Embed Size (px)
Citation preview

7
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
DEBATE DEBATE
An ecosystem approach to health and itsapplications to tropical and emerging diseases
Uma abordagem ecossistêmica à saúde e suasaplicações às doenças tropicais e emergentes
1 Department of PopulationMedicine and Network for Ecosystem Sustainabilityand Health, University of Guelph.Guelph, Ontario,Canada N1G 2W1
David Waltner-Toews 1
Abstract Disease and health outcomes occur within a complex socio-ecological context charac-terized by feedback loops across space and time, self-organization, holarchies, and suddenchanges in organization when thresholds are reached. Disease control programs, even if they aresuccessful, may undermine health; conversely, programs in agriculture and economic develop-ment designed to improve health may simply alter disease patterns. A research and developmentstrategy to promote sustainable health must therefore incorporate multiple scales, multiple per-spectives, and high degrees of uncertainty. The ecosystem approach developed by researchers inthe Great Lakes Basin meets these criteria. This has implications for community involvement inresearch, development policies, and for understanding and controlling tropical and emergingdiseases. Even if unsuccessful in achieving specific outcome targets, however, the requirements ofthis approach for open and democratic communication, negotiation, and ecological awarenessmake its implementation worthwhile.Key words Ecosystem; Tropical Medicine; Public Health; Health
Resumo As manifestações de doença e de saúde ocorrem em contexto socioecológico complexo,caracterizado tanto por circuitos de retroalimentação, que atravessam o espaço e o tempo, quan-to pela auto-organização, holarquias e mudanças bruscas ao nível da organização ao atingir-secertos limiares. Mesmo programas de controle de doenças bem sucedidos podem prejudicar asaúde; inversamente, programas agrícolas e de desenvolvimento econômico projetados para me-lhorar a saúde podem alterar os perfis das doenças. Assim, uma estratégia de pesquisa e desen-volvimento voltada à promoção sustentável da saúde deve incorporar múltiplas escalas e pers-pectivas e elevados graus de incerteza. A abordagem ecossistêmica desenvolvida por pesquisado-res na Bacia dos Grandes Lagos satisfaz tais critérios, com implicações importantes para a parti-cipação comunitária em pesquisa e políticas de desenvolvimento, bem como para a compreen-são e controle de doenças tropicais e emergentes. Ainda quando a abordagem ecossistêmica nãoobtém êxito quanto a metas específicas, exigências de comunicação aberta e democrática, nego-ciação e consciência ecológica justificam sua implementação.Palavras-chave Ecossistema; Medicina Tropical; Saúde Pública; Saúde

Introduction
For several decades after World War II, manyparts of the world undertook committed effortsto eradicate diseases through applied biomed-ical sciences and promote health through pub-lic programs fostering social and economic eq-uity. Both efforts seemed to be successful.Then, in the closing years of the twentieth cen-tury, the efforts to promote health were largelyabandoned in favor of increasing economicactivity per se, at the cost of rapidly rising in-come disparities within and between countries(UNDP, 1999). At the same time, infectious dis-eases once thought to be all but eradicatedhave begun to reemerge as serious problemsthroughout the world (Lederberg et al., 1992;Waltner-Toews, 1995). All of this is occurring ina context of global environmental change oc-curring at speeds and a scale unprecedented inrecent human history. This would appear to bea good time to reconsider how we think abouthuman diseases, health, and their ecologicaland social contexts.
What is health?
Good health, according to the preamble of theWorld Health Organization, is “... a state ofcomplete physical, mental, and social well-be-ing and not merely the absence of disease or in-firmity.” This is clearly a utopian definition, aheaven-on-earth which humanity may wellstrive for, but never – except in rare momentsperhaps when good wine and good friendsconspire together – achieve. MicrobiologistRene Dubos, as an antidote to this utopianism,suggested that good health was simply a“modus vivendi enabling imperfect [people] toachieve a rewarding and not too painful exis-tence while they cope with an imperfect world”(Last, 1988:57). A Dictionary of Epidemiology(Last, 1988:57) also proposes a more pedestri-an, but perhaps more workable, definition ofhealth as: “A state characterized by anatomical,physiological, and psychological integrity, abili-ty to perform personally valued family, work,and community roles; ability to deal with phys-ical, biological, psychological, and social stress;a feeling of well-being; and freedom from therisk of disease and untimely death.”
In general, definitions of the health of plants,animals, people, communities, and ecosystemsinclude some notion of current balance andharmony and some notion of reserve (Waltner-Toews & Wall, 1997) or capacity to respond andadapt to a changing environment (Constanza
WALTNER-TOEWS, D.8
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
et al., 1992). Furthermore, health is directly re-lated to the achievement of desirable and fea-sible goals, and disease is but one constraint onachieving those goals. Thus the achievement ofhealth is a social activity within biophysicalconstraints, rather than a biomedical activitywithin social constraints. Furthermore, thosewho possess the skills required to prevent andtreat disease – analysis, diagnosis, treatment,professional authority – are ill-equipped topromote health. Disease prevention and con-trol programs, in fact, may actually create ill-health. If nothing else, an ecosystem approachto health makes this transparent.
Why do we need approaches to improving or achieving health?
Despite the disclaimer of health being “notmerely the absence of disease” in the WHO defi-nition, nearly all efforts to improve humanhealth in the past century have been aimed atridding the world of various diseases. Indeed,those accomplishments are so remarkable thatone might ask, given the obvious benefits offreedom from smallpox, measles, and polio,why one would even bother to discuss alterna-tives to disease control. Why not simply throwout our vague and luxurious notions of “com-plete physical, social, and mental well-being”and simply redefine health as “absence fromdisease or pathology”? Based on the concept ofhealth as the capacity to achieve culturally de-fined goals, and on the failures of the biomed-ical model, I would like to suggest that thereare sound practical and theoretical reasons fornot doing this.
First, many disease-control programs areno longer effective. The rising tide, globally, ofmulti-resistant organisms and pesticide-resis-tant insect vectors is the direct, unintended re-sult of therapies we use to control or elimi-nate them. One short-term response to these“counter-attacks” is simply more of the same –more vaccines, more drugs, more pesticides –as has been proposed by the Institute of Medi-cine in the United States. In some ways, this islike responding to successful guerrilla warfareby proposing bigger conventional armies andweapons. I suggest that it is time to ponder thewisdom of our bio-military metaphors and lin-ear causal thinking, to address the flaws in rea-soning and tactics we have employed to date,and to use our much vaunted intelligence as aspecies to find more creative solutions.
Second, success in programs which mani-festly promote health in some dimensions –

AN ECOSYSTEM APPROACH TO HEALTH 9
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
such as improvements in agriculture to addressfood shortage – have had unintended negativeeffects on other aspects of health, such as dis-ease. Simple talk of creating “supportive envi-ronments for health” is characterized by theoptimism of a race horse with blinders. Watermanagement programs have had particularlydevastating effects by favoring several tropicaldiseases. Dams are built to generate electricalpower, to control flooding, and to generatewealth (all of which are demonstrably support-ive of health). Nevertheless they also expand orcreate new habitat for flora and fauna whichcause disease, and remove sources of naturalrenewal from farmland (Hunter et al., 1982). InBangladesh, epidemic Kala azar (leishmania-sis) has occurred in populations living withinflood control embankments (Minkin et al.,1996), and malaria epidemics, mad cow dis-ease, and cyclosporiasis have all been associat-ed with aggressive agricultural programs (Walt-ner-Toews, 1999).
More specifically, this cross-sectoral blind-ness means that control of some diseasesthrough, say, environmental restructuring,leads to the emergence of other diseases. Thisis most obvious in foodborne diseases, wherethe industrialization and centralization, whichquite naturally accompanied regulations oncanning and pasteurization to control botu-lism and brucellosis, have resulted in the cre-ation of large ecological niches and associatedlarge-scale epidemics of diseases such as sal-monellosis. In North America, policies andpractices which encourage a voluminous andcheap supply of food, and which on the onehand serve as a preventive against starvation,tend on the other hand to undercut the eco-nomic and ecological sustainability of farmersand to create a whole new array of nutritionaland disease problems associated with obesity.
Disease control programs themselves canalso undermine health in at least two ways.They can disrupt ecological systems whichmake health possible. Thus we are faced withthe dilemma that DDT is useful in bringingmalaria under control, but at the same timeendangers the integrity of the interactionsamong insect pollinators, birds, and food pro-duction which make sustainable livelihoods,and health, possible. Secondly, and less obvi-ously, food supplementation, vaccination, anddrug treatment programs based on a biomed-ical model can undermine the ability of peopleto adapt resourcefully to their own environ-ments. They do this by reinforcing the notionthat it is appropriate for outside experts to de-termine which outcomes – among many possi-
ble competing ones – are appropriate, whichresponses are “correct”, and who should carrythem out. Physicians and veterinarians whoare well equipped to diagnose and treat are ingeneral very poorly trained to promote health,which requires negotiation and adaptation.
Current health and disease control pro-grams often work against each other across or-ganizational scales. Drawing inferences aboutpopulations based on studies of individuals istermed the atomistic fallacy, and is widespreadand widely tolerated in epidemiological stud-ies. Ironically, the converse fallacy – drawinginferences about individuals from populationstudies – is vigorously guarded against. Whatthis means is that all efforts are focused onfinding individual determinants of disease, andthe broad systemic conditions – the very condi-tions which determine whether or not healthyhuman communities are sustainable – arelargely, by design, ignored. Thus we have theabsurdity of governments in some industrial-ized countries giving away groundwater to pri-vate companies, who then wrap it in plasticand sell it back to the original owners of thewater (the citizens of the country) under thepretense that this is good for their individualhealth. Even if the water in the bottle could bedemonstrated to be superior to tap water(which it is not) it would still have major nega-tive consequences for population health be-cause of the energy and resources required formanufacture and disposal of the bottles.
Problems are solved at an individual levelbut become major problems at a regional orglobal level. Thus, saving children through vac-cination without concomitant programs in ed-ucation, nutrition, agriculture, and sustainablelivelihoods undermines the health of wholecommunities and condemns them to slow andpainful death and disintegration (McMichael,1993). Indeed, the tension between sustain-able population health, which requires a cer-tain death and replacement rate, and individ-ual health, for which death is the ultimate neg-ative outcome, has no solution within currentbiomedical models (Waltner-Toews, 2000). Theidea that death and maybe even disease mightin some sense be important for sustainablehealth cannot even be conceptualized in a nor-mal biomedical framework.
Finally, current disciplinary-bound ap-proaches to health, which focus on biomedicaland personal behavioral issues, inhibit healthresearchers and workers from addressing thereal causes – which reflect irreducible interac-tions among economics, politics, and ecosys-tems. This is addressed more fully in a later

WALTNER-TOEWS, D.10
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
section of this paper on emerging infectiousdiseases.
The practical problems, contradictions, anddilemmas that have arisen in our quest for lessdisease and better human health do not simplyreflect lack of investment in public health andscientific infrastructure: sewers, water sup-plies, laboratories, vaccines. These are all im-portant. However, this dis-investment in thepublic good, widespread under conditions ofglobalization, is itself a product of a lack of ap-preciation of the nature and complexity of theproblems we are addressing.
The theoretical basis for a new approach to health
The world we live in can be described as whatRussell Ackoff has called “a mess”, that is, “in-teracting problems or issues that are not easy toappreciate as a whole” (Flood & Carson, 1993:11). Furthermore, it is clear that the complexitywe see in the world around us is not only aproperty of the world we are studying, but alsoa property of the interaction between ourselvesand the world. Normal, conventional scienceassumes an objective, external observer. Forpublic health and ecological issues, where peo-ple – researchers and subjects alike – are inter-nal to the subject being studied, this assump-tion is untenable.
Causal models used by epidemiologists andbiomedical researchers tend to be linear: spe-cific disease outcomes are defined and studiesare designed to identify determinants of thoseoutcomes. In all but a few rare occasions, epi-demiological studies focus on determinants ofdisease in individuals. Models of disease canrarely accommodate the disease outcome itselfas a cause of other outcomes which themselvesconnect back to the disease, or to other dis-eases or health measures. For instance, we havetended to assume that if scientists identifysmoking as a cause of cancer, or tick bites asthe vehicle for infection by a parasite, then thepublic health and behavioral changes neces-sary to prevent these diseases will be madepost haste by an informed public. Cross-scaleinteractions between individual health anddisease outcomes, agricultural and economicpolicies, social expectations created and rein-forced by advertising and entertainment, cul-tural habits of scientists and non-scientists,evolutionary ecology, and epidemic diseasesare rarely studied.
Based on the problems identified above,any new approach to studying and promoting
health must at least encompass multiple eco-logical, social, and health outcomes, and “notjust the absence of disease”. These multipleoutcomes need to be expressed in a context ofa set of interactions, with people inside them,rather than looking at the environment as anexternal “support” or “threat” to health. Sec-ondly, to be adequate to the new tasks facingus, any new theory and plan of action must ac-count for problems of scale and inter-scalarconnections.
Systems theory explicitly addresses theconnections between various elements, andthus provides a useful starting point. A systemis simply a set of elements which interact witheach other within a certain boundary. Manyattempts have been made to reduce people,farms, households, or ecosystems to well-de-fined, machine-like systems which can be sim-ulated mathematically. While such models pro-vide some useful information, those which arethe least realistic tend to provide the strongestimplications for action, while those that are themost realistic provide understanding but sug-gest no obvious solution to the problems beingstudied. Puccia & Levins (1985) suggest thatthere are unavoidable trade-offs in systemsmodeling between generality, realism, and pre-cision. “No model”, they state, “can be general,precise, and realistic”(Puccia & Levins, 1985: 9).
In the face of this intransigence of the messwe are in, some scholars retreat to the detailsof reductionism, with the assurance that if theyare not helping the situation, they may at leastbe supplying data which might be useful. How-ever, the systems literature itself seems to pre-sent us with a kind of post-modern smorgas-bord of systems ideas, ranging from chaos andcatastrophe to soft, dynamic, complex, andecosystems. Some authors (Funtowicz & Ravetz,1994) argue that the interactions between peo-ple and ecosystems reflect an “emergent com-plexity”, which cannot be captured by even ourmost sophisticated complex systems models.This may be true, and should engender humili-ty into all our actions, but does not provide avery useful guide for action itself.
SOHO systems
Among the options available in the new sys-tems smorgasbord is a set of ideas which bringstogether conventional, soft, complex, chaotic,management, participatory, and ecosystems.These ideas, subsumed under an umbrella of“the ecosystem approach”, are based on theview that the mess we live in can be usefully

