Embed Size (px)
Citation preview

www.arquivosonline.com.br Sociedade Brasileira de Cardiologia • ISSN-0066-782X • Volume 102, Nº 5, May 2014
EditorialTrajectories of Cardiovascular Health: Life Course Epidemiology
in Brazil
Special ArticleI Cardiovascular Prevention Guideline of the Brazilian Society of
Cardiology – Executive Summary
Original ArticlesPreclinical Study of a Biodegradable Polymer-based Stent with
Abluminal Sirolimus Release
Effects of Skeletonized versus Pedicled Radial Artery on Postoperative
Graft Patency and Flow
Does C-reactive Protein Add Prognostic Value to GRACE Score in
Acute Coronary Syndromes?
Relationship between Fibrosis and Ventricular Arrhythmias in Chagas
Heart Disease Without Ventricular Dysfunction
Impact of Psychotropic Drugs on QT Interval Dispersion in Adult Patients
Prevalence of Cardiovascular Risk Factors in Hemodialysis Patients –
The CORDIAL Study
LINE-1 Hypomethylation is Associated with the Risk of Coronary
Heart Disease in Chinese Population
Incidence of Ventricular Arrhythmias after Stem Cell Therapy in
Patients with Chagas Cardiomyopathy
Temporal Variation in the Prognosis and Treatment of Advanced Heart
Failure – Before and After 2000
NHETS − Necropsy Heart Transplantation Study
Review ArticleSystems Biology Applied to Heart Failure With Normal Ejection
Fraction
Letter to the EditorObesity and Abnormalities in Echocardiographic Parameters
Extracellular Matrix Turnover: a Balance between MMPs and their Inhibitors
Erratum
Eletronic Pages
Anatomopathological SessionCase 2/2014 – 51-Year Old Patient with Systemic Lupus
Erythematosus and Fever after Valve Replacement
Case ReportProlonged Cardiopulmonary Arrest Treated Successfully in the São
Paulo’s Subway
ViewpointIs Heart Team Fundamental to Aortic Stenosis Transcatheter Treatment?
Figure 3 – Cross-sectional views of porcine coronary arteries on day 28 after bare-metal stent implantation (Group I, left) and biodegradable polymer-coated stent with sirolimus elution on the abluminal surface (Group V) (right). Magnification 40X. Page: 438

Arquivos Brasileiros de Cardiologia - Volume 102, Nº 5, May 2014
REVISTA DA SOCIEDADE BRASILEIRA DE CARDIOLOGIA - Publicada desde 1948
Contents
Editorial
Trajectories of Cardiovascular Health: Life Course Epidemiology in BrazilLucia Campos Pellanda.....................................................................................................................................................................page 418
Special Article
I Cardiovascular Prevention Guideline of the Brazilian Society of Cardiology – Executive SummaryAntonio Felipe Simão, Dalton Bertolim Précoma, Jadelson Pinheiro de Andrade, Harry Correa Filho, José Francisco Kerr Saraiva, Gláucia Maria Moraes de Oliveira.....................................................................................................................................................................page 420
Original Articles
Coronary Angioplasty with and without Stent
Preclinical Study of a Biodegradable Polymer-based Stent with Abluminal Sirolimus ReleaseCelso Kiyochi Takimura, Carlos Augusto Homem M. Campos, Pedro Henrique Magualhães Craveiro Melo, Julliana Carvalho Campos, Paulo Sampaio Gutierrez, Thiago Francisco Costa Borges, Luciano Curado, Spero Penha Morato, Francisco Rafael Martins Laurindo, Pedro Alves Lemos Neto.....................................................................................................................................................................page 432
Heart Surgery - Adults
Effects of Skeletonized versus Pedicled Radial Artery on Postoperative Graft Patency and FlowRômulo C. Arnal Bonini, Rodolfo Staico, Mario Issa, Antoninho Sanfins Arnoni, Paulo Chaccur, Camilo Abdulmassih Neto, Jarbas Jackson Dinkhuysen, Paulo Paredes Paulista, Luiz Carlos Bento de Souza, Luiz Felipe P. Moreira.....................................................................................................................................................................page 441
Acute Coronary Artery Disease
Does C-reactive Protein Add Prognostic Value to GRACE Score in Acute Coronary Syndromes?Luis Cláudio Lemos Correia, Isis Vasconcelos, Guilherme Garcia, Felipe Kalil, Felipe Ferreira, André Silva, Ruan Oliveira, Manuela Carvalhal, Caio Freitas, Márcia Maria Noya-Rabelo.....................................................................................................................................................................page 449
Chagas’ Disease
Relationship between Fibrosis and Ventricular Arrhythmias in Chagas Heart Disease Without Ventricular DysfunctionEduardo Marinho Tassi, Marcelo Abramoff Continentino, Emília Matos do Nascimento, Basílio de Bragança Pereira, Roberto Coury Pedrosa.....................................................................................................................................................................page 456

Arquivos Brasileiros de Cardiologia - Volume 102, Nº 5, May 2014
Electrocardiography
Impact of Psychotropic Drugs on QT Interval Dispersion in Adult PatientsBruno de Queiroz Claudio, Marcelle Azevedo Nossar Costa, Filipe Penna, Mariana Teixeira Konder, Bruno Miguel Jorge Celoria, Luciana Lopes de Souza, Roberto Pozzan, Roberta Siuffo Schneider, Felipe Neves Albuquerque, Denilson Campos Albuquerque.....................................................................................................................................................................page 465
Epidemiology
Prevalence of Cardiovascular Risk Factors in Hemodialysis Patients – The CORDIAL StudyJayme Eduardo Burmeister, Camila Borges Mosmann, Veridiana Borges Costa, Ramiro Tubino Saraiva, Renata Rech Grandi, Juliano Peixoto Bastos, Luiz Felipe Gonçalves, Guido Aranha Rosito.....................................................................................................................................................................page 473
LINE-1 Hypomethylation is Associated with the Risk of Coronary Heart Disease in Chinese PopulationLi Wei, Shuchuan Liu, Zhendong Su, Rongchao Cheng, Xiuping Bai, Xueqi Li.....................................................................................................................................................................page 481
Heart Failure
Incidence of Ventricular Arrhythmias after Stem Cell Therapy in Patients with Chagas CardiomyopathyAdriana Sebba Barroso de Souza, Weimar Kunz Sebba Barroso Souza, Sandra Araujo Costa, Elis Marra de Moreira Freitas, Gustavo Carvalho, Luís Antônio Batista Sá, Salvador Rassi.....................................................................................................................................................................page 489
Temporal Variation in the Prognosis and Treatment of Advanced Heart Failure – Before and After 2000Carlos Henrique Del Carlo, Juliano Novaes Cardoso, Marcelo Eidi Ochia, Mucio Tavares de Oliveira Jr., José Antonio Franchini Ramires, Antonio Carlos Pereira-Barretto.....................................................................................................................................................................page 495
Cardiac Transplantation - Clinical
NHETS − Necropsy Heart Transplantation StudyThiago Ninck Valette, Silvia Moreira Ayub-Ferreira, Luiz Alberto Benvenuti, Victor Sarli Issa, Fernando Bacal, Paulo Roberto Chizzola, Germano Emilio Conceição Souza, Alfredo Inácio Fiorelli, Ronaldo Honorato Barros dos Santos, Edimar Alcides Bocchi.....................................................................................................................................................................page 505
Review Article
Systems Biology Applied to Heart Failure With Normal Ejection FractionEvandro Tinoco Mesquita, Antonio Jose Lagoeiro Jorge, Celso Vale de Souza Junior, João Paulo Pedroza Cassino.....................................................................................................................................................................page 510
Letter to the Editor
Obesity and Abnormalities in Echocardiographic ParametersRoberta Casanova Wilhelms, Eduardo Maffini da Rosa, Mauricio Lizott, Raphael Martin de Melo.....................................................................................................................................................................page 518
Extracellular Matrix Turnover: a Balance between MMPs and their InhibitorsEmre Yalcinkaya, Murat Celik, Baris Bugan.....................................................................................................................................................................page 519
Erratum
.....................................................................................................................................................................page 521

Arquivos Brasileiros de Cardiologia - Volume 102, Nº 5, May 2014
Arquivos Brasileiros de Cardiologia - Eletronic Pages
Anatomopathological Session
Case 2/2014 – 51-Year Old Patient with Systemic Lupus Erythematosus and Fever after Valve ReplacementWilma Noia Ribeiro, Alice Tatsuko Yamada, Paulo Sampaio Gutierrez..................................................................................................................................................................page e44
Case Report
Prolonged Cardiopulmonary Arrest Treated Successfully in the São Paulo’s SubwayRenan Gianotto-Oliveira, Maria Helena Favarato, Maria Margarita Gonzalez, Thiago Liguori, Sergio Timerman, Roberto Kalil Filho..................................................................................................................................................................page e52
Viewpoint
Is Heart Team Fundamental to Aortic Stenosis Transcatheter Treatment?Vitor Emer Egypto Rosa, Antônio Sergio de Santis Andrade Lopes, Tarso Augusto Duenhas Accorsi, Pedro Alves Lemos Neto, Pablo Maria Alberto Pomerantzeff, Flávio Tarasoutchi..................................................................................................................................................................page e55
* Indicate manuscripts only in the electronic version. To view them, visit: http://www.arquivosonline.com.br/2014/english/10205/edicaoatual.asp

Editorial BoardBrazilAguinaldo Figueiredo de Freitas Junior (GO)Alfredo José Mansur (SP)Aloir Queiroz de Araújo Sobrinho (ES)Amanda G. M. R. Sousa (SP)Ana Clara Tude Rodrigues (SP)André Labrunie (PR)Andrei Sposito (SP)Angelo A. V. de Paola (SP)Antonio Augusto Barbosa Lopes (SP) Antonio Carlos C. Carvalho (SP) Antônio Carlos Palandri Chagas (SP) Antonio Carlos Pereira Barretto (SP) Antonio Cláudio L. Nobrega (RJ) Antonio de Padua Mansur (SP)Ari Timerman (SP)Armenio Costa Guimarães (BA)Ayrton Pires Brandão (RJ)Beatriz Matsubara (SP)Brivaldo Markman Filho (PE)Bruno Caramelli (SP)Carisi A. Polanczyk (RS)Carlos Eduardo Rochitte (SP)Carlos Eduardo Suaide Silva (SP) Carlos Vicente Serrano Júnior (SP) Celso Amodeo (SP)Charles Mady (SP)Claudio Gil Soares de Araujo (RJ) Cláudio Tinoco Mesquita (RJ)Cleonice Carvalho C. Mota (MG)Clerio Francisco de Azevedo Filho (RJ)Dalton Bertolim Précoma (PR)Dário C. Sobral Filho (PE)Décio Mion Junior (SP)Denilson Campos de Albuquerque (RJ) Djair Brindeiro Filho (PE)Domingo M. Braile (SP)Edmar Atik (SP)Emilio Hideyuki Moriguchi (RS)
Enio Buffolo (SP)Eulogio E. Martinez Filho (SP) Evandro Tinoco Mesquita (RJ) Expedito E. Ribeiro da Silva (SP)Fábio Vilas-Boas (BA)Fernando Bacal (SP)Flávio D. Fuchs (RS) Francisco Antonio Helfenstein Fonseca (SP)Gilson Soares Feitosa (BA)Glaucia Maria M. de Oliveira (RJ)Hans Fernando R. Dohmann (RJ)Humberto Villacorta Junior (RJ)Ines Lessa (BA)Iran Castro (RS)Jarbas Jakson Dinkhuysen (SP)João Pimenta (SP)Jorge Ilha Guimarães (RS)José Antonio Franchini Ramires (SP)José Augusto Soares Barreto Filho (SE)José Carlos Nicolau (SP)José Lázaro de Andrade (SP)José Péricles Esteves (BA)Leonardo A. M. Zornoff (SP)Leopoldo Soares Piegas (SP)Lucia Campos Pellanda (RS)Luís Eduardo Rohde (RS)Luís Cláudio Lemos Correia (BA)Luiz A. Machado César (SP)Luiz Alberto Piva e Mattos (SP)Marcia Melo Barbosa (MG)Maria da Consolação Moreira (MG)Mario S. S. de Azeredo Coutinho (SC)Maurício I. Scanavacca (SP)Max Grinberg (SP)Michel Batlouni (SP)Murilo Foppa (RS)Nadine O. Clausell (RS)Orlando Campos Filho (SP)Otávio Rizzi Coelho (SP)
Otoni Moreira Gomes (MG)Paulo Andrade Lotufo (SP)Paulo Cesar B. V. Jardim (GO)Paulo J. F. Tucci (SP)Paulo R. A. Caramori (RS)Paulo Roberto B. Évora (SP)Paulo Roberto S. Brofman (PR)Pedro A. Lemos (SP)Protásio Lemos da Luz (SP)Reinaldo B. Bestetti (SP)Renato A. K. Kalil (RS)Ricardo Stein (RS)Salvador Rassi (GO)Sandra da Silva Mattos (PE)Sandra Fuchs (RS)Sergio Timerman (SP)Silvio Henrique Barberato (PR)Tales de Carvalho (SC)Vera D. Aiello (SP)Walter José Gomes (SP)Weimar K. S. B. de Souza (GO)William Azem Chalela (SP)Wilson Mathias Junior (SP)
Exterior
Adelino F. Leite-Moreira (Portugal)Alan Maisel (Estados Unidos)Aldo P. Maggioni (Itália)Cândida Fonseca (Portugal)Fausto Pinto (Portugal)Hugo Grancelli (Argentina)James de Lemos (Estados Unidos) João A. Lima (Estados Unidos)John G. F. Cleland (Inglaterra)Maria Pilar Tornos (Espanha)Pedro Brugada (Bélgica)Peter A. McCullough (Estados Unidos)Peter Libby (Estados Unidos)Piero Anversa (Itália)
Scientific Director Maria da Consolação Vieira Moreira
Chief Editor Luiz Felipe P. Moreira
Associated Editors
Clinical Cardiology José Augusto Barreto-Filho
Surgical Cardiology Paulo Roberto B. Evora
Interventionist Cardiology Pedro A. Lemos
Pediatric/Congenital Cardiology Antonio Augusto Lopes
Arrhythmias/Pacemaker Mauricio Scanavacca
Non-Invasive Diagnostic Methods Carlos E. Rochitte
Basic or Experimental Research Leonardo A. M. Zornoff
Epidemiology/Statistics Lucia Campos Pellanda
Arterial Hypertension Paulo Cesar B. V. Jardim
Ergometrics, Exercise and Cardiac Rehabilitation Ricardo Stein
First Editor (1948-1953) † Jairo Ramos
A JOURNAL OF SOCIEDADE BRASILEIRA DE CARDIOLOGIA - Published since 1948www.arquivosonline.com.br

PresidentAngelo Amato V. de Paola
Vice-PresidentSergio Tavares Montenegro
Financial DirectorJacob Atié
Scientific DirectorMaria da Consolação Vieira Moreira
Administrative DirectorEmilio Cesar Zilli
Assistance Quality DirectorPedro Ferreira de Albuquerque
Communication DirectorMaurício Batista Nunes
Information Technology DirectorJosé Carlos Moura Jorge
Government Liaison DirectorLuiz César Nazário Scala
Director of State and Regional AffairsAbrahão Afiune Neto
Cardiovascular Health Promotion Director - SBC/FuncorCarlos Costa Magalhães
Department DirectorEspecializados - Jorge Eduardo Assef
Research DirectorFernanda Marciano Consolim Colombo
Chief Editor of the Brazilian Archives of CardiologyLuiz Felipe P. Moreira
Special Advisor to the PresidencyFábio Sândoli de Brito
Adjunct Coordination
SBC Newsletter EditorNabil Ghorayeb e Fernando Antonio Lucchese
Continuing Education Coordination Estevão Lanna Figueiredo
Norms and Guidelines Coordination Luiz Carlos Bodanese
Governmental Integration Coordination Edna Maria Marques de Oliveira
Regional Integration Coordination José Luis Aziz
Presidents of State and Regional Brazilian Societies of Cardiology
SBC/AL - Carlos Alberto Ramos Macias
SBC/AM - Simão Gonçalves Maduro
SBC/BA - Mario de Seixas Rocha
SBC/CE - Ana Lucia de Sá Leitão Ramos
SBC/CO - Frederico Somaio Neto
SBC/DF - Wagner Pires de Oliveira Junior
SBC/ES - Marcio Augusto Silva
SBC/GO - Thiago de Souza Veiga Jardim
SBC/MA - Nilton Santana de Oliveira
SBC/MG - Odilon Gariglio Alvarenga de Freitas
SBC/MS - Mércule Pedro Paulista Cavalcante
SBC/MT - Julio César De Oliveira
SBC/NNE - Jose Itamar Abreu Costa
SBC/PA - Luiz Alberto Rolla Maneschy
SBC/PB - Catarina Vasconcelos Cavalcanti
SBC/PE - Helman Campos Martins
SBC/PI - João Francisco de Sousa
SBC/PR - Osni Moreira Filho
SBC/RJ - Olga Ferreira de Souza
SBC/RN - Rui Alberto de Faria Filho
SBC/RS - Carisi Anne Polanczyk
SBC/SC - Marcos Venício Garcia Joaquim
SBC/SE - Fabio Serra Silveira
SBC/SP - Francisco Antonio Helfenstein Fonseca
SBC/TO - Hueverson Junqueira Neves
Sociedade Brasileira de Cardiologia
Presidents of the Specialized Departaments and Study GroupsSBC/DA - José Rocha Faria Neto
SBC/DECAGE - Josmar de Castro Alves
SBC/DCC - José Carlos Nicolau
SBC/DCM - Maria Alayde Mendonça da Silva
SBC/DCC/CP - Isabel Cristina Britto Guimarães
SBC/DIC - Arnaldo Rabischoffsky
SBC/DERC - Nabil Ghorayeb
SBC/DFCVR - Ricardo Adala Benfati
SBC/DHA - Luiz Aparecido Bortolotto
SOBRAC - Luiz Pereira de Magalhães
SBCCV - Marcelo Matos Cascado
SBHCI - Helio Roque Figueira
SBC/DEIC - Dirceu Rodrigues Almeida
GERTC - Clerio Francisco de Azevedo Filho
GAPO - Danielle Menosi Gualandro
GEECG - Joel Alves Pinho Filho
GEECABE - Mario Sergio S. de Azeredo Coutinho
GECETI - Gilson Soares Feitosa Filho
GEMCA - Alvaro Avezum Junior
GECC - Mauricio Wanjgarten
GEPREC - Glaucia Maria Moraes de Oliveira
Grupo de Estudos de Cardiologia Hospitalar - Evandro Tinoco Mesquita
Grupo de Estudos de Cardio-Oncologia - Roberto Kalil Filho
GEEC - Cláudio José Fuganti
GECIP - Gisela Martina Bohns Meyer
GECESP - Ricardo Stein
GECN - Ronaldo de Souza Leão Lima
GERCPM - Artur Haddad Herdy

Arquivos Brasileiros de Cardiologia
Affiliated at the Brazilian Medical Association
Volume 102, Nº 5, May 2014Indexing: ISI (Thomson Scientific), Cumulated Index Medicus (NLM), SCOPUS,
MEDLINE, EMBASE, LILACS, SciELO, PubMed
The ads showed in this issue are of the sole responsibility of advertisers, as well as the concepts expressed in signed articles are of the sole responsibility of their
authors and do not necessarily reflect the views of SBC.
This material is for exclusive distribution to the medical profession. The Brazilian Archives of Cardiology are not responsible for unauthorized access to its contents and
that is not in agreement with the determination in compliance with the Collegiate Board Resolution (DRC) N. 96/08 of the National Sanitary Surveillance Agency
(ANVISA), which updates the technical regulation on Drug Publicity, Advertising, Promotion and Information. According to Article 27 of the insignia, "the advertisement or publicity of prescription drugs should be restricted solely and exclusively to health
professionals qualified to prescribe or dispense such products (...)".
To ensure universal access, the scientific content of the journal is still available for full and free access to all interested parties at:
www.arquivosonline.com.br.
SUPPORT
Commercial Department
Phone: (11) 3411-5500
E-mail: [email protected]
Editorial Production
SBC - Internal Publication Department
Graphic Design and DiagrammingSBC - Internal Design Department
PrintStamppa
Circulation1.500 copies
Address: Av. Marechal Câmara, 160 - 3º andar - Sala 330 20020-907 • Centro • Rio de Janeiro, RJ • Brasil
Phone.: (21) 3478-2700
E-mail: [email protected]
www.arquivosonline.com.br
SciELO: www.scielo.br

Editorial
Trajectories of Cardiovascular Health: Life Course Epidemiology in BrazilLucia Campos PellandaPrograma de Pós-graduação em Ciências da Saúde: cardiologia, Fundação Universitária de Cardiologia. Universidade Federal de Ciências da Saúde, Porto Alegre, RS - Brazil
KeywordsCardiovascular diseases / epidemiology; Life change events;
Risk factors; Periodicals as topic.
DOI: 10.5935/abc.20140065
Cardiovascular epidemiology has advanced enormously in the study of risk factors for atherosclerosis1, as evidenced by publications in Arquivos Brasileiros de Cardiologia (ABC) in the last years2-4.
Based on this information, it is possible to explore new hypotheses and, therefore, new frontiers for prevention. The different perspectives for the study of these risk factors include the life course epidemiology. This perspective considers that the onset of the disease may occur long before the establishment of traditional risk factors in adulthood. Thus, health and diseases can be considered as a result of long-term effects of exposure to different factors throughout the various stages of life, including intrauterine life, childhood, adolescence and adulthood5.
This significantly increases the complexity of analysis6, but also adds dimensions previously little explored in epidemiology and cardiovascular prevention. A basic concept within this line of epidemiological interpretation is that of critical or sensitive periods, that is, the idea that stimulus acting for a certain critical period of development may bring long-lasting consequences on the structure or function of organs. For example, the intrauterine period in which tissues and organs are forming, is critical for the establishment of a risk profile for the rest of the course of life. Metabolic adaptations of the fetus occurred in this period could persist for the rest of life, thus increasing the risk of chronic diseases such as coronary artery disease, diabetes and obesity during adulthood. This process has been called intrauterine programming of chronic diseases7.
The ABC have been publishing interesting articles on this topic, providing insights into the discussions that have been occurring in the international arena8-10.
In a study carried out in Goiânia11, the authors compared the pressures measured by ABPM, of a group of children with low birth weight with those with adequate birth weight, observing that those with underweight had higher blood pressure and abnormal circadian rhythm of blood pressure with reduced nocturnal dipping.
On the other hand, Souza et al.12 studied the association between birth weight and cardiovascular risk factors in adolescents in Salvador, and observed two and a half higher prevalence of obesity and three times higher blood pressure in the group with high birth weight compared to the normal weight group.
These apparently conflicting findings may actually represent a U-shaped curve, in which both low weight and high weight would represent risk over normal weight at birth. In observational studies, newborns weighing less than 2,500 g had a higher incidence of cardiovascular diseases, hypertension and atherosclerosis – and glucose intolerance, – type II diabetes or metabolic syndrome in adulthood. – Babies with birth weight higher than 4 kg, regardless of gestational age or gender, have abnormal metabolism of carbohydrates and lipids associated with later development of obesity, diabetes and dyslipidemia13-15.
Besides the nonlinear association, there are many ways by which intrauterine factors can influence the pattern of disease in later stages. These effects may interact with other stimuli that occur in other periods, undergoing changes throughout life. Therefore, for example, birth weight considered in isolation would not be enough to explain the CAD. It is necessary to consider the relationship between this marker and the events following the moment of birth, such as the rapid recovery of growth in early childhood, that may further promote increased risk16,17.
Therefore, the life course model supports studies on initial exposures and but their potential interaction with other intermediate factors. Gaining acquaintance with this sequence of events and with the idea of critical periods has important consequences in the adoption of preventive strategies, because it helps identify periods of increased need for intervention and helps consider social inequality in health as factors that affect the entire life cycle of many generations5.
The study of Rio de Janeiro18 evaluated the blood pressure of adolescents and, again, the same individuals 18 years later. Adolescents with abnormal blood pressure in the first assessment presented higher average weight, insulin, leptin, apolipoprotein B100 and A1, the highest prevalence of overweight, obesity, increased waist circumference and hypertension in the group with normal blood pressure in adolescence. Adolescence is a phase that deserves special attention. Good nutrition during this phase permanently affects the individual’s life, since in this phase, 25% of adult height and 50% of body mass are acquired. Therefore, it is an important phase for weight control and acquisition of good eating habits.
Mailing Address: Lucia Campos Pellanda •Instituto de Cardiologia / Fundação Universitária de Cardiologia (IC-FUC).Endereço: Avenida Princesa Isabel, 370 / 3º andar, Unidade de Pesquisa. Porto Alegre, Rio Grande do Sul - Brazil. Postal Code: 90620-000.e-mail: [email protected]
418

Editorial
Trajectories of cardiovascular health
Arq Bras Cardiol. 2014; 102(5):418-419
Another interesting study published in ABC19 evaluated individuals at three different times in life. Adults diagnosed with metabolic syndrome presented, as early as in adolescence, significantly higher values for weight, waist circumference and body mass index. This fact has important implications for prevention, since early detection of these risk factors can mean significant benefit in the future20,21.
The aThe adoption of a life course model, therefore, has the potential to significantly change the paradigm
of prevention of cardiovascular diseases, of the current emphasis on control of risk factors in adulthood to a broader approach to prevention of risk factors per se throughout the course of life, including childhood and adolescence. Further Brazilian studies, including potential mechanisms, such as gene expression22, and interactions among the phases of life, body composition and environment23 may add evidence to this set, opening new possibilities of intervention in our community.
1. Schmidt MI, Duncan BB, Azevedo e Silva G, Menezes AM, Monteiro CA, Barreto SM, et al. Chronic non-communicable diseases in Brazil: burden and current challenges. Lancet. 2011;377(9781):1949-61.
2. Fuchs SC, Biolo A, Polanczyk CA. Cardiovascular epidemiology: the legacy of sound national and international studies. Arq Bras Cardiol. 2013;101(2):98-100.
3. Evora PR, Nather JC, Rodrigues AJ. Prevalencia das doenças cardíacas ilustrada em 60 anos dos Arquivos Brasileiros de Cardiologia. Arq Bras Cardiol. 2014;102(1):3-9.
4. Moreira LF. Os Arquivos Brasileiros de Cardiologia e a divulgação da pesquisa em ciencias cardiovasculares no Brasil. Arq Bras Cardiol. 2014;102(1):1-2.
5. Ben-Schlomo Y, Kuh D. A life course approach to chronic disease epidemiology: conceptual models, empirical challenges and interdisciplinary perspectives. Int J Epidemiol. 2002;31(2):285-93.
6. Davey-Smith G, Hart C. Life-course socioeconomic and behavioral influences on cardiovascular mortality: the collaborative study. Am J Public Health. 2002;92(8):1295-8.
7. Barker DJ. The origins of the developmental origins theory. J Intern Med. 2007;261(5):412-7.
8. Desai M, Beall M, Ross MG. Developmental origins of obesity: programmed adipogenesis. Curr Diab Rep. 2013;13(1):27-33.
9. Hallal PC, Dumith SC, Ekelund U, Reichert FF, Menezes AM, Victora CG, et al. Infancy and childhood growth and physical activity in adolescence: prospective birth cohort study from Brazil. Int J Behav Nutr Phys Act. 2012;9:82.
10. Schilithz AO, da Silva CM, Costa AJ, Kale PL. Ecological analysis of the relationship between infant mortality and cardiovascular disease mortality at ages 45-69 in the Brazilian 1935 birth cohort. Prev Med. 2011;52(6):445-7.
11. Salgado CM, Jardim PC, Teles FB, Nunes MC. Baixo peso ao nascer como marcador de alterações na monitorização ambulatorial da pressão arterial. Arq Bras Cardiol. 2009;92(2):107-21.
12. Sousa MA, Guimarães IC, Daltro C, Guimarães AC. Associação entre peso de nascimento e fatores de risco cardiovascular em adolescentes. Arq Bras Cardiol. 2013;101(1):9-17.
13. Victora CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, et al. Maternal and Child Undernutrition Study Group. Maternal and child
undernutrition: consequences for adult health and human capital. Lancet. 2008;371(9609):340-57. Erratum in Lancet. 2008;371(9609):302.
14. Schilithz AO, Silva CM, Costa AJ, Kale PL. Ecological analysis of the relationship between infant mortality and cardiovascular disease mortality at ages 45-69 in the Brazilian 1935 birth cohort. Prev Med. 2011;52(6):445-7.
15. Pereira JA, Rondo PH, Lemos JO, Pacheco de Souza JM, Dias RS. The influence of birthweight on arterial blood pressure of children. Clin Nutr. 2010;29(3):337-40.
16. Dulloo AG. Thrifty energy metabolism in catch-up growth trajectories to insulin and leptin resistance. Best Pract Res Clin Endocrinol Metab. 2008;22(1):155-71.
17. Berends LM, Fernandez-Twinn DS, Martin-Gronert MS, Cripps RL, Ozanne SE. Catch-up growth following intra-uterine growth-restriction programmes an insulin-resistant phenotype in adipose tissue. Int J Obes (Lond). 2013;37(8):1051-7.
18. Campana EM, Brandão AA, Pozzan R, Magalhães ME, Fonseca FL, Pizzi OL, et al. Pressão arterial na adolescencia, adipocinas e inflamação no adulto jovem. Estudo do Rio de Janeiro. Arq Bras Cardiol. 2014;102(1):60-9.
19. Oliveira RM, Franceschini Sdo C, Rosado GP, Priore SE. Influence of prior nutritional status on the development of the metabolic syndrome in adults. Arq Bras Cardiol. 2009 Feb;92(2):101-12.
20. Reilly J J Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. International Journal of Obesity 35, 891-898
21. Giuliano ICB, Caramelli B, Pellanda L, Duncan B, Mattos S, Fonseca FAH et al.. I Diretriz de Prevenção da Aterosclerose na Infância e na Adolescencia. Arq. Bras. Cardiol. 2005, 85(6): 3-36.
22. Lima-Leopoldo Ana Paula, Leopoldo André Soares, Silva Danielle Cristina Tomaz, Nascimento André Ferreira do, Campos Dijon Henrique Salomé de, Luvizotto Renata de Azevedo Melo et al . Influencia de prolongados períodos de obesidade sobre a expressão genica miocárdica. Arq. Bras. Cardiol 2013; 100 (3): 229-237.
23. Bertaso Angela Gallina, Bertol Daniela, Duncan Bruce Bartholow, Foppa Murilo. Epicardial fat: definition, measurements and systematic review of main outcomes. Arq. Bras. Cardiol2013; 101(1): e18-e28.
References
419

Special Article
I Cardiovascular Prevention Guideline of the Brazilian Society of Cardiology – Executive SummaryAntonio Felipe Simão, Dalton Bertolim Précoma, Jadelson Pinheiro de Andrade, Harry Correa Filho, José Francisco Kerr Saraiva, Gláucia Maria Moraes de OliveiraSociedade Brasileira de Cardiologia (SBC) − Brazil
KeywordsCardiovascular Diseases/prevention & control; Risk
Factors; Socioeconomic Factors; Primary Prevention; Health Promotion; Cardiovascular Diseases/guidelines.
Mailing Address: Gláucia Maria Moraes de Oliveira •Visconde de Pirajá 330/1114. Postal Code 22410-000, Rio de Janeiro, RJ – Brazil.E-mail: [email protected]; [email protected] received January 29, 2014; revised manuscript January 30, 2014; accepted January 30, 2014.
DOI: 10.5935/abc.20140067
* To access the complete document with references requested access the link: http://publicacoes.cardiol.br/consenso/2013/Diretriz_Prevencao_Cardiovascular.aspIntroduction
Table 1 – Criteria to identify patients at high risk for coronary events (phase 1)
Atherosclerotic coronary artery, cerebrovascular or obstructive peripheral diseases with clinical manifestations (cardiovascular events) and still in the subclinical form, documented by use of diagnostic methodology;
Arterial revascularization procedures;
Type 1 and type 2 diabetes mellitus;
Chronic kidney disease.
IntroductionBrazil currently faces a major health challenge: the
pandemic scenario of cardiovascular morbidity and mortality. According to Brazilian Health Ministry data, 326,000 deaths due to cardiovascular diseases (CVD) occurred in 2010, corresponding to approximately 1,000 deaths/day, 200,000 deaths due exclusively to ischemic heart and cerebrovascular diseases, reflecting a gloomy scenario far from the minimally acceptable control.
This current scenario can be attributed to many reasons, such as the insufficiency and inadequacy of public health policies for CVD prevention, leading to the well-known lack of infrastructure in primary health care, hindering the fight against preventable affections, mainly in the neediest areas.
In addition, it is worth mentioning the well-known sociocultural factors, such as the excessive consumption of high-caloric foods in association with physical inactivity, and, consequently, the development of obesity and diabetes, and excessive salt intake. Those factors contribute to the development of arterial hypertension, being decisive to the high prevalence of CVD and no opportunity to provide instructions on lifestyle changes.
The medical societies, in partnership with governments and universities, have endeavored to elaborate valuable documents containing strategic plans of CVD prevention and fight. However, simple and objective guidelines, which can be easily accessed and managed by health care personnel, are required to implement that which has been long discussed by specialists and scientists, although with modest results.
For the first time, guidelines and consensus documents, most of which already published in several other guidelines of specialties, have been gathered in a single document to provide the clinician with easy access to the recommendations for primary and secondary CVD prevention. For that, the
Brazilian Society of Cardiology (SBC) has gathered specialized physicians with large experience in preventive actions to elaborate the present document.
Chapter 1 presents the cardiovascular risk stratification for atherosclerosis prevention and treatment. In this chapter, the authors discuss questions such as acute coronary event as the first manifestation of atherosclerotic disease in at least half of the individuals with that complication. Thus, the identification of predisposed asymptomatic individuals is crucial to the effective prevention with correct definition of therapeutic goals, especially the criteria to identify high-risk patients (Table 1). The authors discuss the so-called risk scores, through which the overall risk is calculated, enabling the clinician to quantify and qualify the patients’ individual risk, for both women (Tables 2 and 3) and men (Tables 4 and 5). The combination of those different scores allow the clinician to better estimate the risk, stratifying it gradually: presence of significant atherosclerotic disease or its equivalents; calculation of risk score; aggravating factors (Chart 1) and risk stratification based on lifespan. The authors propose a simplified algorithm for cardiovascular risk stratification, which is exemplified in Figure 1. The recommendations listed as class I and level of evidence A are few, because the other recommendations still require more comprehensive studies with long-term follow-up (Table 6).
Chapter 2 approaches tobacco smoking, the major avoidable risk factor. It is known that 50% of the deaths of smokers, most of which caused by CVD, could be prevented with smoking cessation. In this chapter, the authors discuss preventive measures for tobacco use. Data from the Surveillance of Risk Factors and Protection Against Chronic Diseases via Telephone Inquiry (VIGITEL, in Portuguese), disclosed on April 2012, revealed advances in tobacco use control in Brazil, with 14.8% of smokers older than 18 years. They also approached the primordial prevention of tobacco use, enumerating factors that contribute to smoking initiation and proposing practical strategies for its combat. In addition, the authors discuss techniques to treat the psychological
420

Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Table 2 – Scoring according to overall risk for women
Points Age (years) HDL-C TC SBP (untreated) SBP (treated) Smoking Diabetes
-3 < 120
-2 60+
-1 50-59 < 120
0 30-34 45-49 < 160 120-129 No No
1 35-44 160-199 130-139
2 35-39 < 35 140-149 120-129
3 200-239 130-139 Yes
4 40-44 240-279 150-159 Yes
5 45-49 280+ 160+ 140-149
6 150-159
7 50-54 160+
8 55-59
9 60-64
10 65-69
11 70-74
12 75+
Points Total
HDL-C: high-density lipoprotein cholesterol; TC: total cholesterol; SBP: systolic blood pressure
dependence of smokers with general and specific behavioral approaches. Furthermore, this chapter presents instruments to help to assess and understand the patient’s profile by using universally accepted scales, such as Prochaska and Di Clemente’s and Fagerström’s. Finally, the authors
approach, in a practical way, pharmacological treatment strategies of tobacco use, such as nicotine replacement with bupropion and varenicline, in addition to second-line drugs (nortriptyline), with their possible associations. Table 7 summarizes the classification of recommendation and level of evidence of those strategies.
Chapter 3 discusses the real benefits of primary and secondary CVD prevention, with evident confirmation of diet, supplements and vitamins, aiming at helping the clinician to guide the community in choosing and consuming those products. In addition to supplements, omega-3 fatty acids, vitamins B, C, D and E, folates, alpha-linolenic acids and carotenoids were assessed (Tables 8).
Chapter 4 approaches obesity, overweight and nutrition transition, as well as the consequences for cardiovascular morbidity and mortality of their association with arterial hypertension, dyslipidemias, type 2 diabetes, osteoarthritides and cancer. Tables 9 and 10 list the classification of recommendation and levels of evidence for primary and secondary prevention.
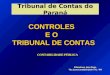
Chapter 5 summarizes the recommendations for systemic arterial hypertension (SAH), emphasizing its importance for the development of several pathologies, such as coronary artery disease, heart failure, cerebrovascular disease and chronic kidney disease. Table 11 shows the routine initial assessment of hypertensive patients, and Table 12, its complementary assessment. Therapeutic decision should consider the patient’s additional risk. Table 13 shows nonpharmacological measures, which are listed according to their recommendation class and level of evidence. Figure 2
Table 3 – Overall cardiovascular risk in 10 years for women
Points Risk (%) Points Risk (%)
≤-2 <1 13 10.0
-1 1.0 14 11.7
0 1.2 15 13.7
1 1.5 16 15.9
2 1.7 17 18.5
3 2.0 18 21.6
4 2.4 19 24.8
5 2.8 20 28.5
6 3.3 21+ > 30
7 3.9
8 4.5
9 5.3
10 6.3
11 7.3
12 8.6
421

Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Table 4 – Scoring according to overall risk for men
Points Age (years) HDL-C TC SBP (untreated) SBP (treated) Smoking Diabetes
-2 60+ < 120
-1 50-59 < 120
0 30-34 45-49 < 160 120-129 No No
1 35-44 160-199 130-139
2 35-39 < 35 200-239 140-159 120-129
3 240-279 160+ 130-139 Yes
4 280+ 140-159 Yes
5 40-44 160+
6 45-49
7
8 50-54
9
10 55-59
11 60-64
12 65-69
13
14 70-74
15 75+
Points Total
HDL-C: high-density lipoprotein cholesterol; TC: total cholesterol; SBP: systolic blood pressure
Table 5 – Overall cardiovascular risk in 10 years for men
Points Risk (%) Points Risk (%)
≤-3 or less <1 13 15.6
-2 1.1 14 18.4
-1 1.4 15 21.6
0 1.6 16 25.3
1 1.9 17 29.4
2 2.3 18+ > 30
3 2.8
4 3.3
5 3.9
6 4.7
7 5.6
8 6.7
9 7.9
10 9.4
11 11.2
12 13.2
shows the algorithm of pharmacological treatment based on the patients’ hypertension stages. Monotherapy can be initiated with any drug class, but SAH control is only achieved in one-third of the cases with that strategy. Chart 2 shows the goals to be met according to patients’ characteristics.
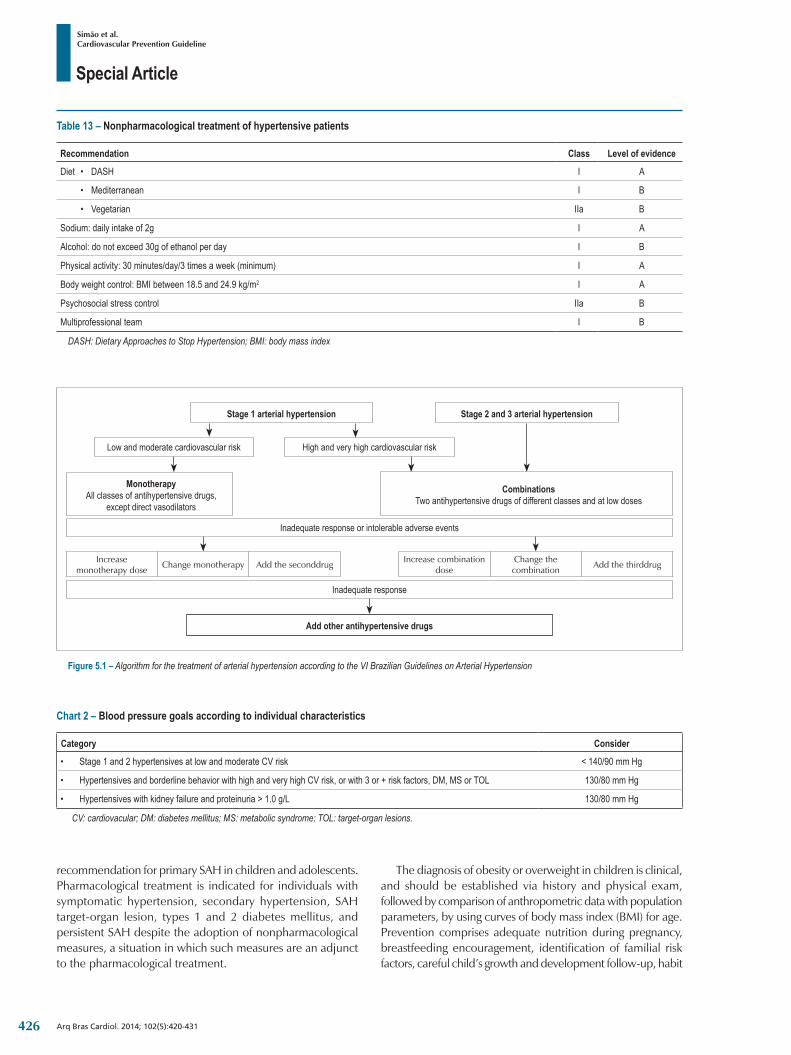
Chapter 6 was aimed at discussing dyslipidemias, in an attempt to, after stratifying the individual risk, establish the therapeutic goals according to the overall risk level (low, intermediate or high). Specific goals are listed for high- and intermediate-risk patients. Patients at low cardiovascular risk should have their goals individualized at their clinician’s discretion and according to lipid reference values. Table 14 presents strategies for lifestyle changes. Table 15 lists the pharmacological alternatives based on their recommendation class and level of evidence.
Chapter 7 discusses diabetes, emphasizing its high prevalence in the adult population, up to 13.5% in some municipalities, which could represent a current population of 17 million individuals with diabetes. Those numbers are increasing due to factors such as population growth and aging, and increasing urbanization, sedentary lifestyle and obesity. This important chapter discusses essential measures for prevention, such as lifestyle changes (Table 16).
422

Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Chart 1 – Aggravating risk factors
• Family history of early coronary artery disease (male first-degree relative < 55 years-old or female first-degree relative < 65 years-old);• Criteria of metabolic syndrome according to the International Diabetes Federation;
• Microalbuminuria (30-300 mg/min) or macroalbuminuria (>300 mg/min);• Left ventricular hypertrophy;• High-sensitivity C-reactive protein > 3 mg/L;• Evidence of subclinical atherosclerotic disease: carotid stenosis/thickening > 1mm coronary calcium score > 100 or > 75th percentile for age or sex ankle-brachial test < 0.9
Table 6 – Classification of recommendation and level of evidence for risk stratification in cardiovascular prevention
Recommendation Class Level of evidence• Clinical manifestations of atherosclerotic disease or equivalents (type 1 or 2 diabetes mellitus and significant chronic kidney disease),
even in primary prevention, have a risk > 20% in 10 years of new cardiovascular events or of the first cardiovascular event I A
• Patients classified as intermediate-risk with a family history of early cardiovascular disease will be reclassified as high-risk IIa B
• Men with a calculated risk for any of the events cited ≥5% and ≤20% and women with that calculated risk ≥5% and ≤10% are considered intermediate-risk I A
• Men with a calculated risk >20% and women with that calculated risk >10% are considered high-risk I A
• For individuals at intermediate risk, aggravating factors should be used, and when present (at least one) reclassify the individual as high-risk IIa B
• Use of risk according to lifespan for low- and intermediate-risk individuals aged >45 years IIa B
Figure 1 – Algorithm for cardiovascular risk stratification. ORS: overall risk stratification; CAD: coronary artery disease; CV: cardiovascular.
ORS < 5% in men and women ORS ≥ 5% and ≤ 20% in men or ≤ 10% in women
HIGH RISKINTERMEDIATE RISK
HIGH RISK
If risk based on lifespan• > 39% for men or• > 20.2 % for women,• High risk of CV events
If family history of early CAD, reclassify Use aggravating: if an aggravating factor is present
LOW RISK INTERMEDIATE RISK
Risk based on lifespan
High-risk condition present or ORS > 20% in men and > 10% in women
Chapter 8 provides a review on metabolic syndrome. There are several versions of the metabolic syndrome definition, and this guideline adopted the joint position paper of several international organizations on the topic. The authors discuss the epidemiological aspects of its
prevalence, approaching different population groups, and aspects related to cardiovascular and metabolic risks, in addition to metabolic syndrome risk factors. Table 17 shows the recommendation class and level of evidence of interventions in metabolic syndrome.
423

Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Table 7 – Classification of recommendation and level of evidence for the treatment of smoking in cardiovascular prevention
Recommendation Class Level of evidence
• Smoking is an independent risk factor for cardiovascular disease, therefore should be avoided I B
• Passive tobacco exposure increases the risk for cardiovascular diseases and should be avoided I B
• Pharmacological treatment of smoking I A
Nicotine replacement I A
Bupropion hydrochloride I A
Varenicline tartrate I A
Table 8 – Summary of the recommendations for not using vitamin supplements to prevent cardiovascular disease (CVD) and recommendations for the consumption of products rich in omega-3 fatty acids
Indication Class Level of evidence
• There is no evidence that supplementation of vitamin A or beta-carotene is beneficial to the primary or secondary prevention of CVD III A
• Supplementations of vitamin B and folic acid are not effective to the primary or secondary prevention of CVD III A
• There is no evidence that supplementation of vitamin C is beneficial to CVD prevention, progression or mortality II A
• Supplementation of vitamin D is not recommended to CVD prevention in individuals with normal serum levels of that vitamin. Likewise, there is no evidence that supplementation in individuals with deficiency of that vitamin will prevent CVD. III C
• Marine omega-3 supplementation (2-4g/day) or even at higher doses should be recommended for severe hypertriglyceridemia (>500mg/dL), at risk for pancreatitis, refractory to nonpharmacological measures and drug treatment I A
• At least two fish-based meals per week, as part of a healthy diet, are recommended to reduce the cardiovascular risk. That is particularly recommended for high-risk individuals, such as those with previous myocardial infarction. I B
• Supplementation of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) is not recommendedfor individuals at risk for cardiovascular disease undergoing evidence-based preventive treatment. III A
• The consumption of polyunsaturated omega-3 fatty acids of vegetable origin, as part of a healthy diet, should be recommended to reduce the cardiovascular risk, although the real benefit of that recommendation is arguable and the evidence is inconclusive. IIb B
• Alpha-linolenic acid (ALA) supplementation is not recommended for cardiovascular disease prevention. III B
Chapter 9 discusses the role played by physical activity, physical exercise and sports in CVD prevention. Physically active individuals tend to be healthier and have better quality of life and longer life expectancy. Table 18 lists the recommended physical exercise levels. In addition, the risks of physical activity are approached, as well as the basic principles for exercise prescription and strategies to encourage referral, implementation and adherence.
Chapter 10 discusses psychosocial factors in CVD prevention. Beginning with the definition of the concept, the chapter discusses the psychosocial conditions frequently associated with cardiovascular risk, such as low socioeconomic status, lack of social support, stress at work place and family life, depression, anxiety, hostility and type D personality. In addition, it assesses the recommendation class and level of evidence of approaching the psychosocial factors in
Table 9 – Summary of the recommendations for obesity and overweight in cardiovascular disease primary prevention
Indication Class Level of evidence
• Three healthy meals (breakfast, lunch and dinner) and two snacks per day II A
• Read food labels and choose those with the lowest amounts of trans fats II A
• Avoid sodas and industrialized juices, cakes, cookies and stuffed cookies, sweet desserts and other sweet treats I A
• Prefer having water between meals II A
• Exercise at least 30 minutes per day, everyday I A
• Individuals with a tendency to obesity or with a familial trend should exercise moderately 45-60 minutes per day; those previously obese, who lost weight, should exercise 60-90 minutes to prevent regaining weight I A
• Avoid the excessive consumption of alcoholic beverages I A
424

Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Table 10 – Summary of the recommendations for obesity and overweight in cardiovascular disease secondary prevention
Indication Class Level of evidence
• Dietary caloric reduction of approximately 500 kcal/day I A
• Intensification of physical activity, such as walking, biking, swimming, aerobic exercises, 30-45 minutes, 3 to 5 times a week. I A
• Reduce sedentary activities, such as being seated for long periods watching TV, at computers or playing video games I B
• Encourage healthy eating for children and adolescents I B
• Sibutramine for weight loss in patients with cardiovascular disease III B
• Bariatric surgery for selected patients I B
Table 11 – Routine initial assessment of the hypertensive patient
Recommendation Class Level of evidence
• Urinalysis I C
• Serum potassium I C
• Serum creatinine I B
• Estimated glomerular filtration rate I B
• Fasting glycemia I C
• Total cholesterol, HDL-C, serum triglycerides I C
• Serum uric acid I C
• Conventional electrocardiogram I B
HDL-C: high-density lipoprotein cholesterol
Table 12 – Complementary assessment of hypertensive patients
Recommendation Class Level of evidence
Chest X-ray IIa C
Echocardiography: • stage 1 and 2 hypertensives without LVH on ECG IIa C
• hypertensives with clinical suspicion of HF I C
Microalbuminuria: • hypertensives and diabetic individuals I A
• hypertensives with metabolic syndrome I C
• hypertensives with 2 or + risk factors I C
Carotid ultrasound IIa B
Treadmill test when coronary artery disease is suspected IIa C
Glycosylated hemoglobin IIa B
Pulse wave velocity IIb C
LVH: left ventricular hypertrophy; ECG: electrocardiogram; HF: heart failure
primary prevention (Table 19) and for adherence (Table 20) by using cognitive-behavioral methods and indicating the ‘ten strategic steps’ to improve counseling for behavioral changes. Interventions on depression, anxiety and distress are also proposed as potential tools for adherence to preventive strategies (Chart 3), which can also be improved with the simple measures.
Chapter 11 approaches dyslipidemia, obesity and SAH in childhood and adolescence. Brazilian population studies have shown a 10%-35% prevalence of dyslipidemia in children and adolescents. Table 21 shows the reference values for lipids and lipoproteins in those age groups.
Table 22 shows the classification of SAH for children and adolescents. Changes in lifestyle are the initial therapeutic
425
Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Table 13 – Nonpharmacological treatment of hypertensive patients
Recommendation Class Level of evidence
Diet • DASH I A
• Mediterranean I B
• Vegetarian IIa B
Sodium: daily intake of 2g I A
Alcohol: do not exceed 30g of ethanol per day I B
Physical activity: 30 minutes/day/3 times a week (minimum) I A
Body weight control: BMI between 18.5 and 24.9 kg/m2 I A
Psychosocial stress control IIa B
Multiprofessional team I B
DASH: Dietary Approaches to Stop Hypertension; BMI: body mass index
Figure 5.1 – Algorithm for the treatment of arterial hypertension according to the VI Brazilian Guidelines on Arterial Hypertension
Stage 1 arterial hypertension Stage 2 and 3 arterial hypertension
Low and moderate cardiovascular risk High and very high cardiovascular risk
MonotherapyAll classes of antihypertensive drugs,
except direct vasodilators
CombinationsTwo antihypertensive drugs of different classes and at low doses
Inadequate response or intolerable adverse events
Increase monotherapy dose Change monotherapy Add the seconddrug Increase combination
doseChange the combination Add the thirddrug
Inadequate response
Add other antihypertensive drugs
Chart 2 – Blood pressure goals according to individual characteristics
Category Consider
• Stage 1 and 2 hypertensives at low and moderate CV risk < 140/90 mm Hg
• Hypertensives and borderline behavior with high and very high CV risk, or with 3 or + risk factors, DM, MS or TOL 130/80 mm Hg
• Hypertensives with kidney failure and proteinuria > 1.0 g/L 130/80 mm Hg
CV: cardiovacular; DM: diabetes mellitus; MS: metabolic syndrome; TOL: target-organ lesions.
recommendation for primary SAH in children and adolescents. Pharmacological treatment is indicated for individuals with symptomatic hypertension, secondary hypertension, SAH target-organ lesion, types 1 and 2 diabetes mellitus, and persistent SAH despite the adoption of nonpharmacological measures, a situation in which such measures are an adjunct to the pharmacological treatment.
The diagnosis of obesity or overweight in children is clinical, and should be established via history and physical exam, followed by comparison of anthropometric data with population parameters, by using curves of body mass index (BMI) for age. Prevention comprises adequate nutrition during pregnancy, breastfeeding encouragement, identification of familial risk factors, careful child’s growth and development follow-up, habit
426
Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Table 14 – Recommendations for the nonpharmacological treatment of dyslipidemia in cardiovascular prevention
Indication Class Level of evidence
• Control LDL-C I A
• Meet the recommended LDL-C level (primary goal) I A
• No goals proposed for HDL-C I A
• Reduce the intake of saturated fatty acids and trans fatty acids, and consume phytosterols (2-3 g/day) and soluble fibers I A
• Increase physical activity I A
• Reduce body weight and increase the ingestion of soy proteins; replace saturated fatty acids with mono- and polyunsaturated fatty acids I B
• Meet the recommended non-HDL-cholesterol level (secondary goal) II A
• Use proper therapy when triglyceride levels > 500 mg/dL to reduce the risk of pancreatitis, and use individualized therapy when triglyceride levels are between 150 and 499 mg/dL II A
• No goals proposed for apolipoproteins or lipoprotein(a) II A
Table 15 – Recommendations for the pharmacological treatment of dyslipidemia
Indication Class Level of evidence
• Statins as the first drug option in primary and secondary prevention I A
• Use fibrates in monotherapy or in association with statins to prevent microvascular disease in patients with type 2 diabetes I A
• Association of ezetimibe or resins with statins when the LDL-C goal is not met IIa C
• Association of niacin with statins III A
• Use omega-3 fatty acids for cardiovascular disease prevention III A
Table 16 – Dietary and physical activity interventions in diabetes mellitus (DM) to prevent cardiovascular disease
Indication Class Level of evidence• Moderate physical exercise for at least 150 minutes in association with moderate diet and energy restriction to prevent DM in
individuals at risk I A
• Because of the effects of obesity on insulin resistance, weight loss is an important therapeutic goal for individuals at risk for DM I A
• Reduction in fat to less than 30% of the energy ingestion and reduced energy ingestion for overweight individuals I A
Table 17 – Interventions in metabolic syndrome (MS) to prevent cardiovascular disease
Indication Class Level of evidence
• A 5%-10% reduction in body weight in one year and long-term maintenance of weight lossare recommended I B
• A diet with low amounts of total, saturated and trans fats, in addition to adequate amounts of fibers, is recommended I B
• Physical activity for at least 30 minutes/day, preferably 45-60 minutes/day, 5 days a week, is recommended I B
• Individuals with impaired glucose tolerance on drug therapy can have a more expressive reduction in the incidence of MS or type 2 diabetes mellitus I B
• Individuals at metabolic risk and with abdominal circumference beyond the recommended limits should undergo a 5%-10% body weight reduction in one year IIa B
• Ingestion of less than 7% of total calories from saturated fat and of less than 200 mg/day of cholesterol in the diet is recommended IIa B
427

Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Table 18 – Recommended exercise levels for health promotion and maintenance
Exercise characteristics Health benefits Comments
• < 150 min/week of mild to moderate intensity some some exercise is certainly better than a sedentary lifestyle
• 150-300 min/week of moderate intensity substantial longer-duration and/or more intense exercise provides more benefits
• > 300 min/week of moderate to high intensity additional Current scientific data specifyan upper limit neither for benefits nor for damages to an apparently healthy individual
Table 19 – Classification of recommendation and level of evidence in approaching psychosocial factors in primary prevention
Recommendation Class Level of evidence
• Behavioral changes with cognitive-behavioral strategy (motivational) I A
• Integration of education and motivational strategies with a multiprofessional team whenever possible I A
• Psychological or psychiatric consultation for more severe cases I C
• Assessment of psychosocial risk factors IIa B
• Pharmacological treatment and psychotherapy for patients with severe depression, anxiety and hostility, aimed at improving the quality of life, despite lack of evidence IIb B
Chart 3 – Clinical strategy to improve adherence
Strategies to improve adherence
• Simplify dosage regimen • Reduce the number of tablets and doses per day
• Reduce costs• Lower cost drug• Generic drugs• Government subsidies and low-cost programs
• Proper communication
• Provide clear information about the benefits, possible adverse effects and duration of treatment• Assess without judging or criticizing the presence of poor adherence• Assess actively the presence of possible side effects (sexual dysfunction, cough, bleeding)• Avoid using technical terms and overloading the patient with a lot of information
• Behavioral strategies
• Incorporate the use of drugs to the patients’ routine, suiting the dosage regimen to activities, meals and bedtime• Use tablet holders, electronic alarm devices, diaries, packages with calendars• Online support groups• Positive reinforcement (incentives, rewards)• Self-monitoring• Motivation counseling
Table 20 – Classification of recommendation and level of evidence of adherence to strategy in cardiovascular prevention, lifestyle and medication
Recommendation Class Level of evidence
• Assess and identify the causes of lack of adherence to define the proper orientation I A
• Use behavioral and motivational strategies for patients with persistent lack of adherence IIa A
changes, especially the adoption of a healthy diet and global increase in physical activity. It is important to involve the child’s entire family, parents, teachers and health care professionals, in addition to count on a multidisciplinary team.
The systematic analysis of studies on the effectiveness of interventions to promote physical activity in the pediatric age group (more particularly adolescents) has shown better results when the actions associate school, family and community,
and when the educational actions involve environmental and health policies.
Table 23 shows the recommendations and their levels of evidence to prevent CVD in children and adolescents.
Chapter 12 discusses topics related to legislation and prevention of CVD risk factors. The authors approach specific sanitary laws, discussing their effective role in health promotion and prevention, by creating healthy environments, in addition
428

Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Table 21 – Reference values for lipids and lipoproteins in children and adolescents
Parameter Acceptable Borderline High (p95) Low (p5)
TC < 170 170-199 > 200
LDL-C < 110 110-129 > 130
n-HDL-C 123 123-143 > 144
TG (0-9a) < 75 75-99 > 100
TG (10-19a) < 90 90-129 > 130
HDL-C > 45 35-45 < 35
Apo A1 > 120 110-120 < 110
Apo B < 90 90-109 > 110
TC: total cholesterol; LDL-C: low-density-lipoprotein cholesterol; n-HDL-C: non-high-density-lipoprotein cholesterol; TG: triglycerides; HDL-C: high-density-lipoprotein cholesterol; Apo A1: apolipoprotein A1; Apo B: apolipoprotein B.
Table 22 – Classification of arterial blood pressure in children and adolescents
Class Percentile of systolic or diastolic blood pressure
Normal < 90
Prehypertension (9)Normal-high (10) 90 to <95 or ≥ 120x80 mm Hg
Stage 1 SAH 95 to 99 increased by 5 mm Hg
Stage 2 SAH > 99 increased by 5 mm Hg
SAH: systemic arterial hypertension
to emphasizing the importance of surveillance, prevention, health care, rehabilitation and health promotion
Chapter 13 discusses specific aspects of prevention of CVD associated with autoimmune diseases, influenza, chronic kidney disease, obstructive arterial disease, socioeconomic factors, obstructive sleep apnea, erectile dysfunction and periodontitis (Table 24).
We provide the medical class with a guideline that gathers, in one single publication, compiled and updated essential prevention topics to be used as a reference in CVD prevention.
Author contributionsConception and design of the research: Simão AF, Précoma
DB, Andrade JP, Correa Filho H, Saraiva JFK, Oliveira GMM; Acquisition of data: Simão AF, Précoma DB, Correa Filho H, Oliveira GMM; Analysis and interpretation of the data: Simão AF, Correa Filho H, Saraiva JFK, Oliveira GMM; Writing of the manuscript: Simão AF, Précoma DB, Correa Filho H, Saraiva JFK, Oliveira GMM; Critical revision of the manuscript for intellectual content: Simão AF, Précoma DB, Andrade JP, Correa Filho H, Saraiva JFK, Oliveira GMM; Revision of the manuscript: Oliveira GMM.
Potential Conflict of InterestThe author Harry Correa Filho declares have conflict with
the companies: Pfizer, Astra Zeneca.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis study is not associated with any thesis or dissertation
work.
429

Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Table 23 – Classification of recommendation and level of evidence for the presence of cardiovascular diseases (CVD) in children and adolescents
Recommendation Class Level of evidence
Obesity screening• Obesity screening by use of BMI in children ≥ 6 years, providing or indicating intensive behavioral interventions directed to
achieving a healthy weight• Ask about early CAD family history to identify children at risk• In the presence of positive family history, assess all family members, especially the parents
I B
• In children aged > 2 years with BMI ≥ 85th percentile: Reinforce preventive instructions (see below) Identify complications and RF: SBP, gallbladder disease symptoms, diabetes, sleep apnea, hypothyroidism, orthopedic disorders,
lipid profile
I C
• In children aged > 2 years with BMI ≥ 85th– 94th percentile,all measures above plus: control of weight gain and fat ingestion, focusing on nutrition and development treatment of RF and complications multidisciplinary approach of moderate to high intensity measure aspartate aminotransferase (AST), alanine aminotransferase (ALT) and blood sugar in children ≥ 10 years of age
I C
• In children aged > 2 years with BMI ≥ 95th percentile, all measures above plus: Long-term objective: maintain BMI < 85 I B
• Consider more aggressive approaches if conservative strategies fail• Check urea and creatinine every 2 years I A
Nutrition – Milk/other beverages
Exclusive maternal breastfeeding for the first 6 months I B
From the 12th to the 24th month, transition to non-aromatic low-fat milk (2% or skim) I B
From 2 to 21 years of age, non-aromatic skim milk should be the major beverage I A
Avoid sugar beverages, encourage water ingestion I B
Dietary fat
Fat ingestion by infants should not be restricted without medical indication I C
From the 12th to the 24th month, transition to family meals with fat corresponding to 30% of the total caloric ingestion, 8%-10% of which of saturated fat I B
From 2 to 21 years of age, fat should correspond to 25%-30% of the total caloric ingestion, 8%-10% of which of saturated fat I A
Avoid trans fat I B
Cholesterol < 300 mg/dL I A
OthersFrom 2 to 21 years of age, encourage fiber ingestion, limit sodium ingestion and encourage healthy life habits: family meals, breakfast, limit fast snacks I B
Physical activity
Parents should create an environment that promotes physical activity and limit sedentary activities, and be role models I C
Limit sedentary activities, especially TV/video I B
Moderate to vigorous physical activity every day I A
BMI: body mass index; CAD: coronary artery disease; RF: risk factors; SBP: systolic blood pressure
430

Special Article
Simão et al.Cardiovascular Prevention Guideline
Arq Bras Cardiol. 2014; 102(5):420-431
Table 24 – Recommendation for approaching special conditions in cardiovascular disease prevention
Recommendation class level of evidence• In the context of preventing cardiovascular events, the benefit of using more strict therapeutic targets, especially due to the
presence of autoimmune diseases, is uncertain. IIb C
• Annual influenza vaccination for patients with established coronary artery or cerebrovascular disease, regardless of age I B
• Annual influenza vaccination for patients at high risk for coronary events, but with no cardiovascular disease, regardless of age. IIa C
• Patients with chronic kidney disease should be considered at very high risk for cardiovascular risk factors, requiring the assessment of glomerular filtration rate reduction and presence of co-morbidities. I C
• Patients with obstructive arterial disease should be considered at very high risk, similarly to that of manifest coronary artery disease, for approaching cardiovascular risk factors. I C
• Socioeconomic indicators should be investigated in clinical assessment and considered when approaching a patient, to improve quality of life and the prognosis of cardiovascular diseases. IIa B
• All patients with obstructive sleep apnea should be considered as potential candidates to primary prevention, undergo cardiovascular risk stratification and be treated according to estimated risk. IIa A
• All men with erectile dysfunction should be considered as potential candidates to primary prevention, undergo cardiovascular risk stratification and be treated according to estimated risk. IIa B
• Patients with periodontitis should be considered for cardiovascular risk stratification and intensive local treatment. IIa B
431

Original Article
Preclinical Study of a Biodegradable Polymer-based Stent with Abluminal Sirolimus ReleaseCelso Kiyochi Takimura1, Carlos Augusto Homem M. Campos1, Pedro Henrique Magualhães Craveiro Melo1, Julliana Carvalho Campos1, Paulo Sampaio Gutierrez1, Thiago Francisco Costa Borges2, Luciano Curado2, Spero Penha Morato3, Francisco Rafael Martins Laurindo1, Pedro Alves Lemos Neto1
Instituto do Coração do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (USP)1; Scitech Produtos Médicos Ltda2; Lasertools Tecnologia Ltda3, São Paulo, SP – Brazil
Mailing Address: Celso Kiyochi Takimura •Avenida Açoce 92, apto. 162, Indianopolis. Postal Code 04075-020, São Paulo, SP – BrazilE-mail: [email protected], [email protected] received September 23, 2013; revised manuscript November 04, 2013; accepted November 13, 2013.
DOI: 10.5935/abc.20140044
Abstract
Background: Bioabsorbable polymer stents with drug elution only on the abluminal surface may be safer than durable polymer drug-eluting stents.
Objective: To report the experimental findings with the Inspiron™ stent – a bioabsorbable polymer-coated stent with sirolimus release from the abluminal surface only, recently approved for clinical use.
Methods: 45 stents were implanted in the coronary arteries of 15 pigs. On day 28 after implantation, angiographic, intracoronary ultrasonographic and histomorphological data were collected. Five groups were analyzed: Group I (nine bare-metal stents); Group II (nine coated with bioabsorbable polymer on the luminal and abluminal surfaces); Group III (eight stents coated with bioabsorbable polymer on the abluminal surface); Group IV (nine stents with bioabsorbable polymer and sirolimus on the luminal and abluminal surfaces); and Group V (ten stents with bioabsorbable polymer and sirolimus only on the abluminal surface).
Results: The following results were observed for Groups I, II, III, IV and V, respectively: percentage stenosis of 29 ± 20; 36 ± 14; 33 ± 19; 22 ± 13 and 26 ± 15 (p = 0.443); late lumen loss (in mm) of 1.02 ± 0.60; 1.24 ± 0.48; 1.11 ± 0.54; 0.72 ± 0.44 and 0.78 ± 0.39 (p = 0.253); neointimal area (in mm2) of 2.60 ± 1.99; 2.74 ± 1.51; 2.74 ± 1.30; 1.30 ± 1.14 and 0.97 ± 0.84 (p = 0.001; Groups IV and V versus Groups I, II and III); and percentage neointimal area of 35 ± 25; 38 ± 18; 39 ± 19; 19 ± 18 and 15 ± 12 (p = 0.001; Groups IV and V versus Groups I, II and III). Injury and inflammation scores were low and with no differences between the groups.
Conclusion: The Inspiron™ stent proved to be safe and was able to significantly inhibit the neointimal hyperplasia observed on day 28 after implantation in porcine coronary arteries. (Arq Bras Cardiol. 2014; 102(5):432-440)
Keywords: Drug-Eluting Stents; Sirolimus; Epidemiology, Experimental.
IntroductionIn the years of 2002 and 2003, the Cypher™ (Cordis
Corp, Miami Lakes, USA) and Taxus™ (Boston Scientific, Natick, USA) drug-eluting coronary stents were approved for clinical use and provided a major breakthrough in the percutaneous treatment of coronary stenoses, thanks to a significant reduction of the incidence of in-stent restenosis and of the need for a new target-vessel revascularization1,2. However, the occurrence of cases of late and very late thrombosis3,4 after implantation was an alert for the safety of these drug-eluting stents.
Among the multiple pathophysiological processes pointed as predisposing factors for late and very late thrombosis are: delayed strut endothelialization; positive remodeling with acquired poor apposition; endothelial dysfunction; and inflammatory reaction due to the presence of a durable polymer5.
With the purpose of overcoming the limitations and adverse events related to first-generation stents, several new drug-eluting stents have been developed. These new stents show variations either in the composition of the alloy, in the strut thickness, in the mesh design, in the drug-carrying polymer, in the drug class and dosage, or in the place on the stent surface from which the drug is released.
We hypothesized that, after drug release and degradation of the biodegradable polymer, only the metallic platform would remain in the arterial wall (like in a bare-metal stent), thus reducing the late and very late thrombosis rates of these stents, without compromising the anti-restenotic efficacy. Drug release from the abluminal surface only (stent surface in contact with the vessel wall) could also prevent delayed endothelialization of the stent struts, which is another mechanism pointed as responsible for thrombosis.
432

Original Article
Takimura et al.Preclinical study of the Inspiron™ stent
Arq Bras Cardiol. 2014; 102(5):432-440
This study presents preclinical data on the Inspiron™ stent (Scitech ® Medical Products Inc., Goiânia, Goiás, Brazil) – a stent composed of a chromium-cobalt L605 alloy, which is coated with a sirolimus and biodegradable polymer mixture only on its abluminal surface, and was recently approved for clinical use.
In this experimental study, the results observed in porcine coronary arteries by means of angiographic, intracoronary ultrasonographic, and histomorphological assessment on day 28 after implantation of the Inspiron™ stent versus stents with polymer and sirolimus on the luminal and abluminal surfaces, and bare-metal stents were compared.
Methods
Ethical AspectsThe study protocol was approved by the Institutional
Research Ethics Committee and was carried out according to the Good Laboratory Practices guidelines.
Animal speciesA total of 15 non-atherosclerotic juvenile pigs from a
commercial farm were used. Their mean weight was 28.9 kg (26 to 31.5 kg), and they received oral acetylsalicylic acid (200 mg) and clopidogrel (300 mg) one day prior to stent implantation.
StentsForty five pre-assembled stents manufactured by Scitech™
Medical Products, Inc., with 2.5, 3.0 and 3.5-mm diameters and 19-mm length were used. These stents are made of a chromium-cobalt L605 alloy, and have a thin strut (75-µm thickness), forming rings with short cells (1.1 mm) linked to each other by 65-µm struts6.
Except for 9 stents with no polymer or drug coating, the other stents were coated with biodegradable polymer, a mixture of poly (lactic acid) and poly (lactic acid-co-glycolic acid); this layer was 5-µm thick, and water- and CO2 degradable within 6 to 9 months (Figure 1).
The drug used in the drug-eluting stents was sirolimus, with 60% release in the first week and 90% within up to 4 weeks. The sirolimus dose used was 8.8 µg per mm of stent in the sirolimus-releasing stent from the luminal and abluminal stent surfaces; or 4.4 µg per mm of stent, on the sirolimus-releasing stent only from the abluminal surface (Inspiron™ stent).
Thus, five types of stents were assessed: nine stents without polymer or antiproliferative drug coating (Group I, bare-metal stent); nine bioabsorbable polymer-coated stents on the luminal and abluminal surfaces (Group II); eight bioabsorbable polymer-coated stents on the abluminal surface (Group III); nine bioabsorbable polymer and sirolimus coated stents on the luminal and abluminal surfaces (Group IV) and ten bioabsorbable polymer- and sirolimus-coated stents only on the abluminal surface (Group V, Inspiron™ stent).
Stent implantation procedureIntramuscular preanesthetic medications were administered
(ketamine 3 mg/kg and midazolam 0.5 mg/kg). Then, after intravenous infusion of thiopental, the animals underwent endotracheal intubation, mechanical ventilation, maintenance of the anesthetic plan with isoflurane and monitoring of their heart rhythms, heart rates, and oxygen saturation.
An arterial line for the stent implantation procedure was obtained by dissecting the common femoral artery, with arterial puncture under direct visualization and insertion of a 6-French valved introducer. Under fluoroscopy (Philips BV – The Netherlands), a 6-French Judkins Right therapeutic catheter was manipulated for selective catheterization of the coronary arteries; next, intracoronary nitroglycerin (200 µg) was administered and coronary angiography was performed in the left anterior oblique view at 45 degrees.
Then, a 0.014-inch Choice PR™ guidewire (Boston Scientific, Natick, USA) was inserted with its distal tip positioned in the target-coronary artery. Following a previous raffle, one stent per artery was implanted, preferably in an arterial segment with few lateral branches and without significant lumen reduction and deployment pressure enough to reach a stent deployment balloon diameter: artery rate of 1.1:1 (Table 1).
Post-Procedure follow-upAfter the procedure, the animals were observed regarding
their anesthetic recovery and were given prophylactic intramuscular antibiotic therapy with benzyl penicillin 1,200,000 units and gentamicin 40 mg. They were extubated when well awake, and sent to individual pens. They later received commercial feed for growing pigs (Cooper™, São José dos Campos, São Paulo, Brazil) and water ad libitum. For 28 days, oral antiplatelet agents were administered (acetylsalicylic acid 100 mg a day and clopidogrel 75 mg a day); the animals were seen daily by veterinarians, who observed them and made notes on their general status, level of physical activity, feed intake, and presence of fever; they also diagnosed and treated occasional surgical wound infections.
On day 28 after stent implantation, the animals were sent back to the animal experimentation laboratory and underwent control coronary angiography with quantitative coronary angiography and intracoronary ultrasonography. They were euthanized by deepening the level of anesthesia and administration of a lethal intravenous injection of potassium chloride (30 to 40 mL).
Histological processingAfter euthanasia and left paramedian thoracotomy, the
heart of each animal was carefully removed, with minimal handling, to prevent external stent compression; the blood in the cardiac chambers was washed out with drinking water and 0.9% saline solution. A 10% formaldehyde solution was then infused in the aortic root at a 100-mmHg pressure for 30 minutes. The arterial segments containing the stents were dissected from the adjacent tissues, removed, and placed in a 10% formaldehyde solution for 24 hours, and later, in
433

Original Article
Takimura et al.Preclinical study of the Inspiron™ stent
Arq Bras Cardiol. 2014; 102(5):432-440
Figure 1 – Detail of the metal mesh (left), strut thickness (top right), and polymer (bottom right) of the chromium-cobalt L605 coronary stent (Scitech© Medical Products Inc., Goiânia, Goiás, Brazil).
70% absolute alcohol. These arterial segments containing the stents were desiccated in alcohol solutions, embedded in methacrylate plastic resins, and subsequently subjected to cross sections (mean thickness of 3.5 µm), with a tungsten knife in a proper microtome (RM 2265, Leica, Germany).
Quantitative Coronary AngiographyAll angiographies of the stent implants and the control
studies performed at day 28 were analyzed by means of off-line quantitative coronary angiography using the CASS II software (Pie Medical, Maastrich, The Nederlands). The minimum lumen diameter (MLD, in mm), reference diameters (RD, in mm), percentage angiographic stenosis (%), and late lumen losses (in mm) were determined.
Intracoronary ultrasonography40-MHZ Atlantis™ SR Pro (Boston Scientific, Natick,
MA, USA) intracoronary sonography catheters were used, with automatic pull back at 0.5 mm/s. The images acquired were analyzed by the built-in measurement software of the intracoronary ultrasound imaging system (Ilab®, Boston Scientific, Natick, MA, USA); using planimetry, the lumen areas (in mm2), stent areas (in mm2), neointimal hyperplasia areas (in mm2), and percentage neointimal hyperplasia areas (%) were determined.
HistomorphologyThree histological slides were obtained per third of stent
segment (proximal, mid-, and distal). These slides were stained with hematoxylin-eosin and Verhoeff’s method for elastic fibers; later, they underwent histomorphological analyses. These analyses were blind as regards the type of
stent implanted and semiquantitative scores were used for the assessment of inflammation7, fibrin deposits8, and degree of injury9.
Statistical AnalysisQuantitative data are expressed as mean ± standard
deviation (SD) or median. After verifying that the data were normally distributed, the simple analysis of variance (one-way ANOVA) was calculated for comparison of the means between the groups; post-hoc analysis was carried out when statistically significant differences were observed between these groups. The Statistical Package for the Social Sciences (SPSS) software, version 20.0, was used for data analysis and the significance level was set at 5%.
Financial disclosureOffice of Science and Technology and Strategic Inputs
(SCTIE)/Department of Science and Tecnnology (DECIT) of the Ministry of Health (MS), National Council of Scientific and Technological Development (CNPq), Studies and Projects Financer (FINEP) of the Ministry of Science and Technology (MCT) and Foundation for Research Support of the State of São Paulo (Fapesp).
ResultsThe stents were successfully implanted in all target coronary
arteries, with no complications during the implantation procedures or in the immediate post-procedure period.
One animal (number 10) died on day six after stent implantation. The death cause determined by pathological study of the heart was acute inferior myocardial infarction due to occlusion of the right coronary artery in which a
434

Original Article
Takimura et al.Preclinical study of the Inspiron™ stent
Arq Bras Cardiol. 2014; 102(5):432-440
Table 1 – Individual data on the stent implantation procedure
Animal number Weight (kg) Target coronary-artery Group Stent size (mm) (diameter x length) Implantation pressure (ATM)
1 31
RC I 3.0 x 19 8
CX III 3.0 x 19 6
AD IV 3.0 x 19 7
2 30
RC I 3.0 x 19 10
CX III 3.5 x 19 8
AD II 3.0 x 19 10
3 30
RC II 3.0 x 19 6
CX IV 3.5 x 19 10
AD III 3.0 x 19 5
4 31.5
RC IV 3.0 x 19 8
CX I 3.0 x 19 6
AD II 3.0 x 19 9
5 28.5
RC IV 3.0 x 19 10
CX II 3.0 x 19 6
AD III 3.0 x 19 7
6 30
RC III 3.0 x 19 10
CX V 3.0 x 19 10
AD I 3.5 x 19 10
7 30
RC V 3.0 x 19 10
CX I 3.0 x 19 12
AD III 3.0 x 19 11
8 26
RC III 3.0 x 19 10
CX V 2.5 x 19 8
AD I 2.5 x 19 9
9 31
RC V 2.5 x 19 6
CX II 3.0 x 19 7
AD IV 2.5 x 19 10
10 27.5
RC II 3.0 x 19 8
CX I 3.5 x 19 8
AD V 2.5 x 19 7
11 26.5
RC IV 3.0 x 19 12
CX IV 3.5 x 19 10
AD V 3.0 x 19 10
12 27.5
RC III 3.5 x 19 7
CX V 3.0 x 19 5
AD II 3.5 x 19 10
13 27
RC II 3.5 x 19 8
CX IV 3.0 x 19 7
AD V 3.0 x 19 11
14 26.5
RC V 3.0 x 19 11
CX III 3.5 x 19 5
AD I 3.0 x 19 7
15 31.5
RC I 3.0 x 19 10
CX IV 3.5 x 19 10
AD V 3.5 x 19 10
RC: right coronary artery; CX: circumflex artery; AD: anterior descending artery; Group I: bare-metal stents; Group II: stents with bioabsorbable polymer on the luminal and abluminal surfaces; Group III: stents with bioabsorbable polymer on the abluminal surface; Group IV: stents with bioabsorbable polymer and sirolimus on the luminal and abluminal surfaces; Group V: stents with bioabsorbable polymer and sirolimus only on the abluminal surface.
435

Original Article
Takimura et al.Preclinical study of the Inspiron™ stent
Arq Bras Cardiol. 2014; 102(5):432-440
Table 2 – Results of quantitative coronary angiography, intracoronary ultrasonography and histomorphology
Groupp value
I (N = 9) II (N = 9) III (N = 8) IV (N = 9) V (N = 10)
Baseline RD (mm) 2.59 ± 0.21 2.62 ± 0.20 2.63 ± 0.30 2.61 ± 0.24 2.50 ± 0.43 0.901
Ballon inflation pressure (ATM) 9.0 ± 1.9 8.0 ± 1.7 7.6 ± 2.2 9.3 ± 1.6 9.0 ± 2.1 0.348
Balloon diameter (mm) 2.76 ± 0.27 2.79 ± 0.24 2.89 ± 0.32 2.83 ± 0.19 2.71 ± 0.26 0.716
Balloon/artery ratio 1.06 ± 0.04 1.06 ± 0.08 1.10 ± 0.07 1.09 ± 0.10 1.10 ± 0.10 0.845
MLD at procedure termination (mm) 2.67 ± 0.23 2.74 ± 0.22 2.69 ± 0.21 2.73 ± 0.22 2.59 ± 0.26 0.749
RD on control angiography (mm) 2.30 ± 0.30 2.49 ± 0.32 2.39 ± 0.30 2.48 ± 0.22 2.54 ± 0.30 0.470
MLD on control angiography (mm) 1.64 ± 0.61 1.59 ± 0.45 1.57 ± 0.49 1.95 ± 0.43 1.85 ± 0.36 0.379
Percentage stenosis (%) 29 ± 20 36 ± 14 33 ± 19 22 ± 13 26 ± 15 0.443
Late lumen loss (mm) 1.02 ± 0.60 1.24 ± 0.48 1.11 ± 0.54 0.72 ± 0.44 0.78 ± 0.39 0.253
Luminal area (mm²) 4.49 ± 2.16 4.29 ± 1.53 4.33 ± 1.40 5.77 ± 3.32 6.03 ± 2.18 0.001*
Vessel area (mm²) 6.95 ± 1.40 6.90 ± 1.27 6.97 ± 0.87 7.00 ± 1.10 7.00 ± 1.58 0.305
Stent area (mm²) 7.09 ± 1.40 7.03 ± 1.27 7.07 ± 0.87 7.07 ± 1.10 7.00 ± 1.70 0.676
Neointimal area (mm²) 2.60 ± 1.99 2.74 ± 1.51 2.74 ± 1.30 1.30 ± 1.14 0.97 ± 0.84 0.001*
Percentage neointimal area (%) 35 ± 25 38 ± 18 39 ± 19 19 ± 18 15 ± 12 0.001*
Inflammation (median) (min-max) 1 (0 - 2) 1 (0 - 2) 1 (0 - 3) 1 (0 - 1) 1 (0 - 1) 0.999
Schwartz injury (median) (min-max) 1 (0 - 3) 1 (0 - 2) 1 (1 - 3) 1 (0 - 2) 1 (0 - 2) 0.999
* Group IV versus Groups I, II, III and Group V versus Groups I, II, III.Group I: bare-metal stents; Group II: stents with bioabsorbable polymer on the luminal and abluminal surfaces; Group III: stents with bioabsorbable polymer on the abluminal surface; Group IV: stents with bioabsorbable polymer and sirolimus on the luminal and abluminal surfaces; Group V: stents with bioabsorbable polymer and sirolimus only on the abluminal surface; RD: reference diameter; MLD: minimum lumen diameter.
stent coated with biodegradable polymer on the luminal and abluminal surfaces had been implanted (Group II stent). The other arteries – anterior descending and circumflex, and the stents implanted in these arteries, were patent, with no firmly adherent intraluminal thrombi. This early death determined an early mortality rate of 6.6% (one in 15 animals), which, according to an Investigators Consensus, is representative of “good implantation technique and stent technology”10 (rate should be lower than 10%).
On day 28 after stent implantation, control coronary angiography performed in the surviving animals showed arterial segments with patent stents and no image suggestive of thrombus.
Findings of quantitative coronary angiography, intracoronary ultrasonography and histopathology are described in Table 2.
Quantitative Coronary AngiographyOn quantitative coronary angiography, the porcine
coronary arteries had a reference diameter of approximately 2.6 mm during the stent implantation procedure. The inflation pressure for stent implantation was, on average, of 8.5 ATM (5 to 12 ATM; p = 0.348), reaching a balloon: artery ratio of 1.1:1 to cause moderate injury to the arterial wall.
Control quantitative coronary angiography on day 28 after the procedure did not show any statistically significant difference between the groups.
Intracoronary ultrasonographyOn intracoronary ultrasonography, adequate stent
strut apposition was observed in all cases on day 28 after implantation. Also, statistically significant larger luminal areas (mm2) were observed in the drug-eluting stents (Groups IV and V) in relation to control stents (Groups I, II and III) (p = 0.001). Likewise, the neointimal area and percentage neointimal area were significantly smaller in these drug-eluting stents in relation to control stents (p = 0.001 for comparisons of Groups IV and V individually versus Groups I, II and III), as shown in Figure 2.
The neointimal hyperplasia observed in the stents coated with bioabsorbable polymer and sirolimus only on the abluminal surface (Group V, Inspiron™ stent) was equivalent to that observed in stents with the same coating on the luminal and abluminal surfaces (Group IV), with no statistically significant difference (p = 0.913).
HistomorphologyThe injury and inflammation scores were low and
showed no statistically significant differences between the groups (p = 0.999). Figure 3 shows histological images of the neointimal hyperplasia on day 28 after implantation of a bare-metal stent (on the left) and of a drug-eluting stent (on the right) in arteries.
436

Original Article
Takimura et al.Preclinical study of the Inspiron™ stent
Arq Bras Cardiol. 2014; 102(5):432-440
Figure 3 – Cross-sectional views of porcine coronary arteries on day 28 after bare-metal stent implantation (Group I, left) and biodegradable polymer-coated stent with sirolimus elution on the abluminal surface (Group V) (right). Magnification 40X.
Figure 2 – Luminal area (mm2), neointimal area (mm2), and percentage neointimal area (%) observed in the experimental groups I to V. * p value < 0.05 for Group IV versus Groups I, II and III, and Group V versus Groups I, II and III.
437

Original Article
Takimura et al.Preclinical study of the Inspiron™ stent
Arq Bras Cardiol. 2014; 102(5):432-440
DiscussionPreclinical studies in laboratory animals for the development
and improvement of coronary stents are important to provide an initial idea of the mechanical performance, safety and efficacy profile of the stents, in addition to being required by regulatory agencies for the approval of these devices for clinical use11.
Despite all the benefits from the first-generation drug-eluting stents which brought a revolution in the treatment of atherosclerotic coronary disease, questions arose on the long-term safety of these devices, especially in relation to late thrombosis12.
After the initial reduction in the number of drug-eluting stents implantation observed at that time, new efforts have focused on the development of stents with the use of different alloys (chromium-cobalt and platinum-chromium), new biocompatible or biodegradable polymers, and the incorporation of new drugs (everolimus, zotarolimus and biolimus A9), aiming to increase the safety of these devices.
Although the pathophysiology of stent thrombosis is multifactorial, several animal and clinical evidences have pointed to the presence of durable polymers as responsible for inflammation and delayed vascular repair13. These evidences have fostered the development of biodegradable polymer-based stents and bioabsorbable stents.
In the present preclinical study on porcine coronary arteries, we observed that biodegradable polymer-coated stents with sirolimus release only from the abluminal surface (Group V, Inspiron™ stent) showed neointimal hyperplasia quantitatively similar to that of polymer and sirolimus-coated stents on the luminal and abluminal surfaces (Group IV). The groups with sirolimus-releasing stents (Groups IV and V) showed lower neointimal area in relation to the bare-metal stents (Groups I, II and III). No difference was observed between the five groups in relation to the injury and inflammation scores, thus showing that both the bioabsorbable polymer and the antiproliferative drug used were safe and effective.
The Inspiron™ eluting-stent is characterized by being composed of a chromium-cobalt L605 alloy, biodegradable polymer coating , and sirolimus elution only on the abluminal surface. Possibly because of being coated with a biodegradable polymer, it is safer than durable-polymer stents. In a meta-analysis of randomized clinical trials comparing stent thrombosis rates up to 4 years after use of the Yukon (Translumina, Hechingen, Germany) and Biomatrix™ Flex (Biosensors International, Singapore) biodegradable polymer-based drug-eluting stents versus the Cypher™ (Cordis Corp, Miami Lakes, Fl, USA) durable-polymer stent, the biodegradable polymer-based stents showed less definitive stent thrombosis, less clinical endpoints and less target-lesion revascularization than the Cypher™ durable-polymer stent14.
An experimental study in a porcine model compared the endothelial activity and inflammation scores in animals undergoing Nobori™ stent implantation – a stent coated with bioabsorbable polymer and biolimus only on its abluminal surface, to that of animals undergoing Cypher™ stent implantation, and found increased endothelial relaxation,
decreased production of superoxide anion, and less inflammation in the coronary segments in the group receiving the Nobori™ stent15.
Recent findings, however, suggest that the presence of a durable polymer per se does not determine a greater risk of late thrombosis16,17. In an experimental study, Kolandaivelu et al18 observed that drug-eluting stents with durable polymer (XIENCE) showed less early thrombogenicity than a corresponding bare-metal stent (Multilink Vision), i.e., polymer and drug coating provided a protective effect for acute thrombogenicity. Factors such as the stent design and strut thickness emerged as other important factors predisposing stent thrombosis.
Several other stents using biodegradable polymer and antiproliferative drugs released only from the abluminal surface have been developed. Examples of these stents are the stainless steel biolimus A9-eluting Nobori™ (Terumo Corp., Japan) and Biomatrix™ (Biosensors International, Singapore) stents ; the stainless steel paclitaxel-eluting JACTAX™ stent (Boston Scientific, Natick, USA) , and the chromium-cobalt sirolimus-eluting Firehawk™ stent (MicroPort Medical, Shanghai, China).
The Inspiron™ stent has been extensively studied in experimental animals with results comparable to those of other drug-eluting stents as regards safety, stent-strut endothelialization, and neointimal hyperplasia19,20.
Clinical studies are underway to evaluate the efficacy of this new drug-eluting stent. The preliminary clinical results of the Inspiron™ stent (INSPIRON I) have shown a good angiographic response, with late lumen loss of 0.18 mm; good ultrasonographic response, with percentage neointimal obstruction of 8.2%; and target-vessel revascularization of 0%.
A randomized clinical trial (DESTINY) comparing the Inspiron™ stent with Biomatrix™ stent is currently being conducted, expected to include 165 randomized patients 2:1 (Inspiron™ stent versus Biomatrix™).
Study limitationsThe model used in the present study was healthy porcine
coronary arteries, which may not represent the progression in a vascular segment with atherosclerotic disease. Atherosclerotic animal models have been developed in rabbits and pigs; however, these models are still uncommonly used in preclinical studies for the development and improvement of coronary stents.
Intracoronary ultrasonography was used only in the control on day 28 after stent implantation with the purpose of assessing in-stent neointimal hyperplasia, and not to guide stent implantation. However, despite the known limitations of quantitative coronary angiography, the findings of this method revealed that the stents were adequately implanted (balloon: artery ratio of 1.1:1) and the intracoronary ultrasonographic findings showed adequate stent strut apposition in all cases.
Optical coherence tomography is a method that has been widely used in preclinical and clinical validation studies of new stents; however, this method was not yet available for experimental animal use in our institution at the time the study was carried out.
438

Original Article
Takimura et al.Preclinical study of the Inspiron™ stent
Arq Bras Cardiol. 2014; 102(5):432-440
1. Morice MC, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E, Perin M et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002;346(23):1773-80.
2. Stone GW, Ellis SG, Cox DA, Hermiller J, O’Shaughnessy C, Mann JT, et al. One-year clinical results with the slow-release, polymer-based, paclitaxel-eluting taxus stent: The TAXUX-IV trial. Circulation. 2004;109(16):1942-7.
3. Pfisterer M, Brunner-La Rocca HP, Buser PT, Rickenbacher P, Hunziker P, Mueller C, et al. Late clinical events after clopidogrel discontinuation may limit the benefit of drug-eluting stents: an observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol. 2006;48(12):2584-91.
4. Stone GW, Moses JW, Ellis SG, Schofer J, Dawkins KD, Morice MC, et al. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N Engl J Med. 2007;356(10):998-1008.
5. Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi GM, Stankovic G, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA. 2005;293(17):2126-30.
6. Lemos PA, Laurindo FR, Morato SP, Takimura C, Campos CA, Gutierrez OS, et al. Stent coronário de liga cobalto-cromo concebido no brasil: Achados histologicos preliminares em modelo experimental porcino. Rev Bras Cardiol Invas. 2007;15(4):378-85.
7. Kornowski R, Hong MK, Tio FO, Bramwell O, Wu H, Leon MB. In-stent restenosis: contributions of inflammatory responses and arterial injury to neointimal hyperplasia. J Am Coll Cardiol. 1998;31(1):224-30.
8. Suzuki T, Kopia G, Hayashi S, Bailey LR, Llanos G, Wilensky R, et al. Stent-based delivery of sirolimus reduces neointimal formation in a porcine coronary model. Circulation. 2001;104(10):1188-93.
9. Schwartz RS, Edelman ER, Carter A, Chronos N, Rogers C, Robinson KA, et al. Drug-eluting stents in preclinical studies recommended evaluation from a consensus group. Circulation. 2002;106(14):1867-73.
10. Schwartz RS, Edelman E, Virmani R, Carter A, Granada JF, Kaluza GL, et al. Drug-eluting stents in preclinical studies: updated consensus recommendations for preclinical evaluation. Circ Cardiovasc Intervent. 2008;1(2):143-53.
11. Suzuki Y, Yeung AC, Ikeno F. The pre-clinical animal model in the translational research of interventional cardiology. JACC Cardiovasc Interv. 2009;2(5):373-83.
12. Camenzind E, Steg PG, Wijns W. Stent thrombosis late after implantation of first-generation drug-eluting stents: a cause for concern. Circulation. 2007;115(11):1440-55.
13. Nakazawa G, Finn AV, Vorpahl M, Ladich ER, Kolodgie FD, Virmani R. Coronary responses and differential mechanisms of late stent thrombosis attributed to first-generation sirolimus- and paclitaxel-eluting stents. J Am Coll Cardiol. 2011;57(4):390-8.
14. Stefanini GG, Byrne RA, Serruys PW, de Waha A, Meier B, Massberg S, et al. Biodegradable polymer drug-eluting stents reduce the risk of stent thrombosis at 4 years in patients undergoing percutaneous coronary intervention: a pooled analysis of individual patient data from the ISAR-test 3, ISAR-test 4, and LEADERS randomized trials. Eur Heart J. 2012;33(10):1214-22.
15. Pendyala LK, Matsumoto D, Shinke T, Iwasaki T, Sugimoto R, Hou D, et al. Nobori stent shows less vascular inflammation and early recovery of endothelial function compared with Cypher stent. JACC Cardiovasc Interv. 2012;5(4):436-44.
16. Sabate M, Cequier A, Iniguez A, Serra A, Hernandez-Antolin R, Mainar V, et al. Everolimus-eluting stent versus bare-metal stent in ST-segment elevation myocardial infarction (examination): 1 year results of a randomised controlled trial. Lancet. 2012;380(9852):1482-90.
17. Palmerini T, Biondi-Zoccai G, Della Riva D, Stettler C, Sangiorgi D, D’Ascenzo F, et al. Stent thrombosis with drug-eluting and bare-metal stents: Evidence from a comprehensive network meta-analysis. Lancet. 2012;379(9824):1393-402.
18. Kolandaivelu K, Swaminathan R, Gibson WJ, Kolachalama VB, Nguyen-Ehrenreich KL, Giddings VL, et al. Stent thrombogenicity early in high-risk interventional settings is driven by stent design and deployment and protected by polymer-drug coatings clinical perspective. Circulation. 2011;123(13):1400-9.
19. Takimura CK, Galon MZ, Lopes Jr A, Carvalho J, Ferreira SK, Chaves MJ, et al. Avaliação pela tomografia de coerencia optica de stent nacional recoberto com polímero biodegradável eluidor de sirolimus vs. Stent eluidor de biolimus a9 em artérias coronárias porcinas. Rev Bras Cardiol Invasiva. 2011;19(2):138-44.
20. Takimura CK, Watanabe IS, Laurindo FR, Gutierrez PS, Aiello VD, Morato SP, et al. Assessment of stent strut endothelialization in iliac arteries of rabbits. Arq Bras Cardiol. 2012;99(6):1123-8.
References
ConclusionsIn this experimental study, the drug-eluting stents
coated with sirolimus and bioabsorbable polymer in porcine coronary arteries showed less neointimal hyperplasia when compared to control bare-metal stents. The bioabsorbable polymer-based stent with sirolimus released only from its abluminal surface (Inspiron™ stent) showed the same neointimal antiproliferative efficacy as the stent with sirolimus released from both the luminal and abluminal surfaces.
Author contributionsConception and design of the research: Takimura CK,
Campos CAH; Acquisition of data: Takimura CK, Campos CAH, Campos JC, Gutierrez PS; Statistical analysis: Takimura CK; Analysis and interpretation of the data: Takimura CK; Writing of the manuscript: Takimura CK, Craveiro PHM; Supervision / as principal investigator: Takimura CK; Critical
revision of the manuscript for intellectual content: Campos CAH, Craveiro PHM, Borges TFC, Curado L, Morato SP, Laurindo FRM, Lemos Neto PA.
Potential Conflict of InterestThe authors Celso Kiyochika Takimura, Francisco Rafael
Martins Laurindo Alves and Pedro Lemos Neto are scientific consultants of Scitech Medical Products. The authors Luciano Spero Penha Morato Curado and are employed of Scitech Medical Products.
Sources of FundingThis study was partially funded by SCTIE/ DECIT do
Ministério da Saúde, CNPQ, FINEP, FAPESP.
Study AssociationThis study is not associated with any thesis or dissertation work.
439

Original Article
Takimura et al.Preclinical study of the Inspiron™ stent
Arq Bras Cardiol. 2014; 102(5):432-440440

Original Article
Effects of Skeletonized versus Pedicled Radial Artery on Postoperative Graft Patency and FlowRômulo C. Arnal Bonini1, Rodolfo Staico2, Mario Issa2, Antoninho Sanfins Arnoni2, Paulo Chaccur2, Camilo Abdulmassih Neto2, Jarbas Jackson Dinkhuysen2, Paulo Paredes Paulista2, Luiz Carlos Bento de Souza2, Luiz Felipe P. Moreira1
Instituto do Coração (Incor), Faculdade de Medicina da Universidade de São Paulo1, São Paulo, SP; Instituto Dante Pazzanese de Cardiologia2, São Paulo, SP - Brazil
Mailing Address: Rômulo César Arnal Bonini •Divisão de Cirurgia Cardiovascular do Hospital Regional. Rua Winston Churchill, 234, apto. 1.402, Jardim Paulistano. Postal Code 19013-710, Presidente Prudente, SP - Brazil E-mail: [email protected] received September 26, 2013; revised manuscript October 04, 2013; accepted October 04, 2013.
DOI: 10.5935/abc.20140016
Abstract
Background: Radial artery (RA) was the second arterial graft introduced in clinical practice for myocardial revascularization. The skeletonization technique of the left internal thoracic artery (LITA) may actually change the graft’s flow capacity with potential advantages. This leads to the assumption that the behavior of the RA, as a coronary graft, is similar to that of the LITA, when skeletonized.
Objective: This study evaluated ‘free’ aortic-coronary radial artery (RA) grafts, whether skeletonized or with adjacent tissues.
Methods: A prospective randomized study comparing 40 patients distributed into two groups was conducted. In group I, we used skeletonized radial arteries (20 patients), and in group II, we used radial arteries with adjacent tissues (20 patients). After the surgical procedure, patients underwent flow velocity measurements.
Results: The main surgical variables were: RA internal diameter, RA length, and free blood flow in the radial artery. The mean RA graft diameters as calculated using quantitative angiography in the immediate postoperative period were similar, as well as the flow velocity measurement variables. On the other hand, coronary cineangiography showed the presence of occlusion in one RA graft and stenosis in five RA grafts in GII, while GI presented stenosis in only one RA graft (p = 0.045).
Conclusion: These results show that the morphological and pathological features, as well as the hemodynamic performance of the free radial artery grafts, whether prepared in a skeletonized manner or with adjacent tissues, are similar. However, a larger number of non-obstructive lesions may be observed when RA is prepared with adjacent tissues. (Arq Bras Cardiol. 2014; 102(5):441-448)
Keywords: Coronary Diseases / surgery; Radial Artery / abnormalities; Radial Artery / surgery; Vascular Patency.
IntroductionRadial artery (RA) was the second arterial graft introduced
in clinical practice for myocardial revascularization1. Initially, it presented unfavorable angiographic results. However, with changes in the surgical technique and the use of spasm-preventing vasodilators, RA started to be used safely and with good results in the treatment of coronary diseases2.
RA skeletonized dissection was introduced by Taggart et al in 20013, based on the good results obtained with skeletonization of the left internal thoracic artery (LITA), which started with Cunningham et al in 19924. There is no question about the effects of pedicled LITA for myocardial revascularization, and notwithstanding these excellent results, the skeletonization technique of LITA may actually change the
graft’s flow capacity with potential advantages4-6. This leads to the assumption that the behavior of the RA, as a coronary graft, is similar to that of the LITA, when skeletonized.
Therefore, the purpose of this study was to randomly compare the hemodynamic and functional performance of RA aorto-coronary grafts, prepared in a skeletonized manner or with adjacent tissues, by means of post-surgical angiography and flowmetry performed in the immediate postoperative period. Morphological and pathological features of these grafts were also compared.
Methods
Study populationThis study was designed as a randomized clinical trial
with distribution of twenty patients per group, according to RA dissection technique and preparation (Group I – skeletonized RA graft and Group II – RA graft with adjacent tissues). Patients diagnosed with stable angina, unstable angina, or a history of non-acute myocardial infarction (with or without ST-segment elevation) were included after free and clear discussion of risks, alternatives, and perceived benefits of the operations. The study protocol was approved by the institutional Research Ethics Committee
441

Original Article
Bonini et al.Skeletonization x Pedicle Preparation of Radial Artery
Arq Bras Cardiol. 2014; 102(5):441-448
and Scientific Review Board, and registered on the National Council of Research Ethics (CONEP). All patients gave written informed consent.
Patients with cineangiographic exams showing coronary stenoses above 70% and good distal anatomy7 in at least two main branches including the circumflex territory, and negative classic and modified Allen test8,9 in the forearm, which is intended for RA dissection, were selected. The following exclusion criteria were applied: (a) age over 70 years; (b) severe obesity; (c) positive Allen test10,11; (d) patients with arteriovenous fistula for hemodialysis, vasculitis, or Raynaud’s disease; (e) RA presenting macroscopically visible calcifications or diffuse atherosclerotic disease; (f) redo operation; (g) additional procedure; (h) severely depressed left ventricular function; (i) contraindications for use of calcium-channel blockers; (j) contraindication for postoperative angiography; (j) acute myocardial infarct with or without ST-segment elevation; (k) patients with kidney failure, or peripheral arterial disease.
Forty patients were selected for this study. All patients had angina class 2–4 according to the Canadian Cardiovascular Society. Previous myocardial infarction (MI), number of diseased vessels, age, gender, diabetes mellitus, hypertension and others characteristics were similar for both groups and are shown in Table 1. All patients were operated on electively.
Surgical technique and pharmacological protocolAll patients were operated on under cardiopulmonary
bypass with mild hypothermia (32-34°C) and intermittent aortic cross-clamping . Soon after discontinuation of cardiopulmonary bypass, intravenous nitroglycerin was administered for 48 hours, and replaced by an oral calcium-channel antagonist after this period.
The RA was dissected and prepared concomitantly with LITA dissection. The RA dissection technique was that proposed by Reyes et al12, and skeletonization, when applied, was performed out of the forearm with the use of scissors; collateral vessels were ligated using 4.0-cotton suture. Intraluminal filling of the RA grafts was performed using heparin-treated blood, and topical papaverine. LITA was used to graft the left anterior descending artery and all RA were used to graft the obtuse marginal artery, the intermediate branch or the first diagonal branch with lesions > 75%. RA grafts were anastomosed proximally in the aorta (retro-aortic), through the orifice performed with a scalpel, using continuous suture with 6.0 or 7.0 polypropylene, and distally to the coronary branches, using continuous end-to-side anastomosis with 7.0 polypropylene suture. The right coronary artery and its branches, as well as arteries with lesions > 75% received saphenous vein grafts.
The following intraoperative variables were analyzed: RA length and free RA flow. Pathological examination of RA endothelial behavior was also performed in both groups.
All patients received isosorbide mononitrate (0.8 mg/kg per min) and diltiazem (2 mg/kg per min) infused intraoperatively and up to 24 h after operation, followed by 20 mg and 180 mg/day orally, respectively, in addition to antiplatelet therapy for at least 6 months. The incidence of MI was monitored by electrocardiograms and serial analyses of serum CK-MB.
Angiography and flowmetry protocolPatients underwent angiography and flowmetry between
postoperative days 7 and 10. The test was performed via the femoral access. The grafts were analyzed by a senior cardiologist and classified according to presence or absence of: non-obstructive stenosis (< 50%), obstructive stenosis (> 50%) and total occlusion.
The average peak velocity and the RA graft flow were recorded in the initial portion (3 cm of the proximal anastomosis) of the RA in both groups. For these measurements, we used a 12-MHz Doppler guide of 0.014 inches (0.035 cm) in diameter, and 175 cm in length (Flowire; Cardiometrics Inc)13. The records were performed at rest and in hyperemia, which was induced by the injection of 30 µg of adenosine directly into the graft. Graft flow reserve consisted of the ratio between the peak velocities in hyperemia and at rest. The blood flow at the proximal portion of the grafts was calculated using the Doucette method13, with the time average of peak velocity and the cross-sectional area of the graft. This area was obtained after determining the diameter by quantitative angiography for the analysis of the margin contour. Absolute dimensions were calculated, using the diagnostic catheter diameter as reference.
Statistical analysisData are expressed as mean ± standard deviation or
as percentages, and were analyzed using Mann-Whitney non-parametric test, chi-square or Fisher’s exact test, when appropriate. The sample size was projected for a 90% power to identify a 10% difference in graft patency, with the significance level set at 5%. P values lower than 0.05 were considered significant, as determined using the SPSS for Windows, version 13.0 (SPSS, Inc., Chicago, IL).
ResultsEach group comprised 20 patients. There was no hospital
mortality. The surgical variables are shown in Table 1. The postoperative complications were: atrial fibrillation (five cases), paroxysmal supraventricular tachycardia (one case), bronchial pneumonia (one case), re-operation due to bleeding in the immediate post-operative period (two cases), surgical wound infection (one case). The length of the RA grafts in the intraoperative period was 171 ± 22.5 mm, on average, in GI, and 163.5 ± 24.4 mm in GII (p = 0.414); and the free RA stroke volume, as calculated with a similar mean blood pressure, was 84.6 ± 53.1 ml/min in GI, and 95.5 ± 63.3 ml/min in GII (p = 0.627). There were no differences between the groups as regards pathological examinations.
Angiographic dataThirty-nine patients underwent cardiac catheterization
in the immediate postoperative period. At the moment of the procedure, there were no variations in blood pressure, heart rate, and hematocrit between the groups. The previous global patency between the groups was similar (p = NS), of 100% in GI (n = 19), and of 95% in GII (n = 20); however, perfect patency was different (p = 0.045) due to the fact
442

