Upload
eduardo-soares
View
213
Download
0
Embed Size (px)
Citation preview
8/13/2019 GrandeQueimado
1/15
http://jic.sagepub.com/Journal of Intensive Care Medicine
http://jic.sagepub.com/content/26/4/223Theonline version of this article can be found at:
DOI: 10.1177/0885066610390869
2011 26: 223J Intensive Care Med
Kevin R. Kasten, Amy T. Makley and Richard J. KaganUpdate on the Critical Care Management of Severe Burns
Published by:
http://www.sagepublications.com
can be found at:Journal of Intensive Care MedicineAdditional services and information for
http://jic.sagepub.com/cgi/alertsEmail Alerts:
http://jic.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://jic.sagepub.com/content/26/4/223.refs.htmlCitations:
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/content/26/4/223http://jic.sagepub.com/content/26/4/223http://jic.sagepub.com/content/26/4/223http://www.sagepublications.com/http://jic.sagepub.com/cgi/alertshttp://jic.sagepub.com/cgi/alertshttp://jic.sagepub.com/subscriptionshttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsPermissions.navhttp://jic.sagepub.com/content/26/4/223.refs.htmlhttp://jic.sagepub.com/content/26/4/223.refs.htmlhttp://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/content/26/4/223.refs.htmlhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsReprints.navhttp://jic.sagepub.com/subscriptionshttp://jic.sagepub.com/cgi/alertshttp://www.sagepublications.com/http://jic.sagepub.com/content/26/4/223http://jic.sagepub.com/8/13/2019 GrandeQueimado
2/15
Update on the Critical CareManagement of Severe Burns
Kevin R. Kasten, MD1
, Amy T. Makley, MD1
, andRichard J. Kagan, MD, FACS1,2
Abstract
Care of the severely injured patient with burn requires correct diagnosis, appropriately tailored resuscitation, and definitivesurgical management to reduce morbidity and mortality. Currently, mortality rates related to severe burn injuries continue to
steadily decline due to the standardization of a multidisciplinary approach instituted at tertiary health care centers. Promptand accurate diagnoses of burn wounds utilizing Lund-Browder diagrams allow for appropriate operative and nonoperative
management. Coupled with diagnostic improvements, advances in resuscitation strategies involving rates, volumes, and fluidtypes have yielded demonstrable benefits related to all aspects of burn care. More recently, identification of comorbid con-
ditions such as inhalation injury and malnutrition have produced appropriate protocols that aid the healing process in severelyinjured patients with burn. As more patients survive larger burn injuries, the early diagnosis and successful treatment of sec-ondary and tertiary complications are becoming commonplace. While advances in this area are exciting, much work to elu-
cidate immune pathways, diagnostic tests, and effective treatment regimens still remain. This review will provide an update onthe critical care management of severe burns, touching on accurate diagnosis, resuscitation, and acute management of this
difficult patient population.
Keywords
burn, ICU, resuscitation, inhalation, sepsis, nutrition
Received January 8, 2010, Received Revised February 19, 2010. Submitted March 25, 2010.
Introduction
Burn injuries account for 500 000 medical visits annually, of
which 40 000 require hospitalization.1 A total of 67% of
reported burns in the United States involve less than 10%
total body surface area (TBSA) with a mortality rate under
0.5%. Proper diagnosis and treatment by emergency room
physicians and general practitioners is vital for good long
term outcomes.1-4 In those patients requiring hospitalization,
appropriate resuscitation, nutritional support, and early surgi-
cal treatment can minimize morbidity and mortality rates,5
especially when treatment occurs in one of the 125 hospitalswith specialized burn centers.1 The evolution of burn
management in the context of specialized care in dedicated
treatment centers has led not only to an overall decrease in
burn-related mortality, but also to a marked increase in the
LA50 (mean extent of burn associated with 50% mortality)
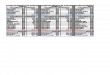
for burn injuries from 40% to >90% TBSA (Figure 1).6-9
Whether treating a burned individual as inpatient or outpati-
ent, appropriate knowledge of burn shock and resuscitation,
nutrition requirements, and wound care will aid the clinician
in the management of the patient.
Evaluation of the Burn Wound
The skin is composed of 2 distinct layers and provides protec-
tion against fluid loss, mechanical damage, and infection. The
epidermis consists of keratinocytes, melanocytes, and
Langerhans cells, while the dermis consists of structural pro-
teins and cells responsible for tensile strength.10 Blood vessels,
hair follicles, and sweat glands are rooted in the dermis. Preser-
vation of these dermal structures following superficial injury is
responsible for the regeneration of epidermal cells required for
primary healing.11
The depth and extent of injury depend on the mechanism ofburn and duration of exposure to the heat source. Scald burns
are associated with a robust pro-inflammatory response leading
1 Department of Surgery, University of Cincinnati, Cincinnati, OH, USA2 Shriners Hospitals for Children-Cincinnati, OH, USA
Corresponding Author:
Richard J. Kagan, Shriners Hospitals for Children, University of Cincinnati
College of Medicine, 3229 Burnet Avenue, Cincinnati, OH 45229, USA
Email: [email protected]
Journal of Intensive Care Medicine
26(4) 223-236
The Author(s) 2011
Reprints and permission:
sagepub.com/journalsPermissions.nav
DOI: 10.1177/0885066610390869
http://jicm.sagepub.com
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
3/15
to increased systemic complications,12 while flame burns are
often associated with an increased incidence of inhalation
injury, an independent risk factor for mortality.5,11 Chemical
burns involve prolonged tissue damage even after removal of the
inciting agent, and in the case of hydrofluoric acid, can produce
life-threatening electrolyte abnormalities. Electrical burns
require close evaluation for cardiac abnormalities and compart-
ment syndrome due to muscle necrosis. Regardless of mechan-
ism, outcomes are directly influenced by burn depth, % TBSA
involvement, patient age, and the ability of the treating clinician
to properly assess and manage all aspects of the burn injury.
First-degree burns are characterized by erythematous
changes, lack of blistering, and significant pain. Wounds
blanch easily on examination and heal within 2 to 3 days fol-
lowing desquamation of dead cells. Scarring is rare and these
injuries should not be included in the estimate of burn size.11
Superficial partial-thickness burns involve the entire
epidermis, typically forming fluid-containing blisters at the
dermal-epidermal junction. Wounds are erythematous, wet-appearing, painful, and blanch with pressure. As the deeper
dermis is left undamaged, wounds heal within 2 weeks without
the need for skin grafting.11 Superficial and deep partial-
thickness burns merit distinction because deep partial-
thickness burns behave clinically like third-degree burns. Deep
partial thickness burns blister, but the blister base will have a
mottled pink and white appearance due to partially damaged
blood vessels. These wounds do not easily blanch and are less
painful than superficial burns due to concomitant nerve injury.
Some burn surgeons advocate initial monitoring of these areas
for up to 14 days to allow wound demarcation, resulting in
fewer operations and less-extensive grafting. Rarely, wounds
heal without surgical intervention, but remain at risk for
developing hypertrophic burn scars and/or contractures.11
Full-thickness, or third-degree, burns are defined by complete
involvement of all skin layers and require definitive surgical
management. These wounds are white, cherry red, brown or
black in color, and do not blanch with pressure. They are typi-
cally insensate from superficial nerve injury.