AN ECOSYSTEM APPROACH TO HEALTH 11
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
understood as self-organizing, holarchic, open(SOHO) systems (Kay et al., 1999).
Holarchy
A SOHO system is characterized by patterns ofinteraction occurring in nested hierarchies(sometimes called holarchies: Checkland & Sc-holes, 1990; Allen & Hoekstra, 1992). Unlike say,a military hierarchy, in which there is a chainof authority, each unit (holon) in a holarchy isboth a whole thing and a part of somethinglarger. For instance, individual people are partsof families, which are parts of neighborhoodsor villages, which in turn make up larger com-munities and so on. This means that an initia-tive, such as improving public hygiene, takenat any given scale (for instance the neighbor-hood) has implications for holons of which it isa part (the city) as well as the holons of which itis comprised (individuals and families). Thespeed of change at one scale (say introductionof genetically engineered crops at a field scale)may disrupt ecological and social systems ofwhich they are a part, and which have co-evolved over much longer periods of time, sothat the expected benefits (improved nutritionto individuals) may not accrue in the expectedway (Giampietro, 1994).
Feedback loops
The interactions in SOHO systems are can berepresented as a mixture of positive and nega-tive feedback loops. For instance, people en-gage in various economic activities – such asclearing land for agriculture, irrigation, mining,house-building – in order to make money toimprove the quality of their lives. Wealth gen-erated by these activities may be used to buildbetter roads, schools, and sewage disposal fa-cilities. People who have more schooling maybe better able to solve social and public healthproblems – at which time they may see thatsome of the activities which made the schoolspossible may themselves be identified as prob-lems. Agricultural activities or manufacturingmay, for instance, result in greater pollution ofthe water supply and the environment, heavierstress on energy use, and general deteriorationof the ecosystem. Some diseases may be pre-vented when swamps are drained or damns arebuilt, even as habitats for new ones are created.
Self-organization, attractors, and surprise
In natural SOHO systems, it appears that, ashigh quality energy (referred to in the thermo-
dynamics literature as exergy) and informationare pumped into the system, the feedback loopsbecome organized in such a way as to makemore effective use of the entering resources,build more structure, and enhance their ownsurvivability. It is this combination of feed-backs, boundaries, and openness which resultsin what is called self-organization. Self-organi-zation is necessary for life to occur. All livingthings – organisms, ecological systems, socio-ecological systems – must remain both bound-ed, with a set of internally relatively stable in-teractions, and open to receiving resources andenergy, and dumping waste, if they are to re-main alive.
Some elements in any ecosystem are moretightly connected than others, and more essen-tial to their mutual well-being and/or the well-being of the system overall. The importance ofconnections is not determined by sector (agri-culture, health, business, social, environmen-tal), but by flows of useful energy, resources,and information related to patterns of self-or-ganization. Thus, activities which enable acommunity to make more effective and elabo-rate use of natural resources and informationare likely to have a greater impact on the via-bility of a given population than health care ac-tivities.
As already suggested, these feedback loopsin SOHO systems tend to organize themselvesin certain patterns which are coherent. Sys-tems researchers call this self-organization “at-tractors”. Most ecosystems – because of the en-ergy and resources available to them – seem tohave a propensity to fall into a certain limitedset of possibilities. Despite advertising claimsto the contrary, not everything is possible, andwe cannot all become whatever we want. We –and the ecosystems and societies we live in –are comprised of physical elements which con-strain our possibilities. Nevertheless, humanintentionality and creativity can push or alterthese constraints, which may result in new sys-tem states – or just in general disintegration. Inthe latter case, if life is to continue, some newsets of mutually supportive interactions needto arise. C. S. Holling, drawing on studies offorest fires and spruce-bud worm infections,has described a normal pattern of develop-ment in many ecosystems which depends on atleast one stage of local disintegration. Accord-ing to his “lazy-eight” model, these ecosystemsfollow a path from exploitation of disconnect-ed resources into greater conservation andstored energy, creative destruction with releaseof biomass (small patches of fires or infesta-tion), reorganization, and then exploitation

WALTNER-TOEWS, D.12
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
again (Holling, 1986). Farmers follow a verycontrolled version of this as they plant, hus-band, harvest, cultivate, and then plant again.
Changes between system states may bequite sudden. Ideas of thresholds and break-points are well-known in both the epidemio-logical and ecological literature (May, 1977; Kayet al., 1999). Disease organisms increase to crit-ical levels at which time the probability of ade-quate contact increases to the point where theepidemic explodes.
There is good evidence that ecosystems canexist in different steady states, reaching criticalpoints and then suddenly reorganizing, duringwhich time there may be drastic changes inspecies composition and diseases. Research onice cores from Greenland has indicated thatglobal temperature changes on the order of 5-16oC have occurred over mere decades duringglobal climatic changes in the past (Severing-haus & Brook, 1999; Taylor, 1999). Such “flips”are attributed to the crossing of temperaturethresholds required to keep global ocean cur-rents moving in particular ways. These kinds ofthreshold effects followed by catastrophicchanges between attractors have been demon-strated for a variety of systems, social as well asecological (Casti, 1994; Kay et al., 1999).
This means that gradualist views of diseasechanges in relation to climate, for instance,may be a very poor basis on which to base or-ganizational response plans, and hence under-mine that part of health which comprises theability to adapt and respond to stress. On theother hand, these insights may also be used tocreate health benefits disproportionately largerelative to the apparent effort. Putting speedbumps on all city streets, and narrowing them,could within a few years result in cleaner air,less respiratory disease, and healthier peoplewho walk more. Of course this would also re-sult in the loss of income from motor-relatedactivities and a change in the physical struc-ture of the cities and in the structure of the na-tional economy. Paying farmers for managinglandscapes sustainably as well as for producingcommodities would change the entire struc-ture of rural communities, migration to cities,international trade, patterns of foodborne dis-ease, and global economic power. While the ex-act outcome in either case could not be pre-dicted, an informed public could at least seethe general shape of the system options.
Multiple perspectives
Because such complex feedback loops haveboth positive and negative effects, different
people will look at the situation (and evaluateit) differently. Where one person sees the ex-citement of economic activity, another personsees deforestation, where one person sees dis-ease control by draining swamps, another per-son sees loss of wildlife and clean water provid-ed by the filtering effects of wetlands. Whereone person sees disease control through metalroofing, another person sees increased eco-nomic and environmental costs and less com-fortable houses. This means that, as the scien-tific description gets better, the problems arenot necessarily resolved, only clarified.
One challenge to creating systems descrip-tions is that of selecting what to put into themand what to leave out. We cannot describe every-thing about everything! Nor does it seem ap-propriate for expert scientists (which scien-tists?) to determine what is important and de-sirable for everyone else. The scientific, ecolog-ical information is important, but not suffi-cient. For this reason, some researchers havedeveloped the idea of extended peer groupsand “post-normal science”. In normal science,one’s disciplinary peers determine the “success”and “quality” of one’s work. If we are talkingabout sustainable, healthy communities, thenclearly there are others who will have some-thing important to contribute. This is especial-ly important given the uncertainty of scientificpredictions with regard to complex systems.
Given this complex theoretical base and theuncertainty of our knowledge, how can we doscientific research and science-based develop-ment in support of health?
What is the ecosystem approach? The practical implications of thinking in terms of complex systems
The concept of an “ecosystem” dates back atleast to British ecologist Arthur Tansley in 1935,and has undergone various permutations inthe decades since then (Bocking, 1994). Theecosystem approach, as described in this paper,is a conceptual and management approach de-veloped and applied by ecologists working withthe International Joint Commission of theGreat Lakes (Allen et al., 1991). These hugefreshwater lakes, which straddle the Canada-US border, are ringed with some of the biggestindustrial cities in North America, such asChicago, Cleveland, Hamilton, and Toronto. Inthis situation, standard approaches to environ-mental management, which were designed forsmaller areas or parks not usually inhabited bypeople, did not seem appropriate.

AN ECOSYSTEM APPROACH TO HEALTH 13
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
Combining insights from ecosystem ecolo-gy, complex systems theory, catastrophe theo-ry, and hierarchy theory, ecosystem researchersand managers developed a process that antici-pates change (without predicting its exact tim-ing and nature) and creates adaptive solutionsin a participatory manner. The process itselfgrew largely out of the work of Peter Check-land, a systems scientist and specialist in busi-ness management (Checkland & Scholes, 1990).Arguing that human activity systems could notbe understood or managed like machines, hedeveloped a seven-step “Soft Systems Method-ology” which focused on how to understandthe goals, perceptions, and transformative ac-tions of people in organizations. This method-ology is best worked out for organizationswhich have definable goals. Allan & Hoekstra(1992), among others, have explored how tocombine such a methodology with the insightsgained from natural sciences and ecology. Stillothers, such as James Kay and members of the“Dirk Gently Group” (The Dirk Gently Group isan informal network of researchers into theproblems of decision-making under conditionsof complexity and uncertainty. Membershipvaries, but includes Silvio Funtowicz, GilbertoGallopin, Mario Giampietro, James Kay, BrunaDe Marchi, Tamsyn Murray, Martin O’Connor,Jerry Ravetz, and David Waltner-Toews) havestruggled with the problems of how to accom-modate human activity systems, multiple per-spectives, and the constraints of ecological andenergy networks.
According to the Ecological Committee ofthe International Joint Commission, in theecosystem approach “there is not one materialecosystem to which our definitions must con-form. Rather, the human actor must accept re-sponsibility for erecting definitions and be pre-pared to change them when the purpose of thedescription changes” (Allen et al., 1991:5). Gen-eralizing this understanding to recognize thatthere are many human actors, with many legit-imate perspectives, Kay & Schneider (1994:38)have argued that using an ecosystem approachmeans “changing in a fundamental way howwe govern ourselves, how we design and operateour decision-making processes and institutions,and how we approach the business of environ-mental science and management.”
Central to an ecosystem approach rooted incomplex systems theories, then, is the notionthat achieving sustainability requires bringingtogether a variety of legitimate stakeholders,drawing on a variety of accepted bodies ofknowledge, to negotiate a learning path basedon a series of conflict resolutions within eco-
logical constraints. Continual learning basedon free flow of information and mutual respect,and investment in democratic local gover-nance, are keys to success (Funtowicz & Ravetz,1994; Roling & Wagemakers, 1998).
This means that, in the ecosystem approach,the practical, social, and institutional dimen-sions are of as much concern to researchers asthe scientific and scholarly concerns. This canget very complicated very quickly, if we re-member that these systems are holarchies.Thus, even if the people in one region can agreeon a common plan of action, they will need topay attention to the larger system of whichthey are a part. On the one hand, urban neigh-borhoods may not be able to solve all their wa-ter problems without help from city or evennational authorities in charge of water distrib-ution systems; on the other hand, if localneighborhoods clean up their streets simplyby shipping garbage elsewhere, this may createa much bigger, more concentrated problemthan the one we started with. Thus local par-ticipatory action, while essential, is alwaysconditional, just as individual freedom insociety is conditional on interactions with oth-er “layers” in the holarchy (Waltner-Toews &Wall, 1997).
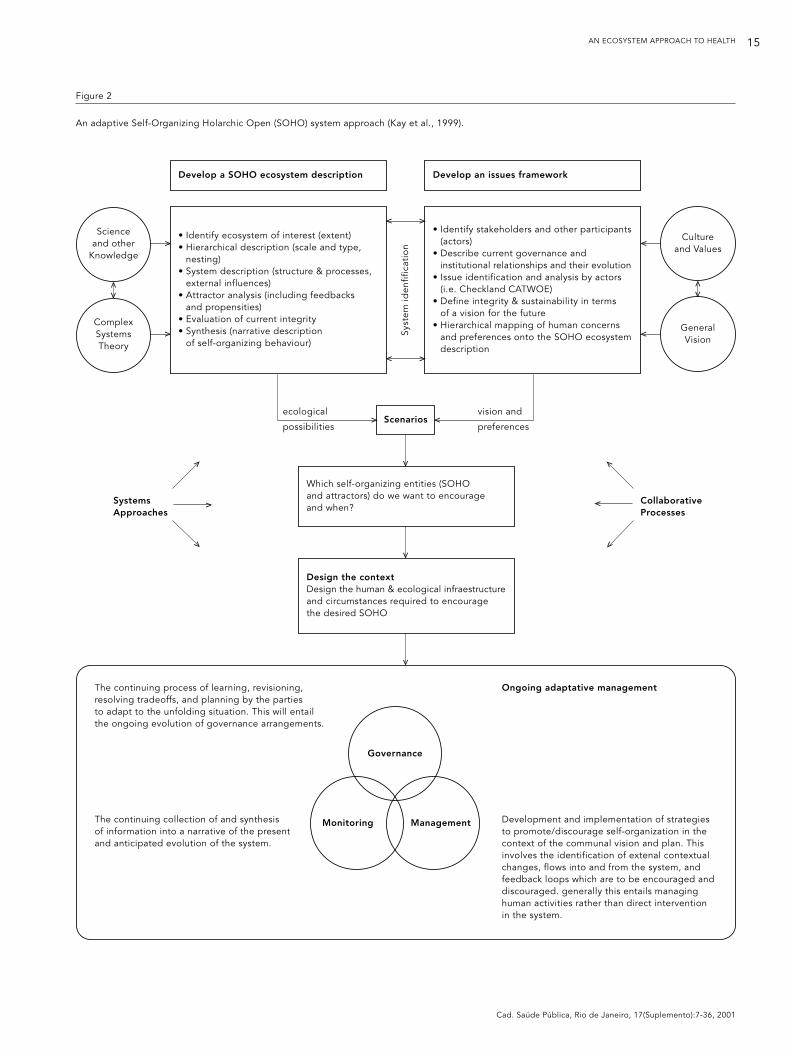
Both scientific studies and participatory ac-tion research (PAR) are necessary ingredientsof an ecosystem approach, and both must bereoriented to a systems understanding of reali-ty. Participatory development without scienceis just politics; science without participatorydevelopment is an academic exercise, andwithout a systems perspective, neither can beused effectively to promote sustainable devel-opment or ecosystem health. There is no singleway to visually represent this kind of multi-lev-el, multiple perspective research (nor is it theintent of this paper to describe the details ofsuch an approach). Several models have beenproposed. A cube with axes representing scale,perspective, and system goals may be used toclassify research and management activities(Figure 1, as adapted from VanLeeuwen et al.,1998). Kay et al. (1999) have proposed a two-armed schematic which emphasizes the inter-actions between natural sciences and socio-cultural visions (Figure 2). Murray and col-leagues (Murray et al., 1999) have proposed aflow diagram, the Adaptive Methodology forEcosystem Sustainability and Health. This putsthe emphasis on process, and may give greaterguidance for planning and action (Figure 3 –Murray et al., 1999).
However this is represented, biomedical re-searchers, sociologists, anthropologists, natur-

