Embed Size (px)
Citation preview

DOENÇA INTESTINAL INFLAMATÓRIA
Profª. Me. Mônica Daiha

Doença Inflamatória Intestinal Crônica
Convivendo com o inimigo...
Msc. Monica Campello DaihaIntituto Qualittas de Pós Graduação
!Definição: !!
Síndrome caracterizada pela resposta exacerbada
e descontrolada do trato digestório
a uma estimulação antigênica !
em consequência à exposição !
excessiva a antígenos.
Doença Inflamatória Intestinal Crônica

Doença Inflamatória Intestinal Crônica
!Ponto Importante: !!
Esta síndrome é responsável !
por, no mínimo, !
50% dos sintomas digestivos !
observados em felinos.
7/13/2016 15 chistosas expresiones de gato que delatan perfectamente lo que están pensando | Upsocl
http://www.upsocl.com/verde/15-chistosas-expresiones-de-gato-que-delatan-perfectamente-lo-que-estan-pensando/ 2/13
Fuente
2. “Te arrepentirás de haberme puesto este ridículo jersey”
Fuente
ESCUCHÓ A UNA MUJER HABLANDODESCARADAMENTE SOBRE SU INFIDELIDAD.ENTONCES PUBLICÓ ESTO EN FACEBOOK
PROBAMOS LOS EXTRAÑOS ATUENDOS DEMANIQUÍES DE GRANDES TIENDAS. LO QUEDESCUBRIMOS NOS DECEPCIONÓ
Fisiopatogenia
Resposta imune aos antígenos
ê
Influxo de células inflamatórias:
!processo inflamatório na mucosa
ê
perda da integridade da mucosa:
ê
alteração de permeabilidade:
!microorganismos da microbiota entérica e os antígenos
adentram na lâmina própria

Fatores Patogênicos
!Dieta ! !Intolerância alimentar ! !Hipersensibilidade alimentar !! !Parasitos ! !Infecções bacterianas ! !Neoplasia !!
Fatores Patogênicos
6
JFMS CLINICAL PRACTICE 445
C L I N I C A L R E V I EW
Journal of Feline Medicine and Surgery (2012) 14, 445–458
Albert E Jergens
FELINE IDIOPATHIC INFLAMMATORYBOWEL DISEASEWhat we know andwhat remains to be unraveled
Practical relevance: Feline idiopathicinflammatory bowel disease (IBD)denotes one form of chronic enteropathythat is immunologically mediated andcharacterized by persistent or recurrentgastrointestinal (GI) signs and histologicinflammation. Signs of vomiting, diarrhea andweight loss generally predominate, and mucosalinflammation may occur in any portion of the GItract (especially the small intestine). Affected catsmay also have concurrent inflammation in otherorgans, such as the pancreas and liver, which mayimpact clinical disease severity.Clinical challenges: The exact etiologies of thisheterogeneous group of disorders have yet to bedetermined, though results from basic science andclinical studies suggest that interplay betweengenetic factors and enteric bacteria is crucial fordisease development. The diagnosis is one ofexclusion and requires intestinal mucosal biopsyto characterize the type and severity of theinflammatory infiltrate, and to differentiate IBD fromother disorders, including alimentary lymphoma.Controversy exists concerning the relativediagnostic accuracy of endoscopic versusfull-thickness specimens for the diagnosis of IBDand its differentiation from alimentary lymphoma.Audience: This article is intended to provideveterinary practitioners with a comprehensiveclinical update on idiopathic IBD in cats. It reviewsthe current evidence-based data, the diagnosticapproach, the evolving histologic criteria, andtreatment options and outcome for feline patientswith this syndrome.
Current understanding of etiologyand pathogenesis
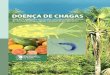
While the exact cause of inflammatory bowel disease (IBD) remainsunknown, current hypotheses suggest that feline IBD, similar to IBDin humans and dogs, involves complex interactions betweenenvironmental factors (ie, intestinal microbial imbalances, dietarycomponents) and the mucosal immune system, resulting in chronicinflammation in susceptible cats (Figure 1).1
Genetic defects in the recognition of commensal versus pathogenicbacteria by the innate immune system play a pivotal role in disease
pathogenesis in humansand dogs with IBD.Mutations in innateimmune receptors ofhumans (NOD2/CARD 15)and dogs (TLR4, TLR5)have now been linked toIBD susceptibility; and inthe presence of an entericmicrobiota may lead toupregulated proinflamma-tory cytokine production(eg, IL-17, TNF-α) andreduced bacterial clearance,
thereby promoting chronic intestinal inflammation.1–3 Whetheror not similar pathomechanisms come into play in the developmentof idiopathic feline IBD has not been fully determined. However,antigens derived from commensal bacteria are likely to be importantin driving disease pathogenesis, as increased populations ofmucosa-associated bacteria (ie, Enterobacteriaceae) have been linked toclinical signs, cytokine mRNA and histopathologic lesions in catswith IBD.4
Other studies have reported increased lamina propria myeloid/histiocyte antigen-positive macrophages, upregulated epithelial majorhistocompatibility complex (MHC) class II molecule expression,and increased antibody reactivity to components of the commensal
DOI: 10.1177/1098612X12451548© ISFM and AAFP 2012
Certain breed predispositions(Siamese and other Asian
breeds) for IBD are recognized,but any breed may be affectedand causal genetic defects have
not been identified to date.
Albert E JergensDVM PhD DACVIM
Department of Veterinary Clinical Sciences,College of Veterinary Medicine,
Iowa State University,Ames, IA 50011, USA
Email: [email protected]
at AMERICAN COLL VET DERMATOLOGY on June 27, 2016jfm.sagepub.comDownloaded from
!Defeitos genéticos: !flora comensal x flora patogênica x hospedeiro !humanos e cães: mutação receptores imunes !microbiota entérica: citocinas proinflamatórias
7/11/2016 Como estudar e lembrar tudo na hora da prova? | Eu Estudo Certo – Blogs A Tribuna
http://blogs.atribuna.com.br/euestudocerto/2014/09/como-estudar-e-lembrar-tudo-na-hora-da-prova/ 1/4
BLAZER
INDIGO
R$ 1.198
SOBRE O BLOG QUEM ESCREVE CONTATO OUTROS BLOGS ACESSE A TRIBUNA.COM.BR ANUNCIE AQUI
Tweetar
Como estudar e lembrar tudo na hora da prova?
29 set, 2014 Estratégia de Estudo Martha Vergine
A pergunta título desse post é uma das mais pesquisadas pelos estudantes.
São muitos os anos que passamos nos bancos escolares e parece que por mais que otempo passe continuamos a sofrer quando o momento da prova chega.
Claro que o mau aluno, aquele que quase nem aparece nas aulas e, se aparece, estáapenas de corpo presente porém sua alma, isto é, concentração, está beeeeemausente, não tem mesmo como gostar do momento da prova, até porque só por ummilagre seria possível ele se lembrar da matéria e conseguir dar qualquer boaresposta.
Sei que essa situação é extremada, pois a maioria dos alunos comparecem às aulas,tentam prestar atenção e em casa ainda dão uma estudada. Entretanto, é só chegaro momento da prova e parece que num passe de mágica esquecem toda a matéria.Para esses também é um sofrimento responder as questões.
Sendo assim, o que fazer?
Sendo bom ou mau aluno parece que não faz diferença na hora da prova, pois essemomento é bem difícil para ambos, então qual a saída?
Ah! Arrisco uma solução.
A solução para qualquer aluno é um CAT ! Isso mesmo um gatinho…
O CAT é uma acrônimo que irá te ajudar a lembrar da TRÍADE DO ESTUDANTEPROFISSIONAL.
Gato??? Estudante pro ssional???
Nossa! Quanta novidade em um post só…
Calma que vou explicar.
0Curtir
SIGA-NOS
PESQUISAR NO BLOG
ASSUNTOS
Desa o #101DiasDeEstudo (3)
Dica de Livros (7)
Dicas de estudo (87)
Dicas motivacionais (142)
Estratégia de Estudo (168)
FÓRMULA PARA APROVAÇÃO (21)
Notícias importantes (78)
Palavrinhas Mágicas (5)
Professores estudantes (5)
Projeto 21 dias para criar o hábito de estudar. (22)
Projeto Meu Diário Virtual de Estudo (22)
Sites e livros interessantes (19)
Vlog (44)
Erro: esta não é uma URL válida de uma Página doFacebook.
JFMS CLINICAL PRACTICE 445
C L I N I C A L R E V I EW
Journal of Feline Medicine and Surgery (2012) 14, 445–458
Albert E Jergens
FELINE IDIOPATHIC INFLAMMATORYBOWEL DISEASEWhat we know andwhat remains to be unraveled
Practical relevance: Feline idiopathicinflammatory bowel disease (IBD)denotes one form of chronic enteropathythat is immunologically mediated andcharacterized by persistent or recurrentgastrointestinal (GI) signs and histologicinflammation. Signs of vomiting, diarrhea andweight loss generally predominate, and mucosalinflammation may occur in any portion of the GItract (especially the small intestine). Affected catsmay also have concurrent inflammation in otherorgans, such as the pancreas and liver, which mayimpact clinical disease severity.Clinical challenges: The exact etiologies of thisheterogeneous group of disorders have yet to bedetermined, though results from basic science andclinical studies suggest that interplay betweengenetic factors and enteric bacteria is crucial fordisease development. The diagnosis is one ofexclusion and requires intestinal mucosal biopsyto characterize the type and severity of theinflammatory infiltrate, and to differentiate IBD fromother disorders, including alimentary lymphoma.Controversy exists concerning the relativediagnostic accuracy of endoscopic versusfull-thickness specimens for the diagnosis of IBDand its differentiation from alimentary lymphoma.Audience: This article is intended to provideveterinary practitioners with a comprehensiveclinical update on idiopathic IBD in cats. It reviewsthe current evidence-based data, the diagnosticapproach, the evolving histologic criteria, andtreatment options and outcome for feline patientswith this syndrome.
Current understanding of etiologyand pathogenesis
While the exact cause of inflammatory bowel disease (IBD) remainsunknown, current hypotheses suggest that feline IBD, similar to IBDin humans and dogs, involves complex interactions betweenenvironmental factors (ie, intestinal microbial imbalances, dietarycomponents) and the mucosal immune system, resulting in chronicinflammation in susceptible cats (Figure 1).1
Genetic defects in the recognition of commensal versus pathogenicbacteria by the innate immune system play a pivotal role in disease
pathogenesis in humansand dogs with IBD.Mutations in innateimmune receptors ofhumans (NOD2/CARD 15)and dogs (TLR4, TLR5)have now been linked toIBD susceptibility; and inthe presence of an entericmicrobiota may lead toupregulated proinflamma-tory cytokine production(eg, IL-17, TNF-α) andreduced bacterial clearance,
thereby promoting chronic intestinal inflammation.1–3 Whetheror not similar pathomechanisms come into play in the developmentof idiopathic feline IBD has not been fully determined. However,antigens derived from commensal bacteria are likely to be importantin driving disease pathogenesis, as increased populations ofmucosa-associated bacteria (ie, Enterobacteriaceae) have been linked toclinical signs, cytokine mRNA and histopathologic lesions in catswith IBD.4
Other studies have reported increased lamina propria myeloid/histiocyte antigen-positive macrophages, upregulated epithelial majorhistocompatibility complex (MHC) class II molecule expression,and increased antibody reactivity to components of the commensal
DOI: 10.1177/1098612X12451548© ISFM and AAFP 2012
Certain breed predispositions(Siamese and other Asian
breeds) for IBD are recognized,but any breed may be affectedand causal genetic defects have
not been identified to date.
Albert E JergensDVM PhD DACVIM
Department of Veterinary Clinical Sciences,College of Veterinary Medicine,
Iowa State University,Ames, IA 50011, USA
Email: [email protected]
at AMERICAN COLL VET DERMATOLOGY on June 27, 2016jfm.sagepub.comDownloaded from

