Embed Size (px)
Citation preview

Abordagem terapêutica da
Litíase
Mauricio Carvalho

Nenhum financiamento ou
conflito de interesse
• Participação em estudos clínicos e/ou
experimentais subvencionados pela indústria;
• Ser palestrante em eventos patrocinados pela
indústria;
• Ser membro do conselho consultivo ou
diretivo da indústria;
• Participar de comitês normativos de estudos
científicos patrocinados pela indústria;
• Receber apoio institucional da indústria;
• Ter ações da indústria;
• Preparo de textos científicos em periódicos
patrocinados pela indústria

1) Tratamento da cólica renal no Pronto-Socorro;2) Tratamento e eliminação da pedra já formada;3) Tratamento da causa, para prevenir novos
cálculos.

HIPEROXALÚRIA
HIPERPARAT. 1o
HIPERCALCEMIA
(5%)
RENAL
ÓSSEA
INTESTINAL
NORMOCALCEMIA
(95%)
HIPERCALCIÚRIA HIPOCITRATÚRIA
Oxalato de cálcio

Tópicos
• Citrato
– Farmacológico
– Dietético
• Tiazídicos
• Hiperuricosuria x cálculos OxCa
• Nutrição na nefrolitíase
– Novos alvos e objetivos

Terapia com Citrato
Farmacológica
Dietética

Citrato
Estudo Paciente Eficácia Observações
1993
Barcelo
citrato
Cálcio N
+ K-Cit
1990
Butz
Não
selecionado
+ Follow-up
1ano/Na-K-
Cit
1994
Hofbauer
Não
selecionado
_ Sem poder /
Na-K-Cit
1997
Ettinger
Não
selecionado
+ RR 0,35 /
K-Mg-Cit

Barcelo P, Wuhl O, Servitge E, Rousaud A, Pak CYC:J Urol 1993; 150: 1761
Randomized double-blind study of potassium citrate in idiopathic
hypocitraturic calcium nephrolithiasis.
24
31
Adverse reactions to potassium citrate were mild. Only 2 patients in the KCit group and 1 in
the placebo group withdraw from the study.

Citrato
Intolerância gastrointestinal
• 60 mEq de Kcit por dia ↑ citrato urinário ~ 400
mg/dia e o ↑ pH em 0,7 unidadesPak CYC, and Resnick MI: Urol Clin North Am 27: 243–253, 2000
• Taxa de abandono de tratamento –
– 3 meses a 3 anos – 25%
• Potencial ulcerogênico. Complicações GI
– Epigastralgia
– Náuseas, vômitos ,diarréia
– Flatulência, obstipação
• Risco de hipercalemia
– Quando usado concomitante a espironolactona ou
amilorida




Tiazídicos

Tiazídicos diminuem a recorrência
FL Coe et al, Kidney Int, 1988

Randomized clinical trials of thiazide treatment in
hypercalciuric stone formers
Abridged
title
Unprocessed bran and
intermittent thiazide in
prevention of recurrent
stones16
Thiazide for calcium
urolithiasis in patients
with hypercalciuria17
Randomized
prospective study of
indapamide in preventing
calcium stone
recurrences18
The role of thiazides
in the prophylaxis of
recurrent calcium
lithiasis19
Year 1987 1992 1993 2006
Exposures Group A: n: 18; Bran (40 g/d).
Group B n: 14; Bran (40 g/d) +
thiazide (50 mg twice a day)
Group A: n: 93
No specific therapy; Group
B: 82: TrichlormeTZD
(4 mg/d)
Group A: n:25; diet and fluid.
Group B: n:25; diet and fluid +
INDA (2.5 mg/d). Group C: n:25;
diet and fluid + INDA (2.5 mg/d)
+ ALOP (300 mg/d)
Group A: n: 17; no specific
therapy; Group B: n: 21;
HCT (50 mg/d) Group C: n:
14; HCT (50 mg/d) +
potassium citrate (20 mL
Eq/d)
Outcomes Stone/year per patient;
stone-free patients (%)
mean urinary excretion of
lithogenic factors
Stone formation rate
(stones/patient/y)
Stone-free patients (%)
Reduction in stone
formation; Remission rate
Total number of newly
formed stones
Stone formation rate
(stones/patient/y);
stone-free patients (%);
reduction in calciuria and
oxaluria
Stone-free patients (%)
Conclusion Thiazide + bran superior.
3/11 (27%) stones compared
with the 11/17 (65%) in the
bran group.
Stones/patient/year
lower in the thiazide
group (0.13 versus
0.31), with statistically
significant difference.
Urinary calcium decreased
to 50% of the
pretreatment values;
stone rate improved more
in the two drugs Tx groups
Recurrence of 19% (4
cases) and 7% (1 case)
in groups B-C,
respectively compared
to 59% (10 cases) of
group A, p=0.003
MAP Pachaly, CP Baena e M Carvalho.
Therapy of nephrolithiasis: where is the evidence from clinical trials?

