Embed Size (px)
Citation preview

� ������������� ��� ������� � �� ���������������� � ����� � ������������ ������ �����������
�� ��!� �������"� �� ��#������$������ ��� ������� � �� ���������������� � ����� � �������% "��������&�#'����������#������$������(���(���(�$������"� �� ����# ������&�# � � ������"� �� ��#������$������ ��� ������� � �� ���������������� � ����
� � �������
) ���� by �� ��*�� � ������#������$
*� $���� ��'(��(����('� ���� ��������� �
Erupções vesicopustulosas benignas no neonato*
+� �����,-� ./����������� %
An Bras Dermatol. 2006;(4):359-66.
!� /���� ��
������� �������� ��'(��(����('� ������'� ���$��('����� �������/ �������� ����� ������(��/������� ���+������� � ���� '������(�� '�� � ����� ��� $�����������0(�(���� ��� � �� 0�� �� � ��� 1� �� ��� ��� � �'�� �0������� '����(���� #������$ ������(���0�0��������$� 2������('� ���3��������� �'�������3����� ����� ������������ �(������ ������� �$����������4�/������ ���5� ��� � � �5� 6�'�� � �'�15� 7�'� $�5� . ���(�� �� /5� ����� �5�/0����5���0 �
Resumo: As erupções vesicopustulosas neonatais compreendem um grupo de desordens quesurgem nas primeiras quatro semanas de vida. Apresentam extensa relação de diagnósti-cos diferenciais e, na maioria das vezes, podem ser identificadas clinicamente ou medianterecursos laboratoriais simples. Os dermatologistas devem reconhecer esses quadros cutâ-neos e, sobretudo, saber diferenciá-los de outras dermatoses graves e potencialmente fatais. Palavras-chave: Acne; Candidíase; Escabiose; Herpes simples; Impetigo; Literatura derevisão; Melanose; Recém-nascido
359
� ��������� 8� ��'(��(��� �('� ���� �� ������� �� ��
������ '� ��3� �� ��� �� ��� � ����9� /��� ��� � ���� ������ ����� ��� $��� �� ��1��� �������� �3� �'�� � $���� �� ������� ��� �� �� � ����� � �$0�/�� ���3� ��� ����� �'�������3� �� �'�� �$���� ��3� 0� $�� '(��(��� �('� ���� ����� �� �(����� ������� �$����� � �����
+�� � � �� ��(� ��� ��� � ����� '���� �$/ ����'(��(����('� ������(��� ���(������(��� ������3� ���(� �$� ��� ���'� �� ���� �(� �$� '�$����3�� ��� � ������ ��� �� �� � ������3� �� ���� ������ ����� ����� ��� $��� ���� $� ��� '����� ��0���� ��� ����� �� ���'����� ��� 0����� � ������� ��������� ��� '����� �� � �� ��'(��(���('� ��� �����������'� ��3��(������������� � �� ����'�� �3� .�$����� ���� � �� ������ �3 ����� ��� � ' $��� 3� ��'� ��(��$��0(� �� :
�������3� ��� ����� ����� ��'�'�� �� +������(�� ������ ������������(���'���'������� � � ���� ���� $�� ��� ������ �� �� ��(��� ��� �(����������� ���� ��(��� � $��� �3� ������3� ��'�����(�� ��������(��� �$��
�����'������� '� �������(����������������� '� ���� �� ��0(���(�� � ���� �� ��� ����/� ������0�'���� ������ �(�3��(�����' �������� �� 0(����3� '�'� $(�� �(�$� �3� ��'�� $��� �� �3������� � ������'�� �����(�� �� �' $������� ��� 0� ��(��� �� ���'���� �� ��(���� �(��� ������������6����
;�������(��� ������ ���0� ���������'����� ��'��� ���1� �� ���'������3���(� ��� $����� �������(������������ ��� ����������$��'���� �� ���0� '������3��(��� �� �+2���� ���3�$���� �3�4;6������ ��0 �'���/���������������0� ��

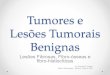
FIGURE 1: Erythema toxicum neonatorum
hing the diagnosis. The discussion below will provideinformation on history, physical and laboratory fin-dings to help distinguish between transient, benigndisorders, mild infections, and serious infectious con-ditions that can occur during the neonatal period.
