Embed Size (px)
Citation preview

1
Universidade Estadual de Montes Claros – Unimontes
Programa de Pós-Graduação em Ciências da Saúde – PPGCS
Mestrado Acadêmico em Ciências da Saúde
Suelleng Maria Cunha Santos
Cirurgiã Dentista
Descrição de uma nova síndrome associada à fibromatose gengival e avaliação
imunohistoquímica de miofibroblastos em fibromatose gengival idiopática.
Dissertação de mestrado acadêmico, apresentada ao Programa de Pós Graduação em Ciências da Saúde, da Universidade Estadual de Montes Claros – Unimontes, como parte das exigências para a obtenção do Título de Mestre em Ciências da Saúde.
Montes Claros – Minas Gerais – Brasil
Maio de 2008

Livros Grátis
http://www.livrosgratis.com.br
Milhares de livros grátis para download.

2
Suelleng Maria Cunha Santos
Cirurgiã Dentista
Descrição de uma nova síndrome associada à fibromatose gengival e avaliação
imunohistoquímica de miofibroblastos em fibromatose gengival idiopática.
Dissertação de mestrado acadêmico, apresentada ao Programa de Pós Graduação em Ciências da Saúde, da Universidade Estadual de Montes Claros – Unimontes, como parte das exigências para a obtenção do Título de Mestre em Ciências da Saúde.
Orientador: Prof. Dr. Hercílio Martelli Júnior
Co-Orientador: Prof. Dr. André Luiz S. Guimarães
Banca examinadora:
Prof. Dr. Hercílio Martelli Júnior
Prof. Dr. Paulo Rogério Ferretti Bonan
Prof. Dr. Antônio Luiz Barbosa Pinheiro
Suplentes:
Profa. Dra Patrícia Furtado Gonçalves
Prof. Dr. Alfredo Maurício B. de Paula
Montes Claros – Minas Gerais – Brasil
Maio de 2008

3
Santos, Suelleng Maria Cunha.
S237d Descrição de uma nova síndrome associada à fibromatose gengival e avaliação imunohistoquímica de miofibroblastos em fibromatose gengival idiopática [Manuscrito] / Suelleng Maria Cunha Santos. – 2008.
79 f. : il. 30 cm.
Referências: f. 63-70.
Dissertação (Mestrado) - Universidade do Estado de Minas Gerais, Programa de Pós-Graduação em Ciências da Saúde, 2008.
Orientador: Prof. Dr. Hercílio Martelli Júnior.
1. Saúde Bucal - gengiva. 2. Fibromatose Gengival.
3. Fibromatose gengival idiopática. I. Universidade do Catalogação: Maria Dalva Ribeiro Lopes – CRB/6 – 2144 e Helena Maria da Silveira – CRB/6 - 1959

4
Substituir pela folha de aprovação

5
DEDICATÓRIA
D edico esta dissertação às pessoas que são para m im exem plos de
vida...aos m eus pais D enilson e L ena, à m inha irm ã Jordana e a
m eu noivo Janir, que sem pre m e estim ularam a dar este grande
passo. E stas pessoas estiveram ao m eu lado m e encorajando nas
horas difíceis e m e aplaudindo nos m om entos de glória. O brigada
por terem acreditado nos m eus sonhos e, ainda m ais, por terem m e
ajudado a transform á-los em realidade!!!

6
AGRADECIMENTOS
Considerando esta dissertação como resultado de uma caminhada que não começou na
Unimontes, agradecer pode não ser tarefa fácil, nem justa. Para não correr o risco da
injustiça, agradeço de antemão a todos que de alguma forma passaram pela minha vida
e contribuíram para a construção de quem sou hoje.
Aos meus pais Denilson e Lena, e a minha irmã Jordana, pelo carinho e força que me
dão, por estarmos sempre juntos nos momentos mais importantes, por "contar" com
vocês!
À Janir, por seu amor, generosidade e apoio irrestrito: emocional e afetivo, por sempre
me estimular a crescer cientifica, ética, profissional e pessoalmente e por estar comigo
desde o início à concretização deste sonho.
Aos amigos Shirlene, Renato, Nanda, Mary e Pedro, amigos que levarei em meu
coração, por terem tornado o período do mestrado tão agradável.
Gostaria de agradecer aos meus antigos professores, que me ensinaram com prazer e
dedicação parte do que sei.
E agradeço, particularmente, a algumas pessoas pela contribuição direta na construção
deste trabalho:

7
Ao Professor Hercílio Martelli Júnior, orientador deste trabalho, pela confiança,
compreensão e apoio demonstrados no seu decorrer. Pela oportunidade que tive de
compartilhar dos seus ensinamentos e dedicação.
Ao professor Paulo Rogério Ferreti Bonan, pelos inestimáveis ensinamentos
transmitidos e principalmente, pela eterna disposição em me atender.
Aos Professores André Luiz Sena Guimarães e Alfredo Maurício Batista de Paula, pela
paciência, dedicação e pelos primeiros contatos com o laboratório, pelo incentivo à
pesquisa científica, por todas as discussões nas reuniões de quarta-feira à noite e por
sempre estarem por perto quando precisei.
À Anamaria e aos colegas do Laboratório de Pesquisa em Saúde, principalmente a
Carlos, Marcos e Erivelton, pela amizade, paciência interminável e por sempre estarem
prontos a ajudar.
Às secretárias do PPGCS, Maria do Carmo Mendes Nobre e Kátia Silene Maia
Azevedo, pelos seus “sim” em todos os momentos de dificuldades, pela dedicação e
competência, pelos auxílios, conversas, pela amizade.
Aos coordenadores do Programa de Pós-Graduação em Ciências da Saúde (PPGCS),
pela oportunidade de crescimento, aprendizado, realização profissional e pessoal e pela
confiança em mim depositada.

8
Ao Reitor da Universidade Estadual de Montes Claros - UNIMONTES, Prof. Paulo
César Gonçalves de Almeida pela estrutura disponibilizada e alta qualidade dos cursos
oferecidos.
À Fundação de Amparo à Pesquisa do Estado de Minas Gerais - FAPEMIG (processo:
2107), que me concedeu bolsa durante a realização deste mestrado.
E finalmente, a Deus, o maior responsável pela minha existência e por sua presença
constante em minha vida.
9
Resumo
Fibromatose gengival (FG) é um termo clínico comumente utilizado para se referir ao
crescimento gengival, decorrente do acúmulo excessivo de proteínas da matriz
extracelular, predominantemente colágeno tipo I e maior proliferação fibroblástica. A
FG pode ser inflamatória, neoplásica, genética e medicamentosa. Porém, em casos onde
a patogênese é desconhecida, o crescimento gengival é denominado FG idiopática
(FGI). A FG de origem genética é denominada fibromatose gengival hereditária (FGH).
A FGH é uma condição rara (1:750.000 nativivos), que manifesta clinicamente por
aumento gengival generalizado. A FGI assemelha-se clínica e histologicamente à FGH,
diferenciando-se apenas pela não existência desta condição em outros indivíduos da
família. Este estudo teve por objetivos: (1) descrever as características clínicas,
genéticas, imaginológicas e microscópicas de uma família portadora de FG associada a
outras alterações e (2) avaliar a presença de miofibroblastos na FGI. Para o primeiro
objetivo, foram realizados estudos clínicos, imaginológicos, microscópicos e genéticos
de portadores da FG associada a alterações dentais e neurológicas. As alterações dentais
foram observadas através de radiografias periapicais, panorâmicas e também por
microscopia eletrônica de varredura, enquanto o tecido gengival foi avaliado através de
imunohistoquímica (actina alfa de músculo liso (α-SMA) e citoqueratina 19) e
microscopia eletrônica de varredura. A análise genética foi feita após a confecção do
heredograma para caracterizar o padrão de herança genética envolvida na condição. Os
resultados demostraram a presença de 70 descendentes diretos, distribuídos em 4
gerações. Desse montante, 11 indivíduos foram afetados, sendo que 3 membros
apresentaram FG e alterações dentais (amelogênese imperfeita, calcificações
intrapulpares, retardo na erupção dentária, dentes impactados, radiolucidez
pericoronária, agenesia dental e dilacerações radiculares), 1 afetado apresentou FG

10
isolada, 1 apresentou FG, alterações dentais e deficiência mental e 6 membros
apresentaram deficiência mental isolada. Na presente família foi verificado a presença
de casamentos consangüíneos e um padrão de herança autossômica recessiva. Análise
histopatológica mostrou tecido gengival com epitélio hiperplásico, com longas e
delgadas cristas que se projetavam para o conjuntivo subjacente, que se apresentou
denso e fibroso. Na imunohistoquímica houve marcação positiva para citoqueratina 19 e
α-SMA, sugerindo, respectivamente, a presença de epitélio odontogênico e de
miofibroblastos. Esses resultados sugerem tratar-se de uma nova condição genética,
com presença simultânea de crescimento gengival, alterações dentais e deficiência
mental. Para o segundo objetivo, foram realizadas avaliações clínicas e microscópicas
da gengiva de portadores de FGI. O tecido gengival apresentava coloração normal, com
consistência firme e fibrosa, causando alterações na erupção e no posicionamento
dental. A história familiar dos pacientes afetados não evidenciou presença de outros
membros afetados na família. Em HE o tecido gengival mostrou moderada hiperplasia
epitelial, com longas e delgadas cristas em direção ao tecido conjuntivo que se mostrou
denso e fibroso. A coloração por Tricrômio de Masson revelou espessos feixes de fibras
colágenas coradas fortemente. A imunohistoquímica mostrou-se negativa para
miofibroblastos (α-SMA). Pelo fato de α-SMA ser um marcador específico de
miofibroblastos, estes resultados sugerem que estas células não estão envolvidas na
patogênese da FGI.
Plavras-chave: Fibromatose gengival, fibromatose gengival idiopática,
miofibroblastos, gengiva, amelogênese imperfeita.

11
Abstract
Gingival fibromatosis (GF) is commonly a clinical term used to refer to the growth
gingival due to the excessive accumulation of matrix extracellular proteins,
predominantly type I collagen and larger proliferation fibroblastic. The GF can be
inflammatory alterations, neoplasic, genetic and systemic drugs, however, in cases
where the pathogenese remains unknown, the growth gingival is denominated GF
idiopathic (IGF). The GF of origin genetic is denominated hereditary gingival
fibromatosis (HGF). The HGF is a rare condition (1:750.000 birth), that manifested
clinically by gingival generalized enlagerment. The IGF resembles each other clinic and
histopathologically to HGF, just differing for the non existence of this condition in other
individuals of the family. This study had for objectives: 1) to describe the clinical
characteristics, genetics, imaginologics and microscopic of a family presenting gingival
fibromatosis associated to other alterations and (2) to evaluate the myofibroblasts
presence in IGF. For the first objective, they were accomplished studies clinical,
imaginologics, microscopic and genetic of bearers of the gingival fibromatosis
associated to dental and neurological alterations. Were the dental alterations observed
through periapical and panoramic radiographs, and also for electronic microscopic of
sweeping, while the tissue gingival was evaluated through immunohistochemistry (α-
smooth muscle actin (α-SMA) and cytokeratin 19), and electronic microscopic of
sweeping. The genetic analysis was made after the making of the pedigree to
characterize the pattern of genetic inheritance involved in the condition. The results
demonstrated the presence of 70 descending direct, distributed in 4 generations. It gave
amount, 11 individuals were affected, and 3 members presented gingival fibromatosis
and dental alterations (imperfect amelogenesis, intrapulpal calcifications, delay on tooth
eruption, unerupted teeth, pericoronal radiolucencies, dental agenesis, and root

12
dilacerations), 1 affected presented GF isolated, 1 presented fibromatose gingival, tooth
alterations and mental deficiency and 6 members presented isolated mental deficiency.
In the present family it was verified the presence of consanguineous marriages and a
pattern of inheritance autosomal recessive. Analysis histopathological showed tissue
gingival with epithelium hyperplasic, with long and thin crests that were projected for
the underlying conjunctive tissue that was dense and fibrous. The coloration for
tricromio of Masson revealed thick bundles of fibers collagen strongly stain. In the
immunohistochemistry there was positive demarcation for cytokeratin 19 and α-SMA,
suggesting, respectively, the presence of epithelium odontogenic and of myofibroblasts.
Those results suggest to treat of a new genetic condition, with simultaneous presence of
growth gingival, dental alterations and mental deficiency. For the second objective,
were accomplished clinical and microscopic evaluations of the gingiva of bearers of
IGF. The tissue gingival presented normal coloration, with firm and fibrous consistence,
causing alterations in the eruption and in the dental positioning. The affected patients'
family history didn't evidence presence of other affected members in the family. In HE
the tissue gingival showed mild hyperplasia epithelial, with long and thin crests in
direction to the conjunctive tissue that was shown dense and fibrous. The coloration for
tricromio of Masson revealed thick bundles of fibers collagen stained strongly. The
immunohistochemistry was shown negative for myofibroblast (α-SMA). For the fact of
α-SMA to be a specific marker of myofibroblast, these results suggest that these cells
are not involved in the pathogenesis of IGF.
Key-words: Gingival fibromatosis, idiopathic gingival fibromatosis, myofibroblasts,
gingiva, imperfect amelogenesis.
13
LISTA DE SIGLAS E ABREVIATURAS
ABC Complexo avidina biotina-peroxidase
AI Amelogênese imperfeita
BSA Albumina de soro bovino
CK19 Citoqueratina 19
CTGF Fator de crescimento do tecido conjuntivo
DA Alterações dentais
EDTA Ácido etilenodiaminotetracético
EGF Fator de crescimento epidérmico
EGF-r Receptor do fator de crescimento epidérmico
ELISA Enzyme Linked Immuno Sorbent Assay
FAS Sintase ácida gordurosa
FG Fibromatose gengival
FGH Fibromatose gengival hereditária
FGI Fibromatose gengival idiopática
GN Gengiva normal
H2O2 Peróxido de Hidrogênio
HE Hematoxilina-eosina
Hsp47 Proteína de choque térmico 47
IL-6 Interleucina 6
INF-γ Interferon-gama
MMP Metaloproteinase da matriz
MR Retardo mental
P4Hs Prolina-quatro hidroxilases
PBS Solução salina tamponada com fosfato
RT-PCR Reação em cadeia polimerase - transcriptase reversa
SOS Son of sevenless
TGF-β Fator de crescimento transformante – beta
TIMP Inibidor tecidual das metaloproteinases
α-SMA Actina alfa de músculo liso
14
SUMÁRIO
1. Introdução 15
1.1. Características clínicas da fibromatose gengival 15
1.2. Características histopatológicas e moleculares da fibromatose gengiva
hereditária
16
1.3. Condições genéticas e síndromes 20
1.4. Alterações dentais relacionadas com a fibromatose gengival 23
1.5. Tratamento da fibromatose gengival 25
1.6. Miofibroblastos 25
2. Proposição 28
2.1. Objetivo Geral 28
2.2. Objetivos Específicos 28
3. Metodologia 29
4. Resultados 30
4.1. Artigo Científico 1 30
4.2. Artigo Científico 2 49
5. Conclusões 62
6. Referências 63
7. Anexos 71
7.1. Figuras do artigo científico 1 71
7.2. Figuras do artigo científico 2 76

15
1. Introdução
1.1. Características clínicas da fibromatose gengival
Fibromatose gengival é um termo clinicamente utilizado para referir-se ao
aumento de volume da gengiva, decorrente do excessivo acúmulo de colágeno e maior
proliferação fibroblástica no tecido gengival (Takagi et al., 1991; Coletta et al., 1998;
Martelli-Júnior et al., 2000). As fibromatoses gengivais podem resultar de condições
locais (inflamatória e neoplásica), medicações sistêmicas e alterações genéticas
(Hakkinen e Csiszar, 2007). Porém, existem casos de aumento gengival, cuja
patogênese permanece desconhecida, sendo a mesma classificada como idiopática e o
crescimento por ela proporcionado, denominado fibromatose gengival idiopática (FGI)
(Gagliano et al. 2005). A fibromatose com etiologia genética é denominada fibromatose
gengival hereditária (FGH) e foi primeiramente descrita por Gross em 1856, tendo o seu
primeiro heredograma elaborado por Nasse em 1895. Posteriormente várias
terminologias foram usadas para esta condição, sendo que em 1961, Zackin e
Weisberger (1961), usaram o termo fibromatose gengival hereditária e desde então o
termo FGH tem sido o mais comumente usado na literatura científica. Essa condição
pode ocorrer como fenótipo isolado, associada às alterações locais e sistêmicas ou como
componente de diversas síndromes (Gorlin et al., 1990; Hakkinen e Csiszar, 2007).
FGH é uma condição bucal rara, 1:750.000 nativivos (Singer et al., 1993), sem
predileção por sexo ou raça (Rushton, 1957), que pode envolver a maxila e a mandíbula.
A manifestação clínica da FGH é bastante heterogênea (Martelli-Júnior et al., 2005). O
crescimento gengival é contínuo, generalizado ou mais raramente localizado, sem
regressão espontânea, podendo resultar na cobertura parcial ou total das coroas clínicas
dentais. A gengiva apresenta-se firme, indolor, não hemorrágica, com coloração rosa e
pontilhado superficial característico (Sciubba e Niebloom, 1986; Bozzo et al., 1992;

