Embed Size (px)
Citation preview

DOUTORADO EM ODONTOLOGIA ÁREA DE CONCENTRAÇÃO EM PERIODONTIA
Maria Josefa Mestnik
ADMINISTRAÇÃO SISTÊMICA DE AMOXICILINA E METRONIDAZOL ASSOCIADA À RASPAGEM E
ALISAMENTO RADICULAR EM INDIVÍDUOS COM PERIODONTITE AGRESSIVA GENERALIZADA:
AVALIAÇÃO LONGITUDINAL
Guarulhos 2012

Maria Josefa Mestnik
ADMINISTRAÇÃO SISTÊMICA DE AMOXICILINA E
METRONIDAZOL ASSOCIADA À RASPAGEM E ALISAMENTO RADICULAR EM INDIVÍDUOS COM
PERIODONTITE AGRESSIVA GENERALIZADA: AVALIAÇÃO LONGITUDINAL
Tese apresentada à Universidade Guarulhos para obtenção do título de Doutor em Odontologia
Área de Concentração: Periodontia Orientador : Prof. Dr. Marcelo de Faveri
Co-orientadora: Profa. Dra. Magda Feres
Guarulhos 2012

Ficha catalográfica elaborada pela Coordenação da Biblioteca Fernando Gay da Fonseca
MESTNIK, Maria Josefa M586a Administração sistêmica de amoxicilina e metronidazol
associada à raspagem e alisamento radicular em indivíduos com periodontite agressiva generalizada: avaliação longitudinal / Maria Josefa Mestink. Guarulhos, 2012.
86 f. : il. ; 31 cm Dissertação (Doutorado em Odontologia) - Centro de pós-
graduação e Pesquisa, Universidade Guarulhos, 2012. Orientador: Prof. Dr. Marcelo de Faveri
Bibliografia: 86 f. 1. periodontite agressiva generalizada, 2. amoxicilina, 3.
metronidazol, 4. clorexidina. 5. terapia periodontal I. Título. II. Universidade Guarulhos.
CDD 22st 617.6


Dedico este trabalho inteiramente aos meus pais Joze e Maria que tenho certeza estão sempre
vibrando por mim, sinto-os latentes em meu ser em todos os momentos da minha vida!

Agradecimentos
Agradeço a Deus pela vida, pela grande oportunidade de estar aqui interagindo, compartilhando experiências, aprimorando-me no vasto mundo da ciência!! Aos meus pais, que continuem a jornada com fé, envoltos na Luz e no Amor do Pai Maior! Saudade! À minha pequena GRANDE família, Jose, João e Antonio, companheiros, tutores, protetores que me apoiam e incentivam sempre! Obrigada por me darem as irmãs Sonia e Carla que torcem pela minha felicidade e sucesso e pelos sobrinhos: Yuri, Kátia, Natália e Helio por me proporcionarem a alegria de ser tia e me sentir tão amada!! Amo vocês!!! Maria de Fátima e Débora,vocês são meu apoio na transição diária entre a vida acadêmica e a clínica. Não encontro palavras para agradecer a dedicação e carinho com que cuidaram dos meus pais e hoje da casa e consultório! Retribuo pedindo a benção de Deus!! Aos meus amigos que entenderam a minha ausência, me enviaram palavras e mensagens de incentivo sempre, me aguardem nos próximos aniversários, shows, casamentos, viagens, etc...!! Sinto-me privilegiada por tudo o que a vida me proporcionou até hoje!! Nestes anos então, nesta universidade, minha família aumentou: 2 filhas, 4 irmãos, 1 irmã e muitos, muitos amigos!!! Gostaria de mencionar todos, mas preciso ser breve. Meu orientador professor Dr. Marcelo de Faveri, outro irmão que a vida me deu! Obrigada por despertar a pesquisadora em mim, mostrando-me o fantástico mundo pelo qual me apaixonei! E por me conduzir com paciência e confiança. Admiro-o como pessoa, professor e pesquisador! À professora Dra. Magda Feres, minha admiração! Tenho muito orgulho em fazer parte de uma equipe que realiza um trabalho com tamanha competência e seriedade! Ao professor Dr. Jamil Shibli, sinônimo de conhecimento e competência! Agradeço todas as oportunidades e incentivo dados durante esses anos do meu ingresso na vida acadêmica. À professora Dra. Luciene Figueiredo, sempre comandando tudo com delicadeza e firmeza! Aprendi muito ao seu lado!!

À professora Dra. Poliana Duarte, sempre amiga, solícita, um grande exemplo de mestre, orientadora, pesquisadora! Admiro-a muito!! Aos professores Drs. do Centro de Pós-Graduação Marta Bastos, Cláudia Ota, Alessandra Acassoni, André Reis, José Augusto Rodrigues e Cézar Arrais que nos passaram o prazer de ensinar! Joyce e Geisla, filhas queridas que Deus me trouxe neste período de tantas alegrias e tristezas! Obrigada pela companhia, carinho, amor, etc... Vanessa, grande amiga que admiro e quero muito bem!! Kelly mesmo sempre ocupada, é amável quando nos encontramos e trocamos algumas palavras! Diogo, Antonio Carlos, Ennyo e Diego, o clube do Bolinha da turma! Vocês são muito divertidos! Rafael e Eduardo, irmãos e companheiros no mundo acadêmico que me mostraram que podemos realizar um trabalho com competência, de forma descontraída e alegre! Obrigada pelo apoio, confiança e pela orientação na informática. Eisla e Daiane, minhas pupilas dedicadas! Vocês estão no caminho certo, associando a prática ao conhecimento! Sucesso! Obrigada Felipe, por nos acalmar nos momentos mais atribulados, com sua tranquilidade e ser sempre tão prestativo! Jadson, irmão do coração, Tamires, Tiago e Thais que bom ter a companhia de vocês na clínica!! À Cinthia Lobo, irmã gêmea, quanta afinidade! Só Deus explica! À Izilvânia Barreto cuja amizade foi fortalecida com a dor da perda, na troca de consolo e saudade!! À Cristina Zoucas, sempre prestativa e carinhosa, resolve todos os nossos problemas burocráticos! À Regina L. da Silva e colegas que deixam tudo limpo e em ordem para que possamos trabalhar com segurança. Aos pacientes que colaboraram para que este trabalho pudesse ser realizado e agradeço a oportunidade de proporcionar-lhes o tratamento que necessitam e não têm condições financeiras para cuidarem da saúde bucal. Muito obrigada, e que Deus abençoe a todos!!!

EU ESCOLHO COMO SERÁ MEU DIA!!!!!
"Hoje levantei cedo pensando no que tenho a fazer antes que o relógio marque meia
noite. É minha função escolher que tipo de dia vou ter hoje. Posso reclamar porque está
chovendo ou agradecer às águas por lavarem a poluição. Posso ficar triste por não ter
dinheiro ou me sentir encorajado para administrar minhas finanças, evitando o
desperdício. Posso reclamar sobre minha saúde ou dar graças por estar vivo. Posso me
queixar dos meus pais por não terem me dado tudo o que eu queria ou posso ser grato
por ter nascido. Posso reclamar por ter que ir trabalhar ou agradecer por ter trabalho.
Posso sentir tédio com o trabalho doméstico ou agradecer a Deus. Posso lamentar
decepções com amigos ou me entusiasmar com a possibilidade de fazer novas
amizades. Se as coisas não saíram como planejei posso ficar feliz por ter hoje para
recomeçar. O dia está na minha frente esperando para ser o que eu quiser. E aqui
estou eu, o escultor que pode dar forma. Tudo depende só de mim."
Charles Chaplin

RESUMO
O objetivo do presente estudo duplo-cego, placebo controlado e randomizado foi avaliar
os efeitos clínicos da raspagem e alisamento radicular (RAR) isoladamente ou em
combinação com metronidazol (MTZ) e amoxicilina (AMX) no tratamento de indivíduos
com periodontite agressiva generalizada (PAG). Foi realizado em 30 indivíduos com
PAG que receberam RAR isoladamente (n=15) ou combinada com antibióticos (n=15;
400mg MTZ e 500mg AMX três vezes ao dia durante 14 dias). Todos os indivíduos
receberam instrução de higiene oral incluindo o uso de enxaguatório bucal contendo
clorexidina 0,12% duas vezes ao dia durante 2 meses. Avaliações clínicas foram
realizadas no momento inicial, aos 6 e 12 meses pós-terapia. Ambos os grupos
apresentaram melhora em todos os parâmetros clínicos 6 e 12 meses após a terapia.
Indivíduos que receberam RAR+MTZ+AMX apresentaram os melhores resultados na
média de profundidade de sondagem (PS; p<0,01) e no nível clínico de inserção
(p<0,05). A associação da terapia antibiótica com a RAR promoveu benefícios clínicos
adicionais em comparação a RAR isoladamente em sítios inicialmente intermediários e
profundos (p<0,05 e p<0,01, respectivamente). Indivíduos do grupo que receberam
MTZ+AMX apresentaram um menor número de bolsas residuais com PS ≥5 mm ou PS
≥ 6 mm, bem como menos indivíduos apresentando nove ou mais sítios com PS ≥ 5
mm ao final do estudo em comparação ao grupo RAR. O tratamento não-cirúrgico
associado à MTZ+AMX promoveu benefícios clínicos adicionais no tratamento de
indivíduos com periodontite agressiva generalizada em 12 meses pós-terapia.
Palavras-chave: periodontite agressiva generalizada; amoxicilina; metronidazol;
clorexidina; terapia periodontal

ABSTRACT
The aim of the present study was to evaluate the clinical effects of scaling and root
planing (SRP) alone or in combination with metronidazole (MTZ) and amoxicillin (AMX)
in the treatment of subjects with generalized aggressive periodontitis (GAgP). A double-
blind, placebo-controlled, randomized clinical trial was conducted in 30 subjects with
GAgP. Subjects received SRP alone (n=15) or combined with antibiotics (n=15; 400mg
MTZ and 500mg AMX three times a day for 14 days). All subjects received oral hygiene
instruction including the use of 0.12% chlorhexidine mouthrinse solution twice a day for
2 months. Clinical examinations were performed at baseline and 6 and 12 months post-
therapy. In both groups, all clinical parameters improved at 6 and 12 months. Subjects
receiving SRP+MTZ+AMX showed the greatest improvements in mean full-mouth
probing depth (p<0,01) and clinical attachment level (p<0,05) at 12 months post. The
antibiotic therapies associated with SRP led to additional clinical benefits over SRP
alone in intermediate and deep sites (p<0,05 and p<0,01, respectively). In addition, the
antibiotic group presented lower mean number of residual sites with PD≥5 mm or ≥6 mm
as well as fewer subjects still presenting nine or more sites with PD≥5 mm at the end of
the study period. The non-surgical treatment of GAgP is markedly improved by the
adjunctive use of MTZ+AMX, up to 1 year post-treatment.
Key words: generalized aggressive periodontitis; amoxicillin; metronidazole;
chlorhexidine; antibiotic therapy

SUMÁRIO
1. Introdução....................................................................................................... 11
1.1 Periodontite..................................................................................................... 11
1.2 Tratamento Periodontal................................................................................... 15
1.3 Antibioticoterapia sistêmica associada à raspagem e alisamento radicular no
tratamento periodontal.....................................................................................
17
1.4 Justificativa....................................................................................................... 23
2. Proposição ..................................................................................................... 24
3. Material e Métodos.......................................................................................... 25
3.1 Seleção da amostra.......................................................................................... 25
3.2 Critérios de inclusão e exclusão....................................................................... 25
3.3 Delineamento do estudo................................................................................... 26
3.4 Monitoramento clínico....................................................................................... 28
3.5 Procedimentos terapêuticos............................................................................. 29
3.5.1 Terapia periodontal básica............................................................................... 29
3.5.2 Bochechos com clorexidina a 0,12%................................................................ 30
3.5.3 Aderência ao tratamento.................................................................................. 30
3.6 Cálculo da amostra........................................................................................... 31
3.7 Análise estatística............................................................................................. 31
4. Artigo científico............................................................................................... 33
5. Conclusão........................................................................................................ 58
Referências bibliográficas............................................................................................59
Anexo A...........................................................................................................................85
Anexo B.......................................................................................................................... 86

11
1.INTRODUÇÃO
1.1. Periodontite
As periodontites tem como característica a destruição do periodonto de
proteção e sustentação dos dentes, causando uma perda progressiva de
inserção, de tecido ósseo e, eventualmente, do elemento dentário (ARMITAGE,
1999). São um grupo de infecções que possuem como fator etiológico primário
as bactérias presentes na cavidade oral, especialmente as que colonizam as
superfícies dos dentes, supra e subgengivalmente, organizadas num biofilme
complexo (SOCRANSKY & HAFFAJEE, 1994). Encontradas na forma Crônica
ou Agressiva, são também classificadas em localizada e generalizada de
acordo com a extensão e a gravidade das lesões teciduais. As principais
características clínicas são edema gengival, sangramento, formação de bolsas
periodontais, mobilidade dentária e em casos mais avançados sua possível
perda (PAGE & SCHROEDER, 1976). A maioria das periodontites são
inflamações crônicas que podem progredir continuamente ou com períodos de
exacerbação e quiescência (LOE et al. 1978; SOCRANSKY et al. 1984;
JEFFCOAT & REDDY, 1991).
A forma crônica das periodontites é a doença de origem bacteriana mais
comum e a maior causa de perda dentária em indivíduos adultos (HAFFAJEE
et al. 1997; ROSLING et al. 2001) e serviu como modelo experimental para a
formulação da patogênese da doença. Com o acúmulo de placa bacteriana, os
tecidos gengivais apresentam sinais de inflamação entre 2 a 4 dias, podendo
ou não progredir para a periodontite (PAGE & SCHROEDER, 1976). Em
relação à microbiota associada a essas infecções, já está bem estabelecido na
literatura que a gengivite é decorrente do acúmulo indiferenciado de bactérias
na margem gengival, enquanto que as periodontites estão associadas ao
aumento nos níveis e proporções de espécies patogênicas, principalmente do
complexo laranja e vermelho, e à concomitante diminuição de espécies
compatíveis com o hospedeiro (TELES et al. 2006). A periodontite crônica é
mais prevalente em adultos, podendo também ocorrer em crianças e
adolescentes, e sua progressão pode variar de lenta a moderada e é

12
normalmente consistente com a presença de fatores locais como cálculo,
biofilme, iatrogenias, etc (ARMITAGE, 1999).
Por outro lado, a periodontite agressiva, também subdividida em
localizada e generalizada, apresenta características clínicas e laboratoriais
claramente identificáveis, o que a torna suficientemente diferente da
periodontite crônica (LANG et al. 1999). É uma infecção que acomete
indivíduos sistemicamente saudáveis, caracterizada por uma grande perda de
inserção clínica associada a uma rápida destruição óssea alveolar, atingindo
normalmente indivíduos jovens, o que indica que o agente etiológico é capaz
de causar um dano tecidual considerável em um período relativamente curto e
também implica ser uma infecção por bactérias altamente virulentas e/ou em
indivíduos altamente suscetíveis (TONETTI e MOMBELI, 1999; ARMITAGE,
1999; LANG et al. 1999). Outra característica da periodontite agressiva usada
como critério para diagnóstico é o histórico familiar de periodontite
(frequentemente há o relato de perda dentária por mobilidade ou de
periodontite em outros membros da família), possivelmente devido a um
componente hereditário (LÓPEZ, 1992; DIEHL et al. 2005; NIBALI et al. 2008).
Muitos artigos tem discutido os fatores de suscetibilidade do hospedeiro para a
periodontite agressiva, tais como polimorfismo de um único nucleotídeo,
neutrófilos polimorfonucleares, anticorpos contra bactérias, fumo, estresse,
fatores anatômicos locais e infecções pelo herpes vírus (MENG et al. 2007).
A prevalência da periodontite agressiva pode variar significativamente
entre os países e etnias. Baixos índices de prevalência que variam de 0,1 e
0,2% foram relatados na Europa (SAXBY, 1984; KRONAUER et al. 1986;
ARMITAGE, 1999), enquanto taxas de prevalência mais elevadas, variando
entre 3 a 10% foram notificadas no Brasil (GJERMO et al. 1984; ALBANDAR et
al. 1991), 5,9% em recrutas de um grupo militar em Israel (LEVIN et al. 2006),
8% no clássico estudo de Loe et al. (1986) com os plantadores de chá do Sri
Lanka, 11,5% no Iraque (ALBANDAR, 1989), 8% na Indonésia (TIMMERMAN
et al. 1998), e nos Estados Unidos encontraram uma prevalência de 10% em
indivíduos afro-americanos, 5% em hispânicos e 1,3% em americanos brancos
(ALBANDAR et al. 1997). Quanto ao gênero, alguns estudos sugerem haver

