Londrina - Paraná 2017
PROGRAMA DE PÓS-GRADUAÇÃO STRICTO SENSU MESTRADO EM EXERCÍCIO FÍSICO NA PROMOÇÃO DA SAÚDE
JEFERSON LUCAS JACINTO
TRAINING CONTROL – APLICATIVO PARA CONTROLE DO
VOLUME DE CARGA EM PROGRAMAS DE EXERCÍCIO
RESISTIDO

JEFERSON LUCAS JACINTO
Cidade ano
AUTOR
Londrina - Paraná
2017
TRAINING CONTROL – APLICATIVO PARA CONTROLE DO VOLUME DE CARGA EM PROGRAMAS DE EXERCÍCIO
RESISTIDO
Relatório Técnico apresentado ao Centro de Pesquisa em Ciências da Saúde, Universidade Norte do Paraná, Unidade Piza, como requisito parcial para a obtenção do título de Mestre Profissional em Exercício Físico na Promoção da Saúde. Orientador: Prof. Dr. Andreo Fernando Aguiar

AUTORIZO A REPRODUÇÃO TOTAL OU PARCIAL DESTE TRABALHO, POR QUALQUER MEIO CONVENCIONAL OU ELETRÔNICO, PARA FINS DE ESTUDO E PESQUISA, DESDE QUE CITADA A FONTE.
Dados Internacionais de catalogação na publicação (CIP) Universidade Pitágoras Unopar
Biblioteca CCBS/CCECA PIZA
Setor de Tratamento da Informação
Jacinto, Jeferson Lucas
J12t Training Control: aplicativo para controle do volume de carga em programas de
exercício resistido. / Jeferson Lucas Jacinto. Londrina: [s.n], 2017.
69f.
Relatório técnico (Mestrado Profissional em Exercício Físico na Promoção da
Saúde).
Universidade Pitágoras Unopar.
Orientador: Prof. Dr. Andreo Fernando Aguiar.
1- Exercício resistido - Relatório técnico de mestrado - UNOPAR 2- Volume
de carga 3- Centros de condicionamento físico 4- Aplicativo 5- Aplicativo -
Android 6- Training control - Aplicativo I- Aguiar, Andreo Fernando; orient. II-
Universidade Pitágoras Unopar.
CDD 613.71 Andressa Fernanda Matos Bonfim - CRB 9/1643

JEFERSON LUCAS JACINTO
TRAINING CONTROL – APLICATIVO PARA CONTROLE DO VOLUME DE CARGA
EM PROGRAMAS DE EXERCÍCIO RESISTIDO
Relatório Técnico apresentado ao Centro de Pesquisa em Ciências da Saúde,
Universidade Norte do Paraná, Unidade Piza, referente ao Curso de Mestrado
Profissional em Exercício Físico na Promoção da Saúde, como requisito parcial para
a obtenção do título de Mestre Profissional conferido pela Banca Examinadora:
_________________________________________ Prof. Dr. Andreo Fernando Aguiar
Universidade Norte do Paraná
_________________________________________ Prof. Dr. Cosme Franklim Buzzachera
Universidade Norte do Paraná
_________________________________________ Prof. Dr. Helio Serassuelo Junior
(Membro Externo)
_________________________________________ Prof. Dr. Dartagnan Pinto Guedes
Coordenador do Curso
Londrina, 01 de dezembro de 2017.

JACINTO, Jeferson Lucas. Training Control – Aplicativo para controle do volume de carga em programas de exercício resistido. 69f. Relatório Técnico. Mestrado Profissional em Exercício Físico na Promoção da Saúde. Centro de Pesquisa em Ciências da Saúde. Universidade Norte do Paraná, Londrina. 2017.
RESUMO
O presente material será apresentado em duas seções distintas, conforme
regimento do Curso de Mestrado Profissional em Exercício Físico na Promoção da
Saúde, da Universidade Norte do Paraná (UNOPAR). A primeira seção corresponde
à produção técnica, na qual apresentamos uma descrição detalhada das fases de
elaboração do aplicativo intitulado “Training Control”. O aplicativo encontra-se
disponível no Google Play Store e poderá ser utilizado em qualquer dispositivo
móvel android (ex: Smartphone), em modo off-line, com a finalidade de analisar e
monitorar o volume de carga (kg) de um ou mais exercícios durante programas de
exercício resistido em equipamentos convencionais encontrados em centros de
condicionamento físico. A segunda seção corresponde à produção científica,
intitulada: ‘Leucine does not improve muscle recovery course after resistance
exercise in untrained young subject’, a ser submetido para publicação no periódico
Amino Acids (Qualis B1). O compilado de informações contidas neste material foi
elaborado para atender as características peculiares do respectivo curso de pós-
graduação, cujo escopo principal é apresentar um produto técnico que possa auxiliar
profissionais e pesquisadores que atuam na área de prescrição e orientação de
programas de exercício físico.
Palavras-chave: Exercício Resistido, Volume de Carga, Centros de
Condicionamento Físico, Aplicativo, Android.

JACINTO, Jeferson Lucas. Training Control –. Mobile application to control the load volume in resistance exercise programs. 69p. Technical Report. Professional Master´s in Exercise in Health Promotion. Research Center in Health Sciences. North University of Parana, Londrina. 2017.
ABSTRACT
The present material will be presented in two distinct sections, according to the
regiment of the Professional Masters Course in Exercise in Health Promotion, from
the North University of Paraná (UNOPAR). The first section corresponds to the
technical production, in which we present a detailed description of the phases of
elaboration of the mobile application entitled "Training of Control". The app is
available on the Google Play Store and can be off-line used on any android mobile
device (e.g., Smartphone) for the purpose of analyzing and monitoring the load
volume (kg) of one or more exercises during resistance exercises on conventional
equipment found in fitness centers. The second section corresponds to the scientific
production, titled: "Leucine does not improve the course of muscle recovery after
resistance exercise in young untrained subject", to be submitted for publication in
Amino Acids (Qualis B1). The compilation of information contained in this material
was prepared to meet the peculiar characteristics of the respective graduate course,
whose main scope is to present a technical product that can assist professionals and
researchers who work in the area of prescription and guidance of physical exercise
programs.
Keywords: Resistance Exercise, Load Volume, Fitness Center, Mobile Application,
Android.

SUMÁRIO
SUMÁRIO 6
1. INTRODUÇÃO ....................................................................................................... 7
2. REVISÃO DE LITERATURA .................................................................................. 9
2.1 BENEFÍCIOS DO EXERCÍCIO RESISTIDO NA SAÚDE ..................................... 9
2.2 PRINCÍPIOS DE PROGRESSÃO APLICADO AO EXERCÍCIO RESISTIDO ...... 9
2.3 VARIÁVEIS ENVOLVIDAS NA PRESCRIÇÃO DO EXERCÍCIO RESISTIDO ....10
2.3.1 Ação muscular ..................................................................................................10
2.3.2 Intensidade utilizada (carga) .............................................................................10
2.3.3 Seleção do exercício ........................................................................................11
2.3.4 Estrutura e sequência dos exercícios ...............................................................11
2.3.5 Intervalo de recuperação ..................................................................................12
2.3.6 Velocidade das repetições ................................................................................12
2.3.7 Frequência ........................................................................................................13
2.3.8 Volume .............................................................................................................13
2.4 RECOMENDAÇÕES PARA A PRESCRIÇÃO DE EXERCÍCIO RESISTIDO ......14
3. DESENVOLVIMENTO ...........................................................................................17
4. DIVULGAÇÃO .......................................................................................................18
5. REFERÊNCIAS .....................................................................................................19
APÊNDICE A – Manual .............................................................................................21
APÊNDICE B – Trabalho Apresentado em Evento Científico ....................................42
APÊNDICE C – Artigo Científico ...............................................................................43

7
1. INTRODUÇÃO
Nas duas últimas décadas a utilização de softwares e aplicativos tem
sido cada vez mais constante no contexto da prescrição, orientação e
monitoramento de programas de exercício físico. A finalidade destas ferramentas é
auxiliar e facilitar as ações cotidianas dos Profissionais de Educação Física e,
consequentemente, melhorar a sua atuação prática no mercado de trabalho. Dentre
as tecnologias mais utilizadas, destacam-se os (i) monitores cardíacos, (ii)
programas de avaliação física, (iii) aplicativos para prescrição de exercício físico, e
(iv) aplicativos para controle de corrida (ex: trajeto e distância percorrida). Apesar
desta ampla variedade de tecnologias, ainda não existem ferramentas para o
monitoramento do volume de carga (VC) durante programas de exercício resistido
em equipamentos convencionais encontrados em centros de condicionamento físico.
O VC é determinado pelo número máximo de repetições (Nrep) nas
séries multiplicado pela carga (kg) aplicada (VC = Nrep x carga), e pode ser calculado
para um ou mais exercícios durante a sessão de treino. Monitorar o VC é parte
fundamental de um programa de prescrição e orientação de exercício resistido (ER)
direcionado a promoção da saúde, pois as modificações nesta variável podem
influenciar diretamente as respostas neurais1, hipertróficas2, metabólicas3, e
hormonais4, refletindo na magnitude das adaptações musculares. Além disso, o
monitoramento do VC pode ser determinante para detecção e prevenção de
possíveis condições de supertreinamento (overtraining)5, diminuindo assim o risco
de lesões futuras.
Entretanto, monitorar o VC no contexto prático pode ser uma tarefa
difícil para a maioria dos profissionais de educação física, devido a vários fatores,
incluindo a 1) necessidade de conhecimento intermediário sobre elaboração de
planilhas, fórmulas e gráficos no programa Microsoft Excel, 2) necessidade de tempo
extra para atualizações das planilhas, e 3) dificuldade para interpretação e
apresentação de gráficos da planilha Excel. Portanto, o desenvolvimento de novas
tecnologias que possam auxiliar no monitoramento do VC durante programas de ER
é fundamental para facilitar as ações cotidianas dos profissionais de educação física.
Portanto, a proposta desta produção técnica será elaborar um
aplicativo para dispositivos móveis (Android), com a finalidade de analisar e
monitorar o volume de carga (kg) de um ou mais exercícios durante programas de
ER.