I. NONINFECTIOUS NEONATAL PUSTULARERUPTIONS1. Erythema Toxicum Neonatorum
Erythema toxicum was originally described byBartholomaeus Melinger in 1472 and named erythe-ma toxicum neonatorum (ETN) by Leiner in 1912.2
ETN is a benign, self-limited condition of the neona-tal period which is very common in term infants, butrare in preterm infants and infants with less than2500g birth weight. It is seen in approximately one-third of all full term newborns.3 There is no racial pre-dilection and males and females are affected equally.In a recently published study, several predisposingfactors for ETN where identified such as female sex,term birth, first-pregnancy birth, birth season (sum-mer and autumn), and vaginal delivery.4
The skin lesions of erythema toxicum (Figure1) are asymptomatic red macules, papules, pustulesor wheals that can affect any area of the body andmost commonly present after 24 to 72 hours of life,but may begin from birth to 2 weeks of age.5 SinceETN is a short lasting dermatosis, prevalence reportsdiffer according to the time of life the neonate is exa-mined.6-10 The sites of predilection are the face,trunk, proximal arms and buttocks whereas palmand sole involvement is unusual. The lesions canlast several days and rarely persist for several weeks.Red macular areas and wheals range from a few mil-limeters to several centimeters with superimposed 1to 2mm papules and pustules. The lesions may befew in number but more often are present in largenumbers and often evolve with crops of waxing andwaning, with spontaneous resolution of individuallesions within hours to days. Cases of recurrent ETNhave been reported as well as cases with only focallesions.5,11,12 The etiology of erythema toxicum neo-natorum is unknown. Unproven causes include ato-pic diathesis, immediate sensitivity to allergens orresponse to thermal, mechanical or chemical stimu-li.13,14 Some authors suggest ETN is a graft versushost-like acute cutaneous reaction triggered bymaternal lymphocytes transferred immediately afterdelivery.5,15
Diagnosis is clinical and a Tzanck smear(Giemsa or Wright stain) of lesional content willreveal numerous eosinophils and confirm the clinicalsuspicion. Laboratory findings may include eosino-philia up to 18% in as many as 15% of the cases.11
KOH and bacterial culture are negative. A skin biopsyis usually unnecessary but if performed it revealsintrafollicular, subcorneal pustules with a dense accu-mulation of eosinophils, hence lack of palmo-plantar
360 de Araujo T, Schachner L.
An Bras Dermatol. 2006;(4):359-66.
CHART 1: Differential diagnosis
Non-infectious: benignAcropustulosis of infancyEosinophilic pustular folliculitisErythema toxicumMilliariaTransient neonatal pustular melanosis
Non-infectious: potentially seriousAcrodermatitis enteropathicaEpidermolysis bullosaEpidermolitic hyperkeratosisIncontinentia pigmentiLangerhans cell histiocytosisUrticaria pigmentosaHerpes gestationis-neonatalPemphigus vulgaris- neonatal
Infectious: usually mildCandidiasis-neonatalImpetigo neonatorumScabies
Infectious: seriousBacterial infections (Chlamydia, Escherichia coli, Hemophilus influenza, Klebsiella pneumoniae, Listeria Monocytogenes, Pseudomonas aeruginosa, Staphilococcus aureus, Streptococcus group A Beta hemolytic)SyphilisCandidiasis-congenitalStaphylococcal scalded skin syndromeViral infections (Cytomegalic, Herpes, Varicella)
RevABDV81N4.qxd 12.08.06 13:11 Page 360

An Bras Dermatol. 2006;(4):359-66.
lesions. Macular lesions show a perivascular eosino-philic infiltrate in the upper dermis.
The differential diagnosis should include tran-sient neonatal pustular melanosis, congenital candi-diasis, miliaria, bacterial infections, herpes simplexinfection, scabies, eosinophilic pustular folliculitisand acropustulosis of infancy. Erythema and onset at1 to 3 days of age may distinguish erythema toxicumfrom transient neonatal pustular melanosis, thoughboth are common and can occur simultaneously.Bacterial infections are usually due to Staphylococcusaureus, but occasional neonatal infections withgroup B Streptococcus, Pseudomonas aeruginosa,Listeria monocytogenes, Hemophylus influenzae andKlebsiella pnemoniae have occurred with pustules.The Gram stain will reveal organisms and the Tzancksmear of all conditions above will reveal predominantneutrophils. Transient neonatal pustular melanosiswill show neutrophil predominance as well.Candidiasis may be differentiated on the basis of apositive potassium hydroxide preparation. Miliariamay be excluded on the basis of its extrafollicularlocation and the presence of lymphocytes on Wrightstain.
Erythema toxicum is self limiting and no treat-ment is necessary other than reassurance to the pa-rents.
2. Transient Neonatal Pustular MelanosisTransient neonatal pustular melanosis (TNPM)
was first described by Ramamurthy in 1976. The inci-dence varies from 0.16 to 15% and the disorder ismore common in black infants.16,17 In Brazil TNPM hasbeen estimated to occur in 9.57% of the newborns.10It is a benign condition of term neonates, characteri-zed by the presence at birth of pustules or vesicles
without surrounding erythema (Figure 2). These vesi-copustules rupture easily, with subsequent formationof pigmented macules that are characteristically sur-rounded by a collarette of scale. These macules maypersist for months but usually fade spontaneouslywithin 3 to 4 weeks. Most commonly affected areasinclude the forehead, posterior ears, chin, neck,upper chest, back, buttocks, abdomen, and thighs,but all areas may be affected, including the palms andsoles. Purely macular forms may indicate an intraute-rine vesico-pustular eruption whereas the vesicle-pus-tular component has resolved in utero.1 The cause ofTNPM is unknown. Genetic influence seems unlikesince the condition has been reported in only one ofidentical twins.18
Wright or Giemsa staining of the pustular con-tents show neutrophils and occasional eosinophils.No organisms are observed and bacterial and viralcultures are negative.19 Skin biopsy shows intracor-neal or subcorneal pustules. The differential diagno-sis is the same as for erythema toxicum neonatorum.No treatment is necessary.