13
diferença na prevalência da periodontite agressiva. Baer (1971) relatou que a
periodontite crônica é mais comum nos homens, enquanto a agressiva é mais
comum nas mulheres. Hormand & Frandsen (1979) relataram que a diferença
em relação ao gênero, diminui com o avanço da idade. Em 1991, Albandar et
al. observaram que houve progressão de perda óssea alveolar nos primeiros
molares, mais prevalente nas meninas da Noruega e em outro estudo entre
estudantes Ugandeses com idade variando de 12 a 25 anos a prevalência foi
maior nos homens (ALBANDAR et al. 2002). Recentemente, Elamin et al.
(2010) observaram um aumento significativo na prevalência de periodontite
agressiva em indivíduos do gênero masculino em comparação ao gênero
feminino (4.9% versus 2.0%) e concluíram que na população do Sudão o
gênero masculino seria um fator de risco para a periodontite agressiva.
Entretanto, não existe até o presente momento uma definição conclusiva
quanto a relação do gênero com a periodontite agressiva.
A microbiota da periodontite agressiva é complexa consistindo
geralmente de bactérias anaeróbias Gram-negativas, tais como
Aggregatibacter actinomycetemcomitans (anteriormente denominado
Actinobacillus actinomycetemcomitans), Porphyromonas gingivalis, Prevotella
intermedia, Tannerella forsythia, Campylobacter rectus, Fusobacterium ssp. e
espécies de Selenomonas (LOESCHE et al. 1985; MULLALLY et al. 2000;
KAMMA et al. 2001, KAMMA et al. 2004; FAVERI et al. 2008). O papel de
bactérias específicas, especialmente do A. actinomycetemcomitans na doença
periodontal agressiva tem sido extensivamente estudado (ZAMBON et al. 1983;
TINOCO et al. 1997; DARBY et al. 2000; CORTELLI et al. 2005; YANG et al.
2005). SLOTS et al. (1980), analisando por meio de cultura microbiana,
amostras de biofilme subgengival de bolsas periodontais profundas de
pacientes portadores de doença periodontal agressiva, detectaram A.
actinomycetemcomitans em 9 dos 10 indivíduos analisados. Outros estudos
detectaram A. actinomycetemcomitans em cerca de 75 a 100% das amostras
de bolsas periodontais ativas na doença periodontal agressiva (MANDELL e
SOCRANSKY, 1981; ZAMBON et al. 1983; CHRISTERSSON et al. 1985;
ZAMBON, 1985; RUSSO et al. 1998; LEE et al. 2003; CORTELLI et al. 2003;
YANG et al. 2005). Embora A. actinomycetemcomitans seja considerado como

14
o principal patógeno na doença periodontal agressiva, existem algumas
controvérsias na literatura (HAN et al. 1991; LOPEZ et al. 1996; MULLALLY et
al. 2000; KAMMA et al. 2001; ISHIKAWA et al. 2002; TREVILATTO et al. 2002;
TAKEUCHI et al. 2003; GAJARDO et al. 2005). MULLALLY et al. (2000) e
KAMMA et al. (2001), estudando populações na Irlanda do Norte e na Grécia,
respectivamente, observaram por meio da técnica do PCR (Reação em cadeia
da polimerase) uma baixa prevalência de A. actinomycetemcomitans (28% e
18,8%, respectivamente) em bolsas periodontais de indivíduos com
periodontite agressiva localizada. Em outro estudo, HAN et al. (1991) não
detectaram por cultura A. actinomycetemcomitans em nenhuma das 23
amostras subgengivais obtidas de indivíduos chineses portadores da forma
agressiva da doença periodontal. TREVILATTO et al. (2002) estudaram uma
família brasileira com periodontite agressiva (n=14) e relataram uma baixa
prevalência de A. actinomycetemcomitans, questionando assim o valor do
isolamento deste microrganismo como forma de diagnóstico. Complementando,
MOMBELLI et al. (2002), em uma revisão sistemática da literatura, relataram
que a presença ou ausência de A. actinomycetemcomitans não pode ser um
parâmetro para diferenciar indivíduos com periodontite agressiva daqueles
com a forma crônica da doença. Assim, estes estudos sugerem que outros
microrganismos, ou então formas mais virulentas de A. actinomycetemcomitans
podem estar associados à etiologia da doença periodontal agressiva.
Entre os fatores de virulência de A. actinomycetemcomitans destacam-
se a capacidade invasiva em células epiteliais (MAYER et al. 1999), e
fibroblastos (ARIRACHAKARAN et al. 2012) e a produção de duas exotoxinas,
a toxina distensora citoletal e a leucotoxina. A toxina distensora citoletal é
capaz de causar parada de ciclo celular na fase G2 levando à distensão das
células epiteliais e fibroblastos, além de agir sobre linfócitos T (SUGAI et al.
1998; MAYER et al. 1999). A leucotoxina, uma proteína membro da família das
RTX, é capaz de lisar neutrófilos e monócitos humanos, prejudicando as
defesas do hospedeiro (KOLODRUBETZ et al. 1989). Assim sendo, a
leucotoxina poderia proteger o A. actinomycetemcomitans contra as células de
defesa do sistema imune do hospedeiro (JOHANSSON et al. 2000). A
expressão da leucotoxina é regulada em muitas cepas, embora determinadas

15
cepas possuam uma deleção de 530 pb na região promotora do gene, afetando
assim a sua transcrição (BROGAN et al. 1994; PAJU et al. 2000). Essas cepas,
chamadas JP2, tem ramificações criticas e tem sido observado uma expressão
mais rápida do gene LTX com a exclusão, levando à produção de uma maior
quantidade da toxina do que em cepas onde a região promotora permanece
intacta (BROGAN et al. 1994). Indivíduos com periodontite agressiva vem
demonstrando uma alta prevalência de cepas extremamente leucotóxicas em
comparação a indivíduos com periodontite crônica e indivíduos saudáveis
(ZAMBON et al. 1996; CORTELLI et al. 2005; ENNIBI et al. 2012; HOGLUND
et al. 2012). Também é verdade que, a colonização oral pelo A.
actinomycetemcomitans é mais diretamente associada com a patogênese da
periodontite agressiva localizada enquanto P. gingivalis, T. forsythia,
Treponema denticola, Campylobacter gracilis, Eubacterium nodatum e
Prevotella intermedia desempenham papel importante na progressão da
doença. O sucesso do tratamento da periodontite agressiva localizada (PAL)
implicaria na redução desses patógenos e um aumento das espécies de
Actinomyces (FAVERI et al. 2009), assim como a identificação precoce e
eliminação do clone JP2 de A. actinomycetemcomitans permitirá aos clínicos
prever de forma eficaz o resultado dos tratamentos aplicados nos pacientes
com doença periodontal (CORTELLI et al. 2009; ENNIBI et al. 2012).
1.2. Tratamento periodontal
O melhor conhecimento da interação entre microbiota e hospedeiro,
perfil microbiológico de cada doença e a distribuição geográfica, podem
propiciar o encontro de uma terapia periodontal adequada, cujos objetivos
principais são a redução da profundidade de sondagem, do sangramento à
sondagem e da supuração, bem como o aumento do nível clínico de inserção,
e a estabilidade desses parâmetros ao longo do tempo. Os estudos científicos
demonstram que esses resultados clínicos satisfatórios são atingidos quando
os níveis, proporções e percentual de sítios colonizados por diferentes
periodontopatógenos são efetivamente reduzidos (SOCRANSKY & HAFFAJEE,
2005; TELES et al. 2006). Subseqüentemente, deve-se estabelecer uma nova

16
comunidade microbiana no biofilme subgengival com níveis e proporções mais
elevadas de microrganismos compatíveis com saúde periodontal.
Aparentemente, esse perfil microbiano compatível com saúde é mais
facilmente instalado na cavidade oral quando a terapia empregada permite uma
rápida e drástica redução dos patógenos, não somente nos sítios profundos,
mas em toda a cavidade oral, incluindo sítios rasos e mucosas. O tratamento
periodontal mais comumente utilizado, a raspagem e alisamento radicular
(RAR), tem como objetivo desorganizar o biofilme dental e suprimir os
patógenos periodontais da cavidade bucal e impedir a progressão da doença
(SOCRANSKY & HAFFAJEE, 2002), e apesar de ser eficaz para uma boa
parcela dos pacientes, muitas vezes não leva às modificações microbiológicas
necessárias para manter os benefícios conseguidos inicialmente, estáveis a
longo prazo, principalmente em indivíduos com periodontite agressiva. Quando
adequadamente executada, a RAR propicia na maioria das vezes, uma
melhora nos parâmetros clínicos periodontais, entretanto é muitas vezes
insuficiente para modificar profundamente o perfil bacteriano patogênico para
um perfil relacionado à saúde periodontal, principalmente em casos de doenças
mais avançadas e generalizadas ou associadas a fatores de risco, como o
fumo (HAFFAJEE et al. 1997; CUGINI et al. 2000; CARVALHO et al. 2004,
2005; MATARAZZO et al. 2008). Com o conhecimento das limitações da
terapia mecânica para o controle da doença periodontal, o entendimento atual
da especificidade do biofilme subgengival e da existência de diferentes
patógenos associados às diferentes formas de infecções periodontais, outras
terapias coadjuvantes à RAR, como os antibióticos sistêmicos, têm sido
propostos com o objetivo de potencializar os efeitos clínicos e microbiológicos
desta forma de terapia (para revisão, ver HERRERA et al. 2002; HAFFAJEE et
al. 2003; HERRERA et al. 2008, MESTNIK et al. 2010).
Além disso, alguns periodontopatógenos relacionados com a doença
periodontal agressiva tem capacidade de invasão tecidual, o que poderia ser
um foco de recolonização dos sítios tratados. Logo, com o objetivo de
potencializar os efeitos da RAR, outras formas de tratamento, como a
associação de antibióticos sistêmicos, têm sido propostas no tratamento de

17
indivíduos com periodontite agressiva (HERRERA et al. 2002; HAFFAJEE et al.
2003).
1.3. Antibioticoterapia sistêmica associada a raspagem e alisamento radicular no tratamento periodontal.
Os antibióticos sistêmicos parecem ter um importante papel no
tratamento das periodontites agressivas, pois muitos desses pacientes não
respondem bem à terapia periodontal mecânica convencional de RAR
(CALIFANO et al. 2003; SLOTS et al. 2004). Três revisões sistemáticas
avaliaram estudos sobre a utilização desses medicamentos em periodontia e
sugerem que os antibióticos sistêmicos potencializam os efeitos da RAR,
principalmente nos indivíduos com periodontite agressiva (HERRERA et al.
2002; HAFFAJEE et al. 2003; SGOLASTRA et al. 2011)
Os antibióticos são substâncias sintéticas e semi-sintéticas, produzidas
por organismos vivos (por exemplo, fungos e bactérias), com ação
antimicrobiana, ou seja, eliminam ou inibem o crescimento de microrganismos.
Somente na década de 70, foram realizados os primeiros estudos controlados
utilizando tetraciclina sistêmica como coadjuvante ao tratamento da
periodontite agressiva localizada (LISTGARTEN et al. 1978; WILLIAMS et al.
1979) e apesar do seu amplo uso, as evidências da qualidade da eficácia da
tetraciclina são escassas. Hayes et al. (1992), na condução de uma meta-
análise, encontraram uma série de falhas metodológicas nos ensaios
publicados até o ano de 1989. Foram os resultados dos estudos de periodontite
agressiva que levaram a uma abordagem terapêutica mais específica
direcionada à eliminação ou supressão do A. actinomycetemcomitans
considerado o fator etiológico da doença (GENCO et al. 1981; LINDHE, 1982;
LINDHE & LILJENBERG, 1984; NOVAK et al. 1988: NOVAK et al. 1992).
Os estudos clínicos controlados sobre a efetividade de antibióticos
sistêmicos no tratamento periodontal tiveram início no final da década de 1970,
com a utilização da tetraciclina no tratamento da periodontite juvenil localizada,
atualmente denominada periodontite agressiva localizada (SLOTS &
ROSLING, 1983). NOVAK et al. (1988) concluíram que a tetraciclina (1g/dia

18
durante 3 a 6 semanas) foi efetiva no tratamento de indivíduos com
periodontite agressiva localizada. Posteriormente, outras investigações clínicas
e microbiológicas mostraram que as tetraciclinas hidroclorídricas ou seus
derivados semi-sintéticos, como a doxiciclina e a minociclina, apresentavam
poucos benefícios no tratamento das periodontites (HAFFAJEE et al. 2007;
XAJIGEORGIOU et al. 2006; BALTACIOGLU et al. 2011) comparado a outros
antimicrobianos.
Outro antibiótico utilizado no tratamento das periodontites é o
metronidazol, que foi administrado primeiramente em 1958 em um ensaio
clínico, por cientistas no laboratório de Rhône-Poulenc - França, como
antitricomonas e, posteriormente utilizado na terapia de outras infecções
parasitárias como amebíase e giardíase. Apesar de ter sido desenvolvido para
ser efetivo contra tricomonas, suas propriedades antimicrobianas em relação
aos anaeróbios estritos e sua aparente habilidade de evitar que
microrganismos susceptíveis tornem-se resistentes ao antimicrobiano têm sido
interessante sob o ponto de vista odontológico (TALLY et al. 1975). Foi
casualmente observado por Shinn em 1962, um alívio nos sintomas de
gengivite ulcerativa necrosante aguda numa mulher que estava em tratamento
da tricomoníase vaginal com o metronidazol e este em seguida, passou a ser
usado no tratamento dessa alteração periodontal (DAVIES et al. 1964;
GLENWRIGHT & SIDAWAY, 1966; LOESCHE et al. 1982), e posteriormente
também na periodontite crônica (LEKOVIC et al. 1983; LOESCHE et al. 1984;
HAFFAJEE et al. 2007). O metronidazol apresenta um amplo espectro de
atividade contra microrganismos anaeróbios estritos in vitro e foi encontrado no
fluído crevicular gengival em concentrações iguais as do soro sanguíneo 1 a 2
horas após a ingestão do medicamento (GIEDRYS-LEEPER et al. 1985).
Estudos que compararam o uso deste antibiótico associado a RAR no
tratamento de indivíduos com periodontite crônica observaram benefícios
clínicos e microbiológicos (SILVA et al. 2011). Apenas um estudo clínico,
placebo controlado avaliou o uso do metronidazol isoladamente no tratamento
da periodontite agressiva generalizada (XAJIGEORGIOU et al. 2006). Os

