Embed Size (px)
Citation preview

PONTIFÍCIA UNIVERSIDADE CATÓLICA DE MINAS GERAIS
Programa de Pós-graduação em Odontologia
Paula Loureiro Cheib Vilefort
AVALIAÇÃO TRIDIMENSIONAL DAS MUDANÇAS DENTOESQUELÉTICAS
APÓS TERAPIA COM O APARELHO HERBST EM DIFERENTES ESTÁGIOS DE
MATURAÇÃO ESQUELÉTICA: um estudo multicêntrico
Belo Horizonte
2018

Paula Loureiro Cheib Vilefort
AVALIAÇÃO TRIDIMENSIONAL DAS MUDANÇAS DENTOESQUELÉTICAS
APÓS TERAPIA COM O APARELHO HERBST EM DIFERENTES ESTÁGIOS DE
MATURAÇÃO ESQUELÉTICA: um estudo multicêntrico
Tese apresentada ao Programa de Pós-graduação em
Odontologia da Pontifícia Universidade Católica de
Minas Gerais, como requisito parcial para a
obtenção do título de Doutor em Odontologia, Área
de Concentração: Clínicas Odontológicas.
Linha de Pesquisa: Métodos de Diagnóstico por
Imagem, Radiobiologia e Radioproteção.
Orientador: Prof. Dr. Bernardo Quiroga Souki
Coorientadora: Profa. Dra. Lucia Helena Soares
Cevidanes
Belo Horizonte
2018

FICHA CATALOGRÁFICA
Elaborada pela Biblioteca da Pontifícia Universidade Católica de Minas Gerais
Vilefort, Paula Loureiro Cheib
V699a Avaliação tridimensional das mudanças dentoesqueléticas após terapia com
o aparelho herbst em diferentes estágios de maturação esquelética: um estudo
multicêntrico / Paula Loureiro Cheib Vilefort. Belo Horizonte, 2018.
168 f. : il.
Orientador: Bernardo Quiroga Souki
Coorientadora: Lucia Helena Soares Cevidanes
Tese (Doutorado) – Pontifícia Universidade Católica de Minas Gerais. Programa
de Pós-Graduação em Odontologia
1. Ortodontia interceptora. 2. Aparelhos ativadores. 3. Má oclusão de angle
classe II. 4. Tomografia computadorizada por raios x. 5. Imagem tridimensional.
6. Traumatismos dentários. I. Souki, Bernardo Quiroga. II. Cevidanes, Lucia
Helena Soares. III. Pontifícia Universidade Católica de Minas Gerais. Programa
de Pós-Graduação em Odontologia. IV. Título.
CDU: 616.314-089.23

Paula Loureiro Cheib Vilefort
AVALIAÇÃO TRIDIMENSIONAL DAS MUDANÇAS DENTOESQUELÉTICAS
APÓS TERAPIA COM O APARELHO HERBST EM DIFERENTES ESTÁGIOS DE
MATURAÇÃO ESQUELÉTICA: um estudo multicêntrico
Tese apresentada ao Programa de Pós-graduação em
Odontologia da Pontifícia Universidade Católica de
Minas Gerais, como requisito parcial para obtenção
do título de Doutor em Odontologia, Área de
Concentração: Clínicas Odontológicas.
COMPOSIÇÃO DA BANCA EXAMINADORA:
1- Prof. Dr. Rogério Lacerda dos Santos – UFJF
2- Prof. Dr. Camilo de Aquino Melgaço – UNINCOR
3- Profa. Dra. Vânia Eloísa de Araújo Silva – PUC Minas
4- Prof. Dr. Amaro Ilídio Vespasiano Silva – PUC Minas
5- Prof. Dr. Bernardo Quiroga Souki – PUC Minas
DATA DA APRESENTAÇÃO E DEFESA: 14 de março de 2018
A tese, nesta identificada, foi aprovada pela Banca Examinadora
Prof. Dr. Bernardo Quiroga Souki Prof. Dr. Rodrigo Villamarim Soares Orientador Coordenador do Programa de Pós-graduação
em Odontologia

Ao meu orientador
que acreditou e me mostrou que eu seria capaz,
e ao meu amado marido
que nunca falha na missão de me apoiar e me sustentar em amor e alegria.

AGRADECIMENTOS
À Deus a minha diária e eterna gratidão pelo dom da vida e por me fazer saber e sentir
que Ele está ao meu lado todo o tempo, me abençoando com saúde, capacidade e disposição.
Aos meus pais por serem minha fonte de apoio e meu porto seguro. À Cida, minha sogra
querida e amiga, que nunca esquece de mim durante suas orações e preces. Tenho certeza de
que elas foram imprescindíveis para que eu chegasse até aqui. Aos meus irmãos, familiares e
amigos queridos. A torcida de vocês é incentivo para mim! Ao Alex por caminhar todos os
dias ao meu lado, mesmo que a milhares de quilômetros de distância, tornando essa
caminhada muito mais leve e feliz; seu amor por mim foi peça fundamental, não me deixando
desanimar diante das dificuldades e fazendo com que elas parecessem muito menores do que
realmente eram para mim. Obrigada por compreender, com paciência, minhas ausências, me
incentivar e me fazer mais forte para correr atrás nos nossos planos. Grande privilégio eu
tenho de te ter como parceiro, ensinando-me sempre sobre alegria, gratidão e esperança.
Ao meu orientador Prof. Bernardo Quiroga Souki que foi meu maior incentivador e
exemplo. Sua inteligência incomum, capacidade de orientar, alegria em ensinar e sua
organização fizeram de mim uma profissional melhor. Facilmente observo e admiro sua
elevada exigência, infinita paciência e persistência, zelo e empenho em tudo o que faz. Serei
eternamente grata por cada passo que dei, onde, de perto ou de longe, agindo ou somente me
vendo agir, me apoiou e me ensinou muito mais que ortodontia.
À Prof. Lucia Helena Soares Cevidanes por tamanho aprendizado de vida e
profissional. Obrigada pela recepção, orientação e oportunidades. Muito grata também pela
parceria e ricos ensinamentos recebidos pelo Prof. Antônio Carlos de Oliveira Ruellas, Dra.
Marília Yatabe, Dr. Marcos Ioshida e Prof. James McNamara.
Agradeço ao Prof. Alexandre Moro e sua aluna de Mestrado Letícia Farah, da
Universidade Positivo, a parceria e confiança depositados em mim, para o desenvolvimento
desse trabalho. E aos alunos do Mestrado em Ortodontia da PUC Minas, Patrícia de Souza
Costa, Juliana Macêdo de Mattos, Karine Sayure Okano, Paula Moreira Oliveira e Lucas
Santana pela preciosa ajuda, e grande parceria.
Agradeço a todos os professores do Programa que de formas distintas e pessoais
transmitiram conhecimento e enriqueceram a minha formação como pesquisadora. Em
especial ao Prof. Dr. Martinho Campolina Rebello Horta e ao Prof. Dr. Rodrigo Villamarim
Soares que conduziram a coordenação do Programa com afinco e dedicação durante o meu
Doutoramento.

Agradeço aos colegas de doutorado e mestrado, pela amizade e parceria. Foi muito
bom poder caminhar com cada um de vocês.
E por fim à CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior),
por me proporcionar uma bolsa de estudo durante meu período no Brasil e durante meu
período na Universidade de Michigan (EUA), através do Programa de Doutorado Sanduíche
no Exterior (PDSE).

“O correr da vida embrulha tudo.
A vida é assim: esquenta e esfria, aperta e daí afrouxa, sossega e depois desinquieta.
O que ela quer da gente é coragem.” (GUIMARÃES ROSA, 1986)

RESUMO
O aparelho Herbst (AH) é um dos dispositivos mais utilizados como opção terapêutica no
tratamento das más oclusões de Classe II. Apesar de já existirem evidências na literatura de
que o tratamento da Classe II deveria incorporar o pico do período puberal de crescimento,
uma parcela dos ortodontistas e dos estudos clínicos científicos da atualidade ainda têm
realizado essa modalidade de tratamento de maneira precoce, durante a fase pré-puberal.
Algumas razões podem ser atribuídas a isto como por exemplo, fator psicossocial e risco
aumentado de traumatismo dentário. Ainda existem alguns questionamentos sobre a eficácia e
eficiência de um tratamento realizado de maneira precoce ou não, em relação a todas as
estruturas do complexo dentofacial, especialmente devido às limitações de metodologia de
imagens bidimensionais (2D) de estudos prévios. O objetivo desse estudo foi investigar as
alterações tridimensionais (3D) dentoesqueléticas do complexo facial (mandíbula, maxila e
relação côndilo-fossa mandibular), após o uso do AH em dois diferentes momentos do estágio
de maturação biológica de crescimento. Uma amostra proveniente de banco de dados de dois
centros universitários foi utilizada e dividida em quatro grupos: (1) Grupo Herbst Puberal –
GHP; 2) Grupo Comparação Puberal – GCP; 3) Grupo Herbst Pre-puberal – GHPP; e 4)
Grupo Comparação Pre-puberal – GCPP. Utilizando software gratuitos (ITK-SNAP 2.2;
Slicer CMF 4.0), modelos virtuais 3D foram construídos a partir de TCFC de crânio
estendido, realizadas em dois tempos; no início do tratamento e após um intervalo de 8 a 12
meses. Superposições em regiões de interesse (base do crânio, maxila, mandíbula e fossa
mandibular) foram realizadas em nível de voxel. Análises utilizando medições entre pontos
anatômicos de referência, superposições com semi-transparências e mapas por código de
cores associados à vetorização foram realizados. Cálculo amostral e análise estatística foram
feitos para cada etapa desse estudo, separadamente. A correlação de concordância intra-classe
foi utilizada para a análise da confiabilidade das leituras. Análises de erro sistemático (teste T
pareado) e aleatório (fórmula de Dahlberg), e a verificação dos pressupostos de normalidade
na distribuição das variáveis (Kolmogorov-Smirnov) foram realizados para a escolha dos
testes de comparação entre os grupos. Pacientes tratados com o AH apresentaram um
significante deslocamento anterior do pogônio (P <0.05), sem giro no sentido horário da
mandíbula. Além disso, o côndilo e porção posterior do ramo apresentaram maior crescimento
superior e posterior (P <0.05). Na maxila, independentemente do estágio de maturação, o AH
promoveu distalização e controle vertical dos molares (P <0.05) e verticalização dos incisivos.
Os efeitos esqueléticos na maxila foram mais expressivos durante o período pré-puberal (P
<0.05). Não foram encontradas mudanças clinicamente significativas, em nenhum dos
estágios de maturação biológica, na relação côndilo-fossa mandibular. Conclui-se que após o
tratamento com o AH realizado durante diferentes estágios do período puberal, distinto padrão
de magnitude e direção de crescimento e deslocamento mandibular e maxilar podem ser
observados. Efeitos dentoalveolares foram mais expressivos e independem do estágio de
maturação esquelética. Efeitos esqueléticos maxilares foram maiores durante o estágio pré-
puberal. A relação côndilo-fossa mandibular não se altera após o uso do AH.
Palavras-chave: Ortodontia interceptora. Aparelhos ativadores. Má oclusão de Angle Classe
II. Tomografia Computadorizada por raios X. Imagem tridimensional.

ABSTRACT
The Herbst appliance (HA) is one of the most frequently used devices worldwide in the
treatment of Class II malocclusion in contemporary orthodontics. Although several studies
have already reported that the treatment of Class II should include puberty in the treatment
plan, a large number of orthodontists still decide for an early approach of Class II, during the
pre-puberty period. Some reasons could be attributed for the decision of early treatment, as
psychosocial factors, and the increased risk of maxillary incisors traumatic injury. Gaps in the
knowledge of the effects of the HA can be attributed to the limitations of the two-dimensional
(2D) methodology. The aim of the current study was to investigate the three-dimensional (3D)
dentoskeletal changes of the facial complex (mandible, maxilla and condyle-glenoid fossa
relationship), after the use of HA at two stages of biological maturation. From the database of
two university centers, the sample was divided into four groups: (1) Herbst pubertal group -
HPG; 2) Comparison pubertal group - CPG; 3) Herbst pre-pubertal group - HPPG; and 4)
Comparison pre-pubertal group - CPPG. Using open-source software (ITK-SNAP 2.2; Slicer
CMF 4.0), 3D virtual models were built from the CBCT’s. Superimpositions in regions of
interest (anterior cranial base, maxilla, mandible, and glenoid fossae) were performed at the
voxel level, and analyzes using point-to-point measurements, semi-transparent overlays, and
color mapping associated with vectorization were done. Sample size calculation and statistic
analysis were done for each section of this study. Intra class correlation coefficients were
performed to test agreement. Random error (Dahlberg`s formula) and systematic error (paired
t-test) were also assessed. Kolmogorov-Smirnov was used to test the normal distribution.
Parametric or non-parametric tests were used accordingly. HA patients showed a significant
anterior displacement of pogonion (P <0.05), with no clockwise mandibular rotation.
Moreover, the condyle and posterior surface of rami presented greater superior and posterior
growth (P <0.05). For the maxilla, independently the stage of biological maturation, the AH
promoted distalization and vertical control of the molars (P <0.05) and uprighting of the
incisors. The maxillary skeletal effects were greater during the pre-pubertal stage (P <0.05).
No clinically significant changes were found in the condyle-fossa relationship during any
biological maturation stages. It was concluded that following HA treatment, performed during
different stages of pubertal period, distinct patterns of magnitude and direction of maxillary
and mandibular growth and displacements could be expected. Dentoalveolar effects were
greater than skeletal ones, independently the skeletal maturation stage. Skeletal maxillary
effects were greater during the pre-pubertal stage. The condyle-glenoid fossa relationship was
not altered after HA treatment, regardless the stage of skeletal maturation.
Keywords: Interceptive orthodontics. Activator appliances. Class II Angle malocclusion.
Cone beam computed tomography. Three-dimensional imaging.

SUMÁRIO
1 INTRODUÇÃO ................................................................................................................... 19
2 REFERENCIAL TEÓRICO .............................................................................................. 23
2.1 Displasia óssea de Classe II: época ideal para a terapia ortopédica ............................ 23
2.2 Ativador mandibular tipo Herbst ................................................................................... 24
2.3 Mudanças na ATM associadas ao uso de ativadores mandibulares ............................ 25
2.4 O uso de Tomografia Computadorizada de Feixes Cônicos na Ortodontia ............... 27
3 HIPÓTESES ........................................................................................................................ 29
4 OBJETIVOS ........................................................................................................................ 31
4.1 Objetivos gerais ................................................................................................................ 31
4.2 Objetivos específicos ......................................................................................................... 31
5 MATERIAL E MÉTODOS ............................................................................................... 33
5.1 Amostra ............................................................................................................................. 33
5.2 Protocolo de instalação e ativação do aparelho ............................................................. 35
5.3 Método de registro ............................................................................................................ 39
5.4 Método de medida ............................................................................................................ 39
5.5 Método de análise ............................................................................................................. 58
6 ARTIGO CIENTÍFICO 1 ................................................................................................... 59
7 ARTIGO CIENTÍFICO 2 ................................................................................................... 85
8 ARTIGO CIENTÍFICO 3 ................................................................................................. 119
9 CONSIDERAÇÕES FINAIS ............................................................................................ 143
REFERÊNCIAS ................................................................................................................... 145
ANEXO A - 1º Parecer Consubstanciado do CEP PUC Minas ....................................... 153
ANEXO B - 2º Parecer Consubstanciado do CEP PUC Minas ........................................ 155
ANEXO C - Artigos científicos publicados ou aceitos em periódicos durante o curso de
Doutorado .............................................................................................................................. 157
ANEXO D - Capítulos de livros publicados durante o curso de Doutorado ................... 163
ANEXO E - Demais produções técnicas feitas durante o curso de Doutorado............... 165
ANEXO F - Trabalhos publicados em anais de eventos (resumo) durante o curso de
Doutorado .............................................................................................................................. 167

19
1 INTRODUÇÃO
As displasias ósseas de Classe II têm elevada prevalência em todo o mundo
(EMRICH; BRODIE; BLAYNEY, 1965; PROFFIT; FIELDS; MORAY, 1998; SANTOS et
al., 2012; LAGANÀ et al., 2013), sendo que a deficiência de crescimento sagital da
mandíbula é o fator etiológico mais associado a este tipo de má oclusão (McNAMARA
JUNIOR, 1981; PANCHERZ; ZIEBER; HOYER, 1997). Tratamentos utilizando dispositivos
ortopédicos removíveis e fixos tem sido preconizados há muitas décadas com o intuito de
normalizar a relação sagital interarcos e obter uma melhora no perfil facial de pacientes em
crescimento (PANCHERZ, 1979; COZZA et al., 2006).
O aparelho Herbst (AH), apresentado por Emil Herbst no início do século XX
(HERBST, 1932), se trata de um ativador mandibular fixo muito utilizado na Europa e
Estados Unidos desde sua reintrodução na literatura por Hans Pancherz algumas décadas mais
tarde (PANCHERZ, 1979). A baixa dependência de colaboração do paciente (PANCHERZ,
1979), bem como a previsibilidade dos resultados clínicos fizeram com que esse aparelho
ganhasse popularidade e aceitação entre os clínicos para a correção da Classe II (RUF;
PANCHERZ, 1999). Diversos aspectos do uso do AH e de seus efeitos biológicos foram
investigados e estão disponíveis na literatura (RUF; PANCHERZ, 1998; PANCHERZ; RUF;
KOHLHAS, 1998; McNAMARA JUNIOR.; PETERSON; PANCHERZ, 2003; KINZINGER;
KOBER; DIEDRICH, 2007; BOOIJ et al., 2013; FRANCHI et al., 2013; PANCHERZ et al.,
2014; SILVA et al., 2014). Existem evidências sobre a remodelação óssea do côndilo e o
aumento do comprimento mandibular após o tratamento com o AH (ALMEIDA et al., 2006;
SERBESIS-TSARUDIS; PANCHERZ, 2008). Além disso, estudos relataram também sobre a
projeção de incisivos inferiores, inclinação lingual dos incisivos superiores, mesialização e
extrusão dos molares inferiores e distalização e intrusão dos molares superiores (SILVA
FILHO; AIELLO; FONTES, 2005; ALMEIDA et al., 2006).
Apesar de extensa literatura ter sido gerada sobre os efeitos dentários e esqueléticos do
tratamento com o AH (PANCHERZ, 1997; HÄGG; DU; RABIE, 2002; HANSEN, 2003;
VANLAECKEN et al., 2006; BARNETT et al., 2008), até o presente momento, a maioria dos
estudos que avaliaram as mudanças associadas ao tratamento com o AH foram baseados em
exames utilizando imagens bidimensionais como radiografias cefalométricas em norma lateral
da face e radiografias transcranianas (PANCHERZ, 1979; PAULSEN, 1997; PANCHERZ;
RUF; KOHLHAS, 1998; PANCHERZ; FISCHER, 2003; ALMEIDA et al., 2006; HÄGG et
al., 2008; SERBESIS-TSARUDIS; PANCHERZ, 2008; PANCHERZ; BJERKLIN;

20
HASHEMI, 2015), ou ainda através de imagens de ressonância magnética (RUF;
PANCHERZ, 1998; RUF; PANCHERZ, 1999; RUF; PANCHERZ, 2000; RUF; WÜSTEN;
PANCHERZ, 2002; AIDAR et al., 2006; KINZINGER et al., 2006; KINZINGER; KOBER;
DIEDRICH, 2007; AIDAR et al., 2009; AIDAR et al., 2010). Sabe-se que métodos de
registro radiográficos bidimensionais estão sujeitos às limitações operacionais como
magnificação da imagem, sobreposição de estruturas ósseas, distorções, posição inadequada
do paciente no momento da tomada radiográfica, e viés do examinador ao sobrepor duas
imagens em tempos diferentes. Dessa maneira, esses métodos de registro têm baixa
reprodutibilidade, não permitindo uma avaliação confiável pelas superposições de estruturas
ósseas (LeCORNU et al., 2013). Para a ressonância magnética, a dificuldade e o desconforto
do paciente ao realizar o exame, o elevado custo e o fato de que esta não é o padrão ouro para
avaliação de tecidos duros, descrevem as limitações desse tipo de exame.
Com o surgimento da tomografia computadorizada de feixes cônicos, um novo campo
na pesquisa surgiu, permitindo entender o que de fato acontece nas estruturas avaliadas após
um tratamento ortodôntico, já que uma superposição volumétrica, e consequentemente, uma
verdadeira avaliação tridimensional é possível com o uso deste tipo de exame. Alguns estudos
(PAULSEN et al., 1995; PAULSEN; KARLE, 2000; VanLAECKEN et al., 2006; MAIA;
RAVELI; SANTOS-PINTO, 2010; BORGES, 2013; LeCORNU et al., 2013; YILDIRIM;
KARACAY; ERKAN, 2014; SESSIRISOMBAT, 2015; CHEN, et al., 2016; WEIWEI et al.,
2016; SAH et al., 2017) utilizaram a TCFC para a avaliação das mudanças esqueléticas após o
uso do AH. Entretanto eles apresentam limitações em sua metodologia já que, em sua grande
maioria, não utilizaram modelos de superposição verdadeiramente tridimensionais (3D) e/ou
apresentaram amostras com tamanho reduzido e ausência de cálculo amostral.
Estudos prévios (RUF; PANCHERZ, 2003; RUF, 2006; PERINETTI et al., 2015;
PERINETTI et al., 2016) relataram que o momento ideal para o tratamento da má oclusão de
Classe II deveria incluir a puberdade, a fim de alcançar um resultado mais eficaz e eficiente.
Existem evidências que o pico de crescimento mandibular coincide com o pico do
crescimento puberal e que o pico do crescimento mandibular ocorre entre os estágios CS3 e
CS4 da maturação das vértebras cervicais (COZZA et al., 2005; BACCETTI; FRANCHI;
McNAMARA JUNIOR, 2005). Logo, o tratamento da Classe II visando o estímulo do
crescimento mandibular se beneficiaria desse estágio biológico de maturação. No entanto,
muitos clínicos continuam tratando seus pacientes portadores de má oclusão de Classe II de
maneira precoce, antes do pico puberal de crescimento (ALMEIDA et al., 2015). Seja por
questões psicossociais, risco aumentado de traumatismo dentário devido a overjet acentuado

21
ou por fatores etiológicos diversos, como por exemplo, má oclusão de Classe II causada por
excesso maxilar.
Outro aspecto ainda pouco documentado e que permanece em discussão entre os
clínicos (IVORRA-CARBONELL et al., 2016) é uma eventual desadaptação do
posicionamento condilar em sua fossa mandibular, após o tratamento com o AH, podendo
levar à mordida dupla, recidivas da correção sagital, e disfunções têmporo-mandibulares.
Considerando que toda a região da articulação temporomandibular sofre modificações por
crescimento e desenvolvimento tridimensional ao longo da maior parte das duas primeiras
décadas de vida (ZARB, 2000; BUMANN; LOTZMANN; MAH, 2002), as avaliações das
mudanças relativas dos côndilos em relação às suas próprias fossas mandibulares precisam
levar em consideração a necessidade de superposições volumétricas 3D.
Sendo assim, justificam-se investigações adicionais por meio de metodologia 3D,
como objetivo de avaliar as mudanças dentoesqueletais no complexo facial, após o período
terapêutico com o AH, tratados em dois momentos diferentes da maturação biológica.


