Embed Size (px)
Citation preview

Universidade de Lisboa
Faculdade de Medicina de Lisboa
Resposta Humoral na Infecção por VIH-2: Impacto no
diagnóstico, prevenção e evolução viral
José Maria Marcelino
Doutoramento em Ciências Biomédicas
2011


Universidade de Lisboa
Faculdade de Medicina de Lisboa
Resposta Humoral na Infecção por VIH-2: Impacto no
diagnóstico, prevenção e evolução viral
José Maria Marcelino
Orientador
Prof. Doutor Nuno Taveira
Co-Orientadores
Charlotta Nilsson, PhD
Prof. Doutor Rui MM Victorino
Especialidade em Ciências Biopatológicas
Todas as afirmações efectuadas no presente documento são da exclusiva
responsabilidade do seu autor, não cabendo qualquer responsabilidade à
Faculdade de Medicina de Lisboa pelos conteúdos nele apresentados.


A impressão desta dissertação foi aprovada pelo Conselho Cientifico da
Faculdade de Medicina de Lisboa em reunião de 22 de Fevereiro de
2011.


Dissertação apresentada à Faculdade de Medicina da Universidade de
Lisboa, para obtenção do grau de Doutor em Ciências Biomédicas.


A presente dissertação foi realizada na Unidade de
Tecnologia de Proteínas e Anticorpos Monoclonais,
Instituto Nacional de Engenharia, Tecnologia e Inovação;
na Unidade de Retrovírus e Infecções Associadas,
Faculdade de Farmácia da Universidade de Lisboa e no
Swedish Institute for Infectious Disease Control,
Estocolmo, Suécia.
O trabalho aqui apresentado foi financiado pelo
POCTI/ESP/48045/2002, Fundação para a Ciência e a
Tecnologia.
Bolsa de Doutoramento da Fundação para a Ciência e a
Tecnologia, (Referência: SFRH/BD/13892/2003).


À minha família


Índice Geral
Agradecimentos .................................................................................. i
Resumo .............................................................................................. v
Summary...........................................................................................xi
Capítulo I
Introdução ......................................................................................... 1
A Pandemia ................................................................................... 3
VIH-2 ................................................................................................. 3
Origem, Estrutura e Replicação .................................................... 3
Patogénese da Infecção VIH .......................................................... 6
Defesas do Hospedeiro na Infecção por VIH .................................. 8
Resposta Celular..................................................................... 9
Resposta Humoral ................................................................ 10
O papel dos anticorpos na infecção VIH ........................... 10
Anticorpos Neutralizantes................................................ 13
Determinantes da neutralização no invólucro do VIH ....... 14
Escape à Neutralização ..................................................... 18
Vacinas para o VIH .......................................................................... 19
Desafios e dificuldades ............................................................... 19
Modelos Animais ......................................................................... 21
Referências ...................................................................................... 22
Capítulo II
Objectivos e Plano de Trabalho ............................................................ 41
Objectivos e Plano de Trabalho ........................................................ 43
Capítulo III
Teste de ELISA específico para o VIH-2 (ELISA-VIH2) .......................... 47
Resumo ........................................................................................... 49
Abstract ........................................................................................... 51
Referências ...................................................................................... 60

Capítulo IV
Resposta de anticorpos IgA e IgG inespecíficos e específicos para as
glicoproteínas gp36 e gp125 do VIH-2 ................................................. 67
Resumo ........................................................................................... 69
Abstract ........................................................................................... 71
Introdução ....................................................................................... 73
Material e Métodos .......................................................................... 74
Resultados....................................................................................... 77
Discussão ........................................................................................ 82
Referências ...................................................................................... 85
CAPÍTULO V
Resposta humoral na evolução molecular das regiões C2, V3 e C3 do
invólucro do VIH-2 em pacientes crónicos ........................................... 93
Resumo ........................................................................................... 95
Abstract ........................................................................................... 97
Introdução ....................................................................................... 99
Material e Métodos ........................................................................ 100
Resultados..................................................................................... 103
Discussão ...................................................................................... 108
Conclusões .................................................................................... 111
Referências .................................................................................... 113
CAPÍTULO VI
Escape à Neutralização na Infecção VIH-2 ......................................... 123
Resumo ......................................................................................... 125
Abstract ......................................................................................... 127
Introdução ..................................................................................... 129
Material e Métodos ........................................................................ 130
Resultados e Discussão ................................................................. 133
Conclusões .................................................................................... 141

Referências .................................................................................... 142
CAPÍTULO VII
Anticorpos neutralizantes contra isolados VIH-2 primários produzidos
em murganhos BALB\c……. .............................................................. 149
Resumo ......................................................................................... 151
Abstract ......................................................................................... 153
Introdução ..................................................................................... 154
Material e Métodos ........................................................................ 155
Resultados..................................................................................... 159
Discussão ...................................................................................... 165
Referências .................................................................................... 167
CAPÍTULO VIII
Discussão Geral e Conclusões ........................................................... 177
Discussão Geral e Conclusões ....................................................... 179
Referências .................................................................................... 189


i
Agradecimentos
Quero agradecer a todos os que contribuíram para a realização deste
trabalho e conclusão da minha tese de doutoramento:
Ewa Bjorling, my initial co-supervisor from Microbiology, Tumor and
Biology Center (MTC) at Karolinska Institutet in Sweden. Thank you
for answer without hesitation to the question I put you by email a
few years ago: “Can you receive me at your lab for some weeks? I
would like to get some practice with your HIV-2 neutralization
method.” You received me without knowing me before and you
opened me a door to share extensive knowledge and experience with
you and your group. Thank you for encouraging my initial work and
for the important support you gave it, which resulted in an important
scientific collaboration along these last years between our
workgroups. I wish you all the luck for your new professional trails.
Charlotta Nilsson, my co-supervisor after Ewa Bjorling and until
now, thank you for sharing with me all your scientific experience and
for your good suggestions and stimulating discussions about my
work. Your enthusiastic new ideas and knowledge on this field have
enriched a lot this thesis. Working with you was excellent and I hope
we’ll have new opportunities to collaborate again in the future.
Rigmor Thorthesson, director of Vaccinology and Immunology
Department of SMI, for having received me and having allowed that
Charlotta Nilsson substituted Ewa Bjorling as my co-supervisor.
All the members of the Swedish group: Qin Lizeng, for nice
discussions about work and for the homemade Chinese food, of
course. Mia, thanks you for receiving me at a weekend in my first
arrival to Stockholm. Kerstin Andersson, for the great support with
PBMC’s at P3 security level. Gunnel Biberfield for your sympathy to
this foreign PhD student. Samer Sourial and Andreas Mörner for all
your support in the months I spent in your lab along these
years….and Sam I will never, never forget the triple mortal jump you
did in front of my eyes when trying to skiing down the Rocky
Mountains in 2002 in Keystone Symposia. If you’ll try to do such
things now you wouldn’t do it better!
Nuno Taveira, obrigado por teres aceitado ser meu orientador deste
fantástico projecto que teve início alguns anos atrás. Terminei uma

ii
fase desse percurso, mas não sei onde e como vai terminar! Foi bom
teres partilhado comigo o teu conhecimento científico numa área tão
delicada e exigente, e teres sido fundamental para a evolução da
minha carreira científica. Nuno, obrigado pela excelente orientação e
pela tua amizade.
Prof. Doutor Rui Victorino (Faculdade de Medicina de Lisboa) é com
satisfação que lhe agradeço não só por ter aceitado ser co-orientador
deste trabalho, como pela disponibilidade que sempre mostrou para
me receber sempre que lho solicitei.
Carlos Novo (director da UTPAM, INETI), gostava de salientar que
independentemente das mudanças que a vida nos trás, vais ser
sempre a pessoa que me abriu “aquela” porta, a porta por onde um
dia entrei para encontrar todas as seguintes, algumas abertas
novamente por ti. Pessoas como tu são pouco comuns nos dias que
correm. Agradeço-te por teres acreditado em mim desde o início e na
confiança que tens depositado em mim ao longo destes anos. A vida
está sempre a mudar, e novos desafios a surgirem, mas a verdadeira
amizade permanece e não desaparece. Obrigado Carlos.
Dra. Alda Fidalgo (Ex-directora da UTPAM, INETI), quero agradecer-
lhe a confiança que depositou em mim e todo o seu empenho em me
abrir a porta de entrada no INETI.
Doutor Roseiro (Director do Departamento de Biotecnologia, INETI),
quero agradecer-lhe as palavras de incentivo que sempre me dirigiu.
Maria Marques, agradeço-te o teu apoio e amizade contínua, as tuas
constantes palavras de encorajamento acerca do meu trabalho e as
várias conversas de “corredor” que tanto ajudavam a manter o
ambiente agradável de trabalho!
Aos restantes colegas da UTPAM, agradeço todo o apoio ao longo do
tempo.
Prof. José Moniz-Pereira (Coordenador da URIA, FFUL), agradeço-lhe
por ter permitido e apoiado o desenvolvimento da maior parte deste
trabalho na URIA.
Prof. Helena Lourenço (Ex-responsável pelo Laboratório de Virologia)
a sua capacidade de fazer pelos outros é também infindável. A sua

iii
disponibilidade para apadrinhar este projecto foi fundamental, pois
sem ela não seria possível realizá-lo. Obrigado pelo seu apoio e
amizade.
No grupo de Microbiologia e na URIA, foram várias as pessoas que de
uma forma ou outra também contribuíram para a realização deste
trabalho, e aos quais quero agradecer a sua amizade e o bom
ambiente de trabalho durante estes anos: Prof. Graciete, Prof. Aida,
João Vital, José Miguel Pereira, Isabel Portugal, Madalena Pimentel,
Elsa Anes, Perpétua Gomes, Ana Clara Ribeiro, Alexandra Maia e
Silva, João Gonçalves (e o seu extenso grupo de colaboradores),
Acilino Freitas, João Pedro Frade, Helena Barroso, Pedro Borrego,
Cheila Rocha, Inês Bártolo, Marta Calado, Paula Matoso, Maria
Espírito Santo, Ofélia, Vera, Lena Brás, Dr.ª Paula Resende, Lavínia,
Nela (Mana!), D. Noémia, D. Fátima, Dina…e todos aqueles que vou
acabar por não mencionar porque a lista já vai longa mas de quem
não esqueci.
À Dra. Manuela Doroana e Prof. Doutor Francisco Antunes, do
serviço de Doenças Infecciosas do Hospital Santa Maria, e ao Dr.
Fernando Maltêz do serviço de doenças infecciosas do Hospital Curry
Cabral, quero agradecer-lhes o empenho no recrutamento dos
doentes e na obtenção das amostras biológicas para que este
trabalho pudesse ter sido realizado.
Aos doentes do Hospital de Santa Maria e do Curry Cabral, a chave
deste estudo, que concordaram em participar neste estudo,
agradeço-vos o vosso empenho, que foi essencial para podermos
compreender mais um pouco desta doença, que afecta milhões de
pessoas.
Aos meus pais e irmãs, a vossa presença na minha vida tem sido
importante não só para partilhar os bons momentos, mas também
para ultrapassar as dificuldades. Os vossos sorrisos e incentivos têm
sido importantes ao longo deste percurso e noutros caminhos. Sem
vocês, tenho a certeza que a vida seria mais difícil.
Aos meus sogros, quero agradecer a disponibilidade que sempre
demonstraram ao longo destes anos, e que em muito contribui para
a realização deste trabalho. Obrigado por tudo.

iv
Aos meus filhos, Sara e João, que me incentivam a acreditar e lutar
por um futuro melhor, e à Xana, não quero deixar de lhe dizer o
quanto a amo e que sem a força e o apoio dela as dificuldades para
realizar este trabalho seriam ainda maiores.
Ao meu irmão Henrique, quero que saibas que este objectivo
alcançado é também teu, pois muito do caminho que já percorri
nesta área, a ti o devo. Queria partilhar contigo este momento, como
partilhamos outros, mas não posso, por isso aqui expresso o meu
muito obrigado por tudo o que passamos juntos.

v
Resumo
Os indivíduos infectados pelo VIH-2 progridem mais lentamente do
que os infectados pelo VIH-1, e estima-se que mais de 95% dos
indivíduos infectados por VIH-2 estejam incluídos na definição
clínica de long-term nonprogressors. Esta diferença faz do VIH-2 um
potencial modelo de estudo de uma infecção VIH atenuada que pode
fornecer uma visão única da patogénese da infecção VIH-1. Até ao
momento, os mecanismos responsáveis pelo fenótipo atenuado do
VIH-2 não são bem conhecidos. A carga viral plasmática é inferior
nos indivíduos infectados pelo VIH-2 do que pelo VIH-1. Isto sugere
que a principal diferença entre os dois tipos de VIH pode estar no
grau de replicação viral, e presume que a resposta imunológica do
hospedeiro contribui directamente para um controlo mais eficiente
da replicação do VIH-2. Actualmente não existem dúvidas de que a
maioria dos indivíduos infectados pelo VIH-1 ou VIH-2 produzem
anticorpos neutralizantes (AcNT) autólogos e heterólogos. Contudo,
existe alguma controvérsia sobre se os AcNT controlam de facto a
replicação viral, uma vez que na maioria dos casos não se observa
correlação inversa entre o título de AcNT e a carga viral plasmática.
Na realidade, tanto no VIH-1 como no VIH-2, parece haver uma
correlação directa entre o título de AcNT e a replicação viral o que
sugere que a replicação viral é essencial para a produção de AcNT.
Neste contexto, uma questão importante é saber como e quando
serão induzidos os AcNT nos indivíduos infectados por VIH-1 e VIH-2
sem carga viral detectável.
Em contraste com o VIH-1, não existem estudos que caracterizem de
forma qualitativa e quantitativa a cinética da resposta humoral anti-
VIH-2 nos primeiros dias da infecção uma vez que a infecção por este
vírus é quase sempre detectada na fase crónica. Obter informação
detalhada sobre os vírus que estabelecem as infecções por VIH-2 e
sobre a natureza da resposta imunológica durante a fase aguda da
infecção por VIH-2 é vital para a produção de uma vacina. Neste
contexto, o principal objectivo desta tese foi caracterizar no decurso
da infecção VIH-2 aguda e crónica, de forma qualitativa e
quantitativa, a natureza e dinâmica da resposta humoral
neutralizante e não neutralizante e caracterizar o impacto destes
anticorpos na evolução molecular e fenotípica do vírus. Também
foram analisados os alvos da resposta neutralizante anti-VIH-2 e o
potencial de dois novos imunogénios VIH-2 para uma vacina.

vi
O primeiro estudo (Capítulo III) teve como objectivo caracterizar em
detalhe a antigenicidade de dois polipéptidos recombinantes
derivados das glicoproteínas de superfície (rpC2-C3) e
transmembranar (rgp36) do VIH-2ALI, o isolado primário de
referência do grupo A. Utilizando estes dois polipéptidos, produziu-se
um novo teste imunoenzimático (ELISA-VIH2) que revelou ter a
sensibilidade e especificidade necessárias para diagnosticar
serologicamente a infecção por VIH-2. A reactividade dos plasmas
VIH-2+ foi significativamente maior para o antigénio rgp36 do que
para o rpC2-C3, sugerindo que o ectodomíno da rgp36 é a região
antigénica imunodominante no invólucro do VIH-2. A resposta de
anticorpos para o rpC2-C3 foi mais variável, permitindo agrupar os
doentes conforme a produção de anticorpos seja baixa ou alta. O
teste permitiu ainda confirmar a infecção VIH-2 em plasmas que
apresentam dupla serologia por testes comerciais. Devido às
características evidenciadas, o teste ELISA-VIH2 poderá ser uma
excelente alternativa aos testes comerciais de diagnóstico serológicos
e de confirmação da infecção por VIH-2. O formato de antigénio
duplo apresentado no teste permite ainda caracterizar em termos
quantitativos e qualitativos a evolução da produção de anticorpos
para as glicoproteínas do invólucro do VIH-2 em doentes infectados.
Os antigénios rpC2-C3 e rgp36 produzidos na primeira fase do
trabalho foram reagentes essenciais para o segundo trabalho
(Capítulo IV), em que a presença de anticorpos IgA e IgG
inespecíficos e específicos para as proteínas do Env do VIH-2 foi
analisada num grupo de doentes VIH-2 na fase aguda (crianças VIH-
2 positivas infectadas via perinatal) e crónica da infecção.
Demonstrou-se que, tal como na infecção VIH-1, a activação
inespecífica das células B também ocorre na infecção VIH-2 crónica
mas só ao nível das células B secretoras de IgG, uma vez que a
concentração total de IgA no plasma dos indivíduos positivos para o
VIH-2 foi idêntica à dos indivíduos saudáveis não infectados por VIH
(grupo controlo). Em relação à resposta humoral específica para as
glicoproteínas do invólucro do VIH-2, observou-se uma associação
inversa entre os anticorpos IgG anti-rpC2-C3 e o número de
linfócitos T CD4+ o que sugere que estes anticorpos reflectem a
progressão da infecção VIH-2. A maioria dos indivíduos também
produziu anticorpos IgA para os dois polipéptidos, o que identifica
pela primeira vez a região C2-C3 como um forte indutor de
anticorpos IgA no soro e confirma a forte antigenicidade do
ectodomíno da gp36. Apesar da amplitude da resposta IgA, não se

vii
observou nenhuma associação entre os anticorpos IgA anti-gp36 ou
anti-gp125 e o estádio da doença como foi descrito para a infecção
VIH-1. Em termos qualitativos (avidez) e quantitativos (titulo e
concentração) a resposta IgG não neutralizante foi maioritariamente
dirigida para a gp36. As subclasses de anticorpos IgG produzidas na
fase crónica da infecção foram IgG1 (reactivos para ambos os
polipéptidos) e IgG3 (reactivo para a gp36). Não se detectou nenhum
efeito protector dos anticorpos IgG1 e IgG3 anti-gp36 na evolução
clínica da SIDA, como foi sugerido para os anticorpos IgG2 anti-gp41
na infecção VIH-1. Contudo, numa análise longitudinal observou-se
uma associação inversa significativa entre os anticorpos IgG anti-C2-
C3 e o número de células T CD4+. Estes resultados são consistentes
com a função imunoprotectora atribuída à região C2-C3 na infecção
VIH-2. Uma vez que a resposta IgG anti-C2-C3 parece reflectir
adequadamente o estado imunológico e a evolução clínica da infecção
VIH-2, a concentração de anticorpos IgG anti-C2-C3 pode ser um
marcador útil para monitorizar a progressão da doença na infecção
VIH-2.
O principal promotor da evolução molecular e fenotípica do VIH-1 é a
pressão selectiva exercida inicialmente pela resposta celular
citotóxica e depois pelos anticorpos neutralizantes. A informação
sobre este assunto no VIH-2 é ainda muito limitada. No Capitulo V
deste trabalho analisou-se longitudinalmente a evolução molecular
das regiões C2, V3 e C3 do Env em 18 doentes VIH-2 recorrendo a
métodos filogenéticos e moleculares e correlacionou-se esta evolução
com a resposta humoral anti-Env. A média da diversidade
nucleotídica intra-hospedeiro aumentou ao longo do curso da
infecção na maioria dos pacientes. A diversidade ao nível dos
aminoácidos foi significativamente mais baixa para a região V3 e
mais elevada para a região C2. A taxa de evolução do VIH-2 na região
que compreende os domínios C2, V3 e C3 região foi de 0,014
substituições/local/ano, que é semelhante à que tem sido referida
para a infecção VIH-1 crónica. O número e posição dos locais
seleccionados positivamente foi muito variável, excepto para os
codões 267 e 270 na região C2 que estiveram sob uma pressão
selectiva forte e persistente na maioria dos doentes. Os locais de
glicosilação ligados á asparagina localizados na C2 e na V3
mantiveram-se conservados em todos os pacientes ao longo do curso
da infecção. A variação intra-hospedeiro da resposta IgG específica
para as regiões C2, V3 e C3, ao longo do tempo, estava inversamente
associada à variação nos nucleótidos e diversidade dos aminoácidos

viii
na região C2-V3-C3. A variação da resposta IgA específica para a C2-
V3-C3 estava inversamente associada à variação no número de locais
N-glicosilação. Os resultados destes estudos demonstram que a
dinâmica evolutiva do invólucro do VIH-2 durante infecções
avirémicas crónicas é semelhante à do VIH-1, o que implica que o
vírus deve estar em replicação activa nos compartimentos celulares.
Contudo, a evolução convergente da N-glicosilação na C2 e V3 e a
diversificação limitada da V3, indicam que existem factores
funcionais importantes que constrangem a potencial diversidade do
invólucro do VIH-2. Na globalidade, os resultados sugerem que: 1) os
anticorpos IgG anti-C2V3C3 são potencialmente eficazes no controlo
da população viral; 2) a região C3 é um alvo importante para os
anticorpos IgA e a N-glicosilação desta região pode prevenir o
reconhecimento de epitopos IgA.
Actualmente, está provado que a maioria dos indivíduos infectados
cronicamente por VIH-2 produz AcNT de largo espectro. No entanto,
conhece-se muito pouco sobre a dinâmica evolutiva desta resposta
neutralizante na infecção VIH-2 crónica e existe informação
controversa sobre o papel dos AcNT no controlo da replicação viral. O
objectivo do trabalho apresentado no Capitulo VI desta tese foi
caracterizar a dinâmica evolutiva da resposta neutralizante na
infecção VIH-2 crónica e a sua relação com a evolução molecular e
fenotípica do VIH-2 e com a evolução da doença. Neste contexto,
analisou-se longitudinalmente ao longo de 3-4 anos a resposta
neutralizante dirigida contra isolados virais primários autólogos e
heterólogos num grupo de doentes VIH-2. A maioria dos doentes
(8/12) estava infectada com vírus que utilizavam o coreceptor CCR5
(R5) e apenas quatro doentes estavam infectados com vírus que
utilizam o coreceptor CXCR4 (X4). Estes resultados confirmam que o
CCR5 é o principal coreceptor utilizado pelo VIH-2 in vivo. A
presença de anticorpos IgG neutralizantes contra isolados autólogos
foi detectada apenas em doentes infectados com vírus R5. È de
realçar que, os quatro doentes infectados com vírus X4 e dois com
vírus R5, não produziram anticorpos capazes de neutralizar os vírus
autólogos. Estes resultados demonstram pela primeira vez que o
escape à neutralização é bastante frequente na infecção crónica por
VIH-2 e que há uma forte relação entre tropismo e neutralização (R5>
sensibilidade e X4> resistência, P <0.0001) do VIH-2. Com uma
única excepção, todos os doentes testados desenvolveram AcNT
contra isolados VIH-2 heterólogos de fenótipo R5. A amplitude desta
resposta neutralizante heteróloga é superior à que se observa
noutros estudos de neutralização em que foram utilizados

ix
pseudovírus e isolados primários de VIH-2. Contudo, tal como
observado anteriormente, nenhum dos doentes produziu anticorpos
neutralizantes contra isolados X4. A ausência de AcNT autólogos e
heterólogos para os isolados X4 sugere fortemente que o escape do
VIH-2 à neutralização in vivo está associado a alterações no tropismo
celular (passagem de R5 para X4). Na infecção VIH-1, os estudos
existentes sobre este assunto sugerem que não há uma relação entre
a susceptibilidade dos vírus e o escape à neutralização e a utilização
de coreceptores.
Demonstrou-se pela primeira, que a potência dos AcNT está
inversamente associada com os anticorpos de ligação para a rpC2-C3
(título e avidez) e não para a rgp36. Estes resultados sugerem
fortemente que os AcNT anti-VIH-2 têm como principal alvo as
regiões C2, V3 e C3 no Env e que a maturidade é um factor
importante na sua actividade neutralizante. As diferenças mais
significativas entre os vírus R5 sensíveis à neutralização e os vírus
X4 resistentes à neutralização ocorreram na região V3. Os vírus
resistentes aos AcNT tinham a região V3 mais longa e um número
maior de aminoácidos carregados positivamente. Estes dados
sugerem que a V3 é o principal alvo dos AcNT dentro do domínio C2-
V3-C3.
Tal como acontece com o VIH-1 são necessárias novas estratégias de
prevenção da infecção VIH-2. O último objectivo desta tese (Capítulo
VII) foi produzir novos imunogénios derivados do isolado de
referência do grupo A, VIH-2ALI e avaliar o seu potencial
neutralizante a nível pré-clínico em ratinhos. As proteínas nativas ou
truncadas do invólucro do VIH-2ALI foram expressas em vírus da
vacina e bactérias. A imunização de murganhos Balb\C com a gp125
truncada (gp125t) ou com o polipéptido rpC2-C3 só induziu uma
resposta de anticorpos de ligação, semelhante à que o VIH-2 induz
no homem, mas não induziu a produção de AcNTs. No entanto, a
indução de AcNTs pelas mesmas proteínas monoméricas foi muito
eficiente quando se imunizou previamente os animais com o vírus da
vacina a expressar quantidades elevadas de gp125t. Os anticorpos
desenvolvidos neutralizaram apenas vírus R5, que são, vírus com
fenótipo igual ao do vírus que originou os imunogénios vacinais (VIH-
2ALI). Os vírus X4 resistentes à neutralização apresentavam
alterações importantes na sequência e estrutura da região V3, que
divergiam significativamente da sequência aminoacídica, da carga
total, tamanho e conformação da região V3 do VIH-2ALI.
Globalmente, os resultados destes estudos demonstraram, pela

x
primeira vez, que AcNT amplamente reactivos contra o VIH-2 podem
ser obtidos utilizando uma estratégia de imunização que consiste
num priming com vírus da vacina recombinante a exprimir a
glicoproteína monomérica gp125 seguida de reforços com o
polipéptido rpC2-C3. Os resultados sugerem ainda que a região V3 é
um domínio neutralizante de largo espectro no VIH-2 e confirmam a
ligação existente entre o escape à neutralização e o tropismo X4 na
infecção VIH-2 (Capítulo VI).
Em conclusão, os resultados obtidos nesta tese permitem evidenciar
o papel central que a região C2-V3-C3 do Env tem na infecção VIH-2
e o impacto que pode ter no diagnóstico, monitorização e prevenção
da infecção por este vírus. Por um lado, esta região é altamente
antigénica, o que se revelou útil no diagnóstico serológico da
infecção. Por outro lado, a associação inversa entre a resposta
humoral contra esta região e o número de linfócitos T CD4+ significa
que o nível de anticorpos anti-C2V3C3 é útil para monitorizar o
estado imunológico e a evolução clínica de indivíduos infectados por
VIH-2. As regiões C2, V3 e C3 contêm os determinantes antigénicos
responsáveis pela indução de AcNT de elevada potência e ampla
reactividade que são comuns nos indivíduos infectados por VIH-2.
Estes resultados, em associação com as experiências de imunização
em ratinho, sugerem fortemente que uma vacina para o VIH-2 deve
direccionar a resposta humoral contra a C2, V3 e C3 na gp125.
Contudo, ao contrário do que se presumia até aqui, a emergência de
vírus resistentes à neutralização é comum na infecção por VIH-2 e
está principalmente associada à emergência de vírus com tropismo
X4 e com maior patogenicidade. Isto deve ser tido em conta na
concepção de uma vacina para o VIH-2. Estes resultados também
são relevantes para a utilização de antagonistas do CCR5 em
pacientes VIH-2.
Palavras-chave: Infecção VIH-2; ELISA específico para VIH-2;
Anticorpos IgA e IgG específicos para o invólucro do VIH-2; Resposta
neutralizante autóloga e heteróloga na infecção VIH-2 crónica;
Escape à neutralização; Indução de anticorpos neutralizantes anti-
VIH-2 em ratinhos.

xi
Summary
Individuals infected with HIV-2 progress more slowly than those
infected by HIV-1, and it is estimated that over 95% of individuals
infected by HIV-2 are included in the clinical definition of long-term
nonprogressors. This difference makes HIV-2 a potential model of an
attenuated HIV infection that can provide a unique insight into the
pathogenesis of HIV-1 infection. So far, the mechanisms responsible
for the attenuated phenotype of HIV-2 are not well known. Plasma
viral load is lower in individuals infected with HIV-2 comparing to
those infected with HIV-1. This suggests that the main difference
between the two types of HIV may be at the level of viral replication,
and assumes that the host immune response contributes
significantly to a more efficient replication control of HIV-2.
Currently, there is no doubt that the majority of individuals infected
with HIV-1 or HIV-2 produce autologous and heterologous
neutralizing antibodies (NAb).However there is some controversy over
whether the NAb effectively control viral replication, since most cases
have not shown an inverse correlation between the titer of NAb and
plasma viral load. In fact, both HIV-1 and HIV-2 seems to show a
direct correlation between the titer of NAb and viral replication
suggesting that viral replication is essential for the production of
NAb. In this context, an important question is how and when the
NAb are induced in individuals infected with HIV-1 and HIV-2
without detectable viral load.
In contrast to HIV-1, there are no studies that characterize both
qualitatively and quantitatively the kinetics of the anti-HIV-2
humoral response in the first days of infection since the infection by
this virus is often detected in chronic phase. To get detailed
information on viruses that establish HIV-2 infections and on the
nature of the immune response during the acute phase of infection
by HIV-2 is vital for the production of a vaccine. In this context, the
main objective of this thesis was to characterize the course of acute
and chronic HIV-2 infection, both qualitatively and quantitatively,
the nature and dynamics of the neutralizing and non-neutralizing
humoral antibody response and characterize the impact of these
antibodies on the molecular and phenotypic evolution of the virus.
We also analyzed the anti-HIV-2 neutralizing response targets and
the potential of two HIV-2 new immunogens for a vaccine.
The first study (Chapter III) aimed to characterize in detail the
antigenicity of two recombinant polypeptides derived from the
surface (rpC2-C3) and transmembrane glycoproteins (rgp36) of HIV-

xii
2ALI, the reference group A primary isolate. Using these two
polypeptides, a new enzyme linked immunoassay (ELISA-HIV2) was
established that had enough sensitivity and specificity to diagnose
HIV-2 infection serologically. The reactivity of HIV-2+ plasma was
significantly higher for antigen rgp36 than for rpC2-C3, suggesting
that the ectodomain of rgp36 is the immunodominant antigenic
region in the envelope of HIV-2. The antibody response to the rpC2-
C3 was more variable, allowing grouping of patients according to low
or high antibody production. The test also allowed us to confirm HIV-
2 in plasma samples that have dual serology result with commercial
tests. Due to the observed characteristics, the ELISA-HIV2 may be a
great alternative to commercial tests for serological diagnosis and for
confirmation of infection by HIV-2. The format of double antigen
presented in the test also allows for characterization, in a
quantitative and qualitative manner, of the evolution of antibody
production against the envelope glycoproteins of HIV-2 in infected
patients.
The rpC2-C3 and rgp36 antigens produced in the first phase of this
study were essential reagents for the second work (Chapter IV) in
which the presence of specific and nonspecific IgA and IgG antibodies
against HIV-2 Env proteins were analyzed in a group of HIV-2
patients in the acute (HIV-2 positive children perinatally infected)
and chronic phase of infection. It was shown that, as in HIV-1
infection, nonspecific activation of B cells also occurs in chronic HIV-
2 infection but only at the level of B cells secreting IgG, since the
total concentration of IgA in the plasma of positive individuals for
HIV-2 was identical to that of healthy individuals not infected with
HIV (control group). Regarding the specific humoral response to the
envelope glycoproteins of HIV-2, we observed an inverse association
between anti rpC2-C3 IgG and the number of CD4+ T lymphocytes
which suggests that these antibodies reflect the progression of HIV-2
infection. Most individuals also produced IgA antibodies against both
polypeptides, which identifies for the first time C2-C3 region as a
strong inducer of IgA antibodies in serum and confirms the strong
antigenicity of the ectodomain of gp36. Despite the magnitude of IgA
response, there was no association between IgA anti-gp36 or anti-
gp125 and the stage of disease as described for the HIV-1 infection.
In qualitative (avidity) and quantitative terms (titer and
concentration) the non-neutralizing IgG response was mainly
directed to the gp36. The subclasses of IgG antibodies produced in
the chronic phase of infection were IgG1 (reactive to both

xiii
polypeptides) and IgG3 (reactive to gp36). Any protective effect of
anti-gp36 IgG1 and IgG3 on clinical AIDS was not detected, as has
been suggested for the anti-gp41 IgG2 in HIV-1 infection. However, a
longitudinal analysis revealed a significant inverse association
between anti-C2-C3 IgG antibodies and the number of CD4+ T cells.
These results are consistent with the immune protective role
assigned to the C2-C3 region in HIV-2 infection. Since the anti-C2-
C3 IgG response seems to adequately reflect the immunological
status and clinical outcome of HIV-2 infection, the concentration of
anti-C2-C3 IgG may be a useful marker for monitoring disease
progression in HIV-2 infection.
The main promoter of molecular and phenotypic evolution of HIV-1 is
the selective pressure exerted initially by cytotoxic cellular response
and thereafter by neutralizing antibodies. In HIV-2, the information
on this subject is still very limited. In Chapter V of this study we
analyzed the molecular evolution of C2, V3 and C3 Env regions
longitudinally, in 18 HIV-2 patients using molecular and
phylogenetic methods and we correlated these changes with anti-Env
humoral response. The mean intra-host nucleotide diversity has
increased over the course of infection in most patients. The diversity
at amino acid level was significantly lower for V3 region and higher
for C2 region. The rate of evolution of HIV-2 in the region comprising
the C2, V3 and C3 domains was 0.014 substitutions/site/year,
which is very similar to what has been referred to for chronic HIV-1
infection. The number and position of positively selected sites was
highly variable, except for codons 267 and 270 in the C2 region that
were under a strong and persistent selective pressure in most
patients. The N-linked glycosylation sites located in C2 and V3
remained preserved in all patients throughout the course of
infection. The intra-host specific IgG response for the regions C2, V3
and C3, over time, was inversely associated with variation in
nucleotide and amino acid diversity in C2-V3-C3 region. The
variation of specific IgA response to C2-V3-C3 was inversely
associated with variation in the number of N-glycosylation sites. The
results of these studies show that the evolutionary dynamics of HIV-
2 envelope during non viremic chronic infections is similar to HIV-1,
which implies that the virus must be actively replicating in cellular
compartments. However, the convergent evolution of N-glycosylation
in C2 and V3 and the limited diversification of V3, indicates that
there are important functional factors that constrain the potential
diversity of HIV-2 envelope. Overall, the results suggest that: 1) anti-

xiv
C2V3C3 IgG antibodies are potentially effective in controlling viral
population; 2) the C3 region is an important target for IgA antibodies
and N-glycosylation of this region can prevent recognition of IgA
epitopes.
Currently, there is evidence that the majority of individuals
chronically infected with HIV-2 produce a wide spectrum of NAb.
However, very little is known about the evolutionary dynamics of
neutralizing response in chronic HIV-2 infection and controversial
information exists on the role of NAb in controlling viral replication.
The aim of the work presented in Chapter VI of this thesis was to
characterize the evolutionary dynamics of neutralizing response in
chronic HIV-2 infection and its relationship with the molecular and
phenotypic evolution of HIV-2 and with the evolution of the disease.
In this context, we analyzed longitudinally over 3-4 years the
neutralizing response directed against autologous and heterologous
primary viral isolates in a group of HIV-2 patients. Most patients (8
out of 12) were infected with viruses that used the CCR5 coreceptor
(R5) and only four patients were infected with viruses that used the
CXCR4 coreceptor (X4). These results confirmed that CCR5 is the
principal coreceptor used by HIV-2 in vivo. The presence of
neutralizing IgG antibodies against autologous isolates was detected
only in patients infected with R5 virus. Remarkably, four patients
infected with X4 virus and two with R5 virus, failed to produce
antibodies capable of neutralizing autologous viruses. These results
show for the first time that neutralization escape is quite common in
chronic infection by HIV-2 and there is a strong correlation between
tropism and neutralization (R5> sensitive and X4> resistant,
P>0.0001) of HIV-2. With only one exception, all patients tested
developed NAb against heterologous HIV-2 isolates with R5
phenotype. The breadth of this heterologous neutralizing response is
higher than that observed in other neutralization studies where
pseudovirus and primary isolates of HIV-2 were used. However, as
noted earlier, none of the patients produced neutralizing antibodies
against X4 isolates. The absence of autologous and heterologous
NAbs against the X4 isolates, strongly suggests that escape of HIV-2
from neutralization in vivo is associated with changes in cell tropism
(transition from R5 to X4). In HIV-1 infection, the existing studies on
this subject suggest that there is no relationship between virus
susceptibility and escape from neutralization and coreceptor usage.
We demonstrated for the first time that the potency of NAb response
was inversely associated with binding antibodies to rpC2-C3 (titer
and avidity) but not to rgp36. These results strongly suggest that the

xv
HIV-2 NAb mostly target the C2, V3 and C3 regions in Env and that
maturity is an important factor in their neutralizing activity. The
most significant differences between the R5 virus sensitive to
neutralization and X4 viruses resistant to neutralization occurred in
the V3 region. NAb-resistant viruses had the longest V3 region and a
larger number of positively charged amino acids. These data suggest
that V3 is the main NAb target within the C2-V3-C3 domain.
As for HIV-1, new strategies for prevention of HIV-2 infection are
required. The final objective of this thesis (Chapter VII) was to
produce new Env immunogens derived from the reference isolate of
group A, HIV-2ALI and evaluate their neutralizing potential at a pre-
clinical level in the mice model. Native or truncated proteins of the
HIV-2ALI envelope were expressed in vaccinia virus and bacteria. The
immunization of Balb\C mice with the truncated gp125 (gp125t) or
with the polypeptide rpC2-C3 induced a binding antibody response,
similar to the one HIV-2 induces in man, but did not induce the
production of NAb. However, the induction of NAb from the same
monomer proteins was highly efficient when the animals were
previously immunized with vaccinia virus expressing high amounts
of gp125t.The antibodies developed neutralized only R5 virus, that is,
virus with the same phenotype of the virus that originated the
vaccine immunogens (HIV-2ALI). X4 viruses resistant to
neutralization showed significant changes in the sequence and
structure of the V3 region, which diverged significantly from the
amino acid sequence, the total charge, size and conformation of the
V3 region of HIV-2ALI. Overall, the results of these studies
demonstrated, for the first time, that NAb broadly reactive against
HIV-2 can be obtained using an immunization strategy consisting of
priming with a recombinant vaccinia virus expressing the monomer
glycoprotein gp125 followed by boosting immunizations with the
polypeptide rpC2-C3. The results also suggest that the V3 region is a
broad spectrum neutralizing domain in HIV-2 and confirm the link
between neutralizing escape and X4 cell tropism in HIV-2 infection
(Chapter VI).
In conclusion, the results obtained in this thesis highlight the central
role that the C2-V3-C3 Env region plays in HIV-2 infection and the
impact that it may have on the diagnosis, monitoring and prevention
of infection by this virus. On one hand, this region is highly
antigenic, which has proved useful in serological diagnosis of
infection. On the other hand, the inverse association between the

xvi
humoral response against this region and the number of CD4+ T
lymphocytes means that the level of anti-C2V3C3 antibodies is
useful for monitoring the immune status and clinical outcome of
infected individuals by HIV-2. The C2, V3 and C3 regions contain the
antigenic determinants responsible for induction of potent and
broadly reactive NAb which are common in individuals infected with
HIV-2. These results, in combination with immunization experiments
in mice strongly suggest that a vaccine against HIV-2 should drive
the humoral response against C2, V3 and C3 in gp125. However,
unlike what was assumed until now, the emergence of neutralization
resistant virus is common in HIV-2 and, most importantly, is
associated with the emergence of viruses with X4 tropism and higher
pathogenicity. This has to be taken into account in the design of a
vaccine against HIV-2. These results are also relevant for the use of
CCR5 antagonists in HIV-2 patients.
Keywords: HIV-2 infection; ELISA specific for HIV-2, IgG and IgA
antibodies specific to the envelope of HIV-2, Autologous and
heterologous neutralizing response in chronic HIV-2 infection;
Neutralization escape; Neutralizing antibodies to HIV-2 in mice
induction.

1
CAPÍTULO I
Introdução

2

3
A PANDEMIA
A Síndrome da Imunodeficiência Adquirida (SIDA) constitui
actualmente um grave problema de Saúde Pública a nível mundial.
Desde que foi descrito o primeiro caso de SIDA nos Estados Unidos
da América em 1981, já morreram aproximadamente 25 milhões de
pessoas em todo o mundo, sendo os países em vias de
desenvolvimento os mais afectados, e estima-se que actualmente
mais de 33.4 milhões de pessoas estejam infectadas com o Vírus da
Imunodeficiência Humana (VIH) em todo o mundo [1].
A SIDA caracteriza-se por uma deterioração progressiva do sistema
imunitário e subsequente aparecimento de infecções oportunistas
que conduzem à morte do hospedeiro [2]. Estudos epidemiológicos e
genéticos confirmam que o VIH é o agente etiológico da SIDA. Há dois
tipos de VIH: VIH-1 e VIH-2. O VIH-1 é responsável pela maioria das
infecções a nível mundial [3], enquanto a infecção VIH-2 está
geograficamente limitada a países da África Ocidental. Portugal é o
país da Europa que tem maior prevalência (3.2%) de casos de SIDA
notificados. Do total de 15.685 casos de SIDA acumulados até 31 de
Dezembro de 2009, 494 foram causados pelo VIH-2 [4].
VIH-2
Origem, Estrutura e Replicação
A colaboração entre clínicos, investigadores portugueses e franceses
em 1985 culminou com a identificação de um novo retrovírus, o VIH-
2 [5]. Estudos filogenéticos indicam que o VIH-2 foi introduzido na
população humana a partir do sooty mangabey, vírus que induz
imunodeficiência no símio, e que o foco inicial (epicentro) terá
acontecido na Costa do Marfim entre 1940 e 1950 [6]. Esta infecção é
considerada endémica, em particular, na Guiné-Bissau, Senegal,
Gâmbia, Gana, Costa do Marfim e Cabo Verde, sendo a Guiné-
Bissau o país em que a prevalência de infecção por VIH-2 é maior.
Os oito grupos de VIH-2 podem ser classificados como epidémicos (A
e B) e não epidémicos (C até H), mas só os vírus do grupo A e B é que
têm relevância clínica [7;8]. O grupo A é predominante em todos os
países e talvez na Costa do Marfim, e o grupo B na Costa do Marfim
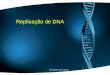
[9]. Estruturalmente, as partículas virais do VIH-2 são constituídas
por um invólucro externo (com origem na membrana da célula
hospedeira), composto pela glicoproteína (gp) transmembranar (TM) e
de superfície (SU), uma matriz interna proteica e uma nucleocápside
proteica em forma de cone onde se encontram as moléculas de ácido

4
ribonucleico (ARN), e as enzimas necessárias à replicação viral
(Figura 1).
Figura 1. Esquema de uma partícula vírica do VIH-2 (Adaptado da
referência [10]).
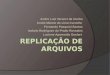
As glicoproteínas de SU e TM desempenham um papel fundamental
na entrada do vírus na célula hospedeira. A infecção inicia-se pela
interacção entre a gp-SU (125kDa, gp125) e o receptor celular CD4,
originando alterações na conformação da gp125 e subsequente
ligação ao coreceptor das quimiocinas, CCR5 (R5) ou CXCR4 (X4). As
alterações conformacionais da gp36 ocorrem após interacção do
péptido de fusão com a membrana citoplasmática da célula
hospedeira (Figura 2). Ao contrário do VIH-1, a maioria dos isolados
Figura 2. Esquema representativo do processo de fusão do VIH
(Adaptado da referência [11]).

5
VIH-2 primários in vitro conseguem infectar células na ausência do
receptor CD4 [12;13] e podem também utilizar uma grande
variedade de outros coreceptores celulares para além do R5 e do X4
[14-17].
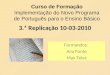
O ciclo de replicação inicia-se (Figura 3) após a fusão entre a
membrana viral e a celular. A cápside viral entra no citoplasma da
célula hospedeira, o seu conteúdo é libertado, e o ARN viral é
transcrito para uma cadeia dupla de ácido desoxirribonucleico (ADN)
pela transcriptase reversa (RT). O ADN proviral é transportado para o
núcleo e inserido no cromossoma da célula hospedeira pela integrase
viral. Depois da integração o ADN proviral é transcrito, produzindo
uma cadeia de ácido ribonucleico (ARN) viral que é transportada do
núcleo para o citoplasma, onde o ARNm (mensageiro) viral é
traduzido originando na maioria das vezes (porque nem sempre se
formam as poliproteínas vif, nef, ver e tat) as poliproteínas que vão
dar origem às proteínas virais. A poliproteína precursora gp160 é
clivada pela protease na gp125 e gp36 sendo depois transportadas
para a membrana plasmática da célula infectada. A associação entre
as poliproteínas do Gag (p55) e Gag-Pol (p160) na superfície interna
da membrana plasmática e o ARN genómico do VIH vai originar à
formação de um novo virião a partir da membrana da célula
hospedeira [18].
Figura 3. Esquema do ciclo replicativo do VIH [18].

6
Patogénese da Infecção VIH
A infecção VIH é geralmente caracterizada por uma fase aguda de
intensa replicação viral e difusão para os tecidos linfóides, uma fase
crónica, muitas vezes assintomática em que a activação imunitária e
a replicação viral se mantêm, e uma fase avançada de depleção
acentuada das células T CD4+, que leva à SIDA [19]. Durante a
infecção VIH ocorre uma depleção profunda de células T CD4+,
principalmente, no tecido associado ao intestino (GALT), que é
acompanhada por níveis elevados de viremia plasmática e
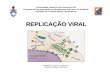
disseminação do vírus para outros órgãos (Figura 4). Neste período,
são estabelecidos reservatórios víricos, de que são exemplo as células
foliculares dendríticas nos centros germinativos, as células T e
macrófagos latentemente infectadas, que possuem o ADN vírico, mas
que não expressam proteínas víricas e, por isso, escapam ao sistema
imunitário. Durante a fase crónica da infecção, a replicação do VIH
também ocorre nos tecidos secundários, resultando numa activação
imunitária generalizada, numa produção sustentada de vírus, numa
renovação elevada de células T e, finalmente, na destruição do
sistema imunitário do hospedeiro e progressão rápida da doença
[20].
Figura 4. Principais eventos na progressão da doença associados à
infecção pelo VIH (Adaptado da referência [20]).

7
Estudos efectuados em modelos animais e no homem sugerem que a
activação imunitária é determinante na imunopatogénese do VIH.
Este processo pode ser originado, aquando da replicação do VIH no
interior do epitélio da mucosa intestinal e consequente danificação,
pela alteração do fenótipo e das múltiplas funções das células T, e
pela indução de vias moduladoras que regulam negativamente certas
funções específicas das células T [21]. Durante o estabelecimento da
viremia (Figura 5), as células de ambos os braços do sistema
imunitário, imunidade inata e adaptativa, são activadas pelas
proteínas virais e pela translocação dos produtos microbianos dos
tecidos associados ao intestino (GALT) para o sangue periférico. As
células activadas vão produzir quantidades de citocinas pró-
inflamatórias, como o factor de necrose tumoral alfa, interferão alfa
Figura 5. Factores associados com a activação imunitária induzida
pelo VIH (Adaptado da referência [20]).
Infecção VIH

8
(IFN-) e interleucina (IL) -1beta e IL-6, que levam a uma activação
imunitária crónica. Além disso, a replicação do VIH e a resposta
imunológica do hospedeiro à infecção contribuem também para a
activação imunitária. Estes eventos promovem níveis elevados de
replicação do VIH, que acabam por levar à exaustão e destruição do
sistema imunitário [20].
O VIH-2 também causa a SIDA no hospedeiro. Contudo, o VIH-2 está
associado a uma progressão mais lenta da doença [22], em que só
25% dos indivíduos infectados progridem para a fase de SIDA [23].
Apesar do grau de activação imunitária ser semelhante na fase
crónica da infecção por VIH-1 e por VIH-2 para o mesmo grau de
depleção de células T CD4+ [24;25], os indivíduos infectados pelo
VIH-2 têm uma taxa de declínio de linfócitos T CD4+ menos
acentuada [26] e uma carga viral plasmática inferior à dos indivíduos
infectados por VIH-1 [27;28]. Vários estudos referem que a carga
proviral é similar em ambas as infecções [22;29-32]. Contudo, dois
estudos recentes sugerem diferenças na carga proviral entre as duas
infecções. Um estudo refere que a carga proviral é superior nos
indivíduos infectados por VIH-2 comparado com os indivíduos
infectados por VIH-1, para contagens de células T CD4+ inferiores a
300 células [33]. O outro estudo refere que a carga proviral é idêntica
nas duas infecções para contagens de células T CD4+ inferiores a
300, mas é superior nos indivíduos infectados por VIH-1 para
contagem de células T CD4+ superiores a 300 [34]. Recentemente, foi
observada uma correlação positiva, entre a frequência de células T
CD4 específicas para o VIH-2 e a activação imunológica, e negativa
entre frequência de células T CD4 e a carga proviral [35]. A
manutenção das células T CD4 durante a infecção VIH-2 crónica
poderá estar correlacionada com uma timopoiese mais eficiente [36].
Ao invés do VIH-1, o VIH-2 não afecta a maturação e diferenciação
das células dendríticas, essenciais à produção de IFN-, uma
citocina importante na estimulação de outras células do sistema
imunitário, com capacidade antiviral, e fundamental na ligação entre
a imunidade inata e adquirida [37].
Defesas do hospedeiro na infecção por VIH
Durante a fase inicial e aguda da infecção por VIH o hospedeiro
desenvolve respostas celulares [38-40] e humorais [41-44] específicas
para o VIH, ainda que a maioria dessas respostas não evite a
replicação do vírus na maioria dos indivíduos infectados. Nesta fase
há selecção de variantes virais que conseguem escapar ao controlo

9
imunitário exercido pela resposta celular [45;46] ou humoral [43;47-
49].
A imunidade inata é a primeira linha de defesa a responder à
infecção antes do desenvolvimento de uma resposta adaptativa
específica [50]. Os macrófagos, as células dendríticas (DC), as células
“natural killer” (NK), as células T γδ, as citocinas (IL-2, IL-12, IFNγ,
IL-4, IL-10 e IL-15), as quimiocinas (CCR5, CXCR4 e IFN γ) e
outras pequenas moléculas circulantes (defensinas) têm um papel
fundamental no controlo e replicação do VIH [51;52]. Existem cada
vez mais evidências sobre o papel do sistema complemento no
controlo da replicação do VIH na fase inicial [53] e em fases
posteriores da infecção [54].
Resposta Celular
Apesar de existir alguma controvérsia quanto ao papel da resposta
celular no controlo da infecção pelo VIH-1, uma vez que em alguns
estudos não foram observadas correlações entre a resposta celular e
a carga viral no plasma [55;56]. Contudo, a maioria dos estudos
sugere que uma resposta de células T CD8+ especifica para
antigénios VIH-1 está associada a um melhor controlo da replicação
do vírus, a uma carga viral mais baixa e a uma progressão mais
lenta da doença nas fases iniciais da infecção por VIH-1 [57-62].
Na infecção VIH-2, as respostas celulares específicas têm sido
documentadas num pequeno número de indivíduos infectados.
Comparando as células T CD8+ especificas para o VIH-2 e para o
VIH-1 quanto à produção de IFN-γ [63-65], capacidade proliferativa
[66], e citoxicidade [64], não foram observadas diferenças
significativas, o que sugere que estes aspectos da resposta
adaptativa para o VIH-2 não contribuem para um maior controlo do
vírus e uma melhor evolução clínica. No entanto, a frequência de
células T CD4+ especificas para o VIH-2 com maior capacidade
proliferativa e uma maior capacidade de produzir IL-2 é mais
frequente na infecção VIH-2 crónica do que na infecção por VIH-1
[65;67;68]. A manutenção da produção de IL-2 pode estar associada
a uma maior capacidade de renovação das células T, bem como à
diminuição da apoptose na infecção VIH-2, uma vez que na infecção
por VIH-1, a diminuição da produção de IL-2 tem sido associada a
uma possível redução da renovação das células T e a um aumento da
susceptibilidade à apoptose celular [69].