WALTNER-TOEWS, D.14
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
al scientists, and ecologists – both professionaland lay – must work together to describe theimportant patterns of natural resource use anddynamics of the ecosystems in which the com-munities live. At best, what emerges from thiscollaboration is an evolutionary understandingof how the current system came to be, what thekey interactions are which determine its cur-rent state, and, based on historical evidence,what kinds of options (attractors) are available.They also describe the system both in terms ofthe functioning of the diverse flora and faunathat are present, and in terms of their functionsfor capturing and disseminating useful energy(exergy) (Kay et al., 1999). Finally, the researchprocess itself involves negotiation of goals andimplementation of desirable and feasible ac-tions. Within the ecosystem approach, policies,programs, and actions serve the same functionas hypotheses and experiments in laboratoryscience.
Where does disease fit into this? One mightbegin by re-thinking disease classification interms of ecological contexts, rather than sim-ply using Linnean classifications. For example,Mara & Alabaster (1995) have devised an envi-ronmental classification of housing-related
diseases in developing countries. It is anotherstep in this process to identify how changinghousing types might modify the evolution ofvirulence in malarial parasites. Ewald (1994),among others, has discussed how enclosedhousing, which removes prostrate victims ofmalaria from the pool on which mosquitoesfeed, will likely lead to an evolution of malariato more benign forms. It is also known thatmetal roofing provides less habitat for Chagasdisease vectors; nevertheless, such roofing car-ries with it ecological costs (use of materialsand energy) as well as economic costs whichmay outweigh their benefits. These pieces ofinformation must be integrated – bringing dis-ease into a health context – as we work inten-sively with communities in specific places tocreate healthy social and ecological systems(Gitau et al., 1996; Murray et al., 1999; Yassi etal., 1999).
Because the ecosystem approach is basedon a holarchic view of reality, part of the re-search is to find ways of creating regional andglobal economic, health, and environmentalpolicies which facilitate, rather than hinder,this work. Health issues need to be put into aholarchic understanding, so we do not run into
Field
Farm
District
Watershed
Ecoregion
Ecozone
Biosphere
Biophysical Social Economic
Dimension
Health
Integrity
Effectiveness
Hie
rarc
hy
Figure 1
A framework for classifying agroecosystem health initiatives.
Adapted from Waltner-Toews & Nielsen, 1995.
AN ECOSYSTEM APPROACH TO HEALTH 15
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
Figure 2
An adaptive Self-Organizing Holarchic Open (SOHO) system approach (Kay et al., 1999).
• Identify ecosystem of interest (extent)• Hierarchical description (scale and type,
nesting)• System description (structure & processes,
external influences)• Attractor analysis (including feedbacks
and propensities)• Evaluation of current integrity• Synthesis (narrative description
of self-organizing behaviour)
• Identify stakeholders and other participants (actors)
• Describe current governance and institutional relationships and their evolution
• Issue identification and analysis by actors (i.e. Checkland CATWOE)
• Define integrity & sustainability in terms of a vision for the future
• Hierarchical mapping of human concerns and preferences onto the SOHO ecosystem description
Develop a SOHO ecosystem description Develop an issues framework
The continuing process of learning, revisioning, resolving tradeoffs, and planning by the parties to adapt to the unfolding situation. This will entailthe ongoing evolution of governance arrangements.
The continuing collection of and synthesis of information into a narrative of the present and anticipated evolution of the system.
Ongoing adaptative management
Development and implementation of strategiesto promote/discourage self-organization in thecontext of the communal vision and plan. Thisinvolves the identification of extenal contextualchanges, flows into and from the system, andfeedback loops which are to be encouraged anddiscouraged. generally this entails managing human activities rather than direct interventionin the system.
Governance
Monitoring...... Management
Science and other
Knowledge
ComplexSystemsTheory
v
v
Culture and Values
General Vision
v
v
vv
vv
vv
vvSy
stem
iden
fific
atio
n
Which self-organizing entities (SOHO and attractors) do we want to encourage and when?
Design the contextDesign the human & ecological infraestructure and circumstances required to encourage the desired SOHO
Scenariosv v
v
v
v
ecological
possibilities
vision and
preferences
SystemsApproaches
v
v
v
CollaborativeProcesses
v
v
v

WALTNER-TOEWS, D.16
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
the situation in which problems are solved atan individual level but become major problemsat a regional or global level, or vice versa. Forinstance, programs which focus on increasingglobal food production often undermine localfood security and health because they fail toaccount for cross-scale issues related to com-munication and control. Conversely, control ofmalaria or the plague in local communitiesmeans that controls must also be put in placeat regional levels to prevent reemergence local-ly. At the same time the cost of control, the ne-cessity for multi-sectoral cooperation, and theconsequences of failure are considerably high-er at the regional level. The only way out of thisbind is through global eradication, or the cre-ation of adaptive strategies to live with the dis-ease through better nutrition, public health in-frastructure, social support networks, and eco-nomic equity, all of have been demonstrated tomitigate the impacts of disease without eradi-cation. Ultimately, local actions will not be sus-tainable if there are not broader supportivepolicy environments; conversely, if local com-munities and ecosystems fail, there will be noglobal economy or healthy global bio-village.
How will the ecosystem approach aid in achieving health ?
Health is related to the ability to achieve desir-able and feasible goals. Therefore, working
with people to identify goals, to understand thesocioeconomic and ecological constraints andopportunities facing them, and to negotiateresolutions rather than “find” solutions, helpsthose people to become healthy by definition.There is no biomedical solution which can beimposed from the outside to promote health.Thus, an ecosystem approach to health pro-motes health in the very means it uses to un-derstand and promote health. Secondly, sincethe ecosystem approach embeds the socialgoals of health within our best understandingof the ecological context, it is more likely to besustainable than an approach to health issueswhich is based on the fantasy of a social realitydisconnected from the biosphere.
Implication of the ecosystem approach for research on tropical and emerging diseases
Emerging, reemerging, and newly recognizeddiseases in both the tropics and in temperatezones, represent failures – failures to under-stand the socio-ecological systems we live in,and failures to respond to new understandingsas they are uncovered. What we learn from thesefailures will largely determine how successfulwe are in creating sustainable and healthy hu-man communities on this planet.
Descriptions of emerging diseases and caus-es of emergence have been reviewed in severalmajor reports and conferences (Lederberg et al.,1992; Levins et al., 1994; Waltner-Toews, 1995;Meslin, 1997). The Institute of Medicine in theUnited States, in a 1992 report, identified half adozen forces which were resulting in the emer-gence of new diseases and the resurgence ofold ones (Table 1 – Lederberg et al., 1992). Pe-ter Drotman of the Centers for Disease Controlhas pointed out that 150 years earlier, in a re-port to the Prussian government regarding a ty-phus epidemic in Upper Silesia, Rudolf Virchowidentified causes and made recommendationswhich are eerily similar to those of the Instituteof Medicine (Table 2 – Drotman, 1998). What isclear from both reports – and remarkable giventhat both men were basic biomedical scientists– is that the causes identified are social, environ-mental and political. This would come as no sur-prise to anyone who has done serious researchin the area (Evans et al., 1994; Farmer, 1996).
Nevertheless, while Virchow’s recommen-dations are overtly social and political – andhence based on the evidence – those of theIOM seem unconnected with the causes (Table3). They are at best technical, and at worst
Historical Reconstruction
Stakeholder Analysis
Policy & Governance Analysis
Multiple System Descriptions
v
v
Figure 3
AMESH: the Research Process.
Adapted from Murray et al., 1999).
Implementation Cross Talk
Seeking Solutions
Monitoring & Evaluation
Issue Analysis
Linking System Descriptions
Analyzing the System Descriptions
Synthesizing theSystem Descriptions
v
v
v v
v
v
v
v v
v

AN ECOSYSTEM APPROACH TO HEALTH 17
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
merely self-serving (at least for biomedical sci-entists). Where, one might ask, are the recom-mendations related to some of the root causesthey have identified – technology and industry,international trade, investment in public healthinfrastructure? Based on the evidence present-ed, should health researchers not be makingstrong health representations to organizationslike the World Trade Organization and theWorld Bank, not on how to clean up the diseasemess after the fact, but on how to prevent themess in the first place? It would almost ap-pear that the ideological lenses through whichemerging diseases – indeed diseases in gener-al – are being studied, preclude acting on theevidence. This, if nothing else, should raise awarning flag that those who study disease arenot necessarily well-equipped to promotehealth, and that new modes of thought are re-quired to promote health at the beginning ofthe new millennium.
Tropical diseases obviously are relatedspecifically to tropical climate, flora, and fau-na. However, if we consider the diseases select-ed by the World Health Organization’s TDR Pro-gram (leishmaniasis, onchocerciasis, Chagasdisease, leprosy, tuberculosis, African try-panosomiasis, schistosomiasis, dengue, lym-phatic filariasis, and malaria), it is also clearthat many of these do not simply occur in thetropics because of climate and landscape. In-deed, even the tropical climate is subject tostrong influences by the climate-changing be-havior of industrialized countries, and land-scapes are being transformed by industrializa-tion processes within tropical countries. Dis-eases such as leprosy and tuberculosis have oc-curred – and continue to occur – in colder cli-mates where poverty creates homes for them.Even those diseases which are likely constrainedby the ecology and climate of the tropics, suchas Chagas disease, can clearly be strongly influ-enced by social and economic practices. Manytropical diseases are thus not only diseases re-lated to climate and environment, but are dis-eases of poverty. In epidemiological terms,conditions of poverty increase the probabilityof adequate contact and hence increase thelikelihood of epidemics. The disappearance ofmany infectious diseases – such as cholera, lep-rosy, tuberculosis, and malaria – has had muchmore to do with housing, nutrition, and watermanagement than with any advances in bio-medical science (Dubos, 1965). This is well es-tablished and, I would hope, non-controver-sial. These public health interventions requirepublic investments. Current drives to evadethese requirements by arguing for more re-
search on drugs and vaccines are largely drivenby private enterprise economics and a post-Cold War fear of seeming to be interested in thepublic good, rather than on the evidence.
Even if the financial powers could be per-suaded to look at the evidence, however, weneed to admit that we are working in a differ-ent context than that which the Europeansfaced at the beginning of the 20th century. Theplanet is considerably more crowded, north-erners are a great deal more insatiable in ourconsumption of resources, and the whole hu-man enterprise now threatens the ecologicalintegrity of the planet which makes our livespossible (UNDP, 1998). So, on the other end ofthe political spectrum, we must say that mas-sive public works programs and environmentalrestructuring of the kind which freed Europeansfrom infectious disease need to be more care-fully considered with regard to their effects onecosystems (which Virchow did not consider).
The ecosystem approach is a way to bringtogether the socioeconomic and biophysicaldimensions of health. Nevertheless, what itbrings to our understanding of emerging dis-eases is not so much a way of identifying newvariables – though it certainly forces us to castour net much broader than in conventional re-
Table 1
Factors in emergence of new diseases (Lederberg et al., 1992).
1) Human demographics and behavior.
2) Technology and industry.
3) Economic development and land use.
4) International travel and commerce.
5) Microbial adaptation and change.
6) Breakdown of public health measures.
Table 2
Some of Virchow’s recommendations to the Prussian government regarding
the typhus epidemic in Upper Silesia, 1848 (adapted from Drotman, 1998).
1) Political reform and local self-government.
2) Education.
3) Economic reform.
4) Agricultural reforms, including development of cooperatives.
5) Road building.
6) Requirement that professionals such as teachers and physicians speak the language of the local people.

WALTNER-TOEWS, D.18
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
search – but a new way of organizing how wethink about them, and how we respond tothem. Emerging diseases demonstrate to ushow our understanding of nature, and ourmanagement responses, have been limited. Inparticular, our understanding of how social andecological variables appear to behave as com-plex adaptive systems changes how we thinkabout social, economic, or environmentalmanagement programs. Some of the lessons tobe learned have been previously reviewed forfoodborne diseases (Waltner-Toews, 1996, 1999)and infectious diseases in general (Levins et al.,1994). This paper will emphasize three particu-lar failures in our understanding and responsewhich have characterized recent discussionson emerging diseases. These failures and in-sights based on them lead directly into a seriesof recommendations (Table 4).
1) The failure to understand non-linear in-teractions, chaotic attractors, and catastrophicthresholds. This failure is apparent in the wayin which economic development, agriculturaltrade policies, and the like are treated, as ifthey were somehow issues separate from socialand mental, as well as physical, well-being. It isalso apparent in current gradualist expecta-tions of the consequences of global warming.The promotion of health in an ecosystem con-text must account for multiple inter-relatedhealth outcomes, of which disease reduction isbut one. Furthermore, it will focus not so muchon linear predictions of health improvementthrough fixed programs (which appears to beimpossible), but on creating adaptive organi-zational responses.
This leads to my recommendations 1a and1b related to system dynamics: 1a) Researchshould be expanded on the changes in ecosys-tems which will most likely push them into thedomains of new attractors. What, researchersshould be asking, are the likely health, environ-mental, and social effects of such reorganiza-
tions? And 1b) That all economic, agriculture,and business policies, approvals of new tech-nologies, and so on be justified in terms of ourbest understanding of their likely systemic ef-fects, and that they not be undertaken unlessthose who live in the system agree that thoseeffects are acceptable and/or that we have inplace adaptive mechanisms to deal with thosechanges.
2) The failure to account for holarchy. Cur-rent efforts aimed at preventing diseases in in-dividuals are currently undertaken with littlethought as to the consequences for popula-tion or ecosystem health. Similarly, population-based programs tend to have a strong autocraticflavor to them which undermines their success.
Failure to account for holarchy has resultedin global trade policies which generate wealthfor the global economy, leading to the destruc-tion of local ecosystems and the maintenanceof local poverty and infectious diseases (Walt-ner-Toews, 2000). This is because global andregional policies often destroy local socio-eco-logical boundaries; individuals whose only loy-alty is to the global market undercut the in-tegrity of local social and ecological systems.Of course, healthy individuals, communities,and ecosystems interact with their surround-ings and change in response to them. However,globalized commercial trade is just anotherform of introducing alien and often invasivespecies into ecosystems; totally free trade iscomparable, at the local community and ecosys-tem level, to pulling the skin off a live animal.Yes, there is more immediate flow of nutri-ents – but this inevitably leads to local death.Some protectionism is simply an act of sur-vival. Indeed, the very idea of interaction withan environment presupposes the integrity ofthe boundaries across which the interactiontakes place. I must underline, however, that ho-larchical thinking drives us not to isolationism,nor to globalism, but to interactions with a pro-
Table 3
Recommendations for action by the Institute of Medicine’s Committee on Emerging Microbial Threats to Health
(adapted from Lederberg et al., 1992).
1) Development and implementation of more effective State, federal, and global surveillance systems.
2) Expansion of National Institutes of Health (NIH)-supported research on agent biology, pathogenesis, and evolution, vectors and their control, vaccines, and antimicrobial drugs.
3) Generation of stockpiles of selected vaccines.
4) Expedite pesticide registration for vector control and stockpile those pesticides.
5) NIH give increased priority to research on personal and community health practices relevant to disease transmission and education “to enhance the health-promoting behavior of diverse target groups.”