19
autores não observaram benefícios clínicos e microbiológicos com o uso desta
terapia adjuvante associada a RAR aos 180 dias pós-terapia.
As penicilinas constituem-se na primeira opção como coadjuvantes no
tratamento das infecções odontológicas leves e moderadas. A amoxicilina têm
um amplo espectro de atividade contra espécies anaeróbias estritas e
facultativas subgengivais (WALKER et al. 1985; KULIK et al. 2008). Atua sobre
microrganismos cocos e bacilos Gram-negativos devido à capacidade de
penetrar nas barreiras lipídicas e na parede celular mais complexa destes
microrganismos, agindo sobre as enzimas situadas na parte externa da
membrana celular bacteriana lipoproteica (MONTGOMERY et al. 2000). Entretanto, o uso da amoxicilina em associação a RAR no tratamento das
periodontites não se mostrou promissor em relação a melhora dos resultados
clínicos e microbiológicos (FERES et al. 2002).
As características benéficas individuais da amoxicilina e do metronidazol
e a possível complementariedade de ação farmacológica para o tratamento da
periodontite têm levado pesquisadores a associar ambas as medicações como
uma terapia adjunta a RAR, com o objetivo de suprimir ou eliminar os
patógenos envolvidos com a doença e obter melhores resultados em longo
prazo. Estudos in vitro demonstraram a efetividade de ação desta combinação
contra o A. actinomycetemcomitans devido a interação entre os antibióticos e o
hidroximetabólito do metronidazol produzido pelo fígado humano. Estas
interações sinérgicas entre estes antibióticos podem explicar a eficácia da
combinação de metronidazol e amoxicilina em várias infecções bacterianas,
incluindo a doença periodontal (PAVICIC et al. 1991, 1992). Van Winkelhoff et
al. (1989) utilizaram a associação de amoxicilina e metronidazol em pacientes
com periodontite agressiva colonizados pelo A. actinomycetemcomitans, e
observaram a eliminação desse patógeno em 21 dos 22 pacientes. Estes
resultados se mantiveram em 16 pacientes por 9-11 meses após o tratamento.
Em 1992 (WINKELHOFF et al.), mostraram que a combinação do metronidazol
(250mg; três vezes ao dia durante 7 dias) e da amoxicilina (500mg; três vezes
ao dia durante 7 dias) era efetiva no tratamento de um grupo de indivíduos com
periodontite colonizados pelo A. actinomycetemcomitans. Aparentemente, a

20
combinação de um antibiótico direcionado para anaeróbios estritos
(metronidazol) e outro para aeróbios ou facultativos (amoxicilina), parece ter
um efeito benéfico no tratamento das periodontites relacionadas à presença do
A. Actinomycetemcomitans, no caso, nas doenças periodontais agressivas.
Estudos subsequentes mostraram excelentes resultados clínicos e
microbiológicos utilizando esta associação de antibióticos sistêmicos no
tratamento das periodontites agressivas (GUERRERO et al. 2005; VIANA
CASARIN, 2012) e na periodontite crônica (PAVICIC et al. 1994; LÓPEZ et al.
1998, 2000; WINKEL et al. 2001; LÓPEZ et al. 2006; DANNEWITZ et al. 2007;
MOEINTAGHAVI et al. 2007; MATARAZZO et al. 2008; SGOLASTRA et al.
2012).
Vários estudos intervencionais sem o uso de um grupo controle foram
realizados utilizando a associação de amoxicilina e metronidazol no tratamento
da periodontite agressiva (van WINKELHOFF et al. 1992; GORDON et al.
1993; WINKEL et al. 1998), porém, os estudos clínicos, randomizados e/ou
placebo controlados, em indivíduos com periodontite agressiva generalizada,
somente começaram a surgir a partir de 2005 (GUERRERO et al. 2005;
XAJIGEORGIOU et al. 2006; HAAS et al. 2008; MESTNIK et al. 2010; VARELA
et al. 2011; BALTACIOĞLU et al. 2011; AIMETTI et al. 2012).
O primeiro estudo clinico placebo-controlado foi realizado por
GUERRERO et al. (2005), os autores selecionaram indivíduos com periodontite
agressiva generalizada, que foram divididos em dois grupos terapêuticos:
Controle- raspagem e alisamento radicular (RAR) associado a placebo e Grupo
Teste- RAR associado à amoxicilina (500mg) e metronidazol (500mg). Um fato
importante deste estudo é que o tratamento de raspagem e alisamento
radicular foi realizado em duas sessões em um intervalo de 24hs, segundo um
protocolo conhecido como “full-mouth disinfection”, além disso, nenhuma
avaliação microbiológica foi realizada. Os autores observaram que a
combinação de metronidazol e amoxicilina levou a resultados clínicos
superiores aos observados no grupo que recebeu apenas a RAR (controle).
Posteriormente, XAJIGEORGIOU et al. (2006) compararam a efetividade de 3
diferentes terapias antibióticas em conjunto com a RAR no tratamento de
indivíduos com periodontite agressiva generalizada. Quarenta e três pacientes

21
participaram do estudo e foram aleatoriamente distribuídos em 4 grupos
terapêuticos: RAR somente (controle) ou em combinação com metronidazol e
amoxicilina (500 mg de cada antibiótico 3x/dia por 7 dias); doxiciclina (200 mg
iniciais, seguida de 100 mg/dia por 14 dias), ou metronidazol (500 mg 3x/dia
por 7 dias). Foram realizadas avaliações clínicas e microbiológicas até 6
meses após as terapias. Amostras de biofilme subgengival foram avaliadas
para a presença de 4 patógenos, A. actinomycetemcomitans, P. gingivalis, T.
denticola e T. forsythia. Os autores observaram que a combinação de
metronidazol e amoxicilina foi a mais eficaz em reduzir o percentual de sítios
com profundidade de sondagem > 6mm, além dos 4 patógenos avaliados. É
interessante observar que nesse estudo, o grupo que recebeu somente RAR foi
o que apresentou os maiores níveis de recolonização pelos
periodontopatógenos avaliados aos 6 meses pós-terapia. Outros estudos vem
corroborar com os benefícios clínicos observados com a associação de
metronidazol e amoxicilina no tratamento da periodontite agressiva
generalizada (GUERRERO et al. 2005; MESTNIK et al. 2010; YEK et al. 2010;
VARELA et al. 2011; BALTACIOĞLU et al. 2011; AIMETTI et al. 2012).
Haas et al. (2008) em um estudo clínico, randomizado e placebo
controlado observaram os efeitos do uso sistêmico de azitromicina associado à
raspagem e alisamento radicular nos parâmetros clínicos periodontais. Foram
selecionados 24 indivíduos e distribuídos aleatoriamente em dois grupos
terapêuticos: RAR somente e RAR associado a azitromicina 500 mg. Os
autores observaram que a associação de azitromicina à terapia básica de
raspagem e alisamento radicular promoveu benefícios clínicos em um período
de avaliação de 12 meses pós terapia em indivíduos com doença periodontal
agressiva generalizada. Não foram observados benefícios microbiológicos com
o uso da azitromicina aos 12 meses pós-terapia (HASS et al. 2012).
De modo geral, os estudos mostram benefícios clínicos e
microbiológicos com a utilização de antibióticos sistêmicos no tratamento das
periodontites; benefícios esses que variam de acordo com o tipo de droga
administrada, com a população estudada e, principalmente, com a adesão dos
pacientes ao protocolo terapêutico (GUERRERO et al. 2007). Os antibióticos
sistêmicos parecem ter um importante papel no tratamento das periodontites

22
agressivas, pois muitos desses pacientes não respondem bem à terapia
periodontal mecânica convencional (CALIFANO et al. 2003; SLOTS et al.
2004). Duas revisões sistemáticas avaliaram estudos sobre a utilização desses
medicamentos em periodontia e sugerem que os antibióticos sistêmicos
potencializam os efeitos da RAR, principalmente nos indivíduos com
periodontite agressiva (HERRERA et al. 2002; HAFFAJEE et al. 2003). Nove
das 10 comparações realizadas na revisão de Haffajee e colaboradores
mostraram que os indivíduos que tomaram um antibiótico sistêmico, em
combinação com a RAR, tiveram um maior ganho na média de nível clínico de
inserção em comparação àqueles indivíduos que receberam RAR somente. Em
uma recente meta análise (SGOLASTRA et al. 2011) sobre o uso de
amoxicilina e metronidazol no tratamento das periodontites agressivas os
autores selecionaram 6 estudos clínicos bem conduzidos para sua avaliação
(GUERRERO et al. 2005; XAJIGEORGIOU et al. 2006; MESTNIK et al. 2010;
YEK et al. 2010; VARELA et al. 2011; BALTACIOĞLU et al. 2011). Os
resultados da meta-análise demonstraram que os indivíduos que receberam a
metronidazol e amoxicilina apresentaram um significativo ganho de inserção
clínica (MD: 0,42; 95% CI: 0,23 -0,61; p < 0,05), além de uma redução
significativa de profundidade de sondagem (MD: 0,58; 95% CI: 0,39-0,77; p <
0,05). Entretanto, os autores relatam que mais estudos, com avaliações
longitudinais são necessárias para confirmar tais achados.
Mestnik et al. (2010) reportaram os resultados clínicos e microbiológicos
preliminares de um estudo clínico placebo-controlado, randomizado e duplo
cego no qual avaliaram o uso de metronidazol e amoxicilina associado a RAR
no tratamento da periodontite agressiva generalizada. Os autores descrevem
que os indivíduos que receberam RAR associada aos antibióticos
apresentaram os melhores resultados na média de profundidade de sondagem
e no nível clínico de inserção. Além disso, a associação da terapia antibiótica
com a RAR promoveu benefícios clínicos adicionais em comparação a RAR
isoladamente em sítios inicialmente intermediários e profundos. Em relação aos
resultados microbiológicos, a terapia de RAR associada ao metronidazol e a
amoxicilina promoveu a alteração mais benéfica no perfil microbiológico
subgengival. Os indivíduos deste grupo demonstraram reduções significativas

23
nos níveis e proporções de periodontopatógenos tais como T. forsythia, P.
gingivalis e T. denticola, e um aumento na proporção de bactérias compatíveis
com o hospedeiro. Para complementar, a terapia de RAR associada aos
antibióticos também reduziu significativamente os níveis de A.
actinomycetemcomitans em sítios profundos. Em conclusão, aos 3 meses pós-
terapia efeitos benéficos foram observados nos parâmetros clínicos e na
composição da microbiota subgengival quando o metronidazol e a amoxicilina
foram associados à RAR.
1.4 Justificativa Como descrito anteriormente, vários estudos observaram benefícios
clínicos adicionais no tratamento da periodontite agressiva generalizada
associando metronidazol e amoxicilina à RAR (GUERRERO et al. 2005;
XAJIGEORGIOU et al. 2006; MESTNIK et al. 2010; YEK et al. 2010; VARELA
et al. 2011; BALTACIOĞLU et al. 2011). Entretanto, a maioria destes estudos
apresentam avaliações clínicas entre 3 e 6 meses pós tratamento. Avaliações
longitudinais são necessárias para confirmar a verdadeira efetividade desta
terapia periodontal. Desta forma, acompanhamentos clínicos por mais de 6
meses ainda faltam na literatura científica e se fazem necessários.

24
2. PROPOSIÇÃO
Avaliar as alterações clínicas promovidas pela terapia de raspagem e
alisamento radicular associada ao uso sistêmico de amoxicilina e metronidazol
em indivíduos com periodontite agressiva generalizada em 1 ano pós-terapia.

25
3. MATERIAL E MÉTODOS 3.1. Seleção da amostra
Trinta indivíduos portadores de periodontite agressiva generalizada que
compareceram na Clínica Odontológica da Universidade Guarulhos foram
selecionados para a participação no estudo. A seleção foi feita por um único
profissional treinado. Os participantes foram informados dos objetivos do
estudo, de seus riscos e benefícios, incluindo os tipos de medições clínicas,
coletas e terapias. Os pacientes que concordaram em participar do estudo
assinaram um Termo de Consentimento Livre e Esclarecido, responderam a
um questionário de saúde/anamnese e receberam a terapia periodontal
gratuitamente, estando de acordo com as diretrizes e normas do Conselho
Nacional de Saúde (Resolução n° 196/96). O projeto foi aprovado pelo Comitê
de Ética em Pesquisa em Seres Humanos da Universidade Guarulhos
(N0156/2007 – Anexo A).
3.2. Critérios de inclusão e exclusão Critérios de inclusão
Para a inclusão no estudo, a seleção dos participantes respeitou os
seguintes critérios (AAP, 1999):
- Voluntários portadores de periodontite agressiva generalizada;
- Apresentar bom estado geral de saúde;
- Idade entre 18-30 anos;
- Possuir no mínimo 20 dentes, excluindo-se os terceiros molares;
- Mínimo de 6 dentes com pelo menos 1 sítio interproximal
apresentando profundidade de sondagem > 5mm e nível clínico de
inserção ≥ 5mm, não contíguos, localizados nos primeiros molares e
incisivos; e mais 6 dentes com as mesmas características clínicas
localizadas em outros grupos dentários.
- Histórico familiar (indivíduos foram questionados quanto a outros
membros da família apresentarem histórico de doença periodontal).

26
Critérios de exclusão
Os critérios de exclusão foram os seguintes:
- Tabagistas;
- Pacientes grávidas ou lactantes;
- História de tratamento periodontal prévio;
- História de antibioticoterapia nos últimos seis meses ou
administração contínua de antinflamatórios;
- História de uso de anti-sépticos bucais nos últimos seis meses;
- História de doença sistêmica que comprometa a resposta do
hospedeiro ou exija medicação profilática ao tratamento;
- Relato de alergia à amoxicilina, metronidazol e clorexidina. 3.3. Delineamento do estudo
Os indivíduos selecionados para participar deste estudo duplo-cego,
placebo controlado, foram aleatoriamente distribuídos por meio de uma tabela
de números equiprováveis, em 2 grupos terapêuticos, cada grupo com 15
indivíduos, sendo 1 grupo controle e 1 grupo teste. Controle (C): Raspagem e alisamento radicular (RAR) associado a placebo;
Teste (T): RAR associado à amoxicilina (500mg, 3x/dia durante 14 dias) e
metronidazol (400mg, 3x/dia durante 14 dias).

27
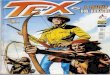
Figura 1. Delineamento experimental.
O protocolo experimental está sumarizado na Figura 1. Inicialmente,
todos os pacientes receberam monitoramento clínico, de acordo com o
protocolo especificado na sessão seguinte (3.4 Monitoramento clínico),
seguido de raspagem supragengival (RSP) de todos os dentes, remoção de
tecido cariado e selamento provisório das cavidades, desgaste de restaurações
em excesso, curativos endodônticos e exodontias. Como instrução de higiene
oral, todos os voluntários foram orientados a utilizar o mesmo dentifrício
contendo triclosan/gantrez (Colgate Total, Anakol Ind. Com. Ltda- Kolynos do
Brasil - Colgate Palmolive Co, São Bernardo do Campo, SP, Brazil), e
receberam escovas Colgate Professional suave (Anakol Ind. Com. Ltda-
Kolynos do Brasil - Colgate Palmolive Co, São Bernardo do Campo, SP, Brazil)
e interdentais HB-Bitufo (Aromaterapia Ind. Com. Ltda., Rua Campos Sales,
953/963, Valinhos, SP, Brasil) nos diâmetros indicados aos espaços entre os
dentes. A terapia básica de RAR foi realizada de 4 a 6 sessões e finalizada, em
RAR: Raspagem e Alisamento Radicular
CLX: Clorexidina 0,12 %/ 2X/dia
Controle (C): RAR + Placebo
Teste (T): RAR + AMX + MTZ

28
14 dias no máximo. Os indivíduos dos 2 grupos experimentais (Controle e
Teste) foram orientados a realizar bochechos com clorexidina 0,12% 2x/dia. O
controle químico do biofilme supragengival foi iniciado em conjunto com a
terapia de RAR e prosseguiu por um período de 45 dias pós-terapia.
Devido à característica duplo-cego do estudo os profissionais
responsáveis pelo tratamento e os indivíduos participantes não tiveram
conhecimento sobre a terapia periodontal recebida. Além disto, o profissional
que realizou os exames clínicos não foi o mesmo que realizou os
procedimentos terapêuticos.
3.4. Monitoramento clínico O monitoramento clínico foi realizado no momento inicial (-14 dias), aos
90, 180 e 360 dias após o término da terapia de RAR por meio de sondas
periodontais manuais (PCPUNC - BR15, HuFriedy do Brasil, RJ, Brasil). Um
examinador foi treinado e calibrado com o objetivo de se conseguir a melhor
reprodutibilidade nas medições realizadas. A metodologia utilizada para a
calibração foi preconizada por Araujo et al. (2003) onde se avaliou o erro
padrão da medida (e.p.m) e o erro médio percentual (e.m.p) para os
parâmetros clínicos periodontais contínuos (profundidade de sondagem e nível
clínico de inserção). O e.p.m e e.m.p intra-examinador demonstrou que o
examinador obteve e.p.m. de 0,13mm e 0,17mm para a profundidade de
sondagem e nível clínico de inserção respectivamente. Esses valores de e.p.m.
indicam uma reprodutibilidade aceitável dentro dos parâmetros de pesquisa
clínica periodontal. Para as variáveis categóricas (índice de placa visível e
índice de sangramento gengival), considerando somente a presença ou a
ausência do parâmetro clínico, foi realizada a média do nível de concordância e
o examinador apresentou uma concordância intra-examinador igual a 92%
(Teste Kappa).
As mensurações clínicas foram realizadas em 6 sítios por dente
(mesiovestibular, vestibular, distovestibular, mesiolingual, lingual, distolingual),
em todos os dentes (exceto terceiros molares). Os seguintes parâmetros
clínicos foram avaliados:

