes as 6h bem como comparar este faacutermaco
com outros compostos que possam ser igualmente eficazes por um raacutecio custo-benefiacutecio
melhor ou vice-versa
22
Relative efficacy of oral analgesics after third molar extraction
Barden Edwards (23)
Relative efficacy of oral analgesics after third molar extraction -
a 2011 update Derry Wiffen (21)
A avaliaccedilatildeo feita e disposta abaixo contemplou tanto a revisatildeo sistemaacutetica que
remonta a 2004 como a sua actualizaccedilatildeo de 2011 Uma vez estando inter-relacionados
consideraacutemos pertinente juntar as apreciaccedilotildees destas revisotildees porque caso contraacuterio
perder-se-ia o contexto de ambas
1 Did the review ask a clearly-focused question
Sim A populaccedilatildeo em estudo comporta pacientes com mais de 15 anos de idade
com uma intensidade de dor basal poacutes-operatoacuteria de moderada a severa apoacutes extracccedilatildeo
de um terceiro molar
A intervenccedilatildeo consistiu no tratamento da dor poacutes-operatoacuteria de intensidade
moderada a severa com doses uacutenicas de analgeacutesicos orais ou placebo sendo que os
analgeacutesicos orais corresponderam a um total de 15 combinaccedilotildees diferentes de faacutermacos
e respectivas dosagens
Os resultados foram obtidos atraveacutes da mediccedilatildeo do aliacutevio total da dor
(TOTPAR) ou da diferenccedila de intensidade da dor (SPID) utilizando uma escala
standard de 5 niacuteveis de aliacutevio da dor uma escala standard de 4 niacuteveis de aliacutevio da dor
ou uma escala visual analoacutegica (VAS) Os efeitos secundaacuterios foram tambeacutem relatados
comparando a proporccedilatildeo de pacientes que apresentaram efeitos generalizados e que
apresentaram efeitos particulares
Actualizaccedilatildeo de 2011
A intervenccedilatildeo consistiu tambeacutem no tratamento da dor poacutes-operatoacuteria de
intensidade moderada a severa com doses uacutenicas de analgeacutesicos orais ou placebo no
entanto os analgeacutesicos utilizados foram diferentes A revisatildeo de 2004 incluiu rofecoxib
and valdecoxib nenhum dos quais se encontra disponiacutevel no mercado Em vez disso
foram utilizadas combinaccedilotildees de ibuprofeno com paracetamol formulaccedilotildees diferentes
de ibuprofeno e diclofenac e etoricoxib
23
2 Did the review include the right type of study
Sim Os estudos que foram incluiacutedos nesta revisatildeo correspondem a ensaios
cliacutenicos aleatorizados duplamente cegos que comparam a eficaacutecia dos diferentes
analgeacutesicos e com placebo na terapecircutica da dor aguda poacutes-operatoacuteria Os grupos
formados possuiacuteam grupos com um miacutenimo de 10 pessoas Em todos os estudos foram
seguidas as guidelines QUORUM e utilizados criteacuterios de inclusatildeo para a dor poacutes-
operatoacuteria em que os resultados satildeo avaliados durante um periacuteodo de 4 a 6 horas apoacutes
medicaccedilatildeo
3 Did the reviewers try to identify all relevant studies
Sim Os autores da revisatildeo tentaram identificar todos os estudos relevantes
pesquisando nas bases de dados electroacutenicas Cochrane Library Biological Abstracts
MEDLINE PubMed e Oxford Pain Relief Para aleacutem disso consultaram a bibliografia
dos artigos de revisatildeo incluiacutedos de modo a encontrar informaccedilatildeo adicional e possiacuteveis
estudos natildeo publicados os quais apresentam na sua maioria datas de pesquisa que
remontam a 2002 No entanto eacute de mencionar que natildeo contactaram os autores e os
fabricantes para recolha de dados nem procuraram estudos com idiomas diferentes do
inglecircs
Actualizaccedilatildeo de 2011
Com o passar dos anos os artigos inseridos na revisatildeo foram actualizados de
forma a incluir outros analgeacutesicos e obter ensaios cliacutenicos adicionais e relevantes Desta
forma a actualizaccedilatildeo da revisatildeo sistemaacutetica de 2004 incluiu 35 revisotildees da Cochrane
com 38 anaacutelises realizadas em diferentes analgeacutesicos de dose uacutenica para determinar a
sua eficaacutecia na dor poacutes-operatoacuteria
4 Did the reviewers assess the quality of the included studies
Sim A qualidade dos estudos incluiacutedos foi avaliada vaacuterios autores
independentes e natildeo cegos (pelo facto de estes conhecerem a literatura existente)
utilizando uma escala de qualidade numerada de 1 a 5 e baseada em 3 criteacuterios
distribuiccedilatildeo aleatorizada dos pacientes se os pacientes e os examinadores se
encontravam cegos se houve remoccedilotildees ou desistecircncias durante o estudo A
classificaccedilatildeo maacutexima de um estudo incluiacutedo foi de 5 e a miacutenima foi de 2
24
Os ensaios cliacutenicos que apresentam uma classificaccedilatildeo igual ou superior a 3
(baixo risco de vieacutes) demonstraram menores efeitos secundaacuterios que os ensaios cliacutenicos
que apresentam uma classificaccedilatildeo igual ou inferior a 2 (alto risco de vieacutes)
5 If the results of the studies have been combined was it reasonable to do so
Sim Os resultados dos diferentes estudos foram apresentados sob a forma de
tabelas nomeadamente a eficaacutecia dos vaacuterios analgeacutesicos e a ocorrecircncia de efeitos
secundaacuterios foram dispostas em tabelas Aqui eram resumidos os resultados o tipo de
intervenccedilatildeo e respectivo nuacutemero total de pacientes e nordm de estudos realizados
Esta revisatildeo sistemaacutetica natildeo incluiu a realizaccedilatildeo de testes heterogeacuteneos nem a
avaliaccedilatildeo do risco de vieacutes das publicaccedilotildees atraveacutes de forest plots dado que na opiniatildeo
dos autores estas abordagens mostraram-se pouco adequados para este tipo de estudos
No entanto a homogeneidade foi avaliada atraveacutes de um modo visual
A resposta a esta questatildeo eacute claramente afirmativa porque a elevada semelhanccedila
das caracteriacutesticas dos diferentes estudos (meacutetodos utilizados tipo de intervenccedilatildeo e
mediccedilatildeo dos resultados) tornou por um lado inadequada a realizaccedilatildeo uma meta-anaacutelise
para avaliar a heterogeneidade mas por outro adequada a realizaccedilatildeo de uma avaliaccedilatildeo
visual da homogeneidade dos mesmos
6 How are the results presented and what is the main result
Os resultados foram medidos atraveacutes da proporccedilatildeo de pacientes do grupo de
tratamento vs placebo que atingiram pelo menos 50 de maxTOTPAR ou seja aliacutevio
de dor A qual foi utilizada para determinar o benefiacutecio relativo e o NNT bem como o
risco relativo dos diferentes estudos incluiacutedos
Atraveacutes da anaacutelise das tabelas eacute possiacutevel tirar 3 conclusotildees principais
1 A proporccedilatildeo de pacientes que atingiram pelo menos 50 de aliacutevio de dor eacute maior
no grupo de tratamento que no grupo placebo agrave excepccedilatildeo do estudo que utilizou
dihidrocodeiacutena 30mg em que as diferenccedilas natildeo foram estatisticamente relevantes
2 Por comparaccedilatildeo ao paracetamol (independentemente das diferentes dosagens) os
anti-inflamatoacuterios natildeo-esteroacuteides inibidores da COX-2 apresentam um maior
benefiacutecio relativo e necessitam do menor nordm de pacientes tratados para atingirem o
objectivo de 50 de aliacutevio de dor
25
3 O paracetamol apresenta um maior risco relativo na medida em que insurgem mais
efeitos secundaacuterios nos estudos em que foi administrado por oposiccedilatildeo aos
NSAIDrsquos
Os anti-inflamatoacuterios natildeo-esteroacuteides inibidores da COX-2 satildeo mais eficazes no
tratamento da dor basal poacutes-operatoacuteria moderada a intensa que o paracetamol
Actualizaccedilatildeo de 2011
Os resultados foram obtidos da mesma forma que na versatildeo de 2004 sendo que
um novo outcome foi considerado ndash tempo meacutedio necessaacuterio para que os pacientes
necessitem de re-medicaccedilatildeo aproximadamente 8 horas Agrave semelhanccedila do que aconteceu
na revisatildeo anterior os dados sobre a dihidrocodeiacutena natildeo foram conclusivos devido agrave
pouca informaccedilatildeo disponiacutevel nos estudos
7 How precise are these results
Os resultados satildeo precisos uma vez que utilizam um intervalo de confianccedila de
95 Eacute de ressalvar que os valores de NNT ou NNH apenas eram calculados quando o
riscobenefiacutecio relativo satildeo significativos isto eacute quando natildeo incluem o valor de 1 No
limite superior do intervalo de confianccedila a intervenccedilatildeo realizada seria a mesma No
entanto dado que o NNH natildeo foi calculado eacute possiacutevel concluir que o risco relativo natildeo
era significativo pelo que permanece uma incerteza se no limite inferior do intervalo de
confianccedila a intervenccedilatildeo realizada seria a mesma
8 Can the results be applied to the local population
Sim Os resultados da revisatildeo sistemaacutetica podem ser aplicados agrave nossa
populaccedilatildeo local porque os criteacuterios de inclusatildeo utilizados correspondem na sua
maioria a mecanismos fisioloacutegicos caracteriacutesticos do ser humano Para aleacutem disso as
teacutecnicas utilizadas satildeo simples e de faacutecil reproduccedilatildeo na medida em que os faacutermacos
utilizados nos ensaios cliacutenicos estatildeo agrave disposiccedilatildeo dos interessados e os meacutetodos
terapecircuticos baacutesicos
No entanto os estudos incluiacutedos nesta revisatildeo incluiacuteram um tratamento com
uma dose uacutenica de analgeacutesico oral que embora reprodutiacutevel difere do paradigma actual
da nossa populaccedilatildeo (em que haacute a tendecircncia para a auto-medicaccedilatildeo e de recorrer a
diferentes faacutermacos)
26
9 Were all important outcomes considered
Natildeo Os resultados enfatizam a eficaacutecia de vaacuterios analgeacutesicos no aliacutevio de 50
dor em comparaccedilatildeo com placebo Eacute focada ainda o benefiacutecio relativo (95 IC) e o NNT
da mesma problemaacutetica Aleacutem deste conjunto de dados satildeo considerados o nuacutemero de
pacientes com efeitos secundaacuterios risco relativo (95 IC) culminando no caacutelculo do
NNH
Contudo natildeo eacute especificado o tipo de efeitos secundaacuterios que podem ser
desencadeados pela toma dos diferentes analgeacutesicos nem aspectos diferenciadores em
analgeacutesicos com eficaacutecia e benefiacutecios idecircnticos (por exemplo custo econoacutemico) Isto
constituiria uma mais-valia para uma escolha mais consciente do analgeacutesico tanto pelos
profissionais como pelos pacientes (individual) e beneficiaria tambeacutem o Sistema
Nacional de Sauacutede (comunidade em geral)
Actualizaccedilatildeo de 2011
Um dos outcomes considerados semelhante ao que foi abordado na revisatildeo de
2004 foi a percentagem de pacientes com dor moderada (30- 60 mm VAS) ou dor
severa (mais de 60 mm) que obtiveram 50 de aliacutevio de dor Contudo foi adicionado
um novo outcome relevante o tempo necessaacuterio para que metade dos pacientes requeriu
re-medicaccedilatildeo
10 Should policy or practice change as a result of the evidence contained in this
review
Natildeo Os resultados desta revisatildeo evidenciam a eficaacutecia dos analgeacutesicos
comparativamente a um placebo nomeadamente que o ibuprofeno e o paracetamol
possuem maior maior o benefiacutecioefeito analgeacutesico quanto maior forem as dosagens
Poreacutem natildeo eacute evidecircncia suficiente para mudar o paradigma de tratamento pois ldquoWhat
these comparisons do not do is to tell dentists what to prescriberdquo Satildeo sim uma
importante ferramenta para a tomada de decisotildees que devem ser adaptadas a cada
paciente tendo presente que 80 dos analgeacutesicos prescritos possuem elevados iacutendices
de eficaacutecia e seguranccedila Em adiccedilatildeo nem todos os analgeacutesicos nesta revisatildeo estatildeo
disponiacuteveis no mercado para serem receitados pelos meacutedicos-dentistas
Conclui-se que para que esta revisatildeo fosse pilar basilar nas prescriccedilotildees de
analgeacutesicos teriam de ser apresentadas evidecircncias de benefiacuteciocusto dos analgeacutesicos
27
com melhores resultados (aspecto econoacutemico e detalhe dos efeitos adversos) Todavia a
informaccedilatildeo presente na mesma sobre a eficaacutecia e efeitos secundaacuterios assim como toda a
bibliografia jaacute existente sobre este assunto eacute uacutetil e deve ser utilizada para tomar inicio agrave
criaccedilatildeo de um formulaacuterio em medicina dentaacuteria
Actualizaccedilatildeo de 2011
Os resultados obtidos da mesma forma que na revisatildeo anterior natildeo foram
suficientemente relevantes para que as poliacuteticas de sauacutede mudassem No entanto a
quantidade de informaccedilatildeo disponiacutevel sobre analgeacutesicos de dose uacutenica para aliacutevio da dor
poacutes-operatoacuteria eacute grande e bastante acessiacutevel Podem assim servir como boas
ferramentas para a formulaccedilatildeo de poliacuteticas e prescriccedilotildees farmacecircuticas para a populaccedilatildeo
quando existirem dados cliacutenicos mais conclusivos
28
AVALIACcedilAtildeO CRIacuteTICA
ENSAIOS CLIacuteNICOS ALEATORIZADOS
Combining paracetamol with a selective cyclooxygenase-2
inhibitor for acute pain relief after third molar surgery a
randomized double-blind placebo-controlled study Haglund and
von Bultzingslowen (25)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo compreende indiviacuteduos saudaacuteveis com idade superior a 18
anos peso entre 50 e 120 kg e com necessidade de extrair terceiros molares inferiores
com remoccedilatildeo oacutessea Foram excluiacutedos pacientes intolerantes ao aacutecido acetilsaliciacutelico
paracetamol eou NSAIDrsquos que estivessem a tomar outro tipo de medicaccedilatildeo (excepto
contraceptivos) graacutevidas ou em periacuteodo de amamentaccedilatildeo problemas com drogas ou
aacutelcool Apenas pacientes que reportaram dor moderada a intensa apoacutes a cirurgia foram
incluiacutedos
Existiram quatro grupos de intervenccedilatildeo
Grupo A rofecoxib 50mg + paracetamol 1g dose uacutenica 155 plusmn 37 minutos apoacutes
cirurgia
Grupo B rofecoxib 50mg dose uacutenica 170 plusmn 45 minutos apoacutes cirurgia
Grupo C paracetamol 1g dose uacutenica 184 plusmn 53 minutos apoacutes cirurgia
Grupo D placebo dose uacutenica 161 plusmn 30 minutos apoacutes cirurgia
Os resultados prenderam-se com a intensidade da dor medida atraveacutes da escala
visual analoacutegica (VAS) de 30 em 30 minutos desde a ingestatildeo do faacutermaco durante 8
horas Atraveacutes destas avaliaccedilotildees da dor foi possiacutevel obter valores de
aliacutevio total da dor TOTPAR
soma da diferenccedila de intensidade da dor SPID nas primeiras trecircs horas
soma da diferenccedila de intensidade da dor SPID ateacute agraves 8 horas
Foram obtidos resultados referentes a uma avaliaccedilatildeo global do tratamento feita
4h e 8h apoacutes a toma do faacutermaco O uso de rescue medication foi tomado em conta bem
como o tempo ateacute agrave sua necessidade Foram ainda avaliados eventuais efeitos
secundaacuterios
29
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim A atribuiccedilatildeo de cada tratamento foi cega para todos os pacientes
investigadores e pessoal envolvido Foi levada a cabo a aleatorizaccedilatildeo pela empresa
farmacecircutica responsaacutevel pela produccedilatildeo das caacutepsulas administradas
Natildeo existindo entraves de teor eacutetico ou de disponibilidade de recursos um
ensaio cliacutenico aleatorizado eacute a escolha mais pertinente quando eacute necessaacuterio comparar
dois ou mais tipos de tratamento O facto de existir um grupo de controlo minimiza o
risco de vieacutes
3 Were participants appropriately allocated to intervention and control groups
A colocaccedilatildeo dos pacientes em cada um dos quarto grupos de tratamento foi
concretizada atraveacutes de tabelas de aleatorizaccedilatildeo
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim Sendo um ensaio cliacutenico duplamente cego tanto o staff investigadores e
pacientes estiveram cegos durante todo o estudo Todas as caacutepsulas eram idecircnticas
sendo que cada embalagem selada continha sempre 6 caacutepsulas Desta forma eacute possiacutevel
garantir que o paciente estaacute cego Sendo cada embalagem feita e selada pela empresa
farmacecircutica eacute igualmente possiacutevel inferir que os investigadores tambeacutem se
encontravam cegos Apenas o investigador principal acedeu aos coacutedigos para fazer os
caacutelculos finais
5 Were all of the participants who entered the trial accounted for at its
conclusion
Os grupos de intervenccedilatildeo foram atribuiacutedos de forma aleatoacuteria e cega os
resultados foram analisados de acordo com o grupo a que inicialmente tinham sido
associados
Inicialmente o desenho do estudo previa 120 participantes
Grupo A n = 40
Grupo B n = 40
Grupo C n = 20
30
Grupo D n = 20 (controlo)
No entanto no final do estudo foram apurados resultados de 107 indiviacuteduos Isto
deve-se a
Apoacutes a cirurgia alguns pacientes (n = 8) natildeo sentiram dor moderada a forte
no entanto quiseram mesmo assim participar sendo os seus resultados
subtraiacutedos aos caacutelculos
Alguns pacientes (n = 5) foram excluiacutedos sendo que um foi drop-out e os
restantes natildeo entregaram ou preencheram os questionaacuterios pedidos
No final a distribuiccedilatildeo de indiviacuteduos por grupos era a seguinte
Grupo A n = 34
Grupo B n = 36
Grupo C n = 20
Grupo D n = 17
Embora se verifique uma ligeira alteraccedilatildeo natildeo eacute motivo relevante de vieacutes
6 Were the participants in all groups followed up and data collected in the same
way
Sim Todos os pacientes tiveram acesso aos mesmos questionaacuterios entregues
pelo investigador Em caso de duacutevida ateacute ao final da duraccedilatildeo do estudo (8 horas) o
paciente podia telefonar ao investigador com quaisquer duacutevidas que surgissem Poreacutem
o paciente era responsaacutevel pelo iniacutecio do estudo ao administrar a si mesmo o faacutermaco
em casa no momento em que o fizesse devia telefonar ao investigador para este ter
conhecimento do iniacutecio do estudo Se o paciente natildeo contactasse o investigador ateacute 3
horas apoacutes a cirurgia o investigador contactaria o paciente Os valores maacuteximo e
miacutenimo de tempo entre a cirurgia e iniacutecio do estudo de foram 118 e 237 minutos a este
facto eacute inerente um risco de vieacutes pois nem todos os pacientes estavam na mesma
condiccedilatildeo quando iniciaram o tratamento podendo reflectir-se nos resultados
7 Did the study have enough participants to minimise the play of chance
Sim Os caacutelculos foram efectuados assumindo que existiria uma diferenccedila na
SPID entre grupos A e B de 20 Foram utilizados testes natildeo-parameacutetricos (Mann-
Whitney U-test) sendo definido que pelo menos 22 pacientes deveriam ser incluiacutedos em
cada um destes grupos
31
8 How are the results presented and what is the main result
Os caacutelculos estatiacutesticos necessaacuterios para a elaboraccedilatildeo dos resultados foram
efectuados no programa Statistical Package for Social Sciences (SPSS) v 12 As
significacircncias entre grupos de tratamento em relaccedilatildeo agraves respostas agrave VAS foram
testadas com t-test de variaacutevel independente em todas as avaliaccedilotildees de dor A mesma
estrateacutegia foi aplicada para a SPID agraves 3 e 8 horas A TOTPAR foi baseada na
assumpccedilatildeo que os resultados satildeo parte de uma escala de intervalos O mesmo teste foi
utilizado para a diferenccedila entre grupos relativamente ao uso de rescue medication Os
testes dos dados provenientes de escalas categoacutericas (PAR e a avaliaccedilatildeo global) foram
realizados atraveacutes de testes natildeo-parameacutetricos (Mann-Whitney U-test)
Intensidade da dor Os resultados favorecem o grupo A ateacute 15h apoacutes o iniacutecio do
tratamento A partir das 2h o grupo A natildeo tem uma eficaacutecia estatisticamente maior que
o grupo B Ambos os grupos tecircm melhores resultados globais que o grupo C O Grupo
D (placebo) eacute notoriamente menos eficaz que todos os outros grupos
Aliacutevio da dor (PAR) Os resultados meacutedios desta afericcedilatildeo satildeo semelhantes aos da
intensidade da dor
TOTPAR Natildeo houve uma diferenccedila significativa entre o grupo A e o grupo B
Ambos foram significativamente melhores que o C todos os grupos de tratamento
activo tiveram melhores resultados que o grupo D (placebo)
SPID Embora o grupo A mostre a maior SPID meacutedia (05 ndash 3h) natildeo foi
estatisticamente diferente do grupo B o grupo C tambeacutem natildeo foi estatisticamente
diferente do grupo B A SPID meacutedia total foi estatisticamente semelhante entre os
grupos A e B mas superior agrave do grupo C O grupo D (placebo) teve resultados
inferiores aos dos restantes grupos
Uso de rescue medication Embora tenha existido um nuacutemero notoriamente
superior de casos entre os grupos A e B comparativamente ao C e ao D esta diferenccedila
natildeo eacute relevante estatisticamente devido ao baixo nuacutemero de pacientes que recorreram a
esta medicaccedilatildeo
Avaliaccedilatildeo global tanto agraves 4 como agraves 8h os grupos A e B receberam avaliaccedilotildees
semelhantes tendo as melhores classificaccedilotildees e sendo significativamente superiores agraves
do grupo C Todos foram melhores que o D (placebo) Agraves 8h as percentagens de
pacientes que avaliaram o tratamento como bom ou excelente foram
Grupo A 90
32
Grupo B 83
Grupo C 42
9 How precise are these results
No artigo natildeo satildeo mencionados intervalos de confianccedila No entanto nos graacuteficos
referentes agrave intensidade da dor eacute possiacutevel ver as barras correspondentes ao intervalo de
confianccedila Existem sempre que necessaacuterio valores de p associados aos resultados
10 Were all important outcomes considered so the results can be applied
Sim A extracccedilatildeo de terceiros molares em Portugal eacute uma praacutetica cliacutenica comum
pelo que o estudo pode ser facilmente reproduzido desde que haja acesso agrave medicaccedilatildeo
utilizada e que esta esteja em formato idecircntico (para garantir que natildeo existe vieacutes)
Poreacutem o facto de ser utilizada uma dose uacutenica poderaacute natildeo ir de encontro com o padratildeo
actual sendo necessaacuteria uma sensibilizaccedilatildeo do paciente diferente para este meacutetodo
Um facto importante foi referido na discussatildeo deste artigo posteriormente agrave
recolha de dados do mesmo surgiram preocupaccedilotildees seacuterias sobre efeitos nocivos
cardiovasculares em tratamentos de longa duraccedilatildeo com rofecoxib embora estes efeito
secundaacuterios tendam a estar relacionados com as doses e natildeo apenas com a selectividade
COX-2 (8 25) Esta informaccedilatildeo eacute altamente relevante de todos os pontos de vista do
paciente e famiacutelia do profissional de sauacutede e oacutergatildeos legislativos
Tendo em conta este facto seriam necessaacuterios estudos adicionais para aferir o
risco de seguir um tratamento como o visado neste ensaio cliacutenico
33
Combined acetaminophen and ibuprofen for pain relief after oral
surgery in adults a randomized controlled trial (13)
1 Did the study ask a clearly-focused question
Sim Foram incluiacutedos pacientes sujeitos a extracccedilatildeo de pelo menos um terceiro
molar inferior Foram excluiacutedos pacientes com idade inferior a 16 anos peso inferior a
50 kg que tivessem tomado NSAIDrsquos (excepto aspirina a 150mg) ou paracetamol 24h
antes da cirurgia entre outros(inserir referencia para a pagina pois sao muitos)
Existiram 3 grupos de intervenccedilatildeo
Grupo A 500mg paracetamol + 150mg ibuprofeno
Grupo B 500mg paracetamol
Grupo C 150mg ibuprofeno
Todos os grupos de intervenccedilatildeo tomaram 2 comprimidos imediatamente antes da
cirurgia e depois 4 comprimidos diariamente (de 6 em 6 horas) durante 48h
Os resultados passaram pela intensidade da dor medida atraveacutes da VAS (mm)
em trecircs momentos distintos antes de tomar qualquer medicaccedilatildeo do estudo
imediatamente apoacutes a cirurgia e de 2 em 2 horas ateacute terminar o periacuteodo de 48 horas A
medida utilizada foi a area under the curve (AUC) dividida pelo tempo resultando em
AUCh Este caacutelculo foi efectuado para encontrar valores ldquomeacutediosrdquo pois houve ligeiras
diferenccedilas no momento da afericcedilatildeo dos valores da VAS Mediu-se tambeacutem o consumo
de rescue medication ao longo das 48 horas
Foram ainda utilizadas escalas categoacutericas de avaliaccedilatildeo global da dor e da
naacuteusea realizadas no final do estudo bem como uma escala VAS para medir os
distuacuterbios no sono apoacutes cada noite
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim A atribuiccedilatildeo de cada tratamento foi cega para todos os pacientes
investigadores e pessoal envolvido O responsaacutevel pela aleatorizaccedilatildeo do estudo foi o
estatiacutestico do estudo O estatiacutestico foi a uacutenica pessoa com acesso agraves informaccedilotildees da
atribuiccedilatildeo de tratamento aos pacientes
34
3 Were participants appropriately allocated to intervention and control groups
A colocaccedilatildeo de pacientes em cada um dos trecircs grupos de tratamento foi
aleatorizada A sequecircncia de aleatorizaccedilatildeo foi gerada por computador pelo estatiacutestico
do estudo Foi utilizada uma proporccedilatildeo de 111 para os trecircs grupos de tratamento isto
foi conseguido atraveacutes de permutaccedilatildeo de blocos com estratificaccedilatildeo para o tipo de
anestesia (local ou geral) e centro de estudo A utilizaccedilatildeo da aleatorizaccedilatildeo por
permutaccedilatildeo de blocos assegura uma distribuiccedilatildeo equilibrada por grupos de tratamento
quando o nuacutemero de indiviacuteduos eacute menor que mil (inserir referencia do artigo de
aleatorizajao MJA)
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim Este ensaio cliacutenico foi duplamente cego Como tal cada tipo de tratamento
consistia em comprimidos idecircnticos colocados num pacote selado as instruccedilotildees sobre
dosagens eram tambeacutem iguais garantindo que o estudo permanecia cego aos
investigadores staff e pacientes prevenindo a existecircncia de vieacuteses
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim O estudo previa um nuacutemero miacutenimo de 120 indiviacuteduos 40 em cada grupo
de tratamento Dos 135 pacientes que concordaram participar apoacutes serem abordados
pelo meacutedico apenas 122 foram incluiacutedos no estudo (os 13 que foram excluiacutedos natildeo
entregaram o diaacuterio de tratamento que lhes foi pedido)
Grupo A n = 40
Grupo B n = 43
Grupo C n = 39
Todos os 122 pacientes incluiacutedos foram seguidos ateacute ao final do estudo
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os pacientes foram abordados primariamente por um cirurgiatildeo e
seguidamente por uma enfermeira responsaacutevel pelo seguimento dos pacientes ao longo
do estudo O seguimento de cada paciente foi realizado de igual forma no hospital e fora
35
dele onde o contacto era estabelecido por telefone de forma a facilitar a recolha de
informaccedilatildeo levada a cabo por meio da entrega de diaacuterios
Em relaccedilatildeo agrave recolha dos dados relativos agrave dor poacutes-operatoacuteria experienciada os
intervalos de tempo utilizados foram semelhantes (imediatamente antes da
administraccedilatildeo da primeira dose logo apoacutes a cirurgia e de 2 em 2 horas durante um
periacuteodo de 48 horas) e a monitorizaccedilatildeo dos pacientes feita utilizando as mesmas
guidelines
7 Did the study have enough participants to minimise the play of chance
Sim Os investigadores do estudo realizaram a power calculation Estimaram
que eram necessaacuterios 120 participantes distribuiacutedos equitativamente pelos 3 grupos O
power foi de 80 na detecccedilatildeo de diferenccedilas entre os grupos de 9 mm (SD de 14mm)
para mediccedilotildees relativas agrave altura de repouso e os de 13mm (SD de 21mm) e para
mediccedilotildees relativas agrave altura de actividade
Dos 135 pacientes incluiacutedos no estudo 13 natildeo devolveram os seus diaacuterios pelo
que ficaram disponiacuteveis 122 participantes a enquadrar a populaccedilatildeo de tratamento (ITT
population) para anaacutelise dos criteacuterios de comparaccedilatildeo primaacuterios (primary endpoints)
Como o criteacuterio de possuir participantes necessaacuterios foi preenchido os
resultados da comparaccedilatildeo do objectivo primaacuterio deste estudo (mediccedilatildeo da intensidade
meacutedia de dor ao longo do estudo) tecircm uma elevada importacircncia cliacutenica Esta
importacircncia eacute equiparaacutevel aos resultados de estudos publicados anteriormente
8 How are the results presented and what is the main result
Os resultados foram apresentados sob a forma de mediccedilotildees nomeadamente as
principais diferenccedilas (mean differences) entre o paracetamolacetaminofeno ibuprofeno
e combinaccedilatildeo dos dois comparando a eficaacutecia farmacocineacutetica e efeitos secundaacuterios
respectivos a cada um Agraves quais estaacute associada uma taxa de erro de 5 (SEM) ou seja
intervalo de confianccedila de 95 (CI) e um valor de P lt001
Foi realizada a mediccedilatildeo da time-adjusted AUC (AUCh) da VAS que
juntamente com a classificaccedilatildeo global de dor revelou-se substancial e
significativamente menor no grupo que utilizou a combinaccedilatildeo do que nos outros dois
grupos (tanto no periacuteodo de repouso como no periacuteodo de actividade)
Apesar de alguns criteacuterios de comparaccedilatildeo secundaacuterios (secondary endpoints) o
uso de medicaccedilatildeo de resgate apoiarem o uso da combinaccedilatildeo do faacutermaco natildeo possuem
36
relevacircncia estatiacutestica Aleacutem disso o tipo de anestesia utilizada na cirurgia e o nordm de
dentes extraiacutedos os paracircmetros farmacocineacuteticos e a ocorrecircncia dos efeitos secundaacuterios
natildeo mostraram diferenccedilas significativas entre os 3 grupos de estudo
Os pacientes medicados com a combinaccedilatildeo de paracetamol e ibuprofeno
experienciaram menos dor poacutes-operatoacuteria durante as 48 horas que os pacientes que
usaram os medicamentos isolados
9 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em conta que foi preacute-
definido um valor para P de 005 de forma determinar se os valores obtidos possuem
relevacircncia estatiacutestica ou natildeo os resultados satildeo precisos
Isto mostra que para que a combinaccedilatildeo dos dois medicamentos possa ser
considerada sem incerteza mais adequada que outros meacutetodos de medicaccedilatildeo seriam
necessaacuterios resultados expliacutecitos e com elevada relevacircncia estatiacutestica
10 Were all important outcomes considered so the results can be applied
Sim O estudo realizado tal como acontece em todos os outros apresenta os
seus pontos fortes e fracos No entanto a pluralidade de criteacuterios utilizados na
comparaccedilatildeo dos vaacuterios grupos de estudo permitiu uma boa percepccedilatildeo da relaccedilatildeo
custobenefiacutecio aqui presente Apesar de certos paracircmetros como a utilizaccedilatildeo de
placebo recrutamento de crianccedilas e avaliaccedilatildeo significativa dos efeitos secundaacuterios natildeo
terem sido explorados estes natildeo apresentam grande peso no que respeita agrave validaccedilatildeo dos
resultados em si Isto acontece pois a bibliografia existente e a praacutetica cliacutenica jaacute nos
permitem deduzir e extrapolar conclusotildees em relaccedilatildeo agravequeles paracircmetros
Deste modo a questatildeo-chave recai sobre o facto de a combinaccedilatildeo de
paracetamol com ibuprofeno ser mais vantajosa e eficaz que a toma de apenas um deles
Caso estes resultados sejam confirmados por estudos de outras entidades a jaacute muito
utilizada combinaccedilatildeo paracetamol+ibuprofeno poderaacute mesmo tornar-se procedimento
padratildeo na terapecircutica da dor aguda moderada (em pacientes sem contra-indicaccedilatildeo para
NSAIDrsquos)
37
Analgesic efficacy of lysine clonixinate paracetamol and
dipyrone in lower third molar extraction a randomized
controlled trial (32)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo em estudo comporta 90 pacientes entre os 18 e 26 anos de
idade com uma indicaccedilatildeo cliacutenica para extracccedilatildeo de um 3ordm molar inferior impactado
(com classe I e II)
A intervenccedilatildeo consistiu no tratamento da dor apoacutes extracccedilatildeo do 3ordm molar atraveacutes
da medicaccedilatildeo com um dos 3 analgeacutesicos em estudo utilizando 8 comprimidos do
respectivo analgeacutesico a serem tomados 1 hora preacute-cirurgia e a cada 6 horas poacutes-cirurgia
durante um periacuteodo de 24 horas
Os resultados foram obtidos atraveacutes da mediccedilatildeo da intensidade da dor utilizando
a escala visual analoacutegica (VAS) mesmo antes da cirurgia e seguidamente 1 2 4 6 8
12 e 24 horas apoacutes a cirurgia Aleacutem disso para cada uma destas mediccedilotildees os pacientes
tinham de relatar o niacutevel de dor em que se encontravam (percepccedilatildeo da dor) atraveacutes de
uma escala decimal com os seguintes criteacuterios
0 cm Sem dor
01- 3 cm Dor ligeira
31-7 cm Dor moderada
71-10 cm Dor intensa
A presenccedila ou ausecircncia de efeitos secundaacuterios foi tambeacutem uma das
preocupaccedilotildees deste estudo e algo avaliado nos resultados Dado que havia a
possibilidade de ocorrecircncia de agranulocitose anemia anafilaxia e complicaccedilotildees
gastrointestinais
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo em questatildeo consiste num ensaio cliacutenico aleatorizado Esta
abordagem foi a mais adequada para a questatildeo colocada uma vez que o objectivo final
eacute comparar a eficaacutecia da lisina clonixinato com o paracetamol e com a dipirona na
analgesia da dor poacutes-operatoacuteria Para obter informaccedilotildees mais completas respeitantes agrave
seguranccedila e eficaacutecia dos faacutermacos comparados eacute necessaacuterio o recrutamento e
aleatorizaccedilatildeo de um determinado nuacutemero de pacientes Eacute necessaacuterio tambeacutem medicaacute-
38
los medir e avaliar os resultados de forma imparcial e objectiva Desta forma eacute mais
provaacutevel chegar a uma conclusatildeo fidedigna e vaacutelida tanto interna como externamente
Pelas razotildees acima enumeradas a realizaccedilatildeo de um ensaio cliacutenico aleatorizado
foi a melhor abordagem a seguir
3 Were participants appropriately allocated to intervention and control groups
Sim Os pacientes foram divididos pelos diferentes grupos de estudo de uma
forma aleatoacuteria utilizando um meacutetodo relativamente simples Os analgeacutesicos foram
repartidos em recipientes brancos opacos e idecircnticos numerados de 1 a 90 Cada
recipiente continha 8 comprimidos de um dos 3 faacutermacos em comparaccedilatildeo (dipirona
500mg paracetamol 750mg lisina clonixinato 125 mg) Por sua vez foi pedido aos
pacientes para retirarem o recipiente agrave sua escolha e ao acaso os quais desconheciam o
seu conteuacutedo
Dos 90 pacientes recrutados de iniacutecio 26 desistiram pelo que os restantes 64
pacientes foram distribuiacutedos por 3 grupos correspondentes a diferentes analgeacutesicos
orais lisina clonixinato composto por 20 indiviacuteduos (8 masculinos 12 femininos)
Paracetamol composto por 23 indiviacuteduos (9M 14F) Dipirona composto por 21
indiviacuteduos (6M 15F)
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Natildeo eacute possiacutevel dizer Os pacientes deste estudo estavam lsquocegosrsquo quanto ao grupo
de estudo em que iriam ser colocados O processo de distribuiccedilatildeo dos indiviacuteduos foi
feito de uma forma aleatoacuteria atraveacutes de um meacutetodo bastante simples de escolha de
recipiente
Quanto aos funcionaacuterios e revisores deste estudo o mesmo pode natildeo ter
acontecido pois nenhuma informaccedilatildeo sobre este aspecto eacute mencionada no artigo
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim No estudo realizado os participantes foram distribuiacutedos por 3 grupos um
de estudo ou intervenccedilatildeo onde foi administrado lisina clonixinato e dois de controlo
onde se administrou paracetamol num e dipirona noutro Natildeo houve redistribuiccedilatildeo dos
39
participantes isto eacute cada participante foi tratado uacutenica e exclusivamente com o faacutermaco
correspondente ao seu grupo
Houve um seguimento dos pacientes durante um periacuteodo de 24 horas de modo a
avaliar a eficaacutecia de cada analgeacutesico na eliminaccedilatildeo da dor poacutes-operatoacuteria de forma
indirecta (quanto maior o aliacutevio de dor ao longo do periacuteodo de estudo maior a eficaacutecia
do respectivo analgeacutesico) Tendo isso em conta os resultados e anaacutelise dos dados foram
realizados em cada grupo e depois comparados com os outros grupos
Os investigadores do estudo poderiam ter formado um grupo placebo e
comparado os seus resultados com os restantes grupos Assim averiguar-se-ia a eficaacutecia
de cada um dos analgeacutesicos e natildeo apenas a eficaacutecia relativa a outros faacutermacos
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os participantes dos diferentes grupos foram seguidos da mesma maneira e
os dados recolhidos de igual forma Os resultados foram avaliados nos mesmos
intervalos de tempo ou seja antes da cirurgia e 1 2 4 6 8 12 e 24 horas apoacutes a
mesma Os pacientes receberam o mesmo tempo de atenccedilatildeo - 24 horas de seguimento e
os dados foram recolhidos utilizando os mesmos paracircmetros a escala visual analoacutegica
para determinar o aliacutevio de dor e a escala decimal para a percepccedilatildeo de dor dos pacientes
e questionaacuterios individuais
Para aleacutem do jaacute referido os investigadores tiveram em atenccedilatildeo a forma como a
cirurgia foi realizada diminuindo o risco de vieacutes
Intervieram 2 cirurgiotildees calibrados entre si na niacutevel da teacutecnica minimizando a
ocorrecircncia de abordagens ciruacutergicas diferentes
o periacuteodo de duraccedilatildeo foi controlado e por isso natildeo influenciou o comportamento
da dor no estudo (meacutedia de 339 minutos com SD plusmn98 min)
Estas cirurgias satildeo bastantes conhecidas e muitas vezes satildeo procedimentos
standard permitindo uma selecccedilatildeo muito mais facilitada e raacutepida de casos cliacutenicos a
incluir no estudo e diminuindo o nuacutemero de eventos de difiacutecil controlo que poderiam
levar a vieacutes dos resultados
7 Did the study have enough participants to minimise the play of chance
Natildeo eacute possiacutevel dizer Dos 90 pacientes inicialmente recrutados para o estudo 26
deles desistiram Os investigadores natildeo referiram o impacto deste nuacutemero de drop-outs
40
na extrapolaccedilatildeo de conclusotildees a partir dos resultados obtidos Igualmente natildeo foram
mencionados quaisquer caacutelculos que determinassem o nuacutemero necessaacuterio de indiviacuteduos
para o estudo ter validade
8 How are the results presented and what is the main result
Os resultados obtidos no estudo foram categorizados por droga e analisados de
acordo com o desenvolvimento da dor poacutes-operatoacuteria Seguidamente foram
apresentados atraveacutes de mediccedilotildees descritivas da variaccedilatildeo da dor as quais utilizaram
paracircmetros como miacutenimo maacuteximo mean median e desvio-padratildeo (SD)
Por sua vez a anaacutelise dos dados foi feita com os testes de Kruskal-Wallis e de
Friedman onde os resultados satildeo considerados estatisticamente relevantes se
culminarem num valor de lsquoprsquo igual ou inferior a 005 (95 IC) e apresentada utilizando
os mesmos paracircmetros de miacutenimo maacuteximo e SD
O valor de P encontra-se claramente acima do valor de referencia preacute-definido
pelo que os resultados natildeo apresentam relevacircncia estatiacutestica suficiente para aferir que
possuem um melhor outcome que o paracetamol
A lisina clonixinato assim como a dipirona e o paracetamol eacute eficiente no
controlo da dor resultante da extracccedilatildeo de um 3ordmmolar inferior pelo que natildeo apresenta
nenhuma diferenccedila significativa dos outros analgeacutesicos mencionados
9 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em conta que os valores de
P obtidos apoacutes anaacutelise dos resultados se encontrarem abaixo de 001 eacute possiacutevel auferir
que os resultados deste estudo satildeo bastante precisos
10 Were all important outcomes considered so the results can be applied
Natildeo Os efeitos gerados pela lisina clonoxinato no tratamento da dor derivada de
extracccedilatildeo do 3ordm molar natildeo foram estatisticamente relevantes quando comparados aos do
paracetamol e dipiridona Apesar de as condiccedilotildees pelas quais o estudo foi realizado
serem reprodutiacuteveis na nossa populaccedilatildeo local (tipo de pessoas localizaccedilatildeo e
reprodutibilidade do tratamento) nada eacute referido em relaccedilatildeo a novas poliacuteticas de sauacutede
nomeadamente na implementaccedilatildeo de uma dose uacutenica culminando numa mudanccedila dos
haacutebitos de sauacutede da comunidade Tambeacutem natildeo foram abordados aspectos econoacutemicos
41
tal como um balanccedilo entre benefiacutecios e encargos de sauacutede que justifique a utilizaccedilatildeo
deste faacutermaco como tratamento preferencial
42
Onset of analgesia with sodium ibuprofen ibuprofen acidin
corporating poloxamer and acetaminophenmdasha single-dose
double-blind placebo-controlled study in patients with post-
operative dental pain Daniels Reader (33)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo em estudo refere-se a pacientes com idade entre os 16 e os 40
anos apresentando uma intensidade de dor basal poacutes-operatoacuteria moderada a severa O
diagnoacutestico para a extracccedilatildeo poderia ser um dos seguintes pelo menos um 3ordm molar
mandibular indicado para remoccedilatildeo (grau de impactaccedilatildeo superior a 4) ou dois terceiros
molares ipsilaretais com pontuaccedilatildeo de impactaccedilatildeo conjunta natildeo superir a 6
A intervenccedilatildeo traduz-se no tratamento da dor poacutes-ciruacutergica com doses uacutenicas de
diferentes faacutermacos Inicialmente cada participante tem a mesma probabilidade de ser
colocado num dos 4 grupos
A ibuprofeno de soacutedio 2x256 mg (ibuprofeno de soacutedio di-hidratado equivalente a
400 mg de ibuprofeno aacutecido + placebos de ibuprofeno poloxamo e
acetaminofeno
B ibuprofenopoloxacircmero (400mg de Ibuprofeno e 120mg de poloxacircmero
surfactante 407) + placebos de ibuprofeno de soacutedio e paracetamol
C 1000mg acetaminofeno + placebos equivalentes
D placebo para as 3 formas de substacircncias activas
O endpoint primaacuterio consistiu no tempo necessaacuterio para um aliacutevio da dor
perceptiacutevel pelos pacientes Foram considerados inuacutemeros endpoints secundaacuterios (foi
utilizada uma escala categoacuterica e VAS para os endpoints 2 3 e 4)
1 Caacutelculo da AUC e SPRID (0 a 6 horas poacutes-tratamento) e tempo necessaacuterio para
um aliacutevio significativo da dor
2 Aliacutevio total da dor (TOTPAR) SPID e SPRID
3 Aliacutevio da dor e intensidade da mesma em termos individuais (5 minutos - 6
horas)
4 PID ao longo do periacuteodo de estudo e o momento em que este foigt ou igual a 1
5 Instante em que os pacientes recorreram a medicaccedilatildeo de recurso
6 Tempo e proporccedilatildeo de pacientes que sentiram 50 aliacutevio da dor
43
7 Abstracccedilatildeo agrave dor (1 e 6 horas) e percepccedilatildeo da interferecircncia causada pela dor nas
actividades quotidianas (escala de Ranvier)
8 Avaliaccedilatildeo qualitativa da medicaccedilatildeo tomada pelos dos participantes
Os efeitos adversos foram obtidos atraveacutes da procura de informaccedilatildeo em
documentaccedilatildeo e relacionados (ou natildeo) com a medicaccedilatildeo do estudo pelo investigador
Foi efectuada uma mediccedilatildeo de sinais vitais 6 horas apoacutes a toma e na visita follow-up na
qual tambeacutem foi realizado um exame fiacutesico
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo em questatildeo eacute descrito como um ensaio cliacutenico duplamente cego e
controlado com placebo Eacute o tipo de estudo indicado para comparar diferentes formas de
tratamento atraveacutes da divisatildeo dos pacientes por grupos Eacute necessaacuterio ter em
consideraccedilatildeo o aspecto eacutetico de tais tratamentos pois ldquoexposing patients to an
intervention believed to be inferior to current treatment is often thought unethicalrdquo (41)
Para garantir a eacutetica dos tratamentos incluiacutedos o estudo foi conduzido de acordo com a
Declaraccedilatildeo de Helsiacutenquia como referido na Directiva da EU de 200120EC e
concordante com a Conferecircncia Internacional de Harmonizaccedilatildeo (ICH) e a GCP (boa
praacutetica cliacutenica)
3 Were participants appropriately allocated to intervention and control groups
Sim Os indiviacuteduos foram divididos aleatoriamente para serem inseridos num
dos 4 grupos de tratamento numa proporccedilatildeo 1111 O meacutetodo de aleatorizaccedilatildeo foi
gerado pelo computador atraveacutes de um randomization Schedule
Para equilibrar a alocaccedilatildeo dos pacientes realizou-se uma estratificaccedilatildeo por sexo
e por intensidade da dor basal O protocolo do estudo foi revisto e aprovado pela
Quorum Review Inc o que leva a querer que a subdivisatildeo foi realmente rigorosa
Os grupos encontram-se equilibrados tanto em nuacutemero como noutras variaacuteveis
particularmente geacutenero intensidade dor basal e idade Deste modo diferenccedilas
reportadas nos resultados natildeo satildeo consequecircncia da heterogeneidade dentro dos grupos
de tratamento
44
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
A aleatorizaccedilatildeo dos participantes foi gerada pelo computador O protocolo do
estudo foi posteriormente revisto como anteriormente referido Agrave partida tanto o
investigador e pacientes natildeo interferiram no processo
Foram usados comprimidos para o ibuprofeno de soacutedio ibuprofenopoloxamero
e caacutepsulas para o paracetamol tanto para as formas activas como placebo
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim Os 322 participantes incluiacutedos de 614 inicialmente recrutados 318
completaram o estudo e 321 foram incluiacutedos na populaccedilatildeo ITT (intended do treat)
No grupo ibuprofeno de soacutedio todos os 80 participantes concluiacuteram a anaacutelise
No grupo B dos 80 inicialmente alocados 76 completaram a anaacutelise Um foi
excluiacutedo perdeu-se o follow-up de outro e os restantes natildeo concluiacuteram por
outros motivos
Dos 81 do grupo do paracetamol um natildeo foi incluiacutedo no ITT (falhou em
providenciar os dados da intensidade da dor basal diaacuteria)
No grupo placebo todos os pacientes concluiacuteram o estudo
Os resultados de cada paciente foram analisados agrave luz do grupo de tratamento
em que estes foram colocados
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os participantes permaneceram nos centros de investigaccedilatildeo cliacutenica apoacutes a
toma durante 8-15h Durante as 6 horas apoacutes o tratamento a eficaacutecia foi medida em
intervalos preacute-determinados Para avaliar a existecircncia de efeitos secundaacuterios foi
realizada uma mediccedilatildeo de sinais vitais conduzido um follow-up poacutes-operativo (5 a 12
dias poacutes-cirurgia) e repetida a avaliaccedilatildeo de efeitos adversos Pode-se considerar anaacutelogo
o acompanhamento entre os vaacuterios pacientes poacutes-cirurgia e medicaccedilatildeo pois constituiu
um seguimento proacuteximo maioritariamente presencial e rigoroso
45
7 Did the study have enough participants to minimise the play of chance
Foram usados dados de estudos preacutevios os quais continham informaccedilatildeo acerca
de AUC e PRID Com estes dados foi determinado que um nuacutemero de 80 pacientes por
grupo providenciaria um power de 90 em detectar diferenccedilas entre os grupos de
tratamento com um niacutevel de significacircncia de 0025 Natildeo foi possiacutevel calcular um power
ldquoformalrdquo para o aliacutevio de dor significativo No entanto a resposta eacute afirmativa para a
questatildeo CASP uma vez que foram realizados esforccedilos para que o nuacutemero das amostras
fosse significativo e correcto
8 How are the results presented and what is the main result
Os resultados satildeo apresentados em termos de percentagens e diferenccedilas meacutedias
(mean differences) alguns com recurso a curvas de Kaplan-Meier (survival curves) Os
efeitos secundaacuterios satildeo apresentados sob a forma de tabela com a percentagem de
pacientes dentro de cada grupo que sofreram os efeitos descritos na mesma
Os grupos A e B exibem resultados substancialmente melhores no que diz
respeito aos seguintes pontos
AUC e SPID satildeo significativamente menores A com 963 e B com 90 face a
C com 675 e D com 25 O tempo para atingir aliacutevio da dor
SPRID Esta eacute semelhante entre os grupos A B e C ateacute aos 45 minutos A partir
deste periacuteodo o ibuprofeno possui uma eficaacutecia superior ao paracetamol
Abstracccedilatildeo agrave dor e percepccedilatildeo da interferecircncia causada pela dor nas actividades
quotidianas (escala de Ranvier)
Utilizaccedilatildeo da medicaccedilatildeo de recurso A com 325 e B com 225 face a C com
438 e D em que a maioria dos pacientes usou a mesma
Avaliaccedilatildeo dos medicamentos por parte dos pacientes (resposta ldquoboardquo ldquomuito
boardquo ou ldquoexcelenterdquo)
No que se refere aos efeitos secundaacuterios 118 da populaccedilatildeo do estudo sofreu
mais efeitos sendo que a maior percentagem ocorreu no grupo do C
Quando comparado com acetaminofeno o ibuprofeno de soacutedio e
Ibuprofenopoloxamero possui uma eficaacutecia analgeacutesica significativamente superior
46
9 How precise are these results
Nos endpoints primaacuterios as diferenccedilas entre as duas formulaccedilotildees de ibuprofeno e
paracetamol foram avaliadas tendo por base o teste de Wilcoxon rank-sum O hazard
ratio e respectivo IC de 975 foram calculados para as comparaccedilotildees entre os
compostos Os endpoints secundaacuterios que agregavam vaacuterios periacuteodos de tempo foram
calculados atraveacutes da AUC Diferenccedilas entre tratamentos foram avaliadas utilizando
valores de α de 005 o intervalo de confianccedila de 95 (CI) foi calculado por meio dos
paracircmetros do modelo adequado
Eacute introduzido o valor de P que na sua generalidade possui valores reduzidos e
menores que 0005 Considerando a homogeneidade dos grupos o caacutelculo do nuacutemero da
amostra com elevado power e os valores de P podemos concluir que no contexto os
resultados satildeo precisos (42)
10 Were all important outcomes considered so the results can be applied
Eacute plausiacutevel que a populaccedilatildeo utilizada no estudo fosse semelhante num estudo
anaacutelogo Tanto o local como o proacuteprio tratamento poderiam ser reproduzidos visto que
os compostos em questatildeo satildeo largamente comercializados
Os resultados satildeo importantes para uma escolha mais consciente por parte dos
indiviacuteduos entre tomar paracetamol ou ibuprofeno apoacutes uma cirurgia de um 3ordm molar Eacute
afirmado na discussatildeo deste estudo que o ibuprofeno possui menores efeitos adversos
gastrointestinais que outros NSAIDrsquos Tendo isso em conta pode conduzir a uma
escolha deste composto no tratamento da dor poacutes ciruacutergica por parte dos profissionais
ldquothese findings support a recommendation for this agent as an analgesic of choice for
the treatment of post-operative dental painrdquo A preocupaccedilatildeo pela comunidade em geral
estaacute impliacutecita neste aspecto se possuir menores efeitos secundaacuterios e benefiacutecio superior
eacute melhor para a populaccedilatildeo em geral O custo financeiro destes medicamentos natildeo se
traduz num ponto diferenciador visto que em Portugal existem geneacutericos de ambos
Eacute uma boa base de comparaccedilatildeo entre o paracetamol e ibuprofeno em muitos
aspectos Na procura da melhor evidecircncia e no sentido de a aplicar eacute importante
completar este estudo com outros que nomeadamente se foquem nos efeitos
secundaacuterios
47
An investigation into the comparative efficacy of soluble aspirin
and solid paracetamol in postoperative pain after third molar
surgery Seymour Hawkesford (22)
1 Did the study ask a clearly-focused question
Sim O estudo em questatildeo trata-se de um ensaio cliacutenico aleatorizado duplamente
cego e controlado por placebo O seu objectivo central eacute comparar a eficaacutecia da aspirina
soluacutevel agrave do paracetamol soacutelido em pacientes com dor poacutes-operatoacuteria apoacutes extracccedilatildeo do
3ordm molar Foi utilizado um grupo placebo como controlo negativo
Soacute foram incluiacutedos pacientes que necessitavam da extracccedilatildeo do 3ordm molar
saudaacuteveis segundo categoria 1 da American Society of Anaesthesiologists (ASA I) ou agrave
discriccedilatildeo do cirurgiatildeo oral categoria 2 Soacute foram abrangidos pacientes que atingiram o
limiar de dor necessaacuterio ou que requeriram analgeacutesicos ateacute 90 minutos apoacutes a cirurgia
Cada paciente incluiacutedo no estudo foi colocado num dos trecircs grupos de
tratamento
Grupo 1 Aspirina soluacutevel 900mg dose uacutenica
Grupo 2 paracetamol soacutelido 1000mg dose uacutenica
Grupo 3 placebo dose uacutenica
Foi utilizado o meacutetodo de double-dummy ndash assim cada grupo recebeu o seu tipo
de tratamento e um placebo do tratamento alternativo No caso do grupo 3 os pacientes
receberam placebos para os dois tipos de tratamento
Os outcomes passaram pela
Comparaccedilatildeo de medidas de intensidade da dor atraveacutes da escala VAS (mm)
entre os grupos de tratamento aos 10 15 20 e 30 minutos apoacutes a dosagem
inicial
Comparaccedilatildeo da AUC240 com recurso a anaacutelise de co-variacircncia usando o
centro do estudo geacutenero baseline pain intensity duraccedilatildeo da cirurgia e
nuacutemero de molares removidos como co-variaacuteveis
Necessidade de recurso a rescue medication
Impressatildeo geral dos pacientes e enfermeiros sobre a medicaccedilatildeo atraveacutes de
uma regressatildeo binomial logiacutestica (em que um resultado positivo se refere a
uma avaliaccedilatildeo ldquomuito boardquo ou ldquoboardquo)
As comparaccedilotildees feitas foram aspirina vs paracetamol e aspirina vs placebo
48
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo apresentado eacute um RCT por vaacuterias razotildees sendo a mais relevante a
aleatorizaccedilatildeo dos grupos de tratamento em que os pacientes incluiacutedos foram
distribuiacutedos com a mesma probabilidade e aleatoriamente para cada grupo de estudo Os
grupos de tratamento tecircm tamanhos semelhantes e satildeo homogeacuteneos e os pacientes
foram seguidos de forma semelhante - as uacutenicas diferenccedilas residem no tratamento
oferecido
A utilizaccedilatildeo deste tipo de estudo foi loacutegica Um ensaio cliacutenico aleatorizado eacute
ideal para comparar efeitos de determinadas intervenccedilotildees e consequentemente ideal
para comparar eficaacutecia entre medicamentos
3 Were participants appropriately allocated to intervention and control groups
Foi realizada uma alocaccedilatildeo aleatoacuteria dos pacientes incluiacutedos assim como uma
aleatorizaccedilatildeo por blocos de cinco para assegurar equiliacutebrio entre grupos de tratamento
ldquoA key advantage of blocked randomization is that treatment groups will be equal in
size and will tend to be uniformly distributed by key outcome-related characteristicsrdquo
(43)
Foi ainda efectuada uma aleatorizaccedilatildeo estratificada por geacutenero de modo a
equilibrar nos trecircs grupos o nuacutemero de mulheres e homens e aumentar a credibilidade
das comparaccedilotildees entre os mesmos (proporccedilatildeo MF 21)
Tabela 2 ndash Dados demograacuteficos dos pacientes do estudo
Variaacutevel Aspirina soluacutevel
900mg
Paracetamol soacutelido
1000 mg
Placebo
Nuacutemero de pacientes 59 62 32
Raacutecio geacutenero MF 1940 1943 1121
Todos os pacientes incluiacutedos receberam anestesia de acordo com a praacutetica
cliacutenica a extracccedilatildeo dos molares impactados foi realizada seguindo a teacutecnica standard
Estes factores contribuem para a semelhanccedila da forma de tratamento dos 3 grupos Com
estes aspectos em comum a todos os pacientes incluiacutedos em adiccedilatildeo agrave homogeneidade
dos grupos nos seus aspectos demograacuteficos diferenccedilas encontradas nos resultados satildeo
consequecircncias de outros factores
49
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim A administraccedilatildeo uacutenica tem a vantagem de natildeo requerer monitorizaccedilatildeo de
um processo ldquodelicadordquo por parte do paciente De facto todo o estudo eacute realizado num
periacuteodo de 4 horas apoacutes a cirurgia e com ajuda de enfermeiros Olhando do ponto de
vista do paciente pode-se consideraacute-lo cego
Se os meacutetodos foram realmente aleatoacuterios o investigador eacute tambeacutem considerado
cego e pode-se afirmar que foram feitos esforccedilos necessaacuterios para o alcanccedilar Tanto a
aspirina soluacutevel como o placebo foram oferecidos sob a forma de uma bebida cor-de-
laranja o paracetamol com substacircncia activa e placebo oferecidos como comprimidos
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim Inicialmente todos os pacientes tinham a mesma probabilidade de serem
incluiacutedos num dos trecircs grupos A distribuiccedilatildeo sendo aleatoacuteria natildeo soacute coloca um
paciente num determinado grupo de tratamento como impossibilita que o mesmo venha
a pertencer a outro O seguimento foi realizado de igual forma para todos os grupos e
intimamente controlado Os resultados foram apresentados separadamente para cada
grupo Dos 167 pacientes foram medicados 153 Dos 14 pacientes natildeo tratados 10 natildeo
desenvolveram dor suficiente para serem incluiacutedos 1 obteve uma reacccedilatildeo adversa agrave
anestesia e 1 natildeo seguiu o protocolo
O grupo da aspirina soluacutevel apresentou melhores resultados que o grupo do
paracetamol e do placebo na medida em que os pacientes reportaram menos dor
apresentou menor intensidade de dor (aos 10 e 30 minutes em comparaccedilatildeo ao
paracetamol e apenas 30 minutos face ao placebo) e os valores de dor global medidos
pela AUC240 foram significativamente menores
6 Were the participants in all groups followed up and data collected in the same
way
Sim A intensidade da dor foi medida frequentemente ao longo de 4 horas
(segundo a VAS) e os pacientes foram informados da possibilidade de tomar medicaccedilatildeo
adicional se necessaacuterio A avaliaccedilatildeo sobre o tratamento dos enfermeiros e dos proacuteprios
pacientes foi tida em consideraccedilatildeo para os resultados
50
Aleacutem disso ao longo do periacuteodo de investigaccedilatildeo a enfermeira do estudo ficou
responsaacutevel por monitorizar os pacientes e registar a ocorrecircncia de quaisquer eventos
adversos Deste modo eacute muito provaacutevel que todos os pacientes tenham recebido o
mesmo niacutevel de atenccedilatildeo
7 Did the study have enough participants to minimise the play of chance
Natildeo eacute possiacutevel dizer No estudo natildeo eacute referida a utilizaccedilatildeo de power calculations
ou outros meacutetodos para determinar o tamanho da amostra Apenas se pode concluir que
o grupo de controlo negativo tem um menor nuacutemero de pacientes consequecircncia de
desistecircncias ou pelo simples facto de agrave partida se conhecerem os resultados
8 How are the results presented and what is the main result
A intensidade da dor foi medida numa escala VAS aos 10 15 20 e 30 minutos
apoacutes a administraccedilatildeo Foi possiacutevel tirar vaacuterias conclusotildees a partir da observaccedilatildeo dos
resultados
A aspirina demonstrou ser significativamente mais eficaz que o paracetamol ou
placebo embora ateacute aos 15 minutos natildeo seja uma diferenccedila muito expressiva
Relativamente agrave AUC240 experiecircncia global da dor no periacuteodo de 4 horas da
investigaccedilatildeo esta foi significativamente menor para o grupo 1
Natildeo existiu diferenccedila significativa entre os grupos no que diz respeito agrave rescue
medication utilizada No entanto o tempo para a administraccedilatildeo da mesma foi
superior no grupo 1 e 2 em relaccedilatildeo ao grupo placebo
Em relaccedilatildeo agrave impressatildeo global natildeo haacute discrepacircncias consideraacuteveis entre grupo 1
e 2 no que diz respeito agrave percentagem de outcomes positivos (58 e 53
respectivamente) O grupo 3 apresentou apenas 31 de outcomes positivos
A tabela com a percentagem de pacientes que desenvolveram efeitos adversos
para cada grupo mostra que 41 dos pacientes apresentaram efeitos secundaacuterios
nos grupos com tratamento activo no entanto muitos destes estavam
relacionados com o procedimento ciruacutergico
A aspirina soluacutevel 900mg providencia uma analgesia mais significante e raacutepida
que o paracetamol 1000mg no periacuteodo imediato apoacutes a cirurgia do 3ordm molar embora natildeo
seja muito expressiva a percepccedilatildeo desta diferenccedila por parte dos pacientes e enfermeiros
51
9 How precise are these results
Os resultados satildeo precisos e apresentados atraveacutes de um intervalo de confianccedila
de 95 satildeo tambeacutem apresentados valores de p
Os valores de p satildeo menores que 005 excepto aos 10 e 15 minutos
Para a intensidade da dor ao longo dos 30 minutos e AUC240 da comparaccedilatildeo
aspirina vs placebo a intervenccedilatildeo utilizada seria a mesma tanto no limite superior
como no inferior excepto aos 10 e 15 minutos Na comparaccedilatildeo aspirina soluacutevel vs
paracetamol soacutelido a decisatildeo seria a mesma independentemente dos limites do intervalo
apenas para os minutos 10 20 e 30
O mesmo aconteceria para a medicaccedilatildeo de recurso (outcome C) e a avaliaccedilatildeo do
tratamento por parte dos pacientes e enfermeiros (outcome D)
Pelo intervalo de confianccedila estar presente e pelo facto de os valores de p serem
bastante reduzidos os resultados satildeo precisos ao ponto de ajudarem a suportar uma
decisatildeo
10 Were all important outcomes considered so the results can be applied
Sim Os pacientes incluiacutedos no estudo o local e o tratamento visados no mesmo
poderiam ser extrapulados e aplicados noutro ambiente O seguimento dos pacientes
durante 4 horas e com ajuda de enfermeiros natildeo se apresenta como muito viaacutevel mas
ainda assim eacute exequiacutevel e seguro
O estudo avalia dados importantes para os profissionais de sauacutede ao afirmar que
a dose (900mg) e a forma (soluacutevel) em que a aspirina eacute tomada conduz a um poder
analgeacutesico superior que o paracetamol No entanto em termos individuais e de poliacuteticas
de sauacutede os efeitos secundaacuterios consequentes da medicaccedilatildeo (excluindo os que se
relacionassem com a cirurgia) deveriam ser completados com estudos suplementares
Segundo este ensaio cliacutenico a incidecircncia de efeitos secundaacuterios natildeo eacute muito
dissemelhante entre aspirina soluacutevel e paracetamol soacutelido nas doses maacuteximas
recomendadas e nestas circunstacircncias a aspirina tem maior poder analgeacutesico Por este
prisma a praacutetica cliacutenica poderia passar pela prescriccedilatildeo de aspirina soluacutevel 900mg para
aliacutevio dor poacutes-operatoacuteria da extracccedilatildeo do terceiro molar Poreacutem eacute necessaacuterio ter em
conta que visa somente a dor nas primeiras quatro horas poacutes-operatoacuterias sendo
importante investigar alternativas eficazes que sejam mais duradouras ou a eficaacutecia e
efeitos secundaacuterios de repetir este tratamento apoacutes as quatro horas iniciais
52
DISCUSSAtildeO
A partir da anaacutelise feita das revisotildees sistemaacuteticas de Weil (19) e de Barden (23)
conclui-se que o paracetamol eacute uma analgeacutesico seguro e eficaz no tratamento da dor
relativa agrave exodontia de terceiros molares pois apresenta um benefiacutecio estatisticamente
significativo quando comparado a placebo Ambas consideram que os melhores valores
de aliacutevio de dor e da diminuiccedilatildeo da intensidade da mesma satildeo alcanccedilados agraves 4 e 6 horas
apoacutes ingestatildeo do faacutermaco
Com base na primeira revisatildeo acima referida o paracetamol exibe uma dose
uacutenica oacuteptima de 1000mg e um periacuteodo de medicaccedilatildeo apropriado de 8 em 8 horas A
maioria dos artigos incluiacutedos apresenta um risco de vieacutes moderado causado
principalmente pela falta de informaccedilatildeo sobre o mecanismo de alocaccedilatildeo de pacientes
podendo levar a uma descredibilidade dos resultados (36)
Na revisatildeo de Barden (23) a comparaccedilatildeo entre os diferentes NSAIDrsquos
demonstrou que este tipo de faacutermacos e particularmente os inibidores da COX-2
exibem os melhores valores de NNT Atraveacutes de uma comparaccedilatildeo indirecta entre
ibuprofeno vs paracetamol os vaacuterios estudos mostraram que o ibuprofeno apresenta
melhores resultados na analgesia da dor poacutes-operatoacuteria (44)
Os estudos de Seymour (22) de Haglund (25) e de Daniels (33) comparam
diferentes compostos activos a um placebo onde o paracetamol estaacute sempre presente
Todos comprovam que enquanto analgeacutesico apresenta uma eficaacutecia largamente
significativa em termos de aliacutevio da dor (usando a escala VAS) Pelo menos 50 dos
indiviacuteduos incluiacutedos que receberam este faacutermaco avaliaram globalmente o tratamento de
forma positiva Poreacutem todos os artigos que
1 Comparam este composto a outro nomeadamente NSAIDrsquos mostram que estes
tecircm uma eficaacutecia significativamente superior agrave do paracetamol tanto em relaccedilatildeo
a valores mais baixos na escala VAS como subjectivamente na avaliaccedilatildeo global
Cerca de 80 dos indiviacuteduos que tomaram NSAIDrsquos classificaram o tratamento
positivamente (agrave excepccedilatildeo dos estudos (32) e (22)) Reportam ainda os efeitos
adversos mais comuns como tonturas naacuteuseas cefaleia e sonolecircncia que
embora de gravidade reduzida tecircm uma incidecircncia superior no paracetamol que
na aspirina e ibuprofeno
53
2 Combinam o paracetamol com NSAIDrsquos provam o efeito aditivo daquele bem
como o facto de estas combinaccedilotildees serem mais eficazes que qualquer um dos
faacutermacos em separado (Merry (13) e Haglund (25))
De acordo com os estudos analisados os NSAIDrsquos aparentam ser uma escolha
preferencial face ao paracetamol porque apresentam uma maior eficaacutecia no aliacutevio da dor
apoacutes extracccedilatildeo de terceiros molares embora disponham de propriedades anti-
inflamatoacuterias notoacuterias (e pertinentes no sucesso do tratamento poacutes-operatoacuterio)
O mecanismo de acccedilatildeo do paracetamol necessita de investigaccedilatildeo adicional que
permita uma melhor compreensatildeo e que traga novas respostas na praacutetica cliacutenica Como
aspecto positivo eacute de acrescentar que natildeo existem diferenccedilas estatisticamente
significantes entre o paracetamol e placebo no que diz respeito a efeitos secundaacuterios
(baixo grau de severidade) podendo ser considerado um composto seguro
A revisatildeo de Barden (23) indica que os resultados da eficaacutecia dos NSAIDrsquos
podem atrair os cliacutenicos a aumentar a sua prescriccedilatildeo sem terem em atenccedilatildeo a sua
relaccedilatildeo com o aumento dos efeitos adversos Isto eacute uma situaccedilatildeo insustentaacutevel na
medida em que nas uacuteltimas duas deacutecadas alguns destes medicamentos foram retirados
do mercado devido a eventos adversos graves posteriormente descobertos Um exemplo
eacute o caso do rofecoxib e valdecoxib que produziram acidentes cardiovasculares seacuterios
provavelmente consequentes da dosagem e natildeo da sua selectividade para a COX-2
(25))
Os efeitos adversos satildeo um motivo de peso para que os pacientes deixem de
tomar determinada substacircncia ou sejam incapazes de tolerar uma dose eficaz da mesma
Informaccedilotildees complementares que englobassem este aspecto seriam ideais e exequiacuteveis
se os autores de ensaios cliacutenicos lhes dessem maior relevo (45)
Outros dados - como custo financeiro e disponibilidade no mercado - poderiam
ser um auxiacutelio na selecccedilatildeo entre paracetamol e outros medicamentos Eacute de ressalvar
que em Portugal os geneacutericos vieram a baixar os preccedilos de analgeacutesicos e NSAIDrsquos
Medicamentos agrave base de ibuprofeno satildeo dos mais dispendiosos (46)
Os NSAIDrsquos tecircm um problema adicional relacionado com a hemostase ndash inibir a
produccedilatildeo de tromboxano A2 e consequentemente aumentar o risco de hemorragia
prolongada (11) No entanto estes efeitos secundaacuterios estatildeo directamente relacionados
com a dosagem pelo que apenas eacute relevante considerar este aspecto em paciente com
problemas de coagulaccedilatildeo
54
Conclui-se que embora a toma de paracetamol seja um procedimento seguro e
eficaz existem no mercado compostos com igual seguranccedila e eficaacutecia superior Apesar
de os inibidores da COX-2 serem os compostos mais eficazes abarcam os efeitos
secundaacuterios mais graves pelo que a realizaccedilatildeo de estudos adicionais eacute imperativo no
sentido de colmatar esta falha
55
RESPOSTA AO PACIENTE
ldquoTendo em conta a evidecircncia cientiacutefica disponiacutevel sobre este assunto e
considerando que natildeo tem problemas gaacutestricos ou de coagulaccedilatildeo sanguiacutenea recomendo
que tome 1g de paracetamol de 8 em 8 horas pois eacute bastante eficaz no aliacutevio da dor
Poreacutem existem outras opccedilotildees como por exemplo combinar o paracetamol a 200mg de
ibuprofeno pode ainda apenas tomar o paracetamol e se sentir necessidade recorrer ao
ibuprofeno 400mg no maacuteximo trecircs vezes ao dia
Tanto o paracetamol como o ibuprofeno tecircm poucos efeitos secundaacuterios e os
mais frequentes satildeo de baixo grau de gravidade Embora existam outros medicamentos
mais eficazes na eliminaccedilatildeo da dor estes tecircm efeitos secundaacuterios mais graves que natildeo
justificam a sua utilizaccedilatildeo
56
REFEREcircNCIAS BIBLIOGRAacuteFICAS
1 Barden J Edwards JE McQuay HJ Andrew Moore R Pain and analgesic
response after third molar extraction and other postsurgical pain Pain 2004107(1-
2)86-90 Epub 20040113
2 Cooper SA Desjardins PJ The value of the dental impaction pain model in drug
development Methods in molecular biology (Clifton NJ) 2010617175-90 Epub
20100326
3 NICE Guidance on the Extraction of Wisdom Teeth2000 13 December 2011
Available from httppublicationsniceorgukguidance-on-the-extraction-of-wisdom-
teeth-ta1clinical-need-and-practice
4 Mettes Dirk TG Nienhuijs Marloes MEL van der Sanden Wil JM Verdonschot
Emiel H Plasschaert A Interventions for treating asymptomatic impacted wisdom teeth
in adolescents and adults Cochrane Database of Systematic Reviews [Internet] 2005
(2) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD003879frameht
ml
5 Seymour RA Use of analgesics in postoperative dental pain a review Journal
of the Royal Society of Medicine 198477(11)949-54 Epub 19841101
6 Berg JM Tymoczko JL Stryer L Biochemistry 5 ed W H Freeman 2002
1050 p
7 Nelson DL Cox MM Lehninger Principles of Biochemistry 5 ed W H
Freeman 2005 1119 p
8 Sciulli MG Capone ML Tacconelli S Patrignani P The future of traditional
nonsteroidal antiinflammatory drugs and cyclooxygenase-2 inhibitors in the treatment
of inflammation and pain Pharmacological reports PR 200557 Suppl66-85 Epub
20060118
9 Devlin TD Devlins Textbook of Biochemistry 6 ed Hoboken NJ Wiley
2006 1208 p
10 Katzung BG Basical and Clinical Pharmacology 10 ed McGraw-Hill 2006
11 Naclerio-Homem Mg Fau - Deboni MCZ Deboni Mc Fau - Rapoport A
Rapoport A Fau - Chin VKL Chin VK Effects of ketoprofen and diclofenac potassium
on blood coagulation tests after removal of third molars (1936-7163 (Electronic))
57
12 Toms L McQuay H Derry S Moore R Single dose oral paracetamol
(acetaminophen) for post-operative pain in adults Cochrane Database of Systematic
Reviews 2008(4)
13 Merry AF Gibbs RD Edwards J Ting GS Frampton C Davies E et al
Combined acetaminophen and ibuprofen for pain relief after oral surgery in adults a
randomized controlled trial British journal of anaesthesia 2010104(1)80-8 Epub
20091217
14 Derry C Derry S Moore R McQuay H Single Dose Oral Ibuprofen for Acute
Post-Operative Pain in Adults Cochrane Database of Systematic Reviews 2009(3)
15 Rang HP Dale MM Ritter JM Moore PK Farmacologia 5 ed Elsevier 2003
Elsevier p
16 Scopel E Alencar M Cruz RM Medidas de avaliaccedilatildeo da dor efdeportes
2007(105)
17 Mata AD Marques D Silveira J Marques J Medicina Dentaacuteria Baseada na
Evidecircncia Novas Opccedilotildees para Velhas Praacuteticas Rev Port Estomatol Cir Maxilofac
200849(1)31-7
18 CASP UK [13 Dezembro 2011] Available from httpwwwcasp-
uknetabout-caspabout-casp
19 Weil K Hooper L Afzal Z Esposito M Worthington Helen V van Wijk A et
al Paracetamol for pain relief after surgical removal of lower wisdom teeth Cochrane
Database of Systematic Reviews [Internet] 2007 (3) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD004487frameht
ml
20 Toms L Derry S Moore RA McQuay Henry J Single dose oral paracetamol
(acetaminophen) with codeine for postoperative pain in adults Cochrane Database of
Systematic Reviews [Internet] 2009 (1) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD001547frameht
ml
21 Derry S Wiffen PJ Moore RA Relative efficacy of oral analgesics after third
molar extraction - a 2011 update Br Dent J 2011211(9)419-20
22 Seymour RA Hawkesford JE Sykes J Stillings M Hill CM An investigation
into the comparative efficacy of soluble aspirin and solid paracetamol in postoperative
pain after third molar surgery Br Dent J 2003194(3)153-7
58
23 Barden J Edwards JE McQuay HJ Wiffen PJ Moore RA Relative efficacy of
oral analgesics after third molar extraction Br Dent J 2004197(7)407-11
24 Saska S Scartezini GR Souza RFd Hochuli-Vieira E Pereira Filho VA
Gabrielli MAC Cloridrato de tramadolparacetamol no controle da dor poacutes-operatoacuteria
em cirurgias de terceiros molares inclusos
Tramadolacetaminophen in the control of postoperative pain for impacted third molar
surgery Rev cir traumatol buco-maxilo-fac 20099(4)
25 Haglund B von Bultzingslowen I Combining paracetamol with a selective
cyclooxygenase-2 inhibitor for acute pain relief after third molar surgery a randomized
double-blind placebo-controlled study European journal of oral sciences
2006114(4)293-301 Epub 20060817
26 Kubitzek F Ziegler G Gold MS Liu JM Ionescu E Analgesic efficacy of low-
dose diclofenac versus paracetamol and placebo in postoperative dental pain Journal of
orofacial pain 200317(3)237-44 Epub 20031003
27 Bjornsson GA Haanaes HR Skoglund LA A randomized double-blind
crossover trial of paracetamol 1000 mg four times daily vs ibuprofen 600 mg effect on
swelling and other postoperative events after third molar surgery British journal of
clinical pharmacology 200355(4)405-12 Epub 20030419
28 Macleod AG Ashford B Voltz M Williams B Cramond T Gorta L et al
Paracetamol versus paracetamol-codeine in the treatment of post-operative dental pain
a randomized double-blind prospective trial Australian dental journal
200247(2)147-51 Epub 20020726
29 Bjornsson GA Haanaes HR Skoglund LA Ketoprofen 75 mg qid versus
acetaminophen 1000 mg qid for 3 days on swelling pain and other postoperative events
after third-molar surgery Journal of clinical pharmacology 200343(3)305-14 Epub
20030318
30 Chopra D Rehan HS Mehra P Kakkar AK A randomized double-blind
placebo-controlled study comparing the efficacy and safety of paracetamol
serratiopeptidase ibuprofen and betamethasone using the dental impaction pain model
International journal of oral and maxillofacial surgery 200938(4)350-5 Epub
20090127
31 Dolci G Ripari M Pacifici L Umile A Evaluation of piroxicam-beta-
cyclodextrin piroxicam paracetamol and placebo in post-operative oral surgery pain
59
International journal of clinical pharmacology research 199414(5-6)185-91 Epub
19940101
32 Noronha VR Gurgel GD Alves LC Noman-Ferreira LC Mendonca LL Aguiar
EG et al Analgesic efficacy of lysine clonixinate paracetamol and dipyrone in lower
third molar extraction a randomized controlled trial Medicina oral patologia oral y
cirugia bucal 200914(8)e411-5 Epub 20090506
33 Daniels S Reader S Berry P Goulder M Onset of analgesia with sodium
ibuprofen ibuprofen acid incorporating poloxamer and acetaminophen--a single-dose
double-blind placebo-controlled study in patients with post-operative dental pain
European journal of clinical pharmacology 200965(4)343-53 Epub 20090303
34 Medve RA Wang J Karim R Tramadol and acetaminophen tablets for dental
pain Anesthesia progress 200148(3)79-81 Epub 20011129
35 Bjornsson GA Haanaes HR Skoglund LA Naproxen 500 mg bid versus
acetaminophen 1000 mg qid effect on swelling and other acute postoperative events
after bilateral third molar surgery Journal of clinical pharmacology 200343(8)849-58
Epub 20030905
36 Marques JF Marques D Silveira J Mata AD Revisotildees Sistemaacuteticas o que satildeo
e para que servem Rev Port Estomatol Cir Maxilofac 200849(3)171-8
37 Rodrigues CL Ziegelmann PK Meta-anaacuteliseum guia praacutetico HCPA
201030(4)436-47
38 Alderson P Absence of evidence is not evidence of absence Bmj
2004328(7438)476-7
39 Berwanger O Suzumura EA Buehler AM Oliveira JB Como Avaliar
Criticamente Revisotildees Sistemaacuteticas e Meta-anaacutelises Revista Brasileira de Terapia
Intensiva 200719(4)475-80
40 Noordzij M Zoccali C Dekker FW Jager KJ Adding up the evidence
systematic reviews and meta-analyses Nephron Clinical practice 2011119(4)c310-6
Epub 20111203
41 Sibbald B Roland M Understanding controlled trials Why are randomised
controlled trials important Bmj 1998316(7126)201
42 Primer on Statistical Significance and P Values Effective Clinical Practice
20014(4)183-4
43 Efird J Blocked randomization with randomly selected block sizes International
journal of environmental research and public health 20118(1)15-20 Epub 20110215
60
44 Cooper S Schachtel B Goldman E Gelb S Cohn P Ibuprofen and
acetaminophen in the relief of acute pain a randomized double blind placebo
controlled study The Journal of Clinical Pharmacology 198929(11)1026-30
45 Edwards JE McQuay HJ Moore RA Collins SL Reporting of Adverse Effects
in Clinical Trials Should Be Improved Lessons from Acute Postoperative Pain Journal
of pain and symptom management 199918(6)427-37
46 Faacutermaco mais vendido versus mais barato Deco Proteste [updated Julho
200919 Dezembro 2011] Available from httpwwwdecoprotesteptservicos-de-
saudefarmaco-mais-vendido-versus-mais-barato-s568081htm
61
ANEXOS
ANEXO A ndash TABELA DE CARACTERIacuteSTICAS DE ARTIGOS EXCLUIacuteDOS
Artigo Fonte Classificaccedilatildeo
inicial Motivo de Exclusatildeo
Toms Derry (20) Cochrane
Library
Possivelmente
Adequado
Natildeo eacute um estudo sobre
extracccedilatildeo de terceiros molares
Saska Scartezini
(24) LILACS
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (27) PubMed Adequado
Estudo natildeo se foca na dor poacutes-
operatoacuteria
Kubitzek Ziegler
(26) PubMed Adequado Artigo natildeo disponiacutevel
Macleod
Ashford (28) PubMed Adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (29) PubMed
Possivelmente
adequado Artigo natildeo disponiacutevel
Chopra Rehan
(30) PubMed
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Dolci Ripari (31) PubMed Possivelmente
adequado Artigo natildeo disponiacutevel
Medve Wang
(34) PubMed
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (35) PubMed
Possivelmente
adequado Artigo natildeo disponiacutevel
62
ANEXO B ndash ARTIGOS INCLUIacuteDOS EM FORMATO
INTEGRALi
i Nota os seguintes artigos estatildeo paginados fora do contexto deste trabalho de acordo com a sua
paginaccedilatildeo original
Paracetamol for pain relief after surgical removal of lower
wisdom teeth (Review)
Weil K Hooper L Afzal Z Esposito M Worthington HV van Wijk A Coulthard P
This is a reprint of a Cochrane review prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2008 Issue 4
httpwwwthecochranelibrarycom
Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
T A B L E O F C O N T E N T S
1HEADER
1ABSTRACT
2PLAIN LANGUAGE SUMMARY
2BACKGROUND
3OBJECTIVES
3METHODS
5RESULTS
8DISCUSSION
9AUTHORSrsquo CONCLUSIONS
9ACKNOWLEDGEMENTS
10REFERENCES
13CHARACTERISTICS OF STUDIES
30DATA AND ANALYSES
Analysis 11 Comparison 1 50 pain relief using pain relief measures Outcome 1 Paracetamol versus placebo number of
people with at least 50 pain relief at 4 hours 31
Analysis 12 Comparison 1 50 pain relief using pain relief measures Outcome 2 Paracetamol versus placebo number of
people with at least 50 pain relief at 6 hours 33
Analysis 21 Comparison 2 50 pain relief using pain intensity measures Outcome 1 Paracetamol versus placebo number
of people with at least 50 pain relief at 4 hours 34
Analysis 22 Comparison 2 50 pain relief using pain intensity measures Outcome 2 Paracetamol versus placebo number
of people with at least 50 pain relief at 6 hours 35
Analysis 31 Comparison 3 Number of people with adverse events Outcome 1 Number of patients with adverse events
paracetamol versus placebo 37
38ADDITIONAL TABLES
42APPENDICES
43WHATrsquoS NEW
43HISTORY
43CONTRIBUTIONS OF AUTHORS
43DECLARATIONS OF INTEREST
44SOURCES OF SUPPORT
44INDEX TERMS
iParacetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
[Intervention Review]
Paracetamol for pain relief after surgical removal of lowerwisdom teeth
Kiaran Weil1 Lee Hooper2 Zahid Afzal3 Marco Esposito1 Helen V Worthington4 Arjen van Wijk5 Paul Coulthard1
1Department of Oral and Maxillofacial Surgery School of Dentistry The University of Manchester Manchester UK 2School of
Medicine Health Policy amp Practice University of East Anglia Norwich UK 3Oral and Maxillofacial Surgery City Hospital Birming-
ham UK 4Cochrane Oral Health Group MANDEC School of Dentistry The University of Manchester Manchester UK 5Social
Dentistry and Behavioural Sciences ACTA Amsterdam Netherlands
Contact address Kiaran Weil Department of Oral and Maxillofacial Surgery School of Dentistry The University of Manchester
Higher Cambridge Street Manchester M15 6FH UK kiaran_weilhotmailcom
Editorial group Cochrane Oral Health Group
Publication status and date Edited (no change to conclusions) published in Issue 4 2008
Review content assessed as up-to-date 21 May 2007
Citation Weil K Hooper L Afzal Z Esposito M Worthington HV van Wijk A Coulthard P Paracetamol for pain relief af-
ter surgical removal of lower wisdom teeth Cochrane Database of Systematic Reviews 2007 Issue 3 Art No CD004487 DOI
10100214651858CD004487pub2
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Paracetamol has been commonly used for the relief of postoperative pain following oral surgery In this review we investigated the
optimal dose of paracetamol and the optimal time for drug administration to provide pain relief taking into account the side effects
of different doses of the drug This will inform dentists and their patients of the best strategy for pain relief after the surgical removal
of wisdom teeth
Objectives
To assess the beneficial and harmful effects of paracetamol for pain relief after surgical removal of lower wisdom teeth compared to
placebo at different doses and administered postoperatively
Search strategy
We searched the Cochrane Oral Health Grouprsquos Trials Register the Cochrane Pain Palliative and Supportive Care Grouprsquos Trials Register
CENTRAL MEDLINE EMBASE and the Current Controlled Trials Register Handsearching included several dental journals We
checked the bibliographies of relevant clinical trials and review articles for studies outside the handsearched journals We wrote to
authors of the identified randomised controlled trials (RCTs) to manufacturers of analgesic pharmaceuticals we searched personal
references in an attempt to identify unpublished or ongoing RCTs No language restriction was applied The last electronic search was
conducted on 24th August 2006
Selection criteria
Randomised parallel group placebo controlled double blind clinical trials of paracetamol for acute pain following third molar surgery
Data collection and analysis
All trials identified were scanned independently and in duplicate by two review authors any disagreements were resolved by discussion
or if necessary a third review author was consulted The proportion of patients with at least 50 pain relief was calculated for both
paracetamol and placebo The number of patients experiencing adverse events andor the total number of adverse events reported were
analysed
1Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Main results
Twenty-one trials met the inclusion criteria A total of 2048 patients were initially enrolled in the trials (1148 received paracetamol
and 892 the placebo) and of these 1968 (96) were included in the meta-analysis (1133 received paracetamol and 835 the placebo)
Paracetamol provided a statistically significant benefit when compared with placebo for pain relief and pain intensity at both 4 and 6
hours Most studies were found to have moderate risk of bias with poorly reported allocation concealment being the main problem
Risk ratio values for pain relief at 4 hours 285 (95 confidence interval (CI) 189 to 429) and at 6 hours 332 (95 CI 188 to 587)
A statistically significant benefit was also found between up to 1000 mg and 1000 mg doses the higher the dose giving greater benefit
for each measure at both time points There was no statistically significant difference between the number of patients who reported
adverse events overall this being 19 in the paracetamol group and 16 in the placebo group
Authorsrsquo conclusions
Paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom teeth
P L A I N L A N G U A G E S U M M A R Y
Paracetamol for pain relief after surgical removal of lower wisdom teeth
The surgical removal of wisdom teeth (third molars) is the most commonly performed surgical procedure undertaken in oral surgery
practice Postoperative complications may include swelling bruising and limited mouth opening but patients are most often concerned
about postoperative pain which may be severe Paracetamol is effective in relieving pain with a low incidence of adverse effects It is one
of the most commonly used analgesics and is widely available without prescription around the world In this review we investigated the
optimal dose of paracetamol and the optimal time for drug administration to provide pain relief after the surgical removal of wisdom
teeth The side effects of different doses of the drug were also explored
Twenty-one trials (with over 2000 participants) were included Paracetamol provided a statistically significant benefit when compared
with placebo for pain relief at both 4 and 6 hours after taking the drug It is most effective at 1000 mg dose and can be taken at six
hourly intervals without compromising safety There was no statistically significant difference between the number of patients who
reported adverse events overall this being 19 in the paracetamol group and 16 in the placebo group It should be noted that most
of the studies were found to have some limitations mainly due to poor reporting of information However the review concludes that
paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom teeth
B A C K G R O U N D
The surgical removal of wisdom teeth is the most commonly per-
formed surgical procedure undertaken in oral surgery practice
Postoperative complications may include swelling bruising and
limited mouth opening but patients are most often concerned
about postoperative pain which may be severe The pain ex-
perienced after oral surgery is a validated and widely used pain
model for the clinical evaluation of analgesic efficacy (Cooper
1976) Tissue damage produced during surgery releases chemicals
that initiate inflammatory pain by activating and sensitising nerve
fibre receptors (Loeser 1999) Chemicals include bradykinin
prostaglandins serotonin and histamine (Dray 1997)
Paracetamol (acetaminophen) is a nonopioid analgesic possessing
antipyretic activity and is effective in relieving pain with a low in-
cidence of adverse effects (Moore 1998) It is one of the most com-
monly used analgesics and is widely available without prescription
around the world Paracetamol is often grouped with the nons-
teroidal anti-inflammatory drug (NSAID) family however it is
considered only to have relatively weak anti-inflammatory activity
(Rang 2003) NSAIDs are assumed largely to produce their anal-
gesia as a result of the inhibition of prostaglandin production by
the enzyme cyclo-oxygenase (Malmberg 1992) The mechanism
of action has not been fully understood Among several theories
it has been suggested that paracetamol is a selective inhibitor of
the newly described COX-3 enzyme a cyclo-oxygenase-1 variant
in the central nervous system This inhibition could represent a
primary central mechanism by which paracetamol decreases pain
and possibly fever (Chandrasekharan 2002) Major evidence has
2Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
been accumulated showing that paracetamol inhibits cyclo-oxy-
genase by reducing the higher oxidative state of the cyclo-oxyge-
nase enzyme by reducing oxygen radical co-substrates (Aronoff
2006) Paracetamol has been shown to be an effective analgesic in
the control of postoperative dental pain in a number of clinical
trials (Bentley 1987 Kiersch 1994 Mehlisch 1990) Pain inten-
sity following third molar surgery has been suggested to reach its
maximum between 3 to 5 hours following surgery (Fisher 1988
Seymour 1985) and therefore this pain model is used to test the
efficacy of a single analgesic dose
A recent systematic review (Barden J 2004) has looked at the ef-
ficacy and safety of paracetamol for postoperative pain manage-
ment and has included the findings of studies involving a wide
variety of types of surgery such as gynaecology surgery abdomi-
nal surgery orthopaedic surgery amongst others including the re-
moval of wisdom teeth There is some debate as to whether dental
pain is different from other pain It has been suggested that the
effect of some analgesics including tramadol were worse for dental
pain than for other types of postsurgical pain (Moore 1997)
In this review we investigated the optimal dose of paracetamol and
the optimal time for drug administration to provide pain relief
taking into account the side effects of different doses of the drug
This will inform dentists and their patients of the best strategy for
best pain relief after the surgical removal of wisdom teeth
O B J E C T I V E S
To assess the beneficial and harmful effects of paracetamol for
pain relief after surgical removal of lower wisdom teeth compared
to placebo at different doses and administered preoperatively or
postoperatively
Primary
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between paracetamol and placebo for pain
relief in patients requiring surgical removal of a lower wisdom
tooth or teeth against the alternative hypothesis of a difference
Secondary
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between different doses of paracetamol for
pain relief in patients requiring surgical removal of a lower
wisdom tooth or teeth against the alternative hypothesis of a
difference
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between different times of administration of
paracetamol for pain relief in patients requiring surgical removal
of a lower wisdom tooth or teeth against the alternative
hypothesis of a difference
M E T H O D S
Criteria for considering studies for this review
Types of studies
All randomised controlled double blind clinical trials
Types of participants
Patients of all health states who required the surgical removal of
a lower wisdom tooth and who had at least had a baseline pain
intensity of moderate to severe pain Patients who also required
removal of an additional tooth or teeth were included Surgery
was undertaken under local anaesthesia intravenous sedation or
general anaesthesia Patients taking concurrent analgesia were ex-
cluded
Types of interventions
Efficacy
bull Paracetamol given as a single dose by mouth in any dose
and in any formulation (for example immediate or slow release)
regardless of when the single dose was given (for example
preoperatively or postoperatively)
Side effects
In order to investigate side effects more thoroughly we included
both single and multiple dose studies
bull Paracetamol given up to 7 days by mouth in any dose and
in any formulation (for example immediate or slow release)
regardless of when the first dose was given (for example
preoperatively or postoperatively)
Types of outcome measures
bull Pain intensity (visual analogue scale (VAS) categorical
verbal rating verbal numerical scale global subjective efficacy
ratings and other categorical rating scales)
bull Pain relief (VAS categorical verbal rating verbal numerical
scale global subjective efficacy ratings and other categorical
rating scales) and derived pain relief outcomes extracted will be
3Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
total pain relief (TOTPAR) summed pain intensity difference
(SPID) over 4 and 6 hours
bull Side effects (for example hepatic and renal) (binary)
Search methods for identification of studies
To identify studies for inclusion or consideration in this review a
detailed search strategy was developed for each database searched
These were based on the search strategy developed for MEDLINE
but revised appropriately for each database The search strategy
combined a sensitive search strategy for randomised controlled
trials (RCTs) revised from phases 1 and 2 of the Cochrane Sensi-
tive Search Strategy for RCTs (as published in Appendix 5b in the
Cochrane Handbook for Systematic Reviews of Interventions 426
(updated September 2006)) The subject search used a combina-
tion of controlled vocabulary and free text terms based on the
search strategy for searching CENTRAL (see Appendix 1)
Databases to be searched
The Cochrane Oral Health Grouprsquos Trials Register (to 24th August
2006)
The Cochrane Central Register of Controlled Trials (CENTRAL)
(The Cochrane Library 2006 Issue 3)
The Cochrane Pain Palliative and Supportive Care Grouprsquos Trials
Register (to 24th August 2006)
MEDLINE (1966 to 24th August 2006)
EMBASE (1980 to 25th August 2006)
Current Controlled Trials Register (wwwcontrolled-trialscom)
(to 24th August 2006)
The bibliographies of papers and review articles were checked for
studies outside the handsearched journals Personal references were
also searched
Language
There were no language restrictions and where necessary transla-
tion into the English language of relevant studies was conducted
Unpublished studies
Authors of RCTs identified were written to in order to obtain
further information about the trial and to attempt to identify
unpublished or ongoing studies We also wrote to manufacturers
of analgesic pharmaceuticals
Handsearching
Several journals relevant to this review were handsearched as part
of the Cochrane Oral Health Grouprsquos ongoing journal hand-
searching programme The list of the dental journals hand-
searched by The Cochrane Collaboration can be found at http
wwwohgcochraneorg
Data collection and analysis
The titles and abstracts (when available) of all reports identified
were scanned independently and in duplicate by two review au-
thors For studies appearing to meet the inclusion criteria or for
which there were insufficient data in the title and abstract to make
a clear decision the full report was obtained and assessed indepen-
dently and in duplicate by two review authors to establish whether
the studies met the inclusion criteria or not Disagreements were
resolved by discussion Where resolution was not possible a third
review author was consulted All studies meeting the inclusion
criteria then underwent quality assessment and data extracted
Studies rejected at this or subsequent stages were recorded in the
Characteristics of excluded studies table and reasons for exclusion
were recorded
Quality assessment
The quality assessment of the included trials was undertaken inde-
pendently and in duplicate by two review authors based on what
is written in the articles
Only double blind trials were included in the review so blinding
was not included in the quality assessment
Two main quality criteria were examined
(1) Allocation concealment recorded as
(A) Adequate -2 points
(B) Unclear - 1 point
(C) Inadequate - 0 points
(2) Completeness of follow up (is there a clear explanation for
withdrawals and drop outs in each treatment group) assessed as
(A) Yes - 1 point
(B) No - 0 points
The agreement for the quality criteria between assessors was de-
termined by Kappa statistics
After taking into account the additional information provided by
the authors of the trials studies were grouped into the following
categories
(A) Low risk of bias - 3 points (plausible bias unlikely to seriously
alter the results) if all criteria were met
(B) Moderate or high risk of bias - 0 to 2 points Moderate risk
of bias - plausible bias that raises some doubt about the results if
one or more criteria are partly met (for example when authors
responded that they had made some attempts to conceal the al-
location of patients to give an explanation for withdrawals but
these attempts were not judged to be ideal these criteria were cat-
egorised as rsquopartlyrsquo) High risk of bias - plausible bias that seriously
weakens confidence in the results if one or more criteria were not
met as described in the Cochrane Handbook for Systematic Reviews
of Interventions 426
We also reported whether the authors of included trials have con-
ducted a sample size calculation
4Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data extraction
Data were extracted by two review authors independently and
in duplicate using specially designed data extraction forms Any
disagreement was discussed and a third review author consulted
where necessary Authors were contacted for clarification of miss-
ing information Data were excluded until further clarification was
available if agreement could not be reached
For each trial the following data were recorded
bull Year of publication country of origin setting and source of
study funding
bull Details of the participants including demographic
characteristics and criteria for inclusion
bull Details on the study design (parallel group or cross-over
design)
bull Details on the type of intervention
bull Details of the outcomes reported including method of
assessment and time intervals
Data synthesis
From the mean total pain relief (TOTPAR) or summed pain in-
tensity difference (SPID) pain indices reported we computed a
dichotomous outcome variable for the number of patients with
at least 50 pain relief according to the methods outlined in a
Cochrane review (Collins 1999) For each of the three objectives
we examined the appropriateness of different continuous outcome
measurements and these were meta-analysed and reported in the
final review
For dichotomous outcomes the estimate of an intervention was
expressed as risk ratios together with 95 confidence intervals
For continuous outcomes mean differences and 95 confidence
intervals were used to summarise the data for each trial
Clinical heterogeneity was assessed by examining the types of par-
ticipants interventions and outcomes in each study Meta-analyses
were conducted only with studies of similar comparisons report-
ing the same outcome measures Risk ratios were used to combine
dichotomous data and mean differences for continuous data us-
ing random-effects models The significance of any discrepancies
in the estimates of the treatment effects from the different trials
was assessed by means of Cochranrsquos test for heterogeneity and any
heterogeneity investigated
Where both visual analogue scale (VAS) and categorical scales were
used to measure pain intensity or pain relief or both the categorical
data were used in the meta-analysis as this was the most frequently
used scale
Subgroup analyses
Subgroup analyses were planned for studies
bull Where patients underwent surgery with local anaesthesia
alone local anaesthesia and intravenous sedation general
anaesthesia alone and general anaesthesia with local anaesthetic
bull Where different types of formulation of paracetamol were
used for instance immediate release versus slow release
bull Where different doses of paracetamol were used (1000 mg
or more and less than 1000 mg)
bull Where time of administration of paracetamol differs
preoperative versus postoperative
bull Where TOTPAR was calculated using pain relief measures
and pain intensity measures
The difference between studies comparing up to 1000 mg doses
with studies comparing 1000 mg or more was examined by per-
forming random-effects metaregression analyses in Stata version
90 (Stata Corporation USA) using the program Metareg
The results of the metaregressions for comparing the two dose
levels up to 1000 mg and 1000 mg or more are presented in
Additional Table 1
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
See Characteristics of included studies and Characteristics of
excluded studies tables
Characteristics of the trial setting and investigators
Of the 67 eligible trials 46 were excluded as shown in the ex-
cluded studies section Of the 21 included studies one was con-
ducted in Denmark (Moller 2000) two in Germany (Kubitzek
2003 Lehnert 1990) one in Italy (Dolci 1994) one in Nor-
way (Skoglund 1991) two in Puerto Rico (Olson 2001 Sunshine
1986) one in Thailand (Vattaraphudej 1986) two in the United
Kingdom (Seymour 1996 Seymour 2003) and 11 in the United
States of America (Cooper 1980 Cooper 1981 Cooper 1988
Cooper 1998 Dionne 1994 Forbes 1984b Forbes 1989 Forbes
1990 Hersh 2000 Kiersch 1994 Mehlisch 1995) Six trials
were conducted at university clinics (Cooper 1998 Hersh 2000
Moller 2000 Olson 2001 Sunshine 1986 Vattaraphudej 1986)
five at private practices (Dionne 1994 Forbes 1984b Forbes
1989 Forbes 1990 Kubitzek 2003) seven did not state a set-
ting (Cooper 1981 Dolci 1994 Kiersch 1994 Mehlisch 1995
Seymour 1996 Seymour 2003 Skoglund 1991) One reported a
single site (Cooper 1988) two reported two sites (Forbes 1989
Seymour 2003) and six specifically stated outpatients (Cooper
1980 Cooper 1988 Forbes 1989 Forbes 1990 Hersh 2000
5Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Lehnert 1990) Seventeen trials were sponsored by industry
(Cooper 1981 Cooper 1988 Cooper 1998 Dionne 1994 Forbes
1984b Forbes 1989 Forbes 1990 Hersh 2000 Kiersch 1994
Kubitzek 2003 Lehnert 1990 Mehlisch 1995 Moller 2000
Olson 2001 Seymour 2003 Skoglund 1991 Sunshine 1986)
one by a university grant (Vattaraphudej 1986) and it was unclear
as whether the remaining three trials (Cooper 1980 Dolci 1994
Seymour 1996) were sponsored but it is likely that they were from
correspondence with some of the authors
Characteristics of interventions
All included interventions were randomised parallel group and
double blind Eleven trials used doses of paracetamol of less than
1000 mg (Cooper 1980 Cooper 1981 Cooper 1988 Dionne
1994 Dolci 1994 Forbes 1984b Forbes 1989 Forbes 1990
Seymour 1996 Sunshine 1986 Vattaraphudej 1986) Eleven tri-
als used doses of 1000 mg (Cooper 1998 Hersh 2000 Kiersch
1994 Kubitzek 2003 Lehnert 1990 Mehlisch 1995 Moller
2000 Olson 2001 Seymour 1996 Seymour 2003 Skoglund
1991) One study (Seymour 1996) used both doses Seven tri-
als used paracetamol in tablet form (Dolci 1994 Forbes 1989
Kubitzek 2003 Mehlisch 1995 Moller 2000 Seymour 2003
Skoglund 1991) Seven trials used capsules (Forbes 1984b Forbes
1989 Forbes 1990 Kiersch 1994 Lehnert 1990 Sunshine 1986
Vattaraphudej 1986) Two trials used caplets (Hersh 2000 Olson
2001) and one trial used effervescent tablets (Moller 2000) Five
trials did not state what formulation was used (Cooper 1980
Cooper 1981 Cooper 1988 Cooper 1998 Dionne 1994) All
trials used placebos in the same formulation as the intervention
Characteristics of outcome measures
For all trials it was possible to calculate the number of patients
with at least 50 total pain relief (TOTPAR) at either 4 hours
6 hours or both Pain intensity was measured in all but one trial
(Kubitzek 2003) pain relief was measured in all but two trials
(Kubitzek 2003 Seymour 2003) Kubitzek 2003 gave a figure for
TOTPAR at six hours and Seymour 2003 measured pain intensity
only Fifteen trials measured pain intensity at 4 hours using a 4-
point categorical scale of 0 to 3 where 0 was no pain at all and 3
was severe pain Five trials measured pain intensity using a visual
analogue scale (VAS) of 0 to 100 mm where 0 was no pain and
100 was the worst pain imaginable Twelve trials measured pain
intensity at 6 hours using a 4-point categorical scale where 0 was
no pain and 3 was severe pain and three trials measured pain
intensity at 6 hours using a VAS of 0 to 100 mm where 0 was no
pain and 100 mm was the worst pain imaginable Sixteen trials
measured pain relief at 4 hours using a 5-point categorical scale
of 0 to 4 where 0 was none and 4 was complete pain relief two
trials measured pain relief at 4 hours using a VAS of 0 to 100 mm
in one trial 0 was none and 100 was complete relief and in the
other trial 0 was complete relief and 100 was no relief (these data
were reversed for statistical purposes) Twelve trials measured pain
relief at 6 hours using a 5-point categorical scale of 0 to 4 where
0 was none and 4 was complete pain relief two trials measured
pain relief at 6 hours using a VAS of 0 to 100 mm in one trial 0
was none and 100 was complete relief and in the other trial 0 was
complete relief and 100 was no relief (these data were reversed for
statistical purposes)
Adverse events and global assessments were recorded in most of
the trials Nineteen trials reported the number of patients with
side effects eight for doses of 1000 mg or more and 15 for doses
of less than 1000 mg Fifteen trials reported the number of adverse
events seven for doses of 1000 mg or more and eight for doses
of less than 1000 mg Fourteen trials recorded global assessment
using a 5-point categorical scale of either 0 to 4 or 1 to 5 where
0 or 1 was poor and 4 or 5 was excellent and four trials used a
4-point categorical scale of 0 to 3 where 0 was poor and 3 was
excellent
Risk of bias in included studies
Details of the quality assessment are presented in Additional Table
2 Seven out of the 21 studies reported adequate concealed al-
location for the remaining studies it was unclear Over half of
the studies (1121) gave clear explanation of withdrawals or drop
outs Taking these two factors into account only three trials were
assessed as being at low risk of bias
Effects of interventions
Comparison 1 Paracetamol versus placebo using
pain relief measurements
(Comparison 1 Outcome 11 amp Comparison 1 Outcome 12)
(Analysis 11 Analysis 12)
There are 16 studies providing pain relief measurements for com-
paring paracetamol versus placebo at 4 hours 11 at doses up to
1000 mg and 5 at doses of 1000 mg Overall there was a highly
statistically significant benefit with the paracetamol with risk ratio
(RR) values for achieving 50 pain relief for all doses of parac-
etamol for 4 hours RR 285 (95 confidence interval (CI) 189
to 429) Chi2 = 6294 degrees of freedom (df ) = 15 P lt 0001
I2 = 76 number needed to treat (to benefit) (NNT) 4 (95
CI 3 to 4) The statistically significant benefit was apparent for
both subgroups with RR for up to 1000 mg 196 (95 CI 134
to 286) Chi2 = 2644 df = 9 P = 0002 I2 = 660 NNT 4
(95 CI 3 to 5) and RR for 1000 mg 456 (95 CI 286 to
727) Chi2 = 544 df = 5 P = 036 I2 = 82 NNT 3 (95
CI 3 to 4) Although both had a statistically significant benefit
6Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
over placebo there was a statistically significant difference between
the two subgroups with an enhanced benefit for the higher doses
(metaregression P lt 0001 Additional Table 3) This subgroup
analysis explained some of the heterogeneity in the overall com-
parison however there is still some unexplained heterogeneity be-
tween the trials in the up to 1000 mg dose comparison
There are 13 studies providing pain relief measurements for com-
paring paracetamol versus placebo at 6 hours 6 doses up to 1000
mg paracetamol and 7 doses of 1000 mg paracetamol Overall
there was a highly statistically significant benefit with the parac-
etamol with RR values for 50 pain relief at 6 hours RR 332
(95 CI 188 to 587) Chi2 = 6335 df = 12 P lt 000001 I2 = 811 NNT 3 (95 CI 3 to 4) The statistically significant
benefit was apparent in both subgroups with RR for up to 1000
mg 189 (95 CI 098 to 367) Chi2 = 1445 df = 5 P = 001
I2 = 654 NNT 6 (95 CI 4 to 10) and RR for 1000 mg
421 (95 CI 297 to 598) Chi2 = 509 df = 6 P = 053 I2 =
0 NNT 3 (95 CI 2 to 3) Although both had a statistically
significant benefit over placebo there was a statistically significant
difference between the two subgroups with an enhanced benefit
for the higher doses (metaregression P lt 0001 Additional Table
3) This subgroup analysis explained some of the heterogeneity in
the overall comparison however there is still some unexplained
heterogeneity between the trials in the up to 1000 mg dose com-
parison
Comparison 2 Paracetamol versus placebo using
pain intensity difference measurements
(Comparison 2 Outcome 21 amp Comparison 2 Outcome 22)
(Analysis 21 Analysis 22)
There are 18 studies providing pain intensity measurements for
comparing paracetamol versus placebo at 4 hours 10 at doses up
to 1000 mg and 8 at doses of 1000 mg Overall there was a highly
statistically significant benefit with paracetamol with RR values
for 50 pain relief at 4 hours RR 487 (95 CI 283 to 837)
Chi2 = 4973 df = 17 P lt 00001 I2 = 658 NNT 3 (95 CI
3 to 5) The statistically significant benefit was apparent in both
subgroups with RR up to 1000 mg 433 (95 CI 219 to 858)
Chi2 = 2622 df = 9 P = 0002 I2 = 657 NNT 3 (95 CI
3 to 4) and RR for 1000 mg 646 (95 CI 234 to 1785) Chi2 = 2347 df = 7 P = 0001 I2 = 702 NNT 4 (95 CI 3
to 5) Both had a statistically significant benefit over placebo but
there was no statistically significant difference between the two
subgroups (metaregression P = 067 Additional Table 3)
There are 14 studies providing pain intensity measurements for
comparing paracetamol versus placebo at 6 hours 6 at doses up
to 1000 mg and 8 at doses of 1000 mg Overall there was a highly
statistically significant benefit with paracetamol with RR values
for 50 pain relief RR 341 (95 CI 234 to 497) Chi2 = 1823
df = 13 P = 015 I2 = 287 NNT 4 (95 CI 3 to 4) The
statistically significant benefit was apparent in both groups with
RR up to 1000 mg 267 (95 CI 146 to 490) Chi2 = 705 df
= 5 P = 022 I2 = 291 NNT 5 (95 CI 3 to 7) and RR for
1000 mg 396 (95 CI 252 to 623) Chi2 = 863 df = 7 P =
028 I2 = 189 NNT 3 (95 CI 3 to 4) Both had a statisti-
cally significant benefit over placebo but there was no statistically
significant difference between the two subgroups (metaregression
P = 015 Additional Table 3)
Comparison 3 Number of patients with adverse
events for paracetamol versus placebo
(Comparison 3 Outcome 31) (Analysis 31)
There are 17 studies that reported the number of patients with
adverse events for paracetamol versus placebo 9 studies used less
than 1000 mg and 8 studies used 1000 mg There was no statisti-
cally significant difference in any group For all doses of paraceta-
mol the RR for an adverse event RR 119 (95 CI 090 to 157)
Chi2 = 2073 df = 15 P = 015 I2 = 276 number needed to
treat to harm (NNTH) 33 (95 CI 143 to infinity) For doses of
less than 1000 mg RR 125 (95 CI 069 to 225) Chi2 = 906
df = 7 P = 025 I2 = 228 NNTH 33 (95 CI 143 to infinity)
For 1000 mg paracetamol RR 116 (95 CI 084 to 160) Chi2
= 1096 df = 7 P = 014 I2 = 362 NNTH 33 (95 CI 125
to infinity)
Subgroup analyses
Where patients underwent surgery with local anaesthesia
alone local anaesthesia and intravenous sedation general
anaesthesia alone and general anaesthesia with local
anaesthetic
When the data were reviewed it was not possible to do a meta-anal-
ysis Of the 21 included studies 7 did not state what anaesthesia
was used 7 used combinations of anaesthesia but were unclear in
reporting which patients received which anaesthesia 4 used local
anaesthetic only and 3 used general anaesthetic only
Where different types of formulation of paracetamol were
used (immediate release versus slow release)
Most included studies did not report on the formulation other
than to say whether it was tablets capsules or caplets Only one
7Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
paper indicated that their study used effervescent tablets (Moller
2000) and their results showed that effervescent tablets gave a faster
onset of pain relief Median value for time to onset of analgesia
was 20 minutes in the effervescent group and 45 minutes in the
tablet group and time to meaningful pain relief was 45 minutes
in the effervescent group and 1 hour in the tablet group However
at the end of a 4-hour period pain relief was better in the tablet
group (44) than the effervescent group (37)
Where different doses of paracetamol were used (1000 mg
or more and less than 1000 mg)
This meta-analysis was conducted 11 studies used doses of 1000
mg or more and 11 studies used doses of less than 1000 mg
(Seymour 1996 used both doses)
NNT for lt 1000 mg of paracetamol is 4 (95 CI 3 to 5) at
4 hours and 6 (95 CI 4 to 10) at 6 hours (using pain relief
measurements)
NNT for lt 1000 mg of paracetamol is 3 (95 CI 3 to 4) at 4 hours
and 5 (95 CI 3 to 7) at 6 hours (using intesity measurements)
NNT for 1000 mg of paracetamol is 3 (95 CI 3 to 4) at 4 hours
and 3 (95 CI 2 to 3) at 6 hours (using pain relief measurements)
NNT for 1000 mg of paracetamol is 4 (95 CI 3 to 5) at 4 hours
and 3 (95 CI 3 to 4) at 6 hours (using intensity measurements)
Where time of administration of paracetamol differs
preoperative versus postoperative
No included study used a preoperative dose as the patients did
not reach moderate or severe pain before the intervention
Where total pain relief (TOTPAR) was calculated using pain
relief measures and pain intensity measures
This meta-analysis was undertaken where the relevant data were
available 16 studies had pain relief data and 17 studies had pain
intensity data
NNT using pain relief scales for lt 1000 mg of paracetamol is 4
(95 CI 3 to 5) at 4 hours and 6 (95 CI 4 to 10) at 6 hours
NNT using pain intensity scales for lt 1000 mg of paracetamol is
3 (95 CI 3 to 4) at 4 hours and 5 (95 CI 3 to 7) at 6 hours
NNT using pain relief scales for 1000 mg of paracetamol is 3 (95
CI 3 to 4) at 4 hours and 3 (95 CI 2 to 3) at 6 hours
NNT using pain intensity scales for 1000 mg of paracetamol is 4
(95 CI 3 to 5) at 4 hours and 3 (95 CI 3 to 4) at 6 hours
D I S C U S S I O N
The results show paracetamol to be an effective analgesia for use
following third molar surgery The number needed to treat (to
benefit) (NNTs) and number needed to treat to harm (NNTHs)
support the use of 1000 mg as an optimal dose It is effective over
both 4 and 6 hours In considering the use of pain relief or pain
intensity difference as a measure of efficacy it was of interest that
metaregression showed that pain relief scales showed a statistically
significant difference for increased dose and pain intensity did
not It is acknowledged that this review only considered single
dose studies when considering efficacy multidosed studies may be
considered when updating the review The NNTs and NNTHs
found in this review are similar to those recorded by a systematic
review (Barden J 2004) where they investigated paracetamol for
pain involving various types of surgery This would confirm yet
again the value of the third molar pain model showing that dental
pain is comparable with pain from other sources The implemen-
tation of NICE (National Institute for Health and Clinical Excel-
lence) Guidelines for removal of third molars has led to a decrease
in the performance of this surgery which may have an adverse
effect on the number of trials able to use the third molar model
In the United States of America such guidelines have not yet been
adopted It is of interest that in striving to provide evidence based
treatment the opportunity for research using the third molar pain
model may be adversely affected
The data available for adverse events show that NNTH for lt 1000
mg of paracetamol is 33 (143 to infinity) for 1000 mg of parac-
etamol is 33 (125 to infinity) and for all doses 33 (143 to infin-
ity) suggesting it is an extremely safe drug Only one severe ad-
verse event was recorded by any researchers and that was a severe
headache (Olson 2001) two other participants stopped taking
paracetamol because of vomiting However there was a high degree
of inconsistency across the trials in the way that adverse events were
recorded raising the concern that only adverse events considered
by the researchers to be attributable to paracetamol were recorded
with some trials recording many AEs and some reporting none
The diverse way in which adverse events were recorded led to there
being over 20 categories of adverse events The main categories
are shown in Additional Table 4 Of interest are adverse events
where placebo scored more highly than paracetamol which could
suggest that paracetamol may possibly have a beneficial effect eg
dry socket but this would require further investigation As all pa-
tients had surgery and various combinations of local anaesthesia
general anaesthesia and sedation making it difficult to ascertain
which effects are directly related to the intervention However the
results strongly support the use of paracetamol in doses up to 1000
mg as a safe effective analgesia
8Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
The efficacy of paracetamol decreases with times and the recom-
mended interval between doses is 8 hours which would suggest
there may be some benefit in a slow release formulation None of
the studies in this trial used a slow release formulation but a trial
(Coulthard 2001) compared sustained release and standard release
formulations of paracetamol and found that the sustained release
was statistically significantly more effective at 6 and 8 hours with
no loss of efficacy at 4 hours Safety for both formulations was
comparable making sustained release paracetamol a safe and ef-
fective choice
The methodology used in the included trials was generally good
This resulted in a large number of participants being included
in this meta-analysis while using only double blind randomised
trials The included trials gave a strong consistent result Many
of the trials were done by researchers with extensive experience
in the field of pain research whose methods have been refined
with experience A large proportion of the trials were done in the
United States and were mostly funded by pharmaceutical com-
panies This seems to be reflected in the methodology However
quality assessment showed there were only three trials with a low
risk of bias and 18 with moderatehigh risk This was mainly the
result of unreported allocation concealment methods In speaking
to some of the authors it is highly likely that the allocation con-
cealment was good in all the trials but that the details were not
well reported Most trials were sponsored by pharmaceutical com-
panies who supplied paracetamol and placebo in identical appear-
ance The reporting of withdrawals and drop outs was sporadic
and even when numbers were cited it was not always clear to which
treatment group the participant had been originally allocated
Mean global assessments (Additional Table 5 Table 6 Table 7
Table 8) all showed higher scores for paracetamol than placebo
It is of interest that despite achieving 50 pain relief participants
did not record 50 on a global assessment scale This again raises
the question of the value of the instruments used to measure the
efficacy of an intervention None of the trials relied on global
assessments as their only measure of efficacy but this information
could be of value to other researchers It raises interesting questions
concerning patientrsquos expectations and the difficulties associated
with quantifying such a subjective experience
A lot of valuable information was gathered incidental to the main
findings in most of the trials So though the topic was concerned
with the use of paracetamol for pain information collected in
many of the trials shed valuable light on subjects such as side effects
measuring instruments and methodology Further appraisal of
the multidisciplinary approach to research a broader view of data
collection and a more accurate reporting of data already collected
could be extremely valuable in the future It would allow research
to be more widely used in various meta-analyses Data from areas
seemingly unrelated to the original null hypothesis eg comparison
of pain relief and pain intensity as a measuring tool adverse event
reporting the significance of global assessments etc could be more
readily available If the third molar trial population does decrease
it would be advantageous to collect as much data as possible from
any trial being undertaken
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
Paracetamol (acetaminophen) is an effective drug to use for post-
operative pain following oral surgery and the reporting of adverse
events shows it to be a safe drug (number needed to treat (to ben-
efit) (NNT) is 3 for 1000 mg of paracetamol at 6 hours number
needed to treat to harm (NNTH) 33) It is most effective at 1000
mg dose and can be taken at six hourly intervals without compro-
mising safety It could be considered more readily by dentist and
patients both as a first choice analgesic or to be taken alternately
with doses of other analgesics such as nonsteroidal anti-inflamma-
tory drugs (NSAIDS)
Implications for research
There is a large body of research in this area and further research
other than as a comparison seems unnecessary However in one
trial (Moller 2000) it was found that an effervescent formulation
appeared to have a faster onset of pain relief which would be
beneficial to patients who are looking for a rapid onset of relief
It may be helpful to undertake some research to confirm these
findings The use of pain relief and pain intensity difference as a
measure of pain relief may be another area for further investigation
It is valuable to have NNTNNTH as a baseline for comparison
with other analgesics Maximizing the third molar pain model
population by multidisciplinary research is another area of interest
highlighted by this review
A C K N O W L E D G E M E N T S
We wish to thank Sylvia Bickley (Cochrane Oral Health Group)
for her assistance with literature searching and Luisa Fernandez
Mauleffinch (Cochrane Oral Health Group) for her help with the
preparation of this review We would also like to thank the follow-
ing referees who reviewed this work at various stages Barry El-
liott Cole Mike Hill Kimito Yamashiro and Lasse Skoglund We
are grateful to Stephen Cooper Donald Mehlisch Philip Moller
Alberto Umile for providing information on their trials and to
Prisana Pripatnanont for translation and information
9Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Cooper 1980 published data only
Cooper SA Precheur H Rauch D Rosenheck A Ladov M
Engel J Evaluation of oxycodone and acetaminophen in
treatment of postoperative dental pain Oral Surgery Oral
Medicine and Oral Pathology 198050(6)496ndash501
Cooper 1981 published data only
Cooper SA Breen JF Giuliani RL The relative efficacy of
indoprofen with opiod-analgesic combinations Journal of
Oral Surgery 198139(1)21ndash5
Cooper 1988 published data only
Cooper SA Firestein A Cohn P Double-blind comparison
of meclofenamate sodium with acetaminophen
acetaminophen with codeine and placebo for relief of
postsurgical dental pain The Journal of Clinical Dentistry
19881(2)31ndash4
Cooper 1998 published data only
Cooper SA Reynolds DC Reynolds B Hersh EV Analgesic
efficacy and safety of (R)- ketoprofen in postoperative dental
pain Journal of Clinical Pharmacology 199838(2 Suppl)
11Sndash18S
Dionne 1994 published data only
Dionne RA Snyder J Hargreaves KM Analgesic efficacy
of flurbiprofen in comparison with acetaminophen
acetaminophen plus codeine and placebo after impacted
third molar removal Journal of Oral and Maxillofacial
Surgery 199452(9)919ndash24
Dolci 1994 published data only
Dolci G Ripari M Pacifici L Umile A Evaluation of
piroxicam-beta-cyclodextrin piroxicam paracetamol and
placebo in post-operative oral surgery pain International
Journal of Clinical Pharmacology Research 199414(5-6)
185ndash91
Forbes 1984b published data only
Forbes JA Barkaszi BA Ragland RN Hankle JJ
Analgesic effect of acetaminophen phenyltoloxamine
and their combination in postoperative oral surgery pain
Pharmacotherapy 19844(4)221ndash6
Forbes 1989 published data only
Forbes JA Butterworth GA Burchfield WH Yorio
CC Selinger LR Rosenmertz SK et alEvaluation of
flurbiprofen acetaminophen an acetaminophen-codeine
combination and placebo in postoperative oral surgery
pain Pharmacotherapy 19899(5)322ndash30
Forbes 1990 published data only
Forbes JA Kehm CJ Grodin CD Beaver WT Evaluation
of ketorolac ibuprofen acetaminophen and an
acetaminophen-codeine combination in postoperative
oral surgery pain Pharmacotherapy 199010(6(Pt 2)))
94Sndash105S
Hersh 2000 published data only
Hersh EV Levin LM Cooper SA Doyle G Waksman J
Wedell D et alIbuprofen liquigel for oral surgery pain
Clinical Therapeutics 200022(11)1306ndash18
Kiersch 1994 published data only
Kiersch TA Halladay SC Hormel PC A single-
dose double-blind comparison of naproxen sodium
acetaminophen and placebo in postoperative dental pain
Clinical Therapeutics 199416(3)394ndash404
Kubitzek 2003 published data only
Kubitzek F Ziegler G Gold MS Liu JM Ionescu E
Analgesic efficacy of low-dose diclofenac versus paracetamol
and placebo in postoperative dental pain Journal of
Orofacial Pain 200317(3)237ndash44
Lehnert 1990 published data only
Lehnert S Reuther J Wahl G Barthel K [The efficacy of
paracetamol (Tylenol) and acetyl salicylic acid (Aspirin)
in treating postoperative pain] Deutsche Zahnarztliche
Zeitschrift 199045(1)23ndash6
Mehlisch 1995 published data only
Mehlisch DR Jasper RD Brown P Korn SH McCarroll K
Murakami AA Comparative study of ibuprofen lysine and
acetaminophen in patients with postoperative dental pain
Clinical Therapeutics 199517(5)852ndash60
Moller 2000 published data only
Moller PL Norholt SE Ganry HE Insuasty JH Vincent
FG Skoglund LA et alTime of onset of analgesia and
analgesic efficacy of effervescent acetaminophen 1000
mg compared to tablet acetominophen 1000 mg in
postoperative dental pain a single-dose double-blind
randomized placebo-controlled study Journal of Clinical
Pharmacology 200040(4)370ndash8
Olson 2001 published data only
Olson NZ Otero AM Marrero I Tirado S Cooper S
Doyle G et alOnset of analgesia for liquigel ibuprofen
400 mg acetaminophen 1000 mg ketoprofen 25 mg
and placebo in the treatment of postoperative dental pain
Journal of Clinical Pharmacology 200141(11)1238ndash47
Seymour 1996 published data only
Seymour RA Kelly PJ Hawkesford JE The efficacy
of ketoprofen and paracetamol (acetaminopen) in
postoperative pain after third molar surgery British Journal
of Clinical Pharmacology 199641(6)581ndash5
Seymour 2003 published data only
Seymour RA Hawkesford JE Sykes J Stillings M Hill
CM An investigation into the comparative efficacy of
soluble aspirin and solid paracetamol in postoperative pain
after third molar surgery British Dental Journal 2003194
(3)153ndash7
Skoglund 1991 published data only
Skoglund LA Skjelbred P Fyllingen G Analgesic efficacy
of acetaminophen 1000 mg acetaminophen 2000 mg and
the combination of acetaminophen 1000 mg and codeine
10Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
phosphate 60 mg versus placebo in acute postoperative
pain Pharmacotherapy 199111(5)364ndash9
Sunshine 1986 published data only
Sunshine A Marrero I Olson N McCormick N Laska
EM Comparative study of flurbiprofen zomepirac sodium
acetaminophen plus codeine and acetaminophen for the
relief of postsurgical dental pain The American Journal of
Medicine 198680(3A)50ndash4
Vattaraphudej 1986 published data only
Vattaraphudej T Thongnoppakao P Koukongviriyapan V
[Comparison of the efficacy of analgesics in pain after oral
surgery] The Journal of the Dental Association of Thailand
198636(6)198ndash206
References to studies excluded from this review
Adame 1979 published data only
Adame C et alPostoperative development of inflammation
after extraction of impacted third molar as a model
for clinical assessment of anti-inflammatory drugs I
Preliminary report Boletin de Estudios Medicos y Biologicos
197930(8)308ndash9
Barden J 2004 published data only
Barden J Edwards J Moore A McQuay H Single dose
oral paracetamol (acetaminophen) for postoperative pain
Cochrane Database of Systematic Reviews 2004 Issue 1
[DOI DOI 10100214651858CD004602]
Becker 1990 published data only
Becker J Beckmann J Bertelt C Gundert-Remy U
Rohmel J Ohlendorf D [Double blind biometric study on
postoperative effects of analgesics] Deutsche Zahnarztliche
Zeitschrift 199045(1)36ndash8
Bentley 1987 published data only
Bentley KC Head TW The additive analgesic efficacy of
acetaminophen 1000 mg and codeine 60 mg in dental
pain Clinical Pharmacology and Therapeutics 198742(6)
634ndash40
Breivik 1998 published data only
Breivik EK Bjornsson GA Variation in surgical trauma and
baseline pain intensity effects on assay sensitivity of an
analgesic trial European Journal of Oral Sciences 1998106
(4)844ndash52
Cooper 1986 published data only
Cooper SA Erlichman MC Mardirossian G Double-
blind comparison of an acetaminophen-codeine-caffeine
combination in oral surgery pain Anesthesia Progress 1986
33(3)139ndash42
Cooper 1989 published data only
Cooper SA Schachtel BP Goldman E Gelb S Cohn P
Ibuprofen and acetaminophen in the relief of acute pain
a randomized double-blind placebo-controlled study
Journal of Clinical Pharmacology 198929(11)1026ndash30
Cooper 1991 published data only
Cooper SA Kupperman A The analgesic efficacy of
flurbiprofen compared to acetaminophen with codeine The
Journal of Clinical Dentistry 19912(3)70ndash4
Dionne 1983 (1) published data only
Dionne RA Campbell RA Cooper SA Hall DL
Buckingham B Suppression of postoperative pain by
preoperative administration of ibuprofen in comparison to
placebo acetaminophen and acetaminophen plus codeine
Journal of Clinical Pharmacology 198323(1)37ndash43
Dionne 1983 (2) published data only
Dionne RA Sisk AL Fox PC Wirdzek PR Gracely
RH Dubner R Suppression of postoperative pain by
preoperative adminsitration of flurbiprofen in comparison
to acetominophen and oxycodone plus acetominophen
Current Therapeutic Research 198334(1)15ndash29
Dionne 1986 published data only
Dionne RA Suppression of dental pain by the preoperative
administration of flurbiprofen The American Journal of
Medicine 198680(3A)41ndash9
Dolci 1993 published data only
Dolci G Ripari M Pacifici L Umile A [Analgesic efficacy
and the tolerance for piroxicam-beta-cyclodextrin compared
to piroxicam paracetamol and placebo in the treatment of
postextraction dental pain] Minerva Stomatologica 199342
(5)235ndash41
Edwards 2002 published data only
Edwards JE McQuay HJ Moore RA Combination
analgesic efficacy individual patient data meta-analysis
of single-dose oral tramadol plus acetaminophen in
acute postoperative pain Journal of Pain and Symptom
Management 200223(2)121ndash30
Forbes 1982 published data only
Forbes JA Beaver WT White EH White RW Neilson GB
Shackleford RW Diflunisal A new oral analgesic with an
unusually long duration of action JAMA 1982248(17)
2139ndash42
Forbes 1984a published data only
Forbes JA Kolodny AL Chachich BM Beaver WT
Nalbuphine acetaminophen and their combination in
postoperative pain Clinical Pharamacology and Therapeutics
198435(6)843ndash51
Gallardo 1990 published data only
Gallardo F Rossi E Analgesic efficacy of flurbiprofen as
compared to acetaminophen and placebo after periodontal
surgery Journal of Periodontology 199061(4)224ndash7
Gustafsson 1983 published data only
Gustafsson I Nystrom E Quiding H Effect of preoperative
paracetamol on pain after oral surgery European Journal of
Clinical Pharmacology 198324(1)63ndash5
Haanaes 1986 published data only
Haanaes HR Benterud UJ Skoglund LA RF 46-790 versus
paracetamol effect on post-operative pain International
Journal of Clinical Pharmacology Therapy and Toxicology
198624(11)598ndash601
Irvine 1982 published data only
Irvine GH Lutterloch MJ Bowerman JE Comparison
of diflunisal and paracetamol in the management of pain
11Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
following wisdom teeth removal British Dental Journal
1982152(1)18ndash20
Laska 1983 published data only
Laska EM Sunshine A Zighelboim I Roure C Marrero
I Wanderling J et alEffect of caffeine on acetaminophen
analgesia Clinical Pharmacology and Therapeutics 198333
(4)498ndash509
Lecointre 1991 published data only
Lecointre C [Efficacy and tolerance of tiaprofenic acid
for extraction complications Results of a randomized
double-blind study tiaprofenic acid versus paracetamol]
LrsquoInformation Dentaire 199173(35)3063ndash6
Liashek 1987 published data only
Liashek P Jr Desjardins PJ Triplett RG Effect of
pretreatment with acetaminophen-propoxyphene for oral
surgery pain Journal of Oral and Maxillofacial Surgery 1987
45(2)99ndash103
Macleod 2002 published data only
Macleod AG Ashford B Voltz M Williams B Cramond T
Gorta L et alParacetamol versus paracetamol-codeine in
the treatment of post-operative dental pain a randomized
double-blind prospective trial Australian Dental Journal
200247(2)147ndash51
Medve 2001 published data only
Medve RA Wang J Karim R Tramadol and acetaminophen
tablets for dental pain Anesthesia Progress 200148(3)
79ndash81
Mehlisch 1984 published data only
Mehlisch DR Frakes LA A controlled comparative
evaluation of acetaminophen and aspirin in the treatment of
postoperative pain Clinical Therapeutics 19847(1)89ndash97
Mehlisch 1990 published data only
Mehlisch DR Sollecito WA Helfrick JF Leibold DG
Markowitz R Schow CE Jr et alMulticenter clinical
trial of ibuprofen and acetaminophen in the treatment of
postoperative dental pain Journal of the American Dental
Association 1990121(2)257ndash63
Moore 1986 published data only
Moore PA Werther JR Seldin EB Stevens CM Analgesic
regimens for third molar surgery pharmacologic and
behavioral considerations Journal of the American Dental
Association 1986113(5)739ndash44
Nystrom 1988 published data only
Nystrom E Gustafsson I Quiding H The pain intensity
at analgesic intake and the efficacy of diflunisal in single
doses and effervescent acetaminophen in single and repeated
doses Pharmacotherapy 19888(3)201ndash9
Petersen 1983 published data only
Petersen JK A double-blind cross-over study of the analgesic
and anti-inflammatory effects of dexamethasone and
paracetamol following surgical removal of lower impacted
third molars International Journal of Oral Surgery 198312
(4)266
Quiding 1981 published data only
Quiding H Oksala E Happonen RP Lehtimaki K Ojala
T The visual analog scale in multiple-dose evaluations of
analgesics The Journal of Clinical Pharmacology 198121
(10)424ndash9
Quiding 1982 (1) published data only
Quiding H Oikarinen V Huitfeldt B Koskimo M
Leikomaa H Nyman C An analgesic study with repeated
doses of phenazone phenazone plus dextropropoxyphene
and paracetamol using a visual analogue scale International
Journal of Oral Surgery 198211(5)304ndash9
Quiding 1982 (2) published data only
Quiding H Persson G Ahlstrom U Bangens S Hellem S
Johansson G et alParacetamol plus supplementary doses
of codeine an analgesic study of repeated doses European
Journal of Clinical Pharmacology 198223(4)315ndash9
Quiding 1984 published data only
Quiding H Oikarinen V Sane J Sjoblad AM Analgesic
efficacy after single and repeated doses of codeine and
acetaminophen Journal of Clinical Pharmacology 198424
(1)27ndash34
Ragot 1991 published data only
Ragot JP [Comparison of analgesic activity of mefenamic
acid and paracetamol in treatment of pain after extraction
of impacted lower 3d molar] LrsquoInformation Dentaire 1991
73(21)1659ndash64
Reijntjes 1987 published data only
Reijntjes RJ Boering G Wesseling H van Rijn LG
Suprofen versus paracetamol after oral surgery International
Journal of Oral and Maxillofacial Surgery 198716(1)45ndash9
Rodrigo 1987 published data only
Rodrigo MR Rosenquist JB Cheung LK Paracetamol
and diflunisal for pain relief following third molar surgery
in Hong Kong Chinese International Journal of Oral and
Maxillofacial Surgery 198716(5)566ndash71
Rodrigo 1989 published data only
Rodrigo C Chau M Rosenquist J A comparison of
paracetamol and diflunisal for pain control following
3rd molar surgery International Journal of Oral and
Maxillofacial Surgery 198918(3)130ndash2
Rosen 1985 published data only
Rosen M Absi EG Webster JA Suprofen compared to
dextropropoxyphene hydrochloride and paracetamol
(Cosalgesic) after extraction of wisdom teeth under general
anaesthesia Anaesthesia 198540(7)639ndash41
Sakata 1989 published data only
Sakata LA Rocha B et alEffects of benzydamine after
surgical removal of impacted teeth [Efeitos da benzidamina
apoacutes a extraccedilaumlo de dentes inclusos] Revista da Associacao
Paulista de Cirurgioes Dentistas 198943(4)167ndash70
Selcuk 1996 published data only
Selcuk E Gomel M Bellibas SE Kose T Tuglular I
Comparison of the analgesic effects of diflunisal and
paracetamol in the treatment of postoperative dental pain
12Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
International Journal of Clinical Pharmacology Research
199616(2-3)57ndash65
Seymour 1981 published data only
Seymour RA Rawlins MD Pharmacokinetics of parenteral
paracetamol and its analgesic effects in post-operative dental
pain European Journal of Clinical Pharmacology 198120
(3)215ndash8
Seymour 1983 published data only
Seymour RA Analgesic efficacy and plasma concentration
of three analgesics in pain after lower third molar removal
SAAD Digest 19835(7)172ndash88
Skjelbred 1979 published data only
Skjelbred P Lokken P Paracetamol versus placebo effects
on post-operative course European Journal of Clinical
Pharmacology 197915(1)27ndash33
Strom 1990 published data only
Strom C Forsberg O Quiding H Engevall S Larsson
O Analgesic efficacy of acetaminophen sustained release
Journal of Clinical Pharmacology 199030(7)654ndash9
Van Aken 2004 published data only
Van Aken H Thys L Veekman L Buerkle H Assessing
analgesia in single and repeated administrations of
propacetamol for postoperative pain comparison with
morphine after dental surgery Anesthesia and Analgesia
200498(1)159ndash65
Winter 1983 published data only
Winter L Appleby F Ciccone PE Pigeon JG A double-
blind comparative evaluation of acetaminophen caffeine
and the combination of acetaminophen and caffeine in
outpatients with postoperative oral surgery pain Current
Therapeutic Research 198333(1)115ndash22
Additional references
Aronoff 2006
Aronoff DM Oates JA Boutaud O New insights into
the mechanism of action of acetaminophen Its clinical
pharmacologic characteristics reflect its inhibition of the
two prostaglandin H2 synthases Clinical Pharmacology and
Therapeutics 200679(1)9ndash19
Chandrasekharan 2002
Chandrasekharan NV Dai H Roos KL Evanson NK
Tomsik J Elton TS et alCOX-3 a cyclooxygenase-1 variant
inhibited by acetaminophen and other analgesicantipyretic
drugs cloning structure and expression Proceedings of the
National Academy of Sciences of the United States of America
200299(21)13926ndash31
Collins 1999
Collins SL Moore RA McQuay HJ Wiffen PJ Edwards JE
Single dose oral ibuprofen and diclofenac for postoperative
pain Cochrane Database of Systematic Reviews 1999
Issue 1 [DOI Art No CD001548 DOI 101002
14651858CD001548]
Cooper 1976
Cooper SA Beaver WT A model to evaluate mild analgesics
in oral surgery outpatients Clinical Pharmacology and
Therapeutics 197620(2)241ndash50
Coulthard 2001
Coulthard P Hill CM Frame JW Barry H Ridge BD
Bacon TH Pain control with paracetamol from a sustained
release formulation and a standard release formulation after
third molar surgery a randomised controlled trial British
Dental Journal 2001191(6)319ndash24
Dray 1997
Dray A Kinins and their receptors in hyperalgesia
Canadian Journal of Physiology and Pharmacology 199775
(6)704ndash12
Fisher 1988
Fisher SE Frame JW Rout PG McEntegart DJ Factors
affecting the onset and severity of pain following the surgical
removal of unilateral impacted mandibular third molar
teeth British Dental Journal 1988164(11)351ndash4
Loeser 1999
Loeser JD Melzack R Pain an overview Lancet 1999353
(9164)1607ndash9
Malmberg 1992
Malmberg AB Yaksh TL Antinociceptive effects of spinal
non-steroidal anti-inflammatory agents on the formalin
test in the rat Journal of Pharmacology and Experimental
Therapeutics 1992263136ndash46
Moore 1997
Moore RA McQuay HJ Single-patient data meta-analysis
of 3453 postoperative patients oral tramadol versus
placebo codeine and combination analgesics Pain 199769
(3)287ndash94
Moore 1998
Moore A Collins S Carroll D McQuay H Edwards
J Single dose paracetamol (acetaminophen) with and
without codeine for postoperative pain Cochrane Database
of Systematic Reviews 1998 Issue 4 [DOI Art No
CD001547 DOI 10100214651858CD001547]
Rang 2003
Rang HP Dale MM Ritter JM Moore PK Anti-
inflammatory and immunosuppresant drugs Pharmacology
5th Edition Churchill Livingstone 2003244ndash61
Seymour 1985
Seymour RA Meechan JG Blair GS An investigation into
post-operative pain after third molar surgery under local
analgesia The British Journal of Oral and Maxillofacial
Surgery 198523(6)410ndash8lowast Indicates the major publication for the study
13Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Cooper 1980
Methods Randomised parallel group double blind study
Participants 298 participants randomised to 6 groups withdrawals unclear (51 from all groups)
Number randomised to intervention male 13 female 24 mean age 225
Number randomised to placebo male 11 female 27 mean age 235
Number of third molars removed mean for intervention and placebo 19
Baseline pain intensity mean for intervention 241 (moderate 22 severe 15) mean for placebo 242
(moderate 22 severe 16)
Setting - outpatients (USA)
Interventions Paracetamol 500 mg versus placebo
Formulation not stated
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse events table
Notes Sponsored unclear
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Cooper 1981
Methods Randomised parallel group double blind study
Participants 248 participants randomised to 5 groups withdrawals unclear (48 from all groups)
Number randomised to intervention male 15 female 22 mean age 222
Number randomised to placebo male 13 female 24 mean age 237
Number of third molars removed not stated
Baseline pain intensity mean for intervention 22 (moderate 29 severe 9) mean for placebo 23 (moderate
26 severe 11)
Setting not stated (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation not stated
Anaesthesia LA or GA
14Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Cooper 1981 (Continued)
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Total number of adverse events and number of people with adverse events reported
Notes Sponsored by
Adria Laboratories
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Cooper 1988
Methods Randomised parallel group double blind study
Participants 165 participants randomised to 4 groups withdrawals unclear (22 from all groups)
Number randomised to intervention male 7 female 29 mean age 246
Number randomised to placebo male 11 female 29 mean age 247
Number of third molars removed mean for intervention 14 mean for placebo 15
Baseline pain intensity mean for intervention 24 (moderate 21 severe 15) mean for placebo 24 (mod-
erate 25 severe 15)
Setting - outpatients - single site (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Total number of adverse events
Notes Sponsored by
Parke-Davis
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
15Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Cooper 1998
Methods Randomised parallel group double blind study
Participants 177 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 23 female 27 mean age 236
Number randomised to placebo male 12 female 14 mean age 227
Number of third molars removed not stated
Baseline pain intensity mean for intervention categorical 23 VAS 603 mean for placebo categorical
22 VAS 628
Setting - Georgetown University Hospital (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe) VAS scale 0-100 mm (none - worst pain
imaginable)
PR at 4 hours and 6 hours categorical scale 0-4 (no relief - complete relief )
Global assessment not stated
Adverse effects table
Notes Sponsored by
Whitehall-Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Dionne 1994
Methods Randomised parallel group double blind study
Participants 135 participants randomised to 5 groups withdrawals unclear (11 from all groups)
Number randomised to intervention male 14 female 13 mean age 296
Number randomised to placebo male 15 female 10 mean age 282
Number of third molars removed not stated
Baseline pain intensity for intervention and placebo not stated
Setting private dental practice (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED or GA
Outcomes PI at 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 1-5 (poor - excellent)
Adverse effects table
16Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Dionne 1994 (Continued)
Notes Sponsored by
Upjohn
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Dolci 1994
Methods Randomised parallel group double blind study
Participants 338 participants enrolled in 4 groups withdrawals unclear (40 from all groups)
Number randomised to intervention male 28 female 44 mean age 279 age range 18-49
Number randomised to placebo male 28 female 48 mean age 272 age range 18-45
Number of third molars removed not stated
Baseline pain intensity range for intervention and placebo given together as average 214 (208 - 219)
Setting not stated (Italy)
Interventions Paracetamol 500 mg versus placebo
Formulation tablets
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (negative - very good)
Adverse effects table
Notes Sponsored - unclear
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Forbes 1984b
Methods Randomised parallel group double blind study
Participants 191 participants randomised to 4 groups withdrawals unclear (43 from all groups 164 used in reporting
of adverse events)
Number randomised to intervention male 19 female 20 mean age 2195
Number of third molars removed mean 244
Number randomised to placebo male 21 female 15 mean age 15-32
Number of third molars removed mean 278
17Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Forbes 1984b (Continued)
Baseline pain intensity mean for intervention 246 (moderate 21 severe 18) mean for placebo 247
(moderate 19 severe 17)
Setting private dental practice (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse effects reported as total number of adverse events and number of patients with adverse events
Notes Sponsored by McNeil Consumer Products
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Forbes 1989
Methods Randomised parallel group double blind study
Participants 107 participants randomised to 5 groups withdrawals unclear (19 from all groups 98 participants used
in reporting of adverse events)
Number randomised to intervention male 9 female 13 mean age 2059 age range 17-31
Number randomised to placebo male 12 female 11 mean age 2374 age range 16-39
Number of third molars removed mean for intervention 259 mean for placebo 209
Baseline pain intensity mean for intervention 245 mean for placebo 239
Setting - 2 sites private dental practice outpatients (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation - 1 tablet amp 1 capsule
Anaesthesia LA and GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects reported by number of patients with adverse events
Notes Sponsored by
Boots Company Ltd GH Besselaar Associates
Risk of bias
Item Authorsrsquo judgement Description
18Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Forbes 1989 (Continued)
Allocation concealment Unclear B - Unclear
Forbes 1990
Methods Randomised parallel group double blind study
Participants 206 participants randomised to 6 groups
Number randomised to intervention male 20 female 16 (5 withdrawals) mean age 225 age range 16-
46
Number randomised to placebo male 18 female 16 (4 withdrawals) mean age 2365 age range 16-45
Number of third molars removed mean for intervention 258 mean for placebo 235
Baseline pain intensity mean for intervention 239 (moderate 22 severe 14) mean for placebo 232
(moderate 23 severe 11)
Setting - private dental practice outpatients (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation capsules
Anaesthesia LA and GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects table
Notes Sponsored by
Syntex Research
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Hersh 2000
Methods Randomised parallel group double blind study
Participants 210 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 20 female 43 mean age 233
Number of third molars removedpatient (11) (26) (35) (451)
Number randomised to placebo male 9 female 8 mean age 237
Number of wisdom teeth removed per patient (11) (25) (33) (418)
Baseline pain intensity mean for intervention 23 (moderate 47 severe 16) mean for placebo 22 (mod-
erate 22 severe 5)
Setting - University of Pennsylvania School of Dental Medicine - outpatients (USA)
19Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hersh 2000 (Continued)
Interventions Paracetamol 1000 mg versus placebo
Formulation caplets
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical 0-3 (none - severe)
PR at 4 hours and 6 hours categorical 0-4 (no relief - complete relief )
Global assessment categorical 0-4 (poor - excellent)
Adverse effects by total number of adverse events and number of patients with adverse events
Notes Sponsored by
Whitehall-Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Kiersch 1994
Methods Randomised parallel group double blind study
Participants 232 participants enrolled in 3 groups
Number randomised to intervention 91 withdrawals 4 (2 before and 2 after randomisation) male 72
female 17 mean age 231 age range 15-39
Number of third molars removedpatient (10) (20) (331) (454)
Number randomised to placebo 47 withdrawals 2 male 35 female 10 mean age 247 age range 15-39
Number of third molars removedpatient (10) (20) (319) (426)
Baseline pain intensity mean for intervention and placebo categorical 212 VAS 5835
Setting not stated (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation capsules
Anaesthesia not stated
Outcomes PI at 4 hours and 6 hours categorical 0-3 (none - severe)
PR at 4 hours and 6 hours categorical 0-4 (none - complete) VAS 0-100 mm (no pain - worst pain I can
imagine)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects reported by total number of adverse events and by number of patients with adverse events
Notes Sponsored by
Syntex Research
Risk of bias
Item Authorsrsquo judgement Description
20Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Kiersch 1994 (Continued)
Allocation concealment Unclear B - Unclear
Kubitzek 2003
Methods Randomised parallel group double blind study
Participants 245 participants randomised to 3 groups no withdrawals
Number randomised to intervention 78
Number randomised to placebo 84 malefemale 40 male over both groups
Number of third molars removed 1 or 2 for each patient
Baseline pain intensity moderate to severe 65-76 in both groups
Setting dental practice (Germany)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia LA
Outcomes PI not stated
PR given as TOTPAR at 6 hours
Global assessment categorical 1-5 (poor - excellent)
Adverse effects not stated
Notes Sponsored by
Novartis Consumer Health
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Lehnert 1990
Methods Randomised parallel group double blind study
Participants 150 participants randomised to 3 groups 50 to each
Number randomised to intervention 1 withdrawal male 23 female 26 mean age 253 age range 17-52
Number randomised to placebo 2 withdrawals male 24 female 18 mean age 251 age range 18-53
Number of hird molars removed not stated
Baseline pain intensity mean for intervention 255 (moderate 22 severe 27) mean for placebo 25
(moderate 21 severe 21)
Setting outpatients (Germany)
Interventions Paracetamol 1000 mg versus placebo
Formulation capsules
Anaesthesia not stated
21Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Lehnert 1990 (Continued)
Outcomes PI at 6 hours categorical scale 0-3 (no pain - severe)
PR at 6 hours categorical scale 0-3 (none - complete)
Global assessment categorical scale 0-3 (poor - excellent)
Adverse effects by number of patients
Notes Sponsored by GH Besselar Associates
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Mehlisch 1995
Methods Randomised parallel group double blind study
Participants 240 participants randomised to 3 groups 1 withdrawal from the acetaminophen group
Number randomised to intervention (1 withdrawal) male 30 female 71 mean age 253 age range 15-
60
Number of third molars removedpatient (10 295 33 43)
Number randomised to placebo male 19 female 21 mean age 242 age range 15-48
Number of third molars removedpatient (10 239 30 41)
Baseline pain intensity mean for intervention 221 (moderate 80 severe 21) mean for placebo 220
(moderate 32 severe 8)
Setting not stated (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation 2 tablets
Anaesthesia not stated
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse events reported by number of patients
Notes Sponsored by
Biomedical Research Group and Merck Research Laboratories
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
22Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Moller 2000
Methods Randomised parallel group double blind study
Participants 242 participants randomised to 4 groups no withdrawals