3. Acropustulosis of infancyAcropustulosis of infancy, or infantile acropus-
tulosis is a chronic or recurrent benign condition ofvery pruritic vesicles and pustules occurring on thehands and feet (Figure 3). It was first described in1979 by Kahn and Rywlin and by Jarret and Ramsdell,and its etiology is unknown and it affects primarilyblack boys.20 The condition may begin during the neo-natal period and continue throughout infancy andearly childhood. Infants and children often presentwith severe prutitus, sleep disturbance, fretfulnessand appetite loss. Clinical manifestations are limitedto the skin, and affected neonates are healthy other-
FIGURE 2: Transient neonatal pustular dermatosis FIGURE 3: Acropustulosis of infancy
Benign vesicopustular eruptions in the neonate 361
RevABDV81N4.qxd 12.08.06 13:11 Page 361

An Bras Dermatol. 2006;(4):359-66.
wise. Cutaneous lesions consist of vesicopustuleswithout surrounding erythema characteristicallyinvolving palms, soles, dorsal hands and feet, andsides of fingers and toes. Crops of lesions may appearin cycles of two to four weeks, with individual lesionslasting three to seven days. The number of lesions isgreatest in the early episodes, becoming less withsubsequent episodes until permanent resolutionoccurs at 2 to 3 years of age.
The etiology remains unknown. Theories sug-gest a reaction pattern in predisposed individuals toinfection or infestation. A history of scabies precedingthe diagnosis of infantile acropustulosis is frequentlyobtained but rarely documented.
Laboratories studies are usually normal, butperipheral eosinophilia has been reported.1,20
A Tzanck smear or Gram’s stain of pustularcontents reveals numerous neutrophils, occasionaleosinophils and no bacteria. Skin biopsy showsintraepidermal or subcorneal pustules filled withneutrophils or eosinophils. Focal vesiculation anddegeneration of keratinocytes with cell necrosis mayalso be seen.
The main differential diagnosis is scabies andmultiple skin scrapings are necessary to rule outactive infestation. Careful examination of patientswith a history of “scabies” have overwhelmingly fai-led to actually confirm infestation.21 Smears forGram and Wright stains, and a potassium hydroxide(KOH) preparations should help eliminate candidia-sis, impetigo, varicella, and herpes simplex infec-tion. Erythema toxicum and transient neonatal pus-tular melanosis may be confused, but both areasymptomatic and transient conditions making thedifferentiation easier.
Acropustulosis of infancy will remit sponta-neously over one or two years. Treatment with potenttopical corticosteroids is usually succesfull for controlof outbreaks. Oral antihistamines may provide reliefof itching in older infants but are contraindicated inneonates because of the undesirable side effect ofsedation. In severe cases dapsone at a dose of 1 to2mg/kg/day may be effective, however this therapyshould be reserved for severe cases unresponsive topotent topical steroids. Baseline glucose-6-phosphatedehydrogenase (G6PD) levels and close monitoringof complete blood cell counts and platelets areappropriate as well as clinical assessment for methe-moglobinemia, fever, jaundice, pallor or purpura.
4. Neonatal AcneNeonatal acne, or neonatal cephalic pustulosis,
has been described as usually beginning at a fewweeks of life and manifested by multiple, inflamma-tory, erythematous papules, comedones and pustules
on the nose forehead and cheeks.22 Although the etio-logy is not clearly defined, neonatal acne appears toresult from stimulation of sebaceous glands by mater-nal and infant androgens. The involvement ofMalassezia spp in the etiopathogenesis has been sug-gested in recent reports.23-25 Lesions spontaneouslyresolve within 1 to 3 months as the sebaceous glandsinvolute, and scarring is absent. Acne initiating at 18months of age versus 18 days is much more worriso-me regarding adrenal-genital-pituitary pathology.Most cases of neonatal acne do not require treatment.Benzoyl peroxide 2.5% lotion or erythromycin 2%solution are safe alternatives.
5. MiliariaMiliaria is a term used to describe obstruc-
tions of the eccrine duct resulting in rupture of theducts and blockage of normal sweating into theskin. The level of obstruction determines the clini-cal manifestations. It can be seen in up to 15% ofneonates, occurring more commonly in warm cli-mates, in nurseries without air-conditioning and infebrile infants.