29
* Índice de Placa Visível – IPV (AINAMO e BAY, 1975): Observou-se a
presença ou ausência de placa dentária supragengival visível, após lavagem e
secagem dos dentes. A ausência de placa recebeu o escore 0 (não-visível) e a
presença de placa recebeu o escore 1 (visível).
* Índice de Sangramento Gengival – ISG (AINAMO e BAY, 1975): Observou-se
a presença ou ausência de sangramento na gengiva marginal após percorrer
levemente com a sonda periodontal ao longo do sulco gengival. A ausência de
sangramento recebeu o escore 0 e a presença de sangramento recebeu escore
1.
* Profundidade de Sondagem – PS: Distância em milímetros, entre a margem
gengival livre e a porção mais apical sondável do sulco/bolsa periodontal.
* Nível Clínico de Inserção – NCI: Distância em milímetros, entre a junção
esmalte-cemento e a porção mais apical sondável do sulco/bolsa periodontal.
* Sangramento à Sondagem – SS: Presença (escore 1) ou ausência (escore 0)
de sangramento até 20 segundos após a sondagem com sonda periodontal
milimetrada.
* Supuração – SUP: Presença (escore 1) ou ausência (escore 0) de supuração
até 20 segundos após a sondagem com sonda periodontal milimetrada.
3.5. Procedimentos terapêuticos 3.5.1. Terapia periodontal básica
Após o exame clínico, os indivíduos foram submetidos à raspagem
supragengival (RSP) e instruções de higiene oral (IHO). Em seguida,
receberam 4 a 6 sessões de RAR com curetas Gracey, números 5/6, 7/8, 11/12
e 13/14 (Hu-Friedy, Chicago, EUA), que tiveram duração de aproximadamente
1 hora dentro dos 14 dias de terapia antibiótica. O tratamento periodontal
recebido foi gratuito durante toda a duração do estudo. As outras necessidades
de tratamento odontológico, quando observadas, foram encaminhadas às
demais disciplinas da Clínica de Odontologia da Universidade Guarulhos.

30
3.5.2. Bochechos com solução de clorexidina a 0,12% Indivíduos dos grupos Controle e Teste receberam RAR e o controle
químico com solução contendo clorexidina 0,12% combinados ou não com o
uso de antibióticos. Os voluntários iniciaram o uso adjuvante do controle
químico em conjunto com a RAR prosseguindo por 45 dias após a terapia
periodontal básica. Os voluntários foram orientados a bochechar 15 ml da
solução duas vezes ao dia (manhã e noite), por 1 minuto, como proposto por
FAVERI et al. (2006). Foi recomendada a não-ingestão de alimentos sólidos ou
líquidos nos 30 minutos subseqüentes aos bochechos, sendo que os mesmos
deveriam ser realizados 40 minutos depois da escovação dentária, para que
não ocorressem interações químicas entre os componentes flúor e Lauril
Sulfato de Sódio (LSS) com o digluconato de clorexidina, diminuindo assim a
efetividade do mesmo (BARKVOLL et al. 1989; OWENS et al. 1997; FAVERI et
al. 2006).
3.5.3. Aderência ao tratamento
Os medicamentos foram manipulados especialmente para esta
pesquisa, na Farmácia de Manipulação da Universidade Guarulhos, com
cápsulas de antibióticos e placebo (talco farmacêutico) da mesma coloração e
tamanho, estocados em frascos leitosos com 21 unidades cada, devidamente
codificados e entregues ao coordenador do estudo. A Clorexidina foi colocada
em frascos de 210 ml, quantidade suficiente para uma semana. Todos os
medicamentos foram fornecidos gratuitamente aos pacientes, que foram
instruídos a relatar eventuais efeitos colaterais ao coordenador, e ao término do
período de administração dos medicamentos/placebo, os indivíduos
responderam a um questionário de possíveis reações adversas e ao final dos
45 dias, outro para o enxaguatório.
A aderência e a motivação do paciente são de suma importância para o
sucesso do tratamento e obtenção de dados confiáveis (GUERRERO et al.
2007; HUGOSON et al. 2007), e neste estudo, houve um acompanhamento via
telefone realizado por um aluno de iniciação científica durante o período de
terapia antibiótica, e os pacientes traziam os frascos vazios para a troca do
enxaguatório e confirmação do término das cápsulas.

31
3.6. Cálculo da Amostra Os dados preliminares deste estudo clinico, randomizado e placebo
controlado foram publicados por Mestnik et al. (2010). O estudo foi
originalmente delineado para comparar o efeito do tratamento de RAR
isoladamente ou associado com o MTZ e AMX no perfil microbiano subgengival
de indivíduos com PAgG. O tamanho da amostra foi baseado na diferença de
6,6% considerando um desvio-padrão de 5% na proporção do complexo
vermelho ao final da terapia periodontal (MATARAZZO et al. 2008). Desta
forma, determinou-se que 13 pacientes por grupo seriam necessários para
obtenção de 80% de poder utilizando um α de 0,05. Com o objetivo de validar
os resultados clínicos do presente estudo foi realizado um cálculo de amostra
post-hoc baseados nas diferenças no ganho de inserção clínica do grupo
controle e teste (1,03 mm) em 1 ano pós-terapia em sítios profundos
(PS>7mm), considerando um desvio padrão médio de 1,17 mm (ver tabela do
artigo). Assim sendo, determinou-se que seriam necessários 17 indivíduos por
grupo para obtenção de um poder de 80% e 14 indivíduos para um poder de
75%. Desta forma, a avaliação clínica apresentada no presente estudo
apresenta um poder entre 75 e 80%.
3.7. Análise estatística A média das medidas clínicas de profundidade de sondagem e nível
clínico de inserção, assim como a média da porcentagem de sítios
apresentando placa visível, sangramento gengival, sangramento à sondagem e
supuração foram computados para cada indivíduo e, posteriormente, dentro de
cada grupo. As alterações na PS e NCI em sítios inicialmente moderados (4-
6mm) e profundos (≥7mm) ou a média do número/porcentagem de sítios com
PS <5mm ou >5mm, ≥6mm, foram avaliados separadamente dentro das
categorias de PS por indivíduo e depois entre os indivíduos de cada grupo. As
diferenças dentro de cada grupo, entre os tempos experimentais foram
avaliadas utilizando o teste Friedman e o teste Dunn. O teste Mann–Whitney foi
utilizado para examinar diferenças entre os 2 grupos terapêuticos entre os

32
tempos, e o teste Qui-quadrado para comparar as diferenças na freqüência de
gênero, de pacientes apresentando diferentes categorias de sítios residuais
após 1 ano de acompanhamento e da auto-percepção de efeitos adversos. Os
dados foram avaliados por meio da intenção de tratar, sendo a última
observação de análise utilizada no exame seguinte. A significância estatística
foi estabelecida em 5% (p<0,05).

33
4. ARTIGO CIENTÍFICO
The effects of adjunctive metronidazole plus amoxicillin in the treatment of
generalized aggressive periodontitis. a 1-year double-blinded, placebo-controlled, randomized clinical trial.
Running title: MTZ plus AMX in the treatment of GAgP.
Maria Josefa MESTNIK1, Magda FERES1, Luciene Cristina FIGUEIREDO1, ,
Ricardo P. TELES2, Poliana Mendes DUARTE1, Marcelo FAVERI1
1 Department of Periodontology, Dental Research Division, Guarulhos University, Guarulhos,
São Paulo, Brazil 2 The Forsyth Institute, Cambridge, MA, USA.
Address for correspondence and reprints (fax number and e-mail can be published)
Marcelo Faveri
Centro de Pós-Graduação e Pesquisa-CEPPE
Universidade Guarulhos
Praça Tereza Cristina, 229 Centro
07023-070 Guarulhos, SP, Brazil
e-mail: [email protected]
Artigo formatado segundo as normas da revista Journal of Clinical Periodontology

34
ABSTRACT
Aim: To evaluate the clinical effects of the adjunctive use of metronidazole
(MTZ) and amoxicillin (AMX) in the treatment of generalized aggressive
periodontitis (GAgP). Methods: 30 subjects were randomly assigned to receive
scaling and root planing (SRP) alone or combined with MTZ (400 mg/TID) and
AMX (500 mg/TID) for 14 days. Subjects were clinically monitored at baseline, 6
months and 1 year post-therapies. Results: Both therapies led to a statistically
significant improvement in all clinical parameters at 1 year post-therapy
(p<0.05). Subjects receiving MTZ plus AMX exhibited the deepest reductions in
mean probing depth (PD) and gain in clinical attachment between baseline and
1 year post-therapy in the full-mouth analysis and in initially intermediate (PD 4-
6 mm) and deep (PD≥7 mm) sites (p<0.01). In addition, the antibiotic group
presented lower mean number of residual sites with PD≥5 mm or ≥6 mm as well
as fewer subjects still presenting nine or more sites with PD≥5 mm or three or
more sites with PD≥6 mm at the end of the study period. Conclusion: The non-
surgical treatment of GAgP is markedly improved by the adjunctive use of
MTZ+AMX, up to 1 year post-treatment.
Key-words: Periodontal disease; Scaling and root planing; Metronidazole,
Amoxicillin; Generalized aggressive periodontitis; Periodontal treatment

35
Clinical Relevance
Scientific rationale for study: It is generally accepted that the association of
MTZ plus AMX as an adjunct to SRP benefits the treatment of GAgP subjects.
However, double-blinded, placebo-controlled RCTs beyond 6 months of follow-
up for this therapy in subjects with GAgP are still missing in the literature.
Principal findings: The antibiotic therapy was significantly better than SRP
alone in improving all clinical parameters evaluated, including the reduction in
the mean number of residual pockets up to 1 year post-treatment. Practical
implications: The adjunctive use of MTZ+AMX offer additional clinical benefit
for the treatment of subjects with GAgP.
Conflict of interest and source of funding statement- The authors declare
that they have no conflict of interests. This study was supported by Research
Grant #2007/55291-9 from Fundação de Amparo à Pesquisa do Estado de São
Paulo (FAPESP, Brazil).

36
INTRODUCTION
Amoxicillin (AMX) and metronidazole (MTZ) adjunctive to scaling and
root planing (SRP) has been originally suggested as a promising treatment for
subjects with periodontitis colonized by Aggregatibacter
actinomycetemcomitans (van Winkelhoff et al. 1989, Pavicić et al. 1992, 1994,
Winkel et al. 2001), mainly due a possible synergistic effect of this combination
of drugs in inhibiting this pathogen. However, randomized controlled clinical
trials (RCT) demonstrated that this treatment protocol improves the clinical and
microbiological effects of SRP, even when prescribed without prior diagnostic of
A. actinomycetemcomitans in subjects exhibiting chronic (Berglundh et al. 1998,
Winkel et al. 2001, Matarazzo et al. 2008, Cionca et al. 2010, Silva et al. 2011)
or aggressive periodontitis (GAgP) (Guerrero et al. 2005, Xajigeorgiou et al.
2006, Kaner et al. 2007, Machtei & Younis 2008, Yek et al. 2010, Mestnik et al.
2010, Baltacioğlu et al. 2011, Aimetti et al. 2012).
Guerrero et al. (2005) published the first RCT evaluating the clinical
effects of MTZ+AMX in the treatment of GAgP up to 6 months post-treatment.
The authors showed that the use of adjunctive antibiotics led to a better clinical
response than that observed with SRP alone. Afterwards, the clinical benefits of
this combination of drugs in the clinical parameters of subjects with GAgP were
corroborated by other studies (Kaner et al. 2007, Machtei & Younis 2008, Yek
et al. 2010, Baltacioğlu et al. 2011, Aimetti et al. 2012). However, double-
blinded, placebo-controlled RCTs beyond 6 months of follow-up for this therapy
in subjects with GAgP are still missing in the literature.
We have recently evaluated the short-term clinical and microbiological
outcomes of the adjunctive use of AMX+MTZ in 30 subjects with GAgP.

37
Subjects taking adjunctive antibiotics showed greater improvements in the
mean full-mouth probing depth (PD) and clinical attachment level (CAL), as well
as in initially intermediate and deep sites in comparison with SRP alone.
Furthermore, these subjects presented fewer sites with PD>5mm than those
treated with SRP alone at 3 months post-therapy. In addition to these favorable
clinical results, the antibiotics led to a more beneficial change in the subgingival
microbial profile (Mestnik et al. 2010). The present study is a longitudinal clinical
evaluation of this investigation. The microbiological data will be presented in a
companion paper (manuscript in preparation).
Therefore, the purpose of this study was to compare the clinical effects of
the adjunctive use of MTZ+AMX by directly comparing the clinical outcomes of
this treatment protocol with those obtained with SRP alone, at 6 months and 1
year post-therapy.
MATERIALS AND METHODS
Sample size calculation
This study is a longitudinal analysis of a RCT (Mestnik et al. 2010) designed
and powered to compare the effects of SRP alone or with MTZ+AMX on the
subgingival microbial profile of subjects with GAgP. The ideal sample size to
assure adequate power for that RCT was calculated considering differences of
at least 6.6 percentage points between groups for the proportion of the red
complex species and a standard deviation of 5. It was determined that 13
subjects per group would be necessary to provide 80% power with an α of 0.05.
In order to validate the clinical comparisons conducted in the present
manuscript we performed a post hoc power calculation based in the observed

38
changes in CAL in initially deep sites (PD>7mm) between the control and test
groups (1.03 mm) at 1 year post-treatment, considering the mean observed
SDs of 1.17 mm (Table 2). Therefore, it was determined that 17 subjects per
group would be necessary to provide 80% power, and 14 to provide 75%
power, with an α of 0.05. Since this study had 15 subjects per group, the power
was considered to lay between 75 and 80%.
Subject Population, Inclusion and Exclusion Criteria
Subjects were selected from the population referred to the Periodontal Clinic of
Guarulhos University (Guarulhos, SP, Brazil) according to the criteria previously
described (Mestnik et al. 2010). In brief, the 30 eligible subjects were thoroughly
informed of the nature, potential risks and benefits of their participation in the
study and signed a Term of Informed Consent. They were in good general
health, had at least 20 teeth excluding third molars and teeth indicated for
extraction and were diagnosed with GAgP based on the current classification of
the American Academy of Periodontology (Armitage 1999). The inclusion
criteria were as follows:
- ≤ 30 years of age;
- minimum of six permanent teeth including incisors and/or first molars
with at least one site each with PD and CAL>5 mm and a minimum of six
teeth other than first molars and incisors with at least one site each with
PD and CAL≥5 mm;
- familial aggregation (during the anamneses the subjects was asked if
they had at least one other member of the family presenting or with
history of periodontal disease)

39
The exclusion criteria were as follows: previous subgingival scaling and root
planing, allergy to amoxicillin and metronidazole, smoking, pregnancy, systemic
diseases that could affect the progression of periodontal disease (e.g. diabetes
and immunological disorders), long-term administration of anti-inflammatory
medication, need of antibiotic coverage for routine dental therapy, antibiotic
therapy in the previous 6 months and allergy to chlorhexidine (CHX).
Experimental design, allocation concealment and treatment protocol
In this double-blinded, randomized, placebo-controlled clinical trial, subjects
were randomly assigned using a computer-generated table to one of the
following treatment groups: Control: SRP + Placebo; and Test: SRP + systemic
MTZ (400 mg) and AMX (500 mg). Subjects in the Control group received MTZ
and AMX placebos. Both antibiotics and placebos were administered T.I.D. for
14 days. Supragingival biofilm control in both groups was achieved by rinsing
with 0.12% CHX solution. All subjects were instructed to gargle with 15 ml of
CHX twice a day for 60 days for 1 min in the morning (30 min after breakfast
and tooth brushing), and at night (before going to sleep).
Before the study began, all subjects received full-mouth supragingival scaling
and instruction on proper home-care techniques. They were also given the
same dentifrice to use during the period of the study (Colgate Total, Anakol Ind.
Com. Ltda- Kolynos do Brasil - Colgate Palmolive Co, São Bernardo do Campo,
SP, Brazil). All subjects received full-mouth SRP performed under local
anesthesia from four to six appointments lasting approximately 1 h each.
Treatment of the entire oral cavity was completed from 10 to 14 days. SRP was

40
performed by one trained periodontist using manual instruments. The antibiotic
or placebo therapies and the CHX rinses started immediately after the first
session of mechanical instrumentation.
Guarulhos University Pharmacy prepared the CHX rinses and the
antibiotics/placebos pills and sent them to the study coordinator (M. Fa.), who
marked the code number of each subject on a set of two packs, according to
the therapy assigned, and gave them to the examiner (M. J. M.). All study
personnel, including the examiner, biostatisticians and participants were kept
blinded as to patient assignment to treatment. All subjects received clinical
monitoring at baseline and at 6 and 12 months post-therapy. Periodontal
maintenance was conducted at 3, 6 and 12 months post-therapy and included
oral hygiene instructions, supragingival plaque control and SRP on residual
sites with PD>5mm. This study protocol was approved by the Guarulhos
University Clinical Research Ethics Committee.
Monitoring of compliance and adverse events
The subjects were asked to bring the packs containing the medication once a
week when compliance was checked. The packs contained 21 capsules of each
placebo or antibiotic, enough for 1 week of medication. During these visits,
subjects returned the old pack containing the placebo or antibiotic and received
a new pack of medication/placebo. They also answered a questionaire about
any self-perceived side-effects of the medication/placebo. Two study assistants
conducted this inquiry, and were also responsible for calling the subjects every
2 days to monitor compliance.