The calculated% TBSA is an independent risk factor corre-
lating with length of hospital stay and mortality5
; however, the
extent of burn injury is overestimated by up to 75% of initial
care providers.13 Incorrect wound extent calculation leads to
over-resuscitation, inappropriate transfer to burn centers, and
poor use of limited resources.14 Burn diagrams, the rule of
nines, and using the palm and fingers of the patients hand
to estimate 1% of normal body surface area are methods for
burn size estimation.15 The rule of nines is a rough estima-
tion of adult body surface area which often overestimates burn
size in children, supporting the need for age-specific body surfacearea charts such as the Lund Browder diagram.16 (Figure 2).
Newer methods to calculateburn surfacearea using computerized
imaging, 2- and 3-dimensional graphics, and body contour repro-
ductions are currently being researched to improve accuracy in
initial wound assessment.17
Early Management and Resuscitation
of Burn Injuries
Approximately 10% of burns present with additional traumatic
injuries, so all patients should be evaluated and managed using
Figure 1. Schematic view of increased LA50over time.A representation of the developments in burn care over the past 70 years thathave allowed for a steady increase in total body surface area (TBSA) burn size from which 50% of patients will survive.
224 Journal of Intensive Care Medicine 26(4)
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
4/15
Advanced Burn Life Support protocols.11 Burn wounds are
initially washed with tepid water18 following removal of the
heat source. Chemical burns are copiously irrigated for a min-
imum of 15 minutes. Ice or iced water increases tissue damage
and is contraindicated due to the risk of hypothermia in patients
sustaining extensive burns.19,20 Electrical injuries mandate tai-
lored evaluation given the propensity for compartment syn-
drome, cardiac dysrhythmias, muscle necrosis, and
multiorgan system involvement.21 Approximately 60% to
70% of burns seen in emergency departments involve less than
10% TBSA and are treated with minor debridement, oral
hydration, topical wound care, and outpatient follow-up.22
Patients who fail outpatient therapy or require supplemental
nutrition or hydration need continued care as inpatients. In such
cases, the optimal treatment and management of large or com-
plicated burn injuries is in a high volume center.11,23 Current
American Burn Association (ABA) guidelines recommend the
transfer of patients meeting specific criteria, including patients
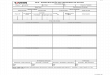
Figure 2. Shriners Hospitals for Children Burn Diagram (Lund-Browder). This adaptation of the Lund-Browder diagram is utilized in ourhospital for estimation of depth and extent of burn in the acute patient.
Kasten et al 225
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
5/15
at extremes of age, large burns, or burns involving critical
anatomy. Prior to transfer, wounds should be covered with
clean, dry material or nonadherent gauze.24 The use of wet
dressings should be avoided to prevent development of
hypothermia in patients with large burn wounds.23 Tetanus pro-
phylaxis, appropriate pain control, and placement of a urinary
catheter in patients being actively resuscitated are all necessary
prior to transport.
Burn Resuscitation
Delay in resuscitation increases mortality following severe
burn injury.5 Intravenous access can be obtained peripherally
with small burns but requires central placement for most burns
greater than 20% TBSA. Balanced crystalloid infusion should
begin after intravenous access is gained, customarily using the
Parkland or modified Brooke formulas as initial guidance. The
Parkland formula was developed in the 1970s by Baxter and
Shires who discovered that resuscitating with a higher volume
in the first 8 hours improved cardiac output.25 Pruitt et al
altered the original Brooke formula to demonstrate that a lower
volume of fluid achieves the same endpoints of resuscitation as
the Parkland formula.25
The modified Brooke formula calls for
2 mL/kg per%TBSA burn of balanced salt solution over the
first 24 hours following injury, while the Parkland formula
recommends 4 mL/kg per %TBSA burn. Although both
formulas call for the subsequent titration of fluid rates, in a
comparative analysis the Parkland formula more often resulted
in over-resuscitation and was an independent risk factor for
mortality.26 However, a separate comparative study found no
clinical differences in outcomes between patients resuscitated
using these 2 formulas.27
Consensus fluid resuscitation by standardized formula has
not been reached.25
At our institution, resuscitation includesthe administration of estimated basal fluid requirements in
addition to the replacement of extensive fluid losses secondary
to burn injury (Table 1). Regardless of the resuscitation for-
mula used, all rely on accurate assessment of extent and depth
of burn and prompt tailoring of the infusion rate to the individ-
ual patient. Resuscitation should be titrated to clinical end-
points including urine output (30-50 mL per hour in adults
and 0.5-1 mL per kg per hour in children26) and hemodynamic
parameters.25 Evaluation of hemodynamic parameters custo-
marily involves cardiac monitoring, continuous pulse oxime-
try, and invasive or noninvasive blood pressure measurement.
Swan-Ganz catheters have fallen out of favor in the
management of ICU patients but may be helpful in monitoring
the resuscitation of the acute burn patient. Newer products such
as the NICO (Philips Respironics) and Vigileo Monitor
(Edwards Lifesciences) allow measurement of cardiac output
and other systemic parameters in patients with burn via
end-tidal carbon dioxide and an arterial line, respectively.28,29
Noninvasive methods of cardiac output measurement include
esophageal Doppler and pulse contour cardiac output, bothdemonstrating results comparable to invasive techniques.30
To help avoid the complications of inadequate or excessive
resuscitation, current research is examining the utility and effi-
cacy of closed-loop autonomous resuscitation.31
Historically, initial resuscitation formulas called for the use
of albumin during the first 24 hours following injury as an
adjunct to crystalloid.25 This was advocated because serum
protein levels decrease rapidly after burn injury, sometimes
resulting in crystalloid resuscitation failure.32 In fact, patients
receiving colloid as part of their resuscitation require less crys-
talloid and total fluid compared to resuscitation with crystalloid
only.33 However, recent evidence demonstrates colloid resusci-
tation does not affect mortality and is more expensive thancrystalloid solutions.34 The theoretical reduction in complica-
tions and mortality from colloid use has not been proven in pro-
spective human trials and is only used in patients unresponsive
to resuscitation with crystalloid.
Complications of Resuscitation
Delayed or inadequate resuscitation results in poor perfusion to
both vital organs and the evolving burn wound itself. This can
lead to necrosis of previously viable tissue, along with progres-
sion of superficial burns to deeper injuries requiring grafting.35
A recent review of the literature demonstrates that a significantproportion of burn injuries are resuscitated with fluid volumes
in excess of that calculated by the Parkland formula, mostly
due to the use of bolus therapy (ie, ATLS, PALS).32,36 The
development of compartment syndromes in the extremities,
torso, or abdomen has been linked to the presence of deep,
full-thickness circumferential burns and the volume of fluid
infused.37 The systemic inflammatory response associated with
larger burns leads to microcirculatory leak, vasodilatation, and
decreased cardiac output and contractility.38 Clinical suspicion
is supported by findings of delayed capillary refill, cyanosis,
paresthesias, and diminished pulses. Compartment pressures
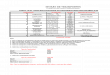
Table 1. Estimated Fluid Resuscitation Requirements for a 12 Year Old Child with 25% Total Body Surface Area Scald Burns. Hourly fluidadministration is guided by the response to treatmenta
Shriners HospitalCincinnati Parkland Formula Modified Brooke Formula
First 8 Hours Second 16 Hours First 8 Hours Second 16 Hours First 8 hours Second 16 Hours
3550 cc/LR 3550 cc/LR 2500 cc/LR 2500 cc/LR 1250 cc/LR 1250 cc/LR
443.8 cc/h 221.9 cc/hr 312.5 cc/h 156.3 cc/h 156.3 cc/h 78.1 cc/ha Initial vital signs in the ER include a weight of 50 kg, height of 145 cm, heart rate of 130 bpm, blood pressure of 90/45, and respiratory rate of 23 with an oxygensaturation of 94% on room air. The following are indicated resuscitation regimens, all titrated based on the patients urine output.