23
2 REFERENCIAL TEÓRICO
2.1 Displasia óssea de Classe II: época ideal para a terapia ortopédica
A displasia óssea de Classe II apresenta uma prevalência de aproximadamente 20%,
sendo a segunda má oclusão mais prevalente (SANTOS et al., 2012; BOURZQUI et al.,
2012). A retrusão mandibular está presente em 70% dos casos contribuindo como fator mais
comum para a discrepância sagital esquelética. Todavia, existem ainda má oclusões de Classe
II causadas pelo excesso de crescimento ântero-posterior da maxila ou ainda pela associação
desses dois fatores (McNAMARA JUNIOR, 1981; TANG; WEI, 1993).
Considerando-se a época do tratamento, dois protocolos de tratamento de Classe II são
utilizados na Ortodontia contemporânea: precoce ou tardio (KING et al., 1990). O tratamento
precoce, feito em duas fases, inicia-se ainda na fase de dentadura mista inicial com uma
abordagem ortopédica, na tentativa de se conseguir uma remodelação esquelética. É
necessária uma contenção dos resultados até que o paciente atinja a fase de dentadura
permanente, onde é feita a fase ortodôntica de finalização (SILVA FILHO; AIELLO;
FONTES, 2005).
No protocolo de tratamento tardio, o início do tratamento é adiado até a fase de
dentadura permanente, coincidindo com o surto puberal de crescimento. Nesse protocolo, a
idade óssea é mais relevante que a idade cronológica ou dentária. Existem evidências que a
incorporação da terapia ortopédica da má oclusão de Classe II na fase puberal de crescimento
favoreça a eficácia e a eficiência. Segundo Baccetti, Franchi e McNamara Junior (2005) este
estágio de maturação corresponde aos estágios de maturação das vértebras cervicais (CS3 e
CS4), avaliado por radiografia lateral cefalométrica. No protocolo de tratamento tardio da má
oclusão de Classe II, também é necessária a segunda fase ortodôntica de finalização.
Entretanto não há um intervalo de tempo entre as fases, excluindo-se a necessidade de
contenção dos resultados parciais da fase ortopédica, e assim diminuindo o tempo total do
tratamento e as chances de recidivas (SILVA FILHO; AIELLO; FONTES, 2005).
Nos pacientes portadores de más oclusões de Classe II por deficiência mandibular, o
deslocamento terapêutico anterior da mandíbula é fator importante na melhora facial. Este
ganho facial é, em tese, alcançado pelo estímulo do crescimento diferencial favorável do
côndilo, ramo e fossa mandibular. Todavia, estudos utilizando avaliação bidimensional
(BURHARDT; McNAMARA JUNIOR; BACCETTI, 2003; BARNETT et al., 2008) e
tridimensional (LeCORNU et al., 2013) relatam não haver crescimento mandibular adicional

24
significante após o uso do AH. Em contrapartida, há na literatura muitos artigos que
utilizaram avaliação bidimensional e avaliação histológica para relatar um crescimento maior
na superfície posterior do côndilo e do ramo mandibular. Peterson e McNamara Junior (2003),
através de um estudo histológico realizado em macacos, relataram ter encontrado significativo
aumento do crescimento na superfície posterior e póstero-superior do côndilo e aumento
significativo da aposição óssea na borda posterior do ramo.
2.2 Ativador mandibular tipo Herbst
Estima-se que o AH seja o mais utilizado na correção das más oclusões esqueléticas
de Classe II na América do Norte (SILVA et al., 2015). Ele foi apresentado por Emil Herbst
no início do século XX (HERBST, 1932) e foi reintroduzido na literatura por Hans Pancherz
no final da década de 1970 (PANCHERZ, 1979). Desde então, esse dispositivo ortopédico
tem sido utilizado por muitos clínicos no tratamento de pacientes portadores de má oclusão de
Classe II com severa deficiência mandibular (RUF; PANCHERZ, 2000). Suas vantagens
clínicas e seus efeitos ortopédicos já têm sido testados e comprovados por muitos
pesquisadores. Por ser um aparelho fixo que mantém a mandíbula continuamente posicionada
anteriormente, sua resposta ortopédica é conseguida através da remodelação da articulação
temporomandibular (ATM) e do aumento no comprimento mandibular (SILVA FILHO;
AIELLO; FONTES, 2005).
Algumas pesquisas avaliaram também seus efeitos maxilares, tanto dentários como
esqueléticos, (HÄGG; DU; RABIE, 2002; HANSEN, 2003; VanLAECKEN et al., 2006;
BARNETT et al., 2008). Há uma concordância na literatura quanto às alterações provocadas
nos componentes dento-alveolares maxilares. Tem-se relatos que os incisivos superiores
foram retruídos e lingualizados (ALMEIDA et al., 2006; NAHÁS et al., 2008). Os molares
superiores foram inclinados para a distal (SILVA FILHO; AIELLO; FONTES, 2005;
NAHÁS et al., 2008) e tiveram sua irrupção restringida no sentido inferior (ALMEIDA et al.,
2006; BARNETT et al., 2008; HAGG et al., 2008; NAHÁS et al., 2008). Porém, a capacidade
do AH causar efeitos esqueléticos ainda é tema de debate na literatura. Alguns estudos
relataram que o AH não induziu uma restrição do crescimento alveolar (ALMEIDA et al.,
2006; NAHÁS et al., 2008; BARNETT et al., 2008). Outros trabalhos discordam com estes
resultados e relatam que o tratamento com o AH provocou uma restrição no comprimento
maxilar (SILVA FILHO; AIELLO; FONTES, 2005; VAN LAECKEN et al., 2006) e no seu

25
deslocamento para frente e para baixo (HÄGG; DU; RABIE, 2002; VAN LAECKEN et al.,
2006). Tal efeito auxiliaria na aquisição de uma melhor relação sagital com a mandíbula.
Não depender da colaboração do paciente é uma vantagem clínica importante
observada no uso desse tipo de aparelho. Em contrapartida, os aparelhos funcionais
removíveis estão sujeitos à cooperação do paciente e, muitas vezes, esse é o motivo que leva
ao insucesso do tratamento (PANCHERZ, 1979).
2.3 Mudanças na ATM associadas ao uso de ativadores mandibulares
O objetivo geral de um tratamento de uma má oclusão de Classe II por deficiência
mandibular é obter um posicionamento mais anterior da mandíbula (PANCHERZ; RUF;
KOHLHAS, 1998; SERBESIS-TSARUDIS; PANCHERZ, 2008). Essas mudanças podem ser
alcançadas através de três mecanismos associados à ATM (separadamente ou a combinação
das três): 1) crescimento mandibular por remodelação condilar; 2) deslocamento anterior da
mandíbula pela remodelação da anatomia da fossa mandibular; e 3) deslocamento anterior da
mandíbula pela rotação e translação condilar dentro da fossa (PANCHERZ; FISCHER, 2003;
SERBESIS-TSARUDIS; PANCHERZ, 2008). Entretanto existem controvérsias acerca dos
mecanismos associados à remodelação côndilo-fossa da ATM após a terapia com o AH
(PANCHERZ, 1979; RUF; PANCHERZ, 1999).
Existem relatos na literatura que afirmam que o tratamento com o AH favorece o
crescimento mandibular em comparação com uma amostra de pacientes sem tratamento
(PANCHERZ, 1979; RUF; PANCHERZ, 1998; HÄGG; DU; RABIE, 2002). Serbesis-
Tsarudise e Pancherz (2008) concluíram que um tratamento com o AH oferece um efeito
ortopédico sagital favorável numa avaliação de curto prazo. Além disso, Ruf e Pancherz
(1998) observaram também que houve uma remodelação óssea durante o período do
tratamento na região anterior da espinha pós-glenóide e, em maior quantidade, na região
póstero-superior do côndilo.
Estudos que utilizaram a radiografia cefalométrica para avaliação das mudanças
encontradas no côndilo após o uso do AH observaram que o crescimento condilar foi dirigido
horizontalmente para trás, com magnitude três vezes maior do que no grupo controle sem
tratamento (PANCHERZ; RUF; KOHLHAS, 1998; SERBESIS-TSARUDIS; PANCHERZ,
2008). Paulsen (1997) observou mudanças na morfologia e presença de um contorno duplo na
parte distoposterior do côndilo e também, em alguns casos, na superfície distal do ramo
interpretando-as como uma remodelação óssea. Nos estudos de Ruf e Pancherz (1998) e Ruf e

26
Pancherz (1999) foi observada uma remodelação óssea na parte mais póstero-superior da
cabeça do côndilo e na superfície anterior da fossa mandibular. Relatou-se que o crescimento
condilar durante o tratamento foi cinco vezes maior e que apresentou uma direção de
crescimento relativamente mais horizontal comparado com o grupo controle que não recebeu
tratamento e que apresentavam uma oclusão ideal. Observou-se, ainda, que a relação côndilo-
fossa não foi afetada pela terapia com o AH.
Ruf e Pancherz (2000), utilizando a ressonância magnética para a avaliação das
mudanças encontradas no crescimento condilar e sua relação com a fossa mandibular,
relataram que o côndilo apresentou um deslocamento estatisticamente significativo mais
anterior na fossa mandibular imediatamente após a remoção do aparelho (T2) em comparação
com a posição inicial em T1 (antes da instalação do aparelho). Entretanto, depois de um ano
que o aparelho havia sido removido (T3), o côndilo retornou para sua posição inicial.
Kinzinger et al. (2006) e Kinzinger, Kober e Diedrich (2007) usaram um aparelho
ortopédico funcional fixo e, através de imagens de ressonância magnética, observaram que o
côndilo se deslocou mais para região inferior e anterior logo que o aparelho foi instalado, mas
que retornou para sua posição original no final do tratamento. Os autores afirmaram que a
reconstrução 3D da superfície do côndilo e suas superposições mostraram que houve um
mecanismo de adaptação e que a melhora na oclusão foi alcançada através de um
reposicionamento fisiológico da ATM (KINZINGER et al., 2006; KINSINGER; KOBER;
DIEDRICH, 2007).
Durante a presente revisão de literatura, foram encontrados alguns artigos publicados e
duas dissertações de mestrado utilizando TC no estudo dos efeitos dentoalveolares do AH
(PAULSEN et al., 1995; PAULSEN; KARLE, 2000; BORGES, 2013; LeCORNU et al.,
2013; YILDIRIM; KARACAY; ERKAN, 2014; SESSIRISOMBAT, 2015; CHEN et al.,
2016; WEIWEI et al., 2016; SAH et al., 2017). Nos relatos de casos de Paulsen et al. (1995) e
Paulsen e Karle (2000) foram avaliados pacientes adultos jovens, após o pico de crescimento
puberal, em que o crescimento endocondral já havia cessado. Foram encontrados contornos
duplos na fossa mandibular e na parte disto-superior dos côndilos durante o tratamento com o
AH, caracterizando uma neoformação óssea dessa região. Yildirim, Karacay e Erkan (2014)
avaliaram a resposta condilar após o uso de 8 meses do aparelho funcional removível Twin-
Block e concluíram que esse aparelho aumenta o volume condilar, o comprimento mandibular
e a distância condilar estimulando o crescimento para cima e para trás do côndilo. Estudos
prévios utilizando avaliação tridimensional de LeCornu et al. (2013) e BORGES (2013)
relataram ter sido observada reabsorção óssea na parede anterior e aposição óssea na parede

27
posterior da fossa, coerentes com a direção de deslocamento condilar após a instalação do
AH. Entretanto, esses estudos apresentam diferenças metodológicas como período de
observação, tipo de aparelho/ancoragem e estágio de maturação dos pacientes em relação ao
modelo de estudo que foi utilizado pela amostra deste pesquisa aqui apresentada.
2.4 O uso de Tomografia Computadorizada de Feixes Cônicos na Ortodontia
Diante do grande avanço científico para o diagnóstico diferencial, a tomografia tem
sido utilizada largamente nas diversas áreas de saúde como um aliado indispensável em casos
de maior complexidade, principalmente por permitir visualizar estruturas com maior acurácia
e uma definição admirável. Permite também, a montagem de secções multiplanares e uma
visão tridimensional, que possibilitam as delimitações de irregularidades e medidas de alta
precisão bem como a representação exata da região avaliada no exame (GARIB et al., 2007).
O surgimento e aumento na acessibilidade das Tomografias Computadorizadas de Feixes
Cônicos (TCFC), especialmente indicadas para a região dentomaxilofacial (HECHLER, 2008;
TYNDALL; RATHORE, 2008) representaram a abertura de novas perspectivas nas
investigações sobre o tema (SMITH; PARK; CEDERBERG, 2011).
Modelagem virtual 3D é conseguida pelo desenvolvimento de uma representação
matemática de estruturas tridimensionais por meio de programas especializados de
computador. Os modelos podem ser criados automaticamente utilizando algorítimos ou
manualmente através de segmentações threshold utilizando as escalas de cinzas de cada
imagem. Esse segundo método consegue reproduzir estruturas mais fiéis à realidade e já é
uma metodologia consolidada (CEVIDANES; STYNER; PROFFIT, 2006). Modelos virtuais
3D representam um objeto ou estrutura anatômica usando uma coleção de pontos no espaço,
conectados por várias formas geométricas como triângulos, linhas e curvas. Atualmente, a
construção e superposição de modelos virtuais 3D permite uma avaliação real da relação
côndilo-fossa e do deslocamento sofrido pelo côndilo após a inserção do AH tanto
qualitativamente como quantitativamente (LeCORNU et al., 2013).


29
3 HIPÓTESES
a) Hipótese Nula 1: após a terapia com o AH, não há diferenças em relação às
mudanças quantitativas e qualitativas na morfologia e posicionamento da mandíbula;
b) Hipótese Alternativa 1: após a terapia com o AH há diferenças em relação às
mudanças quantitativas e qualitativas na morfologia e posicionamento da mandíbula;
c) Hipótese Nula 2: após a terapia com o AH, não há diferenças entre os grupos de
diferentes estágios de maturação esquelética em relação às mudanças quantitativas e
qualitativas na morfologia e posicionamento da maxila;
d) Hipótese Alternativa 2: após a terapia com o AH há diferenças entre os grupos de
diferentes estágios de maturação esquelética em relação às mudanças quantitativas e
qualitativas na morfologia e posicionamento da maxila;
e) Hipótese Nula 3: após a terapia com o AH, não há diferenças entre os grupos de
diferentes estágios de maturação esquelética em relação às mudanças quantitativas e
qualitativas na relação côndilo-fossa mandibular;
f) Hipótese Alternativa 3: após a terapia com o AH há diferenças entre os grupos de
diferentes estágios de maturação esquelética em relação às mudanças quantitativas e
qualitativas na relação côndilo-fossa mandibular.


31
4 OBJETIVOS
4.1 Objetivos gerais
Avaliar tridimensionalmente as mudanças na morfologia e no posicionamento da
maxila, mandíbula, na relação côndilo-fossa mandibular e as alterações dentoalveolares após a
terapia com o AH em diferentes estágios do crescimento puberal.
4.2 Objetivos específicos
a) avaliar e mensurar as mudanças no deslocamento total (3D) e linear
(horizontal, vertical e lateral) bem como na morfologia dos côndilos e ramo
mandibular após a terapia com o AH durante o estágio puberal (ARTIGO
CIENTÍFICO 1);
b) avaliar e mensurar a rotação mandibular após a terapia com o AH durante o
estágio puberal (ARTIGO CIENTÍFICO 1);
c) avaliar e mensurar as mudanças no deslocamento e na morfologia da maxila
após a terapia com o AH durante os estágios pré-puberal e puberal e compará-
las (ARTIGO CIENTÍFICO 2);
d) avaliar e mensurar as alterações dentoalveolares maxilares após a terapia
com o AH durante o estágio pré-puberal e puberal e compará-las (ARTIGO
CIENTÍFICO 2);
e) avaliar e mensurar as mudanças na relação côndilo-fossa mandibular após o
uso do AH, nos estágios pré-puberal e puberal de maturação (ARTIGO
CIENTÍFICO 3).


33
5 MATERIAL E MÉTODOS
A metodologia apresentada nessa seção é o detalhamento de todas as etapas seguidas
para obter os resultados de todos os objetivos dessa pesquisa. Alguns detalhes metodológicos
específicos de cada artigo serão descritos na seção de Materiais e Métodos de cada um deles.
5.1 Amostra
Essa investigação é classificada como um estudo observacional retrospectivo de coorte
e ela foi submetida e aprovada pelo Comitê de ética e pesquisa em humanos da PUC Minas
sob os números CAAE 21534013.8.5137 e 79957417.5.0000.5137 (ANEXOS A e B).
Para cada etapa desta pesquisa foi realizado um cálculo amostral específico, sempre
considerando um alfa (α) de 5% e um beta (β) de 20%, para se atingir uma poder de 80%. Foi
aceito um effect size de até 1. Em cada artigo está descrito detalhadamente essa cálculo.
O banco de dados de duas instituições de ensino (Pontifícia Universidade Católica de
Minas Gerais – PUC Minas; e Universidade Positivo – Curitiba- PR) foi acessado e pacientes
que atendiam aos critérios de inclusão e exclusão desse estudo foram incluídos nessa amostra
(Fig. 1 e 2).
Os critérios de inclusão foram:
a) presença de má oclusão de Classe II com retrognatismo mandibular
identificado pela indicação clínica de avanço terapêutico da mandíbula;
b) overjet ≥ 6 mm;
c) discrepância sagital dentária de no mínimo 4 mm, medida na região dos
primeiros molares permanentes;
d) perfil facial convexo;
e) diferentes estágios de maturação esquelética (puberal ou pré-puberal) avaliado
pelo método das vértebras cervicais (entre CS1 e CS4), sendo essa avaliação
feita pela telerradiografia lateral extraída da TCFC de cada paciente;
f) possuir dois tempos de TCFC com intervalos de 8 a 12 meses entre eles.
Os critérios de exclusão foram:
a) portadores de síndromes, fissuras, deformidades dentofaciais;

34
b) portadores de disfunção temporomandibular;
c) indivíduos que foram submetidos à tratamento ortodôntico prévio onde foi
utilizado Aparelho Extra Bucal e/ou ativadores mandibulares;
Figura 1: Fluxograma de seleção da amostra
Fonte: Elaborada pela autora.

35
Figura 2: Fluxograma da montagem dos grupos avaliados
5.2 Protocolo de instalação e ativação do aparelho
Para as investigações apresentadas nesta tese, os pacientes foram alocados em grupos
de indivíduos tratados com o AH, ou em grupos usados como comparação. Os pacientes dos
grupos “Comparação” também eram portadores de má oclusão de Classe II esquelética mas
não tiveram essa má oclusão corrigida no primeiro momento. Isto ocorreu devido à outras
prioridades de tratamento odontológicos não-ortopédicos, como por exemplo tratamento e
acompanhamento de patologias, tracionamento de dentes impactados ou algum tipo de
tratamento protético/restaurador. Na investigação apresentada no Artigo científico 1, apenas
pacientes em estágio puberal foram incluídos, sendo então gerados os grupos Herbst (GH) e
Comparação (GC). Nos Artigos científicos 2 e 3, foram incluídos os pacientes em estágios
puberal e pré-puberal, formando quatro grupos, sendo denominados Herbst puberal (HP),
Comparação puberal (CP), Herbst pré-puberal (HPP), e Comparação pré-puberal (CPP).
Fonte: Elaborada pela autora.


37
Os pacientes dos grupos Herbst foram tratados utilizando o mesmo protocolo, tanto na
PUC Minas como na Universidade Positivo. O aparelho Herbst possuía um sistema do tipo
telescópio da marca Abzil (São José do Rio Preto, São Paulo). Na arcada maxilar um aparelho
expansor tipo Hyrax da marca Morelli (Sorocaba, São Paulo) e na arcada mandibular um arco
lingual de Nance com fio de aço 1,0mm. Tais acessórios objetivaram o aumento da resistência
do dispositivo e da estabilidade do sistema. Diante da discrepância transversal gerada com o
avanço mandibular, o parafuso expansor foi ativado de acordo com as necessidades
individuais, evitando-se as interferências oclusais. Um fio 0,7 mm de aço na oclusal dos
segundos molares permanentes foi acoplado ao sistema para evitar a extrusão desses dentes,
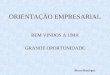
quando presentes (Fig. 3).
Todos os casos seguiram o mesmo protocolo de avanço mandibular, com ativação em
tempo único, objetivando obter uma relação de Classe I de caninos. Aqueles pacientes que
apresentaram interferências no movimento protrusivo e retroinclinação de incisivos
superiores, foram submetidos à alinhamento dentário com aparelho fixo 2x4 na maxila antes
da inserção do AH para permitir a ativação em tempo único.
Figura 3: Design do aparelho Herbst.
Fonte: Elaborada pela autora.


39
5.3 Método de registro
TCFC obtidas antes (T0) e ao final de 8 a 12 meses (T1) (média de 10,2 meses) foram
selecionadas de todos os pacientes. As imagens foram obtidas pelo tomógrafo i-CAT
(Imaging Sciences International, Hatfield, Pennsylvania, Estados Unidos) com FOV de 23 cm
x 17 cm (crânio estendido), voxel de 0,3 x 0,3 x 0,3 mm ou 0,4 x 0,4 x 0,4 mm, 36.90 mA,
120 kV e tempo de exposição de 40 segundos.
5.4 Método de medida
Modelos virtuais tridimensionais (3D), construídos a partir das TCFC, permitiram
mensurar as mudanças entre T0 e T1. O processamento das TCFC e dos modelos virtuais foi
feito através dos software ITK-SNAP 2.2 (software de livre acesso, www.itksnap.org),
SLICER CMF 4.0 (software de livre acesso, www.slicer.org). Para tanto, as tomografias
foram submetidas a uma série de processamentos que incluíram seis etapas:
a) Construção dos modelos 3D: utilizando a ferramenta Intensity Segmenter (Slicer
CMF 4.0), labelmaps (segmentações) das estruturas anatômicas ósseas foram
identificadas baseadas na imagem obtida pela TCFC em uma escala de cinzas, e
modelos tridimensionais volumétricos do crânio foram construídos. Utilizando o
ITK-SNAP 2.2 os ajustes e edições necessárias nos labelmaps foram feitos;
b) Orientação das cabeças: para comparar os dados de todos os pacientes em um
mesmo sistema de coordenadas, o modelo 3D T0 de todos os pacientes foi
posicionado espacialmente utilizando planos de referência padronizados para cada
plano do espaço: o plano axial foi determinado pelos pontos pórion esquerdo e
direito e pela mediana dos pontos orbital direito e esquerdo; o plano sagital
passou pela crista galli e pelo ponto médio da curvatura anterior do forame
magno; e o plano coronal tangenciou o tuberculum da sela túrcica. A orientação
do modelo T0 em uma localização espacial padronizada produziu uma matriz
matemática individual que pode ser aplicada nos scanT1 gerando a mesma
orientação do crânio para todos os dois tempos e para todos os pacientes (Fig. 4);
c) Superposição 3D na base do crânio: a superposição 3D consistiu de duas etapas
(Slicer CMF 4.0): a) aproximação manual dos scans (Fig. 5 e 6) e b) o registro
volumétrico automático baseado em voxel (Fig. 7). Para o registro na base do

40
crânio, os scans T0 e T1 foram manualmente aproximados, tendo como referência
a melhor superposição possível das estruturas da fossa craniana anterior,
especificamente das superfícies endocranianas da região da crista cribiforme do
osso etmóide e na superfície interna do osso frontal. Essas regiões foram
escolhidas já que seu crescimento finaliza-se muito cedo na vida das crianças. A
fase do registro foi feita de maneira totalmente automatizada, baseada em voxels.
O software computou o registro rígido (translação e rotação) que alinha as escalas
de cinzas de T0 e T1 a partir dos dados obtidos pela TCFC, com uma elevada
acurácia, em nível de voxel, na região anterior da base do crânio. Esse registro é
delimitado por uma máscara (uma referência volumétrica) criada a partir do
modelo 3D T0. Essas máscaras volumétricas informam ao software em qual
região os voxels de dois tempos diferentes (T0 e T1) devem se sobrepor;
d) Superposição regional 3D da mandíbula, maxila e fossa craniana: de maneira
similar ao registro feito na base do crânio, a superposição regional da mandíbula,
maxila e fossa mandibular requerem uma aproximação manual prévia dos scans, e
a partir daí um registro automático baseado em voxel (Slicer CMF 4.0). Para a
mandíbula, os scans T0 e T1 foram aproximados tendo como referência a melhor
sobreposição possível das linhas externas do corpo da mandíbula nas três vistas da
tomografia (axial, coronal e sagital). Para a etapa do registro, a máscara utilizada
incluiu o corpo da mandíbula, exceto os dentes e a cortical externa da superfície
inferior do corpo e da sínfise mandibular. O limite posterior da máscara é um
plano adjacente à superfície anterior do ramo, perpendicular à borda inferior da
mandíbula (Fig. 8). Para a maxila, os scans T0 e T1 foram aproximados tendo
como referência a linha inferior do palato duro numa vista sagital e o assoalho da
cavidade nasal numa vista frontal. A máscara utilizada na maxila incluiu a região
do palato duro, excluindo a região dentoalveolar, indo até a linha que passa pelos
forames palatinos (RUELLAS et al., 2016). Para o registro regional na fossa
mandibular, primeiramente os scans T0 e T1 foram aproximados tendo como
referência a borda inferior da fossa mandibular. A máscara foi confeccionada
contendo toda a porção anatômica da fossa mandibular (Fig. 1 do ARTIGO
CIENTÍFICO 3);
e) Avaliações qualitativas utilizando modelos 3D: avaliações qualitativas do
crescimento e do deslocamento maxilar, mandibular e da fossa mandibular, além
das mudanças dentárias, foram feitas através do software SLICER, utilizando a

41
técnica de superposição com semi-transparência de modelos virtuais 3D T0 e T1
(Fig. 9), e mapas por código de cores associados a vetorização de direção e
magnitude de crescimento e deslocamento como exemplificado nas Figuras 10 e
11.
f) Avaliações quantitativas utilizando modelos 3D: a avaliação quantitativa foi
realizada através de uma ferramenta chamada Q3DC (Slicer CMF 4.0). Para tal,
identificação de pontos de referência (landmarks) pelo software ITK-SNAP 2.2
foi realizada previamente. Para evitar erros associados à localização desses pontos
de referência nos modelos virtuais 3D, landmarks tridimensionais, com o tamanho
de um voxel (0,3 mm), foram cuidadosamente plotadas simultaneamente nas três
vistas multiplanares (axial, coronal e sagital), bem como utilizando o modelo 3D
do crânio para conferência final (Fig. 12). Utilizando cores distintas, landmarks
foram colocadas na maxila, mandíbula e fossa mandibular que estarão
especificadas em cada artigo correspondente.