Number randomised to Intervention A male 27 female 33 mean age 245
Number randomised to Intervention B male 26 female 34 mean age 262
Number randomised to Placebo A male 21 female 41 mean age 250
Number randomised to Placebo B male 24 female 36 mean age 246
Number of third molars removed per patient in both groups 1
Mean baseline intensity Intervention A categorical 200 (moderate 60) VAS 494
Mean baseline intensity Intervention B categorical 200 (moderate 60) VAS 473
Mean baseline intensity Placebo A categorical 200 (moderate 61 severe 1) VAS 505
Mean baseline intensity Placebo B categorical 200 (moderate 61) VAS 476
Setting Department of Oral and Maxillofacial Surgery Royal Dental College Aarhus (Denmark)
Interventions Intervention A Paracetamol 1000 mg versus Placebo A
Formulation effervescent tablets
Intervention B Paracetamol 1000 mg versus Placebo B
Formulation tablets
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe) VAS scale 0-100 mm (no pain - worst possible pain)
PR at 4 hours categorical 0-4 (none - complete)
Global assessment categorical 0-3 (poor - excellent)
Adverse effects reported as total number of adverse events and number of patients with adverse events
Notes Sponsored by
Bristol Myers Squibb
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Olson 2001
Methods Randomised parallel group double blind study
Participants 239 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 22 female 44 mean age 222
Number randomised to placebo male 11 female 28 mean age 239
Number of third molars removedpatient intervention - (11) (264) (31) (40) placebo - (11) (2
38) (30) (40)
Baseline pain intensity mean for intervention 286 (moderate 9 severe 57) mean for placebo 29 (moderate
4 severe 35)
Setting University of Puerto Rico School of Dentistry (Puerto Rico)
23Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Olson 2001 (Continued)
Interventions Paracetamol 1000 mg versus placebo
Formulation caplets
Anaesthesia LA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete relief )
Global assessment categorical scale 0-4 (poor - excellent)
Adverse effects table
Notes Sponsored by
Whitehall Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Seymour 1996
Methods Randomised parallel group double blind study
Participants 206 participants randomised to 5 groups
Number randomised to intervention A 1 withdrawal male 12 female 28 mean age 238
Number randomised to intervention B 1 withdrawal male 12 female 28 mean age 277 1 withdrawal
Number randomised to placebo 2 withdrawals male 15 female 24 mean age 246
Number of third molars removedpatient not stated
Baseline pain intensity mean for intervention A VAS 549 mean for intervention B VAS 542 mean
for placebo VAS 565
Setting not stated (UK)
Interventions Intervention A paracetamol 500 mg versus placebo
Intervention B paracetamol 1000 mg versus placebo
Formulation not stated
Anaesthesia GA
Outcomes PI at 6 hours VAS scale 0-100 mm (no pain - unbearable pain)
Global assessment categorical 0 -3 (very good - very poor)
but categories 1 amp 2 and 4 amp 5 not reported separately so unable to include data in tables
Adverse effects - none reported by any participants in any group
Notes Sponsored - unclear
Risk of bias
Item Authorsrsquo judgement Description
24Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Seymour 1996 (Continued)
Allocation concealment Unclear B - Unclear
Seymour 2003
Methods Randomised parallel group double blind study
Participants 167 randomised to 3 groups withdrawals unclear (14 from all groups)
Number randomised to intervention male 19 female 43 mean age 250
Number randomised to placebo male 11 female 21 mean age 251
Number of third molars removedpatient intervention - (12) (214) (312) (434) placebo - (13)
(25) (39) (415)
Baseline pain intensity mean for intervention 506 mean for placebo 541
Setting not clear (2 sites Cardiff and Hexham UK)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia GA
Outcomes PI at 4 hours VAS scale 0-100 mm (none - worst pain imaginable)
PR not stated
Global assessment categorical scale 1-5 (very poor - very good)
Adverse effects table
Notes Sponsored by
Reckitt Benckiser Healthcare
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Skoglund 1991
Methods Randomised parallel group double blind study
Participants 147 participants randomised to 4 groups withdrawals unclear (8 from all groups)
Number randomised to intervention male 16 female 16 mean age 247
Number randomised to placebo male 16 female 17 mean age 244
Number of third molars removed not stated
Baseline pain intensity mean for intervention approx 55 mean for placebo approx 45
Setting not stated (Norway)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia LA
25Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Skoglund 1991 (Continued)
Outcomes PI at 4 hours and 6 hours VAS scale 0-100 mm (none - pain cannot be worse)
PR at 4 hours and 6 hours VAS scale 0-100 mm (complete relief - no relief ) reversed for statistical analysis
Global assessment not stated
Adverse effects table
Notes Sponsored by
Apothekernes Laboratorium
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Sunshine 1986
Methods Randomised parallel group double blind study
Participants 182 participants randomised to 6 groups no withdrawals (only patients with moderate to severe pain
were randomised)
Number randomised to intervention male 6 female 24 mean age 219
Number randomised to placebo male 14 female 16 mean age 23
Number of third molars removed not stated
Baseline pain intensity mean for intervention 200 mean for placebo 200
Setting University of Puerto Rico School of Dentistry Clinic
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia LA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none 0 - complete 100)
Global assessment categorical 0-3 (poor - excellent)
Overall improvement 1-7 (very much worse - very much better)
Adverse effects reported by number of patients with adverse events
Notes Sponsored by
Upjohn
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
26Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Vattaraphudej 1986
Methods Randomised parallel group double blind study
Participants 83 enrolled to 4 groups withdrawals unclear (16 from all groups)
Number randomised to intervention male 8 female 8
Number randomised to placebo male 10 female 9
Number of third molars removed mean for intervention 125 mean for placebo 132
Baseline pain intensity mean for intervention 237 mean for placebo 226
Setting Dept of Oral Surgery Khon Kaen University Thailand
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (no relief - total relief )
Global assessment categorical scale 0-3 (poor - excellent)
Adverse effects none reported
Notes Sponsored by Khon Kaen University Thailand Dr Sompong Thongpradith Merck and Russel
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
GA - general anaesthetic LA - local anaesthetic PI - pain intensity PR - pain relief SED - sedation TOTPAR - total pain relief VAS
- visual analogue scale
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Adame 1979 Title not in journal quoted unable to find paper
Barden J 2004 Meta-analysis dental papers included individually where appropriate
Becker 1990 Not a third molar study
Bentley 1987 Unable to extract data for third molars only written to authors
Breivik 1998 Dose given at 3 hours postoperatively regardless of baseline pain unable to get 4-hour data Study used for side
effects only
27Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Cooper 1986 Unable to extract third molar data written to authors
Cooper 1989 Unable to extract third molar data written to authors
Cooper 1991 Unclear if third molars only written to authors
Dionne 1983 (1) Not single dose administered preoperatively
Dionne 1983 (2) Not placebo controlled not single dose administered preoperatively
Dionne 1986 Not placebo controlled
Dolci 1993 The data for the participants in this study are duplicated in Dolci 1994
Edwards 2002 This was a meta-analysis Need to identify source of data to clarify whether third molar studies and exclude
duplication Written to authors
Forbes 1982 Unable to extract third molar data written to authors
Forbes 1984a Not third molar study
Gallardo 1990 Not third molar study (periodontal surgery)
Gustafsson 1983 Patients given either paracetamol preoperatively and placebo postoperatively or vice versa unable to extract
relevant data
Haanaes 1986 Not placebo controlled Study used for side effects only
Irvine 1982 Not placebo controlled
Laska 1983 Not placebo controlled
Lecointre 1991 Not placebo controlled
Liashek 1987 Multiple doses unable to extract single dose data
Macleod 2002 Not placebo controlled
Medve 2001 Only 8-hour SPID and TOTPAR available need 4-hour andor 6-hour to include in review written to authors
Mehlisch 1984 Unable to extract third molar data written to authors
Mehlisch 1990 Unable to extract third molar data
Moore 1986 Multiple doses given unable to extract single dose data
Nystrom 1988 Not placebo controlled
28Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Petersen 1983 Unable to locate complete article
Quiding 1981 Not placebo controlled
Quiding 1982 (1) Not placebo controlled
Quiding 1982 (2) Not placebo controlled
Quiding 1984 No placebo used
Ragot 1991 Not placebo controlled
Reijntjes 1987 Not placebo controlled
Rodrigo 1987 Mixed parallel and cross-over trial multiple doses unable to extract relevant data
Rodrigo 1989 Not placebo controlled
Rosen 1985 Not placebo controlled multiple doses used unable to extract single dose data
Sakata 1989 Unable to obtain study
Selcuk 1996 Not placebo controlled
Seymour 1981 Cross-over trial baseline pain not stated unable to extract relevant data
Seymour 1983 Acetaminophen administered intravenously
Skjelbred 1979 Multiple doses unable to extract single dose data
Strom 1990 Not placebo controlled
Van Aken 2004 Propacetamol administered intravenously
Winter 1983 Unable to extract third molar data written to authors
SPID - summed pain intensity difference TOTPAR - total pain relief
29Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
Comparison 1 50 pain relief using pain relief measures
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Paracetamol versus placebo
number of people with at least
50 pain relief at 4 hours
16 1498 Risk Ratio (M-H Random 95 CI) 285 [189 429]
11 Up to 1000 mg of
paracetamol
10 710 Risk Ratio (M-H Random 95 CI) 196 [134 286]
12 1000 mg or more 6 788 Risk Ratio (M-H Random 95 CI) 456 [286 727]
2 Paracetamol versus placebo
number of people with at least
50 pain relief at 6 hours
13 1155 Risk Ratio (M-H Random 95 CI) 332 [188 587]
21 Up to 1000 mg of
paracetamol
6 378 Risk Ratio (M-H Random 95 CI) 189 [098 367]
22 1000 mg or more 7 777 Risk Ratio (M-H Random 95 CI) 421 [297 598]
Comparison 2 50 pain relief using pain intensity measures
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Paracetamol versus placebo
number of people with at least
50 pain relief at 4 hours
17 1658 Risk Ratio (M-H Random 95 CI) 487 [283 837]
11 Up to 1000 mg of
paracetamol
10 737 Risk Ratio (M-H Random 95 CI) 433 [219 858]
12 1000 mg or more 8 921 Risk Ratio (M-H Random 95 CI) 646 [234 1785]
2 Paracetamol versus placebo
number of people with at least
50 pain relief at 6 hours
13 1184 Risk Ratio (M-H Random 95 CI) 341 [234 497]
21 Up to 1000 mg of
paracetamol
6 403 Risk Ratio (M-H Random 95 CI) 267 [146 490]
22 1000 mg or more 8 781 Risk Ratio (M-H Random 95 CI) 396 [252 623]
30Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Comparison 3 Number of people with adverse events
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Number of patients with adverse
events paracetamol versus
placebo
17 1645 Risk Ratio (M-H Random 95 CI) 119 [090 157]
11 Up to 1000 mg of
paracetamol
9 672 Risk Ratio (M-H Random 95 CI) 125 [069 225]
12 1000 mg or more 8 973 Risk Ratio (M-H Random 95 CI) 116 [084 160]
Analysis 11 Comparison 1 50 pain relief using pain relief measures Outcome 1 Paracetamol versus
placebo number of people with at least 50 pain relief at 4 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 1 50 pain relief using pain relief measures
Outcome 1 Paracetamol versus placebo number of people with at least 50 pain relief at 4 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Dolci 1994 5472 2576 100 228 [ 161 323 ]
Cooper 1980 1137 1138 82 103 [ 051 207 ]
Forbes 1990 936 134 30 850 [ 114 6357 ]
Forbes 1989 522 023 17 1148 [ 067 19607 ]
Cooper 1988 1636 1240 87 148 [ 081 269 ]
Cooper 1981 2137 637 77 350 [ 160 767 ]
Forbes 1984b 1339 136 30 1200 [ 165 8716 ]
Vattaraphudej 1986 716 219 47 416 [ 100 1726 ]
Sunshine 1986 1830 1530 95 120 [ 076 190 ]
Dionne 1994 2527 1725 102 136 [ 102 182 ]
Subtotal (95 CI) 352 358 667 196 [ 134 286 ]
Total events 179 (Paracetamol better) 90 (Placebo better)
Heterogeneity Tau2 = 018 Chi2 = 2644 df = 9 (P = 0002) I2 =66
Test for overall effect Z = 349 (P = 000048)
2 1000 mg or more
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
31Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Mehlisch 1995 40101 240 49 792 [ 201 3124 ]
Cooper 1998 1850 326 59 312 [ 101 963 ]
Olson 2001 4266 539 74 496 [ 215 1148 ]
Moller 2000 27120 0122 18 5591 [ 345 90627 ]
Hersh 2000 4063 527 75 343 [ 152 773 ]
Kiersch 1994 2589 345 58 421 [ 134 1321 ]
Subtotal (95 CI) 489 299 333 456 [ 286 727 ]
Total events 192 (Paracetamol better) 18 (Placebo better)
Heterogeneity Tau2 = 003 Chi2 = 544 df = 5 (P = 036) I2 =8
Test for overall effect Z = 637 (P lt 000001)
Total (95 CI) 841 657 1000 285 [ 189 429 ]
Total events 371 (Paracetamol better) 108 (Placebo better)
Heterogeneity Tau2 = 040 Chi2 = 6294 df = 15 (Plt000001) I2 =76
Test for overall effect Z = 503 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
32Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 12 Comparison 1 50 pain relief using pain relief measures Outcome 2 Paracetamol versus
placebo number of people with at least 50 pain relief at 6 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 1 50 pain relief using pain relief measures
Outcome 2 Paracetamol versus placebo number of people with at least 50 pain relief at 6 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Forbes 1989 322 023 29 730 [ 040 13375 ]
Cooper 1988 1236 940 99 148 [ 071 310 ]
Forbes 1990 736 034 30 1419 [ 084 23928 ]
Dionne 1994 2427 1825 115 123 [ 093 163 ]
Forbes 1984b 1039 036 31 1943 [ 118 31995 ]
Sunshine 1986 1530 1030 104 150 [ 081 279 ]
Subtotal (95 CI) 190 188 407 189 [ 098 367 ]
Total events 71 (Paracetamol better) 37 (Placebo better)
Heterogeneity Tau2 = 032 Chi2 = 1445 df = 5 (P = 001) I2 =65
Test for overall effect Z = 189 (P = 0058)
2 1000 mg or more
Kubitzek 2003 4569 773 99 680 [ 329 1404 ]
Mehlisch 1995 35101 140 49 1386 [ 196 9779 ]
Kiersch 1994 2089 345 79 337 [ 106 1075 ]
Olson 2001 4166 539 94 485 [ 209 1122 ]
Hersh 2000 3563 527 95 300 [ 132 682 ]
Lehnert 1990 2349 640 96 313 [ 141 693 ]
Cooper 1998 1750 326 81 295 [ 095 914 ]
Subtotal (95 CI) 487 290 593 421 [ 297 598 ]
Total events 216 (Paracetamol better) 30 (Placebo better)
Heterogeneity Tau2 = 00 Chi2 = 509 df = 6 (P = 053) I2 =00
Test for overall effect Z = 806 (P lt 000001)
Total (95 CI) 677 478 1000 332 [ 188 587 ]
Total events 287 (Paracetamol better) 67 (Placebo better)
Heterogeneity Tau2 = 072 Chi2 = 6335 df = 12 (Plt000001) I2 =81
Test for overall effect Z = 412 (P = 0000038)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
33Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 21 Comparison 2 50 pain relief using pain intensity measures Outcome 1 Paracetamol versus
placebo number of people with at least 50 pain relief at 4 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 2 50 pain relief using pain intensity measures
Outcome 1 Paracetamol versus placebo number of people with at least 50 pain relief at 4 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Dolci 1994 4972 576 86 1034 [ 437 2449 ]
Seymour 1996 1940 1039 96 185 [ 099 346 ]
Cooper 1980 737 438 74 180 [ 057 563 ]
Forbes 1990 1036 034 28 1986 [ 121 32639 ]
Forbes 1989 622 023 28 1357 [ 081 22736 ]
Cooper 1988 1236 840 90 167 [ 077 361 ]
Sunshine 1986 1830 630 90 300 [ 138 650 ]
Forbes 1984b 1339 036 28 2498 [ 154 40542 ]
Vattaraphudej 1986 616 119 44 713 [ 095 5317 ]
Cooper 1981 1537 037 28 3100 [ 192 49971 ]
Subtotal (95 CI) 365 372 592 433 [ 219 858 ]
Total events 155 (Paracetamol better) 34 (Placebo better)
Heterogeneity Tau2 = 063 Chi2 = 2622 df = 9 (P = 0002) I2 =66
Test for overall effect Z = 421 (P = 0000026)
2 1000 mg or more
Cooper 1998 1350 026 28 1429 [ 088 23130 ]
Mehlisch 1995 41101 340 75 541 [ 178 1648 ]
Hersh 2000 3663 127 46 1543 [ 223 10685 ]
Skoglund 1991 1632 033 28 3400 [ 213 54391 ]
Seymour 2003 1262 432 78 155 [ 054 442 ]
Seymour 1996 2040 1039 96 195 [ 105 362 ]
Kiersch 1994 989 045 28 971 [ 058 16317 ]
Moller 2000 28120 0122 28 5794 [ 358 93840 ]
Subtotal (95 CI) 557 364 408 646 [ 234 1785 ]
Total events 175 (Paracetamol better) 18 (Placebo better)
Heterogeneity Tau2 = 124 Chi2 = 2347 df = 7 (P = 0001) I2 =70
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
34Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Test for overall effect Z = 360 (P = 000032)
Total (95 CI) 922 736 1000 487 [ 283 837 ]
Total events 330 (Paracetamol better) 52 (Placebo better)
Heterogeneity Tau2 = 070 Chi2 = 4973 df = 17 (P = 000005) I2 =66
Test for overall effect Z = 571 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
Analysis 22 Comparison 2 50 pain relief using pain intensity measures Outcome 2 Paracetamol versus
placebo number of people with at least 50 pain relief at 6 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 2 50 pain relief using pain intensity measures
Outcome 2 Paracetamol versus placebo number of people with at least 50 pain relief at 6 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Seymour 1996 1840 939 152 195 [ 100 380 ]
Forbes 1989 422 023 16 939 [ 054 16485 ]
Cooper 1988 936 640 105 167 [ 066 422 ]
Forbes 1990 836 032 17 1516 [ 091 25267 ]
Forbes 1984b 1139 036 17 2128 [ 130 34843 ]
Sunshine 1986 1430 530 111 280 [ 115 680 ]
Subtotal (95 CI) 203 200 418 267 [ 146 490 ]
Total events 64 (Paracetamol better) 20 (Placebo better)
Heterogeneity Tau2 = 015 Chi2 = 705 df = 5 (P = 022) I2 =29
Test for overall effect Z = 318 (P = 00015)
2 1000 mg or more
Hersh 2000 3163 127 33 1329 [ 191 9242 ]
Mehlisch 1995 39101 340 82 515 [ 169 1571 ]
Olson 2001 4266 739 146 355 [ 177 711 ]
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
35Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Seymour 1996 2140 939 157 228 [ 119 433 ]
Cooper 1998 1250 026 17 1324 [ 081 21504 ]
Kiersch 1994 489 045 16 460 [ 025 8361 ]
Lehnert 1990 2449 542 114 411 [ 172 983 ]
Skoglund 1991 1432 033 17 2988 [ 186 48076 ]
Subtotal (95 CI) 490 291 582 396 [ 252 623 ]
Total events 187 (Paracetamol better) 25 (Placebo better)
Heterogeneity Tau2 = 008 Chi2 = 863 df = 7 (P = 028) I2 =19
Test for overall effect Z = 597 (P lt 000001)
Total (95 CI) 693 491 1000 341 [ 234 497 ]
Total events 251 (Paracetamol better) 45 (Placebo better)
Heterogeneity Tau2 = 013 Chi2 = 1823 df = 13 (P = 015) I2 =29
Test for overall effect Z = 637 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
36Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 31 Comparison 3 Number of people with adverse events Outcome 1 Number of patients with
adverse events paracetamol versus placebo
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 3 Number of people with adverse events
Outcome 1 Number of patients with adverse events paracetamol versus placebo
Study or subgroup Paracetamol more Placebo more Risk Ratio Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Cooper 1980 237 637 033 [ 007 155 ]
Dolci 1994 780 882 090 [ 034 236 ]
Forbes 1990 541 038 1021 [ 058 17873 ]
Forbes 1989 326 226 150 [ 027 825 ]
Sunshine 1986 130 130 100 [ 007 1526 ]
Cooper 1981 1237 438 308 [ 109 869 ]
Dionne 1994 727 525 130 [ 047 356 ]
Vattaraphudej 1986 016 019 00 [ 00 00 ]
Forbes 1984b 143 240 047 [ 004 493 ]
Subtotal (95 CI) 337 335 125 [ 069 225 ]
Total events 38 (Paracetamol more) 28 (Placebo more)
Heterogeneity Tau2 = 016 Chi2 = 906 df = 7 (P = 025) I2 =23
Test for overall effect Z = 074 (P = 046)
2 1000 mg or more
Olson 2001 1066 239 295 [ 068 1279 ]
Cooper 1998 2550 426 325 [ 127 835 ]
Moller 2000 48120 56122 087 [ 065 117 ]
Seymour 2003 2462 932 138 [ 073 260 ]
Mehlisch 1995 1299 440 121 [ 042 354 ]
Kiersch 1994 2691 1347 103 [ 059 182 ]
Hersh 2000 1263 727 073 [ 032 166 ]
Lehnert 1990 549 440 102 [ 029 355 ]
Subtotal (95 CI) 600 373 116 [ 084 160 ]
Total events 162 (Paracetamol more) 99 (Placebo more)
Heterogeneity Tau2 = 007 Chi2 = 1096 df = 7 (P = 014) I2 =36
Test for overall effect Z = 090 (P = 037)
Total (95 CI) 937 708 119 [ 090 157 ]
01 02 05 1 2 5 10
Favours treatment Favours control
(Continued )
37Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol more Placebo more Risk Ratio Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Total events 200 (Paracetamol more) 127 (Placebo more)
Heterogeneity Tau2 = 007 Chi2 = 2073 df = 15 (P = 015) I2 =28
Test for overall effect Z = 121 (P = 023)
01 02 05 1 2 5 10
Favours treatment Favours control
A D D I T I O N A L T A B L E S
Table 1 Number of patients with adverse events (lt 1000 mg ParacetamolPlacebo)
Author Total Paracetamol AEs Paracetamol Total Placebo AEs Placebo
Cooper 1980 37 2 37 6
Cooper 1981 37 12 38 4
Dionne 1994 27 7 25 5
Dolci 1994 80 7 82 8
Forbes 1984b 43 1 40 2
Forbes 1989 26 3 26 2
Forbes 1990 41 5 38 0
Gallardo 1990 15 5 11 3
Seymour 1996 40 0 39 0
Sunshine 1986 30 1 30 1
Vattaraphudej 1986 16 0 19 0
Totals 392 43 385 31
38Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Quality assessment
Author Allocation concealment Follow up Total (Max-3)
Cooper 1980 1 0 1
Cooper 1981 1 0 1
Cooper 1988 1 0 1
Cooper 1998 1 1 2
Dionne 1994 1 0 1
Dolci 1994 1 0 1
Forbes 1984b 2 0 2
Forbes 1989 1 0 1
Forbes 1990 2 0 2
Hersh 2000 1 1 2
Kiersch 1994 1 1 2
Kubitzek 2003 1 1 2
Lehnert 1990 1 1 2
Mehlisch 1995 2 1 3
Moller 2000 1 1 2
Olson 2001 2 1 3
Seymour 1996 1 1 2
Seymour 2003 2 0 2
Skoglund 1991 2 0 2
Sunshine 1986 2 1 3
Vattaraphudej 1986 1 1 2
39Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Random-effects metaregression lt 1000 mg vs 1000 mg Paracetamol vs Placebo
Outcome Number of studies Slope estimate 95 CI Slope interpretation P value
50 pain relief at 4
hours (using pain re-
lief )
16 094 (036 to 152) more pain relief for
higher doses
0001
50 pain relife at 6
hours (using pain re-
lief )
13 114 (071 to 156) more pain relief for
higher doses
lt0001
50 pain relief at
4 hours (using pain
intensity)
16 023 (-084 to 130) more pain relief for
higher doses
067
50 pain relief at
6 hours (using pain
intensity)
14 043 (-015 to 101) more pain relief for
higher doses
015
Table 4 List of adverse events
Adverse events Paracetamol Placebo
Nausea 21 11
Vomiting 11 3
Nausea andor vomiting stomach cramps
abdominal pain
3 3
Headache 47 31
Drowsiness sleepiness somnolence 36 13
Dizziness fainting syncope 9 4
Bleeding 11 7
Chills flushes fever flu-like symptoms 5 0
Paraesthesia 4 2
Jawache 1 0
Swelling 1 6
Cellulitis 1 0
40Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 List of adverse events (Continued)
Dry socket 11 12
Surgical complications 6 13
CNS 5 6
GI 12 2
Body as a whole 8 3
Respiratory 2 0
Psychiatric 0 1
Other hiccups hearingvestibular miosis 5 1
Table 5 Global assessment - 5-point scale(lt 1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Cooper 1980 37 089 38 089
Cooper 1981 37 192 37 062
Cooper 1988 36 238 40 205
Dionne 1994 27 240 25 200
Dolci 1994 72 210 76 217
Forbes 1984 39 126 36 028
Mean 248 183 252 144
Table 6 Global assessment - 4-point scale (lt 1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Forbes 1989 26 100 26 030
Forbes 1990 41 147 38 056
Sunshine 1986 30 120 30 093
Vattaraphudej 1986 16 16 19 116
41Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 6 Global assessment - 4-point scale (lt 1000 mg Paracetamol) (Continued)
Mean 113 131 113 070
Table 7 Global assessment - 5-point scale (1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Kiersch 1994 91 130 47 060
Kubitzek 2003 78 198 84 145
Mehlisch 1995 101 157 40 045
Olson 2001 66 281 39 193
Seymour 2003 62 250 32 214
Mean 398 194 242 129
Table 8 Global assessment - 4-point scale (1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Hersh 2000 63 229 27 085
Moller 2000 120 188 122 154
Mean 183 202 149 141
A P P E N D I C E S
Appendix 1 CENTRAL search strategy
1 MOLAR THIRD single term (MeSH)
2 (wisdom next tooth)
3 (wisdom next teeth)
4 (third near molar)
5 (1 or 2 or 3 or 4)
6 TOOTH EXTRACTION single term (MeSH)
7 (extract near tooth)
8 (extract near teeth)
9 (extract near (third next molar))
10 (extract near (third near molar))
42Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
11 (remov near tooth)
12 (remov near teeth)
13 (surgical near remov)
14 (surgery near remov)
15 (surgical near extract)
16 (surgery near extract)
17 (6 or 7 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16)
18 (5 and 17)
W H A T rsquo S N E W
Last assessed as up-to-date 21 May 2007
Date Event Description
31 July 2008 Amended Converted to new review format
H I S T O R Y
Protocol first published Issue 4 2003
Review first published Issue 3 2007
C O N T R I B U T I O N S O F A U T H O R S
Conceiving designing and co-ordinating the review (Kiaran Weil (KW) Paul Coulthard (PC))
Developing search strategy and undertaking searches (Zahid Afzal (ZA) Arjen van Wijk (AJW) KW)
Screening search results and retrieved papers against inclusion criteria (ZA KW) Marco Esposito (ME) Lee Hooper (LH) PC)
Appraising quality (KW ZA)
Extracting data from papers (KW LH Helen Worthington (HW))
Writing to authors for additional information (KW)
Data management for the review and entering data into RevMan (KW)
Analysis and interpretation of data (KW LH HW)
Writing the review (KW)
Providing general advice on the review (ME LH PC HW)
Performing previous work that was the foundation of current study (PC)
43Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D E C L A R A T I O N S O F I N T E R E S T
None known
S O U R C E S O F S U P P O R T
Internal sources
bull The University of Manchester UK
bull The University of Amsterdam Netherlands
External sources
bull No sources of support supplied
I N D E X T E R M S
Medical Subject Headings (MeSH)
Acetaminophen [adverse effects lowasttherapeutic use] Analgesics Non-Narcotic [adverse effects lowasttherapeutic use] Molar Third [lowastsurgery]
Outcome Assessment (Health Care) Pain Postoperative [lowastdrug therapy] Pain Measurement Randomized Controlled Trials as Topic
Tooth Extraction [lowastadverse effects]
MeSH check words
Humans
44Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 407
Relative efficacy of oral analgesics after thirdmolar extractionJ Barden1 J E Edwards2 H J McQuay3 P J Wiffen4 and R A Moore5
Objectives To compare the relative efficacy of analgesics after thirdmolar extraction from systematic reviews of randomised double blindstudiesData sources Dental trials from systematic reviews of randomiseddouble-blind studies of analgesics in acute painData selection Number of patients with moderate or severe painachieving at least half pain relief over 4 to 6 hours after a single oraldose of analgesicData extraction Independently by two reviewersData synthesis Use of dichotomous information from active andplacebo treatments first to calculate the statistical significance usingrelative risk and then to evaluate the clinical relevance using numberneeded to treat (NNT) Non-steroidal anti-inflammatory drugs (NSAIDs)and cyclo-oxygenase-2 (COX-2) inhibitors had the lowest (best) NNTsfor the outcome of at least half pain relief over 4-6 hours comparedwith placebo With the best performing analgesics 50-70 patients out of100 had good pain relief compared with about 10 out of 100 withplacebo Only paracetamol 600650 mg plus codeine 60 mg wasassociated with any significant increase in any patient experiencing anadverse eventConclusions NSAIDs and COX-2 inhibitors have the lowest (best) NNTsThey may also have fewer adverse effects after third molar surgerythough conclusive evidence is lacking At least 80 of analgesicprescribing by UK dentists is in line with the best available evidence onefficacy and safety
Acute pain has been studied in single dose designs first pro-posed by Beecher and colleagues12 and formalised by Houdeand Wallenstein3 The problem with single trials is that whilethey can demonstrate statistical superiority of analgesic overplacebo variation because of random chance means that if
1Research Associate 2Senior Research Associate 3Professor of Pain Relief 4PrescribingAdvisor 5Research Director Pain Research and Nuffield Department of AnaestheticsUniversity of Oxford Oxford Radcliffe Hospital The Churchill Headington Oxford OX3 7LJ UKCorrespondence to Dr R A MooreE-mail andrewmoorepruoxacuk
Refereed paperReceived 150403 Accepted 121103doi101038sjbdj4811721copy British Dental Journal 2004 197 407ndash411
small they provide a poor estimate of the size of the analgesiceffect4 Combining results from clinically homogeneous trials ina meta-analysis gives an accurate estimate of the extent of theanalgesic effect when sufficient numbers of patients have beenrandomised45
Clinical trials in acute pain normally last 4 to 6 hours becausethat is the duration of effect of most analgesics whether injectedor as tablets and whether simple analgesics NSAIDs or opioidsMeta-analysis in acute pain has concentrated on the use of thearea under the total pain relief versus time curve (TOTPAR)dichotomized into those patients who do or do not achieve atleast half pain relief (at least 50 maximum TOTPAR)6 Thismeasure is the one most frequently reported and it avoids theproblem of reporting continuous pain data as the mean of ahighly skewed distribution7 It has the benefit of being intuitivelymeaningful to patients and professionals as well as being meas-urable
Meta-analyses in acute pain usually combine studies from avariety of pain models and relative efficacy of analgesics inthese studies has been examined6 A majority of studies were inthird molar extraction but any postoperative pain condition islikely to be included In the largest dataset that of aspirin8
pain model (dental or other surgery) made no difference to theNNT
Dentists ask rightly about relative efficacy in dental painThe number of prescription items issued by dentists in Englandwas remarkably consistent between 1998 and 2001 (Table 1)with ibuprofen dihydrocodeine and paracetamol being mostfrequently prescribed This review set out to examine single-dose oral analgesics after third molar extraction from a numberof updated systematic reviews both for the analgesics common-ly prescribed in England and for those for which comparableevidence exists including the newer cyclo-oxygenase-2 selec-tive inhibitors like rofecoxib celecoxib and valdecoxib
METHODSIn all the systematic reviews QUORUM guidelines were fol-lowed9 In the reviews studies for inclusion were soughtthrough searching the Cochrane Library Biological AbstractsMEDLINE PubMed and the Oxford Pain Relief database10 Ref-erence lists and review articles were examined for possible addi-tional references Most had search dates in 2002
This paper reviews the available high quality information on analgesics commonlyprescribed by dentists including COX-2 selective inhibitors
Problems related to chance effects are avoided by combining multiple trials in a meta-analysis
There is good evidence of efficacy for most commonly-prescribed analgesics Standard doses of NSAIDs and COX-2 inhibitors provide the best analgesia and lowest
rate of adverse events
I N B R I E F
RESEARCH
07p407-411qxd 10092004 1518 Page 407
RESEARCH
408 BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004
References for the reviews are as followsAspirin Edwards et al 19998 additional searching in
2002 found no new studiesCelecoxib An unpublished review being submitted as a
Cochrane ReviewDiclofenac An updated version of a Cochrane review11
Dihydrocodeine A Cochrane review12
Ibuprofen An updated version of a Cochrane review11
Paracetamol An updated version of a Cochrane review13
Paracetamol An updated version of a Cochrane review13
plus codeineRofecoxib An updated version of a systematic review14
Valdecoxib A systematic review in preparation
Criteria for inclusion for postoperative dental pain werestudy in third molar extraction full journal publication (exceptvaldecoxib which included information from a poster) ran-domised controlled trials which included single dose treatmentgroups of oral analgesic and placebo double blind designbaseline postoperative pain of moderate to severe intensitypatients over 15 years of age at least 10 patients per group andthe pain outcome measures of total pain relief (TOTPAR) orsummed pain intensity difference (SPID) over 4-6 hours or suf-ficient data to allow their calculation Pain measures allowedfor the calculation of TOTPAR or SPID were a standard fivepoint pain relief scale (none slight moderate good complete)a standard four point pain intensity scale (none mild moder-ate severe) or a standard visual analogue scale (VAS) for pain
relief or pain intensity For adverse events the primary out-come sought was the proportion of patients experiencing anyadverse event with secondary outcomes of patients experienc-ing particular adverse events Although adverse events areoften reported inconsistently in acute pain trials15 the outcomeof any patient experiencing any adverse event was the mostconsistently reported
Each report which could possibly be described as a randomisedcontrolled trial was read independently by several authors andscored using a commonly-used three item 1-5 score qualityscale16 Consensus was then achieved The maximum score of anincluded study was 5 and the minimum score was 2 Authors werenot blinded because they already knew the literature This scoringsystem takes account of randomisation blinding and withdrawalsand drop outs Trials that score 3 or more (less biased) have beenshown repeatedly to have lower treatment effects than those scor-ing 2 or less1718
For each trial mean TOTPAR SPID VAS-TOTPAR or VAS-SPIDvalues for each treatment group were converted to maxTOTPARby division into the calculated maximum value19 The proportionof patients in each treatment group who achieved at least 50maxTOTPAR was calculated using valid equations20-22 The num-ber of patients randomised was taken as the basis for calculationsto produce an intention to treat analysis The number of patientswith at least 50 maxTOTPAR was then used to calculate relativebenefit and NNT for analgesic versus placebo The same methodswere used for adverse events where the number needed to harm(NNH) was calculated
Table 1 Numbers of prescription items issued by dentists and dispensed in EnglandAnalgesic 1998 1999 2000 2001
Ibuprofen 400 mg 107200 110400 109000 103900
Dihydrocodeine 30 mg 53700 50300 49100 46700
Ibuprofen 600 mg 34200 39700 40800 42600
Ibuprofen 200 mg 36300 34600 32000 30600
Paracetamol 500 mg 11100 12800 15400 17200
Paracetamol 500 mg soluble 800 1000 900 900
Pethidine 50 mg 1100 900 700 700
Aspirin 300 mg 200 200 200 200
Source DOH statistics division 2002 calendar year January to December
Dihydrocodeine 30 mgParacetamol 300 mg + codeine 30 mg
Paracetamol 600650 mgAspirin 600650 mg
Paracetamol 9751000 mgCelecoxib 200 mg
Paracetamol 600650 mg + codeine 60 mgIbuprofen 200 mgDiclofenac 50 mgRofecoxib 50 mgIbuprofen 400 mgValdecoxib 20 mgDiclofenac 100 mgValdecoxib 40 mgIbuprofen 600 mg
0 10 20 30 40 50 60 70 80 90 10095 confidence interval of the percent ofpatients achieving at least 50 pain relief
Fig 1 The 95confidence interval ofthe proportion ofpatients with at leasthalf pain relief over 4-6hours compared withplacebo in third molarextraction trials
07p407-411qxd 10092004 1519 Page 408
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 409
of patients had at least half pain relief with active treatment in onesmall trial in dental pain (Table 2)
The adverse event outcome of a patient experiencing anyadverse event is shown in Table 3 from 10113 patients in 107 tri-als Of the 15 drug and dose combinations only paracetamol600650 mg plus codeine 60 mg could be statistically distin-guished from placebo in 10 trials and 824 patients The NNH was53 (41 to 74) indicating that five patients had to be treated withparacetamol 600650 mg plus codeine 60 mg for one of them tohave an adverse event that would not have occurred with placeboFor all other drugs and doses there was no difference betweenanalgesic and placebo
DISCUSSIONSystematic review and meta-analysis both depend on two interde-pendent criteria for them to make sense the quality of the compo-nent individual studies and the total size of the sample availablefor analysis
We know that if trials are of poor reporting quality1718 or notrandomised30 or not blind or both31 then the tendency is to over-estimate the benefits of treatment The reviews included here alldemanded that trials should be both randomised and double-blindas a minimum requirement for inclusion
We also know that even if trials are done well small samplesize can lead to an incorrect answer just because of the randomplay of chance4 For these studies we also know just how muchinformation is needed to be 95 confident of an NNT to withplusmn05 units4 With an NNT of 23 it is 400 patients in the compari-son with an NNT of 29 it is 1000 patients and with an NNT of42 it is many more than with 1000 At NNTs of 4 or more evenwith 1000 patients fewer than 75 of trials will be within plusmn05of the overall NNT
The analgesics for which these two criteria were metunequivocally were valdecoxib (combining 20 mg and 40 mg)rofecoxib 50 mg ibuprofen 400 mg diclofenac 50 mg and prob-ably ibuprofen 200 mg For paracetamol the numbers were bor-derline and for diclofenac 100 mg too small to make any safejudgement There is good evidence of good efficacy for the anal-gesics most commonly prescribed by dentists with the excep-tion of dihydrocodeine where there was little evidence in totaland no convincing evidence of efficacy
Relative benefit and relative risk estimates were calculated with95 confidence intervals using a fixed effects model23 Hetero-geneity tests were not used as they have previously been shown tobe unhelpful2425 though homogeneity was examined visually26
Publication bias was not assessed using funnel plots as these testshave been shown to be unhelpful2728 The number needed to treator harm (NNT and NNH) with confidence intervals was calculatedby the method of Cook and Sackett29 from the sum of all eventsand patients for treatment and placebo
Relative benefit or risk was considered to be statistically signifi-cant when the 95 confidence interval did not include 1 NNT val-ues were only calculated when the relative risk or benefit was sta-tistically significant and are reported with the 95 confidenceinterval Calculations were performed using Microsoft Excel 2001on a Power Macintosh G4
RESULTSTable 2 shows the main results from 14150 patients in 155 trials of15 drug and dose combinations against placebo in third molarextractions Of those 15 drug and dose combinations only dihy-drocodeine 30 mg could not be statistically distinguished fromplacebo because there were no trials with any useful informationin third molar extraction Figure 1 shows the proportion ofpatients achieving at least 50 pain relief with treatment Thesmallest sample for any comparison was 136 patients for celecoxib200 mg Only five of the 14 comparisons had more than 1000patients and seven had fewer than 500 patients In all systematicreviews the majority of trials had quality scores of 3 or more
The lowest (best) NNTs were for NSAIDs and COX-2 inhibitorsat standard or high doses For these NNTs could be as low as about2 (meaning that two patients had to be treated with NSAID orCOXIB for one of them to have an outcome of at least half painrelief that would not have occurred with placebo) Valdecoxib 20mg and 40 mg rofecoxib 50 mg ibuprofen 400 mg and diclofenac50 mg and 100 mg all had NNTs below 24 For all of them about60-70 of patients had at least half pain relief with active treat-ment compared with about 10 with placebo
Paracetamol 9751000 mg aspirin 600650 mg and paraceta-mol 600650 mg had NNTs of between 4 and 5 Fewer than 40 ofpatients with paracetamol at these doses had at least half painrelief with active treatment With dihydrocodeine 30 mg only 16
Table 2 Efficacy of analgesics after third molar extraction from systematic reviews of randomised double blind trials
Number () of patientswith at least 50 pain relief
Drug and dose Treatment Placebo Relative benefit Number needed to treat Total patients Total trials(95 CI) (95 CI)
Valdecoxib 40 mg 204279 (73) 19194 (10) 73 (48 to 112) 16 (14 to 17) 473 4
Diclofenac 100 mg 71102 (70) 8102 (8) 89 (45 to 175) 16 (14 to 19) 204 2
Valdecoxib 20 mg 69101 (68) 8103 (8) 88 (45 to 173) 17 (14 to 20) 204 2
Diclofenac 50 mg 112189 (59) 21178 (12) 49 (33 to 75) 21 (18 to 26) 367 5
Rofecoxib 50 mg 318557 (57) 23262 (9) 66 (44 to 99) 21 (19 to 23) 819 6
Ibuprofen 400 mg 10351835 (56) 1861567 (12) 47 (40 to 54) 22 (21 to 24) 3402 37
Ibuprofen 200 mg 323695 (46) 47499 (9) 46 (35 to 61) 27 (24 to 31) 1194 14
Ibuprofen 600 mg 90114 (79) 3889 (43) 19 (15 to 25) 28 (20 to 43) 203 3
Celecoxib 200 mg 3991 (43) 445 (9) 48 (18 to 127) 29 (21 to 48) 136 1
Paracetamol 9751000 mg 226616 (37) 40422 (9) 38 (28 to 52) 37 (31 to 47) 1038 10
Paracetamol 600650 mg + codeine 60 mg 217532 (48) 64380 (19) 25 (19 to 31) 42 (34 to 55) 911 12
Paracetamol 600650 mg 224630 (36) 76635 (12) 29 (23 to 37) 42 (36 to 52) 1265 10
Aspirin 600650 mg 6271788 (36) 2551847 (15) 25 (22 to 29) 47 (42 to 54) 3635 46
Paracetamol 300 mg + codeine 30 mg 48175 (29) 11124 (9) 33 (18 to 62) 54 (37 to 97) 299 3
Dihydrocodeine 30 mg 849 (16) 250 (4) 41 (09 to 18) not calc 99 1
Shaded areas are those analgesics used by dentists in the UK
07p407-411qxd 10092004 1519 Page 409
RESEARCH
410 BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004
With the information available standard doses of NSAIDs andCOX-2 inhibitors provided the best analgesia (Fig 2) NNTs of 2and below are indicative of very effective medicines32 The indirectcomparisons that allow us to arrive at this conclusion are only sus-tainable because the trials have the same design use patients withthe same entry criterion (moderate or severe pain intensity) withstandard measurements made in the same way over the same peri-od of time and with the same output from each trial and oneknown to be legitimate The validity of the indirect comparisonsare buttressed by the dose response of two doses of ibuprofen (400mg was better than 200 mg) and two doses of paracetamol(9751000 mg was better than 600650 mg) where there were cred-ible amounts of information A systematic review of ibuprofenversus paracetamol in dental studies also concluded that ibuprofenwas superior concordant with the indirect comparison33
The adverse event information we have tells us only aboutpatients experiencing any adverse event With the amount ofinformation available it appears that only higher doses ofcodeine with paracetamol resulted in a significantly higher ratefor this outcome than placebo In Table 3 the rate at which thisadverse event occurred with placebo varied greatly between 2
and 52 This variation will be due partly to small sizes4 butalso because we know that methods of collecting adverse eventdata impact significantly on the reported incidence and becausemethods used varied15
Information about specific adverse events is even more difficultto obtain and very large data sets are required to produce infor-mation about for instance gastric irritation with aspirin use8 Ofinterest to dentists might be the rate of alveolitis or dry socket Thisis reported in some of the newer COXIB studies but not in olderstudies There is just too little information to make a judgement
What these comparisons do not do is to tell dentists what toprescribe They and the products of other systematic reviewsshould not be used as rules but rather as evidence-based toolsto help make better policy decisions and decisions about indi-vidual patients Present prescribing practice (Table 1) showsthat for the most part effective and safe analgesics are beingused in 80 of prescriptions The exception is prescribing dihy-drocodeine 30 mg (20 of prescriptions) for which we lack sin-gle dose evidence of efficacy in dental surgery and which couldnot be distinguished from placebo in other conditions againwith little data6
Paracetamol 300 + codeine 30 mgAspirin 600650 mg
Paracteamol 600650 mgParacetamol 600650 + codeine 60 mg
Paracetamol 9751000 mgCelecoxib 200 mgIbuprofen 200 mgDiclofenac 50 mgIbuprofen 400 mgRofecoxib 50 mg
Valdecoxib 20 mgValdecoxib 40 mgDiclofenac 100 mg
1 2 3 4 5 6 7 8 9 1095 confidence interval of the NNT
Fig 2 The 95confidence interval ofthe number needed totreat (NNT) for at leasthalf pain relief over 4-6hours compared withplacebo in third molarextraction trials
Table 3 Patients experiencing any adverse event with analgesics after third molar extraction from systematic reviews of randomised double blind trials
Number () of patientsharmed with
Drug and dose Treatment Placebo Relative risk Number needed to harm Total patients Total trials(95 CI) (95 CI)
Valdecoxib 40 mg 63180 (35) 76144 (53) 06 (05 to 08) not calc 324 3
Diclofenac 100 mg 252 (4) 252 (4) 10 (12 to 68) not calc 104 1
Valdecoxib 20 mg 36100 (36) 55103 (53) 07 (05 to 09) not calc 203 2
Diclofenac 50 mg 15222 (7) 12210 (6) 12 (06 to 24) not calc 432 4
Rofecoxib 50 mg 105314 (33) 48122 (39) 09 (07 to 11) not calc 436 3
Ibuprofen 400 mg 120972 (13) 91805 (12) 11 (08 to 14) not calc 1777 19
Ibuprofen 200 mg 84554 (15) 69372 (19) 08 (06 to 10) not calc 926 10
Ibuprofen 600 mg no data
Celecoxib 200 mg no data
Paracetamol 9751000 mg 175836 (24) 103464 (20) 11 (09 to 13) not calc 1300 9
Paracetamol 600650 mg + codeine 60 mg 156490 (25) 43333 (14) 18 (13 to 25) 53 (41 to 74) 824 10
Paracetamol 600650 mg 32228 (14) 20229 (9) 16 (09 to 27) not calc 457 7
Aspirin 600650 mg 1551320 (12) 1681422 (12) 10 (08 to 12) not calc 3031 36
Paracetamol 300 mg + codeine 30 mg 29175 (15) 20124 (16) 09 (06 to 16) not calc 299 3
Dihydrocodeine 30 mg 149 (2) 150 (2) 10 (01 to 17) not calc 99 1
Shaded areas are those analgesics used by dentists in the UK
07p407-411qxd 10092004 1520 Page 410
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 411
Not all the analgesics in this review are presently available forprescribing by dentists at least in the UK The information on effi-cacy on harm and on the amount of information available shouldbe useful in any initiative to develop a prescribing formulary indentistry especially as we have growing confidence in the value ofindirect comparisons34
COMPETING INTERESTSRAM has been a consultant for MSD RAM amp HJM have consulted for variouspharmaceutical companies RAM HJM amp JE have received lecture fees frompharmaceutical companies related to analgesics and other healthcareinterventions All authors have received research support from charitiesgovernment and industry sources at various times but no such support wasreceived for this work No author has any direct stock holding in anypharmaceutical company
AUTHORS CONTRIBUTIONSJB was involved with searching data extraction quality scoring analysis andwriting JE was involved with searching data extraction quality scoring andwriting HJM was involved in analysis and writing RAM was involved in dataextraction quality scoring analysis and writing PW was involved with theoriginal concept with researching prescribing data and writing
The work was supported by Pain Research Funds and the Oxford Pain Relief TrustThe authors would like to thank Frances Fairman of the Cochrane Pain Palliativeand Supportive Care systematic review group for bringing this issue to ourattention The Department of Health Statistics Division provided data onprescribing by dentists
1 Beecher H K Keats A S Mosteller F The effectiveness of oral analgesics (morphinecodeine acetylsalicylic acid) and the problem of placebo lsquoreactorsrsquo and lsquononreactorsrsquo J Pharmacol 1953 109 93-400
2 Beecher H K The measurement of pain Pharmacol Rev 1957 9 59-2103 Houde R W Wallenstein S L Beaver W T Clinical measurement of pain In G De
Stevens (ed) Analgetics pp75-122 New York and London Academic Press 1965 4 Moore R A Gavaghan D Tramegraver M R Collins S L McQuay H J Size is everything mdash
large amounts of information are needed to overcome random effects in estimatingdirection and magnitude of treatment effects Pain 98 78 209-216
5 Ioannidis J P A Lau J Evolution of treatment effects over time Empirical insight fromrecursive cumulative metaanalyses PNAS 2001 98 831-836
6 McQuay H J Moore R A An evidence-based resource for pain relief Oxford OxfordUniversity Press 1998
7 McQuay H J Carroll D Moore R A Variation in the placebo effect in randomisedcontrolled trials of analgesics all is as blind as it seems Pain 1996 64 331-335
8 Edwards J E Oldman A Smith L Wiffen P J Carroll D McQuay H J Moore R A Oralaspirin in postoperative pain a quantitative systematic review Pain 1999 81 289-297
9 Moher D Cook D J Eastwood S Olkin I Rennie D Stroup D F Improving the quality ofreports of meta-analyses of randomised controlled the QUOROM statement Lancet1999 354 1896-1900
10 Jadad A R Carroll D Moore A McQuay H Developing a database of published reportsof randomised clinical trials in pain research Pain 1996 66 239-46
11 Collins S L Moore R A McQuay H J Wiffen P J Edward J S Single dose oral ibuprofenand diclofenac for postoperative pain In The Cochrane Library Issue 4 2000 OxfordUpdate Software
12 Edwards J E McQuay H J Moore R A Single-dose dihydrocodeine for acute
postoperative pain In The Cochrane Library Issue 4 2000 Oxford Update Software13 Moore R A Collins S L Carroll D McQuay H J Edwards J Single dose paracetamol
(acetaminophen) with and without codeine for postoperative pain In The CochraneLibrary Issue 4 2000 Oxford Update Software
14 Barden J Edwards J E McQuay H J Moore R A Rofecoxib in acute postoperative painquantitative systematic review BMC Anesthesiol 2002 2 4httpwwwbiomedcentralcom1471-225324
15 Edwards J E McQuay H J Moore R A Collins S L Reporting of adverse effects inclinical trials should be improved Lessons from acute postoperative pain J PainSympt Manage 1999 18 427-437
16 Jadad A R Moore R A Carroll D et al Assessing the quality of reports of randomizedclinical trials is blinding necessary Control Clin Trials 1996 17 1-12
17 Khan K S Daya S Jadad A R The importance of quality of primary studies inproducing unbiased systematic reviews Arch Intern Med 1996 156 661-666
18 Moher D Pham B Jones A et al Does quality of reports of randomised trials affectestimates of intervention efficacy reported in meta-analyses Lancet 1998 352609-613
19 Cooper S A Single-dose analgesic studies the upside and downside of assaysensitivity In Max M B Portenoy R K and Laska E M (eds) The design of analgesicclinical trials (Advances in Pain Research and Therapy Vol 18) pp117-124 New YorkRaven Press 1991
20 Moore A McQuay H Gavaghan D Deriving dichotomous outcome measures fromcontinuous data in randomised controlled trials of analgesics Pain 1996 66 229-237
21 Moore A McQuay H Gavaghan D Deriving dichotomous outcome measures fromcontinuous data in randomised controlled trials of analgesics Verification fromindependent data Pain 1997 69 127-130
22 Moore A Moore O McQuay H Gavaghan D Deriving dichotomous outcome measuresfrom continuous data in randomised controlled trials of analgesics Use of painintensity and visual analogue scales Pain 1997 69 311-315
23 Morris J A Gardner M J Calculating confidence intervals for relative risk odds ratiosand standardised ratios and rates In Gardner M J and Altman D G(eds) Statistics withconfidence mdash confidence intervals and statistical guidelines pp50-63 LondonBritish Medical Journal 1995
24 Gavaghan D J Moore R A McQuay H J An evaluation of homogeneity tests in meta-analyses in pain using simulations of individual patient data Pain 2000 85 415-424
25 Higgins J Thompson S Deeks J Altman D Statistical heterogeneity in systematicreviews of clinical trials a critical appraisal of guidelines and practice J Health SurvRes Policy 2002 7 51-61
26 LAbbeacute K A Detsky A S ORourke K Meta-analysis in clinical research Ann Intern Med1987 107 224-233
27 Sterne J A Gavaghan D Egger M Publication and related bias in meta-analysispower of statistical tests and prevalence in the literature J Clin Epidemiol 2000 531119-1129
28 Tang J-L Liu J L Y Misleading funnel plot for detection of bias in meta-analysis J ClinEpidemiol 2000 53 477-484
29 Cook R J Sackett D L The number needed to treat a clinically useful measure oftreatment effect Br Med J 1995 310 452-454
30 Carroll D Tramegraver M McQuay H Nye B Moore A Randomization is important instudies with pain outcomes systematic review of transcutaneous electrical nervestimulation in acute postoperative pain Br J Anaesth 1996 77 798-803
31 Schulz K F Chalmers I Hayes R J Altman D G Empirical evidence of bias dimensionsof methodological quality associated with estimates of treatment effects incontrolled trials J Am Med Assoc1995 273 408-412
32 McQuay H J Moore R A Using numerical results from systematic reviews in clinicalpractice Ann Intern Med 1997 126 712-720
33 M Hyllested Jones S Pedersen J L Kehlet H Comparative effect of paracetamolNSAIDs or their combination in postoperative pain management a qualitative reviewBr J Anaesth 2002 88 199-214
34 F Song Altman D G Glenny A M Deeks J J Validity of indirect comparison forestimating efficacy of competing interventions empirical evidence from publishedmeta-analyses Br Med J 2003 326 472-476
07p407-411qxd 10092004 1520 Page 411
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
Relative efficacy of oral analgesics after third molar extraction ndash a 2011 updateS Derry1 P J Wiffen2 and R A Moore3
and reporting and were all of high meth-odological quality the relative efficacy of different analgesics is justifiable when established against the common comparator of placebo3 Moreover the methods have been extensively examined and validated using individual patient data analyses45
Several approaches can be used to pre-sent results The percentage of patients who benefit with treatment is one approach obviously the higher the number
In 2004 the British Dental Journal carried a review examining analgesic efficacy meas-ured after third molar extractions1 predom-inantly derived from Cochrane reviews of single dose analgesics in established mod-erate or severe pain In the intervening years the reviews on which it was based have been extended to other analgesics and updated to include relevant additional clinical trials performed in the past decade
The culmination of this work has been the publication by the Cochrane Collaboration of an overview of these updated systematic reviews2 The overview included 35 sepa-rate Cochrane Reviews with 38 analyses of single dose oral analgesics tested in acute postoperative pain models with results from about 45000 participants studied in approximately 350 individual studies About 29000 patients contributed data to trials in dental pain
Each individual review reported results for dental studies where data were avail-able overwhelmingly in the third molar extraction pain model Because all of the reviews used identical methods outcomes
This article provides a summary of the efficacy and relative efficacy of 38 different drugs or drug combinations tested in standard postoperative pain trials It will help clinicians and patients make informed choices about analgesia based on pain relief duration of action and adverse events which can then be put into context for the individual patient depending on local availability This article highlights the fact that no single drug is effective in all patients ndash even the best drugs fail to provide good levels of pain relief in at least 30 These patients should try a different analgesic
the better Another way is to look at the number needed to treat (NNT) for one patient to benefit this is the treatment-specific effect and can be expressed as 100(active - placebo) The ideal NNT is 1 where everyone gets better with treatment and no one does with placebo lower numbers are better In dental tri-als where about 10 of patients benefit with placebo the best possible NNT is 100100 - 10 = 11
13Pain Research and Nuffield Division of Anaesthet-ics Department of Clinical Neurosciences University of Oxford The Churchill Hospital Oxford OX3 7LJ 2UK Cochrane Centre Summertown Pavilion 18-24 Middle Way Oxford OX2 7LG Correspondence to R Andrew Moore Email andrewmoorepruoxacuk
Refereed Paper Accepted 12 September 2011 DOI 101038sjbdj2011905 copyBritish Dental Journal 2011 211 419-420
bull Summarises the known evidence on efficacy of oral analgesics in dental pain
bull Describes shorter term pain relief and time needed before remedication
bull Provides an evidential context for making decisions about individual patients or practice guidelines
I N B R I E F
PRA
CTICE
Table 1 Efficacy results in dental pain studies for a range of commonly used analgesics
Drug and dose (mg)Number of
Percent with at least 50 maxi-mum pain relief NNT
Median time to remedication (hr)
Trials Patients Active Placebo
Aspirin 600650 mg 45 3581 36 14 45 (40 to 52) 30
Aspirin 1000 mg 4 436 35 11 42 (32 to 60) no data
Celecoxib 400 mg 4 620 34 3 25 (22 to 29) 84
Diclofenac 50 mg (Na and K) 9 1119 56 19 27 (24 to 31) 43
Diclofenac 50 mg K 5 622 65 16 21 (19 to 24) no data
Etoriocoxib 120 mg 4 500 71 9 16 (15 to 18) gt24
Ibuprofen 400 mg 49 5428 55 12 23 (22 to 24) 56
Ibuprofen 400 mg soluble 9 959 66 10 18 (17 to 20) no data
Ibuprofen 200 mg + paracetamol 500 mg 2 280 74 10 16 (14 to 18) gt8
Naproxen 500550 mg 5 402 61 7 18 (16 to 21) 89
Paracetamol 1000 mg 19 2157 41 10 32 (29 to 36) 39
Note that data for remedication time were not generally available for dental studies separately and the values reported apply to all postoperative conditions though predominantly third molar extraction
BRITISH DENTAL JOURNAL VOLUME 211 NO 9 NOV 12 2011 419
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
PRACTICE
This brief report describes the main results of interest to dentists using results from the Cochrane overview and from a recent analysis of a combination of ibu-profen and paracetamol5
RESULTSTable 1 reports data for aspirin celecoxib diclofenac etoricoxib ibuprofen ibu-profen plus paracetamol naproxen and paracetamol Widely differing amounts of information were available for individual drugs from as few as 402 patients for nap-roxen 500550 mg and as many as 5428 for ibuprofen 400 mg
One outcome reported is the percentage of patients with initially moderate pain (30-60 mm on a 100 mm VAS) or severe pain (more than 60 mm) who obtained at least 50 of the maximum possible pain relief over a 4-6 hour period after taking the tab-lets This is a high test of efficacy achieved by only about 10 of patients who received no active treatment (placebo) but achieved by 34-74 of those who did get the active drug Ibuprofen 200 mg plus paracetamol 500 mg and etoricoxib 120 mg achieved
response rates above 70 paracetamol 1000 mg achieved only a 41 response rate
Several products had an NNT of about 2 or below the combination of ibupro-fen 200 mg plus paracetamol 500 mg etoricoxib 120 mg ibuprofen 400 mg in a soluble form naproxen 500550 mg and 50 mg of the potassium salt of diclofenac (the sodium salt being much less effective in this assay Fig 1)
A new outcome that some will con-sider relevant is the time required for half the patients to need more analgesia the time to remedication Longer duration is another indicator of greater effect and for a number of analgesics median remedica-tion times are beyond eight hours
DISCUSSIONThe 2004 review included evidence for rofecoxib and valdecoxib neither of which is available today New relevant informa-tion includes data on the ibuprofen plus paracetamol combination different ibu-profen and diclofenac formulations and etoricoxib all of which are among the most efficacious analgesics after third
molar surgery Greater efficacy and longer duration of action tended to go together
For one analgesic relevant to dentistry the evidence is largely silent For dihydrocodeine 30 mg (still commonly used by dentists) only 136 patients were found in trials in dental pain with only 24 obtaining at least 50 maximum pain relief compared with 7 with placebo The resultant NNT was 6 far worse than available for drugs in Table 1 and far worse than ibuprofen 400 mg in the only direct comparison6 The Cochrane overview concluded that the results for dihy-drocodeine were not robust because of the smallness of the data set available and that unpublished results from just 46 patients in zero effect trials would be needed to make any result clinically irrelevant
CONCLUSIONThe amount of evidence available on single dose studies of analgesics in dental pain is large and readily available These results are tools to help formulate policy and pre-scribing for individuals and populations
1 Barden J Edwards J E McQuay H J Wiffen P J Moore R A Relative efficacy of oral analgesics after third molar extraction Br Dent J 2004 197 407ndash411
2 Moore R A Derry S McQuay H J Wiffen P J Single dose oral analgesics for acute postoperative pain in adults Cochrane Database Syst Rev 2011 9 CD008659
3 Song F Altman D G Glenny A M Deeks J J Validity of indirect comparison for estimating efficacy of competing interventions empirical evidence from published meta-analyses BMJ 2003 326 472
4 Moore R A Edwards J E McQuay H J Acute pain individual patient meta-analysis shows the impact of different ways of analysing and presenting results Pain 2005 116 322ndash331
5 Moore R A Straube S Paine J Derry S McQuay H J Minimum efficacy criteria for comparisons between treatments using individual patient meta-analysis of acute pain trials examples of etoricoxib paracetamol ibuprofen and ibuprofenparacetamol combinations after third molar extraction Pain 2011b 152 982ndash989
6 Moore R A Edwards J Derry S McQuay H J Single dose oral dihydrocodeine for acute postop-erative pain Cochrane Database Syst Rev 2000 2 CD002760
Ibuprofen 200mg + paracetamol 500 mg
Ibuprofen 400 mg
Aspirin 600650 mg
Aspirin 1000 mg
Paracetamol 1000
Naproxen 500550
Diclofenac 50 mg (Na and K)
Celecoxib 400 mg
Diclofenac 50 mg K
Ibuprofen 400 mg soluble
Etoriocoxib 120 mg
1 2 3 4 5 6
NNT for at least 50 maximum pain relief (95 CI)
Fig 1 NNTs in dental pain studies for a range of commonly used analgesics
420 BRITISH DENTAL JOURNAL VOLUME 211 NO 9 NOV 12 2011
Combining paracetamol with a selectivecyclooxygenase-2 inhibitor for acutepain relief after third molar surgerya randomized double-blindplacebo-controlled study
Birgitta Haglund12 Inger vonBltzingslccedilwen1
1Public Dental Health Service KarlstadVrmland Sweden 2Department of ClinicalPharmacology Sahlgrenska Academy atGccedilteborg University Sweden
Traditional non-steroidal anti-inflammatory drugs(NSAIDs) [ie non-selective cyclooxygenase (COX)inhibitors such as ibuprofen and diclofenac] have beenwidely used in outpatients for acute pain relief followingoral surgery Their anti-inflammatory and analgesicproperties together with well-established tolerabilitymake them an initial choice for the management of mostforms of mild to moderate pain in outpatients (1 2)However these drugs have well-documented adverseeffects such as gastrointestinal intolerability Further-more they need to be administered several times a dayMore effective and practical pain relief regimes withfewer side-effects are needed for moderate to severe painafter oral surgeryNSAIDs act by inhibiting COX enzymes which are
responsible for the production of prostaglandin fromarachidonic acid This acid emerges from the breakdownof phospholipids in the cell walls of damaged tissue (3)Prostaglandin elicits a number of biological effects someof which contribute to the inflammatory process leading
to pain Multiple COX enzymes have been identifiedCOX-1 is mainly expressed under physiological condi-tions throughout the body for example by platelets (4)and COX-2 is related to inflammation and pain (4ndash6)although COX-1 and COX-2 also have overlappingproperties (7) Improved knowledge on more selectiveCOX enzymes led to the development of specific COX-2inhibitors such as rofecoxib (8) and celecoxib withanalgesic anti-inflammatory and gastroprotective prop-erties Of these drugs rofecoxib has been shown to bemore effective than celecoxib (9ndash11)Rofecoxib has the same analgesic effect as ibuprofen
but with the benefit of a longer duration (9 10 12) It hasa long half-life which makes it suitable for once-dailydosing (12) compared with traditional NSAIDs thatneed to be taken several times per day Rofecoxib hasalso been suggested to be more effective than paracet-amol combined with codeine (13 14) The COX-2inhibitor rofecoxib may be an interesting choice for acutepain relief after oral surgery
Haglund B von Bulzingslowen I Combining paracetamol with a selective cyclooxyge-nase-2 inhibitor for acute pain relief after third molar surgery a randomized double-blind placebo-controlled study Eur J Oral Sci 2006 114 293ndash301 2006 The AuthorsJournal compilation 2006 Eur J Oral Sci
Severe pain after third molar surgery is often encountered and more effective treatmentregimes are warranted The objective of this study was to evaluate if the combinationof paracetamol and rofecoxib a selective cyclooxygenase-2 (COX-2) inhibitorimproves analgesic effects following third molar surgery compared with rofecoxibalone Paracetamol alone was also evaluated Altogether 120 patients with moderate tosevere pain after third molar surgery were given a single postoperative dose of one ofthe following treatments rofecoxib + paracetamol rofecoxib alone paracetamolalone or placebo Patients assessed level of pain and pain relief every 30 min for 8 hafter surgery and made a global evaluation of the medication 4 and 8 h after surgeryParacetamol and rofecoxib combined improved the analgesic effect compared withrofecoxib alone for the first 15 h Rofecoxib alone and the combination of paracet-amol and rofecoxib had a significantly better analgesic effect than paracetamol alonefrom 3 h onwards The early onset of pain relief for the combination of paracetamoland rofecoxib compared with rofecoxib alone could be of great importance whentreating acute pain after third molar surgery After data collection for this studyrofecoxib was withdrawn from the market as a result of reported fatal cardiovascularevents Whether this is relevant for short-term use is unknown but it has to be con-sidered before rofecoxib may be used for pain relief following third molar surgery
Birgitta Haglund Folktandvrden TingvallaBox 577 SE-651 13 Karlstad Sweden
Telefax +46ndash54ndash137435E-mail birgittahaglundlivse
Key words COX-2 inhibitor pain relief para-cetamol randomized trial third molar surgery
Accepted for publication April 2006
Eur J Oral Sci 2006 114 293ndash301Printed in Singapore All rights reserved
2006 The AuthorsJournal compilation 2006 Eur J Oral Sci
European Journal ofOral Sciences
Combining drugs that cause analgesia through differ-ent mechanisms may give additive analgesic effects (15)and lead to dose-sparing effects and improved safety(16) The analgesic mechanism of COX inhibition ispredominantly peripheral Research on paracetamol hasnot been able to delineate a clear mechanism of actionbut it is suggested to lie predominantly in the centralnervous system (17) Some studies indicate that combi-ning a traditional NSAID and paracetamol after oralsurgery may enhance the analgesic effect compared withsingle drug regimes (18 19)The theory of the analgesic effect of traditional
NSAIDs being caused by COX-2 inhibition leads to thethought that an additive effect should be present alsowhen combining rofecoxib and paracetamol The aim ofthis study was therefore to explore in a third molarsurgery pain model (20) if there is an additive analgesiceffect when combining the COX-2 selective inhibitorrofecoxib with paracetamol compared with rofecoxibalone for acute pain relief We also compared the anal-gesic efficiency of rofecoxib and paracetamol becausethis to our knowledge has not been reported followingthird molar surgery
Material and methods
Study design
This study was designed as a multicenter randomizeddouble-blind placebo-controlled study with a single dose ofrofecoxib 50 mg and paracetamol 1 g combined vs rofec-oxib 50 mg alone vs paracetamol 1 g alone vs placebogiven postoperatively to patients stating moderate to severepain after surgical removal of one or two lower third molarsPatients were asked to give written informed consent toparticipate after being told about the procedures A total of120 patients were randomized into four different treatmentgroups as follows 40 patients receiving the combination ofrofecoxib 50 mg and paracetamol 1 g 40 patients receivingrofecoxib 50 mg alone 20 patients receiving paracetamol 1 galone and 20 patients receiving placebo The patientsrsquoevaluations of the treatments were obtained by using aquestionnaire which the patients filled in at home during an8-h study period following intake of the study medicationThe trial was approved by the Regional Ethical Committeeof Medical Research in Orebro Sweden and the MedicalProducts Agency in Uppsala Sweden
Patients
Consecutive patients visiting four general dental practicesand in need of mandibular third molar surgery in accordancewith the National Institutes of Health (NIH) guidelines (21)were screened for enrollment Only patients with thirdmolars needing bone removal were included Other inclusioncriteria were age gt18 yr weight gt50 kg butlt120 kg andan appointment before noon for surgery This was necessaryin order for the patients to have time to fill in the ques-tionnaire for 8 h after intake of the study medication beforebedtime Exclusion criteria were as follows intolerance toacetylsalicylic acid (ASA) paracetamol andor NSAIDsany ongoing medication (except contraceptives) pregnancylactation inadequate contraception alcohol or drug abusePatients with evidence of previous or present cardiovascular
respiratory diabetic hepatic gastric renal neurological orneoplastic diseases were also excluded as were those withongoing pericoronitis or other local oral infections involvingpain Patients with an intake of any analgesics 6 h precedingsurgery was also excluded All patients who met the studycriteria and reported moderate to severe pain after the sur-gery were included in the study
Surgery
The surgery was performed by one of four dentists speciallytrained in dento-alveolar surgery using local anesthesia(lidocaine 20 mg ml)1 plus epinephrine 125 lg ml)1) Theremoval of bone was carried out with a burr under thecooling of saline
Masking randomization and rescue medication
The study medications were masked by being encapsula-ted in identical capsules The capsules contained 50 mg ofrofecoxib 200 mg of paracetamol or placebo All patientswere given a sealed container containing six capsules(Table 1) so that the patients in the different treatmentgroups received the correct amount of medication and stillthe same number of capsules The capsules were manu-factured by Apoteket Production amp Laboratories (APLStockholm Sweden) Randomization of the patients intothe four treatment groups was performed for the group intotal by Apoteket using randomization tables All studypersonnel and participating patients were blinded totreatment assignment for the duration of the study Themain investigator broke the codes for the final calcula-tionsIbuprofen 400 mg was used as a rescue medication in case
patients needed additional analgesia at any time during the8-h study period The rescue medication was kept in aseparate container If patients felt that rescue medicationwas needed they were instructed to wait 90 min if possibleafter intake of their study medication to allow for the studydrug to take effect
Intake of study medication and information about thequestionnaire
After surgery the patients were given their two containerswith study and rescue medications respectively together
Table 1
Distribution of the drug capsules with the different substances percontainer in each study group
Study groups
Rofecoxib50 mg +
paracetamol 1 gRofecoxib50 mg
Paracetamol1 g Placebo
Rofecoxib50 mg
1 1 0 0
Paracetamol200 mg
5 0 5 0
Placebo 0 5 1 6Total no ofcapsules ineach container
6 6 6 6
294 Haglund amp Bultzingslowen
with the questionnaire Routine postoperative informationwas given The patients were instructed to go home and takeno medication before calling the investigator when theyregained full sensibility in the lower lip following the dis-appearance of the local anesthesia If the patient had notcalled the investigatorrsquos mobile phone within 3 h after theend of surgery the investigator called the patientAt the telephone contact the patients were asked to state
their level of pain in the questionnaire using a 3-point scalefrom mild to moderate to severe pain If patients statedmoderate or severe pain they were asked to break the seal ofthe container with their study medication and take all sixcapsules Detailed instructions were provided on how to fill inthe questionnaire To ascertain that patients adhered to theprotocol information was given to contact the investigatorwith any questions regarding medication or other issuesconcerning the studyduring the 8-h postoperative periodThestudy period started at the time of intake of the study medi-cation If patients stated mild pain they were asked if theycould tolerate waiting before taking any medication In suchcases a second telephone contact was made If patients stillstatedmild pain they were asked if it was possible for them toreturn their sealed container with the study medicationPatients who did so were replaced with another patient
Efficacy assessments
The outcome measures of the trial were pain intensity painrelief (PAR) global evaluation score (patientsrsquo overallassessment of the medication) derived summary measuresuse of rescue medication and side-effects experienced allrecorded by the patients in their questionnaire After intakeof the study medication pain intensity and PAR wasassessed by the patient every 30 min for 8 h and the globalevaluation score was measured at 4 and 8 h The startingpoint for each patient was the time for intake of studymedication The final measurement point was the end of theobservation period (ie 8 h later) or the time of intake ofrescue medication If rescue medication was used patientswere asked to assess pain intensity and pain relief and give aglobal evaluation score at the time of intake These scoreswere then used for the rest of the observation period inaccordance with a study by Laska et al (22)Pain intensity was evaluated by the patients using a
horizontal visual analog scale (VAS) of 10 cm marked nopain at 0 and worst possible pain at 10 PAR was meas-ured on a 5-point scale as follows 0 no pain relief 1 somepain relief 2 medium pain relief 3 good pain relief and 4total pain relief Global evaluation score was measured on a4-point scale as follows 0 poor 1 fair 2 good and 3excellent Patients using rescue medication recorded the timeof intake A question about any side-effects experienced wasanswered by yes or no at the end of the study period Ifyes the patients estimated adverse events on a 3-point scale(1 slight 2 moderate 3 severe) and reported what kind ofside-effect was experienced
Analysis
The analgesic effect of the drugs measured every 30 min bypain intensity (VAS) and PAR scores was comparedSummary measures were calculated by the use of the fol-lowing total pain relief (TOTPAR the sum of all PARscores for the whole study period of 05ndash8 h) pain intensitydifference (PID pain intensity at the start minus painintensity at any given observation point) sum of PID for the
05ndash3-h period (SPID05)3 h) and sum of PID for the total05ndash8-h period (SPIDtotal) PID values were not analyzedseparately but used for the calculation of SPIDThe use of rescue medication was compared between the
treatment groups by calculating the percentage of patientsin each group who used rescue Also the mean timebetween intake of the study medication and intake of therescue medication in the different groups was analyzedSide-effects in the treatment groups were compared interms of percentage of patients in each group whoexperienced such problems Median global evaluationscores between the different groups were analyzed as wellas the percentage of patients in each group using the dif-ferent scores
Statistics
The sample size calculations were carried out assuming adifference in SPID outcome between groups using thecombination of rofecoxib + paracetamol and rofecoxibalone amounting to 20 (18) with a power of at least 80and a standard deviation (SD) of 15 using non-para-metric statistics (MannndashWhitney U-test) This calculationestimated that a minimum of 22 patients should be includedin each groupStandard descriptive statistics and tests were used and the
calculations were performed in Statistical Package for SocialSciences (spss) version 12 The principle of last observationcarried forward was used Significances between groupsregarding VAS scores were tested with an independent-samples t-test at each time point for all possible compari-sons as we considered VAS to be a continuous scale inaccordance with Max et al (23) The same applies for thetesting of SPID up to 3 and 8 h The analysis of TOTPARwas based on an assumption that the scores are consideredinterval scaled (23) and significance testing was carried outwith an independent samples t-test The same test was usedfor testing differences between study groups regarding theuse of rescue medication Hypothesis testing of valuesmeasured with categorical ordinal scales (ie PAR andglobal evaluation) was performed with a non-parametrictest (MannndashWhitney U-test) P-values of lt005 were con-sidered statistically significant
Results
Altogether 126 consecutive patients who fulfilled theinclusion criteria gave written informed consent to par-ticipate in the study The majority of the patients whowere asked to participate agreed to do so Patients whodeclined to participate usually did not have a before-noon appointment for the surgery Out of the 126patients six were excluded as they stated their pain asmild at the telephone contacts and were able to returntheir sealed study medication A total of 120 patientsparticipated by taking the randomized study medicationSome patients (n frac14 8) who did not fulfill the criterion ofmoderate to severe pain but nevertheless wanted toparticipate took their study medication but wereexcluded from the calculations Of these patients ahigher proportion was men (75) compared with thestudied population Some patients (n frac14 5) were excludedfor other reasons one patient randomized to the
COX-2 inhibitor and paracetamol after oral surgery 295
rofecoxib group took her rescue medication after only30 min as a result of severe pain and withdrew from thestudy one did not manage to fill in the questionnaireand three did not return their questionnaires althoughthey were repeatedly reminded to do so Final outcomedata were calculated on the following cohort of 107 pa-tients rofecoxib + paracetamol (n frac14 34) rofecoxibalone (n frac1436) paracetamol alone (n frac14 20) and placebo(n frac14 17)The principal investigator and one of the dentists
performed the majority of the operations 43 and 55respectively in total 98 out of 120 The remaining 22operations were performed by the two other dentists oneoperating on 10 and the other on 12 patients as theirstock of patients fulfilling the inclusion criteria wassmaller The principal investigator was in contact withand gave instructions to the 98 patients The 22remaining patients received their instructions from oneof the other two dentists performing the operationsThere were no differences between groups regarding
baseline characteristics and the number of molarsremoved (Tables 2 and 3) In total 56 of the partici-pants were men The mean age of the patients was 27 yr(range 18ndash54) and the mean weight was 73 kg (range 50ndash120) Mean total duration of the surgery was 14 min Intotal 91 patients (85) had one mandibular molar
removed during the operation and 16 (18) had anadditional maxillary molar removed The remaining 16patients (15) had two mandibular molars removed atthe same session (Table 3) There was no difference inpain intensity (VAS) at the start between patients whohad one or two molars removed At the time of intake ofthe study medication 83 of all patients included in theanalysis reported moderate pain and 17 reportedsevere pain There were no major differences in painreported among patients operated on by the differentdentists
Analgesic effect
Pain intensity (VAS) ndash The analgesic effect over the 8-hstudy period recorded by patients using the VAS isshown in Fig 1 Separate curves with confidence inter-vals for study groups are presented in Fig 2 Patientsused the scale from 0 up to 95There was a significant difference in mean VAS score
between the combination group and the rofecoxibgroup at 30 min 1 h and 15 h in favor of thecombination (P lt 005) At 2 h and subsequentlyparacetamol did not show any statistically significantadditive effect when combined with rofecoxib com-pared with rofecoxib aloneWhen comparing rofecoxib and paracetamol after
30 min paracetamol was significantly better regardingeffect on pain intensity (P lt 005) Paracetamol tendedto have a better analgesic effect than rofecoxib (althoughthis was not statistically significant) for another hourafter the starting point From 3 h until the end of thestudy period rofecoxib was significantly better thanparacetamol (P lt 005)Compared with placebo the combination treatment
as well as the single drug treatments resulted in signifi-cantly lower pain intensity scores at all observationpoints except for rofecoxib at 30 min
Pain relief (PAR) ndash The median PAR scores (Fig 3)showed a pattern similar to the mean pain intensityassessment The combination treatment was significantly
Table 2
Baseline characteristics for each study group
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Gender malefemale 1915 2016 128 98Age (yr) 25 (19ndash35) 26 (18ndash41) 29 (19ndash52) 28 (19ndash54)Weight (kg) 73 plusmn 9 70 plusmn 13 79 plusmn 17 72 plusmn 13Volume of local anesthetic (ml) 54 plusmn 2 58 plusmn 1 56 plusmn 1 56 plusmn 1Length of surgery (min) 13 plusmn 7 15 plusmn 8 13 plusmn 7 15 plusmn 6Time from end of surgery tointake of study medication (min)
155 plusmn 37 170 plusmn 45 184 plusmn 53 161 plusmn 30
Pain intensity (VAS) at the start 51 plusmn 18 54 plusmn 16 51 plusmn 18 46 plusmn 15
Mean (range)Mean plusmn SDVAS visual analog scale
Table 3
Number of mandibular and maxillar third molars removed in eachstudy group
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
1 mandibular 24 24 15 122 mandibulars 5 6 3 21 mandibular+ 1 maxillar
5 6 2 3
296 Haglund amp Bultzingslowen
better than rofecoxib alone at 30 min (P lt 005) and at1 h (P lt 001) For the rest of the observation periodthere was no significant difference
Between rofecoxib and paracetamol there was a sig-nificant difference in median PAR score in favor ofparacetamol at 30 min and at 1 h (P lt 005) after drug
Placebo
01234567
0 1 2 3 4 5 6 7 8
Paracetamol 1g
01234567
0 1 2 3 4 5 6 7 8
Rofecoxib 50 mg
01234567
0 1 2 3 4 5 6 7 8
Rofecoxib 50 mg+paracetamol 1 g
01234567
0 1 2 3 4 5 6 7 8
Fig 2 Mean pain intensity recorded on a visual analog scale (VAS) and confidence intervals in study groups during the studyperiod of 8 h
0
1
2
3
4
5
6
0 05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
AV
s S
cr
oe
placebo
paracetamol 1g
rofecoxib 50mg
rofecoxib 50mg +paracetamol 1g
Hours from intake of study medication
Fig 1 Mean pain intensity in study groups recorded on a 10-cm visual analog scale (VAS) at each observation point For signifi-cance tests see the Results
0
05
1
15
2
25
3
35
Pai
n r
elie
f sc
ore
placebo
rofecoxib 50mg
rofecoxib 50mg +
05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
paracetamol 1g
paracetamol 1g
Hours from intake of study medication
Fig 3 Median pain relief (PAR) score in study groups at each observation point Pain relief was assessed using the following scale0 no pain relief 1 some pain relief 2 medium pain relief 3 good pain relief and 4 total pain relief For significance tests see theResults
COX-2 inhibitor and paracetamol after oral surgery 297
intake There was instead a significant difference in favorof rofecoxib from 25 h (P lt 005) and from 3 h(P lt 001) to the end of the observation period Only atthe observation time-points of 15- and 2-h was there nosignificant difference between the two drugs regardingmedian PAR scoresThe combination treatment and the single treatments
were significantly better than placebo throughout thewhole observation period of 8 h
Total pain relief (TOTPAR) ndash There was no significantdifference in mean TOTPAR between the combinationtreatment group and the rofecoxib-alone group (Table 4)However rofecoxib gave significantly better TOTPARthan paracetamol (P lt 005) All the active treatmentgroups gave better TOTPAR than placebo (P lt 0001)
Sum of pain intensity differences (SPID) ndash The combi-nation group had the highest mean SPID05)3 h scorehowever this was not statistically different from rofecoxibalone (Table 4)No significant difference in SPID0)3 h wasseen between rofecoxib and paracetamol All active treat-ments were significantly better than placebo (P lt 0001)
The mean PID over the whole observation period (iemean SPIDtotal) shows that the combination group didnot differ from the rofecoxib group (Table 4) Therofecoxib group was significantly better than paracet-amol alone (P lt 005) All active treatments weresignificantly better than placebo (P lt 0001)
Use of rescue medication ndash The use of rescue medicationmeasured as the cumulative percentage of patients ineach study group needing analgesic rescue at any timeduring the 8-h observation period is shown in Fig 4There was no significant difference regarding the totalpercentage of patients using rescue when comparing thecombination group with the rofecoxib group (Table 4)Figure 4 indicates a major difference between the rofec-oxib and paracetamol groups This difference is how-ever not significant (P frac14 0055) owing to few patientsneeding rescue medication Both the combination groupand the rofecoxib group used significantly less rescuethan the placebo group (P lt 0001) Paracetamol failedto show a significant difference to placebo regardingpercentage of patients using rescue medication (P frac140066)
Table 4
Summary of efficiency measures
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Mean TOTPAR05ndash8 h (SE)
452 (20) 409 (27) 287 (44) 91 (27)
Mean SPID05ndash3 h (SE)
182 (19) 151 (18) 111 (34) )32 (23)
Mean SPIDtotal (SE)
526 (59) 515 (60) 208 (96) )101 (57)
Percentage of patients using rescue medication (SE) 88 (49) 167 (63) 400 (112) 706 (114)Mean time (min) to use of rescue medication (SE) 234 (42) 270 (58) 228 (48) 127 (16)Median global evaluation score (0ndash4) at 4 h 2 2 1 0Median global evaluation score (0ndash4) at 8 h 3 2 1 0
P lt 005 vs placebo P lt 001 vs placebo P lt 0001 vs placeboP lt 005 vs paracetamol P lt 001 vs paracetamol P lt 0001 vs paracetamolSE standard error SPID sum of pain intensity differences TOTPAR total pain relief
0
10
20
30
40
50
60
70
80
05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
Hours from intake of study medication
Cum
ula
itve
perc
enat
geof
paite
nst
taki
gnre
scue
me
idca
tion placebo
paracetamol 1g
rofecoxib 50mg
rofecoxib 50mg +paracetamol 1g
Fig 4 Cumulative percentage of patients in each group using rescue medication during the study period of 8 h For significance testssee the Results
298 Haglund amp Bultzingslowen
There was no statistically significant difference in themean time from intake of study medication to intake ofrescue medication in the different active treatmentgroups However for all active treatments the time wassignificantly longer than for placebo (Table 4)
Side-effects
The majority of all patients 738 reported no adverseevents while 187 experienced side-effects Another75 did not answer this question The majority (789)of the patients with side-effects reported that these wereonly slight while 211 reported moderate side-effectsNo patients reported any severe side-effects No pro-nounced difference was seen between the groupsregarding side-effects The types of side-effects experi-enced are listed in Table 5
Global evaluation
Patientsrsquo median global evaluation scores of their studymedications are shown in Table 4 After 4 h thecombination treatment and rofecoxib alone receivedsimilar evaluations Both groups were significantlybetter than paracetamol (P lt 0001 P lt 001) at thistime All active treatments were significantly betterthan placeboAt 8 h the combination group had the highest score
but the difference from the rofecoxib group was verysmall and not significant (Table 4) Both groups weresignificantly better than paracetamol alone (P lt 0001P lt 001) at 8 h All treatment groups were significantlybetter than placeboThe global evaluation scores are further specified in
Table 6 After 8 h 90 of the patients in the combina-tion group rated their medication as good or excellentFor the rofecoxib group the corresponding value was83 Of the patients treated with paracetamol 42rated their medication as good or excellent after 8 h
Discussion
In this study we showed that for the acute inflammatorypain following third molar surgery there was an additive
analgesic effect when combining rofecoxib with paracet-amol as compared with rofecoxib alone for the first 15 hafter intake After this time point the combination ofrofecoxib and paracetamol gave similar pain relief to thatof the rofecoxib group Paracetamol alone was also moreeffective for the first 15 h while rofecoxib was signifi-cantly better thanparacetamol from3 honwards The factthat rofecoxib and paracetamol were more effective thanplacebo shows that the method used was sensitive enoughto distinguish between different substancesAfter the clinical part of this study was carried out
serious concerns regarding cardiovascular effects of long-term treatment with rofecoxib were raised following re-ports of an increased incidence of myocardial infarctionand stroke among patients treated with rofecoxib in aplacebo-controlled study (24) After a highly significant19-fold increase in the incidence of thrombo-embolicserious adverse events was shown in yet another study(25) rofecoxib was withdrawn from the market Theside-effects of rofecoxib became progressively greaterafter 1 yr of treatment which suggests that the cardio-vascular risk is dose-dependent and not only associatedwith COX-2 selectivity (6) The need for acute pain reliefafter third molar surgery is short and the surgery ismainly performed in otherwise healthy young peopleamong whom the risk for serious cardiovascular events issmall It cannot be ruled out that future further devel-oped selective COX-2 inhibitors may be useful intreating acute pain after third molar surgery in this groupof patients with the advantage of only one dose a dayand minimizing the risk for gastrointestinal symptomsRofecoxib and paracetamol differ in onset time and
patients treated with rofecoxib reach meaningful painrelief after 15 h (8) compared with 05 h for paracet-amol This corresponds well with the results obtained inour study The group treated with paracetamol reportedtheir lowest VAS score by 1 h whereas at this time pointthe rofecoxib group still reported a high VAS scoreThereafter the medium VAS score for the paracetamolgroup increased while patients treated with rofecoxibcontinued to receive good pain relief until the end of theobservation period From these results it is reasonable toassume that the combination grouprsquos significantly betteranalgesic effect between 05 and 1 h compared with
Table 5
Side-effects as stated in patientsrsquo own words
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Fatigue 4 2 3 2Headache 1 2 ndash 2Fever ndash ndash ndash 1Dizziness 1 ndash 2 ndashStomach pains 1 ndash 1 ndashSickness ndash 1 ndash ndashShivers 1 2 ndash ndashPerspirations ndash 1 ndash ndash
Table 6
Percentage of patients in each study group stating their overallexperience of the study medication at 4 and 8 h
Study groups
Rofecoxib+
paracet-amol
(n frac14 34)Rofecoxib(n frac14 36)
Paracet-amol
(n frac14 20)Placebo(n frac14 17)
4 h 8 h 4 h 8 h 4 h 8 h 4 h 8 h
Poor 0 0 7 6 30 32 75 76Fair 6 10 7 11 40 26 18 18Good 47 32 43 36 15 26 7 6Excellent 47 58 43 47 15 16 0 0
COX-2 inhibitor and paracetamol after oral surgery 299
rofecoxib alone was a result of the earlier onset of theeffect of paracetamol The mean VAS scores for thecombination group and the paracetamol group corres-ponds totally at the 30-min observation pointThe peak pain after third molar surgery has been
shown to occur 4ndash6 h postoperatively (26) which coin-cides well with the time for the additive effect of para-cetamol to take effect in our study This supports the useof the combination treatment of rofecoxib and paracet-amol after third molar surgery to gain an early onsetparticularly if pain relief medication is started postop-eratively as it is of great clinical importance to have anearly onset of pain relief when treating acute pain Iftreatment starts pre-operatively the addition of para-cetamol is likely to have less clinical relevance This issupported by a study in which patients were givenrofecoxib and paracetamol before Ear Nose and Throat(ENT) surgery (27) The addition of paracetamol in thatsetting failed to improve the analgesic effects of rofec-oxibRofecoxib and paracetamol also differ in duration
The effect of paracetamol 1 g lasts up to 6 h and the drughas to be administered four times daily while rofecoxib50 mg has an analgesic effect up to 24 h (12) The presentstudy was a single-dose comparison In a normal clinicalsetting another 1 g of paracetamol would probably beprescribed after 6 h which would give another period ofadditive effectThe disparity in effect between rofecoxib and para-
cetamol in the present study from 3 h onwards is inaccordance with the findings of two studies on post-operative pain relief after otolaryngologic surgerycomparing rofecoxib and paracetamol given pre-operatively (11 28) A study regarding inflammatorypain in patients with knee osteoarthritis also showedrofecoxib to be superior to paracetamol (29) The resultof our study from 3 h after baseline and onwards thusconfirms the findings of these studies in a third molarpain modelOur study did not show the same additive effect of
combining rofecoxib and paracetamol as in a study byBreivik et al in which they combined diclofenac andparacetamol (18) These authors demonstrated anadditive effect of paracetamol over the whole studyperiod of 8 h Their study also showed less use of rescuemedication in the combination group compared with thepatients treated with diclofenac alone something alsofound in a study by Matthews et al (19) It would seemreasonable to assume that the additive effect of para-cetamol in our study would be the same as in these twostudies as rofecoxib and ibuprofen have been shown tohave the same analgesic effect following third molarsurgery (9 10 12) and the effects of ibuprofen anddiclofenac are similar (30ndash32) It cannot be ruled out thatthere is a difference in additive effect of paracetamolwhen combining it with rofecoxib compared withdiclofenac This theory is in accordance with the result ofa study by Pickering et al on pain relief after tonsil-lectomy in children in which rofecoxib combined withparacetamol did not significantly alter the need for earlyanalgesia as did ibuprofen combined with paracetamol
(33) Further studies may clarify differences between thetwo drugsIn conclusion the present study indicates that there is
an early additive effect up to 2 h when combiningparacetamol with rofecoxib postoperatively as comparedwith rofecoxib alone which coincides with peak painintensity after the removal of third molars Rofecoxibhad a significantly better analgesic effect than paracet-amol from 3 h onwards Our results indicate that para-cetamol does not enhance the analgesic effect ofrofecoxib over a longer period of time As rofecoxib hasbeen shown to have serious cardiovascular side-effectsfuture studies are needed to determine any serious side-effect during short-term treatment
Acknowledgements ndash This study was supported by grants fromLIV The Country Council of Varmland which made it inde-pendent from all manufacturers of the studied drugs There areno conflicts of interest by any of the authors with any drugcompany We thank Dr Carl-Mauritz Bratt DDS Dr PeterTroberg DDS and Dr Tobias Block DDS for performingsome of the surgery
References1 Cooper SA Five studies on ibuprofen for postsurgical dental
pain Am J Med 1984 77 70ndash772 Dionne RA Campbell RA Cooper SA Hall DL Buck-
ingham B Suppression of postoperative pain by preoperativeadministration of ibuprofen in comparison to placebo acet-aminophen and acetaminophen plus codeine J Clin Pharmacol1983 23 37ndash43
3 Vane JR Inhibition of prostaglandin synthesis as a mechanismof action for the aspirinlike drugs Nature 1971 231 232ndash235
4 Meade EA Smith WL De Witt DL Differential inhibition ofprostaglandin endoperoxide synthase (cyclo-oxygenase) iso-zymes by aspirin and other non-steroidal anti-inflammatorydrugs J Biol Chem 1993 268 6610ndash6614
5 Smith TJ Cyclooxygenase as the principal targets for action ofNSAIDs Rheum Dis Clin North Am 1998 24 501ndash523
6 Sciulli MG Capone ML Tacconelli S Patrignani P Thefuture of traditional nonsteroidal anti-inflammatory drugs andcyclooxygenase-2 inhibitors in the treatment of inflammationand pain Pharmacol Rep 2005 57 66ndash85
7 Spink M Bann S Glickman R Clinical implications of cyclo-oxygenase-2 inhibitors for acute dental pain managementbenefits and risks J Am Dent Assoc 2005 136 1439ndash1448
8 Ehrich EW Dallob A De Lepeleire I Van Hecken ARiendeau D Yuan W Porras A Wittreich J Seibold JRDe Shepper P Mellisch DR Gertz BJ Characterization ofrofecoxib as a cyclooxygenase-2 isoform inhibitor and demon-stration of analgesia in the dental pain model Clin Pharm Ther1999 65 336ndash347
9 Malmstrom K Fricke J Kotey P Kress B Morrisson B Acomparison of rofecoxib versus celecoxib in treating pain afterdental surgery a singlecenter randomized double-blind pla-cebo- and active-comparator-controlled parallel group single-dose study using the dental impaction pain model Clin Ther2002 24 1549ndash1560
10 Malmstrom K Daniels S Kotey P Seidenberg B Desjar-
dins PJ Comparison of rofecoxib and celecoxib two cyclo-oxygenase-2-inhibitors in postoperative dental pain Arandomized placebo- and active-comparator-controlled clinicaltrail Clin Ther 1999 21 1653ndash1663
11 Watcha MF Issioui T Klein KW White PF Costs andeffectiveness of rofecoxib celecoxib and acetaminophen forpreventing pain after ambulatory otolaryngologic surgeryAnesth Analg 2003 96 987ndash994
300 Haglund amp Bultzingslowen
12 Morrisson BW Christensen S Yuan W Brown J Amlani
S Seidenberg B Analgesic efficacy of the cyclooxygenase-2-specific inhibitor rofecoxib in post-dental surgery pain arandomized controlled trial Clin Ther 1999 21 943ndash953
13 Chang DJ Fricke JR Bird RS Bohidar NR Dobbins TWGeba GP Rofecoxib versus codeineacetaminophen in post-operative dental pain a double-blind randomized placebo-and active comparator-controlled clinical trial Clin Ther 200123 1446ndash1455
14 Chang DJ Desjardins PJ Bird SR Black P Chen EPetruschke RA Geba GP Comparison of rofecoxib and amultidose oxycodoneacetaminophen regimen for the treatmentof acute pain following oral surgery a randomized controlledtrial Curr Med Res Opin 2004 20 939ndash949
15 Berenbaum MC What is synergy Pharmacol Rev 1989 4193ndash141
16 Altman RD A rationale for combining acetaminophen andNSAIDs for mild to moderate pain Clin Exp Rheumatol 200422 110ndash117
17 Bjorkman R Hallman KM Hedner J Hedner T Henning
M Acetaminophen blocks spinal hyperalgesia induced byNMDA and substance P Pain 1994 57 259ndash264
18 Breivik EK Barkvoll P Skovlund E Combining diclofenacwith acetaminophen or acetaminophen-codeine after oral sur-gery a randomized double-blind single-dose study ClinPharmacol Ther 1999 66 625ndash635
19 Matthews RW Scully CM Levers BG The efficacy ofdiclofenac sodium (Voltarol) with and without paracetamol inthe control of post-surgical dental pain Br Dent J 1984 157357ndash359
20 Norholt SE Treatment of acute pain following removal ofmandibular third molars use of the dental pain model inpharmacological research and development of a comparableanimal model Int J Oral Maxillofac Surg 1998 27 1ndash41
21 NIH Consensus Development Conference For Removal OfThird Molars J Oral Surg 1980 38 235ndash236
22 Laska EM Siegel C Sunshine A Onset and durationmeasurement and analysis In Max MB Portenoy RKLaska EM eds Advances in pain research and therapy NewYork Raven Press 1991 691ndash698
23 Max MB Laska EM Single-dose analgesic comparisons InMax MB Portenoy RK Laska EM eds Advances in painresearch and therapy New York Raven Press 1991 55ndash97
24 Bombardier C Laine L Reicin A Shapiro D Burgos-Vargas R Davis B Day R Ferraz MB Hawkey CJHochbergMC Kvien TK Schitzer TJ Comparison of uppergastrointestinal toxicity of rofecoxib and naproxen in patientswith rheumatoid arthritis N Engl J Med 2005 343 1520ndash1528
25 Bresalier RS Sandler RS QuanH Bolognese JA Oxenius
B Horgan K Lines C Riddell R Morton D Lanas AKonstam MA Baron JA Cardiovascular events associatedwith rofecoxib in a colorectal adenoma chemoprevention trialN Engl J Med 2005 17 1092ndash1102
26 Szmyd L Shannon ILMohnac AM Control of postoperativesequelae in impacted third molar surgery J Oral Ther Phar-macol 1965 1 491ndash496
27 Issioui T Klein KW White PF Hu J Skrivanek GDAnalgesic efficacy of rofecoxib alone or in combination withacetaminophen in the ambulatory setting Anesthesiology 200195 A35
28 Issioui T KleinKWhite PWatchaM SkrivanekG JonesSHu J BradleyM Caleb I Cost-efficacy of rofecoxib versusacetaminophen for preventing pain after ambulatory surgeryAnesthesiology 2002 97 931ndash937
29 Geba GP Weaver AL Polis AB Dixon ME Schnitzer TJEfficacy of rofecoxib celecoxib and acetaminophen in osteo-arthritis of the knee a randomized trial JAMA 2002 287 64ndash71
30 Joshi A Parara E Macfarlane TV A double-blind rand-omised controlled clinical trial of the effect of preoperativeibuprofen diclofenac paracetamol with codeine and placebotablets for relief of postoperative pain after removal of impac-ted third molars Br J Oral Maxillofac Surg 2004 42 299ndash306
31 Bakshi R Frenkel G Dietlein G Meurer-Witt B Schn-eider B Sinterhauf U A placebo-controlled comparativeevaluation of diclofenac dispersible versus ibuprofen in post-operative pain after third molar surgery J Clin Pharmacol 199434 225ndash230
32 Ahlstrom U Bakshi R Nilsson P Wahlander L Theanalgesic efficacy of diclofenac dispersible and ibuprofen inpostoperative pain after dental extraction Eur J Clin Pharma-col 1993 44 587ndash588
33 Pickering AE Bridge HS Nolan J Stoddart A Double-blind placebo-controlled analgesic study of ibuprofen orrofecoxib in combination with paracetamol for tonsillectomy inchildren Br J Anaesth 2002 88 72ndash77
COX-2 inhibitor and paracetamol after oral surgery 301
Combined acetaminophen and ibuprofen for pain relief after oralsurgery in adults a randomized controlled trial
A F Merry1 2 R D Gibbs3 J Edwards4 G S Ting3 C Frampton5 E Davies1 2
and B J Anderson1
1Department of Anaesthesiology University of Auckland Private Bag 92019 Auckland New Zealand2Department of Anaesthesia Auckland City Hospital Auckland New Zealand 3Oral Health Unit Greenlane
Clinical Centre 214 Greenlane West Epsom Auckland New Zealand 4Oral and Maxillofacial Service Quay
Park Medical Centre 68 Beach Road Auckland Central Auckland New Zealand 5Department of Medicine
Christchurch School of Medicine and Health Sciences University of Otago New Zealand
Corresponding author E-mail amerryaucklandacnz
Background Acetaminophen is often used with a non-steriodal anti-inflammatory drug for
acute pain Hitherto these drugs have had to be given separately typically at different time
intervals Maxigesicw tablets combine acetaminophen and ibuprofen in clinically appropriate
doses to simplify administration and dosage regimen We compared this combination with each
of the constituent drugs for the relief of pain after extraction of third molar teeth
Methods Adults (more than 16 yr) having one or more wisdom teeth removed under general
or local anaesthesia were instructed to take two tablets before operation then two tablets
every 6 h for up to 48 h of (i) a combination of acetaminophen 500 mg and ibuprofen 150 mg
per tablet (Maxigesicw) (ii) acetaminophen 500 mg per tablet alone or (iii) ibuprofen 150 mg
per tablet alone The primary outcome measure was the area under the curve (AUC) of the
100 mm visual analogue scale pain measurements taken for up to 48 h after surgery divided by
time at rest and on activity Pharmacokinetic data were collected in a subset of patients
Results The mean (SEM) time-corrected AUC on rest and activity respectively were combi-
nation group 223 (32) and 284 (34) acetaminophen group 330 (31) and 404 (33) and ibu-
profen group 348 (32) and 402 (34) P001 for each of the four comparisons of combination
vs constituent drug There was no pharmacokinetic interaction between acetaminophen and
ibuprofen administered together
Conclusions Maxigesicw tablets provide superior pain relief after oral surgery to acetamino-
phen or ibuprofen alone
Br J Anaesth 2010 104 80ndash8
Keywords anaesthesia dental analgesia postoperative analgesics non-opioid acetaminophen
analgesics non-opioid ibuprofen non-steroidal anti-inflammatory drugs
Accepted for publication October 16 2009
The relief of pain has been described as a universal human
right but is not always easily achieved1 Opioid analgesics
are effective but have troublesome and potentially danger-
ous side-effects and their potential for abuse may lead to
regulatory and logistical difficulties Non-steroidal anti-
inflammatory drugs (NSAIDs) have fewer regulatory
restrictions but they too have important adverse effects
which are more likely at higher dose or with longer
courses2 Acetaminophen is widely used and is very safe
at the recommended dose of 4 g per day3 but does not
always provide adequate pain relief on its own Combining
analgesics offers the possibility of increasing effectiveness
without increasing dose (and therefore risk)4 5 NSAIDs
are often combined with acetaminophen particularly for
treating postoperative pain6 ndash 10
Prescribing acetaminophen and ibuprofen together is
common in clinical practice6 8 9 11 ndash 13 Ibuprofen has the
advantage of a well-established safety record (particularly
at doses below 15 g per day in adults)14 and in many
countries (including the UK) it is available without
The Author [2010] Published by Oxford University Press on behalf of the British Journal of Anaesthesia
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (httpcreativecommonsorglicensesby-nc25uk)
which permits unrestricted non-commercial use distribution and reproduction in any medium provided the original work is properly cited
British Journal of Anaesthesia 104 (1) 80ndash8 (2010)
doi101093bjaaep338
prescription Typically acetaminophen is given in a dose
regimen of 1 g 6 hourly whereas ibuprofen is given in a
dose of 400 mg 8 hourly3 Compliance with the prescribed
dosing regimen is important for achieving the desired
result with any drug and is often poor with asynchronous
dosing15 A single formulation with a simplified regimen
would probably be appreciated by patients and might
improve compliance
Maxigesicw is a new formulation of acetaminophen 500
mg and ibuprofen 150 mg Taking two tablets 6 hourly
provides the appropriate daily dose of both drugs relatively
simply We have investigated the hypothesis that in adult
patients undergoing a common surgical procedure (extrac-
tion of third molar teeth) this formulation provides
superior analgesia to either of its components alone
Methods
With ethics committee approval we recruited and fol-
lowed up patients between March 2005 and February
2008 Trial registration ANZCTRORGAU (identifier
ACTRN12606000291583)
Setting
This study was conducted at a publicly funded teaching
hospital and a private day-surgical clinic in metropolitan
New Zealand
Participants
We included adults undergoing extraction of at least one
lower wisdom tooth with or without one or more upper
wisdom teeth by one of three participating surgeons We
excluded patients if they were under 16 yr old weighed
50 kg had taken any NSAID (other than aspirin in a
dose of 150 mg daily or less) within 24 h of the operation
had taken acetaminophen or acetaminophen containing
medicines within 12 h of the operation were taking an
angiotensin-converting enzyme inhibitor warfarin steroid
(other than interoperative dexamethasone) or any immu-
nosuppressive drug were intolerant to any NSAID or acet-
aminophen were suffering from a severe local infection
had a history of peptic ulceration asthma or severe hae-
mopoetic renal or hepatic disease were participating in
the investigation of another experimental agent or if the
clinician believed for any other reason that participation in
the study might not be in their best interests
Randomization and blinding
Tablets of identical appearance packaging and dosage
instructions were provided in each of the following formu-
lations (i) acetaminophen 500 mgthornibuprofen 150 mg per
tablet (Maxigesicw Sigma Laboratories Nashik India which
was MHRA approved for manufacturing pharmaceuticals
under GMP) (ii) acetaminophen 500 mg per tablet or
(iii) ibuprofen 150 mg per tablet
Patients were first approached by the surgeon and then
by the study nurse They were given written and verbal
information about the study and invited to participate If
they consented patients were then randomized into one of
the three study groups in a sequential order to receive one
of these formulations in blinded packs The randomization
sequence was computer generated by the study statistician
as a 111 allocation ratio to the three treatments in a
sequence of permuted blocks with stratification for anaes-
thetic type (local or general) and study centre
Stratification by anaesthetic type ensured a balance
between treatments in terms of the number of teeth
extracted as most patients having more than two teeth
extracted have a general anaesthetic Only the statistician
had access to the schedule of patient numbers by drug
allocation Participants and investigators were blinded and
the randomization code was not broken until the final data-
base had been checked and locked
Intervention
Participants were asked to take two tablets of the study
medication before operation (as close as possible to the
start of surgery) and then 4 times a day (as close as poss-
ible to 6 hourly) for up to 48 h after surgery All partici-
pants were given bupivacaine local anaesthetic blocks by
the surgeons For those participants undergoing general
anaesthesia this was induced with propofol and main-
tained with isoflurane and nitrous oxide in oxygen
Monitoring was in accordance with the guidelines of the
Australian and New Zealand College of Anaesthetists16
All extractions were carried out by one of three surgeons
each using his normal technique
If participants required additional postoperative pain
relief while in hospital a rescue dose of fentanyl 10 mg
was given iv as required After discharge to home
codeine was provided (again as rescue medication) in 30
mg tablets one to two to be taken as needed up to
4 hourly
Outcomes
Participants were asked to rate their pain on 100 mm visual
analogue scales (VAS) printed one per double page in a
booklet that they took home Ratings were requested at
baseline (immediately before administration of the first
dose of study medication) after operation (once the partici-
pants were sufficiently awake to respond) and 1ndash2 hourly
thereafter while awake for 48 h The study nurse main-
tained contact with participants by telephone to facilitate
compliance with data collection and the return of diaries
The primary outcome measure was the area under the
curve (AUC) of these VAS ratings divided by time at rest
and on activity The AUC was divided by the period of
the completed assessments to adjust for the fact that some
Combined acetaminophen and ibuprofen for analgesia
81
patients recorded pain for shorter periods than others This
calculation in effect produces a measure of average pain
intensity over the study period
Secondary efficacy outcome measures were a categorical
global pain rating by the participants taken at the end of the
study period rescue analgesia consumption over the study
period a categorical global rating of nausea by the partici-
pants taken at the end of study period the number of epi-
sodes of vomiting over the study period and a rating of
sleep disturbance on a 100 mm VAS assessed after each
night during the study period In addition participants were
asked to rate their experiences of participating in the study
Sample size estimation
We obtained blood samples from the 38 participants
undergoing general anaesthesia in order to have evaluable
pharmacokinetic data for at least 30 patients The first
sample was obtained 30 min after the first dose of study
medication the second sample at the end of anaesthesia
and additional one or two samples after operation in hospi-
tal The plasma concentration of acetaminophen and ibu-
profen were measured by the sponsor and used to form
individual timendashconcentration profiles The analytical
method used an HPLC-DAD (Diode Array Detector) assay
for the simultaneous determination of acetaminophen and
ibuprofen in plasma Precision and accuracy for acetami-
nophen and ibuprofen assay were validated over the con-
centration range 05ndash50 mg ml21 for both drugs The
intra- and inter-batch precision of the assays at low
medium and high concentrations of acetaminophen and
ibuprofen varied from theoretical values by 15 The
lower limit of quantification for each drug was 05 mg
ml21 The sponsor monitored all data collected during the
study and queries and corrections were made when any
inaccuracies or inconsistencies were identified
Sample size estimation
We estimated that 120 participants (40 per group) in the
intention-to-treat (ITT) population would provide 80
power to detect differences between the groups of 9 (SD
14) mm in our primary endpoint for resting assessments
and 13 (SD 21) for measures during activity10 17 with a
one-sided type I error rate of 5 These differences equate
to 25 Differences of this magnitude were considered
clinically important and comparable with differences
typical of previous published studies10
Statistical methods
The data were analysed using SPSS version 150 (SPSS
Inc Chicago IL USA) Efficacy analyses were conducted
on an ITT basis with the additional provision that
there were at least three VAS measurements over at
least 12 h available to calculate the primary endpoint All
participants who were randomized into the study were
included in the safety evaluations As the first dose of
study medication was taken before operation while under
the supervision of the surgeon all randomized patients
took at least a single dose of study medication A last
observation carried forward approach was used for those
subjects who left the study prematurely for non-AUC
based variables
We compared the primary endpoint between the combi-
nation group and each of the acetaminophen and ibuprofen
arms at rest and on activity using a general linear model
(GLM) which included terms for treatment the centre and
anaesthetic stratum Additionally to confirm the consist-
ency of the treatment effects across strata the stratum
treatment interaction terms were tested and included in
the final model The analysis was also checked with
number of teeth extracted as an additional factor
Continuous secondary efficacy endpoints were tested for
significance using the same models as used for the
primary endpoint
A one-tailed P005 was pre-specified to indicate stat-
istical significance We required a statistically significant
result favouring the combination from each of the two
planned comparisons with the constituents to define super-
iority for either rest or on activity measures We used one-
tailed tests as there seemed no theoretical or empirical
basis for expecting that combining these analgesics could
result in a reduction in efficacy and because the require-
ment for each of two comparisons to be significant at
P005 is stringent Secondary categorical efficacy end-
points were compared between the groups using x2 tests
and MannndashWhitney U-tests as appropriate
We used non-linear mixed effect models (NONMEM
VI Globomax LLC Hanover MD USA) to estimate
population pharmacokinetics with a Compaq Digital
Fortran Version 66A compiler on an Intel Celeron 333
MHz CPU (Intel Corp Santa Clara CA USA) under MS
Windows XP (Microsoft Corp Seattle WA USA) This
model allows assessment of inter-individual variability
covariance between pharmacokinetic parameters and
residual error We judged the quality of fit of the pharma-
cokinetic model to data using the NONMEM objective
function examination of plots of observed vs predicted
concentrations and visual predictive checks
Results
After initial screening 189 patients were approached 135
agreed to participate One to four teeth were extracted
with local anaesthetic alone in 69 patients and with local
anaesthetic in combination with general anaesthesia in 66
Thirteen patients did not return their patient diaries so
122 patients were included in the evaluable ITT popu-
lation for the analysis of the primary endpoints (Fig 1)
The treatment groups were adequately matched in baseline
patient and clinical characteristics (Table 1) Of those in
Merry et al
82
the combination group 600 had three or four teeth
extracted compared with 436 for ibuprofen and 535
for acetaminophen
Efficacy
The time-adjusted AUCs were substantially and signifi-
cantly lower at rest and on activity in the combination
group than in either of the other two treatment groups
(Table 2 Figs 2 and 3) with all four P001 The consist-
ency of the treatment effects across strata was confirmed
from the GLM with P-values for the treatment stratum
interaction of 0955 and 0984 for time-adjusted AUCs at
rest and on activity respectively The type of anaesthetic
(local vs general) and number of teeth extracted did not
change the outcome of either analysis
Although all four secondary endpoints favour the com-
bination treatment (Table 3) only the global pain rating
reached statistical significance More participants experi-
enced lsquonilrsquo or lsquomildrsquo pain with the combination (684)
than with either other group this difference was significant
for acetaminophen (375 Pfrac140008) but not for ibupro-
fen (543 Pfrac140263) The use of any rescue medication
also favoured the combination treatment (Table 4) but this
did not reach statistical significance
Pharmacokinetics
There were no significant differences between the combi-
nation group and either constituent group in any of the
estimated pharmacokinetic parameters (Table 5) The
visual predictive plots of individual concentration showed
that 90 of the observations were within the 90 pre-
diction intervals
Twelve participants were given both acetaminophen and
ibuprofen For calculation of the pharmacokinetic vari-
ables a scaling factor was applied to clearance and
volume of distribution in turn for those participants receiv-
ing the combination of acetaminophen and ibuprofen This
scaling factor had no impact on either acetaminophen or
ibuprofen pharmacokinetic parameters indicating that
there was no pharmacokinetic interaction between acetami-
nophen and ibuprofen when administered together
(P005)
Clearance (CLF) and volume of distribution (VF) par-
ameters observed in the study are consistent with those
reported previously (acetaminophen CLFfrac14126ndash210
litre h21 70 kg21 VFfrac14483ndash710 litre 70 kg21 ibupro-
fen CLFfrac1429ndash59 litre h21 70 kg21 VFfrac1464ndash235 litre
70 kg21)18 ndash 20
Adverse effects
The frequency of adverse effects was consistent with the
known effects of the constituent drugs and there were no
Screened(n =189)
Randomized(n =135)
Acetaminophentreatmentgroup(n =47)
Ibuprofentreatment group(n =44)
Combinationtreatment group(n =44)
Patient diariesnot returned(n =4)
Patient diariesnot returned(n =5)
Patient diariesnot returned(n =4)
Included in theanalysis(n =43)
Included in theanalysis(n =39)
Included in theanalysis(n =40)
Fig 1 Flow of participants through trial Not randomized (nfrac1454) (i)
declined to participate (nfrac1415) (ii) did not meet inclusion criteria
(nfrac1414) (iii) other reasons (nfrac1425) other reasons the surgery was
cancelled or rescheduled patient could not be contacted patient was
given the wrong date of the surgery
Table 1 Patient characteristic and baseline information (SD)
Acetaminophen (n547) Ibuprofen (n544) Combination (n544)
Age [mean (range)] (yr) 235 (160ndash404) 237 (168ndash389) 250 (183ndash404)
Weight [mean (SD)] (kg) 713 (156) 808 (201) 711 (135)
Ethnicity [n ()]
Asian 4 (85) 1 (23) 2 (45)
Black 1 (21) 0 (00) 1 (23)
Caucasian 33 (702) 31 (705) 34 (773)
Maori 4 (85) 4 (91) 4 (91)
Pacific Islander 4 (85) 5 (114) 2 (45)
Other 1 (21) 3 (68) 1 (23)
Male [n ()] 13 (277) 21 (477) 13 (295)
Shift workers [n ()] 10 (213) 5 (114) 3 (68)
Preoperative pain scores at rest [mean (SD)] (mm) 19 (51) 21 (52) 26 (68)
Preoperative pain scores on activity [mean (SD)] (mm) 41 (133) 27 (83) 29 (66)
Sleep disturbance for night before surgery as VAS [mean (SD)] (mm) 647 (229) 691 (260) 715 (241)
Combined acetaminophen and ibuprofen for analgesia
83
definitive indications that the adverse event profile is
changed when the two drugs are combined (Table 6)
however the numbers were too small to make meaningful
comparisons between the groups Two participants experi-
enced postoperative bleeding (attributed to surgical
causes) which resolved without readmission to hospital
No gastrointestinal bleeding was reported during the study
Most adverse events were evaluated as mild (574) or
moderate (352) and on review were considered not
related (175) or unlikely to be related (667) to study
medication
General
The majority of participants rated the experience of taking
part in the study as very positive (31) or positive (47)
0
10
20
30
40
50
60
70
80
90
100
ActivityRest
Acetaminophen alone
Ibuprofen alone
Combination
AU
Ch
(m
m)
Fig 2 Mean (thorn95 CI) mm of time-adjusted AUC (AUCtime) for VAS
at rest and on activity by treatment group
Table 2 Mean (SEM 95 CI) of time-adjusted AUC of visual analogue pain
scores at rest and on activity by treatment group The differences between
combination and each constituent were significant at rest (vs acetaminophen
Pfrac140007 and vs ibuprofen Pfrac140003) and on activity (vs acetaminophen
Pfrac140006 and vs ibuprofen Pfrac140007)
Acetaminophen
(n543)
Ibuprofen (n539) Combination
(n540)
At rest 330 (31 279ndash381) 348 (32 294ndash402) 223 (32 170ndash277)
On
activity
404 (33 350ndash458) 402 (34 346ndash459) 284 (34 228ndash341)
0
1020
30
40
5060
70
8090
100A
B
0 4 8 12 16 20 24 28 32 36 40 44 48
0 4 8 12 16 20 24 28 32 36 40 44 48
Hours post-surgery
VA
S s
core
(m
m)
0
10
2030
40
50
60
7080
90
100
Hours post-surgery
VA
S s
core
(m
m)
Acetaminophen aloneIbuprofen aloneCombination
Fig 3 Mean (SE) mm VAS out of 100 at rest (A) and on activity (B)
Table 3 Secondary efficacy endpoints by treatment group The only
significant difference was between the global pain ratings for combination and
acetaminophen (Pfrac140008 MannndashWhitney U-test)
Acetaminophen Ibuprofen Combination
Global pain rating [n ()]
Nil 3 (75) 4 (114) 4 (105)
Mild 12 (300) 15 (429) 22 (579)
Moderate 22 (550) 14 (400) 12 (316)
Severe 3 (75) 2 (57) 0 (00)
Global nausea rating [n ()]
Nil 26 (650) 25 (714) 30 (790)
Mild 10 (250) 8 (229) 7 (184)
Moderate 3 (75) 2 (57) 1 (26)
Severe 1 (25) 0 (00) 0 (00)
Vomiting episodes (n) 5 (in 3 subjects) 0 0
Sleep disturbance night
1 vs baseline VAS
[mean (SD)] (mm)
2219 (292) 2174 (229) 2166 (247)
Sleep disturbance night
2 vs baseline VAS
[mean (SD)] (mm)
2137 (329) 296 (258) 285 (201)
Table 4 Rescue analgesia by group n () none of these differences were
significant
Rescue analgesic Acetaminophen Ibuprofen Combination
Fentanyl in hospital 5 (116) 9 (237) 6 (154)
Codeine in the first 24 h 21 (4770) 16 (4320) 13 (3250)
Codeine in the second 24 h 22 (5370) 14 (4240) 16 (4210)
Any rescue medication over 48 h 25 (625) 18 (5810) 21 (568)
Table 5 Mean (SD) pharmacokinetic parameters (individual Bayesian
estimates used for descriptive statistics) for a one-compartment first-order
absorption first-order elimination model none of the differences for
combination formulations was significant CLF clearance VF volume of
distribution Tabs absorption half-time Cmax maximum concentration Tmax
time to achieve Cmax
Acetaminophen
alone (n515)
Acetaminophen
in combination(n512)
Ibuprofen
alone(n511)
Ibuprofen in
combination(n512)
CLF (litre
h21)
141 (26) 142 (18) 39 (17) 38 (13)
VF (litre) 557 (194) 482 (183) 106 (21) 98 (15)
Tabs (h) 042 (076) 016 (010) 058 (078) 085 (085)
Tmax (h) 109 (112) 064 (031) 116 (090) 144 (093)
Cmax (mg
litre21)
158 (65) 192 (64) 208 (83) 191 (78)
Merry et al
84
and 19 rated the experience as neutral Four participants
(3) found the experience negative and none rated it as
very negative The ratings were not significantly different
between the study groups
Discussion
We found that patients using the combination of acetami-
nophen and ibuprofen experienced less pain during the
first 48 h after oral surgery than those using the same
daily dosage of either agent alone and we think the differ-
ence was clinically relevant There was no evidence of any
pharmacokinetic interaction between acetaminophen and
ibuprofen Patients receiving ibuprofen alone reported the
lowest frequency of adverse events but the numbers are
too small for meaningful comparisons between the groups
and we saw no cause for concern in any group
Our data are consistent with previous evidence showing
that a combination of ibuprofen and acetaminophen pro-
vides better analgesia than acetaminophen alone8 9 13 21
Note however that two of these studies were in children9 13
so data in adults are relatively limited On the other hand
there are many studies supporting the more general point
that the addition of various NSAIDs improves the pain
relief obtainable from acetaminophen alone More impor-
tantly our data add convincingly to the sparse evidence
supporting the more controversial proposition that this
combination is superior to ibuprofen alone12 In a smaller
study in an orthopaedic pain model (which was positive
for the combination in comparison with acetaminophen)
Dahl and colleagues8 showed no such benefit whereas
Viitanen and colleagues13 (in a paediatric tonsillectomy
study) showed an advantage for the combination only in
the period after discharge from hospital The similarity in
efficacy between ibuprofen and acetaminophen on their
own seen in our study contrasts with the findings of
superior pain relief from ibuprofen after dental surgery by
Cooper and colleagues22 but theirs was a single-dose
study
Limitations and strengths of the study
Our results are limited to adults and to the doses and
model of pain studied We think our conclusions are likely
to apply to other age groups and other types of pain but
this will require confirmation We have not explored the
optimal dosage of the combination drug but the dosage
used is consistent with current clinical practice The
inclusion of patients who underwent both general and
local anaesthesia implies that our findings are likely to
apply in either case It is not possible to draw firm con-
clusions on the safety of any drug from a study of only 40
participants per group but acetaminophen and ibuprofen
are well established widely used and considered very safe
in appropriate doses3 23 There is no theoretical reason
Table 6 Adverse events and their relationship with study medication as evaluated by the investigators Postoperative pain was noted as a complication in 2 0
and 1 patient in the acetaminophen ibuprofen and combination groups respectively Some individuals experienced more than one adverse event
Relationship System organ class Acetaminophen Ibuprofen Combination Total
Not related Gastrointestinal disorders (numbness of tongue) 1 0 0 1
General disorders and administration site conditions (swollen arm infusion site
phlebitis)
0 0 2 2
Infections and infestations (dry socket alveolitis of jaw) 1 0 1 2
Injury poisoning and procedural complications (bruising of arm postoperative
pain)
0 0 2 2
Musculoskeletal and connective tissue disorders ( jaw stiffness) 0 0 1 1
Skin and sc tissue disorders (swelling face) 1 1 0 2
Subtotal 3 1 6 10
Unlikely related Blood and lymphatic system disorders (swollen glands) 1 0 0 1
Ear and labyrinth disorders (pain in ear tinnitus) 2 0 0 2
Gastrointestinal disorders (vomiting nausea stomach cramps dry lips) 6 1 2 9
Injury poisoning and procedural complications (postoperative bleeding) 0 0 1 1
Musculoskeletal and connective tissue disorders ( jaw stiffness aches and pains in
legs jaw pain)
2 0 1 3
Nervous system disorders (headache felt faint sleepy balance difficulty light
headiness dizziness drowsiness lethargic)
6 4 4 14
Psychiatric disorders (disorientation) 0 1 0 1
Respiratory thoracic and mediastinal disorders (sore throat pharyngeal ulceration
hypoventilation coughing)
1 1 2 4
Investigations (body temperature increased) 0 0 1 1
Skin and sc tissue disorders (rash redness of external ear swelling face) 0 1 1 2
Subtotal 18 8 12 38
Possibly related Gastrointestinal disorders (stomach cramps abdominal pain constipation stomach
ache vomiting)
3 0 2 5
General disorders and administration site conditions (fever) 1 0 0 1
Injury poisoning and procedural complications (postoperative bleeding) 0 0 1 1
Nervous system disorders (sleepy headache) 1 0 1 2
Subtotal 5 0 4 9
Total 26 9 22 57
Combined acetaminophen and ibuprofen for analgesia
85
and no empirical suggestion from our data to suggest that
the combination would be any less safe than the constitu-
ent drugs on their own Our safety data are observational
rather than based on prospective laboratory investigations
but we followed up participants for adverse events for 3
weeks and it seems unlikely that clinically important
harm would have been missed
Pain after oral surgery can persist for several days10 but
we considered 48 h to be a clinically relevant period and
a longer period of study is likely to have resulted in poorer
compliance with data collection
It could be asked whether a more typical (albeit
complex) regimen for ibuprofen alone might have pro-
vided better analgesia than seen with the 4 hourly
approach used here but this seems unlikely particularly
given that our clinical efficacy data were supported by esti-
mates of population pharmacokinetics We had planned to
correlate drug plasma concentration with pain scores but
the drug plasma concentration results were too sparse and
there were too many confounding variables (such as ethni-
city comparators and rescue analgesia) for this to be
undertaken We did demonstrate a lack of interaction
between the constituent drugs when used in combination
and provided evidence that equivalent and predicted blood
concentrations were achieved (the observations of timendash
concentration profile decreased within 90 of prediction
limits for both acetaminophen and ibuprofen) Furthermore
pharmacokinetic parameter estimates observed in the current
study are very similar to those previously reported18 ndash20
The evaluations used in the efficacy analysis have
established construct validity and are appropriate for
parametric analysis24 25
In designing analgesic studies it is an advantage to
minimize the exposure of participants to inadequate
analgesia while controlling for various sources of bias
Some designs incorporate a placebo group but the efficacy
of both ibuprofen26 and acetaminophen27 in comparison
with placebo are well established by previous research
and we would argue that the use of a placebo in this situ-
ation is unnecessary and perhaps even unethical28 There
would be little value in another lsquome toorsquo analgesic unless
it had clear advantages over established agents Therefore
the question of interest lies in the comparisons between
the new agent (Maxigesicw) and the reference standard of
care and in this case we have actually shown superiority to
both of two possible reference standardsmdashacetaminophen
alone and ibuprofen alone One classic approach to analgesic
studies involves treating established acute pain This has the
alleged advantage that pain relief can be assessed (eg by
using AUC to estimate total pain relief or TOTPAR29 30 or
by calculating a pain reduction index per tablet)31 Our
design in contrast follows the widely accepted clinical prac-
tice of anticipating and treating pain before it occurs which
in our unit at least has long been considered best practice
Furthermore rescue medication was readily available and
those requiring it were evenly distributed between the
groups It is notable that most patients did require rescue
medication suggesting that pain after oral surgery can some-
times be severe enough that even the combination of ibupro-
fen and acetaminophen requires supplementation (and it
might be asked whether it would be a good idea for codeine
for example to be added to the combined formulation)
Nevertheless we think it important that the vast majority of
the participants in all groups reported pain scores that were
reasonably low and that all received analgesic regimens
accepted in contemporary practice The predominantly posi-
tive evaluation by participants of their experience in taking
part in the study provides empirical reassurance on this point
(and also other aspects of the conduct of the study)
The treatment of pain is central to medical practice in
hospitals and in primary care If these results are con-
firmed in other settings the already widely used combi-
nation of acetaminophen and ibuprofen may become the
standard of care for the initial management of moderate
acute pain at least for those patients who do not have
contra-indications to NSAIDs Even using the drugs indi-
vidually the dosage regimen studied here is simpler than
that currently recommended and may well improve com-
pliance with and therefore success with this combination
Providing both drugs in one tablet simplifies this regimen
even further and our data confirm that the specific formu-
lation studied here is effective and that there is no inter-
action between its constituent drugs
Conclusions
Doctors treating pain after oral surgery in hospital and at
home and probably pain in many other situations should
consider using acetaminophen and ibuprofen together four
times a day provided there are no contraindications to
either drug and taking into account the known risks of
NSAIDs The combination formulation studied here sim-
plifies this regimen
Funding
This work was supported by AFT Pharmaceuticals Ltd
assisted by New Zealand Trade and Enterprise
Development Grants
Appendix
Declaration of interest
The Department of Anaesthesiology of the University of
Auckland has received payment from AFT
Pharmaceuticals for conducting this study but none of the
investigators has received payment in their personal
capacity
Merry et al
86
Contributors
AFM BJA CF and Hartley Atkinson designed the
study with input from RDG and JE Hartley Atkinson
obtained funding RDG GST and JE performed the
surgery and contributed to patient recruitment and to the
care of patients during their participation in the study
ED was the study coordinator and was responsible for
patient recruitment and follow-up data collection quality
control and many other logistic aspects of the study The
statistical analysis of clinical data was undertaken by CF
and of the pharmacokinetic data by BJA AFM took
primary responsibility for the manuscript with assistance
from Jennifer Zhang All authors edited and commented
on the manuscript AFM is the guarantor
Chief Executive Officer AFT Pharmaceuticals
Clinical TrialRegulatory Assistant AFT Pharmaceuticals
Ethics approval
This study was approved by the Northern X Regional Ethics
Committee 650 Great South Road Penrose Auckland New
Zealand
Ethics Committee Approval Number AKX0410298
Health Authorities (MEDSAFE) Approval Number
TT50-7316 (458)
Role of the sponsor
The sponsor (AFT Pharmaceuticals Ltd) participated in
the study design and protocol development and provided
logistical support during the trial Monitoring of the
study was performed by the sponsor who also main-
tained the trial database Statistical analyses were
independently performed by the biostatistician and the
results cross-checked by sponsors and investigators The
sponsor assisted with the preparation of the manuscript
and was permitted to review it and to make suggestions
but responsibility for the content of this paper lay with
the academic authors and the style and emphasis is that
of the principle investigator The academic authors had
the explicit right to access all data and publish these
results
Provenance and peer review
This paper was not commissioned informal external peer
review has been obtained before submission to the Journal
Additional contributions
We thank Ms Jenny Rous Pharmacy Manager from the
Mercy Hospital Pharmacy for study drug management
Dr Ralph Richardson Program Manager from Institute of
Environment Science amp Research Limited Wellington in
New Zealand for the plasma sample assays Sally Merry
for proofreading and editing on the manuscript the anaes-
thetists Judy Bent Jack Hill Joanna Rose Joanne Paver
Andrew Warmington and Lisa Chapman at Greenlane
Clinical Centre Kerry Gunn Chris Chambers and
Jonathan Cross at Quay Park Clinic for facilitating the
administration of the study protocol and contributing
substantially to the clinical care of the patients and the
participants for their participation
References1 Cousins MJ Brennan F Carr DB Pain relief a universal human
right Pain 2004 112 1ndash42 Merry A Power I Perioperative NSAIDs towards greater safety
Pain Rev 1995 2 268ndash913 MARTINDALE The Extra Pharmacopoeia London The Royal
Pharmaceutical Society of Great Britain 19964 Mehlisch DR The efficacy of combination analgesic therapy in
relieving dental pain J Am Dent Assoc 2002 133 861ndash71
5 Desmeules J Rollason V Piguet V Dayer P Clinical pharmacologyand rationale of analgesic combinations Eur J Anaesthesiol Suppl2003 20 7ndash11
6 Altman RD A rationale for combining acetaminophen andNSAIDs for mild-to-moderate pain Clin Exp Rheumatol 2004 22
110ndash77 Hyllested M Jones S Pedersen JL Kehlet H Comparative effect
of paracetamol NSAIDs or their combination in postoperativepain management a qualitative review Br J Anaesth 2002 88
199ndash2148 Dahl V Dybvik T Steen T Aune AK Rosenlund EK Raeligder JC
Ibuprofen vs acetaminophen vs ibuprofen and acetaminophenafter arthroscopically assisted anterior cruciate ligament recon-struction Eur J Anaesthesiol 2004 21 471ndash5
9 Gazal G Mackie IC A comparison of paracetamol ibuprofen ortheir combination for pain relief following extractions in childrenunder general anaesthesia a randomized controlled trial Int JPaediatr Dent 2007 17 169ndash77
10 Merry AF Swinburn PF Middleton NG Edwards JL Calder MV
Tenoxicam and paracetamolndashcodeine combination after oralsurgery a prospective randomized double-blind placebo-controlled study Br J Anaesth 1998 81 875ndash80
11 Mitchell A van Zanten SV Inglis K Porter G A randomized con-trolled trial comparing acetaminophen plus ibuprofen versus acet-
aminophen plus codeine plus caffeine after outpatient generalsurgery J Am Coll Surg 2008 206 472ndash9
12 Menhinick KA Gutmann JL Regan JD Taylor SE Buschang PHThe efficacy of pain control following nonsurgical root canal
treatment using ibuprofen or a combination of ibuprofen andacetaminophen in a randomized double-blind placebo-controlledstudy Int Endod J 2004 37 531ndash41
13 Viitanen H Tuominen N Vaaraniemi H Nikanne E Annila PAnalgesic efficacy of rectal acetaminophen and ibuprofen alone
or in combination for paediatric day-case adenoidectomy Br JAnaesth 2003 91 363ndash7
14 Henry D McGettigan P Epidemiology overview of gastrointestinaland renal toxicity of NSAIDs Int J Clin Pract 2003 Suppl (135)43ndash9
15 TGA Medicines Evaluation Committee 2003 Review of non-prescription analgesics Multiple Strength of Oral LiquidsAustralia Therapeutic Goods Administration 2003
Combined acetaminophen and ibuprofen for analgesia
87
16 Australian and New Zealand College of Anaesthetists Monitoringduring anaesthesia (Review P18) Melbourne The College 2008
17 Merry AF Sidebotham DA Middleton NG Calder MV WebsterCS Tenoxicam 20 mg or 40 mg after thoracotomy a prospective
randomized double-blind placebo-controlled study AnaesthIntensive Care 2002 30 160ndash6
18 Davies NM Clinical pharmacokinetics of ibuprofen The first 30years Clin Pharmacokinet 1998 34 101ndash54
19 Prescott LF Pharmacokinetics of paracetamol Paracetamol(Acetaminophen) A Critical Bibliographic Review New York Taylor ampFrancis Inc 2001 205ndash15
20 Rainsford KD The pharmacokinetics of ibuprofen in humans andanimals Ibuprofen A Critical Bibliographic Review London Taylor amp
Francis 1999 92ndash521 Ianiro S Jeansonne B McNeal S Eleazer P The effect of pre-
operative acetaminophen or a combination of acetaminophen andibuprofen on the success of inferior alveolar nerve block forteeth with irreversible pulpitis J Endod 2007 33 11ndash4
22 Cooper SA Schachtel BP Goldman E Gelb S Cohn P Ibuprofenand acetaminophen in the relief of acute pain a randomizeddouble-blind placebo-controlled study J Clin Pharmacol 1989 291026ndash30
23 AHFS Drug Information Bethesda MD American Society of
Health-System Pharmacist 2007
24 Coll AM Ameen JRM Mead D Postoperative pain assessmenttools in day surgery literature review J Adv Nurs 2004 46 124ndash33
25 Philip BK Parametric statistics for evaluation of the visual ana-logue scale Anesth Analg 1990 71 710
26 Schou S Nielsen H Nattestad A et al Analgesic dosendashresponserelationship of ibuprofen 50 100 200 and 400 mg after surgicalremoval of third molars a single-dose randomized placebo-controlled and double-blind study of 304 patients J Clin
Pharmacol 1998 38 447ndash5427 Barden J Edwards J Moore A McQuay H Single dose oral para-
cetamol (acetaminophen) for postoperative pain CochraneDatabase Syst Rev (Online) 2004
28 Anderson B Cranswick N The placebo (I shall please)mdashis it so
pleasing in children Paediatr Anaesth 2005 15 809ndash1329 Australian and New Zealand College of Anaesthetists and Faculty
of Pain Medicine Acute Pain Management Scientific EvidenceAustralian Government National Health and Medical ResearchCouncil 2005
30 Moore RA Edwards JE McQuay HJ Acute pain individualpatient meta-analysis shows the impact of different ways of ana-lysing and presenting results Pain 2005 116 322ndash31
31 Quiding H Oksala E Happonen RP Lehtimaki K Ojala T Thevisual analog scale in multiple-dose evaluations of analgesics J Clin
Pharmacol 1981 21 424ndash9
Merry et al
88
e411
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Journal section Oral Medicine and PathologyPublication Types Research
Analgesic efficacy of Lysine Clonixinate paracetamol and dipyrone in lower third molar extraction A randomized controlled trial
Vladimir-Reimar-Augusto-de Souza Noronha 1 Gladson-de Souza Gurgel 1 Luiz-Ceacutesar-Fonseca Alves 2 Luiz-Claacuteudio Noman-Ferreira 2 Lisette-Lobato Mendonccedila 2 Evandro-Guimaratildees de Aguiar 2 Evandro-Neves Abdo 2
1 Student in Oral and Maxillofacial Surgery and Traummatology Dental School Federal University of Minas Gerais Belo Hori-zonte Brazil2 Senior Lectures of Department of Surgery Pathology and Clinic Dental School Federal University of Minas Gerais Belo Horizonte Brazil
Correspondence Faculdade de Odontologia Universidade Federal de Minas GeraisAv Antonio Carlos 6627Belo Horizonte ndash Minas Gerais - BrasilCEP 31270-901evandroabdogmailcom
Received 18082008Accepted 20032009
Noronha VRA Gurgel GS Alves LCF Noman-Ferreira LC Mendonccedila LL Aguiar EG Abdo EN Analgesic efficacy of lysine clonixinate para-cetamol and dipyrone in lower third molar extraction A randomized con-trolled trial Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 httpwwwmedicinaoralcommedoralfree01v14i8medoralv14i8p412pdf
AbstractObjective The purpose of this study is to compare the analgesic effect of lysine clonixinate paracetamol and dipyrone after lower third molar extraction Material and Methods The sample consisted of 90 individuals with clinical indication for inferior third molars extraction The mean age of the sample was 223 years (DPplusmn25) The individuals received the medication in uni-dentified bottles along with the intake instructions The postoperative pain parameters were measured according to Visual Analogical Scale (VAS) and the data was evaluated using the Kruskal-Wallis Test and Friedman Test with the latter used to test different time intervals for each one of the drugsResults The final sample consisted of 64 individuals including 23 males (459) and 41 females (641) The mean age of the entire sample was 223 years (plusmn25) The average length of the procedures was 339 minutes (plusmn98) The distribution of mean values for this variable showed little variance for the different drugs (p=007) Conclusion Lysine Clonixinate did not show any substantial impact on the postoperative pain control when com-pared to other drugs
Key words Lysine Clonixinate paracetamol dipyrone postoperative pain impacted third molar
Article Number 2409 httpwwwmedicinaoralcomcopy Medicina Oral S L CIF B 96689336 - pISSN 1698-4447 - eISSN 1698-6946eMail medicinamedicinaoralcom Indexed in
-SCI EXPANDED-JOURNAL CITATION REPORTS-Index Medicus MEDLINE PubMed -EMBASE Excerpta Medica-SCOPUS-Indice Meacutedico Espantildeol
e412
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Introduction Surgical extraction of third molars is a very usual clini-cal procedure for controlling problems caused by im-pacted tooth and usually is followed by postoperative pain (1) As a result several studies have been published comparing the drugs used to control postoperative pain after surgical removal of third molars (1-4)Lysine Clonixinate is an analgesic that inhibits prostag-landin synthesis A study comparing Lysine Clonixi-nate with Paracetamol on the oral postoperative pain did not find any significantly difference between them (5) In animals Lysine Clonixinate showed a life span of 3 hours and it is recognized as a non-steroid anti-in-flammatory with the shortest life span when compared to other drugs of its category (6)It bonds to plasma proteins in up to 96-98 and its me-tabolism takes place in the liver four different inactive metabolites being derived Seventy-four percent of its excretion is renal and 25 fecal (7) It holds an ex-cellent bio-tolerance and low incidence of collateral ef-fect in the treatment of painful syndrome such as renal neurogenic muscular and tooth pain (89) and migraine (7) The Visual Analogical Scale (VAS) is considered the best and easiest instrument to measure this type of pain The parameters used by VAS determine the intensity of pain as following no pain mild pain moderate pain and severe pain (10-12) The postoperative pain in dentistry should be controlled even before the surgical procedure itself For that many studies suggest the prescription of anti-inflammatory drugs steroids or not or analgesic drugs with some level of anti-inflammatory properties (1314)Paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom tooth (1516) and dipyrone is similar to other analgesics frequently used in the treatment of moderate to severe postoperative pain (17)Although the drugs under test are safe it is possible the occurrence of adverse effect The estimated ex-cess mortality due to community-acquired agranu-locytosis aplastic anemia anaphylaxis and serious upperrsquogastrointestinal complications was 20 per 100 million for paracetamol 25 per 100 million for dipy-rone (18)Regarding the Paracetamol and Dipyrone large use in Brazil Spain and other countries as well (1719) we decided to use them in order to compare the Lysine Clo-nixinate clinic performance The adverse effects due to the use of Lysine Clonixinate could be nausea vomit-ing allergic reactions vertigo and insomnia (9)
Material and MethodsThe sample of 90 individual consisted of all patients under treatment in that semester at the clinic of Oral
Surgery and Oral Traumatology from Federal Univer-sity of Minas Gerais The following conditions were ob-served in order to select the cases (I) individuals with clinical indication for the removal impacted mandibular third molar in Class I or II positioning A or B accord-ing to Pell et al (20) regardless gender race or social class (II) surgeries that would not extend more than 60 minutes (III) age between 18 and 26 years old (IV) absence of allergies to the drugs under test (V) absence of systemic conditions All surgeries were carried out under local anesthesia-Lidocaine 2 with Felipressine 12500 - Novocoreg (SSWhite Artigos Dentais LTDA Rio de Janeiro Brazil)The patients were informed about the purpose of the research project and were asked to give their written consent The research was approved by the local Ethical CommitteeThe drugs tested were bottled in identical opaque white recipient numbered from 1 to 90 Each recipient con-tained eight tablets of either one of the drugs under test (Dipyrone 500mg Paracetamol 750mg Lysine Clonixi-nate 125 mg) The patients themselves chose the recipi-ent at random and they were unaware of its contentEach patient was told to take one tablet from the given recipient one hour before the surgery and another tablet was taken after the surgery in 6 hours intervals after first dose during 24 hours If the pain persisted the pa-tient was given the liberty to take any other drug and the dentist should be informed The assessment of pain was performed according to VAS Pain was measured just after the surgical proce-dure and 1246812 and 24 hours after the operation For each one of the above options they had also to in-form the level of pain according to a decimal scale The criteria used by the authors to assess patientrsquos pain level were 0 cm no pain 01-3 cm light pain 31-7 cm mo-derate pain 71-10 cm intense pain (9) The descriptive analyses are presented in percentages with mean minimum (min) maximum (max) and standard deviation (SD) Kruskal-Wallis and Friedman tests were used and results were considered statistically significant when value of p was less or equal to 005 at least 95 of the confidence
ResultsThe drop-out in the experiment was of twenty-six cases and therefore the sample was reduced to sixty-four The Lysine Clonixinate group was comprised of 20 in-dividuals (8 males and 12 females) The Paracetamol Group was comprised of 23 individuals (9 males and 14 females) and Dipyrone Group was comprised of 21 individuals (6 males and 15 females) The mean age of the entire sample was 223 years (plusmn25) The length of the procedures was in average 339 min-utes (plusmn98) (Table 1) (Table 2) and (Fig 1) depict each
e413
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Interval drugdescriptive measurement
Pmin max median mean SD
Right after Lysine clonixinate 000 100 000 020 040 09370
Paracetamol 000 300 000 030 070
Dipyrone 000 100 000 010 040
1 hour afterLysine clonixinate 000 200 100 070 060 08130
Paracetamol 000 300 100 060 070
Dipyrone 000 200 100 070 070
2 hours afterLysine clonixinate 000 200 100 080 070 09310
Paracetamol 000 300 100 080 090
Dipyrone 000 300 100 080 080
4 hours afterLysine clonixinate 000 200 100 090 070 08760
Paracetamol 000 200 100 080 070
Dipyrone 000 300 100 100 100
6 horus afterLysine clonixinate 000 200 100 060 060 05330
Paracetamol 000 300 100 080 090
Dipyrone 000 300 000 060 080
8 hours afterLysine clonixinate 000 200 050 060 060 03110
Paracetamol 000 200 000 060 080
Dipyrone 000 300 000 040 080
12 hours afterLysine clonixinate 000 200 000 040 060 05930
Paracetamol 000 200 000 055 070
Dipyrone 000 300 000 040 090
24 hours afterLysine clonixinate 000 200 000 030 060 05820
Paracetamol 000 200 000 040 070
Dipyrone 000 300 000 030 070
Fig 1 Distribution of the scale of pain according to the different time interval for each of the drugs tested
Table 1 Distribution of the variable pain according to VAS in different time period for the tree drugs tested
P refers to Kruskal-Wallis test
e414
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
one of the VAS parameters distributed according to drugs tested No adverse effect was observed with the drugs tested
DiscussionSixty-four individuals underwent surgical removal of their inferior third molars among them 23 (359) were male and 41 (641) female As reported before by Morin et al (21) the variable gender did not play any important role in the distribution of the variable pain after surgery The mean age was 223 years (SDplusmn25 years) and the sample was quite homogeneous in that aspect which is an advantage for the categorization of pain related to age Age can influence the pain control because third molar surgical extraction in older individuals can be-come troublesome due the cortical bone thickness and bone resilience loss (1) Chiapasco et al (1) reported a decrease in morbidity and postoperative complication of third molars in young patients Olmedo-Gaya et al (14) attributed an increase of pain in older patients due to the more bone density and narrower periodontal liga-ment