226 Journal of Intensive Care Medicine 26(4)
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
6/15
can be measured by placement of an 18-g needle connected to
an arterial pressure transducer under the eschar into the subfas-
cial tissue. Pressures above 30 mm Hg in any compartment are
considered diagnostic. Treatment necessitates decompression
via escharotomy and/or fasciotomy by experienced practi-
tioners. Escharotomy includes incision along the full length
of eschar with extension into viable unburned tissue, typicallyusing electrocautery. Fasciotomies involve the surgical open-
ing of the full length of fascial compartments. In both cases,
a tissue bulge is often noted indicating adequate release of com-
partment pressure. The success of these procedures can be
quantified by measuring both prerelease and postrelease pres-
sures using a bedside manometric device. While escharotomies
are commonly performed at the bedside using mild sedation,
fasciotomies may need to be performed in an operating room
under general anesthesia. Due to increased morbidity from
withheld, delayed, or incorrectly executed procedures, these
procedures should only be performed by experienced practi-
tioners at the time of diagnosis.39
Abdominal distention, oliguria, and difficulties withmechanical ventilation may signal development of an abdom-
inal compartment syndrome (ACS). Abdominal compartment
syndrome significantly decreases perfusion to vital organs
including the small and large bowel, liver, and kidneys, contri-
buting to the development of multisystem organ failure.25 Early
recognition of abdominal hypertension through serial bladder
pressure evaluation40 can allow for timely decompressive
laparotomy and avoidance of the sequelae caused by prolonged
tissue ischemia. Percutaneous drainage with peritoneal dialysis
catheters may be an effective alternative to laparotomy, pre-
venting the significantly increased morbidity and mortality
related to fluid loss through an open abdomen.
Inhalation Injury
The development of pulmonary complications has been attrib-
uted to both excessive fluid resuscitation.41 and systemic
inflammation resulting in third spacing, accumulation of inter-
stitial edema, and symptoms of ARDS.42 The presence of inha-
lation injury creates an increased fluid requirement, further
complicating the resuscitation and management of a disease
process predictive of respiratory failure and increased mortal-
ity.5,11,34,43-51
The lower airway, consisting of the tracheobronchial tree
and lung parenchyma, is rarely injured by heated dry air dueto reflexive vocal cord closure and the evaporative cooling
capacity of the upper airway.52,53 Inhaled toxins activate alveo-
lar macrophages, initiating direct cellular damage54 with air-
way hyperemia visible shortly after injury. Inhalants also
induce an inflammatory response in the pulmonary parench-
yma with disruption of surfactant synthesis and worsening lung
compliance.55 Reactive oxygen species (ROS) are molecules
synthesized by phagocytic cells such as macrophages and neu-
trophils that increase vascular permeability with subsequent
extrusion of fluid, increased tissue edema, formation of airway
casts, and ultimately airway obstruction.56 Loss of ciliary
action in the respiratory mucosa can lead to an increased
incidence of pulmonary infections.48
Diagnosis of Inhalation Injury
Closed-space burns involving steam, combustibles, hot gases
or explosions should alert the treating physician to possible air-way injury. Inhalation injury may be present without evidence
of cutaneous injury. The physical exam should include inspec-
tion for soot in the oropharynx, carbonaceous sputum, singed
nasal or facial hairs, and face or neck burns. Signs of respira-
tory distress including wheezing, stridor, tachypnea, or hoarse-
ness, along with altered mental status, agitation, anxiety, or
obtundation, are strongly suggestive of inhalation injury.
Patients may develop progressive respiratory failure upon com-
pletion of resuscitation, so clinical suspicion should remain ele-
vated to allow prompt diagnosis.
As noninvasive monitoring of pulse oximetry in patients
with burn having inhalation injuries can be misleading, labora-
tory and invasive studies are helpful diagnostic adjuncts.Arterial blood gas (ABG) analysis may indicate a component of
inhalation injury with a PaO2:FiO2ratio < 300 upon completion
of resuscitation.57 Albeit controversial, this ratio has been
proposed as an indicator of poor outcome in patients with
burn.58-61 The half-life of carbon monoxide (CO) is 240 to 320
minutes, decreasing to 40 to 80 minutes with 100% normobaric
oxygen,62 so interpretation of carboxyhemoglobin values should
be correlated with elapsed time from injury and oxygen therapy
provided. If concerned, blood cyanide levels should be drawn,
carefully interpreted, and treatment initiated using amyl nitrate
perles, 10% sodium nitrite, and 25% sodium thiosulfate.63,64
Chest x-ray and computed tomography scans are insensitive
for inhalation injury diagnosis due to a relatively normal lung
and airway appearance early in the clinical course.65,66
Fiber-
optic bronchoscopy is the gold standard for diagnosis as direct
visualization of the supra- and infraglottic airway allows for
quantification of hyperemia, edema, and carbonaceous mate-
rial. Fiberoptic bronchoscopy can be therapeutic via removal
of excess exudate, plugs or casts, and placement of an endotra-
cheal tube (ETT) or nasotracheal tube (NTT).67
Management of Inhalation Injury
With suspected inhalation injury, 100% oxygen should be ini-
tiated immediately with the duration of treatment dictated bythe patients condition and the return of the carboxyhemoglo-
bin to normal levels, or below 10%.68,69 Vascular carboxyhe-
moglobin decreases much more rapidly with oxygen therapy
than carboxymyoglobin, especially in the context of continued
treatment with 100% FiO2. This is postulated to promote tissue
washout which may actually increase tissue levels of carbon
monoxide.70 Additionally, as cardiac muscle contains myoglo-
bin, tissue washout may possibly contribute to myocardial
hypoxia.70 Because of this, we do not advocate sustained high
inspiration oxygen concentration in the treatment of CO poi-
soning once carboxyhemoglobin levels have normalized.
Kasten et al 227
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
7/15
Rapid displacement of carboxyhemoglobin through hyper-
baric oxygen (HBO) therapy has also been advocated due to the
neurologic sequelae related to CO poisoning. Unfortunately,
there is a paucity of evidence-based literature for HBO use with
regard to triggers for the initiation of therapy, the duration and
intensity of therapy, and the clinical benefit of such treat-
ment.71 Additionally, the risk of complication from barotrauma
in patients with burn having suspected inhalation injury, com-
bined with the risk of monitoring patients with severe burns
inside the chamber, likely outweighs any perceived benefit
from this therapy. Further studies are needed to fully address
the role of HBO therapy in patients with severe burns and/or
inhalation injuries.