Original Article
Bonini et al.Skeletonization x Pedicle Preparation of Radial Artery
Arq Bras Cardiol. 2014; 102(5):441-448
Table 1 – Clinical and surgical variables
Group I ( n = 20) Group II (n = 20) p-Value
Age (y) 52 ± 6.8 54 ± 5 0.221
Sex (M/F) 17/3 16/4 NS
High Blood Pressure (n) 17 (85%) 19 (95%) 0.605
Dislipidemia (n) 8 (40%) 9 (45%) 0.749
Diabetes (n) 6 (30%) 5 (25%) 0.723
Smoking habit (n) 11 (55%) 10 (50%) 0.752
Stable Angina (n) 17 (85%) 17 (85%) NS
Previous AMI (n) 3 (15%) 3 (15%) NS
CPB Time (min) 86 ± 23.76 89.1 ± 21.3 0.862
Anoxia Time (min) 60.5 ± 13.6 64.7 ± 16.9 0.429
Arterial Graft Revasc. (n) 2.2 ± 0.44 2.2 ± 0.4 NS
Total Revasc. Vessels (n) 3.25 ± 0.8 3.15 ± 0.8 NS
RITA (n) 2 4 NS
Saphenous veins(n) 17 15 NS
M: Male; F: Female; AMI: Acute myocardial infarction; CPB: Cardiopulmonary bypass; RITA: Right Internal Thoracic Artery.
that GI presented only one RA graft with non-obstructive stenosis (< 50%), while GII presented five RA grafts with stenosis (Figure 1), in addition to one occlusion (Figure 2).
Quantitative AngiographyThe mean proximal diameter of the RA was 2.66 ± 0.11 mm
in GI, and 2.53 ± 0.05 mm in GII, with 95% CI (Figure 3).The average peak velocities in the initial portion of the
RA at rest was 18.92 ± 1.75 cm/s in GI, and 18 ± 1.9 cm/s in GII. The RA graft flow reserve was 2.12 ± 0.11 in GI, and 2.01 ± 0.1 in GII (Figure 4). The blood flow in the initial portion of the RA was 54.92 ± 7.66 ml/min in GI, and 44.19 ± 5.13 in GII (Figure 5).
DiscussionThe present study did not demonstrate differences between
the surgical characteristics of RA grafts. Taggart et al3 identified some advantages of the skeletonized RA, anticipating clearly its length, providing an option for the surgeon to choose the type of anastomosis (using it for more than one graft, sequentially, or also serving as an extension for other vessels)3. In this study, although we did not find any statistical differences between the groups regarding the RA length, skeletonization provided us with a better notion of the graft extension. Rukosujem observed the difference in the length of the skeletonized RA in relation to RAs with adjacent tissues, dissected with the use of scissors and clips14.
There were no anatomical and pathological differences between the groups. This includes severe endothelial lesion due to electrocauterization and intimal thickening. Rukosujem observed a larger number of endothelial lesions in patients that had RA skeletonized with ultrasonic scalpels14.
Achouh and Acar15 discussed the follow-up results of 629 radial artery grafts performed over 20 years. Focal stenosis
occurred in 3% of RAs, while string signs were observed in 0.9%. Overall graft patency was 83%. Graft patency decreased exponentially during the first postoperative year, but patency declined at a linear rate with low attrition afterwards, suggesting a lack of radial graft disease15.
In the present study, the postoperative angiography showed evidences of a similar global patency between the groups, but a difference in perfect patency, due to the larger number of non-obstructive stenosis (<50%) and to an occlusion in the RA grafts with adjacent tissues. Skeletonization allows, thorough more faithful visual inspection, the identification of spasms or areas with lesions, which may not be visible in the grafts with adjacent tissues, thus improving the angiographic quality of the graft.
The difference between the global and perfect patency of the RA with adjacent tissues has been demonstrated since the 1990’s by several authors. Parolari et al16 published a literature review presenting an early global average patency of 98.1%, and perfect patency of 90.8% of RA grafts with adjacent tissues17. The authors also reported average global and perfect patency rates of 93.3% and 78.8%, respectively, between 6 and 36 months after surgery. Similar differences were also observed by other authors18,19.
Corroborating the results of our angiographic investigation, Amano et al, in a non-random series of cases, found RA total patency of 98.6% and 98.8%, respectively, for skeletonized RA and with adjacent tissues; while perfect patency was of 96.5% and 84.9%, respectively20. Hirose et al showed early angiographic results of skeletonized RA with ultrasonic scalpels of 96% for perfect patency (free of stenosis), with no differences in comparison to the patency of other arterial grafts21. In 2004, Hirose et al also published angiographic outcomes of a one-year follow-up, showing that 20 patients who received skeletonized RA presented a perfect patency rate of 95.2%22.
443

Original Article
Bonini et al.Skeletonization x Pedicle Preparation of Radial Artery
Arq Bras Cardiol. 2014; 102(5):441-448
Figure 1 – Pedicled radial artery with non-obstructive lesion in the proximal third.
Ali et al concluded that skeletonization of the RA provides valuable patency results. Therefore, if the RA is to be used as a conduit in Coronary Artery Bypass Graft surgery, it may be harvested in either a skeletonized or pedicled fashion, however, their study suggested that skeletonitazion may offer the radial conduit some patency benefit when compared to the pedicled technique23. Tokuda et al24 found that for grafts to the left coronary system, a mean flow < 15 ml/min, and for grafts to the right coronary system, a mean flow < 20 ml/min were predictive of graft failure.
The proximal internal diameters of the RA grafts, as calculated using the quantitative angiographic method were similar in this study. There is no previous information comparing the internal proximal diameter of RAs. However, when this parameter was analyzed in the skeletonized and pediculated LITA using quantitative angiography, a significant increase in the proximal internal diameter with skeletonization was described5.
Webb et al reported a radial artery diameter by quantitative coronary angiography of approximately 2.7 mm in 15 cases after a 5-year follow-up25.
In the analysis of the flow variables (intravascular blood flow, average peak velocity, RA graft flow reserve) using intravascular Doppler flowmetry in the immediate postoperative period, we did not observe any statistical difference between the two study groups. The intravascular Doppler methodology employed in
this study for the collection of data (blood flow velocity) is highly reliable13. The behavior of blood flow of the LITA graft to the left anterior descending artery had already been studied by Akasaka et al using Doppler flowmetry in 199526. They showed that the blood flow was of 62±17 ml/min at rest and the coronary flow reserve, of 1.8 ± 0.3. Similar results were also observed by Gurné et al27. Takami and Ina5 compared two strategies for the dissection of LITA – skeletonized and pediculated, and, using intraoperative flowmetry, they found a superior flow (42.6 ± 29.1 ml/min) of skeletonized LITA in relation to pediculated LITA (26.4 ± 16.1 ml/min)21. On the other hand, Rukosujew et al15 calculated the perivascular free blood flow in 40 patients who received either skeletonized RA or with adjacent tissues, and found no statistical differences between the groups, similar to the results observed in the current study.
Webb et al25 calculated a mean coronary graft volume blood flow baseline of 35 ml/min in graft radial artery. The coronary flow reserve has also been a variable increasingly used for the assessment of coronary lesions and outcomes of percutaneous interventions. Similarly to average peak velocity, this parameter may display large variations in patients with angiographically normal arteries. Based on the experience with the analysis of coronary flow reserve in LITA, and reported by Webb et al25, the mean coronary flow reserve in radial graft was 2.3 with the use of velocity measurements.
444

Original Article
Bonini et al.Skeletonization x Pedicle Preparation of Radial Artery
Arq Bras Cardiol. 2014; 102(5):441-448
Figure 2 – Pedicled radial artery proximally occluded.
Figure 3 – Mean proximal internal angiographic diameter of the radial artery (p = 0.492). Mean ± 95% CI.
445

Original Article
Bonini et al.Skeletonization x Pedicle Preparation of Radial Artery
Arq Bras Cardiol. 2014; 102(5):441-448
Figure 4 – Coronary Flow Reserve of the radial artery (p = 0.624). Mean ± 95%CI.
Figure 5 – Blood flow of the radial artery at rest (p = 0.435). Mean ± 95% CI.
In this study the RA graft flow reserve was 2.12±0.11 in GI, and of 2.01±0.1 in GII. We can conclude that it was satisfactory in this study, thus demonstrating a significant perspective of RA adaptability to different coronary territories.
In conclusion, the results of the present study, with a selected group of patients, allow us to state that the morphologic, functional and hemodynamic performances of RA aorto-coronary grafts to left coronary branches are similar, whether it is prepared
in a skeletonized or pedicled manner. However, the higher frequency of obstruction and stenosis occurring in pedicled grafts may pose a limitation to their long-term performance.
Author contributionsConception and design of the research and Statistical analysis:
Bonini RCA, Moreira, LFP; Acquisition of data and Analysis and interpretation of the data: Bonini RCA, Staico R; Obtaining funding
446

Original Article
Bonini et al.Skeletonization x Pedicle Preparation of Radial Artery
Arq Bras Cardiol. 2014; 102(5):441-448
1. Carpentier A, Guermonprez JL, Deloche A, Frechette C, DuBost C. The aorta-to-coronary radial artery bypass graft: a technique avoiding pathological changes in grafts. Ann Thorac Surg. 1973;16(2):111-21.
2. Acar C, Jebara VA, Portoghese M, Beyssen B, Pagny JY, Grare P, et al. Revival of the radial artery for coronary artery bypass grafting. Ann Thorac Surg. 1992;54(4):652-9.
3. Taggart DP, Mathur MN, Ahmad I. Skeletonization of the radial artery: advantages over the pedicle technique. Ann Thorac Surg. 2001;72(1):298-9.
4. Cunningham JM, Gharavi MA, Fardin R, Meek RA. Considerations in the skeletonization technique of internal thoracic artery dissection. Ann Thorac Surg. 1992;54(5):947-50.
5. Takami Y, Ina H. Effects of skeletonization on intraoperative flow and anastomosis diameter internal thoracic arteries in coronary artery bypass grafting. Ann Thorac Surg. 2002;73(5):1441-5.
6. Gaudino M, Trani C, Glieca F, Mazzari MA, Rigattieri S, Nasso G, et al. Early vasoreactive profile of skeletonized versus pedicle internal thoracic artery grafts. J Thorac Cardiovasc Surg. 2003;125(3):638-41.
7. Moran SV, Baeza R, Guarda E, Zalaquett R, Irarrazaval MJ, Marchant E, et al. Predictors of radial artery patency for coronary bypass operations. Ann Thorac Surg. 2001;72(5):1552-6.
8. Allen EV. Thromboangiitis obliterans: methods of diagnosis of chronic occlusive arterial lesions distal to the wrist illustrative cases. Am J Med Sci. 1929;178:237-44.
9. Ejrup B, Fischer B, Wright IS. Clinical evaluation of blood flow to the hand: the false-positive Allen test. Circulation. 1966;33(5):778-80.
10. Johnson WH 3rd, Cromartie RS 3rd, Arrants JE, Wuamett JD, Holt JB. Simplified method for candidate selection for radial artery harvesting. Ann Thorac Surg. 1998;65(4):1167.
11. Starnes SL, Wolk SW, Lampman RM, Shanley CJ, Prager RL, Kong BK, et al. Nonivasive evaluation of hand circulation before radial artery harvest for coronary artery bypass grafting. J Thorac Cardiovasc Surg. 1999;117(2):261-6.
12. Reyes AT, Frame R, Brodman R. Technique for harvesting the radial artery as a coronary artery bypass graft. Ann Thorac Surg. 1995;59(1):118-26.
13. Doucette JW, Corl D, Payne HM, Flynn AE, Goto M, Nassi M, et al. Validation of a Doppler guide wire for intravascular measurement of coronary artery flow velocity. Circulation. 1992;85(5):1899-911.
14. Rukosujem A, Reichelt R, Fabricius AM, Drees G, Tjan TDT, Rothenburger M, et al. Skeletonization versus pedicle preparation of the radial artery with and without the ultrasonic scalpel. Ann Thorac Surg. 2004;77(1):120-5.
15. Achouh P, Acar C. Twenty-year fate of the radial artery graft. Ann Cardiothorac Surg. 2013;2(4):481-4.
16. Parolari A, Rubini P, Alamanni F, Cannata A, Xin W, Gherli T, et al. The radial artery: which place in coronary operation? Ann Thorac Surg. 2000;69(4):1288-94.
17. Weinschelbaum EE, Gabe ED, Macchia A, Smimmo R, Suárez LD. Total myocardial revascularization with arterial conduits: radial artery combined with internal thoracic arteries. J Thorac Cardiovasc Surg. 1997;114(6):991-6.
18. Acar C, Ramsheyi A, Pagny JY, Jebara V, Barrier P, Fabiani JN, et al. The radial artery coronary for artery after bypass grafting: clinical and angiographic results at for five years. J Thorac Cardiovasc Surg. 1998;116(6):981-9.
19. Possati GF, Gaudino M, Alessandrini F, Luciani N, Glieca F, Trani C, et al. Midterm clinical and angiographic results of radial artery grafts used for myocardial revascularizaton. J Thorac Cardiovasc Surg . 1998;116(6):1015-21.
20. Amano A, Takahashi A, Hirose H. Skeletonized radial artery grafting: improved angiographic results. Ann Thorac Surg. 2002;73(6):1880-7.
21. Hirose H, Amano A. Skeletonized radial artery grafting: one-year patency rate. Heart Surg Forum. 2004;7(4):E277-82.
22. Hirose H, Amano A, Takahashi A, Takanashi S. Skeletonization of the radial artery with the ultrasonic scalpel: clinic angiographic results. Heart Surg Forum. 2003;6(3):E42-7.
23. Ali E, Saso S, Ahmed K, Athanasiou T. When harvested for coronary artery bypass graft surgery does a skeletonized or pedicled radial artery improve conduit patency? Interact Cardiovasc Thorac Surg. 2010;10(2):289-92.
24. Tokuda V, Song MH, Oshima H, Usui A, Ueda Y. Predicting coronary bypass graft failure by intraoperative transit time flow measurement. Ann Thorac Surg. 2007;84(6):1928-33.
25. Webb CM, Moat NE, Chong CF, Collins P. Vascular reactivity and flow characteristics of radial artery and long saphenous vein coronary bypass grafts: a 5-year follow-up. Circulation. 2010;122(9):861-7.
26. Akasaka T, Yoshikawa J, Yoshida K, Maeda K, Hozumi T, Nasu M, et al. Flow capacity of internal mammary artery grafts: early restriction and late improvement assessed by Doppler guide wire: comparison with saphenous vein grafts. J Am Coll Cardiol. 1995;25(3):640-7.
27. Gurné O, Chenu P, Polidori C, Louagie Y, Buche M, Haxhe JP, et al. Functional evaluation of internal mammary artery bypass grafts in the early and late postoperative periods. J Am Coll Cardiol. 1995;25(5):1120-8.
References
and Writing of the manuscript: Bonini RCA; Critical revision of the manuscript for intellectual content: Bonini RCA, Dinkhuysen JJ, Moreira, LFP; Performed surgery: Issa M, Arnoni AS, Chaccur P, Abdulmassih Neto C, Dinkhuysen JJ, Paulista PP, Souza LCB.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
This study was funded by Instituto Dante Pazzanese de Cardiologia.
Study Association
This article is part of the thesis of Doctoral submitted by Rômulo C. Arnal Bonini from Faculdade de Medicina da USP.
447

Original Article
Bonini et al.Skeletonization x Pedicle Preparation of Radial Artery
Arq Bras Cardiol. 2014; 102(5):441-448 448

Original Article
Does C-reactive Protein Add Prognostic Value to GRACE Score in Acute Coronary Syndromes?Luis Cláudio Lemos Correia1,2, Isis Vasconcelos1,2, Guilherme Garcia1,2, Felipe Kalil1,2, Felipe Ferreira1,2, André Silva1,2, Ruan Oliveira1,2, Manuela Carvalhal1,2, Caio Freitas1,2, Márcia Maria Noya-Rabelo1,2
Escola Bahiana de Medicina e Saúde Pública1; Hospital São Rafael2, Salvador, BA - Brazil
Mailing Address: Luis Cláudio Lemos Correia •Av. Princesa Leopoldina 19/402, Graça. Postal Code 40150-080, Salvador, BA – BrazilE-mail: [email protected]; [email protected] received July 30, 2013; revised manuscript October 30, 2013; accepted December 18, 2013.
DOI: 10.5935/abc.20140056
Abstract
Background: The incremental prognostic value of plasma levels of C-reactive protein (CRP) in relation to GRACE score has not been established in patients with acute coronary syndrome (ACS) with non-ST segment elevation.
Objective: To test the hypothesis that CRP measurements at admission increases the prognostic value of GRACE score in patients with ACS.
Methods: A total of 290 subjects, consecutively admitted for ACS, with plasma material obtained upon admission CRP measurement using a high-sensitivity method (nephelometry) were studied. Cardiovascular outcomes during hospitalization were defined by the combination of death, nonfatal myocardial infarction or nonfatal refractory angina.
Results: The incidence of cardiovascular events during hospitalization was 15% (18 deaths, 11 myocardial infarctions, 13 angina episodes) with CRP showing C-statistics of 0.60 (95% CI = 0.51-0.70, p = 0.034) in predicting these outcomes. After adjustment for the GRACE score, elevated CRP (defined as the best cutoff point) tended to be associated with hospital events (OR = 1.89, 95% CI = 0.92 to 3.88, p = 0.08). However, the addition of the variable elevated CRP in the GRACE model did not result in significant increase in C-statistics, which ranged from 0.705 to 0.718 (p = 0.46). Similarly, there was no significant reclassification of risk with the addition of CRP in the predictor model (net reclassification = 5.7 %, p = 0.15).
Conclusion: Although CRP is associated with hospital outcomes, this inflammatory marker does not increase the prognostic value of the GRACE score. (Arq Bras Cardiol. 2014; 102(5):449-455)
Keywords: C-Reactive Protein; Acute Coronary Syndrome; Prognosis; Probability.
IntroductionIn patients with acute coronary syndrome (ACS) with
non-ST-segment elevation, the inflammatory phenomenon hinders the atherosclerotic plaque stabilization, making it vulnerable to recurring coronary events1. This is the rationale for the prognostic value of inflammatory markers in ACS. Among these markers, High-Sensitivity C-Reactive Protein (hs-CRP) is the best studied as a risk predictor in clinical practice2. Actually, several studies have shown an association between CRP and cardiovascular risk in patients with ACS3.
The prognostic association, however, is not a sufficient criterion to define the clinical usefulness. A new biomarker usefulness depends on the demonstration of its incremental value in prognostic models traditionally used in clinical practice4. Our group previously demonstrated that CRP
modestly increases the TIMI risk score5. In recent years, the GRACE score has shown to be the multivariate model with the best accuracy6. However, the incremental value of CRP in relation to GRACE score is yet to be established.
To test the hypothesis that the measurement of CRP increases the prognostic value of the GRACE score, this marker was measured at admission in patients with ACS with non-ST segment elevation and recurrent events were recorded prospectively. Discriminatory analysis (C-statistics) and net reclassification were used as measures of incremental value.
Methods
Sample SelectionIndividuals consecutively admitted to the Coronary
Care Unit of two tertiary hospitals between August 2007 and December 2011, with a diagnosis of unstable angina or myocardial infarction with non-ST segment elevation, were candidates for the Acute Coronary Syndrome Registry (RESCA). The inclusion criteria for this registry is defined by typical chest discomfort and at rest in the past 48 hours, associated with at least one of the following: 1) positive myocardial necrosis marker, defined by troponin T ≥ 0.01 ug/L or troponin I > 0.034 g/L, which
449

Original Article
Correia et al.C-reactive protein and GRACE
Arq Bras Cardiol. 2014; 102(5):449-455
correspond to values above the 99th percentile7,8; 2) ischemic electrocardiographic alterations, consisting of T-wave inversion (≥ 0.1 mV) or transient ST‑segment depression (≥ 0.05 mV); 3) previously documented coronary artery disease, defined as history of myocardial infarction or previous angiography demonstrating coronary obstruction ≥ 50%. We excluded patients whose admission plasma samples were insufficient for CRP measurement and those that refused to participate in the study. The protocol complies with the Declaration of Helsinki and was approved by the Research Ethics Committee of the institution and all patients signed the free and informed consent form.
High-Sensitivity C-Reactive Protein measurementThe measurement of hs-CRP was carried out in a blood
sample collected immediately after hospital admission, aiming at attaining minimum delay between symptom onset and material collection. The plasma was frozen at -70°C for simultaneous measurement of the sample. The nephelometry method (Dade - Behring, Newark, Delaware, USA) was used9. The assistant team was blinded to the CRP values during patient hospitalization.
GRACE scoreTo calculate the GRACE score, patients’ clinical data
collected at the emergency department, electrocardiograms performed within 6 hours of treatment, troponin T measurements related to the first 12 hours of care and the value of the first plasma creatinine were used. Elevation of myocardial necrosis marker as component of the scores was defined as troponin > 99th percentile8. The Killip classification was also applied to patients with unstable angina so that the GRACE score could be calculated. The GRACE score consists of eight variables: five of them are computed semiquantitatively, i.e., different weight for each stratum of age, systolic blood pressure, heart rate, plasma creatinine and Killip class; three of them computed dichotomously (ST-segment depression, myocardial necrosis marker elevation, cardiac arrest on admission). The final score can range from 0 to 37210.
Cardiovascular outcomesThe primary outcome was defined by the combination
of cardiovascular death, nonfatal myocardial infarction or nonfatal refractory angina during hospitalization. Nonfatal myocardial infarction was recorded during hospitalization when there was elevation of troponin > the 99th percentile in patients whose values were negative in the first 24 hours. For patients with infarction on admission, a new CK-MB peak (>50% of the previous value and above the normal value) was required for the definition of reinfarction. Elevation of necrosis markers induced by percutaneous coronary procedure or CABG was not recorded as a recurrent event. Refractory angina during hospitalization was defined by recurrent chest pain at least twice, despite the use of nitrates and controlled double product.
Additionally, patients were contacted by telephone after 30 days, 6 months, and annually thereafter for the detection of combined cardiovascular death, myocardial infarction or
readmission for unstable angina. Readmission was identified by telephone contact and the reason was checked through an interview with the patient and medical record data. Cardiovascular death was defined as sudden death or cardiovascular hospitalization followed by death.
Statistical AnalysisInitially, a Receiver Operating Characteristic (ROC) curve
of CRP levels was constructed to be used as predictors of cardiovascular outcome. Once the accuracy by the ROC curve was demonstrated, the best cutoff point was identified.
This cutoff was used to define elevated CRP, which was entered into a logistic regression model with the GRACE score. If elevated CRP reached statistical significance at the 10% level (p < 0.10), a new GRACE-CRP score would be created, by adding points when CRP was elevated. Additional points were determined by the ratio between the regression coefficient of elevated CRP and the regression coefficient of the GRACE score.
In the discriminant analysis, C-statistics of the GRACE and GRACE-CRP models were compared by the Hanley – McNeil test11. The calibration of the models was described by the Hosmer-Lemeshow test. Furthermore, we evaluated the capacity of the new model (GRACE- CRP) to correctly reclassify information from the traditional GRACE model (high risk versus low risk). The best cutoff from each model in our sample was used for risk definition. The Pencina method (Net Reclassification Improvement-NRI) was used in the net reclassification analysis12 (Figure 1).
CRP values were described as median and interquartile range (IQR) and compared between groups by the non-parametric Mann-Whitney test. Statistically significant p value was defined as < 0.05. SPSS software, version 21 (IBM North America, New York, NY) was used.
Sample size calculationThe sample was sized to provide statistical power for two
predefined statistical analysis. First, the logistic regression analysis, in which we evaluated the predictive value of CRP, regardless of the GRACE score. As this analysis requires two covariates (elevated CRP and GRACE), 20 outcomes are necessary to maintain the recommended ratio of 10 outcomes per covariable13. Second, comparison of the GRACE C-statistics versus GRACE-CRP: assuming a correlation coefficient between the values of two models of 0.95 for a statistical power of 80% (one-tailed alpha of 0.05) in the detection of 0.05 superiority of C-statistics (e.g., 0.65 versus 0.70) of the most complete model (GRACE- CRP) a total of 42 outcomes are required11. Thus, we sequentially included the number of patients necessary to total 42 hospital outcomes, which was enough for both analyses described herein.
Results
Selected sampleA total of 290 patients aged 68 ± 13 years, 52 % females,
53% with a diagnosis of myocardial infarction with non-ST segment elevation and the rest with unstable angina were studied.
450

Original Article
Correia et al.C-reactive protein and GRACE
Arq Bras Cardiol. 2014; 102(5):449-455
The GRACE score showed a median of 115 (IQR = 94-140), with 43% being low risk, 32% medium risk and 25% high risk. The median time between symptom onset and CRP measurement was 6.7 hours (IQR = 3.3 to 24). CRP showed a median of 4.5 mg/L (IQR = 1.4 to 13 mg/L), showing increased inflammatory activity exacerbated by the acute clinical picture. The incidence of cardiovascular outcomes during hospitalization was 15% (18 cardiovascular deaths, 11 nonfatal AMIs, 13 cases of nonfatal refractory angina). After discharge, 244 patients were followed for 518 ± 446 days, with an incidence of cardiovascular outcomes of 24% (11 cardiovascular deaths, 18 hospitalizations for AMI and 28 hospitalizations for angina).
Prognostic value of C-reactive proteinPatients who developed hospital outcome showed median
CRP of 9.1 mg/L (IQR = 2.1 to 22 mg/L), significantly higher than the median of 4.3 mg/L (IQR = 1.3 to 11 mg/ L) observed in patients free of outcomes (p = 0.034). The predictive capacity of CRP in relation to hospital outcomes was characterized by C-statistics of 0.60 (95% CI = 0.51-0.70). In this analysis, the definition of elevated CRP that showed the best accuracy corresponded to a cutoff of 8.83 mg/L.
Analysis of clinical characteristics showed that the group with elevated CRP had modestly older mean age, higher prevalence of positive troponin and Killip > 1, all variables found in the GRACE score, not requiring their entering the multivariate model. Variables not covered by GRACE, as well as treatment variables, were similar between groups (Table 1). When the CRP was adjusted for the GRACE score, statistical significance was reduced to a borderline value (OR = 1.9, 95% CI = 0.92- 3.9, p = 0.08). In this model, the association between the GRACE regression coefficient and the CRP coefficient was 30. Thus,
at the construction of the GRACE-CRP score 30 points were added when CRP was elevated.
Different from the in-hospital phase, CRP values showed no predictive accuracy for cardiovascular outcomes in the late follow-up, with C-statistics of 0.51 (95 % CI = 0.42 to 0.59, p = 0.90). The same occurred when only the hard endpoints of death and nonfatal myocardial infarction were considered (C -statistics = 0.59, 95% CI = 0.49-0.69, p = 0.11).
Incremental value of CRP during hospitalizationThe addition of the variable elevated CRP to the GRACE
model did not result in significant increase in C-statistics, which ranged from 0.705 to 0.718 (p = 0.46) (Figure 2). The GRACE score showed satisfactory calibration with |2 using the Hosmer - Lemeshow test of 7.5 (p = 0.48). After inclusion of elevated CRP in the model, there was no improvement in calibration, which evolved into |2 of 12.1 and p value = 0.15 (Table 2).
Reclassification of the GRACE score by C-reactive proteinAmong the 42 patients who had hospital outcomes, two
were wrongly reclassified from high to low risk, whereas there was no correct reclassification. This resulted in negative net reclassification index for patients with outcomes (- 4.8%).
Among the 248 patients free of hospital outcomes, 26 were correctly reclassified from high to low risk, with no incorrect reclassifications. This resulted in a positive net reclassification index for patients without outcomes (10.5 %).
In the final analysis, when all patients were considered, the net reclassification index was 5.7 % (p = 0.15), indicating that CRP has no value as reclassifying variable of the GRACE score (Table 3).
Figure 1 – Flowchart of data analysis. CRP: C-reactive protein; ROC: Receiver operating characteristic.
ROC curve: prognostic value of CRP
Identification of the best CRP cutoff
Logistic regression: CRP adjustment for GRACE score
GRACE-CRP model: incorporation of CRP into the GRACE model
GRACE versus GRACE-CRP
Comparison of ROCs Analysis of reclassification
451

Original Article
Correia et al.C-reactive protein and GRACE
Arq Bras Cardiol. 2014; 102(5):449-455
Table 1 – Comparison of clinical characteristics between patients with and without elevated C-reactive protein
CRP ≥ 8.83 mg/L CRP < 8.83 mg/L p value
Sample 91 199
Age (years) 71 ± 13 67 ± 13 0.07
Male gender 48 (53%) 90 (45%) 0.23
Diabetes 38 (42%) 77 (39%) 0.62
Positive troponin 62 (68%) 93 (47%) 0.001
ST segment elevation 22 (24%) 35 (18%) 0.19
Killip > 1 29 (32%) 22 (11%) < 0.001
Creatinine clearance (mL/min) 49 ± 25 57 ± 22 0.01
GRACE score 136 ± 39 113 ± 35 < 0.001
In-Hospital treatment
Aspirin 87 (97%) 197 (100%) 0.10
Clopidogrel /Ticagrelor 80 (89%) 184 (93%) 0.25
Subcutaneous enoxaparin 76 (84%) 167 (84%) 1.0
Intravenous unfractionated heparin 3 (88%) 4 (86%) 0.68
GP IIb / IIIa antagonist 6 (6.6%) 7 (3.5%) 0.36
Nitrate 69 (76%) 139 (70%) 0.33
Beta-blocker 67 (74%) 141 (72%) 0.77
Statin 85 (96%) 193 (98%) 0.38
Percutaneous coronary intervention 27 (30%) 60 (30%) 1.0
Coronary artery bypass grafting 10 (11%) 15 (8.0%) 0.30
CRP: C-reactive; GP: Platelet dycoprotein.
Figure 2 – Comparison of ROC curves between GRACE and GRACE-CRP shows similar C-statistics between the two scores (p = 0.46).
452

Original Article
Correia et al.C-reactive protein and GRACE
Arq Bras Cardiol. 2014; 102(5):449-455
Table 2 – Logistic regression model containing GRACE and CRP in predicting hospital outcomes
Variable Coefficient ® Odds Ratio (95%CI) p value
Elevated CRP (dichotomy) 0.638 1.89 (0.92 – 3.9) 0.08
GRACE score (numeri`cal) 0.021 1.02 (1.01 – 1.03) < 0.001
CI: confidence interval
Table 3 – Analysis of net reclassification by CRP-GRACE score in relation to the GRACE score for the definition of high risk
N Reclassification for more Reclassification for less NRI p value
Outcome 42 0 2 - 4.8%
No outcome 248 0 26 10.5%
Total 290 0 28 5.7% 0.15
DiscussionThis prospective cohort study tested the prognostic
value of CRP measured at admission of patients with ACS with non-ST segment elevation. Consistent with previous studies, CRP was associated with cardiovascular outcomes during hospitalization. However, CRP incremental analysis indicated the lack of usefulness for this marker in clinical practice. This apparent contradiction between association with outcome and the lack of incremental value needs to be interpreted.
The strength of the inflammatory hypothesis as a mechanism of genesis and destabilization of atherosclerotic plaques increased in the 1990s, based on experimental studies1, followed by evidence of the association of CRP with cardiovascular risk in the general population14. In the 2000s, several studies were published in journals of high impact, favorable to the prognostic value of CRP in patients with ACS. These studies were analyzed as a systematic review and meta-analysis by our group, which was published in 20103. Unlike the enthusiastic attitude of some authors, our review concluded that there was no conclusive evidence of the incremental prognostic value of CRP. Moreover, only two studies had made incremental evaluation (preliminary studies)5,15, while the remainder was limited to the assessment of independent association .
It is noteworthy that an independent association is not enough to establish the usefulness of a biomarker. To interrupt the predictor evaluation at this stage, considering it validated for clinical use, has been a common error16. The most important question is whether the new risk marker has incremental usefulness in models applied in clinical practice. This response should be obtained by comparing the performance of a predictive model that uses the usual variables with the performance of an alternative model resulting from the incorporation of the new marker into the traditional model. That is, after inserting a new variable to a risk score, how much does the performance of this score improve? The most common way to evaluate this question is to measure the increase in C-statistics after incorporation of the new biomarker, which was not done by most of the
studies in that review. Furthermore, we analyzed the net reclassification, which identifies the correct reclassifications (upwards in a patient that will have an outcome and downwards in a patient without outcome) and subtract from the incorrect ones. This method shows the proportion of patients in which the advent of the new biomarker promoted a correct change in relation to the risk.
Over the past three years, two new studies have been published. A Spanish study where Lopes-Cuenca et al. showed no increase in CRP in the C-statistics of GRACE17 and a French study, in which He et al18 seem to have demonstrated positive data. However, when analyzing the details, one can see that the data of He et al18 suggest the same negative conclusion of our study. As for the discriminatory value, those authors describe a modest increase in C-statistics, from 0.795 to 0.823. Although this difference was statistically significant, its magnitude is of little clinical relevance. Second, the authors take into account a correct reclassification of 12%. However, the net reclassification in which the incorrect are subtracted from the correct is not calculated. If this had been done, absence of reclassification would have been the conclusion. In the present study, we performed C-statistical analysis and correctly applied the Pencina method of reclassification, concluding realistically for the absence of clinical usefulness in incorporating CRP into the routine assessment of patients with ACS.
Thus, the apparent contradiction between the enthusiasm of initial studies and recent evidence is explained by the lack of careful analysis that the first studies performed in their own data. In recent years, the evolution of the scientific community regarding the concept of usefulness of a new biomarker has become stricter regarding data analysis, which ultimately should include incremental value. The CRP is not approved according to this analysis and our study is further evidence in this direction.
The main limitation of this study is its sample size, and thus, our data cannot be considered definitive regarding the lack of any prognosis increment with CRP. On the other hand, we must emphasize that this result is in line with previous studies, which showed no significant improvement
453

Original Article
Correia et al.C-reactive protein and GRACE
Arq Bras Cardiol. 2014; 102(5):449-455
in C-statistics17,18. In addition, our number of outcomes resulted in enough statistical power to identify any clinically relevant increase in C-statistics. As for the late follow-up, there was a loss of 16% in the sample, which is not desirable. Moreover, we emphasize that this follow-up represents a secondary objective of the study and it is unlikely that there would be such difference regarding the characteristics of 46 patients without follow-up to the point of modifying a prior entirely negative result.
We must acknowledge that these data do not definitively rule out the usefulness of other inflammatory markers such as cytokines. In a previous study, our group demonstrated the potential value of a composite score with several inflammatory markers19 and this year a Spanish study showed very significant increase and reclassification with interleukin - 6 in relation to GRACE17.
ConclusionThe limited incremental value of CRP in relation to GRACE
score suggests that the incorporation of this new biomarker in clinical practice for patients with ACS with non-ST-segment elevation is not indicated.
Author contributionsConception and design of the research: Correia LCL, Silva
A, Noya-Rabelo MM; Acquisition of data: Vasconcelos I, Garcia G, Kalil F, Silva A, Oliveira R, Carvalhal M, Freitas C, Ferreira F; Analysis and interpretation of the data: Correia LCL, Carvalhal M, Noya-Rabelo MM; Statistical analysis: Correia LCL; Writing of the manuscript: Correia LCL, Noya-Rabelo MM; Critical revision of the manuscript for intellectual content: Correia LCL, Vasconcelos I, Garcia G, Kalil F, Silva A, Carvalhal M, Ferreira F, Noya-Rabelo MM.
Potential Conflict of InterestNo potential conflict of interest relevant to this article
was reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis study is not associated with any thesis or dissertation work.
1. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation. 2002;105(9):1135-43.
2. Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd, Criqui M, et al; Centers for Disease Control and Prevention; American Heart Association. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003;107(3):499-511.
3. Correia LC, Esteves JP. C-Reactive protein and outcomes in acute coronary syndromes: a systematic review and meta-analysis. Arq Bras Cardiol. 2011;97(1):76-85.
4. Hlatky MA, Greenland P, Arnett DK, Ballantyne CM, Criqui MH, Elkind MS, et al. Criteria for evaluation of novel markers of cardiovascular risk: a scientific statement from the American Heart Association. Circulation. 2009;119(17):2408-16. Erratum in Circulation. 2009;119(25):e606.
5. Correia LC, Lima JC, Rocha MS, D’Oliveira Junior A, Pericles Esteves J. Does high-sensitivity C-reactive protein add prognostic value to the TIMI-Risk Score in individuals with non-ST elevation acute coronary syndromes? Clin Chim Acta. 2007;375(1-2):124-8.
6. Correia LC, Freitas R, Bittencourt AP, Souza AC, Almeida MC, Leal J, et al. [Prognostic value of GRACE scores versus TIMI score in acute coronary syndromes]. Arq Bras Cardiol. 2010;94(5):613-9.
7. Apple FS, Pearce LA, Smith SW, Kaczmarek JM, Murakami MM. Role of monitoring changes in sensitive cardiac troponin I assay results for early diagnosis of myocardial infarction and prediction of risk of adverse events. Clin Chem. 2009;55(5):930-7.
8. Apple FS, Quist HE, Doyle PJ, Otto AP, Murakami MM. Plasma 99th percentile reference limits for cardiac troponin and creatine kinase MB mass for use with European Society of Cardiology/American College of Cardiology consensus recommendations. Clin Chem. 2003;49(8):1331-6.
9. Correia LC, Lima JC, Gerstenblith G, Magalhães LP, Moreira A, Barbosa O Jr, et al. Correlation between turbidimetric and nephelometric methods of measuring C-reactive protein in patients with unstable angina or non-ST elevation acute myocardial infarction. Arq Bras Cardiol. 2003;81(2):133-6, 129-32.
10. Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, Cannon CP, et al; Global Registry of Acute Coronary Events Investigators. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003;163(19):2345-53.
11. Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148(3):839-43.
12. Pencina MJ, D’Agostino RB Sr, D’Agostino RB Jr, Vasan RS. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med. 2008;27(2):157-72.
13. Demidenko E. Sample size and optimal design for logistic regression with binary interaction. Stat Med. 2008;27(1):36-46.
14. Kaptoge S, Di Angelantonio E, Lowe G, Pepys MB, Thompson SG, Collins R, et al; Emerging Risk Factors Collaboration. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet. 2010;375(9709):132-40.
15. Oltrona L, Ardissino D, Merlini PA, Spinola A, Chiodo F, Pezzano A. C-reactive protein elevation and early outcome in patients with unstable angina pectoris. Am J Cardiol. 1997;80(8):1002-6.
16. Tzoulaki I, Liberopoulos G, Ioannidis JP. Assessment of claims of improved prediction beyond the Framingham risk score. JAMA. 2009;302(21):2345-52.
17. Lopez-Cuenca A, Manzano-Fernandez S, Lip GY, Casas T, Sánchez-Martínez M, Mateo-Martínez A, et al. Interleukin-6 and high-sensitivity C-reactive protein for the prediction of outcomes in non-ST-segment elevation acute coronary syndromes. Rev Esp Cardiol. 2013;66(3):185-92.
18. He LP, Tang XY, Ling WH, Chen WQ, Chen YM. Early C-reactive protein in the prediction of long-term outcomes after acute coronary syndromes: a meta-analysis of longitudinal studies. Heart. 2010;96(5):339-46.
19. Correia LC, Andrade BB, Borges VM, Clarencio J, Bittencourt AP, Freitas R, et al. Prognostic value of cytokines and chemokines in addition to the GRACE Score in non-ST-elevation acute coronary syndromes. Clin Chim Acta. 2010;411(7-8):540-5.
References
454

Original Article
Correia et al.C-reactive protein and GRACE
Arq Bras Cardiol. 2014; 102(5):449-455455

Original Article
Relationship between Fibrosis and Ventricular Arrhythmias in Chagas Heart Disease Without Ventricular DysfunctionEduardo Marinho Tassi1, Marcelo Abramoff Continentino2, Emília Matos do Nascimento1,3, Basílio de Bragança Pereira1,3, Roberto Coury Pedrosa1
Instituto de Cardiologia Edson Saad - Universidade Federal do Rio de Janeiro (UFRJ)1; Hospital Frei Galvão, Guaratinguetá, SP2, Coppe – Instituto Alberto Luiz Coimbra de Pós-Graduação e Pesquisa de Engenharia - UFRJ3, Rio de Janeiro, RJ – Brazil
Mailing Address: Eduardo Marinho Tassi •Hospital Universitário Gaffrée e Guinle, Ambulatorio de Cardiologia. Rua Mariz e Barros 775, Tijuca. Postal Code: 20270-004, Rio de Janeiro, RJ - BrazilE-mail: [email protected] received August 22, 2013; revised manuscript December 09, 2013; accepted January 07, 2014
DOI: 10.5935/abc.20140052
Abstract
Background: Patients with Chagas disease and segmental wall motion abnormality (SWMA) have worse prognosis independent of left ventricular ejection fraction (LVEF). Cardiac magnetic resonance (CMR) is currently the best method to detect SWMA and to assess fibrosis.
Objective: To quantify fibrosis by using late gadolinium enhancement CMR in patients with Chagas disease and preserved or minimally impaired ventricular function (> 45%), and to detect patterns of dependence between fibrosis, SWMA and LVEF in the presence of ventricular arrhythmia.
Methods: Electrocardiogram, treadmill exercise test, Holter and CMR were carried out in 61 patients, who were divided into three groups as follows: (1) normal electrocardiogram and CMR without SWMA; (2) abnormal electrocardiogram and CMR without SWMA; (3) CMR with SWMA independently of electrocardiogram.
Results: The number of patients with ventricular arrhythmia in relation to the total of patients, the percentage of fibrosis, and the LVEF were, respectively: Group 1, 4/26, 0.74% and 74.34%; Group 2, 4/16, 3.96% and 68.5%; and Group 3, 11/19, 14.07% and 55.59%. Ventricular arrhythmia was found in 31.1% of the patients. Those with and without ventricular arrhythmia had mean LVEF of 59.87% and 70.18%, respectively, and fibrosis percentage of 11.03% and 3.01%, respectively. Of the variables SWMA, groups, age, LVEF and fibrosis, only the latter was significant for the presence of ventricular arrhythmia, with a cutoff point of 11.78% for fibrosis mass (p < 0.001).
Conclusion: Even in patients with Chagas disease and preserved or minimally impaired ventricular function, electrical instability can be present. Regarding the presence of ventricular arrhythmia, fibrosis is the most important variable, its amount being proportional to the complexity of the groups. (Arq Bras Cardiol. 2014; 102(5):456-464)
Keywords: Arrhythmias, Cardiac; Myocardial Fibrosis; Chagas Heart Disease; Ventricular Dysfunction.
IntroductionChagas disease (CD) remains epidemiologically
important1, because of the high number of infected individuals who can develop severe forms of the disease. In Brazil, two to three million people are estimated to be affected, one third of whom have heart disease, of whom, two thirds are minimally impaired2.
The annual death rate is approximately 24/1,000 patients-year, and most patients have preserved or minimally impaired left ventricular (LV) ejection fraction (LVEF)3. Sudden death is common in CD, can occur in any phase of that disease, and 10% result from a first arrhythmic event. Complex cardiac arrhythmias
(ventricular extrasystoles > 10/hour and/or ventricular tachycardia) are markers of sudden death in CD4.
Patients with CD and normal electrocardiogram (ECG) are known to have survival rate similar to that of the general population, and initial studies have shown that those with CD, segmental wall motion abnormality and preserved LVEF have worse prognosis5,6.
Cardiac magnetic resonance imaging (CMR) is currently the best method to assess ventricular function7 and to detect segmental wall motion abnormalities8; by adding the delayed enhancement technique9, it can assess myocardial fibrosis. The ability of delayed enhancement CMR to detect abnormalities in chronic Chagas heart disease (CCHD) has already been reported10.
Patients with CCHD and ventricular arrhythmia have a worse prognosis, and there is no study correlating the myocardial fibrosis detected on CMR with the severity of arrhythmias in patients with CD and preserved or minimally impaired ventricular function.
MethodsPatients were recruited between March and December
2010 at the CD Outpatient Clinic at our hospital.
456

Original Article
Tassi et al.Fibrosis and ventricular arrhythmias in CD
Arq Bras Cardiol. 2014; 102(5):456-464
All patients from this study provided written informed consent, and the research protocol was approved by the Ethics Committee of our hospital, in accordance with the Declaration of Helsinki.
The inclusion criteria were as follows: asymptomatic patients older than 21 years or those outside an endemic area of CD for more than 20 years with positive serology for CD, preserved or minimally reduced (> 45%) LVEF on echocardiogram, who had undergone ECG, treadmill exercise test (TET) and 24-hour Holter in the previous 12 months.
Patients with the following characteristics were excluded: renal dysfunction (estimated creatinine clearance < 30 mL/min); previous ablation via electrophysiological study; diabetes or more than two risk factors for coronary artery disease; atrial fibrillation; TET compatible with myocardial ischemia; previous myocardial infarction; any myocardial or peripheral revascularization procedure; contraindication to undergo CMR (permanent pacemaker, implanted cardiac defibrillator, neurosurgical clips, or cochlear implants).
Patients were classified according to ECG and CMR findings, and distributed into three groups as follows: 1) Group 1 - normal ECG and no segmental wall motion abnormality on CMR; 2) Group 2 - altered ECG and no segmental wall motion abnormality on CMR; and 3) Group 3 - segmental wall motion abnormality on CMR regardless of ECG. The ECG was considered altered in the presence of any incomplete or complete bundle-branch block, any type of atrioventricular block, mono- or polymorphic ventricular extrasystole , and nonsustained ventricular tachycardia (NSVT). The CMR was considered altered in the presence of any segmental wall motion abnormality.
On Holter, the following situations were considered electrical instability: presence of ventricular extrasystoles > 30/hour; episodes of monomorphic sustained ventricular tachycardia (defined as ventricular rhythm with heart rate > 100 bpm and duration > 30 seconds); and episodes of NSVT (defined as three or more consecutive beats with duration < 30 seconds).
Regarding the TET, only the tests of patients reaching 7 MET, limit defined as a submaximal exercise level (good correlation between the anaerobic threshold achieved and the 7-MET load achieved), were considered for analysis11. Two observers analyzed and compared the ECGs at rest and during exercise (around 7 MET), identifying in both situations the 30-second period with the greatest number of ventricular arrhythmias and/or NSVT episodes. Exertion-induced arrhythmias were defined as the appearance of ventricular arrhythmias on ECG during exercise as compared to rest, or an increase > 10% in their incidence, and/or presence of NSVT12.
The CMR was performed in a 1.5-Tesla GE HDX scanner (Wakeusha, Wisconsin, USA), and two pulse sequences were acquired: the first was a cine-CMR using Steady-State Free Precession (SSFP) in long- and short-axis projections to measure and calculate mass, volumes, LVEF and right ventricular ejection fraction (RVEF). The most basal slice in the short axis was positioned right after the atrioventricular ring, and all subsequent respiratory pauses at maximum exhalation were acquired with 8-mm slice thickness and
2-mm slice spacing up to the LV apex. The parameters used were: field of view (FOV) of 400 mm; matrix of 224 × 224; 20-24 lines/segment; temporal resolution < 50 ms; repetition time (RT) = 3.9 ms, echo time (ET) = 1.5 ms; flip angle of 50°; and NEX of 1.
Three minutes after injecting 0.3 mmol/kg of gadolinium (Dotarem®, Guerbet), an echo-gradient sequence was performed with inversion recovery (delayed enhancement) in the long- and short-axis projections to investigate myocardial fibrosis with the following parameters: FOV of 360 mm; matrix of 224 × 192; 24 lines/segment; ET = 2.9 ms; flip angle of 20°; 8-mm slice thickness; 2-mm slice spacing; and NEX of 2.
Cardiac magnetic resonance postprocessingThe LV and RV measurements and calculations were
performed independently by two researchers blinded to the patient’s groups, at a workstation dedicated to CMR, using specific software (Report CARD®, 3.6 version, GE).
Maximum diastole and systole images were chosen on cinematic display at maximum relaxation and maximum contraction, respectively. Ventricular mass was calculated by using manual tracings of endocardial and epicardial borders at end-systole and end-diastole for each slice for both LV and RV. Papillary muscles were excluded from volume measurements and added to ventricular mass calculation. Such areas were multiplied by slice thickness (8 mm + 2 mm of slice spacing) and added to several slices to obtain end-systolic and end-diastolic volumes, respectively. The EF was calculated as follows: end-systolic volume subtracted from end-diastolic volume and divided by end-diastolic volume. Each of the 17 LV wall segments was classified as normokinetic, hypokinetic, dyskinetic or akinetic.
The calculation of fibrosis mass was performed by using a specific applicative of the software for semiquantitative detection of hyperintense areas compatible with fibrosis on short-axis delayed enhancement sequences. The researcher was free to edit the limits of the area of fibrosis.
Statistical analysisThe statistical analysis comprised a nonparametric
classification tree and survival curves. The nonparametric classification tree method is based on a decision rule approach, implemented with a theory of conditional inference procedures and selection of variables. The node of the classification tree has a p value that corresponds to the log-rank test. The classification tree is aimed at reducing the impurity degree by finding the point that provides greater homogeneity (higher probability of purity) inside a node and greater heterogeneity between nodes. Then, a log-linear model is used to select the most significant variables and to confirm the results obtained by using a regression tree. The 5% significance level was adopted for the entire study.
The presence of ventricular arrhythmias was considered a categorical variable according to ECG, Holter and/or TET findings.
457
Original Article
Tassi et al.Fibrosis and ventricular arrhythmias in CD
Arq Bras Cardiol. 2014; 102(5):456-464
Table 1 – General data
Mean age 62.32 years
BMI 26.02 kg/m2
Group 1 BMI 26.56 kg/m2
Group 2 BMI 25.29 kg/m2
Group 3 BMI 25.24 kg/m2
Number of patients with fibrosis 27 (45.8%)
Group 1 (normal ECG and no SWMA on CMR) 26 (42.6%)
Group 2 (abnormal ECG and no SWMA on CMR) 16 (26.2%)
Group 3 (SWMA on CMR) 19 (31.1%)
Ventricular arrhythmia (TET or Holter) 19 (31.1%)
Patients with fibrosis in Group 1 5 (19.2%)
Patients with fibrosis in Group 2 7 (43.7%)
Patients with fibrosis in Group 3 15 (78.9%)
Patients with fibrosis and ventricular arrhythmia 13 (68.4%)
BMI: body mass index; ECG: electrocardiogram; CMR: cardiac magnetic resonance imaging; SWMA: segmental wall motion abnormality; TET: treadmill exercise test.
Interobserver analysis was performed using the survival analytical technique proposed by Luiz et al13 to assess the reliability of the quantitative measures of EF, LV mass and myocardial fibrosis. That method uses Kaplan-Meier curves without data censoring, in which the failures occur in the absolute difference between the values attributed to the observers. Another improved method proposed by Llorca and Delgado-Rodriguez14 was also used. It considers two groups of different real values rather than global differences. The equivalence of functions of the two observers obtained through Llorca’s method was evaluated by using Tarone-Ware test, a nonparametric weighted log-rank statistic.
Then the explanation coefficient matrix was performed to measure the predictive capacity of a continuous variable to predict another, and the following were assessed: age; LVEF; RVEF; fibrosis; and LV mass. The R software was used for data analysis.
ResultsSixty-one patients (23 men) participated in the study.
Two women did not undergo the post-contrast phase (delayed enhancement) as follows: one due to difficulty in the venous access and another due to history of allergy to gadolinium; they, however, underwent the noncontrast phase (cine-CMR). The patients’ mean age was 62.32 ± 10.43 years. The body mass index of the population studied was 26.02. Four patients showed segmental wall motion abnormality with no ECG abnormalities, being then considered Group 3. Table 1 shows the number of patients with fibrosis in the three groups.
Figure 1 shows the number of patients with segmental wall motion abnormality and fibrosis in each LV wall segment according to the CMR findings. Segmental wall motion abnormality was detected in 19 patients (31.1%). Abnormality
was identified in 113 wall segments (10.89% of the 1,037 possible segments), and the segments most frequently affected were: infero-apical (9.7%); infero-lateral-medial (10.6%); basal (7.9%); and LV apex (9.7%).
On CMR, fibrosis was detected in 27 patients (45.8%) (Figure 1), the mean amount of fibrosis being 15.02 g. Detectable myocardial fibrosis was observed in 87 segments (8.67% of the 1,003 possible segments), the infero-lateral-basal LV wall segment being the most often affected (19.5%).
Electrical instability was detected on Holter or TET in 19 patients (32%), and Graph 1 shows the presence of fibrosis or segmental wall motion abnormality in that group of patients. Of the patients with electrical instability, 78.9% had segmental wall motion abnormality and/or fibrosis on CMR. Of the 42 patients without electrical instability, only 14 patients had myocardial fibrosis and 8 had segmental wall motion abnormality.
Graph 2 shows the amount of fibrosis and the LVEF in each group.
The presence of ventricular arrhythmia in the groups was as follows: four patients in Group 1; four patients in Group 2; and 11 patients in Group 3.
Regarding interobserver agreement to detect ventricular arrhythmias at rest and during exertion, a kappa of 0.87 was obtained [95% confidence interval (95% CI): 0.72-0.92). Kappa for intraobserver agreement was 0.93 (95% CI: 0.74-0.99).
The interobserver disagreement by using Llorca’s method showed that the variables LVEF, RVEF and mass were not significant (0.4 and 0.09 respectively; p = 0.5). Only the variable ‘percentage of fibrosis’ showed significance (p = 0.007) up to 6% of the absolute value of the difference of the result, after which there was no difference.
The categorical analyses of the presence of segmental wall motion abnormality and detection of fibrosis had an interobserver kappa of 0.96. The variables used in the first classification tree (Figure 2) were: segmental wall motion abnormality on CMR; groups (1, 2 and 3); age; LVEF; ventricular arrhythmia; and myocardial fibrosis. Myocardial fibrosis was the only significant variable in the classification tree for the presence of ventricular arrhythmia, with a cutoff point of 11.78% for fibrosis mass (p < 0.001). In addition to segmental wall motion abnormality on CMR and myocardial fibrosis, the second classification tree considered the interactions of those variables with the groups (1, 2 and 3). Group 3 gathered the majority of patients with ventricular arrhythmia (p < 0.001) (Figure 3).
The explanation coefficient matrix was built (Figure 4), enabling R2 calculation of the variables analyzed without using a response variable (ventricular arrhythmia, in the case), and showing that LVEF was inversely proportional to fibrosis (R2 = -0.37), while LVEF and RVEF were proportional to each other (R2 = 0.30).
DiscussionThis study shows objectively that, even in patients with CD
and preserved or minimally impaired LV function, electrical instability can occur. It was demonstrated by the presence of
458
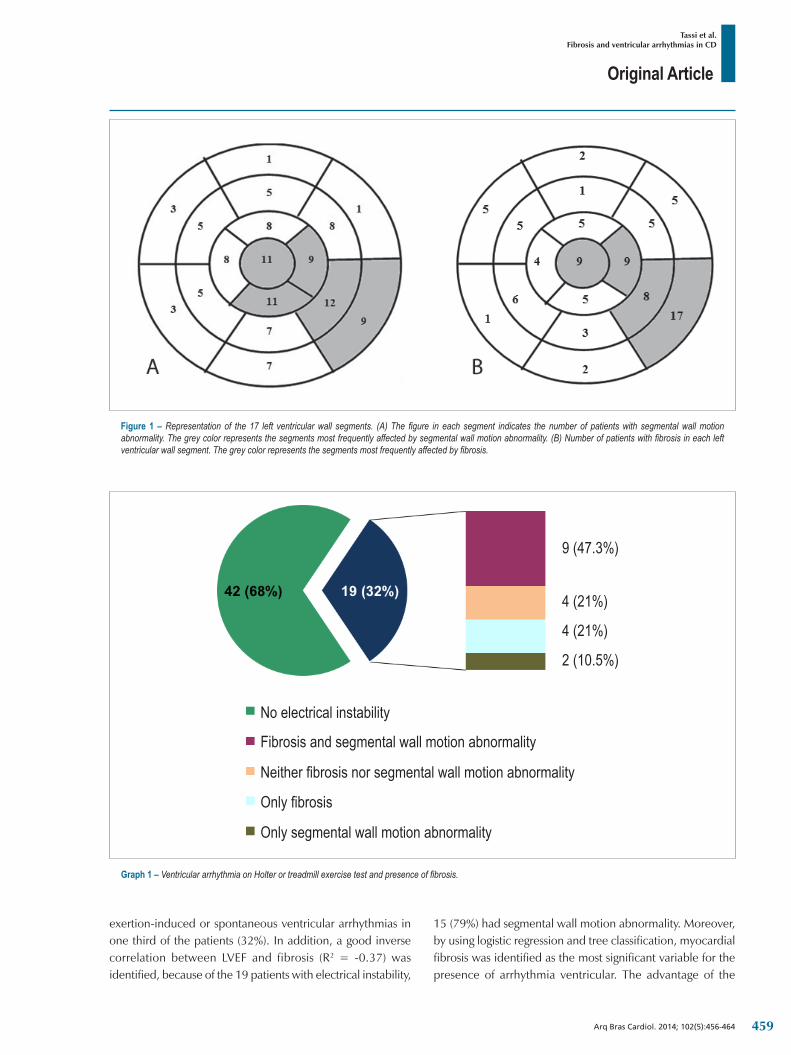
Original Article
Tassi et al.Fibrosis and ventricular arrhythmias in CD
Arq Bras Cardiol. 2014; 102(5):456-464
Figure 1 – Representation of the 17 left ventricular wall segments. (A) The figure in each segment indicates the number of patients with segmental wall motion abnormality. The grey color represents the segments most frequently affected by segmental wall motion abnormality. (B) Number of patients with fibrosis in each left ventricular wall segment. The grey color represents the segments most frequently affected by fibrosis.
Graph 1 – Ventricular arrhythmia on Holter or treadmill exercise test and presence of fibrosis.
No electrical instability
9 (47.3%)
2 (10.5%)
4 (21%)
4 (21%)
Only segmental wall motion abnormality
Only fibrosis
Neither fibrosis nor segmental wall motion abnormality
Fibrosis and segmental wall motion abnormality
exertion-induced or spontaneous ventricular arrhythmias in one third of the patients (32%). In addition, a good inverse correlation between LVEF and fibrosis (R2 = -0.37) was identified, because of the 19 patients with electrical instability,
15 (79%) had segmental wall motion abnormality. Moreover, by using logistic regression and tree classification, myocardial fibrosis was identified as the most significant variable for the presence of arrhythmia ventricular. The advantage of the
459

