-
8/12/2019 Conceitos de Obesidade
1/8
The Concept of Normal Weight Obesity
Estefania Olivero sa , Virend K. Somers a , Ondrej Sochor a , b
,Kashish Goe la , Francisco Lopez-Jimene za ,
a Division of Cardiovascular Diseases, Mayo Clinic, Rochester,
Minnesotab International Clinical Research Center, St. Anne s
University Hospital, Brno, Czech Republic
A R T I C L E I N F O A B S T R A C T
Individuals with normal body weight by body mass index (BMI) and
high body fatpercentage show a high degree of metabolic
dysregulation. This phenomenon, defined asnormal weight obesity, is
associated with a significantly higher risk of developing
metabolicsyndrome, cardiometabolic dysfunction and with higher
mortality. Recently, we have alsoshown that coronary artery disease
patients with normal BMI and central obesity have thehighest
mortality risk as compared to other adiposity patterns. Therefore,
it is important torecognize these high-risk groups for better
adiposity-based risk stratification. There is aneed for an updated
definition of obesity based on adiposity, not on body weight.
2014 Elsevier Inc. All rights reserved.
Keywords:Normal weight obesityObesityMetabolically obese normal
weightCentral obesityBody fat percentage
The Merriam-Webster dictionary defines obesity as a condi-
tion characterized by the excessive accumulation and storageof
fat in the body .1 Obesity is a chronic metabolic disorder
characterized by an increase in the number and/or the size of fat
cells. Global prevalence of obesity has almost doubledsince 1980 2
and has now become an epidemi c3,4 threatening public health. In
2008, more than 1.4 billion adults in theworld were overweight,
from which approximately 200million men and 300 million women were
obese .2 Overweightand obesity represent the fifth leading risk for
global deaths .2
Formerly thought as a problem of high-income
countries,overweight and obesity are becoming more prevalent in
low-and middle-income countries.
The American Heart Association and the American Collegeof
Cardiology guidelines labeled obesity as a major
modifiablecardiovascular disease (CVD) risk factor. Obesity is
associatedwith higher rates of insulin resistance, type 2
diabetesmellitus (DM), hypertension (HTN), dyslipidemia,
coronaryheart disease (CHD), gallbladder disease, obstructive
sleepapnea, non-alcoholic fatty liver disease and some
malignan-cies including endometrial, breast, and colon cancer
.3,4
Obesity is considered an independent risk factor for CVD 5
and is associated with increased mortality in general
healthypopulations .3
Historic perspective of the concept of obesity
Measurement of height and weight was the initial step in
theclinical assessment of overweight and obesity. In 1908,Symonds
reported the results of a large prospective study of weight and
mortality in New Jersey. He registered weight for agiven height and
age, and the influence of excess weight onvitality .6 Subsequently,
obesity was defined in relation todesirable weight, taking in
consideration the actuarial tablesfrom the Metropolitan Life
Insurance Company .7 The conceptused was percent of ideal body
weight. Later on, the Diet andHealth report questioned the approach
of using ideal bodyweigh t8 and suggested that terms like healthy
or good weightranges were associated with decreased mortality .9
After-wards, body mass index (BMI) substituted the assessment of
obesity, calculated as body weight (in kg) divided by height
(in
P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E S
5 6 ( 2 0 1 4 ) 4 2 6 4 3 3
Statement of Conflict of Interest: see page 432. Address reprint
requests to Francisco Lopez-Jimenez, MD, MSc, Division of
Cardiovascular Diseases Mayo Clinic. 200 First St SW
Rochester, MN 55905.E-mail address: [email protected] (F.
Lopez-Jimenez).
0033-0620/$
see front matter 2014 Elsevier Inc. All rights
reserved.http://dx.doi.org/10.1016/j.pcad.2013.10.003
Av a i l a b l e o n l i n e a t w w w. s c i e n c e d i r e c
t . c o m
ScienceDirect
w w w. o n l i n e p c d . c o m
http://dx.doi.org/10.1016/j.pcad.2013.10.003http://dx.doi.org/10.1016/j.pcad.2013.10.003http://dx.doi.org/10.1016/j.pcad.2013.10.003mailto:[email protected]://dx.doi.org/10.1016/j.pcad.2013.10.003http://dx.doi.org/10.1016/j.pcad.2013.10.003mailto:[email protected]://dx.doi.org/10.1016/j.pcad.2013.10.003
-
8/12/2019 Conceitos de Obesidade
2/8
meters) squared. Thei ni ti al u se o f t heindex was in 1842
byQuetelet a Belgianmathematician whonoticed that in peoplehe
considered to have
a normal frame theweight was propor-tional to the heightsquared
.10 In the last3 decades of the 20thcentury, several epi-demiologic
studiesused BMI to prove theassociation betweenadiposity and
mortali-ty, CVD, DM and manyother obesity-relatedcomorbidities.
