Embed Size (px)
Citation preview

MINISTÉRIO DA EDUCAÇÃO E CULTURA
UNIVERSIDADE FEDERAL DE GOIÁS
INSTITUTO DE PATOLOGIA TROPICAL E SAÚDE PÚBLICA
XISTO SENA PASSOS
Caracterização de fungos envolvidos em infecções
nosocomiais
ORIENTADORA: PROFª DRª MARIA DO ROSÁRIO RODRIGUES SILVA
Tese de Doutorado
GOIÂNIA – GO, 2007

UNIVERSIDADE FEDERAL DE GOIÁS INSTITUTO DE PATOLOGIA TROPICAL E SAÚDE PÚBLICA PROGRAMA DE PÓS-GRADUAÇÃO EM MEDICINA TROPICAL
XISTO SENA PASSOS
Caracterização de fungos envolvidos em infecções nosocomiais
ORIENTADORA: PROFª DRª MARIA DO ROSÁRIO RODRIGUES SILVA
Tese de Doutorado apresentada ao Curso de Pós-Graduação em Medicina Tropical do Instituto de Patologia e Saúde Pública da Universidade Federal de Goiás como requisito parcial para obtenção de Grau de Doutor em Medicina Tropical. Área de concentração: Microbiologia.
GOIÂNIA – GO, 2007

Dados Internacionais de Catalogação-na-Publicação (CIP)
(GPT/BC/UFG)
Passos, Xisto Sena. P289c Caracterização de fungos envolvidos em infecções nosocomiais / Xisto Sena Passos . – Goiânia, 2007. xiv,99f. : il., figs., tabs. Orientadora: Maria do Rosário Rodrigues Silva.
1 Tese ( Doutorado ) – Universidade Federal de Goiás, Instituto de Patologia Tropical e Saúde Públi- ca, 2007.
2 Bibliografia: f. 61-78. Inclui lista de abreviaturas, símbolos e unidades. Anexos. 1. Candidíase 2. Candidíase – Mucosa bucal 3. Candidíase – Mucosa vaginal 4. Fungos (Candida) – Tratamento I. Silva, Maria do Rosário Rodrigues II. Universidade Federal de Goiás, Instituto de Patologia Tropical e Saúde Pública III. Título CDU: 616.98:616.934

i
““AA DDeeuuss ppoorr sseemmpprree mmee ddaarr ffoorrççaass,, iilluummiinnaarr ee gguuiiaarr””..

ii
““AAss ttaarreeffaass ddiiáárriiaass jjaammaaiiss iimmppeeddiirraamm aallgguuéémm ddee sseegguuiirr sseeuuss ssoonnhhooss””
PPaauulloo CCooeellhhoo

iii
ÀÀ mmiinnhhaa eessppoossaa AAnnaa LLuuiizzaa ee aaooss mmeeuuss ffiillhhooss,, RRooddoollffoo LLuuccaass ee GGaabbrriieell
AAuugguussttoo,, aa eessssêênncciiaa ddaa mmaaggiiaa qquuee éé aa rraazzããoo ddaa mmiinnhhaa eenneerrggiiaa,,
ppeerrssiissttêênncciiaa ee lluuttaa..

iv
ZZaaiiaa,,
““OO aammoorr éé aa aassaa qquuee DDeeuuss ddeeuu àà aallmmaa ppaarraa qquuee eellaa ppuuddeessssee
ssuubbiirr aattéé EEllee.. QQuueemm éé bboomm tteemm oollhhooss ddee bboonnddaaddee ppaarraa vveerr aattéé ooss eerrrrooss
ddooss oouuttrrooss,, tteemm ccoorraaççããoo ppaarraa ppeerrddooaarr ee tteemm,, ssoobbrreettuuddoo,, ccoorraaggeemm ppaarraa
ddiivviiddiirr aa ssaabbeeddoorriiaa qquuee ppoossssuuii..””
AA vvooccêê nnaa qquuaalliiddaaddee ddee aammiiggaa ee oorriieennttaaddoorraa ssoouu eetteerrnnaammeennttee
ggrraattoo,, ssoobbrreettuuddoo,, ppeelloo pprriivviillééggiioo ddee hhaavveerr ttrraabbaallhhaaddoo ee rreecceebbiiddoo ttaannttoo ddee
vvooccêê nneesssseess aannooss ddee ccoonnvviivvêênncciiaa,, ppooiiss vvooccêê éé aa ssíínntteessee ddaa bboonnddaaddee..
MMuuiittoo oobbrriiggaaddoo ee qquuee DDeeuuss iilluummiinnee sseemmpprree ssuuaa vviiddaa..

v
AGRADECIMENTOS
““DDooiiss hhoommeennss jjuunnttooss ssããoo mmaaiiss ffeelliizzeess qquuee uumm iissoollaaddoo.. SSee uumm vviieerr aa ccaaiirr oo
oouuttrroo oo lleevvaannttaa.. MMaass,, aaii ddoo hhoommeemm ssoolliittáárriioo,, ssee eellee ccaaiirr,, nnããoo hháá nniinngguuéémm
ppaarraa lleevvaannttáá--lloo ((EEccllee 44..11--1100))””..
PPeellaass mmoottiivvaaççõõeess,, ssoommaaddaass àà ggeennoossiiddaaddee ddee vvooccêêss ccoonnsseegguuiimmooss ccoonncclluuiirr
eessttee ttrraabbaallhhoo.. EEssttaa ffooii aa mmaaiioorr aalleeggrriiaa qquuee eexxppeerriimmeenntteeii...... ccoonnttaarr ccoomm ttooddooss
vvooccêêss
OOrriioonnaallddaa ddee FFááttiimmaa LLiissbbooaa FFeennaannddeess
LLúúcciiaa KKiiookkoo HHaassiimmoottoo ee SSoouuzzaa
CCaarroolliinnaa RRooddrriigguueess CCoossttaa
CCrryyssttiiaannee RRooddrriigguueess ddee AArraaúújjoo
JJaanniinnee ddee AAqquuiinnoo LLeemmooss
AAnnaa CCrriissttiinnaa MMaacchhaaddoo ddee SSoouuzzaa
HHiillddeennee MMeenneezzeess ee SSiillvvaa
EElliissaa SSaalleess NNaasscciimmeennttoo
WWeerrtthheerr SSoouuzzaa SSaalleess
PPaattrríícciiaa JJaacckkeelliinnee MMaacciieell
DDeenniissee MMiilliioollii FFeerrrreeiirraa
KKaarrllaa CCaarrvvaallhhoo MMiirraannddaa
MMiirraanniillddeess ddee AAbbrreeuu BBaattiissttaa
JJoosséé CClleemmeennttiinnoo ddee OOlliivveeiirraa NNeettoo
KKaarriinnyy VViieeiirraa SSooaarreess
LLuuiizz AAuugguussttoo PPeerreeiirraa
KKeeiillii SSoouuzzaa

vi
““AAooss pprrooffeessssoorreess ddoo IInnssttiittuuttoo ddee PPaattoollooggiiaa
TTrrooppiiccaall ee SSaaúúddee PPúúbblliiccaa,, uumm aaggrraaddeecciimmeennttoo eessppeecciiaall,, ppeellaa
aaccoollhhiiddaa ee ppeelloo mmuuiittoo qquuee mmee eennssiinnaarraamm aaoo lloonnggoo ddaa
mmiinnhhaa ccaammiinnhhaaddaa””..

vii
ÀÀ UUnniivveerrssiiddaaddee FFeeddeerraall ddee GGooiiááss ppoorr ffoorrnneecceerr
uummaa eexxcceelleennttee eessttrruuttuurraa,, oo qquuee ppoossssiibbiilliittoouu aa rreeaalliizzaaççããoo
ddeessttee ttrraabbaallhhoo..

viii
ÀÀ UUnniivveerrssiiddaaddee PPaauulliissttaa,, rreepprreesseennttaaddaa ppeellooss
pprrooffeessssoorreess ddoo pprrooggrraammaa ddee ppóóss--ggrraadduuççããoo,, qquuee
ssuubbvveenncciioouu rreeccuurrssooss ppaarraa aa eeffeettiivvaaççããoo ddeessttaa ppeessqquuiissaa ee
ppeellaass vvaalliioossaass ssuuggeessttõõeess..

ix
LISTA DE ABREVIATURAS, SÍMBOLOS E UNIDADES.
AIDS Acquired immunodeficiency syndrome
ATCC American type culture colletion
α Alfa
BSI Bloodstream infection
β Beta
°C Grau Celsius
CFU/ml Unidade formadora de colônia por mililitro
CIM Concentração inibitória minima
CLSI Clinical and Laboratory Standards Institute
CVV Candidíase vulvovaginal
DNA Ácido desoxirribonucléico
HAART Highly active anti-retroviral therapy
HC Hospital das Clínicas
HIV Human immunodeficiency virus
ICU Intensive care unit
IgA Imunoglobulina A
MIC Minimal inhibitory concentration
ml Mililitro
μg Micrograma
NCCLS National Committee for Clinical Laboratory Standards
PCR Polymerase Chain Reaction
pH Potencial hidrogeniônico
RAPD Random Amplified Polymorphic DNA
RFLP Restriction Fragment Length Polymorphisms

x
SIDA Síndrome da imunodeficiência adquirida
sp. Espécie
spp. Espécies
SPSS Statistical Programmer for Social Sciences
UFG Universidade Federal de Goiás
USA United State of América
UTI Unidade de terapia intensiva

xi
SUMÁRIO
AGRADECIMENTOS ........................................................................................ v
LISTA DE ABREVIATURAS, SÍMBOLOS E UNIDADES. .............................. ix
RESUMO ........................................................................................................ xiii
ABSTRACT.................................................................................................... xiv
1 INTRODUÇÃO ............................................................................................... 1
1.1 ASPECTOS GERAIS ...................................................................................... 1
1.2 MECANISMO DE PATOGENICIDADE................................................................ 2
1.2.1 Fatores relacionados ao hospedeiro ........................................................ 2
1.2.2 Fatores relacionados ao microrganismo .................................................. 3
1.3 MANIFESTAÇÕES CLÍNICAS .......................................................................... 7
1.3.1 Candidíase superficial .............................................................................. 7
1.3.2 Candidíase sistêmica................................................................................ 9
1.4 INFECÇÕES NOSOCOMAIS POR CANDIDA SPP. ............................................. 10
1.5 TRATAMENTO............................................................................................ 12
1.6 SUSCETIBILIDADE ANTIFÚNGICA IN VITRO .................................................... 15
1.6.1 Resistência aos antifúngicos .................................................................. 18
1.7 MÉTODOS MOLECULARES .......................................................................... 20
2 JUSTIFICATIVA .......................................................................................... 24
3 OBJETIVOS................................................................................................. 26
3.1 OBJETIVO GERAL..................................................................................... 26
3.2 OBJETIVOS ESPECÍFICOS.......................................................................... 26

xii
4 PRODUÇÃO CIENTÍFICA ........................................................................... 27
4.1 ARTIGO 1: CANDIDA COLONIZATION IN INTENSIVE CARE UNIT PATIENST’S
URINE ............................................................................................................. 28
4.2 ARTIGO 2: SPECIES DISTRIBUTION AND ANTIFUNGAL SUSCEPTIBILITY
PATTERNS OF CANDIDA SPP. BLOODSTREAM ISOLATES FROM A BRAZILIAN
TERTIARY CARE HOSPITAL................................................................................ 33
4.3 ARTIGO 3: MOLECULAR EPIDEMIOLOGICAL ANALYSIS OF BLOODSTREAM OF
CANDIDA ALBICANS ......................................................................................... 41
4.4 ARTIGO 4: NOSOCOMIAL INVASIVE INFECTION CAUSED BY CUNNINGHAMELLA
BERTHOLLETIAE: CASE REPORT........................................................................ 55
5 CONCLUSÕES............................................................................................ 59
6 REFERÊNCIAS RELACIONADAS À INTRODUÇÃO ................................ 60
7 ANEXOS ...................................................................................................... 79
7.1 NORMAS PARA PUBLICAÇÃO NA REVISTA MEDICAL MYCOLOGY –
INSTRUCTIONS TO AUTHORS (ARTIGO 3) .......................................................... 79
7.2 PROTOCOLO DO CEPMHA/HC/UFG ....................................................... 92
7.3 TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO................................... 96

xiii
RESUMO
Os pacientes da unidade de terapia intensiva apresentam um índice elevado
de infecções do trato urinário e da corrente sanguínea causadas por Candida
spp. As infecções por esse microrganismo, na maioria das vezes, estão
relacionadas à fonte endógena. Entretanto, fontes exógenas provenientes do
meio ambiente foram descritas como prováveis fontes de candidíase. Neste
trabalho, foram coletadas amostras de sangue, urina, cateter de pacientes e
da superfície da cama e mesa de Meyer da unidade de terapia intensiva de
um hospital terciário, durante o período de um ano para pesquisa e
identificação de fungos. Os potenciais fatores de risco para candidemia e
candidúria foram analisados e o teste de suscetibilidade antifúngica para os
fungos isolados da corrente sanguínea foram realizados usando-se o método
de microdiluição em caldo. A diversidade genética entre isolados de C.
albicans foi avaliada na tentativa de se verificar possíveis correlações de
padrões de DNA das cepas obtidas de amostras clínicas e do meio ambiente
da unidade de terapia intensiva. Dentre as 345 amostras de sangue, Candida
foi detectada em 33 pacientes, e em um paciente foi identicado a presença de
um fungo filamentoso, Cuninghamella bertholetiae. Candida não-albicans foi
responsável por 51,5% dos casos de candidemia. Das 153 amostras de urina
coletadas, candidúria foi verificada em 68 pacientes, sendo que Candida não-
albicans foi identificada em 31,9%. O período de internação relacionado com
candidemia e candidúria foi estatisticamente significante. Uso de antibióticos e
de cateter invasivo foram fatores predominantes nos casos de candidemia e
de candidúria. A suscetibilidade in vitro dos isolados do sangue revelou alta
sensibilidade aos antifúngicos estudados. A análise de RAPD para os 31
isolados de C. albicans do sangue, catheter, urina, superfície de cama e mesa
de Meyer confirmou que os oligonucleotídios Cnd3 e Cnd4 possuem alto valor
discriminatório. Os resultados obtidos permitiram concluir que embora
candidemia estivesse largamente associada à fontes endógenas como
candidúria, a presença de Candida nas superfícies do cateter, cama e da
mesa de Meyer foram consideradas importantes fontes exógenas.

xiv
ABSTRACT
Nosocomial bloodstream and urinary tract infections caused by Candida
spp. are common among the ICU patients. Candida nosocomial infection
has been generally related to the endogenous flora but exogenous infection
originating from the environment has occurred. In this work, we collected
samples of blood, urine, catheter of patients and the surface of bed and
Meyer table from ICU from tertiary hospital during one year period for
research and identification of fungus. It was yet verified the potential risk
factors for candidemia and candiduria and the antifungal susceptibility was
performed by broth microdilution method for Candida isolates recovered
from bloodstream. Additionally, we assessed the genetic diversity among C.
albicans isolates in an effort to establish the relationship between DNA
patterns of the strains recovered from clinical and environment samples
from the ICU. Among 345 blood samples, candidemia was recovered in 33
patients caused by different species of Candida while fungaemia by
Cunninghamella bertholetiae was identified in one patient. Candida non-
albicans was responsible by 51.5% of the cases of candidemia. Among 153
urine samples, candiduria was detected in 68 patients, from which it was
isolated 31.9% of Candida non-albicans. Candida species in the blood and
urine were statiscally associated with long term hospitalization and the most
common risk factors were the use of antibiotics and indwelling urinary
catheter. The majority of Candida isolates from blood were susceptible to
the antifungals tested. The analyses using RAPD among 31 C. albicans
isolates from blood, urine, catheter, surface of bed and Meyer table
confirmed that the Cnd3 and Cnd4 primers have high discriminatory power.
In conclusion, although candidemia was strongly associated to endogenous
sources such as candiduria, it was observed that catheter, surface of bed
and Meyer table were also considered important exogenous sources of
infection.