Continuous pulse oximetry may be accurately utilized once
carboxyhemoglobin levels normalize. Inhalation injuries can
quickly progress to obstruction, hypoxia, and death, with lim-
ited ability to intubate late in the disease course, so timely
establishment of a definitive airway is required (Figure 3).
Early tracheostomy should be considered in any patient with
a projected need for mechanical ventilation longer than 2
weeks. Percutaneous tracheostomy placement in burn patients
was associated with lower complication rates and cost com-
pared to open tracheostomy in a small, historically controlled
study.72
The question of open versus percutaneous tracheost-omy is an important one and requires further exploration
through randomized controlled trials.
Patients with inhalation injury may require nonstandard
methods of ventilation such as volumetric diffusive respiratory
(VDR) and airway pressure release ventilation (APRV) modes.
Volumetric diffusive respiratory involves progressive accumu-
lation of subtidal breaths and passive exhalation once a set air-
way pressure is met.73 Increased PaO2, PaO2:FiO2 ratio, and
decreased mean airway pressure have been demonstrated using
this mode, all without adversely affecting hemodynamics.73,74
This modality may also decrease the incidence of pneumonia
and mortality compared to individuals treated with conven-
tional modes of ventilation.75-77 Airway pressure release venti-
lation uses high and low PEEP to provide adequate
oxygenation and recruitment of closed alveoli. Benefits include
reduced barotrauma, improved oxygenation and ventilation due
to improved V:Q matching, and decreased sedation and paraly-
sis requirement. In those patients refractory to conventionalventilation strategies, the use of venovenous extracorporeal
oxygenation (ECMO) is an option where available. While non-
survivors were shown to have greater peak and mean airway
pressures prior to onset of extracorporeal life support
(ECLS).78 scattered reports throughout the literature show min-
imal improvement in mortality.79-81
Adjunctive therapies such as aggressive pulmonary toilet,
nitric oxide, nebulized heparin, N-acetylcysteine, and/or
bronchodilators should be considered. Inhaled nitric oxide pro-
vides variable improvement in PaO2:FiO2ratios and survival in
patients responding to treatment.82 Therapy should be discon-
tinued due to futility and cost if a response is not demonstrated
between doses of 5 and 20 ppm of nitric oxide within60 minutes.82 Nebulized heparin and tissue plasminogen acti-
vator (TPA) have demonstrated potential efficacy in animal
and human studies through breakdown of fibrin deposition
associated with inhalation injury, maintenance of alveolar
structure, and reduced obstruction.83 Although survival benefit
has not clearly been demonstrated with Mucomyst use follow-
ing pulmonary injury, N-acetylcysteine was noted to decrease
leukocytes in bronchoalveolar lavage.84-86 Aerosolized deliv-
ery of b2-agonists preferentially causes bronchodilation,
attenuation of lung inflammation, and may potentially improve
fluid clearance without systemic cardiac activation.87 While
corticosteroids demonstrate benefit in most chronic pulmonary
diseases, improvement in acute pulmonary inflammation sec-
ondary to inhalation injury and ARDS has not been definitively
demonstrated.68,88-90 Steroids for inhalation injury should be
used with caution until larger prospective studies are
completed.
Nutritional Support in Burns
Burns induce a hypermetabolic state that may persist for up to
12 months following injury.91,92 Many metabolic disturbances
following burn injuries are related to systemic inflammation
and altered hypothalamic function, with resultant increases in
temperature setpoint and production of catecholamines(reviewed in93). This leads to increased protein catabolism and
lipolysis, culminating in decreased lean body mass, poor
wound healing, and weakened host defenses. Most equations
often overestimate the energy requirements of patients with
burn, with indirect calorimetry remaining the gold standard for
calculating resting energy expenditure (REE).94-100 Respira-
tory quotient is unreliable in evaluating the nutrition status of
patients with burn.101 Overfeeding results from excess carbo-
hydrate or fat intake, both detrimental to the critically ill patient
with burn. Excess carbohydrate consumption increases CO2production, fat stores, hepatic dysfunction, hyperglycemia, and
Figure 3. Edema associated with inhalation injury and resuscitation.This photograph depicts facial edema due to severe inhalation injuryand burn shock resuscitation in a pediatric burn patient. Nasotrachealintubation was performed early to prevent accidental loss of airway.
228 Journal of Intensive Care Medicine 26(4)
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
8/15
wound-healing duration.57,93,102 Protein excess does not offset
hypercatabolism, and may actually increase it.102 While some
studies have demonstrated improved survival and reduced hos-
pital stay with underfeeding of nonburned critically ill
patients,102 this strategy is harmful in patients with extensive
burn injuries. Appropriate nutrition is required for wound heal-
ing, mediation of inflammation, suppression of the hypermeta-bolic response, and reduction of sepsis-related morbidity and
mortality.103
Serum albumin levels are often used to monitor nutrition
status in critically ill patients. In the patient with burn, albumin
is a poor surrogate for nutritional status as serum concentra-
tions are known to rapidly fall after burn injury. Replacement
does not stimulate production of endogenous albumin nor has
replacement demonstrated clinical benefits related to pulmon-
ary function, wound healing, gastrointestinal function, or mor-
tality.93 Serial measurement of prealbumin is advocated for
long-term monitoring of nutrition as it is a distinct marker for
protein synthesis, while the one-time measurement of nutri-
tional markers such as transferrin, carotene, iron, and calciumare unreliable indicators of nutrition status.104 Monitoring of
glucose levels remains a central part of nutritional management
in patients with burn. Hyperglycemia occurs in most patients
with burn regardless of injury severity due to an increased rate
of glucose production and impaired tissue glucose extrac-
tion.105,106 Modulation of the inflammatory response with tight
glucose control produces improved survival, sepsis control, and
wound healing.107-109 Interestingly, propranolol also aids in
restoration of glycemic control, in addition to reducing periph-
eral lipolysis and enhancing the immune response to sepsis via
mediation of catecholamine release during severe burn
injury.110 A retrospective review demonstrated a significant
decrease in mortality and healing time for burn patients on beta
blockade therapy prior to injury, an effect not seen when beta
blockade was initiated in the hospital following injury.111
However, in a prospective, randomized trial, decreased healing
time and hospital length of stay was demonstrated after beta
blockade initiation following injury.112 Additionally, beta
blockade in pediatric patients with burn has been associated
with decreased cardiac work, reversal of catabolism,
and attenuation of the inflammatory response without an
increased risk of infection or sepsis.113-115 These findings sup-
port the conclusion that multiple factors play a role in the meta-
bolic response to severe burn trauma and further investigation
with randomized controlled trials is required.