AN ECOSYSTEM APPROACH TO HEALTH 19
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
found respect for boundaries and scales. Con-trolling the emergence of new diseases andcreating healthy human communities dependon maintaining the tension within holarchies.
Recommendations 2a and 2b are thereforethat 2a) Research be expanded on the holarchicboundaries which are important for relative so-cio-ecological stability and 2b) Policies be de-veloped which respect holarchic boundaries,make explicit environment-economy-healthfeedback loops within those boundaries, andwhich encourage trade across those boundaries.
3) The third failure is one of long-term vi-sion, and hence perhaps the most forgivable.On the one hand, this is the failure to take intoaccount the ecological, evolutionary effects ofsocial and economic programs. The obviousexamples are those, like Lyme disease, wherereforestation and expanding deer populations,coupled with encouragement of people to en-joy outdoor life, have also had negative dis-ease-emergence effects. But the failure is morewidespread than that.
This is also evident when apparently nar-rowly focused changes are proposed – such asthe introduction of new genetic varieties ofplants on a wide scale. For instance, the intro-duction of “green revolution” varieties appearsnow to have played an important part in thesystemic changes which have resulted in more
than two billion people worldwide with seriousmicro-nutrient deficiencies, which may beconsidered a major non-infectious emergingdisease (Welch et al., 1997). Farmers chose newvarieties because they grew faster and madethem more money. This displaced a variety ofother crops and in the process restricted the di-et for billions of people. They also became con-siderably more dependent on fossil fuels (forfertilizers and pesticides), contributing to themining of non-renewable resources, globalwarming, and the emergence of new diseases,both infectious and non-infectious. Hence acaloric shortage problem was solved in such away that the system was reorganized in funda-mentally unsustainable ways.
The new wave of genetically modified or-ganisms is being introduced based on the samenaïve view of nature that brought in the firstwave of introductions, with the probabilitythey will further destabilize ecological systems(Giampietro, 1994). This will no doubt result inchanges to micro-flora which will lead to theemergence of new epidemiological patterns ofdisease. Certainly this is what has already hap-pened with regard to many foodborne illness-es, such as bovine spongiform encephalopathy,antibiotic-resistant Salmonella DT 104, andverotoxin-producing E. coli, all of which haveemerged in the agrifood system as unintended
Table 4
Recommendations to understand and control the emergence of new diseases based on an ecosystem
approach to health.
1) Recommendations related to system dynamics:
a) Research should be expanded on the changes in ecosystems which will most likely push them into the domains of new attractors, and what will be the likely health, environmental, and social effects of such reorganizations.
b) That all government policies – economic, business, agriculture, health, new technology approval – be justified in terms of our best understanding of their likely systemic effects, and that they not be undertaken unless those who live in the system agree that those effects are acceptable and/or that we have in place adaptive mechanisms to deal with those changes.
2) Recommendations related to holarchies:
a) Research should be expanded on the holarchic boundaries which are important for relative socio-ecological stability and containment of diseases.
b) Policies should be developed which respect holarchic boundaries, make explicit environment-economy-health feedback loops within those boundaries, and which encourage trade across those boundaries.
3) Recommendations related to long term evolution:
a) Research should be expanded on the co-evolution of ecosystems – including the microbial populations within them – over time.
b) New health, economic, and environmental initiatives take into account possible long-term effects on the system dynamics.
c) That relatively uninhabited ecosystems be protected from further human invasions by economic and political policies until such a time as we have a fuller understanding of the nature of the infectious agents in the system as currently evolved.

WALTNER-TOEWS, D.20
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
side effects – based on naïve and narrow un-derstandings of social and ecological systems –of economic policies intended to promotecheap food. Agricultural and economic devel-opment policies can also be held responsiblefor the (re)emergence of malaria in severalparts of the world.
An understanding of possible long-term ef-fects may not lead us to abandon social pro-jects and policies. Indeed, as Ewald and otherevolutionary ecologists have pointed out formalaria and cholera, these may be used to goodadvantage to devise programs to control dis-ease. But these long-term scenarios should atleast cause us to build into their structure andimplementation mechanisms to detect proba-bly long-term impacts and to compensatorymechanisms for those who are likely to sufferfrom those changes.
This is not only a failure to see the long-term effects of human social projects, however,but a failure to understand that ecosystemshave co-evolved over a long period of time andthat when we invade or disrupt those systems,we do so at some peril, not just to the ecosys-tem (rain forest destruction) but to ourselves,as we become entangled in life cycles thatevolved without us, resulting in the emergenceof diseases like Ebola virus and Kyasanur For-est disease.
Hence, recommendations 3a, 3b, and 3c are:3a) Research be expanded on the co-evolutionof ecosystems – including the microbial popu-lations within them – over time. This will re-quire the establishment of long-term sites invarious parts of the world and incorporatingvarious types of human activities. Such long-term sites have been set up for “pure” ecologi-cal studies; the bases for such teaching-learn-ing sites have already been established in sev-eral on-going projects in various parts of theworld. What is needed now is to rationalizethese, give them some permanent long-termfunding, and expand the range of researchersinvolved; 3b) That new health, economic, andenvironmental initiatives take into accountpossible long-term effects on the system dy-namics; and 3c) That relatively uninhabitedecosystems be protected from further humaninvasions by economic and political policiesuntil such a time as we have a fuller under-standing of the nature of the infectious agentsin the system as currently evolved.
Achieving health for all: Beyond complexity, beyond 2000
Because components of ecosystems interact inways that undermine our ability to make pre-dictions, in particular because of the kinds ofphenomena associated with attractors andthreshold changes, it is essential that anyoneinterested in sustainable health take a broad,ecosystemic approach. Furthermore, becauseof our limited ability to predict outcomes, it isimportant that we maintain our flexibility andour options.
In practical terms, this means that local bio-and social diversity must be maintained as away of maintaining some reserve to respond tothe certain changes ahead. An ecosystem ap-proach to emerging diseases, then, involves, onthe one hand, monitoring changes in the struc-tures of ecosystems which are leading to thecreation of different and often larger nichesfor potential pathogens. On the other hand, itmeans working to stop the most dangerous ofthese changes – working to influence nationaland international economic and political poli-cies which are creating the disease-promotingconditions. It means doing our research insuch a way that the goals such as food security,health, and a convivial life can be achievedwithout threatening the ecosystems which pro-vide the services that make human communi-ties possible.
Because systemic descriptions and resolu-tions are context-specific, and because we aretalking about bringing together multiple sys-tems descriptions, some argue that the amountof time, energy, money, and work required todo this research is impossible in practice toachieve. This criticism is based on outmodedideas of both research and development. Al-though the ecosystem approach to health re-quires a major commitment of people’s activi-ties, these activities are those which should al-ready be going on in any society: planting crops,building bridges, educating children. Within anecosystem approach, every policy decision is ahypothesis, and every management plan is atest of that hypothesis. Research becomes anintegral part of the daily decision-making andevaluating activities of households, commu-nities, regions, and global institutions. Thisis precisely what makes this an adaptive ap-proach; it does not assume that Truth – relativeto sustainability and health – can be estab-lished once-and-for-all with a few definitiveexperiments.
We define health at our boundaries – asindividuals, communities, nations and global-

AN ECOSYSTEM APPROACH TO HEALTH 21
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
ly – and we achieve health by communicatingand negotiating across our boundaries. Thinkecosystemically, act holarchically, should bethe rallying cry of health workers around theworld. There is good evidence that the ecosys-tem approach can help us achieve a global vi-sion of health, but the uncertainty and contra-dictions which it is attempting to accommo-date must ultimately be applied back to itself.If nothing else, the ecosystem approach bringshome the deep understanding that we cannot
“manage” the planet for health, but we canlook for opportunities to better adapt and feelat home – to be healthy – in an uncertain andcontradictory world. Even if our hopes are mis-placed, however, and the specific disease con-trol and health outcomes we seek are notachieved, fundamental requirements of theecosystem approach for open and democraticcommunication, tolerance, negotiation, andecological awareness will surely have made theeffort worthwhile.
Acknowledgments
I would like to thank the International DevelopmentResearch Centre (Montevideo) for their financial sup-port. I would also like to thank James Kay, TamsynMurray, and other members of the Dirk Gently Group( Jerry Ravetz, Silvio Funtowicz, Mario Giampietro,Bruna de Marchi, Martin O’Connor, Gilberto Gallopin,Silvia Tognetti, Henry Regier, George Francis, Nina-Marie Lister et al.) for keeping these debates alive.
References
ALLEN, T.; BANDURKSI, B. & KING, A., 1991. TheEcosystem Approach: Theory and Ecosystem In-tegrity. Report to the Great Lakes Advisory Board,International Joint Commission, USA and Canada.
ALLEN, T. & HOEKSTRA, T. W., 1992. Toward a UnifiedEcology. New York: Columbia University Press.
BOCKING, S., 1994. Visions of nature and society: Ahistory of the ecosystem concept. Alternatives,20:12-18.
CAST, J. L., 1994. Complexification. New York: Harper-Collins Publishers.
CHECKLAND, P. & SCHOLES, P., 1990. Soft SystemsMethodology in Action. John Chichester: Wiley &Sons.
CONSTANZA, R.; NORTON, B. & HASKELL, B., 1992.Ecosystem Health: New Goals for EnvironmentalManagement. Washington, D.C.: Island Press.
DUBOS, R., 1965. Man Adapting. New Haven: YaleUniversity Press.
EVANS, R. G.; BARER, M. L. & MARMOR, T. R., 1994.Why are Some People Healthy and Others Not?The Determinants of Health in Populations. NewYork: Aldine de Gruyter.
EWALD, P., 1994. Evolution of Infectious Disease. Ox-ford: Oxford University Press.
FARMER, P., 1996. Social inequalities and emerginginfectious diseases. Emerging Infectious Diseases,2:259-269.
FUNTOWICZ, S. & RAVETZ, J., 1994. Emergent com-plex systems. Futures, 26:568-582.
GIAMPIETRO, M., 1994. Sustainability and techno-logical development in agriculture: A critical ap-praisal of genetic engineering. Bioscience, 44:677-689.
GITAU, T.; McDERMOTT, J. & WALTNER-TOEWS, D.,1997. Design and implementation of a programto assess the health of an intensively farmedhighlands agroecosystem in Kenya. Epidemiolo-gie et Santé Animale, 31-32:2-7.
HOLLING, C. S., 1986. The resilience of terrestrialecosystems: Local surprise and global change. In:Sustainable Development of the Biosphere (W. M.Clark & R. E. Munn, eds.), pp. 292-320, Cam-bridge: Cambridge University Press.
KAY, J.; REGIER, H.; BOYLE, M. & FRANCIS, G., 1999.An ecosystem approach for sustainability: Ad-dressing the challenge of complexity. Futures,31:721-742.
LAST, J. M., 1988. A Dictionary of Epidemiology. Ox-ford: Oxford University Press.
LEDERBERG, J.; SHOPE, R. & OAKS, S., 1992. Emerg-ing Infections: Microbial Threats to Health in theUnited States. Washington, D.C.: National Acade-my Press.
MARA, D. D. & ALABASTER, G. P., 1995. An environ-mental classification of housing-related diseases

WALTNER-TOEWS, D.22
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
in developing countries. Journal of Tropical Med-icine and Hygiene, 98:41-51.
MAY, R., 1977. Thresholds and breakpoints in ecosys-tems with a multiplicity of stable states. Nature,269:471-477.
MESLIN, F. X., 1997. Global aspects of emerging andpotential zoonoses: A WHO perspective. Emerg-ing Infectious Diseases, 3:223-228.
MINKIN, S. F.; RAHMAN, R. & ISLAM, M. A., 1996.Flood control embankments and epidemic kala-azar in Bangladesh. Ecosystem Health, 2:215-226.
MURRAY, T.; KAY, J.; WALTNER-TOEWS, D. & RAEZ-LUNA, E., 1999. Adaptive Methodology for Ecosys-tem Sustainability and Health (AMESH): An Intro-duction. Conference on Conservation Medicine,White Oak Conservation Center, Florida, April 29-May 2.
PUCCIA, C. & LEVINS, R., 1985. Qualitative Modelingof Complex Systems. Cambridge: Harvard Univer-sity Press.
ROLING, N. G. & WAGEMAKERS, M. A., 1998. Facili-tating Sustainable Agriculture. Cambridge: Cam-bridge University Press.
SEVERINGHAUS, J. P. & BROOK, E. J., 1999. Abruptclimate change at the end of the last glacial peri-od inferred from trapped air in polar ice. Science,286:930-933.
TAYLOR, K., 1999. Rapid climate change. AmericanScientist on the Web, 87 <http://www.amsci.org/articles/99articles/taylor/html>.
UNDP (United Nations’ Development Program), 1998.Overview of Human Development Report 1998.<http://www.undp.org/wdro/e98over.htm>.
UNDP (United Nations’ Development Program), 1999.Human Development Report. Oxford: Oxford Uni-versity Press.
VanLEEUWEN, J.; NIELSEN, N. O. & WALTNER-TOEWS, D., 1998. Ecosystem health: An essentialfield for veterinary medicine. Journal of the Amer-ican Veterinary Association, 212:53-57.
WALTNER-TOEWS, D., 1995. Changing patterns ofcommunicable disease: Who is turning the kalei-doscope? Perspectives in Biology and Medicine,39:43-55.
WALTNER-TOEWS, D., 1996. An agroecosystem per-spective on foodborne illnesses. Ecosystem Health,2:177-185.
WALTNER-TOEWS, D., 1999. Mad Cows and BadBerries. Alternatives Journal: EnvironmentalThought, Policy and Action, 25:38-44.
WALTNER-TOEWS, D., 2000. The end of medicine:The beginning of health. Futures, 312:655-667.
WALTNER-TOEWS, D. & WALL, E., 1997. Emergentperplexity: In search of post-normal questions forcommunity and agroecosystem health. SocialScience and Medicine, 45:1741-1749.
WELCH, R.; COMBS, G. & DUXBURY, J., 1997. Towarda “greener” revolution. Issues in Science and Tech-nology, Fall:50-58.
YASSI, A.; MAS, P.; BONET, M.; TATE, R.; FERNANDEZ,N.; SPEIGEL, J. & PEREZ, M. L., 1999. Applying anecosystem approach to determinants of health inCentro Habana. Ecosystem Health, 5:3-19.

