Embed Size (px)
Citation preview

Caso Clínico / Clinical Case
STREPTOCOCCUS GALLOLYTICUS BACTERAEMIA ASSOCIATED WITHCOLONIC ADENOMATOUS POLYPSA. MURINELLO1, P. MENDONÇA1, C. HO1, P. TAVARES1, H. PERES1, R. RIO TINTO2, A. MORBEY1,C. CAMPOS1, A. LÁZARO1, A. MILHEIRO, M. J. ARIAS, J. OLIVEIRA1, S. BRAZ1
152 A. MURINELLO ET AL GE Vol.13
Recebido para publicação: 26/09/2005Aceite para publicação: 15/02/2006
(1) Departments of Internal Medicine 1, Pathology, Histopathology,Surgery and Gastroenterology, Curry Cabral Hospital, Lisbon, Portugal.(2) Department of Gastroenterology, Stº Antº Capuchos Hospital, Lisbon.Portugal.
Resumo
A bacteriémia por Streptococcus gallolyticus associa-se fre-quentemente ao carcinoma colorrectal, tornando obri-gatória a colonoscopia nestas situações. A endocardite bac-teriana e a artrite séptica são também comuns neste tipo debacteriémias. Tem sido levantada a hipótese das bactériasintestinais poderem ter um papel promotor de hiperproli-feração celular aberrante em lesões cólicas pré-neoplási-cas, aparentemente devido a processos inflamatórios cróni-cos e produção de metabolitos carcinogénicos. Os autoresapresentam o caso dum doente com vários pólipos adeno-matosos tubulares do cólon direito, em dois dos quais sedemonstrou uma área de displasia de alto grau adjacente azona de colite infecciosa bacteriana, associados a quadroclínico de infecção sistémica por Streptococcus gallolyticuse artrite do tornozelo.
Summary
Bacteraemia due to Streptococcus gallolyticus is frequentlyassociated with colorectal carcinoma, making evaluation ofthe gastrointestinal tract by colonoscopy obligatory in suchcases. Bacterial endocarditis and purulent arthritis are alsocommon in patients with these bacteraemias. Intestinalbacteria could behave as promoters of aberrant hyperpro-liferative behaviour in preneoplastic colorectal lesions,apparently due to chronic inflammatory processes and pro-duction of carcinogenic metabolites. The authors treated apatient with several tubular adenomatous polyps of theright colon, two of which showed areas of high-grade dys-plasia adjacent to areas of infectious bacterial colitis asso-ciated with Streptococcus gallolyticus bacteraemia and uni-lateral ankle arthritis.
INTRODUCTION
The aetiology of colon cancer can be related to environ-mental and hereditary factors (1). Bacteria have beenlinked to cancer by two mechanisms: chronic inflamma-tion and production of carcinogenic metabolites (2).Intestinal microflora has been reported to have an actionon the pathogenesis of colon cancer (3). For someauthors it appears to act as a promoter of aberrant hyper-proliferative behaviour in preneoplastic lesions (4). Itwould be of interest to substantiate any relationshipbetween Streptococcus gallolyticcus (formerly known asStreptococcus bovis 1) (5) colonic carriage, colonicpolyps and particularly the type of polyp and its mali-gnant potential. Burns (6) demonstrated that highly pre-malignant polyps were found to be more often associa-ted with Streptococcus gallolyticcus carriage than werebenign polyps. The frequency of involvement ofStreptococcus gallolyticcus bacteraemia in colorectalneoplasia is, however, the subject of controversy, due toits association with both benign (diverticulosis, inflam-matory bowel disease, cecal volvulus, perirectal abscess,
GE - J Port Gastrenterol 2006, 13: 152-156
hemorrhoids, benign polyps) and malignant disease ofthe colon (6,7,8).Enterococci are the predominant Streptococci isolatedfrom human feces, but Streptococcus gallolyticcus hasalso been found in the faecal flora of 10 to 16% ofhealthy human subjects (6,9). In an interesting study byLeport (10) of 77 infections with group D Streptoco-ccusendocarditis, colonic polyps were significantly morefrequent in the Streptococcus gallolyticus group (67%)than in the Enterococcus group (21%). In this study, thefrequency of colonic carcinoma was also significantlyhigher in patients found to have Streptococcus galloly-ticcus endocarditis (18%) than in patients with Ente-rococcus endocarditis (2%). Isolation of Streptococcusgallolyticcus in blood cultures is diagnostically signifi-cant, because this bacteria is a normal inhabitant of thegastrointestinal tract, and bacteraemia and endocarditisdue to these bacteria are often associated with colorectalneoplasia (11,12,13,14). A full evaluation of the gas-trointestinal tract in patients with Streptococcus gallolyt-iccus bacteraemia, with or without endocarditis, ismandatory, due to high frequency of isolation of

Maio/Junho 2006 BACTERIÉMIA POR STREPTOCOCCUS GALLOLYTICUS 153