Enteral and Parenteral Support
Enteral feeding is the ideal route for caloric and nutrient sup-
plementation in patients with burn. Maintenance of gut integ-
rity is hypothesized to reduce the risk of bacterial
translocation and subsequent sepsis.116,117 The role of specialty
amino acids, proteins, and fatty acids present in commercial
enteral formulations for pediatric patients with burn is contro-
versial as studies have demonstrated mixed results.118,119 If
oral caloric intake will be inadequate at 5 to 7 days following
injury, placement of a nasoduodenal feeding tube is recom-
mended. Initial timing of enteral nutrition after burn injury is
controversial, although most burn clinicians advocate starting
feeds within hours of injury unless contraindicated. Studies
demonstrating reversal of hypermetabolism, hypercatabolism,
and systemic inflammation in burn animals receiving early
nutrition have not been replicated in humans, possibly due tothe inability to realistically start early enteral feeding within
1 to 2 hours of burn.103 Improvement in clinical measures such
as decreased length of stay, infection, and mortality have also
not conclusively been shown when compared to later initiation
of enteral feeding (>72 hours).100 The risk of adverse events
including errors in tube placement, aspiration, and intestinal
necrosis underlies arguments to delay initiation of feeding until
burn resuscitation has been completed. In a prospective, rando-
mized trial, Gottschlich et al found 4 out of 5 patients who
developed an abdominal catastrophe from intestinal necrosis
were in the early feeding arm of the study.103 Possible explana-
tions include hypotensive episodes during early burn resuscita-
tion and altered gut perfusion during burn shock, combinedwith the increased intestinal blood flow demand with feed-
ing.103 Despite some of these concerns, initiation of enteral
nutrition upon patient stabilization is considered standard of
care.
Parenteral nutrition (PN), while a mainstay of therapy for
many critically ill patients, is reserved for burn patients unable
to tolerate enteral feedings due to severe diarrhea or an organic
gastrointestinal problem. Increased complication rates in
patients with burn on PN are mostly due to central venous
catheter infections. Peripheral parenteral nutrition (PPN) is
generally not an option due to inadequate calorie delivery and
high risk of peripheral soft tissue damage from extravasation.
Vitamin and Steroid Supplementation
Vitamin A has been shown to aid wound healing following
burn injury and is replaced in patients with >20% TBSA
burns.120 Vitamin C plays a vital role in collagen synthesis and
wound healing, necessitating its supplementation. Wound exu-
dates were found to be the primary site of loss for trace ele-
ments,121 suggesting patients with burn may require
additional supplementation compared to other critically ill
patients. The trace element zinc is necessary for wound heal-
ing, and decreased zinc levels in septic patients may be associ-
ated with subsequent adverse events.57
For these reasons, zincsupplementation is oftentimes included in enteral nutrition for-
mulas. More studies are needed to determine the role of trace
element supplementation in pediatric patients with burn.
Negative nitrogen balance is often seen during the first 1 to
2 weeks postburn due to hypercatabolism in burns and loss of
lean body mass.100 To combat this, the effectiveness of ana-
bolic agents such as oxandrolone in restoration of lean body
mass, improved wound healing, improved nutritional status,
and liver function has been studied.57,122 The impact of ana-
bolic steroids on the course of burn disease is controversial.
A few small, single center studies have been unable to
Kasten et al 229
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
9/15
demonstrate any clear benefits, in contrast to a multicenter trial
stopped prematurely because of significantly fewer hospital
days for patients with severe burn treated with oxandro-
lone.100,123,124 More studies are needed to clarify this conten-
tious treatment question.
Wound Care
Improperly managed burn wounds may convert to deeper
wounds requiring definitive surgical management. Cleansing
and debridement of the wound is accomplished with mild soap
and water or with chlorhexadine/normal saline washes. Most
burn experts recommend debridement of all blisters larger than
0.5 cm to reduce the risk of bacterial colonization or infection.
Burn wounds become colonized in the first few hours with
gram-positive bacteria including Staphylococcus aureus and
epidermidis and are predominantly colonized with gut flora
such as Pseudomonas aeruginosa, Enterobacter cloacae, and
Escherichia coli by 5 days. Health care workers must be vigi-
lant in hand washing and maintenance of a clean environmentaround the wounds for prevention of cross-contamination in
these immunocompromised patients. Culture swabs of all
wound beds should be obtained upon admission and repeated
serially to monitor for changes in colonization. Quantitative
cultures of the burn to diagnose wound invasion are best
obtained by tissue biopsy, either in the operating room or at
bedside. Bacterial colonization of burn wounds does not
require systemic antibiotics but should be managed with early
debridement and/or excision, together with appropriate topical
and/or biologic dressings.
Cleansing and debridement is followed by application of a
topical antimicrobial agent intended to control colonization,
not sterilize the burn wound. Several layers of absorptive gauze
and Kerlix cover the wound to decrease evaporative water
losses.125 Minor burns can be managed with biologic dressings,
silver-coated dressings, or tribiotic ointment covered with non-
adherent gauze. Commonly utilized topical agents include sil-
ver sulfadiazine (Silvadene), mafenide acetate (Sulfamylon),
and silver nitrate. Silvadene continues to demonstrate effective
control of burn wound colonization, while remaining inexpen-
sive and easy to apply. However, eschar penetration is minimal
and complications related to leukopenia and hemolysis have
been reported.126 Mafenide acetate cream (Sulfamylon) is easy
to apply but is painful when applied to superficial partial-
thickness burns. Eschar penetration is greatest with Sulfamy-lon, making it the topical agent of choice in burns where the
eschar will not be excised immediately, or when control of
Pseudomonas aeruginosais required. Metabolic acidosis may
occur with use as Sulfamylon is a carbonic anhydrase inhibitor.
Silver nitrate 0.5% solution has fallen out of favor due to elec-
trolyte abnormalities and poor tissue penetration but may be
used as a reasonably effective agent for treatment of gram-
negative or fungal colonization.
Aside from complications directly related to topical agents,
frequent dressing changes often result in traumatized epithelia-
lization and delayed wound healing. Silvadene has been shown
to delay wound healing due to a direct toxic effect on keratino-
cytes127 (reviewed in ref 128). To combat this, silver-
impregnated dressings such as Acticoat, Aquacel Ag, Mepitel,
and Mepilex have been developed to provide antimicrobial
coverage, adequate humidity, and decreased trauma, all with
less frequent dressing changes. Biosynthetic substitutes like
Biobrane are marketed as epidermal substitutes that allow forfaster re-epithelialization129; however, their use is limited due
to infectious complications.
In addition to topical therapies, deep burns are managed
with surgical excision and placement of xenograft, allograft,
autograft, or cultured skin substitutes (CSS; Figure 4). Skin
substitutes and replacements require adequate wound bed pre-
paration to ensure minimal graft loss. Most experienced burn
surgeons advocate early wound excision within the first 1 to
7 days following thermal injury to attenuate the systemic
inflammatory effects of burns and reduce the risk of sep-
sis.131-135 In fact, no significant difference in infection or mor-
tality rates was found when burn excision was performed at any
point between 2 and 7 days.136 Additionally, in a comparison ofadult patients over 30 years of age sustaining greater than 30%
TBSA injury, no difference in mortality was seen between
excision within the first 72 hours and conservative manage-
ment with grafting after granulation of the wound bed.137 How-
ever, this same study found significantly decreased mortality
and length of hospital stay in pediatric patients and adults aged
17 to 30 years who underwent early excision compared to con-
servative management.137 The appropriate timing for burn
wound excision and grafting involves a number of important
factors including the age of the patient, extent and depth of
burn, comorbidities, hospital resources, and physician prefer-
ence. It is therefore important that the surgeon always assess
the risks and/or benefits of delaying surgical treatment in
burn-injured patients. At our institution, a staged approach is
often taken for more extensive injuries. The burn wound is
excised and bleeding controlled on the first operative day.
Donor site harvest and grafting then occurs on the following
operative day. This approach allows for more extensive exci-
sions, shorter operating times, better temperature control, and
the ability to perform sheet grafting with improved hemostasis.