Principais variáveis da doença inflamatória
!• Sistema imune da mucosa
(mediador e perpetuador dos danos teciduais)
!• Suscetibilidade genética
!• Microbiota entérica:
• Gato: 1.000.000.000/ml ☹
• Cão: 100.000/ml☺
Fisiopatogenia
Histórico
!Emagrecimento progressivo !!Letargia / Depressão !!Polifagia !!Hiporexia ou Anorexia !!Vômito !!Diarréia x Constipação !!
HISTÓRICO
Emagrecimento progressivoLetargia / DepressãoAlterações no apetite:
- hiporexia ou anorexia - polifagia: fase compensada

Diagnóstico Diferencial
Vômito Crônico: !!
45% doença inflamatória intestinal !
18% pancreatite !
5% malignidade gastrointestinal !
3% outras causas
Mimetismo Clínico
!Sem alteração !!Caquexia !!Desidratação !!Mucosas Hipocoradas !!Linfadenopatia mesentérica !!Meteorismo

DIAGNÓSTICO
446 JFMS CLINICAL PRACTICE
RE V IE W / Feline idiopathic IBD
microbiota associated with chronic intestinalinflammation.5 Moreover, a potential role fordietary constituents is suggested by the clini-cal benefit of dietary therapy in some catswith IBD. While a genetic basis for IBD insome cat breeds is suspected, causal geneticdefects have not been identified to date.
Taken together, these studies suggest thatchronic intestinal inflammation of IBD maybe due to overly aggressive T cell responses toenteric bacteria (or fungi)6 in hosts with genet-ic defects that regulate microbial killing,mucosal barrier function or immune respons-es. Environmental factors likely governinflammation onset or reactivation and modu-late genetic susceptibility to disease. Futurestudies are needed to identify possible geneticpredispositions in certain feline breeds thatcontribute to IBD development.
Further unraveling of the pathogenesis ofIBD should facilitate the development ofnovel and more specific treatment options(eg, use of prebiotics or probiotics) for cats.This will require additional clinical trials (andmore research funding) to elucidate whichtherapies are most efficacious in the preven-tion and treatment of chronic IBD.
Figure 1 Chronic intestinal inflammation in feline IBD involves a complex interplaybetween the mucosal immune system and the enteric microbiota in a geneticallysusceptible host. Potential genetic factors affecting barrier function or innate andadaptive immunity may predispose susceptible cats to gastrointestinal (GI) signs, aberranthost responses and microbial imbalances (dysbiosis). Environmental factors (dietaryconstituents, exposure to enteropathogens, NSAID or antibiotic administration, etc) likelygovern inflammation onset or reactivation (disease flares)
Other environmentalfactors
Dysbiosis
Disturbances:✜ GI signs✜ Histologic lesions✜ Immune cells✜ MHC II expression✜ Mucosal cytokines✜ Microbiota imbalances
Rule-outs:✜ Food-responsivecauses✜ Antibiotic-responsiveenteropathy✜ Alimentary lymphoma
Themes:✜ Chronic immune-mediated inflammation✜ Contribution fromgut microbiota✜ Therapeutic responseto diet and drugs
FelineIBD
Proposed pathogenesis of feline IBD
Barrierfunction
Innate andadaptiveimmunity
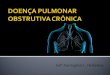
Integrate environment, history and physical examination✜ At-risk breed (?), indoor/outdoor, diet, clinical signs, localizing findings
Investigate for parasites and enteric pathogens✜ Fecal analysis (nematodes, protozoa), fecal culture, PCR (Tritrichomonas foetus)
Perform clinicopathologic testing✜ Detect non-GI disease: CBC, biochemistry profile, urinalysis, fPLI, ± fTLI, bile acids,total T4, FeLV, FIV✜ Detect/characterize GI disease: Hyperproteinemia, hypoalbuminemia (rare), low folateor cobalmin, increased ALT/ALP, fPLI, low phosphorus
Perform advanced diagnostics✜ Detect non-GI disease: Radiography, ultrasonography of intestines, liver, pancreas,mesenteric lymph nodes, masses, effusions; FNA cytology ± biopsy✜ Detect/characterize GI disease: Radiography, ultrasonography to detect intestinalthickening, loss of layering, focal masses, hypoechoic appearance (pancreatitis),hyperechoic appearance (hepatopathy), mesenteric lymphadenopathy;intestinal biopsy via endoscopy, laparoscopy or laparotomy (include ileum);± biopsy of liver, pancreas, lymph nodes
The clinician should first integrate patient history with findings made from the physical examinationand initial diagnostic testing to confirm or refute the presence of primary GI disease. Diagnosticimaging and intestinal mucosal biopsy are then performed to characterize the nature and extent ofmucosal disease.
Modified from references 7 and 26
A diagnosis ofIBD is one ofexclusion and
requires carefulelimination ofIBD mimics.
D i a g n o s t i c a p p r o a c h t o f e l i n e I B D
at AMERICAN COLL VET DERMATOLOGY on June 27, 2016jfm.sagepub.comDownloaded from
JFMS CLINICAL PRACTICE 445
C L I N I C A L R E V I EW
Journal of Feline Medicine and Surgery (2012) 14, 445–458
Albert E Jergens
FELINE IDIOPATHIC INFLAMMATORYBOWEL DISEASEWhat we know andwhat remains to be unraveled
Practical relevance: Feline idiopathicinflammatory bowel disease (IBD)denotes one form of chronic enteropathythat is immunologically mediated andcharacterized by persistent or recurrentgastrointestinal (GI) signs and histologicinflammation. Signs of vomiting, diarrhea andweight loss generally predominate, and mucosalinflammation may occur in any portion of the GItract (especially the small intestine). Affected catsmay also have concurrent inflammation in otherorgans, such as the pancreas and liver, which mayimpact clinical disease severity.Clinical challenges: The exact etiologies of thisheterogeneous group of disorders have yet to bedetermined, though results from basic science andclinical studies suggest that interplay betweengenetic factors and enteric bacteria is crucial fordisease development. The diagnosis is one ofexclusion and requires intestinal mucosal biopsyto characterize the type and severity of theinflammatory infiltrate, and to differentiate IBD fromother disorders, including alimentary lymphoma.Controversy exists concerning the relativediagnostic accuracy of endoscopic versusfull-thickness specimens for the diagnosis of IBDand its differentiation from alimentary lymphoma.Audience: This article is intended to provideveterinary practitioners with a comprehensiveclinical update on idiopathic IBD in cats. It reviewsthe current evidence-based data, the diagnosticapproach, the evolving histologic criteria, andtreatment options and outcome for feline patientswith this syndrome.
Current understanding of etiologyand pathogenesis
While the exact cause of inflammatory bowel disease (IBD) remainsunknown, current hypotheses suggest that feline IBD, similar to IBDin humans and dogs, involves complex interactions betweenenvironmental factors (ie, intestinal microbial imbalances, dietarycomponents) and the mucosal immune system, resulting in chronicinflammation in susceptible cats (Figure 1).1
Genetic defects in the recognition of commensal versus pathogenicbacteria by the innate immune system play a pivotal role in disease
pathogenesis in humansand dogs with IBD.Mutations in innateimmune receptors ofhumans (NOD2/CARD 15)and dogs (TLR4, TLR5)have now been linked toIBD susceptibility; and inthe presence of an entericmicrobiota may lead toupregulated proinflamma-tory cytokine production(eg, IL-17, TNF-α) andreduced bacterial clearance,
thereby promoting chronic intestinal inflammation.1–3 Whetheror not similar pathomechanisms come into play in the developmentof idiopathic feline IBD has not been fully determined. However,antigens derived from commensal bacteria are likely to be importantin driving disease pathogenesis, as increased populations ofmucosa-associated bacteria (ie, Enterobacteriaceae) have been linked toclinical signs, cytokine mRNA and histopathologic lesions in catswith IBD.4
Other studies have reported increased lamina propria myeloid/histiocyte antigen-positive macrophages, upregulated epithelial majorhistocompatibility complex (MHC) class II molecule expression,and increased antibody reactivity to components of the commensal
DOI: 10.1177/1098612X12451548© ISFM and AAFP 2012
Certain breed predispositions(Siamese and other Asian
breeds) for IBD are recognized,but any breed may be affectedand causal genetic defects have
not been identified to date.
Albert E JergensDVM PhD DACVIM
Department of Veterinary Clinical Sciences,College of Veterinary Medicine,
Iowa State University,Ames, IA 50011, USA
Email: [email protected]
at AMERICAN COLL VET DERMATOLOGY on June 27, 2016jfm.sagepub.comDownloaded from
Alterações Laboratoriais
!Anemia normocítica normocrômica !!Leucocitose neutrofílica sem desvio !!Hipoalbuminemia !!Sorologia FIV/FeLV !!Parasitológico !