The patients underwent all the surgical procedures by 2 surgeons with calibration of the techniques avoiding therefore different approaches The surgeries length was controlled and therefore did not influence the be-havior of pain in this study- 339 min (SDplusmn98 min) Regarding this the authors believe there is no bias con-cerning the time-period of surgery on the results here presentedThe surgery of third molar is a well known procedure It allows a standardization of case selection reducing therefore the number of uncontrolled events that may lead to biasQuestionnaire and VAS were used to obtain the data The data bank was categorized by drug and analyzed according to the development of the postoperative con-dition as presented in (Table 1)The results in this study show no statistically significant difference between the drugs under test for controlling postoperative pain Martiacute et al (5) found similar results comparing Paracetamol and Lysine ClonixinateThe high number of patients without any pain in the postoperative period can be related to the local anesthe-sia The number of patients without pain in the postop-
DescriptionDrug Interval min Max median mean SD p
Lisyne clonixinate
Right after 00 10 00 02 04
lt 0001
1 hour after 00 20 10 07 062 hours after 00 20 10 08 074 hours after 00 20 10 09 076 hours after 00 20 10 06 068 hours after 00 20 05 06 0612 hours after 00 20 00 04 0624 hours after 00 20 00 03 06
Paracetamol
Right after 00 30 00 03 07
lt 0001
1 hour after 00 30 10 06 072 hours after 00 30 10 08 094 hours after 00 20 10 08 076 hours after 00 30 10 08 098 hours after 00 20 00 06 0812 hours after 00 20 00 05 0724 hours after 00 20 00 04 07
Dipyrone
Right after 00 10 00 01 04
lt 0001
1 hour after 00 20 10 07 072 hours after 00 30 10 08 084 hours after 00 30 10 10 106 hours after 00 30 00 06 088 hours after 00 30 00 04 0812 hours after 00 30 00 04 0924 hours after 00 30 00 03 07
Table 2 Distribution of pain perception in the different time intervals after surgery according to VAS
P refers to Friedman test
e415
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
erative period decreases with the passing of time Four hours after the surgery this percentage was the smallest and it increases slightly on the 6th and 8th hour after surgery reaching its peak with 24 hours The results presented here are similar to those of Olme-do-Gaya et al (14) who found out that the postoperative pain reaches its higher intensity during the first 8 hours after the surgery The moderate postoperative pain is re-ported when the production of pain mediator increases and also when the effect of local anesthesia is fading away After the 8th hour and during the subsequently days the pain decreases progressivelyThe results of this study show that the Lysine Clonixi-nate as well as Dipyrone and Paracetamol are efficient in controlling the postoperative pain in the surgery of inferior impacted third molars Lysine Clonixinate pos-sesses an analgesic activity similar to that of Dipyrone and Paracetamol and did not show any substantial im-pact on the control of postoperative pain when com-pared to those drugs
References1 Chiapasco M De Cicco L Marrone G Side effects and complica-tions associated with third molar surgery Oral Surg Oral Med Oral Pathol 199376412-20 2 Laureano Filho JR Maurette PE Allais M Cotinho M Fernandes C Clinical comparative study of the effectiveness of two dosages of Dexamethasone to control postoperative swelling trismus and pain after the surgical extraction of mandibular impacted third molars Med Oral Patol Oral Cir Bucal 200813E129-32 3 Loacutepez-Carriches C Martiacutenez-Gonzaacutelez JM Donado-Rodriacuteguez M Analgesic efficacy of diclofenac versus methylprednisolone in the control of postoperative pain after surgical removal of lower third molars Med Oral Patol Oral Cir Bucal 200510432-9 4 Esteller-Martiacutenez V Paredes-Garciacutea J Valmaseda-Castelloacuten E Berini-Ayteacutes L Gay-Escoda C Analgesic efficacy of diclofenac sodium versus ibuprofen following surgical extraction of impacted lower third molars Med Oral Patol Oral Cir Bucal 20049448-53 444-8 5 Martiacute ML De los Santos AR Di Girolamo G Gil M Manero EO Fraga C Lysine clonixinate in minor dental surgery double-blind randomized parallel study versus paracetamol Int J Tissue React 199315207-13 6 Gonzaacutelez-Martin G Cattan C Zuntildeiga S Pharmacokinetics of lysine clonixinate in children in postoperative care Int J Clin Phar-macol Ther 199634396-9 7 Krymchantowski AV Peixoto P Higashi R Silva A Jr Schutz V Lysine clonixinate vs naproxen sodium for the acute treatment of mi-graine a double-blind randomized crossover study MedGenMed 2005769 8 Ortiacute E Coirini H Pico JC Site-specific effects of the nonsteroidal anti-inflammatory drug lysine clonixinate on rat brain opioid recep-tors Pharmacology 199958190-9 9 Krymchantowski AV Barbosa JS Cheim C Alves LA Oral lysine clonixinate in the acute treatment of migraine a double-blind place-bo-controlled study Arq Neuropsiquiatr 20015946-9 10 Kremer E Atkinson JH Ignelzi RJ Measurement of pain patient preference does not confound pain measurement Pain 198110241-8 11 Price DD McGrath PA Rafii A Buckingham B The validation of visual analogue scales as ratio scale measures for chronic and ex-perimental pain Pain 19831745-56 12 Collins SL Moore RA McQuay HJ The visual analogue
pain intensity scale what is moderate pain in millimetres Pain 19977295-7 13 Seymour RA Walton JG Pain control after third molar surgery Int J Oral Surg 198413457-85 14 Olmedo-Gaya MV Vallecillo-Capilla M Galvez-Mateos R Rela-tion of patient and surgical variables to postoperative pain and inflam-mation in the extraction of third molars Med Oral 20027360-9 15 Weil K Hooper L Afzal Z Esposito M Worthington HV Van Wijk AJ et al Paracetamol for pain relief after surgical removal of lower wisdom teeth Cochrane Database Syst Rev 20073CD004487 16 Moore A Collins S Carroll D McQuay H Paracetamol with and without codeine in acute pain a quantitative systematic review Pain 199770193-201 17 Edwards JE Meseguer F Faura CC Moore RA McQuay HJ Single-dose dipyrone for acute postoperative pain Cochrane Data-base Syst Rev 20013CD003227 18 Andrade SE Martinez C Walker AM Comparative safety evalu-ation of non-narcotic analgesics J Clin Epidemiol 1998511357-65 19 Lorenzetti BB Ferreira SH Mode of analgesic action of dipy-rone direct antagonism of inflammatory hyperalgesia Eur J Phar-macol 1985114375-81 20 Pell GJ Gregory BT Impacted mandibular third molars clas-sification and modified techniques for removal Dent Digest 193339330-821 Morin C Lund JP Villarroel T Clokie CM Feine JS Differences between the sexes in post-surgical pain Pain 20008579-85
CLINICAL TRIAL
Onset of analgesia with sodium ibuprofen ibuprofen acidincorporating poloxamer and acetaminophenmdasha single-dosedouble-blind placebo-controlled study in patientswith post-operative dental pain
Stephen Daniels amp Sandie Reader amp Phillip Berry amp
Michael Goulder
Received 24 September 2008 Accepted 6 January 2009 Published online 28 February 2009 Springer-Verlag 2009
AbstractObjective To compare the onset of action and efficacy ofsodium ibuprofen (ibuprofen sodium dihydrate) and ibu-profen acid incorporating poloxamer (ibuprofenpoloxamer)with that of acetaminophen and placebo in patients withpost-operative dental painMethods A double-blind randomised placebo-controlledactive comparator two-centre study assessing the analgesicefficacy of sodium ibuprofen (512 mg equivalent to400 mg ibuprofen acid) ibuprofenpoloxamer (containing400 mg ibuprofen acid and 120 mg poloxamer 407)acetaminophen (1000 mg) and placebo in patients withmoderate-to-severe pain after third molar extraction (n=322) Onset of action was assessed using the two-stopwatchtechnique and pain intensity and relief were measuredusing validated traditional descriptor scales
Results Significantly more patients achieved confirmedperceptible pain relief and meaningful pain relief withsodium ibuprofen (963 Plt00001) and ibuprofenpoloxamer (900 P=00005) than with acetaminophen(675) The onset of action of both ibuprofen formula-tions was comparable with that of acetaminophen up to45 min post-dose a marked divergence in onset times infavour of the ibuprofen formulations occurred from45 min onward Mean values for the area under the painrelief and pain intensity differences curve (0ndash6 h) weresignificantly greater for sodium ibuprofen (346) andibuprofen acid (349) than for acetaminophen (225) (Plt0001) Other pain relief and pain intensity endpointsfavoured both ibuprofen formulations over acetamino-phen Distractibility from pain (6 h) was significantlygreater with the ibuprofen formulations than with acet-aminophen (P=0008 for sodium ibuprofen P=003 foribuprofenpoloxamer) In patients receiving ibuprofenpain interfered less with daily activities (at 1 and 6 h)than in those receiving acetaminophen (Ple0015) Bothibuprofen formulations had significantly better meanglobal assessment scores than acetaminophen (Plt0001)Tolerability profiles of the ibuprofen formulations werecomparable with that of acetaminophenConclusions Compared with acetaminophen sodiumibuprofen was associated with significantly greateranalgesic efficacy pain relief in a greater proportion ofpatients and greater patient satisfaction
Keywords Acetaminophen Dental pain
Ibuprofenpoloxamer Impacted teeth Post-operative pain
Sodium ibuprofen
Eur J Clin Pharmacol (2009) 65343ndash353DOI 101007s00228-009-0614-y
S DanielsPremier Research Group Clinical Research Center3200 Red RiverAustin TX 78705 USA
S Reader P Berry ()Reckitt Benckiser Healthcare UKDansom LaneHull HU8 7DS UKe-mail phillipberryreckittbenckisercom
M GoulderWorldwide Clinical Trials UK Ltd Isaac Newton CentreNottingham Science and Technology ParkNottingham NG7 2RH UK
Introduction
Ibuprofen [2-(4-isobutylphenyl) propionic acid] is awidely used non-steroidal anti-inflammatory drug(NSAID) currently licensed and marketed worldwide Itexhibits anti-inflammatory analgesic and antipyreticeffects in humans by working as a potent inhibitor of thecyclooxygenase enzyme system and is used to treat painresulting from a wide variety of ailments There is anextensive amount of published literature describing theefficacy of ibuprofen [1ndash7]
Patients with acute pain require rapid relief from over-the-counter (OTC) analgesics Rapidly absorbed ibuprofenformulations have been developed [8] and it was antici-pated that this rapid absorption would result in early onsetof analgesia This placebo-controlled double-blind rando-mised single-dose study was conducted to measure thetime to onset and degree of analgesia from two investiga-tional ibuprofen formulations The first investigationalibuprofen formulation contains the sodium salt of the drugibuprofen sodium dihydrate (sodium ibuprofen) Theformulation used in this study contains 256 mg of theibuprofen sodium salt equivalent to 200 mg ibuprofen acidIt is well documented that ibuprofen salts such asibuprofen sodium lysine and arginate are more rapidlyabsorbed than formulations of free ibuprofen acid [9] andseveral studies have shown that faster absorbed formula-tions lead to faster onset of analgesia [10ndash12] The saltdissolves rapidly in the gastrointestinal tract leading tofaster absorption Pharmacokinetic analyses show that thetime to peak plasma concentration (Tmax) with ibuprofensodium dihydrate is achieved in approximately 30ndash40 min[8] in contrast to the 1ndash2 h reported for standard ibuprofentablets [13 14] The second investigational ibuprofenformulation contains ibuprofen acid plus the surfactantpoloxamer 407 [from the poloxamer family of polymericnon-ionic surface active agents (ibuprofenpoloxamer)]mdashtoincrease the rate of dissolution of the tablet and enable morerapid absorption relative to standard ibuprofen formula-tions Acetaminophen another widely used OTC analgesicand antipyretic indicated for the same mild-to-moderatepain conditions as ibuprofen was included in the study as areference
The dental pain model was used because it is the mostappropriate model to investigate onset of analgesic actionIt is an established post-surgical pain model that involvesextraction of impacted third molars (wisdom teeth) arelatively consistent surgical technique that predictablyproduces moderate-to-severe pain The model is widelyaccepted and has a proven record of assay sensitivity (ieseparating active drugs from each other as well as fromplacebo) [11 12 15ndash18] The model is sensitive enough todemonstrate a correlation between plasma levels of ibupro-
fen and onset of analgesia with faster absorbed formula-tions such as ibuprofen arginate having a faster clinicalresponse time than standard ibuprofen [11 12 19] Theresults from dental pain studies have been widely extrap-olated to other general pain conditions including mostcommon OTC conditions
Onset of analgesic action was assessed using the two-stopwatch technique [11 12 19] and pain intensity andpain relief at each of the assessment timepoints wereassessed using traditional descriptor scales Exploratoryanalyses were conducted to give additional informationabout the rate of onset of action of the medications and tocompare the extent of relief provided by each of the activeformulations
Both ibuprofen formulations were given at a doseequivalent to 400 mg ibuprofen acid The acetaminophenproduct included in the study was Tylenol Extra Strength(1000 mg) a commercially available product The brandedprinting was removed from the Tylenol caplets to enable amatched placebo to be produced The doses of both drugsare the maximum licensed OTC doses in the USA and mostother countries and they have well-established safety andefficacy profiles
The primary objective of the study was to determine thetime to onset of analgesia following dosing with sodiumibuprofen tablets (2times256 mg ibuprofen sodium dihydrate)and ibuprofen acid tablets incorporating poloxamer (2times200 mg ibuprofen plus 60 mg poloxamer 407) hereafterreferred to as ibuprofenpoloxamer in patients with post-operative dental pain The secondary objective was tocompare the efficacy of the two ibuprofen formulationswith that of 1000 mg acetaminophen and placebo in termsof onset peak and duration of analgesic action
The study was conducted in accordance with theDeclaration of Helsinki [20] as referenced in EU Directive200120EC [21] and complies with International Confer-ence on Harmonisation (ICH) Good Clinical Practice(GCP) and applicable regulatory requirements
Methods
Study design
This study was a randomised double-blind placebo-controlled single-dose parallel-group study using thedental pain model It was conducted in two clinical researchcentres (Austin Texas and San Marcos Texas)
Patients andor their legal guardians provided informedconsent before the conduct of study-related proceduresPatients were screened within the 28 days before surgeryOn the day of surgery patients underwent surgical removalof one partially or full bone impacted mandibular third
344 Eur J Clin Pharmacol (2009) 65343ndash353
molar or two ipsilateral third molars with a total impactionscore of 4 5 or 6
Degree of impaction Points
Erupted 0Soft tissue 1Partial bone 2Complete (full) bone 3Unusual impaction (horizontalinverted or posterior-anterior) 4
Surgery was performed under local anaesthetic (approx-imately 100 mg lidocaine 2 with 110000 epinephrine)with conscious sedation (35 lmin 50 nitrous oxide for15 min) using standard surgical techniques Followingsurgery patients who fulfilled the inclusion criteria regard-ing baseline pain intensity were randomly allocated to oneof four treatment groups (sodium ibuprofen ibuprofenpoloxamer acetaminophen or placebo) in a 1111 ratioaccording to a computer-generated randomisation schedulethat stratified patients by sex and baseline pain intensityAfter dosing patients remained in the centre for 8ndash15 hOnset of action and efficacy assessments were recorded atpre-determined intervals during the 6 h post-dose A post-operative follow-up was conducted 5ndash12 days after surgery
The study protocol and its amendments together with thepatient information and consent documents were reviewedand approved by Quorum Review Inc (Seattle WA)
Patients
Patients were recruited from the Premier Research GroupClinical Research Centers database via advertising andpractitioner referral Eligible patients were males andfemales 16ndash40 years of age with a primary diagnosis of
amp at least one mandibular third molar (with full bonyimpaction and an impaction score of ge4 on a 5-pointscale) indicated for removal
amp two ipsilateral third molars with a combined totalimpaction score no greater than 6
In either case patients were required to have moderate orsevere baseline pain intensity as assessed using a 4-pointcategorical pain intensity scale and confirmed with a visualanalogue scale (VAS) score of ge50 mm but le85 mm (where0=no pain and 100 mm=worst pain)
The main exclusion criteria were history of significantdisease that rendered the patient unsuitable for inclusionsignificant ongoing painful conditions other than thatassociated with third molar surgery any ongoing conditionthat may have interfered with the absorption distributionmetabolism or excretion of study medications history ofallergy gastrointestinal complaints (including ulcers heart-burn dyspepsia and indigestion) migraine headaches
within the last year psychotic illness or drug abuse useof concomitant medication that may have confoundedassessments of pain relief (eg psychotropic drugs anti-depressants or sedative-hypnotics) pregnancylactationingestion of any analgesic or anti-inflammatory drug frommidnight of the night before surgery
Sample size determination
For the primary endpoint data were available for the time toperceptible relief from three studies using ibuprofen arginate[11 12 19] These data suggested that the time to perceptiblerelief would be 9 to 14 min for the two test formulationsassuming a similar onset of action to that of ibuprofen arginateSince it was assumed that the majority of placebo patientswould not achieve meaningful relief it was planned that thetime to confirmed perceptible relief for these patients would becensored at 4 h Although the spread of observations was notprovided for the arginate formulation it was assumed conser-vatively that the standard deviation (SD) for time to confirmedperceptible relief would be 1 h (based on the possible rangebeing 0ndash4 h and covering plusmn 2 SD) Hence this study was highlypowered (gt99) to detect such a large difference for the time toconfirmed perceptible relief using the Wilcoxon test
For the area under the curve (AUC) (pain relief intensitydifference [PRID] from 0 to 6 h) data were available fromtwo previous studies which compared ibuprofen lysine [22]and liquigel [23] ibuprofen with acetaminophen In the formerstudy PRID to 6 h was not provided but the sum of painintensity differences (SPID) to 6 h was given This gave adifference of 251 between ibuprofen lysine and acetamino-phen The within-group SD for acetaminophen was 447Using these data it was calculated that with 80 patients pergroup this study would have a 90 power to detect adifference between the ibuprofen formulations and acetamin-ophen at a significance level of 0025 If the data from theliquigel paper were used for sum of the measures of pain reliefand pain intensity difference (SPRID) to 6 h a slightly higherpower would be achieved It was not possible to performformal power calculations for the second endpoint in the closedtest procedure namely time to meaningful relief
Study and concomitant treatments
Following surgery eligible patients received a single oraldose (four tablets and two caplets) of one of the followingfour study treatments
amp sodium ibuprofen 2times256 mg ibuprofen sodium dihy-drate tablets (each tablet equivalent to 200 mg ibupro-fen acid) plus two matched placebo for ibuprofenpoloxamer tablets plus two matched placebo for 500 mgacetaminophen caplets
Eur J Clin Pharmacol (2009) 65343ndash353 345
amp ibuprofenpoloxamer 2times200 mg ibuprofen acid tabletseach tablet incorporating 60 mg of the surfactantpoloxamer 407 plus two matched placebo for sodiumibuprofen tablets plus two matched placebo for 500 mgacetaminophen caplets
amp acetaminophen 2times500 mg acetaminophen (TylenolExtra Strength) caplets plus two matched placebo forsodium ibuprofen tablets plus two matched placebo foribuprofenpoloxamer tablets
amp placebo two matched placebo for sodium ibuprofentablets plus two matched placebo for ibuprofenpolox-amer tablets plus two matched placebo for 500 mgacetaminophen caplets
Patients were encouraged to wait at least 90 min afterreceiving the study treatment before consuming rescuemedication although rescue medication was available atany time after dosing If rescue medication was neededwithin the first 4 h of dosing an intra-muscular injection ofketorolac tromethamine (60 mg) was administered Ifrescue medication was needed later than 4 h after studydrug administration acetaminophen 500 mghydrocodone5 mg or ketorolac tromethamine was given A prescriptionfor acetaminophen 500 mghydrocodone 5 mg was provid-ed to patients for home use at the time of discharge
The use of intravenous oral or inhaled (nitrous)sedation during surgery was prohibited Analgesic andanti-inflammatory drugs (except for the permitted rescuemedications antibiotics and anaesthetics) were not per-mitted during the 6-h post-dose assessment periodPenicillins macrolide antibiotics clindamycin and topicaltetracycline gelfoam were permitted the use of selectiveserotonin-reuptake inhibitors (SSRIs) and selective nor-epinephrine-reuptake inhibitors (SNRIs) was also accept-able in patients who had maintained a stable dose for atleast 4 weeks prior to the first visit Caffeine-containingfoods and drinks were to be discontinued from midnightprior to surgery until the end of the 6-h post-doseassessment period Ice packs were not allowed for thefirst 3 h after dosing
Efficacy endpoints
Patients were queried at pre-determined intervals by thestudy staff and all pain assessments were recorded by thepatient in their diary
Pain intensity (categorical and VAS)
Pain intensity (PI) was assessed at the following timesbaseline (0 h) and at 5 10 15 20 25 30 35 40 45 60 90120 180 240 300 and 360 min after dosing The PI wasmeasured on a categorical scale in response to the question
ldquoWhat is your pain level at this timerdquo with patient responsechoices of none=0 mild=1 moderate=2 and severe=3 Inaddition patients were also asked to draw a single vertical lineto indicate their current level of PI on the 100-mm VASPatients were randomised to treatment when they rated theirbaseline PI as moderate or severe and the score on the VASwas ge50 mm but le85 mm
Pain relief and pain half-gone
Pain relief (PR) was assessed at the same times as PI (withthe exception of 0 h) in response to the question ldquoHowmuch relief have you had from your starting painrdquo withpatient response choices of none=0 a little=1 some=2 alot=3 and complete=4 In addition patients were alsoasked ldquoIs your starting pain at least half gonerdquo withpatient responses as no=0 or yes=1
Perceptible and meaningful PR
Two stopwatches were started at the time of dosing Eachpatient was instructed ldquoStop the first stopwatch when you firstfeel any pain relief whatsoever This does not mean you feelcompletely better although you might but when you first feelany relief in the pain you have nowrdquo The patient wasinstructed ldquoStop the second stopwatch when the pain relief ismeaningful to yourdquo If the patient did not press thestopwatches within the first 4 h of the treatment period or ifrescue medication was required the patients were no longerrequired to use the stopwatches
Distractibility from pain
Distractibility from pain was assessed at baseline and at 60and 360 min after dosing in response to the question ldquoHoweasy is it for you to distract yourself from your painrdquoPatients responded using a 100-mm VAS scale where 0 =very easy and 100 = impossible
Rainier scale
Patients completed the Rainier scale at baseline and at 60and 360 min after dosing This assessed perceivedfunctional impairment of activities of daily living (ieeating driving sleeping reading working and speaking)Patients rated the perceived pain interference with eachactivity on a scale of 1 to 10 where 1 = would not interfereat all and 10 = would completely interfere
Rescue medication
The time of rescue medication was recorded Patientstaking rescue medication completed all pain intensity and
346 Eur J Clin Pharmacol (2009) 65343ndash353
pain relief assessments immediately before rescue medica-tion and continued to record their pain assessmentsthroughout the 6-h assessment period
Global evaluation
At the end of 6 h or at the time of rescue medication patientswere asked ldquoHow effective do you think the study medicationis as a treatment for painrdquo Response choices were 1 =excellent 2 = very good 3 = good 4 = fair or 5 = poor
The primary efficacy endpoint was the time to firstconfirmed perceptible pain relief There were two keysecondary endpoints (1) the AUC for SPRID from 0 to 6 hand (2) the time to meaningful pain relief
Other secondary endpoints included (1) total pain relief(TOTPAR) SPID (categorical and VAS) SPRID from 0 to4 h (2) TOTPAR SPID (categorical and VAS) from 0 to6 h (3) individual pain relief and pain intensity (categoricaland VAS) readings at each timepoint from 5 min to 6 h (4)peak pain relief and pain intensity difference (PID)(categorical and VAS) throughout the 6-h evaluation period(5) first time at which PID was ge1 (6) time to first use ofrescue medication (7) time to and proportion of patientswith pain half-gone (8) distractibility from pain at baselineand at 1 and 6 h post-dose and perceived pain interferencewith daily activities (Rainier scale) at 1 and 6 h post-dose(9) patientrsquos overall assessment of the medication
Safety assessments
Adverse events (AEs) were assessed by non-directedquestioning recorded in the source documentation andthen assessed by the Investigator with respect to severityand relationship to study medication Vital signs (bloodpressure heart rate and oral temperature) were assessed atscreening baseline (pre-dose) at 6 h post-dose and at thefollow-up visit A physical examination was also conductedat screening and at the follow-up visit 5ndash12 days aftersurgery
Statistical analyses
All calculations and figures were produced using SAS ver91 or S-PLUS 62 (SAS Institute Cary NC) The analysisof the primary endpoints was performed via a closed testprocedure The actual protocol-defined primary endpointwas the time to first confirmed perceptible pain reliefPairwise differences between the two ibuprofen formula-tions and placebo were assessed at a significance level of25 so the overall alpha-level of 5 was maintained Forthe primary endpoint pairwise differences between the twoibuprofen formulations and placebo were assessed using theWilcoxon rank-sum test A sensitivity analysis was also
performed where differences between the ibuprofen for-mulations and placebo were assessed using a Cox regres-sion analysis with treatment group study site gender andbaseline pain intensity (categorical) included in the modelThe hazard ratio and associated 975 confidence intervals(CIs) were calculated for the pairwise comparisons
It was planned that if either of the primary pairwisecomparisons were significant at the 25 level the keysecondary endpoints (SPRID 0ndash6 h and time to meaningfulpain relief) were to be assessed for that formulation under aclosed-test procedure Each endpoint was assessed in theorder specified and only if the previous assessments for thatformulation were significant were the subsequent end-points assessed in a confirmatory sense Once the endpointwas not significant then all subsequent assessments wereconsidered exploratory
Endpoints aggregated over several time points werecalculated using AUC as per the secondary endpointDifferences between the treatments were assessed at atwo-sided alpha of 005 A 95 CI for the pairwisedifferences between the treatments was calculated fromthe parameter estimates of the fitted model The pairwisecomparisons of interest were between each of the ibuprofenformulations and placebo and between each of theibuprofen formulations and acetaminophen For the time-to-event parameters such as time to first (unconfirmed)perceptible pain relief differences between the treatmentgroups were assessed as per the primary endpoint
Differences between each of the two ibuprofen formu-lations and acetaminophen in the key secondary endpointsand in the majority of the other secondary endpoints wereanalysed by analysis of covariance (ANCOVA) includingtreatment group study site gender and baseline painintensity (categorical scale) as factors
All assessments completed after the patient had takenrescue medication were considered to be missing For bothpain relief and pain intensity differences missing valuesbetween two available assessments were linearly interpo-lated Missing readings that could not be interpolated werereplaced with the baseline pain intensity or zero relief
All enrolled patients who received a dose of studymedication were included in the safety population All AEswere listed and tabulated by treatment severity relationshipto therapy and body system according to the MedicalDictionary for Regulatory Activities (MedDRA) Version81
Results
Between June and October 2005 a total of 322 patients(mean age 213 years) were randomised to receive studytreatment Of the 322 randomised patients 318 (988)
Eur J Clin Pharmacol (2009) 65343ndash353 347
completed the study The trial profile including the totalnumber of patients withdrawn and analysed is illustrated inFig 1 A total of 321 patients all of whom were balancedacross treatment groups with respect to baseline demo-graphics pain intensity and clinical characteristics (Table 1)were included in the intent-to-treat (ITT) population
Primary efficacy endpoint
Significantly more patients reported confirmed perceptiblepain relief with sodium ibuprofen (963) and ibuprofenpoloxamer (900) than with acetaminophen (675) (Plt00001 and P=00005 respectively) In the placebo grouponly 259 patients reported confirmed perceptible painrelief KaplanndashMeier median times to confirmed perceptiblepain relief were 170 min for sodium ibuprofen 185 minfor ibuprofenpoloxamer and 201 min for acetaminophen(Fig 2) Median time could not be estimated for placebo asfewer than 50 of patients assigned to this groupexperienced confirmed perceptible pain relief Comparisonsof pairwise differences between the two ibuprofen formu-lations and placebo using Wilcoxon rank-sum tests and Coxregression analysis were highly significant (Plt0001 forboth analyses)
Key secondary efficacy endpoints
Mean SPRID (0ndash6 h) values were 346 349 225 and073 for the sodium ibuprofen ibuprofenpoloxamer
acetaminophen and placebo groups respectively Pair-wise comparisons of ibuprofen and acetaminophen werehighly significant in favour of both ibuprofen formula-tions (Plt0001)
Significantly more patients reported meaningful painrelief with sodium ibuprofen (963) or ibuprofenpolox-amer (900) than with acetaminophen (675) (Plt00001and P=00005 respectively) (Fig 3) Of the patientsreceiving placebo 259 reported meaningful pain reliefThe KaplanndashMeier median times to meaningful relief were451 min (sodium ibuprofen) 447 min (ibuprofenpolox-amer) and 541 min (acetaminophen) Neither of the twoWilcoxon rank-sum comparisons between the ibuprofenformulations and acetaminophen were statistically signifi-cant whereas pairwise comparisons obtained via Coxregression analysis were statistically significantly different(P le 0002) The KaplanndashMeier survival curves were similarfor the ibuprofen and acetaminophen groups up to 45 minbut the degree of separation from 45 min onward wasmarked with more patients achieving meaningful painrelief with ibuprofen
Sitendashtreatment interactions
In general site was a statistically significant factor subjectsfrom the SanMarcos site had less favourable outcomes For theprimary efficacy endpoint and for the key secondary efficacyendpoints of SPRID (0ndash6 h) and time to meaningful pain reliefsite was statistically significantly For all three measures the
Withdrawn from ITT (failure toprovide baseline diary data) 1Withdrawn from ITT (failure toprovide baseline diary data) 1Withdrawn from ITT (failure toprovide baseline diary data) 1
IBUPROFENPOLOXAMER
Total screened 614
Total randomised 322
Excluded prior to surgery (n=240)
Excluded prior to dosing (n=52)
Failure to meet inclusion criteria (n=292)
Allocated to intervention 80
ACETAMINOPHEN
Allocated to intervention 81
PLACEBO
Allocated to intervention 81
Completed 80 Completed 81 Completed 81
Total analysed (ITTa) 80 Total analysed (ITTa) 80 Total analysed (ITTa) 81
Completed 76
Withdrew consent 1Lost to follow-up 1Other reasons 2
Withdrawn 0 Withdrawn 0 Withdrawn 0
Total analysed (ITTa) 80
SODIUM IBUPROFEN
Not included in ITT (failure to provide baseline diary data) 1
Allocated to intervention 80
Fig 1 Flow diagram illustrat-ing patient inclusion and exclu-sion throughout the study ITTIntent to treat aThe ITT popula-tion consisted of all patientswho were randomised whocompleted the baseline efficacyassessments and who had atleast one post-baseline assess-ment (primary efficacy set)
348 Eur J Clin Pharmacol (2009) 65343ndash353
interaction between site and treatment was formally investigat-ed In all cases the interaction term was not statisticallysignificant implying that treatment group responses wereconsistent between the sites
Exploratory secondary efficacy endpoints
Pain relief andor reduction in pain intensity
All summary endpoints related to pain relief andor PIDwere significantly more favourable for the two ibuprofenformulations than for acetaminophen or placebo (Plt0001for both ibuprofen formulations vs acetaminophen orplacebo in all comparisons)
A summary of pain relief scores at specified time pointsfrom 5 min to 6 h is displayed in Fig 4 The superiority of
the two ibuprofen formulations over acetaminophen canclearly be seen from 45 min post-dose onward A summaryof PID (categorical) scores at specified time points from5 min to 6 h is displayed in Fig 5 The superiority of thetwo ibuprofen formulations over acetaminophen can beclearly seen from 60 min post-dose onward
Individual PR and PID
The pain relief and PID (categorical and VAS) scores showthat sodium ibuprofen provided more effective pain reliefthan placebo at 15 min [P=0021 (PR) P=004 (PIDcategorical) P=0036 (PID VAS)] Similarly ibuprofenpoloxamer provided more effective relief than placebo at25 min [P=0002 (PR) P=0002 (PID categorical)] and at20 min [P=0008 (PID VAS)]
Timepoint (mins)
a
ttain
ing
conf
irmed
per
cept
ible
rel
ief
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 2 KaplanndashMeier curves for time to first confirmed perceptiblepain relief
Timepoint (mins)
a
ttain
ing
mea
ning
ful r
elie
f
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 3 KaplanndashMeier curves for time to meaningful pain relief
Table 1 Patient demographics and clinical characteristics at baseline (ITT population)
Baseline patient characteristics Treatment group
Sodium ibuprofen(n=80)
Ibuprofenpoloxamer(n=80)
Acetaminophen(n=80)
Placebo(n=81)
Total(n=321)
Age (years) mean (SD) 214 (388) 214 (360) 212 (443) 211 (408) 213 (399)Sex n ()Male 31 (388) 31 (388) 30 (375) 31 (383) 123 (383)Female 49 (613) 49 (613) 50 (625) 50 (617) 198 (617)
Baseline pain intensity (categorical) n ()Moderate 61 (763) 60 (750) 60 (750) 62 (765) 243 (757)Severe 19 (238) 20 (250) 20 (250) 19 (235) 78 (243)
Baseline pain intensity (VAS) mean (SD)Mean (SD) 6816 (874) 6881 (949) 6703 (932) 6737 (1003) 6784 (939)Range 51ndash85 50ndash89 52ndash84 50ndash85 50ndash89
ITT intent-to-treat SD standard deviation VAS visual analogue scaleTreatment definitions sodium ibuprofen=2times256 mg ibuprofen sodium dihydrate tablets (each tablet equivalent to 200 mg ibuprofen acid)ibuprofenpoloxamer=2times200 mg ibuprofen acid tablets acetaminophen=2times500 mg acetaminophen caplets
Eur J Clin Pharmacol (2009) 65343ndash353 349
First time to PID ge 1
There were no significant differences between the activetreatment groups in the proportion of the time to reportingof PID ge 1
Time to first use of rescue medication
Rescue medication was required by significantly fewerpatients in the sodium ibuprofen group (325) and theibuprofenpoloxamer group (225) than in the acetamin-ophen (438) group Owing to the relatively smallproportion of patients reporting the use of rescue medica-tion KaplanndashMeier median times to first use of rescuemedication could not be calculated The pairwise compar-isons between the two ibuprofen formulations and acet-aminophen were both statistically significant using theWilcoxon rank-sum test with P=0019 and P=0001 forsodium ibuprofen and the ibuprofenpoloxamer formula-tion respectively (Fig 6) The vast majority of patientsrandomised to placebo took rescue medication (827)
Time to and proportion of patients with pain half-gone
The proportion of patients reporting pain half-gone were938 888 75 and 370 for sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo re-spectively The median time to pain half-gone wassimilar for all three active treatment groupsmdash350 min(sodium ibuprofen) 375 min (ibuprofenpoloxamer) and450 min (acetaminophen) The Wilcoxon rank-sumcomparisons between the ibuprofen formulations andacetaminophen were not statistically significant (P=007and P=018 for sodium ibuprofen and ibuprofenpolox-amer respectively) but the two equivalent comparisonswere statistically significant when the Cox regression wasused (P=0013 and P=002 for sodium ibuprofen andibuprofenpoloxamer respectively) This may be explainedin terms of a greater proportion of patients randomised toeither of the ibuprofen formulations reporting the endpointscompared with acetaminophen However as for time tomeaningful relief the separation in onset times in favour ofibuprofen was only apparent from 45 min post-doseonward
Distractibility from pain (VAS)
At 1-h post-dose the mean values for the distractibilityfrom pain (VAS) scores were 290 321 381 and657 mm for sodium ibuprofen ibuprofenpoloxameracetaminophen and placebo respectively Both ibuprofenformations had lower (more favourable) scores thanplacebo (Plt0001) and sodium ibuprofen versus acetamin-ophen was statistically significant (P=0010) whereas theibuprofenpoloxamer versus acetaminophen comparisonswere non-significant (P=0083)
At 6 h post-dose both ibuprofen formulations hadmore favourable distractibility from pain scores thanacetaminophen (P=0008 and P=003 sodium ibuprofen
Timepoint (minutes)
Mea
n pa
in in
tens
ity d
iffer
ence
s
00
05
10
15
0 15 35 60 90 120 180 240 300 360
Sodium ibuprofen IbuprofenpoloxamerAcetaminophenPlacebo
Fig 5 Mean pain intensity difference (categorical) at each timepoint
Timepoint (mins)
ta
ken
resc
ue m
edic
atio
n
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 6 KaplanndashMeier curves for time to first use of rescue medication
Fig 4 Mean pain relief at each timepoint
350 Eur J Clin Pharmacol (2009) 65343ndash353
and ibuprofenpoloxamer respectively) The vast majorityof patients randomised to placebo took rescue medicationso only 14 patients provided valid data within this grouphence this analysis was not performed for the placebogroup
Pain interference with daily activities (Rainier scale)
At 1-h post-dose the mean values on the Rainier scale were188 223 268 and 432 for the sodium ibuprofen ibuprofenpoloxamer acetaminophen and placebo groups respectivelyThe scores were statistically significantly lower for bothibuprofen formulations than for placebo (Plt0001) andacetaminophen [P=0001 (sodium ibuprofen) and P=0015(ibuprofenpoloxamer)] At 6-h post-dose the mean valueswere 151 171 224 and 163 for the sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo groupsrespectively Both ibuprofen formulations maintained signif-icantly lower (more favourable) values on the Rainier scalethan acetaminophen (P=0004 and P=0011 for sodiumibuprofen and ibuprofenpoloxamer) Placebo treatment wasnot analysed for this comparison as only 14 patients in thisgroup provided valid data
Patientrsquos overall assessment of medication as a treatmentfor pain
Significantly more patients in the sodium ibuprofen (813)and ibuprofenpoloxamer (848) groups rated the studymedication as good very good or excellent than in the groupsthat received acetaminophen (538) or placebo (173)Furthermore the mean global assessment scores weresignificantly lower (more favourable) for both ibuprofenformulationsmdash240 (sodium ibuprofen) and 244 (ibuprofenpoloxamer)mdashthan for acetaminophen or for placebo (341 and446 respectively Plt0001)
Safety findings
A total of 118 of all patients had AEs that were consideredby the investigators to be possibly related to study medicationno events were classified as definitely or probably related tostudy treatment Adverse events were experienced by 300238 309 and 296 of patients receiving sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo respec-tively The majority of AEs (73) were mild-to-moderate inseverity and the most frequently reported AEs includednausea headache vomiting and dizziness Adverse eventsoccurring in at least 5 of all patients in any treatment groupare summarised in Table 2 Severe AEs (including vomitingnausea dizziness abdominal pain and headache) occurred atrates of 63 (sodium ibuprofen) 25 (ibuprofenpolox-amer) 123 (acetaminophen) and 99 (placebo) therewere no deaths or withdrawals attributable to AEs during thestudy period There were no significant differences betweenstudy medications in terms of tolerability
Discussion
This placebo-controlled study demonstrated excellent assaysensitivity for every measure of efficacy with bothibuprofen formulations and acetaminophen showing clini-cally and statistically significant analgesia that was superiorto placebo Furthermore the overall analgesic efficacy(duration and total effect) of both ibuprofen formulationswas shown to be superior to acetaminophen
Data from this study showed statistically significant differ-ences between both the ibuprofen test formulations andplacebo for the primary endpoint ie the time to firstconfirmed perceptible pain relief In addition a significantlygreater proportion of patients receiving ibuprofen experiencedconfirmed perceptible pain relief than those receiving acet-
Table 2 Adverse events occurring in gt5 of patients in any treatment group
Sodium ibuprofen (n=80) Ibuprofenpoloxamer (n=80) Acetaminophen (n=81) Placebo (n=81)
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Any AE 43 24 (300) 27 19 (238) 41 25 (309) 39 24 (296)GastrointestinalNausea 10 9 (113) 5 5 (63) 8 8 (99) 14 14 (173)Vomiting 2 2 (25) 1 1 (13) 6 6 (74) 8 8 (99)Nervous systemDizziness 4 4 (50) 0 0 (00) 6 5 (62) 5 5 (62)Headache 11 11 (138) 5 4 (50) 4 4 (49) 3 3 (37)
AE Adverse eventTreatment definitions sodium ibuprofen=2times256 mg ibuprofen sodium dihydrate tablets (each tablet equivalent to 200 mg ibuprofen acid)ibuprofenpoloxamer=2times200 mg ibuprofenpoloxamer tablets acetaminophen=2times500 mg acetaminophen capletsa Percentages based on total number of patients per treatment group
Eur J Clin Pharmacol (2009) 65343ndash353 351
aminophen The median time to meaningful pain relief was45 min for both ibuprofen formulations and 54 min foracetaminophen Although a much greater proportion ofpatients reported relief on the two ibuprofen formulationsthe divergence in onset times was only apparent from 45 minpost-dose onward ie there was a much higher proportion ofresponders from 45 min onward for the ibuprofen treatmentsthan for acetaminophen Because of this late divergence theWilcoxon rank-sum test was not sensitive enough to detectsignificant differences whereas the Cox proportional hazardsregression analysis showed significant differences in favour ofibuprofen over acetaminophen In terms of SPRID over 6 hboth ibuprofen test formulations were significantly moreefficacious than acetaminophen
Previous studies using the post-operative dental painmodel have demonstrated that treatment with a differentibuprofen salt formulation ibuprofen arginate (l-argininesalt of ibuprofen) resulted in faster onset times to analgesiaand greater overall efficacy than treatment with conven-tional (standard) ibuprofen [11 12 19] The pharmacoki-netic profile of the ibuprofen sodium formulation used inthis study has been shown to be similar to that of ibuprofenarginate with peak plasma concentrations achieved atapproximately 30ndash40 min compared with 1ndash2 h forstandard ibuprofen [8 13 14] Therefore it was anticipatedthat the rapid absorption associated with sodium ibuprofenwould result in early onset of analgesia similar to thatobserved for ibuprofen arginate This study was notintended nor was it sufficiently powered to compare thetwo ibuprofen formulations
When comparing the median time to meaningful painrelief data from this study with previous studies bothibuprofen test formulations in this study were found to be atthe upper end of the range for ibuprofen arginate andibuprofen lysine data (range 24ndash42 min) [11 12 19 22]ie 451 min (sodium ibuprofen) and 447 min (ibuprofenpoloxamer) In the earlier studies where ibuprofen arginatewas compared with conventional ibuprofen the mediantime to meaningful pain relief obtained for ibuprofenarginate was approximately half that of the conventionalibuprofen [11 12 19] A recent bioavailability study hasalso shown that the Tmax for sodium ibuprofen was lessthan half that of standard ibuprofen (ie 35 min vs 90 minrespectively) [8] Therefore it was not unexpected thatsodium ibuprofen had a fast onset of analgesic effect in thisstudy that was in a similar order of magnitude as thosepreviously reported for faster absorbed formulations
The analyses of secondary endpoints related to degreeof pain relief andor reduction in pain intensity (TOT-PAR SPRID SPID peak PID and peak PR) consistentlyfavoured both ibuprofen formulations over acetamino-phen Only in terms of time to PID of at least 1 werethere no statistically significant differences observed
compared with acetaminophen Measures of analgesicdurationmdashthe proportion of patients taking rescue med-ication and the time to rescue medicationmdashshowed thatthose in the acetaminophen group received rescuemedication sooner than those in either of the twoibuprofen groups This suggests that both ibuprofenformulations had a longer duration of action thanacetaminophen which is in keeping with that previouslyreported for ibuprofen lysine [22] and ibuprofen liquigel[23] In terms of pain relief and PID the timepoint at whicha significant difference was first observed between either ofthe ibuprofen formulations and placebo was 15 min(sodium ibuprofen) a significant difference between eitherof the ibuprofen formulations and acetaminophen was firstobserved at 45 min (sodium ibuprofen) In comparison withpreviously published data studies with ibuprofen arginateand ibuprofen lysine demonstrated significant differences inpain relief and PID between ibuprofen and placebo at 10ndash15 min [11 12 19 23] Furthermore significant differ-ences between ibuprofen lysine and acetaminophen wereobserved at 15 min much sooner than the 45 min observedin our study [22] These differences could be explained bythe different formulations of ibuprofen the fact that adifferent brand of acetaminophen was used in each of therespective studies or the inherent variability associated witha small sample size
Patients in both ibuprofen groups were able to distractthemselves from their pain at 1 and 6 h after dosingsignificantly more easily than those in the placebo andacetaminophen groups (6 h only) Patients in both ibupro-fen groups also reported that pain would interfere with theirdaily activities significantly less than patients in theacetaminophen group Patients in the two ibuprofen groupsrated the study medication as good very good or excellentmore frequently than those in the acetaminophen andplacebo groups
Ibuprofen is a well-tolerated NSAID at low doses [24]However even at prescribed doses ibuprofen is associatedwith the least risk of gastrointestinal complications com-pared with other NSAIDs [25ndash27] No new safety concernswere raised by the current study treatment with singledoses of sodium ibuprofen and ibuprofenpoloxamer werewell tolerated with AE profiles comparable to that ofacetaminophen The most frequently reported AEs consid-ered to be related to study treatment (ie nausea headachevomiting and dizziness) are not unexpected in patientsrecovering from dental surgery
In conclusion these results suggest that compared withacetaminophen both the sodium ibuprofen and ibuprofenacid incorporating poloxamer formulations are more effi-cacious in providing rapid and sustained analgesia and areassociated with pain relief in a greater proportion ofpatients undergoing surgical removal of impacted third
352 Eur J Clin Pharmacol (2009) 65343ndash353
molars Together with the favourable safety profile ofibuprofen these findings support a recommendation forthis agent as an analgesic of choice for the treatment ofpost-operative dental pain
Acknowledgements The authors would like to acknowledgeFranklin S Bonasso DDS and R Dean Jasper DDS (Central OralSurgery Group) Barbara Hernandez MA CCRC Michael Goulder(Worldwide Clinical Trials UK Ltd) for statistical support andVandana Sahajpal PhD and Quyen Chu PhD (Sudler amp HennesseyLondon) for medical writing support
Conflict of interest This study was funded by Reckitt BenckiserGroup plc Stephen Daniels (Premier Research Group ClinicalResearch Centers USA) is the Co-ordinating Investigator SandieReader and Phillip Berry are employees of Reckitt Benckiser Group plc
References
1 Sweetman SC (ed) (2002) Ibuprofen In Martindale the completedrug reference 33rd edn Pharmaceutical Press London
2 Mehlisch DR Sollecito WA Helfrick JF et al (1990) Multicenterclinical trial of ibuprofen and acetaminophen in the treatment ofpostoperative dental pain J Am Dent Assoc 121257ndash263
3 Roy S (1983) A double-blind comparison of propionic acidderivative (ibuprofen) and a fenamate (mefanamic acid) in thetreatment of dysmenorrhoea Obstet Gynecol 61628ndash632
4 Moran M (1991) Double-blind comparison of diclofenac potassi-um ibuprofen and placebo in the treatment of ankle sprain J IntMed Res 19121ndash130
5 Goswick CB (1983) Ibuprofen versus propoxyphene hydrochlo-ride and placebo in acute musculoskeletal trauma Curr Ther ResClin Exp 34685ndash692
6 Schachtel BP Thoden WR (1988) Onset of action of ibuprofenin the treatment of muscle-contraction headache Headache28471ndash474
7 Pearce I Frank GJ Pearce JMS (1983) Ibuprofen compared withacetaminophen in migraine Practitioner 227465ndash467
8 Dewland P Reader S Berry P (2008) Bioavailability of ibuprofenfollowing oral administration of standard ibuprofen sodiumibuprofen or ibuprofen acid incorporating poloxamer in healthyvolunteers Eur J Clin Pharmacol (submitted)
9 Geisslinger G Menzel S Wissel K Brune K (1993) Single dosepharmacokinetics of different formulations of ibuprofen andaspirin Drug Invest 5238ndash242
10 Schleier P Prochnau A Schmidt-Westhausen AM et al (2007)Ibuprofen sodium dihydrate an ibuprofen formulation withimproved absorption characteristics provides faster and great-er pain relief than ibuprofen acid Int J Clin Pharmacol Ther4589ndash97
11 Black P Max MB Desjardins P et al (2002) A randomizeddouble-blind placebo-controlled comparison of the analgesic
efficacy onset of action and tolerability of ibuprofen arginateand ibuprofen in postoperative dental pain Clin Ther241072ndash1089
12 Desjardins P Black P Papageorge M et al (2002) Ibuprofenarginate provides effective relief from postoperative dental painwith a more rapid onset of action than ibuprofen Eur J ClinPharmacol 58387ndash394
13 Albert KS Gernaat CM (1984) Pharmacokinetics of ibuprofenAm J Med 7740ndash46
14 Davies NM (1998) Clinical pharmacokinetics of ibuprofen Thefirst 30 years Clin Pharmacokinet 34101ndash114
15 Cooper SA Precheur H Rauch D et al (1984) The analgesicefficacy of ibuprofen compared to acetaminophen with codeine(abstract) Clin Pharmacol Ther 35232
16 Mehlisch D Frakes L (1984) A controlled comparative evaluationof acetaminophen and aspirin in the treatment of post-operativepain Clin Ther Exerpta Med 789ndash97
17 Mehlisch D Markenson J Schnitzer T (1999) The efficacy ofnonsteroidal anti-inflammatory drugs for acute pain CancerControl 65ndash9
18 Daniels SE Desjardins PJ Talwalker S et al (2002) The analgesicefficacy of valdecoxib vs oxycodoneacetaminophen after oralsurgery J Am Dental Assoc 133611ndash621
19 Mehlisch DR Ardia A Pallotta T (2002) A controlled compar-ative study of ibuprofen arginate versus conventional ibuprofen inthe treatment of postoperative dental pain J Clin Pharmacol42904ndash911
20 World Medical Association (1964) Declaration of HelsinkiEthical principles for medical research involving human patientsAdopted by the 18th WMA General Assembly 1964 and amendedby the 29th 35th 41st and 48th WMA General Assemblies
21 European Parliament and Council of 4 April 2001 (2001)Directive 200120EC of the approximation of the laws regu-lations and administrative provisions of the Member Statesrelating to the implementation of good clinical practice in theconduct of clinical trials on medicinal products for human useOfficial Journal of the European Communities Brussels
22 Mehlisch DR Jasper RD Brown P et al (1995) Comparativestudy of ibuprofen lysine and acetaminophen in patients withpostoperative dental pain Clin Ther 17852ndash860
23 Olson NZ Otero AM Marrero I et al (2001) Onset of analgesiafor liquigel ibuprofen 400 mg acetaminophen 1000 mg ketopro-fen 25 mg and placebo in the treatment of postoperative dentalpain J Clin Pharmacol 411238ndash1247
24 Sachs C (2005) Oral analgesics for acute nonspecific pain AmFam Physician 71913ndash918
25 Doyle G Furey S Berlin R et al (1999) Gastrointestinal safetyand tolerance of ibuprofen at maximum over-the-counter doseAliment Pharmacol Ther 13897ndash906
26 Henry D Lim LL Garcia Rodriguez LA et al (1996) Variability inrisk of gastrointestinal complications with individual non-steroidalanti-inflammatory drugs results of collaborative met-analysis BrMed J 3121563ndash1566
27 Henry D McGettigan P (2003) Epidemiology overview ofgastrointestinal and renal toxicity of NSAIDs Int J Clin Pract13543ndash49
Eur J Clin Pharmacol (2009) 65343ndash353 353
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 153
RESEARCH
An investigation into the comparative efficacyof soluble aspirin and solid paracetamol inpostoperative pain after third molar surgeryR A Seymour1 J E Hawkesford2 J Sykes3 M Stillings4 and C M Hill5
Objective To compare the efficacy of soluble aspirin 900 mg andparacetamol 1000 mg in patients with postoperative pain after thirdmolar surgeryDesign A randomised placebo controlled double-blind studySetting Day stay units of Oral and Maxillofacial Surgery at CardiffDental Hospital and Hexham General Hospital NorthumberlandSubjects and methods One hundred and sixty-seven (104 female)patients who required the removal of their impacted third molars undergeneral anaesthesiaIntervention In the early postoperative period patients were medicatedwith either a single dose of soluble aspirin 900 mg solid paracetamol1000 mg or placebo Main outcome measures Pain intensity was measured on 100 mmvisual analogue scales at 0 5 10 15 20 30 45 60 90 120 and 240minutes after dosing Other efficacy variables evaluated included time torescue medication and an overall assessment of the study medicationefficacy by the patient on completion of the studyResults One hundred and sixty-seven patients consented to take part inthe study but only 153 were medicated Of the 14 patients not treated10 failed to develop sufficient pain to enter the study two withdrewconsent one had an adverse reaction to the general anaesthetic and onewas a protocol violator Over the four hour investigation period patientstreated with soluble aspirin reported significantly less pain whencompared with those treated with paracetamol (mean difference inAUC0-240 = -2001 95 CI ndash3893 to ndash109 p=0038) and placebo (meandifference in AUC0-240 = -3470 95 CI ndash5719 to ndash1221 p=0003)
1Head of Department Professor of Restorative Dentistry Department of RestorativeDentistry Dental School University of Newcastle Newcastle upon Tyne 2Consultant Oraland Maxillofacial Surgeon Department of Oral and Maxillofacial Surgery NewcastleGeneral Hospital Newcastle upon Tyne 3Clinical Statistician Reckitt Benckiser Healthcare(UK) Hull 4Head of Global Professional Relations Reckitt Benckiser Healthcare (UK) Hull5Consultant Oral and Maxillofacial Surgeon Department of Oral Surgery Dental SchoolUniversity of Wales College of Medicine Cardiff Correspondence to Professor R A Seymour Department of Restorative Dentistry DentalSchool University of Newcastle upon Tyne Framlington Place Newcastle upon TyneEngland NE2 4BWE-mail R A Seymournclacuk
Refereed paperReceived 080302 Accepted 060902copy British Dental Journal 2003 194 153ndash157
Similarly at 20 and 30 minutes after dosing patients in the solubleaspirin group were reporting significantly less pain than those in theparacetamol treatment group (mean difference in pain intensity at 20minutes ndash79 95 CI ndash153 to ndash06 p=0035 at 30 minutes ndash106 95CI ndash186 to ndash26 p=0010) There were no significant differences betweentreatment groups with respect to the number of patients requiringrescue medication however the time to dosing was significantly longerfor those taking soluble aspirin when compared with placebo (hazardratio 234 95 CI 141 to 388 plt0001) Conclusion The findings from this study showed that soluble aspirin900 mg provides significant and more rapid analgesia than paracetamol1000 mg in the early postoperative period after third molar surgery
INTRODUCTIONBoth aspirin (acetylsalicylic acid) and paracetamol (acetamino-phen) are widely available analgesics The drugs are used exten-sively in dentistry either self-prescribed by the patient or recom-mended by the dental surgeon Despite such use there have beenfew comparative studies on these analgesics and the studies pub-lished seem to suggest that the drugs are equi-analgesic1 Morerecent evidence suggests that many factors appear to influence theefficacy of aspirin in postoperative dental pain These include for-mulation dose and plasma concentration of acetylsalicylate2-5
The latter appears to be determined by plasma aspirin esteraseactivity By contrast there is limited information on the efficacy ofparacetamol in postoperative dental pain
Historically there have been many studies comparing the effi-cacy of a whole range of analgesics which have used aspirin as thestandard treatment (positive control) In such studies the formula-tion chosen has invariably been a solid format of the drug This hasled to the impression that aspirin is relatively weak and slow act-ing Previous studies34 have shown that soluble aspirin provides agreater onset of action and is overall more effective than solidaspirin However up to the present time there has been no studycomparing the efficacy of soluble aspirin with solid paracetamolThe present study was designed to investigate whether the superi-ority of soluble aspirin over solid aspirin would be reproducedwhen compared with solid paracetamol The doses chosen for each
This study has shown the benefits of soluble aspirin (900 mg) over solid paracetamol (1000 mg)in the control of postoperative pain after third molar extractions
The aspirin preparation provided an earlier onset of pain relief when compared with paracetamol Most patients in the study did require additional analgesia in the early postoperative period
but the time to remedication was significantly longer in soluble aspirin group whencompared with the placebo
Adverse events due to the medication were few and showed no differences between treatmentgroups
Soluble aspirin 900 mg appears to be a more useful analgesic than paracetamol in the controlof postoperative pain after third molar surgery
I N B R I E F
RESEARCH
154 BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003
preparation used in this study is the maximum recommendedwhen purchased as over the counter (OTC) medications
Removal of impacted third molars remains a common dentalsurgical procedure that results in a significant level of postopera-tive pain6 Pain is usually of short duration and reaches its maxi-mum intensity in the early postoperative period7 It is during thistime period that analgesics are frequently prescribed The nature ofthe pain and its duration make the third molar pain model usefulfor evaluation of analgesic efficacy
The overall aim of the present study was to directly compare theefficacy of soluble aspirin with that of solid paracetamol tablets inpatients with postoperative pain after third molar surgery A place-bo group was also used to act as a negative control Within thisoverall remit the primary aim of the study was to compare theonset of efficacy between the two preparations
MATERIAL AND METHODSAdult patients who required the removal of at least one impactedlower third molar were invited to participate in the study Patientswere enrolled from two centres (Cardiff and Hexham) Informedwritten consent was obtained from each patient prior to theirentry into the study which had received ethical approval from theappropriate local Health Authority Ethical Committees Patientsenrolled into the study were fit and healthy and complied with thecriteria of the American Society of Anaesthesiologists categoryone or at the discretion of the dental surgeon category two Allpatients attended a screening clinic prior to their participation inthe study The pre-screening was held up to a maximum of threeweeks before surgery Patients were asked to abstain from takingany analgesics for 24 hours prior to their third molar extractions
Patients underwent the removal of their impacted third molarsunder general anaesthesia The anaesthetic regimen was accord-ing to routine clinical practice at the dental centre and includedinduction with intravenous propofol Muscle relaxation wasachieved with vecuronium atracurium pancurium mivacuriumor suxamethonium Anaesthesia was maintained with nitrousoxide oxygen and either isoflurane enflurane or sevofluranePerioperative analgesia was provided by fentanyl or alfentanyl
Impacted third molars were removed following a standard tech-nique Bone removal was carried out with a drill under saline sprayThe operating time (from first incision to completion of last suture)was recorded for each patient On completion of the surgical proce-dure time was allowed for the patients to recover fully from theeffects of the anaesthetic They were then returned to the wardwhere they were monitored by the study nurse and their pain inten-sity assessed on 100 mm visual analogue scales (VAS) The bound-aries of the scale were marked lsquono painrsquo and lsquoworst pain imaginablersquoWhen patientsrsquo pain intensity reached a level in excess of 30 mm onthe VAS they were randomised to study medication Patients whosepain intensity did not reach the required level or who did notrequest analgesia within 1frac12 hours post-operatively were with-drawn from the study Each eligible patient was randomly allocatedto one of the following treatment groups soluble aspirin (Disprinreg)900 mg solid paracetamol tablets BP 1000 mg or placebo In order
to double-blind the study a double-dummy technique was usedEach patient assigned to receive active soluble aspirin or activesolid paracetamol also received a placebo for the alternative treat-ment and placebo patients received a placebo for both formula-tions Soluble aspirin and the aspirin placebo were presented as anorange drink Paracetamol active and placebo were given as tabletsPatients were randomised to treatment groups in the ratio of 2aspirin2 paracetamol1 placebo The randomisation was stratifiedfor gender A randomisation block size of five was used to ensurebalance between the treatment groups
Pain assessmentThe following measures were used to evaluate efficacya) Pain intensity measures were recorded immediately pre-dose (0
minutes) and at 5 10 15 20 30 45 60 90 120 and 240 minutesafter dosing Onset of analgesia was primarily assessed by painintensity measures at 10 15 20 and 30 minutes
b)Pain intensity over the four hour investigation period The serial VAS measures of the four hour investigation periodwere compiled into a graph of pain (mm) versus time (minutes)The area under the graph (AUC) was calculated using the trape-zoidal method and denoted as AUC240 Such a measure gives anoverall assessment of each patientrsquos pain experience throughoutthe four hour investigation period8
c) Use of rescue medicationIn the event of poor pain control patients were allowed access toalternative analgesia (ibuprofen 400 mg) Patients were encour-aged not to request re-medication in the first hour post-dosingin order to give the study medication time to work For thosetaking additional analgesics the time was recorded and theirlast pre-rescue medication intensity score was extrapolated overthe remaining time points9
d)Overall evaluation At the end of the four hour investigation period (or prior to tak-ing rescue medication) the study nurses and the patients wereasked to provide an overall evaluation of the efficacy of thestudy medication The categories were lsquovery goodrsquo lsquogoodrsquo lsquosatis-factoryrsquo lsquopoorrsquo and lsquovery poorrsquo
Throughout the investigation period a study nurse was respon-sible for monitoring the patients and recording any adverse events
Statistical methodsA previous study in postoperative pain after removal of impactedthird molars4 suggested that mean VAS differences between solu-ble aspirin and placebo and soluble aspirin and solid paracetamolof 26 mm and 14 mm respectively might be anticipated at 20 min-utes post treatment Using a randomisation of 2 soluble aspirin 2paracetamol 1 placebo a total sample size of 150 patients had atleast 80 power to detect this difference
The VAS pain intensity measurements at 10 15 20 and 30minutes after dosing and AUC240 were compared between treat-ment groups using an analysis of covariance using centre gen-der baseline pain intensity operation duration and number of
Table 1 Demographic details of patients who were medicated for the study Where appropriate results are expressed as mean (SD)Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo
Number of patients 59 62 32Gender ratio MF 1940 1943 1121Age (years) 256 (56) 250 (53) 251 (47)Weight (kg) 702 (16) 719 (145) 743 (149)Mean operating time (mins) 173 (101) 165 (101) 130 (130)Number of molars removed 1 3 (5) 2 (3) 3 (9)[ patients ()] 2 15 (25) 14 (23) 5 (16)
3 11 (19) 12 (19) 9 (28)4 30 (51) 34 (55) 15 (47)
Mean baseline pain score on 100 mm VAS 574 (176) 506 (142) 541 (144)
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 155
in Hexham and the remainder in Cardiff Of the 14 patients nottreated 10 failed to develop sufficient pain to enter the studytwo withdrew consent one had an adverse reaction to the anaes-thesia and one was a protocol violator Demographic details ofthe patients are shown in Table 1 The three groups were bal-anced for demographic variables
The primary aim of the study was to compare the rate of onset ofanalgesia and the 20-minute time was considered to be appropriatefor such an assessment Pain scores as recorded on the VAS at eachtime point are illustrated in Figure 1 and Tables 2a and 2b VASscores decreased in all treatment groups during the first 15 minutespost dosing (Figure 1) At 20 minutes post dosing patients in the sol-
molars removed as covariates Use of rescue medication and thestudy nursesrsquo and patientsrsquo overall impression of their medicationwere analysed using binomial logistic regression with a lsquopositiversquooutcome defined as a response of lsquovery goodrsquo or lsquogoodrsquo Time toadministration of rescue medication was compared betweentreatment groups using Coxrsquos proportional hazard model Com-parisons were performed for soluble aspirin versus solid paraceta-mol and soluble aspirin versus placebo
RESULTSOne hundred and sixty seven patients consented to take part inthe study and 153 were medicated Of these 29 were medicated
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 30 45 60 90 120 240
Time (mins)
Pain
(mm
)
Soluble AspirinParacetamolPlacebo
Figure 1 Graph to show mean pain scores (mm) versus time (mins) for patients after treatment with placebo solid paracetamol 1000 mg and solubleaspirin 900 mg
Table 2a Summary of efficacy parameters recorded during the investigation period pain scoresBetween treatment comparisons
Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Mean difference (95 CI) p-value Mean difference (95 CI) p-value
Pain score (in mm) 10 mins after dosing 412 (28) 482 (29) 474 (33) -61 (-133 to 10) 0092 -70 (-130 to ndash09) 0024Pain score (in mm) 15 mins after dosing 407 (32) 458 (33) 445 (38) -39 (-120 to 43) 0350 -51 (-120 to 18) 0143Pain score (in mm) 20 mins after dosing 402 (34) 481 (35) 500 (40) -98 (-186 to ndash11) 0028 -79 (-153 to ndash06) 0035Pain score (in mm) 30 mins after dosing 356 (37) 462 (38) 476 (44) -120 (-216 to ndash25) 0014 -106 (-186 to ndash26) 0010Overall pain - AUC240(mmmins) 8001 (871) 10002 (898) 11471 (1035) -3470 (-5719 to ndash1221) 0003 -2001 (-3893 to ndash109) 0038
data presented are adjusted (least squares) mean (standard error of the mean)
Table 2b Summary of efficacy parameters recorded during the investigation period use of escape medicationBetween treatment comparisons
Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds (hazard) ratio (95 CI) p-value Odds (hazard) ratio (95 CI) p-value
Number of patients 48 (81) 46 (74) 29 (91) 0172 (0020 to 1052) 0078 1485 (0455 to 5197) 0518taking escape analgesics
Time (minutes) to 115 (63 - 165) 94 (47 - ++) 64 (42 ndash 117) 234 (141 to 388) lt0001 130 (084 to 203) 0236remedication
data presented are median (Inter Quartile Range)++ Upper quartile cannot be estimated
RESEARCH
156 BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003
uble aspirin group reported significantly less pain than those treatedwith solid paracetamol (p=0035) or placebo (p=0028) Similarlypain intensity was significantly less at 10 and 30 minutes post dos-ing for patients treated with soluble aspirin when compared withsolid paracetamol (p=0024 and 0010 respectively) Pain intensitywas also significantly less for patients treated with soluble aspirinwhen compared with placebo at 30 minutes post dosing (p=0014)but was not significant at 10 minutes post-dosing (p=0092) By con-trast to these findings at 15 minutes after dosing pain scores werenot significantly different between soluble aspirin and placebo(p=0350) or between soluble aspirin and solid paracetamol(p=0143) Overall pain scores as assessed by the AUC240 were sig-nificantly lower in the soluble aspirin group when compared withsolid paracetamol (p=0038) and placebo (p=0003) There was nosignificant centre difference for any of the pain intensity variables
The use of rescue medication and time to requesting such med-ication is also shown in Table 2b There was no significant differ-ence between soluble aspirin and solid paracetamol or placebowith respect to the number of patients requiring rescue medicationduring the four hour investigation period (pgt005) However thetime to administration of rescue medication was significantlylonger for those patients taking soluble aspirin when comparedwith placebo (plt0001) There was no significant difference in timeto rescue medication between the soluble aspirin treated patientsand those treated with solid paracetamol (p=0236) The time toadministration of rescue medication did show a significant centreeffect with those patients enrolled in Cardiff requiring rescueanalgesia at an earlier time point than those in Hexham (plt0001)
The study nursesrsquo and patientsrsquo overall assessment of the effica-cy of the medication is shown in Tables 3a and 3b There was nosignificant difference between soluble aspirin and solid paraceta-mol (p=0285) with respect to the percentage of lsquopositiversquo outcomesassessed by the patients however soluble aspirin was favoured incomparison with placebo (p=0010) Results were similar for thestudy nursesrsquo assessment (p=0387 p=0024)
Adverse events were reported by 41 of patients with a higheroverall incidence in the active treatment groups (Table 4) Many ofthese events were related to the procedure The most commonadverse events were in the central and peripheral nervous system(primarily dizziness) and the gastro-intestinal system (primarilynausea) The incidence of dizziness was similar in the soluble
aspirin and placebo groups (14 and 13 respectively) and wasgreater than in the solid paracetamol group (6) The incidence ofnausea was comparable in the soluble aspirin and solid paraceta-mol groups (15 and 16 respectively) and was greater than thatin the placebo group (6) Gingival bleeding (the only adverseevent recorded under lsquohaemostasisrsquo) had a slightly lower incidencein the soluble aspirin group (8) than in the solid paracetamolgroup (13) and was only slightly higher than that reported in theplacebo group (3) This finding is contrary to any expectationsthat aspirin might exacerbate post-operative bleeding
DISCUSSIONThe present study has shown that soluble aspirin 900 mg is an effec-tive analgesic in the control of postoperative pain after the removalof impacted third molars confirming the evidence from previousstudies34 In addition soluble aspirin provided better pain controlthan solid paracetamol 1000 mg This superior efficacy is reflectedin the overall pain score (Table 2a and Figure 1) and also in the painscores reported during the first 30 minutes post dosing The datasuggest that soluble aspirin is providing a more rapid reduction inpain in the early postoperative period when compared with solidparacetamol If the pain scores are examined in terms of percentagereduction when compared with baseline the results show that solu-ble aspirin is twice as effective as solid paracetamol (at 20 and 30minutes the percentage reduction for soluble aspirin is 310 and406 respectively whilst the figures for solid paracetamol are142 and 204) From the perspective of patient management arapid reduction in pain is an important requisite of any analgesicformulation10 The exception to this pattern is the pain scores at 15minutes post dosing At this time point pain intensity scores aftersoluble aspirin are not significantly different from either placebo orsolid paracetamol mdash the reason for this finding is unclear
Previous comparative efficacy studies between aspirin andparacetamol in postoperative dental pain have revealed somewhatequivocal results11112 The consensus view1 is that both aspirin andparacetamol are both equi-analgesic and equipotent The studiesuse a solid tablet formulation of aspirin at a dose of 650 mg Studiesusing similar methodology have shown that the efficacy of aspirinin postoperative dental pain is related to dose and formulation34
The use of a soluble formulation and the 900 mg dose may explainthe superior efficacy of aspirin in this study
Table 3b Distribution of scores from study nursesrsquo global assessment of the medication (number ())Score Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds Ratio (95 CI) p-value Odds Ratio (95 CI) p-value
Positive outcome 32 (54) 32 (52) 10 (31) 2974 (1179 to 7951) 0024 1403 (0655 to 3054) 0387Very good 15 (25) 11 (18) 3 (9)Good 17 (29) 21 (34) 7 (22)Satisfactory 17 (29) 14 (23) 12 (38)Poor 8 (14) 14 (23) 7 (22)Very poor 2 (3) 2 (3) 3 (9)Total 59 62 32
positive outcome = response of lsquovery goodrsquo or lsquogoodrsquo
Table 3a Distribution of scores from patientsrsquo global assessment of the medication (number ())Score Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds Ratio (95 CI) p-value Odds Ratio (95 CI) p-value
Positive outcome 34 (58) 33 (53) 10 (31) 3591 (1402 to 9828) 0010 1530 (0706 to 3380) 0285Very good 15 (25) 12 (19) 3 (9)Good 19 (32) 21 (34) 7 (22)Satisfactory 15 (25) 12 (19) 10 (31)Poor 8 (14) 15 (24) 9 (28)Very poor 2 (3) 2 (3) 3 (9)Total 59 62 32
positive outcome = response of lsquovery goodrsquo or lsquogoodrsquo
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 157
The primary aim of this investigation was to compare both anal-gesics with respect to onset of action Early time points were chosenfor this comparison as they represent a suitable period from dosingwhen patients would expect to experience meaningful pain reliefSoluble aspirin was significantly superior to both placebo and solidparacetamol at both 20 and 30 minutes post dosing and there wereindications of superiority as early as at 10 minutes In part this maybe due to the rapid absorption of soluble aspirin and the subsequentpeak concentrations of acetylsalicylate (Tmax) that occurs at thesetime points It has been previously shown that plasma concentra-tions of acetylsalicylate are also important determinants of aspirinrsquosefficacy in postoperative dental pain2 By contrast the absorption ofsolid paracetamol tablets is slow with a Tmax of 60 minutes13 Thusdifferences in pharmacokinetics may account for the differences inonset of analgesia observed in the present study
It is now well established that aspirin exerts both analgesic andanti-inflammatory action by inhibiting prostaglandin synthesis14
Aspirin irreversibly inhibits both cyclo-oxygenase 1 and 2 (Cox-1and Cox-2) by acetylating serine 530 thus preventing the bindingof arachidonic acid to the active sites of the enzyme The pharma-codynamics of paracetamol are uncertain and by comparison withaspirin the drug exhibits weak anti-inflammatory action This lackof a pronounced anti-inflammatory effect may also explain theweaker efficacy of this drug in postoperative dental pain
We can conclude from this study that a single dose of solubleaspirin 900 mg provides significant and more rapid analgesia thansolid paracetamol 1000 mg in the early postoperative period afterthird molar surgery This study confirms the value of soluble aspirinin the management of pain after dental surgical procedures
The authors are grateful to Reckitt Benckiser Healthcare for their support inthis study
1 Cooper S A Comparative analgesic efficacies of aspirin and acetaminophen ArchIntern Med 1981 141 282-285
2 Seymour R A Williams F M Ward A Rawlins M D Aspirin metabolism and efficacyin postoperative dental pain Br J Clin Pharmacol 1984 17 697-701
3 Seymour R A Williams F M Luyk N M et al Comparative efficacy of soluble aspirinand aspirin tablets in postoperative dental pain Eur J Clin Pharmacol 1986 30495-498
4 Holland I S Seymour R A Ward-Booth R P Ord R A Lim K L Hoare R C Anevaluation of different doses of soluble aspirin and aspirin tablets in postoperativedental pain Br J Clin Pharmacol 1988 26 463-468
5 Seymour R A Weldon M Kelly P Nicholson E Hawkesford J E An evaluation ofbuffered aspirin and aspirin tablets in postoperative pain after third molar surgeryBr J Clin Pharmacol 1992 33 395-399
6 Seymour R A Blair G S Wyatt F A Post-operative dental pain and analgesicefficacy Part I Br J Oral Surg 1983 21 290-297
7 Seymour R A Meechan J G Blair G S An investigation into post-operative painafter third molar surgery under local analgesia Br J Oral Maxillofac Surg 1985 23410-418
8 Matthews J N Altman D G Campbell M J Royston P Analysis of serialmeasurements in medical research Br Med J 1990 300 230-235
9 Lasagna L Analgesic methodology a brief history and commentary J ClinPharmacol 1980 20 373-376
10 Meechan J G Seymour R A The use of third molar surgery in clinicalpharmacology Br J Oral Maxillofac Surg 1993 31 360-365
11 Skjelbred P Album B Lokken P Acetylsalicylic acid vs paracetamol effects onpost-operative course Eur J Clin Pharmacol 1977 12 257-264
12 Mehlisch D R Frakes L A A controlled comparative evaluation of acetaminophenand aspirin in the treatment of postoperative pain Clin Ther 1984 7 89-97
13 Muir N Nichols J D Stillings M R Sykes J Comparative bioavailability of aspirinand paracetamol following single dose administration of soluble and plain tabletsCurr Med Res Opin 1997 13 491-500
14 Vane J Botting R Inflammation and the mechanism of action of anti-inflammatory drugs Faseb J 1987 1 89-96
Table 4 Incidence and distribution of adverse events for each treatment groupPercentage of patients reporting events (number of events)
Body system Soluble aspirin (n=59) Solid paracetamol (n=62) Placebo (n=32) Total (n=153)
CNS 20 (14) 8 (5) 19 (6) 15 (25)GI 17 (12) 16 (12) 6 (2) 14 (26)Body as a whole 7 (4) 13 (8) 6 (3) 9 (15)Haemostasis 8 (7) 13 (8) 3 (1) 9 (16)Respiratory 7 (4) 3 (2) 0 (0) 4 (6)Psychiatric 2 (1) 0 (0) 3 (1) 1 (2)Hearingvestibular 0 (0) 2 (1) 0 (0) 1 (1)Skinappendages 2 (1) 0 (0) 0 (0) 1 (1)Vision 2 (1) 0 (0) 0 (0) 1 (1)Total 51 (44) 39 (36) 28 (13) 41 (93)

ABSTRACT
Aims To investigate the efficacy and side effects of paracetamol (1000mg) on
the lower third molar extraction post-operative pain relief to compare it to other
NSAIDrsquos efficacy as well as the combination of both
Methods Searches were conducted in secondary databases (Cochrane Database
of Systematic Reviews Evidentista CEBD EBD and Lilacs) as well as in primary
databases (Medline atraveacutes dos motores de busca PubMed e NICE) between 7 and
November 19 The encountered articles were initially evaluated based on their titles and
abstracts in order to assess their relevance This was done according to a classification
system ldquoadequaterdquo ldquoprobably adequaterdquo ldquoinadequaterdquo
Results A total of 161 records were found including systematic reviews and
randomized clinical trials only 31 were classified as ldquoadequaterdquo or ldquoprobably
adequaterdquo After a more thorough analysis of each abstract in addition to further
reading of the papers only 8 articles fulfilled the inclusion criteria Thus they were
evaluated according to the CASP critical appraisal sheets
Conclusions Paracetamol is a safe and effective analgesic which presents a
statistical significant advantage when compared to a placebo However paracetamol
shows less efficacy when compared to other NSAIDrsquos such as ibuprofen The
combination of paracetamol + other NSAID also shows to be more effective displaying
the additive effect of this compound Although NSAIDrsquos show the best pain relief
scores some can cause severe side effects as opposed to paracetamol Further studies
are needed in order to better investigate the adverse effects of these drugs as well as the
mechanism of action of paracetamol which still remains unclear Other data such as
financial cost and market availability should be approached in future studies
Keywords Paracetamol NSAIDrsquos lower third molar tooth extraction post-operative
pain pain relief Visual Analogic Scale
5
IacuteNDICE
PERGUNTA FORMULADA PELO PACIENTE 6
QUESTAtildeO PICO 6
OBJECTIVOS 6
INTRODUCcedilAtildeO 7
PESQUISA 12
Criteacuterios de Selecccedilatildeo 12
Tipos de Estudos escolhidos participantes intervenccedilatildeo e de mediccedilatildeo 12
Avaliaccedilatildeo dos Estudos 13
Estrateacutegias de Pesquisa 12
Cochrane Database for Systematic Reviews helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 13
Evidence-Based Dentistry (EBD) helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 14
National Institute of Health and Clinical Excellence (NICE) helliphelliphelliphelliphelliphellip 14
Literatura Latino-Americana e do Caribe em Ciecircncias da Sauacutede (LILACS) 14
PubMed 15
AVALIACcedilAtildeO CRIacuteTICA 17
Revisotildees Sistemaacuteticas 17
Ensaios Cliacutenicos Aleatorizados 28
DISCUSSAtildeO 52
RESPOSTA DADA AO PACIENTE 55
REFEREcircNCIAS BIBLIOGRAacuteFICAS 56
ANEXOS 61
Anexo A ndash Tabela de Artigos Excluiacutedos 61
Anexo B ndash Artigos Incluiacutedos em formato integral 62
6
PERGUNTA FORMULADA PELO PACIENTE
Apoacutes uma exodontia de um terceiro molar inferior ldquoDoutor natildeo me vai passar
mais nada aleacutem do paracetamol para as dores Eacute eficaz Natildeo vou ter doresrdquo
QUESTAtildeO PICO
Com base na questatildeo apresentada pelo paciente eacute possiacutevel identificar
Populaccedilatildeo ndash Pacientes adultos com pelo menos um terceiro molar inferior
Intervenccedilatildeo ndash administraccedilatildeo poacutes-operatoacuteria de paracetamol (1000g) aquando
duma exodontia do terceiro molar inferior
Comparaccedilatildeo ndash outros analgeacutesicos e NSAIDrsquos (Non-Steroidal Anti-
Inflammatory Drugs) convencionais
Outcome ndash Eliminaccedilatildeo ou atenuaccedilatildeo da dor medida atraveacutes da escala visual
analoacutegica de dor
Em pacientes adultos apoacutes exodontia do 3ordm molar inferior a administraccedilatildeo
de paracetamol eacute mais eficaz na terapecircutica analgeacutesica comparativamente a outros
analgeacutesicos e anti-inflamatoacuterios natildeo esteroacuteides convencionais utilizando uma
escala visual analoacutegica de dor
OBJECTIVOS
Primaacuterios
Investigar a eficaacutecia do paracetamol (1000mg) na eliminaccedilatildeo da dor dentaacuteria
poacutes-operatoacuteria e comparaacute-la com outros NSAIDrsquos comparando os efeitos secundaacuterios
associados a cada faacutermaco
Secundaacuterios
Aferir a eficaacutecia relativa dos vaacuterios NSAIDrsquos bem como combinaccedilotildees de
paracetamol com outros compostos
7
INTRODUCcedilAtildeO
EXODONTIA DE TERCEIROS MOLARES INFERIORES
A extracccedilatildeo de terceiros molares eacute um procedimento ciruacutergico no campo da
sauacutede oral amplamente praticado e difundido A dor poacutes-operatoacuteria desta intervenccedilatildeo
tornou-se o modelo mais frequentemente usado em ensaios sobre dor aguda por ser um
procedimento comum com dor moderada a severa e com um nuacutemero suficiente de
pacientes para se realizar um estudo de forma relativamente faacutecil (1 2)
Os motivos que conduzem agrave exodontia de terceiros molares devem ser
considerados cuidadosamente natildeo soacute na sua dimensatildeo cliacutenica como no encontro dos
interesses do paciente econoacutemicos e outros Algumas situaccedilotildees constituem uma razatildeo
largamente aceite para a extracccedilatildeo sendo descritas em normas de orientaccedilatildeo cliacutenica
Natildeo se pode excluir poreacutem uma selecccedilatildeo e procura cuidadosa por parte do cliacutenico da
melhor evidecircncia cientiacutefica
Segundo as normas de orientaccedilatildeo cliacutenica NICE a extracccedilatildeo de sisos impactados
deve ser limitada a pacientes que evidenciam patologia como caacuteries irrestauraacuteveis
patologias pulpares ou periapicais natildeo trataacuteveis abcesso e osteomielite reabsorccedilatildeo
internaexterna do dente ou dentes adjacentes fractura dentaacuteria quistos tumores e
outros (3) Terceiros molares impactados mas livres de patologia natildeo devem ser
extraiacutedos pois natildeo haacute evidecircncia de que sugira que traria benefiacutecios para os pacientes
Iria tambeacutem sujeitar pacientes saudaacuteveis aos riscos que acompanha este tipo de
procedimento e os efeitos poacutes-operatoacuterios do mesmo Existe controveacutersia em redor
deste assunto e sobre se existe algum benefiacutecio na extraccedilatildeo profilaacutetica ldquoNo evidence
was found to support or refute routine prophylactic removal of asymptomatic impacted
wisdom teeth in adults There is some reliable evidence that suggests that the
prophylactic removal of asymptomatic impacted wisdom teeth in adolescents neither
reduces nor prevents late incisor crowdingrdquo (4) A extracccedilatildeo de um dente natildeo impactado
deve ser executada quando a natildeo extracccedilatildeo do mesmo eacute ou potencialmente viraacute a
constituir uma situaccedilatildeo patoloacutegica Este procedimento ciruacutergico conduz a um niacutevel
significante de dor poacutes-operatoacuteria sendo esta mais severa nas primeiras doze horas apoacutes
o procedimento com o pico de intensidade nas 6-8 horas poacutes-operatoacuterias (5)
8
ETIOLOGIA DA DOR
Os tecidos lesados ou traumatizados na sequecircncia da remoccedilatildeo do terceiro molar
conduzem agrave libertaccedilatildeo de mediadores bioquiacutemicos (celulares e soluacuteveis) A inflamaccedilatildeo
aguda surge como resposta ao stress tecidual e passa por um aumento da irrigaccedilatildeo
sanguiacutenea - vasodilataccedilatildeo e aumento de permeabilidade vascular Pode-se enfatizar os
papeacuteis das histamina e a bradiquinina (recruta NO) como mediadores soluacuteveis
importantes na vasodilataccedilatildeo
Os prostanoacuteides ndash moleacuteculas envolvidas nos processos de inflamaccedilatildeo- satildeo
ecosanoacuteides ou seja derivados de precursores de aacutecidos gordos e sintetizados via
cascata do aacutecido araquidoacutenico (6 p 503 7 p 800 8) em condiccedilotildees fisioloacutegicas tecircm
um papel preponderante na citoprotecccedilatildeo da mucosa gaacutestrica hemostase e
hemodinacircmica renal A este grupo pertencem as prostaglandinas prostaciclinas
tromboxanos e leucotrienos Enquanto que as prostaglandinas satildeo sintetizadas a partir
do aacutecido araquidoacutenico por acccedilatildeo de enzimas como as ciclo-oxigenases (COX) os
leucotrienos resultam da acccedilatildeo da lipoxigenase Havendo stress tecidual a membrana
celular eacute danificada conduzindo agrave actividade da enzima fosfolipase Esta ao iniciar a
lipoacutelise possibilita a obtenccedilatildeo do percursor dos prostanoacuteides o aacutecido araquidoacutenico Por
um lado os produtos da acccedilatildeo da lipoxigenase podem estar envolvidos na formaccedilatildeo do
edema por outro os produtos da ciclo-oxigenase nomeadamente prostaglandinas estatildeo
envolvidos no processo de dor e pirexia
A ciclo-oxigenase possui 2 isoenzimas COX-1 e COX-2 (7 p 800)
A COX-1 eacute constitutiva da maioria dos tecidos humanos mas com especial
relevacircncia para mediar a integridade da mucosa gaacutestrica endoteacutelio vascular rins e
plaquetas
A COX-2 eacute expressa apoacutes lesatildeo e aquando a libertaccedilatildeo de mediadores como a
Interleucina-1 o Factor de Activaccedilatildeo de Plaquetas (PAF) ou endotoxinas
lipopolissacaacuterido (LPS) (9) Contribui para o processo inflamatoacuterio e hiperalgesia pois
ao formar prostaglandinas sensibiliza as terminaccedilotildees nervosas locais livres
nociceptivas
PARACETAMOL
O paracetamol eacute uma das drogas mais importantes usadas no tratamento da dor
aguda moderada a severa quando natildeo eacute necessaacuterio um efeito anti-inflamatoacuterio (10)
Classificado como analgeacutesico actua no sistema nervoso pela activaccedilatildeo indirecta de
9
receptores canabinoacuteides (11) embora este mecanismo ainda natildeo esteja totalmente
esclarecido (12) secundariamente inibe a COX-1 e COX-2 e por consequente a
siacutentese das prostaglandinas Como antipireacutetico age no centro hipotalacircmico que regula a
temperatura produzindo vasodilataccedilatildeo perifeacuterica e aumento do fluxo sanguiacuteneo
diminuindo a temperatura pela sudorese e perda de calor pela pele
O paracetamol eacute usualmente administrado oralmente (10) Apresenta uma meia-
vida de 2-3 horas Apesar de ser comparaacutevel agrave aspirina como analgeacutesico e antipireacutetico
eficaz o paracetamol difere no facto de natildeo possuir propriedades anti-inflamatoacuterias
(10) Difere dos analgeacutesicos opioacuteides porque natildeo provoca euforia nem altera o estado
de humor do doente Da mesma forma que os (NSAIDrsquos) natildeo causa problemas de
dependecircncia toleracircncia e siacutendrome de abstinecircncia Eacute muito utilizado e seguro com a
dosagem recomendada de 4g por dia mas nem sempre oferece um aliacutevio adequado da
dor aguda por si soacute (13)
NSAIDrsquoS
Os NSAIDrsquos satildeo dos agentes terapecircuticos mais utilizados no mundo inteiro
inclui-se neste grupo o ibuprofeno importante no tratamento da dor aguda e croacutenica
(14) Dos inibidores selectivos da COX-2 mais recentes nomeadamente rofecoxib
valdecoxib e celecoxib apenas este uacuteltimo foi comercializado nos EUA devido aos
restantes terem sido associados a eventos tromboacuteticos cardiovasculares (15 pp 277-
281) Apresentam trecircs acccedilotildees principais que resultam da inibiccedilatildeo da COX-2 e da
consequente reduccedilatildeo da siacutentese de prostanoacuteides
Acccedilatildeo anti-inflamatoacuteria a modificaccedilatildeo da resposta inflamatoacuteria ocorre pela
reduccedilatildeo do nordm de prostaglandinas vasodilatadoras (PGE2 prostaciclina)
associada a menor vasodilataccedilatildeo e indirectamente a menos edema No entanto a
acumulaccedilatildeo de ceacutelulas inflamatoacuterias natildeo eacute diminuiacuteda
Efeito analgeacutesico a reduccedilatildeo da siacutentese de prostaglandinas diminui a
sensibilizaccedilatildeo das terminaccedilotildees nervosas nociceptivas a mediadores da
inflamaccedilatildeo (como bradicinina e 5-hidroxitriptamina) provoca tambeacutem a reduccedilatildeo
da vasodilataccedilatildeo e desse modo o aliacutevio da cefaleia
10
Efeito antipireacutetico deve-se em parte agrave diminuiccedilatildeo da prostaglandina
mediadora a interleucina-1 responsaacutevel pela estimulaccedilatildeo do hipotaacutelamo e
consequente aumento de temperatura ndash febre (10 pp 1056-1061)
Eacute de referir ainda que todos os NSAIDrsquos agrave excepccedilatildeo dos inibidores selectivos da
COX-2 e salicilatos natildeo-acetilados tecircm um efeito inibitoacuterio na agregaccedilatildeo de plaquetas
(15 pp 277-281)
Os efeitos secundaacuterios resultam em grande parte da inibiccedilatildeo da COX-1 Entre
os mais frequentes encontram-se Dispepsia naacuteuseas e voacutemitos associados a lesotildees
gaacutestricas provocadas pela anulaccedilatildeo do efeito protector da prostaglandina sobre a mucosa
gaacutestrica Insuficiecircncia renal Reacccedilotildees cutacircneas Distuacuterbios hepaacuteticos Riscos
cardiovasculares e outros (10)
ESCALAS DE MEDICcedilAtildeO DE DOR - ESCALA VISUAL ANALOacuteGICA
A dor sendo um fenoacutemeno subjectivo compreende um grande conjunto de
componentes - componentes fisioloacutegicos cognitivos sensoriais comportamentais entre
outros Avaliar a dor utilizando uma medida que abranja todas as suas facetas e seja
fidedigna tem-se demonstrado impossiacutevelldquoUm instrumento ideal para a mensuraccedilatildeo da
dor deveria ter propriedades de uma escala de razatildeo fornecer informaccedilatildeo imediata
sobre a fidedignidade do desempenho dos pacientes ser relativamente livre de vieacuteses
ser simples de utilizar com pacientes () demonstrar utilidade tanto para a dor
experimental quanto para a dor cliacutenica permitindo comparaccedilotildees confiaacuteveis entre ambos
os tipos de dorrdquo(16)
A Escala Visual Analoacutegica (VAS) consiste numa mediccedilatildeo da dor em mm (0-
100mm) em que agrave extremidade 0 corresponde ldquonenhuma dorrdquo e agrave extremidade
antagoacutenica ldquopior dor possiacutevelrdquo Eacute uma forma simples eficaz - dentro das limitaccedilotildees - e
faacutecil de reproduzir ldquoou seja pode ser compreendida em distintas situaccedilotildees onde haacute
diferenccedilas culturais ou de linguagem do avaliador cliacutenico ou examinadorrdquo(16)
Para responder agrave questatildeo colocada pelo paciente eacute necessaacuterio a procura da
melhor evidecircncia cientiacutefica integrando-a com o proacuteprio interesse do paciente e a
expertise do cliacutenico Estes objectivos da Medicina Dentaacuteria Baseada na Evidecircncia satildeo
em parte consequecircncia de uma actualizaccedilatildeo constante de praacuteticas cliacutenicas consequentes
de novas evidecircncias cientiacuteficas e com a noccedilatildeo de que nenhum tratamento eacute completo
11
sem que ldquoas expectativas exigecircncias e direitos legiacutetimos dos pacientes sejam integrados
nos processos de decisatildeo cliacutenica sendo tal facto reconhecidamente essencial para a
melhoria da qualidade de vidardquo(17)
12
PESQUISA
CRITEacuteRIOS DE SELECCcedilAtildeO
Tipos de Estudos Escolhidos
Para este trabalho foram escolhidos apenas ensaios cliacutenicos aleatorizados cegos
(preferencialmente duplamente cegos) controlados ou natildeo por placebo e revisotildees
sistemaacuteticas
Tipos de participantes
Indiviacuteduos com idade superior a 15 anos
Sujeitos a cirurgia para extracccedilatildeo unilateral ou bilateral do 3ordm molar inferior
Que natildeo estivessem a tomar qualquer outro tipo de medicaccedilatildeo com efeitos
idecircnticos ou semelhantes aos faacutermacos em estudo
Sem patologias orais que provoquem dor moderada a forte ou outras patologias
que afectem a percepccedilatildeo da dor
Tipos de intervenccedilatildeo
Administraccedilatildeo apenas por via oral de
Paracetamol (1000mg) vs placebo
Paracetamol (1000mg) vs outro(s) NSAIDrsquos
Paracetamol ( 1000mg) vs outro(s) NSAIDrsquos vs placebo
Paracetamol (1000mg) + outro(s) NSAIDrsquos
ou Paracetamol (1000mg) + outro(s) NSAIDrsquos vs placebo
Estudos com outros tipos de intervenccedilatildeo natildeo foram incluiacutedos Os estudos que
apenas incluiacuteram o paracetamol sob a forma de proacute-farmaco foram excluiacutedos
Mediccedilatildeo de Resultados
A mediccedilatildeo de resultados foi obtida atraveacutes da escala visual analoacutegica (VAS ndash
visual analogic scale)
13
Avaliaccedilatildeo dos Estudos
Todos os estudos foram avaliados segundo fichas CASP (Critical Appraisal
Skills Programme) Estas consistem num conjunto de questotildees que permitem avaliar um
artigo cientiacutefico no seu todo para em uacuteltima anaacutelise aferir a sua aplicabilidade validade
e fiabilidade (18) Estas fichas existem para vaacuterios tipos de estudo as CASP utilizadas
neste trabalho foram as referentes a revisotildees sistemaacuteticas e ensaios cliacutenicos
aleatorizados
ESTRATEacuteGIAS DE PESQUISA
Apoacutes cada pesquisa os artigos encontrados foram avaliados numa fase inicial
com base nos seus tiacutetulos e abstracts para averiguar a sua relevacircncia A seguinte escala
foi utilizada adequado possivelmente adequado inadequado Toda a pesquisa foi
efectuada entre 7 e 19 de Novembro de 2011
Primeiramente foram consultadas bases de dados secundaacuterias apoacutes pesquisa
nestas fontes seguiram-se bases de dados primaacuterias
Cochrane Database for Systematic Reviews
Na pesquisa avanccedilada desta base de dados secundaacuteria foi introduzida a seguinte
combinaccedilatildeo de termos utilizando conectores boleanos e seleccionando as opccedilotildees
ldquosearch all textrdquo e ldquoCochrane Database of Systematic Reviewsrdquo
paracetamol AND third molar removal AND pain relief AND analgesicrdquo
Foram encontrados 14 resultados (3 protocolos e 11 revisotildees sistemaacuteticas) dos
quais uma revisatildeo foi categorizada como ldquoadequadardquo
Paracetamol for pain relief after surgical removal of lower wisdom teeth Weil
Hooper (19) Esta revisatildeo foi novamente encontrada na base de dados EBD bem
como na NICE e no PubMed
E outra classificada como ldquopossivelmente adequadardquo mas posteriormente
excluiacuteda (20)
14
Evidence-Based Dentistry (EBD)
Nesta base de dados foi introduzida a combinaccedilatildeo de termos
ldquoParacetamol OR acetaminophen AND third molar AND painrdquo utilizando os
filtros ldquoBritish Dental Journalrdquo e ldquoEvidence-Based Dentistryrdquo
Foram encontrados 28 resultados dos quais uma revisatildeo foi classificada como
ldquoadequadardquo
Relative efficacy of oral analgesics after third molar extraction ndash a 2011 update
Derry Wiffen (21)
E ainda dois artigos classificados como ldquopossivelmente adequadordquo
An investigation into the comparative efficacy of soluble aspirin and solid
paracetamol in postoperative pain after third molar surgery Seymour
Hawkesford (22)
Relative efficacy of oral analgesics after third molar extraction Barden
Edwards (23)
National Institute of Health and Clinical Excellence (NICE)
Nesta base de dados foi introduzida a seguinte combinaccedilatildeo de termos
ldquoParacetamol and third molar removal and pain and analgesicrdquo
Dos 28 resultados obtidos 1 foi previamente encontrado e classificado (19)
Dos restantes 27 artigos nenhum foi classificado como adequado ou possivelmente
adequado
LILACS
Nesta base de dados primaacuteria foi introduzida a seguinte combinaccedilatildeo de termos
ldquoParacetamol terceiro molar dorrdquo
Dos 3 resultados obtidos um foi classificado como possivelmente adequado mas
posteriormente excluiacutedo (24)
15
PUBMED
Nesta base de dados primaacuteria foram efectuadas duas pesquisas com termos
diferentes Apenas foram utilizados termos MeSH foram utilizados conectores
boleanos em ambas as pesquisas
Pesquisa 1
Search ((((Acetaminophen[Mesh]) AND Anti-Inflammatory Agents[Mesh])
AND Molar Third[Mesh]) AND Tooth Extraction[Mesh]) AND Pain
Postoperative[Mesh]
Limits only items with abstracts Humans Clinical Trial Meta-Analysis
Randomized Controlled Trial Review Comparative Study Controlled Clinical
Trial English Spanish Portuguese
Foram obtidos 32 resultados dos quais 5 artigos foram classificados como
ldquoadequadosrdquo
Combining paracetamol with a selective cyclooxygenase-2 inhibitor for acute
pain relief after third molar surgery a randomized double-blind placebo-
controlled study Haglund and von Bultzingslowen (25)
Dos restantes quatro artigos um (22) era repetido e os outros trecircs (26-28) foram
posteriormente excluiacutedos
Quatro foram considerados ldquopossivelmente adequadosrdquo dos quais trecircs (29-31)
foram posteriormente excluiacutedos O artigo remanescente foi
Analgesic efficacy of lysine clonixinate paracetamol and dipyrone in lower
third molar extraction a randomized controlled trial (32)
Pesquisa 2
Search (((Acetaminophen[Mesh]) AND Analgesics[Mesh]) AND Molar
Third[Mesh]) AND Tooth Extraction[Mesh]
Limits only items with abstracts Humans Clinical Trial Meta-Analysis
Randomized Controlled Trial Review English
16
Obtiveram-se 56 resultados em que sete foram seleccionados como sendo
ldquoadequadosrdquo
Combined acetaminophen and ibuprofen for pain relief after oral surgery in
adults a randomized controlled trial Merry Gibbs (13)
Destes artigos seis (19 22 23 25 28 32) eram repetidos
Oito artigos foram classificados como ldquopossivelmente adequadosrdquo
Onset of analgesia with sodium ibuprofen ibuprofen acid incorporating poloxamer
and acetaminophen--a single-dose double-blind placebo-controlled study in
patients with post-operative dental pain Daniels Reader (33)
Dos oito artigos cinco foram repetidos (26 27 29-31) dois (34 35) foi
posteriormente excluiacutedo
No anexo A encontra-se uma tabela de artigos excluiacutedos cujas razotildees satildeo
discriminadas
Eacute de notar que este tipo de estrateacutegia de pesquisa traz associada grande
quantidade de resultados irrelevantes superior agrave de artigos de interesse mas facilita a
aquisiccedilatildeo de todos os artigos importantes colocando em primeiro plano a sensibilidade
e natildeo a especificidade (36) A utilizaccedilatildeo de conectores boleanos e de filtros especiacuteficos
foi uma forma de minimizar o nuacutemero de resultados natildeo relacionados (17) preservando
os de interesse
17
AVALIACcedilAtildeO CRIacuteTICA
REVISOtildeES SISTEMAacuteTICAS
Paracetamol for pain relief after surgical removal of lower
wisdom teeth Weil Hooper (19)
1 Did the review ask a clearly-focused question
Sim A populaccedilatildeo em estudo compreende pacientes de qualquer estado de sauacutede
que necessitem de uma exodontia do terceiro molar inferior e que apresentam uma
intensidade de dor basal moderada a forte Foram excluiacutedos pacientes que estivessem a
tomar outro analgeacutesico A intervenccedilatildeo foi baseada em dois aspectos ndash eficaacutecia e efeitos
secundaacuterios
A terapecircutica usada para avaliar a eficaacutecia consistiu na administraccedilatildeo de uma
dose uacutenica de paracetamol por via oral independentemente da formulaccedilatildeo ou do
momento em que o faacutermaco foi tomado
Em relaccedilatildeo aos efeitos secundaacuterios foram incluiacutedos estudos natildeo soacute de dose
uacutenica como tambeacutem de doses muacuteltiplas de acetaminofeno consideraram-se estudos em
que este composto foi tomado ateacute 7 dias apoacutes a primeira toma Para este trabalho apenas
seratildeo considerados os resultados com base na administraccedilatildeo poacutes-operatoacuteria do
paracetamol
Os resultados ndash intensidade da dor e aliacutevio da dor ndash foram medidos usando as
escalas visual analoacutegica categoacuterica verbal numeacuterica verbal global subjectiva de
avaliaccedilatildeo de eficaacutecia e outras categoacutericas Os outcomes derivados do aliacutevio da dor
contabilizados foram total pain relief (TOTPAR) e summed pain intensity difference
(SPID) durante 4 e 6 horas Foram ainda contabilizados os efeitos secundaacuterios
2 Did the review include the right type of study
Os uacutenicos estudos incluiacutedos foram ensaios cliacutenicos aleatorizados duplamente
cegos que comparam o paracetamol a um placebo bem como dosagens diferentes
avaliando efeitos agraves 4 e 6 horas Este tipo de estudo eacute adequado pois implica um baixo
risco de vieacutes
18
3 Did the reviewers try to identify all relevant studies
Sim Os autores utilizaram estudos de todos os idiomas recorrendo agrave sua
traduccedilatildeo quando necessaacuterio Foram consultadas bases de dados bibliograacuteficas
electroacutenicas The Cochrane Oral Health Grouprsquos Trials Register The Cochrane Central
Register of Controlled Trials The Cochrane Pain Palliative and Supportive Care
Grouprsquos Trials Register MEDLINE EMBASE e Current Controlled Trials Register
Tambeacutem foram realizadas pesquisas manuais em revistas como parte do Cochrane Oral
Health Grouprsquos ongoing journal handsearching programme A pesquisa visou estudos
publicados entre 1966 e 25 de Agosto de 2006
Foram enviadas cartas a autores de ensaios cliacutenicos aleatorizados com vista a
obter estudos natildeo publicados bem como a empresas farmacecircuticas fabricantes de
analgeacutesicos
Os autores deste estudo consultaram ainda referecircncias bibliograacuteficas de papers
reviews e referecircncias pessoais
4 Did the reviewers asses the quality of the included studies
Sim Foi utilizada uma estrateacutegia clara e bem definida para a determinaccedilatildeo dos
estudos a incluir Este processo foi realizado independentemente por dois autores da
revisatildeo ndash natildeo cegos ndash baseando-se em dois criteacuterios centrais atribuiccedilatildeo oculta do
faacutermaco e a existecircncia de um follow-up completo Para estes criteacuterios foi utilizado um
sistema de pontuaccedilatildeo Desta forma a cada estudo foi-lhe atribuiacuteda uma pontuaccedilatildeo
formando-se dois grupos
Baixo risco de vieacutes
Moderado ou alto risco de vieacutes
5 If the results of the studies have been combined was it reasonable to do so
Sim os resultados foram apresentados de forma combinada e loacutegica Em
primeiro lugar foram apresentadas tabelas uma para cada artigoestudo incluiacutedo em
que se encontravam discriminados os meacutetodos participantes intervenccedilotildees resultados e
outras notas Os resultados dos diferentes estudos foram agrupados em 2 outcomes
tendo cada outcome 2 divisotildees
Outcome 1 ndash TOTPAR agraves 4h
A ndash Dosagem de paracetamol ateacute 1000mg vs placebo
B ndash Dosagem de paracetamol igual ou superior a 1000mg vs placebo
19
Outcome 2 ndash TOTPAR agraves 6h
A ndash Dosagem de paracetamol ateacute 1000mg vs placebo
B ndash Dosagem de paracetamol igual ou superior a 1000mg vs placebo
Todos estes grupos foram analisados e comparados segundos 2 paracircmetros
Comparaccedilatildeo 1- Medidas de aliacutevio da dor
Comparaccedilatildeo 2- Medidas de intensidade da dor
Tendo em conta todas estas variaacuteveis foram realizadas meta-anaacutelises por
subgrupo (pp 29-40) utilizando graacuteficos forest plot
Anaacutelise 11 ndash Comparaccedilatildeo 1 de A vs B ndash Outcome 1
Anaacutelise 12 ndash Comparaccedilatildeo 1 de A vs B ndash Outcome 2
Anaacutelise 21 ndash Comparaccedilatildeo 2 de A vs B ndash Outcome 1
Anaacutelise 22 ndash Comparaccedilatildeo 2 de A vs B ndash Outcome 2
Anaacutelise 3 ndash Comparaccedilatildeo do nuacutemero de efeitos adversos de paracetamol vs
placebo comparando ainda as duas dosagens diferentes
Valores de heterogeneidade (representados por I2) proacuteximos de 25 indicam
baixa discrepacircncia 50 satildeo indicadores de heterogeneidade moderada e valores
proacuteximos de 75 satildeo sinal de alta heterogeneidade entre os estudos (37)
Olhando para os valores de I2 dois possuem alta heterogeneidade um moderada
e dois baixa Nos grupos que apresentam uma discrepacircncia estatiacutestica significativa dos
resultados a aglutinaccedilatildeo dos mesmos natildeo foi muito bem sucedida Nestes grupos ainda
que a heterogeneidade seja elevada a apresentaccedilatildeo dos resultados de cada estudo foram
correcta e individualmente apresentados Aleacutem deste aspecto os diferentes meacutetodos ndash
dosagem e tempo - foram agrupados exactamente para que as formas de intervenccedilatildeo e
meacutetodos com o menor risco de vieacutes
Tabela 1 ndash Valores de heterogeneidade (I2) de cada anaacutelise
Total de I2
()
Anaacutelise 11 Anaacutelise 12 Anaacutelise 21 Anaacutelise 22 Anaacutelise 3
76 81 66 29 28
Natildeo foram discutidas as variaccedilotildees nos resultados
20
6 How are the results presented and what is the main result
A meta-anaacutelise por subgrupos foi realizada com recurso agrave medida de eficaacutecia de
intervenccedilatildeo Risco Relativo (RR) Analisando o graacutefico forest plot os ldquoquadradosrdquo a azul
representam o RR e o poliacutegono (semelhante a um losango) sumariza todas as
informaccedilotildees (provenientes dos vaacuterios estudos) sobre o efeito do paracetamol (38)
ldquoQuando o IC natildeo ultrapassa a linha de nulidade pode-se afirmar que o resultado eacute
estatisticamente significativo Estudos maiores possuem IC mais estreitos ou seja
resultados mais precisos e maior contribuiccedilatildeo para a meta-anaacutelise que tambeacutem eacute repre-
sentada graficamente (quanto maior a aacuterea do quadrado maior o peso) e valor
percentualrdquo (39) A significacircncia aumenta com a distacircncia do poliacutegono da linha de natildeo
efeito
Independentemente do tempo (4 ou 6h) dosagens ateacute 1000mg de paracetamol
apresentam uma pequena discrepacircncia nos resultados sendo que o paracetamol eacute
ligeiramente mais eficaz que o placebo Doses iguais ou superiores a 1000mg de
paracetamol traduzem-se num maior aliacutevio da dor poacutes-operatoacuteria (poliacutegono afastado da
linha de natildeo-efeito)
Em relaccedilatildeo agrave anaacutelise 3 ateacute doses de 1 g de paracetamol nuacutemero de casos de
efeitos adversos eacute muito semelhante entre placebo e a substacircncia activa Para
concentraccedilotildees superiores a 1000 mg o nuacutemero de efeiros adversos eacute superior para
paracetamol Eacute possiacutevel concluir que natildeo haacute uma diferenccedila notoacuteria no nuacutemero de casos
de efeitos adversos O poliacutegono cruza sempre a linha de natildeo efeito
O paracetamol eacute consideravelmente mais eficaz que o placebo no aliacutevio de 50
da dor principalmente em doses iguais ou superiores a 1000mg Natildeo haacute diferenccedila
significativa em relaccedilatildeo aos efeitos adversos
7 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em consideraccedilatildeo que o
poliacutegono natildeo intersecta a linha de natildeo efeito os resultados satildeo precisos (anaacutelise 1 a 2)
Na anaacutelise 3 mesmo com um IC 95 o poliacutegono cruza a linha de natildeo efeito logo natildeo eacute
possiacutevel tirar conclusotildees semelhantes em relaccedilatildeo aos limites inferior e superior do IC
Eacute de notar que a elaboraccedilatildeo de uma meta-anaacutelise contribui para a robustez dos
resultados daiacute provenientes combinar os resultados de cada estudo individual numa
meta-anaacutelise aumenta o poder estatiacutestico gerando resultados mais precisos (40)
21
8 Can the results be applied to the local population
Sim A extracccedilatildeo de terceiros molares inferiores eacute uma praacutetica cliacutenica comum
em Portugal O paracetamol eacute um analgeacutesico largamente comercializado e administrado
(sendo natildeo sujeito a receita meacutedica) pelo que era possiacutevel reproduzir esta forma de
tratamento
No entanto os estudos incluiacutedos na revisatildeo referem-se a uma dose uacutenica que
embora reproduziacutevel na populaccedilatildeo local seria necessaacuteria uma modificaccedilatildeo do
paradigma cultural em relaccedilatildeo agrave toma de medicamentos
9 Were all important outcomes considered
Natildeo A revisatildeo considera a eficaacutecia do paracetamol vs placebo no aliacutevio da dor
e simultaneamente a ocorrecircncia de efeitos secundaacuterios Satildeo abordados directamente
dois aspectos ndash o da praacutetica cliacutenica e o da investigaccedilatildeo Ambos satildeo relativos ao
profissional de sauacutede e implicitamente ao proacuteprio indiviacuteduo e aos familiares (ao serem
referidas as doses periacuteodos entre tomas e combinaccedilotildees com outros NSAIDrsquos mais
eficazes e simultaneamente seguras)
Poreacutem nada eacute referido em relaccedilatildeo a novas poliacuteticas de sauacutede nomeadamente na
implementaccedilatildeo de uma dose uacutenica culminando numa mudanccedila dos haacutebitos de sauacutede da
comunidade Tambeacutem natildeo foram abordados aspectos econoacutemicos tal como um balanccedilo
entre benefiacutecios e encargos de sauacutede que justifique a utilizaccedilatildeo deste faacutermaco como
tratamento preferencial
10 Should policy or practice change as a result of the evidence contained in this
review
Natildeo Esta revisatildeo demonstra que comparativamente a um placebo o paracetamol
eacute mais eficaz principalmente em doses elevadas e que natildeo haacute diferenccedila estatiacutestica
significativa no nuacutemero de efeitos secundaacuterios Poreacutem natildeo eacute possiacutevel tirar conclusotildees
sobre a dor depois do periacuteodo considerado de 6h Desta forma implementar uma dose
uacutenica de paracetamol a 1000mg seria imprudente sem previamente realizar estudos
complementares sobre a evoluccedilatildeo da dor apoacutes as 6h bem como comparar este faacutermaco
com outros compostos que possam ser igualmente eficazes por um raacutecio custo-benefiacutecio
melhor ou vice-versa
22
Relative efficacy of oral analgesics after third molar extraction
Barden Edwards (23)
Relative efficacy of oral analgesics after third molar extraction -
a 2011 update Derry Wiffen (21)
A avaliaccedilatildeo feita e disposta abaixo contemplou tanto a revisatildeo sistemaacutetica que
remonta a 2004 como a sua actualizaccedilatildeo de 2011 Uma vez estando inter-relacionados
consideraacutemos pertinente juntar as apreciaccedilotildees destas revisotildees porque caso contraacuterio
perder-se-ia o contexto de ambas
1 Did the review ask a clearly-focused question
Sim A populaccedilatildeo em estudo comporta pacientes com mais de 15 anos de idade
com uma intensidade de dor basal poacutes-operatoacuteria de moderada a severa apoacutes extracccedilatildeo
de um terceiro molar
A intervenccedilatildeo consistiu no tratamento da dor poacutes-operatoacuteria de intensidade
moderada a severa com doses uacutenicas de analgeacutesicos orais ou placebo sendo que os
analgeacutesicos orais corresponderam a um total de 15 combinaccedilotildees diferentes de faacutermacos
e respectivas dosagens
Os resultados foram obtidos atraveacutes da mediccedilatildeo do aliacutevio total da dor
(TOTPAR) ou da diferenccedila de intensidade da dor (SPID) utilizando uma escala
standard de 5 niacuteveis de aliacutevio da dor uma escala standard de 4 niacuteveis de aliacutevio da dor
ou uma escala visual analoacutegica (VAS) Os efeitos secundaacuterios foram tambeacutem relatados
comparando a proporccedilatildeo de pacientes que apresentaram efeitos generalizados e que
apresentaram efeitos particulares
Actualizaccedilatildeo de 2011
A intervenccedilatildeo consistiu tambeacutem no tratamento da dor poacutes-operatoacuteria de
intensidade moderada a severa com doses uacutenicas de analgeacutesicos orais ou placebo no
entanto os analgeacutesicos utilizados foram diferentes A revisatildeo de 2004 incluiu rofecoxib
and valdecoxib nenhum dos quais se encontra disponiacutevel no mercado Em vez disso
foram utilizadas combinaccedilotildees de ibuprofeno com paracetamol formulaccedilotildees diferentes
de ibuprofeno e diclofenac e etoricoxib
23
2 Did the review include the right type of study
Sim Os estudos que foram incluiacutedos nesta revisatildeo correspondem a ensaios
cliacutenicos aleatorizados duplamente cegos que comparam a eficaacutecia dos diferentes
analgeacutesicos e com placebo na terapecircutica da dor aguda poacutes-operatoacuteria Os grupos
formados possuiacuteam grupos com um miacutenimo de 10 pessoas Em todos os estudos foram
seguidas as guidelines QUORUM e utilizados criteacuterios de inclusatildeo para a dor poacutes-
operatoacuteria em que os resultados satildeo avaliados durante um periacuteodo de 4 a 6 horas apoacutes
medicaccedilatildeo
3 Did the reviewers try to identify all relevant studies
Sim Os autores da revisatildeo tentaram identificar todos os estudos relevantes
pesquisando nas bases de dados electroacutenicas Cochrane Library Biological Abstracts
MEDLINE PubMed e Oxford Pain Relief Para aleacutem disso consultaram a bibliografia
dos artigos de revisatildeo incluiacutedos de modo a encontrar informaccedilatildeo adicional e possiacuteveis
estudos natildeo publicados os quais apresentam na sua maioria datas de pesquisa que
remontam a 2002 No entanto eacute de mencionar que natildeo contactaram os autores e os
fabricantes para recolha de dados nem procuraram estudos com idiomas diferentes do
inglecircs
Actualizaccedilatildeo de 2011
Com o passar dos anos os artigos inseridos na revisatildeo foram actualizados de
forma a incluir outros analgeacutesicos e obter ensaios cliacutenicos adicionais e relevantes Desta
forma a actualizaccedilatildeo da revisatildeo sistemaacutetica de 2004 incluiu 35 revisotildees da Cochrane
com 38 anaacutelises realizadas em diferentes analgeacutesicos de dose uacutenica para determinar a
sua eficaacutecia na dor poacutes-operatoacuteria
4 Did the reviewers assess the quality of the included studies
Sim A qualidade dos estudos incluiacutedos foi avaliada vaacuterios autores
independentes e natildeo cegos (pelo facto de estes conhecerem a literatura existente)
utilizando uma escala de qualidade numerada de 1 a 5 e baseada em 3 criteacuterios
distribuiccedilatildeo aleatorizada dos pacientes se os pacientes e os examinadores se
encontravam cegos se houve remoccedilotildees ou desistecircncias durante o estudo A
classificaccedilatildeo maacutexima de um estudo incluiacutedo foi de 5 e a miacutenima foi de 2
24
Os ensaios cliacutenicos que apresentam uma classificaccedilatildeo igual ou superior a 3
(baixo risco de vieacutes) demonstraram menores efeitos secundaacuterios que os ensaios cliacutenicos
que apresentam uma classificaccedilatildeo igual ou inferior a 2 (alto risco de vieacutes)
5 If the results of the studies have been combined was it reasonable to do so
Sim Os resultados dos diferentes estudos foram apresentados sob a forma de
tabelas nomeadamente a eficaacutecia dos vaacuterios analgeacutesicos e a ocorrecircncia de efeitos
secundaacuterios foram dispostas em tabelas Aqui eram resumidos os resultados o tipo de
intervenccedilatildeo e respectivo nuacutemero total de pacientes e nordm de estudos realizados
Esta revisatildeo sistemaacutetica natildeo incluiu a realizaccedilatildeo de testes heterogeacuteneos nem a
avaliaccedilatildeo do risco de vieacutes das publicaccedilotildees atraveacutes de forest plots dado que na opiniatildeo
dos autores estas abordagens mostraram-se pouco adequados para este tipo de estudos
No entanto a homogeneidade foi avaliada atraveacutes de um modo visual
A resposta a esta questatildeo eacute claramente afirmativa porque a elevada semelhanccedila
das caracteriacutesticas dos diferentes estudos (meacutetodos utilizados tipo de intervenccedilatildeo e
mediccedilatildeo dos resultados) tornou por um lado inadequada a realizaccedilatildeo uma meta-anaacutelise
para avaliar a heterogeneidade mas por outro adequada a realizaccedilatildeo de uma avaliaccedilatildeo
visual da homogeneidade dos mesmos
6 How are the results presented and what is the main result
Os resultados foram medidos atraveacutes da proporccedilatildeo de pacientes do grupo de
tratamento vs placebo que atingiram pelo menos 50 de maxTOTPAR ou seja aliacutevio
de dor A qual foi utilizada para determinar o benefiacutecio relativo e o NNT bem como o
risco relativo dos diferentes estudos incluiacutedos
Atraveacutes da anaacutelise das tabelas eacute possiacutevel tirar 3 conclusotildees principais
1 A proporccedilatildeo de pacientes que atingiram pelo menos 50 de aliacutevio de dor eacute maior
no grupo de tratamento que no grupo placebo agrave excepccedilatildeo do estudo que utilizou
dihidrocodeiacutena 30mg em que as diferenccedilas natildeo foram estatisticamente relevantes
2 Por comparaccedilatildeo ao paracetamol (independentemente das diferentes dosagens) os
anti-inflamatoacuterios natildeo-esteroacuteides inibidores da COX-2 apresentam um maior
benefiacutecio relativo e necessitam do menor nordm de pacientes tratados para atingirem o
objectivo de 50 de aliacutevio de dor
25
3 O paracetamol apresenta um maior risco relativo na medida em que insurgem mais
efeitos secundaacuterios nos estudos em que foi administrado por oposiccedilatildeo aos
NSAIDrsquos
Os anti-inflamatoacuterios natildeo-esteroacuteides inibidores da COX-2 satildeo mais eficazes no
tratamento da dor basal poacutes-operatoacuteria moderada a intensa que o paracetamol
Actualizaccedilatildeo de 2011
Os resultados foram obtidos da mesma forma que na versatildeo de 2004 sendo que
um novo outcome foi considerado ndash tempo meacutedio necessaacuterio para que os pacientes
necessitem de re-medicaccedilatildeo aproximadamente 8 horas Agrave semelhanccedila do que aconteceu
na revisatildeo anterior os dados sobre a dihidrocodeiacutena natildeo foram conclusivos devido agrave
pouca informaccedilatildeo disponiacutevel nos estudos
7 How precise are these results
Os resultados satildeo precisos uma vez que utilizam um intervalo de confianccedila de
95 Eacute de ressalvar que os valores de NNT ou NNH apenas eram calculados quando o
riscobenefiacutecio relativo satildeo significativos isto eacute quando natildeo incluem o valor de 1 No
limite superior do intervalo de confianccedila a intervenccedilatildeo realizada seria a mesma No
entanto dado que o NNH natildeo foi calculado eacute possiacutevel concluir que o risco relativo natildeo
era significativo pelo que permanece uma incerteza se no limite inferior do intervalo de
confianccedila a intervenccedilatildeo realizada seria a mesma
8 Can the results be applied to the local population
Sim Os resultados da revisatildeo sistemaacutetica podem ser aplicados agrave nossa
populaccedilatildeo local porque os criteacuterios de inclusatildeo utilizados correspondem na sua
maioria a mecanismos fisioloacutegicos caracteriacutesticos do ser humano Para aleacutem disso as
teacutecnicas utilizadas satildeo simples e de faacutecil reproduccedilatildeo na medida em que os faacutermacos
utilizados nos ensaios cliacutenicos estatildeo agrave disposiccedilatildeo dos interessados e os meacutetodos
terapecircuticos baacutesicos
No entanto os estudos incluiacutedos nesta revisatildeo incluiacuteram um tratamento com
uma dose uacutenica de analgeacutesico oral que embora reprodutiacutevel difere do paradigma actual
da nossa populaccedilatildeo (em que haacute a tendecircncia para a auto-medicaccedilatildeo e de recorrer a
diferentes faacutermacos)
26
9 Were all important outcomes considered
Natildeo Os resultados enfatizam a eficaacutecia de vaacuterios analgeacutesicos no aliacutevio de 50
dor em comparaccedilatildeo com placebo Eacute focada ainda o benefiacutecio relativo (95 IC) e o NNT
da mesma problemaacutetica Aleacutem deste conjunto de dados satildeo considerados o nuacutemero de
pacientes com efeitos secundaacuterios risco relativo (95 IC) culminando no caacutelculo do
NNH
Contudo natildeo eacute especificado o tipo de efeitos secundaacuterios que podem ser
desencadeados pela toma dos diferentes analgeacutesicos nem aspectos diferenciadores em
analgeacutesicos com eficaacutecia e benefiacutecios idecircnticos (por exemplo custo econoacutemico) Isto
constituiria uma mais-valia para uma escolha mais consciente do analgeacutesico tanto pelos
profissionais como pelos pacientes (individual) e beneficiaria tambeacutem o Sistema
Nacional de Sauacutede (comunidade em geral)
Actualizaccedilatildeo de 2011
Um dos outcomes considerados semelhante ao que foi abordado na revisatildeo de
2004 foi a percentagem de pacientes com dor moderada (30- 60 mm VAS) ou dor
severa (mais de 60 mm) que obtiveram 50 de aliacutevio de dor Contudo foi adicionado
um novo outcome relevante o tempo necessaacuterio para que metade dos pacientes requeriu
re-medicaccedilatildeo
10 Should policy or practice change as a result of the evidence contained in this
review
Natildeo Os resultados desta revisatildeo evidenciam a eficaacutecia dos analgeacutesicos
comparativamente a um placebo nomeadamente que o ibuprofeno e o paracetamol
possuem maior maior o benefiacutecioefeito analgeacutesico quanto maior forem as dosagens
Poreacutem natildeo eacute evidecircncia suficiente para mudar o paradigma de tratamento pois ldquoWhat
these comparisons do not do is to tell dentists what to prescriberdquo Satildeo sim uma
importante ferramenta para a tomada de decisotildees que devem ser adaptadas a cada
paciente tendo presente que 80 dos analgeacutesicos prescritos possuem elevados iacutendices
de eficaacutecia e seguranccedila Em adiccedilatildeo nem todos os analgeacutesicos nesta revisatildeo estatildeo
disponiacuteveis no mercado para serem receitados pelos meacutedicos-dentistas
Conclui-se que para que esta revisatildeo fosse pilar basilar nas prescriccedilotildees de
analgeacutesicos teriam de ser apresentadas evidecircncias de benefiacuteciocusto dos analgeacutesicos
27
com melhores resultados (aspecto econoacutemico e detalhe dos efeitos adversos) Todavia a
informaccedilatildeo presente na mesma sobre a eficaacutecia e efeitos secundaacuterios assim como toda a
bibliografia jaacute existente sobre este assunto eacute uacutetil e deve ser utilizada para tomar inicio agrave
criaccedilatildeo de um formulaacuterio em medicina dentaacuteria
Actualizaccedilatildeo de 2011
Os resultados obtidos da mesma forma que na revisatildeo anterior natildeo foram
suficientemente relevantes para que as poliacuteticas de sauacutede mudassem No entanto a
quantidade de informaccedilatildeo disponiacutevel sobre analgeacutesicos de dose uacutenica para aliacutevio da dor
poacutes-operatoacuteria eacute grande e bastante acessiacutevel Podem assim servir como boas
ferramentas para a formulaccedilatildeo de poliacuteticas e prescriccedilotildees farmacecircuticas para a populaccedilatildeo
quando existirem dados cliacutenicos mais conclusivos
28
AVALIACcedilAtildeO CRIacuteTICA
ENSAIOS CLIacuteNICOS ALEATORIZADOS
Combining paracetamol with a selective cyclooxygenase-2
inhibitor for acute pain relief after third molar surgery a
randomized double-blind placebo-controlled study Haglund and
von Bultzingslowen (25)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo compreende indiviacuteduos saudaacuteveis com idade superior a 18
anos peso entre 50 e 120 kg e com necessidade de extrair terceiros molares inferiores
com remoccedilatildeo oacutessea Foram excluiacutedos pacientes intolerantes ao aacutecido acetilsaliciacutelico
paracetamol eou NSAIDrsquos que estivessem a tomar outro tipo de medicaccedilatildeo (excepto
contraceptivos) graacutevidas ou em periacuteodo de amamentaccedilatildeo problemas com drogas ou
aacutelcool Apenas pacientes que reportaram dor moderada a intensa apoacutes a cirurgia foram
incluiacutedos
Existiram quatro grupos de intervenccedilatildeo
Grupo A rofecoxib 50mg + paracetamol 1g dose uacutenica 155 plusmn 37 minutos apoacutes
cirurgia
Grupo B rofecoxib 50mg dose uacutenica 170 plusmn 45 minutos apoacutes cirurgia
Grupo C paracetamol 1g dose uacutenica 184 plusmn 53 minutos apoacutes cirurgia
Grupo D placebo dose uacutenica 161 plusmn 30 minutos apoacutes cirurgia
Os resultados prenderam-se com a intensidade da dor medida atraveacutes da escala
visual analoacutegica (VAS) de 30 em 30 minutos desde a ingestatildeo do faacutermaco durante 8
horas Atraveacutes destas avaliaccedilotildees da dor foi possiacutevel obter valores de
aliacutevio total da dor TOTPAR
soma da diferenccedila de intensidade da dor SPID nas primeiras trecircs horas
soma da diferenccedila de intensidade da dor SPID ateacute agraves 8 horas
Foram obtidos resultados referentes a uma avaliaccedilatildeo global do tratamento feita
4h e 8h apoacutes a toma do faacutermaco O uso de rescue medication foi tomado em conta bem
como o tempo ateacute agrave sua necessidade Foram ainda avaliados eventuais efeitos
secundaacuterios
29
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim A atribuiccedilatildeo de cada tratamento foi cega para todos os pacientes
investigadores e pessoal envolvido Foi levada a cabo a aleatorizaccedilatildeo pela empresa
farmacecircutica responsaacutevel pela produccedilatildeo das caacutepsulas administradas
Natildeo existindo entraves de teor eacutetico ou de disponibilidade de recursos um
ensaio cliacutenico aleatorizado eacute a escolha mais pertinente quando eacute necessaacuterio comparar
dois ou mais tipos de tratamento O facto de existir um grupo de controlo minimiza o
risco de vieacutes
3 Were participants appropriately allocated to intervention and control groups
A colocaccedilatildeo dos pacientes em cada um dos quarto grupos de tratamento foi
concretizada atraveacutes de tabelas de aleatorizaccedilatildeo
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim Sendo um ensaio cliacutenico duplamente cego tanto o staff investigadores e
pacientes estiveram cegos durante todo o estudo Todas as caacutepsulas eram idecircnticas
sendo que cada embalagem selada continha sempre 6 caacutepsulas Desta forma eacute possiacutevel
garantir que o paciente estaacute cego Sendo cada embalagem feita e selada pela empresa
farmacecircutica eacute igualmente possiacutevel inferir que os investigadores tambeacutem se
encontravam cegos Apenas o investigador principal acedeu aos coacutedigos para fazer os
caacutelculos finais
5 Were all of the participants who entered the trial accounted for at its
conclusion
Os grupos de intervenccedilatildeo foram atribuiacutedos de forma aleatoacuteria e cega os
resultados foram analisados de acordo com o grupo a que inicialmente tinham sido
associados
Inicialmente o desenho do estudo previa 120 participantes
Grupo A n = 40
Grupo B n = 40
Grupo C n = 20
30
Grupo D n = 20 (controlo)
No entanto no final do estudo foram apurados resultados de 107 indiviacuteduos Isto
deve-se a
Apoacutes a cirurgia alguns pacientes (n = 8) natildeo sentiram dor moderada a forte
no entanto quiseram mesmo assim participar sendo os seus resultados
subtraiacutedos aos caacutelculos
Alguns pacientes (n = 5) foram excluiacutedos sendo que um foi drop-out e os
restantes natildeo entregaram ou preencheram os questionaacuterios pedidos
No final a distribuiccedilatildeo de indiviacuteduos por grupos era a seguinte
Grupo A n = 34
Grupo B n = 36
Grupo C n = 20
Grupo D n = 17
Embora se verifique uma ligeira alteraccedilatildeo natildeo eacute motivo relevante de vieacutes
6 Were the participants in all groups followed up and data collected in the same
way
Sim Todos os pacientes tiveram acesso aos mesmos questionaacuterios entregues
pelo investigador Em caso de duacutevida ateacute ao final da duraccedilatildeo do estudo (8 horas) o
paciente podia telefonar ao investigador com quaisquer duacutevidas que surgissem Poreacutem
o paciente era responsaacutevel pelo iniacutecio do estudo ao administrar a si mesmo o faacutermaco
em casa no momento em que o fizesse devia telefonar ao investigador para este ter
conhecimento do iniacutecio do estudo Se o paciente natildeo contactasse o investigador ateacute 3
horas apoacutes a cirurgia o investigador contactaria o paciente Os valores maacuteximo e
miacutenimo de tempo entre a cirurgia e iniacutecio do estudo de foram 118 e 237 minutos a este
facto eacute inerente um risco de vieacutes pois nem todos os pacientes estavam na mesma
condiccedilatildeo quando iniciaram o tratamento podendo reflectir-se nos resultados
7 Did the study have enough participants to minimise the play of chance
Sim Os caacutelculos foram efectuados assumindo que existiria uma diferenccedila na
SPID entre grupos A e B de 20 Foram utilizados testes natildeo-parameacutetricos (Mann-
Whitney U-test) sendo definido que pelo menos 22 pacientes deveriam ser incluiacutedos em
cada um destes grupos
31
8 How are the results presented and what is the main result
Os caacutelculos estatiacutesticos necessaacuterios para a elaboraccedilatildeo dos resultados foram
efectuados no programa Statistical Package for Social Sciences (SPSS) v 12 As
significacircncias entre grupos de tratamento em relaccedilatildeo agraves respostas agrave VAS foram
testadas com t-test de variaacutevel independente em todas as avaliaccedilotildees de dor A mesma
estrateacutegia foi aplicada para a SPID agraves 3 e 8 horas A TOTPAR foi baseada na
assumpccedilatildeo que os resultados satildeo parte de uma escala de intervalos O mesmo teste foi
utilizado para a diferenccedila entre grupos relativamente ao uso de rescue medication Os
testes dos dados provenientes de escalas categoacutericas (PAR e a avaliaccedilatildeo global) foram
realizados atraveacutes de testes natildeo-parameacutetricos (Mann-Whitney U-test)
Intensidade da dor Os resultados favorecem o grupo A ateacute 15h apoacutes o iniacutecio do
tratamento A partir das 2h o grupo A natildeo tem uma eficaacutecia estatisticamente maior que
o grupo B Ambos os grupos tecircm melhores resultados globais que o grupo C O Grupo
D (placebo) eacute notoriamente menos eficaz que todos os outros grupos
Aliacutevio da dor (PAR) Os resultados meacutedios desta afericcedilatildeo satildeo semelhantes aos da
intensidade da dor
TOTPAR Natildeo houve uma diferenccedila significativa entre o grupo A e o grupo B
Ambos foram significativamente melhores que o C todos os grupos de tratamento
activo tiveram melhores resultados que o grupo D (placebo)
SPID Embora o grupo A mostre a maior SPID meacutedia (05 ndash 3h) natildeo foi
estatisticamente diferente do grupo B o grupo C tambeacutem natildeo foi estatisticamente
diferente do grupo B A SPID meacutedia total foi estatisticamente semelhante entre os
grupos A e B mas superior agrave do grupo C O grupo D (placebo) teve resultados
inferiores aos dos restantes grupos
Uso de rescue medication Embora tenha existido um nuacutemero notoriamente
superior de casos entre os grupos A e B comparativamente ao C e ao D esta diferenccedila
natildeo eacute relevante estatisticamente devido ao baixo nuacutemero de pacientes que recorreram a
esta medicaccedilatildeo
Avaliaccedilatildeo global tanto agraves 4 como agraves 8h os grupos A e B receberam avaliaccedilotildees
semelhantes tendo as melhores classificaccedilotildees e sendo significativamente superiores agraves
do grupo C Todos foram melhores que o D (placebo) Agraves 8h as percentagens de
pacientes que avaliaram o tratamento como bom ou excelente foram
Grupo A 90
32
Grupo B 83
Grupo C 42
9 How precise are these results
No artigo natildeo satildeo mencionados intervalos de confianccedila No entanto nos graacuteficos
referentes agrave intensidade da dor eacute possiacutevel ver as barras correspondentes ao intervalo de
confianccedila Existem sempre que necessaacuterio valores de p associados aos resultados
10 Were all important outcomes considered so the results can be applied
Sim A extracccedilatildeo de terceiros molares em Portugal eacute uma praacutetica cliacutenica comum
pelo que o estudo pode ser facilmente reproduzido desde que haja acesso agrave medicaccedilatildeo
utilizada e que esta esteja em formato idecircntico (para garantir que natildeo existe vieacutes)
Poreacutem o facto de ser utilizada uma dose uacutenica poderaacute natildeo ir de encontro com o padratildeo
actual sendo necessaacuteria uma sensibilizaccedilatildeo do paciente diferente para este meacutetodo
Um facto importante foi referido na discussatildeo deste artigo posteriormente agrave
recolha de dados do mesmo surgiram preocupaccedilotildees seacuterias sobre efeitos nocivos
cardiovasculares em tratamentos de longa duraccedilatildeo com rofecoxib embora estes efeito
secundaacuterios tendam a estar relacionados com as doses e natildeo apenas com a selectividade
COX-2 (8 25) Esta informaccedilatildeo eacute altamente relevante de todos os pontos de vista do
paciente e famiacutelia do profissional de sauacutede e oacutergatildeos legislativos
Tendo em conta este facto seriam necessaacuterios estudos adicionais para aferir o
risco de seguir um tratamento como o visado neste ensaio cliacutenico
33
Combined acetaminophen and ibuprofen for pain relief after oral
surgery in adults a randomized controlled trial (13)
1 Did the study ask a clearly-focused question
Sim Foram incluiacutedos pacientes sujeitos a extracccedilatildeo de pelo menos um terceiro
molar inferior Foram excluiacutedos pacientes com idade inferior a 16 anos peso inferior a
50 kg que tivessem tomado NSAIDrsquos (excepto aspirina a 150mg) ou paracetamol 24h
antes da cirurgia entre outros(inserir referencia para a pagina pois sao muitos)
Existiram 3 grupos de intervenccedilatildeo
Grupo A 500mg paracetamol + 150mg ibuprofeno
Grupo B 500mg paracetamol
Grupo C 150mg ibuprofeno
Todos os grupos de intervenccedilatildeo tomaram 2 comprimidos imediatamente antes da
cirurgia e depois 4 comprimidos diariamente (de 6 em 6 horas) durante 48h
Os resultados passaram pela intensidade da dor medida atraveacutes da VAS (mm)
em trecircs momentos distintos antes de tomar qualquer medicaccedilatildeo do estudo
imediatamente apoacutes a cirurgia e de 2 em 2 horas ateacute terminar o periacuteodo de 48 horas A
medida utilizada foi a area under the curve (AUC) dividida pelo tempo resultando em
AUCh Este caacutelculo foi efectuado para encontrar valores ldquomeacutediosrdquo pois houve ligeiras
diferenccedilas no momento da afericcedilatildeo dos valores da VAS Mediu-se tambeacutem o consumo
de rescue medication ao longo das 48 horas
Foram ainda utilizadas escalas categoacutericas de avaliaccedilatildeo global da dor e da
naacuteusea realizadas no final do estudo bem como uma escala VAS para medir os
distuacuterbios no sono apoacutes cada noite
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim A atribuiccedilatildeo de cada tratamento foi cega para todos os pacientes
investigadores e pessoal envolvido O responsaacutevel pela aleatorizaccedilatildeo do estudo foi o
estatiacutestico do estudo O estatiacutestico foi a uacutenica pessoa com acesso agraves informaccedilotildees da
atribuiccedilatildeo de tratamento aos pacientes
34
3 Were participants appropriately allocated to intervention and control groups
A colocaccedilatildeo de pacientes em cada um dos trecircs grupos de tratamento foi
aleatorizada A sequecircncia de aleatorizaccedilatildeo foi gerada por computador pelo estatiacutestico
do estudo Foi utilizada uma proporccedilatildeo de 111 para os trecircs grupos de tratamento isto
foi conseguido atraveacutes de permutaccedilatildeo de blocos com estratificaccedilatildeo para o tipo de
anestesia (local ou geral) e centro de estudo A utilizaccedilatildeo da aleatorizaccedilatildeo por
permutaccedilatildeo de blocos assegura uma distribuiccedilatildeo equilibrada por grupos de tratamento
quando o nuacutemero de indiviacuteduos eacute menor que mil (inserir referencia do artigo de
aleatorizajao MJA)
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim Este ensaio cliacutenico foi duplamente cego Como tal cada tipo de tratamento
consistia em comprimidos idecircnticos colocados num pacote selado as instruccedilotildees sobre
dosagens eram tambeacutem iguais garantindo que o estudo permanecia cego aos
investigadores staff e pacientes prevenindo a existecircncia de vieacuteses
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim O estudo previa um nuacutemero miacutenimo de 120 indiviacuteduos 40 em cada grupo
de tratamento Dos 135 pacientes que concordaram participar apoacutes serem abordados
pelo meacutedico apenas 122 foram incluiacutedos no estudo (os 13 que foram excluiacutedos natildeo
entregaram o diaacuterio de tratamento que lhes foi pedido)
Grupo A n = 40
Grupo B n = 43
Grupo C n = 39
Todos os 122 pacientes incluiacutedos foram seguidos ateacute ao final do estudo
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os pacientes foram abordados primariamente por um cirurgiatildeo e
seguidamente por uma enfermeira responsaacutevel pelo seguimento dos pacientes ao longo
do estudo O seguimento de cada paciente foi realizado de igual forma no hospital e fora
35
dele onde o contacto era estabelecido por telefone de forma a facilitar a recolha de
informaccedilatildeo levada a cabo por meio da entrega de diaacuterios
Em relaccedilatildeo agrave recolha dos dados relativos agrave dor poacutes-operatoacuteria experienciada os
intervalos de tempo utilizados foram semelhantes (imediatamente antes da
administraccedilatildeo da primeira dose logo apoacutes a cirurgia e de 2 em 2 horas durante um
periacuteodo de 48 horas) e a monitorizaccedilatildeo dos pacientes feita utilizando as mesmas
guidelines
7 Did the study have enough participants to minimise the play of chance
Sim Os investigadores do estudo realizaram a power calculation Estimaram
que eram necessaacuterios 120 participantes distribuiacutedos equitativamente pelos 3 grupos O
power foi de 80 na detecccedilatildeo de diferenccedilas entre os grupos de 9 mm (SD de 14mm)
para mediccedilotildees relativas agrave altura de repouso e os de 13mm (SD de 21mm) e para
mediccedilotildees relativas agrave altura de actividade
Dos 135 pacientes incluiacutedos no estudo 13 natildeo devolveram os seus diaacuterios pelo
que ficaram disponiacuteveis 122 participantes a enquadrar a populaccedilatildeo de tratamento (ITT
population) para anaacutelise dos criteacuterios de comparaccedilatildeo primaacuterios (primary endpoints)
Como o criteacuterio de possuir participantes necessaacuterios foi preenchido os
resultados da comparaccedilatildeo do objectivo primaacuterio deste estudo (mediccedilatildeo da intensidade
meacutedia de dor ao longo do estudo) tecircm uma elevada importacircncia cliacutenica Esta
importacircncia eacute equiparaacutevel aos resultados de estudos publicados anteriormente
8 How are the results presented and what is the main result
Os resultados foram apresentados sob a forma de mediccedilotildees nomeadamente as
principais diferenccedilas (mean differences) entre o paracetamolacetaminofeno ibuprofeno
e combinaccedilatildeo dos dois comparando a eficaacutecia farmacocineacutetica e efeitos secundaacuterios
respectivos a cada um Agraves quais estaacute associada uma taxa de erro de 5 (SEM) ou seja
intervalo de confianccedila de 95 (CI) e um valor de P lt001
Foi realizada a mediccedilatildeo da time-adjusted AUC (AUCh) da VAS que
juntamente com a classificaccedilatildeo global de dor revelou-se substancial e
significativamente menor no grupo que utilizou a combinaccedilatildeo do que nos outros dois
grupos (tanto no periacuteodo de repouso como no periacuteodo de actividade)
Apesar de alguns criteacuterios de comparaccedilatildeo secundaacuterios (secondary endpoints) o
uso de medicaccedilatildeo de resgate apoiarem o uso da combinaccedilatildeo do faacutermaco natildeo possuem
36
relevacircncia estatiacutestica Aleacutem disso o tipo de anestesia utilizada na cirurgia e o nordm de
dentes extraiacutedos os paracircmetros farmacocineacuteticos e a ocorrecircncia dos efeitos secundaacuterios
natildeo mostraram diferenccedilas significativas entre os 3 grupos de estudo
Os pacientes medicados com a combinaccedilatildeo de paracetamol e ibuprofeno
experienciaram menos dor poacutes-operatoacuteria durante as 48 horas que os pacientes que
usaram os medicamentos isolados
9 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em conta que foi preacute-
definido um valor para P de 005 de forma determinar se os valores obtidos possuem
relevacircncia estatiacutestica ou natildeo os resultados satildeo precisos
Isto mostra que para que a combinaccedilatildeo dos dois medicamentos possa ser
considerada sem incerteza mais adequada que outros meacutetodos de medicaccedilatildeo seriam
necessaacuterios resultados expliacutecitos e com elevada relevacircncia estatiacutestica
10 Were all important outcomes considered so the results can be applied
Sim O estudo realizado tal como acontece em todos os outros apresenta os
seus pontos fortes e fracos No entanto a pluralidade de criteacuterios utilizados na
comparaccedilatildeo dos vaacuterios grupos de estudo permitiu uma boa percepccedilatildeo da relaccedilatildeo
custobenefiacutecio aqui presente Apesar de certos paracircmetros como a utilizaccedilatildeo de
placebo recrutamento de crianccedilas e avaliaccedilatildeo significativa dos efeitos secundaacuterios natildeo
terem sido explorados estes natildeo apresentam grande peso no que respeita agrave validaccedilatildeo dos
resultados em si Isto acontece pois a bibliografia existente e a praacutetica cliacutenica jaacute nos
permitem deduzir e extrapolar conclusotildees em relaccedilatildeo agravequeles paracircmetros
Deste modo a questatildeo-chave recai sobre o facto de a combinaccedilatildeo de
paracetamol com ibuprofeno ser mais vantajosa e eficaz que a toma de apenas um deles
Caso estes resultados sejam confirmados por estudos de outras entidades a jaacute muito
utilizada combinaccedilatildeo paracetamol+ibuprofeno poderaacute mesmo tornar-se procedimento
padratildeo na terapecircutica da dor aguda moderada (em pacientes sem contra-indicaccedilatildeo para
NSAIDrsquos)
37
Analgesic efficacy of lysine clonixinate paracetamol and
dipyrone in lower third molar extraction a randomized
controlled trial (32)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo em estudo comporta 90 pacientes entre os 18 e 26 anos de
idade com uma indicaccedilatildeo cliacutenica para extracccedilatildeo de um 3ordm molar inferior impactado
(com classe I e II)
A intervenccedilatildeo consistiu no tratamento da dor apoacutes extracccedilatildeo do 3ordm molar atraveacutes
da medicaccedilatildeo com um dos 3 analgeacutesicos em estudo utilizando 8 comprimidos do
respectivo analgeacutesico a serem tomados 1 hora preacute-cirurgia e a cada 6 horas poacutes-cirurgia
durante um periacuteodo de 24 horas
Os resultados foram obtidos atraveacutes da mediccedilatildeo da intensidade da dor utilizando
a escala visual analoacutegica (VAS) mesmo antes da cirurgia e seguidamente 1 2 4 6 8
12 e 24 horas apoacutes a cirurgia Aleacutem disso para cada uma destas mediccedilotildees os pacientes
tinham de relatar o niacutevel de dor em que se encontravam (percepccedilatildeo da dor) atraveacutes de
uma escala decimal com os seguintes criteacuterios
0 cm Sem dor
01- 3 cm Dor ligeira
31-7 cm Dor moderada
71-10 cm Dor intensa
A presenccedila ou ausecircncia de efeitos secundaacuterios foi tambeacutem uma das
preocupaccedilotildees deste estudo e algo avaliado nos resultados Dado que havia a
possibilidade de ocorrecircncia de agranulocitose anemia anafilaxia e complicaccedilotildees
gastrointestinais
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo em questatildeo consiste num ensaio cliacutenico aleatorizado Esta
abordagem foi a mais adequada para a questatildeo colocada uma vez que o objectivo final
eacute comparar a eficaacutecia da lisina clonixinato com o paracetamol e com a dipirona na
analgesia da dor poacutes-operatoacuteria Para obter informaccedilotildees mais completas respeitantes agrave
seguranccedila e eficaacutecia dos faacutermacos comparados eacute necessaacuterio o recrutamento e
aleatorizaccedilatildeo de um determinado nuacutemero de pacientes Eacute necessaacuterio tambeacutem medicaacute-
38
los medir e avaliar os resultados de forma imparcial e objectiva Desta forma eacute mais
provaacutevel chegar a uma conclusatildeo fidedigna e vaacutelida tanto interna como externamente
Pelas razotildees acima enumeradas a realizaccedilatildeo de um ensaio cliacutenico aleatorizado
foi a melhor abordagem a seguir
3 Were participants appropriately allocated to intervention and control groups
Sim Os pacientes foram divididos pelos diferentes grupos de estudo de uma
forma aleatoacuteria utilizando um meacutetodo relativamente simples Os analgeacutesicos foram
repartidos em recipientes brancos opacos e idecircnticos numerados de 1 a 90 Cada
recipiente continha 8 comprimidos de um dos 3 faacutermacos em comparaccedilatildeo (dipirona
500mg paracetamol 750mg lisina clonixinato 125 mg) Por sua vez foi pedido aos
pacientes para retirarem o recipiente agrave sua escolha e ao acaso os quais desconheciam o
seu conteuacutedo
Dos 90 pacientes recrutados de iniacutecio 26 desistiram pelo que os restantes 64
pacientes foram distribuiacutedos por 3 grupos correspondentes a diferentes analgeacutesicos
orais lisina clonixinato composto por 20 indiviacuteduos (8 masculinos 12 femininos)
Paracetamol composto por 23 indiviacuteduos (9M 14F) Dipirona composto por 21
indiviacuteduos (6M 15F)
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Natildeo eacute possiacutevel dizer Os pacientes deste estudo estavam lsquocegosrsquo quanto ao grupo
de estudo em que iriam ser colocados O processo de distribuiccedilatildeo dos indiviacuteduos foi
feito de uma forma aleatoacuteria atraveacutes de um meacutetodo bastante simples de escolha de
recipiente
Quanto aos funcionaacuterios e revisores deste estudo o mesmo pode natildeo ter
acontecido pois nenhuma informaccedilatildeo sobre este aspecto eacute mencionada no artigo
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim No estudo realizado os participantes foram distribuiacutedos por 3 grupos um
de estudo ou intervenccedilatildeo onde foi administrado lisina clonixinato e dois de controlo
onde se administrou paracetamol num e dipirona noutro Natildeo houve redistribuiccedilatildeo dos
39
participantes isto eacute cada participante foi tratado uacutenica e exclusivamente com o faacutermaco
correspondente ao seu grupo
Houve um seguimento dos pacientes durante um periacuteodo de 24 horas de modo a
avaliar a eficaacutecia de cada analgeacutesico na eliminaccedilatildeo da dor poacutes-operatoacuteria de forma
indirecta (quanto maior o aliacutevio de dor ao longo do periacuteodo de estudo maior a eficaacutecia
do respectivo analgeacutesico) Tendo isso em conta os resultados e anaacutelise dos dados foram
realizados em cada grupo e depois comparados com os outros grupos
Os investigadores do estudo poderiam ter formado um grupo placebo e
comparado os seus resultados com os restantes grupos Assim averiguar-se-ia a eficaacutecia
de cada um dos analgeacutesicos e natildeo apenas a eficaacutecia relativa a outros faacutermacos
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os participantes dos diferentes grupos foram seguidos da mesma maneira e
os dados recolhidos de igual forma Os resultados foram avaliados nos mesmos
intervalos de tempo ou seja antes da cirurgia e 1 2 4 6 8 12 e 24 horas apoacutes a
mesma Os pacientes receberam o mesmo tempo de atenccedilatildeo - 24 horas de seguimento e
os dados foram recolhidos utilizando os mesmos paracircmetros a escala visual analoacutegica
para determinar o aliacutevio de dor e a escala decimal para a percepccedilatildeo de dor dos pacientes
e questionaacuterios individuais
Para aleacutem do jaacute referido os investigadores tiveram em atenccedilatildeo a forma como a
cirurgia foi realizada diminuindo o risco de vieacutes
Intervieram 2 cirurgiotildees calibrados entre si na niacutevel da teacutecnica minimizando a
ocorrecircncia de abordagens ciruacutergicas diferentes
o periacuteodo de duraccedilatildeo foi controlado e por isso natildeo influenciou o comportamento
da dor no estudo (meacutedia de 339 minutos com SD plusmn98 min)
Estas cirurgias satildeo bastantes conhecidas e muitas vezes satildeo procedimentos
standard permitindo uma selecccedilatildeo muito mais facilitada e raacutepida de casos cliacutenicos a
incluir no estudo e diminuindo o nuacutemero de eventos de difiacutecil controlo que poderiam
levar a vieacutes dos resultados
7 Did the study have enough participants to minimise the play of chance
Natildeo eacute possiacutevel dizer Dos 90 pacientes inicialmente recrutados para o estudo 26
deles desistiram Os investigadores natildeo referiram o impacto deste nuacutemero de drop-outs
40
na extrapolaccedilatildeo de conclusotildees a partir dos resultados obtidos Igualmente natildeo foram
mencionados quaisquer caacutelculos que determinassem o nuacutemero necessaacuterio de indiviacuteduos
para o estudo ter validade
8 How are the results presented and what is the main result
Os resultados obtidos no estudo foram categorizados por droga e analisados de
acordo com o desenvolvimento da dor poacutes-operatoacuteria Seguidamente foram
apresentados atraveacutes de mediccedilotildees descritivas da variaccedilatildeo da dor as quais utilizaram
paracircmetros como miacutenimo maacuteximo mean median e desvio-padratildeo (SD)
Por sua vez a anaacutelise dos dados foi feita com os testes de Kruskal-Wallis e de
Friedman onde os resultados satildeo considerados estatisticamente relevantes se
culminarem num valor de lsquoprsquo igual ou inferior a 005 (95 IC) e apresentada utilizando
os mesmos paracircmetros de miacutenimo maacuteximo e SD
O valor de P encontra-se claramente acima do valor de referencia preacute-definido
pelo que os resultados natildeo apresentam relevacircncia estatiacutestica suficiente para aferir que
possuem um melhor outcome que o paracetamol
A lisina clonixinato assim como a dipirona e o paracetamol eacute eficiente no
controlo da dor resultante da extracccedilatildeo de um 3ordmmolar inferior pelo que natildeo apresenta