AN ECOSYSTEM APPROACH TO HEALTH 23
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
Pavlovsky revisited. New clothes for ecology inepidemiology. A commentary on An EcosystemApproach to Health and its Applications toTropical and Emerging Diseases, by DavidWaltner-Toews.
The ecological approach to understanding dis-ease dynamics in populations is at least as oldas Hippocrates (Hippocrates, s.d.). From Hip-pocrates until the dawn of the bacteriologicalera, disease theory was mostly ecological in na-ture (Galen, s.d.). In fact, not truly ecologicalaccording to the current scientific definition,but ecological in nature. According to the Hip-pocratic definition, an endemic was a diseasedetermined by the nature of a certain place.Demos had a broad meaning, and could be un-derstood as people or population, but also asplace, home. Under this definition, climatic,hydrological, and behavioral determinantswere seen as the main forces. This view of dis-ease occurrence and distribution persisted forcenturies. Hippocrates’ writings were recycledby Galen (Galen, s.d.) in the early Christian eraand resisted even the Galilean modernizationof science during the Renaissance, surviving asthe mainstay of medical and public health sci-ence until the late 18th century. Hippocratesand Galen are not the main subject of discus-sion here, but it must be noted that their con-cept of disease was ecological. Disease was aconsequence of local conditions, which had tobe favorable for a particular disease to occur.Diseases were named after the respective sce-narios in which they occurred, such that differ-ent scenarios gave rise to different diseases.
Pavlovsky (Pavlovsky, s.d.), a little-knownparasitologist from what was then the SovietUnion, can be considered one of the first topropose a reasonably well-structured theory ofinfectious disease ecology. Unfortunately, inthe late 1930s Soviet epidemiology (and indeedSoviet science as a whole) were not very wellknown in the West, and Pavlovsky’s theory ofthe natural nidality of transmissible diseaseshad a very restricted circulation (Audy, 1958;Marr, 1995). Nonetheless, Pavlovsky succeededin furthering the understanding of disease oc-currence and the consequences of ecosystem
Debate on the paper by David Waltner-ToewsDebate sobre o artigo de David Waltner-Toews
Departamento of Medicina,Faculdade de Ciências Médicas, Universidade Estadual de Campinas.Superintendência de Controle de Endemias,Secretaria Estadual da Saúde, São [email protected]
Luiz Jacintho da Silva
modification. Unfortunately Pavlovsky did ven-ture too far forward, since he appeared to besatisfied with understanding leishmaniasis andthe then-emerging tick-borne encephalitis.
We can, with reasonable confidence, acceptthat the ecosystem approach to infectious dis-eases began with Pavlovsky. Waltner-Toews’ ar-ticle presents ecosystem analysis as a recentinvention, which it is not. A large number ofresearchers have employed one or anothermethod of ecosystem analysis for understand-ing and controlling infectious diseases (Audy,1958; May, 1958; Burnet et al., 1972; Croll et al.,1983; Blower et al., 1991). In fact, the extensiveuse of the term “tropical” to define a broad ar-ray of diseases is inappropriate. Globalizationhas erased boundaries between endemic anddisease-free areas; these diseases are not a pre-rogative of tropical ecosystems, albeit the latterare doubtless extremely favorable to their oc-currence.
What distinguishes contemporary ecosys-tem analysis of diseases is the ecological para-digm adopted (Science et Vie, 1996; Earn et al.,1998). Virchow, cited by Waltner-Toews, con-cluded the obvious. Appalling living conditionsin mid-19th century Silesia made the associa-tion obvious; it was not the result of scientificreasoning, but only of sound common sense.The failure of post-War economic developmentprojects in the Third World and of large dis-ease-control programs preceded the late 1970sdebt crisis. The Marshall Plan had been a suc-cess in Europe; malaria eradication was also asuccess in Southern Europe and the Southeast-ern United States, but fell short of its objectivesin the Third World. Worse yet, many develop-ment projects, like irrigation schemes and hy-droelectric dams, caused diseases to spread(Hughes et al., 1970; Gordon-Smith, 1975). Cul-tural traits of target groups conflicted with be-havioral changes needed for disease control. Itgradually became obvious that infectious dis-ease control programs demanded a more com-prehensive approach than the prevailing linearreasoning.
The ecosystem approach proposed by Walt-ner-Toews is no doubt interesting, but the the-oretical basis is not clearly presented. Modernecological theory differs from Pavlovsky’s.Modern science has abandoned the passion forprecision to embrace a love of the imprecise,the uncertain. Chaos theory is finding its placein virtually all scientific disciplines (Hénon,1989; Casti, 1995; Science Illustrée, 1996; Earnet al., 1998). Waltner-Toews commits a Freudi-an slip when he discusses attractors and cata-strophic changes, which are an integral part of

WALTNER-TOEWS, D.24
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
chaos theory. Waltner-Toews’ ecosystem ap-proach is more than a cookbook recipe for un-derstanding and controlling infectious diseases,but this is not made clear as he expounds on itstheoretical base. Public health needs a soundertheoretical base, and ecosystem analysis is amajor step towards raising epidemiology to thesame level of philosophical soundness asphysics. Public health must be wary of “new”approaches. Infectious disease control has ad-vanced enormously in its technical aspects, butthe latter have still proven to be insufficient. Amore appropriate understanding of disease isneeded, and Waltner-Toews comes close. How-ever, he appears to be distracted by the siren’ssong of the biased world view still prevailing inmany scientific circles in industrialized coun-tries. Infectious diseases must be seen as awhole, not divided into tropical and non-tropi-cal, meaning in fact underdeveloped and de-veloped. Waltner-Toews proposes a distinctionbetween tropical and non-tropical diseases,according to which the former frequently “oc-cur in settings where the links between localecosystems and local communities are intenseand obvious.”[quoted from a preliminary ver-sion of the article]. Links between ecosystemsand communities are hard to understand, ascommunities are integral parts of ecosystems.Here lies another Freudian slip, since ecosys-tem is seen as merely the natural ecosystem,detached from human presence.
The ecosystem approach presented by Walt-ner-Toews is appealing, but unfortunately in-fected by a biased view of the developing world.
AUDY, J. R., 1958. The localisation of disease with spe-cial reference to the zoonoses. Transactions of theRoyal Society of Tropical Medicine and Hygiene,52:308-328.
BLOWER, S. M. & McLEAN, A. R., 1991. Mixing ecolo-gy and epidemiology. Proceedings of the Royal So-ciety of London B Biological Sciences, 245:187-192.
BURNET, M. & WHITE, D. O., 1972. The ecologicalpoint of view. In: Natural History of InfectiousDisease (M. Burnet & D. O. White, eds.), pp. 1-21,4th Ed., Cambridge: Cambridge University Press.
CASTI, J. L., 1995. Complexification. Explaining aParadoxical World Through the Science of Sur-prise. New York: Harper Perennial.
CROLL, N. A. & CROSS, J. H., 1983. Human Ecology andInfectious Diseases. New York: Academic Press.
EARN, D. J.; ROHANI, P. & GRENFELL, B. T., 1998. Per-sistence, chaos and synchrony in ecology andepidemiology. Proceedings of the Royal Society ofLondon B Biological Sciences, 265:7-10.
GALEN, s.d. On the Natural Faculties. <http://classics.mit.edu/galen/natfac.html>.
GORDON-SMITH, C. E., 1975. Changing patterns ofdisease in the tropics. In: Man – Made Lakes andHuman Health (N. F. Stanley & M. P. Alpers, eds.),
pp. 345–362, London: Academic Press.HÉNON, M., 1989. La diffusion chaotique. La Récher-
che, 20:490-498.HIPPOCRATES, s.d. On Airs, Waters, and Places. <http:
//www.classics.mit.edu/Hippocrates/airwatpl.html>.
HUGHES, C. C. & HUNTER, J. M., 1970. Disease and“development” in Africa. Social Science and Med-icine, 3:443-493.
MARR, J., 1995. The natural nidality of transmissiblediseases: Searching for the “MacGuffin”. <http://www.medscape.com/medscape/f...es/1997/ms001.marr/ms001.marr.html>.
MAY, J. M., 1958. The Ecology of Human Disease. NewYork: M. D. Publications.
PAVLOVSKY, E. N., s.d. Natural Nidality of Transmis-sible Diseases. Moscow: Peace Publishers.
SCIENCE ET VIE, 1996. L’écologie. Cent ans d’adoles-cence. Science et Vie, 949 (octobre):84-87.
SCIENCE ILLUSTRÉE, 1996. Nous vivons au bord duchaos. Science Illustrée, 12 (décembre):50-55.
David Waltner-Toews (W-T) has chosen to dis-cuss an issue of fundamental importance, therole of environmental change and how it re-lates to human health, i. e., how to combine thesocioeconomic and biophysical dimensionsof human health. It is a complex challenge tograsp how relations between ecosystems areconnected and influence the everyday life,health, and welfare of human beings. W-T ap-plies an ecosystem approach to this task in hisarticle.
In the introduction he asks, “What ishealth”? He mentions the World Health Orga-nization’s definition “...as a state of completephysical, mental, and social well-being, and notmerely the absence of disease”. W-T is critical ofthis definition. What he suggests is a redefini-tion of health as “absence from disease andpathology”. I find this confusing in relation tothe holistic ecosystem approach presented lat-er in the article. For me, the above statement isa perception of health as a static and biomed-ical condition. I would have preferred anotherintroduction, since this definition certainlystands apart from the rest of the article, and henever really returns to the meaning behind thisredefinition.
If W-T intends to discuss the WHO policystarting with the 1948 founding document,such a discussion must be placed in some formof historical context, since the document isclearly biomedical and born within Western
Ibero-American Institute,Göteborg [email protected]
Maj-Lis Follér

AN ECOSYSTEM APPROACH TO HEALTH 25
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
tradition. For W-T’s overall global and ecosys-tem approach to health, I find more relevanta continuation of the Alma-Ata Declaration,which is now more than 20 years old, but whichcertainly focuses more on the importance ofcommunity involvement for improving healthconditions. In a world of limited resources,mass unemployment, and health standards thatare socially and economically far removed fromsuch aims for the majority of the world popula-tion, neither the idealistic WHO definition northat proposed by W-T provides a realistic start-ing point. Such ideal statements sound strangeand dangerous in relation to my way of dealingwith today’s reality. They have the potential ofcreating new problems in establishing for whomand on what level in society the absence of dis-ease or pathology can be defined. The WHOdefinition of health is part of the Western tradi-tion and implies the notion of perfectibility. Iwould suggest a more processual view of thecontinuum between health and disease in theintroduction, since this is what the author em-phasizes later on in the article. We are all born,live, and die, and during this process we mustdeal with physical, emotional, and psychologi-cal strain. This is part of life, and only on an in-dividual level can one decide whether to defineone’s situation as illness. This is valid for peo-ple with disabilities, those defined by societyas mentally ill or abnormal, and persons withstress-related disease.
At any rate, W-T applies an ecosystem ap-proach to health in the rest of the article. Hedefines a system as a set of elements which in-teract with each other within certain bound-aries. He elaborates on the concepts of hol-archy, attractor, and complex feedback loops,all central to understanding an ecosystem ap-proach. Systems that are hierarchically nestedwithin each other are called holarchical. As Iunderstand the ecosystem approach, the pointwith concepts such as holarchies is to showthat there is always interdependence betweensubsystems and supersystems. Central to thisapproach is that there is a systematic function;the supersystem is dependent on continuouscooperation with the subsystem. This is trans-lated into another terminology by which every-thing is related to everything else, and the fo-cus of this article is the relationship betweenglobal and local concerns in today’s world. W-Tmakes these relations more transparent by giv-ing examples of the importance of local activi-ties and how they interfere with and influenceglobal activities. That is to say, there is an inter-connectedness between the holarchy of theecosphere, ecosystems, and human systems,
hence the connections between human healthand ecosystem health.
I agree that we need some form of holisticapproach for the integration of social, econom-ic, and environmental interests in relation tohuman health in a systematic way. But evenwith this very broad approach to connectecosystem health and human health, W-T doesnot talk about interdisciplinarity or how to es-tablish cooperation between scientists. W-Twrites, “Both scientific studies and participato-ry action research (PAR) are necessary ingredi-ents of an ecosystem approach, and both mustbe reoriented to a systems understanding of re-ality.” This is a huge task, but I agree that wehave to begin the dialogue. The question is howto elaborate communications between peopleliving in rural communities around the globeand researchers in a two-tier way. On the onehand, taking local knowledge seriously, and onthe other, translating and making scientificknowledge understandable to people in ruralareas of the world. W-T also writes, “How canwe do scientific research and science-based de-velopment in support of health?” W-T gives ex-amples to show that medical sciences bothsolve and create problems, displaying a certainhumbleness of mind, which I like.
I believe that we need broad scientific co-operation among scientists from ecology, med-icine, and social and cultural disciplines tosolve many of today’s health problems. But lo-cal participation and elaboration of dialoguewith people in the communities are just as im-portant. They often have concepts of healththat go beyond merely the physical functioningof individuals. As I interpret it, this is also theintention behind W-T’s approach, but he miss-es some of the “soft” aspects, such as the be-havioral and cultural dimensions of people liv-ing in the communities. They are the ones af-fected by tropical, emerging, and other dis-eases.
Still, the author has taken an important stepin this article in attempting to connect an ecosys-tem approach to different aspects of health-re-lated issues, even though he deals largely withpatterns of infectious and emerging diseases.W-T attempts to cross borders between ecolog-ical, sociological, and medical sciences andparticipatory action research. We know thatthere are linkages between human activitiesand alterations in ecosystem functions andservices with direct consequences for diseasetransmission and some more indirect effects,and W-T highlights some of these connections.
We are now more than 6 billion people liv-ing on the planet Earth. If we want a sustain-