Streptococcus gallolyticcus in the blood of patients withvarious gastrointestinal diseases (6,7,8). Pyogenicarthritis as a complication of colonic neoplasia was alsoreferred to by some authors (15,16,17).Recently it was reported that patients with colorectalcancer have increased faecal carriage of Streptococcusgallolyticcus (56%) compared to normal individuals andpatients with benign diseases of the colon, such ascolonic diverticulosis, inflammatory bowel disease,cecal volvulus, perirectal abscess and hemorrhoids (10-23%) (6,7,8). The lower percentages of faecal carriageof Streptococcus gallolyticcus found by Burns (6) wereattributed by the author to the different methodology ofthe study, but even so, a statistical significant, progres-sively higher percentage of faecal carriage of Strepto-coccus gallolyticcus was demonstrated between normalindividuals and patients with tubular adenomas,tubulovillous adenomas, villous adenomas and patientswith colorectal cancer. These results raise the questionof whether it is the malignant milieu of the colon thatpromotes the growth of Streptococcus gallolyticcus or ifStreptococcus gallolyticcus contributes in some way tothe malignant milieu. (6).In addition to colorectal cancer, there have been a fewreports of Streptococcus gallolyticcus bacteraemia asso-ciated with colonic adenoma (6, 18). The authors treateda patient with several tubular adenomatous polyps of theright colon, two with areas of superficial high-gradedysplasia, one of which was ulcerated. However, surgi-cal sampling did not reveal high-grade dysplasia, ratherit showed only several tubular adenomas with low-gradedysplasia, together with adjacent apparent features ofinfectious colitis on the ulcerated polyp. No malignanttissue was detected, and the patient is well and shows nosigns of malignant evolution one year after right hemi-colectomy, although we recently found four other ade-nomatous polyps that probably went undetected in theprevious colonoscopy. Two of these were tubulovillousadenomas with low-grade dysplasia and two were tubu-lar adenomas, one with high-grade dysplasia occupying5% of the glandular area.
CLINICAL REPORT
A 55 year old Caucasian man was admitted to our Unitin October 2004 complaining of a fever (37.8-38.5º C)almost every evening, of three weeks duration, alongwith nocturnal diaphoresis and intermittent arthralgia ofthe right ankle. He denied any other symptoms. Hereported frequent consumption of cottage cheese andthat he had been to Tunisia the month before. Heappeared well nourished and somewhat pale.
Temperature was 38.2ºC, blood pressure 130/70 mm Hg,heart rate 100 beats p/min. Thoracic and abdominalexaminations were normal. There were no signs ofanaemia. Painful swelling of the right ankle was appa-rent, although without other signs of inflammation andinfection. Digital rectal touch was normal. LAB tests revealed: slight normocytic, normochromicanaemia (Hgb 10.8 g/dL), no leucocytosis, normalplatelets, ESR 79 mm/1st hour, normal coagulation tests;normal SMA-12 biochemical profile; normal serumimmunoglobulins; negative ANA, DNA and Coombstests; slightly elevated C3, C4 and haptoglobin levels.Serology for HAV, HBV, HCV, HIV, CMV, EBV, Herpesvirus, Yersinia, Brucella, Borrelia and C. burnetti wereall negative; CEA and CA 19.9 levels were normal.Meanwhile, x-ray of the ankle and CT scans of the tho-rax and abdomen were normal. No endocarditic vegeta-tions were detected on echocardiogram. A completecolonoscopy revealed several sessile and pediculatedpolyps on the right colon of varying sizes, one morula-ted polyp at 70 cm (8 mm), one sessile polyp at 80 cm(1,5 cm) and two contiguous sessile polyps at 100 cm (3cm) (Figure 1). Biopsies of the polyps showed featuresof tubular adenomas with low-grade dysplasia on thepolyp at 70 cm and high-grade dysplasia on the polypsat 80 and 100 cm. After this examination we decided tobegin empirical antibiotic therapy with gentamicin andceftriaxone. The patient became apyretic after the se-cond day of therapy and the arthritis was promptlyresolved. Seven days after the colonoscopy, five bloodcultures taken the day of admission were all positive forStreptococcus gallolyticcus, sensitive to penicillin G,ampicillin, cefotaxime, erythromycin and clindamycin.Nevertheless, we decided to continue the previouslyinstituted empiric therapy for a complete course of 15days, due to the good response to therapy. Two consult-ing gastroenterologists decided on definitive surgical
Figura 1 - HEx10: Colon biopsy: tubular adenoma with high-grade dysplasia.