41
Clinical Monitoring
Clinical monitoring was performed by one calibrated examiner and the
treatment was carried out by another clinician. Thus, the examiner and the
clinician were masked as to the nature of the treatment groups. Visible plaque
(presence or absence), gingival bleeding (presence or absence), bleeding on
probing (BOP; presence or absence), suppuration (presence or absence), PD
(mm) and CAL (mm) were measured at six sites per tooth (mesiobuccal, buccal,
distobuccal, distolingual, lingual and mesiolingual) in all teeth, excluding third
molars. The PD and CAL measurements were recorded to the nearest
millimeter using a North Carolina periodontal probe (Hu-Friedy, Chicago, IL,
USA).
Investigator’ Calibration
The examiner participated in a calibration exercise that was performed in 10
non-study subjects with periodontitis. The calibration exercise was previously
described in Mestnik et al. (2010). In brief, the standard error of measurement
was calculated and the intra-examiner variability was 0.15 mm for PD and 0.19
mm for CAL.
Primary and secondary outcome variables
It was defined that the primary outcome variable to determine the superiority of
one treatment over the other would be differences between groups for mean
CAL changes at 12 months post-treatment in sites with baseline PD≥7 mm. The

42
secondary outcome variables were differences between groups for the following
parameters: mean PD change in sites with baseline PD≥7 mm, mean CAL and
PD changes in the full-mouth as well as in sites with baseline PD between 4
and 6 mm, mean changes in individual full-mouth mean CAL, difference in the
number of sites with PD≥5mm or PD≤5mm and PD≥6mm, as well as the
prevalence of subjects with low, moderate or higher risk of disease progression.
Statistical Analysis
Each individual clinical parameter was computed per subject and then across
subjects in both groups. Changes in PD and CAL in sites with initial PD 4–6 mm
and ≥7mm or the mean number/percentage of sites with PD<5 mm or >5 mm,
>6 mm, were averaged separately within the PD categories per subject and
then across subjects in each group. The significance of differences within each
group (over the course of the study) was sought using Friedman and Dunn’s
multiple comparison tests, and between groups (at each time point) using the
Mann-Whitney test. Chi-square test was used to compare the differences in the
frequency of gender, of subjects exhibiting different categories of residual sites
at 1 year of follow-up and of self-perceived adverse effects. The data were
evaluated using intention-to-treat analysis with last observation carried forward.
The level of significance was set at 5%.
Results
Subject retention, compliance and adverse effects

43
The study was conducted between July 2007 and December 2010. Figure 1
presents the flow chart of the study design. Two subjects per group did not
return for the 12 month follow-up visit. Adverse events were reported previously
by Mestnik et al. (2010). No statistically significant differences were observed
between groups for the number of subjects reporting adverse events. All
subjects reported that they would start the treatment again if necessary. All
subjects reported that they completed the course of the antibiotics, and this
information was confirmed by pill counts.
Clinical Findings
Table 1 presents demographic characteristics and full-mouth mean data for the
clinical parameters evaluated at baseline, and at 6 months and 1 year post-
therapies. The baseline and 3-month data were reported previously (Mestnik et
al., 2010). There were no statistically significant differences between groups for
any parameter at baseline (p>0.05). All therapies led to a statistically significant
decrease in mean PD, CAL and in the percentage of sites with visible plaque,
gingival bleeding, BOP and suppuration. At 6 months and 1 year the full-mouth
mean PD was statistically significantly lower in the Test group in comparison
with the Control group. The mean PD reduction and clinical attachment (CA)
gain between baseline and 6 months or 1 year post-therapy are presented in
Table 2. Subjects taking MTZ+AMX exhibited a greater reduction in PD and
gain in CA in comparison with those receiving SRP-only; in the full-mouth
analysis and in initially intermediate (PD 4-6 mm) and deep (PD≥7 mm) sites
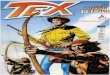
(p<0.01). Figure 2 presents changes in mean full-mouth CAL for individual

44
subjects at 1 year post-SRP. The median of CAL change for the 30 subjects of
the study was 0.93 mm. The number of subjects showing CAL gain within or
above this value (0.93 to 2.30) was 10 and 6 in the Test and Control groups,
respectively. Conversely, the number of subjects presenting CAL change below
0.93 (0.93 to -0.45) was 5 and 9, for Test and Control groups, respectively.
Table 3 shows the mean number and percentage of sites with PD ≥5 mm and
PD ≥6 mm over the course of the study. Both treatments were effective in
reducing the number/percentage of deep sites (PD≥5 mm and PD≥6 mm)
during the course of the study (p<0.05). At 1 year post-treatment the Test group
had less sites with PD≥5 mm and ≥6 mm in comparison with the Control group
(p<0.001). Data for residual sites at subject level are presented in Table 4. The
upper panel of Table 4 was organized according to the individual risk profile for
periodontal disease progression proposed by Lang & Tonetti (2003), as follows:
low risk: ≤4 sites with PD≥5mm; moderate risk: 5-8 sites with PD≥5mm and
high risk: ≥9 sites with PD≥5 mm. Fewer subjects in the Test group (n=4) still
had high risk for disease progression at 1 year (≥ 9 sites with PD>5 mm), in
comparison with the Control group (n=12). Conversely, 8 subjects in the Test
group and only 1 in the SRP group showed low risk for disease progression (≤ 4
sites with PD>5 mm) at the end of the study period. This same trend was
observed for PD≥6mm. At 12 months post-treatment, 6 subjects in the
MTZ+AMX group had ≥ 3 sites with PD≥6 mm, as opposed to 13 subjects in the
control group

45
DISCUSSION
To our knowledge, this was the first double-blinded placebo-controlled RCT to
provide data up to 1 year of the adjunctive use of MTZ+AMX in the treatment of
GAgP. The results indicated that the clinical benefits observed with the use of
this therapeutic protocol in the short-term analysis (Mestnik et al. 2010) were
maintained and even extended at 6 months and 1 year post-treatment.
Subjects taking MTZ+AMX exhibited significantly greater reductions in PD and
gain in CA than those receiving SRP alone, in the full-mouth analysis as well as
in initially intermediate or deep sites. All these differences were statistically
significant at 6 months and 1 year post-therapies (Table 2). Interesting
information was also provided by the results of gain in CA at the subject level
(Figure 2). From the 15 subjects taking antibiotics, 9 were among those who
have gained more CA at 1 year, a totally inverse trend seen in the SRP group,
which had 9 subjects among those who gained less CA. These added benefit of
MTZ+AMX in improving mean PD and CA agree and extend data from previous
RCTs (Guerrero et al. 2005, Xajigeorgiou et al. 2006, Yek et al, 2010, Aimetti et
al. 2012).
While the mean changes in PD and CA were overall maintained from the 3
months to 1 year of follow-up some important clinical differences were observed
between the short-term and the long-term analysis on the number of sites with
PD≥5 mm (Tables 3 and 4). At 3 months post-treatment, the difference in mean
number of these residual sites between control and test groups was 6.8 (18.2
and 11.4, respectively; p<0.05) (Mestnik et al. 2010), while at 1 year this

46
difference was greatly accentuated to 16.9 sites (23.3 and 6.4, respectively;
p<0.00). This is probably the most striking finding of the present study, since
the presence of sites with PD≥5 mm after treatment has been indicated as one
of the most important parameters to evaluate treatment success and to predict
disease recurrence and the need of further treatment (Lang & Tonetti, 2003;
Renvert & Persson, 2002, Matuliene et al. 2008, 2010). Curiously, the
frequency of these residual sites decreased in the test group from 3 months
(Mestnik et al. 2010), to 1 year, while an increase was detected in the control
group. One plausible explanation for this opposite clinical trend may be
differences on the effect of the two treatments in changing the subgingival
microbial profile. As clearly demonstrated in the short-term analysis (Mestnik et
al. 2010), at 3 months post-treatment the group receiving adjunctive MTZ+AMX
had significantly lower levels and proportions of all pathogens from the red
complex and some putative periodontal pathogens from the orange complex in
comparison with those receiving SRP alone. The remaining presence of high
proportion of pathogens at the end of the periodontal therapy may increase the
risk of future disease progression (Teles et al. 2008, Kinney et al. 2011). The
longitudinal microbiological effects of these treatments will be presented in a
second paper and will certainly contribute to the better understanding of this
and other clinical trends.
The data for remaining deep sites at the subject level were also rather
enlightening (Table 4). At the end of the study period, 12 subjects (86.6%) from
the control group against only 4 (26.7%) from the test group presented high risk
for future disease recurrence according to Lang & Tonetti (2003), i.e. 9 or more
sites with PD≥5mm. The only study that did not found added benefits for the

47
adjunctive use of MTZ+AMX in reducing the frequency of residual pockets used
a lower dose of MTZ, 250 mg (Varela et al. 2011), as opposed to 400-500 mg
applied in all other investigations (Guerrero et al. 2005, Xajigeorgiou et al. 2006,
Yek et al 2010, Aimetti et al. 2012). However, the impact of different doses and
durations of this antibiotic protocol still needs to be further explored.
One limitation of the present investigation was the low number of
subjects in each group, which conferred a power of 75% to this study, below
80% that, by convention, is a more acceptable level of power. This occurred
because this RCT was originally designed and powered to compare the effects
of SRP alone or with MTZ+AMX in the subgingival microbial profile. So, 15
subjects per group would be enough to provide 80% of power using the
microbiological primary outcome variable (differences between groups for
proportion of red complex), but not for the clinical outcome variable used in the
present study. The main problem of low powered RCTs is the increased
probability of type II error (false negative), that is the study might have been too
small to detect actual differences between groups. This was clearly not a
problem in the present study since the majority of the clinical results and the
primary outcome variable evaluated were statistically significantly different
between the two groups, always in favor of the antibiotic treatment. Apparently,
this combination of therapies is so potent in comparison to the mechanical
treatment alone that its benefits are evident even in a trial with 75% of chances
of detecting them.
The longitudinal results presented in this manuscript, together with those
reported in previous RCTs of 3 and 6-month (Guerrero et al. 2005, Mestnik et
al. 2010, Yek et al. 2010, Baltacioğlu et al. 2011, Aimetti et al. 2012) or in a

48
recent meta-analysis (Sgolastra et al. 2011) demonstrated that this treatment
protocol (SRP+MTZ+AMX) is of great benefit for subjects with GAgP. In
addition, none of these studies reported the occurrence of serious adverse
events with the use of this combination of drugs.
In conclusion, the results of this study indicate that the non-surgical
treatment of GAgP is markedly improved by the adjunctive use of MTZ+AMX,
up to 1 year post-treatment.
References Armitage, G. C. (1999) Development of a classification and conditions. Annals
of Periodontology 4, 1-6.
Baltacioğlu, E., Aslan, M., Saraç, Ö., Saybak, A. & Yuva, P.(2011) Analysis of
clinical results of systemic antimicrobials combined with nonsurgical periodontal
treatment for generalized aggressive periodontitis: a pilot study. Journal
Canadian Dental Association 77, b97.
Berglundh, T., Krok, L., Liljenberg, B., Westfelt, E., Serino, G. & Lindhe, J.
(1998) The use of metronidazole and amoxicillin in the treatment of advanced
periodontal disease. A prospective, controlled clinical trial. Journal of Clinical
Periodontology 25, 354-62.
Cionca, N., Giannopoulou, C., Ugolotti, G. & Mombelli, A. (2010) Microbiologic
testing and outcomes of full-mouth scaling and root planing with or without
amoxicillin/metronidazole in chronic periodontitis. Journal of Periodontology 81, 15-23.
Guerrero, A., Griffiths, G. S., Nibali, L., Suvan, J., Moles, D. R., Laurell, L. &
Tonetti, M. S. (2005) Adjunctive benefits of systemic amoxicillin and
metronidazole in non-surgical treatment of generalized aggressive periodontitis:

49
a randomized placebo-controlled clinical trial. Journal of Clinical Periodontology
32, 1096–1107.
Kaner, D., Bernimoulin, J. P., Hopfenmuller, W., Kleber, B. M. & Friedmann, A.
(2007) Controlled-delivery chlorhexidine chip versus amoxicillin/metronidazole
as adjunctive antimicrobial therapy for generalized aggressive periodontitis: a
randomized controlled clinical trial. Journal of Clinical Periodontology 34, 880–
891.
Kinney, J.S., Morelli, T., Braun, T., Ramseier, C.A., Herr, A.E., Sugai, J.V.,
Shelburne, C.E., Rayburn, L.A., Singh, A.K. & Giannobile, W.V. (2011)
Saliva/pathogen biomarker signatures and periodontal disease progression.
Journal of Dental Research 90, 752-8.
Lang, N.P. & Tonetti, M.S. (2003) Periodontal risk assessment (PRA) for
patients in supportive periodontal therapy (SPT). Oral Health & Preventive
Dentistry 1, 7-16.
Machtei, E.E. & Younis, M.N. (2008) The use of 2 antibiotic regimens in
aggressive periodontitis: comparison of changes in clinical parameters and
gingival crevicular fluid biomarkers. Quintessence International 39:811-819
Matarazzo, F., Figueiredo, L. C., Cruz, S. E., Faveri, M. & Feres, M. (2008)
Clinical and microbiological benefits of systemic metronidazole and amoxicillin
in the treatment of smokers with chronic periodontitis: a randomized placebo-
controlled study. Journal of Clinical Periodontology 35, 885-896.
Matuliene, G., Pjetursson, B.E., Salvi, G.E., Schmidlin, K., Brägger, U.,
Zwahlen, M. & Lang, N.P. (2008) Influence of residual pockets on progression
of periodontitis and tooth loss: results after 11 years of maintenance. Journal of
Clinical Periodontology 35, 685-695.
Matuliene , G., Studer, R., Lang, N.P., Schmidlin, K., Pjetursson, B.E., Salvi,
G.E., Brägger, U. & Zwahlen, M. (2010) Significance of Periodontal Risk

50
Assessment in the recurrence of periodontitis and tooth loss. Journal of Clinical
Periodontology 37, 191-9.
Mestnik, M.J., Feres, M., Figueiredo, L.C., Duarte, P.M., Lira, E.A. & Faveri, M.
Short-term benefits of the adjunctive use of metronidazole plus amoxicillin in the
microbial profile and in the clinical parameters of subjects with generalized
aggressive periodontitis. Journal of Clinical Periodontology 37, 353-65.
Pavicić, M.J., van Winkelhoff, A.J. & de Graaff, J. (1992) In vitro susceptibilities
of Actinobacillus actinomycetemcomitans to a number of antimicrobial
combinations. Antimicrobial. Agents and Chemotherapy 36, 2634-2638.
Pavicić, M.J., van Winkelhoff, A.J., Pavicić-Temming, Y.A. & de Graaff, J.
(1994) Amoxycillin causes an enhanced uptake of metronidazole in
Actinobacillus actinomycetemcomitans: a mechanism of synergy. Journal of
Antimicrobial Chemotherapy 34, 1047-1050.
Renvert, S. & Persson, G.R. (2002) A systematic review on the use of residual
probing depth, bleeding on probing and furcation status following initial
periodontal therapy to predict further attachment and tooth loss. Journal of
Clinical Periodontology 29, (Suppl 3) 82-89.
Sgolastra, F., Petrucci, A., Gatto, R. & Monaco, A. (2011) Effectiveness of
Systemic Amoxicillin/Metronidazole as an Adjunctive Therapy to Full-Mouth
Scaling and Root Planing in the Treatment of Aggressive Periodontitis: A
Systematic Review and Meta-Analysis. Journal of Periodontology Nov 3. [Epub
ahead of print]
Silva M.P., Feres M., Sirotto T.A., Soares G.M., Mendes J.A., Faveri M.,
Figueiredo L.C. (2011) Clinical and microbiological benefits of metronidazole
alone or with amoxicillin as adjuncts in the treatment of chronic periodontitis: a
randomized placebo-controlled clinical trial. Journal of Clinical Periodontology
38, 828-37.
Teles, R.P., Patel, M., Socransky, S.S. & Haffajee, A.D. (2008) Disease
progression in periodontally healthy and maintenance subjects. Journal of
Periodontology 79, 784-94.