Withthe help of expertsfrom around the worldwho formed The
Inter-national Obesity TaskForce , in 1997 theWorld Health
Organi-
zation (WHO) came up with the definition of obesity as aBMI 30
kg/m 2.11,12 The definition also described other degrees of
adiposity like overweight and obesity grade 1 and2, although the
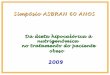
cutoffs chosen were arbitrary. Fig 1shows the classification of
obesity modified by the NationalHeart, Lung and Blood Institute
task force, along with
the associated disease risk with increasing BMI .13
Obesity can be also measured using direct and indirectmeasures
of fatness other than BMI. The methods to estimatebody fat (BF)
include bioelectrical impedance, hydrostaticplethysmography,
isotope dilution techniques, dual x-rayabsorptiometry, skinfold
method, body impedance measureswith over the counter scales, and
air displacementplethysmography .14 Epidemiologic studies have also
demon-strated that central fat distribution, measured with
waistcircumference (WC), waist-to-hip ratio (WHR) and
weight-to-height ratio, is also an important measure of
adiposity-related risk .15
Pitfalls of current BF mass measurements
BMI as a measure of BF became popular and widely usedbecause of
its simplicity and validation in multiple epidemi-ologic studies.
Surprisingly, even though obesity is defined asexcessive adiposity,
there is no consensus on how to defineobesity using fat mass
calculation or fat percentage, other than the effort by the
American Society of Endocrinologistswho defined obesity by BF
percent as >35% in women and>25% in men .16 Direct
measurement of adipose tissue using methods like water-displacement
plethysmography or mag-
netic resonance is too cumbersome to be used in largepopulations
or in clinical practice. Newer methods to measure
fat content like air-displacement plethysmography, DEXA or
electrical bioimpedance have shown to be valid and notnecessarily
expensive.
Although several studies have demonstrated a highcorrelation
between BMI and directly-measured BF, thediagnostic performance of
BMI is not optimal to identifyleanness or excessive BF. We have
tested the accuracy of BMI
for diagnosing obesity in the adult general population using
data from 13,601 individuals from the Third National Healthand
Nutrition Examination Survey .17 Using bioimpedance tocalculate BF
and a BMI >30 kg/m 2 to define obesity, BMI had avery high
specificity (97%) but poor sensitivity (42%) to detectobesity 17,18
Therefore, more than half of the individuals withincreased BF
percentage may be misclassified by BMI. Inindividuals with BMI of
25 kg/m 2, the index had 86%sensitivity and a specificity of 73%. A
meta-analysis of thediagnostic performance of BMI to detect
excessive adiposityusing different techniques as the gold standard
showedsimilar results .18 A recent study demonstrated a wide
rangeof BF % using dual energy x-ray absorptiometry in people
withnormal BMI, ranging from 5.6 to 31.2% in men and from 4.6
to51.1% among women .19 The main limitation of BMI is that itcannot
differentiate BF from lean mass, and central fromperipheral fat.
Therefore, athletes with enhanced bodymuscle mass may be
misclassified as obese when using onlyBMI to diagnose obesity,
whereas people with low lean massbut high BF content may still have
a normal BMI .20
Challenging the simplistic concept of obesity asdefined by
BMI
Over the last 30 years, there have been several new
conceptschallenging the simplistic concept that obesity can
bediagnosed based on weight and height. Numerous studieshave
proposed definitions of the obesity subtypes ( Table 1 ).