Exames por Imagem
!Ultrassonografia Abdominal !
!Alteração da ecogenicidade !
!Espessamento da parede !
!Perda da definição das camadas da parede intestinal !
!Aumento de volume dos linfonodos mesentéricos !
M.V. Juliana Derenne
Diagnóstico
!Ponto Importante: !!
Doença Inflamatória Intestinal? !
x !
NEOPLASIA???7/13/2016 gato+pensando.jpg (395×500)
http://1.bp.blogspot.com/_6ubWbERxZ7s/TScoP3OvuZI/AAAAAAAAAjU/Y5VeXi-XwxY/s1600/gato+pensando.jpg 1/1
7/13/2016 15 chistosas expresiones de gato que delatan perfectamente lo que están pensando | Upsocl
http://www.upsocl.com/verde/15-chistosas-expresiones-de-gato-que-delatan-perfectamente-lo-que-estan-pensando/ 4/13
Fuente
6. Esperemos que ese perro disfrute de sus últimos minutos devida
SAPATILHA SUEDECRYSTAL PEARL
BLUSA ESTAMPASAMARKAND
OXFORDPLATAFORMAPALHA
Fuente
7. El famoso “grumpy cat” o gato gruñón

186 JFMS CLINICAL PRACTICE
R E V I E W / Feline AL: classification, clinical signs and non-invasive diagnostics
neutrophilic leukocytosis is usually present,which may be accompanied by a regenerativeleft shift.31–33 A peripheral lymphocytosis(with LGL morphology) was documentedin over 80% of cats with LGLL in twostudies.31,35 However, in two other studies
D i a g n o s t i c i n v e s t i g a t i o n
Tests to rule out other primary and secondarygastrointestinal diseases in older cats with chronic
weight loss, vomiting and/or diarrhoea
Blood and urine tests✜ Complete blood count✜ Serum biochemical profile✜ Serum total T4
✜ Serum cobalamin and folate✜ FIV and FeLV serology✜ Feline pancreatic lipase (Spec fPL;
Idexx Laboratories)✜ Urinalysis
Therapeutic trials✜ Fenbendazole (50 mg/kg PO q24h for 5 days)
Diagnostic imaging✜ Abdominal ultrasonography✜ Thoracic radiography
Dietary elimination trialsTo investigate possible adverse food reactions:✜ Single novel protein + carbohydrate✜ Hydrolysed protein diet
Faecal tests
If small bowel diarrhoea is predominant:✜ Faecal flotation assays✜ Faecal immunoassays/direct fluorescent antigen tests/
PCR assays for detection of:– Giardia species– Cryptosporidium species– Campylobacter species– Enteropathogenic bacterial toxins
If mixed/large bowel diarrhoea is predominant:✜ Faecal smears/culture/PCR assays for detection of
Tritrichomonas fetus
If there is bloody diarrhoea, especially in cats with feverand an inflammatory leukogram:✜ Faecal culture for enteropathogenic bacteria (Salmonella
species, Clostridium species, Campylobacter species)
lymphocytosis was uncommon in cats withLGLL, although peripheral lymphoblastswere present in 15% of cats.32,33 Since LGLscan be identified with routine haematologicalstains, peripheral blood smears should beexamined thoroughly in the assessment ofall cats where AL is suspected.✜ Serum albumin The most commonserum biochemical abnormality in AL ishypoalbuminaemia. In intestinal disease,hypoalbuminaemia occurs when loss ofalbumin into the lumen through acompromised intestinal wall exceeds thecapacity of the liver to synthesise albumin.Hypoalbuminaemia is less common in catswith LGAL than in other forms of AL,probably because the integrity of theintestinal wall can be maintained until late inthe disease process.3,19,23,32,33,63 Elevations inbilirubin or liver enzymes, or azotaemia, mayoccur in cats with AL with hepatic or renalinvolvement.23,24,32,60,63
✜ Serum cobalamin Up to 80% of cats withLGAL are hypocobalaminaemic.25 Thisfinding is not unexpected since cobalamin isabsorbed from the ileum, and the ileum andjejunum are the most common locations forLGAL.22,23,27 Utilisation of cobalamin byproliferating intestinal microflora in theproximal intestine can further reduceavailable cobalamin.64
✜ Serum folate Folate levels may be low,normal or high in cats with LGAL.24,25 Folatedeconjugase, a brush border enzyme, and acarrier protein required for folate absorptionare located only in proximal intestinalenterocytes. Hence, low serum folate levelsoccur with proximal intestinal disease due toreduced mucosal absorption. High serumfolate levels can occur due to proliferation ofintestinal microflora that synthesise folate.64
Serum folate levels were low in 4% and highin 37% of cats with LGAL in one report.25
The frequency of perturbations in serumfolate and cobalamin with other forms of ALhas not been evaluated.
Abdominal ultrasonographyAbdominal ultrasonography facilitates evalua-tion of the gastrointestinal tract by assessmentof wall thickness, layering, motility and lumi-nal content. Normal intestinal wall appears as afive-layered image, with alternating hyper- andhypoechoic layers corresponding to the lumi-nal surface, mucosa, submucosa, muscularisand serosa. Normal ultrasonographic intestinalwall thicknesses are: duodenum and jejunum≤2.8 mm, ileum ≤3.2 mm and colon ≤1.7 mm.65
Mesenteric lymph node diameter is generally≤5 mm.66 Mural thickening can be further char-acterised by symmetry, anatomical location andwhether it is focal, multifocal or diffuse.
by guest on April 15, 2012jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/Journal of Feline Medicine and Surgery
http://jfm.sagepub.com/content/14/3/182The online version of this article can be found at:
DOI: 10.1177/1098612X12439265
2012 14: 182Journal of Feline Medicine and SurgeryVanessa Barrs and Julia Beatty
Feline alimentary lymphoma : 1. Classification, risk factors, clinical signs and non-invasive diagnostics
Published by:
International Society of Feline Medicine
American Association of Feline Practitioners
and http://www.sagepublications.com
can be found at:Journal of Feline Medicine and SurgeryAdditional services and information for
http://jfm.sagepub.com/cgi/alertsEmail Alerts:
http://jfm.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Feb 27, 2012Version of Record >>
by guest on April 15, 2012jfm.sagepub.comDownloaded from
16
186 JFMS CLINICAL PRACTICE
RE V IE W / Feline AL: classification, clinical signs and non-invasive diagnostics
neutrophilic leukocytosis is usually present,which may be accompanied by a regenerativeleft shift.31–33 A peripheral lymphocytosis(with LGL morphology) was documentedin over 80% of cats with LGLL in twostudies.31,35 However, in two other studies
D i a g n o s t i c i n v e s t i g a t i o n
Tests to rule out other primary and secondarygastrointestinal diseases in older cats with chronic
weight loss, vomiting and/or diarrhoea
Blood and urine tests✜ Complete blood count✜ Serum biochemical profile✜ Serum total T4
✜ Serum cobalamin and folate✜ FIV and FeLV serology✜ Feline pancreatic lipase (Spec fPL;
Idexx Laboratories)✜ Urinalysis
Therapeutic trials✜ Fenbendazole (50 mg/kg PO q24h for 5 days)
Diagnostic imaging✜ Abdominal ultrasonography✜ Thoracic radiography
Dietary elimination trialsTo investigate possible adverse food reactions:✜ Single novel protein + carbohydrate✜ Hydrolysed protein diet
Faecal tests
If small bowel diarrhoea is predominant:✜ Faecal flotation assays✜ Faecal immunoassays/direct fluorescent antigen tests/
PCR assays for detection of:– Giardia species– Cryptosporidium species– Campylobacter species– Enteropathogenic bacterial toxins
If mixed/large bowel diarrhoea is predominant:✜ Faecal smears/culture/PCR assays for detection of
Tritrichomonas fetus
If there is bloody diarrhoea, especially in cats with feverand an inflammatory leukogram:✜ Faecal culture for enteropathogenic bacteria (Salmonella
species, Clostridium species, Campylobacter species)
lymphocytosis was uncommon in cats withLGLL, although peripheral lymphoblastswere present in 15% of cats.32,33 Since LGLscan be identified with routine haematologicalstains, peripheral blood smears should beexamined thoroughly in the assessment ofall cats where AL is suspected.✜ Serum albumin The most commonserum biochemical abnormality in AL ishypoalbuminaemia. In intestinal disease,hypoalbuminaemia occurs when loss ofalbumin into the lumen through acompromised intestinal wall exceeds thecapacity of the liver to synthesise albumin.Hypoalbuminaemia is less common in catswith LGAL than in other forms of AL,probably because the integrity of theintestinal wall can be maintained until late inthe disease process.3,19,23,32,33,63 Elevations inbilirubin or liver enzymes, or azotaemia, mayoccur in cats with AL with hepatic or renalinvolvement.23,24,32,60,63
✜ Serum cobalamin Up to 80% of cats withLGAL are hypocobalaminaemic.25 Thisfinding is not unexpected since cobalamin isabsorbed from the ileum, and the ileum andjejunum are the most common locations forLGAL.22,23,27 Utilisation of cobalamin byproliferating intestinal microflora in theproximal intestine can further reduceavailable cobalamin.64
✜ Serum folate Folate levels may be low,normal or high in cats with LGAL.24,25 Folatedeconjugase, a brush border enzyme, and acarrier protein required for folate absorptionare located only in proximal intestinalenterocytes. Hence, low serum folate levelsoccur with proximal intestinal disease due toreduced mucosal absorption. High serumfolate levels can occur due to proliferation ofintestinal microflora that synthesise folate.64
Serum folate levels were low in 4% and highin 37% of cats with LGAL in one report.25
The frequency of perturbations in serumfolate and cobalamin with other forms of ALhas not been evaluated.
Abdominal ultrasonographyAbdominal ultrasonography facilitates evalua-tion of the gastrointestinal tract by assessmentof wall thickness, layering, motility and lumi-nal content. Normal intestinal wall appears as afive-layered image, with alternating hyper- andhypoechoic layers corresponding to the lumi-nal surface, mucosa, submucosa, muscularisand serosa. Normal ultrasonographic intestinalwall thicknesses are: duodenum and jejunum≤2.8 mm, ileum ≤3.2 mm and colon ≤1.7 mm.65
Mesenteric lymph node diameter is generally≤5 mm.66 Mural thickening can be further char-acterised by symmetry, anatomical location andwhether it is focal, multifocal or diffuse.
by guest on April 15, 2012jfm.sagepub.comDownloaded from


