Embed Size (px)
Citation preview
Prasugrel como antiagregante único en la Angioplastia
Primaria.
MARIO SADABA HOSPITAL DE GALDAKAO.

Prasugrel como antiagregante único ICP
1ª.

Elevación STElevación ST
Sindrome Coronario AgudoSindrome Coronario Agudo
Dolor tipo isquémicoDolor tipo isquémicoPresentaciónPresentación
ECG-Enfoque ECG-Enfoque Dx- ACTITUD Dx- ACTITUD
TTOTTO
TRATAMIENTOTRATAMIENTO
TROMBOLISISTROMBOLISISTROMBOLISISTROMBOLISISICP 1ªICP 1ªICP 1ªICP 1ª
AAS + CLOPIAAS + CLOPIAAS + CLOPIAAS + CLOPI
PRASUGREL (60/10) if no contraindication.PRASUGREL (60/10) if no contraindication. TICAGRELOR (180/90) if no contraindication.TICAGRELOR (180/90) if no contraindication. CLOPIDOGREL (600/75) CLOPIDOGREL (600/75) only only when PRASUGREL o when PRASUGREL o TICAGRELOR are not available or contraindicatedTICAGRELOR are not available or contraindicated

Farmacodinámica Tica-prasu-clopi.
Ticagrelor y prasugrel más rápidos en el inicio de acción y menor variabilidad que el clopidogrel

Farmacodinámica Tica-prasu SCAEST.
En el contexto de SCA tanto Ticagrelor como prasugrel tardan más de 2 horas en tener niveles de
antiagregación adecuados
•High residual platelet reactivity (HRPR) was defined as a PRU ≥ 240.

TRITON STEMI vs PLATO STEMI
N=7544P=0.07
0
Primary Efficacy Endpoint
2
4
8
12
6
10
0
ClopidogrelTicagrelor
6 8 10 12
Cum
ula
tive inci
dence
(%
)
42
Primary Efficacy Endpoint
Time (Days)
5
10
15
0
0 50 100 150 200 250 300 350 400 450
Pro
port
ion o
f pati
en
ts (
%)
9.5
12.4
10.0
HR=0.79 (0.65–0.97) NNT=41
p=0.02RRR=21%
p=0.002
RRR=32%
6.5
N=3534P=0.02
ClopidogrelPrasugrel
Time (Months)
TRITON PLATO
HR=0.87 (0.75 to 1.01) NNT=71
10.8
9.4
p=0.07RRR=13%