51
van Winkelhoff, A. J., Rodenburg, J. P., Goene´, R. J., Abbas, F., Winkel, E. G.
& de Graaff, J. (1989) Metronidazole plus amoxycillin in the treatment of
Actinobacillus actinomycetemcomitans associated periodontitis. Journal of
Clinical Periodontology 16, 128–131
Varela VM, Heller D, Silva-Senem MX, Torres MC, Colombo AP, Feres-Filho
EJ. (2011). Systemic antimicrobials adjunctive to a repeated mechanical and
antiseptic therapy for aggressive periodontitis: a 6-month randomized controlled
trial. Journal of Periodontology 82:1121-30
Winkel, E. G., van Winkelhoff, A. J., Timmerman, M. F., van der Velden, U. &
van der Weijden, G. A. (2001) Amoxicillin plus metronidazole in the treatment of
adult periodontitis patients. A double-blind placebo controlled study. Journal of
Clinical Periodontology 28, 296–305.
Xajigeorgiou, C., Sakellari, D., Slini, T., Baka, A. & Konstantinidis, A. (2006)
Clinical and microbiological effects of different antimicrobials on generalized
aggressive periodontitis. Journal of Clinical Periodontology 33, 254–264.
Yek, E.C., Cintan, S., Topcuoglu, N., Kulekci, G., Issever, H. & Kantarci, A.
(2010) Efficacy of amoxicillin and metronidazole combination for the
management of generalized aggressive periodontitis. Journal of Periodontology
81, 964-974. Figures legends: Figure 1. Flow chart of the study design.
Figure 2. Plots of the mean changes in individual full-mouth mean clinical
attachment level between baseline and 1 year post-SRP of subjects in the two
treatment groups. The circles represent the mean value of each subject. The
line represents the median of change of this clinical parameter in all 30
subjects. Positive values represent a gain in clinical attachment level (CAL),
while negative values represent a loss in CAL at 1 year post-SRP. SRP, scaling
and root planing; MTZ, metronidazole; AMX, amoxicillin.

52
Table 1. Demographic characteristics and mean (± SD) full-mouth clinical parameters at baseline and at follow-up visits. Treatment groups Variable Time-point SRP
(n=15) SRP+MTZ+AMX
(n=15) MW
(p-value) Gender (male/female)* Baseline 4/11 6/9 0.56711 Age (years) Baseline 27.6 ± 3.5 26.8 ± 3.9 0.23423 Baseline 4.09 ± 0.62a 4.27 ± 0.71 a 0.66311 PD (mm) 6 months 3.16 ± 0.52 b 2.64 ± 0.35 b 0.00246 1 year 3.17 ± 0.46 b 2.64 ± 0.42 b 0.00264 CAL (mm) Baseline 4.23 ± 0.50 a 4.47 ± 0.84 a 0.39516 6 months 3.50 ± 0.63 b 3.23 ± 0.54 b 0.19136 1 year 3.63 ± 0.58 b 3.32 ± 0.74 b 0.14089 % sites with Baseline 62.7 ± 22.4 a 61.3 ± 19.8 a 0.93389 Plaque accumulation 6 months 34.0 ± 14.0 b 35.9 ± 13.7 b 0.70889 1 year 33.3 ± 13.2 b 35.9 ± 13.6 b 0.77153 Baseline 23.7 ± 20.4 a 37.3 ± 27.2 a 0.64817 Gingival bleeding 6 months 7.5 ± 9.1 b 3.4 ± 3.8 b 0.21281 1 year 7.9 ± 7.5 b 9.3 ± 8.7 b 0.69310 Baseline 63.8 ± 21.3 a 77.7 ± 19.7 a 0.17093 Bleeding on probing 6 months 16.4 ± 13.5 b 10.7 ± 8.8 b 0.30947 1 year 13.7 ± 10.3 b 10.0 ± 7.1 b 0.35058 Baseline 3.8 ± 9.3 a 1.8 ±3 .8 a 0.11869 Suppuration 6 months 0.3 ± 0.8 b 0.5 ± 1.1 b 0.63186 1 year 0.4 ± 0.9 b 0.3 ± 0.6 b 0.78988 The significance of differences between baseline and the follow-up visits was assessed using Friedman and Dunn’s multiple comparison tests (different letters indicate significant differences between time points). The significance of differences between groups at each time point was assessed using the Mann-Whitney (MW) and Chi-square Test (*). SRP, scaling and root planing; MTZ, metronidazole; AMX, amoxicillin; PD, probing depth; CAL, clinical attachment level; SD, standard deviation.

53
Table 2. Mean PD reduction and CA gain between baseline and 6 months and 1 year post-therapy. Treatment groups
Baseline PD
Variable Time-point SRP
(n=15)
SRP+MTZ+AMX
(n=15)
MW
(p-value)
Full-mouth
PD reduction 0-6 months 0.94 ± 0.38 1.58 ± 0.51 0.00084
0-1 year 0.92 ± 0.47 1.61 ± 0.60 0.00230
CA gain 0-6 months 0.78 ± 0.41 1.23 ± 0.41 0.01074
0-1 year 0.93 ± 0.47 1.61 ± 0.60 0.00230
4-6mm
PD reduction 0-6 months 1.33 ± 0.41 2.09 ± 0.40 0.00021
0-1 year 1.41 ± 0.47 2.30 ± 0.29 0.00002
CA gain 0-6 months 1.12 ± 0.50 1.72 ± 0.41 0.00302
0-1 year 1.11 ± 0.63 1.96 ± 0.44 0.00072
≥7mm
PD reduction 0-6 months 2.79 ± 0.74 4.27 ± 1.34 0.00017
0-1 year 2.78 ± 1.09 4.18 ± 1.42 0.00139
CA gain 0-6 months 2.34 ± 0.81 3.43 ± 1.14 0.00024
0-1 year 2.32 ± 1.11 3.35 ± 1.23 0.00227
The significance of differences between groups at each time point was assessed using the Mann-Whitney test (MW).
SRP, scaling and root planing; MTZ, metronidazole; AMX, amoxicillin; PD, probing depth; PD, probing depht; CA, clinical attachment; SD, standard deviation

54
Table 3. Mean number and (mean percentage) ± SD of sites with PD ≥ 5mm and PD ≥ 6mm at baseline and at follow-up visits. Treatment groups Variable Time-point SRP
(n=15) SRP+MTZ+AMX
(n=15) MW
(p-value)
Baseline 52.2 ± 18.0a (34.8 ± 10.9)
52.5 ± 17.9 a (37.3 ± 12.7 )
0.98348
PD≥5mm 6 months 19.0 ± 16.0b (12.9 ± 10.6)
7.6 ± 8.9 b (5.8± 6.8)
0.00606
1 year 23.1 ± 13.4b (16.0 ± 8.8)
6.4 ± 7.2 b (5.2 ± 6.1)
0.00028
Baseline 25.5 ± 17.5 a
(17.0 ± 11.1)
33.5 ± 18.4a (24.3 ± 13.2)
0.22861
PD≥6mm 6 months 8.7 ± 13.3 b (5.9 ± 8.3)
3.7 ± 6.5b (2.8 ± 4.5)
0.01637
1 year 9.9 ± 11.9 b (6.7 ± 7.9)
3.3 ± 5.1 b (2.7 ± 4.4)
0.00338
The significance of differences between baseline and the follow-up visits was assessed using Friedman and Dunn’s multiple comparison tests (different letters indicate significant differences between time points). The significance of differences between groups at each time point was assessed using the Mann-Whitney test (MW). SRP, scaling and root planing; MTZ, metronidazole; AMX, amoxicillin; PD, probing depth; BOP, bleeding on probing.

55
Table 4. Number and percentage of subjects presenting low (<4 sites with PD≥5 mm), moderate (5-8 sites with PD≥5 mm) or high (≥9 sites with PD≥5 mm) risk for disease progression according to Lang & Tonetti (2003) as well as presenting 0, 1-2 or ≥3 sites with PD≥6 mm at 1 year post-treatment.
Treatment groups Chi-square
p-value Variable Categories SRP SRP+MTZ+AMX
Risk for disease progression
Low risk 1 (6.6%) 8 (53.3%)
Moderate risk 02 (13.4%) 3 (20.0%) 0.008
High risk 12 (80.0%) 4(26.7%)
Number of PD
>6mm
0 0 (0.0%) 5 (33.3%)
1-2 2 (13.4%) 4 (26.7%) 0.031
≥3 13 (86.6%) 6 (40.0%)
The significance of differences between groups was assessed using Chi-Square Test.
SRP, scaling and root planing; MTZ, metronidazole; AMX, amoxicillin; PD, probing
depth

56
200 subjects assessed for eligibility
30 subjects randomized
170 excluded. Reason: Not meeting inclusion
criteria
SRP
n=15
SRP+MTZ+AMX
n=15
Lost to follow up: n=2
Reason: could not be contacted
n=13 with complete data
n=15 analyzed
Lost to follow up: n=2
Reason: could not be contacted
n=13 with complete data
n=15 analyzed
Screening
Allocation
6 months
1 year
Figure 1.
Lost to follow up: n=0
n=15 with complete data
n=15 analysed
Lost to follow up: n=0
n=15 with complete data
n=15 analysed
Lost to follow up: n=0
n=15 with complete data
n=15 analysed

57
Figure 2.
SRP
SRP+MTZ+AMX

58
5. CONCLUSÃO A associação de metronidazol e amoxicilina à RAR apresentou
benefícios clínicos adicionais na terapia de indivíduos com doença periodontal
agressiva generalizada comparada à RAR apenas, mantendo esses
parâmetros durante 1 ano.

59
REFERÊNCIAS BIBLIOGRÁFICAS
AIMETTI M, ROMANO F, GUZZI N, CARNEVALE G. Full-mouth disinfection
and systemic antimicrobial therapy in generalized aggressive periodontitis: a
randomized, placebo-controlled trial. J Clin Periodontol v. 39, p. 284-294,
2012.
AINAMO J, BAY I. Problems and proposals for recording gingivitis and plaque.
Int Dent J. v.25, n. 4, p. 229-35, Dec. 1975.
ALBANDAR JM. Prevalence of incipient radiographic periodontal lesions in
relation to ethnic background and dental care provisions in young adults. J Clin
Periodontol. v. 16, n. 10, p. 625-9, Nov. 1989.
ALBANDAR JM, BUISCHI YA, BARBOSA MF. Destructive forms of periodontal
disease in adolescents. A 3-year longitudinal study. J Periodontol. v. 62, n. 6,
p. 370-6, Jun. 1991.
ALBANDAR JM, BROWN LJ, LÖE H. Clinical features of early-onset
periodontitis. J Am Dent Assoc. v. 128, n. 10, p. 1393-9, Oct. 1997.

60
ALBANDAR JM, MURANGA MB, RAMS TE. Prevalence of aggressive
periodontitis in school attendees in Uganda. J Clin Periodontol. v. 29, n. 9, p.
823-31, Sep. 2002.
ARAUJO MW, HOVEY KM, BENEDEK JR, GROSSI SG, DORN J,
WACTAWSKI-WENDE J, GENCO RJ, TREVISAN M. Reproducibility of
probing depth measurement using a constant-force electronic probe: analysis of
inter- and intraexaminer variability. J Periodontol. v. 74, n. 12, p. 1736-40, Dec.
2003.
ARIRACHAKARAN P, APINHASMIT W, PAUNGMALIT P, JERAMETHAKUL
P, RERKYEN P, MAHANONDA R. Infection of human gingival fibroblasts with
Aggregatibacter actinomycetemcomitans: An in vitro study. Arch Oral Biol. Feb
18, 2012 - [Epub ahead of print]
ARMITAGE GC. Development of a classification system for periodontal
diseases and conditions. Ann Periodontol. v. 4, n. 1, p. 1-6, Dec. 1999.
BAER PN. The case for periodontosis as a clinical entity. J Periodontol. v. 42,
n. 8, p. 516-20, Aug. 1971.

61
BALTACIOGLU E, ASLAN M, SARAÇ Ö, SAYBAK A, YUVA P. Analysis of
clinical results of systemic antimicrobials combined with nonsurgical periodontal
treatment for generalized aggressive periodontitis: a pilot study. J Can Dent
Assoc. v. 77, n. b97, 2011.
BARKVOLL P, ROLLA G, SVENDSEN K. Interaction between chlorhexidine
digluconate and sodium lauryl sulfate in vivo. J Clin Periodontol. v. 16, n. 9, p.
593-5, Oct. 1989.
BROGAN JM, LALLY ET, POULSEN K, KILIAN M, DEMUTH DR. Regulation
of Actinobacillus actinomycetemcomitans leukotoxin expression: analysis of the
promoter regions of leukotoxic and minimally leukotoxic strains. Infect Immun.
v. 62, n. 2, p. 501-8, Feb. 1994.
CALIFANO JV. Research, Science and Therapy Committee American Academy
of Periodontology. Position paper: periodontal diseases of children and
adolescents. J Periodontol. v. 74, n. 11, p. 1696-704, Nov. 2003.
CARVALHO LH, D'AVILA GB, LEÃO A, HAFFAJEE AD, SOCRANSKY SS,
FERES M. Scaling and root planing, systemic metronidazole and professional
plaque removal in the treatment of chronic periodontitis in a Brazilian
population. I. clinical results. J Clin Periodontol. v. 31, n. 12, p. 1070-6, Dec.
2004.