Miliaria crystalina (sudamina) is the mostcommon type of miliaria and is manifested byminute, non-inflammatory vesicles without sur-rounding erythema. These lesions are asymptoma-tic, superficial and may appear like dewdrops onthe skin. Commonly affected sites include the fore-head and upper trunk. Miliaria crystalina repre-sents rupture of the eccrine duct at the level of thestratum corneum.
Miliaria rubra (prickly heat) is due to intraepi-dermal obstruction of the sweat duct with sweat lea-kage into the duct and a secondary local inflammatoryresponse. Lesions are 1-3mm erythematous, non-folli-cular papules, vesicles or pustules. Common sitesinclude the face, neck and trunk. Miliaria rubraoccurs later than miliaria crystalina, usually beyondthe second week of life. Occasionally it can progressto pustular lesions (miliaria profunda), most promi-nent on the trunk and extremities, and reflects eccri-ne ductal occlusion at the dermo-epidermal junction.Miliaria profunda is rare in neonates.
The diagnosis of miliaria is made by clinicalobservation. The precise cause is unknown. There issome support for an extracellular polysaccharidesubstance produced by some strains ofStaphylococcus epidermidis being involved in sweatduct obstruction and poral occlusion by epidermalcellular edema may be an initial event.
The use of very thick emollients can result in amiliaria profunda picture in infants, especially thosewith atopic dermatitis.
362 de Araujo T, Schachner L.
RevABDV81N4.qxd 16.08.06 15:32 Page 362

An Bras Dermatol. 2006;(4):359-66.
6. Eosinophilic pustular folliculitisEosinophilic pustular folliculitis (or eosinophi-
lic pustulosis) was first described in adults by Ofugi etal and in infants by Lucky et al in 1984.26 It may pre-sent at birth or in the first few days of life with yello-wish pustules predominantly on the scalp and face,but also trunk and extremities. The pustules generallycrust within two or three days of onset and may recurin crops.27 The waxing and waning course of thedisease may last for several years. Pruritus and irrita-bility in younger infants is common.
A Tzanck smear or Gram’s stain of the pustularcontents demonstrates numerous eosinophils. Somepatients have eosinophilia as well as leukocytosis onblood counts obtained during outbreaks. Biopsy spe-cimens of the pustules show eosinophils and eosino-philic spongiosis in the epidermis, with a dense der-mal perifollicular infiltrate of eosinophils, histiocytes,and lymphocytes. Cultures for bacteria, fungus, andviruses are all negative.28
The etiology is unknown. It has been suggestedthat it may represent a more persistent form of ery-thema toxicum neonatorum, based on histopatholo-gic similarities. Differential diagnosis includes scalppyoderma, erythema toxicum, transient neonatal pus-tular melanosis, acropustulosis of infancy, bacterial orfungal folliculitis, scabies, candidiasis, andLangerhans cell histiocytosis. The clinical presenta-tion, location, and histology of these lesions allow dif-ferentiation from all these entities.
A persistent generalized, non-remitting EPF hasbeen seen in infants with severe AIDS and is conside-red a marker of worse prognosis.
Treatment is moderately successful with low ormid-potency topical corticosteroids and/or antibiotictherapy. Antihistamines may be helpful in controllingpruritus. Other therapies that may be useful includedapsone, oral cimetidine and systemic prednisone.
II. INFECTIOUS NEONATAL PUSTULAR ERUPTIONSII.a. Bacterial Infections
1. Impetigo BullosaImpetigo bullosa is characterized by flaccid
vesicles, pustules or bullae on erythematous basesthat rupture easily leaving a narrow rim of scale at theedge of a moist erosion. It may appear as early as thesecond or third day of life. These lesions re-epithelia-lize rapidly and do not result in scars. The diaper areaand folds of the skin are commonly involved.
Certain strains of Staphylococcus aureus(Phage group II, lysotypes 3A, 3C, 55 or 71) have theability to produce an exfoliative exotoxin which cau-ses bullous impetigo. When the toxins enter the syste-mic circulation, there is potential for generalizedinvolvement of the skin, also called staphylococcal
scalded skin syndrome.29 Staphylococcal scalded skinsyndrome lesions have a negative Gram stain butoften bacterial cultures are positive.
Diagnosis of impetigo is easily made by Gram’sstain of a pustule, which reveals neutrophils andGram- positive cocci in clusters. Bacterial culturesconfirm the diagnosis.
Localized infections can be treated with a topi-cal antibiotic such as mupirocin or fucidic acid. Morewidespread lesions require systemic therapy.
2. Other bacterial infectionsBacterial infections can be acquired prenatally,
during delivery, or after birth. Group B beta-hemoly-tic streptococcus, Listeria monocytogenes,Hemophilus influenza and Pseudomonas aeruginosaare bacterial pathogens that may produce pustulesand sepsis in the neonate.