WALTNER-TOEWS, D.26
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
Indiana University.Blomington,Indiana, United States of America.
Emilio F. Moran The discussion by David Waltner-Toews coversconsiderable ground and is stimulating as awhole. It correctly diagnoses our contemporaryproblems as stemming from sectoral and disci-plinary thinking, with all the inevitable blinders.Indeed, he reviews the frequent failures that re-sult when we mean to do good but fail to foreseethe consequences of our interventions at high-er or lower levels in complex system hierarchies.
I was particularly taken by his Table 4 of rec-ommendations, which seem to be sensible andappropriate as first steps to health in the newmillennium. There can be little quarrel with theauthor that we need more complex systemsthinking or that this approach (together withparticipation by the populations affected in theprocess) is likely to lead to better health out-comes. My main critique of the author is thathe fails to provide either details on how hisGreat Lakes Basin program or the Dirk GentlyGroup are attempting to implement this ap-proach or evidence for improved outcomesfrom such efforts.
Without evidence for how a SOHO approachleads to improved health and well-being, it isunlikely that its adoption will follow. There aremany inherent difficulties in the approach thatmust be dealt with (and the author only rarelyalludes to them): divergent and/or competinginterests among sectors of the human commu-nity; the free-rider problem; the challenge ofbuilding robust institutions based on trust andreciprocity (in a world where these are increas-ingly scarce); mechanisms for allocating costsin multi-tier systems, etc.
In other words, the sectoral model has pre-vailed because it makes it easier to managesimple, single-tier systems created to facili-tate operations, allocate charges, and producereasonable results (while ignoring upstreamand downstream consequences). The proposedSOHO approach is conceptually more attrac-tive but riddled with all kinds of new chal-lenges for its “managers” or modelers. Particu-larly if such systems are non-linear and chaotic(as they must be), the uncertainty of outcomein itself is a political challenge for those whowish to implement it. Most human communi-ties are not likely to be receptive to outcomescharacterized by uncertainty. The author andhis colleagues need to move from the appeal-ing conceptual and diagnostic stage to an op-erational model if we are to hope for imple-mentation of this idealistic goal in the 21st cen-tury. We certainly need alternatives to healthand business as usual.
able future, different strata in society mustwork together. As scientists, we have to crossdisciplinary borders to find new connectionsand black holes in our knowledge and under-standing of the relationship between globalprocesses, local impact, and individual behav-ior. W-T has taken one step in this direction,and more discussion is needed. The debate thattook place in Rio de Janeiro during the IDRCmeeting in November 1999 between ecolo-gists, human ecologists, social scientists, med-ical scientists, development organizations, andPAHO representatives was a good initiative. Itis through the creation of interdisciplinary fo-rums and an open dialogue that we will realizethat no one has a single all-encompassingcompetence for a sustainable future. We haveto learn from each other and hopefully be partof a process which moves the contemporaryand future ecosystem and human health situa-tion in a positive direction.

AN ECOSYSTEM APPROACH TO HEALTH 27
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
In this interesting article Waltner-Toews dis-cusses the notion of ecosystem health and theinsights it can provide for confronting theemergence and complexity of infectious dis-eases. According to him, those who possess theskills required to prevent and treat disease areill-equipped to promote health. As some au-thors have pointed out before (Levins et al.,1994) he notes that disease prevention and con-trol programs tend to ignore complexity andmay, in fact, create ill-health. In his view, thesefailures result from our limited ability to pre-dict outcomes and from our incapacity to ac-count for holarchy and to understand non-lin-ear interactions, chaotic attractors, and cata-strophic thresholds in complex ecosystems.
Background information is necessary tounderstand the contributions and possiblelimitations of the ecosystem health approachproposed in this article. The notion of ecosystemhealth was first introduced by Rapport (1989) inan international meeting of the Association forGreat Lakes Research and was developed laterin other publications. In 1994, an internationalworkshop on Agrosystem Health was organizedby the University of Guelph with the support ofIDRC. The discussions focused then on the con-tributions of the health paradigms to understandagroecosystems: vigor, resilience, and systemorganization, as suggested by Constanza (1994),and on the comparative advantages of theecosystem. health concept over sustainability.
According to some authors (Smit & Smithers,1994), for practical purposes the concepts wereessentially the same, while other authors (Walt-ner-Toews, 1994) suggested that the health par-adigm could provide a more appropriate basisfor thought and action in agroecosystems. Inthis workshop, it was noted that sustainabilityand ecosystem health are tightly connected butare distinct concepts and that their more exactrelationship remained to be determined.
Simultaneously, in the health field, some re-search groups developed ecosystem approach-es to emergence and resurgence of infectiousdiseases worldwide. In 1991, in the UnitedStates, the Harvard New Diseases Group start-ed a transdisciplinary research agenda in thisarea. Contributions were published later in theAnnals of the New York Academy of Sciences(Wilson et al., 1994) and in other publications.
The issues discussed in Waltner-Toews’ ar-ticle can therefore be explored from two dis-tinct epistemological perspectives: the ecolo-gist’s viewpoint, the contribution and useful-ness of the health paradigm to understand and
Cristina de AlbuquerquePossas
Escola Nacional de Saúde Pública,Fundação Oswaldo Cruz.
intervene on complex ecosystems; the publichealth perspective, the contribution of theecosystem health notion (or metaphor, as sug-gested by Gallopín, 1994), to understandingand confronting the complexity of epidemio-logical profiles and the emergence of diseases.
First, some ecologists view the incorpora-tion of the health paradigm for ecosystem re-search and monitoring change to maximizeecosystem health as problematic (Gallopín,1994). The definition of health is crucial here. Ifhealth is defined as something that might bekept constant (“people die and ecosystemsevolve”), then the notion of ecosystem healthwould not be appropriate to deal with sustain-ability in a dynamic and changing world. Incontrast, other arguments, as proposed byWaltner-Toews in this article, provide a defini-tion of health that can be broader, incorporat-ing into this approach the notions of balanceand harmony on the one hand and capacity torespond to changing environments on the oth-er. From this perspective, the notion of ecosys-tem health can provide interesting insights.
Second, from the public health perspectivethe issues concerning the contributions ofecosystem health are even more complex. Onthe one hand, the ecosystem health notion canprovide a crucial and missing ecosystem ap-proach to understand the complexity of epi-demiological profiles and the emergence ofdiseases. On the other, in a world where theeconomy and societies are being transformedby accelerating globalization and local policycommunities are gaining political and econom-ic power, it is important to stress that the con-ceptual force of the ecosystem health approachwill certainly depend on our capacity to incor-porate these social and political dimensionsinto a new theoretical framework.
Ecosystems have become complex socialecosystems (agro-industrial ecosystems and ur-ban ecosystems) increasingly transformed byhuman activities, interacting and expanding inways never before imagined. Globalization isincreasing local demands for political powerand participation, stimulating pressures for so-cial inclusion in sustainable development, par-ticularly in developing countries where socialexclusion and poverty are dramatic. Therefore,monitoring change in the structures of ecosys-tems leading to niches for potential pathogensto emerging diseases, as proposed by Waltner-Toews, requires a new approach. On the onehand, ecological frameworks consider the vari-ability of the physical and biotic environmentbut tend to homogenize people without takinginto account different social systems, classes,

WALTNER-TOEWS, D.28
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
or even the commodity as a physically power-ful social construct, tending to omit social as-pects of survival. On the other, the social sci-ences correspondingly make use of social dif-ferentiation without linking it to patterns of ex-posure and vulnerability to the biological andphysical environment.
Contributions by the social and political sci-ences to understanding and dealing with themacro-processes permeating ecosystems andhealth reform strategies should be integratedinto a new “social ecosystem health” paradigm(Levins et al., 1994; Possas & Marques, 1994;Levins & Lopez, 1999). Bringing together thesocioeconomic and biophysical dimensions ofhealth and trying to understand how social andecological variables appear to behave in com-plex systems, as Waltner-Toews has suggested,require more than incorporating these new el-ements into theory. It is necessary to bridge ina new theoretical framework the conceptualand methodological gaps between paradigmsfrom social sciences and ecology, which havehistorically been kept apart.
CONSTANZA, R., 1994. Supplementary comments onthe concept of ecosystem health. In: Agroecosys-tem Health: Proceedings of an International Work-shop (N. O. Nielsen, ed.), pp. 29-30, Ottawa: Uni-versity of Guelph/IDRC/CGIAR.
GALOPIN, G. C., 1994 Agrosystem health: A guidingconcept for agricultural research?. In: Agroecosys-tem Health: Proceedings of an International Work-shop (N. O. Nielsen, ed.), pp. 51-65, Ottawa: Uni-versity of Guelph/IDRC/CGIAR.
LEVINS, R.; AWERBUCH, T.; BRINKMAN, U.;ECKARDT, I.; EPSTEIN, P.; MAKHOUL, N.; POS-SAS, C. A.; PUCCIA, C.; SPIELMAN, A. & WILSON,M. E., 1994. The emergence of new diseases.American Scientist, 52:60.
LEVINS, R. & LOPEZ, C., 1999. Toward an ecosocialview of health. International Journal of HealthServices, 29:261-293.
POSSAS, C. A. & MARQUES, M. B., 1994. Health tran-sitions and complex systems: A challenge to pre-diction? Annals of the New York Academy of Sci-ences, 740:285-296.
RAPPORT, D. J., 1989. What constitutes ecosystemhealth? Perspectives in Biology and Medicine, 33:120-132.
SMIT, B. & SMITHERS, J., 1994. Sustainable Agricul-ture and Agroecosystem Health. In: Agroecosys-tem Health: Proceedings of an International Work-shop (N. O. Nielsen, ed.), pp. 31-38, Ottawa: Uni-versity of Guelph/IDRC/CGIAR.
WALTNER-TOEWS, D., 1994. Ecosystem health: Aframework for implementing sustainability in agri-culture. In: Agroecosystem Health: Proceedings of anInternational Workshop (N. O. Nielsen, ed.), pp. 8-20, Ottawa: University of Guelph/IDRC/CGIAR.
WILSON, M.; LEVINS, R. & SPIELMAN, A., 1994. Dis-ease in Evolution. Annals of the New York Acade-my of Sciences, 740.
Universidade de Brasília.
José Maria G.de Almeida Jr.
There are three main types of world views:holistic, fragmentary, and fractal (Almeida Jr.,1994; Almeida Jr., in press). The ecosystem ap-proach is by definition holistic, because it takesabiotic, biotic, and cultural factors into ac-count, along with a flow of matter and energyacross space and time. Accordingly, the con-cept of holistic health (or, for that matter,ecosystem health) involves all the patient’smental and family circumstances (social, eco-nomic, etc.) rather than just the physical andbiological aspects of disease.
There is no doubt that Waltner-Toews’ecosystem approach to health deals with thesubject as a whole rather than merely examin-ing it in a fragmentary way. But what aboutmind in his model? The lack of this dimensionis, in my opinion, the central weakness of hisotherwise intelligent, instructive, and usefulpaper.
It seems to me that the author fails to takethe reality of mind into account (at least in anexplicit way) in keeping with the scientific tra-dition of not dealing with elusive categories.This is a regrettable mistake. For example, whatcan be said of hard epidemiological data onhigh blood pressure caused by hidden emo-tions (Mann, 1999)? Or eye movement desensi-tization and reprocessing (EMDR) as a power-ful psychological procedure, developed mainlyby Shapiro (1995) as a therapy for overcominganxiety, stress, and trauma?.
The fact is that the role of mind-body inter-action in health and disease is so well recog-nized today (Benson & Marg, 1996) that it mustbe incorporated into any health-disease mod-el, especially a holistic one.
In addition to the above general remark, Iwish to propose some questions to the author:
1) How does the ecosystem approach tohealth relate to (1) gene therapy, (2) transgen-ics, and (3) cloning?.
2) “Many tropical diseases are thus not onlydiseases related to climate and environment,but are diseases of poverty.” In making this con-flictive affirmation, it seems that Waltner-Toewsdoes not really believe in tropical diseases asdiseases of poverty.
3) How does the author fully explain Dubos’formidable “mirage of health” concept (Dubos,1959) in light of the proposed ecosystem ap-proach to health, particularly with respect toemerging diseases?
4) Waltner-Toews’ ecosystem model of healthis part of an overall view of sustainable devel-opment. It would be interesting to know the