PRASUGREL. TRITON STEMI-ICP 1ª
All ACS/PCI patients
N=13608UA/NSTEMI
patients
N=10074
STEMI patients
N=3534
Primary PCI
N=2438 (69%)
Secondary PCI
N=1094 (31%)*
ClopidogreClopidogrell
N=1235N=1235
PrasugrePrasugrell
N=1203N=1203Lancet 2009; 373: 723–31
MEDIANA TIEMPO SINTOMAS ICP1ª
4,2h (2,7-7)
Aceeso Femoral 91%
Uso Inh IIb-IIIa 64%
Duración de tto 15,2 meses
Seguimiento 15 meses.
Abandono de tto 2,5%
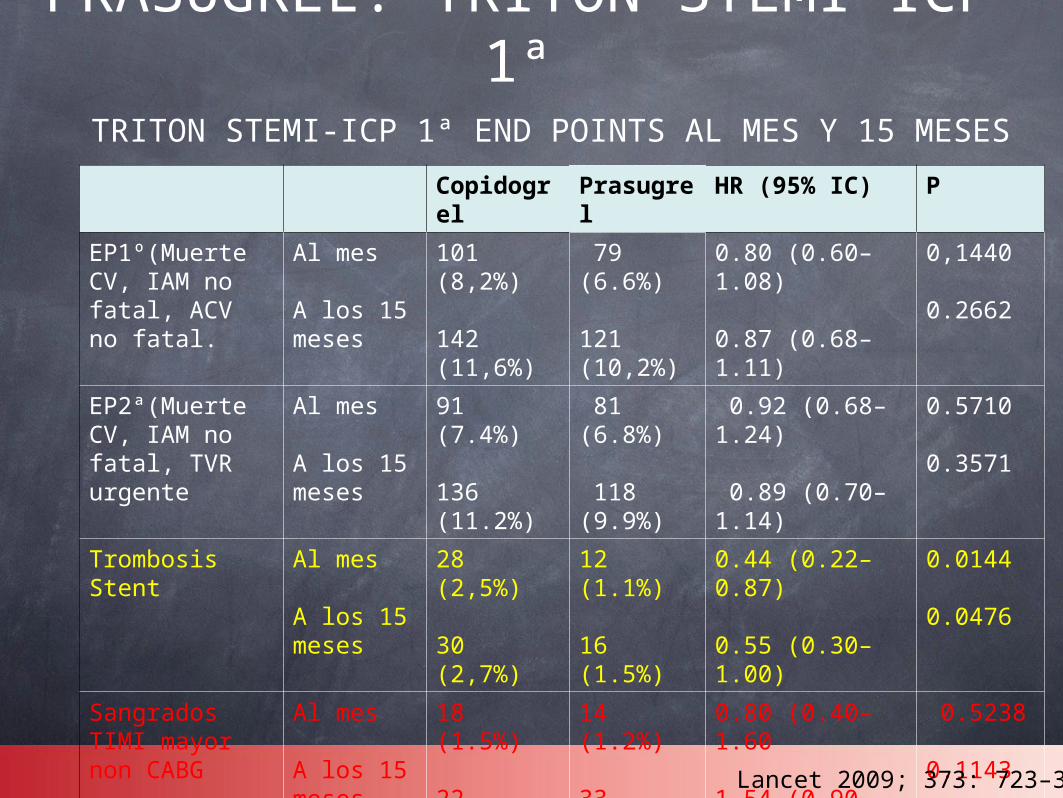
Copidogrel
Prasugrel
HR (95% IC) P
EP1º(Muerte CV, IAM no fatal, ACV no fatal.
Al mes
A los 15 meses
101 (8,2%)
142 (11,6%)
79 (6.6%)
121 (10,2%)
0.80 (0.60–1.08)
0.87 (0.68–1.11)
0,1440
0.2662
EP2ª(Muerte CV, IAM no fatal, TVR urgente
Al mes
A los 15 meses
91 (7.4%)
136 (11.2%)