8
Assim esperamos que este aplicativo, facilite: (1) o controle e
monitoramento do VC durante programas de orientação e prescrição de ER para
diferentes populações, (2) a apresentação dos dados e gráficos referentes ao
histórico do VC junto aos clientes, possibilitando a visualização da progressão do
treino, (3) os possíveis ajustes das variáveis de treino (séries, repetições e carga)
em tempo real, no próprio ambiente de trabalho, possibilitando maior controle do
protocolo de treino, (4) o controle e monitoramento do VC de diversos clientes ao
mesmo tempo, e (5) o armazenamento e apresentação dos dados referente ao
histórico de treino de cada cliente.

9
2. REVISÃO DE LITERATURA
2.1 BENEFÍCIOS DO EXERCÍCIO RESISTIDO NA SAÚDE
A prática de ER é uma das atividades que mais cresceu nas duas
últimas décadas, devido a seus inúmeros benefícios à saúde, incluindo o aumento
da força e massa muscular, potência e velocidade, resistência, desempenho motor,
equilíbrio e coordenação6. Além disso, a prática de ER em combinação com
exercícios cardiorrespiratórios e de flexibilidade pode resultar na (a) melhora da
função cardiovascular, (b) redução dos fatores de risco associados à doença
coronariana e diabetes, (c) prevenir a osteoporose, (d) reduzir os riscos de câncer
de cólon, (e) promover a manutenção e perda de peso, (f) melhorar a estabilidade
dinâmica, (g) preservar a capacidade funcional, e (h) promover o bem-estar
psicológico7.
Os programas de ER devem ser elaborados e orientados por
Profissionais de Educação Física, e podem ser praticados por diversas populações,
incluindo adolescentes, adultos, idosos e pessoas com algumas patologias (por
exemplo, doença cardiovascular, doença neuromuscular, síndrome metabólica,
diabetes e HIV)5. Todavia, para uma adequada prescrição e orientação de ER os
profissionais devem respeitar a individualidade biológica, e monitorar as variáveis
básicas que norteiam a prática destes exercícios, como a intensidade (carga), o
número de repetições, a velocidade e amplitude do movimento, o intervalo entre as
séries e exercícios, o número de exercícios, e o volume de carga dos exercícios e da
sessão de treino.
2.2 PRINCÍPIOS DE PROGRESSÃO APLICADO AO EXERCÍCIO RESISTIDO
A progressão do ER pode ser definida como o ato de avançar em
direção a um objetivo até alcançar a meta pré-estabelecida. Os princípios básicos de
progressão para maximizar os ganhos do ER são três: (1) sobrecarga, (2)
especificidade e (3) variação. O princípio de sobrecarga pode ser definido como o
aumento gradual do estresse aplicado sobre o corpo durante o ER. Considerando
que a adaptação fisiológica do programa ER pode ocorrer em um período de tempo
curto, são necessárias alterações em uma ou mais variáveis do programa para
promover “novas” adaptações. Tais alterações incluem o aumento da carga
(intensidade), aumento do número de repetições, alteração da velocidade das
repetições com carga submáxima, e redução do período de descanso5,7.

10
O princípio de especificidade refere-se as adaptações fisiológicas
específicas do estímulo aplicado, e é determinado por vários fatores, incluindo a
ação muscular envolvida, a velocidade do movimento, a amplitude de movimento, o
grupo muscular treinado, o sistema energético envolvido, e a intensidade e volume
de treino. Já o princípio de variação ou periodização implica nas alterações
sistemáticas de uma ou mais variáveis ao longo do tempo, permitindo que o estimulo
do ER permaneça desafiador e eficaz5.
2.3 VARIÁVEIS ENVOLVIDAS NA PRESCRIÇÃO DO EXERCÍCIO RESISTIDO
Segundo as recomendações do American College of Sport Medicine
(ACSM)7, um programa de ER é composto por diversas variáveis, incluindo a ação
muscular, intensidade utilizada (carga), volume, seleção de exercícios, estrutura e
sequência dos exercícios, intervalo de recuperação (descanso), velocidade das
repetições e frequência.
2.3.1 Ação muscular
A maioria dos programas de ER incluem principalmente repetições
dinâmicas, com ações musculares concêntricas e excêntricas, enquanto as ações
musculares isométricas desempenham um papel secundário5. As ações excêntricas
apresentam maior força produzida por área muscular, e envolvem menor
recrutamento de unidades motoras, apresentam menor exigência metabólica e são
favoráveis à promoção das adaptações hipertróficas. Os progressos relacionados a
manipulação da ação muscular durante o programa de ER é mínima, considerado
que a maioria dos programas incluem ações concêntricas e excêntricas. No entanto,
programas avançados que incluem exercícios isométricos podem ser benéficos para
maximizar os ganhos de força e hipertrofia5,7.
2.3.2 Intensidade utilizada (carga)
A alteração da carga no ER (quantidade de peso levantado ou
resistência ao exercício) pode afetar diretamente as respostas agudas metabólicas3,
hormonais8, neurais9,10 e cardiovasculares11, e dependem de outras variáveis, como
a ordem dos exercícios, volume, frequência, ação muscular, velocidade das
repetições e o intervalo de descanso5-7. Dependendo do objetivo, experiência e nível
de aptidão física do indivíduo, a progressão de carga do ER pode seguir um ou mais
aspectos: (1) aumentar a carga com base em uma porcentagem de 1RM, (2)

11
aumentar a carga com base em um número de repetições alvo, (3) aumentar a carga
dentro de uma zona alvo prescrita (Ex: 8-12 RM)7. Abaixo encontra-se a Tabela 1
com as recomendações apresentada pelo ACSM 7.
Tabela 1. Recomendações do ACSM
% 1RM Indivíduo Resposta
60-70 % Iniciante ↑ força muscular dinâmica
60-85 % Intermediário ↑ força muscular
> 80 % Avançado ↑ força muscular
Fonte: American College of Sports Medicine7
2.3.3 Seleção do exercício
Os exercícios de articulação única e múltipla demostram ser efetivos
no aumento de força muscular. Exercícios de múltiplas articulações, evidenciam
mais de uma articulação ou grupo muscular principal e requerem respostas neurais
complexas, e são considerados mais efetivos no aumento de força muscular. Já os
exercícios de articulação única, enfatizam uma única articulação ou grupo muscular,
e são utilizados para trabalhar grupos musculares específicos e apresentam nível
reduzido de habilidades e envolvimento técnico. Outra maneira de variar a seleção
do exercício é incluir ao programa exercícios unilaterais e bilaterais, podendo variar
os equipamentos utilizados, como: pesos livres, cordas cabos, máquinas, bolas de
estabilidade, bosu, prancha de equilíbrio5,12.
2.3.4 Estrutura e sequência dos exercícios
Para obter resultados efetivos o programa de ER deve ser elaborado
com base na quantidade de grupos musculares exigidos em cada sessão13. Por
exemplo, existem três estruturas de exercícios: (1) exercício para todo o corpo
(envolve a realização de exercícios que enfatizam todos os principais grupos
musculares, ou seja, um ou dois exercícios para cada grupo muscular na mesma
sessão), (2) exercícios para a região superior e inferior do corpo (em sessões
distintas realiza-se exercícios para os grupos musculares superiores, e exercícios
para os grupos musculares inferiores), (3) um ou mais grupos musculares isolados
por sessão (envolve a realização de exercícios para grupos musculares específicos,
por exemplo, exercícios para peito e costas). Todas estas estruturas são eficazes
para melhorar a força, hipertrofia e resistência muscular, o que determinará a