182 JFMS CLINICAL PRACTICE
C L I N I C A L R E V I EW
Journal of Feline Medicine and Surgery (2012) 14, 182–190
Vanessa R BarrsBVSc (Hons) MVetClinStud MANZCVSc (Small Animal)
FANZCVSc (Feline Med) GradCertEd (Higher Ed)*Julia A Beatty
BSc (Hons) BVetMed PhD FANZCVSc (Feline Med)GradCertEd (Higher Ed) MRCVS
Valentine Charlton Cat Centre,Faculty of Veterinary Science,
University of Sydney,Sydney NSW 2006, Australia
*Corresponding author.Email: [email protected]
DOI: 10.1177/1098612X12439265© ISFM and AAFP 2012
Vanessa Barrs and Julia Beatty
FELINE ALIMENTARY LYMPHOMA1. Classification, risk factors,clinical signs and non-invasivediagnostics
Practical relevance Alimentarylymphoma (AL) occurscommonly in cats and existsas distinct subtypes that differin their clinical course,response to treatment andprognosis. Accurate diagnosis isimportant to guide appropriatetreatment.Clinical challenges Differentiation of low-gradealimentary lymphoma from lymphoplasmacyticenteritis can be challenging, especially whereendoscopic intestinal biopsies, which sample onlythe mucosa and submucosa, are used. The majordifferentials for intermediate- and high-gradealimentary lymphoma are other neoplasticand non-neoplastic intestinal mass lesions.The diagnosis of large granular lymphocytelymphoma requires vigilance as it may be missedwith routine diagnostics.Patient group AL affects predominantly middle-to old-aged domestic crossbred cats (median age10–13 years).Evidence base The evidence supporting thisreview is grade II, III and IV, derived fromprospective studies, retrospective case series,reviews, extrapolation from other species,pathophysiological justification and the combinedclinical experience of those working in the field.
PART 2Part 2 of this two-part article, reviewingthe benefits and limitations of various
biopsy techniques, treatment options andprognosis for different subtypes
of alimentary lymphoma, appearson pages 191–201 of this issue of
J Feline Med Surg and atDOI: 10.1177/1098612X12439266
Alimentary lymphoma – and its three clinical entities
Alimentary lymphoma (AL), the most common anatomical form oflymphoma in cats, comprises a group of diseases centred on the gastro-intestinal tract, with variable extraintestinal involvement. Three histo-logical grades of AL are recognised: low (LGAL), intermediate (IGAL)and high (HGAL). A separate histological subclassification of AL, largegranular lymphocyte lymphoma (LGLL), which can be of any grade,is also described. Although these different subtypes of lymphomashare features related to gastrointestinal dysfunction, such as weightloss, vomiting and diarrhoea, there are major differences in clinicalpresentation, techniques required for diagnosis, treatment and progno-sis (Table 1). From a clinical perspective, LGAL and LGLL can be con-sidered as separate entities and IGAL and HGAL can be consideredtogether as a third entity because, other than histological grade, theclinical features of IGAL and HGAL are similar.1 Accurate diagnosis isessential to differentiate these lymphomas from each other and fromother primary and secondary gastrointestinal diseases so that appro-priate treatment can be initiated.
Classification and prevalence
Lymphoma is the most common intestinal neoplasm of cats, followedby adenocarcinoma and then mast cell tumour. In a study of 1129 felineintestinal neoplasms diagnosed histologically, 55% were lymphomas,32% were adenocarcinomas and 4% were mast cell tumours.2 Felinelymphoma can be classified by anatomical location, histological gradeand immunophenotype.
Anatomical classificationThe traditional anatomical classification recognises mediastinal, multi-centric, alimentary and extranodal forms. Of these, AL is the most com-mon anatomical form identified.3–10 The declining influence of felineleukaemia virus (FeLV) worldwide has resulted in an increase in therelative prevalence of AL, since AL has the weakest association withFeLV antigenaemia. Some studies suggest that the absolute incidence
by guest on April 15, 2012jfm.sagepub.comDownloaded from
182 JFMS CLINICAL PRACTICE
C L I N I C A L R E V I EW
Journal of Feline Medicine and Surgery (2012) 14, 182–190
Vanessa R BarrsBVSc (Hons) MVetClinStud MANZCVSc (Small Animal)
FANZCVSc (Feline Med) GradCertEd (Higher Ed)*Julia A Beatty
BSc (Hons) BVetMed PhD FANZCVSc (Feline Med)GradCertEd (Higher Ed) MRCVS
Valentine Charlton Cat Centre,Faculty of Veterinary Science,
University of Sydney,Sydney NSW 2006, Australia
*Corresponding author.Email: [email protected]
DOI: 10.1177/1098612X12439265© ISFM and AAFP 2012
Vanessa Barrs and Julia Beatty
FELINE ALIMENTARY LYMPHOMA1. Classification, risk factors,clinical signs and non-invasivediagnostics
Practical relevance Alimentarylymphoma (AL) occurscommonly in cats and existsas distinct subtypes that differin their clinical course,response to treatment andprognosis. Accurate diagnosis isimportant to guide appropriatetreatment.Clinical challenges Differentiation of low-gradealimentary lymphoma from lymphoplasmacyticenteritis can be challenging, especially whereendoscopic intestinal biopsies, which sample onlythe mucosa and submucosa, are used. The majordifferentials for intermediate- and high-gradealimentary lymphoma are other neoplasticand non-neoplastic intestinal mass lesions.The diagnosis of large granular lymphocytelymphoma requires vigilance as it may be missedwith routine diagnostics.Patient group AL affects predominantly middle-to old-aged domestic crossbred cats (median age10–13 years).Evidence base The evidence supporting thisreview is grade II, III and IV, derived fromprospective studies, retrospective case series,reviews, extrapolation from other species,pathophysiological justification and the combinedclinical experience of those working in the field.
PART 2Part 2 of this two-part article, reviewingthe benefits and limitations of various
biopsy techniques, treatment options andprognosis for different subtypes
of alimentary lymphoma, appearson pages 191–201 of this issue of
J Feline Med Surg and atDOI: 10.1177/1098612X12439266
Alimentary lymphoma – and its three clinical entities
Alimentary lymphoma (AL), the most common anatomical form oflymphoma in cats, comprises a group of diseases centred on the gastro-intestinal tract, with variable extraintestinal involvement. Three histo-logical grades of AL are recognised: low (LGAL), intermediate (IGAL)and high (HGAL). A separate histological subclassification of AL, largegranular lymphocyte lymphoma (LGLL), which can be of any grade,is also described. Although these different subtypes of lymphomashare features related to gastrointestinal dysfunction, such as weightloss, vomiting and diarrhoea, there are major differences in clinicalpresentation, techniques required for diagnosis, treatment and progno-sis (Table 1). From a clinical perspective, LGAL and LGLL can be con-sidered as separate entities and IGAL and HGAL can be consideredtogether as a third entity because, other than histological grade, theclinical features of IGAL and HGAL are similar.1 Accurate diagnosis isessential to differentiate these lymphomas from each other and fromother primary and secondary gastrointestinal diseases so that appro-priate treatment can be initiated.
Classification and prevalence
Lymphoma is the most common intestinal neoplasm of cats, followedby adenocarcinoma and then mast cell tumour. In a study of 1129 felineintestinal neoplasms diagnosed histologically, 55% were lymphomas,32% were adenocarcinomas and 4% were mast cell tumours.2 Felinelymphoma can be classified by anatomical location, histological gradeand immunophenotype.
Anatomical classificationThe traditional anatomical classification recognises mediastinal, multi-centric, alimentary and extranodal forms. Of these, AL is the most com-mon anatomical form identified.3–10 The declining influence of felineleukaemia virus (FeLV) worldwide has resulted in an increase in therelative prevalence of AL, since AL has the weakest association withFeLV antigenaemia. Some studies suggest that the absolute incidence
by guest on April 15, 2012jfm.sagepub.comDownloaded from
JFMS CLINICAL PRACTICE 185
of AL has been established in humans.In genetically predisposed individuals,enteropathy-associated T cell lymphoma(EATCL) can arise from clonal transformationof intestinal IELs after chronic antigenicstimulation.54,55 EATCL is the most commonneoplastic complication of coeliac disease.Several lines of evidence support theproposition that intestinal inflammation isa risk factor for the development of T celllymphoma (of any histological grade) andLGLL in cats. In two studies, 60% of catswith intestinal T cell lymphoma and 33%of cats with LGLL had chronic clinicalillnesses suggestive of pre-existinginflammatory disease.31,56
Concurrent lymphoplasmacyticenteritis (LPE) has been identifiedin other regions of the alimentarytract in up to 41% of catswith LGAL of T cellimmunophenotype,22–24 andapparent histological progression ofLPE to AL has been documented inindividual cases.57,58
Differential diagnosis
The presenting signs of AL are common tomany primary and secondary gastrointestinaldiseases. LPE is a major differential diagnosisfor LGAL in particular. A comparison betweencats with LPE and LGAL found no correlationbetween clinical findings and the final diagno-sis.61 In cats with intestinal mural masslesions, epithelial and mast cell neoplasia aremajor differentials. Diagnostic tests recom-mended to rule out other primary and second-ary gastrointestinal diseases are listed in thebox on page 186.
Non-invasive diagnostics
Routine laboratory testing✜ Haematology The most commonhaematological abnormalities in cats withAL are anaemia, due to chronic diseaseand/or gastrointestinal blood loss, andneutrophilia.3,24,25,31,32,63 While routinehaematology is of low diagnostic yield forLGAL and I/HGAL, careful evaluation of aperipheral blood film is an essential step forthe diagnosis of LGLL. In LGLL, marked
REV IEW / Feline AL: classification, clinical signs and non-invasive diagnostics
LGALThe most common clinical signs of LGAL are weight loss (Figure 1;≥80%), vomiting (≥70%), diarrhoea (≥60%) and partial or com-plete anorexia (≥50%). The appetite may be normal or, occasion-ally, polyphagia isnoted. Less fre-quently reportedsigns include lethar-gy and polydip-sia.19,23–25,61 In themajority of cases,clinical signs arechronic (present for>1 month).23,24,61
Abdominal palpationis often abnormal(Figure 2); diffuselythickened intestinalloops are detected ina third to more thanhalf of affected cats.An abdominal massis palpable in20–30% of cases, attributable to mesenteric lymph nodeenlargement or, rarely, to a focal intestinal mass.19,23,24
I/HGAL and LGLLClinical signs in cats with I/HGAL and LGLL are similar to thosefor LGAL but tend to be more acute and/or severe. A majorclinical difference, compared with LGAL, is the presence of apalpable abdominal mass at diagnosis in the majority of cases
of I/HGAL and LGLL. The mass comprises focal intestinal thick-ening and/or extraintestinal lesions, such as mesenteric lymph-adenomegaly, hepatomegaly or renomegaly. Intussusception,intestinal obstruction and intestinal perforation are more com-mon in cases of I/HGAL than in LGAL.3,12,19,31,32,35,62
Figure 1 Weight lossis present in 80% ormore of cats withlow-grade alimentarylymphoma (LGAL)
Figure 2 Abdominal palpation can be normal in cats with LGAL,but common abnormalities include diffusely thickened intestinal loopsor a palpably enlarged mesenteric lymph node
H i s t o r y a n d c l i n i c a l s i g n s
Abdominal palpation can be normalin cats with LGAL . . . By contrast an
abdominal mass is palpable in most catswith I/HGAL and LGLL.
SignalmentAll forms of AL typically affect middle- toold-aged domestic crossbred cats with amedian age at diagnosis of 10–13 years.A slight male predisposition (1.5:1 maleto female ratio) for HGAL identified
in some reports, has not beenidentified for LGAL or
LGLL.4–7,12,13,15,16,19,23–26,32,59,60
by guest on April 15, 2012jfm.sagepub.comDownloaded from
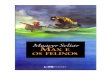
cells, necrosis, oedema and/or haemorrhage(Figure 3).3,67,68 Transmural intestinalthickening in I/HGAL is usually symmetricalor concentric, in contrast to intestinal mast celltumours and adenocarcinomas whereintestinal wall thickening is often asymmetricalor eccentric.69,70 Ultrasonographically, evidenceof extraintestinal involvement is common inI/HGAL.3,12
JFMS CLINICAL PRACTICE 187
REV IEW / Feline AL: classification, clinical signs and non-invasive diagnostics
Figure 4 (a) Mild diffusesmall intestinal wallthickening (wall thickness3.4 mm) in a cat with LGAL;(b and c) severe smallintestinal wall thickeningin a cat with LGAL (wallthickness 4.9 mm in b, and4 mm in c). Note that thealternating hyperechoic andhypoechoic appearance ofintestinal layers seen inhealthy cats is preserved incats with LGAL
