Embed Size (px)
Citation preview

Abordagem de Massas Cervicais Pediátricas
Dr. Leonardo Guimarães Rangel Cirurgião de Cabeça e Pescoço
Staff do HUPE-UERJ Doutorando em Cirurgia

Abordagem Inicial
3 Perguntas
Quando ?
Aonde ?
De Onde ? ?

Abordagem Inicial

Abordagem Inicial
Quando

Abordagem Inicial

Abordagem Inicial

Abordagem Inicial

Abordagem Inicial

Abordagem Inicial
Aonde

Abordagem Inicial

tipos de massas cervicais
Congênitas Inflamatórias
Neoplásicas

tipos de massas cervicais
Congênitas Inflamatórias
Neoplásicas De Onde

Quando De Onde
Aonde

Quando De Onde
Aonde

Quando De Onde
Aonde
DX

Inflamatórias Linha Média ∆ anterior ∆ posterior
Adenites Adenites Adenites
1ª Viral 2ª Bacteriana
3ª granulomatosa
1ª Viral 2ª Bacteriana
3ª granulomatosa1ª Viral
2ª Bacteriana 3ª granulomatosaSialoadenites
Parotidea Submandibular

Congênitas
Linha Média ∆ anterior ∆ posterior
Cisto Tireoglosso
Cisto Dermóide
Cistos Branquiais
Laringocele
Cisto Tímico
Linfangioma
Lipoma

NeoplásicasLinha Média ∆ anterior ∆ posterior
Linfomas
Ca Tireóide
Linfomas
Linfangiomas
Lipomas
Metástases
Trato aerodigestivo
Face
Glomus
Tumor Corpo Carotídeo
Hemangiomas
Neurogênicos

Anamnese
Infecções Respiratórias
Viagens Recentes
Contato com animais
Tratamentos dentários e saúde bucal

Exame Físico
Carácterísticas da Lesão
Tamanho
Posição
Consistência
Aderência
Pulsátil
Ulcerada
Dor

Avaliação Laboratorial
Hemograma Completo
Pesquisa de HIV 1 e 2
VDRL
VHS, PCR-t
LDH
Teste de Mantoux (PPD)
sorologia para CMV
sorologia para EBV
VDRL + FTA-abs
sorologia para Toxoplasmose
sorologia para Tularemia
sorologia para Histoplasmose
sorologia para Bartonela Henselae (arranhadura do Gato)
Dç Lyme ( IGM Borrelia)

Exames de Imagem
Ultrassom
Custo x Benefício
Sólido x Líquido
Pús

Exames de ImagemTC
Radiação Ionizante Contraste Iodado Sedação Mais Rápido
RNM
sem Radiação Sedação Mais Demorado

Cisto Branquial

Cisto Branquial

Cisto Branquial

Cisto Branquial

Cisto Branquial

Cisto tireoglosso

Cisto tireoglosso

Cisto tireoglosso

Linfangioma

Linfangioma

Linfangioma

Linfangioma

Linfangioma

Linfangioma

Linfangioma

Glândulas Salivares Tumores
São Raros
Parótida (+ comum)
65% benignos
hemangioma
linfangioma
35% malignos
ca mucoepidermóide

Glândulas Salivares Tumores
São Raros
Parótida (+ comum)
65% benignos
hemangioma
linfangioma
35% malignos
ca mucoepidermóide

Glândulas Salivares Tumores
São Raros
Parótida (+ comum)
65% benignos
hemangioma
linfangioma
35% malignos
ca mucoepidermóide

Glândulas Salivares Tumores
São Raros
Parótida (+ comum)
65% benignos
hemangioma
linfangioma
35% malignos
ca mucoepidermóide

Glândulas Salivares Tumores
São Raros
Parótida (+ comum)
65% benignos
hemangioma
linfangioma
35% malignos
ca mucoepidermóide

Glândulas Salivares Tumores
São Raros
Parótida (+ comum)
65% benignos
hemangioma
linfangioma
35% malignos
ca mucoepidermóide

Glândulas Salivares Tumores
São Raros
Parótida (+ comum)
65% benignos
hemangioma
linfangioma
35% malignos
ca mucoepidermóide