81 (6.8%)
118 (9.9%)
0.92 (0.68–1.24)
0.89 (0.70–1.14)
0.5710
0.3571
Trombosis Stent
Al mes
A los 15 meses
28 (2,5%)
30 (2,7%)
12 (1.1%)
16 (1.5%)
0.44 (0.22–0.87)
0.55 (0.30–1.00)
0.0144
0.0476
Sangrados TIMI mayor non CABG
Al mes
A los 15 meses
18 (1.5%)
22 (1.9%)
14 (1.2%)
33 (3.1%)
0.80 (0.40–1.60
1.54 (0.90–2.64)
0.5238
0.1143
TRITON STEMI-ICP 1ª END POINTS AL MES Y 15 MESES
Lancet 2009; 373: 723–31
PRASUGREL. TRITON STEMI-ICP 1ª
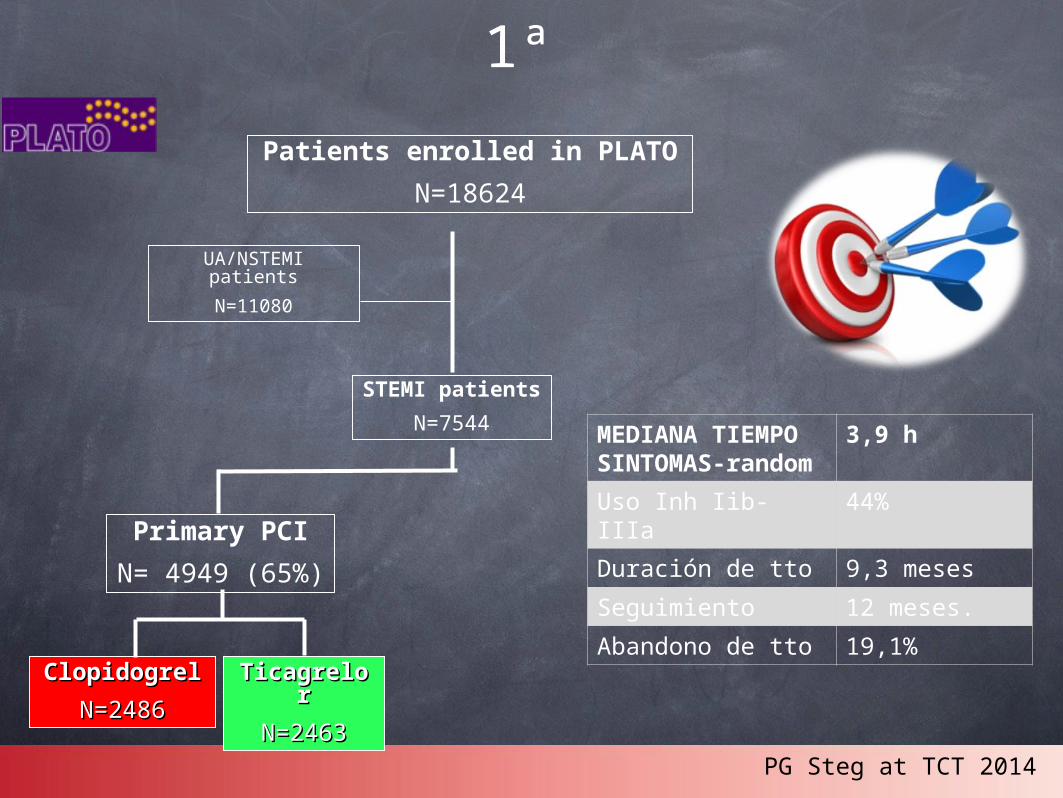
TICAGRELOR. PLATO STEMI-ICP 1ª
Patients enrolled in PLATO
N=18624
UA/NSTEMI patients
N=11080
STEMI patients
N=7544
Primary PCI
N= 4949 (65%)
ClopidogrelClopidogrel
N=2486N=2486
TicagrelorTicagrelor
N=2463N=2463
MEDIANA TIEMPO SINTOMAS-random
3,9 h