c
✜ I/HGAL The ultrasonographic featuresof I/HGAL include transmural intestinalthickening with disruption of normal walllayering, reduced wall echogenicity,localised hypomotility and abdominallymphadenomegaly. Loss of intestinal walllayering occurs due to infiltration of theintestinal wall with neoplastic or inflammatory
a
b
Figure 3 (a) Ultrasonographicand (b) gross appearanceof a focal jejunal mass dueto high-grade alimentarylymphoma (HGAL). Theintestinal wall is thickened(1 cm) and has lost its normalalternating hyperechoic andhypoechoic wall layeringpattern. The symmetricalconcentrically thickenedintestinal wall is visualised in(c) and vascularity identifiedusing power Doppler.Extraintestinal involvement,such as concurrent renal (d)and hepatic (e) masses,is common in HGAL.Images (a), (c), (d) and (e)courtesy of Karon Hoffman,University Veterinary TeachingHospital, Sydney
a b c
d e
Transmural intestinal thickening in I/HGALis usually symmetrical or concentric.
by guest on April 15, 2012jfm.sagepub.comDownloaded from
188 JFMS CLINICAL PRACTICE
RE V IE W / Feline AL: classification, clinical signs and non-invasive diagnostics
Funding
The authors received no specific grant from any funding agencyin the public, commercial or not-for-profit sectors for the prepara-tion of this review article.
Conflict of interest
The authors declare that there is no conflict of interest.
References
1 Valli VE, Jacobs RM, Norris A, Couto CG, Morrison WB, et al.The histologic classification of 602 cases of feline lympho-proliferative disease using the National Cancer Instituteworking formulation. J Vet Diagn Invest 2000; 12: 295–306.
2 Rissetto K, Villamil JA, Selting KA, Tyler J and Henry CJ.Recent trends in feline intestinal neoplasia: an epidemio-logic study of 1129 cases in the Veterinary Medical Databasefrom 1964 to 2004. J Am Anim Hosp Assoc 2011; 47: 28–36.
3 Mahony OM, Moore AS, Cotter SM, Engler SJ, Brown D andPenninck DG. Alimentary lymphoma in cats: 28 cases(1988–1993). J Am Vet Med Assoc 1995; 207: 1593–1598.
✜ LGAL In LGAL, intestinal wall thicknessis normal or increased, with preservation ofwall layering (Figure 4). In one study of catswith LGAL and diffuse small intestinalthickening, mean wall thickness was 4.3 mm(median 4.5 mm, range 3.4–5.0 mm).23
Mesenteric lymph node enlargement was alsocommon. In another report, 81% of cats withLGAL had evidence of intestinal thickeningon abdominal ultrasonography.26 Importantly,the ultrasonographic features of LGAL donot distinguish it from LPE or otherenteropathies.61,71 Thickening of themuscularis propria layer, which was foundto be significantly associated with LGALand not LPE or normal small intestine,may assist in the ranking of differentials.72
It should be emphasised that the finding ofnormal intestinal wall thickness and normalmesenteric lymph nodes on abdominalultrasonography does not rule out adiagnosis of LGAL; in patients withconsistent clinical signs, intestinal biopsyis indicated. Less common findings onultrasonographic examination of cats withLGAL include a focal intestinal mass orintussusception.23,24 Diffuse infiltration of theliver may be present histologically but is notreadily identifiable ultrasonographically.23
✜ LGLL The ultrasonographic features ofLGLL in cats have not been described indetail but appear similar to I/HGAL.32
KEY POINTS
The finding of normal intestinal wall thickness andnormal mesenteric lymph nodes on ultrasonography
does not rule out a diagnosis of LGAL.
4 Gabor LJ, Malik R and Canfield PJ. Clinical and anatomicalfeatures of lymphosarcoma in 118 cats. Aust Vet J 1998; 76:725–732.
5 Vail DM, Moore AS, Ogilvie GK and Volk LM. Felinelymphoma (145 cases): proliferation indices, cluster of dif-ferentiation 3 immunoreactivity, and their association withprognosis in 90 cats. J Vet Intern Med 1998; 12: 349–354.
6 Louwerens M, London CA, Pedersen NC and Lyons LA.Feline lymphoma in the post-feline leukemia virus era. J VetIntern Med 2005; 19: 329–335.
7 Milner RJ, Peyton J, Cooke K, Fox LE, Gallagher A, Gordon P,et al. Response rates and survival times for cats with lym-phoma treated with the University of Wisconsin–Madisonchemotherapy protocol: 38 cases (1996–2003). J Am Vet MedAssoc 2005; 227: 1118–1122.
8 Stutzer B, Lutz H, Majzoub M, Hermans W, Hirschberger J,Sauter-Louis C, et al. Incidence of persistent viraemia andlatent feline leukemia virus infection in cats with lym-phoma. J Feline Med Surg 2011; 13: 81–87.
9 Vezzali E, Parodi AL, Marcato PS and Bettini G.Histopathologic classification of 171 cases of canine andfeline non-Hodgkin lymphoma according to the WHO.Vet Comp Oncol 2010; 8: 38–49.
✜ I/HGAL typically presents acutely and can often be diagnosed byaspirate cytology of a mural intestinal mass or mesenteric lymph node.
✜ The clinical course of LGAL is chronic and LPE is a majordifferential. Definitive diagnosis may not be possible onhistological evaluation of intestinal biopsy specimens alone.Immunohistochemistry and clonality testing, in addition to routinehistopathology, can assist in differentiating LGAL frominflammatory disease.
✜ LGLL is the least common subtype and runs an acute clinicalcourse. An index of suspicion is required to diagnose LGLL.Cytological evaluation of peripheral blood films and fine-needleaspirate biopsies is useful for diagnosis. For histological diagnosis,Giemsa-stained plastic-embedded biopsy specimens arenecessary for reliable detection of granules within neoplasticlymphocytes. Alternatively, immunohistochemistry can beperformed to detect the cytotoxic granule protein, granzyme B.
✜ Where the REAL/WHO histological classification schemeis used for diagnosis of AL, clinicians should additionallyrequest that pathologists include the histologicalgrade of the lymphoma to help guide therapeuticdecisions.
by guest on April 15, 2012jfm.sagepub.comDownloaded from
JFMS CLINICAL PRACTICE 185
of AL has been established in humans.In genetically predisposed individuals,enteropathy-associated T cell lymphoma(EATCL) can arise from clonal transformationof intestinal IELs after chronic antigenicstimulation.54,55 EATCL is the most commonneoplastic complication of coeliac disease.Several lines of evidence support theproposition that intestinal inflammation isa risk factor for the development of T celllymphoma (of any histological grade) andLGLL in cats. In two studies, 60% of catswith intestinal T cell lymphoma and 33%of cats with LGLL had chronic clinicalillnesses suggestive of pre-existinginflammatory disease.31,56
Concurrent lymphoplasmacyticenteritis (LPE) has been identifiedin other regions of the alimentarytract in up to 41% of catswith LGAL of T cellimmunophenotype,22–24 andapparent histological progression ofLPE to AL has been documented inindividual cases.57,58
Differential diagnosis
The presenting signs of AL are common tomany primary and secondary gastrointestinaldiseases. LPE is a major differential diagnosisfor LGAL in particular. A comparison betweencats with LPE and LGAL found no correlationbetween clinical findings and the final diagno-sis.61 In cats with intestinal mural masslesions, epithelial and mast cell neoplasia aremajor differentials. Diagnostic tests recom-mended to rule out other primary and second-ary gastrointestinal diseases are listed in thebox on page 186.
Non-invasive diagnostics
Routine laboratory testing✜ Haematology The most commonhaematological abnormalities in cats withAL are anaemia, due to chronic diseaseand/or gastrointestinal blood loss, andneutrophilia.3,24,25,31,32,63 While routinehaematology is of low diagnostic yield forLGAL and I/HGAL, careful evaluation of aperipheral blood film is an essential step forthe diagnosis of LGLL. In LGLL, marked
REV IEW / Feline AL: classification, clinical signs and non-invasive diagnostics
LGALThe most common clinical signs of LGAL are weight loss (Figure 1;≥80%), vomiting (≥70%), diarrhoea (≥60%) and partial or com-plete anorexia (≥50%). The appetite may be normal or, occasion-ally, polyphagia isnoted. Less fre-quently reportedsigns include lethar-gy and polydip-sia.19,23–25,61 In themajority of cases,clinical signs arechronic (present for>1 month).23,24,61
Abdominal palpationis often abnormal(Figure 2); diffuselythickened intestinalloops are detected ina third to more thanhalf of affected cats.An abdominal massis palpable in20–30% of cases, attributable to mesenteric lymph nodeenlargement or, rarely, to a focal intestinal mass.19,23,24
I/HGAL and LGLLClinical signs in cats with I/HGAL and LGLL are similar to thosefor LGAL but tend to be more acute and/or severe. A majorclinical difference, compared with LGAL, is the presence of apalpable abdominal mass at diagnosis in the majority of cases
of I/HGAL and LGLL. The mass comprises focal intestinal thick-ening and/or extraintestinal lesions, such as mesenteric lymph-adenomegaly, hepatomegaly or renomegaly. Intussusception,intestinal obstruction and intestinal perforation are more com-mon in cases of I/HGAL than in LGAL.3,12,19,31,32,35,62
Figure 1 Weight lossis present in 80% ormore of cats withlow-grade alimentarylymphoma (LGAL)
Figure 2 Abdominal palpation can be normal in cats with LGAL,but common abnormalities include diffusely thickened intestinal loopsor a palpably enlarged mesenteric lymph node
H i s t o r y a n d c l i n i c a l s i g n s
Abdominal palpation can be normalin cats with LGAL . . . By contrast an
abdominal mass is palpable in most catswith I/HGAL and LGLL.
SignalmentAll forms of AL typically affect middle- toold-aged domestic crossbred cats with amedian age at diagnosis of 10–13 years.A slight male predisposition (1.5:1 maleto female ratio) for HGAL identified
in some reports, has not beenidentified for LGAL or
LGLL.4–7,12,13,15,16,19,23–26,32,59,60
by guest on April 15, 2012jfm.sagepub.comDownloaded from
192 JFMS CLINICAL PRACTICE
histological demonstration of disruption ofnormal lymph node architecture by the neo-plastic infiltrate.
This contrasts with the diagnosis ofI/HGAL and LGLL, which can often be madeon the basis of aspiration cytology of focalintestinal wall masses, enlarged mesenteric
R EV I EW / Feline AL: biopsy techniques, treatment options and prognosis
Figure 2 (a) Ileocaecocolichigh-grade alimentarylymphoma (HGAL) and (b) acut surface from the samespecimen. Diagnosis ofHGAL can often be basedon cytology of ultrasound-guided fine-needle aspiratesfrom a focal intestinal massor an enlarged mesentericlymph node. (c) Diff Quikcytology of a concurrentabdominal effusion, showingneoplastic round cells and amitotic figure. Image (c)courtesy of Dr Patricia Martin,Veterinary PathologyDiagnostic Services,University of Sydneya
a
b c
Figure 3 (a) Diff Quikstained smear of a fine-needle aspirate biopsy froman enlarged mesentericlymph node (b) and intestinalmass (c) in a cat with largegranular lymphocytelymphoma (LGLL). In (a)neoplastic round cells havea basophilic cytoplasmand contain large purpleintracytoplasmic granules(arrows). Image (a) courtesyof Dr Patricia Martin, VeterinaryPathology Diagnostic Services,University of Sydney
b
c
lymph nodes or extraintestinal mass lesions(Figure 2).2–6 This is because of the characteris-tic morphology of the neoplastic infiltrate(large lymphoblastic cells or large granularlymphocytes [LGLs]), which facilitates differ-entiation from the background population oflymphocytes. Also, modified Wright-Giemsastains (eg, Diff Quik; Dade Shearing) used forcytological specimens are more sensitive fordetecting LGLs than haematoxylin and eosin(HE) stains used for histological specimens.On cytology, LGLs are identified as largemononuclear cells with moderate amountsof deeply basophilic cytoplasm containingmultiple blue or purple granules (Figure 3).5,7
On HE sections, LGLL may be erroneouslyreported as I/HGAL. Reliable identification ofcytoplasmic granules in fixed tissues requiresevaluation of Giemsa-stained, plastic-embed-ded tissue or immunohistochemistry to detectthe cytotoxic granule protein, granzyme B.8,9
Diagnostic considerationsfor LGAL
Intestinal biopsy procurementHistological evaluation of intestinal biopsiesis required for diagnosis of LGAL and forother forms of AL where cytological evalua-tion is not definitive (Figures 4 and 5). LGALis typically a diffuse or multifocal diseaseaffecting more than one region of the gastro-intestinal tract. There is jejunal and ilealinvolvement in over 90% of cases, duodenalinvolvement in over 70% and gastric involve-ment in 7–40% of cases.1,10,11 The distributionof gastrointestinal involvement in lympho-plasmacytic enteritis (LPE) is similar to LGALexcept that gastric involvement is morecommon in LPE.11
by guest on April 15, 2012jfm.sagepub.comDownloaded from