43
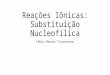
Figura 4: Orientação do crânio nas três vistas: sagital, coronal e axial (Software
SLICER).
Fonte: Elaborada pela autora.


45
Figura 5: Tomografias sobrepostas antes da aproximação (Software SLICER).
Fonte: Elaborada pela autora.


47
Figura 6: Tomografias sobrepostas após a aproximação na base do crânio (Software
SLICER).
Fonte: Elaborada pela autora.


49
Figura 7: Registro em nível de voxel da base do crânio T0. A) T0; B) T1; C) registro de
T1 em T0.
Fonte: Elaborada pela autora.


51
Figura 8: Região de sínfise mandibular funcionando como máscara para realizar o
registro regional da mandíbula em nível de voxel.
Fonte: Elaborada pela autora.


53
Figura 9: Método de superposição com semi-transparência dos modelos virtuais T0 e T1
demonstrando mudanças que ocorreram imediatamente após à instalação do AH.
Fonte: Elaborada pela autora.


55
Figura 10: Mapas por código de cores.
Fonte: Elaborada pela autora.


57
Figura 11: Associação do método por mapas por código de cores com o método de
correspondência por forma: vetores indicando direção e magnitude de crescimento.
Figura 12: Identificação de landmarks nos dentes, nas três vistas e no modelo 3D
(Software ITK-Snap).
Fonte: Elaborada pela autora.
Fonte: Elaborada pela autora.

58
5.5 Método de análise
A análise dos dados foi conduzida utilizando o software estatístico SPSS (versão 21.0;
SPSS, Chicago, IL, EUA). Foi realizada uma exploração geral dos dados com estatística
descritiva. O teste Kolmogorov-Smirnov indicou que a maioria das variáveis não atendia aos
pressupostos de normalidade e, por isso, para a comparação entre os grupos foi utilizada uma
estatística não-paramétrica (testes de Mann-Whitney, Kruskall-Wallis e Wilcoxon). A
concordância entre as leituras intra e inter-examinadores foi feita utilizando o teste ICC. As
análises de erro foram feitas com o teste t pareado (erro sistemático), e a fórmula de Dalhberg
(erro aleatório). Para isto, foram feitas releituras dos dados de 15 pacientes com intervalo de 1
mês para cada seção desta pesquisa (mandíbula, maxila, relação côndilo-fossa mandibular). O
nível de significância foi estabelecido em 5%.

59
6 ARTIGO CIENTÍFICO 1
Three-dimensional skeletal mandibular changes associated with Herbst appliance
treatment
Publicado no periódico Orthodontics Craniofacial Research em Maio de 2017.
Esse artigo foi formatado respeitando as normas da revista presente no link abaixo:
http://onlinelibrary.wiley.com/journal/10.1111/(ISSN)1601-6343

60
Three-dimensional skeletal mandibular changes associated with Herbst appliance
treatment
BQ Souki1, PLC Vilefort
1, DD Oliveira
1, I Andrade Junior
1, AC Ruellas
2, MS Yatabe
3, T
Nguyen4, L Franchi
5, JA McNamara Jr
6, LHS Cevidanes
6
Pontifical Catholic University of Minas Gerais, Belo Horizonte, Brazil1
Federal University of Rio de Janeiro, Rio de Janeiro, Brazil2
University of Sao Paulo, Bauru, Brazil3
University of North Carolina, Chapel Hill, USA4
University of Florence, Florence, Italy5
University of Michigan, Ann Arbor, USA6
Correspondence to:
Bernardo Souki
Pontifical Catholic University of Minas Gerais
Av. Dom José Gaspar, 500 Coração Eucarístico Belo Horizonte Brazil (30535-901).
Phone: 55-31-32455108
E-mail: [email protected]

61
Abstract
Objectives: Three-dimensional evaluation of skeletal mandibular changes following Herbst
appliance treatment. Setting and Sample Population: Retrospective case–control study, based
on a sample size calculation. Twenty-five pubertal patients treated with Herbst appliance
(HAG), and 25 matched Class II patients who received other non-orthopaedic dental
treatments (CG). Material and Methods: Three-dimensional models were generated from pre-
treatment (T0) and post-treatment (T1) cone beam computed tomograms. Volumetric
registration on the cranial base was used to assess mandibular displacement; volumetric
regional registration was performed to evaluate mandibular growth. Quantitative
measurements of X, Y, Z and 3D Euclidian changes, and also qualitative visualization by
colour-mapping and semi-transparent overlays were obtained. Results: Downward
displacement of the mandible was observed in both HAG and CG (2.4 mm and 1.5 mm,
respectively). Significant forward displacement of the mandible was observed in the HAG
(1.7 mm). HAG showed greater 3D superior and posterior condylar growth than the CG
(3.5 mm and 2.0 mm, respectively). Greater posterior growth of the ramus was noted in the
HAG than in CG. Conclusions: Immediately after Herbst therapy, a significant mandibular
forward displacement was achieved, due to increased bone remodelling of the condyles and
rami compared to a comparison group. Three-dimensional changes in the direction and
magnitude of condylar growth were observed in Herbst patients.

62
Introduction
The primary goal of Herbst appliance therapy is to correct Class II malocclusion and
improve facial convexity (1-3). Numerous clinical studies (4-9) have reported a short-term
increase in mandible length and forward displacement of the mandible. Furthermore,
histological animal studies corroborated these findings by showing growth modification of the
mandibular condyle and ramus following Herbst treatment (10-11). Much debate still exists,
however, as to whether the bite jumping mechanism has the capacity of stimulating greater
mandibular growth and consequently forward displacement of the mandible (12-15).
To date, the majority of Herbst studies were performed using two-dimensional (2D)
cephalometric imaging, an approach that cannot explain adequately the complex interactions
of three-dimensional (3D) changes that occur with growth and treatment (16). In a recently
published systematic review (14) concerning the changes in the TMJ morphology in Class II
patients treated with fixed mandibular repositioning evaluated with 3D imaging, the authors
concluded that previous literature has “failed to establish conclusive evidence of the exact
nature of TMJ tissue response”. The authors suggested the development of an adequate
sample size CBCT 3D investigation, using valid and reliable superimposition technique to
quantify bone remodeling.
Therefore, the aim of this retrospective study was to compare the mandibular skeletal
changes in pubertal Class II patients treated with Herbst appliance versus orthopedically-
untreated Class II controls, using a 3D virtual modeling protocol.
Materials and methods
Sampling
This investigation is a retrospective study that followed the ethical standards of the
institutional review board of Pontifical Catholic University of Minas Gerais, Belo Horizonte,

63
Brazil. The primary focus was to evaluate increases in condylar growth during Herbst therapy.
Based on the standard deviation of 1.85 mm reported by Pancherz et al. (17), an alpha
significance level of 0.05 and a power of 0.80 to detect changes of 1.5 mm, a sample size of
25 patients per group was calculated. The total sample included 50 skeletal Class II pubertal
patients.
Patients had been treated at the graduate program in orthodontics of the Pontifical
Catholic University of Minas Gerais and were considered eligible for this study when they
had routine pre-treatment (T0) and post-treatment (T1) CBCTs acquired for the purpose of the
orthodontic or dental diagnosis and treatment planning. Moreover, the patients at T0 were: 1)
in the permanent dentition; 2) age between 12 and 16 years old; 3) in the pubertal growth
period, as determined by the Cervical Vertebrae Maturation Method (18); 4) with Class II
division 1 malocclusion characterized by full Class II molar relationships, and canines that
had at least 4 mm sagittal discrepancy to achieve a Class I relationship; 5) and an improved
facial profile when the mandible was postured in a forward position (19).
Twenty-five patients who had received one-step mandibular activation with a
cantilever Herbst to obtain a Class I canines relationship were included in the Herbst
appliance group (HAG). The remaining 25 subjects were assigned to the comparison group
(CG). The patients in the CG had the need for other dental treatments or an orthodontic
leveling and alignment of maxillary teeth, without dentofacial orthopedic effects. At T0, no
significant different morphologic characteristics were detected between HAG and CG patients
(p>0.05). The Herbst patients presented with an ANB of 6.4°±1.2°, SNB of 72.4°±2.1°, and
SNGoGn of 32.1°±2.2°. The Comparison Group patients had an ANB of 5.9°±1.0°, SNB of
73.0°±3.0° and SNGoGn of 32.0°±2.6°.

64
Image Acquisition
Cone Beam Computed Tomographic (CBCT) scans had been taken for all subjects,
using an iCat machine (Imaging Sciences International, Hatfield, PA), with a 40-second scan,
a 23 x 17 cm field of view (FOV), and a voxel size of 0.3 mm. In the HAG, the scans were
taken before HA delivery (T0) and after 7.9 ± 0.4 months of treatment (T1). In the CG, the
scans were taken at two time-points: at baseline (T0), and at the end of the orthodontic or
prosthetic treatment, during the follow-up of impacted canine treatment, or after maxillary
cyst marsupialization. The average time between films in CG was 8.4 ± 1.3 months. All
patients had been instructed to bite into centric occlusion during scan acquisition.
Image analysis
The 3D image analysis procedures followed the protocol that has been published
elsewhere (20-23), which included the following: (1) construction of 3D surface models (20);
(2) 3D model orientation in the Cartesian planes (20-21); (3) 3D cranial base superimposition
for the mandibular displacement analysis (20); (4) 3D mandibular regional superimposition
(manual approximation and automated registration on the body of the mandible) for the
mandibular growth analysis (22); (5) qualitative assessments using 3D mesh surface models
(20, 23); and (6) quantitative measurements using Pick-n’-Paint and Q3DC tools of 3D Slicer
(20, 24).
Statistical analysis
Fourteen scans were selected randomly, and models were rebuilt and re-measured by
two blinded investigators after a two-week interval. Random error was measured according to
Dahlberg’s formula, and both intra and inter-observer agreement measurements were tested
using intraclass correlation coefficients (ICC).

65
Systematic error was assessed using the paired t-test. To evaluate the differences
between the Herbst and Comparison groups with regard to T1-T0 changes, independent
sample t-tests with Holm-Bonferroni correction for multiple tests were used. Analysis of
covariance (ANCOVA) was conducted with the mean T0-T1 change in the several ROI’s as
the dependent variables, group of treatment as the independent variable, and SNGoGn angle
as the covariate. Chi-square test was used to assess differences in the gender distribution. The
level of significance was set at 0.05.
Results
The two groups were matched by gender (HAG, 11 males vs. CG 15 males, chi-square
P > 0.05), chronological age (13.7 ± 1.8 years for HAG vs. 13.9 ± 1.2 years for CG), stage of
dental development, stage of skeletal maturation (88% in CS3 or CS4), and by length of
observational period (8 months). In each group, 2 patients were in stage CS2 and 1 patient
was in stage CS5.
The ICCs were greater than 0.89 for both intra- and inter-observer repeated
measurements. There were no statistically significant systematic errors between the 2
measurements performed by the same operator (p>0.05), and random error values varied
between 0.07 mm (3D condyle anterior) and 0.18 mm (3D condyle superior).
Mandibular displacement and rotation in HAG and CG is shown in Table 1. The
condylar and ramal growth changes in the right and left side were symmetrical, with no
statistically significant difference between sides in both groups (Table 2). Mean differences in
mandibular and ramal growth between the HAG and CG are reported in Table 3.
Fig. 1 shows the mandibular displacement with the cranial base superimposition of
HAG and CG individuals, while Figures 2 and 3 show the pattern of growth of the condyle

66
and rami with color-coded with regional superimposition. The skeletal mandibular changes
associated with Herbst treatment can be summarized as follows:
The forward displacement of the mandible was greater in the HAG
Pogonion showed a significant anterior displacement (Y axis) in the HAG (HAG, 2.2
mm vs. CG, 0.5 mm; mean difference, 1.7 mm; Table 1, Figure 1). The 3D displacement was
significantly greater in the HAG (HAG, 3.7 mm vs. CG, 2.2 mm; mean difference, 1.5 mm).
Both groups showed a similar (p>0.05) downward (Z axis) mandibular displacement (2.4 mm
vs. 1.5 mm in the HAG and CG, respectively). Changes in mandibular pitch were minimal in
both groups (mean 0.1° clockwise; 95% CI from -2.1° to 2.3° in the HAG vs. 0.3°
counterclockwise 95% CI from -2.5° to 2.0° in the CG group). Fifteen patients in the HAG
showed clockwise pitch, while 11 patients in the CG showed clockwise pitch.
Patients in the HAG presented a different pattern of condylar growth
The 3D net growth of condyles in all surfaces was significantly greater in the HAG
(superior, 1.4 mm; lateral 1.1 mm; medial, 0.5 mm; anterior 1.3 mm; posterior, 1.2 mm; Table
3, Figs. 2 and 3), with the exception of the medial pole. Patients in the HAG showed more
posterior and superior condylar growth than the CG (p<0.05), with the exception of the
vertical growth of the medial condylar pole (Table 3). The right-left lateral skeletal changes
did not show statistically significant differences between groups.
The posterior surface of the rami in the HAG showed greater amounts of posterior
growth
The Herbst group showed a statistically significant greater net change for the lower
region of the ramus in the projected Y component (0.6 mm; Fig. 3). The vertical and lateral

67
growth of the mandibular ramus (Z and X axis, respectively) was not significantly different
between the groups. 3D net changes in the superior (neck) region of the rami did not show
statistically significant differences between HAG and CG.
Discussion
Previous reports on the net gain of mandibular advancement are controversial.
Pancherz (8) reported 2.5 mm of Pogonion advancement when compared to an untreated
sample of Class II sample after 6 months of HA treatment. However, 16 years later, Pancherz
et al. (17) reported only a 0.9mm gain in the position of Pogonion in the Herbst group in
comparison to values from the Bolton Standards (2.2 mm vs. 1.3 mm). De Almeida et al. (25)
did not find statistical difference in the Pogonion position between treated and control
patients. In our study, the net mean of 1.5 mm increment (HAG 3.7 mm vs. CG 2.2 mm) in
mandibular anterior displacement in the projected y-axis may have contributed to facial
profile improvement, as well as correction of the malocclusion that was observed clinically in
all HAG patients.
Our findings concerning the 3D directional components of the mandibular growth and
displacement relative to the cranial base revealed 2.4 mm downward displacement of the
Pogonion region. Pancherz et al. (17) reported that Herbst treatment produced 3.9 mm of
downward displacement of the Pogonion region. Differences in appliance design using
mandibular first premolars as anchorage in the Pancherz study (17) versus first molars in the
present study may have resulted in differences on the point of force application and improved
control of vertical growth in the present study.
The results of this investigation suggest that condylar and ramal growth are modified
with Herbst appliance treatment. Our findings indicated that in the superior region and the
posterior surface of the condyles showed 1.4 mm and 1.2 mm greater growth in the HAG than

68
the CG over an 8-month period. The 3D components of bone remodeling, however, were not
uniform along the whole condylar surface. As was expected from a morphological and
functional standpoint, changes in the shape of the mandible typically take place during normal
growth. Such morphological changes in the shape and position of the condyles were observed
in most of the HAG and CG subjects.
The amount of effective condylar growth in Herbst subjects found in the current 3D
investigation (1.4 mm in the superior aspect of the condyles) was very close to data reported
previously in 2D cephalometric studies that used Condylion as reference landmark. Pancherz
(17) reported 1.8 mm of effective condylar growth in the Herbst groups. Another study (25)
found 2.5 mm of supplementary mandibular length increase in Herbst patients. The relatively
smaller net differences in condylar growth observed in the present study can be explained by:
1) the stage of skeletal maturation of the patients; 2) differences in the control groups; and 3)
the methods of registration and measurement.
The short observational period in the current investigation could account for the
relatively small skeletal changes. However, previous Herbst studies using 2D imaging have
shown greater skeletal changes with even shorter observational periods (6 months). The 3D
condylar growth, ranging between 2 and 3 mm observed in the HAG in this study cannot be
considered small. As the CG showed 3D condylar growth ranging between 1 and 2 mm,
however, the net differences were not as high as described previously in the literature. The
growth of the rami posteriorly was significantly greater in the HAG. Although 0.6 mm in the
inferior region of the rami might be considered small from a clinical point of view, this
perspective can change if the short observation period is taken into account. Significant bone
deposition along the posterior border of the ramus has been reported in experimental studies
with juvenile rhesus monkey (11).

69
Conclusions
Immediately after Herbst therapy, significant more mandibular forward displacement
without pitch was achieved, due to increased bone remodeling of the condyles and rami
compared to an untreated sample. Herbst patients presented different magnitude and direction
of condylar growth as contrasted to comparison patients.
Acknowledgment
The authors would like to acknowledge the CAPES (Coordenação de Aperfeiçoamento de
Pessoal de Nível Superior – “Coordination for higher Education Staff Development”) and
CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico – “National Counsel
of Technological and Scientific Development”) for their financial support.
References
1. Flores-Mir C, Major MP, Major PW. Soft tissue changes with fixed functional
appliances in Class II division 1. Angle Orthod 2006;76:712-20.
2. Baysal A, Uysal T. Soft tissue effects of Twin Block and Herbst appliances in patients
with Class II division 1 mandibular retrognathy. Eur J Orthod 2013;35:71-81.
3. Cozza P, Baccetti T, Franchi L, De Toffol L, McNamara JA Jr. Mandibular changes
produced by functional appliances in Class II malocclusion: a systematic review. Am J
Orthod Dentofacial Orthop 2006;129:599.e1-12.
4. Baltromejus S, Ruf S, Pancherz H. Effective temporomandibular joint growth and chin
position changes: Activator versus Herbst treatment. A cephalometric roentgenographic
study. Eur J Orthod 2002;24:627-37.
5. McGuinness N. Fixed functional appliances show definite skeletal and dental changes
in the short term. Eur J Orthod 2016;38,127-8.

70
6. Yang X, Zhu Y, Long H, et al. The effectiveness of the Herbst appliance for patients
with Class II malocclusion: a meta-analysis. Eur J Orthod 2016; 38,324-23.
7. Deen E, Woods MG. Effects of the Herbst appliance in growing orthodontic patients
with different underlying vertical patterns. Aust Orthod J 2015;31:59-68.
8. Pancherz H. The mechanism of Class II correction in Herbst appliance treatment. A
cephalometric investigation. Am J Orthod 1982;82:104-13.
9. Serbesis-Tsarudis C, Pancherz H. “Effective” TMJ and chin position changes in Class
II treatment. Angle Orthod 2008;78:813–8.
10. Chayanupatkul A, Rabie ABM, Hägg U. Temporomandibular response to early and
late removal of bite-jumping devices. Eur J Orthod 2003;25:465-70.
11. Peterson JE, McNamara JA. Temporomandibular joint adaptations associated with
Herbst appliance treatment in juvenile rhesus monkeys (Macaca mulatta). Semin
Orthod 2003;9:12-25.
12. Baysal A, Uysal T. Dentoskeletal effects of Twin Block and Herbst appliances in
patients with Class II division 1 mandibular retrognathy. Eur J Orthod 2014;36:164-72.
13. Zymperdikas VF, Koretsi V, Papageorgiou SN, Papadopoulos MA. Treatment effects
of fixed functional appliances in patients with Class II malocclusion: a systematic
review and meta-analysis. Eur J Orthod 2016:38,113-26.
14. Al-Saleh MAQ, Alsufyani N, Flores-Mir C, Nebbe B, Major PW. Changes in
temporomandibular joint morphology in class II patients treated with fixed mandibular
repositioning and evaluated through 3D imaging: a systematic review. Orthod
Craniofac Res 2015;18:185–201.
15. D’Antò V, Bucci R, Franchi L, Rongo R, Michelotti A, Martina R. Class II functional
orthopaedic treatment: a systematic review of systematic reviews. J Oral Rehabil
2015;42:624–42.

71
16. Durão AR, Pittayapat P, Rockenbach MIB, et al. Validity of 2D lateral cephalometry in
orthodontics: a systematic review. Prog Orthod 2013;14:31.
17. Pancherz H, Ruf S, Kohlhas P. “Effective condylar growth” and chin position changes
in Herbst treatment: a cephalometric roentgenographic long-term study. Am J Orthod
Dentofacial Orthop 1998;114:437-46.
18. Baccetti T, Franchi L, McNamara JA Jr. The Cervical Vertebral Maturation (CVM)
method for the assessment of optimal treatment timing in dentofacial orthopedics.
Semin Orthod 2005;11:119-129.
19. Martina R, Cioffi I, Galeotti A, et al. Efficacy of the Sander bite-jumping appliance in
growing patients with mandibular retrusion: a randomized controlled trial. Orthod
Craniofac Res 2013;16:116-26.
20. Yatabe M, Garib D, Faco R, de Clerck H, Souki B, Janson G, Nguyen T, Cevidanes L,
Ruellas A. Mandibular and glenoid fossa changes after bone-anchored maxillary
protraction therapy in patients with UCLP: A 3-D preliminary assessment. Angle
Orthod 2016; e-pub ahead of print Sep 26.
21. Ruellas AC, Tonello C, Gomes LR, Yatabe MS, Macron L, Lopinto J, Goncalves JR,
Garib Carreira DG, Alonso N, Souki BQ, Coqueiro RS, Cevidanes LH. Common 3-
dimensional coordinate system for assessment of directional changes. Am J Orthod
Dentofacial Orthop 2016;149:645-56.
22. Ruellas AC, Yatabe MS, Souki BQ, Benavides E, Nguyen T, Luiz RR, Franchi L,
Cevidanes LH. 3D Mandibular superimposition: Comparison of regions of reference for
voxel-based registration. PLoS One 2016;11:e0157625.
23. Solem RC, Ruellas A, Miller A, Kelly K, Ricks-Oddie JL, Cevidanes L. Congenital and
acquired mandibular asymmetry: Mapping growth and remodeling in 3 dimensions. Am
J Orthod Dentofacial Orthop 2016;150:238-51.

72
24. Nguyen T, Cevidanes L, Paniagua B, Zhu H, Koerich L, De Clerck H. Use of shape
correspondence analysis to quantify skeletal changes associated with bone-anchored
Class III correction. Angle Orthod 2014;84:329-36.
25. de Almeida MR, Henriques JFC, de Almeida RR, Weber U, McNamara JA Jr. Short-
term treatment effects produced by the Herbst appliance in the mixed dentition. Angle
Orthod 2005;75:540-7.

73
Figures
Fig. 1. Cranial base volumetric superimposition and the 3D models semi-transparent overlays.
A) Anterior cranial base superimposition mask. B) Full face displacement after Herbst
appliance treatment. C) Mandibular displacement in comparison group individual. D)
Mandibular displacement after Herbst appliance treatment.


75
Fig. 2. Semi-transparent overlays of the 3D models (T0, red; and T1, black mesh), and closest
point color maps in the qualitative assessment of the condylar growth (mandibular regional
superimposition). A) Herbst appliance patient. B) Comparison group patient.


77
Fig. 3 Shape correspondence color mapping with vectors in the qualitative assessment of the
condylar and rami growth (mandibular regional superimposition). A) Herbst appliance
patient. B) Comparison group subject.