Uso Inh Iib-IIIa 44%
Duración de tto 9,3 meses
Seguimiento 12 meses.
Abandono de tto 19,1%
PG Steg at TCT 2014
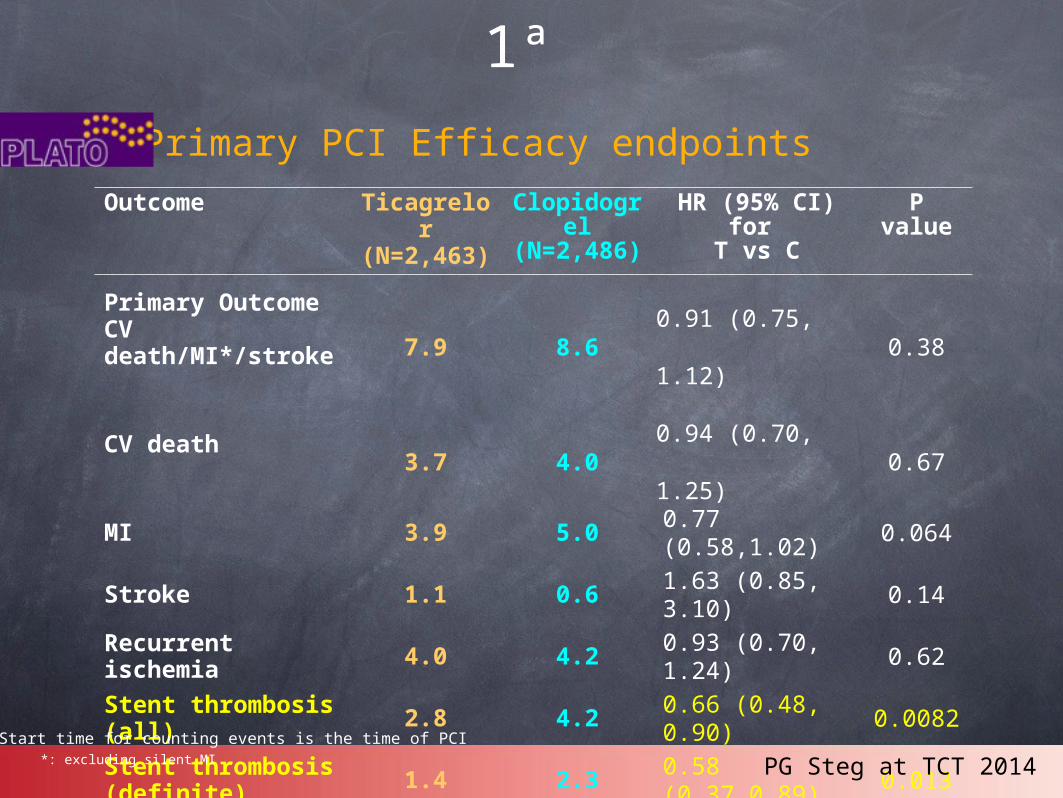
Primary PCI Efficacy endpoints
Outcome Ticagrelor
(N=2,463)
Clopidogrel
(N=2,486)
HR (95% CI) for
T vs C
P value
Primary OutcomeCV death/MI*/stroke 7.9 8.6 0.91 (0.75, 1.12) 0.38
CV death3.7 4.0 0.94 (0.70, 1.25) 0.67
MI 3.9 5.0 0.77 (0.58,1.02)
0.064
Stroke 1.1 0.6 1.63 (0.85, 3.10)
0.14
Recurrent ischemia 4.0 4.2 0.93 (0.70,
1.24)0.62
Stent thrombosis (all) 2.8 4.2 0.66 (0.48,
0.90)0.0082
Stent thrombosis (definite) 1.4 2.3 0.58
(0.37,0.89)0.013
*: excluding silent MI
Start time for counting events is the time of PCI
TICAGRELOR. PLATO STEMI-ICP 1ª
PG Steg at TCT 2014