12
escolha de uma delas serão os objetivos, tempo disponível, frequência e as
preferências pessoais do praticante5.
As diferenças encontradas entre essas estruturas são: (1) grau de
especialização (Ex: três a quatro exercícios para um grupo muscular específico
podem ser realizados em uma sessão de ER por grupamentos musculares em
comparação com um ou dois exercícios para cada grupo muscular em uma sessão
para corpo inteiro), (2) período de recuperação entre as sessões (um grupo
muscular maior pode ser trabalhado de forma isolada uma a duas vezes por
semana, de duas a três vezes por semana quando a sessão for dividida em superior
e inferior, e três ou mais vezes na semana em sessões de exercício que envolva
todo o corpo)5.
A sequência dos exercícios e o número de grupos musculares
exigidos durante a sessão de ER afeta diretamente a força muscular. Portanto,
recomenda-se para indivíduos iniciantes, intermediários e avançados (para todas as
estruturas do programa de ER) que exercícios com grandes grupos musculares
devem ser treinados antes dos exercícios com pequenos grupos musculares,
exercícios multiarticulares antes dos exercícios monoarticulares, exercícios de alta
intensidade antes dos exercícios de baixa intensidade ou rodízio de exercícios
(região superior e inferior do corpo ou agonistas e antagonistas)7.
2.3.5 Intervalo de recuperação
O intervalo de descanso entre as séries e exercícios afeta
diretamente as respostas metabólicas, hormonais e cardiovasculares durante o ER,
bem como o desempenho nas subsequentes séries e as adaptações ao exercício.
Para indivíduos iniciantes, intermediários e avançados, recomenda-se um período
de recuperação de 2-3 minutos para exercícios principais com carga elevada (Ex:
agachamento e supino), e para exercícios complementares um período de descanso
de 1-2 minutos7.
O período de descanso pode variar de acordo com a complexidade
do exercício (por exemplo, levantamento olímpico requer um período de descanso
mais longo), e com o objetivo principal do programa de ER (ou seja, nem todo
exercício usará o mesmo intervalo de descanso)7.
2.3.6 Velocidade das repetições
A velocidade que a contração muscular de uma série de exercício é

13
realizada pode afetar diretamente as respostas neurais14, hipertróficas15 e
metabólicas16. Para o ER dinâmico e constante (também chamado de isotônico)
observa-se redução na produção de força quando se trabalha em baixa velocidade.
Ao interpretar os efeitos da realização de repetições lentas, é
importante notar que existem dois tipos, a intencional e não intencional. Contrações
com velocidade lenta intencional, são usadas com cargas submáximas o que
permite ao indivíduo ter maior controle da velocidade e do tempo em que os
músculos estão sob tensão. Por outro lado, as contrações com velocidade lenta não
intencional ocorrem quando os indivíduos tentam exercer força máxima, mas devido
a carga elevada ou fadiga, a execução se realiza com velocidade lenta7.
Em comparação com velocidades lentas, as velocidades moderadas
(1-2:1-2) e rápidas (<1:1), mostram ser mais eficazes para maiores capacidades de
desempenho muscular (Ex: volume, número de repetições realizadas) e no aumento
da taxa de ganho de força. O ACSM recomenda para indivíduos iniciantes a
utilização de velocidades lentas e moderadas, para indivíduos intermediários
velocidade moderada, já para os indivíduos avançados recomenda-se a inclusão de
um contínuo de velocidades a partir de velocidades não intencionais lentas a
rápidas5,7.
2.3.7 Frequência
O número de sessões realizadas durante um período específico de
tempo pode influenciar as adaptações ao ER. A frequência ideal depende de alguns
fatores, como o volume, intensidade, seleção de exercícios, nível de
condicionamento, capacidade de recuperação e a quantidade de grupos musculares
trabalhados durante a sessão, tempo disponível, objetivos do programa5,7.
O ACSM7 recomenda que indivíduos iniciantes no programa de ER
treinem o corpo todo 2-3 vezes por semana, a progressão para o treinamento
intermediário usa-se uma frequência de 3-4 dias por semana (3 dias se estiver
usando o treino para corpo todo, e 4 dias se estiver utilizando uma rotina com
divisão de grupos musculares). Os indivíduos avançados podem treinar de 4-6 vezes
por semana, já os halterofilistas e bodybuilders podem utilizar alta frequência, por
exemplo 2 treinos por dia, durante 4-5 dias por semana.
2.3.8 Volume
O VC (também chamado de volume de treino) é determinado pela

14
soma do número total de repetições realizadas durante um exercício ou sessão de
ER multiplicado pela resistência utilizada (Kg)7. O VC mostrou alterar as respostas
de diversos sistemas fisiológicos, incluindo o sistema nervoso1, muscular2,
metabólico3 e hormonal4. Durante um programa de ER, pode ser calculado vários
VC, como por exemplo o VC por exercício (número de séries vs. número de
repetições vs. carga), VC por grupo muscular (soma de todos os volumes de cada
exercício por um determinado grupo muscular), VC global da sessão (soma de todos
os volumes dos exercícios realizados na sessão). Para alterar o VC é necessário
modificar uma das seguintes variáveis, número de exercícios realizados na sessão,
o número de repetições realizadas por séries, o número de séries do exercício ou a
carga utilizada5,7.
Existe uma relação inversamente proporcional entre o volume e
intensidade. Controlar e monitorar o VC é essencial, pois assim reduz os riscos de
supertreinamento (overtraining). O treinamento de força envolve alta intensidade
(carga) e baixo número de séries e repetições, ou seja, baixo volume. O treino de
hipertrofia e resistência muscular envolve em cargas leves a moderadas, com
múltiplas séries e alto número de repetições, ou seja, com alto volume5.
Assim o VC deve basear-se nos objetivos individuais, pois existem
numerosas possibilidades para uma progressão efetiva dentro do programa de ER.
2.4 RECOMENDAÇÕES PARA A PRESCRIÇÃO DE EXERCÍCIO RESISTIDO
Tabela 2. Recomendações do ACSM para o aumento da potência muscular
Variável Iniciantes Intermediário Avançado
Carga 30-60% 1RM1
60% 1RM2
30-60% 1RM1
0-60% 1RM2 85-100% 1RM
Séries 1-3 3-6 3-6
Repetições 3-6 1-6 1-6
Exercício Monoarticular
Multiarticular
Monoarticular
Multiarticular
Monoarticular
Multiarticular
Período de Recuperação
2-3 min.
1-2 min. Exercício complementar
2-3 min.
1-2 min. Exercício complementar
2-3 min.
1-2 min. Exercício complementar
Velocidade das Repetições Rápida Rápida Rápida
Frequência 2-33 d/semana 3-44 d/semana 4-53,2 d/semana
Fonte: American College of Sports Medicine7

15
1 Parte superior do o corpo; 2 Parte inferior do corpo; 3 Todos os grupos musculares (todo o
corpo); 4 Divisão por grupos musculares.
Tabela 3. Recomendações do ACSM para hipertrofia muscular
Variável Iniciantes Intermediário Avançado
Ação Muscular
Concêntrica
Excêntrica
Isométrica
Concêntrica
Excêntrica
Isométrica
Concêntrica
Excêntrica
Isométrica
Carga 70-85% 1RM 70-85% 1RM 70-100% 1RM
Séries 1-3 1-3 3-6
Repetições 8-12 8-12 1-12
Exercício Monoarticular
Multiarticular
Monoarticular
Multiarticular
Monoarticular
Multiarticular
Período de Recuperação 1-2 min. 1-2 min.
2-3 min.
(Alta intensidade)
1-2 min. (Intensidade moderada)
Velocidade das Repetições Lento
Moderado
Lento
Moderado
Lenta
Moderada
Rápida
Frequência 2-31 d/semana 2-31 d/semana
2-42 d/semana 4-62 d/semana
Fonte: American College of Sports Medicine7
1 Todos os grupos musculares (todo o corpo); 2 Divisão por grupos musculares.

16
Tabela 4. Recomendações do ACSM para o aumento da resistência muscular
Variável Iniciantes Intermediário Avançado
Carga Leve Leve Leve
Séries Múltiplas Múltiplas Múltiplas
Repetições 10-15 10-15 10-25 ou Mais
Exercício
Unilateral
Bilateral
Monoarticular
Multiarticular
Unilateral
Bilateral
Monoarticular
Multiarticular
Unilateral
Bilateral
Monoarticular
Multiarticular
Período de Recuperação < 1 min. < 1 min. < 1-2 min.
Velocidade das Repetições Intencionalmente
lenta Intencionalment
e lenta Moderadas a rápidas
Frequência 2-31 d/semana 31 d/semana
42 d/semana 4-62 d/semana
Fonte: American College of Sports Medicine7
1 Todos os grupos musculares (todo o corpo); 2 Divisão por grupos musculares.

17
3. DESENVOLVIMENTO
Uma empresa especializada foi contratada para desenvolver o
aplicativo (APÊNDICE A), conforme os passos abaixo:
(1) Reunião para levantamento de informações do projeto
Reunião para apresentação do idealizador do produto.
Discussão das funcionalidades e suas particularidades do projeto considerando
as premissas levantadas pelo idealizador.
Apresentação de um escopo inicial do MVP (Minimum Viable Product) a ser
produzido.
(2) Análise e projeção
Exposição da análise de viabilidade do projeto composto de seu escopo e
funcionalidades.
Planejamento de desenvolvimento das funcionalidades do MVP e de alterações
do projeto.
(3) Prototipação e apresentação
Apresentação do design das telas e seus componentes exemplificando a
navegação e usabilidade do aplicativo.
Validação de regras aplicadas nos cálculos que serão gerados nos gráficos.
Readequação de funcionalidades do projeto conforme a necessidade.
(4) Desenvolvimento
Fase de implementação das funcionalidades (programação).
(5) Testes
Validação do aplicativo conforme escopo e funcionalidades.
Aprimoramento de detalhes de navegação, fluxo e ergonomia.
(6) Homologação
Liberação de uma versão beta para homologação com o cliente, validando
todas as funcionalidades levantadas e realizadas.
(7) Publicação
Ao final foi gerado um arquivo APK (Android Package) com a criação do

18
certificado digital e disponibilizado a versão pronta para publicação na loja
Google Play.
4. DIVULGAÇÃO
O aplicativo será divulgado através das mídias sociais, por meio de
anúncios no Facebook, Instagram e Google, também será oferecido cursos de curta
duração e workshops em universidades, faculdades e centros educacionais que
oferecem o curso de graduação em educação física.