79
Table 1. Comparison of mandibular displacement (T1-T0) in Herbst appliance and Comparison groups (t-test and ANCOVAa). Cranial base superimposition.
ROI Coordinates Groups Mean SD Mean difference CI 95% T-test p value
F Groups
F SNGoGn
Pogonion X
Herbst -0.37 0.65 -0.29 -0.85 0.25 0.279 2.056 0.073
Comparison -0.08 0.46
Y Herbst 2.20 1.31 1.66 0.74 2.60
0.001** 14.396** 0.088 Comparison 0.54 1.34
Z Herbst 2.37 1.6 0.90 -0.21 2.03
0.110 2.134 1.897 Comparison 1.47 1.64
3D Herbst 3.68 1.55 1.46 0.42 2.49
0.007** 8.052** 1.833
Comparison 2.22 0.43
Mandible
Pitch Herbst 0.06 0.6 0.35 -0.20 0.90
0.207 1.853 0.926 Comparison -0.29 0.95
Notes: a ANCOVA indicates analysis of covariance; SD, standard deviation; CI 95%, confidence interval of 95%; X, mesial-lateral; Y, anterior-posterior; Z superior-inferior; (+), rightward, forward, downward, clockwise
rotation; (-), leftward, backward, upward, counterclockwise rotation.
* p<0.05; ** p<0.01
Pitch is defined as clockwise and/or counterclockwise rotation in a lateral view.

80
Table 2. Condylar and rami growth after Herbst appliance therapy with the comparison between right and left sides (t-test). Mandibular regional superimposition.
Continuação
Herbst Group Comparison Group
Right Side Left Side Right Side Left Side
ROI Coordinates Mean SD Mean SD T-test
p value Mean SD Mean SD T-test
p value
Condyle Superior
X 0.53 0.48
0.53 0.49 0.948
0.44 0.31
0.49 0.29 0.684
Y 1.87 1.13
1.95 0.99 0.473
0.72 0.95
0.67 1.16 0.603
Z 2.55 0.95
2.61 1.17 0.783
1.67 1.28
1.64 1.08 0.820
3D 3.39 1.18
3.50 1.28 0.599
2.03 1.4
2 1.43 0.866
Condyle Lateral
X 0.87 0.55
0.54 0.60 0.103
0.42 0.34
0.5 0.58 0.621
Y 0.97 0.58
0.95 0.61 0.869
0.33 0.38
0.31 0.37 0.846
Z 2.56 0.87
2.62 1.03 0.823
1.56 1.2
1.56 1.1 0.819
3D 2.4 1.41
2.01 1.1 0.194
1.17 0.92
1.29 1.04 0.598
Condyle Medial
X 0.97 0.45
0.86 0.66 0.425
0.63 0.44
0.77 0.71 0.214
Y 2.19 1.5
2.47 1.35 0.092
0.85 0.96
1.08 1.3 0.152
Z 1.81 0.75
1.77 1.03 0.856
1.3 0.89
1.24 0.77 0.649
3D 2.21 1.31
2.55 1.6 0.297
1.63 1.12
2.01 1.5 0.122
Condyle Anterior
X 0.43 0.38
0.47 0.39 0.717
0.53 0.42
0.44 0.48 0.569
Y 1.80 1.22
1.89 1.04 0.542
0.66 0.76
0.82 1.11 0.244
Z 1.83 0.77
1.80 1.18 0.906
1.16 0.98
1.07 0.62 0.653
3D 2.70 1.16
2.71 1.31 0.975
1.43 0.98
1.37 1.25 0.784
Condyle Posterior
X 1.30 0.86
1.19 0.83 0.361
0.71 0.62
0.85 0.78 0.193
Y 1.16 0.95
1.23 0.82 0.625
0.5 0.5
0.54 0.76 0.768
Z 2.26 0.87
2.20 0.83 0.746
1.49 0.75
1.5 0.77 0.639
3D 2.80 1.27
2.68 1.02 0.532
1.51 1.15
1.62 1.29 0.689
Rami Neck X 0.97 0.56
0.80 0.67 0.385
0.64 0.4
0.77 0.73 0.375

81
Y 0.70 0.60
0.74 0.51 0.625
0.26 0.26
0.24 0.18 0.139
Z 1.03 0.71
0.90 0.48 0.659
1.03 1.08
0.76 0.63 0.423
3D 1.40 1.16
1.37 0.74 0.851
1.22 1.16
1.04 0.95 0.515
Rami Posterior
X 0.63 0.62
0.62 0.85 0.912
0.44 0.26
0.46 0.36 0.999
Y 0.82 0.48
0.86 0.57 0.751
0.20 0.15
0.26 0.21 0.996
Z 0.95 0.93
0.91 0.82 0.703
0.72 0.79
0.54 0.45 0.954
3D 1.52 1.11
1.47 0.96 0.754
1.21 1.16
1.03 0.95 0.976
Notes:
X: mesial-lateral, Y: anterior-posterior; Z: superior-inferior
(+): lateral, backward, upward

82
Table 3. Comparison of condylar and rami changes (T1-T0) in Herbst appliance and Comparison groups (t-test and ANCOVAa) Continuação

83
Conclusão
Notes: a ANCOVA indicates analysis of covariance; SD, standard deviation; CI 95%, confidence interval of 95%; X, mesial-lateral; Y, anterior-posterior; Z superior-inferior; (+), rightward, forward,
downward, clockwise rotation; (-), leftward, backward, upward, counterclockwise rotation, *p<0.05; **p<0.01.,


85
7 ARTIGO CIENTÍFICO 2
Maxillary dentoskeletal changes following Herbst appliance treatment in pre-
pubertal and pubertal stages
Esse artigo será submetido para publicação no periódico The Angle Orthodontist
(Qualis A2) e ele foi formatado respeitando as normas da revista presente no link abaixo:
http://www.angle.org/page/submit?code=angf-site

86
Maxillary dentoskeletal changes following Herbst appliance treatment in pre-pubertal
and pubertal stages
Paula Loureiro Cheib-Vileforta; Lucia Helena Soares Cevidanes
b; Patricia de Souza Costa
c;
Marilia Sayako Yatabed; Antonio Carlos de Oliveira Ruellas
b; James A. McNamara Jr.
e;
Alexandre Morof, Bernardo Quiroga Souki
g
aPhD Student, Graduate Program in Dentistry, Pontifical Catholic University of Minas Gerais, Belo
Horizonte, Brazil. bAssociate Professor, Department of Orthodontics and Pediatric Dentistry, School of Dentistry,
University of Michigan, Ann Arbor, Mich. cPrivate Practice, Former resident of Orthodontics, Pontifical Catholic University of Minas Gerais,
Belo Horizonte, Brazil. dResearch Fellow, Department of Orthodontics and Pediatric Dentistry, School of Dentistry,
University of Michigan, Ann Arbor, Mich. e Thomas M. and Doris Graber Endowed Professor of Dentistry Emeritus, Department of
Orthodontics and Pediatric Dentistry, School of Dentistry; Professor Emeritus of Cell and
Developmental Biology, School of Medicine; Research Professor Emeritus, Center for Human
Growth and Development, The University of Michigan, Ann Arbor, Mich; and Private Practice, Ann
Arbor, Mich. fAssociate Professor, Federal University of Parana, Graduate Program in Dentistry, University
Positivo; and Private Practice, Curitiba, Brazil. gAssociate Professor, Graduate Program in Dentistry, Pontifical Catholic University of Minas Gerais,
Belo Horizonte, Brazil; and Private Practice, Belo Horizonte, Brazil.
Mailing address:
Bernardo Quiroga Souki
Av. Dom José Gaspar 500 – Coração Eucarístico
Belo Horizonte – MG – Brazil - CEP 30535-901
Phone: +55 31 3319-4414
Email: [email protected]

87
ABSTRACT
Objective: To assess the maxillary dentoskeletal changes associated with the Herbst
appliance (HA) treatment. Materials and Methods: 3D virtual surface models were
generated from CBCT scans of 41 Class II patients treated with HA, and 37 Class II
comparison patients. According to the skeletal age, four groups were composed: 1) Pubertal
Herbst Group – PHG, n=21; 2) Pubertal Comparison Group – PCG, n=16; 3) Pre-pubertal
Herbst Group – PPHG, n=20; and 4) Pre-pubertal Comparison Group – PPCG; n=21. Total
and regional volumetric superimpositions of the scans were performed. Point-to-point
measurements of the displacements of dental and skeletal landmarks, in the X, Y, Z and 3D
perspectives, provided the quantitative data. Color maps and semitransparent overlays
offered the qualitative analysis. Non-parametric statistics were used. Results: Restriction of
the forward displacement of A-point (0.7 mm), and restriction of the downward
displacement of ANS (0.6 mm) was found in PPHG (P < .05). No significant skeletal
maxillary changes were found in the PHG. HA did not impact the maxillary downward
displacement of PHG and PPHG patients. Relative to the maxilla, the molars of HA patients
had a significant vertical control. Incisors were uprighted (approximately 2.3 degrees, P >
.05) and molars were distalized (approximately 1.2 mm, P < .05) in both HA groups. In the
Herbst groups, pre-pubertal patients showed greater dental compensations, but without
significant statistical difference. Conclusions: HA treatment provided some restriction of
the anterior and inferior maxillary growth and the effects were more evident in the pre-
pubertal patients than in the pubertal patients. Maxillary dentoalveolar changes were
observed in all patients regardless the stage of maturation.
KEYWORDS: Angle Class II Malocclusion; Maxilla; Herbst Appliance; Cone Beam
Computed Tomography.

88
INTRODUCTION
The Herbst appliance (HA) treatment aims to correct the convex profile of Class II
malocclusion patients associated with mandibular deficiency. Notable scientific efforts have
been already applied in order to understand the biological effects of this appliance.1–3
Due to
the fact that the mechanism of action of the HA is focused on the mandible, the literature
about this topic is mostly dedicated to the mandibular dentoskeletal effects.4–6
Only few
reports are available about the maxillary HA effects.7–9
Critics have been raised on the
effective exclusive mandibular improvements, and in the opinion of some researchers, the
maxillary effects would overcome the mandibular ones, at least in the long term.10,11
There is evidence that the ideal timing to treat mandibular deficiency of Class II
malocclusion patients, using fixed mandibular advancement devices, should include puberty,
in order to achieve a more effective and efficient outcome.12,13
However, the ideal treatment
timing to target maxillary effects could be different, since significant maxillary growth
occurs earlier.14
Regarding the maxilla, the HA effects are skeletal or dentoalveolar? Is there
any difference if the HA treatment is performed before or during the peak of pubertal
growth?
Most findings about HA dentoskeletal effects were based on two-dimensional
analysis.3,7,13,15,16
Such registration method, however, is subject to operational limitations as
bone structures overlap, imaging distortions and examiner`s bias by overlapping two images
from different time-point exams.17,18
Volumetric CBCT superimpositions, in the other hand,
allows a comprehensive assessment of the three-dimensional (3D) dentoskeletal changes
associated with treatments and or facial growth.18–20
A previous 3D pilot study reported a
significant restriction of the maxillary growth after the use of HA by pubertal patients,
comparatively to a group of Class II elastic patients.17
Therefore, this study aims to assess the 3D maxillary dentoskeletal changes associated
with the HA in groups of patients treated in the pre-pubertal and pubertal stages of
maturation.
MATERIALS AND METHODS
Sampling
This study was approved by the Institutional Review Board of the Pontifical Catholic
University of Minas Gerais (PUC Minas), in Belo Horizonte, Brazil. A retrospective cohort
was conducted from February 2011 to December 2014, by means of the database review

89
from graduate programs in orthodontics of two universities in Brazil. The sample size
calculation was based on the standard deviation value of 1.49 mm presented by Manfredi et
al.21
related to the primary aim of this study (A-point sagittal displacement). Considering α
of 5%, and a power of 80%, and to detect maxillary changes greater than 0.6 mm (effect-size
of 0.4), using ANOVA F-test, it was recommended the minimum of 19 individuals in each
group.
Seventy-eight skeletal Class II malocclusion patients who met the eligibility criteria
were included in this cohort. All of them had CBCT scans taken before treatment (T0) and at
the end of the observation period (T1 – mean of 10.2 months later); 37 treated in the pre-
pubertal and 41 in the pubertal stage of maturation. Forty patients had been treated with
cantilever HA (3M Abzil, São José do Rio Preto, Brazil).
The sample was grouped in pubertal (Pubertal Herbst Group – PHG; n=20; 9 girls vs.
11 boys) and pre-pubertal (Pre-pubertal Herbst Group – PPHG; n=20; 7 girls vs. 13 boys)
patients that received HA; and pubertal (Pubertal Comparison Group – PCG; n=16; 8 girls
vs. 8 boys) and pre-pubertal (Pre-pubertal Comparison Group – PCG; n=21; 3 girls vs. 18
boys) comparison patients. Pubertal patients had a mean age of 13.6 years old, and pre-
pubertal patients has a mean age of 9.5 years old. The comparison groups consisted of
patients that received others dental treatments before the orthopedic Class II correction, as
the follow up of impacted tooth, pathological cyst marsupialization treatment, or prosthetic
treatments. The inclusion criteria were that at T0 individuals had: 1) to present full molars
and canines in Class II division 1 relationship; 2) at least, 4 mm of mandibular advancement
to reach a first molar Class I relationship after HA insertion; 3) facial aspect of mandibular
retrusion, 4) to be at pubertal stages of CS3 or CS4 for the pubertal groups, and at stages
CS1 or CS2 for the pre-pubertal groups, 5) presenting CBCT scans before and after HA
treatment (for HA groups). Individuals with craniofacial anomalies were not included in the
sample.
Image Acquisition
All CBCT scans were taken using an iCat machine (Imaging Sciences International,
LLC, Hatfield, PA), with 40 seconds of digitalization, a field of view (FOV) of 23 cm x 17
cm, and a voxel of 0.3 or 0.4 mm. In the pubertal groups, the exams were carried out before
the HA insertion (T0) and 8 to 10 months (SD 1.2 months) after the HA treatment (T1). In
pre-pubertal groups, the exams were carried out at some time point (T0) and 10 to 12

90
months later (SD 1.5 months) (T1). All patients were instructed to bite in centric occlusion
during the acquisition of CBCTs.
Image Analysis
Image analysis protocol has been previously described.22–24
The methodology allows
the volumetric voxel based registration in the anterior cranial base,25
as well in regional
areas of interest. Maxillary regional registration has been described elsewhere.22
The 3D
virtual models of the heads were oriented in the same coordinate system, allowing reliable
comparisons between several patients.26
Open-source software (Slicer CMF 4.0 and ITK-
Snap 2.2) were used. The quantitative assessment of maxillary dentoskeletal changes was
carried out using the Q3DC tool on the Slicer CMF 4.0. From anatomic landmarks
accurately and simultaneously identified and pre-labeled in the multiplanar views (sagittal,
axial and coronal), and confirmed on the 3D surface model, point-to-point measurements
were carried out, quantifying the X, Y, Z and 3D displacements between the T0 and T1
models, relative to the anterior cranial base (ACB). The maxillary dental changes were also
measured relative to the maxillary regional superimposition. Maxillary rotations (pitch, roll,
and yaw) were also evaluated.
A total of seven landmarks were pre-labeled19
in each time-point scan. Three skeletal
landmarks were identified on the maxilla: (1) at anterior nasal spine (ANS); (2) at A-point
(AP); and (3) at the posterior nasal spine (PNS). Four dental landmarks were identified at:
(4) the mid-point of the incisal edge of the permanent right upper central incisor (IE); (5) the
root apex of the permanent right upper central incisor (IRA); (6) the mesio-buccal cusp tip
of the first permanent maxillary molars (MC); and (7) the mesio-buccal root apex of the
same molar (MRA).
Qualitative assessments of the maxillary growth and displacement were carried out
using semi-transparent overlays and shape-correspondence color maps (Figures 1 to 5), with
3D Slicer software tools.
Statistical analysis
The data analysis was carried out using SPSS version 20.0. To determine the errors in
the identification of landmarks, and in the measurements of the virtual models, 10 scans
were randomly selected, models were rebuilt, and re-measured by two investigators after an
interval of two weeks. The random error was measured according to Dahlberg’s formula34
and an analysis of the reproducibility of the intra-observer and inter-observer measurements

91
was tested using intraclass correlation coefficients (ICC), with a confidence level of 95%.
The systematic error (bias) was assessed using paired t-test. The normality and
homoscedasticity assumptions inspection was carried out by means of Kolmogorov-Smirnov
e Levene tests, respectively. Because most of the variables did not present normal
distribution and same variance, non-parametric comparison of the median values for
independent samples test (Mann-Whitney) was used. It was chosen the level of significance
of 5%.
RESULTS
The ICCs were greater than 0.87 for both intra and inter-observer repeated
measurements. There were no statistically significant systematic errors between the two
measurements performed by the same operator (P > .05).
Descriptive data relative to the maxillary skeletal and dental displacements are
presented in Table 1. The difference between HA groups (PPHG and PHG), and the
differences between these groups and their matched comparison groups (PPCG and PCG,
respectively) are shown in Table 2.
Based on the current findings, the following results can be presented:
Herbst appliance promoted a restriction of the anterior displacement of A-point in pre-
pubertal patients
The A-point showed statistically significant anterior-posterior (Y component)
displacement (P < .01) during the pre-pubertal period (HPPG, 0.28 mm vs. CPPG, 0.96 mm)
but not during the pubertal period (HPG, 0.12 mm vs. CPG, 0.22 mm) (Tables 1 and 2).
ANS and PNS did not show statistically significant anterior-posterior displacement (Table
2). The ANS of pubertal patients moved forward 0.43 mm and 0.54 mm (for Herbst and
Comparison groups, respectively), and 0.47 mm vs. 0.83 mm for the pre-pubertal patients
(Table 1), with P > .05 in the comparison of these groups (Table 2). PNS displaced
backward in all groups (HPG, -0.03 mm; CPG, -0.13 mm; HPPG, -0.24 mm; CPPG, -0.15
mm; P > .05). In Tables 1 and 2, positive signals means that the landmark displaced
anteriorly, while negative signals means that landmarks had posterior displacement between
T0 and T1. Figures 1 to 4 show the visual analysis of the pattern of maxillary displacement
of the four groups. Figures 6 and 7 summarize the difference between HA and comparison
groups, during pubertal and pre-pubertal stages respectively.

92
The Herbst appliance did not influence the downward displacement of the maxilla
ANS, A point and PNS moved downward in all groups, and no major differences were
found in the values of vertical displacement of skeletal landmarks, except to the ANS in the
pre-pubertal period (HPPG, -1.09 mm vs. CPPG, -1.67 mm (Table 1); P < .05 (Table 2)).
The negative signals in all groups means that landmarks had downward displacement
between T0 and T1. Maxillary vertical displacement can be observed in the semi-transparent
overlays and color mapping in the four groups (Figures 1 to 4).
Incisors moved backward in Herbst groups
Relative to the cranial base superimposition the maxillary incisors of treated groups
were statistically significant moved backward (P < .05), (HPG vs. CPG, 0.69 mm; HPPG vs.
CPPG, 1.44 mm), without pitch rotation (clockwise). Relative to the regional maxillary
superimposition the maxillary incisors were distalized 0.55 mm in the comparison of
pubertal groups (PHG vs. CPG), and 0.33 mm in the comparison of pre-pubertal groups
(PPHG vs. CPPG), but without statistically significant differences (P > .05) (Tables 1 and 2,
Figure 6 and 7). No statistically significant pitch rotation was found in the incisors
angulation in the maxillary regional superimposition analysis.
No vertical changes in the position of the incisors were observed
Relative to the cranial base (HPG, -1.84 mm; CPG, -1.53 mm; HPPG, -1.99 mm;
CPPG, -2.62 mm), and to the regional superimposition (HPG, -0.92 mm; CPG, -0.62 mm;
HPPG, -0.69 mm; CPPG, -0.22 mm), the Y component (superior-inferior) of the IE did not
show statistically significant differences (P > .05).
The amount of the molar distalization and tipback were not influenced by the pubertal
stage
Table 1 shows that molars were moved backward approximately 0.9 mm in the
pubertal groups (HPG, -0.86 mm vs. CPG, -0.15 mm – right side; HPG, -1.17 mm vs. CPG,
-0.13 mm – left side); and approximately 1.5 mm in the pre-pubertal groups (HPPG, -1.35
mm vs. CPPG, 0.15 mm – right side; HPG, -1.11 mm vs. CPG, 0.40 mm – left side). The
distalization was greater on the crown than on the root, with a pitch rotation (tipback) of
approximately 3.0 degrees in PHG and 5 degrees in PPHG. No significant differences in the
distalization of the molars were observed between PHG and PPHG.
A vertical control of the molars was observed in the Herbst patients

93
Molars moved downward relative to the cranial base in all groups (Table 1). However,
a statistically significant difference was observed in the amount of the downward
displacement between the HA and comparison groups within the two stages of skeletal
maturation (Table 2). Despite the downward maxilla displacement relative to the cranial
base in all groups, vertical control of the molars was observed in the HA patients. Relative
to the maxillary regional registration, the molars had less vertical displacement in PHG
(right side, 0.70 mm difference HPG vs. CPG; left side, 0.96 mm difference HPG vs. CPG).
These differences (average between sides of 0.84 mm) were statistically significant (P <
.05). Also relative to the maxillary regional registration, the molars in PPHG were vertically
stable (0.00 mm) and in PPCG, they extruded 0.64 mm in PPCG. The difference (0.63 mm)
was also statistically significant.
DISCUSSION
Previous studies on the dentoskeletal effects of the HA treatment have been mainly
focused on the mandibular effects.4–6
But, some researchers have questioned if in fact
maxillary effects would overcome mandibular gains.10,11
Recently, Rogers et al.11
affirmed
that “the primary effect of the Herbst in terms of maxillomandibular correction was in the
maxilla”. Wieslander10
reported a significant maxillary effect of the headgear-Herbst
appliance, concluding that the maxillary sutural remodeling might be more receptive to
long-term orthopedic treatment than the mandibular condylar growth process. But, due to
their small sample size, different orthopedic approach, and individual variability, such
findings should be interpreted with caution. Moreover, these studies used only 2D
assessments and no maxillary regional superimposition. Even with the possible maxillary
dentoskeletal contribution of the HA on the treatment of the Class II malocclusion, most of
the debate about mandibular versus maxillary effects have been presented based on believes
and personal thoughts. The current paper reports the first 3D investigation of the maxillary
effects of HA.
This study findings revealed that pre-pubertal Class II patients treated with the HA
presented more maxillary sagittal influence than pubertal individuals. Pre-pubertal patients
presented a restriction of 0.7 mm of sagittal displacement of A-point relative to the matched
comparison group, while pubertal individuals showed only 0.1 mm of net change. In
agreement, with a sample of 30 pre-pubertal patients, de Almeida et al.27
also found 0.7mm
of A-point restraint after 12 months of HA treatment. But, with a sample of 10 patients,

94
Pancherz28
described that patients treated with HA had 0.4 mm of distalization from the A-
point. Otherwise, some investigations did not find significant maxillary skeletal changes
after HA treatment. A recent systematic review reported that publication bias was detected
in A point measurements.29
And in another systematic review, Barnett et al.30
concluded that
minimal effects were demonstrated on the maxilla. Phan et al.31
reported no restraint of
maxillary growth in patients treated with HA. In the current study, we found 0.5 mm of ANS
growth restriction in pre-pubertal patients treated with HA, but without statistical difference.
However, de Almeida et al27
reported significant 0.8 mm of ANS restraint in their pre-
pubertal patients. As differences are small they may be explained by individual variability
in the different study samples.
The qualitative assessments using overlays with semitransparency, as well as the
color-maps, allow clear visualization of maxillary growth changes with the HA. In these
images, a restriction of the anterior region of the maxilla is observed in the HA groups, and a
forward displacement of the maxilla took place in the comparison groups (Figures 1 to 5).
These findings represent individual findings, while Tables 1 and 2 reveal that only A-point
in the PPHG showed statistically significant result.
For the assessment of 3D skeletal maxillary changes, this study utilized classic
landmarks in cephalometrics as fiducials for skeletal structures, due to their location are at
well-defined areas of maximum surface curvature. Another previous CBCT investigation
have also used ANS, PNS, A-point.17
The assessment of maxillary skeletal displacement as
measures at such landmarks must be carefully interpreted, as it may be a source of error
when maxillary growth changes are expected to happen. Because ANS, PNS and A-point
present independent and variable changes along time, they do not necessarily indicate the
behavior of the whole maxillary growth. The ANS forward displacement does not mean that
the maxillary body moved forward. Moreover, the A-point localization in the alveolar bone
exposes the landmark location to changes associated with the incisors movement. In the
sample of pubertal patients, several individuals had maxillary incisors aligned and leveled
with edgewise brackets, what might have influenced the displacement of A-point. However,
as both HA and comparison groups had similar number of patients with such condition, it
probably did not brought differences between groups.
Evidence-based reports have indicated puberty as the gold-standard timing to
effectively correct the Class II malocclusion using dentofacial orthopedic appliances.13
However, clinicians may need to begin the correction of the excessive overjet due to
psychosocial problems or the increased risk of traumatic injuries in the pre-pubertal stage.32–