Definitive surgical management requires appropriate topical
antimicrobial therapy postoperatively for prevention of graft
loss and burn wound infection.
Sepsis in the Burn Patient
Improvements in resuscitation strategies and supportive care
have shifted the underlying cause of morbidity and mortality
in patients with burn from burn shock to infection. Unfortu-
nately, sepsis is an independent risk factor of mortality follow-
ing thermal injury, especially when multiorgan system failure
(MOSF) is present.138,139 Open wounds, injured lungs, central
venous catheters, and urinary catheters place the patient with
burn at constant risk of infection and sepsis. Diagnostic uncer-
tainty due to altered physiology affecting clinical and labora-
tory parameters complicates therapeutic intervention. Signs
230 Journal of Intensive Care Medicine 26(4)
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
10/15
of sepsis, including elevated temperature, tachycardia, tachyp-
nea, and leukocytosis, may be present in the burned patient
without underlying infection. Laboratory markers including
peripheral white blood cell (WBC) levels, procalcitonin, C
reactive protein, and others have been proposed as early indi-
cators of sepsis in the burn patient, all with mixed results.
Absolute values and trends in WBC, neutrophil percentage,
and body temperature are unable to predict bloodstream
infection in the burn patient.139 Although controversial, use
of procalcitonin level has been advocated due to its sensitiv-
ity, specificity, and mortality correlation in patients with burn
having sepsis.140 However, procalcitonin was reported insuffi-
cient as a single diagnostic marker for sepsis in patients with
burn141 and inferior to monitoring trends in CRP and platelet
count.142 As another marker, decreased Human Leukocyte
Antigen DR expression showed an inverse correlation between
and mortality in sepsis.143
Continued research is needed toclarify the immune response to sepsis, ultimately aiding in
accurate diagnosis of infection.
Early markers of infection can alert physicians to initiate
treatment of unconfirmed but potentially fatal infections.
Breakdown of barrier function following burn injury provides
the largest entrance point for infection. Careful attention and
documentation by physicians and nursing staff of open wounds,
together with weekly or biweekly cultures, can prevent pro-
gression of superficial colonization to invasive sepsis. In addi-
tion, the topical and surgical therapies enumerated above are
first lines of care for the prevention of burn wound infections,
the most serious of which is invasive burn wound sepsis.
Pneumonia, while not as common as burn wound infection,
occurs in 4.5% of flame-injured patients and is associated with
increased days of mechanical ventilation, longer ICU stay,
and higher hospital cost.1,144 Aggressive bronchoscopy with
BAL confirms the infectious agent, provides antibiotic
sensitivity information for quick tailoring of antibiotics, and
subsequently decreases ventilator and ICU days.146 Following
recently released ABA guidelines for prevention, diagnosis
and treatment of pneumonia can reduce the complications
related to this disease process.146
Bloodstream and urinary tract infections are of constant
concern due to prolonged duration of catheter use.148 Newer
technologies have yielded silver-impregnated, chlorhexadine/
silver sulfadiazine coated, and antibiotic-coated catheters tar-
geted to reduce catheter infection.149,150 Unfortunately, the
ability of antiseptic/antibiotic impregnated catheters to preventbloodstream infection was found to have no effect beyond that
of a comprehensive education strategy involving proper eva-
luation and maintenance of indwelling catheters.151 Timing
of central access exchange in the patient with burn is deter-
mined by the risk of colonization, need for placement through
burned versus unburned tissue, and physician preference.152
Prompt removal of all indwelling catheters when no longer
warranted provides the best prevention for infection in the
patient with burn. Blood and urinary tract infections are treated
with removal of the catheter whenever possible and appropri-
ately tailored antibiotic therapy.
Figure 4.Burn wounds healed with culture skin substitute (CSS). Shown is the back of a pediatric patient grafted with CSS (outlined by dashedlines) and split-thickness skin autograft. A, At 2 weeks after grafting, the borders of the CSS were discernable but the wound was mostly closed.B, At 10 weeks post-grafting, the healed CSS was pliable and hypopigmented observation of some pigmented foci. Reprinted from Clinics inDermatology, Volume 23, Dorothy M. Supp, Steven T. Boyce, Engineered skin substitutes: practices and potentials, Pages 403-412, Copyright(2005), with permission from Elsevier.
Kasten et al 231
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
11/15
Conclusion
Dedication and research over the past 5 decades has produced
an enviable reduction in mortality for burn-injured patients
treated in the United States. With appropriate and tailored
resuscitation regimens, early enteral nutrition, quick and effec-
tive management of the burn wound with topical and surgical
therapies, the severely injured burn patient can not only survivebut experience minimal short and long-term morbidities. Suc-
cess in these areas involves a multidisciplinary team trained
in current state-of-the-art interventions and therapies, with ulti-
mate goal of restoring function and allowing psychosocial
reintegration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect
to the authorship and/or publication of this article.
FundingThe author(s) received no financial support for the research and/or
authorship of this article.
References
1. National Burn Repository 2009 Report: Dataset 5.0 American
Burn Association, Chicago, IL http://www.ameriburn.org/
2009NBRAnnualReport.pdf.
2. Wibbenmeyer LA, Amelon MJ, Torner JC, et al. Population-
based assessment of burn injury in southern iowa: Identification
of children and young-adult at-risk groups and behaviors. J Burn
Care Rehabil. 2003;24(4):192-202.
3. Ryan CM, Schoenfeld DA, Thorpe WP, Sheridan RL,
Cassem EH, Tompkins RG. Objective estimates of the probability
of death from burn injuries. N Engl J Med. 1998;338(6):362-366.
4. DeKoning EP, Hakenewerth A, Platts-Mills TF, Tintinalli JE.
Epidemiology of burn injuries presenting to north carolina emer-
gency departments in 2006-2007. Burns. 2009;35(6):776-782.
5. Wolf SE, Rose JK, Desai MH, Mileski JP, Barrow RE,
Herndon DN. Mortality determinants in massive pediatric burns.
An analysis of 103 children with > or 80% tbsa burns (> or
70% full-thickness).Ann Surg. 1997;225(5):554-565; discussion
565-559.
6. Esselman PC. Burn rehabilitation: an overview.Arch Phys Med
Rehabil. 2007;88(12 suppl 2):S3-S6.7. Harrington DT. Burn injuries and burn care. Med Health R I.
2009;92(5):179-180.
8. Mann R, Heimbach D. Prognosis and treatment of burns. West
J Med. 1996;165(4):215-220.
9. McGwin G Jr, Cross JM, Ford JW, Rue LW 3rd. Long-term
trends in mortality according to age among adult burn patients.
J Burn Care Rehabil. 2003;24(1):21-25.
10. Church D, Elsayed S, Reid O, Winston B, Lindsay R. Burn wound
infections.Clin Microbiol Rev. 2006;19(2):403-434.
11. Grunwald TB, Garner WL. Acute burns. Plast Reconstr Surg.
2008;121(5):311e-319e.
12. Tschop J, Martignoni A, Reid MD, et al. Differential immunolo-
gical phenotypes are exhibited after scald and flame burns.Shock.
2009;31(2):157-163.
13. Cone JB. Whats new in general surgery: burns and metabolism.
J Am Coll Surg. 2005;200(4):607-615.