19
5. REFERÊNCIAS
1. Häkkinen K, Pakarinen A, Alén M, Kauhanen H, Komi PV. Neuromuscular and
hormonal responses in elite athletes to two successive strength training sessions
in one day. Eur J Appl Physiol Occup Physiol 1988;57(2):133-139.
2. Tesch PA, Komi PV, Häkkinen K. Enzymatic adaptations consequent to long-term
strength training. Int J Sports Med 1987;8(Suppl1):66-69.
3. Ratamess NA, Falvo MJ, Mangine GT, Hoffman JR, Faigenbaum AD, Kang J. The
effect of rest interval length on metabolic responses to the bench press exercise.
Eur J Appl Physiol 2007;100(1):1-17.
4. Ratamess NA, Kraemer WJ, Volek JS, Maresh CM, Vanheest JL, Sharman MJ, et
al. Androgen receptor content following heavy resistance exercise in men. J
Steroid Biochem Mol Biol 2005;93(1):35-42.
5. Kraemer WJ, Ratamess NA. Fundamentals of resistance training: progression and
exercise prescription. Med Sci Sports Exerc 2004;36(4):674-688.
6. Kraemer WJ, Ratamess NA. Physiology of resistance training: current issues.
Philadelphia: Saunders; 2000.
7. ACSM. American College of Sports Medicine position stand. Progression models
in resistance training for healthy adults. Med Sci Sports Exerc 2009;41(3):687-708.
8. Raastad T, Bjøro T, Hallén J. Hormonal responses to high- and moderate-intensity
strength exercise. Eur J Appl Physiol 2000;82(1-2):121-128.
9. Häkkinen K, Alén M, Komi PV. Changes in isometric force- and relaxation-time,
electromyographic and muscle fibre characteristics of human skeletal muscle
during strength training and detraining. Acta Physiol Scand 1985;125(4):573-585.
10. Komi PV. Strength and Power in Sport. Oxford: Blackwell Scientific; 1992.
11. Fleck SJ. Cardiovascular adaptations to resistance training. Med Sci Sports
Exerc 1988;20(5):S146-S151.
12. Cronin J, McNair PJ, Marshall RN. The effects of bungy weight training on
muscle function and functional performance. J Sports Sci 2003;21(1):59-71.

20
13. Sforzo GA, Touey PR. Manipulating Exercise Order Affects Muscular
Performance During a Resistance Exercise Training Session. J Strength Cond
Res 1996;10:20–24.
14. Häkkinen K, Komi PV, Alén M. Effect of explosive type strength training on
isometric force- and relaxation-time, electromyographic and muscle fibre
characteristics of leg extensor muscles. Acta Physiol Scand 1985;125(4):587-
600.
15. Shepstone TN, Tang JE, Dallaire S, Schuenke MD, Staron RS, Phillips SM.
Short-term high- vs. low-velocity isokinetic lengthening training results in greater
hypertrophy of the elbow flexors in young men. J Appl Physiol 2005;98(5):1768-
1776.
16. Mazzetti S, Douglass M, Yocum A, Harber M. Effect of explosive versus slow
contractions and exercise intensity on energy expenditure. Med Sci Sports Exerc
2007;39(8):1291-1301.

21
APÊNDICE A – Manual

22

23

24

25

26

27

28

29

30

31

32

33

34

35

36

37

38

39

40

41

42
APÊNDICE B – Trabalho Apresentado em Evento Científico
EFEITOS DA SUPLEMENTAÇÃO DE LEUCINA SOBRE OS NÍVEIS DE CREATINA QUINASE DURANTE A RECUPERAÇÃO MUSCULAR APÓS EXERCÍCIO RESISTIDO INTRODUÇÃO: A suplementação nutricional tem sido utilizada como uma estratégia não farmacológica para acelerar o processo de recuperação muscular após exercício resistido (ER). Neste contexto, prévios estudos sugerem que a suplementação de leucina (LEU) pode ser benéfica para aumentar a taxa de síntese proteica via estimulação da proteína mTOR e, consequentemente, acelerar o processo de recuperação muscular. No entanto, os efeitos atenuantes da suplementação de LEU sobre os níveis de creatina quinase (CK) após uma sessão de ER permanecem não esclarecidos. OBJETIVOS: Investigar os efeitos da suplementação isolada de LEU sobre os níveis plasmáticos de CK após uma única sessão de ER. MÉTODOS: Foi empregado um desenho crossover e duplo cego, na qual 11 homens e 3 mulheres (24 ± 3,3 anos) não treinados foram suplementados com LEU (6 g/dia) e placebo (PLA, 6 g/dia), em dois momentos, separados por um período washout de 1 semana. Em cada momento, os participantes foram submetidos a 1 sessão de ER (3 séries de 12 repetições à 70% de 1RM) envolvendo os exercícios de leg press e agachamento hack, e 3 subsequentes sessões (24, 48, e 72 horas após a sessão de ER) de teste de fadiga muscular (1 série até a fadiga voluntária à 50% de 1RM). Os suplementos foram fracionados em duas doses de 3 g que foram ingeridas 30 minutos antes e imediatamente após a sessão de ER e testes de fadiga. Os níveis de CK foram analisados nos momentos pré e pós a sessão de ER, e imediatamente após os testes de fadiga. Os dados foram analisados por meio de testes de ANOVA para medidas repetidas, complementado
pelo teste post-hoc de Bonferroni. O nível de significância foi estabelecido em P < 0,05. RESULTADOS: Os níveis plasmáticos de CK aumentaram (P < 0.05) em ambos os tratamentos (LEU e PLA) após a sessão de ER. Este aumento permaneceu elevado até o período de 24 h, e retornou gradualmente aos níveis basais após 48h de recuperação. Entretanto, nenhuma diferença significante (P > 0.05) foi observada entre os tratamentos com LEU e PLA. CONCLUSÃO: A suplementação isolada de LEU não alterou os níveis de CK após uma única sessão de ER de alta intensidade, sugerindo que a utilização deste suplemento pode não ser eficaz para acelerar o processo de recuperação muscular. Jacinto JL, Andrade WB, Oliveira DB, Aguiar AF. Efeitos da suplementação de leucina sobre os níveis de creatina quinase durante a recuperação muscular após exercício resistido. 40º Simpósio Internacional de Ciências do Esporte (Celafiscs). São Paulo, Brasil. 2017. p.8.

43
APÊNDICE C – Artigo Científico
Free leucine supplementation does not improve functional muscle recovery
after resistance exercise in young adult subjects
Jeferson Lucas Jacinto1, Andreo Fernando Aguiar1,
1 Center of Research in Health Sciences, North University of Paraná (UNOPAR),
Londrina, Paraná, Brazil
Corresponding author: Andreo Fernando Aguiar ()
Center of Research in Health Sciences, North University of Paraná (UNOPAR),
Avenue Paris, 675, Jardim Piza, CEP: 86041-120, Londrina, PR, Brazil. Tel: +55
4399523813, Fax: +55 4333717725, email: [email protected]

44
ABSTRACT
Purpose: The effects of free leucine (LEU) supplementation on muscle recovery
from resistance exercise (RE) remains unknown. We aimed to determine whether
free LEU supplementation improves muscle recovery after a single session of high-
intensity RE in untrained young adults. Methods: Fourteen young adults (23.9 ± 3.6
yr.) participated in a double-blind crossover study in which they received 6 g of LEU
or placebo (PLA) on 2 different occasions, separated by a 7-d washout period. Each
occasion consisted of a single session of high-intensity RE (0 h) involving quadriceps
muscle, and 3 subsequent fatigue tests sessions (at 24, 48 and 72 h) to assess the
time course of muscle recovery. During the tests sessions, we assessed the following
variables: number of maximum repetitions, electromyography signal (i.e., root mean
square [RMS] and frequency median [MF]), muscle soreness and perceived exertion,
as well as blood levels of creatine kinase (CK) and lactate. Results: CK levels
increased at post-exercise and remained elevate at 24 h, which progressively
returned to baseline at 48 h post-exercise in both conditions. Lactate levels increased
immediately post-exercise and remained elevated at 24, 48, and 72 h post-exercise
in both conditions. No significant treatment x time interaction was found for all
dependents variables (maximum repetitions, perceived exertion, muscle soreness,
CPK, lactate, RMS, and MF) during the recovery period. Conclusion: Our data
indicates that free LEU supplementation does not improve the muscle recovery
process following a high-intensity RE session in untrained young subjects.
Keywords: Dietary supplements; amino acids; leucine; skeletal muscle; resistance
training; function recovery.