1 INTRODUÇÃO
1.1 Aspectos gerais
Candidíase é uma infecção normalmente secundária aguda ou crônica,
com manifestações clínicas extremamente diversificadas podendo produzir
lesões que variam de uma simples irritação no tecido cutâneo até uma
resposta granulomatosa. As lesões podem ser superficiais com localização
principalmente nas mucosas bucal e vaginal, ou sistêmica, verificando-se em
alguns casos, septicemia por Candida (Menezes et al. 2005).
As leveduras do gênero Candida incluem aproximadamente 200
espécies, dentre as quais C. albicans, C. dubliniensis, C. famata, C. glabrata,
C. guilliermondii, C. haemualaii, C. inconspicua, C. kefyr, C. krusei, C. lambica,
C. lipolytica, C. lusitaniae, C. novergensis, C. parapsilosis, C. pelliculosa, C.
rugosa, C. sake, C. spharice, C. tropicalis e C. zeylanoides estão associadas
com candidíase no homem e/ou em animais (Hajjeh et al 2004; Segal, 2004;
Almirante et al. 2005; Colombo et al. 2006). Candida albicans é a espécie
patogênica de maior prevalência na maioria das casuísticas estudadas (Richet
et al. 2002). Espécies não-albicans, entretanto têm aumentado
gradativamente, sendo que C. tropicalis, C. glabrata e C. parapsilosis são
comumente isoladas em casos de candidíase relatadas por diferentes
pesquisadores (Pfaller et al. 1999; Sota et al. 1999; Cantón et al. 2001; Galván
& Mariscal 2006).

2
O gênero Candida faz parte da microbiota da pele, das mucosas, do trato
digestivo e geniturinário humano ou de animais, encontrando-se também
saprofiticamente em plantas, objetos inanimados e no meio ambiente
havendo, portanto fatores ligados ao hospedeiro ou ao microrganismo que
influenciam na transformação dessas leveduras de saprófitas para parasitas
(Galván & Mariscal, 2006).
1.2 Mecanismo de patogenicidade
1.2.1 Fatores relacionados ao hospedeiro
A capacidade de produção de infecção por espécies de Candida depende
mais do hospedeiro do que do fungo. A candidíase pode ocorrer pelo
rompimento do equilíbrio parasita-hospedeiro, que pode ser desencadeado
pelas alterações das barreiras teciduais, da microbiota autóctone e da
resposta imune (Drago et al. 2000; Calderone & Fronzi, 2001).
Alterações na superfície da pele ou mucosas possibilitam a proliferação
ou mudança do sítio anatômico da levedura contribuindo para a instalação de
Candida no organismo do hospedeiro. Esse fator é comum em pacientes que
sofrem constantemente traumatismo devido a procedimentos invasivos, como
sondas e cateteres, e em pacientes com extensas queimaduras (Pulcini et al.
2006).
Espécies de Candida, especialmente C. albicans, consideradas como
pertencentes à microbiota autóctone humana, de orofaringe, dobras da pele,
secreções brônquicas, vagina, urina e fezes (Odds, 1988; Macphail et al.
2002) podem, em determinadas circunstâncias como uso de antibioticoterapia

3
prolongada, proliferarem desencadeando infecção. Pacientes de unidade de
terapia intensiva, que geralmente recebem altas doses de antibióticos, tornam-
se mais propensos à produção de infecção por estas leveduras (Safdar et al.
2002).
Mecanismos mediados por imunidade celular e humoral constituem uma
eficiente proteção contra infecções por fungos do gênero Candida (Richardson
& Warnock, 1994). O papel da atividade de neutrófilos contra infecções
sistêmicas pode ser evidenciado pelo aumento de infecções disseminadas em
pacientes submetidos à quimioterapia (Merz, 1990). Neutrófilos e macrófagos
participam na defesa do hospedeiro devido à sua ação microbicida
(Greenfield, 1992). Por outro lado, a importância das células T na prevenção
do desenvolvimento de candidíase mucocutânea tem sido demonstrada.
Candidíase é freqüente em crianças com problemas no timo, principal órgão
formador de linfócitos T, e em pacientes com a síndrome da imunodeficiência
humana adquirida (AIDS ou SIDA), em que se observa uma acentuada
diminuição dessas células (Merz, 1990). A imunidade humoral pode auxiliar na
defesa do hospedeiro através da formação de anticorpos, que associados ao
sistema complemento, atuam como opsonizadores para as células
fagocitárias, ou impedem a adesão do microrganismo às células do
hospedeiro (IgA secretora) (Odds, 1988; Samaranayake & MacFarlane, 1990).
1.2.2 Fatores relacionados ao microrganismo
Candida albicans e outras espécies do gênero possuem características
celulares e moleculares que possibilitam a produção de infecções. Estas

4
características estão relacionadas principalmente à adesão, ao dimorfismo
(variação de antígenos de superfície), à variabilidade fenotípica (fenômeno
switching), e à produção de toxinas e exoenzimas, como proteases e
fosfolipases produzidas pelos microrganismos (Hellstein et al. 1993; Vargas et
al. 2000; Fotedar & Al-Hedaithy, 2003).
Os mecanismos de patogenicidade das espécies de Candida variam de
acordo com o tipo de infecção. A invasão da corrente sangüínea e
crescimento nos tecidos podem requerer determinados fatores de virulência
que podem ser diferentes daqueles para causar doenças na superfície das
mucosas (De Bernardis et al. 1993; Venkatesan et al. 2005). No
estabelecimento da infecção sistêmica os patógenos oportunistas são
capazes de evadirem do sistema imune, sobreviverem e iniciarem o seu
processo de divisão, difundindo-se para os órgãos internos do hospedeiro
(Casadevall & Piorfski, 2001). O mecanismo de produção de lesões por
fungos do gênero Candida não é totalmente conhecido. Não há evidências se
a invasão da levedura está mais relacionada à falhas no sistema de defesa do
hospedeiro ou a propriedades específicas da levedura (Venkatesan et al.
2005).
A capacidade que o microrganismo tem de se aderir a superfícies das
células do hospedeiro representa o primeiro mecanismo da patogênese
(Calderone & Fronzi, 2001). As doenças infecciosas, de uma maneira geral,
são conhecidas por começar com a fixação do patógeno a um alvo particular
no hospedeiro, como ocorre com a candidíase. A parede das leveduras do

5
gênero Candida, como C. albicans, não possui apenas a propriedade de
conferir a forma estrutural à célula, mas também é o local onde se inicia a
interação entre esse fungo e o meio ambiente (Calderone & Fronzi, 2001).
Isso ocorre porque estas leveduras apresentam proteínas denominadas
adesinas que permitem a sua adesão a elementos extracelulares,
considerados receptores, como fibrinogênio, fibronectina e laminina, presentes
nos tecidos humanos (Vardar-Ünlü, 1998, Calderone & Fronzi, 2001; Yang,
2003).
Candida albicans pode se apresentar sob a forma de levedura ou
filamentosa, o que caracteriza o seu dimorfismo (Brown & Gow, 1999; Ernst,
2000). A formação de hifas é considerada importante fator de virulência não
apenas por promover a invasão da célula para o interior da mucosa, mas
também por impedir que as células de Candida sejam englobadas por
macrófagos e neutrófilos (Yang et al. 2003). A transição de leveduras para
hifas pode ser influenciada pela temperatura, pH, fontes de carbono e
substâncias químicas (Odds, 1988, Lan et al. 2002). Sua capacidade de
mudar de fase de levedura para filamentosa é importante para uma maior
interação com o hospedeiro, facilitando a adesão, e aumentando assim a sua
virulência (Cutler, 1991). As células em forma de leveduras e de hifas podem
estar presentes no hospedeiro não somente durante o processo de infecção,
mas também durante o processo de colonização do fungo (Souza et al. 1990;
Bartie et al. 2001).

6
As variações na morfologia de colônias de espécies de Candida,
descritas principalmente em C. albicans, caracterizadas como fenômeno
switching, parecem estar envolvidas no mecanismo de virulência dessas
leveduras. Nesse fenômeno, a mudança fenotípica que se expressa pela
morfologia, induz provavelmente alteração na fisiologia e na patogenicidade
do microrganismo (Lian et al. 2003, Laffey & Butler, 2005). Esse mecanismo
pode permitir que um organismo adaptado ao meio ambiente altere, através
da expressão de um gene seletivo, a resposta fúngica frente aos agentes
antifúngicos (Lachke et al. 2002; Miller et al. 2006).
A produção de proteinase e da fosfolipase tem sido relatada como sendo
um importante determinante de patogenicidade de C. albicans (Cutler, 1991;
Pincus et al. 1999, Menezes et al. 2005). As proteinases têm afinidade por
substratos tais como queratina, colágeno desnaturado, hemoglobinas, matriz
celular e albumina (Rüchel et al. 1982; McDonalds & Odds, 1983; Ghannoun &
Abu-Elteen, 1990; Culter 1991; Odds 1994, Ibrahim et al. 1995, Calderone &
Fronzi, 2001) envolvidas em vários processos bioquímicos. Esses atributos
estão associados a diversos fatores de virulência como formação de
pseudomicélio, adesão e fenômeno “switching”, tornando mais complexos os
mecanismos de patogenicidade de leveduras (Naglik et al. 2003, Naglik et al.
2004). O primeiro relato de fosfolipase em C. albicans foi publicado em 1966
(Werner, 1966). A presença de fosfolipases na superfície da levedura e na
extremidade do pseudomicélio propicia a lesão tecidual por alterar os
constituintes lipídicos da membrana celular do hospedeiro. Esta enzima tem

7
sido detectada em poucas espécies, como C. albicans e C. glabrata
(Samaranayake et al. 1984; Banno et al. 1985; Hube, 1996; Ghannoum, 1998;
Ghannoum, 2000). Williams et al. (1990) verificaram que 94% de C. albicans
isoladas da cavidade bucal de pacientes com AIDS, foram produtoras de
fosfolipase. Outras enzimas, como glucoamilase, fosfatase ácida e
metalopeptidase, provavelmente correlacionadas com virulência podem ser
encontradas em leveduras do gênero Candida (Naglik et al. 2003).
1.3 Manifestações clínicas
As infecções decorrentes da ação patogênica de fungos do gênero
Candida, denominadas candidíases, podem envolver a pele, as mucosas e
órgãos internos atingindo algumas vezes o sistema sanguíneo. De acordo
com o envolvimento do organismo no hospedeiro, a candidíase pode ser
classificada em superficial e sistêmica.
1.3.1 Candidíase superficial
A candidíase com envolvimento superficial acomete pele, unhas e
mucosas orofaríngeas e genitais (Ghannoum, 2001).
As infecções da pele se localizam principalmente em áreas intertriginosas
úmidas, como os espaços interdigitais, os sulcos submamários, axilas e
pregas suprapúbicas. As lesões se caracterizam por se apresentarem
eritematosas, úmidas, com bordos mal definidos e escamosos formados por
vesículas que se rompem precocemente. Em alguns casos, observa-se a
presença de placas secas, escamosas e pústulas (Samanarayake et al. 2002).

8
A onicomicose, definida como infecção fúngica ungueal, representa 20%
das doenças das unhas, sendo uma das mais freqüentes causas de
onicopatias em todo o mundo (Arena & Ruiz-Esmenjaud, 2004). Essa infecção
pode manifestar-se como um edema eritematoso da prega ungueal
(paroníquia), ou como uma separação da placa ungueal do seu leito
(onicólise). Esse tipo de infecção, segundo as recomendações da
nomenclatura das infecções fúngicas proposta pela "Sociedade Internacional
de Micologia Humana e Animal", quando o agente causal se trata de
leveduras do gênero Candida, deve ser denominada candidoses ungueais
(López-Jodra et al. 1999). Onicomicose por Candida spp afeta
aproximadamente 5% da população mundial, sendo altamente freqüentes na
América Latina (Arenas & Ocego 1997; Murray & Dawber, 2002) e representa
em torno de 30% de todas as infecções micóticas superficiais (Migdley et al.
1994).
A candidíase de mucosa bucal pode se apresentar sob quatro formas
clínicas. A forma eritematosa, a qual é representada por áreas avermelhadas,
localizadas principalmente no palato, língua e mucosa bucal. A
pseudomembranosa, onde se observa a formação de lesões membranosas de
cor branca à amarelada em toda a mucosa, a queilite angular que acomete as
comissuras labiais com aspectos clínicos, que variam desde os fissurais a
ulcerados e a candidíase hiperplásica que se apresenta sob a forma de placas
ou nódulos esbranquiçados, firmemente aderidos às áreas da mucosa,
podendo ocorrer na língua e ser confundida com a leucoplasia pilosa

9
(Cavassani et al. 2002). Lesões de mucosa bucal são frequentemente
relatadas em pacientes imunocomprometidos, particularmente em AIDS.
Candidíase vulvovaginal (CVV), processo inflamatório que acarreta
corrimentos, pruridos, além de incômodos como ardência e dor ao urinar
podem ser decorrentes de diversos fatores, como o abafamento da área
vaginal, higiene pessoal inadequada, mudança de pH ou até mesmo o uso de
contraceptivos (Ferrazza et al. 2005). A freqüência de CVV tem aumentado
gradativamente, evoluindo de 0,5% em 1968 para 22,5% em 1998, época em
que se tornou a causa mais comum de infecção vaginal (Adad et al. 2001).
Atualmente, CVV está entre os principais problemas ginecológicos que afetam
mulheres em idade reprodutiva, atingindo milhares de pessoas no mundo
(Costa et al. 2004). Há estimativas de que provavelmente 55,7% de todas as
mulheres terão pelo menos um episódio de vulvovaginite por Candida spp ao
longo de suas vidas (Foxman et al. 2000).
1.3.2 Candidíase sistêmica
Esse tipo de infecção ocorre quando o fungo se instala em diferentes
órgãos do hospedeiro, com localização mais freqüente nos pulmões e trato
urinário, sendo que em determinados indivíduos podem levar a candidemia
(Galván & Mariscal, 2006).
Uma das características mais importantes com relação à candidíase
sistêmica é sua associação à altas taxas de mortalidade. A taxa média de
mortalidade em pacientes com essa patologia nos Estados Unidos é de
aproximadamente 38% (Beck-Sagué & Jarvis 1993), em Israel de 21,5%

10
(Rennert et al. 2000), na Espanha oscila entre 22 e 33,3% (Sota et al. 1999;
Saballs et al. 2000), enquanto no Brasil é de aproximadamente 50% (Colombo
et al. 1999).
Em pacientes hospitalizados a combinação de vários fatores constitui
riscos para candidíase invasiva e candidemia (Cantón et al. 2001). O uso de
cateter, de antibióticos, nutrição parenteral, freqüentementes utilizados em
pacientes internados contribuem para uma maior capacidade de invasão por
leveduras do gênero Candida (Frazer et al. 1992; Franklin & Metry 1992;
Fridkin & Jarvis, 1996).
A incidência das infecções sistêmicas por Candida tem sido descrita
principalmente em indivíduos hospitalizados, particularmente em unidade de
terapia intensiva (Vincent et al. 1998), verificando-se um grande aumento nas
últimas décadas. Segundo Schwesinger et al. (2005), em um hospital terciário
alemão, de necropsias realizadas no período de 1994 – 1998, verificou-se
uma incidência de 3% de candidíases invasivas e no período compreendido
entre 1999 – 2003, a mesma passou a ser de 10%.
1.4 Infecções nosocomais por Candida spp.
Infecções invasivas são consideradas importantes causas de morbidade
e mortalidade em hospitais (Saleh & Al-Hedaithy, 2003, Boo et al. 2005). A
tecnologia disponível na área médica e laboratorial, para diagnóstico e
tratamento, além do aprimoramento das medidas de suporte de vida a
pacientes críticos, particularmente os de unidade de terapia intensiva,
possibilitaram uma maior sobrevida de portadores de doenças degenerativas

11
e neoplásicas, pós-cirúrgicos e de crianças prematuras, aumentando o risco à
aquisição de infecções (Araújo, 1998, Antunes et al. 2005). Alterações na
resposta imune do hospedeiro, rompimento de barreiras e exposição a vários
antibióticos, rendem aos pacientes de UTI altamente suscetíveis, infecções da
corrente sangüínea, do trato respiratório e urinário (Arantes et al. 2003). Um
estudo realizado por Appelgren et al. 2001, em unidades de terapia intensiva,
mostrou que 35% dos pacientes tiveram infecção nosocomial, sendo que 17%
eram infecções da corrente sanguínea.
Espécies de fungos pertencentes aos gêneros Candida e Aspergillus e a
classe dos Zygomycetos são os responsáveis pela maioria dessas infecções
(Anaisse et al. 1989; Wingard et al. 1991). É de grande interesse a elevada
freqüência de candidíase detectada nos grandes hospitais. Diversos fatores
concorrem para o aumento de infecções nosocomiais por Candida. Colombo &
Guimarães (2003) identificaram azotemia, uso de cateter venoso central, uso
de esteróides, cirurgia de grande porte, colonização por Candida spp. e
hemodiálise, como fatores de risco associados em pacientes hospitalizados.
Segundo esses autores, considerando os fatores de riscos mencionados, é
possível entender porque a maior freqüência de candidemia tem sido
documentada em indivíduos críticos admitidos em unidade de terapia
intensiva.
C. albicans é a principal espécie capaz de produzir candidemia (Colombo
& Guimarães, 2003), mas outras espécies não-albicans, como C. parapsilosis,
C. glabrata, C. krusei e C. tropicalis estão implicadas como agentes dessa