95
34 Thus, our sample included patients within the two stages of skeletal maturity (pre-pubertal
and pubertal), in order to understand if maxillary effects of the HA were different in patients
treated with different timing. We have found that pre-pubertal patients in our comparison
group presented more forward and downward maxillary displacement than pubertal subjects
in the comparison group, indicating that maxillary growth is more active during early stages
of maturity. Probably due to the greater maxillary growth potential during pre-puberty,
greater maxillary growth restriction was found in patients treated early with HA. Thus, the
decision for early treatment with the HA can have an additional indication, besides the
previously described special recommendations (risk of trauma, or psychosocial effects), to
achieve maxillary sagittal growth control.
The maxillary anterior region present a downward displacement on the HA groups, of
approximately 1 mm (0.8 mm in PHG, and 1.1 mm in PPHG), while the posterior region
suffered a smaller vertical displacement (0.4 mm in PHG, and 0.6 mm in PPHG). Maxillary
clockwise rotation has been previously reported. Pancherz28
described the clockwise rotation
on the palatine plan, reporting 0.6 degrees in relation to the cranial base. In another study,
Pancherz and Anehus-Pancherz7 confirmed such findings, and reported 2 degrees of occlusal
plane inclination, and 0.2 degrees of palatal plane rotation. In the present study, the
maxillary incisors were vertically displaced 0.45 mm downward in PHG and 0.83 mm in
PPHG, according Table 1. In Pancherz’s study28
, a downward movement of 0.9 mm of the
incisors was described.
The molars vertical behavior in the HA groups was not similar to the comparison
groups. In the superior-inferior direction, we hypothesized that the direction of the forces
generated by the appliance, would lead to molar intrusion. This study results show that the
HA caused a relative intrusion of the molars relative to the cranial base, since in the HA
patients the molars were vertically stable while in the CG patients molars erupted. Such
finding is in accordance with previous 2D studies.14,28
The first permanent molars displaced
laterally significantly (coordinate X), in the Herbst groups (P < .05) due to the rapid
maxillary expansion (RME) included in HA preparation for the mandibular advancement.
A limiting aspect of the current investigation was the inclusion of comparison patients,
instead of control patients. The teeth alignment before HA treatment, as well as the RME
might have influenced the results. The alignment of the incisors and the RME are routinely
performed in order to allow the mandibular advancement. But, because they were performed
in 60% of the Herbst and also comparison patients, it is possible that they were not a bias in
that sample. We can infer that comparison Class II patients who had received tooth

96
movements, other than that target primarily to correct the molars sagittal relationship, might
present some degree of mandibular spontaneous growth aid. If a real control group were
used, probably the differences between HA and comparison groups would be greater.
Moreover, the minor intrusion of the molars observed in the current sample after HA
treatment would be greater if RME had not been carried out in several HA patients.
The significant maxillary molars distalization (puberal, 0.9 mm; pre-pubertal, 1.5 mm)
and tipback crown rotation (puberal, 3°; pre-pubertal, 6.5°), and also to the minor maxillary
skeletal changes helped the correction of the dental Class II relationship. These
measurements were small as Table 1 shows, but are clearly visible with the qualitative 3D
tools. These findings are in accordance with prior studies that compared the HA to the high-
pull headgear appliance, as to restriction effect of the development on the vertical direction
of the upper molars.7,31
Pancherz and Anehus-Pancherz7 concluded that HA had therapeutic
action similar to the headgear conventional applicance.29
Clinically, with the current design
of HA, was not noticed a so remarkable inclination, as with the use of a cervical headgear.
CONCLUSIONS
HA treatment provided some restriction of the anterior and inferior maxillary growth
and the effects were more evident in the pre-pubertal patients than in the pubertal patients.
Maxillary dentoalveolar changes were observed in all patients regardless the stage of
maturation.
ACKNOWLEDGMENT
The authors would like to acknowledge the CAPES and FIP PUC Minas for their financial
support.
REFERENCES
1. Ruf S, Pancherz H. Temporomandibular joint growth adaptation in Herbst treatment: a
prospective magnetic resonance imaging and cephalometric roentgenographic study. Eur.
J. Orthod. 1998;20:375-388.
2. McNamara JA, Peterson JE, Pancherz H. Histologic changes associated with the Herbst
appliance in adult rhesus monkeys (Macaca mulatta). Semin. Orthod. 2003;9:26-40.
3. Cozza P, Baccetti T, Franchi L, De Toffol L, McNamara J a. Mandibular changes produced

97
by functional appliances in Class II malocclusion: a systematic review. Am. J. Orthod.
Dentofacial Orthop. 2006;129:599.e1-599.e12.
4. Pancherz H, Ruf S, Kohlhas P. “Effective condylar growth” and chin position changes in
Herbst treatment: a cephalometric roentgenographic long-term study. Am. J. Orthod.
Dentofacial Orthop. 1998;114:437-446.
5. Pancherz H, Fischer S. Amount and direction of temporomandibular joint growth changes
in Herbst treatment: a cephalometric long-term investigation. Angle Orthod.
2003;73:493-501.
6. Serbesis-Tsarudis C, Pancherz H. “Effective” TMJ and chin position changes in Class II
treatment. Angle Orthod. 2008;78:813-818.
7. Pancherz H, Anehus-Pancherz M. The headgear effect of the herbst appliance: A
cephalometric long-term study. Am. J. Orthod. Dentofac. Orthop. 1993;103:510-520.
8. Lai M. Molar distalization with the Herbst appliance. Semin. Orthod. 2000;6:119-128.
9. Hdgg U, Du X, Rabie ABM, Bendeus M. What Does Headgear Add to Herbst Treatment
and to Retention? Semin. Orthod. 2003;9:57-66.
10. Wieslander L. Long-term effect of treatment with the headgear-Herbst appliance in the
early mixed dentition. Stability or relapse? Am. J. Orthod. Dentofac. Orthop.
1993;104:319-329.
11. Rogers K, Campbell PM, Tadlock L, Schneiderman E, Buschang PH. Treatment changes
of hypo- and hyperdivergent Class II Herbst patients. Angle Orthod. 2018;88:3-9.
12. Ruf S, Pancherz H. When is the ideal period for Herbst therapy-early or late? Semin.
Orthod. 2003;9:47-56.
13. Perinetti G, Primozic J, Furlani G, Franchi L, Contardo L. Treatment effects of fixed
functional appliances alone or in combination with multibracket appliances: A systematic
review and meta-analysis. Angle Orthod. 2015;85:480-492.
14. Enlow DH, Bang S. Growth and remodeling of the human maxilla. Am. J. Orthod.
1965;51:446-464.
15. Hägg U, Du X, Rabie ABM. Initial and late treatment effects of headgear-Herbst
appliance with mandibular step-by-step advancement. Am. J. Orthod. Dentofacial
Orthop. 2002;122:477-485.
16. Pancherz H. The effects, limitations, and long-termdentofacial adaptations to treatment
with the herbst appliance. Semin. Orthod. 1997;3:232-243.
17. LeCornu M, Cevidanes LHS, Zhu H, Wu C-D, Larson B, Nguyen T. Three-dimensional
treatment outcomes in Class II patients treated with the Herbst appliance: a pilot study.

98
Am. J. Orthod. Dentofacial Orthop. 2013;144:818-830.
18. Kula TJ, Ghoneima A, Eckert G, Parks ET, Utreja A, Kula K. Two-dimensional vs 3-
dimensional comparison of alveolar bone over maxillary incisors with A-point as a
reference. Am. J. Orthod. Dentofac. Orthop. 2017;152:836-847.e2.
19. Cevidanes LHC, Oliveira AEF, Grauer D, Styner M, Proffit WR. Clinical application of
3D imaging for assessment of treatment outcomes. Semin. Orthod. 2011;17:72-80.
20. Ghoneima A, Kula K. Accuracy and reliability of cone-beam computed tomography for
airway volume analysis. Eur. J. Orthod. 2013;35:256-261.
21. Manfredi C, Cimino R, Trani A, Pancherz H. Skeletal changes of Herbst appliance
therapy investigated with more conventional cephalometrics and European norms. Angle
Orthod. 2001;71:170-176.
22. De Oliveira Ruellas AC, Huanca Ghislanzoni LT, Gomes MR, et al. Comparison and
reproducibility of 2 regions of reference for maxillary regional registration with cone-
beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2016;149:533-542.
23. Souki BQ, Vilefort PLC, Oliveira DD, et al. Three-dimensional skeletal mandibular
changes associated with Herbst appliance treatment. Orthod. Craniofac. Res.
2017;20:111-118.
24. Yatabe M, Garib DG, Faco RA de S, et al. Bone-anchored maxillary protraction therapy
in patients with unilateral complete cleft lip and palate: 3-dimensional assessment of
maxillary effects. Am. J. Orthod. Dentofacial Orthop. 2017;152:327-335.
25. Cevidanes LHS, Styner M a, Proffit WR. Image analysis and superimposition of 3-
dimensional cone-beam computed tomography models. Am. J. Orthod. Dentofacial
Orthop. 2006;129:611-618.
26. Ruellas AC de O, Tonello C, Gomes LR, et al. Common 3-dimensional coordinate system
for assessment of directional changes. Am. J. Orthod. Dentofac. Orthop. 2016;149:645-
656.
27. de Almeida MR, Henriques JFC, de Almeida RR, Weber U, McNamara JAJ. Short-term
treatment effects produced by the Herbst appliance in the mixed dentition. Angle Orthod.
2005;75:540-547.
28. Pancherz H. The effect of continuous bite jumping on the dentofacial complex: a follow-
up study after Herbst appliance treatment of class II malocclusions. Eur. J. Orthod.
1981;3:49-60.
29. Yang X, Zhu Y, Long H, et al. The effectiveness of the Herbst appliance for patients with
Class II malocclusion: A meta-analysis. Eur. J. Orthod. 2016;38:324-333.

99
30. Barnett G a, Higgins DW, Major PW, Flores-Mir C. Immediate skeletal and dentoalveolar
effects of the crown- or banded type Herbst appliance on Class II division 1
malocclusion. Angle Orthod. 2008;78:361-369.
31. Phan KLD, Bendeus M, Hagg U, Hansen K, Rabie ABM. Comparison of the headgear
activator and Herbst appliance--effects and post-treatment changes. Eur. J. Orthod.
2006;28:594-604.
32. O’Brien K, Wright J, Conboy F, et al. Effectiveness of early orthodontic treatment with
the Twin-block appliance: a multicenter, randomized, controlled trial. Part 2:
Psychosocial effects. Am. J. Orthod. Dentofacial Orthop. 2003;124:488-495.
33. O’Brien K. Is early treatment for Class II malocclusion effective? Results from a
randomized controlled trial. Am. J. Orthod. Dentofacial Orthop. 2006;129:64-65.
34. O’Brien K, Macfarlane T, Wright J, et al. Early treatment for Class II malocclusion and
perceived improvements in facial profile. Am. J. Orthod. Dentofac. Orthop.
2009;135:580–585.


101
FIGURES
Figure 1 – Semitransparent overlays of T0 (red) and T1 (black mesh) virtual models of a
pubertal Herbst appliance patient. (A) Cranial base registration, showing a minor backward
and major downward maxillary displacement. (B) Regional maxillary registration, showing
minor backward and downward displacements. Transversal dimensional gain can be
observed associated with RME. The distalization and vertical control of molars can be
observed in semitransparency and color map with shape correspondence method.


103
Figure 2 – Semitransparent overlays of T0 (red) and T1 (black mesh) virtual models of a
pubertal comparison patient. (A) Cranial base registration, showing a minor forward
displacement. (B) Regional maxillary registration, showing no skeletal changes and the
color map with shape correspondence method presented minor forward dental displacement.


105
Figure 3 - Semitransparent overlays of T0 (red) and T1 (black mesh) virtual models of a
pre-pubertal Herbst appliance patient. (A) Cranial base registration, showing minor
backward and major downward maxillary displacement. (B) Regional maxillary registration,
showing the real backward and downward displacement of the maxilla, with no association
with cranial base growth or displacement. Transversal growth could not be observed. The
distalization and vertical control of molars could be observed in semitransparency and color
map with shape correspondence method.


107
Figure 4 - Semitransparent overlays of T0 (red) and T1 (black mesh) virtual models of a
pre-pubertal comparison patient. (A) Cranial base registration, showing minor forward and
downward maxillary displacement relative to the cranial base. (B) Regional maxillary
registration, showing minor skeletal changes. Color map with shape correspondence method
presented an uprighting of the incisors, probably due to the RME. No dental changes of the
molars were found.


109
Figure 5 – Shape Correspondence color mapping with vectorization of the four groups.
Relative to the cranial base, all groups showed downward maxillary displacement but with
different pattern of magnitude. (A) HPG showing minor backward maxillary displacement.
(B) CPG showing minor forward maxillary displacement. (C) HPPG showing more
backward maxillary displacement than HPG. (D) CPPG showing more forward maxillary
displacement that CPG.


111
Figure 6 – Differences between HPG and CPG. The positive sign means that Herbst group
presented greater changes than Comparison group. Negative sign means that Herbst group
presented smaller changes than comparison group. The arrows indicate the net changes
direction for the Herbst groups. The red numbers indicate statistically significant changes.


113
Figure 7 - Differences between HPPG and CPPG. The positive sign means that Herbst
group presented greater changes than Comparison group. Negative sign means that Herbst
group presented smaller changes than comparison group. The arrows indicate the net
changes direction for the Herbst group. The red numbers indicate statistically significant
changes.


115
Table 1. Descriptive data of the skeletal and dental maxillary changes relative to the cranial base, for the four groups (T1 – T0).
PHG PCG PPHG PPCG
Landmarks Coordinate Mean SD Median Mean SD Median Mean SD Median Mean SD Median
ANS
Y 0.43 1.13 0.30 0.54 0.81 0.61 0.47 0.78 0.41 0.83 0.75 0.69
Z -0.98 0.89 -0.75 -1.06 0.63 -0.90 -1.09 0.68 -0.93 -1.67 0.90 -1.94
3D 1.40 1.14 0.79 1.39 0.72 1.27 1.42 0.67 1.20 1.95 1.01 2.34
A Point
Y 0.12 0.39 0.06 0.22 0.82 0.15 0.28 0.62 0.30 0.96 0.77 0.81
Z -0.79 0.90 -1.05 -0.83 0.47 -0.82 -1.05 0.61 -1.14 -1.60 1.06 -1.55
3D 1.10 0.67 1.21 1.17 0.45 1.08 1.29 0.48 1.33 2.01 1.07 2.20
PNS
Y -0.03 0.55 -0.09 -0.13 0.76 0.00 -0.24 0.47 -0.30 -0.15 0.39 -0.09
Z -0.28 0.70 -0.36 -0.72 0.63 -0.66 -0.61 0.77 -0.60 -0.87 0.79 -0.73
3D 0.75 0.51 0.64 0.98 0.73 0.78 1.10 1.16 0.68 1.03 0.70 0.88
ANS-PNS Yaw 0.00 0.04 0.00 0.02 0.06 0.00 0.03 0.07 0.01 -0.03 0.09 -0.01
Pitch -0.35 1.67 -0.36 -0.38 0.57 -0.57 -0.56 0.88 -0.87 -0.94 0.98 -0.77
Incisal Edge
Y -0.44 1.77 -0.64 0.25 1.09 0.60 -0.13 1.60 0.01 1.30 1.16 1.28
Z -1.84 1.31 -1.73 -1.53 1.15 -1.20 -1.99 0.91 -2.10 -2.62 1.42 -2.90
3D 2.53 1.62 2.24 1.97 1.12 1.92 2.72 0.75 2.65 3.10 1.61 3.19
CM
X 1.33 1.20 1.20 0.71 1.21 0.49 0.79 1.10 0.54 0.20 0.56 0.02
Y -0.87 1.91 -1.50 0.25 0.99 0.45 -1.36 1.36 -1.30 1.19 1.01 1.06
Z -0.75 2.08 -0.15 -1.57 1.07 -1.51 -0.90 1.16 -1.05 -2.26 1.37 -2.44
3D 2.83 2.06 2.44 2.29 1.10 2.07 2.57 0.96 2.55 2.82 1.30 2.90
LAI Pitch -3.63 4.24 -4.09 -1.26 3.78 -0.14 -2.95 4.27 -3.90 -0.16 2.71 -0.57
LAM Pitch -3.43 3.78 -3.73 -0.19 2.51 0.33 -5.98 5.20 -4.80 1.25 2.23 1.56
Roll 0.69 2.45 0.02 -0.34 2.87 -0.08 1.26 2.65 0.98 -1.05 1.48 -0.92
Notes:
SD. Standard Deviation; Incisal Edge. Mid-point of the incisal edge of the permanent right upper central incisor; CM. mesio-buccal cusp tip of the permanent maxillary first molar; LAI. Long axis of the permanent right upper central incisor; LAM. Long axis of the permanent maxillary first molar; X. mesial-lateral; Y. anterior-posterior; Z superior-inferior; (+). Rightward; forward; upward; clockwise rotation; (-). Leftward; backward;
downward; counterclockwise rotation.

116
Table 2. Descriptive data of the dental maxillary changes relative to the maxillary superimposition for the four groups (T1 – T0).
PHG PCG PPHG PPCG
Landmarks Coordinate Mean SD Median Mean SD Median Mean SD Median Mean SD Median
Incisal edge
Y -0.43 1.69 -0.78 0.12 1.07 -0.30 -0.07 1.40 0.08 0.26 1.21 0.15
Z -0.92 0.90 -0.62 -0.62 0.43 -0.75 -0.69 0.74 -0.90 -0.22 1.33 -0.58
3D 1.75 1.39 1.32 1.20 0.66 1.08 1.69 0.66 1.63 1.57 1.00 1.34
R CM
X 1.40 1.06 1.38 0.59 1.05 0.45 0.77 0.89 0.49 0.11 0.54 0.00
Y -0.86 1.86 -1.02 -0.15 0.53 0.00 -1.35 1.28 -1.19 0.15 0.78 0.00
Z 0.08 1.80 0.43 -0.63 0.62 -0.62 0.00 1.10 -0.10 -0.30 1.25 -0.46
3D 2.57 1.92 2.25 1.38 0.76 1.38 2.15 1.15 2.02 1.42 0.71 1.42
L CM
X -1.10 0.82 -0.90 -0.54 0.97 -0.60 -0.51 1.14 -0.60 -0.21 0.37 -0.26
Y -1.17 1.13 -1.05 -0.13 0.49 -0.30 -1.11 1.58 -0.84 0.40 0.55 0.30
Z 0.44 0.74 0.53 -0.52 0.43 -0.60 -0.02 1.29 -0.15 -0.97 0.53 -1.02
3D 2.05 0.99 1.98 1.21 0.65 1.12 2.27 1.27 2.00 1.25 0.53 1.37
LAI Pitch -3.44 4.39 -3.64 -1.65 4.27 -0.56 -1.22 5.68 -1.01 0.12 3.09 -0.09
R LAM Pitch -2.92 4.00 -2.73 -0.08 2.45 0.48 -5.52 5.08 -5.06 0.62 2.26 0.36
Roll 0.82 2.46 0.68 -0.40 2.82 -0.39 1.70 3.12 0.61 -0.84 1.50 -0.70
L LAM Pitch -3.54 4.08 -3.24 -0.38 2.37 0.00 -5.45 6.78 -3.75 1.37 1.53 1.01
Roll -0.58 1.95 -0.46 -0.62 2.35 -0.04 -0.23 4.43 -1.82 -0.04 2.13 0.09
Notes:
Incisal Edge. mid-point of the incisal edge of the permanent right upper central incisor; R CM. mesio-buccal cusp tip of the right permanent maxillary first molar; L CM. mesio-buccal cusp tip of the left permanent
maxillary first molar LAI. Long axis of the permanent right upper central incisor; R LAM. Long axis of the right permanent maxillary first molar; L LAM. Long axis of the left permanent maxillary first molar X.
mesial-lateral; Y. anterior-posterior; Z superior-inferior; (+). Rightward; forward; upward; clockwise rotation; (-). Leftward; backward; downward; counterclockwise rotation.

117
Table 3. The mean differences of the skeletal and dental maxillary changes relative to the cranial base in the comparison between the groups.
PHG vs. PCG PHG vs. PPHG PPHG vs. PPCG
Landmarks Coordinates Mean difference SE 95% CI P Value
Mean difference SE 95% CI P Value
Mean difference SE 95% CI P Value
ANS Y -0.11 0.33 -0.79 0.56 0.679 0.20 0.29 -0.40 0.80 0.845 -0.51 0.25 -1.02 0.01 0.179 Z 0.07 0.25 -0.44 0.58 0.342 0.33 0.25 -0.19 0.84 0.328 0.63 0.26 0.10 1.16 0.042
3D 0.01 0.31 -0.61 0.63 0.342 -0.19 0.30 -0.80 0.42 0.163 -0.67 0.27 -1.23 -0.11 0.054
A Point Y -0.10 0.22 -0.56 0.36 0.842 -0.17 0.21 -0.60 0.26 0.425 -0.69 0.25 -1.21 -0.18 0.003 Z 0.03 0.23 -0.43 0.50 0.976 0.34 0.29 -0.25 0.93 0.354 0.57 0.29 -0.03 1.16 0.062
3D -0.07 0.19 -0.46 0.32 0.358 -0.26 0.21 -0.70 0.18 0.201 -0.71 0.27 -1.28 -0.15 0.011
PNS Y 0.10 0.22 -0.34 0.54 0.723 0.29 0.16 -0.03 0.61 0.241 -0.12 0.15 -0.44 0.19 0.674 Z 0.44 0.22 -0.02 0.89 0.060 0.49 0.26 -0.04 1.02 0.042 0.19 0.25 -0.31 0.69 0.441
3D -0.22 0.21 -0.64 0.19 0.356 -0.16 0.22 -0.61 0.30 0.372 -0.20 0.23 -0.67 0.26 0.845
ANS-PNS Yaw -0.02 0.02 -0.06 0.01 0.448 -0.02 0.02 -0.06 0.01 0.094 0.05 0.03 0.00 0.10 0.030 Pitch 0.03 0.44 -0.86 0.92 0.297 -0.14 0.29 -0.73 0.44 0.865 0.50 0.33 -0.17 1.17 0.426
Incisal
Edge
Y -0.69 0.73 -2.20 0.83 0.192 -0.61 0.52 -1.68 0.46 0.345 -1.44 0.45 -2.37 -0.52 0.009 Z -0.32 0.57 -1.51 0.88 0.423 0.52 0.35 -0.20 1.24 0.398 0.52 0.40 -0.30 1.35 0.121
3D 0.56 0.68 -0.85 1.96 0.462 -0.52 0.37 -1.29 0.25 0.389 -0.36 0.42 -1.23 0.52 0.302
CM
X 0.63 0.40 -0.19 1.44 0.141 0.64 0.42 -0.22 1.50 0.130 0.55 0.33 -0.14 1.24 0.106 Y -1.12 0.53 -2.19 -0.05 0.002 -0.19 0.46 -1.13 0.75 0.734 -2.41 0.41 -3.24 -1.58 0.000 Z 0.82 0.57 -0.34 1.98 0.004 0.91 0.43 0.03 1.79 0.060 1.29 0.42 0.44 2.13 0.003
3D 0.55 0.57 -0.61 1.70 0.172 -0.13 0.37 -0.88 0.62 0.784 -0.27 0.39 -1.06 0.51 0.473 LAI Pitch -2.37 1.86 -6.25 1.51 0.285 -0.93 1.50 -4.01 2.15 0.640 -3.13 1.22 -5.65 -0.62 0.075
LAM Pitch -3.25 1.09 -5.47 -1.02 0.001 1.72 1.65 -1.67 5.10 0.137 -7.41 1.49 -10.52 -4.31 0.000 Roll 1.02 0.88 -0.76 2.80 0.232 -0.20 0.91 -2.06 1.65 0.449 1.99 0.79 0.34 3.64 0.002
Notes:
SE. Standard Error of Mean; 95% CI. 95% confidence interval; Incisal Edge. Mid-point of the incisal edge of the permanent right upper central incisor; CM. mesio-buccal cusp tip of the permanent maxillary first molar; LAI. Long axis of the permanent right upper central incisor; LAM. Long axis of the permanent maxillary first molar; X. mesial-lateral; Y. anterior-posterior; Z superior-inferior; (+). Rightward; forward; upward; clockwise rotation; (-). Leftward; backward; downward; counterclockwise rotation.