treatment. This decision was based on the size andhistopathology of the biggest polyp and its unresectabi-lity, the friability of the right hemicolon, and alsobecause it was associated with bacteraemia in five bloodcultures, due to the risk of recurrent bacteraemia andpossible complications, such as endocarditis. A righthemicolectomy was performed, the surgical specimenrevealing a greater number of polyps than were seen onthe colonoscopy - both sessile and pediculated polyps atvarious distances from the distal border: at 5 cm (sessilepolyp 4x2x1.5 cm), 6.5 cm (depression area with efface-ment of the mucosal folds 3x2x0.9 cm) (area of previousbiopsy?), 11 cm (two pediculated polyps: 2x1 cm and2.6x0.5 cm); 14.5 cm (sessile polyp 0.5x0.3 cm), 16 cm(sessile polyp 4.5x3x1 cm), 21.5 cm (sessile polyp 0.3cm) and 29 cm (sessile polyp 0.9x0.5 cm). On micro-scopic view the polyps were all tubular adenomas withlow-grade dysplasia (Figure 2). No areas of high-gradedysplasia were found in the surgical sample. The biggestof the polyps was ulcerated and had intense transmuralneutrophil inflammatory infiltrate (Figure 3) with phle-gmonous areas, abscesses and tissue necrosis. Theepithelium of the polyps showed areas of accentuatedcrypt reduction and foci with crypt abscesses (Figura 4),due to infectious colitis, and ischemic colitis. Acute peri-intestinal lymphadenitis with sinus hystiocytosis wascons-picuous, but no neoplastic tissue was identified.These histopathological features suggested a continuinglocal infectious process despite the apparen-tly goodresponse to antibiotic the-rapy. No history of prior colondisease was elicited and nor was there any family histo-ry of colonic polyposis or colorectal cancer. One yearafter surgery the patient was doing well, but a follow upcolonoscopy done at that time showed four other pedi-culated polyps, which in retrospect we believe, based ontheir size, had probably been missed on the previouscolonoscopy due to less than optimal bowel cleansing.
These were located at 30 cm (10 mm) on the sigmoidcolon, at 60 cm (1x0.5 cm), at 62 cm (0.8x0.5 cm) andat 65 cm (2mm) on the transverse colon. All the polypswere removed by colonoscopic polypectomy. The firstpolyp was a tubular adenoma with low-grade dysplasia,the second and the fourth polyps were tubulovillous ade-nomas with low-grade dysplasia, but the third polyp wasa tubular adenoma with focal high-grade dysplasia occu-pying 5% of the glandular area. The basal areas of all thepolyps did not reveal dysplasia and neoplasic tissue. A follow up colonoscopy will be done in one year's timeand, if normal, again within two to three years. If it con-tinues to be normal, future monitoring will be done withcolonoscopies every 3 to 5 years.
DISCUSSION
Due to the common association between Streptococcusgallolyticcus bacteraemia and colorectal cancer and
154 A. MURINELLO ET AL GE Vol.13
Figura 2 - HEx5: Surgical sample of right colon: tubular adeno-mas with low-grade dysplasia.