10
Resposta Humoral
O papel dos anticorpos na infecção VIH
Não existem dúvidas quanto ao papel que os anticorpos têm no
diagnóstico da infecção VIH [70;71]. Os anticorpos específicos para o
VIH podem ser detectados em vários compartimentos como, no
sangue, nas mucosas e fluidos genitais. Os primeiros anticorpos
surgem aproximadamente 15 dias após o início da infecção (Figura 6)
e são a base para a maioria dos testes de despiste da infecção (ex.
Elisa). Mais tarde, quando se observa uma redução na virémia e na
antigenémia, detectam-se os anticorpos neutralizantes autólogos. Os
anticorpos no plasma reagem contra as proteínas do Env, gag, Pol e
proteínas reguladoras – vpr, tat, nef. [72]. Durante a infecção VIH
são produzidas imunoglobulinas (Igs) do tipo M (IgM), G (IgG) e A
(IgA).
Figura 6. Cinética da resposta humoral na fase aguda da infecção
pelo VIH quanto à evolução da carga viral, anticorpos não
neutralizante e anticorpos neutralizantes (Adaptado da referência
[73]).
A IgM é a primeira Ig a ser produzida, mas apresenta uma baixa
afinidade para o antigénio e encontra-se apenas no sangue [74].
A IgA é a Ig predominante na superfície das mucosas no homem e na
maioria dos mamíferos, e é a segunda Ig mais abundante em
circulação no homem. As múltiplas formas moleculares e as

11
diferentes subclasses da IgA fazem com que seja a mais heterogénea
das Ig [75]. No homem existem 3 formas: a monomérica (mIgA)
representa mais de 80-90% da IgA no soro; a dimérica (dIgA) ou
polimérica (pIgA) e a forma secretora (sIgA). Os dois subtipos de IgA
presentes no soro são a IgA1 e a IgA2. A IgA1 representa 85% das IgA
totais. Em termos funcionais as IgA podem ser divididas em IgA
secretoras em (compartimento da mucosa), ou IgA plasmáticas
(compartimento sistémico). Vários estudos têm sugerido que os
anticorpos IgA presentes nas mucosas (secreções vaginais e saliva)
protegem contra a infecção VIH-1 e VIH-2 [76-81].
A IgG1 é a subclasse predominante no soro de pacientes infectados
por VIH-1 [82;83]. Na infecção VIH-1 o título de anticorpos IgG1
contra a p24 e a gp120 é significantemente maior nos pacientes que
controlam a replicação comparado com progressores crónicos [82]. A
neutralização de isolados VIH-1 R5, X4 ou R5X4 é mais eficaz com a
IgG3 do que com a IgG1 ou IgG2, isto deve-se á região que liga o
fragmento Fc ao fragmento variável ser maior [82]. Em alguns
indivíduos VIH-1 assintomáticos ocorre a produção de anticorpos
anti-Tat e a sua presença tem sido correlacionada com o estado de
LTNP [84].
Os anticorpos desempenham um papel fundamental no controlo e
eliminação das partículas virais e células infectadas pelo VIH. Os
anticorpos que se ligam às proteínas do invólucro e inibem
directamente a entrada do vírus na célula são denominados de
anticorpos neutralizantes (AcNT). A figura 7 exemplifica o modo de
Figura 7. Esquema do modo de acção de alguns AcNT humanos
como o b12 (B), 17b e 2G12 (C) e 2F5 e 4E10 (D), em várias fases do
processo de entrada do VIH na célula (Adaptado da referência [85]).

12
acção de alguns AcNT humanos de largo espectro e com uma elevada
potência neutralizante. O anticorpo b12 interfere no local de ligação
da gp120 ao receptor CD4; o 2G12 é dirigido para um epitopo
glicosilado na gp120, o 17b liga-se ao domínio de ligação ao
coreceptor que fica exposto após a ligação da gp120 ao receptor CD4,
e os anticorpos 2F5 e 4E10 evitam a fusão entre a membrana do
vírus e da célula ao ligar-se à gp41 [85].
Os anticorpos não formalmente neutralizantes podem também ter
actividade antiviral que é mediada pela região constante (Fc) do
anticorpo, e resulta da interacção entre a região Fc do anticorpo e os
receptores da região Fc expressos na membrana celular de vários
tipos de células (ex. NK, macrófagos, dendríticas e neutrófilos). Estes
anticorpos actuam através de um ou mais dos seguintes mecanismos
antivirais (Figura 8): citoxicidade dependente do complemento (CDC),
citoxicidade celular dependente do anticorpo (ADCC), inibição viral
mediada por células e dependente dos anticorpos (ADCVI), e
fagocitose [86-91]. O mecanismo de acção antiviral da ADCVI é
semelhante ao da ADCC, só que em vez de ocorrer a lise da célula
infectada, ocorre a inibição da saída dos viriões das células
infectadas [92;93]
Figura 8. Mecanismos antivirais mediados pela região Fc do
anticorpo (Adaptado da referência [94]).

13
Numerosos estudos têm demonstrado uma associação inversa entre
resposta ADCC e ADCVI e progressão da doença, e uma associação
directa com o número de células CD4 e a carga viral em indivíduos
positivos para VIH-1 [95].
Anticorpos Neutralizantes
A resposta neutralizante desenvolvida pela maioria dos indivíduos
durante a infecção pelo VIH é dirigida contra as glicoproteínas do
invólucro do VIH (gp-TM e SU) [96-100]. A presença de AcNT (Figura
9) autólogos no plasma é detectada normalmente ao fim de seis
meses após a infecção, enquanto os AcNT heterólogos são
normalmente detectados na fase mais avançada da infecção e apenas
uma minoria de indivíduos infectados produz AcNT heterólogos com
actividade neutralizante para múltiplos isolados VIH-1 primários
[85;96;96;101]. Há estudos que associam a presença de anticorpos
neutralizantes específicos para o VIH-1 (de amplitude e potencia
elevada) com a não progressão da infecção [102-104]. Contudo,
noutros estudos não foi possível observar esse efeito no controlo da
replicação [105;106]. A progressão da doença VIH-1 tem sido
associada à perda da actividade neutralizante, escape viral e a
ausência de anticorpos neutralizantes [103;107;108]. A presença de
AcNT no plasma de indivíduos infectados por VIH-2 foi demonstrada
pela primeira vez por Robin Weiss e colaboradores [109]. Os vários
estudos realizados sobre neutralização do VIH-2 têm apresentado
algumas lacunas no que respeita ao número de amostras utilizadas
nos ensaios, à utilização de isolados adaptados em vez de isolados
primários, à falta de correlação clínica e à não utilização de ensaios
de neutralização padronizados [110-112].
Figura 9. Evolução da viremia, resposta celular citotóxica e
anticorpos neutralizantes (AcNT) durante a infecção VIH (Adaptado
da referência [113]).

14
Apesar destas limitações, os resultados obtidos sugerem que o VIH-2
tem uma menor capacidade de escapar aos AcNT comparado com o
VIH-1 [47]. A glicosilação da glicoproteína externa do invólucro,
gp125, a infecção não dependente do CD4 e a utilização de
coreceptores alternativos in vitro parecem ser factores determinantes
para um melhor controlo dos isolados VIH-2 primários pelos AcNT
[112;114;115].
A resposta neutralizante autóloga e heteróloga em indivíduos
infectados pelo VIH-2 ou pelo VIH-1 tem sido analisada e comparada
em vários estudos. Os AcNT contra isolados primários autólogos são
mais comuns na infecção VIH-2 do que na infecção VIH-1 [111;116].
Um estudo recente sugere que os indivíduos VIH-2 positivos
desenvolvem uma resposta neutralizante heteróloga de grande
amplitude, mas com uma potência de neutralização mais baixa [117].
Esta maior amplitude no VIH-2 pode não ter sido originada pela
diversidade viral ou pelo escape à neutralização como no VIH-1, mas
sim devido a uma propriedade intrínseca do VIH-2 como antigénio. A
existência de um repertório de anticorpos neutralizantes mais amplo
nos indivíduos VIH-2 positivos pode também ser consequência de um
sistema imunitário mais bem preservado. Os AcNT com actividade
neutralizante contra isolados VIH-1 primários heterólogos só são
encontrados nas fases finais da infecção VIH-1, e a maioria dos
indivíduos infectados não conseguem desenvolver uma resposta
neutralizante heteróloga que neutralize múltiplos vírus diferentes
durante o primeiro da infecção [118].
Existem indivíduos infectados por VIH-1 que se mantêm saudáveis
na ausência de terapia anti-retroviral. Estes indivíduos denominados
de “long-term non-progressors” [LTNPs] mantêm o número de células
T CD4+ dentro dos valores normais durante mais de 10 anos, e
representam entre 5 a 15% da população de indivíduos VIH-1
positivos crónicos. Os níveis de ARN viral no plasma dos LTNP são
frequentemente baixos. Entre os indivíduos LTNP foram identificados
dois subgrupos, os "elite controllers" [ECs] que mantêm a carga viral
abaixo do limite de detecção (50 cópias de ARN/ml) dos testes
comerciais [119] e os "viremic controllers" que persistentemente têm
carga viral detectável, mas em níveis muito baixos. Os EC
representam menos de 1% da população infectada por VIH-1 [120].
Determinantes da neutralização no invólucro do VIH
A glicoproteína de SU do VIH é composta por 5 regiões hipervariáveis
(V1 a V5) separadas por 5 regiões relativamente mais conservadas,
regiões C1 a C5 (Figura 10). Nos últimos anos a região V3,
denominada o principal determinante da neutralização (PDN), tem

15
merecido especial atenção, uma vez que para além de conter o PDN,
esta região também está envolvida na fusão viral e no tropismo
celular [121;122]. Durante a fase aguda e crónica da infecção VIH-1
o título de anticorpos específicos contra a região V3 é muito elevado
[122].
Figura 10. Estrutura secundária representativa das regiões
constantes e variáveis da glicoproteína de superfície do VIH
(Adaptado da referência [123]).
Apesar de esta região ser muito imunogénica, a actividade
neutralizante dos anticorpos anti-V3 é muito baixa contra isolados
VIH-1 primários, enquanto os isolados adaptados são facilmente
neutralizados [124-126].
Figura 11. Desenho esquemático das regiões variáveis da gp120 de
isolados VIH-1 primários A) e adaptados B) com os locais de ligação
ao receptor CD4 (R) e ao coreceptor (CoR) R5 ou X4. (Adaptado da
referência [126] ).

16
Os epitopos conformacionais presentes na região V3 da gp120 dos
isolados VIH-1 primários induzem AcNT com elevada potência
neutralizante, frequentemente abaixo de ng/ml, comparado com os
anticorpos induzidos por epitopos lineares [127;128].
Está bem definido que a ligação da gp120 do VIH-1 ao receptor CD4
altera as posições das regiões V1/V2 e V3, expondo desta forma as
regiões conservadas adjacentes à região V3 [129-131]. Os glicanos
existentes nas regiões V1/V2 e na base da V3 restringem o acesso
dos anticorpos à região V3 [132-134]. A deleção da região V1/V2
redirecciona a resposta humoral para a região V3 alterando a
imunogenicidade da gp120 [135-137]. Estes dados sugerem a
existência de dois estados conformacionais da gp-SU. O primeiro
estado corresponde a uma estrutura fechada, em que os epitopos
nos locais de ligação ao CD4 e ao coreceptor R5 ou X4 não estão
expostos aos anticorpos; o segundo estado é uma estrutura aberta,
em que os epitopos nos locais de ligação ao CD4 e ao R5 ou X4 ficam
expostos aos anticorpos (Figura 11) [126].
Os determinantes da neutralização do VIH-2 não estão tão bem
caracterizados como os do VIH-1. Apesar da região V3 do VIH-2
apresentar um elevado grau de similaridade entre os diferentes
grupos [138] e da região central da V3 ser muito conservada, o papel
da V3 na indução de anticorpos neutralizantes no VIH-2 não tem
sido consensual. Alguns trabalhos descrevem que no VIH-2 a
utilização de péptidos lineares é suficiente para induzir anticorpos
neutralizantes contra a região V3 [139-141]. No entanto, outros
estudos não lhe atribuem esse papel [142;143].
As regiões V1/V2 da gp125 dos isolados VIH-2 primários parecem
não interferir com a ligação dos anticorpos à região V3, como
acontece no VIH-1, uma vez que a deleção desta região não aumenta
o acesso dos anticorpos à região V3 do VIH-2 [144]. Os isolados VIH-
2 primários mais sensíveis aos AcNT são os que não precisam do
receptor celular CD4 para infectar as células [12], enquanto nos
isolados VIH-1 primários só a deleção da região V1/V2 é que torna os
isolados mais sensíveis à neutralização. As diferenças estruturais
entre as glicoproteínas nativas do invólucro de ambos os vírus
sugerem que no VIH-2 a gp125 dos isolados primários terá uma
estrutura aberta, permitindo deste modo que o domínio de ligação ao
coreceptor celular na região V3 fique parcial ou totalmente exposta
aos anticorpos (Figura 11) [145]. No entanto este assunto ainda é

17
controverso porque indivíduos infectados por VIH-2 não produzem
anticorpos anti-V3.
As características estruturais que as glicoproteínas de SU (gp120) do
VIH-1 apresentam, como uma forte glicosilação (50% de glicanos),
uma grande variabilidade ao nível da sequência de aminoácidos
[47;124;146;147], assim como a não exposição dos locais de ligação
ao receptor, têm sido grandes obstáculos à indução de AcNT
protectivos de largo espectro para o VIH-1 [47]. A produção de AcNT
de amplitude elevada nos indivíduos VIH-1+ é geralmente baixa.
Apenas 10 a 30% dos indivíduos VIH-1 infectados desenvolvem AcNT
de amplitude elevada [148]. Apesar de terem sido isolados vários
anticorpos monoclonais humanos contra o invólucro do VIH, apenas
uma pequena percentagem deles neutraliza múltiplos isolados VIH-1
primários [128;149]. Estes anticorpos (Tabela 1) reconhecem
epitopos conformacionais no domínio externo da gp120 e na região
externa da gp41 próxima da membrana [128;149] Até ao momento
não foram ainda isolados anticorpos monoclonais neutralizantes
humanos para o VIH-2.
Tabela 1. Anticorpos monoclonais humanos neutralizantes de largo
espectro de neutralização (Adaptado da referência [96]).
Anticorpos
neutralizantes
Epitopo
(local)
Características do
epitopo
4E10 MPER da gp41 do VIH-1 Região NWFNIT pode ter
reactividade cruzada com a
cardiolipina
2F5 MPER da gp41 do VIH-1 Região ELDKWA pode ter
reactividade cruzada com a
cardiolipina
Z13 MPER da gp41 do VIH-1 WNWFDITN
447-52D gp120 Epitopo conformacional
conservado no domínio
externo da gp120
PG9 e PG16 Regiões V1/V2 e V3 na
gp120
Conformacional
VCR01 Local de ligação ao
receptor CD4
Conformacional
B12 gp120 Epitopo conformacional
conservado no domínio
externo da gp120
MPER: região externa próxima da membrana

18
Escape à Neutralização
Um dos maiores desafios que o VIH tem colocado à investigação é a
forma como consegue superar e ultrapassar as respostas imunes
mediadas pelas células T e anticorpos, e finalmente induzir
imunodeficiência no hospedeiro. Os anticorpos dirigidos contra a
glicoproteína do invólucro podem ser detectados no início da infecção
e são capazes de neutralizar as variantes dos vírus autólogos com os
títulos de neutralização a aumentarem ao longo do tempo na maioria
dos pacientes [150-152]. No entanto, a elevada variabilidade genética
do VIH, especialmente ao nível das glicoproteínas do invólucro (gp41e
gp120) e uma rápida evolução do invólucro permite aos vírus escapar
aos AcNT produzidos pelo hospedeiro, originando deste modo ciclos
sucessivos de produção de novos anticorpos e consequente escape
viral [47;152-154].
Devido à pressão exercida pelos AcNT, a quantidade e/ as posições
dos glicanos evoluem de forma a criar um escudo protector que
muda continuamente sobre a superfície do invólucro de forma a
proteger determinadas regiões do invólucro essenciais para a entrada
do vírus na célula hospedeira [155;156]. As variações observadas nas
sequências de aminoácidos das regiões variáveis (ex. inserções e
deleções, e mudanças no número de potenciais locais de glicosilação
ligados à asparagina) têm sido associadas com o escape viral aos
AcNT [157;158]. Em particular, o comprimento e as características
da glicosilação nas regiões V1/V2 parecem desempenhar um papel
na resistência aos AcNT [102;159-162], evitando desta forma que
regiões subjacentes do invólucro sejam reconhecidas pelos
anticorpos [163].
A maioria dos estudos sugere que o escape aos AcNT é um
acontecimento frequente na infecção VIH-1 [164-166]. Na infecção
VIH-2 este assunto não está estudado de forma efectiva como no
VIH-1. O escape aos AcNT foi apenas observado num estudo
efectuado por Shi e colaboradores, mas utilizando um pequeno
número de amostras [112]. Compreender os mecanismos que estão
na base do controlo imunológico e de que forma o VIH consegue
escapar ao controlo imunitário, poderá num futuro próximo ser a
chave para o desenvolvimento de vacinas para o VIH-2.

19
Vacinas para o VIH
Desafios e dificuldades
A disseminação mundial do VIH representa um sério problema ao
desenvolvimento global e à saúde pública. O desenvolvimento de
uma vacina segura, eficaz e protectora acessível a nível mundial, é a
melhor forma para controlar a pandemia no futuro. Nos últimos anos
foram feitos progressos significativos nas áreas da virologia,
imunologia, patogénese do VIH/SIDA e também no desenvolvimento
de medicamentos anti-retrovirais. No entanto, o desenvolvimento de
uma vacina contra o VIH-1 enfrenta enormes desafios científicos
devido à grande variabilidade genética do vírus, à ausência de
correlatos de uma resposta imunológica protectora, dificuldade na
construção e apresentação dos imunogénios neutralizantes,
limitações com os modelos animais existentes e ainda problemas
logísticos associados com a realização dos ensaios clínicos [167].
Apesar da necessidade urgente de uma vacina para o VIH-1, apenas
dois conceitos de vacinas completaram os estudos de eficácia clínica.
O primeiro conceito desenvolvido pela VaxGen utilizava subunidades
recombinantes da gp120 de subtipos B e E do VIH-1 para induzir
uma resposta humoral, mas os anticorpos neutralizantes obtidos não
protegiam contra a infecção VIH-1 e não tinham um largo espectro.
O segundo conceito utilizava um adenovírus recombinante do
serotipo 5 (Ad5) para expressar as proteínas dos genes Gag, Pol e
Nef, e induzir células T CD8+ específicas para o VIH-1, que fossem
capazes de prevenir ou reduzir a carga viral após a infecção. Na Fase
2b dos estudos de eficácia do Ad5 da Merck, apesar da maioria dos
indivíduos ter desenvolvido uma resposta celular, houve indivíduos
em que esse efeito foi suprimido pela pré-existência de anticorpos
neutralizantes contra o Ad5, e alguns adquiriram a infecção pelo
VIH-1. [168]. Os quatro principais ensaios clínicos para avaliar a
eficácia de uma vacina para o VIH-1, AIDSVAX 003 e AIDSVAX 004
(conduzidos pela Empresa VaxGen) e HVTN 502 e HTVN 503 (HIV
Vaccine Trials Network financiado pelo NIH) não foram bem-
sucedidos.
No entanto, um ensaio recente conduzido na Tailândia (RV144)
demonstrou que é possível induzir uma resposta imunitária
esterilizante (apesar de reduzida) por anticorpos não neutralizantes

20
[169], renovando assim o optimismo quanto à obtenção de uma
vacina para o VIH-1 [170]. A tabela 2 resume as diferentes
estratégias utilizadas para estimular uma resposta humoral e
celular. Resume também as vantagens e desvantagens de cada tipo
de vacina, as implicações caso sejam vacinas vivas atenuadas,
subunidades proteicas da gp120, vacinas baseadas em vectores
vivos, vacinas ADN, vacinas vírus inactivados e combinação de
produtos [167].
Tabela 2. Tipo de vacinas produzidas para o VIH-1.
Vacina Características Vantagens Desvantagens
Viva ou
atenuada
Deficiente no gene
Nef e em LTR
Resposta
CTL
Potencialmente
patogénica
Recombinante Usa proteínas do
VIH para induzir
anticorpos
Induz
anticorpos
in vitro
Não induz CTL e
os anticorpos são
ineficazes
Viva (baseada
em vectores)
Inserção de parte
do genoma em
bactérias ou vírus
Resposta
celular e
humoral
Potencialmente
patogénica
ADN Inserção de genes
num plasmídeo
bacteriano
Baratas e
fáceis de
transportar
Potencialmente
patogénica
Inactivada Vírus inactivado
por métodos
químicos e/ou UV
Segura (se
inactivada)
Resposta contra
células em vez dos
vírus
Pseudovírus Expressam
proteínas VIH:
ausência de ARN
viral e genes
replicativos
Resposta
celular e
humoral;
segura
Não protege
contra a infecção
A vacinação é um processo complexo e a sua eficácia pode ser
influenciada por múltiplos factores como: a) vector utilizado, b) dose
da vacina, c) intervalo entre a primeira imunização e o reforço, d)
tropismo do vírus e espécie do hospedeiro, e) imunidade prévia que
não teve origem na vacina, f) tipo de imunidade pretendida (humoral
ou celular) e g) tempo de duração da resposta imunitária [168].
As diferentes estratégias utilizadas para a produção de uma vacina
para o VIH-2 não têm conseguido induzir uma resposta neutralizante
protectora, e as respostas neutralizantes obtidas são fracas e não
evitam que os animais sejam infectados (Tabela 2).

21
Tabela 3. Imunogénios e vectores utilizados na indução de uma
vacina para o VIH-2.
VIH-2
[Referência]
Imunogénios Modelo
Animal
Resposta
SBL6669 [139;171;172]
SBL6669 [173-176]
gp125 e regiãoV3
Canarypox e Vírus da Vacina atenuado (expressão de várias proteínas), e reforço com gp160, gp125 e péptidos da V3
Murganho e porquinho Guiné Macaco Cynomolgus e Rhesus
AcNT autólogos e heterólogos. Neutralização fraca; protecção parcial contra isolados VIH-2 autólogos.
BEN [177]
Subunidades da gp130 (em micelas)
Macaco Cynomolgus
Neutralização fraca de isolados autólogos e heterólogos.
ROD [178]
Vírus Vacina (expressa gene Env e Gag)
Macaco Rhesus
Ausência de AcNT e resposta protectora.
UC2 [179]
ADN (gene Tat, Nef, Gag e Env)
Babuíno Protecção parcial para isolados autólogos; não induz AcNT
Modelos Animais
Os primatas não humanos têm sido o modelo animal mais utilizado
para estudar o desenvolvimento de uma vacina para o VIH. Os
chimpanzés, (Pan troglodytes) e os macacos de rabo de porco,
(Macaca nemestrina), são susceptíveis à infecção pelo VIH, mas
mantêm baixos níveis de carga viral e não desenvolvem sintomas
clínicos da SIDA. Os macacos africanos são hospedeiros naturais de
uma grande variedade de vírus dos símios (VISagm, VISsm, VISsyk,
VIScol, etc.), mas não desenvolvem doença clínica após serem
infectados [180]. Os babuínos (Papio cynocephalus) têm sido
essenciais para estudar a patogénese da infecção VIH-2 uma vez que
o VIH-2 causa uma infecção crónica que progride durante vários
anos antes do aparecimento da fase de SIDA [181].

22
Por outro lado a avaliação da eficácia das vacinas utilizando o
macaco implica infectar os animais com doses elevadas de vírus
(entre 103 e 105 TCID50), o equivalente a 5x107 cópias de ARN/ml.
Estas doses elevadas de vírus são necessárias para garantir 100% de
infecção nos animais controlo. No entanto, estas doses elevadas de
vírus utilizadas nos ensaios não correspondem à exposição natural
por parte do homem ao VIH, onde têm sido observadas
concentrações no plasma seminal de 103 a 105 cópias de ARN/ml
[182;183].
Estudos efectuados em modelos animais sugerem que uma vacina
eficaz que proteja os indivíduos da infecção por VIH deverá ser capaz
de estimular a produção de anticorpos neutralizantes e as respostas
mediadas por células.
Referências
[1] UNAIDS/WHO global AIDS statistics. AIDS Care 2003 Feb;15(1):144.
[2] Pantaleo G, Fauci AS. Immunopathogenesis of HIV infection. Annu Rev Microbiol 1996;50:825-54.
[3] Greene WC. A history of AIDS: looking back to see ahead. Eur J Immunol 2007 Nov;37 Suppl 1:S94-102.
[4] de Silva TI, Cotten M, Rowland-Jones SL. HIV-2: the forgotten AIDS virus. Trends Microbiol 2008 Dec;16(12):588-95.
[5] Clavel F, Guetard D, Brun-Vezinet F, et al. Isolation of a new human retrovirus from West African patients with AIDS. Science 1986 Jul 18;233(4761):343-6.
[6] Lemey P, Pybus OG, Wang B, Saksena NK, Salemi M, Vandamme AM. Tracing the origin and history of the HIV-2 epidemic. Proc Natl Acad Sci U S A 2003 May 27;100(11):6588-92.
[7] Damond F, Worobey M, Campa P, et al. Identification of a highly divergent HIV type 2 and proposal for a change in HIV type 2 classification. AIDS Res Hum Retroviruses 2004 Jun;20(6):666-72.

23
[8] Jaffar S, Grant AD, Whitworth J, Smith PG, Whittle H. The natural history of HIV-1 and HIV-2 infections in adults in Africa: a literature review. Bull World Health Organ 2004 Jun;82(6):462-9.
[9] Ntemgwa ML, d'Aquin TT, Brenner BG, Camacho RJ, Wainberg MA. Antiretroviral drug resistance in human immunodeficiency virus type 2. Antimicrob Agents Chemother 2009 Sep;53(9):3611-9.
[10] Sierra S, Kupfer B, Kaiser R. Basics of the virology of HIV-1 and its replication. J Clin Virol 2005 Dec;34(4):233-44.
[11] O'Hara BM, Olson WC. HIV entry inhibitors in clinical development. Curr Opin Pharmacol 2002 Oct;2(5):523-8.
[12] Thomas ER, Shotton C, Weiss RA, Clapham PR, McKnight A. CD4-dependent and CD4-independent HIV-2: consequences for neutralization. AIDS 2003 Feb 14;17(3):291-300.
[13] Reeves JD, Hibbitts S, Simmons G, et al. Primary human immunodeficiency virus type 2 (HIV-2) isolates infect CD4-negative cells via CCR5 and CXCR4: comparison with HIV-1 and simian immunodeficiency virus and relevance to cell tropism in vivo. J Virol 1999 Sep;73(9):7795-804.
[14] Morner A, Bjorndal A, Albert J, et al. Primary human immunodeficiency virus type 2 (HIV-2) isolates, like HIV-1 isolates, frequently use CCR5 but show promiscuity in coreceptor usage. J Virol 1999 Mar;73(3):2343-9.
[15] McKnight A, Dittmar MT, Moniz-Periera J, et al. A broad range of chemokine receptors are used by primary isolates of human immunodeficiency virus type 2 as coreceptors with CD4. J Virol 1998 May;72(5):4065-71.
[16] Azevedo-Pereira JM, Santos-Costa Q, Moniz-Pereira J. HIV-2 infection and chemokine receptors usage - clues to reduced virulence of HIV-2. Curr HIV Res 2005 Jan;3(1):3-16.
[17] McKnight A, Dittmar MT, Moniz-Periera J, et al. A broad range of chemokine receptors are used by primary isolates of human immunodeficiency virus type 2 as coreceptors with CD4. J Virol 1998 May;72(5):4065-71.
[18] Adamson CS, Freed EO. Novel approaches to inhibiting HIV-1 replication. Antiviral Res 2010 Jan;85(1):119-41.
[19] Levy JA. HIV pathogenesis: 25 years of progress and persistent challenges. AIDS 2009 Jan 14;23(2):147-60.

24
[20] Moir S, Chun TW, Fauci AS. Pathogenic Mechanisms of HIV Disease. Annu Rev Pathol 2010 Jan 15.
[21] Douek DC, Roederer M, Koup RA. Emerging concepts in the immunopathogenesis of AIDS. Annu Rev Med 2009;60:471-84.
[22] Bock PJ, Markovitz DM. Infection with HIV-2. AIDS 2001;15 Suppl 5:S35-S45.
[23] de Silva TI, Cotten M, Rowland-Jones SL. HIV-2: the forgotten AIDS virus. Trends Microbiol 2008 Dec;16(12):588-95.
[24] Sousa AE, Carneiro J, Meier-Schellersheim M, Grossman Z, Victorino RM. CD4 T cell depletion is linked directly to immune activation in the pathogenesis of HIV-1 and HIV-2 but only indirectly to the viral load. J Immunol 2002 Sep 15;169(6):3400-6.
[25] Grossman Z, Meier-Schellersheim M, Sousa AE, Victorino RM, Paul WE. CD4+ T-cell depletion in HIV infection: are we closer to understanding the cause? Nat Med 2002 Apr;8(4):319-23.
[26] Jaffar S, Wilkins A, Ngom PT, et al. Rate of decline of percentage CD4+ cells is faster in HIV-1 than in HIV-2 infection. J Acquir Immune Defic Syndr Hum Retrovirol 1997 Dec 15;16(5):327-32.
[27] Shanmugam V, Switzer WM, Nkengasong JN, et al. Lower HIV-2 plasma viral loads may explain differences between the natural histories of HIV-1 and HIV-2 infections. J Acquir Immune Defic Syndr 2000 Jul 1;24(3):257-63.
[28] MacNeil A, Sarr AD, Sankale JL, Meloni ST, Mboup S, Kanki P. Direct evidence of lower viral replication rates in vivo in human immunodeficiency virus type 2 (HIV-2) infection than in HIV-1 infection. J Virol 2007 May;81(10):5325-30.
[29] Ariyoshi K, Berry N, Wilkins A, et al. A community-based study of human immunodeficiency virus type 2 provirus load in rural village in West Africa. J Infect Dis 1996 Jan;173(1):245-8.
[30] Sarr AD, Popper S, Thior I, et al. Relation between HIV-2 proviral load and CD4+ lymphocyte count differs in monotypic and dual HIV infections. J Hum Virol 1999 Jan;2(1):45-51.
[31] Soares R, Foxall R, Albuquerque A, et al. Increased frequency of circulating CCR5+ CD4+ T cells in human immunodeficiency virus type 2 infection. J Virol 2006 Dec;80(24):12425-9.

25
[32] Gomes P, Taveira NC, Pereira JM, Antunes F, Ferreira MO, Lourenco MH. Quantitation of human immunodeficiency virus type 2 DNA in peripheral blood mononuclear cells by using a quantitative-competitive PCR assay. J Clin Microbiol 1999 Feb;37(2):453-6.
[33] Gottlieb GS, Hawes SE, Kiviat NB, Sow PS. Differences in proviral DNA load between HIV-1-infected and HIV-2-infected patients. AIDS 2008 Jul 11;22(11):1379-80.
[34] Gueudin M, Damond F, Braun J, et al. Differences in proviral DNA load between HIV-1- and HIV-2-infected patients. AIDS 2008 Jan 11;22(2):211-5.
[35] Foxall RB, Cortesao CS, Albuquerque AS, Soares RS, Victorino RM, Sousa AE. Gag-specific CD4+ T-cell frequency is inversely correlated with proviral load and directly correlated with immune activation in infection with human immunodeficiency virus type 2 (HIV-2) but not HIV-1. J Virol 2008 Oct;82(19):9795-9.
[36] Gautier D, Beq S, Cortesao CS, Sousa AE, Cheynier R. Efficient thymopoiesis contributes to the maintenance of peripheral CD4 T cells during chronic human immunodeficiency virus type 2 infection. J Virol 2007 Nov;81(22):12685-8.
[37] Cavaleiro R, Brunn GJ, Albuquerque AS, Victorino RM, Platt JL, Sousa AE. Monocyte-mediated T cell suppression by HIV-2 envelope proteins. Eur J Immunol 2007 Dec;37(12):3435-44.
[38] McMichael AJ, Rowland-Jones SL. Cellular immune responses to HIV. Nature 2001 Apr 19;410(6831):980-7.
[39] Wick WD, Yang OO, Corey L, Self SG. How many human immunodeficiency virus type 1-infected target cells can a cytotoxic T-lymphocyte kill? J Virol 2005 Nov;79(21):13579-86.
[40] Douek DC, Picker LJ, Koup RA. T cell dynamics in HIV-1 infection. Annu Rev Immunol 2003;21:265-304.
[41] Cao H, Walker BD. Immunopathogenesis of HIV-1 infection. Clin Dermatol 2000 Jul;18(4):401-10.
[42] Trkola A, Kuster H, Leemann C, et al. Humoral immunity to HIV-1: kinetics of antibody responses in chronic infection reflects capacity of immune system to improve viral set point. Blood 2004 Sep 15;104(6):1784-92.
[43] Bunnik EM, Pisas L, van Nuenen AC, Schuitemaker H. Autologous neutralizing humoral immunity and evolution of the viral

26
envelope in the course of subtype B human immunodeficiency virus type 1 infection. J Virol 2008 Aug;82(16):7932-41.
[44] Burke B, Barnett SW. Broadening our view of protective antibody responses against HIV. Curr HIV Res 2007 Nov;5(6):625-41.
[45] Oxenius A, Price DA, Trkola A, et al. Loss of viral control in early HIV-1 infection is temporally associated with sequential escape from CD8+ T cell responses and decrease in HIV-1-specific CD4+ and CD8+ T cell frequencies. J Infect Dis 2004 Aug 15;190(4):713-21.
[46] Stebbings R, Berry N, Waldmann H, et al. CD8+ lymphocytes do not mediate protection against acute superinfection 20 days after vaccination with a live attenuated simian immunodeficiency virus. J Virol 2005 Oct;79(19):12264-72.
[47] Wei X, Decker JM, Wang S, et al. Antibody neutralization and escape by HIV-1. Nature 2003 Mar 20;422(6929):307-12.
[48] Stevceva L, Yoon V, Anastasiades D, Poznansky MC. Immune responses to HIV Gp120 that facilitate viral escape. Curr HIV Res 2007 Jan;5(1):47-54.
[49] van Gils MJ, Bunnik EM, Burger JA, et al. Rapid escape from preserved cross-reactive neutralizing humoral immunity without loss of viral fitness in HIV-1-infected progressors and long-term nonprogressors. J Virol 2010 Apr;84(7):3576-85.
[50] Janeway CA, Jr., Medzhitov R. Innate immune recognition. Annu Rev Immunol 2002;20:197-216.
[51] Lehner T, Wang Y, Pido-Lopez J, Whittall T, Bergmeier LA, Babaahmady K. The emerging role of innate immunity in protection against HIV-1 infection. Vaccine 2008 Jun 6;26(24):2997-3001.
[52] Suresh P, Wanchu A. Chemokines and chemokine receptors in HIV infection: role in pathogenesis and therapeutics. J Postgrad Med 2006 Jul;52(3):210-7.
[53] Stoiber H. Complement, Fc receptors and antibodies: a Trojan horse in HIV infection? Curr Opin HIV AIDS 2009 Sep;4(5):394-9.
[54] Stoiber H, Banki Z, Wilflingseder D, Dierich MP. Complement-HIV interactions during all steps of viral pathogenesis. Vaccine 2008 Jun 6;26(24):3046-54.
[55] Addo MM, Yu XG, Rathod A, et al. Comprehensive epitope analysis of human immunodeficiency virus type 1 (HIV-1)-specific T-

27
cell responses directed against the entire expressed HIV-1 genome demonstrate broadly directed responses, but no correlation to viral load. J Virol 2003 Feb;77(3):2081-92.
[56] Kaufmann DE, Bailey PM, Sidney J, et al. Comprehensive analysis of human immunodeficiency virus type 1-specific CD4 responses reveals marked immunodominance of gag and nef and the presence of broadly recognized peptides. J Virol 2004 May;78(9):4463-77.
[57] Rosenberg ES, Billingsley JM, Caliendo AM, et al. Vigorous HIV-1-specific CD4+ T cell responses associated with control of viremia. Science 1997 Nov 21;278(5342):1447-50.
[58] Norris PJ, Rosenberg ES. CD4(+) T helper cells and the role they play in viral control. J Mol Med 2002 Jul;80(7):397-405.
[59] Norris PJ, Rosenberg ES. Cellular immune response to human immunodeficiency virus. AIDS 2001 Feb;15 Suppl 2:S16-S21.
[60] McMichael AJ, Rowland-Jones SL. Cellular immune responses to HIV. Nature 2001 Apr 19;410(6831):980-7.
[61] Kim GJ, Lee HS, Hong KJ, Kim SS. Dynamic correlation between CTL response and viral load in primary human immunodeficiency virus-1 infected Koreans. Virol J 2010;7:239.
[62] Edwards BH, Bansal A, Sabbaj S, Bakari J, Mulligan MJ, Goepfert PA. Magnitude of functional CD8+ T-cell responses to the gag protein of human immunodeficiency virus type 1 correlates inversely with viral load in plasma. J Virol 2002 Mar;76(5):2298-305.
[63] Gillespie GM, Pinheiro S, Sayeid-Al-Jamee M, et al. CD8+ T cell responses to human immunodeficiency viruses type 2 (HIV-2) and type 1 (HIV-1) gag proteins are distinguishable by magnitude and breadth but not cellular phenotype. Eur J Immunol 2005 May;35(5):1445-53.
[64] Jaye A, Sarge-Njie R, Schim vdL, et al. No differences in cellular immune responses between asymptomatic HIV type 1- and type 2-infected Gambian patients. J Infect Dis 2004 Feb 1;189(3):498-505.
[65] Zheng NN, Kiviat NB, Sow PS, et al. Comparison of human immunodeficiency virus (HIV)-specific T-cell responses in HIV-1- and HIV-2-infected individuals in Senegal. J Virol 2004 Dec;78(24):13934-42.

28
[66] Duvall MG, Jaye A, Dong T, et al. Maintenance of HIV-specific CD4+ T cell help distinguishes HIV-2 from HIV-1 infection. J Immunol 2006 Jun 1;176(11):6973-81.
[67] Pinto LA, Covas MJ, Victorino RM. T-helper cross reactivity to viral recombinant proteins in HIV-2-infected patients. AIDS 1993 Oct;7(10):1389-91.
[68] Sousa AE, Chaves AF, Loureiro A, Victorino RM. Comparison of the frequency of interleukin (IL)-2-, interferon-gamma-, and IL-4-producing T cells in 2 diseases, human immunodeficiency virus types 1 and 2, with distinct clinical outcomes. J Infect Dis 2001 Sep 1;184(5):552-9.
[69] Jaleco AC, Covas MJ, Victorino RM. Analysis of lymphocyte cell death and apoptosis in HIV-2-infected patients. Clin Exp Immunol 1994 Nov;98(2):185-9.
[70] Azevedo-Pereira JM, Lourenco MH, Barin F, et al. Multicenter evaluation of a fully automated screening test, VIDAS HIV 1 + 2, for antibodies to human immunodeficiency virus types 1 and 2. J Clin Microbiol 1994 Oct;32(10):2559-63.
[71] Kannangai R, Ramalingam S, Prakash KJ, et al. A peptide enzyme linked immunosorbent assay (ELISA) for the detection of human immunodeficiency virus type-2 (HIV-2) antibodies: an evaluation on polymerase chain reaction (PCR) confirmed samples. J Clin Virol 2001 Aug;22(1):41-6.
[72] Gaines H, von Sydow M, Sonnerborg A, et al. Antibody response in primary human immunodeficiency virus infection. Lancet 1987 May 30;1(8544):1249-53.
[73] Tomaras GD, Haynes BF. HIV-1-specific antibody responses during acute and chronic HIV-1 infection. Curr Opin HIV AIDS 2009 Sep;4(5):373-9.
[74] Tomaras GD, Yates NL, Liu P, et al. Initial B-cell responses to transmitted human immunodeficiency virus type 1: virion-binding immunoglobulin M (IgM) and IgG antibodies followed by plasma anti-gp41 antibodies with ineffective control of initial viremia. J Virol 2008 Dec;82(24):12449-63.
[75] Russell MW, Lue C, van den Wall Bake AW, Moldoveanu Z, Mestecky J. Molecular heterogeneity of human IgA antibodies during an immune response. Clin Exp Immunol 1992 Jan;87(1):1-6.

29
[76] Barassi C, Lazzarin A, Lopalco L. CCR5-specific mucosal IgA in saliva and genital fluids of HIV-exposed seronegative subjects. Blood 2004 Oct 1;104(7):2205-6.
[77] Devito C, Broliden K, Kaul R, et al. Mucosal and plasma IgA from HIV-1-exposed uninfected individuals inhibit HIV-1 transcytosis across human epithelial cells. J Immunol 2000 Nov 1;165(9):5170-6.
[78] Devito C, Hinkula J, Kaul R, et al. Cross-clade HIV-1-specific neutralizing IgA in mucosal and systemic compartments of HIV-1-exposed, persistently seronegative subjects. J Acquir Immune Defic Syndr 2002 Aug 1;30(4):413-20.
[79] Ferre AL, Hunt PW, Critchfield JW, et al. Mucosal immune responses to HIV-1 in elite controllers: a potential correlate of immune control. Blood 2009 Apr 23;113(17):3978-89.
[80] Lehner T. Innate and adaptive mucosal immunity in protection against HIV infection. Vaccine 2003 Jun 1;21 Suppl 2:S68-S76.
[81] Lizeng Q, Skott P, Sourial S, et al. Serum immunoglobulin A (IgA)-mediated immunity in human immunodeficiency virus type 2 (HIV-2) infection. Virology 2003 Apr 10;308(2):225-32.
[82] Banerjee K, Klasse PJ, Sanders RW, et al. IgG subclass profiles in infected HIV type 1 controllers and chronic progressors and in uninfected recipients of Env vaccines. AIDS Res Hum Retroviruses 2010 Apr;26(4):445-58.
[83] Cavacini LA, Kuhrt D, Duval M, Mayer K, Posner MR. Binding and neutralization activity of human IgG1 and IgG3 from serum of HIV-infected individuals. AIDS Res Hum Retroviruses 2003 Sep;19(9):785-92.
[84] Rezza G, Fiorelli V, Dorrucci M, et al. The presence of anti-Tat antibodies is predictive of long-term nonprogression to AIDS or severe immunodeficiency: findings in a cohort of HIV-1 seroconverters. J Infect Dis 2005 Apr 15;191(8):1321-4.
[85] Humbert M, Dietrich U. The role of neutralizing antibodies in HIV infection. AIDS Rev 2006 Apr;8(2):51-9.
[86] Forthal DN, Moog C. Fc receptor-mediated antiviral antibodies. Curr Opin HIV AIDS 2009 Sep;4(5):388-93.
[87] Gomez-Roman VR, Patterson LJ, Venzon D, et al. Vaccine-elicited antibodies mediate antibody-dependent cellular cytotoxicity correlated with significantly reduced acute viremia in rhesus

30
macaques challenged with SIVmac251. J Immunol 2005 Feb 15;174(4):2185-9.
[88] Lambotte O, Ferrari G, Moog C, et al. Heterogeneous neutralizing antibody and antibody-dependent cell cytotoxicity responses in HIV-1 elite controllers. AIDS 2009 May 15;23(8):897-906.
[89] Klein JS, Webster A, Gnanapragasam PN, Galimidi RP, Bjorkman PJ. A dimeric form of the HIV-1 antibody 2G12 elicits potent antibody-dependent cellular cytotoxicity. AIDS 2010 Jul 17;24(11):1633-40.
[90] Ng CT, Jaworski JP, Jayaraman P, et al. Passive neutralizing antibody controls SHIV viremia and enhances B cell responses in infant macaques. Nat Med 2010 Oct;16(10):1117-9.
[91] Hessell AJ, Hangartner L, Hunter M, et al. Fc receptor but not complement binding is important in antibody protection against HIV. Nature 2007 Sep 6;449(7158):101-4.
[92] Forthal DN, Landucci G, Bream J, Jacobson LP, Phan TB, Montoya B. FcgammaRIIa genotype predicts progression of HIV infection. J Immunol 2007 Dec 1;179(11):7916-23.
[93] Hidajat R, Xiao P, Zhou Q, et al. Correlation of vaccine-elicited systemic and mucosal nonneutralizing antibody activities with reduced acute viremia following intrarectal simian immunodeficiency virus SIVmac251 challenge of rhesus macaques. J Virol 2009 Jan;83(2):791-801.
[94] Marasco WA, Sui J. The growth and potential of human antiviral monoclonal antibody therapeutics. Nat Biotechnol 2007 Dec;25(12):1421-34.
[95] Chung A, Rollman E, Johansson S, Kent SJ, Stratov I. The utility of ADCC responses in HIV infection. Curr HIV Res 2008 Nov;6(6):515-9.
[96] Baum LL. Role of humoral immunity in host defense against HIV. Curr HIV /AIDS Rep 2010 Feb;7(1):11-8.
[97] Lagenaur LA, Villarroel VA, Bundoc V, Dey B, Berger EA. sCD4-17b bifunctional protein: extremely broad and potent neutralization of HIV-1 Env pseudotyped viruses from genetically diverse primary isolates. Retrovirology 2010;7:11.