12
infecção (Colombo et al. 1999; Ellis et al. 2003; Marchetti et al. 2004, Medrano
et al. 2006). O aumento de espécies não-albicans como agentes importantes
de candidemia está ligado ao uso profilático, ou empírico, de agentes
antifúngicos, com menor suscetibilidade a esses (Rodriguez & Moreira, 1999;
Lewis & Klepser, 1999; Pfaller, 2000).
As espécies de Candida podem causar o mesmo tipo de enfermidade, no
entanto, a gravidade e as opções terapêuticas diferem entre as distintas
espécies e dentro da mesma espécie (Sandven, 2000; Cantón, 2001),
justificando o uso dos testes de suscetibilidade in vitro para uma terapia
adequada.
1.5 Tratamento
Anfotericina B é considerada o padrão ouro da terapia antifúngica. Esse
fármaco é um antibiótico macrolideo com atividade antifúngica frente a
numerosas espécies de fungos como Candida, Cryptococcus, Histoplasma
capsulatum, Paracoccidioides brasiliensis e Aspergillus. É um antifúngico
altamente lipofílico, sendo administrado em associação à desoxicolato. A sua
principal limitação no emprego clínico é decorrente de seus efeitos
secundários, dos quais um dos mais graves é a nefrotoxicidade (López-
Medrado et al. 2005).
O tratamento das infecções fúngicas tem sido também realizado com
derivados azólicos, como fluconazol, itraconazol, voriconazol, ou ainda com
cancidas, como caspofungina, equinocandina e micafungina, os quais
apresentam maior facilidade na sua administração, e menores efeitos

13
colaterais do que os observados para anfotericina B (Ayeni et al. 1999;
Berrouane et al. 1999; Sheehan et al. 1999). A pouca toxicidade, fácil
administração e eficácia no tratamento têm resultado no uso abusivo de
fluconazol, o que provavelmente possibilitou o desenvolvimento da resistência
desse antifúngico em espécies de Candida (Rex et al. 1995; Rex & Pfaller
2002). As infecções invasivas por C. glabrata, principalmente em indivíduos
transplantados, têm ocorrido com altos índices de mortalidade devido ao uso
de fluconazol como profilático. Candida krusei é considerada intrinsecamente
resistente a este derivado azólico (Abi-Said et al. 1997; Bodey et al. 2002). Em
casos de candidíase que não respondem ao tratamento com fluconazol e
itraconazol, tem sido instituído o uso de voriconazol com boa eficácia (Lozano-
Chiu et al. 1999; Pfaller et al. 2002).
Voriconazol é um agente antifúngico triazólico de segunda geração, com
amplo espectro, sendo derivado sintético do fluconazol. As modificações
introduzidas na molécula de voriconazol resultaram em uma maior afinidade à
enzima 14-α-lanosterol demetilase e no aumento do espectro de ação.
Voriconazol exibe um amplo e potente espectro de ação contra os fungos: C.
albicans, Aspergillus sp, Cryptococcus neoformans, Histoplasma capsulatum,
Coccidioides immitis, Scedosporium spp., Fusarium spp., Penicillium
marneffei, Trichosporon spp. e Saccharomyces cerevisae (Sabo & Abdel-
Rahmanl, 2000; Bizarro & Dinis, 2003, Gimeno & Martinez, 2007), podendo
apresentar atividade contra isolados que são resistentes ao fluconazol,
itraconazol e anfotericina B.

14
As equinocandinas, pertencente ao grupo das candinas, possuem três
agentes antifúngicos, caspofungina, micafungina e anidulafungina, sendo
fármacos que inibem a síntese da β-1,3-D glucana, componente da parede
celular de muitos fungos filamentosos e de leveduras (Bergold & Georgiadis
2004). A sua ação na parede faz com que esses agentes antifúngicos tenham
maior facilidade de ação sobre os fungos sem haver interferência no
hospedeiro e dessa forma são menos tóxicos para o paciente (Gimeno &
Martinez, 2007).
A caspofungina, licenciada para uso clínico, é um derivado semi-sintético
da pneumonocandina B, única equinocandina aprovada nos Estados Unidos,
indicada no tratamento de candidíase, onde as espécies de Candida
respondem a este antifúngico, inclusive as resistentes ao fluconazol
(Deresinski & Stevens, 2003). Resultados de estudos de caspofungina na
candidíase invasiva e na candidemia sugerem equivalente eficácia à
anfotericina B, mas com menos efeitos tóxicos (Abuhammour & Habte-Gaber,
2004).
Em um estudo realizado por Odio et al. (2004) foi avaliado o tratamento
com caspofungina em 10 recém-nascidos, com candidíase invasiva, causada
por C. albicans, C. tropicalis, C. parapsilosis e C. glabrata. Embora tivesse
sido registrada resistência ao fluconazol nas espécies não-albicans e em dois
casos de C. albicans, bem como resistência a anfotericina por C. glabrata, a
caspofungina mostrou-se com elevada eficácia, no tratamento da candidíase
destas crianças.

15
Embora haja boa resposta às terapias com diferentes agentes
antifúngicos no tratamento de candidíase, para pacientes de UTI há uma
enorme dificuldade na eficácia, pois além da sintomatologia das infecções
fúngicas ser totalmente inespecífica nesses pacientes dificultando o
diagnóstico, a debilidade do hospedeiro leva a uma diminuição na resposta ao
agente antifúngico (Muñoz et al. 2000). Nesses pacientes, a utilização de
antifúngicos se tem restringido àqueles com infecções fúngicas documentadas
ou com um alto risco de apresentar infecções por esses fungos (Wade, 1993;
Pizzo, 2000), para evitar o desenvolvimento de resistência aos antifúngicos.
Com a crescente incidência das infecções fúngicas sistêmicas, o
aumento do número de agentes antifúngicos além do aparecimento de
isolados resistentes, torna-se necessário à seleção adequada do antifúngico,
o que pode ser realizado através dos testes de suscetibilidade.
1.6 Suscetibilidade antifúngica in vitro
A utilização dos testes de suscetibilidade antifúngica in vitro para que seja
realizado um tratamento rápido, adequado e eficaz, tornou-se necessária
devido às constantes resistências detectadas em diferentes fungos (Colombo,
1994; Zardo & Mezzan, 2004; Yang et al. 2005; Magill et al. 2006)
Na última década, foram padronizados vários métodos para provas de
sensibilidade in vitro a antifúngicos e alguns deles são atualmente indicados
como referência, servindo para validar outras provas, incluindo àquelas
comerciais.

16
Alguns testes preconizados para detectar resistência a antifúngicos, têm
mostrado boa reprodutibilidade intra e interlaboratorial, além de correlação
com a evolução clínica dos pacientes. O National Committee for Clinical
Laboratory Standards (NCCLS), atual Clinical and Laboratory Standards
Institute (CLSI), publicou o documento M27-A2, para provas de suscetibilidade
a antifúngicos em leveduras como método de referência (NCCLS/CLSI, 2002).
Esse documento contém técnicas de macro e microdiluição em caldo para
determinar a concentração inibitória mínima (CIM). Elas foram desenvolvidas
para testes com leveduras dos gêneros Candida e Cryptococcus, frente à
anfotericina B, 5-fluorocitosina e azólicos, incluindo cetoconazol, fluconazol,
itraconazol, posaconazol, ravuconazol e voriconazol. Os possíveis fatores
como meio de cultura, pH, temperatura de incubação e leitura do teste, que
podem causar erros na determinação da CIM são padronizados neste método
(NCCLS/CLSI, 2002).
Um outro método do CLSI foi descrito no documento M44-A que
descreve uma prova sensível e prática, validada para testes de suscetibilidade
em Candida spp., utilizando discos impregnados com fluconazol ou com
voriconazol. O documento inclui critério de interpretação para os diâmetros de
halos obtidos com discos de fluconazol e valores esperados para cepas-
padrão permitindo verificar a concentração inibitória mínima (NCCLS/CLSI,
2004).
Testes de suscetibilidade in vitro aos antifúngicos são realizados por
vários sistemas comerciais, incluindo, dentre outros, ASTY (Kyokyuto Pharma-

17
Centical, Japão), ATB Fungus 2 (Api-bioMérieux, França), Candifast
(International Microbio, Itália), Etest (AB-Biodisck, Suécia), Fungitest (Bio-Rad,
Farança), Integral Systems Yeast (Liofilchen Diagnostics, Itália), Mycostandard
(Institut Pasteur, França), Mycototal (Behring Diagnostic, França) e Sensititre
®YeastOne (Trek Diagnostic System, EUA) (Arikan & Akova, 1997; Morace et
al. 2002; Bae et al. 2004; Durussel et al. 2004; Lombardi et al. 2004; Carrillo-
Muñoz et al. 2006).
Dentre os sistemas comerciais estudados, apenas alguns demonstraram
potencial suficiente para se constituir em uma alternativa para os laboratórios
assistenciais, como o Sensititre ®YeastOne e o Etest, os quais mostraram boa
reprodutibilidade e indiscutível capacidade em detectar a resistência in vitro
aos azóis, sobretudo ao fluconazol, quando comparados aos métodos de
macro e microdiluição para leveduras (Lombardi et al. 2004; Carrillo-Muñoz et
al. 2006).
Sensititre ®YeastOne é um método de microdiluição em caldo baseado
no documento M27-A2, que consiste de uma placa de microtitulação
descartável, que contém diluições seriadas desidratadas de seis agentes
antifúngicos, incluindo anfotericina B, fluconazol, itraconazol, cetoconazol,
voriconazol e 5-fluorocitosina, em cavidades individuais. As cavidades contêm
azul de Alamar como indicador colorimétrico, o qual melhora a leitura do ponto
de corte mediante mudança de cor azul para rosa. Os resultados são
expressos em CIM e estudos comparativos com os métodos NCCLS/CLSI
mostraram-se concordantes (Chaturvedi et al. 2004).

18
O Etest, método de difusão em ágar, utiliza uma tira contendo um
gradiente de concentração do agente antimicrobiano em estudo permitindo a
determinação de CIM. Este método é disponível para detectar a CIM de
anfotericina B, 5-fluorocitosina, cetoconazol, itraconazol, voriconazol,
fluconazol e caspofungina para leveduras dos gêneros Candida e
Cryptococcus e para alguns fungos filamentosos (Denning et al. 1997; Clancy
& Nguyen, 1999; Fernandes et al. 2003; Costa et al. 2004). Trabalhos
experimentais têm demonstrado concordância de Etest com os resultados
encontrados pelo NCCLS/CLSI (Hazen et al., 2003; Pfaller et al., 2003).
1.6.1 Resistência aos antifúngicos
Os derivados azólicos, como fluconazol e itraconazol, largamente
utilizados para o tratamento de candidíase, atuam inibindo a C14α–
demetilase, uma citocromo P-450 acarretando o acúmulo de esteróides
metilados e diminuição da síntese do ergosterol. Essa enzima inibe a
produção de ergosterol, que é o principal constituinte da membrana celular do
fungo, com conseqüente inibição do crescimento celular (Hitchocock et al.
1993; Vanden Bossche, 1997; Manavathu et al. 1999, Nenoff et al. 1999;
Burgess et al. 2000; Bizarro & Dinis, 2003). Alguns isolados de fungos podem
apresentar resistência aos derivados azólicos. São conhecidos três
mecanismos de resistência aos azólicos. 1- Redução do acúmulo intracelular
do fármaco resultante da utilização reduzida deste agente antifúngico ou do
aumento da efluxo do fármaco devido à ação de produtos de genes de
resistência aos antifúngicos, 2- Alteração estrutural da enzima C14α-

19
demetilase, resultando em uma diminuição na sua ligação aos azólicos, 3-
Aumento da produção de 14α-demetilase, superando o efeito inibidor dos
azólicos (Nenoff et al. 1999; Gao et al. 2003).
A resistência aos derivados azólicos pode ser influenciada pela
imunossupressão dos pacientes e uso prolongado do agente antifúngico
(Yang et al. 2003). O uso freqüente de terapia antifúngica em pacientes
imunocomprometidos, em decorrência de constantes recidivas de candidíase,
é o fator que provavelmente tenha maior influencia na ocorrência de
resistência a diferentes fármacos e selecionando espécies. Espécies de
Candida como C. glabrata e C. krusei, têm se mostrado resistentes ao
fluconazol devido ao uso prolongado desse agente antifúngico (Abbas et al.
2000; Kauffman et al. 2000; Taylor et al. 2000; Colombo et al. 2002; Trick et al.
2002). Segundo Barchiesi et al. (2002), pacientes infectados pelo HIV que
fazem uso de terapia antiretroviral altamente ativa (HAART) freqüentemente
apresentam leveduras na cavidade bucal resistentes ao fluconazol.
Há poucos relatos de resistência de espécies de Candida frente ao
voriconazol. Takakura et al. (2004) relataram que 100% dos isolados de C.
krusei e 60% de outras espécies não-albicans, com baixa suscetibilidade ao
fluconazol, foram suscetíveis ao voriconazol.
A anfotericina B pertence à ampla família dos macrolídeos poliênicos e
atua ligando-se ao ergosterol da membrana celular fúngica, alterando sua
permeabilidade o que acarreta desequilíbrio osmótico, pela perda de íons
intracelulares e conseqüentemente lise e morte das células (Vanden Bossche,

20
1997). A resistência de leveduras à anfotericina B é raramente detectada. A
resistência a anfotericina B por isolados de C. lusitaniae e C. tropicalis, assim
como de alguns fungos filamentosos como Trichosporon spp. e Fusarium spp
tem sido descrita (Vanden Bossche, 1997; Godoy et al. 2003; Antunes et al.
2005).
Diferenças na suscetibilidade, importante característica fenotípica de um
determinado patógeno aos agentes terapêuticos, pode ser detectada pela
variabilidade genética existente entre os isolados (Cirak et al. 2003; Schaller et
al. 2005).
1.7 Métodos moleculares
Várias técnicas de tipagem molecular têm sido utilizadas para
caracterização de diferentes microrganismos produtores de infecções no ser
humano (Voss et al. 1995; Lian et al. 2003). Esses procedimentos podem
responder questões relacionadas à patogênese do fungo, detecção de
microepidemias, distinção de infecção primária ou recidiva, à similaridade
entre as diferentes cepas e a tentativa de relacionar o isolado à fonte de
infecção (Merz, 1990; Voss et al. 1995; Soll, 2000; Lian et al. 2003).
A caracterização dos isolados de leveduras inclui métodos de tipagem
molecular, análise do DNA polimórfico amplificado aleatoricamente (RAPD),
métodos de fingerprinting, análise de fragmentos de DNA gerados por
enzimas de restrição (RFLPs) e hibridação por Southern blot do DNA
(Andrigheto et al. 2000; Dassanayake et al. 2000; Ergon & Gülay, 2004).