118
Table 4. The mean differences of the dental maxillary changes relative to the maxillary superimposition in the comparison between the groups.
PHG vs. PCG PHG vs. PPHG PPHG vs. PPCG
Landmarks Coordinates Mean difference SE 95% CI P Value
Mean difference SE 95% CI P Value
Mean difference SE 95% CI P Value
Incisal
Edge
Y 0.55 0.70 -1.54 1.38 0.481 -0.63 0.44 -1.53 0.27 0.282 -0.33 0.42 -1.20 0.54 0.670
Z -0.30 0.36 -1.05 0.45 0.622 0.00 0.24 -0.49 0.49 0.822 -0.47 0.36 -1.18 0.24 0.207
3D 0.56 0.56 -0.61 1.72 0.397 -0.15 0.27 -0.70 0.39 0.395 0.12 0.29 -0.44 0.62 0.447
R CM
X 0.80 0.35 0.09 1.52 0.050 0.75 0.36 0.02 1.48 0.056 0.62 0.28 0.04 1.19 0.014
Y -0.71 0.48 -1.69 0.27 0.005 -0.08 0.42 -0.94 0.78 0.490 -1.34 0.35 -2.07 -0.62 0.000
Z 0.70 0.47 -0.26 1.66 0.000 0.56 0.35 -0.16 1.28 0.093 0.13 0.42 -0.72 0.97 0.303
3D 1.20 0.51 0.16 2.24 0.011 0.14 0.40 -0.68 0.96 0.516 0.79 0.31 0.15 1.43 0.045
L CM
X -0.55 0.30 -1.16 0.06 0.078 -0.94 0.36 -1.67 -0.21 0.106 -0.13 0.29 -0.74 0.49 0.215
Y -1.04 0.28 -1.61 -0.46 0.005 -0.54 0.54 -1.65 0.56 0.607 -1.30 0.44 -2.21 -0.38 0.001
Z 0.96 0.21 0.54 1.38 0.000 0.75 0.40 -0.07 1.57 0.042 0.80 0.36 0.03 1.56 0.005
3D 0.84 0.27 0.28 1.40 0.012 0.22 0.44 -0.68 1.12 0.685 0.86 0.37 0.08 1.63 0.003 LAI Pitch -1.80 1.99 -5.95 2.36 0.378 -2.11 1.64 -5.47 1.25 0.323 -1.98 1.41 -4.90 0.93 0.485
R LAM Pitch -2.84 1.14 -5.16 -0.52 0.003 1.71 1.60 -1.58 4.99 0.105 -6.27 1.43 -9.26 -3.28 0.000
Roll 1.22 0.88 -0.57 3.01 0.171 -0.69 1.04 -2.82 1.44 0.589 2.48 0.92 0.55 4.40 0.004
L LAM Pitch -3.16 1.09 -5.38 -0.94 0.018 -0.10 2.19 -4.58 4.38 0.449 -6.07 1.82 -9.92 -2.23 0.000
Roll 0.04 0.72 -1.42 1.49 0.987 -0.81 1.18 -3.25 1.63 0.626 0.33 1.15 -2.07 1.52 0.297 Notes: SE. Standard Error of Mean; 95% CI. 95% confidence interval; Incisal Edge. Mid-point of the incisal edge of the permanent right upper central incisor; R CM. mesio-buccal cusp tip of the right permanent maxillary first molar; L CM. mesio-buccal cusp tip of the left permanent maxillary first molar LAI. Long axis of the permanent right upper central incisor; R LAM. Long axis of the right permanent maxillary first molar; L LAM. Long axis of the left permanent maxillary first molar X. mesial-lateral; Y. anterior-posterior; Z superior-inferior; (+). Rightward; forward; upward; clockwise rotation; (-). Leftward; backward; downward; counterclockwise rotation.

119
8 ARTIGO CIENTÍFICO 3
Changes of the condyle-glenoid fossa relationship after Herbst appliance
treatment. Do they really happen?
Esse artigo será submetido para publicação no periódico The Angle Orthodontist
(Qualis A2) e ele foi formatado respeitando as normas da revista presente no link abaixo:
http://www.angle.org/page/submit?code=angf-site

120
Changes of the condyle-glenoid fossa relationship after Herbst appliance treatment. Do
they really happen?
Paula Loureiro Cheib Vileforta, Leticia Orefice Farah
b, Alexandre Moro
c, Antonio Carlos de
Oliveira Ruellasd, Bernardo Quiroga Souki
e, Lorenzo Franchi
f, James A McNamara Jr
g, Lucia
Helena Soares Cevidanesd
aPhD Student, Graduate Program in Dentistry, Pontifical Catholic University of Minas Gerais, Belo
Horizonte, Brazil. bPrivate Practice, Former resident of Orthodontics, University Positivo, Curitiba, Brazil.
cAssociate Professor, Federal University of Paraná, Graduate Program in Dentistry, University
Positivo; and Private Practice, Curitiba, Brazil. dAssociate Professor, Department of Orthodontics and Pediatric Dentistry, School of Dentistry,
University of Michigan, Ann Arbor, Mich. eAssociate Professor, Graduate Program in Dentistry, Pontifical Catholic University of Minas Gerais,
Belo Horizonte, Brazil; and Private Practice, Belo Horizonte, Brazil. fAssociate Professor, Graduate Program in Orthodontics, University of Florence, Florence, Italy.
g Thomas M. and Doris Graber Endowed Professor of Dentistry Emeritus, Department of Orthodontics
and Pediatric Dentistry, School of Dentistry; Professor Emeritus of Cell and Developmental Biology,
School of Medicine; Research Professor Emeritus, Center for Human Growth and Development, The
University of Michigan, Ann Arbor, Mich; and Private Practice, Ann Arbor, Mich.
Mailing address:
Bernardo Quiroga Souki
Av. Dom José Gaspar 500 – Coração Eucarístico
Belo Horizonte – MG – Brazil- CEP 30535-901
Telephone: +55 31 3319-4414
Email: [email protected]

121
ABSTRACT
Objective: To evaluate the spatial position of the mandibular condyles relative to their
glenoid fossae in Class II malocclusion patients after Herbst appliance (HA) treatment.
Materials and Methods: CBCT scans of 41 patients treated with cantilever HA were
compared with scans of 30 comparison individuals. Patients were grouped according to their
stage of skeletal maturation at baseline. Pubertal Herbst Group (PHG; n=24, mean age 14.5
years, CS 3-4) and Pre-pubertal Herbst Group (PPHG; n=17, mean age 9.9 years, CS 1-2)
were compared with Class II individuals in pubertal (PCG; n=12, mean age 13.9 years), and
pre-pubertal stage (PPCG; n=18, mean age 10.6 years) whose dental treatment did not include
dentofacial orthopedics. CBCT scans had been taken before treatment (T0), and after 8 to 12
months (T1). 3D surface models were constructed from scans to allow the volumetrically
superimposing of each independently glenoid fossa. Point-to-point measurements of pre-
labeled anatomic landmarks located in the condyles, and at the fossae were performed relative
to the X, Y, Z and 3D projected displacements. Qualitative assessment using semi-transparent
overlays and color-mapping were also run. Results: Relative to the glenoid fossa, condylar
position at T1 was similar to T0, in all groups (P > .05). The displacement of the condyles
within the glenoid fossae was very small (≤ 1.04 mm). Conclusion: Regardless the stage of
skeletal maturation, HA treatment did not change the original condyle-glenoid fossa
relationship.
KEYWORDS: Herbst appliance, mandibular condyles, Temporomandibular Joint, Imaging
three-dimensional

122
INTRODUCTION
Since its re-introduction in the late 1970´s1, dentoskeletal effects of the Herbst
appliance (HA) treatment have been extensively reported in the literature2–6
. The high
predictability of its clinical outcome, and the requirement of low patient`s compliance favored
the popularity of HA among orthodontists for the correction of the Class II malocclusion7.
However, an aspect on HA that still generates concern among clinicians is the hypothetical
changes in the original spatial position of the condyle within the glenoid fossa after the
mandibular therapeutic advancement, what would lead to temporomandibular (TMJ)
disorders, to dual bites, and/or to a relapse of the sagittal correction. Nevertheless, do they
really happen?
During the first two decades of life, the TMJ region and the posterior region of the
cranial base undergo three-dimensional (3D) changes associated with normal growth and
development. Significant transverse gain occurs in the TMJ, to compensate the V-shaped
growth of the mandible.8 Thus, the longitudinal spatial changes assessment of the relative
position of the condyles within their glenoid fossae should take into consideration the need for
a volumetric registration (superimpositions) of models at each glenoid fossa independently,
avoiding the bias of the transverse changes. But most studies on the condylar positional
changes following HA treatment have been performed using two-dimensional (2D)
cephalometric imaging9–13
or magnetic resonance imaging (MRI) and/or computed
tomography, but all with 2D methods.9,13–20
Unfortunately, 2D methods have low validity and
reproducibility due to magnification, distortion, and problems with the patient positioning.
Based on the assumption that the ideal situation would be, to have the condyles in their
original relationship within the glenoid fossae at the end of HA treatment, the superimposition
of two time-point scans should be performed using the volumetric best-fit of the inner contour
of the fossa. The increase in the accessibility of cone-beam computed tomography (CBCT),
and the lower radiation doses in current CBCT equipment, additional investigations on
craniofacial growth could be designed.21
Therefore, the aim of this investigation was to evaluate the condylar position relative
to the glenoid fossa after the HA treatment, comparing the spatial changes of the condyle
position of patients treated during pubertal and pre-pubertal stages of biological maturation.

123
MATERIALS AND METHODS
Sample
This retrospective clinical study was based on patient’s orthodontic records from two
universities databases (Pontifical Catholic University of Minas Gerais - Belo Horizonte,
Minas Gerais, Brazil; and Positivo University - Curitiba, Parana, Brazil). Sample size
calculation was based on the standard deviation of 0.6 mm, presented by Kinzinger, Kober
and Diedrich,18
associated with spatial position of the anterior surface of the condyles relative
to the glenoid fossa, which was the target primary outcome to be evaluated. Considering α of
5%, and β of 20%, in order to achieve a power of 80% and to detect condylar position
changes greater than 0.6 mm, it was recommended 17 individuals in each group for an effect-
size of 1.
Forty-one Class II patients with mandibular retrognatism treated effectively with HA
were allocated in HA groups. Thirty matched Class II patients served as comparison
individuals. Patients with syndromes, clefts, dentofacial deformities or temporomandibular
dysfunction were excluded from this investigation.
The skeletal maturation was assessed with the maturation of cervical vertebrae,
according to Baccetti et al.22
, and patients were grouped as pre-pubertal individuals (CS1 and
CS2) or pubertal individuals (CS3 and CS4). Patients of the PHG (pubertal Herbst group)
received the HA during the CS3 and CS4 maturation stages, while patients at PPHG (pre-
pubertal Herbst group) were treated during CS1 and CS2 maturation stages.
In PHG (n=24, mean 14.5 years old – ranging from 12 to 16 years old), and in PPHG
(n=17, mean 10.8 years old – ranging from 9 to 13 years old), the treatment duration was 8 to
12 months (mean 10 months). For all HA patients the Class II was treated and molars and
canines Class I relationship were obtained.
Comparison patients received other dental treatments that did not include dentofacial
orthopedic effects (e.g. orthodontic traction of impacted teeth, dentigerous cyst
marsupialization, prosthetic treatment or occlusal interferences in the region of the incisors
with the indication for orthodontic treatment for prior dental decompensation). The
observation period of PCG (pubertal comparison group – n=12, mean 14.1 years old – ranging
from 12 to 16 years old), and PPCG (pre-pubertal comparison group – n=18, mean 10.4 years
old – ranging from 10 to 11 years old) also ranged from 8 to 12 months (mean 10 months).
All Herbst patients were treated with a cantilever HA design with a ‘one step’
mandibular advancement (varied between 3 to 10mm, depending on the patient’s sagittal

124
discrepancy), to achieve a Class I canines and first molar relationship at the day of the HA
insertion.
Image acquisition
CBCT’s were performed using the i-Cat machine (Imaging Sciences International,
LLC, Hatfield, PA, USA) with isotropic 0.3 x 0.3 x 0.3 mm voxel. During CBCT
acquisitions, the head position had been standardized (Frankfurt plane parallel to the ground).
All patients were instructed to bite into maximum occlusal contacts. The CBCT were
performed before HA installation (T0) and after 8 to 12 months of treatment (T1). HA
patients had their T1 scans taken shortly after HA removal. Analysis of serial CBCT images
to evaluate changes between T0 and T1 included 3D analysis procedures using ITK-SNAP
(open-source software, www.itksnap.org), and 3D SLICER CMF (open-source software,
www.slicer.org). The image analysis procedures included: (1) virtual 3D surface models
construction: automatic segmentation of the anatomical structures of the patients' head were
performed using the "Intensity Segmenter" tool in 3D Slicer CMF 3.0 software; (2) head
orientation in the same Cartesian coordinate system, as described by Ruellas et al.23
(3)
manual approximation (best fit) of T0 and T1 scans using the lowest surface of right glenoid
fossa roof as reference; (4) semi-automatic and manual segmentation of the right glenoid
fossa for the construction of virtual 3D surface models of glenoid fossa that it served as
reference region for the automatic voxel based registration (Figure 1); (5) automated voxel-
based registration, of T0 and T1 scans, with the region of interest defined as the most inferior
surface of the right glenoid fossa roof, and (6) quantitative and qualitative measurements.
Methods of Measurements
Quantitative assessment of the changes of the position of the right side condyle at T1,
relative to the most inferior surface of the glenoid fossa, was performed using a 3D
volumetric registration. 3D point-to-point measurements, using ITK-SNAP for the
identification of landmarks, and the Q3DC tool of 3D Slicer for the quantification of T1
displacements in the X, Y, Z projections, and the Euclidean 3D distance were assessed. Thus,
T0 and T1 landmarks identification and pre-labeling were conducted by the same investigator,
using two independent screens, simultaneously, using the multiplanar views (sagittal, axial,
coronal) of oriented T0 grayscale scan, and registered T1 grayscale scan. Fourteen landmarks
were constructed with 0.5 mm 3D spheres (Figure 2) in each time-point scan (T0 and T1). In
the sagittal view it was marked seven spheres (Figure 2A): the most superior point of the

125
inner surface of the glenoid fossa; the most inferior point of the articular eminence; the mid-
point between spheres 1 and 2; the most posterior point of the glenoid fossa; the most superior
point of the condyle; the most anterior point of the condyle; the most posterior point of the
condyle. In the coronal view it was marked 4 spheres (Figure 2B): the most lateral point of the
glenoid fossa; the most medial point of the glenoid fossa; the most lateral point of the
condyle; the most medial point of the condyle. In the axial view it was measured the greatest
condylar diameter using the medial and lateral poles of the condyle (Figure 2C).
In order to select the sagittal slice to be used as the reference for sagittal view
measurements (named in this study as mater sagittal slice), it was identified in the axial view
the first slice that includes the full roof of the right glenoid fossa, running the mouse scroll
from top to bottom. It is a very thin bone layer. After selecting the geometric center of the
contour of the glenoid fossa roof (axial view), it was generated the mater sagittal slice (Figure
2A).
Six linear measurements from the condyle to the glenoid fossa were performed in each
time-point scan. It was also evaluated the condylar rotations (Pitch, Roll and Yaw) from T0 to
T1 (Figure 2) using the measurement #7.
Qualitative visual analysis of the displacement of the T1 condyle was performed using
semi-transparent overlays and closest-point color mapping (Figure 3). It was used 3D Slice
tools (Model maker, Model-to-model distance, and Shape Population Viewer) to calculate and
visualize the changes in the position of T1 condyle in comparison with T0 condyle, relative to
the glenoid fossa.
Statistical analysis
Data analysis was performed with the SPSS statistical software package (version 21.0;
SPSS, Chicago, IL). To determine the errors in landmark identification, and in the
displacements of the 3D spheres measurements, 30 scans were randomly selected, the models
were rebuilt, and re-measured by two investigators after a two-week interval. The random
error was measured according to Dahlberg’s formula16
and both intra and inter-observer
agreement measurements were tested using intraclass correlation coefficients (ICC), with a
confidence level of 95%. The systematic error (bias) was assessed using the paired t-test.
Some variables did not show normal distribution, and thus, the non-parametric Mann-
Whitney test was used to compare the medians. The level of significance was set at 0.05.

126
RESULTS
The ICCs were greater than 0.88 for both intra and inter-observer repeated
measurements. There were no statistically significant systematic errors between the two
measurements performed by the same operator (P > .05), and random error values varied
between 0.07 mm and 0.6 mm.
Despite the sample size calculation recommended 17 individuals in each group, it was
not possible to collect data of 17 comparison patients in the pubertal stage of maturation
(PCG). However, with the 12 individuals in that group, the post-hoc assessment computed
78.5% of achieved power (G*Power 3.1, open-source software, Dusseldorf, Germany).
Table 1 shows the descriptive data, including the median, mean and standard deviation
for the linear and rotational angular changes of the condylar position within the glenoid fossa
of treated and comparison groups, during the pubertal and pre-pubertal stages of maturation.
Changes were very small. The greatest sagittal displacement of the condyle was observed in
measurement #1 of the PPHG (0.60 mm) while the greatest vertical displacement was found
in measurement #5 of the PPHG (0.59mm).
The mean differences between groups, including the 95% confidence interval, and
standard error of the mean are shown in Table 2. The maximum displacement from T0 to T1
was found in the HPG (0.6 mm; P < .05) in measurement #3, which represents the distance
from the most posterior point of the condyle to the posterior internal surface of the glenoid
fossa. All other comparisons did not show statistically significance, and were smaller than 0.6
mm.
The difference of Pitch, Roll, and Yaw in the three comparison of the four groups
(Table 2) showed that condylar rotations after HA treatment happened. During the pubertal
period condylar pitch and roll were close to 3 degrees, while in the pre-pubertal period they
were smaller (Pitch, 1.65 degrees; Roll, 2.27 degrees). Yaw was very small, despite the stage
of skeletal maturation. None of the observed rotations presented statistical significance. In the
comparison between HA patients treated in the two stages of maturation (HPG vs. HPPG),
condylar rotations were small (≤ 1.4 degrees).
DISCUSSION
Using a novel imaging methodology, our findings corroborate previous 2D reports that
dentofacial orthopedics, using fixed mandibular advancement, in the effective treatment of
Class II malocclusion does not change the position of the condyles, relative to the glenoid
fossa. Ruf e Pancherz12
had analyzed MRI images of 15 Class II patients treated with HA for

127
7 months. They reported that “the condyle-fossa relationship was, on average unaffected by
Herbst therapy”. Kinzinger et al.17
and Kinzinger, Kober, Diedrich18
evaluated MRI’s of 20
Class II patients treated with fixed mandibular advancement device (FMA, Forestadent
Pforzheim, Germany) and found that “the improved dental occlusion was not achieved at the
price of a change to an unphysiological position in the temporomandibular joints”. The
current investigation adds to the literature a more robust sample size, with adequate statistical
power to affirm that the absence of statistical difference in the previous reports was not due to
small samples. It was also added the information that regardless the stage of maturation,
growing individuals in pre-pubertal and pubertal stages present the same result.
Despite the current knowledge on timing for an effective and efficient approach of
skeletal Class II malocclusion indicates puberty as the gold-standard,24,25
some severe Class II
patients, due to psychological problems or the increased risk of traumatic injury, need early
treatment. 26–30
Thus, we have included in our sample pre-pubertal children who had been
treated in very young age (mean age 8.6 years old). This pioneer information is important to
the clinicians, because even knowing that a significant effective condylar growth at early ages
is not likely to happen, at least an iatrogenic displacement of the condyles will not occur. Ruf
and Pancherz12
had evaluated only older patients, from 11.1 years-old to 17.6 years-old (mean
age 13.6); similar to Kinzinger and co-workers, who had also included adolescents and young
adults from 12 to 25.7 years old (mean age 15.6).18
Spatial changes of condylar position are expected during some modalities of
orthodontic treatment. Melgaço et al.31
reported a statistically significant anterior and inferior
displacements and a lateral inclination of the condyles three weeks after RME. In regard HA,
previous reports had used 2D assessments and measurements of the condylar spatial changes.
9–20 We have performed a full 3D evaluation, including the right-left (X projection), anterior-
posterior (Y projection), superior-inferior (Z), and 3D Euclidean distance measurements.
Also, it was used visual analytics tools as semi-transparent overlays of 3D models, and color
mappings, which provide a qualitative tool to comprehend what the numbers had shown.
To improve the validity of the measurements, it was performed a novel method for
regional volumetric superimposition specific for the glenoid fossa, avoiding the problems
associated with the head transversal growth, which negatively impact superimpositions based
on the mid-sagittal structures. We have decided to use only the right side, because the
mandibular advancement was similar in both sides, and it was inferred that the changes in the
right side must be similar to those in the left. In Figure 3, it is clear that condyles and rami
changed their morphology by means of bone remodeling along the HA treatment, with bone

128
apposition in the lateral surfaces (red color), and bone removal in the medial aspect (blue
color), but that the condyles kept their original position within the glenoid fossa (green color).
Bone remodeling in the superior and posterior regions of the condyle and fossa may
have been one of the factors that contributed to the maintenance of the condyle-fossa
relationship. However, with the methodology used in the present study, this cannot be
confirmed. Recent 3D studies have also suggested compensatory TMJ bone growth after HA
treatment. LeCornu et al.32
showed significant bone remodeling activity within the glenoid
fossae of HA patients. Souki et al.33
found a significant increase and change in the pattern of
bone remodeling of the condyles and mandibular ramus compared to a comparison group. It
was found that the HA patients presented a different magnitude and direction condylar growth
from comparison patients.
According to Buschang and Santos-Pinto,8 the glenoid fossa in normal growth
untreated young patients moves posterior-inferiorly along with the growth of the posterior
base of the skull, mainly by the activity of the spheno-occipital synchondrosis. In addition, the
displacement is twice greater posteriorly than inferiorly. In a period of 4 years, the
displacement reported by these authors was 3 to 4 millimeters. Therefore, displacement of the
fossa in the posterior direction is almost twice larger than the posterior condyle growth, which
would result in a posterior positioning of the mandible. Moreover, in Class II patients, the
glenoid fossa is positioned more posteriorly.8 Faced with this, it could be affirmed that the
normal growth and displacement pattern presented by the condyle and fossa occurs in an
opposite way to the direction that they need to undergo in order to maintain their relationship
as in the beginning of HA treatment. Therefore, it is suggested that the maintenance of the
condyle-fossa relationship after HA treatment is due to a combination of condyle return to the
original position due to ligament and muscle traction and a small portion of bone remodeling
with bone neoformation in the superior and posterior regions condyle, according some studies
with animals showed34,35
It is recommended additional 3D studies, with the aim to understand
the remodeling changes within the glenoid fossa and the mechanism for such a significant
rebound effect of the condyles in their glenoid fossa during HA treatment.
Differently to the current findings, Ruf and Pancherz14
used MRI and reported that the
condyles had a statistically significant anterior displacement in the glenoid fossa, immediately
after removal of the HA, in comparison with their initial position, prior to the appliance
insertion. However, one year after the appliance had been removed, the condyles returned to
its initial position.
Thus, orthodontists should not be concerned about the anterior displacement of the

129
mandibular condyles, immediately after Herbst insertion. The rebound effect is likely to
happen, and at the end of the treatment, condyles will be sited in their original position.
CONCLUSIONS
HA treatment did not change the condyle-fossa relationship, regardless the stage of
skeletal maturation. The condyles remained spatially stable relative to their glenoid fossae
after 8-12 months of treatment.
ACKNOWLEDGMENT
The authors would like to acknowledge the CAPES and FIP PUC Minas for their financial
support.
REFERENCES
1. Pancherz H. Treatment of Class II malocclusions by jumping the bite with the Herbst
appliance. A cephalometric investigation. Am. J. Orthod. Dentofac. Orthop. 1979;76:423-
442.
2. Pancherz H. The effects, limitations, and long-term dentofacial adaptations to treatment
with the Herbst appliance. Semin. Orthod. 1997;3:232-243.
3. Pancherz H, Malmgren O, Hägg U, Omblus J, Hansen K. Class II correction in Herbst and
Bass therapy. Eur. J. Orthod. 1989;11:17-30.
4. Voudouris JC, Woodside DG, Altuna G, Kuftinec MM, Angelopoulos G, Bourque PJ.
Condyle-fossa modifications and muscle interactions during herbst treatment, part 1. new
technological methods. Am. J. Orthod. Dentofac. Orthop. 2003;123:604-613.
5. VanLaecken R, Martin C a, Dischinger T, Razmus T, Ngan P. Treatment effects of the
edgewise Herbst appliance: a cephalometric and tomographic investigation. Am. J.
Orthod. Dentofacial Orthop. 2006;130:582-593.
6. Ruf S, Pancherz H. The mechanism of Class II correction during Herbst therapy in relation
to the vertical jaw base relationship: a cephalometric roentgenographic study. Angle
Orthod. 1997;67:271-276.
7. Silva JFE, Gerszewski C, Moresca RC, Correr GM, Flores-Mir C, Moro A. Retrospective
study of clinical complications during orthodontic treatment with either a removable

130
mandibular acrylic splint Herbst or with a cantilever Herbst. Angle Orthod. 2015;85:64-
71.
8. Buschang PH, Santos-Pinto A. Condylar growth and glenoid fossa displacement during
childhood and adolescence. Am. J. Orthod. Dentofacial Orthop. 1998;113:437-442.
9. Pancherz H, Ruf S, Kohlhas P. “Effective condylar growth” and chin position changes in
Herbst treatment: a cephalometric roentgenographic long-term study. Am. J. Orthod.
Dentofacial Orthop. 1998;114:437-446.
10. Pancherz H, Fischer S. Amount and direction of temporomandibular joint growth changes
in Herbst treatment: a cephalometric long-term investigation. Angle Orthod.
2003;73:493-501.
11. Serbesis-Tsarudis C, Pancherz H. “Effective” TMJ and chin position changes in Class II
treatment. Angle Orthod. 2008;78:813-818.
12. Ruf S, Pancherz H. Temporomandibular joint growth adaptation in Herbst treatment: a
prospective magnetic resonance imaging and cephalometric roentgenographic study. Eur.
J. Orthod. 1998;20:375-388.
13. Ruf S, Pancherz H. Temporomandibular joint remodeling in adolescents and young adults
during Herbst treatment: A prospective longitudinal magnetic resonance imaging and
cephalometric radiographic investigation. Am. J. Orthod. Dentofacial Orthop.
1999;115(6):607-618.
14. Ruf S, Pancherz H. Does bite-jumping damage the TMJ? A prospective longitudinal
clinical and MRI study of Herbst patients. Angle Orthod. 2000;70:183-199.
15. Popowich K, Nebbe B, Major PW. Effect of Herbst treatment on temporomandibular joint
morphology: a systematic literature review. Am. J. Orthod. Dentofacial Orthop.
2003;123:388-394.
16. VanLaecken R, Martin C a, Dischinger T, Razmus T, Ngan P. Treatment effects of the
edgewise Herbst appliance: a cephalometric and tomographic investigation. Am. J.
Orthod. Dentofacial Orthop. 2006;130:582-593.
17. Kinzinger GSM, Roth a, Gülden N, Bücker a, Diedrich PR. Effects of orthodontic
treatment with fixed functional orthopaedic appliances on the condyle-fossa relationship
in the temporomandibular joint: a magnetic resonance imaging study (Part I).
Dentomaxillofac. Radiol. 2006;35:339-346.