IIb. Viral infections1. Herpes simplex infection (HSV)Approximately 5% of neonatal HSV is a truly
intrauterine infection, resulting in a baby infected atbirth.1 Since the primary period of viral inoculation isintrapartum, and given the variable incubation time,neonatal HSV may be present any time in the first 4 to6 weeks of life. Up to one quarter of infected neona-tes will have signs of infection on the first day of life.30
Most (70%) neonatal herpes simplex virus aredue to HSV type 2. HSV-2 may be acquired by the neo-nate transplacentally, by viremia during gestation,intranatally by passage through an infected birth canal,or postnatally by direct contact with infected humans.About 16% to 30% of women in the United States areseropositive for HSV-2, and 0.3% to 2% of womenshed HSV from the vagina at the time of delivery.
The initial symptoms of disseminated HSVinfection are lethargy, hypo- or hyperthermia, irritabi-lity and poor feeding. Cutaneous findings are the firstvisible sign in about two-thirds of neonates infectedwith HSV. Grouped or single vesicles or pustules onerythematous bases appear in crops on the skin andmucous membranes. The eyes may also be affected.Neonatal herpes may spread quickly to involve thecentral nervous system and/or multiple internalorgans. The neonate’s condition may deterioraterapidly, therefore prompt and accurate diagnosis ismore than desirable.
A Tzanck smear of vesicles bases reveal multi-nucleated giant epithelial cells, indicating a herpeticinfection. Viral culture and direct immunofluorescen-ce testing may be used to confirm the diagnosis.Biopsy specimens reveal an intraepidermal vesicleproduced by ballooning and reticular degeneration ofepidermal cells. Marked acantholysis is present.
Benign vesicopustular eruptions in the neonate 363
RevABDV81N4.qxd 16.08.06 15:32 Page 363

An Bras Dermatol. 2006;(4):359-66.
wise. Cutaneous lesions consist of vesicopustuleswithout surrounding erythema characteristicallyinvolving palms, soles, dorsal hands and feet, andsides of fingers and toes. Crops of lesions may appearin cycles of two to four weeks, with individual lesionslasting three to seven days. The number of lesions isgreatest in the early episodes, becoming less withsubsequent episodes until permanent resolutionoccurs at 2 to 3 years of age.
The etiology remains unknown. Theories sug-gest a reaction pattern in predisposed individuals toinfection or infestation. A history of scabies precedingthe diagnosis of infantile acropustulosis is frequentlyobtained but rarely documented.
Laboratories studies are usually normal, butperipheral eosinophilia has been reported.1,20
A Tzanck smear or Gram’s stain of pustularcontents reveals numerous neutrophils, occasionaleosinophils and no bacteria. Skin biopsy showsintraepidermal or subcorneal pustules filled withneutrophils or eosinophils. Focal vesiculation anddegeneration of keratinocytes with cell necrosis mayalso be seen.
The main differential diagnosis is scabies andmultiple skin scrapings are necessary to rule outactive infestation. Careful examination of patientswith a history of “scabies” have overwhelmingly fai-led to actually confirm infestation.21 Smears forGram and Wright stains, and a potassium hydroxide(KOH) preparations should help eliminate candidia-sis, impetigo, varicella, and herpes simplex infec-tion. Erythema toxicum and transient neonatal pus-tular melanosis may be confused, but both areasymptomatic and transient conditions making thedifferentiation easier.
Acropustulosis of infancy will remit sponta-neously over one or two years. Treatment with potenttopical corticosteroids is usually succesfull for controlof outbreaks. Oral antihistamines may provide reliefof itching in older infants but are contraindicated inneonates because of the undesirable side effect ofsedation. In severe cases dapsone at a dose of 1 to2mg/kg/day may be effective, however this therapyshould be reserved for severe cases unresponsive topotent topical steroids. Baseline glucose-6-phosphatedehydrogenase (G6PD) levels and close monitoringof complete blood cell counts and platelets areappropriate as well as clinical assessment for methe-moglobinemia, fever, jaundice, pallor or purpura.
4. Neonatal AcneNeonatal acne, or neonatal cephalic pustulosis,
has been described as usually beginning at a fewweeks of life and manifested by multiple, inflamma-tory, erythematous papules, comedones and pustules
on the nose forehead and cheeks.22 Although the etio-logy is not clearly defined, neonatal acne appears toresult from stimulation of sebaceous glands by mater-nal and infant androgens. The involvement ofMalassezia spp in the etiopathogenesis has been sug-gested in recent reports.23-25 Lesions spontaneouslyresolve within 1 to 3 months as the sebaceous glandsinvolute, and scarring is absent. Acne initiating at 18months of age versus 18 days is much more worriso-me regarding adrenal-genital-pituitary pathology.Most cases of neonatal acne do not require treatment.Benzoyl peroxide 2.5% lotion or erythromycin 2%solution are safe alternatives.