Thiazides
• Intestinal calcium absorption may ↓ during long-term
thiazide administration
• During the first few days of administration, there is
frequently a slight rise in total serum calcium
• 20 to 30% increase in UMg excretion which is evident
during the initial period of administration
• A marked ↑ of approximately 50% in zinc excretion
• A marked ↓ in UOx excretion occurred with the
administration of 50 mg of hydrochlorothiazide daily
• HCT dose employed is 50 mg, twice daily (↓ Uca 150
mg/day)

Diminuição da solubilidade do OxCa
pelo ácido úrico
(Salting-out)
Hiperuricosuria x cálculos OxCa

60 pts; Hiperuricosuria; Normocalciuria; Alopurinol 100mg X 3/dia

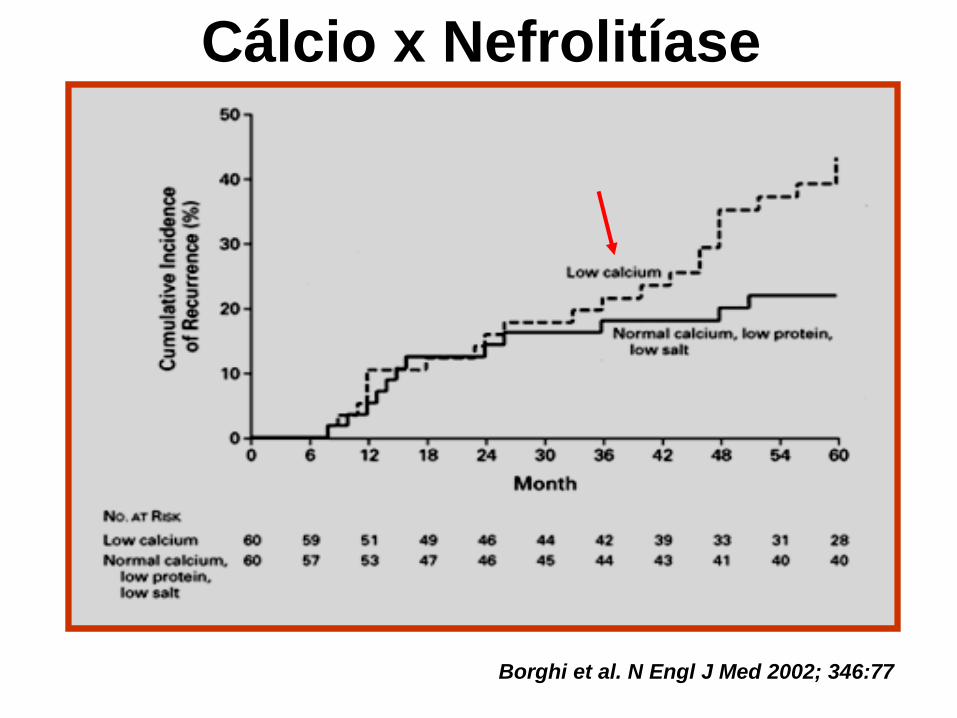
Borghi et al. N Engl J Med 2002; 346:77
Cálcio x Nefrolitíase
Nutrição na nefrolitíase
Novos alvos e objetivos

DASH Score and Stone Risk
0,2
0,4
0,6
0,8
1,0
Q1 Q2 Q3 Q4 Q5
HPFS
NHS I
NHS II
Re
lative
Ris
k
DASH Score
P trend <
0.001
17 21 24 27 31
J Am Soc Nephrol. 2009
Oct; 20(10): 2253–2259.