Original Article
Tassi et al.Fibrosis and ventricular arrhythmias in CD
Arq Bras Cardiol. 2014; 102(5):456-464
Graph 2 – Ejection fraction and amount of fibrosis in the different groups. LVEF: left ventricular ejection fraction.
Figure 2 – Classification tree showing that fibrosis is the most significant variable for the presence of ventricular arrhythmia, with a cutoff point of 11.78%.
classification tree is that, in addition to identifying the most relevant variable, it calculates the cutoff point (11.78% for fibrosis mass). In the group with fibrosis > 11.78%, only two
patients had no ventricular arrhythmia (p < 0.001), which might mean that patients with a greater percentage of fibrosis have an increased risk for frequent ventricular arrhythmia.
460

Original Article
Tassi et al.Fibrosis and ventricular arrhythmias in CD
Arq Bras Cardiol. 2014; 102(5):456-464
Figure 3 – Classification tree per group, showing that the group with segmental wall motion abnormality (Group 3) had the majority of patients with ventricular arrhythmia.
According to Myerburg et al15, three factors are required for electrical sudden death: arrhythmogenic substrate; triggering events; and functional changes. Fibrosis plays a relevant role in the first factor. In patients with CD, those three factors can be clearly identified: the arrhythmogenic substrate is represented by the myocardial fibrosis and inflammation; the triggering events, by the frequent ventricular extrasystoles; and the functional changes, by the autonomous nervous system physiological changes.
Ventricular arrhythmia in CD is associated with ventricular dysfunction, and patients with ventricular dysfunction and complex ventricular arrhythmias have worse prognosis. The presence of ventricular electrical instability in patients with preserved LVEF and segmental wall motion abnormality is little studied.
It is possible that the 19.2% of Group 1 patients who had myocardial fibrosis detectable on CMR could be in an initial phase of CCHD, especially because four of them had ventricular arrhythmia. According to pathological studies16,17, the initial process is myocarditis with fibrosis, which can progress to segmental wall motion abnormality and ventricular dysfunction.
Our population is considered of low risk according to any prognostic score. Nevertheless, 45.7% of them have myocardial fibrosis detectable on CMR. The presence and
amount of fibrosis were higher in Group 3 patients. That group also had more patients with ventricular arrhythmia, which could indirectly mean a higher arrhythmogenic potential.
Prospective studies on CCHD using CMR are scarce. Recently, Regueiro et al18, in a descriptive study, have shown the association of ECG changes (with segmental wall motion abnormality) with the increase in fibrosis mass and right and left ventricular dysfunctions. Mello et al19, assessing patients with CCHD on CMR, have shown that transmural fibrosis in more than two LV myocardial segments was more often associated with ventricular tachycardia.
In the present study, the segments most often affected by fibrosis were also those with more segmental wall motion abnormalities. This suggests a topographical relationship between sympathetic denervation, fibrosis and hypokinesia. The temporal relationship between those variables can help to understand the pathophysiological process and should be the object of future studies.
It is worth noting the reliability of the imaging test. Echocardiography is examiner-dependent and its interobserver variability is a well-known limitation. The CMR is known for its high reproducibility. In this study, the interobserver variability was < 5% for LVEF and RVEF, thus, not significant (p = 0.5 and 0.4, respectively). The percentage of fibrosis mass showed
461

Original Article
Tassi et al.Fibrosis and ventricular arrhythmias in CD
Arq Bras Cardiol. 2014; 102(5):456-464
Figure 4 – Correlation matrix (values as R2). The more oval the tracing, the better the correlation. LV: left ventricular; LVEF: left ventricular ejection fraction; RVEF: right ventricular ejection fraction.
0.03
0.30 -0.37 -0.05
-0.10
0.03
LVEF.1
RVEF.1
fibrosis.1
LVmass.1
Age
a statistical difference of 6%; however, a variability of such magnitude, regarding the small mean fibrosis amount found (15.02 g), can be of little clinical and scientific relevance, because, considering the standard deviation, it would be 15.02g ± 0.9 g. In addition, if regarded as categorical variable, it would have an excellent correlation (kappa = 0.96).
Study limitationsThe patients in this study have not undergone coronary
cineangiography to exclude coronary arterial disease as the cause of myocardial fibrosis. However, patients with diabetes and two or more risk factors for coronary arterial disease were excluded, thus reducing that probability. In addition, no patients with abnormalities suggestive of coronary arterial disease on TET or CMR were identified. Recently, Carvalho et al20 have shown a small prevalence of coronary arterial disease in patients with CD.
Most episodes of sudden death occur between the ages of 20 and 50 years in men. This differs from our population,
mainly comprised by women with a mean age of 63 years, a fact that can underestimate prognostic events. Nevertheless, in that low-risk group, there was significant substrate for the presence of arrhythmias (segmental wall motion abnormality and presence of myocardial fibrosis).
The definition of ventricular arrhythmia includes the presence of frequent ventricular extrasystoles > 30/h, which can be considered of little clinical relevance. However, this study was aimed at assessing the triggering mechanism of early ventricular instability (fibrosis and segmental wall motion abnormality), rather than the immediate clinical impact.
ConclusionsOn CMR, both myocardial fibrosis and segmental wall
motion abnormality were associated with ventricular arrhythmia in patients with CCHD.
462

Original Article
Tassi et al.Fibrosis and ventricular arrhythmias in CD
Arq Bras Cardiol. 2014; 102(5):456-464
Even in patients with CCHD and preserved or minimally impaired ventricular function, the arrhythmogenic substrate can be present. Myocardial fibrosis detected on CMR is the most important variable associated with ventricular arrhythmia.
AcknowledgementsWe thank Dr. Marco Lauzi, from Guerbet, for providing
the gadolinium (Dotarem®) used in this study.
Author contributionsConception and design of the research: Tassi EM, Pereira BB,
Pedrosa RC; Acquisition of data: Tassi EM, Continentino MA; Analysis and interpretation of the data: Tassi EM, Continentino MA, Nascimento EM, Pereira BB, Pedrosa RC; Statistical analysis: Nascimento EM, Pereira BB; Writing of the manuscript:
Tassi EM, Continentino MA, Pedrosa RC; Critical revision of the manuscript for intellectual content: Tassi EM, Pedrosa RC.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
This study was partially funded by FAPESP.
Study Association
This article is part of the thesis of master submitted by Eduardo Marinho Tassi from Faculdade de Medicina da Universidade Federal do Rio de Janeiro.
1. Dias JC. Elimination of Chagas disease transmission: perspectives. Mem Inst Oswaldo Cruz. 2009;104 Suppl 1:41-5.
2. Dias JC, Prata A, Correia D. Problems and perspectives for Chagas disease control: in search of a realistic analysis. Rev Soc Bras Med Trop. 2008;41(2):193-6.
3. Rassi A Jr, Rassi A, Little WC, Xavier SS, Rassi SG, Rassi AG, et al. Development and validation of a risk score for predicting death in Chagas’ heart disease. N Engl J Med. 2006;355(8):799-808.
4. Rassi A Jr, Rassi JG, Rassi A. Sudden death in Chagas’ disease. Arq Bras Cardiol. 2001;76(1):75-96.
5. Pazin-Filho A, Romano MM, Almeida Filho OC, Furuta MS, Viviani LF, Schimidt A, et al. Minor segmental wall motion abnormalities detected in patients with Chagas’ disease have adverse prognostic implications. Braz J Med Biol Res. 2006;39(4):483-7.
6. Terzi FV, Siqueira Filho AG, Nascimento EM, Pereira Bde B, Pedrosa RC. Regional left ventricular dysfunction and its association with complex ventricular arrhythmia, in chagasic patients with normal or borderline electrocardiogram. Rev Soc Bras Med Trop. 2010;43(5):557-61.
7. Grothues F, Smith GC, Moon JC, Bellenger NG, Collins P, Klein HU. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol. 2002;90(1):29-34.
8. Peshock RM, Rokey R, Malloy GM, McNamee P, Biya LM, Parkey RW, et al. Assessment of myocardial systolic wall thickening using nuclear magnetic resonance imaging. J Am Coll Cardiol. 1989;14(3):653-9.
9. Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu F, Bundy JM, et al. An improved MR imaging technique for the visualization of myocardial infarction. Radiology. 2001;218(1):215-23.
10. Rochitte CE, Oliveira PF, Andrade JM, Ianni BM, Parga JR, Avila LF, et al., Myocardial delayed enhancement by magnetic resonance imaging in patients with Chagas’ disease: a marker of disease severity. J Am Coll Cardiol. 2005;46(8):1553-8.
11. Oliveira FP, Pedrosa RC, Giannella-Neto A. Gas exchange during exercise in different evolutional stages of chronic Chagas’ heart disease. Arq Bras Cardiol. 2000;75(6):481-98.
12. Pedrosa RC, Salles JH, Magnanini MM, Bezerra DC, Bloch KV. Prognostic value of exercise-induced ventricular arrhythmia in Chagas’ heart disease. Pacing Clin Electrophysiol. 2011;34(11):1492-7.
13. Luiz RR, Costa AJ, Kale PL, Werneck BL. Assessment of agreement of a quantitative variable: a new graphical approach. J Clin Epidemiol. 2003;56(10):963-7.
14. Llorca J, Delgado-Rodriguez M. Survival analytical techniques were used to assess agreement of a quantitative variable. J Clin Epidemiol. 2005;58(3):314-5.
15. Myerburg RJ, Kessler KM, Bassett AL, Castellanos A. A biological approach to sudden cardiac death: structure, function and cause. Am J Cardiol. 1989;63(20):1512-6.
16. Higuchi ML, Fukasawa S, de Brito T, Parzianello LC, Bellotti G, Ramires JA. Different microcirculatory and interstitial matrix patterns in idiopathic dilated cardiomyopathy and Chagas’ disease: a three dimensional confocal microscopy study. Heart. 1999;82(3):279-85.
17. Mady C, Ianni BM, Arteaga E, Montes GS, Caldini EG, Andrade G, et al. Relation between interstitial myocardial collagen and the degree of clinical impairment in Chagas’ disease. Am J Cardiol. 1999;84(3):354-6. Erratum in Am J Cardiol. 1999;84(12):1456.
18. Regueiro A, Garcia-Alvarez A, Sitges M, Ortoz-Perez JT, De Coralt MT, Pinazo MJ, et al. Myocardial involvement in Chagas disease: insights from cardiac magnetic resonance. Int J Cardiol. 2011;165(1):107-12.
19. Mello RP, Szarf G, Schvartzman PR, Nakano FM, Espinosa MM, Szenfeld D, et al. Delayed enhancement cardiac magnetic resonance imaging can identify the risk for ventricular tachycardia in chronic Chagas’ heart disease. Arq Bras Cardiol. 2012;98(5):421-30.
20. Carvalho G, Rassi S, Bastos JM, Camara SS. Asymptomatic coronary artery disease in chagasic patients. Arq Bras Cardiol. 2011;97(5):408-12.
References
463

Original Article
Tassi et al.Fibrosis and ventricular arrhythmias in CD
Arq Bras Cardiol. 2014; 102(5):456-464464

Original Article
Impact of Psychotropic Drugs on QT Interval Dispersion in Adult PatientsBruno de Queiroz Claudio1,2, Marcelle Azevedo Nossar Costa1, Filipe Penna1, Mariana Teixeira Konder1, Bruno Miguel Jorge Celoria1, Luciana Lopes de Souza1, Roberto Pozzan2, Roberta Siuffo Schneider2, Felipe Neves Albuquerque2, Denilson Campos Albuquerque1,2
Hospital Copa D’Or/IDOR1; Universidade do Estado do Rio de Janeiro – UERJ2, Rio de Janeiro, RJ - Brazil
Mailing Address: Bruno de Queiroz Claudio •Rua Presidente João Pessoa, 95, apto. 801, bloco 1, Icaraí. Postal Code: 24220-330, Niteroi, RJ - BrazilE-mail: [email protected], [email protected] received September 12, 2013; revised manuscript November 01, 2013, accepted November 26, 2013.
DOI: 10.5935/abc.20140055
Abstract
Background: Drug-induced increase in QT dispersion has been associated with potentially fatal ventricular arrhythmias. Little is known about the use of psychotropic substances, alone or in combination with other drugs on QT dispersion.
Objectives: To evaluate the impact of psychotropic drugs on QT interval dispersion in adults.
Methods: An observational cohort study was designed involving 161 patients hospitalized from an emergency department at a tertiary hospital, divided into psychotropic users or non-users. Demographic, clinical, laboratory data and drugs used on a regular basis were collected on admission, in addition to 12-lead electrocardiogram with QT dispersion measurement.
Results: QT dispersion was significantly higher in the psychotropic user group compared to non-users (69.25 ± 25.5 ms vs. 57.08 ± 23.4 ms; p = 0.002). The QT interval corrected by Bazzett formula was also higher in the psychotropic drugs user group, with statistical significance. (439.79 ± 31.14 ms vs. 427.71 ± 28.42 ms; p = 0.011). A regression analysis model showed a positive association between the number of psychotropic drugs used and QT interval dispersion, with r = 0.341 and p < 0.001.
Conclusions: The use of psychotropic drugs was associated with increased QT dispersion and this increase was accentuated, as the number of psychotropic drugs used was higher. (Arq Bras Cardiol. 2014; 102(5):465-472)
Keywords: Electrocardiography; Cardiovascular diseases; Torsades de Pointes; Ventricular fibrillation; Death, Sudden.
IntroductionThe perception and interest in unexpected death are
secular. Sudden cardiac death received its first scientific definition in 1707 with Giovanni Lancisi1, in his work De mortibus subitaneis. The most prevalent cause of sudden death is coronary artery disease, followed by cardiomyopathies and primarily electrical cardiac causes, especially the long QT syndrome, either congenital or acquired – the latter induced by drugs, in most cases. Data indicate that QT prolongation is a major contributor to the genesis of polymorphic ventricular tachycardia or torsades de pointes, even in structurally normal hearts2. This prolongation is not a pharmacological property attributed only to antiarrhythmic drugs. A recent American cohort showed that 5 million Americans are exposed to drugs that prolong the QT interval, with antibiotics and psychotropic drugs, especially antipsychotics, being the most common2,3.
However, not all drugs that prolong the QT interval increase the risk of ventricular arrhythmias4. It is currently accepted that the electrical disturbance genesis is related to blockage of ionic currents of potassium channels, notably in M cells of the human ventricle, with subsequent QT interval prolongation and dispersion (QTD) on the electrocardiogram (ECG), closely related to the onset of torsades de pointes4-7.
The concept of "QT interval dispersion", defined as the difference between the maximum and minimum QT interval measured at the 12-lead ECG, was introduced by Higham and Campbell8 in the early 1990s. Initially proposed as an index of electrical instability, it represents the expression of physiological regional variation of myocardial excitability recovery.
Since then, the analysis of QTD was accepted as a noninvasive method for the detection of ventricular repolar izat ion heterogenei ty, being a marker of arrhythmogenesis, especially in the presence of an ischemic substrate and drug-induced ventricular arrhythmias. Additionally, there have been studies associating it as a prognostic index in heart failure and hypertrophic cardiomyopathy8,9.
Little is known about the impact on QTD with the specific use of antipsychotics and its associations with other drugs acting on the central nervous or cardiovascular system.
465

Original Article
Claudio et al.Impact of psychotropic drugs on QT interval dispersion
Arq Bras Cardiol. 2014; 102(5):465-472
Methods
Study characterizationThe present was a prospective, multicenter, observational
cohort study, carried out in a private hospital in Rio de Janeiro, with an open emergency room, from September 2009 to January 2013. The research protocol was approved by the Institutional Research Ethics Committee (REC) (number 148/09).
Study populationOf the total number of patients admitted at the institution,
necessarily admitted through the emergency room, 194 met the initial eligibility criteria for the study. After careful evaluation, 33 patients were excluded and population sample comprised 161 patients.
The subjects of the investigation were not submitted to any interventions resulting from the study. A liability form was completed by the main investigator on the use of information contained in medical records and database, thus making it unnecessary for patients to sign the Informed Consent form.
Inclusion criteriaThe following inclusion criteria were used: age > 40 years;
emergency care and subsequent hospital admission for more than 24 hours, regardless of the reason for admission; performance of ECG with at least 12 leads in the emergency room; performance of basic complementary laboratory tests (glucose, potassium and magnesium).
Exclusion criteriaThe exclusion criteria were: patients with artificial
cardiac pacing, either temporary or permanent; patients with congenital long-QT syndrome; patients with calcium metabolism alterations; patients with atrial fibrillation of any cause and/or frequent ventricular arrhythmia; patients using antiemetics, prokinetics and antibiotics that alter ventricular repolarization.
According to the study design and construction of methodology, the use of concomitant drugs that would influence QT interval and its dispersion was cause for careful analysis. Thus, we excluded patients on continuous use of other drugs that prolong the QT interval, especially domperidone, bromopride and metoclopramide.
The sample population was stratified into two groups according to the use or nonuse of psychotropic drugs. Group 1 (G1) consisted of patients who were not taking psychotropic drugs, while Group 2 (G2) consisted of patients taking psychotropic drugs.
Investigation proceduresDemographic data, present and past medical history,
information on regular use of drugs and diagnostic hypotheses were collected on admission. Any drug that had more than seven days of uninterrupted use before hospital admission was defined as continuous use.
All antipsychotics, anticonvulsants, antidepressants and drugs used in dementia syndromes used by the sample population were taken into account. All drugs subject to classification according to Vaughan Williams were considered antiarrhythmic drugs.
A 12-lead ECG was performed on patient admission, while still in the emergency department, being a routine procedure for any patient older than 40 years of age, symptomatic or not (hospital accreditation process protocol by the Joint Commission).
Laboratory assessmentLaboratory evaluation consisted of measurements of
plasma glucose, potassium and magnesium, also assessed on admission. Glycemia levels did not take into account any criterion of fasting. Calcium ion was measured when requested by the emergency team. A Vitros 250 analyzer (Johnson & Johnson, New Brunswick, USA) was used for biochemical measurement of magnesium and glucose, with the dry-chemical method. The measurements of potassium and calcium ion were performed using a Gem Premier 3000 analyzer (Instrumentation Laboratory, Bedford, USA) using the selective electrode method. Normal values of these tests were determined according to the institution protocols.
QT dispersion measurementEach patient’s ECG was recorded in three-channel
conventional ECG equipment (HP - Hewlett Packard Company, Palo Alto, United States) with recording speed of 25 mm/s and recording of the 12 leads considered as conventional (D1, D2, D3, aVR , aVL, aVF, V1, V2, V3, V4, V5, V6). ECGs that did not have at least nine leads with a QT interval technically capable of being measured were excluded. The QT interval is measured from the first deflection of the QRS complex to the end of the T wave, defined as the meeting point of the descending branch of T to the isoelectric line. In the presence of a U wave, the end of the T wave is considered as the base of deflection formed by the two waves. The presence of bundle branch block did not exclude patients from the study.
Cardiac cycles succeeding early beats (extrasystoles) were abandoned10. "QT interval dispersion" is defined as the difference between the maximum and minimum QT interval measured on the 12-lead (at least nine leads).
The digitized ECGs were analyzed with the help of Preview® software, version 5.5.2 (719.25) (Apple Inc ®, Cupertino, USA). Tracings were submitted to a 300% magnification and QT measurement was made digitally. All ECG tracings were digitalized with a 200 dpi resolution and saved in JPEG format to allow use of the Preview® program measuring tool. ECGs were captured by an Epson Stylus TX105 scanner (Long Beach, United States) and amplified during digitalization.
However, in daily clinical practice, the measurements of QT interval and QTD can be performed simply with the aid of a triplicate magnifying glass8,9. Two QT interval and QTD measures were performed by four examiners blinded to the clinical characteristics of patients and the arithmetic mean of the values were considered for the analysis.
466

Original Article
Claudio et al.Impact of psychotropic drugs on QT interval dispersion
Arq Bras Cardiol. 2014; 102(5):465-472
Several methodologies have been described for the measurement of QT interval 10, 11. In this study, we used the difference between the second largest and the second smallest QT interval (minimum of nine leads)10,11 to measure QTD, a methodology also used by Campbell et al12. Studies can be found in the literature13,14 that used the standard measure of QTD or that corrected by heart rate. In the present study, we used the default QT dispersion.
Statistical AnalysisUnivariate, bivariate, covariance and multivariate analysis
were used for the statistical analysis of the data.Univariate analysis was used for the description of the
studied variables, using simple frequency and percentage tables for discrete variables and mean (minimum-maximum), and graphical representation of histograms and box-plots for continuous variables. Bivariate analysis was used for discrete variables, using contingency tables and chi-square, Fisher exact and ML chi-square tests, when indicated; the Student’s t test, paired or not, and Mann-Whitney test were used for continuous variables,.
Levene's test was used to test whether the studied samples had homoscedasticity, that is, whether they had the same variance. A significant F ratio in this test indicates that the differences in mean, or effects, probably exist between the groups. In the case of heteroscedastic samples, non-parametric tests were used according to the characteristics of the studied variable. Welch and Brown-Forsythe tests were used in the assessment of the mean magnesium levels between groups.
Analysis of covariance was used with regression models and analysis of variance (ANOVA), using the partial ETA squared (η2), which allows inferring what proportion of the total variance is attributed to the studied variable (effect size). Multivariate analysis was used from a log-linear model for discrete variables aiming to detect and resolve the confusion effects. Pearson’s correlation coefficient was used to demonstrate the correlation between two or more variables. The ANOVA model was chosen for the analysis of variance between the studied groups.
Results
Sample populationOf a total of 194 initially selected patients, 161 met the
inclusion criteria and constituted the sample population of this study. The most prevalent cause of exclusion was the presence of atrial fibrillation (11) in the electrocardiogram, followed by artificial cardiac stimulation (7), calcium replacement without the measured serum level of calcium ion (5), frequent ventricular extrasystoles (4), incapacity of analyzing the ECG due to technical problems (3), and documented hypercalcemia.
The sample population (n = 161) was stratified into two groups according to the use or nonuse of psychotropic drugs: G1 consisting of patients who did not use psychotropic drugs (n = 85 patients) and G2 consisting of users of psychotropic drugs (n = 76 patients).
The reasons for hospital admission of patients are shown in Table 1, per group. There was no statistical significance between the groups.
Drugs used by the sample populationTables 2 and 3 show the frequency of psychotropic drugs
and antiarrhythmic drugs used by the sample population. This use may have been isolated or in associations. None of the patients from the sample population used digitalis.
Clinical and epidemiologic characteristics of the sample population
Female gender were more prevalent in G2, with statistical significance (p = 0.04). We sought to determine whether, in G2, the gender difference would have an impact the QTD, as there was no difference between men and women regarding psychotropic drug use (p = 0.642). There was a positive correlation between age and the use of psychotropic drugs.
The prevalence of hypertension, diabetes mellitus and known coronary artery disease showed no statistically significant difference between G1 and G2.
Regarding the laboratory variables, all patients (n = 161) had serum potassium, magnesium and glucose levels measured on admission at the emergency service, with no statistical difference between the two groups. The study excluded patients with hyper- and hypocalcemia. It is noteworthy that plasma glucose levels were not measured in fasting. Levene’s test was used to better understand the behavior of variance in the two groups.
Therefore, glucose and potassium showed a homoscedastic distribution, whereas magnesium had a heteroscedastic distribution, after using the appropriate statistical test for each situation. The results are shown in Table 4.
QT interval dispersion behaviorQTD was significantly higher in the group of psychotropic
drug users compared to non-users (p = 0.002). The QT interval corrected by the Bazett’s formula was also higher in the group using psychotropic drugs, with statistical significance (p = 0.011), as shown in Table 5. The variance was homogeneous in QTD, in the corrected QT interval and heart rate between the groups.
The analysis of covariance between age and use of psychotropic drugs was performed aiming to determine the adjusted mean of the QTD. As measure of analysis of variance, η2 was used. After adjusting the mean (G2 = 68.38 ± 8.11 milliseconds - ms and G1 = 57.85 ± 7.22 ms), the difference between the groups remained significant (p = 0.009).
Analysis of use of multiple psychotropic drugs on QT dispersion
In the sample population, 85 patients were not taking any psychotropic drugs, 52 used one drug, 16 patients used two drugs simultaneously, three patients used three drugs, four used four psychotropic drugs and one patient in the study used five psychotropic drugs simultaneously.
467

Original Article
Claudio et al.Impact of psychotropic drugs on QT interval dispersion
Arq Bras Cardiol. 2014; 102(5):465-472
A linear regression model showed a positive association between the number of psychotropic drugs used and QTD, with r = 0.341. (Chart 1)
The intensity of the linear association between variables was quantified. Pearson’s linear correlation showed a positive correlation between the number of psychotropic drugs and patient age in QTD (Table 6). In the regression model, when the data are analyzed together, R = 0.329.
To better understand the association between these two variables in QTD, a regression model was proposed, followed by an ANOVA model, to allow the measurement of the adjusted Beta of the number of psychotropic drugs and age, with QTD being the dependent variable.
When the coefficients are adjusted, only the number of psychotropic drugs shows statistical significance with QTD (p <0.001).
Of the original sample population, the impact of concurrent use of psychotropic and antiarrhythmic drugs was evaluated, compared to the isolated use of antiarrhythmics. Table 3 details the type of antiarrhythmic drug used according to the classification of Vaughan Williams, with no statistical difference between the studied subgroups. The combined use of both classes of drugs showed a statistically significant increase in the QT interval. However, there was no statistical difference in QTD between the two subgroups (Table 7).
DiscussãoAiming to assess the impact of psychotropic drug use on
QTD, it was necessary to study separately the clinical and demographic variables, identifying the isolated and combined action of these drugs with other cardiovascular action drugs.
Table 1 – Distribution of groups according to the reasons for hospital admission
Reasons for hospital admission Total Group 1 n (%) Group 2 n (%) Chi-square
Orthopedic surgical admissions 96 51 (60) 45 (59.21) p = 0.19
Admissions for general and urological surgery 32 20 (23.53) 13 (17.11) p = 0.065
Pulmonary sepsis 21 8 (9.41) 12 (15.79) p = 0.085
Urinary sepsis 12 6 (7.06) 6 (7.89) p = 0.32
Total 161 85 (100) 76 (100)
Table 2 – Psychotropics used by the sample population
Salt name Patients using it Salt name Patients using it
Haloperidol 1 Phenobarbital 1
Chlorpromazine 1 Phenytoin 2
Levomepromazine 3 Lamotrigine 2
Risperidone 3 Carbamazepine 4
Clozapine 1 Oxcarbazepine 2
Quetiapine 23 Gabapentin 6
Olanzapine 2 Valproic acid 4
Ziprasidone 0 Topiramate 2
Aripiprazole 0 Venlafaxine 4
Promethazine 3 Memantine 7
Amitriptyline 3 Mirtazapine 4
Imipramine 1 Duloxetine 3
Clomipramine 2 Fluoxetine 3
Doxepin 1 Paroxetine 1
Desipramine 0 Sertraline 4
Nortriptyline 1 Citalopram 6
Trazodone 1 Citalopram 3
Bupropion 2 Donepezil 2
Maprotiline 1 Rivastigmine 4
Nefazodone 0 Galantamine 1
468

Original Article
Claudio et al.Impact of psychotropic drugs on QT interval dispersion
Arq Bras Cardiol. 2014; 102(5):465-472
Over the past 25 years, the QTD has been studied by several authors in different clinical scenarios, in normal subjects and patients with heart disease. Tran et al15 in a study that evaluated the influence of age and sex on QTD, concluded that estrogen, athoughit does not change the QT interval, significantly reduces its dispersion. In a healthy population, Alici et al16 also confirmed these findings. In the population evaluated in this study, the results were similar.
The use of psychotropic drugs is more common in elderly women17,18 and this population had a significantly higher number of women in G2.
In this context, we expected to find a higher number of females in the group of psychotropic drug users. For this reason, the QTD was analyzed separately in men and women in the group of psychotropic drug users and it was greater in men (71.15 ± 26.91 ms) than in women (68.26 ± 24.96 ms), with no statistical significance. It is known that in the age range of the female population, estrogen protection is not as present any more. Thus, other mechanisms were studied to understand this phenomenon.
Table 3 – Antiarrhythmic drugs used by the sample population
Vaughan-Williams Class I Class II Class III Class IVTotal
---- Beta-blockers Amiodarone Sotalol Diltiazen Verapamil
Psychotropics + Antiarrhythmics 0 9 6 1 4 0 20
Antiarrhythmics 0 7 4 1 2 1 15
Table 4 – Demographic, clinical and laboratory data
Variable G1 (n = 85) G2 (n = 76) Statistical test p value
Age (years), mean ± standard deviation 67.68 ± 12.68 74.43 ± 11.37 t = 3.540 0.001
Male gender, % 50.60 34.20 Χ2 = 4.395 0.04
Female gender, % 49.40 65.80
SAH, % 40 39.50 Χ2 = 0.005 1
DM, % 25.90 23.70 Χ2 = 0.104 0.885
CAD, % 21.20 13.20 Χ2 = 1.796 0.214
Potassium, mean ± standard deviation (mEq/L) 4.29 ± 0.55 4.31 ± 0.69 F = 0.493 0.852
Magnesium, mean ± standard deviation (mg/dL) 1.88 ± 0.21 1.95 ± 0.34 F = 6.444* 0.109
Glycemia, mean ± standard deviation (mg/dL) 115 ± 40 123 ± 46 F = 1.194 0.191
* Heteroscedastic sample. SAH: systemic arterial hypertension; DM: diabetes mellitus; CAD: coronary artery disease; F: Levene F ratio.
Table 5 – Electrocardiographic data and behavior of QT interval dispersion
Variable Group 1 (n = 85) Group 2 (n = 76)t Test
p value
QT interval dispersion, mean ± standard deviation (ms) 57.08 ± 23.4 69.25 ± 25.5 0.002
Corrected QT interval, mean ± standard deviation (ms) 427.71 ± 28.42 439.79 ± 31.14 0.011
Heart rate, mean ± standard deviation (bpm) 79 ± 15 77 ± 18 0.379
Ebert et al19 demonstrated in an animal model that ionic currents in females, specifically in potassium channels, are significantly smaller than in males of the same species of rats. This effect is accentuated in the presence of class III antiarrhythmic drugs, increasing the QTD. Therefore, elderly women are particularly susceptible to changes in the QT interval and this fact should be considered when prescribing psychotropic drugs.
Regarding comorbidities found in the population, there was no statistical difference between the groups of non-users and users of psychotropic drugs on the prevalence of hypertension, diabetes mellitus and coronary artery disease. There was a high prevalence of these comorbidities in this population, respectively 60.2%, 24.8% and 17.4%. This may be related to the age of the sample, as well as the patient selection method, carried out in the emergency room. The profile of emergency patients and institution alignment explain the high number of orthopedic surgical patients. It is noteworthy that no patient was admitted for acute coronary syndrome, which is therefore, not a bias.
469
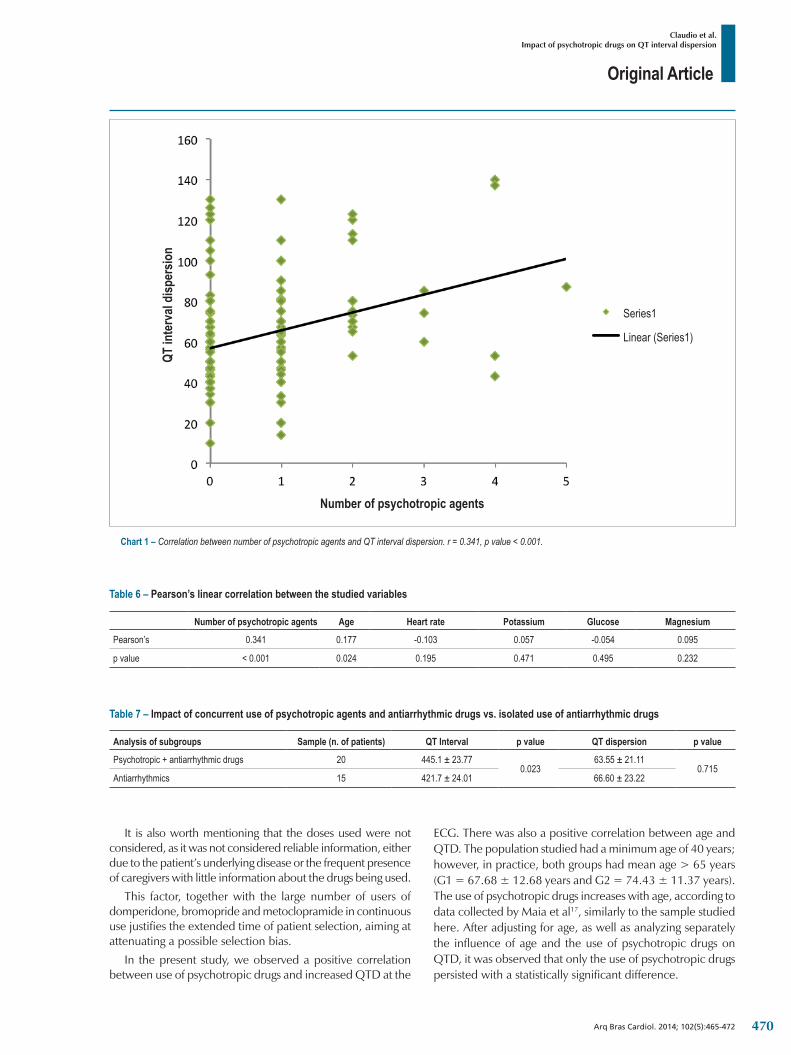
Original Article
Claudio et al.Impact of psychotropic drugs on QT interval dispersion
Arq Bras Cardiol. 2014; 102(5):465-472
Chart 1 – Correlation between number of psychotropic agents and QT interval dispersion. r = 0.341, p value < 0.001.
Series1
Linear (Series1)
Number of psychotropic agents
QT in
terv
al di
sper
sion
Table 6 – Pearson’s linear correlation between the studied variables
Number of psychotropic agents Age Heart rate Potassium Glucose Magnesium
Pearson’s 0.341 0.177 -0.103 0.057 -0.054 0.095
p value < 0.001 0.024 0.195 0.471 0.495 0.232
Table 7 – Impact of concurrent use of psychotropic agents and antiarrhythmic drugs vs. isolated use of antiarrhythmic drugs
Analysis of subgroups Sample (n. of patients) QT Interval p value QT dispersion p value
Psychotropic + antiarrhythmic drugs 20 445.1 ± 23.770.023
63.55 ± 21.110.715
Antiarrhythmics 15 421.7 ± 24.01 66.60 ± 23.22
It is also worth mentioning that the doses used were not considered, as it was not considered reliable information, either due to the patient’s underlying disease or the frequent presence of caregivers with little information about the drugs being used.
This factor, together with the large number of users of domperidone, bromopride and metoclopramide in continuous use justifies the extended time of patient selection, aiming at attenuating a possible selection bias.
In the present study, we observed a positive correlation between use of psychotropic drugs and increased QTD at the
ECG. There was also a positive correlation between age and QTD. The population studied had a minimum age of 40 years; however, in practice, both groups had mean age > 65 years (G1 = 67.68 ± 12.68 years and G2 = 74.43 ± 11.37 years). The use of psychotropic drugs increases with age, according to data collected by Maia et al17, similarly to the sample studied here. After adjusting for age, as well as analyzing separately the influence of age and the use of psychotropic drugs on QTD, it was observed that only the use of psychotropic drugs persisted with a statistically significant difference.
470

Original Article
Claudio et al.Impact of psychotropic drugs on QT interval dispersion
Arq Bras Cardiol. 2014; 102(5):465-472
1. Timerman S, Ramires JA. Morte súbita: aspectos epidemiologicos. Rev Soc Cardiol Estado de São Paulo. 2006;16(1):8-23.
2. Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med. 2004;350(10):1013-22.
3. Curtis LH, Østbye T, Sendersky V, Hutchison S, Allen LaPointe NM, Al-Khatib SM, et al. Prescription of QT-prolonging drugs in a cohort of about 5 million outpatients. Am J Med. 2003;114(2):135-41.
4. Antzelevitch C, Shimizu W, Yan GX, Sicouri S, Weissenburger J, Nesterenko VV, et al. The M cell: its contribution to the ECG and to normal and abnormal electrical function of the heart. J Cardiovasc Electrophysiol. 1999;10(8):1124-52.
5. Antzelevitch C. The role of spatial dispersion of repolarization in inherited and acquired sudden cardiac death syndromes. Am J Physiol Heart Circ Physiol. 2007;293(4):H2024-38.
6. Restivo M, Caref EB, Kozhevnikov DO, El-Sherif N. Spatial dispersion of repolarization is a key factor in the arrythmogenicity of long QT syndrome. J Cardiovasc Electrophysiol. 2004;15(3):323-31.
7. Antzelevitch C, Shimizu W. Cellular mechanisms underlying the long QT syndrome. Curr Opin Cardiol. 2002;17(1):43-51.
8. Higham PD, Campbell RW. QT dispersion. Br Heart J. 1994;71(6):508-10.
9. Day CP, McComb JM, Campbell RW. QT dispersion: an indication of arrhythmia risk in patients with long QT intervals. Br Heart J. 1990;63(6):342-4.
10. Day CP, McComb JM, Campbell RW. QT dispersion in sinus beats and ventricular extrasystoles in normal hearts. Br Heart J. 1992;67(1):39-41.
11. Murray A, McLaughlin NB, Campbell RW. Measuring QT dispersion: man versus machine. Heart. 1997;77(6):539-42.
12. Campbell RW, Gardiner P, Amos PA, Chadwick D, Jordan RS. Measurement of the QT interval. Eur Heart J. 1985;6 Suppl D:81-3.
13. Murray A, McLaughlin NB, Bourke JP, Doig JC, Furniss SS, Campbell RW. Errors in manual measurement of QT intervals. Br Heart J. 1994;71(4):386-90.
14. McLaughin NB, Campbell RW, Murray A. Accuracy of four automatic QT measurement techniques in cardiac patients and healthy subjects. Heart. 1996;76(5):422-6.
15. Tran H, White CM, Chow MS, Kluger J. An evaluation of the impact of gender and age on QT dispersion in healthy subjects. Ann Noninvasive Electrocardiol. 2001;6(2):129-33.
References
Other authors also confirmed these findings. Mangoni et al20 demonstrated that age has no association with QTD. In the present sample, both the use of psychotropic drugs and the number of psychotropic drugs had a positive correlation with QTD. Of the 76 patients in the psychotropic user group, 24 used a combination of more than one psychotropic drug, corresponding to 31.5% of the group. Thus 114 uses were documented, with the most frequent drug being Quetiapine (20%).
Dispersion values > 60 ms were found in the group using psychotropic drugs, which, in most studies performed to date, are associated with increased cardiovascular death. The Rotterdam Study21 evaluated a cohort of 2,358 men and 3,454 women during a mean period of four years and observed that the presence of QTD > 60 ms was associated with a 2.5-fold higher risk of cardiac death, 1.9-fold higher risk of sudden death and a 40% higher risk of overall death than in the group with QTD <60 ms.
In our study, after adjusting for age, the mean QT interval dispersion was 57.85 ± 7.22 ms in the group of non-users and 68.38 ± 8.11 ms in the group of psychotropic drug users, confirming the risk involved in using these drugs.
It is noteworthy that digitalization, followed by enlargement of electrocardiographic recordings, allowed a high level of resolution, enabling a manual, easy, quick and effective acquisition of the QT interval and its subsequent dispersion, with negligible interobserver variation.
Thus, the QTc interval and its dispersion should be thoroughly investigated in the general population, in outpatient, as well as surgical and emergency settings22,23. Health professionals involved in drug prescription and monitoring of patients taking psychotropic drugs, especially the elderly, should routinely include the ECG in the diagnosis routine of this population, in addition to carefully assess the combination of drugs used.
ConclusionIn the sample population studied, the use of psychotropic
drugs, used alone or with other drugs, is associated with increased QT interval dispersion. The greater the number of psychotropic drugs used, the greater the QT dispersion. There was a positive correlation between the number of psychotropic drugs used per patient and increased QT dispersion. The simultaneous use of psychotropic and antiarrhythmic drugs is associated with the increase in the corrected QT interval, but not QT dispersion, when compared to the subgroup of patients that use only antiarrhythmic drugs.
Author contributionsConception and design of the research: Claudio BQ,
Albuquerque DC; Acquisition of data: Claudio BQ, Penna F, Konder MT, Celoria BMJ, Souza LL; Analysis and interpretation of the data: Claudio BQ, Costa MAN, Penna F, Celoria BMJ, Souza LL, Schneider RS, Albuquerque DC; Statistical analysis: Claudio BQ, Pozzan R, Albuquerque FN, Albuquerque DC; Writing of the manuscript: Claudio BQ, Albuquerque DC; Critical revision of the manuscript for intellectual content: Claudio BQ, Costa MAN, Albuquerque DC.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of Funding There were no external funding sources for this study.
Study AssociationThis article is part of the thesis of master submitted by
Bruno de Queiroz Claudio from Universidade do Estado do Rio de Janeiro.
471

Original Article
Claudio et al.Impact of psychotropic drugs on QT interval dispersion
Arq Bras Cardiol. 2014; 102(5):465-472
16. Alici G, Sahin M, Ozkan B, Acar G, Acar RD, Yazicioglu MV, et al. The comparison in reduction of QT dispersion after primary percutaneous coronary intervention according to existence of thrombectomy in ST-segment elevation myocardial infarction. Clin Cardiol. 2013;36(5):276-9.
17. Maia LC, Durante AM, Ramos LR. Prevalencia de transtornos mentais em área urbana no norte de Minas Gerais, Brasil. Rev Saúde Pública. 2004;38(5):650-6.
18. Gazalle FK, Hallal PC, Lima MS. Depressão na população idosa: os médicos estão investigando? Rev Bras Psiquiatr. 2004;26(3):145-9.
19. Ebert SN, Liu XK, Woosley RL. Female gender as a risk factor for drug-induced cardiac arrhythmias: evaluation of clinical and experimental evidence. J Womens Health. 1998;7(5):547-57.
20. Mangoni AA, Kinirons MT, Swift CG, Jackson SH. Impact of age on QT interval and QT dispersion in healthy subjects: a regression analysis. Age Ageing. 2003;32(3):326-31.
21. de Bruyne MC, Hoes AW, Kors JA, Hofman A, van Bemmel JH, Grobbee DE. Prolonged QT interval predicts cardiac and all-cause mortality in the eldery. The Rotterdam Study. Eur Heart J. 1999;20(4):278-84.
22. Hancı V, Yurtlu S, Karabağ T, Okyay D, Hakimoğlu S, Kayhan G, et al. Effects of esmolol, lidocaine and fentanyl on P wave dispersion,QT, QTc intervals and hemodynamic responses to endotracheal intubation during propofol induction: a comparative study. Rev Bras Anestesiol. 2013;63(3):235-44.
23. Hanci V, Yurtlu S, Aydin M, Bilir S, Erdoğan G, Okyay RD, et al. Preoperative abnormal P and QTc dispersion intervals in patients with metabolic syndrome. Anesth Analg. 2011;112(4):824-7.
472

Original Article
Prevalence of Cardiovascular Risk Factors in Hemodialysis Patients – The CORDIAL StudyJayme Eduardo Burmeister1,2, Camila Borges Mosmann2, Veridiana Borges Costa5, Ramiro Tubino Saraiva2, Renata Rech Grandi2, Juliano Peixoto Bastos2, Luiz Felipe Gonçalves3,4, Guido Aranha Rosito1,2
Universidade Federal de Ciências da Saúde de Porto Alegre - Programa de Pós-graduação em Ciências da Saúde1; Universidade Luterana do Brasil - Curso de Medicina2; Universidade Federal do Rio Grande do Sul - Faculdade de Medicina3; Hospital Mãe de Deus - Departamento de Nefrologia4; Universidade Federal de Ciências da Saúde de Porto Alegre - Faculdade de Medicina5, Porto Alegre, RS – Brazil
Mailing Address: Jayme Eduardo Burmeister •Rua Cel. Lucas de Oliveira, 1270, Apto 301, Bela Vista. Postal Code 90440-010, Porto Alegre, RS - BrazilE-mail: [email protected] received July 25, 2013; revised manuscript November 11, 2013; accepted November 29, 2013.
DOI: 10.5935/abc.20140048
Abstract
Background: There are scarce epidemiological data on cardiovascular risk profile of chronic hemodialysis patients in Brazil.
Objective: The CORDIAL study was designed to evaluate cardiovascular risk factors and follow up a hemodialysis population in a Brazilian metropolitan city.
Methods: All patients undergoing regular hemodialysis for chronic renal failure in all fifteen nephrology centers of Porto Alegre were considered for inclusion in the baseline phase of the CORDIAL study. Clinical, laboratory and demographic data were obtained in medical records and in structured individual interviews performed in all patients by trained researchers.
Results: A total of 1215 patients were included (97.3% of all hemodialysis patients in the city of Porto Alegre). Their average age was 58.3 years old, 59.5% were male and 62.8% were white. The prevalence of cardiovascular risk factors observed was 87.5% for hypertension, 84.7% for dyslipidemia, 73.1% for sedentary lifestyle, 53.7% for tobacco use, and 35.8% for diabetes. In a multivariate adjusted analysis, we found that sedentary lifestyle (p = 0.032, PR 1.08 – 95%CI: 1.01-1.15), dyslipidemia (p = 0.019, PR 1.08 – 95%CI: 1.01-1.14), and obesity (p < 0.001, PR 1.96 – 95%CI: 1.45-2.63) were more frequent in women; and hypertension (p = 0.018, PR 1.06 – 95%CI: 1.01-1.11) and tobacco use (p = 0.006, PR 2.7 – 95%CI: 1.79-4.17) were more often found among patients under 65 years old. Sedentary lifestyle was independently associated with time in dialysis less than 12 months (p < 0.001, PR 1.23 – 95% CI: 1.14-1.33).
Conclusion: Hemodialysis patients in this southern metropolitan Brazilian city have a high prevalence of cardiovascular risk factors resembling many northern countries. (Arq Bras Cardiol. 2014; 102(5):473-480)
Keywords: Patients; Renal dialysis; Risk factors; Prevalence.
IntroductionCardiovascular diseases (CVD) are the main cause of death
in chronic kidney disease (CKD) patients on hemodialysis1-3. In these patients, cardiovascular mortality is 10- to 20-fold higher when compared to individuals from the general population of the same sex, age and race2-5 and can be up to 44 times higher in the presence of diabetes6. CVD are present since the early stages of chronic kidney disease and reach around 30 to 44% of those beginning hemodialysis7-10. Strikingly, occult ischemic CVD are present in up to 50% of asymptomatic dialysis patients7,11,12.
This high amount of CVD can be attributed to the high prevalence of cardiovascular risk factors13. Although traditional risk factors alone could not entirely explain such a high CVD
burden4,14, they seem to be highly predictive of cardiovascular events12, especially in the elderly15. Likewise, cardiovascular profile seems to allow risk stratification in CKD16.
A large percentage of patients entering dialysis have a clustering of non-controlled risk factors for CVD14 leading to an even higher chance of adverse outcomes17.
This high prevalence of traditional CVD risk factors on chronic hemodialysis patients has been reported in several studies in different world countries8-10,12,14,18-20. However, there is a lack of consistent epidemiological data in our country for this population, both for methodological biases and the use of small samples restricted to a single hospital or clinic.
The main objective of this study was to evaluate the prevalence of traditional cardiovascular risk factors in the population of CKD outpatients on chronic hemodialysis in a southern metropolitan city of Brazil.
Methods
Study Design and Research PopulationThe CORDIAL (Cardiovascular Outcomes Registry in
Dialysis Patients) study was designed to collect data on
473