nenhuma diferenccedila significativa dos outros analgeacutesicos mencionados
9 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em conta que os valores de
P obtidos apoacutes anaacutelise dos resultados se encontrarem abaixo de 001 eacute possiacutevel auferir
que os resultados deste estudo satildeo bastante precisos
10 Were all important outcomes considered so the results can be applied
Natildeo Os efeitos gerados pela lisina clonoxinato no tratamento da dor derivada de
extracccedilatildeo do 3ordm molar natildeo foram estatisticamente relevantes quando comparados aos do
paracetamol e dipiridona Apesar de as condiccedilotildees pelas quais o estudo foi realizado
serem reprodutiacuteveis na nossa populaccedilatildeo local (tipo de pessoas localizaccedilatildeo e
reprodutibilidade do tratamento) nada eacute referido em relaccedilatildeo a novas poliacuteticas de sauacutede
nomeadamente na implementaccedilatildeo de uma dose uacutenica culminando numa mudanccedila dos
haacutebitos de sauacutede da comunidade Tambeacutem natildeo foram abordados aspectos econoacutemicos
41
tal como um balanccedilo entre benefiacutecios e encargos de sauacutede que justifique a utilizaccedilatildeo
deste faacutermaco como tratamento preferencial
42
Onset of analgesia with sodium ibuprofen ibuprofen acidin
corporating poloxamer and acetaminophenmdasha single-dose
double-blind placebo-controlled study in patients with post-
operative dental pain Daniels Reader (33)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo em estudo refere-se a pacientes com idade entre os 16 e os 40
anos apresentando uma intensidade de dor basal poacutes-operatoacuteria moderada a severa O
diagnoacutestico para a extracccedilatildeo poderia ser um dos seguintes pelo menos um 3ordm molar
mandibular indicado para remoccedilatildeo (grau de impactaccedilatildeo superior a 4) ou dois terceiros
molares ipsilaretais com pontuaccedilatildeo de impactaccedilatildeo conjunta natildeo superir a 6
A intervenccedilatildeo traduz-se no tratamento da dor poacutes-ciruacutergica com doses uacutenicas de
diferentes faacutermacos Inicialmente cada participante tem a mesma probabilidade de ser
colocado num dos 4 grupos
A ibuprofeno de soacutedio 2x256 mg (ibuprofeno de soacutedio di-hidratado equivalente a
400 mg de ibuprofeno aacutecido + placebos de ibuprofeno poloxamo e
acetaminofeno
B ibuprofenopoloxacircmero (400mg de Ibuprofeno e 120mg de poloxacircmero
surfactante 407) + placebos de ibuprofeno de soacutedio e paracetamol
C 1000mg acetaminofeno + placebos equivalentes
D placebo para as 3 formas de substacircncias activas
O endpoint primaacuterio consistiu no tempo necessaacuterio para um aliacutevio da dor
perceptiacutevel pelos pacientes Foram considerados inuacutemeros endpoints secundaacuterios (foi
utilizada uma escala categoacuterica e VAS para os endpoints 2 3 e 4)
1 Caacutelculo da AUC e SPRID (0 a 6 horas poacutes-tratamento) e tempo necessaacuterio para
um aliacutevio significativo da dor
2 Aliacutevio total da dor (TOTPAR) SPID e SPRID
3 Aliacutevio da dor e intensidade da mesma em termos individuais (5 minutos - 6
horas)
4 PID ao longo do periacuteodo de estudo e o momento em que este foigt ou igual a 1
5 Instante em que os pacientes recorreram a medicaccedilatildeo de recurso
6 Tempo e proporccedilatildeo de pacientes que sentiram 50 aliacutevio da dor
43
7 Abstracccedilatildeo agrave dor (1 e 6 horas) e percepccedilatildeo da interferecircncia causada pela dor nas
actividades quotidianas (escala de Ranvier)
8 Avaliaccedilatildeo qualitativa da medicaccedilatildeo tomada pelos dos participantes
Os efeitos adversos foram obtidos atraveacutes da procura de informaccedilatildeo em
documentaccedilatildeo e relacionados (ou natildeo) com a medicaccedilatildeo do estudo pelo investigador
Foi efectuada uma mediccedilatildeo de sinais vitais 6 horas apoacutes a toma e na visita follow-up na
qual tambeacutem foi realizado um exame fiacutesico
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo em questatildeo eacute descrito como um ensaio cliacutenico duplamente cego e
controlado com placebo Eacute o tipo de estudo indicado para comparar diferentes formas de
tratamento atraveacutes da divisatildeo dos pacientes por grupos Eacute necessaacuterio ter em
consideraccedilatildeo o aspecto eacutetico de tais tratamentos pois ldquoexposing patients to an
intervention believed to be inferior to current treatment is often thought unethicalrdquo (41)
Para garantir a eacutetica dos tratamentos incluiacutedos o estudo foi conduzido de acordo com a
Declaraccedilatildeo de Helsiacutenquia como referido na Directiva da EU de 200120EC e
concordante com a Conferecircncia Internacional de Harmonizaccedilatildeo (ICH) e a GCP (boa
praacutetica cliacutenica)
3 Were participants appropriately allocated to intervention and control groups
Sim Os indiviacuteduos foram divididos aleatoriamente para serem inseridos num
dos 4 grupos de tratamento numa proporccedilatildeo 1111 O meacutetodo de aleatorizaccedilatildeo foi
gerado pelo computador atraveacutes de um randomization Schedule
Para equilibrar a alocaccedilatildeo dos pacientes realizou-se uma estratificaccedilatildeo por sexo
e por intensidade da dor basal O protocolo do estudo foi revisto e aprovado pela
Quorum Review Inc o que leva a querer que a subdivisatildeo foi realmente rigorosa
Os grupos encontram-se equilibrados tanto em nuacutemero como noutras variaacuteveis
particularmente geacutenero intensidade dor basal e idade Deste modo diferenccedilas
reportadas nos resultados natildeo satildeo consequecircncia da heterogeneidade dentro dos grupos
de tratamento
44
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
A aleatorizaccedilatildeo dos participantes foi gerada pelo computador O protocolo do
estudo foi posteriormente revisto como anteriormente referido Agrave partida tanto o
investigador e pacientes natildeo interferiram no processo
Foram usados comprimidos para o ibuprofeno de soacutedio ibuprofenopoloxamero
e caacutepsulas para o paracetamol tanto para as formas activas como placebo
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim Os 322 participantes incluiacutedos de 614 inicialmente recrutados 318
completaram o estudo e 321 foram incluiacutedos na populaccedilatildeo ITT (intended do treat)
No grupo ibuprofeno de soacutedio todos os 80 participantes concluiacuteram a anaacutelise
No grupo B dos 80 inicialmente alocados 76 completaram a anaacutelise Um foi
excluiacutedo perdeu-se o follow-up de outro e os restantes natildeo concluiacuteram por
outros motivos
Dos 81 do grupo do paracetamol um natildeo foi incluiacutedo no ITT (falhou em
providenciar os dados da intensidade da dor basal diaacuteria)
No grupo placebo todos os pacientes concluiacuteram o estudo
Os resultados de cada paciente foram analisados agrave luz do grupo de tratamento
em que estes foram colocados
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os participantes permaneceram nos centros de investigaccedilatildeo cliacutenica apoacutes a
toma durante 8-15h Durante as 6 horas apoacutes o tratamento a eficaacutecia foi medida em
intervalos preacute-determinados Para avaliar a existecircncia de efeitos secundaacuterios foi
realizada uma mediccedilatildeo de sinais vitais conduzido um follow-up poacutes-operativo (5 a 12
dias poacutes-cirurgia) e repetida a avaliaccedilatildeo de efeitos adversos Pode-se considerar anaacutelogo
o acompanhamento entre os vaacuterios pacientes poacutes-cirurgia e medicaccedilatildeo pois constituiu
um seguimento proacuteximo maioritariamente presencial e rigoroso
45
7 Did the study have enough participants to minimise the play of chance
Foram usados dados de estudos preacutevios os quais continham informaccedilatildeo acerca
de AUC e PRID Com estes dados foi determinado que um nuacutemero de 80 pacientes por
grupo providenciaria um power de 90 em detectar diferenccedilas entre os grupos de
tratamento com um niacutevel de significacircncia de 0025 Natildeo foi possiacutevel calcular um power
ldquoformalrdquo para o aliacutevio de dor significativo No entanto a resposta eacute afirmativa para a
questatildeo CASP uma vez que foram realizados esforccedilos para que o nuacutemero das amostras
fosse significativo e correcto
8 How are the results presented and what is the main result
Os resultados satildeo apresentados em termos de percentagens e diferenccedilas meacutedias
(mean differences) alguns com recurso a curvas de Kaplan-Meier (survival curves) Os
efeitos secundaacuterios satildeo apresentados sob a forma de tabela com a percentagem de
pacientes dentro de cada grupo que sofreram os efeitos descritos na mesma
Os grupos A e B exibem resultados substancialmente melhores no que diz
respeito aos seguintes pontos
AUC e SPID satildeo significativamente menores A com 963 e B com 90 face a
C com 675 e D com 25 O tempo para atingir aliacutevio da dor
SPRID Esta eacute semelhante entre os grupos A B e C ateacute aos 45 minutos A partir
deste periacuteodo o ibuprofeno possui uma eficaacutecia superior ao paracetamol
Abstracccedilatildeo agrave dor e percepccedilatildeo da interferecircncia causada pela dor nas actividades
quotidianas (escala de Ranvier)
Utilizaccedilatildeo da medicaccedilatildeo de recurso A com 325 e B com 225 face a C com
438 e D em que a maioria dos pacientes usou a mesma
Avaliaccedilatildeo dos medicamentos por parte dos pacientes (resposta ldquoboardquo ldquomuito
boardquo ou ldquoexcelenterdquo)
No que se refere aos efeitos secundaacuterios 118 da populaccedilatildeo do estudo sofreu
mais efeitos sendo que a maior percentagem ocorreu no grupo do C
Quando comparado com acetaminofeno o ibuprofeno de soacutedio e
Ibuprofenopoloxamero possui uma eficaacutecia analgeacutesica significativamente superior
46
9 How precise are these results
Nos endpoints primaacuterios as diferenccedilas entre as duas formulaccedilotildees de ibuprofeno e
paracetamol foram avaliadas tendo por base o teste de Wilcoxon rank-sum O hazard
ratio e respectivo IC de 975 foram calculados para as comparaccedilotildees entre os
compostos Os endpoints secundaacuterios que agregavam vaacuterios periacuteodos de tempo foram
calculados atraveacutes da AUC Diferenccedilas entre tratamentos foram avaliadas utilizando
valores de α de 005 o intervalo de confianccedila de 95 (CI) foi calculado por meio dos
paracircmetros do modelo adequado
Eacute introduzido o valor de P que na sua generalidade possui valores reduzidos e
menores que 0005 Considerando a homogeneidade dos grupos o caacutelculo do nuacutemero da
amostra com elevado power e os valores de P podemos concluir que no contexto os
resultados satildeo precisos (42)
10 Were all important outcomes considered so the results can be applied
Eacute plausiacutevel que a populaccedilatildeo utilizada no estudo fosse semelhante num estudo
anaacutelogo Tanto o local como o proacuteprio tratamento poderiam ser reproduzidos visto que
os compostos em questatildeo satildeo largamente comercializados
Os resultados satildeo importantes para uma escolha mais consciente por parte dos
indiviacuteduos entre tomar paracetamol ou ibuprofeno apoacutes uma cirurgia de um 3ordm molar Eacute
afirmado na discussatildeo deste estudo que o ibuprofeno possui menores efeitos adversos
gastrointestinais que outros NSAIDrsquos Tendo isso em conta pode conduzir a uma
escolha deste composto no tratamento da dor poacutes ciruacutergica por parte dos profissionais
ldquothese findings support a recommendation for this agent as an analgesic of choice for
the treatment of post-operative dental painrdquo A preocupaccedilatildeo pela comunidade em geral
estaacute impliacutecita neste aspecto se possuir menores efeitos secundaacuterios e benefiacutecio superior
eacute melhor para a populaccedilatildeo em geral O custo financeiro destes medicamentos natildeo se
traduz num ponto diferenciador visto que em Portugal existem geneacutericos de ambos
Eacute uma boa base de comparaccedilatildeo entre o paracetamol e ibuprofeno em muitos
aspectos Na procura da melhor evidecircncia e no sentido de a aplicar eacute importante
completar este estudo com outros que nomeadamente se foquem nos efeitos
secundaacuterios
47
An investigation into the comparative efficacy of soluble aspirin
and solid paracetamol in postoperative pain after third molar
surgery Seymour Hawkesford (22)
1 Did the study ask a clearly-focused question
Sim O estudo em questatildeo trata-se de um ensaio cliacutenico aleatorizado duplamente
cego e controlado por placebo O seu objectivo central eacute comparar a eficaacutecia da aspirina
soluacutevel agrave do paracetamol soacutelido em pacientes com dor poacutes-operatoacuteria apoacutes extracccedilatildeo do
3ordm molar Foi utilizado um grupo placebo como controlo negativo
Soacute foram incluiacutedos pacientes que necessitavam da extracccedilatildeo do 3ordm molar
saudaacuteveis segundo categoria 1 da American Society of Anaesthesiologists (ASA I) ou agrave
discriccedilatildeo do cirurgiatildeo oral categoria 2 Soacute foram abrangidos pacientes que atingiram o
limiar de dor necessaacuterio ou que requeriram analgeacutesicos ateacute 90 minutos apoacutes a cirurgia
Cada paciente incluiacutedo no estudo foi colocado num dos trecircs grupos de
tratamento
Grupo 1 Aspirina soluacutevel 900mg dose uacutenica
Grupo 2 paracetamol soacutelido 1000mg dose uacutenica
Grupo 3 placebo dose uacutenica
Foi utilizado o meacutetodo de double-dummy ndash assim cada grupo recebeu o seu tipo
de tratamento e um placebo do tratamento alternativo No caso do grupo 3 os pacientes
receberam placebos para os dois tipos de tratamento
Os outcomes passaram pela
Comparaccedilatildeo de medidas de intensidade da dor atraveacutes da escala VAS (mm)
entre os grupos de tratamento aos 10 15 20 e 30 minutos apoacutes a dosagem
inicial
Comparaccedilatildeo da AUC240 com recurso a anaacutelise de co-variacircncia usando o
centro do estudo geacutenero baseline pain intensity duraccedilatildeo da cirurgia e
nuacutemero de molares removidos como co-variaacuteveis
Necessidade de recurso a rescue medication
Impressatildeo geral dos pacientes e enfermeiros sobre a medicaccedilatildeo atraveacutes de
uma regressatildeo binomial logiacutestica (em que um resultado positivo se refere a
uma avaliaccedilatildeo ldquomuito boardquo ou ldquoboardquo)
As comparaccedilotildees feitas foram aspirina vs paracetamol e aspirina vs placebo
48
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo apresentado eacute um RCT por vaacuterias razotildees sendo a mais relevante a
aleatorizaccedilatildeo dos grupos de tratamento em que os pacientes incluiacutedos foram
distribuiacutedos com a mesma probabilidade e aleatoriamente para cada grupo de estudo Os
grupos de tratamento tecircm tamanhos semelhantes e satildeo homogeacuteneos e os pacientes
foram seguidos de forma semelhante - as uacutenicas diferenccedilas residem no tratamento
oferecido
A utilizaccedilatildeo deste tipo de estudo foi loacutegica Um ensaio cliacutenico aleatorizado eacute
ideal para comparar efeitos de determinadas intervenccedilotildees e consequentemente ideal
para comparar eficaacutecia entre medicamentos
3 Were participants appropriately allocated to intervention and control groups
Foi realizada uma alocaccedilatildeo aleatoacuteria dos pacientes incluiacutedos assim como uma
aleatorizaccedilatildeo por blocos de cinco para assegurar equiliacutebrio entre grupos de tratamento
ldquoA key advantage of blocked randomization is that treatment groups will be equal in
size and will tend to be uniformly distributed by key outcome-related characteristicsrdquo
(43)
Foi ainda efectuada uma aleatorizaccedilatildeo estratificada por geacutenero de modo a
equilibrar nos trecircs grupos o nuacutemero de mulheres e homens e aumentar a credibilidade
das comparaccedilotildees entre os mesmos (proporccedilatildeo MF 21)
Tabela 2 ndash Dados demograacuteficos dos pacientes do estudo
Variaacutevel Aspirina soluacutevel
900mg
Paracetamol soacutelido
1000 mg
Placebo
Nuacutemero de pacientes 59 62 32
Raacutecio geacutenero MF 1940 1943 1121
Todos os pacientes incluiacutedos receberam anestesia de acordo com a praacutetica
cliacutenica a extracccedilatildeo dos molares impactados foi realizada seguindo a teacutecnica standard
Estes factores contribuem para a semelhanccedila da forma de tratamento dos 3 grupos Com
estes aspectos em comum a todos os pacientes incluiacutedos em adiccedilatildeo agrave homogeneidade
dos grupos nos seus aspectos demograacuteficos diferenccedilas encontradas nos resultados satildeo
consequecircncias de outros factores
49
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim A administraccedilatildeo uacutenica tem a vantagem de natildeo requerer monitorizaccedilatildeo de
um processo ldquodelicadordquo por parte do paciente De facto todo o estudo eacute realizado num
periacuteodo de 4 horas apoacutes a cirurgia e com ajuda de enfermeiros Olhando do ponto de
vista do paciente pode-se consideraacute-lo cego
Se os meacutetodos foram realmente aleatoacuterios o investigador eacute tambeacutem considerado
cego e pode-se afirmar que foram feitos esforccedilos necessaacuterios para o alcanccedilar Tanto a
aspirina soluacutevel como o placebo foram oferecidos sob a forma de uma bebida cor-de-
laranja o paracetamol com substacircncia activa e placebo oferecidos como comprimidos
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim Inicialmente todos os pacientes tinham a mesma probabilidade de serem
incluiacutedos num dos trecircs grupos A distribuiccedilatildeo sendo aleatoacuteria natildeo soacute coloca um
paciente num determinado grupo de tratamento como impossibilita que o mesmo venha
a pertencer a outro O seguimento foi realizado de igual forma para todos os grupos e
intimamente controlado Os resultados foram apresentados separadamente para cada
grupo Dos 167 pacientes foram medicados 153 Dos 14 pacientes natildeo tratados 10 natildeo
desenvolveram dor suficiente para serem incluiacutedos 1 obteve uma reacccedilatildeo adversa agrave
anestesia e 1 natildeo seguiu o protocolo
O grupo da aspirina soluacutevel apresentou melhores resultados que o grupo do
paracetamol e do placebo na medida em que os pacientes reportaram menos dor
apresentou menor intensidade de dor (aos 10 e 30 minutes em comparaccedilatildeo ao
paracetamol e apenas 30 minutos face ao placebo) e os valores de dor global medidos
pela AUC240 foram significativamente menores
6 Were the participants in all groups followed up and data collected in the same
way
Sim A intensidade da dor foi medida frequentemente ao longo de 4 horas
(segundo a VAS) e os pacientes foram informados da possibilidade de tomar medicaccedilatildeo
adicional se necessaacuterio A avaliaccedilatildeo sobre o tratamento dos enfermeiros e dos proacuteprios
pacientes foi tida em consideraccedilatildeo para os resultados
50
Aleacutem disso ao longo do periacuteodo de investigaccedilatildeo a enfermeira do estudo ficou
responsaacutevel por monitorizar os pacientes e registar a ocorrecircncia de quaisquer eventos
adversos Deste modo eacute muito provaacutevel que todos os pacientes tenham recebido o
mesmo niacutevel de atenccedilatildeo
7 Did the study have enough participants to minimise the play of chance
Natildeo eacute possiacutevel dizer No estudo natildeo eacute referida a utilizaccedilatildeo de power calculations
ou outros meacutetodos para determinar o tamanho da amostra Apenas se pode concluir que
o grupo de controlo negativo tem um menor nuacutemero de pacientes consequecircncia de
desistecircncias ou pelo simples facto de agrave partida se conhecerem os resultados
8 How are the results presented and what is the main result
A intensidade da dor foi medida numa escala VAS aos 10 15 20 e 30 minutos
apoacutes a administraccedilatildeo Foi possiacutevel tirar vaacuterias conclusotildees a partir da observaccedilatildeo dos
resultados
A aspirina demonstrou ser significativamente mais eficaz que o paracetamol ou
placebo embora ateacute aos 15 minutos natildeo seja uma diferenccedila muito expressiva
Relativamente agrave AUC240 experiecircncia global da dor no periacuteodo de 4 horas da
investigaccedilatildeo esta foi significativamente menor para o grupo 1
Natildeo existiu diferenccedila significativa entre os grupos no que diz respeito agrave rescue
medication utilizada No entanto o tempo para a administraccedilatildeo da mesma foi
superior no grupo 1 e 2 em relaccedilatildeo ao grupo placebo
Em relaccedilatildeo agrave impressatildeo global natildeo haacute discrepacircncias consideraacuteveis entre grupo 1
e 2 no que diz respeito agrave percentagem de outcomes positivos (58 e 53
respectivamente) O grupo 3 apresentou apenas 31 de outcomes positivos
A tabela com a percentagem de pacientes que desenvolveram efeitos adversos
para cada grupo mostra que 41 dos pacientes apresentaram efeitos secundaacuterios
nos grupos com tratamento activo no entanto muitos destes estavam
relacionados com o procedimento ciruacutergico
A aspirina soluacutevel 900mg providencia uma analgesia mais significante e raacutepida
que o paracetamol 1000mg no periacuteodo imediato apoacutes a cirurgia do 3ordm molar embora natildeo
seja muito expressiva a percepccedilatildeo desta diferenccedila por parte dos pacientes e enfermeiros
51
9 How precise are these results
Os resultados satildeo precisos e apresentados atraveacutes de um intervalo de confianccedila
de 95 satildeo tambeacutem apresentados valores de p
Os valores de p satildeo menores que 005 excepto aos 10 e 15 minutos
Para a intensidade da dor ao longo dos 30 minutos e AUC240 da comparaccedilatildeo
aspirina vs placebo a intervenccedilatildeo utilizada seria a mesma tanto no limite superior
como no inferior excepto aos 10 e 15 minutos Na comparaccedilatildeo aspirina soluacutevel vs
paracetamol soacutelido a decisatildeo seria a mesma independentemente dos limites do intervalo
apenas para os minutos 10 20 e 30
O mesmo aconteceria para a medicaccedilatildeo de recurso (outcome C) e a avaliaccedilatildeo do
tratamento por parte dos pacientes e enfermeiros (outcome D)
Pelo intervalo de confianccedila estar presente e pelo facto de os valores de p serem
bastante reduzidos os resultados satildeo precisos ao ponto de ajudarem a suportar uma
decisatildeo
10 Were all important outcomes considered so the results can be applied
Sim Os pacientes incluiacutedos no estudo o local e o tratamento visados no mesmo
poderiam ser extrapulados e aplicados noutro ambiente O seguimento dos pacientes
durante 4 horas e com ajuda de enfermeiros natildeo se apresenta como muito viaacutevel mas
ainda assim eacute exequiacutevel e seguro
O estudo avalia dados importantes para os profissionais de sauacutede ao afirmar que
a dose (900mg) e a forma (soluacutevel) em que a aspirina eacute tomada conduz a um poder
analgeacutesico superior que o paracetamol No entanto em termos individuais e de poliacuteticas
de sauacutede os efeitos secundaacuterios consequentes da medicaccedilatildeo (excluindo os que se
relacionassem com a cirurgia) deveriam ser completados com estudos suplementares
Segundo este ensaio cliacutenico a incidecircncia de efeitos secundaacuterios natildeo eacute muito
dissemelhante entre aspirina soluacutevel e paracetamol soacutelido nas doses maacuteximas
recomendadas e nestas circunstacircncias a aspirina tem maior poder analgeacutesico Por este
prisma a praacutetica cliacutenica poderia passar pela prescriccedilatildeo de aspirina soluacutevel 900mg para
aliacutevio dor poacutes-operatoacuteria da extracccedilatildeo do terceiro molar Poreacutem eacute necessaacuterio ter em
conta que visa somente a dor nas primeiras quatro horas poacutes-operatoacuterias sendo
importante investigar alternativas eficazes que sejam mais duradouras ou a eficaacutecia e
efeitos secundaacuterios de repetir este tratamento apoacutes as quatro horas iniciais
52
DISCUSSAtildeO
A partir da anaacutelise feita das revisotildees sistemaacuteticas de Weil (19) e de Barden (23)
conclui-se que o paracetamol eacute uma analgeacutesico seguro e eficaz no tratamento da dor
relativa agrave exodontia de terceiros molares pois apresenta um benefiacutecio estatisticamente
significativo quando comparado a placebo Ambas consideram que os melhores valores
de aliacutevio de dor e da diminuiccedilatildeo da intensidade da mesma satildeo alcanccedilados agraves 4 e 6 horas
apoacutes ingestatildeo do faacutermaco
Com base na primeira revisatildeo acima referida o paracetamol exibe uma dose
uacutenica oacuteptima de 1000mg e um periacuteodo de medicaccedilatildeo apropriado de 8 em 8 horas A
maioria dos artigos incluiacutedos apresenta um risco de vieacutes moderado causado
principalmente pela falta de informaccedilatildeo sobre o mecanismo de alocaccedilatildeo de pacientes
podendo levar a uma descredibilidade dos resultados (36)
Na revisatildeo de Barden (23) a comparaccedilatildeo entre os diferentes NSAIDrsquos
demonstrou que este tipo de faacutermacos e particularmente os inibidores da COX-2
exibem os melhores valores de NNT Atraveacutes de uma comparaccedilatildeo indirecta entre
ibuprofeno vs paracetamol os vaacuterios estudos mostraram que o ibuprofeno apresenta
melhores resultados na analgesia da dor poacutes-operatoacuteria (44)
Os estudos de Seymour (22) de Haglund (25) e de Daniels (33) comparam
diferentes compostos activos a um placebo onde o paracetamol estaacute sempre presente
Todos comprovam que enquanto analgeacutesico apresenta uma eficaacutecia largamente
significativa em termos de aliacutevio da dor (usando a escala VAS) Pelo menos 50 dos
indiviacuteduos incluiacutedos que receberam este faacutermaco avaliaram globalmente o tratamento de
forma positiva Poreacutem todos os artigos que
1 Comparam este composto a outro nomeadamente NSAIDrsquos mostram que estes
tecircm uma eficaacutecia significativamente superior agrave do paracetamol tanto em relaccedilatildeo
a valores mais baixos na escala VAS como subjectivamente na avaliaccedilatildeo global
Cerca de 80 dos indiviacuteduos que tomaram NSAIDrsquos classificaram o tratamento
positivamente (agrave excepccedilatildeo dos estudos (32) e (22)) Reportam ainda os efeitos
adversos mais comuns como tonturas naacuteuseas cefaleia e sonolecircncia que
embora de gravidade reduzida tecircm uma incidecircncia superior no paracetamol que
na aspirina e ibuprofeno
53
2 Combinam o paracetamol com NSAIDrsquos provam o efeito aditivo daquele bem
como o facto de estas combinaccedilotildees serem mais eficazes que qualquer um dos
faacutermacos em separado (Merry (13) e Haglund (25))
De acordo com os estudos analisados os NSAIDrsquos aparentam ser uma escolha
preferencial face ao paracetamol porque apresentam uma maior eficaacutecia no aliacutevio da dor
apoacutes extracccedilatildeo de terceiros molares embora disponham de propriedades anti-
inflamatoacuterias notoacuterias (e pertinentes no sucesso do tratamento poacutes-operatoacuterio)
O mecanismo de acccedilatildeo do paracetamol necessita de investigaccedilatildeo adicional que
permita uma melhor compreensatildeo e que traga novas respostas na praacutetica cliacutenica Como
aspecto positivo eacute de acrescentar que natildeo existem diferenccedilas estatisticamente
significantes entre o paracetamol e placebo no que diz respeito a efeitos secundaacuterios
(baixo grau de severidade) podendo ser considerado um composto seguro
A revisatildeo de Barden (23) indica que os resultados da eficaacutecia dos NSAIDrsquos
podem atrair os cliacutenicos a aumentar a sua prescriccedilatildeo sem terem em atenccedilatildeo a sua
relaccedilatildeo com o aumento dos efeitos adversos Isto eacute uma situaccedilatildeo insustentaacutevel na
medida em que nas uacuteltimas duas deacutecadas alguns destes medicamentos foram retirados
do mercado devido a eventos adversos graves posteriormente descobertos Um exemplo
eacute o caso do rofecoxib e valdecoxib que produziram acidentes cardiovasculares seacuterios
provavelmente consequentes da dosagem e natildeo da sua selectividade para a COX-2
(25))
Os efeitos adversos satildeo um motivo de peso para que os pacientes deixem de
tomar determinada substacircncia ou sejam incapazes de tolerar uma dose eficaz da mesma
Informaccedilotildees complementares que englobassem este aspecto seriam ideais e exequiacuteveis
se os autores de ensaios cliacutenicos lhes dessem maior relevo (45)
Outros dados - como custo financeiro e disponibilidade no mercado - poderiam
ser um auxiacutelio na selecccedilatildeo entre paracetamol e outros medicamentos Eacute de ressalvar
que em Portugal os geneacutericos vieram a baixar os preccedilos de analgeacutesicos e NSAIDrsquos
Medicamentos agrave base de ibuprofeno satildeo dos mais dispendiosos (46)
Os NSAIDrsquos tecircm um problema adicional relacionado com a hemostase ndash inibir a
produccedilatildeo de tromboxano A2 e consequentemente aumentar o risco de hemorragia
prolongada (11) No entanto estes efeitos secundaacuterios estatildeo directamente relacionados
com a dosagem pelo que apenas eacute relevante considerar este aspecto em paciente com
problemas de coagulaccedilatildeo
54
Conclui-se que embora a toma de paracetamol seja um procedimento seguro e
eficaz existem no mercado compostos com igual seguranccedila e eficaacutecia superior Apesar
de os inibidores da COX-2 serem os compostos mais eficazes abarcam os efeitos
secundaacuterios mais graves pelo que a realizaccedilatildeo de estudos adicionais eacute imperativo no
sentido de colmatar esta falha
55
RESPOSTA AO PACIENTE
ldquoTendo em conta a evidecircncia cientiacutefica disponiacutevel sobre este assunto e
considerando que natildeo tem problemas gaacutestricos ou de coagulaccedilatildeo sanguiacutenea recomendo
que tome 1g de paracetamol de 8 em 8 horas pois eacute bastante eficaz no aliacutevio da dor
Poreacutem existem outras opccedilotildees como por exemplo combinar o paracetamol a 200mg de
ibuprofeno pode ainda apenas tomar o paracetamol e se sentir necessidade recorrer ao
ibuprofeno 400mg no maacuteximo trecircs vezes ao dia
Tanto o paracetamol como o ibuprofeno tecircm poucos efeitos secundaacuterios e os
mais frequentes satildeo de baixo grau de gravidade Embora existam outros medicamentos
mais eficazes na eliminaccedilatildeo da dor estes tecircm efeitos secundaacuterios mais graves que natildeo
justificam a sua utilizaccedilatildeo
56
REFEREcircNCIAS BIBLIOGRAacuteFICAS
1 Barden J Edwards JE McQuay HJ Andrew Moore R Pain and analgesic
response after third molar extraction and other postsurgical pain Pain 2004107(1-
2)86-90 Epub 20040113
2 Cooper SA Desjardins PJ The value of the dental impaction pain model in drug
development Methods in molecular biology (Clifton NJ) 2010617175-90 Epub
20100326
3 NICE Guidance on the Extraction of Wisdom Teeth2000 13 December 2011
Available from httppublicationsniceorgukguidance-on-the-extraction-of-wisdom-
teeth-ta1clinical-need-and-practice
4 Mettes Dirk TG Nienhuijs Marloes MEL van der Sanden Wil JM Verdonschot
Emiel H Plasschaert A Interventions for treating asymptomatic impacted wisdom teeth
in adolescents and adults Cochrane Database of Systematic Reviews [Internet] 2005
(2) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD003879frameht
ml
5 Seymour RA Use of analgesics in postoperative dental pain a review Journal
of the Royal Society of Medicine 198477(11)949-54 Epub 19841101
6 Berg JM Tymoczko JL Stryer L Biochemistry 5 ed W H Freeman 2002
1050 p
7 Nelson DL Cox MM Lehninger Principles of Biochemistry 5 ed W H
Freeman 2005 1119 p
8 Sciulli MG Capone ML Tacconelli S Patrignani P The future of traditional
nonsteroidal antiinflammatory drugs and cyclooxygenase-2 inhibitors in the treatment
of inflammation and pain Pharmacological reports PR 200557 Suppl66-85 Epub
20060118
9 Devlin TD Devlins Textbook of Biochemistry 6 ed Hoboken NJ Wiley
2006 1208 p
10 Katzung BG Basical and Clinical Pharmacology 10 ed McGraw-Hill 2006
11 Naclerio-Homem Mg Fau - Deboni MCZ Deboni Mc Fau - Rapoport A
Rapoport A Fau - Chin VKL Chin VK Effects of ketoprofen and diclofenac potassium
on blood coagulation tests after removal of third molars (1936-7163 (Electronic))
57
12 Toms L McQuay H Derry S Moore R Single dose oral paracetamol
(acetaminophen) for post-operative pain in adults Cochrane Database of Systematic
Reviews 2008(4)
13 Merry AF Gibbs RD Edwards J Ting GS Frampton C Davies E et al
Combined acetaminophen and ibuprofen for pain relief after oral surgery in adults a
randomized controlled trial British journal of anaesthesia 2010104(1)80-8 Epub
20091217
14 Derry C Derry S Moore R McQuay H Single Dose Oral Ibuprofen for Acute
Post-Operative Pain in Adults Cochrane Database of Systematic Reviews 2009(3)
15 Rang HP Dale MM Ritter JM Moore PK Farmacologia 5 ed Elsevier 2003
Elsevier p
16 Scopel E Alencar M Cruz RM Medidas de avaliaccedilatildeo da dor efdeportes
2007(105)
17 Mata AD Marques D Silveira J Marques J Medicina Dentaacuteria Baseada na
Evidecircncia Novas Opccedilotildees para Velhas Praacuteticas Rev Port Estomatol Cir Maxilofac
200849(1)31-7
18 CASP UK [13 Dezembro 2011] Available from httpwwwcasp-
uknetabout-caspabout-casp
19 Weil K Hooper L Afzal Z Esposito M Worthington Helen V van Wijk A et
al Paracetamol for pain relief after surgical removal of lower wisdom teeth Cochrane
Database of Systematic Reviews [Internet] 2007 (3) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD004487frameht
ml
20 Toms L Derry S Moore RA McQuay Henry J Single dose oral paracetamol
(acetaminophen) with codeine for postoperative pain in adults Cochrane Database of
Systematic Reviews [Internet] 2009 (1) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD001547frameht
ml
21 Derry S Wiffen PJ Moore RA Relative efficacy of oral analgesics after third
molar extraction - a 2011 update Br Dent J 2011211(9)419-20
22 Seymour RA Hawkesford JE Sykes J Stillings M Hill CM An investigation
into the comparative efficacy of soluble aspirin and solid paracetamol in postoperative
pain after third molar surgery Br Dent J 2003194(3)153-7
58
23 Barden J Edwards JE McQuay HJ Wiffen PJ Moore RA Relative efficacy of
oral analgesics after third molar extraction Br Dent J 2004197(7)407-11
24 Saska S Scartezini GR Souza RFd Hochuli-Vieira E Pereira Filho VA
Gabrielli MAC Cloridrato de tramadolparacetamol no controle da dor poacutes-operatoacuteria
em cirurgias de terceiros molares inclusos
Tramadolacetaminophen in the control of postoperative pain for impacted third molar
surgery Rev cir traumatol buco-maxilo-fac 20099(4)
25 Haglund B von Bultzingslowen I Combining paracetamol with a selective
cyclooxygenase-2 inhibitor for acute pain relief after third molar surgery a randomized
double-blind placebo-controlled study European journal of oral sciences
2006114(4)293-301 Epub 20060817
26 Kubitzek F Ziegler G Gold MS Liu JM Ionescu E Analgesic efficacy of low-
dose diclofenac versus paracetamol and placebo in postoperative dental pain Journal of
orofacial pain 200317(3)237-44 Epub 20031003
27 Bjornsson GA Haanaes HR Skoglund LA A randomized double-blind
crossover trial of paracetamol 1000 mg four times daily vs ibuprofen 600 mg effect on
swelling and other postoperative events after third molar surgery British journal of
clinical pharmacology 200355(4)405-12 Epub 20030419
28 Macleod AG Ashford B Voltz M Williams B Cramond T Gorta L et al
Paracetamol versus paracetamol-codeine in the treatment of post-operative dental pain
a randomized double-blind prospective trial Australian dental journal
200247(2)147-51 Epub 20020726
29 Bjornsson GA Haanaes HR Skoglund LA Ketoprofen 75 mg qid versus
acetaminophen 1000 mg qid for 3 days on swelling pain and other postoperative events
after third-molar surgery Journal of clinical pharmacology 200343(3)305-14 Epub
20030318
30 Chopra D Rehan HS Mehra P Kakkar AK A randomized double-blind
placebo-controlled study comparing the efficacy and safety of paracetamol
serratiopeptidase ibuprofen and betamethasone using the dental impaction pain model
International journal of oral and maxillofacial surgery 200938(4)350-5 Epub
20090127
31 Dolci G Ripari M Pacifici L Umile A Evaluation of piroxicam-beta-
cyclodextrin piroxicam paracetamol and placebo in post-operative oral surgery pain
59
International journal of clinical pharmacology research 199414(5-6)185-91 Epub
19940101
32 Noronha VR Gurgel GD Alves LC Noman-Ferreira LC Mendonca LL Aguiar
EG et al Analgesic efficacy of lysine clonixinate paracetamol and dipyrone in lower
third molar extraction a randomized controlled trial Medicina oral patologia oral y
cirugia bucal 200914(8)e411-5 Epub 20090506
33 Daniels S Reader S Berry P Goulder M Onset of analgesia with sodium
ibuprofen ibuprofen acid incorporating poloxamer and acetaminophen--a single-dose
double-blind placebo-controlled study in patients with post-operative dental pain
European journal of clinical pharmacology 200965(4)343-53 Epub 20090303
34 Medve RA Wang J Karim R Tramadol and acetaminophen tablets for dental
pain Anesthesia progress 200148(3)79-81 Epub 20011129
35 Bjornsson GA Haanaes HR Skoglund LA Naproxen 500 mg bid versus
acetaminophen 1000 mg qid effect on swelling and other acute postoperative events
after bilateral third molar surgery Journal of clinical pharmacology 200343(8)849-58
Epub 20030905
36 Marques JF Marques D Silveira J Mata AD Revisotildees Sistemaacuteticas o que satildeo
e para que servem Rev Port Estomatol Cir Maxilofac 200849(3)171-8
37 Rodrigues CL Ziegelmann PK Meta-anaacuteliseum guia praacutetico HCPA
201030(4)436-47
38 Alderson P Absence of evidence is not evidence of absence Bmj
2004328(7438)476-7
39 Berwanger O Suzumura EA Buehler AM Oliveira JB Como Avaliar
Criticamente Revisotildees Sistemaacuteticas e Meta-anaacutelises Revista Brasileira de Terapia
Intensiva 200719(4)475-80
40 Noordzij M Zoccali C Dekker FW Jager KJ Adding up the evidence
systematic reviews and meta-analyses Nephron Clinical practice 2011119(4)c310-6
Epub 20111203
41 Sibbald B Roland M Understanding controlled trials Why are randomised
controlled trials important Bmj 1998316(7126)201
42 Primer on Statistical Significance and P Values Effective Clinical Practice
20014(4)183-4
43 Efird J Blocked randomization with randomly selected block sizes International
journal of environmental research and public health 20118(1)15-20 Epub 20110215
60
44 Cooper S Schachtel B Goldman E Gelb S Cohn P Ibuprofen and
acetaminophen in the relief of acute pain a randomized double blind placebo
controlled study The Journal of Clinical Pharmacology 198929(11)1026-30
45 Edwards JE McQuay HJ Moore RA Collins SL Reporting of Adverse Effects
in Clinical Trials Should Be Improved Lessons from Acute Postoperative Pain Journal
of pain and symptom management 199918(6)427-37
46 Faacutermaco mais vendido versus mais barato Deco Proteste [updated Julho
200919 Dezembro 2011] Available from httpwwwdecoprotesteptservicos-de-
saudefarmaco-mais-vendido-versus-mais-barato-s568081htm
61
ANEXOS
ANEXO A ndash TABELA DE CARACTERIacuteSTICAS DE ARTIGOS EXCLUIacuteDOS
Artigo Fonte Classificaccedilatildeo
inicial Motivo de Exclusatildeo
Toms Derry (20) Cochrane
Library
Possivelmente
Adequado
Natildeo eacute um estudo sobre
extracccedilatildeo de terceiros molares
Saska Scartezini
(24) LILACS
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (27) PubMed Adequado
Estudo natildeo se foca na dor poacutes-
operatoacuteria
Kubitzek Ziegler
(26) PubMed Adequado Artigo natildeo disponiacutevel
Macleod
Ashford (28) PubMed Adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (29) PubMed
Possivelmente
adequado Artigo natildeo disponiacutevel
Chopra Rehan
(30) PubMed
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Dolci Ripari (31) PubMed Possivelmente
adequado Artigo natildeo disponiacutevel
Medve Wang
(34) PubMed
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (35) PubMed
Possivelmente
adequado Artigo natildeo disponiacutevel
62
ANEXO B ndash ARTIGOS INCLUIacuteDOS EM FORMATO
INTEGRALi
i Nota os seguintes artigos estatildeo paginados fora do contexto deste trabalho de acordo com a sua
paginaccedilatildeo original
Paracetamol for pain relief after surgical removal of lower
wisdom teeth (Review)
Weil K Hooper L Afzal Z Esposito M Worthington HV van Wijk A Coulthard P
This is a reprint of a Cochrane review prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2008 Issue 4
httpwwwthecochranelibrarycom
Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
T A B L E O F C O N T E N T S
1HEADER
1ABSTRACT
2PLAIN LANGUAGE SUMMARY
2BACKGROUND
3OBJECTIVES
3METHODS
5RESULTS
8DISCUSSION
9AUTHORSrsquo CONCLUSIONS
9ACKNOWLEDGEMENTS
10REFERENCES
13CHARACTERISTICS OF STUDIES
30DATA AND ANALYSES
Analysis 11 Comparison 1 50 pain relief using pain relief measures Outcome 1 Paracetamol versus placebo number of
people with at least 50 pain relief at 4 hours 31
Analysis 12 Comparison 1 50 pain relief using pain relief measures Outcome 2 Paracetamol versus placebo number of
people with at least 50 pain relief at 6 hours 33
Analysis 21 Comparison 2 50 pain relief using pain intensity measures Outcome 1 Paracetamol versus placebo number
of people with at least 50 pain relief at 4 hours 34
Analysis 22 Comparison 2 50 pain relief using pain intensity measures Outcome 2 Paracetamol versus placebo number
of people with at least 50 pain relief at 6 hours 35
Analysis 31 Comparison 3 Number of people with adverse events Outcome 1 Number of patients with adverse events
paracetamol versus placebo 37
38ADDITIONAL TABLES
42APPENDICES
43WHATrsquoS NEW
43HISTORY
43CONTRIBUTIONS OF AUTHORS
43DECLARATIONS OF INTEREST
44SOURCES OF SUPPORT
44INDEX TERMS
iParacetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
[Intervention Review]
Paracetamol for pain relief after surgical removal of lowerwisdom teeth
Kiaran Weil1 Lee Hooper2 Zahid Afzal3 Marco Esposito1 Helen V Worthington4 Arjen van Wijk5 Paul Coulthard1
1Department of Oral and Maxillofacial Surgery School of Dentistry The University of Manchester Manchester UK 2School of
Medicine Health Policy amp Practice University of East Anglia Norwich UK 3Oral and Maxillofacial Surgery City Hospital Birming-
ham UK 4Cochrane Oral Health Group MANDEC School of Dentistry The University of Manchester Manchester UK 5Social
Dentistry and Behavioural Sciences ACTA Amsterdam Netherlands
Contact address Kiaran Weil Department of Oral and Maxillofacial Surgery School of Dentistry The University of Manchester
Higher Cambridge Street Manchester M15 6FH UK kiaran_weilhotmailcom
Editorial group Cochrane Oral Health Group
Publication status and date Edited (no change to conclusions) published in Issue 4 2008
Review content assessed as up-to-date 21 May 2007
Citation Weil K Hooper L Afzal Z Esposito M Worthington HV van Wijk A Coulthard P Paracetamol for pain relief af-
ter surgical removal of lower wisdom teeth Cochrane Database of Systematic Reviews 2007 Issue 3 Art No CD004487 DOI
10100214651858CD004487pub2
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Paracetamol has been commonly used for the relief of postoperative pain following oral surgery In this review we investigated the
optimal dose of paracetamol and the optimal time for drug administration to provide pain relief taking into account the side effects
of different doses of the drug This will inform dentists and their patients of the best strategy for pain relief after the surgical removal
of wisdom teeth
Objectives
To assess the beneficial and harmful effects of paracetamol for pain relief after surgical removal of lower wisdom teeth compared to
placebo at different doses and administered postoperatively
Search strategy
We searched the Cochrane Oral Health Grouprsquos Trials Register the Cochrane Pain Palliative and Supportive Care Grouprsquos Trials Register
CENTRAL MEDLINE EMBASE and the Current Controlled Trials Register Handsearching included several dental journals We
checked the bibliographies of relevant clinical trials and review articles for studies outside the handsearched journals We wrote to
authors of the identified randomised controlled trials (RCTs) to manufacturers of analgesic pharmaceuticals we searched personal
references in an attempt to identify unpublished or ongoing RCTs No language restriction was applied The last electronic search was
conducted on 24th August 2006
Selection criteria
Randomised parallel group placebo controlled double blind clinical trials of paracetamol for acute pain following third molar surgery
Data collection and analysis
All trials identified were scanned independently and in duplicate by two review authors any disagreements were resolved by discussion
or if necessary a third review author was consulted The proportion of patients with at least 50 pain relief was calculated for both
paracetamol and placebo The number of patients experiencing adverse events andor the total number of adverse events reported were
analysed
1Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Main results
Twenty-one trials met the inclusion criteria A total of 2048 patients were initially enrolled in the trials (1148 received paracetamol
and 892 the placebo) and of these 1968 (96) were included in the meta-analysis (1133 received paracetamol and 835 the placebo)
Paracetamol provided a statistically significant benefit when compared with placebo for pain relief and pain intensity at both 4 and 6
hours Most studies were found to have moderate risk of bias with poorly reported allocation concealment being the main problem
Risk ratio values for pain relief at 4 hours 285 (95 confidence interval (CI) 189 to 429) and at 6 hours 332 (95 CI 188 to 587)
A statistically significant benefit was also found between up to 1000 mg and 1000 mg doses the higher the dose giving greater benefit
for each measure at both time points There was no statistically significant difference between the number of patients who reported
adverse events overall this being 19 in the paracetamol group and 16 in the placebo group
Authorsrsquo conclusions
Paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom teeth
P L A I N L A N G U A G E S U M M A R Y
Paracetamol for pain relief after surgical removal of lower wisdom teeth
The surgical removal of wisdom teeth (third molars) is the most commonly performed surgical procedure undertaken in oral surgery
practice Postoperative complications may include swelling bruising and limited mouth opening but patients are most often concerned
about postoperative pain which may be severe Paracetamol is effective in relieving pain with a low incidence of adverse effects It is one
of the most commonly used analgesics and is widely available without prescription around the world In this review we investigated the
optimal dose of paracetamol and the optimal time for drug administration to provide pain relief after the surgical removal of wisdom
teeth The side effects of different doses of the drug were also explored
Twenty-one trials (with over 2000 participants) were included Paracetamol provided a statistically significant benefit when compared
with placebo for pain relief at both 4 and 6 hours after taking the drug It is most effective at 1000 mg dose and can be taken at six
hourly intervals without compromising safety There was no statistically significant difference between the number of patients who
reported adverse events overall this being 19 in the paracetamol group and 16 in the placebo group It should be noted that most
of the studies were found to have some limitations mainly due to poor reporting of information However the review concludes that
paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom teeth
B A C K G R O U N D
The surgical removal of wisdom teeth is the most commonly per-
formed surgical procedure undertaken in oral surgery practice
Postoperative complications may include swelling bruising and
limited mouth opening but patients are most often concerned
about postoperative pain which may be severe The pain ex-
perienced after oral surgery is a validated and widely used pain
model for the clinical evaluation of analgesic efficacy (Cooper
1976) Tissue damage produced during surgery releases chemicals
that initiate inflammatory pain by activating and sensitising nerve
fibre receptors (Loeser 1999) Chemicals include bradykinin
prostaglandins serotonin and histamine (Dray 1997)
Paracetamol (acetaminophen) is a nonopioid analgesic possessing
antipyretic activity and is effective in relieving pain with a low in-
cidence of adverse effects (Moore 1998) It is one of the most com-
monly used analgesics and is widely available without prescription
around the world Paracetamol is often grouped with the nons-
teroidal anti-inflammatory drug (NSAID) family however it is
considered only to have relatively weak anti-inflammatory activity
(Rang 2003) NSAIDs are assumed largely to produce their anal-
gesia as a result of the inhibition of prostaglandin production by
the enzyme cyclo-oxygenase (Malmberg 1992) The mechanism
of action has not been fully understood Among several theories
it has been suggested that paracetamol is a selective inhibitor of
the newly described COX-3 enzyme a cyclo-oxygenase-1 variant
in the central nervous system This inhibition could represent a
primary central mechanism by which paracetamol decreases pain
and possibly fever (Chandrasekharan 2002) Major evidence has
2Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
been accumulated showing that paracetamol inhibits cyclo-oxy-
genase by reducing the higher oxidative state of the cyclo-oxyge-
nase enzyme by reducing oxygen radical co-substrates (Aronoff
2006) Paracetamol has been shown to be an effective analgesic in
the control of postoperative dental pain in a number of clinical
trials (Bentley 1987 Kiersch 1994 Mehlisch 1990) Pain inten-
sity following third molar surgery has been suggested to reach its
maximum between 3 to 5 hours following surgery (Fisher 1988
Seymour 1985) and therefore this pain model is used to test the
efficacy of a single analgesic dose
A recent systematic review (Barden J 2004) has looked at the ef-
ficacy and safety of paracetamol for postoperative pain manage-
ment and has included the findings of studies involving a wide
variety of types of surgery such as gynaecology surgery abdomi-
nal surgery orthopaedic surgery amongst others including the re-
moval of wisdom teeth There is some debate as to whether dental
pain is different from other pain It has been suggested that the
effect of some analgesics including tramadol were worse for dental
pain than for other types of postsurgical pain (Moore 1997)
In this review we investigated the optimal dose of paracetamol and
the optimal time for drug administration to provide pain relief
taking into account the side effects of different doses of the drug
This will inform dentists and their patients of the best strategy for
best pain relief after the surgical removal of wisdom teeth
O B J E C T I V E S
To assess the beneficial and harmful effects of paracetamol for
pain relief after surgical removal of lower wisdom teeth compared
to placebo at different doses and administered preoperatively or
postoperatively
Primary
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between paracetamol and placebo for pain
relief in patients requiring surgical removal of a lower wisdom
tooth or teeth against the alternative hypothesis of a difference
Secondary
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between different doses of paracetamol for
pain relief in patients requiring surgical removal of a lower
wisdom tooth or teeth against the alternative hypothesis of a
difference
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between different times of administration of
paracetamol for pain relief in patients requiring surgical removal
of a lower wisdom tooth or teeth against the alternative
hypothesis of a difference
M E T H O D S
Criteria for considering studies for this review
Types of studies
All randomised controlled double blind clinical trials
Types of participants
Patients of all health states who required the surgical removal of
a lower wisdom tooth and who had at least had a baseline pain
intensity of moderate to severe pain Patients who also required
removal of an additional tooth or teeth were included Surgery
was undertaken under local anaesthesia intravenous sedation or
general anaesthesia Patients taking concurrent analgesia were ex-
cluded
Types of interventions
Efficacy
bull Paracetamol given as a single dose by mouth in any dose
and in any formulation (for example immediate or slow release)
regardless of when the single dose was given (for example
preoperatively or postoperatively)
Side effects
In order to investigate side effects more thoroughly we included
both single and multiple dose studies
bull Paracetamol given up to 7 days by mouth in any dose and
in any formulation (for example immediate or slow release)
regardless of when the first dose was given (for example
preoperatively or postoperatively)
Types of outcome measures
bull Pain intensity (visual analogue scale (VAS) categorical
verbal rating verbal numerical scale global subjective efficacy
ratings and other categorical rating scales)
bull Pain relief (VAS categorical verbal rating verbal numerical
scale global subjective efficacy ratings and other categorical
rating scales) and derived pain relief outcomes extracted will be
3Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
total pain relief (TOTPAR) summed pain intensity difference
(SPID) over 4 and 6 hours
bull Side effects (for example hepatic and renal) (binary)
Search methods for identification of studies
To identify studies for inclusion or consideration in this review a
detailed search strategy was developed for each database searched
These were based on the search strategy developed for MEDLINE
but revised appropriately for each database The search strategy
combined a sensitive search strategy for randomised controlled
trials (RCTs) revised from phases 1 and 2 of the Cochrane Sensi-
tive Search Strategy for RCTs (as published in Appendix 5b in the
Cochrane Handbook for Systematic Reviews of Interventions 426
(updated September 2006)) The subject search used a combina-
tion of controlled vocabulary and free text terms based on the
search strategy for searching CENTRAL (see Appendix 1)
Databases to be searched
The Cochrane Oral Health Grouprsquos Trials Register (to 24th August
2006)
The Cochrane Central Register of Controlled Trials (CENTRAL)
(The Cochrane Library 2006 Issue 3)
The Cochrane Pain Palliative and Supportive Care Grouprsquos Trials
Register (to 24th August 2006)
MEDLINE (1966 to 24th August 2006)
EMBASE (1980 to 25th August 2006)
Current Controlled Trials Register (wwwcontrolled-trialscom)
(to 24th August 2006)
The bibliographies of papers and review articles were checked for
studies outside the handsearched journals Personal references were
also searched
Language
There were no language restrictions and where necessary transla-
tion into the English language of relevant studies was conducted
Unpublished studies
Authors of RCTs identified were written to in order to obtain
further information about the trial and to attempt to identify
unpublished or ongoing studies We also wrote to manufacturers
of analgesic pharmaceuticals
Handsearching
Several journals relevant to this review were handsearched as part
of the Cochrane Oral Health Grouprsquos ongoing journal hand-
searching programme The list of the dental journals hand-
searched by The Cochrane Collaboration can be found at http
wwwohgcochraneorg
Data collection and analysis
The titles and abstracts (when available) of all reports identified
were scanned independently and in duplicate by two review au-
thors For studies appearing to meet the inclusion criteria or for
which there were insufficient data in the title and abstract to make
a clear decision the full report was obtained and assessed indepen-
dently and in duplicate by two review authors to establish whether
the studies met the inclusion criteria or not Disagreements were
resolved by discussion Where resolution was not possible a third
review author was consulted All studies meeting the inclusion
criteria then underwent quality assessment and data extracted
Studies rejected at this or subsequent stages were recorded in the
Characteristics of excluded studies table and reasons for exclusion
were recorded
Quality assessment
The quality assessment of the included trials was undertaken inde-
pendently and in duplicate by two review authors based on what
is written in the articles
Only double blind trials were included in the review so blinding
was not included in the quality assessment
Two main quality criteria were examined
(1) Allocation concealment recorded as
(A) Adequate -2 points
(B) Unclear - 1 point
(C) Inadequate - 0 points
(2) Completeness of follow up (is there a clear explanation for
withdrawals and drop outs in each treatment group) assessed as
(A) Yes - 1 point
(B) No - 0 points
The agreement for the quality criteria between assessors was de-
termined by Kappa statistics
After taking into account the additional information provided by
the authors of the trials studies were grouped into the following
categories
(A) Low risk of bias - 3 points (plausible bias unlikely to seriously
alter the results) if all criteria were met
(B) Moderate or high risk of bias - 0 to 2 points Moderate risk
of bias - plausible bias that raises some doubt about the results if
one or more criteria are partly met (for example when authors
responded that they had made some attempts to conceal the al-
location of patients to give an explanation for withdrawals but
these attempts were not judged to be ideal these criteria were cat-
egorised as rsquopartlyrsquo) High risk of bias - plausible bias that seriously
weakens confidence in the results if one or more criteria were not
met as described in the Cochrane Handbook for Systematic Reviews
of Interventions 426
We also reported whether the authors of included trials have con-
ducted a sample size calculation
4Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data extraction
Data were extracted by two review authors independently and
in duplicate using specially designed data extraction forms Any
disagreement was discussed and a third review author consulted
where necessary Authors were contacted for clarification of miss-
ing information Data were excluded until further clarification was
available if agreement could not be reached
For each trial the following data were recorded
bull Year of publication country of origin setting and source of
study funding
bull Details of the participants including demographic
characteristics and criteria for inclusion
bull Details on the study design (parallel group or cross-over
design)
bull Details on the type of intervention
bull Details of the outcomes reported including method of
assessment and time intervals
Data synthesis
From the mean total pain relief (TOTPAR) or summed pain in-
tensity difference (SPID) pain indices reported we computed a
dichotomous outcome variable for the number of patients with
at least 50 pain relief according to the methods outlined in a
Cochrane review (Collins 1999) For each of the three objectives
we examined the appropriateness of different continuous outcome
measurements and these were meta-analysed and reported in the
final review
For dichotomous outcomes the estimate of an intervention was
expressed as risk ratios together with 95 confidence intervals
For continuous outcomes mean differences and 95 confidence
intervals were used to summarise the data for each trial
Clinical heterogeneity was assessed by examining the types of par-
ticipants interventions and outcomes in each study Meta-analyses
were conducted only with studies of similar comparisons report-
ing the same outcome measures Risk ratios were used to combine
dichotomous data and mean differences for continuous data us-
ing random-effects models The significance of any discrepancies
in the estimates of the treatment effects from the different trials
was assessed by means of Cochranrsquos test for heterogeneity and any
heterogeneity investigated
Where both visual analogue scale (VAS) and categorical scales were
used to measure pain intensity or pain relief or both the categorical
data were used in the meta-analysis as this was the most frequently
used scale
Subgroup analyses
Subgroup analyses were planned for studies
bull Where patients underwent surgery with local anaesthesia
alone local anaesthesia and intravenous sedation general
anaesthesia alone and general anaesthesia with local anaesthetic
bull Where different types of formulation of paracetamol were
used for instance immediate release versus slow release
bull Where different doses of paracetamol were used (1000 mg
or more and less than 1000 mg)
bull Where time of administration of paracetamol differs
preoperative versus postoperative
bull Where TOTPAR was calculated using pain relief measures
and pain intensity measures
The difference between studies comparing up to 1000 mg doses
with studies comparing 1000 mg or more was examined by per-
forming random-effects metaregression analyses in Stata version
90 (Stata Corporation USA) using the program Metareg
The results of the metaregressions for comparing the two dose
levels up to 1000 mg and 1000 mg or more are presented in
Additional Table 1
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
See Characteristics of included studies and Characteristics of
excluded studies tables
Characteristics of the trial setting and investigators
Of the 67 eligible trials 46 were excluded as shown in the ex-
cluded studies section Of the 21 included studies one was con-
ducted in Denmark (Moller 2000) two in Germany (Kubitzek
2003 Lehnert 1990) one in Italy (Dolci 1994) one in Nor-
way (Skoglund 1991) two in Puerto Rico (Olson 2001 Sunshine
1986) one in Thailand (Vattaraphudej 1986) two in the United
Kingdom (Seymour 1996 Seymour 2003) and 11 in the United
States of America (Cooper 1980 Cooper 1981 Cooper 1988
Cooper 1998 Dionne 1994 Forbes 1984b Forbes 1989 Forbes
1990 Hersh 2000 Kiersch 1994 Mehlisch 1995) Six trials
were conducted at university clinics (Cooper 1998 Hersh 2000
Moller 2000 Olson 2001 Sunshine 1986 Vattaraphudej 1986)
five at private practices (Dionne 1994 Forbes 1984b Forbes
1989 Forbes 1990 Kubitzek 2003) seven did not state a set-
ting (Cooper 1981 Dolci 1994 Kiersch 1994 Mehlisch 1995
Seymour 1996 Seymour 2003 Skoglund 1991) One reported a
single site (Cooper 1988) two reported two sites (Forbes 1989
Seymour 2003) and six specifically stated outpatients (Cooper
1980 Cooper 1988 Forbes 1989 Forbes 1990 Hersh 2000
5Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Lehnert 1990) Seventeen trials were sponsored by industry
(Cooper 1981 Cooper 1988 Cooper 1998 Dionne 1994 Forbes
1984b Forbes 1989 Forbes 1990 Hersh 2000 Kiersch 1994
Kubitzek 2003 Lehnert 1990 Mehlisch 1995 Moller 2000
Olson 2001 Seymour 2003 Skoglund 1991 Sunshine 1986)
one by a university grant (Vattaraphudej 1986) and it was unclear
as whether the remaining three trials (Cooper 1980 Dolci 1994
Seymour 1996) were sponsored but it is likely that they were from
correspondence with some of the authors
Characteristics of interventions
All included interventions were randomised parallel group and
double blind Eleven trials used doses of paracetamol of less than
1000 mg (Cooper 1980 Cooper 1981 Cooper 1988 Dionne
1994 Dolci 1994 Forbes 1984b Forbes 1989 Forbes 1990
Seymour 1996 Sunshine 1986 Vattaraphudej 1986) Eleven tri-
als used doses of 1000 mg (Cooper 1998 Hersh 2000 Kiersch
1994 Kubitzek 2003 Lehnert 1990 Mehlisch 1995 Moller
2000 Olson 2001 Seymour 1996 Seymour 2003 Skoglund
1991) One study (Seymour 1996) used both doses Seven tri-
als used paracetamol in tablet form (Dolci 1994 Forbes 1989
Kubitzek 2003 Mehlisch 1995 Moller 2000 Seymour 2003
Skoglund 1991) Seven trials used capsules (Forbes 1984b Forbes
1989 Forbes 1990 Kiersch 1994 Lehnert 1990 Sunshine 1986
Vattaraphudej 1986) Two trials used caplets (Hersh 2000 Olson
2001) and one trial used effervescent tablets (Moller 2000) Five
trials did not state what formulation was used (Cooper 1980
Cooper 1981 Cooper 1988 Cooper 1998 Dionne 1994) All
trials used placebos in the same formulation as the intervention
Characteristics of outcome measures
For all trials it was possible to calculate the number of patients
with at least 50 total pain relief (TOTPAR) at either 4 hours
6 hours or both Pain intensity was measured in all but one trial
(Kubitzek 2003) pain relief was measured in all but two trials
(Kubitzek 2003 Seymour 2003) Kubitzek 2003 gave a figure for
TOTPAR at six hours and Seymour 2003 measured pain intensity
only Fifteen trials measured pain intensity at 4 hours using a 4-
point categorical scale of 0 to 3 where 0 was no pain at all and 3
was severe pain Five trials measured pain intensity using a visual
analogue scale (VAS) of 0 to 100 mm where 0 was no pain and
100 was the worst pain imaginable Twelve trials measured pain
intensity at 6 hours using a 4-point categorical scale where 0 was
no pain and 3 was severe pain and three trials measured pain
intensity at 6 hours using a VAS of 0 to 100 mm where 0 was no
pain and 100 mm was the worst pain imaginable Sixteen trials
measured pain relief at 4 hours using a 5-point categorical scale
of 0 to 4 where 0 was none and 4 was complete pain relief two
trials measured pain relief at 4 hours using a VAS of 0 to 100 mm
in one trial 0 was none and 100 was complete relief and in the
other trial 0 was complete relief and 100 was no relief (these data
were reversed for statistical purposes) Twelve trials measured pain
relief at 6 hours using a 5-point categorical scale of 0 to 4 where
0 was none and 4 was complete pain relief two trials measured
pain relief at 6 hours using a VAS of 0 to 100 mm in one trial 0
was none and 100 was complete relief and in the other trial 0 was
complete relief and 100 was no relief (these data were reversed for
statistical purposes)
Adverse events and global assessments were recorded in most of
the trials Nineteen trials reported the number of patients with
side effects eight for doses of 1000 mg or more and 15 for doses
of less than 1000 mg Fifteen trials reported the number of adverse
events seven for doses of 1000 mg or more and eight for doses
of less than 1000 mg Fourteen trials recorded global assessment
using a 5-point categorical scale of either 0 to 4 or 1 to 5 where
0 or 1 was poor and 4 or 5 was excellent and four trials used a
4-point categorical scale of 0 to 3 where 0 was poor and 3 was
excellent
Risk of bias in included studies
Details of the quality assessment are presented in Additional Table
2 Seven out of the 21 studies reported adequate concealed al-
location for the remaining studies it was unclear Over half of
the studies (1121) gave clear explanation of withdrawals or drop
outs Taking these two factors into account only three trials were
assessed as being at low risk of bias
Effects of interventions
Comparison 1 Paracetamol versus placebo using
pain relief measurements
(Comparison 1 Outcome 11 amp Comparison 1 Outcome 12)
(Analysis 11 Analysis 12)
There are 16 studies providing pain relief measurements for com-
paring paracetamol versus placebo at 4 hours 11 at doses up to
1000 mg and 5 at doses of 1000 mg Overall there was a highly
statistically significant benefit with the paracetamol with risk ratio
(RR) values for achieving 50 pain relief for all doses of parac-
etamol for 4 hours RR 285 (95 confidence interval (CI) 189
to 429) Chi2 = 6294 degrees of freedom (df ) = 15 P lt 0001
I2 = 76 number needed to treat (to benefit) (NNT) 4 (95
CI 3 to 4) The statistically significant benefit was apparent for
both subgroups with RR for up to 1000 mg 196 (95 CI 134
to 286) Chi2 = 2644 df = 9 P = 0002 I2 = 660 NNT 4
(95 CI 3 to 5) and RR for 1000 mg 456 (95 CI 286 to
727) Chi2 = 544 df = 5 P = 036 I2 = 82 NNT 3 (95
CI 3 to 4) Although both had a statistically significant benefit
6Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
over placebo there was a statistically significant difference between
the two subgroups with an enhanced benefit for the higher doses
(metaregression P lt 0001 Additional Table 3) This subgroup
analysis explained some of the heterogeneity in the overall com-
parison however there is still some unexplained heterogeneity be-
tween the trials in the up to 1000 mg dose comparison
There are 13 studies providing pain relief measurements for com-
paring paracetamol versus placebo at 6 hours 6 doses up to 1000
mg paracetamol and 7 doses of 1000 mg paracetamol Overall
there was a highly statistically significant benefit with the parac-
etamol with RR values for 50 pain relief at 6 hours RR 332
(95 CI 188 to 587) Chi2 = 6335 df = 12 P lt 000001 I2 = 811 NNT 3 (95 CI 3 to 4) The statistically significant
benefit was apparent in both subgroups with RR for up to 1000
mg 189 (95 CI 098 to 367) Chi2 = 1445 df = 5 P = 001
I2 = 654 NNT 6 (95 CI 4 to 10) and RR for 1000 mg
421 (95 CI 297 to 598) Chi2 = 509 df = 6 P = 053 I2 =
0 NNT 3 (95 CI 2 to 3) Although both had a statistically
significant benefit over placebo there was a statistically significant
difference between the two subgroups with an enhanced benefit
for the higher doses (metaregression P lt 0001 Additional Table
3) This subgroup analysis explained some of the heterogeneity in
the overall comparison however there is still some unexplained
heterogeneity between the trials in the up to 1000 mg dose com-
parison
Comparison 2 Paracetamol versus placebo using
pain intensity difference measurements
(Comparison 2 Outcome 21 amp Comparison 2 Outcome 22)
(Analysis 21 Analysis 22)
There are 18 studies providing pain intensity measurements for
comparing paracetamol versus placebo at 4 hours 10 at doses up
to 1000 mg and 8 at doses of 1000 mg Overall there was a highly
statistically significant benefit with paracetamol with RR values
for 50 pain relief at 4 hours RR 487 (95 CI 283 to 837)
Chi2 = 4973 df = 17 P lt 00001 I2 = 658 NNT 3 (95 CI
3 to 5) The statistically significant benefit was apparent in both
subgroups with RR up to 1000 mg 433 (95 CI 219 to 858)
Chi2 = 2622 df = 9 P = 0002 I2 = 657 NNT 3 (95 CI
3 to 4) and RR for 1000 mg 646 (95 CI 234 to 1785) Chi2 = 2347 df = 7 P = 0001 I2 = 702 NNT 4 (95 CI 3
to 5) Both had a statistically significant benefit over placebo but
there was no statistically significant difference between the two
subgroups (metaregression P = 067 Additional Table 3)
There are 14 studies providing pain intensity measurements for
comparing paracetamol versus placebo at 6 hours 6 at doses up
to 1000 mg and 8 at doses of 1000 mg Overall there was a highly
statistically significant benefit with paracetamol with RR values
for 50 pain relief RR 341 (95 CI 234 to 497) Chi2 = 1823
df = 13 P = 015 I2 = 287 NNT 4 (95 CI 3 to 4) The
statistically significant benefit was apparent in both groups with
RR up to 1000 mg 267 (95 CI 146 to 490) Chi2 = 705 df
= 5 P = 022 I2 = 291 NNT 5 (95 CI 3 to 7) and RR for
1000 mg 396 (95 CI 252 to 623) Chi2 = 863 df = 7 P =
028 I2 = 189 NNT 3 (95 CI 3 to 4) Both had a statisti-
cally significant benefit over placebo but there was no statistically
significant difference between the two subgroups (metaregression
P = 015 Additional Table 3)
Comparison 3 Number of patients with adverse
events for paracetamol versus placebo
(Comparison 3 Outcome 31) (Analysis 31)
There are 17 studies that reported the number of patients with
adverse events for paracetamol versus placebo 9 studies used less
than 1000 mg and 8 studies used 1000 mg There was no statisti-
cally significant difference in any group For all doses of paraceta-
mol the RR for an adverse event RR 119 (95 CI 090 to 157)
Chi2 = 2073 df = 15 P = 015 I2 = 276 number needed to
treat to harm (NNTH) 33 (95 CI 143 to infinity) For doses of
less than 1000 mg RR 125 (95 CI 069 to 225) Chi2 = 906
df = 7 P = 025 I2 = 228 NNTH 33 (95 CI 143 to infinity)
For 1000 mg paracetamol RR 116 (95 CI 084 to 160) Chi2
= 1096 df = 7 P = 014 I2 = 362 NNTH 33 (95 CI 125
to infinity)
Subgroup analyses
Where patients underwent surgery with local anaesthesia
alone local anaesthesia and intravenous sedation general
anaesthesia alone and general anaesthesia with local
anaesthetic
When the data were reviewed it was not possible to do a meta-anal-
ysis Of the 21 included studies 7 did not state what anaesthesia
was used 7 used combinations of anaesthesia but were unclear in
reporting which patients received which anaesthesia 4 used local
anaesthetic only and 3 used general anaesthetic only
Where different types of formulation of paracetamol were
used (immediate release versus slow release)
Most included studies did not report on the formulation other
than to say whether it was tablets capsules or caplets Only one
7Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
paper indicated that their study used effervescent tablets (Moller
2000) and their results showed that effervescent tablets gave a faster
onset of pain relief Median value for time to onset of analgesia
was 20 minutes in the effervescent group and 45 minutes in the
tablet group and time to meaningful pain relief was 45 minutes
in the effervescent group and 1 hour in the tablet group However
at the end of a 4-hour period pain relief was better in the tablet
group (44) than the effervescent group (37)
Where different doses of paracetamol were used (1000 mg
or more and less than 1000 mg)
This meta-analysis was conducted 11 studies used doses of 1000
mg or more and 11 studies used doses of less than 1000 mg
(Seymour 1996 used both doses)
NNT for lt 1000 mg of paracetamol is 4 (95 CI 3 to 5) at
4 hours and 6 (95 CI 4 to 10) at 6 hours (using pain relief
measurements)
NNT for lt 1000 mg of paracetamol is 3 (95 CI 3 to 4) at 4 hours
and 5 (95 CI 3 to 7) at 6 hours (using intesity measurements)
NNT for 1000 mg of paracetamol is 3 (95 CI 3 to 4) at 4 hours
and 3 (95 CI 2 to 3) at 6 hours (using pain relief measurements)
NNT for 1000 mg of paracetamol is 4 (95 CI 3 to 5) at 4 hours
and 3 (95 CI 3 to 4) at 6 hours (using intensity measurements)
Where time of administration of paracetamol differs
preoperative versus postoperative
No included study used a preoperative dose as the patients did
not reach moderate or severe pain before the intervention
Where total pain relief (TOTPAR) was calculated using pain
relief measures and pain intensity measures
This meta-analysis was undertaken where the relevant data were
available 16 studies had pain relief data and 17 studies had pain
intensity data
NNT using pain relief scales for lt 1000 mg of paracetamol is 4
(95 CI 3 to 5) at 4 hours and 6 (95 CI 4 to 10) at 6 hours
NNT using pain intensity scales for lt 1000 mg of paracetamol is
3 (95 CI 3 to 4) at 4 hours and 5 (95 CI 3 to 7) at 6 hours
NNT using pain relief scales for 1000 mg of paracetamol is 3 (95
CI 3 to 4) at 4 hours and 3 (95 CI 2 to 3) at 6 hours
NNT using pain intensity scales for 1000 mg of paracetamol is 4
(95 CI 3 to 5) at 4 hours and 3 (95 CI 3 to 4) at 6 hours
D I S C U S S I O N
The results show paracetamol to be an effective analgesia for use
following third molar surgery The number needed to treat (to
benefit) (NNTs) and number needed to treat to harm (NNTHs)
support the use of 1000 mg as an optimal dose It is effective over
both 4 and 6 hours In considering the use of pain relief or pain
intensity difference as a measure of efficacy it was of interest that
metaregression showed that pain relief scales showed a statistically
significant difference for increased dose and pain intensity did
not It is acknowledged that this review only considered single
dose studies when considering efficacy multidosed studies may be
considered when updating the review The NNTs and NNTHs
found in this review are similar to those recorded by a systematic
review (Barden J 2004) where they investigated paracetamol for
pain involving various types of surgery This would confirm yet
again the value of the third molar pain model showing that dental
pain is comparable with pain from other sources The implemen-
tation of NICE (National Institute for Health and Clinical Excel-
lence) Guidelines for removal of third molars has led to a decrease
in the performance of this surgery which may have an adverse
effect on the number of trials able to use the third molar model
In the United States of America such guidelines have not yet been
adopted It is of interest that in striving to provide evidence based
treatment the opportunity for research using the third molar pain
model may be adversely affected
The data available for adverse events show that NNTH for lt 1000
mg of paracetamol is 33 (143 to infinity) for 1000 mg of parac-
etamol is 33 (125 to infinity) and for all doses 33 (143 to infin-
ity) suggesting it is an extremely safe drug Only one severe ad-
verse event was recorded by any researchers and that was a severe
headache (Olson 2001) two other participants stopped taking
paracetamol because of vomiting However there was a high degree
of inconsistency across the trials in the way that adverse events were
recorded raising the concern that only adverse events considered
by the researchers to be attributable to paracetamol were recorded
with some trials recording many AEs and some reporting none
The diverse way in which adverse events were recorded led to there
being over 20 categories of adverse events The main categories
are shown in Additional Table 4 Of interest are adverse events
where placebo scored more highly than paracetamol which could
suggest that paracetamol may possibly have a beneficial effect eg
dry socket but this would require further investigation As all pa-
tients had surgery and various combinations of local anaesthesia
general anaesthesia and sedation making it difficult to ascertain
which effects are directly related to the intervention However the
results strongly support the use of paracetamol in doses up to 1000
mg as a safe effective analgesia
8Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
The efficacy of paracetamol decreases with times and the recom-
mended interval between doses is 8 hours which would suggest
there may be some benefit in a slow release formulation None of
the studies in this trial used a slow release formulation but a trial
(Coulthard 2001) compared sustained release and standard release
formulations of paracetamol and found that the sustained release
was statistically significantly more effective at 6 and 8 hours with
no loss of efficacy at 4 hours Safety for both formulations was
comparable making sustained release paracetamol a safe and ef-
fective choice
The methodology used in the included trials was generally good
This resulted in a large number of participants being included
in this meta-analysis while using only double blind randomised
trials The included trials gave a strong consistent result Many
of the trials were done by researchers with extensive experience
in the field of pain research whose methods have been refined
with experience A large proportion of the trials were done in the
United States and were mostly funded by pharmaceutical com-
panies This seems to be reflected in the methodology However
quality assessment showed there were only three trials with a low
risk of bias and 18 with moderatehigh risk This was mainly the
result of unreported allocation concealment methods In speaking
to some of the authors it is highly likely that the allocation con-
cealment was good in all the trials but that the details were not
well reported Most trials were sponsored by pharmaceutical com-
panies who supplied paracetamol and placebo in identical appear-
ance The reporting of withdrawals and drop outs was sporadic
and even when numbers were cited it was not always clear to which
treatment group the participant had been originally allocated
Mean global assessments (Additional Table 5 Table 6 Table 7
Table 8) all showed higher scores for paracetamol than placebo
It is of interest that despite achieving 50 pain relief participants
did not record 50 on a global assessment scale This again raises
the question of the value of the instruments used to measure the
efficacy of an intervention None of the trials relied on global
assessments as their only measure of efficacy but this information
could be of value to other researchers It raises interesting questions
concerning patientrsquos expectations and the difficulties associated
with quantifying such a subjective experience
A lot of valuable information was gathered incidental to the main
findings in most of the trials So though the topic was concerned
with the use of paracetamol for pain information collected in
many of the trials shed valuable light on subjects such as side effects
measuring instruments and methodology Further appraisal of
the multidisciplinary approach to research a broader view of data
collection and a more accurate reporting of data already collected
could be extremely valuable in the future It would allow research
to be more widely used in various meta-analyses Data from areas
seemingly unrelated to the original null hypothesis eg comparison
of pain relief and pain intensity as a measuring tool adverse event
reporting the significance of global assessments etc could be more
readily available If the third molar trial population does decrease
it would be advantageous to collect as much data as possible from
any trial being undertaken
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
Paracetamol (acetaminophen) is an effective drug to use for post-
operative pain following oral surgery and the reporting of adverse
events shows it to be a safe drug (number needed to treat (to ben-
efit) (NNT) is 3 for 1000 mg of paracetamol at 6 hours number
needed to treat to harm (NNTH) 33) It is most effective at 1000
mg dose and can be taken at six hourly intervals without compro-
mising safety It could be considered more readily by dentist and
patients both as a first choice analgesic or to be taken alternately
with doses of other analgesics such as nonsteroidal anti-inflamma-
tory drugs (NSAIDS)
Implications for research
There is a large body of research in this area and further research
other than as a comparison seems unnecessary However in one
trial (Moller 2000) it was found that an effervescent formulation
appeared to have a faster onset of pain relief which would be
beneficial to patients who are looking for a rapid onset of relief
It may be helpful to undertake some research to confirm these
findings The use of pain relief and pain intensity difference as a
measure of pain relief may be another area for further investigation
It is valuable to have NNTNNTH as a baseline for comparison
with other analgesics Maximizing the third molar pain model
population by multidisciplinary research is another area of interest
highlighted by this review
A C K N O W L E D G E M E N T S
We wish to thank Sylvia Bickley (Cochrane Oral Health Group)
for her assistance with literature searching and Luisa Fernandez
Mauleffinch (Cochrane Oral Health Group) for her help with the
preparation of this review We would also like to thank the follow-
ing referees who reviewed this work at various stages Barry El-
liott Cole Mike Hill Kimito Yamashiro and Lasse Skoglund We
are grateful to Stephen Cooper Donald Mehlisch Philip Moller
Alberto Umile for providing information on their trials and to
Prisana Pripatnanont for translation and information
9Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Cooper 1980 published data only
Cooper SA Precheur H Rauch D Rosenheck A Ladov M
Engel J Evaluation of oxycodone and acetaminophen in
treatment of postoperative dental pain Oral Surgery Oral
Medicine and Oral Pathology 198050(6)496ndash501
Cooper 1981 published data only
Cooper SA Breen JF Giuliani RL The relative efficacy of
indoprofen with opiod-analgesic combinations Journal of
Oral Surgery 198139(1)21ndash5
Cooper 1988 published data only
Cooper SA Firestein A Cohn P Double-blind comparison
of meclofenamate sodium with acetaminophen
acetaminophen with codeine and placebo for relief of
postsurgical dental pain The Journal of Clinical Dentistry
19881(2)31ndash4
Cooper 1998 published data only
Cooper SA Reynolds DC Reynolds B Hersh EV Analgesic
efficacy and safety of (R)- ketoprofen in postoperative dental
pain Journal of Clinical Pharmacology 199838(2 Suppl)
11Sndash18S
Dionne 1994 published data only
Dionne RA Snyder J Hargreaves KM Analgesic efficacy
of flurbiprofen in comparison with acetaminophen
acetaminophen plus codeine and placebo after impacted
third molar removal Journal of Oral and Maxillofacial
Surgery 199452(9)919ndash24
Dolci 1994 published data only
Dolci G Ripari M Pacifici L Umile A Evaluation of
piroxicam-beta-cyclodextrin piroxicam paracetamol and
placebo in post-operative oral surgery pain International
Journal of Clinical Pharmacology Research 199414(5-6)
185ndash91
Forbes 1984b published data only
Forbes JA Barkaszi BA Ragland RN Hankle JJ
Analgesic effect of acetaminophen phenyltoloxamine
and their combination in postoperative oral surgery pain
Pharmacotherapy 19844(4)221ndash6
Forbes 1989 published data only
Forbes JA Butterworth GA Burchfield WH Yorio
CC Selinger LR Rosenmertz SK et alEvaluation of
flurbiprofen acetaminophen an acetaminophen-codeine
combination and placebo in postoperative oral surgery
pain Pharmacotherapy 19899(5)322ndash30
Forbes 1990 published data only
Forbes JA Kehm CJ Grodin CD Beaver WT Evaluation
of ketorolac ibuprofen acetaminophen and an
acetaminophen-codeine combination in postoperative
oral surgery pain Pharmacotherapy 199010(6(Pt 2)))
94Sndash105S
Hersh 2000 published data only
Hersh EV Levin LM Cooper SA Doyle G Waksman J
Wedell D et alIbuprofen liquigel for oral surgery pain
Clinical Therapeutics 200022(11)1306ndash18
Kiersch 1994 published data only
Kiersch TA Halladay SC Hormel PC A single-
dose double-blind comparison of naproxen sodium
acetaminophen and placebo in postoperative dental pain
Clinical Therapeutics 199416(3)394ndash404
Kubitzek 2003 published data only
Kubitzek F Ziegler G Gold MS Liu JM Ionescu E
Analgesic efficacy of low-dose diclofenac versus paracetamol
and placebo in postoperative dental pain Journal of
Orofacial Pain 200317(3)237ndash44
Lehnert 1990 published data only
Lehnert S Reuther J Wahl G Barthel K [The efficacy of
paracetamol (Tylenol) and acetyl salicylic acid (Aspirin)
in treating postoperative pain] Deutsche Zahnarztliche
Zeitschrift 199045(1)23ndash6
Mehlisch 1995 published data only
Mehlisch DR Jasper RD Brown P Korn SH McCarroll K
Murakami AA Comparative study of ibuprofen lysine and
acetaminophen in patients with postoperative dental pain
Clinical Therapeutics 199517(5)852ndash60
Moller 2000 published data only
Moller PL Norholt SE Ganry HE Insuasty JH Vincent
FG Skoglund LA et alTime of onset of analgesia and
analgesic efficacy of effervescent acetaminophen 1000
mg compared to tablet acetominophen 1000 mg in
postoperative dental pain a single-dose double-blind
randomized placebo-controlled study Journal of Clinical
Pharmacology 200040(4)370ndash8
Olson 2001 published data only
Olson NZ Otero AM Marrero I Tirado S Cooper S
Doyle G et alOnset of analgesia for liquigel ibuprofen
400 mg acetaminophen 1000 mg ketoprofen 25 mg
and placebo in the treatment of postoperative dental pain
Journal of Clinical Pharmacology 200141(11)1238ndash47
Seymour 1996 published data only
Seymour RA Kelly PJ Hawkesford JE The efficacy
of ketoprofen and paracetamol (acetaminopen) in
postoperative pain after third molar surgery British Journal
of Clinical Pharmacology 199641(6)581ndash5
Seymour 2003 published data only
Seymour RA Hawkesford JE Sykes J Stillings M Hill
CM An investigation into the comparative efficacy of
soluble aspirin and solid paracetamol in postoperative pain
after third molar surgery British Dental Journal 2003194
(3)153ndash7
Skoglund 1991 published data only
Skoglund LA Skjelbred P Fyllingen G Analgesic efficacy
of acetaminophen 1000 mg acetaminophen 2000 mg and
the combination of acetaminophen 1000 mg and codeine
10Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
phosphate 60 mg versus placebo in acute postoperative
pain Pharmacotherapy 199111(5)364ndash9
Sunshine 1986 published data only
Sunshine A Marrero I Olson N McCormick N Laska
EM Comparative study of flurbiprofen zomepirac sodium
acetaminophen plus codeine and acetaminophen for the
relief of postsurgical dental pain The American Journal of
Medicine 198680(3A)50ndash4
Vattaraphudej 1986 published data only
Vattaraphudej T Thongnoppakao P Koukongviriyapan V
[Comparison of the efficacy of analgesics in pain after oral
surgery] The Journal of the Dental Association of Thailand
198636(6)198ndash206
References to studies excluded from this review
Adame 1979 published data only
Adame C et alPostoperative development of inflammation
after extraction of impacted third molar as a model
for clinical assessment of anti-inflammatory drugs I
Preliminary report Boletin de Estudios Medicos y Biologicos
197930(8)308ndash9
Barden J 2004 published data only
Barden J Edwards J Moore A McQuay H Single dose
oral paracetamol (acetaminophen) for postoperative pain
Cochrane Database of Systematic Reviews 2004 Issue 1
[DOI DOI 10100214651858CD004602]
Becker 1990 published data only
Becker J Beckmann J Bertelt C Gundert-Remy U
Rohmel J Ohlendorf D [Double blind biometric study on
postoperative effects of analgesics] Deutsche Zahnarztliche
Zeitschrift 199045(1)36ndash8
Bentley 1987 published data only
Bentley KC Head TW The additive analgesic efficacy of
acetaminophen 1000 mg and codeine 60 mg in dental
pain Clinical Pharmacology and Therapeutics 198742(6)
634ndash40
Breivik 1998 published data only
Breivik EK Bjornsson GA Variation in surgical trauma and
baseline pain intensity effects on assay sensitivity of an
analgesic trial European Journal of Oral Sciences 1998106
(4)844ndash52
Cooper 1986 published data only
Cooper SA Erlichman MC Mardirossian G Double-
blind comparison of an acetaminophen-codeine-caffeine
combination in oral surgery pain Anesthesia Progress 1986
33(3)139ndash42
Cooper 1989 published data only
Cooper SA Schachtel BP Goldman E Gelb S Cohn P
Ibuprofen and acetaminophen in the relief of acute pain
a randomized double-blind placebo-controlled study
Journal of Clinical Pharmacology 198929(11)1026ndash30
Cooper 1991 published data only
Cooper SA Kupperman A The analgesic efficacy of
flurbiprofen compared to acetaminophen with codeine The
Journal of Clinical Dentistry 19912(3)70ndash4
Dionne 1983 (1) published data only
Dionne RA Campbell RA Cooper SA Hall DL
Buckingham B Suppression of postoperative pain by
preoperative administration of ibuprofen in comparison to
placebo acetaminophen and acetaminophen plus codeine
Journal of Clinical Pharmacology 198323(1)37ndash43
Dionne 1983 (2) published data only
Dionne RA Sisk AL Fox PC Wirdzek PR Gracely
RH Dubner R Suppression of postoperative pain by
preoperative adminsitration of flurbiprofen in comparison
to acetominophen and oxycodone plus acetominophen
Current Therapeutic Research 198334(1)15ndash29
Dionne 1986 published data only
Dionne RA Suppression of dental pain by the preoperative
administration of flurbiprofen The American Journal of
Medicine 198680(3A)41ndash9
Dolci 1993 published data only
Dolci G Ripari M Pacifici L Umile A [Analgesic efficacy
and the tolerance for piroxicam-beta-cyclodextrin compared
to piroxicam paracetamol and placebo in the treatment of
postextraction dental pain] Minerva Stomatologica 199342
(5)235ndash41
Edwards 2002 published data only
Edwards JE McQuay HJ Moore RA Combination
analgesic efficacy individual patient data meta-analysis
of single-dose oral tramadol plus acetaminophen in
acute postoperative pain Journal of Pain and Symptom
Management 200223(2)121ndash30
Forbes 1982 published data only
Forbes JA Beaver WT White EH White RW Neilson GB
Shackleford RW Diflunisal A new oral analgesic with an
unusually long duration of action JAMA 1982248(17)
2139ndash42
Forbes 1984a published data only
Forbes JA Kolodny AL Chachich BM Beaver WT
Nalbuphine acetaminophen and their combination in
postoperative pain Clinical Pharamacology and Therapeutics
198435(6)843ndash51
Gallardo 1990 published data only
Gallardo F Rossi E Analgesic efficacy of flurbiprofen as
compared to acetaminophen and placebo after periodontal
surgery Journal of Periodontology 199061(4)224ndash7
Gustafsson 1983 published data only
Gustafsson I Nystrom E Quiding H Effect of preoperative
paracetamol on pain after oral surgery European Journal of
Clinical Pharmacology 198324(1)63ndash5
Haanaes 1986 published data only
Haanaes HR Benterud UJ Skoglund LA RF 46-790 versus
paracetamol effect on post-operative pain International
Journal of Clinical Pharmacology Therapy and Toxicology
198624(11)598ndash601
Irvine 1982 published data only
Irvine GH Lutterloch MJ Bowerman JE Comparison
of diflunisal and paracetamol in the management of pain
11Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
following wisdom teeth removal British Dental Journal
1982152(1)18ndash20
Laska 1983 published data only
Laska EM Sunshine A Zighelboim I Roure C Marrero
I Wanderling J et alEffect of caffeine on acetaminophen
analgesia Clinical Pharmacology and Therapeutics 198333
(4)498ndash509
Lecointre 1991 published data only
Lecointre C [Efficacy and tolerance of tiaprofenic acid
for extraction complications Results of a randomized
double-blind study tiaprofenic acid versus paracetamol]
LrsquoInformation Dentaire 199173(35)3063ndash6
Liashek 1987 published data only
Liashek P Jr Desjardins PJ Triplett RG Effect of
pretreatment with acetaminophen-propoxyphene for oral
surgery pain Journal of Oral and Maxillofacial Surgery 1987
45(2)99ndash103
Macleod 2002 published data only
Macleod AG Ashford B Voltz M Williams B Cramond T
Gorta L et alParacetamol versus paracetamol-codeine in
the treatment of post-operative dental pain a randomized
double-blind prospective trial Australian Dental Journal
200247(2)147ndash51
Medve 2001 published data only
Medve RA Wang J Karim R Tramadol and acetaminophen
tablets for dental pain Anesthesia Progress 200148(3)
79ndash81
Mehlisch 1984 published data only
Mehlisch DR Frakes LA A controlled comparative
evaluation of acetaminophen and aspirin in the treatment of
postoperative pain Clinical Therapeutics 19847(1)89ndash97
Mehlisch 1990 published data only
Mehlisch DR Sollecito WA Helfrick JF Leibold DG
Markowitz R Schow CE Jr et alMulticenter clinical
trial of ibuprofen and acetaminophen in the treatment of
postoperative dental pain Journal of the American Dental
Association 1990121(2)257ndash63
Moore 1986 published data only
Moore PA Werther JR Seldin EB Stevens CM Analgesic
regimens for third molar surgery pharmacologic and
behavioral considerations Journal of the American Dental
Association 1986113(5)739ndash44
Nystrom 1988 published data only
Nystrom E Gustafsson I Quiding H The pain intensity
at analgesic intake and the efficacy of diflunisal in single
doses and effervescent acetaminophen in single and repeated
doses Pharmacotherapy 19888(3)201ndash9
Petersen 1983 published data only
Petersen JK A double-blind cross-over study of the analgesic
and anti-inflammatory effects of dexamethasone and
paracetamol following surgical removal of lower impacted
third molars International Journal of Oral Surgery 198312
(4)266
Quiding 1981 published data only
Quiding H Oksala E Happonen RP Lehtimaki K Ojala
T The visual analog scale in multiple-dose evaluations of
analgesics The Journal of Clinical Pharmacology 198121
(10)424ndash9
Quiding 1982 (1) published data only
Quiding H Oikarinen V Huitfeldt B Koskimo M
Leikomaa H Nyman C An analgesic study with repeated
doses of phenazone phenazone plus dextropropoxyphene
and paracetamol using a visual analogue scale International
Journal of Oral Surgery 198211(5)304ndash9
Quiding 1982 (2) published data only
Quiding H Persson G Ahlstrom U Bangens S Hellem S
Johansson G et alParacetamol plus supplementary doses
of codeine an analgesic study of repeated doses European
Journal of Clinical Pharmacology 198223(4)315ndash9
Quiding 1984 published data only
Quiding H Oikarinen V Sane J Sjoblad AM Analgesic
efficacy after single and repeated doses of codeine and
acetaminophen Journal of Clinical Pharmacology 198424
(1)27ndash34
Ragot 1991 published data only
Ragot JP [Comparison of analgesic activity of mefenamic
acid and paracetamol in treatment of pain after extraction
of impacted lower 3d molar] LrsquoInformation Dentaire 1991
73(21)1659ndash64
Reijntjes 1987 published data only
Reijntjes RJ Boering G Wesseling H van Rijn LG
Suprofen versus paracetamol after oral surgery International
Journal of Oral and Maxillofacial Surgery 198716(1)45ndash9
Rodrigo 1987 published data only
Rodrigo MR Rosenquist JB Cheung LK Paracetamol
and diflunisal for pain relief following third molar surgery
in Hong Kong Chinese International Journal of Oral and
Maxillofacial Surgery 198716(5)566ndash71
Rodrigo 1989 published data only
Rodrigo C Chau M Rosenquist J A comparison of
paracetamol and diflunisal for pain control following
3rd molar surgery International Journal of Oral and
Maxillofacial Surgery 198918(3)130ndash2
Rosen 1985 published data only
Rosen M Absi EG Webster JA Suprofen compared to
dextropropoxyphene hydrochloride and paracetamol
(Cosalgesic) after extraction of wisdom teeth under general
anaesthesia Anaesthesia 198540(7)639ndash41
Sakata 1989 published data only
Sakata LA Rocha B et alEffects of benzydamine after
surgical removal of impacted teeth [Efeitos da benzidamina
apoacutes a extraccedilaumlo de dentes inclusos] Revista da Associacao
Paulista de Cirurgioes Dentistas 198943(4)167ndash70
Selcuk 1996 published data only
Selcuk E Gomel M Bellibas SE Kose T Tuglular I
Comparison of the analgesic effects of diflunisal and
paracetamol in the treatment of postoperative dental pain
12Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
International Journal of Clinical Pharmacology Research
199616(2-3)57ndash65
Seymour 1981 published data only
Seymour RA Rawlins MD Pharmacokinetics of parenteral
paracetamol and its analgesic effects in post-operative dental
pain European Journal of Clinical Pharmacology 198120
(3)215ndash8
Seymour 1983 published data only
Seymour RA Analgesic efficacy and plasma concentration
of three analgesics in pain after lower third molar removal
SAAD Digest 19835(7)172ndash88
Skjelbred 1979 published data only
Skjelbred P Lokken P Paracetamol versus placebo effects
on post-operative course European Journal of Clinical
Pharmacology 197915(1)27ndash33
Strom 1990 published data only
Strom C Forsberg O Quiding H Engevall S Larsson
O Analgesic efficacy of acetaminophen sustained release
Journal of Clinical Pharmacology 199030(7)654ndash9
Van Aken 2004 published data only
Van Aken H Thys L Veekman L Buerkle H Assessing
analgesia in single and repeated administrations of
propacetamol for postoperative pain comparison with
morphine after dental surgery Anesthesia and Analgesia
200498(1)159ndash65
Winter 1983 published data only
Winter L Appleby F Ciccone PE Pigeon JG A double-
blind comparative evaluation of acetaminophen caffeine
and the combination of acetaminophen and caffeine in
outpatients with postoperative oral surgery pain Current
Therapeutic Research 198333(1)115ndash22
Additional references
Aronoff 2006
Aronoff DM Oates JA Boutaud O New insights into
the mechanism of action of acetaminophen Its clinical
pharmacologic characteristics reflect its inhibition of the
two prostaglandin H2 synthases Clinical Pharmacology and
Therapeutics 200679(1)9ndash19
Chandrasekharan 2002
Chandrasekharan NV Dai H Roos KL Evanson NK
Tomsik J Elton TS et alCOX-3 a cyclooxygenase-1 variant
inhibited by acetaminophen and other analgesicantipyretic
drugs cloning structure and expression Proceedings of the
National Academy of Sciences of the United States of America
200299(21)13926ndash31
Collins 1999
Collins SL Moore RA McQuay HJ Wiffen PJ Edwards JE
Single dose oral ibuprofen and diclofenac for postoperative
pain Cochrane Database of Systematic Reviews 1999
Issue 1 [DOI Art No CD001548 DOI 101002
14651858CD001548]
Cooper 1976
Cooper SA Beaver WT A model to evaluate mild analgesics
in oral surgery outpatients Clinical Pharmacology and
Therapeutics 197620(2)241ndash50
Coulthard 2001
Coulthard P Hill CM Frame JW Barry H Ridge BD
Bacon TH Pain control with paracetamol from a sustained
release formulation and a standard release formulation after
third molar surgery a randomised controlled trial British
Dental Journal 2001191(6)319ndash24
Dray 1997
Dray A Kinins and their receptors in hyperalgesia
Canadian Journal of Physiology and Pharmacology 199775
(6)704ndash12
Fisher 1988
Fisher SE Frame JW Rout PG McEntegart DJ Factors
affecting the onset and severity of pain following the surgical
removal of unilateral impacted mandibular third molar
teeth British Dental Journal 1988164(11)351ndash4
Loeser 1999
Loeser JD Melzack R Pain an overview Lancet 1999353
(9164)1607ndash9
Malmberg 1992
Malmberg AB Yaksh TL Antinociceptive effects of spinal
non-steroidal anti-inflammatory agents on the formalin
test in the rat Journal of Pharmacology and Experimental
Therapeutics 1992263136ndash46
Moore 1997
Moore RA McQuay HJ Single-patient data meta-analysis
of 3453 postoperative patients oral tramadol versus
placebo codeine and combination analgesics Pain 199769
(3)287ndash94
Moore 1998
Moore A Collins S Carroll D McQuay H Edwards
J Single dose paracetamol (acetaminophen) with and
without codeine for postoperative pain Cochrane Database
of Systematic Reviews 1998 Issue 4 [DOI Art No
CD001547 DOI 10100214651858CD001547]
Rang 2003
Rang HP Dale MM Ritter JM Moore PK Anti-
inflammatory and immunosuppresant drugs Pharmacology
5th Edition Churchill Livingstone 2003244ndash61
Seymour 1985
Seymour RA Meechan JG Blair GS An investigation into
post-operative pain after third molar surgery under local
analgesia The British Journal of Oral and Maxillofacial
Surgery 198523(6)410ndash8lowast Indicates the major publication for the study
13Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Cooper 1980
Methods Randomised parallel group double blind study
Participants 298 participants randomised to 6 groups withdrawals unclear (51 from all groups)
Number randomised to intervention male 13 female 24 mean age 225
Number randomised to placebo male 11 female 27 mean age 235
Number of third molars removed mean for intervention and placebo 19
Baseline pain intensity mean for intervention 241 (moderate 22 severe 15) mean for placebo 242
(moderate 22 severe 16)
Setting - outpatients (USA)
Interventions Paracetamol 500 mg versus placebo
Formulation not stated
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse events table
Notes Sponsored unclear
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Cooper 1981
Methods Randomised parallel group double blind study
Participants 248 participants randomised to 5 groups withdrawals unclear (48 from all groups)
Number randomised to intervention male 15 female 22 mean age 222
Number randomised to placebo male 13 female 24 mean age 237
Number of third molars removed not stated
Baseline pain intensity mean for intervention 22 (moderate 29 severe 9) mean for placebo 23 (moderate
26 severe 11)
Setting not stated (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation not stated
Anaesthesia LA or GA
14Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Cooper 1981 (Continued)
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Total number of adverse events and number of people with adverse events reported
Notes Sponsored by
Adria Laboratories
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Cooper 1988
Methods Randomised parallel group double blind study
Participants 165 participants randomised to 4 groups withdrawals unclear (22 from all groups)
Number randomised to intervention male 7 female 29 mean age 246
Number randomised to placebo male 11 female 29 mean age 247
Number of third molars removed mean for intervention 14 mean for placebo 15
Baseline pain intensity mean for intervention 24 (moderate 21 severe 15) mean for placebo 24 (mod-
erate 25 severe 15)
Setting - outpatients - single site (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Total number of adverse events
Notes Sponsored by
Parke-Davis
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
15Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Cooper 1998
Methods Randomised parallel group double blind study
Participants 177 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 23 female 27 mean age 236
Number randomised to placebo male 12 female 14 mean age 227
Number of third molars removed not stated
Baseline pain intensity mean for intervention categorical 23 VAS 603 mean for placebo categorical
22 VAS 628
Setting - Georgetown University Hospital (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe) VAS scale 0-100 mm (none - worst pain
imaginable)
PR at 4 hours and 6 hours categorical scale 0-4 (no relief - complete relief )
Global assessment not stated
Adverse effects table
Notes Sponsored by
Whitehall-Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Dionne 1994
Methods Randomised parallel group double blind study
Participants 135 participants randomised to 5 groups withdrawals unclear (11 from all groups)
Number randomised to intervention male 14 female 13 mean age 296
Number randomised to placebo male 15 female 10 mean age 282
Number of third molars removed not stated
Baseline pain intensity for intervention and placebo not stated
Setting private dental practice (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED or GA
Outcomes PI at 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 1-5 (poor - excellent)
Adverse effects table
16Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Dionne 1994 (Continued)
Notes Sponsored by
Upjohn
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Dolci 1994
Methods Randomised parallel group double blind study
Participants 338 participants enrolled in 4 groups withdrawals unclear (40 from all groups)
Number randomised to intervention male 28 female 44 mean age 279 age range 18-49
Number randomised to placebo male 28 female 48 mean age 272 age range 18-45
Number of third molars removed not stated
Baseline pain intensity range for intervention and placebo given together as average 214 (208 - 219)
Setting not stated (Italy)
Interventions Paracetamol 500 mg versus placebo
Formulation tablets
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (negative - very good)
Adverse effects table
Notes Sponsored - unclear
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Forbes 1984b
Methods Randomised parallel group double blind study
Participants 191 participants randomised to 4 groups withdrawals unclear (43 from all groups 164 used in reporting
of adverse events)
Number randomised to intervention male 19 female 20 mean age 2195
Number of third molars removed mean 244
Number randomised to placebo male 21 female 15 mean age 15-32
Number of third molars removed mean 278
17Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Forbes 1984b (Continued)
Baseline pain intensity mean for intervention 246 (moderate 21 severe 18) mean for placebo 247
(moderate 19 severe 17)
Setting private dental practice (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse effects reported as total number of adverse events and number of patients with adverse events
Notes Sponsored by McNeil Consumer Products
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Forbes 1989
Methods Randomised parallel group double blind study
Participants 107 participants randomised to 5 groups withdrawals unclear (19 from all groups 98 participants used
in reporting of adverse events)
Number randomised to intervention male 9 female 13 mean age 2059 age range 17-31
Number randomised to placebo male 12 female 11 mean age 2374 age range 16-39
Number of third molars removed mean for intervention 259 mean for placebo 209
Baseline pain intensity mean for intervention 245 mean for placebo 239
Setting - 2 sites private dental practice outpatients (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation - 1 tablet amp 1 capsule
Anaesthesia LA and GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects reported by number of patients with adverse events
Notes Sponsored by
Boots Company Ltd GH Besselaar Associates
Risk of bias
Item Authorsrsquo judgement Description
18Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Forbes 1989 (Continued)
Allocation concealment Unclear B - Unclear
Forbes 1990
Methods Randomised parallel group double blind study
Participants 206 participants randomised to 6 groups
Number randomised to intervention male 20 female 16 (5 withdrawals) mean age 225 age range 16-
46
Number randomised to placebo male 18 female 16 (4 withdrawals) mean age 2365 age range 16-45
Number of third molars removed mean for intervention 258 mean for placebo 235
Baseline pain intensity mean for intervention 239 (moderate 22 severe 14) mean for placebo 232
(moderate 23 severe 11)
Setting - private dental practice outpatients (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation capsules
Anaesthesia LA and GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects table
Notes Sponsored by
Syntex Research
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Hersh 2000
Methods Randomised parallel group double blind study
Participants 210 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 20 female 43 mean age 233
Number of third molars removedpatient (11) (26) (35) (451)
Number randomised to placebo male 9 female 8 mean age 237
Number of wisdom teeth removed per patient (11) (25) (33) (418)
Baseline pain intensity mean for intervention 23 (moderate 47 severe 16) mean for placebo 22 (mod-
erate 22 severe 5)
Setting - University of Pennsylvania School of Dental Medicine - outpatients (USA)
19Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hersh 2000 (Continued)
Interventions Paracetamol 1000 mg versus placebo
Formulation caplets
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical 0-3 (none - severe)
PR at 4 hours and 6 hours categorical 0-4 (no relief - complete relief )
Global assessment categorical 0-4 (poor - excellent)
Adverse effects by total number of adverse events and number of patients with adverse events
Notes Sponsored by
Whitehall-Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Kiersch 1994
Methods Randomised parallel group double blind study
Participants 232 participants enrolled in 3 groups
Number randomised to intervention 91 withdrawals 4 (2 before and 2 after randomisation) male 72
female 17 mean age 231 age range 15-39
Number of third molars removedpatient (10) (20) (331) (454)
Number randomised to placebo 47 withdrawals 2 male 35 female 10 mean age 247 age range 15-39
Number of third molars removedpatient (10) (20) (319) (426)
Baseline pain intensity mean for intervention and placebo categorical 212 VAS 5835
Setting not stated (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation capsules
Anaesthesia not stated
Outcomes PI at 4 hours and 6 hours categorical 0-3 (none - severe)
PR at 4 hours and 6 hours categorical 0-4 (none - complete) VAS 0-100 mm (no pain - worst pain I can
imagine)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects reported by total number of adverse events and by number of patients with adverse events
Notes Sponsored by
Syntex Research
Risk of bias
Item Authorsrsquo judgement Description
20Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Kiersch 1994 (Continued)
Allocation concealment Unclear B - Unclear
Kubitzek 2003
Methods Randomised parallel group double blind study
Participants 245 participants randomised to 3 groups no withdrawals
Number randomised to intervention 78
Number randomised to placebo 84 malefemale 40 male over both groups
Number of third molars removed 1 or 2 for each patient
Baseline pain intensity moderate to severe 65-76 in both groups
Setting dental practice (Germany)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia LA
Outcomes PI not stated
PR given as TOTPAR at 6 hours
Global assessment categorical 1-5 (poor - excellent)
Adverse effects not stated
Notes Sponsored by
Novartis Consumer Health
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Lehnert 1990
Methods Randomised parallel group double blind study
Participants 150 participants randomised to 3 groups 50 to each
Number randomised to intervention 1 withdrawal male 23 female 26 mean age 253 age range 17-52
Number randomised to placebo 2 withdrawals male 24 female 18 mean age 251 age range 18-53
Number of hird molars removed not stated
Baseline pain intensity mean for intervention 255 (moderate 22 severe 27) mean for placebo 25
(moderate 21 severe 21)
Setting outpatients (Germany)
Interventions Paracetamol 1000 mg versus placebo
Formulation capsules
Anaesthesia not stated
21Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Lehnert 1990 (Continued)
Outcomes PI at 6 hours categorical scale 0-3 (no pain - severe)
PR at 6 hours categorical scale 0-3 (none - complete)
Global assessment categorical scale 0-3 (poor - excellent)
Adverse effects by number of patients
Notes Sponsored by GH Besselar Associates
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Mehlisch 1995
Methods Randomised parallel group double blind study
Participants 240 participants randomised to 3 groups 1 withdrawal from the acetaminophen group
Number randomised to intervention (1 withdrawal) male 30 female 71 mean age 253 age range 15-
60
Number of third molars removedpatient (10 295 33 43)
Number randomised to placebo male 19 female 21 mean age 242 age range 15-48
Number of third molars removedpatient (10 239 30 41)
Baseline pain intensity mean for intervention 221 (moderate 80 severe 21) mean for placebo 220
(moderate 32 severe 8)
Setting not stated (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation 2 tablets
Anaesthesia not stated
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse events reported by number of patients
Notes Sponsored by
Biomedical Research Group and Merck Research Laboratories
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
22Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Moller 2000
Methods Randomised parallel group double blind study
Participants 242 participants randomised to 4 groups no withdrawals
Number randomised to Intervention A male 27 female 33 mean age 245
Number randomised to Intervention B male 26 female 34 mean age 262
Number randomised to Placebo A male 21 female 41 mean age 250
Number randomised to Placebo B male 24 female 36 mean age 246
Number of third molars removed per patient in both groups 1
Mean baseline intensity Intervention A categorical 200 (moderate 60) VAS 494
Mean baseline intensity Intervention B categorical 200 (moderate 60) VAS 473
Mean baseline intensity Placebo A categorical 200 (moderate 61 severe 1) VAS 505
Mean baseline intensity Placebo B categorical 200 (moderate 61) VAS 476
Setting Department of Oral and Maxillofacial Surgery Royal Dental College Aarhus (Denmark)
Interventions Intervention A Paracetamol 1000 mg versus Placebo A
Formulation effervescent tablets
Intervention B Paracetamol 1000 mg versus Placebo B
Formulation tablets
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe) VAS scale 0-100 mm (no pain - worst possible pain)
PR at 4 hours categorical 0-4 (none - complete)
Global assessment categorical 0-3 (poor - excellent)
Adverse effects reported as total number of adverse events and number of patients with adverse events
Notes Sponsored by
Bristol Myers Squibb
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Olson 2001
Methods Randomised parallel group double blind study
Participants 239 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 22 female 44 mean age 222
Number randomised to placebo male 11 female 28 mean age 239
Number of third molars removedpatient intervention - (11) (264) (31) (40) placebo - (11) (2
38) (30) (40)
Baseline pain intensity mean for intervention 286 (moderate 9 severe 57) mean for placebo 29 (moderate
4 severe 35)
Setting University of Puerto Rico School of Dentistry (Puerto Rico)
23Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Olson 2001 (Continued)
Interventions Paracetamol 1000 mg versus placebo
Formulation caplets
Anaesthesia LA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete relief )
Global assessment categorical scale 0-4 (poor - excellent)
Adverse effects table
Notes Sponsored by
Whitehall Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Seymour 1996
Methods Randomised parallel group double blind study
Participants 206 participants randomised to 5 groups
Number randomised to intervention A 1 withdrawal male 12 female 28 mean age 238
Number randomised to intervention B 1 withdrawal male 12 female 28 mean age 277 1 withdrawal
Number randomised to placebo 2 withdrawals male 15 female 24 mean age 246
Number of third molars removedpatient not stated
Baseline pain intensity mean for intervention A VAS 549 mean for intervention B VAS 542 mean
for placebo VAS 565
Setting not stated (UK)
Interventions Intervention A paracetamol 500 mg versus placebo
Intervention B paracetamol 1000 mg versus placebo
Formulation not stated
Anaesthesia GA
Outcomes PI at 6 hours VAS scale 0-100 mm (no pain - unbearable pain)
Global assessment categorical 0 -3 (very good - very poor)
but categories 1 amp 2 and 4 amp 5 not reported separately so unable to include data in tables
Adverse effects - none reported by any participants in any group
Notes Sponsored - unclear
Risk of bias
Item Authorsrsquo judgement Description
24Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Seymour 1996 (Continued)
Allocation concealment Unclear B - Unclear
Seymour 2003
Methods Randomised parallel group double blind study
Participants 167 randomised to 3 groups withdrawals unclear (14 from all groups)
Number randomised to intervention male 19 female 43 mean age 250
Number randomised to placebo male 11 female 21 mean age 251
Number of third molars removedpatient intervention - (12) (214) (312) (434) placebo - (13)
(25) (39) (415)
Baseline pain intensity mean for intervention 506 mean for placebo 541
Setting not clear (2 sites Cardiff and Hexham UK)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia GA
Outcomes PI at 4 hours VAS scale 0-100 mm (none - worst pain imaginable)
PR not stated
Global assessment categorical scale 1-5 (very poor - very good)
Adverse effects table
Notes Sponsored by
Reckitt Benckiser Healthcare
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Skoglund 1991
Methods Randomised parallel group double blind study
Participants 147 participants randomised to 4 groups withdrawals unclear (8 from all groups)
Number randomised to intervention male 16 female 16 mean age 247
Number randomised to placebo male 16 female 17 mean age 244
Number of third molars removed not stated
Baseline pain intensity mean for intervention approx 55 mean for placebo approx 45
Setting not stated (Norway)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia LA
25Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Skoglund 1991 (Continued)
Outcomes PI at 4 hours and 6 hours VAS scale 0-100 mm (none - pain cannot be worse)
PR at 4 hours and 6 hours VAS scale 0-100 mm (complete relief - no relief ) reversed for statistical analysis
Global assessment not stated
Adverse effects table
Notes Sponsored by
Apothekernes Laboratorium
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Sunshine 1986
Methods Randomised parallel group double blind study
Participants 182 participants randomised to 6 groups no withdrawals (only patients with moderate to severe pain
were randomised)
Number randomised to intervention male 6 female 24 mean age 219
Number randomised to placebo male 14 female 16 mean age 23
Number of third molars removed not stated
Baseline pain intensity mean for intervention 200 mean for placebo 200
Setting University of Puerto Rico School of Dentistry Clinic
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia LA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none 0 - complete 100)
Global assessment categorical 0-3 (poor - excellent)
Overall improvement 1-7 (very much worse - very much better)
Adverse effects reported by number of patients with adverse events
Notes Sponsored by
Upjohn
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
26Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Vattaraphudej 1986
Methods Randomised parallel group double blind study
Participants 83 enrolled to 4 groups withdrawals unclear (16 from all groups)
Number randomised to intervention male 8 female 8
Number randomised to placebo male 10 female 9
Number of third molars removed mean for intervention 125 mean for placebo 132
Baseline pain intensity mean for intervention 237 mean for placebo 226
Setting Dept of Oral Surgery Khon Kaen University Thailand
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (no relief - total relief )
Global assessment categorical scale 0-3 (poor - excellent)
Adverse effects none reported
Notes Sponsored by Khon Kaen University Thailand Dr Sompong Thongpradith Merck and Russel
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
GA - general anaesthetic LA - local anaesthetic PI - pain intensity PR - pain relief SED - sedation TOTPAR - total pain relief VAS
- visual analogue scale
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Adame 1979 Title not in journal quoted unable to find paper
Barden J 2004 Meta-analysis dental papers included individually where appropriate
Becker 1990 Not a third molar study
Bentley 1987 Unable to extract data for third molars only written to authors
Breivik 1998 Dose given at 3 hours postoperatively regardless of baseline pain unable to get 4-hour data Study used for side
effects only
27Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Cooper 1986 Unable to extract third molar data written to authors
Cooper 1989 Unable to extract third molar data written to authors
Cooper 1991 Unclear if third molars only written to authors
Dionne 1983 (1) Not single dose administered preoperatively
Dionne 1983 (2) Not placebo controlled not single dose administered preoperatively
Dionne 1986 Not placebo controlled
Dolci 1993 The data for the participants in this study are duplicated in Dolci 1994
Edwards 2002 This was a meta-analysis Need to identify source of data to clarify whether third molar studies and exclude
duplication Written to authors
Forbes 1982 Unable to extract third molar data written to authors
Forbes 1984a Not third molar study
Gallardo 1990 Not third molar study (periodontal surgery)
Gustafsson 1983 Patients given either paracetamol preoperatively and placebo postoperatively or vice versa unable to extract
relevant data
Haanaes 1986 Not placebo controlled Study used for side effects only
Irvine 1982 Not placebo controlled
Laska 1983 Not placebo controlled
Lecointre 1991 Not placebo controlled
Liashek 1987 Multiple doses unable to extract single dose data
Macleod 2002 Not placebo controlled
Medve 2001 Only 8-hour SPID and TOTPAR available need 4-hour andor 6-hour to include in review written to authors
Mehlisch 1984 Unable to extract third molar data written to authors
Mehlisch 1990 Unable to extract third molar data
Moore 1986 Multiple doses given unable to extract single dose data
Nystrom 1988 Not placebo controlled
28Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Petersen 1983 Unable to locate complete article
Quiding 1981 Not placebo controlled
Quiding 1982 (1) Not placebo controlled
Quiding 1982 (2) Not placebo controlled
Quiding 1984 No placebo used
Ragot 1991 Not placebo controlled
Reijntjes 1987 Not placebo controlled
Rodrigo 1987 Mixed parallel and cross-over trial multiple doses unable to extract relevant data
Rodrigo 1989 Not placebo controlled
Rosen 1985 Not placebo controlled multiple doses used unable to extract single dose data
Sakata 1989 Unable to obtain study
Selcuk 1996 Not placebo controlled
Seymour 1981 Cross-over trial baseline pain not stated unable to extract relevant data
Seymour 1983 Acetaminophen administered intravenously
Skjelbred 1979 Multiple doses unable to extract single dose data
Strom 1990 Not placebo controlled
Van Aken 2004 Propacetamol administered intravenously
Winter 1983 Unable to extract third molar data written to authors
SPID - summed pain intensity difference TOTPAR - total pain relief
29Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
Comparison 1 50 pain relief using pain relief measures
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Paracetamol versus placebo
number of people with at least
50 pain relief at 4 hours
16 1498 Risk Ratio (M-H Random 95 CI) 285 [189 429]
11 Up to 1000 mg of
paracetamol
10 710 Risk Ratio (M-H Random 95 CI) 196 [134 286]
12 1000 mg or more 6 788 Risk Ratio (M-H Random 95 CI) 456 [286 727]
2 Paracetamol versus placebo
number of people with at least
50 pain relief at 6 hours
13 1155 Risk Ratio (M-H Random 95 CI) 332 [188 587]
21 Up to 1000 mg of
paracetamol
6 378 Risk Ratio (M-H Random 95 CI) 189 [098 367]
22 1000 mg or more 7 777 Risk Ratio (M-H Random 95 CI) 421 [297 598]
Comparison 2 50 pain relief using pain intensity measures
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Paracetamol versus placebo
number of people with at least
50 pain relief at 4 hours
17 1658 Risk Ratio (M-H Random 95 CI) 487 [283 837]
11 Up to 1000 mg of
paracetamol
10 737 Risk Ratio (M-H Random 95 CI) 433 [219 858]
12 1000 mg or more 8 921 Risk Ratio (M-H Random 95 CI) 646 [234 1785]
2 Paracetamol versus placebo
number of people with at least
50 pain relief at 6 hours
13 1184 Risk Ratio (M-H Random 95 CI) 341 [234 497]
21 Up to 1000 mg of
paracetamol
6 403 Risk Ratio (M-H Random 95 CI) 267 [146 490]
22 1000 mg or more 8 781 Risk Ratio (M-H Random 95 CI) 396 [252 623]
30Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Comparison 3 Number of people with adverse events
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Number of patients with adverse
events paracetamol versus
placebo
17 1645 Risk Ratio (M-H Random 95 CI) 119 [090 157]
11 Up to 1000 mg of
paracetamol
9 672 Risk Ratio (M-H Random 95 CI) 125 [069 225]
12 1000 mg or more 8 973 Risk Ratio (M-H Random 95 CI) 116 [084 160]
Analysis 11 Comparison 1 50 pain relief using pain relief measures Outcome 1 Paracetamol versus
placebo number of people with at least 50 pain relief at 4 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 1 50 pain relief using pain relief measures
Outcome 1 Paracetamol versus placebo number of people with at least 50 pain relief at 4 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Dolci 1994 5472 2576 100 228 [ 161 323 ]
Cooper 1980 1137 1138 82 103 [ 051 207 ]
Forbes 1990 936 134 30 850 [ 114 6357 ]
Forbes 1989 522 023 17 1148 [ 067 19607 ]
Cooper 1988 1636 1240 87 148 [ 081 269 ]
Cooper 1981 2137 637 77 350 [ 160 767 ]
Forbes 1984b 1339 136 30 1200 [ 165 8716 ]
Vattaraphudej 1986 716 219 47 416 [ 100 1726 ]
Sunshine 1986 1830 1530 95 120 [ 076 190 ]
Dionne 1994 2527 1725 102 136 [ 102 182 ]
Subtotal (95 CI) 352 358 667 196 [ 134 286 ]
Total events 179 (Paracetamol better) 90 (Placebo better)
Heterogeneity Tau2 = 018 Chi2 = 2644 df = 9 (P = 0002) I2 =66
Test for overall effect Z = 349 (P = 000048)
2 1000 mg or more
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
31Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Mehlisch 1995 40101 240 49 792 [ 201 3124 ]
Cooper 1998 1850 326 59 312 [ 101 963 ]
Olson 2001 4266 539 74 496 [ 215 1148 ]
Moller 2000 27120 0122 18 5591 [ 345 90627 ]
Hersh 2000 4063 527 75 343 [ 152 773 ]
Kiersch 1994 2589 345 58 421 [ 134 1321 ]
Subtotal (95 CI) 489 299 333 456 [ 286 727 ]
Total events 192 (Paracetamol better) 18 (Placebo better)
Heterogeneity Tau2 = 003 Chi2 = 544 df = 5 (P = 036) I2 =8
Test for overall effect Z = 637 (P lt 000001)
Total (95 CI) 841 657 1000 285 [ 189 429 ]
Total events 371 (Paracetamol better) 108 (Placebo better)
Heterogeneity Tau2 = 040 Chi2 = 6294 df = 15 (Plt000001) I2 =76
Test for overall effect Z = 503 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
32Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 12 Comparison 1 50 pain relief using pain relief measures Outcome 2 Paracetamol versus
placebo number of people with at least 50 pain relief at 6 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 1 50 pain relief using pain relief measures
Outcome 2 Paracetamol versus placebo number of people with at least 50 pain relief at 6 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Forbes 1989 322 023 29 730 [ 040 13375 ]
Cooper 1988 1236 940 99 148 [ 071 310 ]
Forbes 1990 736 034 30 1419 [ 084 23928 ]
Dionne 1994 2427 1825 115 123 [ 093 163 ]
Forbes 1984b 1039 036 31 1943 [ 118 31995 ]
Sunshine 1986 1530 1030 104 150 [ 081 279 ]
Subtotal (95 CI) 190 188 407 189 [ 098 367 ]
Total events 71 (Paracetamol better) 37 (Placebo better)
Heterogeneity Tau2 = 032 Chi2 = 1445 df = 5 (P = 001) I2 =65
Test for overall effect Z = 189 (P = 0058)
2 1000 mg or more
Kubitzek 2003 4569 773 99 680 [ 329 1404 ]
Mehlisch 1995 35101 140 49 1386 [ 196 9779 ]
Kiersch 1994 2089 345 79 337 [ 106 1075 ]
Olson 2001 4166 539 94 485 [ 209 1122 ]
Hersh 2000 3563 527 95 300 [ 132 682 ]
Lehnert 1990 2349 640 96 313 [ 141 693 ]
Cooper 1998 1750 326 81 295 [ 095 914 ]
Subtotal (95 CI) 487 290 593 421 [ 297 598 ]
Total events 216 (Paracetamol better) 30 (Placebo better)
Heterogeneity Tau2 = 00 Chi2 = 509 df = 6 (P = 053) I2 =00
Test for overall effect Z = 806 (P lt 000001)
Total (95 CI) 677 478 1000 332 [ 188 587 ]
Total events 287 (Paracetamol better) 67 (Placebo better)
Heterogeneity Tau2 = 072 Chi2 = 6335 df = 12 (Plt000001) I2 =81
Test for overall effect Z = 412 (P = 0000038)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
33Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 21 Comparison 2 50 pain relief using pain intensity measures Outcome 1 Paracetamol versus
placebo number of people with at least 50 pain relief at 4 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 2 50 pain relief using pain intensity measures
Outcome 1 Paracetamol versus placebo number of people with at least 50 pain relief at 4 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Dolci 1994 4972 576 86 1034 [ 437 2449 ]
Seymour 1996 1940 1039 96 185 [ 099 346 ]
Cooper 1980 737 438 74 180 [ 057 563 ]
Forbes 1990 1036 034 28 1986 [ 121 32639 ]
Forbes 1989 622 023 28 1357 [ 081 22736 ]
Cooper 1988 1236 840 90 167 [ 077 361 ]
Sunshine 1986 1830 630 90 300 [ 138 650 ]
Forbes 1984b 1339 036 28 2498 [ 154 40542 ]
Vattaraphudej 1986 616 119 44 713 [ 095 5317 ]
Cooper 1981 1537 037 28 3100 [ 192 49971 ]
Subtotal (95 CI) 365 372 592 433 [ 219 858 ]
Total events 155 (Paracetamol better) 34 (Placebo better)
Heterogeneity Tau2 = 063 Chi2 = 2622 df = 9 (P = 0002) I2 =66
Test for overall effect Z = 421 (P = 0000026)
2 1000 mg or more
Cooper 1998 1350 026 28 1429 [ 088 23130 ]
Mehlisch 1995 41101 340 75 541 [ 178 1648 ]
Hersh 2000 3663 127 46 1543 [ 223 10685 ]
Skoglund 1991 1632 033 28 3400 [ 213 54391 ]
Seymour 2003 1262 432 78 155 [ 054 442 ]
Seymour 1996 2040 1039 96 195 [ 105 362 ]
Kiersch 1994 989 045 28 971 [ 058 16317 ]
Moller 2000 28120 0122 28 5794 [ 358 93840 ]
Subtotal (95 CI) 557 364 408 646 [ 234 1785 ]
Total events 175 (Paracetamol better) 18 (Placebo better)
Heterogeneity Tau2 = 124 Chi2 = 2347 df = 7 (P = 0001) I2 =70
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
34Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Test for overall effect Z = 360 (P = 000032)
Total (95 CI) 922 736 1000 487 [ 283 837 ]
Total events 330 (Paracetamol better) 52 (Placebo better)
Heterogeneity Tau2 = 070 Chi2 = 4973 df = 17 (P = 000005) I2 =66
Test for overall effect Z = 571 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
Analysis 22 Comparison 2 50 pain relief using pain intensity measures Outcome 2 Paracetamol versus
placebo number of people with at least 50 pain relief at 6 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 2 50 pain relief using pain intensity measures
Outcome 2 Paracetamol versus placebo number of people with at least 50 pain relief at 6 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Seymour 1996 1840 939 152 195 [ 100 380 ]
Forbes 1989 422 023 16 939 [ 054 16485 ]
Cooper 1988 936 640 105 167 [ 066 422 ]
Forbes 1990 836 032 17 1516 [ 091 25267 ]
Forbes 1984b 1139 036 17 2128 [ 130 34843 ]
Sunshine 1986 1430 530 111 280 [ 115 680 ]
Subtotal (95 CI) 203 200 418 267 [ 146 490 ]
Total events 64 (Paracetamol better) 20 (Placebo better)
Heterogeneity Tau2 = 015 Chi2 = 705 df = 5 (P = 022) I2 =29
Test for overall effect Z = 318 (P = 00015)
2 1000 mg or more
Hersh 2000 3163 127 33 1329 [ 191 9242 ]
Mehlisch 1995 39101 340 82 515 [ 169 1571 ]
Olson 2001 4266 739 146 355 [ 177 711 ]
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
35Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Seymour 1996 2140 939 157 228 [ 119 433 ]
Cooper 1998 1250 026 17 1324 [ 081 21504 ]
Kiersch 1994 489 045 16 460 [ 025 8361 ]
Lehnert 1990 2449 542 114 411 [ 172 983 ]
Skoglund 1991 1432 033 17 2988 [ 186 48076 ]
Subtotal (95 CI) 490 291 582 396 [ 252 623 ]
Total events 187 (Paracetamol better) 25 (Placebo better)
Heterogeneity Tau2 = 008 Chi2 = 863 df = 7 (P = 028) I2 =19
Test for overall effect Z = 597 (P lt 000001)
Total (95 CI) 693 491 1000 341 [ 234 497 ]
Total events 251 (Paracetamol better) 45 (Placebo better)
Heterogeneity Tau2 = 013 Chi2 = 1823 df = 13 (P = 015) I2 =29
Test for overall effect Z = 637 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
36Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 31 Comparison 3 Number of people with adverse events Outcome 1 Number of patients with
adverse events paracetamol versus placebo
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 3 Number of people with adverse events
Outcome 1 Number of patients with adverse events paracetamol versus placebo
Study or subgroup Paracetamol more Placebo more Risk Ratio Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Cooper 1980 237 637 033 [ 007 155 ]
Dolci 1994 780 882 090 [ 034 236 ]
Forbes 1990 541 038 1021 [ 058 17873 ]
Forbes 1989 326 226 150 [ 027 825 ]
Sunshine 1986 130 130 100 [ 007 1526 ]
Cooper 1981 1237 438 308 [ 109 869 ]
Dionne 1994 727 525 130 [ 047 356 ]
Vattaraphudej 1986 016 019 00 [ 00 00 ]
Forbes 1984b 143 240 047 [ 004 493 ]
Subtotal (95 CI) 337 335 125 [ 069 225 ]
Total events 38 (Paracetamol more) 28 (Placebo more)
Heterogeneity Tau2 = 016 Chi2 = 906 df = 7 (P = 025) I2 =23
Test for overall effect Z = 074 (P = 046)
2 1000 mg or more
Olson 2001 1066 239 295 [ 068 1279 ]
Cooper 1998 2550 426 325 [ 127 835 ]
Moller 2000 48120 56122 087 [ 065 117 ]
Seymour 2003 2462 932 138 [ 073 260 ]
Mehlisch 1995 1299 440 121 [ 042 354 ]
Kiersch 1994 2691 1347 103 [ 059 182 ]
Hersh 2000 1263 727 073 [ 032 166 ]
Lehnert 1990 549 440 102 [ 029 355 ]
Subtotal (95 CI) 600 373 116 [ 084 160 ]
Total events 162 (Paracetamol more) 99 (Placebo more)
Heterogeneity Tau2 = 007 Chi2 = 1096 df = 7 (P = 014) I2 =36
Test for overall effect Z = 090 (P = 037)
Total (95 CI) 937 708 119 [ 090 157 ]
01 02 05 1 2 5 10
Favours treatment Favours control
(Continued )
37Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol more Placebo more Risk Ratio Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Total events 200 (Paracetamol more) 127 (Placebo more)
Heterogeneity Tau2 = 007 Chi2 = 2073 df = 15 (P = 015) I2 =28
Test for overall effect Z = 121 (P = 023)
01 02 05 1 2 5 10
Favours treatment Favours control
A D D I T I O N A L T A B L E S
Table 1 Number of patients with adverse events (lt 1000 mg ParacetamolPlacebo)
Author Total Paracetamol AEs Paracetamol Total Placebo AEs Placebo
Cooper 1980 37 2 37 6
Cooper 1981 37 12 38 4
Dionne 1994 27 7 25 5
Dolci 1994 80 7 82 8
Forbes 1984b 43 1 40 2
Forbes 1989 26 3 26 2
Forbes 1990 41 5 38 0
Gallardo 1990 15 5 11 3
Seymour 1996 40 0 39 0
Sunshine 1986 30 1 30 1
Vattaraphudej 1986 16 0 19 0
Totals 392 43 385 31
38Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Quality assessment
Author Allocation concealment Follow up Total (Max-3)
Cooper 1980 1 0 1
Cooper 1981 1 0 1
Cooper 1988 1 0 1
Cooper 1998 1 1 2
Dionne 1994 1 0 1
Dolci 1994 1 0 1
Forbes 1984b 2 0 2
Forbes 1989 1 0 1
Forbes 1990 2 0 2
Hersh 2000 1 1 2
Kiersch 1994 1 1 2
Kubitzek 2003 1 1 2
Lehnert 1990 1 1 2
Mehlisch 1995 2 1 3
Moller 2000 1 1 2
Olson 2001 2 1 3
Seymour 1996 1 1 2
Seymour 2003 2 0 2
Skoglund 1991 2 0 2
Sunshine 1986 2 1 3
Vattaraphudej 1986 1 1 2
39Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Random-effects metaregression lt 1000 mg vs 1000 mg Paracetamol vs Placebo
Outcome Number of studies Slope estimate 95 CI Slope interpretation P value
50 pain relief at 4
hours (using pain re-
lief )
16 094 (036 to 152) more pain relief for
higher doses
0001
50 pain relife at 6
hours (using pain re-
lief )
13 114 (071 to 156) more pain relief for
higher doses
lt0001
50 pain relief at
4 hours (using pain
intensity)
16 023 (-084 to 130) more pain relief for
higher doses
067
50 pain relief at
6 hours (using pain
intensity)
14 043 (-015 to 101) more pain relief for
higher doses
015
Table 4 List of adverse events
Adverse events Paracetamol Placebo
Nausea 21 11
Vomiting 11 3
Nausea andor vomiting stomach cramps
abdominal pain
3 3
Headache 47 31
Drowsiness sleepiness somnolence 36 13
Dizziness fainting syncope 9 4
Bleeding 11 7
Chills flushes fever flu-like symptoms 5 0
Paraesthesia 4 2
Jawache 1 0
Swelling 1 6
Cellulitis 1 0
40Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 List of adverse events (Continued)
Dry socket 11 12
Surgical complications 6 13
CNS 5 6
GI 12 2
Body as a whole 8 3
Respiratory 2 0
Psychiatric 0 1
Other hiccups hearingvestibular miosis 5 1
Table 5 Global assessment - 5-point scale(lt 1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Cooper 1980 37 089 38 089
Cooper 1981 37 192 37 062
Cooper 1988 36 238 40 205
Dionne 1994 27 240 25 200
Dolci 1994 72 210 76 217
Forbes 1984 39 126 36 028
Mean 248 183 252 144
Table 6 Global assessment - 4-point scale (lt 1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Forbes 1989 26 100 26 030
Forbes 1990 41 147 38 056
Sunshine 1986 30 120 30 093
Vattaraphudej 1986 16 16 19 116
41Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 6 Global assessment - 4-point scale (lt 1000 mg Paracetamol) (Continued)
Mean 113 131 113 070
Table 7 Global assessment - 5-point scale (1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Kiersch 1994 91 130 47 060
Kubitzek 2003 78 198 84 145
Mehlisch 1995 101 157 40 045
Olson 2001 66 281 39 193
Seymour 2003 62 250 32 214
Mean 398 194 242 129
Table 8 Global assessment - 4-point scale (1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Hersh 2000 63 229 27 085
Moller 2000 120 188 122 154
Mean 183 202 149 141
A P P E N D I C E S
Appendix 1 CENTRAL search strategy
1 MOLAR THIRD single term (MeSH)
2 (wisdom next tooth)
3 (wisdom next teeth)
4 (third near molar)
5 (1 or 2 or 3 or 4)
6 TOOTH EXTRACTION single term (MeSH)
7 (extract near tooth)
8 (extract near teeth)
9 (extract near (third next molar))
10 (extract near (third near molar))
42Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
11 (remov near tooth)
12 (remov near teeth)
13 (surgical near remov)
14 (surgery near remov)
15 (surgical near extract)
16 (surgery near extract)
17 (6 or 7 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16)
18 (5 and 17)
W H A T rsquo S N E W
Last assessed as up-to-date 21 May 2007
Date Event Description
31 July 2008 Amended Converted to new review format
H I S T O R Y
Protocol first published Issue 4 2003
Review first published Issue 3 2007
C O N T R I B U T I O N S O F A U T H O R S
Conceiving designing and co-ordinating the review (Kiaran Weil (KW) Paul Coulthard (PC))
Developing search strategy and undertaking searches (Zahid Afzal (ZA) Arjen van Wijk (AJW) KW)
Screening search results and retrieved papers against inclusion criteria (ZA KW) Marco Esposito (ME) Lee Hooper (LH) PC)
Appraising quality (KW ZA)
Extracting data from papers (KW LH Helen Worthington (HW))
Writing to authors for additional information (KW)
Data management for the review and entering data into RevMan (KW)
Analysis and interpretation of data (KW LH HW)
Writing the review (KW)
Providing general advice on the review (ME LH PC HW)
Performing previous work that was the foundation of current study (PC)
43Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D E C L A R A T I O N S O F I N T E R E S T
None known
S O U R C E S O F S U P P O R T
Internal sources
bull The University of Manchester UK
bull The University of Amsterdam Netherlands
External sources
bull No sources of support supplied
I N D E X T E R M S
Medical Subject Headings (MeSH)
Acetaminophen [adverse effects lowasttherapeutic use] Analgesics Non-Narcotic [adverse effects lowasttherapeutic use] Molar Third [lowastsurgery]
Outcome Assessment (Health Care) Pain Postoperative [lowastdrug therapy] Pain Measurement Randomized Controlled Trials as Topic
Tooth Extraction [lowastadverse effects]
MeSH check words
Humans
44Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 407
Relative efficacy of oral analgesics after thirdmolar extractionJ Barden1 J E Edwards2 H J McQuay3 P J Wiffen4 and R A Moore5
Objectives To compare the relative efficacy of analgesics after thirdmolar extraction from systematic reviews of randomised double blindstudiesData sources Dental trials from systematic reviews of randomiseddouble-blind studies of analgesics in acute painData selection Number of patients with moderate or severe painachieving at least half pain relief over 4 to 6 hours after a single oraldose of analgesicData extraction Independently by two reviewersData synthesis Use of dichotomous information from active andplacebo treatments first to calculate the statistical significance usingrelative risk and then to evaluate the clinical relevance using numberneeded to treat (NNT) Non-steroidal anti-inflammatory drugs (NSAIDs)and cyclo-oxygenase-2 (COX-2) inhibitors had the lowest (best) NNTsfor the outcome of at least half pain relief over 4-6 hours comparedwith placebo With the best performing analgesics 50-70 patients out of100 had good pain relief compared with about 10 out of 100 withplacebo Only paracetamol 600650 mg plus codeine 60 mg wasassociated with any significant increase in any patient experiencing anadverse eventConclusions NSAIDs and COX-2 inhibitors have the lowest (best) NNTsThey may also have fewer adverse effects after third molar surgerythough conclusive evidence is lacking At least 80 of analgesicprescribing by UK dentists is in line with the best available evidence onefficacy and safety
Acute pain has been studied in single dose designs first pro-posed by Beecher and colleagues12 and formalised by Houdeand Wallenstein3 The problem with single trials is that whilethey can demonstrate statistical superiority of analgesic overplacebo variation because of random chance means that if
1Research Associate 2Senior Research Associate 3Professor of Pain Relief 4PrescribingAdvisor 5Research Director Pain Research and Nuffield Department of AnaestheticsUniversity of Oxford Oxford Radcliffe Hospital The Churchill Headington Oxford OX3 7LJ UKCorrespondence to Dr R A MooreE-mail andrewmoorepruoxacuk
Refereed paperReceived 150403 Accepted 121103doi101038sjbdj4811721copy British Dental Journal 2004 197 407ndash411
small they provide a poor estimate of the size of the analgesiceffect4 Combining results from clinically homogeneous trials ina meta-analysis gives an accurate estimate of the extent of theanalgesic effect when sufficient numbers of patients have beenrandomised45
Clinical trials in acute pain normally last 4 to 6 hours becausethat is the duration of effect of most analgesics whether injectedor as tablets and whether simple analgesics NSAIDs or opioidsMeta-analysis in acute pain has concentrated on the use of thearea under the total pain relief versus time curve (TOTPAR)dichotomized into those patients who do or do not achieve atleast half pain relief (at least 50 maximum TOTPAR)6 Thismeasure is the one most frequently reported and it avoids theproblem of reporting continuous pain data as the mean of ahighly skewed distribution7 It has the benefit of being intuitivelymeaningful to patients and professionals as well as being meas-urable
Meta-analyses in acute pain usually combine studies from avariety of pain models and relative efficacy of analgesics inthese studies has been examined6 A majority of studies were inthird molar extraction but any postoperative pain condition islikely to be included In the largest dataset that of aspirin8
pain model (dental or other surgery) made no difference to theNNT
Dentists ask rightly about relative efficacy in dental painThe number of prescription items issued by dentists in Englandwas remarkably consistent between 1998 and 2001 (Table 1)with ibuprofen dihydrocodeine and paracetamol being mostfrequently prescribed This review set out to examine single-dose oral analgesics after third molar extraction from a numberof updated systematic reviews both for the analgesics common-ly prescribed in England and for those for which comparableevidence exists including the newer cyclo-oxygenase-2 selec-tive inhibitors like rofecoxib celecoxib and valdecoxib
METHODSIn all the systematic reviews QUORUM guidelines were fol-lowed9 In the reviews studies for inclusion were soughtthrough searching the Cochrane Library Biological AbstractsMEDLINE PubMed and the Oxford Pain Relief database10 Ref-erence lists and review articles were examined for possible addi-tional references Most had search dates in 2002
This paper reviews the available high quality information on analgesics commonlyprescribed by dentists including COX-2 selective inhibitors
Problems related to chance effects are avoided by combining multiple trials in a meta-analysis
There is good evidence of efficacy for most commonly-prescribed analgesics Standard doses of NSAIDs and COX-2 inhibitors provide the best analgesia and lowest
rate of adverse events
I N B R I E F
RESEARCH
07p407-411qxd 10092004 1518 Page 407
RESEARCH
408 BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004
References for the reviews are as followsAspirin Edwards et al 19998 additional searching in
2002 found no new studiesCelecoxib An unpublished review being submitted as a
Cochrane ReviewDiclofenac An updated version of a Cochrane review11
Dihydrocodeine A Cochrane review12
Ibuprofen An updated version of a Cochrane review11
Paracetamol An updated version of a Cochrane review13
Paracetamol An updated version of a Cochrane review13
plus codeineRofecoxib An updated version of a systematic review14
Valdecoxib A systematic review in preparation
Criteria for inclusion for postoperative dental pain werestudy in third molar extraction full journal publication (exceptvaldecoxib which included information from a poster) ran-domised controlled trials which included single dose treatmentgroups of oral analgesic and placebo double blind designbaseline postoperative pain of moderate to severe intensitypatients over 15 years of age at least 10 patients per group andthe pain outcome measures of total pain relief (TOTPAR) orsummed pain intensity difference (SPID) over 4-6 hours or suf-ficient data to allow their calculation Pain measures allowedfor the calculation of TOTPAR or SPID were a standard fivepoint pain relief scale (none slight moderate good complete)a standard four point pain intensity scale (none mild moder-ate severe) or a standard visual analogue scale (VAS) for pain
relief or pain intensity For adverse events the primary out-come sought was the proportion of patients experiencing anyadverse event with secondary outcomes of patients experienc-ing particular adverse events Although adverse events areoften reported inconsistently in acute pain trials15 the outcomeof any patient experiencing any adverse event was the mostconsistently reported
Each report which could possibly be described as a randomisedcontrolled trial was read independently by several authors andscored using a commonly-used three item 1-5 score qualityscale16 Consensus was then achieved The maximum score of anincluded study was 5 and the minimum score was 2 Authors werenot blinded because they already knew the literature This scoringsystem takes account of randomisation blinding and withdrawalsand drop outs Trials that score 3 or more (less biased) have beenshown repeatedly to have lower treatment effects than those scor-ing 2 or less1718
For each trial mean TOTPAR SPID VAS-TOTPAR or VAS-SPIDvalues for each treatment group were converted to maxTOTPARby division into the calculated maximum value19 The proportionof patients in each treatment group who achieved at least 50maxTOTPAR was calculated using valid equations20-22 The num-ber of patients randomised was taken as the basis for calculationsto produce an intention to treat analysis The number of patientswith at least 50 maxTOTPAR was then used to calculate relativebenefit and NNT for analgesic versus placebo The same methodswere used for adverse events where the number needed to harm(NNH) was calculated
Table 1 Numbers of prescription items issued by dentists and dispensed in EnglandAnalgesic 1998 1999 2000 2001
Ibuprofen 400 mg 107200 110400 109000 103900
Dihydrocodeine 30 mg 53700 50300 49100 46700
Ibuprofen 600 mg 34200 39700 40800 42600
Ibuprofen 200 mg 36300 34600 32000 30600
Paracetamol 500 mg 11100 12800 15400 17200
Paracetamol 500 mg soluble 800 1000 900 900
Pethidine 50 mg 1100 900 700 700
Aspirin 300 mg 200 200 200 200
Source DOH statistics division 2002 calendar year January to December
Dihydrocodeine 30 mgParacetamol 300 mg + codeine 30 mg
Paracetamol 600650 mgAspirin 600650 mg
Paracetamol 9751000 mgCelecoxib 200 mg
Paracetamol 600650 mg + codeine 60 mgIbuprofen 200 mgDiclofenac 50 mgRofecoxib 50 mgIbuprofen 400 mgValdecoxib 20 mgDiclofenac 100 mgValdecoxib 40 mgIbuprofen 600 mg
0 10 20 30 40 50 60 70 80 90 10095 confidence interval of the percent ofpatients achieving at least 50 pain relief
Fig 1 The 95confidence interval ofthe proportion ofpatients with at leasthalf pain relief over 4-6hours compared withplacebo in third molarextraction trials
07p407-411qxd 10092004 1519 Page 408
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 409
of patients had at least half pain relief with active treatment in onesmall trial in dental pain (Table 2)
The adverse event outcome of a patient experiencing anyadverse event is shown in Table 3 from 10113 patients in 107 tri-als Of the 15 drug and dose combinations only paracetamol600650 mg plus codeine 60 mg could be statistically distin-guished from placebo in 10 trials and 824 patients The NNH was53 (41 to 74) indicating that five patients had to be treated withparacetamol 600650 mg plus codeine 60 mg for one of them tohave an adverse event that would not have occurred with placeboFor all other drugs and doses there was no difference betweenanalgesic and placebo
DISCUSSIONSystematic review and meta-analysis both depend on two interde-pendent criteria for them to make sense the quality of the compo-nent individual studies and the total size of the sample availablefor analysis
We know that if trials are of poor reporting quality1718 or notrandomised30 or not blind or both31 then the tendency is to over-estimate the benefits of treatment The reviews included here alldemanded that trials should be both randomised and double-blindas a minimum requirement for inclusion
We also know that even if trials are done well small samplesize can lead to an incorrect answer just because of the randomplay of chance4 For these studies we also know just how muchinformation is needed to be 95 confident of an NNT to withplusmn05 units4 With an NNT of 23 it is 400 patients in the compari-son with an NNT of 29 it is 1000 patients and with an NNT of42 it is many more than with 1000 At NNTs of 4 or more evenwith 1000 patients fewer than 75 of trials will be within plusmn05of the overall NNT
The analgesics for which these two criteria were metunequivocally were valdecoxib (combining 20 mg and 40 mg)rofecoxib 50 mg ibuprofen 400 mg diclofenac 50 mg and prob-ably ibuprofen 200 mg For paracetamol the numbers were bor-derline and for diclofenac 100 mg too small to make any safejudgement There is good evidence of good efficacy for the anal-gesics most commonly prescribed by dentists with the excep-tion of dihydrocodeine where there was little evidence in totaland no convincing evidence of efficacy
Relative benefit and relative risk estimates were calculated with95 confidence intervals using a fixed effects model23 Hetero-geneity tests were not used as they have previously been shown tobe unhelpful2425 though homogeneity was examined visually26
Publication bias was not assessed using funnel plots as these testshave been shown to be unhelpful2728 The number needed to treator harm (NNT and NNH) with confidence intervals was calculatedby the method of Cook and Sackett29 from the sum of all eventsand patients for treatment and placebo
Relative benefit or risk was considered to be statistically signifi-cant when the 95 confidence interval did not include 1 NNT val-ues were only calculated when the relative risk or benefit was sta-tistically significant and are reported with the 95 confidenceinterval Calculations were performed using Microsoft Excel 2001on a Power Macintosh G4
RESULTSTable 2 shows the main results from 14150 patients in 155 trials of15 drug and dose combinations against placebo in third molarextractions Of those 15 drug and dose combinations only dihy-drocodeine 30 mg could not be statistically distinguished fromplacebo because there were no trials with any useful informationin third molar extraction Figure 1 shows the proportion ofpatients achieving at least 50 pain relief with treatment Thesmallest sample for any comparison was 136 patients for celecoxib200 mg Only five of the 14 comparisons had more than 1000patients and seven had fewer than 500 patients In all systematicreviews the majority of trials had quality scores of 3 or more
The lowest (best) NNTs were for NSAIDs and COX-2 inhibitorsat standard or high doses For these NNTs could be as low as about2 (meaning that two patients had to be treated with NSAID orCOXIB for one of them to have an outcome of at least half painrelief that would not have occurred with placebo) Valdecoxib 20mg and 40 mg rofecoxib 50 mg ibuprofen 400 mg and diclofenac50 mg and 100 mg all had NNTs below 24 For all of them about60-70 of patients had at least half pain relief with active treat-ment compared with about 10 with placebo