21
Low-grade alimentary lymphoma: clinicopathologicalfindings and response to treatment in 17 cases
Amy E Lingard BVSc (Hons), MACVSc (Feline Medicine)1,a, Katherine Briscoe BVSc (Hons), MACVSc
(Feline Medicine)1, Julia A Beatty BSc (Hons), BVetMed, PhD, FACVSc (Feline Medicine), MRCVS
1, Antony SMoore BVSc, MVSc, DACVIM (Oncology)
2, Ann M Crowley BVSc (Hons), MACVSc, Diplomate American
College of Veterinary Pathologists3, Mark Krockenberger BSc (Vet), BVSc, PhD, MACVSc (Pathobiology),
MASM4, Richard K Churcher BVSc, FACVSc (Canine Medicine)
5, Paul J Canfield DVSc, PhD,
GradCertEdStud, FRCPath (Veterinary Pathology), FACVSc (Clinical Pathology), MRCVS4, Vanessa R Barrs BVSc
(Hons), MVetClinStud, FACVSc (Feline Medicine), GradCertEd1*
1Valentine Charlton Cat Centre,Faculty of Veterinary Science, TheUniversity of Sydney, NSW 2006,Australia2Veterinary Oncology Consultants,379 Lake Innes Drive, WauchopeNSW 2446, Australia3Anapath, PO Box 504, NewportNSW 2106, Australia4Veterinary Pathology DiagnosticServices, Faculty of VeterinaryScience, The University of Sydney,NSW 2006, Australia5North Shore Veterinary SpecialistCentre, 64 Atchison Street, CrowsNest NSW 2065, Australia
Low-grade alimentary lymphoma (LGAL) was diagnosed by histological andimmunohistochemical evaluation of full-thickness biopsies from multipleregions of the gastrointestinal tract collected during exploratory laparotomy in17 cats. The most common clinical signs were weight loss (n¼ 17) and vomitingand/or diarrhoea (n¼ 15). Clinical signs were chronic in 11 cases. Abdominalpalpation was abnormal in 12 cats, including diffuse intestinal thickening (n¼ 8),an abdominal mass due to mesenteric lymph node enlargement (n¼ 5) anda focal mural intestinal mass (n¼ 1). The most common ultrasonographic findingwas normal or increased intestinal wall thickness with preservation of layering.Ultrasound-guided fine-needle aspirates of mesenteric lymph nodes (n¼ 9) wereincorrectly identified as benign lymphoid hyperplasia in eight cats, in which thehistological diagnosis from biopsies was lymphoma. There was neoplasticinfiltration of more than one anatomic region of the gastrointestinal tract in16/17 cats. The jejunum (15/15 cats) and ileum (13/14 cats), followed by theduodenum (10/12 cats), were the most frequently affected sites. Twelve catswere treated with oral prednisolone and high-dose pulse chlorambucil, two witha modified MadisoneWisconsin multiagent protocol and three witha combination of both protocols. Thirteen of the 17 cats (76%) had completeclinical remission with a median remission time of 18.9 months. Cats thatachieved complete remission had significantly longer median survival times(19.3 months) than cats that did not achieve complete remission (n¼ 4)(4.1 months; P¼ 0.019). The prognosis for cats with LGAL treated with oralprednisolone in combination with high-dose pulse chlorambucil is good toexcellent.
Date accepted: 15 May 2009 ! 2009 ESFM and AAFP. Published by Elsevier Ltd. All rights reserved.
A limentary lymphoma is the most commonanatomic form of lymphoma in the cat.1e3
It is characterised by infiltration of the gas-trointestinal tract with neoplastic lymphocytes, withor without mesenteric lymph node involvement.4e6
Feline alimentary lymphoma can be histologicallyclassified by the National Cancer Institute WorkingFormulation (NCIWF) as high-grade, intermediate-
grade or low-grade with the latter being common inthe diffuse form.7e11 A less commonly describedform of alimentary lymphoma is large granular lym-phocytic lymphoma.12,13
Low-grade alimentary lymphoma (LGAL) was firstdescribed as a clinical entity in cats in a retrospectivestudy of 29 cases.10 The diagnosis was based on histol-ogy of haematoxylin and eosin (HE)-stained sectionsfrom gastroduodenal endoscopic biopsies (EB).10
Cats with LGAL were reported to have a more favour-able outcome when treated with oral prednisoloneand high-dose pulse chlorambucil compared to cats
*Corresponding author. E-mail: [email protected] address: The Cat Clinic, 1 Miller Street, Prahran VIC3181, Australia.
ARTICLE IN PRESS
Journal of Feline Medicine and Surgery (2009) --, --e--
doi:10.1016/j.jfms.2009.05.021
1098-612X/09/------+-- $36.00/0 ! 2009 ESFM and AAFP. Published by Elsevier Ltd. All rights reserved.
Please cite this article in press as: Amy E Lingard et al., Low-grade alimentary lymphoma: clinicopathological findings and re-sponse to treatment in 17 cases, J Feline Med Surg (2009), doi:10.1016/j.jfms.2009.05.021
Perdadepeso:17gatosVômitoe;ouDiarréia:15gatosPalpaçãoanormal:12gatos
Espessamentoparedeintestinal:8gatosMassaabdominal+Aumentolinfonodo:5gatos
Massafocal:1gato
JAmVetMedAssoc.2013Nov15;243(10):1455-61.doi:10.2460/javma.243.10.1455.
!Diagnosisofchronicsmallboweldiseaseincats:100cases
(2008-2012).!
NorsworthyGD1,ScotEstepJ,KiupelM,OlsonJC,GasslerLN.!OBJECTIVE: To determinewhether a diagnosis of chronic small bowel disease could beestablished in a subset of cats that had clinical signs of chronic vomiting, chronic smallbowel diarrhea, weight loss, or a combination of these, combined withultrasonographicallydeterminedthickeningofthesmallbowel.!PROCEDURES:Medicalrecordsofcatswithclinicalsignsofchronicvomiting,chronicsmallbowel diarrhea, weight loss, or a combination of these, combined withultrasonographicallydeterminedsmallbowelthickening,thatunderwentlaparotomyandmultiplesmallbowelbiopsiesbetween2008and2012wereexamined.Biopsyspecimenswere submitted for histologic evaluation, immunohistochemical evaluation, and, whenfindingswereambiguous,PCRassayforantigenreceptorrearrangement.!RESULTS:Chronicsmallboweldiseasewasdiagnosedin99ofthe100cats.The
mostcommondiagnoseswerechronicenteritisandintestinallymphoma.