Original Article
Burmeister et al.Cardiovascular risk factors in hemodialysis
Arq Bras Cardiol. 2014; 102(5):473-480
cardiovascular risk profile and carry out the follow-up of all CKD patients enrolled in a regular outpatient hemodialysis program in the city of Porto Alegre, Brazil. The present article describes the baseline phase data and reports a cross-sectional analysis of this population.
Eligibility criteria for enrollment included age 18 years or more, being in chronic outpatient dialysis for more than 30 days, and ability to provide informed consent for participation. The study complies with the Declaration of Helsinki and the protocol was approved by the Ethics Committee for Research of Universidade Federal de Ciencias da Saúde de Porto Alegre (UFCSPA) and by the review boards of the clinical centers included.
From August 2010 to March 2011, all CKD patients on hemodialysis in each of the fifteen dialysis centers of the city of Porto Alegre (Appendix 1) were considered for enrollment and 1215 (97.3% of all) matched the inclusion criteria and agreed to provide informed consent.
CORDIAL Data CollectionTo collect the CORDIAL baseline data we used a standardized
case report form adapted and extended to our needs from the REACH registry, a study performed in several countries including Brazil21. The form was comprehensively filled after visits to each center where patients, health care staff and electronic clinical records were accessed.
Weight, height and blood pressure measured before and after the dialysis session (mean of the last 3 sessions) were obtained from reviewing the patients’ medical records. Prevalence of atherosclerotic cardiovascular disease, diabetes, and hypertension were established by reviewing all history and physical data in the dialysis clinic medical charts and other available medical documents. Furthermore, we considered as hypertensive any patient in use of antihypertensive drugs, or those with mean pre dialysis blood pressure in the stage 1 or up of the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) classification22.
The definition of diabetes included both type 1 and type 2, with or without oral hypoglycemic medication or insulin. Tobacco use was registered as past or present. In accordance with the Kidney Disease Outcomes Quality Initiative of the National Kidney Foundation (K/DOQI-NKF)23, dyslipidemia was defined as the presence of any of the following – total cholesterol > 200 mg/dL, low-density lipoprotein (LDL)-cholesterol > 100 mg/dL, high-density lipoprotein (HDL)-cholesterol < 40 mg/dL, triglycerides > 150 mg/dL, or the use of statin. Current physical activity was established by an inquiry asking about “any moderate activity (as light walking, bicycling, or gardening) or hard one (running, playing football – soccer, hard swimming) at least 30 min two times per week” and “how many minutes in a week”.
Laboratory data were obtained from the medical chart as the most recent result in the six preceding months.
Data about gender were available for all CORDIAL participants, about age for 1213 (99.8%), and race, height and weight for 1206 (99.3%) each.
Information about hypertension status, cardiovascular disease, physical activity, smoking and lipid profile were available respectively for 1210 (99.6%), 1170 (96.3%), 1150 (94.7%), 1147 (94.4%), and 1121 (92.3%) of the individuals in the cohort.
StatisticsStatistical analyses were carried out in STATA 9.0.
Descriptive statistics were used to characterize the sample. Unadjusted and adjusted prevalence ratios were calculated separately for each dependent variable (hypertension, diabetes, dyslipidemia, tobacco use, sedentary lifestyle, and obesity) with independent variables (gender, age, race, time in dialysis, and diagnosis of cardiovascular disease). All tests were two-tailed and the significance level used was 0.05.
ResultsThe present study included 1215 subjects (97.3%
population on chronic outpatient hemodialysis) with a mean age of 58.3 years old, being 59.5% males and 62.8 % white.
Table 1 presents demographic and clinical data for all the patients in the CORDIAL study and also stratified by gender.
The prevalence of traditional cardiovascular risk factors displayed in Table 2 reaches almost 90% for hypertension and dyslipidemia, and about 75% of the subjects were sedentary. Diabetes has a prevalence of 35.8 % in the hemodialysis population of Porto Alegre (Table 2).
In a multivariate analysis (Table 3), older patients presented a higher prevalence of diabetes and sedentary lifestyle. Hypertension, tobacco use, and obesity, however, were more prevalent in the younger ones. Tobacco use was more prevalent in males, while obesity, dyslipidemia, and sedentary lifestyle were more common in females. Sedentary lifestyle was more prevalent in those who were on dialysis for less than 12 months (linear tendency). Hypertension, diabetes, dyslipidemia, and low physical activity were more prevalent among those with diagnosis of cardiovascular disease.
DiscussionThe 1215 individuals included in our study represent
97.3 % of all outpatients on hemodialysis for chronic renal failure during the collecting data period in Porto Alegre. The demographic characteristics of our study population were similar to other studies in several countries9,10,12,14,18,19. The mean age was close to 60 years old (with 35% over 65 years old) and almost 60% of the participants were men. Overall, the baseline cross-sectional phase of the CORDIAL study describes a high prevalence of various traditional cardiovascular risk factors. Prevalence of hypertension (87.5%), dyslipidemia (84.7%), sedentary lifestyle (73.1%), smoking (53.7%) and diabetes (35.8%) were similar to recent studies developed all over the world9,12,14,18,19,24 and also comparable to findings in pre-dialysis CKD patients4.
474

Original Article
Burmeister et al.Cardiovascular risk factors in hemodialysis
Arq Bras Cardiol. 2014; 102(5):473-480
Table 1 – Clinical and demographic data for the patients in the CORDIAL study
All Male Female
(n = 1215) (n = 723) (n = 492)
DemographicsAge (years) – mean(SD) 58.3 (15.0) 59.1 (14.6) 57.1 (15.4)
Race – %White 62.8 66.2 57.8
Black 25.9 23.1 30.1
Other 11.3 10.7 12.1
Time in dialysis (months) – median (interquartile range) 34 (12-71) 35 (12-67) 34 (12-72)
Age of beginning dialysis (years-old) – mean (SD) 54.1 (15.9) 54.9 (15.6) 53.0 (16.2)
Clinical data
Diabetes
DM 1 – n (%) 27 15 (55.6) 12 (44.4)
DM 2 – n (%) 407 239 (58.7) 168 (41.3)
BMI (kg/m2) – mean (SD) 24.7 (4.7) 24.3 (4.2) 25.2 (5.4)< 18.5 (kg/m2) - % 6.1 5.0 7.8
18.5 to 24.9 (kg/m2) - % 52.1 56.2 46.2
25 to 29.9 (kg/m2) - % 29.4 30.0 28.3
≥ 30 (kg/m2) - % 12.4 8.8 17.7
Pre-dialysis blood pressureSystolic (mmHg) – mean (SD) 146.9 (23.4) 147.3 (23.3) 146.4 (23.5)
Diastolic (mmHg) – mean (SD) 82.5 (14.0) 82.8 (13.9) 81.9 (14.1)
Systolic ≥ 140 mmHg – % 70.2 71.6 68.6
Diastolic ≥ 90 mmHg – % 34.7 36.0 32.9
Systolic ≥ 140 mmHg and/or diastolic ≥ 90mmHg – % 72.2 74.7 70.0
Lipid profileCholesterol, total (mg/dL) – mean (SD) 168.2 (48.3) 159.0 (44.1) 183.1 (50.6)
HDL-cholesterol (mg/dL) – mean (SD) 40.1 (14.8) 37.6 (12.6) 43,7 (16.8)
LDL-cholesterol (mg/dL – mean (SD) 94.3 (38.1) 88.6 (35.4) 102.4 (40.4)
Triglycerides (mg/dL) – mean (SD) 171.7 (133.0) 167.8 (145.3) 177.5 (112.6)
Total cholesterol >200 mg/dL – % 22.5 16.3 31.5
HDL-cholesterol <40 mg/dL – % 60.3 64.5 49.5
LDL-cholesterol >100 mg/dL – % 39.4 32.2 49.5
Triglycerides >150 mg/dL - % 45.2 41.6 50.6
Tobacco useEx-smokers - % 40.5 46.8 31.2
Active smokers - % 13.2 15.2 10.2
Years of tobacco use for active smokers – mean (SD) 30.8 (15.0) 31.2 (14.9) 30.0 (15.3)
Number of cig/day for active smokers – mean (SD) 12.5 (10.8) 12.7 (11.2) 12.0 (10.0)
Physical activityNone - % 73.1 71.1 76.2
Up to 60 minutes/week - % 9.6 10.6 8.0
From 60 to 90 min/week - % 5.6 5.5 5.8
From 90 to 120 min/week - % 4.9 5.2 4.3
Over 120 min/week - % 6.8 7.6 5.6
DM: diabetes mellitus; BMI: body mass index; SD: standard deviation; HDL: high density lipoprotein; LDL: low density lipoprotein.
475

Original Article
Burmeister et al.Cardiovascular risk factors in hemodialysis
Arq Bras Cardiol. 2014; 102(5):473-480
Table 2 – Prevalence of cardiovascular risk factors in CORDIAL (%)
Hypertension 87.5
Diabetes 35.8
Dyslipidemia 84.7
Tobacco use 53.7
Sedentary lifestyle 73.1
Elderly (≥ 65 years) 34.9
Male 59.5
Obesity (BMI ≥ 30) 12.4
HypertensionHypertension was found in 87.5 % of our patients, a result
higher than that found by Portolés et al. (the MAR study) in a multicenter cohort in Spain a decade ago (75.8 %)19, but similar to others, like 87.1 % in the study by Ohsawa et al. in Japan (KAREN Study, 2005)18, 86 % in a cohort of 2535 patients in the USA (Agarwal, 2003)25, and around 86 % in two studies in Spain9,12. The CHOICE study found a higher prevalence
Table 3 – Adjusted prevalence rates (PR) of each cardiovascular risk factor in CORDIAL study
Hypertension Diabetes Dyslipidemia Tobacco Sedentary lifestyle Obesity
PR(95%CI) p PR
(95%CI) p PR(95%CI) p PR
(95%CI) p PR(95%CI) p PR
(95%CI) p
Gender 0.883 0.453 0.019 0.006 0.032 < 0.001
Female 1.00 1.00 1.00 1.00 1.00 1.00
Male 1.00 (0.96-1.05)
0.94 (0.81-1.10)
0.93 (0.88-0.99)
1.57 (1.14-2.15)
0.93 (0.87-0.99)
0.51 (0.38-0.69)
Age – years-old 0.018 < 0.001 0.645 < 0.001 < 0.001 < 0.001
< 65 1.00 1.00 1.00 1.00 1.00 1.00
≥ 65 0.94 (0.90-0.99)
1.46 (1.26-1.69)
1.01 (0.95-1.08)
0.37 (0.24-0.56)
1.16 (1.09-1.24)
0.53 (0.37-0.77)
Race 0.232 0.753 0.534 0.057 0.884 0.840
White 1.00 1.00 1.00 1.00 1.00 1.00
Other 0.97 (0.93-1.02)
0.97 (0.83-1.14)
1.02 (0.96-1.08)
1.33 (0.99-1.78)
1.01 (0.94-1.08)
0.97 (0.71-1.31)
Time in dialysis – months 0.384 0.334 0.442 0.091 < 0.001 0.936
1 – 12 1.00 1.00 1.00 1.00 1.00 1.00
13 – 24 1.01 (0.95-1.07)
1.09 (0.89-1.34)
1.04 (0.95-1.15)
1.23 (0.75-2.03)
0.86 (0.77-0.95)
0.98 (0.61-1.58)
25 – 36 0.98 (0.91-1.06)
1.05 (0.83-1.33)
1.06 (0.96-1.18)
1.60 (0.96-2.66)
0.90 (0.81-1.00)
0.72 (0.39-1.35)
> 36 0.98 (0.93-1.03)
0.92 (0.76-1.12)
1.03 (0.96-1.11)
1.39 (0.94-2.06)
0.81 (0.75-0.88)
1.03 (0.70-1.51)
Diagnosis of cardiovascular disease
< 0.001 < 0.001 0.009 0.564 0.049 0.230
No 1.00 1.00 1.00 1.00 1.00 1.00
Yes 1.14 (1.09-1.18)
1.42 (1.22-1.66)
1.08 (1.02-1.15)
0.91 (0.67-1.25)
1.07 (1.00-1.15)
1.21 (0.89-1.65)
(96.0 % among 1041 individuals)14. Pre dialysis mean blood pressure in our population (about 147/82 mmHg) is similar to other studies (149/79 mmHg in CHOICE, and 147/80 mmHg in DMMS Wave2)10,14. Uncontrolled blood pressure in the pre dialysis measurements is 72 % in our cohort (Table 1), similar to the 70 % in the study of Agarwal et al25 and to the 69 % in the CHOICE study14. In CORDIAL, a multivariate adjusted analysis found that patients under 65 years-old presented a higher prevalence of hypertension.
Hypertension has been related to higher mortality in hemodialysis patients26 and the importance of treating high blood pressure in these individuals was highlighted in two recent meta-analysis suggesting a reduction in cardiovascular events and all-cause mortality in those treated with antihypertensive drugs27,28.
DyslipidemiaAmong our patients, the prevalence of dyslipidemia was
84.7 %, a higher rate comparing to other studies like 50% in CHOICE14. The different criteria in each study preclude a more accurate comparison. Our mean LDL-cholesterol (94.3 mg/L) was similar to others9,12,14,18,19, with Kronnnenberg reporting a higher value (115 mg/dL)24.
476

Original Article
Burmeister et al.Cardiovascular risk factors in hemodialysis
Arq Bras Cardiol. 2014; 102(5):473-480
The prevalence of elevated triglycerides was 45.2 % in our cohort, higher than the study by Collado et al12 and the CHOICE study (36.9 % over 200mg/dL)14. Mean values were 171.7 mg/dL in CORDIAL, higher than in KAREN and ANSWER, similar to the MAR study and Kronenberg et al24, and lower than CHOICE (199mg/dL)9,14,18,19,24. HDL-cholesterol under 40 mg/dL was more prevalent in our cohort (60.3 %) than in others9,14,18,19. An exception was the 66 % reported by Kronenberg et al24.
In CORDIAL, there was a higher adjusted prevalence of dyslipidemia in female patients, while Ohsawa et al. reported an opposite finding18. Although there is not a proven association between serum lipids and the development CVD outcomes in dialysis patients29, lipid measurements and treatment remains a cornerstone approach to prevent CVD even in CKD patients24.
Smoking
Tobacco use is associated with a markedly increased risk of heart disease in dialysis patients8,16. Smoking (past or present) was described in 53.7 % of our patients, in accordance to others studies9,10,12,14,19. Thirteen percent of our patients were current smokers, similar to other authors9,14,19, except for the KAREN study, with 28.2%18. In CORDIAL, the adjusted prevalence of tobacco use was higher in males and in those with less than 65 years.
Sedentary lifestyle
Sedentary lifestyle was identified in 73.1% of our patients. In the CHOICE study14, only 14 % reported physical activity to perspiration at least 3 times a week. Tentori et al. (2010)30 described results of 20,920 patients in the DOPPS study with a self-reported regular physical activity of 47.4 %. Comorbidities and physical limitations could explain the low adherence of haemodialysis patients to exercise programs31. Besides, older age could represent another limitation to physical activity – among our patients, adjusted prevalence of physical inactivity was higher in those over 65 years than in younger patients (Table 3).
DiabetesDiabetes prevalence among dialysis patients is already
high and increasing32. The 5-year survival rate among diabetic patients on hemodialysis is worse than in non-diabetics. A recent study in Brazil found 41.1 versus 62.7 %, respectively33. According to the 2009 United States Renal Data System (USRDS) database, only 30 % of the diabetic patients survived five years after beginning hemodialysis1.
In CORDIAL, diabetics were 35.8 % of the population, a lower rate than the one presented in CHOICE (54%)14, but similar to the 38.5% in the 2012 USRDS Annual Report34, with others ranging from 26 to 43 %9,10,18-20.
ObesityObesity estimated by body mass index (BMI) was present
in 12.4% of individuals in CORDIAL. The MAR study19 reported obesity in 14% of their patients, while in ANSWER
and CHOICE the prevalence was higher (20 and 26%, respectively)9,14. Unlike the general population, overweight dialysis patients have better prognosis, supposedly due to a better nutritional status35. Recently, BMI has been considered a non-efficient tool in the assessment of excess body fat content and thereafter obesity36. Reverse epidemiology and inadequate assessment of fat accumulation could explain the “obesity paradox” in CKD37.
AgeIn CKD patients on hemodialysis, older age confers a
cardiovascular risk that parallels the relationship described in the general population38. There is a growing prevalence of elderly in the hemodialysis population all-over the world9,10,19. In the Brazilian dialysis census of 2000, those with age 60 or more were 26 %39, while in 2011 there were 31.5 % with age 65 or more40. In CORDIAL, also in 2011, we found a rate of 34.9 %.
LimitationsOur data presents the usual drawbacks of cross-sectional
studies limiting causal inferences. We had to rely on clinical laboratory measurements of 15 dialysis centers instead of using a core lab. We described similar rates observed in other studies, but our data cannot be generalized to other cities in our country. Our data, however, has the strength of having been acquired from a large population with few dropouts and double-checking structured individual interviews and clinical charts.
ConclusionThe population in chronic hemodialysis in this large
metropolitan south-American city described in the CORDIAL study presents a high prevalence of cardiovascular risk factors. These findings confirm in Brazil what has been previously verified in northern hemisphere countries, the high-risk cardiovascular profile of hemodialysis patients. Prospective studies and clinical trials are needed to further clarify interventions that can be transformed in public health strategies to prevent cardiovascular death in hemodialysis patients.
Acknowledgement The authors thank the medical directors of all dialysis units
in the city of Porto Alegre for their consent and assistance to this study.
Appendix 1 – Dialysis clinical centers of Porto Alegre, BrazilCentro de Dialise e Transplante, CliniRim, Clinica Nefron,
Clinica Vita Rim, Hospital das Clinicas de Porto Alegre, Hospital Divina Providencia, Hospital Ernesto Dornelles, Hospital Mãe de Deus, Hospital Moinhos de Vento, Hospital N. Sra. da Conceição, Hospital Parque Belém, Hospital Santa Casa Porto Alegre, Hospital São Lucas, Hospital Vila Nova, Mãe de Deus Center.
477

Original Article
Burmeister et al.Cardiovascular risk factors in hemodialysis
Arq Bras Cardiol. 2014; 102(5):473-480
Appendix 2 – Associated researchers to the CORDIAL studyAmanda Galdino Macolmes, Camila Borges Mosmann,
Daiane Jaqueline Nascimento, Debora Wassaf Youssef, Eduardo Hoffmann Miranda, Felipe Borsu Salles, Fernando Mendonça Alvares, Fernando Augusto Dannebrock, Gabriela Dotta Dornelles, Gisiane Munaro, Jaime Fracasso Jr, Japão Drose Pereira, Jean Pierre W. Youssef, Liana Pilau Abreu, Liz Lopes Sombrio, Luana Bringhenti, Luzia Gross Lague, Maikel Alf Klein, Mariano Feraboli Fontana, Mauricio Rodrigues, Natalia Fiorentin Caramori, Ramiro Tubino Saraiva, Renata Rech Grandi, Renato Budzyn David, Veridiana Borges Costa.
Author contributionsConception and design of the research: Burmeister JE,
Rosito GA; Acquisition of data: Burmeister JE, Mosmann CB, Costa VB, Saraiva RT, Grandi RR, Bastos JP; Analysis and interpretation of the data: Burmeister JE, Mosmann CB, Costa VB, Bastos JP, Gonçalves LF, Rosito GA; Statistical analysis:
Burmeister JE, Bastos JP, Gonçalves LF, Rosito GA; Writing of the manuscript: Burmeister JE, Mosmann CB, Costa VB, Saraiva RT, Grandi RR, Bastos JP, Rosito GA; Critical revision of the manuscript for intellectual content: Burmeister JE, Mosmann CB, Costa VB, Bastos JP, Gonçalves LF, Rosito GA; Coordination work of collecting and recording data: Burmeister JE; General Coordinator of the Project: Rosito GA.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any thesis or dissertation work.
1. United States Renal Data System, Excerpts from USRDS 2009 Annual Data Report. U.S. Department of Health and Human Services. The National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. Am J Kidney Dis. 2010;55(Suppl 1):S1-420.
2. Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32(Suppl.3):S112-9.
3. Levey AS, Beto JA, Coronado BE, Eknoyan G, Foley RN, Kasiske BL, et al. Controlling the epidemic of cardiovascular disease in chronic renal disease: what do we know? What do we need to learn, where do we go from here? Am J Kidney Dis. 1998;32(5):853-906.
4. Sarnak MJ, Coronado BE, Greene T, Wang SR, Kusek JW, Beck GJ, et al. Cardiovascular disease risk factors in chronic renal insufficiency. Clin Nephrol. 2002;57(5):327-35.
5. Weiner DE, Tabatabai S, Tighiouart H, Elsayed E, Bansal N, Griffith J, et al. Cardiovascular outcomes and all-cause mortality: exploring the interaction between CKD and cardiovascular disease. Am J Kidney Dis. 2006;48(3):392-401.
6. Brown JH, Hunt LP, Vites NP, Short CD, Gokal R, Mallick NP. Comparative mortality from cardiovascular disease in patients with chronic renal failure. Nephrol Dial Transplant. 1994;9(8):1136-42.
7. Ohtake T, Kobayashi S, Moriya H, Negishi K, Okamoto K, Maesato K, et al. High prevalence of occult coronary artery stenosis in patients with chronic kidney disease at the initiation of renal replacement therapy: an angiographic examination. J Am Soc Nephrol. 2005;16(4):1141-8.
8. Di Benedetto A, Marcelli D, D’Andrea A, Cice G, D’Isa S, Cappabianca S, et al. Risk factors and underlying cardiovascular diseases in incident ESRD patients. J Nephrol. 2005;18(5):592-8.
9. Pérez-Garcia R, Martín-Malo A, Fort J, Cuevas X, Llados F, Lozano J, et al. Baseline characteristics of an incident haemodialysis population in Spain: results from ANSWER – a multicentre, prospective, observational cohort study. Nephrol Dial Transplant. 2009;24(2):578-88.
10. Stack AG, Bloembergen W. Prevalence and clinical correlates of coronary artery disease among new dialysis patients in the United States: a cross-sectional study. J Am Soc Nephrol. 2001;12(7):1516-23.
11. Charytan D, Kuntz RE, Mauri L, DeFilippi C. Distribution of coronary artery disease and relation to mortality in asymptomatic hemodialysis patients. Am J Kidney Dis. 2007;48(3):409-16.
12. Collado S, Coll E, Deulofeu R, Guerrero L, Pons M, Cruzado JM, et al. Prevalence of cardiovascular disease in uraemia and relevance of cardiovascular risk factors. Nefrologia. 2010;30(3):342-8.
13. Levin A, Djurdjev O, Barrett B, Burgess E, Carlisle E, Ethier J, et al. Cardiovascular disease in patients with chronic kidney disease: getting to the heart of the matter. Am J Kidney Dis. 2001;38(6):1398-407.
14. Longenecker JC, Coresh J, Powe NR, LeveyAS, FinkNE, Martin A et al. Traditional cardiovascular disease risk factors in dialysis patients compared with the general population: The CHOICE Study. J Am Soc Nephrol. 2002;13(7):1918-27.
15. Shlipak MG, Fried LF, Cushman M, Manollo TA, Peterson D, Stehman-Breen C et al. Cardiovascular mortality risk in chronic kidney disease: comparison of traditional and novel risk factors. JAMA. 2005;293(14):1737-45.
16. Shah DS, Polkinghorne KR, Pellicano R, Kerr PG. Are traditional risk factors valid for assessing cardiovascular risk in end-stage renal failure patients? Nephrology (Carlton). 2008;13(8):667-71.
17. Xue JL, Frazier ET, Herzog CA, Collins AJ. Association of heart disease with diabetes and hypertension in patients with ESRD. Am J Kidney Dis. 2005;45(2):316-23.
18. Ohsawa M, KatoK, Itai K, Onoda T, Konda R, Fujioka T, et al; KAREN Study Group. Cardiovascular risk factors in hemodialysis patients: results from baseline data of kaleidoscopic aproaches to patients with end-stage renal disease study. J Epidemiol. 2005;15(3):96-105.
19. Portolés J, Lopez-Gomez JM, Aljama P. Cardiovascular risk in hemodialysis in Spain: prevalence, management and target results (MAR study). Nefrología.2005;25(3):297-306.
20. Furth S, Hermann J, Powe N. Cardiovascular risk factors, comorbidity and survival outcomes in black and white dialysis patients. Semin Dial. 1998;11(2):102-5.
21. Bhatt DL, Steg PG, Ohman EM, Hirsch AT, Ikeda Y, Mas JL, et al; REACH Registry Investigators. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 2006;295(2):180-9.
References
478

Original Article
Burmeister et al.Cardiovascular risk factors in hemodialysis
Arq Bras Cardiol. 2014; 102(5):473-480
22. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. National Heart, Lung and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure:National Hoigh Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560-72.
23. Kidney Disease Outcomes Quality Initiative (K/DOQI) Group. K/DOQI clinical practice guidelines for management of dyslipidemias in patients with kidney disease. Am J Kidney Dis. 2003;41(Suppl 3):S1-92.
24. Kronenberg F, Lingenhel A, Neyer U, Lhotta K, König P, Auinger M, et al. Prevalence of dyslipidemic risk factors in hemodialysis and CAPD patientes. Kidney Int. 2003;63(Suppl 84):S113-6.
25. Agarwal R, NissensonAR, Battle D, Coyne DW, Trout JR, Warnock DG. Prevalence, treatment, and control of hypertension in chronic hemodialysis patients in the United States. Am J Med. 2003;115(4):291-7.
26. Amar J, Vernier I, Rossignol E, Bongard V, Arnaud C, Conte JJ, et al. Nocturnal blood pressure and 24-hour pulse pressure are potent indicators of mortality in hemodialysis patients. Kidney Int. 2000;57(6):2485-91.
27. Heerspink HJ, Ninomiya T, Zoungas S, de Zeeuw D, Grobbe DE, Jardine MJ, et al. Effect of lowering blood pressure on cardiovascular events and mortality in patients on dialysis: a systematic review and meta-analysis of randomised controlled trials. Lancet. 2009;373(9668):1009-15.
28. Agarwal R, Sinha AD. Cardiovascular protection and antihypertensive drugs dialysis patients: a systematic review and meta-analysis. Hypertension. 2009;53(5):860-6.
29. Heymann EP, Kassimatis TI, Goldsmith DJ. Dyslipidemia, statins, and CKD patients’ outcomes – review of the evidence in the post-sharp era. J Nephrol. 2012;25(4):460-72.
30. Tentori F, Elder SJ, Thumma J, Pisoni RL, Bommer J, Fissell RB, et al. Physical exercise among participants in the Dialysis Outcomes and Practice Patterns Study (DOPPS): correlates and associated outcomes. Nephrol Dial Transplant. 2010;25(9):3050-62.
31. Miller BW, Cress CL, Johnson ME, Nichols DH, Schnitzler MA. Exercise during hemodialysis decreases the use of antihypertensive medications. Am J Kidney Dis. 2002;39(4):828-33.
32. Van Dijk PC, Jager KJ, Stengel B, Grönhagen-Riska C, Feest TG, Briggs JD. Renal replacement therapy for diabetic end-stage renal disease: data from 10 registries in Europe (1991-2000). Kidney Int. 2005;67(4):1489-99.
33. Matos JP, Almeida JR, Guinsburg A, Marelli C, Barra AB, Vasconcellos MS, et al. Assessment of a five-year survival on hemodialysis in Brazil: a cohort of 3,082 incident patients. J Bras Nefrol. 2011;33(4):436-41.
34. U. S. Renal Data System, USRDS 2012 Annual Data Report.: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD;2012.
35. Leavey SF, McCullough K, Hecking E, Goodkin D, Port FK, Young EW. Body mass index and mortality in “healthier” as compared with “sicker” haemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol Dial Transplant. 2001;16(12):2386-94.
36. Okorodudu DO, Jumean MF, Montori VM, Romero-Corral A, Somers VK, Erwin PJ, et al. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: a systematic review and meta-analysis. Int J Obes (Lond). 2010;34(5):791-9.
37. Agarwal R, Bills JE, Light RP. Diagnosing obesity by body mass index in chronic kidney disease: an explanation for the “obesity paradox”? Hypertension. 2010,56(5):893-900.
38. Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108(17):2154-69.
39. Sesso R. Inquérito epidemiologico em unidades de diálise do Brasil. J Bras Nefrol. 2000;22(3 Supl 2):23-6.
40. Sesso RC, Lopes AA, Thomé FS, Lugon JR, Santos DR. Diálise crônica no Brasil - relatorio do Censo Brasileiro de Diálise, 2011. J Bras Nefrol. 2012;34(3):272-7.
479

Original Article
Burmeister et al.Cardiovascular risk factors in hemodialysis
Arq Bras Cardiol. 2014; 102(5):473-480 480

Original Article
LINE-1 Hypomethylation is Associated with the Risk of Coronary Heart Disease in Chinese PopulationLi Wei1, Shuchuan Liu2, Zhendong Su1, Rongchao Cheng1, Xiuping Bai1, Xueqi Li1Department of Cardiology, The Fourth Affiliated Hospital of Harbin Medical University1; Department of Hematology, The First Affiliated Hospital of Harbin Medical University2, Harbin – China
Mailing Address: Xueqi Li •No. 37 Yiyuan Street, Nan Gang. Postal Code 150001, HarbinE-mail: [email protected] received Octobrer 20, 2013; revised manuscript Decembrer 12, 2013; acceptea Decembrer 13, 2013.
DOI: 10.5935/abc.20140054
Abstract
Background: Global methylation level in blood leukocyte DNA has been associated with the risk of coronary heart disease (CHD), with inconsistent results in various populations. Similar data are lacking in Chinese population where different genetic, lifestyle and environmental factors may affect DNA methylation and its risk relationship with CHD.
Objectives: To examine whether global methylation is associated with the risk of CHD in Chinese population.
Methods: A total of 334 cases with CHD and 788 healthy controls were included. Global methylation in blood leukocyte DNA was estimated by analyzing LINE-1 repeats using bisulfite pyrosequencing.
Results: In an initial analysis restricted to control subjects, LINE-1 level reduced significantly with aging, elevated total cholesterol, and diagnosis of diabetes. In the case-control analysis, reduced LINE-1 methylation was associated with increased risk of CHD; analysis by quartile revealed odds ratios (95%CI) of 0.9 (0.6-1.4), 1.9 (1.3-2.9) and 2.3 (1.6-3.5) for the third, second and first (lowest) quartile (Ptrend < 0.001), respectively, compared to the fourth (highest) quartile. Lower (<median) LINE-1 methylation was associated with a 2.2-fold (95%CI = 1.7-3.0) increased risk of CHD. The lower LINE-1-related CHD risk estimates tended to be stronger among subjects with the highest tertile of homocysteine (Pinteraction = 0.042) and those with diagnosis of hypertension (Pinteraction = 0.012).
Conclusion: LINE-1 hypomethylation is associated with the risk of CHD in Chinese population. Potential CHD risk factors such as older age, elevated total cholesterol, and diagnosis of diabetes may have impact on global DNA methylation, whereby exerting their effect on CHD risk. (Arq Bras Cardiol. 2014; 102(5):481-488)
Keywords: Epigenetics; Coronary Heart Disease; Global Methylation; LINE-1; Blood Leukocyte DNA
IntroductionCoronary heart disease (CHD) constitutes 90-95% of
all cases with cardiovascular diseases, which rank the leading cause of death in the world1,2. Age, sex, diets, cigarette smoking, hypertension, diabetes, dyslipidemia, homocysteine, obesity, family history of CHD and genetic factors have been characterized to play a major role in the CHD etiology2-4.
Epigenetic modification, especially aberrant global DNA methylation pattern, is increasingly recognized as a key factor in the development of CHD. Global DNA hypomethylation may induce genomic instability and deregulate gene transcription, thereby contributing to the development of various human diseases including CHD5. In animal models, global DNA hypomethylation has been
associated with aortic lipid deposition, a predictor of future atherosclerosis6,7. Further, an association between global DNA hypomethylation and susceptibility to subclinical atherosclerosis has been reported in young adults8. In addition, in healthy subjects, global methylation level measured in blood leukocyte DNA has been associated with risk factors for CHD, such as aging, cigarette smoking, folate deficiency, hyperhomocysteinemia, higher levels of low density lipoprotein and lower levels of high density lipoprotein9-14. Several epidemiological studies have reported that global methylation level could be a determinant risk factor for CHD, but the results were inconsistent in various populations15-17. Similar data are lacking in Chinese population where different genetic, lifestyle and environmental factors may affect DNA methylation and its risk relationship with CHD18, 19.
About 55% of human genome consists of repetitive elements20, including approximately 500,000 LINE-1 repeats which represent approximately 17% of the human genome21. Because of high representation throughout the genome and heavy methylation in normal tissue, LINE-1 has been used as a surrogate marker for estimating global DNA methylation levels22,23.
In the present study, we have investigated the relationship between LINE-1 methylation and the risk of CHD in a Chinese
481

Original Article
Wei et al.LINE-1 hypomethylation and CHD risk
Arq Bras Cardiol. 2014; 102(5):481-488
population. We also examined the association between LINE-1 methylation and potential risk factors for CHD including age, sex, body mass index (BMI), total cholesterol, triglyceride, homocysteine, smoking status, hypertension and diabetes, as well as their modifying effect on the LINE-1-related risk estimate for CHD.
Methods
Study participantsThis case-control study enrolled 334 patients with CHD
and 788 control subjects from the Fourth Affiliated Hospital, Harbin Medical University, Harbin, China from March 2007 to September 2010. All participants were unrelated individuals from the Chinese Han population, and the controls were frequency-matched to the cases by age (± 5 years) and sex. The diagnosis of CHD was established by angiographic evidence of ≥70% stenosis of 1 major coronary artery, or ≥ 50% of the left main coronary artery. The controls filled a regular health survey and their detailed examination by history analysis, physical examination, electrocardiography, and echocardiography revealed absence of CHD or other heart diseases. For both CHD and control groups, subjects with spastic angina pectoris, peripheral artery disease, and any kind of autoimmune-related disease or cancers were excluded. Information on age, sex, height, weight, cigarette smoking, and diagnosis of hypertension and diabetes was obtained by using a structured questionnaire through in-person interviews. An ever-smoker was defined as a smoker of at least 1 cigarette per day for at least 6 months. BMI was calculated using the formula: body weight in kilograms divided by the square of body height in meters (kg/m2). Information on serum total cholesterol, triglyceride and plasma homocysteine was collected on the basis of medical records. Written informed consent was obtained from each participant. The study protocol was approved by the ethics review committee of the Institutional Review Board of the participant hospital.
DNA methylation analysis of LINE-1 repetitive elements Genomic DNA was extracted from blood leukocytes using
the QIAamp DNA Blood Extraction kit (Qiagen, Shanghai, China), and then modified by treatment with sodium bisulfite using the Zymo EZ DNA Methylation kit (Zymo, CA, USA), following the manufacturer’s protocol. A modified method of PCR-based pyrosequencing originally described by Yang et al22 was performed to quantitate methylation of the LINE-1 repetitive elements. In brief, PCR was carried out in a 50-µl reaction volume containing 25 µl of GoTaq Green Master mix (Promega, WI, USA), 1 pmol of forward primer (TTT TGA GTT AGG TGT GGG ATA TA), 1 pmol of biotinylated reverse primer (biotin-AAA ATC AAA AAA TTC CCT TTC), and 50 ng of bisulfite-treated genomic DNA. PCR cycling conditions were 95°C for 30 s, 50°C for 30 s and 72°C for 30 s for 40 cycles. PCR product was bound to streptavidin sepharose beads (Amersham Biosciences, Uppsala, Sweden). These sepharose beads containing the bound PCR product were purified, washed, denatured and washed again. Then, 0.3-µM pyrosequencing
primer (AGT TAG GTG TGG GAT ATA GT) was annealed to the purified single-stranded PCR product. Pyrosequencing was performed using the PSQ HS 96 Pyrosequencing System. For all assays we used built-in controls to verify bisulfite conversion. Each sample was assayed in duplicate and their average was used in final analysis. The degree of LINE-1 methylation was expressed as % 5-methylated cytosines (%5mC) over total (methylated + unmethylated) cytosines.
Statistical analysisChi-square test was used to examine the differences in the
distributions of categorical variables and Student’s t-test for the differences in means of continuous variables between CHD cases and control subjects. Linear regression models were used to evaluate LINE-1 differences among controls in relation to age, sex, BMI, total cholesterol, triglyceride, homocysteine, smoking status, hypertension and diabetes. Unconditional logistic regression was used to estimate odds ratio (OR) for CHD and 95% confidence interval (CI). Quartile and median cut-points were based on LINE-1 distributions among controls. All models were adjusted for age (as a continuous variable), sex, and smoking status (ever-smoker: yes vs no). Further adjustment by other potential confounding variables, including BMI, total cholesterol, triglyceride, homocysteine, hypertension and diabetes, did not materially alter the risk estimates. Therefore, these variables were not included in the final models. Effect modification by individual covariates was assessed using likelihood-ratio tests. All tests were two-sided and a P value of <0.05 was considered significant. Statistical analyses were conducted using the Stata 10.1 (Stata Corporation, College Station, TX).
ResultsThe potential risk factors of study subjects by case and
control status are shown in Table 1. No significant differences between CHD cases and control subjects were found in the distributions of age, sex, BMI, or triglyceride. When compared with the controls, CHD cases were more likely to be ever-smoker, and tended to have higher levels of total cholesterol and homocysteine. Cases also were likely to have diagnosis of hypertension and diabetes.
The effects of potential risk factors on LINE-1 methylation level among control subjects are shown in Table 2. As expected, LINE-1 level reduced significantly with increasing age (p = 0.016). We also observed that total cholesterol (p < 0.001) and diagnosis of diabetes (p < 0.001) were inversely associated with LINE-1 methylation levels. No statistically significant relationships were observed between LINE-1 methylation level and sex, smoking status, BMI, triglyceride, homocysteine, or diagnosis of hypertension.
CHD cases had significantly reduced LINE-1 methylation level than controls (mean (standard deviation, SD): 80.96 (2.40) vs 81.67 (2.46), p < 0.001) (Table 1). Analyses of LINE-1 in quartiles, based on the distribution in controls, show that the LINE-1 methylation level was inversely associated with the risk of CHD (Table 3). Relative to subjects in the fourth (highest) quartile of LINE-1 methylation, ORs
482

Original Article
Wei et al.LINE-1 hypomethylation and CHD risk
Arq Bras Cardiol. 2014; 102(5):481-488
for CHD were 0.9 (95% CI, 0.6-1.4), 1.9 (95% CI, 1.3-2.9) and 2.3 (95% CI, 1.6-3.5) for the subjects with methylation in the third, second and first (lowest) quartile (Ptrend < 0.001), respectively. When using the alternative cut-point based on the median, individuals with lower (<median) LINE-1 methylation had a 2.2-fold (95% CI, 1.7-3.0) increased risk of CHD compared with subjects with higher (> median) LINE-1 methylation.
When stratified by potential risk factors, the lower LINE-1-related CHD risk estimates tended to be stronger among subjects with the highest tertile of homocysteine (OR = 3.2, 95% CI, 3.2-5.2) and those with diagnosis of hypertension (OR = 3.1, 95 %CI, 2.1-4.8) (Table 4). Statistically significant interactions in relation to CHD risk were observed between LINE-1 methylation and homocysteine level (P interaction = 0.042), and between
Table 1 – Potential risk factors of study subjects
Potential risk factors Cases, n (%) Controls, n (%) p value*
Age (tertile), years
< 59 96 (28.7) 266 (33.8)
60-65 119 (35.6) 236 (29.9)
> 65 119 (35.6) 286 (36.3) 0.12
Sex
Female 66 (19.8) 150 (19.0)
Male 268 (80.2) 638 (81.0) 0.78
Ever-smoker
No 156 (47.4) 590 (75.4)
Yes 173 (52.6) 193 (24.6) < 0.001
Body mass index (tertile), kg/m2
< 22.0 97 (29.1) 262 (33.2)
22.0-25.4 122 (36.5) 264 (33.6)
> 25.4 115 (34.4) 262 (33.2) 0.36
Total cholesterol (tertile), mmol/L
< 2.9 57 (17.1) 262 (33.2)
2.9-4.8 123 (36.8) 263 (33.4)
> 4.8 154 (46.1) 263 (33.4) < 0.001
Triglyceride (tertile), mmol/L
< 1.1 113 (33.8) 265 (33.7)
1.1-1.6 111 (33.2) 258 (32.8)
> 1.6 110 (33.0) 263 (33.5) 0.98
Homocysteine (tertile), μmol/L
< 9 70 (21.6) 241 (32.3)
9-11 106 (32.7) 252 (33.7)
> 11 148 (45.7) 254 (34.0) < 0.001
Hypertension
No 128 (38.3) 520 (66.0)
Yes 206 (61.7) 268 (34.0) < 0.001
Diabetes
No 212 (63.5) 638 (81.0)
Yes 122 (36.5) 150 (19.0) < 0.001
Mean LINE-1 (SD) 80.96 (2.40) 81.67 (2.46) < 0.001†
SD: standard deviation. *P value obtained from a X2-test comparing cases and controls. †P value obtained from a Student’s t-test comparing cases and controls.
483

Original Article
Wei et al.LINE-1 hypomethylation and CHD risk
Arq Bras Cardiol. 2014; 102(5):481-488
LINE-1 methylation and hypertension (Pinteraction = 0.012). Stratification by other potential risk factors including age (tertile), sex (female, male), smoking status (ever-smoker: no, yes), BMI (tertile), total cholesterol (tertile), triglyceride (tertile), and diagnosis of diabetes (no, yes), produced comparable risk estimates (data not shown). The interactions between LINE-1 methylation and these factors on CHD risk were not statistically significant (data not shown).
DiscussionIn the present study, we demonstrated a statistically
significant, inverse relationship between LINE-1 methylation level and CHD risk in the Chinese population. Homocysteine level and diagnosis of hypertension modified this inverse relationship. Considering that CHD is one of the most common diseases, along with its severity24, the risk factor
Table 2 – Relation of potential CHD risk factors to LINE-1 methylation levels among control subjects
Potential risk factors n LINE-1, mean (95% CI)* P value*
Age (tertile), years†
< 59 266 81.58 (81.33-81.83)
60-65 236 81.47 (81.22-81.72)
> 65 286 81.21 (80.97-81.45) 0.016
Sex‡
Female 150 81.47 (81.14-81.81)
Male 638 81.40 (81.24-81.56) 0.46
Ever smoker§
No 590 81.59 (81.41-81.76)
Yes 193 81.05 (80.80-81.31) 0.35
Body mass index (tertile), kg/m2
< 22.0 262 81.41 (81.16-81.66)
22.0-25.4 264 81.24 (80.99-81.48)
> 25.4 262 81.58 (81.34-81.83) 0.54
Total cholesterol (tertile), mmol/L
< 2.9 262 81.83 (81.57-82.10)
2.9-4.8 263 81.57 (81.34-81.81)
> 4.8 263 80.95 (80.72-81.18) < 0.001
Triglyceride (tertile), mmol/L
< 1.1 265 81.39 (81.15-81.64)
1.1-1.6 258 81.43 (81.18-81.68)
> 1.6 263 81.42 (81.18-81.67) 0.42
Homocysteine (tertile), μmol/L
< 9 241 81.53 (81.26-81.80)
9-11 252 81.37 (81.12-81.63)
> 11 254 81.41 (81.17-81.65) 0.91
Hypertension
No 520 81.53 (81.34-81.72)
Yes 268 81.25 (81.03-81.47) 0.59
Diabetes
No 638 81.59 (81.43-81.75)
Yes 150 80.85 (80.56-81.14) < 0.001
CHD: Coronary heart disease; CI: Confidence interval. *Adjusted for age, sex, and smoking status. †Only adjusted for sex and smoking status. ‡Only adjusted for age and smoking status. §Only adjusted for age and sex.
484

Original Article
Wei et al.LINE-1 hypomethylation and CHD risk
Arq Bras Cardiol. 2014; 102(5):481-488
Table 3 – LINE-1 methylation levels in relation to CHD risk
LINE-1 (%5mC) Cases, n (%) Controls, n (%) OR (95% CI)*
Quartile†
Q4(> 82.73) 55 (16.5) 197 (25.0) 1.0 (reference)
Q3(81.52-82.72) 49 (14.7) 194 (24.6) 0.9 (0.6-1.4)
Q2(80.17-81.51) 101 (30.2) 199 (25.3) 1.9 (1.3-2.9)
Q1(< 80.16) 129 (38.6) 198 (25.1) 2.3 (1.6-3.5)
Ptrend < 0.001
Median†
High(≥ 81.52) 104 (31.1) 391 (49.6) 1.0 (reference)
Low(< 81.52) 230 (68.9) 397 (50.4) 2.2 (1.7-3.0)
%5mC: % 5-methylated cytosines; CHD: coronary heart disease; CI: confidence interval; OR: odds ratio.*Adjusted for age, sex, and smoking status. †The quartiles and the median of LINE-1 measures were based on values among control subjects.
Table 4 – LINE-1 level in relation to CHD risk, by homocysteine level and diagnosis of hypertension
Potential risk factors LINE-1* Cases, n (%) Controls, n (%) OR (95% CI) †
Homocysteine, μmol/L
< 9High 24 (34.3) 126 (52.3) 1.0 (reference)
Low 46 (65.7) 115 (47.7) 2.2 (1.2-4.0)
9-11High 41 (38.7) 115 (45.6) 1.0 (reference)
Low 65 (61.3) 137 (54.4) 1.4 (0.9-2.3)
> 11High 36 (24.3) 135 (53.1) 1.0 (reference)
Low 112 (75.7) 119 (46.9) 3.2 (2.0-5.2)
Hypertension
NoHigh 51 (39.8) 251 (48.3) 1.0 (reference)
Low 77 (60.2) 269 (51.7) 1.5 (1.0-2.3)
YesHigh 53 (25.7) 140 (52.2) 1.0 (reference)
Low 153 (74.3) 128 (47.8) 3.1 (2.1-4.8)
CHD: coronary heart disease; CI: confidence interval; OR: odds ratio. *The median of LINE-1 measure was based on values among control subjects. High: ≥ 81.52 (%5mC); Low: < 81.52 (%5mC). †Adjusted for age, sex, and smoking status.
of global hypomethylation could have a sizable impact on public health. Because DNA methylation is a reversible epigenetic mechanism, this blood-based marker could offer exciting new opportunities for population-based CHD prevention as well as risk assessment25.
Global DNA methylation levels, assessed in repeat regions from leukocyte-derived DNA, have been reported to be associated with risk of CHD in American, Singapore, and Indian populations, with inconsistent observations15-17. In a cohort of 712 elderly men from American population, LINE-1 hypomethylation was associated with increased risk for ischemic heart disease in both cross-sectional and longitudinal analyses15. This is consistent with the findings in the present study. However, in our data, there were also significant relationships among women as well as in different age groups between LINE-1 methylation and CHD risk, which provide further data to
what was previously observed in the American population15. On the other hand, in a Singapore population, higher methylation levels of Alu/Sat2 repeats were reported in males with a history of myocardial infarction or stroke (n = 8) than in control males (n = 121)16; In an Indian population, higher methylation levels of CCGG sequences were reported in cases with coronary artery disease (n = 137) than in controls (n = 150)17. The different lifestyle, environmental exposures, and genetic backgrounds among the populations, and differences in sample size and repetitive elements of DNA targeted for measuring global hypomethylation levels26-28, might contributed to the different findings across these studies.
The modifying effect of age on global DNA methylation levels, consistent with previous data29, may reflect age-related cumulative effects of enviromental exposures to risk factors for CHD. Global hypomethylation in leukocyte DNA has been
485

Original Article
Wei et al.LINE-1 hypomethylation and CHD risk
Arq Bras Cardiol. 2014; 102(5):481-488
associated with exposure to multiple types of enviromental pollutants such as polycyclic aromatic hydrocarbons, particulate air pollution, black carbon and sulfates30-32. The present study also showed that two recognized CHD risk factors, elevated total cholesterol and diagnosis of diabetes, were related to reduced LINE-1 methylation levels, further supporting a role of DNA hypomethylation in the development of CHD.
In our data, there was a lack of association between LINE-1 methylation and homocysteine level or diagnosis of hypertension, which differs somewhat from what was observed previously10,33. However, we observed that both homocysteine level and diagnosis of hypertension modified the inverse relationship between LINE-1 methylation and CHD risk. Further studies are warranted to replicate these findings and to elucidate the underlying mechanism of homocysteine level and diagnosis of hypertension on their modifying role in the association between global hypomethylation and CHD risk.
Our study had the advantages of being based on a relatively large sample size, diagnosis of CHD by angiographic evidence, and accurate quantitative analysis using pyrosequencing methodology, which is suitable for measuring subtle changes in DNA methylation. The chief limitation of the present study was the retrospective nature of the study design, i.e., the collection of blood samples from CHD patients took place after their CHD diagnosis. If the diagnosis of CHD had any direct or indirect impact on global DNA methylation through changing subject’s lifestyle or environmental exposure, we could have observed a confounded or biased association between LINE-1 methylation and CHD risk. However, similar risk estimates were observed when the logistic regression analysis was restricted to 212 newly diagnosed CHD cases as compared to controls (data not shown). Moreover, our finding that LINE-1 methylation levels were reduced in control subjects with CHD risk factors such as older age, elevated total cholesterol, and diagnosis of diabetes, indicates that reduced LINE-1 methylation in high-risk control subjects may result
from exposures related to the risk of CHD. In addition, in the longitudinal analyses in the study by Baccarelli et al31, lower LINE-1-related increased risk of ischemic heart disease has been observed.
ConclusionThe findings of the present study support global DNA
hypomethylation measured in LINE-1 repeats is associated with the risk of CHD in the Chinese population. Potential CHD risk factors such as older age, elevated total cholesterol and diagnosis of diabetes may have impact on global DNA methylation, whereby exerting their effect on CHD risk.
Author contributionsConception and design of the research and Analysis and
interpretation of the data: Wei L, Liu S, Su Z, Cheng R, Bai X, Li X; Acquisition of data: Wei L, Su Z, Cheng R; Statistical analysis: Wei L, Bai X, Li X; Writing of the manuscript: Wei L, Liu S, Su Z, Cheng R, Bai X; Critical revision of the manuscript for intellectual content: Li X.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part of the thesis of master submitted by Li
Wei, from the Fourth Affiliated Hospital of Harbin Medical University.
1. Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, et al. Executive summary: heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127(1):143-52.
2. Pranavchand R, Reddy BM. Current status of understanding of the genetic etiology of coronary heart disease. J Postgrad Med. 2013;59(1):30-41.
3. Garcia-Rios A, Delgado-Lista J, Alcala-Diaz JF, Lopez-Miranda J, Perez-Martinez P. Nutraceuticals and coronary heart disease. Curr Opin Cardiol. 2013;28(4):475-82.
4. Marti-Carvajal AJ, Sola I, Lathyris D, Karakitsiou DE, Simancas-Racines D. Homocysteine-lowering interventions for preventing cardiovascular events. Cochrane Database Syst Rev. 2013;1:CD006612.
5. Kulis M, Esteller M. DNA methylation and cancer. Adv Genet. 2010;70:27-56.
6. Lund G, Andersson L, Lauria M, Lindholm M, Fraga MF, Villar-Garea A, et al. DNA methylation polymorphisms precede any histological sign of atherosclerosis in mice lacking apolipoprotein E. J Biol Chem. 2004;279(28):29147-54.
7. Chen Z, Karaplis AC, Ackerman SL, Pogribny IP, Melnyk S, Lussier-Cacan S, et al. Mice deficient in methylenetetrahydrofolate reductase exhibit hyperhomocysteinemia and decreased methylation capacity, with neuropathology and aortic lipid deposition. Hum Mol Genet. 2001;10(5):433-43.
8. Bressler J, Shimmin LC, Boerwinkle E, Hixson JE. Global DNA methylation and risk of subclinical atherosclerosis in young adults: the Pathobiological Determinants of Atherosclerosis in Youth (PDAY) study. Atherosclerosis. 2011;219(2):958-62.
9. Wang TC, Song YS, Wang H, Zhang J, Yu SF, Gu YE, et al. Oxidative DNA damage and global DNA hypomethylation are related to folate deficiency in chromate manufacturing workers. J Hazard Mater. 2012;213-214:440-6.
10. Zacho J, Yazdanyar S, Bojesen SE, Tybjaerg-Hansen A, Nordestgaard BG. Hyperhomocysteinemia, methylenetetrahydrofolate reductase c.677C>T polymorphism and risk of cancer: cross-sectional and prospective studies and meta-analyses of 75,000 cases and 93,000 controls. Int J Cancer. 2011;128(3):644-52.
References
486