21
A cariotipagem por eletroforese de campo pulsado é considerada útil
devido ao seu alto poder discriminatório, sendo utilizada para diferenciação
intra e interespecífica de leveduras, devido a grande variedade no tamanho e
número de seus cromossomos (Dassanayake et al. 2000; Cirak et al. 2003).
Dentre as técnicas moleculares, o RAPD tem sido usado no estudo da
variabilidade entre espécies (Uijthof et al. 1994; Molnár et al. 1996). A
detecção e exploração de seqüências de polimorfismos de DNA ocorridos
naturalmente representam um dos mais significativos desenvolvimentos na
biologia molecular. O método RAPD tem sido bastante utilizado principalmente
pela vantagem de ser simples e rápido (Tavares et al. 1992).
O RAPD requer uma pequena quantidade de DNA e permite a
visualização de um grande número de marcas polimórficas. O uso de RAPD
tem-se mostrado útil nos estudos de microrganismos para o quais não se tem
muita informação genética. A técnica é baseada na amplificação de
fragmentos não específicos de DNA, em reações sucessivas de
polimerização. Como descrito por Williams et al. (1990), os oligonucleotídios
são construídos com seqüências aleatórias, ao contrário da PCR
fingerprinting, revelando polimorfismos em toda a extensão do genoma. Tais
polimorfismos são reconhecidos pela presença de um fragmento amplificado
em um dos genomas em relação à ausência desse mesmo fragmento em
outro.
O desenvolvimento da técnica de RAPD representou um marco na
caracterização molecular de diversos microrganismos, especialmente para

22
identificação de espécies microbianas, quando pequenas seqüências
genômicas são avaliadas (Ergon & Gülay, 2004; Pinto et al. 2004). A análise
de RAPD é projetada para caracterizar isolados dentro de uma mesma
espécie (Melo et al. 1998; Cirak et al. 2003) e para enfoques epidemiológicos
evidenciando uma relação entre fonte ambiental e manifestações clínicas
(Soll, 2000; Lian et al. 2003). Essa técnica, além de gastar menos tempo, é de
fácil aplicabilidade e os resultados têm demonstrado o alto poder
discriminatório e eficácia (Soll, 2000). A análise de RAPD tem também sido
usada em vários estudos em que é investigada a relação clonal entre
diferentes espécies de Candida obtidas de vários espécimes de pacientes
hospitalizados em diferentes unidades hospitalares, incluindo unidade de
terapia intensiva (Arif et al. 1996; Hedderwick et al. 2000).
A análise de RAPD foi usada por Pinto et al. (2004), para verificar a
variabilidade genômica de 37 isolados obtidos de diferentes regiões do corpo
de 11 pacientes imunocomprometidos infectados com o HIV, permitindo
verificar polimorfismo intra e inter específicos entre isolados de um mesmo
paciente e entre os isolados de diferentes pacientes.
Em experimentos utilizando diferentes materiais clínicos de um mesmo
indivíduo, usando RAPD para tipagem de C. albicans isoladas de pacientes de
UTI, Vrion & Matsiota-Bernard (2001) conseguiram estabelecer a natureza
endógena de 17 isolados desta espécie. Em isolados clínicos de C.
parapsilosis, Dassanayake et al. (2000) observaram através de RAPD
variações genéticas intra-espécies, as quais foram verificadas pelos padrões

23
diferentes de bandas. Esses experimentos demonstram a capacidade desse
método em determinar a epidemiologia de infecções por Candida.
PCR fingerprinting utiliza oligonucleotídeos que são específicos para
seqüências curtas e repetitivas hipervariáveis de leveduras, permitindo que
isolados sejam identificados com sensibilidade suficiente para detectar
diferenças inter e intra espécies (Dassanayake et al. 2000; Meyer et al. 2001).
Esse método, devido à sua eficácia, é usado com freqüência, pois permite
verificar a epidemiologia de fungos envolvidos em infecções nosocomiais
(Schönian et al. 1993; Dassanayake et al. 2000).
A técnica de RFLP é utilizada para caracterizar microrganismos pelos
padrões derivados da clivagem de seu DNA, cujos comprimentos dos
fragmentos produzidos podem diferir quando o DNA é digerido com diferentes
enzimas de restrição. Os padrões de bandas gerados podem ser usados para
diferenciar uma espécie de outra (Irobi et al. 1999; Mirhendi et al. 2005).

24
2 JUSTIFICATIVA Como exposto anteriormente, o aumento da incidência das infecções
fúngicas nosocomiais nas últimas décadas, faz com que esse tema seja
abordado por muitos pesquisadores. O registro de maior incidência dessas
infecções é observado principalmente em indivíduos imunocomprometidos,
como pacientes com AIDS, transplantados de medula óssea e órgãos sólidos,
nos submetidos à quimioterapia e naqueles que permanecem longos períodos
em hospitais essencialmente nos pacientes de UTI (Hazen 1995, Voss et al.
1995). A maior sobrevivência detectada nestes indivíduos induz a aquisição
de infecções oportunísticas como a candidíase. Em pacientes
imunocomprometidos com granulocitopenia acentuada, há um risco maior de
infecções sistêmicas por Candida, como a candidemia (Medrano et al. 2006).
A identificação da espécie de Candida, nos últimos anos, tem-se
mostrado de grande importância, pois tem sido verificada uma tendência de
mudança de etiologia da candidíase. Apesar de C. albicans ser o agente
etiológico mais comumente identificado, espécies não-albicans, têm-se
mostrado predominantes (Brilhante et al. 2005, Menezes et al. 2005). As
infecções observadas em diferentes casuísticas estudadas em pacientes de
unidade de terapia intensiva mostram as espécies de Candida não-albicans
como responsáveis por altas taxas de morbidade e mortalidade (Aquino et al.
2005).
O tratamento rápido de candidíase, provavelmente faz com que diminua
os casos de mortalidade. A eficácia do agente antifúngico pode ser detectada
através da realização prévia de testes de suscetibilidade in vitro, pois há

25
alguns microrganismos que podem ser resistentes aos diferentes antifúngicos.
O teste de suscetibilidade de diluição em caldo, preconizado pelo CLSI,
proporciona na maioria das vezes, bons resultados de leitura de end-point.
Tem sido descrito que há uma concordância in vitro e in vivo dos resultados
de suscetibilidade, principalmente quando se refere a detecção de resistência.
Há vários fatores que interferem na aquisição de candidíase nos
pacientes de UTI. Eliminar os fatores endógenos é uma tarefa difícil, mas
fatores exógenos podem perfeitamente serem contornados, o que
provavelmente evitaria vários casos de candidíase nosocomial. Sendo assim,
a verificação das características moleculares, usando testes como o RAPD,
que permite diferenciação intra-espécie torna-se de grande valia para o auxílio
de determinação dessas fontes exógenas ou endógenas, contribuindo na
prevenção de candidíase.

26
3 OBJETIVOS
3.1 Objetivo Geral
Identificar e caracterizar leveduras do gênero Candida de fômites
(cateter, mesa de Meyer e cama) e amostras clínicas (sangue e urina) de
pacientes da unidade de terapia intensiva do Hospital das Clínicas da
Universidade Federal de Goiás.
3.2 Objetivos específicos
a. Isolar e identificar fungos presentes na corrente sangüínea e urina de
pacientes da UTI.
b. Avaliar a prevalência das espécies de Candida presentes na corrente
sangüínea e na urina e detectar os fatores de riscos para candidemia e
candidúria em pacientes da UTI.
c. Avaliar o padrão de suscetibilidade in vitro de amostras de Candida
isoladas do sangue dos pacientes frente à anfotericina B, fluconazol,
itraconazol e voriconazol.
d. Analisar os isolados de C. albicans genotipicamente, tentando
correlacionar os padrões de DNA obtidos de amostras clínicas e
ambientais da Unidade de Terapia Intensiva.

27
4 PRODUÇÃO CIENTÍFICA
a. ARTIGO 1: Candida colonization in intensive care unit patienst’s urine
b. ARTIGO 2: Species distribution and antifungal susceptibility patterns of
Candida spp. bloodstream isolates from a Brazilian tertiary care hospital
c. ARTIGO 3: Molecular epidemiological analysis of bloodstream of
Candida albicans
d. ARTIGO 4: Nosocomial invasive infection caused by Cunninghamella
bertholletiae: case report

28
4.1 ARTIGO 1: Candida colonization in intensive care unit patienst’s urine

29

30

31

32

33
4.2 ARTIGO 2: Species distribution and antifungal susceptibility patterns of Candida spp. bloodstream isolates from a Brazilian tertiary care hospital.

34

35

36

37

38

39

40

41
4.3 ARTIGO 3: Molecular epidemiological analysis of bloodstream of Candida albicans

42
Molecular epidemiological analysis of bloodstream of Candida albicans
Xisto Sena Passos1, Werther Souza Sales2, Carolina Rodrigues Costa2, Janine de
Aquino Lemos2, Lúcia Kioko Hasimoto e Souza2, Keili Souza2, Luiz Augusto Pereira3,
Maria do Rosário Rodrigues Silva2,4
1Universidade Paulista, Goiânia, GO; Brazil; 2Instituto de Patologia e Saúde Pública
da Universidade Federal de Goiás, GO, Brazil, 3Instituto de Ciências Biológicas da
Universidade Federal de Goiás, 4Rua 15, no. 108 Apto. 700, Setor Oeste, Goiânia,
GO, 74.140-090, Brazil
Summary: Candidemia is generally related to the endogenous flora but exogenous
infection originating from hospital staff or from the environment has been determined
as occurring. The randomly amplified polymorphic DNA (RAPD) method can reveal
strain specific variation. In this work, we used a RAPD assay to assess genetic
diversity among C. albicans isolates in an effort to find the relatedness between DNA
patterns of the strains recovered from clinical and environment samples from the ICU
from the Hospital das Clínicas da Universidade Federal de Goiás. The primers
named Cnd3 (5´-CCAGATGCAC-3`) and Cnd4 (5’-ACGGTACACT-3`) were used as
single primers in the PCR. RAPD profiles from blood and urine from the same patient
were identical in almost all samples studied, except for one patient. The bed of this
patient had the same genotype from his blood. Although most of C. albicans isolates
probably had had an endogenous origin, the finding of isolates from the patients with
same profile as the environment isolates suggest that the candidemia may be
resulted from an exogenous source.
Key words: Candida albicans, PCR, RAPD, nosocomial infection Correspondence: Dra. Maria do Rosário Rodrigues Silva. Rua 15, no. 108 Apto. 700, Setor Oeste. 74.140-090 Goiânia – GO, Brasil. Phone: 55 62 3209-6127; Fax: 55 62 3202-3022. E-mail: [email protected]

43
Introduction
Candida septicemia is considered as fungal major nosocomial infection and it is
largely associated with a least a 50% mortality rate [1,2,3]. ICU patients are
particularly susceptible to systemic infection because they are seriously ill and are
subjected to a number of therapeutic and supportive interventions (central venous
catheters, mechanical ventilations and tracheostomy), which breach physiological
barriers to infection [4,5].
Although the yeast species are considered important nosocomial pathogens,
little is known of their epidemiology. Candidemia is generally related to the
endogenous flora but exogenous infection originating from hospital staff or from the
environment has been determined as occurring [5]. In cases in which an exogenous
source is involved, the sanitary measures are mandatory to prevent the cross-
transmission of C. albicans.
Molecular typing system can be employed to characterize the pathogen to the
subspecies level or still to determine whether the infections studied are due to same
strain or due to different strains [3,6,7]. The randomly amplified polymorphic DNA
(RAPD) method, that use specific short oligonucleotide primers which can be
arbitrarily primed at multiple positions of the yeast genome, can reveal strain specific
variation. This method has been used to characterize the genetic relations among
Candida species isolates [8,9].
In this work, we used a RAPD assay to assess genetic diversity among C.
albicans isolates in an effort to find the relationship between DNA patterns of the
strains recovered from clinical and environment samples from the ICU from the same
hospital over a period of one year.

44
Materials and Methods
Isolates and patients. A total of 10 C. albicans isolates recovered from blood
specimens of 10 patients of the ICU from a tertiary hospital between March 2004 and
April 2005 were included in this study. Isolates of the same species recovered from
other sources related to these patients such as urine, catheter besides isolates from
environmental sources as of surface of bed and from Meyer table collected on the
same day were also taken in this study. The sources of isolates studied are related in
table 1.
The isolates were identified by conventional sugar assimilation and
fermentation methods and the germ-tube formation and confirmed by the
commercially available API 20C identification test (API Laboratory Products Ltd.,
Grafton Way, Basingstoke, Hants, England). All isolates were maintained in sterile
water at – 20oC and the purity of cultures was ensured by regular identification using
standard techniques.
Genotypic characterization
Preparation of DNA for randomly amplified polymorphic DNA (RAPD).
Yeasts obtained from stock cultures were sub-cultured on yeast-peptone dextrose
medium (1% yeast extract peptone, 2% glucose, 1.2% agar) at 37oC for 24 to 48
hours.
Genomic DNA extraction was based on the method described by Del Poeta et
al. 1999 [10] modified by Casali et al. 2003 [11]. Briefly, a heavy inoculum of C.
albicans strains grown in YEPD agar (Yeast Extract Peptone Dextrose) were
suspended in 0.5 ml TENTS (10 mM Tris, pH 7.5, 1 mM EDTA pH 8.0, 200 mM NaCl,
2% Triton, 1% SDS) containing 0.2 ml of 0.45 mm glass beads and 0.5 ml of

45
phenol:chloroform and vortexed for 2 min. After the centrifugation for 10 min at 13000
g, the aqueous phase transferred to a new tube and the same volume of 100%
ethanol was added and incubated at -20oC for 1 h for DNA precipitation. The
precipitated DNA was resuspended in 0.5 ml TE (10 mM Tris HCl pH 8, 1 mM EDTA
pH 8.0) containing 50 µg/mL RNAse A, and incubated at 37oC for 30 min. The yeast
DNA was deproteinated and extracted from the sample by adding equal volume of
phenol and chloroform. Finally, the DNA was precipitated with 70% ethanol and after
dryed, stored at-20oC in 100 μl of TE buffer until further processing for PCR.
RAPD analysis
The primers named Cnd3 (5´-CCAGATGCAC-3`) and Cnd4 (5’-ACGGTACACT-3`)
were used as single primers in the PCR. Amplifications reactions as described by
Ergon & Gülay [12], were performed in volumes of 25 μl including about 25 ng of the
DNA template; 10 mM Tris-HCl, pH 8.3, 50 mM KCl, 1.5 mM MgCl, 0.2 mM each of
the dATP, dCTP, dGTP and dTTP and 2.5 U Taq DNA polymerase (Invitrogen). The
primers were used at a concentration of 30 ng. Amplification was performed in a PCR
MJ Research Thermal Cycler model PTC-100 TM programmed for denaturation at
94ºC for 3 min; 45 cycles of 1 min at 94ºC, 1 min at 36ºC and 2 min at 72ºC, and
extension at 720C for 7 min. Amplification products were separated by
electrophoresis in 1.2% agarose gel containing 1x tris-borate-EDTA (TBE) buffer,
stained with ethidium bromide at 0.5 μg/ml and visualized under UV light. All
amplifications were reapeated at least twice.