Diagnóstico
!Biópsia endoscópica: amostras pequenas (máx. 2,8mm) !!Biópsia cirúrgica: mucosa, submucosa e muscular !!!!
JFMS CLINICAL PRACTICE 451
RE V IEW / Feline idiopathic IBD
– so-called ‘lymphoplasmacytic enteritis’ (LPE)– is the most frequently reported form of felineIBD.10,35,36 However, the appropriateness andclinical relevance of the term lymphocytic/plasmacytic enteritis is a contentious issue. Forexample, LPE may also be associated withintestinal parasites, dietary sensitivity andfeline hyperthyroidism.8 Moreover, cats withand without signs of intestinal disease havesimilar numbers of lymphocytes and plasmacells in tissues.5 In hyperthyroid cats with LPE,successful treatment (via I131) of the hyper-thyroidism has resulted in remission ofclinical signs but follow-up biopsies werenot performed to assess for eradication ofmucosal inflammation (author’s unpublishedobservations).
Recent studies indicate that changes inmucosal architecture, such as villous morphol-ogy and fibrosis, are related to the presence andseverity of GI disease. These studies have usedquantitative observer-independent variables(eg, proinflammatory cytokines, mucosal bacte-ria) to identify histopathological correlates ofdisease. In cats with signs of GI disease, villusatrophy and fusion correlated with severity ofclinical signs and degree of proinflammatorycytokine upregulation in the duodenal mucosa.In a separate investigation, histopathologicinflammation was correlated with clinicalsigns, endoscopic lesions (ie, mucosal friability,granularity and/or erosions), and clinicopatho-logic abnormalities (ie, increased total proteinconcentration, elevated ALT/ALP activities,hypophosphatemia, hypocobalaminemia,and/or increased fPLI) in cats with IBD.26
Surgical versus endoscopically obtainedbiopsiesBiopsies for histopathologic diagnosis of IBDare obligatory and they may be obtainedendoscopically (mucosal sample) or bylaparoscopy or exploratory laparotomy (full-thickness sample). Controversy exists con-cerning the relative diagnostic accuracy ofendoscopic versus full-thickness specimensfor the diagnosis of IBD and alimentary lym-phoma. Making a correct diagnosis is furthercomplicated by the fact that these disordersshare a variety of overlapping features (eg,clinical signs, physical examination findings,abdominal ultrasonographic abnormalitiesand histopathologic lesions) and that chronicmucosal inflammation (eg, gastric Helicobacterheilmannii infection) may progress to lym-phoma in some instances.40
Endoscopic biopsy specimens of the stom-ach and duodenum were considered inade-quate compared with full-thickness biopsiesfor differentiating IBD from lymphoma in onestudy.14 However, duodenal (endoscopic)assessment was limited to only 50% of the catsand mucosal biopsy was performed blindly(with only three specimens obtained per cat) in8/22 (36%) of the cats. Because none of the catsin this study had endoscopic biopsy of theileum performed, malignant infiltrates in thisorgan could only be confirmed in full-thickness specimens obtained by laparotomy.In another study, the likelihood for diagnosisof alimentary lymphoma was greatest in catsundergoing multi-organ biopsy from all seg-ments of the intestine and the mesenteric
Eosinophilic enteropathyEosinophilic enterocolitis (EE) is characterized by markedmucosal infiltration of eosinophils in the intestinal lamina propria.Eosinophilic enteritis may occur alone, as a component of EE, orin association with hypereosinophilic syndrome in cats.37 Thisdisorder may result from dietary sensitivity or endoparasitism,and lesions may be focal or diffuse in distribution. Similar to LPE,diagnostic criteria vary and there is considerable controversy asto the magnitude of the normal eosinophilic population in smalland large intestine and what is considered excessive. A diagno-sis of EE is strengthened by the observation of eosinophils in thesubmucosa and the presence of infiltrates in the mesentericlymph nodes.38 Clinical signs include small or large bowel diar-rhea, vomiting, anorexia and weight loss. Physical examinationmay detect palpably thickened intestinal loops (presumably dueto the submusosal eosinophilic infiltrates) but these may also bea feature of non-EE intestinal infiltrative diseases. Peripherallymphadenopathy and hepatosplenomegaly are also reported in
cats with hypereosinophilic syndrome. Laboratory testing mayreveal eosinophilia in some cats. The endoscopic findings for EEare similar to those described for LPE.
Neutrophilic enteropathyNeutrophils are usually only a minor component of the inflamma-tory response in IBD and are primarily seen with erosive mucosallesions. Suppurative colitis may occur in young cats but is anuncommon IBD variant.39 Clinical signs include large boweldiarrhea, hematochezia, or tenesmus of variable severity.Histopathologic lesions include dense infiltrates of neutrophilsaccompanied by lesser numbers of lymphocytes and plasmacells. The cause is unknown but this disorder may be associatedwith enteropathogenic bacteria, including Clostridium speciesand Campylobacter jejuni. Neutrophilic forms of IBD are rare andthe suspicion for a primary bacterial etiopathogenesis is basedon the abundant and complex intestinal microbiota present in thecolon.
U n u s u a l f o r m s o f f e l i n e I B D
Chronic enteropathies characterized by eosinophilic or neutrophilic inflammation are much less commonly diagnosed in catsthan LPE. There are no apparent gender or breed predispositions for these unusual forms of feline IBD.
Biopsies forhistopathologic
diagnosis ofIBD are
obligatory . . .The ileum
seems to be aconsistently
affected organand shouldalways be
biopsied whenlymphoma or
IBD issuspected.
at AMERICAN COLL VET DERMATOLOGY on June 27, 2016jfm.sagepub.comDownloaded from
JFMS CLINICAL PRACTICE 445
C L I N I C A L R E V I EW
Journal of Feline Medicine and Surgery (2012) 14, 445–458
Albert E Jergens
FELINE IDIOPATHIC INFLAMMATORYBOWEL DISEASEWhat we know andwhat remains to be unraveled
Practical relevance: Feline idiopathicinflammatory bowel disease (IBD)denotes one form of chronic enteropathythat is immunologically mediated andcharacterized by persistent or recurrentgastrointestinal (GI) signs and histologicinflammation. Signs of vomiting, diarrhea andweight loss generally predominate, and mucosalinflammation may occur in any portion of the GItract (especially the small intestine). Affected catsmay also have concurrent inflammation in otherorgans, such as the pancreas and liver, which mayimpact clinical disease severity.Clinical challenges: The exact etiologies of thisheterogeneous group of disorders have yet to bedetermined, though results from basic science andclinical studies suggest that interplay betweengenetic factors and enteric bacteria is crucial fordisease development. The diagnosis is one ofexclusion and requires intestinal mucosal biopsyto characterize the type and severity of theinflammatory infiltrate, and to differentiate IBD fromother disorders, including alimentary lymphoma.Controversy exists concerning the relativediagnostic accuracy of endoscopic versusfull-thickness specimens for the diagnosis of IBDand its differentiation from alimentary lymphoma.Audience: This article is intended to provideveterinary practitioners with a comprehensiveclinical update on idiopathic IBD in cats. It reviewsthe current evidence-based data, the diagnosticapproach, the evolving histologic criteria, andtreatment options and outcome for feline patientswith this syndrome.
Current understanding of etiologyand pathogenesis
While the exact cause of inflammatory bowel disease (IBD) remainsunknown, current hypotheses suggest that feline IBD, similar to IBDin humans and dogs, involves complex interactions betweenenvironmental factors (ie, intestinal microbial imbalances, dietarycomponents) and the mucosal immune system, resulting in chronicinflammation in susceptible cats (Figure 1).1
Genetic defects in the recognition of commensal versus pathogenicbacteria by the innate immune system play a pivotal role in disease
pathogenesis in humansand dogs with IBD.Mutations in innateimmune receptors ofhumans (NOD2/CARD 15)and dogs (TLR4, TLR5)have now been linked toIBD susceptibility; and inthe presence of an entericmicrobiota may lead toupregulated proinflamma-tory cytokine production(eg, IL-17, TNF-α) andreduced bacterial clearance,
thereby promoting chronic intestinal inflammation.1–3 Whetheror not similar pathomechanisms come into play in the developmentof idiopathic feline IBD has not been fully determined. However,antigens derived from commensal bacteria are likely to be importantin driving disease pathogenesis, as increased populations ofmucosa-associated bacteria (ie, Enterobacteriaceae) have been linked toclinical signs, cytokine mRNA and histopathologic lesions in catswith IBD.4
Other studies have reported increased lamina propria myeloid/histiocyte antigen-positive macrophages, upregulated epithelial majorhistocompatibility complex (MHC) class II molecule expression,and increased antibody reactivity to components of the commensal
DOI: 10.1177/1098612X12451548© ISFM and AAFP 2012
Certain breed predispositions(Siamese and other Asian
breeds) for IBD are recognized,but any breed may be affectedand causal genetic defects have
not been identified to date.
Albert E JergensDVM PhD DACVIM
Department of Veterinary Clinical Sciences,College of Veterinary Medicine,
Iowa State University,Ames, IA 50011, USA
Email: [email protected]
at AMERICAN COLL VET DERMATOLOGY on June 27, 2016jfm.sagepub.comDownloaded from
TRATAMENTO