Firstly, Ruderman et a l21 challenged the notion thatstandard
weight height tables were the proper way todetermine high-risk
groups for obesity associated disorders.They observed normal weight
individuals suffering from type2 DM, premature CHD, HTN and
hypertriglyceridemia withassociated hyperinsulinemia. They pointed
out that theseabnormalities could not be explained by skinfold
thicknessor adipose mass and hypothesized that it was due to larger
fat cells. The identified metabolically obese, normal
weightindividuals had benefits when they went through programsof
energy restriction and weight loss. If patients werechallenged to a
4 12 week period of diet and exercise therewas metabolic
improvement .22 Some studies suggested thatthe main issue to
explain the metabolic abnormalities inindividuals not particularly
overweight was fat distribution.On the basis of these studies, it
was proposed a scoring method to identify a metabolically obese
normal weightindividual. Depending on the presence of associated
diseasesor biochemical abnormalities related to insulin
resistance,individuals would be assigned a score to base the
diagnosisof metabolically obese normal weight. All of these
mentioned
disturbances predispose the individual to suffer from ,23
as well as making them a susceptible population to suffer
Abbreviations and Acronyms
BF = body fat
BMI = body mass index
CHD = coronary heart disease
CVD = cardiovascular disease
DM = diabetes mellitus
HDL = high-density lipoproteincholesterol
HF = heart failure
HOMA = Homeostasis ModelAssessment
HTN = hypertension
LDL = low-density lipoprotein
NWO = normal weight obesity
WC = waist circumferenceWHO = World HealthOrganization
WHR = waist-to-hip ratio
427P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E
S 5 6 ( 2 0 1 4 ) 4 2 6 4 3 3
-
8/12/2019 Conceitos de Obesidade
3/8
from type 2 DM with a three to four-fold time higher riskthan
control non-obese individuals .24 Specific reversiblefactors appear
to predispose metabolically-obese normal-weight individuals, like
decreased aerobic fitness, physicalactivity energy expenditure
25,26 and a lower level of dietaryrestraint .23
Karelis et a l27 and Dvorak et a l25 realized that insulin
sensitivity was related to body composition and that
bodycomposition could be a major determinant for the
metabolicbehavior of individuals ( Table 2 ). In their review
Karelis et a l27
addressed the differences among the metabolically healthyobese,
the metabolically obese normal weight, the individualat risk of
obesity and the metabolically healthy individual(Table 3 ).
Metabolically healthy obese subjects when com-pared with obese
insulin resistant adults have a healthier metabolic risk profile
and higher disposition index (insulinsensitivity insulin secretion)
.28 These findings challenge theconcept that obesity itself
produces -cell dysfunction. Mostmetabolically obese normal weight
subjects can be identifiedwith risk factors in the familial
background, birth weight,adult onset weight gain and central
adiposity, physicalactivity status, and the presence of related
pathologies .22
In addition to the metabolically obese normal weightphenotype,
other subclassifications of obesity have beendescribed, like
metabolically normal obesity and NWO.
Normal weight obesity: a distinct phenotype linkedto metabolic
dysregulation and inflammation
In 2006, De Lorenzo et a l29 described the association
betweennormal weight and high fat content with metabolic abnor-
malities. The term
NWO
described those individuals withnormal body weight and BMI
(30%). Despite the fact that obesity is defined as excessivebody
adiposity according to the etymology of the word, thereis no
consensus about how to define obesity based on BFcontent or %. Some
investigators have proposed sex- and age-adjusted cut-off values
for NWO. These were defined as thecombination of a normal BMI and
increased BF%: 20 39 years,>19% and >32%; 40 59 years,
>21% and 33% and 60 79 years,
> 24% and 35% for men and women, respectively .30
A currentchallenge when evaluating BF is that there is no
consensusabout thebest cutoff for percent of BF to
defineexcessfatness.The different proposed cutoff points of BF vary
between 20and 25% for men and 30 and 37% for women .20,31,32
Importantly, metabolically obese normal weight individ-uals
likely represent a subset of all NWO people. It is clear thatnot
everybody with NWO has the cluster of metabolicabnormalities.
However, what has not been clearly deter-mined is what extent of
the metabolic dysregulation inmetabolically obese normal weight
people could be solelyexplained by increased amounts of total fat,
a high BF percentor increased visceral fat.
Relationship between NWO, metabolicdysregulation and
inflammation
There is strong evidence linking NWO and metabolicdysregulation.
De Lorenzo et a l29 evaluated 74 women andanalyzed anthropometric
variables, body composition, resting metabolic rate and biohumoral
variables. They found signif-icant differences in high-density
lipoprotein (HDL) betweennormal weight obese and pre-obese-obese
individuals. Therewere significant correlations among CVD risk
indexes, lean of
the right part of the trunk and total cholesterol/HDL (R = 0.69,
p < 0.001) and LDL/HDL (R = 0.72, p < 0.001) and lean
Fig 1 Classification of obesity developed by the National Heart,
Lung and Blood Institute task force, along with the
associateddisease risk with increasing BMI, waist circumference and
waist to hip ratio.