31
[98] Gray ES, Madiga MC, Moore PL, et al. Broad neutralization of human immunodeficiency virus type 1 mediated by plasma antibodies against the gp41 membrane proximal external region. J Virol 2009 Nov;83(21):11265-74.
[99] Binley J. Specificities of broadly neutralizing anti-HIV-1 sera. Curr Opin HIV AIDS 2009 Sep;4(5):364-72.
[100] Sather DN, Armann J, Ching LK, et al. Factors associated with the development of cross-reactive neutralizing antibodies during human immunodeficiency virus type 1 infection. J Virol 2009 Jan;83(2):757-69.
[101] van Gils MJ, Euler Z, Schweighardt B, Wrin T, Schuitemaker H. Prevalence of cross-reactive HIV-1-neutralizing activity in HIV-1-infected patients with rapid or slow disease progression. AIDS 2009 Nov 27;23(18):2405-14.
[102] Cao J, Sullivan N, Desjardin E, et al. Replication and neutralization of human immunodeficiency virus type 1 lacking the V1 and V2 variable loops of the gp120 envelope glycoprotein. J Virol 1997 Dec;71(12):9808-12.
[103] Cecilia D, Kleeberger C, Munoz A, Giorgi JV, Zolla-Pazner S. A longitudinal study of neutralizing antibodies and disease progression in HIV-1-infected subjects. J Infect Dis 1999 Jun;179(6):1365-74.
[104] Zhang YJ, Fracasso C, Fiore JR, et al. Augmented serum neutralizing activity against primary human immunodeficiency virus type 1 (HIV-1) isolates in two groups of HIV-1-infected long-term nonprogressors. J Infect Dis 1997 Nov;176(5):1180-7.
[105] Bailey JR, Williams TM, Siliciano RF, Blankson JN. Maintenance of viral suppression in HIV-1-infected HLA-B*57+ elite suppressors despite CTL escape mutations. J Exp Med 2006 May 15;203(5):1357-69.
[106] Harrer T, Harrer E, Kalams SA, et al. Strong cytotoxic T cell and weak neutralizing antibody responses in a subset of persons with stable nonprogressing HIV type 1 infection. AIDS Res Hum Retroviruses 1996 May 1;12(7):585-92.
[107] Jolly PE, Weiss HL. Neutralization and enhancement of HIV-1 infection by sera from HIV-1 infected individuals who progress to disease at different rates. Virology 2000 Jul 20;273(1):52-9.
[108] Bartolo I, Camacho R, Barroso H, Bezerra V, Taveira N. Rapid clinical progression to AIDS and death in a persistently seronegative

32
HIV-1 infected heterosexual young man. AIDS 2009 Nov 13;23(17):2359-62.
[109] Weiss RA, Clapham PR, Weber JN, et al. HIV-2 antisera cross-neutralize HIV-1. AIDS 1988 Apr;2(2):95-100.
[110] Schulz TF, Whitby D, Hoad JG, Corrah T, Whittle H, Weiss RA. Biological and molecular variability of human immunodeficiency virus type 2 isolates from The Gambia. J Virol 1990 Oct;64(10):5177-82.
[111] Bjorling E, Scarlatti G, von Gegerfelt A, et al. Autologous neutralizing antibodies prevail in HIV-2 but not in HIV-1 infection. Virology 1993 Mar;193(1):528-30.
[112] Shi Y, Brandin E, Vincic E, et al. Evolution of human immunodeficiency virus type 2 coreceptor usage, autologous neutralization, envelope sequence and glycosylation. J Gen Virol 2005 Dec;86(Pt 12):3385-96.
[113] Mascola JR, Montefiori DC. The role of antibodies in HIV vaccines. Annu Rev Immunol 2010 Mar;28:413-44.
[114] de Silva TI, Cotten M, Rowland-Jones SL. HIV-2: the forgotten AIDS virus. Trends Microbiol 2008 Dec;16(12):588-95.
[115] Reeves JD, Hibbitts S, Simmons G, et al. Primary human immunodeficiency virus type 2 (HIV-2) isolates infect CD4-negative cells via CCR5 and CXCR4: comparison with HIV-1 and simian immunodeficiency virus and relevance to cell tropism in vivo. J Virol 1999 Sep;73(9):7795-804.
[116] Tamalet C, Simon F, Dhiver C, et al. Autologous neutralizing antibodies and viral load in HIV-2-infected individuals. AIDS 1995 Jan;9(1):90-1.
[117] Rodriguez SK, Sarr AD, MacNeil A, et al. Comparison of heterologous neutralizing antibody responses of human immunodeficiency virus type 1 (HIV-1)- and HIV-2-infected Senegalese patients: distinct patterns of breadth and magnitude distinguish HIV-1 and HIV-2 infections. J Virol 2007 May;81(10):5331-8.
[118] Chenna R, Sugawara H, Koike T, et al. Multiple sequence alignment with the Clustal series of programs. Nucleic Acids Res 2003 Jul 1;31(13):3497-500.

33
[119] O'Connell KA, Bailey JR, Blankson JN. Elucidating the elite: mechanisms of control in HIV-1 infection. Trends Pharmacol Sci 2009 Dec;30(12):631-7.
[120] Deeks SG, Walker BD. Human immunodeficiency virus controllers: mechanisms of durable virus control in the absence of antiretroviral therapy. Immunity 2007 Sep;27(3):406-16.
[121] Laakso MM, Lee FH, Haggarty B, et al. V3 loop truncations in HIV-1 envelope impart resistance to coreceptor inhibitors and enhanced sensitivity to neutralizing antibodies. PLoS Pathog 2007 Aug 24;3(8):e117.
[122] Davis KL, Gray ES, Moore PL, et al. High titer HIV-1 V3-specific antibodies with broad reactivity but low neutralizing potency in acute infection and following vaccination. Virology 2009 May 10;387(2):414-26.
[123] Pikora CA. Glycosylation of the ENV spike of primate immunodeficiency viruses and antibody neutralization. Curr HIV Res 2004 Jul;2(3):243-54.
[124] Burton DR, Desrosiers RC, Doms RW, et al. HIV vaccine design and the neutralizing antibody problem. Nat Immunol 2004 Mar;5(3):233-6.
[125] Spenlehauer C, Saragosti S, Fleury HJ, Kirn A, Aubertin AM, Moog C. Study of the V3 loop as a target epitope for antibodies involved in the neutralization of primary isolates versus T-cell-line-adapted strains of human immunodeficiency virus type 1. J Virol 1998 Dec;72(12):9855-64.
[126] Wyatt R, Kwong PD, Desjardins E, et al. The antigenic structure of the HIV gp120 envelope glycoprotein. Nature 1998 Jun 18;393(6686):705-11.
[127] Gorny MK, Williams C, Volsky B, et al. Human monoclonal antibodies specific for conformation-sensitive epitopes of V3 neutralize human immunodeficiency virus type 1 primary isolates from various clades. J Virol 2002 Sep;76(18):9035-45.
[128] Pinter A. Roles of HIV-1 Env variable regions in viral neutralization and vaccine development. Curr HIV Res 2007 Nov;5(6):542-53.
[129] Mbah HA, Burda S, Gorny MK, et al. Effect of soluble CD4 on exposure of epitopes on primary, intact, native human

34
immunodeficiency virus type 1 virions of different genetic clades. J Virol 2001 Aug;75(16):7785-8.
[130] Wyatt R, Moore J, Accola M, Desjardin E, Robinson J, Sodroski J. Involvement of the V1/V2 variable loop structure in the exposure of human immunodeficiency virus type 1 gp120 epitopes induced by receptor binding. J Virol 1995 Sep;69(9):5723-33.
[131] Sullivan N, Sun Y, Sattentau Q, et al. CD4-Induced conformational changes in the human immunodeficiency virus type 1 gp120 glycoprotein: consequences for virus entry and neutralization. J Virol 1998 Jun;72(6):4694-703.
[132] Losman B, Bolmstedt A, Schonning K, et al. Protection of neutralization epitopes in the V3 loop of oligomeric human immunodeficiency virus type 1 glycoprotein 120 by N-linked oligosaccharides in the V1 region. AIDS Res Hum Retroviruses 2001 Jul 20;17(11):1067-76.
[133] Ly A, Stamatatos L. V2 loop glycosylation of the human immunodeficiency virus type 1 SF162 envelope facilitates interaction of this protein with CD4 and CCR5 receptors and protects the virus from neutralization by anti-V3 loop and anti-CD4 binding site antibodies. J Virol 2000 Aug;74(15):6769-76.
[134] Schonning K, Jansson B, Olofsson S, Nielsen JO, Hansen JS. Resistance to V3-directed neutralization caused by an N-linked oligosaccharide depends on the quaternary structure of the HIV-1 envelope oligomer. Virology 1996 Apr 1;218(1):134-40.
[135] Barnett SW, Lu S, Srivastava I, et al. The ability of an oligomeric human immunodeficiency virus type 1 (HIV-1) envelope antigen to elicit neutralizing antibodies against primary HIV-1 isolates is improved following partial deletion of the second hypervariable region. J Virol 2001 Jun;75(12):5526-40.
[136] Kim YB, Han DP, Cao C, Cho MW. Immunogenicity and ability of variable loop-deleted human immunodeficiency virus type 1 envelope glycoproteins to elicit neutralizing antibodies. Virology 2003 Jan 5;305(1):124-37.
[137] Srivastava IK, VanDorsten K, Vojtech L, Barnett SW, Stamatatos L. Changes in the immunogenic properties of soluble gp140 human immunodeficiency virus envelope constructs upon partial deletion of the second hypervariable region. J Virol 2003 Feb;77(4):2310-20.
[138] Plantier JC, Damond F, Souquieres S, Brun-Vezinet F, Simon F, Barin F. V3 serological subtyping of human immunodeficiency

35
virus type 2 infection is not relevant. J Clin Microbiol 2001 Oct;39(10):3803-7.
[139] Bjorling E, Chiodi F, Utter G, Norrby E. Two neutralizing domains in the V3 region in the envelope glycoprotein gp125 of HIV type 2. J Immunol 1994 Feb 15;152(4):1952-9.
[140] Matsushita S, Matsumi S, Yoshimura K, Morikita T, Murakami T, Takatsuki K. Neutralizing monoclonal antibodies against human immunodeficiency virus type 2 gp120. J Virol 1995 Jun;69(6):3333-40.
[141] McKnight A, Shotton C, Cordell J, Jones I, Simmons G, Clapham PR. Location, exposure, and conservation of neutralizing and nonneutralizing epitopes on human immunodeficiency virus type 2 SU glycoprotein. J Virol 1996 Jul;70(7):4598-606.
[142] Babas T, Benichou S, Guetard D, Montagnier L, Bahraoui E. Specificity of antipeptide antibodies produced against V2 and V3 regions of the external envelope of human immunodeficiency virus type 2. Mol Immunol 1994 Apr;31(5):361-9.
[143] Robert-Guroff M, Aldrich K, Muldoon R, et al. Cross-neutralization of human immunodeficiency virus type 1 and 2 and simian immunodeficiency virus isolates. J Virol 1992 Jun;66(6):3602-8.
[144] Sourial S, Nilsson C, Warnmark A, Achour A, Harris RA. Deletion of the V1/V2 region does not increase the accessibility of the V3 region of recombinant gp125. Curr HIV Res 2006 Apr;4(2):229-37.
[145] Bhattacharya J, Peters PJ, Clapham PR. Human immunodeficiency virus type 1 envelope glycoproteins that lack cytoplasmic domain cysteines: impact on association with membrane lipid rafts and incorporation onto budding virus particles. J Virol 2004 May;78(10):5500-6.
[146] Kwong PD, Doyle ML, Casper DJ, et al. HIV-1 evades antibody-mediated neutralization through conformational masking of receptor-binding sites. Nature 2002 Dec 12;420(6916):678-82.
[147] Mascola JR, Montefiori DC. HIV-1: nature's master of disguise. Nat Med 2003 Apr;9(4):393-4.
[148] Walker LM, Simek MD, Priddy F, et al. A limited number of antibody specificities mediate broad and potent serum neutralization in selected HIV-1 infected individuals. PLoS Pathog 2010 Aug;6(8).

36
[149] Pantophlet R, Burton DR. GP120: target for neutralizing HIV-1 antibodies. Annu Rev Immunol 2006;24:739-69.
[150] Albert J, Abrahamsson B, Nagy K, et al. Rapid development of isolate-specific neutralizing antibodies after primary HIV-1 infection and consequent emergence of virus variants which resist neutralization by autologous sera. AIDS 1990 Feb;4(2):107-12.
[151] Pilgrim AK, Pantaleo G, Cohen OJ, et al. Neutralizing antibody responses to human immunodeficiency virus type 1 in primary infection and long-term-nonprogressive infection. J Infect Dis 1997 Oct;176(4):924-32.
[152] Richman DD, Wrin T, Little SJ, Petropoulos CJ. Rapid evolution of the neutralizing antibody response to HIV type 1 infection. Proc Natl Acad Sci U S A 2003 Apr 1;100(7):4144-9.
[153] Moog C, Fleury HJ, Pellegrin I, Kirn A, Aubertin AM. Autologous and heterologous neutralizing antibody responses following initial seroconversion in human immunodeficiency virus type 1-infected individuals. J Virol 1997 May;71(5):3734-41.
[154] Mahalanabis M, Jayaraman P, Miura T, et al. Continuous viral escape and selection by autologous neutralizing antibodies in drug-naive human immunodeficiency virus controllers. J Virol 2009 Jan;83(2):662-72.
[155] Raska M, Novak J. Involvement of envelope-glycoprotein glycans in HIV-1 biology and infection. Arch Immunol Ther Exp (Warsz ) 2010 Jun;58(3):191-208.
[156] Quinones-Kochs MI, Buonocore L, Rose JK. Role of N-linked glycans in a human immunodeficiency virus envelope glycoprotein: effects on protein function and the neutralizing antibody response. J Virol 2002 May;76(9):4199-211.
[157] Draenert R, Allen TM, Liu Y, et al. Constraints on HIV-1 evolution and immunodominance revealed in monozygotic adult twins infected with the same virus. J Exp Med 2006 Mar 20;203(3):529-39.
[158] Frost SD, Wrin T, Smith DM, et al. Neutralizing antibody responses drive the evolution of human immunodeficiency virus type 1 envelope during recent HIV infection. Proc Natl Acad Sci U S A 2005 Dec 20;102(51):18514-9.
[159] Chackerian B, Rudensey LM, Overbaugh J. Specific N-linked and O-linked glycosylation modifications in the envelope V1 domain

37
of simian immunodeficiency virus variants that evolve in the host alter recognition by neutralizing antibodies. J Virol 1997 Oct;71(10):7719-27.
[160] Pinter A, Honnen WJ, He Y, Gorny MK, Zolla-Pazner S, Kayman SC. The V1/V2 domain of gp120 is a global regulator of the sensitivity of primary human immunodeficiency virus type 1 isolates to neutralization by antibodies commonly induced upon infection. J Virol 2004 May;78(10):5205-15.
[161] Rong R, Bibollet-Ruche F, Mulenga J, Allen S, Blackwell JL, Derdeyn CA. Role of V1V2 and other human immunodeficiency virus type 1 envelope domains in resistance to autologous neutralization during clade C infection. J Virol 2007 Feb;81(3):1350-9.
[162] Sagar M, Wu X, Lee S, Overbaugh J. Human immunodeficiency virus type 1 V1-V2 envelope loop sequences expand and add glycosylation sites over the course of infection, and these modifications affect antibody neutralization sensitivity. J Virol 2006 Oct;80(19):9586-98.
[163] Gray ES, Moore PL, Choge IA, et al. Neutralizing antibody responses in acute human immunodeficiency virus type 1 subtype C infection. J Virol 2007 Jun;81(12):6187-96.
[164] Rong R, Li B, Lynch RM, et al. Escape from autologous neutralizing antibodies in acute/early subtype C HIV-1 infection requires multiple pathways. PLoS Pathog 2009 Sep;5(9):e1000594.
[165] Bosch KA, Rainwater S, Jaoko W, Overbaugh J. Temporal analysis of HIV envelope sequence evolution and antibody escape in a subtype A-infected individual with a broad neutralizing antibody response. Virology 2010 Mar 1;398(1):115-24.
[166] Parren PW, Wang M, Trkola A, et al. Antibody neutralization-resistant primary isolates of human immunodeficiency virus type 1. J Virol 1998 Dec;72(12):10270-4.
[167] Girard MP, Osmanov SK, Kieny MP. A review of vaccine research and development: the human immunodeficiency virus (HIV). Vaccine 2006 May 8;24(19):4062-81.
[168] Barouch DH. Challenges in the development of an HIV-1 vaccine. Nature 2008 Oct 2;455(7213):613-9.
[169] Alter G, Moody MA. The humoral response to HIV-1: new insights, renewed focus. J Infect Dis 2010 Oct 15;202 Suppl 2:S315-S322.

38
[170] Bansal GP, Malaspina A, Flores J. Future paths for HIV vaccine research: Exploiting results from recent clinical trials and current scientific advances. Curr Opin Mol Ther 2010 Feb;12(1):39-46.
[171] Bjorling E, Broliden K, Bernardi D, et al. Hyperimmune antisera against synthetic peptides representing the glycoprotein of human immunodeficiency virus type 2 can mediate neutralization and antibody-dependent cytotoxic activity. Proc Natl Acad Sci U S A 1991 Jul 15;88(14):6082-6.
[172] Gilljam G. Envelope glycoproteins of HIV-1, HIV-2, and SIV purified with Galanthus nivalis agglutinin induce strong immune responses. AIDS Res Hum Retroviruses 1993 May;9(5):431-8.
[173] Andersson S, Makitalo B, Thorstensson R, et al. Immunogenicity and protective efficacy of a human immunodeficiency virus type 2 recombinant canarypox (ALVAC) vaccine candidate in cynomolgus monkeys. J Infect Dis 1996 Nov;174(5):977-85.
[174] Franchini G, Robert-Guroff M, Tartaglia J, et al. Highly attenuated HIV type 2 recombinant poxviruses, but not HIV-2 recombinant Salmonella vaccines, induce long-lasting protection in rhesus macaques. AIDS Res Hum Retroviruses 1995 Aug;11(8):909-20.
[175] Myagkikh M, Alipanah S, Markham PD, et al. Multiple immunizations with attenuated poxvirus HIV type 2 recombinants and subunit boosts required for protection of rhesus macaques. AIDS Res Hum Retroviruses 1996 Jul 20;12(11):985-92.
[176] Patterson LJ, Peng B, Abimiku AG, et al. Cross-protection in NYVAC-HIV-1-immunized/HIV-2-challenged but not in NYVAC-HIV-2-immunized/SHIV-challenged rhesus macaques. AIDS 2000 Nov 10;14(16):2445-55.
[177] Luke W, Voss G, Stahl-Hennig C, et al. Protection of cynomolgus macaques (Macaca fascicularis) against infection with the human immunodeficiency virus type 2 strain ben (HIV-2ben) by immunization with the virion-derived envelope glycoprotein gp130. AIDS Res Hum Retroviruses 1993 May;9(5):387-94.
[178] Vogt G, le Grand R, Vaslin B, et al. Heterologous HIV-2 challenge of rhesus monkeys immunized with recombinant vaccinia viruses and purified recombinant HIV-2 proteins. Vaccine 1995 Feb;13(2):202-8.
[179] Locher CP, Witt SA, Ashlock BM, et al. Human immunodeficiency virus type 2 DNA vaccine provides partial

39
protection from acute baboon infection. Vaccine 2004 Jun 2;22(17-18):2261-72.
[180] Peeters M, Courgnaud V, Abela B, et al. Risk to human health from a plethora of simian immunodeficiency viruses in primate bushmeat. Emerg Infect Dis 2002 May;8(5):451-7.
[181] Locher CP, Witt SA, Herndier BG, Tenner-Racz K, Racz P, Levy JA. Baboons as an animal model for human immunodeficiency virus pathogenesis and vaccine development. Immunol Rev 2001 Oct;183:127-40.
[182] Chakraborty H, Sen PK, Helms RW, et al. Viral burden in genital secretions determines male-to-female sexual transmission of HIV-1: a probabilistic empiric model. AIDS 2001 Mar 30;15(5):621-7.
[183] Gray RH, Wawer MJ, Brookmeyer R, et al. Probability of HIV-1
transmission per coital act in monogamous, heterosexual, HIV-1-
discordant couples in Rakai, Uganda. Lancet 2001 Apr
14;357(9263):1149-53.

40

CAPÍTULO II
Objectivos e Plano de Trabalho

42

43
Objectivos e Plano de Trabalho
Em contraste com a quase generalidade dos indivíduos infectados
por VIH-1, a maior parte dos indivíduos infectados por VIH-2 não
tem carga viral plasmática detectável e não progridem para SIDA
mesmo na ausência de tratamento antiretrovírico. Os determinantes
do aparente equilíbrio existente entre o VIH-2 e o hospedeiro são
ainda desconhecidos e a sua compreensão poderá contribuir para o
desenvolvimento de uma vacina.
Pensa-se que a resposta imunitária humoral contribui directamente
para o controlo da replicação na infecção VIH-2. De facto, os poucos
estudos existentes, todos efectuados em doentes crónicos, indicam
que a maioria dos indivíduos infectados por VIH-2 produz anticorpos
neutralizantes de largo espectro. Contudo, existe ainda muita
controvérsia sobre o exacto papel destes anticorpos in vivo uma vez
que nos doentes VIH-2 a correlação inversa entre o título de
anticorpos neutralizantes e a carga viral plasmática é mais a
excepção do que a regra.
O papel dos anticorpos neutralizantes na infecção VIH-2 poderá ser
clarificado, analisando a cinética evolutiva da resposta humoral anti-
VIH-2 ao longo da infecção e caracterizando o seu impacto na
evolução do vírus. Neste contexto, o primeiro objectivo desta tese foi
caracterizar, no decurso da infecção VIH-2 aguda e crónica, a
natureza e dinâmica da resposta humoral neutralizante e não
neutralizante. O segundo objectivo foi caracterizar e analisar o
impacto destes anticorpos na evolução molecular e fenotípica do VIH-
2. O terceiro e último objectivo foi analisar, em modelo animal, o
potencial neutralizante de novos imunogénios derivados do Env do
VIH-2.
Para cumprir o primeiro objectivo, uma vez que os anticorpos
neutralizantes bem como grande parte dos não neutralizantes têm
como alvo epitopos localizados no invólucro, decidiu-se caracterizar
apenas a resposta humoral dirigida contra as duas glicoproteínas do
invólucro, gp125 e gp36. Foram identificadas na literatura as duas
regiões potencialmente mais antigénicas do invólucro do VIH-2 e
desenhou-se dois polipéptidos contendo, presumivelmente, estas
regiões. A primeira fase experimental desta tese destinou-se à
clonagem, expressão, purificação e análise da antigenicidade destes
dois novos polipéptidos (designados rpC3-C3 e rgp36). Os métodos
escolhidos para a análise da antigenicidade foram o ensaio
imunoenzimático ELISA e o Western blot e as amostras de plasma

44
utilizadas neste processo foram colhidas de um número significativo
(≥100) de doentes infectados por VIH-2 e/ou por VIH-1, e também de
um número igualmente significativo de indivíduos não infectados
(Capítulo III).
Para investigar a natureza e dinâmica da resposta humoral no
decurso da infecção por VIH-2 (Objectivo 1), foram seleccionadas
duas crianças infectadas por via perinatal (infecção aguda por VIH-2)
e um conjunto significativo de doentes com infecção crónica
apresentando diferentes graus de comprometimento imunológico e
clínico. Estes doentes foram seguidos durante um período de 3-4
anos, em média. A análise qualitativa dos anticorpos IgG e IgA anti-
VIH-2 baseou-se na medição da sua reactividade específica e avidez
para os dois antigénios do invólucro (rpC2-C3 e rgp36); o título e a
concentração de anticorpos no plasma constituíram os parâmetros
quantitativos analisados (Capítulo IV). A resposta neutralizante foi
investigada com anticorpos IgG purificados do plasma e vírus
autólogos e heterólogos isolados dos doentes (Capítulo VI). Todos os
isolados foram classificados quanto ao seu tropismo R5 ou X4 de
forma a permitir investigar também a associação entre neutralização
e tropismo na infecção VIH-2 (Objectivo 2).
O impacto dos anticorpos neutralizantes e não neutralizantes na
evolução molecular do VIH-2 (Objectivo 2) foi investigado a partir de
sequências clonais do Env (regiões C2, V3 e C3) dos isolados de um
subgrupo de doentes seguidos ao longo de alguns anos. Os
parâmetros analisados, seleccionados a partir de trabalhos análogos
efectuados no VIH-1, foram os seguintes: diversidade nucleotídica e
aminoacídica, taxa de evolução anual, grau de glicosilação, pressão
positiva, e dimensão e carga da região V3. Para este trabalho foram
utilizados métodos filogenéticos e moleculares previamente validados
em estudos efectuados em doentes infectados por VIH-1 (Capítulo V).
O último objectivo desta tese foi produzir e analisar a nível pré-
clínico o potencial neutralizante de novos imunogénios baseados no
Env do VIH-2. Neste trabalho pretendeu-se contribuir para tentar
ultrapassar o principal obstáculo à produção de uma vacina contra o
VIH: a inexistência de imunogénios capazes de induzir a produção de
anticorpos neutralizantes de largo espectro contra múltiplos
isolados. O isolado primário de referência VIH-2ALI (tropismo R5) foi
seleccionado para a partir dele se exprimir as glicoproteínas do
invólucro num vector vivo, o vírus da vacina. Com base em estudos
anteriores, o animal seleccionado para realizar os ensaios de
imunogenicidade foi o murganho Balb/C e a modalidade de
imunização o prime-boosting em que o prime foi efectuado com vírus

45
da vacina a exprimir a gp125 do VIH-2ALI e o boost foi efectuado com
a proteína rpC2-C3, cuja elevada antigenicidade tinha sido
comprovada no Capítulo III. A resposta neutralizante gerada por
estes novos imunogénios irá ser analisada contra o extenso painel de
isolados virais VIH-2 obtidos nas primeiras fases deste trabalho
(Capítulo III) onde se incluíram isolados com tropismo R5 e X4.
Conforme previsto no Decreto-Lei 388/70, art. 8º, parágrafo 2, parte
integral dos resultados apresentados encontra-se publicada ou
submetida para publicação nos seguintes artigos:
José Maria Marcelino, Helena Barroso, Fátima Gonçalves, Sofia
Marques Silva, Carlos Novo, Perpétua Gomes, Ricardo Camacho, and
Nuno Taveira. Use of a New Dual-Antigen Enzyme-Linked
Immunosorbent Assay To Detect and Characterize the Human
Antibody Response to the Human Immunodeficiency Virus Type 2
Envelope gp125 and gp36 Glycoproteins. Journal of Clinical
Microbiology, 2006, 44: 607–611.
José Maria Marcelino, Charlotta Nilsson, Helena Barroso, Perpétua
Gomes, Pedro Borrego, Fernando Maltez, Lino Rosado, Manuela
Doroana, Francisco Antunes and Nuno Taveira. Envelope-specific
antibody response in HIV-2 infection: C2V3C3-specific IgG response
is associated with disease progression. AIDS, 2008, 22: 2257–2265.
Pedro Borrego, José Maria Marcelino, Cheila Rocha, Manuela
Doroana, Francisco Antunes, Fernando Maltez, Perpétua Gomes,
Carlos Novo, Helena Barroso and Nuno Taveira. The role of the
humoral immune response in the molecular evolution of the envelope
C2, V3 and C3 regions in chronically HIV-2 infected patients.
Retrovirology, 2008, 5:78.
José Maria Marcelino, Pedro Borrego, Charlotta Nilsson, Helena
Barroso, Manuela Doroana, Francisco Antunes, Carlos Novo, and
Nuno Taveira. Escape from neutralization is a frequent event in HIV-
2 infection and is strongly associated with X4 tropism. (Submitted).
José Maria Marcelino, Pedro Borrego, Cheila Rocha, Helena
Barroso, Alexandre Quintas, Carlos Novo and Nuno Taveira. Potent
and broadly reactive HIV-2 neutralizing antibodies elicited by a
Vaccinia virus vector-prime C2V3C3 polypeptide boost immunization
strategy. J Virol. 2010, 84: 12429-12436.

46

CAPÍTULO III
Teste de ELISA específico para o VIH-2
(ELISA-VIH2).

48

49
Desenvolvimento de um novo teste imunoenzimático
específico para o VIH-2 (ELISA-VIH-2)
Publicação: Use of a New Dual-Antigen Enzyme-Linked
Immunosorbent Assay To Detect and Characterize the
Human Antibody Response to the Human
Immunodeficiency Virus Type 2 Envelope gp125 and
gp36 Glycoproteins.
José Maria Marcelino, Helena Barroso, Fátima
Gonçalves, Sofia Marques Silva, Carlos Novo, Perpétua
Gomes, Ricardo Camacho, and Nuno Taveira.
Journal of Clinical Microbiology, 2006, 44: 607–611.
Sumário
Foi desenvolvido um novo teste imunoenzimático de duplo antigénio
específico para proteínas do invólucro do vírus da imunodeficiência
humana do tipo 2 (VIH-2), ELISA-VIH2, utilizando dois novos
polipeptídeos recombinantes, rpC2-C3 e rgp36, derivados do
invólucro do VIH-2. O desempenho do diagnóstico foi determinado
com amostras VIH-2, VIH-1, e VIH-1/2. Ambos os polipeptídeos
mostraram 100% de especificidade clínica. A sensibilidade clínica foi
de 100% para o rgp36 e 93,4% para o rpC2-C3. O teste ELISA-VIH2
pode ser útil para diagnosticar e confirmar a infecção pelo VIH-2.

50

51
Use of a New Dual-Antigen Enzyme-Linked Immunosorbent
Assay To Detect and Characterize the Human Antibody
Response to the Human Immunodeficiency Virus Type 2
Envelope gp125 and gp36 Glycoproteins.
ABSTRACT
A dual-antigen enzyme-linked immunosorbent assay specific for
human immunodeficiency virus type 2 (HIV-2) envelope proteins,
ELISA-HIV2, was developed with two new recombinant polypeptides,
rpC2-C3 and rgp36, derived from the HIV-2 envelope. The diagnostic
performance was determined with HIV-2, HIV-1, and HIV-1/2
samples. Both polypeptides showed 100% specificity. Clinical
sensitivity was 100% for rgp36 and 93.4% for rpC2-C3. ELISA-HIV2
may be used for the specific diagnosis and confirmation of HIV-2
infection.

52

53
Human immunodeficiency virus type 2 (HIV-2), the second AIDS
virus isolated from West African patients in 1985 (8), is now present
in all continents (20, 21, 23). The highest prevalence of HIV-2 in
West Africa is found in Guinea-Bissau, where prevalence rates of
between 5 and 10% of the adult urban population have been
reported (39). The highest prevalence of HIV-2 outside West Africa is
found in Portugal, where a prevalence rate of 3.4% has been reported
among AIDS cases (9).
Six immunogenic regions were identified in the HIV-2 envelope
glycoproteins: three in gp125 (amino acids 234 to 248 in C2, 296 to
337 in V3, and 472 to 507 in C5) and three in the gp36 ectodomain
(amino acids 573 to 595, 634 to 649, and 644 to 658) (11, 13, 18, 27,
30, 34, 40, 50). The gp36 ectodomain is highly conserved and elicits
a type-specific antibody response (13, 33). Hence, most licensed
diagnostic assays incorporate gp36-derived antigens to detect HIV-2-
specific antibodies (1, 4, 12, 28, 29, 38, 42, 45, 48). The sensitivity of
these assays to detect HIV-2 seroconversions has not been formally
tested. However, the sensitivity of several fourth-generation HIV1/2
assays was low with diluted HIV-2-positive samples (29), suggesting
that some screening assays may not detect low levels of HIV-2
antibodies (32). The reduced sensitivity of these kits may be caused
by inappropriate antigen selection and/or reduced antibody levels in
the HIV-2 patients (19, 26, 45).
It is important to differentiate between single infection with either
HIV-1 or HIV-2 and dual infection. Dual HIV-1 and HIV-2
seroreactivity is relatively frequent in countries where both HIV-1
and HIV-2 are endemic, such as Portugal (1.4%), Guinea-Bissau
(0.7%), Senegal (0.4%), and India (up to 2%) (9, 17, 24, 35). However,
the true rate of dual infections in these countries is generally
unknown. This is in part due to the lack of sensitive and specific
HIV-2 antibody tests. In fact, only two enzyme-linked
immunosorbent assays (ELISAs) of low specificity (92%) are currently
available for the diagnosis of HIV-2 infection, both of which use the
same viral lysate antigen (2, 7). Most often, reactivity with gp36- or
gp125-derived antigens (peptides or recombinant proteins)
incorporated into Western blot (WB) and immunoblot assays is used
to distinguish between HIV-2 and HIV-1 infections (41). However, the
sensitivity of these tests is generally low, and serological
crossreactivity between the HIV-1 and HIV-2 Env glycoproteins has
been described, which may complicate the final diagnosis (10, 37,
49).
In this study, we produced a new HIV-2 ELISA (ELISAHIV2) using
two new recombinant proteins, rgp36 and rpC2-C3, derived from the
reference primary isolate HIV-2ALI (44). Using pSK7.3 plasmid as a

54
template, which contains the HIV-2ALI env gene (44), a PCR was
performed with primers Hepit 11 (5’-TTT AGATACTGTGCACC-3’) and
Hepit 12 (5’-TTAGTCCAC ATATATAC-3’) to obtain a C2-C3 env
fragment with 497 bp (positions 661 to 1157 in HIV-2 ALI env). The
thermal cycling conditions were as follows: denaturation at 94°C for
1 min, annealing 60°C for 1 min, and extension at 72°C for 1 min for
45 cycles. Another PCR was performed with primers Hepit 15 (5’-
GGCACGGCAGCTTTAACGC-3’) and Hepit 17 (5’-GTC
CCTGCAGTTATTTTTGTAGTTCATATG-3) to obtain a gp36 fragment
with 385 bp (positions 1578 to 1963 in HIV- 2ALI env). The thermal
cycling conditions were as follows: denaturation at 94°C for 1 min,
annealing at 65°C for 1 min, and extension at 72°C for 1 min for 40
cycles. The resulting fragments were cloned into the bacterial
expression vector pTrcHis (Invitrogen), generating recombinant
plasmids pTrcC2-C3 and pTrcgp36. The expression of both
recombinant polypeptides rpC2-C3 and rgp36 in Escherichia coli
strain TOP10 was induced with isopropyl--D-thiogalactopyranoside
following the instructions from the manufacturer. Purification of the
histidinated rgp36 and rpC2-C3 polypeptides was done using a fast
protein liquid chromatography system (Pharmacia). The purified
recombinant polypeptides were analyzed by sodium dodecyl sulfate-
12% polyacrylamide gel electrophoresis under reducing conditions to
determine the size of the fusion proteins. Quantification of the
purified proteins was done with the Bio-Rad protein assay. The
recombinant histidinated polypeptides rgp36 and rpC2-C3 were
purified to 95% homogeneity, and final concentrations of 7 and 3.4
mg/liter were obtained for rgp36 and rpC2-C3, respectively.
A microplate ELISA, ELISA-HIV2, was developed using rgp36 and
rpC2-C3 polypeptides as independent capture antigens. Polystyrene
immune module microwells (Maxisorp; Nalgen Nunc International)
were independently coated (100 l/well) with each recombinant
polypeptide at a concentration of 2.5 lg/ml in 0.05 M bicarbonate
buffer, pH 9.4, and incubated overnight at 4°C. After one wash with
0.01 M Tris and 0.15 M NaCl, pH 7.4 (TBS), microwells were blocked
with 1% gelatin (Bio-Rad) for 1 h and washed twice with TBS buffer.
One hundred milliliters of a 1/100 dilution of each HIV-positive and
negative plasma sample in TBS containing 0.05% Tween-20 (TBS-T),
0.1% gelatin, and 5% goat serum (Sigma-Aldrich) was added, and
this mixture was then incubated for 1 h at room temperature. After
five washes with TBS-T, a 1:2,000 dilution of goat anti-human
immunoglobulin G (Fc specific) conjugated to alkaline phosphatase
(Sigma-Aldrich) in TBS-T was added and incubated for 1 h at room
temperature. The color was developed using p-nitrophenylphosphate

55
tablets (Sigma-Aldrich) as a chromogenic substrate, and the optical
density (OD) was measured with an automated LP 400 microplate
reader (Bio-Rad) at 405 nm against a reference wavelength of 620
nm. The clinical cutoff value of the assay, calculated as the mean OD
value of HIV-seronegative samples more 3 times the standard
deviation [SD], was determined using samples from healthy HIV-
seronegative subjects (n = 60). The results of the assay are expressed
quantitatively as ODclinical sample/ODcut-off (S/CO) ratios. For
ratio values of >1, the sample is considered seroreactive.
The clinical specificity of ELISA-HIV2 was evaluated against a panel
of plasma samples from healthy HIV-seronegative subjects. These
included samples from blood donors (n = 130) and from pregnant
women (n = 30). Two samples reacted weakly against rgp36 (mean
S/CO ratio, 1.21 [SD, 0.27]); eight samples reacted weakly against
rpC2-C3 (mean S/CO ratio, 1.18 [SD, 0.23]). Upon retesting in
duplicate, all samples gave negative results. Therefore, 100% clinical
specificity was obtained for both polypeptides. The 100% specificity
of the ELISA-HIV2 assay compares favorably to the specificity of the
two licensed HIV-2 serodiagnosis assays (<92%) (2, 7) and to the
specificity of most mixed HIV-1/HIV-2 assays (mean, 99%; range,
94.6% to 100% for assays based on recombinant proteins; mean,
98%; range 90.4% to 100% for assays based on synthetic peptides)
(1, 4, 5, 12, 14, 22, 28, 31, 38, 42, 43, 45, 48).
A panel of samples from 106 HIV-2-positive and 95 HIV-1-positive
patients was used to determine the clinical sensitivity of the ELISA-
HIV2 assay. HIV seropositivity was first determined by using the kit
VIDAS HIV DUO (Bio Merieux). Positive samples were subsequently
tested by Peptilav 1-2, an immunoblot assay containing a single
peptide antigen from the transmembrane glycoprotein of HIV-1 and
HIV-2. Depending on the Peptilav results, samples were further
tested by WB using the HIV-1 kit WB 2.2 and/or the HIV-2 kit New
LAV Blot II. Patients with samples reacting positive in HIV-1 and
HIV-2 Western blots were considered dually seroreactive. WB results
were considered positive when two Env bands with or without Gag
and/or Pol bands were present (16). WB results were considered
negative when no HIV-specific band was present and indeterminate
when any band pattern shown was not considered positive or
negative.
All 106 HIV-2 samples reacted with rgp36, and 99 (93.4%) samples
reacted also with rpC2-C3 (Fig. 1A and B). The 100% clinical
sensitivity and specificity obtained with rgp36 indicate that the
ELISA-HIV2 assay can be used in the serodiagnosis of HIV-2
infection. The mean S/CO ratio was significantly higher for the rgp36
antigen than that for rpC2-C3 (8.27 [SD, 1.49] versus 4.89 [SD,

56
2.51]; P < 0.0001). These results suggest that the gp36 ectodomain is
the immunodominant antigenic region in the HIV-2 envelope and are
consistent with previous studies showing that recombinant gp36
proteins derived from several laboratory strains of HIV-2 are highly
immunogenic (18, 40, 50). Most commercial and homemade ELISAs
report similar sensitivities using substantially more sera per reaction
compared to our assay (50 to 200 l versus 1 l) (38, 43, 48).
However, several fourth-generation mixed HIV-1/2 assays performed
poorly with diluted (up to 1:1,000) HIV-2 samples, suggesting that
FIG. 1. Patterns of reactivity of HIV plasma samples with rgp36 and
rpC2-C3. Reactivity of HIV-1 and HIV-2 samples with rgp36 (A) and
rpC2-C3 (B). (C) Low (LR) and high (HR) rpC2-C3 responders. S/CO,
ODsample/ODcutoff ratio. Reactivity to rgp36 and rpC2-C3 is
indicated by open ( ) and black (■) squares, respectively. The
horizontal solid line represents the cutoff value; samples with S/CO
values of ≥1 are considered reactive. The dotted line represents the
lower S/CO value obtained with HIV-2 samples for rgp36. Student’s t
test was used to compare mean S/CO OD values obtained for both
antigens.
they may not detect the low levels of antibodies present at
seroconversion and early infection (29). The higher sensitivity of the
ELISA-HIV2 assay suggests that it may permit improved detection of
HIV-2 seroconversions and recent infections. Testing of longitudinal

57
specimens from recently infected individuals would be needed to
support this claim. Such studies are, however, difficult to perform
due to the low incidence of HIV-2 infection (20).
The finding that 93.4% of the HIV-2 samples reacted also with the
rpC2-C3 polypeptide contrasts with the low immunoreactivity (below
81%) reported for recombinant proteins encoded by corresponding
sequences in HIV-2 strains SBL6669 (6), ROD (40), NIHZ (50), and
ST (18). One explanation for this discrepancy is that rpC2-C3 may
comprise epitopes which are more antigenic than the corresponding
regions in HIV-2 strains SBL6669, ROD, NIHZ, and ST, all of which
are laboratory- adapted isolates. Therefore, antibodies present in the
infected immune sera may recognize the HIV-2ALI antigen better.
HIV-2 patients could be clustered into high immune responders and
low immune responders according to the level of antibodies to rpC2-
C3 (Fig. 1C). Conflicting reports exist on the prognostic value of
gp120 antibody responses. Nevertheless, high gp120 binding
antibody titers were negatively correlated to immune functions and
viremia control in chronically HIV-1-infected patients (46). It will be
important to investigate the correlations between the titer of C2-C3
binding antibodies, viremia, and immune functions, including
neutralizing antibody response, in HIV-2 infection.
Antibodies to the envelope gp41 develop early in HIV-1 infection,
while antibodies to the V3 region of gp120 develop later in infection.
Therefore, the different antibody responses to rpC2-C3 may also be
due to the timing of infection (32, 36). Further testing of longitudinal
specimens from seroconverters will be needed to study the kinetics of
antibody responses to this envelope protein and to assess the
usefulness of this information to date the timing of HIV-2 infection.
All 95 HIV-1 samples analyzed with ELISA-HIV2 gave negative
results with rpC2-C3. Thirty-one (32.6%) samples crossreacted with
rgp36, but the reactivity was significantly weaker than that of HIV-2
samples (mean S/CO ratio, 2.42 [SD, 0.85] versus 8.27 [SD, 1.49]; P
≤ 0.0001) (Fig. 1A). These results suggested that the ELISA-HIV2
assay could be useful to discriminate between HIV-1 and HIV-2
infection in individuals with dual-positive serology. Seven HIV-1 and
HIV-2 dually reactive serum samples were analyzed by ELISA-HIV2
and PCR amplification of HIV gag and/or env genes. For PCR,
proviral DNA was extracted from uncultured peripheral blood
mononuclear cells with the Wizard genomic DNA purification kit
(Promega). For HIV-1, nested PCR was used to amplify a 409-bp
fragment from the C2-C3 env region, using outer primer pair JA167
and JA170 and inner primers JA168 and JA169, and a 582-bp
fragment from the p17 gag region, using outer primer pair JA152
and JA155 and inner primers JA153 and JA154. Thermal cycling

58
conditions for PCR and primer numbers and positions have been
described previously (25). For HIV-2, nested PCR was used to amplify
a 378-bp fragment from the HIV-2 C2-C3 env gene region (positions
6949 to 7327 in HIV-2ALI) as described elsewhere (3). The amplified
PCR products were visualized by electrophoresis in 2% agarose gel.
For each patient, at least two independent PCRs were performed
under identical conditions. HIV-1 plasma viral load was determined
using the Quantiplex HIV RNA 3.0 (bDNA) kit (Bayer Diagnostics).
TABLE 1. Type of infection in dually HIV-1 and HIV-2 seroreactive
individuals determined with ELISA-HIV2 and PCR amplification.
The PCR and ELISA-HIV2 results indicated that none of the patients
was dually infected, four patients being infected with HIV-2 and
three with HIV-1 (Table 1). Therefore, the ELISA-HIV2 assay can be
used to discriminate between HIV-1 and HIV-2 infections in dually
seroreactive patients. In Portugal, the reported rate of dual HIV-
1/HIV-2 seropositivity is 1.4% but the true rate of dual infections is
unknown (9). The finding that none of the dually seroreactive
patients was dually infected suggests that dual HIV-1/HIV-2
infections are rare in Portugal. Earlier reports suggested that most
dually seropositive individuals from Guinea-Bissau (78 to 86%) (47),
Ivory Coast, and the Gambia (72%) (19) were indeed dually infected.
In more recent studies performed in India (22) and Senegal (15), a
40% rate of dual infections was reported among dually seroreactive
patients. Although the number of patients was small in all studies,
the declining prevalence of dual infections that they document is
consistent with the worldwide decreasing incidence and prevalence
rates of HIV-2 infection (9, 20). Reactivity against two envelope

59
glycoproteins is the World Health Organization criterion used for the
WB confirmation of HIV infection (16).
TABLE 2- Diagnostic performance of ELISA-HIV2 with HIV-1
samples classified as indeterminate in HIV-2 Western blot (New LAV
Blot II).
To further investigate the reliability of ELISA-HIV2 as a confirmatory
test, we tested a panel of samples (n = 56) that were reactive in the
screening assay VIDAS HIV DUO and in the confirmatory assay New
LAV Blot II (51 positive and 5 indeterminate). All 51 WB-positive
samples reacted as HIV-2 samples in ELISA- HIV2, whereas the
indeterminate samples were HIV-2 negative in ELISA-HIV2 (Table 2).
Four indeterminate samples reacted as HIV-1 in the HIV-1 Western
blot and Peptilav 1-2. One indeterminate sample, which reacted also
as HIV-1 in WB, was dually HIV-1/HIV-2 seroreactive in Peptilav 1-2.
These results demonstrate that ELISA-HIV2 can be used as a
confirmatory assay for the serodiagnosis of HIV-2 infection.
In conclusion, the highly sensitive and specific ELISA-HIV2 is an
excellent alternative to the available tests for the serologic diagnosis
and confirmation of HIV-2 infection. The dual-antigen format
adopted in ELISA-HIV2 will permit the qualitative and quantitative
characterization of the antibody response to the envelope gp125 and
gp36 glycoproteins in HIV-2-infected patients.
This work was supported by grant POCTI/ESP/48045/2002 from
Fundação para a Ciência e Tecnologia (FCT), Portugal.

60
References
1. Andersson, S., Z. da Silva, H. Norrgren, F. Dias, G. Biberfeld.
1997. Field evaluation of alternative testing strategies for diagnosis
and differentiation of HIV-1 and HIV-2 infections in an HIV-1 and
HIV-2-prevalent area. AIDS 11:1815-1822.
2. Azevedo-Pereira, J. M., M. H. Lourenço, F. Barin, R. Cisterna, F.
Denis, P. Moncharmont, R. Grillo and M. O. Santos-Ferreira. 1994.
Multicenter evaluation of a fully automated screening test, VIDAS
HIV 1+ 2, for antibodies to human Immunodeficiency virus types 1
and 2. J. Clin. Microbiol. 32:2559-2563.
3. Barroso, H., F. Araújo, M. H. Gomes, A. Mota-Miranda, N. Taveira.
2004. Phylogenetic demonstration of two cases of perinatal Human
Immunodeficiency Virus Type 2 infection diagnosed in adulthood.
AIDS Res. Hum. Retroviruses 20:1373-1376.
4. Beelaert, G., G. Vercauteren, K. Fransen, M. Mangelschots, M. De
Rooy, S. Garcia-Ribas, G. van der Groen. 2002. Comparative
evaluation of eight commercial enzyme linked immunosorbent assays
and 14 simple assays for detection of antibodies to HIV. J. Virol.
Methods 105:197-206.
5. Benitez, J., D. Palenzuela, J. Rivero, J. V. Gavilondo. 1998. A
recombinant protein based immunoassay for the combined detection
of antibodies to HIV-1, HIV-2 and HTLV-I. J. Virol. Methods 70:85-
91.
6. Bottiger, B., A. Karlsson, P. A. Andreasson, A. Naucler, C. M.
Costa, E. Norrby, G. Biberfeld. 1990. Envelope cross-reactivity
between human immunodeficiency virus types 1 and 2 detected by
different serological methods: correlation between cross-
neutralization and reactivity against the main neutralizing site. J.
Virol. 64:3492-3499.
7. Center for Disease Control. 1990. Current trends in surveillance
for HIV-2 infection in blood donors: United States, 1987-1989.
MMWR 39:829-831.
8. Clavel, F., D. Guetard, F. Brun-Vezinet, S. Chamaret, M. A. Rey,
M. O. Santos-Ferreira, A. G. Laurent, C. Dauguet, C. Katlama, C.
Rouzioux, D. Klatzman, J. L. Champalimaud, and L. Montagnier.

61
1986. Isolation of a new human retrovirus from West African
patients with AIDS. Science 233:343-346.
9. Comissão Nacional de Luta Contra a Sida. 2004. A situação em
Portugal a 30 de Dezembro de 2004.Documento SIDA 133/CVEDT.
10. Decker, J. M., F. Bibollet-Ruche, X. Wei, S. Wang, D. N. Levy, W.
Wang, E. Delaporte, M. Peeters, C. A. Derdeyn, S. Allen, E. Hunter,
M. S. Saag, J. A. Hoxie, B. H. Hahn, P. D. Kwong, J. E. Robinson,
and G. M. Shaw. 2005. Antigenic conservation and immunogenicity
of the HIV coreceptor binding site. J.Exp.Med. 201:1407-1419.
11. de Wolf, F., R. H. Meloen, M. Bakker, F. Barin, J. Goudsmit.
1991. Characterization of human antibody-binding sites on the
external envelope glycoprotein of human immunodeficiency virus
type 2. J. Gen. Virol. 72:1261-1267.
12. Galli, R. A., S. Castriciano, M. Fearon, C. Major, K. W. Choi, J.
Mahony, M. Chernesky. 1997. Performance characteristics of
recombinant enzyme immunoassay to detect antibodies to human
immunodeficiency virus type 1 (HIV-1) and HIV-2 and to measure
early antibody responses in seroconverting patients. J. Clin.
Microbiol. 34:999-1002.
13. Gnann, J. W., J. B. McCormick, S. Mitchell, J. A. Nelson, M. B.
A. Oldstone. 1987. Synthetic peptide immunoassay distinguishes
HIV type 1 and HIV type 2 infections. Science 237:1346-1349.
14. Gonzalez, L., R. W. Boyle, M. Zhang, J. Castillo, S. Whittier, P.
Della-Latta, L. M. Clarke, J. R. George, X. Fang, J. G. Wang, B.
Hosein, C. Y. Wang. 1997. Synthetic-peptide-based enzyme-linked
immunosorbent assay for screening human serum or plasma for
antibodies to human immunodeficiency virus type 1 and type 2. Clin.
Diagn. Lab. Immunol. 4:598-603.
15. Gottlieb, G. S., P. S. Sow, S. E. Hawes, I. Ndoye, A. M. Coll-Seck,
M. E. Curlin, C. W. Critchlow, N. B. Kiviat, J. I. Mullins. 2003.
Molecular epidemiology of dual HIV-1/HIV-2 seropositive adults from
Senegal, West Africa. AIDS Res. Hum. Retroviruses 19:575-584.
16. Guèye-Ndiaye, A. 2002. Serodiagnosis of HIV Infection, p. 121-
138. In Max Essex, Souleymane Mboup, P. J. Kanki, R. G. Marlink,
and S. D. Tlou (ed.), AIDS in Africa, 2nd ed. Kluer Academic/Plenum
Publishers, New York.