Paracetamol 9751000 mg aspirin 600650 mg and paraceta-mol 600650 mg had NNTs of between 4 and 5 Fewer than 40 ofpatients with paracetamol at these doses had at least half painrelief with active treatment With dihydrocodeine 30 mg only 16
Table 2 Efficacy of analgesics after third molar extraction from systematic reviews of randomised double blind trials
Number () of patientswith at least 50 pain relief
Drug and dose Treatment Placebo Relative benefit Number needed to treat Total patients Total trials(95 CI) (95 CI)
Valdecoxib 40 mg 204279 (73) 19194 (10) 73 (48 to 112) 16 (14 to 17) 473 4
Diclofenac 100 mg 71102 (70) 8102 (8) 89 (45 to 175) 16 (14 to 19) 204 2
Valdecoxib 20 mg 69101 (68) 8103 (8) 88 (45 to 173) 17 (14 to 20) 204 2
Diclofenac 50 mg 112189 (59) 21178 (12) 49 (33 to 75) 21 (18 to 26) 367 5
Rofecoxib 50 mg 318557 (57) 23262 (9) 66 (44 to 99) 21 (19 to 23) 819 6
Ibuprofen 400 mg 10351835 (56) 1861567 (12) 47 (40 to 54) 22 (21 to 24) 3402 37
Ibuprofen 200 mg 323695 (46) 47499 (9) 46 (35 to 61) 27 (24 to 31) 1194 14
Ibuprofen 600 mg 90114 (79) 3889 (43) 19 (15 to 25) 28 (20 to 43) 203 3
Celecoxib 200 mg 3991 (43) 445 (9) 48 (18 to 127) 29 (21 to 48) 136 1
Paracetamol 9751000 mg 226616 (37) 40422 (9) 38 (28 to 52) 37 (31 to 47) 1038 10
Paracetamol 600650 mg + codeine 60 mg 217532 (48) 64380 (19) 25 (19 to 31) 42 (34 to 55) 911 12
Paracetamol 600650 mg 224630 (36) 76635 (12) 29 (23 to 37) 42 (36 to 52) 1265 10
Aspirin 600650 mg 6271788 (36) 2551847 (15) 25 (22 to 29) 47 (42 to 54) 3635 46
Paracetamol 300 mg + codeine 30 mg 48175 (29) 11124 (9) 33 (18 to 62) 54 (37 to 97) 299 3
Dihydrocodeine 30 mg 849 (16) 250 (4) 41 (09 to 18) not calc 99 1
Shaded areas are those analgesics used by dentists in the UK
07p407-411qxd 10092004 1519 Page 409
RESEARCH
410 BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004
With the information available standard doses of NSAIDs andCOX-2 inhibitors provided the best analgesia (Fig 2) NNTs of 2and below are indicative of very effective medicines32 The indirectcomparisons that allow us to arrive at this conclusion are only sus-tainable because the trials have the same design use patients withthe same entry criterion (moderate or severe pain intensity) withstandard measurements made in the same way over the same peri-od of time and with the same output from each trial and oneknown to be legitimate The validity of the indirect comparisonsare buttressed by the dose response of two doses of ibuprofen (400mg was better than 200 mg) and two doses of paracetamol(9751000 mg was better than 600650 mg) where there were cred-ible amounts of information A systematic review of ibuprofenversus paracetamol in dental studies also concluded that ibuprofenwas superior concordant with the indirect comparison33
The adverse event information we have tells us only aboutpatients experiencing any adverse event With the amount ofinformation available it appears that only higher doses ofcodeine with paracetamol resulted in a significantly higher ratefor this outcome than placebo In Table 3 the rate at which thisadverse event occurred with placebo varied greatly between 2
and 52 This variation will be due partly to small sizes4 butalso because we know that methods of collecting adverse eventdata impact significantly on the reported incidence and becausemethods used varied15
Information about specific adverse events is even more difficultto obtain and very large data sets are required to produce infor-mation about for instance gastric irritation with aspirin use8 Ofinterest to dentists might be the rate of alveolitis or dry socket Thisis reported in some of the newer COXIB studies but not in olderstudies There is just too little information to make a judgement
What these comparisons do not do is to tell dentists what toprescribe They and the products of other systematic reviewsshould not be used as rules but rather as evidence-based toolsto help make better policy decisions and decisions about indi-vidual patients Present prescribing practice (Table 1) showsthat for the most part effective and safe analgesics are beingused in 80 of prescriptions The exception is prescribing dihy-drocodeine 30 mg (20 of prescriptions) for which we lack sin-gle dose evidence of efficacy in dental surgery and which couldnot be distinguished from placebo in other conditions againwith little data6
Paracetamol 300 + codeine 30 mgAspirin 600650 mg
Paracteamol 600650 mgParacetamol 600650 + codeine 60 mg
Paracetamol 9751000 mgCelecoxib 200 mgIbuprofen 200 mgDiclofenac 50 mgIbuprofen 400 mgRofecoxib 50 mg
Valdecoxib 20 mgValdecoxib 40 mgDiclofenac 100 mg
1 2 3 4 5 6 7 8 9 1095 confidence interval of the NNT
Fig 2 The 95confidence interval ofthe number needed totreat (NNT) for at leasthalf pain relief over 4-6hours compared withplacebo in third molarextraction trials
Table 3 Patients experiencing any adverse event with analgesics after third molar extraction from systematic reviews of randomised double blind trials
Number () of patientsharmed with
Drug and dose Treatment Placebo Relative risk Number needed to harm Total patients Total trials(95 CI) (95 CI)
Valdecoxib 40 mg 63180 (35) 76144 (53) 06 (05 to 08) not calc 324 3
Diclofenac 100 mg 252 (4) 252 (4) 10 (12 to 68) not calc 104 1
Valdecoxib 20 mg 36100 (36) 55103 (53) 07 (05 to 09) not calc 203 2
Diclofenac 50 mg 15222 (7) 12210 (6) 12 (06 to 24) not calc 432 4
Rofecoxib 50 mg 105314 (33) 48122 (39) 09 (07 to 11) not calc 436 3
Ibuprofen 400 mg 120972 (13) 91805 (12) 11 (08 to 14) not calc 1777 19
Ibuprofen 200 mg 84554 (15) 69372 (19) 08 (06 to 10) not calc 926 10
Ibuprofen 600 mg no data
Celecoxib 200 mg no data
Paracetamol 9751000 mg 175836 (24) 103464 (20) 11 (09 to 13) not calc 1300 9
Paracetamol 600650 mg + codeine 60 mg 156490 (25) 43333 (14) 18 (13 to 25) 53 (41 to 74) 824 10
Paracetamol 600650 mg 32228 (14) 20229 (9) 16 (09 to 27) not calc 457 7
Aspirin 600650 mg 1551320 (12) 1681422 (12) 10 (08 to 12) not calc 3031 36
Paracetamol 300 mg + codeine 30 mg 29175 (15) 20124 (16) 09 (06 to 16) not calc 299 3
Dihydrocodeine 30 mg 149 (2) 150 (2) 10 (01 to 17) not calc 99 1
Shaded areas are those analgesics used by dentists in the UK
07p407-411qxd 10092004 1520 Page 410
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 411
Not all the analgesics in this review are presently available forprescribing by dentists at least in the UK The information on effi-cacy on harm and on the amount of information available shouldbe useful in any initiative to develop a prescribing formulary indentistry especially as we have growing confidence in the value ofindirect comparisons34
COMPETING INTERESTSRAM has been a consultant for MSD RAM amp HJM have consulted for variouspharmaceutical companies RAM HJM amp JE have received lecture fees frompharmaceutical companies related to analgesics and other healthcareinterventions All authors have received research support from charitiesgovernment and industry sources at various times but no such support wasreceived for this work No author has any direct stock holding in anypharmaceutical company
AUTHORS CONTRIBUTIONSJB was involved with searching data extraction quality scoring analysis andwriting JE was involved with searching data extraction quality scoring andwriting HJM was involved in analysis and writing RAM was involved in dataextraction quality scoring analysis and writing PW was involved with theoriginal concept with researching prescribing data and writing
The work was supported by Pain Research Funds and the Oxford Pain Relief TrustThe authors would like to thank Frances Fairman of the Cochrane Pain Palliativeand Supportive Care systematic review group for bringing this issue to ourattention The Department of Health Statistics Division provided data onprescribing by dentists
1 Beecher H K Keats A S Mosteller F The effectiveness of oral analgesics (morphinecodeine acetylsalicylic acid) and the problem of placebo lsquoreactorsrsquo and lsquononreactorsrsquo J Pharmacol 1953 109 93-400
2 Beecher H K The measurement of pain Pharmacol Rev 1957 9 59-2103 Houde R W Wallenstein S L Beaver W T Clinical measurement of pain In G De
Stevens (ed) Analgetics pp75-122 New York and London Academic Press 1965 4 Moore R A Gavaghan D Tramegraver M R Collins S L McQuay H J Size is everything mdash
large amounts of information are needed to overcome random effects in estimatingdirection and magnitude of treatment effects Pain 98 78 209-216
5 Ioannidis J P A Lau J Evolution of treatment effects over time Empirical insight fromrecursive cumulative metaanalyses PNAS 2001 98 831-836
6 McQuay H J Moore R A An evidence-based resource for pain relief Oxford OxfordUniversity Press 1998
7 McQuay H J Carroll D Moore R A Variation in the placebo effect in randomisedcontrolled trials of analgesics all is as blind as it seems Pain 1996 64 331-335
8 Edwards J E Oldman A Smith L Wiffen P J Carroll D McQuay H J Moore R A Oralaspirin in postoperative pain a quantitative systematic review Pain 1999 81 289-297
9 Moher D Cook D J Eastwood S Olkin I Rennie D Stroup D F Improving the quality ofreports of meta-analyses of randomised controlled the QUOROM statement Lancet1999 354 1896-1900
10 Jadad A R Carroll D Moore A McQuay H Developing a database of published reportsof randomised clinical trials in pain research Pain 1996 66 239-46
11 Collins S L Moore R A McQuay H J Wiffen P J Edward J S Single dose oral ibuprofenand diclofenac for postoperative pain In The Cochrane Library Issue 4 2000 OxfordUpdate Software
12 Edwards J E McQuay H J Moore R A Single-dose dihydrocodeine for acute
postoperative pain In The Cochrane Library Issue 4 2000 Oxford Update Software13 Moore R A Collins S L Carroll D McQuay H J Edwards J Single dose paracetamol
(acetaminophen) with and without codeine for postoperative pain In The CochraneLibrary Issue 4 2000 Oxford Update Software
14 Barden J Edwards J E McQuay H J Moore R A Rofecoxib in acute postoperative painquantitative systematic review BMC Anesthesiol 2002 2 4httpwwwbiomedcentralcom1471-225324
15 Edwards J E McQuay H J Moore R A Collins S L Reporting of adverse effects inclinical trials should be improved Lessons from acute postoperative pain J PainSympt Manage 1999 18 427-437
16 Jadad A R Moore R A Carroll D et al Assessing the quality of reports of randomizedclinical trials is blinding necessary Control Clin Trials 1996 17 1-12
17 Khan K S Daya S Jadad A R The importance of quality of primary studies inproducing unbiased systematic reviews Arch Intern Med 1996 156 661-666
18 Moher D Pham B Jones A et al Does quality of reports of randomised trials affectestimates of intervention efficacy reported in meta-analyses Lancet 1998 352609-613
19 Cooper S A Single-dose analgesic studies the upside and downside of assaysensitivity In Max M B Portenoy R K and Laska E M (eds) The design of analgesicclinical trials (Advances in Pain Research and Therapy Vol 18) pp117-124 New YorkRaven Press 1991
20 Moore A McQuay H Gavaghan D Deriving dichotomous outcome measures fromcontinuous data in randomised controlled trials of analgesics Pain 1996 66 229-237
21 Moore A McQuay H Gavaghan D Deriving dichotomous outcome measures fromcontinuous data in randomised controlled trials of analgesics Verification fromindependent data Pain 1997 69 127-130
22 Moore A Moore O McQuay H Gavaghan D Deriving dichotomous outcome measuresfrom continuous data in randomised controlled trials of analgesics Use of painintensity and visual analogue scales Pain 1997 69 311-315
23 Morris J A Gardner M J Calculating confidence intervals for relative risk odds ratiosand standardised ratios and rates In Gardner M J and Altman D G(eds) Statistics withconfidence mdash confidence intervals and statistical guidelines pp50-63 LondonBritish Medical Journal 1995
24 Gavaghan D J Moore R A McQuay H J An evaluation of homogeneity tests in meta-analyses in pain using simulations of individual patient data Pain 2000 85 415-424
25 Higgins J Thompson S Deeks J Altman D Statistical heterogeneity in systematicreviews of clinical trials a critical appraisal of guidelines and practice J Health SurvRes Policy 2002 7 51-61
26 LAbbeacute K A Detsky A S ORourke K Meta-analysis in clinical research Ann Intern Med1987 107 224-233
27 Sterne J A Gavaghan D Egger M Publication and related bias in meta-analysispower of statistical tests and prevalence in the literature J Clin Epidemiol 2000 531119-1129
28 Tang J-L Liu J L Y Misleading funnel plot for detection of bias in meta-analysis J ClinEpidemiol 2000 53 477-484
29 Cook R J Sackett D L The number needed to treat a clinically useful measure oftreatment effect Br Med J 1995 310 452-454
30 Carroll D Tramegraver M McQuay H Nye B Moore A Randomization is important instudies with pain outcomes systematic review of transcutaneous electrical nervestimulation in acute postoperative pain Br J Anaesth 1996 77 798-803
31 Schulz K F Chalmers I Hayes R J Altman D G Empirical evidence of bias dimensionsof methodological quality associated with estimates of treatment effects incontrolled trials J Am Med Assoc1995 273 408-412
32 McQuay H J Moore R A Using numerical results from systematic reviews in clinicalpractice Ann Intern Med 1997 126 712-720
33 M Hyllested Jones S Pedersen J L Kehlet H Comparative effect of paracetamolNSAIDs or their combination in postoperative pain management a qualitative reviewBr J Anaesth 2002 88 199-214
34 F Song Altman D G Glenny A M Deeks J J Validity of indirect comparison forestimating efficacy of competing interventions empirical evidence from publishedmeta-analyses Br Med J 2003 326 472-476
07p407-411qxd 10092004 1520 Page 411
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
Relative efficacy of oral analgesics after third molar extraction ndash a 2011 updateS Derry1 P J Wiffen2 and R A Moore3
and reporting and were all of high meth-odological quality the relative efficacy of different analgesics is justifiable when established against the common comparator of placebo3 Moreover the methods have been extensively examined and validated using individual patient data analyses45
Several approaches can be used to pre-sent results The percentage of patients who benefit with treatment is one approach obviously the higher the number
In 2004 the British Dental Journal carried a review examining analgesic efficacy meas-ured after third molar extractions1 predom-inantly derived from Cochrane reviews of single dose analgesics in established mod-erate or severe pain In the intervening years the reviews on which it was based have been extended to other analgesics and updated to include relevant additional clinical trials performed in the past decade
The culmination of this work has been the publication by the Cochrane Collaboration of an overview of these updated systematic reviews2 The overview included 35 sepa-rate Cochrane Reviews with 38 analyses of single dose oral analgesics tested in acute postoperative pain models with results from about 45000 participants studied in approximately 350 individual studies About 29000 patients contributed data to trials in dental pain
Each individual review reported results for dental studies where data were avail-able overwhelmingly in the third molar extraction pain model Because all of the reviews used identical methods outcomes
This article provides a summary of the efficacy and relative efficacy of 38 different drugs or drug combinations tested in standard postoperative pain trials It will help clinicians and patients make informed choices about analgesia based on pain relief duration of action and adverse events which can then be put into context for the individual patient depending on local availability This article highlights the fact that no single drug is effective in all patients ndash even the best drugs fail to provide good levels of pain relief in at least 30 These patients should try a different analgesic
the better Another way is to look at the number needed to treat (NNT) for one patient to benefit this is the treatment-specific effect and can be expressed as 100(active - placebo) The ideal NNT is 1 where everyone gets better with treatment and no one does with placebo lower numbers are better In dental tri-als where about 10 of patients benefit with placebo the best possible NNT is 100100 - 10 = 11
13Pain Research and Nuffield Division of Anaesthet-ics Department of Clinical Neurosciences University of Oxford The Churchill Hospital Oxford OX3 7LJ 2UK Cochrane Centre Summertown Pavilion 18-24 Middle Way Oxford OX2 7LG Correspondence to R Andrew Moore Email andrewmoorepruoxacuk
Refereed Paper Accepted 12 September 2011 DOI 101038sjbdj2011905 copyBritish Dental Journal 2011 211 419-420
bull Summarises the known evidence on efficacy of oral analgesics in dental pain
bull Describes shorter term pain relief and time needed before remedication
bull Provides an evidential context for making decisions about individual patients or practice guidelines
I N B R I E F
PRA
CTICE
Table 1 Efficacy results in dental pain studies for a range of commonly used analgesics
Drug and dose (mg)Number of
Percent with at least 50 maxi-mum pain relief NNT
Median time to remedication (hr)
Trials Patients Active Placebo
Aspirin 600650 mg 45 3581 36 14 45 (40 to 52) 30
Aspirin 1000 mg 4 436 35 11 42 (32 to 60) no data
Celecoxib 400 mg 4 620 34 3 25 (22 to 29) 84
Diclofenac 50 mg (Na and K) 9 1119 56 19 27 (24 to 31) 43
Diclofenac 50 mg K 5 622 65 16 21 (19 to 24) no data
Etoriocoxib 120 mg 4 500 71 9 16 (15 to 18) gt24
Ibuprofen 400 mg 49 5428 55 12 23 (22 to 24) 56
Ibuprofen 400 mg soluble 9 959 66 10 18 (17 to 20) no data
Ibuprofen 200 mg + paracetamol 500 mg 2 280 74 10 16 (14 to 18) gt8
Naproxen 500550 mg 5 402 61 7 18 (16 to 21) 89
Paracetamol 1000 mg 19 2157 41 10 32 (29 to 36) 39
Note that data for remedication time were not generally available for dental studies separately and the values reported apply to all postoperative conditions though predominantly third molar extraction
BRITISH DENTAL JOURNAL VOLUME 211 NO 9 NOV 12 2011 419
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
PRACTICE
This brief report describes the main results of interest to dentists using results from the Cochrane overview and from a recent analysis of a combination of ibu-profen and paracetamol5
RESULTSTable 1 reports data for aspirin celecoxib diclofenac etoricoxib ibuprofen ibu-profen plus paracetamol naproxen and paracetamol Widely differing amounts of information were available for individual drugs from as few as 402 patients for nap-roxen 500550 mg and as many as 5428 for ibuprofen 400 mg
One outcome reported is the percentage of patients with initially moderate pain (30-60 mm on a 100 mm VAS) or severe pain (more than 60 mm) who obtained at least 50 of the maximum possible pain relief over a 4-6 hour period after taking the tab-lets This is a high test of efficacy achieved by only about 10 of patients who received no active treatment (placebo) but achieved by 34-74 of those who did get the active drug Ibuprofen 200 mg plus paracetamol 500 mg and etoricoxib 120 mg achieved
response rates above 70 paracetamol 1000 mg achieved only a 41 response rate
Several products had an NNT of about 2 or below the combination of ibupro-fen 200 mg plus paracetamol 500 mg etoricoxib 120 mg ibuprofen 400 mg in a soluble form naproxen 500550 mg and 50 mg of the potassium salt of diclofenac (the sodium salt being much less effective in this assay Fig 1)
A new outcome that some will con-sider relevant is the time required for half the patients to need more analgesia the time to remedication Longer duration is another indicator of greater effect and for a number of analgesics median remedica-tion times are beyond eight hours
DISCUSSIONThe 2004 review included evidence for rofecoxib and valdecoxib neither of which is available today New relevant informa-tion includes data on the ibuprofen plus paracetamol combination different ibu-profen and diclofenac formulations and etoricoxib all of which are among the most efficacious analgesics after third
molar surgery Greater efficacy and longer duration of action tended to go together
For one analgesic relevant to dentistry the evidence is largely silent For dihydrocodeine 30 mg (still commonly used by dentists) only 136 patients were found in trials in dental pain with only 24 obtaining at least 50 maximum pain relief compared with 7 with placebo The resultant NNT was 6 far worse than available for drugs in Table 1 and far worse than ibuprofen 400 mg in the only direct comparison6 The Cochrane overview concluded that the results for dihy-drocodeine were not robust because of the smallness of the data set available and that unpublished results from just 46 patients in zero effect trials would be needed to make any result clinically irrelevant
CONCLUSIONThe amount of evidence available on single dose studies of analgesics in dental pain is large and readily available These results are tools to help formulate policy and pre-scribing for individuals and populations
1 Barden J Edwards J E McQuay H J Wiffen P J Moore R A Relative efficacy of oral analgesics after third molar extraction Br Dent J 2004 197 407ndash411
2 Moore R A Derry S McQuay H J Wiffen P J Single dose oral analgesics for acute postoperative pain in adults Cochrane Database Syst Rev 2011 9 CD008659
3 Song F Altman D G Glenny A M Deeks J J Validity of indirect comparison for estimating efficacy of competing interventions empirical evidence from published meta-analyses BMJ 2003 326 472
4 Moore R A Edwards J E McQuay H J Acute pain individual patient meta-analysis shows the impact of different ways of analysing and presenting results Pain 2005 116 322ndash331
5 Moore R A Straube S Paine J Derry S McQuay H J Minimum efficacy criteria for comparisons between treatments using individual patient meta-analysis of acute pain trials examples of etoricoxib paracetamol ibuprofen and ibuprofenparacetamol combinations after third molar extraction Pain 2011b 152 982ndash989
6 Moore R A Edwards J Derry S McQuay H J Single dose oral dihydrocodeine for acute postop-erative pain Cochrane Database Syst Rev 2000 2 CD002760
Ibuprofen 200mg + paracetamol 500 mg
Ibuprofen 400 mg
Aspirin 600650 mg
Aspirin 1000 mg
Paracetamol 1000
Naproxen 500550
Diclofenac 50 mg (Na and K)
Celecoxib 400 mg
Diclofenac 50 mg K
Ibuprofen 400 mg soluble
Etoriocoxib 120 mg
1 2 3 4 5 6
NNT for at least 50 maximum pain relief (95 CI)
Fig 1 NNTs in dental pain studies for a range of commonly used analgesics
420 BRITISH DENTAL JOURNAL VOLUME 211 NO 9 NOV 12 2011
Combining paracetamol with a selectivecyclooxygenase-2 inhibitor for acutepain relief after third molar surgerya randomized double-blindplacebo-controlled study
Birgitta Haglund12 Inger vonBltzingslccedilwen1
1Public Dental Health Service KarlstadVrmland Sweden 2Department of ClinicalPharmacology Sahlgrenska Academy atGccedilteborg University Sweden
Traditional non-steroidal anti-inflammatory drugs(NSAIDs) [ie non-selective cyclooxygenase (COX)inhibitors such as ibuprofen and diclofenac] have beenwidely used in outpatients for acute pain relief followingoral surgery Their anti-inflammatory and analgesicproperties together with well-established tolerabilitymake them an initial choice for the management of mostforms of mild to moderate pain in outpatients (1 2)However these drugs have well-documented adverseeffects such as gastrointestinal intolerability Further-more they need to be administered several times a dayMore effective and practical pain relief regimes withfewer side-effects are needed for moderate to severe painafter oral surgeryNSAIDs act by inhibiting COX enzymes which are
responsible for the production of prostaglandin fromarachidonic acid This acid emerges from the breakdownof phospholipids in the cell walls of damaged tissue (3)Prostaglandin elicits a number of biological effects someof which contribute to the inflammatory process leading
to pain Multiple COX enzymes have been identifiedCOX-1 is mainly expressed under physiological condi-tions throughout the body for example by platelets (4)and COX-2 is related to inflammation and pain (4ndash6)although COX-1 and COX-2 also have overlappingproperties (7) Improved knowledge on more selectiveCOX enzymes led to the development of specific COX-2inhibitors such as rofecoxib (8) and celecoxib withanalgesic anti-inflammatory and gastroprotective prop-erties Of these drugs rofecoxib has been shown to bemore effective than celecoxib (9ndash11)Rofecoxib has the same analgesic effect as ibuprofen
but with the benefit of a longer duration (9 10 12) It hasa long half-life which makes it suitable for once-dailydosing (12) compared with traditional NSAIDs thatneed to be taken several times per day Rofecoxib hasalso been suggested to be more effective than paracet-amol combined with codeine (13 14) The COX-2inhibitor rofecoxib may be an interesting choice for acutepain relief after oral surgery
Haglund B von Bulzingslowen I Combining paracetamol with a selective cyclooxyge-nase-2 inhibitor for acute pain relief after third molar surgery a randomized double-blind placebo-controlled study Eur J Oral Sci 2006 114 293ndash301 2006 The AuthorsJournal compilation 2006 Eur J Oral Sci
Severe pain after third molar surgery is often encountered and more effective treatmentregimes are warranted The objective of this study was to evaluate if the combinationof paracetamol and rofecoxib a selective cyclooxygenase-2 (COX-2) inhibitorimproves analgesic effects following third molar surgery compared with rofecoxibalone Paracetamol alone was also evaluated Altogether 120 patients with moderate tosevere pain after third molar surgery were given a single postoperative dose of one ofthe following treatments rofecoxib + paracetamol rofecoxib alone paracetamolalone or placebo Patients assessed level of pain and pain relief every 30 min for 8 hafter surgery and made a global evaluation of the medication 4 and 8 h after surgeryParacetamol and rofecoxib combined improved the analgesic effect compared withrofecoxib alone for the first 15 h Rofecoxib alone and the combination of paracet-amol and rofecoxib had a significantly better analgesic effect than paracetamol alonefrom 3 h onwards The early onset of pain relief for the combination of paracetamoland rofecoxib compared with rofecoxib alone could be of great importance whentreating acute pain after third molar surgery After data collection for this studyrofecoxib was withdrawn from the market as a result of reported fatal cardiovascularevents Whether this is relevant for short-term use is unknown but it has to be con-sidered before rofecoxib may be used for pain relief following third molar surgery
Birgitta Haglund Folktandvrden TingvallaBox 577 SE-651 13 Karlstad Sweden
Telefax +46ndash54ndash137435E-mail birgittahaglundlivse
Key words COX-2 inhibitor pain relief para-cetamol randomized trial third molar surgery
Accepted for publication April 2006
Eur J Oral Sci 2006 114 293ndash301Printed in Singapore All rights reserved
2006 The AuthorsJournal compilation 2006 Eur J Oral Sci
European Journal ofOral Sciences
Combining drugs that cause analgesia through differ-ent mechanisms may give additive analgesic effects (15)and lead to dose-sparing effects and improved safety(16) The analgesic mechanism of COX inhibition ispredominantly peripheral Research on paracetamol hasnot been able to delineate a clear mechanism of actionbut it is suggested to lie predominantly in the centralnervous system (17) Some studies indicate that combi-ning a traditional NSAID and paracetamol after oralsurgery may enhance the analgesic effect compared withsingle drug regimes (18 19)The theory of the analgesic effect of traditional
NSAIDs being caused by COX-2 inhibition leads to thethought that an additive effect should be present alsowhen combining rofecoxib and paracetamol The aim ofthis study was therefore to explore in a third molarsurgery pain model (20) if there is an additive analgesiceffect when combining the COX-2 selective inhibitorrofecoxib with paracetamol compared with rofecoxibalone for acute pain relief We also compared the anal-gesic efficiency of rofecoxib and paracetamol becausethis to our knowledge has not been reported followingthird molar surgery
Material and methods
Study design
This study was designed as a multicenter randomizeddouble-blind placebo-controlled study with a single dose ofrofecoxib 50 mg and paracetamol 1 g combined vs rofec-oxib 50 mg alone vs paracetamol 1 g alone vs placebogiven postoperatively to patients stating moderate to severepain after surgical removal of one or two lower third molarsPatients were asked to give written informed consent toparticipate after being told about the procedures A total of120 patients were randomized into four different treatmentgroups as follows 40 patients receiving the combination ofrofecoxib 50 mg and paracetamol 1 g 40 patients receivingrofecoxib 50 mg alone 20 patients receiving paracetamol 1 galone and 20 patients receiving placebo The patientsrsquoevaluations of the treatments were obtained by using aquestionnaire which the patients filled in at home during an8-h study period following intake of the study medicationThe trial was approved by the Regional Ethical Committeeof Medical Research in Orebro Sweden and the MedicalProducts Agency in Uppsala Sweden
Patients
Consecutive patients visiting four general dental practicesand in need of mandibular third molar surgery in accordancewith the National Institutes of Health (NIH) guidelines (21)were screened for enrollment Only patients with thirdmolars needing bone removal were included Other inclusioncriteria were age gt18 yr weight gt50 kg butlt120 kg andan appointment before noon for surgery This was necessaryin order for the patients to have time to fill in the ques-tionnaire for 8 h after intake of the study medication beforebedtime Exclusion criteria were as follows intolerance toacetylsalicylic acid (ASA) paracetamol andor NSAIDsany ongoing medication (except contraceptives) pregnancylactation inadequate contraception alcohol or drug abusePatients with evidence of previous or present cardiovascular
respiratory diabetic hepatic gastric renal neurological orneoplastic diseases were also excluded as were those withongoing pericoronitis or other local oral infections involvingpain Patients with an intake of any analgesics 6 h precedingsurgery was also excluded All patients who met the studycriteria and reported moderate to severe pain after the sur-gery were included in the study
Surgery
The surgery was performed by one of four dentists speciallytrained in dento-alveolar surgery using local anesthesia(lidocaine 20 mg ml)1 plus epinephrine 125 lg ml)1) Theremoval of bone was carried out with a burr under thecooling of saline
Masking randomization and rescue medication
The study medications were masked by being encapsula-ted in identical capsules The capsules contained 50 mg ofrofecoxib 200 mg of paracetamol or placebo All patientswere given a sealed container containing six capsules(Table 1) so that the patients in the different treatmentgroups received the correct amount of medication and stillthe same number of capsules The capsules were manu-factured by Apoteket Production amp Laboratories (APLStockholm Sweden) Randomization of the patients intothe four treatment groups was performed for the group intotal by Apoteket using randomization tables All studypersonnel and participating patients were blinded totreatment assignment for the duration of the study Themain investigator broke the codes for the final calcula-tionsIbuprofen 400 mg was used as a rescue medication in case
patients needed additional analgesia at any time during the8-h study period The rescue medication was kept in aseparate container If patients felt that rescue medicationwas needed they were instructed to wait 90 min if possibleafter intake of their study medication to allow for the studydrug to take effect
Intake of study medication and information about thequestionnaire
After surgery the patients were given their two containerswith study and rescue medications respectively together
Table 1
Distribution of the drug capsules with the different substances percontainer in each study group
Study groups
Rofecoxib50 mg +
paracetamol 1 gRofecoxib50 mg
Paracetamol1 g Placebo
Rofecoxib50 mg
1 1 0 0
Paracetamol200 mg
5 0 5 0
Placebo 0 5 1 6Total no ofcapsules ineach container
6 6 6 6
294 Haglund amp Bultzingslowen
with the questionnaire Routine postoperative informationwas given The patients were instructed to go home and takeno medication before calling the investigator when theyregained full sensibility in the lower lip following the dis-appearance of the local anesthesia If the patient had notcalled the investigatorrsquos mobile phone within 3 h after theend of surgery the investigator called the patientAt the telephone contact the patients were asked to state
their level of pain in the questionnaire using a 3-point scalefrom mild to moderate to severe pain If patients statedmoderate or severe pain they were asked to break the seal ofthe container with their study medication and take all sixcapsules Detailed instructions were provided on how to fill inthe questionnaire To ascertain that patients adhered to theprotocol information was given to contact the investigatorwith any questions regarding medication or other issuesconcerning the studyduring the 8-h postoperative periodThestudy period started at the time of intake of the study medi-cation If patients stated mild pain they were asked if theycould tolerate waiting before taking any medication In suchcases a second telephone contact was made If patients stillstatedmild pain they were asked if it was possible for them toreturn their sealed container with the study medicationPatients who did so were replaced with another patient
Efficacy assessments
The outcome measures of the trial were pain intensity painrelief (PAR) global evaluation score (patientsrsquo overallassessment of the medication) derived summary measuresuse of rescue medication and side-effects experienced allrecorded by the patients in their questionnaire After intakeof the study medication pain intensity and PAR wasassessed by the patient every 30 min for 8 h and the globalevaluation score was measured at 4 and 8 h The startingpoint for each patient was the time for intake of studymedication The final measurement point was the end of theobservation period (ie 8 h later) or the time of intake ofrescue medication If rescue medication was used patientswere asked to assess pain intensity and pain relief and give aglobal evaluation score at the time of intake These scoreswere then used for the rest of the observation period inaccordance with a study by Laska et al (22)Pain intensity was evaluated by the patients using a
horizontal visual analog scale (VAS) of 10 cm marked nopain at 0 and worst possible pain at 10 PAR was meas-ured on a 5-point scale as follows 0 no pain relief 1 somepain relief 2 medium pain relief 3 good pain relief and 4total pain relief Global evaluation score was measured on a4-point scale as follows 0 poor 1 fair 2 good and 3excellent Patients using rescue medication recorded the timeof intake A question about any side-effects experienced wasanswered by yes or no at the end of the study period Ifyes the patients estimated adverse events on a 3-point scale(1 slight 2 moderate 3 severe) and reported what kind ofside-effect was experienced
Analysis
The analgesic effect of the drugs measured every 30 min bypain intensity (VAS) and PAR scores was comparedSummary measures were calculated by the use of the fol-lowing total pain relief (TOTPAR the sum of all PARscores for the whole study period of 05ndash8 h) pain intensitydifference (PID pain intensity at the start minus painintensity at any given observation point) sum of PID for the
05ndash3-h period (SPID05)3 h) and sum of PID for the total05ndash8-h period (SPIDtotal) PID values were not analyzedseparately but used for the calculation of SPIDThe use of rescue medication was compared between the
treatment groups by calculating the percentage of patientsin each group who used rescue Also the mean timebetween intake of the study medication and intake of therescue medication in the different groups was analyzedSide-effects in the treatment groups were compared interms of percentage of patients in each group whoexperienced such problems Median global evaluationscores between the different groups were analyzed as wellas the percentage of patients in each group using the dif-ferent scores
Statistics
The sample size calculations were carried out assuming adifference in SPID outcome between groups using thecombination of rofecoxib + paracetamol and rofecoxibalone amounting to 20 (18) with a power of at least 80and a standard deviation (SD) of 15 using non-para-metric statistics (MannndashWhitney U-test) This calculationestimated that a minimum of 22 patients should be includedin each groupStandard descriptive statistics and tests were used and the
calculations were performed in Statistical Package for SocialSciences (spss) version 12 The principle of last observationcarried forward was used Significances between groupsregarding VAS scores were tested with an independent-samples t-test at each time point for all possible compari-sons as we considered VAS to be a continuous scale inaccordance with Max et al (23) The same applies for thetesting of SPID up to 3 and 8 h The analysis of TOTPARwas based on an assumption that the scores are consideredinterval scaled (23) and significance testing was carried outwith an independent samples t-test The same test was usedfor testing differences between study groups regarding theuse of rescue medication Hypothesis testing of valuesmeasured with categorical ordinal scales (ie PAR andglobal evaluation) was performed with a non-parametrictest (MannndashWhitney U-test) P-values of lt005 were con-sidered statistically significant
Results
Altogether 126 consecutive patients who fulfilled theinclusion criteria gave written informed consent to par-ticipate in the study The majority of the patients whowere asked to participate agreed to do so Patients whodeclined to participate usually did not have a before-noon appointment for the surgery Out of the 126patients six were excluded as they stated their pain asmild at the telephone contacts and were able to returntheir sealed study medication A total of 120 patientsparticipated by taking the randomized study medicationSome patients (n frac14 8) who did not fulfill the criterion ofmoderate to severe pain but nevertheless wanted toparticipate took their study medication but wereexcluded from the calculations Of these patients ahigher proportion was men (75) compared with thestudied population Some patients (n frac14 5) were excludedfor other reasons one patient randomized to the
COX-2 inhibitor and paracetamol after oral surgery 295
rofecoxib group took her rescue medication after only30 min as a result of severe pain and withdrew from thestudy one did not manage to fill in the questionnaireand three did not return their questionnaires althoughthey were repeatedly reminded to do so Final outcomedata were calculated on the following cohort of 107 pa-tients rofecoxib + paracetamol (n frac14 34) rofecoxibalone (n frac1436) paracetamol alone (n frac14 20) and placebo(n frac14 17)The principal investigator and one of the dentists
performed the majority of the operations 43 and 55respectively in total 98 out of 120 The remaining 22operations were performed by the two other dentists oneoperating on 10 and the other on 12 patients as theirstock of patients fulfilling the inclusion criteria wassmaller The principal investigator was in contact withand gave instructions to the 98 patients The 22remaining patients received their instructions from oneof the other two dentists performing the operationsThere were no differences between groups regarding
baseline characteristics and the number of molarsremoved (Tables 2 and 3) In total 56 of the partici-pants were men The mean age of the patients was 27 yr(range 18ndash54) and the mean weight was 73 kg (range 50ndash120) Mean total duration of the surgery was 14 min Intotal 91 patients (85) had one mandibular molar
removed during the operation and 16 (18) had anadditional maxillary molar removed The remaining 16patients (15) had two mandibular molars removed atthe same session (Table 3) There was no difference inpain intensity (VAS) at the start between patients whohad one or two molars removed At the time of intake ofthe study medication 83 of all patients included in theanalysis reported moderate pain and 17 reportedsevere pain There were no major differences in painreported among patients operated on by the differentdentists
Analgesic effect
Pain intensity (VAS) ndash The analgesic effect over the 8-hstudy period recorded by patients using the VAS isshown in Fig 1 Separate curves with confidence inter-vals for study groups are presented in Fig 2 Patientsused the scale from 0 up to 95There was a significant difference in mean VAS score
between the combination group and the rofecoxibgroup at 30 min 1 h and 15 h in favor of thecombination (P lt 005) At 2 h and subsequentlyparacetamol did not show any statistically significantadditive effect when combined with rofecoxib com-pared with rofecoxib aloneWhen comparing rofecoxib and paracetamol after
30 min paracetamol was significantly better regardingeffect on pain intensity (P lt 005) Paracetamol tendedto have a better analgesic effect than rofecoxib (althoughthis was not statistically significant) for another hourafter the starting point From 3 h until the end of thestudy period rofecoxib was significantly better thanparacetamol (P lt 005)Compared with placebo the combination treatment
as well as the single drug treatments resulted in signifi-cantly lower pain intensity scores at all observationpoints except for rofecoxib at 30 min
Pain relief (PAR) ndash The median PAR scores (Fig 3)showed a pattern similar to the mean pain intensityassessment The combination treatment was significantly
Table 2
Baseline characteristics for each study group
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Gender malefemale 1915 2016 128 98Age (yr) 25 (19ndash35) 26 (18ndash41) 29 (19ndash52) 28 (19ndash54)Weight (kg) 73 plusmn 9 70 plusmn 13 79 plusmn 17 72 plusmn 13Volume of local anesthetic (ml) 54 plusmn 2 58 plusmn 1 56 plusmn 1 56 plusmn 1Length of surgery (min) 13 plusmn 7 15 plusmn 8 13 plusmn 7 15 plusmn 6Time from end of surgery tointake of study medication (min)
155 plusmn 37 170 plusmn 45 184 plusmn 53 161 plusmn 30
Pain intensity (VAS) at the start 51 plusmn 18 54 plusmn 16 51 plusmn 18 46 plusmn 15
Mean (range)Mean plusmn SDVAS visual analog scale
Table 3
Number of mandibular and maxillar third molars removed in eachstudy group
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
1 mandibular 24 24 15 122 mandibulars 5 6 3 21 mandibular+ 1 maxillar
5 6 2 3
296 Haglund amp Bultzingslowen
better than rofecoxib alone at 30 min (P lt 005) and at1 h (P lt 001) For the rest of the observation periodthere was no significant difference
Between rofecoxib and paracetamol there was a sig-nificant difference in median PAR score in favor ofparacetamol at 30 min and at 1 h (P lt 005) after drug
Placebo
01234567
0 1 2 3 4 5 6 7 8
Paracetamol 1g
01234567
0 1 2 3 4 5 6 7 8
Rofecoxib 50 mg
01234567
0 1 2 3 4 5 6 7 8
Rofecoxib 50 mg+paracetamol 1 g
01234567
0 1 2 3 4 5 6 7 8
Fig 2 Mean pain intensity recorded on a visual analog scale (VAS) and confidence intervals in study groups during the studyperiod of 8 h
0
1
2
3
4
5
6
0 05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
AV
s S
cr
oe
placebo
paracetamol 1g
rofecoxib 50mg
rofecoxib 50mg +paracetamol 1g
Hours from intake of study medication
Fig 1 Mean pain intensity in study groups recorded on a 10-cm visual analog scale (VAS) at each observation point For signifi-cance tests see the Results
0
05
1
15
2
25
3
35
Pai
n r
elie
f sc
ore
placebo
rofecoxib 50mg
rofecoxib 50mg +
05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
paracetamol 1g
paracetamol 1g
Hours from intake of study medication
Fig 3 Median pain relief (PAR) score in study groups at each observation point Pain relief was assessed using the following scale0 no pain relief 1 some pain relief 2 medium pain relief 3 good pain relief and 4 total pain relief For significance tests see theResults
COX-2 inhibitor and paracetamol after oral surgery 297
intake There was instead a significant difference in favorof rofecoxib from 25 h (P lt 005) and from 3 h(P lt 001) to the end of the observation period Only atthe observation time-points of 15- and 2-h was there nosignificant difference between the two drugs regardingmedian PAR scoresThe combination treatment and the single treatments
were significantly better than placebo throughout thewhole observation period of 8 h
Total pain relief (TOTPAR) ndash There was no significantdifference in mean TOTPAR between the combinationtreatment group and the rofecoxib-alone group (Table 4)However rofecoxib gave significantly better TOTPARthan paracetamol (P lt 005) All the active treatmentgroups gave better TOTPAR than placebo (P lt 0001)
Sum of pain intensity differences (SPID) ndash The combi-nation group had the highest mean SPID05)3 h scorehowever this was not statistically different from rofecoxibalone (Table 4)No significant difference in SPID0)3 h wasseen between rofecoxib and paracetamol All active treat-ments were significantly better than placebo (P lt 0001)
The mean PID over the whole observation period (iemean SPIDtotal) shows that the combination group didnot differ from the rofecoxib group (Table 4) Therofecoxib group was significantly better than paracet-amol alone (P lt 005) All active treatments weresignificantly better than placebo (P lt 0001)
Use of rescue medication ndash The use of rescue medicationmeasured as the cumulative percentage of patients ineach study group needing analgesic rescue at any timeduring the 8-h observation period is shown in Fig 4There was no significant difference regarding the totalpercentage of patients using rescue when comparing thecombination group with the rofecoxib group (Table 4)Figure 4 indicates a major difference between the rofec-oxib and paracetamol groups This difference is how-ever not significant (P frac14 0055) owing to few patientsneeding rescue medication Both the combination groupand the rofecoxib group used significantly less rescuethan the placebo group (P lt 0001) Paracetamol failedto show a significant difference to placebo regardingpercentage of patients using rescue medication (P frac140066)
Table 4
Summary of efficiency measures
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Mean TOTPAR05ndash8 h (SE)
452 (20) 409 (27) 287 (44) 91 (27)
Mean SPID05ndash3 h (SE)
182 (19) 151 (18) 111 (34) )32 (23)
Mean SPIDtotal (SE)
526 (59) 515 (60) 208 (96) )101 (57)
Percentage of patients using rescue medication (SE) 88 (49) 167 (63) 400 (112) 706 (114)Mean time (min) to use of rescue medication (SE) 234 (42) 270 (58) 228 (48) 127 (16)Median global evaluation score (0ndash4) at 4 h 2 2 1 0Median global evaluation score (0ndash4) at 8 h 3 2 1 0
P lt 005 vs placebo P lt 001 vs placebo P lt 0001 vs placeboP lt 005 vs paracetamol P lt 001 vs paracetamol P lt 0001 vs paracetamolSE standard error SPID sum of pain intensity differences TOTPAR total pain relief
0
10
20
30
40
50
60
70
80
05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
Hours from intake of study medication
Cum
ula
itve
perc
enat
geof
paite
nst
taki
gnre
scue
me
idca
tion placebo
paracetamol 1g
rofecoxib 50mg
rofecoxib 50mg +paracetamol 1g
Fig 4 Cumulative percentage of patients in each group using rescue medication during the study period of 8 h For significance testssee the Results
298 Haglund amp Bultzingslowen
There was no statistically significant difference in themean time from intake of study medication to intake ofrescue medication in the different active treatmentgroups However for all active treatments the time wassignificantly longer than for placebo (Table 4)
Side-effects
The majority of all patients 738 reported no adverseevents while 187 experienced side-effects Another75 did not answer this question The majority (789)of the patients with side-effects reported that these wereonly slight while 211 reported moderate side-effectsNo patients reported any severe side-effects No pro-nounced difference was seen between the groupsregarding side-effects The types of side-effects experi-enced are listed in Table 5
Global evaluation
Patientsrsquo median global evaluation scores of their studymedications are shown in Table 4 After 4 h thecombination treatment and rofecoxib alone receivedsimilar evaluations Both groups were significantlybetter than paracetamol (P lt 0001 P lt 001) at thistime All active treatments were significantly betterthan placeboAt 8 h the combination group had the highest score
but the difference from the rofecoxib group was verysmall and not significant (Table 4) Both groups weresignificantly better than paracetamol alone (P lt 0001P lt 001) at 8 h All treatment groups were significantlybetter than placeboThe global evaluation scores are further specified in
Table 6 After 8 h 90 of the patients in the combina-tion group rated their medication as good or excellentFor the rofecoxib group the corresponding value was83 Of the patients treated with paracetamol 42rated their medication as good or excellent after 8 h
Discussion
In this study we showed that for the acute inflammatorypain following third molar surgery there was an additive
analgesic effect when combining rofecoxib with paracet-amol as compared with rofecoxib alone for the first 15 hafter intake After this time point the combination ofrofecoxib and paracetamol gave similar pain relief to thatof the rofecoxib group Paracetamol alone was also moreeffective for the first 15 h while rofecoxib was signifi-cantly better thanparacetamol from3 honwards The factthat rofecoxib and paracetamol were more effective thanplacebo shows that the method used was sensitive enoughto distinguish between different substancesAfter the clinical part of this study was carried out
serious concerns regarding cardiovascular effects of long-term treatment with rofecoxib were raised following re-ports of an increased incidence of myocardial infarctionand stroke among patients treated with rofecoxib in aplacebo-controlled study (24) After a highly significant19-fold increase in the incidence of thrombo-embolicserious adverse events was shown in yet another study(25) rofecoxib was withdrawn from the market Theside-effects of rofecoxib became progressively greaterafter 1 yr of treatment which suggests that the cardio-vascular risk is dose-dependent and not only associatedwith COX-2 selectivity (6) The need for acute pain reliefafter third molar surgery is short and the surgery ismainly performed in otherwise healthy young peopleamong whom the risk for serious cardiovascular events issmall It cannot be ruled out that future further devel-oped selective COX-2 inhibitors may be useful intreating acute pain after third molar surgery in this groupof patients with the advantage of only one dose a dayand minimizing the risk for gastrointestinal symptomsRofecoxib and paracetamol differ in onset time and
patients treated with rofecoxib reach meaningful painrelief after 15 h (8) compared with 05 h for paracet-amol This corresponds well with the results obtained inour study The group treated with paracetamol reportedtheir lowest VAS score by 1 h whereas at this time pointthe rofecoxib group still reported a high VAS scoreThereafter the medium VAS score for the paracetamolgroup increased while patients treated with rofecoxibcontinued to receive good pain relief until the end of theobservation period From these results it is reasonable toassume that the combination grouprsquos significantly betteranalgesic effect between 05 and 1 h compared with
Table 5
Side-effects as stated in patientsrsquo own words
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Fatigue 4 2 3 2Headache 1 2 ndash 2Fever ndash ndash ndash 1Dizziness 1 ndash 2 ndashStomach pains 1 ndash 1 ndashSickness ndash 1 ndash ndashShivers 1 2 ndash ndashPerspirations ndash 1 ndash ndash
Table 6
Percentage of patients in each study group stating their overallexperience of the study medication at 4 and 8 h
Study groups
Rofecoxib+
paracet-amol
(n frac14 34)Rofecoxib(n frac14 36)
Paracet-amol
(n frac14 20)Placebo(n frac14 17)
4 h 8 h 4 h 8 h 4 h 8 h 4 h 8 h
Poor 0 0 7 6 30 32 75 76Fair 6 10 7 11 40 26 18 18Good 47 32 43 36 15 26 7 6Excellent 47 58 43 47 15 16 0 0
COX-2 inhibitor and paracetamol after oral surgery 299
rofecoxib alone was a result of the earlier onset of theeffect of paracetamol The mean VAS scores for thecombination group and the paracetamol group corres-ponds totally at the 30-min observation pointThe peak pain after third molar surgery has been
shown to occur 4ndash6 h postoperatively (26) which coin-cides well with the time for the additive effect of para-cetamol to take effect in our study This supports the useof the combination treatment of rofecoxib and paracet-amol after third molar surgery to gain an early onsetparticularly if pain relief medication is started postop-eratively as it is of great clinical importance to have anearly onset of pain relief when treating acute pain Iftreatment starts pre-operatively the addition of para-cetamol is likely to have less clinical relevance This issupported by a study in which patients were givenrofecoxib and paracetamol before Ear Nose and Throat(ENT) surgery (27) The addition of paracetamol in thatsetting failed to improve the analgesic effects of rofec-oxibRofecoxib and paracetamol also differ in duration
The effect of paracetamol 1 g lasts up to 6 h and the drughas to be administered four times daily while rofecoxib50 mg has an analgesic effect up to 24 h (12) The presentstudy was a single-dose comparison In a normal clinicalsetting another 1 g of paracetamol would probably beprescribed after 6 h which would give another period ofadditive effectThe disparity in effect between rofecoxib and para-
cetamol in the present study from 3 h onwards is inaccordance with the findings of two studies on post-operative pain relief after otolaryngologic surgerycomparing rofecoxib and paracetamol given pre-operatively (11 28) A study regarding inflammatorypain in patients with knee osteoarthritis also showedrofecoxib to be superior to paracetamol (29) The resultof our study from 3 h after baseline and onwards thusconfirms the findings of these studies in a third molarpain modelOur study did not show the same additive effect of
combining rofecoxib and paracetamol as in a study byBreivik et al in which they combined diclofenac andparacetamol (18) These authors demonstrated anadditive effect of paracetamol over the whole studyperiod of 8 h Their study also showed less use of rescuemedication in the combination group compared with thepatients treated with diclofenac alone something alsofound in a study by Matthews et al (19) It would seemreasonable to assume that the additive effect of para-cetamol in our study would be the same as in these twostudies as rofecoxib and ibuprofen have been shown tohave the same analgesic effect following third molarsurgery (9 10 12) and the effects of ibuprofen anddiclofenac are similar (30ndash32) It cannot be ruled out thatthere is a difference in additive effect of paracetamolwhen combining it with rofecoxib compared withdiclofenac This theory is in accordance with the result ofa study by Pickering et al on pain relief after tonsil-lectomy in children in which rofecoxib combined withparacetamol did not significantly alter the need for earlyanalgesia as did ibuprofen combined with paracetamol
(33) Further studies may clarify differences between thetwo drugsIn conclusion the present study indicates that there is
an early additive effect up to 2 h when combiningparacetamol with rofecoxib postoperatively as comparedwith rofecoxib alone which coincides with peak painintensity after the removal of third molars Rofecoxibhad a significantly better analgesic effect than paracet-amol from 3 h onwards Our results indicate that para-cetamol does not enhance the analgesic effect ofrofecoxib over a longer period of time As rofecoxib hasbeen shown to have serious cardiovascular side-effectsfuture studies are needed to determine any serious side-effect during short-term treatment
Acknowledgements ndash This study was supported by grants fromLIV The Country Council of Varmland which made it inde-pendent from all manufacturers of the studied drugs There areno conflicts of interest by any of the authors with any drugcompany We thank Dr Carl-Mauritz Bratt DDS Dr PeterTroberg DDS and Dr Tobias Block DDS for performingsome of the surgery
References1 Cooper SA Five studies on ibuprofen for postsurgical dental
pain Am J Med 1984 77 70ndash772 Dionne RA Campbell RA Cooper SA Hall DL Buck-
ingham B Suppression of postoperative pain by preoperativeadministration of ibuprofen in comparison to placebo acet-aminophen and acetaminophen plus codeine J Clin Pharmacol1983 23 37ndash43
3 Vane JR Inhibition of prostaglandin synthesis as a mechanismof action for the aspirinlike drugs Nature 1971 231 232ndash235
4 Meade EA Smith WL De Witt DL Differential inhibition ofprostaglandin endoperoxide synthase (cyclo-oxygenase) iso-zymes by aspirin and other non-steroidal anti-inflammatorydrugs J Biol Chem 1993 268 6610ndash6614
5 Smith TJ Cyclooxygenase as the principal targets for action ofNSAIDs Rheum Dis Clin North Am 1998 24 501ndash523
6 Sciulli MG Capone ML Tacconelli S Patrignani P Thefuture of traditional nonsteroidal anti-inflammatory drugs andcyclooxygenase-2 inhibitors in the treatment of inflammationand pain Pharmacol Rep 2005 57 66ndash85
7 Spink M Bann S Glickman R Clinical implications of cyclo-oxygenase-2 inhibitors for acute dental pain managementbenefits and risks J Am Dent Assoc 2005 136 1439ndash1448
8 Ehrich EW Dallob A De Lepeleire I Van Hecken ARiendeau D Yuan W Porras A Wittreich J Seibold JRDe Shepper P Mellisch DR Gertz BJ Characterization ofrofecoxib as a cyclooxygenase-2 isoform inhibitor and demon-stration of analgesia in the dental pain model Clin Pharm Ther1999 65 336ndash347
9 Malmstrom K Fricke J Kotey P Kress B Morrisson B Acomparison of rofecoxib versus celecoxib in treating pain afterdental surgery a singlecenter randomized double-blind pla-cebo- and active-comparator-controlled parallel group single-dose study using the dental impaction pain model Clin Ther2002 24 1549ndash1560
10 Malmstrom K Daniels S Kotey P Seidenberg B Desjar-
dins PJ Comparison of rofecoxib and celecoxib two cyclo-oxygenase-2-inhibitors in postoperative dental pain Arandomized placebo- and active-comparator-controlled clinicaltrail Clin Ther 1999 21 1653ndash1663
11 Watcha MF Issioui T Klein KW White PF Costs andeffectiveness of rofecoxib celecoxib and acetaminophen forpreventing pain after ambulatory otolaryngologic surgeryAnesth Analg 2003 96 987ndash994
300 Haglund amp Bultzingslowen
12 Morrisson BW Christensen S Yuan W Brown J Amlani
S Seidenberg B Analgesic efficacy of the cyclooxygenase-2-specific inhibitor rofecoxib in post-dental surgery pain arandomized controlled trial Clin Ther 1999 21 943ndash953
13 Chang DJ Fricke JR Bird RS Bohidar NR Dobbins TWGeba GP Rofecoxib versus codeineacetaminophen in post-operative dental pain a double-blind randomized placebo-and active comparator-controlled clinical trial Clin Ther 200123 1446ndash1455
14 Chang DJ Desjardins PJ Bird SR Black P Chen EPetruschke RA Geba GP Comparison of rofecoxib and amultidose oxycodoneacetaminophen regimen for the treatmentof acute pain following oral surgery a randomized controlledtrial Curr Med Res Opin 2004 20 939ndash949
15 Berenbaum MC What is synergy Pharmacol Rev 1989 4193ndash141
16 Altman RD A rationale for combining acetaminophen andNSAIDs for mild to moderate pain Clin Exp Rheumatol 200422 110ndash117
17 Bjorkman R Hallman KM Hedner J Hedner T Henning
M Acetaminophen blocks spinal hyperalgesia induced byNMDA and substance P Pain 1994 57 259ndash264
18 Breivik EK Barkvoll P Skovlund E Combining diclofenacwith acetaminophen or acetaminophen-codeine after oral sur-gery a randomized double-blind single-dose study ClinPharmacol Ther 1999 66 625ndash635
19 Matthews RW Scully CM Levers BG The efficacy ofdiclofenac sodium (Voltarol) with and without paracetamol inthe control of post-surgical dental pain Br Dent J 1984 157357ndash359
20 Norholt SE Treatment of acute pain following removal ofmandibular third molars use of the dental pain model inpharmacological research and development of a comparableanimal model Int J Oral Maxillofac Surg 1998 27 1ndash41
21 NIH Consensus Development Conference For Removal OfThird Molars J Oral Surg 1980 38 235ndash236
22 Laska EM Siegel C Sunshine A Onset and durationmeasurement and analysis In Max MB Portenoy RKLaska EM eds Advances in pain research and therapy NewYork Raven Press 1991 691ndash698
23 Max MB Laska EM Single-dose analgesic comparisons InMax MB Portenoy RK Laska EM eds Advances in painresearch and therapy New York Raven Press 1991 55ndash97
24 Bombardier C Laine L Reicin A Shapiro D Burgos-Vargas R Davis B Day R Ferraz MB Hawkey CJHochbergMC Kvien TK Schitzer TJ Comparison of uppergastrointestinal toxicity of rofecoxib and naproxen in patientswith rheumatoid arthritis N Engl J Med 2005 343 1520ndash1528
25 Bresalier RS Sandler RS QuanH Bolognese JA Oxenius
B Horgan K Lines C Riddell R Morton D Lanas AKonstam MA Baron JA Cardiovascular events associatedwith rofecoxib in a colorectal adenoma chemoprevention trialN Engl J Med 2005 17 1092ndash1102
26 Szmyd L Shannon ILMohnac AM Control of postoperativesequelae in impacted third molar surgery J Oral Ther Phar-macol 1965 1 491ndash496
27 Issioui T Klein KW White PF Hu J Skrivanek GDAnalgesic efficacy of rofecoxib alone or in combination withacetaminophen in the ambulatory setting Anesthesiology 200195 A35
28 Issioui T KleinKWhite PWatchaM SkrivanekG JonesSHu J BradleyM Caleb I Cost-efficacy of rofecoxib versusacetaminophen for preventing pain after ambulatory surgeryAnesthesiology 2002 97 931ndash937
29 Geba GP Weaver AL Polis AB Dixon ME Schnitzer TJEfficacy of rofecoxib celecoxib and acetaminophen in osteo-arthritis of the knee a randomized trial JAMA 2002 287 64ndash71
30 Joshi A Parara E Macfarlane TV A double-blind rand-omised controlled clinical trial of the effect of preoperativeibuprofen diclofenac paracetamol with codeine and placebotablets for relief of postoperative pain after removal of impac-ted third molars Br J Oral Maxillofac Surg 2004 42 299ndash306
31 Bakshi R Frenkel G Dietlein G Meurer-Witt B Schn-eider B Sinterhauf U A placebo-controlled comparativeevaluation of diclofenac dispersible versus ibuprofen in post-operative pain after third molar surgery J Clin Pharmacol 199434 225ndash230
32 Ahlstrom U Bakshi R Nilsson P Wahlander L Theanalgesic efficacy of diclofenac dispersible and ibuprofen inpostoperative pain after dental extraction Eur J Clin Pharma-col 1993 44 587ndash588
33 Pickering AE Bridge HS Nolan J Stoddart A Double-blind placebo-controlled analgesic study of ibuprofen orrofecoxib in combination with paracetamol for tonsillectomy inchildren Br J Anaesth 2002 88 72ndash77
COX-2 inhibitor and paracetamol after oral surgery 301
Combined acetaminophen and ibuprofen for pain relief after oralsurgery in adults a randomized controlled trial
A F Merry1 2 R D Gibbs3 J Edwards4 G S Ting3 C Frampton5 E Davies1 2
and B J Anderson1
1Department of Anaesthesiology University of Auckland Private Bag 92019 Auckland New Zealand2Department of Anaesthesia Auckland City Hospital Auckland New Zealand 3Oral Health Unit Greenlane
Clinical Centre 214 Greenlane West Epsom Auckland New Zealand 4Oral and Maxillofacial Service Quay
Park Medical Centre 68 Beach Road Auckland Central Auckland New Zealand 5Department of Medicine
Christchurch School of Medicine and Health Sciences University of Otago New Zealand
Corresponding author E-mail amerryaucklandacnz
Background Acetaminophen is often used with a non-steriodal anti-inflammatory drug for
acute pain Hitherto these drugs have had to be given separately typically at different time
intervals Maxigesicw tablets combine acetaminophen and ibuprofen in clinically appropriate
doses to simplify administration and dosage regimen We compared this combination with each
of the constituent drugs for the relief of pain after extraction of third molar teeth
Methods Adults (more than 16 yr) having one or more wisdom teeth removed under general
or local anaesthesia were instructed to take two tablets before operation then two tablets
every 6 h for up to 48 h of (i) a combination of acetaminophen 500 mg and ibuprofen 150 mg
per tablet (Maxigesicw) (ii) acetaminophen 500 mg per tablet alone or (iii) ibuprofen 150 mg
per tablet alone The primary outcome measure was the area under the curve (AUC) of the
100 mm visual analogue scale pain measurements taken for up to 48 h after surgery divided by
time at rest and on activity Pharmacokinetic data were collected in a subset of patients
Results The mean (SEM) time-corrected AUC on rest and activity respectively were combi-
nation group 223 (32) and 284 (34) acetaminophen group 330 (31) and 404 (33) and ibu-
profen group 348 (32) and 402 (34) P001 for each of the four comparisons of combination
vs constituent drug There was no pharmacokinetic interaction between acetaminophen and
ibuprofen administered together
Conclusions Maxigesicw tablets provide superior pain relief after oral surgery to acetamino-
phen or ibuprofen alone
Br J Anaesth 2010 104 80ndash8
Keywords anaesthesia dental analgesia postoperative analgesics non-opioid acetaminophen
analgesics non-opioid ibuprofen non-steroidal anti-inflammatory drugs
Accepted for publication October 16 2009
The relief of pain has been described as a universal human
right but is not always easily achieved1 Opioid analgesics
are effective but have troublesome and potentially danger-
ous side-effects and their potential for abuse may lead to
regulatory and logistical difficulties Non-steroidal anti-
inflammatory drugs (NSAIDs) have fewer regulatory
restrictions but they too have important adverse effects
which are more likely at higher dose or with longer
courses2 Acetaminophen is widely used and is very safe
at the recommended dose of 4 g per day3 but does not
always provide adequate pain relief on its own Combining
analgesics offers the possibility of increasing effectiveness
without increasing dose (and therefore risk)4 5 NSAIDs
are often combined with acetaminophen particularly for
treating postoperative pain6 ndash 10
Prescribing acetaminophen and ibuprofen together is
common in clinical practice6 8 9 11 ndash 13 Ibuprofen has the
advantage of a well-established safety record (particularly
at doses below 15 g per day in adults)14 and in many
countries (including the UK) it is available without
The Author [2010] Published by Oxford University Press on behalf of the British Journal of Anaesthesia
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (httpcreativecommonsorglicensesby-nc25uk)
which permits unrestricted non-commercial use distribution and reproduction in any medium provided the original work is properly cited
British Journal of Anaesthesia 104 (1) 80ndash8 (2010)
doi101093bjaaep338
prescription Typically acetaminophen is given in a dose
regimen of 1 g 6 hourly whereas ibuprofen is given in a
dose of 400 mg 8 hourly3 Compliance with the prescribed
dosing regimen is important for achieving the desired
result with any drug and is often poor with asynchronous
dosing15 A single formulation with a simplified regimen
would probably be appreciated by patients and might
improve compliance
Maxigesicw is a new formulation of acetaminophen 500
mg and ibuprofen 150 mg Taking two tablets 6 hourly
provides the appropriate daily dose of both drugs relatively
simply We have investigated the hypothesis that in adult
patients undergoing a common surgical procedure (extrac-
tion of third molar teeth) this formulation provides
superior analgesia to either of its components alone
Methods
With ethics committee approval we recruited and fol-
lowed up patients between March 2005 and February
2008 Trial registration ANZCTRORGAU (identifier
ACTRN12606000291583)
Setting
This study was conducted at a publicly funded teaching
hospital and a private day-surgical clinic in metropolitan
New Zealand
Participants
We included adults undergoing extraction of at least one
lower wisdom tooth with or without one or more upper
wisdom teeth by one of three participating surgeons We
excluded patients if they were under 16 yr old weighed
50 kg had taken any NSAID (other than aspirin in a
dose of 150 mg daily or less) within 24 h of the operation
had taken acetaminophen or acetaminophen containing
medicines within 12 h of the operation were taking an
angiotensin-converting enzyme inhibitor warfarin steroid
(other than interoperative dexamethasone) or any immu-
nosuppressive drug were intolerant to any NSAID or acet-
aminophen were suffering from a severe local infection
had a history of peptic ulceration asthma or severe hae-
mopoetic renal or hepatic disease were participating in
the investigation of another experimental agent or if the
clinician believed for any other reason that participation in
the study might not be in their best interests
Randomization and blinding
Tablets of identical appearance packaging and dosage
instructions were provided in each of the following formu-
lations (i) acetaminophen 500 mgthornibuprofen 150 mg per
tablet (Maxigesicw Sigma Laboratories Nashik India which
was MHRA approved for manufacturing pharmaceuticals
under GMP) (ii) acetaminophen 500 mg per tablet or
(iii) ibuprofen 150 mg per tablet
Patients were first approached by the surgeon and then
by the study nurse They were given written and verbal
information about the study and invited to participate If
they consented patients were then randomized into one of
the three study groups in a sequential order to receive one
of these formulations in blinded packs The randomization
sequence was computer generated by the study statistician
as a 111 allocation ratio to the three treatments in a
sequence of permuted blocks with stratification for anaes-
thetic type (local or general) and study centre
Stratification by anaesthetic type ensured a balance
between treatments in terms of the number of teeth
extracted as most patients having more than two teeth
extracted have a general anaesthetic Only the statistician
had access to the schedule of patient numbers by drug
allocation Participants and investigators were blinded and
the randomization code was not broken until the final data-
base had been checked and locked
Intervention
Participants were asked to take two tablets of the study
medication before operation (as close as possible to the
start of surgery) and then 4 times a day (as close as poss-
ible to 6 hourly) for up to 48 h after surgery All partici-
pants were given bupivacaine local anaesthetic blocks by
the surgeons For those participants undergoing general
anaesthesia this was induced with propofol and main-
tained with isoflurane and nitrous oxide in oxygen
Monitoring was in accordance with the guidelines of the
Australian and New Zealand College of Anaesthetists16
All extractions were carried out by one of three surgeons
each using his normal technique
If participants required additional postoperative pain
relief while in hospital a rescue dose of fentanyl 10 mg
was given iv as required After discharge to home
codeine was provided (again as rescue medication) in 30
mg tablets one to two to be taken as needed up to
4 hourly
Outcomes
Participants were asked to rate their pain on 100 mm visual
analogue scales (VAS) printed one per double page in a
booklet that they took home Ratings were requested at
baseline (immediately before administration of the first
dose of study medication) after operation (once the partici-
pants were sufficiently awake to respond) and 1ndash2 hourly
thereafter while awake for 48 h The study nurse main-
tained contact with participants by telephone to facilitate
compliance with data collection and the return of diaries
The primary outcome measure was the area under the
curve (AUC) of these VAS ratings divided by time at rest
and on activity The AUC was divided by the period of
the completed assessments to adjust for the fact that some
Combined acetaminophen and ibuprofen for analgesia
81
patients recorded pain for shorter periods than others This
calculation in effect produces a measure of average pain
intensity over the study period
Secondary efficacy outcome measures were a categorical
global pain rating by the participants taken at the end of the
study period rescue analgesia consumption over the study
period a categorical global rating of nausea by the partici-
pants taken at the end of study period the number of epi-
sodes of vomiting over the study period and a rating of
sleep disturbance on a 100 mm VAS assessed after each
night during the study period In addition participants were
asked to rate their experiences of participating in the study
Sample size estimation
We obtained blood samples from the 38 participants
undergoing general anaesthesia in order to have evaluable
pharmacokinetic data for at least 30 patients The first
sample was obtained 30 min after the first dose of study
medication the second sample at the end of anaesthesia
and additional one or two samples after operation in hospi-
tal The plasma concentration of acetaminophen and ibu-
profen were measured by the sponsor and used to form
individual timendashconcentration profiles The analytical
method used an HPLC-DAD (Diode Array Detector) assay
for the simultaneous determination of acetaminophen and
ibuprofen in plasma Precision and accuracy for acetami-
nophen and ibuprofen assay were validated over the con-
centration range 05ndash50 mg ml21 for both drugs The
intra- and inter-batch precision of the assays at low
medium and high concentrations of acetaminophen and
ibuprofen varied from theoretical values by 15 The
lower limit of quantification for each drug was 05 mg
ml21 The sponsor monitored all data collected during the
study and queries and corrections were made when any
inaccuracies or inconsistencies were identified
Sample size estimation
We estimated that 120 participants (40 per group) in the
intention-to-treat (ITT) population would provide 80
power to detect differences between the groups of 9 (SD
14) mm in our primary endpoint for resting assessments
and 13 (SD 21) for measures during activity10 17 with a
one-sided type I error rate of 5 These differences equate
to 25 Differences of this magnitude were considered
clinically important and comparable with differences
typical of previous published studies10
Statistical methods
The data were analysed using SPSS version 150 (SPSS
Inc Chicago IL USA) Efficacy analyses were conducted
on an ITT basis with the additional provision that
there were at least three VAS measurements over at
least 12 h available to calculate the primary endpoint All
participants who were randomized into the study were
included in the safety evaluations As the first dose of
study medication was taken before operation while under
the supervision of the surgeon all randomized patients
took at least a single dose of study medication A last
observation carried forward approach was used for those
subjects who left the study prematurely for non-AUC
based variables
We compared the primary endpoint between the combi-
nation group and each of the acetaminophen and ibuprofen
arms at rest and on activity using a general linear model
(GLM) which included terms for treatment the centre and
anaesthetic stratum Additionally to confirm the consist-
ency of the treatment effects across strata the stratum
treatment interaction terms were tested and included in
the final model The analysis was also checked with
number of teeth extracted as an additional factor
Continuous secondary efficacy endpoints were tested for
significance using the same models as used for the
primary endpoint
A one-tailed P005 was pre-specified to indicate stat-
istical significance We required a statistically significant
result favouring the combination from each of the two
planned comparisons with the constituents to define super-
iority for either rest or on activity measures We used one-
tailed tests as there seemed no theoretical or empirical
basis for expecting that combining these analgesics could
result in a reduction in efficacy and because the require-
ment for each of two comparisons to be significant at
P005 is stringent Secondary categorical efficacy end-
points were compared between the groups using x2 tests
and MannndashWhitney U-tests as appropriate
We used non-linear mixed effect models (NONMEM
VI Globomax LLC Hanover MD USA) to estimate
population pharmacokinetics with a Compaq Digital
Fortran Version 66A compiler on an Intel Celeron 333
MHz CPU (Intel Corp Santa Clara CA USA) under MS
Windows XP (Microsoft Corp Seattle WA USA) This
model allows assessment of inter-individual variability
covariance between pharmacokinetic parameters and
residual error We judged the quality of fit of the pharma-
cokinetic model to data using the NONMEM objective
function examination of plots of observed vs predicted
concentrations and visual predictive checks
Results
After initial screening 189 patients were approached 135
agreed to participate One to four teeth were extracted
with local anaesthetic alone in 69 patients and with local
anaesthetic in combination with general anaesthesia in 66
Thirteen patients did not return their patient diaries so
122 patients were included in the evaluable ITT popu-
lation for the analysis of the primary endpoints (Fig 1)
The treatment groups were adequately matched in baseline
patient and clinical characteristics (Table 1) Of those in
Merry et al
82
the combination group 600 had three or four teeth
extracted compared with 436 for ibuprofen and 535
for acetaminophen
Efficacy
The time-adjusted AUCs were substantially and signifi-
cantly lower at rest and on activity in the combination
group than in either of the other two treatment groups
(Table 2 Figs 2 and 3) with all four P001 The consist-
ency of the treatment effects across strata was confirmed
from the GLM with P-values for the treatment stratum
interaction of 0955 and 0984 for time-adjusted AUCs at
rest and on activity respectively The type of anaesthetic
(local vs general) and number of teeth extracted did not
change the outcome of either analysis
Although all four secondary endpoints favour the com-
bination treatment (Table 3) only the global pain rating
reached statistical significance More participants experi-
enced lsquonilrsquo or lsquomildrsquo pain with the combination (684)
than with either other group this difference was significant
for acetaminophen (375 Pfrac140008) but not for ibupro-
fen (543 Pfrac140263) The use of any rescue medication
also favoured the combination treatment (Table 4) but this
did not reach statistical significance
Pharmacokinetics
There were no significant differences between the combi-
nation group and either constituent group in any of the
estimated pharmacokinetic parameters (Table 5) The
visual predictive plots of individual concentration showed
that 90 of the observations were within the 90 pre-
diction intervals
Twelve participants were given both acetaminophen and
ibuprofen For calculation of the pharmacokinetic vari-
ables a scaling factor was applied to clearance and
volume of distribution in turn for those participants receiv-
ing the combination of acetaminophen and ibuprofen This
scaling factor had no impact on either acetaminophen or
ibuprofen pharmacokinetic parameters indicating that
there was no pharmacokinetic interaction between acetami-
nophen and ibuprofen when administered together
(P005)
Clearance (CLF) and volume of distribution (VF) par-
ameters observed in the study are consistent with those
reported previously (acetaminophen CLFfrac14126ndash210
litre h21 70 kg21 VFfrac14483ndash710 litre 70 kg21 ibupro-
fen CLFfrac1429ndash59 litre h21 70 kg21 VFfrac1464ndash235 litre
70 kg21)18 ndash 20
Adverse effects
The frequency of adverse effects was consistent with the
known effects of the constituent drugs and there were no
Screened(n =189)
Randomized(n =135)
Acetaminophentreatmentgroup(n =47)
Ibuprofentreatment group(n =44)
Combinationtreatment group(n =44)
Patient diariesnot returned(n =4)
Patient diariesnot returned(n =5)
Patient diariesnot returned(n =4)
Included in theanalysis(n =43)
Included in theanalysis(n =39)
Included in theanalysis(n =40)
Fig 1 Flow of participants through trial Not randomized (nfrac1454) (i)
declined to participate (nfrac1415) (ii) did not meet inclusion criteria
(nfrac1414) (iii) other reasons (nfrac1425) other reasons the surgery was
cancelled or rescheduled patient could not be contacted patient was
given the wrong date of the surgery
Table 1 Patient characteristic and baseline information (SD)
Acetaminophen (n547) Ibuprofen (n544) Combination (n544)
Age [mean (range)] (yr) 235 (160ndash404) 237 (168ndash389) 250 (183ndash404)
Weight [mean (SD)] (kg) 713 (156) 808 (201) 711 (135)
Ethnicity [n ()]
Asian 4 (85) 1 (23) 2 (45)
Black 1 (21) 0 (00) 1 (23)
Caucasian 33 (702) 31 (705) 34 (773)
Maori 4 (85) 4 (91) 4 (91)
Pacific Islander 4 (85) 5 (114) 2 (45)
Other 1 (21) 3 (68) 1 (23)
Male [n ()] 13 (277) 21 (477) 13 (295)
Shift workers [n ()] 10 (213) 5 (114) 3 (68)
Preoperative pain scores at rest [mean (SD)] (mm) 19 (51) 21 (52) 26 (68)
Preoperative pain scores on activity [mean (SD)] (mm) 41 (133) 27 (83) 29 (66)
Sleep disturbance for night before surgery as VAS [mean (SD)] (mm) 647 (229) 691 (260) 715 (241)
Combined acetaminophen and ibuprofen for analgesia
83
definitive indications that the adverse event profile is
changed when the two drugs are combined (Table 6)
however the numbers were too small to make meaningful
comparisons between the groups Two participants experi-
enced postoperative bleeding (attributed to surgical
causes) which resolved without readmission to hospital
No gastrointestinal bleeding was reported during the study
Most adverse events were evaluated as mild (574) or
moderate (352) and on review were considered not
related (175) or unlikely to be related (667) to study
medication
General
The majority of participants rated the experience of taking
part in the study as very positive (31) or positive (47)
0
10
20
30
40
50
60
70
80
90
100
ActivityRest
Acetaminophen alone
Ibuprofen alone
Combination
AU
Ch
(m
m)
Fig 2 Mean (thorn95 CI) mm of time-adjusted AUC (AUCtime) for VAS
at rest and on activity by treatment group
Table 2 Mean (SEM 95 CI) of time-adjusted AUC of visual analogue pain
scores at rest and on activity by treatment group The differences between
combination and each constituent were significant at rest (vs acetaminophen
Pfrac140007 and vs ibuprofen Pfrac140003) and on activity (vs acetaminophen
Pfrac140006 and vs ibuprofen Pfrac140007)
Acetaminophen
(n543)
Ibuprofen (n539) Combination
(n540)
At rest 330 (31 279ndash381) 348 (32 294ndash402) 223 (32 170ndash277)
On
activity
404 (33 350ndash458) 402 (34 346ndash459) 284 (34 228ndash341)
0
1020
30
40
5060
70
8090
100A
B
0 4 8 12 16 20 24 28 32 36 40 44 48
0 4 8 12 16 20 24 28 32 36 40 44 48
Hours post-surgery
VA
S s
core
(m
m)
0
10
2030
40
50
60
7080
90
100
Hours post-surgery
VA
S s
core
(m
m)
Acetaminophen aloneIbuprofen aloneCombination
Fig 3 Mean (SE) mm VAS out of 100 at rest (A) and on activity (B)
Table 3 Secondary efficacy endpoints by treatment group The only
significant difference was between the global pain ratings for combination and
acetaminophen (Pfrac140008 MannndashWhitney U-test)
Acetaminophen Ibuprofen Combination
Global pain rating [n ()]
Nil 3 (75) 4 (114) 4 (105)
Mild 12 (300) 15 (429) 22 (579)
Moderate 22 (550) 14 (400) 12 (316)
Severe 3 (75) 2 (57) 0 (00)
Global nausea rating [n ()]
Nil 26 (650) 25 (714) 30 (790)
Mild 10 (250) 8 (229) 7 (184)
Moderate 3 (75) 2 (57) 1 (26)
Severe 1 (25) 0 (00) 0 (00)
Vomiting episodes (n) 5 (in 3 subjects) 0 0
Sleep disturbance night
1 vs baseline VAS
[mean (SD)] (mm)
2219 (292) 2174 (229) 2166 (247)
Sleep disturbance night
2 vs baseline VAS
[mean (SD)] (mm)
2137 (329) 296 (258) 285 (201)
Table 4 Rescue analgesia by group n () none of these differences were
significant
Rescue analgesic Acetaminophen Ibuprofen Combination
Fentanyl in hospital 5 (116) 9 (237) 6 (154)
Codeine in the first 24 h 21 (4770) 16 (4320) 13 (3250)
Codeine in the second 24 h 22 (5370) 14 (4240) 16 (4210)
Any rescue medication over 48 h 25 (625) 18 (5810) 21 (568)
Table 5 Mean (SD) pharmacokinetic parameters (individual Bayesian
estimates used for descriptive statistics) for a one-compartment first-order
absorption first-order elimination model none of the differences for
combination formulations was significant CLF clearance VF volume of
distribution Tabs absorption half-time Cmax maximum concentration Tmax
time to achieve Cmax
Acetaminophen
alone (n515)
Acetaminophen
in combination(n512)
Ibuprofen
alone(n511)
Ibuprofen in
combination(n512)
CLF (litre
h21)
141 (26) 142 (18) 39 (17) 38 (13)
VF (litre) 557 (194) 482 (183) 106 (21) 98 (15)
Tabs (h) 042 (076) 016 (010) 058 (078) 085 (085)
Tmax (h) 109 (112) 064 (031) 116 (090) 144 (093)
Cmax (mg
litre21)
158 (65) 192 (64) 208 (83) 191 (78)
Merry et al
84
and 19 rated the experience as neutral Four participants
(3) found the experience negative and none rated it as
very negative The ratings were not significantly different
between the study groups
Discussion
We found that patients using the combination of acetami-
nophen and ibuprofen experienced less pain during the
first 48 h after oral surgery than those using the same
daily dosage of either agent alone and we think the differ-
ence was clinically relevant There was no evidence of any
pharmacokinetic interaction between acetaminophen and
ibuprofen Patients receiving ibuprofen alone reported the
lowest frequency of adverse events but the numbers are
too small for meaningful comparisons between the groups
and we saw no cause for concern in any group
Our data are consistent with previous evidence showing
that a combination of ibuprofen and acetaminophen pro-
vides better analgesia than acetaminophen alone8 9 13 21
Note however that two of these studies were in children9 13
so data in adults are relatively limited On the other hand
there are many studies supporting the more general point
that the addition of various NSAIDs improves the pain
relief obtainable from acetaminophen alone More impor-
tantly our data add convincingly to the sparse evidence
supporting the more controversial proposition that this
combination is superior to ibuprofen alone12 In a smaller
study in an orthopaedic pain model (which was positive
for the combination in comparison with acetaminophen)
Dahl and colleagues8 showed no such benefit whereas
Viitanen and colleagues13 (in a paediatric tonsillectomy
study) showed an advantage for the combination only in
the period after discharge from hospital The similarity in
efficacy between ibuprofen and acetaminophen on their
own seen in our study contrasts with the findings of
superior pain relief from ibuprofen after dental surgery by
Cooper and colleagues22 but theirs was a single-dose
study
Limitations and strengths of the study
Our results are limited to adults and to the doses and
model of pain studied We think our conclusions are likely
to apply to other age groups and other types of pain but
this will require confirmation We have not explored the
optimal dosage of the combination drug but the dosage
used is consistent with current clinical practice The
inclusion of patients who underwent both general and
local anaesthesia implies that our findings are likely to
apply in either case It is not possible to draw firm con-
clusions on the safety of any drug from a study of only 40
participants per group but acetaminophen and ibuprofen
are well established widely used and considered very safe
in appropriate doses3 23 There is no theoretical reason
Table 6 Adverse events and their relationship with study medication as evaluated by the investigators Postoperative pain was noted as a complication in 2 0
and 1 patient in the acetaminophen ibuprofen and combination groups respectively Some individuals experienced more than one adverse event
Relationship System organ class Acetaminophen Ibuprofen Combination Total
Not related Gastrointestinal disorders (numbness of tongue) 1 0 0 1
General disorders and administration site conditions (swollen arm infusion site
phlebitis)
0 0 2 2
Infections and infestations (dry socket alveolitis of jaw) 1 0 1 2
Injury poisoning and procedural complications (bruising of arm postoperative
pain)
0 0 2 2
Musculoskeletal and connective tissue disorders ( jaw stiffness) 0 0 1 1
Skin and sc tissue disorders (swelling face) 1 1 0 2
Subtotal 3 1 6 10
Unlikely related Blood and lymphatic system disorders (swollen glands) 1 0 0 1
Ear and labyrinth disorders (pain in ear tinnitus) 2 0 0 2
Gastrointestinal disorders (vomiting nausea stomach cramps dry lips) 6 1 2 9
Injury poisoning and procedural complications (postoperative bleeding) 0 0 1 1
Musculoskeletal and connective tissue disorders ( jaw stiffness aches and pains in
legs jaw pain)
2 0 1 3
Nervous system disorders (headache felt faint sleepy balance difficulty light
headiness dizziness drowsiness lethargic)
6 4 4 14
Psychiatric disorders (disorientation) 0 1 0 1
Respiratory thoracic and mediastinal disorders (sore throat pharyngeal ulceration
hypoventilation coughing)
1 1 2 4
Investigations (body temperature increased) 0 0 1 1
Skin and sc tissue disorders (rash redness of external ear swelling face) 0 1 1 2
Subtotal 18 8 12 38
Possibly related Gastrointestinal disorders (stomach cramps abdominal pain constipation stomach
ache vomiting)
3 0 2 5
General disorders and administration site conditions (fever) 1 0 0 1
Injury poisoning and procedural complications (postoperative bleeding) 0 0 1 1
Nervous system disorders (sleepy headache) 1 0 1 2
Subtotal 5 0 4 9
Total 26 9 22 57
Combined acetaminophen and ibuprofen for analgesia
85
and no empirical suggestion from our data to suggest that
the combination would be any less safe than the constitu-
ent drugs on their own Our safety data are observational
rather than based on prospective laboratory investigations
but we followed up participants for adverse events for 3
weeks and it seems unlikely that clinically important
harm would have been missed
Pain after oral surgery can persist for several days10 but
we considered 48 h to be a clinically relevant period and
a longer period of study is likely to have resulted in poorer
compliance with data collection
It could be asked whether a more typical (albeit
complex) regimen for ibuprofen alone might have pro-
vided better analgesia than seen with the 4 hourly
approach used here but this seems unlikely particularly
given that our clinical efficacy data were supported by esti-
mates of population pharmacokinetics We had planned to
correlate drug plasma concentration with pain scores but
the drug plasma concentration results were too sparse and
there were too many confounding variables (such as ethni-
city comparators and rescue analgesia) for this to be
undertaken We did demonstrate a lack of interaction
between the constituent drugs when used in combination
and provided evidence that equivalent and predicted blood
concentrations were achieved (the observations of timendash
concentration profile decreased within 90 of prediction
limits for both acetaminophen and ibuprofen) Furthermore
pharmacokinetic parameter estimates observed in the current
study are very similar to those previously reported18 ndash20
The evaluations used in the efficacy analysis have
established construct validity and are appropriate for
parametric analysis24 25
In designing analgesic studies it is an advantage to
minimize the exposure of participants to inadequate
analgesia while controlling for various sources of bias
Some designs incorporate a placebo group but the efficacy
of both ibuprofen26 and acetaminophen27 in comparison
with placebo are well established by previous research
and we would argue that the use of a placebo in this situ-
ation is unnecessary and perhaps even unethical28 There
would be little value in another lsquome toorsquo analgesic unless
it had clear advantages over established agents Therefore
the question of interest lies in the comparisons between
the new agent (Maxigesicw) and the reference standard of
care and in this case we have actually shown superiority to
both of two possible reference standardsmdashacetaminophen
alone and ibuprofen alone One classic approach to analgesic
studies involves treating established acute pain This has the
alleged advantage that pain relief can be assessed (eg by
using AUC to estimate total pain relief or TOTPAR29 30 or
by calculating a pain reduction index per tablet)31 Our
design in contrast follows the widely accepted clinical prac-
tice of anticipating and treating pain before it occurs which
in our unit at least has long been considered best practice
Furthermore rescue medication was readily available and
those requiring it were evenly distributed between the
groups It is notable that most patients did require rescue
medication suggesting that pain after oral surgery can some-
times be severe enough that even the combination of ibupro-
fen and acetaminophen requires supplementation (and it
might be asked whether it would be a good idea for codeine
for example to be added to the combined formulation)
Nevertheless we think it important that the vast majority of
the participants in all groups reported pain scores that were
reasonably low and that all received analgesic regimens
accepted in contemporary practice The predominantly posi-
tive evaluation by participants of their experience in taking
part in the study provides empirical reassurance on this point
(and also other aspects of the conduct of the study)
The treatment of pain is central to medical practice in
hospitals and in primary care If these results are con-
firmed in other settings the already widely used combi-
nation of acetaminophen and ibuprofen may become the
standard of care for the initial management of moderate
acute pain at least for those patients who do not have
contra-indications to NSAIDs Even using the drugs indi-
vidually the dosage regimen studied here is simpler than
that currently recommended and may well improve com-
pliance with and therefore success with this combination
Providing both drugs in one tablet simplifies this regimen
even further and our data confirm that the specific formu-
lation studied here is effective and that there is no inter-
action between its constituent drugs
Conclusions
Doctors treating pain after oral surgery in hospital and at
home and probably pain in many other situations should
consider using acetaminophen and ibuprofen together four
times a day provided there are no contraindications to
either drug and taking into account the known risks of
NSAIDs The combination formulation studied here sim-
plifies this regimen
Funding
This work was supported by AFT Pharmaceuticals Ltd
assisted by New Zealand Trade and Enterprise
Development Grants
Appendix
Declaration of interest
The Department of Anaesthesiology of the University of
Auckland has received payment from AFT
Pharmaceuticals for conducting this study but none of the
investigators has received payment in their personal
capacity
Merry et al
86
Contributors
AFM BJA CF and Hartley Atkinson designed the
study with input from RDG and JE Hartley Atkinson
obtained funding RDG GST and JE performed the
surgery and contributed to patient recruitment and to the
care of patients during their participation in the study
ED was the study coordinator and was responsible for
patient recruitment and follow-up data collection quality
control and many other logistic aspects of the study The
statistical analysis of clinical data was undertaken by CF
and of the pharmacokinetic data by BJA AFM took
primary responsibility for the manuscript with assistance
from Jennifer Zhang All authors edited and commented
on the manuscript AFM is the guarantor
Chief Executive Officer AFT Pharmaceuticals
Clinical TrialRegulatory Assistant AFT Pharmaceuticals
Ethics approval
This study was approved by the Northern X Regional Ethics
Committee 650 Great South Road Penrose Auckland New
Zealand
Ethics Committee Approval Number AKX0410298
Health Authorities (MEDSAFE) Approval Number
TT50-7316 (458)
Role of the sponsor
The sponsor (AFT Pharmaceuticals Ltd) participated in
the study design and protocol development and provided
logistical support during the trial Monitoring of the
study was performed by the sponsor who also main-
tained the trial database Statistical analyses were
independently performed by the biostatistician and the
results cross-checked by sponsors and investigators The
sponsor assisted with the preparation of the manuscript
and was permitted to review it and to make suggestions
but responsibility for the content of this paper lay with
the academic authors and the style and emphasis is that
of the principle investigator The academic authors had
the explicit right to access all data and publish these
results
Provenance and peer review
This paper was not commissioned informal external peer
review has been obtained before submission to the Journal
Additional contributions
We thank Ms Jenny Rous Pharmacy Manager from the
Mercy Hospital Pharmacy for study drug management
Dr Ralph Richardson Program Manager from Institute of
Environment Science amp Research Limited Wellington in
New Zealand for the plasma sample assays Sally Merry
for proofreading and editing on the manuscript the anaes-
thetists Judy Bent Jack Hill Joanna Rose Joanne Paver
Andrew Warmington and Lisa Chapman at Greenlane
Clinical Centre Kerry Gunn Chris Chambers and
Jonathan Cross at Quay Park Clinic for facilitating the
administration of the study protocol and contributing
substantially to the clinical care of the patients and the
participants for their participation
References1 Cousins MJ Brennan F Carr DB Pain relief a universal human
right Pain 2004 112 1ndash42 Merry A Power I Perioperative NSAIDs towards greater safety
Pain Rev 1995 2 268ndash913 MARTINDALE The Extra Pharmacopoeia London The Royal
Pharmaceutical Society of Great Britain 19964 Mehlisch DR The efficacy of combination analgesic therapy in
relieving dental pain J Am Dent Assoc 2002 133 861ndash71
5 Desmeules J Rollason V Piguet V Dayer P Clinical pharmacologyand rationale of analgesic combinations Eur J Anaesthesiol Suppl2003 20 7ndash11
6 Altman RD A rationale for combining acetaminophen andNSAIDs for mild-to-moderate pain Clin Exp Rheumatol 2004 22
110ndash77 Hyllested M Jones S Pedersen JL Kehlet H Comparative effect
of paracetamol NSAIDs or their combination in postoperativepain management a qualitative review Br J Anaesth 2002 88
199ndash2148 Dahl V Dybvik T Steen T Aune AK Rosenlund EK Raeligder JC
Ibuprofen vs acetaminophen vs ibuprofen and acetaminophenafter arthroscopically assisted anterior cruciate ligament recon-struction Eur J Anaesthesiol 2004 21 471ndash5
9 Gazal G Mackie IC A comparison of paracetamol ibuprofen ortheir combination for pain relief following extractions in childrenunder general anaesthesia a randomized controlled trial Int JPaediatr Dent 2007 17 169ndash77
10 Merry AF Swinburn PF Middleton NG Edwards JL Calder MV
Tenoxicam and paracetamolndashcodeine combination after oralsurgery a prospective randomized double-blind placebo-controlled study Br J Anaesth 1998 81 875ndash80
11 Mitchell A van Zanten SV Inglis K Porter G A randomized con-trolled trial comparing acetaminophen plus ibuprofen versus acet-
aminophen plus codeine plus caffeine after outpatient generalsurgery J Am Coll Surg 2008 206 472ndash9
12 Menhinick KA Gutmann JL Regan JD Taylor SE Buschang PHThe efficacy of pain control following nonsurgical root canal
treatment using ibuprofen or a combination of ibuprofen andacetaminophen in a randomized double-blind placebo-controlledstudy Int Endod J 2004 37 531ndash41
13 Viitanen H Tuominen N Vaaraniemi H Nikanne E Annila PAnalgesic efficacy of rectal acetaminophen and ibuprofen alone
or in combination for paediatric day-case adenoidectomy Br JAnaesth 2003 91 363ndash7
14 Henry D McGettigan P Epidemiology overview of gastrointestinaland renal toxicity of NSAIDs Int J Clin Pract 2003 Suppl (135)43ndash9
15 TGA Medicines Evaluation Committee 2003 Review of non-prescription analgesics Multiple Strength of Oral LiquidsAustralia Therapeutic Goods Administration 2003
Combined acetaminophen and ibuprofen for analgesia
87
16 Australian and New Zealand College of Anaesthetists Monitoringduring anaesthesia (Review P18) Melbourne The College 2008
17 Merry AF Sidebotham DA Middleton NG Calder MV WebsterCS Tenoxicam 20 mg or 40 mg after thoracotomy a prospective
randomized double-blind placebo-controlled study AnaesthIntensive Care 2002 30 160ndash6
18 Davies NM Clinical pharmacokinetics of ibuprofen The first 30years Clin Pharmacokinet 1998 34 101ndash54
19 Prescott LF Pharmacokinetics of paracetamol Paracetamol(Acetaminophen) A Critical Bibliographic Review New York Taylor ampFrancis Inc 2001 205ndash15
20 Rainsford KD The pharmacokinetics of ibuprofen in humans andanimals Ibuprofen A Critical Bibliographic Review London Taylor amp
Francis 1999 92ndash521 Ianiro S Jeansonne B McNeal S Eleazer P The effect of pre-
operative acetaminophen or a combination of acetaminophen andibuprofen on the success of inferior alveolar nerve block forteeth with irreversible pulpitis J Endod 2007 33 11ndash4
22 Cooper SA Schachtel BP Goldman E Gelb S Cohn P Ibuprofenand acetaminophen in the relief of acute pain a randomizeddouble-blind placebo-controlled study J Clin Pharmacol 1989 291026ndash30
23 AHFS Drug Information Bethesda MD American Society of
Health-System Pharmacist 2007
24 Coll AM Ameen JRM Mead D Postoperative pain assessmenttools in day surgery literature review J Adv Nurs 2004 46 124ndash33
25 Philip BK Parametric statistics for evaluation of the visual ana-logue scale Anesth Analg 1990 71 710
26 Schou S Nielsen H Nattestad A et al Analgesic dosendashresponserelationship of ibuprofen 50 100 200 and 400 mg after surgicalremoval of third molars a single-dose randomized placebo-controlled and double-blind study of 304 patients J Clin
Pharmacol 1998 38 447ndash5427 Barden J Edwards J Moore A McQuay H Single dose oral para-
cetamol (acetaminophen) for postoperative pain CochraneDatabase Syst Rev (Online) 2004
28 Anderson B Cranswick N The placebo (I shall please)mdashis it so
pleasing in children Paediatr Anaesth 2005 15 809ndash1329 Australian and New Zealand College of Anaesthetists and Faculty
of Pain Medicine Acute Pain Management Scientific EvidenceAustralian Government National Health and Medical ResearchCouncil 2005
30 Moore RA Edwards JE McQuay HJ Acute pain individualpatient meta-analysis shows the impact of different ways of ana-lysing and presenting results Pain 2005 116 322ndash31
31 Quiding H Oksala E Happonen RP Lehtimaki K Ojala T Thevisual analog scale in multiple-dose evaluations of analgesics J Clin
Pharmacol 1981 21 424ndash9
Merry et al
88
e411
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Journal section Oral Medicine and PathologyPublication Types Research
Analgesic efficacy of Lysine Clonixinate paracetamol and dipyrone in lower third molar extraction A randomized controlled trial
Vladimir-Reimar-Augusto-de Souza Noronha 1 Gladson-de Souza Gurgel 1 Luiz-Ceacutesar-Fonseca Alves 2 Luiz-Claacuteudio Noman-Ferreira 2 Lisette-Lobato Mendonccedila 2 Evandro-Guimaratildees de Aguiar 2 Evandro-Neves Abdo 2
1 Student in Oral and Maxillofacial Surgery and Traummatology Dental School Federal University of Minas Gerais Belo Hori-zonte Brazil2 Senior Lectures of Department of Surgery Pathology and Clinic Dental School Federal University of Minas Gerais Belo Horizonte Brazil
Correspondence Faculdade de Odontologia Universidade Federal de Minas GeraisAv Antonio Carlos 6627Belo Horizonte ndash Minas Gerais - BrasilCEP 31270-901evandroabdogmailcom
Received 18082008Accepted 20032009
Noronha VRA Gurgel GS Alves LCF Noman-Ferreira LC Mendonccedila LL Aguiar EG Abdo EN Analgesic efficacy of lysine clonixinate para-cetamol and dipyrone in lower third molar extraction A randomized con-trolled trial Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 httpwwwmedicinaoralcommedoralfree01v14i8medoralv14i8p412pdf
AbstractObjective The purpose of this study is to compare the analgesic effect of lysine clonixinate paracetamol and dipyrone after lower third molar extraction Material and Methods The sample consisted of 90 individuals with clinical indication for inferior third molars extraction The mean age of the sample was 223 years (DPplusmn25) The individuals received the medication in uni-dentified bottles along with the intake instructions The postoperative pain parameters were measured according to Visual Analogical Scale (VAS) and the data was evaluated using the Kruskal-Wallis Test and Friedman Test with the latter used to test different time intervals for each one of the drugsResults The final sample consisted of 64 individuals including 23 males (459) and 41 females (641) The mean age of the entire sample was 223 years (plusmn25) The average length of the procedures was 339 minutes (plusmn98) The distribution of mean values for this variable showed little variance for the different drugs (p=007) Conclusion Lysine Clonixinate did not show any substantial impact on the postoperative pain control when com-pared to other drugs
Key words Lysine Clonixinate paracetamol dipyrone postoperative pain impacted third molar
Article Number 2409 httpwwwmedicinaoralcomcopy Medicina Oral S L CIF B 96689336 - pISSN 1698-4447 - eISSN 1698-6946eMail medicinamedicinaoralcom Indexed in
-SCI EXPANDED-JOURNAL CITATION REPORTS-Index Medicus MEDLINE PubMed -EMBASE Excerpta Medica-SCOPUS-Indice Meacutedico Espantildeol
e412
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Introduction Surgical extraction of third molars is a very usual clini-cal procedure for controlling problems caused by im-pacted tooth and usually is followed by postoperative pain (1) As a result several studies have been published comparing the drugs used to control postoperative pain after surgical removal of third molars (1-4)Lysine Clonixinate is an analgesic that inhibits prostag-landin synthesis A study comparing Lysine Clonixi-nate with Paracetamol on the oral postoperative pain did not find any significantly difference between them (5) In animals Lysine Clonixinate showed a life span of 3 hours and it is recognized as a non-steroid anti-in-flammatory with the shortest life span when compared to other drugs of its category (6)It bonds to plasma proteins in up to 96-98 and its me-tabolism takes place in the liver four different inactive metabolites being derived Seventy-four percent of its excretion is renal and 25 fecal (7) It holds an ex-cellent bio-tolerance and low incidence of collateral ef-fect in the treatment of painful syndrome such as renal neurogenic muscular and tooth pain (89) and migraine (7) The Visual Analogical Scale (VAS) is considered the best and easiest instrument to measure this type of pain The parameters used by VAS determine the intensity of pain as following no pain mild pain moderate pain and severe pain (10-12) The postoperative pain in dentistry should be controlled even before the surgical procedure itself For that many studies suggest the prescription of anti-inflammatory drugs steroids or not or analgesic drugs with some level of anti-inflammatory properties (1314)Paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom tooth (1516) and dipyrone is similar to other analgesics frequently used in the treatment of moderate to severe postoperative pain (17)Although the drugs under test are safe it is possible the occurrence of adverse effect The estimated ex-cess mortality due to community-acquired agranu-locytosis aplastic anemia anaphylaxis and serious upperrsquogastrointestinal complications was 20 per 100 million for paracetamol 25 per 100 million for dipy-rone (18)Regarding the Paracetamol and Dipyrone large use in Brazil Spain and other countries as well (1719) we decided to use them in order to compare the Lysine Clo-nixinate clinic performance The adverse effects due to the use of Lysine Clonixinate could be nausea vomit-ing allergic reactions vertigo and insomnia (9)
Material and MethodsThe sample of 90 individual consisted of all patients under treatment in that semester at the clinic of Oral
Surgery and Oral Traumatology from Federal Univer-sity of Minas Gerais The following conditions were ob-served in order to select the cases (I) individuals with clinical indication for the removal impacted mandibular third molar in Class I or II positioning A or B accord-ing to Pell et al (20) regardless gender race or social class (II) surgeries that would not extend more than 60 minutes (III) age between 18 and 26 years old (IV) absence of allergies to the drugs under test (V) absence of systemic conditions All surgeries were carried out under local anesthesia-Lidocaine 2 with Felipressine 12500 - Novocoreg (SSWhite Artigos Dentais LTDA Rio de Janeiro Brazil)The patients were informed about the purpose of the research project and were asked to give their written consent The research was approved by the local Ethical CommitteeThe drugs tested were bottled in identical opaque white recipient numbered from 1 to 90 Each recipient con-tained eight tablets of either one of the drugs under test (Dipyrone 500mg Paracetamol 750mg Lysine Clonixi-nate 125 mg) The patients themselves chose the recipi-ent at random and they were unaware of its contentEach patient was told to take one tablet from the given recipient one hour before the surgery and another tablet was taken after the surgery in 6 hours intervals after first dose during 24 hours If the pain persisted the pa-tient was given the liberty to take any other drug and the dentist should be informed The assessment of pain was performed according to VAS Pain was measured just after the surgical proce-dure and 1246812 and 24 hours after the operation For each one of the above options they had also to in-form the level of pain according to a decimal scale The criteria used by the authors to assess patientrsquos pain level were 0 cm no pain 01-3 cm light pain 31-7 cm mo-derate pain 71-10 cm intense pain (9) The descriptive analyses are presented in percentages with mean minimum (min) maximum (max) and standard deviation (SD) Kruskal-Wallis and Friedman tests were used and results were considered statistically significant when value of p was less or equal to 005 at least 95 of the confidence
ResultsThe drop-out in the experiment was of twenty-six cases and therefore the sample was reduced to sixty-four The Lysine Clonixinate group was comprised of 20 in-dividuals (8 males and 12 females) The Paracetamol Group was comprised of 23 individuals (9 males and 14 females) and Dipyrone Group was comprised of 21 individuals (6 males and 15 females) The mean age of the entire sample was 223 years (plusmn25) The length of the procedures was in average 339 min-utes (plusmn98) (Table 1) (Table 2) and (Fig 1) depict each
e413
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Interval drugdescriptive measurement
Pmin max median mean SD
Right after Lysine clonixinate 000 100 000 020 040 09370
Paracetamol 000 300 000 030 070
Dipyrone 000 100 000 010 040
1 hour afterLysine clonixinate 000 200 100 070 060 08130
Paracetamol 000 300 100 060 070
Dipyrone 000 200 100 070 070
2 hours afterLysine clonixinate 000 200 100 080 070 09310
Paracetamol 000 300 100 080 090
Dipyrone 000 300 100 080 080
4 hours afterLysine clonixinate 000 200 100 090 070 08760
Paracetamol 000 200 100 080 070
Dipyrone 000 300 100 100 100
6 horus afterLysine clonixinate 000 200 100 060 060 05330
Paracetamol 000 300 100 080 090
Dipyrone 000 300 000 060 080
8 hours afterLysine clonixinate 000 200 050 060 060 03110
Paracetamol 000 200 000 060 080
Dipyrone 000 300 000 040 080
12 hours afterLysine clonixinate 000 200 000 040 060 05930
Paracetamol 000 200 000 055 070
Dipyrone 000 300 000 040 090
24 hours afterLysine clonixinate 000 200 000 030 060 05820
Paracetamol 000 200 000 040 070
Dipyrone 000 300 000 030 070
Fig 1 Distribution of the scale of pain according to the different time interval for each of the drugs tested
Table 1 Distribution of the variable pain according to VAS in different time period for the tree drugs tested
P refers to Kruskal-Wallis test
e414
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
one of the VAS parameters distributed according to drugs tested No adverse effect was observed with the drugs tested
DiscussionSixty-four individuals underwent surgical removal of their inferior third molars among them 23 (359) were male and 41 (641) female As reported before by Morin et al (21) the variable gender did not play any important role in the distribution of the variable pain after surgery The mean age was 223 years (SDplusmn25 years) and the sample was quite homogeneous in that aspect which is an advantage for the categorization of pain related to age Age can influence the pain control because third molar surgical extraction in older individuals can be-come troublesome due the cortical bone thickness and bone resilience loss (1) Chiapasco et al (1) reported a decrease in morbidity and postoperative complication of third molars in young patients Olmedo-Gaya et al (14) attributed an increase of pain in older patients due to the more bone density and narrower periodontal liga-ment
The patients underwent all the surgical procedures by 2 surgeons with calibration of the techniques avoiding therefore different approaches The surgeries length was controlled and therefore did not influence the be-havior of pain in this study- 339 min (SDplusmn98 min) Regarding this the authors believe there is no bias con-cerning the time-period of surgery on the results here presentedThe surgery of third molar is a well known procedure It allows a standardization of case selection reducing therefore the number of uncontrolled events that may lead to biasQuestionnaire and VAS were used to obtain the data The data bank was categorized by drug and analyzed according to the development of the postoperative con-dition as presented in (Table 1)The results in this study show no statistically significant difference between the drugs under test for controlling postoperative pain Martiacute et al (5) found similar results comparing Paracetamol and Lysine ClonixinateThe high number of patients without any pain in the postoperative period can be related to the local anesthe-sia The number of patients without pain in the postop-
DescriptionDrug Interval min Max median mean SD p
Lisyne clonixinate
Right after 00 10 00 02 04
lt 0001
1 hour after 00 20 10 07 062 hours after 00 20 10 08 074 hours after 00 20 10 09 076 hours after 00 20 10 06 068 hours after 00 20 05 06 0612 hours after 00 20 00 04 0624 hours after 00 20 00 03 06
Paracetamol
Right after 00 30 00 03 07
lt 0001
1 hour after 00 30 10 06 072 hours after 00 30 10 08 094 hours after 00 20 10 08 076 hours after 00 30 10 08 098 hours after 00 20 00 06 0812 hours after 00 20 00 05 0724 hours after 00 20 00 04 07
Dipyrone
Right after 00 10 00 01 04
lt 0001
1 hour after 00 20 10 07 072 hours after 00 30 10 08 084 hours after 00 30 10 10 106 hours after 00 30 00 06 088 hours after 00 30 00 04 0812 hours after 00 30 00 04 0924 hours after 00 30 00 03 07
Table 2 Distribution of pain perception in the different time intervals after surgery according to VAS
P refers to Friedman test
e415
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
erative period decreases with the passing of time Four hours after the surgery this percentage was the smallest and it increases slightly on the 6th and 8th hour after surgery reaching its peak with 24 hours The results presented here are similar to those of Olme-do-Gaya et al (14) who found out that the postoperative pain reaches its higher intensity during the first 8 hours after the surgery The moderate postoperative pain is re-ported when the production of pain mediator increases and also when the effect of local anesthesia is fading away After the 8th hour and during the subsequently days the pain decreases progressivelyThe results of this study show that the Lysine Clonixi-nate as well as Dipyrone and Paracetamol are efficient in controlling the postoperative pain in the surgery of inferior impacted third molars Lysine Clonixinate pos-sesses an analgesic activity similar to that of Dipyrone and Paracetamol and did not show any substantial im-pact on the control of postoperative pain when com-pared to those drugs
References1 Chiapasco M De Cicco L Marrone G Side effects and complica-tions associated with third molar surgery Oral Surg Oral Med Oral Pathol 199376412-20 2 Laureano Filho JR Maurette PE Allais M Cotinho M Fernandes C Clinical comparative study of the effectiveness of two dosages of Dexamethasone to control postoperative swelling trismus and pain after the surgical extraction of mandibular impacted third molars Med Oral Patol Oral Cir Bucal 200813E129-32 3 Loacutepez-Carriches C Martiacutenez-Gonzaacutelez JM Donado-Rodriacuteguez M Analgesic efficacy of diclofenac versus methylprednisolone in the control of postoperative pain after surgical removal of lower third molars Med Oral Patol Oral Cir Bucal 200510432-9 4 Esteller-Martiacutenez V Paredes-Garciacutea J Valmaseda-Castelloacuten E Berini-Ayteacutes L Gay-Escoda C Analgesic efficacy of diclofenac sodium versus ibuprofen following surgical extraction of impacted lower third molars Med Oral Patol Oral Cir Bucal 20049448-53 444-8 5 Martiacute ML De los Santos AR Di Girolamo G Gil M Manero EO Fraga C Lysine clonixinate in minor dental surgery double-blind randomized parallel study versus paracetamol Int J Tissue React 199315207-13 6 Gonzaacutelez-Martin G Cattan C Zuntildeiga S Pharmacokinetics of lysine clonixinate in children in postoperative care Int J Clin Phar-macol Ther 199634396-9 7 Krymchantowski AV Peixoto P Higashi R Silva A Jr Schutz V Lysine clonixinate vs naproxen sodium for the acute treatment of mi-graine a double-blind randomized crossover study MedGenMed 2005769 8 Ortiacute E Coirini H Pico JC Site-specific effects of the nonsteroidal anti-inflammatory drug lysine clonixinate on rat brain opioid recep-tors Pharmacology 199958190-9 9 Krymchantowski AV Barbosa JS Cheim C Alves LA Oral lysine clonixinate in the acute treatment of migraine a double-blind place-bo-controlled study Arq Neuropsiquiatr 20015946-9 10 Kremer E Atkinson JH Ignelzi RJ Measurement of pain patient preference does not confound pain measurement Pain 198110241-8 11 Price DD McGrath PA Rafii A Buckingham B The validation of visual analogue scales as ratio scale measures for chronic and ex-perimental pain Pain 19831745-56 12 Collins SL Moore RA McQuay HJ The visual analogue
pain intensity scale what is moderate pain in millimetres Pain 19977295-7 13 Seymour RA Walton JG Pain control after third molar surgery Int J Oral Surg 198413457-85 14 Olmedo-Gaya MV Vallecillo-Capilla M Galvez-Mateos R Rela-tion of patient and surgical variables to postoperative pain and inflam-mation in the extraction of third molars Med Oral 20027360-9 15 Weil K Hooper L Afzal Z Esposito M Worthington HV Van Wijk AJ et al Paracetamol for pain relief after surgical removal of lower wisdom teeth Cochrane Database Syst Rev 20073CD004487 16 Moore A Collins S Carroll D McQuay H Paracetamol with and without codeine in acute pain a quantitative systematic review Pain 199770193-201 17 Edwards JE Meseguer F Faura CC Moore RA McQuay HJ Single-dose dipyrone for acute postoperative pain Cochrane Data-base Syst Rev 20013CD003227 18 Andrade SE Martinez C Walker AM Comparative safety evalu-ation of non-narcotic analgesics J Clin Epidemiol 1998511357-65 19 Lorenzetti BB Ferreira SH Mode of analgesic action of dipy-rone direct antagonism of inflammatory hyperalgesia Eur J Phar-macol 1985114375-81 20 Pell GJ Gregory BT Impacted mandibular third molars clas-sification and modified techniques for removal Dent Digest 193339330-821 Morin C Lund JP Villarroel T Clokie CM Feine JS Differences between the sexes in post-surgical pain Pain 20008579-85
CLINICAL TRIAL
Onset of analgesia with sodium ibuprofen ibuprofen acidincorporating poloxamer and acetaminophenmdasha single-dosedouble-blind placebo-controlled study in patientswith post-operative dental pain
Stephen Daniels amp Sandie Reader amp Phillip Berry amp
Michael Goulder
Received 24 September 2008 Accepted 6 January 2009 Published online 28 February 2009 Springer-Verlag 2009
AbstractObjective To compare the onset of action and efficacy ofsodium ibuprofen (ibuprofen sodium dihydrate) and ibu-profen acid incorporating poloxamer (ibuprofenpoloxamer)with that of acetaminophen and placebo in patients withpost-operative dental painMethods A double-blind randomised placebo-controlledactive comparator two-centre study assessing the analgesicefficacy of sodium ibuprofen (512 mg equivalent to400 mg ibuprofen acid) ibuprofenpoloxamer (containing400 mg ibuprofen acid and 120 mg poloxamer 407)acetaminophen (1000 mg) and placebo in patients withmoderate-to-severe pain after third molar extraction (n=322) Onset of action was assessed using the two-stopwatchtechnique and pain intensity and relief were measuredusing validated traditional descriptor scales
Results Significantly more patients achieved confirmedperceptible pain relief and meaningful pain relief withsodium ibuprofen (963 Plt00001) and ibuprofenpoloxamer (900 P=00005) than with acetaminophen(675) The onset of action of both ibuprofen formula-tions was comparable with that of acetaminophen up to45 min post-dose a marked divergence in onset times infavour of the ibuprofen formulations occurred from45 min onward Mean values for the area under the painrelief and pain intensity differences curve (0ndash6 h) weresignificantly greater for sodium ibuprofen (346) andibuprofen acid (349) than for acetaminophen (225) (Plt0001) Other pain relief and pain intensity endpointsfavoured both ibuprofen formulations over acetamino-phen Distractibility from pain (6 h) was significantlygreater with the ibuprofen formulations than with acet-aminophen (P=0008 for sodium ibuprofen P=003 foribuprofenpoloxamer) In patients receiving ibuprofenpain interfered less with daily activities (at 1 and 6 h)than in those receiving acetaminophen (Ple0015) Bothibuprofen formulations had significantly better meanglobal assessment scores than acetaminophen (Plt0001)Tolerability profiles of the ibuprofen formulations werecomparable with that of acetaminophenConclusions Compared with acetaminophen sodiumibuprofen was associated with significantly greateranalgesic efficacy pain relief in a greater proportion ofpatients and greater patient satisfaction
Keywords Acetaminophen Dental pain
Ibuprofenpoloxamer Impacted teeth Post-operative pain
Sodium ibuprofen
Eur J Clin Pharmacol (2009) 65343ndash353DOI 101007s00228-009-0614-y
S DanielsPremier Research Group Clinical Research Center3200 Red RiverAustin TX 78705 USA
S Reader P Berry ()Reckitt Benckiser Healthcare UKDansom LaneHull HU8 7DS UKe-mail phillipberryreckittbenckisercom
M GoulderWorldwide Clinical Trials UK Ltd Isaac Newton CentreNottingham Science and Technology ParkNottingham NG7 2RH UK
Introduction
Ibuprofen [2-(4-isobutylphenyl) propionic acid] is awidely used non-steroidal anti-inflammatory drug(NSAID) currently licensed and marketed worldwide Itexhibits anti-inflammatory analgesic and antipyreticeffects in humans by working as a potent inhibitor of thecyclooxygenase enzyme system and is used to treat painresulting from a wide variety of ailments There is anextensive amount of published literature describing theefficacy of ibuprofen [1ndash7]
Patients with acute pain require rapid relief from over-the-counter (OTC) analgesics Rapidly absorbed ibuprofenformulations have been developed [8] and it was antici-pated that this rapid absorption would result in early onsetof analgesia This placebo-controlled double-blind rando-mised single-dose study was conducted to measure thetime to onset and degree of analgesia from two investiga-tional ibuprofen formulations The first investigationalibuprofen formulation contains the sodium salt of the drugibuprofen sodium dihydrate (sodium ibuprofen) Theformulation used in this study contains 256 mg of theibuprofen sodium salt equivalent to 200 mg ibuprofen acidIt is well documented that ibuprofen salts such asibuprofen sodium lysine and arginate are more rapidlyabsorbed than formulations of free ibuprofen acid [9] andseveral studies have shown that faster absorbed formula-tions lead to faster onset of analgesia [10ndash12] The saltdissolves rapidly in the gastrointestinal tract leading tofaster absorption Pharmacokinetic analyses show that thetime to peak plasma concentration (Tmax) with ibuprofensodium dihydrate is achieved in approximately 30ndash40 min[8] in contrast to the 1ndash2 h reported for standard ibuprofentablets [13 14] The second investigational ibuprofenformulation contains ibuprofen acid plus the surfactantpoloxamer 407 [from the poloxamer family of polymericnon-ionic surface active agents (ibuprofenpoloxamer)]mdashtoincrease the rate of dissolution of the tablet and enable morerapid absorption relative to standard ibuprofen formula-tions Acetaminophen another widely used OTC analgesicand antipyretic indicated for the same mild-to-moderatepain conditions as ibuprofen was included in the study as areference
The dental pain model was used because it is the mostappropriate model to investigate onset of analgesic actionIt is an established post-surgical pain model that involvesextraction of impacted third molars (wisdom teeth) arelatively consistent surgical technique that predictablyproduces moderate-to-severe pain The model is widelyaccepted and has a proven record of assay sensitivity (ieseparating active drugs from each other as well as fromplacebo) [11 12 15ndash18] The model is sensitive enough todemonstrate a correlation between plasma levels of ibupro-
fen and onset of analgesia with faster absorbed formula-tions such as ibuprofen arginate having a faster clinicalresponse time than standard ibuprofen [11 12 19] Theresults from dental pain studies have been widely extrap-olated to other general pain conditions including mostcommon OTC conditions
Onset of analgesic action was assessed using the two-stopwatch technique [11 12 19] and pain intensity andpain relief at each of the assessment timepoints wereassessed using traditional descriptor scales Exploratoryanalyses were conducted to give additional informationabout the rate of onset of action of the medications and tocompare the extent of relief provided by each of the activeformulations
Both ibuprofen formulations were given at a doseequivalent to 400 mg ibuprofen acid The acetaminophenproduct included in the study was Tylenol Extra Strength(1000 mg) a commercially available product The brandedprinting was removed from the Tylenol caplets to enable amatched placebo to be produced The doses of both drugsare the maximum licensed OTC doses in the USA and mostother countries and they have well-established safety andefficacy profiles
The primary objective of the study was to determine thetime to onset of analgesia following dosing with sodiumibuprofen tablets (2times256 mg ibuprofen sodium dihydrate)and ibuprofen acid tablets incorporating poloxamer (2times200 mg ibuprofen plus 60 mg poloxamer 407) hereafterreferred to as ibuprofenpoloxamer in patients with post-operative dental pain The secondary objective was tocompare the efficacy of the two ibuprofen formulationswith that of 1000 mg acetaminophen and placebo in termsof onset peak and duration of analgesic action
The study was conducted in accordance with theDeclaration of Helsinki [20] as referenced in EU Directive200120EC [21] and complies with International Confer-ence on Harmonisation (ICH) Good Clinical Practice(GCP) and applicable regulatory requirements
Methods
Study design
This study was a randomised double-blind placebo-controlled single-dose parallel-group study using thedental pain model It was conducted in two clinical researchcentres (Austin Texas and San Marcos Texas)
Patients andor their legal guardians provided informedconsent before the conduct of study-related proceduresPatients were screened within the 28 days before surgeryOn the day of surgery patients underwent surgical removalof one partially or full bone impacted mandibular third
344 Eur J Clin Pharmacol (2009) 65343ndash353
molar or two ipsilateral third molars with a total impactionscore of 4 5 or 6
Degree of impaction Points
Erupted 0Soft tissue 1Partial bone 2Complete (full) bone 3Unusual impaction (horizontalinverted or posterior-anterior) 4
Surgery was performed under local anaesthetic (approx-imately 100 mg lidocaine 2 with 110000 epinephrine)with conscious sedation (35 lmin 50 nitrous oxide for15 min) using standard surgical techniques Followingsurgery patients who fulfilled the inclusion criteria regard-ing baseline pain intensity were randomly allocated to oneof four treatment groups (sodium ibuprofen ibuprofenpoloxamer acetaminophen or placebo) in a 1111 ratioaccording to a computer-generated randomisation schedulethat stratified patients by sex and baseline pain intensityAfter dosing patients remained in the centre for 8ndash15 hOnset of action and efficacy assessments were recorded atpre-determined intervals during the 6 h post-dose A post-operative follow-up was conducted 5ndash12 days after surgery
The study protocol and its amendments together with thepatient information and consent documents were reviewedand approved by Quorum Review Inc (Seattle WA)
Patients
Patients were recruited from the Premier Research GroupClinical Research Centers database via advertising andpractitioner referral Eligible patients were males andfemales 16ndash40 years of age with a primary diagnosis of
amp at least one mandibular third molar (with full bonyimpaction and an impaction score of ge4 on a 5-pointscale) indicated for removal
amp two ipsilateral third molars with a combined totalimpaction score no greater than 6
In either case patients were required to have moderate orsevere baseline pain intensity as assessed using a 4-pointcategorical pain intensity scale and confirmed with a visualanalogue scale (VAS) score of ge50 mm but le85 mm (where0=no pain and 100 mm=worst pain)
The main exclusion criteria were history of significantdisease that rendered the patient unsuitable for inclusionsignificant ongoing painful conditions other than thatassociated with third molar surgery any ongoing conditionthat may have interfered with the absorption distributionmetabolism or excretion of study medications history ofallergy gastrointestinal complaints (including ulcers heart-burn dyspepsia and indigestion) migraine headaches
within the last year psychotic illness or drug abuse useof concomitant medication that may have confoundedassessments of pain relief (eg psychotropic drugs anti-depressants or sedative-hypnotics) pregnancylactationingestion of any analgesic or anti-inflammatory drug frommidnight of the night before surgery
Sample size determination
For the primary endpoint data were available for the time toperceptible relief from three studies using ibuprofen arginate[11 12 19] These data suggested that the time to perceptiblerelief would be 9 to 14 min for the two test formulationsassuming a similar onset of action to that of ibuprofen arginateSince it was assumed that the majority of placebo patientswould not achieve meaningful relief it was planned that thetime to confirmed perceptible relief for these patients would becensored at 4 h Although the spread of observations was notprovided for the arginate formulation it was assumed conser-vatively that the standard deviation (SD) for time to confirmedperceptible relief would be 1 h (based on the possible rangebeing 0ndash4 h and covering plusmn 2 SD) Hence this study was highlypowered (gt99) to detect such a large difference for the time toconfirmed perceptible relief using the Wilcoxon test
For the area under the curve (AUC) (pain relief intensitydifference [PRID] from 0 to 6 h) data were available fromtwo previous studies which compared ibuprofen lysine [22]and liquigel [23] ibuprofen with acetaminophen In the formerstudy PRID to 6 h was not provided but the sum of painintensity differences (SPID) to 6 h was given This gave adifference of 251 between ibuprofen lysine and acetamino-phen The within-group SD for acetaminophen was 447Using these data it was calculated that with 80 patients pergroup this study would have a 90 power to detect adifference between the ibuprofen formulations and acetamin-ophen at a significance level of 0025 If the data from theliquigel paper were used for sum of the measures of pain reliefand pain intensity difference (SPRID) to 6 h a slightly higherpower would be achieved It was not possible to performformal power calculations for the second endpoint in the closedtest procedure namely time to meaningful relief
Study and concomitant treatments
Following surgery eligible patients received a single oraldose (four tablets and two caplets) of one of the followingfour study treatments
amp sodium ibuprofen 2times256 mg ibuprofen sodium dihy-drate tablets (each tablet equivalent to 200 mg ibupro-fen acid) plus two matched placebo for ibuprofenpoloxamer tablets plus two matched placebo for 500 mgacetaminophen caplets
Eur J Clin Pharmacol (2009) 65343ndash353 345
amp ibuprofenpoloxamer 2times200 mg ibuprofen acid tabletseach tablet incorporating 60 mg of the surfactantpoloxamer 407 plus two matched placebo for sodiumibuprofen tablets plus two matched placebo for 500 mgacetaminophen caplets
amp acetaminophen 2times500 mg acetaminophen (TylenolExtra Strength) caplets plus two matched placebo forsodium ibuprofen tablets plus two matched placebo foribuprofenpoloxamer tablets
amp placebo two matched placebo for sodium ibuprofentablets plus two matched placebo for ibuprofenpolox-amer tablets plus two matched placebo for 500 mgacetaminophen caplets
Patients were encouraged to wait at least 90 min afterreceiving the study treatment before consuming rescuemedication although rescue medication was available atany time after dosing If rescue medication was neededwithin the first 4 h of dosing an intra-muscular injection ofketorolac tromethamine (60 mg) was administered Ifrescue medication was needed later than 4 h after studydrug administration acetaminophen 500 mghydrocodone5 mg or ketorolac tromethamine was given A prescriptionfor acetaminophen 500 mghydrocodone 5 mg was provid-ed to patients for home use at the time of discharge
The use of intravenous oral or inhaled (nitrous)sedation during surgery was prohibited Analgesic andanti-inflammatory drugs (except for the permitted rescuemedications antibiotics and anaesthetics) were not per-mitted during the 6-h post-dose assessment periodPenicillins macrolide antibiotics clindamycin and topicaltetracycline gelfoam were permitted the use of selectiveserotonin-reuptake inhibitors (SSRIs) and selective nor-epinephrine-reuptake inhibitors (SNRIs) was also accept-able in patients who had maintained a stable dose for atleast 4 weeks prior to the first visit Caffeine-containingfoods and drinks were to be discontinued from midnightprior to surgery until the end of the 6-h post-doseassessment period Ice packs were not allowed for thefirst 3 h after dosing
Efficacy endpoints
Patients were queried at pre-determined intervals by thestudy staff and all pain assessments were recorded by thepatient in their diary
Pain intensity (categorical and VAS)
Pain intensity (PI) was assessed at the following timesbaseline (0 h) and at 5 10 15 20 25 30 35 40 45 60 90120 180 240 300 and 360 min after dosing The PI wasmeasured on a categorical scale in response to the question
ldquoWhat is your pain level at this timerdquo with patient responsechoices of none=0 mild=1 moderate=2 and severe=3 Inaddition patients were also asked to draw a single vertical lineto indicate their current level of PI on the 100-mm VASPatients were randomised to treatment when they rated theirbaseline PI as moderate or severe and the score on the VASwas ge50 mm but le85 mm
Pain relief and pain half-gone
Pain relief (PR) was assessed at the same times as PI (withthe exception of 0 h) in response to the question ldquoHowmuch relief have you had from your starting painrdquo withpatient response choices of none=0 a little=1 some=2 alot=3 and complete=4 In addition patients were alsoasked ldquoIs your starting pain at least half gonerdquo withpatient responses as no=0 or yes=1
Perceptible and meaningful PR
Two stopwatches were started at the time of dosing Eachpatient was instructed ldquoStop the first stopwatch when you firstfeel any pain relief whatsoever This does not mean you feelcompletely better although you might but when you first feelany relief in the pain you have nowrdquo The patient wasinstructed ldquoStop the second stopwatch when the pain relief ismeaningful to yourdquo If the patient did not press thestopwatches within the first 4 h of the treatment period or ifrescue medication was required the patients were no longerrequired to use the stopwatches
Distractibility from pain
Distractibility from pain was assessed at baseline and at 60and 360 min after dosing in response to the question ldquoHoweasy is it for you to distract yourself from your painrdquoPatients responded using a 100-mm VAS scale where 0 =very easy and 100 = impossible
Rainier scale
Patients completed the Rainier scale at baseline and at 60and 360 min after dosing This assessed perceivedfunctional impairment of activities of daily living (ieeating driving sleeping reading working and speaking)Patients rated the perceived pain interference with eachactivity on a scale of 1 to 10 where 1 = would not interfereat all and 10 = would completely interfere
Rescue medication
The time of rescue medication was recorded Patientstaking rescue medication completed all pain intensity and
346 Eur J Clin Pharmacol (2009) 65343ndash353
pain relief assessments immediately before rescue medica-tion and continued to record their pain assessmentsthroughout the 6-h assessment period
Global evaluation
At the end of 6 h or at the time of rescue medication patientswere asked ldquoHow effective do you think the study medicationis as a treatment for painrdquo Response choices were 1 =excellent 2 = very good 3 = good 4 = fair or 5 = poor
The primary efficacy endpoint was the time to firstconfirmed perceptible pain relief There were two keysecondary endpoints (1) the AUC for SPRID from 0 to 6 hand (2) the time to meaningful pain relief
Other secondary endpoints included (1) total pain relief(TOTPAR) SPID (categorical and VAS) SPRID from 0 to4 h (2) TOTPAR SPID (categorical and VAS) from 0 to6 h (3) individual pain relief and pain intensity (categoricaland VAS) readings at each timepoint from 5 min to 6 h (4)peak pain relief and pain intensity difference (PID)(categorical and VAS) throughout the 6-h evaluation period(5) first time at which PID was ge1 (6) time to first use ofrescue medication (7) time to and proportion of patientswith pain half-gone (8) distractibility from pain at baselineand at 1 and 6 h post-dose and perceived pain interferencewith daily activities (Rainier scale) at 1 and 6 h post-dose(9) patientrsquos overall assessment of the medication
Safety assessments
Adverse events (AEs) were assessed by non-directedquestioning recorded in the source documentation andthen assessed by the Investigator with respect to severityand relationship to study medication Vital signs (bloodpressure heart rate and oral temperature) were assessed atscreening baseline (pre-dose) at 6 h post-dose and at thefollow-up visit A physical examination was also conductedat screening and at the follow-up visit 5ndash12 days aftersurgery
Statistical analyses
All calculations and figures were produced using SAS ver91 or S-PLUS 62 (SAS Institute Cary NC) The analysisof the primary endpoints was performed via a closed testprocedure The actual protocol-defined primary endpointwas the time to first confirmed perceptible pain reliefPairwise differences between the two ibuprofen formula-tions and placebo were assessed at a significance level of25 so the overall alpha-level of 5 was maintained Forthe primary endpoint pairwise differences between the twoibuprofen formulations and placebo were assessed using theWilcoxon rank-sum test A sensitivity analysis was also
performed where differences between the ibuprofen for-mulations and placebo were assessed using a Cox regres-sion analysis with treatment group study site gender andbaseline pain intensity (categorical) included in the modelThe hazard ratio and associated 975 confidence intervals(CIs) were calculated for the pairwise comparisons
It was planned that if either of the primary pairwisecomparisons were significant at the 25 level the keysecondary endpoints (SPRID 0ndash6 h and time to meaningfulpain relief) were to be assessed for that formulation under aclosed-test procedure Each endpoint was assessed in theorder specified and only if the previous assessments for thatformulation were significant were the subsequent end-points assessed in a confirmatory sense Once the endpointwas not significant then all subsequent assessments wereconsidered exploratory
Endpoints aggregated over several time points werecalculated using AUC as per the secondary endpointDifferences between the treatments were assessed at atwo-sided alpha of 005 A 95 CI for the pairwisedifferences between the treatments was calculated fromthe parameter estimates of the fitted model The pairwisecomparisons of interest were between each of the ibuprofenformulations and placebo and between each of theibuprofen formulations and acetaminophen For the time-to-event parameters such as time to first (unconfirmed)perceptible pain relief differences between the treatmentgroups were assessed as per the primary endpoint
Differences between each of the two ibuprofen formu-lations and acetaminophen in the key secondary endpointsand in the majority of the other secondary endpoints wereanalysed by analysis of covariance (ANCOVA) includingtreatment group study site gender and baseline painintensity (categorical scale) as factors
All assessments completed after the patient had takenrescue medication were considered to be missing For bothpain relief and pain intensity differences missing valuesbetween two available assessments were linearly interpo-lated Missing readings that could not be interpolated werereplaced with the baseline pain intensity or zero relief
All enrolled patients who received a dose of studymedication were included in the safety population All AEswere listed and tabulated by treatment severity relationshipto therapy and body system according to the MedicalDictionary for Regulatory Activities (MedDRA) Version81
Results
Between June and October 2005 a total of 322 patients(mean age 213 years) were randomised to receive studytreatment Of the 322 randomised patients 318 (988)
Eur J Clin Pharmacol (2009) 65343ndash353 347
completed the study The trial profile including the totalnumber of patients withdrawn and analysed is illustrated inFig 1 A total of 321 patients all of whom were balancedacross treatment groups with respect to baseline demo-graphics pain intensity and clinical characteristics (Table 1)were included in the intent-to-treat (ITT) population
Primary efficacy endpoint
Significantly more patients reported confirmed perceptiblepain relief with sodium ibuprofen (963) and ibuprofenpoloxamer (900) than with acetaminophen (675) (Plt00001 and P=00005 respectively) In the placebo grouponly 259 patients reported confirmed perceptible painrelief KaplanndashMeier median times to confirmed perceptiblepain relief were 170 min for sodium ibuprofen 185 minfor ibuprofenpoloxamer and 201 min for acetaminophen(Fig 2) Median time could not be estimated for placebo asfewer than 50 of patients assigned to this groupexperienced confirmed perceptible pain relief Comparisonsof pairwise differences between the two ibuprofen formu-lations and placebo using Wilcoxon rank-sum tests and Coxregression analysis were highly significant (Plt0001 forboth analyses)
Key secondary efficacy endpoints
Mean SPRID (0ndash6 h) values were 346 349 225 and073 for the sodium ibuprofen ibuprofenpoloxamer
acetaminophen and placebo groups respectively Pair-wise comparisons of ibuprofen and acetaminophen werehighly significant in favour of both ibuprofen formula-tions (Plt0001)
Significantly more patients reported meaningful painrelief with sodium ibuprofen (963) or ibuprofenpolox-amer (900) than with acetaminophen (675) (Plt00001and P=00005 respectively) (Fig 3) Of the patientsreceiving placebo 259 reported meaningful pain reliefThe KaplanndashMeier median times to meaningful relief were451 min (sodium ibuprofen) 447 min (ibuprofenpolox-amer) and 541 min (acetaminophen) Neither of the twoWilcoxon rank-sum comparisons between the ibuprofenformulations and acetaminophen were statistically signifi-cant whereas pairwise comparisons obtained via Coxregression analysis were statistically significantly different(P le 0002) The KaplanndashMeier survival curves were similarfor the ibuprofen and acetaminophen groups up to 45 minbut the degree of separation from 45 min onward wasmarked with more patients achieving meaningful painrelief with ibuprofen
Sitendashtreatment interactions
In general site was a statistically significant factor subjectsfrom the SanMarcos site had less favourable outcomes For theprimary efficacy endpoint and for the key secondary efficacyendpoints of SPRID (0ndash6 h) and time to meaningful pain reliefsite was statistically significantly For all three measures the
Withdrawn from ITT (failure toprovide baseline diary data) 1Withdrawn from ITT (failure toprovide baseline diary data) 1Withdrawn from ITT (failure toprovide baseline diary data) 1
IBUPROFENPOLOXAMER
Total screened 614
Total randomised 322
Excluded prior to surgery (n=240)
Excluded prior to dosing (n=52)
Failure to meet inclusion criteria (n=292)
Allocated to intervention 80
ACETAMINOPHEN
Allocated to intervention 81
PLACEBO
Allocated to intervention 81
Completed 80 Completed 81 Completed 81
Total analysed (ITTa) 80 Total analysed (ITTa) 80 Total analysed (ITTa) 81
Completed 76
Withdrew consent 1Lost to follow-up 1Other reasons 2
Withdrawn 0 Withdrawn 0 Withdrawn 0
Total analysed (ITTa) 80
SODIUM IBUPROFEN
Not included in ITT (failure to provide baseline diary data) 1
Allocated to intervention 80
Fig 1 Flow diagram illustrat-ing patient inclusion and exclu-sion throughout the study ITTIntent to treat aThe ITT popula-tion consisted of all patientswho were randomised whocompleted the baseline efficacyassessments and who had atleast one post-baseline assess-ment (primary efficacy set)
348 Eur J Clin Pharmacol (2009) 65343ndash353
interaction between site and treatment was formally investigat-ed In all cases the interaction term was not statisticallysignificant implying that treatment group responses wereconsistent between the sites
Exploratory secondary efficacy endpoints
Pain relief andor reduction in pain intensity
All summary endpoints related to pain relief andor PIDwere significantly more favourable for the two ibuprofenformulations than for acetaminophen or placebo (Plt0001for both ibuprofen formulations vs acetaminophen orplacebo in all comparisons)
A summary of pain relief scores at specified time pointsfrom 5 min to 6 h is displayed in Fig 4 The superiority of
the two ibuprofen formulations over acetaminophen canclearly be seen from 45 min post-dose onward A summaryof PID (categorical) scores at specified time points from5 min to 6 h is displayed in Fig 5 The superiority of thetwo ibuprofen formulations over acetaminophen can beclearly seen from 60 min post-dose onward
Individual PR and PID
The pain relief and PID (categorical and VAS) scores showthat sodium ibuprofen provided more effective pain reliefthan placebo at 15 min [P=0021 (PR) P=004 (PIDcategorical) P=0036 (PID VAS)] Similarly ibuprofenpoloxamer provided more effective relief than placebo at25 min [P=0002 (PR) P=0002 (PID categorical)] and at20 min [P=0008 (PID VAS)]
Timepoint (mins)
a
ttain
ing
conf
irmed
per
cept
ible
rel
ief
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 2 KaplanndashMeier curves for time to first confirmed perceptiblepain relief
Timepoint (mins)
a
ttain
ing
mea
ning
ful r
elie
f
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 3 KaplanndashMeier curves for time to meaningful pain relief
Table 1 Patient demographics and clinical characteristics at baseline (ITT population)
Baseline patient characteristics Treatment group
Sodium ibuprofen(n=80)
Ibuprofenpoloxamer(n=80)
Acetaminophen(n=80)
Placebo(n=81)
Total(n=321)
Age (years) mean (SD) 214 (388) 214 (360) 212 (443) 211 (408) 213 (399)Sex n ()Male 31 (388) 31 (388) 30 (375) 31 (383) 123 (383)Female 49 (613) 49 (613) 50 (625) 50 (617) 198 (617)
Baseline pain intensity (categorical) n ()Moderate 61 (763) 60 (750) 60 (750) 62 (765) 243 (757)Severe 19 (238) 20 (250) 20 (250) 19 (235) 78 (243)
Baseline pain intensity (VAS) mean (SD)Mean (SD) 6816 (874) 6881 (949) 6703 (932) 6737 (1003) 6784 (939)Range 51ndash85 50ndash89 52ndash84 50ndash85 50ndash89
ITT intent-to-treat SD standard deviation VAS visual analogue scaleTreatment definitions sodium ibuprofen=2times256 mg ibuprofen sodium dihydrate tablets (each tablet equivalent to 200 mg ibuprofen acid)ibuprofenpoloxamer=2times200 mg ibuprofen acid tablets acetaminophen=2times500 mg acetaminophen caplets
Eur J Clin Pharmacol (2009) 65343ndash353 349
First time to PID ge 1
There were no significant differences between the activetreatment groups in the proportion of the time to reportingof PID ge 1
Time to first use of rescue medication
Rescue medication was required by significantly fewerpatients in the sodium ibuprofen group (325) and theibuprofenpoloxamer group (225) than in the acetamin-ophen (438) group Owing to the relatively smallproportion of patients reporting the use of rescue medica-tion KaplanndashMeier median times to first use of rescuemedication could not be calculated The pairwise compar-isons between the two ibuprofen formulations and acet-aminophen were both statistically significant using theWilcoxon rank-sum test with P=0019 and P=0001 forsodium ibuprofen and the ibuprofenpoloxamer formula-tion respectively (Fig 6) The vast majority of patientsrandomised to placebo took rescue medication (827)
Time to and proportion of patients with pain half-gone
The proportion of patients reporting pain half-gone were938 888 75 and 370 for sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo re-spectively The median time to pain half-gone wassimilar for all three active treatment groupsmdash350 min(sodium ibuprofen) 375 min (ibuprofenpoloxamer) and450 min (acetaminophen) The Wilcoxon rank-sumcomparisons between the ibuprofen formulations andacetaminophen were not statistically significant (P=007and P=018 for sodium ibuprofen and ibuprofenpolox-amer respectively) but the two equivalent comparisonswere statistically significant when the Cox regression wasused (P=0013 and P=002 for sodium ibuprofen andibuprofenpoloxamer respectively) This may be explainedin terms of a greater proportion of patients randomised toeither of the ibuprofen formulations reporting the endpointscompared with acetaminophen However as for time tomeaningful relief the separation in onset times in favour ofibuprofen was only apparent from 45 min post-doseonward
Distractibility from pain (VAS)
At 1-h post-dose the mean values for the distractibilityfrom pain (VAS) scores were 290 321 381 and657 mm for sodium ibuprofen ibuprofenpoloxameracetaminophen and placebo respectively Both ibuprofenformations had lower (more favourable) scores thanplacebo (Plt0001) and sodium ibuprofen versus acetamin-ophen was statistically significant (P=0010) whereas theibuprofenpoloxamer versus acetaminophen comparisonswere non-significant (P=0083)
At 6 h post-dose both ibuprofen formulations hadmore favourable distractibility from pain scores thanacetaminophen (P=0008 and P=003 sodium ibuprofen
Timepoint (minutes)
Mea
n pa
in in
tens
ity d
iffer
ence
s
00
05
10
15
0 15 35 60 90 120 180 240 300 360
Sodium ibuprofen IbuprofenpoloxamerAcetaminophenPlacebo
Fig 5 Mean pain intensity difference (categorical) at each timepoint
Timepoint (mins)
ta
ken
resc
ue m
edic
atio
n
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 6 KaplanndashMeier curves for time to first use of rescue medication
Fig 4 Mean pain relief at each timepoint
350 Eur J Clin Pharmacol (2009) 65343ndash353
and ibuprofenpoloxamer respectively) The vast majorityof patients randomised to placebo took rescue medicationso only 14 patients provided valid data within this grouphence this analysis was not performed for the placebogroup
Pain interference with daily activities (Rainier scale)
At 1-h post-dose the mean values on the Rainier scale were188 223 268 and 432 for the sodium ibuprofen ibuprofenpoloxamer acetaminophen and placebo groups respectivelyThe scores were statistically significantly lower for bothibuprofen formulations than for placebo (Plt0001) andacetaminophen [P=0001 (sodium ibuprofen) and P=0015(ibuprofenpoloxamer)] At 6-h post-dose the mean valueswere 151 171 224 and 163 for the sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo groupsrespectively Both ibuprofen formulations maintained signif-icantly lower (more favourable) values on the Rainier scalethan acetaminophen (P=0004 and P=0011 for sodiumibuprofen and ibuprofenpoloxamer) Placebo treatment wasnot analysed for this comparison as only 14 patients in thisgroup provided valid data
Patientrsquos overall assessment of medication as a treatmentfor pain
Significantly more patients in the sodium ibuprofen (813)and ibuprofenpoloxamer (848) groups rated the studymedication as good very good or excellent than in the groupsthat received acetaminophen (538) or placebo (173)Furthermore the mean global assessment scores weresignificantly lower (more favourable) for both ibuprofenformulationsmdash240 (sodium ibuprofen) and 244 (ibuprofenpoloxamer)mdashthan for acetaminophen or for placebo (341 and446 respectively Plt0001)