46
PCR profile analysis
The banding profiles for each isolate were compared visually. Bands were recorded
as present (1) or absent (0). Simple matching´s similarity coefficient (SM) values for
each pair wise comparison between isolates were calculated and a similarity
coefficient matrix was constructed. An SM value of 1.00 represented the same
genotype; SM values between 0.80 and 0.99 represented clonally related isolates
and SM under 0.80 represented distinct strains [12]. Clonally related isolates are
presented as of the same pattern added of ` (e.g. A’ and A’’ for Cnd3 and 1’ and 1’’
for Cnd4).
Results
A total of 31 C. albicans isolates (10 of blood, 9 of urine, 5 of catheter, 4 of Meyer
table and 3 of bed) were submitted to molecular typing using the RAPD method. Both
two primers (Cnd3 and Cnd 4) used in this study were successful in eliciting banding
profiles for each isolate. Amplification products obtained were specific to each primer
and ranged from 4 to 8 bands with fragment size from 350 bp to 2000 bp for Cnd3
and from 3 to 6 bands with fragment size from 300 bp to a 3500 bp for Cnd4. Most of
the major bands were present in all isolates studied and almost all strains had a
conserved fragment: 650 Kb for both primers (Figs 1 and 2).
Both two primers had high discriminatory power. Among 31 C. albicans
isolates, 12 patterns were detected with primer Cnd3 and 14 patterns with Cnd4
(Table 1). The similarity coefficients for Cnd3 between profiles A-L were calculated
and ranged from 28% to 85%. Some strains had closely related patterns. The isolate
7 (A’) had high similarity with the isolates 4, 5 and 6 (A), the isolate 24 (F’) with
isolates 23 and 25 (F) and the isolate 34 (B’) with the isolates 10 and 11 (B). The

47
similarity coefficients for Cnd 4 between the profiles 1-14 ranged from 16 to 80%.
Profiles 1 to 15 were clearly different from 15 previously identified.
RAPD profiles from blood and urine from the same patient were identical in
almost all sample studied, except for patient 5, where the two clinical samples were
different by using the two primers. However it was observed that the isolate from the
bed of this patient (5) had a similar genotype as the one isolated from his blood.
Another interesting fact was verified with isolates 12 (surface of Meyer table of patient
3) and 40 (bed of patient 8) of C. albicans. These isolates presented had the same
genotype when isolated from blood and urine of their patients. Additionally, it was
detected the same genotype in isolates, 19 (catheter from patient 4), 32 (bed from
patient 6) and 42 (catheter from patient 9)
Discussion
Although nosocomial candidemia constitutes a growing issue, [3] it is quite difficult to
achieve a precise understanding of its epidemiology. Colonization precedes
candidemia and it is considered to be an important risk factor in endogenous
infections [13]. Tortorano et al. 2004 [14] showed a previous colonization of the
alimentary tract by the same Candida specie causing fungaemia. Candidemia has
been relationship with previous colonization of the urinary tract [15]. Urinary tract
colonization deserves consideration, because it is a common event in hospitalized
patients affecting 6.5-20% of patients [16]. In this work, molecular typing
demonstrated that the paired isolates from blood and urine were identical for patients
with C. albicans, suggesting an endogenous origin of candidemia.
It is well known that exogenous sources of C. albicans may be involved in the
development of nosocomial candidiasis [17]. In this study, it was found that strains of

48
C. albicans isolated from the blood of patients 5 and 8 were identicals to isolated from
surface of their beds. Besides, identical strains were isolated from blood of patient 3
and surface of Meyer table (table 1). These samples from environment were collected
on the same day of blood collection of patients with candidemia. Robert et al. 1995
[18] characterized strains of C. albicans colonized on admission as identical to other
patient that was culture negative on admission and acquired the yeast after 25 days,
suggesting cross infection. The epidemiology of nosocomial C. albicans isolates
infection is complex and the mechanism by which the patients in our study acquired
their strains remains not totally clear. However the finding of three isolates from the
blood of patients with the same molecular profile as the ones isolated from the
environment isolates suggest that the candidemia may be resulted from exogenous
source.
Exogenous acquisition of candidemia is also postulated to be associated with
intravascular devices and parenteral nutrition. The candidemia related to catheter has
been suggested by some researchers [19, 20]. The isolates from catheter and blood
of patient 6 had the same genotype, suggesting that the portal of entry of C. albicans
was via the catheter.
Interestingly, molecular typing, demonstrated that isolates of catheter from
patient 4 (isolate 19), of bed from patient 6 (isolate 32) and of catheter from patient 9
(isolate 42) also had the same genotypes. These results may infere in cross infection.
It is possible that C. albicans strains recovered in catheter or surface of bed was
arised from hands of hospital coworkers.
The 12 and 14 different patterns presented by primers Cnd3 and Cnd4
respectively, confirm the discriminatory value of RAPD, which is considered quite
similar to other powerful genotyping methods [3,5]. The RAPD assay using primers

49
Cnd3 and Cnd4 can be an important tool to identify the intra-specific genetic
variability among C. albicans isolates.
In conclusion, although candidemia was strongly associated to endogenous
sources as candiduria, it was indicated that catheter, surface of bed and Meyer table
can also be considered important exogenous sources of infection.
ACKNOWLEDGMENTS
The financial help received by the first author from the Universidade Paulista – Brazil.
REFERENCE
1. Meunier F, Aoun M, Bitar N. Candidemia in immunocompromised patients. Clin
Infect Dis 1992; 14:120-125.
2. Giammanco GM, Lopes MM, Coimbra RS, Pignato S, Grimont PAD, Grimont F, et
al. Value of morphotyping for the characterization of Candida albicans clinical
isolates. Mem Inst Oswaldo Cruz 2005; 100: 483-490.
3. Shin JH, Og YG, Cho D, Kee SJ, Shin MG, Suh SP et al. Molecular
Epidemiological Analysis of Bloodstream Isolates of Candida albicans from a
University Hospital over a Five-Year Period. J Microbiol 2005; 43:546-554.
4. Pfaller MA. Epidemiology of Nosocomial candidiasis: the importance of molecular
typing. Brazilian J Infect Dis 2000; 4:161-167.
5. Vrioni G, Matsiota-Bernard P. Molecular typing of Candida isolates from patients
hospitalized in an intensive care unit. 2001; J Infect. 42:50-56.
6. Mehta SK, Stevens DA; Mishra S, Feroze F, Pierson DL. Distribution of Candida
albicans genotypes among family members - demonstration by sequential DNA
fingerprinting with probes Ca3, C1 and CARE2. Diag Microbiol Infect Dis 1999;
34:19-25.

50
7. Andrighetto C, Psomas E, Tzanetakis N, Suzzi G, Lombardi A. Randomly amplified
polymorphic DNA (RAPD) PCR for the identification of yeasts isolated from dairy
products. Letters in Applied Microbiology 2000; 30, 5-9.
8. Dassanayake RS, Samaranayake YH, Samaranayake LP. Genomic diversity of
oral Candida krusei isolates as revealed by DNA fingerprinting and electrophoretic
karyotyping. Acta Patho Microbiol et Immun Scand. 2000; 108:697-704.
9. Pinto PM, Resende MA, Koga-Ito CY, Tendler M. Genetic variability analysis
among clinical Candida spp. isolates using random amplified polymorphic DNA.
Mem Inst Oswaldo Cruz 2004; 99:147-152.
10. Del Poeta M, Toffaletti DL, Rude TH, Dykstra CC, Heitman J, Perfect JR.
Topoisomerase I is essential in Cryptococcus neoformans: role in pathology and
as an antifungal target. Genetics 1999; 152:176-178.
11. Casali AK, Goulart L, Silva LKR, Ribeiro AM, Amaral AA, Alves SH, Schrank A,
Meyer W, Vainstein MH. Molecular typing of clinical and environmental
Cryptococcus neoformans isolates in the Brasilian state Rio Grande do Sul. FEMS
Yeast Resear 2003; 33:405-415.
12. Ergon MC, Gülay Z. Molecular epidemiology of Candida species isolated from
urine at an intensive care unit. Mycoses 2005; 48:126-131.
13. Eggimann P, Garbino J, Pitter D. Epidemiology of Candida species infections in
critically ill non-immunosuppressed patients. Lancet Infect Dis 2003; 3:685-702.
14. Torturano AM, Peman J, Bernhardt H, et al.; the ECMM Working Group on
Candidaemia. Epidemiology of candidaemia in Europe: results of 28-month
European Confederation of Medical Mycology (ECMM) hospital-based surveillance
study. Eur J Clin Microbiol Infect Dis 2004; 23:317-322.
15. Binelli CA, Moretti ML, Assis RS, Sauaia N, Menezes PR, Ribeiro E, Geiger DCP,
Mikami Y, Miyaji M, Oliveira MS, Barone AA, Levin AS. Investigation of the
possible association between nosocomial candiduria and candidaemia. Eur Clin
Microbiol Infect Dis 2006; 12:538-543.

51
16. Pegano L, Antinori A, Ammassari A et al. Retrospective study of candidaemia in
patients with hematological malignancies. Eru J Haemat 1999; 63:77-85.
17. Schonian G, Meusel O, Tietz HJ, Meyer W, Graser Y, Tausch I, et al.
Identification of clinical strains of Candida albicans by DNA fingerprinting with the
polymerase chain reaction. Mycoses 1993; 36:171-179.
18. Robert F, Lebreton F, Bougnoux ME, Paugam A, Wassermann D, Schlotterer M,
et al. Use of random amplified polymorphic DNA as a typing method for Candida
albicans in epidemiological surveillance of a burn unit. J Clin Microb1995; 33:2366-
2371.
19. Shin JH, Park MR, Song JW, Shin DH, Jung SI, Cho D, Kee SJ, Shin MG, Suh
SP, Ryang DW. Microevolution of Candida albicans strains during catheter-related
candidemia. J Clin Microbiol 2004; 42:4025-4031.
20. Torturano AM, Kibbler C, Peman J, Bernhardt H, Klingspor L, Grillot R.
Candidaemia in Europe: epidemiology and resistance. Int J Antimicrobiol Agents
2006; 27:359-366.

52
Table 1. Candida albicans isolates recovered from 10 ICU patients with candidemia and from other clinical and environment materials relationship to these patients.
Genotype (patterns) Patients Isolation date (mo/day/yr) Isolates Sources of isolates Cnd3 Cnd4
1. 09/12/2003 4-112A3E Catheter A 1
09/26/2003 5-112C6E Blood A 1
09/19/2003 6-112B7E Urine A 1
09/23/2003 7-112C1A Meyer table A’ 2
2. 12/18/2003 10-159C6A Blood B 3
12/12/2003 11-159B7A Urine B 3
3. 12/15/2003 12-164A1A Meyer table C 4
12/15/2003 13-164A6A Blood C 4
12/15/2003 14-164A7A Urine C 4
4. 01/06/2004 15-174B1E Meyer table C 4
01/06/2004 17-174B6A Blood D 5
01/06/2004 18-174B7A Urine D 5
01/06/2004 19-174B2A Catheter E 6
5. 05/31/2004 23-231I6A Blood F 7
05/17/2004 24-231G7A Urine F’ 8
05/31/2004 25-231I2E Bed F 7
6. 04/05/2004 30-234A3E Catheter G 9
04/05/2004 31-234F6A Blood G 9
04/05/2004 32-234A2A Bed E 6
7. 08/11/2004 34-280C1E Meyer table B’ 10
08/18/2004 35-280D6A Blood H 11
08/04/2004 36-280B7E Urine H 11
8. 10/29/2004 37-315A6E Blood I 12
11/19/2004 38-315D7E Urine I 12
10/29/2004 39-315A3E Catheter J 12
10/29/2004 40-315A2E Bed I 12
9. 11/10/2004 42-320A3E Catheter E 6
11/10/2004 43-320A6E Blood K 13
11/10/2004 44-320A7A Urine K 13
10. 05/04/2005 45-365B6A Blood L 14
05/04/2005 46-365B7A Urine L 14

53
12000 5000 2000 1650 1000 850 650 500 400
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 MM
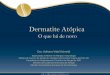
Figure1. RAPD Profiles of 31 Candida albicans isolates obtained with primer Cnd3. Profile A (lines 1-3:
catheter, blood and urine related with patient 1); profile A´(line 4: table Meyer related with patient 1);
profile B (lines 5, 6: blood and urine related with patient 2); profile C (lines 7, 8, 9 and 10: table Meyer,
blood and urine related with patient 3 and table Meyer related with patient 4); profile D (lines 11, 12
blood and urine related with patient 4); profile E (lines 13 ,19, 27: catheter related with patient 4, 19
bed related with patient 6, 27 catheter related with patient 9, respectively); profile F (lines 14, 16: blood
and bed related with patient 5); profile F’ (line 15: urine related with patient 5); profile G (lines 17, 18:
catheter and blood related with patient 6); profile H (lines 21, 22: blood and urine related with patient
7); profile I (lines 23, 24, 26: blood, urine and bed related with patient 8); profile J (line 25: catheter
related with patient 8); profile K (lines 28, 29: blood and urine related with patient 9), and profile L
(lines 30, 31: blood and urine related with patient 10).

54
12000 5000 2000 1650 1000 850 650 500 400 300
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 MM
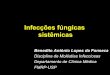
Figure 2. RAPD Profiles of 31 Candida albicans isolates obtained with primer Cnd4. Profile 1 (lines 1,
2, 3: catheter, blood and urine related with patient 1), profile 2 (line 4: Meyer table related with patient
1); profile 3 (lines 5, 6: blood and urine related with patient 2); profile 4 (lines 7, 8, 9 and 10: Meyer
table, blood and urine related with patient 3 and Meyer table related with patient 4); profile 5 (lines 11,
12: blood and urine related with patient 4), profile 6 (line 13, 19, 27: catheter related with patient 4, bed
related with patient 6; catheter related with patient 9, respectively); profile 7 (lines 14, 16: blood and
bed related with patient 5), profile 8 (line 15: urine related with patient 5); profile 9 (lines 17, 18:
catheter and blood related with patient 6); profile 10 (line 20: Meyer table related with patient 7); profile
11 (lines 21, 22: blood and urine related with patient 7); profile 12 (lines 23, 24, 25, 26 blood, urine,
catheter and bed related with patient 8); profile 13 ( lines 28, 29: blood and urine related with patient
9); and profile 14 (lines 30, 31: blood and urine related with patient 10).

55
4.4 ARTIGO 4: Nosocomial invasive infection caused by Cunninghamella bertholletiae: case report

56

57

58

59
5 CONCLUSÕES
1. Foi observada uma elevada freqüência de candidúria em pacientes da UTI
(44,4%).
2. Candidúria e candidemia podem ser adquiridas após um longo período de
internação.
3. Espécies de Candida não-albicans estavam presentes no sangue e urina
com um percentual elevado.
4. A atividade in vitro de voriconazol foi maior do que a do itraconazol,
fluconazol e anfotericina B, sugerindo que voriconazol pode ser o azólico
mais efetivo no tratamento de infecções por Candida na corrente
sangüínea.
5. O encontro de isolados resistentes a diferentes antifúngicos mostra a
importância do uso dos testes de suscetibilidade in vitro para a terapia
adequada.
6. O ensaio de RAPD usando os primers Cnd3 e Cnd4 podem ser uma
ferramenta importante para identificar a variabilidade genética intra-
específica entre isolados de C. albicans.
7. A possível fonte de transmissão ambiental de candidíase encontrada em
três casos justifica a importância de maiores cuidados na UTI para evitar a
transmissão da infecção.
8. O achado de infecção por C. bertholletiae causando fungemia em pacientes
imunocomprometidos foi muito importante, porque este microrganismo é
normalmente um contaminante. Este achado mostra que tem que se ter um
grande cuidado no isolamento de fungos não usualmente causadores de
infecção.

60
6 REFERÊNCIAS RELACIONADAS À INTRODUÇÃO
Abbas J, Bodey GP, Hanna HA, Mardini M, Girgawy E, Abi-Said D, Whimbey
E, Hachem R, Raad I 2000. Candida krusei fungemia. An escalating
serious infection in immunocompromised patients. Arch Intern Med
160:2659-2664.
Abi-Said D, Anaissie E, Uzun O, Raad I, Pinzcowski H, Vartivarian S 1997. The
epidemiology of hematogenous candidiasis caused by different Candida
species. Clin Infect Dis 24:1122-1128.
Abuhammour W, Habte-Gaber E 2004. Newer antifungal agents. Indian J
Pediatr 71:253-259.
Adad SJ, Lima RV, Sawan ZTE 2001. Frequency of Trichomonas vaginalis,
Candida sp and Gardnerella vaginalis in cervical-vaginal smears in four
different decades. São Paulo Med J 119:200-205.
Almirante B, Rodríguez D, Park BJ, Cuenca-Estrella M, Planes AM, Almela M,
Mensa J, Sanchez F, Ayants J, Gimenez M, Saballs P, Fridkin SK, Morgan
J, Rodriguez-Tudela JL, Warnock DW, Pahissa A 2005. Epidemiology and
predictors of mortality in cases of Candida bloodstream infection: results
from population-based sureveillance, Barcelona, Spain, from 2002 to 2003.
J Clin Microbiol 43:1826-1835.
Anaisse EJ, Bodey GP, Kantarjan H 1989. New spectrum of fungal infection in
patients with cancer. Rev Infect Dis 11:369-378.
Andrighetto C, Psomas E, Tzanetakis N, Suzzi G, Lombardi A 2000. Randomly
amplified polymorphic DNA (RAPD) PCR for the identification of yeasts
isolated from dairy products. Let Appl Microbiology 30:5-9.
Antunes AGV, Pasqualotto AC, Diaz MC, D'azevedo PA, Severo LC 2005.
Candidemia in a Brazilian tertiary care hospital: species distribution and

61
antifungal susceptibility patterns. Rev. Inst. Med. trop. S. Paulo, 46: 239-
241.
Appelgren P, Heliström I, Wetzberg E, Söderlund V, Bundslev L, Ransjö U
2001. Risk factors for nosocomial intensive care infection: a long-term
prospective analysis. Acta Anaesthesiol Scand 45:710-719.
Aquino VR, Lunardi LW, Goldani LZ, Barth AF 2005. Prevalence, susceptibility
profile for fluconazole and risk factors for candidemia in a tertiary care
hospital in Southern Brazil. Braz J Infect Dis 9:411-418.
Arantes A, Carvalho ES, Medeiros EAS, Farhat CK, Mantese OC 2003. Uso de
diagramas de controle na vigilância epidemiológica das infecções
hospitalares. Rev Saúde Pública 37:768-774.
Araújo MAE. Infecções fúngicas nosocomiais. Revista do Idipa nº 1/outubro
1998.
Arenas R, Ocejo D 1997. Onicomicosis: frecuencia actual en un departamento
de dermatología de la Ciudad de Mexico. Dermatol Rev Mex 41:171-176.
Arenas R, Ruiz-Esmenjaud J 2004. Onicomicose na infância: uma perspectiva
atual com ênfase na revisão do tratamento. An Bras Dermatol 79:225-232.
Arif S, Barkham T, Power BG, Howell SA 1996. Techniques for investigation of
on apparent outbreak of infections with Candida glabrata. J Clin Microbiol
34:2205-2209.
Arikan S, Gur D, Akova M 1997. Comparison of Etest, microdilution and
colorimetric dilution with reference broth macrodilution method for
antifungal susceptibility testing of clinically significant Candida species
isolated from immunocompromised patients. Mycoses, 40: 291-296.
Ayeni O, Riederer KM, Wilson FM, Khath R 1999. Clinicians reactions to
positive urine culture for Candida organisms. Mycoses 42:285-289.