Original Article
Wei et al.LINE-1 hypomethylation and CHD risk
Arq Bras Cardiol. 2014; 102(5):481-488
11. Flom JD, Ferris JS, Liao Y, Tehranifar P, Richards CB, Cho YH, et al. Prenatal smoke exposure and genomic DNA methylation in a multiethnic birth cohort. Cancer Epidemiol Biomarkers Prev. 2011;20(12):2518-23.
12. Terry MB, Delgado-Cruzata L, Vin-Raviv N, Wu HC, Santella RM. DNA methylation in white blood cells: association with risk factors in epidemiologic studies. Epigenetics. 2011;6(7):828-37.
13. Hsiung DT, Marsit CJ, Houseman EA, Eddy K, Furniss CS, McClean MD, et al. Global DNA methylation level in whole blood as a biomarker in head and neck squamous cell carcinoma. Cancer Epidemiol Biomarkers Prev. 2007;16(1):108-14.
14. Cash HL, McGarvey ST, Houseman EA, Marsit CJ, Hawley NL, Lambert-Messerlian GM, et al. Cardiovascular disease risk factors and DNA methylation at the LINE-1 repeat region in peripheral blood from Samoan Islanders. Epigenetics. 2011;6(10):1257-64.
15. Baccarelli A, Wright R, Bollati V, Litonjua A, Zanobetti A, Tarantini L, et al. Ischemic heart disease and stroke in relation to blood DNA methylation. Epidemiology. 2010;21(6):819-28.
16. Kim M, Long TI, Arakawa K, Wang R, Yu MC, Laird PW. DNA methylation as a biomarker for cardiovascular disease risk. PLoS One. 2010;5(3):e9692.
17. Sharma P, Kumar J, Garg G, Kumar A, Patowary A, Karthikeyan G, et al. Detection of altered global DNA methylation in coronary artery disease patients. DNA Cell Biol. 2008;27(7):357-65.
18. Terry MB, Ferris JS, Pilsner R, Flom JD, Tehranifar P, Santella RM, et al. Genomic DNA methylation among women in a multiethnic New York City birth cohort. Cancer Epidemiol Biomarkers Prev. 2008;17(9):2306-10.
19. Zhang FF, Cardarelli R, Carroll J, Fulda KG, Kaur M, Gonzalez K, et al. Significant differences in global genomic DNA methylation by gender and race/ethnicity in peripheral blood. Epigenetics. 2011;6(5):623-9.
20. Lander ES, Linton LM, Birren B, Nusbaum C, Zody MC, Baldwin J, et al. Initial sequencing and analysis of the human genome. Nature. 2001; 409(6822):860-921.
21. Cordaux R, Batzer MA. The impact of retrotransposons on human genome evolution. Nat Rev Genet. 2009;10(10):691-703.
22. Yang AS, Estecio MR, Doshi K, Kondo Y, Tajara EH, Issa JP. A simple method for estimating global DNA methylation using bisulfite PCR of repetitive DNA elements. Nucleic Acids Res. 2004;32(3):e38.
23. Zhu ZZ, Hou L, Bollati V, Tarantini L, Marinelli B, Cantone L, et al. Predictors of global methylation levels in blood DNA of healthy subjects: a combined analysis. Int J Epidemiol. 2012;41(1):126-39.
24. He J, Gu D, Wu X, Reynolds K, Duan X, Yao C, et al. Major causes of death among men and women in China. N Engl J Med. 2005;353(11):1124-34.
25. Feinberg AP. Phenotypic plasticity and the epigenetics of human disease. Nature. 2007;447(7143):433-40.
26. Tehranifar P, Wu HC, Fan X, Flom JD, Ferris JS, Cho YH, et al. Early life socioeconomic factors and genomic DNA methylation in mid-life. Epigenetics. 2013; 8(1):23-7.
27. Virani S, Dolinoy DC, Halubai S, Jones TR, Domino SE, Rozek LS, et al. Delivery type not associated with global methylation at birth. Clin Epigenetics. 2012;4(1):8.
28. Zhu ZZ, Sparrow D, Hou L, Tarantini L, Bollati V, Litonjua AA, et al. Repetitive element hypomethylation in blood leukocyte DNA and cancer incidence, prevalence, and mortality in elderly individuals: the Normative Aging Study. Cancer Causes Control. 2011;22(3):437-47.
29. Bollati V, Schwartz J, Wright R, Litonjua A, Tarantini L, Suh H, et al. Decline in genomic DNA methylation through aging in a cohort of elderly subjects. Mech Ageing Dev. 2009;130(4):234-9.
30. Herbstman JB, Tang D, Zhu D, Qu L, Sjodin A, Li Z, et al. Prenatal exposure to polycyclic aromatic hydrocarbons, benzo[a]pyrene-DNA adducts, and genomic DNA methylation in cord blood. Environ Health Perspect. 2012;120(5):733-8.
31. Baccarelli A, Wright RO, Bollati V, Tarantini L, Litonjua AA, Suh HH, et al. Rapid DNA methylation changes after exposure to traffic particles. Am J Respir Crit Care Med. 2009; 179(7):572-8.
32. Madrigano J, Baccarelli A, Mittleman MA, Wright RO, Sparrow D, Vokonas PS, et al. Prolonged exposure to particulate pollution, genes associated with glutathione pathways, and DNA methylation in a cohort of older men. Environ Health Perspect. 2011;119(7):977-82.
33. Alexeeff SE, Baccarelli AA, Halonen J, Coull BA, Wright RO, Tarantini L, et al. Association between blood pressure and DNA methylation of retrotransposons and pro-inflammatory genes. Int J Epidemiol. 2013;42(1):270-80.
487

Original Article
Wei et al.LINE-1 hypomethylation and CHD risk
Arq Bras Cardiol. 2014; 102(5):481-488 488

Original Article
Incidence of Ventricular Arrhythmias after Stem Cell Therapy in Patients with Chagas CardiomyopathyAdriana Sebba Barroso de Souza, Weimar Kunz Sebba Barroso Souza, Sandra Araujo Costa, Elis Marra de Moreira Freitas, Gustavo Carvalho, Luís Antônio Batista Sá, Salvador RassiHospital das Clínicas da Universidade Federal de Goiás, Goiânia (GO) − Brazil
Mailing Address: Adriana Sebba Barroso de Souza •Universidade Federal de Goiás, - Av. Esperança, s/n - Setor Itatiaia. Postal Code 74001-970, Goiânia, GO – BrazilE-mail: [email protected] received September 22, 2013, revised manuscript December 17, 2013, accepted December 18, 2013.
DOI: 10.5935/abc.20140053
Abstract
Background: Treatment with stem cells in several cardiomyopathies may be related to the increase in arrhythmias.
Objectives: To determine whether intracoronary injection of stem cells in patients with Chagas cardiomyopathy is associated with increased incidence of ventricular arrhythmias, compared to the Control Group.
Methods: A retrospective cohort study that evaluated the medical records of 60 patients who participated in a previous cross-sectional study. The following data were collected: age, gender, drugs used and Holter variables that demonstrated the presence of arrhythmias. Holter was performed in four stages: randomization, 2, 6 and 12 months segments. The Control Group received medical treatment and intracoronary injection of placebo and the Study Group had drug treatment and autologous stem cell implant.
Results: There was no difference between Control Group and Study Group when analyzing the arrhythmia criteria. In the intra-group analysis, significant difference was found between the Holter tests of the Study Group for the variable total ventricular premature beats when compared with baseline, with p = 0.014 between Holter at randomization and Holter at 2 months, p = 0.004 between Holter at randomization and Holter at 6 months, and p = 0.014 between Holter at randomization and Holter at 12 months. The variable non-sustained ventricular tachycardia between Holter at randomization and Holter at 6 months showed p = 0.036.
Conclusion: The intracoronary injection of stem cells did not increase the incidence of ventricular arrhythmias in patients with Chagas cardiomyopathy compared to the Control Group. (Arq Bras Cardiol. 2014; 102(5):489-494)
Keywords: Arrhythmias, Cardiac; Stem Cell Transplantation; Chagas Cardiomyopathy.
IntroductionIn the past decades, heart failure (HF) has emerged as a
public health problem. Kannel, based on epidemiological studies obtained in the Framingham Heart Study, estimated that in the United States, there are 5 million HF patients, with approximately 400,000 new cases per year. The problem is presumed to be of the same magnitude in Brazil1.
According to data from the World Health Organization (WHO), although vectorial transmission has been interrupted in countries such as Brazil, Chile and Uruguay, the prevalence of patients with chronic chagasic cardiopathy was estimated between 18 and 20 million people in Latin America, with 300,000 new cases each year, and 50,000 annual deaths associated with the disease2.
Despite the widely positive impact with new drugs for the treatment of HF, the disease progresses and patient prognosis remains reserved, with reduced quality of life and survival. Thus, there is an enormous interest and need to seek new therapies that may offer beneficial effects in the evolution of these patients3.
Of the new therapeutic procedures, the most promising seems to be stem cell therapy.
In Brazil, preliminary studies including a limited number of patients have shown that the use of stem cells from bone marrow is safe and potentially effective in patients with HF4,5.
Stem cells have an intrinsic potential for arrhythmia, mainly related to their common lack of electromechanical integration in the recipient myocardium; it is also important to recognize that patients eligible for cell replacement therapy are likely to develop arrhythmias due to underlying heart disease6.
The study by Satsuki Fukushima provided experimental evidence that direct intramyocardial injection of stem cells from bone marrow can induce severe ventricular arrhythmias in the first 14 days after the injection in chronic HF models7.
The aim of this study was to compare the frequency of ventricular arrhythmia in a group of patients who received intracoronary injection of stem cells with a control group.
489

Original Article
Souza et al.Arrhythmias after stem cell injection
Arq Bras Cardiol. 2014; 102(5):489-494
MethodsThis study was approved by the Ethics and Research
Committee of Hospital das Clinicas of Universidade Federal de Goiás, protocol number 179/2011.
This is a retrospective analysis of a cohort of patients enrolled in a prospective, double-blind, randomized clinical trial, included in the Multicenter Randomized Study of Cell Therapy in Cardiopathies (EMRTCC) - chagasic cardiopathy arm, carried out at the Heart Failure Service of Hospital das Clinicas of Universidade Federal de Goiás.
The sample consisted of 60 patients included in the abovementioned protocol from April 2006 to November 2009, followed for at least 1 year after randomization. This was a convenience sample. Inclusion criteria were: having been included in the study and undergone Holter monitoring during the follow-up period. Patients were divided into two groups in a double-blind fashion: the control group (CG) received appropriate medical treatment and optimized for HF and intracoronary injection of placebo; the Study Group (SG) received, in addition to adequate drug treatment, autologous stem cell transplant obtained from bone marrow aspirate.
A total of 34 patients were randomly assigned to the SG and 26 to the CG. Data collection was performed from January to July 2012 from medical records. This randomization was carried out by the EMRTCC national study, which explains the fact that the groups ended up with different samples at the Heart Failure Service, Hospital das Clinicas, Universidade Federal de Goiás.
Data regarding age (in years), gender (male or female); death (yes or no), medications used (renin-angiotensin system blocker, digitalis, angiotensin-converting enzyme inhibitors, spironolactone, diuretics, amiodarone, beta-blockers), and the number and viability of stem cells used for transplant were collected.
The presence of arrhythmia was assessed from Holter results. Holter monitoring was performed at randomization (baseline - Holter 1) and after 2 (Holter 2), 6 (Holter 3) and 12 (Holter 4) months of follow-up.
The criteria assessed by Holter were total number of beats, ventricular premature beats, supraventricular premature beats, total episodes of Nonsustained Ventricular Tachycardia (NSVT), and Sustained Ventricular Tachycardia (SVT). The presence of three or more consecutive ventricular premature beats in a 30-second interval with heart rate above one hundred beats per minute was considered NSVT, while SVT was considered in the presence of ventricular premature beats for a period greater than 30 seconds or causing hemodynamic instability at any time interval with heart rate above one hundred beats per minute. For this study, ventricular arrhythmia was considered as an increase in the total incidence of NSVT and SVT episodes.
Statistical AnalysisData were entered in Excel for Windows software
spreadsheets and analyzed using the Statistical Package for Social Sciences (SPSS), releases 17.0 and 19.0.
Age was shown as mean and standard deviation and gender as absolute and relative frequency.
Fisher’s test was used to compare the frequency of medication use between the SG and the CG.
After applying the Kolmogorov-Smirnov test for quantitative variables obtained at Holter, Student’s t test was performed for normally distributed variables and the Mann Whitney’s test for those with non-normal distribution. These tests were used to compare the groups.
To compare the Holter variables at different intragroup moments, the Student’s t test or Wilcoxon test was used for choosing data distribution. Wilcoxon’s test was used to compare the percentages of the findings in relation to the total number of beats of the variables: salvos of NSVT and total SVT episodes, in relation to Holter at different intragroup moments, to verify whether there was a significant difference between the Holter results.
A 95% level of confidence was established for all analyses, i.e., p < 0.05 was considered significant.
ResultsPatients included in the study had a mean age of
50.7 ± 9.6 years; 70% (42) were males and 30% (18) females. There were ten deaths in the SG and nine in the CG during the 12-month follow-up.
Stem cell viability was 98% in both groups. The amount of cells in the CG was on average 2.75 x 108 and in the SG, 2.62 x 108. There was no significant difference between the groups.
Holter data are shown in Table 1, with no difference between groups regarding the variables that demonstrated the presence of arrhythmia on Holter examinations at any time (randomization, 2 months, 6 months and 12 months of follow-up).
When comparing Holter 1 (randomization) to the others, in the SG, there was a significant difference between total ventricular premature beats in all comparisons, differences in total number of beats and NSVT between Holter monitoring tests 1 and 3 (Table 2). The same analysis was performed in the CG (Table 3), which showed no statistical significance.
A statistical evaluation of the SG was carried out with the variables NSVT and SVT, percentage-wise, in relation to the total number of beats at Holter monitoring, which showed no significance in the intragroup analysis (Table 4). This evaluation was performed due to the observation that the total number of beats, as well as the NSVT, increased at Holter monitoring in the follow-up.
There was no statistical difference in terms of medications for the treatment of HF used by the patients in both groups, at the time of randomization (Table 5).
DiscussionThe present study found no increase in numbers of
isolated ventricular premature beats compared with the CG, in agreement with studies by Vilas Boas et al4,8. The studies by Vilas Boas et al4,8 had a patient profile similar to ours. We studied 28 chagasic patients in functional class III and IV
490

Original Article
Souza et al.Arrhythmias after stem cell injection
Arq Bras Cardiol. 2014; 102(5):489-494
Table 2 – Comparison between Holter tests performed in the Study Group during the 12-month follow-up, n = 60, Goiânia, Goiás, 2010
Variable Total number of beats* Total number of ventricular premature beats** Salvos of NSVT** Total episodes of SVT**
Holter 1 vs. Holter 2 0.524 0.014*** 0.070 1.000
Holter 1 vs. Holter 3 0.024*** 0.004*** 0.036*** 0.317
Holter 1 vs. Holter 4 0.083 0.014*** 0.375 0.102
* Student test was used; ** in total heartbeats and Wilcoxon test; p < 0.05. ***: in total ventricular extrasystoles NSVT and SVT episodes and was found significance p < 0,05 for both items. Holter 1: performed at randomization; Holter 2: performed at 2 months of follow-up; Holter 3: performed at 6 months of follow-up; Holter 4: performed at 12 months of follow-up. NSVT: nonsustained ventricular tachycardia; SVT: sustained ventricular tachycardia.
Table 3 – Comparison between Holter tests performed in the Control Group during the 12-month follow-up, n = 60, Goiânia, Goiás, 2010
Variable Total number of beats* Total number of ventricular premature beats** Salvos of NSVT** Total episodes of SVT**
Holter 1 vs. Holter 2 0.026*** 0.239 0.984 1.000
Holter 1 vs. Holter 3 0.014*** 0.161 0.975 0.317
Holter 1 vs. Holter 4 0.015*** 0.128 0.061 1.000
* Student test was used; ** in total heartbeats and Wilcoxon test; p < 0.05. ***: in total ventricular extrasystoles NSVT and SVT episodes and was found significance p < 0,05 for both items. Holter 1: performed at randomization; Holter 2: performed at 2 months of follow-up; Holter 3: performed at 6 months of follow-up; Holter 4: performed at 12 months of follow-up. NSVT: nonsustained ventricular tachycardia; SVT: sustained ventricular tachycardia.
Table 1 – Variables obtained by Holter performed at randomization (Holter 1), 2 months (Holter 2), 6 months (Holter 3) and 12 months (Holter 4) of study follow-up, n = 60, Goiânia, Goiás, 2010
Variable Study Group Control Group p value
Holter 1 (n = 34) (n = 26)
Total number of beats 81,209.33 ± 17,417.57 86,343.54 ± 17,474.21 0.189
Total ventricular premature beats 2,685.18 ± 3,052.48 2,640.06 ± 3,412.12 0.435
Total supraventricular premature beats 926.77 ± 3,659.93 2.330.33 ± 9,875.09 0.514
NSVT 5.15 ± 12.02 3.79 ± 5.68 0.744
Total SVT episodes 0.00 ± 0.0 0.0 ± 0.0 -
Holter 2 (n = 32) (n = 26)
Total number of beats 89,474.62 ± 10,906.01 88,457.09 ± 20,175.04 0.994
Total ventricular premature beats 3,764.00 ± 5,313.65 3,611.22 ± 4,549.22 0.478
Total supraventricular premature beats 1.363.07 ± 4,609.85 457.41 ± 1,703.04 0.994
NSVT 29.92 ± 135.33 14.77 ± 33.31 0.456
Total SVT episodes 0.0 ± 0.0 0.0 ± 0.0 -
Holter 3 (n = 28) (n = 21)
Total number of beats 92,394.25 ± 11,519.21 94,715.06 ± 19,856.30 0.836
Total ventricular premature beats 4,817.48 ± 6,152.71 5,072.41 ± 7,508.33 0.379
Total supraventricular premature beats 1,893.07 ± 5,341.60 2,580.45 ± 9,623.00 0.809
NSVT 30.11 ± 135.37 24.12 ± 56.53 0.956
Total SVT episodes 2.11 ± 10.96 0.0 ± 0.0 0.277
Holter 4 (n = 26) (n = 16)
Total number of beats 96,965.00 ± 10,386.72 91,487.25 ± 16,403.77 0.255
Total ventricular premature beats 9,713.17 ± 1,8607.40 4,234.29 ± 4,010.05 0.459
Total supraventricular premature beats 1,480.58 ± 2,957.37 2,477.79 ± 8,422.73 0.862
NSVT 19.17 ± 36.47 2.25 ± 4.59 0.117
Total SVT episodes 0.12 ± 0.61 0.0 ± 0.0 0.400
Mann-Whitney test; p < 0.05. NSVT: nonsustained ventricular tachycardia; SVT: sustained ventricular tachycardia.
491

Original Article
Souza et al.Arrhythmias after stem cell injection
Arq Bras Cardiol. 2014; 102(5):489-494
Table 4 – Comparison test of the variables: nonsustained ventricular tachycardia (NSVT) and sustained ventricular tachycardia (SVT) as percentages in Holter examinations at 2 months, 6 months and 12 months of follow-up, n = 60, Goiânia, Goiás, 2010
ComparisonControl group Study group
Salvos of NSVT (p) Total episodes of SVT (p) Salvos of NSVT (p) Total episodes of SVT (p)
Holter 1 vs. Holter 2 0.904 1.000 0.286 1.000
Holter 1 vs. Holter 3 0.796 0.317 0.198 1.000
Holter 1 vs. Holter 4 0.753 1.000 0.381 0.317
Wilcoxon Test; p < 0.05. Holter 1: performed at randomization; Holter 2: performed at 2 months of follow-up; Holter 3: performed at 6 months of follow-up; Holter 4: performed at 12 months of follow-up. NSVT: nonsustained ventricular tachycardia; SVT: sustained ventricular tachycardia.
Table 5 – Analysis of medications taken by patients at the time of randomization, n = 60, Goiânia, Goiás, 2010
Variable Study Group (n = 34) n (%) Control Group (n = 26) n (%) p value
ARB 7 (25.9) 10 (30.3) 0.212
Digitalis 14 (51.9) 14 (42.4) 0.158
ACEI 8 (29.6) 10 (30.3) 0.222
Spironolactone 19 (70.4) 21 (63.6) 0.188
Diuretics 19 (70.4) 25 (75.8) 0.206
Amiodarone 10 (37.0) 11 (33.3) 0.204
Beta-blockers 2 (7.4) 12 (36.4) 0.171
Source: patients’ files. Fisher’s test. ARB: angiotensin-II receptor blocker; ACEI: angiotensin-converting enzyme inhibitor.
of the New York Heart Association (NYHA). Vilas Boas et al4,8, similarly to this study, evaluated patients with advanced-stage cardiomyopathy and demonstrated the safety regarding the genesis of arrhythmias in this group of patients.
In the SG, which received the stem cell therapy, it is possible to observe an increase in the density of ventricular premature beats, when comparing the baseline Holter monitoring with those subsequently performed after 2, 6 and 12 months of follow-up, with a statistically significant difference. Thus, it is possible to consider that there was an increase in the incidence of ventricular premature beats when compared with the group baseline assessment. In disagreement with the HEBE study9 carried out in Holland, which evaluated 200 ischemic patients who received cell therapy and stem cell infusion within 12 hours of the ischemic event, with excellent safety profile, the present study showed no severe arrhythmia events.
When we analyzing the presence of NSVT, compared with baseline of the SG itself, a difference was observed between Holter 1 and Holter 3, with statistical significance. This fact is in disagreement with the randomized multicenter STAR-HEART study10, which analyzed 191 patients with ischemic cardiomyopathy, of which follow-up showed improvement of arrhythmia in those treated with stem cells.
At the analysis of NSVT and SVT data, percentage-wise when compared to the total number of beats, it became clear that this increase was proportional and without statistical significance, exactly as in the multicenter studies BOOST11
and TOPCARE-AMI12, which evaluated patients with ischemic cardiomyopathy and found no increase in the number of ventricular arrhythmia events.
Stem cell therapy has been used in several different diseases, showing a good safety profile13.
ConclusionChronic heart failure is a progressive disease, in spite
of intensive pharmacological treatment, and remains a severe health problem worldwide. Therefore, in addition to conventional therapy, treatment regimens are needed that can improve quality of life and increase ventricular performance and survival.
Treatment with bone marrow cells does not cure Chagas disease, but attempts to repair the damage that results from years or even decades of aggression to the myocardium.
Our data suggest that patients with heart failure due to Chagas disease and class III and IV heart failure submitted to transplantation of stem cells from bone marrow to the myocardium, showed no increase in the incidence of sustained ventricular tachycardia, but showed increase in nonsustained ventricular tachycardia between Holter at randomization and Holter at 6 months in the Study Group, as well as increased VPB density in the Study group. At the percentage analysis, there was no significant increase of nonsustained ventricular tachycardia, or sustained ventricular tachycardia.
492

Original Article
Souza et al.Arrhythmias after stem cell injection
Arq Bras Cardiol. 2014; 102(5):489-494
1. Kannel WB. Incidence and epidemiology of heart failure. Heart Fail Rev. 2000;5(2):167-73.
2. Engels D, Savioli L. Reconsidering the underestimated burden caused by neglected tropical diseases. Trends Parasitol. 2006;22(8):363-6.
3. Almeida DR. Avanços no tratamento clínico da insuficiencia cardíaca. In: Barreto AC, Bocchi EA. Insuficiencia cardíaca, Local: Segmento, 2003. p. 251-67.
4. Vilas-Boas F, Feitosa GS, Soares MB, Pinho-Filho JA, Mota AC, Almeida AJ, et al. Bone marrow cell transplantation in chagas’ disease heart failure: report of the first human experience. Arq Bras Cardiol. 2011; 96(4):325-31.
5. Bocchi EA, Bacal F, Guimarães G, Mendroni A, Mocelin A, Filho AE, et al. Granulocyte-colony stimulating factor or granulocyte-colony stimulating factor associated to stem cell intracoronary infusion effects in non ischemic refractory heart failure. Int J Cardiol. 2010;138(1):94-7.
6. Menasché P. Stem cell therapy for heart failure: are arrhythmias a real safety concern? Circulation. 2009;119(20):2735-2740.
7. Fukushima S, Varela-Carver A, Coppen SR, Yamahara K, Felkin LE, Lee J, et al. Direct intramyocardial but not intracoronary injection of bone marrow cells induces ventricular arrhythmias in a rat chronic ischemic heart failure model. Circulation. 2007;115(17):2254-61.
8. Vilas-Boas F, Feitosa GS, Soares MB, Mota A, Pinho-Filho JA, Almeida AJ, et al. Early results of bone marrow cell transplantation to the myocardium
of patients with heart failure due to Chagas disease. Arq Bras Cardiol. 2006;87(2):159-66.
9. Hirsch A, Nijveldt R, van der Vleuten PA, Tijssen JG, van der Giessen WJ, Tio RA, et al; HEBE Investigators. Intracoronary infusion of mononuclear cells from bone marrow or peripheral blood compared with standard therapy in patients after acute myocardial infarction treated by primary percutaneous coronary intervention: results of the randomized controlled HEBE Trial. Eur Heart J. 2011;32(14):1736-47.
10. Strauer BE, Yousef M, Schannwell CM. The acute and long-term effects of intracoronary Stem cell Transplantation in 191 patients with chronic heARt failure: the STAR-HEART study. Eur J Heart Fail. 2010;12(7):721-9.
11. Meyer GP, Wollert KC, Lotz J, Pirr J, Rager U, Lippolt P, et al. Intracoronary bone marrow cell transfer after myocardial infarction: 5-year follow-up from the randomized-controlled BOOST Trial. Eur Heart J. 2009;30(24):2978-984.
12. Britten MB, Abolmaali ND, Assmus B, Lehmann R, Honold J, Schmitt J, et al. Infarct remodeling after intracoronary progenitor cell treatment in patients with acute myocardial infarction (TOPCARE-AMI): mechanistic insights from serial contrast-enhanced magnetic resonance imaging. Circulation. 2003;108(18):2212-8.
13. Martin-Rendon E, Brunskill SJ, Hyde CJ, Stanworth SJ, Mathur A, Watt SM. Autologous bone marrow stem cells to treat acute myocardial infarction: a systematic review. Eur Heart J. 2008;29(15):1807-18.
References
Author contributionsAcquisition of data:Costa SA, Freitas EMM, Carvalho G;
Analysis and interpretation of the data: Souza ASB, Sá LAB; Statistical analysis: Souza ASB; Writing of the manuscript: Souza ASB; Critical revision of the manuscript for intellectual content: Souza WKSB, Souza ASB, Rassi S.
Potential Conflict of InterestNo potential conflict of interest relevant to this article
was reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part of the thesis of master submitted by Adriana
Sebba Barroso de Souza from Universidade Federal de Goiás.
493

Original Article
Souza et al.Arrhythmias after stem cell injection
Arq Bras Cardiol. 2014; 102(5):489-494 494

Original Article
Temporal Variation in the Prognosis and Treatment of Advanced Heart Failure – Before and After 2000Carlos Henrique Del Carlo1, Juliano Novaes Cardoso1,2, Marcelo Eidi Ochia1,2, Mucio Tavares de Oliveira Jr.1, José Antonio Franchini Ramires1, Antonio Carlos Pereira-Barretto1
Instituto do Coração - Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo (USP)1, São Paulo, SP; Hospital Auxiliar de Cotoxó/Instituto do Coração - Hospital das Clínicas - Faculdade de Medicina - Universidade de São Paulo (USP)2, São Paulo, SP − Brazil
Mailing Address: Carlos Henrique Del Carlo •Instituto do Coração, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, Avenida Dr. Enéas de Carvalho Aguiar, 44, Cerqueira César. Postal Code 05403-900, São Paulo, SP, Brazil.E-mail: [email protected]; [email protected] received September 22, 2013, revised manuscript November 24, 2013, accepted December 17, 2013.
DOI: 10.5935/abc.20140050
Abstract
Background: The treatment of heart failure has evolved in recent decades suggesting that survival is increasing.
Objective: To verify whether there has been improvement in the survival of patients with advanced heart failure.
Methods: We retrospectively compared the treatment and follow-up data from two cohorts of patients with systolic heart failure admitted for compensation up to 2000 (n = 353) and after 2000 (n = 279). We analyzed in-hospital death, re-hospitalization and death in 1 year of follow-up. We used Mann-Whitney U test and chi-square test for comparison between groups. The predictors of mortality were identified by regression analysis through Cox proportional hazards model and survival analysis by the Kaplan-Meier survival analysis.
Results: The patients admitted until 2000 were younger, had lower left ventricular impairment and received a lower proportion of beta-blockers at discharge. The survival of patients hospitalized before 2000 was lower than those hospitalized after 2000 (40.1% vs. 67.4%; p < 0.001). The independent predictors of mortality in the regression analysis were: Chagas disease (hazard ratio: 1.9; 95% confidence interval: 1.3-3.0), angiotensin-converting-enzyme inhibitors (hazard ratio: 0.6; 95% confidence interval: 0.4-0.9), beta-blockers (hazard ratio: 0.3; 95% confidence interval: 0.2-0.5), creatinine ≥ 1.4 mg/dL (hazard ratio: 2.0; 95% confidence interval: 1.3-3.0), serum sodium ≤ 135 mEq/L (hazard ratio: 1.8; 95% confidence interval: 1.2-2.7).
Conclusions: Patients with advanced heart failure showed a significant improvement in survival and reduction in re-hospitalizations. The neurohormonal blockade, with angiotensin-converting-enzyme inhibitors and beta-blockers, had an important role in increasing survival of these patients with advanced heart failure. (Arq Bras Cardiol. 2014; 102(5):495-504)
Keywords: Heart Failure / therapy; Prognosis; Heart Failure / mortality; Chagas Disease.
IntroductionHeart failure (HF) is a clinical syndrome of which
evolution is known to have high morbidity and mortality1,2. In epidemiological studies, HF patients showed a significant reduction in quality of life and a worse evolution than many types of cancer3.
Treatment with neurohormonal blockers has modified this history, reducing the high mortality, the rate of re-hospitalizations and improving quality of life in patients with this syndrome4. This improvement has been demonstrated
in clinical trials and controlled studies, but we do not know whether this improvement has also been observed in the real world, among patients in the institutions, clinics and offices, and particularly, we have no data on the Brazilian population4.
Working in a tertiary hospital in São Paulo, we followed the evolution of HF patients in the last two decades and observed that the population we treated during these years has not changed substantially regarding characteristics, as the admission criteria have not changed. This fact allowed us to compares the outcome of patients, considering two periods: before and after the year 2000.
This study sought to assess whether the outcomes of patients with HF changed when comparing the two periods and verify, among the studied variables, which were associated with prognosis of this syndrome.
MethodsA total of 632 hospitalized patients were prospectively
studied in a tertiary hospital in São Paulo, all with advanced HF, systolic dysfunction with ejection fraction < 40%, in
495

Original Article
Del Carlo et al.Improvement in Heart Failure Prognosis
Arq Bras Cardiol. 2014; 102(5):495-504
NYHA (New York Heart Association) III / IV. Patients in this hospital came from the emergency room and were transferred there when they did not compensate after the first measures or because they required inotropic support for compensation. These selection criteria for hospitalization led to the admission of more severe patients with severe clinical manifestation.
All patients underwent clinical and laboratory assessment, including biochemical analysis, CBC, echocardiography and radiological examinations. Regarding the etiology of heart disease, patients were divided into three groups: those with chagasic etiology, those with ischemic etiology and those with nonischemic etiology. The diagnosis of Chagasic heart disease was established by the presence of positive serological reactions, and ischemic heart disease was confirmed by the presence of a history of heart attack, angina or confirmed by coronary angiography. In the absence of these characteristics, the patient was considered to have non-ischemic heart disease.
These patients are part of a prospective study database of patients hospitalized in our service, due to advanced, decompensated HF and all met the same abovementioned inclusion criteria2,5-8. Patients were included in different years, which allowed us to perform a temporal analysis regarding the evolution of prognosis and treatment of this syndrome. For the purpose of this analysis, performed retrospectively, the patients were divided into two groups: those admitted until December 31, 2000 and those admitted after that date. Patients included in the study admitted before 2000 were part of prospective studies in the years 1992, 1994, 1996 and 19995-8. Patients enrolled after 2000 were studied in 2005 and 20062. We compared the characteristics of the two groups, considering clinical, laboratory, and evolution aspects.
Patients were followed for 1 year, and the vital status of the patients, number of visits to the emergency room and need for rehospitalization were determined by telephone or by reviewing electronic medical records. The clinical outcome analyzed was mortality from all causes during the follow-up period.
Among these patients, a subgroup had the treatment analyzed during and after discharge, and predictors of mortality were assessed in this subgroup, consisting of 333 patients (52.7% of total)2,8. This subgroup was selected based on the availability of data on drug therapy used during hospitalization and pre-hospital discharge.
Continuous variables were shown as means ± standard deviation and categorical variables as frequencies and percentages. We compared the characteristics of patients regarding mortality at the end of follow-up. Continuous variables were analyzed by Mann-Whitney U test and categorical variables by the chi-square test or Fisher exact test.
Predictors of mortality were determined by uni- and multivariate analysis, using the Cox proportional hazards method. A regression model was constructed for the primary endpoint, adjusted for clinical and laboratory characteristics as well as those of administered drugs. The criterion for model
variable selection was a p value < 0.200 in the univariate analysis. The final model was built using a stepwise forward procedure. All predictor variables with p < 0.05 were mantained in the final model. Hazard ratio was shown, with the corresponding confidence interval of 95% (95% CI) and p value.
Based on the follow-up data, survival curves were constructed using the Kaplan-Meier method. All statistical analyses were performed using the statistical software Statistical Package for Social Sciences (SPSS).
P values are two-tailed and the significance level was set at 5%.
ResultsThe mean age of patients was 54.8 ± 15.1 years and
most were males, 435 (68.8%). The mean left ventricular ejection fraction (LVEF) was 28.2 ± 7.2% and mean Systolic Blood Pressure (SBP) was 104.6 ± 22.9 mmHg. The most frequent cause of heart disease was non-ischemic, followed by chagasic and ischemic.
Most patients had non-dialytic kidney failure.A total of 353 patients hospitalized from 1992 to
December 31, 2000, and 279 patients hospitalized between 2005 and 2006 were included in the study.
Table 1, shows the comparison of baseline characteristics between patients admitted until 2000 and after 2000.
Patients hospitalized until the year 2000 were 7.5 years younger than those admitted after 2000 and had a less impaired LVEF and lower levels of plasma sodium. The percentage of patients with Chagas disease was higher in admissions until 2000.
The survival of patients hospitalized until the year 2000 was 40.1% and 67.4%, among those hospitalized after the year 2000, with a 68% increase in the survival rate in the first year of follow-up (Figure 1).
To analyze the possible variables related to survival, we evaluated the data of 333 patients (52.7% of the total). These data are shown in Table 2. This analysis showed that 209 patients (62.8%) needed inotropes in the compensation period. At discharge, most patients were receiving a prescription of renin-angiotensin system blocker (72.4%) and a beta-blocker (59.8%). A total of 186 (55.9%) patients were treated with carvedilol and 13 patients (3.9%) with metoprolol succinate. When comparing the two groups, patients admitted until 2000 received a lower proportion of beta-blocker prescriptions and a higher proportion of digoxin.
In this analysis, patients admitted until the year 2000 had higher in-hospital mortality (20.0% vs 8.7%, p = 0.008) and a higher number of re-hospitalizations than those admitted after 2000 (51.4% vs. 27.9%, p < 0.001). At 1 year of follow up, mortality of those admitted until the year 2000 was 62.9% vs. 23.6% for those hospitalized after 2000 (p < 0.001).
The length of hospital stay did not differ between the two groups, being 28.3 ± 21.1 days in those admitted until 2000 and 25.1 ± 16.7 days (p = 0.251) in those hospitalized after the year 2000.
496

Original Article
Del Carlo et al.Improvement in Heart Failure Prognosis
Arq Bras Cardiol. 2014; 102(5):495-504
Tables 3 and 4 show the comparison of patient characteristics regarding mortality at 1 year of follow up and the univariate and multivariate regression analysis of predictors of death in this period. Chagasic etiology, presence of renal impairment (higher
urea levels and creatinine), lower levels of sodium and nitrate use were predictors of increased mortality. Variables associated with reduced mortality were the prescription of Angiotensin-Converting Enzyme Inhibitor (ACEI) and beta-blockers. In the multivariate
Table 1 – Comparison of characteristics between the groups before and after 2000
Characteristics Population (n = 632)Year of treatment
p valueBefore 2000 (n = 353) After 2000 (n = 279)
Age (years) 54.8 ± 15.1 59.0 ± 14.8 51.5 ± 14.5 < 0.001
Male gender 435 (68.8) 255 (72.2) 180 (64.5) 0.037
Etiology:
Ischemic 132 (20.9) 56 (15.0) 76 (27.2) < 0.001
Non-ischemic (non- chagasic) 312 (49.4) 173 (49.0) 139 (49.8) 0.839
Chagasic 188 (29.7) 124 (35.1) 64 (22.9) 0.001
LVEF (%) 28.2 ± 7.2 30.8 ± 5.9 24.7 ± 7.3 < 0.001
Creatinine (mg/dL) 1.5 ± 0.7 1.5 ± 0.5 1.5 ± 0.5 0.239
Sodium (mEq/L) 135.7 ± 5.0 136.7 ± 4.7 134.9 ± 5.1 < 0.001
SBP (mmHg) 103.6 (25.4) 102.6 ± 21.9 105.0 ± 30.1 0.163
Mortality (1 year) 264 (41.8) 200 (56.7) 63 (22.8) < 0.001
LVEF: left ventricular ejection fraction; SBP: systolic blood pressure.
Figure 1 – Survival of patients hospitalized for decompensated heart failure before and after the year 2000. The probability of survival at 1 year of follow-up was 40.1% in hospitalized patients before 2000 and 67.4% in hospitalized patients after 2000 (p < 0.001).
Prob
abilit
y of s
urviv
al
Days
After the year 2000
Before the year 2000
1.0
0.8
0.6
0.4
0.2
0.0
0 100 200 300 400 500 600
Log-Rank (Chi-square) = 23.82 - p<0.001
497

Original Article
Del Carlo et al.Improvement in Heart Failure Prognosis
Arq Bras Cardiol. 2014; 102(5):495-504
Table 2 – Comparison of patients in relation to the year of treatment
Characteristics Population (n = 333)Year of treatment
p valueBefore 2000 (n = 70) After 2000 (n = 263)
Age (years) 58.7 ± 15.4 54.2 ± 15.8 59.9 ± 15.1 0.011
Male gender 213 (64.0) 48 (68.6) 165 (62.7) 0.366
Etiology:
Ischemic 94 (28.2) 18 (25.7) 76 (28.9) 0.599
Non-ischemic (non-chagasic) 163 (48.9) 33 (47.1) 130 (49.4) 0.734
Chagasic 76 (22.8) 19 (27.1) 57 (21.7) 0.333
LVEF (%) 28.0 ± 11.4 31.3 ± 8.4 27.1 ± 11.9 < 0.001
Hemoglobin (g/L) 13.2 ± 2.0 13.9 ± 2.1 13.0 ± 1.9 0.001
Urea (mg/dL) 74.7 ± 42.5 72.9 ± 35.2 75.1 ± 44.2 0.842
Creatinine (mg/dL) 1.5 ± 0.7 1.4 ± 0.5 1.5 ± 0.8 0.699
Sodium (mEq/L) 136.6 ± 4.9 135.9 ± 5.4 136.7 ± 4.7 0.083
SBP (mmHg) 105.3 ± 23.3 111.7 ± 25.4 103.5 ± 22.4 0.017
DBP (mmHg) 68.7 ± 18.1 76.7 ± 17.9 66.3 ± 17.5 < 0.001
Medications:
Dobutamine 187 (57.9) 36 (51.4) 151 (57.4) 0.216
Milrinone 6 (1.9) 0 (0.0) 6 (2.3) 0.346
Levosimendan 16 (5.0) 0 (0.0) 16 (6.1) 0.028
ACEI 241 (72.4) 60 (85.7) 181 (68.8) 0.005
Beta-blockers 199 (59.8) 8 (11.4) 191 (72.6) < 0.001
Losartan 42 (12.7) 0 (0.0) 42 (16.0) < 0.001
Nitrates 117 (35.2) 39 (55.7) 78 (29.7) < 0.001
Hydralazine 108 (32.5) 16 (22.9) 92 (35.0) 0.052
Digoxin 194 (58.6) 64 (92.8) 130 (49.4) < 0.001
Spironolactone 48 (14.5) 0 (0.0) 48 (18.3) < 0.001
Furosemide 261 (78.6) 70 (100.0) 191 (72.6) < 0.001
Hydrochlorothiazide 59 (17.8) 0 (0.0) 59 (22.4) < 0.001
Clinical results:
Mortality in-Hospital 37 (11.1) 14 (20.0) 23 (8.7) 0.008
Mortality at follow-up (1 year) 106 (31.8) 44 (62.9) 62 (23.6) < 0.001
Rehospitalization 109 (32.8) 36 (51.4) 73 (27.9) < 0.001
Clinical events 168 (49.2) 56 (80.0) 108 (41.1) < 0.001
Data are expressed as mean ± standard deviation or number (percentage). LVEF: left ventricular ejection fraction; SBP: systolic blood pressure; DBP: diastolic blood pressure; ACEI: angiotensin-converting enzyme inhibitor.Clinical events, death or rehospitalization within 1 year.
regression analysis, five variables were identified as independent predictors of mortality, with three being associated with worse prognosis (Chagas disease, creatinine ≥ 1.4 mg/dL, and sodium ≤ 135 mEq/L) and two associated with improved prognosis: the prescription of ACEI and beta-blockers.
Figures 2 and 3 show survival curves stratified for ACEI and beta-blockers. In Figure 4, the survival curve was stratified for the combined use of ACEI and beta-blockers, demonstrating
improvement in survival of patients who received the combined therapy with the two medications.
DiscussionAccording to the results of this observational study, we
observed that in this new century, the survival of patients with advanced HF has improved significantly, as well as the rates of
498

Original Article
Del Carlo et al.Improvement in Heart Failure Prognosis
Arq Bras Cardiol. 2014; 102(5):495-504
Table 3 – Comparison of patients in relation to 1-year mortality
Characteristics1-year mortality
p valueYes (n = 106) No (n = 227)
Age (years) 58.2 ± 17.3 58.9 ± 14.5 0.928
Male gender 63 (59.4) 150 (66.1) 0.239
Etiology:
Ischemic 27 (25.5) 67 (29.5) 0.445
Non-ischemic (non-chagasic) 44 (41.5) 119 (52.4) 0.063
Chagasic 35 (33.0) 41 (18.1) 0.002
LVEF (%) 28.9 ± 9.5 27.6 ± 12.1 0.116
Hemoglobin (g/L) 13.3 ± 2.2 13.1 ± 1.8 0.311
Urea (mg/dL) 80.8 ± 42.8 71.8 ± 42.1 0.016
Creatinine (mg/dL) 1.5 ± 0.5 1.5 ± 0.8 0.043
Sodium (mEq/L) 135.3 ± 4.9 137.1 ± 4.8 0.001
SBP (mmHg) 103.1 ± 20.7 106.4 ± 24.5 0.505
DBP (mmHg) 69.3 ± 15.3 68.4 ± 19.3 0.503
Medications
Inotropic agents 75 (71.4) 127 (57.5) 0.015
ACEI 69 (65.1) 172 (75.8) 0.042
Beta-blocker 36 (34.0) 163 (71.8) < 0.001
Losartan 12 (11.3) 30 (13.2) 0.649
Nitrates 47 (44.3) 70 (30.8) 0.014
Hydralazine 38 (35.8) 70 (30.8) 0.333
Digoxin 76 (71.7) 118 (52.0) < 0.001
Spironolactone 11 (10.4) 37 (16.3) 0.161
Furosemide 90 (84.9) 171 (75.3) 0.032
Hydrochlorothiazide 18 (17.0) 41 (18.1) 0.839
Data are expressed as mean ± standard deviation or number (percentage). LVEF: left ventricular ejection fraction; SBP: systolic blood pressure; DBP: diastolic blood pressure; ACEI: angiotensin-converting enzyme inhibitor.
re-hospitalization. Treatment with neurohormonal blockers, especially ACEI and beta-blockers, was associated with this increase in survival rates.
Heart failure, in its advanced form, is a malignant disease with a higher mortality rate than a few types of cancer3. Even with the current treatment, mortality can be high in the most severe forms, as it has an association with the intensity of the heart disease and its clinical manifestations9. Patients with advanced disease are referred to our institution, a tertiary hospital in São Paulo, which results in higher mortality than that observed in other institutions. Our current mortality rate is approximately 8% and we observed that approximately a quarter of patients who were discharged died in the first year of follow-up2.
Although this mortality rate is still high, when we compared data from patients hospitalized until the year 2000, we found a significant reduction. It should be noted that when comparing the characteristics of the study population in two periods, before and after 2000, we observed that they are quite similar, but the hospitalized population after
2000 shows alterations that indicate more pronounced clinical manifestations, such as higher levels of urea and creatinine at admission and lower LVEF. Despite these signs of greater severity, when comparing the two periods, there was a significant reduction in mortality, which decreased from 20% to the current 8.8%2. This reduction was probably due to more aggressive management of cardiac decompensation and the higher proportion of patients currently being treated with ACEI and beta-blockers10,11.
In our institution, ACEI and beta-blockers are not systematically withdrawn at hospitalization for cardiac decompensation12. In general, ACEI have their dose increased, as vasoconstriction is the major pathophysiological alteration in cardiac decompensation. The beta-blocker is maintained and in cases that need inotropes, the dose of the beta-blocker is halved, which results in the fact many patients continue taking 6.25 mg or 12.5 mg of carvedilol twice daily. In the multivariate analysis, the prescription of ACEI and beta-blockers was associated with reduced mortality.
499

Original Article
Del Carlo et al.Improvement in Heart Failure Prognosis
Arq Bras Cardiol. 2014; 102(5):495-504
Table 4 – Univariate and multivariate analysis regression (Cox) of predictors of death
Predictor (univariate analysis) Hazard ratio 95% Confidence Interval (95%CI) p value
Age > 60 years 1.0 0.7 – 1.5 0.998
Male gender 0.8 0.5 – 1.2 0.247
Etiology:
Ischemic 0.8 0.5 – 1.3 0.389
Non-ischemic (non-chagasic) 0.7 0.5 – 1.1 0.124
Chagasic 1.8 1.2 – 2.7 0.008
LVEF < 0.25 0.8 0.6 – 1.3 0.382
Anemia 1.0 0.7 – 1.6 0.939
Urea ≥ 60 mg/dL 1.7 1.1 – 2.5 0.013
Creatinine ≥ 1.4 mg/dL 1.6 1.1 – 2.4 0.013
Sodium ≤ 135 mEq/L 1.8 1.2 – 2.6 0.004
SBP < 90 mmHg 0.9 0.5 – 1.5 0.640
Medications
Inotropic agents 1.7 1.1 – 2.7 0.008
ACEI 0.6 0.4 – 0.9 0.020
Beta-blocker 0.3 0.2 – 0.5 < 0.001
Losartan 1.1 0.6 – 2.0 0.788
Nitrates 1.6 1.1 – 2.4 0.017
Hydralazine 1.4 0.9 – 2.1 0.097
Digoxin 1.4 0.9 – 2.2 0.106
Spironolactone 0.7 0.4 – 1.3 0.274
Hydrochlorothiazide 1.2 0.7 – 2.0 0.483
Furosemide 1.4 0.8 – 2.4 0.205
Predictor (multivariate analysis) Hazard ratio 95% confidence Interval p value
Creatinine ≥ 1,4 mg/dL 2.0 1.3 – 3.0 0.002
Chagasic etiology 1.9 1.3 – 3.0 0.002
ACEI 0.6 0.4 – 0.9 0.040
Beta-blocker 0.3 0.2 – 0.5 < 0.001
Sodium ≤ 135 mEq/L 1.8 1.2 – 2.7 0.003
LVEF: left ventricular ejection fraction; SBP: systolic blood pressure; ACEI: angiotensin-converting enzyme inhibitor.
Therefore, the most intense neurohormonal blockade played an important role in this increase in in-hospital survival. Thus, although the mortality rate is still high, it is decreasing, when one considers the data from the two periods at our institution. It is noteworthy the fact that data from the National Health System (SUS) do not show the occurrence of the reduction we observed, but showing in fact, an increase in mortality (5.41 % to 6.97 %) from 1992 to 2002, when analyzing all hospitalizations for HF in Brazil2.
When comparing our rates with data from Europe and the United States in different registries of HF, mortality in our hospitals is higher in general. But much of this high mortality is probably due to the greater severity of patients admitted to our service. When comparing the characteristics
of hospitalized patients, this greater severity can be observed among Brazilian patients.
For instance, when we compare our data with those of the U.S. ADHERE registry, it can be seen that 74.9% of hospitalized patients in our hospital had systolic BP < 115 mm Hg, whereas in the ADHERE registry only 18.5% were hypotensive9. Low BP is an important prognostic marker in several studies, including the ADHERE registry. An important point to note is that, despite the higher overall mortality rate of our patients, when we analyzed the total number of more severe patients (BUN > 43 mg/dL, BP < 115 mmHg and creatinine > 2.75 mg/dL), mortality did not differ significantly, with our patient population being numerically lower than that of the American study
500
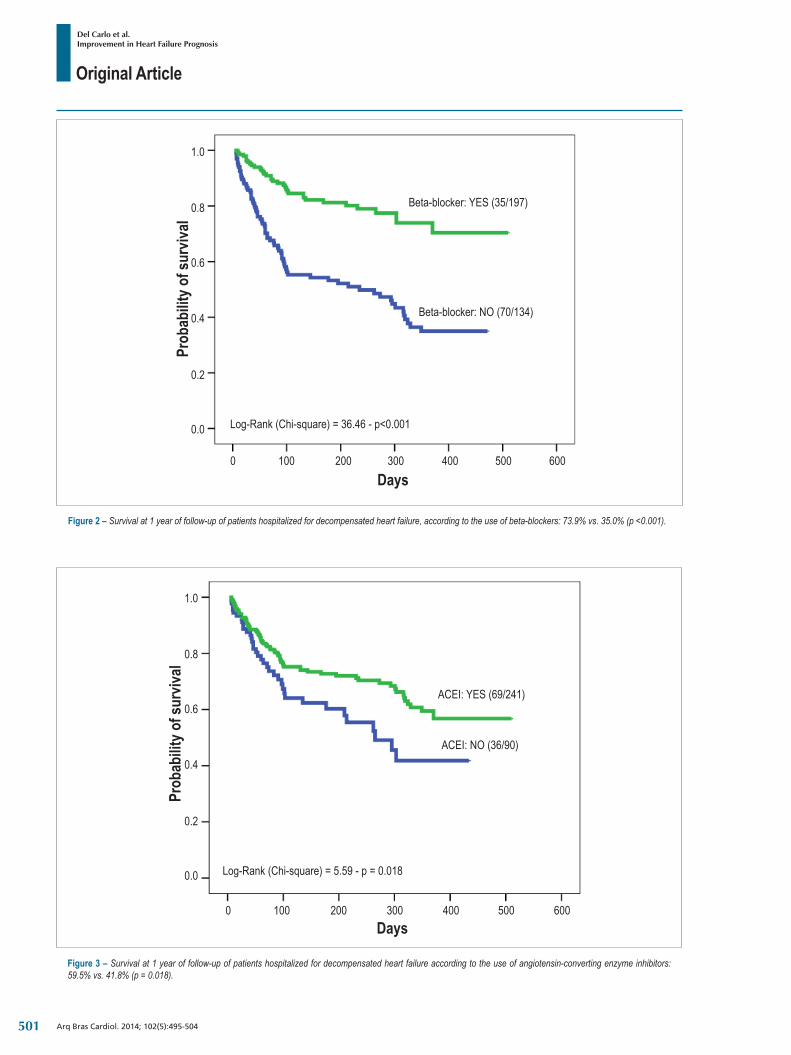
Original Article
Del Carlo et al.Improvement in Heart Failure Prognosis
Arq Bras Cardiol. 2014; 102(5):495-504
Figure 2 – Survival at 1 year of follow-up of patients hospitalized for decompensated heart failure, according to the use of beta-blockers: 73.9% vs. 35.0% (p <0.001).
Prob
abilit
y of s
urviv
al
Days
Beta-blocker: YES (35/197)
Beta-blocker: NO (70/134)
1.0
0.8
0.6
0.4
0.2
0.0
0 100 200 300 400 500 600
Log-Rank (Chi-square) = 36.46 - p<0.001
Figure 3 – Survival at 1 year of follow-up of patients hospitalized for decompensated heart failure according to the use of angiotensin-converting enzyme inhibitors: 59.5% vs. 41.8% (p = 0.018).
ACEI: YES (69/241)
ACEI: NO (36/90)
Days
Prob
abilit
y of s
urviv
al
1.0
0.8
0.6
0.4
0.2
0.0
0 100 200 300 400 500 600
Log-Rank (Chi-square) = 5.59 - p = 0.018
501
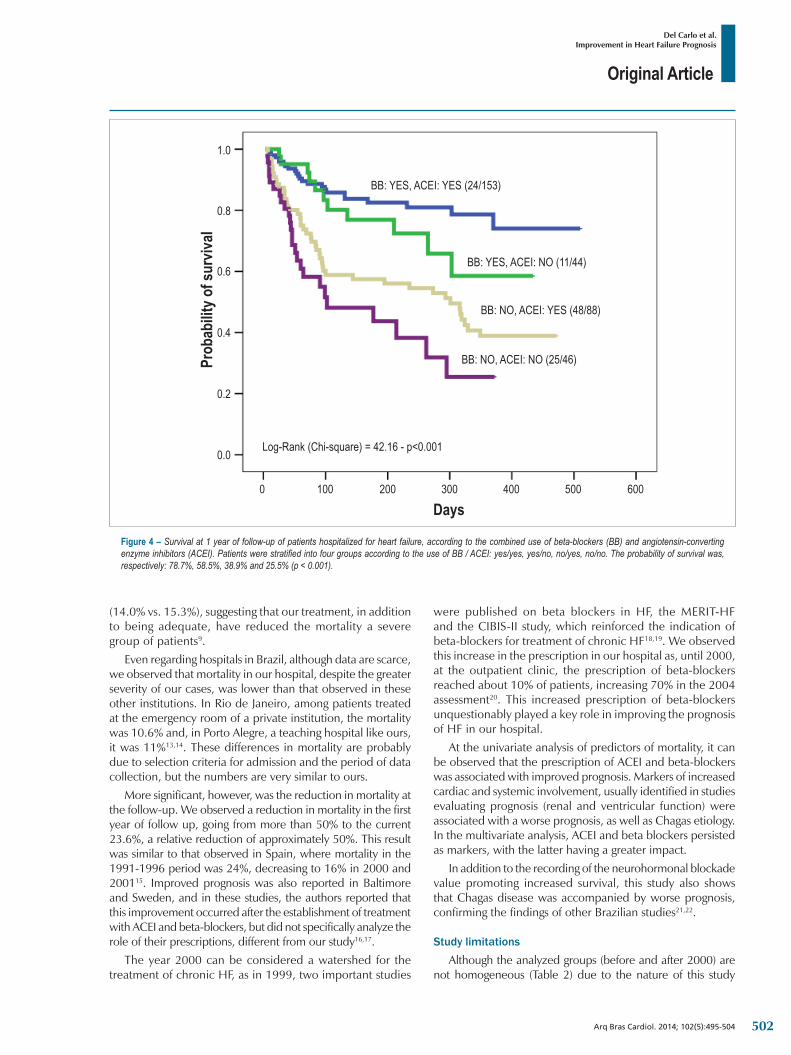
Original Article
Del Carlo et al.Improvement in Heart Failure Prognosis
Arq Bras Cardiol. 2014; 102(5):495-504
(14.0% vs. 15.3%), suggesting that our treatment, in addition to being adequate, have reduced the mortality a severe group of patients9.
Even regarding hospitals in Brazil, although data are scarce, we observed that mortality in our hospital, despite the greater severity of our cases, was lower than that observed in these other institutions. In Rio de Janeiro, among patients treated at the emergency room of a private institution, the mortality was 10.6% and, in Porto Alegre, a teaching hospital like ours, it was 11%13,14. These differences in mortality are probably due to selection criteria for admission and the period of data collection, but the numbers are very similar to ours.
More significant, however, was the reduction in mortality at the follow-up. We observed a reduction in mortality in the first year of follow up, going from more than 50% to the current 23.6%, a relative reduction of approximately 50%. This result was similar to that observed in Spain, where mortality in the 1991-1996 period was 24%, decreasing to 16% in 2000 and 200115. Improved prognosis was also reported in Baltimore and Sweden, and in these studies, the authors reported that this improvement occurred after the establishment of treatment with ACEI and beta-blockers, but did not specifically analyze the role of their prescriptions, different from our study16,17.
The year 2000 can be considered a watershed for the treatment of chronic HF, as in 1999, two important studies
were published on beta blockers in HF, the MERIT-HF and the CIBIS-II study, which reinforced the indication of beta-blockers for treatment of chronic HF18,19. We observed this increase in the prescription in our hospital as, until 2000, at the outpatient clinic, the prescription of beta-blockers reached about 10% of patients, increasing 70% in the 2004 assessment20. This increased prescription of beta-blockers unquestionably played a key role in improving the prognosis of HF in our hospital.
At the univariate analysis of predictors of mortality, it can be observed that the prescription of ACEI and beta-blockers was associated with improved prognosis. Markers of increased cardiac and systemic involvement, usually identified in studies evaluating prognosis (renal and ventricular function) were associated with a worse prognosis, as well as Chagas etiology. In the multivariate analysis, ACEI and beta blockers persisted as markers, with the latter having a greater impact.
In addition to the recording of the neurohormonal blockade value promoting increased survival, this study also shows that Chagas disease was accompanied by worse prognosis, confirming the findings of other Brazilian studies21,22.
Study limitationsAlthough the analyzed groups (before and after 2000) are
not homogeneous (Table 2) due to the nature of this study
Figure 4 – Survival at 1 year of follow-up of patients hospitalized for heart failure, according to the combined use of beta-blockers (BB) and angiotensin-converting enzyme inhibitors (ACEI). Patients were stratified into four groups according to the use of BB / ACEI: yes/yes, yes/no, no/yes, no/no. The probability of survival was, respectively: 78.7%, 58.5%, 38.9% and 25.5% (p < 0.001).
Prob
abilit
y of s
urviv
al
Days
BB: NO, ACEI: NO (25/46)
BB: NO, ACEI: YES (48/88)
BB: YES, ACEI: NO (11/44)
BB: YES, ACEI: YES (24/153)
1.0
0.8
0.6
0.4
0.2
0.0
0 100 200 300 400 500 600
Log-Rank (Chi-square) = 42.16 - p<0.001
502