16
Bozzo et al., 1994; Martelli-Júnior et al., 2005). Normalmente o crescimento gengival
inicia-se no período de erupção da dentição permanente, podendo também desenvolver-
se durante a dentição decídua, e mais raramente, estar presente antes da erupção dental,
verificando espessamento da mucosa do rebordo alveolar (Singer et al., 1993; Bozzo et
al., 2000).
FGI refere-se ao crescimento gengival cujas características clínicas e
histopatológicas se assemelham bastante à FGH, sendo a não existência de outros casos
na família o fator diferencial. Não obstante, alguns autores como Clocheret et al. (2003)
preferem classificar como FGH, as alterações cujo locus genético já se encontra bem
definido, devendo todos os outros crescimentos gengivais sem causas conhecidas serem
denominados de FGI, até mesmo se o crescimento é observado em mais de um membro
da mesma família, na ausência de qualquer outro sinal ou sintoma.
O aumento gengival resulta em alterações funcionais e estéticas, como
diastemas, retardo na erupção dental, má posicionamento dos dentes, dificuldade na
higiene bucal e no vedamento labial (Bozzo et al., 2000). Pode ainda levar à retenção da
dentição decídua, dificuldades na mastigação, fonação e problemas psicológicos
(Martelli-Júnior et al., 2005; Coletta e Graner, 2006). Embora não afete diretamente o
osso alveolar, o aumento tecidual pode favorecer o acúmulo de placa bacteriana,
induzindo a periodontite e conseqüentemente a reabsorção dental e halitose (Coletta e
Graner, 2006).
1.2. Características histopatológicas e moleculares da fibromatose gengival
hereditária
A FGH foi descrita em microscopia óptica, pela primeira vez, por Tomes em
1879. Esta condição é caracterizada histologicamente por epitélio pavimentoso

17
estratificado queratinizado, mostrando áreas de acantose (Johnson et al., 1986; Andrade,
2001) e longas e delgadas projeções epiteliais que se estendem em direção ao tecido
conjuntivo subjacente (Singer et al., 1993). O tecido conjuntivo apresenta densos e
espessos feixes de fibras colágenas entremeadas por fibroblastos e discreto infiltrado
inflamatório nas áreas perivasculares (Redman et al., 1985). Pequenos e múltiplos focos
de calcificação distrófica, ilhas de metaplasia óssea, áreas de ulceração e focos de
células inflamatórias também foram descritos (Gunhan et al., 1995). Através de análises
de microscopia eletrônica e de ultra-estrutura do tecido conjuntivo da FGH, observou-se
presença de fibrilas colágenas, com estruturas anormais, incluindo variações de
diâmetro, assim como aumento na presença de fibras oxitalânicas e diminuição das
fibras elásticas (Barros et al., 2001).
Embora diversos estudos tenham sido realizados sobre o tecido conjuntivo da
FGH, poucos estudos avaliaram o comportamento do tecido epitelial (Coletta e Graner,
2006). O tecido epitelial da FGH apresenta-se bem estruturado, com longas e delgadas
cristas que se projetam em direção ao conjuntivo subjacente (Araújo et al., 2003).
Farrer-Brown et al. (1972) relataram presença de hiperplasia epitelial na FGH, porém,
em estudos utilizando espécimes de FGH associados com inflamação crônica. Raeste et
al. (1978) encontraram hiperplasia epitelial e papilas proeminentes em áreas com
intenso infiltrado inflamatório crônico. Araújo et al. (2003) demonstraram que as áreas
do epitélio da FGH (sem infiltrado inflamatório) e da gengiva clinicamente normal
foram similares. Análises histopatológicas de tecidos provenientes da FGI revelam
moderada hiperplasia epitelial, e uma quantidade aumentada de feixes de fibras
colágenas no tecido conjuntivo (Clocheret et al., 2003; Gagliano et al., 2005),
características que se assemelham às da FGH.

18
É interessante verificar que em aumentos gengivais medicamentosos, a
hiperplasia epitelial observada é provavelmente decorrente da resposta inflamatória
desencadeada pelos efeitos do medicamento (Brown et al., 1991).
Os mecanismos bioquímicos e moleculares que levam à formação excessiva de
tecido gengival são desconhecidos e os estudos enfocando os principais eventos em
cultura de células são controversos. Johnson et al. (1986) estudando fibroblastos
gengivais em cultura, obtidos de uma criança de 13 anos de idade, portadora de aumento
gengival acentuado, sem que qualquer outro membro da família apresentasse a
condição, demonstraram uma taxa de crescimento menor que as células obtidas de um
adulto jovem normal e uma quantidade de colágeno menor que as células controle.
Araújo et al. (2003), mostraram que a proliferação de células epiteliais da FGH é
significantemente maior, comparado à gengiva normal. Observaram ainda a presença de
cristas epiteliais profundas que se dirigem para o tecido conjuntivo, sendo que os
padrões de expressão do fator de crescimento epidérmico (EGF) e o receptor
correspondente (EGF-r) foram correlatos com o potencial proliferativo das células
epiteliais na região das cristas epiteliais.
Morfologicamente, em condições de subconfluência celular, os fibroblastos da
FGH foram similares aos da gengiva normal (GN). Exibiram formato fusiforme com
núcleo central e típicos prolongamentos citoplasmáticos. Porém, em condições de
confluência celular, os fibroblastos da FGH demonstraram tamanhos e largura menores
que os fibroblastos da GN (Martelli-Júnior et al., 2000). A coloração das células pela
técnica convencional de HE e análise de microscopia de luz demonstrou que, a redução
no volume celular dos fibroblastos da FGH em condições de confluência celular é
resultado da redução do volume citoplasmático e não do volume nuclear. Embora,
alguns aspectos da FGH sejam descritos em estudos com cultura de células e

19
microscopia de luz, poucos estudos têm sido realizados utilizando-se imunomarcadores
para FGH (Martelli-Júnior et al., 2000; 2003; Wright et al., 2001).
O aumento na capacidade proliferativa de fibroblastos pode contribuir para o
aumento gengival observado na FGH, devido a uma maior atividade sintética de maior
número de células no tecido (Coletta et al., 1999). Resultados obtidos por diferentes
ensaios bioquímicos demonstraram uma produção e expressão reduzida de MMP-1 e
MMP-2 em fibroblastos de FGH, comparado a fibroblastos de gengiva clinicamente
normal (Coletta et al., 1999). Tipton et al. (1997), mostraram uma proliferação mais
rápida dos fibroblastos e uma síntese aumentada de colágeno e fibronectina em células
de FGH, comparadas a células de gengiva normal, o que foi ratificado num estudo com
quatro diferentes linhagens de fibroblastos de FGH, utilizando diferentes marcadores de
proliferação celular (Coletta et al., 1998). Contudo, em um estudo analisando os
aspectos morfológicos e moleculares da FGI, Gagliano et al., (2005) observaram maior
expressão de colágeno tipo I, assim como maiores taxas de MMP-1 e MMP-9 na FGI
quando comparada com tecido gengival normal. Estes resultados parecem sugerir que
neste caso o acúmulo de colágeno no tecido conjuntivo não estava associado com
aumento da síntese ou diminuição da degradação. Já Martelli-Júnior et al. (2003),
estudando uma família autossômica dominante portadora de FGH (Bozzo et al., 1994),
mostraram utilizando diferentes ensaios de RT-PCR, ELISA, Western blot e
enzimografia, maior expressão e produção de colágeno tipo I e Hsp47 em fibroblastos
de FGH comparado a fibroblastos de gengiva normal (GN), enquanto a expressão e
produção de MMP-1 e MMP-2 foram menores em fibroblastos de FGH comparado a
GN. Adicionalmente, quando do condicionamento de fibroblastos de FGH com
diferentes citocinas, verificou-se que TGF-β1 e IL-6 estimularam aumento na expressão
de colágeno tipo I e Hsp47, enquanto INF-γ reduziu a expressão e produção de colágeno
20
tipo I e Hsp47, tendo pouco efeito na expressão de MMP-1 e MMP-2. Sobral et al.
(2007) verificaram os efeitos do TGF-β1 e INF-γ na transdiferenciação de
miofibroblastos em culturas de células humanas e demonstraram que o TGF-β1 foi
capaz de induzir, dose e tempo-dependente, a expressão de α-SMA, enquanto o INF-γ
além de inibir a transdiferenciação fibroblastos-miofibroblastos, via TGF-β1 e a
expressão de α-SMA e colágeno tipo I em culturas gengivais normais (GN), também
alterou o metabolismo dos miofibroblastos FGH, ocasionando uma diminuição da
expressão de α-SMA e colágeno tipo I e estimulando a expressão de SMAD7, inibindo
assim, o fator de crescimento do tecido conjuntivo (CTGF), que tem sido considerado
molécula chave na transdiferenciação via ativação de TGF-β1.
Vários trabalhos têm procurado elucidar os eventos biomoleculares envolvidos
na etiopatogênese da FGH. Almeida et al. (2005) avaliaram o papel da sintase ácida
gordurosa (FAS), enzima anabólica que tem sido relacionada à patogênese de várias
neoplasias malignas, na FGH e GN e, observaram que esta enzima era produzida em
maior quantidade por fibroblastos da FGH comparada a gengiva normal.
Meng et al. (2007) investigando as P4Hs, MMP-1, MMP-3 e TIMP-1 na
patogênese da FGH, mostraram que não houve diferenças no padrão de proliferação
fibroblástica entre os fibroblastos FGH e de GN. Porém, ao verificarem a expressão de
colágeno tipo I e dos subtipos de P4Hs, observaram que além das taxas de colágeno
somente as taxas da enzima P4Hα (I) foram maiores para fibroblastos FGH em relação à
GN.
1.3. Condições genéticas e síndromes
Na maioria dos casos, a FGH é transmitida como herança autossômica
dominante, embora padrões recessivos tenham sido descritos (Singer et al., 1993). Os

21
relatos de fenótipos autossômicos recessivos, que são minoria em relação ao fenótipo
dominante, segundo Nevin et al. (1971), provém de casamentos cosangüíneos. Porém, a
cosangüinidade não é a única e nem a explicação mais aceita. Descendente de pessoas
não aparentadas, cada qual portadora de um gene mutante, parece ser responsável pela
maioria dos casos de doenças autossômicas recessivas, principalmente se o caráter
recessivo apresentar alta freqüência na população (Coletta et al., 1998).
A FGH pode ocorrer como fenótipo clínico isolado ou mais raramente como
componente de variadas síndromes (Gorlin et al., 1990). Nesse caso, as associações
mais comuns são: múltiplos fibromas e infecções recorrentes (síndrome de Murray-
Puretic-Drescher), retardo na erupção dental e opacidade da córnea (síndrome de
Rutheford), displasia do nariz, orelhas e unhas, hepatoesplenomegalia e
hiperflexibilidade das articulações (síndrome de Zimmerman-Laband), perda
progressiva da audição (síndrome de Jones), querubismo, retardo mental, hipertricose e
epilepsia (síndrome de Ramon) e microftalmia e hipopigmentação (síndrome de Cross)
(Bakeen e Scully, 1991; Coletta e Graner, 2006).
A FGH pode ainda ocorrer como nova mutação. Nesses casos, os indivíduos são
classificados como portadores de fibromatose gengival idiopática, pelo fato de não se
verificar história de envolvimento familial e evidências de transmissão genética (Coletta
e Graner, 2006). A síndrome de Prune-Belly, caracterizada por ser uma condição
autossômica recessiva, ligada ao sexo, foi descrita como apresentando fibromatose
gengival, dismorfismo facial, defeitos na musculatura abdominal e dilatação no trato
urinário (Ramasamy et al., 2005).
Bozzo et al. (1994) mostraram em uma família portadora de FGH da região de
Piracicaba (SP), que a penetrância da FGH é completa, pois em nenhuma ocasião
indivíduos não afetados, tiveram filhos afetados. Além disso, há evidências de

22
expressão variável, sendo que irmãos de uma mesma família apresentavam graus
variados de aumento gengival. Recentemente, Martelli-Júnior et al. (2007) comparando
características clínicas e biológicas de duas famílias distintas portadoras de FGH
isolada, observaram haver diferenças quanto à manifestação clínica, penetrância e no
padrão de proliferação celular, demonstrando assim, heterogeneidade clínica e genética
desta condição.
Embora fatores genéticos tenham uma efetiva participação na FGH, os
mecanismos bioquímicos e os genes responsáveis por esta alteração são pouco
conhecidos (Shashi et al., 1999). Hart et al. (1998), estudando uma família de 32
pessoas, sendo 12 membros afetados para FGH, mostrou relação da FGH com o
cromossomo 2p21, entre os locus D2S1788 e D2S441. Entretanto, técnicas de
alinhamento genético, similares àquelas realizadas por Hart et al. (1998), na família
descrita por Bozzo et al. (1994) não confirmaram os mesmos achados (Hart et al.,
2000). A identificação das bases genéticas da FGH proverá uma melhor compreensão
dos mecanismos envolvidos e possibilitarão perspectivas para terapias mais eficientes
nestes pacientes.
Embora a FGH tenha sido descrita há mais de um século (Gross, 1856), as
primeiras análises genéticas foram feitas há poucos anos. Foram descritos 4 diferentes
locus associados com a forma isolada da FGH; 2 mapeados no cromossomo 2 (2p21-22
e 2p22.3-p23.3) (Hart et al., 1998; Xiao et al., 2000; Ye et al., 2005), 1 no cromossomo
5 (5q13-q22) (Xiao et al., 2000) e recentemente uma alteração no cromossomo 11
(11p15) (Zhu et al., 2007). Hart et al. (2002), identificaram no cromossomo 2p21-p22
uma alteração no domínio carboxila-terminal da proteína SOS1 em indivíduos afetados
pela FGH, sugerindo assim, que este gene seria responsável pela FGH. Alterações nesta