Safety findings
A total of 118 of all patients had AEs that were consideredby the investigators to be possibly related to study medicationno events were classified as definitely or probably related tostudy treatment Adverse events were experienced by 300238 309 and 296 of patients receiving sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo respec-tively The majority of AEs (73) were mild-to-moderate inseverity and the most frequently reported AEs includednausea headache vomiting and dizziness Adverse eventsoccurring in at least 5 of all patients in any treatment groupare summarised in Table 2 Severe AEs (including vomitingnausea dizziness abdominal pain and headache) occurred atrates of 63 (sodium ibuprofen) 25 (ibuprofenpolox-amer) 123 (acetaminophen) and 99 (placebo) therewere no deaths or withdrawals attributable to AEs during thestudy period There were no significant differences betweenstudy medications in terms of tolerability
Discussion
This placebo-controlled study demonstrated excellent assaysensitivity for every measure of efficacy with bothibuprofen formulations and acetaminophen showing clini-cally and statistically significant analgesia that was superiorto placebo Furthermore the overall analgesic efficacy(duration and total effect) of both ibuprofen formulationswas shown to be superior to acetaminophen
Data from this study showed statistically significant differ-ences between both the ibuprofen test formulations andplacebo for the primary endpoint ie the time to firstconfirmed perceptible pain relief In addition a significantlygreater proportion of patients receiving ibuprofen experiencedconfirmed perceptible pain relief than those receiving acet-
Table 2 Adverse events occurring in gt5 of patients in any treatment group
Sodium ibuprofen (n=80) Ibuprofenpoloxamer (n=80) Acetaminophen (n=81) Placebo (n=81)
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Any AE 43 24 (300) 27 19 (238) 41 25 (309) 39 24 (296)GastrointestinalNausea 10 9 (113) 5 5 (63) 8 8 (99) 14 14 (173)Vomiting 2 2 (25) 1 1 (13) 6 6 (74) 8 8 (99)Nervous systemDizziness 4 4 (50) 0 0 (00) 6 5 (62) 5 5 (62)Headache 11 11 (138) 5 4 (50) 4 4 (49) 3 3 (37)
AE Adverse eventTreatment definitions sodium ibuprofen=2times256 mg ibuprofen sodium dihydrate tablets (each tablet equivalent to 200 mg ibuprofen acid)ibuprofenpoloxamer=2times200 mg ibuprofenpoloxamer tablets acetaminophen=2times500 mg acetaminophen capletsa Percentages based on total number of patients per treatment group
Eur J Clin Pharmacol (2009) 65343ndash353 351
aminophen The median time to meaningful pain relief was45 min for both ibuprofen formulations and 54 min foracetaminophen Although a much greater proportion ofpatients reported relief on the two ibuprofen formulationsthe divergence in onset times was only apparent from 45 minpost-dose onward ie there was a much higher proportion ofresponders from 45 min onward for the ibuprofen treatmentsthan for acetaminophen Because of this late divergence theWilcoxon rank-sum test was not sensitive enough to detectsignificant differences whereas the Cox proportional hazardsregression analysis showed significant differences in favour ofibuprofen over acetaminophen In terms of SPRID over 6 hboth ibuprofen test formulations were significantly moreefficacious than acetaminophen
Previous studies using the post-operative dental painmodel have demonstrated that treatment with a differentibuprofen salt formulation ibuprofen arginate (l-argininesalt of ibuprofen) resulted in faster onset times to analgesiaand greater overall efficacy than treatment with conven-tional (standard) ibuprofen [11 12 19] The pharmacoki-netic profile of the ibuprofen sodium formulation used inthis study has been shown to be similar to that of ibuprofenarginate with peak plasma concentrations achieved atapproximately 30ndash40 min compared with 1ndash2 h forstandard ibuprofen [8 13 14] Therefore it was anticipatedthat the rapid absorption associated with sodium ibuprofenwould result in early onset of analgesia similar to thatobserved for ibuprofen arginate This study was notintended nor was it sufficiently powered to compare thetwo ibuprofen formulations
When comparing the median time to meaningful painrelief data from this study with previous studies bothibuprofen test formulations in this study were found to be atthe upper end of the range for ibuprofen arginate andibuprofen lysine data (range 24ndash42 min) [11 12 19 22]ie 451 min (sodium ibuprofen) and 447 min (ibuprofenpoloxamer) In the earlier studies where ibuprofen arginatewas compared with conventional ibuprofen the mediantime to meaningful pain relief obtained for ibuprofenarginate was approximately half that of the conventionalibuprofen [11 12 19] A recent bioavailability study hasalso shown that the Tmax for sodium ibuprofen was lessthan half that of standard ibuprofen (ie 35 min vs 90 minrespectively) [8] Therefore it was not unexpected thatsodium ibuprofen had a fast onset of analgesic effect in thisstudy that was in a similar order of magnitude as thosepreviously reported for faster absorbed formulations
The analyses of secondary endpoints related to degreeof pain relief andor reduction in pain intensity (TOT-PAR SPRID SPID peak PID and peak PR) consistentlyfavoured both ibuprofen formulations over acetamino-phen Only in terms of time to PID of at least 1 werethere no statistically significant differences observed
compared with acetaminophen Measures of analgesicdurationmdashthe proportion of patients taking rescue med-ication and the time to rescue medicationmdashshowed thatthose in the acetaminophen group received rescuemedication sooner than those in either of the twoibuprofen groups This suggests that both ibuprofenformulations had a longer duration of action thanacetaminophen which is in keeping with that previouslyreported for ibuprofen lysine [22] and ibuprofen liquigel[23] In terms of pain relief and PID the timepoint at whicha significant difference was first observed between either ofthe ibuprofen formulations and placebo was 15 min(sodium ibuprofen) a significant difference between eitherof the ibuprofen formulations and acetaminophen was firstobserved at 45 min (sodium ibuprofen) In comparison withpreviously published data studies with ibuprofen arginateand ibuprofen lysine demonstrated significant differences inpain relief and PID between ibuprofen and placebo at 10ndash15 min [11 12 19 23] Furthermore significant differ-ences between ibuprofen lysine and acetaminophen wereobserved at 15 min much sooner than the 45 min observedin our study [22] These differences could be explained bythe different formulations of ibuprofen the fact that adifferent brand of acetaminophen was used in each of therespective studies or the inherent variability associated witha small sample size
Patients in both ibuprofen groups were able to distractthemselves from their pain at 1 and 6 h after dosingsignificantly more easily than those in the placebo andacetaminophen groups (6 h only) Patients in both ibupro-fen groups also reported that pain would interfere with theirdaily activities significantly less than patients in theacetaminophen group Patients in the two ibuprofen groupsrated the study medication as good very good or excellentmore frequently than those in the acetaminophen andplacebo groups
Ibuprofen is a well-tolerated NSAID at low doses [24]However even at prescribed doses ibuprofen is associatedwith the least risk of gastrointestinal complications com-pared with other NSAIDs [25ndash27] No new safety concernswere raised by the current study treatment with singledoses of sodium ibuprofen and ibuprofenpoloxamer werewell tolerated with AE profiles comparable to that ofacetaminophen The most frequently reported AEs consid-ered to be related to study treatment (ie nausea headachevomiting and dizziness) are not unexpected in patientsrecovering from dental surgery
In conclusion these results suggest that compared withacetaminophen both the sodium ibuprofen and ibuprofenacid incorporating poloxamer formulations are more effi-cacious in providing rapid and sustained analgesia and areassociated with pain relief in a greater proportion ofpatients undergoing surgical removal of impacted third
352 Eur J Clin Pharmacol (2009) 65343ndash353
molars Together with the favourable safety profile ofibuprofen these findings support a recommendation forthis agent as an analgesic of choice for the treatment ofpost-operative dental pain
Acknowledgements The authors would like to acknowledgeFranklin S Bonasso DDS and R Dean Jasper DDS (Central OralSurgery Group) Barbara Hernandez MA CCRC Michael Goulder(Worldwide Clinical Trials UK Ltd) for statistical support andVandana Sahajpal PhD and Quyen Chu PhD (Sudler amp HennesseyLondon) for medical writing support
Conflict of interest This study was funded by Reckitt BenckiserGroup plc Stephen Daniels (Premier Research Group ClinicalResearch Centers USA) is the Co-ordinating Investigator SandieReader and Phillip Berry are employees of Reckitt Benckiser Group plc
References
1 Sweetman SC (ed) (2002) Ibuprofen In Martindale the completedrug reference 33rd edn Pharmaceutical Press London
2 Mehlisch DR Sollecito WA Helfrick JF et al (1990) Multicenterclinical trial of ibuprofen and acetaminophen in the treatment ofpostoperative dental pain J Am Dent Assoc 121257ndash263
3 Roy S (1983) A double-blind comparison of propionic acidderivative (ibuprofen) and a fenamate (mefanamic acid) in thetreatment of dysmenorrhoea Obstet Gynecol 61628ndash632
4 Moran M (1991) Double-blind comparison of diclofenac potassi-um ibuprofen and placebo in the treatment of ankle sprain J IntMed Res 19121ndash130
5 Goswick CB (1983) Ibuprofen versus propoxyphene hydrochlo-ride and placebo in acute musculoskeletal trauma Curr Ther ResClin Exp 34685ndash692
6 Schachtel BP Thoden WR (1988) Onset of action of ibuprofenin the treatment of muscle-contraction headache Headache28471ndash474
7 Pearce I Frank GJ Pearce JMS (1983) Ibuprofen compared withacetaminophen in migraine Practitioner 227465ndash467
8 Dewland P Reader S Berry P (2008) Bioavailability of ibuprofenfollowing oral administration of standard ibuprofen sodiumibuprofen or ibuprofen acid incorporating poloxamer in healthyvolunteers Eur J Clin Pharmacol (submitted)
9 Geisslinger G Menzel S Wissel K Brune K (1993) Single dosepharmacokinetics of different formulations of ibuprofen andaspirin Drug Invest 5238ndash242
10 Schleier P Prochnau A Schmidt-Westhausen AM et al (2007)Ibuprofen sodium dihydrate an ibuprofen formulation withimproved absorption characteristics provides faster and great-er pain relief than ibuprofen acid Int J Clin Pharmacol Ther4589ndash97
11 Black P Max MB Desjardins P et al (2002) A randomizeddouble-blind placebo-controlled comparison of the analgesic
efficacy onset of action and tolerability of ibuprofen arginateand ibuprofen in postoperative dental pain Clin Ther241072ndash1089
12 Desjardins P Black P Papageorge M et al (2002) Ibuprofenarginate provides effective relief from postoperative dental painwith a more rapid onset of action than ibuprofen Eur J ClinPharmacol 58387ndash394
13 Albert KS Gernaat CM (1984) Pharmacokinetics of ibuprofenAm J Med 7740ndash46
14 Davies NM (1998) Clinical pharmacokinetics of ibuprofen Thefirst 30 years Clin Pharmacokinet 34101ndash114
15 Cooper SA Precheur H Rauch D et al (1984) The analgesicefficacy of ibuprofen compared to acetaminophen with codeine(abstract) Clin Pharmacol Ther 35232
16 Mehlisch D Frakes L (1984) A controlled comparative evaluationof acetaminophen and aspirin in the treatment of post-operativepain Clin Ther Exerpta Med 789ndash97
17 Mehlisch D Markenson J Schnitzer T (1999) The efficacy ofnonsteroidal anti-inflammatory drugs for acute pain CancerControl 65ndash9
18 Daniels SE Desjardins PJ Talwalker S et al (2002) The analgesicefficacy of valdecoxib vs oxycodoneacetaminophen after oralsurgery J Am Dental Assoc 133611ndash621
19 Mehlisch DR Ardia A Pallotta T (2002) A controlled compar-ative study of ibuprofen arginate versus conventional ibuprofen inthe treatment of postoperative dental pain J Clin Pharmacol42904ndash911
20 World Medical Association (1964) Declaration of HelsinkiEthical principles for medical research involving human patientsAdopted by the 18th WMA General Assembly 1964 and amendedby the 29th 35th 41st and 48th WMA General Assemblies
21 European Parliament and Council of 4 April 2001 (2001)Directive 200120EC of the approximation of the laws regu-lations and administrative provisions of the Member Statesrelating to the implementation of good clinical practice in theconduct of clinical trials on medicinal products for human useOfficial Journal of the European Communities Brussels
22 Mehlisch DR Jasper RD Brown P et al (1995) Comparativestudy of ibuprofen lysine and acetaminophen in patients withpostoperative dental pain Clin Ther 17852ndash860
23 Olson NZ Otero AM Marrero I et al (2001) Onset of analgesiafor liquigel ibuprofen 400 mg acetaminophen 1000 mg ketopro-fen 25 mg and placebo in the treatment of postoperative dentalpain J Clin Pharmacol 411238ndash1247
24 Sachs C (2005) Oral analgesics for acute nonspecific pain AmFam Physician 71913ndash918
25 Doyle G Furey S Berlin R et al (1999) Gastrointestinal safetyand tolerance of ibuprofen at maximum over-the-counter doseAliment Pharmacol Ther 13897ndash906
26 Henry D Lim LL Garcia Rodriguez LA et al (1996) Variability inrisk of gastrointestinal complications with individual non-steroidalanti-inflammatory drugs results of collaborative met-analysis BrMed J 3121563ndash1566
27 Henry D McGettigan P (2003) Epidemiology overview ofgastrointestinal and renal toxicity of NSAIDs Int J Clin Pract13543ndash49
Eur J Clin Pharmacol (2009) 65343ndash353 353
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 153
RESEARCH
An investigation into the comparative efficacyof soluble aspirin and solid paracetamol inpostoperative pain after third molar surgeryR A Seymour1 J E Hawkesford2 J Sykes3 M Stillings4 and C M Hill5
Objective To compare the efficacy of soluble aspirin 900 mg andparacetamol 1000 mg in patients with postoperative pain after thirdmolar surgeryDesign A randomised placebo controlled double-blind studySetting Day stay units of Oral and Maxillofacial Surgery at CardiffDental Hospital and Hexham General Hospital NorthumberlandSubjects and methods One hundred and sixty-seven (104 female)patients who required the removal of their impacted third molars undergeneral anaesthesiaIntervention In the early postoperative period patients were medicatedwith either a single dose of soluble aspirin 900 mg solid paracetamol1000 mg or placebo Main outcome measures Pain intensity was measured on 100 mmvisual analogue scales at 0 5 10 15 20 30 45 60 90 120 and 240minutes after dosing Other efficacy variables evaluated included time torescue medication and an overall assessment of the study medicationefficacy by the patient on completion of the studyResults One hundred and sixty-seven patients consented to take part inthe study but only 153 were medicated Of the 14 patients not treated10 failed to develop sufficient pain to enter the study two withdrewconsent one had an adverse reaction to the general anaesthetic and onewas a protocol violator Over the four hour investigation period patientstreated with soluble aspirin reported significantly less pain whencompared with those treated with paracetamol (mean difference inAUC0-240 = -2001 95 CI ndash3893 to ndash109 p=0038) and placebo (meandifference in AUC0-240 = -3470 95 CI ndash5719 to ndash1221 p=0003)
1Head of Department Professor of Restorative Dentistry Department of RestorativeDentistry Dental School University of Newcastle Newcastle upon Tyne 2Consultant Oraland Maxillofacial Surgeon Department of Oral and Maxillofacial Surgery NewcastleGeneral Hospital Newcastle upon Tyne 3Clinical Statistician Reckitt Benckiser Healthcare(UK) Hull 4Head of Global Professional Relations Reckitt Benckiser Healthcare (UK) Hull5Consultant Oral and Maxillofacial Surgeon Department of Oral Surgery Dental SchoolUniversity of Wales College of Medicine Cardiff Correspondence to Professor R A Seymour Department of Restorative Dentistry DentalSchool University of Newcastle upon Tyne Framlington Place Newcastle upon TyneEngland NE2 4BWE-mail R A Seymournclacuk
Refereed paperReceived 080302 Accepted 060902copy British Dental Journal 2003 194 153ndash157
Similarly at 20 and 30 minutes after dosing patients in the solubleaspirin group were reporting significantly less pain than those in theparacetamol treatment group (mean difference in pain intensity at 20minutes ndash79 95 CI ndash153 to ndash06 p=0035 at 30 minutes ndash106 95CI ndash186 to ndash26 p=0010) There were no significant differences betweentreatment groups with respect to the number of patients requiringrescue medication however the time to dosing was significantly longerfor those taking soluble aspirin when compared with placebo (hazardratio 234 95 CI 141 to 388 plt0001) Conclusion The findings from this study showed that soluble aspirin900 mg provides significant and more rapid analgesia than paracetamol1000 mg in the early postoperative period after third molar surgery
INTRODUCTIONBoth aspirin (acetylsalicylic acid) and paracetamol (acetamino-phen) are widely available analgesics The drugs are used exten-sively in dentistry either self-prescribed by the patient or recom-mended by the dental surgeon Despite such use there have beenfew comparative studies on these analgesics and the studies pub-lished seem to suggest that the drugs are equi-analgesic1 Morerecent evidence suggests that many factors appear to influence theefficacy of aspirin in postoperative dental pain These include for-mulation dose and plasma concentration of acetylsalicylate2-5
The latter appears to be determined by plasma aspirin esteraseactivity By contrast there is limited information on the efficacy ofparacetamol in postoperative dental pain
Historically there have been many studies comparing the effi-cacy of a whole range of analgesics which have used aspirin as thestandard treatment (positive control) In such studies the formula-tion chosen has invariably been a solid format of the drug This hasled to the impression that aspirin is relatively weak and slow act-ing Previous studies34 have shown that soluble aspirin provides agreater onset of action and is overall more effective than solidaspirin However up to the present time there has been no studycomparing the efficacy of soluble aspirin with solid paracetamolThe present study was designed to investigate whether the superi-ority of soluble aspirin over solid aspirin would be reproducedwhen compared with solid paracetamol The doses chosen for each
This study has shown the benefits of soluble aspirin (900 mg) over solid paracetamol (1000 mg)in the control of postoperative pain after third molar extractions
The aspirin preparation provided an earlier onset of pain relief when compared with paracetamol Most patients in the study did require additional analgesia in the early postoperative period
but the time to remedication was significantly longer in soluble aspirin group whencompared with the placebo
Adverse events due to the medication were few and showed no differences between treatmentgroups
Soluble aspirin 900 mg appears to be a more useful analgesic than paracetamol in the controlof postoperative pain after third molar surgery
I N B R I E F
RESEARCH
154 BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003
preparation used in this study is the maximum recommendedwhen purchased as over the counter (OTC) medications
Removal of impacted third molars remains a common dentalsurgical procedure that results in a significant level of postopera-tive pain6 Pain is usually of short duration and reaches its maxi-mum intensity in the early postoperative period7 It is during thistime period that analgesics are frequently prescribed The nature ofthe pain and its duration make the third molar pain model usefulfor evaluation of analgesic efficacy
The overall aim of the present study was to directly compare theefficacy of soluble aspirin with that of solid paracetamol tablets inpatients with postoperative pain after third molar surgery A place-bo group was also used to act as a negative control Within thisoverall remit the primary aim of the study was to compare theonset of efficacy between the two preparations
MATERIAL AND METHODSAdult patients who required the removal of at least one impactedlower third molar were invited to participate in the study Patientswere enrolled from two centres (Cardiff and Hexham) Informedwritten consent was obtained from each patient prior to theirentry into the study which had received ethical approval from theappropriate local Health Authority Ethical Committees Patientsenrolled into the study were fit and healthy and complied with thecriteria of the American Society of Anaesthesiologists categoryone or at the discretion of the dental surgeon category two Allpatients attended a screening clinic prior to their participation inthe study The pre-screening was held up to a maximum of threeweeks before surgery Patients were asked to abstain from takingany analgesics for 24 hours prior to their third molar extractions
Patients underwent the removal of their impacted third molarsunder general anaesthesia The anaesthetic regimen was accord-ing to routine clinical practice at the dental centre and includedinduction with intravenous propofol Muscle relaxation wasachieved with vecuronium atracurium pancurium mivacuriumor suxamethonium Anaesthesia was maintained with nitrousoxide oxygen and either isoflurane enflurane or sevofluranePerioperative analgesia was provided by fentanyl or alfentanyl
Impacted third molars were removed following a standard tech-nique Bone removal was carried out with a drill under saline sprayThe operating time (from first incision to completion of last suture)was recorded for each patient On completion of the surgical proce-dure time was allowed for the patients to recover fully from theeffects of the anaesthetic They were then returned to the wardwhere they were monitored by the study nurse and their pain inten-sity assessed on 100 mm visual analogue scales (VAS) The bound-aries of the scale were marked lsquono painrsquo and lsquoworst pain imaginablersquoWhen patientsrsquo pain intensity reached a level in excess of 30 mm onthe VAS they were randomised to study medication Patients whosepain intensity did not reach the required level or who did notrequest analgesia within 1frac12 hours post-operatively were with-drawn from the study Each eligible patient was randomly allocatedto one of the following treatment groups soluble aspirin (Disprinreg)900 mg solid paracetamol tablets BP 1000 mg or placebo In order
to double-blind the study a double-dummy technique was usedEach patient assigned to receive active soluble aspirin or activesolid paracetamol also received a placebo for the alternative treat-ment and placebo patients received a placebo for both formula-tions Soluble aspirin and the aspirin placebo were presented as anorange drink Paracetamol active and placebo were given as tabletsPatients were randomised to treatment groups in the ratio of 2aspirin2 paracetamol1 placebo The randomisation was stratifiedfor gender A randomisation block size of five was used to ensurebalance between the treatment groups
Pain assessmentThe following measures were used to evaluate efficacya) Pain intensity measures were recorded immediately pre-dose (0
minutes) and at 5 10 15 20 30 45 60 90 120 and 240 minutesafter dosing Onset of analgesia was primarily assessed by painintensity measures at 10 15 20 and 30 minutes
b)Pain intensity over the four hour investigation period The serial VAS measures of the four hour investigation periodwere compiled into a graph of pain (mm) versus time (minutes)The area under the graph (AUC) was calculated using the trape-zoidal method and denoted as AUC240 Such a measure gives anoverall assessment of each patientrsquos pain experience throughoutthe four hour investigation period8
c) Use of rescue medicationIn the event of poor pain control patients were allowed access toalternative analgesia (ibuprofen 400 mg) Patients were encour-aged not to request re-medication in the first hour post-dosingin order to give the study medication time to work For thosetaking additional analgesics the time was recorded and theirlast pre-rescue medication intensity score was extrapolated overthe remaining time points9
d)Overall evaluation At the end of the four hour investigation period (or prior to tak-ing rescue medication) the study nurses and the patients wereasked to provide an overall evaluation of the efficacy of thestudy medication The categories were lsquovery goodrsquo lsquogoodrsquo lsquosatis-factoryrsquo lsquopoorrsquo and lsquovery poorrsquo
Throughout the investigation period a study nurse was respon-sible for monitoring the patients and recording any adverse events
Statistical methodsA previous study in postoperative pain after removal of impactedthird molars4 suggested that mean VAS differences between solu-ble aspirin and placebo and soluble aspirin and solid paracetamolof 26 mm and 14 mm respectively might be anticipated at 20 min-utes post treatment Using a randomisation of 2 soluble aspirin 2paracetamol 1 placebo a total sample size of 150 patients had atleast 80 power to detect this difference
The VAS pain intensity measurements at 10 15 20 and 30minutes after dosing and AUC240 were compared between treat-ment groups using an analysis of covariance using centre gen-der baseline pain intensity operation duration and number of
Table 1 Demographic details of patients who were medicated for the study Where appropriate results are expressed as mean (SD)Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo
Number of patients 59 62 32Gender ratio MF 1940 1943 1121Age (years) 256 (56) 250 (53) 251 (47)Weight (kg) 702 (16) 719 (145) 743 (149)Mean operating time (mins) 173 (101) 165 (101) 130 (130)Number of molars removed 1 3 (5) 2 (3) 3 (9)[ patients ()] 2 15 (25) 14 (23) 5 (16)
3 11 (19) 12 (19) 9 (28)4 30 (51) 34 (55) 15 (47)
Mean baseline pain score on 100 mm VAS 574 (176) 506 (142) 541 (144)
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 155
in Hexham and the remainder in Cardiff Of the 14 patients nottreated 10 failed to develop sufficient pain to enter the studytwo withdrew consent one had an adverse reaction to the anaes-thesia and one was a protocol violator Demographic details ofthe patients are shown in Table 1 The three groups were bal-anced for demographic variables
The primary aim of the study was to compare the rate of onset ofanalgesia and the 20-minute time was considered to be appropriatefor such an assessment Pain scores as recorded on the VAS at eachtime point are illustrated in Figure 1 and Tables 2a and 2b VASscores decreased in all treatment groups during the first 15 minutespost dosing (Figure 1) At 20 minutes post dosing patients in the sol-
molars removed as covariates Use of rescue medication and thestudy nursesrsquo and patientsrsquo overall impression of their medicationwere analysed using binomial logistic regression with a lsquopositiversquooutcome defined as a response of lsquovery goodrsquo or lsquogoodrsquo Time toadministration of rescue medication was compared betweentreatment groups using Coxrsquos proportional hazard model Com-parisons were performed for soluble aspirin versus solid paraceta-mol and soluble aspirin versus placebo
RESULTSOne hundred and sixty seven patients consented to take part inthe study and 153 were medicated Of these 29 were medicated
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 30 45 60 90 120 240
Time (mins)
Pain
(mm
)
Soluble AspirinParacetamolPlacebo
Figure 1 Graph to show mean pain scores (mm) versus time (mins) for patients after treatment with placebo solid paracetamol 1000 mg and solubleaspirin 900 mg
Table 2a Summary of efficacy parameters recorded during the investigation period pain scoresBetween treatment comparisons
Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Mean difference (95 CI) p-value Mean difference (95 CI) p-value
Pain score (in mm) 10 mins after dosing 412 (28) 482 (29) 474 (33) -61 (-133 to 10) 0092 -70 (-130 to ndash09) 0024Pain score (in mm) 15 mins after dosing 407 (32) 458 (33) 445 (38) -39 (-120 to 43) 0350 -51 (-120 to 18) 0143Pain score (in mm) 20 mins after dosing 402 (34) 481 (35) 500 (40) -98 (-186 to ndash11) 0028 -79 (-153 to ndash06) 0035Pain score (in mm) 30 mins after dosing 356 (37) 462 (38) 476 (44) -120 (-216 to ndash25) 0014 -106 (-186 to ndash26) 0010Overall pain - AUC240(mmmins) 8001 (871) 10002 (898) 11471 (1035) -3470 (-5719 to ndash1221) 0003 -2001 (-3893 to ndash109) 0038
data presented are adjusted (least squares) mean (standard error of the mean)
Table 2b Summary of efficacy parameters recorded during the investigation period use of escape medicationBetween treatment comparisons
Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds (hazard) ratio (95 CI) p-value Odds (hazard) ratio (95 CI) p-value
Number of patients 48 (81) 46 (74) 29 (91) 0172 (0020 to 1052) 0078 1485 (0455 to 5197) 0518taking escape analgesics
Time (minutes) to 115 (63 - 165) 94 (47 - ++) 64 (42 ndash 117) 234 (141 to 388) lt0001 130 (084 to 203) 0236remedication
data presented are median (Inter Quartile Range)++ Upper quartile cannot be estimated
RESEARCH
156 BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003
uble aspirin group reported significantly less pain than those treatedwith solid paracetamol (p=0035) or placebo (p=0028) Similarlypain intensity was significantly less at 10 and 30 minutes post dos-ing for patients treated with soluble aspirin when compared withsolid paracetamol (p=0024 and 0010 respectively) Pain intensitywas also significantly less for patients treated with soluble aspirinwhen compared with placebo at 30 minutes post dosing (p=0014)but was not significant at 10 minutes post-dosing (p=0092) By con-trast to these findings at 15 minutes after dosing pain scores werenot significantly different between soluble aspirin and placebo(p=0350) or between soluble aspirin and solid paracetamol(p=0143) Overall pain scores as assessed by the AUC240 were sig-nificantly lower in the soluble aspirin group when compared withsolid paracetamol (p=0038) and placebo (p=0003) There was nosignificant centre difference for any of the pain intensity variables
The use of rescue medication and time to requesting such med-ication is also shown in Table 2b There was no significant differ-ence between soluble aspirin and solid paracetamol or placebowith respect to the number of patients requiring rescue medicationduring the four hour investigation period (pgt005) However thetime to administration of rescue medication was significantlylonger for those patients taking soluble aspirin when comparedwith placebo (plt0001) There was no significant difference in timeto rescue medication between the soluble aspirin treated patientsand those treated with solid paracetamol (p=0236) The time toadministration of rescue medication did show a significant centreeffect with those patients enrolled in Cardiff requiring rescueanalgesia at an earlier time point than those in Hexham (plt0001)
The study nursesrsquo and patientsrsquo overall assessment of the effica-cy of the medication is shown in Tables 3a and 3b There was nosignificant difference between soluble aspirin and solid paraceta-mol (p=0285) with respect to the percentage of lsquopositiversquo outcomesassessed by the patients however soluble aspirin was favoured incomparison with placebo (p=0010) Results were similar for thestudy nursesrsquo assessment (p=0387 p=0024)
Adverse events were reported by 41 of patients with a higheroverall incidence in the active treatment groups (Table 4) Many ofthese events were related to the procedure The most commonadverse events were in the central and peripheral nervous system(primarily dizziness) and the gastro-intestinal system (primarilynausea) The incidence of dizziness was similar in the soluble
aspirin and placebo groups (14 and 13 respectively) and wasgreater than in the solid paracetamol group (6) The incidence ofnausea was comparable in the soluble aspirin and solid paraceta-mol groups (15 and 16 respectively) and was greater than thatin the placebo group (6) Gingival bleeding (the only adverseevent recorded under lsquohaemostasisrsquo) had a slightly lower incidencein the soluble aspirin group (8) than in the solid paracetamolgroup (13) and was only slightly higher than that reported in theplacebo group (3) This finding is contrary to any expectationsthat aspirin might exacerbate post-operative bleeding
DISCUSSIONThe present study has shown that soluble aspirin 900 mg is an effec-tive analgesic in the control of postoperative pain after the removalof impacted third molars confirming the evidence from previousstudies34 In addition soluble aspirin provided better pain controlthan solid paracetamol 1000 mg This superior efficacy is reflectedin the overall pain score (Table 2a and Figure 1) and also in the painscores reported during the first 30 minutes post dosing The datasuggest that soluble aspirin is providing a more rapid reduction inpain in the early postoperative period when compared with solidparacetamol If the pain scores are examined in terms of percentagereduction when compared with baseline the results show that solu-ble aspirin is twice as effective as solid paracetamol (at 20 and 30minutes the percentage reduction for soluble aspirin is 310 and406 respectively whilst the figures for solid paracetamol are142 and 204) From the perspective of patient management arapid reduction in pain is an important requisite of any analgesicformulation10 The exception to this pattern is the pain scores at 15minutes post dosing At this time point pain intensity scores aftersoluble aspirin are not significantly different from either placebo orsolid paracetamol mdash the reason for this finding is unclear
Previous comparative efficacy studies between aspirin andparacetamol in postoperative dental pain have revealed somewhatequivocal results11112 The consensus view1 is that both aspirin andparacetamol are both equi-analgesic and equipotent The studiesuse a solid tablet formulation of aspirin at a dose of 650 mg Studiesusing similar methodology have shown that the efficacy of aspirinin postoperative dental pain is related to dose and formulation34
The use of a soluble formulation and the 900 mg dose may explainthe superior efficacy of aspirin in this study
Table 3b Distribution of scores from study nursesrsquo global assessment of the medication (number ())Score Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds Ratio (95 CI) p-value Odds Ratio (95 CI) p-value
Positive outcome 32 (54) 32 (52) 10 (31) 2974 (1179 to 7951) 0024 1403 (0655 to 3054) 0387Very good 15 (25) 11 (18) 3 (9)Good 17 (29) 21 (34) 7 (22)Satisfactory 17 (29) 14 (23) 12 (38)Poor 8 (14) 14 (23) 7 (22)Very poor 2 (3) 2 (3) 3 (9)Total 59 62 32
positive outcome = response of lsquovery goodrsquo or lsquogoodrsquo
Table 3a Distribution of scores from patientsrsquo global assessment of the medication (number ())Score Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds Ratio (95 CI) p-value Odds Ratio (95 CI) p-value
Positive outcome 34 (58) 33 (53) 10 (31) 3591 (1402 to 9828) 0010 1530 (0706 to 3380) 0285Very good 15 (25) 12 (19) 3 (9)Good 19 (32) 21 (34) 7 (22)Satisfactory 15 (25) 12 (19) 10 (31)Poor 8 (14) 15 (24) 9 (28)Very poor 2 (3) 2 (3) 3 (9)Total 59 62 32
positive outcome = response of lsquovery goodrsquo or lsquogoodrsquo
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 157
The primary aim of this investigation was to compare both anal-gesics with respect to onset of action Early time points were chosenfor this comparison as they represent a suitable period from dosingwhen patients would expect to experience meaningful pain reliefSoluble aspirin was significantly superior to both placebo and solidparacetamol at both 20 and 30 minutes post dosing and there wereindications of superiority as early as at 10 minutes In part this maybe due to the rapid absorption of soluble aspirin and the subsequentpeak concentrations of acetylsalicylate (Tmax) that occurs at thesetime points It has been previously shown that plasma concentra-tions of acetylsalicylate are also important determinants of aspirinrsquosefficacy in postoperative dental pain2 By contrast the absorption ofsolid paracetamol tablets is slow with a Tmax of 60 minutes13 Thusdifferences in pharmacokinetics may account for the differences inonset of analgesia observed in the present study
It is now well established that aspirin exerts both analgesic andanti-inflammatory action by inhibiting prostaglandin synthesis14
Aspirin irreversibly inhibits both cyclo-oxygenase 1 and 2 (Cox-1and Cox-2) by acetylating serine 530 thus preventing the bindingof arachidonic acid to the active sites of the enzyme The pharma-codynamics of paracetamol are uncertain and by comparison withaspirin the drug exhibits weak anti-inflammatory action This lackof a pronounced anti-inflammatory effect may also explain theweaker efficacy of this drug in postoperative dental pain
We can conclude from this study that a single dose of solubleaspirin 900 mg provides significant and more rapid analgesia thansolid paracetamol 1000 mg in the early postoperative period afterthird molar surgery This study confirms the value of soluble aspirinin the management of pain after dental surgical procedures
The authors are grateful to Reckitt Benckiser Healthcare for their support inthis study
1 Cooper S A Comparative analgesic efficacies of aspirin and acetaminophen ArchIntern Med 1981 141 282-285
2 Seymour R A Williams F M Ward A Rawlins M D Aspirin metabolism and efficacyin postoperative dental pain Br J Clin Pharmacol 1984 17 697-701
3 Seymour R A Williams F M Luyk N M et al Comparative efficacy of soluble aspirinand aspirin tablets in postoperative dental pain Eur J Clin Pharmacol 1986 30495-498
4 Holland I S Seymour R A Ward-Booth R P Ord R A Lim K L Hoare R C Anevaluation of different doses of soluble aspirin and aspirin tablets in postoperativedental pain Br J Clin Pharmacol 1988 26 463-468
5 Seymour R A Weldon M Kelly P Nicholson E Hawkesford J E An evaluation ofbuffered aspirin and aspirin tablets in postoperative pain after third molar surgeryBr J Clin Pharmacol 1992 33 395-399
6 Seymour R A Blair G S Wyatt F A Post-operative dental pain and analgesicefficacy Part I Br J Oral Surg 1983 21 290-297
7 Seymour R A Meechan J G Blair G S An investigation into post-operative painafter third molar surgery under local analgesia Br J Oral Maxillofac Surg 1985 23410-418
8 Matthews J N Altman D G Campbell M J Royston P Analysis of serialmeasurements in medical research Br Med J 1990 300 230-235
9 Lasagna L Analgesic methodology a brief history and commentary J ClinPharmacol 1980 20 373-376
10 Meechan J G Seymour R A The use of third molar surgery in clinicalpharmacology Br J Oral Maxillofac Surg 1993 31 360-365
11 Skjelbred P Album B Lokken P Acetylsalicylic acid vs paracetamol effects onpost-operative course Eur J Clin Pharmacol 1977 12 257-264
12 Mehlisch D R Frakes L A A controlled comparative evaluation of acetaminophenand aspirin in the treatment of postoperative pain Clin Ther 1984 7 89-97
13 Muir N Nichols J D Stillings M R Sykes J Comparative bioavailability of aspirinand paracetamol following single dose administration of soluble and plain tabletsCurr Med Res Opin 1997 13 491-500
14 Vane J Botting R Inflammation and the mechanism of action of anti-inflammatory drugs Faseb J 1987 1 89-96
Table 4 Incidence and distribution of adverse events for each treatment groupPercentage of patients reporting events (number of events)
Body system Soluble aspirin (n=59) Solid paracetamol (n=62) Placebo (n=32) Total (n=153)
CNS 20 (14) 8 (5) 19 (6) 15 (25)GI 17 (12) 16 (12) 6 (2) 14 (26)Body as a whole 7 (4) 13 (8) 6 (3) 9 (15)Haemostasis 8 (7) 13 (8) 3 (1) 9 (16)Respiratory 7 (4) 3 (2) 0 (0) 4 (6)Psychiatric 2 (1) 0 (0) 3 (1) 1 (2)Hearingvestibular 0 (0) 2 (1) 0 (0) 1 (1)Skinappendages 2 (1) 0 (0) 0 (0) 1 (1)Vision 2 (1) 0 (0) 0 (0) 1 (1)Total 51 (44) 39 (36) 28 (13) 41 (93)

5
IacuteNDICE
PERGUNTA FORMULADA PELO PACIENTE 6
QUESTAtildeO PICO 6
OBJECTIVOS 6
INTRODUCcedilAtildeO 7
PESQUISA 12
Criteacuterios de Selecccedilatildeo 12
Tipos de Estudos escolhidos participantes intervenccedilatildeo e de mediccedilatildeo 12
Avaliaccedilatildeo dos Estudos 13
Estrateacutegias de Pesquisa 12
Cochrane Database for Systematic Reviews helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 13
Evidence-Based Dentistry (EBD) helliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip 14
National Institute of Health and Clinical Excellence (NICE) helliphelliphelliphelliphelliphellip 14
Literatura Latino-Americana e do Caribe em Ciecircncias da Sauacutede (LILACS) 14
PubMed 15
AVALIACcedilAtildeO CRIacuteTICA 17
Revisotildees Sistemaacuteticas 17
Ensaios Cliacutenicos Aleatorizados 28
DISCUSSAtildeO 52
RESPOSTA DADA AO PACIENTE 55
REFEREcircNCIAS BIBLIOGRAacuteFICAS 56
ANEXOS 61
Anexo A ndash Tabela de Artigos Excluiacutedos 61
Anexo B ndash Artigos Incluiacutedos em formato integral 62
6
PERGUNTA FORMULADA PELO PACIENTE
Apoacutes uma exodontia de um terceiro molar inferior ldquoDoutor natildeo me vai passar
mais nada aleacutem do paracetamol para as dores Eacute eficaz Natildeo vou ter doresrdquo
QUESTAtildeO PICO
Com base na questatildeo apresentada pelo paciente eacute possiacutevel identificar
Populaccedilatildeo ndash Pacientes adultos com pelo menos um terceiro molar inferior
Intervenccedilatildeo ndash administraccedilatildeo poacutes-operatoacuteria de paracetamol (1000g) aquando
duma exodontia do terceiro molar inferior
Comparaccedilatildeo ndash outros analgeacutesicos e NSAIDrsquos (Non-Steroidal Anti-
Inflammatory Drugs) convencionais
Outcome ndash Eliminaccedilatildeo ou atenuaccedilatildeo da dor medida atraveacutes da escala visual
analoacutegica de dor
Em pacientes adultos apoacutes exodontia do 3ordm molar inferior a administraccedilatildeo
de paracetamol eacute mais eficaz na terapecircutica analgeacutesica comparativamente a outros
analgeacutesicos e anti-inflamatoacuterios natildeo esteroacuteides convencionais utilizando uma
escala visual analoacutegica de dor
OBJECTIVOS
Primaacuterios
Investigar a eficaacutecia do paracetamol (1000mg) na eliminaccedilatildeo da dor dentaacuteria
poacutes-operatoacuteria e comparaacute-la com outros NSAIDrsquos comparando os efeitos secundaacuterios
associados a cada faacutermaco
Secundaacuterios
Aferir a eficaacutecia relativa dos vaacuterios NSAIDrsquos bem como combinaccedilotildees de
paracetamol com outros compostos
7
INTRODUCcedilAtildeO
EXODONTIA DE TERCEIROS MOLARES INFERIORES
A extracccedilatildeo de terceiros molares eacute um procedimento ciruacutergico no campo da
sauacutede oral amplamente praticado e difundido A dor poacutes-operatoacuteria desta intervenccedilatildeo
tornou-se o modelo mais frequentemente usado em ensaios sobre dor aguda por ser um
procedimento comum com dor moderada a severa e com um nuacutemero suficiente de
pacientes para se realizar um estudo de forma relativamente faacutecil (1 2)
Os motivos que conduzem agrave exodontia de terceiros molares devem ser
considerados cuidadosamente natildeo soacute na sua dimensatildeo cliacutenica como no encontro dos
interesses do paciente econoacutemicos e outros Algumas situaccedilotildees constituem uma razatildeo
largamente aceite para a extracccedilatildeo sendo descritas em normas de orientaccedilatildeo cliacutenica
Natildeo se pode excluir poreacutem uma selecccedilatildeo e procura cuidadosa por parte do cliacutenico da
melhor evidecircncia cientiacutefica
Segundo as normas de orientaccedilatildeo cliacutenica NICE a extracccedilatildeo de sisos impactados
deve ser limitada a pacientes que evidenciam patologia como caacuteries irrestauraacuteveis
patologias pulpares ou periapicais natildeo trataacuteveis abcesso e osteomielite reabsorccedilatildeo
internaexterna do dente ou dentes adjacentes fractura dentaacuteria quistos tumores e
outros (3) Terceiros molares impactados mas livres de patologia natildeo devem ser
extraiacutedos pois natildeo haacute evidecircncia de que sugira que traria benefiacutecios para os pacientes
Iria tambeacutem sujeitar pacientes saudaacuteveis aos riscos que acompanha este tipo de
procedimento e os efeitos poacutes-operatoacuterios do mesmo Existe controveacutersia em redor
deste assunto e sobre se existe algum benefiacutecio na extraccedilatildeo profilaacutetica ldquoNo evidence
was found to support or refute routine prophylactic removal of asymptomatic impacted
wisdom teeth in adults There is some reliable evidence that suggests that the
prophylactic removal of asymptomatic impacted wisdom teeth in adolescents neither
reduces nor prevents late incisor crowdingrdquo (4) A extracccedilatildeo de um dente natildeo impactado
deve ser executada quando a natildeo extracccedilatildeo do mesmo eacute ou potencialmente viraacute a
constituir uma situaccedilatildeo patoloacutegica Este procedimento ciruacutergico conduz a um niacutevel
significante de dor poacutes-operatoacuteria sendo esta mais severa nas primeiras doze horas apoacutes
o procedimento com o pico de intensidade nas 6-8 horas poacutes-operatoacuterias (5)
8
ETIOLOGIA DA DOR
Os tecidos lesados ou traumatizados na sequecircncia da remoccedilatildeo do terceiro molar
conduzem agrave libertaccedilatildeo de mediadores bioquiacutemicos (celulares e soluacuteveis) A inflamaccedilatildeo
aguda surge como resposta ao stress tecidual e passa por um aumento da irrigaccedilatildeo
sanguiacutenea - vasodilataccedilatildeo e aumento de permeabilidade vascular Pode-se enfatizar os
papeacuteis das histamina e a bradiquinina (recruta NO) como mediadores soluacuteveis
importantes na vasodilataccedilatildeo
Os prostanoacuteides ndash moleacuteculas envolvidas nos processos de inflamaccedilatildeo- satildeo
ecosanoacuteides ou seja derivados de precursores de aacutecidos gordos e sintetizados via
cascata do aacutecido araquidoacutenico (6 p 503 7 p 800 8) em condiccedilotildees fisioloacutegicas tecircm
um papel preponderante na citoprotecccedilatildeo da mucosa gaacutestrica hemostase e
hemodinacircmica renal A este grupo pertencem as prostaglandinas prostaciclinas
tromboxanos e leucotrienos Enquanto que as prostaglandinas satildeo sintetizadas a partir
do aacutecido araquidoacutenico por acccedilatildeo de enzimas como as ciclo-oxigenases (COX) os
leucotrienos resultam da acccedilatildeo da lipoxigenase Havendo stress tecidual a membrana
celular eacute danificada conduzindo agrave actividade da enzima fosfolipase Esta ao iniciar a
lipoacutelise possibilita a obtenccedilatildeo do percursor dos prostanoacuteides o aacutecido araquidoacutenico Por
um lado os produtos da acccedilatildeo da lipoxigenase podem estar envolvidos na formaccedilatildeo do
edema por outro os produtos da ciclo-oxigenase nomeadamente prostaglandinas estatildeo
envolvidos no processo de dor e pirexia
A ciclo-oxigenase possui 2 isoenzimas COX-1 e COX-2 (7 p 800)
A COX-1 eacute constitutiva da maioria dos tecidos humanos mas com especial
relevacircncia para mediar a integridade da mucosa gaacutestrica endoteacutelio vascular rins e
plaquetas
A COX-2 eacute expressa apoacutes lesatildeo e aquando a libertaccedilatildeo de mediadores como a
Interleucina-1 o Factor de Activaccedilatildeo de Plaquetas (PAF) ou endotoxinas
lipopolissacaacuterido (LPS) (9) Contribui para o processo inflamatoacuterio e hiperalgesia pois
ao formar prostaglandinas sensibiliza as terminaccedilotildees nervosas locais livres
nociceptivas
PARACETAMOL
O paracetamol eacute uma das drogas mais importantes usadas no tratamento da dor
aguda moderada a severa quando natildeo eacute necessaacuterio um efeito anti-inflamatoacuterio (10)
Classificado como analgeacutesico actua no sistema nervoso pela activaccedilatildeo indirecta de
9
receptores canabinoacuteides (11) embora este mecanismo ainda natildeo esteja totalmente
esclarecido (12) secundariamente inibe a COX-1 e COX-2 e por consequente a
siacutentese das prostaglandinas Como antipireacutetico age no centro hipotalacircmico que regula a
temperatura produzindo vasodilataccedilatildeo perifeacuterica e aumento do fluxo sanguiacuteneo
diminuindo a temperatura pela sudorese e perda de calor pela pele
O paracetamol eacute usualmente administrado oralmente (10) Apresenta uma meia-
vida de 2-3 horas Apesar de ser comparaacutevel agrave aspirina como analgeacutesico e antipireacutetico
eficaz o paracetamol difere no facto de natildeo possuir propriedades anti-inflamatoacuterias
(10) Difere dos analgeacutesicos opioacuteides porque natildeo provoca euforia nem altera o estado
de humor do doente Da mesma forma que os (NSAIDrsquos) natildeo causa problemas de
dependecircncia toleracircncia e siacutendrome de abstinecircncia Eacute muito utilizado e seguro com a
dosagem recomendada de 4g por dia mas nem sempre oferece um aliacutevio adequado da
dor aguda por si soacute (13)
NSAIDrsquoS
Os NSAIDrsquos satildeo dos agentes terapecircuticos mais utilizados no mundo inteiro
inclui-se neste grupo o ibuprofeno importante no tratamento da dor aguda e croacutenica
(14) Dos inibidores selectivos da COX-2 mais recentes nomeadamente rofecoxib
valdecoxib e celecoxib apenas este uacuteltimo foi comercializado nos EUA devido aos
restantes terem sido associados a eventos tromboacuteticos cardiovasculares (15 pp 277-
281) Apresentam trecircs acccedilotildees principais que resultam da inibiccedilatildeo da COX-2 e da
consequente reduccedilatildeo da siacutentese de prostanoacuteides
Acccedilatildeo anti-inflamatoacuteria a modificaccedilatildeo da resposta inflamatoacuteria ocorre pela
reduccedilatildeo do nordm de prostaglandinas vasodilatadoras (PGE2 prostaciclina)
associada a menor vasodilataccedilatildeo e indirectamente a menos edema No entanto a
acumulaccedilatildeo de ceacutelulas inflamatoacuterias natildeo eacute diminuiacuteda
Efeito analgeacutesico a reduccedilatildeo da siacutentese de prostaglandinas diminui a
sensibilizaccedilatildeo das terminaccedilotildees nervosas nociceptivas a mediadores da
inflamaccedilatildeo (como bradicinina e 5-hidroxitriptamina) provoca tambeacutem a reduccedilatildeo
da vasodilataccedilatildeo e desse modo o aliacutevio da cefaleia
10
Efeito antipireacutetico deve-se em parte agrave diminuiccedilatildeo da prostaglandina
mediadora a interleucina-1 responsaacutevel pela estimulaccedilatildeo do hipotaacutelamo e
consequente aumento de temperatura ndash febre (10 pp 1056-1061)
Eacute de referir ainda que todos os NSAIDrsquos agrave excepccedilatildeo dos inibidores selectivos da
COX-2 e salicilatos natildeo-acetilados tecircm um efeito inibitoacuterio na agregaccedilatildeo de plaquetas
(15 pp 277-281)
Os efeitos secundaacuterios resultam em grande parte da inibiccedilatildeo da COX-1 Entre
os mais frequentes encontram-se Dispepsia naacuteuseas e voacutemitos associados a lesotildees
gaacutestricas provocadas pela anulaccedilatildeo do efeito protector da prostaglandina sobre a mucosa
gaacutestrica Insuficiecircncia renal Reacccedilotildees cutacircneas Distuacuterbios hepaacuteticos Riscos
cardiovasculares e outros (10)
ESCALAS DE MEDICcedilAtildeO DE DOR - ESCALA VISUAL ANALOacuteGICA
A dor sendo um fenoacutemeno subjectivo compreende um grande conjunto de
componentes - componentes fisioloacutegicos cognitivos sensoriais comportamentais entre
outros Avaliar a dor utilizando uma medida que abranja todas as suas facetas e seja
fidedigna tem-se demonstrado impossiacutevelldquoUm instrumento ideal para a mensuraccedilatildeo da
dor deveria ter propriedades de uma escala de razatildeo fornecer informaccedilatildeo imediata
sobre a fidedignidade do desempenho dos pacientes ser relativamente livre de vieacuteses
ser simples de utilizar com pacientes () demonstrar utilidade tanto para a dor
experimental quanto para a dor cliacutenica permitindo comparaccedilotildees confiaacuteveis entre ambos
os tipos de dorrdquo(16)
A Escala Visual Analoacutegica (VAS) consiste numa mediccedilatildeo da dor em mm (0-
100mm) em que agrave extremidade 0 corresponde ldquonenhuma dorrdquo e agrave extremidade
antagoacutenica ldquopior dor possiacutevelrdquo Eacute uma forma simples eficaz - dentro das limitaccedilotildees - e
faacutecil de reproduzir ldquoou seja pode ser compreendida em distintas situaccedilotildees onde haacute
diferenccedilas culturais ou de linguagem do avaliador cliacutenico ou examinadorrdquo(16)
Para responder agrave questatildeo colocada pelo paciente eacute necessaacuterio a procura da
melhor evidecircncia cientiacutefica integrando-a com o proacuteprio interesse do paciente e a
expertise do cliacutenico Estes objectivos da Medicina Dentaacuteria Baseada na Evidecircncia satildeo
em parte consequecircncia de uma actualizaccedilatildeo constante de praacuteticas cliacutenicas consequentes
de novas evidecircncias cientiacuteficas e com a noccedilatildeo de que nenhum tratamento eacute completo
11
sem que ldquoas expectativas exigecircncias e direitos legiacutetimos dos pacientes sejam integrados
nos processos de decisatildeo cliacutenica sendo tal facto reconhecidamente essencial para a
melhoria da qualidade de vidardquo(17)
12
PESQUISA
CRITEacuteRIOS DE SELECCcedilAtildeO
Tipos de Estudos Escolhidos
Para este trabalho foram escolhidos apenas ensaios cliacutenicos aleatorizados cegos
(preferencialmente duplamente cegos) controlados ou natildeo por placebo e revisotildees
sistemaacuteticas
Tipos de participantes
Indiviacuteduos com idade superior a 15 anos
Sujeitos a cirurgia para extracccedilatildeo unilateral ou bilateral do 3ordm molar inferior
Que natildeo estivessem a tomar qualquer outro tipo de medicaccedilatildeo com efeitos
idecircnticos ou semelhantes aos faacutermacos em estudo
Sem patologias orais que provoquem dor moderada a forte ou outras patologias
que afectem a percepccedilatildeo da dor
Tipos de intervenccedilatildeo
Administraccedilatildeo apenas por via oral de
Paracetamol (1000mg) vs placebo
Paracetamol (1000mg) vs outro(s) NSAIDrsquos
Paracetamol ( 1000mg) vs outro(s) NSAIDrsquos vs placebo
Paracetamol (1000mg) + outro(s) NSAIDrsquos
ou Paracetamol (1000mg) + outro(s) NSAIDrsquos vs placebo
Estudos com outros tipos de intervenccedilatildeo natildeo foram incluiacutedos Os estudos que
apenas incluiacuteram o paracetamol sob a forma de proacute-farmaco foram excluiacutedos
Mediccedilatildeo de Resultados
A mediccedilatildeo de resultados foi obtida atraveacutes da escala visual analoacutegica (VAS ndash
visual analogic scale)
13
Avaliaccedilatildeo dos Estudos
Todos os estudos foram avaliados segundo fichas CASP (Critical Appraisal
Skills Programme) Estas consistem num conjunto de questotildees que permitem avaliar um
artigo cientiacutefico no seu todo para em uacuteltima anaacutelise aferir a sua aplicabilidade validade
e fiabilidade (18) Estas fichas existem para vaacuterios tipos de estudo as CASP utilizadas
neste trabalho foram as referentes a revisotildees sistemaacuteticas e ensaios cliacutenicos
aleatorizados
ESTRATEacuteGIAS DE PESQUISA
Apoacutes cada pesquisa os artigos encontrados foram avaliados numa fase inicial
com base nos seus tiacutetulos e abstracts para averiguar a sua relevacircncia A seguinte escala
foi utilizada adequado possivelmente adequado inadequado Toda a pesquisa foi
efectuada entre 7 e 19 de Novembro de 2011
Primeiramente foram consultadas bases de dados secundaacuterias apoacutes pesquisa
nestas fontes seguiram-se bases de dados primaacuterias
Cochrane Database for Systematic Reviews
Na pesquisa avanccedilada desta base de dados secundaacuteria foi introduzida a seguinte
combinaccedilatildeo de termos utilizando conectores boleanos e seleccionando as opccedilotildees
ldquosearch all textrdquo e ldquoCochrane Database of Systematic Reviewsrdquo
paracetamol AND third molar removal AND pain relief AND analgesicrdquo
Foram encontrados 14 resultados (3 protocolos e 11 revisotildees sistemaacuteticas) dos
quais uma revisatildeo foi categorizada como ldquoadequadardquo
Paracetamol for pain relief after surgical removal of lower wisdom teeth Weil
Hooper (19) Esta revisatildeo foi novamente encontrada na base de dados EBD bem
como na NICE e no PubMed
E outra classificada como ldquopossivelmente adequadardquo mas posteriormente
excluiacuteda (20)
14
Evidence-Based Dentistry (EBD)
Nesta base de dados foi introduzida a combinaccedilatildeo de termos
ldquoParacetamol OR acetaminophen AND third molar AND painrdquo utilizando os
filtros ldquoBritish Dental Journalrdquo e ldquoEvidence-Based Dentistryrdquo
Foram encontrados 28 resultados dos quais uma revisatildeo foi classificada como
ldquoadequadardquo
Relative efficacy of oral analgesics after third molar extraction ndash a 2011 update
Derry Wiffen (21)
E ainda dois artigos classificados como ldquopossivelmente adequadordquo
An investigation into the comparative efficacy of soluble aspirin and solid
paracetamol in postoperative pain after third molar surgery Seymour
Hawkesford (22)
Relative efficacy of oral analgesics after third molar extraction Barden
Edwards (23)
National Institute of Health and Clinical Excellence (NICE)
Nesta base de dados foi introduzida a seguinte combinaccedilatildeo de termos
ldquoParacetamol and third molar removal and pain and analgesicrdquo
Dos 28 resultados obtidos 1 foi previamente encontrado e classificado (19)
Dos restantes 27 artigos nenhum foi classificado como adequado ou possivelmente
adequado
LILACS
Nesta base de dados primaacuteria foi introduzida a seguinte combinaccedilatildeo de termos
ldquoParacetamol terceiro molar dorrdquo
Dos 3 resultados obtidos um foi classificado como possivelmente adequado mas
posteriormente excluiacutedo (24)
15
PUBMED
Nesta base de dados primaacuteria foram efectuadas duas pesquisas com termos
diferentes Apenas foram utilizados termos MeSH foram utilizados conectores
boleanos em ambas as pesquisas
Pesquisa 1
Search ((((Acetaminophen[Mesh]) AND Anti-Inflammatory Agents[Mesh])
AND Molar Third[Mesh]) AND Tooth Extraction[Mesh]) AND Pain
Postoperative[Mesh]
Limits only items with abstracts Humans Clinical Trial Meta-Analysis
Randomized Controlled Trial Review Comparative Study Controlled Clinical
Trial English Spanish Portuguese
Foram obtidos 32 resultados dos quais 5 artigos foram classificados como
ldquoadequadosrdquo
Combining paracetamol with a selective cyclooxygenase-2 inhibitor for acute
pain relief after third molar surgery a randomized double-blind placebo-
controlled study Haglund and von Bultzingslowen (25)
Dos restantes quatro artigos um (22) era repetido e os outros trecircs (26-28) foram
posteriormente excluiacutedos
Quatro foram considerados ldquopossivelmente adequadosrdquo dos quais trecircs (29-31)
foram posteriormente excluiacutedos O artigo remanescente foi
Analgesic efficacy of lysine clonixinate paracetamol and dipyrone in lower
third molar extraction a randomized controlled trial (32)
Pesquisa 2
Search (((Acetaminophen[Mesh]) AND Analgesics[Mesh]) AND Molar
Third[Mesh]) AND Tooth Extraction[Mesh]
Limits only items with abstracts Humans Clinical Trial Meta-Analysis
Randomized Controlled Trial Review English
16
Obtiveram-se 56 resultados em que sete foram seleccionados como sendo
ldquoadequadosrdquo
Combined acetaminophen and ibuprofen for pain relief after oral surgery in
adults a randomized controlled trial Merry Gibbs (13)
Destes artigos seis (19 22 23 25 28 32) eram repetidos
Oito artigos foram classificados como ldquopossivelmente adequadosrdquo
Onset of analgesia with sodium ibuprofen ibuprofen acid incorporating poloxamer
and acetaminophen--a single-dose double-blind placebo-controlled study in
patients with post-operative dental pain Daniels Reader (33)
Dos oito artigos cinco foram repetidos (26 27 29-31) dois (34 35) foi
posteriormente excluiacutedo
No anexo A encontra-se uma tabela de artigos excluiacutedos cujas razotildees satildeo
discriminadas
Eacute de notar que este tipo de estrateacutegia de pesquisa traz associada grande
quantidade de resultados irrelevantes superior agrave de artigos de interesse mas facilita a
aquisiccedilatildeo de todos os artigos importantes colocando em primeiro plano a sensibilidade
e natildeo a especificidade (36) A utilizaccedilatildeo de conectores boleanos e de filtros especiacuteficos
foi uma forma de minimizar o nuacutemero de resultados natildeo relacionados (17) preservando
os de interesse
17
AVALIACcedilAtildeO CRIacuteTICA
REVISOtildeES SISTEMAacuteTICAS
Paracetamol for pain relief after surgical removal of lower
wisdom teeth Weil Hooper (19)
1 Did the review ask a clearly-focused question
Sim A populaccedilatildeo em estudo compreende pacientes de qualquer estado de sauacutede
que necessitem de uma exodontia do terceiro molar inferior e que apresentam uma
intensidade de dor basal moderada a forte Foram excluiacutedos pacientes que estivessem a
tomar outro analgeacutesico A intervenccedilatildeo foi baseada em dois aspectos ndash eficaacutecia e efeitos
secundaacuterios
A terapecircutica usada para avaliar a eficaacutecia consistiu na administraccedilatildeo de uma
dose uacutenica de paracetamol por via oral independentemente da formulaccedilatildeo ou do
momento em que o faacutermaco foi tomado
Em relaccedilatildeo aos efeitos secundaacuterios foram incluiacutedos estudos natildeo soacute de dose
uacutenica como tambeacutem de doses muacuteltiplas de acetaminofeno consideraram-se estudos em
que este composto foi tomado ateacute 7 dias apoacutes a primeira toma Para este trabalho apenas
seratildeo considerados os resultados com base na administraccedilatildeo poacutes-operatoacuteria do
paracetamol
Os resultados ndash intensidade da dor e aliacutevio da dor ndash foram medidos usando as
escalas visual analoacutegica categoacuterica verbal numeacuterica verbal global subjectiva de
avaliaccedilatildeo de eficaacutecia e outras categoacutericas Os outcomes derivados do aliacutevio da dor
contabilizados foram total pain relief (TOTPAR) e summed pain intensity difference
(SPID) durante 4 e 6 horas Foram ainda contabilizados os efeitos secundaacuterios
2 Did the review include the right type of study
Os uacutenicos estudos incluiacutedos foram ensaios cliacutenicos aleatorizados duplamente
cegos que comparam o paracetamol a um placebo bem como dosagens diferentes
avaliando efeitos agraves 4 e 6 horas Este tipo de estudo eacute adequado pois implica um baixo
risco de vieacutes
18
3 Did the reviewers try to identify all relevant studies
Sim Os autores utilizaram estudos de todos os idiomas recorrendo agrave sua
traduccedilatildeo quando necessaacuterio Foram consultadas bases de dados bibliograacuteficas
electroacutenicas The Cochrane Oral Health Grouprsquos Trials Register The Cochrane Central
Register of Controlled Trials The Cochrane Pain Palliative and Supportive Care
Grouprsquos Trials Register MEDLINE EMBASE e Current Controlled Trials Register
Tambeacutem foram realizadas pesquisas manuais em revistas como parte do Cochrane Oral
Health Grouprsquos ongoing journal handsearching programme A pesquisa visou estudos
publicados entre 1966 e 25 de Agosto de 2006
Foram enviadas cartas a autores de ensaios cliacutenicos aleatorizados com vista a
obter estudos natildeo publicados bem como a empresas farmacecircuticas fabricantes de
analgeacutesicos
Os autores deste estudo consultaram ainda referecircncias bibliograacuteficas de papers
reviews e referecircncias pessoais
4 Did the reviewers asses the quality of the included studies
Sim Foi utilizada uma estrateacutegia clara e bem definida para a determinaccedilatildeo dos
estudos a incluir Este processo foi realizado independentemente por dois autores da
revisatildeo ndash natildeo cegos ndash baseando-se em dois criteacuterios centrais atribuiccedilatildeo oculta do
faacutermaco e a existecircncia de um follow-up completo Para estes criteacuterios foi utilizado um
sistema de pontuaccedilatildeo Desta forma a cada estudo foi-lhe atribuiacuteda uma pontuaccedilatildeo
formando-se dois grupos
Baixo risco de vieacutes
Moderado ou alto risco de vieacutes
5 If the results of the studies have been combined was it reasonable to do so
Sim os resultados foram apresentados de forma combinada e loacutegica Em
primeiro lugar foram apresentadas tabelas uma para cada artigoestudo incluiacutedo em
que se encontravam discriminados os meacutetodos participantes intervenccedilotildees resultados e
outras notas Os resultados dos diferentes estudos foram agrupados em 2 outcomes
tendo cada outcome 2 divisotildees
Outcome 1 ndash TOTPAR agraves 4h
A ndash Dosagem de paracetamol ateacute 1000mg vs placebo
B ndash Dosagem de paracetamol igual ou superior a 1000mg vs placebo
19
Outcome 2 ndash TOTPAR agraves 6h
A ndash Dosagem de paracetamol ateacute 1000mg vs placebo
B ndash Dosagem de paracetamol igual ou superior a 1000mg vs placebo
Todos estes grupos foram analisados e comparados segundos 2 paracircmetros
Comparaccedilatildeo 1- Medidas de aliacutevio da dor
Comparaccedilatildeo 2- Medidas de intensidade da dor
Tendo em conta todas estas variaacuteveis foram realizadas meta-anaacutelises por
subgrupo (pp 29-40) utilizando graacuteficos forest plot
Anaacutelise 11 ndash Comparaccedilatildeo 1 de A vs B ndash Outcome 1
Anaacutelise 12 ndash Comparaccedilatildeo 1 de A vs B ndash Outcome 2
Anaacutelise 21 ndash Comparaccedilatildeo 2 de A vs B ndash Outcome 1
Anaacutelise 22 ndash Comparaccedilatildeo 2 de A vs B ndash Outcome 2
Anaacutelise 3 ndash Comparaccedilatildeo do nuacutemero de efeitos adversos de paracetamol vs
placebo comparando ainda as duas dosagens diferentes
Valores de heterogeneidade (representados por I2) proacuteximos de 25 indicam
baixa discrepacircncia 50 satildeo indicadores de heterogeneidade moderada e valores
proacuteximos de 75 satildeo sinal de alta heterogeneidade entre os estudos (37)
Olhando para os valores de I2 dois possuem alta heterogeneidade um moderada
e dois baixa Nos grupos que apresentam uma discrepacircncia estatiacutestica significativa dos
resultados a aglutinaccedilatildeo dos mesmos natildeo foi muito bem sucedida Nestes grupos ainda
que a heterogeneidade seja elevada a apresentaccedilatildeo dos resultados de cada estudo foram
correcta e individualmente apresentados Aleacutem deste aspecto os diferentes meacutetodos ndash
dosagem e tempo - foram agrupados exactamente para que as formas de intervenccedilatildeo e
meacutetodos com o menor risco de vieacutes
Tabela 1 ndash Valores de heterogeneidade (I2) de cada anaacutelise
Total de I2
()
Anaacutelise 11 Anaacutelise 12 Anaacutelise 21 Anaacutelise 22 Anaacutelise 3
76 81 66 29 28
Natildeo foram discutidas as variaccedilotildees nos resultados
20
6 How are the results presented and what is the main result
A meta-anaacutelise por subgrupos foi realizada com recurso agrave medida de eficaacutecia de
intervenccedilatildeo Risco Relativo (RR) Analisando o graacutefico forest plot os ldquoquadradosrdquo a azul
representam o RR e o poliacutegono (semelhante a um losango) sumariza todas as
informaccedilotildees (provenientes dos vaacuterios estudos) sobre o efeito do paracetamol (38)
ldquoQuando o IC natildeo ultrapassa a linha de nulidade pode-se afirmar que o resultado eacute
estatisticamente significativo Estudos maiores possuem IC mais estreitos ou seja
resultados mais precisos e maior contribuiccedilatildeo para a meta-anaacutelise que tambeacutem eacute repre-
sentada graficamente (quanto maior a aacuterea do quadrado maior o peso) e valor
percentualrdquo (39) A significacircncia aumenta com a distacircncia do poliacutegono da linha de natildeo
efeito
Independentemente do tempo (4 ou 6h) dosagens ateacute 1000mg de paracetamol
apresentam uma pequena discrepacircncia nos resultados sendo que o paracetamol eacute
ligeiramente mais eficaz que o placebo Doses iguais ou superiores a 1000mg de
paracetamol traduzem-se num maior aliacutevio da dor poacutes-operatoacuteria (poliacutegono afastado da
linha de natildeo-efeito)
Em relaccedilatildeo agrave anaacutelise 3 ateacute doses de 1 g de paracetamol nuacutemero de casos de
efeitos adversos eacute muito semelhante entre placebo e a substacircncia activa Para
concentraccedilotildees superiores a 1000 mg o nuacutemero de efeiros adversos eacute superior para
paracetamol Eacute possiacutevel concluir que natildeo haacute uma diferenccedila notoacuteria no nuacutemero de casos
de efeitos adversos O poliacutegono cruza sempre a linha de natildeo efeito
O paracetamol eacute consideravelmente mais eficaz que o placebo no aliacutevio de 50
da dor principalmente em doses iguais ou superiores a 1000mg Natildeo haacute diferenccedila
significativa em relaccedilatildeo aos efeitos adversos
7 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em consideraccedilatildeo que o
poliacutegono natildeo intersecta a linha de natildeo efeito os resultados satildeo precisos (anaacutelise 1 a 2)
Na anaacutelise 3 mesmo com um IC 95 o poliacutegono cruza a linha de natildeo efeito logo natildeo eacute
possiacutevel tirar conclusotildees semelhantes em relaccedilatildeo aos limites inferior e superior do IC
Eacute de notar que a elaboraccedilatildeo de uma meta-anaacutelise contribui para a robustez dos
resultados daiacute provenientes combinar os resultados de cada estudo individual numa
meta-anaacutelise aumenta o poder estatiacutestico gerando resultados mais precisos (40)
21
8 Can the results be applied to the local population
Sim A extracccedilatildeo de terceiros molares inferiores eacute uma praacutetica cliacutenica comum
em Portugal O paracetamol eacute um analgeacutesico largamente comercializado e administrado
(sendo natildeo sujeito a receita meacutedica) pelo que era possiacutevel reproduzir esta forma de
tratamento
No entanto os estudos incluiacutedos na revisatildeo referem-se a uma dose uacutenica que
embora reproduziacutevel na populaccedilatildeo local seria necessaacuteria uma modificaccedilatildeo do
paradigma cultural em relaccedilatildeo agrave toma de medicamentos
9 Were all important outcomes considered
Natildeo A revisatildeo considera a eficaacutecia do paracetamol vs placebo no aliacutevio da dor
e simultaneamente a ocorrecircncia de efeitos secundaacuterios Satildeo abordados directamente
dois aspectos ndash o da praacutetica cliacutenica e o da investigaccedilatildeo Ambos satildeo relativos ao
profissional de sauacutede e implicitamente ao proacuteprio indiviacuteduo e aos familiares (ao serem
referidas as doses periacuteodos entre tomas e combinaccedilotildees com outros NSAIDrsquos mais
eficazes e simultaneamente seguras)
Poreacutem nada eacute referido em relaccedilatildeo a novas poliacuteticas de sauacutede nomeadamente na
implementaccedilatildeo de uma dose uacutenica culminando numa mudanccedila dos haacutebitos de sauacutede da
comunidade Tambeacutem natildeo foram abordados aspectos econoacutemicos tal como um balanccedilo
entre benefiacutecios e encargos de sauacutede que justifique a utilizaccedilatildeo deste faacutermaco como
tratamento preferencial
10 Should policy or practice change as a result of the evidence contained in this
review
Natildeo Esta revisatildeo demonstra que comparativamente a um placebo o paracetamol
eacute mais eficaz principalmente em doses elevadas e que natildeo haacute diferenccedila estatiacutestica
significativa no nuacutemero de efeitos secundaacuterios Poreacutem natildeo eacute possiacutevel tirar conclusotildees
sobre a dor depois do periacuteodo considerado de 6h Desta forma implementar uma dose
uacutenica de paracetamol a 1000mg seria imprudente sem previamente realizar estudos
complementares sobre a evoluccedilatildeo da dor apoacutes as 6h bem como comparar este faacutermaco
com outros compostos que possam ser igualmente eficazes por um raacutecio custo-benefiacutecio
melhor ou vice-versa
22
Relative efficacy of oral analgesics after third molar extraction
Barden Edwards (23)
Relative efficacy of oral analgesics after third molar extraction -
a 2011 update Derry Wiffen (21)
A avaliaccedilatildeo feita e disposta abaixo contemplou tanto a revisatildeo sistemaacutetica que
remonta a 2004 como a sua actualizaccedilatildeo de 2011 Uma vez estando inter-relacionados
consideraacutemos pertinente juntar as apreciaccedilotildees destas revisotildees porque caso contraacuterio
perder-se-ia o contexto de ambas
1 Did the review ask a clearly-focused question
Sim A populaccedilatildeo em estudo comporta pacientes com mais de 15 anos de idade
com uma intensidade de dor basal poacutes-operatoacuteria de moderada a severa apoacutes extracccedilatildeo
de um terceiro molar
A intervenccedilatildeo consistiu no tratamento da dor poacutes-operatoacuteria de intensidade
moderada a severa com doses uacutenicas de analgeacutesicos orais ou placebo sendo que os
analgeacutesicos orais corresponderam a um total de 15 combinaccedilotildees diferentes de faacutermacos
e respectivas dosagens
Os resultados foram obtidos atraveacutes da mediccedilatildeo do aliacutevio total da dor
(TOTPAR) ou da diferenccedila de intensidade da dor (SPID) utilizando uma escala
standard de 5 niacuteveis de aliacutevio da dor uma escala standard de 4 niacuteveis de aliacutevio da dor
ou uma escala visual analoacutegica (VAS) Os efeitos secundaacuterios foram tambeacutem relatados
comparando a proporccedilatildeo de pacientes que apresentaram efeitos generalizados e que
apresentaram efeitos particulares
Actualizaccedilatildeo de 2011
A intervenccedilatildeo consistiu tambeacutem no tratamento da dor poacutes-operatoacuteria de
intensidade moderada a severa com doses uacutenicas de analgeacutesicos orais ou placebo no
entanto os analgeacutesicos utilizados foram diferentes A revisatildeo de 2004 incluiu rofecoxib
and valdecoxib nenhum dos quais se encontra disponiacutevel no mercado Em vez disso
foram utilizadas combinaccedilotildees de ibuprofeno com paracetamol formulaccedilotildees diferentes
de ibuprofeno e diclofenac e etoricoxib
23
2 Did the review include the right type of study
Sim Os estudos que foram incluiacutedos nesta revisatildeo correspondem a ensaios
cliacutenicos aleatorizados duplamente cegos que comparam a eficaacutecia dos diferentes
analgeacutesicos e com placebo na terapecircutica da dor aguda poacutes-operatoacuteria Os grupos
formados possuiacuteam grupos com um miacutenimo de 10 pessoas Em todos os estudos foram
seguidas as guidelines QUORUM e utilizados criteacuterios de inclusatildeo para a dor poacutes-
operatoacuteria em que os resultados satildeo avaliados durante um periacuteodo de 4 a 6 horas apoacutes
medicaccedilatildeo
3 Did the reviewers try to identify all relevant studies
Sim Os autores da revisatildeo tentaram identificar todos os estudos relevantes
pesquisando nas bases de dados electroacutenicas Cochrane Library Biological Abstracts
MEDLINE PubMed e Oxford Pain Relief Para aleacutem disso consultaram a bibliografia
dos artigos de revisatildeo incluiacutedos de modo a encontrar informaccedilatildeo adicional e possiacuteveis
estudos natildeo publicados os quais apresentam na sua maioria datas de pesquisa que
remontam a 2002 No entanto eacute de mencionar que natildeo contactaram os autores e os
fabricantes para recolha de dados nem procuraram estudos com idiomas diferentes do
inglecircs
Actualizaccedilatildeo de 2011
Com o passar dos anos os artigos inseridos na revisatildeo foram actualizados de
forma a incluir outros analgeacutesicos e obter ensaios cliacutenicos adicionais e relevantes Desta
forma a actualizaccedilatildeo da revisatildeo sistemaacutetica de 2004 incluiu 35 revisotildees da Cochrane
com 38 anaacutelises realizadas em diferentes analgeacutesicos de dose uacutenica para determinar a
sua eficaacutecia na dor poacutes-operatoacuteria
4 Did the reviewers assess the quality of the included studies
Sim A qualidade dos estudos incluiacutedos foi avaliada vaacuterios autores
independentes e natildeo cegos (pelo facto de estes conhecerem a literatura existente)
utilizando uma escala de qualidade numerada de 1 a 5 e baseada em 3 criteacuterios
distribuiccedilatildeo aleatorizada dos pacientes se os pacientes e os examinadores se
encontravam cegos se houve remoccedilotildees ou desistecircncias durante o estudo A
classificaccedilatildeo maacutexima de um estudo incluiacutedo foi de 5 e a miacutenima foi de 2
24
Os ensaios cliacutenicos que apresentam uma classificaccedilatildeo igual ou superior a 3
(baixo risco de vieacutes) demonstraram menores efeitos secundaacuterios que os ensaios cliacutenicos
que apresentam uma classificaccedilatildeo igual ou inferior a 2 (alto risco de vieacutes)
5 If the results of the studies have been combined was it reasonable to do so
Sim Os resultados dos diferentes estudos foram apresentados sob a forma de
tabelas nomeadamente a eficaacutecia dos vaacuterios analgeacutesicos e a ocorrecircncia de efeitos
secundaacuterios foram dispostas em tabelas Aqui eram resumidos os resultados o tipo de
intervenccedilatildeo e respectivo nuacutemero total de pacientes e nordm de estudos realizados
Esta revisatildeo sistemaacutetica natildeo incluiu a realizaccedilatildeo de testes heterogeacuteneos nem a
avaliaccedilatildeo do risco de vieacutes das publicaccedilotildees atraveacutes de forest plots dado que na opiniatildeo
dos autores estas abordagens mostraram-se pouco adequados para este tipo de estudos
No entanto a homogeneidade foi avaliada atraveacutes de um modo visual
A resposta a esta questatildeo eacute claramente afirmativa porque a elevada semelhanccedila
das caracteriacutesticas dos diferentes estudos (meacutetodos utilizados tipo de intervenccedilatildeo e
mediccedilatildeo dos resultados) tornou por um lado inadequada a realizaccedilatildeo uma meta-anaacutelise
para avaliar a heterogeneidade mas por outro adequada a realizaccedilatildeo de uma avaliaccedilatildeo
visual da homogeneidade dos mesmos
6 How are the results presented and what is the main result
Os resultados foram medidos atraveacutes da proporccedilatildeo de pacientes do grupo de
tratamento vs placebo que atingiram pelo menos 50 de maxTOTPAR ou seja aliacutevio
de dor A qual foi utilizada para determinar o benefiacutecio relativo e o NNT bem como o
risco relativo dos diferentes estudos incluiacutedos
Atraveacutes da anaacutelise das tabelas eacute possiacutevel tirar 3 conclusotildees principais
1 A proporccedilatildeo de pacientes que atingiram pelo menos 50 de aliacutevio de dor eacute maior
no grupo de tratamento que no grupo placebo agrave excepccedilatildeo do estudo que utilizou
dihidrocodeiacutena 30mg em que as diferenccedilas natildeo foram estatisticamente relevantes
2 Por comparaccedilatildeo ao paracetamol (independentemente das diferentes dosagens) os
anti-inflamatoacuterios natildeo-esteroacuteides inibidores da COX-2 apresentam um maior
benefiacutecio relativo e necessitam do menor nordm de pacientes tratados para atingirem o
objectivo de 50 de aliacutevio de dor
25
3 O paracetamol apresenta um maior risco relativo na medida em que insurgem mais
efeitos secundaacuterios nos estudos em que foi administrado por oposiccedilatildeo aos
NSAIDrsquos
Os anti-inflamatoacuterios natildeo-esteroacuteides inibidores da COX-2 satildeo mais eficazes no
tratamento da dor basal poacutes-operatoacuteria moderada a intensa que o paracetamol
Actualizaccedilatildeo de 2011
Os resultados foram obtidos da mesma forma que na versatildeo de 2004 sendo que
um novo outcome foi considerado ndash tempo meacutedio necessaacuterio para que os pacientes
necessitem de re-medicaccedilatildeo aproximadamente 8 horas Agrave semelhanccedila do que aconteceu
na revisatildeo anterior os dados sobre a dihidrocodeiacutena natildeo foram conclusivos devido agrave
pouca informaccedilatildeo disponiacutevel nos estudos
7 How precise are these results
Os resultados satildeo precisos uma vez que utilizam um intervalo de confianccedila de
95 Eacute de ressalvar que os valores de NNT ou NNH apenas eram calculados quando o
riscobenefiacutecio relativo satildeo significativos isto eacute quando natildeo incluem o valor de 1 No
limite superior do intervalo de confianccedila a intervenccedilatildeo realizada seria a mesma No
entanto dado que o NNH natildeo foi calculado eacute possiacutevel concluir que o risco relativo natildeo
era significativo pelo que permanece uma incerteza se no limite inferior do intervalo de
confianccedila a intervenccedilatildeo realizada seria a mesma
8 Can the results be applied to the local population
Sim Os resultados da revisatildeo sistemaacutetica podem ser aplicados agrave nossa
populaccedilatildeo local porque os criteacuterios de inclusatildeo utilizados correspondem na sua
maioria a mecanismos fisioloacutegicos caracteriacutesticos do ser humano Para aleacutem disso as
teacutecnicas utilizadas satildeo simples e de faacutecil reproduccedilatildeo na medida em que os faacutermacos
utilizados nos ensaios cliacutenicos estatildeo agrave disposiccedilatildeo dos interessados e os meacutetodos
terapecircuticos baacutesicos
No entanto os estudos incluiacutedos nesta revisatildeo incluiacuteram um tratamento com
uma dose uacutenica de analgeacutesico oral que embora reprodutiacutevel difere do paradigma actual
da nossa populaccedilatildeo (em que haacute a tendecircncia para a auto-medicaccedilatildeo e de recorrer a
diferentes faacutermacos)
26
9 Were all important outcomes considered
Natildeo Os resultados enfatizam a eficaacutecia de vaacuterios analgeacutesicos no aliacutevio de 50
dor em comparaccedilatildeo com placebo Eacute focada ainda o benefiacutecio relativo (95 IC) e o NNT
da mesma problemaacutetica Aleacutem deste conjunto de dados satildeo considerados o nuacutemero de
pacientes com efeitos secundaacuterios risco relativo (95 IC) culminando no caacutelculo do
NNH
Contudo natildeo eacute especificado o tipo de efeitos secundaacuterios que podem ser
desencadeados pela toma dos diferentes analgeacutesicos nem aspectos diferenciadores em
analgeacutesicos com eficaacutecia e benefiacutecios idecircnticos (por exemplo custo econoacutemico) Isto
constituiria uma mais-valia para uma escolha mais consciente do analgeacutesico tanto pelos
profissionais como pelos pacientes (individual) e beneficiaria tambeacutem o Sistema
Nacional de Sauacutede (comunidade em geral)
Actualizaccedilatildeo de 2011
Um dos outcomes considerados semelhante ao que foi abordado na revisatildeo de
2004 foi a percentagem de pacientes com dor moderada (30- 60 mm VAS) ou dor
severa (mais de 60 mm) que obtiveram 50 de aliacutevio de dor Contudo foi adicionado
um novo outcome relevante o tempo necessaacuterio para que metade dos pacientes requeriu
re-medicaccedilatildeo
10 Should policy or practice change as a result of the evidence contained in this
review
Natildeo Os resultados desta revisatildeo evidenciam a eficaacutecia dos analgeacutesicos
comparativamente a um placebo nomeadamente que o ibuprofeno e o paracetamol
possuem maior maior o benefiacutecioefeito analgeacutesico quanto maior forem as dosagens
Poreacutem natildeo eacute evidecircncia suficiente para mudar o paradigma de tratamento pois ldquoWhat
these comparisons do not do is to tell dentists what to prescriberdquo Satildeo sim uma
importante ferramenta para a tomada de decisotildees que devem ser adaptadas a cada
paciente tendo presente que 80 dos analgeacutesicos prescritos possuem elevados iacutendices
de eficaacutecia e seguranccedila Em adiccedilatildeo nem todos os analgeacutesicos nesta revisatildeo estatildeo
disponiacuteveis no mercado para serem receitados pelos meacutedicos-dentistas
Conclui-se que para que esta revisatildeo fosse pilar basilar nas prescriccedilotildees de
analgeacutesicos teriam de ser apresentadas evidecircncias de benefiacuteciocusto dos analgeacutesicos
27
com melhores resultados (aspecto econoacutemico e detalhe dos efeitos adversos) Todavia a
informaccedilatildeo presente na mesma sobre a eficaacutecia e efeitos secundaacuterios assim como toda a
bibliografia jaacute existente sobre este assunto eacute uacutetil e deve ser utilizada para tomar inicio agrave
criaccedilatildeo de um formulaacuterio em medicina dentaacuteria
Actualizaccedilatildeo de 2011
Os resultados obtidos da mesma forma que na revisatildeo anterior natildeo foram
suficientemente relevantes para que as poliacuteticas de sauacutede mudassem No entanto a
quantidade de informaccedilatildeo disponiacutevel sobre analgeacutesicos de dose uacutenica para aliacutevio da dor
poacutes-operatoacuteria eacute grande e bastante acessiacutevel Podem assim servir como boas
ferramentas para a formulaccedilatildeo de poliacuteticas e prescriccedilotildees farmacecircuticas para a populaccedilatildeo
quando existirem dados cliacutenicos mais conclusivos
28
AVALIACcedilAtildeO CRIacuteTICA
ENSAIOS CLIacuteNICOS ALEATORIZADOS
Combining paracetamol with a selective cyclooxygenase-2
inhibitor for acute pain relief after third molar surgery a
randomized double-blind placebo-controlled study Haglund and
von Bultzingslowen (25)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo compreende indiviacuteduos saudaacuteveis com idade superior a 18
anos peso entre 50 e 120 kg e com necessidade de extrair terceiros molares inferiores
com remoccedilatildeo oacutessea Foram excluiacutedos pacientes intolerantes ao aacutecido acetilsaliciacutelico
paracetamol eou NSAIDrsquos que estivessem a tomar outro tipo de medicaccedilatildeo (excepto
contraceptivos) graacutevidas ou em periacuteodo de amamentaccedilatildeo problemas com drogas ou
aacutelcool Apenas pacientes que reportaram dor moderada a intensa apoacutes a cirurgia foram
incluiacutedos
Existiram quatro grupos de intervenccedilatildeo
Grupo A rofecoxib 50mg + paracetamol 1g dose uacutenica 155 plusmn 37 minutos apoacutes
cirurgia
Grupo B rofecoxib 50mg dose uacutenica 170 plusmn 45 minutos apoacutes cirurgia
Grupo C paracetamol 1g dose uacutenica 184 plusmn 53 minutos apoacutes cirurgia
Grupo D placebo dose uacutenica 161 plusmn 30 minutos apoacutes cirurgia
Os resultados prenderam-se com a intensidade da dor medida atraveacutes da escala
visual analoacutegica (VAS) de 30 em 30 minutos desde a ingestatildeo do faacutermaco durante 8
horas Atraveacutes destas avaliaccedilotildees da dor foi possiacutevel obter valores de
aliacutevio total da dor TOTPAR
soma da diferenccedila de intensidade da dor SPID nas primeiras trecircs horas
soma da diferenccedila de intensidade da dor SPID ateacute agraves 8 horas
Foram obtidos resultados referentes a uma avaliaccedilatildeo global do tratamento feita
4h e 8h apoacutes a toma do faacutermaco O uso de rescue medication foi tomado em conta bem
como o tempo ateacute agrave sua necessidade Foram ainda avaliados eventuais efeitos
secundaacuterios
29
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim A atribuiccedilatildeo de cada tratamento foi cega para todos os pacientes
investigadores e pessoal envolvido Foi levada a cabo a aleatorizaccedilatildeo pela empresa
farmacecircutica responsaacutevel pela produccedilatildeo das caacutepsulas administradas
Natildeo existindo entraves de teor eacutetico ou de disponibilidade de recursos um
ensaio cliacutenico aleatorizado eacute a escolha mais pertinente quando eacute necessaacuterio comparar
dois ou mais tipos de tratamento O facto de existir um grupo de controlo minimiza o
risco de vieacutes
3 Were participants appropriately allocated to intervention and control groups
A colocaccedilatildeo dos pacientes em cada um dos quarto grupos de tratamento foi
concretizada atraveacutes de tabelas de aleatorizaccedilatildeo
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim Sendo um ensaio cliacutenico duplamente cego tanto o staff investigadores e
pacientes estiveram cegos durante todo o estudo Todas as caacutepsulas eram idecircnticas
sendo que cada embalagem selada continha sempre 6 caacutepsulas Desta forma eacute possiacutevel
garantir que o paciente estaacute cego Sendo cada embalagem feita e selada pela empresa
farmacecircutica eacute igualmente possiacutevel inferir que os investigadores tambeacutem se
encontravam cegos Apenas o investigador principal acedeu aos coacutedigos para fazer os
caacutelculos finais
5 Were all of the participants who entered the trial accounted for at its
conclusion
Os grupos de intervenccedilatildeo foram atribuiacutedos de forma aleatoacuteria e cega os
resultados foram analisados de acordo com o grupo a que inicialmente tinham sido
associados
Inicialmente o desenho do estudo previa 120 participantes
Grupo A n = 40
Grupo B n = 40
Grupo C n = 20
30
Grupo D n = 20 (controlo)
No entanto no final do estudo foram apurados resultados de 107 indiviacuteduos Isto
deve-se a
Apoacutes a cirurgia alguns pacientes (n = 8) natildeo sentiram dor moderada a forte
no entanto quiseram mesmo assim participar sendo os seus resultados
subtraiacutedos aos caacutelculos
Alguns pacientes (n = 5) foram excluiacutedos sendo que um foi drop-out e os
restantes natildeo entregaram ou preencheram os questionaacuterios pedidos
No final a distribuiccedilatildeo de indiviacuteduos por grupos era a seguinte
Grupo A n = 34
Grupo B n = 36
Grupo C n = 20
Grupo D n = 17
Embora se verifique uma ligeira alteraccedilatildeo natildeo eacute motivo relevante de vieacutes
6 Were the participants in all groups followed up and data collected in the same
way
Sim Todos os pacientes tiveram acesso aos mesmos questionaacuterios entregues
pelo investigador Em caso de duacutevida ateacute ao final da duraccedilatildeo do estudo (8 horas) o
paciente podia telefonar ao investigador com quaisquer duacutevidas que surgissem Poreacutem
o paciente era responsaacutevel pelo iniacutecio do estudo ao administrar a si mesmo o faacutermaco
em casa no momento em que o fizesse devia telefonar ao investigador para este ter
conhecimento do iniacutecio do estudo Se o paciente natildeo contactasse o investigador ateacute 3
horas apoacutes a cirurgia o investigador contactaria o paciente Os valores maacuteximo e
miacutenimo de tempo entre a cirurgia e iniacutecio do estudo de foram 118 e 237 minutos a este
facto eacute inerente um risco de vieacutes pois nem todos os pacientes estavam na mesma
condiccedilatildeo quando iniciaram o tratamento podendo reflectir-se nos resultados
7 Did the study have enough participants to minimise the play of chance
Sim Os caacutelculos foram efectuados assumindo que existiria uma diferenccedila na
SPID entre grupos A e B de 20 Foram utilizados testes natildeo-parameacutetricos (Mann-
Whitney U-test) sendo definido que pelo menos 22 pacientes deveriam ser incluiacutedos em
cada um destes grupos
31
8 How are the results presented and what is the main result
Os caacutelculos estatiacutesticos necessaacuterios para a elaboraccedilatildeo dos resultados foram
efectuados no programa Statistical Package for Social Sciences (SPSS) v 12 As
significacircncias entre grupos de tratamento em relaccedilatildeo agraves respostas agrave VAS foram
testadas com t-test de variaacutevel independente em todas as avaliaccedilotildees de dor A mesma
estrateacutegia foi aplicada para a SPID agraves 3 e 8 horas A TOTPAR foi baseada na
assumpccedilatildeo que os resultados satildeo parte de uma escala de intervalos O mesmo teste foi
utilizado para a diferenccedila entre grupos relativamente ao uso de rescue medication Os
testes dos dados provenientes de escalas categoacutericas (PAR e a avaliaccedilatildeo global) foram
realizados atraveacutes de testes natildeo-parameacutetricos (Mann-Whitney U-test)
Intensidade da dor Os resultados favorecem o grupo A ateacute 15h apoacutes o iniacutecio do
tratamento A partir das 2h o grupo A natildeo tem uma eficaacutecia estatisticamente maior que
o grupo B Ambos os grupos tecircm melhores resultados globais que o grupo C O Grupo
D (placebo) eacute notoriamente menos eficaz que todos os outros grupos
Aliacutevio da dor (PAR) Os resultados meacutedios desta afericcedilatildeo satildeo semelhantes aos da
intensidade da dor
TOTPAR Natildeo houve uma diferenccedila significativa entre o grupo A e o grupo B
Ambos foram significativamente melhores que o C todos os grupos de tratamento
activo tiveram melhores resultados que o grupo D (placebo)
SPID Embora o grupo A mostre a maior SPID meacutedia (05 ndash 3h) natildeo foi
estatisticamente diferente do grupo B o grupo C tambeacutem natildeo foi estatisticamente
diferente do grupo B A SPID meacutedia total foi estatisticamente semelhante entre os
grupos A e B mas superior agrave do grupo C O grupo D (placebo) teve resultados
inferiores aos dos restantes grupos
Uso de rescue medication Embora tenha existido um nuacutemero notoriamente
superior de casos entre os grupos A e B comparativamente ao C e ao D esta diferenccedila
natildeo eacute relevante estatisticamente devido ao baixo nuacutemero de pacientes que recorreram a
esta medicaccedilatildeo
Avaliaccedilatildeo global tanto agraves 4 como agraves 8h os grupos A e B receberam avaliaccedilotildees
semelhantes tendo as melhores classificaccedilotildees e sendo significativamente superiores agraves
do grupo C Todos foram melhores que o D (placebo) Agraves 8h as percentagens de
pacientes que avaliaram o tratamento como bom ou excelente foram
Grupo A 90
32
Grupo B 83
Grupo C 42
9 How precise are these results
No artigo natildeo satildeo mencionados intervalos de confianccedila No entanto nos graacuteficos
referentes agrave intensidade da dor eacute possiacutevel ver as barras correspondentes ao intervalo de
confianccedila Existem sempre que necessaacuterio valores de p associados aos resultados
10 Were all important outcomes considered so the results can be applied
Sim A extracccedilatildeo de terceiros molares em Portugal eacute uma praacutetica cliacutenica comum
pelo que o estudo pode ser facilmente reproduzido desde que haja acesso agrave medicaccedilatildeo
utilizada e que esta esteja em formato idecircntico (para garantir que natildeo existe vieacutes)
Poreacutem o facto de ser utilizada uma dose uacutenica poderaacute natildeo ir de encontro com o padratildeo
actual sendo necessaacuteria uma sensibilizaccedilatildeo do paciente diferente para este meacutetodo
Um facto importante foi referido na discussatildeo deste artigo posteriormente agrave
recolha de dados do mesmo surgiram preocupaccedilotildees seacuterias sobre efeitos nocivos
cardiovasculares em tratamentos de longa duraccedilatildeo com rofecoxib embora estes efeito
secundaacuterios tendam a estar relacionados com as doses e natildeo apenas com a selectividade
COX-2 (8 25) Esta informaccedilatildeo eacute altamente relevante de todos os pontos de vista do
paciente e famiacutelia do profissional de sauacutede e oacutergatildeos legislativos
Tendo em conta este facto seriam necessaacuterios estudos adicionais para aferir o
risco de seguir um tratamento como o visado neste ensaio cliacutenico
33
Combined acetaminophen and ibuprofen for pain relief after oral
surgery in adults a randomized controlled trial (13)
1 Did the study ask a clearly-focused question
Sim Foram incluiacutedos pacientes sujeitos a extracccedilatildeo de pelo menos um terceiro
molar inferior Foram excluiacutedos pacientes com idade inferior a 16 anos peso inferior a
50 kg que tivessem tomado NSAIDrsquos (excepto aspirina a 150mg) ou paracetamol 24h
antes da cirurgia entre outros(inserir referencia para a pagina pois sao muitos)
Existiram 3 grupos de intervenccedilatildeo
Grupo A 500mg paracetamol + 150mg ibuprofeno
Grupo B 500mg paracetamol
Grupo C 150mg ibuprofeno
Todos os grupos de intervenccedilatildeo tomaram 2 comprimidos imediatamente antes da
cirurgia e depois 4 comprimidos diariamente (de 6 em 6 horas) durante 48h
Os resultados passaram pela intensidade da dor medida atraveacutes da VAS (mm)
em trecircs momentos distintos antes de tomar qualquer medicaccedilatildeo do estudo
imediatamente apoacutes a cirurgia e de 2 em 2 horas ateacute terminar o periacuteodo de 48 horas A
medida utilizada foi a area under the curve (AUC) dividida pelo tempo resultando em
AUCh Este caacutelculo foi efectuado para encontrar valores ldquomeacutediosrdquo pois houve ligeiras
diferenccedilas no momento da afericcedilatildeo dos valores da VAS Mediu-se tambeacutem o consumo
de rescue medication ao longo das 48 horas
Foram ainda utilizadas escalas categoacutericas de avaliaccedilatildeo global da dor e da
naacuteusea realizadas no final do estudo bem como uma escala VAS para medir os
distuacuterbios no sono apoacutes cada noite
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim A atribuiccedilatildeo de cada tratamento foi cega para todos os pacientes
investigadores e pessoal envolvido O responsaacutevel pela aleatorizaccedilatildeo do estudo foi o
estatiacutestico do estudo O estatiacutestico foi a uacutenica pessoa com acesso agraves informaccedilotildees da
atribuiccedilatildeo de tratamento aos pacientes
34
3 Were participants appropriately allocated to intervention and control groups
A colocaccedilatildeo de pacientes em cada um dos trecircs grupos de tratamento foi
aleatorizada A sequecircncia de aleatorizaccedilatildeo foi gerada por computador pelo estatiacutestico
do estudo Foi utilizada uma proporccedilatildeo de 111 para os trecircs grupos de tratamento isto
foi conseguido atraveacutes de permutaccedilatildeo de blocos com estratificaccedilatildeo para o tipo de
anestesia (local ou geral) e centro de estudo A utilizaccedilatildeo da aleatorizaccedilatildeo por
permutaccedilatildeo de blocos assegura uma distribuiccedilatildeo equilibrada por grupos de tratamento
quando o nuacutemero de indiviacuteduos eacute menor que mil (inserir referencia do artigo de
aleatorizajao MJA)
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim Este ensaio cliacutenico foi duplamente cego Como tal cada tipo de tratamento
consistia em comprimidos idecircnticos colocados num pacote selado as instruccedilotildees sobre
dosagens eram tambeacutem iguais garantindo que o estudo permanecia cego aos
investigadores staff e pacientes prevenindo a existecircncia de vieacuteses
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim O estudo previa um nuacutemero miacutenimo de 120 indiviacuteduos 40 em cada grupo
de tratamento Dos 135 pacientes que concordaram participar apoacutes serem abordados
pelo meacutedico apenas 122 foram incluiacutedos no estudo (os 13 que foram excluiacutedos natildeo
entregaram o diaacuterio de tratamento que lhes foi pedido)
Grupo A n = 40
Grupo B n = 43
Grupo C n = 39
Todos os 122 pacientes incluiacutedos foram seguidos ateacute ao final do estudo
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os pacientes foram abordados primariamente por um cirurgiatildeo e
seguidamente por uma enfermeira responsaacutevel pelo seguimento dos pacientes ao longo
do estudo O seguimento de cada paciente foi realizado de igual forma no hospital e fora
35
dele onde o contacto era estabelecido por telefone de forma a facilitar a recolha de
informaccedilatildeo levada a cabo por meio da entrega de diaacuterios
Em relaccedilatildeo agrave recolha dos dados relativos agrave dor poacutes-operatoacuteria experienciada os
intervalos de tempo utilizados foram semelhantes (imediatamente antes da
administraccedilatildeo da primeira dose logo apoacutes a cirurgia e de 2 em 2 horas durante um
periacuteodo de 48 horas) e a monitorizaccedilatildeo dos pacientes feita utilizando as mesmas
guidelines
7 Did the study have enough participants to minimise the play of chance
Sim Os investigadores do estudo realizaram a power calculation Estimaram
que eram necessaacuterios 120 participantes distribuiacutedos equitativamente pelos 3 grupos O
power foi de 80 na detecccedilatildeo de diferenccedilas entre os grupos de 9 mm (SD de 14mm)
para mediccedilotildees relativas agrave altura de repouso e os de 13mm (SD de 21mm) e para
mediccedilotildees relativas agrave altura de actividade
Dos 135 pacientes incluiacutedos no estudo 13 natildeo devolveram os seus diaacuterios pelo
que ficaram disponiacuteveis 122 participantes a enquadrar a populaccedilatildeo de tratamento (ITT
population) para anaacutelise dos criteacuterios de comparaccedilatildeo primaacuterios (primary endpoints)
Como o criteacuterio de possuir participantes necessaacuterios foi preenchido os
resultados da comparaccedilatildeo do objectivo primaacuterio deste estudo (mediccedilatildeo da intensidade
meacutedia de dor ao longo do estudo) tecircm uma elevada importacircncia cliacutenica Esta
importacircncia eacute equiparaacutevel aos resultados de estudos publicados anteriormente
8 How are the results presented and what is the main result
Os resultados foram apresentados sob a forma de mediccedilotildees nomeadamente as
principais diferenccedilas (mean differences) entre o paracetamolacetaminofeno ibuprofeno
e combinaccedilatildeo dos dois comparando a eficaacutecia farmacocineacutetica e efeitos secundaacuterios
respectivos a cada um Agraves quais estaacute associada uma taxa de erro de 5 (SEM) ou seja
intervalo de confianccedila de 95 (CI) e um valor de P lt001
Foi realizada a mediccedilatildeo da time-adjusted AUC (AUCh) da VAS que
juntamente com a classificaccedilatildeo global de dor revelou-se substancial e
significativamente menor no grupo que utilizou a combinaccedilatildeo do que nos outros dois
grupos (tanto no periacuteodo de repouso como no periacuteodo de actividade)
Apesar de alguns criteacuterios de comparaccedilatildeo secundaacuterios (secondary endpoints) o
uso de medicaccedilatildeo de resgate apoiarem o uso da combinaccedilatildeo do faacutermaco natildeo possuem
36
relevacircncia estatiacutestica Aleacutem disso o tipo de anestesia utilizada na cirurgia e o nordm de
dentes extraiacutedos os paracircmetros farmacocineacuteticos e a ocorrecircncia dos efeitos secundaacuterios
natildeo mostraram diferenccedilas significativas entre os 3 grupos de estudo
Os pacientes medicados com a combinaccedilatildeo de paracetamol e ibuprofeno
experienciaram menos dor poacutes-operatoacuteria durante as 48 horas que os pacientes que
usaram os medicamentos isolados
9 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em conta que foi preacute-
definido um valor para P de 005 de forma determinar se os valores obtidos possuem
relevacircncia estatiacutestica ou natildeo os resultados satildeo precisos
Isto mostra que para que a combinaccedilatildeo dos dois medicamentos possa ser
considerada sem incerteza mais adequada que outros meacutetodos de medicaccedilatildeo seriam
necessaacuterios resultados expliacutecitos e com elevada relevacircncia estatiacutestica
10 Were all important outcomes considered so the results can be applied
Sim O estudo realizado tal como acontece em todos os outros apresenta os
seus pontos fortes e fracos No entanto a pluralidade de criteacuterios utilizados na
comparaccedilatildeo dos vaacuterios grupos de estudo permitiu uma boa percepccedilatildeo da relaccedilatildeo
custobenefiacutecio aqui presente Apesar de certos paracircmetros como a utilizaccedilatildeo de
placebo recrutamento de crianccedilas e avaliaccedilatildeo significativa dos efeitos secundaacuterios natildeo
terem sido explorados estes natildeo apresentam grande peso no que respeita agrave validaccedilatildeo dos
resultados em si Isto acontece pois a bibliografia existente e a praacutetica cliacutenica jaacute nos
permitem deduzir e extrapolar conclusotildees em relaccedilatildeo agravequeles paracircmetros
Deste modo a questatildeo-chave recai sobre o facto de a combinaccedilatildeo de
paracetamol com ibuprofeno ser mais vantajosa e eficaz que a toma de apenas um deles
Caso estes resultados sejam confirmados por estudos de outras entidades a jaacute muito
utilizada combinaccedilatildeo paracetamol+ibuprofeno poderaacute mesmo tornar-se procedimento
padratildeo na terapecircutica da dor aguda moderada (em pacientes sem contra-indicaccedilatildeo para
NSAIDrsquos)
37
Analgesic efficacy of lysine clonixinate paracetamol and
dipyrone in lower third molar extraction a randomized
controlled trial (32)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo em estudo comporta 90 pacientes entre os 18 e 26 anos de
idade com uma indicaccedilatildeo cliacutenica para extracccedilatildeo de um 3ordm molar inferior impactado
(com classe I e II)
A intervenccedilatildeo consistiu no tratamento da dor apoacutes extracccedilatildeo do 3ordm molar atraveacutes
da medicaccedilatildeo com um dos 3 analgeacutesicos em estudo utilizando 8 comprimidos do
respectivo analgeacutesico a serem tomados 1 hora preacute-cirurgia e a cada 6 horas poacutes-cirurgia
durante um periacuteodo de 24 horas
Os resultados foram obtidos atraveacutes da mediccedilatildeo da intensidade da dor utilizando
a escala visual analoacutegica (VAS) mesmo antes da cirurgia e seguidamente 1 2 4 6 8
12 e 24 horas apoacutes a cirurgia Aleacutem disso para cada uma destas mediccedilotildees os pacientes
tinham de relatar o niacutevel de dor em que se encontravam (percepccedilatildeo da dor) atraveacutes de
uma escala decimal com os seguintes criteacuterios
0 cm Sem dor
01- 3 cm Dor ligeira
31-7 cm Dor moderada
71-10 cm Dor intensa
A presenccedila ou ausecircncia de efeitos secundaacuterios foi tambeacutem uma das
preocupaccedilotildees deste estudo e algo avaliado nos resultados Dado que havia a
possibilidade de ocorrecircncia de agranulocitose anemia anafilaxia e complicaccedilotildees
gastrointestinais
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo em questatildeo consiste num ensaio cliacutenico aleatorizado Esta
abordagem foi a mais adequada para a questatildeo colocada uma vez que o objectivo final
eacute comparar a eficaacutecia da lisina clonixinato com o paracetamol e com a dipirona na
analgesia da dor poacutes-operatoacuteria Para obter informaccedilotildees mais completas respeitantes agrave
seguranccedila e eficaacutecia dos faacutermacos comparados eacute necessaacuterio o recrutamento e
aleatorizaccedilatildeo de um determinado nuacutemero de pacientes Eacute necessaacuterio tambeacutem medicaacute-
38
los medir e avaliar os resultados de forma imparcial e objectiva Desta forma eacute mais
provaacutevel chegar a uma conclusatildeo fidedigna e vaacutelida tanto interna como externamente
Pelas razotildees acima enumeradas a realizaccedilatildeo de um ensaio cliacutenico aleatorizado
foi a melhor abordagem a seguir
3 Were participants appropriately allocated to intervention and control groups
Sim Os pacientes foram divididos pelos diferentes grupos de estudo de uma
forma aleatoacuteria utilizando um meacutetodo relativamente simples Os analgeacutesicos foram
repartidos em recipientes brancos opacos e idecircnticos numerados de 1 a 90 Cada
recipiente continha 8 comprimidos de um dos 3 faacutermacos em comparaccedilatildeo (dipirona
500mg paracetamol 750mg lisina clonixinato 125 mg) Por sua vez foi pedido aos
pacientes para retirarem o recipiente agrave sua escolha e ao acaso os quais desconheciam o
seu conteuacutedo
Dos 90 pacientes recrutados de iniacutecio 26 desistiram pelo que os restantes 64
pacientes foram distribuiacutedos por 3 grupos correspondentes a diferentes analgeacutesicos
orais lisina clonixinato composto por 20 indiviacuteduos (8 masculinos 12 femininos)
Paracetamol composto por 23 indiviacuteduos (9M 14F) Dipirona composto por 21
indiviacuteduos (6M 15F)
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Natildeo eacute possiacutevel dizer Os pacientes deste estudo estavam lsquocegosrsquo quanto ao grupo
de estudo em que iriam ser colocados O processo de distribuiccedilatildeo dos indiviacuteduos foi
feito de uma forma aleatoacuteria atraveacutes de um meacutetodo bastante simples de escolha de
recipiente
Quanto aos funcionaacuterios e revisores deste estudo o mesmo pode natildeo ter
acontecido pois nenhuma informaccedilatildeo sobre este aspecto eacute mencionada no artigo
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim No estudo realizado os participantes foram distribuiacutedos por 3 grupos um
de estudo ou intervenccedilatildeo onde foi administrado lisina clonixinato e dois de controlo
onde se administrou paracetamol num e dipirona noutro Natildeo houve redistribuiccedilatildeo dos
39
participantes isto eacute cada participante foi tratado uacutenica e exclusivamente com o faacutermaco
correspondente ao seu grupo
Houve um seguimento dos pacientes durante um periacuteodo de 24 horas de modo a
avaliar a eficaacutecia de cada analgeacutesico na eliminaccedilatildeo da dor poacutes-operatoacuteria de forma
indirecta (quanto maior o aliacutevio de dor ao longo do periacuteodo de estudo maior a eficaacutecia
do respectivo analgeacutesico) Tendo isso em conta os resultados e anaacutelise dos dados foram
realizados em cada grupo e depois comparados com os outros grupos
Os investigadores do estudo poderiam ter formado um grupo placebo e
comparado os seus resultados com os restantes grupos Assim averiguar-se-ia a eficaacutecia
de cada um dos analgeacutesicos e natildeo apenas a eficaacutecia relativa a outros faacutermacos
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os participantes dos diferentes grupos foram seguidos da mesma maneira e
os dados recolhidos de igual forma Os resultados foram avaliados nos mesmos
intervalos de tempo ou seja antes da cirurgia e 1 2 4 6 8 12 e 24 horas apoacutes a
mesma Os pacientes receberam o mesmo tempo de atenccedilatildeo - 24 horas de seguimento e
os dados foram recolhidos utilizando os mesmos paracircmetros a escala visual analoacutegica
para determinar o aliacutevio de dor e a escala decimal para a percepccedilatildeo de dor dos pacientes
e questionaacuterios individuais
Para aleacutem do jaacute referido os investigadores tiveram em atenccedilatildeo a forma como a
cirurgia foi realizada diminuindo o risco de vieacutes
Intervieram 2 cirurgiotildees calibrados entre si na niacutevel da teacutecnica minimizando a
ocorrecircncia de abordagens ciruacutergicas diferentes
o periacuteodo de duraccedilatildeo foi controlado e por isso natildeo influenciou o comportamento
da dor no estudo (meacutedia de 339 minutos com SD plusmn98 min)
Estas cirurgias satildeo bastantes conhecidas e muitas vezes satildeo procedimentos
standard permitindo uma selecccedilatildeo muito mais facilitada e raacutepida de casos cliacutenicos a
incluir no estudo e diminuindo o nuacutemero de eventos de difiacutecil controlo que poderiam
levar a vieacutes dos resultados
7 Did the study have enough participants to minimise the play of chance
Natildeo eacute possiacutevel dizer Dos 90 pacientes inicialmente recrutados para o estudo 26
deles desistiram Os investigadores natildeo referiram o impacto deste nuacutemero de drop-outs
40
na extrapolaccedilatildeo de conclusotildees a partir dos resultados obtidos Igualmente natildeo foram
mencionados quaisquer caacutelculos que determinassem o nuacutemero necessaacuterio de indiviacuteduos
para o estudo ter validade
8 How are the results presented and what is the main result
Os resultados obtidos no estudo foram categorizados por droga e analisados de
acordo com o desenvolvimento da dor poacutes-operatoacuteria Seguidamente foram
apresentados atraveacutes de mediccedilotildees descritivas da variaccedilatildeo da dor as quais utilizaram
paracircmetros como miacutenimo maacuteximo mean median e desvio-padratildeo (SD)
Por sua vez a anaacutelise dos dados foi feita com os testes de Kruskal-Wallis e de
Friedman onde os resultados satildeo considerados estatisticamente relevantes se
culminarem num valor de lsquoprsquo igual ou inferior a 005 (95 IC) e apresentada utilizando
os mesmos paracircmetros de miacutenimo maacuteximo e SD
O valor de P encontra-se claramente acima do valor de referencia preacute-definido
pelo que os resultados natildeo apresentam relevacircncia estatiacutestica suficiente para aferir que
possuem um melhor outcome que o paracetamol
A lisina clonixinato assim como a dipirona e o paracetamol eacute eficiente no
controlo da dor resultante da extracccedilatildeo de um 3ordmmolar inferior pelo que natildeo apresenta
nenhuma diferenccedila significativa dos outros analgeacutesicos mencionados
9 How precise are these results
Utilizando um intervalo de confianccedila de 95 e tendo em conta que os valores de
P obtidos apoacutes anaacutelise dos resultados se encontrarem abaixo de 001 eacute possiacutevel auferir
que os resultados deste estudo satildeo bastante precisos
10 Were all important outcomes considered so the results can be applied
Natildeo Os efeitos gerados pela lisina clonoxinato no tratamento da dor derivada de
extracccedilatildeo do 3ordm molar natildeo foram estatisticamente relevantes quando comparados aos do
paracetamol e dipiridona Apesar de as condiccedilotildees pelas quais o estudo foi realizado
serem reprodutiacuteveis na nossa populaccedilatildeo local (tipo de pessoas localizaccedilatildeo e
reprodutibilidade do tratamento) nada eacute referido em relaccedilatildeo a novas poliacuteticas de sauacutede
nomeadamente na implementaccedilatildeo de uma dose uacutenica culminando numa mudanccedila dos
haacutebitos de sauacutede da comunidade Tambeacutem natildeo foram abordados aspectos econoacutemicos
41
tal como um balanccedilo entre benefiacutecios e encargos de sauacutede que justifique a utilizaccedilatildeo
deste faacutermaco como tratamento preferencial
42
Onset of analgesia with sodium ibuprofen ibuprofen acidin
corporating poloxamer and acetaminophenmdasha single-dose
double-blind placebo-controlled study in patients with post-
operative dental pain Daniels Reader (33)
1 Did the study ask a clearly-focused question
Sim A populaccedilatildeo em estudo refere-se a pacientes com idade entre os 16 e os 40
anos apresentando uma intensidade de dor basal poacutes-operatoacuteria moderada a severa O
diagnoacutestico para a extracccedilatildeo poderia ser um dos seguintes pelo menos um 3ordm molar
mandibular indicado para remoccedilatildeo (grau de impactaccedilatildeo superior a 4) ou dois terceiros
molares ipsilaretais com pontuaccedilatildeo de impactaccedilatildeo conjunta natildeo superir a 6
A intervenccedilatildeo traduz-se no tratamento da dor poacutes-ciruacutergica com doses uacutenicas de
diferentes faacutermacos Inicialmente cada participante tem a mesma probabilidade de ser
colocado num dos 4 grupos
A ibuprofeno de soacutedio 2x256 mg (ibuprofeno de soacutedio di-hidratado equivalente a
400 mg de ibuprofeno aacutecido + placebos de ibuprofeno poloxamo e
acetaminofeno
B ibuprofenopoloxacircmero (400mg de Ibuprofeno e 120mg de poloxacircmero
surfactante 407) + placebos de ibuprofeno de soacutedio e paracetamol
C 1000mg acetaminofeno + placebos equivalentes
D placebo para as 3 formas de substacircncias activas
O endpoint primaacuterio consistiu no tempo necessaacuterio para um aliacutevio da dor
perceptiacutevel pelos pacientes Foram considerados inuacutemeros endpoints secundaacuterios (foi
utilizada uma escala categoacuterica e VAS para os endpoints 2 3 e 4)
1 Caacutelculo da AUC e SPRID (0 a 6 horas poacutes-tratamento) e tempo necessaacuterio para
um aliacutevio significativo da dor
2 Aliacutevio total da dor (TOTPAR) SPID e SPRID
3 Aliacutevio da dor e intensidade da mesma em termos individuais (5 minutos - 6
horas)
4 PID ao longo do periacuteodo de estudo e o momento em que este foigt ou igual a 1
5 Instante em que os pacientes recorreram a medicaccedilatildeo de recurso
6 Tempo e proporccedilatildeo de pacientes que sentiram 50 aliacutevio da dor
43
7 Abstracccedilatildeo agrave dor (1 e 6 horas) e percepccedilatildeo da interferecircncia causada pela dor nas
actividades quotidianas (escala de Ranvier)
8 Avaliaccedilatildeo qualitativa da medicaccedilatildeo tomada pelos dos participantes
Os efeitos adversos foram obtidos atraveacutes da procura de informaccedilatildeo em
documentaccedilatildeo e relacionados (ou natildeo) com a medicaccedilatildeo do estudo pelo investigador
Foi efectuada uma mediccedilatildeo de sinais vitais 6 horas apoacutes a toma e na visita follow-up na
qual tambeacutem foi realizado um exame fiacutesico
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo em questatildeo eacute descrito como um ensaio cliacutenico duplamente cego e
controlado com placebo Eacute o tipo de estudo indicado para comparar diferentes formas de
tratamento atraveacutes da divisatildeo dos pacientes por grupos Eacute necessaacuterio ter em
consideraccedilatildeo o aspecto eacutetico de tais tratamentos pois ldquoexposing patients to an
intervention believed to be inferior to current treatment is often thought unethicalrdquo (41)
Para garantir a eacutetica dos tratamentos incluiacutedos o estudo foi conduzido de acordo com a
Declaraccedilatildeo de Helsiacutenquia como referido na Directiva da EU de 200120EC e
concordante com a Conferecircncia Internacional de Harmonizaccedilatildeo (ICH) e a GCP (boa
praacutetica cliacutenica)
3 Were participants appropriately allocated to intervention and control groups
Sim Os indiviacuteduos foram divididos aleatoriamente para serem inseridos num
dos 4 grupos de tratamento numa proporccedilatildeo 1111 O meacutetodo de aleatorizaccedilatildeo foi
gerado pelo computador atraveacutes de um randomization Schedule
Para equilibrar a alocaccedilatildeo dos pacientes realizou-se uma estratificaccedilatildeo por sexo
e por intensidade da dor basal O protocolo do estudo foi revisto e aprovado pela
Quorum Review Inc o que leva a querer que a subdivisatildeo foi realmente rigorosa
Os grupos encontram-se equilibrados tanto em nuacutemero como noutras variaacuteveis
particularmente geacutenero intensidade dor basal e idade Deste modo diferenccedilas
reportadas nos resultados natildeo satildeo consequecircncia da heterogeneidade dentro dos grupos
de tratamento
44
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
A aleatorizaccedilatildeo dos participantes foi gerada pelo computador O protocolo do
estudo foi posteriormente revisto como anteriormente referido Agrave partida tanto o
investigador e pacientes natildeo interferiram no processo
Foram usados comprimidos para o ibuprofeno de soacutedio ibuprofenopoloxamero
e caacutepsulas para o paracetamol tanto para as formas activas como placebo
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim Os 322 participantes incluiacutedos de 614 inicialmente recrutados 318
completaram o estudo e 321 foram incluiacutedos na populaccedilatildeo ITT (intended do treat)
No grupo ibuprofeno de soacutedio todos os 80 participantes concluiacuteram a anaacutelise
No grupo B dos 80 inicialmente alocados 76 completaram a anaacutelise Um foi
excluiacutedo perdeu-se o follow-up de outro e os restantes natildeo concluiacuteram por
outros motivos
Dos 81 do grupo do paracetamol um natildeo foi incluiacutedo no ITT (falhou em
providenciar os dados da intensidade da dor basal diaacuteria)
No grupo placebo todos os pacientes concluiacuteram o estudo
Os resultados de cada paciente foram analisados agrave luz do grupo de tratamento
em que estes foram colocados
6 Were the participants in all groups followed up and data collected in the same
way
Sim Os participantes permaneceram nos centros de investigaccedilatildeo cliacutenica apoacutes a
toma durante 8-15h Durante as 6 horas apoacutes o tratamento a eficaacutecia foi medida em
intervalos preacute-determinados Para avaliar a existecircncia de efeitos secundaacuterios foi
realizada uma mediccedilatildeo de sinais vitais conduzido um follow-up poacutes-operativo (5 a 12
dias poacutes-cirurgia) e repetida a avaliaccedilatildeo de efeitos adversos Pode-se considerar anaacutelogo
o acompanhamento entre os vaacuterios pacientes poacutes-cirurgia e medicaccedilatildeo pois constituiu
um seguimento proacuteximo maioritariamente presencial e rigoroso
45
7 Did the study have enough participants to minimise the play of chance
Foram usados dados de estudos preacutevios os quais continham informaccedilatildeo acerca
de AUC e PRID Com estes dados foi determinado que um nuacutemero de 80 pacientes por
grupo providenciaria um power de 90 em detectar diferenccedilas entre os grupos de
tratamento com um niacutevel de significacircncia de 0025 Natildeo foi possiacutevel calcular um power
ldquoformalrdquo para o aliacutevio de dor significativo No entanto a resposta eacute afirmativa para a
questatildeo CASP uma vez que foram realizados esforccedilos para que o nuacutemero das amostras
fosse significativo e correcto
8 How are the results presented and what is the main result
Os resultados satildeo apresentados em termos de percentagens e diferenccedilas meacutedias
(mean differences) alguns com recurso a curvas de Kaplan-Meier (survival curves) Os
efeitos secundaacuterios satildeo apresentados sob a forma de tabela com a percentagem de
pacientes dentro de cada grupo que sofreram os efeitos descritos na mesma
Os grupos A e B exibem resultados substancialmente melhores no que diz
respeito aos seguintes pontos
AUC e SPID satildeo significativamente menores A com 963 e B com 90 face a
C com 675 e D com 25 O tempo para atingir aliacutevio da dor
SPRID Esta eacute semelhante entre os grupos A B e C ateacute aos 45 minutos A partir
deste periacuteodo o ibuprofeno possui uma eficaacutecia superior ao paracetamol
Abstracccedilatildeo agrave dor e percepccedilatildeo da interferecircncia causada pela dor nas actividades
quotidianas (escala de Ranvier)
Utilizaccedilatildeo da medicaccedilatildeo de recurso A com 325 e B com 225 face a C com
438 e D em que a maioria dos pacientes usou a mesma
Avaliaccedilatildeo dos medicamentos por parte dos pacientes (resposta ldquoboardquo ldquomuito
boardquo ou ldquoexcelenterdquo)
No que se refere aos efeitos secundaacuterios 118 da populaccedilatildeo do estudo sofreu
mais efeitos sendo que a maior percentagem ocorreu no grupo do C
Quando comparado com acetaminofeno o ibuprofeno de soacutedio e
Ibuprofenopoloxamero possui uma eficaacutecia analgeacutesica significativamente superior
46
9 How precise are these results
Nos endpoints primaacuterios as diferenccedilas entre as duas formulaccedilotildees de ibuprofeno e
paracetamol foram avaliadas tendo por base o teste de Wilcoxon rank-sum O hazard
ratio e respectivo IC de 975 foram calculados para as comparaccedilotildees entre os
compostos Os endpoints secundaacuterios que agregavam vaacuterios periacuteodos de tempo foram
calculados atraveacutes da AUC Diferenccedilas entre tratamentos foram avaliadas utilizando
valores de α de 005 o intervalo de confianccedila de 95 (CI) foi calculado por meio dos
paracircmetros do modelo adequado
Eacute introduzido o valor de P que na sua generalidade possui valores reduzidos e
menores que 0005 Considerando a homogeneidade dos grupos o caacutelculo do nuacutemero da
amostra com elevado power e os valores de P podemos concluir que no contexto os
resultados satildeo precisos (42)
10 Were all important outcomes considered so the results can be applied
Eacute plausiacutevel que a populaccedilatildeo utilizada no estudo fosse semelhante num estudo
anaacutelogo Tanto o local como o proacuteprio tratamento poderiam ser reproduzidos visto que
os compostos em questatildeo satildeo largamente comercializados
Os resultados satildeo importantes para uma escolha mais consciente por parte dos
indiviacuteduos entre tomar paracetamol ou ibuprofeno apoacutes uma cirurgia de um 3ordm molar Eacute
afirmado na discussatildeo deste estudo que o ibuprofeno possui menores efeitos adversos
gastrointestinais que outros NSAIDrsquos Tendo isso em conta pode conduzir a uma
escolha deste composto no tratamento da dor poacutes ciruacutergica por parte dos profissionais
ldquothese findings support a recommendation for this agent as an analgesic of choice for
the treatment of post-operative dental painrdquo A preocupaccedilatildeo pela comunidade em geral
estaacute impliacutecita neste aspecto se possuir menores efeitos secundaacuterios e benefiacutecio superior
eacute melhor para a populaccedilatildeo em geral O custo financeiro destes medicamentos natildeo se
traduz num ponto diferenciador visto que em Portugal existem geneacutericos de ambos
Eacute uma boa base de comparaccedilatildeo entre o paracetamol e ibuprofeno em muitos
aspectos Na procura da melhor evidecircncia e no sentido de a aplicar eacute importante
completar este estudo com outros que nomeadamente se foquem nos efeitos
secundaacuterios
47
An investigation into the comparative efficacy of soluble aspirin
and solid paracetamol in postoperative pain after third molar
surgery Seymour Hawkesford (22)
1 Did the study ask a clearly-focused question
Sim O estudo em questatildeo trata-se de um ensaio cliacutenico aleatorizado duplamente
cego e controlado por placebo O seu objectivo central eacute comparar a eficaacutecia da aspirina
soluacutevel agrave do paracetamol soacutelido em pacientes com dor poacutes-operatoacuteria apoacutes extracccedilatildeo do
3ordm molar Foi utilizado um grupo placebo como controlo negativo
Soacute foram incluiacutedos pacientes que necessitavam da extracccedilatildeo do 3ordm molar
saudaacuteveis segundo categoria 1 da American Society of Anaesthesiologists (ASA I) ou agrave
discriccedilatildeo do cirurgiatildeo oral categoria 2 Soacute foram abrangidos pacientes que atingiram o
limiar de dor necessaacuterio ou que requeriram analgeacutesicos ateacute 90 minutos apoacutes a cirurgia
Cada paciente incluiacutedo no estudo foi colocado num dos trecircs grupos de
tratamento
Grupo 1 Aspirina soluacutevel 900mg dose uacutenica
Grupo 2 paracetamol soacutelido 1000mg dose uacutenica
Grupo 3 placebo dose uacutenica
Foi utilizado o meacutetodo de double-dummy ndash assim cada grupo recebeu o seu tipo
de tratamento e um placebo do tratamento alternativo No caso do grupo 3 os pacientes
receberam placebos para os dois tipos de tratamento
Os outcomes passaram pela
Comparaccedilatildeo de medidas de intensidade da dor atraveacutes da escala VAS (mm)
entre os grupos de tratamento aos 10 15 20 e 30 minutos apoacutes a dosagem
inicial
Comparaccedilatildeo da AUC240 com recurso a anaacutelise de co-variacircncia usando o
centro do estudo geacutenero baseline pain intensity duraccedilatildeo da cirurgia e
nuacutemero de molares removidos como co-variaacuteveis
Necessidade de recurso a rescue medication
Impressatildeo geral dos pacientes e enfermeiros sobre a medicaccedilatildeo atraveacutes de
uma regressatildeo binomial logiacutestica (em que um resultado positivo se refere a
uma avaliaccedilatildeo ldquomuito boardquo ou ldquoboardquo)
As comparaccedilotildees feitas foram aspirina vs paracetamol e aspirina vs placebo
48
2 Was this a randomised controlled trial (RCT) and was it appropriately so
Sim O estudo apresentado eacute um RCT por vaacuterias razotildees sendo a mais relevante a
aleatorizaccedilatildeo dos grupos de tratamento em que os pacientes incluiacutedos foram
distribuiacutedos com a mesma probabilidade e aleatoriamente para cada grupo de estudo Os
grupos de tratamento tecircm tamanhos semelhantes e satildeo homogeacuteneos e os pacientes
foram seguidos de forma semelhante - as uacutenicas diferenccedilas residem no tratamento
oferecido
A utilizaccedilatildeo deste tipo de estudo foi loacutegica Um ensaio cliacutenico aleatorizado eacute
ideal para comparar efeitos de determinadas intervenccedilotildees e consequentemente ideal
para comparar eficaacutecia entre medicamentos
3 Were participants appropriately allocated to intervention and control groups
Foi realizada uma alocaccedilatildeo aleatoacuteria dos pacientes incluiacutedos assim como uma
aleatorizaccedilatildeo por blocos de cinco para assegurar equiliacutebrio entre grupos de tratamento
ldquoA key advantage of blocked randomization is that treatment groups will be equal in
size and will tend to be uniformly distributed by key outcome-related characteristicsrdquo
(43)
Foi ainda efectuada uma aleatorizaccedilatildeo estratificada por geacutenero de modo a
equilibrar nos trecircs grupos o nuacutemero de mulheres e homens e aumentar a credibilidade
das comparaccedilotildees entre os mesmos (proporccedilatildeo MF 21)
Tabela 2 ndash Dados demograacuteficos dos pacientes do estudo
Variaacutevel Aspirina soluacutevel
900mg
Paracetamol soacutelido
1000 mg
Placebo
Nuacutemero de pacientes 59 62 32
Raacutecio geacutenero MF 1940 1943 1121
Todos os pacientes incluiacutedos receberam anestesia de acordo com a praacutetica
cliacutenica a extracccedilatildeo dos molares impactados foi realizada seguindo a teacutecnica standard
Estes factores contribuem para a semelhanccedila da forma de tratamento dos 3 grupos Com
estes aspectos em comum a todos os pacientes incluiacutedos em adiccedilatildeo agrave homogeneidade
dos grupos nos seus aspectos demograacuteficos diferenccedilas encontradas nos resultados satildeo
consequecircncias de outros factores
49
4 Were participants staff and study personnel lsquoblindrsquo to participantsrsquo study
group
Sim A administraccedilatildeo uacutenica tem a vantagem de natildeo requerer monitorizaccedilatildeo de
um processo ldquodelicadordquo por parte do paciente De facto todo o estudo eacute realizado num
periacuteodo de 4 horas apoacutes a cirurgia e com ajuda de enfermeiros Olhando do ponto de
vista do paciente pode-se consideraacute-lo cego
Se os meacutetodos foram realmente aleatoacuterios o investigador eacute tambeacutem considerado
cego e pode-se afirmar que foram feitos esforccedilos necessaacuterios para o alcanccedilar Tanto a
aspirina soluacutevel como o placebo foram oferecidos sob a forma de uma bebida cor-de-
laranja o paracetamol com substacircncia activa e placebo oferecidos como comprimidos
5 Were all of the participants who entered the trial accounted for at its
conclusion
Sim Inicialmente todos os pacientes tinham a mesma probabilidade de serem
incluiacutedos num dos trecircs grupos A distribuiccedilatildeo sendo aleatoacuteria natildeo soacute coloca um
paciente num determinado grupo de tratamento como impossibilita que o mesmo venha
a pertencer a outro O seguimento foi realizado de igual forma para todos os grupos e
intimamente controlado Os resultados foram apresentados separadamente para cada
grupo Dos 167 pacientes foram medicados 153 Dos 14 pacientes natildeo tratados 10 natildeo
desenvolveram dor suficiente para serem incluiacutedos 1 obteve uma reacccedilatildeo adversa agrave
anestesia e 1 natildeo seguiu o protocolo
O grupo da aspirina soluacutevel apresentou melhores resultados que o grupo do
paracetamol e do placebo na medida em que os pacientes reportaram menos dor
apresentou menor intensidade de dor (aos 10 e 30 minutes em comparaccedilatildeo ao
paracetamol e apenas 30 minutos face ao placebo) e os valores de dor global medidos
pela AUC240 foram significativamente menores
6 Were the participants in all groups followed up and data collected in the same
way
Sim A intensidade da dor foi medida frequentemente ao longo de 4 horas
(segundo a VAS) e os pacientes foram informados da possibilidade de tomar medicaccedilatildeo
adicional se necessaacuterio A avaliaccedilatildeo sobre o tratamento dos enfermeiros e dos proacuteprios
pacientes foi tida em consideraccedilatildeo para os resultados
50
Aleacutem disso ao longo do periacuteodo de investigaccedilatildeo a enfermeira do estudo ficou
responsaacutevel por monitorizar os pacientes e registar a ocorrecircncia de quaisquer eventos
adversos Deste modo eacute muito provaacutevel que todos os pacientes tenham recebido o
mesmo niacutevel de atenccedilatildeo
7 Did the study have enough participants to minimise the play of chance
Natildeo eacute possiacutevel dizer No estudo natildeo eacute referida a utilizaccedilatildeo de power calculations
ou outros meacutetodos para determinar o tamanho da amostra Apenas se pode concluir que
o grupo de controlo negativo tem um menor nuacutemero de pacientes consequecircncia de
desistecircncias ou pelo simples facto de agrave partida se conhecerem os resultados
8 How are the results presented and what is the main result
A intensidade da dor foi medida numa escala VAS aos 10 15 20 e 30 minutos
apoacutes a administraccedilatildeo Foi possiacutevel tirar vaacuterias conclusotildees a partir da observaccedilatildeo dos
resultados
A aspirina demonstrou ser significativamente mais eficaz que o paracetamol ou
placebo embora ateacute aos 15 minutos natildeo seja uma diferenccedila muito expressiva
Relativamente agrave AUC240 experiecircncia global da dor no periacuteodo de 4 horas da
investigaccedilatildeo esta foi significativamente menor para o grupo 1
Natildeo existiu diferenccedila significativa entre os grupos no que diz respeito agrave rescue
medication utilizada No entanto o tempo para a administraccedilatildeo da mesma foi
superior no grupo 1 e 2 em relaccedilatildeo ao grupo placebo
Em relaccedilatildeo agrave impressatildeo global natildeo haacute discrepacircncias consideraacuteveis entre grupo 1
e 2 no que diz respeito agrave percentagem de outcomes positivos (58 e 53
respectivamente) O grupo 3 apresentou apenas 31 de outcomes positivos
A tabela com a percentagem de pacientes que desenvolveram efeitos adversos
para cada grupo mostra que 41 dos pacientes apresentaram efeitos secundaacuterios
nos grupos com tratamento activo no entanto muitos destes estavam
relacionados com o procedimento ciruacutergico
A aspirina soluacutevel 900mg providencia uma analgesia mais significante e raacutepida
que o paracetamol 1000mg no periacuteodo imediato apoacutes a cirurgia do 3ordm molar embora natildeo
seja muito expressiva a percepccedilatildeo desta diferenccedila por parte dos pacientes e enfermeiros
51
9 How precise are these results
Os resultados satildeo precisos e apresentados atraveacutes de um intervalo de confianccedila
de 95 satildeo tambeacutem apresentados valores de p
Os valores de p satildeo menores que 005 excepto aos 10 e 15 minutos
Para a intensidade da dor ao longo dos 30 minutos e AUC240 da comparaccedilatildeo
aspirina vs placebo a intervenccedilatildeo utilizada seria a mesma tanto no limite superior
como no inferior excepto aos 10 e 15 minutos Na comparaccedilatildeo aspirina soluacutevel vs
paracetamol soacutelido a decisatildeo seria a mesma independentemente dos limites do intervalo
apenas para os minutos 10 20 e 30
O mesmo aconteceria para a medicaccedilatildeo de recurso (outcome C) e a avaliaccedilatildeo do
tratamento por parte dos pacientes e enfermeiros (outcome D)
Pelo intervalo de confianccedila estar presente e pelo facto de os valores de p serem
bastante reduzidos os resultados satildeo precisos ao ponto de ajudarem a suportar uma
decisatildeo
10 Were all important outcomes considered so the results can be applied
Sim Os pacientes incluiacutedos no estudo o local e o tratamento visados no mesmo
poderiam ser extrapulados e aplicados noutro ambiente O seguimento dos pacientes
durante 4 horas e com ajuda de enfermeiros natildeo se apresenta como muito viaacutevel mas
ainda assim eacute exequiacutevel e seguro
O estudo avalia dados importantes para os profissionais de sauacutede ao afirmar que
a dose (900mg) e a forma (soluacutevel) em que a aspirina eacute tomada conduz a um poder
analgeacutesico superior que o paracetamol No entanto em termos individuais e de poliacuteticas
de sauacutede os efeitos secundaacuterios consequentes da medicaccedilatildeo (excluindo os que se
relacionassem com a cirurgia) deveriam ser completados com estudos suplementares
Segundo este ensaio cliacutenico a incidecircncia de efeitos secundaacuterios natildeo eacute muito
dissemelhante entre aspirina soluacutevel e paracetamol soacutelido nas doses maacuteximas
recomendadas e nestas circunstacircncias a aspirina tem maior poder analgeacutesico Por este
prisma a praacutetica cliacutenica poderia passar pela prescriccedilatildeo de aspirina soluacutevel 900mg para
aliacutevio dor poacutes-operatoacuteria da extracccedilatildeo do terceiro molar Poreacutem eacute necessaacuterio ter em
conta que visa somente a dor nas primeiras quatro horas poacutes-operatoacuterias sendo
importante investigar alternativas eficazes que sejam mais duradouras ou a eficaacutecia e
efeitos secundaacuterios de repetir este tratamento apoacutes as quatro horas iniciais
52
DISCUSSAtildeO
A partir da anaacutelise feita das revisotildees sistemaacuteticas de Weil (19) e de Barden (23)
conclui-se que o paracetamol eacute uma analgeacutesico seguro e eficaz no tratamento da dor
relativa agrave exodontia de terceiros molares pois apresenta um benefiacutecio estatisticamente
significativo quando comparado a placebo Ambas consideram que os melhores valores
de aliacutevio de dor e da diminuiccedilatildeo da intensidade da mesma satildeo alcanccedilados agraves 4 e 6 horas
apoacutes ingestatildeo do faacutermaco
Com base na primeira revisatildeo acima referida o paracetamol exibe uma dose
uacutenica oacuteptima de 1000mg e um periacuteodo de medicaccedilatildeo apropriado de 8 em 8 horas A
maioria dos artigos incluiacutedos apresenta um risco de vieacutes moderado causado
principalmente pela falta de informaccedilatildeo sobre o mecanismo de alocaccedilatildeo de pacientes
podendo levar a uma descredibilidade dos resultados (36)
Na revisatildeo de Barden (23) a comparaccedilatildeo entre os diferentes NSAIDrsquos
demonstrou que este tipo de faacutermacos e particularmente os inibidores da COX-2
exibem os melhores valores de NNT Atraveacutes de uma comparaccedilatildeo indirecta entre
ibuprofeno vs paracetamol os vaacuterios estudos mostraram que o ibuprofeno apresenta
melhores resultados na analgesia da dor poacutes-operatoacuteria (44)
Os estudos de Seymour (22) de Haglund (25) e de Daniels (33) comparam
diferentes compostos activos a um placebo onde o paracetamol estaacute sempre presente
Todos comprovam que enquanto analgeacutesico apresenta uma eficaacutecia largamente
significativa em termos de aliacutevio da dor (usando a escala VAS) Pelo menos 50 dos
indiviacuteduos incluiacutedos que receberam este faacutermaco avaliaram globalmente o tratamento de
forma positiva Poreacutem todos os artigos que
1 Comparam este composto a outro nomeadamente NSAIDrsquos mostram que estes
tecircm uma eficaacutecia significativamente superior agrave do paracetamol tanto em relaccedilatildeo
a valores mais baixos na escala VAS como subjectivamente na avaliaccedilatildeo global
Cerca de 80 dos indiviacuteduos que tomaram NSAIDrsquos classificaram o tratamento
positivamente (agrave excepccedilatildeo dos estudos (32) e (22)) Reportam ainda os efeitos
adversos mais comuns como tonturas naacuteuseas cefaleia e sonolecircncia que
embora de gravidade reduzida tecircm uma incidecircncia superior no paracetamol que
na aspirina e ibuprofeno
53
2 Combinam o paracetamol com NSAIDrsquos provam o efeito aditivo daquele bem
como o facto de estas combinaccedilotildees serem mais eficazes que qualquer um dos
faacutermacos em separado (Merry (13) e Haglund (25))
De acordo com os estudos analisados os NSAIDrsquos aparentam ser uma escolha
preferencial face ao paracetamol porque apresentam uma maior eficaacutecia no aliacutevio da dor
apoacutes extracccedilatildeo de terceiros molares embora disponham de propriedades anti-
inflamatoacuterias notoacuterias (e pertinentes no sucesso do tratamento poacutes-operatoacuterio)
O mecanismo de acccedilatildeo do paracetamol necessita de investigaccedilatildeo adicional que
permita uma melhor compreensatildeo e que traga novas respostas na praacutetica cliacutenica Como
aspecto positivo eacute de acrescentar que natildeo existem diferenccedilas estatisticamente
significantes entre o paracetamol e placebo no que diz respeito a efeitos secundaacuterios
(baixo grau de severidade) podendo ser considerado um composto seguro
A revisatildeo de Barden (23) indica que os resultados da eficaacutecia dos NSAIDrsquos
podem atrair os cliacutenicos a aumentar a sua prescriccedilatildeo sem terem em atenccedilatildeo a sua
relaccedilatildeo com o aumento dos efeitos adversos Isto eacute uma situaccedilatildeo insustentaacutevel na
medida em que nas uacuteltimas duas deacutecadas alguns destes medicamentos foram retirados
do mercado devido a eventos adversos graves posteriormente descobertos Um exemplo
eacute o caso do rofecoxib e valdecoxib que produziram acidentes cardiovasculares seacuterios
provavelmente consequentes da dosagem e natildeo da sua selectividade para a COX-2
(25))
Os efeitos adversos satildeo um motivo de peso para que os pacientes deixem de
tomar determinada substacircncia ou sejam incapazes de tolerar uma dose eficaz da mesma
Informaccedilotildees complementares que englobassem este aspecto seriam ideais e exequiacuteveis
se os autores de ensaios cliacutenicos lhes dessem maior relevo (45)
Outros dados - como custo financeiro e disponibilidade no mercado - poderiam
ser um auxiacutelio na selecccedilatildeo entre paracetamol e outros medicamentos Eacute de ressalvar
que em Portugal os geneacutericos vieram a baixar os preccedilos de analgeacutesicos e NSAIDrsquos
Medicamentos agrave base de ibuprofeno satildeo dos mais dispendiosos (46)
Os NSAIDrsquos tecircm um problema adicional relacionado com a hemostase ndash inibir a
produccedilatildeo de tromboxano A2 e consequentemente aumentar o risco de hemorragia
prolongada (11) No entanto estes efeitos secundaacuterios estatildeo directamente relacionados
com a dosagem pelo que apenas eacute relevante considerar este aspecto em paciente com
problemas de coagulaccedilatildeo
54
Conclui-se que embora a toma de paracetamol seja um procedimento seguro e
eficaz existem no mercado compostos com igual seguranccedila e eficaacutecia superior Apesar
de os inibidores da COX-2 serem os compostos mais eficazes abarcam os efeitos
secundaacuterios mais graves pelo que a realizaccedilatildeo de estudos adicionais eacute imperativo no
sentido de colmatar esta falha
55
RESPOSTA AO PACIENTE
ldquoTendo em conta a evidecircncia cientiacutefica disponiacutevel sobre este assunto e
considerando que natildeo tem problemas gaacutestricos ou de coagulaccedilatildeo sanguiacutenea recomendo
que tome 1g de paracetamol de 8 em 8 horas pois eacute bastante eficaz no aliacutevio da dor
Poreacutem existem outras opccedilotildees como por exemplo combinar o paracetamol a 200mg de
ibuprofeno pode ainda apenas tomar o paracetamol e se sentir necessidade recorrer ao
ibuprofeno 400mg no maacuteximo trecircs vezes ao dia
Tanto o paracetamol como o ibuprofeno tecircm poucos efeitos secundaacuterios e os
mais frequentes satildeo de baixo grau de gravidade Embora existam outros medicamentos
mais eficazes na eliminaccedilatildeo da dor estes tecircm efeitos secundaacuterios mais graves que natildeo
justificam a sua utilizaccedilatildeo
56
REFEREcircNCIAS BIBLIOGRAacuteFICAS
1 Barden J Edwards JE McQuay HJ Andrew Moore R Pain and analgesic
response after third molar extraction and other postsurgical pain Pain 2004107(1-
2)86-90 Epub 20040113
2 Cooper SA Desjardins PJ The value of the dental impaction pain model in drug
development Methods in molecular biology (Clifton NJ) 2010617175-90 Epub
20100326
3 NICE Guidance on the Extraction of Wisdom Teeth2000 13 December 2011
Available from httppublicationsniceorgukguidance-on-the-extraction-of-wisdom-
teeth-ta1clinical-need-and-practice
4 Mettes Dirk TG Nienhuijs Marloes MEL van der Sanden Wil JM Verdonschot
Emiel H Plasschaert A Interventions for treating asymptomatic impacted wisdom teeth
in adolescents and adults Cochrane Database of Systematic Reviews [Internet] 2005
(2) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD003879frameht
ml
5 Seymour RA Use of analgesics in postoperative dental pain a review Journal
of the Royal Society of Medicine 198477(11)949-54 Epub 19841101
6 Berg JM Tymoczko JL Stryer L Biochemistry 5 ed W H Freeman 2002
1050 p
7 Nelson DL Cox MM Lehninger Principles of Biochemistry 5 ed W H
Freeman 2005 1119 p
8 Sciulli MG Capone ML Tacconelli S Patrignani P The future of traditional
nonsteroidal antiinflammatory drugs and cyclooxygenase-2 inhibitors in the treatment
of inflammation and pain Pharmacological reports PR 200557 Suppl66-85 Epub
20060118
9 Devlin TD Devlins Textbook of Biochemistry 6 ed Hoboken NJ Wiley
2006 1208 p
10 Katzung BG Basical and Clinical Pharmacology 10 ed McGraw-Hill 2006
11 Naclerio-Homem Mg Fau - Deboni MCZ Deboni Mc Fau - Rapoport A
Rapoport A Fau - Chin VKL Chin VK Effects of ketoprofen and diclofenac potassium
on blood coagulation tests after removal of third molars (1936-7163 (Electronic))
57
12 Toms L McQuay H Derry S Moore R Single dose oral paracetamol
(acetaminophen) for post-operative pain in adults Cochrane Database of Systematic
Reviews 2008(4)
13 Merry AF Gibbs RD Edwards J Ting GS Frampton C Davies E et al
Combined acetaminophen and ibuprofen for pain relief after oral surgery in adults a
randomized controlled trial British journal of anaesthesia 2010104(1)80-8 Epub
20091217
14 Derry C Derry S Moore R McQuay H Single Dose Oral Ibuprofen for Acute
Post-Operative Pain in Adults Cochrane Database of Systematic Reviews 2009(3)
15 Rang HP Dale MM Ritter JM Moore PK Farmacologia 5 ed Elsevier 2003
Elsevier p
16 Scopel E Alencar M Cruz RM Medidas de avaliaccedilatildeo da dor efdeportes
2007(105)
17 Mata AD Marques D Silveira J Marques J Medicina Dentaacuteria Baseada na
Evidecircncia Novas Opccedilotildees para Velhas Praacuteticas Rev Port Estomatol Cir Maxilofac
200849(1)31-7
18 CASP UK [13 Dezembro 2011] Available from httpwwwcasp-
uknetabout-caspabout-casp
19 Weil K Hooper L Afzal Z Esposito M Worthington Helen V van Wijk A et
al Paracetamol for pain relief after surgical removal of lower wisdom teeth Cochrane
Database of Systematic Reviews [Internet] 2007 (3) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD004487frameht
ml
20 Toms L Derry S Moore RA McQuay Henry J Single dose oral paracetamol
(acetaminophen) with codeine for postoperative pain in adults Cochrane Database of
Systematic Reviews [Internet] 2009 (1) Available from
httpwwwmrwintersciencewileycomcochraneclsysrevarticlesCD001547frameht
ml
21 Derry S Wiffen PJ Moore RA Relative efficacy of oral analgesics after third
molar extraction - a 2011 update Br Dent J 2011211(9)419-20
22 Seymour RA Hawkesford JE Sykes J Stillings M Hill CM An investigation
into the comparative efficacy of soluble aspirin and solid paracetamol in postoperative
pain after third molar surgery Br Dent J 2003194(3)153-7
58
23 Barden J Edwards JE McQuay HJ Wiffen PJ Moore RA Relative efficacy of
oral analgesics after third molar extraction Br Dent J 2004197(7)407-11
24 Saska S Scartezini GR Souza RFd Hochuli-Vieira E Pereira Filho VA
Gabrielli MAC Cloridrato de tramadolparacetamol no controle da dor poacutes-operatoacuteria
em cirurgias de terceiros molares inclusos
Tramadolacetaminophen in the control of postoperative pain for impacted third molar
surgery Rev cir traumatol buco-maxilo-fac 20099(4)
25 Haglund B von Bultzingslowen I Combining paracetamol with a selective
cyclooxygenase-2 inhibitor for acute pain relief after third molar surgery a randomized
double-blind placebo-controlled study European journal of oral sciences
2006114(4)293-301 Epub 20060817
26 Kubitzek F Ziegler G Gold MS Liu JM Ionescu E Analgesic efficacy of low-
dose diclofenac versus paracetamol and placebo in postoperative dental pain Journal of
orofacial pain 200317(3)237-44 Epub 20031003
27 Bjornsson GA Haanaes HR Skoglund LA A randomized double-blind
crossover trial of paracetamol 1000 mg four times daily vs ibuprofen 600 mg effect on
swelling and other postoperative events after third molar surgery British journal of
clinical pharmacology 200355(4)405-12 Epub 20030419
28 Macleod AG Ashford B Voltz M Williams B Cramond T Gorta L et al
Paracetamol versus paracetamol-codeine in the treatment of post-operative dental pain
a randomized double-blind prospective trial Australian dental journal
200247(2)147-51 Epub 20020726
29 Bjornsson GA Haanaes HR Skoglund LA Ketoprofen 75 mg qid versus
acetaminophen 1000 mg qid for 3 days on swelling pain and other postoperative events
after third-molar surgery Journal of clinical pharmacology 200343(3)305-14 Epub
20030318
30 Chopra D Rehan HS Mehra P Kakkar AK A randomized double-blind
placebo-controlled study comparing the efficacy and safety of paracetamol
serratiopeptidase ibuprofen and betamethasone using the dental impaction pain model
International journal of oral and maxillofacial surgery 200938(4)350-5 Epub
20090127
31 Dolci G Ripari M Pacifici L Umile A Evaluation of piroxicam-beta-
cyclodextrin piroxicam paracetamol and placebo in post-operative oral surgery pain
59
International journal of clinical pharmacology research 199414(5-6)185-91 Epub
19940101
32 Noronha VR Gurgel GD Alves LC Noman-Ferreira LC Mendonca LL Aguiar
EG et al Analgesic efficacy of lysine clonixinate paracetamol and dipyrone in lower
third molar extraction a randomized controlled trial Medicina oral patologia oral y
cirugia bucal 200914(8)e411-5 Epub 20090506
33 Daniels S Reader S Berry P Goulder M Onset of analgesia with sodium
ibuprofen ibuprofen acid incorporating poloxamer and acetaminophen--a single-dose
double-blind placebo-controlled study in patients with post-operative dental pain
European journal of clinical pharmacology 200965(4)343-53 Epub 20090303
34 Medve RA Wang J Karim R Tramadol and acetaminophen tablets for dental
pain Anesthesia progress 200148(3)79-81 Epub 20011129
35 Bjornsson GA Haanaes HR Skoglund LA Naproxen 500 mg bid versus
acetaminophen 1000 mg qid effect on swelling and other acute postoperative events
after bilateral third molar surgery Journal of clinical pharmacology 200343(8)849-58
Epub 20030905
36 Marques JF Marques D Silveira J Mata AD Revisotildees Sistemaacuteticas o que satildeo
e para que servem Rev Port Estomatol Cir Maxilofac 200849(3)171-8
37 Rodrigues CL Ziegelmann PK Meta-anaacuteliseum guia praacutetico HCPA
201030(4)436-47
38 Alderson P Absence of evidence is not evidence of absence Bmj
2004328(7438)476-7
39 Berwanger O Suzumura EA Buehler AM Oliveira JB Como Avaliar
Criticamente Revisotildees Sistemaacuteticas e Meta-anaacutelises Revista Brasileira de Terapia
Intensiva 200719(4)475-80
40 Noordzij M Zoccali C Dekker FW Jager KJ Adding up the evidence
systematic reviews and meta-analyses Nephron Clinical practice 2011119(4)c310-6
Epub 20111203
41 Sibbald B Roland M Understanding controlled trials Why are randomised
controlled trials important Bmj 1998316(7126)201
42 Primer on Statistical Significance and P Values Effective Clinical Practice
20014(4)183-4
43 Efird J Blocked randomization with randomly selected block sizes International
journal of environmental research and public health 20118(1)15-20 Epub 20110215
60
44 Cooper S Schachtel B Goldman E Gelb S Cohn P Ibuprofen and
acetaminophen in the relief of acute pain a randomized double blind placebo
controlled study The Journal of Clinical Pharmacology 198929(11)1026-30
45 Edwards JE McQuay HJ Moore RA Collins SL Reporting of Adverse Effects
in Clinical Trials Should Be Improved Lessons from Acute Postoperative Pain Journal
of pain and symptom management 199918(6)427-37
46 Faacutermaco mais vendido versus mais barato Deco Proteste [updated Julho
200919 Dezembro 2011] Available from httpwwwdecoprotesteptservicos-de-
saudefarmaco-mais-vendido-versus-mais-barato-s568081htm
61
ANEXOS
ANEXO A ndash TABELA DE CARACTERIacuteSTICAS DE ARTIGOS EXCLUIacuteDOS
Artigo Fonte Classificaccedilatildeo
inicial Motivo de Exclusatildeo
Toms Derry (20) Cochrane
Library
Possivelmente
Adequado
Natildeo eacute um estudo sobre
extracccedilatildeo de terceiros molares
Saska Scartezini
(24) LILACS
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (27) PubMed Adequado
Estudo natildeo se foca na dor poacutes-
operatoacuteria
Kubitzek Ziegler
(26) PubMed Adequado Artigo natildeo disponiacutevel
Macleod
Ashford (28) PubMed Adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (29) PubMed
Possivelmente
adequado Artigo natildeo disponiacutevel
Chopra Rehan
(30) PubMed
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Dolci Ripari (31) PubMed Possivelmente
adequado Artigo natildeo disponiacutevel
Medve Wang
(34) PubMed
Possivelmente
adequado
Estudo natildeo visa o tipo de
intervenccedilatildeo considerada
Bjornsson
Haanaes (35) PubMed
Possivelmente
adequado Artigo natildeo disponiacutevel
62
ANEXO B ndash ARTIGOS INCLUIacuteDOS EM FORMATO
INTEGRALi
i Nota os seguintes artigos estatildeo paginados fora do contexto deste trabalho de acordo com a sua
paginaccedilatildeo original
Paracetamol for pain relief after surgical removal of lower
wisdom teeth (Review)
Weil K Hooper L Afzal Z Esposito M Worthington HV van Wijk A Coulthard P
This is a reprint of a Cochrane review prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2008 Issue 4
httpwwwthecochranelibrarycom
Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
T A B L E O F C O N T E N T S
1HEADER
1ABSTRACT
2PLAIN LANGUAGE SUMMARY
2BACKGROUND
3OBJECTIVES
3METHODS
5RESULTS
8DISCUSSION
9AUTHORSrsquo CONCLUSIONS
9ACKNOWLEDGEMENTS
10REFERENCES
13CHARACTERISTICS OF STUDIES
30DATA AND ANALYSES
Analysis 11 Comparison 1 50 pain relief using pain relief measures Outcome 1 Paracetamol versus placebo number of
people with at least 50 pain relief at 4 hours 31
Analysis 12 Comparison 1 50 pain relief using pain relief measures Outcome 2 Paracetamol versus placebo number of
people with at least 50 pain relief at 6 hours 33
Analysis 21 Comparison 2 50 pain relief using pain intensity measures Outcome 1 Paracetamol versus placebo number
of people with at least 50 pain relief at 4 hours 34
Analysis 22 Comparison 2 50 pain relief using pain intensity measures Outcome 2 Paracetamol versus placebo number
of people with at least 50 pain relief at 6 hours 35
Analysis 31 Comparison 3 Number of people with adverse events Outcome 1 Number of patients with adverse events
paracetamol versus placebo 37
38ADDITIONAL TABLES
42APPENDICES
43WHATrsquoS NEW
43HISTORY
43CONTRIBUTIONS OF AUTHORS
43DECLARATIONS OF INTEREST
44SOURCES OF SUPPORT
44INDEX TERMS
iParacetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
[Intervention Review]
Paracetamol for pain relief after surgical removal of lowerwisdom teeth
Kiaran Weil1 Lee Hooper2 Zahid Afzal3 Marco Esposito1 Helen V Worthington4 Arjen van Wijk5 Paul Coulthard1
1Department of Oral and Maxillofacial Surgery School of Dentistry The University of Manchester Manchester UK 2School of