5. MiliariaMiliaria is a term used to describe obstructions
of the eccrine duct resulting in rupture of the ductsand blockage of normal sweating into the skin. Thelevel of obstruction determines the clinical manifesta-tions. It can be seen in up to 15% of neonates, occur-ring more commonly in warm climates, in nurserieswithout air-conditioning and in febrile infants.
Miliaria crystalina (sudamina) is the mostcommon type of miliaria and is manifested byminute, non-inflammatory vesicles without sur-rounding erythema. These lesions are asymptoma-tic, superficial and may appear like dewdrops onthe skin. Commonly affected sites include the fore-head and upper trunk. Miliaria crystalina repre-sents rupture of the eccrine duct at the level of thestratum corneum.
Miliaria rubra (prickly heat) is due to intraepi-dermal obstruction of the sweat duct with sweat lea-kage into the duct and a secondary local inflammatoryresponse. Lesions are 1-3mm erythematous, non-folli-cular papules, vesicles or pustules. Common sitesinclude the face, neck and trunk. Miliaria rubraoccurs later than miliaria crystalina, usually beyondthe second week of life. Occasionally it can progressto pustular lesions (miliaria profunda), most promi-nent on the trunk and extremities, and reflects eccri-ne ductal occlusion at the dermo-epidermal junction.Miliaria profunda is rare in neonates.
The diagnosis of miliaria is made by clinicalobservation. The precise cause is unknown. There issome support for an extracellular polysaccharidesubstance produced by some strains ofStaphylococcus epidermidis being involved in sweatduct obstruction and poral occlusion by epidermalcellular edema may be an initial event.
The use of very thick emollients can result in amiliaria profunda picture in infants, especially thosewith atopic dermatitis.
6. Eosinophilic pustular folliculitis
362 de Araujo T, Schachner L.
RevABDV81N4.qxd 12.08.06 13:11 Page 362

An Bras Dermatol. 2006;(4):359-66.
Multinicleated cells and eosinophilic inclusion bodiescan be seen.
If left untreated, disseminated HSV infection isfatal in many cases. Although it has been demonstra-ted that vidarabine is as effective as acyclovir in theHSV-infected neonate, most experts utilize acyclovirin these patients because of relative ease of adminis-tration.
If active genital herpetic lesions are present ina pregnant woman at the time of labor, a cesarean sec-tion is recommend if the fetal membranes have beenruptured for less than 6 hours. Prevention is the besttreatment, and newborns should be protected fromexposure to HSV whenever possible.
IIc. Fungal Infections 1. CandidiasisCandida infection can be divided in two forms,
congenital and neonatal. Congenital candidiasis is anintrauterine infection, while neonatal candidiasis isacquired as the infant passes through a contaminatedbirth canal. In both forms the causative organism isCandida albicans, a pathogen found in the vaginalcanal of 20 to 25% of pregnant women. A possibleway in which intrauterine infection may occur is byCandida organisms ascending via the vagina andcrossing ruptured or intact fetal membranes.
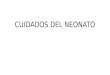
In congenital candidiasis lesions are present atbirth or usually within 12 hours following delivery(Figure 4). The rash is usually diffusely scattered overthe whole body, including the face, chest, back andextremities. Oral and diaper area involvement is gene-rally absent. The congenital form usually starts as ery-thematous macules and vesicles, which quickly evolveinto pustules. A pronounced desquamation followsthe acute phase with exfoliated crusted lesions. Signs
of systemic disease and hematologic abnormalitiesare generally absent.30
Neonatal candidiasis is usually seen after theseventh day of life, occurring as oral trush and pustu-les and vesicles with satellite lesions confined to thediaper area. The intergluteal and cervical folds(Figure 5), perineum, genitalia, suprapubic area, but-tocks, and inner thighs are frequently involved. Inthese areas candidiasis evolves into scaling, bright redplaques, with distinct pustular and vesicular satellitelesions at the periphery. Constitutional symptoms areabsent. In neonatal candidiasis, C. albicans can oftenbe isolated from the feces.
Diagnosis of candidiasis is made by findingpseudohyphae and spores with a potassium hydroxi-de preparation of a pustule or scale and confirmed bya fungal culture.
Candidiasis is treated topically with imidazolederivatives, such as miconazole, clotrimazole, or keto-conazole cream. Lesions last approximately 2 weeks,desquamate and resolve without residua. Trush istreated by oral nystatin.
Disseminated systemic candidiasis may occurrarely and is primarily an infection of preterm, lowbirth weight infants, immunologically compromisedpatients, and neonates requiring intensive care withinvasive procedures. It may affect the lungs, menin-ges, kidneys, bladder, joints, and less commonly theliver, heart and eyes. Disseminated candidiasis is asso-ciated with significant morbidity and mortality. Thespreading of a candidal diaper rash to the trunk andextremities should alert the clinician to the possibilityof dissemination of infection. Intermittent fever thatis resitant to anti pyretics, with cutaneous candidallesions or cellulitis at the site of an intravenous cathe-ter, and persistent candidemia or candiduria, even in
364 de Araujo T, Schachner L.