62
17. Holmgren, B., Z. da Silva, O. Larsen, P. Vastrup, S. Andersson,
P. Aaby. 2003. Dual infections with HIV-1, HIV-2 and HTLV-I are
more common in older women than in men in Guinea-Bissau. AIDS
17:241-253.
18. Huang, M. L., M. Essex, T. H. Lee. 1991. Localization of
immunogenic domains in the human immunodeficiency virus type 2
envelope. J. Virol. 65:5073-5079.
19. Ishikawa, K., K. Fransen, K. Ariyoshi, J. N. Nkengasong, W.
Janssens, L. Heyndrickx, H. Whittle, M. O. Diallo, P. D. Ghys, I. M.
Coulibaly, A. E. Greenberg, J. Piedade, W. Canas-Ferreira, G. van der
Groen. 1998. Improved detection of HIV-2 proviral DNA in dually
seroreactive individuals by PCR. AIDS 12:1419-1425.
20. Jaffar, S., A. D. Grant, J. Whitworth, P. G. Smith, and H.
Whittle. 2004. The natural history of HIV-1 and HIV-2 infections in
adults in Africa: a literature review. Bull.World Health Organ.
82:462-469.
21. Kanki, P. J., J-L. Sankalé and S. Mboup. 2002. Biology of
Human Immunodeficiency Virus Type 2 (HIV-2), p. 74-103. In Max
Essex, Souleymane Mboup, P. J. Kanki, R. G. Marlink, and S. D.
Tlou (ed.), AIDS in Africa, 2nd ed. Kluer Academic/Plenum
Publishers, New York.
22. Kannangai, R., S. Ramalingam, K. J. Prakash, O. C. Abraham,
R. George, R. C. Castillo, D. H. Schwartz, M. V. Jesudason, G.
Sridharan. 2001. A peptide enzyme linked immunosorbent assay
(ELISA) for the detection of human immunodeficiency virus type-2
(HIV-2) antibodies: an evaluation on polymerase chain reaction (PCR)
confirmed samples. J. Clin. Virol. 22:41-46.
23. Kulkarni, S., S. Tripathy, K. Agnihotri, N. Jatkar, S. Jadhav, W.
Umakanth, K. Dhande, P. Tondare, R. Gangakhedkar, R. Paranjape.
2005. Indian primary HIV-2 isolates and relationship between V3
genotype, biological phenotype and coreceptor usage. Virology
337:68-75.
24. Laurent, C., K. Seck, N. Coumba, T. Kane, N. Samb, A. Wade, F.
Liegeois, S. Mboup, I. Ndoye, E. Delaporte. 2003. Prevalence of HIV
and other sexually transmitted infections, and risk behaviours in
unregistered sex workers in Dakar, Senegal. AIDS 17:1811-1816.

63
25. Leitner, T., D. Escanilla, S. Marquina, J. Wahlberg, C. Brostrom,
H. B. Hansson, M. Uhlen, J. Albert. 1995. Biological and molecular
characterization of subtype D, G, and A/D recombinant HIV-1
transmissions in Sweden. Virology 10:136-146.
26. Lizeng, Q., C. Nilsson, S. Sourial, S. Andersson, O. Larsen, P.
Aaby, M. Ehnlund, E. Bjorling. 2004. Potent neutralizing serum
immunoglobulin A (IgA) in human immunodeficiency virus type 2-
exposed IgG-seronegative individuals. J. Virol. 78:7016-7022.
27. Lizeng, Q., P. Skott, S. Sourial, C. Nilsson, S. Andersson, M.
Ehnlund, N. Taveira, E. Bjorling. 2003. Serum immunoglobulin A
(IgA)-mediated immunity in human immunodeficiency virus type 2
(HIV-2) infection. Virology 308:225-232.
28. Ly, T. D., S. Laperche, C. Brennan, A. Vallari, A. Ebel, J. Hunt,
L. Martin, D. Daghfal, G. Schochetman, S. Devare. 2004. Evaluation
of the sensitivity and specificity of six HIV combined p24 antigen and
antibody assays. J. Virol. Methods 122:185-194.
29. Ly, T. D., L. Martin, D. Daghfal, A. Sandridge, D. West, R.
Bristow, L. Chalouas, X. Qiu, S. C. Lou, J. C. Hunt, G. Schochetman,
S. G. Devare. 2001. Seven human immunodeficiency virus (HIV)
antigen-antibody combination assays: evaluation of HIV
seroconversion sensitivity and subtype detection. J. Clin. Microbiol.
39:3122-3128.
30. Mannervik, M., P. Putkonen, V. Ruden, K. A. Kent, E. Norrby, B.
Wahren, P. A. Broliden. 1992. Identification of B-cell antigenic sites
on HIV-2 gp125. AIDS 5:177-187.
31. Manocha, M., K. T. Chitralekha, M. Thakar, D. Shashikiran, R.
S. Paranjape, D. N. Rao. 2003. Comparing modified and plain peptide
linked enzyme immunosorbent assay (ELISA) for detection of human
immunodeficiency virus type-1 (HIV-1) and type-2 (HIV-2) antibodies.
Immunol. Lett. 85:275-278.
32. McDougal, J. S., C. D. Pilcher, B. S. Parekh, G. Gershy-Damet,
B. M. Branson, K. Marsh, S. Z.Wiktor. 2005. Surveillance for HIV-1
incidence using tests for recent infection in resource-constrained
countries. AIDS. Suppl 2:S25-30.
33. Norrby, E., G. Biberfeld, F. Chiodi, A. von Gegerfeldt, A. Naucler,
E. Parks, R. Lerner. 1987. Discrimination between antibodies to HIV

64
and to related retroviruses using site-directed serology. Nature
329:248-250.
34. Norrby, E., P. Putkonen, B. Bottiger, G. Utter, G. Biberfeld.
1991. Comparison of linear antigenic sites in the envelope proteins of
human immunodeficiency virus (HIV) type 2 and type 1. AIDS Res.
Hum. Retroviruses 7:279-285.
35. Paranjape, R. S., S. P. Tripathy, P. A. Menon, S. M. Mehendale,
P. Khatavkar, D. R. Joshi, U. Patil, D. A. Gadkari, and J. J.
Rodrigues. 1997. Increasing trend of HIV seroprevalence among
pulmonary tuberculosis patients in Pune, India. Indian J. Med. Res.
106:207-211.
36. Pilcher, C. D., S. A. Fiscus, T. Q. Nguyen, E. Foust, L. Wolf, D.
Williams, R. Ashby, J. O. O'Dowd, J. T. McPherson, B. Stalzer, L.
Hightow, W. C. Miller, J. J. Eron, Jr., M. S. Cohen, P. A. Leone.
2005. Detection of acute infections during HIV testing in North
Carolina. N. Engl. J. Med. 352:1873-1883.
37. Robert-Guroff, M., K. Aldrich, R. Muldoon, T. L. Stern, G. P.
Bansal, T. J. Matthews, P. D. Markham, R. C. Gallo, G. Franchini,.
1992. Cross-neutralization of human immunodeficiency virus type 1
and 2 and simian immunodeficiency virus isolates. J. Virol. 66:3602-
3608.
38. Saville, R. D., N. T. Constantine, F. R. Cleghorn, N. Jack, C.
Bartholomew, J. Edwards, P. Gomez, W. A. Blattner. 2001. Fourth-
generation enzyme-linked immunosorbent assay for the
simultaneous detection of human immunodeficiency virus antigen
and antibody. J. Clin. Microbiol. 39:2518-2524.
39. Schim van der Loeff, M. F., P. Aaby. 1999. Towards a better
understanding of the epidemiology of HIV-2. AIDS 13:S69-84.
40. Schulz, T. F., W. Oberhuber, J. M. Hofbauer, P. Hengster, C.
Larcher, L. C. Gurtler, R. Tedder, H. Wachter, M. P. Dierich. 1989.
Recombinant peptides derived from the env-gene of HIV-2 in the
serodiagnosis of HIV-2 infections. AIDS 3:165-172.
41. Schupbach, J. 1999. Human immunodeficiency viruses, p. 847-
870. In Eds Murray, P. R., Baron, E. J., Pfaller, M. A., Tenover, F. C.
Yolken, R. H. (ed), Manual of clinical microbiology, 7th ed. American
Society for Microbiology.

65
42. Sickinger, E., M. Stieler, B. Kaufman, H. P. Kapprell, D. West, A.
Sandridge, S. Devare, G. Schochetman, J. C. Hunt, D. Daghfal;
AxSYM Clinical Study Group. 2004. Multicenter evaluation of a new,
automated enzyme-linked immunoassay for detection of human
immunodeficiency virus-specific antibodies and antigen. J. Clin.
Microbiol. 42:21-29.
43. Simon, F., S. Souquiere, F. Damond, A. Kfutwah, M. Makuwa, E.
Leroy, P. Rouquet, J. L. Berthier, J. Rigoulet, A. Lecu, P. T. Telfer, I.
Pandrea, J. C. Plantier, F. Barre-Sinoussi, P. Roques, M. C. Muller-
Trutwin, C. Apetrei. 2001. Synthetic peptide strategy for the
detection of and discrimination among highly divergent primate
lentiviruses. AIDS Res. Hum. Retroviruses 17:937-952.
44. Taveira, N. C., F. Bex, A. Burny, D. Robertson, M. O. Ferreira, J.
Moniz-Pereira. 1994. Molecular characterization of the env gene from
a non-syncytium-inducing HIV-2 isolate (HIV-2ALI). AIDS Res. Hum.
Retroviruses 10:223-224.
45. Thorstensson, R., S. Andersson, S. Lindback, F. Dias, F. Mhalu,
H. Gaines, G. Biberfeld. 1998. Evaluation of 14 commercial HIV-
1/HIV-2 antibody assays using serum panels of different
geographical origin and clinical stage including a unique
seroconversion panel. J. Virol. Methods 70:139-151.
46. Trkola, A., H. Kuster, C. Leemann, A. Oxenius, C. Fagard, H.
Furrer, M. Battegay, P. Vernazza, E. Bernasconi, R. Weber, B.
Hirschel, S. Bonhoeffer, and H. F. Gunthard. 2004. Humoral
immunity to HIV-1: kinetics of antibody responses in chronic
infection reflects capacity of immune system to improve viral set
point. Blood 104:1784-1792.
47. Walther-Jallow, L., S. Andersson, Z. da Silva, G. Biberfeld. 1999.
High concordance between polymerase chain reaction and antibody
testing of specimens from individuals dually infected with HIV types
1 and 2 in Guinea-Bissau, West Africa. AIDS Res. Hum. Retroviruses
15:957-962.
48. Weber, B., M. Moshtaghi-Boronjeni, M. Brunner, W. Preiser, M.
Breiner, H. W. Doerr. 1995. Evaluation of the reliability of 6 current
anti-HIV-1/HIV-2 enzyme immunoassays. J. Virol. Methods 55:97-
104.

66
49. Weiss, R. A., P. R. Clapham, J. N. Weber, D. Whitby, R. S.
Tedder, T. O'Connor, S. Chamaret, L. Montagnier. 1998. HIV-2
antisera cross-neutralize HIV-1. AIDS 2:95-100.
50. Zuber, M., K. P. Samuel, J. A. Lautenberger, P. J. Kanki, T. S.
Papas. 1990. Bacterially produced HIV-2 env polypeptides specific for
distinguishing HIV-2 from HIV-1 infections. AIDS Res. Hum.
Retroviruses 6:525-534.

CAPÍTULO IV
Resposta de anticorpos IgA e IgG
inespecíficos e específicos para as
glicoproteínas gp36 e gp125 do VIH-2.

68

69
Análise da Resposta IgA e IgG Inespecífica e
Caracterização da Cinética, Isotipo e Avidez dos
Anticorpos IgA e IgG Específicos das Glicoproteínas gp36 e
gp125 do VIH-2.
Publicação: Envelope-specific antibody response in HIV-2
infection: C2V3C3-specific IgG response is associated
with disease progression.
José Maria Marcelino, Charlotta Nilsson, Helena
Barroso, Perpétua Gomes, Pedro Borrego, Fernando
Maltez, Lino Rosado, Manuela Doroana, Francisco
Antunes and Nuno Taveira.
AIDS, 2008, 22: 2257 – 2265.
Sumário
Objectivos: Estudar as respostas IgA e IgG inespecíficas e
específicas do invólucro na infecção VIH-2 aguda e crónica.
Métodos: Foram estudados 28 indivíduos adultos com infecção VIH-
2 crónica e duas crianças infectadas via perinatal. As concentrações
totais de IgA e IgG no plasma foram determinadas por nefelometria.
A reactividade dos anticorpos IgA e IgG contra a região
imunodominante na gp36 e a região C2V3C3 na gp125 foi analisada
com o ensaio imunoenzimático, ELISA-VIH2. Obtiveram-se as
sequências clonais da região C2V3C3 do env da maioria dos
pacientes.
Resultados: A concentração total de IgG no plasma, ao contrário da
IgA, foi significativamente mais elevada nos pacientes VIH-2+ do que
nos indivíduos saudáveis, e revelou uma correlação inversa
relativamente às contagens de células T CD4+. A seroconversão
relativa à gp36 ocorreu durante o primeiro ano de vida em ambas as
crianças. A criança que apresentou uma rápida progressão da
doença não produziu anticorpos específicos contra a região C2V3C3.
A maioria dos pacientes cronicamente infectados produziu
anticorpos IgG1, IgG3 e IgA contra a gp36 e a C2V3C3. A ausência
de resposta IgG específica contra a C2V3C3 em dois pacientes
mostrou estar associada a uma alteração major na região V3. Através
de uma análise longitudinal, verificou-se a existência de uma
associação inversa significativa entre a resposta de anticorpos
específica para a C2V3C3 e a contagem de células T CD4+.

70
Conclusão: O VIH-2 induz inicialmente uma forte e ampla resposta
de anticorpos IgG e IgA específicos para a C2V3C3 e gp36. O
aumento na resposta IgG contra a região C2V3C3 do invólucro está
associado a uma perda elevada de células T CD4 + nos pacientes
cronicamente infectados. Estes resultados fornecem um maior
suporte ao papel imune protector da região C2V3C3 do invólucro
durante a infecção VIH-2 e tem implicações directas no diagnóstico
do VIH-2, e na gestão clínica e na patogénese.

71
Envelope-specific Antibody Response in HIV-2 Infection:
C2V3C3-specific IgG Response is Associated with Disease
Progression.
Abstract
Objective: To examine the unspecific and envelope-specific IgA and
IgG responses in acute and chronic HIV-2 infection.
Methods: Twenty-eight chronically infected adults and two children
with perinatal infection were studied. Total plasma concentrations of
IgA and IgG were determined by nephelometry. IgA and IgG reactivity
against the immunodominant region in gp36 and the C2V3C3 region
in gp125 was tested with the enzyme-linked immunosorbent assay
(ELISA)–HIV-2 assay. Clonal sequences of the C2V3C3 env region
were obtained for most patients.
Results: Total plasma IgG concentration, but not IgA, was
significantly higher than normal in HIV-2 patients and correlated
inversely with CD4+ T-cell counts. Seroconversion to gp36 occurred
during the first year of life in both infants. The infant with rapid
disease progression did not elicit C2V3C3-specific antibodies. Most
chronically infected patients produced plasma IgG1, IgG3 and IgA
antibodies against gp36 and C2V3C3. Lack of C2V3C3-specific IgG
response in two patients was associated with a major antigenic
change in the V3 region. In longitudinal analysis, there was a
significant inverse association between the C2V3C3-specific IgG
antibody response and the number of CD4+ T cells.
Conclusion: HIV-2 promotes an early, strong and broad gp36 and
C2V3C3-specific IgG and IgA response. Increase in the IgG response
against the envelope C2V3C3 region is associated with increased loss
of CD4+ T cells in chronically infected patients. These results provide
further support for the immune protective role of the C2V3C3
envelope region during HIV-2 infection and have direct implications
for HIV-2 diagnosis, clinical management and pathogenesis.

72

73
Introduction
HIV-2 causes localized infections in Western African countries,
mostly in Guinea-Bissau, Gambia and Senegal, and in a few other
countries with former colonial ties with these countries, including
Portugal and France. There is limited knowledge on the natural
history of HIV-2 infection because no study has investigated the full
course of infection from the time of seroconversion. The available
data indicate that the majority of HIV-2-infected individuals behave
like HIV-1 controllers (long-term nonprogressors and elite
suppressors) having normal CD4+ T-cell counts, low or absent
plasma viremia and absence of clinical disease [1,2]. Not
surprisingly, HIV-2 infection has a minor effect on survival in most
adults [3,4]. The low or absent plasma viremia in most HIV-2
patients [5–9] probably determines low HIV-2 heterosexual and
vertical transmission rates [10–12] and explains the declining
prevalence of HIV-2 infection worldwide [13,14].
The mechanisms underlying immune control of HIV-2 replication and
disease progression are still not fully understood. Robust
polyfunctional T-cell responses, mainly directed to the Gag protein,
have been recently associated with viremia control in HIV-2 infection
[15,16]. Lower capacity to infect dendritic cells [17], lower in-vitro
replication rates and replication kinetics in peripheral blood
lymphocytes [5] and macrophages [18], and lower replication rate in
vivo [9] have also been implicated in the lower plasma viremia and
pathogenesis of HIV-2 compared with HIV-1. Finally, compared with
HIV-1, HIV-2- infected individuals may have higher titers of IgG and
IgA neutralizing antibodies that may contribute for the better control
of viral replication in these patients [19–21].
Chronic immune activation is a characteristic of HIV disease
progression and an important driving force of HIV-1 and HIV-2
pathogenesis [22–27]. Immune activation provides the virus with
activated CD4 T-cell targets and it predicts disease progression
better than either the peripheral blood CD4 T-cell count or the viral
load in plasma [28–31]. A lower rate of CD4 and CD8 cells immune
activation and dysfunction has been described in HIV-2 patients with
normal CD4 cell counts compared with their HIV-1-infected
counterparts [1]. More recently, this has been associated with the
CD4 and CD8 cells immunosuppressive activity of the C2V3C3
envelope region [32].
Very few studies have been published on the nature and dynamics of
the antibody response against HIV-2. In general, the antibody

74
response against the viral proteins in HIV-2 chronically infected
patients does not seem to be different from that of HIV-1 infection.
Indeed, the majority of HIV-2 patients produce IgG antibodies
against the structural proteins of the virus and this forms the basis
for their serologic diagnosis [33–35].
B-cell activation, however, may be less pronounced in chronic HIV-2
infection compared with HIV-1 infection. This has been suggested in
one study [36] in which total serum IgG concentration was
significantly higher in HIV-2-infected patients from Senegal
compared with uninfected controls but lower than in HIV-1 patients.
The magnitude and kinetics of the IgA and IgG-antibody response
against the envelope glycoproteins have so far not been investigated
in the course of HIV-2 infection.
Previously, we have used the new enzyme-linked immunosorbent
assay (ELISA)–HIV2 assay to show that the majority of HIV-2 patients
produce IgG antibodies against rpC2–C3 and rgp36, two recombinant
polypeptides representing the gp125 and gp36 envelope glycoproteins
[33]. We have also shown that HIV-2 patients could be divided into
high and low-immune responders according to the level of antibodies
produced against the C2–C3 envelope region suggesting that the
antibody response against this region could be a marker of clinical
condition. In the present study, we examine in detail, the magnitude
and dynamics of the unspecific and env-specific IgA and IgG
responses in chronic and acute HIV-2 infection.
Patients, samples and methods
We analyzed 30 HIV-2-infected patients from three hospitals in
Lisbon and 50 seronegative individuals (blood donors). Two patients
were children with perinatal HIV-2 infection. The characteristics of
the patients enrolled in the study are described in Table 1. Patients
were born in Portugal (16), Guinea Bissau (12), Cape Vert Islands (1)
and Mozambique (1). All patients are living in Lisbon for over a
decade.
HIV seropositivity was determined with VIDAS HIV DUO (Bio-
Mérieux, Lyon, France). HIV-1 and HIV-2 differentiation was done by
Western Blot 2.2 (Genelabs Diagnostics, Science Park, Singapore),
New LAV Blot II and Peptilav 1-2 (Bio-Rad, Hercules, California,
USA). HIV-2 infection in children was determined by virus isolation,
as described previously [37]. Ethical approval was obtained from
each hospital ethics committee and each participant or their parents,
in the case of the children, gave informed consent before entry into
the study.

75
Table 1. Characteristics of the HIV-2-infected adults and children
included in this study.
Quantification of CD4R T cells, plasma virémia and IgA and IgG.
CD4+ T-cell counts were determined in total blood samples by flow
cytometric analysis using FACSCalibur (Becton Dickinson, Franklin
Lakes, New Jersey, USA). HIV-2 viremia in the plasma was quantified
with a quantitative-competitive reverse transcriptase-PCR assay as
described elsewhere [38]. IgA and IgG nephelometry Turbox kits
(Orion Diagnostica’s Turbox plus, Finland) were used to evaluate the
total concentrations of IgA and IgG in plasma, following the
manufacturer’s instructions.
IgA and IgG antibody reactivity against the HIV-2 antigens rgp36
and rpC2–C3. The location of the recombinant rpC2–C3 (165 amino
acids in gp125) and rgp36 (128 amino acids in the gp36 ectodomain)
polypeptides used in this work was described previously [33]. IgG
reactivity against rgp36 and rpC2–C3 was determined using the
ELISA-HIV-2 test also as described previously [33]. IgA reactivity was
determined with horseradish peroxidase (HRP)-conjugated rabbit
antihuman IgA. The clinical cutoff value of the assay was determined
using samples from healthy HIV-seronegative individuals. The results
of the assay are expressed quantitatively as optical density of the
clinical sample (ODcs)/optical density of the cutoff (ODco) ratios. For
ratio values above 1, the sample was considered as seroreactive.

76
Rgp36 and rpC2–C3-specific antibodies in plasma were titrated with
the ELISA-HIV-2 test using six serial four-fold dilutions (initial
dilution of 1:100). Antibody titers were defined by linear regression
analysis as the higher antibody dilution giving a positive reaction.
IgG subclass reactivity against rgp36 and rpC2–C3. Reactivity of
the different IgG subclasses against rgp36 and rpC2–C3 was
determined with ELISA-HIV-2 test with the following modifications.
After incubation of plasma samples, HRP-conjugated sheep
antihuman IgG1, IgG2, IgG3 or IgG4 antibody (The Binding Site Ltd.,
Birmingham, UK) was added and incubated at room temperature.
The anti-IgG1 antibody was diluted at 1:6000 and the others at
1:3000.
Envelope glycoprotein-specific antibody avidity. The avidity index
values of rgp36 and rpC2–C3-specific IgG1 antibodies were
determined by measuring the resistance of IgG1–rgp36 or IgG1–
rpC2–C3 complexes to dissociation with 6 mol/l urea as previously
described [39]. ELISA-HIV2 test was used with the following
modifications. A 6 mol/l urea solution in phosphate buffered saline
(PBS) was added to duplicate wells incubated previously with HIV-2-
positive and negative samples. In control wells, PBS was added
instead of urea. After 10 min incubation, the wells were washed and
incubated with sheep antihuman IgG1 HRP-conjugated for 1 h. The
reaction was revealed with SIGMA FAST OPD solution (Sigma, St.
Louis, Missouri, USA) as described previously. The cutoff value for
this avidity test was calculated as the mean optical density value of
HIV-seronegative samples incubated with urea or PBS alone and
three times the SD. Sample/cutoff ratios were calculated and the
avidity index of HIV antibodies was then calculated as the following
ratio: (sample/cutoff ratio of the urea aliquot)/ (sample/cutoff ratio
of the PBS aliquot) [40].
DNA extraction, PCR amplification, cloning and sequencing.
Proviral DNA was extracted from peripheral blood mononuclear cells
(PBMCs) with the Wizard Genomic DNA Purification kit (Promega,
Madison, Wisconsin, USA). A fragment of the C2V3C3 region (394 bp)
of the HIV-2 env gene was amplified by PCR, cloned and sequenced
as described previously [41]. For each patient, an average of 13
clones was sequenced.
Statistical analysis. Statistical analyses were performed with
GraphPad Prism 4.02. Nonparametric tests were used to compare
means between variables: Mann–Whitney U-test was used to

77
compare IgA and IgG antibody response against both polypeptides
and the correlation between antibody concentration, titer and avidity
to rgp36 and rpC2–C3 was determined using the Spearman rank
test. Deming linear regression was used to study the overall variation
(slopes) of dynamics of CD4 cells and IgG response against rpC2–C3
of each patient as a function of time (longitudinal analysis). All P
values are two tailed and P values below 0.05 were considered
significant.
Results
Total concentrations of plasma IgA and IgG in HIV-2 infection.
The total IgG and IgA plasma concentrations were determined in 50
healthy controls (blood donors) and 28 HIV-2-infected adult patients
Fig. 1. Total and envelope-specific antibody response in HIV-2
infection. (a) Correlation between CD4+ T-cell counts in peripheral
blood and total concentration of IgA and IgG in plasma of HIV-2-
infected patients; (b) level of IgA and IgG antibodies produced against
the polypeptides rgp36 and rpC2–C3; (c) reactivity of the four human
IgG subclasses (IgG1, IgG2, IgG3 and IgG4) against rgp36 and rpC2–
C3; (d) avidity index of rgp36 and rpC2–C3–IgG1-specific antibodies.
residing in Portugal showing different clinical, virologic and
epidemiologic features (Table 1). Total IgG plasma concentrations
were significantly higher in HIV-2 patients compared with uninfected
controls (mean 19.2 ± 6.3 vs. 10.1 ± 2.3 g/l, P<0.0001). Total IgA
concentrations were similar in HIV-2 patients and uninfected

78
controls (mean 2.4 ± 1.1 vs. 2.1 ± 0.8 g/l, P = 0.1626). In HIV-2-
infected patients, total IgG concentration was negatively correlated to
the number of CD4+ T cells (r = -0.5829, P<0.0001) (Fig. 1a). No
association was found between the total IgA concentration and the
number of CD4+ T cells (r = 0.1392, P = 0.2540). Total IgA and IgG
concentrations were positively correlated in healthy individuals (r =
0.4132, P = 0.0039). In HIV-2 patients, there was no correlation
between the total IgA and IgG concentrations (r = -0.1927; P = 0.1).
IgG and IgA antibody response against the HIV-2 envelope
glycoproteins. The presence of envelope-specific IgG and IgA
antibodies was investigated in 28 HIV-2-infected patients by using
the ELISA-HIV-2 test [33]. With the exception of patient number 27
showing only IgG antibodies against rgp36 in two consecutive
samples, all patients had IgA antibodies binding to the recombinant
polypeptides rgp36 and rpC2–C3. IgG antibodies against rgp36 were
detected in all 28 patients; IgG antibodies against rpC2–C3 were
detected in 26 patients (Fig. 1b). The magnitude of the IgG response
was significantly higher against rgp36 than against rpC2–C3 (median
optical density/cutoff 16.09 for rpC2–C3 vs. 34.22 for rgp36,
P<0.0001).
The IgA response against both polypeptides was significantly lower
when compared with the IgG response (P<0.0001) (Fig. 1b). There
was, however, no significant difference in IgA reactivity against both
polypeptides (P = 0.3988). IgA and IgG antibody responses against
both polypeptides were not directly correlated (data not shown). The
level of reactivity of the different IgG subclasses produced against the
two polypeptides was also investigated (Fig. 1c). All patients had IgG1
antibodies binding to rgp36; 26 (92.8%) patients also produced IgG1
to rpC2–C3. The response against rgp36 was significantly stronger as
compared with rpC2–C3 (mean optical density/cutoff 29.24 for rgp36
vs. 16.14 for rpC2–C3, P<0.0001). Ten patients produced IgG2
against rgp36; six patients produced also IgG2 to rpC2–C3. However,
the antibody reactivity against both polypeptides was very weak
(mean optical density/cutoff 1.43 for rgp36 and 1.48 for rpC2–C3).
Twenty patients produced IgG3 antibodies against rgp36; only three
patients produced IgG3 against rpC2–C3. Similar to IgG1, IgG3
reactivity was stronger against rgp36 as compared with rpC2–C3
(mean optical density/cutoff 8.23 for rgp36 vs. 1.51 for rpC2–C3,
P<0.0001). IgG4 antibodies against rgp36 were detected in two
patients only (patient numbers 4 and 11).

79
Correlation between antibody concentration, titer and avidity to
rgp36 and rpC2–C3. The titer (log10) of the IgG antibodies produced
against rpC2–C3 ranged from 3.08 to 4.32 and ranged from 3.65 to
5.45 to rgp36.
Fig. 2. Longitudinal analysis of anti-rpC2–C3 IgG response and
CD4+ T-cell counts in HIV-2-infected patients. Anti-C2–C3 antibody
response was plotted as a function of the number of CD4+ T cells in
patients with at least 500 CD4+ T cells/ml (a), patients with less
than 500 CD4+ T cells/ml (b); Deming regression analysis of the
dynamics of the C2–C3-specific IgG response and CD4+ T-cell counts
along the course of HIV-2 infection (c); comparison of the annual
variation (slopes) in the number of CD4+ T cells/ml in antiretroviral-
treated and untreated patients (Mann–Whitney test) (d). Dotted lines
indicate C2–C3-specific IgG level.
Significantly higher IgG antibody titers were obtained against rgp36
than rpC2–C3 (median titer 4.57 for rgp36 vs. 3.27 for rpC2–C3,
P<0.0001). There was a positive correlation between the antibody
titers against both polypeptides (r = 0.5641, P = 0.0027).
The avidity index of the IgG1 antibodies binding to rgp36 was
significantly higher as compared with rpC2–C3 (mean avidity index
0.96 for rgp36 vs. 0.89 for rpC2–C3; P = 0.0032) (Fig. 1d). The
relationship between IgG antibody titer, concentration and avidity

80
was investigated. There was a strong positive correlation between
antibody titer and concentration for rpC2–C3 (r = 0.8779, P<0.0001)
and rgp36 (r = 0.4875, P = 0.0099). Antibody titer and avidity were
marginally associated only for rpC2–C3 (r = 0.3703, P = 0.0626).
Fig. 3. Kinetics of IgG antibody response against rgp36 and rpC2–C3
and CD4+ T-cell counts in two children infected by mother-to-child
transmission.
The antibody response against the HIV-2 Env C2–C3 region is a
sensitive marker of disease progression. The antibody response
against rpC2–C3 and rgp36 and the number of CD4+ T cells was
investigated prospectively for a period of 4 years in 16 adult HIV-2
patients (Table 1; Fig. 2a and b). There was a significant inverse
correlation between the dynamics of CD4 cell counts and IgG
response against rpC2–C3 over time (Deming regression analysis, F =
5.817; P = 0.0345) (Fig. 2c). No such correlation was found for the
IgG response against rgp36 (data not shown).
Antiretroviral therapy (ART) has a modest impact on CD4 cell
recovery in HIV-2 patients [42,43]. In the present study, ART also
had no significant impact in the within-patient annual variation of
the number of CD4+ T cells (ART patients, median variation = -21.24
CD4+ cells per year; range -187.0–50.26 vs. drug-naïve patients,
median = -11.58; range -49.61–83.50; Mann–Whitney test, P = 0.154)
(Fig. 2d). ART also did not impact the within-patient evolution of the
C2–C3-IgG response (data not shown).
The IgG response against the C2–C3 and rgp36 antigens was
measured retrospectively in two children with perinatal infection for
a mean period of 7.5 years (Fig. 3). Both children exhibited a rapid
decline in the number of CD4+ T cells and progressed rapidly to
AIDS, children C1 dying at the age of 8 years (Table 1) [44].

81
Clinical condition of patient C2 remains stable up to this day with
undetectable viral load. In the first year of infection, the antibody
response against gp36 was in the same order of magnitude in both
patients, waning significantly only in patient C1 in association with a
sharp decline in the number of CD4+ T cells (Fig. 3a).
Antibody response against rpC2–C3 was always weak in patient C1
being almost undetectable at the time of death. Patient C2 produced
a strong antibody response against gp36 and C2–C3 in a setting of
significant decline in the number of CD4+ T cells (Fig. 3b).
Sequencing of the env C2V3C3 regions .Clonal sequences were
obtained from the env C2–C3 region of most patients. To try to find
an explanation for the absence of IgG antibodies binding to the
rpC2–C3 polypeptide in patient numbers 27 and 28, we compared
the C2–C3 amino acid sequence of these patients with those of the
other patients and of the HIV-2ALI isolate that was used to produce
the rpC2–C3 polypeptide [33] (Fig. 4).
Fig. 4. Alignment of the consensus C2V3C3 amino acid sequences of
patient numbers 27 and 28 with the reference HIV-2ALI sequence
and with a consensus sequence of all the remaining patients
included in this study. The polymorphisms found exclusively in
patient numbers 27 and 28 sequences are shown in bold letters.
Nine unique amino acid substitutions and one insertion were found
in the C2–C3 regions of patient numbers 27 and 28. These
polymorphisms occurred mostly (six out of 10) at the core of the V3
region.
Discussion
In this study, we examined, for the first time, the unspecific and
Env-specific IgA and IgG responses in acute and chronic HIV-2
infection. As previously found in Senegalese patients [36], total
serum IgG concentrations were significantly higher in chronic HIV-2

82
adult patients than in uninfected controls. These results indicate
that, similar to chronic HIV-1 infection, unspecific B-cell activation
also occurs in chronic HIV-2 infection. Total IgG concentration
correlated inversely with CD4+ T-cell counts establishing, for the first
time, a link between CD4 cell loss and B-cell activation in HIV-2
infection. However, this is not a polyclonal activation as contrary to
HIV-1 infection in which the levels of all immunoglobulin isotypes are
increased in association with immunological and/or virological
failure [45,46], total IgA antibody production was not affected in our
patients. Importantly, as most IgA-producing B cells are activated in
intestinal lymphoid tissue [47], the normal production of total IgA
and HIV-specific IgA (see below) in HIV-2 infection suggests that the
gastrointestinal immune system is not as severely affected in HIV-2
as it is in HIV-1 infection [23,48].
The human antibody response against rpC2–C3 and rgp36, two
polypeptides representing the most antigenic regions of the HIV-2
gp125 and gp36 envelope glycoproteins, was analyzed in two infants
infected with HIV-2 by their mothers and in 28 chronically infected
adults. In both infants, seroconversion to gp36 occurred during the
first year of age but at different levels. For the infant who is still
controlling the infection (patient C2) antibody response to gp36 and
C2V3C3 rose to levels similar to those found in chronic patients,
even in a context of progressive CD4 cell count decline. In contrast,
de-novo production of anti-C2V3C3 antibodies did not occur in
infant C1 who progressed quickly to AIDS and death. Hence, these
results indicate that an early, strong and sustained antibody
response to C2V3C3 in gp125 is important to prevent progression to
AIDS and death. It is likely that patient C1 was infected in early
pregnancy and that this prevented the adequate development of the
immune system. The weakened antibody response may have
contributed significantly for the rapid evolution of the infecting virus
to a highly aggressive phenotype, which caused rapid immune
deficiency and death [44, 49, 50].
In two patients (number 27 and 28), we could not detect IgG
antibodies reacting with the rpC2–C3 polypeptide. A high number of
amino acid changes were detected in the C2–C3 region of these
patients compared with the other patients and with the rpC2–C3
antigen used in the ELISA-HIV2 assay. These occurred mostly at the
core of the V3 region, which is the principal antigenic determinant in
the HIV-2 surface glycoprotein [51]. Therefore, it is likely that the
type-specific antibodies produced against this divergent C2V3C3
region fail to recognize the particular rpC2–C3 antigen used in the
ELISA-HIV2 assay.

83
All but one patient that exclusively produced antigp36 IgA, produced
IgA antibodies reacting with both the C2–C3 and gp36 polypeptides.
These findings are consistent with a healthy gastrointestinal immune
system in HIV-2 infection (see above) and signal an important
difference for HIV-1 infection as only 32–91% of HIV-1 patients
produce serum IgA antibodies against the gp41 and/or gp120
envelope glycoproteins, this being inversely related to the stage of
disease [45,52–54]. Our results confirm the strong IgA antigenicity of
the gp36 ectodomain in HIV-2 infection [20] and identify, for the first
time, the C2–C3 region as a strong inducer of serum IgA antibodies.
The finding that the C2–C3 region and the gp36 ectodomain contain
highly antigenic IgA epitopes and that these are different from the
IgG epitopes may inform the production of better HIV-2
serodiagnostic tests (e.g. rapid tests using mucosal samples).
IgG titers against rgp36 and rpC2–C3 were strongly correlated, which
indicates that in the native envelope glycoprotein complexes the
corresponding epitopes are presented in a similar way to the B
lymphocytes. Nonetheless, the IgG response was predominantly
directed to gp36 both qualitatively (avidity) and quantitatively (titer
and concentration). Gp36 also induces higher levels of all IgG
subclasses when compared with gp125. Together, these results
extend our previous observations providing definitive evidence for the
immunodominant role of the gp36 ectodomain in HIV-2 infection
[20,33].
We found that IgG1 is the predominant antibody subclass produced
against both HIV-2 envelope glycoproteins. However, unlike in HIV-1
infection, IgG3 and not IgG2 was the second most reactive subclass
to gp36 [55–59]. In HIV-1 infection, the inverse relationship between
gp41- specific IgG2 antibody levels and clinical progression to AIDS
suggests that this type of antibodies may be protective [55,56,59–61].
For HIV-2, such a protective effect could instead be attributed to
IgG1 or IgG3 [62]. We investigated this hypothesis in our longitudinal
adult cohort and could not find any association between IgG1 and
IgG3 response against the gp36 polypeptide and disease progression
measured by the loss of CD4+ T cells. Instead, we found a significant
inverse association between C2 and C3-specific IgG antibody
production and the number of CD4+ T cells. Importantly, this
association was also found in one pediatric patient with progressive
infection. How can the loss of CD4+ T cells be associated with the
IgG response against the C2V3C3 region? Cavaleiro et al. [32,63]
have recently demonstrated that the C2V3C3 region of the HIV-2
envelope exerts an immunosuppressive activity on the CD4 and CD8
cells and suggested that this may be associated with the low rate of

84
immune activation and CD4 cell loss observed in most HIV-2
patients. In this context, increasing levels of anti-C2V3C3 antibodies
are expected to decrease the immunosuppressive function of this
region leading to higher immune activation and the associated CD4
cell loss. Overall, our results provide further support for the immune
protective function of the C2V3C3 envelope region during HIV-2
infection [32].
In agreement with most HIV-2 reports, we have shown here that
chronic HIV-2 infection usually courses without evidence for viral
replication in the plasma [9]. The number of CD4+ T cells is the only
available marker to monitor disease progression in these patients.
However, as shown here and elsewhere [9], HIV-2 patients may live
many years with low CD4+ T-cell counts without sign of disease
progression. Our results show that the anti-C2–C3 IgG response
adequately reflects the immunological and clinical progression in the
HIV-2 patients. We suggest, therefore, that antibody concentration
against the C2–C3 envelope region should be a useful marker to
monitor disease progression in HIV-2 infection.
Acknowledgements
The present work was supported by Fundação para a Ciência e
Tecnologia (project POCTI/ESP/48045). José Marcelino is the
recipient of a PhD scholarship from Fundação para a Ciência e
Tecnologia (FCT), Portugal. The Instituto Português do Sangue (IPS),
Portugal, is gratefully acknowledged for the provision of seronegative
plasma samples. We thank Luisa Papoila for statistical support.
J.M.M., C.N. and N.T. designed the study. J.M.M. performed all
antibody assays. H.B. and P.B. provided analytical reagents and
nucleotide sequences. F.M., L.R., F.A. and M.D. contributed clinical
data from the patients. P.G. performed the viral load assays. H.B.,
P.B., F.M., L.R., F.A., M.D. and P.G. assisted in data analysis.
J.M.M., C.N. and N.T. analyzed the data and wrote the paper.
References
1. Rowland-Jones S. Protective immunity against HIV infection:
lessons from HIV-2 infection. Future Microbiol 2006; 1:427– 433.
2. Rowland-Jones SL, Whittle HC. Out of Africa: what can we learn
from HIV-2 about protective immunity to HIV-1? Nat Immunol 2007;
8:329–331.

85
3. Holmgren B, da Silva Z, Vastrup P, Larsen O, Andersson S, Ravn
H, et al. Mortality associated with HIV-1, HIV-2, and HTLV-I single
and dual infections in a middle-aged and older population in Guinea-
Bissau. Retrovirology 2007; 4:85.
4. Poulsen AG, Aaby P, Gottschau A, Kvinesdal BB, Dias F, Molbak
K, et al. HIV-2 infection in Bissau, West Africa, 1987–1989:
incidence, prevalences, and routes of transmission. J Acquir Immune
Defic Syndr 1993; 6:941–948.
5. Blaak H, van der Ende ME, Boers PH, Schuitemaker H, Osterhaus
AD. In vitro replication capacity of HIV-2 variants from long-term
aviremic individuals. Virology 2006; 353:144–154.
6. Arien KK, Abraha A, Quinones-Mateu ME, Kestens L, Vanham G,
Arts EJ. The replicative fitness of primary human immunodeficiency
virus type 1 (HIV-1) group M, HIV-1 group O, and HIV-2 isolates. J
Virol 2005; 79:8979–8990.
7. Soriano V, Gomes P, Heneine W, Holguin A, Doruana M, Antunes
R, et al. Human immunodeficiency virus type 2 (HIV-2) in Portugal:
clinical spectrum, circulating subtypes, virus isolation, and plasma
viral load. J Med Virol 2000; 61:111– 116.
8. Gueudin M, Damond F, Braun J, Taieb A, Lemee V, Plantier JC, et
al. Differences in proviral DNA load between HIV-1- and HIV-2-
infected patients. AIDS 2008; 22:211–215.
9. MacNeil A, Sarr AD, Sankale JL, Meloni ST, Mboup S, Kanki P.
Direct evidence of lower viral replication rates in vivo in human
immunodeficiency virus type 2 (HIV-2) infection than in HIV-1
infection. J Virol 2007; 81:5325–5330.
10. Kanki PJ, Travers KU, Mboup S, Hsieh CC, Marlink RG, Gueye-
Ndiaye A, et al. Slower heterosexual spread of HIV-2 than HIV-1.
Lancet 1994; 343:943–946.
11. Adjorlolo-Johnson G, De Cock KM, Ekpini E, Vetter KM, Sibailly
T, Brattegaard K, et al. Prospective comparison of mother-tochild
transmission of HIV-1 and HIV-2 in Abidjan, Ivory Coast. JAMA
1994; 272:462–466.

86
12. Quinn TC, Wawer MJ, Sewankambo N, Serwadda D, Li C,
Wabwire-Mangen F, et al. Viral load and heterosexual transmission
of human immunodeficiency virus type 1. Rakai Project Study
Group. N Engl J Med 2000; 342:921–929.
13. Mansson F, Alves A, Silva ZJ, Dias F, Andersson S, Biberfeld G,
et al. Trends of HIV-1 and HIV-2 prevalence among pregnant women
in Guinea-Bissau, West Africa: possible effect of the civil war 1998–
1999. Sex Transm Infect 2007; 83:463–467.
14. Marcelino JM, Novo C, Pereira JM, Picotez F, Clemente A, Taveira
N. Production and characterization of a mouse monoclonal antibody
against the Gag p26 protein of human immunodeficiency virus type
2: identification of a new antigenic epitope. AIDS Res Hum
Retroviruses 2001; 17:1279–1283.
15. Leligdowicz A, Yindom LM, Onyango C, Sarge-Njie R, Alabi A,
Cotten M, et al. Robust Gag-specific T cell responses characterize
viremia control in HIV-2 infection. J Clin Invest 2007; 117:3067–
3074.
16. Duvall MG, Precopio ML, Ambrozak DA, Jaye A, McMichael AJ,
Whittle HC, et al. Polyfunctional T cell responses are a hallmark of
HIV-2 infection. Eur J Immunol 2008; 38:350–363.
17. Duvall MG, Lore K, Blaak H, Ambrozak DA, Adams WC, Santos
K, et al. Dendritic cells are less susceptible to human
immunodeficiency virus type 2 (HIV-2) infection than to HIV-1
infection. J Virol 2007; 81:13486–13498.
18. Marchant D, Neil SJ, McKnight A. Human immunodeficiency
virus types 1 and 2 have different replication kinetics in human
primary macrophage culture. J Gen Virol 2006; 87:411–418.
19. Rodriguez SK, Sarr AD, MacNeil A, Thakore-Meloni S, Gueye-
Ndiaye A, Traore I, et al. Comparison of heterologous neutralizing
antibody responses of human immunodeficiency virus type 1 (HIV-1)-
and HIV-2-infected Senegalese patients: distinct patterns of breadth
and magnitude distinguish HIV-1 and HIV-2 infections. J Virol 2007;
81:5331–5338.
20. Lizeng Q, Skott P, Sourial S, Nilsson C, Andersson SS, Ehnlund
M, et al. Serum immunoglobulin A (IgA)-mediated immunity in

87
human immunodeficiency virus type 2 (HIV-2) infection. Virology
2003; 308:225–232.
21. Tamalet C, Simon F, Dhiver C, Matheron S, de Micco P, Gastao
JA, et al. Autologous neutralizing antibodies and viral load in HIV-2-
infected individuals. AIDS 1995; 9:90–91.
22. Brenchley JM, Price DA, Douek DC. HIV disease: fallout from a
mucosal catastrophe? Nat Immunol 2006; 7:235–239.
23. Douek D. HIV disease progression: immune activation, microbes,
and a leaky gut. Top HIV Med 2007; 15:114–117.
24. Sousa AE, Carneiro J, Meier-Schellersheim M, Grossman Z,
Victorino RM. CD4 T cell depletion is linked directly to immune
activation in the pathogenesis of HIV-1 and HIV-2 but only indirectly
to the viral load. J Immunol 2002; 169:3400–3406.
25. Grossman Z, Meier-Schellersheim M, Paul WE, Picker LJ.
Pathogenesis of HIV infection: what the virus spares is as important
as what it destroys. Nat Med 2006; 12:289–295.
26. Hunt PW. Role of immune activation in HIV pathogenesis. Curr
HIV/AIDS Rep 2007; 4:42–47.
27. Grossman Z, Meier-Schellersheim M, Sousa AE, Victorino RM,
Paul WE. CD4RT-cell depletion in HIV infection: are we closer to
understanding the cause? Nat Med 2002; 8:319–323.
28. Deeks SG, Kitchen CM, Liu L, Guo H, Gascon R, Narvaez AB, et
al. Immune activation set point during early HIV infection predicts
subsequent CD4R T-cell changes independent of viral load. Blood
2004; 104:942–947.
29. Giorgi JV, Hultin LE, McKeating JA, Johnson TD, Owens B,
Jacobson LP, et al. Shorter survival in advanced human
immunodeficiency virus type 1 infection is more closely associated
with T lymphocyte activation than with plasma virus burden or virus
chemokine coreceptor usage. J Infect Dis 1999; 179:859–870.
30. Hazenberg MD, Otto SA, van Benthem BH, Roos MT, Coutinh
RA, Lange JM, et al. Persistent immune activation in HIV-1 infection
is associated with progression to AIDS. AIDS 2003; 17:1881–1888.