Medicine Health Policy amp Practice University of East Anglia Norwich UK 3Oral and Maxillofacial Surgery City Hospital Birming-
ham UK 4Cochrane Oral Health Group MANDEC School of Dentistry The University of Manchester Manchester UK 5Social
Dentistry and Behavioural Sciences ACTA Amsterdam Netherlands
Contact address Kiaran Weil Department of Oral and Maxillofacial Surgery School of Dentistry The University of Manchester
Higher Cambridge Street Manchester M15 6FH UK kiaran_weilhotmailcom
Editorial group Cochrane Oral Health Group
Publication status and date Edited (no change to conclusions) published in Issue 4 2008
Review content assessed as up-to-date 21 May 2007
Citation Weil K Hooper L Afzal Z Esposito M Worthington HV van Wijk A Coulthard P Paracetamol for pain relief af-
ter surgical removal of lower wisdom teeth Cochrane Database of Systematic Reviews 2007 Issue 3 Art No CD004487 DOI
10100214651858CD004487pub2
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Paracetamol has been commonly used for the relief of postoperative pain following oral surgery In this review we investigated the
optimal dose of paracetamol and the optimal time for drug administration to provide pain relief taking into account the side effects
of different doses of the drug This will inform dentists and their patients of the best strategy for pain relief after the surgical removal
of wisdom teeth
Objectives
To assess the beneficial and harmful effects of paracetamol for pain relief after surgical removal of lower wisdom teeth compared to
placebo at different doses and administered postoperatively
Search strategy
We searched the Cochrane Oral Health Grouprsquos Trials Register the Cochrane Pain Palliative and Supportive Care Grouprsquos Trials Register
CENTRAL MEDLINE EMBASE and the Current Controlled Trials Register Handsearching included several dental journals We
checked the bibliographies of relevant clinical trials and review articles for studies outside the handsearched journals We wrote to
authors of the identified randomised controlled trials (RCTs) to manufacturers of analgesic pharmaceuticals we searched personal
references in an attempt to identify unpublished or ongoing RCTs No language restriction was applied The last electronic search was
conducted on 24th August 2006
Selection criteria
Randomised parallel group placebo controlled double blind clinical trials of paracetamol for acute pain following third molar surgery
Data collection and analysis
All trials identified were scanned independently and in duplicate by two review authors any disagreements were resolved by discussion
or if necessary a third review author was consulted The proportion of patients with at least 50 pain relief was calculated for both
paracetamol and placebo The number of patients experiencing adverse events andor the total number of adverse events reported were
analysed
1Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Main results
Twenty-one trials met the inclusion criteria A total of 2048 patients were initially enrolled in the trials (1148 received paracetamol
and 892 the placebo) and of these 1968 (96) were included in the meta-analysis (1133 received paracetamol and 835 the placebo)
Paracetamol provided a statistically significant benefit when compared with placebo for pain relief and pain intensity at both 4 and 6
hours Most studies were found to have moderate risk of bias with poorly reported allocation concealment being the main problem
Risk ratio values for pain relief at 4 hours 285 (95 confidence interval (CI) 189 to 429) and at 6 hours 332 (95 CI 188 to 587)
A statistically significant benefit was also found between up to 1000 mg and 1000 mg doses the higher the dose giving greater benefit
for each measure at both time points There was no statistically significant difference between the number of patients who reported
adverse events overall this being 19 in the paracetamol group and 16 in the placebo group
Authorsrsquo conclusions
Paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom teeth
P L A I N L A N G U A G E S U M M A R Y
Paracetamol for pain relief after surgical removal of lower wisdom teeth
The surgical removal of wisdom teeth (third molars) is the most commonly performed surgical procedure undertaken in oral surgery
practice Postoperative complications may include swelling bruising and limited mouth opening but patients are most often concerned
about postoperative pain which may be severe Paracetamol is effective in relieving pain with a low incidence of adverse effects It is one
of the most commonly used analgesics and is widely available without prescription around the world In this review we investigated the
optimal dose of paracetamol and the optimal time for drug administration to provide pain relief after the surgical removal of wisdom
teeth The side effects of different doses of the drug were also explored
Twenty-one trials (with over 2000 participants) were included Paracetamol provided a statistically significant benefit when compared
with placebo for pain relief at both 4 and 6 hours after taking the drug It is most effective at 1000 mg dose and can be taken at six
hourly intervals without compromising safety There was no statistically significant difference between the number of patients who
reported adverse events overall this being 19 in the paracetamol group and 16 in the placebo group It should be noted that most
of the studies were found to have some limitations mainly due to poor reporting of information However the review concludes that
paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom teeth
B A C K G R O U N D
The surgical removal of wisdom teeth is the most commonly per-
formed surgical procedure undertaken in oral surgery practice
Postoperative complications may include swelling bruising and
limited mouth opening but patients are most often concerned
about postoperative pain which may be severe The pain ex-
perienced after oral surgery is a validated and widely used pain
model for the clinical evaluation of analgesic efficacy (Cooper
1976) Tissue damage produced during surgery releases chemicals
that initiate inflammatory pain by activating and sensitising nerve
fibre receptors (Loeser 1999) Chemicals include bradykinin
prostaglandins serotonin and histamine (Dray 1997)
Paracetamol (acetaminophen) is a nonopioid analgesic possessing
antipyretic activity and is effective in relieving pain with a low in-
cidence of adverse effects (Moore 1998) It is one of the most com-
monly used analgesics and is widely available without prescription
around the world Paracetamol is often grouped with the nons-
teroidal anti-inflammatory drug (NSAID) family however it is
considered only to have relatively weak anti-inflammatory activity
(Rang 2003) NSAIDs are assumed largely to produce their anal-
gesia as a result of the inhibition of prostaglandin production by
the enzyme cyclo-oxygenase (Malmberg 1992) The mechanism
of action has not been fully understood Among several theories
it has been suggested that paracetamol is a selective inhibitor of
the newly described COX-3 enzyme a cyclo-oxygenase-1 variant
in the central nervous system This inhibition could represent a
primary central mechanism by which paracetamol decreases pain
and possibly fever (Chandrasekharan 2002) Major evidence has
2Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
been accumulated showing that paracetamol inhibits cyclo-oxy-
genase by reducing the higher oxidative state of the cyclo-oxyge-
nase enzyme by reducing oxygen radical co-substrates (Aronoff
2006) Paracetamol has been shown to be an effective analgesic in
the control of postoperative dental pain in a number of clinical
trials (Bentley 1987 Kiersch 1994 Mehlisch 1990) Pain inten-
sity following third molar surgery has been suggested to reach its
maximum between 3 to 5 hours following surgery (Fisher 1988
Seymour 1985) and therefore this pain model is used to test the
efficacy of a single analgesic dose
A recent systematic review (Barden J 2004) has looked at the ef-
ficacy and safety of paracetamol for postoperative pain manage-
ment and has included the findings of studies involving a wide
variety of types of surgery such as gynaecology surgery abdomi-
nal surgery orthopaedic surgery amongst others including the re-
moval of wisdom teeth There is some debate as to whether dental
pain is different from other pain It has been suggested that the
effect of some analgesics including tramadol were worse for dental
pain than for other types of postsurgical pain (Moore 1997)
In this review we investigated the optimal dose of paracetamol and
the optimal time for drug administration to provide pain relief
taking into account the side effects of different doses of the drug
This will inform dentists and their patients of the best strategy for
best pain relief after the surgical removal of wisdom teeth
O B J E C T I V E S
To assess the beneficial and harmful effects of paracetamol for
pain relief after surgical removal of lower wisdom teeth compared
to placebo at different doses and administered preoperatively or
postoperatively
Primary
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between paracetamol and placebo for pain
relief in patients requiring surgical removal of a lower wisdom
tooth or teeth against the alternative hypothesis of a difference
Secondary
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between different doses of paracetamol for
pain relief in patients requiring surgical removal of a lower
wisdom tooth or teeth against the alternative hypothesis of a
difference
bull To test the null hypothesis of no difference in the beneficial
and harmful effects between different times of administration of
paracetamol for pain relief in patients requiring surgical removal
of a lower wisdom tooth or teeth against the alternative
hypothesis of a difference
M E T H O D S
Criteria for considering studies for this review
Types of studies
All randomised controlled double blind clinical trials
Types of participants
Patients of all health states who required the surgical removal of
a lower wisdom tooth and who had at least had a baseline pain
intensity of moderate to severe pain Patients who also required
removal of an additional tooth or teeth were included Surgery
was undertaken under local anaesthesia intravenous sedation or
general anaesthesia Patients taking concurrent analgesia were ex-
cluded
Types of interventions
Efficacy
bull Paracetamol given as a single dose by mouth in any dose
and in any formulation (for example immediate or slow release)
regardless of when the single dose was given (for example
preoperatively or postoperatively)
Side effects
In order to investigate side effects more thoroughly we included
both single and multiple dose studies
bull Paracetamol given up to 7 days by mouth in any dose and
in any formulation (for example immediate or slow release)
regardless of when the first dose was given (for example
preoperatively or postoperatively)
Types of outcome measures
bull Pain intensity (visual analogue scale (VAS) categorical
verbal rating verbal numerical scale global subjective efficacy
ratings and other categorical rating scales)
bull Pain relief (VAS categorical verbal rating verbal numerical
scale global subjective efficacy ratings and other categorical
rating scales) and derived pain relief outcomes extracted will be
3Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
total pain relief (TOTPAR) summed pain intensity difference
(SPID) over 4 and 6 hours
bull Side effects (for example hepatic and renal) (binary)
Search methods for identification of studies
To identify studies for inclusion or consideration in this review a
detailed search strategy was developed for each database searched
These were based on the search strategy developed for MEDLINE
but revised appropriately for each database The search strategy
combined a sensitive search strategy for randomised controlled
trials (RCTs) revised from phases 1 and 2 of the Cochrane Sensi-
tive Search Strategy for RCTs (as published in Appendix 5b in the
Cochrane Handbook for Systematic Reviews of Interventions 426
(updated September 2006)) The subject search used a combina-
tion of controlled vocabulary and free text terms based on the
search strategy for searching CENTRAL (see Appendix 1)
Databases to be searched
The Cochrane Oral Health Grouprsquos Trials Register (to 24th August
2006)
The Cochrane Central Register of Controlled Trials (CENTRAL)
(The Cochrane Library 2006 Issue 3)
The Cochrane Pain Palliative and Supportive Care Grouprsquos Trials
Register (to 24th August 2006)
MEDLINE (1966 to 24th August 2006)
EMBASE (1980 to 25th August 2006)
Current Controlled Trials Register (wwwcontrolled-trialscom)
(to 24th August 2006)
The bibliographies of papers and review articles were checked for
studies outside the handsearched journals Personal references were
also searched
Language
There were no language restrictions and where necessary transla-
tion into the English language of relevant studies was conducted
Unpublished studies
Authors of RCTs identified were written to in order to obtain
further information about the trial and to attempt to identify
unpublished or ongoing studies We also wrote to manufacturers
of analgesic pharmaceuticals
Handsearching
Several journals relevant to this review were handsearched as part
of the Cochrane Oral Health Grouprsquos ongoing journal hand-
searching programme The list of the dental journals hand-
searched by The Cochrane Collaboration can be found at http
wwwohgcochraneorg
Data collection and analysis
The titles and abstracts (when available) of all reports identified
were scanned independently and in duplicate by two review au-
thors For studies appearing to meet the inclusion criteria or for
which there were insufficient data in the title and abstract to make
a clear decision the full report was obtained and assessed indepen-
dently and in duplicate by two review authors to establish whether
the studies met the inclusion criteria or not Disagreements were
resolved by discussion Where resolution was not possible a third
review author was consulted All studies meeting the inclusion
criteria then underwent quality assessment and data extracted
Studies rejected at this or subsequent stages were recorded in the
Characteristics of excluded studies table and reasons for exclusion
were recorded
Quality assessment
The quality assessment of the included trials was undertaken inde-
pendently and in duplicate by two review authors based on what
is written in the articles
Only double blind trials were included in the review so blinding
was not included in the quality assessment
Two main quality criteria were examined
(1) Allocation concealment recorded as
(A) Adequate -2 points
(B) Unclear - 1 point
(C) Inadequate - 0 points
(2) Completeness of follow up (is there a clear explanation for
withdrawals and drop outs in each treatment group) assessed as
(A) Yes - 1 point
(B) No - 0 points
The agreement for the quality criteria between assessors was de-
termined by Kappa statistics
After taking into account the additional information provided by
the authors of the trials studies were grouped into the following
categories
(A) Low risk of bias - 3 points (plausible bias unlikely to seriously
alter the results) if all criteria were met
(B) Moderate or high risk of bias - 0 to 2 points Moderate risk
of bias - plausible bias that raises some doubt about the results if
one or more criteria are partly met (for example when authors
responded that they had made some attempts to conceal the al-
location of patients to give an explanation for withdrawals but
these attempts were not judged to be ideal these criteria were cat-
egorised as rsquopartlyrsquo) High risk of bias - plausible bias that seriously
weakens confidence in the results if one or more criteria were not
met as described in the Cochrane Handbook for Systematic Reviews
of Interventions 426
We also reported whether the authors of included trials have con-
ducted a sample size calculation
4Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Data extraction
Data were extracted by two review authors independently and
in duplicate using specially designed data extraction forms Any
disagreement was discussed and a third review author consulted
where necessary Authors were contacted for clarification of miss-
ing information Data were excluded until further clarification was
available if agreement could not be reached
For each trial the following data were recorded
bull Year of publication country of origin setting and source of
study funding
bull Details of the participants including demographic
characteristics and criteria for inclusion
bull Details on the study design (parallel group or cross-over
design)
bull Details on the type of intervention
bull Details of the outcomes reported including method of
assessment and time intervals
Data synthesis
From the mean total pain relief (TOTPAR) or summed pain in-
tensity difference (SPID) pain indices reported we computed a
dichotomous outcome variable for the number of patients with
at least 50 pain relief according to the methods outlined in a
Cochrane review (Collins 1999) For each of the three objectives
we examined the appropriateness of different continuous outcome
measurements and these were meta-analysed and reported in the
final review
For dichotomous outcomes the estimate of an intervention was
expressed as risk ratios together with 95 confidence intervals
For continuous outcomes mean differences and 95 confidence
intervals were used to summarise the data for each trial
Clinical heterogeneity was assessed by examining the types of par-
ticipants interventions and outcomes in each study Meta-analyses
were conducted only with studies of similar comparisons report-
ing the same outcome measures Risk ratios were used to combine
dichotomous data and mean differences for continuous data us-
ing random-effects models The significance of any discrepancies
in the estimates of the treatment effects from the different trials
was assessed by means of Cochranrsquos test for heterogeneity and any
heterogeneity investigated
Where both visual analogue scale (VAS) and categorical scales were
used to measure pain intensity or pain relief or both the categorical
data were used in the meta-analysis as this was the most frequently
used scale
Subgroup analyses
Subgroup analyses were planned for studies
bull Where patients underwent surgery with local anaesthesia
alone local anaesthesia and intravenous sedation general
anaesthesia alone and general anaesthesia with local anaesthetic
bull Where different types of formulation of paracetamol were
used for instance immediate release versus slow release
bull Where different doses of paracetamol were used (1000 mg
or more and less than 1000 mg)
bull Where time of administration of paracetamol differs
preoperative versus postoperative
bull Where TOTPAR was calculated using pain relief measures
and pain intensity measures
The difference between studies comparing up to 1000 mg doses
with studies comparing 1000 mg or more was examined by per-
forming random-effects metaregression analyses in Stata version
90 (Stata Corporation USA) using the program Metareg
The results of the metaregressions for comparing the two dose
levels up to 1000 mg and 1000 mg or more are presented in
Additional Table 1
R E S U L T S
Description of studies
See Characteristics of included studies Characteristics of excluded
studies
See Characteristics of included studies and Characteristics of
excluded studies tables
Characteristics of the trial setting and investigators
Of the 67 eligible trials 46 were excluded as shown in the ex-
cluded studies section Of the 21 included studies one was con-
ducted in Denmark (Moller 2000) two in Germany (Kubitzek
2003 Lehnert 1990) one in Italy (Dolci 1994) one in Nor-
way (Skoglund 1991) two in Puerto Rico (Olson 2001 Sunshine
1986) one in Thailand (Vattaraphudej 1986) two in the United
Kingdom (Seymour 1996 Seymour 2003) and 11 in the United
States of America (Cooper 1980 Cooper 1981 Cooper 1988
Cooper 1998 Dionne 1994 Forbes 1984b Forbes 1989 Forbes
1990 Hersh 2000 Kiersch 1994 Mehlisch 1995) Six trials
were conducted at university clinics (Cooper 1998 Hersh 2000
Moller 2000 Olson 2001 Sunshine 1986 Vattaraphudej 1986)
five at private practices (Dionne 1994 Forbes 1984b Forbes
1989 Forbes 1990 Kubitzek 2003) seven did not state a set-
ting (Cooper 1981 Dolci 1994 Kiersch 1994 Mehlisch 1995
Seymour 1996 Seymour 2003 Skoglund 1991) One reported a
single site (Cooper 1988) two reported two sites (Forbes 1989
Seymour 2003) and six specifically stated outpatients (Cooper
1980 Cooper 1988 Forbes 1989 Forbes 1990 Hersh 2000
5Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Lehnert 1990) Seventeen trials were sponsored by industry
(Cooper 1981 Cooper 1988 Cooper 1998 Dionne 1994 Forbes
1984b Forbes 1989 Forbes 1990 Hersh 2000 Kiersch 1994
Kubitzek 2003 Lehnert 1990 Mehlisch 1995 Moller 2000
Olson 2001 Seymour 2003 Skoglund 1991 Sunshine 1986)
one by a university grant (Vattaraphudej 1986) and it was unclear
as whether the remaining three trials (Cooper 1980 Dolci 1994
Seymour 1996) were sponsored but it is likely that they were from
correspondence with some of the authors
Characteristics of interventions
All included interventions were randomised parallel group and
double blind Eleven trials used doses of paracetamol of less than
1000 mg (Cooper 1980 Cooper 1981 Cooper 1988 Dionne
1994 Dolci 1994 Forbes 1984b Forbes 1989 Forbes 1990
Seymour 1996 Sunshine 1986 Vattaraphudej 1986) Eleven tri-
als used doses of 1000 mg (Cooper 1998 Hersh 2000 Kiersch
1994 Kubitzek 2003 Lehnert 1990 Mehlisch 1995 Moller
2000 Olson 2001 Seymour 1996 Seymour 2003 Skoglund
1991) One study (Seymour 1996) used both doses Seven tri-
als used paracetamol in tablet form (Dolci 1994 Forbes 1989
Kubitzek 2003 Mehlisch 1995 Moller 2000 Seymour 2003
Skoglund 1991) Seven trials used capsules (Forbes 1984b Forbes
1989 Forbes 1990 Kiersch 1994 Lehnert 1990 Sunshine 1986
Vattaraphudej 1986) Two trials used caplets (Hersh 2000 Olson
2001) and one trial used effervescent tablets (Moller 2000) Five
trials did not state what formulation was used (Cooper 1980
Cooper 1981 Cooper 1988 Cooper 1998 Dionne 1994) All
trials used placebos in the same formulation as the intervention
Characteristics of outcome measures
For all trials it was possible to calculate the number of patients
with at least 50 total pain relief (TOTPAR) at either 4 hours
6 hours or both Pain intensity was measured in all but one trial
(Kubitzek 2003) pain relief was measured in all but two trials
(Kubitzek 2003 Seymour 2003) Kubitzek 2003 gave a figure for
TOTPAR at six hours and Seymour 2003 measured pain intensity
only Fifteen trials measured pain intensity at 4 hours using a 4-
point categorical scale of 0 to 3 where 0 was no pain at all and 3
was severe pain Five trials measured pain intensity using a visual
analogue scale (VAS) of 0 to 100 mm where 0 was no pain and
100 was the worst pain imaginable Twelve trials measured pain
intensity at 6 hours using a 4-point categorical scale where 0 was
no pain and 3 was severe pain and three trials measured pain
intensity at 6 hours using a VAS of 0 to 100 mm where 0 was no
pain and 100 mm was the worst pain imaginable Sixteen trials
measured pain relief at 4 hours using a 5-point categorical scale
of 0 to 4 where 0 was none and 4 was complete pain relief two
trials measured pain relief at 4 hours using a VAS of 0 to 100 mm
in one trial 0 was none and 100 was complete relief and in the
other trial 0 was complete relief and 100 was no relief (these data
were reversed for statistical purposes) Twelve trials measured pain
relief at 6 hours using a 5-point categorical scale of 0 to 4 where
0 was none and 4 was complete pain relief two trials measured
pain relief at 6 hours using a VAS of 0 to 100 mm in one trial 0
was none and 100 was complete relief and in the other trial 0 was
complete relief and 100 was no relief (these data were reversed for
statistical purposes)
Adverse events and global assessments were recorded in most of
the trials Nineteen trials reported the number of patients with
side effects eight for doses of 1000 mg or more and 15 for doses
of less than 1000 mg Fifteen trials reported the number of adverse
events seven for doses of 1000 mg or more and eight for doses
of less than 1000 mg Fourteen trials recorded global assessment
using a 5-point categorical scale of either 0 to 4 or 1 to 5 where
0 or 1 was poor and 4 or 5 was excellent and four trials used a
4-point categorical scale of 0 to 3 where 0 was poor and 3 was
excellent
Risk of bias in included studies
Details of the quality assessment are presented in Additional Table
2 Seven out of the 21 studies reported adequate concealed al-
location for the remaining studies it was unclear Over half of
the studies (1121) gave clear explanation of withdrawals or drop
outs Taking these two factors into account only three trials were
assessed as being at low risk of bias
Effects of interventions
Comparison 1 Paracetamol versus placebo using
pain relief measurements
(Comparison 1 Outcome 11 amp Comparison 1 Outcome 12)
(Analysis 11 Analysis 12)
There are 16 studies providing pain relief measurements for com-
paring paracetamol versus placebo at 4 hours 11 at doses up to
1000 mg and 5 at doses of 1000 mg Overall there was a highly
statistically significant benefit with the paracetamol with risk ratio
(RR) values for achieving 50 pain relief for all doses of parac-
etamol for 4 hours RR 285 (95 confidence interval (CI) 189
to 429) Chi2 = 6294 degrees of freedom (df ) = 15 P lt 0001
I2 = 76 number needed to treat (to benefit) (NNT) 4 (95
CI 3 to 4) The statistically significant benefit was apparent for
both subgroups with RR for up to 1000 mg 196 (95 CI 134
to 286) Chi2 = 2644 df = 9 P = 0002 I2 = 660 NNT 4
(95 CI 3 to 5) and RR for 1000 mg 456 (95 CI 286 to
727) Chi2 = 544 df = 5 P = 036 I2 = 82 NNT 3 (95
CI 3 to 4) Although both had a statistically significant benefit
6Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
over placebo there was a statistically significant difference between
the two subgroups with an enhanced benefit for the higher doses
(metaregression P lt 0001 Additional Table 3) This subgroup
analysis explained some of the heterogeneity in the overall com-
parison however there is still some unexplained heterogeneity be-
tween the trials in the up to 1000 mg dose comparison
There are 13 studies providing pain relief measurements for com-
paring paracetamol versus placebo at 6 hours 6 doses up to 1000
mg paracetamol and 7 doses of 1000 mg paracetamol Overall
there was a highly statistically significant benefit with the parac-
etamol with RR values for 50 pain relief at 6 hours RR 332
(95 CI 188 to 587) Chi2 = 6335 df = 12 P lt 000001 I2 = 811 NNT 3 (95 CI 3 to 4) The statistically significant
benefit was apparent in both subgroups with RR for up to 1000
mg 189 (95 CI 098 to 367) Chi2 = 1445 df = 5 P = 001
I2 = 654 NNT 6 (95 CI 4 to 10) and RR for 1000 mg
421 (95 CI 297 to 598) Chi2 = 509 df = 6 P = 053 I2 =
0 NNT 3 (95 CI 2 to 3) Although both had a statistically
significant benefit over placebo there was a statistically significant
difference between the two subgroups with an enhanced benefit
for the higher doses (metaregression P lt 0001 Additional Table
3) This subgroup analysis explained some of the heterogeneity in
the overall comparison however there is still some unexplained
heterogeneity between the trials in the up to 1000 mg dose com-
parison
Comparison 2 Paracetamol versus placebo using
pain intensity difference measurements
(Comparison 2 Outcome 21 amp Comparison 2 Outcome 22)
(Analysis 21 Analysis 22)
There are 18 studies providing pain intensity measurements for
comparing paracetamol versus placebo at 4 hours 10 at doses up
to 1000 mg and 8 at doses of 1000 mg Overall there was a highly
statistically significant benefit with paracetamol with RR values
for 50 pain relief at 4 hours RR 487 (95 CI 283 to 837)
Chi2 = 4973 df = 17 P lt 00001 I2 = 658 NNT 3 (95 CI
3 to 5) The statistically significant benefit was apparent in both
subgroups with RR up to 1000 mg 433 (95 CI 219 to 858)
Chi2 = 2622 df = 9 P = 0002 I2 = 657 NNT 3 (95 CI
3 to 4) and RR for 1000 mg 646 (95 CI 234 to 1785) Chi2 = 2347 df = 7 P = 0001 I2 = 702 NNT 4 (95 CI 3
to 5) Both had a statistically significant benefit over placebo but
there was no statistically significant difference between the two
subgroups (metaregression P = 067 Additional Table 3)
There are 14 studies providing pain intensity measurements for
comparing paracetamol versus placebo at 6 hours 6 at doses up
to 1000 mg and 8 at doses of 1000 mg Overall there was a highly
statistically significant benefit with paracetamol with RR values
for 50 pain relief RR 341 (95 CI 234 to 497) Chi2 = 1823
df = 13 P = 015 I2 = 287 NNT 4 (95 CI 3 to 4) The
statistically significant benefit was apparent in both groups with
RR up to 1000 mg 267 (95 CI 146 to 490) Chi2 = 705 df
= 5 P = 022 I2 = 291 NNT 5 (95 CI 3 to 7) and RR for
1000 mg 396 (95 CI 252 to 623) Chi2 = 863 df = 7 P =
028 I2 = 189 NNT 3 (95 CI 3 to 4) Both had a statisti-
cally significant benefit over placebo but there was no statistically
significant difference between the two subgroups (metaregression
P = 015 Additional Table 3)
Comparison 3 Number of patients with adverse
events for paracetamol versus placebo
(Comparison 3 Outcome 31) (Analysis 31)
There are 17 studies that reported the number of patients with
adverse events for paracetamol versus placebo 9 studies used less
than 1000 mg and 8 studies used 1000 mg There was no statisti-
cally significant difference in any group For all doses of paraceta-
mol the RR for an adverse event RR 119 (95 CI 090 to 157)
Chi2 = 2073 df = 15 P = 015 I2 = 276 number needed to
treat to harm (NNTH) 33 (95 CI 143 to infinity) For doses of
less than 1000 mg RR 125 (95 CI 069 to 225) Chi2 = 906
df = 7 P = 025 I2 = 228 NNTH 33 (95 CI 143 to infinity)
For 1000 mg paracetamol RR 116 (95 CI 084 to 160) Chi2
= 1096 df = 7 P = 014 I2 = 362 NNTH 33 (95 CI 125
to infinity)
Subgroup analyses
Where patients underwent surgery with local anaesthesia
alone local anaesthesia and intravenous sedation general
anaesthesia alone and general anaesthesia with local
anaesthetic
When the data were reviewed it was not possible to do a meta-anal-
ysis Of the 21 included studies 7 did not state what anaesthesia
was used 7 used combinations of anaesthesia but were unclear in
reporting which patients received which anaesthesia 4 used local
anaesthetic only and 3 used general anaesthetic only
Where different types of formulation of paracetamol were
used (immediate release versus slow release)
Most included studies did not report on the formulation other
than to say whether it was tablets capsules or caplets Only one
7Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
paper indicated that their study used effervescent tablets (Moller
2000) and their results showed that effervescent tablets gave a faster
onset of pain relief Median value for time to onset of analgesia
was 20 minutes in the effervescent group and 45 minutes in the
tablet group and time to meaningful pain relief was 45 minutes
in the effervescent group and 1 hour in the tablet group However
at the end of a 4-hour period pain relief was better in the tablet
group (44) than the effervescent group (37)
Where different doses of paracetamol were used (1000 mg
or more and less than 1000 mg)
This meta-analysis was conducted 11 studies used doses of 1000
mg or more and 11 studies used doses of less than 1000 mg
(Seymour 1996 used both doses)
NNT for lt 1000 mg of paracetamol is 4 (95 CI 3 to 5) at
4 hours and 6 (95 CI 4 to 10) at 6 hours (using pain relief
measurements)
NNT for lt 1000 mg of paracetamol is 3 (95 CI 3 to 4) at 4 hours
and 5 (95 CI 3 to 7) at 6 hours (using intesity measurements)
NNT for 1000 mg of paracetamol is 3 (95 CI 3 to 4) at 4 hours
and 3 (95 CI 2 to 3) at 6 hours (using pain relief measurements)
NNT for 1000 mg of paracetamol is 4 (95 CI 3 to 5) at 4 hours
and 3 (95 CI 3 to 4) at 6 hours (using intensity measurements)
Where time of administration of paracetamol differs
preoperative versus postoperative
No included study used a preoperative dose as the patients did
not reach moderate or severe pain before the intervention
Where total pain relief (TOTPAR) was calculated using pain
relief measures and pain intensity measures
This meta-analysis was undertaken where the relevant data were
available 16 studies had pain relief data and 17 studies had pain
intensity data
NNT using pain relief scales for lt 1000 mg of paracetamol is 4
(95 CI 3 to 5) at 4 hours and 6 (95 CI 4 to 10) at 6 hours
NNT using pain intensity scales for lt 1000 mg of paracetamol is
3 (95 CI 3 to 4) at 4 hours and 5 (95 CI 3 to 7) at 6 hours
NNT using pain relief scales for 1000 mg of paracetamol is 3 (95
CI 3 to 4) at 4 hours and 3 (95 CI 2 to 3) at 6 hours
NNT using pain intensity scales for 1000 mg of paracetamol is 4
(95 CI 3 to 5) at 4 hours and 3 (95 CI 3 to 4) at 6 hours
D I S C U S S I O N
The results show paracetamol to be an effective analgesia for use
following third molar surgery The number needed to treat (to
benefit) (NNTs) and number needed to treat to harm (NNTHs)
support the use of 1000 mg as an optimal dose It is effective over
both 4 and 6 hours In considering the use of pain relief or pain
intensity difference as a measure of efficacy it was of interest that
metaregression showed that pain relief scales showed a statistically
significant difference for increased dose and pain intensity did
not It is acknowledged that this review only considered single
dose studies when considering efficacy multidosed studies may be
considered when updating the review The NNTs and NNTHs
found in this review are similar to those recorded by a systematic
review (Barden J 2004) where they investigated paracetamol for
pain involving various types of surgery This would confirm yet
again the value of the third molar pain model showing that dental
pain is comparable with pain from other sources The implemen-
tation of NICE (National Institute for Health and Clinical Excel-
lence) Guidelines for removal of third molars has led to a decrease
in the performance of this surgery which may have an adverse
effect on the number of trials able to use the third molar model
In the United States of America such guidelines have not yet been
adopted It is of interest that in striving to provide evidence based
treatment the opportunity for research using the third molar pain
model may be adversely affected
The data available for adverse events show that NNTH for lt 1000
mg of paracetamol is 33 (143 to infinity) for 1000 mg of parac-
etamol is 33 (125 to infinity) and for all doses 33 (143 to infin-
ity) suggesting it is an extremely safe drug Only one severe ad-
verse event was recorded by any researchers and that was a severe
headache (Olson 2001) two other participants stopped taking
paracetamol because of vomiting However there was a high degree
of inconsistency across the trials in the way that adverse events were
recorded raising the concern that only adverse events considered
by the researchers to be attributable to paracetamol were recorded
with some trials recording many AEs and some reporting none
The diverse way in which adverse events were recorded led to there
being over 20 categories of adverse events The main categories
are shown in Additional Table 4 Of interest are adverse events
where placebo scored more highly than paracetamol which could
suggest that paracetamol may possibly have a beneficial effect eg
dry socket but this would require further investigation As all pa-
tients had surgery and various combinations of local anaesthesia
general anaesthesia and sedation making it difficult to ascertain
which effects are directly related to the intervention However the
results strongly support the use of paracetamol in doses up to 1000
mg as a safe effective analgesia
8Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
The efficacy of paracetamol decreases with times and the recom-
mended interval between doses is 8 hours which would suggest
there may be some benefit in a slow release formulation None of
the studies in this trial used a slow release formulation but a trial
(Coulthard 2001) compared sustained release and standard release
formulations of paracetamol and found that the sustained release
was statistically significantly more effective at 6 and 8 hours with
no loss of efficacy at 4 hours Safety for both formulations was
comparable making sustained release paracetamol a safe and ef-
fective choice
The methodology used in the included trials was generally good
This resulted in a large number of participants being included
in this meta-analysis while using only double blind randomised
trials The included trials gave a strong consistent result Many
of the trials were done by researchers with extensive experience
in the field of pain research whose methods have been refined
with experience A large proportion of the trials were done in the
United States and were mostly funded by pharmaceutical com-
panies This seems to be reflected in the methodology However
quality assessment showed there were only three trials with a low
risk of bias and 18 with moderatehigh risk This was mainly the
result of unreported allocation concealment methods In speaking
to some of the authors it is highly likely that the allocation con-
cealment was good in all the trials but that the details were not
well reported Most trials were sponsored by pharmaceutical com-
panies who supplied paracetamol and placebo in identical appear-
ance The reporting of withdrawals and drop outs was sporadic
and even when numbers were cited it was not always clear to which
treatment group the participant had been originally allocated
Mean global assessments (Additional Table 5 Table 6 Table 7
Table 8) all showed higher scores for paracetamol than placebo
It is of interest that despite achieving 50 pain relief participants
did not record 50 on a global assessment scale This again raises
the question of the value of the instruments used to measure the
efficacy of an intervention None of the trials relied on global
assessments as their only measure of efficacy but this information
could be of value to other researchers It raises interesting questions
concerning patientrsquos expectations and the difficulties associated
with quantifying such a subjective experience
A lot of valuable information was gathered incidental to the main
findings in most of the trials So though the topic was concerned
with the use of paracetamol for pain information collected in
many of the trials shed valuable light on subjects such as side effects
measuring instruments and methodology Further appraisal of
the multidisciplinary approach to research a broader view of data
collection and a more accurate reporting of data already collected
could be extremely valuable in the future It would allow research
to be more widely used in various meta-analyses Data from areas
seemingly unrelated to the original null hypothesis eg comparison
of pain relief and pain intensity as a measuring tool adverse event
reporting the significance of global assessments etc could be more
readily available If the third molar trial population does decrease
it would be advantageous to collect as much data as possible from
any trial being undertaken
A U T H O R S rsquo C O N C L U S I O N SImplications for practice
Paracetamol (acetaminophen) is an effective drug to use for post-
operative pain following oral surgery and the reporting of adverse
events shows it to be a safe drug (number needed to treat (to ben-
efit) (NNT) is 3 for 1000 mg of paracetamol at 6 hours number
needed to treat to harm (NNTH) 33) It is most effective at 1000
mg dose and can be taken at six hourly intervals without compro-
mising safety It could be considered more readily by dentist and
patients both as a first choice analgesic or to be taken alternately
with doses of other analgesics such as nonsteroidal anti-inflamma-
tory drugs (NSAIDS)
Implications for research
There is a large body of research in this area and further research
other than as a comparison seems unnecessary However in one
trial (Moller 2000) it was found that an effervescent formulation
appeared to have a faster onset of pain relief which would be
beneficial to patients who are looking for a rapid onset of relief
It may be helpful to undertake some research to confirm these
findings The use of pain relief and pain intensity difference as a
measure of pain relief may be another area for further investigation
It is valuable to have NNTNNTH as a baseline for comparison
with other analgesics Maximizing the third molar pain model
population by multidisciplinary research is another area of interest
highlighted by this review
A C K N O W L E D G E M E N T S
We wish to thank Sylvia Bickley (Cochrane Oral Health Group)
for her assistance with literature searching and Luisa Fernandez
Mauleffinch (Cochrane Oral Health Group) for her help with the
preparation of this review We would also like to thank the follow-
ing referees who reviewed this work at various stages Barry El-
liott Cole Mike Hill Kimito Yamashiro and Lasse Skoglund We
are grateful to Stephen Cooper Donald Mehlisch Philip Moller
Alberto Umile for providing information on their trials and to
Prisana Pripatnanont for translation and information
9Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies included in this review
Cooper 1980 published data only
Cooper SA Precheur H Rauch D Rosenheck A Ladov M
Engel J Evaluation of oxycodone and acetaminophen in
treatment of postoperative dental pain Oral Surgery Oral
Medicine and Oral Pathology 198050(6)496ndash501
Cooper 1981 published data only
Cooper SA Breen JF Giuliani RL The relative efficacy of
indoprofen with opiod-analgesic combinations Journal of
Oral Surgery 198139(1)21ndash5
Cooper 1988 published data only
Cooper SA Firestein A Cohn P Double-blind comparison
of meclofenamate sodium with acetaminophen
acetaminophen with codeine and placebo for relief of
postsurgical dental pain The Journal of Clinical Dentistry
19881(2)31ndash4
Cooper 1998 published data only
Cooper SA Reynolds DC Reynolds B Hersh EV Analgesic
efficacy and safety of (R)- ketoprofen in postoperative dental
pain Journal of Clinical Pharmacology 199838(2 Suppl)
11Sndash18S
Dionne 1994 published data only
Dionne RA Snyder J Hargreaves KM Analgesic efficacy
of flurbiprofen in comparison with acetaminophen
acetaminophen plus codeine and placebo after impacted
third molar removal Journal of Oral and Maxillofacial
Surgery 199452(9)919ndash24
Dolci 1994 published data only
Dolci G Ripari M Pacifici L Umile A Evaluation of
piroxicam-beta-cyclodextrin piroxicam paracetamol and
placebo in post-operative oral surgery pain International
Journal of Clinical Pharmacology Research 199414(5-6)
185ndash91
Forbes 1984b published data only
Forbes JA Barkaszi BA Ragland RN Hankle JJ
Analgesic effect of acetaminophen phenyltoloxamine
and their combination in postoperative oral surgery pain
Pharmacotherapy 19844(4)221ndash6
Forbes 1989 published data only
Forbes JA Butterworth GA Burchfield WH Yorio
CC Selinger LR Rosenmertz SK et alEvaluation of
flurbiprofen acetaminophen an acetaminophen-codeine
combination and placebo in postoperative oral surgery
pain Pharmacotherapy 19899(5)322ndash30
Forbes 1990 published data only
Forbes JA Kehm CJ Grodin CD Beaver WT Evaluation
of ketorolac ibuprofen acetaminophen and an
acetaminophen-codeine combination in postoperative
oral surgery pain Pharmacotherapy 199010(6(Pt 2)))
94Sndash105S
Hersh 2000 published data only
Hersh EV Levin LM Cooper SA Doyle G Waksman J
Wedell D et alIbuprofen liquigel for oral surgery pain
Clinical Therapeutics 200022(11)1306ndash18
Kiersch 1994 published data only
Kiersch TA Halladay SC Hormel PC A single-
dose double-blind comparison of naproxen sodium
acetaminophen and placebo in postoperative dental pain
Clinical Therapeutics 199416(3)394ndash404
Kubitzek 2003 published data only
Kubitzek F Ziegler G Gold MS Liu JM Ionescu E
Analgesic efficacy of low-dose diclofenac versus paracetamol
and placebo in postoperative dental pain Journal of
Orofacial Pain 200317(3)237ndash44
Lehnert 1990 published data only
Lehnert S Reuther J Wahl G Barthel K [The efficacy of
paracetamol (Tylenol) and acetyl salicylic acid (Aspirin)
in treating postoperative pain] Deutsche Zahnarztliche
Zeitschrift 199045(1)23ndash6
Mehlisch 1995 published data only
Mehlisch DR Jasper RD Brown P Korn SH McCarroll K
Murakami AA Comparative study of ibuprofen lysine and
acetaminophen in patients with postoperative dental pain
Clinical Therapeutics 199517(5)852ndash60
Moller 2000 published data only
Moller PL Norholt SE Ganry HE Insuasty JH Vincent
FG Skoglund LA et alTime of onset of analgesia and
analgesic efficacy of effervescent acetaminophen 1000
mg compared to tablet acetominophen 1000 mg in
postoperative dental pain a single-dose double-blind
randomized placebo-controlled study Journal of Clinical
Pharmacology 200040(4)370ndash8
Olson 2001 published data only
Olson NZ Otero AM Marrero I Tirado S Cooper S
Doyle G et alOnset of analgesia for liquigel ibuprofen
400 mg acetaminophen 1000 mg ketoprofen 25 mg
and placebo in the treatment of postoperative dental pain
Journal of Clinical Pharmacology 200141(11)1238ndash47
Seymour 1996 published data only
Seymour RA Kelly PJ Hawkesford JE The efficacy
of ketoprofen and paracetamol (acetaminopen) in
postoperative pain after third molar surgery British Journal
of Clinical Pharmacology 199641(6)581ndash5
Seymour 2003 published data only
Seymour RA Hawkesford JE Sykes J Stillings M Hill
CM An investigation into the comparative efficacy of
soluble aspirin and solid paracetamol in postoperative pain
after third molar surgery British Dental Journal 2003194
(3)153ndash7
Skoglund 1991 published data only
Skoglund LA Skjelbred P Fyllingen G Analgesic efficacy
of acetaminophen 1000 mg acetaminophen 2000 mg and
the combination of acetaminophen 1000 mg and codeine
10Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
phosphate 60 mg versus placebo in acute postoperative
pain Pharmacotherapy 199111(5)364ndash9
Sunshine 1986 published data only
Sunshine A Marrero I Olson N McCormick N Laska
EM Comparative study of flurbiprofen zomepirac sodium
acetaminophen plus codeine and acetaminophen for the
relief of postsurgical dental pain The American Journal of
Medicine 198680(3A)50ndash4
Vattaraphudej 1986 published data only
Vattaraphudej T Thongnoppakao P Koukongviriyapan V
[Comparison of the efficacy of analgesics in pain after oral
surgery] The Journal of the Dental Association of Thailand
198636(6)198ndash206
References to studies excluded from this review
Adame 1979 published data only
Adame C et alPostoperative development of inflammation
after extraction of impacted third molar as a model
for clinical assessment of anti-inflammatory drugs I
Preliminary report Boletin de Estudios Medicos y Biologicos
197930(8)308ndash9
Barden J 2004 published data only
Barden J Edwards J Moore A McQuay H Single dose
oral paracetamol (acetaminophen) for postoperative pain
Cochrane Database of Systematic Reviews 2004 Issue 1
[DOI DOI 10100214651858CD004602]
Becker 1990 published data only
Becker J Beckmann J Bertelt C Gundert-Remy U
Rohmel J Ohlendorf D [Double blind biometric study on
postoperative effects of analgesics] Deutsche Zahnarztliche
Zeitschrift 199045(1)36ndash8
Bentley 1987 published data only
Bentley KC Head TW The additive analgesic efficacy of
acetaminophen 1000 mg and codeine 60 mg in dental
pain Clinical Pharmacology and Therapeutics 198742(6)
634ndash40
Breivik 1998 published data only
Breivik EK Bjornsson GA Variation in surgical trauma and
baseline pain intensity effects on assay sensitivity of an
analgesic trial European Journal of Oral Sciences 1998106
(4)844ndash52
Cooper 1986 published data only
Cooper SA Erlichman MC Mardirossian G Double-
blind comparison of an acetaminophen-codeine-caffeine
combination in oral surgery pain Anesthesia Progress 1986
33(3)139ndash42
Cooper 1989 published data only
Cooper SA Schachtel BP Goldman E Gelb S Cohn P
Ibuprofen and acetaminophen in the relief of acute pain
a randomized double-blind placebo-controlled study
Journal of Clinical Pharmacology 198929(11)1026ndash30
Cooper 1991 published data only
Cooper SA Kupperman A The analgesic efficacy of
flurbiprofen compared to acetaminophen with codeine The
Journal of Clinical Dentistry 19912(3)70ndash4
Dionne 1983 (1) published data only
Dionne RA Campbell RA Cooper SA Hall DL
Buckingham B Suppression of postoperative pain by
preoperative administration of ibuprofen in comparison to
placebo acetaminophen and acetaminophen plus codeine
Journal of Clinical Pharmacology 198323(1)37ndash43
Dionne 1983 (2) published data only
Dionne RA Sisk AL Fox PC Wirdzek PR Gracely
RH Dubner R Suppression of postoperative pain by
preoperative adminsitration of flurbiprofen in comparison
to acetominophen and oxycodone plus acetominophen
Current Therapeutic Research 198334(1)15ndash29
Dionne 1986 published data only
Dionne RA Suppression of dental pain by the preoperative
administration of flurbiprofen The American Journal of
Medicine 198680(3A)41ndash9
Dolci 1993 published data only
Dolci G Ripari M Pacifici L Umile A [Analgesic efficacy
and the tolerance for piroxicam-beta-cyclodextrin compared
to piroxicam paracetamol and placebo in the treatment of
postextraction dental pain] Minerva Stomatologica 199342
(5)235ndash41
Edwards 2002 published data only
Edwards JE McQuay HJ Moore RA Combination
analgesic efficacy individual patient data meta-analysis
of single-dose oral tramadol plus acetaminophen in
acute postoperative pain Journal of Pain and Symptom
Management 200223(2)121ndash30
Forbes 1982 published data only
Forbes JA Beaver WT White EH White RW Neilson GB
Shackleford RW Diflunisal A new oral analgesic with an
unusually long duration of action JAMA 1982248(17)
2139ndash42
Forbes 1984a published data only
Forbes JA Kolodny AL Chachich BM Beaver WT
Nalbuphine acetaminophen and their combination in
postoperative pain Clinical Pharamacology and Therapeutics
198435(6)843ndash51
Gallardo 1990 published data only
Gallardo F Rossi E Analgesic efficacy of flurbiprofen as
compared to acetaminophen and placebo after periodontal
surgery Journal of Periodontology 199061(4)224ndash7
Gustafsson 1983 published data only
Gustafsson I Nystrom E Quiding H Effect of preoperative
paracetamol on pain after oral surgery European Journal of
Clinical Pharmacology 198324(1)63ndash5
Haanaes 1986 published data only
Haanaes HR Benterud UJ Skoglund LA RF 46-790 versus
paracetamol effect on post-operative pain International
Journal of Clinical Pharmacology Therapy and Toxicology
198624(11)598ndash601
Irvine 1982 published data only
Irvine GH Lutterloch MJ Bowerman JE Comparison
of diflunisal and paracetamol in the management of pain
11Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
following wisdom teeth removal British Dental Journal
1982152(1)18ndash20
Laska 1983 published data only
Laska EM Sunshine A Zighelboim I Roure C Marrero
I Wanderling J et alEffect of caffeine on acetaminophen
analgesia Clinical Pharmacology and Therapeutics 198333
(4)498ndash509
Lecointre 1991 published data only
Lecointre C [Efficacy and tolerance of tiaprofenic acid
for extraction complications Results of a randomized
double-blind study tiaprofenic acid versus paracetamol]
LrsquoInformation Dentaire 199173(35)3063ndash6
Liashek 1987 published data only
Liashek P Jr Desjardins PJ Triplett RG Effect of
pretreatment with acetaminophen-propoxyphene for oral
surgery pain Journal of Oral and Maxillofacial Surgery 1987
45(2)99ndash103
Macleod 2002 published data only
Macleod AG Ashford B Voltz M Williams B Cramond T
Gorta L et alParacetamol versus paracetamol-codeine in
the treatment of post-operative dental pain a randomized
double-blind prospective trial Australian Dental Journal
200247(2)147ndash51
Medve 2001 published data only
Medve RA Wang J Karim R Tramadol and acetaminophen
tablets for dental pain Anesthesia Progress 200148(3)
79ndash81
Mehlisch 1984 published data only
Mehlisch DR Frakes LA A controlled comparative
evaluation of acetaminophen and aspirin in the treatment of
postoperative pain Clinical Therapeutics 19847(1)89ndash97
Mehlisch 1990 published data only
Mehlisch DR Sollecito WA Helfrick JF Leibold DG
Markowitz R Schow CE Jr et alMulticenter clinical
trial of ibuprofen and acetaminophen in the treatment of
postoperative dental pain Journal of the American Dental
Association 1990121(2)257ndash63
Moore 1986 published data only
Moore PA Werther JR Seldin EB Stevens CM Analgesic
regimens for third molar surgery pharmacologic and
behavioral considerations Journal of the American Dental
Association 1986113(5)739ndash44
Nystrom 1988 published data only
Nystrom E Gustafsson I Quiding H The pain intensity
at analgesic intake and the efficacy of diflunisal in single
doses and effervescent acetaminophen in single and repeated
doses Pharmacotherapy 19888(3)201ndash9
Petersen 1983 published data only
Petersen JK A double-blind cross-over study of the analgesic
and anti-inflammatory effects of dexamethasone and
paracetamol following surgical removal of lower impacted
third molars International Journal of Oral Surgery 198312
(4)266
Quiding 1981 published data only
Quiding H Oksala E Happonen RP Lehtimaki K Ojala
T The visual analog scale in multiple-dose evaluations of
analgesics The Journal of Clinical Pharmacology 198121
(10)424ndash9
Quiding 1982 (1) published data only
Quiding H Oikarinen V Huitfeldt B Koskimo M
Leikomaa H Nyman C An analgesic study with repeated
doses of phenazone phenazone plus dextropropoxyphene
and paracetamol using a visual analogue scale International
Journal of Oral Surgery 198211(5)304ndash9
Quiding 1982 (2) published data only
Quiding H Persson G Ahlstrom U Bangens S Hellem S
Johansson G et alParacetamol plus supplementary doses
of codeine an analgesic study of repeated doses European
Journal of Clinical Pharmacology 198223(4)315ndash9
Quiding 1984 published data only
Quiding H Oikarinen V Sane J Sjoblad AM Analgesic
efficacy after single and repeated doses of codeine and
acetaminophen Journal of Clinical Pharmacology 198424
(1)27ndash34
Ragot 1991 published data only
Ragot JP [Comparison of analgesic activity of mefenamic
acid and paracetamol in treatment of pain after extraction
of impacted lower 3d molar] LrsquoInformation Dentaire 1991
73(21)1659ndash64
Reijntjes 1987 published data only
Reijntjes RJ Boering G Wesseling H van Rijn LG
Suprofen versus paracetamol after oral surgery International
Journal of Oral and Maxillofacial Surgery 198716(1)45ndash9
Rodrigo 1987 published data only
Rodrigo MR Rosenquist JB Cheung LK Paracetamol
and diflunisal for pain relief following third molar surgery
in Hong Kong Chinese International Journal of Oral and
Maxillofacial Surgery 198716(5)566ndash71
Rodrigo 1989 published data only
Rodrigo C Chau M Rosenquist J A comparison of
paracetamol and diflunisal for pain control following
3rd molar surgery International Journal of Oral and
Maxillofacial Surgery 198918(3)130ndash2
Rosen 1985 published data only
Rosen M Absi EG Webster JA Suprofen compared to
dextropropoxyphene hydrochloride and paracetamol
(Cosalgesic) after extraction of wisdom teeth under general
anaesthesia Anaesthesia 198540(7)639ndash41
Sakata 1989 published data only
Sakata LA Rocha B et alEffects of benzydamine after
surgical removal of impacted teeth [Efeitos da benzidamina
apoacutes a extraccedilaumlo de dentes inclusos] Revista da Associacao
Paulista de Cirurgioes Dentistas 198943(4)167ndash70
Selcuk 1996 published data only
Selcuk E Gomel M Bellibas SE Kose T Tuglular I
Comparison of the analgesic effects of diflunisal and
paracetamol in the treatment of postoperative dental pain
12Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
International Journal of Clinical Pharmacology Research
199616(2-3)57ndash65
Seymour 1981 published data only
Seymour RA Rawlins MD Pharmacokinetics of parenteral
paracetamol and its analgesic effects in post-operative dental
pain European Journal of Clinical Pharmacology 198120
(3)215ndash8
Seymour 1983 published data only
Seymour RA Analgesic efficacy and plasma concentration
of three analgesics in pain after lower third molar removal
SAAD Digest 19835(7)172ndash88
Skjelbred 1979 published data only
Skjelbred P Lokken P Paracetamol versus placebo effects
on post-operative course European Journal of Clinical
Pharmacology 197915(1)27ndash33
Strom 1990 published data only
Strom C Forsberg O Quiding H Engevall S Larsson
O Analgesic efficacy of acetaminophen sustained release
Journal of Clinical Pharmacology 199030(7)654ndash9
Van Aken 2004 published data only
Van Aken H Thys L Veekman L Buerkle H Assessing
analgesia in single and repeated administrations of
propacetamol for postoperative pain comparison with
morphine after dental surgery Anesthesia and Analgesia
200498(1)159ndash65
Winter 1983 published data only
Winter L Appleby F Ciccone PE Pigeon JG A double-
blind comparative evaluation of acetaminophen caffeine
and the combination of acetaminophen and caffeine in
outpatients with postoperative oral surgery pain Current
Therapeutic Research 198333(1)115ndash22
Additional references
Aronoff 2006
Aronoff DM Oates JA Boutaud O New insights into
the mechanism of action of acetaminophen Its clinical
pharmacologic characteristics reflect its inhibition of the
two prostaglandin H2 synthases Clinical Pharmacology and
Therapeutics 200679(1)9ndash19
Chandrasekharan 2002
Chandrasekharan NV Dai H Roos KL Evanson NK
Tomsik J Elton TS et alCOX-3 a cyclooxygenase-1 variant
inhibited by acetaminophen and other analgesicantipyretic
drugs cloning structure and expression Proceedings of the
National Academy of Sciences of the United States of America
200299(21)13926ndash31
Collins 1999
Collins SL Moore RA McQuay HJ Wiffen PJ Edwards JE
Single dose oral ibuprofen and diclofenac for postoperative
pain Cochrane Database of Systematic Reviews 1999
Issue 1 [DOI Art No CD001548 DOI 101002
14651858CD001548]
Cooper 1976
Cooper SA Beaver WT A model to evaluate mild analgesics
in oral surgery outpatients Clinical Pharmacology and
Therapeutics 197620(2)241ndash50
Coulthard 2001
Coulthard P Hill CM Frame JW Barry H Ridge BD
Bacon TH Pain control with paracetamol from a sustained
release formulation and a standard release formulation after
third molar surgery a randomised controlled trial British
Dental Journal 2001191(6)319ndash24
Dray 1997
Dray A Kinins and their receptors in hyperalgesia
Canadian Journal of Physiology and Pharmacology 199775
(6)704ndash12
Fisher 1988
Fisher SE Frame JW Rout PG McEntegart DJ Factors
affecting the onset and severity of pain following the surgical
removal of unilateral impacted mandibular third molar
teeth British Dental Journal 1988164(11)351ndash4
Loeser 1999
Loeser JD Melzack R Pain an overview Lancet 1999353
(9164)1607ndash9
Malmberg 1992
Malmberg AB Yaksh TL Antinociceptive effects of spinal
non-steroidal anti-inflammatory agents on the formalin
test in the rat Journal of Pharmacology and Experimental
Therapeutics 1992263136ndash46
Moore 1997
Moore RA McQuay HJ Single-patient data meta-analysis
of 3453 postoperative patients oral tramadol versus
placebo codeine and combination analgesics Pain 199769
(3)287ndash94
Moore 1998
Moore A Collins S Carroll D McQuay H Edwards
J Single dose paracetamol (acetaminophen) with and
without codeine for postoperative pain Cochrane Database
of Systematic Reviews 1998 Issue 4 [DOI Art No
CD001547 DOI 10100214651858CD001547]
Rang 2003
Rang HP Dale MM Ritter JM Moore PK Anti-
inflammatory and immunosuppresant drugs Pharmacology
5th Edition Churchill Livingstone 2003244ndash61
Seymour 1985
Seymour RA Meechan JG Blair GS An investigation into
post-operative pain after third molar surgery under local
analgesia The British Journal of Oral and Maxillofacial
Surgery 198523(6)410ndash8lowast Indicates the major publication for the study
13Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Cooper 1980
Methods Randomised parallel group double blind study
Participants 298 participants randomised to 6 groups withdrawals unclear (51 from all groups)
Number randomised to intervention male 13 female 24 mean age 225
Number randomised to placebo male 11 female 27 mean age 235
Number of third molars removed mean for intervention and placebo 19
Baseline pain intensity mean for intervention 241 (moderate 22 severe 15) mean for placebo 242
(moderate 22 severe 16)
Setting - outpatients (USA)
Interventions Paracetamol 500 mg versus placebo
Formulation not stated
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse events table
Notes Sponsored unclear
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Cooper 1981
Methods Randomised parallel group double blind study
Participants 248 participants randomised to 5 groups withdrawals unclear (48 from all groups)
Number randomised to intervention male 15 female 22 mean age 222
Number randomised to placebo male 13 female 24 mean age 237
Number of third molars removed not stated
Baseline pain intensity mean for intervention 22 (moderate 29 severe 9) mean for placebo 23 (moderate
26 severe 11)
Setting not stated (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation not stated
Anaesthesia LA or GA
14Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Cooper 1981 (Continued)
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Total number of adverse events and number of people with adverse events reported
Notes Sponsored by
Adria Laboratories
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Cooper 1988
Methods Randomised parallel group double blind study
Participants 165 participants randomised to 4 groups withdrawals unclear (22 from all groups)
Number randomised to intervention male 7 female 29 mean age 246
Number randomised to placebo male 11 female 29 mean age 247
Number of third molars removed mean for intervention 14 mean for placebo 15
Baseline pain intensity mean for intervention 24 (moderate 21 severe 15) mean for placebo 24 (mod-
erate 25 severe 15)
Setting - outpatients - single site (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Total number of adverse events
Notes Sponsored by
Parke-Davis
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
15Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Cooper 1998
Methods Randomised parallel group double blind study
Participants 177 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 23 female 27 mean age 236
Number randomised to placebo male 12 female 14 mean age 227
Number of third molars removed not stated
Baseline pain intensity mean for intervention categorical 23 VAS 603 mean for placebo categorical
22 VAS 628
Setting - Georgetown University Hospital (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe) VAS scale 0-100 mm (none - worst pain
imaginable)
PR at 4 hours and 6 hours categorical scale 0-4 (no relief - complete relief )
Global assessment not stated
Adverse effects table
Notes Sponsored by
Whitehall-Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Dionne 1994
Methods Randomised parallel group double blind study
Participants 135 participants randomised to 5 groups withdrawals unclear (11 from all groups)
Number randomised to intervention male 14 female 13 mean age 296
Number randomised to placebo male 15 female 10 mean age 282
Number of third molars removed not stated
Baseline pain intensity for intervention and placebo not stated
Setting private dental practice (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation not stated
Anaesthesia LA or LA and SED or GA
Outcomes PI at 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 1-5 (poor - excellent)
Adverse effects table
16Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Dionne 1994 (Continued)
Notes Sponsored by
Upjohn
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Dolci 1994
Methods Randomised parallel group double blind study
Participants 338 participants enrolled in 4 groups withdrawals unclear (40 from all groups)
Number randomised to intervention male 28 female 44 mean age 279 age range 18-49
Number randomised to placebo male 28 female 48 mean age 272 age range 18-45
Number of third molars removed not stated
Baseline pain intensity range for intervention and placebo given together as average 214 (208 - 219)
Setting not stated (Italy)
Interventions Paracetamol 500 mg versus placebo
Formulation tablets
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (negative - very good)
Adverse effects table
Notes Sponsored - unclear
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Forbes 1984b
Methods Randomised parallel group double blind study
Participants 191 participants randomised to 4 groups withdrawals unclear (43 from all groups 164 used in reporting
of adverse events)
Number randomised to intervention male 19 female 20 mean age 2195
Number of third molars removed mean 244
Number randomised to placebo male 21 female 15 mean age 15-32
Number of third molars removed mean 278
17Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Forbes 1984b (Continued)
Baseline pain intensity mean for intervention 246 (moderate 21 severe 18) mean for placebo 247
(moderate 19 severe 17)
Setting private dental practice (USA)
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse effects reported as total number of adverse events and number of patients with adverse events
Notes Sponsored by McNeil Consumer Products
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Forbes 1989
Methods Randomised parallel group double blind study
Participants 107 participants randomised to 5 groups withdrawals unclear (19 from all groups 98 participants used
in reporting of adverse events)
Number randomised to intervention male 9 female 13 mean age 2059 age range 17-31
Number randomised to placebo male 12 female 11 mean age 2374 age range 16-39
Number of third molars removed mean for intervention 259 mean for placebo 209
Baseline pain intensity mean for intervention 245 mean for placebo 239
Setting - 2 sites private dental practice outpatients (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation - 1 tablet amp 1 capsule
Anaesthesia LA and GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects reported by number of patients with adverse events
Notes Sponsored by
Boots Company Ltd GH Besselaar Associates
Risk of bias
Item Authorsrsquo judgement Description
18Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Forbes 1989 (Continued)
Allocation concealment Unclear B - Unclear
Forbes 1990
Methods Randomised parallel group double blind study
Participants 206 participants randomised to 6 groups
Number randomised to intervention male 20 female 16 (5 withdrawals) mean age 225 age range 16-
46
Number randomised to placebo male 18 female 16 (4 withdrawals) mean age 2365 age range 16-45
Number of third molars removed mean for intervention 258 mean for placebo 235
Baseline pain intensity mean for intervention 239 (moderate 22 severe 14) mean for placebo 232
(moderate 23 severe 11)
Setting - private dental practice outpatients (USA)
Interventions Paracetamol 600 mg versus placebo
Formulation capsules
Anaesthesia LA and GA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects table
Notes Sponsored by
Syntex Research
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Hersh 2000
Methods Randomised parallel group double blind study
Participants 210 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 20 female 43 mean age 233
Number of third molars removedpatient (11) (26) (35) (451)
Number randomised to placebo male 9 female 8 mean age 237
Number of wisdom teeth removed per patient (11) (25) (33) (418)
Baseline pain intensity mean for intervention 23 (moderate 47 severe 16) mean for placebo 22 (mod-
erate 22 severe 5)
Setting - University of Pennsylvania School of Dental Medicine - outpatients (USA)
19Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Hersh 2000 (Continued)
Interventions Paracetamol 1000 mg versus placebo
Formulation caplets
Anaesthesia LA or LA and SED
Outcomes PI at 4 hours and 6 hours categorical 0-3 (none - severe)
PR at 4 hours and 6 hours categorical 0-4 (no relief - complete relief )
Global assessment categorical 0-4 (poor - excellent)
Adverse effects by total number of adverse events and number of patients with adverse events
Notes Sponsored by
Whitehall-Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Kiersch 1994
Methods Randomised parallel group double blind study
Participants 232 participants enrolled in 3 groups
Number randomised to intervention 91 withdrawals 4 (2 before and 2 after randomisation) male 72
female 17 mean age 231 age range 15-39
Number of third molars removedpatient (10) (20) (331) (454)
Number randomised to placebo 47 withdrawals 2 male 35 female 10 mean age 247 age range 15-39
Number of third molars removedpatient (10) (20) (319) (426)
Baseline pain intensity mean for intervention and placebo categorical 212 VAS 5835
Setting not stated (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation capsules
Anaesthesia not stated
Outcomes PI at 4 hours and 6 hours categorical 0-3 (none - severe)
PR at 4 hours and 6 hours categorical 0-4 (none - complete) VAS 0-100 mm (no pain - worst pain I can
imagine)
Global assessment categorical 0-4 (poor - excellent)
Adverse effects reported by total number of adverse events and by number of patients with adverse events
Notes Sponsored by
Syntex Research
Risk of bias
Item Authorsrsquo judgement Description
20Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Kiersch 1994 (Continued)
Allocation concealment Unclear B - Unclear
Kubitzek 2003
Methods Randomised parallel group double blind study
Participants 245 participants randomised to 3 groups no withdrawals
Number randomised to intervention 78
Number randomised to placebo 84 malefemale 40 male over both groups
Number of third molars removed 1 or 2 for each patient
Baseline pain intensity moderate to severe 65-76 in both groups
Setting dental practice (Germany)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia LA
Outcomes PI not stated
PR given as TOTPAR at 6 hours
Global assessment categorical 1-5 (poor - excellent)
Adverse effects not stated
Notes Sponsored by
Novartis Consumer Health
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Lehnert 1990
Methods Randomised parallel group double blind study
Participants 150 participants randomised to 3 groups 50 to each
Number randomised to intervention 1 withdrawal male 23 female 26 mean age 253 age range 17-52
Number randomised to placebo 2 withdrawals male 24 female 18 mean age 251 age range 18-53
Number of hird molars removed not stated
Baseline pain intensity mean for intervention 255 (moderate 22 severe 27) mean for placebo 25
(moderate 21 severe 21)
Setting outpatients (Germany)
Interventions Paracetamol 1000 mg versus placebo
Formulation capsules
Anaesthesia not stated
21Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Lehnert 1990 (Continued)
Outcomes PI at 6 hours categorical scale 0-3 (no pain - severe)
PR at 6 hours categorical scale 0-3 (none - complete)
Global assessment categorical scale 0-3 (poor - excellent)
Adverse effects by number of patients
Notes Sponsored by GH Besselar Associates
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Mehlisch 1995
Methods Randomised parallel group double blind study
Participants 240 participants randomised to 3 groups 1 withdrawal from the acetaminophen group
Number randomised to intervention (1 withdrawal) male 30 female 71 mean age 253 age range 15-
60
Number of third molars removedpatient (10 295 33 43)
Number randomised to placebo male 19 female 21 mean age 242 age range 15-48
Number of third molars removedpatient (10 239 30 41)
Baseline pain intensity mean for intervention 221 (moderate 80 severe 21) mean for placebo 220
(moderate 32 severe 8)
Setting not stated (USA)
Interventions Paracetamol 1000 mg versus placebo
Formulation 2 tablets
Anaesthesia not stated
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete)
Global assessment categorical scale 0-4 (poor - excellent)
Adverse events reported by number of patients
Notes Sponsored by
Biomedical Research Group and Merck Research Laboratories
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
22Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Moller 2000
Methods Randomised parallel group double blind study
Participants 242 participants randomised to 4 groups no withdrawals
Number randomised to Intervention A male 27 female 33 mean age 245
Number randomised to Intervention B male 26 female 34 mean age 262
Number randomised to Placebo A male 21 female 41 mean age 250
Number randomised to Placebo B male 24 female 36 mean age 246
Number of third molars removed per patient in both groups 1
Mean baseline intensity Intervention A categorical 200 (moderate 60) VAS 494
Mean baseline intensity Intervention B categorical 200 (moderate 60) VAS 473
Mean baseline intensity Placebo A categorical 200 (moderate 61 severe 1) VAS 505
Mean baseline intensity Placebo B categorical 200 (moderate 61) VAS 476
Setting Department of Oral and Maxillofacial Surgery Royal Dental College Aarhus (Denmark)
Interventions Intervention A Paracetamol 1000 mg versus Placebo A
Formulation effervescent tablets
Intervention B Paracetamol 1000 mg versus Placebo B
Formulation tablets
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe) VAS scale 0-100 mm (no pain - worst possible pain)
PR at 4 hours categorical 0-4 (none - complete)
Global assessment categorical 0-3 (poor - excellent)
Adverse effects reported as total number of adverse events and number of patients with adverse events
Notes Sponsored by
Bristol Myers Squibb
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
Olson 2001
Methods Randomised parallel group double blind study
Participants 239 participants randomised to 4 groups no withdrawals
Number randomised to intervention male 22 female 44 mean age 222
Number randomised to placebo male 11 female 28 mean age 239
Number of third molars removedpatient intervention - (11) (264) (31) (40) placebo - (11) (2
38) (30) (40)
Baseline pain intensity mean for intervention 286 (moderate 9 severe 57) mean for placebo 29 (moderate
4 severe 35)
Setting University of Puerto Rico School of Dentistry (Puerto Rico)
23Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Olson 2001 (Continued)
Interventions Paracetamol 1000 mg versus placebo
Formulation caplets
Anaesthesia LA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none - complete relief )
Global assessment categorical scale 0-4 (poor - excellent)
Adverse effects table
Notes Sponsored by
Whitehall Robins
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Seymour 1996
Methods Randomised parallel group double blind study
Participants 206 participants randomised to 5 groups
Number randomised to intervention A 1 withdrawal male 12 female 28 mean age 238
Number randomised to intervention B 1 withdrawal male 12 female 28 mean age 277 1 withdrawal
Number randomised to placebo 2 withdrawals male 15 female 24 mean age 246
Number of third molars removedpatient not stated
Baseline pain intensity mean for intervention A VAS 549 mean for intervention B VAS 542 mean
for placebo VAS 565
Setting not stated (UK)
Interventions Intervention A paracetamol 500 mg versus placebo
Intervention B paracetamol 1000 mg versus placebo
Formulation not stated
Anaesthesia GA
Outcomes PI at 6 hours VAS scale 0-100 mm (no pain - unbearable pain)
Global assessment categorical 0 -3 (very good - very poor)
but categories 1 amp 2 and 4 amp 5 not reported separately so unable to include data in tables
Adverse effects - none reported by any participants in any group
Notes Sponsored - unclear
Risk of bias
Item Authorsrsquo judgement Description
24Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Seymour 1996 (Continued)
Allocation concealment Unclear B - Unclear
Seymour 2003
Methods Randomised parallel group double blind study
Participants 167 randomised to 3 groups withdrawals unclear (14 from all groups)
Number randomised to intervention male 19 female 43 mean age 250
Number randomised to placebo male 11 female 21 mean age 251
Number of third molars removedpatient intervention - (12) (214) (312) (434) placebo - (13)
(25) (39) (415)
Baseline pain intensity mean for intervention 506 mean for placebo 541
Setting not clear (2 sites Cardiff and Hexham UK)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia GA
Outcomes PI at 4 hours VAS scale 0-100 mm (none - worst pain imaginable)
PR not stated
Global assessment categorical scale 1-5 (very poor - very good)
Adverse effects table
Notes Sponsored by
Reckitt Benckiser Healthcare
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Skoglund 1991
Methods Randomised parallel group double blind study
Participants 147 participants randomised to 4 groups withdrawals unclear (8 from all groups)
Number randomised to intervention male 16 female 16 mean age 247
Number randomised to placebo male 16 female 17 mean age 244
Number of third molars removed not stated
Baseline pain intensity mean for intervention approx 55 mean for placebo approx 45
Setting not stated (Norway)
Interventions Paracetamol 1000 mg versus placebo
Formulation tablets
Anaesthesia LA
25Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Skoglund 1991 (Continued)
Outcomes PI at 4 hours and 6 hours VAS scale 0-100 mm (none - pain cannot be worse)
PR at 4 hours and 6 hours VAS scale 0-100 mm (complete relief - no relief ) reversed for statistical analysis
Global assessment not stated
Adverse effects table
Notes Sponsored by
Apothekernes Laboratorium
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
Sunshine 1986
Methods Randomised parallel group double blind study
Participants 182 participants randomised to 6 groups no withdrawals (only patients with moderate to severe pain
were randomised)
Number randomised to intervention male 6 female 24 mean age 219
Number randomised to placebo male 14 female 16 mean age 23
Number of third molars removed not stated
Baseline pain intensity mean for intervention 200 mean for placebo 200
Setting University of Puerto Rico School of Dentistry Clinic
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia LA
Outcomes PI at 4 hours and 6 hours categorical scale 0-3 (none - severe)
PR at 4 hours and 6 hours categorical scale 0-4 (none 0 - complete 100)
Global assessment categorical 0-3 (poor - excellent)
Overall improvement 1-7 (very much worse - very much better)
Adverse effects reported by number of patients with adverse events
Notes Sponsored by
Upjohn
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Yes A - Adequate
26Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Vattaraphudej 1986
Methods Randomised parallel group double blind study
Participants 83 enrolled to 4 groups withdrawals unclear (16 from all groups)
Number randomised to intervention male 8 female 8
Number randomised to placebo male 10 female 9
Number of third molars removed mean for intervention 125 mean for placebo 132
Baseline pain intensity mean for intervention 237 mean for placebo 226
Setting Dept of Oral Surgery Khon Kaen University Thailand
Interventions Paracetamol 650 mg versus placebo
Formulation capsules
Anaesthesia not stated
Outcomes PI at 4 hours categorical scale 0-3 (none - severe)
PR at 4 hours categorical scale 0-4 (no relief - total relief )
Global assessment categorical scale 0-3 (poor - excellent)
Adverse effects none reported
Notes Sponsored by Khon Kaen University Thailand Dr Sompong Thongpradith Merck and Russel
Risk of bias
Item Authorsrsquo judgement Description
Allocation concealment Unclear B - Unclear
GA - general anaesthetic LA - local anaesthetic PI - pain intensity PR - pain relief SED - sedation TOTPAR - total pain relief VAS
- visual analogue scale
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Adame 1979 Title not in journal quoted unable to find paper
Barden J 2004 Meta-analysis dental papers included individually where appropriate
Becker 1990 Not a third molar study
Bentley 1987 Unable to extract data for third molars only written to authors
Breivik 1998 Dose given at 3 hours postoperatively regardless of baseline pain unable to get 4-hour data Study used for side
effects only
27Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Cooper 1986 Unable to extract third molar data written to authors
Cooper 1989 Unable to extract third molar data written to authors
Cooper 1991 Unclear if third molars only written to authors
Dionne 1983 (1) Not single dose administered preoperatively
Dionne 1983 (2) Not placebo controlled not single dose administered preoperatively
Dionne 1986 Not placebo controlled
Dolci 1993 The data for the participants in this study are duplicated in Dolci 1994
Edwards 2002 This was a meta-analysis Need to identify source of data to clarify whether third molar studies and exclude
duplication Written to authors
Forbes 1982 Unable to extract third molar data written to authors
Forbes 1984a Not third molar study
Gallardo 1990 Not third molar study (periodontal surgery)
Gustafsson 1983 Patients given either paracetamol preoperatively and placebo postoperatively or vice versa unable to extract
relevant data
Haanaes 1986 Not placebo controlled Study used for side effects only
Irvine 1982 Not placebo controlled
Laska 1983 Not placebo controlled
Lecointre 1991 Not placebo controlled
Liashek 1987 Multiple doses unable to extract single dose data
Macleod 2002 Not placebo controlled
Medve 2001 Only 8-hour SPID and TOTPAR available need 4-hour andor 6-hour to include in review written to authors
Mehlisch 1984 Unable to extract third molar data written to authors
Mehlisch 1990 Unable to extract third molar data
Moore 1986 Multiple doses given unable to extract single dose data
Nystrom 1988 Not placebo controlled
28Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Petersen 1983 Unable to locate complete article
Quiding 1981 Not placebo controlled
Quiding 1982 (1) Not placebo controlled
Quiding 1982 (2) Not placebo controlled
Quiding 1984 No placebo used
Ragot 1991 Not placebo controlled
Reijntjes 1987 Not placebo controlled
Rodrigo 1987 Mixed parallel and cross-over trial multiple doses unable to extract relevant data
Rodrigo 1989 Not placebo controlled
Rosen 1985 Not placebo controlled multiple doses used unable to extract single dose data
Sakata 1989 Unable to obtain study
Selcuk 1996 Not placebo controlled
Seymour 1981 Cross-over trial baseline pain not stated unable to extract relevant data
Seymour 1983 Acetaminophen administered intravenously
Skjelbred 1979 Multiple doses unable to extract single dose data
Strom 1990 Not placebo controlled
Van Aken 2004 Propacetamol administered intravenously
Winter 1983 Unable to extract third molar data written to authors
SPID - summed pain intensity difference TOTPAR - total pain relief
29Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
Comparison 1 50 pain relief using pain relief measures
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Paracetamol versus placebo
number of people with at least
50 pain relief at 4 hours
16 1498 Risk Ratio (M-H Random 95 CI) 285 [189 429]
11 Up to 1000 mg of
paracetamol
10 710 Risk Ratio (M-H Random 95 CI) 196 [134 286]
12 1000 mg or more 6 788 Risk Ratio (M-H Random 95 CI) 456 [286 727]
2 Paracetamol versus placebo
number of people with at least
50 pain relief at 6 hours
13 1155 Risk Ratio (M-H Random 95 CI) 332 [188 587]
21 Up to 1000 mg of
paracetamol
6 378 Risk Ratio (M-H Random 95 CI) 189 [098 367]
22 1000 mg or more 7 777 Risk Ratio (M-H Random 95 CI) 421 [297 598]
Comparison 2 50 pain relief using pain intensity measures
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Paracetamol versus placebo
number of people with at least
50 pain relief at 4 hours
17 1658 Risk Ratio (M-H Random 95 CI) 487 [283 837]
11 Up to 1000 mg of
paracetamol
10 737 Risk Ratio (M-H Random 95 CI) 433 [219 858]
12 1000 mg or more 8 921 Risk Ratio (M-H Random 95 CI) 646 [234 1785]
2 Paracetamol versus placebo
number of people with at least
50 pain relief at 6 hours
13 1184 Risk Ratio (M-H Random 95 CI) 341 [234 497]
21 Up to 1000 mg of
paracetamol
6 403 Risk Ratio (M-H Random 95 CI) 267 [146 490]
22 1000 mg or more 8 781 Risk Ratio (M-H Random 95 CI) 396 [252 623]
30Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Comparison 3 Number of people with adverse events
Outcome or subgroup titleNo of
studies
No of
participants Statistical method Effect size
1 Number of patients with adverse
events paracetamol versus
placebo
17 1645 Risk Ratio (M-H Random 95 CI) 119 [090 157]
11 Up to 1000 mg of
paracetamol
9 672 Risk Ratio (M-H Random 95 CI) 125 [069 225]
12 1000 mg or more 8 973 Risk Ratio (M-H Random 95 CI) 116 [084 160]
Analysis 11 Comparison 1 50 pain relief using pain relief measures Outcome 1 Paracetamol versus
placebo number of people with at least 50 pain relief at 4 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 1 50 pain relief using pain relief measures
Outcome 1 Paracetamol versus placebo number of people with at least 50 pain relief at 4 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Dolci 1994 5472 2576 100 228 [ 161 323 ]
Cooper 1980 1137 1138 82 103 [ 051 207 ]
Forbes 1990 936 134 30 850 [ 114 6357 ]
Forbes 1989 522 023 17 1148 [ 067 19607 ]
Cooper 1988 1636 1240 87 148 [ 081 269 ]
Cooper 1981 2137 637 77 350 [ 160 767 ]
Forbes 1984b 1339 136 30 1200 [ 165 8716 ]
Vattaraphudej 1986 716 219 47 416 [ 100 1726 ]
Sunshine 1986 1830 1530 95 120 [ 076 190 ]
Dionne 1994 2527 1725 102 136 [ 102 182 ]
Subtotal (95 CI) 352 358 667 196 [ 134 286 ]
Total events 179 (Paracetamol better) 90 (Placebo better)
Heterogeneity Tau2 = 018 Chi2 = 2644 df = 9 (P = 0002) I2 =66
Test for overall effect Z = 349 (P = 000048)
2 1000 mg or more
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
31Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Mehlisch 1995 40101 240 49 792 [ 201 3124 ]
Cooper 1998 1850 326 59 312 [ 101 963 ]
Olson 2001 4266 539 74 496 [ 215 1148 ]
Moller 2000 27120 0122 18 5591 [ 345 90627 ]
Hersh 2000 4063 527 75 343 [ 152 773 ]
Kiersch 1994 2589 345 58 421 [ 134 1321 ]
Subtotal (95 CI) 489 299 333 456 [ 286 727 ]
Total events 192 (Paracetamol better) 18 (Placebo better)
Heterogeneity Tau2 = 003 Chi2 = 544 df = 5 (P = 036) I2 =8
Test for overall effect Z = 637 (P lt 000001)
Total (95 CI) 841 657 1000 285 [ 189 429 ]
Total events 371 (Paracetamol better) 108 (Placebo better)
Heterogeneity Tau2 = 040 Chi2 = 6294 df = 15 (Plt000001) I2 =76
Test for overall effect Z = 503 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
32Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 12 Comparison 1 50 pain relief using pain relief measures Outcome 2 Paracetamol versus
placebo number of people with at least 50 pain relief at 6 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 1 50 pain relief using pain relief measures
Outcome 2 Paracetamol versus placebo number of people with at least 50 pain relief at 6 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Forbes 1989 322 023 29 730 [ 040 13375 ]
Cooper 1988 1236 940 99 148 [ 071 310 ]
Forbes 1990 736 034 30 1419 [ 084 23928 ]
Dionne 1994 2427 1825 115 123 [ 093 163 ]
Forbes 1984b 1039 036 31 1943 [ 118 31995 ]
Sunshine 1986 1530 1030 104 150 [ 081 279 ]
Subtotal (95 CI) 190 188 407 189 [ 098 367 ]
Total events 71 (Paracetamol better) 37 (Placebo better)
Heterogeneity Tau2 = 032 Chi2 = 1445 df = 5 (P = 001) I2 =65
Test for overall effect Z = 189 (P = 0058)
2 1000 mg or more
Kubitzek 2003 4569 773 99 680 [ 329 1404 ]
Mehlisch 1995 35101 140 49 1386 [ 196 9779 ]
Kiersch 1994 2089 345 79 337 [ 106 1075 ]
Olson 2001 4166 539 94 485 [ 209 1122 ]
Hersh 2000 3563 527 95 300 [ 132 682 ]
Lehnert 1990 2349 640 96 313 [ 141 693 ]
Cooper 1998 1750 326 81 295 [ 095 914 ]
Subtotal (95 CI) 487 290 593 421 [ 297 598 ]
Total events 216 (Paracetamol better) 30 (Placebo better)
Heterogeneity Tau2 = 00 Chi2 = 509 df = 6 (P = 053) I2 =00
Test for overall effect Z = 806 (P lt 000001)
Total (95 CI) 677 478 1000 332 [ 188 587 ]
Total events 287 (Paracetamol better) 67 (Placebo better)
Heterogeneity Tau2 = 072 Chi2 = 6335 df = 12 (Plt000001) I2 =81
Test for overall effect Z = 412 (P = 0000038)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
33Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 21 Comparison 2 50 pain relief using pain intensity measures Outcome 1 Paracetamol versus
placebo number of people with at least 50 pain relief at 4 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 2 50 pain relief using pain intensity measures
Outcome 1 Paracetamol versus placebo number of people with at least 50 pain relief at 4 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Dolci 1994 4972 576 86 1034 [ 437 2449 ]
Seymour 1996 1940 1039 96 185 [ 099 346 ]
Cooper 1980 737 438 74 180 [ 057 563 ]
Forbes 1990 1036 034 28 1986 [ 121 32639 ]
Forbes 1989 622 023 28 1357 [ 081 22736 ]
Cooper 1988 1236 840 90 167 [ 077 361 ]
Sunshine 1986 1830 630 90 300 [ 138 650 ]
Forbes 1984b 1339 036 28 2498 [ 154 40542 ]
Vattaraphudej 1986 616 119 44 713 [ 095 5317 ]
Cooper 1981 1537 037 28 3100 [ 192 49971 ]
Subtotal (95 CI) 365 372 592 433 [ 219 858 ]
Total events 155 (Paracetamol better) 34 (Placebo better)
Heterogeneity Tau2 = 063 Chi2 = 2622 df = 9 (P = 0002) I2 =66
Test for overall effect Z = 421 (P = 0000026)
2 1000 mg or more
Cooper 1998 1350 026 28 1429 [ 088 23130 ]
Mehlisch 1995 41101 340 75 541 [ 178 1648 ]
Hersh 2000 3663 127 46 1543 [ 223 10685 ]
Skoglund 1991 1632 033 28 3400 [ 213 54391 ]
Seymour 2003 1262 432 78 155 [ 054 442 ]
Seymour 1996 2040 1039 96 195 [ 105 362 ]
Kiersch 1994 989 045 28 971 [ 058 16317 ]
Moller 2000 28120 0122 28 5794 [ 358 93840 ]
Subtotal (95 CI) 557 364 408 646 [ 234 1785 ]
Total events 175 (Paracetamol better) 18 (Placebo better)
Heterogeneity Tau2 = 124 Chi2 = 2347 df = 7 (P = 0001) I2 =70
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
34Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Test for overall effect Z = 360 (P = 000032)
Total (95 CI) 922 736 1000 487 [ 283 837 ]
Total events 330 (Paracetamol better) 52 (Placebo better)
Heterogeneity Tau2 = 070 Chi2 = 4973 df = 17 (P = 000005) I2 =66
Test for overall effect Z = 571 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
Analysis 22 Comparison 2 50 pain relief using pain intensity measures Outcome 2 Paracetamol versus
placebo number of people with at least 50 pain relief at 6 hours
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 2 50 pain relief using pain intensity measures
Outcome 2 Paracetamol versus placebo number of people with at least 50 pain relief at 6 hours
Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Seymour 1996 1840 939 152 195 [ 100 380 ]
Forbes 1989 422 023 16 939 [ 054 16485 ]
Cooper 1988 936 640 105 167 [ 066 422 ]
Forbes 1990 836 032 17 1516 [ 091 25267 ]
Forbes 1984b 1139 036 17 2128 [ 130 34843 ]
Sunshine 1986 1430 530 111 280 [ 115 680 ]
Subtotal (95 CI) 203 200 418 267 [ 146 490 ]
Total events 64 (Paracetamol better) 20 (Placebo better)
Heterogeneity Tau2 = 015 Chi2 = 705 df = 5 (P = 022) I2 =29
Test for overall effect Z = 318 (P = 00015)
2 1000 mg or more
Hersh 2000 3163 127 33 1329 [ 191 9242 ]
Mehlisch 1995 39101 340 82 515 [ 169 1571 ]
Olson 2001 4266 739 146 355 [ 177 711 ]
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
(Continued )
35Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol better Placebo better Risk Ratio Weight Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Seymour 1996 2140 939 157 228 [ 119 433 ]
Cooper 1998 1250 026 17 1324 [ 081 21504 ]
Kiersch 1994 489 045 16 460 [ 025 8361 ]
Lehnert 1990 2449 542 114 411 [ 172 983 ]
Skoglund 1991 1432 033 17 2988 [ 186 48076 ]
Subtotal (95 CI) 490 291 582 396 [ 252 623 ]
Total events 187 (Paracetamol better) 25 (Placebo better)
Heterogeneity Tau2 = 008 Chi2 = 863 df = 7 (P = 028) I2 =19
Test for overall effect Z = 597 (P lt 000001)
Total (95 CI) 693 491 1000 341 [ 234 497 ]
Total events 251 (Paracetamol better) 45 (Placebo better)
Heterogeneity Tau2 = 013 Chi2 = 1823 df = 13 (P = 015) I2 =29
Test for overall effect Z = 637 (P lt 000001)
01 02 05 1 2 5 10
Favours placebo Favours paracetamol
36Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Analysis 31 Comparison 3 Number of people with adverse events Outcome 1 Number of patients with
adverse events paracetamol versus placebo
Review Paracetamol for pain relief after surgical removal of lower wisdom teeth
Comparison 3 Number of people with adverse events
Outcome 1 Number of patients with adverse events paracetamol versus placebo
Study or subgroup Paracetamol more Placebo more Risk Ratio Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
1 Up to 1000 mg of paracetamol
Cooper 1980 237 637 033 [ 007 155 ]
Dolci 1994 780 882 090 [ 034 236 ]
Forbes 1990 541 038 1021 [ 058 17873 ]
Forbes 1989 326 226 150 [ 027 825 ]
Sunshine 1986 130 130 100 [ 007 1526 ]
Cooper 1981 1237 438 308 [ 109 869 ]
Dionne 1994 727 525 130 [ 047 356 ]
Vattaraphudej 1986 016 019 00 [ 00 00 ]
Forbes 1984b 143 240 047 [ 004 493 ]
Subtotal (95 CI) 337 335 125 [ 069 225 ]
Total events 38 (Paracetamol more) 28 (Placebo more)
Heterogeneity Tau2 = 016 Chi2 = 906 df = 7 (P = 025) I2 =23
Test for overall effect Z = 074 (P = 046)
2 1000 mg or more
Olson 2001 1066 239 295 [ 068 1279 ]
Cooper 1998 2550 426 325 [ 127 835 ]
Moller 2000 48120 56122 087 [ 065 117 ]
Seymour 2003 2462 932 138 [ 073 260 ]
Mehlisch 1995 1299 440 121 [ 042 354 ]
Kiersch 1994 2691 1347 103 [ 059 182 ]
Hersh 2000 1263 727 073 [ 032 166 ]
Lehnert 1990 549 440 102 [ 029 355 ]
Subtotal (95 CI) 600 373 116 [ 084 160 ]
Total events 162 (Paracetamol more) 99 (Placebo more)
Heterogeneity Tau2 = 007 Chi2 = 1096 df = 7 (P = 014) I2 =36
Test for overall effect Z = 090 (P = 037)
Total (95 CI) 937 708 119 [ 090 157 ]
01 02 05 1 2 5 10
Favours treatment Favours control
(Continued )
37Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
( Continued)Study or subgroup Paracetamol more Placebo more Risk Ratio Risk Ratio
nN nN M-HRandom95 CI M-HRandom95 CI
Total events 200 (Paracetamol more) 127 (Placebo more)
Heterogeneity Tau2 = 007 Chi2 = 2073 df = 15 (P = 015) I2 =28
Test for overall effect Z = 121 (P = 023)
01 02 05 1 2 5 10
Favours treatment Favours control
A D D I T I O N A L T A B L E S
Table 1 Number of patients with adverse events (lt 1000 mg ParacetamolPlacebo)
Author Total Paracetamol AEs Paracetamol Total Placebo AEs Placebo
Cooper 1980 37 2 37 6
Cooper 1981 37 12 38 4
Dionne 1994 27 7 25 5
Dolci 1994 80 7 82 8
Forbes 1984b 43 1 40 2
Forbes 1989 26 3 26 2
Forbes 1990 41 5 38 0
Gallardo 1990 15 5 11 3
Seymour 1996 40 0 39 0
Sunshine 1986 30 1 30 1
Vattaraphudej 1986 16 0 19 0
Totals 392 43 385 31
38Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Quality assessment
Author Allocation concealment Follow up Total (Max-3)
Cooper 1980 1 0 1
Cooper 1981 1 0 1
Cooper 1988 1 0 1
Cooper 1998 1 1 2
Dionne 1994 1 0 1
Dolci 1994 1 0 1
Forbes 1984b 2 0 2
Forbes 1989 1 0 1
Forbes 1990 2 0 2
Hersh 2000 1 1 2
Kiersch 1994 1 1 2
Kubitzek 2003 1 1 2
Lehnert 1990 1 1 2
Mehlisch 1995 2 1 3
Moller 2000 1 1 2
Olson 2001 2 1 3
Seymour 1996 1 1 2
Seymour 2003 2 0 2
Skoglund 1991 2 0 2
Sunshine 1986 2 1 3
Vattaraphudej 1986 1 1 2
39Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Random-effects metaregression lt 1000 mg vs 1000 mg Paracetamol vs Placebo
Outcome Number of studies Slope estimate 95 CI Slope interpretation P value
50 pain relief at 4
hours (using pain re-
lief )
16 094 (036 to 152) more pain relief for
higher doses
0001
50 pain relife at 6
hours (using pain re-
lief )
13 114 (071 to 156) more pain relief for
higher doses
lt0001
50 pain relief at
4 hours (using pain
intensity)
16 023 (-084 to 130) more pain relief for
higher doses
067
50 pain relief at
6 hours (using pain
intensity)
14 043 (-015 to 101) more pain relief for
higher doses
015
Table 4 List of adverse events
Adverse events Paracetamol Placebo
Nausea 21 11
Vomiting 11 3
Nausea andor vomiting stomach cramps
abdominal pain
3 3
Headache 47 31
Drowsiness sleepiness somnolence 36 13
Dizziness fainting syncope 9 4
Bleeding 11 7
Chills flushes fever flu-like symptoms 5 0
Paraesthesia 4 2
Jawache 1 0
Swelling 1 6
Cellulitis 1 0
40Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 List of adverse events (Continued)
Dry socket 11 12
Surgical complications 6 13
CNS 5 6
GI 12 2
Body as a whole 8 3
Respiratory 2 0
Psychiatric 0 1
Other hiccups hearingvestibular miosis 5 1
Table 5 Global assessment - 5-point scale(lt 1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Cooper 1980 37 089 38 089
Cooper 1981 37 192 37 062
Cooper 1988 36 238 40 205
Dionne 1994 27 240 25 200
Dolci 1994 72 210 76 217
Forbes 1984 39 126 36 028
Mean 248 183 252 144
Table 6 Global assessment - 4-point scale (lt 1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Forbes 1989 26 100 26 030
Forbes 1990 41 147 38 056
Sunshine 1986 30 120 30 093
Vattaraphudej 1986 16 16 19 116
41Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 6 Global assessment - 4-point scale (lt 1000 mg Paracetamol) (Continued)
Mean 113 131 113 070
Table 7 Global assessment - 5-point scale (1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Kiersch 1994 91 130 47 060
Kubitzek 2003 78 198 84 145
Mehlisch 1995 101 157 40 045
Olson 2001 66 281 39 193
Seymour 2003 62 250 32 214
Mean 398 194 242 129
Table 8 Global assessment - 4-point scale (1000 mg Paracetamol)
Author Total Paracetamol Global assessment Total Placebo Global assessment
Hersh 2000 63 229 27 085
Moller 2000 120 188 122 154
Mean 183 202 149 141
A P P E N D I C E S
Appendix 1 CENTRAL search strategy
1 MOLAR THIRD single term (MeSH)
2 (wisdom next tooth)
3 (wisdom next teeth)
4 (third near molar)
5 (1 or 2 or 3 or 4)
6 TOOTH EXTRACTION single term (MeSH)
7 (extract near tooth)
8 (extract near teeth)
9 (extract near (third next molar))
10 (extract near (third near molar))
42Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
11 (remov near tooth)
12 (remov near teeth)
13 (surgical near remov)
14 (surgery near remov)
15 (surgical near extract)
16 (surgery near extract)
17 (6 or 7 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16)
18 (5 and 17)
W H A T rsquo S N E W
Last assessed as up-to-date 21 May 2007
Date Event Description
31 July 2008 Amended Converted to new review format
H I S T O R Y
Protocol first published Issue 4 2003
Review first published Issue 3 2007
C O N T R I B U T I O N S O F A U T H O R S
Conceiving designing and co-ordinating the review (Kiaran Weil (KW) Paul Coulthard (PC))
Developing search strategy and undertaking searches (Zahid Afzal (ZA) Arjen van Wijk (AJW) KW)
Screening search results and retrieved papers against inclusion criteria (ZA KW) Marco Esposito (ME) Lee Hooper (LH) PC)
Appraising quality (KW ZA)
Extracting data from papers (KW LH Helen Worthington (HW))
Writing to authors for additional information (KW)
Data management for the review and entering data into RevMan (KW)
Analysis and interpretation of data (KW LH HW)
Writing the review (KW)
Providing general advice on the review (ME LH PC HW)
Performing previous work that was the foundation of current study (PC)
43Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D E C L A R A T I O N S O F I N T E R E S T
None known
S O U R C E S O F S U P P O R T
Internal sources
bull The University of Manchester UK
bull The University of Amsterdam Netherlands
External sources
bull No sources of support supplied
I N D E X T E R M S
Medical Subject Headings (MeSH)
Acetaminophen [adverse effects lowasttherapeutic use] Analgesics Non-Narcotic [adverse effects lowasttherapeutic use] Molar Third [lowastsurgery]
Outcome Assessment (Health Care) Pain Postoperative [lowastdrug therapy] Pain Measurement Randomized Controlled Trials as Topic
Tooth Extraction [lowastadverse effects]
MeSH check words
Humans
44Paracetamol for pain relief after surgical removal of lower wisdom teeth (Review)
Copyright copy 2008 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 407
Relative efficacy of oral analgesics after thirdmolar extractionJ Barden1 J E Edwards2 H J McQuay3 P J Wiffen4 and R A Moore5
Objectives To compare the relative efficacy of analgesics after thirdmolar extraction from systematic reviews of randomised double blindstudiesData sources Dental trials from systematic reviews of randomiseddouble-blind studies of analgesics in acute painData selection Number of patients with moderate or severe painachieving at least half pain relief over 4 to 6 hours after a single oraldose of analgesicData extraction Independently by two reviewersData synthesis Use of dichotomous information from active andplacebo treatments first to calculate the statistical significance usingrelative risk and then to evaluate the clinical relevance using numberneeded to treat (NNT) Non-steroidal anti-inflammatory drugs (NSAIDs)and cyclo-oxygenase-2 (COX-2) inhibitors had the lowest (best) NNTsfor the outcome of at least half pain relief over 4-6 hours comparedwith placebo With the best performing analgesics 50-70 patients out of100 had good pain relief compared with about 10 out of 100 withplacebo Only paracetamol 600650 mg plus codeine 60 mg wasassociated with any significant increase in any patient experiencing anadverse eventConclusions NSAIDs and COX-2 inhibitors have the lowest (best) NNTsThey may also have fewer adverse effects after third molar surgerythough conclusive evidence is lacking At least 80 of analgesicprescribing by UK dentists is in line with the best available evidence onefficacy and safety
Acute pain has been studied in single dose designs first pro-posed by Beecher and colleagues12 and formalised by Houdeand Wallenstein3 The problem with single trials is that whilethey can demonstrate statistical superiority of analgesic overplacebo variation because of random chance means that if
1Research Associate 2Senior Research Associate 3Professor of Pain Relief 4PrescribingAdvisor 5Research Director Pain Research and Nuffield Department of AnaestheticsUniversity of Oxford Oxford Radcliffe Hospital The Churchill Headington Oxford OX3 7LJ UKCorrespondence to Dr R A MooreE-mail andrewmoorepruoxacuk
Refereed paperReceived 150403 Accepted 121103doi101038sjbdj4811721copy British Dental Journal 2004 197 407ndash411
small they provide a poor estimate of the size of the analgesiceffect4 Combining results from clinically homogeneous trials ina meta-analysis gives an accurate estimate of the extent of theanalgesic effect when sufficient numbers of patients have beenrandomised45
Clinical trials in acute pain normally last 4 to 6 hours becausethat is the duration of effect of most analgesics whether injectedor as tablets and whether simple analgesics NSAIDs or opioidsMeta-analysis in acute pain has concentrated on the use of thearea under the total pain relief versus time curve (TOTPAR)dichotomized into those patients who do or do not achieve atleast half pain relief (at least 50 maximum TOTPAR)6 Thismeasure is the one most frequently reported and it avoids theproblem of reporting continuous pain data as the mean of ahighly skewed distribution7 It has the benefit of being intuitivelymeaningful to patients and professionals as well as being meas-urable
Meta-analyses in acute pain usually combine studies from avariety of pain models and relative efficacy of analgesics inthese studies has been examined6 A majority of studies were inthird molar extraction but any postoperative pain condition islikely to be included In the largest dataset that of aspirin8
pain model (dental or other surgery) made no difference to theNNT
Dentists ask rightly about relative efficacy in dental painThe number of prescription items issued by dentists in Englandwas remarkably consistent between 1998 and 2001 (Table 1)with ibuprofen dihydrocodeine and paracetamol being mostfrequently prescribed This review set out to examine single-dose oral analgesics after third molar extraction from a numberof updated systematic reviews both for the analgesics common-ly prescribed in England and for those for which comparableevidence exists including the newer cyclo-oxygenase-2 selec-tive inhibitors like rofecoxib celecoxib and valdecoxib
METHODSIn all the systematic reviews QUORUM guidelines were fol-lowed9 In the reviews studies for inclusion were soughtthrough searching the Cochrane Library Biological AbstractsMEDLINE PubMed and the Oxford Pain Relief database10 Ref-erence lists and review articles were examined for possible addi-tional references Most had search dates in 2002
This paper reviews the available high quality information on analgesics commonlyprescribed by dentists including COX-2 selective inhibitors
Problems related to chance effects are avoided by combining multiple trials in a meta-analysis
There is good evidence of efficacy for most commonly-prescribed analgesics Standard doses of NSAIDs and COX-2 inhibitors provide the best analgesia and lowest
rate of adverse events
I N B R I E F
RESEARCH
07p407-411qxd 10092004 1518 Page 407
RESEARCH
408 BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004
References for the reviews are as followsAspirin Edwards et al 19998 additional searching in
2002 found no new studiesCelecoxib An unpublished review being submitted as a
Cochrane ReviewDiclofenac An updated version of a Cochrane review11
Dihydrocodeine A Cochrane review12
Ibuprofen An updated version of a Cochrane review11
Paracetamol An updated version of a Cochrane review13
Paracetamol An updated version of a Cochrane review13
plus codeineRofecoxib An updated version of a systematic review14
Valdecoxib A systematic review in preparation
Criteria for inclusion for postoperative dental pain werestudy in third molar extraction full journal publication (exceptvaldecoxib which included information from a poster) ran-domised controlled trials which included single dose treatmentgroups of oral analgesic and placebo double blind designbaseline postoperative pain of moderate to severe intensitypatients over 15 years of age at least 10 patients per group andthe pain outcome measures of total pain relief (TOTPAR) orsummed pain intensity difference (SPID) over 4-6 hours or suf-ficient data to allow their calculation Pain measures allowedfor the calculation of TOTPAR or SPID were a standard fivepoint pain relief scale (none slight moderate good complete)a standard four point pain intensity scale (none mild moder-ate severe) or a standard visual analogue scale (VAS) for pain
relief or pain intensity For adverse events the primary out-come sought was the proportion of patients experiencing anyadverse event with secondary outcomes of patients experienc-ing particular adverse events Although adverse events areoften reported inconsistently in acute pain trials15 the outcomeof any patient experiencing any adverse event was the mostconsistently reported
Each report which could possibly be described as a randomisedcontrolled trial was read independently by several authors andscored using a commonly-used three item 1-5 score qualityscale16 Consensus was then achieved The maximum score of anincluded study was 5 and the minimum score was 2 Authors werenot blinded because they already knew the literature This scoringsystem takes account of randomisation blinding and withdrawalsand drop outs Trials that score 3 or more (less biased) have beenshown repeatedly to have lower treatment effects than those scor-ing 2 or less1718
For each trial mean TOTPAR SPID VAS-TOTPAR or VAS-SPIDvalues for each treatment group were converted to maxTOTPARby division into the calculated maximum value19 The proportionof patients in each treatment group who achieved at least 50maxTOTPAR was calculated using valid equations20-22 The num-ber of patients randomised was taken as the basis for calculationsto produce an intention to treat analysis The number of patientswith at least 50 maxTOTPAR was then used to calculate relativebenefit and NNT for analgesic versus placebo The same methodswere used for adverse events where the number needed to harm(NNH) was calculated
Table 1 Numbers of prescription items issued by dentists and dispensed in EnglandAnalgesic 1998 1999 2000 2001
Ibuprofen 400 mg 107200 110400 109000 103900
Dihydrocodeine 30 mg 53700 50300 49100 46700
Ibuprofen 600 mg 34200 39700 40800 42600
Ibuprofen 200 mg 36300 34600 32000 30600
Paracetamol 500 mg 11100 12800 15400 17200
Paracetamol 500 mg soluble 800 1000 900 900
Pethidine 50 mg 1100 900 700 700
Aspirin 300 mg 200 200 200 200
Source DOH statistics division 2002 calendar year January to December
Dihydrocodeine 30 mgParacetamol 300 mg + codeine 30 mg
Paracetamol 600650 mgAspirin 600650 mg
Paracetamol 9751000 mgCelecoxib 200 mg
Paracetamol 600650 mg + codeine 60 mgIbuprofen 200 mgDiclofenac 50 mgRofecoxib 50 mgIbuprofen 400 mgValdecoxib 20 mgDiclofenac 100 mgValdecoxib 40 mgIbuprofen 600 mg
0 10 20 30 40 50 60 70 80 90 10095 confidence interval of the percent ofpatients achieving at least 50 pain relief
Fig 1 The 95confidence interval ofthe proportion ofpatients with at leasthalf pain relief over 4-6hours compared withplacebo in third molarextraction trials
07p407-411qxd 10092004 1519 Page 408
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 409
of patients had at least half pain relief with active treatment in onesmall trial in dental pain (Table 2)
The adverse event outcome of a patient experiencing anyadverse event is shown in Table 3 from 10113 patients in 107 tri-als Of the 15 drug and dose combinations only paracetamol600650 mg plus codeine 60 mg could be statistically distin-guished from placebo in 10 trials and 824 patients The NNH was53 (41 to 74) indicating that five patients had to be treated withparacetamol 600650 mg plus codeine 60 mg for one of them tohave an adverse event that would not have occurred with placeboFor all other drugs and doses there was no difference betweenanalgesic and placebo
DISCUSSIONSystematic review and meta-analysis both depend on two interde-pendent criteria for them to make sense the quality of the compo-nent individual studies and the total size of the sample availablefor analysis
We know that if trials are of poor reporting quality1718 or notrandomised30 or not blind or both31 then the tendency is to over-estimate the benefits of treatment The reviews included here alldemanded that trials should be both randomised and double-blindas a minimum requirement for inclusion
We also know that even if trials are done well small samplesize can lead to an incorrect answer just because of the randomplay of chance4 For these studies we also know just how muchinformation is needed to be 95 confident of an NNT to withplusmn05 units4 With an NNT of 23 it is 400 patients in the compari-son with an NNT of 29 it is 1000 patients and with an NNT of42 it is many more than with 1000 At NNTs of 4 or more evenwith 1000 patients fewer than 75 of trials will be within plusmn05of the overall NNT
The analgesics for which these two criteria were metunequivocally were valdecoxib (combining 20 mg and 40 mg)rofecoxib 50 mg ibuprofen 400 mg diclofenac 50 mg and prob-ably ibuprofen 200 mg For paracetamol the numbers were bor-derline and for diclofenac 100 mg too small to make any safejudgement There is good evidence of good efficacy for the anal-gesics most commonly prescribed by dentists with the excep-tion of dihydrocodeine where there was little evidence in totaland no convincing evidence of efficacy
Relative benefit and relative risk estimates were calculated with95 confidence intervals using a fixed effects model23 Hetero-geneity tests were not used as they have previously been shown tobe unhelpful2425 though homogeneity was examined visually26
Publication bias was not assessed using funnel plots as these testshave been shown to be unhelpful2728 The number needed to treator harm (NNT and NNH) with confidence intervals was calculatedby the method of Cook and Sackett29 from the sum of all eventsand patients for treatment and placebo
Relative benefit or risk was considered to be statistically signifi-cant when the 95 confidence interval did not include 1 NNT val-ues were only calculated when the relative risk or benefit was sta-tistically significant and are reported with the 95 confidenceinterval Calculations were performed using Microsoft Excel 2001on a Power Macintosh G4
RESULTSTable 2 shows the main results from 14150 patients in 155 trials of15 drug and dose combinations against placebo in third molarextractions Of those 15 drug and dose combinations only dihy-drocodeine 30 mg could not be statistically distinguished fromplacebo because there were no trials with any useful informationin third molar extraction Figure 1 shows the proportion ofpatients achieving at least 50 pain relief with treatment Thesmallest sample for any comparison was 136 patients for celecoxib200 mg Only five of the 14 comparisons had more than 1000patients and seven had fewer than 500 patients In all systematicreviews the majority of trials had quality scores of 3 or more
The lowest (best) NNTs were for NSAIDs and COX-2 inhibitorsat standard or high doses For these NNTs could be as low as about2 (meaning that two patients had to be treated with NSAID orCOXIB for one of them to have an outcome of at least half painrelief that would not have occurred with placebo) Valdecoxib 20mg and 40 mg rofecoxib 50 mg ibuprofen 400 mg and diclofenac50 mg and 100 mg all had NNTs below 24 For all of them about60-70 of patients had at least half pain relief with active treat-ment compared with about 10 with placebo
Paracetamol 9751000 mg aspirin 600650 mg and paraceta-mol 600650 mg had NNTs of between 4 and 5 Fewer than 40 ofpatients with paracetamol at these doses had at least half painrelief with active treatment With dihydrocodeine 30 mg only 16
Table 2 Efficacy of analgesics after third molar extraction from systematic reviews of randomised double blind trials
Number () of patientswith at least 50 pain relief
Drug and dose Treatment Placebo Relative benefit Number needed to treat Total patients Total trials(95 CI) (95 CI)
Valdecoxib 40 mg 204279 (73) 19194 (10) 73 (48 to 112) 16 (14 to 17) 473 4
Diclofenac 100 mg 71102 (70) 8102 (8) 89 (45 to 175) 16 (14 to 19) 204 2
Valdecoxib 20 mg 69101 (68) 8103 (8) 88 (45 to 173) 17 (14 to 20) 204 2
Diclofenac 50 mg 112189 (59) 21178 (12) 49 (33 to 75) 21 (18 to 26) 367 5
Rofecoxib 50 mg 318557 (57) 23262 (9) 66 (44 to 99) 21 (19 to 23) 819 6
Ibuprofen 400 mg 10351835 (56) 1861567 (12) 47 (40 to 54) 22 (21 to 24) 3402 37
Ibuprofen 200 mg 323695 (46) 47499 (9) 46 (35 to 61) 27 (24 to 31) 1194 14
Ibuprofen 600 mg 90114 (79) 3889 (43) 19 (15 to 25) 28 (20 to 43) 203 3
Celecoxib 200 mg 3991 (43) 445 (9) 48 (18 to 127) 29 (21 to 48) 136 1
Paracetamol 9751000 mg 226616 (37) 40422 (9) 38 (28 to 52) 37 (31 to 47) 1038 10
Paracetamol 600650 mg + codeine 60 mg 217532 (48) 64380 (19) 25 (19 to 31) 42 (34 to 55) 911 12
Paracetamol 600650 mg 224630 (36) 76635 (12) 29 (23 to 37) 42 (36 to 52) 1265 10
Aspirin 600650 mg 6271788 (36) 2551847 (15) 25 (22 to 29) 47 (42 to 54) 3635 46
Paracetamol 300 mg + codeine 30 mg 48175 (29) 11124 (9) 33 (18 to 62) 54 (37 to 97) 299 3
Dihydrocodeine 30 mg 849 (16) 250 (4) 41 (09 to 18) not calc 99 1
Shaded areas are those analgesics used by dentists in the UK
07p407-411qxd 10092004 1519 Page 409
RESEARCH
410 BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004
With the information available standard doses of NSAIDs andCOX-2 inhibitors provided the best analgesia (Fig 2) NNTs of 2and below are indicative of very effective medicines32 The indirectcomparisons that allow us to arrive at this conclusion are only sus-tainable because the trials have the same design use patients withthe same entry criterion (moderate or severe pain intensity) withstandard measurements made in the same way over the same peri-od of time and with the same output from each trial and oneknown to be legitimate The validity of the indirect comparisonsare buttressed by the dose response of two doses of ibuprofen (400mg was better than 200 mg) and two doses of paracetamol(9751000 mg was better than 600650 mg) where there were cred-ible amounts of information A systematic review of ibuprofenversus paracetamol in dental studies also concluded that ibuprofenwas superior concordant with the indirect comparison33
The adverse event information we have tells us only aboutpatients experiencing any adverse event With the amount ofinformation available it appears that only higher doses ofcodeine with paracetamol resulted in a significantly higher ratefor this outcome than placebo In Table 3 the rate at which thisadverse event occurred with placebo varied greatly between 2
and 52 This variation will be due partly to small sizes4 butalso because we know that methods of collecting adverse eventdata impact significantly on the reported incidence and becausemethods used varied15
Information about specific adverse events is even more difficultto obtain and very large data sets are required to produce infor-mation about for instance gastric irritation with aspirin use8 Ofinterest to dentists might be the rate of alveolitis or dry socket Thisis reported in some of the newer COXIB studies but not in olderstudies There is just too little information to make a judgement
What these comparisons do not do is to tell dentists what toprescribe They and the products of other systematic reviewsshould not be used as rules but rather as evidence-based toolsto help make better policy decisions and decisions about indi-vidual patients Present prescribing practice (Table 1) showsthat for the most part effective and safe analgesics are beingused in 80 of prescriptions The exception is prescribing dihy-drocodeine 30 mg (20 of prescriptions) for which we lack sin-gle dose evidence of efficacy in dental surgery and which couldnot be distinguished from placebo in other conditions againwith little data6
Paracetamol 300 + codeine 30 mgAspirin 600650 mg
Paracteamol 600650 mgParacetamol 600650 + codeine 60 mg
Paracetamol 9751000 mgCelecoxib 200 mgIbuprofen 200 mgDiclofenac 50 mgIbuprofen 400 mgRofecoxib 50 mg
Valdecoxib 20 mgValdecoxib 40 mgDiclofenac 100 mg
1 2 3 4 5 6 7 8 9 1095 confidence interval of the NNT
Fig 2 The 95confidence interval ofthe number needed totreat (NNT) for at leasthalf pain relief over 4-6hours compared withplacebo in third molarextraction trials
Table 3 Patients experiencing any adverse event with analgesics after third molar extraction from systematic reviews of randomised double blind trials
Number () of patientsharmed with
Drug and dose Treatment Placebo Relative risk Number needed to harm Total patients Total trials(95 CI) (95 CI)
Valdecoxib 40 mg 63180 (35) 76144 (53) 06 (05 to 08) not calc 324 3
Diclofenac 100 mg 252 (4) 252 (4) 10 (12 to 68) not calc 104 1
Valdecoxib 20 mg 36100 (36) 55103 (53) 07 (05 to 09) not calc 203 2
Diclofenac 50 mg 15222 (7) 12210 (6) 12 (06 to 24) not calc 432 4
Rofecoxib 50 mg 105314 (33) 48122 (39) 09 (07 to 11) not calc 436 3
Ibuprofen 400 mg 120972 (13) 91805 (12) 11 (08 to 14) not calc 1777 19
Ibuprofen 200 mg 84554 (15) 69372 (19) 08 (06 to 10) not calc 926 10
Ibuprofen 600 mg no data
Celecoxib 200 mg no data
Paracetamol 9751000 mg 175836 (24) 103464 (20) 11 (09 to 13) not calc 1300 9
Paracetamol 600650 mg + codeine 60 mg 156490 (25) 43333 (14) 18 (13 to 25) 53 (41 to 74) 824 10
Paracetamol 600650 mg 32228 (14) 20229 (9) 16 (09 to 27) not calc 457 7
Aspirin 600650 mg 1551320 (12) 1681422 (12) 10 (08 to 12) not calc 3031 36
Paracetamol 300 mg + codeine 30 mg 29175 (15) 20124 (16) 09 (06 to 16) not calc 299 3
Dihydrocodeine 30 mg 149 (2) 150 (2) 10 (01 to 17) not calc 99 1
Shaded areas are those analgesics used by dentists in the UK
07p407-411qxd 10092004 1520 Page 410
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 197 NO 7 OCTOBER 9 2004 411
Not all the analgesics in this review are presently available forprescribing by dentists at least in the UK The information on effi-cacy on harm and on the amount of information available shouldbe useful in any initiative to develop a prescribing formulary indentistry especially as we have growing confidence in the value ofindirect comparisons34
COMPETING INTERESTSRAM has been a consultant for MSD RAM amp HJM have consulted for variouspharmaceutical companies RAM HJM amp JE have received lecture fees frompharmaceutical companies related to analgesics and other healthcareinterventions All authors have received research support from charitiesgovernment and industry sources at various times but no such support wasreceived for this work No author has any direct stock holding in anypharmaceutical company
AUTHORS CONTRIBUTIONSJB was involved with searching data extraction quality scoring analysis andwriting JE was involved with searching data extraction quality scoring andwriting HJM was involved in analysis and writing RAM was involved in dataextraction quality scoring analysis and writing PW was involved with theoriginal concept with researching prescribing data and writing
The work was supported by Pain Research Funds and the Oxford Pain Relief TrustThe authors would like to thank Frances Fairman of the Cochrane Pain Palliativeand Supportive Care systematic review group for bringing this issue to ourattention The Department of Health Statistics Division provided data onprescribing by dentists
1 Beecher H K Keats A S Mosteller F The effectiveness of oral analgesics (morphinecodeine acetylsalicylic acid) and the problem of placebo lsquoreactorsrsquo and lsquononreactorsrsquo J Pharmacol 1953 109 93-400
2 Beecher H K The measurement of pain Pharmacol Rev 1957 9 59-2103 Houde R W Wallenstein S L Beaver W T Clinical measurement of pain In G De
Stevens (ed) Analgetics pp75-122 New York and London Academic Press 1965 4 Moore R A Gavaghan D Tramegraver M R Collins S L McQuay H J Size is everything mdash
large amounts of information are needed to overcome random effects in estimatingdirection and magnitude of treatment effects Pain 98 78 209-216
5 Ioannidis J P A Lau J Evolution of treatment effects over time Empirical insight fromrecursive cumulative metaanalyses PNAS 2001 98 831-836
6 McQuay H J Moore R A An evidence-based resource for pain relief Oxford OxfordUniversity Press 1998
7 McQuay H J Carroll D Moore R A Variation in the placebo effect in randomisedcontrolled trials of analgesics all is as blind as it seems Pain 1996 64 331-335
8 Edwards J E Oldman A Smith L Wiffen P J Carroll D McQuay H J Moore R A Oralaspirin in postoperative pain a quantitative systematic review Pain 1999 81 289-297
9 Moher D Cook D J Eastwood S Olkin I Rennie D Stroup D F Improving the quality ofreports of meta-analyses of randomised controlled the QUOROM statement Lancet1999 354 1896-1900
10 Jadad A R Carroll D Moore A McQuay H Developing a database of published reportsof randomised clinical trials in pain research Pain 1996 66 239-46
11 Collins S L Moore R A McQuay H J Wiffen P J Edward J S Single dose oral ibuprofenand diclofenac for postoperative pain In The Cochrane Library Issue 4 2000 OxfordUpdate Software
12 Edwards J E McQuay H J Moore R A Single-dose dihydrocodeine for acute
postoperative pain In The Cochrane Library Issue 4 2000 Oxford Update Software13 Moore R A Collins S L Carroll D McQuay H J Edwards J Single dose paracetamol
(acetaminophen) with and without codeine for postoperative pain In The CochraneLibrary Issue 4 2000 Oxford Update Software
14 Barden J Edwards J E McQuay H J Moore R A Rofecoxib in acute postoperative painquantitative systematic review BMC Anesthesiol 2002 2 4httpwwwbiomedcentralcom1471-225324
15 Edwards J E McQuay H J Moore R A Collins S L Reporting of adverse effects inclinical trials should be improved Lessons from acute postoperative pain J PainSympt Manage 1999 18 427-437
16 Jadad A R Moore R A Carroll D et al Assessing the quality of reports of randomizedclinical trials is blinding necessary Control Clin Trials 1996 17 1-12
17 Khan K S Daya S Jadad A R The importance of quality of primary studies inproducing unbiased systematic reviews Arch Intern Med 1996 156 661-666
18 Moher D Pham B Jones A et al Does quality of reports of randomised trials affectestimates of intervention efficacy reported in meta-analyses Lancet 1998 352609-613
19 Cooper S A Single-dose analgesic studies the upside and downside of assaysensitivity In Max M B Portenoy R K and Laska E M (eds) The design of analgesicclinical trials (Advances in Pain Research and Therapy Vol 18) pp117-124 New YorkRaven Press 1991
20 Moore A McQuay H Gavaghan D Deriving dichotomous outcome measures fromcontinuous data in randomised controlled trials of analgesics Pain 1996 66 229-237
21 Moore A McQuay H Gavaghan D Deriving dichotomous outcome measures fromcontinuous data in randomised controlled trials of analgesics Verification fromindependent data Pain 1997 69 127-130
22 Moore A Moore O McQuay H Gavaghan D Deriving dichotomous outcome measuresfrom continuous data in randomised controlled trials of analgesics Use of painintensity and visual analogue scales Pain 1997 69 311-315
23 Morris J A Gardner M J Calculating confidence intervals for relative risk odds ratiosand standardised ratios and rates In Gardner M J and Altman D G(eds) Statistics withconfidence mdash confidence intervals and statistical guidelines pp50-63 LondonBritish Medical Journal 1995
24 Gavaghan D J Moore R A McQuay H J An evaluation of homogeneity tests in meta-analyses in pain using simulations of individual patient data Pain 2000 85 415-424
25 Higgins J Thompson S Deeks J Altman D Statistical heterogeneity in systematicreviews of clinical trials a critical appraisal of guidelines and practice J Health SurvRes Policy 2002 7 51-61
26 LAbbeacute K A Detsky A S ORourke K Meta-analysis in clinical research Ann Intern Med1987 107 224-233
27 Sterne J A Gavaghan D Egger M Publication and related bias in meta-analysispower of statistical tests and prevalence in the literature J Clin Epidemiol 2000 531119-1129
28 Tang J-L Liu J L Y Misleading funnel plot for detection of bias in meta-analysis J ClinEpidemiol 2000 53 477-484
29 Cook R J Sackett D L The number needed to treat a clinically useful measure oftreatment effect Br Med J 1995 310 452-454
30 Carroll D Tramegraver M McQuay H Nye B Moore A Randomization is important instudies with pain outcomes systematic review of transcutaneous electrical nervestimulation in acute postoperative pain Br J Anaesth 1996 77 798-803
31 Schulz K F Chalmers I Hayes R J Altman D G Empirical evidence of bias dimensionsof methodological quality associated with estimates of treatment effects incontrolled trials J Am Med Assoc1995 273 408-412
32 McQuay H J Moore R A Using numerical results from systematic reviews in clinicalpractice Ann Intern Med 1997 126 712-720
33 M Hyllested Jones S Pedersen J L Kehlet H Comparative effect of paracetamolNSAIDs or their combination in postoperative pain management a qualitative reviewBr J Anaesth 2002 88 199-214
34 F Song Altman D G Glenny A M Deeks J J Validity of indirect comparison forestimating efficacy of competing interventions empirical evidence from publishedmeta-analyses Br Med J 2003 326 472-476
07p407-411qxd 10092004 1520 Page 411
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
Relative efficacy of oral analgesics after third molar extraction ndash a 2011 updateS Derry1 P J Wiffen2 and R A Moore3
and reporting and were all of high meth-odological quality the relative efficacy of different analgesics is justifiable when established against the common comparator of placebo3 Moreover the methods have been extensively examined and validated using individual patient data analyses45
Several approaches can be used to pre-sent results The percentage of patients who benefit with treatment is one approach obviously the higher the number
In 2004 the British Dental Journal carried a review examining analgesic efficacy meas-ured after third molar extractions1 predom-inantly derived from Cochrane reviews of single dose analgesics in established mod-erate or severe pain In the intervening years the reviews on which it was based have been extended to other analgesics and updated to include relevant additional clinical trials performed in the past decade
The culmination of this work has been the publication by the Cochrane Collaboration of an overview of these updated systematic reviews2 The overview included 35 sepa-rate Cochrane Reviews with 38 analyses of single dose oral analgesics tested in acute postoperative pain models with results from about 45000 participants studied in approximately 350 individual studies About 29000 patients contributed data to trials in dental pain
Each individual review reported results for dental studies where data were avail-able overwhelmingly in the third molar extraction pain model Because all of the reviews used identical methods outcomes
This article provides a summary of the efficacy and relative efficacy of 38 different drugs or drug combinations tested in standard postoperative pain trials It will help clinicians and patients make informed choices about analgesia based on pain relief duration of action and adverse events which can then be put into context for the individual patient depending on local availability This article highlights the fact that no single drug is effective in all patients ndash even the best drugs fail to provide good levels of pain relief in at least 30 These patients should try a different analgesic
the better Another way is to look at the number needed to treat (NNT) for one patient to benefit this is the treatment-specific effect and can be expressed as 100(active - placebo) The ideal NNT is 1 where everyone gets better with treatment and no one does with placebo lower numbers are better In dental tri-als where about 10 of patients benefit with placebo the best possible NNT is 100100 - 10 = 11
13Pain Research and Nuffield Division of Anaesthet-ics Department of Clinical Neurosciences University of Oxford The Churchill Hospital Oxford OX3 7LJ 2UK Cochrane Centre Summertown Pavilion 18-24 Middle Way Oxford OX2 7LG Correspondence to R Andrew Moore Email andrewmoorepruoxacuk
Refereed Paper Accepted 12 September 2011 DOI 101038sjbdj2011905 copyBritish Dental Journal 2011 211 419-420
bull Summarises the known evidence on efficacy of oral analgesics in dental pain
bull Describes shorter term pain relief and time needed before remedication
bull Provides an evidential context for making decisions about individual patients or practice guidelines
I N B R I E F
PRA
CTICE
Table 1 Efficacy results in dental pain studies for a range of commonly used analgesics
Drug and dose (mg)Number of
Percent with at least 50 maxi-mum pain relief NNT
Median time to remedication (hr)
Trials Patients Active Placebo
Aspirin 600650 mg 45 3581 36 14 45 (40 to 52) 30
Aspirin 1000 mg 4 436 35 11 42 (32 to 60) no data
Celecoxib 400 mg 4 620 34 3 25 (22 to 29) 84
Diclofenac 50 mg (Na and K) 9 1119 56 19 27 (24 to 31) 43
Diclofenac 50 mg K 5 622 65 16 21 (19 to 24) no data
Etoriocoxib 120 mg 4 500 71 9 16 (15 to 18) gt24
Ibuprofen 400 mg 49 5428 55 12 23 (22 to 24) 56
Ibuprofen 400 mg soluble 9 959 66 10 18 (17 to 20) no data
Ibuprofen 200 mg + paracetamol 500 mg 2 280 74 10 16 (14 to 18) gt8
Naproxen 500550 mg 5 402 61 7 18 (16 to 21) 89
Paracetamol 1000 mg 19 2157 41 10 32 (29 to 36) 39
Note that data for remedication time were not generally available for dental studies separately and the values reported apply to all postoperative conditions though predominantly third molar extraction
BRITISH DENTAL JOURNAL VOLUME 211 NO 9 NOV 12 2011 419
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
copy 2011 Macmillan Publishers Limited All rights reserved
PRACTICE
This brief report describes the main results of interest to dentists using results from the Cochrane overview and from a recent analysis of a combination of ibu-profen and paracetamol5
RESULTSTable 1 reports data for aspirin celecoxib diclofenac etoricoxib ibuprofen ibu-profen plus paracetamol naproxen and paracetamol Widely differing amounts of information were available for individual drugs from as few as 402 patients for nap-roxen 500550 mg and as many as 5428 for ibuprofen 400 mg
One outcome reported is the percentage of patients with initially moderate pain (30-60 mm on a 100 mm VAS) or severe pain (more than 60 mm) who obtained at least 50 of the maximum possible pain relief over a 4-6 hour period after taking the tab-lets This is a high test of efficacy achieved by only about 10 of patients who received no active treatment (placebo) but achieved by 34-74 of those who did get the active drug Ibuprofen 200 mg plus paracetamol 500 mg and etoricoxib 120 mg achieved
response rates above 70 paracetamol 1000 mg achieved only a 41 response rate
Several products had an NNT of about 2 or below the combination of ibupro-fen 200 mg plus paracetamol 500 mg etoricoxib 120 mg ibuprofen 400 mg in a soluble form naproxen 500550 mg and 50 mg of the potassium salt of diclofenac (the sodium salt being much less effective in this assay Fig 1)
A new outcome that some will con-sider relevant is the time required for half the patients to need more analgesia the time to remedication Longer duration is another indicator of greater effect and for a number of analgesics median remedica-tion times are beyond eight hours
DISCUSSIONThe 2004 review included evidence for rofecoxib and valdecoxib neither of which is available today New relevant informa-tion includes data on the ibuprofen plus paracetamol combination different ibu-profen and diclofenac formulations and etoricoxib all of which are among the most efficacious analgesics after third
molar surgery Greater efficacy and longer duration of action tended to go together
For one analgesic relevant to dentistry the evidence is largely silent For dihydrocodeine 30 mg (still commonly used by dentists) only 136 patients were found in trials in dental pain with only 24 obtaining at least 50 maximum pain relief compared with 7 with placebo The resultant NNT was 6 far worse than available for drugs in Table 1 and far worse than ibuprofen 400 mg in the only direct comparison6 The Cochrane overview concluded that the results for dihy-drocodeine were not robust because of the smallness of the data set available and that unpublished results from just 46 patients in zero effect trials would be needed to make any result clinically irrelevant
CONCLUSIONThe amount of evidence available on single dose studies of analgesics in dental pain is large and readily available These results are tools to help formulate policy and pre-scribing for individuals and populations
1 Barden J Edwards J E McQuay H J Wiffen P J Moore R A Relative efficacy of oral analgesics after third molar extraction Br Dent J 2004 197 407ndash411
2 Moore R A Derry S McQuay H J Wiffen P J Single dose oral analgesics for acute postoperative pain in adults Cochrane Database Syst Rev 2011 9 CD008659
3 Song F Altman D G Glenny A M Deeks J J Validity of indirect comparison for estimating efficacy of competing interventions empirical evidence from published meta-analyses BMJ 2003 326 472
4 Moore R A Edwards J E McQuay H J Acute pain individual patient meta-analysis shows the impact of different ways of analysing and presenting results Pain 2005 116 322ndash331
5 Moore R A Straube S Paine J Derry S McQuay H J Minimum efficacy criteria for comparisons between treatments using individual patient meta-analysis of acute pain trials examples of etoricoxib paracetamol ibuprofen and ibuprofenparacetamol combinations after third molar extraction Pain 2011b 152 982ndash989
6 Moore R A Edwards J Derry S McQuay H J Single dose oral dihydrocodeine for acute postop-erative pain Cochrane Database Syst Rev 2000 2 CD002760
Ibuprofen 200mg + paracetamol 500 mg
Ibuprofen 400 mg
Aspirin 600650 mg
Aspirin 1000 mg
Paracetamol 1000
Naproxen 500550
Diclofenac 50 mg (Na and K)
Celecoxib 400 mg
Diclofenac 50 mg K
Ibuprofen 400 mg soluble
Etoriocoxib 120 mg
1 2 3 4 5 6
NNT for at least 50 maximum pain relief (95 CI)
Fig 1 NNTs in dental pain studies for a range of commonly used analgesics
420 BRITISH DENTAL JOURNAL VOLUME 211 NO 9 NOV 12 2011
Combining paracetamol with a selectivecyclooxygenase-2 inhibitor for acutepain relief after third molar surgerya randomized double-blindplacebo-controlled study
Birgitta Haglund12 Inger vonBltzingslccedilwen1
1Public Dental Health Service KarlstadVrmland Sweden 2Department of ClinicalPharmacology Sahlgrenska Academy atGccedilteborg University Sweden
Traditional non-steroidal anti-inflammatory drugs(NSAIDs) [ie non-selective cyclooxygenase (COX)inhibitors such as ibuprofen and diclofenac] have beenwidely used in outpatients for acute pain relief followingoral surgery Their anti-inflammatory and analgesicproperties together with well-established tolerabilitymake them an initial choice for the management of mostforms of mild to moderate pain in outpatients (1 2)However these drugs have well-documented adverseeffects such as gastrointestinal intolerability Further-more they need to be administered several times a dayMore effective and practical pain relief regimes withfewer side-effects are needed for moderate to severe painafter oral surgeryNSAIDs act by inhibiting COX enzymes which are
responsible for the production of prostaglandin fromarachidonic acid This acid emerges from the breakdownof phospholipids in the cell walls of damaged tissue (3)Prostaglandin elicits a number of biological effects someof which contribute to the inflammatory process leading
to pain Multiple COX enzymes have been identifiedCOX-1 is mainly expressed under physiological condi-tions throughout the body for example by platelets (4)and COX-2 is related to inflammation and pain (4ndash6)although COX-1 and COX-2 also have overlappingproperties (7) Improved knowledge on more selectiveCOX enzymes led to the development of specific COX-2inhibitors such as rofecoxib (8) and celecoxib withanalgesic anti-inflammatory and gastroprotective prop-erties Of these drugs rofecoxib has been shown to bemore effective than celecoxib (9ndash11)Rofecoxib has the same analgesic effect as ibuprofen
but with the benefit of a longer duration (9 10 12) It hasa long half-life which makes it suitable for once-dailydosing (12) compared with traditional NSAIDs thatneed to be taken several times per day Rofecoxib hasalso been suggested to be more effective than paracet-amol combined with codeine (13 14) The COX-2inhibitor rofecoxib may be an interesting choice for acutepain relief after oral surgery
Haglund B von Bulzingslowen I Combining paracetamol with a selective cyclooxyge-nase-2 inhibitor for acute pain relief after third molar surgery a randomized double-blind placebo-controlled study Eur J Oral Sci 2006 114 293ndash301 2006 The AuthorsJournal compilation 2006 Eur J Oral Sci
Severe pain after third molar surgery is often encountered and more effective treatmentregimes are warranted The objective of this study was to evaluate if the combinationof paracetamol and rofecoxib a selective cyclooxygenase-2 (COX-2) inhibitorimproves analgesic effects following third molar surgery compared with rofecoxibalone Paracetamol alone was also evaluated Altogether 120 patients with moderate tosevere pain after third molar surgery were given a single postoperative dose of one ofthe following treatments rofecoxib + paracetamol rofecoxib alone paracetamolalone or placebo Patients assessed level of pain and pain relief every 30 min for 8 hafter surgery and made a global evaluation of the medication 4 and 8 h after surgeryParacetamol and rofecoxib combined improved the analgesic effect compared withrofecoxib alone for the first 15 h Rofecoxib alone and the combination of paracet-amol and rofecoxib had a significantly better analgesic effect than paracetamol alonefrom 3 h onwards The early onset of pain relief for the combination of paracetamoland rofecoxib compared with rofecoxib alone could be of great importance whentreating acute pain after third molar surgery After data collection for this studyrofecoxib was withdrawn from the market as a result of reported fatal cardiovascularevents Whether this is relevant for short-term use is unknown but it has to be con-sidered before rofecoxib may be used for pain relief following third molar surgery
Birgitta Haglund Folktandvrden TingvallaBox 577 SE-651 13 Karlstad Sweden
Telefax +46ndash54ndash137435E-mail birgittahaglundlivse
Key words COX-2 inhibitor pain relief para-cetamol randomized trial third molar surgery
Accepted for publication April 2006
Eur J Oral Sci 2006 114 293ndash301Printed in Singapore All rights reserved
2006 The AuthorsJournal compilation 2006 Eur J Oral Sci
European Journal ofOral Sciences
Combining drugs that cause analgesia through differ-ent mechanisms may give additive analgesic effects (15)and lead to dose-sparing effects and improved safety(16) The analgesic mechanism of COX inhibition ispredominantly peripheral Research on paracetamol hasnot been able to delineate a clear mechanism of actionbut it is suggested to lie predominantly in the centralnervous system (17) Some studies indicate that combi-ning a traditional NSAID and paracetamol after oralsurgery may enhance the analgesic effect compared withsingle drug regimes (18 19)The theory of the analgesic effect of traditional
NSAIDs being caused by COX-2 inhibition leads to thethought that an additive effect should be present alsowhen combining rofecoxib and paracetamol The aim ofthis study was therefore to explore in a third molarsurgery pain model (20) if there is an additive analgesiceffect when combining the COX-2 selective inhibitorrofecoxib with paracetamol compared with rofecoxibalone for acute pain relief We also compared the anal-gesic efficiency of rofecoxib and paracetamol becausethis to our knowledge has not been reported followingthird molar surgery
Material and methods
Study design
This study was designed as a multicenter randomizeddouble-blind placebo-controlled study with a single dose ofrofecoxib 50 mg and paracetamol 1 g combined vs rofec-oxib 50 mg alone vs paracetamol 1 g alone vs placebogiven postoperatively to patients stating moderate to severepain after surgical removal of one or two lower third molarsPatients were asked to give written informed consent toparticipate after being told about the procedures A total of120 patients were randomized into four different treatmentgroups as follows 40 patients receiving the combination ofrofecoxib 50 mg and paracetamol 1 g 40 patients receivingrofecoxib 50 mg alone 20 patients receiving paracetamol 1 galone and 20 patients receiving placebo The patientsrsquoevaluations of the treatments were obtained by using aquestionnaire which the patients filled in at home during an8-h study period following intake of the study medicationThe trial was approved by the Regional Ethical Committeeof Medical Research in Orebro Sweden and the MedicalProducts Agency in Uppsala Sweden
Patients
Consecutive patients visiting four general dental practicesand in need of mandibular third molar surgery in accordancewith the National Institutes of Health (NIH) guidelines (21)were screened for enrollment Only patients with thirdmolars needing bone removal were included Other inclusioncriteria were age gt18 yr weight gt50 kg butlt120 kg andan appointment before noon for surgery This was necessaryin order for the patients to have time to fill in the ques-tionnaire for 8 h after intake of the study medication beforebedtime Exclusion criteria were as follows intolerance toacetylsalicylic acid (ASA) paracetamol andor NSAIDsany ongoing medication (except contraceptives) pregnancylactation inadequate contraception alcohol or drug abusePatients with evidence of previous or present cardiovascular
respiratory diabetic hepatic gastric renal neurological orneoplastic diseases were also excluded as were those withongoing pericoronitis or other local oral infections involvingpain Patients with an intake of any analgesics 6 h precedingsurgery was also excluded All patients who met the studycriteria and reported moderate to severe pain after the sur-gery were included in the study
Surgery
The surgery was performed by one of four dentists speciallytrained in dento-alveolar surgery using local anesthesia(lidocaine 20 mg ml)1 plus epinephrine 125 lg ml)1) Theremoval of bone was carried out with a burr under thecooling of saline
Masking randomization and rescue medication
The study medications were masked by being encapsula-ted in identical capsules The capsules contained 50 mg ofrofecoxib 200 mg of paracetamol or placebo All patientswere given a sealed container containing six capsules(Table 1) so that the patients in the different treatmentgroups received the correct amount of medication and stillthe same number of capsules The capsules were manu-factured by Apoteket Production amp Laboratories (APLStockholm Sweden) Randomization of the patients intothe four treatment groups was performed for the group intotal by Apoteket using randomization tables All studypersonnel and participating patients were blinded totreatment assignment for the duration of the study Themain investigator broke the codes for the final calcula-tionsIbuprofen 400 mg was used as a rescue medication in case
patients needed additional analgesia at any time during the8-h study period The rescue medication was kept in aseparate container If patients felt that rescue medicationwas needed they were instructed to wait 90 min if possibleafter intake of their study medication to allow for the studydrug to take effect
Intake of study medication and information about thequestionnaire
After surgery the patients were given their two containerswith study and rescue medications respectively together
Table 1
Distribution of the drug capsules with the different substances percontainer in each study group
Study groups
Rofecoxib50 mg +
paracetamol 1 gRofecoxib50 mg
Paracetamol1 g Placebo
Rofecoxib50 mg
1 1 0 0
Paracetamol200 mg
5 0 5 0
Placebo 0 5 1 6Total no ofcapsules ineach container
6 6 6 6
294 Haglund amp Bultzingslowen
with the questionnaire Routine postoperative informationwas given The patients were instructed to go home and takeno medication before calling the investigator when theyregained full sensibility in the lower lip following the dis-appearance of the local anesthesia If the patient had notcalled the investigatorrsquos mobile phone within 3 h after theend of surgery the investigator called the patientAt the telephone contact the patients were asked to state
their level of pain in the questionnaire using a 3-point scalefrom mild to moderate to severe pain If patients statedmoderate or severe pain they were asked to break the seal ofthe container with their study medication and take all sixcapsules Detailed instructions were provided on how to fill inthe questionnaire To ascertain that patients adhered to theprotocol information was given to contact the investigatorwith any questions regarding medication or other issuesconcerning the studyduring the 8-h postoperative periodThestudy period started at the time of intake of the study medi-cation If patients stated mild pain they were asked if theycould tolerate waiting before taking any medication In suchcases a second telephone contact was made If patients stillstatedmild pain they were asked if it was possible for them toreturn their sealed container with the study medicationPatients who did so were replaced with another patient
Efficacy assessments
The outcome measures of the trial were pain intensity painrelief (PAR) global evaluation score (patientsrsquo overallassessment of the medication) derived summary measuresuse of rescue medication and side-effects experienced allrecorded by the patients in their questionnaire After intakeof the study medication pain intensity and PAR wasassessed by the patient every 30 min for 8 h and the globalevaluation score was measured at 4 and 8 h The startingpoint for each patient was the time for intake of studymedication The final measurement point was the end of theobservation period (ie 8 h later) or the time of intake ofrescue medication If rescue medication was used patientswere asked to assess pain intensity and pain relief and give aglobal evaluation score at the time of intake These scoreswere then used for the rest of the observation period inaccordance with a study by Laska et al (22)Pain intensity was evaluated by the patients using a
horizontal visual analog scale (VAS) of 10 cm marked nopain at 0 and worst possible pain at 10 PAR was meas-ured on a 5-point scale as follows 0 no pain relief 1 somepain relief 2 medium pain relief 3 good pain relief and 4total pain relief Global evaluation score was measured on a4-point scale as follows 0 poor 1 fair 2 good and 3excellent Patients using rescue medication recorded the timeof intake A question about any side-effects experienced wasanswered by yes or no at the end of the study period Ifyes the patients estimated adverse events on a 3-point scale(1 slight 2 moderate 3 severe) and reported what kind ofside-effect was experienced
Analysis
The analgesic effect of the drugs measured every 30 min bypain intensity (VAS) and PAR scores was comparedSummary measures were calculated by the use of the fol-lowing total pain relief (TOTPAR the sum of all PARscores for the whole study period of 05ndash8 h) pain intensitydifference (PID pain intensity at the start minus painintensity at any given observation point) sum of PID for the
05ndash3-h period (SPID05)3 h) and sum of PID for the total05ndash8-h period (SPIDtotal) PID values were not analyzedseparately but used for the calculation of SPIDThe use of rescue medication was compared between the
treatment groups by calculating the percentage of patientsin each group who used rescue Also the mean timebetween intake of the study medication and intake of therescue medication in the different groups was analyzedSide-effects in the treatment groups were compared interms of percentage of patients in each group whoexperienced such problems Median global evaluationscores between the different groups were analyzed as wellas the percentage of patients in each group using the dif-ferent scores
Statistics
The sample size calculations were carried out assuming adifference in SPID outcome between groups using thecombination of rofecoxib + paracetamol and rofecoxibalone amounting to 20 (18) with a power of at least 80and a standard deviation (SD) of 15 using non-para-metric statistics (MannndashWhitney U-test) This calculationestimated that a minimum of 22 patients should be includedin each groupStandard descriptive statistics and tests were used and the
calculations were performed in Statistical Package for SocialSciences (spss) version 12 The principle of last observationcarried forward was used Significances between groupsregarding VAS scores were tested with an independent-samples t-test at each time point for all possible compari-sons as we considered VAS to be a continuous scale inaccordance with Max et al (23) The same applies for thetesting of SPID up to 3 and 8 h The analysis of TOTPARwas based on an assumption that the scores are consideredinterval scaled (23) and significance testing was carried outwith an independent samples t-test The same test was usedfor testing differences between study groups regarding theuse of rescue medication Hypothesis testing of valuesmeasured with categorical ordinal scales (ie PAR andglobal evaluation) was performed with a non-parametrictest (MannndashWhitney U-test) P-values of lt005 were con-sidered statistically significant
Results
Altogether 126 consecutive patients who fulfilled theinclusion criteria gave written informed consent to par-ticipate in the study The majority of the patients whowere asked to participate agreed to do so Patients whodeclined to participate usually did not have a before-noon appointment for the surgery Out of the 126patients six were excluded as they stated their pain asmild at the telephone contacts and were able to returntheir sealed study medication A total of 120 patientsparticipated by taking the randomized study medicationSome patients (n frac14 8) who did not fulfill the criterion ofmoderate to severe pain but nevertheless wanted toparticipate took their study medication but wereexcluded from the calculations Of these patients ahigher proportion was men (75) compared with thestudied population Some patients (n frac14 5) were excludedfor other reasons one patient randomized to the
COX-2 inhibitor and paracetamol after oral surgery 295
rofecoxib group took her rescue medication after only30 min as a result of severe pain and withdrew from thestudy one did not manage to fill in the questionnaireand three did not return their questionnaires althoughthey were repeatedly reminded to do so Final outcomedata were calculated on the following cohort of 107 pa-tients rofecoxib + paracetamol (n frac14 34) rofecoxibalone (n frac1436) paracetamol alone (n frac14 20) and placebo(n frac14 17)The principal investigator and one of the dentists
performed the majority of the operations 43 and 55respectively in total 98 out of 120 The remaining 22operations were performed by the two other dentists oneoperating on 10 and the other on 12 patients as theirstock of patients fulfilling the inclusion criteria wassmaller The principal investigator was in contact withand gave instructions to the 98 patients The 22remaining patients received their instructions from oneof the other two dentists performing the operationsThere were no differences between groups regarding
baseline characteristics and the number of molarsremoved (Tables 2 and 3) In total 56 of the partici-pants were men The mean age of the patients was 27 yr(range 18ndash54) and the mean weight was 73 kg (range 50ndash120) Mean total duration of the surgery was 14 min Intotal 91 patients (85) had one mandibular molar
removed during the operation and 16 (18) had anadditional maxillary molar removed The remaining 16patients (15) had two mandibular molars removed atthe same session (Table 3) There was no difference inpain intensity (VAS) at the start between patients whohad one or two molars removed At the time of intake ofthe study medication 83 of all patients included in theanalysis reported moderate pain and 17 reportedsevere pain There were no major differences in painreported among patients operated on by the differentdentists
Analgesic effect
Pain intensity (VAS) ndash The analgesic effect over the 8-hstudy period recorded by patients using the VAS isshown in Fig 1 Separate curves with confidence inter-vals for study groups are presented in Fig 2 Patientsused the scale from 0 up to 95There was a significant difference in mean VAS score