14. Collis N, Smith G, Fenton OM. Accuracy of burn size estimation
and subsequent fluid resuscitation prior to arrival at the yorkshire
regional burns unit. A three year retrospective study. Burns. 1999;
25(4):345-351.
15. Perry RJ, Moore CA, Morgan BD, Plummer DL. Determining the
approximate area of a burn: an inconsistency investigated and re-
evaluated.BMJ. 1996;312(7042):1338.
16. Wachtel TL, Berry CC, Wachtel EE, Frank HA. The inter-rater
reliability of estimating the size of burns from various burn area
chart drawings. Burns. 2000;26(2):156-170.
17. Neuwalder JM, Sampson C, Breuing KH, Orgill DP. A review of
computer-aided body surface area determination: Sage ii and
epris 3d burn vision. J Burn Care Rehabil. 2002;23(1):55-59;
discussion 54.
18. Cuttle L, Pearn J, McMillan JR, Kimble RM. A review of first aidtreatments for burn injuries. Burns. 2009;35(6):768-775.
19. Sawada Y, Urushidate S, Yotsuyanagi T, Ishita K. Is prolonged
and excessive cooling of a scalded wound effective? Burns.
1997;23(1):55-58.
20. Ofeigsson OJ, Mitchell R, Patrick RS. Observations on the cold
water treatment of cutaneous burns. J Pathol. 1972;108(2):
145-150.
21. Koumbourlis AC. Electrical injuries. Crit Care Med. 2002;30
(11 suppl):S424-S430.
22. Latenser BA, Miller SF, Bessey PQ, et al. National burn reposi-
tory 2006: a ten-year review. J Burn Care Res. 2007;28(5):
635-658.
23. Latenser BA. Critical care of the burn patient: the first 48 hours.
Crit Care Med. 2009;37(10):2819-2826.
24. Armour AD, Billmire DA. Pediatric thermal injury: acute care
and reconstruction update. Plast Reconstr Surg. 2009;124
(1 suppl):117e-127e.
25. Pruitt, BA Jr. Fluid and Electrolyte Replacement in the Burned
Patient.Surg Clin N Am 1978; (58):1291-1312.
26. Chung KK, Wolf SE, Cancio LC, et al. Resuscitation of severely
burned military casualties: fluid begets more fluid. J Trauma.
2009;67(2):231-237; discussion 237.
27. Cancio LC, Chavez S, Alvarado-Ortega M, et al. Predicting
increased fluid requirements during the resuscitation of thermally
injured patients. J Trauma. 2004;56(2):404-413; discussion 413-404.
28. Reid RD, Jayamaha J. The use of a cardiac output monitor to
guide the initial fluid resuscitation in a patient with burns. Emerg
Med J. 2007;24(5):e32.
29. Jaffe MB. Partial CO2 rebreathing cardiac outputoperating prin-
ciples of the nico system. J Clin Monit Comput. 1999;15(6):
387-401.
30. Berton C, Cholley B. Equipment review: new techniques for car-
diac output measurementoesophageal doppler, fick principle
using carbon dioxide, and pulse contour analysis. Crit Care.
2002;6(3):216-221.
232 Journal of Intensive Care Medicine 26(4)
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
12/15
31. Salinas J, Drew G, Gallagher J, et al. Closed-loop and decision-
assist resuscitation of burn patients. J Trauma. 2008;64
(4 suppl):S321-332.
32. Warden GD. Burn shock resuscitation.World J Surg. 1992;16(1):
16-23.
33. Goodwin CW, Dorethy J, Lam V, Pruitt BA Jr. Randomized trial
of efficacy of crystalloid and colloid resuscitation on hemody-
namic response and lung water following thermal injury. Ann
Surg. 1983;197(5):520-531.
34. Alderson P, Bunn F, Lefebvre C, et al. Human albumin solution
for resuscitation and volume expansion in critically ill patients.
Cochrane Database Syst Rev. 2004;(4):CD001208.
35. Nisanci M, Eski M, Sahin I, Ilgan S, Isik S. Saving the zone of
stasis in burns with activated protein C: an experimental study
in rats. Burns. 2010;36(3):397-402.
36. Dulhunty JM, Boots RJ, Rudd MJ, Muller MJ, Lipman J.
Increased fluid resuscitation can lead to adverse outcomes in
major-burn injured patients, but low mortality is achievable.
Burns. 2008;34(8):1090-1097.
37. Ivy ME, Atweh NA, Palmer J, Possenti PP, Pineau M, DAiuto M.Intra-abdominal hypertension and abdominal compartment syn-
drome in burn patients. J Trauma. 2000;49(3):387-391.
38. Tricklebank S. Modern trends in fluid therapy for burns.Burns.
2009;35(6):757-767.
39. Brown RL, Greenhalgh DG, Kagan RJ, Warden GD. The ade-
quacy of limb escharotomies-fasciotomies after referral to a major
burn center. J Trauma. 1994;37(6):916-920.
40. Hershberger RC, Hunt JL, Arnoldo BD, Purdue GF. Abdominal
compartment syndrome in the severely burned patient. J Burn
Care Res. 2007;28(5):708-714.
41. Klein MB, Hayden D, Elson C, et al. The association between
fluid administration and outcome following major burn: A multi-
center study. Ann Surg. 2007;245(4):622-628.
42. Steinvall I, Bak Z, Sjoberg F. Acute respiratory distress syn-
drome is as important as inhalation injury for the development
of respiratory dysfunction in major burns. Burns. 2008;34(4):
441-451.
43. Maybauer DM, Maybauer MO, Traber DL. Resuscitation with
hypertonic saline in burn shock and sepsis. Crit Care Med.
2006;34(6):1849-1850.
44. Herndon DN, Thompson PB, Traber DL. Pulmonary injury in
burned patients.Crit Care Clin. 1985;1(1):79-96.
45. Shirani KZ, Pruitt BA Jr, Mason AD Jr. The influence of inhala-
tion injury and pneumonia on burn mortality. Ann Surg. 1987;
205(1):82-87.46. Palmieri TL, Warner P, Mlcak RP, et al. Inhalation injury in chil-
dren: a 10 year experience at shriners hospitals for children.
J Burn Care Res. 2009;30(1):206-208.
47. Craft B, Kagan RJ. Current management of burns. Medical
Update for Psychiatrists. 1998;3(2):53-57.
48. Hanumadass ML, Kagan RJ, and Matsuda T. Management of
Pediatric Burns. In Vidyasagar, D and Sarnaik AP, ed. Neonatal
and Pediatric Intensive Care. PSG Publishing Co. Littleton,
MA; 1985:215-226.
49. McAuliffe PF and Mozingo DW. Inhalation Injury and Ventilator
Management. In: Soper NJ, Saffle JR, eds.Problems in General
Surgery: Thermal Injuries. Philadelphia, PA: Lippincott, Wil-
liams and Wilkins; 2002;20:97-105.
50. Robb BW and Kagan RJ: Outpatient and Emergency Department
Management of Thermal Injuries. Probl Gen Surg. 2003;7-15.
51. Ware LB, Matthay MA. The acute respiratory distress syndrome.
N Engl J Med. 2000;342(18):1334-1349.