88
31. Choudhary SK, Vrisekoop N, Jansen CA, Otto SA, Schuitemaker
H, Miedema F, et al. Low immune activation despite high levels of
pathogenic human immunodeficiency virus type 1 results in long-
term asymptomatic disease. J Virol 2007; 81:8838–8842.
32. Cavaleiro R, Brunn GJ, Albuquerque AS, Victorino RM, Platt JL,
Sousa AE. Monocyte-mediated T cell suppression by HIV-2 envelope
proteins. Eur J Immunol 2007; 37:3435–3444. 33.
33. Marcelino JM, Barroso H, Goncalves F, Silva SM, Novo C, Gomes
P, et al. Use of a new dual-antigen enzyme-linked immunosorbent
assay to detect and characterize the human antibody response to the
human immunodeficiency virus type 2 envelope gp125 and gp36
glycoproteins. J Clin Microbiol 2006; 44:607–611.
34. Azevedo-Pereira JM, Lourenco MH, Barin F, Cisterna R, Denis F,
Moncharmont P, et al. Multicenter evaluation of a fully automated
screening test, VIDAS HIV 1 R 2, for antibodies to human
immunodeficiency virus types 1 and 2. J Clin Microbiol 1994;
32:2559–2563.
35. Clavel F, Mansinho K, Chamaret S, Guetard D, Favier V, Nina J,
et al.Human immunodeficiency virus type 2 infection associated with
AIDS in West Africa. N Engl J Med 1987; 316:1180–1185.
36. Michel P, Balde AT, Roussilhon C, Aribot G, Sarthou JL,
Gougeon ML. Reduced immune activation and T cell apoptosis in
human immunodeficiency virus type 2 compared with type 1:
correlation of T cell apoptosis with beta2 microglobulin concentration
and disease evolution. J Infect Dis 2000; 181:64–75.
37. Cavaco-Silva P, Taveira NC, Rosado L, Lourenco MH, Moniz-
Pereira J, Douglas NW, et al. Virological and molecular
demonstration of human immunodeficiency virus type 2 vertical
transmission. J Virol 1998; 72:3418–3422.
38. Gomes P, Taveira NC, Pereira JM, Antunes F, Ferreira MO,
Lourenco MH. Quantitation of human immunodeficiency virus type 2
DNA in peripheral blood mononuclear cells by using a quantitative-
competitive PCR assay. J Clin Microbiol 1999; 37:453–456.
39. Levett PN, Sonnenberg K, Sidaway F, Shead S, Niedrig M,
Steinhagen K, et al. Use of immunoglobulin G avidity assays for

89
differentiation of primary from previous infections with West Nile
virus. J Clin Microbiol 2005; 43:5873–5875.
40. Martro E, Suligoi B, Gonzalez V, Bossi V, Esteve A, Mei J, et al.
Comparison of the avidity index method and the serologic testing
algorithm for recent human immunodeficiency virus (HIV)
seroconversion, two methods using a single serum sample for
identification of recent HIV infections. J Clin Microbiol 2005;
43:6197–6199.
41. Barroso H, Taveira N. Evidence for negative selective pressure in
HIV-2 evolution in vivo. Infect Genet Evol 2005; 5:239– 246.
42. Matheron S, Damond F, Benard A, Taieb A, Campa P, Peytavin
G, et al. CD4 cell recovery in treated HIV-2-infected adults is lower
than expected: results from the French ANRS CO5 HIV-2 cohort.
AIDS 2006; 20:459–462.
43. Drylewicz J, Matheron S, Lazaro E, Damond F, Bonnet F, Simon
F, et al. Comparison of viro-immunological marker changes between
HIV-1 and HIV-2-infected patients in France. AIDS 2008; 22:457–
468.
44. Cavaco-Silva P, Taveira NC, Lourenco MH, Santos Ferreira MO,
Daniels RS. Vertical transmission of HIV-2. Lancet 1997; 349:177–
178.
45. Cartry O, Moja P, Quesnel A, Pozzetto B, Lucht FR, Genin C.
Quantification of IgA and IgG and specificities of antibodies to viral
proteins in parotid saliva at different stages of HIV-1 infection. Clin
Exp Immunol 1997; 109:47–53.
46. Lugada ES, Mermin J, Asjo B, Kaharuza F, Downing R,
Langeland N, et al. Immunoglobulin levels amongst persons with and
without human immunodeficiency virus type 1 infection in Uganda
and Norway. Scand J Immunol 2004; 59:203– 208.
47. Macpherson AJ, Gatto D, Sainsbury E, Harriman GR, Hengartner
H, Zinkernagel RM. A primitive T cell-independent mechanism of
intestinal mucosal IgA responses to commensal bacteria. Science
2000; 288:2222–2226.

90
48. Gordon SN, Klatt NR, Bosinger SE, Brenchley JM, Milush JM,
Engram JC, et al. Severe depletion of mucosal CD4R T cells in AIDS-
free simian immunodeficiency virus-infected sooty mangabeys. J
Immunol 2007; 179:3026–3034.
49. Richman DD, Wrin T, Little SJ, Petropoulos CJ. Rapid evolution
of the neutralizing antibody response to HIV type 1 infection. Proc
Natl Acad Sci U S A 2003; 100:4144–4149.
50. Zhang ZQ, Casimiro DR, Schleif WA, Chen M, Citron M, Davies
ME, et al. Early depletion of proliferating B cells of germinal center in
rapidly progressive simian immunodeficiency virus infection. Virology
2007; 361:455–464.
51. Taveira NC, Ferreira MO, Pereira JM. Amplification of fulllength
HIV-2 envelope genes. Mol Cell Probes 1996; 10:91– 98.
52. Wu X, Jackson S. Plasma and salivary IgA subclasses and IgM in
HIV-1-infected individuals. J Clin Immunol 2002; 22:106– 115.
53. Raux M, Finkielsztejn L, Salmon-Ceron D, Bouchez H, Excler JL,
Dulioust E, et al. Comparison of the distribution of IgG and IgA
antibodies in serum and various mucosal fluids of HIV type 1-
infected subjects. AIDS Res Hum Retroviruses 1999; 15: 1365–1376.
54. Mestecky J, Jackson S, Moldoveanu Z, Nesbit LR, Kulhavy R,
Prince SJ, et al. Paucity of antigen-specific IgA responses in sera and
external secretions of HIV-type 1-infected individuals. AIDS Res Hum
Retroviruses 2004; 20:972–988.
55. Ngo-Giang-Huong N, Candotti D, Goubar A, Autran B, Maynart
M, Sicard D, et al. HIV type 1-specific IgG2 antibodies: markers of
helper T cell type 1 response and prognostic marker of
longtermnonprogression. AIDS Res Hum Retroviruses 2001;
17:1435–1446.
56. Chiodi F, Mathiesen T, Albert J, Parks E, Norrby E, Wahren B.
IgG subclass responses to a transmembrane protein (gp41) peptide
in HIV infection. J Immunol 1989; 142: 3809–3814.
57. Raux M, Finkielsztejn L, Salmon-Ceron D, Bouchez H, Excler JL,
Dulioust E, et al. IgG subclass distribution in serum and various

91
mucosal fluids of HIV type 1-infected subjects. AIDS Res Hum
Retroviruses 2000; 16:583–594.
58. Wu X, Jackson S. Plasma and salivary IgG subclasses in HIV
type 1 infection: evidence of both transudation and local synthesis of
IgG in parotid saliva. AIDS Res Hum Retroviruses 2000; 16:1423–
1431.
59. Forthal DN, Landucci G, Bream J, Jacobson LP, Phan TB,
Montoya B. FcgammaRIIa genotype predicts progression of HIV
infection. J Immunol 2007; 179:7916–7923.
60. Lal RB, Heiba IM, Dhawan RR, Smith ES, Perine PL. IgG
subclass responses to human immunodeficiency virus-1 antigens:
lack of IgG2 response to gp41 correlates with clinical manifestation
of disease. Clin Immunol Immunopathol 1991; 58:267–277.
61. Martinez V, Costagliola D, Bonduelle O, N’go N, Schnuriger A,
Theodorou I, et al. Combination of HIV-1-specific CD4 Th1 cell
responses and IgG2 antibodies is the best predictor for persistence of
long-term nonprogression. J Infect Dis 2005; 191:2053–2063.
62. Scharf O, Golding H, King LR, Eller N, Frazier D, Golding B, et al.
Immunoglobulin G3 from polyclonal human immunodeficiency virus
(HIV) immune globulin is more potent than other subclasses in
neutralizing HIV type 1. J Virol 2001; 75:6558– 6565.
63. Cavaleiro R, Sousa AE, Loureiro A, Victorino RM. Marked
immunosuppressive effects of the HIV-2 envelope protein in spite of
the lower HIV-2 pathogenicity. AIDS 2000; 14:2679– 2686.


93
CAPÍTULO V
Resposta Humoral na Evolução Molecular
das Regiões C2, V3 e C3 do Invólucro do
VIH-2 em Pacientes Crónicos

94

95
O Papel da Resposta Humoral na Evolução Molecular das
Regiões C2, V3 e C3 do Invólucro do VIH-2 em Pacientes
Cronicamente Infectados.
Publicação: The role of the humoral immune response in the
molecular evolution of the envelope C2, V3 and C3
regions in chronically HIV-2 infected patients.
Pedro Borrego, José Maria Marcelino, Cheila Rocha,
Manuela Doroana, Francisco Antunes, Fernando
Maltez, Perpétua Gomes, Carlos Novo, Helena Barroso
and Nuno Taveira.
Retrovirology, 2008, 5:78
Sumário
Introdução: Este estudo foi planeado para investigar, pela primeira
vez, a evolução molecular num curto período, as regiões C2, V3 e C3
do invólucro do VIH-2 e a sua associação com a resposta imune. A
partir de uma coorte de dezoito pacientes infectados com VIH-2,
seguidos prospectivamente ao longo de 2-4 anos, foram obtidas
sequências clonais da região C2V3C3 do env. Na região C2V3C3
foram analisadas a diversidade genética, divergência, selecção
positiva e glicosilação em função do número de células T CD4+ e da
reactividade dos anticorpos IgG e IgA contra a C2V3C3.
Resultados: A média da diversidade nucleotídica intra-hospedeiro foi
2,1% (DP, 1,1%), aumentando ao longo do curso da infecção na
maioria dos pacientes. A diversidade ao nível dos aminoácidos foi
significativamente mais baixa para a região V3 e mais elevada para a
região C2. A taxa média de divergência foi 0,014
substituições/local/ano, que é semelhante à que tem sido referida
para a infecção VIH-1 crónica. O número e posição dos locais
seleccionados positivamente foi muito variável, excepto para os
codões 267 e 270 na região C2 que estiveram sob uma pressão
selectiva forte e persistente na maioria dos pacientes. Os locais de
glicosilação ligados á asparagina (N-glicosilação) localizados na C2 e
na V3 mantiveram-se conservados em todos os pacientes ao longo do
curso da infecção. A variação intra-hospedeiro da resposta IgG
específica para a C2V3C3, ao longo do tempo, mostrou estar
inversamente associada à variação nos nucleótidos e diversidade dos
aminoácidos na região C2V3C3. A variação da resposta IgA específica

96
para a C2V3C3 mostrou estar inversamente associada à variação no
número de locais N-glicosilação.
Conclusão: A dinâmica evolucionária do invólucro do VIH-2 durante
infecções avirémicas crónicas é semelhante à do VIH-1, o que implica
que o vírus deve estar em replicação activa nos compartimentos
celulares. A evolução convergente da N-glicosilação na C2 e V3, e a
diversificação limitada da V3, indicam que existem factores
funcionais importantes na potencial diversidade do invólucro do VIH-
2. Os anticorpos IgG específicos para a C2V3C3 são eficazes na
redução da dimensão da população viral limitando o número de vírus
mutantes com capacidade de escape. A região C3 parece ser um alvo
para os anticorpos IgA e a N-glicosilação elevada pode prevenir o
reconhecimento do invólucro do VIH-2 por parte destes anticorpos.
Os nossos resultados trazem novas reflexões sobre a biologia do VIH-
2 e a sua relação com o hospedeiro humano e podem ter importantes
implicações na concepção de uma vacina.

97
The Role of the Humoral Immune Response in the
Molecular Evolution of the C2, V3 and C3 Regions in
Chronically HIV-2 Infected Patients
Abstract
Background: This study was designed to investigate, for the first
time, the short-term molecular evolution of the HIV-2 C2, V3 and C3
envelope regions and its association with the immune response.
Clonal sequences of the env C2V3C3 region were obtained from a
cohort of eighteen HIV-2 chronically infected patients followed
prospectively during 2–4 years. Genetic diversity, divergence, positive
selection and glycosylation in the C2V3C3 region were analysed as a
function of the number of CD4+ T cells and the anti-C2V3C3 IgG and
IgA antibody reactivity
Results: The mean intra-host nucleotide diversity was 2.1% (SD,
1.1%), increasing along the course of infection in most patients.
Diversity at the amino acid level was significantly lower for the V3
region and higher for the C2 region. The average divergence rate was
0.014 substitutions/site/year, which is similar to that reported in
chronic HIV-1 infection. The number and position of positively
selected sites was highly variable, except for codons 267 and 270 in
C2 that were under strong and persistent positive selection in most
patients. N-glycosylation sites located in C2 and V3 were conserved
in all patients along the course of infection. Intra-host variation of
C2V3C3-specific IgG response over time was inversely associated
with the variation in nucleotide and amino acid diversity of the
C2V3C3 region. Variation of the C2V3C3-specific IgA response was
inversely associated with variation in the number of N-glycosylation
sites.
Conclusion: The evolutionary dynamics of HIV-2 envelope during
chronic aviremic infection is similar to HIV-1 implying that the virus
should be actively replicating in cellular compartments. Convergent
evolution of N-glycosylation in C2 and V3, and the limited
diversification of V3, indicates that there are important functional
constraints to the potential diversity of the HIV-2 envelope. C2V3C3-
specific IgG antibodies are effective at reducing viral population size
limiting the number of virus escape mutants. The C3 region seems to
be a target for IgA antibodies and increasing N-linked glycosylation
may prevent HIV-2 envelope recognition by these antibodies. Our
results provide new insights into the biology of HIV-2 and its relation

98
with the human host and may have important implications for
vaccine design.

99
Background
The etiologic agents of AIDS, HIV-1 and HIV-2, are two distinct
human lentiviruses with similar structural and genomic organization
but sharing only 50% of genetic similarity [1]. Compared to HIV-1,
the infection by HIV-2 is associated with better prognosis, slower
disease progression and transmission, longer latency period and
reduced mortality rate [2-6]. Moreover, most HIV-2 patients have
normal CD4+ T cell counts and low or undetectable plasmatic viral
levels [7,8]. Two possible explanations for these differences may be
the slower replication capacity of HIV-2 and a more efficient immune
control of HIV-2 [9-13].
The env gene codes for the viral envelope glycoproteins, which are
responsible for HIV entry into cells [14]. Rapid evolutionary changes
and high genetic variability are two major characteristics of the HIV
env gene [15]. In HIV-1 infection, conflicting associations have been
reported between disease status and within-patient env gene
evolution. Hence, some studies have shown that genetic diversity and
divergence from the infecting strain increase during HIV-1 infection
but become stable or even decrease in the advanced stage of disease,
with the lower CD4+ T cell counts and progression to AIDS [16-18].
Other authors have shown that higher genetic diversity and
divergence are found in patients with rapid progression to disease
than in slow- or non-progressors [19,20]. There is also a positive
correlation between viral replication and intrahost HIV-1 evolution in
elite controllers and long-term nonprogressors [21].
The number of studies investigating within-patient HIV-2 molecular
evolution and their association with clinical and immunological
evolution is limited. In one transversal study, we have shown that
the genetic diversity of the HIV-2 env may be directly related to the
period of infection [22]. Longitudinal studies performed in Senegal
have shown that higher variability in the env V3 region is generally
found in patients with faster disease progression to AIDS [23] and
that in elite controllers (patients infected for ≈ 10 years with normal
CD4+ T cell counts without antiretroviral therapy and with low or
undetectable viral load) the rate of env gene diversification may be
positively associated with the rate of CD4+ T cell number decrease
[24].
Higher rate of molecular evolution, with predominance of
nonsynonymous amino acid substitutions, tends to occur in regions
of the HIV-1 env gene submitted to strong selective pressure from the
immune system [15,25-28]. A structure of particular importance in
this process is the V3 loop of the surface glycoprotein which is
essential for HIV coreceptor usage [29-32] and for inducing the

100
production of neutralizing and nonneutralizing antibodies in HIV
infected individuals [33]. Neutralizing antibody responses, both
autologous [34-36] and heterologous [36,37] may be more common in
HIV-2 than in HIV-1 infection. Still, little is known about the role of
humoral immunity in the evolution of the HIV-2 env gene. In the
present study we analyze, for the first time, the molecular evolution
of the env C2V3C3 regions in chronically HIV-2 infected patients over
a two to four year period in the context of their antibody response
(IgG and IgA) against the same envelope region.
Methods
Patients. Eighteen HIV-2 patients attending different hospitals in
Lisbon, Portugal, were followed prospectively during 2–4 years (Table
1). Fourteen patients were taking reverse transcriptase and/or
protease inhibitors. During the follow-up period three patients
(PTHCC20, PTHSM9 and PTHSM10) had detectable plasma viral
load. Eight patients had < 200 CD4+ T cells/μl (AIDS defining
condition).
Quantification of HIV-2 plasma virémia. HIV-2 viremia in the
plasma was quantified with a quantitative-competitive RT-PCR assay
as described elsewhere [38].
DNA extraction, PCR amplification, cloning and sequencing.
PBMCs from all patients were co-cultivated with normal PBMCs to
try to isolate virus [39]. At the end of the culture period, which is
when the culture was positive (mean, 15 days), cells were harvested
and DNA was extracted with the Wizard® Genomic DNA Purification
kit (Promega) for subsequent analysis. A fragment of the C2V3C3
region (378 bp) of the HIV-2 env gene was amplified in a nested
Polymerase Chain Reaction (PCR) as described previously [22]. PCR
fragments were cloned into pCR®4-TOPO® vector (Invitrogen) and
transformed into One Shot® Match1™-T1R competent cells
(Invitrogen). Cloned plasmids were extracted [40], purified and
sequenced using BigDye Terminator Cycle sequencing kit (Applied
Biosystems), with M13 Forward and Reverse primers, and an
automated sequencer (ABI Prism 3100, Applied Biosystems). For
each patient an average of 13 clones (range 7–21) was sequenced per
sampling year.

101
Table 1: Virological and immunological characterization of the
patients.
Sequence analysis and phylogenetic studies. The nucleotide
sequences were aligned using Clustal X [41] and manual
adjustments were made using Genedoc [42]. Genetic distances
between sequences were calculated using the maximum composite
likelihood method implemented in the MEGA version 4 [43]. Inter-
and intra-sample synonymous (dS) and nonsynonymous (dN)
distances were estimated using the modified Nei-Gojobory method
with the Jukes-Cantor correction, also implemented in the MEGA
software package.
Maximum likelihood analyses [44] were performed using the best-fit
model of molecular evolution estimated by Model test under the
Akaike information criterion [45]. The chosen model was TVM+G+I.
Tree searches were conducted in PAUP version 4.0 using the nearest-
neighbor interchange (NNI) and tree bisection and reconnection (TBR)
heuristic search strategies [46], and bootstrap resampling [47]. The
nucleotide divergence rate was estimated using an adaptation of the
methodology previously described by Salazar-Gonzalez et al. [48].
Firstly, maximum likelihood trees were constructed for each patient

102
using all clonal sequences from each time point and rooted with the
consensus sequences from other patients. Then, assuming a
molecular clock, the branch lengths between the leafs and the root of
the tree were calculated by using Branchlength Calculator [49] and
plotted against time in years.
Natural selection of specific amino acids was examined using
Codeml, models M0 and M3, with the HYPHY package [50]. Potential
N-glycosylation sites were identified using N-Glycosite [51]. The
entropy at each position in protein alignment was measured with
Shannon Entropy [52].
Humoral antibody response against the env C2V3C3 regions. IgG
and IgA antibody response against the env C2V3C3 region was
quantified with the ELISA-HIV2 test developed in our laboratory, as
described elsewhere with some modifications [53]. Briefly, microtiter
plates (96-well) were coated with rgp36 and rpC2-C3 by overnight
incubation at 4°C and blocked with 1% gelatine in Tris-buffered
saline (TBS). HIV-2-positive plasma samples were added to the
antigen coated wells at a 1:100 dilution. Bound antibodies were
detected by using alkaline phosphatase (AP)-conjugated goat anti-
human IgG (diluted 1:2000 in TBS) or horseradish peroxidase (HPR)-
conjugated rabbit anti-human IgA (diluted 1:2000 in phosphate-
buffer saline) (Sigma-Aldrich). The colour was developed using p-
nitrophenilphosphate (p-NPP Tablets, Sigma-Aldrich) as chromogenic
substrate to AP and o-phenylenediamine dihydrochloride (OPD) to
HPR. Optical density (OD) was measured with an automated
microplate reader LP 400 (Bio-Rad) at 405 and 492 nm against a
reference wavelength of 620 nm. The clinical cut-off value of the
assay, calculated as the mean OD value of HIV-seronegative samples
plus three times the standard deviation [SD], was determined using
samples from healthy HIV-seronegative subjects. The results of the
assay are expressed quantitatively as ODclinical sample(S)/ODcut-
off (CO) ratios. For ratio values >1 the sample is considered as
seroreactive.
Statistical analysis. Statistical analysis was performed in GraphPad
Prism version 4.00 for Windows (GraphPad Software), with a level of
significance of 5%. For the inter-patient statistical analysis across
time, only information obtained from one time point (one sample) per
patient was considered in order to guarantee the independence of the
data analyzed. Thus, to maximize the number of observations in the
analysis, we chose the first sample (first time point) available for
each patient. Nonparametric tests were used to compare means and

103
medians between variables: paired data was analyzed with Wilcoxon-
matched pairs test and Friedman test; unpaired variables were
tested with Mann Whitney U test and Kruskal-Wallis test. To study
how two variables varied together linear regression was performed
and Spearman correlation coefficients were computed. Finally,
Deming linear regression was used to study the overall variation
(slopes) of intra-patient data with time (longitudinal analysis).
GenBank accession numbers. Sequences have been assigned the
following GenBank accession numbers: EU358115–EU358499,
EU358501, EU358504, EU358507, EU358509, EU358513,
EU358517, EU358519–EU358521, EU358524, EU358525,
EU358527–EU358531, EU358533, EU358536–EU358538,
EU358541, EU358543, EU358546–EU358549, EU358551–
EU358567, EU360797–EU360799.
Results
Phylogenetic relationships, genetic diversity and divergence. To
investigate the molecular evolution of the HIV-2 env gene we have
amplified, cloned and sequenced the env gene fragment coding for
the C2, V3 and C3 regions using yearly samples collected from 18
patients followed prospectively for 2–4 years. A total of 431 clonal
sequences were obtained from 18 patients (average of 13 sequences
per patient per sampling year). Phylogenetic analysis showed that all
sequences clustered together within HIV-2 group A and that each
patient sequences formed monophyletic sub-clusters with high
bootstrap supporting values (Figure 1). Phylogenetic analysis also
showed that with the exceptions of patients PTHCC1, PTHCC5 and
PTHCC20, sequences from most patients were not segregated
according to sampling years, a clear indication that there were no
major shifts in virus population structure from one year to the other.
The mean evolutionary distance between different nucleotide
sequences from each sample/year (nucleotide diversity) was 2.1%
(standard deviation = 1.1) (additional file 1). Nucleotide diversity was
neither associated with clinical status (2.1% mean median genetic
distance in AIDS patients vs 1.4% in the other patients; p = 0.203)
nor with plasma viremia (2.3% in viremic patients vs 1.8% in
aviremic patients; p = 0.386) (n = 18).

104
Figure 1. Maximum-likelihood phylogenetic analysis. The
phylogenetic tree was constructed with reference sequences from
HIV-2 groups A, B and G, under the TVM+G+I evolutionary model,
using the NNI heuristic search strategy and 1000 bootstrap
replications. The triangles represent the compressed subtrees
containing clonal sequences obtained from all samples collected for
each patient. The length of the triangle represents the intra-patient
nucleotide diversity and its thickness is proportional to the number
of sequences. The bootstrap values supporting the internal The scale
bar represents evolutionary distances in and higher for the C2 region
(p < 0.005) (additional file 1). The inset contains the subtrees of
patient PTHCC1 (A), PTHCC20 (B) and PTHCC5 C) (Yellow circle –
2003; green circle – 2004; blue circle – 2005).
Considering the first and the last samples of each patient, nucleotide
diversity increased along the course of infection in all patients,

105
except for patient PTHCC5 (additional file 1). Shannon's entropy was
used to measure the relative amino acid variability in our set of
sequences [52]. The sum of entropy values of the amino acid
alignments varied between regions (p < 0.001), being significantly
lower for the V3 region (p < 0.001) and higher for the C2 region (p <
0.005) (additional file 1).
Within-patient nucleotide divergence rate was on average 0.014
substitutions per site per year for the C2V3C3 region, but it varied
widely between patients (SD = 0.011). There was no association
between the divergence rate and the variation in the number of CD4+
T cells over time (Deming regression analysis, F = 0.058, p = 0.816).
Likewise, the divergence rate of the C2V3C3 regions was not related
with the level of IgG antibodies produced against the homologous
peptide over time (F = 0.192, p = 0.675).
Selection analysis and adaptation rate of the C2, V3, and C3
regions. Intra-patient analysis showed that the overall C2V3C3
region was under purifying selection (dN/dS ratio < 1) along the
course of infection in all patients (additional file 1). Analysis of the
number and location of positively selected codons is useful to identify
particular amino acids that may be under the selective pressure of
the immune system, regions that can define potential neutralizing
epitopes or that are functionally important for the protein [15, 25-
28]. In the present study, higher number of sites under positive
selection tended to be found in patients with detectable viremia
compared to patients with undetectable viremia (median, 15 sites vs
2; p = 0.061) (n = 18) (additional file 1). Otherwise, the number of
positively selected sites was highly variable in number and position
in most patients (Figure 2). Notable exceptions were amino acids at
positions 267 and 270 in C2 (numbered according to the reference
HIV-2ALI strain) that were under strong positive selection in all
patients. Selection at these two sites persisted for at least two years
in 9 patients (Figure 2). Because of these two sites, the median
number of positively selected codons per sample was higher in the
C2 region compared with the other regions (p < 0.005) (n = 18).
Finally, using linear regression analysis we found that within each
patient an average of 1.0 (SD = 3.8) positively selected site varied per
year (adaptation rate).

106
y,itensity and distribution of positively
Figure 2. Frequency, intensity and distribution of positively selected
sites in the C2, V3 and C3 regions along the course of HIV-2
infection. Positively selected codons (obtained with Codeml, model
M3) were classified in two categories according to the ω ratio:ω>6,
codons under strong selective pressure; 1<ω<6, codons under weak
selective pressure. The frequency and distribution of positively
selected sites in the C2, V3 and C3 regions are shown in each
infection year. Higher frequency positively selected sites are shown in
bold letters. Sites were numbered according to the reference HIV-
2ALI strain. (na, not available).
Glycosylation of the HIV-2 env C2-C3 region. Since the
glycosylation pattern of the HIV-1 env gene may influence
neutralization escape to the immune system, viral tropism and
clinical progression [32,36,54-57], we determined the number of
potential N-glycosylation sites in our sequences and examined its
variation as a function of time and other parameters analyzed in this
study. The number of N-glycosylation sites ranged from 5 to 8
(median, 7) and tended to be conserved along the infection in each
patient, the exception being patient PTHCC1 with an increase in two
sites over the three years of follow up (Figure 3). The number of
glycosylation sites varied significantly between C2, V3 and C3 (p <
0.001), being concentrated particularly in C2 (p < 0.001) (n = 18). At
the intra- and inter-patient level, the most conserved N-glycosylation
sites were located in C2 and V3. With one exception, all sites that
varied over time were located in C3. The number of N-linked
glycosylation sites was directly associated with the number of
positively selected sites (r2 = 0.301; p = 0.018).

107
Figure 3. Frequency and distribution of potential N-glycosylation
sites in the C2, V3 and C3 regions along the course of infection. The
frequency and distribution of potential N-linked glycosylation sites in
the C2, V3 and C3 regions are shown in each infection year. Higher
frequency glycosylation sites are shown in bold letters. Sites were
numbered according to the reference HIV-2ALI strain. (na, not
available).
Molecular evolution of the C2, V3 and C3 regions as a function
of the antibody response. All patients produced IgA antibodies
against the C2V3C3 region whereas IgG antibodies were detected in
all but two patients, PTHSM9 and PTHSM10 (Table 1). Intrapatient
analysis revealed that along the course of the infection the variation
of C2V3C3-specific IgG response was inversely associated with the
variation of nucleotide diversity (F = 22.09; p = 0.002) as well as with
the dN rate (F = 22.800; p = 0.002) and amino acid diversity
(Shannon's entropy, F = 23.610; p = 0.002), particularly in the V3 (F
= 11.660; p = 0.014) and C3 regions (F = 6.214; p = 0.041) (n = 9)
(Figure 4).

108
Figure 4. C2V3C3 sequence evolution along the course of infection
as a function of antibody response. Deming regression analysis. (A)
Annual variation (slope) of the C2V3C3-IgG response vs annual
variation (slope) of the mean nucleotide diversity; (B) Annual
variation (slope) of the C2V3C3-IgA response vs annual variation
(slope) of the number of potential N-glycosylation sites.
Variation of the C2V3C3-specific IgA response over time was
inversely associated with variation in the number of N-linked
glycosylation sites (F = 22.090; p = 0.042; n = 4) which occurred in
four patients particularly in the C3 region (Figure 4).evolution along
the course of infection as a function of antibody response
Discussion
In this study we have examined, for the first time, the molecular
evolution of the envelope C2, V3 and C3 regions during chronic HIV-
2 infection and its correlation with the antibody response against the
same regions. Our cohort was constituted by long-term infected
patients showing, in general, low CD4+ T cell counts and
undetectable plasma viremia.
Nucleotide diversity increased with time in all but one patient with
values similar to those obtained in an earlier study performed with
HIV-2 elite controllers (2.1%, this study, vs 1.7%; p = 0.3440) [24].
This value is also similar to the 2.5% median diversity reported for
chronically HIV-1 infected patients [58] and to the 3.0% mean
diversity reported for some long-term nonprogressors with low viral
load [21].
In phylogenetic analysis we found low quasispecies complexity in
most patients, i.e. virus populations from most patients were mostly
homogeneous during the follow up period. This was expected since
HIV-2 is generally seen as a slowly evolving virus and over a short
period of time one would expect to observe few evolutionary changes
[22,24,59]. However, in three patients there was evidence for
segregation of virus quasispecies according to the year of infection,

109
which implies high rate of evolutionary change and immune selection
in these patients [15,60]. Consistent with this, we found that the
nucleotide divergence rate varied widely between patients. Moreover,
the average nucleotide divergence rate (0.014 substitutions per site
per year) was very high when compared to that reported for HIV-2
elite controllers (mean, 0.23%) [24] and for HIV-1 long-term non
progressors with low plasma viral load (mean, 0.27%) [21]. Even
though we could not detect any association between nucleotide
divergence and the number of CD4+ T cells, the higher net
divergence observed in our patients might be related to their high
immune deterioration, as higher genetic divergence is generally
found in HIV-1 rapid progressors compared to slow- or non-
progressors [19,20]. In fact, the 0.014 annual divergence rate found
in our patients is similar to that found in chronically HIV-1 infected
patients (between 1.0% and 1.5% per year) [17,58]. In conclusion,
the sampling schedule used in our study, and possibly the fact that
we have analyzed the virus present inside the cells and not in the
plasma, has enabled us to demonstrate that the evolutionary
dynamics of HIV-2 during chronic infection is surprisingly similar to
HIV-1. This implies that HIV-2 is actively replicating during chronic
infection, possibly in the lymphoid tissue, as in HIV-2 patients the
mononuclear cells in the lymph nodes are heavily infected, even
more than the mononuclear cells in the peripheral blood [61,62].
Future studies of HIV-2 nucleotide divergence should include also
the virus populations present in the lymphoid tissue and other
cellular compartments (e.g. GI tract).
Despite the high nucleotide divergence rate, most of the
substitutions were of a synonymous nature such that the dN/dS
ratio of the C2V3C3 region was always below one and, most
importantly, it decreased over time in most patients. These results
are in agreement with previous reports that have examined the
C2V3C3 region [22,24] and with the observation that, globally, the
HIV-2 env gene is under purifying selection [25]. Consistent with
previous studies of a cross-sectional nature, we found that C2 and
C3, but not V3, were the fastest evolving regions at the nucleotide
and amino acid level contributing significantly to the high within-
patient nucleotide divergence rate [22,63]. The conservation of the V3
region in vivo implies that in HIV-2, as in HIV-1, this region is
submitted to strong structural and conformational constraints which
are probably related to its crucial functional roles at the level of
coreceptor binding and cell entry [29-32].
It is probable that adaptation to immune pressure is the main driver
of the rapid intra-host evolution of the C2 and C3 regions in HIV-2

110
[15,25,58,60,64-66]. Indeed, we found that most of the amino acids
under selection are located in C2, including the two amino acids that
are under strongest positive selection in all patients (positions 267
and 270). Moreover, selection at these two sites persisted for at least
two years in the majority of the patients which is a clear indication
that they are under continued immune pressure in vivo [60,67]. The
equivalent amino acids in HIV-1 are not under positive selection [67],
are located in the hidden surface of envelope glycoprotein complex
[58] and define a cytotoxic T cell epitope [68]. Thus, our results also
suggest that the antigenic presentation of the C2, and perhaps the
C3 region (see below), in the envelope complex of HIV-2 differs
substantially from that of HIV-1.
Glycans on HIV-1 envelope protein play an important role in the
folding of the glycoproteins, in infection and in evasion from the host
immune response (reviewed in [69]). We found that, as for HIV-1
[51,58], the majority of potential N-glycosylation sites were
concentrated in the C2 region. The four N-glycosylation sites in C2
and the site in the beginning of V3 were highly conserved in all
patients throughout infection which is strongly indicative of
convergent evolution at these glycosylation hotspots and suggests an
unexpected constraint on the potential diversity of the HIV-2
envelope [70,71]. The convergent evolution of glycosylation sites may
have important implications for both vaccine design and antiviral
therapeutic [69].
To try to identify the immune correlates of the molecular evolution of
HIV-2 C2, V3 and C3 regions we have looked into all possible
associations between the number of CD4+ T cells or the IgA and IgG
antibody levels and different parameters that reflect viral molecular
evolution. In longitudinal analysis there was no significant
association between the number of CD4+ T cells and nucleotide
diversity, amino acid entropy, nucleotide divergence, dN/dS ratio and
number of positively selected sites. These results are in partial
contrast to those of MacNeil et al. [24], who found a direct
association between the rates of HIV-2 diversification and rates of
CD4+ T cell decline in long term non progressors followed for a
decade in Senegal. The short term follow-up and the associated
modest variation in the number of CD4 + T cells might have
prevented the detection of this type of association in our patients.
Strikingly, however, there was a close relationship between virus
diversification and evolution and C2V3C3-specific antibody response
over time. In fact, higher IgG response was significantly associated
with lower viral variability at the nucleotide and amino acid levels as
well as with lower frequency of nonsynonymous substitutions. These

111
results imply that the anti-C2V3C3 IgG antibodies are effective at
reducing viral population size limiting the number of virus escape
mutants [72]. This is in striking contrast to the majority of acute and
chronic HIV-1 infections where the virus quickly escapes from anti-
V3 and anti-C3 autologous neutralizing antibodies [33,73-76].
Consistent with the lower capacity of HIV-2 to escape from C2V3C3-
neutralizing antibodies when compared to HIV-1, we found that on
average HIV-2 has a five-fold lower adaptation rate in vivo than HIV-1
(1 positively selected site per year vs 5 sites per year) [60,77]. The
HIV-2 low adaptation rate may be related to its low replicative
capacity and low plasma viral load [12,13,78]. Overall, these results
provide support for a crucial role of neutralizing antibody response in
the effective containment of viral replication in HIV-2 infection in vivo
[36].
Surprisingly, in some patients addition of glycans to the C3 region
was associated with a reduction in the IgA immunogenicity of the
C2V3C3 region. Envelope-specific plasma IgA antibodies, mostly
binding to the gp36 transmembrane glycoprotein, have been found to
neutralize HIV-2 [79]. Increasing the number of N-glycans in the
envelope gp120 surface glycoprotein, or varying the position of
glycosylation sites, has been associated with escape from IgG
neutralizing antibody response in simian immunodeficiency virus
(SIV) and HIV-1 infection [57,80-82]. Hence, one plausible
explanation for the inverse association between IgA response and N-
glycosylation is that the C3 envelope region induces IgA neutralizing
antibodies to which HIV-2 escapes through the occlusion of the C3
region with N-linked glycans. This may have important implications
for vaccine design. Ongoing studies will determine whether C2V3C3-
specific IgA antibodies present in these patients effectively neutralize
their autologous virus.
Conclusion
The evolutionary dynamics of HIV-2 envelope during chronic and
highly suppressed infection is surprisingly similar to HIV-1 implying
that the virus is actively replicating in cellular compartments.
Convergent evolution of N-glycosylation in C2 and V3, as well as the
limited diversification of V3, indicates however that there are
important functional constraints to the potential diversity of the HIV-
2 envelope. HIV-2 envelope diversification is inversely related to the
C2V3C3-specific IgG antibody response over time implying that these
antibodies are effective at reducing viral population size, limiting the
number of virus escape mutants. The C3 region seems to be a target
for IgA antibodies and increasing N-linked glycosylation may prevent

112
HIV-2 envelope recognition by these antibodies. Our results provide
new insights into the biology of HIV-2 and its relation with the
human host and may have important implications for vaccine design.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
NT designed and coordinated the study. PB performed most of the
cloning and sequencing experiments. JMM isolated the viruses and
quantified the antibody responses. HB and CR participated in virus
isolation and in the sequencing analysis of some patients. MD, FA
and FM recruited the patients and were responsible for collecting the
blood samples and the clinical data. PG quantified the plasma
viremia. CN and PG helped with the interpretation of data and
revision of the manuscript. PB and NT preformed statistical analysis.
PB and NT interpreted the data and wrote the manuscript. All
authors reviewed and accepted the final manuscript.
Additional material file 1
Table 2. Results from sequence and phylogenetic analysis. adN/dS –
ratio of nonsynonymous and synonymous substitutions, obtained with
Codeml (model M0). bdN/dS – ratio of nonsynonymous and
synonymous substitutions between the first and the last time point,
obtained with Codeml (model M0), when applicable. c Sum of
Shannon's entropy values at each position in protein alignment. d
Number of positively selected codons in the nucleotide alignment,
obtained with Codeml (model M3). SD – Standard deviation. Click here
for file
http://www.biomedcentral.com/content/supplementary/1 42-4690-
5-78-S1.xls]
Acknowledgements
This work was supported by Fundação para a Ciência e Tecnologia
(project POCTI/ESP/48045). Pedro Borrego is supported by a PhD
grant from Fundação para a Ciência e Tecnologia.
References
1. Hu DJ, Dondero TJ, Rayfield MA, George JR, Schochetman G,
Jaffe HW, Luo CC, Kalish ML, Weniger BG, Pau CP, et al.: The
emerging genetic diversity of HIV. The importance of global

113
surveillance for diagnostics, research, and prevention. JAMA 1996,
275:210-216.
2. Andersson S, Norrgren H, da Silva Z, Biague A, Bamba S, Kwok S,
Christopherson C, Biberfeld G, Albert J: Plasma viral load in HIV-1
and HIV-2 singly and dually infected individuals in Guinea-Bissau,
West Africa: significantly lower plasma virus set point in HIV-2
infection than in HIV-1 infection. Arch Intern Med 2000, 160:3286-
3293.
3. Kanki PJ, Travers KU, S MB, Hsieh CC, Marlink RG, Gueye NA,
Siby T, Thior I, Hernandez-Avila M, Sankale JL, et al.: Slower
heterosexual spread of HIV-2 than HIV-1. Lancet 1994, 343:943-946.
4. Marlink R, Kanki P, Thior I, Travers K, Eisen G, Siby T, Traore I,
Hsieh CC, Dia MC, Gueye EH, et al.: Reduced rate of disease
development after HIV-2 infection as compared to HIV-1. Science
1994, 265:1587-1590.
5. Whittle H, Morris J, Todd J, Corrah T, Sabally S, Bangali J, Ngom
PT, Rolfe M, Wilkins A: HIV-2-infected patients survive longer than
HIV-1-infected patients. AIDS 1994, 8:1617-1620.
6. Reeves JD, Doms RW: Human immunodeficiency virus type 2. J
Gen Virol 2002, 83:1253-1265.
7. Berry N, Ariyoshi K, Jaffar S, Sabally S, Corrah T, Tedder R,
Whittle H: Low peripheral blood viral HIV-2 RNA in individuals with
high CD4 percentage differentiates HIV-2 from HIV-1 infection. J
Hum Virol 1998, 1:457-468.
8. Soares R, Foxall R, Albuquerque A, Cortesao C, Garcia M,
Victorino RM, Sousa AE: Increased frequency of circulating CCR5+
CD4+ T cells in human immunodeficiency virus type 2 infection. J
Virol 2006, 80:12425-12429.
9. Anderson DE, Llenado RA, Torres JV: Humoral immunity and the
evolution of HIV-2. Viral Immunol 2004, 17:436-439.
10. Berry N, Jaffar S, Schim van der Loeff M, Ariyoshi K, Harding E,
N'Gom PT, Dias F, Wilkins A, Ricard D, Aaby P, et al.: Low level
viremia and high CD4% predict normal survival in a cohort of HIV

114
type-2-infected villagers. AIDS Res Hum Retroviruses 2002, 18:1167-
1173.
11. Lizeng Q, Nilsson C, Sourial S, Andersson S, Larsen O, Aaby P,
Ehnlund M, Bjorling E: Potent neutralizing serum immunoglobulin A
(IgA) in human immunodeficiency virus type 2-exposed IgG-
seronegative individuals. J Virol 2004, 78:7016-7022.
12. MacNeil A, Sarr AD, Sankale JL, Meloni ST, Mboup S, Kanki P:
Direct evidence of lower viral replication rates in vivo in human
immunodeficiency virus type 2 (HIV-2) infection than in HIV-1
infection. J Virol 2007, 81:5325-5330.
13. Blaak H, Ende ME van der, Boers PH, Schuitemaker H,
Osterhaus AD: In vitro replication capacity of HIV-2 variants from
longterm aviremic individuals. Virology 2006, 353:144-154.
14. Levy JA: HIV and the pathogenesis of AIDS 2nd edition.
Washington, D.C.: ASM Press; 1998.
15. Lemey P, Rambaut A, Pybus OG: HIV evolutionary dynamics
within and among hosts. AIDS Rev 2006, 8:125-140.
16. Delwart EL, Pan H, Sheppard HW, Wolpert D, Neumann AU,
Korber B, Mullins JI: Slower evolution of human immunodeficiency
virus type 1 quasispecies during progression to AIDS. J Virol 1997,
71:7498-7508.
17. Shankarappa R, Margolick JB, Gange SJ, Rodrigo AG, Upchurch
D, Farzadegan H, Gupta P, Rinaldo CR, Learn GH, He X, et al.:
Consistent viral evolutionary changes associated with the
progression of human immunodeficiency virus type 1 infection. J
Virol 1999, 73:10489-10502.
18. Williamson S, Perry SM, Bustamante CD, Orive ME, Stearns MN,
Kelly JK: A statistical characterization of consistent patterns of
human immunodeficiency virus evolution within infected patients.
Mol Biol Evol 2005, 22:456-468.
19. Castiglione F, Poccia F, D'Offizi G, Bernaschi M: Mutation,
fitness, viral diversity, and predictive markers of disease progression
in a computational model of HIV type 1 infection. AIDS Res Hum
Retroviruses 2004, 20:1314-1323.

115
20. Markham RB, Wang WC, Weisstein AE, Wang Z, Munoz A,
Templeton A, Margolick J, Vlahov D, Quinn T, Farzadegan H, Yu XF:
Patterns of HIV-1 evolution in individuals with differing rates of CD4
T cell decline. Proc Natl Acad Sci USA 1998, 95:12568-12573.
21. Bello G, Casado C, Sandonis V, Alvaro-Cifuentes T, Dos Santos
CA, Garcia S, Rodriguez C, Del Romero J, Pilotto JH, Grinsztejn B, et
al.: Plasma viral load threshold for sustaining intrahost HIV type 1
evolution. AIDS Res Hum Retroviruses 2007, 23:1242-1250.
22. Barroso H, Taveira N: Evidence for negative selective pressure in
HIV-2 evolution in vivo. Infect Genet Evol 2005, 5:239-246.
23. Sankale JL, de la Tour RS, Renjifo B, Siby T, Mboup S, Marlink
RG, Essex ME, Kanki PJ: Intrapatient variability of the human
immunodeficiency virus type 2 envelope V3 loop. AIDS Res Hum
Retroviruses 1995, 11:617-623.
24. MacNeil A, Sankale JL, Meloni ST, Sarr AD, Mboup S, Kanki P:
Longterm intrapatient viral evolution during HIV-2 infection. J Infect
Dis 2007, 195:726-733.
25. Choisy M, Woelk CH, Guegan JF, Robertson DL: Comparative
study of adaptive molecular evolution in different human
immunodeficiency virus groups and subtypes. J Virol 2004, 78:1962-
1970.
26. Mikhail M, Wang B, Lemey P, Beckthold B, Vandamme AM, Gill
MJ, Saksena NK: Role of viral evolutionary rate in HIV-1 disease
progression in a linked cohort. Retrovirology 2005, 2:41.
27. Yamaguchi Y, Gojobori T: Evolutionary mechanisms and
population dynamics of the third variable envelope region of HIV
within single hosts. Proc Natl Acad Sci USA 1997, 94:1264-1269.
28. Zhang H, Hoffmann F, He J, He X, Kankasa C, Ruprecht R, West
JT, Orti G, Wood C: Evolution of subtype C HIV-1 Env in a slowly
progressing Zambian infant. Retrovirology 2005, 2:67.
29. De Jong JJ, De Ronde A, Keulen W, Tersmette M, Goudsmit J:
Minimal requirements for the human immunodeficiency virus type 1
V3 domain to support the syncytium-inducing phenotype: analysis
by single amino acid substitution. J Virol 1992, 66:6777-6780.

116
30. Delobel P, Nugeyre MT, Cazabat M, Pasquier C, Marchou B,
Massip P, Barre-Sinoussi F, Israel N, Izopet J: Population-based
sequencing of the V3 region of env for predicting the coreceptor
usage of human immunodeficiency virus type 1 quasispecies. J Clin
Microbiol 2007, 45:1572-1580.
31. Huang CC, Tang M, Zhang MY, Majeed S, Montabana E,
Stanfield RL, Dimitrov DS, Korber B, Sodroski J, Wilson IA, et al.:
Structure of a V3-containing HIV-1 gp120 core. Science 2005,
310:1025-1028.
32. Isaka Y, Sato A, Miki S, Kawauchi S, Sakaida H, Hori T,
Uchiyama T, Adachi A, Hayami M, Fujiwara T, Yoshie O: Small
amino acid changes in the V3 loop of human immunodeficiency virus
type 2 determines the coreceptor usage for CXCR4 and CCR5.
Virology 1999, 264:237-243.
33. Zolla-Pazner S: Improving on nature: focusing the immune
response on the V3 loop. Hum Antibodies 2005, 14:69-72.
34. Bjorling E, Scarlatti G, von Gegerfelt A, Albert J, Biberfeld G,
Chiodi F, Norrby E, Fenyo EM: Autologous neutralizing antibodies
prevail in HIV-2 but not in HIV-1 infection. Virology 1993, 193:528-
530.
35. Andersson S: HIV-2 and the immune response. AIDS Reviews
2001, 3:11-23.
36. Shi Y, Brandin E, Vincic E, Jansson M, Blaxhult A, Gyllensten
K, Moberg L, Brostrom C, Fenyo EM, Albert J: Evolution of human
immunodeficiency virus type 2 coreceptor usage, autologous
neutralization, envelope sequence and glycosylation. J Gen Virol
2005, 86:3385-3396.
37. Rodriguez SK, Sarr AD, MacNeil A, Thakore-Meloni S, Gueye-
Ndiaye A, Traore I, Dia MC, Mboup S, Kanki PJ: Comparison of
heterologous neutralizing antibody responses of human
immunodeficiency virus type 1 (HIV-1)- and HIV-2-infected
Senegalese patients: distinct patterns of breadth and magnitude
distinguish HIV-1 and HIV-2 infections. J Virol 2007, 81:5331-5338.
38. Soriano V, Gomes P, Heneine W, Holguin A, Doruana M,
Antunes R, Mansinho K, Switzer WM, Araujo C, Shanmugam V, et

117
al.: Human immunodeficiency virus type 2 (HIV-2) in Portugal:
clinical spectrum, circulating subtypes, virus isolation, and plasma
viral load. J Med Virol 2000, 61:111-116.
39. Cavaco-Silva P, Taveira NC, Rosado L, Lourenco MH, Moniz-
Pereira J, Douglas NW, Daniels RS, Santos-Ferreira MO: Virological
and molecular demonstration of human immunodeficiency vírus type
2 vertical transmission. J Virol 1998, 72:3418-3422.
40. Sambrook J, Maniatis T, Fritsch EF: Molecular cloning: a
laboratory manual 2nd edition. Cold Spring Harbor, N.Y.: Cold Spring
Harbor Laboratory; 1989.
41. Thompson JD, Gibson TJ, Plewniak F, Jeanmougin F, Higgins
DG: The CLUSTAL_X windows interface: flexible strategies for
multiple sequence alignment aided by quality analysis tools. Nucleic
Acids Res 1997, 25:4876-4882.
42. Nicholas KB, Nicholas Hugh B Jr: GeneDoc: a tool for editing
and annotating multiple sequence alignments. Distributed by the
author. 1997.
43. Tamura K, Dudley J, Nei M, Kumar S: MEGA4: Molecular
Evolutionary Genetics Analysis (MEGA) software version 4.0. Mol Biol
Evol 2007, 24:1596-1599.
44. Felsenstein J: Evolutionary trees from DNA sequences: a
maximum likelihood approach. J Mol Evol 1981, 17:368-376.
45. Posada D, Crandall KA: MODELTEST: testing the model of DNA
substitution. Bioinformatics 1998, 14:817-818.
46. Swofford DL: PAUP*. Phylogenetic Analysis using Parsimony
(*and other Methods). Version 4. Sinauer-Associates, Sunderland,
Massachusetts; 1998.
47. Felsenstein J: Confidence limits on phylogenies: An approach
using the bootstrap. Evolution 1985, 39:783-791.
48. Salazar-Gonzalez JF, Bailes E, Pham KT, Salazar MG, Guffey MB,
Keele BF, Derdeyn CA, Farmer P, Hunter E, Allen S, et al.:
Deciphering human immunodeficiency virus type 1 transmission and

118
early envelope diversification by single-genome amplification and
sequencing. J Virol 2008, 82:3952-3970.
49.BranchlengtCalculator[http://www.hiv.lanl.gov/content/sequenc
e/BRANCHLENGTH/branchlength.html]
50. Pond SL, Frost SD, Muse SV: HyPhy: hypothesis testing
usingphylogenies. Bioinformatics 2005, 21:676-679.
51. Zhang M, Gaschen B, Blay W, Foley B, Haigwood N, Kuiken C,
Korber B: Tracking global patterns of N-linked glycosylation site
variation in highly variable viral glycoproteins: HIV, SIV, and HCV
envelopes and influenza hemagglutinin. Glycobiology 2004, 14:1229-
1246.
52. Korber BT, Kunstman KJ, Patterson BK, Furtado M, McEvilly
MM, Levy R, Wolinsky SM: Genetic differences between blood- and
brain-derived viral sequences from human immunodeficiency virus
type 1-infected patients: evidence of conserved elements in the V3
region of the envelope protein of brain derived sequences. J Virol
1994, 68:7467-7481.
53. Marcelino JM, Barroso H, Goncalves F, Silva SM, Novo C, Gomes
P, Camacho R, Taveira N: Use of a new dual-antigen enzymelinked
immunosorbent assay to detect and characterize the human
antibody response to the human immunodeficiency virus type 2
envelope gp125 and gp36 glycoproteins. J Clin Microbiol 2006,
44:607-611.
54. Botarelli P, Houlden BA, Haigwood NL, Servis C, Montagna D,
Abrignani S: N-glycosylation of HIV-gp120 may constrain recognition
by T lymphocytes. J Immunol 1991, 147:3128-3132.
55. Clevestig P, Pramanik L, Leitner T, Ehrnst A: CCR5 use by
human immunodeficiency virus type 1 is associated closely with the
gp120 V3 loop N-linked glycosylation site. J Gen Virol 2006, 87:607-
612.
56. Pollakis G, Kang S, Kliphuis A, Chalaby MI, Goudsmit J, Paxton
WA: N-linked glycosylation of the HIV type-1 gp120 envelope
glycoprotein as a major determinant of CCR5 and CXCR4 coreceptor
utilization. J Biol Chem 2001, 276:13433-13441.