23
proteína conduzem a uma prolongada ativação de sinalizadores, como o Ras/MAPK,
envolvidos no processo de controle e diferenciação celular (Jang et al., 2007).
Quando da avaliação genética da FGH associada a outras alterações, poucos
estudos foram realizados e com resultados bastante variados. Alterações
cromossômicas, incluindo duplicações, deleções e/ou outras anormalidades dos
cromossomos 2p13-16, 4q, 14q, 19p e 19q foram relatadas (Macias-Flores et al., 1984;
Fryns, 1996; Hart et al., 2000; Stefanova et al., 2003). Mangino et al. (2003),
descreveram uma família italiana com FGH associada com hipertricose e excluíram à
ligação aos locus nos cromossomos 2 e 5, sugerindo assim que a FGH associada à
hipertricose é geneticamente distinta da FGH isolada. Esses achados genéticos sugerem
que as formas de FGH são heterogêneas e que provavelmente diversos mecanismos
biológicos estão envolvidos na sua etiologia (Coletta e Graner, 2006). Zhu et al. (2007),
estudando duas famílias chinesas, portadoras de FGH isolada, identificaram um novo
locus no cromossomo 11p15, associado à FGH, ratificando o conceito de
heterogeneidade genética da doença. Alterações nessa região cromossômica descrita
têm sido também associadas com tumor de Wilms, rabdomiosarcoma (Falls et al., 1999)
e carcinoma adrenocortical (Henry et al., 1989).
1.4. Alterações dentais relacionadas com a fibromatose gengival
Dentre as alterações dentais relacionadas com a FG encontra-se a amelogênese
imperfeita (AI). Esta condição representa um grupo genético e clinicamente
heterogêneo de desordens hereditárias que afetam a formação do esmalte dentário
(Nusier et al., 2004). Defeitos de esmalte em AI são variáveis, desde deficiência na
formação a defeitos na mineralização e conteúdos protéicos. Normalmente, as AI
24
podem se apresentar como herança autossômica dominante, autossômica recessiva ou
ligada ao cromossomo X (Crawford et al., 2007).
Alguns trabalhos têm descrito casos de várias alterações dentais em combinação
com os defeitos de esmalte, incluindo, não erupção dentária, calcificações pulpares,
reabsorções radiculares e coronárias, hipercementose e taurodontismo. Estudo realizado
por Collins et al. (1999) estabeleceram que a prevalência de anormalidades dentárias
como ausência dental congênita, demora na erupção dental, reabsorção coronária,
reabsorção radicular e calcificações pulpares, assim como densidade quantitativamente
reduzida do esmalte dental foi mais comumente observado nos grupos de indivíduos
com AI comparado aos não afetados.
Aumento gengival também tem sido descrito em associação com AI em poucos
e isolados relatos de casos. Macedo et al. (2005) descreveram um caso de associação
entre AI hipoplásica e hiperplasia gengival. Clinicamente eles observaram vários dentes
apresentando alterações na superfície do esmalte e um aumento gengival generalizado
em ambos os arcos. Histopatologicamente visualizaram um epitélio de revestimento
escamoso estratificado paraceratinizado e um tecido conjuntivo denso, fibroso vascular,
apresentando moderado infiltrado inflamatório, corpos calcificados e ilhas de epitélio
odontogênico. Esses achados não são muito comuns em hiperplasia gengival, o que leva
a se pensar que poderiam estar presentes pela associação desta com a AI. Gunhan et al.
(1995) relataram a ocorrência de numerosas calcificações, depósitos amilóides e ilhas de
epitélio odontogênico na gengiva de três irmãos com FGH, características
microscópicas até então não relatadas em pacientes com esta condição. Recentemente,
Feller et al. (2006) relataram um caso isolado com uma combinação de displasia do
esmalte, múltiplos dentes não erupcionados com extensas lesões pericoronárias,
maloclusão com mordida aberta anterior e pequeno aumento gengival.
25
1.5. Tratamento da fibromatose gengival
Embora, o tratamento realizado para portadores de FGH seja consenso, existem
controvérsias entre os autores com relação ao período exato para se iniciar o tratamento
(Coletta e Graner, 2006). De maneira geral, acredita-se que o melhor momento para se
iniciar os procedimentos cirúrgicos para redução do crescimento gengival, seja após a
completa erupção da dentição permanente (Cuestas-Carnero e Bornancini, 1988).
Contudo, em muitos casos, a não realização do procedimento cirúrgico prévio a erupção
da dentição permanente, pode gerar diversas conseqüências, como retenção da dentição,
dificuldades de fonação e mastigação, estética e má posicionamento dental, além de
dificuldade na higiene bucal (Bozzo et al., 2000).
O tratamento da FGH depende da extensão de envolvimento propiciado pelo
crescimento gengival. Quando o aumento gengival é discreto, a efetiva higiene bucal
profissional e doméstica é suficiente para manter a boa aparência do tecido gengival.
Em crescimentos gengivais moderados e graves, o tratamento atual recomendado é a
combinação de técnicas cirúrgicas periodontais, de gengivectomia e gengivoplastia,
sendo no passado preconizado a extração de todos os dentes para redução do aumento
gengival (Coletta e Graner, 2006).
Tem sido demonstrado que a taxa de recorrência do aumento gengival, após
procedimentos cirúrgicos é mais freqüente em crianças e adolescentes, comparado com
adultos e idosos e também mais comuns em áreas com acúmulo de placa bacteriana
(Kavvadia et al., 2005).
1.6. Miofibroblastos
Miofibroblastos são células mesenquimais que exibem fenótipo híbrido com
características de fibroblastos e de células musculares lisas e caracterizam-se pela

26
elevada expressão de isoformas de α-actina (α-SMA) (Gabbiani, 1992). Essas células
foram primeiramente observadas em tecido de granulação durante os processos de
cicatrização e, posteriormente, em numerosos processos patológicos, incluindo
quelóides e fibromatoses (Desmouliere et al., 2005).
Os miofibroblastos se formam a partir da diferenciação de células
indiferenciadas ou da transdiferenciação de fibroblastos, processo que se inicia com a
aquisição de fibras do estresse composta por actina citoplasmática e a produção de
fibronectina celular; uma variante da fibronectina que está presente durante o
desenvolvimento de muitos órgãos e, com raras exceções, não é encontrada em tecidos
adultos (Desmouliere et al., 2003). Os miofibroblastos quando ativados sintetizam
níveis elevados de proteínas da matriz extracelular, particularmente colágeno, e
reduzidos níveis de metaloproteinases da matriz. Morfologicamente, os miofibroblastos
são caracterizados pela presença de intenso aparato contrátil, contendo um
empacotamento de actina, principalmente α-SMA, associado às proteínas como miosina
e fibras do estresse (Desmouliere et al., 2005).
Diversos estudos demonstraram a presença de células com características de
miofibroblastos em tecidos normais especializados e em uma variedade de condições
alteradas, como na doença de Dupuytren, na pancreatite fibrosa induzida por
ciclosporina A e nas fibroses pulmonar, renal e hepática (Vaquero et al., 1999; Qi et al.,
2005 e Willis et al., 2006). A doença de Dupuytren é uma alteração miofibroblástica
proliferativa caracterizada pelo espessamento de bandas fibrosas da superfície palmar
das mãos e dedos, onde os efeitos proliferativos e fibrinogênicos de TGF-β1 se
apresentam exacerbados (Tomasek et al., 2002). Existem evidências de que a produção
de colágeno por fibroblastos, estimulados por TGF-β1, seja conseqüência da

27
diferenciação em miofibroblastos, que é a aquisição fenotípica necessária para o
aumento da produção de colágeno (Petrov et al. 2002).
Os mecanismos que desencadeiam a transdiferenciação dos miofibroblastos
permanecem desconhecidos, porém estudos demonstraram importante papel para TGF-
β1 neste processo (Fan et al., 1999; Smith et al., 2006). Fan et al. (1999), demonstraram
que TGF-β1 é capaz de promover a transdiferenciação de linhagens celulares de células
epiteliais tubulares de ratos em miofibroblastos. Esses autores demonstraram ainda que
o tratamento com TGF-β1 é acompanhado pela expressão do marcador específico de
miofibroblastos (α-SMA) e uma diminuição na expressão do marcador epitelial E-
caderina. Métodos de bloqueio da síntese de TGF-β1 vêm sendo testados como forma
de tratamento de doenças causadas por fibroses intersticiais (Gressner et al., 2002).
Assim, a maioria dos estudos tem focado nos aspectos da sinalização do TGF-β
que dá origem ao fenótipo diferenciado, com interesse central na expressão do gene
marcador, α-actina de músculo liso (Phan et al. 2008).

28
2. Proposição
2.1. Objetivo Geral
Avaliar as características clínicas, genéticas, imaginológicas e microscópicas da
fibromatose gengival associada a alterações dentais e deficiência mental e a presença de
miofibroblastos na fibromatose gengival idiopática.
2.2. Objetivos Específicos
1. Avaliar as características clínicas da fibromatose gengival associada a alterações
dentais e deficiência mental;
2. Avaliar o padrão de herança genética, por meio da confecção do heredograma da
família em estudo;
3. Avaliar as características imaginológicas da fibromatose gengival associada a
alterações dentais e deficiência mental;
4. Avaliar as características microscópicas da fibromatose gengival associada a
alterações dentais e deficiência mental;
5. Avaliar imunohistoquimicamente a presença de miofibroblastos no tecido gengival de
portadores de fibromatose gengival idiopática.

29
3. Metodologia
O capítulo de “Metodologia” apresenta-se suprimido aqui, pois a presente
dissertação foi confeccionada com a inserção de artigos científicos. Os aspectos
metodológicos encontram-se nos próprios artigos científicos.
O 1º artigo científico intitula-se: “Case reports of a new syndrome associating
gingival fibromatosis and dental abnormalities in a consanguineous family”, enquanto o
2º artigo intitula-se “Idiopathic gingival fibromatosis: clinical features and
immunohistochemical evaluation of myofibroblasts”.

30
4. Resultados
4.1 – Artigo Científico 1
Case reports of a new syndrome associating gingival fibromatosis and dental
abnormalities in a consanguineous family
Key findings
This case series describes a new autosomal recessive syndrome characterized by
gingival fibromatosis, hypoplastic amelogenesis imperfecta, intrapulpal calcifications,
and pericoronal radiolucencies in unerupted teeth.
Abstract
Background/Aim: Gingival fibromatosis (GF) is characterized by fibrotic enlargement
of the gingiva that can be inherited as an isolated trait (named hereditary gingival
fibromatosis) or as component of a syndrome. This article reports one kindred affected
by a syndrome characterized by GF associated with dental abnormalities (DA),
including generalized thin hypoplastic amelogenesis imperfecta (AI).
Methods: To characterize the pattern of inheritance and the clinical features, 70 family
members were examined. Hematoxylin and eosin stain, immunohistochemistry, and
scanning electronic microscopy (SEM) were performed to identify the alterations on
gingiva, teeth and dental follicles.
Results: Examination of the family pedigree demonstrated multiple consanguineous
first cousin marriages and an autosomal recessive trait of inheritance. Four members
demonstrated mild GF in association with DA, including generalized thin hypoplastic
AI, intrapulpal calcifications, delay on tooth eruption, and pericoronal radiolucencies
31
involving unerupted teeth. One out of those 4 patients also had mental retardation (MR).
MR as an isolated feature was observed in 6 members, whereas isolated GF was found
in 1 individual. Combination of gingivectomy and gingivoplasty followed by regular
dental procedures were performed in these patients. Histological examination of the
gingival enlargement revealed a dense connective tissue containing myofibroblasts,
islands of odontogenic epithelium, and calcified psammomatous deposits that by SEM
resembling cementicle-like structures. Pericoronal lesions also showed calcified
psammomatous deposits in association with islands of odontogenic epithelium. Enamel
ultrastructure analysis revealed normal surface alternated by irregular and porous areas.
Conclusion: We propose that these cases represent a new syndrome within the
spectrum of those including GF.
Key words: Gingival fibromatosis; dental abnormalities; generalized thin hypoplastic
amelogenesis imperfecta; autosomal recessive.
Running title: Gingival fibromatosis and dental abnormalities syndrome.
32
Introduction
Gingival fibromatosis (GF) is the overgrowth of the gingiva characterized by na
expansion and accumulation of the connective tissue with occasional presence of
increased number of cells.1 It is induced as a side-effect of systemic drugs, including the
anti-seizure drug phenytoin, the immunesuppressor cyclosporine, and the calcium-
channel-blocker with anti-hypertensive activity nifedipine, or it is hereditary.2,3 As an
inherited disorder, GF may be isolated, in which it is referred as hereditary gingival
fibromatosis (HGF), or part of a genetic syndrome.4 HGF is traditionally considered an
autosomal dominant disease, whereas pedigree analyses of GF syndromic forms are
consistent with either dominant or recessive Mendelian transmission pattern.3 GF as
part of a syndrome is related to hyperthricosis and/or metal retardation syndrome,
Zimmermann-Laband syndrome, Murray-Puretic-Drescher syndrome (juvenile hyaline
fibromatosis), Rutherfurd syndrome, GF with distinctive fácies syndrome, Ramon
syndrome, Cross syndrome, Jones syndrome, and Pune Belly syndrome.3 GF in
association with growth hormone deficiency,5,6 hypothyroidism,7 hearing loss and
supernumerary teeth,8 and more recently, generalized aggressive periodontitis9 were
also described. Amelogenesis imperfecta (AI) is a general term for a number of
conditions that affects enamel formation and/or calcification.10 In most of the cases, an
autosomal dominant mode of inheritance is involved, however, the disease is frequently
found as an autosomal recessive or X-linked disorder.11 Enamel defects in AI are highly
variables, ranging from deficiency on enamel formation to defects in the mineral and
protein content.12 Furthermore, some case reports have described numerous dental
alterations in combination with AI, including unerupted teeth, pulpal calcifications, root
and crown resorption, hypercementosis, and taurodontism.13-15 Gingival enlargement
has also been described in association with AI in few and isolated case reports.16-18

33
Recently, Feller et al.19 reported a single case showing enamel dysplasia, multiple
unerupted teeth with large pericoronal lesions, anterior open bite malocclusion and mild
gingival overgrowth. The present study reports a family spanning 3 generation with
members from consanguineous marriage manifesting a new autosomal recessive
syndrome characterized by GF associated with dental abnormalities (DA), including
generalized thin hypoplastic AI, intrapulpal calcifications, delay of tooth eruption,
pericoronal radiolucencies in unerupted teeth, dental agenesis, and root dilacerations.
Interestingly, 1 individual showed GF and DA in combination with mental retardation
(MR).
Report of cases
The pedigree of the kindred could be reliably constructed for the 3 latest generations
and is depicted in Figure 1. All members were clinically examined, and photographs
and family histories permitted the diagnosis of 4 deceased individuals. The clinical
examination of the 70 descendants revealed that 1 (male) was affected by isolated GF, 3
(1 male and 2 females) showed GF associated with DA, and 1 (female) member had GF
and DA in association with MR. Six members (1 male and 5 females) presented with
isolated MR. All affected members came from consanguineous marriage, except for the
member with isolated GF. The member with isolated GF is married with a first cousin
and has 5 daughters (1 with MR) without signs of GF. Pedigree analysis provides ample
evidence that GF and DA were transmitted together by an autosomal recessive gene.
Patients described in this study are numbered in Figure 1, and a summary of the clinical
features is depicted in Table 1.

34
Patient 1: The proband, a 19-year-old female, was referred to the University of Montes
Claros Dental Clinic for complete dental treatment. Her mother stated that she has never
seen a dentist before. She is the second of 5 siblings (3 affected by MR) of a first cousin
marriage (Fig. 1). She was born at full term after normal pregnancy, and there were no
perinatal complications. She was hypotonic as an infant and showed a delay in
acquiring developmental milestones. Her speech was significantly delayed. She has
MR, but her social development and bonding skills are satisfactory. She had never
experienced seizures or suffered from deafness. There were no signs of hypertricosis or
history of renal problems. Intraoral examination detected a generalized enlargement of
the gingival tissue and the absence of several permanent teeth. The gingival overgrowth
was mild without significant degree of inflammation, and was most evident in the molar
region. Her mother informed that the gingiva started to overgrowth after eruption of the
permanent dentition. The erupted teeth showed a yellow discoloration with thin enamel
of normal hardness. The erupted teeth were spaced and the molars showed a significant
reduction in size. The upper central incisors presented a semi-lunar shaped defect. The
radiographic examination showed upper right third molar agenesis, microdontia of the
other third molars, and delayed eruption of several teeth. No density differences
between enamel and dentin was observed. Intrapulpal calcifications in both erupted and
unerupted teeth were evident. Unerupted teeth had large and well-defined pericoronal
radiolucencies. The roots of the lower left premolars appeared dilacerated, and the lower
second molars showed distorted and poorly developed roots.
Patient 2: The patient 2 is a 13-year-old young woman cousin of the patient 1, who was
born with 32 weeks of gestational development via cesarean. There were no perinatal
complications. She has a twin sister and 1 brother similarly affected, 2 healthy twin

35
brothers, and 1 deceased (undetermined) brother (Fig. 1). The systemic exploration was
normal, and her parents were first degree cousin. Her medical history was unremarkable
and she never taken any medication associated with gingival overgrowth. She did not
present with any mental impairment or hypertrichosis. Intraoral examination showed a
dentition with yellow discolored teeth with diasthemas and thin enamel of normal
hardness. The gingiva was enlarged in both arches, and the posterior áreas were more
severely affected (Fig. 2). Radiographically, it was impossible to visualize enamel or
differentiate it from dentin. Obvious coronal and radicular pulpal calcifications were
present in numerous teeth. The upper and lower second molars had pericoronal
radiolucent zones delineated by sclerotic borders. Periapical radiograph of the posterior
lower left area demonstrated a calcificated material in the gingiva located between the
second pre-molar and the first molar.
Patient 3: Patient 3 is twin sister of the patient 2 and cousin of the patient 1. Her mother
described the pregnancy as normal, without risk of fetal loss or use of medications. Her
weight and height were considered to be within normal limits for a 32-week girl. Her
medical history was unremarkable. She did not show any mental impairment. Clinical
examination revealed generalized, but mild gingival overgrowth involving both the
maxillary and mandibular arches, with morphologically altered teeth. Gingival
enlargement had normal color, fibrous consistency, and was most evident in the anterior
region. The permanent dentition showed yellow color, thin enamel and large inter-
proximal spaces. Radiographic examination revealed no density difference between
enamel and dentin, but the dentin showed normal radiodensity. Periapical radiographs
demonstrated coronal and radicular intrapulpal calcifications, which were needle-shaped