Tratamento
!Mudança da Dieta & Terapia Farmacológica ! !Controle dietético ! !Antibioticoterapia ! !Corticoterapia ! !Imunossupressores !
Tratamento
!Dieta ! !Restrição de gordura
! !Proteína inexperiente
! !Proteína ultra-hidrolisada
!!

Tratamento
!Prednisolona (Prelone®3mg/ml-humano) dose: 2mg/kg PO q.24hd redução dose 25% q.30dias duração do tto: 3 a 6 meses!!! !!Metronidazol (Flagyl®250mg-humano) dose: 15mg/kg PO q.24h por 14 dias redução dose 25% mais 14 dias !!Clorambucil (Leukeran®-humano) dose: 2mg/gato PO q.72h por 21 dias !!Ciclosporina (Genuxal®-humano) dose: 5mg/gato/PO/por 21dias
JFMS CLINICAL PRACTICE 445
C L I N I C A L R E V I EW
Journal of Feline Medicine and Surgery (2012) 14, 445–458
Albert E Jergens
FELINE IDIOPATHIC INFLAMMATORYBOWEL DISEASEWhat we know andwhat remains to be unraveled
Practical relevance: Feline idiopathicinflammatory bowel disease (IBD)denotes one form of chronic enteropathythat is immunologically mediated andcharacterized by persistent or recurrentgastrointestinal (GI) signs and histologicinflammation. Signs of vomiting, diarrhea andweight loss generally predominate, and mucosalinflammation may occur in any portion of the GItract (especially the small intestine). Affected catsmay also have concurrent inflammation in otherorgans, such as the pancreas and liver, which mayimpact clinical disease severity.Clinical challenges: The exact etiologies of thisheterogeneous group of disorders have yet to bedetermined, though results from basic science andclinical studies suggest that interplay betweengenetic factors and enteric bacteria is crucial fordisease development. The diagnosis is one ofexclusion and requires intestinal mucosal biopsyto characterize the type and severity of theinflammatory infiltrate, and to differentiate IBD fromother disorders, including alimentary lymphoma.Controversy exists concerning the relativediagnostic accuracy of endoscopic versusfull-thickness specimens for the diagnosis of IBDand its differentiation from alimentary lymphoma.Audience: This article is intended to provideveterinary practitioners with a comprehensiveclinical update on idiopathic IBD in cats. It reviewsthe current evidence-based data, the diagnosticapproach, the evolving histologic criteria, andtreatment options and outcome for feline patientswith this syndrome.
Current understanding of etiologyand pathogenesis
While the exact cause of inflammatory bowel disease (IBD) remainsunknown, current hypotheses suggest that feline IBD, similar to IBDin humans and dogs, involves complex interactions betweenenvironmental factors (ie, intestinal microbial imbalances, dietarycomponents) and the mucosal immune system, resulting in chronicinflammation in susceptible cats (Figure 1).1
Genetic defects in the recognition of commensal versus pathogenicbacteria by the innate immune system play a pivotal role in disease
pathogenesis in humansand dogs with IBD.Mutations in innateimmune receptors ofhumans (NOD2/CARD 15)and dogs (TLR4, TLR5)have now been linked toIBD susceptibility; and inthe presence of an entericmicrobiota may lead toupregulated proinflamma-tory cytokine production(eg, IL-17, TNF-α) andreduced bacterial clearance,
thereby promoting chronic intestinal inflammation.1–3 Whetheror not similar pathomechanisms come into play in the developmentof idiopathic feline IBD has not been fully determined. However,antigens derived from commensal bacteria are likely to be importantin driving disease pathogenesis, as increased populations ofmucosa-associated bacteria (ie, Enterobacteriaceae) have been linked toclinical signs, cytokine mRNA and histopathologic lesions in catswith IBD.4
Other studies have reported increased lamina propria myeloid/histiocyte antigen-positive macrophages, upregulated epithelial majorhistocompatibility complex (MHC) class II molecule expression,and increased antibody reactivity to components of the commensal
DOI: 10.1177/1098612X12451548© ISFM and AAFP 2012
Certain breed predispositions(Siamese and other Asian
breeds) for IBD are recognized,but any breed may be affectedand causal genetic defects have
not been identified to date.
Albert E JergensDVM PhD DACVIM
Department of Veterinary Clinical Sciences,College of Veterinary Medicine,
Iowa State University,Ames, IA 50011, USA
Email: [email protected]
at AMERICAN COLL VET DERMATOLOGY on June 27, 2016jfm.sagepub.comDownloaded from
e o gordo? idoso? renal? cardiopata?
!Budesonida ! !corticóide de ação local
! !redução dos efeitos sistêmicos
! !dose: 1mg/gato/dia (manipular)
!!!

Suplementos
!Cobalamina (vitamina B12-hidrossolúvel) ! !deficiência B12:
! !mudança da permeabilidade da mucosa
! !redução absorção de nutrientes
!anemia em humanos ! !dose: 250mcg/gato/semana/6sem !!!
Suplementos
!FIBRAS SOLÚVEIS (Colite) ! !Psylium
! !substrato para simbiose colonica
!!PROBIÓTICOS ! !corrigir desequilíbrio e reduzir inflamação !
!!

Prognóstico
☺ Favorável ☺ !
☹ Exceto com linfoma intestinal ! !!
DODÓI
Obrigada! 32