Original Article
Del Carlo et al.Improvement in Heart Failure Prognosis
Arq Bras Cardiol. 2014; 102(5):495-504
1. Cleland JG, Khand A, Clark A. The heart failure epidemic: exactly how big is it? Eur Heart J. 2001;22(8):623-6.
2. Pereira-Barretto AC, Del Carlo CH, Cardoso JN, Morgado PC, Munhoz RT, Eid MO, et al. Re-hospitalizações e morte por insuficiencia cardíaca: índices ainda alarmantes. Arq Bras Cardiol. 2008;91(5):335-41.
3. McMurray JJ, Stewart S. The burden of heart failure. Eur Heart J. 2002; 4 (Suppl D):50-8.
4. Fonarow GC, Heywood T, Heidenreich PA, Lopatin M, Yancy CW. Temporal trends in clinical characteristics, treatments, and outcomes for heart failure hospitalizations, 2002 to 2004: findings from acute decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2007;153(6):1021-8.
5. Veloso LG, de Oliveira MT Jr, Munhoz RT, Morgado PC, Ramires JA, Barretto AC. Repercussão nutricional na insuficiencia cardíaca avançada e seu valor na avaliação prognostica. Arq Bras Cardiol. 2005;84(6):480-5.
6. de Oliveira MT Jr, Canesin MF, Munhoz RT, Del Carlo CH, Scipioni AR, Ramires JA, et al. Principais características clínicas de pacientes que sobrevivem 24 meses ou mais apos uma hospitalização devido a descompensação cardíaca. Arq Bras Cardiol. 2005;84(2):161-6.
7. Canesin MF, Giorgi D, Oliveira MT Jr, Wajngarten M, Mansur A, Ramires JA, et al. Ambulatory blood pressure monitoring of patients with heart failure: a new prognosis marker. Arq Bras Cardiol. 2002;78(1):83-9.
8. Del Carlo CH, Pereira-Barretto AC, Cassaro-Strunz C, Latorre Mdo R, Ramires JA. Serial measure of cardiac troponin T levels for prediction of clinical events in decompensated heart failure. J Card Fail. 2004;10(1):43-8.
9. Fonarow GC, Adams KJ Jr, Abraham WT, Yancy CW, Boscardin WJ; ADHERE Scientific advisory committee, study group and investigators. Risk stratification for in-hospital mortality in acutely decompensated heart failure: classification and regression tree analysis. JAMA. 2005;293(5):572-80.
10. Bocchi EA, Marcondes-Braga FG, Ayub-Ferreira SM, Rohde LE, Oliveira WA, Almeida DR, et al.; Sociedade Brasileira de Cardiologia. III Diretriz brasileira de insuficiencia cardíaca crônica. Arq Bras Cardiol. 2009;93(1 supl.1):1-71.
11. Bocchi EA, Marcondes-Braga FG, Bacal F, Ferraz AS, Albuquerque D, Rodrigues D, et al. Sociedade Brasileira de Cardiologia. Atualização da Diretriz Brasileira de Insuficiencia Cardíaca Crônica - 2012. Arq Bras Cardiol. 2012;98(1 supl. 1):1-33.
12. Lima MV, Cardoso JN, Ochiai ME, Grativol KM, Grativol OS, Brancalhão EC, et al. É necessário suspender o betabloqueador na insuficiencia cardíaca descompensada com baixo débito? Arq Bras Cardiol. 2010;95(4):530-5.
13. VillaCorta H, Mesquita ET, Cardoso R, Bonates T, Maia ER, Silva AC, et al. Preditores de sobrevida obtidos na unidade de emergencia em pacientes atendidos por insuficiencia cardíaca descompensada. Rev Port Cardiol. 2003;22(4):495-507.
14. Rohde LE, Clausell N, Ribeiro JP, Goldraich L, Netto R, William Dec GW, et al. Heath outcomes in decompensated congestive heart failure: a comparison of tertiary hospitals in Brazil and United States. Int J Cardiol. 2005;102(1):71-7.
15. Grigorian Shamagian L, Gonzalez-Juanatey JR, Roman AV, Acuna JM, Lamela AV. The death rate among hospitalized heart failure patients with normal and depressed left ventricular ejection fraction in the year following discharge: evolution over a 10-year period. Eur Heart J. 2005;26(21):2251-8.
16. Feinglass J, Martin GJ, Lin E, Johnson MR, Gheorghiade M. Is heart failure survival improving? Evidence from 2323 elederly patients hospitalized between 1989-2000. Am Heart J. 2003;146(1):111-4.
17. Schaufelberger M, Swedberg K, Koster M, Rosen M, Rosengren A. Decreasing one-year mortality and hospitalization rates for heart failure in Sweden. Data from Swedish Hospital discharge Registry 1988 to 2000. Eur Heart J. 2004;25(4):300-7.
References
(observational and retrospective), it is noteworthy the fact that, although patients in the group after 2000 were more severe (older mean age, lower LVEF and lower mean SBP), this group - the most severe - was precisely the one that had the best clinical outcomes at follow-up with lower mortality and lower rates of re-hospitalization. One must consider that these results are observational and that other factors such as improved treatment adherence and cointerventions (e.g., cardiac surgery and interventional procedures), after discharge, were not quantified and may have influenced the improvement in prognosis, in addition to the higher rate of prescription of neurohormonal blockers, particularly beta-blockers. It should be noted that a possible selection bias was the fact that we performed analyses of survival in little more than 50% of the study patients, of which data regarding therapy used was available. Moreover, regarding therapy, we performed the qualitative analysis, while the quantitative analysis of the dose at discharge and at follow-up would be important to evaluate the influence of optimized dose of these medications on patients' prognosis. However, these issues could be addressed in future studies.
ConclusionThis study provided some evidence that, in the real world,
the survival of patients with heart failure has increased and
that treatment optimization with neurohormonal blockers have had an important role in improving prognosis.
Author contributionsConception and design of the research, Analysis and
interpretation of the data and Critical revision of the manuscript for intellectual content: Del Carlo CH, Cardoso JN, Ochia ME, Oliveira Jr. MT, Ramires JAF, Pereira-Barretto AC; Acquisition of data: Del Carlo CH, Cardoso JN, Ochia ME, Oliveira Jr. MT; Statistical analysis: Del Carlo CH; Writing of the manuscript: Del Carlo CH, Ramires JAF, Pereira-Barretto AC.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any post-graduation program.
503

Original Article
Del Carlo et al.Improvement in Heart Failure Prognosis
Arq Bras Cardiol. 2014; 102(5):495-504
18. The cardiac insufficiency bisoprolol study II (CIBIS-II): a randomized trial. Lancet. 1999;353(9146):9-13.
19. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet. 1999;353(9169):2001-7.
20. Pereira-Barretto AC. Tratamento da insuficiencia cardíaca crônica. In: Nobre F, Serrano Jr CV. Tratado de cardiologia SOCESP. Barueri (São Paulo): Editora Manole; 2009. p 1065-74.
21. Freitas HG, Chizzola PR, Paes AT, Lima AC, Mansur AJ. Risk stratification in a Brazilian hospital-based cohort of 1220 outpatients with heart failure: role of Chagas’ disease. Int J Cardiol. 2005;102(2):239-47.
22. Silva CP, Del Carlo CH, Oliveira Jr MT, Scipioni A, Strunz-Cassaro C, Ramires JAF, et al. Porque o portadores de cardiomiopatia chagásica tem pior evolução que os não chagásicos? Arq Bras Cardiol. 2008;91(6):389-94.
504

Original Article
NHETS − Necropsy Heart Transplantation StudyThiago Ninck Valette, Silvia Moreira Ayub-Ferreira, Luiz Alberto Benvenuti, Victor Sarli Issa, Fernando Bacal, Paulo Roberto Chizzola, Germano Emilio Conceição Souza, Alfredo Inácio Fiorelli, Ronaldo Honorato Barros dos Santos, Edimar Alcides BocchiInstituto do Coração do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (USP), São Paulo, SP – Brazil
DOI: 10.5935/abc.20140039
Abstract
Background: Discrepancies between pre and post-mortem diagnoses are reported in the literature, ranging from 4.1 to 49.8 % in cases referred for necropsy, with important impact on patient treatment.
Objective: To analyze patients who died after cardiac transplantation and to compare the pre- and post-mortem diagnoses.
Methods: Perform a review of medical records and analyze clinical data, comorbidities, immunosuppression regimen, laboratory tests, clinical cause of death and cause of death at the necropsy. Then, the clinical and necroscopic causes of death of each patient were compared.
Results: 48 deaths undergoing necropsy were analyzed during 2000-2010; 29 (60.4 %) had concordant clinical and necroscopic diagnoses, 16 (33.3%) had discordant diagnoses and three (6.3%) had unclear diagnoses. Among the discordant ones, 15 (31.3%) had possible impact on survival and one (2.1%) had no impact on survival. The main clinical misdiagnosis was infection, with five cases (26.7 % of discordant), followed by hyperacute rejection, with four cases (20 % of the discordant ones), and pulmonary thromboembolism, with three cases (13.3% of discordant ones).
Conclusion: Discrepancies between clinical diagnosis and necroscopic findings are commonly found in cardiac transplantation. New strategies to improve clinical diagnosis should be made, considering the results of the necropsy, to improve the treatment of heart failure by heart transplantation. (Arq Bras Cardiol. 2014; 102(5):505-509)
Keywords: Heart Transplantation; Autopsy.
Mailing Address: Thiago Ninck Valette •Avenida Interlagos, 871, bloco 7, apto. 43, Jardim Marajoara. Postal Code 04661-100, São Paulo, SP – Brazil E-mail: [email protected], [email protected] revised August 20, 2013, revised manuscript November 17, 2013, accepted November 18, 2013.
analyzing the causes of death and comparing the pre- and post-mortem diagnoses.
MethodsRetrospective study was carried out by analysis of medical
records of deaths from heart transplantation that were submitted necropsy in the period 2000-2010. Clinical data for analysis of comorbidities, immunosuppression regimen, laboratory test results, clinical cause of death and cause of death at the necropsy were collected.
The pre-mortem death diagnosis was compared with the post-mortem one and then the discrepancies between the two diagnoses were classified according to Goldman et al2 criteria adapted by Battle et al3, while some cases were not classified4. The classification was as follows:
• Major discrepancies:- class I: discrepancies in major diagnosis, with impact on survival;- class II: discrepancies in major diagnosis, with no impact on survival;
• Minor discrepancies:- class III: discrepancies in minor diagnoses not directly related to cause of death;- class IV: discrepancies in minor occult diagnoses (non-
IntroductionThe necroscopic examination has contributed to the
evolution of medical knowledge. However, the frequency at which medical centers perform necropsies has been declining in recent decades, in different series. The assumed reasons for this phenomenon are diverse and include cultural aspects, lack of authorization by families, lack of financial resources for the procedure, an aging population and less interest in necropsy findings in the elderly, a decrease in the scientific interest in the necroscopic findings and hesitation facing the possibility of medical error detection. Considering this historical trend, discrepancies between pre and post-mortem diagnoses continue to be reported, ranging from 4.1 to 49.8% of cases referred for necroscopic examination1. A recent study did not evaluate the diagnoses obtained through pre-mortem clinical data with the necroscopic diagnoses of patients undergoing cardiac transplantation.
This study aimed to assess patients who died after cardiac transplantation and were submitted to necropsy,
505

Original Article
Valette et al.Necropsy in heart transplantation
Arq Bras Cardiol. 2014; 102(5):505-509
diagnosable), but with possible epidemiological or genetic importance;
• Non-discrepancy:- class V: non-discrepant diagnoses;
• Non-classifiable cases:- class VI: patients whose clinical or necroscopic diagnoses cannot be performed adequately.
Deaths were also differentiated as early or late, with early being those that occurred up to 1 year after transplantation and late the ones that occurred after 12 months. Discrepancies were evaluated in these two groups, verifying the causes of death.
This study was approved by the Research Ethics Committee. It was not necessary to obtain the signed free and informed consent, as this was a retrospective study based on the analysis of medical records.
The study received financial support from Fundação de Amparo à Pesquisa do Estado de São Paulo, process #2010/12278-5.
ResultsFrom 2000 to 2010, 124 patients submitted to cardiac
transplantation died. Cardiac transplantation of the 124 patients occurred from February 1987 to March 2010. Of these 124 patients, 48 were submitted to necropsy, which comprise the study sample. Figure 1 shows the case selection flowchart of the study.
The mean age was 41 years and 67% were men. The mean post-transplantation follow-up duration was 991 ± 1,728 days. The most frequent etiology of the disease (before transplantation) was chagasic heart disease. Regarding comorbidities, 44% of the
patients had hypertension, 31% dyslipidemia, and 18% diabetes mellitus. Table 1 shows the general characteristics of the patients.
Of the 48 analyzed cases, 29 (60.4 %) had concordant clinical and necroscopic diagnoses (class V), 16 (33.3 %) had discordant diagnoses and three (6.3%) had an unclear diagnosis (class VI). Among the discordant ones, 15 (31.3%) had possible impact on survival (class I) and one (2.1%) had no impact on survival (class II). The main clinical misdiagnosis was infection, with five cases (26.7% of discordant ones), followed by hyperacute rejection, with four cases (20% of discordant ones) and pulmonary thromboembolism with three cases (13.3% of discordant ones). Figure 2 shows the chart distribution of necropsies, based on the classification of discrepancies. Figure 3 and Table 2 compare the clinical and necroscopic diagnoses of class I discordant cases.
A total of 62.5 % (30 cases) were classified as early deaths and 37.5 % as late ones (18 cases). Among the early cases, 56% were concordant with impact on survival (class V), 33% discordant with impact on survival (class I), Figure 1 - Flowchart of case selection.
384 Heart transplantations from 02/1987 to 03/2010
239 deaths
124 deaths from 2000-2010
48 Deaths with necropsy fromde 2000-2010
139 alive
6 retransplantation
115 deaths before 2000
76 Necropsies Not permitted or Non-authorized
Table 1 - Clinical characteristics of studied patients
Characteristics n = 48
Age (years ) 41 ± 16
Male gender (%) 67
Follow-up after transplantation (days) 991 ± 1,728
Etiology (%)
Ischemic 14.6
Idiopathic 29.2
Hypertensive 2.1
Chagas disease 31.3
Others 13
Systemic Arterial Hypertension (%) 44
Diabetes mellitus (%) 18
Dyslipidemia (%) 31
Leukocytes 8,590 ± 4,972
Sodium (mEq/L) 136 ± 4
Creatinine (mg/dL) 1.9 ± 0.6
Urea (mg/dL) 79 ± 56
Potassium (mEq/L) 4.5 ± 0.6
Hemoglobin (g/dL) 12.5 ± 2.17
Medications (%)
Cyclosporine 50
Tacrolimus 14.6
Mycophenolate mofetil 54
Corticosteroids 77
Azathioprine 29.2
Sirolimus 14.6
506

Original Article
Valette et al.Necropsy in heart transplantation
Arq Bras Cardiol. 2014; 102(5):505-509
Figure 2 - Distribution of discrepancies between clinical and necroscopic diagnoses.
general hospitals, there were 6-37 % of major discrepancies and 25-28 % of minor ones7-9.
The most difficult necroscopic diagnosis to be clinically hypothesized was acute graft dysfunction. In this series, it was misdiagnosed as hyperacute rejection, hemorrhagic shock and septic shock. These data show the difficulty to confirm this diagnosis in clinical practice, as it depends on situations related to the perioperative period (the donor’s conditions, time of ischemia, myocardial protection and the recipient’s prior pulmonary hypertension) and the degree of suspicion of the attending physician, as there is no specific marker for the diagnosis.
Another premortem unsuspected necroscopic diagnosis was GVD. This was confused with other conditions that lead to ventricular dysfunction with cellular rejection and pulmonary thromboembolism. Although GVD is one of the main late causes of post-transplantation death10 a dose of clinical suspicion is also needed to initiate the appropriate diagnostic method.
Finally, another common diagnostic error was acute humoral rejection, which is known by its diagnostic difficulties, requiring advanced immunohistological methods, such as immunofluorescence and immunoperoxidase, in addition to the fact that the patient needs to be capable of being submitted to endomyocardial biopsy procedure.
Taking into account only the necroscopic cause of death, the data from this study are similar to those in the literature11,12, with emphasis on acute graft dysfunction, infection, rejection and GVD. Separating the deaths in early and late cases, acute graft dysfunction and GVD stood out, respectively.
Regarding the cause of cardiomyopathy that led to transplantation, this sample differs from that found in the
3% discordant with no impact on survival (class II) and 6 % had unclear diagnoses (Class VI). Among the late, 67% were concordant with impact on survival (class V), 28% discordant with impact on survival (class I) and 5.6% had unclear diagnoses (Class VI).
The causes of death verified at the necropsies were acute graft dysfunction (22.9%), acute rejection (20.8 %), infection (18.8%), Graft Vascular Disease (GVD-16.7%), other causes (14.6%) and unknown causes (6.3%).
In the group classified as early death, 37 % of deaths were due to acute graft dysfunction, 20% acute humoral rejection, 16.7% septic shock, 16.7% from other causes, and 6% of unknown causes.
In the late group, 45% of deaths were due to GVD, 17% to acute cellular rejection, 11% to septic shock, 22% from other causes and 5% of unknown causes.
DiscussionOur study showed a significant frequency of discrepancies
between clinical and necroscopic diagnoses of the cause of death, most often with a possible impact on survival.
In the literature, no recent studies were found comparing the clinical and necroscopic causes of death in patients undergoing cardiac transplantation, making this work a current tool for information analysis.
On the other hand, the rate of discordance in the present sample, on average, was higher than that observed in other series of patients unrelated to heart transplantation. Discrepancies values of 7.5 to 23 %, classified as major, were found in patients admitted to the intensive care unit, with 11-13% for minor discrepancies5,6. For patients admitted to
507

Original Article
Valette et al.Necropsy in heart transplantation
Arq Bras Cardiol. 2014; 102(5):505-509
Table 2 - Comparison between clinical and necroscopic diagnoses of class I discordant cases
Clinical Diagnosis
Necr
osco
pic D
iagno
sis
HR ACR AHR SS CS PTE HS MOSF
GVD 2 1
PTE 1
MS 1
DIC 1
AGD 3 1 1 1
AHR 2 1
HR: hyperacute rejection; ACR: acute cellular rejection; AHR: acute humoral rejection, SS: septic shock, CS: cardiogenic shock; PTE: pulmonary thromboembolism, HS: Hemorrhagic shock; MOSF: multiple organ and system failure; GVD: graft vascular disease, MS: mixed shock, DIC: disseminated intravascular coagulation; AGD: acute graft dysfunction.
Figure 3 - Comparison between clinical and necroscopic diagnoses of class I discordant cases.
Clinical diagnosis
Necroscopic
diagnosis
hype
racu
te re
jectio
n
Acute
cell r
ejecti
on
Humo
ral re
jectio
n
Septi
c sho
ck
Card
iogen
ic sh
ock
Pulm
onar
y thr
ombo
embo
lism
Hemo
rrhag
ic sh
ock
Multip
le or
gan a
nd sy
stem
failur
e
Humoral rejectionAcute graft dysfunction
Disseminated intravascular coagulationMixed shock
Pulmonary thromboembolism
Graft vascular disease
3
2
1
0
508

Original Article
Valette et al.Necropsy in heart transplantation
Arq Bras Cardiol. 2014; 102(5):505-509
1. Shojania KG, Burton EC, McDonald KM, Goldman L. Changes in rates of autopsy-detected diagnostic errors over time: a systematic review. JAMA. 2003;289(21):2849-56.
2. Goldman L, Sayson R, Robbins S, Cohn LH, Bettmann M, Weisberg M. The value of the autopsy in three medical eras. N Engl J Med. 1983;308(17):1000-5.
3. Battle RM, Pathak D, Humble CG, Key CR, Vanatta PR, Hill RB, et al. Factors influencing discrepancies between premortem and postmortem diagnoses. JAMA. 1987;258(3):339-44.
4. Bellwald M. [Autopsies with unsatisfactory results]. Schweiz Med Wochenschr. 1982;112(3):75-82.
5. Mort TC, Yeston NS. The relationship of pre mortem diagnoses and post mortem findings in a surgical intensive care unit. Crit Care Med. 1999;27(2):299-303.
6. Tejerina E, Esteban A, Fernández-Segoviano P, María Rodríguez-Barbero J, Gordo F, Frutos-Vivar F, et al. Clinical diagnoses and autopsy findings: discrepancies in critically ill patients. Crit Care Med. 2012;40(3):842-6.
References7. De Escalante Yangüela B, Oncins Torres R, Sampedro Felíu JA, Lacasa Marzo
J, Figueras Ara C, Nájar Subías M. [Descriptive study of autopsies of internal medicine department at the hospital of barbastro and clinico-pathological correlation]. An Med Interna. 2000;17(9):460-4.
8. Kotovicz F, Mauad T, Saldiva PH. Clinico-pathological discrepancies in a general university hospital in São Paulo, Brazil. Clinics (Sao Paulo). 2008;63(5):581-8.
9. Bürgesser MV, Camps D, Calafat P, Diller A. [Discrepancies between clinical diagnoses and autopsy findings]. Medicina (B Aires). 2011;71(2):135-8.
10. Stehlik J, Edwards LB, Kucheryavaya AY, Benden C, Christie JD, Dipchand AI, et al; International Society of Heart and Lung Transplantation. The Registry of the International Society for Heart and Lung Transplantation: 29th official adult heart transplant report--2012. J Heart Lung Transplant. 2012;31(10):1052-64.
11. Alexander RT, Steenbergen C. Cause of death and sudden cardiac death after heart transplantation: an autopsy study. Am J Clin Pathol. 2003;119(5):740-8.
12. Zuppan CW, Wells LM, Kerstetter JC, Johnston JK, Bailey LL, Chinnock RE. Cause of death in pediatric and infant heart transplant recipients: review of a 20-year, single-institution cohort. J Heart Lung Transplant. 2009;28(6):579-84.
International Society of Heart and Lung Transplantation Annual Report, 2012. While the most prevalent etiology in this study was Chagas’ disease, followed by idiopathic dilated cardiomyopathy, the global data showed the most prevalent etiology was idiopathic dilated cardiomyopathy (54 %), followed by ischemic heart disease (37 %)10. This difference is due to the prevalence of Chagas disease in our country, unlike what occurs in Europe and North America.
Among the limitations of this study is sample size, which reflects the decrease in the number of necropsies in recent decades, as mentioned before. Consequently, only 38.7 % of deaths between 2000 and 2010 were submitted to necropsy and were included in the study, which may interfere with the results.
Moreover, the analysis of records may not accurately reveal the clinical cause of death, as factors such as incomplete filling out of medical records and difficulties in understanding older records, which were not yet electronic, can interfere with the impression of the presumed clinical cause of death.
ConclusionDiscrepancies between clinical diagnosis and necroscopic
findings are commonly found in cardiac transplantation. New strategies to improve clinical diagnosis should be made,
considering necroscopic results to improve the treatment of heart failure by heart transplantation.
Author contributionsConception and design of the research: Ayub-Ferreira SM,
Bocchi EA; Acquisition of data: Valette TN, Ayub-Ferreira SM, Benvenuti LA, Issa VS, Bacal F, Chizzola PR, Souza GEC, Fiorelli AI, Santos RHB; Analysis and interpretation of the data: Valette TN, Ayub-Ferreira SM, Benvenuti LA, Issa VS, Bacal F, Chizzola PR, Souza GEC, Fiorelli AI, Santos RHB; Statistical analysis: Ayub-Ferreira SM; Writing of the manuscript: Valette TN; Critical revision of the manuscript for intellectual content: Ayub-Ferreira SM, Benvenuti LA, Bocchi EA; Supervision / as principal investigator: Bocchi EA.
Potential Conflict of InterestNo potential conflict of interest relevant to this article
was reported.
Sources of FundingThis study was partially funded by FAPESP. Study AssociationThis study is not associated with any thesis or dissertation work.
509

Review Article
Systems Biology Applied to Heart Failure With Normal Ejection FractionEvandro Tinoco Mesquita, Antonio Jose Lagoeiro Jorge, Celso Vale de Souza Junior, João Paulo Pedroza CassinoUniversidade Federal Fluminense, Niterói, RJ - Brazil
AbstractHeart failure with normal ejection fraction (HFNEF) is
currently the most prevalent clinical phenotype of heart failure. However, the treatments available have shown no reduction in mortality so far. Advances in the omics sciences and techniques of high data processing used in molecular biology have enabled the development of an integrating approach to HFNEF based on systems biology.
This study aimed at presenting a systems-biology-based HFNEF model using the bottom-up and top-down approaches.
A literature search was conducted for studies published between 1991 and 2013 regarding HFNEF pathophysiology, its biomarkers and systems biology. A conceptual model was developed using bottom-up and top-down approaches of systems biology.
The use of systems-biology approaches for HFNEF, a complex clinical syndrome, can be useful to better understand its pathophysiology and to discover new therapeutic targets.
IntroductionHeart failure (HF) is a complex clinical syndrome, and the
final pathway of different forms of aggression to the cardiac muscle. It manifests as two distinct phenotypes: HF with reduced ejection fraction (HFREF) and HF with normal ejection fraction (HFNEF).
The HFNEF prevalence has increased, so that HFNEF will become the most prevalent phenotype of HF in this decade, affecting mainly elderly individuals of the female sex with multiple co-morbidities1. Its pathophysiology has been mainly centered on the presence of left ventricular (LV) structural and diastolic functional changes, which cause an increase in LV filling pressures and intolerance to physical exertion2-4.
The results of different randomized clinical studies, using drug treatment directed at improving diastolic function, have shown neutral results regarding patients’ survival5-7. The oslerian approach classically used to describe the
mechanisms of disease, as well as the construction of the reasoning that is the basis of treatment for HFNEF might need to be replaced by a new approach that uses systems biology, recently introduced into other areas of internal medicine, such as infectology and oncology. That new approach has led to the development of successful new drugs in those areas, allowing the construction of the so-called personalized medicine, which has propitiated the advance of that concept. That is important mainly because HFNEF is a cardiovascular syndrome with multiple abnormalities of the pathophysiological pathways, which interact through a complex network8-9.
This review was aimed at presenting recent concepts of systems biology and its potential use in complex cardiovascular diseases, such as HFNEF, a syndrome with multiple pathophysiological abnormalities and still limited therapeutic arsenal in the light of current knowledge.
HFNEF and its pathophysiological complexityFrom the clinical and epidemiological viewpoints, compared
to patients with HFREF, those with the HFNEF phenotype are usually older, more obese, of the female sex and have a history of arterial hypertension and atrial fibrillation 1,10,11.
The diagnosis of HFNEF is currently made from a clinical suspicion (intolerance to exercise) in association with the following Doppler echocardiographic findings, by using tissue Doppler: LV ejection fraction ≥ 50%; final LV indexed diastolic volume < 97 mL/m²; and diastolic functional abnormalities12,13.
Patients with HFNEF have shown different subcellular abnormalities, such as changes in the extracellular matrix with increased deposits of advanced glycation end-products, collagen profile changes, sarcomeric protein titin isoform switch and hypophosphorilation, increased inflammatory response, and reduced SERCA2 pump activity14,15. The changes observed at cellular level were apoptosis, cardiomyocyte stiffness and hypertrophy, which might be responsible for concentric remodeling, even in the absence of LV hypertrophy. Macroscopically, LV hypertrophy and increased left atrial volume are observed, characterizing the major structural changes of patients with HFNEF. Finally, all changes lead to disorder of the cardiovascular system, which, integrated with other systems, will cause or aggravate multisystem abnormalities known as co-morbidities14 (Figure 1).
Briefly, such structural and functional changes increase the risk of LV diastolic dysfunction. Although patients with HFNEF have LV ejection fraction values considered normal, they have changes in systolic performance, which can be assessed through different systolic function indices, such as
KeywordsHeart Failure; Stroke Volume; Ventricular Dysfunction,
Left; Aged.Mailing Address: Antonio Jose Lagoeiro Jorge •Rua Coronel Bittencourt, 66, Boa Vista. Postal Code: 24900-000, Marica, RJ - BrasilE-mail:[email protected] , [email protected] received june 26, 2013; revised manuscript september 24, 2013; accepted september 26, 2013.
DOI: 10.5935/abc.20140062
510

Review Article
Mesquita et al.Systems Biology and HFNEF
Arq Bras Cardiol. 2014; 102(5):510-517
LV contractility, systolic volume, cardiac output and axial systolic shortening velocity (S’). Abnormality of relaxation and increased ventricular stiffness lead to increased LV filling pressures, which are diastolic dysfunction markers2.
Changes in arterial stiffness and endothelial function are present in different degrees in individuals with HFNEF, contributing to aggravate diastolic dysfunction, increasing afterload and causing or intensifying myocardial ischemia. In addition, abnormalities of the microcirculation can also contribute to intolerance to exercise by hindering the perfusion of skeletal and respiratory muscles, which has been studied in individuals with HFNEF.
Mesquita et al. and Matsubara have provided a more detailed discussion of the pathophysiology of HFNEF in two recent reviews published in the Arquivos Brasileiros de Cardiologia3,4.
Defining the systems-biology approachThe contemporary translational model of developing
scientific knowledge in the medical area has allowed the large-scale use of new effective treatments for diseases. That model, derived from the oslerian system, has established that the presence of a certain disease should be defined as changes in a tissue (anatomico-clinical correlation), from which its pathophysiology can be pursued and a specific therapeutic target developed16,17. Based on the advances of molecular biology and using the oslerian view, the identification of individual genes, proteins and cells has been sought, as well as the study of their functions, providing limited information on complex diseases.
Systems biology allows, through the construction of mathematical models, simulations and data processing techniques, the integration of information from the omics sciences and clinical-epidemiological data, to provide better understanding of the interactions between the components of live systems and their biological processes18-20.
Systems biology has its roots in the formulation of the internal environment stability principle by Claude Bernard in 1865, and has gained quantitative formalism with the mathematical description of the potential of action biophysics, first delineated by Hodgkin and Huxley in nervous cells, and soon after extended to the cardiac potential of action by Denis Noble21. That approach has been applied in medicine since before the molecular biology revolution. However, in the pregenomic era, systems biology was naturally hindered by the lack of technologies necessary to reach that integration and by the inability to investigate such systems in details21. However, in the past decades, scientific advances in the areas of molecular biology, engineering, bioinformatics, and physics, in association with the omics sciences (Table 1), enabled the acquisition of more complete information with a greater capacity to define more detailed approaches.
Systems biology, whose major characteristics are shown in Table 2, can be understood as the interaction of different biological systems activated at the molecular, cellular, tissular and organic levels, which can be assessed by use of tools, many of which available in clinical practice8,22.
Systems biology allows a new understanding of the concept of disease, which can be defined as the lack of cooperation between some of the biological parts in an organic system, resulting in impairment of the entire functioning of the organism14.
Figure 1 – HFNEF – pathophysiology and co-morbidities. HFNEF – Heart failure with normal ejection fraction.
ICFEN
Disfunção VentricularPiora do relaxamentoPiora da rigidez
Disfunção Atrial
Disfunção AutonômicaIncompetência cronotrópica
Disfunção VascularRigidez vascularAcoplamento ventrículo arterial
Doença valvular
Hipertensão pulmonar
Doença Pulmonar
Deficiência de ferro e anemia
Disfunção renal e sobrecarga de volume
Idade , sexo e Descondicionamento
físico
Obesidade e sarcopenia
DepressãoDisfunção Endotelial
HFNEF
pulmonary disease
iron deficiency and anemia
iron deficiencyand anemia
kidney dysfunction and volume overload
age, sex and physical unfitness
obesity and sarcopenia
depressionheart valve disease
endothelial dysfunction
pulmonary hypertension
vascular dysfunctionvascular stiffness
ventricular-arterial coupling
chronotropic incompetenceincompetência cronotrópica
atrial dysfunction
ventricular dysfunctionworse relaxation
stiffness aggravation
511

Review Article
Mesquita et al.Systems Biology and HFNEF
Arq Bras Cardiol. 2014; 102(5):510-517
Table 2 - Major characteristics of Systems Biology
• Studies biological systems globally, at molecular level;
• Distinguishes from the classical linear theory: one gene, one protein;
• Integrates knowledge from different disciplines;
• Proposes mathematical models to explain some biological phenomena;
• Manipulates a large amount of data from experimental studies;
• Performs studies that verify the quality of the models described by comparing numerical simulations and experimental data.
Table 1 - Omics sciences
Genomics Science that studies all genes, and analyzes their interactions and influences on biological pathways and networks.
TranscriptomicsScience that studies the phenomena involved in mRNA transcription. Through microarray technology, it accesses the expression of thousands of transcribed genes and identifies gene patterns (molecular signature) that can be used as biomarkers for etiology identification, prognostic assessment, and HF treatment.
Proteomics Science that studies all proteins encoded in the genome; can be used to identify HF prior to the appearance of symptoms, therefore increasing the chances of an earlier and more effective treatment.
Metabolomics Science that studies the molecular metabolites found in cells, tissues and organs, identifying their regulatory effects on genes and proteins. Used to identify biomarkers in HF.
Epigenomics Science that studies the mechanisms capable of influencing the reading and interpreting of a chain of genes based on environmental factors on the genome.
Microbiomics Science that studies the genomes of microbes and their interactions in a certain ecosystem. It is worth noting the study on interactions of intestinal bacteria and trimethylamine-N-oxide production, which propitiate the development of atherosclerosis.
HF: heart failure.
According to that concept of disease, two study approaches can be identified: the bottom-up approach, aimed at defining the specificities that compose a structure, enumerating elements and identifying their individual characteristics to obtain an image of the point to be studied; and the top-down approach, which does not need to provide details of the network components, but to understand the general principles of the network to better understand it and to guide the identification of unpredicted elements. Similarly, the bottom-up approach could be compared to a ‘link the dots’ image, in which the real picture can only be revealed when each dot is duly recognized and linked to the others. The top-down approach can be understood as an impressionist painting, which, when seen from a short distance, does not allow us to identify the whole picture; it has to be seen from a distance, with a more comprehensive view, not requiring excessive details to reveal the image completely. Combining both characteristics, the knowledge on the system analyzed is amplified, allowing the identification of new proposals and pathways14,19.
The network concept is aimed at providing a structure in which its forming and functional components interact in a self-organized biological network. The networks, rather than the components themselves, create the physiological behavior and disease. Each knot in a network represents a component (a gene, a protein), and the interconnection of the components describes the typical architecture imposed by biological selection and evolution21 (Figure 2).
Working with networks simplifies complex systems, synthesizing the elements as knots and their interactions as
lines between them, and identifies functional groups as module. Many of those biological networks have a topology described as scale-free, in which knots with few connections have priority; when linked to knots that have an elevated number of connections, those are called hubs (Figure 2). That architecture provides a biologically strong evolutionary advantage, considering that there are multiple alternative pathways to go from one knot to the other. In addition, that ‘redundancy’ enables the networks to more easily adapt to environmental changes. At each level, the network obtains new properties not previewed in the preceding levels, demonstrating the concept of emergent property8,18. Failure of the biological networks or incapacity to obtain emergent property at the following level causes disruptions in the physiological mechanisms, generating complex pathological phenotypes.
The network approach might allow a change of paradigm in HF treatment, because, instead of trying to adapt different patients to one single treatment (reductionism), it is aimed at directing the treatment profile at the different patients based on their individual networks (personalized medicine)23.
The development of that approach is usually centered on a molecular target. However, in complex human diseases, that target is neither easily identified nor directed by one single factor23.
Recent analyses have shown that a large number of traditional medications do not reach target proteins, but only proteins of the neighboring networks, which can be a reason for the modest effects obtained when some drugs are used for patients with HFNEF8.
512

Review Article
Mesquita et al.Systems Biology and HFNEF
Arq Bras Cardiol. 2014; 102(5):510-517
Figure 2 – Overview of a biological network. Adapted from Chan SY, Loscalzo J. The emerging paradigm of network medicine in the study of human disease. Circulation Res. 2012 Jul 20;111(3):359-74.
Hub
knot
line (interaction)
In contrast, a new pharmacology based on biological systems begins to develop aimed at creating new drugs that can be directed at one or more targets involved in the pathophysiological processes of the most relevant networks. That approach begins to be used in cancer and HIV/AIDS, and can become useful for HFNEF, making a new view of HFNEF under the systems biology perspective critical8.
An HFNEF model using the systems-biology approachThe HFNEF is obviously a complex syndrome, whose
pathophysiology and progression remain unclear, which makes the construction of a network model for HFNEF potentially useful and challenging in the current state of knowledge.
The heart involves different structural and functional hierarchic scales, which, through multiple interactions of subsystems, allow normal heart to achieve uniformity despite its structural and functional complexities at different levels24 (Figure 3). That approach has identified different structural and functional abnormalities of the heart in humans and other animals7.
From the mechanistic viewpoint, HFNEF can be defined as a complex condition, thus requiring an approach that encompasses the current concepts of systems biology. The analysis of omic data is crucial for understanding the factors involved in HFNEF and for identifying biomarkers with diagnostic and prognostic properties for clinical use5.
By using the systems-biology approach and integrating different abnormalities observed in HFNEF, we propose a model that combines environmental and genetic factors, cardiac and vascular morphofunctional changes, abnormalities in other systems, and interaction with different co-morbidities,
developing a holistic view of that syndrome and integrating the bottom-up and top-down methodologies (Figure 4).
The HFNEF results from systemic diseases, such as hypertension, diabetes, obesity and coronary artery disease, in association with the female sexual dimorphism. In addition, the aging process influences different cellular and subcellular pathways, promoting functional and structural abnormalities in the heart and great vessels. Recently, abnormalities in the protein folding process have been observed during the abnormal aging of the heart, and can contribute to HFNEF, a phenomenon called “Alzheimer’s of the heart”.
In addition, experimental evidence has shown that, in the heart of elderly rats, a reduction in the growth differentiation factor 11 (GDF11), which modulates the ligand-receptor activity in cardiomyocytes, contributes to cardiac hypertrophy and to the decreased SERCA2 functional activity, also causing an elevation in B-type natriuretic peptide (BNP) levels. However, when GDF11 levels are restored, a reduction in cardiac hypertrophy and an increase in the SERCA2 pump activity are observed, with consequent restoration of diastolic heart function25.
Eventually those abnormalities cause intolerance to physical exertion, systemic and/or pulmonary congestion, tissue hypoperfusion and cardiac arrhythmias, such as atrial fibrillation, leading to HF signs and symptoms26.
Another important concept influenced by the systems biology paradigm is that of the biomarker, considered a clinical status indicator that can be obtained from the integration of multiple biological activity levels in the network. That approach is responsible for guiding the identification of the biomarker based on deep understanding of its biological
513

Review Article
Mesquita et al.Systems Biology and HFNEF
Arq Bras Cardiol. 2014; 102(5):510-517
Figure 3 – Model of the left ventricle as a dissipative structure with emergent properties. Adapted from De Keulenaer GW, Brutsaert DL. Systolic and diastolic heart failure are overlapping phenotypes within the heart failure spectrum. Circulation.2011;123(18):1996-2004.
uniformitythrough
non-uniformity
communication between cells
systemic level
organic level
tissue level
tissue hypoperfusionintolerance to exertion
volume overload
emergent property
emergent property
emergent property
emergent property
vascular stiffnessconcentric remodeling
hypertrophy cardiomyocyte
stiffness
celllevel
titinSERCA 2Acollagen
TIMPSIL-6
mRNA
cross-bridges
sarcomeric protein interaction ion flow
epigenomics
sarcoplasmic reticulum
genomics proteomics transcriptomics metabolomics
mechanism. The BNP, released in the presence of increased intraventricular pressure, is used for diagnostic confirmation and prognosis in HFNEF, and, more recently, has shown therapeutic usefulness in HFREF18.
Other biomarkers that assess fibrosis, inflammation and necrosis have been studied in HFNEF. Current strategies using micro RNA have shown promise to better characterize patients with HFNEF. In addition, the use of multiple biomarkers in clinical research has introduced an approach similar to that of a system, and can significantly contribute to prognostic assessment and therapeutic response in HFNEF27.
Understanding the pathophysiological abnormalities in multiple pathways in HFNEF has led to the development of new drugs directed at more than one pathway identified as critical to HFNEF. The LCZ696 is a dual-acting angiotensin receptor-neprilysin inhibitor composed of a neprilysin inhibitor prodrug, AHU 377, and the angiotensin receptor antagonist valsartan. Neprilysin degrades biologically active natriuretic peptides, such as atrial natriuretic peptide (ANP), BNP, and C-type natriuretic peptide, but not NT-pro-BNP, which is biologically inactive. By increasing active natriuretic peptides,
neprilysin inhibitor increases the myocardial generation of cyclic guanosine, which enhances myocardial relaxation and reduces hypertrophy. In addition, natriuretic peptides stimulate natriuresis, diuresis and vasodilation, and can have an additional anti-fibrotic and anti-sympathetic effect. Furthermore, neprilysin contributes to angiotensin collapse, which is the rationale for the dual action of the compound, which inhibits that enzyme and blocks angiotensin action or generation28 (Figure 5).
The LCZ696 has been tested in patients with HFNEF (PARAMOUNT Study – phase 2) and has shown a more marked reduction in NT-pro-BNP than that caused by the isolated valsartan use. In addition, LCZ696 was better than valsartan to promote left atrial reverse remodeling and to improve those patients’ functional class28.
Briefly, HF understanding from the systems-biology perspective is still limited by the difficulty to integrate data from that complex information system into a biopathological model, mainly because of the several variables that interfere with the existing relationships, such as the genetic variations of each individual and the environmental influence on organisms8.
514

Review Article
Mesquita et al.Systems Biology and HFNEF
Arq Bras Cardiol. 2014; 102(5):510-517
Figu
re 4
– Sch
emat
ic m
odel
of a
biol
ogica
l net
work
for H
FNEF
.
515

Review Article
Mesquita et al.Systems Biology and HFNEF
Arq Bras Cardiol. 2014; 102(5):510-517
Figure 5 – Mechanisms of action of the new drug LCZ696 that inhibits neprilysin and blocks the angiotensin receptor. Solomon SD, Zile M, Pieske B, et al; Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection fraction (PARAMOUNT) Investigators.Lancet;2012;380:1387-95.
natriuretic peptide system renin-angiotensin systemheart failure
pro-BNP angiotensinogen(liver secretion)
angiotensin I
angiotensin II
AT1 receptor
NT-pro-BNP
inactive fragments
LCZ696
AHU377↓
LBQ657
Valsartanvasodilation ↓ blood pressure↓ sympathetic tone ↓ aldosterone level↓ fibrosis↓ hypertrophynatriuresis / diuresis
vasoconstriction↑ blood pressure↑ sympathetic tone ↑ aldosterone level↑ fibrosis↑ hypertrophy
BNP
neprilysin
ConclusionThe systems-biology approach in HFNEF is at an
initial stage and can offer the possibility to widen the knowledge on pathophysiology, to refine the diagnosis and to lead to the development of new biomarkers and therapeutic targets.
Currently, the combination of a reductionist view with a holistic view is still necessary to better understand HFNEF, which involves a network of complex interactions between biological entities in different scales.
Thus, the complex pathophysiology of HFNEF and the lack of a treatment capable of reducing its impact on mortality make it the ideal cardiovascular condition for a new approach using systems biology, allowing the development of future therapeutic targets.
Author contributionsConception and design of the research: Mesquita ET;
Writing of the manuscript: Mesquita ET, Jorge AJL, Souza Junior CV, Cassino JPP; Critical revision of the manuscript for intellectual content: Mesquita ET, Jorge AJL.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis study is not associated with any thesis or dissertation work.
References1. Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends
in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355(3):251-9.
2. Mesquita ET, Jorge AJ. Insuficiencia cardíaca com fração de ejeção normal – novos critérios diagnosticos e avanços fisiopatologicos. Arq Bras Cardiol. 2009;93(2):180-7.
3. Roscani MG, Matsubara LS, Matsubara BB. Heart failure with normal ejection fraction. Arq Bras Cardiol. 2010;94(5):652-60.
4. Mesquita ET, Socrates J, Rassi S, Villacorta H, Mady C. Heart failure with preserved systolic function. Arq Bras Cardiol. 2004;82(5):494-500.
5. Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ, et al. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet. 2003;362(9386):777-81.
6. Cleland JG, Tendera M, Adamus J, Freemantle N, Pçonski L, Taylor J, et al. The perindopril in elderly people with chronic heart failure (PEP-CHF) study. Eur Heart J. 2006;27(19):2338-45.
516
Review Article
Mesquita et al.Systems Biology and HFNEF
Arq Bras Cardiol. 2014; 102(5):510-517
7. Massie BM, Carson PE, McMurray JJ, Komajda M, McKelvie R, Zile MR, et al. Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med. 2008;359(23):2456-67.
8. Chan SY, White K, Loscalzo J. Deciphering the molecular basis or human cardiovascular disease through network biology. Curr Opin Cardiol. 2012;27(3):202-9.
9. Chan SY, Loscalzo J. The emerging paradigm of network medicine in the study of human disease. Circ Res. 2012;111(3):359-74.
10. Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006;355(3):260-9.
11. Redfield MM, Jacobsen SJ, Burnett Jr JC, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. J Am Med Assoc. 2003;289(2):194-202.
12. Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28(20):2539-50.
13. Tschope C, Kasner M, Westermann D, Gaub R, Poller WC, Schultheiss HP. The role of NT-proBNP in the diagnostics of isolated diastolic dysfunction: correlation with echocardiographic and invasive measurements. Eur Heart J. 2005;26(21):2277-84.
14. Louridas GE, Lourida KG. A conceptual paradigm of heart failure and systems biology approach. Int J Cardiol. 2012;159(1):5-13.
15. Borbély A, Papp Z, Edes I, Paulus WJ. Molecular determinants of heart failure with normal left ventricular ejection fraction. Pharmacol Rep. 2009;61(1):139-45.
16. Norman G. Medical education: past, present and future. Perspect Med Educ. 2012;1(1):6-14.
17. Chen R, Snyder M. Systems biology: personalized medicine for the future? Curr Opin Pharmacol. 2012;12(5):623-8.
18. Lusis AJ, Weiss JN. Cardiovascular networks: systems-based approaches to cardiovascular disease. Circulation. 2010;121(1):157-70.
19. Barabasi AL, Gulbahce N, Loscalzo J. Network medicine: a network-based approach to human disease. Nat Rev Genet. 2011;12(1):56-68.
20. Maclellan WR, Wang Y, Lusis, AJ.Systems-based approaches to cardiovascular disease. Nat Rev Cardiol. 2012;9(3):172-84.
21. Dewey FE, Wheeler MT, Ashley EA. Systems biology of heart failure, challenges and hopes. Curr Opin Cardiol. 2011;26(4):314-21.
22. De Keulenaer GW, Brutsaert DL. Systolic and diastolic heart failure are overlapping phenotypes within the heart failure spectrum. Circulation. 2011;123(18):1996-2004.
23. Voora D, Ginsburg GS. Cl inical appl icat ion of cardiovascular pharmacogenetics. J Am Coll Cardiol. 2012;60(1):9-20
24. Brutsaert DL. Cardiac dysfunction in heart failure: the cardiologist’s love affair with time. Prog Cardiovasc Dis. 2006;49(3):157-81.
25. Lee RT, Loffredo FS, Steinhauser ML, Jay SM, Gannon IJ, Paancoast JR, Yalamanchi P, et al. Growth differentiation factor 11 is a circulating factor that reverses age-related cardiac hypertrophy. Cell. 2013;153(4):828-39.
26. Willis MS, Patterson C. Proteotoxicity and cardiac dysfunction--Alzheimer’s disease of the heart? N Engl J Med. 2013;368(5):455-64.
27. Azuaje FJ, Dewey FE, Brutsaert DL, Devaux Y, Ashley EA, Wagner DR. Systems-based approaches to cardiovascular biomarker discovery. Circ Cardiovasc Genet. 2012;5(3):360-7.
28. Solomon SD, Zile M, Pieske B, Voors A, Shah A, Kraigher-Krainer E, et al; Prospective comparison of ARNI with ARB on Management Of heart failUre with preserved ejectioN fracTion (PARAMOUNT) Investigators. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet. 2012;380(98):1387-95.
517