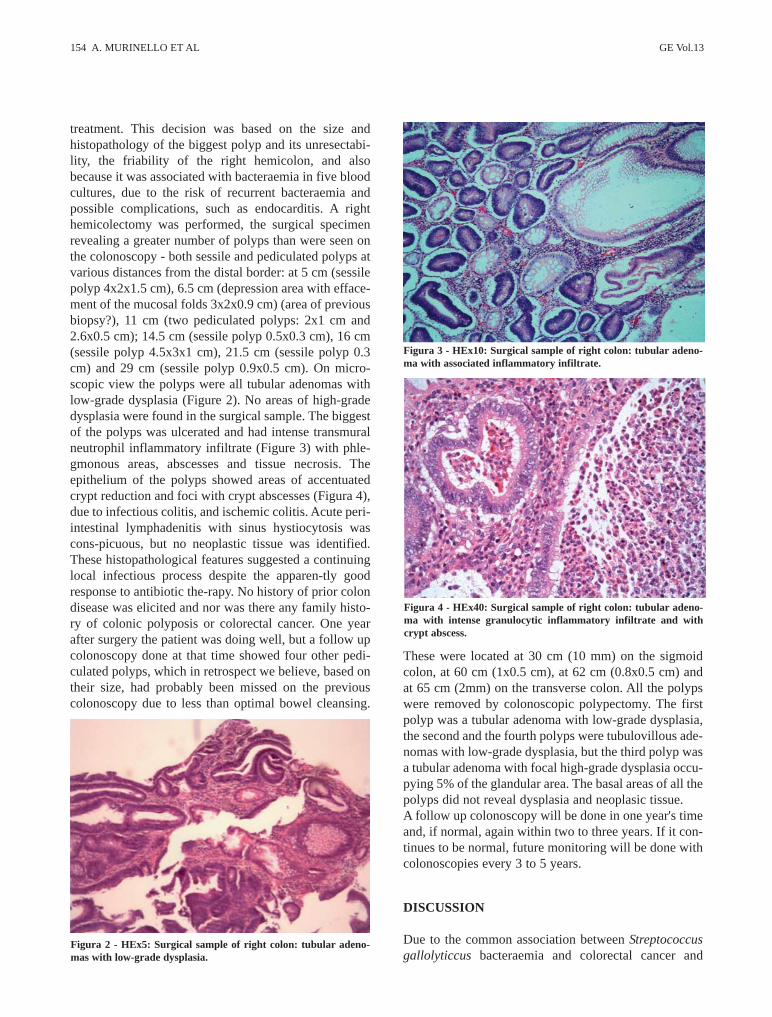
Figura 3 - HEx10: Surgical sample of right colon: tubular adeno-ma with associated inflammatory infiltrate.
Figura 4 - HEx40: Surgical sample of right colon: tubular adeno-ma with intense granulocytic inflammatory infiltrate and withcrypt abscess.

Maio/Junho 2006 BACTERIÉMIA POR STREPTOCOCCUS GALLOLYTICUS 155
tubulovillous and villous adenomas, even in patientswithout previous bowel symptoms, it is recommendedthat these patients undergo full colonoscopy to screenfor colorectal cancer (12,16,17). Changes in local condi-tions and disruption of capillary channels at the site ofco-lorectal neoplasias allow Streptococcus gallolyticcusto proliferate and gain entry into the blood stream.Cells that line the mucosal surface of the bowel form amajor mechanical barrier that separates the host's inter-nal milieu from the external environment and function asan integral component of the mucosal immune system.There is intercellular functioning and an amplifyingcommunication network through delivered signalsinduced by cytokines produced by a number of differentcells at the level of bowel mucosa. These cytokinesdeliver signals that influence the activation, growth, dif-ferentiation, or migration of the target cells upon whichthey act. Individual cells can produce multiple cytoki-nes. Microbial entry is important in the activation of thiscytokine signalling network (19). Since the cytokines expressed in response to bacterialinvasion or to other pro-inflammatory agonists have awell documented role in chemotaxis and activation ofinflammatory cells, colon epithelial cells appear to beprogrammed to provide a set of signals for activation ofthe mucosal inflammatory response in the earliest pha-ses after microbial invasion. Some cytokines andchemokynes activate a spectrum of pro-inflammatoryeffects (IL-1, IL-8, TNF-α, GM-CSF, monocyte chemo-tactic protein-1), whereas others downregulate inflam-matory responses (IL-10, TGF ß1). Invasion of the intes-tinal mucosa by pathogenic bacteria leads to a markedacute mucosal inflammatory response, induced by thecytokine system network, which is characterized histo-logically by infiltration with neutrophils and macro-phages/monocytes (19). The adherence of Streptococcus gallolyticcus to intesti-nal epithelial cells seems to be the initial process in co-lonization and subsequent infection of the host. Theadhesion of several opportunistic bacteria to host tissue,mediated through binding to various human cell surfacesor extracellular matrix components (fibronectin, colla-gen and laminin) is correlated with pathogenicity and, inthe case of Streptococcus gallolyticcus, the relationshipbetween bacteraemia/endocarditis and carcinoma of thecolon suggests the existence of Streptococcus gallolytic-cus adhesins which allow colonization of both colonicand vascular tissues (4). Bacterial adherence to various human cells induces syn-thesis of pro-inflammatory cytokines and chemokynes,and promotes the upregulation of adhesion molecules byengaging bacterial surface adhesins of the modulineclass (20). The ability of Streptococcus gallolyticcus to
adhere to human tumour cells has not been demonstra-ted. However, the close relationship between Strepto-coccus gallolyticcus bacteraemia and endocarditis andcarcinoma suggests the existence of such a mechanisminvolving the reaction of bacterial adhesins with tumourcell surface receptors (21). In addition, cytokines alsoappear to promote and enhance bacterial adherence tovarious cells (22). Recent data show that TNF-α pro-vides a microenvironment conductive to the prolifera-tion of anaerobic bacteria, including Streptococcus ga-llolyticcus, and that IL-8 secretion by colon