AN ECOSYSTEM APPROACH TO HEALTH 29
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
author’s opinion of an international effort to-wards that end.
ALMEIDA Jr., J. M. G., 1994. Desenvolvimento eco-logicamente auto-sustentável: Conceitos, princí-pios e implicações. Humanidades, 38:284-299.
ALMEIDA Jr., J. M. G. Holística: Por Uma Visão Estra-tégica de Desenvolvimento Ecologicamente Auto-Sustentável. (in press)
BENSON, H. & STARK, M., 1996. Timeless Healing.New York: Scribner.
DUBOS, R., 1959. Mirage of Health. New York: Harper.MANN, S. J., 1999. The Hidden Cause of High Blood
Pressure – Changing the Myths. London: Thor-sons.
SHAPIRO, F., 1995. Eye Movement Desensitization andReprocessing – Basic Principles, Protocols, andProcedures. New York: Guilford.
London School of Hygiene and TropicalMedicine.
Anthony J.McMichael
This paper addresses a complex topic: the“ecosystem approach to health”. We health sci-entists can readily lose our way among some ofthe concepts in this unfamiliar domain. We are,frankly, not used to thinking of health and dis-ease within an ecosystem-based framework;we prefer to attribute disease causation toevents or processes that arise and act at thelevel of the individual. This, for half a century,has been the dominant expectation of epidemi-ologists, and their methods are well-honed tothis expectation.
Scientists in the Western world are the in-tellectual heirs to three centuries of a very dif-ferent conceptual framework, that is, Newton-ian science that views the world as a mechani-cal system amenable to reductive analysis. Thishas been the science of disaggregation, quan-tification, and assumed orderliness; the sci-ence that assumes a gradualist relationship,wherein a small change in the initial condi-tions of some process will cause a small effect,while larger changes will induce larger effects.This is the scientific tradition within which doc-tors “have sought to localize disease within thebody, to identify specific pathological lesions,first in organs, then in tissues, then cells andnow molecules... A germ, toxin, or gene can beheld to account for most ailments, and the im-portance of predisposition, constitution, and so-cial or environmental circumstances has di-minished” (Anderson, 1999:49).
This conventional biomedical view is notwrong. But it is only part of the story – and per-
haps not even the most important part. A larg-er question for epidemiologists is to under-stand why disease rates rise and fall over time,why some populations have different ratesfrom others. Such questions are best answeredwhen there is recognition that the health of apopulation is an ecological index – that is, ittells us about the balance between that popu-lation’s biological needs and the capacity of theenvironment to meet those needs. In the longerterm the level of a population’s health reflectsthe adequacy of the carrying capacity of theenvironment. If we are slow to appreciate this,it is largely because humankind’s cultural de-vices, especially technological adaptations andthe buffering effects of imports, modulate theenvironmental carrying capacity; for humans(in contrast to other wild species) the carryingcapacity is not externally fixed.
This paper alludes to the ecological dimen-sion of human health. It describes, for exam-ple, how environmental interventions by hu-man societies alter the risks of transmission ofvarious infectious diseases. The theoretical basefor “ecosystem health” is presented in terms ofnested relationships – holarchies – and the in-terdependencies between levels and compo-nents. Nevertheless, the paper fails to makequite clear just what is the “ecosystem ap-proach”. Is this because that approach cannotbe defined so much as intuited from a genericunderstanding of how ecological systems andprocesses work? Is this a phenomenon that issubject to multiple interpretations, one thattakes us into the uncertain and chameleon-likerealm of non-normal science (Funtowicz &Ravetz, 1994)?
Elsewhere, Waltner-Toews and colleagueshave surveyed the historical progression of at-tempts to model influences on human states ofhealth (VanLeeuwen et al., 1999). The earliestmodel, from the 1930s, was the classical trian-gular host-agent-environment model whichelaborated the specific, one-agent-one-diseaseGerm Theory. In the 1950s, the British epidemi-ologist Jerry Morris propounded a social-eco-logical model in which the host was differenti-ated into genetic and experiential components,the environment was differentiated into physi-cal and social, and the “agent” became behav-iors of the person. Here was a pioneering inte-grative view of how diseases such as heart dis-ease arose within modern urban society – thiswas social realism, but with no explicit recog-nition of the role of the natural environmentand its life-support systems. In the 1970s and1980s various attempts were made to extendthese models, within a social-environmental

WALTNER-TOEWS, D.30
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
context. These mandala-like models recog-nized nested layers of influence, interactiveprocesses between those layered factors, andthe several dimensions of “health” – physical,mental, and spiritual. In the 1990s a more elas-tic, permissive, “butterfly” model of biophysi-cal and social-psychological influences onphysical, mental, and spiritual health has beenpropounded (Bormann, 1996).
And so we enter the 21st century, havingprogressed from simplicity, linearity, and box-es-and-arrows to complexity, multidirectional-ity, and porous, interacting spheres of influ-ence. This leads us to talk more comfortablyof “life course epidemiology” and to seek an“ecosystem approach” to health. The Newton-ian mold has been broken, though not discard-ed. This is what Wulff (1999:50) has referred toas the impending return of biomedicine to-wards the Aristotelian world view, “the theoriesabout open self-organizing systems, chaos, frac-tals and non-linear dynamics [that] have al-ready provided new and important insight intothe mechanisms of nature”.
We get further clues later in this paper. Walt-ner-Toews says we must use both current de-scription and an evolutionary understanding.Positivism is inappropriate. We must have a“feel” for why the system is like it is, and a feelfor what “health” (as an index of biological func-tioning within the system context) signifies.The issue is clarified as he explores the mean-ing of “ecosystem health” for infectious dis-ease: “What distinguishes many so-called tropi-cal diseases is that they occur in settings wherethe links between local ecosystems and localcommunities are intense and obvious.” [quotedfrom a preliminary version of the article].Wecan, he says, replace Linnaean branching clas-sification with generic groupings based oncommon ecological origins, e.g., housing-relat-ed infectious diseases in developing countries.We can see more clearly the interplay betweenlocal and global needs. We see the environmentas an interactive medium; like Heraclitus’ river,it is never the same twice. We also begin to seethat disease and death are part of a larger,healthy, ongoing ecological narrative, with thesuccession of generations.
Finally we see more explicitly the politicaldimension to all of this, the dimension thatgoes beyond phenomenological description.This may shock the purist ecologist. But, then,we are talking about the human animal, thespecies that supplements “nature” (genes) with“nurture” (cumulative culture). Waltner-Toewssays that: “The ecosystem approach is a way tobring together the socioeconomic and biophysi-
cal dimensions of health. Nevertheless, what itbrings to our understanding of emerging dis-eases is not so much a way of identifying newvariables – though it certainly forces us to castour net much broader than in conventional re-search – but a new way of organizing how wethink about them and respond to them.”
We are not yet very good at thinking interms of complex systems dynamics, in termsof holarchical relationships, nor within a long-term time frame. Striving for an ecosystem viewof human health and disease requires us to un-derstand these concepts. Faced by the chal-lenge of finding ecologically sustainable waysof living for over six billion people, this under-standing of human population health is essen-tial. This paper helps us along that path – apath that requires some large-frame humility,not small-frame biomedical hubris. In Waltner-Toews’ words: “Within an ecosystem approach,every policy decision is a hypothesis and everymanagement plan is a test of that hypothesis.”
ANDERSON, W. H., 1999. Perception of disease andits meanings. Lancet, 354(Sup.4):49.
BORMANN, F. H., 1996. Ecology: A personal history.Annual Review of Energetics and Environment,21:1-29.
FUNTOWICZ, S. & RAVETZ, J. R., 1994. Emergentcomplex systems. Futures, 26:568-582.
VAN LEEUWEN, J. A.; WALTNER-TOEWS, D.; ABER-NATHY, T. & SMIT, B., 1999. Evolving models ofhuman health towards an ecosystem context.Ecosystem Health, 3:204-219.
WULFF, H. R., 1999. The concept of disease: FromNewton back to Aristotle. Lancet, 354:SIV49.
School of Communityand Regional Planning,University of British Columbia.
William E. Rees Commentary: an ecosystem approach to survival
“…human civilization – primarily Western tech-noindustrial urban society – will self-destruct,producing massive ecological damage, socialchaos, and megadeath.” (Smith & Sauer-Thomp-son, 1998).
David Waltner-Toews presents a strong casefor ecosystemic thinking – indeed socio-ecosys-temic thinking – in the future control of tropi-cal and emerging diseases. Several key pointsstand out, particularly the association of manydiseases with poverty (exposure to vectors un-der crowded, unsanitary conditions); the mul-tiple disease-favoring effects of the ecosystem

AN ECOSYSTEM APPROACH TO HEALTH 31
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
disruption accompanying the expansion of hu-man activities, and the growing recognitionthat “normal” predictive (Newtonian) scienceis an inadequate foundation for either popula-tion heath or ecosystem management. Indeed,the behavior of complex dynamic systems de-mands humble recognition that the best strate-gies for maintaining population health are like-ly to be those that enable society to adapt withminimal damage to unanticipated systemschange.
If the paper has a major substantive flaw itlies in its paradoxically near-static approach tothe dynamic systems it is analyzing. There islittle reference to the rate or nature of globalchange. Certainly the ecosystemic approachwould be a powerful tool if the world were inecological steady-state, but Waltner-Toews’ ar-guments are all the more compelling in the realworld of dynamic change.
And this is definitely a world of dynamicchange – the past two centuries have seen themassive expansion of the human enterprise onthe one hand, accompanied by the precipitouserosion of ecosystems and the life-supportservices they provide, on the other. Most criti-cally from the perspective of socio-ecologicaldisease control, this anthropogenic explosion/implosion continues unabated. Much of thecontemporary world is currently ‘enjoying’ anunprecedented stretch of continuous materialgrowth. Indeed, the global economy has tripledin size and the human population has bal-looned by 30% to six billion since 1980. Mean-while in the course of industrialization, half theworld’s forests have been logged or converted(rate:130,000 km2 yr-1); half the land on earthhas been modified for human use; half theworld’s wetlands have been lost; 70% of its ma-jor fish-stocks have been placed in jeopardy;atmospheric carbon dioxide has risen 30% andclimate change is upon us; and biodiversityloss is accelerating (extinction is now at least1000 times the “background” rate).
Mindful of the emerging possibility of cata-strophic systems “flips”, Waltner-Toews recom-mends research that will identify and protect“holarchic boundaries” to avoid critical systemsbeing drawn into “new attractors”, and policiesthat will protect relatively pristine ecosystemsfrom “human invasion”. He also recognizes thatwe must address the chronic poverty that ex-poses ever greater absolute numbers of peopleto new and emerging diseases. However, heprovides no indication of how these policiesmight be implemented or whether they cansucceed on a finite planet dedicated to materi-al growth.
These are not trivial questions. Should pre-vailing growth rates continue, we can expect anadditional five-fold expansion of economicoutput and up to four billion more members ofthe human family by 2050. Given the prevailingvalues of consumer society, the massive expan-sion of the human enterprise necessarily meansthe continuing dismantling and contraction ofnature (Rees, in press). Feeding the expandingpopulation requires the invasion and destruc-tion of pristine ecosystems; globalization com-moditizes nature while marginalizing the non-market – but vital – life-support functions itprovides; liberalized global trade and export-led ‘development’ create economic incentivesto over-exploit resource systems; productionagriculture and forestry homogenize naturalecosystems and impose unstable monocul-tures that can be maintained only at great eco-nomic and material cost. Meanwhile, despitethe unprecedented expansion of the economy,a quarter of humanity still lives in abject pover-ty and is increasingly at risk from environmen-tal collapse and accompanying disease. (Thewidening income gap poses an unprecedentedmoral challenge to the world. In 1960, the rich-est fifth of humanity earned ‘only’ thirty timesas much as the poorest fifth; by 1990 the ratiowas about 60:1 (UNDP, 1994) and is on its wayto 90:1 today.) In short, all the factors Waltner-Toews identifies as favoring ecosystems col-lapse and new diseases, are running amokacross the planet.
The destabilizing effect on the ecosphere isbeginning to show. According to the Interna-tional Red Cross’s 1999 World Disasters Report,singular events such as Hurricane Mitch andthe El Niño weather phenomenon, plus declin-ing soil fertility and deforestation, drove arecord 25 million people from the countrysideinto crowded, under-serviced, disease-riddenshantytowns around the developing world’srapidly growing cities. This is 58% of the world’stotal refugees. The Report predicts that devel-oping countries in particular will continue tobe hit by super-disasters driven by human-in-duced atmospheric and climatic change, eco-logical degradation, and rising populationpressures. This is a recipe for a global popula-tion health calamity. As Waltner-Toews writes,“the ecosystem approach brings home thedeep understanding that we cannot “‘manage’the planet for health…” (my emphasis). Let ushope it also brings home the understandingthat humanity’s best chance for survival withdignity rests with our learning better to man-age ourselves.

WALTNER-TOEWS, D.32
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
REES, W. E. Patch disturbance, eco-footprints, and bi-ological integrity: Revisiting the limits to growth.In: Ecological Integrity: Integrating Environment,Conservation and Health (D. Pimentel & R. Nosseds.). Washington, D.C.: Island Press. (in press)
SMITH, J. W. & SAUER-THOMPSON, G., 1998. Civi-lization’s wake: Ecology, economics and the rootsof environmental destruction and neglect. Popu-lation and Environment, 19:541-575.
Instituto de Saúde Coletiva, UniversidadeFederal da Bahia.
Maurício L.Barreto
Interventions in the environment and society in the quest for health:how scientific can we be?
There is no doubt that one of the current char-acteristics of many scientific fields is to seekall-encompassing models capable of providingmore convincing and useful explanations forthe phenomena under study. No matter howmuch I reflect on the notion that science candevelop itself on its own strengths, I take a firmstand with those who view science as funda-mentally tied to the search for solutions to con-crete problems, even though this may requireinvestigative projects in the short, medium,long, and very long terms. Such effort can beunderstood as one of the most useful exercisesin strategic planning, and as such the under-taking entails risks, since of course part of theeffort fails to materialize in the form of actualproducts. At any rate, we may always ask: a so-lution to what? a solution for whom? The arti-cle under debate aims a cutting but fair cri-tique at the biomedical models flourishingaround disease. In such models the idea ofhealth, no matter how embellished it may be,is never understood beyond the notion of cure(or prevention of disease at most). Such mod-els are hardly useful whenever one thinks ofhealth as something positive (and here it is un-necessary to repeat the well-known WHO defi-nition) rather than as the mere absence of dis-ease. If we do think along these lines, we canonly ask what should be done by all those whocriticize, find fault, or even abhor such models?Of course this question is asked frequently, butthe answer is not at all easy (Barreto, 1998). Forexample, in a recent review of the child healthissue, Ehiri & Prowse (1999) discuss the extentto which preventive and promotional pro-grams reflect the Western medical care model,with little emphasis on child health’s environ-
mental and social dimensions, even though itis the object of extensive discussion and appar-ent consensus.
The biomedical model is reaffirmed dailyby immense research and intervention struc-tures, based on an enormous and lucrative in-dustrial and services framework, worshippedby many, but considered scarcely useful andeven iatrogenic by (a few) others. Consideringthe scientific research component alone in theUnited States, the National Institute of Healthalone invests 14 billion dollars a year. But wedo not have to look that far for examples, sincein Brazil the scarce resources for health allocat-ed through the Ministry of Health and its affili-ated institutions basically serve to reaffirm thissame Western biomedical model.
With recent advances in molecular genet-ics, more than a few believe that human ills (in-cluding health problems) are located in thegenes and the molecules coded by them. Forthose who so believe, issues like the environ-ment, society, and other blah-blah-blahs aremerely ideological elements that feed the polit-ical action of a handful of upstarts, or in a moreuseful way, when properly presented, to serveas an enticing introduction to the discourse ofeven the very proponents of the biomedicalmodel. This reminds us of Pasteur’s Revolution,a transcendental moment in the progress ofscientific knowledge; however, when it wascontextualized within the philosophical hue ofPositivism it transmuted the idea of microbialcausality of disease (a huge step forward in late19th-century scientific knowledge) into dog-ma, a fact with repercussions that are still felttoday and that have hampered (if not com-pletely impeded) other approaches to healthand human diseases. An analysis of recent ad-vances in biology and molecular genetics showshow these fields have spawned a new revolu-tion in knowledge of the human body, but thatthey have simultaneously fed a growing legionof ideas that once again seek to reduce humanhealth to its biological determinants, consider-ing discussions of man and the environment orman and society as merely ideological, with noscientific basis.
The paper currently under debate toucheson these and other discussions and proposes amodel, the “ecosystem approach”, which is cer-tainly appealing since it “brings together the so-cioeconomic and biophysical approach tohealth”. Obviously, if the biomedical model cur-rently predominates when the issue is knowl-edge concerning the causes of health and dis-eases, what can we expect from the interven-tions to be conducted vis-à-vis supposedly