428 P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S
E S 5 6 ( 2 0 1 4 ) 4 2 6 4 3 3
-
8/12/2019 Conceitos de Obesidade
4/8
and resting metabolic rate (R = 0.44, p = 0.022) in normalweight
obese women. Twenty-eight women with high BF(>30%) had
significantly lower metabolic rate and oxygenconsumption compared
to the 20 women with normal BMIand no excess in BF defined as
-
8/12/2019 Conceitos de Obesidade
5/8
obese group, and the concentrations of interleukin-6 andtumor
necrosis factor- were correlated with fat masspercentage in the
normal weight obese .33 The cytokinesconcentrations had an
intermediate value in the NWOindividuals suggesting that this group
was in an earlyinflammatory state .33 Tumor necrosis factor- ,
interleukin-1and interleukin-6 are related to the adipose mass;
conse-quently they are increased in the obese individuals .34
DiRenzo et a l35 studied 60 white Italian women subdivided
asfollows: 20 normal-weight individuals (BMI < 25 kg/m 2 ; FM%25
kg/m 2; FM% >30%). Theydemonstrated that NWO women were in early
inflammatorystatus, as well as in an oxidative stress related to
metabolicdysfunction related to obesity. Reduced glutathione and
nitric
oxide metabolites were significantly lower in
pre-obese-obese(BMI > 25 kg/m2 ; Fat mass > 30%) and normal
weight obesecompared to normal weight individuals .35
Glutathioneshowed a protective role against oxidative and free
radical-mediated injury.
There also was a strong association with reduced gluta-thione
levels and body weight, BMI and fat mass percentage
(R = 0.45, at least p < 0.05); WC (R = 0.33, p < 0.05);
free fatmass (FFM) % (R = 0.45; p < 0.01); interleukin-1 ,
interleukin-6, interleukin-10, interleukin-15 (R = 0.39, 0.33,
0.36, 0.34, respectively, p < 0.05); and triglycerides (R =
0.416,p < 0.05). Lipid peroxide levels negatively correlated to
FFM %(R = 0.413, p < 0.05) and positively correlated to fat
masspercentage (R = 0.408), interleukin-15 (R = 0.502), tumor
ne-
crosis factor- (R = 0.341), insulin (R = 0.412), total
cholesterol(R = 0.4036), low-density lipoprotein cholesterol (R =
0.405),and triglycerides (R = 0.405) [p < 0.05].35
There is a known association between left ventricular
dysfunction and heart failure (HF). However, Kosmala et a l36
realized that most of the studies relating HF and
leftventricular dysfunction did not assess individuals withnormal
BMI but with increased BF content. They designeda study with 168
individuals, from which the normalweight obese subjects
demonstrated left ventricle systolicand diastolic dysfunction,
increased fibrosis intensity(assessed through procollagen type I
carboxyl-terminalpropeptide), impaired insulin sensitivity, and
augmentedpro-inflammatory activation in comparison to the
individualswith normal BF. Those results were consistent with older
studies assessing the link between obesity as measured withBMI, and
changes in myocardial performance .37
Marques-Vidal et a l38 conducted a cross-sectional study in3,213
women and 2,912 men and defined normal weightobesity as a BMI
-
8/12/2019 Conceitos de Obesidade
6/8
dependent on the total amount of BF mass rather than on theBF %.
On the other hand, adiponectin levels were similar between lean and
NWO women .38 Females with NWO hadhigher levels of interleukin-1 ,
interleukin-1 , andinterleukin-8, but similar values of C-reactive
protein,suggesting that the relationship between NWO and
inflam-mation is a complex one. Other studies have shown a
polymorphism within interleukin-1 receptor antagonist genesecond
intron (A2) associated with an increase in interleukin-1 plasma
levels in NWO syndrome .39
Relationship between NWO and metabolicsyndrome(MetS)
There is increased risk for MetS and each one of itscomponents
with NWO. Romero-Corral et a l20 demonstratedthat individuals
classified as NWO had a prevalence of MetS 4-fold higher than
people also with normal BMI but normal BF %.NWO adults also had an
increased prevalence of dyslipidemia,DM, hyperglycemia without DM,
central obesity and HTN.When divided by sex, women were
particularly affected, aswomen in the highest tertile were about 8
times more likely tohave MetS than those in the lowest tertile of
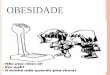
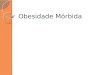
BF. This study alsoproved that the prevalence of MetS and of its
individualcomponents increased as the BF content increased in
menand women ( Figs2 and 3 ). After adjusting forsex, age, and
race/ethnicity, body fat was associated with higher odds of having
MetS (OR = 1.11, 95% CI 1.09 1.14, for each % point of BF).