FIGURE 5: Neonatal candidiasisFIGURE 4: Congenital candidiasis
RevABDV81N4.qxd 12.08.06 13:11 Page 364

An Bras Dermatol. 2006;(4):359-66.
the absenceof skin findings or systemic symptoms,indicate the presence of disseminated disease.
Confirming the diagnosis of suspected dissemi-nated candidiasis is difficult. Widespread infectiondespite negative cultures is common. The diagnosis isconfirmed by isolating Candida albicans from blood,abscesses, urine, or other body fluids, or by demons-tration of the organism in a cutaneous biopsy. Theearly institution of treatment is the critical prognosticfactor. Amphotericin B or 5-flucytosine intravenouslyare the drugs of choice. The use of these medicationsrequires careful monitoring of side effects. The pre-term infant may suffer a devastatingly lethal candidalscalded skin syndrome.
2. Ptyrosporum folliculitisPityrosporum yeasts (Malassezia furfur) are
the cause of pityriasis versicolor, which is usually seenas a disorder of adolescents and young adults, butmay be a very rare cause of folliculitis in neonates.Cutaneous lesions consist of follicular papules andsparse pustules on the face and scalp. The diagnosisis based on a positive KOH and culture of pustularcontents. Treatment is achieved with topical imidazo-le derivatives such as miconazole, clotrimazole, orketoconazole cream.
II.c Parasitic Infections1. ScabiesScabies is a contagious disorder caused by
Sarcoptes scabiei, a parasitic mite, which invades thestratum corneum. After an incubation period of 2 to 6weeks, an extremely pruritic rash develops. If theinfestation occurs soon after the delivery, the disordermay be seen in the neonate.
Scabies is a distinct clinical eruption characte-rized by pruritic papules, vesicles, and linear bur-rows mixed with excoriations, eczematization, crus-ting, or secondary infection. The clinical pattern of
scabies in newborns differs from that seen in olderinfants, children, and adults. In older children andadults most of the lesions are concentrated on thefinger webs, wrist, axillae, arm flexure, beltline, peri-neum and genitals. In infants and young children theinfestation rapidly becomes more generalized, usual-ly involving the palms, soles, head, neck and face.Vesicles are common in neonates, and there is a ten-dency for pustule formation early in the course of theinfestation. Irritability, poor feeding, and failure togain weight are also quite characteristic. A careful his-tory and examination of the baby’s caretakers willfrequently disclose a history or pruritus and/or typi-cal scabies lesions. Frequent maternal sites are peria-reolar regions of the breasts, as well as the wrists andfingers.
Definitive diagnosis is made by microscopicexamination of scrapings from unexcoriated lesionsin a mineral oil preparation. The presence of adultmite, ova, larva or stool confirms the diagnosis.
The treatment of choice is permethrin 5%cream applied from head to toes for 6 hours. Whenpermethrin cream is not available, neonates can alsobe treated with 5% sulfur in petrolatum. Sulfur-con-taining preparations are messy, staining, and malodo-rous, and must be applied for three nights. It’s crucialto treat all family members and other caretakers at thesame time and launder clothing and bedding in hightemperature water. It’s important to differentiatenodular neonatal scabies from hystiocytosis X, whichit can simulate clinically.
CONCLUSIONSPustular eruptions in the neonate can have
many clinical presentations and significance. Simplediagnostic methods can aid in differentiating betweenthem, and most importantly, in separating transient,benign pustular eruptions from serious and life-threa-tening conditions. �
Benign vesicopustular eruptions in the neonate 365
ACKNOWLEDGEMENTClinical picture of this article have been
provided by Luciana Pereira, MD and BernardoGontijo, MD.
RevABDV81N4.qxd 12.08.06 13:11 Page 365

An Bras Dermatol. 2006;(4):359-66.
MAILING ADDRESS:Lawrence SchachnerPO Box 016250 (R 250) - Miami Fl 33101Phone: (305)243-6742 - Fax: (305)243-6191E-mail: [email protected]
REFERENCES1. Schachner L, Hansen RC. Pediatric Dermatology. 3rd
ed. Philadelphia: Mosby; 2003.2. Carr JA, Hodgman JE, Freedman RI, Levan NE.
Relationship between toxic erythema and infant maturity.Am J Dis Child. 1966;112:129-34.
3. Rahm S. Erythema toxicum neonatorum. Pediatr Dermatol. 2001;18:177-87.
4. Liu C, Feng J, R Qu, Zhou H, Ma H, Niu X, et al. Epidemiologic study of the predisposing factors inerythema toxicum neonatorum. Dermatology. 2005; 210:269-72.