45
INTRODUCTION
Nutritional supplements are a common strategy used by athletes and recreationally
active adults to improve physical performance and muscle recovery. Among the
supplements, the amino acids branched-chain (BCAA), in particular leucine (LEU),
has been received special attention for their contribution in increasing muscle protein
synthesis (MPS) rates (Anthony et al. 2000; Koopman et al. 2006; Dreyer et al. 2008)
through a mainly process regulated by mammalian target of rapamycin (mTOR)
signaling pathway (Wang and Proud 2006). Additionally, it has also been suggested
that LEU supplementation may suppress muscle proteolysis (Zanchi et al. 2008) and
reduce protein oxidation (Shimomura et al. 2010) after resistance exercise.
Nevertheless, most of the previous studies that showed positive effects used
supplementation LEU in combination with other amino acids (e.g., BCAA), precluding
the analysis of their isolated effects (Coombes and McNaughton 2000; Greer et al.
2007; Howatson et al. 2012; Nosaka et al. 2006). For example, Howatson et al.
(2012) showed that BCAA administration during 12 days (10 g twice a day,
containing a ratio of 2:1:1 leucine, isoleucine and valines, respectively) promoted
reduction in CK levels, muscle soreness and greater recovery of maximal voluntary
contraction (MVC) during recovery period after five sets of 20 drop-jumps, compared
to the placebo group. Nosaka et al. (2006) reported that intake 4.5 g of an amino acid
mixture (3.6 g; 60% were essential amino acids with the major portion being BCAA) +
0.5 g CHO + 10 vitamins + 2 minerals + 0.045 g fat 30 min prior, immediately after
exercise and after dinner, may attenuates muscle damage over a 4-day recovery
period. These authors also showed a reduction in CK levels, aldolase activity,
myoglobin concentration and muscle soreness in untrained male that performed an
arm curl exercise.

46
Additionality, Coombes and McNaughton (2000) demonstrated significantly
reduced levels of lactate dehydrogenase (LDH) and CK during the recovery (up to 5
d post exercise) from a 120-min exercise in cycle ergometer at 70% VO2max in man
supplemented with BCAA (12 g/day) during 14 days. Consistent with these findings,
Greer et al. (2007) demonstrated a reduction in CK, LDH and soreness levels in
untrained men supplemented with BCAA (1.22 g leucine, 480 mg isoleucine and 730
mg valine) after performed 90 min exercise in cycle ergometer at 55% VO2peak.
While there is strong evidence to demonstrate that amino acid
supplementation containing LEU may be beneficial for decrease several recovery
markers after exercise, no study to date has examined whether free LEU
supplementation improves recovery of muscle function after high-intensity RE in
young adult subjects. Therefore, the aim of this study was to investigate the effects of
free LEU supplementation on recovery of muscle function after a single session of
high-intensity RE in untrained young adult subjects. Given that LEU has been shown
to improves several recovery markers (e.g., CK, LDH, myoglobin, muscle soreness)
and stimulate anabolic pathways (e.g., mTOR), we hypothesized that free LEU
supplementation would enhance muscle recovery from RE in young adult subjects.

47
METHODS
Subjects
Seventeen healthy, recreationally active subjects were recruited from a university
population, and 14 (11 men and 3 woman) of then completed the study (3 withdrew
by factor not related to the study). An a priori power analysis was conducted
(G*Power v. 3.1.9.2) for an F test (repeated measures, within- between interaction
factors for five-time points) to assess the required number of participants. On the
basis of a statistical power (1 – β) of 0.90, a moderate effect size (0.5), and an overall
level of significance of 0.05, least 8 subjects were required for this study. Participants
were excluded if they: (1) were smoker, (2) had ingested any ergogenic supplement
or anabolic steroids for the 6 months prior to the start of study, (3) were talking any
medication that could affect muscle recovery or the ability to train intensely, (4) had
participated in a exercise training program (more than 2 days per week, for 6 months
prior to the beginning of the study), (5) were unable to provide a detailed description
of their lifestyle and daily food intake, and (6) did not have medical approval to
perform physical exercise. The participants’ characteristics are presented in Table 1.
All subjects were informed of the procedures, risks, and benefits of the investigation
and signed an informed consent document approved by the Institutional Review
Board of the University (protocol no: 1.748.002). All procedures were performed
according to the principles in the latest version Declaration of Helsinki, revised in
2008.

48
Table 1. Participant characteristics
Age, y 23.9 ± 3.6
Height, cm 170.0 ± 8.0
Weight, kg 75.4 ± 8.7
BMI, kg/m2 26.1 ± 2.8
Glucose, mg/dL
Insulin, µg/dL
80.9 ± 10.1
11.7 ± 8.5
Cholesterol, mg/dL 166.1 ± 30.6
Values are means ± SD
Experimental design
A double-blind random crossover design was performed to examine the effects of
LEU supplementation on the time course of muscle recovery after a single session of
high-intensity RE in young subjects (Fig. 1). All subjects were randomly
supplemented with 1 of 2 treatments [leucine (LEU) or placebo (PLA)] on 2 occasions
(T1 and T2) separated by a 7-day washout period in order to ensure complete LEU
elimination from the body. Before T1, all subject completed 3 sessions of
familiarization and 2 sessions 1-repetition maximum (1RM) tests for leg press and
hack squat exercise. During T1 and T2, all subjects underwent a single session of
RE (0 h) and 3 subsequent sessions (at 24, 48 and 72 h) of fatigue tests (to assess
the time course of muscle recovery), performed at 30 minutes after supplementation.
In each session of the fatigue test, functional (i.e., number of maximum repetitions,
muscle soreness, and perceived exertion), metabolic (i.e., CK and lactate), and
physiological (i.e., RMS and MF signal) indicators of muscle recovery were
assessed. All participants completed a 3-day dietary intake record (including 1
weekend day) during each study moment. All subjects had adequate protein (> 1.2
g/kg/day) and carbohydrate (> 3 g/kg/day) intake during the study period (Table 2),
according to the recommendations proposed by the ACSM (2016).

49
We used a crossover design because of its advantages over a parallel group
design. First, crossover designs are not influenced by intersubject variability (e.g.,
genetic, food intake, motivation, and life style) because the participants acts as its
own control. Second, crossover designs are statistically efficient and require fewer
subjects than parallel designs. Finally, crossover designs allow the experiment to the
performed in a shorter time than a parallel group study, thereby increasing
participant’s adherence.
Figure 1. Experimental design.
Familiarization protocol
Before T1, all subjects completed 3 familiarization sessions with leg press and hack
squat exercises in order to minimize any learning effects and establish the reliability
of the testing protocols (Fig. 1). The protocol consisted of 3 sets of 8-12 repetitions,
with 2 min rest between sets and exercises. Qualified personnel individually
supervised each participant during the familiarization period. All sessions of
familiarization were performed at the same location, between 8 and 10 a.m.

50
Determination of one-repetition maximum load
After the familiarization, the participants completed 2 sessions of 1RM test for leg
press and hack squat exercises (Fig. 1). Standard testing protocol as previously
documented by Baechle and Earle (2008). The 1RM test was preceded by a set of
warm-up exercise (~15 repetitions) for each exercise. After 2 min of rest, the 1RM
attempts were performed with a progressively increasing load for each attempt, and
were separated by 4 to 5 min rest intervals to allow adequate recovery. Only 3
attempts were allowed in each testing session. Verbal encouragement was provided
during all 1RM attempts. The exercise was standardized and continuously monitored
by the same experienced rater in an attempt to assure the data quality and determine
the 1RM within 3 attempts. The interclass correlation coefficients (ICC) test-retest
were 0.94 for each 1RM test, indicating the elimination of the learning curve for the
subjects. All session of 1RM tests were performed at the same location, between 8
and 10 a.m.
Resistance training
During T1 and T2, all subjects were submitted to a single session of high-intensity
RE (3 sets of 8-12 repetitions at 70% of 1RM with 2 min rest between sets and
exercises), involving the leg press and hack squat exercise (bilateral), using
commercial machines (Nakagym equipment, São Paulo, Brazil). The cadence of
muscle action was 1 s concentric: 2 s eccentric according metronome. This protocol
was designed to maximize the recruitment of quadriceps muscle, and the training
stimulus was similar to a conventional RE session (3 sets of 8-12 repetitions at 70-
75% of 1RM) for novice individuals (ACSM, 2009). RE session began with general
(moderate walking on treadmill for 10 min) and specific (1 set of 12 repetitions with a
self-selected load) warm-up exercises for quadriceps muscle. Qualified personnel
supervised each participant individually during every workout. The RE session were

51
performed at the same location, between 8 and 10 a.m.
Supplementation protocol
During T1 and T2, the subjects orally ingested an identical appearance and
equivalent amount (6 g/d) of LEU or PLA dissolved in 200 mL of water. The LEU and
PLA were analyzed and confirmed for purity prior to the study. We have chosen to
use a dose of 6 g because similar doses (i.e., 3 – 5 g) has been reported to increase
the MPS rate in young subjects (Stark et al. 2012; Churchward-Venne et al. 2014).
The supplements were consumed in two equal doses (30 min before and
immediately after RE session and fatigue tests). It has been reported that the peak
concentration of plasma LEU is reached within 30 min (Katsanos et al. 2006;
Wilkinson et al. 2013). To ensure the double-blind design, an individual who was not
involved in the study was responsible for placing the supplements into bags and
labeling the capsules with the subjects´ names according to the randomization list.
Dietary intake
Participant completed a 3-day dietary intake record (including 1 weekend day) during
the T1 and T2 moments. The macronutrient composition of the diets was calculated
using software for nutritional assessment (Avanutri, version 3.1.4, Rio de Janeiro-RJ,
Brazil). Participants were instructed to maintain their habitual daily diet, and to refrain
from any strenuous activity during experimental period. The participants were also
instructed to report any adverse events from the supplements. No discomfort or
adverse effect were reported after LEU ingestion.
Perceived exertion
Rating of perceived exertion was measured immediately after muscular fatigue tests
(24, 48, and 72 h after RE session) during T1 and T2 using the OMNI-RES scale
(Robertson et al. 2003) (Fig. 1). The subjects were instructed to report the perceived
exertion value indicating a number of the OMNI-RES scale (0 “no effort” and 10