Glândulas Salivares Tumores
São Raros
Parótida (+ comum)
65% benignos
hemangioma
linfangioma
35% malignos
ca mucoepidermóide

Processo inflamatório recorrente das glândulas salivares.
Aumento de volume
Dor
Febre
Mal estar
Saliva mucopurulenta
Fluxo salivar Diminuido
Glândulas Salivares Parotidite Recorente da Infância

Processo inflamatório recorrente das glândulas salivares.
Aumento de volume
Dor
Febre
Mal estar
Saliva mucopurulenta
Fluxo salivar Diminuido
Glândulas Salivares Parotidite Recorente da Infância
Unilateral

Glândulas Salivares Parotidite Recorente da Infância
Entidade Rara
Início: 8 meses – 16 anos
♂ > ♀
Episódios ao ano : 2-10
Evolução : remissão após adolescência

Hemangiomas
Capilares
Mistos
Cavernoso

Hemangiomas
Capilares
Mistos
Cavernoso

Hemangiomas
Capilares
Mistos
Cavernoso

Hemangiomas
Capilares
Mistos
Cavernoso

Hemangiomas
Capilares
Mistos
Cavernoso

Linfonodos !

http://histology.medicine.umich.edu/resources/lymphatic-system

Junqueira, 12ªed

Anatomia Ultrassonográfica
Anatomy 59
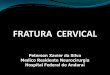
Fig. 6.1 Histology of a typical cervical lymph node. The trabeculae extending centrally from the periphery represent the lymph node hilum and contain, among other things, the blood vessels (asterisk). (Reproduced with kind permission of A. Agaimy MD, Institute of Pathology, Erlangen University Hospital, Germany.)
Fig. 6.2a Right side of the neck, transverse, level II. An oval lymph node in acute lymphadenitis colli (RF); the node has a delicate internal echo pattern with well-defined margins and measures 30 mm × 15 mm in both short-axis diameters. A clearly visible incidental finding is the nerve bundle of the vagus nerve seen in cross-section between the internal (ACI) and external (ACE) carotid arteries (asterisk). GSM, submandibular gland.
Homogeneity of the intranodal EchotextureAccording to classical teaching, the lymph node cortex (hypoechoic) and hilum (echogenic) show a homogeneous structure on ultrasound (Fig. 6.18). The presence of a markedly inhomogeneous echotexture is a relevant criterion of malignancy (Figs. 6.19, 6.20, 6.21).
Pearls and PitfallsIt is becoming problematic that the latest ultrasound scanners with higher resolution and improved displays hardly ever show completely homogeneous lymph nodes; rather they nearly always demonstrate some inhomogeneous—but not actually malignant—textural elements.
If the lymph node structure is altered as the result of a malignant trans-formation, the distinction between cortex and hilum is lost (Fig. 6.22). The echotexture is inhomogeneous with anechoic areas indicating necrosis and reduced perfusion of the center of the tumor (Figs. 6.23, 6.24).
On the other hand, a central anechoic area in a reactive cervical lymph node is typical of abscess formation. Liquefaction with a cen-tral anechoic area is seen particularly in mycobacteria infections and actinomycosis (see below). In contrast, echogenic reflections or calci-fication are characteristically seen in tuberculosis and in the case of metastases of papillary carcinoma of the thyroid.
Lymph Node Distribution
Level in the NeckIf there is an inflammatory process, the lymph nodes in the drainage channels of the affected organs show reactive changes. Hugely enlarged cervical lymph nodes in the lower neck are relatively less often affected by inflammation and are therefore detectable more often in the pres-ence of malignancy. The overall clinical situation must also be taken into account to be able to make an appropriate assessment (Fig. 6.25).
Noting the distribution of lymphadenopathy helps in narrowing down the differential diagnosis (Figs. 6.26, 6.27). Lymph node metas-tases from solid tumors are usually found initially in groups sited in the relevant lymphatic drainage channels. Particularly in cervical cases, the manifestation of many types of malignant lymphoma tends to appear in a conglomerate pattern.
*
*
Pearls and PitfallsThe ultrasound criteria for assessing whether or not a cervical lymph node is malignant are:
1. Size and three-dimensional proportions2. Detectability of a lymph node hilus, perfusion pattern3. Lymph node shape4. Border of the lymph node5. Homogeneity of the intranodal structure6. Distribution of the lymph nodes