Outcome Ticagrelor
(N=2,460)
Clopidogrel
(N=2,483)
HR (95% CI) for T vs C
P value
Major bleeding6.7 6.8
0.97 (0.77,
1.22)0.79
Fatal/Life-threatening bleed 3.1 3.3
0.94 (0.68,
1.31)0.71
Non-CABG major bleed 3.3 2.8 1.14 (0.81,
1.6)0.45
CABG-related major bleed 3.3 4.2 0.79 (0.58,
1.08)0.14
Major/minor bleed 9.8 9.1 1.05 (0.86, 1.27)
0.63
Dyspnea 12.7 8.2 1.65 (1.37, 1.99)
<0.0001
Start time for counting events is the time of PCI PG Steg at TCT 2014
TICAGRELOR. PLATO STEMI-ICP 1ª
Primary PCI Safety endpoints

TICAGRELOR. PLATO STEMI-ICP 1ª
PRASUGREL. TRITON STEMI-ICP 1ª
• No potenciados para ver diferencias en end point primario.
• tasa de trombosis.
• = sangrados mayores.

Beneficios clinicos netos.Beneficios clinicos netos.Subgrupos de riesgo de Subgrupos de riesgo de
sangrado sangrado
OVERALLOVERALL
>=60 kg< 60 kg
< 75>=75
NoSi
0.50.5 11 22
ACV/AIT
previo
Edad
Peso
Risk (%)Risk (%)
+ 54+ 54-16-16
-1-1-16-16
+3+3-14-14-13-13
Prasugrel BetterPrasugrel Better Clopidogrel BetterHRHR
PPint int = =
0.0060.006
PPint int = =
0.180.18
PPint int = =
0.360.36
Post-hoc analisisPost-hoc analisis
No beneficio clínico y aumento de sangrados
beneficio clínico y aumento de sangrados
beneficio clínico y aumento de sangrados
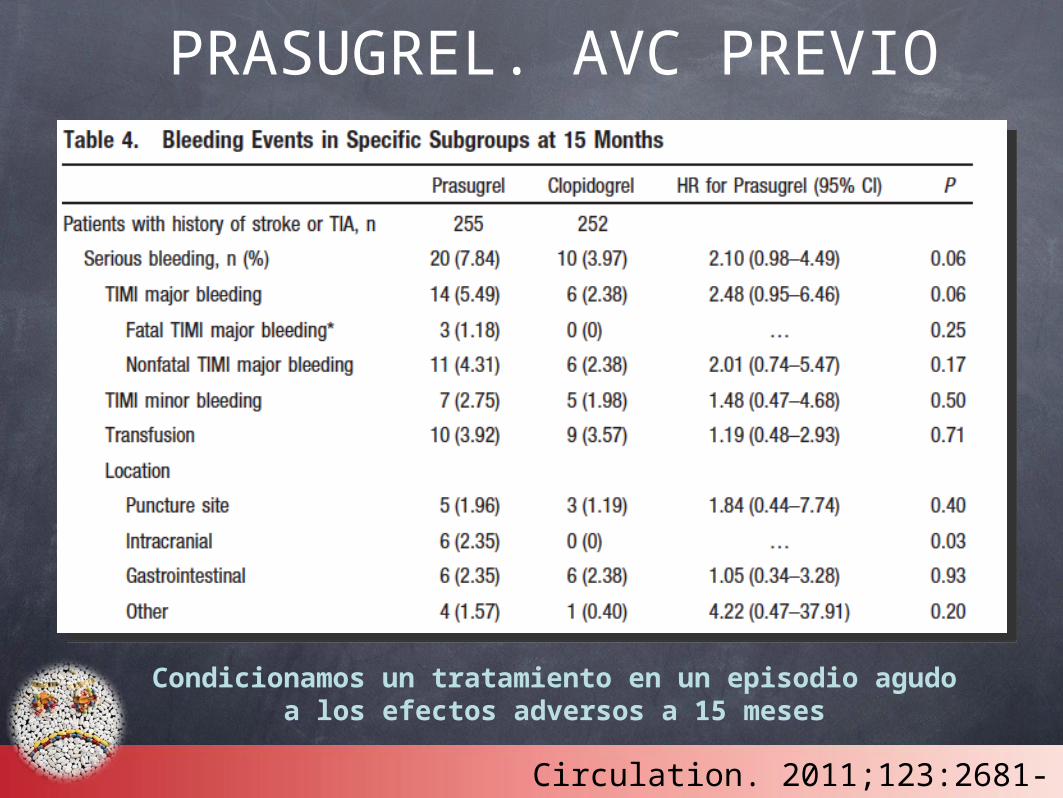
PRASUGREL. AVC PREVIO
Condicionamos un tratamiento en un episodio agudo a los efectos adversos a 15 meses
Circulation. 2011;123:2681-2689