36
in the anterior teeth. Left upper third molar was absent, and lower second molars had
radiolucent pericoronal lesions with partially sclerotic margins.
Patient 4: This patient is an 18-year-old man, the older brother of the patient 2 and 3.
He was born at full term by a normal spontaneous vertex delivery. There were no
perinatal complications. All physical findings were within normal limits, and he denied
to have taken any medication associated with gingival overgrowth. He has previous
history of several dental extractions. Clinical examination revealed a mild generalized
gingival overgrowth and a disturbed eruption pattern, with retention of deciduous teeth.
Both deciduous and permanent teeth that were visible had a distinct yellow color and
their surfaces were thin but hard. The teeth were widely spaced without contact points.
The lower left first molar crown was partially destroyed and a periapical lesion was
evident (Fig. 3). Similar to the other cases, it was impossible to differentiate enamel
from dentin, coronal and radicular pulpal calcifications were observed, and some
unerupted teeth had pericoronal radiolucent areas delineated by sclerotic borders.
Treatment
The initial treatment consisted of oral hygiene orientation and plaque control. An
improvement in oral hygiene was observed for all patients with the exception of patient
1, whose mental and motor impairment contributed to continued plaque accumulation.
The conservative surgical treatment consists of quadrant-byquadrant internal bevel
gingivectomy in association with gingivoplasty, followed by 0.12% chlorhexidine oral
rinses twice a day for 2 weeks after each surgery. The interval between surgeries was of
2-3 months. After the last gingivectomy and post-surgical follow-up visit, the patient
returned periodically for observation and regular dental treatment, including dental

37
filling, dental extractions and prosthesis rehabilitation. Implant therapy is under
consideration for patient 4. Scaling and prophylaxis are performed every six months.
There was no recurrence of the gingival enlargement after 18 months. Genetic
counseling was given to all affected family members and their parents. Information
regarding the pattern of gene transmission, possible ways of expression, and
consequences of phenotypes were emphasized.
Histopathological and ultrastructural features
The tissues removed during the surgical procedures, gingiva and hyperplastic dental
follicles, were fixed in formalin, embedded in paraffin, and sections used for
hematoxylin and eosin (HE) stain or immunostaining as previously described.20 Teeth
were cut sagittally in two halves in a mesio-distal direction with a low-speed saw
microtome. One half was decalcified in 5% nitric acid prior paraffin embedded, and the
other half was analyzed by scanning electron microscopy (SEM) at 15 kV*. The
histological features of the overgrowth gingiva were very similar among affected
members. The microscopic analysis showed a well-structured epithelium with elongated
and thin papillae inserted in fibrous connective tissue. Areas with mild chronic
inflammatory infiltrates were observed in the subepithelial connective tissue. The
connective tissue showed an increased amount of collagen fiber bundles running in all
directions (Fig. 4A). Immunohistochemical analysis against α-SMA showed a broadly
presence of myofibroblasts in the lesional connective tissue (Fig. 4D). Large numbers of
spherical and laminated calcified structures resembling dysplastic enamel or
cementicles, and nests of epithelium resembling odontogenic epithelium rests were
observed (Fig. 4B). The nest cells were strongly reactive for the monotypic antibody
anti-CK19, confirming the odontogenic origin (Fig. 4C). We also performed a SEM

38
examination using 5 µm paraffin section etched or not with 2% EDTA as previously
described by Kodaka & Debari.21 Untreated calcified structures demonstrated a globular
outside surface and a glass-like aspect with several cracks in the inside portion (Fig. 5A
and B). After EDTA etching, the calcified structures demonstrated appositional
laminations with an increased porosity in the center, revealing a cementoid origin for
the calcifications (Fig. 5C and D). The histopathological analysis of the hyperplastic
follicles of the impacted teeth showed mature fibrous connective tissue containing
various odontogenic epithelial islands associated with psammomatus calcifications.
Those features were quite similar to those observed in the gingival tissue. Three teeth
were selected for histological and SEM examination. One tooth was extracted due to a
carious lesion, whereas the other two were unerupted ones. In all teeth, HE staining of
the decalcified halves revealed normal dentin and cementum, and an obliteration of the
pulpal chambers. The pulpal chamber of the decay tooth was filled in part by reparative
dentin and in part by abnormal dentin, characterized by few and irregular tubules and
áreas of globular appearance (Fig. 6A and B). The unerupted teeth showed the pulpal
chambers only obliterated by amorphous dentin (Fig. 6C and D). Enamel ultrastructure
of the unerupted teeth revealed a thin irregular enamel layer with normal structure
alternated by rough areas with severe porosity and irregularly shaped empty spaces (Fig.
7A and B). The irregular areas of enamel have a laminated and shedding appearance
with unrecognizable ultrastructure (Fig. 7C). Enamel was present only at the cervical
area of the erupted tooth.
* Scanning electron microscope Jeol JSM 5600 LV, Japan.

39
Discussion
This report documents a large family affected by an undescribed syndrome
characterized by GF and DA with thin generalized hypoplastic AI as the main dental
feature. Other variant features included pulpal calcifications, root dilacerations,
hypodontia, delay of tooth eruption, and pericoronal radiolucencies in unerupted teeth.
In this family, there was no presence of DA in family members without GF, while 1
subject was diagnosed with isolated GF. The presence of GF in association with DA, in
particular hypoplastic amelogenesis imperfecta, intrapulpal calcifications and
pericoronal radiolucencies in unerupted teeth, in 4 family members suggests that these
traits are segregating together and represent the expression of a single condition. It is
known that isolated GF may result from a single gene mutation, whereas syndromic
forms may result from alterations of multiple genes or single gene dosage effect.22 On
the other hand, MR was superimposed with GF and DA in 1 patient, and was detected
as an isolated feature in 6 descendants, suggesting that the coexistence of MR and GF
plus DA may represent a coincidence of 2 conditions in the same family with multiple
consanguineous marriages. MR in the offspring is a common feature in consanguineous
marriages.23 GF as an inheritance disorder shows a heterogeneous pattern of
transmission. Chromosomal abnormalities reported for syndromes with GF include
duplications, deletions, and/or other anomalies of chromosomes 2p13-16, 4q, 8, 14q,
19p, 19q, and Xq.24-28 Mangino et al.29 described an Italian family affected by GF in
association with hypertrichosis, and linkage genetic analysis excluded a connection to
previously mapped HGF loci on chromosomes 2 (GINGF on 2p21-22 and GINGF3 on
2p22.3-p23.3) and 5 (GINGF2 on 5q13-q22), suggesting that syndromes with GF are
genetically different from isolated GF which are traditionally transmitted by an
autosomal dominant gene.30 The family described here is consistent with an autosomal

40
recessive mode of inheritance of GF and DA with history of consanguinity in all
affected members. The clinical findings of the patients described here were consistent
with genetic GF. GF can vary from focal sites of gingival enlargement to generalized
involvement, and the degree of overgrowth may vary from slight to severe.31 The
gingival enlargement may result in both esthetic and functional problems for affected
individuals.3 The patients exhibited a generalized but mild gingival overgrowth, and the
posterior region of both maxilla and mandible were severely affected in patients 1 and
2, while that in patients 3 and 4 was mainly evident in the anterior region. None of the
affected patients show functional discomforts, but they were unhappy with the
appearance of their gingiva, particularly the twins. In all 4 examined cases, their
mothers stated that the gingival enlargement was seen during eruption of the permanent
teeth. It is known from previous reported cases that the condition usually begins at the
time of eruption of the permanent dentition 32, but can develop with the eruption of the
deciduous dentition and rarely is seen at birth.33 The histological features of the gingiva
were also consistent with previous reported cases.34 The gingival tissues were composed
of fibrous connective tissue with collagen fiber bundles running in all directions, and all
samples contained a significant proportion of myofibroblasts as revealed by α-SMA
immunohistochemical staining. We have previous demonstrated that myofibroblasts, the
main cellular type involved in extracellular matrix deposition in fibrotic diseases, is
associated with HGF etiopathology.35,36 We have also observed a broadly distribution of
calcified psammomatous structures associated with odontogenic epithelial remnants in
the overgrown gingiva. There is only one case report describing the occurrence of
numerous calcifications and islands of odontogenic epithelium in the gingiva of patients
affected by isolated GF.37 SEM examination of the calcified structures revealed
appositional laminations with a globular and porous central core which is often

41
observed in cementicles in the root furcations.21 Regarding the formation of these
cementicle-like structures, it is presumed that they were formed by the activity of the
odontogenic epithelial cells, which were in close contact with the calcifications. Other
possible origin would be bone metaplasia or dystrophic calcifications, but no necrotic
tissue was observed in these cases. Farrer-Brown et al.38 described the presence of
numerous trabeculae of metaplastic bone and few small calcified particles in the gingiva
of 4 members from one family affected by HGF. Enamel alterations were compatible
with generalized thin hypoplastic autosomal recessive AI.12 Affected members showed
teeth with yellow color, smooth surface, lack of contact points, no enamel apparent
radiographically, and thin enamel layer with normal structure alternated by rough areas
with severe porosity and irregularly shaped empty spaces. AI has been described to
occur as part of several syndromes,10 but there are only few reports in the literature
demonstrating the association between AI and gingival overgrowth.16-18 However, those
were isolated cases and inflammation caused by plaque accumulation seems to be the
inductor of the gingival enlargement in most of the cases. Generalized gingival
overgrowth has also been described in a patient affected by the syndrome associating AI
with nephrocalcinosis.39 None of our patients had any history of renal impairment, and
all of them had normal renal ultrasound scans and normal calcium levels in the serum.
Recently, Feller et al.19 reported a case quite similar to ours, affecting a 12-year-old
male who had enamel dysplasia, odontogenic fibroma-like hamartomas, teeth with
pulpal calcifications, and mild and generalized gingival overgrowth. The authors
reported that the patient has 5 siblings and the mother stated that none of them or any
other family member has any similar oral manifestations. Previous reports of this
association reported by Feller et al.19 have been described in the literature, but that was
the first one to identify gingival enlargement.15,40,41 Interestingly enough, all 5 reports of
42
this association are single cases originated from South Africa. The histopathological
features of the gingival tissue presented here were very similar to those reported by
Feller et al.19 with the exception of intense mixed acute and chronic inflammatory
infiltrate extending into the epithelium, which was associated with hyperplastic
changes, presented in their case. Previous evaluation of the morphological pattern of the
gingival epithelium of isolated GF tissues demonstrated that hyperplastic alterations are
only found in inflamed specimens, whereas áreas without inflammation showed only
long and deep epithelial papillae.34 Microscopic examination of the dental follicles of
the impacted te named as odontogenic fibroma-like hamartomas. The hyperplastic
dental follicles consisted of fibrous connective tissue with odontogenic remnants and
cementicle-like structures similar to that in the gingival overgrowth. Furthermore, the
presence of unerupted teeth in the affected patients is probably due to the obstruction
caused by the pericoronal lesions. Similar hyperplastic alterations in the dental follicles
were observed in AI, nephrocalcinosis and hypocalciuria syndrome.39 A notable feature
in our patients was the intrapulpal calcifications affecting most of the teeth, whether
erupted or unerupted. Most of the calcifications were limited to coronal pulpal chamber,
and presented a needleshaped. In erupted teeth, the pulpal chamber was filled by an
association of reparative dentin, caused probably by the enamel attrition, and abnormal
dentin, characterized by few and irregular tubules and areas of globular appearance,
whereas unerupted teeth were filled by this amorphous dentin only. Intrapulpal
calcification in AI patients is a common feature, although those are most likely caused
by reparative dentin deposition or pulpal degeneration due to vascular insufficiency
resulting from hypercementosis.13,19 In the examined teeth, dentin and cementum were
normal, and the presence of intrapulpal calcifications in unerupted teeth suggest that the
pulpal morphogenesis is also affected in this syndrome. However, further investigation

43
is needed to elucidate the mechanisms behind this phenotype. GF may result in both
esthetic and functional problems for affected individuals, and the only treatment
available is surgical resection of the overgrowth tissue, but recurrence is anticipated.3
Recently, we demonstrated in vitro that interferon gamma inhibits significantly HGF
myofibroblastic cell metabolism as revealed by the decreased synthesis of type I
collagen, supporting that locally delivery of this cytokine may be useful to prevent the
gingival overgrowth of affected patients.36 Our patients were unhappy with the
appearance of their gingiva and were surgically treated by a combination of
gingivectomy and gingivoplasty. Since it has been demonstrated that recurrence is faster
in areas with dental plaque accumulation,42,43 we put the patients in a combination of
monthly examination with professional cleaning and oral hygiene instructions, and
recurrence has not been seen after 18 months. Restorative and rehabilitation dentistry
are more complex and extensive in patients affected by AI. In conclusion, one previous
report of gingival overgrowth associated with enamel dysplasia, odontogenic fibroma-
like hamartomas and intrapulpal calcifications shows similarities to this family.
Nevertheless, it was a single case report. If so doing, we believe that the above-
mentioned features are sufficiently unique to characterize a new autosomal recessive
syndrome associating GF and DA, including generalized thin hypoplastic AI. MR
participation needs further analysis. Finally, genetic investigation is essential to clarify
the defect behind this syndrome.
44
References
1. Takagi M, Yamamoto H, Mega H, Hsieh KJ, Shioda S, Enomoto S. Heterogeneity in
the gingival fibromatoses. Cancer 1991;68:2202-2212.
2. Dongari-Bagtzoglou A. Drug-associated gingival enlargement. J Periodontol
2004;75:1424-1431.
3. Coletta RD, Graner E. Hereditary gingival fibromatosis: a systematic review. J
Periodontol 2006;77:753-764.
4. Gorlin R, Cohen M, Henekam R. Syndromes of the head and neck., ed. 4th. New
York: Oxford University Press (Oxford Monographs on Medical Genetics); 2001:847-
857.
5. Bhowmick SK, Gidvani VK, Rettig KR. Hereditary gingival fibromatosis and growth
retardation. Endocr Pract 2001;7:383-387.
6. Oikarinen K, Salo T, Kaar ML, Lahtela P, Altonen M. Hereditary gingival
fibromatosis associated with growth hormone deficiency. Br J Oral Maxillofac Surg
1990;28:335-339.
7. Chaikin BS. Report of a case of fibromatosis of the gingivae associated with a
hypothyroidism. Periodontics 1965;3:306-309.
8. Wynne SE, Aldred MJ, Bartold PM. Hereditary gingival fibromatosis associated with
hearing loss and supernumerary teeth--a new syndrome. J Periodontol 1995;66:75-79.
9. Casavecchia P, Uzel MI, Kantarci A, et al. Hereditary gingival fibromatosis
associated with generalized aggressive periodontitis: a case report. J Periodontol
2004;75:770-778.
10. Crawford PJ, Aldred M, Bloch-Zupan A. Amelogenesis imperfecta. Orphanet J
Rare Dis 2007;2:1-11.