52
“maximal effort”) that best represented their overall muscular effort (Robertson et al.
2003; Day et al. 2004).
Delayed-onset muscle soreness
Muscle soreness was measured before muscular endurance tests (24, 48 and 72 h
after RE session) during T1 and T2 using a visual analog scale (VAS) (Fig. 1). The
VAS consists of a 10 cm line whose and points were labeled with “no pain” (left) and
“unbearable pain” (right). The subjects were instructed to palpate their quadriceps
muscle and mark a vertical line at the scale that best represented their rating of
momentary soreness. The score was the distance (in cm) from the left side of the
scale to the point marked (Mattacolla et al. 1997).
Muscular endurance tests and electromyography (EMG) signal recordings
During T1 and T2, all subjects were submitted to a muscular fatigue test (1 set at
50% of 1RM until failure) in the leg press exercise at 24, 48 and 72 h after RE
session (Fig. 1), in order to examine the muscular endurance recovery. During the
leg press test, surface EMG signals were recorded from the vastus lateralis (VL)
muscle using a pre-amplified (gain: 1000) active bipolar surface electrode (Model
EMG System Brazil Ltda, São José dos Campos, SP, Brazil) at a sampling rate of
2000 Hz. The subject’s skin was prepared by removing the superficial dead skin and
was sterilized with an alcohol swab. The Electrodes was placed at 2/3 on the line
from the anterior spina iliaca superior to the lateral side of the patella according to the
SENIAM (Surface EMG for Non-Invasive Assessment of Muscles) recommendation
and the reference electrode was fixed at the right styloid process. The EMG signals
were filtered with a band-pass digital filter between 10 and 500 Hz to remove high
frequency noise as well as low-frequency movement.
To determine the muscle activation and fatigue, two EMG parameters were
computed: Root mean square (RMS) and Median frequency (MF). RMS corresponds

53
to the muscular activation of the second and before last contractions of the
endurance test (e.g., to avoid the acceleration and the deceleration portions of the
concentric leg contractions during the extension phase of movement). This
parameter was computed by a moving RMS method executed on successive 250 ms
(512 points) time-series windows (50% overlap) to obtain the RMS average values
during the entire leg press exercise. MF corresponds to muscle fatigue from the
magnitude of the electromyography spectral content evaluated by the MF value of
the power spectra (Short-fast Fourier transform, Hanning windows processing) during
successive time windows (50% overlap) of 250 ms for the total time of the fatigue
test. Least squares linear regression analysis was applied to the MF time series to
calculate the rate of decline in MF over time (MF/time slope as a muscle fatigue
index), as supported by previous studies (Larivière et al. 2002; Kienbacher et al.
2014; da Silva et al. 2015). All EMG signals and estimates (RMS and MF) were
processed using MATLAB sub-routines for data computation from subsequent
analysis (Version 8.0, Mathworks®, South Natick, MA, USA).
Blood collection and analysis
Blood sample were collected at pre- and post-exercise as well as immediately after
muscular fatigue tests (24, 48, and 72 h after RE session) during T1 and T2 for
analyses of CK, lactate, insulin, glucose and cholesterol concentrations (Fig. 1). The
blood samples were allowed to coagulate at room temperature for 60 min and then
centrifuged at 2,000 g for 15 min, and the serum was frozen at -80ºC until analysis.
All analyses were performed in a laboratory equipped with automated systems using
commercial kits for chemiluminescence (insulin), kinetic (CK and lactate), and
enzymatic (cholesterol and glucose) techniques.
Statistical analysis
Data are expressed as means standard deviation (SD). The normality and

54
homogeneity for outcome measures were tested using the Shapiro-Wilk’s and
Levene’s tests, respectively. Independent variables included the supplementation
protocol (i.e., LEU and PLA) and time (i.e., 24, 48 and 72 h). Dependent variables
included number of maximum repetitions, perceived exertion, muscle soreness, EMG
signs (i.e., RMS and MF), and blood analysis (i.e., CK, and lactate). Food intake
(during T1 and T2) and area under curve (AUC) were analyzed using a paired t-test.
Two-way (treatment x time) analysis of variance (ANOVA) with repeated measures
was used to evaluate changes over time and between group for all dependent
variables. Violation of sphericity was adjusted by Greenhouse-Geisser. When
significant differences were confirmed with ANOVA, multiple comparisons testing
were performed using Bonferroni post hoc correction to identify these differences.
The significance level was set at P 0.05. Statistical analyses were performed using
SPSS statistical analysis software (SPSS version 20.0; Chicago, IL, USA).
Effect size (ES) and confidential interval (CI) have been recommended as a
more appropriate analysis for evidence the magnitude of an intervention (treatment
effect) (Nakagawa and Cuthill, 2007; Page, 2014) due their biological importance to
make clinical decision (Page, 2014), and elimination of confounding factors such as
sample size and measure variability (Batterham and Hopkins, 2006; Wilkinson, 2014;
Hopkins et al. 2009). Thus, we also analyzed ES and 95% CI (Cohen, 1977) to
ensure a more realistic biological interpretation of data and to provide practical
information on the magnitude or direction of the difference (treatment effect).

55
RESULTS
Dietary intake. The macronutrient intake is presented in Table 2. No significant
difference in the daily dietary intake were observed between T1 and T2 moments,
and all participants had adequate protein (>1.2 g/kg/day) and CHO (>3 g/kg/day)
intake during the study period, according to the recommendations proposed by
ACSM (2016). Participants throughout study reported no adverse effect.
Table 2. Macronutrient dietary intake between T1 and T2 moments
T1 T2 p value
Protein, g/kg/d 1.3 ± 0.4 1.3 ± 0.4 0.44
Carbohydrate, g/kg/d 3.6 ± 1.5 3.2 ± 1.1 0.44
Fat, g/kg/d 0.8 ± 0.3 0.8 ± 0.2 0.94
Total energy, kcal 2037.8 ± 778.8 1888.8 ± 500.4 0.58
Values are means ± SD. There were no differences between T1 and T2
moments.
Total repetitions and perceived exertion in the fatigue tests during recovery. The total
number of repetitions and perceived exertion for leg press (Fig. 2) fatigue tests during
recovery at 24, 48 and 72 h post-exercise did not differ over time between LEU and
PLA conditions (treatment x time P > 0.05; time P > 0.05). Both LEU and PLA
conditions achieved maximum perceived effort (OMNI scale score) in leg press (LEU:
10 0.1 vs. PLA: 10 0.1; P > 0.05) fatigue tests. AUC over 3 days of recovery was
similar (P > 0.05) between groups (Fig. 2; Left upper figure). The ES (95% CI) for
total repetitions over the 3 days of recovery is shown (Fig. 2; Right upper figure). The
data shown no positive effect in favor of LEU group.

56
Figure 2. Number of maximum repetitions in the leg press fatigue tests between LEU and
PLA groups during 3-d recovery period (24, 48, and 72h post-exercise). Data are means ± SD.
Left upper figure indicates the area-under-curve (AUC) during 3-d recovery period.
(Repeated-measures ANOVA: time P > 0.05; Group x time P > 0.05). Right upper figure
indicates the effect size (95% CI) between LEU and PLA groups during 3-d recovery period.
Note: The point “0” indicates the PLA group. When CI is further from “0” represent more
difference between groups (positive or negative), and the CI closer to “0” represent less group
difference or effect. When CI contains “0” means that there is no effect of treatment or
difference between groups. The data show no positive effect in favor of LEU.
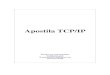
CK and lactate blood levels after fatigue tests during recovery. Serum CK levels
increased (time P < 0.05) at post-exercise and remained elevate at 24 h (Fig. 3A),
with no differences between LEU and PLA conditions (treatment x time P > 0.05). CK
levels returned to baseline at 48 h post-exercise (Fig. 3A). Plasma lactate levels
increased (time P < 0.05) immediately post-exercise and remained elevated at 24,
48, and 72 h post-exercise (Fig. 3B), with no differences between LEU and PLA

57
conditions (treatment x time P > 0.05). AUC for CK (Fig. 3A; Left upper figure) and
lactate (Fig. 3B; Left upper figure) over 3 days of recovery were similar (P > 0.05)
between groups. The ES (95% CI) for CK (Fig. 3A; Right upper figure) and lactate
(Fig. 3B; Right upper figure) over the 3 days of recovery shown no positive effect in
favor of LEU group compared to PLA group.
Figure 3. Blood CK (A) and lactate (B) levels between LEU and PLA groups at pre- and
post-exercise, and immediately after fatigue tests during 3-d recovery period (24, 48, and 72h
post-exercise). Data are means ± SD. Left upper figure indicates the area-under-curve (AUC)
during 3-d recovery period. (Repeated-measures ANOVA: *P < 0.05 compared to Pre; Group
x time P > 0.05). Right upper figure indicates the effect size (95% CI) between LEU and PLA
groups during 3-d recovery period. Note: The point “0” indicates the PLA group. When CI is
further from “0” represent more difference between groups (positive or negative), and the CI
closer to “0” represent less group difference or effect. When CI contains “0” means that there
is no effect of treatment or difference between groups. The data show no positive effect in
favor of LEU.