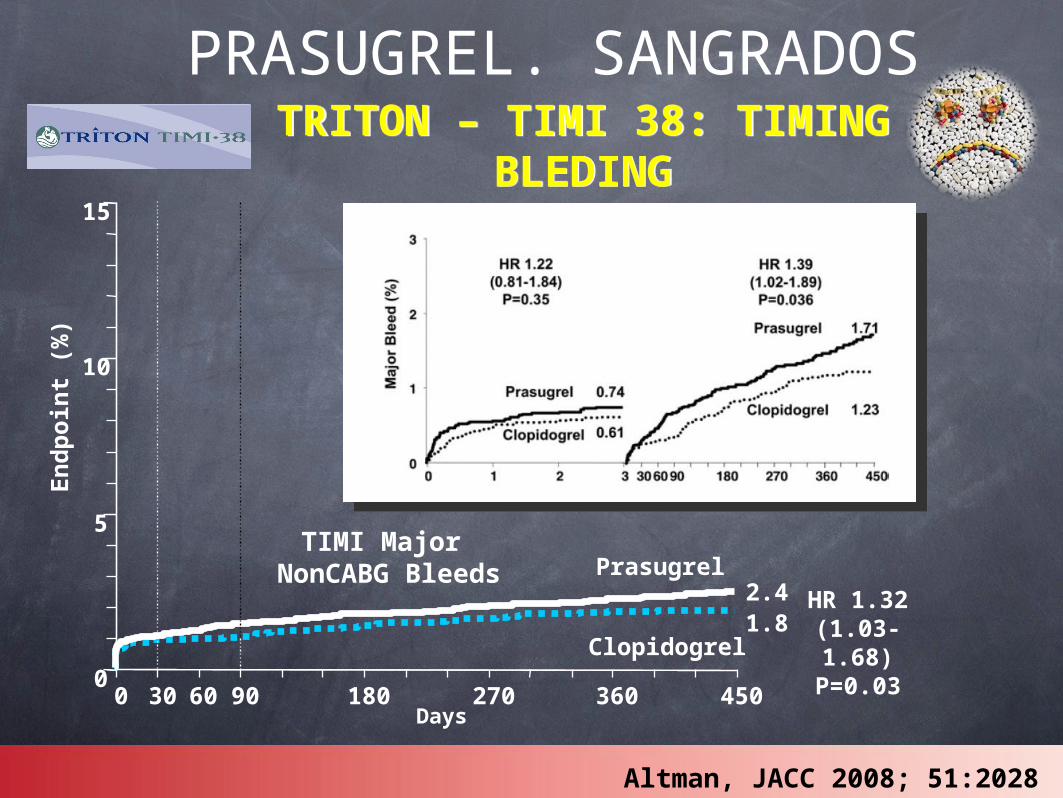
0
5
10
15
0 30 60 90 180 270 360 450Days
En
dp
oin
t (%
)
HR 1.32(1.03-1.68)
P=0.03
Prasugrel
Clopidogrel1.82.4
TIMI Major NonCABG Bleeds
Altman, JACC 2008; 51:2028
TRITON – TIMI 38: TIMING BLEDING
TRITON – TIMI 38: TIMING BLEDING
PRASUGREL. SANGRADOS
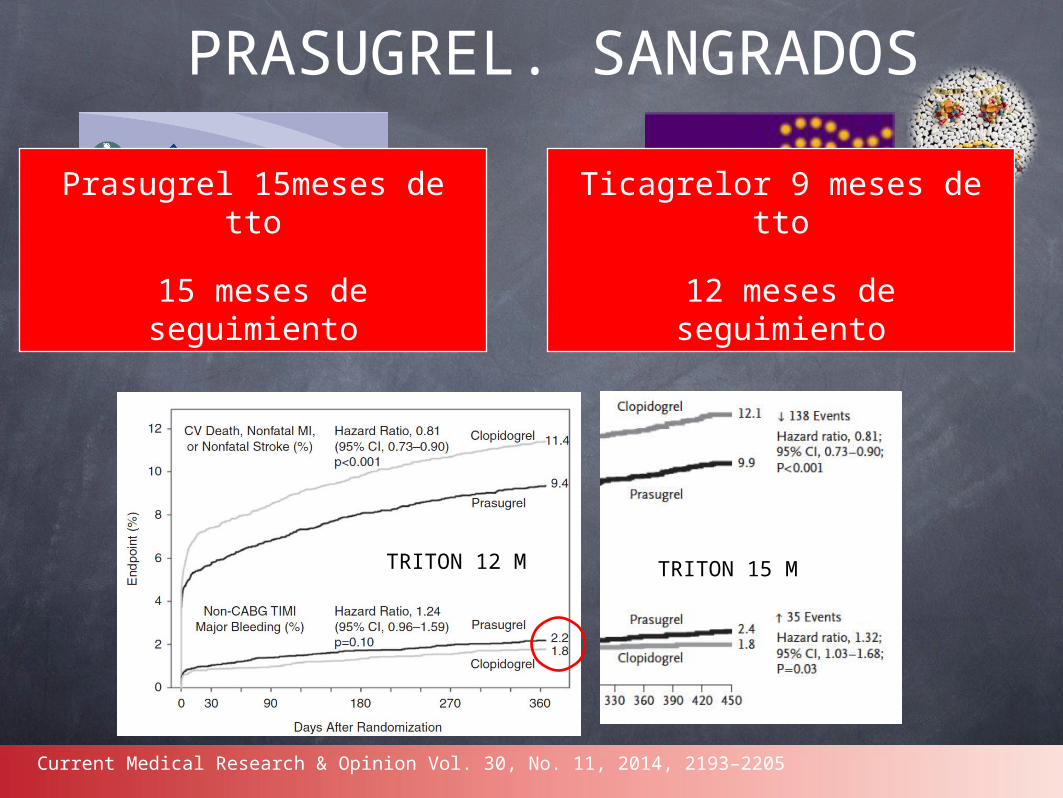
PRASUGREL. SANGRADOS
Prasugrel 15meses de tto
15 meses de seguimiento
Ticagrelor 9 meses de tto
12 meses de seguimiento
Current Medical Research & Opinion Vol. 30, No. 11, 2014, 2193–2205
TRITON 12 M TRITON 15 M
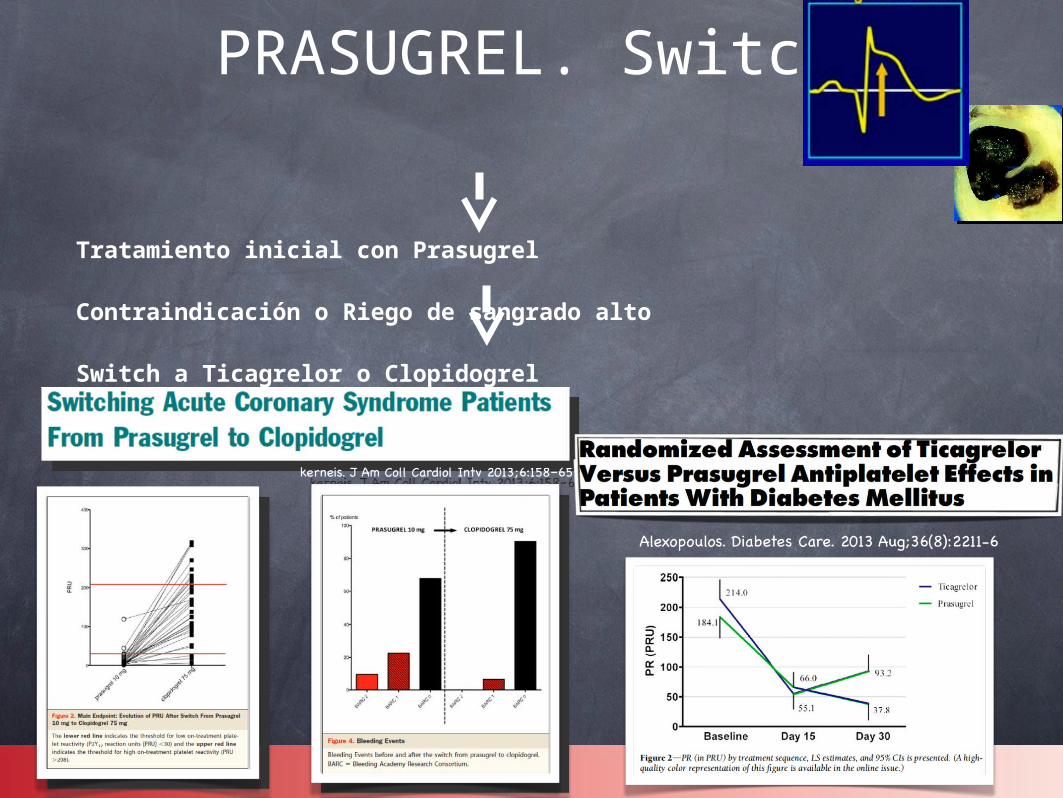
Tratamiento inicial con Prasugrel
Contraindicación o Riego de sangrado alto
Switch a Ticagrelor o Clopidogrel
PRASUGREL. Switch.