45
11. Aldred MJ, Savarirayan R, Crawford PJ. Amelogenesis imperfecta: a classification
and catalogue for the 21st century. Oral Dis 2003;9:19-23.
12. Nusier M, Yassin O, Hart TC, Samimi A, Wright JT. Phenotypic diversity and
revision of the nomenclature for autosomal recessive amelogenesis imperfecta. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 2004;97:220-230.
13. Lykogeorgos T, Duncan K, Crawford PJ, Aldred MJ. Unusual manifestations in X-
linked amelogenesis imperfecta. Int J Paediatr Dent 2003;13:356-361.
14. Collins MA, Mauriello SM, Tyndall DA, Wright JT. Dental anomalies associated
with amelogenesis imperfecta: a radiographic assessment. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 1999;88:358-364.
15. Peters E, Cohen M, Altini M. Rough hypoplastic amelogenesis imperfecta with
follicular hyperplasia. Oral Surg Oral Med Oral Pathol 1992;74:87-92.
16. Macedo GO, Tunes RS, Motta AC, et al. Amelogenesis imperfecta and unusual
gingival hyperplasia. J Periodontol 2005;76:1563-1566.
17. Atasu M, Biren S, Mumcu G. Hypocalcification type amelogenesis imperfecta in
permanent dentition in association with heavily worn primary teeth, gingival
hyperplasia, hypodontia and impacted teeth. J Clin Pediatr Dent 1999;23:117-121.
18. Brennan MT, O'Connell BC, Rams TE, O'Connell AC. Management of gingival
overgrowth associated with generalized enamel defects in a child. J Clin Pediatr Dent
1999;23:97-101.
19. Feller L, Jadwat Y, Bouckaert M, Buskin A, Raubenheimer EJ. Enamel dysplasia
with odontogenic fibroma-like hamartomas: review of the literature and report of a case.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:620-624.

46
20. Coletta RD, Cotrim P, Almeida OP, Alves VA, Wakamatsu A, Vargas PA. Basaloid
squamous carcinoma of oral cavity: a histologic and immunohistochemical study. Oral
Oncol 2002;38:723-729.
21. Kodaka T, Debari K. Scanning electron microscopy and energy-dispersive X-ray
microanalysis studies of afibrillar cementum and cementicle-like structures in human
teeth. J Electron Microsc (Tokyo) 2002;51:327-335.
22. Hart TC, Pallos D, Bozzo L, et al. Evidence of genetic heterogeneity for hereditary
gingival fibromatosis. J Dent Res 2000;79:1758-1764.
23. Abdulrazzaq YM, Bener A, al-Gazali LI, al-Khayat AI, Micallef R, Gaber T. A
study of possible deleterious effects of consanguinity. Clin Genet 1997;51:167-173.
24. Macias-Flores MA, Garcia-Cruz D, Rivera H, et al. A new form of hypertrichosis
inherited as an X-linked dominant trait. Hum Genet 1984;66:66-70.
25. Shashi V, Pallos D, Pettenati MJ, et al. Genetic heterogeneity of gingival
fibromatosis on chromosome 2p. J Med Genet 1999;36:683-686.
26. Hart TC, Zhang Y, Gorry MC, et al. A mutation in the SOS1 gene causes hereditary
gingival fibromatosis type 1. Am J Hum Genet 2002;70:943-954.
27. Fryns JP. Gingival fibromatosis and partial duplication of the short arm of
chromosome 2 (dup(2)(p13-->p21)). Ann Genet 1996;39:54-55.
28. Stefanova M, Atanassov D, Krastev T, Fuchs S, Kutsche K. Zimmermann-Laband
syndrome associated with a balanced reciprocal translocation t(3;8)(p21.2;q24.3) in
mother and daughter: molecular cytogenetic characterization of the breakpoint regions.
Am J Med Genet A 2003;117:289-294.
29. Mangino M, Pizzuti A, Dallapiccola B, Bonfante A, Saccilotto D, Cucchiara E.
Hereditary gingival fibromatosis (HGF) with hypertrichosis is unlinked to the HGF1
and HGF2 loci. Am J Med Genet A 2003;116:312-314.

47
30. Martelli-Junior H, Lemos DP, Silva CO, Graner E, Coletta RD. Hereditary gingival
fibromatosis: report of a five-generation family using cellular proliferation analysis. J
Periodontol 2005;76:2299-2305.
31. Bozzo L, Machado MA, de Almeida OP, Lopes MA, Coletta RD. Hereditary
gingival fibromatosis: report of three cases. J Clin Pediatr Dent 2000;25:41-46.
32. Baptista IP. Hereditary gingival fibromatosis: a case report. J Clin Periodontol
2002;29:871-874.
33. Bozzo L, de Almedia OP, Scully C, Aldred MJ. Hereditary gingival fibromatosis.
Report of an extensive four-generation pedigree. Oral Surg Oral Med Oral Pathol
1994;78:452-454.
34. Araujo CS, Graner E, Almeida OP, Sauk JJ, Coletta RD. Histomorphometric
characteristics and expression of epidermal growth factor and its receptor by epithelial
cells of normal gingiva and hereditary gingival fibromatosis. J Periodontal Res
2003;38:237-241.
35. Bitu CC, Sobral LM, Kellermann MG, et al. Heterogeneous presence of
myofibroblast in hereditary gingival fibromatosis. J Clin Periodontol 2005;33:393-400.
36. Sobral LM, Montan PF, Martelli-Junior H, Graner E, Coletta RD. Opposite effects
of TGF-beta1 and IFN-gamma on transdifferentiation of myofibroblast in human
gingival cell cultures. J Clin Periodontol 2007;34:397-406.
37. Gunhan O, Gardner DG, Bostanci H, Gunhan M. Familial gingival fibromatosis
with unusual histologic findings. J Periodontol 1995;66:1008-1011.
38. Farrer-Brown G, Lucas RB, Winstock D. Familial gingival fibromatosis: na unusual
pathology. J Oral Pathol 1972;1:76-83.
48
39. Paula LM, Melo NS, Silva Guerra EN, Mestrinho DH, Acevedo AC. Case report of
a rare syndrome associating amelogenesis imperfecta and nephrocalcinosis in a
consanguineous family. Arch Oral Biol 2005;50:237-242.
40. van Heerden WF, Raubenheimer EJ, Dreyer AF, Benn AM. Amelogenesis
imperfecta: multiple impactions associated with odontogenic fibromas (WHO) type. J
Dent Assoc S Afr 1990;45:467-471.
41. Raubenheimer EJ, Noffke CE. Central odontogenic fibroma-like tumors,
hypodontia, and enamel dysplasia: review of the literature and report of a case. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:74-77.
42. Kavvadia K, Pepelassi E, Alexandridis C, Arkadopoulou A, Polyzois G, Tossios K.
Gingival fibromatosis and significant tooth eruption delay in an 11-year-old male: a 30-
month follow-up. Int J Paediatr Dent 2005;15:294-302.
43. Ramer M, Marrone J, Stahl B, Burakoff R. Hereditary gingival fibromatosis:
identification, treatment, control. J Am Dent Assoc 1996;127:493-495.

49
4.2 – Artigo Científico 2
Idiopathic gingival fibromatosis: clinical features and immunohistochemical
evaluation of myofibroblasts
Abstract
Backgroung/Aim: Gingival fibromatosis is an enlargement of the gingival tissue
characterized by an excessive accumulation of extracellular matrix, predominantly type
I collagen. It is induced as a side-effect of systemic drugs, including the anti-seizure
drug phenytoin, the immunesuppressor cyclosporine, and the calcium-channel-blocker
with anti-hypertensive activity nifedipine, or it is hereditary. However, in some cases,
the overgrowth of the gingival is idiopathic; these cases its pathogenesis remains
unknown. Myofibroblasts are cells related to fibroblasts and exhibit a hybrid phenotype
between fibroblasts and smooth muscle cells. These cells are characterized by
expression of the specific smooth muscle isoform of α-actin (α-SMA) and, when
activated, synthesize high levels of extracellular matrix proteins, particularly collagen.
This paper reports two cases of idiophatic gingival fibromatosis, and discusses the
diagnosis, histopathological features, treatment and immunohistochemical evaluation of
myofibroblasts this condition.
Materials and Methods: Two patients (one children and one adult) was diagnosed as
having idiophatic gingival fibromatosis because her medical and family histories were
unremarkable, her medical history was not indicative of drug-induced gingival
enlargement or hormonal changes and there was no evidence of history of consanguinity
to suggest autosomal recessive inheritance or genetic transmission. Both were referred
to the Stomatology Clinic at State University of Montes Claros, Dental School, Montes
50
Claros – Minas Gerais, due to fibrous gingival overgrowth. The treatment of patients
consisted of quadrant-by-quadrant gingivectomy/gingivoplasty technique, followed by
0.25% chlorhexidine oral rinses twice a day for two weeks after each surgery. The
tissues removed during surgical procedures were fixed in formalin, embedded in
paraffin, and sections used for hematoxylin and eosin and Mason tricromic stain. To
determine the presence of myofibroblasts in the overgrowth tissues we performed
immunohistochemistry against α-SMA protein.
Results: The histological examination of the gingival tissues from both cases revealed
mild epithelial hyperplasia with long rete pegs and marked increase in the dense fibrous
connective tissue. The Mason tricromic technique revealed wide bundles of collagen
strongly stained. These analysis of immunohistochemistry revealed that idiophatic
gingival fibromatosis tissue samples were negative for α-SMA in the connective tissue,
except in the smooth muscle of the blood vessel walls (internal positive control).
Conclusions: In all two cases, we trended toward a more conservative approach. In
both cases, there no recurrence of gingival enlargement. The first case postsurgical
follow-up is of 4 years and second case the follow-up is of 1 year. Recently, we
demonstrated that the presence of myofibroblasts is heterogeneous in two families with
hereditary gingival fibromatosis. In our two cases of idiophatic gingival fibromatosis
gingival tissues as revealed by immunohistochemical were negative for α-SMA in the
connective tissue, except in the smooth muscle of the blood vessel walls (internal
positive control). Such variations may be attributed to subsets of fibroblasts that exist in
the gingival and periodontum. Given the fact that α-SMA is the specific marker of
myofibroblasts, these results strongly suggest that myofibroblasts are involved not in
gingival overgrowth in two cases reported here of idiophatic gingival fibromatosis.

51
Keywords: Idiopathic gingival fibromatosis; gingival overgrowth;
immunohistochemistry, myofibroblasts.
52
Introduction
Gingival fibromatosis (GF) is the overgrowth of the gingival characterized by an
expansion and accumulation of the connective tissue with occasional presence of
increased number cells.24 It is induced as a side-effect of systemic drugs, including the
anti-seizure drug phenytoin, the immunesuppressor cyclosporine, and the calcium-
channel-blocker with anti-hypertensive activity nifedipine, or it is hereditary.11
However, in some cases, the overgrowth of the gingival is idiopathic; this cases its
pathogenesis remains unknown.23
Most idiopathic hyperplasias are probably caused by a genetic disorder and
should, therefore, not be called idiopathic, as the cause is “a genetic disorder”.
However, for the moment it has not been proven on which gene this genetic disorder is
located, so all hyperplasia without cause should still be described as idiopathic, even if
the hyperplasia is seen in the same family without any other symptoms.7
Myofibroblasts are cells related to fibroblasts and exhibit a hybrid phenotype
between fibroblasts and smooth muscle cells. 12 These cells are characterized by
expression of the specific smooth muscle isoform of α-actin (α-SMA) and, when
activated, synthesize high levels of extracellular matrix proteins, particularly collagen.12
Several reports have shown the presence of cells with myofibroblastic features in
specialized normal tissues and in a variety of pathological situations, such as
Dupuytren’s disease, cyclosporine-induced pancreatic fibrosis, and pulmonary, renal
and hepatic fibrosis.1,4,13 Recently, we showed for first time the presence of
myofibroblasts in hereditary gingival fibromatosis (HGF) and sindromic gingival
fibromatosis (SGF).5,19
Many studies have shown increased transcriptional and translational levels of
type I collagen in both tissue and fibroblasts cultures derived from of HGF patients.8,20
53
Furthermore, HGF fibroblasts produce excessive amounts of TGF-β120 which is, in
association with an elevated synthesis of collagen, an intrinsic characteristic of
myofibroblasts.12 As overgrowth of the gingival tissue provides an excellent model for
study of connective tissue fibrosis. This paper reports two cases of idiophatic gingival
fibromatosis, and discusses the diagnosis, histopathological features, treatment and
immunohistochemical evaluation of myofibroblasts this condition.
Case report 1
A ten-year-old brown boy was referred to the Stomatology Clinic at State
University of Montes Claros, Dental School, Montes Claros – Minas Gerais, due to
pronounced fibrous gingival overgrowth. Clinical examination revealed generalized and
severe gingival overgrowth involving both the maxillary and mandibular arches, with
morphologically normal teeth (Fig. 1). The gingiva was pink, and its firm, dense,
fibrous consistency caused difficulty in tooth eruption and inadequate position dental.
The patient had difficulty maintaining adequate oral self care hygiene. Gingival
enlargement had first been noticed months after birth, but it was evident during the
period of deciduous dentition. Panoramic radiograph did not reveal any bone alteration.
He had a marked open and cross bite with dramatic flaring prevented normal lip closure
(Fig. 2).
The systemic exploration the patient was normal. The mother described the
pregnancy as normal, without risk of fetal loss or use of medications. He denied taking
any medications associated with gingival overgrowth and his weight and height were
considered to be within normal limits. He did not appear to have any mental
impairment. The patient was unhappy with the appearance of his gingiva. His mother

54
and father had absence of a relevant medical history. The patient has two brothers and
without gingival alteration presence in both.
The treatment of boy consisted of quadrant-by-quadrant
gingivectomy/gingivoplasty technique with periodontal, followed by 0.25%
chlorhexidine oral rinses twice a day for two weeks after each surgery. After the last
gingivectomy and post-surgical follow-up visit, the patient returned periodically for
observation. Scaling and prophylaxis are performed every six months.
Case report 2
A thirty-year-old caucasian man was referred for evaluation in Service due to
gingival fibrous enlargement varying from mild to moderate. The overgrowth tissue
affected buccal and lingual/palatal aspects, involving both the maxilla and mandible
(Fig 3). The mucosa was pink and firm to probing. The gingival hyperplasia caused
difficulties to dental biofilm removal and in these areas was observed signals of
inflammation. The patient had difficulty maintaining adequate oral self care hygiene.
The panoramic radiographic does not show any misformed teeth and anodontia. The
systemic exploration was normal. His medical history was unremarkable and he never
taken any medication associated with gingival overgrowth. He did not appear to have
any mental impairment or hypertrichosis. He has three brothers any without alteration
gingival. The mother and father not have history of consanguineous wedding. The
treatment was similar patient case 1.
Histopathological features
The tissues removed during gingivectomy/gingivoplasty surgical procedures
were fixed in formalin, embedded in paraffin, and sections used for hematoxylin and

55
eosin (H&E) stain. The histological examination of gingival overgrowth tissue
specimens revealed mild epithelial hyperplasia with longs rete pegs and marked
increase in the dense fibrous connective tissue in both cases (Fig 4). The Mason
Tricromic technique revealed wide bundles of collagen strongly stained in blue (Fig 5).
To determine the presence or not of myofibroblasts in IGF tissue specimens, we
performed immunohistochemistry against α-SMA protein. Immunostaining was
performed using 3-µm sections from 10% formalin-fixed, paraffin-embedded
specimens. After dewaxing and hydration in graded alcohol solutions, the sections were
treated with 3% H2O2, followed by incubation with 10 mM citric acid, pH 6.0, in a
microwave for 24 min., divided into two cycles for antigen retrieval. After washing with
phosphate-buffered saline (PBS), the sections were treated with 1% bovine serum
albumin (BSA) in PBS for 1 h and then incubated with monoclonal mouse anti-α-SMA
diluted 1:200, followed by the ABC method (Dako Corp.). Reactions were developed
by incubating the sections with 0.6 mg/ml 3,3”-diaminobenzidine tetrahydrochloride
(Sigma, St. Louis, MO, USA) containing 0.01% H2O2. Control reactions performed by
the omission of the primary antibodies did not show any staining. This analysis of
immunohistochemistry revealed that IGF tissue samples (n=2) were negative for α-
SMA in the connective tissue, except in the smooth muscle of the blood vessel walls
(internal positive control) (Fig 6).
Discussion
Although the underlying mechanisms of the gingival fibrosis that characterize
HGF and IFG remain unclear, it been proposed that gingival overgrowth develops
through activation or selection of resident tissue fibroblasts, phenotypically
characterized by increased proliferation, low levels of extracellular matrix-degrading