119
57. Polzer S, Dittmar MT, Schmitz H, Schreiber M: The N-linked
glycan g15 within the V3 loop of the HIV-1 external glycoprotein
gp120 affects coreceptor usage, cellular tropism, and neutralization.
Virology 2002, 304:70-80.
58. Joos B, Fischer M, Schweizer A, Kuster H, Boni J, Wong JK,
Weber R, Trkola A, Gunthard HF: Positive in vivo selection of the
HIV-1 envelope protein gp120 occurs at surface-exposed regions. J
Infect Dis 2007, 196:313-320.
59. Barroso H, Araujo F, Gomes MH, Mota-Miranda A, Taveira N:
Phylogenetic demonstration of two cases of perinatal human
immunodeficiency virus type 2 infection diagnosed in adulthood.
AIDS Res and Hum Retroviruses 2004, 20:1373-1376.
60. Rambaut A, Posada D, Crandall KA, Holmes EC: The causes and
consequences of HIV evolution. Nat Rev Genet 2004, 5:52-61.
61. Gomes P, Taveira NC, Pereira JM, Antunes F, Ferreira MO,
Lourenco MH: Quantitation of human immunodeficiency virus type 2
DNA in peripheral blood mononuclear cells by using a quantitative-
competitive PCR assay. J Clin Microbiol 1999, 37:453-456.
62. Jobe O, Ariyoshi K, Marchant A, Sabally S, Corrah T, Berry N,
Jaffar S, Whittle H: Proviral load and immune function in blood and
lymph node during HIV-1 and HIV-2 infection. Clin Exp Immunol
1999, 116:474-478.
63. Parreira R, Esteves A, Santos C, Piedade J, Venenno T, Canas-
Ferreira WF: Genetic variability of human immunodeficiency virus
type 2 C2V3 region within and between individuals from Bissau,
Guinea-Bissau, West Africa. AIDS Res and Hum Retroviruses 2000,
16:1307-1312.
64. Yamaguchi-Kabata Y, Gojobori T: Reevaluation of amino acid
variability of the human immunodeficiency virus type 1 gp120
envelope glycoprotein and prediction of new discontinuous epitopes.
J Virol 2000, 74:4335-4350.
65. Yang W, Bielawski JP, Yang Z: Widespread adaptive evolution in
the human immunodeficiency virus type 1 genome. J Mol Evol 2003,
57:212-221.

120
66. Lemey P, Kosakovsky Pond SL, Drummond AJ, Pybus OG,
Shapiro B, Barroso H, and Taveira N, Rambaut A: Synonymous
substitution rates predict HIV disease progression as a result of
underlying replication dynamics. PLoS Comput Biol 2007, 3:e29.
67. Ross HA, Rodrigo AG: Immune-mediated positive selection drives
human immunodeficiency virus type 1 molecular variation and
predicts disease duration. J Virol 2002, 76:11715-11720.
68. Korber BT M, Brander C, Haynes BF, Koup R, Moore JP, Walker
BD, Watkins DI: HIV Molecular Immunology 2006/2007. Los Alamos
National Laboratory, Theoretical Biology and Biophysics, Los Alamos,
New Mexico. LA-UR 07-4752.
69. Scanlan CN, Offer J, Zitzmann N, Dwek RA: Exploiting the
defensive sugars of HIV-1 for drug and vaccine design. Nature 2007,
446:1038-1045.
70. Fischer PB, Karlsson GB, Butters TD, Dwek RA, Platt FM:
Nbutyldeoxynojirimycin-mediated inhibition of human
immunodeficiency virus entry correlates with changes in antibody
recognition of the V1/V2 region of gp120. J Virol 1996, 70:7143-
7152.
71. Poon AF, Lewis FI, Pond SL, Frost SD: Evolutionary interactions
between N-linked glycosylation sites in the HIV-1 envelope. PLoS
Comput Biol 2007, 3:e11.
72. Grenfell BT, Pybus OG, Gog JR, Wood JL, Daly JM, Mumford JA,
Holmes EC: Unifying the epidemiological and evolutionary dynamics
of pathogens. Science 2004, 303:327-332.
73. Zolla-Pazner S: Identifying epitopes of HIV-1 that induce
protective antibodies. Nat Rev Immunol 2004, 4:199-210.
74. Richman DD, Wrin T, Little SJ, Petropoulos CJ: Rapid evolution
of the neutralizing antibody response to HIV type 1 infection. Proc
Natl Acad Sci USA 2003, 100:4144-4149.
75. Frost SD, Wrin T, Smith DM, Kosakovsky Pond SL, Liu Y,
Paxinos E, Chappey C, Galovich J, Beauchaine J, Petropoulos CJ, et
al.: Neutralizing antibody responses drive the evolution of human

121
immunodeficiency virus type 1 envelope during recent HIV infection.
Proc Natl Acad Sci USA 2005, 102:18514-18519.
76. Moore PL, Gray ES, Choge IA, Ranchobe N, Mlisana K, Abdool
Karim SS, Williamson C, Morris L: The c3-v4 region is a major target
of autologous neutralizing antibodies in human immunodeficiency
virus type 1 subtype C infection. J Virol 2008, 82:1860-1869.
77. Williamson S: Adaptation in the env gene of HIV-1 and
evolutionary theories of disease progression. Mol Biol Evol 2003,
20:1318-1325.
78. Marchant D, Neil SJ, McKnight A: Human immunodeficiency
virus types 1 and 2 have different replication kinetics in human
primary macrophage culture. J Gen Virol 2006, 87:411-418.
79. Lizeng Q, Skott P, Sourial S, Nilsson C, Andersson SS, Ehnlund
M, Taveira N, Bjorling E: Serum immunoglobulin A (IgA)-mediated
immunity in human immunodeficiency virus type 2 (HIV-2) infection.
Virology 2003, 308:225-232.
80. Chackerian B, Rudensey LM, Overbaugh J: Specific N-linked
and O-linked glycosylation modifications in the envelope V1 domain
of simian immunodeficiency virus variants that evolve in the host
alter recognition by neutralizing antibodies. J Virol 1997, 71:7719-
7727.
81. Wei X, Decker JM, Wang S, Hui H, Kappes JC, Wu X, Salazar-
Gonzalez JF, Salazar MG, Kilby JM, Saag MS, et al.: Antibody
neutralization and escape by HIV-1. Nature 2003, 422:307-312.
82. Sagar M, Wu X, Lee S, Overbaugh J: Human immunodeficiency
virus type 1 V1-V2 envelope loop sequences expand and add
glycosylation sites over the course of infection, and these
modifications affect antibody neutralization sensitivity. J Virol 2006,
80:9586-959

122

CAPÍTULO VI
Escape à Neutralização na Infecção VIH-2

124

125
Escape à Neutralização é um Evento Frequente na Infecção
VIH-2 e está Fortemente Associado com o Tropismo X4
Publicação: Escape from neutralization is a frequent event in HIV-
2 infection and is strongly associated with X4 tropism.
José Maria Marcelino, Pedro Borrego, Charlotta
Nilsson, Helena Barroso, Manuela Doroana, Francisco
Antunes, Carlos Novo, and Nuno Taveira.
Submitted, 2010
Sumário
Introdução: A infecção VIH-2 induz a produção de anticorpos
neutralizantes (AcNT) de largo espectro. No entanto, pouco se
conhece sobre os alvos neutralizantes, a dinâmica dos AcNT e o
escape à neutralização durante a infecção VIH-2. Este estudo foi
realizado para investigar estes assuntos.
Método: Um coorte de 28 pacientes infectados por VIH-2 foi seguido
e estudado durante 4 anos. A actividade neutralizante autóloga e
heteróloga foi determinada com isolados VIH-2 primários e
anticorpos IgG purificados num ensaio de neutralização utilizando
células TZM-bl. A utilização de coreceptores foi determinada em
células GHOST. A sequência das regiões C2, V3 e C3 foi determinada
para todos os pacientes. O teste de ELISA-VIH2 foi utilizado para
determinar o título de anticorpos de ligação reactivos para os
polipeptidos que representam, a gp125 (rpC2-C3) e a gp36 (rgp36),
subunidades do invólucro.
Resultados: Foram isolados 24 novos isolados primários de 12
pacientes. A maioria dos pacientes (8 em 12) estava infectada com
vírus R5, e os restantes 4 com vírus X4. A presença de AcNT
autólogos (mediana IC50 = 3.91 g/ml) só foi detectada em 6
pacientes, todos infectados com vírus R5. A maioria dos pacientes (4
em 6) que não produziram AcNT autólogos estava infectada com
vírus X4. Com excepção de um paciente todos produziram anticorpos
contra os vírus R5. A resposta de anticorpos heterólogos diferiu
muito em termos de potência entre os pacientes (mediana IC50 = 4.14
g/ml, variação = 0.049-49.08 g/ml). A potência dos anticorpos
neutralizantes estava inversamente associada com os anticorpos de
ligação e a avidez para o rpC2-C3 e não para a gp36.
Surpreendentemente nenhum dos pacientes produziu anticorpos

126
neutralizantes contra isolados X4. A carga e o tamanho da ansa V3
estavam fortemente associados com o tropismo e a resistência à
neutralização.
Conclusões: Anticorpos neutralizantes heterólogos de elevada
potência e espectro são produzidos na maioria dos pacientes VIH-2
com infecção crónica, mas parecem ser restritos apenas aos vírus
R5. O escape à neutralização é um acontecimento frequente na
infecção VIH-2 e está fortemente associado com o tropismo X4. Uma
resposta de anticorpos forte e bem desenvolvida é essencial para a
produção de anticorpos neutralizantes potentes contra a região C2,
V3 e C3 da gp125 do invólucro. Os determinantes virais para a
resistência à neutralização e o tropismo X4 parecem estar localizados
principalmente na região V3. Estes resultados têm implicações claras
para o desenho de imunogénios vacinais capazes de induzir a
produção de anticorpos neutralizantes de reactividade alargada.

127
Escape from Neutralization is a Frequent Event in HIV-2
Infection and is strongly associated with X4
ABSTRACT
Background: HIV-2 infection induces the production of a broad
neutralizing antibody (NAb) response. However, little is known about
the neutralizing targets and the dynamics of the NAb response and
viral escape from neutralization during HIV-2 infection. This study
was set out to investigate these issues.
Methods: A cohort of 28 HIV-2 infected patients followed during 4
years was analyzed. Autologous and heterologous neutralizing
activities were determined with primary isolates and purified IgG
antibodies in a TZM-bl cells-based assay. Coreceptor usage of the
viruses was determined in GHOST cells. The sequence of the C2, V3
and C3 env regions was determined for all patients. The ELISA-HIV2
assay was used to determine the binding antibody titter against
polypeptides representing gp125 (rpC2-C3) and gp36 (rgp36)
envelope subunits.
Results: Twenty four new primary isolates were obtained from 12
patients. Most patients (8 out of 12) were infected with R5-viruses;
the remaining 4 patients harbored X4-viruses. Autologous NAbs
(median IC50 = 3.91 µg/ml; range = 0.049-38 µg/ml) were detected
only in 6 patients, all infected with R5-viruses. Most (4/6) patients
unable to produce autologous NAbs were infected with X4-viruses.
All but one patient produced NAbs targeting heterologous R5
isolates. The heterologous NAb response differed widely in potency
between patients (median IC50 = 4.14 µg/ml; range= 0.049-49.08
µg/ml). Potency of the neutralizing antibodies was inversely
associated with binding antibody titters and avidity to rpC2-C3 but
not to rgp36. Strikingly, none of the patients produced neutralizing
antibodies against X4 isolates. The charge and size of the V3 loop
was strongly associated with X4 tropism and resistance to
neutralization.
Conclusions: Potent and broadly reactive heterologous neutralizing
antibodies are elicited in most chronically infected HIV-2 patients but
they seem to be restricted to R5 isolates. Escape from neutralization
is a frequent event in HIV-2 infection and is strongly associated with
X4 tropism. A strong and mature antibody response is required for
the production of potent neutralizing antibodies targeting the C2, V3
and C3 regions in the gp125 envelope. Viral determinants of
neutralization resistance and X4 tropism seem to be located mostly

128
in the V3 region. These results have clear implications for the design
of HIV-2 vaccine immunogens able to elicit the production of broadly
reactive neutralizing antibodies.

129
Introduction
In contrast to the HIV-1 pandemic, HIV-2 is only prevalent in West
Africa where it seems to have been present since the 1940s (21). In
Europe, infection with HIV-2 remains rare (2-3% of all AIDS cases),
being observed mainly in France and Portugal (14, 39, 45). Eight
different HIV-2 groups named A through H have been reported but
only groups A and B cause human epidemics (12, 13, 18, 47).
Isolates from group A are, however, responsible for the vast majority
of HIV-2 infections worldwide (38).
For reasons that are still not clear, HIV-1 and HIV-2 infections lead
to very different immunological and clinical outcomes. In contrast to
HIV-1 infected patients, the majority of HIV-2-infected individuals
have reduced general immune activation, normal CD4+ T cell counts,
low or absent viremia and absence of clinical disease (2, 15, 25, 42).
This may be related with a more effective immune response produced
against HIV-2. In fact, most HIV-2 infected individuals have strong
cytotoxic responses to Env and Gag proteins and raise autologous
and heterologous neutralizing antibodies (5, 14, 22, 37, 40). The
attenuated course of HIV-2 infection compared to HIV-1 has also
been associated to a lower state of immune activation, which may be
related to the immunosuppressive activity of the C2-V3-C3 envelope
region (10, 11, 20). Similar immunosuppressive activity has not been
found in the homologous C2-V3-C3 region in the HIV-1 envelope
(11). Finally, the transmission rate of HIV-2 is also significantly lower
than that of HIV-1 and this has been associated with the low or
absent viremia found in most HIV-2 patients (7, 23).
It is now well established that HIV-2 infection elicits the production
of broadly reactive neutralizing antibodies (NAb) (5, 22, 37, 40).
However, little is known about the dynamics of the NAb response in
chronic HIV-2 infection and no information exists regarding the role
of this NAbs in control of viral replication. One study found that
there was a significant positive correlation between heterologous NAb
titer and viral load in chronically HIV-2 infected patients, suggesting
that heterologous antibodies may be driven by viral replication (37).
Interestingly, this would imply that HIV-2 escapes easily from the
neutralizing antibodies. However, a recent study did not find
evidence of viral escape from neutralizing antibodies and instead
suggested that highly effective NAbs, together with low viral
replicative capacity, prevents HIV-2 from escaping the neutralizing
response (40). A better understanding of the dynamics of the NAb

130
response and viral escape from neutralization during HIV-2 infection
is clearly needed.
The antibody specificities that mediate HIV-2 neutralization are still
elusive. The V3 region in the envelope gp125 has been identified as a
neutralizing target by some but not by all investigators (1, 3, 4, 9, 26,
36, 44). Other weakly neutralizing epitopes were identified in V1, V2,
V4 and C5 regions in gp125 and in the COOH-terminal region of the
gp41 ectodomain (3, 4, 28). The identification of the most important
neutralizing determinants in the HIV-2 Env will provide crucial
information for vaccine design. The aims of this study were to
characterize the evolution and dynamics of the NAb response
(autologous and heterologous) and escape in chronically HIV-2
infected patient and identify neutralizing targets and determinants.
Material and Methods
Study population. Twenty eight HIV-2 patients attending different
hospital in Lisbon were followed prospectively during 4 years. The
characteristic of the patients enrolled in the study have been
reported previously (8). HIV seropositivity was determined with
VIDAS HIV DUO (Bio-Mérieux, Lyon, France). HIV-1 and HIV-2
differentiation was done by Western Blot 2.2 (Genelabs Diagnostics,
Science Park, Singapore), New LAV Blot II and Peptilav 1-2 (Bio-Rad,
Hercules, California, USA). HIV-2 viremia in the plasma was
quantified with a quantitative-competitive reverse transcriptase-PCR
assay as described elsewhere(19). Ethical approval was obtained
from each hospital ethics committee and each participant gave
informed consent before entry into the study.
Cloning and sequencing. DNA extraction, PCR amplification,
cloning and sequencing analysis of the C2V3C3 region (378 bp) of
the HIV-2 env gene was done as described elsewhere (8).
Purification and quantification of IgGs. The serum samples were
diluted (1:1 ratio) in 500 mM NaCl (binding buffer) and mixed with
equal volume (200 l) of protein G SepharoseTm 4 Fast Flow (GE
Healthcare Europe). The beads were washed three times with binding
buffer and one time with buffer phosphate saline (PBS), and the
antibodies were eluted by mixing 200 ml of 100 mM glycine-HCl
elution buffer (pH 2.7) for 30 s. The beads were then
microcentrifuged for 30 seconds and held in place on the bottom of
the tube. The acid-eluted solution containing IgG was quickly

131
removed and placed into a separate tube containing 1 M Tris (pH 9.0)
buffer to reach pH 7.0 to 7.4.
IgG nephelometry Turbox kits (Orion Diagnostica’s Turbox plus,
Finland) were used to evaluate the concentrations of IgG fractions,
following the manufacturer’s instruction.
Determination of coreceptor usage. Coreceptor usage of the HIV-2
isolates was determined by using GHOST cells expressing CCR1,
CCR2, CCR3, CCR4, CCR5, CXCR4, Bonzo/STRL33 or BOB/GPR15.
Parental GHOST cells without coreceptors were also included. Fifty
thousand cells per well were seeded in 24-well dishes and infected
with 50 l of reporter virus containing 2 to 15 nanograms (ng) of p24
antigen and incubated during 3 hr in an volume of 0,25 ml of
Dulbecco’s modified essential medium (D-MEM) containing 10%
heat-inactivated fetal calf serum (FCS), 2% penicillin-streptomycin,
1% L-glutamine, 500 g/ml geneticin, 50 g/ml hygromycin, 1 g/ml
puromycin, and 20 g/ml polybrene. The cells were maintained in 1
ml of D-MEM medium and incubated at 37°C overnight. The parental
GOSTH cell line medium no contains puromycin. On next day the
virus/plasma mixture was removed, the cells were washed once with
1 ml of phosphate-buffered saline (PBS) followed by the addition of 1
ml D-MEM medium and incubated at 37°C for 72 hours. The culture
supernatants were collected and analyzed in an in-house enzyme-
linked immunosorbent assay (ELISA) for detection of HIV-2/SIV
antigen (43).
Assay to measuring neutralization antibodies. The neutralizing
activity of IgG antibodies against HIV-2 primary isolates was
analyzed in a sensitive, single-round viral infectivity assay using a
Luciferase Reporter Gene Assay in TZM-bl cells (also called JC53BL-
13) (30, 46). We first demonstrated that all primary HIV-2 isolates
replicated efficiently in TZM-bl cells after 48h hours of infection (Fig.
1). These results indicated that we could use these cells in the
neutralization assays. For the neutralization assays, the cells (15,000
cells in 100 l of complete growth medium (GM) that consist of D-
MEM supplemented with 10% fetal bovine serum (FBS, heat-
inactivated), 25 mM HEPES and 50 g/ml gentamicin) were added to
each well of 96-well flat-bottom culture plates (Nunc) and allowed to
adhere overnight before addition of equals parts of IgG antibodies
and virus. T he eluted IgG samples (concentrations tested between
100 to 0.05 g/ml) were mixed with 2 to 15 ng of HIV-2 isolates,
previously quantified for p24 content using a commercial enzyme-
linked immunosorbent assay (INNOTEST HIV Antigen mAb;

132
INNOGENETICS N. V., Belgium) and incubated for 1 h at 37°C in a
total volume of 200 l of GM containing polybrene (20 g/ml).
FIG. 1. Infectivity of HIV-2 isolates. Virus stocks were produced in
PBMC. Infectivity was determined by infection of TZM-
bl/CD4/CCR5/CXCR4-expressing cells and measurement of
luciferase light signals in target cell lysates per nanogram of p24.
Error bars represent standard errors from a five independent
experiments to each isolate. HIV-1Bal and TZM-bl cells alone were
used as control.
Forty-eight hours later, cells were lysed directly in the neutralization
plate during 2 min, 100 l of culture medium was removed from each
well and added 100 l of One-Glo luciferase assay substrate reagent
(Promega, Madison, WI). Plates were immediately analyzed for
luciferase activity on a luminometer read. Background luminescence
was measured using control wells that contained only target cells
and medium. Neutralizing activity was displayed as the percent
inhibition of viral infection (luciferase activity) at each antibody
concentration compared to an antibody-negative control: percent
inhibition = [1 - (luciferase with antibody/luciferase without
antibody)] X 100. Fifty percent inhibitory concentrations (IC50s) of
purified immunoglobulin G (IgG) were derived by determination of

133
antibody concentrations that 50% of the infectious virus was
neutralized. Values were calculated through a dose-response curve
fit with nonlinear function (four-parameter logistic equations) using
GraphPad prism software (San Diego, CA). To monitor the amount of
neutralization activity that is not HIV Env protein specific, each IgG
sample was also tested against a pseudovirus carrying the vesicular
stomatitis virus (VSV) envelope protein (obtained through the NIH
AIDS Research and Reference Reagent Program). These VSV envelope
proteins are able to mediate virus entry into the target cells used but
are not inhibited by anti-HIV Env antibodies. Assays for heterologous
neutralization were performed as described above against six HIV-2
virus isolates from the panel studied.
Statistical analyses. Statistical analyses were performed using the
GraphPad Prism version 5.01 for Windows (San Diego, CA) with a
level of significance of 5%. The Mann Whitney U was used to
compare means between variables. Contingency tables were analyzed
with Fisher’s exact test. To study how two variables varied together,
linear regression was performed and Spearman correlation
coefficients were computed against the transmembrane glycoprotein
gp36 and neutralization potency.
Results and Discussion
CXCR4 tropism may be a marker of disease progression in HIV-2
infection. Between 2003 and 2006 twenty-five primary HIV-2
isolates were obtained from twelve Portuguese HIV-2 patients living
in Portugal. Only patient PT11 was naïve to antiretroviral therapy
(Table 1). Eight patients harbored viruses that preferentially used
CCR5 whereas viruses from the remaining 4 patients used mainly
CXCR4. Overall, these results confirm that CCR5 is the major co-
receptor used by HIV-2 in vivo (6, 32, 33, 40). Consistent with
previous reports, R5 and X4 isolates were able to infect GHOST-
CD4+ cells expressing a number of alternative coreceptores; X4
isolates showed a broader coreceptor usage compared with R5
isolates (Table 1) (6, 32, 33, 40).

134
Table 1. Characteristics of patients and coreceptor usage by primary
HIV-2 isolates.
*, patient age in 2003; †, values > 1 indicate coreceptor use with base on antigen production; -
, values < 1 no coreceptor use; S, yes; N, no; B, black; C, Caucasian; F, female; M, male; ND,
not done.
The median CD4+ T-cell counts in patients infected with X4 isolates
was five times lower when compared with patients infected with R5
isolates (median [interquartile range] = 66 [21.5 to 210] vs [IQR] =
333 [209.5 to 402]; P = 0.0727). These results are consistent with the
positive association between plasma viremia and CXCR4 usage in
HIV-2 patients (6) and provide further support for a potential
association between HIV-2 disease progression and CXCR4 usage
(40).
Autologous neutralization and escape is frequent in HIV-2
patients and is related to cell tropism. Autologous neutralization
was investigated in 12 HIV-2 patients. A durable autologous
neutralizing response was found in six patients (50%) all infected
with R5 isolates (Fig. 2A). The four patients infected with X4 isolates
and two R5 infected patients did not produce antibodies able to
neutralize the autologous isolates. These results reveal a significant
association between R5 tropism and neutralization sensitivity and
between X4 tropism and neutralization resistance (Fisher’s exact
test, P = 0.001).

135
FIG. 2. Autologous neutralizing IgG response against HIV-2 isolates-
R5 [white bars] or X4 [black bars] A) and potency of IgG antibodies to
R5 isolates (B).
Regarding the potency of the neutralizing response, there were major
differences between patients (Fig. 2B). Some patients produced very
potent NAbs able to neutralize their autologous isolates at very low
concentrations (patient V18-03, IC50, 0.049 g/ml) whereas for other
patients 100-fold more antibodies was required to neutralize the
autologous isolate (see patient V11-03 in Fig 2B). There was no
association between the autologous neutralization response and the
CD4 T-cell count or viral load of the patients. In all, these results
confirm and extend previous results indicating that a potent and
durable autologous neutralizing response is relatively common in
chronic HIV-2 patients (5, 40) and provide strong evidence indicating
that escape to neutralization is a frequent event in HIV-2 infection,
especially in patients infected with X4 isolates. In contrast to us, Shi
et al (40) found HIV-2 escape from autologous neutralizing antibodies
to be a rare event. However, these authors studied only four patients
and only one of them harbored an X4 isolate. The different results
can also be due to the use of different neutralization methods and
cell lines. Frequent HIV-2 escape from neutralization is, however,
highly consistent with the positive association between plasma
viremia and neutralization potency found in one study (37) and with
the remarkably high evolutionary rate of HIV-2 envelope gene in
chronically infected patients (41) .The striking association between
X4 tropism and resistance to neutralization suggests that HIV-2
escape from antibody neutralization in vivo is mostly driven by a
change in cell tropism associated with a change from R5 to X4 co-
receptor usage. In HIV-1, escape from neutralization has only rarely
been associated with changes in viral tropism (27, 29).
A B

136
HIV-2 patients produce a very broad and potent heterologous
NAb response against R5 isolates. Plasma IgGs were purified from
28 patient samples (one time point per patient, year 2003) and their
neutralizing activity was tested against two X4 isolates and six
heterologous primary HIV-2 isolates (all R5). No neutralization was
observed against the X4 isolates. In contrast, with one exception
(patient PT28), all patients produced IgG antibodies that neutralized
at least three R5 isolates; the majority of the patients (18/27; 67.8%)
could neutralized all six R5-isolates (Table 2).
Table 2. Heterologous neutralizing antibody IgG response against R5
isolates.
Nd; not determined
Viruses were neutralized at a median IgG concentration of 4.1 g/ml
(range, 0.05-49.080 g/ml) but there were some differences between
isolates (Fig. 3). These results confirm and extend previous findings
indicating that HIV-2 patients produce a very broad (37) and
sometimes potent heterologous NAb response and demonstrate, for

137
the first time, that this response is restricted to R5 isolates.
Moreover, they confirm our previous finding that X4 HIV-2 isolates
are inherently resistant to antibody neutralization. As neutralization
sensitivity of HIV-1 seems is generally unrelated to co-receptor usage
(31), our results may signal a new and fundamental difference
between the HIV-2 and HIV-1 envelope.
FIG. 3. Potency of IgG neutralizing antibodies against HIV-2 R5-
isolates.
ART therapy has no impact in the neutralizing activity in HIV-2
infection. Most HIV-2 patients are elite controllers and are no taking
any antiretroviral medication. Purified IgG antibodies from plasma of
drun naïve (n = 9) and undergoing ART (n = 19) patients were
analyzed in terms of neutralization response. To investigate the
impact of ART on the neutralizing activity, we analyzed the
heterologous neutralizing potency in patients undergoing ART (n =
18) and drug-naïve patients (n = 9). No statistic difference was
observed between neutralizing activity of the two groups of patients
against all six primary isolates (Fig. 4). These results demonstrate
that ART therapy has no role in neutralizing response against HIV-2
and suggest that little or no viral replication in the plasma is needed
to maintain the production of neutralizing antibodies against this
virus.

138
FIG. 4. Potency of IgG neutralizing antibodies purified from plasma
patients under antiretroviral therapy (grey column) and drug-naïve
patients (black column) against primary HIV-2 R5-isolates.
The NAb response in HIV-2 patients is directed to the C2, V3 and
C3 regions in gp125. Previously, we have obtained data suggesting
that the binding antibody reactivity against a polypeptide comprising
the C2, V3 and C3 envelope regions (rpC2-C3 polypeptide) was
inversely related with the evolution of number of the CD4+ T cells in
HIV-2 patients (24). Here we decided to investigate the nature of the
association between the neutralizing and binding antibody response
in the same patients. Remarkably, a significant inverse association
was detected between the potency of heterologous NAbs and the titer
(Spearman r = -0.4729; P = 0.0262) and avidity (Spearman r = -
0.6136; P = 0.0024) of binding IgG antibodies produced against a
polypeptide comprising the C2, V3 and C3 envelope regions (rpC2-C3
polypeptide) (Fig. 5). However, there was no association between the
binding antibody response against the transmembrane glycoprotein
gp36 and neutralization potency (titer, Spearman r = -0.3968; P =
0.0675; avidity, Spearman r = -0.3199; P = 0.1466). These results
strongly suggest, on the one hand, that the NAb IgG response in HIV-
2 patients is mostly directed to the C2, V3 and C3 regions in gp125
and, on the other hand, that a strong and mature antibody response
is required for the production of potent neutralizing antibodies
targeting these envelope regions. It should be noted that in contrast
to the NAb IgG response, NAb IgA response in HIV-2 patients

139
response seem to target preferentially the transmembrane gp36
glycoprotein (22).
FIG. 5. Relation between the potency of heterologous neutralizing
IgG antibodies and binding IgG titer and avidity against rpC2-C3.
V3 region is the most important IgG neutralizing target in HIV-2
infection. To investigate the interplay between the NAb response
and the virus isolates in each individual and try to determine the
molecular basis of neutralization sensitivity and escape, the C2, V3
and C3 env regions of the patient isolates were sequenced and
aligned with the reference HIV-2ALI sequence (Fig. 6). Despite the
high variability found in the C2 and C3 regions, the most interesting
amino acid changes possibly associated with neutralizing phenotype
were found in the V3 loop. Neutralizable isolates had a V3 loop
median net charge of 7 (range, 6-7) which was well inferior to the V3
loop charge of non-neutralizable isolates (R5 and X4) (median 9,
range 8-11) (Table 3).

140
FIG. 6. Tropism and amino acid sequence of C2, V3 and C3 domains
of the HIV-2 envelope protein of sequential isolates from the twelve
study subjects. Potential N-linked glycosilation sites are shaded in
green. Charged amino acids that are present in the neutralization
resistant isolates and absent from the neutralization sensitive
isolates are shaded in blue. Insertions are indicated by bold red
letters.
However, these differences did not reach statistical significance
indicating that the charge of the V3 loop is not the sole determinant
of neutralization phenotype. Strikingly, however, we found that all
non-neutralizable X4 isolates had a 1-3 amino acid insertion at the
tip of the V3 loop. Thus, the increase in charge and size may lead to
significant changes in V3 loop conformation which may decrease its
exposure and/or its binding affinity to the neutralizing antibodies. In
HIV-1, escape from neutralization has been associated with multiple
amino acid substitutions in different regions of the envelope
glycoproteins including but not limited to the V3 loop (16, 17, 35,
46). Resistance to neutralization in HIV-1 has also been associated
with a decrease in net positive charge in the V3 loop (34) and an
increase in the size and glycan content of the variable regions,
specially V1 and V2, in the surface glycoprotein (46).

141
Table 3. Tropism, neutralization susceptibility and size and charge of
the V3 region.
Conclusions
Potent and broadly reactive heterologous neutralizing antibodies are
elicited in most chronically infected HIV-2 patients but they seem to
be restricted to R5 isolates. Escape from neutralization is a frequent
event in HIV-2 infection and is strongly associated with X4 tropism.
A strong and mature antibody response is required for the
production of potent neutralizing antibodies targeting the C2, V3 and
C3 regions in the gp125 envelope. Viral determinants of
neutralization resistance and X4 tropism seem to be located mostly
in the V3 region. These results strongly suggest that escape from the
neutralizing antibodies is the major selective force driving the
molecular and phenotypic evolution of HIV-2 in vivo. These results
have clear implications for the design of HIV-2 vaccine immunogens

142
able to elicit the production of broadly reactive neutralizing
antibodies.
References
1. Babas, T., S. Benichou, D. Guetard, L. Montagnier, and E.
Bahraoui. 1994. Specificity of antipeptide antibodies produced
against V2 and V3 regions of the external envelope of human
immunodeficiency virus type 2. Mol Immunol 31:361-9.
2. Berry, N., K. Ariyoshi, S. Jaffar, S. Sabally, T. Corrah, R. Tedder,
and H. Whittle. 1998. Low peripheral blood viral HIV-2 RNA in
individuals with high CD4 percentage differentiates HIV-2 from HIV-
1 infection. J Hum Virol 1:457-68.
3. Bjorling, E., K. Broliden, D. Bernardi, G. Utter, R. Thorstensson,
F. Chiodi, and E. Norrby. 1991. Hyperimmune antisera against
synthetic peptides representing the glycoprotein of human
immunodeficiency virus type 2 can mediate neutralization and
antibody-dependent cytotoxic activity. Proc Natl Acad Sci U S A
88:6082-6.
4. Bjorling, E., F. Chiodi, G. Utter, and E. Norrby. 1994. Two
neutralizing domains in the V3 region in the envelope glycoprotein
gp125 of HIV type 2. J Immunol 152:1952-9.
5. Bjorling, E., G. Scarlatti, A. von Gegerfelt, J. Albert, G. Biberfeld,
F. Chiodi, E. Norrby, and E. M. Fenyo. 1993. Autologous neutralizing
antibodies prevail in HIV-2 but not in HIV-1 infection. Virology
193:528-30.
6. Blaak, H., P. H. Boers, R. A. Gruters, H. Schuitemaker, M. E. van
der Ende, and A. D. Osterhaus. 2005. CCR5, GPR15, and CXCR6 are
major coreceptors of human immunodeficiency virus type 2 variants
isolated from individuals with and without plasma viremia. J Virol
79:1686-700.
7. Blaak, H., M. E. van der Ende, P. H. Boers, H. Schuitemaker, and
A. D. Osterhaus. 2006. In vitro replication capacity of HIV-2 variants
from long-term aviremic individuals. Virology 353:144-54.
8. Borrego, P., J. M. Marcelino, C. Rocha, M. Doroana, F. Antunes,
F. Maltez, P. Gomes, C. Novo, H. Barroso, and N. Taveira. 2008. The

143
role of the humoral immune response in the molecular evolution of
the envelope C2, V3 and C3 regions in chronically HIV-2 infected
patients. Retrovirology 5:78.
9. Bottiger, B., A. Karlsson, P. A. Andreasson, A. Naucler, C. M.
Costa, E. Norrby, and G. Biberfeld. 1990. Envelope cross-reactivity
between human immunodeficiency virus types 1 and 2 detected by
different serological methods: correlation between cross-
neutralization and reactivity against the main neutralizing site. J
Virol 64:3492-9.
10. Cavaleiro, R., G. J. Brunn, A. S. Albuquerque, R. M. Victorino, J.
L. Platt, and A. E. Sousa. 2007. Monocyte-mediated T cell
suppression by HIV-2 envelope proteins. Eur J Immunol 37:3435-44.
11. Cavaleiro, R., A. E. Sousa, A. Loureiro, and R. M. Victorino.
2000. Marked immunosuppressive effects of the HIV-2 envelope
protein in spite of the lower HIV-2 pathogenicity. AIDS 14:2679-86.
12. Chen, Z., A. Luckay, D. L. Sodora, P. Telfer, P. Reed, A. Gettie, J.
M. Kanu, R. F. Sadek, J. Yee, D. D. Ho, L. Zhang, and P. A. Marx.
1997. Human immunodeficiency virus type 2 (HIV-2) seroprevalence
and characterization of a distinct HIV-2 genetic subtype from the
natural range of simian immunodeficiency virus-infected sooty
mangabeys. J Virol 71:3953-60.
13. Damond, F., M. Worobey, P. Campa, I. Farfara, G. Colin, S.
Matheron, F. Brun-Vezinet, D. L. Robertson, and F. Simon. 2004.
Identification of a highly divergent HIV type 2 and proposal for a
change in HIV type 2 classification. AIDS Res Hum Retroviruses
20:666-72.
14. de Silva, T. I., M. Cotten, and S. L. Rowland-Jones. 2008. HIV-2:
the forgotten AIDS virus. Trends Microbiol 16:588-95.
15. Drylewicz, J., S. Matheron, E. Lazaro, F. Damond, F. Bonnet, F.
Simon, F. Dabis, F. Brun-Vezinet, G. Chene, and R. Thiebaut. 2008.
Comparison of viro-immunological marker changes between HIV-1
and HIV-2-infected patients in France. AIDS 22:457-68.
16. Frost, S. D., Y. Liu, S. L. Pond, C. Chappey, T. Wrin, C. J.
Petropoulos, S. J. Little, and D. D. Richman. 2005. Characterization
of human immunodeficiency virus type 1 (HIV-1) envelope variation

144
and neutralizing antibody responses during transmission of HIV-1
subtype B. J Virol 79:6523-7.
17. Frost, S. D., T. Wrin, D. M. Smith, S. L. Kosakovsky Pond, Y.
Liu, E. Paxinos, C. Chappey, J. Galovich, J. Beauchaine, C. J.
Petropoulos, S. J. Little, and D. D. Richman. 2005. Neutralizing
antibody responses drive the evolution of human immunodeficiency
virus type 1 envelope during recent HIV infection. Proc Natl Acad Sci
U S A 102:18514-9.
18. Gao, F., L. Yue, D. L. Robertson, S. C. Hill, H. Hui, R. J. Biggar,
A. E. Neequaye, T. M. Whelan, D. D. Ho, G. M. Shaw, and et al.
1994. Genetic diversity of human immunodeficiency virus type 2:
evidence for distinct sequence subtypes with differences in virus
biology. J Virol 68:7433-47.
19. Gomes, P., N. C. Taveira, J. M. Pereira, F. Antunes, M. O.
Ferreira, and M. H. Lourenco. 1999. Quantitation of human
immunodeficiency virus type 2 DNA in peripheral blood mononuclear
cells by using a quantitative-competitive PCR assay. J Clin Microbiol
37:453-6.
20. Grossman, Z., M. Meier-Schellersheim, A. E. Sousa, R. M.
Victorino, and W. E. Paul. 2002. CD4+ T-cell depletion in HIV
infection: are we closer to understanding the cause? Nat Med 8:319-
23.
21. Lemey, P., O. G. Pybus, B. Wang, N. K. Saksena, M. Salemi, and
A. M. Vandamme. 2003. Tracing the origin and history of the HIV-2
epidemic. Proc Natl Acad Sci U S A 100:6588-92.
22. Lizeng, Q., P. Skott, S. Sourial, C. Nilsson, S. S. Andersson, M.
Ehnlund, N. Taveira, and E. Bjorling. 2003. Serum immunoglobulin
A (IgA)-mediated immunity in human immunodeficiency virus type 2
(HIV-2) infection. Virology 308:225-32.
23. MacNeil, A., A. D. Sarr, J. L. Sankale, S. T. Meloni, S. Mboup,
and P. Kanki. 2007. Direct evidence of lower viral replication rates in
vivo in human immunodeficiency virus type 2 (HIV-2) infection than
in HIV-1 infection. J Virol 81:5325-30.
24. Marcelino, J. M., C. Nilsson, H. Barroso, P. Gomes, P. Borrego,
F. Maltez, L. Rosado, M. Doroana, F. Antunes, and N. Taveira. 2008.

145
Envelope-specific antibody response in HIV-2 infection: C2V3C3-
specific IgG response is associated with disease progression. Aids
22:2257-65.
25. Marlink, R., P. Kanki, I. Thior, K. Travers, G. Eisen, T. Siby, I.
Traore, C. C. Hsieh, M. C. Dia, E. H. Gueye, and et al. 1994. Reduced
rate of disease development after HIV-2 infection as compared to
HIV-1. Science 265:1587-90.
26. Matsushita, S., S. Matsumi, K. Yoshimura, T. Morikita, T.
Murakami, and K. Takatsuki. 1995. Neutralizing monoclonal
antibodies against human immunodeficiency virus type 2 gp120. J
Virol 69:3333-40.
27. McKnight, A., and P. R. Clapham. 1995. Immune escape and
tropism of HIV. Trends Microbiol 3:356-61.
28. McKnight, A., C. Shotton, J. Cordell, I. Jones, G. Simmons, and
P. R. Clapham. 1996. Location, exposure, and conservation of
neutralizing and nonneutralizing epitopes on human
immunodeficiency virus type 2 SU glycoprotein. J Virol 70:4598-606.
29. McKnight, A., R. A. Weiss, C. Shotton, Y. Takeuchi, H. Hoshino,
and P. R. Clapham. 1995. Change in tropism upon immune escape
by human immunodeficiency virus. J Virol 69:3167-70.
30. Montefiori, D. C. 2009. Measuring HIV Neutralization in a
Luciferase Reporter Gene Assay. Methods Mol Biol 485:395-405.
31. Montefiori, D. C., R. G. Collman, T. R. Fouts, J. Y. Zhou, M.
Bilska, J. A. Hoxie, J. P. Moore, and D. P. Bolognesi. 1998. Evidence
that antibody-mediated neutralization of human immunodeficiency
virus type 1 by sera from infected individuals is independent of
coreceptor usage. J Virol 72:1886-93.
32. Morner, A., A. Bjorndal, J. Albert, V. N. Kewalramani, D. R.
Littman, R. Inoue, R. Thorstensson, E. M. Fenyo, and E. Bjorling.
1999. Primary human immunodeficiency virus type 2 (HIV-2)
isolates, like HIV-1 isolates, frequently use CCR5 but show
promiscuity in coreceptor usage. J Virol 73:2343-9.
33. Morner, A., A. Bjorndal, A. C. Leandersson, J. Albert, E. Bjorling,
and M. Jansson. 2002. CCR5 or CXCR4 is required for efficient

146
infection of peripheral blood mononuclear cells by promiscuous
human immunodeficiency virus type 2 primary isolates. AIDS Res
Hum Retroviruses 18:193-200.
34. Naganawa, S., M. Yokoyama, T. Shiino, T. Suzuki, Y.
Ishigatsubo, A. Ueda, A. Shirai, M. Takeno, S. Hayakawa, S. Sato, O.
Tochikubo, S. Kiyoura, K. Sawada, T. Ikegami, T. Kanda, K.
Kitamura, and H. Sato. 2008. Net positive charge of HIV-1 CRF01_AE
V3 sequence regulates viral sensitivity to humoral immunity. PLoS
One 3:e3206.
35. O'Rourke, S. M., B. Schweighardt, P. Phung, D. P. Fonseca, K.
Terry, T. Wrin, F. Sinangil, and P. W. Berman. 2010. Mutation at a
Single Position in the V2 Domain of the HIV-1 Envelope Protein
Confers Neutralization Sensitivity to a Highly Neutralization-
Resistant Virus. J Virol 84:11200-9.
36. Robert-Guroff, M., K. Aldrich, R. Muldoon, T. L. Stern, G. P.
Bansal, T. J. Matthews, P. D. Markham, R. C. Gallo, and G.
Franchini. 1992. Cross-neutralization of human immunodeficiency
virus type 1 and 2 and simian immunodeficiency virus isolates. J
Virol 66:3602-8.
37. Rodriguez, S. K., A. D. Sarr, A. MacNeil, S. Thakore-Meloni, A.
Gueye-Ndiaye, I. Traore, M. C. Dia, S. Mboup, and P. J. Kanki. 2007.
Comparison of heterologous neutralizing antibody responses of
human immunodeficiency virus type 1 (HIV-1)- and HIV-2-infected
Senegalese patients: distinct patterns of breadth and magnitude
distinguish HIV-1 and HIV-2 infections. J Virol 81:5331-8.
38. Rowland-Jones, S. 2006. Protective immunity against HIV
infection: lessons from HIV-2 infection. Future Microbiol 1:427-33.
39. Semaille, C., F. Barin, F. Cazein, J. Pillonel, F. Lot, D. Brand, J.
C. Plantier, P. Bernillon, S. Le Vu, R. Pinget, and J. C. Desenclos.
2007. Monitoring the dynamics of the HIV epidemic using assays for
recent infection and serotyping among new HIV diagnoses:
experience after 2 years in France. J Infect Dis 196:377-83.
40. Shi, Y., E. Brandin, E. Vincic, M. Jansson, A. Blaxhult, K.
Gyllensten, L. Moberg, C. Brostrom, E. M. Fenyo, and J. Albert.
2005. Evolution of human immunodeficiency virus type 2 coreceptor

147
usage, autologous neutralization, envelope sequence and
glycosylation. J Gen Virol 86:3385-96.
41. Skar, H., P. Borrego, J. M. Marcelino, M. Mild, H. Barroso, N.
Taveira, T. Leitner, and J. Albert. 2010. HIV-2 genetic evolution in
patients with advanced disease is faster than in matched HIV-1
patients. J Virol. In press.
42. Soares, R., R. Foxall, A. Albuquerque, C. Cortesao, M. Garcia, R.
M. Victorino, and A. E. Sousa. 2006. Increased frequency of
circulating CCR5+ CD4+ T cells in human immunodeficiency virus
type 2 infection. J Virol 80:12425-9.
43. Thorstensson, R., L. Walther, P. Putkonen, J. Albert, and G.
Biberfeld. 1991. A capture enzyme immunoassay for detection of
HIV-2/SIV antigen. J Acquir Immune Defic Syndr 4:374-9.
44. Traincard, F., M. A. Rey-Cuille, I. Huon, S. Dartevelle, J. C.
Mazie, and S. Benichou. 1994. Characterization of monoclonal
antibodies to human immunodeficiency virus type 2 envelope
glycoproteins. AIDS Res Hum Retroviruses 10:1659-67.
45. Valadas, E., L. Franca, S. Sousa, and F. Antunes. 2009. 20
years of HIV-2 infection in Portugal: trends and changes in
epidemiology. Clin Infect Dis 48:1166-7.
46. Wei, X., J. M. Decker, S. Wang, H. Hui, J. C. Kappes, X. Wu, J.
F. Salazar-Gonzalez, M. G. Salazar, J. M. Kilby, M. S. Saag, N. L.
Komarova, M. A. Nowak, B. H. Hahn, P. D. Kwong, and G. M. Shaw.
2003. Antibody neutralization and escape by HIV-1. Nature 422:307-
12.
47. Yamaguchi, J., S. G. Devare, and C. A. Brennan. 2000.
Identification of a new HIV-2 subtype based on phylogenetic analysis
of full-length genomic sequence. AIDS Res Hum Retroviruses 16:925-
30.