131
18. Kinzinger G, Kober C, Diedrich P. Topography and morphology of the mandibular
condyle during fixed functional orthopedic treatment --a magnetic resonance imaging
study. J. Orofac. Orthop. 2007;68:124-147.
19. Aidar LADA, Abrahão M, Yamashita HK, Dominguez GC. Herbst appliance therapy and
temporomandibular joint disc position: a prospective longitudinal magnetic resonance
imaging study. Am. J. Orthod. Dentofacial Orthop. 2006;129:486-496.
20. Aidar LADA, Dominguez GC, Yamashita HK, Abrahão M. Changes in
temporomandibular joint disc position and form following Herbst and fixed orthodontic
treatment. Angle Orthod. 2010;80:843-852.
21. Smith BR, Park JH, Cederberg RA. An evaluation of cone-beam computed tomography
use in postgraduate orthodontic programs in the United States and Canada. J. Dent. Educ.
2011;75:98-106.
22. Baccetti T, Franchi L, McNamara JA. The Cervical Vertebral Maturation (CVM) Method
for the Assessment of Optimal Treatment Timing in Dentofacial Orthopedics. Semin.
Orthod. 2005;11:119-129.
23. Ruellas ACO, Tonello C, Gomes LR, et al. Common 3-dimensional coordinate system
for assessment of directional changes. Am J Orthod Dentofac. Orthop 2017;149:645-656.
24. Perinetti G, Primožič J, Furlani G, Franchi L, Contardo L. Treatment effects of fixed
functional appliances alone or in combination with multibracket appliances: A systematic
review and meta-analysis. Angle Orthod. 2015;85:480-492.
25. Perinetti G, Primožič J, Franchi L, Contardo L. Treatment effects of removable functional
appliances in pre-pubertal and pubertal Class II patients: A systematic review and meta-
analysis of controlled studies. PLoS One 2015;10:1-35.
26. O’Brien K, Wright J, Conboy F, et al. Effectiveness of early orthodontic treatment with
the Twin-block appliance: a multicenter, randomized, controlled trial. Part 2:
Psychosocial effects. Am. J. Orthod. Dentofacial Orthop. 2003;124:488-95.
27. O’Brien K, Macfarlane T, Wright J, et al. Early treatment for Class II malocclusion and
perceived improvements in facial profile. Am. J. Orthod. Dentofac. Orthop.
2009;135:580-585.
28. O’Brien K. Is early treatment for Class II malocclusion effective? Results from a
randomized controlled trial. Am. J. Orthod. Dentofacial Orthop. 2006;129:S64-65.

132
29. Thiruvenkatachari B, Harrison JE, Worthington H V, O’Brien KD. Orthodontic treatment
for prominent upper front teeth (Class II malocclusion) in children. Cochrane Database
Syst. Rev. 2013;CD003452.
30. Petti S. Over two hundred million injuries to anterior teeth attributable to large overjet: A
meta-analysis. Dent. Traumatol. 2015;31:1-8.
31. Melgaço CA, Neto JC, Jurach EM, Nojima MDCG, Nojima LI. Immediate changes in
condylar position after rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop.
2014;145:771-779.
32. LeCornu M, Cevidanes LHS, Zhu H, Wu C-D, Larson B, Nguyen T. Three-dimensional
treatment outcomes in Class II patients treated with the Herbst appliance: a pilot study.
Am. J. Orthod. Dentofacial Orthop. 2013;144:818-830.
33. Souki BQ, Vilefort PLC, Oliveira DD, et al. Three-dimensional skeletal mandibular
changes associated with Herbst appliance treatment. Orthod. Craniofac. Res.
2017;20:111-118.
34. Voudouris JC, Woodside DG, Altuna G, Angelopoulos G, Bourque PJ, Lacouture CY.
Condyle-fossa modifications and muscle interactions during Herbst treatment, Part 2.
Results and conclusions. Am. J. Orthod. Dentofacial Orthop. 2003;124:13-29.
35. Peterson JE, Mcnamara JA. Temporomandibular Joint Adaptations Associated With
Herbst Appliance Treatment in Juvenile Rhesus Monkeys (Macaca mulata). Semin.
Orthod. 2003;9:12-25.

133
FIGURES
Figure 1 – At the ITK-Snap software, label maps at axial (A), sagittal (B) and coronal (D)
views for the semi-automatic and manual segmentation of the right glenoid fossa for the
construction of virtual 3D surface model of glenoid fossa (C) that it served as mask (reference
region) for the automatic voxel based registration.


135
Figure 2 – 0.5 mm diameter landmarks selection at condyles and glenoid fossae, in two time
points, T0 and T1, in sagittal (A), coronal (B) and axial (C) view simultaneously allowed the
following measurements: 1 - Displacement of the most superior point of the condyle relative
to the internal superior surface of the glenoid fossa; 2 - Displacement of the most anterior
point of the condyle relative to the articular eminence; 3 - Displacement of the most posterior
point of the condyle relative to the posterior internal surface of the glenoid fossa; 4 -
Displacement of the most anterior point of the condyle relative to the anterior internal surface
of the glenoid fossa; 5 - Displacement of the most lateral point of the condyle relative to the
lateral internal surface of the glenoid fossa; 6 - Displacement of the most medial point of the
condyle relative to the medial internal portion of the glenoid fossa; 7 - Angular changes of the
most superior point of the condyle.


137
Figure 3 - A - Overlay; B and C - Color map, lateral and medial view respectively.


139
Table 1. Descriptive data and the comparison among the four groups relative to the landmarks changes. Kruskal-Wallis test.
HPG CPG HPPG CPPG P value
Landmarks Coordinates Median Mean SD Median Mean SD Median Mean SD Median Mean SD
1
X 0.00 0.00 0.01 0.00 0.00 0.01 -0.03 -0.03 0.07 0.02 0.07 0.13 0.016
Y -0.01 -0.06 0.72 0.03 0.08 0.82 0.60 0.26 1.52 -0.15 -0.09 0.42 0.247
Z -0.02 0.05 0.52 -0.09 -0.05 0.46 0.48 0.31 1.17 0.09 0.09 0.74 0.485
3D 0.07 0.12 0.57 0.15 0.24 0.59 0.63 0.29 1.54 0.06 0.06 0.70 0.674
2
X 0.00 0.00 0.07 0.00 -0.01 0.06 -0.01 0.00 0.07 0.03 0.57 2.10 0.021
Y -0.30 -0.34 0.76 -0.03 -0.08 0.72 -0.29 -0.22 1.33 -0.55 -0.65 0.92 0.301
Z 0.16 0.13 0.74 -0.44 -0.28 0.58 -0.58 -0.43 0.87 0.01 0.29 0.99 0.129
3D -0.05 -0.04 0.84 0.19 0.30 0.65 -0.37 -0.37 1.11 -0.51 -0.42 0.62 0.037
3
X -0.01 -0.02 0.07 0.00 -0.02 0.06 0.01 0.01 0.11 0.02 0.04 0.16 0.271
Y 0.29 0.32 0.62 -0.09 0.24 1.07 0.09 -0.02 1.46 -0.31 -0.11 0.90 0.245
Z 0.37 0.29 0.91 0.31 0.48 0.83 0.00 0.02 1.46 1.04 0.75 1.03 0.319
3D 0.46 0.38 0.84 -0.31 -0.22 0.66 0.08 -0.01 1.90 0.30 0.43 1.06 0.182
X 0.00 -0.02 0.04 0.00 0.02 0.05 -0.01 -0.01 0.07 0.04 0.07 0.11 0.000
4 Y -0.07 -0.07 0.59 -0.05 -0.09 0.58 -0.22 -0.20 1.26 -0.29 0.04 0.91 0.996
Z 0.24 0.22 0.99 0.17 -0.13 1.02 0.37 -0.15 1.63 0.32 0.40 1.02 0.757
3D 0.13 0.36 0.68 0.09 -0.11 1.01 -0.01 -0.48 1.66 0.14 0.36 1.08 0.289
X 0.00 0.03 0.84 -0.16 0.17 0.43 0.34 -0.12 1.77 -0.55 -0.40 0.64 0.238
5 Y 0.01 0.01 0.04 0.00 0.01 0.03 0.00 0.00 0.04 0.03 0.06 0.08 0.060
Z -0.07 0.04 0.79 -0.24 -0.38 1.03 0.59 -0.04 2.01 0.44 0.51 1.11 0.310
3D 0.26 0.21 0.76 0.18 0.18 1.20 0.89 0.27 2.53 -0.15 0.20 1.14 0.732

140
Continued
HPG CPG HPPG CPPG P value
Landmarks Coordinates Median Mean SD Median Mean SD Median Mean SD Median Mean SD
X 0.24 0.04 0.81 -0.04 0.04 0.67 -0.02 -0.23 1.00 0.07 0.41 1.32 0.648
6 Y 0.00 -0.01 0.04 0.00 -0.01 0.08 0.00 0.01 0.04 0.04 0.07 0.07 0.001
Z 0.09 0.19 0.87 0.16 0.05 0.59 0.35 0.28 1.56 0.70 1.32 2.63 0.356
3D 0.02 0.07 0.94 0.12 0.22 0.51 0.12 0.39 1.42 0.73 1.62 2.85 0.249
Pitch 2.36 2.97 4.63 1.08 -0.13 6.93 3.01 4.58 6.11 5.53 6.23 4.87 0.058
7 Roll 1.62 4.46 8.77 1.97 1.57 4.42 4.29 3.99 3.62 4.62 6.26 5.07 0.144
Yaw 0.94 0.86 3.12 1.60 1.44 1.47 1.88 2.34 1.71 3.44 3.65 1.83 0.003
Notes:
P value = Kruskal-Wallis test
Measurement 1 - Displacement of the most superior point of the condyle relative to the internal superior surface of the glenoid fossa
Measurement 2 - Displacement of the most anterior point of the condyle relative to the articular eminence
Measurement 3 - Displacement of the most posterior point of the condyle relative to the posterior internal surface of the glenoid fossa
Measurement 4 - Displacement of the most anterior point of the condyle relative to the anterior internal surface of the glenoid fossa
Measurement 5 - Displacement of the most lateral point of the condyle relative to the lateral internal surface of the glenoid fossa
Measurement 6 - Displacement of the most medial point of the condyle relative to the medial internal portion of the glenoid fossa
Measurement 7 - Angular changes of the most superior point of the condyle

141
Table 2. The mean differences in the comparison between the groups, including Standard Error of Mean, and the 95% confidence interval.
HPG vs CPG HPG vs. HPPG HPPG vs. CPPG
Measurements Coordinates Mean diff SEM 95% CI P value
Mean diff SEM 95% CI P value
Mean diff SEM 95% CI P value
X 0,00 0,00 -0,01 0,01 0,658
0,03 0,02 -0,01 0,07 0,073
-0,11 0,04 -0,18 0,03 0,058
1 Y -0,15 0,28 -0,72 0,43 0,432
-0,32 0,42 -1,20 0,56 0,167
0,34 0,40 -0,52 1,20 0,055
Z 0,10 0,17 -0,24 0,45 0,802
-0,25 0,32 -0,92 0,42 0,167
0,22 0,35 -0,50 0,93 0,329
3D -0,12 0,20 -0,54 0,30 0,730
-0,17 0,41 -1,05 0,70 0,343
0,23 0,43 -0,67 1,13 0,294
X 0,01 0,02 -0,03 0,06 0,789
0,00 0,02 -0,05 0,04 0,924
-0,57 0,50 -1,61 0,48 0,010
2 Y -0,25 0,26 -0,78 0,27 0,279
-0,11 0,37 -0,90 0,67 0,839
0,43 0,41 -0,41 1,26 0,437
Z 0,40 0,22 -0,05 0,86 0,132
0,55 0,27 0,00 1,10 0,062
-0,72 0,32 -1,38 -0,06 0,089
3D -0,34 0,25 -0,85 0,17 0,132
0,33 0,33 -0,35 1,01 0,343
0,05 0,32 -0,62 0,72 0,759
X 0,00 0,02 -0,05 0,05 0,518
-0,03 0,03 -0,09 0,04 0,249
-0,03 0,05 -0,12 0,06 0,514
3 Y 0,08 0,33 -0,63 0,79 0,198
0,34 0,40 -0,50 1,18 0,401
0,08 0,43 -0,81 0,98 0,575
Z -0,18 0,30 -0,80 0,44 0,851
0,27 0,42 -0,60 1,14 0,417
-0,73 0,45 -1,65 0,20 0,065
3D 0,60 0,25 0,09 1,12 0,022
0,39 0,52 -0,70 1,48 0,417
-0,44 0,55 -1,58 0,71 0,664
X -0,04 0,02 -0,07 0,04 0,139
-0,01 0,02 -0,05 0,03 0,785
-0,08 0,03 -0,15 0,20 0,079
4 Y 0,02 0,20 -0,40 0,44 0,875
0,13 0,35 -0,60 0,86 0,978
-0,24 0,39 -1,04 0,57 0,772
Z 0,34 0,35 -0,39 1,08 0,500
0,37 0,46 -0,60 1,33 0,695
-0,55 0,48 -1,55 0,46 0,470
3D 0,47 0,32 -0,21 1,15 0,272
0,84 0,45 -0,11 1,78 0,093
-0,84 0,50 -1,87 0,19 0,133
X -0,24 0,32 -0,03 0,04 0,265
0,15 0,49 -0,87 1,18 0,808
0,28 0,48 -0,74 1,29 0,164
5 Y 0,00 0,01 -0,03 0,02 0,900
0,01 0,01 -0,01 0,03 0,303
-0,07 0,02 -0,11 0,02 0,094
Z 0,41 0,33 -0,29 1,12 0,245
0,08 0,54 -1,06 1,23 0,756
-0,56 0,58 -1,76 0,65 0,625
3D 0,03 0,38 -0,78 0,83 0,802
-0,06 0,67 -1,48 1,36 0,357
0,06 0,70 -1,41 1,54 0,329

142
Continued
HPG vs CPG HPG vs. HPPG HPPG vs. CPPG
Measurements Coordinates Mean diff SEM 95% CI P value Mean diff SEM 95% CI P value Mean diff SEM 95% CI P value
X 0,00 0,25 -0,52 0,51 0,604 0,26 0,30 -0,36 0,89 0,372 -0,64 0,40 -1,46 0,19 0,270
6 Y -0,01 0,02 -0,06 0,04 0,285
-0,02 0,01 -0,05 0,00 0,297
-0,06 0,02 -0,10 0,02 0,098
Z 0,14 0,24 -0,35 0,64 0,660
-0,08 0,44 -1,00 0,83 0,725
-1,04 0,74 -2,55 0,47 0,294
3D -0,14 0,24 -0,62 0,34 0,683
-0,32 0,41 -1,17 0,54 0,499
-1,23 0,77 -2,81 0,34 0,262
Pitch 3,10 2,20 -1,56 7,77 0,362
-1,61 1,82 -5,38 2,15 0,357
-1,65 1,95 -5,65 2,36 0,426
7 Roll 2,89 2,14 -1,45 7,24 0,851
0,47 1,96 -3,50 4,45 0,291
-2,27 1,52 -5,37 0,82 0,311
Yaw -0,58 0,74 -2,09 0,93 0,572 -1,48 0,75 -3,01 0,04 0,116 -1,32 0,62 -2,57 0,06 0,133
Notes:
P value = Mann Whitney test
Measurement 1 - Displacement of the most superior point of the condyle relative to the internal superior surface of the glenoid fossa
Measurement 2 - Displacement of the most anterior point of the condyle relative to the articular eminence
Measurement 3 - Displacement of the most posterior point of the condyle relative to the posterior internal surface of the glenoid fossa
Measurement 4 - Displacement of the most anterior point of the condyle relative to the anterior internal surface of the glenoid fossa
Measurement 5 - Displacement of the most lateral point of the condyle relative to the lateral internal surface of the glenoid fossa
Measurement 6 - Displacement of the most medial point of the condyle relative to the medial internal portion of the glenoid fossa

143
9 CONSIDERAÇÕES FINAIS
As hipóteses nulas #1 e #2 foram rejeitadas, permanecendo as hipóteses alternativas de
que há diferenças em relação às mudanças quantitativas e qualitativas na morfologia e
posicionamento da mandíbula e maxila. Entretanto não se rejeitou a hipótese nula #3 em que
não há diferenças entre os grupos de diferentes estágios de maturação esquelética em relação
às mudanças quantitativas e qualitativas na relação côndilo-fossa mandibular.
Baseando-se na experiência clínica do corpo de pesquisadores desse estudo, e em
alguns artigos prévios sobre o tema, ao iniciarmos essa investigação existia uma expectativa
de se encontrar um maior impacto esquelético do AH, principalmente quando este fosse
utilizado durante o surto de crescimento puberal. Entretanto, pôde-se observar que, apesar da
diferença estatística estar presente em algumas variáveis testadas, os efeitos esqueléticos da
terapia com o HA foram discretos em comparação com os efeitos dento-alveolares que
tiveram grande peso na correção da má oclusão da Classe II. Mesmo assim, achamos que esse
efeito esquelético, mesmo que discreto, foi fundamental para atingirmos resultados mais
eficientes.
Diante dos resultados encontrados, podemos concluir de maneira geral que:
a) pacientes do grupo Herbst apresentaram diferente magnitude e direção de
crescimento condilar e da superfície posterior do ramo, contrastando com os
pacientes do grupo comparação. Um significativo deslocamento anterior da
mandíbula, sem rotação no sentido horário, foi observado nos pacientes que
usaram o aparelho Herbst;
b) o aparelho Herbst restringiu parcialmente o deslocamento anterior e inferior da
maxila em pacientes pré-puberais mas não em pacientes puberais. Distalização
de molares permanentes, com controle vertical, foi observado em pacientes
pré-puberais e puberais tratados;
c) o tratamento com o aparelho de Herbst não alterou a relação côndilo-fossa
mandibular, independente do estágio de maturação.
Nesse estudo procurou-se responder uma série de perguntas à respeito dos efeitos do
AH. Dividiu-se o conteúdo em três artigos. No primeiro, em que foi avaliado os efeitos
mandibulares após a instalação do AH, o acesso ao banco de dados do grupo de pacientes pré-
puberais ainda não tinha ocorrido. Logo, não foi feita a comparação desses resultados entre os

144
Grupos puberais e pré-puberais. Planeja-se rodar essa análise futuramente. Entretanto, essa
variável temporal não é uma preocupação para a comunidade ortodôntica atualmente, já que é
sabido que resultados mais eficazes e eficientes se tratando da mandíbula são alcançados
quando o tratamento ocorre durante o pico da fase puberal de crescimento.
Contrariamente, os efeitos maxilares e a relação côndilo-fossa mandibular após a
terapia com o AH, ainda não estava bem documentado na literatura se existe diferença em
relação ao estágio de maturação biológica em que o tratamento é realizado. Assim, o segundo
e terceiro artigos trazem uma contribuição acerca deste conhecimento. Encontrou-se nesse
estudo, e foi relatado pela primeira vez na literatura, que os efeitos de um aparelho de tração
extra-oral do AH são maiores em pacientes que se encontram na fase pré-puberal. E que, após
a correção eficaz da má oclusão de Classe II utilizando o aparelho Herbst, a relação côndilo-
fossa mandibular não é alterada independentemente do estágio de maturação em que o
paciente se encontra durante o tratamento.
Dentro deste projeto de estudo, teve-se também como um dos objetivos iniciais a
avaliação das mudanças na morfologia da fossa mandibular após o uso do AH. Entretanto,
devido ao enorme consumo de tempo para rodar essa análise, utilizando a metodologia
escolhida, e considerando que a doutoranda cumpriu todo o programa em 3 anos, esse
objetivo não foi possível de ser alcançado por questões temporais. Esperamos que esse estudo
possa ter continuidade com outros alunos e que essa avaliação seja feita em breve.
Ao longo do desenvolvimento deste projeto obteve-se aprovação de fomento de
pesquisa (FIP PUC Minas #2014/8545-S1) e a doutoranda foi contemplada com uma bolsa
CAPES durante sua permanência no Brasil e também uma bolsa CAPES durante sua
permanência no exterior através do Programa Doutorado-Sanduíche no Exterior (PDSE – no
88881.134753/2016-01). Durante o curso de doutorado, outras atividades foram e estão sendo
desenvolvidas paralelamente à linha de pesquisa apresentada nessa tese (ANEXOS C, D, E,
F).