5. Chang MW, Jiang SB, Orlow SJ. Atypical erythema toxicumneonatorum of delayed onset in a term infant. Pediatr Dermatol. 1999;16:137-41.
6. Desmons F, Chevillard Y. Fréquence des diversesdermatoses du nuveau-né et du nourrisson pendant les dix premiers jours de la vie. Bull Soc Fr Dermatol Syphiligr. 1974;81:169-258.
7. Nascimento LV, Rozo EM, Yarak S, Coimbra SD, Porto JA. Prevalência de dermatoses em recém-nascidos no berçário de um hospital universitário. An Bras Dermatol. 1992;67:305-7.
8. Osburn K, Schosser RH, Everett MA. Congenitalpigmented and vascular lesions in newborn infants. J Am Acad Dermatol. 1987;16:788-92.
9. Rohr JB. The skin of the newborn. Aust J Dermatol. 1975;16:118-20.
10. Pereira LB. Prevalência de dermatoses no recém-nascido: estudo comparativo entre dois hospitais de Belo Horizonte, Brasil [tese]. Belo Horizonte (MG): Universidade Federal de Minas Gerais; 1997.
11. Van Praag MC, Van Rooij RW, Folkers E, Spritzer R, Menke HE, Oranje AP. Diagnosis and treatment ofpustular eruptions in the neonate. Pediatr Dermatol. 1997;14:131-43.
12. Schwartz RA, Janniger CK. Erythema toxicumneonatorum. Cutis. 1996;58:153-5.
13. Maffei FA, Michaels MG, Wald ER. An unusal presentationof erythema toxicum scrotal pustules. Arch Pedatr Adolesc Med. 1996;150:649-50.
14. Berg FJ, Solomon LM. Erythem neonatorum toxicum. Arch Dis Child. 1987;62:327-8.
15. Schwartz RA, Janniger CK. Erythema toxicum neonatorum.Cutis. 1996;58:153-5.
16. Barr RJ, Globerman LM, Weber FA. Transient neonatal pustular melanosis. Int J Dermatol. 1979;18:636-8.
17. Fox JN, Walton RG, Gottlieb B. Pigmented skin lesions in black newborn infants. Cutis. 1979;24:399-402.
18. Merlob P, Metzker A, Reisner SH. Transient neonatal pustular melanosis. Am J Dis Child. 1982;136:521-2.
19. Chabrolle JP, Le Luyer B. Vésiculo-pustules et mélanose transitory du neouveau-né: une affection bénigne. Ann Pediatr. 1987;34:169-70.
20. Newton JA, Salisbury J, Marsden A, McGibbon DH. Acropustulosis of infancy. Br J Dermatol. 1986;115:735-9.
21. Mancini AJ, Frieden IJ, Paller AS. Infantile acropustulosisrevisited: history of scabies and response to topical
corticosteroids. Pediatr Dermatol. 1998;15:337-41.22. Mengesha YM, Bennett ML. Pustular skin disorders.
Am J Clin Dermatol. 2002;3:389-400.23. Rapelanoro R, Mortureux P, Couprie B, Maleville J,
Thaieb A. Neonatal Malassezia furfur pustulosis. Arch Dermatol. 1996;132:190-3.
24. Niamba P, Weill FX, Sarlangue J, Labreze C, Couprie B, Thaieb A. Is common neonatal cephalic pustulosis (neonatal acne) triggered by Malassezia sympodalis? Arch Dermatol. 1998;134:995-8.
25. Bernier V, Weill FX, Hirigouyen V, Eleau C, Feyler A, Labreze C, et al. Skin colonization by Malassezia species in neonates. A prospective study and relationship with neonatal cephalic pustulosis. Arch Dermatol. 2002;138:215-8.
26. Lucky AW, Esterly NB, Heskel N, Krafchik BR, Solomon LM. Eosinophilic pustular folliculitis in infancy. Pediatr Dermatol. 1984;1:202-6.
27. Buckely DA, Munn SE, Higgins EM. Neonatal eosinophilic pustular folliculitis. Clin Exp Dermatol. 2001;26:251-5.
28. Duarte AM, Kramer J, Yusk JW, Paller A, Schachner LA. Eosinophilic pustular folliculitis in infancy andchildhood. Am J Dis Chil. 1993;147:197-200.
29. Amagai M, Matsuyoshi N, Wang Z, Andl C, Stanley J. Toxins in bullous impetigo and staphylococcal scalded-skin syndrome targets desmoglein1. Nature Med. 200;6:1275-7.
30. Conlon JD, Drolet BA. Skin lesions in the neonate. Pediatr Clin North Am. 2004;51:863-88.
How to cite this article: de Araujo T, Schachner L. Benign vesicopustular eruptions in the neonate. An Bras Dermatol.2006;81(4):359-66.
366 de Araujo T, Schachner L.
RevABDV81N4.qxd 12.08.06 13:11 Page 366