56
metalloproteinases l (MMP-1 and MMP-2), and abnormally high collagen
production.9,10 Futhermore, the autocrine stimulation by excessive amounts of TGF-β1
produced by HGF cells seems to contribute to these phenotypes.2,20 Morphologic and
quantitative analysis of the IGF biopsies showed a higher collagen content in the
gingival connective compartment in IGF than normal gingival. This finding may
account for the enlargement of the gingival tissue.15 Recently, Kather et al. (17)
indicated that there is a significant increase in the area fraction of collagen in 3 HGF
families. However, the relative numbers of gingival fibroblasts differ in the different
HGF types. These differences may reflect different forms of HGF, consistent with the
genetic heterogeneity that characterizes HGF conditions.17
Myofibroblasts are very specialized cells with a hybrid phenotype between
fibroblasts and smooth muscle cells, and are characterized by expression of the specific
smooth muscle isoform of α-actin (α-SMA).14 Those cells are present transiently during
wound healing, where they play essential roles in wound contraction and connective
tissue restoration.12 In contrast, they are persistent in fibrotic lesions leading for the
excessive collagen accumulation.13 As summarized above, myofibroblasts could play a
role in HGF, because HGF fibroblasts display several features that are intrinsic of
myofibroblasts including activated phenotype in the presence of elevated levels of TGF-
β1.
Recently, we demonstrated that the presence of myofibroblasts is heterogeneous
in two families with HGF.5 Interestingly, α-SMA was detected in low levels in vitro in
cultures from HGF family 1 and normal gingival but not in vivo, which is probably due
to the stress fiber induction associated with cellular cultures. In family 2, all HGF
gingival tissues as revealed by immunohistochemical staining against α-SMA and was
detected in high levels in vitro in cultures from HGF family 2. In our two cases of IGF
57
gingival tissues as revealed by immunohistochemical were negative for α-SMA in the
connective tissue, except in the smooth muscle of the blood vessel walls (internal
positive control). Such variations may be attributed to subsets of fibroblasts that exist in
the gingival and periodontum.21 Given the fact that α-SMA is the specific marker of
myofibroblasts, these results strongly suggest that myofibroblasts are involved not in
gingival overgrowth in two cases reported here of IGF.
Two patients (one children and one adult) was diagnosed as having “idiophatic”
gingival fibromatosis because her medical and family histories were unremarkable, her
medical history was not indicative of drug-induced gingival enlargement or hormonal
changes and there was no evidence of history of consanguinity to suggest autosomal
recessive inheritance or genetic transmission.
Nevertheless, the features clinical and microscopic observed were similar in
every way to those described by other authors.3,6 GF, particularly HGF may occur as an
isolated feature or rarely as part of a syndrome.11 The syndromic characteristic most
commonly seen in association with HGF is hypertricosis, which is occasionally
associated with mental retardation. This association of extreme hirsutism with gingival
fibromatosis follows a dominant pattern of inheritance.11 Association of gingival
fibromatosis, ear, nose, bone, and nail defects and hepatosplenomegaly characterizes the
Zimmermann-Laband syndrome.18 Jones et al. (16) described a family with gingival
fibromatosis associated with progressive deafness in five generation. This association is
described as Jones syndrome.16 Murray-Peretic-Drescher syndrome (juvenile hyaline
fibromatosis) is characterized by gingival fibromatosis, multiple hyaline fibromas,
osteolysis of terminal phalanges, recurrent infections stunted growth, and premature
death.22 Recently, we describe gingival fibromatosis associated with dental
abnormalities in a consanguineous family.19

58
The gingival enlargement results in both esthetic and functional problems for
affected individuals. The most common effects are diastemas, malpositioning of teeth,
prolonged retention of primary dentition, delayed eruption, cross and open bites,
prominent lips, and open lip posture.3,6 Although the gingival enlargement does not
directly affect the alveolar bone, the gingival swelling increases the biofilm
accumulation, inducing periodontitis, bone resorption and halitosis.11 The gingival
enlargement usually begins at the time of eruption of the permanent dentition or, less
frequently, with the eruption of the deciduous dentition.11 The first case here, the
mother’s patients noticed gingival enlargement after birth, but it was evident during the
period of deciduous dentition. The second case, the patient only noted the enlargement
in the last 5-6 years. GF can't be cured but can be controlled with varying degrees of
success. When the enlargement is minimal, good scaling of teeth and oral homecare
may be all that is required to maintain good appearance.11 When the excess tissue
increases and appearance and function were compromised, there are indicated the
surgical intervention. Several authors have reported the recurrence of hyperplasic tissue
in HGF following gingivectomy, however, the psychological benefits of even temporary
cosmetic improvement must not be underestimated and may outweigh the probability of
recurrences in such a severe case.11 In all two cases, we trended toward a more
conservative approach. In both cases reported here, there no recurrence of gingival
enlargement. The first case postsurgical follow-up is of 4 years and second case the
follow-up is of 1 year.
In conclusion, this study evaluated for first time the presence of myofibroblasts
in IGF. Although we results were obtained from two cases clinical only, may contribute
to identification of biological mechanisms leading to gingival overgrowth, particularly
IGF. Future studies will be necessary to determine the pathogenesis of IGF.

59
References
1. Ahmed A, Huang L, Raftery A, Ahmed AK, Fahmy H, El Nahas AM, Haylor JL.
Cyclosporine A sensitizes the kidney to tubulointerstitial fibrosis induced by renal warm
ischemia. Transplant 77: 686-692, 2004.
2. Andrade CR, Cotrim P, Graner E, Almeida OP, Sauk JJ, Coletta RD. Transforming
growth factor beta 1, autocrine stimulation regulates fibroblast proliferation in
hereditary gingival fibromatosis. J Periodontol 72: 1726-1733, 2001.
3. Baptista IP. Hereditary gingival fibromatosis: a case report. J Clin Periodontol 29:
871-874, 2002.
4. Bisson MA, McGrouther DA, Mudera V, Grobbelaar DA. The different
characteristics of Dupuytren’s disease fibroblasts derived from either nodule or cord:
expression of alpha-smooth muscle actin and the response to stimulation by TGF-beta1.
J Hand Surg 28: 351-356, 2003.
5. Bitu CC, Sobral LM, Kelemann MG, Martelli-Júnior H, Zecckin KG, Graner E,
Coletta RD. Heterogeneous presence of myofibroblasts in hereditary gingival
fibromatosis. J Clin Periodontol 33: 393-400, 2006.
6. Bozzo L, Machado MAN, Almeida OP, Lopes MA, Coletta RD. Hereditary gingival
fibromatosis: report of three cases. J Clin Pediatr Dent 25: 41-46, 2000.
7. Clocheret K, Dekeyser C, Carels C, Willens G. Idiophatic gingival hyperplasia and
orthodontic treatment: a case report. J O 30: 13-19, 2003.
8. Coletta RD, Almeida OP, Ferreira LR, Reynolds MA, Sauk JJ. Increase in expression
of Hsp47 and collagen in hereditary gingival fibromatosis is modulated by stress and
terminal procollagen N-propeptides. Conn Tis Res 40: 237-249, 1999.
60
9. Coletta RD, Almeida OP, Graner E, Page RC, Bozzo L. Differential proliferation of
fibroblasts cultured from hereditary gingival fibromatosis and normal gingiva. J
Periodont Res 33: 469-475, 1998.
10. Coletta RD, Almeida OP, Reynolds MA, Sauk JJ. Alteration in expression of MMP-
1 and MMP-2 but not TIMP-1 and TIMP-2 in hereditary gingival fibromatosis is
mediated by TGF-β1 autocrine stimulation. J Periodont Res 34: 1-7, 1999.
11. Coletta RD, Graner E. Hereditary gingival fibromatosis: a systematic review. J
Periodontol 77:753-764, 2006.
12. Desmouliere A, Chaponnier C, Gabbiani G. Tissue repair, contraction, and
myofibroblasts. Wound Repair Regen 13: 7-12, 2005
13. Desmouliere A, Darby IA, Gabbiani G. Normal and pathology soft tissue
remodeling: role of the myofibroblasts, with special emphasis on liver and kidney
fibrosis. Lab Invest 33: 393-400, 2003.
14. Gabbiani G. The biology of the myofibroblasts. Kidney International 41: 530-532,
1992.
15. Gagliano N, Moscheni C, Dellavia C, Masiero S, Torri C, Grizzi F, Stabellini G,
Giola M. Morphological and molecular analysis of idiophatic gingival fibromatosis: a
case report. J Clin Periodontol 32: 1116-1121, 2005.
16. Jones G, Wilroy RS, McHaney V. Familial gingival fibromatosis associated with
progressive deafness in five generations of a family. Birth Defects Orig Artic Ser 13:
195-201, 1977.
17. Kather J, Salgado MAC, Salgado UFL, Cortelli JR, Pallos D. Clinical and
histomorphometric characteristics of three different families with hereditary gingival
fibromatosis. Oral Surg Oral Med Oral Pathol, 105: 348-352, 2008.
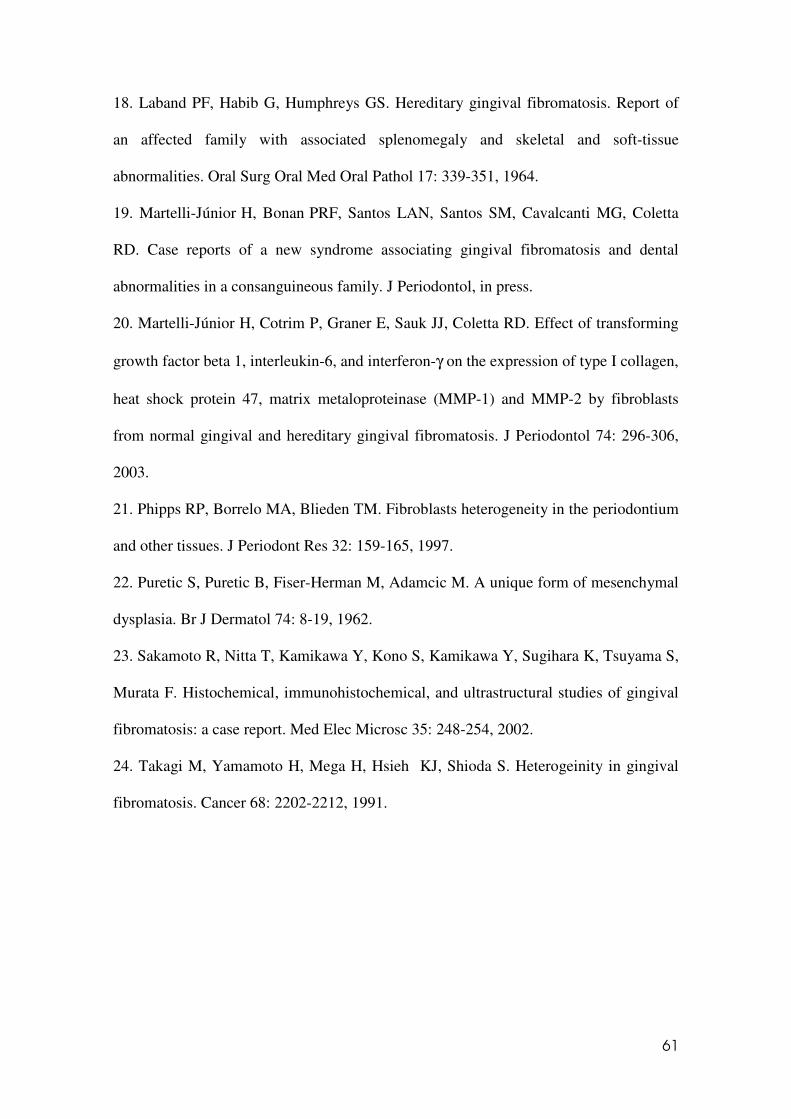
61
18. Laband PF, Habib G, Humphreys GS. Hereditary gingival fibromatosis. Report of
an affected family with associated splenomegaly and skeletal and soft-tissue
abnormalities. Oral Surg Oral Med Oral Pathol 17: 339-351, 1964.
19. Martelli-Júnior H, Bonan PRF, Santos LAN, Santos SM, Cavalcanti MG, Coletta
RD. Case reports of a new syndrome associating gingival fibromatosis and dental
abnormalities in a consanguineous family. J Periodontol, in press.
20. Martelli-Júnior H, Cotrim P, Graner E, Sauk JJ, Coletta RD. Effect of transforming
growth factor beta 1, interleukin-6, and interferon-γ on the expression of type I collagen,
heat shock protein 47, matrix metaloproteinase (MMP-1) and MMP-2 by fibroblasts
from normal gingival and hereditary gingival fibromatosis. J Periodontol 74: 296-306,
2003.
21. Phipps RP, Borrelo MA, Blieden TM. Fibroblasts heterogeneity in the periodontium
and other tissues. J Periodont Res 32: 159-165, 1997.
22. Puretic S, Puretic B, Fiser-Herman M, Adamcic M. A unique form of mesenchymal
dysplasia. Br J Dermatol 74: 8-19, 1962.
23. Sakamoto R, Nitta T, Kamikawa Y, Kono S, Kamikawa Y, Sugihara K, Tsuyama S,
Murata F. Histochemical, immunohistochemical, and ultrastructural studies of gingival
fibromatosis: a case report. Med Elec Microsc 35: 248-254, 2002.
24. Takagi M, Yamamoto H, Mega H, Hsieh KJ, Shioda S. Heterogeinity in gingival
fibromatosis. Cancer 68: 2202-2212, 1991.

62
5. Conclusões
Após a realização dos dois objetivos propostos no presente estudo concluiu-se
que:
1. Pela primeira vez foi observada na literatura científica a associação da fibromatose
gengival com alterações dentais e deficiência mental, aspectos estes compatíveis com a
descrição de uma nova condição genética.
2. Em nenhuma geração do heredograma analisado, observou-se indivíduos com
alterações dentais sem a presença da fibromatose gengival simultaneamente.
3. Análise imunohistoquímica para miofibroblastos (α-SMA) mostrou-se negativa em
portadores de fibromatose gengival idiopática, sugerindo que estas células não
participam da patogênese deste crescimento gengival.

63
6. Referências
1. Almeida JP, Coletta RD, Silva SD, Agostini M, Vargas PA, Bozzo L, Graner E.
(2005) Proliferation of fibroblasts cultured from normal gingiva and hereditary gingival
fibromatosis is dependent on fatty acid synthase activity. J Periodontol 76: 272-278.
2. Andrade CR. (2001) Análise do efeito autócrino do fator de crescimento
transformante beta 1 na proliferação celular de fibroblastos gengivais em pacientes com
fibromatose gengival hereditária. Dissertação de Mestrado. Faculdade de Odontologia –
Universidade Estadual de Campinas – Unicamp.
3. Araújo CS, Graner E, Almeida OP, Sauk JJ, Coletta RD. (2003) Histomorphometric
characteristics and expression of epidermal growth factors and its receptor by epithelial
cells of normal gingival and hereditary gingival fibromatosis. J Periodontal Res 38: 237-
241.
4. Bakeen G, Scully C. (1991) Hereditary gingival fibromatosis in a family with the
Zimmermann-Laband syndrome. J Oral Pathol Med 20: 457-459.
5. Barros SP, Merzel J, Araújo VC, Almeida OP, Bozzo L. (2001) Ultrastructural
aspects of connective tissue in hereditary gingival fibromatosis. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod 92: 78-82.
6. Bozzo L, Almeida OP, Scully C, Aldred MJ. (1994) Hereditary gingival fibromatosis:
report of an extensive four generation pedigree. Oral Surg Oral Med Oral Pathol 78:
452-454.
7. Bozzo L, Almeida OP, Scully C. (1992) Familial gingival hyperplasia: a case of
pseudo-Laband syndrome. Periodont Clin Invest 14: 23-24.
8. Bozzo L, Machado MA, Almeida OP, Lopes MA, Coletta RD. (2000) Hereditary
gingival fibromatosis: report of three cases. J Clin Pediatr Dent 25: 41-46.