58
Muscle soreness during recovery. Perceived intensity of muscle soreness before
fatigue tests during recovery at 24 h (LEU: 3.3 ± 1.8 vs. PLA: 3.8 ± 2.8), 48 h (LEU:
4.0 ± 2.5 vs. PLA: 4.1 ± 2.8) and 72 h (LEU: 2.9 ± 2.7 vs. PLA: 3.4 ± 2.7) post-
exercise did not differ over time between LEU and PLA conditions (treatment x time
P > 0.05; time P > 0.05).
EMG signal in the fatigue tests during recovery. RMS (Fig. 4A) and MF slope (Fig.
4B) in the leg press fatigue test during the recovery period (24, 48, and 72 h after
RE) did not change over time between LEU and PLA conditions (treatment x time P >
0.05; time P > 0.05), recovery were similar between conditions. AUC for RMS and
MF slope (Fig. 4A and B, respectively; Left upper panel) over 3 days of recovery
were similar (P > 0.05) between LEU and PLA groups. The ES (95% CI) for RMS and
MF slope over the 3 days of recovery are shown in Fig. 4A and B, respectively (Right
upper panel). The data show a positive effect in the MF slope 24 and 48 h post-
exercise in favor of LEU group and 72 h after shown a negative effect for this group.

59
Figure 4. RMS (A) and MF slope (B) values between LEU and PLA groups in the leg press
fatigue test during 3-d recovery period (24, 48, and 72 h post-exercise). Data are means ± SD.
Left upper figure indicates the area-under-curve (AUC) during 3-d recovery period.
(Repeated-measures ANOVA: time P > 0.05; Group x time P > 0.05). Right upper figure
indicates the effect size (95% CI) between LEU and PLA groups during 3-d recovery period.
Note: The point “0” indicates the PLA group. When CI is further from “0” represent more
difference between groups (positive or negative), and the CI closer to “0” represent less group
difference or effect. When CI contains “0” means that there is no effect of treatment or
difference between groups. The data show a positive effect in 24 and 48 h in the MF slope in
favor of LEU group, 72 h after shown a negative effect for this group.

60
DISCUSSION
To our knowledge, this is the first study to examine the effects of free LEU
supplementation on the time course of muscle recovery after a single session of
high-intensity RE in untrained young adult subjects. Based on the physiological
properties and beneficial effects of LEU on recovery markers (e.g., protein synthesis,
CK, and soreness), we hypothesized that LEU supplementation would enhance
muscle recovery process after RE by improving the muscular functional, metabolic,
anabolic, and physiological responses. In contrast to our hypothesis, we observed
that LEU supplementation 30 min prior and immediately after exercise (6 g total)
does not improvement functional (i.e., number of maximum repetitions, muscle
soreness, and perceived exertion), metabolic (i.e., CK and lactate), and physiological
(i.e., RMS and MF signal) indicators of muscle recovery in untrained young adult
subjects.
Leucine supplementation has been shown to increase MPS rate (Anthony et
al. 2000; Koopman et al. 2006; Dreyer et al. 2008), through a mainly process
regulated by mammalian target of rapamycin (mTOR) signaling pathway (Wang and
Proud 2006). This positive effect on MPS may be favorable for enhancing
regeneration of muscle damage after exercise (Kirby et al. 2012) and then improving
muscle function during recovery process. Nevertheless, we have shown that free
LEU supplementation does not promote any improvements in number of maximum
repetitions during recovery from RE (24, 48, and 72 h). According to our results,
Stock et al. (2010) showed that LEU addition in a carbohydrate beverage 30 min
before and immediately after exercise (45 mg/kg LEU + 0,50 g/kg CHO total) in
subjects trained does not increase performance (i.e., number of maximum repetition)
during 6 sets of squats to fatigue 30 min after beverage ingestion and 72 h later.

61
In addition, the RE session resulted in similar increase in plasma CK (post-
exercise and remained elevate at 24 h) and lactate (immediately post-exercise)
levels in both the LEU and PLA conditions, which typically indicates muscle damage
and impaired muscle function. Consistent with our results, Kirby et al. (2012) showed
no significant differences in CK levels between LEU and PLA groups, and LEU had
greater soreness levels over the five times of recovery after 5 sets of 20 drop jumps
and 6 sets of 10 repetitions of eccentric-only leg press in untrained males. Similarly,
Stock et al. (2010) reported no beneficial effects of LEU supplementation on CK and
lactate dehydrogenase levels. These results are consistent with no beneficial effect
of BCAA (containing 3.5 g leucine) on muscle soreness and plasma CK
concentration during 2 days after completed 12 sets of 10 repetitions of eccentric
knee extension in untrained males (Jackman et al. (2010). On the other hand,
previous studies shown that BCAA supplementation can reduce muscle soreness
(Howatson et al. 2012; Nosaka et al. 2006; Greer et al. 2007), CK levels (Howatson
et al. 2012; Nosaka et al. 2006; Coombes and McNaughton 2000) and LDH
(Coombes and McNaughton 2000; Greer et al. 2007). Therefore, a possible
explanation for our results may be the inability of LEU to attenuate muscle damage
during recovery period. The effect of LEU may have such a minimum contribution,
disappearing in the recovery period, due to the adverse conditions that muscle is
found after high-intensity RE with making differences difficult to be identify.
Additionally, we showed no differences in electromyography (EMG) indicators
of muscle activation (RMS) and fatigue (MF) between LEU and PLA conditions. To
our knowledge, this is the first study to examine the effects of LEU supplementation
on EMG indicators of RMS and MF during recovery from high-intensity RE.
Considering that the decline in MF and increase in RMS are typically associated with
muscle fatigue during isometric and dynamic contraction (De Luca 1993; Arab and

62
Salavati, 2007; da Silva et al. 2008; Adam and De Luca 2003), we expected an
inverse effect of LEU supplementation on these factors in the fatigue tests during
recovery period. However, no differences were observed between the LEU and PLA
conditions, which is line with the lack of a beneficial effect of LEU supplementation on
muscle functions (i.e., number of repetitions performed). This indicates that LEU
supplementation is not effective in improving the neuromuscular responses during
recovery from RE. This result is consistent with no difference in the muscle soreness
between LEU and PLA conditions during the recovery period. Although muscle
soreness may a poor indicator of exercise-induced muscle damage during recovery
(Nosaka et al. 2002), it usually reflects muscle fatigue. This supports the findings of
the present study that LEU supplementation does not attenuate muscle fatigue
during the period of recovery. Therefore, any possible beneficial effects of LEU
supplementation on muscle protein synthesis rates (Anthony et al. 2000; Koopman et
al. 2006; Dreyer et al. 2008), increase to muscle proteolysis (Zanchi et al. 2008;
Waldron et al. 2017) and reduced protein oxidation (Shimomura et al. 2010; Waldron
et al. 2017) may not be sufficient to improve muscle recovery in untrained young
subjects. It is noteworthy that a dose ~ 3 g is sufficient to increase blood LEU levels
(Katsanos et al. 2006), and MPS rate in young subjects (Stark et al. 2012;
Churchward-Venne et al. 2014). In addition, it has been demonstrated that after
administration of LEU (~ 3 g), time to reach maximum concentration (Tmax) was ~30
min and decreased to baseline by 2-3 h (Katsanos et al. 2006; Wilkinson et al. 2013).
Thus, the lack of a positive effect of free LEU supplementation on muscle recovery
from RE does not necessarily indicate that our subjects did not experience an
increase in the plasma LEU levels after exercise.
A few limitations of this study must be mentioned. First, we did not analyze
plasma LEU concentrations. However, previous studies that used the same dose of

63
LEU (i.e., 1.7 g; 2,8 g and 3.4 g) showed an increase in plasma LEU concentrations
(Katsanos et al. 2006; Wilkinson et al. 2013). Second, we did not collect muscle
biopsies for analysis of muscle tissue markers of regeneration (e.g., protein synthesis
and anabolic factors such as insulin-like growth factor [IGF-I], hepatocyte growth
factor [HGF], mTOR, and ribosomal protein S6 kinase [p70S6k]) and damage (e.g.,
histological changes); however, we analyzed the major plasma markers of muscle
regeneration (i.e., CK) as well as functional outcome measures (i.e., number of
repetitions performed, perceived exertion, muscle soreness, and EMG signs). Finally,
we did not standardize the subjects’ diet; however, we did instruct subjects to
duplicate their food intake for the 24 h proceeding each session.
In conclusion, LEU supplementation 30 min before and immediately post-
exercise (6 g total) does not improve muscle recovery from a single session of high-
intensity RE in untrained young subjects. Therefore, it is premature to recommend
free LEU supplementation as an ergogenic aid to improve muscle recovery after RE.
Future studies are required to assess the effects of LEU in individuals with different
training status (e.g., recreational practitioners and/or athletes).
Conflict of interest
No conflicts of interest, financial, or otherwise, are declared by the author(s).

