Embed Size (px)
Citation preview

Fenômeno de RaynaudFenômeno de RaynaudDisciplina Reumatologia
2015

Fenômeno de RaynaudFenômeno de Raynaud
Resposta fisiológica exagerada em resposta a exposição ao frio e ao estresse
Isquemia Cianose Cianose
Reperfusão
Herrick, A. L. Nat. Rev. Rheumatol. 2012


Fenômeno de RaynaudFenômeno de Raynaud
NATURE REVIEWS | RHEUMATOLOGY VOLUME 8 | AUGUST 2012 | 471
NO-mediated vasodilatation in Raynaud phenomenon is highly complex.14 NO relaxes smooth muscle cells. In sclerodermatous skin, endo thelial NO synthase (NOS) is initially increased, whereas in advanced disease, induc-ible NOS is increased.15 The roles of the different isoforms of NOS in cutaneous vasodilatation are currently unclear10 and reduced NO production via neuronal NOS could also have a role, at least in SSc,16 demonstrating the interplay between ‘vascular’ and ‘neural’ abnormalities. Further complicating the role of NO, in patients with SSc, the plasma levels of an endogenous inhibitor of endothelial NOS—asymmetric dimethylarginine—are increased.17 However, irrespec tive of whether there is underproduc-tion or overproduc tion of NO in the digits of patients with SSc (which could be disease-stage-dependent), NO supplementation (for example, via topical application of glyceryl trinitrate) results in vasodilatation. This response could be as good in patients with SSc as in patients with primary Raynaud phenomenon and healthy controls.18
Increased vasoconstrictionOverproduction of vasoconstrictors by endothelial cells (in particular endothelin-1 and angiotensin II) most likely contributes to SSc-related Raynaud phenomenon. The expression of endothelin-1 is increased in sclero-dermatous skin.19 An imbalance in the renin– angiotensin system, in favour of angiotensin II, is thought to occur in SSc.20 Although some studies implicated a role for endothelin-1 in primary Raynaud phe nomenon,11,21 this evidence is much weaker than that for SSc. One excit-ing development in recent years has been the increased understanding of signal transduction pathways in vas-cular smooth muscle, as discussed below briefly, which highlights the fact that ‘vascular’ and ‘neural’ mechanisms cannot be considered in isolation.
Structural abnormalitiesStructural abnormalities of both the microvasculature and the digital arteries are well studied in SSc,22,23 and undoubtedly, contribute to impaired digital perfusion. The microangiopathy of SSc can be clearly demonstrated non-invasively by capillaroscopy (Figure 2). Typical changes are enlarged, widened capillaries (through which the red blood cells move sluggishly) with areas of avascularity (Figure 2b). The most striking change in the digital artery is intimal hyperplasia (Figure 3). The ulnar artery may also be affected in SSc,24 and it has been suggested that the prevalence of proximal large vessel disease is increased in patients with SSc compared to control population;25 however, this finding remains controversial.
The pathogenesis of SSc-related microvascular and digital artery structural vascular disease is well studied.14,26–28 Although the pathogenesis is not fully under stood, pro-gress is being made and possible contributors include endothelial injury (of unknown cause) as a potential early or initiating mechanism, endothelial cell apoptosis (which might promote fibrosis29), abnormal expression of tran-scription factors,28 aberrant production of growth factors and cytokines, activation of pericytes,30 and abnormalities of both angiogenesis and vasculo genesis (with a reduction
in bone- marrow-derived endothelial precursors).31 A recent study has shown that the anti-angiogenic vascular endothelial growth factor (VEGF) isoform VEGF165b is over expressed in SSc.32 This finding could explain, at least in part, the marked attrition of microvessels.
By contrast, structural abnormalities do not occur in primary Raynaud phenomenon: any reported abnor-malities have been subtle changes33 and could possi-bly relate to the unclear distinction between primary Raynaud phenomenon and SSc. A small proportion of patients (1–2% per year) with what appears to be primary Ray naud phenomenon progress to an SSc-spectrum dis-order or other underlying disease.34 The thumb is less affected by Raynaud phenomenon than other digits:35 the reason for this reduced effect is unknown, but could imply that its shorter length is in some way protective for structural (and possibly functional) change.
Neural abnormalitiesSeveral different neurotransmitters and their receptors are implicated in the pathogenesis of Raynaud phenom-enon, as many of these neurotransmitters mediate either vasodilatation or vasoconstriction. Both autonomic and small sensory nerve fibres are likely to be involved.
Nerve bres(sympatheticand sensory)
Smooth muscle cell
Endothelial cell
Endothelin-1from endothelial cells
Oxidative stress
Endothelial damageReduced blood ow/
procoagulant tendency
NOfrom endothelial cells
Platelet activation/aggregation
Reactivity of smooth muscleα2-adrenoceptors (via
Rho/Rho kinase activation)
Thrombin
Viscosity
Fibrinolysis
Red blood celldeformability
Vasoconstriction Vasodilatation
Vasodilatatory neuropeptides (e.g. CGRP) from sensor y
afferents
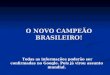
Figure 1 | Schematic representation of some of the key elements and mechanisms contributing to the pathogenesis of Raynaud phenomenon. Some of the mediators contribute to disease pathogenesis via different mechanisms. For example, reactive oxygen species (resulting in oxidative stress) may damage the endothelium via lipid peroxidation, but may also activate Rho/Rho kinase resulting in increased vasoconstriction. Abbreviations: CGRP, calcitonin gene-related peptide; NO, nitric oxide. Modified from Herrick, A. L. Pathogenesis of Raynaud’s phenomenon, Rheumatology 44, 587–596 (2005), by permission of Oxford University Press.
R E V I E W S
© 2012 Macmillan Publishers Limited. All rights reserved