62
Bae HG, Sohn YH, Shin JH, Kim MN 2004. The evaluation of clinical utility of
ATB Fungus 2 for antifungal susceptibility testing in Candida species.
Korean J. Clin. Microbiol 7: 156-163.
Banno Y, Yamada T, Nozawa Y 1985. Secreted phospholipase of the
dimorphic fungus Candida albicans; separation of three enzymes and
some biological properties. Sabouraudia 47-54.
Barchiesi F, Maracci M, Radi B, Arzeni D, Baldassarri I, Giacometti A, Scalise
G 2002. Point prevalence, microbiology and fluconazole susceptibility
patterns of yeast isolates colonizing the oral cavities of HIV-infected
patients in the era of highly active antiretroviral therapy. J Antimicrob
Chemother 50: 999-1002.
Bartie LK, Williams DW, Wilson MJ, Potts JC, Lewis MAO 2001. PCR
fingerprinting of Candida albicans associated with chronic hyperplastic
candidoses and other oral conditions. J Clin Microbiol 39:4066-4075.
Beck-Sagué CM, Jarvis WR 1993. The National Nosocomial Fungal
Surveillance Systen. Secular Trends in the Epidemiology of Nosocomial
Fungal Infections in the United States, 1980-1990. J Infec Dis 167:1247-
1251.
Bered F, Barbosa Neto JF, Carvalho FIF 1997. Marcadores moleculares e sua
aplicação no melhoramento genético de plantas. Ciên Rur 27:513-520.
Bergold AM, Georgiadis S 2004. Novidades em fármacos antifúngicos: uma
revisão. Visão Acad 5:159-172.
Berrouane YF, Herwaldt IA, Pfaller MA 1999. Trends in antifungal use and
epidemiology of nosocomial yeast infections in a university hospital. J Clin
Microbiol 37:531-537.
Bizarro A, Dinis AP 2003. Tratamento de infecções fúngicas sistêmicas: novas
perspectivas farmacológicas. Rev Org Farmcol Iberoam 13:23-31.

63
Bodey GP, Mardani M, Hanna HA 2002. The epidemiology of Candida glabrata
and Candida albicans fungemia in immunocompromised patients with
cancer. Am J Med 1125:380-385.
Boo TW, Reilly BO, Leary JO, Cryan B 2005. Candidemia in an Irish tertiary
referral hospital: epidemiology and prognostic factors. Mycoses 48:251-
259.
Brilhante RS, Cordeiro RA, Medanno DJ 2005. Onychomycosis in Ceara
(Northeast Brazil): epidemiological and laboratory aspects. Mem Inst
Oswaldo Cruz 100:131-135.
Brown AJ, Gow NA 1999. Regulatory networks controlling Candida albicans
morphogenesis. Trends Microbiol 7:333-338.
Burgess DS, Hastings RW, Summers KK, Hardin TC, Rinaldi MG 2000.
Pharmacodynamics of fluconazole, itraconazole and amphotericin B
against Candida albicans. Diagn Microbiol Infect Dis 36:13-18.
Calderone RA, Fonzi WA 2001. Virulence factores of Candida albicans. Trends
Microb 9:327-335.
Cantón E, Viudes A, Pemán J 2001. Infección sistémica nosocomial por
levaduras. Rev Iberoam Micol 18:51-55.
Carrillo-Muñoz AJ, Quindós G, Ruesga M, Del Valle O, Cantón E Hernández-
Molina JM, Santos P 2006. In vitro antifungal susceptibility testing of
filamentous fungi with Sensitre YeastOne™. Mycoses 49:293-297.
Casadevall A, Pirofski L 2001. Host-pathogen interactions: the attributes of
virulence. J Infect Dis 184:337-344.
Cavassani VGS, Sobrinho JA, Homem MGN, Rapoport A 2002. Candidíase
oral como marcador de prognóstico em pacientes portadores do HIV. Rev
Bras Otorrinolaringol 68:630-634.

64
Chaturvedi V, Ramani R, Pfaller MA 2004. Collaborative study of the NCCLS
and flow cytometry methods for antifungal susceptibility testing of Candida
albicans. J Clin Microbiol 42:2249-2251.
Cirak MY, Kalkanci A, Kustimur S 2003. Use of molecular methods in
identification of Candida species and evoluation of fluconazole resistance.
Mem Inst Oswaldo Cruz 98:1027-1032.
Clancy CJ, Nguyen MH 1999 Correlation between in vitro susceptibility
determined by E-test and response to therapy with amphotericin B: results
from a multicenter prospective study of candidemia. Antimicrob Agents
Chemother 43:1289-1290.
Colombo AL 1994. Avaliação in vitro, por três métodos diferentes da
sensibilidade de leveduras a antifúngicos azólicos. São Paulo, 72p (Tese
de Doutorado, Escola Paulista de Medicina).
Colombo AL, Da Matta D, De Almeida LP, Rosas R 2002. Fluconazole
susceptibility of Brazilian Candida isolates assessed by a disk diffusion
method. Braz J Infec. Dis 6:118-123.
Colombo AL, Guimarães T 2003. Epidemiologia das infecções hematogênicas
por Candida spp. Rev Soc Bras Med Trop 36:599-607.
Colombo AL, Nucci M, Park BJ, Nouer AS, Arthington-Skaggs B, da Mata DA,
Warnock DW, Morgan J 2006. Epidemiology of candidemia in Brazil: a
nationwide sentinel surveillance of candidemia in eleven medical centers. J
Clin Microbiol 44:2816-2823.
Colombo AL, Nucci M, Salomao R 1999. High rate of non-albicans candidemia
in Brazilian tertiary care hospitals. Dia Microbiol Infect Dis 34:281-286.
Costa M, Passos XS, Miranda ATB, Araújo RSC, Paula CR, Silva MRR 2004.
Correlation of in vitro itraconazole and fluconazole susceptibility with

65
clinical outcome for patients with vulvovaginal candidiasis. Mycophatol 157:
43-47.
Cutler JE 1991. Putative virulence factors of Candida albicans. Annu Rev
Microbiol 45:187-218.
Dassanayake RS, Samaranayake YH, Samaranayake LP 2000. Genomic
diversity of oral Candida krusei isolates as revealed by DNA fingerprinting
and eletrophoretic karyotyping. APMIS 108:697-704.
De Bernardis F, Adriani D, Lorenzini R, Pontieri E, Carruba G, Cassone A
1993. Filamentous growth and elevated vaginopathic potential of a non-
germinative variant of Candida albicans expressing low virulence in
systemic infection. Infect immune 61:1500-1508.
Denning DW, Radford SA, Oakley KL, Hall L, Johnson EM, Warnock DW 1997.
Correlation between in vitro susceptibility testing to itraconazole and in vivo
outcome of Aspergillus fumigatus infection. J Antimicrob Chemother
40:401-414.
Deresinski SC, Stevens DA 2003. Caspofungin. Clin Infect Dis 36:1445-1457.
Drago L, Mombelli B, DE Vecchi E, Bonaccorso C, Fassina MC, Gismondo MR
2000. Candida albicans cellular internalization: a new pathogenic factor?
Int J. Antimic. Agents, 16:545-547.
Durussel, C. Comparative study of various methods, NCCLS, M27-A2,
EUCAST, and ATB Fungus 2 (bio-Merieux) for the in vitro antifungal
susceptibility testing of Candida sp. 14th European Congress of Clinical
Microbiology and Infectious Diseases, Prague, 2004, p.902.
Ellis D, Marriott D, Hajjeh RA, Warnock D, Meyer W, Barton R 2003.
Epidemiology: surveillance of fungal infections. Med Mycol 38:173-182.

66
Ergon MC, Gülay Z 2004. Molecular epidemiology of Candida species isolated
from urine at an intensive care unit. Mycoses 48:126-131.
Ernst JF 2000. Transcription factors in Candida albicans-environmental control
of morphogenesis. Microbiology 146: 1763-1774.
Fernandes OFL, Passos XS, Souza LKH, Miranda ATB, Cerqueira CHPV, Silva
MRR 2003. In vitro susceptibility characteristics of Cryptococcus
neoformans varieties from AIDS patients in Goiania, Brazil. Mem Inst
Oswaldo Cruz 98:839-841.
Ferrazza MHSH, Maluf MLF, Consolaro MEL, Shinobu CS, Svidzinski TIE,
Batista MR 2005. Caracterização de leveduras isoladas da vagina e sua
associação com candidíase vulvovaginal em duas cidades do sul do Brasil.
Rev Bras Gineco Obstet 27:58-63.
Fotedar R, Al-Hedaithy S 2003. Comparison of phospholipase and proteinase
activity in Candida albicans and C. dubliniensis. Mycoses 48:62-67.
Foxman B, Barlow R, D'Arcy H, Gillespie B, Sobel JD 2000. Candida vaginitis:
self-reported incidence and associated costs. Sex Transm Dis 27:230-235.
Franklin C, Metry M 1992. Life-threatening Candida infections in the intensive
care unit. J Intensive Care Med 7: 127-137.
Frazer VJ, Jones M, Dunkel J, Strofer S, Medoff G, Dunagan WC 1992.
Candidemia in a tertiary care hospital: epidemiology, risk factors, and
predictors of mortality. Clin Infect Dis 15:414-421.
Fridkin SK, Jarvis WR 1996. Epidemiology of nosocomial fungal infections. Clin
Microbiol Rev 9:499-511.
Galván B, Mariscal F 2006. Epidemiologia de la candidemia em UCI. Rev
Iberoam Micol 23:12-15.

67
Gao H, Pennsi M, Shah K, Qiao X, Hariprasol SM, Mieler WF, Samuel M, Holz
ER 2003. Safety of itravitreal voriconazole: electinographic and
histopathologic studies. Trans Am Ophtalmol Soc 101:183:189.
Ghannoum MA & Abu Elteen KH 1990. Pathogenicity determinants of Candida.
Mycoses 33: 265-282.
Ghannoum MA 2000. Potential role of phospholipases in virulence and fungal
pathogenesis. Clin Microbiol Rev 13: 122-143
Ghannoum MA 2001. Candida: a causative agent of an emerging infection. Soc
Invest Dermatol 6:188-196.
Ghannoum MA1998. Extracellular phospholipases as universal virulence factor
in pathogenic fungi. J Med Mycol 39: 55-59
Gimeno RB, Martínez MJM 2007. Respuesta terapéutica prolongada a
voriconazol en un caso de broncoaspergilosis alérgica. Arch
Bronconeumol 43:49-51.
Godoy P, Tiraboschi IN, Severo LC, Bustamante B, Calvo B, Almeida LP,
Matta DA, Colombo AL 2003. Species distribution and antifungal
susceptibility profile of Candida spp bloodstream isolates from Latin
American Hospitals. Mem Inst Oswaldo Cruz, 98: 401-405.
Greenfield RA 1992. Host defense system interactions with Candida albicans. J
Med Vet Mycol 30: 89-104.
Hajjeh RA, Safair AN, Harrison LH, Lyon GM, Athington-Skaggs BA, Mirza SA,
Phelan M, Morgan J, Lee-Yang W, Ciblak MA, Benjamin LE, Sanza LA,
Huie S, Yeo SF, Brandt ME, Warnock DW 2004. Incidence of bloodstream
infections due to Candida species and In vitro susceptibilities of isolates
collected from 1998 to 2000 in a population-based active Surveillance
Program. J Clin Microbiol 42:1519-1527.

68
Hazen KC 1995. New and emerging yeast pathogens. Rev Clin Microbiol
8:462-478.
Hazen KC, Baron EJ, Colombo AL, Girmenia C, Sanchez-Sousa A, Del
Palacio A, Bedout C, Gibbs DL and the Global antifungal Surveillance
Group 2003. Comparison of the susceptibilities of Candida spp. to
fluconazole and voriconazole in a 4-year global evaluation using disk
diffusion. J Clin Microbiol 41:5623-5632.
Hedderwick SA, Lyons MJ, Liu M, Vazquez JA, Kauffman CA 2000.
Epidemiology of yeast colonization in the intensive care unit. Eur J Clin
Microbiol Infect Dis 19:663-670.
Hellstein J, Vawter-Hugart H, Fotos P, Schmid J, Soll DR 1993. Genetic
similarity and phenotypic diversity of commensal and pathogenic strains of
Candida albicans isolated from the oral cavity. J Clin Microbiol 31:3190-
3199.
Hitchocock CA, Pye GW, Troka PF 1993. Fluconazole resistance in Candida
glabrata. Antimicrobiol Agents Chemother 37:1962-1965.
Hube B 1996. Candida albicans secreted aspartyl proteinases. Curr Trop Med
Mycol 7: 55-69.
Ibrahim AS, Mirbord F, Filler SG 1995. Evidence implicating phospholipase as
a virulence factor of Candida albicans. Infect Immun 63: 1993-1998.
Irobi J, Schoofs A, Goossens H 1999. Genetic identification of Candida species
in HIV-positive patients using the polymerase chain reaction and restriction
fragment length polymorphism analysis of its DNA. Mol Cell Probes
14:401-406.
Kauffman CA, Vasquez JA, Solel JD, Gallis HA, McKinser DS, Karelmar AW,
Sugar AM, Sharkey PK, Wise GJ, Mangi R, Mosher A, Lee JY, Dismukes

69
WE 2000. Prospective multicenter surveillance study of funguria in
hospitalized patients. Clin Infect Dis 30:14-18.
Lachke SA, Joly S, Daniels K, Soll DR 2002. Phenotypic switching and
filamentation in Candida glabrata. Microbiology 148:2661-2674.
Laffey SF, Butler G 2005. Phenotype switching affects biolfilm formation by
Candida parapsilosis. Microbiology 151:1073-1081.
Lan CY, Newport G, Murillo LA, Jones T, Scherer S, Davis RW, Agabian N
2002. Metabolic specialization associated with phenotypic switching in
Candida albicans. PNAS 99:14907-14912.
Lewis RE & Klepser ME 1999. The changing face of nosocomial candidemia:
epidemiology, resistance, and drug therapy. Am J Health Syst Pharm
56:525-533.
Lian C, Zhao J, Zhang Z, Liu W 2003. Genotype of Candida species associated
with different conditions of vulvovaginal candidosis. Mycosis 47:495-502.
Lombardi G, Farina C, Andreoni S, Fazii P, Faggi E, Manso E, Nanetti A,
Mazzoni A. 2004 Comparative evaluation of Sensititre®YeastOne vs
NCCLS M27A protocol and E-test for antifungal susceptibility testing of
yeasts. Mycoses 47:397-401.
López-Jodra O, Torres-Rodriguez JM 1999. Especies fúngicas poco comunes
responsables de onicomicosis. Rev Iberoam Micol 16:11-15.
López-Medrado F, Díaz-Pedroche C, Lumbreras C, Aguado JM 2005. Utilidad
de la amfotericina B liposomal para la prevención de la infección fúngica
en receptores de un trasplante de órgano sólido. Rev Esp Quimioterap
18:14-20.
Lozano-Chiu M, Arikan S, Paetzick VL, Anaisse EJ, Rex JH 1999. Optimizing
voriconazole susceptibility testing of Candida effects of incubation time,