64
REFERENCES
1. ACSM. American College of Sports Medicine position stand (2009) Progression
models in resistance training for healthy adults. Med Sci Sports Exerc 41:687-708.
2. ACSM. American College of Sports Medicine Joint Position Statement (2016)
Nutrition and Athletic Performance. Med Sci Sports Exerc 48:543-568.
3. Adam A, De Luca CJ (2003) Recruitment order of motor units in human vastus
lateralis muscle is maintained during fatiguing contractions. J Neurophysiol
90:2919-2927.
4. Anthony JC, Yoshizawa F, Anthony TG, Vary TC, Jefferson LS, Kimball SR (2000)
Leucine stimulates translation initiation in skeletal muscle of postabsorptive rats
via a rapamycin-sensitive pathway. J Nutr 130:2413-2419.
5. Arab AM, Salavati M, Ebrahimi I, Ebrahim Mousavi M (2007) Sensitivity, specificity
and predictive value of the clinical trunk muscle endurance tests in low back pain.
Clin Rehabil 21:640-647.
6. Baechle TR, Earle RW (2008) Resistance training and spotting techniques. In:
Earle RW, Baechle TR (eds) Essentials of strength and training and conditioning:
national strength and conditioning association, 3rd edn. Human Kinetics,
Champaign, pp 326-376.
7. Batterham AM, Hopkins WG (2006) Making meaningful inferences about
magnitudes. Int J Sports Physiol Perform 1:50-57.
8. Cohen J (1977) Statistical Power Analysis for Behavioral Sciences, 1rd edn.
Academic Press, New York, pp 490.
9. Churchward-Venne TA, Breen L, Di Donato DM, Hector AJ, Mitchell CJ, Moore
DR, Stellingwerff T, Breuille D, Offord EA, Baker SK, Phillips SM (2014) Leucine

65
supplementation of a low-protein mixed macronutrient beverage enhances
myofibrillar protein synthesis in young men: a double-blind, randomized trial. Am J
Clin Nutr 99:276-286.
10. Coombes JS, McNaughton LR (2000) Effects of branched-chain amino acid
supplementation on serum creatine kinase and lactate dehydrogenase after
prolonged exercise. J Sports Med Phys Fitness 40:240-246.
11. da Silva RA, Lariviere C, Arsenault AB, Nadeau S, Plamondon A (2008) The
comparison of wavelet- and Fourier-based electromyographic indices of back
muscle fatigue during dynamic contractions: validity and reliability results.
Electromyogr Clin Neurophysiol 48:147-162.
12. da Silva RA, Vieira ER, Cabrera M, Altimari LR, Aguiar AF, Nowotny AH,
Carvalho AF, Oliveira MR (2015) Back muscle fatigue of younger and older
adults with and without chronic low back pain using two protocols: A case-control
study. J Electromyogr Kinesiol 25:928-936.
13. Day ML, McGuigan MR, Brice G, Foster C (2004) Monitoring exercise intensity
during resistance training using the session RPE scale. J Strength Cond Res
18:353-358.
14. De Luca CJ (1993) Use of the surface EMG signal for performance evaluation of
back muscles. Muscle Nerve 16:210-216.
15. Dreyer HC, Drummond MJ, Pennings B, Fujita S, Glynn EL, Chinkes DL,
Dhanani S, Volpi E, Rasmussen BB (2008) Leucine-enriched essential amino
acid and carbohydrate ingestion following resistance exercise enhances mTOR
signaling and protein synthesis in human muscle. Am J Physiol Endocrinol Metab
294:E392-E400.

66
16. Greer BK, Woodard JL, White JP, Arguello EM, Haymes EM (2007) Branched-
chain amino acid supplementation and indicators of muscle damage after
endurance exercise. Int J Sport Nutr Exerc Metab 17:595-607.
17. Hopkins WG, Marshall SW, Batterham AM, Hanin J (2009) Progressive statistics
for studies in sports medicine and exercise science. Med Sci Sports Exerc 41:3-
13.
18. Howatson G, Hoad M, Goodall S, Tallent J, Bell PG, French DN (2012) Exercise-
induced muscle damage is reduced in resistance-trained males by branched
chain amino acids: a randomized, double-blind, placebo controlled study. J Int
Soc Sports Nutr 9:20.
19. Jackman SR, Witard OC, Jeukendrup AE, Tipton KD (2010) Branched-chain
amino acid ingestion can ameliorate soreness from eccentric exercise. Med Sci
Sports Exerc 42:962-970.
20. Katsanos CS, Kobayashi H, Sheffield-Moore M, Aarsland A, Wolfe RR (2006) A
high proportion of leucine is required for optimal stimulation of the rate of muscle
protein synthesis by essential amino acids in the elderly. Am J Physiol Endocrinol
Metab 291:E381-E387.
21. Kienbacher T, Habenicht R, Starek C, Mair P, Wolf M, Paul B, Riegler S,
Kollmitzer J, Ebenbichler G (2014) The potential use of spectral
electromyographic fatigue as a screening and outcome monitoring tool of
sarcopenic back muscle alterations. J Neuroeng Rehabil 11:106.
22. Kirby TJ, Triplett NT, Haines TL, Skinner JW, Fairbrother KR, McBride JM (2012)
Effect of leucine supplementation on indices of muscle damage following drop
jumps and resistance exercise. Amino Acids 42:1987-1996.

67
23. Koopman R, Verdijk L, Manders RJ, Gijsen AP, Gorselink M, Pijpers E,
Wagenmakers AJ, van Loon LJ (2006) Co-ingestion of protein and leucine
stimulates muscle protein synthesis rates to the same extent in young and elderly
lean men. Am J Clin Nutr 84:623-632.
24. Larivière C, Arsenault AB, Gravel D, Gagnon D, Loisel P (2002) Evaluation of
measurement strategies to increase the reliability of EMG indices to assess back
muscle fatigue and recovery. J Electromyogr Kinesiol 12:91-102.
25. Mattacola CG, Perrin DH, Gansneder BM, Allen JD, Mickey CA (1997) A
Comparison of Visual Analog and Graphic Rating Scales for Assessing Pain
Following Delayed Onset Muscle Soreness. Journal of Sport Rehabilitation 6:38-
46.
26. Nakagawa S, Cuthill IC (2007) Effect size, confidence interval and statistical
significance: a practical guide for biologists. Biol Rev Camb Philos Soc 82:591-
605.
27. Nosaka K, Newton M, Sacco P (2002) Delayed-onset muscle soreness does not
reflect the magnitude of eccentric exercise-induced muscle damage. Scand J
Med Sci Sports 12:337-346.
28. Nosaka K, Sacco P, Mawatari K (2006) Effects of amino acid supplementation on
muscle soreness and damage. Int J Sport Nutr Exerc Metab 16:620-635.
29. Page P (2014) Beyond statistical significance: clinical interpretation of
rehabilitation research literature. Int J Sports Phys Ther 9:726-736.
30. Robertson RJ, Goss FL, Rutkowski J, Lenz B, Dixon C, Timmer J, Frazee K,
Dube J, Andreacci J (2003) Concurrent validation of the OMNI perceived exertion
scale for resistance exercise. Med Sci Sports Exerc 35:333-341.

68
31. Shimomura Y, Inaguma A, Watanabe S, Yamamoto Y, Muramatsu Y, Bajotto G,
Sato J, Shimomura N, Kobayashi H, Mawatari K (2010) Branched-chain amino
acid supplementation before squat exercise and delayed-onset muscle soreness.
Int J Sport Nutr Exerc Metab 20:236-244.
32. Stark M, Lukaszuk J, Prawitz A, Salacinski A (2012) Protein timing and its effects
on muscular hypertrophy and strength in individuals engaged in weight-training. J
Int Soc Sports Nutr 9:54.
33. Stock MS, Young JC, Golding LA, Kruskall LJ, Tandy RD, Conway-Klaassen JM,
Beck TW (2010) The effects of adding leucine to pre and postexercise
carbohydrate beverages on acute muscle recovery from resistance training. J
Strength Cond Res 24:2211-2219.
34. Waldron M, Whelan K, Jeffries O, Burt D, Howe L, Patterson SD (2017) The
effects of acute branched-chain amino acid supplementation on recovery from a
single bout of hypertrophy exercise in resistance-trained athletes. Appl Physiol
Nutr Metab 42:630-636.
35. Wang X, Proud CG (2006) The mTOR pathway in the control of protein
synthesis. Physiology (Bethesda) 21:362-369.
36. Wilkinson DJ, Hossain T, Hill DS, Phillips BE, Crossland H, Williams J, Loughna
P, Churchward-Venne TA, Breen L, Phillips SM, Etheridge T, Rathmacher JA,
Smith K, Szewczyk NJ, Atherton PJ (2013) Effects of leucine and its metabolite
β-hydroxy-β-methylbutyrate on human skeletal muscle protein metabolism. J
Physiol 591:2911-2923.

69
37. Wilkinson M (2014) Distinguishing between statistical significance and
practical/clinical meaningfulness using statistical inference. Sports Med 44:295-
301.
38. Zanchi NE, Nicastro H, Lancha AH Jr (2008) Potential antiproteolytic effects of L-
leucine: observations of in vitro and in vivo studies. Nutr Metab (Lond) 5:20.
Recommended