A cohort study from Brazil including 1,222 subjectsbetween 23
and 25 years old proved the earlier findings thatNWO was associated
with MetS and insulin resistance .40 In
this study, NWO was significantly associated with risk for MetS
(OR = 6.83; 95% CI 2.84 16.47) and with the homeostasismodel
assessment (HOMA) 2 insulin resistance (OR = 3.81;95% CI 1.57
9.28), low insulin sensitivity (OR = 3.89; 95% CI2.39 6.33) and
high insulin secretion (OR = 2.17; 95% CI1.24 3.80). This study
also showed significant associationbetween NWO and some elements of
the MetS, such as highWC (OR = 8.46; 95% CI 5.09 14.04), low HDL
cholesterol (OR =1.65; 95% CI 1.11 2.47) and high triglyceride
levels (OR = 1.93;95% CI 1.02 3.64).
Normal weight with central obesity and prognosisin coronary
artery disease
Increasing central obesity is linked to higher mortality
inadults with or without CHD, even in those with normal BMI .41
Normal weight with central obesity as determined by WC or
WHR in adults with CHD is associated with the highest risk of
mortality ,41,42 compared with subjects with normal BMI andno
central obesity and with obese patients by BMI regardlessof their
central obesity status. Furthermore, the obesityparadox, where
people with CHD and obesity by BMI haveshown better prognosis than
those with normal weight, doesnot occur when obesity is determined
by the fat distribution .41
While higher BMI relates to better prognosis in CHD
patients,higher WC or WHR is directly related to higher mortality
risk.Those findings may be explained at least in part because
BMIhas shown a poor diagnostic accuracy to identify
excessiveadiposity in adults with CHD .43 Hence, WC and WHRmeasured
in CHD patients will better help to stratify anddevelop therapeutic
guidelines for fat loss .41
NWO and mortality.
We have demonstrated that NWO has been associated withincreased
CVD and all-cause mortality .20 Women with NWOwere 2.2 times more
likely to die from CVDs compared withthose with low BF. When women
were classified by tertiles of BF %, the mortality risk increased
as the BF %increased. Theincreased mortality risk was independent
from HTN, DM anddyslipidemia, suggesting that the increased
mortality risk
implicates pathways beyond the traditional
obesity-relatedcomorbidities.
Future directions
NWOmaybe present in approximately 30 million Americans .20
The prevalence of NWO varies from 2% to 28% in women andlessthan
3%in men .32,38 We havescarce information regarding the
determinants of NWO in the general population. Although
Fig 2 Normal weight obesity: metabolic syndrome criteria by body
fat group: men. Fig 3 Normal weight obesity: metabolic syndrome
criteria by body fat group: women.
431P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E
S 5 6 ( 2 0 1 4 ) 4 2 6 4 3 3
http://localhost/var/www/apps/conversion/tmp/scratch_5/image%20of%20Fig%E0%B3%80http://localhost/var/www/apps/conversion/tmp/scratch_5/image%20of%20Fig%E0%B2%80
-
8/12/2019 Conceitos de Obesidade
7/8
environmental factors are probably implicated in the origin of
normal weight central obesity, genetic factors cannot beexcluded.
There is a need for epidemiologic studies assessing the prevalence
of NWO among different ethnic groups andstudies with genotypic and
phenotypic characterization of subjects to elucidate the potential
role of genes in the causeand treatment of NWO.
The definition of obesity has become a dynamic conceptthat has
evolved for the past 5 decades, as the understanding of adipose
tissue continues to evolve too.
However, current evidence suggests that the diagnosis of obesity
at the individual level will at some point include somemeasurement
of BF content and information on fat distribu-tion. The decision
about the diagnostic threshold for fat massor BF % will depend on
optimal cutoffs based on epidemio-logic studies with long-term
follow-up and information onobesity related comorbidities and
mortality.
ConclusionsThediagnosisof obesity hasbeen evolvingover
time.Thecurrentdefinition of obesity by weight and height has been
challengedwith recent evidence showing that BMI-defined obesity may
notaccurately identify all the obesity-related CVD risk. People
withnormal BMI and high BF content are at increased risk for
metabolic dysregulation, systemic inflammation and mortality.The
concept of metabolic obese normal weight overlaps withthe NWO. It
is possible that the metabolic dysregulation seen inmetabolic obese
normal weight individuals may be all related toincreased body
adipositynot detected by BMI. There is a need for studies
addressing the complex interaction among fat content,
distribution and activity, and muscle mass content, and their
effect on metabolism, CVD risk and survival.
Statement of Conflict of Interest
All authors declare that there are no conflicts of interest.