149
CAPÍTULO VII
Anticorpos Neutralizantes contra isolados
VIH-2 Primários Produzidos em Murganhos
BALB\c

150

151
Anticorpos Neutralizantes de Elevada Potência e Grande
Reactividade para Isolados VIH-2 Induzidos via uma
Estratégia de Imunização que utiliza como Priming o Vírus
da Vacina e como Reforço o polipeptido C3V3C3
Publicação: Potent and broadly reactive HIV-2 neutralizing
antibodies elicited by a Vaccinia virus vector-prime
C2V3C3 polypeptide boost immunization strategy.
José Maria Marcelino, Pedro Borrego, Cheila Rocha,
Helena Barroso, Alexandre Quintas, Carlos Novo and
Nuno Taveira.
J Virol. 2010: 84, 2: 12429-12436
Sumário
A infecção com o Vírus da Imunodeficiência Humana tipo 2 (VIH-2)
afecta cerca de 1-2 milhões de indivíduos, na sua maioria da África
Ocidental, Europa e Índia. Tal como acontece com o VIH-1 são
necessárias novas estratégias de prevenção da infecção VIH-2. O
nosso objectivo foi produzir novos imunogénios para vacinas que
induzissem a produção de anticorpos neutralizantes (AcNT) de largo
espectro contra o VIH-2. A partir do isolado de referência HIV-2ALI
expressaram-se, no vírus da vacina e em bactérias, proteínas nativas
ou truncadas do invólucro. Este isolado foi utilizado devido às suas
características fenotípicas únicas, que combinam a independência do
receptor CD4 e a utilização do CCR5. Os AcNT não foram obtidos nos
murganhos BALB/c através de imunização simples com a gp125 do
invólucro truncada (gp125t) ou com o polipéptido recombinante
(rpC2-C3) que incluía as regiões C2, V3 e C3 do invólucro. Contudo,
uma forte e ampla resposta de AcNT foi obtida em murganhos
inicialmente imunizados com a gp125t expressa em vírus da vacina e
sujeitos a um reforço com rpC2-C3. O soro destes animais
neutralizou potentemente (mediana do título de neutralização de
50% = 3.200) 6/6 isolados primários VIH-2 altamente divergentes. A
utilização de co-receptores e a sequência V3 dos isolados
susceptíveis aos AcNT revelaram-se semelhantes aos do imunogénio
da vacina (HIV-2ALI). Em contraste, os AcNT não reagiram contra os
3 isolados X4 que apresentavam alterações major na sequência e
estrutura da ansa da V3. No seu conjunto, estes resultados
demonstram que os AcNT amplamente reactivos contra o VIH-2
podem ser obtidos utilizando uma estratégia de imunização, que
consiste numa imunização inicial com o vírus da vacina e depois

152
reforços com o rpC2-C3, e sugerem também uma potencial relação
entre o escape à neutralização e o tropismo celular.

153
Potent and Broadly Reactive HIV-2 Neutralizing Antibodies
Elicited by a Vaccinia Virus Vector-Prime C2V3C3
Polypeptide Boost Immunization Strategy
Abstract
Human immunodeficiency virus type 2 (HIV-2) infection affects about
1 to 2 million individuals, the majority living in West Africa, Europe,
and India. As for HIV-1, new strategies for the prevention of HIV-2
infection are needed. Our aim was to produce new vaccine
immunogens that elicit the production of broadly reactive HIV-2
neutralizing antibodies (NAbs). Native and truncated envelope
proteins from the reference HIV-2ALI isolate were expressed in
vaccinia virus or in bacteria. This source isolate was used due to its
unique phenotype combining CD4 independence and CCR5 usage.
NAbs were not elicited in BALB/c mice by single immunization with a
truncated and fully glycosylated envelope gp125 (gp125t) or a
recombinant polypeptide comprising the C2, V3, and C3 envelope
regions (rpC2-C3). A strong and broad NAb response was, however,
elicited in mice primed with gp125t expressed in vaccinia virus and
boosted with rpC2-C3. Serum from these animals potently
neutralized (median 50% neutralizing titer, 3,200) six of six highly
divergent primary HIV-2 isolates. Coreceptor usage and the V3
sequence of NAb-sensitive isolates were similar to that of the
vaccinating immunogen (HIV-2ALI). In contrast, NAbs were not
reactive on three X4 isolates that displayed major changes in V3 loop
sequence and structure. Collectively, our findings demonstrate that
broadly reactive HIV-2 NAbs can be elicited by using a vaccinia virus
vector-prime/rpC2-C3–boost immunization strategy and suggest a
potential relationship between escape to neutralization and cell
tropism.

154

155
Introduction
Human immunodeficiency virus type 2 (HIV-2) infection affects 1 to 2
million individuals, most of whom live in India, West Africa, and
Europe (17). HIV-2 has diversified into eight genetic groups named A
to H, of which group A is by far the most prevalent worldwide.
Nucleotide sequences of Env can differ up to 21% within a particular
group and by over 35% between groups.
The mortality rate in HIV-2-infected patients is at least twice that of
uninfected individuals (26). Nonetheless, the majority of HIV-2-
infected individuals survive as elite controllers (17). In the absence of
antiretroviral therapy, the numbers of infected cells (39) and viral
loads (36) are much lower among HIV-2-infected individuals than
among those who are HIV-1 infected. This may be related to a more
effective immune response produced against HIV-2. In fact, most
HIV-2-infected individuals have proliferative T-cell responses and
strong cytotoxic responses to Env and Gag proteins (17, 31).
Moreover, autologous and heterologous neutralizing antibodies
(NAbs) are raised in most HIV-2-infected individuals (8, 32, 48, 52),
and the virus seems unable to escape from these antibodies (52). As
for HIV-1, the antibody specificities that mediate HIV-2
neutralization and control are still elusive. The V3 region in the
envelope gp125 has been identified as a neutralizing target by some
but not by all investigators (3, 6, 7, 11, 40, 47, 54). Other weakly
neutralizing epitopes were identified in the V1, V2, V4, and C5
regions in gp125 and in the COOH terminal region of the gp41
ectodomain (6, 7, 41). A better understanding of the neutralizing
determinants in the HIV-2 Env will provide crucial information
regarding the most relevant targets for vaccine design.
The development of immunogens that elicit the production of broadly
reactive NAbs is considered the number one priority for the HIV-1
vaccine field (4, 42). Most current HIV-1 vaccine candidates intended
to elicit such broadly reactive NAbs are based on purified envelope
constructs that mimic the structure of the most conserved
neutralizing epitopes in the native trimeric Env complex and/or on
the expression of wild-type or modified envelope glycoproteins by
different types of expression vectors (4, 5, 29, 49, 58). With respect to
HIV-2, purified gp125 glycoprotein or synthetic peptides representing
selected V3 regions from HIV-2 strain SBL6669 induced autologous
and heterologous NAbs in mice or guinea pigs (6, 7, 22). However,
immunization of cynomolgus monkeys with a subunit vaccine
consisting of gp130 (HIV-2BEN) micelles offered little protection
against autologous or heterologous challenge (34). Immunization of
rhesus (19, 44, 45) and cynomolgus (1) monkeys with canarypox or

156
attenuated vaccinia virus expressing several HIV-2 SBL6669
proteins, including the envelope glycoproteins, in combination with
booster immunizations with gp160, gp125, or V3 synthetic peptides,
elicited a weak neutralizing response and partial protection against
autologous HIV-2 challenge. Likewise, vaccination of rhesus monkeys
with immunogens derived from the historic HIV-2ROD strain failed to
generate neutralizing antibodies and to protect against heterologous
challenge (55). Finally, baboons inoculated with a DNA vaccine
expressing the tat, nef, gag, and env genes of the HIV-2UC2 group B
isolate were partially protected against autologous challenge without
the production of neutralizing antibodies (33). These studies
illustrate the urgent need for new vaccine immunogens and/or
vaccination strategies that elicit the production of broadly reactive
NAbs against HIV-2. The present study was designed to investigate in
the mouse model the immunogenicity and neutralizing response
elicited by novel recombinant envelope proteins derived from the
reference primary HIV-2ALI isolate, when administered alone or in
different prime-boost combinations.
MATERIALS AND METHODS
Cells, plasmids, viruses, and antibodies. HeLa and Rat-2 (TK-) cells
were purchased from American Type Culture Collection (Rockville,
MD). The Western Reserve strain of vaccinia virus (vWR),
recombinant vaccinia virus expressing HIV-2ROD Env (rVV/ROD)
(43), and GHOST/CD4/CXCR4 and GHOST/ CD4/CCR5 cells were
provided by the AIDS Research and Reference Reagent Program,
National Institutes of Health. T-cell lines and peripheral blood
mononuclear cells were grown in RPMI 1640 medium with 10% fetal
calf serum. HeLa, Rat2, GHOST/CD4/CXCR4, and
GHOST/CD4/CCR5 cells were grown in Dulbecco minimal essential
medium (DMEM) with 10% fetal calf serum and antibiotics. Plasmid
pMJ601 was a gift from Bernard Moss (16). HIV-2 antisera were
obtained from infected individuals.
Cloning of native and mutated HIV-2ALI env genes. The HIV-2ALI
env gene was amplified by PCR as described previously (53) and
cloned into the SalI site of the vaccinia virus insertion vector
pMJ601. This procedure generated the recombinant plasmid pMJALI
(Fig. 1A). In this vector, protein expression is driven by a strong
synthetic late vaccinia virus promoter (16). Using the megaprimer
method of site-directed mutagenesis (50), a TAG stop codon was
introduced at position 8143 in the HIV-2ALI env gene. In the first
PCR the left outside primer was 5’-ATTGGGGATTATAAATTAG-3’

157
(nucleotides [nt] 8124 to 8143 of HIV-2ALI) and the right outside
primer was 5’-TCACAGGAGGG CAATTTCTGC-3’ (nt 9262 to 9282).
PCR product (mega primer) was isolated and purified by agarose gel
electrophoresis. For the second PCR amplification, the left outside
primer was 5’-CGAAAGGGCAGACGAAGAAGGACTCC-3’ (nt 6623 to
6648, in the rev gene) and the right outside primer was the mega-
primer. The vaccinia virus insertion plasmid containing HIV-2ALI
mutated env gene was named pMJALIM2.
Production of recombinant vaccinia viruses. Recombinant
vaccinia viruses were obtained as previously described (35). In brief,
pMJALI or pMJALIM2 were transfected into the thymidine kinase-
negative Rat2 (TK) cells by the calcium orthophosphate method, and
cells were simultaneously infected with vaccinia virus strain WR.
Recombinant vaccinia viruses, both 5-bromodeoxyuridine resistant
and -galactosidase positive, were selected for further studies. The
recombinant vaccinia viruses were named rVV/ALI and rVV/ALIM2.
Radiolabeling and immunoprecipitations. Confluent monolayers of
HeLa cells were infected with 5 PFU of recombinant vaccinia
virus/cell and labeled for 16 to 18 h with 100 Ci of
[35S]methionine/ml. For pulse-chase studies, the cells were pulsed
with 100 Ci of [35S]methionine/ml for 30 min and chased for various
periods with DMEM containing 10% fetal calf serum. Labeled cells
were lysed, and proteins from the cell lysate and from the cell-free
supernatant were immunoprecipitated with 10 l of human anti-HIV-
2 sera and adsorbed to protein A-Sepharose. Immunoprecipitated
proteins were characterized by SDS-PAGE at 7.5% and visualized by
autoradiography after fluorographic enhancement (Amersham
Amplify; GE Healthcare).
Mouse immunizations. Four groups (I, II, III, and V) of 6-week-old
female BALB/c mice were immunized intraperitoneally (i.p.) with 2 x
107 PFU of vaccinia virus vWR or rVV/ALIM2 in 100 l of phosphate-
buffered saline (PBS). Another two groups (IV and VI) of mice were
immunized by the i.p. route with 10 g of the rpC2-C3 polypeptide
(37) or soluble gp125t emulsified in complete Freund adjuvant
(priming) or incomplete Freund adjuvant (boosts). Four mice were
used in each group. For all mice, the schedule of immunization
included one priming and two boosts at days 14 and 28 (see Table S1
in the supplemental material). Mice were bled 14 days after each
immunization to assay for binding and neutralizing antibodies.

158
ELISAs. Enzyme-linked immunosorbent assay (ELISA) plates were
coated with the rpC2-C3 polypeptide as described previously (37). To
produce gp125t for ELISAs, 293 cells were infected with rVV/ALIM2
(4 PFU per cell). The infecting virus was replaced with serum-free
DMEM at 3 h postinfection. The medium containing gp125t was
collected at 24 h postinfection, clarified by centrifugation at 2,000 x g
for 5 min, and passed through a 0.2-m-pore-size filter. Immuno
MaxiSorp 96-well microplates (Nunc) were coated with the gp125t
supernatant (1:5 dilution) or recombinant polypeptide rpC2-C3 (2.5
g/ml) both diluted in 0.05 M bicarbonate buffer (pH 9.4) and
blocked with 1% gelatin (Bio-Rad). Mouse antiserum at serial 2-fold
dilutions (starting at 1:100) was added to the microplates and, after
1 h of incubation at room temperature, alkaline phosphatase (AP)-
conjugated goat anti-mouse IgG was added as a secondary antibody.
Colorimetric reaction was developed with p-nitrophenylphosphate
(pNPP) and read at 405 nm on a microplate reader. Negative controls
were serum from preimmune mice and mice immunized with vWR.
Positive control was serum from HIV-2-infected individuals. In this
case, the secondary antibody was AP-conjugated anti-human IgG.
Sera with an optical density (OD) above the cutoff (mean OD of the
preimmune mice serum plus two times the standard deviation) were
considered positive.
Neutralization assays. Primary virus isolates were obtained from
nine unrelated HIV-2-infected Portuguese patients by using the
cocultivation method as described previously (13). The neutralizing
activity of mice serum against these HIV-2 primary isolates was
analyzed in a single-round viral infectivity assay using a luciferase
reporter gene assay in TZM-bl cells (56, 57). The cells (15,000 cells in
100 l of complete growth medium (GM) that consists of DMEM
supplemented with 10% fetal bovine serum (heat inactivated), 25 mM
HEPES, and 50 g of gentamicin/ml were added to each well of 96-
well flat-bottom culture plates (Nunc) and allowed to adhere
overnight before addition of equals parts of serum and virus
dilutions. Next, 100-l portions of 5-fold serial dilutions (beginning at
1:40) of heat-inactivated mouse sera were mixed with 100 l of each
virus (corresponding to 5 to 15 ng of capsid p26, as quantified by
Innotest HIV antigen MAb [Innogenetics N.V., Belgium]) and
incubated for 1 h at 37°C in a total volume of 200 l of GM
containing Polybrene (20 g/ml). After 48 h, culture medium was
removed from each well, and cells were lysed directly in the plate
during 2 min with 100 l of One-Glow luciferase assay substrate
reagent (Promega, Madison, WI). Plates were immediately analyzed

159
for luciferase activity on a luminometer (TECAN). Background
luminescence was measured by using control wells that contained
only target cells and medium. Virus neutralization titer was defined
as the maximal dilution of plasma required to reduce virus
production by 50% on day 2 after infection. Neutralizing titer was
displayed as the percent inhibition of viral infection (luciferase
activity) at each serum dilution: % inhibition = [1 - (luciferase serum
samples/luciferase without serum samples)] x 100. To monitor the
amount of neutralization activity that is not HIV-2 specific, each
serum sample was also tested against a pseudovirus carrying the
vesicular stomatitis virus (VSV) envelope protein. These VSV
envelope proteins are able to mediate virus entry into the target cells
used but are not inhibited by anti-HIV Env antibodies. The reduction
of VSV infection by different sera was 15% at a 1:40 dilution, 5% at a
1:100 dilution, and 0% at a dilution of >1:100. The different mice
sera were also tested against an HIV-1 isolate (HIV-1BAL), and no
reduction in virus infectivity was observed.
Molecular and evolutionary analysis of C2-V3-C3 Env sequences.
Maximum likelihood phylogenetic trees were constructed with
alignments of C2, V3, and C3 consensus nucleotide sequences
obtained from all primary isolates used in the present study.
GenBank accession number for PTHCC6.03 is GU591163. Accession
numbers for all other sequences can be found elsewhere (10).
Reference HIV-2 sequences were obtained from GenBank.
Evolutionary distances between sequences were calculated by using
the HKY model of nucleotide substitution. Maximum-likelihood tree
searches were conducted using Treefinder (28) with bootstrap
resampling. Three-dimensional (3D) structural homology modeling of
C2, V3, and C3 amino acid sequences from HIV-2 isolates was
performed using SWISS-MODEL (2). This tool maps linear amino
acid sequences to 3D structures of proteins. This is done by
comparing the source protein sequence to that of proteins with
known 3D structures in the Protein Data Bank (PDB). The tool
generates an alignment between the query sequence and a
homologous sequence from the PDB and allows visualizing the
result.
Data analysis. The statistical significance of differences between
groups was determined by using the Mann-Whitney test within the
program GraphPad Prism (version 4.00). A P value of <0.05 was
considered statistically significant.

160
RESULTS
Expression of native and truncated HIV-2ALI Env glycoproteins
in vaccinia virus. HIV-2 ALI, considered the prototypic group A
primary isolate, uses predominantly the CCR5 coreceptor to enter
cells and is relatively CD4 independent (46). The full-length env gene
of this isolate was cloned into the pMJ601 vaccinia virus insertion
vector generating pMJALI (Fig. 1A) and recombinant vaccinia virus
rVV/ALI was produced as described previously (35).
FIG. 1. Immunoprecipitation analysis of HIV-2ALI envelope
glycoproteins expressed by recombinant vaccinia viruses. (A)
Schematic representation of the pMJALI plasmid used to produce
rVV/ALI. The env gene from HIV-2ALI was cloned into the unique
SalI site of the pMJ601 plasmid, which is located adjacent to the
synthetic late promoter within the X region (16). (B) HIV-2ALI and
HIV-2ROD envelope glycoproteins expressed in HeLa cells by
recombinant vaccinia viruses rVV/ALI and rVV/ROD (positive
control), respectively. (C) Schematic representation of gp125t protein
expressed by rVV/ALIM2, with the sizes and approximate locations
of the conserved and variable domains indicated. (D) Pulsechase
analysis of gp125t expression. HeLa cells infected with rVV/ALIM2
were metabolically labeled for 30 min with [35S]methionine and
chased for 1, 3, and 18 h. In panels C and D, viral glycoproteins were
immunoprecipitated from cell lysates (E) and supernatant (S) with
antiserum from an HIV-2-infected individual and analyzed by SDS-
PAGE and fluorography. Mock, uninfected cells; vWR, cells infected
with the WR strain of vaccinia virus (negative control). Standard
molecular mass markers are indicated in kilodaltons.

161
Immunoprecipitation assays with human HIV-2 antiserum showed
that rVV/ALI expresses high levels of HIV-2 precursor envelope
glycoprotein (gp140) that is processed to originate the surface
(gp125) and transmembrane (gp36) glycoproteins that are then
transported to the cell surface (Fig. 1B). In these assays,
recombinant vaccinia virus expressing the Env glycoproteins of the
historical HIV-2ROD isolate (rVV/ROD) was used as a positive
control. Cell-to-cell fusion assays showed that rVV/ALI only induced
syncytium formation in CCR5-positive cells (GHOST/CD4/ CCR5)
(see Table S1 in the supplemental material). To be able to produce
high amounts of gp125, a stop codon was inserted by site-directed
mutagenesis at the end of the corresponding env coding region. The
mutated env gene should code for a truncated gp125 (gp125t)
lacking 26 amino acids at the carboxyl terminus of the C5 region
(Fig. 1C). As anticipated, recombinant vaccinia virus rVV/ALIM2
secreted gp125t into the cell supernatant in high levels (95% of total
amount after 18 h of chase, as determined by densitometric analysis
of the bands), and no gp140 or gp36 was produced (Fig. 1D).
Secreted gp125t bound poorly to cellular CD4 (data not shown).
Together, these results are consistent with the relative CD4
independence and CCR5 usage of HIV-2ALI (46), indicating that the
envelope glycoproteins expressed in vaccinia virus maintain the
structure and function of the original viral isolate.
HIV-2ALI Env-based immunogens elicit a strong and broad NAb
response in mice. To investigate the humoral immunogenicity of
HIV-2ALI-derived envelope gp125t and rpC2-C3 polypeptide (37),
BALB/c mice were inoculated with one or more of the following
immunogens: rVV/ALIM2, gp125t or rpC2-C3 polypeptide (see Table
S2 in the supplemental material). The binding antibody response to
each immunogen was analyzed with the ELISA-HIV2 assay (37),
which uses the rpC2-C3 polypeptide as antigen, and with a newly
derived ELISA using gp125t as a capture antigen. All mice produced
IgG antibodies reacting with gp125t or rpC2-C3 polypeptide (Fig. 2).
Mice immunized solely with rpC2-C3 produced the strongest rpC2-
C3-specific binding antibody responses (endpoint titer, 1:25,600) but
did not produce antibodies against gp125t. Conversely, mice
immunized solely with gp125t produced a strong IgG response
against gp125t (endpoint titer, 25,600) but not against rpC2-C3 (Fig.
2).

162
FIG. 2. Binding IgG response against the rpC2-C3 polypeptide and
gp125t in BALB/c mice immunized with different HIV-2ALI antigens.
Four mice were immunized with each vaccine regimen. For all mice,
the schedule of immunization included one priming and two boosting
at days 14 and 28. Fourteen days after each immunization, sera were
collected and assayed for the presence of binding IgG antibodies to
rpC2-C3 polypeptide and soluble gp125t. Mice antiserum at a 1:100
dilution was added to rpC2-C3 polypeptide (A) or gp125t (B) coated
microplates, and alkaline phosphatase (AP)-conjugated goat anti-
mouse IgG was added as a secondary antibody. (C) Endpoint
antibody titers against rpC2-C3 after the last immunization (boost II).
(D) Endpoint antibody titers against gp125t after the last
immunization (boost II). The boxes in panels A and B indicate the
median antibody responses and standard deviations. The lines in
panels C and D indicate the median antibody responses.
Importantly, mice primed with rVV/ALIM2 and boosted with rpC2-C3
produced IgG antibodies that bound strongly to rpC2- C3 (median
titer, 19,200; range, 12,800 to 25,600) and gp125t (median titer,
9,600; range, 6,400 to 25,600).
The neutralizing properties of mice antiserum were tested against
nine highly divergent heterologous isolates of HIV-2 group A (see Fig.

163
S1 in the supplemental material), of which six used the CCR5
coreceptor and three used the CXCR4 coreceptor (Table 1).
The genetic diversity of the primary virus isolates was significantly
higher compared to the reference isolates (median number of
nucleotide substitutions per site, 0.2399 versus 0.1657 [P = 0.0013])
(see Table S3 in the supplemental material). The median divergence
from the vaccinating ALI strain was also very high (0.2146 nucleotide
substitutions per site), and this was independent of coreceptor
usage.
Mice inoculated with rVV/ALIM2 alone and mice inoculated with
prime-boost regimens containing rVV/ALIM2 and rpC2-C3
polypeptide or rVV/ALIM2 and gp125t, generated antibodies
neutralizing the R5 isolates (Table 1). In contrast, mice immunized
Table 1. Neutralization of primary HIV-2 isolates by antiserum from
mice immunized with envelope proteins derived from HIV-2ALI
solely with rpC2-C3 or gp125t did not produce neutralizing
antibodies. The strongest and broadest neutralizing responses were
found in mice primed with rVV/ ALIM2 and boosted with rpC2-C3.
Sera from these animals potently neutralized (50% median
neutralizing titers, 3,200; range, 1,280 to 10,240) all primary isolates
of the CCR5 phenotype. However, none of the immunogens generated
neutralizing antibodies reactive against the X4 isolates. Together,
these results demonstrate that a potent and broad HIV-2
neutralizing response can be elicited with a vaccinia virus vector
prime/ rpC2-C3-boost vaccination strategy that direct the antibody
response to the central C2, V3, and C3 envelope regions in the native
HIV-2 envelope complex.
Sequence and structure markers of viral susceptibility to
antibody-mediated neutralization. Considering the C2, V3, and C3
regions, ALI differed from the other isolates by a median of 16 amino
acids (magnitude range, 11 to 30) (Fig. 3). C2 was the most
conserved region reference HIV-2ALI strain and the other primary

164
HIV-2 isolates analyzed in the present study. Amino acids only
present in the V3 region of the X4 neutralization resistant isolates
are shown in boldface letters. (median number of amino acid
replacements, 3; range, 2 to 5), whereas C3 was the most divergent
region (median, 11; range, 8 to 17).
Table 1. Neutralization of primary HIV-2 isolates by antiserum from
mice immunized with envelope proteins derived from HIV-2ALI.
This was unrelated with the tropism of the virus isolates. However,
the V3 loop of neutralization-sensitive R5 (NS-R5) isolates differed
only by 1 amino acid from ALI (magnitude, 0 to 1), whereas those
from neutralization-resistant X4 (NR-X4) isolates differed by an
average of 8 amino acids (magnitude, 7 to 9) (P = 0.0238). Compared
to ALI and with the NS-R5 isolates, the V3 loop of the NR-X4 isolates
was longer, due to the insertion of 1 to 3 amino acids at the tip of the
loop, and had a higher number of charged amino acids, mostly
arginine, leading to a higher overall net charge (Fig. 3 and Table 1).
Superimposed 3D structures of C2, V3, and C3 regions derived from
the primary isolates and HIV-2ALI were obtained by homology
modeling with the conformational structure of an unliganded SIV
gp120 envelope glycoprotein (PDB ID 2bf1) (14). Not surprisingly, the
V3 loop structure from NS-R5 isolates was similar to ALI and differed
significantly from the V3 loop structure of the NR-X4 isolates (Fig. 4).
Taken together, these results suggest that the V3 loop is a major
neutralization determinant in the HIV-2 envelope. Since X4 usage
evolves from R5 usage, the results also suggest a potential
relationship between HIV-2 escape to neutralization, coreceptor
usage and cell tropism.

165
FIG. 4. Conformational structure of the C2-V3-C3 domains from the
primary HIV-2 isolates, as determined by homology modeling. (A) V3
loop conformation of reference HIV-2ALI and neutralization sensitive
isolates (PTHCC2.03, PTHCC6.03, PTHCC7.03, PTHCC12.03,
PTHCC17.03, and PTHCC19.03). Two different patterns are
predicted: a conformational pattern similar to the reference HIV-2
ALI (PTHCC6.03, PTHCC7.03, PTHCC12.03, and PTHCC17.03) and a
pattern slightly more exposed than the reference (PTHCC2.03 and
PTHCC19.03). (B) V3 loop structure conformation of reference and of
neutralization resistant isolates (PTHCC20.03, PTHSM9.03, and
PTHSM10.03). All of the conformational patterns are structurally
different from the reference HIV-2ALI. The V3 loop is highlighted by a
red color gradient, while the C2 and C3 domains are shown in white.
DISCUSSION
We show here, for the first time, that a potent and broad HIV-2
neutralizing response can be elicited in mice using a vaccinia virus
vector-prime/rpC2-C3-polypeptide boost vaccination strategy. All

166
immunogens used in the present study were derived from the
envelope gene of HIV-2ALI. We used this source isolate for three
main reasons. First, because it is the prototypic primary isolate of
HIV-2 group A, the most prevalent group worldwide. Second, because
it uses predominantly the CCR5 coreceptor to enter cells (46), a
phenotypic feature that is shared by most HIV-2 isolates found in
asymptomatic patients (9) and that is commonly found in
transmitted HIV isolates (30). Third, because HIV-2 ALI is as CD4
independent as many other primary HIV-2 isolates (46), and this has
been associated with an increased likelihood of exposition of broadly
neutralizing epitopes in vivo (58). Based on the published
information, we reasoned that the combination of these three
features would make this an appropriate source isolate for the
production of Env-based vaccine immunogens aimed at eliciting
neutralizing antibodies targeting the most commonly transmitted
strains of HIV-2. A new recombinant vaccinia virus, rVV/ALIM2, was
produced expressing high levels of a truncated version of gp125 from
HIV-2ALI. Mice immunized with this virus elicited a binding IgG
antibody response that is similar to natural HIV-2 infection (37, 38)
and elicited the production of low levels of NAbs. In contrast, animals
vaccinated solely with monomeric gp125t or rpC2-C3, despite
eliciting a binding IgG antibody response that was even stronger
than that attained in natural infection (4.4 log10 versus 3.3 log10)
(38), could not raise the production of NAbs. These results indicating
that NAb epitopes are not formed or presented effectively by our
monomeric Env immunogens are consistent with previous data
showing poor induction of HIV NAbs by envelope subunits (12, 18,
51). Strikingly, however, elicitation of NAbs by the same monomeric
Env proteins was highly effective in animals primed with rVV/ALIM2
expressing truncated gp125t. To our knowledge, this is the first
demonstration that a robust and broad HIV neutralizing response
can be elicited with a prime-boost vaccination strategy based on
replicating competent poxvirus vectors and monomeric Env
subunits.
Replication-competent poxvirus vectors, in contrast to nonreplicating
poxvirus such as MVA, NYVAC, or canarypox, allows sustained and
high-level transgene expression in vivo, and this has been related
with strong CD8 (21, 27) and CD4 (27) T-cell responses.
Recent evidence indicates that the generation and persistence of a
strong antiviral antibody response depends on the previous
induction of a strong Th2 type-specific cellular immune response
(20). Thus, the high-level expression of Env glycoproteins ascribed by
the strong late promoter present in our recombinant vaccinia virus

167
vector may have been a determinant for the generation of a strong
Th2 type-specific response and B-cell activation, which then enabled
an effective NAb production following the booster immunizations with
either gp125t or rpC2-C3. Of note, the specific cellular immune
response triggered by nonreplicating poxvirus vectors is of the Th1
type, which may explain the weak antibody response elicited by these
vectors (23, 25). Our results therefore provide support for the use of
replicating competent recombinant vaccinia virus as a component of
an HIV vaccine. To this end, new recombinant vaccinia virus vectors
may need to be produced using highly attenuated smallpox vaccine
strains such as, for instance, ACAM2000 (24).
The data also demonstrate that directing the antibody response to
the central C2, V3, and C3 envelope regions in the native HIV-2
envelope complex was determinant for the elicitation of high levels of
broadly reactive NAbs. These core Env regions contain highly
antigenic and immunodominant HIV-2 epitopes, and most HIV-2-
infected patients produce IgG and IgA antibodies reacting with them
(37, 38). We have recently shown that the V3 and C3 regions in the
HIV-2 envelope are remarkably stable over the course of infection
and that C2V3C3-specific IgG antibodies may contribute to reduce
viral population size and limit the number of virus escape mutants
(10). Collectively, therefore, the results suggest that a therapeutic or
sterilizing vaccine strategy targeting the C2, V3, and C3 envelope
regions may lead to a sustained neutralizing response and durable
control of HIV-2 replication (15).
We noticed that all neutralizable HIV-2 isolates used the CCR5
coreceptor and that the V3 amino acid sequence and structure of
these isolates was remarkably conserved and diverged very little from
that of the vaccine isolate (HIV-2ALI). In contrast, X4-tropic viruses
were resistant to neutralization and their V3 loop diverged
significantly from ALI in amino acid sequence, net charge (higher
charge), size (longer), and structural conformation. These results
suggest that the V3 loop is the broadly neutralizing domain
contained within the C2, V3, and C3 envelope regions and establish
a possible link between neutralization escape and tropism in HIV-2.
These results also provide important new leads for the design of new
vaccine immunogens aimed at eliciting antibodies that neutralize
both R5 and X4 HIV-2 isolates.
In conclusion, a prime-boost immunization strategy with
recombinant vaccinia virus expressing the envelope gp125 of HIV-
2ALI, a CD4-independent R5 primary isolate, and a polypeptide
comprising the C2, V3, and C3 envelope regions of the same isolate
induces in mice a strong and broadly neutralizing antibody response,

168
possibly targeting the V3 region of the vast majority of primary HIV-2
isolates (R5 isolates of group A). Our findings provide support for
testing these new HIV -2 immunogens in vaccine trials in other
animal models. Finally, our findings provide proof-of-concept for a
new type of HIV vaccine aimed at eliciting high levels of broadly
NAbs, one that uses replication-competent recombinant vaccinia
virus vectors to prime the cellular immune response and activate B
cells and monomeric polypeptides comprising broadly neutralizing
epitopes to boost the neutralizing B-cell response.
ACKNOWLEDGMENTS
This study was supported by grant PTDC/SAU-FCF/67673/2006
from Fundação para a Ciência e Tecnologia (Portugal). The following
reagents were obtained through the AIDS Research and Reference
Reagent Program, Division of AIDS, NIAID, NIH: rVV/ROD from Mark
J. Mulligan and TZM-bl from John C. Kappes, Xiaoyun Wu, and
Tranzyme, Inc.
We do not have a commercial or other association that might pose a
conflict of interest.
References
1. Andersson, S., B. Makitalo, R. Thorstensson, G. Franchini, J.
Tartaglia, K. Limbach, E. Paoletti, P. Putkonen, and G. Biberfeld.
1996. Immunogenicity and protective efficacy of a human
immunodeficiency virus type 2 recombinant canarypox (ALVAC)
vaccine candidate in cynomolgus monkeys. J. Infect. Dis. 174:977–
985.
2. Arnold, K., L. Bordoli, J. Kopp, and T. Schwede. 2006. The SWISS-
MODEL workspace: a web-based environment for protein structure
homology modeling. Bioinformatics 22:195–201.
3. Babas, T., S. Benichou, D. Guetard, L. Montagnier, and E.
Bahraoui. 1994. Specificity of antipeptide antibodies produced
against V2 and V3 regions of the external envelope of human
immunodeficiency virus type 2. Mol. Immunol. 31:361–369.
4. Barouch, D. H. 2008. Challenges in the development of an HIV-1
vaccine. Nature 455:613 619.
5. Barouch, D. H., K. L. O’Brien, N. L. Simmons, S. L. King, P.
Abbink, L. F. Maxfield, Y. H. Sun, A. La Porte, A. M. Riggs, D. M.

169
Lynch, S. L. Clark, K. Backus, J. R. Perry, M. S. Seaman, A. Carville,
K. G. Mansfield, J. J. Szinger, W. Fischer, M. Muldoon, and B.
Korber. Mosaic HIV-1 vaccines expand the breadth and depth of
cellular immune responses in rhesus monkeys. Nat. Med. 16:319–
323.
6. Bjorling, E., K. Broliden, D. Bernardi, G. Utter, R. Thorstensson,
F. Chiodi, and E. Norrby. 1991. Hyperimmune antisera against
synthetic peptides representing the glycoprotein of human
immunodeficiency virus type 2 can mediate neutralization and
antibody-dependent cytotoxic activity. Proc. Natl. Acad. Sci. U. S. A.
88:6082–6086.
7. Bjorling, E., F. Chiodi, G. Utter, and E. Norrby. 1994. Two
neutralizing domains in the V3 region in the envelope glycoprotein
gp125 of HIV type 2. J. Immunol. 152:1952–1959.
8. Bjorling, E., G. Scarlatti, A. von Gegerfelt, J. Albert, G. Biberfeld,
F. Chiodi, E. Norrby, and E. M. Fenyo. 1993. Autologous neutralizing
antibodies prevail in HIV-2 but not in HIV-1 infection. Virology
193:528–530.
9. Blaak, H., P. H. Boers, R. A. Gruters, H. Schuitemaker, M. E. van
der Ende, and A. D. Osterhaus. 2005. CCR5, GPR15, and CXCR6 are
major coreceptors of human immunodeficiency virus type 2 variants
isolated from individuals with or without plasma viremia. J. Virol.
79:1686–1700.
10. Borrego, P., J. M. Marcelino, C. Rocha, M. Doroana, F. Antunes,
F. Maltez, P. Gomes, C. Novo, H. Barroso, and N. Taveira. 2008. The
role of the humoral immune response in the molecular evolution of
the envelope C2, V3, and C3 regions in chronically HIV-2-infected
patients. Retrovirology 5:78.
11. Bottiger, B., A. Karlsson, P. A. Andreasson, A. Naucler, C. M.
Costa, E. Norrby, and G. Biberfeld. 1990. Envelope cross-reactivity
between human immunodeficiency virus types 1 and 2 detected by
different serological methods: correlation between cross-
neutralization and reactivity against the main neutralizing site. J.
Virol. 64:3492–3499.
12. Buonaguro, L., L. Racioppi, M. L. Tornesello, C. Arra, M. L.
Visciano, B. Biryahwaho, S. D. Sempala, G. Giraldo, and F. M.
Buonaguro. 2002. Induction of neutralizing antibodies and cytotoxic

170
T lymphocytes in BALB/c mice immunized with virus-like particles
presenting a gp120 molecule from a HIV-1 isolate of clade A. Antivir.
Res. 54:189–201.
13. Cavaco-Silva, P., N. C. Taveira, L. Rosado, M. H. Lourenco, J.
Moniz- Pereira, N. W. Douglas, R. S. Daniels, and M. O. Santos-
Ferreira. 1998. Virological and molecular demonstration of human
immunodeficiency virus type 2 vertical transmission. J. Virol.
72:3418–3422.
14. Chen, B., E. M. Vogan, H. Gong, J. J. Skehel, D. C. Wiley, and S.
C. Harrison. 2005. Structure of an unliganded simian
immunodeficiency virus gp120 core. Nature 433:834–841.
15. Davenport, M. P., L. Loh, J. Petravic, and S. J. Kent. 2008. Rates
of HIV immune escape and reversion: implications for vaccination.
Trends Microbiol. 16:561–566.
16. Davison, A. J., and B. Moss. 1990. New vaccinia virus
recombination plasmids incorporating a synthetic late promoter for
high level expression of foreign proteins. Nucleic Acids Res. 18:4285–
4286.
17. de Silva, T. I., M. Cotten, and S. L. Rowland-Jones. 2008. HIV-2:
the forgotten AIDS virus. Trends Microbiol. 16:588–595.
18. Dey, B., M. Pancera, K. Svehla, Y. Shu, S. H. Xiang, J.
Vainshtein, Y. Li, J. Sodroski, P. D. Kwong, J. R. Mascola, and R.
Wyatt. 2007. Characterization of human immunodeficiency virus
type 1 monomeric and trimeric gp120 glycoproteins stabilized in the
CD4-bound state: antigenicity, biophysics, and immunogenicity. J.
Virol. 81:5579–5593.
19. Franchini, G., M. Robert-Guroff, J. Tartaglia, A. Aggarwal, A.
Abimiku, J. Benson, P. Markham, K. Limbach, G. Hurteau, J. Fullen,
et al. 1995. Highly attenuated HIV type 2 recombinant poxviruses,
but not HIV-2 recombinant Salmonella vaccines, induce long-lasting
protection in rhesus macaques. AIDS Res. Hum. Retrovir. 11:909–
920.
20. Gaucher, D., R. Therrien, N. Kettaf, B. R. Angermann, G.
Boucher, A. Filali-Mouhim, J. M. Moser, R. S. Mehta, D. R. Drake III,
E. Castro, R. Akondy, A. Rinfret, B. Yassine-Diab, E. A. Said, Y.
Chouikh, M. J. Cameron, R. Clum, D. Kelvin, R. Somogyi, L. D.

171
Greller, R. S. Balderas, P. Wilkinson, G. Pantaleo, J. Tartaglia, E. K.
Haddad, and R. P. Sekaly. 2008. Yellow fever vaccine induces
integrated multilineage and polyfunctional immune responses. J.
Exp. Med. 205:3119–3131.
21. Geiben-Lynn, R., J. R. Greenland, K. Frimpong-Boateng, and N.
L. Letvin. 2008. Kinetics of recombinant adenovirus type 5, vaccinia
virus, modified vaccinia Ankara virus, and DNA antigen expression
in vivo and the induction of memory T-lymphocyte responses. Clin.
Vaccine Immunol. 15:691–696.
22. Gilljam, G. 1993. Envelope glycoproteins of HIV-1, HIV-2, and
SIV purified with Galanthus nivalis agglutinin induce strong immune
responses. AIDS Res. Hum. Retrovir. 9:431–438.
23. Gomez, C. E., J. L. Najera, V. Jimenez, K. Bieler, J. Wild, L.
Kostic, S. Heidari, M. Chen, M. J. Frachette, G. Pantaleo, H. Wolf, P.
Liljestrom, R. Wagner, and M. Esteban. 2007. Generation and
immunogenicity of novel HIV/AIDS vaccine candidates targeting HIV-
1 Env/Gag-Pol-Nef antigens of clade C. Vaccine 25:1969–1992.
24. Handley, L., R. M. Buller, S. E. Frey, C. Bellone, and S. Parker.
2009. The new ACAM2000 vaccine and other therapies to control
orthopoxvirus outbreaks and bioterror attacks. Expert Rev. Vaccines
8:841–850.
25. Harari, A., P. A. Bart, W. Stohr, G. Tapia, M. Garcia, E. Medjitna-
Rais, S. Burnet, C. Cellerai, O. Erlwein, T. Barber, C. Moog, P.
Liljestrom, R. Wagner, H. Wolf, J. P. Kraehenbuhl, M. Esteban, J.
Heeney, M. J. Frachette, J. Tartaglia, S. McCormack, A. Babiker, J.
Weber, and G. Pantaleo. 2008. An HIV-1 clade C DNA prime, NYVAC
boost vaccine regimen induces reliable, polyfunctional, and long-
lasting T-cell responses. J. Exp. Med. 205: 63–77.
26. Holmgren, B., Z. da Silva, P. Vastrup, O. Larsen, S. Andersson,
H. Ravn, and P. Aaby. 2007. Mortality associated with HIV-1, HIV-2,
and HTLV-1 single and dual infections in a middle-aged and older
population in Guinea- Bissau. Retrovirology 4:85.
27. Hovav, A. H., M. W. Panas, C. E. Osuna, M. J. Cayabyab, P.
Autissier, and N. L. Letvin. 2007. The impact of a boosting
immunogen on the differentiation of secondary memory CD8 T
cells. J. Virol. 81:12793–12802.

172
28. Jobb, G. 2008. TREEFINDER version of October 2008 ed.
Distributed by the author. G. Jobb, Munich, Germany.
29. Johnston, M. I., and A. S. Fauci. 2007. An HIV vaccine: evolving
concepts. N. Engl. J. Med. 356:2073–2081.
30. Keele, B. F., E. E. Giorgi, J. F. Salazar-Gonzalez, J. M. Decker, K.
T. Pham, M. G. Salazar, C. Sun, T. Grayson, S. Wang, H. Li, X. Wei,
C. Jiang, J. L. Kirchherr, F. Gao, J. A. Anderson, L. H. Ping, R.
Swanstrom, G. D. Tomaras, W. A. Blattner, P. A. Goepfert, J. M.
Kilby, M. S. Saag, E. L. Delwart, M. P. Busch, M. S. Cohen, D. C.
Montefiori, B. F. Haynes, B. Gaschen, G. S. Athreya, H. Y. Lee, N.
Wood, C. Seoighe, A. S. Perelson, T. Bhattacharya, B. T. Korber, B.
H. Hahn, and G. M. Shaw. 2008. Identification and characterization
of transmitted and early founder virus envelopes in primary HIV-1
infection. Proc. Natl. Acad. Sci. U. S. A. 105:7552–7557.
31. Leligdowicz, A., and S. Rowland-Jones. 2008. Tenets of
protection from progression to AIDS: lessons from the immune
responses to HIV-2 infection. Expert Rev. Vaccines 7:319–331.
32. Lizeng, Q., P. Skott, S. Sourial, C. Nilsson, S. S. Andersson, M.
Ehnlund, N. Taveira, and E. Bjorling. 2003. Serum immunoglobulin
A (IgA)-mediated immunity in human immunodeficiency virus type 2
(HIV-2) infection. Virology 308:225–232.
33. Locher, C. P., S. A. Witt, B. M. Ashlock, P. Polacino, S. L. Hu, S.
Shiboski, A. M. Schmidt, M. B. Agy, D. M. Anderson, S. I. Staprans,
J. zur Megede, and J. A. Levy. 2004. Human immunodeficiency virus
type 2 DNA vaccine provides partial protection from acute baboon
infection. Vaccine 22:2261– 2272.
34. Luke, W., G. Voss, C. Stahl-Hennig, C. Coulibaly, P. Putkonen,
H. Petry, and G. Hunsmann. 1993. Protection of cynomolgus
macaques (Macaca fascicularis) against infection with the human
immunodeficiency virus type 2 strain ben (HIV-2ben) by
immunization with the virion-derived envelope glycoprotein gp130.
AIDS Res. Hum. Retrovir. 9:387–394.
35. Mackett, M., G. L. Smith, and B. Moss. 1985. The construction
and characterization of vaccinia virus recombinants expressing
foreign genes, p. 191– 212. In D. M. Glover (ed.), DNA cloning. IRL
Press, Oxford, United Kingdom.

173
36. MacNeil, A., A. D. Sarr, J. L. Sankale, S. T. Meloni, S. Mboup,
and P. Kanki. 2007. Direct evidence of lower viral replication rates in
vivo in human immunodeficiency virus type 2 (HIV-2) infection than
in HIV-1 infection. J. Virol. 81:5325–5330.
37. Marcelino, J. M., H. Barroso, F. Goncalves, S. M. Silva, C. Novo,
P. Gomes, R. Camacho, and N. Taveira. 2006. Use of a new dual-
antigen enzyme-linked immunosorbent assay to detect and
characterize the human antibody response to the human
immunodeficiency virus type 2 envelope gp125 and gp36
glycoproteins. J. Clin. Microbiol. 44:607–611.
38. Marcelino, J. M., C. Nilsson, H. Barroso, P. Gomes, P. Borrego, F.
Maltez, L. Rosado, M. Doroana, F. Antunes, and N. Taveira. 2008.
Envelope-specific antibody response in HIV-2 infection: C2V3C3-
specific IgG response is associated with disease progression. AIDS
22:2257-2265.
39. Matheron, S., S. Pueyo, F. Damond, F. Simon, A. Lepretre, P.
Campa, R. Salamon, G. Chene, and F. Brun-Vezinet. 2003. Factors
associated with clinical progression in HIV-2 infected-patients: the
French ANRS cohort. AIDS 17:2593–2601.
40. Matsushita, S., S. Matsumi, K. Yoshimura, T. Morikita, T.
Murakami, and K. Takatsuki. 1995. Neutralizing monoclonal
antibodies against human immunodeficiency virus type 2 gp120. J.
Virol. 69:3333–3340.
41. McKnight, A., C. Shotton, J. Cordell, I. Jones, G. Simmons, and
P. R. Clapham. 1996. Location, exposure, and conservation of
neutralizing and nonneutralizing epitopes on human
immunodeficiency virus type 2 SU glycoprotein. J. Virol. 70:4598–
4606.
42. Montefiori, D., Q. Sattentau, J. Flores, J. Esparza, and J.
Mascola. 2007. Antibody-based HIV-1 vaccines: recent developments
and future directions. PLoS Med. 4:e348.
43. Mulligan, M. J., G. D. Ritter, Jr., M. A. Chaikin, G. V.
Yamshchikov, P. Kumar, B. H. Hahn, R. W. Sweet, and R. W.
Compans. 1992. Human immunodeficiency virus type 2 envelope
glycoprotein: differential CD4 interactions of soluble gp120 versus
the assembled envelope complex. Virology 187:233–241.

174
44. Myagkikh, M., S. Alipanah, P. D. Markham, J. Tartaglia, E.
Paoletti, R. C. Gallo, G. Franchini, and M. Robert-Guroff. 1996.
Multiple immunizations with attenuated poxvirus HIV type 2
recombinants and subunit boosts required for protection of rhesus
macaques. AIDS Res. Hum. Retrovir. 12: 985–992.
45. Patterson, L. J., B. Peng, A. G. Abimiku, K. Aldrich, L. Murty, P.
D. Markham, V. S. Kalyanaraman, W. G. Alvord, J. Tartaglia, G.
Franchini, and M. Robert-Guroff. 2000. Cross-protection in NYVAC-
HIV-1-immunized/ HIV-2-challenged but not in NYVAC-HIV-2-
immunized/SHIV-challenged rhesus macaques. AIDS 14:2445–2455.
46. Reeves, J. D., S. Hibbitts, G. Simmons, A. McKnight, J. M.
Azevedo-Pereira, J. Moniz-Pereira, and P. R. Clapham. 1999. Primary
human immunodeficiency virus type 2 (HIV-2) isolates infect CD4-
negative cells via CCR5 and CXCR4: comparison with HIV-1 and
simian immunodeficiency virus and relevance to cell tropism in vivo.
J. Virol. 73:7795–7804.
47. Robert-Guroff, M., K. Aldrich, R. Muldoon, T. L. Stern, G. P.
Bansal, T. J. Matthews, P. D. Markham, R. C. Gallo, and G.
Franchini. 1992. Crossneutralization of human immunodeficiency
virus type 1 and 2 and simian immunodeficiency virus isolates. J.
Virol. 66:3602–3608.
48. Rodriguez, S. K., A. D. Sarr, A. MacNeil, S. Thakore-Meloni, A.
Gueye- Ndiaye, I. Traore, M. C. Dia, S. Mboup, and P. J. Kanki.
2007. Comparison of heterologous neutralizing antibody responses of
human immunodeficiency virus type 1 (HIV-1)- and HIV-2-infected
Senegalese patients: distinct patterns of breadth and magnitude
distinguish HIV-1 and HIV-2 infections. J. Virol. 81:5331–5338.
49. Santra, S., H. X. Liao, R. Zhang, M. Muldoon, S. Watson, W.
Fischer, J. Theiler, J. Szinger, H. Balachandran, A. Buzby, D. Quinn,
R. J. Parks, C. Y. Tsao, A. Carville, K. G. Mansfield, G. N. Pavlakis, B.
K. Felber, B. F. Haynes, B. T. Korber, and N. L. Letvin. Mosaic
vaccines elicit CD8 T lymphocyte responses that confer enhanced
immune coverage of diverse HIV strains in monkeys. Nat. Med.
16:324–328.
50. Sarkar, G., and S. S. Sommer. 1990. The “megaprimer” method
of sitedirected mutagenesis. Biotechniques 8:404–407.