62
CARVALHO LH, D'AVILA GB, LEÃO A, GONÇALVES C, HAFFAJEE AD,
SOCRANSKY SS, FERES M. Scaling and root planing, systemic metronidazole
and professional plaque removal in the treatment of chronic periodontitis in a
Brazilian population II--microbiological results. J Clin Periodontol. v. 32, n. 4,
p. 406-11, Apr. 2005.
CHRISTERSSON LA, SLOTS J, ZAMBON JJ, GENCO RJ. Transmission and
colonization of Actinobacillus actinomycetemcomitans in localized juvenile
periodontitis patients. J Periodontol. v. 56, n. 3, p. 127-31, Mar. 1985.
CORTELLI SC, JORGE AO, CORTELLI JR, JORDAN SF, HARASZTHY VI.
Detection of highly and minimally leukotoxic Actinobacillus
actinomycetemcomitans strains in patients with periodontal disease. Pesqui
Odontol Bras. v. 17, n. 2, p. 183-8, Apr-Jun, 2003.
CORTELLI JR, CORTELLI SC, JORDAN S, HARASZTHY VI, ZAMBON JJ.
Prevalence of periodontal pathogens in Brazilians with aggressive or chronic
periodontitis. J Clin Periodontol. v. 32, n. 8, p. 860-6, Aug. 2005.
CORTELLI SC, COSTA FO, KAWAI T, AQUINO DR, FRANCO GC, OHARA K,
ROMAN-TORRES CV, CORTELLI JR. Diminished treatment response of
periodontally diseased patients infected with the JP2 clone of Aggregatibacter

63
(Actinobacillus) actinomycetemcomitans. J Clin Microbiol. v. 47, n. 7, p. 2018-
25, Jul. 2009.
CUGINI MA, HAFFAJEE AD, SMITH C, KENT RL Jr, SOCRANSKY SS. The
effect of scaling and root planing on the clinical and microbiological parameters
of periodontal diseases: 12-month results. J Clin Periodontol. v. 27, n. 1, p.
30-6, Jan. 2000.
DANNEWITZ B, POHL S, EICKHOLZ P, KIM TS. Clinical and microbiological
effects of a combined mechanic-antibiotic therapy in subjects with Actinobacillus
actinomycetemcomitans-associated periodontitis. Am J Dent. v. 20, n. 3, p.
153-6, Jun. 2007.
DARBY IB, HODGE PJ, RIGGIO MP, KINANE DF. Microbial comparison of
smoker and non-smoker adult and early-onset periodontitis patients by
polymerase chain reaction. J Clin Periodontol. v. 27, n. 6, p. 417-24, Jun.
2000.
DAVIES AH, McFADZEN JA, SQUIRES S. Treatment of Vicent´s stomatitis with
metronidazole. Br Med. v. 1, n. 5391, p. 1149-50, May. 1964.

64
DIEHL SR, Wu T, MICHALOWICZ BS, BROOKS CN, CALIFANO JV,
BURMEISTER JA, SCHENKEIN HA. Quantitative measures of aggressive
periodontitis show substantial heritability and consistency with traditional
diagnoses. J Periodontol. v. 76, n. 2, p. 279-88, Feb. 2005.
ELAMIN AM, SKAUG N, ALI RW, BAKKEN V, ALBANAR JM. Ethnic disparities
in the prevalence of periodontitis among high school students in Sudan. J
Periodontol. v. 81, n. 6, p. 891-6, Jun. 2010.
ENNIBI OK, BENRACHADI L, BOUZIANE A, HAUBEK D, POULSEN K. The
highly leukotoxic JP2 clone of Aggregatibacter actinomycetemcomitans in
localized and generalized forms of aggressive periodontitis. Acta Odontol
Scand. Jan 18. 2012 [Epub ahead of print]
FAVERI M, GURSKY LC, FERES M, SHIBLI JA, SALVADOR SL, de
FIGUEIREDO LC. Scaling and root planing and chlorhexidine mouthrinses in
the treatment of chronic periodontitis: a randomized, placebo-controlled clinical
trial. J Clin Periodontol v. 33, n. 11, p. 819-828, Nov. 2006.
FAVERI M, MAYER MP, FERES M, de FIGUEIREDO LC, DEWHIRST FE,
PASTER BJ. Microbiological diversity of generalized aggressive periodontitis
by 16S rRNA clonal analysis. Oral Microbiol Immunol. v. 23, n. 2, p. 112-8,
Apr. 2008.

65
FAVERI M, FIGUEIREDO LC, DUARTE PM, MESTNIK MJ, MAYER MP,
FERES M. Microbiological profile of untreated subjects with localized
aggressive periodontitis. J Clin Periodontol. v. 36, n. 9, p. 739-49, Sep, 2009.
FERES M, HAFFAJEE AD, ALLARD K, SOM S, GOODSON JM, SOCRANSKY
SS. Antibiotic resistance of subgingival species during and after antibiotic
therapy. J Clin Periodontol. V.29, n. 8, p. 724-35, Aug, 2002.
GAJARDO M, SILVA N, GÓMEZ L, LEÓN R, PARRA B, CONTRERAS A,
GAMONAL J. Prevalence of periodontopathic bacteria in aggressive
periodontitis patients in a Chilean population. J Periodontol. v. 76, n. 2, p. 289-
94, Feb. 2005.
GENCO RJ, CIANCIOLA L, ROSLING B. Treatment of localized juvenile
periodontitis. J Dent Res. V. 60, Spec. Issue, P. 527(Abstr. 872), 1981.
GIEDRYS-LEEPER E, SELIPSKY H, WILLIANS BL. Effects of short-term
administration of metronidazole on the subgingival microflora. J Clin
Periodontol. v. 12, n. 10, p. 797-814, Nov. 1985.

66
GJERMO P, BELLINI HT, PEREIRA SANTOS V, MARTINS JG, FERRACYOLI
JR. Prevalence of bone loss in a group of Brazilian teenagers assessed on bite-
wing radiographs. J Clin Periodontol. v. 11, n. 2, p. 104-13, Fev. 1984.
GLENWRIGHT HD, SIDAWAY DA. The use of metronidazole in treatment of
acute ulcerative gingivits. Br Dent J. v. 121, n. 4, p. 174–7, Aug. 1966.
GORDON JM, WALKER CB. Current status of systemic antibiotic usage in
destructive periodontal disease. J Periodontol. v. 64, n. 8, Suppl, p. 760-71,
Aug. 1993.
GUERRERO A, GRIFFITHS GS, NIBALI L, SUVAN J, MOLES DR, LAURELL
L, TONETTI MS. Adjunctive benefits of systemic amoxicillin and metronidazole
in non-surgical treatment of generalized aggressive periodontitis: a randomized
placebo-controlled clinical trial. J Clin Periodontol. v. 32, n. 10, p. 1096-107,
Oct. 2005.
GUERRERO A, ECHEVERRÍA JJ, TONETTI MS. Incomplete adherence to an
adjunctive systemic antibiotic regimen decreases clinical outcomes in
generalized aggressive periodontitis patients: a pilot retrospective study. J Clin
Periodontol. v. 34, n. 10, p. 897-902, Oct. 2007.

67
HAAS AN, CASTRO GD, MORENO T, SUSIN C, ALBANDAR JM,
OPPERMANN R, RÖSING K. Azitromycin as an adjunctive treatment of
aggressive periodontitis: 12-months randomized clinical Trial. J Clin
Periodontol. v. 35, p. 696-704, May. 2008.
HAAS AN, SILVA-BOGHOSSIAN CM, COLOMBO AP, SUSIN C, ALBANDAR
JM, OPPERMANN RV, RÖSING CK. Adjunctive Azithromycin in the Treatment
of Aggressive Periodontitis: Microbiological Findings of a 12-Month Randomized
Clinical Trial. J Dent. Mar 20, 2012. [Epub ahead of print]
HAFFAJEE AD, CUGINI MA, DIBART S, SMITH C, KENT RL Jr, SOCRANSKY
SS. The effect of SRP on the clinical and microbiological parameters of
periodontal diseases. J Clin Periodontol. v. 24, n. 5, p. 324-34, May. 1997.
HAFFAJEE AD, SOCRANSKY SS, GUNSOLLEY JC. Systemic anti-infective
periodontal therapy. A systemic review. Ann Periodontol v. 8, p. 15-181, Dec.
2003.
HAFFAJEE AD, TORRESYAP G, SOCRANSKY SS. Clinical changes following
four different periodontal therapies for the treatment of chronic periodontitis: 1-
year results. J Clin Periodontol. v. 34, n. 3, p. 243-53, 2007.

68
HAN NM, XIAO XR, ZHANG LS, RI XQ, ZHANG JZ, TONG YH, YANG MR,
XIAO ZR. Bacteriological study of juvenile periodontitis in China. J Periodontal
Res. v. 26, n. 5, p. 409-14, Sep. 1991.
HAYES C, ANTCZAK-BOUCKOMS A, BURDICK E. Quality assessment and
meta-analysis of systemic tetracycline use in chronic adult periodontitis. J Clin
Periodontol. v. 19, n. 3, p. 164-8. Mar. 1992.
HERRERA D, SANZ M, JEPSEN S, NEEDLE,AN I, ROLDÁN S. A systematic
review on the effect of systemic antimicrobials as an adjunct to scaling and root
planing in periodontitis patients. J Clin Periodontol. v. 29, Suppl, p. 3:136-59,
2002.
HERRERA D, ALONSO B, LEÓN R, ROLDÁN S, SANZ M. Antimicrobial
therapy in periodontitis: the use of systemic antimicrobials against the
subgingival bofilm. Review. J Clin Periodontol. v. 35, n. 8, Suppl, p. 45-66,
Sep. 2008.
HÖGLUND ÅBERG C, KWAMIN F, CLAESSPM R, JOHANSSON A, HAUBEK
D. Presence of JP2 and Non-JP2 Genotypes of Aggregatibacter
actinomycetemcomitans and Periodontal Attachment Loss in Adolescents in
Ghana. J Periodontol. Mar 1. 2012 [Epub ahead of print]

69
HORMAND J, FRANDSEN A. Juvenile periodontitis. Localization of bone loss in
relation to age, sex, and teeth. J Clin Periodontol. v. 6, n. 6, p. 407-16, Dec.
1979.
HUGOSON A, LUNDGREN D, ASKLÖW B, BORGKLINT G. Effect of three
different dental health preventive programmes on young adult individuals: a
randomized, blinded, parallel group, controlled evaluation of oral hygiene
behaviour on plaque and gingivitis. J Clin Periodontol. v. 34, n. 5, p. 407-15,
May. 2007.
ISHIKAWA I, KAWASHIMA Y, ODA S, IWATA T, ARAKAWA S. Three case
reports of aggressive periodontitis associated with Porphyromonas gingivalis in
younger patients. J Periodontal Res. v. 37, n. 5, p. 324-32, Oct. 2002.
JEFFCOAT MK, REDDY MS. Progression of probing attachment loss in adult
periodontitis. J Periodontol. v. 62, n. 3, p. 185-9, Mar. 1991.
JOHANSSON A, CLAESSON R, HANSTROM L, SANDSTROM G, KALFAS S.
Polymorphonuclear leukocyte degranulation induced by leukotoxin from
Actinobacillus actinomycetemcomitans. J Periodontal Res. v. 35, n. 2, p. 85-
92, Apr. 2000.

70
KAMMA JJ, NAKOU M, PERSSON RG. Association of early onset periodontitis
microbiota with aspartate aminotransferase activity in gingival crevicular fluid. J
Clin Periodontol. v. 28, n. 12, p. 1096-105, Dec. 2001.
KAMMA JJ, NAKOU M, GMÜR R, BAEHNI PC. Microbiological profile of early
onset/aggressive periodontitis patients. Oral Microbiol Immunol.v. 19, n. 5, p.
314-21, Oct. 2004.
KOLODRUBETZ D, DAILEY T, EBERSOLE J, KRAIG E. Cloning and
expression of the leukotoxin gene from Actinobacillus actinomycetemcomitans.
Infect Immun. v. 57, n. 5, p. 1465-9, May. 1989.
KRONAUER E, BORSA G, LANG NP. Prevalence of incipient juvenile
periodontitis at age 16 years in Switzerland. J Clin Periodontol. v. 13, n. 2, p.
103-8, Feb. 1986.
KULIK EM, LENKEIT K, CHENAUX S, MEYER J. Antimicrobial susceptibility of
periodontopathogenic bacteria. J Antimicrob Chemother. v. 61, n. 5, p. 1087-
91, May. 2008.

71
LANG N, BARTHOLD, PM CULLIMAN M, et al. Consensus Report: Aggressive
periodontitis. Annais of Periodontology n. 4, p. 53, Dec. 1999.
LEE JW, CHOI BK, YOO YJ, CHOI SH, CHO KS, CHAI JK, KIM CK.
Distribution of periodontal pathogens in Korean aggressive periodontitis. J
Periodontol. v. 74, n. 9, p. 1329-35, Sep. 2003.
LEKOVIC V, KENNEY EB, CARRANZA FAJ, ENDRES B. The effect of
metronidazole on human periodontal disease: a clinical and bacteriological
study. J Periodontol. v. 54, n. 8, p. 476-80, Aug. 1983.
LEVIN L, ELI I, ASHKENAZI M. Dental anxiety among young Israeli male adults
as related to treatment received during childhood. J Public Health Dent. v. 66,
n. 2, p. 147-51, Spring. 2006.
LINDHE J. Treatment of localized periodontitis. In: Genco RJ, Mergenhagen
SE, (ed.). Host-parasite interactions in periodontal diseases. American Society
for Microbiology. p. 382–394, 1982.
LINDHE J, LILJENBERG B. Treatment of localized juvenile periodontitis.
Results after 5 years. J Clin Periodontol. v. 11, n. 6, p. 399-410, Jul. 1984.

72
LISTGARTEN MA, LINDHE J, HELLDEN L. Effect of tetracycline and/or scaling
on human periodontal disease. Clinical, microbiological, and histological
observations. J Clin Periodontol. v. 5, n. 4, p. 246-71, nov. 1978.
LÖE H, ANERUD A, BOYSEN H, SMITH M. The natural history periodontal
disease in man: the rate of periodontal destruction before 40 years of age. J
Periodontol. v. 49, n. 12, p. 607-20, Dec. 1978.
LÖE H, ANERUD A, BOYSEN H, MORRISON E. Natural history of periodontal
disease in man: rapid, moderate and no loss of attachment in Sri Lankan
laborers 14 to 46 years of age. J Clin Periodontol. v. 13, n. 5, p. 431-45, 1986.
LOESCHE WJ, SYED SA, LAUGHON BE, STOLL J. The bacteriology of acute
necrotizing ulcerative gingivitis. J Periodontol. v. 53, n. 4, p. 223-30, Apr. 1982.
LOESCHE WJ, SYED SA, MORRISON EC, KERRY GA, HIGGINS T, STOLL J.
Metronidazole in periodontitis. I. Clinical and bacteriological results after 15 to
30 weeks. J Periodontol. v. 55, n. 6, p. 325-35, Jun. 1984.
LOESCHE WJ, SYED SA, Schmidt E, Morrison EC. Bacterial profiles of
subgingival plaques in periodontitis. J Periodontol. v. 56, n. 8, p. 447-56, Aug.
1985.

73
LÓPEZ NJ. Clinical, laboratory, and immunological studies of a family with a
high prevalence of generalized prepubertal and juvenile periodontitis. J
Periodontol. v. 63, n. 5, p. 457-68, May. 1992.
LÓPEZ NJ, MELLADO JC, LEIGHTON GX. Occurrence of Actinobacillus
actinomycetemcomitans, Porphyromonas gingivalis and Prevotella intermedia in
juvenile periodontitis. J Clin Periodontol. v. 23, n. 2, p. 101-5, Feb. 1996.
LÓPEZ NJ, GAMONAL JA. Effects of metronidazole plus amoxicillin in
progressive untreated adult periodontitis: Results of a single 1-week course
after 2 and 4 months. J Periodontol. v. 69, n. 11, p. 1291-8, Nov. 1998.
LÓPEZ NJ, GAMONAL JA, MARTINEZ B. Repeated metronidazole and
amoxicillin treatment of periodontitis. A follow-up study. J Periodontol. v. 71, n.
1, p. 79-89, Jan. 2000.
LÓPEZ NJ, SOCRANSKY SS, Da SILVA I, JAPLIT MR, HAFFAJEE AD. Effects
of metronidazole plus amoxicillin as the only therapy on the microbiological and
clinical parameters of untreated chronic periodontitis. J Clin Periodontol. v. 33,
n. 9, p. 648-60, Sep. 2006.
MANDELL Rl, SOCRANSKY SS. A selective medium for Actinobacillus
actinomycetemcomitans and the incidence of the organism in juvenile
periodontitis. J Periodontol. v. 52, n. 10, p. 593-8, Oct. 1981.