64
9. Brown RS, Beaver WT, Bottomley WK. (1991) On mechanism of drug-induced
gingival hyperplasia. J Oral Pathol Med 20: 201-209.
10. Clocheret K, Dekeyser C, Carels C, Willems G. (2003). Idiopathic gingival
hyperplasia and orthodontic treatment: a case report. Journal of Orthodontics 30: 13-19.
11. Coletta RD, Almeida OP, Graner E, Page RC, Bozzo L. (1998) Differential
proliferation of fibroblasts cultured from hereditary gingival fibromatosis and normal
gingiva. J Period Res 33: 469-475.
12. Coletta RD, Almeida OP, Reynolds MA, Sauk JJ. (1999) Alteration in expression of
MMP-1 and TIMP-2 in hereditary gingival fibromatosis is mediated by TGF-β1
autocrine stimulation. J Periodont Res 34: 457-463.
13. Coletta RD, Graner E. (2006) Hereditary gingival fibromatosis. J Periodontol 33:
469-475.
14. Collins MA, Mauriello SM, Tyndall DA, Wright JT. (1999) Dental anomalies
associated with amelogenesis imperfecta. A radiographic assessment. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 88: 358-364.
15. Crawford PJM, Aldred M, Bloch-Zupan A. (2007) Amelogenesis imperfecta.
Orphanet Journal of Rare Diseases 2:1-11.
16. Cuestas-Carnero R, Bornancini CA. (1988) Hereditary generalized gengival
fibromatosis associated with hypertricosis: report of five cases in one family. J Oral
Maxillofac Surg 46: 415-442.
17. Desmouliere A, Chaponnier C, Gabbiani G. (2005) Tissue repair, contraction, and
myofibroblasts. Wound Repair Regen 13: 7-12.
18. Desmouliere A, Darby IA, Gabbiani G. (2003) Normal and pathology soft tissue
remodeling: role of the myofibroblasts, with special emphasis on liver and kidney
fibrosis. Lab Invest 33: 393-400.

65
19. Falls JG, Pulford DJ, Wylie AA, Jirtle RL. (1999) Genomic imprinting: implications
for human disease. Am J Pathol 154: 635-647.
20. Fan JM, Ng YY, Hill PA, Mu W, Atkins RC. (1999) Transforming growth factor
beta regulates tubular ephitelial-myofibroblast transdifferentiation in vitro. Kidney Int
56: 1455-1467.
21. Farrer-Brown G, Lucas RB, Winstock D. (1972) Familial gingival fibromatosis: an
unusual pathology. J Oral Pathol 1: 76-83.
22. Feller L, Jadwat Y, Bouckaert M, Buskin A, Raubenheimer EJ. (2006) Enamel
dysplasia with odontogenic fibroma-like hamartomas: review of the literature and report
of a case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101(5):620-624.
23. Fryns JP. (1996) Gingival fibromatosis and partial duplication of the short arm of
chromosome 2 (dup(2)(p13-p21)). Ann Genet 39: 54-55.
24. Gabbiani G. (1992) The biology of the myofibroblasts. Kidney Int 41: 530-532.
25. Gagliano N, Moscheni C, Dellavia C, Masiero S, Torri C, Grizzi F, Stabellini G,
Gioia M. (2005) Morphological and molecular analysis of idiopathic gingival
fibromatosis: a case report. J. Clin. Periodontol 32: 1116-1121.
26. Gorlin RJ, Cohen MMJ, Levin LS. (1990) Syndromes of the head and neck. 1a ed.,
p.977.
27. Gressner AM, Weiskirchen R, Breitkopf K, Dooley S. (2002) Roles of TGF-beta in
hepatic fibrosis. Front Biosci 7: 793-807.
28. Gross (1856). apud Takagi M, Yamamoto H, Mega H, Hsieh KJ, Shioda S. (1991)
Heterogeneity in gingival fibromatosis. Cancer 68: 2202-2212.
29. Gunhan O, Gardner DG, Bostanci H, Gunhan M. (1995) Familial gingival
fibromatosis with unusual histologic findings. J Periodontol 66: 1008-1011.

66
30. Hakkinen L, Csiszar A. (2007) Hereditary gingival fibromatosis: characteristics and
novel putative pathogenic mechanisms. J Dent Res 86: 25-34.
31. Hart TC, Pallos D, Bowden DW, Bolyard J, Pettenati MJ, Cortelli JR. (1998)
Genetic linkage of hereditary gingival fibromatosis to chromosome 2p21. Am J Hum
Genet 62: 876-883.
32. Hart TC, Pallos D, Bozzo L, Almeida OP, Marazita ML, O’Connell JR, Cortelli JR.
(2000) Evidence of genetic heterogeneity for hereditary gingival fibromatosis. J Dent
Res 79: 1758-1764.
33. Hart TC, Zhang Y, Gorry MC, Hart PS, Cooper M, Marazita ML, Marks JM,
Cortelli JR, Pallos D. (2002) A Mutation in the SOS1 gene causes hereditary gingival
fibromatosis type 1. Am J Hum Genet 70: 943-954.
34. Henry I, Grandjouan S, Couillin P, Barichard F, Huerre-Jeanpierre C, Glaser T,
Philip T, Lenoir G, Chaussain JL, Junien C. (1989) Tumor-specific loss of 11p15.5
allels in del11p13 Wilms tumor and in familial adrenocortical carcinoma. Proc Natl
Acad Sci USA 86: 3247-3251.
35. Jang SY, Lee EJ, Hart PS, Ramaswami M, Pallos D, Hart TC. (2007) Germline
gain-of-function with SOS1 mutation in hereditary gingival fibromatosis. Biol Chem
282: 20245-20255.
36. Johnson BD, El-Guingy M, Ammons WF, Narayanan S, Page RC. (1986) A dectect
in fibroblasts from an unidentified syndrome with gingival hyperplasia as the
predominant feature. J Periodontol Res 21: 403-413.
37. Kavvadia K, Pepelassi E, Alexandridis C, Arkadopoulou A, Polyzois G, Tossios K.
(2005) Gingival fibromatosis and significant tooth eruption delay in an 11-year-old
male: a 30-month follow-up. Int J Paediatr Dent 15: 294-302.

67
38. Macedo GO, Tunes RS, Motta AC, Passador-Santos F, Grisi MM, Souza SL, et al.
(2005) Amelogenesis imperfecta and unusual gingival hyperplasia. J Periodontol
76(9):1563-6.
39. Macias-Flores MA, Garcia-Cruz D, Rivera H. (1984) A new form of hypertrichosis
inherited as an X-linked dominant trait. Hum Genet 66: 66-70.
40. Mangino M, Pizzuti A, Dallapiccola B, Bonfante A, Saccilotto D, Cucchiara E.
(2003) Hereditary gingival fibromatosis (HGF) with hypertrichosis is unlinked to the
HGF1 and HGF2 loci. Am J Med Genet 116: 312-314.
41. Martelli-Júnior H, Bolzani G, Graner E, Bozzo L, Coletta RD. (2000) Microscopic
and proliferative comparasion of gingival fibroblasts from patients with normal gingiva
and with hereditary gingival fibromatosis. Pesq Odont Bras 14: 123-129.
42. Martelli-Júnior H, Cotrim P, Graner E, Sauk JJ, Coletta RD. (2003) Effect of
transforming growth factor beta 1, interleukin-6, and interferon-γ on the expression of
type I collagen, heat shock protein 47, matrix metaloproteinase (MMP-1) and MMP-2
by fibroblasts from normal gingival and hereditary gingival fibromatosis. J Periodontol
74: 296-306.
43. Martelli-Júnior H, Lemos DP, Silva CO, Graner E, Coletta RD. (2005) Hereditary
gingival fibromatosis: report of a five generation family with cellular proliferation
analysis. J Periodontol 76: 2299-2305.
44. Martelli-Júnior H, Ferreira ST, Bonan PRF, Barbosa DR, Bitu CC, Coletta RD.
(2007) Comparação clínica, histopatológica e genética entre duas famílias afetadas por
fibromatose gengival hereditária. Rev Bras Odontol 64: 62-63.
45. Meng LY, Huang M, Ye XQ, Fan MW, Bian Z. (2007) Increased expression of
collagen prolyl 4-hydroxylases in chinese patients with hereditary gingival fibromatosis.
Archives of Oral Biology 52: 1209-1214.

68
46. Nasse (1895). apud Rushton MA. (1957) Hereditary or idiophatic hyperplasia of the
gums. Dent Pract 7: 136-146.
47. Nevin NC. (1971) Hereditary gingival fibromatosis. J Ment Defic Res 15: 130-135.
48. Nusier M, Yassin O, Hart TC, Samimi A, Wright T. (2004) Phenotypic diversity
and revision of the nomenclature for autosomal recessive amelogenesis imperfecta. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 97: 220-230.
49. Petrov VV, Fagard RH, Lijnen PJ. (2002). apud Phan SH. Biology of fibroblasts and
myofibroblasts. (2008) Proceedings of the American Thoracic Society 3: 334-337.
50. Pfeiffer P, Clausen PP, Andersen K, Rose C. (1996) Lack of prognostic significance
of epidermal growth factor receptor and the oncoprotein p185 in patients with
systemically untreated no-small-cell lung cancer: an immunohistochemical study on
cryosections. Br J Cancer 74: 86-91.
51. Phan SH. Biology of fibroblasts and myofibroblasts. (2008) Proceedings of the
American Thoracic Society 3: 334-337.
52. Qi W, Twigg S, Chen X, Polhill TS, Gilbert RE. (2005) Integrated actions of
transforming growth factor beta 1 and connective tissue growth factor in renal fibrosis.
Am J Physiol Renal Physiol 288: 800-809.
53. Raeste AM, Collan Y, Kipilen E. (1978) Hereditary fibrous hyperplasia of the
gingival with varying penetrance and expressivity. Scand J Dent Res 86: 357-365.
54. Ramasamy R, Haviland M, Woodard JR, Barone JG. (2005) Patters of inheritance in
familial prune belly syndrome. Urology 65: 1227.
55. Redman RS, Ward CC, Patterson RH. (1985) Focus of epithelial dysplasia arising in
hereditary gingival fibromatosis. J Periodontol 56: 158-162.
56. Rushton MA. (1957) Hereditary or idiopathic hyperplasia of the gums. Dent Pract 7:
136-146.
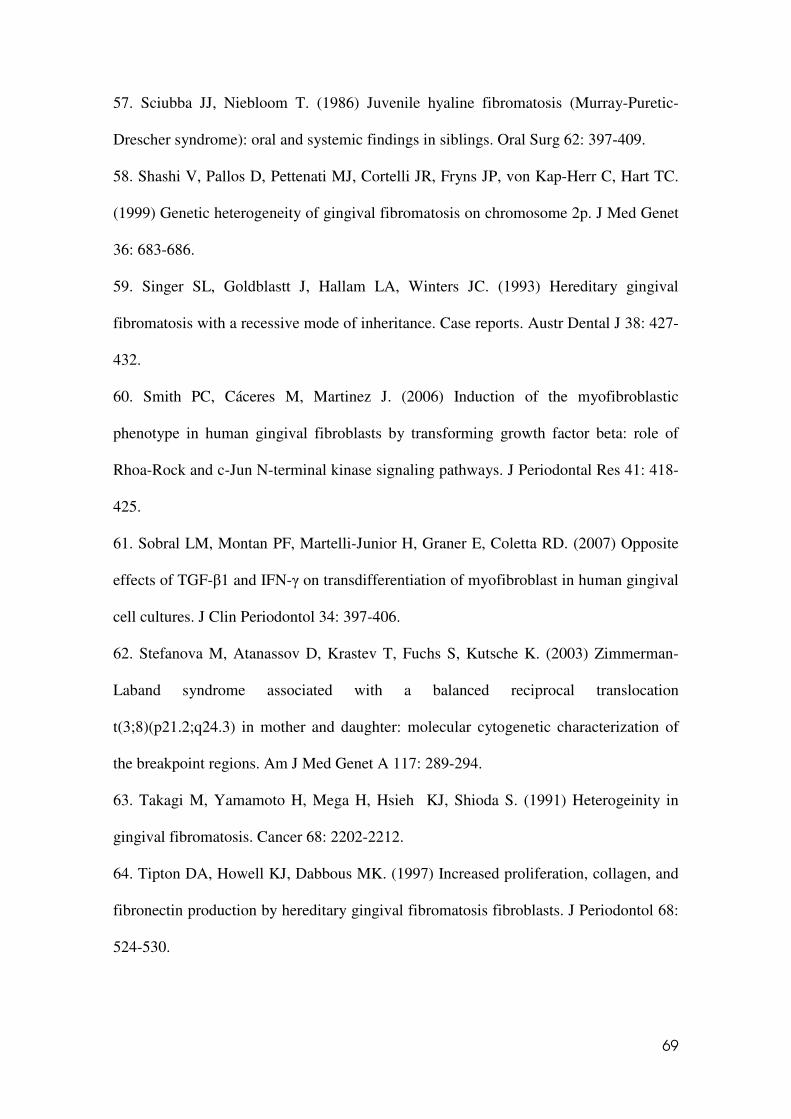
69
57. Sciubba JJ, Niebloom T. (1986) Juvenile hyaline fibromatosis (Murray-Puretic-
Drescher syndrome): oral and systemic findings in siblings. Oral Surg 62: 397-409.
58. Shashi V, Pallos D, Pettenati MJ, Cortelli JR, Fryns JP, von Kap-Herr C, Hart TC.
(1999) Genetic heterogeneity of gingival fibromatosis on chromosome 2p. J Med Genet
36: 683-686.
59. Singer SL, Goldblastt J, Hallam LA, Winters JC. (1993) Hereditary gingival
fibromatosis with a recessive mode of inheritance. Case reports. Austr Dental J 38: 427-
432.
60. Smith PC, Cáceres M, Martinez J. (2006) Induction of the myofibroblastic
phenotype in human gingival fibroblasts by transforming growth factor beta: role of
Rhoa-Rock and c-Jun N-terminal kinase signaling pathways. J Periodontal Res 41: 418-
425.
61. Sobral LM, Montan PF, Martelli-Junior H, Graner E, Coletta RD. (2007) Opposite
effects of TGF-β1 and IFN-γ on transdifferentiation of myofibroblast in human gingival
cell cultures. J Clin Periodontol 34: 397-406.
62. Stefanova M, Atanassov D, Krastev T, Fuchs S, Kutsche K. (2003) Zimmerman-
Laband syndrome associated with a balanced reciprocal translocation
t(3;8)(p21.2;q24.3) in mother and daughter: molecular cytogenetic characterization of
the breakpoint regions. Am J Med Genet A 117: 289-294.
63. Takagi M, Yamamoto H, Mega H, Hsieh KJ, Shioda S. (1991) Heterogeinity in
gingival fibromatosis. Cancer 68: 2202-2212.
64. Tipton DA, Howell KJ, Dabbous MK. (1997) Increased proliferation, collagen, and
fibronectin production by hereditary gingival fibromatosis fibroblasts. J Periodontol 68:
524-530.

70
65. Tomasek JJ, Gabbiani G, Hinz B, Chaponnier C, Brown RA. (2002) Myofibroblast
and mechano-regulation of connective tissue remodelling. Nat Rev Mol Cell Biol 3:
349-363.
66. Vaquero E, Molero X, Tian X, Salas A, Malagelada JR. (1999) Myofibroblast
proliferation, fibrosis, and defective pancreatic repair by cyclosporine in rats. Gut 45:
269-277.
67. Willis BC, duBois RM, Borok Z. (2006) Ephitelial origin of myofibroblasts during
fibrosis in the lung. Proc Am Thorac Soc 3: 377-382.
68. Wise GE, Lin F, Fan W. (1992) Localization of EGF and its receptor in mandibular
molar of the rat prior to and during prefunctional tooth eruption. Dev Dyn 195: 121-
126.
69. Wrigth HJ, Chapple IL, Matthews JB. (2001) TGF-beta isoforms and TGF-beta
receptors in drug-induced and hereditary gingival overgrowth. J Oral Pathol Med 30:
281-289.
70. Xiao S, Wang X, Qu B. (2000) Refinement of the locus for autosomal dominant
hereditary gingival fibromatosis (GINGF) to a 3.8-cM region on 2p21. Genomics 68:
247-252.
71. Ye X, Shi L, Cheng Y. (2005) A novel locus for autosomal dominant hereditary
gingival fibromatosis, GINGF3, maps to chromosome 2p22.3-p23.3. Clin Genet 68:
239-244.
72. Zackin SJ, Weisberger D. (1961) Hereditary gingival fibromatosis: report of a
family. J Oral Pathol 14: 828-836.
73. Zhu Y, Zhang W, Huo Z, Xia Y, Li B, Kong X, Hu L. (2007) A novel locus for
maternally inherited human gingival fibromatosis at chromosome 11p15. Hum Genet
121: 113-123.

71
7. ANEXOS
7.1: Figuras e legendas referentes ao artigo 1: Case reports of a new syndrome
associating gingival fibromatosis and dental abnormalities in a consanguineous
family.