145
REFERÊNCIAS
AIDAR, L.A.A. et al. Herbst appliance therapy and the temporomandibular joint disc
position: a prospective longitudinal MRI study. American Journal of Orthodontics and
Dentofacial Orthopedics, v.129, n.4, p. 486-496, Apr. 2006.
AIDAR, L.A.A. et al. Effects of Herbst appliance treatment on temporomandibular joint disc
position and morphology: A prospective magnetic resonance imaging study. American
Journal of Orthodontics and Dentofacial Orthopedics, v.136, n.3, p. 412-424, Sept. 2009.
AIDAR, L.A.A. et al. Changes in temporomandibular joint disc position and form following
Herbst and fixed orthodontic treatment. The Angle Orthodontist, v.80, n.5, p. 843-852, Sept.
2010.
ALMEIDA, M.R. et al. Efeitos dentoesqueléticos produzidos pelo aparelho de Herbst na
dentadura mista. Revista Dental Press de Ortodontia e Ortopedia Facial, v.11, n.5, p. 21-
34, set./out. 2006.
ALMEIDA, S.A. Do orthodontists recommend Class II treatment according to evidence-
based knowledge? Revista de odontologia da UNESP, v.44, p. 305-312, May 2015.
BACCETTI, T.; FRANCHI, L.; MCNAMARA, JUNIOR J.A. The Cervical Vertebral
Maturation (CVM) Method for the Assessment of Optimal Treatment Timing in Dentofacial
Orthopedics. Seminars in Orthodontics, v.11, n.3, p. 119-129, 2005.
BANKS, P.; WRIGHT, J.; O’BRIEN, K. Incremental versus maximum bite advancement
during Twin-block therapy: a randomized controlled clinical trial. American Journal of
Orthodontics and Dentofacial Orthopedics, v.126, n.5, p. 583-588, 2004.
BARNETT, G.A. et al. Immediate skeletal and dentoalveolar effects of the crown- or banded
type Herbst appliance on Class II division 1 malocclusion. The Angle Orthodontist, v.78,
n.2, p. 361–369, 2008.
BOOIJ, J.W. et al. Class II treatment by extraction of maxillary first molars or Herbst
appliance: dentoskeletal and soft tissue effects in comparison. Journal of Orofacial
Orthopedics, v.74, n.1, p. 52–63, 2013.
BORGES, S.W. Avaliação tridimensional do tratamento da má olusão de Classe II com o
aparelho de Herbst. 2013. (Dissertação de Mestrado) – Departamento de odontologia,
Universidade Positivo, 2013.
BOURZQUI, F. et al. Prevalence of malocclusions and orthodontic treatment need in 8- to
12-year-old schoolchildren in Casablanca, Morocco. Progress in Orthodontics, v.13, n.2, p.
164-172, Sept. 2012.
BUMANN, A.; LOTZMANN, U.; MAH, J. TMJ disorders and orofacial pain: the role of
the dentistry in a multidisciplinary diagnostic approach (Color Atlas of Dental Medicine).
Stuttgart: Thieme, 2002.

146
BURKHARDT, D.R., McNAMARA, JUNIOR J.A.; BACCETTI, T. Maxillary molar
distalization or mandibular enhancement: a cephalometric comparison of comprehensive
orthodontic treatment including the pendulum and the Herbst appliances. American Journal
of Orthodontics and Dentofacial Orthopedics, v.123, n.2, p. 108-116, Feb. 2003.
CEVIDANES, L.H.S.; STYNER, M.A.; PROFFIT, W.R. Image analysis and superimposition
of 3-dimensional cone-beam computed tomograph models. American Journal of
Orthodontics and Dentofacial Orthopedics, v.129, n.5, p. 611-618, May 2006.
CHEIB, P.L. et al. Displacement of the mandibular condyles immediately after Herbst
appliance insertion: 3D assessment. Turkish Journal of Orthodontics, v.29, p. 31-37, Oct.
2016.
CHEN, W.W. et al. A cone-beam CT investigation on the effect of two-
phase treatment and fixed appliancetreatment only on temporomandibular joint. Zhonghua
Kou Qiang Yi Xue Za Zhi, v.51, p. 410-414, July 2016.
COZZA, P. et al. Mandibular changes produced by functional appliances in Class II
malocclusion: a systematic review. American Journal of Orthodontics and Dentofacial
Orthopedics, v.129, p. 599e1-599-e12, May 2006.
DE MATTOS, J. et al. Three-Dimensional Positional Assessment of Glenoid Fossae and
Mandibular Condyles in Patients with Class II Subdivision Malocclusion. The Angle
Orthodontist, v.87, p. 847-854, Nov. 2017.
DU, X.; HÄGG, U.; RABIE, A.B. Effects of headgear Herbst and mandibular step-by-step
advancement versus conventional Herbst appliance and maximal jumping of the mandible.
European Journal of Orthodontics, v.24, n.2, p. 167-174, 2002.
DeVINCENZO, J.P.; WINN, M.W. Orthopedic and orthodontic effects resulting from the use
of a functional appliance with different amounts of protrusive activation. American Journal
ofOrthodontics andDentofacialOrthopedics, v.96, n.3, p. 181-190, 1989.
EMRICH, R.E.; BRODIE, A.G.; BLAYNEY, J.R. Prevalence of Class I, Class II, and Class
III Malocclusions (Angle) in an Urban Population An Epidemiological Study. Journal of
Dental Research, v.44, n.5, p. 947–953, 1965.
FRANCHI, L. et al. Long-term skeletal and dental effects and treatment timing for functional
appliances in Class II malocclusion. The Angle Orthodontist, v.83, n.2, p. 334–340, 2013.
GARIB, D. G. et al. Tomografia Computadorizada de feixe cônico (cone beam): entendendo
este novo método de diagnóstico por imagem com promissora aplicabilidade na Ortodontia.
Dental Press de Ortodontia e Ortopedia Facial, v.12, p. 139-205, 2007.
HÄGG, U.; DU, X.; RABIE, A.B.M. Initial and late treatment effects of headgear-Herbst
appliance with mandibular step-by-step advancement. American Journal of Orthodontics
and Dentofacial Orthopedics, v.122, n.5, p. 477-485, 2002.

147
HÄGG, U. et al. Condylar growth and mandibular positioning with stepwise vs maximum
advancement. American Journal of Orthodontics and Dentofacial Orthopedics, v.134,
n.4, p. 525-536, Oct. 2008.
HANSEN, K. Treatment and posttreatment effects of the Herbst appliance on the dental
arches and arch relationships. Seminars in Orthodontics, v.9, n.1, p. 67–73, 2003.
HATCHER, D.C.; ABOUDARA, C.L. Diagnosis goes digital. American Journal of
Orthodontics and Dentofacial Orthopedics, v.125, n.4, p. 512-515, Apr. 2004.
HECHLER, S.L. Cone-Beam CT: Applications in Orthodontics. Dental Clinics of North
America, v.52, p. 809–823, 2008.
HERBST, E. New ideas and apparatus in orthodontics. International Journal of
Orthodontics, Oral Surgery and Radiography, v.18, n.9, p. 962–969, 1932.
HERBST, E. DreiBigjährigeErfahrungenmitdem Retentions-Scharnier.
ZahnärztlRundschau, v.43, p. 1515-1524; 1563-1568; 1611-1616, 1934.
IVORRA-CARBONELL, L. et al. Impact of functional mandibular advancement appliances
on the temporomandibular joint - a systematic review. Medicina Oral Patologia Oral y
Cirugia Bucal, v.21, n.5, p. e565-e572, 2016.
KING, G.J. et al. The timing of treatment for Class II malocclusions in children: a literature
review. The Angle Orthodontist, v.60, p. 87-97, July 1990.
KINZINGER, G.; KOBER, C.; DIEDRICH, P. Topography and morphology of the
mandibular condyle during fixed functional orthopedic treatment – a magnetic resonance
imaging study. Journal of Orofacial Orthopedics, v.68, n.2, p. 124-147, 2007.
KINZINGER, G.S.M. et al. Effects of orthodontic treatment with fixed functional orthopaedic
appliances on the condyle-fossa relationship in the temporomandibular joint: a magnetic
resonance imaging study (Part I). Dentomaxillofacial Radiology, v.35, p. 339–346, 2006.
LAGANÀ, G. et al. Prevalence of malocclusions, oral habits and orthodontic treatment need
in a 7- to 15-year-old schoolchildren population in Tirana. Progress in Orthodontics, v.14,
n.12, p. 186-196, 2013.
LeCORNU, M. et al. Three-dimensional treatment outcomes in Class II patients treated with
the Herbst appliance: a pilot study. American Journal of Orthodontics and Dentofacial
Orthopedics, v.144, n.6, p. 818–830, 2013.
McNAMARA, JUNIOR J.A. Components of Class II malocclusion in children 8 - 10 years of
age. The Angle Orthodontist, v.51, n.3, p. 177-202, 1981.
McNAMARA, JUNIOR, J.A.; PETERSON, J.E.; PANCHERZ, H. Histologic changes
associated with the Herbst appliance in adult rhesus monkeys (Macaca mulatta). Seminars in
Orthodontics, v.9, n.1, p. 26-40, 2003.

148
ÖMBLUS, J. et al. Long-term effects of Class II correction in Herbst and Bass therapy.
European Journal of Orthodontics, v.19, n.2, p.185-193, 1997.
PANCHERZ, H. The effects, limitations, and long-term dentofacial adaptations to treatment
with the Herbst appliance. Seminars in Orthodontics, v.3, n.4, p. 232-243, 1997.
PANCHERZ, H. Treatment of Class II malocclusions by jumping the bite with the Herbst
appliance: a cephalometric investigation. American Journal of Orthodontics and
Dentofacial Orthopedics, v.76, n.4, p. 423-442, Oct. 1979.
PANCHERZ, H.; ANEHUS-PANCHERZ, M. The effect of continuous bite jumping with the
Herbst appliance on the masticatory system: a functional analysis of treated class II
malocclusions. European Journal of Orthodontics, v.4, n.1, p. 37-44, 1982.
PANCHERZ, H.; BJERKLIN, K.; HASHEMI, K. Late adult skeletofacial
growth after adolescent Herbst therapy: A 32-year longitudinal follow-up study. American
Journal of Orthodontics and Dentofacial Orthopedics, v.147, n.1, p. 19-28, Jan. 2015.
PANCHERZ, H. et al. Thirty-two-year follow-up study of Herbst therapy: a biometric dental
cast analysis. American Journal of Orthodontics and Dentofacial Orthopedics, v.145, n.1,
p. 15-27, 2014.
PANCHERZ, H.; FISCHER, S. Amount and Direction of Temporomandibular Joint Growth
Changes in Herbst Treatment: A Cephalometric Long-Term Investigation. The Angle
Orthodontist, v.73, n.5, p. 493-501, 2003.
PANCHERZ, H.; RUF, S. When is the ideal period for Herbst therapy - early or late?
Seminars in Orthodontics, v.9, p. 47-45, Mar. 2003.
PANCHERZ, H.; RUF, S.; KOHLHAS, P. “Effective condylar growth” and chin position
changes in Herbst treatment: A cephalometric roentgenographic long-term study. American
Journal of Orthodontics and Dentofacial Orthopedics, v.144, n.4, p. 437-446, Oct. 1998.
PANCHERZ, H.; ZIEBER, K.; HOYER, B. Cephalometric characteristics of Class II division
1 and Class II division 2 malocclusions: a comparative study in children. The Angle
Orthodontist, v.67, p. 111-120, 1997.
PAULSEN, H.U. Morphological changes of the TMJ condyles of 100 patients treated with the
Herbst appliance in the period of puberty to adulthood: Along-term radiographic study.
European Journal of Orthodontics, v.19, p. 657-668, 1997.
PAULSEN, H.U.; KARLE, A. Computer tomographic and radiographic changes in the
temporomandibular joints of two young adults with occlusal asymmetry, treated with the
Herbst appliance. European Journal of Orthodontics, v.22, n.6, p. 649-656, 2000.
PAULSEN, H.U. et al. CT-scanning and radiographic analysis of temporomandibular joints
and cephalometric analysis in a case of Herbst treatment in late puberty. European Journal
of Orthodontics, v.17, n.3, p. 165-175, 1995.

149
PERINNETTI, G. et al. Treatment effects of removable functional appliances in pre-pubertal
and pubertal Class II patients: a systematic review and meta-analysis of controlled studies.
Plos One, v.10, p. 1-36, Oct. 2015.
PERINNETTI, G. et al. Diagnostic reliability of the cervical vertebral maturation method and
standing height in the identification of the mandibular growth spurt. The Angle
Orthodontist, v.86, p. 599-609, July 2016.
PETERSON, J.E.; McNAMARA, JUNIOR J.A. Temporomandibular joint adaptations
associated with herbst appliance treatment in juvenile rhesus monkeys (Macaca mulatta).
Seminars in Orthodontics, v.9, n.1, p. 12-25, Mar. 2003.
PROFFIT, W.R.; FIELDS, H.W.; MORAY, L.J. Prevalence of malocclusion and orthodontic
treatment need in the United States: estimates from the NHANES III survey. The
International Journal of Adult Orthodontics and Orthognathic Surgery, v.13, n.2, p. 97-
106, 1998.
RABIE, A.B. et al. The correlation of replicating cells and osteogenesis in the condyle during
stepwise advancement. The Angle Orthodontist, v.73, n.4, p. 457-465, 2003.
GUIMARÃES ROSA, J. Grande sertão: veredas. Rio de Janeiro: Nova Fronteira, 1986.
RUELLAS, A.C.O. et al. Comparison and reproducibility of 2 regions of reference for
maxillary regional registration with cone-beam computed tomography. American Journal of
Orthodontics and Dentofacial Orthopedics, v.149, n.4, p. 533-542, Apr. 2016.
RUF, S. Optimal time for treatment with the Herbst appliance. L' Orthodontie française,
v.77, p. 163-167, Mar. 2006.
RUF, S.; PANCHERZ, H. Does bite-jumping damage the TMJ? A prospective longitudinal
clinical and MRI study of Herbst patients. The Angle Orthodontist, v.70, n.3, p. 183-199,
2000.
RUF, S.; PANCHERZ, H. Temporomandibular joint growth adaptation in Herbst treatment: a
prospective magnetic resonance imaging and cephalometric roentgenographic study.
European Journal of Orthodontics, v.20, n.4, p. 375-388, Aug. 1998.
RUF, S.; PANCHERZ, H. Temporomandibular joint remodeling in adolescents and young
adults during Herbst treatment: A prospective longitudinal magnetic resonance imaging and
cephalometric radiographic investigation. American Journal of Orthodontics and
Dentofacial Orthopedics, v.115, n.6, p. 607-618, 1999.
RUF, S.; WÜSTEN, B.; PANCHERZ, H. Temporomandibular joint effects of activator
treatment: a prospective longitudinal magnetic resonance imaging and clinical study. The
Angle Orthodontist, v.72, n.6, p. 527-540, Dec. 2002.

150
SAH, K. et al. The effect of Herbst treatment on amount and direction changes of
temporomandibular join growth: a short-term investigation of cone-beam computed
tomography. International Journal of Oral & Maxillofacial Surgery, v.46, p. 237-237,
Mar. 2017.
SANTOS, R.R. et al. Prevalence of malocclusion and related oral habits in 5- to 6-year-old
children. Oral Health & Preventive Dentistry, v.10, n.4, p. 311-318, 2012.
SERBESIS-TSARUDIS, C.; PANCHERZ, H. ‘‘Effective’’ TMJ and chin position changes in
Class II treatment. The Angle Orthodontist, v.78, n.5, p. 813-818, 2008.
SESSIRISOMBAT, C. A three-dimensional study of craniofacial and airway structures in
skeletal class II treated with RME and Herbst appliance. 2015. (Dissertação de Mestrado).
The University of Sydney, 2015.
SILVA FILHO, O.G.; AIELLO, C.A.; FONTES, M.V. Aparelho Herbst: protocolos de
tratamento precoce e tardio. Revista Dental Press de Ortodontia e Ortopedia Facial, v.10,
n.1, p. 30-45, Jan./Fev.2005.
SILVA, J. et al. Retrospective study of clinical complications during orthodontic treatment
with either a removable mandibular acrylic splint Herbst or with a cantilever Herbst. The
Angle Orthodontist, v.85, n.1, p. 64-71, 2014.
SMITH, B.R.; PARK, J.H.; CEDERBERG, R.A. An evaluation of cone-beam computed
tomography use in postgraduate orthodontic programs in the United States and Canada.
Journal of Dental Education, v.75, n.1, p. 98-106, Jan. 2011.
SOUKI, B.Q. et al. Three-dimensional changes in the mandible and articular fossae
following Herbst appliance therapy: A preliminary CBCT study. Interdisciplinary
Therapy: Using Contemporary Approaches for Complex Cases. Kapila, S e
Goonewardene. Ann Arbor: The University of Michigan, v.51, p.113-134, 2016.
TANG, E.L.; WEI, S.H. Recording and measuring malocclusion: a review of the literature.
American Journal of Orthodontics and Dentofacial Orthopedics, v.103, p. 344-351, 1993.
TYNDALL, D.A.; RATHORE, S. Cone-beam CT diagnostic applications: caries, periodontal
bone assessment, and endodontic applications. Dental Clinics of North America, v.52, p.
825-841, 2008.
VANLAECKEN, R. et al. Treatment effects of the edgewise Herbst appliance: a
cephalometric and tomographic investigation. American Journal of Orthodontics and
Dentofacial Orthopedics, v.130, n.5, p. 582-593, 2006.
WEIWEI, C. et al. Cone beam computed tomography analysis of the bony structure of the
temporomandibular joint during two phase treatment with Herbst appliance. Hua Xi Kou
Qiang Yi Xue Za Zhi, v.34, p. 498-501, Oct. 2016.
WEY, M.C. et al. Stepwise advancement versus maximum jumping with headgear activator.
European Journal of Orthodontics, v.29, n.3, p. 283-293, 2008.

151
YILDIRIM, E.; KARACAY, S.; ERKAN, M. Condylar response to functional therapy with
Twin-Block as shown by cone-beam computed tomography. The Angle Orthodontist, v.84,
n.6, p. 1018-1025, 2014.
ZARB, G.A. et al. O crescimento da articulação temporomandibular e dos músculos da
mastigação. Copenhaga: Editora Santos, 2000.


153
ANEXO A – 1º Parecer Consubstanciado do CEP PUC Minas


155
ANEXO B - 2º Parecer Consubstanciado do CEP PUC Minas


157
ANEXO C - Artigos científicos publicados ou aceitos em periódicos durante o curso de
Doutorado
1. CHEIB, P. L.; CEVIDANES, L. H. S.; RUELLAS, A. C. O.; FRANCHI, L.; OLIVEIRA,
D. D.; BRAGA, W. M.; SOUKI, B. Q. Displacement of the mandibular condyles immediately
after Herbst appliance insertion - 3D assessment. Turkish Journal of Orthodontics, 2016.

158
2. SOUSA, A. A.; CHEIB, P. L.; ANDRADE JUNIOR, I.; OLIVEIRA, D. D.; SOUKI, B.
Q.; CEVIDANES, L. H. S. Comparação de 2 disjuntores na expansão maxilar em pacientes
com fenda labiopalatina: relato de 2 casos. Revista da Sociedade Portuguesa de Estomatologia
e Medicina Dentária, p.116 - 124, 2016.

159
3. SOUKI, B.Q.; VILEFORT, P.L.C.; OLIVEIRA, D.D.; ANDRADE JUNIOR, I.;
RUELLAS, A.C.O.; YATABE, M.S.; NGUYEN, T.; FRANCHI, L.; McNAMARA JUNIOR,
J.A.; CEVIDANES, L.H.S. Three-dimensional skeletal mandibular changes associated with
Herbst appliance treatment. Orthodontics cranio-facial research, v. 20, p. 111-118, May 2017.

160
4. SOUKI, B.Q.; CHEIB, P.L.; ARAUJO, L.F.F.; GONTIJO, H.P.; RUELLAS, A.C.O.;
CEVIDANES, L.H.S. O uso de tomografia computadorizada por feixe cônico em ortodontia:
informações básicas para o clínico. Orthoscience, v.10 (39), p.32-50, Set 2017.

161
5. DE MATTOS, J.M.; PALOMO J.M.; RUELLAS, A.C.O.; CHEIB, P.L.; ELILIWI,
M.; SOUKI, B.Q. Three-dimensional positional assessment of glenoid fossae and mandibular
condyles in patients with Class II subdivision malocclusion. Angle Orthodontist, v. 87, p.
847-854, 2017.

162
6. OKANO, K.S.; CEVIDANES, L.H.S.; CHEIB, P.L.; RUELLAS, A.C.O.; YATABE, M.;
NGUYEN, T.; FRANCHI L.; MCNAMARA J.A.; SOUKI, B.Q. Three-dimensional
assessment of the posterior region of the cranial base following Herbst appliance treatment.
Angle Orthodontist, in press, 2018. (Aceito para publicação).

163
ANEXO D - Capítulos de livros publicados durante o curso de Doutorado
1. SOUKI, BERNARDO Q.; CEVIDANES, L. H. S.; CHEIB, P. L.; MOYSES-BRAGA,
WAGNER FERNANDO; RUELLAS, A. C. O.; FRANCHI, L.; MCNAMARA JUNIOR, J.
Three-dimensional changes in the mandible and articular fossae following Herbst appliance
therapy: A preliminary CBCT study. In: Kapila, S & Goonewardene M. (Org.).
Interdisciplinary Therapy: Using Contemporary Approaches for Complex Cases.1ed, 2016,
v.51, p. 113-134.


165
ANEXO E - Demais produções técnicas feitas durante o curso de Doutorado
1. CHEIB, PAULA L.; SOUKI, B. Q.; ARAUJO, L. F. F.
Odontodrops #1 Dicas clínicas e laboratoriais na confecção do aparelho Herbst, 2016.
(Desenvolvimento de material didático ou instrucional)


167
ANEXO F - Trabalhos publicados em anais de eventos (resumo) durante o curso de
Doutorado
1. VILLORIA, E. M.; CHEIB, P. L.; LEAO, P. L. R.; SOUZA, P. E. A.; SOUKI, B. Q.
ACOMPANHAMENTO TOMOGRÁFICO DA REGRESSÃO DE CISTO
ODONTOGÊNICO APÓS MARSUPIALIZAÇÃO: RELATO DE CASO In: X CONABRO,
2016, Porto de Galinhas. Revista ABRO. Associação Brasileira de Radiologia Odontológica,
2016. v.16. p.154 - 154
2. BARROS, H. M. P.; SOUKI, B. Q.; MATTOS, J. M.; RUELLAS, A. C. O.; PALOMO, J.
M.; CHEIB, P. L. Avaliação 3D da posição da fossa glenóide e côndilos mandibulares em
pacientes com má oclusão de Classe II subdivisão In: 33 Reunião Anual da Sociedade
Brasileira de Pesquisa Odontológica, 2016, Campinas. Brazilian Oral Research. São Paulo:
Faculdade de Odontologia da Universidade de São Paulo, 2016. v.30. p.415-415

168
3. OKANO, K. S.; SOUKI, B. Q.; CHEIB, P. L.; RUELLAS, A. C. O.; CEVIDANES, L. H.
S. Avaliação tridimensional da base posterior do crânio após o uso do aparelho Herbst In: 33
Reunião Anual da Sociedade Brasileira de Pesquisa Odontológica, 2016, Campinas.
Brazilian Oral Research. São Paulo: Faculdade de Odontologia da Universidade de São
Paulo, 2016. v.30. p.418-418
4. SANGALLI, K. L.; FARAH, L. O.; RUELLAS, A. C. O.; CHEIB, P. L.; GRANDE, I. M.
P.; SOUKI, B. Q.; MORO, A. Avaliação tridimensional do posicionamento do côndilo
mandibular após o tratamento com o aparelho Herbst In: 33 Reunião Anual da Sociedade
Brasileira de Pesquisa Odontológica, 2016, Campinas. Brazilian Oral Research. São Paulo:
Faculdade de Odontologia da Universidade de São Paulo, 2016. v.30. p.424-424
5. CHEIB, P. L.; CEVIDANES, L. H. S.; RUELLAS, A. C. O.; SOUKI, B. Q. Mudanças 3D
dentoesqueléticas mandibulares associadas ao aparelho Herbst: um estudo retrospectivo de
caso-controle. In: 33 Reunião Anual da Sociedade Brasileira de Pesquisa Odontológica, 2016,
Campinas. Brazilian Oral Research. São Paulo: Universidade de São Paulo, 2016. v.30.
p.485-485
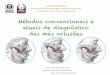


![Dicionário Filosófico [extratos] - cairu.br · 5 7 6ah e˘ ah ˇ e˘ !l ˘˝ ˘ ah9ˇ e.˘˛ ˛˘ ahh e// ahh˙ e/qah 9 # 6 ah # /ahi #˘ ahi #˘ ( ˘0#˘ ˘($ ˘ah # "˘ ah h](https://img.document.onl/doc/110x75/5ba50ecd09d3f2db298c7dd9/dicionario-filosofico-extratos-cairubr-5-7-6ah-e-ah-e-l-.jpg)