Acknowledgments
Supported in part by the European Regional DevelopmentFund,
project FNUSA-ICRC (Z.1.05/1.1.00/02.0123) and CzechMinistry of
Health (NT13434-4/2012).
R E F E R E N C E S
1. Obesity. (Accessed 6/5/2013, 2013, at
http://www.merriam-webster.com/dictionary/obesity .).
2. Obesity and overweight. Fact sheet No. 311. March
2013.(Accessed 6/5/2013, 2013, at
http://www.who.int/mediacentre/factsheets/fs311/en/ .).
3. Poirier P, Giles TD, Bray GA, et al. Obesity and
cardiovas-cular disease: pathophysiology, evaluation, and effect of
weight loss: an update of the 1997 American HeartAssociation
Scientific Statement on Obesity and Heart
Disease from the Obesity Committee of the Council onNutrition,
Physical Activity, and Metabolism.
Circulation.2006;113:898-918.
4. Pi-Sunyer FX. The obesity epidemic: pathophysiologyand
consequences of obesity. Obes Res. 2002;10(Suppl 2):97S 104S.
5. Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity asan
independent risk factor for cardiovascular disease: a
26-year follow-up of participants in the Framingham HeartStudy.
Circulation. 1983;67:968-977.6. Symonds B. The influence of
overweight and underweight on
vitality. 1908. Int J Epidemiol. 2010;39:951-957.7. Metropolitan
Life Insurance Company. Overweight: its
prevention and significance. Stat Bull Metropol Life Insur
Co.1960;41:6.
8. National Research Council. Diet and health, implications for
reducing chronic disease risk, National Research
Council.Washington, DC: National Academy Press. 1989.
9. Nutrition and your health: dietary guidelines for
Americans.US Department of Agriculture and USDepartment of Health
and Human Services, Home andGarden Bulletin No. 232. In. 3 ed.
Washington, DC.; 1990:273 930.
10. Quetelet LAJ. A Treatise on Man and the Development of
HisFaculties. New York: Burt Franklin. 1968.
11. World Health Organization. Physical status: the use
andinterpretation of anthropometry. Report of a WHO
ExpertCommittee. World Health Organ Tech Rep Ser.
1995;854:1-452.
12. WHO. Obesity: preventing and managing the global
epidemic.Report of a WHO Consultation. WHO Technical Report
Series894. Geneva: World Health Organization. 2000.
13. NHLBI Obesity Education Initiative Expert Panel on
theIdentification, Evaluation, and Treatment of Overweightand
Obesity in Adults. Clinical Guidelines on theIdentification,
Evaluation, and Treatment of Overweightand Obesity in Adults The
Evidence Report. NationalInstitutes of Health. Obes Res.
1998;6(Suppl 2):51S 209S.
14. Cornier MA, Despres JP, Davis N, et al. Assessing adiposity:
ascientific statement from the American Heart
Association.Circulation. 2011;124:1996-2019.
15. Mathieu P, Poirier P, Pibarot P, Lemieux I, Despres JP.
Visceralobesity: the link among inflammation, hypertension,
andcardiovascular disease. Hypertension. 2009;53:577-584.
16. AACE/ACE Obesity Task Force. AACE/ACE position statementon
the prevention, diagnosis, and treatment of obesity.(1998
revision). Endocr Pract. 1998;4:297-349.
17. Romero-Corral A, Somers VK, Sierra-Johnson J, et al.
Accuracyof body mass index in diagnosing obesity in the adult
generalpopulation. Int J Obes. 2008;32:959-966.
18. Okorodudu DO, Jumean MF, Montori VM, et al.
Diagnosticperformance of body mass index to identify obesity as
definedby body adiposity: a systematic review and meta-analysis.
Int J Obes. 2010;34:791-799.
19. Kennedy AP, Shea JL, Sun G. Comparison of the
classificationof obesity by BMI vs. dual-energy X-ray
absorptiometry inthe Newfoundland population. Obesity (Silver
Spring). 2009;17:2094-2099.
20. Romero-Corral A, Somers VK, Sierra-Johnson J, et al.Normal
weight obesity: a risk factor for cardiometabolicdysregulation and
cardiovascular mortality. Eur Heart J.2010;31:737-746.
21. Ruderman NB, Schneider SH, Berchtold P. The
metabolically-obese, normal-weight individual. Am J Clin Nutr.
1981;34:1617-1621.
22. Ruderman N, Chisholm D, Pi-Sunyer X, Schneider S.
Themetabolically obese, normal-weight individual
revisited.Diabetes. 1998;47:699-713.