72
3 children
6 grandchildrenNo GF, DA and
MR cases
1 child
No GF, DA
and MR cases
5 children (1 MR)
7 grandchildren3 children
No GF, DA
and MR cases
3 children
No GF, DA
and MR cases
3 children
1 MR
2 children
No GF, DAand MR cases
1 child
No GF, DAand MR cases
No Affected
Gingival Fibromatosis (GF)
Dental Abnormalities (DA)
Mental Retardation (MR)
I
II
III
1
2 3 4
All Three features
1
?
Tabel 1. Summary of the clinical features of the patients of this study
GF AI Pericoronal radioluciences + unerupted
teeth
Intrapulpal calcifications
Retetion of
deciduous
Dental
agenesis
Root
dilaceration
Microdontia
Patient 1 Yes Yes Yes Yes No Yes (#1) Yes Yes (molars)
Patient 2 Yes Yes Yes Yes Yes No No No
Patient 3 Yes Yes Yes Yes Yes Yes (#16) No No
Patient 4 Yes Yes Yes Yes Yes No No No
GF: gingival fibromatosis, AI: generelized thin hypoplastic amelogenesis imperfecta.
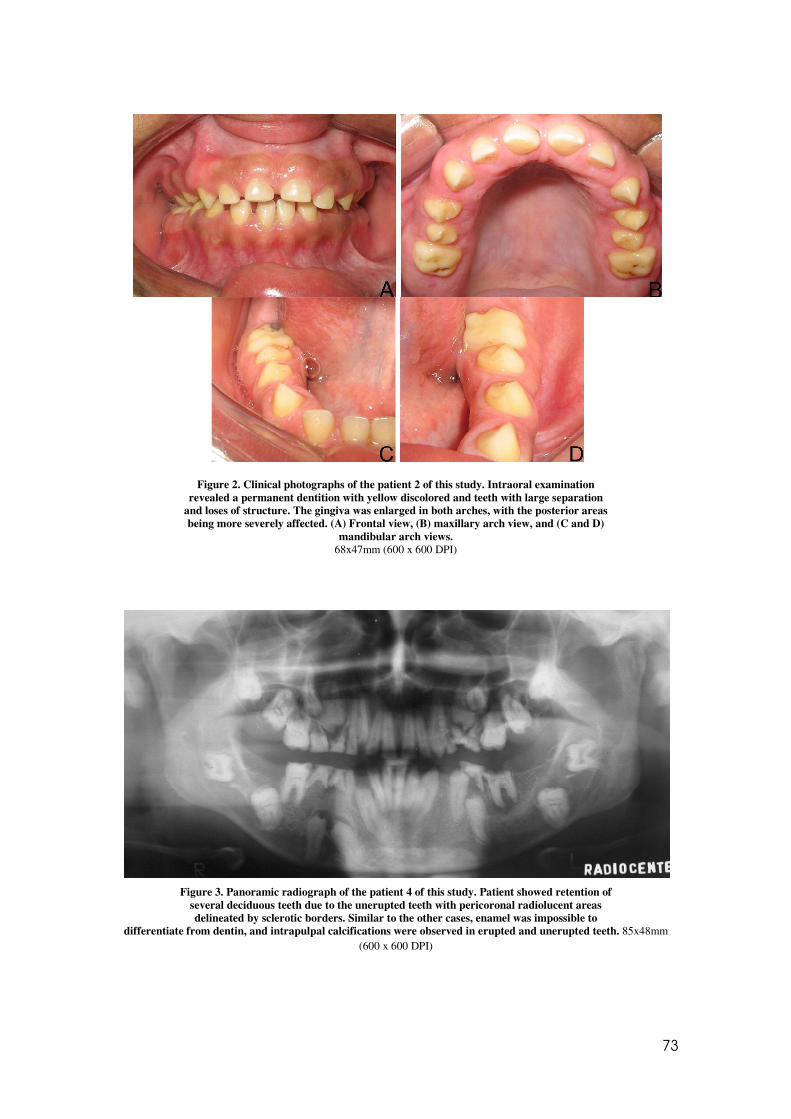
73
Figure 2. Clinical photographs of the patient 2 of this study. Intraoral examination
revealed a permanent dentition with yellow discolored and teeth with large separation and loses of structure. The gingiva was enlarged in both arches, with the posterior areas being more severely affected. (A) Frontal view, (B) maxillary arch view, and (C and D)
mandibular arch views. 68x47mm (600 x 600 DPI)
Figure 3. Panoramic radiograph of the patient 4 of this study. Patient showed retention of several deciduous teeth due to the unerupted teeth with pericoronal radiolucent areas delineated by sclerotic borders. Similar to the other cases, enamel was impossible to
differentiate from dentin, and intrapulpal calcifications were observed in erupted and unerupted teeth. 85x48mm (600 x 600 DPI)
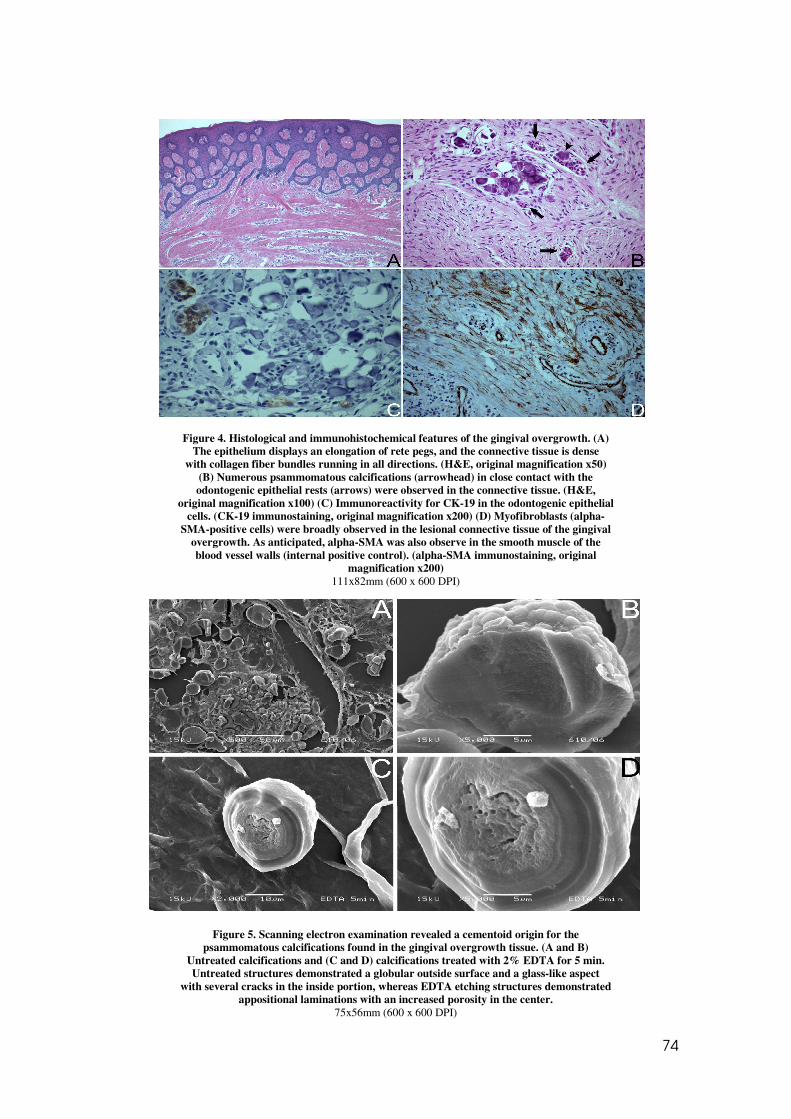
74
Figure 4. Histological and immunohistochemical features of the gingival overgrowth. (A) The epithelium displays an elongation of rete pegs, and the connective tissue is dense
with collagen fiber bundles running in all directions. (H&E, original magnification x50) (B) Numerous psammomatous calcifications (arrowhead) in close contact with the odontogenic epithelial rests (arrows) were observed in the connective tissue. (H&E,
original magnification x100) (C) Immunoreactivity for CK-19 in the odontogenic epithelial cells. (CK-19 immunostaining, original magnification x200) (D) Myofibroblasts (alpha-
SMA-positive cells) were broadly observed in the lesional connective tissue of the gingival overgrowth. As anticipated, alpha-SMA was also observe in the smooth muscle of the blood vessel walls (internal positive control). (alpha-SMA immunostaining, original
magnification x200) 111x82mm (600 x 600 DPI)
Figure 5. Scanning electron examination revealed a cementoid origin for the psammomatous calcifications found in the gingival overgrowth tissue. (A and B)
Untreated calcifications and (C and D) calcifications treated with 2% EDTA for 5 min. Untreated structures demonstrated a globular outside surface and a glass-like aspect
with several cracks in the inside portion, whereas EDTA etching structures demonstrated appositional laminations with an increased porosity in the center.
75x56mm (600 x 600 DPI)

75
Figure 6. Histological features of the intrapulpal calcification in an erupted tooth with decay (A and B) and in an unerupted tooth (C and D). (A) Pulpal chamber was filled in
part by reparative dentin and in part by amorphous dentin. (B) High power view of amorphous calcified tissue revealed few and irregular dentinal tubules and areas of
globular appearance (arrows). (C) Pulpal tissue was replaced by an amorphous calcified tissue resembling dentin. (D) High power view of the intrapulpal calcification showing areas of globular dentin (arrows) associated with areas containing few and irregular
dentinal tubules (arrowhead). D: dentin, RD: reparative dentin, and ACT: amorphous calcified tissue. (HE, original magnification in A x100, B x200, C x25, and D x400)
119x90mm (381 x 381 DPI)
Figure 7. Scanning electronic microscopy micrographs of an unerupted tooth affected by AI. (A) Enamel surface was thin and irregular in all extension of the crown. (B) Normal
areas of enamel were alternated by rough areas with severe porosity and irregularly shaped empty spaces (arrows). (C) Irregular areas of enamel have a laminated,
descamative and porous appearance. 24x6mm (600 x 600 DPI)

76
7.2: Figuras e legendas referentes ao artigo 2: Idiopathic gingival fibromatosis:
clinical features and immunohistochemical evaluation of myofibroblasts
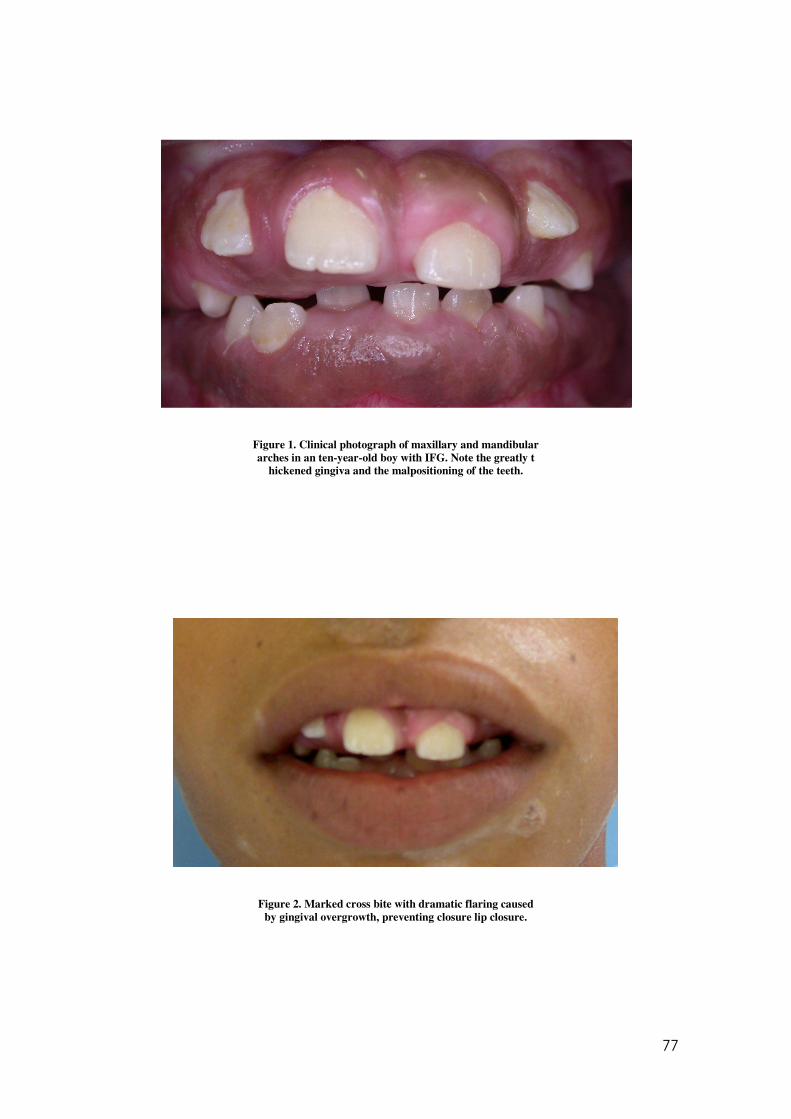
77
Figure 1. Clinical photograph of maxillary and mandibular arches in an ten-year-old boy with IFG. Note the greatly t
hickened gingiva and the malpositioning of the teeth.
Figure 2. Marked cross bite with dramatic flaring caused by gingival overgrowth, preventing closure lip closure.

78
Figure 3. Clinical view showing a mild gingival hyperplasia affecting maxilla and mandible in a thirty-year-old-man.
Figure 4. Histologically, the IGF is characterized by a mucosa in which the epithelium contains slender rete pegs that extend
into a dense connective tissue that is rich in collagen fibers. (HE, x 40).

79
Figure 5. The Mason Tricromic technique revealed wide bundles of collagen strongly stained in blue (TM x 40).
Figure 6. Histological features of αααα-SMA immunohistochemical was negative for αααα-SMA in the connective tissue, except in the
smooth muscle of the blood vessel walls (internal positive control). (α-SMA x 40).

Livros Grátis( http://www.livrosgratis.com.br )
Milhares de Livros para Download: Baixar livros de AdministraçãoBaixar livros de AgronomiaBaixar livros de ArquiteturaBaixar livros de ArtesBaixar livros de AstronomiaBaixar livros de Biologia GeralBaixar livros de Ciência da ComputaçãoBaixar livros de Ciência da InformaçãoBaixar livros de Ciência PolíticaBaixar livros de Ciências da SaúdeBaixar livros de ComunicaçãoBaixar livros do Conselho Nacional de Educação - CNEBaixar livros de Defesa civilBaixar livros de DireitoBaixar livros de Direitos humanosBaixar livros de EconomiaBaixar livros de Economia DomésticaBaixar livros de EducaçãoBaixar livros de Educação - TrânsitoBaixar livros de Educação FísicaBaixar livros de Engenharia AeroespacialBaixar livros de FarmáciaBaixar livros de FilosofiaBaixar livros de FísicaBaixar livros de GeociênciasBaixar livros de GeografiaBaixar livros de HistóriaBaixar livros de Línguas

Baixar livros de LiteraturaBaixar livros de Literatura de CordelBaixar livros de Literatura InfantilBaixar livros de MatemáticaBaixar livros de MedicinaBaixar livros de Medicina VeterináriaBaixar livros de Meio AmbienteBaixar livros de MeteorologiaBaixar Monografias e TCCBaixar livros MultidisciplinarBaixar livros de MúsicaBaixar livros de PsicologiaBaixar livros de QuímicaBaixar livros de Saúde ColetivaBaixar livros de Serviço SocialBaixar livros de SociologiaBaixar livros de TeologiaBaixar livros de TrabalhoBaixar livros de Turismo









![vfg]kfgL ;'/Iff of]hgf xft] k'l:tsf€¦ · vfg]kfgL ;'/Iff of]hgf xft] k'l:tsf g]kfn ;/sf/;x/L ljsf; dGqfno vfg]kfgL tyf 9n lgsf; ljefu @)&) g]kfn ;/sf/ vfg]kfgL tyf ;/;kmfO dGqfno](https://img.document.onl/doc/110x75/5f87fa2a65e23b2a8528fc4e/vfgkfgl-iff-ofhgf-xft-kltsf-vfgkfgl-iff-ofhgf-xft-kltsf-gkfn-sfxl.jpg)









![Vof ;DaGwL bL3 {sfnLg of ]hgf @)^&–@)*&](https://img.document.onl/doc/110x75/629a64b84e728d43975dd1d7/vof-dagwl-bl3-sfnlg-of-hgf-ampamp.jpg)