TICA-PRASU. Switch.

Switch. Normas generales.
PRASUGREL
CLOPIDOGREL: 75mg.
TICAGRELOR: 90 mg.
TICAGRELOR
CLOPIDOGREL: 300 mg.
PRASUGREL: 60 mg.

Tica vs Prasu. Adherencia al tto
Duración media de tratamiento – 14,5 mesesPérdida de seguimiento – 14 pacientes (0.1%)Discontinuación– prasugrel 2.5% y clopidogrel 1.4%
Wiviott SD et al. Am Heart J 2006;152(4):627-635

PRASUGREL vs TICAGRELOR.ADHERENCIA AL TRATAMIENTO
PLATO: 7,4% DE ABANDONO DE TICAGRELOR POR EFECTOS ADVERSOS
Abandono de DAPT en los primeros 12 meses aumenta el riesgo de eventos isquémicos.
TRITON: 2,5% DE ABANDONO DE PRASUGREL

Copago por parte del asegurado Efient 10 mg 28 comp
Ticagrelor 90 mg
56 comp
Diferencia Efient -
Ticagrelor
63,38 € 89,61 € -26,23 € Activos rentas <18.000€/año
40% 25,35 € 35,84 € -10,49 €
Activos con rentas entre 18.000€ - 100.000€/año
50% 31,69 € 44,81 € -13,12 €
Activos rentas >100.000€/año
60% 38,03 € 53,77 € -15,74 €
Aportación por el paciente por cada mes de tto antiagregante según el porcentaje de
copago que le correponda sobre el PVPIVA
PRASUGREL vs TICAGRELOR.€€€€€
PRASUGREL MÁS BARATO AL PACIENTE Y AL SISTEMA SANITARIO
Prasugrel como antiagregante único ICP
1ª.
Eficacia Pocos efectos adversos iniciales
Adherencia al tratamiento €€€€€




J. of Cardiovasc. Trans. Res. (2014) 7:91–100

The primary objective of this study is to test the hypothesis that ticagrelor is superior to prasugrel in ACS patients with planned invasive strategy. Primary efficacy endpoint is the composite of death, myocardial infarction, or stroke at 12 months after randomization.
1,895 patients in each group.
10 % incidence of the primary endpoint in the ticagrelor group [10], 12.9 % in the prasugrel group (22.5 % relative risk reduction with ticagrelor)
ISAR-REACT 5


0%
2%
4%
6%
8%
10%
12%
14%
16%
0 90 180 270 360 450Days after Randomization
0%
2%
4%
6%
8%
10%
12%
14%
16%
0 90 180 270 360 450Days after Randomization
End P
oint (
%)
0%
2%
4%
6%
8%
10%
12%
14%
16%
0 90 180 270 360 450Days after Randomization
0%
2%
4%
6%
8%
10%
12%
14%
16%
0 90 180 270 360 450Days after Randomization
End P
oint (
%)
CV Death/MI/Stroke — Clopidogrel — PrasugrelCV Death/MI/Stroke — Clopidogrel — Prasugrel
CV Death/Spontaneous MI/Stroke
Secondary PCISecondary PCI
14.2
9.6
Primary PCIPrimary PCI
15 m: HR 0.65 (0.46-0.93) p=0.02
30d: HR 0.51 (0.34-0.76) p=0.000830d HR 0.81 (0.60-1.09) p=0.17
15m: HR 0.89 (0.69-1.31) p=0.3
15 m P-interaction = 0.96
30d P-interaction = 0.68
11.6
10.3
8.4
6.5
CV Death/Spont. MI/Stroke — Clopidogrel — PrasugrelCV Death/Spont. MI/Stroke — Clopidogrel — Prasugrel
7.2
5.5
15 m: HR 0.75 (0.46-1.21) p=0.23
30d: HR 0.44 (0.22-0.88) p=0.0230d HR 0.53 (0.34-0.81) p=0.003
15m: HR 0.76 (0.56-1.03) p=0.08
Udell JA et al. JACC Cardiovasc Interv. 2014 ;7:604-12.





clopi.
farmacodinamia. disperse, rapid.
triton icp. plato icp y tto médico.
precio tica y prasu al mes.
abandono de tratamiento.
riesgo sangrado inicial. Riesgo de sangrado seguimiento. diferencia del seguimiento 9 meses, 15 meses.
diseño estudios. Diff, seguimiento, adherencia, plato tenía antecedente del triton.
Revisar el articulo de Steg del 2010. Mortalidad. Efectos pleiotropicos también dan disnea. Polimorfismos.