432 P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S
E S 5 6 ( 2 0 1 4 ) 4 2 6 4 3 3
http://www.merriam-webster.com/dictionary/obesityhttp://www.merriam-webster.com/dictionary/obesityhttp://www.who.int/mediacentre/factsheets/fs311/en/http://www.who.int/mediacentre/factsheets/fs311/en/http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0010http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0010http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0010http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0010http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0010http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0010http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0010http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0015http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0015http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0015http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0015http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0015http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0015http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0020http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0020http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0020http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0020http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0175http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0175http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0175http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0175http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0025http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0025http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0025http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0180http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0180http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0185http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0185http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0185http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0185http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0185http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0190http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0190http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0190http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0030http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0030http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0030http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0030http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0035http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0035http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0035http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0035http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0035http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0040http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0040http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0040http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0040http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0040http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0200http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0200http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0200http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0200http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0200http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0045http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0045http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0045http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0045http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0045http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0045http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0050http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0050http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0050http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0050http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0050http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0050http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0055http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0055http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0055http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0055http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0055http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0065http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0065http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0065http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0065http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0065http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0065http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0065http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0060http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0055http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0055http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0055http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0055http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0050http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0050http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0050http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0050http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0045http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0045http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0045http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0045http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0200http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0200http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0200http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0040http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0040http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0040http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0035http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0035http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0035http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0030http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0030http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0030http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0195http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0190http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0190http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0190http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0185http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0185http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0185http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0180http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0180http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0025http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0025http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0025http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0175http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0175http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0175http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0020http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0020http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0015http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0015http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0015http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0015http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0010http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0010http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0010http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0005http://www.who.int/mediacentre/factsheets/fs311/en/http://www.who.int/mediacentre/factsheets/fs311/en/http://www.merriam-webster.com/dictionary/obesityhttp://www.merriam-webster.com/dictionary/obesity
-
8/12/2019 Conceitos de Obesidade
8/8
23. Conus F, Allison DB, Rabasa-Lhoret R, et al. Metabolicand
behavioral characteristics of metabolically obese butnormal-weight
women. J Clin Endocrinol Metab. 2004;89:5013-020.
24. Meigs JB, Wilson PW, Fox CS, et al. Body mass
index,metabolic syndrome, and risk of type 2 diabetes or
cardiovascular disease. J Clin Endocrinol Metab.
2006;91:2906-2912.
25. Dvorak RV, DeNino WF, Ades PA, Poehlman ET.
Phenotypiccharacteristics associated with insulin resistance in
meta-bolically obese but normal-weight young women.
Diabetes.1999;48:2210-2214.
26. Ruderman NB, Berchtold P, Schneider S.
Obesity-associateddisorders in normal-weight individuals: some
speculations.Int J Obes. 1982;6(Suppl 1):151-157.
27. Karelis AD, St-Pierre DH, Conus F, Rabasa-Lhoret R,
PoehlmanET. Metabolic and body composition factors in subgroups of
obesity: what do we know? J Clin Endocrinol Metab.
2004;89:2569-2575.
28. Succurro E, Marini MA, Frontoni S, et al. Insulin secretion
inmetabolically obese, but normal weight, and in
metabolicallyhealthy but obese individuals. Obesity (Silver
Spring). 2008;16:1881-1886.
29. De Lorenzo A, Martinoli R, Vaia F, Di Renzo L. Normal
weightobese (NWO) women: an evaluation of a candidate newsyndrome.
Nutr Metab Cardiovasc Dis. 2006;16:513-523.
30. Gallagher D, Heymsfield SB, Heo M, Jebb SA, Murgatroyd
PR,Sakamoto Y. Healthy percentage body fat ranges: an approachfor
developing guidelines based on body mass index. Am J ClinNutr.
2000;72:694-701.
31. Romero-Corral A, Montori VM, Somers VK, et al. Associationof
bodyweight with total mortality and with cardiovascular events in
coronary artery disease: a systematic review of cohort studies.
Lancet. 2006;368:666-678.
32. Marques-Vidal P, Pecoud A, Hayoz D, et al. Prevalence of
normal weight obesity in Switzerland: effect of variousdefinitions.
Eur J Nutr. 2008;47:251-257.
33. De Lorenzo A, Del Gobbo V, Premrov MG, Bigioni M, Galvano
F,Di Renzo L. Normal-weight obese syndrome: earlyinflammation? Am J
Clin Nutr. 2007;85:40-45.
34. Hauner H. Secretory factors from human adipose tissue
andtheir functional role. Proc Nutr Soc. 2005;64:163-169.