70
endpoint rule, species of Candida, and level of fluconzaole susceptibility. J
Clin Microbiol 37:2755-2759.
Macphail GLP, Taylon GD, Burchanan-Chell M, Ross C, Wilson S Kureishi A
2002. Epidemiology, treatment and outcome of candidemia: a fiver-year
review at three Canadian hospitals. Mycoses 45:141-145.
Magill SS, Shields C, Sears CL, Choti M, Merz WG 2006. Triazole cross-
resistance among Candida spp.: case report, occurrence among
bloodstream isolates, and implications for antifungal therapy. J Clin
Microbiol 44:529-535.
Manavathu EK, Kallakuri S, Arganoza MT, Vázquez JA 1999. Amino acid
variations of cytochrome P-450 lanosterol 14α-demethylase (CYP51A1)
from fluconzole-resistant clinical isolates of Candida albicans. Rev Iberoam
Micol 16:198-203.
Marchetti O, Bille J, Fluckger U 2004. Epidemiology of candidemia in Swiss
tertiary care hospitals: secular trends, 1991-2000. Clin Infect Dis 38:311-
320.
McDonalds F, Odds FC 1983. Virulence for mice of a proteinase secreting
strain o Candida and a proteinase-deficient mutant. J Gen Microbiol
129:431-438.
Medrano DJA, Brilhante RSN, Cordeiro RA, Rocha MFG, Rabenhorst SHB,
Sidrim JJC 2006. Candidemia in a Brazilian hospital: the importance of
Candida parapsilosis. Rev Inst Med Trop S. Paulo 48:17-20.
Melo SA, Almeida LP, Colombo AL, Briones MRS 1998. Evolutionary distance
and identification of Candida species in clinical isolates by randomly
amplified polymorphic DNA (RAPD). 142:57-66.
Menezes EA, Cavalcante MS, Farias RB, Teixeira AB, Pinheiro FG, Bezerra
BP, Torres JCN, Cunha FA 2005. Freqüência e atividade enzimática de

71
Candida albicans isoladas da mucosa bucal de crianças de uma creche da
periferia de Fortaleza. J Bras Patol Med Lab 41:9-13.
Merz WG 1990. Candida albicans strain delineation. Clin Microbiol 3: 321-334.
Meyer W, Maszewska K, Sorrell TC 2001. PCR fingerprinting: a convenent
molecular tool to distinguish between Candida dubliniensis and Candida
albicans. Med Mycology 39:185-193.
Migdley G, Moore MK, Cookk, JC, Phan QG 1994. Mycology of nail disorders.
J Am Acad Derm 31: 68-74.
Miller NS, Dick JD, Merz WG 2006. Phenotypic switiching in Candida lusitaniae
on copper sulfate indicator agar: association with amphotericin B
resistance and filamentation. J Clin Microbiol 44:1536-1539.
Mirhendi H, Makimura K, Zomorodian K, Maeda N, Ohshima T, Yamaguchi H
2005. Differentiation of Candida albicans and Candida dubliniensis using a
single-enzyme PCR-RFLP method. J Infect Dis 58:235-237.
Molnár O, Prillinger H, Lopandic K 1996. Analysis of coenzyme Q systems,
monosaccharide patterns of purified cell walls, and RAPD-PCR patterns in
the genus Kluyveromyces. Ant van Leeuwenhoek 70:67-68.
Morace G, Amato G, Bistoni F, Fadda G, Marone P, Montagna MT, Oliveri S,
Polonelli L, Rigoli R, Mancuso I, La Face S, Masucci L, Romano L, Napoli
C, Tatò D, Buscema MG, Belli CMC, Piccirillo MM, Conti S, Covan S, Fanti
F, Cavanna C, Alò FD, Pitzurra L 2002. Multicenter comparative evaluation
of six commercial systems and the National Committee for Clinical
Laboratory Standards M27-A Broth Microdilution Method for fluconazole
susceptibility testing of Candida species. J Clin Microbiol 40:2953-2958.
Mullis K, Faloona F 1987. Specific synthesis of DNA in vitro a polymerase
catalyzed chain reaction. Meth Enzym 155:335-335.

72
Munõz P, Burillo A, Bouza Emilio 2000. Criteria used when initiating antifungal
therapy against Candida spp. In the intensive care unit. Int J Antim
Agents15:83-90.
Murray SC, Dawber RP 2002. Onychomycosis of toenails: orthopaedic and
podiatric considerations. Australas J Dermatol 43: 105-112.
Naglik JR, Albrecht A, Bader O, Hube B 2004. Candida albicans proteinase
and host/pathogen interations. Cel Microbiol 6:915-926.
Naglik JR, Challacombe SJ, Hube B 2003. Candida albicans secreted aspartyl
proteinases in virulence and pathogenesis. Microbiol Mol Biol Rev 67: 400-
428.
National Committee for Clinical Laboratory Standards 2002. Reference method
for broth dilution antifungal susceptibility testing of yeasts: approved
standardsecond edition. National Committee for Clinical Laboratory
Standards document M27-A2. Villanova, PA, v. 17, n. 9.
National Committee for Clinical Laboratory Standards. Method for antifungal
disk diffusion susceptibility testing of yeasts: approved guideline M44-A.
National Committee for Clinical Laboratory Standards. Wayne, Pa, 2004.
Nenoff P, Oswald U, Haustein UF 1999. In vitro susceptibility of yeasts for
fluconazole and itraconazole. Evaluation of a microdilution test. Mycosis
42:629-639.
Odds FC 1988. Candida and candidosis 2a ed. London, Bailliére Tindall, 468p.
Odds FC 1994. Candida species and virulence. ASM News; 60: 31-38.
Odio CM, Araya R, Pinto LE, Castro CE, Vasquez S, Alfaro B, Saenz A,
Herrera CE, Walsh TJ 2004. Caspofungin therapy of neonates with
invasive candidíases. Pedriatr Infect Dis J 23:1093-1097.

73
Pfaller MA 2000. Epidemiologic of nosocomial candidiasis: the importance of
molecular typing. Braz Jour Infect Dis 4:161-167.
Pfaller MA, Diekema DJ, Messer SA, Boyken L, Hollis RJ 2003. Activities of
fluconazole and voriconazole against 1,586 recent clinical isolates of
Candida species determined by broth microdilution, disk diffusion, and
Etest methods: report from the ARTEMIS Global Antifungal Suscetibility
Program, 2001. J Clin Microbiol 41:1440-1446.
Pfaller MA, Messer SA, Hollis RJ 1999. Trends in species distribution and
susceptibility to fluconazole among bloodstream isolates of Candida
species in the United States. Diagn Microbiol Infect Dis 33:217-222.
Pfaller MA, Messer SA, Hollis RJ, Jones RN, Diekema DJ 2002. In vitro
activities of ravuconazole and voriconazole compared with those of four
approved systemic antifungal agents against 6.970 clinical isolates of
Candida spp. Antimicrob Agents Chemother 46:1723-1727.
Pincus DH, Coleman DC, Pruitt WR 1999. Rapid identification of Candida
dubliniensis with commercial yeast identification systems. J Clin Microbiol
37:3533-3539.
Pinto PM, Resende MA, Koga-Ito CY, Tendler M 2004. Genetic variability
analysis among clinical Candida spp. Isolates using random amplified
polymorphic DNA. Mem Inst Oswaldo Cruz 99:147-152.
Pizzo PA 2000. Empirical therapy and prevention of infection in the
immunocompromised host. En: Mandell GL, Douglas GR, Bennett JE, editors.
Principales and practice of infectious diseases. New York Churchill Livingstone,
p.3102-11.
Pulcine C, Pradier C, Samat-Long C, Hyvernat H, Bernardin G, Ichai C,
Dellamonica P, Roger PM 2006. Factors associated with adherence to
infectious diseases advice in two intensive care units. J Antimicrobil
Chemoth 57:546-550.

74
Rennert G, Pitilik S, Finkelstein R, Kitzes-Cohen R 2000. Epidemiology of
candidemia. A nationwide survey in Israel. Infection, 20:26-29.
Rex JH, Pfaller MA 2002. Has antifungal susceptibility testing come of age?
Clin Infect Dis 35:982-989.
Rex, JH, Pfaller MA, Barry AL, Nelson PW, Webb CD 1995. Antifungal
susceptibility testing of isolates from a randomized multicenter trial of
fluconazol versus amphotericin B as treatment of nonneutropenic patients
with candidemia. Antimicrobiol Agents Chemother 39:40-44.
Richardson MD, Warnock, DW 1994. Fungal Infection Diagnosis and
management. 4ª ed. Blackwell Scientific Publication, Oxford, 207p.
Richet H, Roux P, Des Champs C, Esmult Y, Andremont A and the French
Candidemia Study Group 2002. Candidemia in French hospitals: incidence
rates and characteristics. Clin Microbiol Infect 2002, 8:405-412.
Richet H, Roux P, Des Champs C, Esnault Y, Andremont A, and the French
Candidemia Study Group 2002. Candidemia in French hospitals: incidence
rates and characteristics. Clin Microbiol Infect Dis 8:405-412.Rodriguez
JLN, Moreira JLB 1999. Infecções fúngicas nosocomiais. In: Sidrim JJC &
Rocha MFC, ed. Fundamentos Clínicos de Laboratoriais da Micologia
Médica. Rio de Janeiro. Guanabra Koogan p.212-214.
Rodriguez JLN, Moreira JLB 1999. Infecções fúngicas nosocomiais. In: sidrim
JJC & Rocha MFC, ed. Fundamentos Clínicos de Laboratoriais da
Micologia Médica. Rio de Janeiro. Guanabara Koogan p.212-214.
Rüchel R, Tegeler R, Trost TM 1982. A comparison of secretory proteinases
from different strains of Candida albicans. Sabouraudia 20: 233-244.
Saballs P, Torres-Rodríguez JM, Salvadó M, Sales P, Gimeno Bayón JL,
Knobel H, Colomés JLL, Serrano C, Drobnic L 2000. La candidemia en el

75
sindrome de inmunodeficiencia adquirida. Estudo retrospectivo de nueve
casos. Rev Iberoam Micol 17:2-5.
Sabo JA, Abdel-Rahman SM 2000. Voriconazole: a new triazole antifungal.
Ann Pharmacother 34:1032-1043.
Safdar A, Perlin DS, Armstrong D 2002. Hemoatogenous infections due to C.
parapsilosis, changing trends in fungemia patients at a comprehensive
cancer center during the last four decades. Diagn Microbiol Infect Dis
44:11-16.
Saleh S, Al-Hedaithy A 2003. The yeast species causing fungemia at a
university hospital in Riyath, Saudi Arábia, during a 10-year period.
Mycoses 46:275-280.
Samaranayake LP, Fidel PL, Naglik JR, Sweet SP, Teanpaisan R, Coogan
MM, Blignaut E, Wanzala P 2002. Fungal infections associated with HIV
infection. Oral Diseases 8:151-160.
Samaranayake LP, MacFarlane TW 1990. Oral candidosis, Boston, Wright.
p265
Samaranayake LP, Raeside JM, Macfarlane TW 1984. Factors affecting the
phospholipase activity of Candida species in vitro. Sabouraudia 22:201-
207.
Sandven P 2000. Epidemiology of candidemia. Rev Iberoam Micol 17:73-81.
Schaller M, Borelli C, Korting HC, Hube B 2005. Hydrolytic enzymes as
virulence factors of Candida albicans. Mycoses 48:365-377.
Schönian G, Meusel O, Tietz HJ, Meyer W, Graser Y, Tausch I, Presber W,
Mitchell TG 1993. Identification of clinical strains of Candida albicans by
DNA fingerprinting with the polymerase chain reaction. Mycoses 36:171-
179.

76
Schwesinger G, Junghans D, Schroder G, Bernhardt H, Knoke M 2005.
Candidosis and aspergillosis as autopsy findings from 1994 to 2003.
Mycoses 48: 176-180.
Segal E 2004. Candida, still number one-what do we know and where are we
going from there? Mycoses 48:3-11.
Sheehan DJ, Hitchocock CA, Sobley CM 1999. Current and emerging azole
antifungal agents. Clin Microbiol Rev 12:40-79.
Soll DR 2000. The ins and outs of DNA fingerprinting the infectious fungi. Rev
Clin Microbiol 13:332-370.
Sota M, Ezpeleta C, Cisterna R 1999. Description of 165 of fungemia: a
multicenter study. Rev Iberoam Micol 16:30-35.
Souza EMB, Paula CR, Purchio A, Gambale W, Corrêa B, Cury AE 1990.
Aspectos morfológicos, fatores de virulêcia e sensibilidade a antifúngicos
de amostras de Candida albicans, sorotipos A e B, isoladas em São Paulo,
Brasil. Rev Microbiol 21:247-253.
Takakura S, Fujihama N, Saito T, Kudo T, Iinuma Y, Ichiyama S, and the Japan
Invasive Mycosis Surveillance Study Group 2004. National surveillance of
species distribuition in blood isolated of Candida species in Japan and their
susceptibility to six antifungal agents including voriconazole and
micafungin. J Antimicrobiol Chemother 53:283-289.
Tavares FCA, Echeverrigaray S, Gomes LH 1992. Identificação molecular de
leveduras de fermentação. Stab: Açúcar, Álcool e Sub-Produtos 10:34-39.
Taylor BN, Fichtenbaum C, Saavedra M, Slavinski J, Swoboda R, Wozniak K,
Arribas A, Powderly W, Fidel PL Jr 2000. In vivo virulence of Candida
albicans isolates causing mucosal infections in people infected with the
human Immunodeficiency Virus. J Infect Dis 182: 955-959.

77
Trick WE, Fridkin SK, Edwards JR, Hajjeh RA, Gaynes RP, and the National
Nosocomial Infections Surveillance System Hospitals 2002. Secular trends
of hospital-acquired candidemia among intensive care unit patients in the
United States during 1989-1999. Clin Infect Dis 35:627-630.
Uijthof JMJ, Hoog GS, Cock AWAM 1994. Patogenicity of strains of the black
yeast Exophiala (Wangiella) dermatitidis: an evolution based on
polymerase chain reaction. Mycosis 37:235-242.
Vanden Bossche H 1997. Mechanisms of antifungal resistance. Rev Iberoamer
Micol 14: 44-49.
Vardar-Ünlü G 1998. Identification of fibronectin adhesin on Candida albicans.
J Med Sciences 28:475-480.
Vargas K, Messer SA, Pfaller M, Lockhart SR, Stapleton JT, Hellstein J, Soll
DR 2000. Elevated phenotypic swintching and drug resistance of Candida
albicans from human immunodeficiency virus-positive individuals prior to
first thrust episode. J Clin Microbiol 38:3595-3607.
Venkatesan P, Perfect JR, Myers SA 2005. Evaluation and management of
fungal infections in immunocompromised patients. Dermatol Therapy
18:44-57.
Vincent JL, Anaissie E; Bruining H, Demajo W, el-Ebiary M; Haber J, Hiramatsu
Y, Nitenberg G, Nystrom PO, Pittet D, Rogers T, Sandven P, Sganga G,
Schaller MD, Solomkin J 1998. Epidemiology, diagnosis and treatment of
systemic Candida infection in surgical patients under intensive care.
Intensive Care Med 24: 206-216.
Voss A, Pfaller MA, Hollis RJ, Rhine-Chalberg J, Doebbeling BN 1995.
Investigation of Candida albicans transmission in a surgical intensive care
unit cluster by using genomic DNA typing methods. J Clin Microbiol
33:576-580.

78
Vrion G, Matsiota-Bernard P 2001. Molecular typing of Candida isolates from
patients hospitalized in an intensive care unit. J Infection 42:50-56.
Wade JC 1993. Management of infections in patients with acute leukemia.
Hematol Oncol Clin North Am 7:293-315.
Werner H 1966. Untersuchunger uber die lipase-aktivitat bei hefen und
hefeahnliehen pilzen. ZbL Bakt Hyg I Abt A 200:113-124.
Williams JGK, Kubelik AR, Livak KJ 1990. DNA polymorphisms amplified by
arbitrary primers are useful as genetics markers. Nucl Ac Researc
18:6531-6535.
Wingard JR, Merz WG, Rinaldi MG, Johnson TR, Karp JE, Saral R 1991.
Increase in Candida krusei infection among patients with bone marrow
transplantation and neutropenia treated prophylactically with fluconazole. N
Engl J Med 325:1274-1277.
Yang YL 2003. Virulence factors of Candida species. J Microbiol Immunol
Infect 36:223-228.
Yang YL, Cheng HH, Ho YA, Hsiao CF, Lo HJ 2003. Fluconazole resistance
rate of Candida species from different regions and hospital types in
Taiwan. J Microbiol Immunol Infect 36:187-191.
Yang YL, Li SY, Cheng HH, Lo HJ 2005. The trend of susceptibilities to
amphotericin B and fluconazole of Candida species from 1999 to 2002 in
Taiwan. Inf Dis 5:1-5.
Zardo V, Mezzan A 2004. Os antifúngicos nas infecções por Candida sp.
NewLab 63:136-146.