175
51. Schneider, J. A., S. A. Alam, M. Ackers, B. Parekh, H. Y. Chen, P.
Graham, M. Gurwith, K. Mayer, and R. M. Novak. 2007. Mucosal
HIV-binding antibody and neutralizing activity in high-risk HIV-
uninfected female participants in a trial of HIV-vaccine efficacy. J.
Infect. Dis. 196:1637–1644.
52. Shi, Y., E. Brandin, E. Vincic, M. Jansson, A. Blaxhult, K.
Gyllensten, L. Moberg, C. Brostrom, E. M. Fenyo, and J. Albert.
2005. Evolution of human immunodeficiency virus type 2 coreceptor
usage, autologous neutralization, envelope sequence and
glycosylation. J. Gen. Virol. 86:3385–3396.
53. Taveira, N. C., F. Bex, A. Burny, D. Robertson, M. O. Ferreira,
and J. Moniz-Pereira. 1994. Molecular characterization of the env
gene from a non-syncytium-inducing HIV-2 isolate (HIV-2ALI). AIDS
Res. Hum. Retrovir. 10:223–224.
54. Traincard, F., M. A. Rey-Cuille, I. Huon, S. Dartevelle, J. C.
Mazie, and S. Benichou. 1994. Characterization of monoclonal
antibodies to human immunodeficiency virus type 2 envelope
glycoproteins. AIDS Res. Hum. Retrovir. 10:1659–1667.
55. Vogt, G., R. le Grand, B. Vaslin, F. Boussin, M. H. Auboyer, Y.
Riviere, P. Putkonen, P. Sonigo, M. P. Kieny, M. Girard, et al. 1995.
Heterologous HIV-2 challenge of rhesus monkeys immunized with
recombinant vaccinia viruses and purified recombinant HIV-2
proteins. Vaccine 13:202–208.
56. Wei, X., J. M. Decker, H. Liu, Z. Zhang, R. B. Arani, J. M. Kilby,
M. S. Saag, X. Wu, G. M. Shaw, and J. C. Kappes. 2002. Emergence
of resistant human immunodeficiency virus type 1 in patients
receiving fusion inhibitor (T-20) monotherapy. Antimicrob. Agents
Chemother. 46:1896–1905.
57. Wei, X., J. M. Decker, S. Wang, H. Hui, J. C. Kappes, X. Wu, J.
F. Salazar- Gonzalez, M. G. Salazar, J. M. Kilby, M. S. Saag, N. L.
Komarova, M. A. Nowak, B. H. Hahn, P. D. Kwong, and G. M. Shaw.
2003. Antibody neutralization and escape by HIV-1. Nature 422:307–
312.
58. Zhang, P. F., F. Cham, M. Dong, A. Choudhary, P. Bouma, Z.
Zhang, Y. Shao, Y. R. Feng, L. Wang, N. Mathy, G. Voss, C. C.
Broder, and G. V. Quinnan, Jr. 2007. Extensively cross-reactive anti-

176
HIV-1 neutralizing antibodies induced by gp140 immunization. Proc.
Natl. Acad. Sci. U. S. A. 104:10193–10198

177
CAPÍTULO VIII
Discussão Geral e Conclusões

178

179
Discussão Geral e Conclusões
Na infecção VIH-2 só uma minoria dos indivíduos infectados
desenvolve a SIDA. A carga viral plasmática e a taxa de depleção das
células T CD4 são significativamente mais baixas nos indivíduos
infectados por VIH-2 do que por VIH-1 [1-3]. Os estudos já realizados
sugerem que a resposta humoral e celular produzida pelos
indivíduos infectados por VIH-2 são mais eficazes no controlo da
replicação viral do que a desenvolvida pelos indivíduos infectados por
VIH-1 [4-11]. Neste contexto, o VIH-2 tem sido descrito como um
modelo natural de infecção atenuada por VIH de grande utilidade
para investigar as correlações imunológicas protectoras da infecção
VIH.
O estudo apresentado nesta tese teve como objectivo contribuir para
um melhor conhecimento da resposta humoral nas fases aguda e
crónica da infecção VIH-2. Primeiro, desenvolveu-se um novo teste
imunoenzimático (ELISA-HIV2) para determinar o potencial
antigénico e aplicação em diagnóstico de proteínas recombinantes
derivadas da glicoproteína de superfície gp125 e da proteína
transmembranar gp36 (Capítulo III). A resposta humoral contra o
VIH-2 foi analisada de forma qualitativa e quantitativa em 28
doentes com infecção crónica e duas crianças infectadas por via
perinatal durante um período aproximado de 4 anos. Avaliou-se a
concentração de anticorpos IgA e IgG total (resposta inespecífica) e
caracterizou-se a cinética, isotipo e avidez da resposta IgA e IgG
dirigida especificamente para as glicoproteínas gp36 e gp125
(Capítulo IV). Determinou-se o impacto dos anticorpos IgA e IgG na
evolução molecular das regiões C2, V3 e C3 da glicoproteína gp125
(Capítulo V). Caracterizou-se a dinâmica evolutiva da resposta
neutralizante autóloga e heteróloga na infecção VIH-2 (Capítulo VI).
Finalmente, avaliou-se a resposta neutralizante induzida por duas
proteínas recombinantes derivadas do invólucro do isolado primário
de referência VIH-2ALI em murganhos Balb/C (Capítulo VII).
O diagnóstico serológico da infecção VIH-2 baseia-se na detecção de
anticorpos para as proteínas do VIH-2. A especificidade da maioria
dos testes comerciais de diagnóstico serológico licenciados para a
infecção VIH-2 é inferior a 100% e a sensibilidade clínica varia
consideravelmente quando se testam diluições de amostras de
plasma positivas para VIH-2 [12]. A existência de reactividade entre
plasmas de VIH-1 e a glicoproteína transmembranar (gp36) do
invólucro do VIH-2 pode interferir com o diagnóstico da infecção por
VIH-2 [13-16]. A maioria dos antigénios recombinantes usados nos

180
testes de diagnóstico serológicos tem origem em isolados de
laboratório, sobretudo do VIH-2ROD. A procura de novos antigénios
derivados de isolados VIH-2 primários é determinante para o
desenvolvimento de métodos de diagnóstico mais específicos e de
novas vacinas. Um dos primeiros objectivos deste trabalho foi
produzir por métodos recombinantes novos antigénios derivados das
regiões imunodominantes do invólucro do isolado primário de
referência do grupo A, o VIH-2ALI. As proteínas rgp36 e rpC2-C3
correspondentes, respectivamente, à região mais imunogénica da
gp36 e gp125 do VIH-2 [17, 18] foram purificadas e utilizadas no
desenvolvimento de um teste de ELISA (ELISA-VIH2) para detectar a
presença de anticorpos específicos das glicoproteínas do invólucro do
VIH-2 [16]. A avaliação do teste foi aferida com amostras de plasmas
positivas para VIH-2 e VIH-1, e plasmas de indivíduos saudáveis não
infectados por VIH. A especificidade do teste para os antigénios
rgp36 e rpC2-C3 foi superior à dos testes de serodiagnóstico
licenciados para o VIH-2, e da maioria dos testes mistos (testes
baseados em proteínas recombinantes e péptidos sintéticos) para
VIH-1/VIH-2, quando foram analisadas amostras negativas para VIH
[19-26]. A sensibilidade clínica (100%) obtida no teste ELISA-VIH2
com o antigénio rgp36 é idêntica à dos testes de ELISA comerciais e
aos desenvolvidos em laboratório que usam a gp36 como antigénio.
Contudo, os testes comerciais necessitam de usar maiores volumes
de plasma por reacção (50 a 200µl) comparado com o ELISA-VIH2
(1µl). Os resultados de sensibilidade e especificidade obtidos com a
rgp36 sugerem que o teste pode ser útil no serodiagnóstico da
infecção por VIH-2. Por outro lado, a forte antigenicidade da proteína
rgp36 em relação à rpC2-C3, sugere que o ectodomíno da gp36 é a
região antigénica imunodominante no invólucro do VIH-2, e está de
acordo com estudos anteriores que mostraram que as proteínas gp36
recombinantes provenientes de estirpes VIH-2 laboratoriais são
altamente imunogénicas [27, 28].
Ao invés da proteína rpC2-C3, em que trinta e uma das amostras
VIH-1 eram positivas com a rgp36 (reactividade quatro vezes inferior
à das amostras VIH-2), nenhuma das amostras VIH-1 apresentou
reactividade com o rpC2-C3. Estes resultados sugerem que o teste
pode ser útil para discriminar entre a infecção por VIH-1 e VIH-2 em
indivíduos com dupla serologia positiva. Para investigar esta
possibilidade, analisou-se por PCR e ELISA-VIH2 sete amostras de
plasma positivas para VIH-1 e VIH-2 (com base em testes serológicos
comerciais). Com base no teste de ELISA-VIH-2 e confirmado por
PCR verificou-se que quatro amostras eram positivas para VIH-2 e
três para VIH-1. Estes resultados sugerem que o teste pode ser útil

181
para discriminar entre infecção por VIH-1 ou VIH-2 em pacientes
duplamente seroreactivos. Segundo dados do Núcleo de Vigilância
Laboratorial de Doenças Infecciosas do Instituto Nacional de Saúde,
I.P, a taxa de indivíduos infectados por VIH-1/VIH-2 é de 1,4%.
Tendo em atenção aos resultados obtidos com o teste e à taxa de
duplas infecções reportadas [16], seria importante testar mais
amostras de pacientes referenciados como duplamente infectados
para se poder determinar qual a taxa de duplas infecções em
Portugal.
A reactividade contra as duas glicoproteínas do invólucro do VIH é o
critério definido pela Organização Mundial de Saúde para a
confirmação por WB da infecção por VIH [29]. A avaliação do ELISA-
VIH2 como um teste de confirmação da infecção VIH-2 foi efectuado
com 56 amostras testadas previamente pelos testes, VIDAS VIH DUO
(teste de triagem), e New LAV Blot II (teste confirmatório), 51 das 56
amostras testadas apresentaram resultados positivas para VIH-2 e 5
apresentaram resultados indeterminadas. As 51 amostras
consideradas positivas em WB reagiram positivamente no teste
ELISA-VIH2, enquanto as cinco amostras indeterminadas
apresentaram resultados negativos no teste ELISA-VIH2. Quatro das
cinco amostras indeterminadas reagiram como amostras positivas
para VIH-1 no WB VIH-1 e no Peptilav 1 e 2. A outra amostra que
deu indeterminado, e que era positiva para VIH-1 no WB, foi
considerada positiva para VIH-1/VIH-2 no teste Peptilav 1-2. Em
conclusão, neste estudo demonstrámos: 1) a antigenicidade das
proteínas recombinantes, rgp36 e rpC2-C3; 2) que estas regiões são
imunodominantes nos pacientes VIH-2 e 3) que a elevada
sensibilidade e especificidade obtida com o teste ELISA-VIH2 poderia
constituir uma alternativa aos testes serológicos disponíveis para
diagnosticar e confirmar a infecção por VIH-2.
Os antigénios rpC2-C3 e rgp36 usados no teste ELISA-VIH2 foram
essenciais para a caracterização qualitativa e quantitativa da
resposta de anticorpos para a gp125 e gp36 em pacientes infectados
pelo VIH-2.
A hiperactivação dos linfócitos B e níveis elevados de
imunoglobulinas (hipergamaglobulinémia) são características
patogénicas das infecções crónicas persistentes e estão bem
caracterizadas nos indivíduos infectados por VIH-1 [30]. As
concentrações elevadas de anticorpos IgG (principalmente IgG1 e
IgG3) e IgA não específicas das proteínas do VIH-1 presentes no soro
são comuns nos indivíduos infectados e resultam de uma activação
policlonal das células B pelo VIH-1 [31]. Neste trabalho, a resposta

182
humoral inespecífica foi analisada longitudinalmente em 28
pacientes VIH-2+ crónicos ao longo de 4 anos. Os resultados obtidos
sugerem que a activação inespecífica das células B também ocorre
na infecção VIH-2 crónica, mas só ao nível das células B secretoras
de IgG, uma vez que a concentração total de IgA no soro é idêntica à
dos indivíduos não infectados [32]. Esta diferença pode estar
relacionada com uma melhor preservação do sistema gastrointestinal
na infecção VIH-2. Contudo, um estudo recente sugere que a
translocação microbiana para o sangue periférico também ocorre nos
indivíduos infectados pelo VIH-2, contribuindo para a activação
imunitária tanto nos indivíduos infectados por VIH-1 como por VIH-2
[33]. Seria importante investigar qual o mecanismo que regula a
diferenciação e proliferação das células B produtoras de anticorpos
IgA na infecção por VIH-2.
Existem vários estudos que correlacionam a resposta humoral com o
ritmo de progressão da infecção VIH-1. Anticorpos anti-p24 estão
correlacionados com uma progressão mais lenta enquanto os
anticorpos anti-gp120 estão correlacionados com uma progressão
rápida [34-36]. Na infecção VIH-2 crónica não existem dados sobre o
papel da resposta humoral na progressão da infecção VIH-2. Neste
trabalho, a magnitude e a cinética da resposta IgA e IgG contra a
gp36 e a gp125 do invólucro do VIH-2 foram analisadas
longitudinalmente em 28 pacientes adultos positivos para VIH-2 e
duas crianças infectadas pelas mães. Nas duas crianças a
seroconversão para a gp36 ocorreu durante o primeiro ano de vida.
Na criança em que não houve progressão da infecção (paciente C2),
os níveis de anticorpos IgG anti-gp36 e gp125 eram semelhantes aos
observados nos pacientes adultos crónicos, mesmo num contexto de
declínio progressivo das células CD4. Em contrapartida, a criança
(paciente C1) que progrediu rapidamente para SIDA e faleceu não
produziu anticorpos anti-gp125. Uma resposta de anticorpos forte e
sustentada anti-gp125 na fase inicial da infecção pode ser
determinante na progressão da infecção. Por outro lado, uma
resposta humoral debilitada pode ter contribuído para o
desenvolvimento de isolados com fenótipo mais agressivo.
A presença de anticorpos IgG específicos para o antigénio
representativo da gp125 (rpC2-C3) também não foi detectada nos
pacientes 27 e 28. A região C2-V3-C3 dos isolados virais desses
pacientes apresentava um elevado número de aminoácidos alterados
quando comparadas com as regiões homólogas dos isolados dos
outros pacientes e com o antigénio rpC2-C3 utilizado no teste ELISA-
VIH2. A ausência de reactividade para a região C2-C3 nestes
pacientes pode ser consequência das alterações ocorridas

183
principalmente nos determinantes antigénicos da região V3 dos
respectivos vírus [37, 38]. Á excepção de um paciente que produziu
exclusivamente IgA para a gp36, todos os outros produziram
anticorpos IgA que reagiram contra ambos os polipéptidos, C2-C3 e
gp36. Na infecção VIH-1 apenas uma fracção reduzida de pacientes
produzem anticorpos IgA anti-gp41 e / ou anti-gp120, estando esta
produção relacionada inversamente com o estádio da doença [39,
40]. Os nossos resultados confirmam a antigenicidade do ectodomíno
da gp36 na infecção VIH-2, e identificam pela primeira vez a região
C2-C3 como indutora de anticorpos IgA no soro. Constatou-se que a
região C2-C3 e a gp36 contêm epitopos que induzem anticorpos IgA,
o que, pode ser relevante para a produção de novos testes de
diagnóstico serológico para a infecção VIH-2 (por exemplo, testes
rápidos utilizando amostras de saliva).
A forte correlação entre os títulos de anticorpos IgG para a gp36 e
gp125 nos pacientes VIH-2 (P = 0.0027) sugere que as duas
proteínas são muito imunogénicas. No entanto, a resposta IgG foi
dirigida predominantemente para a gp36 em termos qualitativos
(avidez) e quantitativos (título e concentração). A gp36 também
induziu níveis mais elevados de todas as subclasses de IgG, ao invés
da gp125.
A IgG1 foi a subclasse mais produzida contra as duas glicoproteínas
do invólucro do VIH-2. Na infecção VIH-1, o anticorpo IgG3 foi a
segunda subclasse mais reactiva contra a gp36 em vez do IgG2 [41,
42]. A correlação inversa entre os níveis de anticorpos IgG2 anti-gp41
e a evolução clínica da SIDA observada na infecção VIH-1 sugere que
os anticorpos IgG2 podem ter um papel protectivo [43]. Na infecção
VIH-2 não encontrámos qualquer associação entre a resposta IgG1 e
IgG3 anti-gp36 e a progressão da doença, tendo como base a
depleção de células T CD4+. O que realmente observámos foi uma
correlação inversa significativa entre anticorpos IgG anti-C2-C3 e a
contagem de células T CD4+. Esta correlação também foi observada
numa das crianças estudada. Pode a diminuição de células T CD4+
estar associada com a resposta IgG anti-C2V3C3? Cavaleiro e
colaboradores sugerem que a região C2V3C3 do invólucro do VIH-2
exerce uma actividade imunosupressora sobre as células T CD4 e
CD8, e que pode estar associado com uma baixa taxa de activação
imunitária e com a reduzida perda de células T CD4+ observada na
maioria dos pacientes VIH-2 [44]. Os nossos resultados fornecem
apoio adicional para a função imunoprotectora da região C2V3C3 do
invólucro do VIH-2 durante a infecção, uma vez que a resposta de
anticorpos IgG anti-C2-C3 parece reflectir o estado imunológico e a
evolução clínica dos pacientes VIH-2. Neste contexto, pode dizer-se

184
que se justificava investigar se a concentração de anticorpos IgG
para anti-C2-C3 poderia ser mais um marcador para monitorizar a
progressão da doença na infecção VIH-2.
O principal promotor da evolução molecular e fenotípica do VIH-1 é a
pressão selectiva exercida pela resposta imunitária humoral
(anticorpos neutralizantes) e pela resposta celular citotóxica [45-47].
A informação existente sobre este assunto no VIH-2 é muito limitada.
Com o objectivo de determinar, pela primeira vez, a taxa de evolução
molecular do VIH-2 in vivo e caracterizar os seus potenciais
determinantes, analisámos longitudinalmente as sequências
nucleotídicas e aminoacídicas das regiões C2, V3 e C3 de 18
pacientes recorrendo a métodos filogenéticos e moleculares (Capítulo
V).
Com excepção de um paciente, os valores de diversidade nucleotídica
observados nos pacientes estudados foram semelhantes aos
encontrados nos EC para o VIH-2, nos indivíduos VIH-1 LTNP com
cargas virais baixas e nos indivíduos VIH-1 com infecções crónicas
[48, 49]. A taxa de divergência nucleotídica nos pacientes estudados
foi bastante elevada quando comparada com os pacientes infectados
por VIH-1 (1.4% versus 0.27%). Estes resultados confirmados
posteriormente num maior número de doentes ao nível da região C2-
V3-C3 e da glicoproteína de superfície [50] sugerem uma replicação
activa do VIH-2 durante a fase crónica da infecção, podendo esta
ocorrer no tecido linfoíde, uma vez que a carga proviral é maior nas
células mononucleadas dos nódulos linfáticos do que nas células do
sangue periférico [51, 52]. Novos estudos que analisem a divergência
nucleotídica na infecção VIH-2 devem incluir também a população
viral presente no tecido linfoíde e noutros compartimentos celulares
(por exemplo, do trato gastrointestinal).
Apesar das taxas elevadas de divergência nucleotídica, a maioria das
substituições foram de natureza sinónima e diminuíram ao longo do
tempo na maioria dos pacientes. Os resultados obtidos estão de
acordo com estudos anteriores sobre a região C2-V3-C3 e que
indicam que, globalmente, o gene env do VIH-2 está sob selecção
negativa ou purificadora [53]. Verificámos ainda que foram as regiões
C2 e C3 que evoluíram a taxas mais elevadas ao nível dos
nucleótidos e dos aminoácidos, contribuindo significativamente para
a elevada taxa de divergência nucleotídica observada em cada
paciente. A conservação da região V3 in vivo implica que, tanto no
VIH-2 como no VIH-1, esta região está submetida a fortes restrições
estruturais e conformacionais, relacionadas provavelmente com as

185
funções cruciais que desempenha ao nível da ligação aos co-
receptores e entrada nas células [54, 55].
Será que a rápida evolução das regiões C2 e C3 resulta da adaptação
do VIH-2 à pressão imunitária do hospedeiro? A maioria dos
aminoácidos que estão sob selecção positiva concentra-se na região
C2, incluindo dois aminoácidos (posições 267 e 270) que estão sob
forte selecção positiva em todos os pacientes. Além disso, a selecção
nestas duas posições persistiu durante pelo menos dois anos na
maioria dos pacientes, o que indica que estiveram continuamente
sob pressão imunológica in vivo. No VIH-1, os aminoácidos
equivalentes definem um epitopo para as células T citotóxicas e não
estão sob selecção positiva, uma vez que se encontram localizados na
face oculta da gp120 [49]. No VIH-2, a maioria dos locais de
glicosilação concentra-se na C2 e na V3 e mantêm-se conservados ao
longo do tempo que é indicativo de uma evolução convergente e
sugere restrições inesperadas à diversidade do invólucro do VIH-2.
MacNeil e colaboradores [56] encontraram uma associação directa
entre as taxas de diversificação do VIH-2 e as taxas do declínio das
células T CD4+ em indivíduos seguidos durante mais de uma década
no Senegal. Nos nossos resultados não encontrámos nenhuma
correlação entre a contagem de células T CD4+ e a diversidade
nucleotídica, a entropia dos aminoácidos, a divergência nucleotídica,
o rácio dN/dS e o número de locais seleccionados positivamente.
Estes resultados podem estar relacionados com um curto período de
acompanhamento dos pacientes. No entanto, observámos uma
relação inversa entre a diversidade e evolução dos vírus e a resposta
de anticorpos específicos da C2V3C3 ao longo do tempo. A forte
resposta de anticorpos IgG específicos da C2V3C3 está
significativamente associada com uma menor variabilidade viral ao
nível dos nucleótidos e dos aminoácidos e com uma menor
frequência de substituições sinónimas. Observámos também uma
correlação inversa significativa entre a resposta IgA e a glicosilação
da região C3 da gp125. No VIH-1, o aumento ou alteração dos locais
de glicosilação na gp120 está associado com o escape do vírus aos
anticorpos IgG neutralizantes [57]. Assim, os nossos resultados
sugerem que a região C3 do VIH-2 poderá conter epitopos
neutralizantes para os anticorpos IgA.
Na infecção VIH-1 a maioria dos pacientes desenvolve AcNT contra
vírus autólogos, mas à medida que a infecção progride os novos
isolados não são neutralizados talvez devido ao desenvolvimento de
vírus autólogos resistentes muito rapidamente. Os invólucros dos
isolados autólogos resistentes à neutralização, em geral, sofreram
uma selecção positiva maior, um aumento da gp160 e do número de

186
locais de glicosilação [47, 58]. Os anticorpos neutralizantes autólogos
estão presentes em doentes crónicos não progressores, evidenciando
o papel que têm no controlo da replicação viral [59]. Os anticorpos
neutralizantes heterólogos de largo espectro surgem apenas em
alguns pacientes ao fim do primeiro ano após a infecção e parece
haver uma associação entre a potência e o espectro destes anticorpos
com o tempo de infecção, a carga viral plasmática e a avidez de
ligação ao Env [60, 61]. No caso da infecção VIH-2 os estudos são
limitados e sugerem que a resposta neutralizante autóloga é
frequente nos doentes VIH-2 [62] e que a resposta heteróloga é de
maior espectro, mas de menor potência do que no VIH-1 [4, 63].
Contudo, apenas um estudo, utilizando um número muito pequeno
de doentes, analisou a dinâmica evolutiva da resposta neutralizante
na infecção VIH-2 e correlacionou-a com a replicação e evolução do
vírus e a progressão da doença. Neste estudo não se detectou escape
à neutralização pelo VIH-2 [5].
O objectivo do Capítulo 6 foi caracterizar a dinâmica da resposta
neutralizante na infecção VIH-2 crónica e relaciona-la com a
evolução viral e a evolução da doença. Neste contexto, analisámos
longitudinalmente ao longo de 3-4 anos a resposta neutralizante
dirigida contra isolados virais primários autólogos e heterólogos num
grupo de 28 pacientes positivos para VIH-2. A mediana da contagem
de células T CD4+, a idade dos pacientes e os anos de infecção após
o diagnóstico foram respectivamente de 363 células (variando entre
15 e 1523 células), 48 anos (variação entre 25 e 77 anos) e 8 anos
após o diagnóstico da infecção (variação entre 2 e 19 anos). Apenas
dois pacientes tinham carga viral detectável. Os vírus isolados de
cada paciente foram caracterizados quanto à utilização de
coreceptores e a sequência aminoacídica da região C2, V3 e C3 dos
vários isolados foi determinada.
A presença de anticorpos IgG com actividade neutralizante específica
para isolados autólogos foi detectada em apenas 6 dos 12 pacientes
(50% dos pacientes), todos eles infectados com isolados de fenótipo
R5. Estes resultados mostram que o escape à neutralização é
frequente na infecção crónica por VIH-2. Tendo em conta os dados
sobre a resposta neutralizante heteróloga obtidos em estudos
anteriores e comparando com os nossos resultados podemos sugerir
que a resposta neutralizante heteróloga tem realmente uma
amplitude maior na infecção VIH-2 do que na infecção VIH-1. É
importante realçar que, há excepção e um doente, todos os outros
desenvolveram AcNT IgG contra isolados heterólogos de fenótipo R5
mas não contra isolados X4. O facto de não se ter detectado AcNT

187
contra isolados X4 sugere que o escape do VIH-2 à neutralização
poderá estar associado a alterações no tropismo. Na infecção VIH-1,
os poucos estudos existentes sobre este assunto sugerem que não há
uma relação entre a neutralização e a utilização de coreceptores [64-
66].
Observou-se uma correlação inversa entre a resposta neutralizante
heteróloga e o título de anticorpos de ligação e a avidez apenas para
o polipéptido rpC2-C3. A análise das sequências aminoacídicas das
regiões C2, V3 e C3 do Env dos vírus R5 sensíveis à neutralização
(R5-SN) e dos vírus X4 resistentes à neutralização (X4-RN) revelou
diferenças significativas na região V3. Os vírus X4-RN tinham a
região V3 mais longa, (inserções entre 1 e 3 aminoácidos) e um
número maior de aminoácidos carregados (maioria arginina). A
estrutura conformacional da região V3 dos isolados R5-SN é bem
diferente dos X4-RN.
Um dos objectivos no desenvolvimento de uma vacina para o VIH é a
produção de anticorpos neutralizantes que neutralizem todos os
subtipos virais [67, 68]. Contudo, as várias estratégias desenvolvidas
até hoje para induzir AcNT contra isolados VIH-1 ou VIH-2 primários
têm-se revelado ineficazes [69]. A principal dificuldade tem sido o
desenho e a produção de imunogénios que induzam a produção de
títulos elevados de anticorpos neutralizantes de largo espectro [70,
71]. Deste modo, a produção de novos imunogénios é uma das
prioridades no desenvolvimento de uma vacina para o VIH. O
trabalho inicial deste estudo mostrou que os indivíduos infectados
por VIH-2 produzem níveis elevados de anticorpos que têm como alvo
a região extracelular da gp36, a gp125 e, dentro desta, a região C2-
V3-C3 [16, 32].
Posteriormente, mostramos in vitro que os anticorpos testado são de
largo espectro neutralizante e que as regiões C2, V3 e C3 evoluem a
uma taxa muito elevada nos pacientes VIH-2 possivelmente em
resposta à pressão selectiva imposta pelos anticorpos neutralizantes
[72, 73]. Em conjunto, estes resultados sugerem que a resposta
neutralizante anti-C2-V3-C3 tem um papel determinante no controlo
da replicação viral in vivo. Assim, na parte final deste trabalho
testámos se a região C2-V3-C3 seria um bom imunogénio vacinal.
Verificámos que os murganhos imunizados só com a proteína rpC2-
C3 não desenvolveram uma resposta neutralizante. Contudo,
murganhos imunizados primeiro com vírus da vacina recombinante
exprimindo a proteína gp125t e depois com a proteína rpC2-C3
desenvolveram uma resposta neutralizante de largo espectro e
superior à que ocorre numa infecção normal por VIH-2 [4, 74]. Estes

188
resultados mostraram que a proteína rpC2-C3 é um bom antigénio
de reforço, e que a imunização primária com a gp125t glicosilada
expressa por um vector viral replicativo é fundamental para a
indução de uma forte resposta neutralizante. Verificámos que todos
os isolados VIH-2 primários neutralizados utilizavam o coreceptor
CCR5. O fenótipo CCR5 é uma característica comum à maioria dos
isolados VIH-2 encontrados em pacientes assintomáticos [75] e nos
isolados VIH que são transmitidos [76]. A sequência de aminoácidos
e a estrutura da região V3 divergiram muito pouco do isolado vacinal
que também usa o CCR5 (VIH-2ALI). Pelo contrário, os vírus com
fenótipo X4 foram resistentes à neutralização e as regiões V3
divergiam significativamente em relação à do ALI na sequência de
aminoácidos, na carga total (carga superior), tamanho (maior) e
conformação estrutural. Estes resultados sugerem: 1) que o alvo dos
anticorpos neutralizantes induzidos nos murganhos está localizado
na região V3 e é de natureza conformacional; 2) a existência de uma
potencial correlação entre a utilização de co-receptores e a resposta
neutralizante e 3) novas abordagens para a produção de uma vacina
para o VIH-2 e podem ser essenciais também para a produção de
uma vacina para o VIH-1.
Em conclusão, os resultados apresentados nesta tese sugerem que
as glicoproteínas do invólucro do VIH-2, em comparação com as do
VIH-1, são mais eficazes na estimulação e manutenção de respostas
imunológicas humorais mais consistentes e com menor variabilidade
entre a maioria dos indivíduos infectados por VIH-2, permitindo
deste modo desenvolver novos antigénios essências para o
diagnóstico, prevenção e progressão da infecção por VIH-2.
Referências
[1] Andersson S, Norrgren H, da Silva Z, et al. Plasma viral load in
HIV-1 and HIV-2 singly and dually infected individuals in Guinea-
Bissau, West Africa: significantly lower plasma virus set point in
HIV-2 infection than in HIV-1 infection. Arch.Intern.Med.
2000;160(21):3286-93.
[2] Jaffar S, Grant AD, Whitworth J, Smith PG, Whittle H. The
natural history of HIV-1 and HIV-2 infections in adults in Africa: a
literature review. Bull.World Health Organ 2004;82(6):462-9.
[3] Popper SJ, Sarr AD, Travers KU, et al. Lower human
immunodeficiency virus (HIV) type 2 viral load reflects the difference

189
in pathogenicity of HIV-1 and HIV-2. J.Infect.Dis.
1999;180(4):1116-21.
[4] Rodriguez SK, Sarr AD, MacNeil A, et al. Comparison of
heterologous neutralizing antibody responses of human
immunodeficiency virus type 1 (HIV-1)- and HIV-2-infected
Senegalese patients: distinct patterns of breadth and magnitude
distinguish HIV-1 and HIV-2 infections. J.Virol. 2007;81(10):5331-
8.
[5] Shi Y, Brandin E, Vincic E, et al. Evolution of human
immunodeficiency virus type 2 coreceptor usage, autologous
neutralization, envelope sequence and glycosylation. J.Gen.Virol.
2005;86(Pt 12):3385-96.
[6] Rowland-Jones S. Protective immunity against HIV infection:
lessons from HIV-2 infection. Future.Microbiol. 2006;1:427-33.
[7] Rowland-Jones SL, Whittle HC. Out of Africa: what can we learn
from HIV-2 about protective immunity to HIV-1? Nat.Immunol.
2007;8(4):329-31.
[8] Sousa AE, Chaves AF, Loureiro A, Victorino RM. Comparison of
the frequency of interleukin (IL)-2-, interferon-gamma-, and IL-4-
producing T cells in 2 diseases, human immunodeficiency virus
types 1 and 2, with distinct clinical outcomes. J.Infect.Dis.
2001;184(5):552-9.
[9] Sousa AE, Carneiro J, Meier-Schellersheim M, Grossman Z,
Victorino RM. CD4 T cell depletion is linked directly to immune
activation in the pathogenesis of HIV-1 and HIV-2 but only indirectly
to the viral load. J.Immunol. 2002;169(6):3400-6.
[10] Foxall RB, Cortesao CS, Albuquerque AS, Soares RS, Victorino
RM, Sousa AE. Gag-specific CD4+ T-cell frequency is inversely
correlated with proviral load and directly correlated with immune
activation in infection with human immunodeficiency virus type 2
(HIV-2) but not HIV-1. J.Virol. 2008;82(19):9795-9.
[11] Leligdowicz A, Yindom LM, Onyango C, et al. Robust Gag-
specific T cell responses characterize viremia control in HIV-2
infection. J.Clin.Invest 2007;117(10):3067-74.

190
[12] Ly TD, Martin L, Daghfal D, et al. Seven human
immunodeficiency virus (HIV) antigen-antibody combination assays:
evaluation of HIV seroconversion sensitivity and subtype detection.
J.Clin.Microbiol. 2001;39(9):3122-8.
[13] Weiss RA, Clapham PR, Weber JN, et al. HIV-2 antisera cross-
neutralize HIV-1. AIDS 1988;2(2):95-100.
[14] Robert-Guroff M, Aldrich K, Muldoon R, et al. Cross-
neutralization of human immunodeficiency virus type 1 and 2 and
simian immunodeficiency virus isolates. J.Virol. 1992;66(6):3602-8.
[15] Nyambi PN, Willems B, Janssens W, et al. The neutralization
relationship of HIV type 1, HIV type 2, and SIVcpz is reflected in the
genetic diversity that distinguishes them. AIDS
Res.Hum.Retroviruses 1997;13(1):7-17.
[16] Marcelino JM, Barroso H, Goncalves F, et al. Use of a new dual-
antigen enzyme-linked immunosorbent assay to detect and
characterize the human antibody response to the human
immunodeficiency virus type 2 envelope gp125 and gp36
glycoproteins. J.Clin.Microbiol. 2006;44(2):607-11.
[17] Huang ML, Essex M, Lee TH. Localization of immunogenic
domains in the human immunodeficiency virus type 2 envelope.
J.Virol. 1991;65(9):5073-9.
[18] Chiodi F, Bjorling E, Samuelsson A, Norrby E. Antigenic and
immunogenic sites of HIV-2 glycoproteins. Chem.Immunol.
1993;56:61-77.
[19] Andersson S, da Silva Z, Norrgren H, Dias F, Biberfeld G. Field
evaluation of alternative testing strategies for diagnosis and
differentiation of HIV-1 and HIV-2 infections in an HIV-1 and HIV-2-
prevalent area. AIDS 1997;11(15):1815-22.
[20] Benitez J, Palenzuela D, Rivero J, Gavilondo JV. A recombinant
protein based immunoassay for the combined detection of antibodies
to HIV-1, HIV-2 and HTLV-I. J.Virol.Methods 1998;70(1):85-91.
[21] Galli RA, Castriciano S, Fearon M, et al. Performance
characteristics of recombinant enzyme immunoassay to detect
antibodies to human immunodeficiency virus type 1 (HIV-1) and HIV-

191
2 and to measure early antibody responses in seroconverting
patients. J.Clin.Microbiol. 1996;34(4):999-1002.
[22] Gonzalez L, Boyle RW, Zhang M, et al. Synthetic-peptide-based
enzyme-linked immunosorbent assay for screening human serum or
plasma for antibodies to human immunodeficiency virus type 1 and
type 2. Clin.Diagn.Lab Immunol. 1997;4(5):598-603.
[23] Kannangai R, Ramalingam S, Prakash KJ, et al. A peptide
enzyme linked immunosorbent assay (ELISA) for the detection of
human immunodeficiency virus type-2 (HIV-2) antibodies: an
evaluation on polymerase chain reaction (PCR) confirmed samples.
J.Clin.Virol. 2001;22(1):41-6.
[24] Manocha M, Chitralekha KT, Thakar M, Shashikiran D,
Paranjape RS, Rao DN. Comparing modified and plain peptide linked
enzyme immunosorbent assay (ELISA) for detection of human
immunodeficiency virus type-1 (HIV-1) and type-2 (HIV-2) antibodies.
Immunol.Lett. 2003;85(3):275-8.
[25] Simon F, Souquiere S, Damond F, et al. Synthetic peptide
strategy for the detection of and discrimination among highly
divergent primate lentiviruses. AIDS Res.Hum.Retroviruses
2001;17(10):937-52.
[26] Thorstensson R, Andersson S, Lindback S, et al. Evaluation of
14 commercial HIV-1/HIV-2 antibody assays using serum panels of
different geographical origin and clinical stage including a unique
seroconversion panel. J.Virol.Methods 1998;70(2):139-51.
[27] Zuber M, Samuel KP, Lautenberger JA, Kanki PJ, Papas TS.
Bacterially produced HIV-2 env polypeptides specific for
distinguishing HIV-2 from HIV-1 infections. AIDS
Res.Hum.Retroviruses 1990;6(4):525-34.
[28] Schulz TF, Oberhuber W, Hofbauer JM, et al. Recombinant
peptides derived from the env-gene of HIV-2 in the serodiagnosis of
HIV-2 infections. AIDS 1989;3(3):165-72.
[29] AIDS: proposed WHO criteria for interpreting western blot assays
for HIV-1, HIV-2, and HTLV-I/HTLV-II. Bull.World Health Organ
1991;69(1):127-3.

192
[30] Swingler S, Zhou J, Swingler C, et al. Evidence for a pathogenic
determinant in HIV-1 Nef involved in B cell dysfunction in HIV/AIDS.
Cell Host.Microbe 2008;4(1):63-76.
[31] Abelian A, Burling K, Easterbrook P, Winter G.
Hyperimmunoglobulinemia and rate of HIV type 1 infection
progression. AIDS Res.Hum.Retroviruses 2004;20(1):127-8.
[32] Marcelino JM, Nilsson C, Barroso H, et al. Envelope-specific
antibody response in HIV-2 infection: C2V3C3-specific IgG response
is associated with disease progression. AIDS 2008;22(17):2257-65.
[33] Nowroozalizadeh S, Mansson F, da Silva Z, et al. Microbial
translocation correlates with the severity of both HIV-1 and HIV-2
infections. J.Infect.Dis. 2010;201(8):1150-4.
[34] Forthal DN, Gilbert PB, Landucci G, Phan T. Recombinant gp120
vaccine-induced antibodies inhibit clinical strains of HIV-1 in the
presence of Fc receptor-bearing effector cells and correlate inversely
with HIV infection rate. J.Immunol. 2007;178(10):6596-603.
[35] Trkola A, Kuster H, Leemann C, et al. Humoral immunity to
HIV-1: kinetics of antibody responses in chronic infection reflects
capacity of immune system to improve viral set point. Blood
2004;104(6):1784-92.
[36] Tang S, Zhao J, Wang A, et al. Characterization of immune
responses to capsid protein p24 of human immunodeficiency virus
type 1 and implications for detection. Clin.Vaccine Immunol.
2010;17(8):1244-51.
[37] McKnight A, Shotton C, Cordell J, Jones I, Simmons G, Clapham
PR. Location, exposure, and conservation of neutralizing and
nonneutralizing epitopes on human immunodeficiency virus type 2
SU glycoprotein. J.Virol. 1996;70(7):4598-606.
[38] Sourial S, Nilsson C. HIV-2 neutralization by intact V3-specific
Fab fragments. Virol.J. 2008;5:96
[39] Cartry O, Moja P, Quesnel A, Pozzetto B, Lucht FR, Genin C.
Quantification of IgA and IgG and specificities of antibodies to viral
proteins in parotid saliva at different stages of HIV-1 infection.
Clin.Exp.Immunol. 1997;109(1):47-53.

193
[40] Mestecky J, Jackson S, Moldoveanu Z, et al. Paucity of antigen-
specific IgA responses in sera and external secretions of HIV-type 1-
infected individuals. AIDS Res.Hum.Retroviruses 2004;20(9):972-
88.
[41] Ngo-Giang-Huong N, Candotti D, Goubar A, et al. HIV type 1-
specific IgG2 antibodies: markers of helper T cell type 1 response and
prognostic marker of long-term nonprogression. AIDS
Res.Hum.Retroviruses 2001;17(15):1435-46.
[42] Forthal DN, Landucci G, Bream J, Jacobson LP, Phan TB,
Montoya B. FcgammaRIIa genotype predicts progression of HIV
infection. J.Immunol. 2007;179(11):7916-23.
[43] Lal RB, Heiba IM, Dhawan RR, Smith ES, Perine PL. IgG
subclass responses to human immunodeficiency virus-1 antigens:
lack of IgG2 response to gp41 correlates with clinical manifestation
of disease. Clin.Immunol.Immunopathol. 1991;58(2):267-77.
[44] Cavaleiro R, Sousa AE, Loureiro A, Victorino RM. Marked
immunosuppressive effects of the HIV-2 envelope protein in spite of
the lower HIV-2 pathogenicity. AIDS 2000;14(17):2679-86.
[45] O'Connell KA, Brennan TP, Bailey JR, Ray SC, Siliciano RF,
Blankson JN. Control of HIV-1 in elite suppressors despite ongoing
replication and evolution in plasma virus. J.Virol.
2010;84(14):7018-28.
[46] Bailey JR, Brennan TP, O'Connell KA, Siliciano RF, Blankson JN.
Evidence of CD8+ T-cell-mediated selective pressure on human
immunodeficiency virus type 1 nef in HLA-B*57+ elite suppressors.
J.Virol. 2009;83(1):88-97.
[47] Bunnik EM, Pisas L, van Nuenen AC, Schuitemaker H.
Autologous neutralizing humoral immunity and evolution of the viral
envelope in the course of subtype B human immunodeficiency virus
type 1 infection. J.Virol. 2008;82(16):7932-41.
[48] Bello G, Casado C, Sandonis V, et al. Plasma viral load threshold
for sustaining intrahost HIV type 1 evolution. AIDS
Res.Hum.Retroviruses 2007;23(10):1242-50.

194
[49] Joos B, Fischer M, Schweizer A, et al. Positive in vivo selection of
the HIV-1 envelope protein gp120 occurs at surface-exposed regions.
J.Infect.Dis. 2007;196(2):313-20.
[50] Skar H, Borrego P, Wallstrom TC, et al. HIV-2 genetic evolution
in patients with advanced disease is faster than that in matched
HIV-1 patients. J.Virol. 2010;84(14):7412-5.
[51] Jobe O, Ariyoshi K, Marchant A, et al. Proviral load and immune
function in blood and lymph node during HIV-1 and HIV-2 infection.
Clin.Exp.Immunol. 1999;116(3):474-8.
[52] Gomes P, Taveira NC, Pereira JM, Antunes F, Ferreira MO,
Lourenco MH. Quantitation of human immunodeficiency virus type 2
DNA in peripheral blood mononuclear cells by using a quantitative-
competitive PCR assay. J.Clin.Microbiol. 1999;37(2):453-6.
[53] Choisy M, Woelk CH, Guegan JF, Robertson DL. Comparative
study of adaptive molecular evolution in different human
immunodeficiency virus groups and subtypes. J.Virol.
2004;78(4):1962-70.
[54] Isaka Y, Sato A, Miki S, et al. Small amino acid changes in the
V3 loop of human immunodeficiency virus type 2 determines the
coreceptor usage for CXCR4 and CCR5. Virology 1999;264(1):237-
43.
[55] Delobel P, Nugeyre MT, Cazabat M, et al. Population-based
sequencing of the V3 region of env for predicting the coreceptor
usage of human immunodeficiency virus type 1 quasispecies.
J.Clin.Microbiol. 2007;45(5):1572-80.
[56] MacNeil A, Sankale JL, Meloni ST, Sarr AD, Mboup S, Kanki P.
Long-term intrapatient viral evolution during HIV-2 infection.
J.Infect.Dis. 2007;195(5):726-33.
[57] Pantophlet R, Burton DR. GP120: target for neutralizing HIV-1
antibodies. Annu.Rev.Immunol. 2006;24:739-69.
[58] Richman DD, Wrin T, Little SJ, Petropoulos CJ. Rapid evolution
of the neutralizing antibody response to HIV type 1 infection.
Proc.Natl.Acad.Sci.U.S.A 2003;100(7):4144-9.

195
[59] Mahalanabis M, Jayaraman P, Miura T, et al. Continuous viral
escape and selection by autologous neutralizing antibodies in drug-
naive human immunodeficiency virus controllers. J.Virol.
2009;83(2):662-72.
[60] Gray ES, Moore PL, Choge IA, et al. Neutralizing antibody
responses in acute human immunodeficiency virus type 1 subtype C
infection. J.Virol. 2007;81(12):6187-96.
[61] Sather DN, Armann J, Ching LK, et al. Factors associated with
the development of cross-reactive neutralizing antibodies during
human immunodeficiency virus type 1 infection. J.Virol.
2009;83(2):757-69.
[62] Bjorling E, Scarlatti G, von Gegerfelt A, et al. Autologous
neutralizing antibodies prevail in HIV-2 but not in HIV-1 infection.
Virology 1993;193(1):528-30.
[63] Lizeng Q, Skott P, Sourial S, et al. Serum immunoglobulin A
(IgA)-mediated immunity in human immunodeficiency virus type 2
(HIV-2) infection. Virology 2003;308(2):225-32.
[64] Lacasse RA, Follis KE, Moudgil T, et al. Coreceptor utilization by
human immunodeficiency virus type 1 is not a primary determinant
of neutralization sensitivity. J.Virol. 1998;72(3):2491-5.
[65] McKnight A, Clapham PR. Immune escape and tropism of HIV.
Trends Microbiol. 1995;3(9):356-61.
[66] McKnight A, Weiss RA, Shotton C, Takeuchi Y, Hoshino H,
Clapham PR. Change in tropism upon immune escape by human
immunodeficiency virus. J.Virol. 1995;69(5):3167-70.
[67] Sather DN, Stamatatos L. Epitope specificities of broadly
neutralizing plasmas from HIV-1 infected subjects. Vaccine 2010;28
Suppl 2:B8-12.
[68] Sather DN, Armann J, Ching LK, et al. Factors associated with
the development of cross-reactive neutralizing antibodies during
human immunodeficiency virus type 1 infection. J.Virol.
2009;83(2):757-69.

196
[69] Montefiori D, Sattentau Q, Flores J, Esparza J, Mascola J.
Antibody-based HIV-1 vaccines: recent developments and future
directions. PLoS.Med. 2007;4(12):e348
[70] Walker LM, Phogat SK, Chan-Hui PY, et al. Broad and potent
neutralizing antibodies from an African donor reveal a new HIV-1
vaccine target. Science 2009;326(5950):285-9.
[71] Trkola A, Kuster H, Rusert P, et al. In vivo efficacy of human
immunodeficiency virus neutralizing antibodies: estimates for
protective titers. J.Virol. 2008;82(3):1591-9.
[72] Borrego P, Marcelino JM, Rocha C, et al. The role of the humoral
immune response in the molecular evolution of the envelope C2, V3
and C3 regions in chronically HIV-2 infected patients. Retrovirology.
2008;5:78
[73] Skar H, Borrego P, Wallstrom TC, et al. HIV-2 genetic evolution
in patients with advanced disease is faster than that in matched
HIV-1 patients. J.Virol. 2010;84(14):7412-5.
[74] Marcelino JM, Novo C, Pereira JM, Picotez F, Clemente A, Taveira
N. Production and characterization of a mouse monoclonal antibody
against the Gag p26 protein of human immunodeficiency virus type
2: identification of a new antigenic epitope. AIDS
Res.Hum.Retroviruses 2001;17(13):1279-83.
[75] Blaak H, Boers PH, Gruters RA, Schuitemaker H, van der Ende
ME, Osterhaus AD. CCR5, GPR15, and CXCR6 are major coreceptors
of human immunodeficiency virus type 2 variants isolated from
individuals with and without plasma viremia. J.Virol.
2005;79(3):1686-700.
[76] Keele BF, Giorgi EE, Salazar-Gonzalez JF, et al. Identification
and characterization of transmitted and early founder virus
envelopes in primary HIV-1 infection. Proc.Natl.Acad.Sci.U.S.A
2008;105(21):7552-7.