74
MATARAZZO F, FIGUEIREDO LC, CRUZ SE, FAVERI M, FERES M. Clinical
and microbiological benefits of systemic metronidazole and amoxicillin in the
treatment of smokers with chronic periodontitis: a randomized placebo-
controlled study. J Clin Periodontol. v. 35, n. 10, p. 885-96, Oct. 2008.
MAYER MP, BUENO LC, HANSEN EJ, DiRIENZO JM. Identification of a
cytolethal distending toxin gene locus and features of a virulence-associated
region in Actinobacillus actinomycetemcomitans. Infect Immun. v. 67, n. 3, p.
1227-37, Mar. 1999.
MENGH, XU L, LI Q, HAN J, ZHAO Y. Determinants of host susceptibility in
aggressive periodontitis. Review. Periodontol 2000. n. 43, p. 133-59, 2007.
MESTNIK MJ, FERES M, FIGUEIREDO LC, DUARTE PM, LIRA EA, FAVERI
M. Short-term benefits of the adjunctive use of metronidazole plus amoxicillin in
the microbial profile and in the clinical parameters of subjects with generalized
aggressive periodontitis. J Clin Periodontol. v. 37, n. 4, p. 353-65, Apr. 2010.
MOMBELLI A, CASAGNI F, MADIANOS PN. Can presence or absence of
periodontal pathogens distinguish between subjects with chronic and
aggressive periodontitis? A systematic review. J Clin Periodontol. v. 29, n. 3,
Suppl, p. 10-21, 2002.

75
MOEINTAGHAVI A, TALEBI-ARDAKANI MR, HAERIAN-ARDAKANI A, ZANDI
H, TAGHIPOUR S, FALLAHZADEH H, PAKZAD A, FAHAMI N. Adjunctive
effects of systemic amoxicillin and metronidazole with scaling and root planing:
a randomized, placebo controlled clinical trial. J Contemp Dent Pract. v. 8, n.
5, p. 51-9, Jul. 2007.
MONTGOMERY EH. Antibióticos antibacterianos. In: Yagiela JA, Neidle EA,
Dowd FJ. Farmacologia e terapêutica para dentistas. Rio de Janeiro:
Guanabara Koogan, p. 468-502, 2000.
MULLALLY BH, DACE B, SHELBURNE CE, WOLFF LF, COULTER WA.
Prevalence of periodontal pathogens in localized and generalized forms of
early-onset periodontitis. J Periodontal Res. v. 35, n. 4, p. 232-41, Aug. 2000.
NIBALI L, DONOS N, BRETT PM, PARKAR M, ELLINAS T, LLORENTE M,
GRIFFITHS GS. A familial analysis of aggressive periodontitis - clinical and
genetic findings. J Periodontal Res. v. 43, n. 6, p. 627-34, Dec. 2008.
NOVAK MJ, POLSON AM, ADAIR SM. Tetracycline therapy in patients with
early juvenile periodontitis. J Periodontol. v. 59, n. 6, p. 366-72, Jun. 1988.
NOVAK MJ, STAMATELAKYS C, ADAIR SM. Resolution of early lesions of
juvenile periodontitis with tetracycline therapy alone: long-term observations of

76
4 cases. J Periodontol. v. 62, n. 10, p. 628-33, Oct. 1991. Erratum in: J
Periodontol. v. 63, n. 2, p. 148, Feb. 1992.
OWENS J, ADDY M, FAULKNER J, LOCKWOOD C, Adair R. A short-term
clinical study design to investigate the chemical plaque inhibitory properties of
mouthrinses when used as adjuncts to toothpastes: applied to chlorhexidine. J
Clin Periodontol. v. 24, n. 10, p. 732-7, Oct. 1997.
PAGE RC, SCHROEDER HE. Pathogenesis of inflammatory periodontal
disease. A summary of current work. Review. Lab Invest. v. 34, n. 3, p. 235-49,
Mar. 1976.
PAJU S, GOULHEN F, ASIKAINEN S, GRENIER D, MAYRAND D, UITTO V.
Localization of heat shock proteins in clinical Actinobacillus
actinomycetemcomitans strains and their effects on epithelial cell proliferation.
FEMS Microbiol Lett. v. 182, n. 2, p. 231-5, Jan. 2000.
PAVICIC MJ, van WINKELHOFF AJ, de GRAAFF J. Synergistic effects
between amoxicillin, metronidazole, and the hydroxymetabolite of
metronidazole against Actinobacillus actinomycetemcomitans. Antimicrob
Agents Chemother. v. 35, n. 5, p. 961-6, May. 1991.

77
PAVICIC MJ, van WINKELHOFF AJ, de GRAAFF J. In vitro susceptibilities of
Actinobacillus actinomycetemcomitans to a number of antimicrobial
combinations. Antimicrob Agents Chemother. v. 36, n. 12, p. 2634-8, Dec.
1992.
PAVICIC MJ, van WINKELHOFF AJ, DOUQUÉ NH, STEURES RW, de
GRAAFF J. Microbiological and clinical effects of metronidazole and amoxicillin
in Actinobacillus actinomycetemcomitans-associated periodontitis. A 2-year
evaluation. J Clin Periodontol. v. 21, n. 2, p. 107-12, Feb. 1994.
ROSLING B, SERINO G, HELLSTROM Mk, SOCRANSKY SS, LINDHE J.
Longitudinal periodontal tissue alterations during supportive therapy: findings
from subjects with normal and high suscepyibility to periodontal disease. J Clin
Periodontol. v. 28, n. 3, p. 241-9, Mar. 2001.
RUSSO PA, NOWZARI H, SLOTS J. Transmission and persistence of
Actinobacillus actinomycetemcomitans in twins with advanced periodontitis. J
Calif Dent Assoc. v. 26, n. 4, p. 290-4, Apr. 1998.
SAXBY M. Prevalence of juvenile periodontitis in a British school population.
Community Dent Oral Epidemiol. v. 12, n. 3, p. 185-7, Jun. 1984.
SGOLASTRA F, PETRUCCI A, GATTO R, MONACO A. Effectiveness of
Systemic Amoxicillin/Metronidazole as an Adjunctive Therapy to Full-Mouth

78
Scaling and Root Planing in the Treatment of Aggressive Periodontitis: A
Systematic Review and Meta-Analysis. J Periodontol. Nov 3. 2011. [Epub
ahead of print]
SGOLASTRA F, GATTO R, PETRUCCI A, MONACO A. Effectiveness of
Systemic Amoxicillin/Metronidazole as Adjunctive Therapy to Scaling and Root
Planing in the Treatment of Chronic Periodontitis: A Systematic Review and
Meta-Analysis. J Periodontol. Feb 14. 2012. [Epub ahead of print]
SILVA MP, FERES M, SIROTTO TA, SOARES GM, MENDES JA, FAVERI M,
FIGUEIREDO LC. Clinical and microbiological benefits of metronidazole alone
or with amoxicillin as adjuncts in the treatment of chronic periodontitis: a
randomized placebo-controlled clinical trial. J Clin Periodontol. V. 38, n. 9, p.
828-37, Sep. 2011.
SLOTS J, REYNOLDS HS, GENCO RJ. Actinobacillus
actinomycetemcomitans in human periodontal disease: a cross-sectional
microbiological investigation. Infect Immun. v. 29, n. 3, p. 1013-20, Sep. 1980.
SLOTS J, ROSLING BG. Suppression of the periodontopathic microflora in
localized juvenile periodontitis by systemic tetracycline. J Clin Periodontol. v.
10, n. 5, p. 465-86, Sep. 1983.

79
SLOTS J. Research, Science and Therapy Committee. Systemic antibiotics in
periodontics. J Periodontol. v. 75, n. 11, p. 1553-65, Nov. 2004.
SOCRANSKY SS, HAFFAJEE AD, GOODSON JM, LINDHE J. New concepts
of destructive periodontal disease. J Clin Periodontol. v. 11, n. 1, p. 21-32,
Jan. 1984.
SOCRANSKY SS, HAFFAJEE AD. Evidence of bacterial etiology: a historical
perspective. Rewiew. Periodontol 2000. n. 5, p. 7-25, Jun. 1994.
SOCRANSKY SS, HAFFAJEE AD. Dental biofilms: difficult therapeutic targets.
Review. Periodontol 2000. n. 28, p. 12-55, 2002.
SOCRANSKY SS, HAFFAJEE AD. Periodontal microbial ecology. Review.
Periodontol 2000. n. 38, p. 135-87, 2005.
SUGAI M, KAWAMOTO T, PÉRÈS SY, UENO Y, KOMATSUZAWA H,
FUJIWARA T, KURIHARA H, SUGINAKA H, OSWALD E. The cell cycle-
specific growth-inhibitory factor produced by Actinobacillus
actinomycetemcomitans is a cytolethal distending toxin. Infect Immun. v. 66, n.
10, p. 5008-19, Oct. 1998.

80
TAKEUCHI Y, UMEDA M, ISHIZUKA M, HUANG Y, ISHIKAWA I. Prevalence
of periodontopathic bacteria in aggressive periodontitis patients in a Japanese
population. J Periodontol. v. 74, n. 10, p. 1460-9, Oct. 2003.
TALLY FP, SUTTER VL, FINEGOLD SM. Treatment of anaerobic infections
with metronidazole. Antimicrob Agents Chemother. v. 7, n. 5, p. 672-5, May.
1975.
TELES RP, HAFFAJEE AD, SOCRANSKY SS. Microbiological goals of
periodontal therapy. Rewiew. Periodontol 2000. n. 42, p. 180-218, 2006.
TIMMERMAN MF, Van der WEIJDEN GA, ARMAND S, ABBAS F, WINKEL
EG, Van WINKELHOFF AJ, Van der VELDEN U. Untreated periodontal disease
in Indonesian adolescents. Clinical and microbiological baseline data. J Clin
Periodontol. v. 25, n. 3, p. 215-24, Mar. 1998.
TINOCO EM, BELDI MI, LOUREIRO CA, LANA M, CAMPEDELLI F, TINOCO
NM, GJERMO P, PREUS HR. Localized juvenile periodontitis and
Actinobacillus actinomycetemcomitans in a Brazilian population. Eur J Oral Sci.
v. 105, n. 1, p. 9-14, Feb. 1997.

81
TONETTI MS, MOMBELLI A. Early-onset periodontitis. Ann Periodontol. v. 4,
n. 1, p. 39-53, Dec. 1999.
TREVILATTO PC, TRAMONTINA VA, MACHADO MA, GONÇALVES RB,
SALLUM AW, LINE SR. Clinical, genetic and microbiological findings in a
Brazilian family with aggressive periodontitis. J Clin Periodontol. v. 29, n. 3, p.
233-9, Mar. 2002.
VARELA VM, HELLER D, SILVA-SENEM MX, TORRES MC, COLOMBO AP,
FERES-FILHO EJ. Systemic antimicrobials adjunctive to a repeated mechanical
and antiseptic therapy for aggressive periodontitis: a 6-month randomized
controlled trial. J Periodontol. v. 82, n. 8, p. 1121-30, Aug. 2011.
VIANA CASARIN RC, RIBEIRO ED, SALLUM EA, NOCITI-Jr FH,
GONÇALVES RB, CASATI MZ. Amoxicillin/Metronidazole Improves Clinical
and Microbiological Results of One-Stage, Full Mouth, Ultrasonic Debridement
in Aggressive Periodontitis Treatment. J Periodontol. Jan 2012. [Epub ahead
of print]
WALKER CB, PAPPAS JD, TYLER KZ, COHEN S, GORDON JM. Antibiotic
susceptibilities of periodontal bacteria. In vitro susceptibilities to eight
antimicrobial agents. J Periodontol. v. 56, Suppl.,n. 11, p. 67-74, Nov. 1985.

82
WILLIAMS BL, OSTERBERG KA, JORGENSEN J. Subgingival microflora of
periodontal patients on tetracycline therapy. J Clin Periodontol. v. 6, n. 4, p.
210-21, Aug. 1979.
WINKEL EG, van WINKELHOFF AJ, van der VELDEN U. Additional clinical and
microbiological effects of amoxicillin and metronidazole after initial periodontal
therapy. J Clin Periodontol. v. 25, n. 11Pt 1, p. 857-64, Nov. 1998.
WINKEL EG, van WINKELHOFF AJ, TIMMERMAN MF, Van der VELDEN U,
Van der WEIJDEN GA. Amoxicillin plus metronidazole in the treatment of adult
periodontitis patients. A double-blind placebo-controlled study. J Clin
Periodontol. v. 28, n. 4, p. 296-305, Apr. 2001.
van WINKELHOFF AJ, RODENBURG JP, GOENÉ RJ, ABBAS F, WINKEL EG,
de GRAAFF J. Metronidazole plus amoxycillin in the treatment of Actinobacillus
actinomycetemcomitans associated periodontitis. J Clin Periodontol. v. 16, n.
2, p. 128-31, Feb. 1989.
van WINKELHOFF AJ, TIJHOF CJ, de GRAAFF J. Microbiological and clinical
results of metronidazole plus amoxicillin therapy in Actinobacillus

83
actinomycetemcomitans-associated periodontitis. J Periodontol. v. 63, n. 1, p.
52-7, Jan. 1992.
XAJIGEORGIOU C, SAKELLARI D, SLINI T, BAKA A, KONSTANTINIDIS A.
Clinical and microbiological effects of different antimicrobials on generalized
aggressive periodontitis. J Clin Periodontol. v. 33, n. 4, p. 254-64, Apr. 2006.
YANG HW, HUANG YF, CHAN Y, CHOU MY. Relationship of Actinobacillus
actinomycetemcomitans serotypes to periodontal condition: prevalence and
proportions in subgingival plaque. Eur J Oral Sci. v. 113, n. 1, p. 28-33, Feb.
2005.
YEK EC, CINTAN S, TOPCUOGLU N, KULEKCI G, ISSEVER H, KANTARCI A.
Efficacy of amoxicillin and metronidazole combination for the management of
generalized aggressive periodontitis. J Periodontol. v. 81, n. 7, p. 964-74, Jul.
2010.
ZAMBON JJ, CHRISTERSSON LA, SLOTS J. Actinobacillus
actinomycetemcomitans in human periodontal disease. Prevalence in patient
groups and distribution of biotypes and serotypes within families. J
Periodontol. v. 54, n. 12, p. 707-11, Dec. 1983.

84
ZAMBON JJ. Actinobacillus actinomycetemcomitans in human periodontal
disease. J Clin Periodontol. v. 12, n. 1, p. 1-20, Jan. 1985.
ZAMBON JJ. Periodontal diseases: microbial factors. Ann Periodontol. v. 1, n.
1, p. 879-925, Nov. 1996.

85
ANEXO A

86
ANEXO B
PRODUÇÃO CIENTÍFICA DISCENTE VINCULADA À PESQUISA
a) Bastos MF, Lima JA, Vieira PM, Mestnik MJ, Faveri M, Duarte PM. TNF-
alpha and IL-4 levels in generalized aggressive periodontitis subjects. Oral Dis.
2009 Jan;15(1):82-7.
b) Faveri M, Figueiredo LC, Duarte PM, Mestnik MJ, Mayer MP, Feres M.
Microbiological profile of untreated subjects with localized aggressive
periodontitis. J Clin Periodontol. 2009 Sep;36(9):739-49.
c) Duarte PM, da Rocha M, Sampaio E, Mestnik MJ, Feres M, Figueiredo LC,
Bastos MF, Faveri M. Serum levels of cytokines in subjects with generalized
chronic and aggressive periodontitis before and after non-surgical periodontal
therapy: a pilot study. J Periodontol. 2010 Jul;81(7):1056-63.
d) Mestnik MJ, Feres M, Figueiredo LC, Duarte PM, Lira EA, Faveri M. Short-
term benefits of the adjunctive use of metronidazole plus amoxicillin in the
microbial profile and in the clinical parameters of subjects with generalized
aggressive periodontitis. J Clin Periodontol. 2010 Apr;37(4):353-65.
e) de Lima Oliveira AP, de Faveri M, Gursky LC, Mestnik MJ, Feres M, Haffajee
AD, Socransky SS, Teles RP. Effects of periodontal therapy on GCF cytokines
in generalized aggressive periodontitis subjects. J Clin Periodontol. 2012
Mar;39(3):295-302.