between the combination group and the rofecoxibgroup at 30 min 1 h and 15 h in favor of thecombination (P lt 005) At 2 h and subsequentlyparacetamol did not show any statistically significantadditive effect when combined with rofecoxib com-pared with rofecoxib aloneWhen comparing rofecoxib and paracetamol after
30 min paracetamol was significantly better regardingeffect on pain intensity (P lt 005) Paracetamol tendedto have a better analgesic effect than rofecoxib (althoughthis was not statistically significant) for another hourafter the starting point From 3 h until the end of thestudy period rofecoxib was significantly better thanparacetamol (P lt 005)Compared with placebo the combination treatment
as well as the single drug treatments resulted in signifi-cantly lower pain intensity scores at all observationpoints except for rofecoxib at 30 min
Pain relief (PAR) ndash The median PAR scores (Fig 3)showed a pattern similar to the mean pain intensityassessment The combination treatment was significantly
Table 2
Baseline characteristics for each study group
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Gender malefemale 1915 2016 128 98Age (yr) 25 (19ndash35) 26 (18ndash41) 29 (19ndash52) 28 (19ndash54)Weight (kg) 73 plusmn 9 70 plusmn 13 79 plusmn 17 72 plusmn 13Volume of local anesthetic (ml) 54 plusmn 2 58 plusmn 1 56 plusmn 1 56 plusmn 1Length of surgery (min) 13 plusmn 7 15 plusmn 8 13 plusmn 7 15 plusmn 6Time from end of surgery tointake of study medication (min)
155 plusmn 37 170 plusmn 45 184 plusmn 53 161 plusmn 30
Pain intensity (VAS) at the start 51 plusmn 18 54 plusmn 16 51 plusmn 18 46 plusmn 15
Mean (range)Mean plusmn SDVAS visual analog scale
Table 3
Number of mandibular and maxillar third molars removed in eachstudy group
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
1 mandibular 24 24 15 122 mandibulars 5 6 3 21 mandibular+ 1 maxillar
5 6 2 3
296 Haglund amp Bultzingslowen
better than rofecoxib alone at 30 min (P lt 005) and at1 h (P lt 001) For the rest of the observation periodthere was no significant difference
Between rofecoxib and paracetamol there was a sig-nificant difference in median PAR score in favor ofparacetamol at 30 min and at 1 h (P lt 005) after drug
Placebo
01234567
0 1 2 3 4 5 6 7 8
Paracetamol 1g
01234567
0 1 2 3 4 5 6 7 8
Rofecoxib 50 mg
01234567
0 1 2 3 4 5 6 7 8
Rofecoxib 50 mg+paracetamol 1 g
01234567
0 1 2 3 4 5 6 7 8
Fig 2 Mean pain intensity recorded on a visual analog scale (VAS) and confidence intervals in study groups during the studyperiod of 8 h
0
1
2
3
4
5
6
0 05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
AV
s S
cr
oe
placebo
paracetamol 1g
rofecoxib 50mg
rofecoxib 50mg +paracetamol 1g
Hours from intake of study medication
Fig 1 Mean pain intensity in study groups recorded on a 10-cm visual analog scale (VAS) at each observation point For signifi-cance tests see the Results
0
05
1
15
2
25
3
35
Pai
n r
elie
f sc
ore
placebo
rofecoxib 50mg
rofecoxib 50mg +
05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
paracetamol 1g
paracetamol 1g
Hours from intake of study medication
Fig 3 Median pain relief (PAR) score in study groups at each observation point Pain relief was assessed using the following scale0 no pain relief 1 some pain relief 2 medium pain relief 3 good pain relief and 4 total pain relief For significance tests see theResults
COX-2 inhibitor and paracetamol after oral surgery 297
intake There was instead a significant difference in favorof rofecoxib from 25 h (P lt 005) and from 3 h(P lt 001) to the end of the observation period Only atthe observation time-points of 15- and 2-h was there nosignificant difference between the two drugs regardingmedian PAR scoresThe combination treatment and the single treatments
were significantly better than placebo throughout thewhole observation period of 8 h
Total pain relief (TOTPAR) ndash There was no significantdifference in mean TOTPAR between the combinationtreatment group and the rofecoxib-alone group (Table 4)However rofecoxib gave significantly better TOTPARthan paracetamol (P lt 005) All the active treatmentgroups gave better TOTPAR than placebo (P lt 0001)
Sum of pain intensity differences (SPID) ndash The combi-nation group had the highest mean SPID05)3 h scorehowever this was not statistically different from rofecoxibalone (Table 4)No significant difference in SPID0)3 h wasseen between rofecoxib and paracetamol All active treat-ments were significantly better than placebo (P lt 0001)
The mean PID over the whole observation period (iemean SPIDtotal) shows that the combination group didnot differ from the rofecoxib group (Table 4) Therofecoxib group was significantly better than paracet-amol alone (P lt 005) All active treatments weresignificantly better than placebo (P lt 0001)
Use of rescue medication ndash The use of rescue medicationmeasured as the cumulative percentage of patients ineach study group needing analgesic rescue at any timeduring the 8-h observation period is shown in Fig 4There was no significant difference regarding the totalpercentage of patients using rescue when comparing thecombination group with the rofecoxib group (Table 4)Figure 4 indicates a major difference between the rofec-oxib and paracetamol groups This difference is how-ever not significant (P frac14 0055) owing to few patientsneeding rescue medication Both the combination groupand the rofecoxib group used significantly less rescuethan the placebo group (P lt 0001) Paracetamol failedto show a significant difference to placebo regardingpercentage of patients using rescue medication (P frac140066)
Table 4
Summary of efficiency measures
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Mean TOTPAR05ndash8 h (SE)
452 (20) 409 (27) 287 (44) 91 (27)
Mean SPID05ndash3 h (SE)
182 (19) 151 (18) 111 (34) )32 (23)
Mean SPIDtotal (SE)
526 (59) 515 (60) 208 (96) )101 (57)
Percentage of patients using rescue medication (SE) 88 (49) 167 (63) 400 (112) 706 (114)Mean time (min) to use of rescue medication (SE) 234 (42) 270 (58) 228 (48) 127 (16)Median global evaluation score (0ndash4) at 4 h 2 2 1 0Median global evaluation score (0ndash4) at 8 h 3 2 1 0
P lt 005 vs placebo P lt 001 vs placebo P lt 0001 vs placeboP lt 005 vs paracetamol P lt 001 vs paracetamol P lt 0001 vs paracetamolSE standard error SPID sum of pain intensity differences TOTPAR total pain relief
0
10
20
30
40
50
60
70
80
05 1 15 2 25 3 35 4 45 5 55 6 65 7 75 8
Hours from intake of study medication
Cum
ula
itve
perc
enat
geof
paite
nst
taki
gnre
scue
me
idca
tion placebo
paracetamol 1g
rofecoxib 50mg
rofecoxib 50mg +paracetamol 1g
Fig 4 Cumulative percentage of patients in each group using rescue medication during the study period of 8 h For significance testssee the Results
298 Haglund amp Bultzingslowen
There was no statistically significant difference in themean time from intake of study medication to intake ofrescue medication in the different active treatmentgroups However for all active treatments the time wassignificantly longer than for placebo (Table 4)
Side-effects
The majority of all patients 738 reported no adverseevents while 187 experienced side-effects Another75 did not answer this question The majority (789)of the patients with side-effects reported that these wereonly slight while 211 reported moderate side-effectsNo patients reported any severe side-effects No pro-nounced difference was seen between the groupsregarding side-effects The types of side-effects experi-enced are listed in Table 5
Global evaluation
Patientsrsquo median global evaluation scores of their studymedications are shown in Table 4 After 4 h thecombination treatment and rofecoxib alone receivedsimilar evaluations Both groups were significantlybetter than paracetamol (P lt 0001 P lt 001) at thistime All active treatments were significantly betterthan placeboAt 8 h the combination group had the highest score
but the difference from the rofecoxib group was verysmall and not significant (Table 4) Both groups weresignificantly better than paracetamol alone (P lt 0001P lt 001) at 8 h All treatment groups were significantlybetter than placeboThe global evaluation scores are further specified in
Table 6 After 8 h 90 of the patients in the combina-tion group rated their medication as good or excellentFor the rofecoxib group the corresponding value was83 Of the patients treated with paracetamol 42rated their medication as good or excellent after 8 h
Discussion
In this study we showed that for the acute inflammatorypain following third molar surgery there was an additive
analgesic effect when combining rofecoxib with paracet-amol as compared with rofecoxib alone for the first 15 hafter intake After this time point the combination ofrofecoxib and paracetamol gave similar pain relief to thatof the rofecoxib group Paracetamol alone was also moreeffective for the first 15 h while rofecoxib was signifi-cantly better thanparacetamol from3 honwards The factthat rofecoxib and paracetamol were more effective thanplacebo shows that the method used was sensitive enoughto distinguish between different substancesAfter the clinical part of this study was carried out
serious concerns regarding cardiovascular effects of long-term treatment with rofecoxib were raised following re-ports of an increased incidence of myocardial infarctionand stroke among patients treated with rofecoxib in aplacebo-controlled study (24) After a highly significant19-fold increase in the incidence of thrombo-embolicserious adverse events was shown in yet another study(25) rofecoxib was withdrawn from the market Theside-effects of rofecoxib became progressively greaterafter 1 yr of treatment which suggests that the cardio-vascular risk is dose-dependent and not only associatedwith COX-2 selectivity (6) The need for acute pain reliefafter third molar surgery is short and the surgery ismainly performed in otherwise healthy young peopleamong whom the risk for serious cardiovascular events issmall It cannot be ruled out that future further devel-oped selective COX-2 inhibitors may be useful intreating acute pain after third molar surgery in this groupof patients with the advantage of only one dose a dayand minimizing the risk for gastrointestinal symptomsRofecoxib and paracetamol differ in onset time and
patients treated with rofecoxib reach meaningful painrelief after 15 h (8) compared with 05 h for paracet-amol This corresponds well with the results obtained inour study The group treated with paracetamol reportedtheir lowest VAS score by 1 h whereas at this time pointthe rofecoxib group still reported a high VAS scoreThereafter the medium VAS score for the paracetamolgroup increased while patients treated with rofecoxibcontinued to receive good pain relief until the end of theobservation period From these results it is reasonable toassume that the combination grouprsquos significantly betteranalgesic effect between 05 and 1 h compared with
Table 5
Side-effects as stated in patientsrsquo own words
Study groups
Rofecoxib +paracetamol(n frac14 34)
Rofecoxib(n frac14 36)
Paracetamol(n frac14 20)
Placebo(n frac14 17)
Fatigue 4 2 3 2Headache 1 2 ndash 2Fever ndash ndash ndash 1Dizziness 1 ndash 2 ndashStomach pains 1 ndash 1 ndashSickness ndash 1 ndash ndashShivers 1 2 ndash ndashPerspirations ndash 1 ndash ndash
Table 6
Percentage of patients in each study group stating their overallexperience of the study medication at 4 and 8 h
Study groups
Rofecoxib+
paracet-amol
(n frac14 34)Rofecoxib(n frac14 36)
Paracet-amol
(n frac14 20)Placebo(n frac14 17)
4 h 8 h 4 h 8 h 4 h 8 h 4 h 8 h
Poor 0 0 7 6 30 32 75 76Fair 6 10 7 11 40 26 18 18Good 47 32 43 36 15 26 7 6Excellent 47 58 43 47 15 16 0 0
COX-2 inhibitor and paracetamol after oral surgery 299
rofecoxib alone was a result of the earlier onset of theeffect of paracetamol The mean VAS scores for thecombination group and the paracetamol group corres-ponds totally at the 30-min observation pointThe peak pain after third molar surgery has been
shown to occur 4ndash6 h postoperatively (26) which coin-cides well with the time for the additive effect of para-cetamol to take effect in our study This supports the useof the combination treatment of rofecoxib and paracet-amol after third molar surgery to gain an early onsetparticularly if pain relief medication is started postop-eratively as it is of great clinical importance to have anearly onset of pain relief when treating acute pain Iftreatment starts pre-operatively the addition of para-cetamol is likely to have less clinical relevance This issupported by a study in which patients were givenrofecoxib and paracetamol before Ear Nose and Throat(ENT) surgery (27) The addition of paracetamol in thatsetting failed to improve the analgesic effects of rofec-oxibRofecoxib and paracetamol also differ in duration
The effect of paracetamol 1 g lasts up to 6 h and the drughas to be administered four times daily while rofecoxib50 mg has an analgesic effect up to 24 h (12) The presentstudy was a single-dose comparison In a normal clinicalsetting another 1 g of paracetamol would probably beprescribed after 6 h which would give another period ofadditive effectThe disparity in effect between rofecoxib and para-
cetamol in the present study from 3 h onwards is inaccordance with the findings of two studies on post-operative pain relief after otolaryngologic surgerycomparing rofecoxib and paracetamol given pre-operatively (11 28) A study regarding inflammatorypain in patients with knee osteoarthritis also showedrofecoxib to be superior to paracetamol (29) The resultof our study from 3 h after baseline and onwards thusconfirms the findings of these studies in a third molarpain modelOur study did not show the same additive effect of
combining rofecoxib and paracetamol as in a study byBreivik et al in which they combined diclofenac andparacetamol (18) These authors demonstrated anadditive effect of paracetamol over the whole studyperiod of 8 h Their study also showed less use of rescuemedication in the combination group compared with thepatients treated with diclofenac alone something alsofound in a study by Matthews et al (19) It would seemreasonable to assume that the additive effect of para-cetamol in our study would be the same as in these twostudies as rofecoxib and ibuprofen have been shown tohave the same analgesic effect following third molarsurgery (9 10 12) and the effects of ibuprofen anddiclofenac are similar (30ndash32) It cannot be ruled out thatthere is a difference in additive effect of paracetamolwhen combining it with rofecoxib compared withdiclofenac This theory is in accordance with the result ofa study by Pickering et al on pain relief after tonsil-lectomy in children in which rofecoxib combined withparacetamol did not significantly alter the need for earlyanalgesia as did ibuprofen combined with paracetamol
(33) Further studies may clarify differences between thetwo drugsIn conclusion the present study indicates that there is
an early additive effect up to 2 h when combiningparacetamol with rofecoxib postoperatively as comparedwith rofecoxib alone which coincides with peak painintensity after the removal of third molars Rofecoxibhad a significantly better analgesic effect than paracet-amol from 3 h onwards Our results indicate that para-cetamol does not enhance the analgesic effect ofrofecoxib over a longer period of time As rofecoxib hasbeen shown to have serious cardiovascular side-effectsfuture studies are needed to determine any serious side-effect during short-term treatment
Acknowledgements ndash This study was supported by grants fromLIV The Country Council of Varmland which made it inde-pendent from all manufacturers of the studied drugs There areno conflicts of interest by any of the authors with any drugcompany We thank Dr Carl-Mauritz Bratt DDS Dr PeterTroberg DDS and Dr Tobias Block DDS for performingsome of the surgery
References1 Cooper SA Five studies on ibuprofen for postsurgical dental
pain Am J Med 1984 77 70ndash772 Dionne RA Campbell RA Cooper SA Hall DL Buck-
ingham B Suppression of postoperative pain by preoperativeadministration of ibuprofen in comparison to placebo acet-aminophen and acetaminophen plus codeine J Clin Pharmacol1983 23 37ndash43
3 Vane JR Inhibition of prostaglandin synthesis as a mechanismof action for the aspirinlike drugs Nature 1971 231 232ndash235
4 Meade EA Smith WL De Witt DL Differential inhibition ofprostaglandin endoperoxide synthase (cyclo-oxygenase) iso-zymes by aspirin and other non-steroidal anti-inflammatorydrugs J Biol Chem 1993 268 6610ndash6614
5 Smith TJ Cyclooxygenase as the principal targets for action ofNSAIDs Rheum Dis Clin North Am 1998 24 501ndash523
6 Sciulli MG Capone ML Tacconelli S Patrignani P Thefuture of traditional nonsteroidal anti-inflammatory drugs andcyclooxygenase-2 inhibitors in the treatment of inflammationand pain Pharmacol Rep 2005 57 66ndash85
7 Spink M Bann S Glickman R Clinical implications of cyclo-oxygenase-2 inhibitors for acute dental pain managementbenefits and risks J Am Dent Assoc 2005 136 1439ndash1448
8 Ehrich EW Dallob A De Lepeleire I Van Hecken ARiendeau D Yuan W Porras A Wittreich J Seibold JRDe Shepper P Mellisch DR Gertz BJ Characterization ofrofecoxib as a cyclooxygenase-2 isoform inhibitor and demon-stration of analgesia in the dental pain model Clin Pharm Ther1999 65 336ndash347
9 Malmstrom K Fricke J Kotey P Kress B Morrisson B Acomparison of rofecoxib versus celecoxib in treating pain afterdental surgery a singlecenter randomized double-blind pla-cebo- and active-comparator-controlled parallel group single-dose study using the dental impaction pain model Clin Ther2002 24 1549ndash1560
10 Malmstrom K Daniels S Kotey P Seidenberg B Desjar-
dins PJ Comparison of rofecoxib and celecoxib two cyclo-oxygenase-2-inhibitors in postoperative dental pain Arandomized placebo- and active-comparator-controlled clinicaltrail Clin Ther 1999 21 1653ndash1663
11 Watcha MF Issioui T Klein KW White PF Costs andeffectiveness of rofecoxib celecoxib and acetaminophen forpreventing pain after ambulatory otolaryngologic surgeryAnesth Analg 2003 96 987ndash994
300 Haglund amp Bultzingslowen
12 Morrisson BW Christensen S Yuan W Brown J Amlani
S Seidenberg B Analgesic efficacy of the cyclooxygenase-2-specific inhibitor rofecoxib in post-dental surgery pain arandomized controlled trial Clin Ther 1999 21 943ndash953
13 Chang DJ Fricke JR Bird RS Bohidar NR Dobbins TWGeba GP Rofecoxib versus codeineacetaminophen in post-operative dental pain a double-blind randomized placebo-and active comparator-controlled clinical trial Clin Ther 200123 1446ndash1455
14 Chang DJ Desjardins PJ Bird SR Black P Chen EPetruschke RA Geba GP Comparison of rofecoxib and amultidose oxycodoneacetaminophen regimen for the treatmentof acute pain following oral surgery a randomized controlledtrial Curr Med Res Opin 2004 20 939ndash949
15 Berenbaum MC What is synergy Pharmacol Rev 1989 4193ndash141
16 Altman RD A rationale for combining acetaminophen andNSAIDs for mild to moderate pain Clin Exp Rheumatol 200422 110ndash117
17 Bjorkman R Hallman KM Hedner J Hedner T Henning
M Acetaminophen blocks spinal hyperalgesia induced byNMDA and substance P Pain 1994 57 259ndash264
18 Breivik EK Barkvoll P Skovlund E Combining diclofenacwith acetaminophen or acetaminophen-codeine after oral sur-gery a randomized double-blind single-dose study ClinPharmacol Ther 1999 66 625ndash635
19 Matthews RW Scully CM Levers BG The efficacy ofdiclofenac sodium (Voltarol) with and without paracetamol inthe control of post-surgical dental pain Br Dent J 1984 157357ndash359
20 Norholt SE Treatment of acute pain following removal ofmandibular third molars use of the dental pain model inpharmacological research and development of a comparableanimal model Int J Oral Maxillofac Surg 1998 27 1ndash41
21 NIH Consensus Development Conference For Removal OfThird Molars J Oral Surg 1980 38 235ndash236
22 Laska EM Siegel C Sunshine A Onset and durationmeasurement and analysis In Max MB Portenoy RKLaska EM eds Advances in pain research and therapy NewYork Raven Press 1991 691ndash698
23 Max MB Laska EM Single-dose analgesic comparisons InMax MB Portenoy RK Laska EM eds Advances in painresearch and therapy New York Raven Press 1991 55ndash97
24 Bombardier C Laine L Reicin A Shapiro D Burgos-Vargas R Davis B Day R Ferraz MB Hawkey CJHochbergMC Kvien TK Schitzer TJ Comparison of uppergastrointestinal toxicity of rofecoxib and naproxen in patientswith rheumatoid arthritis N Engl J Med 2005 343 1520ndash1528
25 Bresalier RS Sandler RS QuanH Bolognese JA Oxenius
B Horgan K Lines C Riddell R Morton D Lanas AKonstam MA Baron JA Cardiovascular events associatedwith rofecoxib in a colorectal adenoma chemoprevention trialN Engl J Med 2005 17 1092ndash1102
26 Szmyd L Shannon ILMohnac AM Control of postoperativesequelae in impacted third molar surgery J Oral Ther Phar-macol 1965 1 491ndash496
27 Issioui T Klein KW White PF Hu J Skrivanek GDAnalgesic efficacy of rofecoxib alone or in combination withacetaminophen in the ambulatory setting Anesthesiology 200195 A35
28 Issioui T KleinKWhite PWatchaM SkrivanekG JonesSHu J BradleyM Caleb I Cost-efficacy of rofecoxib versusacetaminophen for preventing pain after ambulatory surgeryAnesthesiology 2002 97 931ndash937
29 Geba GP Weaver AL Polis AB Dixon ME Schnitzer TJEfficacy of rofecoxib celecoxib and acetaminophen in osteo-arthritis of the knee a randomized trial JAMA 2002 287 64ndash71
30 Joshi A Parara E Macfarlane TV A double-blind rand-omised controlled clinical trial of the effect of preoperativeibuprofen diclofenac paracetamol with codeine and placebotablets for relief of postoperative pain after removal of impac-ted third molars Br J Oral Maxillofac Surg 2004 42 299ndash306
31 Bakshi R Frenkel G Dietlein G Meurer-Witt B Schn-eider B Sinterhauf U A placebo-controlled comparativeevaluation of diclofenac dispersible versus ibuprofen in post-operative pain after third molar surgery J Clin Pharmacol 199434 225ndash230
32 Ahlstrom U Bakshi R Nilsson P Wahlander L Theanalgesic efficacy of diclofenac dispersible and ibuprofen inpostoperative pain after dental extraction Eur J Clin Pharma-col 1993 44 587ndash588
33 Pickering AE Bridge HS Nolan J Stoddart A Double-blind placebo-controlled analgesic study of ibuprofen orrofecoxib in combination with paracetamol for tonsillectomy inchildren Br J Anaesth 2002 88 72ndash77
COX-2 inhibitor and paracetamol after oral surgery 301
Combined acetaminophen and ibuprofen for pain relief after oralsurgery in adults a randomized controlled trial
A F Merry1 2 R D Gibbs3 J Edwards4 G S Ting3 C Frampton5 E Davies1 2
and B J Anderson1
1Department of Anaesthesiology University of Auckland Private Bag 92019 Auckland New Zealand2Department of Anaesthesia Auckland City Hospital Auckland New Zealand 3Oral Health Unit Greenlane
Clinical Centre 214 Greenlane West Epsom Auckland New Zealand 4Oral and Maxillofacial Service Quay
Park Medical Centre 68 Beach Road Auckland Central Auckland New Zealand 5Department of Medicine
Christchurch School of Medicine and Health Sciences University of Otago New Zealand
Corresponding author E-mail amerryaucklandacnz
Background Acetaminophen is often used with a non-steriodal anti-inflammatory drug for
acute pain Hitherto these drugs have had to be given separately typically at different time
intervals Maxigesicw tablets combine acetaminophen and ibuprofen in clinically appropriate
doses to simplify administration and dosage regimen We compared this combination with each
of the constituent drugs for the relief of pain after extraction of third molar teeth
Methods Adults (more than 16 yr) having one or more wisdom teeth removed under general
or local anaesthesia were instructed to take two tablets before operation then two tablets
every 6 h for up to 48 h of (i) a combination of acetaminophen 500 mg and ibuprofen 150 mg
per tablet (Maxigesicw) (ii) acetaminophen 500 mg per tablet alone or (iii) ibuprofen 150 mg
per tablet alone The primary outcome measure was the area under the curve (AUC) of the
100 mm visual analogue scale pain measurements taken for up to 48 h after surgery divided by
time at rest and on activity Pharmacokinetic data were collected in a subset of patients
Results The mean (SEM) time-corrected AUC on rest and activity respectively were combi-
nation group 223 (32) and 284 (34) acetaminophen group 330 (31) and 404 (33) and ibu-
profen group 348 (32) and 402 (34) P001 for each of the four comparisons of combination
vs constituent drug There was no pharmacokinetic interaction between acetaminophen and
ibuprofen administered together
Conclusions Maxigesicw tablets provide superior pain relief after oral surgery to acetamino-
phen or ibuprofen alone
Br J Anaesth 2010 104 80ndash8
Keywords anaesthesia dental analgesia postoperative analgesics non-opioid acetaminophen
analgesics non-opioid ibuprofen non-steroidal anti-inflammatory drugs
Accepted for publication October 16 2009
The relief of pain has been described as a universal human
right but is not always easily achieved1 Opioid analgesics
are effective but have troublesome and potentially danger-
ous side-effects and their potential for abuse may lead to
regulatory and logistical difficulties Non-steroidal anti-
inflammatory drugs (NSAIDs) have fewer regulatory
restrictions but they too have important adverse effects
which are more likely at higher dose or with longer
courses2 Acetaminophen is widely used and is very safe
at the recommended dose of 4 g per day3 but does not
always provide adequate pain relief on its own Combining
analgesics offers the possibility of increasing effectiveness
without increasing dose (and therefore risk)4 5 NSAIDs
are often combined with acetaminophen particularly for
treating postoperative pain6 ndash 10
Prescribing acetaminophen and ibuprofen together is
common in clinical practice6 8 9 11 ndash 13 Ibuprofen has the
advantage of a well-established safety record (particularly
at doses below 15 g per day in adults)14 and in many
countries (including the UK) it is available without
The Author [2010] Published by Oxford University Press on behalf of the British Journal of Anaesthesia
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (httpcreativecommonsorglicensesby-nc25uk)
which permits unrestricted non-commercial use distribution and reproduction in any medium provided the original work is properly cited
British Journal of Anaesthesia 104 (1) 80ndash8 (2010)
doi101093bjaaep338
prescription Typically acetaminophen is given in a dose
regimen of 1 g 6 hourly whereas ibuprofen is given in a
dose of 400 mg 8 hourly3 Compliance with the prescribed
dosing regimen is important for achieving the desired
result with any drug and is often poor with asynchronous
dosing15 A single formulation with a simplified regimen
would probably be appreciated by patients and might
improve compliance
Maxigesicw is a new formulation of acetaminophen 500
mg and ibuprofen 150 mg Taking two tablets 6 hourly
provides the appropriate daily dose of both drugs relatively
simply We have investigated the hypothesis that in adult
patients undergoing a common surgical procedure (extrac-
tion of third molar teeth) this formulation provides
superior analgesia to either of its components alone
Methods
With ethics committee approval we recruited and fol-
lowed up patients between March 2005 and February
2008 Trial registration ANZCTRORGAU (identifier
ACTRN12606000291583)
Setting
This study was conducted at a publicly funded teaching
hospital and a private day-surgical clinic in metropolitan
New Zealand
Participants
We included adults undergoing extraction of at least one
lower wisdom tooth with or without one or more upper
wisdom teeth by one of three participating surgeons We
excluded patients if they were under 16 yr old weighed
50 kg had taken any NSAID (other than aspirin in a
dose of 150 mg daily or less) within 24 h of the operation
had taken acetaminophen or acetaminophen containing
medicines within 12 h of the operation were taking an
angiotensin-converting enzyme inhibitor warfarin steroid
(other than interoperative dexamethasone) or any immu-
nosuppressive drug were intolerant to any NSAID or acet-
aminophen were suffering from a severe local infection
had a history of peptic ulceration asthma or severe hae-
mopoetic renal or hepatic disease were participating in
the investigation of another experimental agent or if the
clinician believed for any other reason that participation in
the study might not be in their best interests
Randomization and blinding
Tablets of identical appearance packaging and dosage
instructions were provided in each of the following formu-
lations (i) acetaminophen 500 mgthornibuprofen 150 mg per
tablet (Maxigesicw Sigma Laboratories Nashik India which
was MHRA approved for manufacturing pharmaceuticals
under GMP) (ii) acetaminophen 500 mg per tablet or
(iii) ibuprofen 150 mg per tablet
Patients were first approached by the surgeon and then
by the study nurse They were given written and verbal
information about the study and invited to participate If
they consented patients were then randomized into one of
the three study groups in a sequential order to receive one
of these formulations in blinded packs The randomization
sequence was computer generated by the study statistician
as a 111 allocation ratio to the three treatments in a
sequence of permuted blocks with stratification for anaes-
thetic type (local or general) and study centre
Stratification by anaesthetic type ensured a balance
between treatments in terms of the number of teeth
extracted as most patients having more than two teeth
extracted have a general anaesthetic Only the statistician
had access to the schedule of patient numbers by drug
allocation Participants and investigators were blinded and
the randomization code was not broken until the final data-
base had been checked and locked
Intervention
Participants were asked to take two tablets of the study
medication before operation (as close as possible to the
start of surgery) and then 4 times a day (as close as poss-
ible to 6 hourly) for up to 48 h after surgery All partici-
pants were given bupivacaine local anaesthetic blocks by
the surgeons For those participants undergoing general
anaesthesia this was induced with propofol and main-
tained with isoflurane and nitrous oxide in oxygen
Monitoring was in accordance with the guidelines of the
Australian and New Zealand College of Anaesthetists16
All extractions were carried out by one of three surgeons
each using his normal technique
If participants required additional postoperative pain
relief while in hospital a rescue dose of fentanyl 10 mg
was given iv as required After discharge to home
codeine was provided (again as rescue medication) in 30
mg tablets one to two to be taken as needed up to
4 hourly
Outcomes
Participants were asked to rate their pain on 100 mm visual
analogue scales (VAS) printed one per double page in a
booklet that they took home Ratings were requested at
baseline (immediately before administration of the first
dose of study medication) after operation (once the partici-
pants were sufficiently awake to respond) and 1ndash2 hourly
thereafter while awake for 48 h The study nurse main-
tained contact with participants by telephone to facilitate
compliance with data collection and the return of diaries
The primary outcome measure was the area under the
curve (AUC) of these VAS ratings divided by time at rest
and on activity The AUC was divided by the period of
the completed assessments to adjust for the fact that some
Combined acetaminophen and ibuprofen for analgesia
81
patients recorded pain for shorter periods than others This
calculation in effect produces a measure of average pain
intensity over the study period
Secondary efficacy outcome measures were a categorical
global pain rating by the participants taken at the end of the
study period rescue analgesia consumption over the study
period a categorical global rating of nausea by the partici-
pants taken at the end of study period the number of epi-
sodes of vomiting over the study period and a rating of
sleep disturbance on a 100 mm VAS assessed after each
night during the study period In addition participants were
asked to rate their experiences of participating in the study
Sample size estimation
We obtained blood samples from the 38 participants
undergoing general anaesthesia in order to have evaluable
pharmacokinetic data for at least 30 patients The first
sample was obtained 30 min after the first dose of study
medication the second sample at the end of anaesthesia
and additional one or two samples after operation in hospi-
tal The plasma concentration of acetaminophen and ibu-
profen were measured by the sponsor and used to form
individual timendashconcentration profiles The analytical
method used an HPLC-DAD (Diode Array Detector) assay
for the simultaneous determination of acetaminophen and
ibuprofen in plasma Precision and accuracy for acetami-
nophen and ibuprofen assay were validated over the con-
centration range 05ndash50 mg ml21 for both drugs The
intra- and inter-batch precision of the assays at low
medium and high concentrations of acetaminophen and
ibuprofen varied from theoretical values by 15 The
lower limit of quantification for each drug was 05 mg
ml21 The sponsor monitored all data collected during the
study and queries and corrections were made when any
inaccuracies or inconsistencies were identified
Sample size estimation
We estimated that 120 participants (40 per group) in the
intention-to-treat (ITT) population would provide 80
power to detect differences between the groups of 9 (SD
14) mm in our primary endpoint for resting assessments
and 13 (SD 21) for measures during activity10 17 with a
one-sided type I error rate of 5 These differences equate
to 25 Differences of this magnitude were considered
clinically important and comparable with differences
typical of previous published studies10
Statistical methods
The data were analysed using SPSS version 150 (SPSS
Inc Chicago IL USA) Efficacy analyses were conducted
on an ITT basis with the additional provision that
there were at least three VAS measurements over at
least 12 h available to calculate the primary endpoint All
participants who were randomized into the study were
included in the safety evaluations As the first dose of
study medication was taken before operation while under
the supervision of the surgeon all randomized patients
took at least a single dose of study medication A last
observation carried forward approach was used for those
subjects who left the study prematurely for non-AUC
based variables
We compared the primary endpoint between the combi-
nation group and each of the acetaminophen and ibuprofen
arms at rest and on activity using a general linear model
(GLM) which included terms for treatment the centre and
anaesthetic stratum Additionally to confirm the consist-
ency of the treatment effects across strata the stratum
treatment interaction terms were tested and included in
the final model The analysis was also checked with
number of teeth extracted as an additional factor
Continuous secondary efficacy endpoints were tested for
significance using the same models as used for the
primary endpoint
A one-tailed P005 was pre-specified to indicate stat-
istical significance We required a statistically significant
result favouring the combination from each of the two
planned comparisons with the constituents to define super-
iority for either rest or on activity measures We used one-
tailed tests as there seemed no theoretical or empirical
basis for expecting that combining these analgesics could
result in a reduction in efficacy and because the require-
ment for each of two comparisons to be significant at
P005 is stringent Secondary categorical efficacy end-
points were compared between the groups using x2 tests
and MannndashWhitney U-tests as appropriate
We used non-linear mixed effect models (NONMEM
VI Globomax LLC Hanover MD USA) to estimate
population pharmacokinetics with a Compaq Digital
Fortran Version 66A compiler on an Intel Celeron 333
MHz CPU (Intel Corp Santa Clara CA USA) under MS
Windows XP (Microsoft Corp Seattle WA USA) This
model allows assessment of inter-individual variability
covariance between pharmacokinetic parameters and
residual error We judged the quality of fit of the pharma-
cokinetic model to data using the NONMEM objective
function examination of plots of observed vs predicted
concentrations and visual predictive checks
Results
After initial screening 189 patients were approached 135
agreed to participate One to four teeth were extracted
with local anaesthetic alone in 69 patients and with local
anaesthetic in combination with general anaesthesia in 66
Thirteen patients did not return their patient diaries so
122 patients were included in the evaluable ITT popu-
lation for the analysis of the primary endpoints (Fig 1)
The treatment groups were adequately matched in baseline
patient and clinical characteristics (Table 1) Of those in
Merry et al
82
the combination group 600 had three or four teeth
extracted compared with 436 for ibuprofen and 535
for acetaminophen
Efficacy
The time-adjusted AUCs were substantially and signifi-
cantly lower at rest and on activity in the combination
group than in either of the other two treatment groups
(Table 2 Figs 2 and 3) with all four P001 The consist-
ency of the treatment effects across strata was confirmed
from the GLM with P-values for the treatment stratum
interaction of 0955 and 0984 for time-adjusted AUCs at
rest and on activity respectively The type of anaesthetic
(local vs general) and number of teeth extracted did not
change the outcome of either analysis
Although all four secondary endpoints favour the com-
bination treatment (Table 3) only the global pain rating
reached statistical significance More participants experi-
enced lsquonilrsquo or lsquomildrsquo pain with the combination (684)
than with either other group this difference was significant
for acetaminophen (375 Pfrac140008) but not for ibupro-
fen (543 Pfrac140263) The use of any rescue medication
also favoured the combination treatment (Table 4) but this
did not reach statistical significance
Pharmacokinetics
There were no significant differences between the combi-
nation group and either constituent group in any of the
estimated pharmacokinetic parameters (Table 5) The
visual predictive plots of individual concentration showed
that 90 of the observations were within the 90 pre-
diction intervals
Twelve participants were given both acetaminophen and
ibuprofen For calculation of the pharmacokinetic vari-
ables a scaling factor was applied to clearance and
volume of distribution in turn for those participants receiv-
ing the combination of acetaminophen and ibuprofen This
scaling factor had no impact on either acetaminophen or
ibuprofen pharmacokinetic parameters indicating that
there was no pharmacokinetic interaction between acetami-
nophen and ibuprofen when administered together
(P005)
Clearance (CLF) and volume of distribution (VF) par-
ameters observed in the study are consistent with those
reported previously (acetaminophen CLFfrac14126ndash210
litre h21 70 kg21 VFfrac14483ndash710 litre 70 kg21 ibupro-
fen CLFfrac1429ndash59 litre h21 70 kg21 VFfrac1464ndash235 litre
70 kg21)18 ndash 20
Adverse effects
The frequency of adverse effects was consistent with the
known effects of the constituent drugs and there were no
Screened(n =189)
Randomized(n =135)
Acetaminophentreatmentgroup(n =47)
Ibuprofentreatment group(n =44)
Combinationtreatment group(n =44)
Patient diariesnot returned(n =4)
Patient diariesnot returned(n =5)
Patient diariesnot returned(n =4)
Included in theanalysis(n =43)
Included in theanalysis(n =39)
Included in theanalysis(n =40)
Fig 1 Flow of participants through trial Not randomized (nfrac1454) (i)
declined to participate (nfrac1415) (ii) did not meet inclusion criteria
(nfrac1414) (iii) other reasons (nfrac1425) other reasons the surgery was
cancelled or rescheduled patient could not be contacted patient was
given the wrong date of the surgery
Table 1 Patient characteristic and baseline information (SD)
Acetaminophen (n547) Ibuprofen (n544) Combination (n544)
Age [mean (range)] (yr) 235 (160ndash404) 237 (168ndash389) 250 (183ndash404)
Weight [mean (SD)] (kg) 713 (156) 808 (201) 711 (135)
Ethnicity [n ()]
Asian 4 (85) 1 (23) 2 (45)
Black 1 (21) 0 (00) 1 (23)
Caucasian 33 (702) 31 (705) 34 (773)
Maori 4 (85) 4 (91) 4 (91)
Pacific Islander 4 (85) 5 (114) 2 (45)
Other 1 (21) 3 (68) 1 (23)
Male [n ()] 13 (277) 21 (477) 13 (295)
Shift workers [n ()] 10 (213) 5 (114) 3 (68)
Preoperative pain scores at rest [mean (SD)] (mm) 19 (51) 21 (52) 26 (68)
Preoperative pain scores on activity [mean (SD)] (mm) 41 (133) 27 (83) 29 (66)
Sleep disturbance for night before surgery as VAS [mean (SD)] (mm) 647 (229) 691 (260) 715 (241)
Combined acetaminophen and ibuprofen for analgesia
83
definitive indications that the adverse event profile is
changed when the two drugs are combined (Table 6)
however the numbers were too small to make meaningful
comparisons between the groups Two participants experi-
enced postoperative bleeding (attributed to surgical
causes) which resolved without readmission to hospital
No gastrointestinal bleeding was reported during the study
Most adverse events were evaluated as mild (574) or
moderate (352) and on review were considered not
related (175) or unlikely to be related (667) to study
medication
General
The majority of participants rated the experience of taking
part in the study as very positive (31) or positive (47)
0
10
20
30
40
50
60
70
80
90
100
ActivityRest
Acetaminophen alone
Ibuprofen alone
Combination
AU
Ch
(m
m)
Fig 2 Mean (thorn95 CI) mm of time-adjusted AUC (AUCtime) for VAS
at rest and on activity by treatment group
Table 2 Mean (SEM 95 CI) of time-adjusted AUC of visual analogue pain
scores at rest and on activity by treatment group The differences between
combination and each constituent were significant at rest (vs acetaminophen
Pfrac140007 and vs ibuprofen Pfrac140003) and on activity (vs acetaminophen
Pfrac140006 and vs ibuprofen Pfrac140007)
Acetaminophen
(n543)
Ibuprofen (n539) Combination
(n540)
At rest 330 (31 279ndash381) 348 (32 294ndash402) 223 (32 170ndash277)
On
activity
404 (33 350ndash458) 402 (34 346ndash459) 284 (34 228ndash341)
0
1020
30
40
5060
70
8090
100A
B
0 4 8 12 16 20 24 28 32 36 40 44 48
0 4 8 12 16 20 24 28 32 36 40 44 48
Hours post-surgery
VA
S s
core
(m
m)
0
10
2030
40
50
60
7080
90
100
Hours post-surgery
VA
S s
core
(m
m)
Acetaminophen aloneIbuprofen aloneCombination
Fig 3 Mean (SE) mm VAS out of 100 at rest (A) and on activity (B)
Table 3 Secondary efficacy endpoints by treatment group The only
significant difference was between the global pain ratings for combination and
acetaminophen (Pfrac140008 MannndashWhitney U-test)
Acetaminophen Ibuprofen Combination
Global pain rating [n ()]
Nil 3 (75) 4 (114) 4 (105)
Mild 12 (300) 15 (429) 22 (579)
Moderate 22 (550) 14 (400) 12 (316)
Severe 3 (75) 2 (57) 0 (00)
Global nausea rating [n ()]
Nil 26 (650) 25 (714) 30 (790)
Mild 10 (250) 8 (229) 7 (184)
Moderate 3 (75) 2 (57) 1 (26)
Severe 1 (25) 0 (00) 0 (00)
Vomiting episodes (n) 5 (in 3 subjects) 0 0
Sleep disturbance night
1 vs baseline VAS
[mean (SD)] (mm)
2219 (292) 2174 (229) 2166 (247)
Sleep disturbance night
2 vs baseline VAS
[mean (SD)] (mm)
2137 (329) 296 (258) 285 (201)
Table 4 Rescue analgesia by group n () none of these differences were
significant
Rescue analgesic Acetaminophen Ibuprofen Combination
Fentanyl in hospital 5 (116) 9 (237) 6 (154)
Codeine in the first 24 h 21 (4770) 16 (4320) 13 (3250)
Codeine in the second 24 h 22 (5370) 14 (4240) 16 (4210)
Any rescue medication over 48 h 25 (625) 18 (5810) 21 (568)
Table 5 Mean (SD) pharmacokinetic parameters (individual Bayesian
estimates used for descriptive statistics) for a one-compartment first-order
absorption first-order elimination model none of the differences for
combination formulations was significant CLF clearance VF volume of
distribution Tabs absorption half-time Cmax maximum concentration Tmax
time to achieve Cmax
Acetaminophen
alone (n515)
Acetaminophen
in combination(n512)
Ibuprofen
alone(n511)
Ibuprofen in
combination(n512)
CLF (litre
h21)
141 (26) 142 (18) 39 (17) 38 (13)
VF (litre) 557 (194) 482 (183) 106 (21) 98 (15)
Tabs (h) 042 (076) 016 (010) 058 (078) 085 (085)
Tmax (h) 109 (112) 064 (031) 116 (090) 144 (093)
Cmax (mg
litre21)
158 (65) 192 (64) 208 (83) 191 (78)
Merry et al
84
and 19 rated the experience as neutral Four participants
(3) found the experience negative and none rated it as
very negative The ratings were not significantly different
between the study groups
Discussion
We found that patients using the combination of acetami-
nophen and ibuprofen experienced less pain during the
first 48 h after oral surgery than those using the same
daily dosage of either agent alone and we think the differ-
ence was clinically relevant There was no evidence of any
pharmacokinetic interaction between acetaminophen and
ibuprofen Patients receiving ibuprofen alone reported the
lowest frequency of adverse events but the numbers are
too small for meaningful comparisons between the groups
and we saw no cause for concern in any group
Our data are consistent with previous evidence showing
that a combination of ibuprofen and acetaminophen pro-
vides better analgesia than acetaminophen alone8 9 13 21
Note however that two of these studies were in children9 13
so data in adults are relatively limited On the other hand
there are many studies supporting the more general point
that the addition of various NSAIDs improves the pain
relief obtainable from acetaminophen alone More impor-
tantly our data add convincingly to the sparse evidence
supporting the more controversial proposition that this
combination is superior to ibuprofen alone12 In a smaller
study in an orthopaedic pain model (which was positive
for the combination in comparison with acetaminophen)
Dahl and colleagues8 showed no such benefit whereas
Viitanen and colleagues13 (in a paediatric tonsillectomy
study) showed an advantage for the combination only in
the period after discharge from hospital The similarity in
efficacy between ibuprofen and acetaminophen on their
own seen in our study contrasts with the findings of
superior pain relief from ibuprofen after dental surgery by
Cooper and colleagues22 but theirs was a single-dose
study
Limitations and strengths of the study
Our results are limited to adults and to the doses and
model of pain studied We think our conclusions are likely
to apply to other age groups and other types of pain but
this will require confirmation We have not explored the
optimal dosage of the combination drug but the dosage
used is consistent with current clinical practice The
inclusion of patients who underwent both general and
local anaesthesia implies that our findings are likely to
apply in either case It is not possible to draw firm con-
clusions on the safety of any drug from a study of only 40
participants per group but acetaminophen and ibuprofen
are well established widely used and considered very safe
in appropriate doses3 23 There is no theoretical reason
Table 6 Adverse events and their relationship with study medication as evaluated by the investigators Postoperative pain was noted as a complication in 2 0
and 1 patient in the acetaminophen ibuprofen and combination groups respectively Some individuals experienced more than one adverse event
Relationship System organ class Acetaminophen Ibuprofen Combination Total
Not related Gastrointestinal disorders (numbness of tongue) 1 0 0 1
General disorders and administration site conditions (swollen arm infusion site
phlebitis)
0 0 2 2
Infections and infestations (dry socket alveolitis of jaw) 1 0 1 2
Injury poisoning and procedural complications (bruising of arm postoperative
pain)
0 0 2 2
Musculoskeletal and connective tissue disorders ( jaw stiffness) 0 0 1 1
Skin and sc tissue disorders (swelling face) 1 1 0 2
Subtotal 3 1 6 10
Unlikely related Blood and lymphatic system disorders (swollen glands) 1 0 0 1
Ear and labyrinth disorders (pain in ear tinnitus) 2 0 0 2
Gastrointestinal disorders (vomiting nausea stomach cramps dry lips) 6 1 2 9
Injury poisoning and procedural complications (postoperative bleeding) 0 0 1 1
Musculoskeletal and connective tissue disorders ( jaw stiffness aches and pains in
legs jaw pain)
2 0 1 3
Nervous system disorders (headache felt faint sleepy balance difficulty light
headiness dizziness drowsiness lethargic)
6 4 4 14
Psychiatric disorders (disorientation) 0 1 0 1
Respiratory thoracic and mediastinal disorders (sore throat pharyngeal ulceration
hypoventilation coughing)
1 1 2 4
Investigations (body temperature increased) 0 0 1 1
Skin and sc tissue disorders (rash redness of external ear swelling face) 0 1 1 2
Subtotal 18 8 12 38
Possibly related Gastrointestinal disorders (stomach cramps abdominal pain constipation stomach
ache vomiting)
3 0 2 5
General disorders and administration site conditions (fever) 1 0 0 1
Injury poisoning and procedural complications (postoperative bleeding) 0 0 1 1
Nervous system disorders (sleepy headache) 1 0 1 2
Subtotal 5 0 4 9
Total 26 9 22 57
Combined acetaminophen and ibuprofen for analgesia
85
and no empirical suggestion from our data to suggest that
the combination would be any less safe than the constitu-
ent drugs on their own Our safety data are observational
rather than based on prospective laboratory investigations
but we followed up participants for adverse events for 3
weeks and it seems unlikely that clinically important
harm would have been missed
Pain after oral surgery can persist for several days10 but
we considered 48 h to be a clinically relevant period and
a longer period of study is likely to have resulted in poorer
compliance with data collection
It could be asked whether a more typical (albeit
complex) regimen for ibuprofen alone might have pro-
vided better analgesia than seen with the 4 hourly
approach used here but this seems unlikely particularly
given that our clinical efficacy data were supported by esti-
mates of population pharmacokinetics We had planned to
correlate drug plasma concentration with pain scores but
the drug plasma concentration results were too sparse and
there were too many confounding variables (such as ethni-
city comparators and rescue analgesia) for this to be
undertaken We did demonstrate a lack of interaction
between the constituent drugs when used in combination
and provided evidence that equivalent and predicted blood
concentrations were achieved (the observations of timendash
concentration profile decreased within 90 of prediction
limits for both acetaminophen and ibuprofen) Furthermore
pharmacokinetic parameter estimates observed in the current
study are very similar to those previously reported18 ndash20
The evaluations used in the efficacy analysis have
established construct validity and are appropriate for
parametric analysis24 25
In designing analgesic studies it is an advantage to
minimize the exposure of participants to inadequate
analgesia while controlling for various sources of bias
Some designs incorporate a placebo group but the efficacy
of both ibuprofen26 and acetaminophen27 in comparison
with placebo are well established by previous research
and we would argue that the use of a placebo in this situ-
ation is unnecessary and perhaps even unethical28 There
would be little value in another lsquome toorsquo analgesic unless
it had clear advantages over established agents Therefore
the question of interest lies in the comparisons between
the new agent (Maxigesicw) and the reference standard of
care and in this case we have actually shown superiority to
both of two possible reference standardsmdashacetaminophen
alone and ibuprofen alone One classic approach to analgesic
studies involves treating established acute pain This has the
alleged advantage that pain relief can be assessed (eg by
using AUC to estimate total pain relief or TOTPAR29 30 or
by calculating a pain reduction index per tablet)31 Our
design in contrast follows the widely accepted clinical prac-
tice of anticipating and treating pain before it occurs which
in our unit at least has long been considered best practice
Furthermore rescue medication was readily available and
those requiring it were evenly distributed between the
groups It is notable that most patients did require rescue
medication suggesting that pain after oral surgery can some-
times be severe enough that even the combination of ibupro-
fen and acetaminophen requires supplementation (and it
might be asked whether it would be a good idea for codeine
for example to be added to the combined formulation)
Nevertheless we think it important that the vast majority of
the participants in all groups reported pain scores that were
reasonably low and that all received analgesic regimens
accepted in contemporary practice The predominantly posi-
tive evaluation by participants of their experience in taking
part in the study provides empirical reassurance on this point
(and also other aspects of the conduct of the study)
The treatment of pain is central to medical practice in
hospitals and in primary care If these results are con-
firmed in other settings the already widely used combi-
nation of acetaminophen and ibuprofen may become the
standard of care for the initial management of moderate
acute pain at least for those patients who do not have
contra-indications to NSAIDs Even using the drugs indi-
vidually the dosage regimen studied here is simpler than
that currently recommended and may well improve com-
pliance with and therefore success with this combination
Providing both drugs in one tablet simplifies this regimen
even further and our data confirm that the specific formu-
lation studied here is effective and that there is no inter-
action between its constituent drugs
Conclusions
Doctors treating pain after oral surgery in hospital and at
home and probably pain in many other situations should
consider using acetaminophen and ibuprofen together four
times a day provided there are no contraindications to
either drug and taking into account the known risks of
NSAIDs The combination formulation studied here sim-
plifies this regimen
Funding
This work was supported by AFT Pharmaceuticals Ltd
assisted by New Zealand Trade and Enterprise
Development Grants
Appendix
Declaration of interest
The Department of Anaesthesiology of the University of
Auckland has received payment from AFT
Pharmaceuticals for conducting this study but none of the
investigators has received payment in their personal
capacity
Merry et al
86
Contributors
AFM BJA CF and Hartley Atkinson designed the
study with input from RDG and JE Hartley Atkinson
obtained funding RDG GST and JE performed the
surgery and contributed to patient recruitment and to the
care of patients during their participation in the study
ED was the study coordinator and was responsible for
patient recruitment and follow-up data collection quality
control and many other logistic aspects of the study The
statistical analysis of clinical data was undertaken by CF
and of the pharmacokinetic data by BJA AFM took
primary responsibility for the manuscript with assistance
from Jennifer Zhang All authors edited and commented
on the manuscript AFM is the guarantor
Chief Executive Officer AFT Pharmaceuticals
Clinical TrialRegulatory Assistant AFT Pharmaceuticals
Ethics approval
This study was approved by the Northern X Regional Ethics
Committee 650 Great South Road Penrose Auckland New
Zealand
Ethics Committee Approval Number AKX0410298
Health Authorities (MEDSAFE) Approval Number
TT50-7316 (458)
Role of the sponsor
The sponsor (AFT Pharmaceuticals Ltd) participated in
the study design and protocol development and provided
logistical support during the trial Monitoring of the
study was performed by the sponsor who also main-
tained the trial database Statistical analyses were
independently performed by the biostatistician and the
results cross-checked by sponsors and investigators The
sponsor assisted with the preparation of the manuscript
and was permitted to review it and to make suggestions
but responsibility for the content of this paper lay with
the academic authors and the style and emphasis is that
of the principle investigator The academic authors had
the explicit right to access all data and publish these
results
Provenance and peer review
This paper was not commissioned informal external peer
review has been obtained before submission to the Journal
Additional contributions
We thank Ms Jenny Rous Pharmacy Manager from the
Mercy Hospital Pharmacy for study drug management
Dr Ralph Richardson Program Manager from Institute of
Environment Science amp Research Limited Wellington in
New Zealand for the plasma sample assays Sally Merry
for proofreading and editing on the manuscript the anaes-
thetists Judy Bent Jack Hill Joanna Rose Joanne Paver
Andrew Warmington and Lisa Chapman at Greenlane
Clinical Centre Kerry Gunn Chris Chambers and
Jonathan Cross at Quay Park Clinic for facilitating the
administration of the study protocol and contributing
substantially to the clinical care of the patients and the
participants for their participation
References1 Cousins MJ Brennan F Carr DB Pain relief a universal human
right Pain 2004 112 1ndash42 Merry A Power I Perioperative NSAIDs towards greater safety
Pain Rev 1995 2 268ndash913 MARTINDALE The Extra Pharmacopoeia London The Royal
Pharmaceutical Society of Great Britain 19964 Mehlisch DR The efficacy of combination analgesic therapy in
relieving dental pain J Am Dent Assoc 2002 133 861ndash71
5 Desmeules J Rollason V Piguet V Dayer P Clinical pharmacologyand rationale of analgesic combinations Eur J Anaesthesiol Suppl2003 20 7ndash11
6 Altman RD A rationale for combining acetaminophen andNSAIDs for mild-to-moderate pain Clin Exp Rheumatol 2004 22
110ndash77 Hyllested M Jones S Pedersen JL Kehlet H Comparative effect
of paracetamol NSAIDs or their combination in postoperativepain management a qualitative review Br J Anaesth 2002 88
199ndash2148 Dahl V Dybvik T Steen T Aune AK Rosenlund EK Raeligder JC
Ibuprofen vs acetaminophen vs ibuprofen and acetaminophenafter arthroscopically assisted anterior cruciate ligament recon-struction Eur J Anaesthesiol 2004 21 471ndash5
9 Gazal G Mackie IC A comparison of paracetamol ibuprofen ortheir combination for pain relief following extractions in childrenunder general anaesthesia a randomized controlled trial Int JPaediatr Dent 2007 17 169ndash77
10 Merry AF Swinburn PF Middleton NG Edwards JL Calder MV
Tenoxicam and paracetamolndashcodeine combination after oralsurgery a prospective randomized double-blind placebo-controlled study Br J Anaesth 1998 81 875ndash80
11 Mitchell A van Zanten SV Inglis K Porter G A randomized con-trolled trial comparing acetaminophen plus ibuprofen versus acet-
aminophen plus codeine plus caffeine after outpatient generalsurgery J Am Coll Surg 2008 206 472ndash9
12 Menhinick KA Gutmann JL Regan JD Taylor SE Buschang PHThe efficacy of pain control following nonsurgical root canal
treatment using ibuprofen or a combination of ibuprofen andacetaminophen in a randomized double-blind placebo-controlledstudy Int Endod J 2004 37 531ndash41
13 Viitanen H Tuominen N Vaaraniemi H Nikanne E Annila PAnalgesic efficacy of rectal acetaminophen and ibuprofen alone
or in combination for paediatric day-case adenoidectomy Br JAnaesth 2003 91 363ndash7
14 Henry D McGettigan P Epidemiology overview of gastrointestinaland renal toxicity of NSAIDs Int J Clin Pract 2003 Suppl (135)43ndash9
15 TGA Medicines Evaluation Committee 2003 Review of non-prescription analgesics Multiple Strength of Oral LiquidsAustralia Therapeutic Goods Administration 2003
Combined acetaminophen and ibuprofen for analgesia
87
16 Australian and New Zealand College of Anaesthetists Monitoringduring anaesthesia (Review P18) Melbourne The College 2008
17 Merry AF Sidebotham DA Middleton NG Calder MV WebsterCS Tenoxicam 20 mg or 40 mg after thoracotomy a prospective
randomized double-blind placebo-controlled study AnaesthIntensive Care 2002 30 160ndash6
18 Davies NM Clinical pharmacokinetics of ibuprofen The first 30years Clin Pharmacokinet 1998 34 101ndash54
19 Prescott LF Pharmacokinetics of paracetamol Paracetamol(Acetaminophen) A Critical Bibliographic Review New York Taylor ampFrancis Inc 2001 205ndash15
20 Rainsford KD The pharmacokinetics of ibuprofen in humans andanimals Ibuprofen A Critical Bibliographic Review London Taylor amp
Francis 1999 92ndash521 Ianiro S Jeansonne B McNeal S Eleazer P The effect of pre-
operative acetaminophen or a combination of acetaminophen andibuprofen on the success of inferior alveolar nerve block forteeth with irreversible pulpitis J Endod 2007 33 11ndash4
22 Cooper SA Schachtel BP Goldman E Gelb S Cohn P Ibuprofenand acetaminophen in the relief of acute pain a randomizeddouble-blind placebo-controlled study J Clin Pharmacol 1989 291026ndash30
23 AHFS Drug Information Bethesda MD American Society of
Health-System Pharmacist 2007
24 Coll AM Ameen JRM Mead D Postoperative pain assessmenttools in day surgery literature review J Adv Nurs 2004 46 124ndash33
25 Philip BK Parametric statistics for evaluation of the visual ana-logue scale Anesth Analg 1990 71 710
26 Schou S Nielsen H Nattestad A et al Analgesic dosendashresponserelationship of ibuprofen 50 100 200 and 400 mg after surgicalremoval of third molars a single-dose randomized placebo-controlled and double-blind study of 304 patients J Clin
Pharmacol 1998 38 447ndash5427 Barden J Edwards J Moore A McQuay H Single dose oral para-
cetamol (acetaminophen) for postoperative pain CochraneDatabase Syst Rev (Online) 2004
28 Anderson B Cranswick N The placebo (I shall please)mdashis it so
pleasing in children Paediatr Anaesth 2005 15 809ndash1329 Australian and New Zealand College of Anaesthetists and Faculty
of Pain Medicine Acute Pain Management Scientific EvidenceAustralian Government National Health and Medical ResearchCouncil 2005
30 Moore RA Edwards JE McQuay HJ Acute pain individualpatient meta-analysis shows the impact of different ways of ana-lysing and presenting results Pain 2005 116 322ndash31
31 Quiding H Oksala E Happonen RP Lehtimaki K Ojala T Thevisual analog scale in multiple-dose evaluations of analgesics J Clin
Pharmacol 1981 21 424ndash9
Merry et al
88
e411
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Journal section Oral Medicine and PathologyPublication Types Research
Analgesic efficacy of Lysine Clonixinate paracetamol and dipyrone in lower third molar extraction A randomized controlled trial
Vladimir-Reimar-Augusto-de Souza Noronha 1 Gladson-de Souza Gurgel 1 Luiz-Ceacutesar-Fonseca Alves 2 Luiz-Claacuteudio Noman-Ferreira 2 Lisette-Lobato Mendonccedila 2 Evandro-Guimaratildees de Aguiar 2 Evandro-Neves Abdo 2
1 Student in Oral and Maxillofacial Surgery and Traummatology Dental School Federal University of Minas Gerais Belo Hori-zonte Brazil2 Senior Lectures of Department of Surgery Pathology and Clinic Dental School Federal University of Minas Gerais Belo Horizonte Brazil
Correspondence Faculdade de Odontologia Universidade Federal de Minas GeraisAv Antonio Carlos 6627Belo Horizonte ndash Minas Gerais - BrasilCEP 31270-901evandroabdogmailcom
Received 18082008Accepted 20032009
Noronha VRA Gurgel GS Alves LCF Noman-Ferreira LC Mendonccedila LL Aguiar EG Abdo EN Analgesic efficacy of lysine clonixinate para-cetamol and dipyrone in lower third molar extraction A randomized con-trolled trial Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 httpwwwmedicinaoralcommedoralfree01v14i8medoralv14i8p412pdf
AbstractObjective The purpose of this study is to compare the analgesic effect of lysine clonixinate paracetamol and dipyrone after lower third molar extraction Material and Methods The sample consisted of 90 individuals with clinical indication for inferior third molars extraction The mean age of the sample was 223 years (DPplusmn25) The individuals received the medication in uni-dentified bottles along with the intake instructions The postoperative pain parameters were measured according to Visual Analogical Scale (VAS) and the data was evaluated using the Kruskal-Wallis Test and Friedman Test with the latter used to test different time intervals for each one of the drugsResults The final sample consisted of 64 individuals including 23 males (459) and 41 females (641) The mean age of the entire sample was 223 years (plusmn25) The average length of the procedures was 339 minutes (plusmn98) The distribution of mean values for this variable showed little variance for the different drugs (p=007) Conclusion Lysine Clonixinate did not show any substantial impact on the postoperative pain control when com-pared to other drugs
Key words Lysine Clonixinate paracetamol dipyrone postoperative pain impacted third molar
Article Number 2409 httpwwwmedicinaoralcomcopy Medicina Oral S L CIF B 96689336 - pISSN 1698-4447 - eISSN 1698-6946eMail medicinamedicinaoralcom Indexed in
-SCI EXPANDED-JOURNAL CITATION REPORTS-Index Medicus MEDLINE PubMed -EMBASE Excerpta Medica-SCOPUS-Indice Meacutedico Espantildeol
e412
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Introduction Surgical extraction of third molars is a very usual clini-cal procedure for controlling problems caused by im-pacted tooth and usually is followed by postoperative pain (1) As a result several studies have been published comparing the drugs used to control postoperative pain after surgical removal of third molars (1-4)Lysine Clonixinate is an analgesic that inhibits prostag-landin synthesis A study comparing Lysine Clonixi-nate with Paracetamol on the oral postoperative pain did not find any significantly difference between them (5) In animals Lysine Clonixinate showed a life span of 3 hours and it is recognized as a non-steroid anti-in-flammatory with the shortest life span when compared to other drugs of its category (6)It bonds to plasma proteins in up to 96-98 and its me-tabolism takes place in the liver four different inactive metabolites being derived Seventy-four percent of its excretion is renal and 25 fecal (7) It holds an ex-cellent bio-tolerance and low incidence of collateral ef-fect in the treatment of painful syndrome such as renal neurogenic muscular and tooth pain (89) and migraine (7) The Visual Analogical Scale (VAS) is considered the best and easiest instrument to measure this type of pain The parameters used by VAS determine the intensity of pain as following no pain mild pain moderate pain and severe pain (10-12) The postoperative pain in dentistry should be controlled even before the surgical procedure itself For that many studies suggest the prescription of anti-inflammatory drugs steroids or not or analgesic drugs with some level of anti-inflammatory properties (1314)Paracetamol is a safe effective drug for the treatment of postoperative pain following the surgical removal of lower wisdom tooth (1516) and dipyrone is similar to other analgesics frequently used in the treatment of moderate to severe postoperative pain (17)Although the drugs under test are safe it is possible the occurrence of adverse effect The estimated ex-cess mortality due to community-acquired agranu-locytosis aplastic anemia anaphylaxis and serious upperrsquogastrointestinal complications was 20 per 100 million for paracetamol 25 per 100 million for dipy-rone (18)Regarding the Paracetamol and Dipyrone large use in Brazil Spain and other countries as well (1719) we decided to use them in order to compare the Lysine Clo-nixinate clinic performance The adverse effects due to the use of Lysine Clonixinate could be nausea vomit-ing allergic reactions vertigo and insomnia (9)
Material and MethodsThe sample of 90 individual consisted of all patients under treatment in that semester at the clinic of Oral
Surgery and Oral Traumatology from Federal Univer-sity of Minas Gerais The following conditions were ob-served in order to select the cases (I) individuals with clinical indication for the removal impacted mandibular third molar in Class I or II positioning A or B accord-ing to Pell et al (20) regardless gender race or social class (II) surgeries that would not extend more than 60 minutes (III) age between 18 and 26 years old (IV) absence of allergies to the drugs under test (V) absence of systemic conditions All surgeries were carried out under local anesthesia-Lidocaine 2 with Felipressine 12500 - Novocoreg (SSWhite Artigos Dentais LTDA Rio de Janeiro Brazil)The patients were informed about the purpose of the research project and were asked to give their written consent The research was approved by the local Ethical CommitteeThe drugs tested were bottled in identical opaque white recipient numbered from 1 to 90 Each recipient con-tained eight tablets of either one of the drugs under test (Dipyrone 500mg Paracetamol 750mg Lysine Clonixi-nate 125 mg) The patients themselves chose the recipi-ent at random and they were unaware of its contentEach patient was told to take one tablet from the given recipient one hour before the surgery and another tablet was taken after the surgery in 6 hours intervals after first dose during 24 hours If the pain persisted the pa-tient was given the liberty to take any other drug and the dentist should be informed The assessment of pain was performed according to VAS Pain was measured just after the surgical proce-dure and 1246812 and 24 hours after the operation For each one of the above options they had also to in-form the level of pain according to a decimal scale The criteria used by the authors to assess patientrsquos pain level were 0 cm no pain 01-3 cm light pain 31-7 cm mo-derate pain 71-10 cm intense pain (9) The descriptive analyses are presented in percentages with mean minimum (min) maximum (max) and standard deviation (SD) Kruskal-Wallis and Friedman tests were used and results were considered statistically significant when value of p was less or equal to 005 at least 95 of the confidence
ResultsThe drop-out in the experiment was of twenty-six cases and therefore the sample was reduced to sixty-four The Lysine Clonixinate group was comprised of 20 in-dividuals (8 males and 12 females) The Paracetamol Group was comprised of 23 individuals (9 males and 14 females) and Dipyrone Group was comprised of 21 individuals (6 males and 15 females) The mean age of the entire sample was 223 years (plusmn25) The length of the procedures was in average 339 min-utes (plusmn98) (Table 1) (Table 2) and (Fig 1) depict each
e413
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
Interval drugdescriptive measurement
Pmin max median mean SD
Right after Lysine clonixinate 000 100 000 020 040 09370
Paracetamol 000 300 000 030 070
Dipyrone 000 100 000 010 040
1 hour afterLysine clonixinate 000 200 100 070 060 08130
Paracetamol 000 300 100 060 070
Dipyrone 000 200 100 070 070
2 hours afterLysine clonixinate 000 200 100 080 070 09310
Paracetamol 000 300 100 080 090
Dipyrone 000 300 100 080 080
4 hours afterLysine clonixinate 000 200 100 090 070 08760
Paracetamol 000 200 100 080 070
Dipyrone 000 300 100 100 100
6 horus afterLysine clonixinate 000 200 100 060 060 05330
Paracetamol 000 300 100 080 090
Dipyrone 000 300 000 060 080
8 hours afterLysine clonixinate 000 200 050 060 060 03110
Paracetamol 000 200 000 060 080
Dipyrone 000 300 000 040 080
12 hours afterLysine clonixinate 000 200 000 040 060 05930
Paracetamol 000 200 000 055 070
Dipyrone 000 300 000 040 090
24 hours afterLysine clonixinate 000 200 000 030 060 05820
Paracetamol 000 200 000 040 070
Dipyrone 000 300 000 030 070
Fig 1 Distribution of the scale of pain according to the different time interval for each of the drugs tested
Table 1 Distribution of the variable pain according to VAS in different time period for the tree drugs tested
P refers to Kruskal-Wallis test
e414
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
one of the VAS parameters distributed according to drugs tested No adverse effect was observed with the drugs tested
DiscussionSixty-four individuals underwent surgical removal of their inferior third molars among them 23 (359) were male and 41 (641) female As reported before by Morin et al (21) the variable gender did not play any important role in the distribution of the variable pain after surgery The mean age was 223 years (SDplusmn25 years) and the sample was quite homogeneous in that aspect which is an advantage for the categorization of pain related to age Age can influence the pain control because third molar surgical extraction in older individuals can be-come troublesome due the cortical bone thickness and bone resilience loss (1) Chiapasco et al (1) reported a decrease in morbidity and postoperative complication of third molars in young patients Olmedo-Gaya et al (14) attributed an increase of pain in older patients due to the more bone density and narrower periodontal liga-ment
The patients underwent all the surgical procedures by 2 surgeons with calibration of the techniques avoiding therefore different approaches The surgeries length was controlled and therefore did not influence the be-havior of pain in this study- 339 min (SDplusmn98 min) Regarding this the authors believe there is no bias con-cerning the time-period of surgery on the results here presentedThe surgery of third molar is a well known procedure It allows a standardization of case selection reducing therefore the number of uncontrolled events that may lead to biasQuestionnaire and VAS were used to obtain the data The data bank was categorized by drug and analyzed according to the development of the postoperative con-dition as presented in (Table 1)The results in this study show no statistically significant difference between the drugs under test for controlling postoperative pain Martiacute et al (5) found similar results comparing Paracetamol and Lysine ClonixinateThe high number of patients without any pain in the postoperative period can be related to the local anesthe-sia The number of patients without pain in the postop-
DescriptionDrug Interval min Max median mean SD p
Lisyne clonixinate
Right after 00 10 00 02 04
lt 0001
1 hour after 00 20 10 07 062 hours after 00 20 10 08 074 hours after 00 20 10 09 076 hours after 00 20 10 06 068 hours after 00 20 05 06 0612 hours after 00 20 00 04 0624 hours after 00 20 00 03 06
Paracetamol
Right after 00 30 00 03 07
lt 0001
1 hour after 00 30 10 06 072 hours after 00 30 10 08 094 hours after 00 20 10 08 076 hours after 00 30 10 08 098 hours after 00 20 00 06 0812 hours after 00 20 00 05 0724 hours after 00 20 00 04 07
Dipyrone
Right after 00 10 00 01 04
lt 0001
1 hour after 00 20 10 07 072 hours after 00 30 10 08 084 hours after 00 30 10 10 106 hours after 00 30 00 06 088 hours after 00 30 00 04 0812 hours after 00 30 00 04 0924 hours after 00 30 00 03 07
Table 2 Distribution of pain perception in the different time intervals after surgery according to VAS
P refers to Friedman test
e415
Med Oral Patol Oral Cir Bucal 2009 Aug 114 (8)e411-5 Lysine Clonixinate paracetamol and dipyrone to control postoperative pain
erative period decreases with the passing of time Four hours after the surgery this percentage was the smallest and it increases slightly on the 6th and 8th hour after surgery reaching its peak with 24 hours The results presented here are similar to those of Olme-do-Gaya et al (14) who found out that the postoperative pain reaches its higher intensity during the first 8 hours after the surgery The moderate postoperative pain is re-ported when the production of pain mediator increases and also when the effect of local anesthesia is fading away After the 8th hour and during the subsequently days the pain decreases progressivelyThe results of this study show that the Lysine Clonixi-nate as well as Dipyrone and Paracetamol are efficient in controlling the postoperative pain in the surgery of inferior impacted third molars Lysine Clonixinate pos-sesses an analgesic activity similar to that of Dipyrone and Paracetamol and did not show any substantial im-pact on the control of postoperative pain when com-pared to those drugs
References1 Chiapasco M De Cicco L Marrone G Side effects and complica-tions associated with third molar surgery Oral Surg Oral Med Oral Pathol 199376412-20 2 Laureano Filho JR Maurette PE Allais M Cotinho M Fernandes C Clinical comparative study of the effectiveness of two dosages of Dexamethasone to control postoperative swelling trismus and pain after the surgical extraction of mandibular impacted third molars Med Oral Patol Oral Cir Bucal 200813E129-32 3 Loacutepez-Carriches C Martiacutenez-Gonzaacutelez JM Donado-Rodriacuteguez M Analgesic efficacy of diclofenac versus methylprednisolone in the control of postoperative pain after surgical removal of lower third molars Med Oral Patol Oral Cir Bucal 200510432-9 4 Esteller-Martiacutenez V Paredes-Garciacutea J Valmaseda-Castelloacuten E Berini-Ayteacutes L Gay-Escoda C Analgesic efficacy of diclofenac sodium versus ibuprofen following surgical extraction of impacted lower third molars Med Oral Patol Oral Cir Bucal 20049448-53 444-8 5 Martiacute ML De los Santos AR Di Girolamo G Gil M Manero EO Fraga C Lysine clonixinate in minor dental surgery double-blind randomized parallel study versus paracetamol Int J Tissue React 199315207-13 6 Gonzaacutelez-Martin G Cattan C Zuntildeiga S Pharmacokinetics of lysine clonixinate in children in postoperative care Int J Clin Phar-macol Ther 199634396-9 7 Krymchantowski AV Peixoto P Higashi R Silva A Jr Schutz V Lysine clonixinate vs naproxen sodium for the acute treatment of mi-graine a double-blind randomized crossover study MedGenMed 2005769 8 Ortiacute E Coirini H Pico JC Site-specific effects of the nonsteroidal anti-inflammatory drug lysine clonixinate on rat brain opioid recep-tors Pharmacology 199958190-9 9 Krymchantowski AV Barbosa JS Cheim C Alves LA Oral lysine clonixinate in the acute treatment of migraine a double-blind place-bo-controlled study Arq Neuropsiquiatr 20015946-9 10 Kremer E Atkinson JH Ignelzi RJ Measurement of pain patient preference does not confound pain measurement Pain 198110241-8 11 Price DD McGrath PA Rafii A Buckingham B The validation of visual analogue scales as ratio scale measures for chronic and ex-perimental pain Pain 19831745-56 12 Collins SL Moore RA McQuay HJ The visual analogue
pain intensity scale what is moderate pain in millimetres Pain 19977295-7 13 Seymour RA Walton JG Pain control after third molar surgery Int J Oral Surg 198413457-85 14 Olmedo-Gaya MV Vallecillo-Capilla M Galvez-Mateos R Rela-tion of patient and surgical variables to postoperative pain and inflam-mation in the extraction of third molars Med Oral 20027360-9 15 Weil K Hooper L Afzal Z Esposito M Worthington HV Van Wijk AJ et al Paracetamol for pain relief after surgical removal of lower wisdom teeth Cochrane Database Syst Rev 20073CD004487 16 Moore A Collins S Carroll D McQuay H Paracetamol with and without codeine in acute pain a quantitative systematic review Pain 199770193-201 17 Edwards JE Meseguer F Faura CC Moore RA McQuay HJ Single-dose dipyrone for acute postoperative pain Cochrane Data-base Syst Rev 20013CD003227 18 Andrade SE Martinez C Walker AM Comparative safety evalu-ation of non-narcotic analgesics J Clin Epidemiol 1998511357-65 19 Lorenzetti BB Ferreira SH Mode of analgesic action of dipy-rone direct antagonism of inflammatory hyperalgesia Eur J Phar-macol 1985114375-81 20 Pell GJ Gregory BT Impacted mandibular third molars clas-sification and modified techniques for removal Dent Digest 193339330-821 Morin C Lund JP Villarroel T Clokie CM Feine JS Differences between the sexes in post-surgical pain Pain 20008579-85
CLINICAL TRIAL
Onset of analgesia with sodium ibuprofen ibuprofen acidincorporating poloxamer and acetaminophenmdasha single-dosedouble-blind placebo-controlled study in patientswith post-operative dental pain
Stephen Daniels amp Sandie Reader amp Phillip Berry amp
Michael Goulder
Received 24 September 2008 Accepted 6 January 2009 Published online 28 February 2009 Springer-Verlag 2009
AbstractObjective To compare the onset of action and efficacy ofsodium ibuprofen (ibuprofen sodium dihydrate) and ibu-profen acid incorporating poloxamer (ibuprofenpoloxamer)with that of acetaminophen and placebo in patients withpost-operative dental painMethods A double-blind randomised placebo-controlledactive comparator two-centre study assessing the analgesicefficacy of sodium ibuprofen (512 mg equivalent to400 mg ibuprofen acid) ibuprofenpoloxamer (containing400 mg ibuprofen acid and 120 mg poloxamer 407)acetaminophen (1000 mg) and placebo in patients withmoderate-to-severe pain after third molar extraction (n=322) Onset of action was assessed using the two-stopwatchtechnique and pain intensity and relief were measuredusing validated traditional descriptor scales
Results Significantly more patients achieved confirmedperceptible pain relief and meaningful pain relief withsodium ibuprofen (963 Plt00001) and ibuprofenpoloxamer (900 P=00005) than with acetaminophen(675) The onset of action of both ibuprofen formula-tions was comparable with that of acetaminophen up to45 min post-dose a marked divergence in onset times infavour of the ibuprofen formulations occurred from45 min onward Mean values for the area under the painrelief and pain intensity differences curve (0ndash6 h) weresignificantly greater for sodium ibuprofen (346) andibuprofen acid (349) than for acetaminophen (225) (Plt0001) Other pain relief and pain intensity endpointsfavoured both ibuprofen formulations over acetamino-phen Distractibility from pain (6 h) was significantlygreater with the ibuprofen formulations than with acet-aminophen (P=0008 for sodium ibuprofen P=003 foribuprofenpoloxamer) In patients receiving ibuprofenpain interfered less with daily activities (at 1 and 6 h)than in those receiving acetaminophen (Ple0015) Bothibuprofen formulations had significantly better meanglobal assessment scores than acetaminophen (Plt0001)Tolerability profiles of the ibuprofen formulations werecomparable with that of acetaminophenConclusions Compared with acetaminophen sodiumibuprofen was associated with significantly greateranalgesic efficacy pain relief in a greater proportion ofpatients and greater patient satisfaction
Keywords Acetaminophen Dental pain
Ibuprofenpoloxamer Impacted teeth Post-operative pain
Sodium ibuprofen
Eur J Clin Pharmacol (2009) 65343ndash353DOI 101007s00228-009-0614-y
S DanielsPremier Research Group Clinical Research Center3200 Red RiverAustin TX 78705 USA
S Reader P Berry ()Reckitt Benckiser Healthcare UKDansom LaneHull HU8 7DS UKe-mail phillipberryreckittbenckisercom
M GoulderWorldwide Clinical Trials UK Ltd Isaac Newton CentreNottingham Science and Technology ParkNottingham NG7 2RH UK
Introduction
Ibuprofen [2-(4-isobutylphenyl) propionic acid] is awidely used non-steroidal anti-inflammatory drug(NSAID) currently licensed and marketed worldwide Itexhibits anti-inflammatory analgesic and antipyreticeffects in humans by working as a potent inhibitor of thecyclooxygenase enzyme system and is used to treat painresulting from a wide variety of ailments There is anextensive amount of published literature describing theefficacy of ibuprofen [1ndash7]
Patients with acute pain require rapid relief from over-the-counter (OTC) analgesics Rapidly absorbed ibuprofenformulations have been developed [8] and it was antici-pated that this rapid absorption would result in early onsetof analgesia This placebo-controlled double-blind rando-mised single-dose study was conducted to measure thetime to onset and degree of analgesia from two investiga-tional ibuprofen formulations The first investigationalibuprofen formulation contains the sodium salt of the drugibuprofen sodium dihydrate (sodium ibuprofen) Theformulation used in this study contains 256 mg of theibuprofen sodium salt equivalent to 200 mg ibuprofen acidIt is well documented that ibuprofen salts such asibuprofen sodium lysine and arginate are more rapidlyabsorbed than formulations of free ibuprofen acid [9] andseveral studies have shown that faster absorbed formula-tions lead to faster onset of analgesia [10ndash12] The saltdissolves rapidly in the gastrointestinal tract leading tofaster absorption Pharmacokinetic analyses show that thetime to peak plasma concentration (Tmax) with ibuprofensodium dihydrate is achieved in approximately 30ndash40 min[8] in contrast to the 1ndash2 h reported for standard ibuprofentablets [13 14] The second investigational ibuprofenformulation contains ibuprofen acid plus the surfactantpoloxamer 407 [from the poloxamer family of polymericnon-ionic surface active agents (ibuprofenpoloxamer)]mdashtoincrease the rate of dissolution of the tablet and enable morerapid absorption relative to standard ibuprofen formula-tions Acetaminophen another widely used OTC analgesicand antipyretic indicated for the same mild-to-moderatepain conditions as ibuprofen was included in the study as areference
The dental pain model was used because it is the mostappropriate model to investigate onset of analgesic actionIt is an established post-surgical pain model that involvesextraction of impacted third molars (wisdom teeth) arelatively consistent surgical technique that predictablyproduces moderate-to-severe pain The model is widelyaccepted and has a proven record of assay sensitivity (ieseparating active drugs from each other as well as fromplacebo) [11 12 15ndash18] The model is sensitive enough todemonstrate a correlation between plasma levels of ibupro-
fen and onset of analgesia with faster absorbed formula-tions such as ibuprofen arginate having a faster clinicalresponse time than standard ibuprofen [11 12 19] Theresults from dental pain studies have been widely extrap-olated to other general pain conditions including mostcommon OTC conditions
Onset of analgesic action was assessed using the two-stopwatch technique [11 12 19] and pain intensity andpain relief at each of the assessment timepoints wereassessed using traditional descriptor scales Exploratoryanalyses were conducted to give additional informationabout the rate of onset of action of the medications and tocompare the extent of relief provided by each of the activeformulations
Both ibuprofen formulations were given at a doseequivalent to 400 mg ibuprofen acid The acetaminophenproduct included in the study was Tylenol Extra Strength(1000 mg) a commercially available product The brandedprinting was removed from the Tylenol caplets to enable amatched placebo to be produced The doses of both drugsare the maximum licensed OTC doses in the USA and mostother countries and they have well-established safety andefficacy profiles
The primary objective of the study was to determine thetime to onset of analgesia following dosing with sodiumibuprofen tablets (2times256 mg ibuprofen sodium dihydrate)and ibuprofen acid tablets incorporating poloxamer (2times200 mg ibuprofen plus 60 mg poloxamer 407) hereafterreferred to as ibuprofenpoloxamer in patients with post-operative dental pain The secondary objective was tocompare the efficacy of the two ibuprofen formulationswith that of 1000 mg acetaminophen and placebo in termsof onset peak and duration of analgesic action
The study was conducted in accordance with theDeclaration of Helsinki [20] as referenced in EU Directive200120EC [21] and complies with International Confer-ence on Harmonisation (ICH) Good Clinical Practice(GCP) and applicable regulatory requirements
Methods
Study design
This study was a randomised double-blind placebo-controlled single-dose parallel-group study using thedental pain model It was conducted in two clinical researchcentres (Austin Texas and San Marcos Texas)
Patients andor their legal guardians provided informedconsent before the conduct of study-related proceduresPatients were screened within the 28 days before surgeryOn the day of surgery patients underwent surgical removalof one partially or full bone impacted mandibular third
344 Eur J Clin Pharmacol (2009) 65343ndash353
molar or two ipsilateral third molars with a total impactionscore of 4 5 or 6
Degree of impaction Points
Erupted 0Soft tissue 1Partial bone 2Complete (full) bone 3Unusual impaction (horizontalinverted or posterior-anterior) 4
Surgery was performed under local anaesthetic (approx-imately 100 mg lidocaine 2 with 110000 epinephrine)with conscious sedation (35 lmin 50 nitrous oxide for15 min) using standard surgical techniques Followingsurgery patients who fulfilled the inclusion criteria regard-ing baseline pain intensity were randomly allocated to oneof four treatment groups (sodium ibuprofen ibuprofenpoloxamer acetaminophen or placebo) in a 1111 ratioaccording to a computer-generated randomisation schedulethat stratified patients by sex and baseline pain intensityAfter dosing patients remained in the centre for 8ndash15 hOnset of action and efficacy assessments were recorded atpre-determined intervals during the 6 h post-dose A post-operative follow-up was conducted 5ndash12 days after surgery
The study protocol and its amendments together with thepatient information and consent documents were reviewedand approved by Quorum Review Inc (Seattle WA)
Patients
Patients were recruited from the Premier Research GroupClinical Research Centers database via advertising andpractitioner referral Eligible patients were males andfemales 16ndash40 years of age with a primary diagnosis of
amp at least one mandibular third molar (with full bonyimpaction and an impaction score of ge4 on a 5-pointscale) indicated for removal
amp two ipsilateral third molars with a combined totalimpaction score no greater than 6
In either case patients were required to have moderate orsevere baseline pain intensity as assessed using a 4-pointcategorical pain intensity scale and confirmed with a visualanalogue scale (VAS) score of ge50 mm but le85 mm (where0=no pain and 100 mm=worst pain)
The main exclusion criteria were history of significantdisease that rendered the patient unsuitable for inclusionsignificant ongoing painful conditions other than thatassociated with third molar surgery any ongoing conditionthat may have interfered with the absorption distributionmetabolism or excretion of study medications history ofallergy gastrointestinal complaints (including ulcers heart-burn dyspepsia and indigestion) migraine headaches
within the last year psychotic illness or drug abuse useof concomitant medication that may have confoundedassessments of pain relief (eg psychotropic drugs anti-depressants or sedative-hypnotics) pregnancylactationingestion of any analgesic or anti-inflammatory drug frommidnight of the night before surgery
Sample size determination
For the primary endpoint data were available for the time toperceptible relief from three studies using ibuprofen arginate[11 12 19] These data suggested that the time to perceptiblerelief would be 9 to 14 min for the two test formulationsassuming a similar onset of action to that of ibuprofen arginateSince it was assumed that the majority of placebo patientswould not achieve meaningful relief it was planned that thetime to confirmed perceptible relief for these patients would becensored at 4 h Although the spread of observations was notprovided for the arginate formulation it was assumed conser-vatively that the standard deviation (SD) for time to confirmedperceptible relief would be 1 h (based on the possible rangebeing 0ndash4 h and covering plusmn 2 SD) Hence this study was highlypowered (gt99) to detect such a large difference for the time toconfirmed perceptible relief using the Wilcoxon test
For the area under the curve (AUC) (pain relief intensitydifference [PRID] from 0 to 6 h) data were available fromtwo previous studies which compared ibuprofen lysine [22]and liquigel [23] ibuprofen with acetaminophen In the formerstudy PRID to 6 h was not provided but the sum of painintensity differences (SPID) to 6 h was given This gave adifference of 251 between ibuprofen lysine and acetamino-phen The within-group SD for acetaminophen was 447Using these data it was calculated that with 80 patients pergroup this study would have a 90 power to detect adifference between the ibuprofen formulations and acetamin-ophen at a significance level of 0025 If the data from theliquigel paper were used for sum of the measures of pain reliefand pain intensity difference (SPRID) to 6 h a slightly higherpower would be achieved It was not possible to performformal power calculations for the second endpoint in the closedtest procedure namely time to meaningful relief
Study and concomitant treatments
Following surgery eligible patients received a single oraldose (four tablets and two caplets) of one of the followingfour study treatments
amp sodium ibuprofen 2times256 mg ibuprofen sodium dihy-drate tablets (each tablet equivalent to 200 mg ibupro-fen acid) plus two matched placebo for ibuprofenpoloxamer tablets plus two matched placebo for 500 mgacetaminophen caplets
Eur J Clin Pharmacol (2009) 65343ndash353 345
amp ibuprofenpoloxamer 2times200 mg ibuprofen acid tabletseach tablet incorporating 60 mg of the surfactantpoloxamer 407 plus two matched placebo for sodiumibuprofen tablets plus two matched placebo for 500 mgacetaminophen caplets
amp acetaminophen 2times500 mg acetaminophen (TylenolExtra Strength) caplets plus two matched placebo forsodium ibuprofen tablets plus two matched placebo foribuprofenpoloxamer tablets
amp placebo two matched placebo for sodium ibuprofentablets plus two matched placebo for ibuprofenpolox-amer tablets plus two matched placebo for 500 mgacetaminophen caplets
Patients were encouraged to wait at least 90 min afterreceiving the study treatment before consuming rescuemedication although rescue medication was available atany time after dosing If rescue medication was neededwithin the first 4 h of dosing an intra-muscular injection ofketorolac tromethamine (60 mg) was administered Ifrescue medication was needed later than 4 h after studydrug administration acetaminophen 500 mghydrocodone5 mg or ketorolac tromethamine was given A prescriptionfor acetaminophen 500 mghydrocodone 5 mg was provid-ed to patients for home use at the time of discharge
The use of intravenous oral or inhaled (nitrous)sedation during surgery was prohibited Analgesic andanti-inflammatory drugs (except for the permitted rescuemedications antibiotics and anaesthetics) were not per-mitted during the 6-h post-dose assessment periodPenicillins macrolide antibiotics clindamycin and topicaltetracycline gelfoam were permitted the use of selectiveserotonin-reuptake inhibitors (SSRIs) and selective nor-epinephrine-reuptake inhibitors (SNRIs) was also accept-able in patients who had maintained a stable dose for atleast 4 weeks prior to the first visit Caffeine-containingfoods and drinks were to be discontinued from midnightprior to surgery until the end of the 6-h post-doseassessment period Ice packs were not allowed for thefirst 3 h after dosing
Efficacy endpoints
Patients were queried at pre-determined intervals by thestudy staff and all pain assessments were recorded by thepatient in their diary
Pain intensity (categorical and VAS)
Pain intensity (PI) was assessed at the following timesbaseline (0 h) and at 5 10 15 20 25 30 35 40 45 60 90120 180 240 300 and 360 min after dosing The PI wasmeasured on a categorical scale in response to the question
ldquoWhat is your pain level at this timerdquo with patient responsechoices of none=0 mild=1 moderate=2 and severe=3 Inaddition patients were also asked to draw a single vertical lineto indicate their current level of PI on the 100-mm VASPatients were randomised to treatment when they rated theirbaseline PI as moderate or severe and the score on the VASwas ge50 mm but le85 mm
Pain relief and pain half-gone
Pain relief (PR) was assessed at the same times as PI (withthe exception of 0 h) in response to the question ldquoHowmuch relief have you had from your starting painrdquo withpatient response choices of none=0 a little=1 some=2 alot=3 and complete=4 In addition patients were alsoasked ldquoIs your starting pain at least half gonerdquo withpatient responses as no=0 or yes=1
Perceptible and meaningful PR
Two stopwatches were started at the time of dosing Eachpatient was instructed ldquoStop the first stopwatch when you firstfeel any pain relief whatsoever This does not mean you feelcompletely better although you might but when you first feelany relief in the pain you have nowrdquo The patient wasinstructed ldquoStop the second stopwatch when the pain relief ismeaningful to yourdquo If the patient did not press thestopwatches within the first 4 h of the treatment period or ifrescue medication was required the patients were no longerrequired to use the stopwatches
Distractibility from pain
Distractibility from pain was assessed at baseline and at 60and 360 min after dosing in response to the question ldquoHoweasy is it for you to distract yourself from your painrdquoPatients responded using a 100-mm VAS scale where 0 =very easy and 100 = impossible
Rainier scale
Patients completed the Rainier scale at baseline and at 60and 360 min after dosing This assessed perceivedfunctional impairment of activities of daily living (ieeating driving sleeping reading working and speaking)Patients rated the perceived pain interference with eachactivity on a scale of 1 to 10 where 1 = would not interfereat all and 10 = would completely interfere
Rescue medication
The time of rescue medication was recorded Patientstaking rescue medication completed all pain intensity and
346 Eur J Clin Pharmacol (2009) 65343ndash353
pain relief assessments immediately before rescue medica-tion and continued to record their pain assessmentsthroughout the 6-h assessment period
Global evaluation
At the end of 6 h or at the time of rescue medication patientswere asked ldquoHow effective do you think the study medicationis as a treatment for painrdquo Response choices were 1 =excellent 2 = very good 3 = good 4 = fair or 5 = poor
The primary efficacy endpoint was the time to firstconfirmed perceptible pain relief There were two keysecondary endpoints (1) the AUC for SPRID from 0 to 6 hand (2) the time to meaningful pain relief
Other secondary endpoints included (1) total pain relief(TOTPAR) SPID (categorical and VAS) SPRID from 0 to4 h (2) TOTPAR SPID (categorical and VAS) from 0 to6 h (3) individual pain relief and pain intensity (categoricaland VAS) readings at each timepoint from 5 min to 6 h (4)peak pain relief and pain intensity difference (PID)(categorical and VAS) throughout the 6-h evaluation period(5) first time at which PID was ge1 (6) time to first use ofrescue medication (7) time to and proportion of patientswith pain half-gone (8) distractibility from pain at baselineand at 1 and 6 h post-dose and perceived pain interferencewith daily activities (Rainier scale) at 1 and 6 h post-dose(9) patientrsquos overall assessment of the medication
Safety assessments
Adverse events (AEs) were assessed by non-directedquestioning recorded in the source documentation andthen assessed by the Investigator with respect to severityand relationship to study medication Vital signs (bloodpressure heart rate and oral temperature) were assessed atscreening baseline (pre-dose) at 6 h post-dose and at thefollow-up visit A physical examination was also conductedat screening and at the follow-up visit 5ndash12 days aftersurgery
Statistical analyses
All calculations and figures were produced using SAS ver91 or S-PLUS 62 (SAS Institute Cary NC) The analysisof the primary endpoints was performed via a closed testprocedure The actual protocol-defined primary endpointwas the time to first confirmed perceptible pain reliefPairwise differences between the two ibuprofen formula-tions and placebo were assessed at a significance level of25 so the overall alpha-level of 5 was maintained Forthe primary endpoint pairwise differences between the twoibuprofen formulations and placebo were assessed using theWilcoxon rank-sum test A sensitivity analysis was also
performed where differences between the ibuprofen for-mulations and placebo were assessed using a Cox regres-sion analysis with treatment group study site gender andbaseline pain intensity (categorical) included in the modelThe hazard ratio and associated 975 confidence intervals(CIs) were calculated for the pairwise comparisons
It was planned that if either of the primary pairwisecomparisons were significant at the 25 level the keysecondary endpoints (SPRID 0ndash6 h and time to meaningfulpain relief) were to be assessed for that formulation under aclosed-test procedure Each endpoint was assessed in theorder specified and only if the previous assessments for thatformulation were significant were the subsequent end-points assessed in a confirmatory sense Once the endpointwas not significant then all subsequent assessments wereconsidered exploratory
Endpoints aggregated over several time points werecalculated using AUC as per the secondary endpointDifferences between the treatments were assessed at atwo-sided alpha of 005 A 95 CI for the pairwisedifferences between the treatments was calculated fromthe parameter estimates of the fitted model The pairwisecomparisons of interest were between each of the ibuprofenformulations and placebo and between each of theibuprofen formulations and acetaminophen For the time-to-event parameters such as time to first (unconfirmed)perceptible pain relief differences between the treatmentgroups were assessed as per the primary endpoint
Differences between each of the two ibuprofen formu-lations and acetaminophen in the key secondary endpointsand in the majority of the other secondary endpoints wereanalysed by analysis of covariance (ANCOVA) includingtreatment group study site gender and baseline painintensity (categorical scale) as factors
All assessments completed after the patient had takenrescue medication were considered to be missing For bothpain relief and pain intensity differences missing valuesbetween two available assessments were linearly interpo-lated Missing readings that could not be interpolated werereplaced with the baseline pain intensity or zero relief
All enrolled patients who received a dose of studymedication were included in the safety population All AEswere listed and tabulated by treatment severity relationshipto therapy and body system according to the MedicalDictionary for Regulatory Activities (MedDRA) Version81
Results
Between June and October 2005 a total of 322 patients(mean age 213 years) were randomised to receive studytreatment Of the 322 randomised patients 318 (988)
Eur J Clin Pharmacol (2009) 65343ndash353 347
completed the study The trial profile including the totalnumber of patients withdrawn and analysed is illustrated inFig 1 A total of 321 patients all of whom were balancedacross treatment groups with respect to baseline demo-graphics pain intensity and clinical characteristics (Table 1)were included in the intent-to-treat (ITT) population
Primary efficacy endpoint
Significantly more patients reported confirmed perceptiblepain relief with sodium ibuprofen (963) and ibuprofenpoloxamer (900) than with acetaminophen (675) (Plt00001 and P=00005 respectively) In the placebo grouponly 259 patients reported confirmed perceptible painrelief KaplanndashMeier median times to confirmed perceptiblepain relief were 170 min for sodium ibuprofen 185 minfor ibuprofenpoloxamer and 201 min for acetaminophen(Fig 2) Median time could not be estimated for placebo asfewer than 50 of patients assigned to this groupexperienced confirmed perceptible pain relief Comparisonsof pairwise differences between the two ibuprofen formu-lations and placebo using Wilcoxon rank-sum tests and Coxregression analysis were highly significant (Plt0001 forboth analyses)
Key secondary efficacy endpoints
Mean SPRID (0ndash6 h) values were 346 349 225 and073 for the sodium ibuprofen ibuprofenpoloxamer
acetaminophen and placebo groups respectively Pair-wise comparisons of ibuprofen and acetaminophen werehighly significant in favour of both ibuprofen formula-tions (Plt0001)
Significantly more patients reported meaningful painrelief with sodium ibuprofen (963) or ibuprofenpolox-amer (900) than with acetaminophen (675) (Plt00001and P=00005 respectively) (Fig 3) Of the patientsreceiving placebo 259 reported meaningful pain reliefThe KaplanndashMeier median times to meaningful relief were451 min (sodium ibuprofen) 447 min (ibuprofenpolox-amer) and 541 min (acetaminophen) Neither of the twoWilcoxon rank-sum comparisons between the ibuprofenformulations and acetaminophen were statistically signifi-cant whereas pairwise comparisons obtained via Coxregression analysis were statistically significantly different(P le 0002) The KaplanndashMeier survival curves were similarfor the ibuprofen and acetaminophen groups up to 45 minbut the degree of separation from 45 min onward wasmarked with more patients achieving meaningful painrelief with ibuprofen
Sitendashtreatment interactions
In general site was a statistically significant factor subjectsfrom the SanMarcos site had less favourable outcomes For theprimary efficacy endpoint and for the key secondary efficacyendpoints of SPRID (0ndash6 h) and time to meaningful pain reliefsite was statistically significantly For all three measures the
Withdrawn from ITT (failure toprovide baseline diary data) 1Withdrawn from ITT (failure toprovide baseline diary data) 1Withdrawn from ITT (failure toprovide baseline diary data) 1
IBUPROFENPOLOXAMER
Total screened 614
Total randomised 322
Excluded prior to surgery (n=240)
Excluded prior to dosing (n=52)
Failure to meet inclusion criteria (n=292)
Allocated to intervention 80
ACETAMINOPHEN
Allocated to intervention 81
PLACEBO
Allocated to intervention 81
Completed 80 Completed 81 Completed 81
Total analysed (ITTa) 80 Total analysed (ITTa) 80 Total analysed (ITTa) 81
Completed 76
Withdrew consent 1Lost to follow-up 1Other reasons 2
Withdrawn 0 Withdrawn 0 Withdrawn 0
Total analysed (ITTa) 80
SODIUM IBUPROFEN
Not included in ITT (failure to provide baseline diary data) 1
Allocated to intervention 80
Fig 1 Flow diagram illustrat-ing patient inclusion and exclu-sion throughout the study ITTIntent to treat aThe ITT popula-tion consisted of all patientswho were randomised whocompleted the baseline efficacyassessments and who had atleast one post-baseline assess-ment (primary efficacy set)
348 Eur J Clin Pharmacol (2009) 65343ndash353
interaction between site and treatment was formally investigat-ed In all cases the interaction term was not statisticallysignificant implying that treatment group responses wereconsistent between the sites
Exploratory secondary efficacy endpoints
Pain relief andor reduction in pain intensity
All summary endpoints related to pain relief andor PIDwere significantly more favourable for the two ibuprofenformulations than for acetaminophen or placebo (Plt0001for both ibuprofen formulations vs acetaminophen orplacebo in all comparisons)
A summary of pain relief scores at specified time pointsfrom 5 min to 6 h is displayed in Fig 4 The superiority of
the two ibuprofen formulations over acetaminophen canclearly be seen from 45 min post-dose onward A summaryof PID (categorical) scores at specified time points from5 min to 6 h is displayed in Fig 5 The superiority of thetwo ibuprofen formulations over acetaminophen can beclearly seen from 60 min post-dose onward
Individual PR and PID
The pain relief and PID (categorical and VAS) scores showthat sodium ibuprofen provided more effective pain reliefthan placebo at 15 min [P=0021 (PR) P=004 (PIDcategorical) P=0036 (PID VAS)] Similarly ibuprofenpoloxamer provided more effective relief than placebo at25 min [P=0002 (PR) P=0002 (PID categorical)] and at20 min [P=0008 (PID VAS)]
Timepoint (mins)
a
ttain
ing
conf
irmed
per
cept
ible
rel
ief
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 2 KaplanndashMeier curves for time to first confirmed perceptiblepain relief
Timepoint (mins)
a
ttain
ing
mea
ning
ful r
elie
f
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 3 KaplanndashMeier curves for time to meaningful pain relief
Table 1 Patient demographics and clinical characteristics at baseline (ITT population)
Baseline patient characteristics Treatment group
Sodium ibuprofen(n=80)
Ibuprofenpoloxamer(n=80)
Acetaminophen(n=80)
Placebo(n=81)
Total(n=321)
Age (years) mean (SD) 214 (388) 214 (360) 212 (443) 211 (408) 213 (399)Sex n ()Male 31 (388) 31 (388) 30 (375) 31 (383) 123 (383)Female 49 (613) 49 (613) 50 (625) 50 (617) 198 (617)
Baseline pain intensity (categorical) n ()Moderate 61 (763) 60 (750) 60 (750) 62 (765) 243 (757)Severe 19 (238) 20 (250) 20 (250) 19 (235) 78 (243)
Baseline pain intensity (VAS) mean (SD)Mean (SD) 6816 (874) 6881 (949) 6703 (932) 6737 (1003) 6784 (939)Range 51ndash85 50ndash89 52ndash84 50ndash85 50ndash89
ITT intent-to-treat SD standard deviation VAS visual analogue scaleTreatment definitions sodium ibuprofen=2times256 mg ibuprofen sodium dihydrate tablets (each tablet equivalent to 200 mg ibuprofen acid)ibuprofenpoloxamer=2times200 mg ibuprofen acid tablets acetaminophen=2times500 mg acetaminophen caplets
Eur J Clin Pharmacol (2009) 65343ndash353 349
First time to PID ge 1
There were no significant differences between the activetreatment groups in the proportion of the time to reportingof PID ge 1
Time to first use of rescue medication
Rescue medication was required by significantly fewerpatients in the sodium ibuprofen group (325) and theibuprofenpoloxamer group (225) than in the acetamin-ophen (438) group Owing to the relatively smallproportion of patients reporting the use of rescue medica-tion KaplanndashMeier median times to first use of rescuemedication could not be calculated The pairwise compar-isons between the two ibuprofen formulations and acet-aminophen were both statistically significant using theWilcoxon rank-sum test with P=0019 and P=0001 forsodium ibuprofen and the ibuprofenpoloxamer formula-tion respectively (Fig 6) The vast majority of patientsrandomised to placebo took rescue medication (827)
Time to and proportion of patients with pain half-gone
The proportion of patients reporting pain half-gone were938 888 75 and 370 for sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo re-spectively The median time to pain half-gone wassimilar for all three active treatment groupsmdash350 min(sodium ibuprofen) 375 min (ibuprofenpoloxamer) and450 min (acetaminophen) The Wilcoxon rank-sumcomparisons between the ibuprofen formulations andacetaminophen were not statistically significant (P=007and P=018 for sodium ibuprofen and ibuprofenpolox-amer respectively) but the two equivalent comparisonswere statistically significant when the Cox regression wasused (P=0013 and P=002 for sodium ibuprofen andibuprofenpoloxamer respectively) This may be explainedin terms of a greater proportion of patients randomised toeither of the ibuprofen formulations reporting the endpointscompared with acetaminophen However as for time tomeaningful relief the separation in onset times in favour ofibuprofen was only apparent from 45 min post-doseonward
Distractibility from pain (VAS)
At 1-h post-dose the mean values for the distractibilityfrom pain (VAS) scores were 290 321 381 and657 mm for sodium ibuprofen ibuprofenpoloxameracetaminophen and placebo respectively Both ibuprofenformations had lower (more favourable) scores thanplacebo (Plt0001) and sodium ibuprofen versus acetamin-ophen was statistically significant (P=0010) whereas theibuprofenpoloxamer versus acetaminophen comparisonswere non-significant (P=0083)
At 6 h post-dose both ibuprofen formulations hadmore favourable distractibility from pain scores thanacetaminophen (P=0008 and P=003 sodium ibuprofen
Timepoint (minutes)
Mea
n pa
in in
tens
ity d
iffer
ence
s
00
05
10
15
0 15 35 60 90 120 180 240 300 360
Sodium ibuprofen IbuprofenpoloxamerAcetaminophenPlacebo
Fig 5 Mean pain intensity difference (categorical) at each timepoint
Timepoint (mins)
ta
ken
resc
ue m
edic
atio
n
0 50 100 150 200 250
020
4060
8010
0
Sodium ibuprofenIbuprofenpoloxamerAcetaminophenPlacebo
Fig 6 KaplanndashMeier curves for time to first use of rescue medication
Fig 4 Mean pain relief at each timepoint
350 Eur J Clin Pharmacol (2009) 65343ndash353
and ibuprofenpoloxamer respectively) The vast majorityof patients randomised to placebo took rescue medicationso only 14 patients provided valid data within this grouphence this analysis was not performed for the placebogroup
Pain interference with daily activities (Rainier scale)
At 1-h post-dose the mean values on the Rainier scale were188 223 268 and 432 for the sodium ibuprofen ibuprofenpoloxamer acetaminophen and placebo groups respectivelyThe scores were statistically significantly lower for bothibuprofen formulations than for placebo (Plt0001) andacetaminophen [P=0001 (sodium ibuprofen) and P=0015(ibuprofenpoloxamer)] At 6-h post-dose the mean valueswere 151 171 224 and 163 for the sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo groupsrespectively Both ibuprofen formulations maintained signif-icantly lower (more favourable) values on the Rainier scalethan acetaminophen (P=0004 and P=0011 for sodiumibuprofen and ibuprofenpoloxamer) Placebo treatment wasnot analysed for this comparison as only 14 patients in thisgroup provided valid data
Patientrsquos overall assessment of medication as a treatmentfor pain
Significantly more patients in the sodium ibuprofen (813)and ibuprofenpoloxamer (848) groups rated the studymedication as good very good or excellent than in the groupsthat received acetaminophen (538) or placebo (173)Furthermore the mean global assessment scores weresignificantly lower (more favourable) for both ibuprofenformulationsmdash240 (sodium ibuprofen) and 244 (ibuprofenpoloxamer)mdashthan for acetaminophen or for placebo (341 and446 respectively Plt0001)
Safety findings
A total of 118 of all patients had AEs that were consideredby the investigators to be possibly related to study medicationno events were classified as definitely or probably related tostudy treatment Adverse events were experienced by 300238 309 and 296 of patients receiving sodium ibuprofenibuprofenpoloxamer acetaminophen and placebo respec-tively The majority of AEs (73) were mild-to-moderate inseverity and the most frequently reported AEs includednausea headache vomiting and dizziness Adverse eventsoccurring in at least 5 of all patients in any treatment groupare summarised in Table 2 Severe AEs (including vomitingnausea dizziness abdominal pain and headache) occurred atrates of 63 (sodium ibuprofen) 25 (ibuprofenpolox-amer) 123 (acetaminophen) and 99 (placebo) therewere no deaths or withdrawals attributable to AEs during thestudy period There were no significant differences betweenstudy medications in terms of tolerability
Discussion
This placebo-controlled study demonstrated excellent assaysensitivity for every measure of efficacy with bothibuprofen formulations and acetaminophen showing clini-cally and statistically significant analgesia that was superiorto placebo Furthermore the overall analgesic efficacy(duration and total effect) of both ibuprofen formulationswas shown to be superior to acetaminophen
Data from this study showed statistically significant differ-ences between both the ibuprofen test formulations andplacebo for the primary endpoint ie the time to firstconfirmed perceptible pain relief In addition a significantlygreater proportion of patients receiving ibuprofen experiencedconfirmed perceptible pain relief than those receiving acet-
Table 2 Adverse events occurring in gt5 of patients in any treatment group
Sodium ibuprofen (n=80) Ibuprofenpoloxamer (n=80) Acetaminophen (n=81) Placebo (n=81)
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Numberof events
Number ofpatients n ()a
Any AE 43 24 (300) 27 19 (238) 41 25 (309) 39 24 (296)GastrointestinalNausea 10 9 (113) 5 5 (63) 8 8 (99) 14 14 (173)Vomiting 2 2 (25) 1 1 (13) 6 6 (74) 8 8 (99)Nervous systemDizziness 4 4 (50) 0 0 (00) 6 5 (62) 5 5 (62)Headache 11 11 (138) 5 4 (50) 4 4 (49) 3 3 (37)
AE Adverse eventTreatment definitions sodium ibuprofen=2times256 mg ibuprofen sodium dihydrate tablets (each tablet equivalent to 200 mg ibuprofen acid)ibuprofenpoloxamer=2times200 mg ibuprofenpoloxamer tablets acetaminophen=2times500 mg acetaminophen capletsa Percentages based on total number of patients per treatment group
Eur J Clin Pharmacol (2009) 65343ndash353 351
aminophen The median time to meaningful pain relief was45 min for both ibuprofen formulations and 54 min foracetaminophen Although a much greater proportion ofpatients reported relief on the two ibuprofen formulationsthe divergence in onset times was only apparent from 45 minpost-dose onward ie there was a much higher proportion ofresponders from 45 min onward for the ibuprofen treatmentsthan for acetaminophen Because of this late divergence theWilcoxon rank-sum test was not sensitive enough to detectsignificant differences whereas the Cox proportional hazardsregression analysis showed significant differences in favour ofibuprofen over acetaminophen In terms of SPRID over 6 hboth ibuprofen test formulations were significantly moreefficacious than acetaminophen
Previous studies using the post-operative dental painmodel have demonstrated that treatment with a differentibuprofen salt formulation ibuprofen arginate (l-argininesalt of ibuprofen) resulted in faster onset times to analgesiaand greater overall efficacy than treatment with conven-tional (standard) ibuprofen [11 12 19] The pharmacoki-netic profile of the ibuprofen sodium formulation used inthis study has been shown to be similar to that of ibuprofenarginate with peak plasma concentrations achieved atapproximately 30ndash40 min compared with 1ndash2 h forstandard ibuprofen [8 13 14] Therefore it was anticipatedthat the rapid absorption associated with sodium ibuprofenwould result in early onset of analgesia similar to thatobserved for ibuprofen arginate This study was notintended nor was it sufficiently powered to compare thetwo ibuprofen formulations
When comparing the median time to meaningful painrelief data from this study with previous studies bothibuprofen test formulations in this study were found to be atthe upper end of the range for ibuprofen arginate andibuprofen lysine data (range 24ndash42 min) [11 12 19 22]ie 451 min (sodium ibuprofen) and 447 min (ibuprofenpoloxamer) In the earlier studies where ibuprofen arginatewas compared with conventional ibuprofen the mediantime to meaningful pain relief obtained for ibuprofenarginate was approximately half that of the conventionalibuprofen [11 12 19] A recent bioavailability study hasalso shown that the Tmax for sodium ibuprofen was lessthan half that of standard ibuprofen (ie 35 min vs 90 minrespectively) [8] Therefore it was not unexpected thatsodium ibuprofen had a fast onset of analgesic effect in thisstudy that was in a similar order of magnitude as thosepreviously reported for faster absorbed formulations
The analyses of secondary endpoints related to degreeof pain relief andor reduction in pain intensity (TOT-PAR SPRID SPID peak PID and peak PR) consistentlyfavoured both ibuprofen formulations over acetamino-phen Only in terms of time to PID of at least 1 werethere no statistically significant differences observed
compared with acetaminophen Measures of analgesicdurationmdashthe proportion of patients taking rescue med-ication and the time to rescue medicationmdashshowed thatthose in the acetaminophen group received rescuemedication sooner than those in either of the twoibuprofen groups This suggests that both ibuprofenformulations had a longer duration of action thanacetaminophen which is in keeping with that previouslyreported for ibuprofen lysine [22] and ibuprofen liquigel[23] In terms of pain relief and PID the timepoint at whicha significant difference was first observed between either ofthe ibuprofen formulations and placebo was 15 min(sodium ibuprofen) a significant difference between eitherof the ibuprofen formulations and acetaminophen was firstobserved at 45 min (sodium ibuprofen) In comparison withpreviously published data studies with ibuprofen arginateand ibuprofen lysine demonstrated significant differences inpain relief and PID between ibuprofen and placebo at 10ndash15 min [11 12 19 23] Furthermore significant differ-ences between ibuprofen lysine and acetaminophen wereobserved at 15 min much sooner than the 45 min observedin our study [22] These differences could be explained bythe different formulations of ibuprofen the fact that adifferent brand of acetaminophen was used in each of therespective studies or the inherent variability associated witha small sample size
Patients in both ibuprofen groups were able to distractthemselves from their pain at 1 and 6 h after dosingsignificantly more easily than those in the placebo andacetaminophen groups (6 h only) Patients in both ibupro-fen groups also reported that pain would interfere with theirdaily activities significantly less than patients in theacetaminophen group Patients in the two ibuprofen groupsrated the study medication as good very good or excellentmore frequently than those in the acetaminophen andplacebo groups
Ibuprofen is a well-tolerated NSAID at low doses [24]However even at prescribed doses ibuprofen is associatedwith the least risk of gastrointestinal complications com-pared with other NSAIDs [25ndash27] No new safety concernswere raised by the current study treatment with singledoses of sodium ibuprofen and ibuprofenpoloxamer werewell tolerated with AE profiles comparable to that ofacetaminophen The most frequently reported AEs consid-ered to be related to study treatment (ie nausea headachevomiting and dizziness) are not unexpected in patientsrecovering from dental surgery
In conclusion these results suggest that compared withacetaminophen both the sodium ibuprofen and ibuprofenacid incorporating poloxamer formulations are more effi-cacious in providing rapid and sustained analgesia and areassociated with pain relief in a greater proportion ofpatients undergoing surgical removal of impacted third
352 Eur J Clin Pharmacol (2009) 65343ndash353
molars Together with the favourable safety profile ofibuprofen these findings support a recommendation forthis agent as an analgesic of choice for the treatment ofpost-operative dental pain
Acknowledgements The authors would like to acknowledgeFranklin S Bonasso DDS and R Dean Jasper DDS (Central OralSurgery Group) Barbara Hernandez MA CCRC Michael Goulder(Worldwide Clinical Trials UK Ltd) for statistical support andVandana Sahajpal PhD and Quyen Chu PhD (Sudler amp HennesseyLondon) for medical writing support
Conflict of interest This study was funded by Reckitt BenckiserGroup plc Stephen Daniels (Premier Research Group ClinicalResearch Centers USA) is the Co-ordinating Investigator SandieReader and Phillip Berry are employees of Reckitt Benckiser Group plc
References
1 Sweetman SC (ed) (2002) Ibuprofen In Martindale the completedrug reference 33rd edn Pharmaceutical Press London
2 Mehlisch DR Sollecito WA Helfrick JF et al (1990) Multicenterclinical trial of ibuprofen and acetaminophen in the treatment ofpostoperative dental pain J Am Dent Assoc 121257ndash263
3 Roy S (1983) A double-blind comparison of propionic acidderivative (ibuprofen) and a fenamate (mefanamic acid) in thetreatment of dysmenorrhoea Obstet Gynecol 61628ndash632
4 Moran M (1991) Double-blind comparison of diclofenac potassi-um ibuprofen and placebo in the treatment of ankle sprain J IntMed Res 19121ndash130
5 Goswick CB (1983) Ibuprofen versus propoxyphene hydrochlo-ride and placebo in acute musculoskeletal trauma Curr Ther ResClin Exp 34685ndash692
6 Schachtel BP Thoden WR (1988) Onset of action of ibuprofenin the treatment of muscle-contraction headache Headache28471ndash474
7 Pearce I Frank GJ Pearce JMS (1983) Ibuprofen compared withacetaminophen in migraine Practitioner 227465ndash467
8 Dewland P Reader S Berry P (2008) Bioavailability of ibuprofenfollowing oral administration of standard ibuprofen sodiumibuprofen or ibuprofen acid incorporating poloxamer in healthyvolunteers Eur J Clin Pharmacol (submitted)
9 Geisslinger G Menzel S Wissel K Brune K (1993) Single dosepharmacokinetics of different formulations of ibuprofen andaspirin Drug Invest 5238ndash242
10 Schleier P Prochnau A Schmidt-Westhausen AM et al (2007)Ibuprofen sodium dihydrate an ibuprofen formulation withimproved absorption characteristics provides faster and great-er pain relief than ibuprofen acid Int J Clin Pharmacol Ther4589ndash97
11 Black P Max MB Desjardins P et al (2002) A randomizeddouble-blind placebo-controlled comparison of the analgesic
efficacy onset of action and tolerability of ibuprofen arginateand ibuprofen in postoperative dental pain Clin Ther241072ndash1089
12 Desjardins P Black P Papageorge M et al (2002) Ibuprofenarginate provides effective relief from postoperative dental painwith a more rapid onset of action than ibuprofen Eur J ClinPharmacol 58387ndash394
13 Albert KS Gernaat CM (1984) Pharmacokinetics of ibuprofenAm J Med 7740ndash46
14 Davies NM (1998) Clinical pharmacokinetics of ibuprofen Thefirst 30 years Clin Pharmacokinet 34101ndash114
15 Cooper SA Precheur H Rauch D et al (1984) The analgesicefficacy of ibuprofen compared to acetaminophen with codeine(abstract) Clin Pharmacol Ther 35232
16 Mehlisch D Frakes L (1984) A controlled comparative evaluationof acetaminophen and aspirin in the treatment of post-operativepain Clin Ther Exerpta Med 789ndash97
17 Mehlisch D Markenson J Schnitzer T (1999) The efficacy ofnonsteroidal anti-inflammatory drugs for acute pain CancerControl 65ndash9
18 Daniels SE Desjardins PJ Talwalker S et al (2002) The analgesicefficacy of valdecoxib vs oxycodoneacetaminophen after oralsurgery J Am Dental Assoc 133611ndash621
19 Mehlisch DR Ardia A Pallotta T (2002) A controlled compar-ative study of ibuprofen arginate versus conventional ibuprofen inthe treatment of postoperative dental pain J Clin Pharmacol42904ndash911
20 World Medical Association (1964) Declaration of HelsinkiEthical principles for medical research involving human patientsAdopted by the 18th WMA General Assembly 1964 and amendedby the 29th 35th 41st and 48th WMA General Assemblies
21 European Parliament and Council of 4 April 2001 (2001)Directive 200120EC of the approximation of the laws regu-lations and administrative provisions of the Member Statesrelating to the implementation of good clinical practice in theconduct of clinical trials on medicinal products for human useOfficial Journal of the European Communities Brussels
22 Mehlisch DR Jasper RD Brown P et al (1995) Comparativestudy of ibuprofen lysine and acetaminophen in patients withpostoperative dental pain Clin Ther 17852ndash860
23 Olson NZ Otero AM Marrero I et al (2001) Onset of analgesiafor liquigel ibuprofen 400 mg acetaminophen 1000 mg ketopro-fen 25 mg and placebo in the treatment of postoperative dentalpain J Clin Pharmacol 411238ndash1247
24 Sachs C (2005) Oral analgesics for acute nonspecific pain AmFam Physician 71913ndash918
25 Doyle G Furey S Berlin R et al (1999) Gastrointestinal safetyand tolerance of ibuprofen at maximum over-the-counter doseAliment Pharmacol Ther 13897ndash906
26 Henry D Lim LL Garcia Rodriguez LA et al (1996) Variability inrisk of gastrointestinal complications with individual non-steroidalanti-inflammatory drugs results of collaborative met-analysis BrMed J 3121563ndash1566
27 Henry D McGettigan P (2003) Epidemiology overview ofgastrointestinal and renal toxicity of NSAIDs Int J Clin Pract13543ndash49
Eur J Clin Pharmacol (2009) 65343ndash353 353
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 153
RESEARCH
An investigation into the comparative efficacyof soluble aspirin and solid paracetamol inpostoperative pain after third molar surgeryR A Seymour1 J E Hawkesford2 J Sykes3 M Stillings4 and C M Hill5
Objective To compare the efficacy of soluble aspirin 900 mg andparacetamol 1000 mg in patients with postoperative pain after thirdmolar surgeryDesign A randomised placebo controlled double-blind studySetting Day stay units of Oral and Maxillofacial Surgery at CardiffDental Hospital and Hexham General Hospital NorthumberlandSubjects and methods One hundred and sixty-seven (104 female)patients who required the removal of their impacted third molars undergeneral anaesthesiaIntervention In the early postoperative period patients were medicatedwith either a single dose of soluble aspirin 900 mg solid paracetamol1000 mg or placebo Main outcome measures Pain intensity was measured on 100 mmvisual analogue scales at 0 5 10 15 20 30 45 60 90 120 and 240minutes after dosing Other efficacy variables evaluated included time torescue medication and an overall assessment of the study medicationefficacy by the patient on completion of the studyResults One hundred and sixty-seven patients consented to take part inthe study but only 153 were medicated Of the 14 patients not treated10 failed to develop sufficient pain to enter the study two withdrewconsent one had an adverse reaction to the general anaesthetic and onewas a protocol violator Over the four hour investigation period patientstreated with soluble aspirin reported significantly less pain whencompared with those treated with paracetamol (mean difference inAUC0-240 = -2001 95 CI ndash3893 to ndash109 p=0038) and placebo (meandifference in AUC0-240 = -3470 95 CI ndash5719 to ndash1221 p=0003)
1Head of Department Professor of Restorative Dentistry Department of RestorativeDentistry Dental School University of Newcastle Newcastle upon Tyne 2Consultant Oraland Maxillofacial Surgeon Department of Oral and Maxillofacial Surgery NewcastleGeneral Hospital Newcastle upon Tyne 3Clinical Statistician Reckitt Benckiser Healthcare(UK) Hull 4Head of Global Professional Relations Reckitt Benckiser Healthcare (UK) Hull5Consultant Oral and Maxillofacial Surgeon Department of Oral Surgery Dental SchoolUniversity of Wales College of Medicine Cardiff Correspondence to Professor R A Seymour Department of Restorative Dentistry DentalSchool University of Newcastle upon Tyne Framlington Place Newcastle upon TyneEngland NE2 4BWE-mail R A Seymournclacuk
Refereed paperReceived 080302 Accepted 060902copy British Dental Journal 2003 194 153ndash157
Similarly at 20 and 30 minutes after dosing patients in the solubleaspirin group were reporting significantly less pain than those in theparacetamol treatment group (mean difference in pain intensity at 20minutes ndash79 95 CI ndash153 to ndash06 p=0035 at 30 minutes ndash106 95CI ndash186 to ndash26 p=0010) There were no significant differences betweentreatment groups with respect to the number of patients requiringrescue medication however the time to dosing was significantly longerfor those taking soluble aspirin when compared with placebo (hazardratio 234 95 CI 141 to 388 plt0001) Conclusion The findings from this study showed that soluble aspirin900 mg provides significant and more rapid analgesia than paracetamol1000 mg in the early postoperative period after third molar surgery
INTRODUCTIONBoth aspirin (acetylsalicylic acid) and paracetamol (acetamino-phen) are widely available analgesics The drugs are used exten-sively in dentistry either self-prescribed by the patient or recom-mended by the dental surgeon Despite such use there have beenfew comparative studies on these analgesics and the studies pub-lished seem to suggest that the drugs are equi-analgesic1 Morerecent evidence suggests that many factors appear to influence theefficacy of aspirin in postoperative dental pain These include for-mulation dose and plasma concentration of acetylsalicylate2-5
The latter appears to be determined by plasma aspirin esteraseactivity By contrast there is limited information on the efficacy ofparacetamol in postoperative dental pain
Historically there have been many studies comparing the effi-cacy of a whole range of analgesics which have used aspirin as thestandard treatment (positive control) In such studies the formula-tion chosen has invariably been a solid format of the drug This hasled to the impression that aspirin is relatively weak and slow act-ing Previous studies34 have shown that soluble aspirin provides agreater onset of action and is overall more effective than solidaspirin However up to the present time there has been no studycomparing the efficacy of soluble aspirin with solid paracetamolThe present study was designed to investigate whether the superi-ority of soluble aspirin over solid aspirin would be reproducedwhen compared with solid paracetamol The doses chosen for each
This study has shown the benefits of soluble aspirin (900 mg) over solid paracetamol (1000 mg)in the control of postoperative pain after third molar extractions
The aspirin preparation provided an earlier onset of pain relief when compared with paracetamol Most patients in the study did require additional analgesia in the early postoperative period
but the time to remedication was significantly longer in soluble aspirin group whencompared with the placebo
Adverse events due to the medication were few and showed no differences between treatmentgroups
Soluble aspirin 900 mg appears to be a more useful analgesic than paracetamol in the controlof postoperative pain after third molar surgery
I N B R I E F
RESEARCH
154 BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003
preparation used in this study is the maximum recommendedwhen purchased as over the counter (OTC) medications
Removal of impacted third molars remains a common dentalsurgical procedure that results in a significant level of postopera-tive pain6 Pain is usually of short duration and reaches its maxi-mum intensity in the early postoperative period7 It is during thistime period that analgesics are frequently prescribed The nature ofthe pain and its duration make the third molar pain model usefulfor evaluation of analgesic efficacy
The overall aim of the present study was to directly compare theefficacy of soluble aspirin with that of solid paracetamol tablets inpatients with postoperative pain after third molar surgery A place-bo group was also used to act as a negative control Within thisoverall remit the primary aim of the study was to compare theonset of efficacy between the two preparations
MATERIAL AND METHODSAdult patients who required the removal of at least one impactedlower third molar were invited to participate in the study Patientswere enrolled from two centres (Cardiff and Hexham) Informedwritten consent was obtained from each patient prior to theirentry into the study which had received ethical approval from theappropriate local Health Authority Ethical Committees Patientsenrolled into the study were fit and healthy and complied with thecriteria of the American Society of Anaesthesiologists categoryone or at the discretion of the dental surgeon category two Allpatients attended a screening clinic prior to their participation inthe study The pre-screening was held up to a maximum of threeweeks before surgery Patients were asked to abstain from takingany analgesics for 24 hours prior to their third molar extractions
Patients underwent the removal of their impacted third molarsunder general anaesthesia The anaesthetic regimen was accord-ing to routine clinical practice at the dental centre and includedinduction with intravenous propofol Muscle relaxation wasachieved with vecuronium atracurium pancurium mivacuriumor suxamethonium Anaesthesia was maintained with nitrousoxide oxygen and either isoflurane enflurane or sevofluranePerioperative analgesia was provided by fentanyl or alfentanyl
Impacted third molars were removed following a standard tech-nique Bone removal was carried out with a drill under saline sprayThe operating time (from first incision to completion of last suture)was recorded for each patient On completion of the surgical proce-dure time was allowed for the patients to recover fully from theeffects of the anaesthetic They were then returned to the wardwhere they were monitored by the study nurse and their pain inten-sity assessed on 100 mm visual analogue scales (VAS) The bound-aries of the scale were marked lsquono painrsquo and lsquoworst pain imaginablersquoWhen patientsrsquo pain intensity reached a level in excess of 30 mm onthe VAS they were randomised to study medication Patients whosepain intensity did not reach the required level or who did notrequest analgesia within 1frac12 hours post-operatively were with-drawn from the study Each eligible patient was randomly allocatedto one of the following treatment groups soluble aspirin (Disprinreg)900 mg solid paracetamol tablets BP 1000 mg or placebo In order
to double-blind the study a double-dummy technique was usedEach patient assigned to receive active soluble aspirin or activesolid paracetamol also received a placebo for the alternative treat-ment and placebo patients received a placebo for both formula-tions Soluble aspirin and the aspirin placebo were presented as anorange drink Paracetamol active and placebo were given as tabletsPatients were randomised to treatment groups in the ratio of 2aspirin2 paracetamol1 placebo The randomisation was stratifiedfor gender A randomisation block size of five was used to ensurebalance between the treatment groups
Pain assessmentThe following measures were used to evaluate efficacya) Pain intensity measures were recorded immediately pre-dose (0
minutes) and at 5 10 15 20 30 45 60 90 120 and 240 minutesafter dosing Onset of analgesia was primarily assessed by painintensity measures at 10 15 20 and 30 minutes
b)Pain intensity over the four hour investigation period The serial VAS measures of the four hour investigation periodwere compiled into a graph of pain (mm) versus time (minutes)The area under the graph (AUC) was calculated using the trape-zoidal method and denoted as AUC240 Such a measure gives anoverall assessment of each patientrsquos pain experience throughoutthe four hour investigation period8
c) Use of rescue medicationIn the event of poor pain control patients were allowed access toalternative analgesia (ibuprofen 400 mg) Patients were encour-aged not to request re-medication in the first hour post-dosingin order to give the study medication time to work For thosetaking additional analgesics the time was recorded and theirlast pre-rescue medication intensity score was extrapolated overthe remaining time points9
d)Overall evaluation At the end of the four hour investigation period (or prior to tak-ing rescue medication) the study nurses and the patients wereasked to provide an overall evaluation of the efficacy of thestudy medication The categories were lsquovery goodrsquo lsquogoodrsquo lsquosatis-factoryrsquo lsquopoorrsquo and lsquovery poorrsquo
Throughout the investigation period a study nurse was respon-sible for monitoring the patients and recording any adverse events
Statistical methodsA previous study in postoperative pain after removal of impactedthird molars4 suggested that mean VAS differences between solu-ble aspirin and placebo and soluble aspirin and solid paracetamolof 26 mm and 14 mm respectively might be anticipated at 20 min-utes post treatment Using a randomisation of 2 soluble aspirin 2paracetamol 1 placebo a total sample size of 150 patients had atleast 80 power to detect this difference
The VAS pain intensity measurements at 10 15 20 and 30minutes after dosing and AUC240 were compared between treat-ment groups using an analysis of covariance using centre gen-der baseline pain intensity operation duration and number of
Table 1 Demographic details of patients who were medicated for the study Where appropriate results are expressed as mean (SD)Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo
Number of patients 59 62 32Gender ratio MF 1940 1943 1121Age (years) 256 (56) 250 (53) 251 (47)Weight (kg) 702 (16) 719 (145) 743 (149)Mean operating time (mins) 173 (101) 165 (101) 130 (130)Number of molars removed 1 3 (5) 2 (3) 3 (9)[ patients ()] 2 15 (25) 14 (23) 5 (16)
3 11 (19) 12 (19) 9 (28)4 30 (51) 34 (55) 15 (47)
Mean baseline pain score on 100 mm VAS 574 (176) 506 (142) 541 (144)
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 155
in Hexham and the remainder in Cardiff Of the 14 patients nottreated 10 failed to develop sufficient pain to enter the studytwo withdrew consent one had an adverse reaction to the anaes-thesia and one was a protocol violator Demographic details ofthe patients are shown in Table 1 The three groups were bal-anced for demographic variables
The primary aim of the study was to compare the rate of onset ofanalgesia and the 20-minute time was considered to be appropriatefor such an assessment Pain scores as recorded on the VAS at eachtime point are illustrated in Figure 1 and Tables 2a and 2b VASscores decreased in all treatment groups during the first 15 minutespost dosing (Figure 1) At 20 minutes post dosing patients in the sol-
molars removed as covariates Use of rescue medication and thestudy nursesrsquo and patientsrsquo overall impression of their medicationwere analysed using binomial logistic regression with a lsquopositiversquooutcome defined as a response of lsquovery goodrsquo or lsquogoodrsquo Time toadministration of rescue medication was compared betweentreatment groups using Coxrsquos proportional hazard model Com-parisons were performed for soluble aspirin versus solid paraceta-mol and soluble aspirin versus placebo
RESULTSOne hundred and sixty seven patients consented to take part inthe study and 153 were medicated Of these 29 were medicated
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 30 45 60 90 120 240
Time (mins)
Pain
(mm
)
Soluble AspirinParacetamolPlacebo
Figure 1 Graph to show mean pain scores (mm) versus time (mins) for patients after treatment with placebo solid paracetamol 1000 mg and solubleaspirin 900 mg
Table 2a Summary of efficacy parameters recorded during the investigation period pain scoresBetween treatment comparisons
Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Mean difference (95 CI) p-value Mean difference (95 CI) p-value
Pain score (in mm) 10 mins after dosing 412 (28) 482 (29) 474 (33) -61 (-133 to 10) 0092 -70 (-130 to ndash09) 0024Pain score (in mm) 15 mins after dosing 407 (32) 458 (33) 445 (38) -39 (-120 to 43) 0350 -51 (-120 to 18) 0143Pain score (in mm) 20 mins after dosing 402 (34) 481 (35) 500 (40) -98 (-186 to ndash11) 0028 -79 (-153 to ndash06) 0035Pain score (in mm) 30 mins after dosing 356 (37) 462 (38) 476 (44) -120 (-216 to ndash25) 0014 -106 (-186 to ndash26) 0010Overall pain - AUC240(mmmins) 8001 (871) 10002 (898) 11471 (1035) -3470 (-5719 to ndash1221) 0003 -2001 (-3893 to ndash109) 0038
data presented are adjusted (least squares) mean (standard error of the mean)
Table 2b Summary of efficacy parameters recorded during the investigation period use of escape medicationBetween treatment comparisons
Variable Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds (hazard) ratio (95 CI) p-value Odds (hazard) ratio (95 CI) p-value
Number of patients 48 (81) 46 (74) 29 (91) 0172 (0020 to 1052) 0078 1485 (0455 to 5197) 0518taking escape analgesics
Time (minutes) to 115 (63 - 165) 94 (47 - ++) 64 (42 ndash 117) 234 (141 to 388) lt0001 130 (084 to 203) 0236remedication
data presented are median (Inter Quartile Range)++ Upper quartile cannot be estimated
RESEARCH
156 BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003
uble aspirin group reported significantly less pain than those treatedwith solid paracetamol (p=0035) or placebo (p=0028) Similarlypain intensity was significantly less at 10 and 30 minutes post dos-ing for patients treated with soluble aspirin when compared withsolid paracetamol (p=0024 and 0010 respectively) Pain intensitywas also significantly less for patients treated with soluble aspirinwhen compared with placebo at 30 minutes post dosing (p=0014)but was not significant at 10 minutes post-dosing (p=0092) By con-trast to these findings at 15 minutes after dosing pain scores werenot significantly different between soluble aspirin and placebo(p=0350) or between soluble aspirin and solid paracetamol(p=0143) Overall pain scores as assessed by the AUC240 were sig-nificantly lower in the soluble aspirin group when compared withsolid paracetamol (p=0038) and placebo (p=0003) There was nosignificant centre difference for any of the pain intensity variables
The use of rescue medication and time to requesting such med-ication is also shown in Table 2b There was no significant differ-ence between soluble aspirin and solid paracetamol or placebowith respect to the number of patients requiring rescue medicationduring the four hour investigation period (pgt005) However thetime to administration of rescue medication was significantlylonger for those patients taking soluble aspirin when comparedwith placebo (plt0001) There was no significant difference in timeto rescue medication between the soluble aspirin treated patientsand those treated with solid paracetamol (p=0236) The time toadministration of rescue medication did show a significant centreeffect with those patients enrolled in Cardiff requiring rescueanalgesia at an earlier time point than those in Hexham (plt0001)
The study nursesrsquo and patientsrsquo overall assessment of the effica-cy of the medication is shown in Tables 3a and 3b There was nosignificant difference between soluble aspirin and solid paraceta-mol (p=0285) with respect to the percentage of lsquopositiversquo outcomesassessed by the patients however soluble aspirin was favoured incomparison with placebo (p=0010) Results were similar for thestudy nursesrsquo assessment (p=0387 p=0024)
Adverse events were reported by 41 of patients with a higheroverall incidence in the active treatment groups (Table 4) Many ofthese events were related to the procedure The most commonadverse events were in the central and peripheral nervous system(primarily dizziness) and the gastro-intestinal system (primarilynausea) The incidence of dizziness was similar in the soluble
aspirin and placebo groups (14 and 13 respectively) and wasgreater than in the solid paracetamol group (6) The incidence ofnausea was comparable in the soluble aspirin and solid paraceta-mol groups (15 and 16 respectively) and was greater than thatin the placebo group (6) Gingival bleeding (the only adverseevent recorded under lsquohaemostasisrsquo) had a slightly lower incidencein the soluble aspirin group (8) than in the solid paracetamolgroup (13) and was only slightly higher than that reported in theplacebo group (3) This finding is contrary to any expectationsthat aspirin might exacerbate post-operative bleeding
DISCUSSIONThe present study has shown that soluble aspirin 900 mg is an effec-tive analgesic in the control of postoperative pain after the removalof impacted third molars confirming the evidence from previousstudies34 In addition soluble aspirin provided better pain controlthan solid paracetamol 1000 mg This superior efficacy is reflectedin the overall pain score (Table 2a and Figure 1) and also in the painscores reported during the first 30 minutes post dosing The datasuggest that soluble aspirin is providing a more rapid reduction inpain in the early postoperative period when compared with solidparacetamol If the pain scores are examined in terms of percentagereduction when compared with baseline the results show that solu-ble aspirin is twice as effective as solid paracetamol (at 20 and 30minutes the percentage reduction for soluble aspirin is 310 and406 respectively whilst the figures for solid paracetamol are142 and 204) From the perspective of patient management arapid reduction in pain is an important requisite of any analgesicformulation10 The exception to this pattern is the pain scores at 15minutes post dosing At this time point pain intensity scores aftersoluble aspirin are not significantly different from either placebo orsolid paracetamol mdash the reason for this finding is unclear
Previous comparative efficacy studies between aspirin andparacetamol in postoperative dental pain have revealed somewhatequivocal results11112 The consensus view1 is that both aspirin andparacetamol are both equi-analgesic and equipotent The studiesuse a solid tablet formulation of aspirin at a dose of 650 mg Studiesusing similar methodology have shown that the efficacy of aspirinin postoperative dental pain is related to dose and formulation34
The use of a soluble formulation and the 900 mg dose may explainthe superior efficacy of aspirin in this study
Table 3b Distribution of scores from study nursesrsquo global assessment of the medication (number ())Score Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds Ratio (95 CI) p-value Odds Ratio (95 CI) p-value
Positive outcome 32 (54) 32 (52) 10 (31) 2974 (1179 to 7951) 0024 1403 (0655 to 3054) 0387Very good 15 (25) 11 (18) 3 (9)Good 17 (29) 21 (34) 7 (22)Satisfactory 17 (29) 14 (23) 12 (38)Poor 8 (14) 14 (23) 7 (22)Very poor 2 (3) 2 (3) 3 (9)Total 59 62 32
positive outcome = response of lsquovery goodrsquo or lsquogoodrsquo
Table 3a Distribution of scores from patientsrsquo global assessment of the medication (number ())Score Soluble aspirin 900 mg Solid paracetamol 1000 mg Placebo Soluble aspirin vs placebo Soluble aspirin vs solid paracetamol
Odds Ratio (95 CI) p-value Odds Ratio (95 CI) p-value
Positive outcome 34 (58) 33 (53) 10 (31) 3591 (1402 to 9828) 0010 1530 (0706 to 3380) 0285Very good 15 (25) 12 (19) 3 (9)Good 19 (32) 21 (34) 7 (22)Satisfactory 15 (25) 12 (19) 10 (31)Poor 8 (14) 15 (24) 9 (28)Very poor 2 (3) 2 (3) 3 (9)Total 59 62 32
positive outcome = response of lsquovery goodrsquo or lsquogoodrsquo
RESEARCH
BRITISH DENTAL JOURNAL VOLUME 194 NO 3 FEBRUARY 8 2003 157
The primary aim of this investigation was to compare both anal-gesics with respect to onset of action Early time points were chosenfor this comparison as they represent a suitable period from dosingwhen patients would expect to experience meaningful pain reliefSoluble aspirin was significantly superior to both placebo and solidparacetamol at both 20 and 30 minutes post dosing and there wereindications of superiority as early as at 10 minutes In part this maybe due to the rapid absorption of soluble aspirin and the subsequentpeak concentrations of acetylsalicylate (Tmax) that occurs at thesetime points It has been previously shown that plasma concentra-tions of acetylsalicylate are also important determinants of aspirinrsquosefficacy in postoperative dental pain2 By contrast the absorption ofsolid paracetamol tablets is slow with a Tmax of 60 minutes13 Thusdifferences in pharmacokinetics may account for the differences inonset of analgesia observed in the present study
It is now well established that aspirin exerts both analgesic andanti-inflammatory action by inhibiting prostaglandin synthesis14
Aspirin irreversibly inhibits both cyclo-oxygenase 1 and 2 (Cox-1and Cox-2) by acetylating serine 530 thus preventing the bindingof arachidonic acid to the active sites of the enzyme The pharma-codynamics of paracetamol are uncertain and by comparison withaspirin the drug exhibits weak anti-inflammatory action This lackof a pronounced anti-inflammatory effect may also explain theweaker efficacy of this drug in postoperative dental pain
We can conclude from this study that a single dose of solubleaspirin 900 mg provides significant and more rapid analgesia thansolid paracetamol 1000 mg in the early postoperative period afterthird molar surgery This study confirms the value of soluble aspirinin the management of pain after dental surgical procedures
The authors are grateful to Reckitt Benckiser Healthcare for their support inthis study
1 Cooper S A Comparative analgesic efficacies of aspirin and acetaminophen ArchIntern Med 1981 141 282-285
2 Seymour R A Williams F M Ward A Rawlins M D Aspirin metabolism and efficacyin postoperative dental pain Br J Clin Pharmacol 1984 17 697-701
3 Seymour R A Williams F M Luyk N M et al Comparative efficacy of soluble aspirinand aspirin tablets in postoperative dental pain Eur J Clin Pharmacol 1986 30495-498
4 Holland I S Seymour R A Ward-Booth R P Ord R A Lim K L Hoare R C Anevaluation of different doses of soluble aspirin and aspirin tablets in postoperativedental pain Br J Clin Pharmacol 1988 26 463-468
5 Seymour R A Weldon M Kelly P Nicholson E Hawkesford J E An evaluation ofbuffered aspirin and aspirin tablets in postoperative pain after third molar surgeryBr J Clin Pharmacol 1992 33 395-399
6 Seymour R A Blair G S Wyatt F A Post-operative dental pain and analgesicefficacy Part I Br J Oral Surg 1983 21 290-297
7 Seymour R A Meechan J G Blair G S An investigation into post-operative painafter third molar surgery under local analgesia Br J Oral Maxillofac Surg 1985 23410-418
8 Matthews J N Altman D G Campbell M J Royston P Analysis of serialmeasurements in medical research Br Med J 1990 300 230-235
9 Lasagna L Analgesic methodology a brief history and commentary J ClinPharmacol 1980 20 373-376
10 Meechan J G Seymour R A The use of third molar surgery in clinicalpharmacology Br J Oral Maxillofac Surg 1993 31 360-365
11 Skjelbred P Album B Lokken P Acetylsalicylic acid vs paracetamol effects onpost-operative course Eur J Clin Pharmacol 1977 12 257-264
12 Mehlisch D R Frakes L A A controlled comparative evaluation of acetaminophenand aspirin in the treatment of postoperative pain Clin Ther 1984 7 89-97
13 Muir N Nichols J D Stillings M R Sykes J Comparative bioavailability of aspirinand paracetamol following single dose administration of soluble and plain tabletsCurr Med Res Opin 1997 13 491-500
14 Vane J Botting R Inflammation and the mechanism of action of anti-inflammatory drugs Faseb J 1987 1 89-96
Table 4 Incidence and distribution of adverse events for each treatment groupPercentage of patients reporting events (number of events)
Body system Soluble aspirin (n=59) Solid paracetamol (n=62) Placebo (n=32) Total (n=153)
CNS 20 (14) 8 (5) 19 (6) 15 (25)GI 17 (12) 16 (12) 6 (2) 14 (26)Body as a whole 7 (4) 13 (8) 6 (3) 9 (15)Haemostasis 8 (7) 13 (8) 3 (1) 9 (16)Respiratory 7 (4) 3 (2) 0 (0) 4 (6)Psychiatric 2 (1) 0 (0) 3 (1) 1 (2)Hearingvestibular 0 (0) 2 (1) 0 (0) 1 (1)Skinappendages 2 (1) 0 (0) 0 (0) 1 (1)Vision 2 (1) 0 (0) 0 (0) 1 (1)Total 51 (44) 39 (36) 28 (13) 41 (93)