epithelialcells from different sites is enhanced in various infla-mmatory diseases. Thus, the ability of Streptococcusgallolyticcus to adhere to and stimulate human cells maycontribute to the pathogenicity of the bacteria (22). It was reported that the local action of cytokines or ofchemical mediators able to promote vasodilatation andenhancement of capillary permeability may support bac-terial entry at the tumour site and increase bacterialadherence to various cells (23). Some authors refer to thepotential involvement of Streptococcus gallolyticcus inintestinal carcinogenesis. Ellmerich (4), in a very inter-esting experimental study in rats, demonstrated thatStreptococcus gallolyticcus or its antigens promotedprogression of pre-neoplastic lesions through increasedformation of hyperproliferative aberrant colonic crypts,enhanced expression of proliferative markers andincreased production of IL-8 in the colonic mucosa.Bacterial cell wall proteins were found to be more potentinducers of neoplastic transformation than the intact bac-teria. On the other hand, these abnormalities were onlydemonstrated when pre-neoplastic lesions were alreadypresent and not in normal mucosa (4).Production of inflammatory cytokines, such as TNF-α,IL-1ß and IL-6, and the chemokine IL-8, contribute tothe normal host defence mechanisms (24), leading to theformation of nitric oxide and free radicals, such as super-oxide, peroxynitrites and hydroxyl radicals, as well asalkylperoxy radicals (25). Owing to their potent muta-genicity, all these molecular species can contribute toneoplastic processes by modifying cellular DNA. Inaddition, the production of angiogenic factors, such asIL-8 triggered by Streptococcus gallolyticcus antigens,in the colonic mucosa may also favour the progressionof colon carcinogenesis (26,27).Contrary to the more commonly reported associationbetween Streptococcus gallolyticcus bacteraemia andcolorectal cancer, a link to pre-neoplastic adenomatouspolyps was rarely reported (4,6,18). Although we cannotassume a cause and effect relationship in the case of ourpatient, the clinical report includes several commonlyassumed criteria that support the hypothesised relation-ship between colorectal Streptococcus gallolyticcus

infection and the progressive development of malignantdisease in pre-neoplastic adenomatous polyps. Pyogenicarthritis in a patient with colonic neoplasia is alsodescribed by several authors (14,15,16). In our case thearthritis was probably related to Streptococcus galloly-ticcus bacteraemia but without the development of pyo-genic arthritis, and it behaved as a reactive-type arthritis.
Correspondência:António Guilherme Neves MurinelloAvª Engº Antº Azevedo Coutinho, Lt 8 r/c - dto2750-644 Cascaise-mail: [email protected] or [email protected]
REFERENCES
1. Armstrong B, Doll R. Environmental factors and cancer incidenceand mortality in different countries with special reference todietary practice. Int J Cancer 1975; 15: 617-31.
2. Parsonnet J. Bacterial infection as a cause of cancer. EnvironHealth Perspect 1995; 103: 263-8.
3. Hill MJ, Drasar BS, Hawksworth G, Aries V, Crowther JS,Williams RE. Bacteria and etiology of cancer of large bowel.Lancet 1970; i: 95-100.
4. Ellmerich S, Scholler M, Duranton B, Gossé F, Galluser M, KleinJP, et al. Promotion of intestinal carcinogenesis by Streptococcusbovis. Carcinogenesis 2000; 21: 753-6.
5. Schlegel L, Grimont F, Grimont PA, Bouvet A. New group Dstreptococcal species. Indian J Med Res 2004; 119: 252-6.
6. Burns CA, McCaughey R, Lauter CB. The association ofStreptococcus bovis carriage and colon neoplasia: possible rela-tionship with polyps and their premalignant potential. Am JGastrenterol 1985; 80: 42-6.