Características Ultrassonográficas
Tamanho
referência : menor eixo
Níveis IB e II =8mm , IA, III, IV e V = 5mm
limite da detecção de metástases 3mm - para qualquer método

Características Ultrassonográficas
Formato
Solbati Index : maior/menor eixo
normal (1,5-2,0)
LFN inflamados aumentam mas mantém a forma
linfonodos metastáticos são redondos

Características Ultrassonográficas
Sinal Do Hilo
Benignidade
60 6 Neck Lymph Nodes
II So
nogr
aphi
c An
atom
y an
d Pa
thol
ogy
Fig. 6.4 Left side of the neck, transverse, CCDS. A round, clearly defined lymph node lateral to the common carotid artery (ACC), with a classical “hilar sign” and hilar perfusion seen on CCDS. The afferent and efferent hilar vessels can also be identified at the right border of the node. In this case, the massive enlargement of the node with maintenance of the normal vascular and hilar structures was due to non-Hodgkin lymphoma. A cystic mass in the lower neck area may also be found with metastases of papillary thyroid carcinomas.
Fig. 6.2b Right side of the neck, longitudinal, level II. The oval lymph node seen in acute lymphadenitis colli measures 32 mm on its long axis.
Fig. 6.3 Left side of the neck, transverse, level V. This lymph node shows a characteristic pattern of inflammation (kidney shape, hilar sign, homo-geneous texture). MSCM, stemocleidomastoid muscle, VJI, internal jugular vein, WS, vertebral spine.
60 6 Neck Lymph Nodes
II So
nogr
aphi
c An
atom
y an
d Pa
thol
ogy
Fig. 6.4 Left side of the neck, transverse, CCDS. A round, clearly defined lymph node lateral to the common carotid artery (ACC), with a classical “hilar sign” and hilar perfusion seen on CCDS. The afferent and efferent hilar vessels can also be identified at the right border of the node. In this case, the massive enlargement of the node with maintenance of the normal vascular and hilar structures was due to non-Hodgkin lymphoma. A cystic mass in the lower neck area may also be found with metastases of papillary thyroid carcinomas.
Fig. 6.2b Right side of the neck, longitudinal, level II. The oval lymph node seen in acute lymphadenitis colli measures 32 mm on its long axis.
Fig. 6.3 Left side of the neck, transverse, level V. This lymph node shows a characteristic pattern of inflammation (kidney shape, hilar sign, homo-geneous texture). MSCM, stemocleidomastoid muscle, VJI, internal jugular vein, WS, vertebral spine.

Características Ultrassonográficas
Bordas
Bem demarcadas
Movimento livre

Características Ultrassonográficas
Homogeniedade
Hilo hiperecóico
cortex Hipoecóico
Anatomy 67
Fig. 6.23 Left side of the neck, longitudinal, level III. A round lymph node metastasis with irregular borders has an anechoic center, which is indicative of necrosis caused by the metastatic transformation. VJI, internal jugular vein; MSCM, sternocleidomastoid muscle.
Fig. 6.24 Left side of the neck, level II. Medial to the internal and external carotid arteries, the round metastasis has an anechoic center consistent with central necrosis; this is considered to be a sign of malignancy. To the left, medial in the image, is an ill-defined hypoechoic primary tumor (TU) of the left side of the oropharynx. The internal jugular vein (VJI) is compromised and can be seen between the anterior border of the sternocleidomastoid muscle (MSCM) and the internal carotid artery (ACI). The vein can be demonstrated better with a Valsalva maneuver. ACE, external carotid artery.
Fig. 6.25 Split screen, right side of the floor of the mouth. The two round paramedian lymph nodes with inhomogeneous internal echoes lie on the right in level IA. If there were an acute dental infection, these two lymph nodes (RF1 and RF2), both showing a weak “hilar sign” and clearly defined margins, would be consistent with reactive enlargement; however, both lymph nodes can definitely be considered possible metastases when there is clinical suspicion of cancer of the floor of the mouth, tongue, or sinonasal area. MD, digastric muscle; MGH, geniohyoid muscle; MM, mylohyoid muscle. Histological diagnosis: Lymph node metastasis.