35. Di Renzo L, Galvano F, Orlandi C, et al. Oxidative stress
innormal-weight obese syndrome. Obesity (Silver
Spring).2010;18:2125-2130.
36. Kosmala W, Jedrzejuk D, Derzhko R, Przewlocka-Kosmala
M,Mysiak A, Bednarek-Tupikowska G. Left ventricular
functionimpairment in patients with normal-weight
obesity:contribution of abdominal fat deposition, profibrotic
state,reduced insulin sensitivity, and proinflammatory
activation.
Circ Cardiovasc Imaging. 2012;5:349-356.37. Wong CY,
O'Moore-Sullivan T, Leano R, Byrne N, Beller E,Marwick TH.
Alterations of left ventricular myocardialcharacteristics
associated with obesity. Circulation. 2004;110:3081-3087.
38. Marques-Vidal P, Pecoud A, Hayoz D, et al. Normal
weightobesity: relationship with lipids, glycaemic status, liver
enzymes and inflammation. Nutr Metab Cardiovasc
Dis.2010;20:669-675.
39. Di Renzo L, Bigioni M, Del Gobbo V, et al. Interleukin-1
(IL-1)receptor antagonist gene polymorphism in normal weightobese
syndrome: relationship to body composition and IL-1alpha and beta
plasma levels. Pharmacol Res. 2007;55:131-138.
40. Madeira FB, Silva AA, Veloso HF, et al. Normal weight
obesityis associated with metabolic syndrome and insulin
resistancein young adults from a middle-income country. PLoS
One.2013;8:e60673.
41. Coutinho T, Goel K, Correa de Sa D, et al. Central obesity
andsurvival in subjects with coronary artery disease: a
systematicreview of the literature and collaborative analysis
withindividual subject data. J Am Coll Cardiol.
2011;57:1877-1886.
42. Coutinho T, Goel K, Correa de Sa D, et al. Combining
bodymass index with measures of central obesity in theassessment of
mortality in subjects with coronary disease:role of normal weight
central obesity . J Am Coll Cardiol.2013;61:553-560.
43. Romero-Corral A, Somers VK, Sierra-Johnson J, et al.
Diag-nostic performance of body mass index to detect obesity
inpatients with coronary artery disease. Eur Heart J. 2007;28:
2087-2093.44. Kim JY, Han SH, Yang BM. Implication of
high-body-fat
percentage on cardiometabolic risk in middle-aged,
healthy,normal-weight adults. Obesity (Silver Spring).
2013;21(8):1571-1577.
433P R O G R E S S I N C A R D I O V A S C U L A R D I S E A S E
S 5 6 ( 2 0 1 4 ) 4 2 6 4 3 3
http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0070http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0070http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0070http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0070http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0070http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0070http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0075http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0075http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0075http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0075http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0075http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0075http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0080http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0080http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0080http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0080http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0080http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0085http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0085http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0085http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0085http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0090http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0090http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0090http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0090http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0090http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0090http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0095http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0095http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0095http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0095http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0095http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0095http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0100http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0100http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0100http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0100http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0100http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0105http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0105http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0105http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0105http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0105http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0105http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0110http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0110http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0110http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0110http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0110http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0110http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0115http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0115http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0115http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0115http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0115http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0120http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0120http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0120http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0120http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0120http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0125http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0125http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0125http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0125http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0130http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0130http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0130http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0130http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0140http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0140http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0140http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0140http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0140http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0140http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0145http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0145http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0145http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0145http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0145http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0150http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0150http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0150http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0150http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0150http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0150http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0155http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0155http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0155http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0155http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0155http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0160http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0160http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0160http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0160http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0160http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0160http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0170http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0170http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0170http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0170http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0170http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0170http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0205http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0205http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0205http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0205http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0205http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0205http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0205http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0205http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0205http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0205http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0170http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0170http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0170http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0170http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0165http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0160http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0160http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0160http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0160http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0155http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0155http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0155http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0155http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0150http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0150http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0150http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0150http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0145http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0145http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0145http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0145http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0140http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0140http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0140http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0140http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0135http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0130http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0130http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0130http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0125http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0125http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0120http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0120http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0120http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0115http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0115http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0115http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0110http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0110http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0110http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0110http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0105http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0105http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0105http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0105http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0100http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0100http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0100http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0095http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0095http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0095http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0095http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0090http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0090http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0090http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0090http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0085http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0085http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0085http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0080http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0080http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0080http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0080http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0075http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0075http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0075http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0075http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0070http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0070http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0070http://refhub.elsevier.com/S0033-0620(13)00176-X/rf0070