7. Reynolds JG, Silva E, McCormack WH. Association ofStreptococcus bovis bacteraemia with bowel disease. J ClinMicrobiol 1983; 17: 696-7.
8. Klein RS, Catalano MT, Edberg SC, Casey JI, Steigbigel NH.Streptococcus bovis septicaemia and carcinoma of the colon. AnnInt Med 1979; 91: 560-2.
9. Klein RS, Recco RA, Catalano MT, Edberg SC, Casey JL,Steigbrigel NH. Association of Streptococcus bovis with carcino-ma of the colon. New Engl J Med 1977; 297: 800-2.
10. Leport C, Bure A, Leport J, Vilde JL. Incidence of colonic lesions inStreptococcus bovis and Enterococcus endocarditis. The Lancet 1987; 1: 748
11. Beebe JL, Koneman EW. Recovery of uncommon bacteria fromblood: association with neoplasic disease. Clin Microbiol Rev1995; 8: 336-56.
12. Hossenbux K, Dale BA, Walls AD, Lawrence JR. Streptococcusbovis endocarditis and colonic carcinoma: a neglected association.Brit Med J 1983; 287: 21.
13. Douglas GW, Levin RH, Sokoloff L. Infectious arthritis compli-cating neoplasic disease. New Engl J Med 1964; 270: 298-302.
14. Moellering RC, Watson KB, Kuntz LJ. Endocarditis due to groupD Streptococci: comparison of disease caused by Streptococcusbovis with that produced by Enterococci. Am J Med 1974; 57:239-50.
15. Lyon LJ, Nevine MA. Carcinoma of the colon presenting as pyo-genic arthritis. JAMA 1979; 241: 2060.
16. Murinello A, Loureiro Mª, Joana A, Van-Dunen F, Mota L,Lamarão P, et al. Carcinoma of the colon associated with purulentarthritis. Rev Gastrent Cirurg (Portuguese) 1996; XIII: 23-9.
17. Syngal S, Bandipalliam P, Boland R. Surveillance of patients at highrisk for colorectal cancer. Med Clin North Amer 2005; 89: 61-84.
18. Beeching NJ, Christmas TI, Ellis-Pegler RB, Nicholson GI.Streptococcus bovis bacteremia requires rigorous exclusion ofcolonic neoplasia and endocarditis. Quart J Med 1985; 56: 439-40.
19. Jung HC, Eckmann L, Yan S-K, Panja A, Fierer J, Mozycka-Wroblenska E, et al. A distinct array of proinflammatory cytokinesis expressed in human colon epithelial cells in response to bacte-rial invasion. J Clin Invest 1995; 95: 55-65.
20. Hirota K, Osawa R, Nemoto K, Ono T, Micycke Y. Highlyexpressed human syalic Lewis x antigen on cell surface ofStreptococcus gallolyticcus. The Lancet 1996; 347: 760.
21. Ellmerich S, Djouder N, Scholler M, Klein JP. Production ofcytokines by monocytes, epithelial and endothelial cells activatedby Streptococcus bovis. Cytokine 2000; 12: 26-31.
22. Cheung AL, Koomey JM, Lee S, Jaffe EA, Fischetti VA.Recombinant human tumor necrosis factor alpha promotes adhe-rence of Staphylococcus aureus to cultured human epitheliodcells. Infect Immunolog 1991; 59: 3827-31.
23. Wancke CA, Bistrian B. Recombinant human tumour necrosis fac-tor and recombinant murine interleukin-1 alter the binding ofEscherichia coli to intestine, mucin glycoprotein, and the HT29-C1 intestinal cell line. Nutrition 1997; 13: 959-64.
24. Janeway CA, Travers P. Immunobiology: The Immune System inHealth and Disease. Garland Publishing Inc. New York andLondon. 1997.
25. Oshima H, Bartsch H. Chronic infections and inflammatoryprocesses as cancer risk factors: possible role of nitric oxide incarcinogenesis. Mutat Res 1994; 305: 253-64.
26. Norrby K. Interleukin-8 and "de novo" mammalian angiogenesis.Cell Prolif 1996; 29: 315-23.
27. Eisma RJ, Spiro JD, Kreutzer DL. Role of angiogenic factors:coexpression of interleukin-8 and vascular endothelial growth fac-tor in patients with head and neck squamous carcinoma.Laryngoscope 1999; 109: 687-93.
156 A. MURINELLO ET AL GE Vol.13