Letter to the Editor
Obesity and Abnormalities in Echocardiographic ParametersRoberta Casanova Wilhelms, Eduardo Maffini da Rosa, Mauricio Lizott, Raphael Martin de MeloUniversidade de Caxias do Sul – UCS, Caxias do Sul, RS - Brazil
Dear Editor,
We congratulate the authors of the manuscript published under the title “The Impact of Isolated Obesity on Right Ventricular Function in Young Adults”1. We believe that the hemodynamic changes that characterize obesity could
modify the echocardiographic parameters found abnormal in this study, that is, increased volemia would readjust the parameters of ventricular function without any concomitant changes in ventricular function. What is the authors’ opinion about this analysis?2.
Mailing Address: Roberta Casanova Wilhelms •Rua Humberto de Campos, 1113, Cristo Redentor. Postal Code: 95084-440, Caxias do Sul, RS - BrazilE-mail: [email protected], [email protected] received October 13, 2013; revised manuscript October 16, 2013; accepted November 29, 2013.
KeywordsObesity; Echocardiography.
1. Sokmen A, Sokmen G, Acar G, Akcay A, Koroglu S, Koleoglu M, et al. The impact of isolated obesity on right ventricular function in young adults. Arq Bras Cardiol. 2013;101(2):160-8.
2. Schusterova I, Jurko A, Minarik M. Left ventricular systolic and diastolic function in children with overweight and obesity. Bratisl Lek Listy. 2013;114(9):526-30.
References
DOI: 10.5935/abc.20140059
518

Letter to the Editor
Extracellular Matrix Turnover: a Balance between MMPs and their InhibitorsEmre Yalcinkaya1, Murat Celik2, Baris Bugan3
Aksaz Military Hospital - Departamento de Cardiologia1, Mugla, Turquia; Gulhane Military Medical Faculty - Departamento de Cardiologia2, Ankara, Turquia; Malatya Military Hospital - Departamento de Cardiologia3, Malatya, Turkey
Mailing Address: EmreYalcinkaya •Aksaz Military Hospital Department of Cardiology; Aksaz Asker Hastanesi, Kardiyoloji Bolumu, 48750, Aksaz/Marmaris/Mugla, TurkeyEmail: [email protected] received December 13, 2013; revised manuscript January 7, 2014; accepted January 7, 2014.
KeywordsMatrix Metalloproteinase 1; Matrix metalloproteinase
inhibitors; Metabolic X Syndrome; Extracellular matrix.
1. Santos AB, Junges M, Silvello D, Macari A, Araújo BS, Seligman BG, et al. Early change of extracellular matrix and diastolic parameters in metabolic syndrome. Arq Bras Cardiol. 2013;101(4):311-6.
2. Roderfeld M, Graf J, Giese B, Salguero-Palacios R, Tschuschner A, Müller-Newen G, et al. Latent MMP-9 is bound to TIMP-1 before secretion. Biol Chem. 2007;388(11):1227-34.
3. Avădanei R, Căruntu ID, Amălinei C, Lozneanu L, Balan R, Grigoraş A, et al. High variability in MMP2/TIMP2 and MMP9/TIMP1 expression in secondary liver tumors. Rom J Morphol Embryol. 2013;54(3):479-85.
4. Cogni AL, Farah E, Minicucci MF, Azevedo PS, Okoshi K, Matsubara BB, et al. Metalloproteinases-2 and -9 predict left ventricular remodeling after myocardial infarction. Arq Bras Cardiol. 2013;100(4):315-21.
5. Kim Y, Remacle AG, Chernov AV, Liu H, Shubayev I, Lai C, et al. The MMP-9/TIMP-1 axis controls the status of differentiation and function of myelin-forming Schwann cells in nerve regeneration. PLoS One. 2012;7(3):e33664.
References
DOI: 10.5935/abc.20140061
To the Editor,We read with great interest the article by Santos et
al1, entitled “Early Change of Extracellular Matrix and Diastolic Parameters in Metabolic Syndrome”, which was published in october of Arquivos Brasileiros de Cardiologia. The authors1 aimed to compare diastolic function, biomarkers representing extracellular matrix activity (MMP9 and TIMP1), inflammation and cardiac hemodynamic stress in patients with the metabolic syndrome and healthy controls. We thank authors for their excellent data and valuable study but some comments may be of beneficial.
Matrix metalloproteinases (MMPs) play major roles in tissue development, matrix collagen turnover, repair and remodeling2-5. The TIMPs are usually secreted together with
variable amounts of their MMPs and regulate MMPs’ proteolytic activities by binding tightly to their catalytic sites2.
Extracellular matrix (ECM) turnover is largely modulated by the interaction between MMPs and their TIMPs.2-5A correlation and reciprocal influences between MMP and their TIMP determines the combined effect on ECM turnover4,5.
Expression patterns of MMP9 andTIMP1 (a specific inhibitor of MMP9), are closely correlated with physiological, pathological and micro-environmental processes characterized by the degradation and accumulation of the ECM3. A balance between MMP9 and TIMP1 is a major parameter in regulating both the enzyme activation and functionality in the tissue3-5. Consequently, MMP9/TIMP1 ratio could be viewed as a more reliable, useful and determinative marker in the evaluation of their potential prognostic capacities compared with MMP9 and TIMP1 separately. Determining the changes in the ECM balance and activity with a more appropriate method could give a chance to observe the influences on the results more precisely.
519

Letter to the Editor
Yalcinkaya et al.Determination of an extracellular matrix turnover
ReplyWe appreciate the thoughtful and valuable comments. It is
currently known that the balance between metalloproteinase (MMP) and their tissue inhibitors (TIMP) partly regulates the myocardial extracel lular matr ix homeostasis . The commenters suggested that the description of the MMP/TIMP ratio would provide additional information about degradation and modulation of collagen synthesis.i,ii. This could be inferred from our previous analysis where patients with Metabolic Syndrome (MS) had higher levels of MMP9 compared to healthy controls, despite similar levels of TIMP1.iii We primarily opted to show these biomarkers individually providing a more comprehensive description
of the scenario, considering the individual response and interplay between these biomarkers.
Performing the suggested analysis, the MMP9/TIMP1 ratio was higher in MS compared to controls (2.4 ± 1.1 in MS vs. 1.5± 0.6 in control group, p < 0.001), reflecting the original findings. Additionally, in multivariate analysis, higher MMP9/TIMP1 remained associated with MS (p = 0.006), independently of the remaining relevant covariates. The higher MMP9/TIMP1 ratio reinforces the concept that an increased turnover of collagen is associated with MS even in this young population. Whether changes in MMP9 individually or in MMP9/TIMP1 ratio have prognostic value in MS remains to be determined.
Arq Bras Cardiol. 2014; 102(5):519-520 520

Erratum
Edition of September 2013, vol. 101 (3), Suppl. 3, page 1-93The “Brazilian Guidelines on Antiplatelet Agents and Anticoagulants in Cardiology,” published as supplement number three
to the September 2013 edition of the Arquivos Brasileiros de Cardiologia [Arq Bras Cardiol. 2013;101 (3Suppl.3):1-93], was fixed as follows:
On page 17, Table 2, change the Class of recommendation of “Exchange of heparins (UFH and enoxaparin)” to III.On page 31, Table 5, last line, consider correct the wording “In situations of CHADSVasc zero or up to 1 (if it is only by the
female sex), the non-use of oral anticoagulation (such as rivaroxaban) may be considered,” Class of recommendation: II and Level of evidence: A.
On page 47, table 13, consider as correct the wording “Indications”: “Treatment of acute and chronic VTE at a dose of 15 mg twice a day in the first 21 days followed by 20 mg once a day for 3, 6, or 12 months or for a longer time at the physician’s discretion.”
Edition of December 2013, vol. 101 (6), Suppl. 3, page 1-63In “I Brazilian Guidelines on Cardiovascular Prevention”, consider Izar MC as the correct form for the name of the author
Maria Cristina de Oliveira Izar.
DOI: 10.5935/abc.2013S009e
521
Anatomopathological Session
Case 2/2014 – 51-Year Old Patient with Systemic Lupus Erythematosus and Fever after Valve ReplacementWilma Noia Ribeiro, Alice Tatsuko Yamada, Paulo Sampaio GutierrezInstituto do Coração (InCor), HC-FMUSP, São Paulo, SP – Brazil
Mailing Address: Vera Demarchi Aiello •Avenida Dr. Enéas de Carvalho Aguiar, 44, subsolo, bloco I, Cerqueira César. Postal Code 05403-000, São Paulo, SP – BrazilE-mail: [email protected], [email protected]
KeywordsSystemic lupus erythematosus; Hypertension; Dyslipidemia;
Aortic valve stenosis / surgery.
Section editor: Alfredo José Mansur ([email protected])
Associated editors: Desidério Favarato ([email protected])
Vera Demarchi Aiello ([email protected])
DOI: 10.5935/abc.20140069
A 51-year old female patient presented with precordial pain and dyspnea at moderate exertion, being diagnosed with severe aortic stenosis, with indication for surgical treatment.
The patient had arterial hypertension, mixed dyslipidemia, was a smoker and had systemic lupus erythematosus, which initiated at the age of 16, as well as nephritis. She reported anemia and seizures, which were attributed to lupus. In the past months, she had presented with pleuritic precordial pain, which became worse in the decubitus position and improved at the sitting position, which was attributed to pericarditis.
The physical examination (25/10/2011) revealed the patient had good general status, was hydrated, eupneic, with 60 bpm heart rate, and 110 x 70 mmHg blood pressure. Pulmonary auscultation was normal, and cardiac auscultation revealed rhythmic sounds, hypophonesis of the aortic component of the second sound and systolic murmur ++++/6+. The abdominal examination was normal, with no edema, and wrists were symmetric.
ECG (31/10/2011) revealed sinus rhythm, 48 bpm heart rate, 200 ms PR interval, 113 ms QRS duration, 464 ms QT, disorder in the intraventricular conduction of the stimulus, and changes in ventricular repolarization (Figure 1).
Laboratory examinations (24/10/2011) revealed; hemoglobin, 7 g/dL; hematocrit level, 21%; MCV, 95 fL; leukocytes, 6,940/mm3 (72% neutrophils, 1% eosinophils, 1% basophils, 22% lymphocytes, and 4% monocytes); platelets, 303,000/mm3; urea, 62 mg/dL; creatinine, 1.21 mg/dL (glomerular filtration, 50 mL/min/1.73m2); AST, 36 UI/L; ALT, 42 UI/L; calcium, 4.3 mEq/L; magnesium, 2.30 mEq/L; total protein, 7.4 g/dL; lactate dehydrogenase, 447 U/L; sodium, 138 mEq/L; and potassium, 4.7 mEq/L; PT (INR), 1.1; TTPA (rel), 0.99; total cholesterol, 301 mg/dL; HDL-c, 46 mg/dL; LDL-c, 169 mg/dL; and triglycerides, 378 mg/dL.
The echocardiogram (26/10/2011) showed left atrium of 40 mm, aorta of 32 mm, septum of 16 mm, posterior wall of 15 mm, left ventricle of 50/32 mm (diastole/systole), ejection fraction of 65%, left ventricle with normal dimensions and severe hypertrophy; mitral valve with discrete thickening, with a 3.7 cm2 valve area; aortic valve with severe calcification, 0.5 cm2 valve area; maximal systolic gradient of 138 mmHg, mean gradient of 83 mmHg; the relationship between the velocity of the exit path of the left ventricle and the aortic valve was of 0.14 (severe stenosis when <0,25); there was discrete pericardial stroke.
The patient received transfusion of red cell concentrate.High digestive endoscopy (3/11/2011) revealed mild antral
gastritis and erosive duodenitis.Cardiac catheterization and cinecoronariography
(7/11/2011) showed severe calcification of the aortic and coronary valves; there was a 70% lesion in the medium third of the right coronary and irregularities in the other coronaries.
The consulted rheumatologist indicated pulse therapy with 1 mg/kg of methylprednisolone for nine days due to probable lupus activity, and, afterwards, 40 mg of daily prednisone were maintained.
The patient was submitted to surgery for aortic valve replacement by bovine pericardial bioprosthesis and myocardial revascularization with right aortocoronary saphenous graft (23/11/2011). At the end of the surgery, she presented with bradycardia and severe hypotension, and needed to use an epicardial pacemaker to revert the picture.
Decreasing doses of vasoactive drugs were necessary to control hypotension, and examinations on the third post-operative day (26/11/2011) showed hemoglobin levels at 7.2 g/dL; hematocrit, 23%; leukocytes, 13,900/mm2, with 92% of neutrophils, 122,000/mm3 of platelets, urea of 71 mg/dL, creatinine of 1.4 mg/dL, sodium of 143 mEq/L, and potassium of 3 mEq/L.
The patient was delusional and with pulmonary congestion. Antibiotic therapy was initiated with tazobactam and piperacillin, and, two days later, vancomycin was added. The symptoms of delirium and pulmonary congestion improved, and she was discharged from cardiac recovery on the seventh post-operative day.
Hemocultures and urocultures were negative (29/11/2011).ECG (30/11/2011) revealed sinus rhythm and inactive
septal area (Figure 2).A new laboratory evaluation (5/12/2011) revealed
hemoglobin levels at 8.8 g/dL; hematocrits, 28%; leukocytes, 9,240/mm3; platelets, 34,800/mm3; urea, 50 mg/dL; creatinine, 2.92 mg/dL; sodium, 139 mEq/L; potassium, 3.6 mEq/L; PCR, 97 mg/L.
e44

Anatomopathological Session
Ribeiro et al.Correlação AnatomoclínicaAnatomoclinical correlation
Arq Bras Cardiol. 2014; 102(5):e44-e51
A new echocardiogram (5/12/2011) revealed aorta of 37 mm, left atrium of 41 mm, right ventricle of 25 mm, septum of 13 mm, left atrium of 41 mm, left ventricle of 53/41, ejection fraction of 35%. There was severe hypertrophy in the left ventricle, apical akinesis of the other walls and atypical movements of the interventricular septum. The prosthesis was normofunctional, with maximal gradient of 19 mmHg and mean gradient of 12 mmHg, and the relationship of velocities of exit path LV/aortic prosthesis was of 0.43.
Uroculture (7/12/2012) was negative.Laboratory examinations (9/12/2011) revealed: hemoglobin
levels at 7.8 g/dL; hematrocrit, 25%; MCV, 100 fL; leukocytes,
9,040/mm3 (bands, 1%; segmented, 76%; lymphocytes, 21%; and monocytes, 2%); platelets, 330,000/mm3; urea, 60 mg/dL; creatinine, 2.48 mg/dL (FG = 22 mL/min/1.73 m2); sodium, 138 mEq/L; potassium, 3.8 mEq/L; PCR, 91.5 mg/L; PT (INR), 1.0; and TTPA rel, 1.11.
The patient was discharged with a prescription for hydralazine, carvedilol, furosemide, prednisone, chloroquine, atorvastatin, ferrous sulfate, folic acid, ASA.
The physical examination at hospital discharge showed serous secretion in the scar from the saphenous vein stripping in the left lower limb.
Figure 1 – Electrocardiogram - Sinus bradycardia, intraventricular conduction disorder and ST-T segment changes.
Figure 2 – Eletrocardiogram - Sinus rhythm, septal inactive area, ST-T segment changes.
e45

Anatomopathological Session
Ribeiro et al.Correlação AnatomoclínicaAnatomoclinical correlation
Arq Bras Cardiol. 2014; 102(5):e44-e51
The patient was readmitted on 20/1/2012 (about one month after hospital discharge) due to an infection in the surgery wound from the saphenous vein stripping. Hemocultures were positive for multi sensitive Enterococcus sp, and the patient received intravenous ampicillin for 14 days.
The transesophageal echocardiogram (24/1/2012) revealed aorta of 35 mm, left atrium of 41mm, right ventricle of 28 mm, septum of 13 mm, posterior wall of 12 mm, left ventricle of 53 mm, and ejection fraction of 35%. The left ventricle was hypertrophic, and presented apical akinesis and diffuse hypokinesis; the aortic prosthesis was normofunctional, with no changes, with maximal gradient of 22 mmHg and mean gradient of 12 mmHg. The other valves were normal.
Thoracic tomography (20/1/2012) did not show signs of mediastinitis, osteomyelitis or pneumonia.
The left lower extremity Doppler was negative for deep vein thrombosis (27/1/2012).
The patient was discharged from the hospital on 3/2/2012, and the lower limb infection was considered as healed, and the wound would be healed by second intention.
The prescribed medications were: 100 mg ASA, 50 mg carvedilol, 100 mg losartan, 25 mg spironolactone, 20 mg atorvastatin, 20 mg omeprazole, 20 mg prednisone, 400 mg hydroxychloroquine, 5 mg folic acid, 120 mg ferrous sulfate per day.
In a doctor’s appointment (28/3/2012), the patient complained of asthenia, and prednisone increased to 60 mg; the administration of ivermectin was added.
Thoracic radiography (in March, 2012) – Figures 3 and 4 – revealed cardiomegaly +++/4+ and free lungs.
The left lower extremity Doppler was negative for deep vein thrombosis (17/4/2012).
Three months later, she came to the emergency room of the hospital in shock, with 40 bpm heart rate and inaudible pressure, so the use of vasoactive amines and orotracheal intubation were necessary for respiratory support.
Laboratory examinations (on May, 8) revealed: erythrocytes, 1,900,000/mm3; blood cell count, 5.8 g/dL; hematocrits, 19%; reticulocyte, 12.1%; MCV, 100 fL; leukocytes, 12,500/mm3 (bands, 15%; segmented, 79%; lymphocytes, 5%; monocytes, 1%); sodium, 139 mEq/L; potassium, 4.5 mEq/L; calcium, 4 mEq/L; ionized calcium, 1.16; magnesium, 1.8 mEq/L; arterial lactate, 14 mg/dL; PT (INR) 1; TTPA (rel) 0.76; ALT, 57 U/L; AST, 26 U/L; gamma-GT, 153 U/L; lactate dehydrogenase, 560 U/L; total bilirubin, 0.35 mg/dL; right bilirubin, 0;10 mg/dL; urine I, normal. Arterial gasometry showed: pH, 7;46; CO2p, 32 mmHg; O2p, 104 mmHg; O2 saturation, 97.5%; bicarbonate, 22.2 mEq/L; and base excess (-) 1.1 mEq/L.ENTRAM FIGURAS 3 E 4
Echocardiogram (8/5/2012) showed aorta of 37 mm, left atrium of 43 mm, septum of 13 mm, posterior wall of 11 mm, left ventricle of 51/39 mm, ejection fraction of 50%, and moderate hypertrophy of the left ventricle and apical akinesis. The aortic graft presented thickened leaflets, minimum central regurgitation, and maximal transvalvular gradient was 58 mm Hg, mean gradient was 39 mm Hg; the other valves were normal.
Some hours later, the patient presented cardiac arrest caused by ventricular fibrillation. After recovery, there were three more cardiac arrests with pulseless electrical activity, which were reversed. Afterwards, there was a new cardiac arrest with irreversible pulseless electrical activity, and the patient passed away (8/5/2012).
Clinical aspectsThe clinical case reports a 51-year old patient with
systemic lupus erythematosus, arterial hypertension and mixed dyslipidemia, who went to the emergency room with fever and in shock.
The systemic lupus erythematosus (SLE) is an autoimmune inflammatory disease, which is characterized by the immune complex deposition in the involved organs, including the heart. Its clinical picture is determined by periods of exacerbations and remission, with variable clinical course and prognosis.
It affects around 20-150 per 100,000 inhabitants, being mostly prevalent among women (8:1) and black people; 65% of the patients present with symptoms between the ages of 16 and 65 years old. In the reported clinical case, there is a patient who first presented the clinical picture with lupus nephritis at the age of 16, which is in accordance with findings in literature1.
Even though kidneys are classically the organs that are mostly affected by SLE, the heart and the heart/lung circulation can also be significantly affected2. This disease can have an impact on the heart by means of several manifestations, which include arrhythmia and conduction disorders, pericardiopathies, myocardiopathies and coronariopathy.
These manifestations can be simultaneous and should be rapidly recognized in order to establish the proper immunosuppression combined with specific cardiology therapy. The clinical recognition of cardiovascular aggression can be difficult due to the common existence of multiple clinical problems in patients with lupus, such as infections and renal insufficiency.
The pathogenesis of the heart disease in systemic lupus erythematosus is not clear yet. The model that is traditionally considered for the pathogenesis of lupus carditis is very similar to that of other sites affected by lupus, so it is believed that the immune complex deposition and the activation of the complement would lead to acute, chronic or recurring inflammation in the vascular endothelium, pericardium, myocardium, endocardium, conduction system and valve leaflets, which can be supported by the common finding of immune complexes, complement and antinuclear antibodies in the affected tissues3.
Pericarditis is the most common cardiac manifestation, which is clinically present in up to 25% of the patients. Series of autopsies and imaging methods demonstrated the pericardial involvement in more than 60% of the patients2. It can occur as an initial manifestation of SLE, or at any point of the course of the disease, as was the case of the mentioned patient, or it can be a complication from chronic kidney disease.
e46

Anatomopathological Session
Ribeiro et al.Correlação AnatomoclínicaAnatomoclinical correlation
Arq Bras Cardiol. 2014; 102(5):e44-e51
Figure 3 – Chest x-ray (postero-anterior view)- Metallic sutures in the sternum, normal lungs and enlarged heart image.
Figure 4 – Chest x-ray (lateral view)- Metallic sutures in the sternum, prosthetic valvar ring.
e47

Anatomopathological Session
Ribeiro et al.Correlação AnatomoclínicaAnatomoclinical correlation
Arq Bras Cardiol. 2014; 102(5):e44-e51
Clinical picture is usually typical, and it can be manifested by fever, tachycardia, substernal pain (which is aggravated by the act of breathing, coughing or bending over), and by the presence of pericardial friction at auscultation; the electrocardiographic evaluation, with peaked T waves and increasing ST segment, usually does not differ from other causes of pericarditis3.
Despite the young age presented by most patients with lupus, atherosclerosis remains as the most common cause of ischemic heart disease. In these patients, it is possible to observe the occurrence of accelerated atherosclerosis associated with the presence of its habitual risk factors, which makes this disease an independent risk factor for the cardiovascular disease, as well as rheumatoid arthritis4.
It presents coronariopathy prevalence of up to 10%, and eight times more chances in relation to the general population4. Some studies suggest that the acute myocardial infarction can be the cause of death in up to 25% of the cases, especially among patients who have had the disease for longer. The risk of this complication can be 52 times higher in relation to the population that is free of disease, when the time of disease evolution is longer than five years4.
In the reported case, the patient presented not only SLE, but also other risk factors that contributed with the development of coronary artery disease: systemic arterial hypertension, smoking and mixed dyslipidemia.
Additional causes of acute coronary syndromes in the SLE include thrombosis – usually correlated to the presence of antiphospholipid antibodies –, embolism resulting from nonbacterial vegetative endocarditis (Liebman-Sacks), and coronary arteritis.
The myocardial dysfunction of SLE is usually multifactorial, and it can result from immunological lesion, ischemia, valve disease or coexisting problems, such as systemic arterial hypertension. The clinically evident acute myocarditis is not common, and it can present itself by the presence of thoracic pain and tachycardia, being disproportional to the presence of fever. Clinical signs and symptoms of cardiac insufficiency are uncommon, being present in only 5-10% of the patients5.
Arrhythmia and conduction disorders can occur in the course of the disease, usually concomitantly to other cardiac manifestations, such as pericarditis, myocarditis and coronary ischemia6.
Sinus tachycardia is the most common manifestation, being present in approximately 50% of the cases7. In this case, the patient presented with sinus bradycardia, with prolonged QT interval of 464 ms. The expected corrected QT interval for that patient would be of less than 415 ms. According to Okin et al8, the presence of this finding can be a predictive of morbidity and mortality.
Valve involvement is common, being demonstrated in transesophageal studies in more than 50% of the patients with LSE9. Valve thickening is the most common echographic finding, followed by vegetation and valve insufficiency. Even though the severity of valve compromise is usually mild and asymptomatic, in this clinical case we observed severe valvular stenosis.
The patient was submitted to myocardial revascularization and valve replacement, in November, 2011, and on the third post-operative day, she presented with a suggestive picture of decompensated heart failure with clinical signs of low cardiac output associated with pulmonary congestion. Clinical measures were taken to compensate the picture, including the use of antibiotics, with clinical progress.
The main differential diagnoses for the clinical picture of the patient were infectious process, myocardial ischemia and lupus myocarditis.
The hypothesis of infection should be considered because the patient was in the post-operative period and had SLE, cardiopathy and nephropathy, and such conditions made her more prone to infections. The absence of fever and negative cultures made this diagnosis less likely.
Another diagnostic hypothesis to be considered in this context is coronary ischemia, since the patient had already had a previous coronary disease. Besides, the electrocardiogram and the echocardiogram presented new segmental changes, septal inactive area, and septal akinesis, respectively. In this case, thromboembolic ischemic events and/or coronary arteritis cannot be ruled out.
It is usually difficult to tell coronary arteritis from accelerated atherosclerosis. In cinecoronariography, arteritis is suggested when we find coronary aneurysms, focal lesions or ones that develop rapidly, which could have been the case of the patient assessed in this clinical case10.
Based on the presented case, the factor that apparently triggered the clinical picture of the patient was lupus myocarditis, since the patient presented with new ventricular systolic dysfunction. The improved ventricular function shown in the echocardiogram conducted in May, 2012, seemed to corroborate this diagnosis, after the immunosuppressive therapy began, in the appointment of March, 2012.
The diagnosis of lupus myocarditis is usually difficult, since it normally progresses to mild and little symptomatic myocardial dysfunction, and mainly due to the concomitance of other factors that are potentially responsible for myocardial damage, such as ischemia, anemia, and secondary water retention to renal disease or to the use of corticosteroids.
On 8/5/2012, the patient was in shock and presented with bradycardia. Clinical measures to compensate the clinical picture were initiated, including the use of vasoactive amines and respiratory support. However, the patient had clinical worsening and cardiorespiratory arrest on this same day.
The main differential diagnoses for the final clinical picture were cardiogenic shock, hypovolemic shock and septic shock, to be discussed afterwards.
The hypothesis of cardiogenic shock caused by myocardial ischemia should be considered. This diagnosis is less likely because, in the echocardiogram conducted in May, 2012, no segmental changes were observed. In fact, it was possible to observe improvements in ventricular function, in relation to the echocardiogram performed in January, 2012. This improved cardiac performance can be attributed to the optimized treatment of lupus cardiomyopathy.
e48

Anatomopathological Session
Ribeiro et al.Correlação AnatomoclínicaAnatomoclinical correlation
Arq Bras Cardiol. 2014; 102(5):e44-e51
This echocardiogram also detected moderate aortic stenosis. Some level of valve dysfunction could also be present in the immediate post-operative period, as a result of the sub-stenosing graft implanted in a patient with a small caliber aorta, which, in this patient, was masked by the moderate ventricular dysfunction that occurred in the post-operative period. Another factor that could justify aortic stenosis would be a thrombotic process, especially if the patient had antiphospholipid antibodies and not under full anticoagulation. Another hypothesis is the one of hypovolemic shock due to hemorrhage. Even though the patient did not present exteriorization of bleeding, we observed important decrease in hemoglobin levels (from 7.8 to 5.8). The high levels of reticulocytes associated with low levels of bilirubin makes the peripheral destruction of erythrocytes less likely as a causative factor for this anemia.
For the presented case, the factor that apparently was the main trigger of the final clinical picture of this patient was infectious, which is corroborated by the increasing count of young neutrophils and by the reported fever, which was mentioned in the beginning of the clinical case.
Among all possible focuses for this septic scenario, we cannot rule out the hypothesis of acute infective endocarditis. Infective endocarditis is the infectious process of the cardiac endothelium, which can affect any cardiac structure: septal defects, tendinous cords, mural endocardium and intracavitary and arteriovenous shunts. However, these are the most commonly involved cardiac valves, especially the mitral (40%) and the aortic valve (34%)11.
Currently, for the diagnosis, modified Duke criteria are used, which are based on clinical, laboratory and echocardiographic findings11. The transesophageal echocardiogram became the method of choice to visualize vegetation, especially at the presence of degenerated and calcified valves or mechanical prosthesis. Therefore, in the patient of this clinical case, the absence of vegetation at the transthoracic echocardiogram does not rule out that diagnosis.
In spite of the advancements in clinical diagnosis, of the advent of new antibiotics and the improvement of surgical techniques, bacterial endocarditis still presents high morbimortality, and its prognosis depends on the etiological agent and on cardiac status before the infectious picture12 (Dr. Wilma Noia Ribeiro, Dr. Alice Tatsuko Yamada).
Diagnostic hypothesesSyndromic diagnosis: congestive heart failure; etiology:
lúpus cardiomyopathy; final event: septic shock (Dr. Wilma Noia Ribeiro, Dr. Alice Tatsuko Yamada).
NecropsyThe patient had two diseases: atherosclerosis and lupus
erythematosus.Atherosclerosis was mild in the aorta, moderate in the
branches of the left coronary, and reaching 70% levels of obstruction in the right coronary artery, therefore being submitted to revascularization with saphenous vein interposition graft. At necropsy, the graft was obstructed in the ostium and fibrosed, which means the premature closure after surgery. In spite of that, there was no significant myocardial ischemia injury, only areas of non-abundant myocardial sclerosis, compatible with what usually occurs at the presence of myocardial hypertrophy due to ay cause.
The lupus diagnosis is based on clinical and laboratory data. Under the morphological focus, several aspects can be attributed to the disease, and there is nothing characteristic enough to allow the diagnosis. Therefore, the surgically replaced valve had non-specific chronic valvulitis (Figure 5), which could also have had another cause, such as rheumatic disease, for example.
Necropsy showed the existence of bacterial endocarditis, caused by Gram-positive cocci that affected the aortic valve prosthesis and the ring around it (Figures 6 and 7), as well as abundant abdominal bleeding, which was the final responsible for the death of the patient.
In other organs, the most relevant finding was segmental and focal glomerulopathy (Dr. Paulo Sampaio Gutierrez).
Main disease: bacterial endocarditis in biological aortic valve prosthesis. Baseline disease: systemic lupus erythematosus with aortic valvulopathy and arterial hypertension. Secondary disease: coronary atherosclerosis. Causa mortis: abdominal hemorrhage (Dr. Paulo Sampaio Gutierrez).
CommentThe cause of hemorrhage was not determined: nothing
was found in the arterial territory that is normally examined during necropsies; possibly, there could be a downstream lesion, in the circulatory tree. By considering the existence of endocarditis, the main possibility is the occurrence of secondary arteritis (mycotic aneurysm). Another possibility is that the vascular lesion could be iatrogenic, since a catheter passed through that region, but at hospital admission the patient presented aggravation of previous anemia and certain level of abdominal distension.
Segmental and focal glomerulopathy are usually a result of immune complex deposition; in this case, it can be a consequence both of lupus and endocarditis.
Even with necropsy, it was not clear why the patient presented worsened cardiac function after surgery.
e49

Anatomopathological Session
Ribeiro et al.Correlação AnatomoclínicaAnatomoclinical correlation
Arq Bras Cardiol. 2014; 102(5):e44-e51
Figure 5 – Histological cut of native aortic valve removed in surgery. It is possible to observe non-specific chronic valvulitis with calcification points. Hematoxylin and eosin staining method; 5x objective lens.
Figure 6 – Left ventricular outflow tract and aortic root with aortic valve prosthesis of biological material partially detached. It is possible to observe the presence of inflammatory tissue, both in the prosthesis (blue arrow) and in the ring around it (red arrow). It is also possible to see the occlusion in the ostium of the right aortocoronary saphenous graft (white arrow).
e50

Anatomopathological Session
Ribeiro et al.Correlação AnatomoclínicaAnatomoclinical correlation
1. Shur PH, Hahn BH. Epidemiology and pathogenesis ofsystemic lupus erythematosus. Up to date. [Internet] 2010 Jun 16. [Acessao do em 2010 out 25/10/.]. Disponível em: http://www.uptodate.com
2. Doria A, Iaccarino L, Sarzi-Puttini P, Atzeni F, Turriel 3. M, Petri M. Cardiac involvement in systemic lupus erythematosus. Lupus. 2005; 14(9):683-6.
3. Falcão CA, Lucena N, lves IC, Pessoa AL, Godoi ET. Cardite lúpica. Arq Bras Cardiol. 2000; 74(1):55-63.
4. Simão AF, Precoma DB, Andrade JP, Correa Filho H, Saraiva JF, Oliveira GM, et al; Sociedade Brasileira de Cardiologia. I Diretriz brasileira de prevenção cardiovascular. Arq Bras Cardiol. 2013;101(6 supl 2):1-52.
5. Law WG, Thong BY, Lian TY, Kong KO, Chng HH. 5. Acute lupus myocarditis: clinical features and outcome of an oriental case series. Lupus. 2005; 14(10):827-31.
6. Cardoso CR, Sales MA, Papi JA, Salles GF. QT-interval parameters are increased in systemic lupus erythematosus patients. Lupus. 2005; 14(10):846-52.
7. Hejtmancik MR, Wright JC, Quint R, Jennings FL. The cardiovascular manifestations of systemic lupus erythematosus. Am Heart J. 1964; 68:119-30.
8. Okin PM, Devereux RB, Howard BV, Fabsitz RR, Lee ET, Welty TK. Assessment of QT interval and QT dispersion for prediction of all-cause and cardiovascular mortality in American Indians: The Strong Heart Study. Circulation. 2000; 101(1):61-6.
9. Roldan CA, Crawford MH. Connective tissue diseases and the heart. In: Crawford MH (ed). Current diagnosis & treatment in cardiology. Rio de Janeiro: Prentice Hall do Brasil; 1995. p. 428-47.
10. Petri M. Cardiovascular systemic lupus erythematosus, systemic lupus erythematosus. In: Lahita RG (ed). Systemic lupus erithematosus. Amsterdam: Elsevier Academic Press; 2004. p. 913-42.Elsevier. 2004; ..
11. Anguera IJM, Cabell CH, Chen AY, Stafford JA, Corey GR, et al; International Collaboration on Endocarditis Merged Database Study Group. Staphylococcus aureus native valve infective endocarditis: report of 566 episodes from the International Collaboration on Endocarditis Merged Database. Clin Infect Dis. 2005; 41(4):507-14.
12. Mansur AJ, Grinberg M, Galluci SD, Bellotti G, Jatene A, Pileggi F. Infective endocarditis: analysis of 300 episodes. Arq Bras Cardiol. 1990;54(1):13-21.
References
Arq Bras Cardiol. 2014; 102(5):e44-e51
Figure 7 – Panel of histological cuts of the aortic valve ring (A and B) and of the vegetation in the aortic prosthesis (C and D), both with bacterial endocarditis. In A and C, little enlargement (objective magnification: 5x), with general view of the inflammatory process, including fibrin deposition (F). In B, more enlargement (objective enlargement: 20x), showing inflammatory infiltrate with prevalence of polymorphonuclear neutrophils. D, staining showing, in purple, the presence of Gram-positive cocci (Brown and Hopps stain, objective magnification: 40x). A, B and C: hematoxylin and eosin staining method.
e51

Case Report
Prolonged Cardiopulmonary Arrest Treated Successfully in the São Paulo’s SubwayRenan Gianotto-Oliveira, Maria Helena Favarato, Maria Margarita Gonzalez, Thiago Liguori, Sergio Timerman, Roberto Kalil FilhoInstituto do Coração - Hospital das Clínicas - Faculdade de Medicina - Universidade de São Paulo, São Paulo, SP - Brazil
Mailing Address: Renan Gianotto-Oliveira •Laboratório de Simulação em Emerg. Cardiovasculares (LTSEC) - Av. Dr. Enéas de Carvalho Aguiar, 44 - 2º andar, Postal Code 05403-900, São Paulo, SP - BrazilE-mail: [email protected] received June 02, 2013; revised manuscript August 20, 2013; accepted August 20, 2013.
KeywordsOut-of-Hospital Cardiac Arrest; Ventricular Fibrillation;
Cardiopulmonary Resuscitation; Heart Massage; Electric Countershock.
DOI: 10.5935/abc.20140058
IntroductionIn Brazi l , c i rculatory diseases, including CPA
(Cardiopulmonary Arrests), were the leading cause of death in 20101. Estimates are that, in Brazil, around 220,000 CPAs happen every year, including ventricular fibrillation, 180,000 in pre-hospital environment and 40,000 in-hospital2.
Recent observational studies of victims of CPA in extra-hospital environment revealed that only CCC (Continuous Chest Compressions) – hands-only CPR – were equivalent or higher than conventional CPR (Cardiopulmonary Resuscitation) (using a 30:2 ratio of compressions/ventilations) in adult patients, mainly with regard to neurological benefits3-5.
We present a case of PCA occurred in Companhia do Metropolitano de São Paulo (São Paulo’s Subway) attended by lay rescuers who performed CCC and applied shocks by means of AED (Automatic External Defibrillator).
Case ReportMan, 55, Japanese origin, trader, with a history of
hypertension. He was in one of the São Paulo’s Subway stations when he felt sharp and constant pain in chest, accompanied by dizziness and progressing to loss of consciousness. The users triggered the subway employees (laypersons trained in CPR) who identified the CPA and started to assist him. They requested the AED and started applying CCC immediately. In two minutes, the AED was in place, with paddles applied to the chest of the victim. The rhythm (ventricular fibrillation) was analyzed and shock was indicated in less than 20 seconds. Chest compressions were immediately resumed and the AED showed four shocks over 8 minutes, all of them followed by CCC. After the fifth shock, the victim was breathing again, though unconscious, and defibrillation was no longer indicated in subsequent analyzes. Assessing the AED reading after the last shock,
the patient evolved into sinus rhythm, which is the reason why no more shocks were indicated (Figure 1). Rescuers alternated at each two minutes of CCC. With the arrival of SAMU (Emergency Mobile Healthcare Service), tracheal intubation, medications and special care were administered.
The victim was sent to a secondary hospital, admitted unconscious in sinus rhythm with a heart rate of 130 bpm, blood pressure of 160 x 100 mmHg, respiratory rate of 16 rpm, and isochoric and reactive pupils, presenting vesicular murmur, flaccid abdomen on palpation and Glasgow of level 6. The acute myocardial infarction was confirmed by ST segment elevation in lower leads and elevation of troponin and CKMB. The patient underwent thrombolytic therapy with streptokinase, under myocardial reperfusion criteria. During hospitalization, he acquired pneumonia associated with mechanical ventilation. He was discharged after 19 days without neurological sequelae. After one year, the patient was asymptomatic, with active life and undergoing outpatient follow-up.
DiscussionThe most common CPA rhythm in extra-hospital environment
is the fibrillation6. The probability of success in resuscitation decreases significantly over time, from 7 to 10% by minute in which defibrillation is delayed6,7. The performance of chest compressions increases the time for effective defibrillation. Needless to say that training laypersons on CPR skills and structuring mobile emergency services is crucial for the approach and, although the response time of emergency services is critical to a successful resuscitation, the laypersons training in CPR and handling of AED boost the success possibilities6-8.
Globally, the percentage of lay witnesses who initiate CPR ranges from 20 to 70%, averaging 50%. The lowest percentages are usually associated with delayed onset of resuscitation and a worse prognosis, whereas the early initiation of chest compressions results in higher number of hospital admissions and up to three times higher hospital discharges with survival6-9.
New international recommendations allow the practice of CPR with CCC, without ventilation, in certain circumstances. This practice has been called cardiocerebral resuscitation4. It indicates that the quick start of CPR and early defibrillation are associated with better neurological prognosis4,7,9.
Based on animal studies, the concept that the addition of ventilations to compressions, made by witnesses, does not increase the survival of ventricular fibrillation or myocardial infarction has been increasingly accepted. Clinical studies in humans have also shown the efficacy of CCC7-9.
e52

Case Report
Gianotto-Oliveira et al.Cardiopulmonary Arrest in the São Paulo’s Subway
Arq Bras Cardiol. 2014; 102(5):e48-e50
Figure 1 - Application of five automated external defibrillator shocks followed by return of sinus rhythm and tachycardia.
Regarding the characteristics of training, CPR only with compressions is associated with greater knowledge retention and greater willingness of laypersons to perform it. Furthermore, regardless of the cause and duration of CPA and the availability of AED on site, CPR with CCC is better than no CPR7-9.
In São Paulo’s Subway, staff is trained at least every two years in resuscitation skills attending a standardized course of AHA (American Heart Association), with practical training on mannequins and handling of AED. During training, only CCC is practiced without pauses for ventilation, according to international guidelines. Systematic training is necessary, as studies show that a larger number of courses and the short time interval between them are predictors for obtaining rapid and early compressions, thus improving the patient’s prognosis. Public awareness programs should also be on the agenda of public policies for reducing mortality from sudden cardiac death6.
Another link in the chain of the survival of out-of-hospital cardiac CPA is the easy access to AED by the rescuer. The early defibrillation, before the arrival of the emergency
service, should be a priority6,10. The early defibrillation with use of AED can improve the prognosis of patients, including higher survival and better neurological between survivors. The use of AED is extremely simple, and a trained layperson can perform the defibrillation procedure with the same fitness and safety of a healthcare professional. Since 1991, AHA has encouraged the provision of easily accessible AEDs in public places, in addition to courses on CPR and on using AED10.
According to large population studies, PAD (Public Access to Defibrillation), putting AEDs at the disposal of laymen trained in its use, has the potential to be the intervention which represents the greatest breakthrough in the treatment of CPA in ventricular fibrillation, since the development of CPR, as it allows the victims to be defibrillated within the first minutes of CPA10. There is evidence that the handling of AEDs, within PAD programs, may double the survival of victims compared to access to SAMU. The early defibrillation provided by PAD is still associated to better neurological prognosis6,10. The Brazilian precedents is gradually evolving to establish that the said devices be mandatory in several places.
e53

Case Report
Gianotto-Oliveira et al.Cardiopulmonary Arrest in the São Paulo’s Subway
Arq Bras Cardiol. 2014; 102(5):e48-e50
1. Ministério da Saúde. Datasus: Indicadores de mortalidade: mortalidade proporcional por grupos de causas. [Acesso em 2012 Jan 22]. Disponível em: http://tabnet.datasus.gov.br/cgi/ tabcgi.exe?idb2010/c04.def
2. Canesin MF, Timerman S, Nazima W. Treinamento em emergências cardiovasculares avançado da Sociedade Brasileira de Cardiologia. Barueri (SP): Manole; 2013.
3. Bohm K, Rosenqvist M, Herlitz J, Hollenberg J, Svensson L. Survival is similar after standard treatment and chest compression only in out-of-hospital bystander cardiopulmonary resuscitation. Circulation. 2007;116(25):2908-12.
4. Kern KB, Timerman S, Gonzalez MM, Ramires JA. Optimized approach in cardiocerebral resuscitation. Arq Bras Cardiol. 2011;96(4):e77-80.
5. Sayre MS, Berg RA, Cave DM, Page RL, Potts J, White RD, et al. Hands-only (compression-only) cardiopulmonary resuscitation: a call to action for bystander response to adults who experience out-of-hospital sudden cardiac arrest: a science advisory for the public from the American Heart Association Emergency Cardiovascular Care Committee. Circulation. 2008;117(16):2162-7.
6. Sasaki M, Iwami T, Kitamura T, Nomoto S, Nishiyama C, Sakai T, et. al. Incidence and outcome of out-of-hospital cardiac arrest with public access defibrillation- a descriptive epidemiological study in a large urban community. Circ J. 2011;75(12):2821-6.
7. Ewy GA, Sanders AB. Alternative approach to improving survival of patients with out-of-hospital primary cardiac arrest. J Am Coll Cardiol. 2013;61(2):113-8.
8. Iwami Y, Kitamura T, Kawamura T, Mitamura H, Nagao K, Takayama M, et. al; Japanese Circulation Society Resuscitation Science Study (JCS-ReSS) Group. Chest compression only cardiopulmonary resuscitation for out-of-hospital cardiac arrest with public-access defibrillation: a nationwide cohort study. Circulation. 2012:126(24):2844-51.
9. Lee K. Cardiopulmonary resuscitation: new concept. Tuberc Respir Dis (Seoul). 2012;72(5):401-8.
10. Atkins DL. Realistic expectations for public access defibrillation programs. Curr Opin Crit Care. 2010;16(3):191-5.
References
In conclusion, as exemplified in this case, the implementation of programs of access to defibrillation, in concert with laypersons’ training in CPR with CCC and in the use of AED actually contributes to reducing mortality and improves the neurological prognosis in out-of-hospital CPA. Programs like this should be mandatory in our country, especially in the coming years, when Brazil will host major events, such as the FIFA World Cup and the Olympics.
Author contributionsConception and design of the research: Gianotto-Oliveira
R, Liguori T; Acquisition of data: Gianotto-Oliveira R, Gonzalez MM; Analysis and interpretation of the data: Favarato MH; Writing of the manuscript: Gianotto-Oliveira R, Favarato
MH, Gonzalez MM; Critical revision of the manuscript for intellectual content: Timerman S, Kalil Filho R.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any thesis or dissertation work.
e54

Viewpoint
Is Heart Team Fundamental to Aortic Stenosis Transcatheter Treatment?Vitor Emer Egypto Rosa, Antônio Sergio de Santis Andrade Lopes, Tarso Augusto Duenhas Accorsi, Pedro Alves Lemos Neto, Pablo Maria Alberto Pomerantzeff, Flávio TarasoutchiInstituto do Coração - InCor – HC FMUSP, São Paulo, SP - Brazil
Mailing Address: Vitor Emer Egypto Rosa •Rua da Cristiano Viana, Cerqueira Cesar. Postal Code 05411-000, São Paulo, SP - BrazilE-mail: [email protected] received October 29, 2013; revised manuscript November 26, 2013; accepted November 27, 2013.
KeywordsAortic valve stenosis / surgery; Patient care team; Heart failure.
DOI: 10.5935/abc.20140060
Demographic projections have shown that the contingent of elderly people in Brazil will double within the next 20 years1, with a consequent increase in the prevalence of aging-related diseases, such as degenerative aortic valve stenosis (AoS), diagnosed in 3% to 5% of the population older than 75 yeas2,3. New modalities of treatment for AoS have been recently developed, mainly represented by the transcatheter implantation of aortic prosthesis (TAVI – Transcatheter Aortic Valve Implantation), which has become a therapeutic option for patients whose conventional surgical treatment is not feasible. In the current scenario, characterized by the high demand of the increasing elderly population, the availability of new treatment methods provides clinical expertise for the accurate diagnosis of heart valve disease, assessment of the comorbidities and risks of interventions, in addition to the rationalization of resources, considering the complexity and high costs involved in TAVI.
Clinical practice has shown that the adequate selection of the best therapeutic method for high surgical-risk AoS requires multidisciplinary medical interaction, contemplating all the patients’ biopsychosocial characteristics. Thus, several medical centers have continuously incorporated the ‘Heart Team’ concept for decision-making. The Heart Team, a group composed by different specialists involved in managing heart valve disease, gathers opinions for the individualized analysis of those patients, from eligibility criteria and technical adequacy of the procedure to post-TAVI care. Each cardiological sub-specialty also plays particular roles in the procedure performance. The clinical cardiologist is responsible for patients’ selection and indication and for pre-and post-procedure follow-up. The cardiovascular surgeon is responsible for performing the transaortic and transapical procedure, helping with the transfemoral approach, and treating possible complications. The radiologist is responsible for assessing the access path and valve diameters, and helping choosing the adequate prosthesis. The echocardiographer is responsible for the anatomical and functional characterization of the valve disease and intraoperative assessment of the adequate position of the prosthesis and post-procedure complications. The interventional cardiologist is responsible
for indicating the procedure and performing it. In addition, the Heart Team also comprises other professionals, such as nurses, physical therapists, nutritionists, and psychologists. Worldwide, there is an increasing incorporation of the Heart Team into cardiological centers, in accordance with the considerations of the last guidelines on heart valve diseases4,5. There is consensus about not encouraging the performance of TAVI at sites lacking a Heart Team, which emphasizes the importance of institutional alignment with the new recommendations.
So far, TAVI indications have been restricted to subgroups of patients with AoS considered inoperable or at high surgical risk, supported by the results of the Placement of Aortic Transcatheter Valves (PARTNER) trial (cohorts B and A, respectively)6,7. In cohort B, published in 2010, patients with inoperable AoS were randomized to either TAVI or standard treatment (clinical or balloon-catheter valvuloplasty), and a surprising 20% reduction in mortality in one year was observed6. It is worth noting that few medical interventions assessed in randomized studies have yielded similar results. Cohort A, a non-inferiority study, however, has compared TAVI with the surgical aortic valve replacement in patients at high surgical risk, and has shown similar one-year survival rates7. In that study, the preoperative risk has been established by use of the Society for Thoracic Surgeons (STS) score8. However, on daily practice the use of scores for high-risk patients has been criticized, because they have not been developed on populations submitted to TAVI, in addition to the exclusion of the clinical variables that could significantly increase morbidity and mortality. Of the risk variables for the elderly, frailty, characterized as a weakened physiological reserve9, still represents a challenge in preoperative assessment, despite its high prevalence (one third of patients older than 80 years) and impact on postoperative morbidity10. To define and standardize a phenotype of frailty, Fried et al9 have developed a score using data from the Cardiovascular Health Study (CHS) with 5,317 patients older than 65 years, and have assessed the following items: unintentional weight loss; self-reported exhaustion; weakness; slow walking speed; and low physical activity. Individuals meeting at least three of those criteria were considered frail, being at higher risk for postoperative complications, including mortality10. However, scores should be used as aiding tools (second opinion) to clinical impression rather than absolute classification tools (mathematization of Medicine)11. It is worth noting that hematological changes, advanced liver and lung diseases, malnourishment, aortic calcification grade, difficult surgical approach, and surgical experience/volume of the center are characteristics rarely included in risk scores and known to have a large impact on the increase of surgical risks.
e55

Viewpoint
Rosa et al.The Heart Team Importance
Arq Bras Cardiol. 2014; 102(5):e51-e52
1. Instituto Brasileiro de Geografia e Estatística (IBGE). [Internet]. Acesso em em 2013 Out 22]. Disponível em: http://www.ibge.gov.br/home/
2. Lindroos M, Kupari M, Heikkila J, Tilvis R. Prevalence of aortic valve abnormalities in the elderly: an echocardiographic study of a random population sample. J Am Coll Cardiol. 1993;21(5):1220-5.
3. Freeman RV, Otto CM. Spectrum of calcific aortic valve disease: pathogenesis, disease progression, and treatment strategies. Circulation. 2005;111(24):3316-26.
4. Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012;33(19):2451-96.
5. Holmes Jr DR, Mack MJ. Transcatheter valve therapy: a professional society overview from the American College of Cardiology Foundation and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;58(4):445-55.
6. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who can not undergo surgery. N Engl J Med. 2010;363(17):1597-607.
7. Kodali SK, Williams MR, Smith CR, Svensson LG, Webb JG, Makkar RR, et al. Two-year outcomes after transcatheter or surgical aortic-valve replacement. N Engl J Med. 2012;366(18):1686-95.
8. O’Brien SM, Shahian DM, Filardo G, Ferraris VA, Haan CK, Rich JB, et al; Society of Thoracic Surgeons Quality Measurement Task Force. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 2--isolated valve surgery. Ann Thorac Surg. 2009;88(1 Suppl):S23-42.
9. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146-56.
10. Ahmed N, Mandel R, Fain MJ. Frailty: an emerging geriatric syndrome. Am J Med. 2007;120(9):748-53.
11. Van Mieghem NM, Serruys PW. The art of risk stratification in TAVI. Eur Heart J. 2013;34(25):1859-61.
12. Nashef SA, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR, et al; EuroSCORE II. Eur J Cardiothorac Surg. 2012;41(4):734-44.
13. Wenaweser P, Stortecky S, Schwander S, Heg D, Huber C, Pilgrim T, et al. Clinical outcomes of Patients with estimated low or intermediate surgical risk undergoing transcatheter. Aortic valve implantation. Eur Heart J. 2013;34(25):1894-905.
14. Tarasoutchi F, Montera MW, Grinberg M, Barbosa MR, Piñeiro DJ, Sánchez CR, et al. Diretriz Brasileira de Valvopatias - SBC 2011 / I Diretriz Interamericana de Valvopatias - SIAC 2011. Arq Bras Cardiol. 2011;97(5 supl. 1):1-67.
References
The increasing experience with the use of TAVI has made it safer and has encouraged widening its indications also for patients with AoS at intermediate surgical risk, classified according to the EuroSCORE II12 and STS score8, in addition to those with dysfunctional aortic bioprosthesis (valve-in-valve). However, in most cases, those patients had other variables not contemplated in those scores, which added risk to surgery or even contraindicated it13. Ignoring the durability of the prosthesis and the possible benefit of surgical valve replacement makes the TAVI indication to that group exceptional. Therefore, the results of large ongoing randomized trials, such as the SURTAVI and PARTNER 2, are awaited to extend TAVI indication for those patients. Currently, the 2011 Brazilian and Inter-American Guidelines on Valve Diseases14, one of the first to consider TAVI as a therapeutic option for AoS, consider that procedure only to patients to whom conventional aortic prosthesis implantation is contraindicated.
In conclusion, symptomatic patients with important AoS have complex cardiac disease, which is life-threatening in the short run, in addition to frequent multiple comorbidities. Approximately 30% of those patients are not eligible for conventional cardiac surgery, due to their prohibitive surgical risk. For that subgroup of patients to benefit from a possible TAVI, careful assessment should precede decision-making.
That scenario is compounded by the scarcity of scientific data definitively guiding that question and the high heterogeneity of patients. Thus, the Heart Team undoubtedly benefits the management of those patients. So far, the message is “there is no TAVI if there is no Heart Team”4,11,13.
Author contributionsConception and design of the research, Writing of the
manuscript and Critical revision of the manuscript for intellectual content: Rosa VEE, Lopes ASSA, Accorsi TADA, Lemos Neto PA, Pomerantzeff PMA, Tarasoutchi F.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any thesis or dissertation work.
e56