Características Ultrassonográficas
Homogeniedade
Hilo hiperecóico
cortex Hipoecóico
Anatomy 67
Fig. 6.23 Left side of the neck, longitudinal, level III. A round lymph node metastasis with irregular borders has an anechoic center, which is indicative of necrosis caused by the metastatic transformation. VJI, internal jugular vein; MSCM, sternocleidomastoid muscle.
Fig. 6.24 Left side of the neck, level II. Medial to the internal and external carotid arteries, the round metastasis has an anechoic center consistent with central necrosis; this is considered to be a sign of malignancy. To the left, medial in the image, is an ill-defined hypoechoic primary tumor (TU) of the left side of the oropharynx. The internal jugular vein (VJI) is compromised and can be seen between the anterior border of the sternocleidomastoid muscle (MSCM) and the internal carotid artery (ACI). The vein can be demonstrated better with a Valsalva maneuver. ACE, external carotid artery.
Fig. 6.25 Split screen, right side of the floor of the mouth. The two round paramedian lymph nodes with inhomogeneous internal echoes lie on the right in level IA. If there were an acute dental infection, these two lymph nodes (RF1 and RF2), both showing a weak “hilar sign” and clearly defined margins, would be consistent with reactive enlargement; however, both lymph nodes can definitely be considered possible metastases when there is clinical suspicion of cancer of the floor of the mouth, tongue, or sinonasal area. MD, digastric muscle; MGH, geniohyoid muscle; MM, mylohyoid muscle. Histological diagnosis: Lymph node metastasis.

Características Ultrassonográficas
Distribuição
número
distruição de acordo com a queixas

Características Ultrassonográficas
Distribuição
número
distruição de acordo com a queixas

Características Ultrassonográficas
Distribuição
número
distruição de acordo com a queixas

Características Ultrassonográficas
66 6 Neck Lymph Nodes
II So
nogr
aphi
c An
atom
y an
d Pa
thol
ogy
Fig. 6.21 Split screen, right side of the neck, level III. A lymph node (RF) in a patient being followed up for malignant disease; the caudal margins show marked extension. Compared with the normal architecture, there is marked inhomogeneity. ACC, common carotid artery; VJI, internal jugular vein; MSCM, sternocleidomastoid muscle. Diagnosis: Lymph node metastasis recurrence, 6 months after initial multimodal treatment.
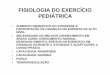
Fig. 6.22 A schematic representation of morphological changes in metastases. These morphological transfornations within a lymph node illustrate sonographic findings of malignancy.
Fig. 6.20 Split screen, right side of the neck, level IV, CCDS. The space-occupying lesion (RF) with an inhomogeneous echo pattern is sited laterally to the common carotid artery (ACC) and the internal jugular vein (VJI). The perfusion is peripheral and decentralized: in addition, irregular echogenic internal echoes are consistent with metastasis. MSCM, sternocleidomastoid muscle. Diagnosis: Lymph node metastasis.
Lymph nodeand its capsule
Fatty hilum composed offatty tissues surroundingthe hilum and medullaof a lymph node
Metastatic focus
Necrotic area withinthe metastatic focus
No changes in the size or formof the lymph node are evident.
Thickness is first affected(6 mm or greater in thickness).
The capsule also becomes thicker.
Although the entire lymphnode becomes enlarged,the capsule is retained.
A metastatic focus occupiesalmost the entire lymph node.
A border is clearly observed(10–20 mm in thickness;
can be identified even by CT).
The metastatic focusextends beyond the capsule
of the lymph node intosurrounding tissues. The border
becomes poorly demarcated.
1 2 3
7 6 5
4

Características Ultrassonográficas
Lembrar
Tamanho e proporções
Hilo
formato
Borda
Homogeniedade
Distribuição

Conclusão
Diversas etiologias
Avaliar melhor momento para abordagem
Evitar procedimentos desnecessários