Fenômeno de RaynaudFenômeno de Raynaud
• Primário ou idiopático:
Mulher jovem Ataques simétricos/ curta duração Prevalência: 19-11% Ausência de cicatriz, ulcera ou gangrena digital Capilaroscopia normal FAN negativo PAIs normais Exame físico normal Ausência de sintomas sugestivos de DTC
Herrick, A. L. Nat. Rev. Rheumatol. 2012

Fenômeno de RaynaudFenômeno de Raynaud
•Secundário• DTC:
• ESCLEROSE SISTÊMICAESCLEROSE SISTÊMICA
• Miopatias infamatórias
• Lúpus Eritematoso Sistêmico
• Síndrome de Sjogren
• Vasculite

Úlcera digitalÚlcera digital

Cicatriz e Úlcera DigitalCicatriz e Úlcera Digital

Gangrena Gangrena DigitalDigital

Fenômeno de RaynaudFenômeno de Raynaud

Esclerodermia Esclerodermia LocalizadaLocalizada

Esclerodermia LocalizadaEsclerodermia Localizada• Morféia
• mais comum
• placas de pele espessada com graus variados de pigmentação
• “gutata” e “subcutânea”
• Morféia generalizada• Área extensa
• Esclerodermia linear• Podem apresentar envolvimento profundo da pele até atingir os músculos.
• mais comuns nas pernas e nos braços e, quando acometem as articulações, podem acarretar limitações da função articular.
• Esclerodermia “em golpe de sabre”• face ou o couro cabeludo
• ocasionalmente pode causar atrofia da face (inclusive língua e a boca)

MorféiaMorféia


Esclerodermia LinearEsclerodermia Linear

Esclerodermia LinearEsclerodermia Linear

Golpe de SabreGolpe de Sabre

Síndrome de Parry- RombergSíndrome de Parry- Romberg

Síndrome de Parry- Romberg
• A síndrome de Parry-Romberg, também denominada atrofia hemifacial progressiva, consiste em uma rara condição na qual há degeneração progressiva e encolhimento dos tecidos situados abaixo da pele da face, incluindo, em muitos casos, os ossos.

Esclerose SistêmicaEsclerose Sistêmica

Esclerose SistêmicaEsclerose Sistêmica
• Prevalência: 1 a 2 casos por 100.000
• Predominio feminino 4:1
• 30-50 anos
• Fatores genéticos
• Fatores ambientais• Sínd. Erasmus (silicose+ES)
• Sínd. ASIA

Esclerose SistêmicaEsclerose Sistêmica
• FORMA PRECOCE• F. Raynaud• Capilaroscopia SD• ACA ou SCl-70 +
• SINE ESCLERODERMA• F. Raynaud• FAN positivo• Manifestações viscerais
• LIMITADA• DIFUSA• SÍNDROMES DE SUPERPOSIÇÃO

Esclerose Sistêmica LimitadaEsclerose Sistêmica Limitada
• Subtipo mais prevalente
• Não acomete: abdome, dorso, braços ou coxa
• Evolução mais lenta
• Mais frequente:
• Dismotilidade Esofágica
• Hipertensão Arterial Pulmonar
• Calcinose
• Telangiectasia
• ACA (padrão de FAN centromérico)

Esclerose Sistêmica DifusaEsclerose Sistêmica Difusa
• Subtipo mais grave
• Evolução mais rápida
• Maior mortalidade
• Forma mais comum em crianças
• Mais frequente:
• Fibrose pulmonar
• Miocardite fibrosante
• Crise renal esclerodermica
• SCL-70 (Antitopoisomerase)

Esclerose Sistêmica Esclerose Sistêmica LimitadaLimitada(CREST)(CREST)