AN ECOSYSTEM APPROACH TO HEALTH 33
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
known problems? A question that remains tobe answered is whether we can propose effec-tive and scientifically sound interventionswithout a clear causal model for health prob-lems. Elementary scientific logic tells us thatwhen we intervene in reality we must avail our-selves of reasonable models on which to testthe intervention, but that each intervention al-so needs to be empirically tested. Herein liesan imperfection left by incomplete scientificprogress, that is, the scarcity of resources forevaluation of interventions. If we now some-times spend decades discussing whether a giv-en vaccine is effective, we can only imaginetackling the daunting task of evaluating a com-plex and much less clearly outlined interven-tion as proposed under the “ecosystem ap-proach”.
Of course the ideas laid out here may sug-gest a paralyzing and backward-thinking typeof “scientism”, as opposed to the “progres-sivism” of the “ecosystem approach”. No, Iwould never think that actions should neces-sarily be governed from beginning to end byscientific rationality, as indeed is the status thatthe “ecosystem approach” seeks. However, I be-lieve that interventions in human populationsare politically defined, with a greater or lesserdegree of rationality and scientific basis. Thereis no doubt that human health underwent in-terventions before scientific knowledge exist-ed, and sometimes even with great success.
In short, I do not believe that we have “sci-entific” answers to many of the main issues af-fecting human health. We know that manythings are wrong, we share in the criticism con-tained in the paper, and we agree with the ur-gent need to “address the flaws in reasoningand tactics we have employed to date”. Howev-er, all this serves more to orient the agenda fora scientific program and less to orient scientifi-cally based interventions. Meanwhile, thereis a wide range of evidence suggesting thatchanges are needed in society and the environ-ment to achieve better health standards, butthat this agenda is far from being defined inmerely scientific terms. At most, the sciencesin their current stage can provide clues for po-litically organized societies to choose the bestactions, or sometimes the lesser of two evils,with a view towards solving their health prob-lems. It was no coincidence that the report byan expert committee named by the UK Min-istry of Health to recommend policies for re-ducing existing health inequalities noted thatinterventions in this field had rarely been sub-mitted to controlled evaluation methods; how-ever, this did not keep the committee from
seeking its own alternatives in order to issueopinions on the effectiveness of existing healthinterventions and thus offer scientifically basedalternatives to bolster the country’s socialhealth policies (Acheson et al., 1998). Some be-lieve that epidemiology’s multifactorial causalmodels only serve as a counterpoint to tradi-tional biomedical models when they are basedon the idea that health (as a biologically basedevent) is, in the final analysis, a social phenom-enon (Tesh, 1998) and that in order to be effec-tive, proposals generated from the perspectiveof social epidemiology must seek not only sci-entific support but above all social and politi-cal backing (Heymann, 2000).
ACHESON, D.; BARKER, D.; CHAMBERS, J.; GRA-HAM, H.; MARMOT, M. & WHITEHEAD, M., 1998.Independent Inquiry into Health Inequalities.London: The Stationery Office.
BARRETO, M. L., 1998. Por uma epidemiologia desaúde coletiva. Revista Brasileira de Epidemiolo-gia, 1:104-130.
EHIRI, J. E. & PROWSE, J. M., 1999. Child health pro-motion in developing countries: The case for in-tegration of environmental and social interven-tions? Health Policy and Planning, 14:1-10.
HEYMANN, S. J., 2000. Health and social policy. In:Social Epidemiology (L. F. Berkman & J. Kawachi,eds.), pp. 368-382, New York: Oxford UniversityPress.
TESH, S. N., 1988. Hidden Arguments: Political Ideol-ogy and Disease Prevention Policy. New Brunswick:Rutgers University Press.

WALTNER-TOEWS, D.34
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
I am grateful to the respondents for their cri-tiques both of the arguments I have made, andof the less-than-clear way in which I presentedthem. They have been generous in making al-lowances for my own struggle with understand-ing and presenting the theory and the practiceof an ecosystem approach to health. I havetried to incorporate the editorial comments in-to the article itself in such a way as to clarify myarguments but not, in the interests of real de-bate, to change them.
I feel the need to clarify the context of thearticle and make a few general comments. Iwas invited to take the ecosystem approach tohealth and apply it to how we think about trop-ical and emerging diseases. I have elsewherediscussed concepts and models of health insome detail, and in this article focused only onthe tension between health – which I describeas a negotiated construct within biophysicalconstraints – and disease, which is merelyone of many constraints (Waltner-Toews &Wall, 1997; Waltner-Toews, 2000). Secondly, theecosystem approach to health, which is a par-ticipatory research and management method-ology, firmly rooted in complex systems theo-ries (which include elements of chaos and cat-astrophe theory), needs to be distinguishedfrom ecosystem health, which is an attempt toapply health management ideas to ecosystems.Whereas the ecosystem approach states that“there is not one material system to which ourdefinitions must conform”, ecosystem healthtends to take a more biomedical view that thereis indeed one material system on which we canagree, and whose health we can assess. Thusecosystem health tends to focus on outcomes,and the ecosystem approach tends to focus onprocess. This is obviously not a clear division,rather a difference of focus.
Luiz Jacintho da Silva is quite correct in cit-ing the historical antecedents of viewing dis-eases in ecological context. What distinguishesHippocrates, the 19th-century sanitarians,Pavlovsky, and Virchow from this current effortis a changed understanding of the naturalworld and our place in it. We have gone from apurely empirical sense of inter-relatedness, tomiasma theories, to a focus on specific etiolog-
The author repliesO autor responde
ic agents, back to the agent-host-environmenttriad, and now to a more complex and sophis-ticated understanding of inter-relatedness.From both da Silva’s and Foller’s comments, itis clear that I have not communicated with suf-ficient clarity that the ecosystem approach, be-cause it requires local participation to definethe elements and relationships of interest in agiven ecosystem, is necessarily rooted in cul-ture as well as nature. However, as Cristina deAlbuquerque Possas points out, there are ten-sions between the scientific tendency to ho-mogenize, and the cultural tendency to partic-ularize. The ecosystem approach, drawing onwhat has been called Post Normal Science(Funtowicz & Ravetz, 1994), incorporates thesetensions by requiring negotiation and whatJames Kay has called “cross talk” (Kay et al.,1999). Because of this, implementing “ecosys-tem approach to health” programs must facenot only deficits in our understanding of socio-ecological systems, but very real and oftendaunting political power struggles. We contin-ue to debate these issues, and how to deal withthem, in workshops sponsored by the Networkfor Ecosystem Sustainability and Health (NESH),as well as on our web-site (www.nesh.ca).
Given the practical issues of competing in-terests, governance, and uncertainties not justamong disciplines, but among researchers andnon-researchers, both Foller and Moran won-der about implementing this approach. Theyare quite correct to see these as challenges, butI think Moran is unduly pessimistic. Conflictresolution in the development context has re-ceived considerable attention in recent years(see, for instance, Buckles, 1999). Furthermore,we have found, at least at the local communitylevel, that many people understand, accept,and can work with uncertainty and compro-mise if they are part of the investigative andmanagement process. Many government insti-tutions have problems implementing policieson public health and environmental issues be-cause they assume that their “experts” can ade-quately define the risks and hence impose so-lutions on the public. The public will shoulderrisks they have chosen, but not those imposed.In this context, the major practical constraintsto implementing this approach relate to democ-racy, a sense of a common good beyond the in-dividual household, and knowledge (not nec-essarily formal education, but the ability to ar-ticulate understanding and argument). In manypoor countries, the third component is miss-ing. In North America, a lack of the secondcomponent has proven to be the major prob-lem. Again, there are exceptions; some of us
David Waltner-Toews

AN ECOSYSTEM APPROACH TO HEALTH 35
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
have found modern students of science inNorth America to be unable to clearly articu-late understandings and arguments. I did notdiscuss specific methodological tools in the ar-ticle, but the process invariably involves trian-gulating results from a combination of meth-ods, ranging from those developed by partici-patory action practitioners (which are usuallycentral), to those used in conventional scholar-ly inquiry, Soft Systems Methodology (Check-land & Scholes, 1991), influence diagrams, andnewer dynamic simulation models and Geo-graphic Information Systems. The specific toolsused are determined by the questions beingasked by the participants.
José Maria G. de Almeida Jr. raises severalinteresting and important points. Since mywife is a counselor-therapist, I am well awareof EMDR (which links mind and body at an in-dividual level), as well as the broader literaturelinking mental and social conditions to bio-physical health at more encompassing sys-temic levels in the socio-ecological holarchies(e.g. Evans et al., 1994). Health in the tropicshas both socioeconomic (e.g., poverty) and eco-logical (e.g., climate) constraints. One of theways we have dealt with that in implementingthe ecosystem approach is to require local,public participation defining the research ques-tions and the management options. The processitself empowers people and promotes health;this is what I mean by saying that the meansachieve the ends.
I consider gene therapy to be a medical pro-cedure and not a health promotion technique,and cloning faces the same problems as othergenetic engineering of organisms, in that (amongother things) it changes the rate of change at aparticular scale (the individual) and hence cre-ates serious disturbances at other, co-evolvingscales which cannot adapt as quickly (Giampi-etro, 1994). Bill Reese makes this point muchmore forcefully in his comments. If I have down-played the rapidity of change and the potentialfor catastrophe it is because, from a practicalpoint of view, I have found that such descrip-tions of the situation, while probably true, tendto foster some combination of panic with de-spair, numbness, or totalitarianism. Indeed, Iwould argue that many of the lists of quantita-tive indicators of sustainability generated by in-ternational agencies reflect these tendencies.Faced with the urgency of systemic breakdownand hemorrhaging of species, my veterinarytraining tells me that calm, considered inter-ventions may get us further toward our goals.
Still, Dubos’ “mirage of health” can be dis-couraging for anyone working in the health
field, since it quite clearly demonstrates thathealth, as a state, is a moving, probably unat-tainable, target. Studies using the ecosystemapproach may be classified in static form (Fig-ure 1), and portions of it may be teased apartand made to appear linear (Figure 2), but theprocess overall is always, in practice, an itera-tive one of continuous re-negotiation of goalsdefined from different perspectives, actions,assessments, changed understandings, and re-negotiation (Figure 3). This is not a process witha beginning and an end, and reflects the factthat good health is a function of both the out-comes and how they are achieved. Health inthis context is not so much a mirage as a senseof well-being that we need to continually rede-fine and renew as the world changes.
Dr. Lima Barreto’s comments raise thequestion of whether the ecosystem approach,as here defined, is science at all. John Robin-son, Director of the Sustainable DevelopmentResearch Institute at the University of BritishColumbia, has argued that what we are talkingabout is “co-generation of knowledge”, and thatby referring to it as a kind of “post-normal sci-ence” we are giving unwarranted credit to sci-entists (personal communication). People likeFuntowicz and Ravetz tend to see this as an en-richment or expansion in the nature of science,in which the primary task of scientists is tohelp us find ways to live with what appears tobe irreducible uncertainty. That is, in address-ing questions marked by epistemological andethical conflicts and where the stakes and un-certainties are high, a new kind of public sci-ence, responding to an expanded peer group,is required. This is still, I think they would ar-gue, a systematic gathering of knowledge in thepursuit of general laws, open to scrutiny andevaluation and verification by peers, and thusqualifies as a kind of science. One could arguethat this is simply a sort of “rational politics”, apolitics informed by science. Barreto’s responseto this is that political interventions are onlypartly rational and scientific. As, I would add,is the very notion of health. Indeed, one mem-ber of our NESH group – not coincidentally, Ithink, a Peruvian – has argued that we pay fartoo little attention to the forces of politicaleconomy in our ecosystem approach. Survey-ing the political and health landscape at thebeginning of the 21st century, I have no con-vincing response to this. The struggle to findreasonable resolutions to complex and oftentragically absurd situations is a struggle, I think,worth pursuing.
Barreto wonders how we can measure suc-cess. The ecosystem approach is focused on re-

WALTNER-TOEWS, D.36
Cad. Saúde Pública, Rio de Janeiro, 17(Suplemento):7-36, 2001
solving the practical, complex problems of howwe can live well (with health), as one speciesamong many, on this planet. In a constantlychanging context, how can we know if we havesucceeded? In at least one of our projects (inKenya) we derived two sets of indicators formeasuring success – one created by the researchteam, and one created primarily by the vil-lagers. The latter, we found, were the more use-ful – though much more difficult for researchersto measure – because they reflected the quali-ties of life that people actually cared about.Nevertheless, health is also a concept full ofcontradictions, in which for instance, globalhealth may dictate restrictions on local health,and population health in a context of ecologi-cal constraints requires the death of some indi-viduals. Indeed, we face many tragedies whichhave no technical solutions. As both a scientist
and an activist, I think that the ecosystem ap-proach to health, as defined in this paper,which struggles as much with process as withoutcome, offers (at least to the extent to whichthe ideal is realized) some hope for dealing withquestions where conventional science and pol-itics appear to be at an impasse. Nevertheless, Ido not believe that we will ever find a definitiveway of coping with the uncertainty, tragedy,and wonder of the human condition. For thisreason, music, poetry, stories, and rituals willalways be essential for achieving health. Butthat is another paper.
BUCKLES, D., 1999. Conflict and Collaboration inNatural Resource Management. Ottawa/Washing-ton, D.C.: IDRC/World Bank Institute.
See the original article for all other references.





