79
7 ANEXOS
7.1 Normas para publicação na revista Medical Mycology –
Instructions to Authors (Artigo 3)
The official publication of the International Society for Human and
Animal Mycology, Medical Mycology is an international journal which
focuses on original and innovative studies of all aspects of medical,
veterinary and environmental mycology. The topics include, but are not
limited to mycological, biochemical and molecular investigations of
etiological agents of mycoses; aspects of pathogenesis, immunology,
and epidemiology of mycotic diseases; case reports of unusual medical
or veterinary fungal infections; laboratory approaches to the identification
of fungal pathogens, antifungal therapy and prophylaxis; mode of action,
pharmacokinetics and assessments of new antifungal agents;
investigations of the mycological aspects of the indoor environment, with
a focus on human and animal health. The aim of the journal is to present
the best scientific reports from throughout the world and in so doing to
provide a comprehensive reference base for medical mycologists,
microbiologists, clinicians, and environ-mental specialists.
Further information about the Journal including links to the online
sample copy, contents pages and copyright assignment form can be
found on the Journal homepage.

80
Please note that you and your co-authors in submitting this
manuscript are confirming that all authors have (a) made a substantial
contribution to the information or material submitted for publication, (b)
read and approved the final manuscript, and (c) no direct or indirect
financial incentive associated with publishing the article. In addition, by
submitting your work, you and your co-authors are stipulating that the
manuscript is not, either in whole or in part, currently under consideration
by any other scientific journal or has been previously published in either
hard copy or electronic format.
Types of Papers
Original papers. These may be of any length, but must have; (a) a
Cover-Page listing all authors and their affiliations and contact
information for the corresponding author, (b) a separate page for a
Summary, (c) text consisting of Introduction, Materials & Methods,
Results, and Discussion, (d) References, (e) Tables with footnoted
descriptions of all abbreviations contained in the table, and (f) Figures,
with appropriate figure legends allowing a reader to understand their
content without reference to the text. Manuscripts should be in English,
double-spaced, in no less than size 12 font. Pages should be numbered
consecutively, beginning with the cover-page. References are to be

81
numbered, in brackets, e.g., [1], in order of their citation in the text and
listed in the Reference section by their appearance in the text.
Reviews. Authors must first electronically submit an outline of their
proposed article for evaluation by the Editor. The outline should be no
more than two, double-spaced pages in 12 font, in which the authors
describe the objectives and contents of the report. The outline must be
submitted to the Reviews Editor, Francoise Dromer: [email protected].
Once the proposal has been evaluated, the authors will be informed of
the results of the Review Editor’s initial consideration of their proposal.
NOTE - the journal does NOT accept uncommisioned reviews for
publication.
Case Reports. Such articles must make a distinct, novel contribution to
the understanding of the etiologic agents, its clinical manifestations,
and/or its treatment. They should NOT be based merely on the first
incidence of a known cosmopolitan or widely distributed etiologic agent in
the nations of the authors’ residence. Reports of unusual etiologic agents
MUST be substantiated with a living culture deposited in an
internationally recognized professional culture collection, defined as a
collection that has full-time staff dedicated to receiving, preserving and
shipping of culture cultures. Manuscripts MUST be in English and

82
prepared as is an original article, EXCEPT that the text should consist of
an Introduction, Case Report and Discussion.
Short Communications. These manuscripts are to provide an
opportunity for the presentation of preliminary or brief observations that
do not warrant a full paper. The manuscript should be prepared as is an
original article, except they may be no more than 10 double-spaced
pages in no less than size 12 font (including cover-page, abstract, text,
references, and tables/figures).
Letters. Letters to the Editor are intended to provide an opportunity to
discuss issues related to previous published original articles, case
reports or short communications and should not be used for the
presentation of the authors’ preliminary data from their own
investigations. Letters should be no more than 2 double-spaced pages, in
no less than size 12 font, including references.
Submission of manuscripts
All submissions to this journal should be made via the Manuscript
Central site: http://mc.manuscriptcentral.com/tmmy. Users who have not
used the site before must create an account from the link on the login
page. Assistance with this and all other areas of the site are available in

83
the User Guide, which is accessed via the ‘Get Help Now’ button at the
top right of all Manuscript Central web pages.
Preparation of manuscripts
1. Manuscripts must be written in English and submitted as a Word for
Windows (PC) file.
2. Manuscripts must be prepared in 12pt font with one (1) inch
margins all around and double spaced.
3. Papers should be organized as follows: Full title and Short title;
Name(s) and affiliations of author(s); Full postal address, telephone
and fax numbers, and email address for the corresponding author;
Summary (maximum 200 words); Keywords (up to five); Introduction;
Materials and Methods; Results; Discussion (as appropriate to the
article); Acknowledgements; References; Tables; Figure captions.
4. Statistics and measurements should be given in numerals when
followed by a unit (e.g., 2 mg but two patients). SI units must be used.
5. Abbreviations should be defined when first used in the text.
References
Use the Vancouver system in preparing the references. They should
be numbered sequentially in the order in which they first appear in the
text. References should be cited in the text within brackets. e.g., [1]. In

84
preparing your reference list, please note that works with six (6) or more
authors should be cited by the names of the first three (3) authors, with
the remaining authors included by et al. Journal names must be
abbreviated without the use of periods and should be in italic font. The
journal number should be in bold font and issue numbers should not be
included. In addition, include all page numbers of the citations. The
following examples illustrate the correct style for the different types of
references:
1. Journal article
Author AB, Author CD, Author EF, et al. [if six or more] Title of paper. J
Title Abbrev 1995; 00: 000-000.
2. Book chapter
Author AB, Author CD, Author EF, et al. [if six or more] Chapter title. In:
Editor AB, Editor CD, eds. Book Title With Initial Uppercase Letters, 5th
edn. Place: Publisher, 1995: 000-000.
3. Book
Author AB, Author CD (eds). Book Title With Initial Uppercase Letters,
5th edn. Place: Publisher, 1995.

85
4. Thesis
Author AB. Paper title with lowercase initials to all words. PhD thesis,
University, 1995.
5. Conference proceedings
Author AB. Paper title. In: Editor AB, ed. Proceedings Title, place, date.
Place: publisher, 1995: 000-000 (for abstracts the abstract number
should be cited instead of the page number).
6. Personal communications, Unpublished results etc References to
personal communications, unpublished results and papers submitted for
publication (but not yet accepted) should only appear in the text, and in
the following form: [A. B. Author, unpublished results]. [C. D. Author,
personal communication].
7. Journal article on the Internet
Abood S. Quality improvement initiative in nursing homes: the ANA acts
in an advisory role. Am J Nurs [serial on the Internet]. 2002 Jun [cited
2002 Aug 12];102(6):[about3 p.]. Available from:
<http://www. nursingworld.org/AJN/2002/june/Wawatch.htm>

86
8. Monograph on the Internet
Foley KM, Gelband H, editors. Improving palliative care for cancer
[monograph on the Internet]. Washington: National Academy Press; 2001
[cited 2002 Jul 9]. Available from:
<http://www.nap.edu/books/0309074029/html>
9. Homepage/Web site
Cancer-Pain.org [homepage on the Internet].
New York: Association of Cancer Online Resources, Inc.; c2000-01
[updated 2002 May 16; cited 2002 Jul 9]. Available from:
<http://www.cancer-pain.org>
10. Part of a homepage/Web site
American Medical Association [homepage on the Internet]. Chicago: The
Association; c1995-2002 [updated 2001 Aug 23; cited 2002 Aug 12].
AMA Office of Group Practice Liaison; [about 2 screens]. Available from:
<http://www.ama-assn.org/ama/pub/category/1736. html>
11. Database on the Internet
Open database:
Who’s Certified [database on the Internet]. Evanston (IL): The American
Board of Medical Specialists. c2000-[cited 2001 Mar 8]. Available from:
<http://www.abms.org/newsearch.asp_/www.abms.org/newsearch.asp>

87
Closed database:
Jablonski S. Online Multiple Congential Anomaly/Mental Retardation
(MCA/MR) Syndromes [database on the Internet]. Bethesda (MD):
National Library of Medicine (US). c1999 [updated 2001 Nov 20; cited
2002 Aug 12]. Available from:
<http://www.nlm.nih.gov/mesh/jablonski/syndrome_title.html>
12. Part of a database on the InternetMeSH Browser [database on the
Internet]. Bethesda (MD): National Library of Medicine (US); 2002-[cited
2003 Jun 10]. Meta-analysis; unique ID: D015201; [about 3 p.]. Available
from:
<http://www.nlm.nih.gov/mesh/MBrowser_/www.www.nlm.nih.gov/mesh/
MBrowser> Files updated weekly.
Tables
Tables should be numbered according to their sequence in the text;
all tables should be referred to in the text. Each table should be supplied
on a separate sheet, never within the body of the text. The table heading
should be brief and self explanatory. Column headings should be brief
and include units in parentheses where applicable. Only horizontal rules
should be used.

88
Figures
Graphics must be submitted as JPEG, GIF or BMP files. Scanned
images should be of a sufficient resolution: 300 dpi for halftones/color;
500 dpi for combination halftones; 1000–1200 dpi for line art. Illustrations
should be submitted separate from the manuscript text file, either as
individual files or together in a single file. The journal has a limited
number of free colour pages within its annual page allowance. Authors
should consult the editorial office with respect to colour reproduction at
submission stage. Authors may be required to pay to guarantee colour
reproduction. Any figure submitted as a colour original may appear in
colour within the journal’s online edition.
Nomenclature
Proposals for names of new taxa of fungi must conform with the
requirements of the current International Code of Botanical
Nomenclature, as should the scientific names used for fungi. Binomials
should appear in italic; each must be spelt out in full at first mention in
both the abstract and text (thereafter, the generic name may be
appropriately abbreviated) and whenever used in the titles of figures and
tables.

89
Animals in research
Manuscripts containing information related to the experimental use
of animals must clearly state that the studies complied with relevant
professional and institutional animal welfare policies. Specifically, that
procedures involving animals conformed to the ILAR Guide for the Care
and Use of
Laboratory Animals (1996 and later editions) of the Institute of
Laboratory Animal Research, Commission on Life Sciences, National
Research Council (http://www.nap.edu/catalog/5140.html).
Disclosures of potential conflicts of interest
Authors of research articles should disclose at the time of
submission any financial arrangement they may have with a company
whose product is pertinent to the manuscript or with a company making a
competing product. Such information will be held in confidence while the
paper is under review and will not influence the editorial decision, but if
the article is accepted for publication, a disclosure statement will appear
in the journal. The intent of this policy is not to prevent authors with these
relationships from publishing work, but rather to adopt transparency such
that readers can make objective judgements on conclusions drawn.

90
Authorship contributions
Contributions must be substantial in order to warrant authorship.
Each author should have participated sufficiently in the work to take
public responsibility for the content. All other contributors should be listed
in the acknowledgements.
Electronic proofs
When proofs are ready, corresponding authors will receive e-mail
notification with a password and Web address from which to download a
PDF. Hard copies of proofs will not be mailed. To avoid delays in
publication, corrections to proofs must be returned within 48 hours, by
electronic transmittal, fax or mail.
Offprints
Corresponding authors will receive either fifty printed offprints or a
PDF of the final version of the paper. Preferences should be stipulated
when returning proofs.
Copyright
It is a condition of publication that authors assign copyright or licence
the publication rights in their articles, including abstracts, to ISHAM. This
enables us to ensure full copyright protection and to disseminate the

91
article, and the journal, to the widest possible readership in print and
electronic formats as appropriate. Authors may, of course, use the article
elsewhere after publication without prior permission from Informa UK
Ltd., provided that acknowledgement is given to the journal as the
original source of publication, and that Informa Healthcare is notified so
that our records show that its use is properly authorised. Authors retain a
number of other rights under the Informa UK Ltd. rights policies
documents. These policies are referred to at the Copyright FAQs page.

92
7.2 Protocolo do CEPMHA/HC/UFG

93

94

95

96
7.3 Termo de consentimento livre e esclarecido
Você está sendo convidado (a) para participar, com voluntário, em uma
pesquisa intitulada “Caracterização de fungos envolvidos em infecções nosocomiais”. Após ser esclarecido (a) sobre as informações a
seguir, no caso de aceitar fazer parte do estudo, assine ao final deste
documento, que está em duas vias. Uma delas é sua e a outra é do
pesquisador responsável. Em caso de recusa você não será penalizado (a) de
forma alguma. Se aceitar participar e decidir retirar seu consentimento, não
será prejudicado em seu tratamento. Em caso de dúvida sobre a pesquisa,
você poderá entrar em contato com o pesquisador responsável Ms. Xisto
Sena Passos nos telefones: 3255-9858 / 9972-4158.
INFORMAÇÕES SOBRE A PESQUISA
“Caracterização de fungos envolvidos em infecções nosocomiais”.
PESQUISADORES PARTICIPANTES
Dra. Maria do Rosário Rodrigues Silva – Investigadora responsável
Fone: (0XX62) 3209-6127
Ms. Xisto Sena Passos – Biólogo / Pesquisador
Fones: (0XX62) 3209-6127 / 3255-9858 / 9972-4158
OBJETIVO DO ESTUDO
Será avaliado um grande grupo de pacientes, os quais se encontram
internados na UTI do Hospital das Clínicas da Universidade Federal de Goiás,
durante o período de fevereiro de 2003 a dezembro de 2004.
Provavelmente você já deve ter ouvido falar em micose. Esta doença é
causada por fungos que produzem lesões na pele ou em qualquer parte do

97
organismo humano, através deste estudo o responsável pelo paciente terá
acesso aos exames laboratoriais que ajudará o médico a tratá-la.
Neste trabalho, após a devida identificação e caracterização do fungo,
será realizado um teste, chamado suscetibilidade, no qual será verificado a
sensibilidade do fungo isolado frente a três medicamentos, anfotericina B,
itraconazol e fluconazol.
Através das informações obtidas no laboratório e com ajuda do médico,
nós tentaremos controlar melhor a doença e possivelmente evitar que outros
indivíduos a adquiram.
CONDUÇÃO DO ESTUDO
O paciente será submetido inicialmente à colheita de sangue e urina, pelo
profissional responsável pela UTI, assim que for internado.
Durante a permanência do paciente na UTI serão realizadas colheitas de
sangue e urina a cada sete dias. O material coletado será levado para o
laboratório de Micologia do Instituto de Patologia Tropical e Saúde Publica da
UFGO, onde será submetido a exame micológico.
Estes exames não serão pagos pelo paciente.
PARTICIPAÇÃO AUTORIZADA
Participar deste estudo será uma decisão autorizada pela responsável e
este poderá se recusar a participar ou desistir deste estudo a qualquer
momento, sem explicar o porquê.

98
PACIENTES PARTICIPANTES DO ESTUDO
Neste estudo serão incluídos todos os pacientes (autorizados), que
apresentarem características ou não de fungemia internados na UTI do
Hospital das Clínicas da UFGO.
RISCOS
Não há riscos para o paciente. Nenhum tipo de medicamento será
utilizado por nós.
Para colheita do material, o paciente não será maltratado. A colheita do
sangue e da urina, não implicará em mal estar para o paciente.
BENEFÍCIOS
O estudo realizado por nós possivelmente contribuirá enormemente para
a redução de infecções nos hospitais por fungos.
CONFIDENCIALIDADE
Se o responsável concordar com a participação do paciente, as
informações clínicas e laboratoriais relacionadas ao paciente serão
confidencialmente mantidas em sigilo o tempo todo, nem o nome ou mesmo
iniciais irão constar em qualquer registro nesta pesquisa. O Comitê de Ética
poderá necessitar ter acesso aos seus registros médicos para verificação dos
formulários de estudo, no entanto, sua identidade será mantida em sigilo
absoluto.

99
RESPONSÁVEL
Este estudo será conduzido por:
Dra. Maria do Rosário Rodrigues Silva pelo fone (0XX62) 3209-6127.
(Investigadora responsável)
Ms. Xisto Sena Passos pelo fone (0XX62) 209-6127(Biólogo / Pesquisador)