Envolvimento Cutâneo DifusoEnvolvimento Cutâneo Difuso

CalcinoseCalcinose

TelangiectasiasTelangiectasias

Capilaroscopia padrão SDCapilaroscopia padrão SD
NATURE REVIEWS | RHEUMATOLOGY VOLUME 6 | OCTOBER 2010 | 581
Raynaud phenomenon (Figure 3c). It has been estimated that the number of normal capillaries is reduced to 20% in patients with active SSc.24 The extensive disappearance of capillaries can generate large avascular areas, which have a desert-like appearance in the nail-bed micro-vascular array. Loss of capillaries could be relevant in determining the severe tissue hypoxia that is involved in the development of digital skin ulcers.11 In patients with recent onset of Raynaud phenomenon, the appearance of rapidly prog ressive capillary loss can represent the first dramatic capillaro scopic evidence of destruction of the micro vessels and the development of severe SSc.
Ramified capillariesCapillary loss induces local hypoxia and the consequent local production of vessel growth factors (such as vascular endothelial growth factor), which in turn stimulating the formation of new capillaries—neoangiogenesis.25 A range of morphological features of the micro vasculature attribu table to neoangiogenesis is seen almost exclusively in patients with late SSc and secondary Raynaud phe-nomenon (Figure 3d). The main morphological hallmark
of angiogenesis in advanced SSc is the clustering of twisted capillaries, with pronounced heterogeneity in shape and size, winding together with bushy capillaries. Highly con-voluted and branched capillary loop clusters, surrounded by loss of normal capillary loops, are characteristic features of neoangiogenesis in advanced SSc.
Characterization of SSc-specific patternsHistorically, the capillaroscopic aspects of vascular damage in SSc were partially graded into two major pat-terns: active and slow.26 Since the year 2000, new classifi-cations related to selected characteristics of disease progression have been proposed to improve the diag-nostic and prognostic power of capillaroscopic analysis.27 Consequently, microvascular lesions detected by NVC in patients with SSc can be reclassified into three different NVC patterns, ‘early’, ‘active’ and ‘late’, which are clearly distinguishable from the ‘normal’ pattern (Figure 4).28
The ‘early’ SSc pattern is considered the most important since it is fundamental to the differentiation of primary and secondary Raynaud phenomenon. This pattern is characterized by the presence of a small number of giant
a
c d
b
Figure 3 | Markers of scleroderma patterns. Images obtained by routine nailfold videocapillaroscopy analysis of patients with systemic sclerosis (magnification × 200) reveal the morphological markers of microvascular disorganization that characterize overt systemic sclerosis and related nailfold videocapillaroscopy patterns (‘early’,‘active’ and ‘late’ systemic sclerosis) in the presence of secondary Raynaud phenomenon. a | Giant capillaries (arrows), the earliest and most striking morphological feature of secondary Raynaud phenomenon, are homogeneously enlarged microvascular loops that serve as potential markers of microangiopathy. b | Microhemorrhages (arrows) result from the microvascular extravasation of red blood cells from damaged capillaries. c | Loss of capillaries (arrows) can lead to the presence of avascular areas in the nailfold bed and subsequent local tissue hypoxia. d | Neoangiogenesis is characterized by the clustering of twisted and bushy capillaries (arrows) and represents a local reaction to tissue hypoxia.
R E V I E W S
nrrheum_104_OCT10.indd 581 10/9/10 15:29:00
© 20 Macmillan Publishers Limited. All rights reserved10
Ectasia
Micro hemorragia
Perda de capilarCapilar em arbusto

Esclerose SistêmicaEsclerose Sistêmica

Esclerose Esclerose SistêmicaSistêmica
• Manifestações clínicas:• F. Raynaud (95%)
• Capilaroscopia padrão SD
• Músculo esqueléticas
• artralgia e artrite
• espessamento tendíneo
• miopatia e fraqueza muscular
• Gastrointestinal (90%)
• Dismotilidade esofágica
• Incontinência fecal
• Diarreia crônica e desnutrição
GAVE

Esclerose SistêmicaEsclerose Sistêmica
• Manifestações clínicas:Manifestações clínicas:
• PulmonarPulmonar
• Doença intersticial pulmonar (70%)Doença intersticial pulmonar (70%)
• Hipertensão arterial pulmonarHipertensão arterial pulmonar
• CoraçãoCoração
• Derrame pericárdicoDerrame pericárdico
• Miocardite fibrosanteMiocardite fibrosante
• Crise Renal esclerodérmicaCrise Renal esclerodérmica
• OutrasOutras
• Síndrome SiccaSíndrome Sicca
• Neuropatia trigêmeoNeuropatia trigêmeo
• Túnel do CarpoTúnel do Carpo
• Mononeurite múltipla e polineuropatiaMononeurite múltipla e polineuropatia

TratamentoTratamento• Fenômeno de Raynaud:
- orientações gerais para evitar o frio
- bloqueadores de canais de cálcio (nifedipina, diltiazem)
- inibidores da enzima conversora da angiotensina
- inibidor seletivo serotonina
- inibidor da fosfodiesterase
- antagonista do receptor de endotelina 1
- prostanóide
- simpatectomia
• Pele: • ciclofosfamida em casos graves
• metotrexato

TratamentoTratamento• Doença pulmonar: • ciclofosfamida
• azatioprina
• Micofenolato mofetil
• Trato gastrointestinal: - mudar hábitos
- procinéticos
- inibidores de bomba de prótons
• Doença renal: inibidor da ECA
• Transplante Medula Óssea casos graves

![Dedo Isquemico [Modo de Compatibilidade] · • Diagnóstico diferencial • Raynaud Primário – Fisiopatologia • Raynaud Secundário Dedo Isquêmico – Causas – Fisiopatologia](https://img.document.onl/doc/110x75/5c615a2d09d3f21b6a8cfdde/dedo-isquemico-modo-de-compatibilidade-diagnostico-diferencial-raynaud.jpg)