52. Pruitt BA Jr, Erickson DR, Morris A. Progressive pulmonary
insufficiency and other pulmonary complications of thermal
injury.J Trauma. 1975;15(5):369-379.
53. Moritz AR, Henriques FC. Studies of thermal injury II: the rela-
tive importance of time and surface temperature in the causation
of cutaneous burns. Am J Pathol. 1947;23(5):695-720.
54. Miller K, Chang A. Acute inhalation injury. Emerg Med Clin
North Am. 2003;21(2):533-557.
55. Nieman GF, Clark WR Jr, Wax SD, Webb SR. The effect of
smoke inhalation on pulmonary surfactant. Ann Surg. 1980;
191(2):171-181.
56. Herndon DN, Traber LD, Linares H, et al. Etiology of the pul-
monary pathophysiology associated with inhalation injury.Resus-
citation. 1986;14(1-2):43-59.57. MakG AS,Kagan R.Pediatricburns. In:Wheeler D WH, ShanleyT,
ed.Pediatric Critical Care Medicine. Springer-Verlag; 2007:1597-
1606.
58. Gauglitz GG, Finnerty CC, Herndon DN, Mlcak RP, Jeschke MG.
Mak G, Allen S, and Kagan RJ: Pediatric Burns. In: Wheeler D,
Wong H, Shandley T, eds. Pediatric Critical Care Medicine:
Basic Science and Clinical Evidence. London, UK: Springer-
Verlag; 2007;1597-1606.
59. Gonzalez-Castro A, Llorca J, Buron J, Suberviola B, Vallejo A,
Minambres E. Evaluation of the oxygenation ratio as long-term
prognostic marker after lung transplantation. Transplant Proc.
2007;39(7):2422-2424.
60. Krafft P, Fridrich P, Pernerstorfer T, et al. The acute respiratory
distress syndrome: definitions, severity and clinical outcome.
An analysis of 101 clinical investigations. Intensive Care Med.
1996;22(6):519-529.
61. Yilmaz M, Iscimen R, Keegan MT, et al. Six-month survival of
patients with acute lung injury: prospective cohort study. Crit
Care Med. 2007;35(10):2303-2307.
62. Weaver LK, Howe S, Hopkins R, Chan KJ. Carboxyhemoglobin
half-life in carbon monoxide-poisoned patients treated with 100%
oxygen at atmospheric pressure. Chest. 2000;117(3):801-808.
63. Baud FJ, Barriot P, Toffis V, et al. Elevated blood cyanide con-
centrations in victims of smoke inhalation. N Engl J Med. 1991;
325(25):1761-1766.64. Barillo DJ. Diagnosis and treatment of cyanide toxicity. J Burn
Care Res. 2009;30(1):148-152.
65. Reske A, Bak Z, Samuelsson A, Morales O, Seiwerts M,
Sjoberg F. Computed tomographya possible aid in the diagnosis
of smoke inhalation injury?Acta Anaesthesiol Scand. 2005;49(2):
257-260.
66. Wittram C, Kenny JB. The admission chest radiograph after acute
inhalation injury and burns.Br J Radiol. 1994;67(800):751-754.
67. Nugent N and Herndon D. Diagnosis and Treatment of Inhalation
Injury. In: Herndon, ed.Total Burn Care. Saunders; Philadelphia,
PA; 2007.
Kasten et al 233
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
13/15
68. Rabinowitz PM, Siegel MD. Acute inhalation injury.Clin Chest
Med. 2002;23(4):707-715.
69. Ernst A, Zibrak JD. Carbon monoxide poisoning. N Engl J Med.
1998;339(22):1603-1608.
70. Erupaka K, Bruce EN, Bruce MC. Prediction of extravascular
burden of carbon monoxide (co) in the human heart. Ann Biomed
Eng. 2010;38(2):403-438.
71. Kealey GP. Carbon monoxide toxicity.J Burn Care Res. 2009;
30(1):146-147.
72. Gravvanis AI, Tsoutsos DA, Iconomou TG, Papadopoulos SG.
Percutaneous versus conventional tracheostomy in burned
patients with inhalation injury. World J Surg. 2005;29(12):
1571-1575.
73. Rodeberg DA, Housinger TA, Greenhalgh DG, Maschinot NE,
Warden GD. Improved ventilatory function in burn patients using
volumetric diffusive respiration. J Am Coll Surg. 1994;179(5):
518-522.
74. Carman B, Cahill T, Warden G, McCall J. A prospective, rando-
mized comparison of the volume diffusive respirator vs conven-
tional ventilation for ventilation of burned children. 2001 abapaper. J Burn Care Rehabil. 2002;23(6):444-448.
75. Cioffi WG, Graves TA, McManus WF, Pruitt BA Jr. High-
frequency percussive ventilation in patients with inhalation
injury.J Trauma. 1989;29(3):350-354.
76. Cioffi WG Jr, Rue LW 3rd, Graves TA, McManus WF,
Mason AD Jr, Pruitt BA Jr. Prophylactic use of high-
frequency percussive ventilation in patients with inhalation
injury.Ann Surg. 1991;213(6):575-580; discussion 580-572.
77. Rue LW 3rd, Cioffi WG, Mason AD, McManus WF, Pruitt BA
Jr. Improved survival of burned patients with inhalation injury.
Arch Surg. 1993;128(7):772-778; discussion 778-780.
78. Kane TD, Greenhalgh DG, Warden GD, Goretsky MJ,
Ryckman FC, Warner BW. Pediatric burn patients with respira-
tory failure: predictors of outcome with the use of extracorporeal
life support. J Burn Care Rehabil. 1999;20(2):145-150.
79. Alpard SK, Zwischenberger JB. Extracorporeal membrane oxy-
genation for severe respiratory failure. Chest Surg Clin N Am.
2002;12(2):355-378, vii.
80. Nehra D, Goldstein AM, Doody DP, Ryan DP, Chang Y,
Masiakos PT. Extracorporeal membrane oxygenation for nonneo-
natal acute respiratory failure: The massachusetts general hospital
experience from 1990 to 2008.Arch Surg. 2009;144(5):427-432;
discussion 432.
81. Thompson JT, Molnar JA,Hines MH,Chang MC,PranikoffT. Suc-
cessful management of adult smoke inhalation with extracorporealmembrane oxygenation.J Burn Care Rehabil. 2005;26(1):62-66.
82. Sheridan RL, Hess D. Inhaled nitric oxide in inhalation injury.
J Burn Care Res. 2009;30(1):162-164.
83. Enkhbaatar P, Murakami K, Cox R, et al. Aerosolized tissue plas-
minogen inhibitor improves pulmonary function in sheep with
burn and smoke inhalation.Shock. 2004;22(1):70-75.
84. FuZ, YangZ, Liu L,Liu Z,He B,Wu J.[theinfluenceof n-acetyl-l-
cysteine on pulmonary injury and oxygen stress after smoke inhala-
tion injury].Zhonghua Shao Shang Za Zhi. 2002;18:152-154.
85. Miller AC, Rivero A, Ziad S, Smith DJ, Elamin EM. Influence of
nebulized unfractionated heparin and n-acetylcysteine in acute
lung injury after smoke inhalation injury. J Burn Care Res.
2009;30(2):249-256.
86. Adhikari N, Burns KE, Meade MO. Pharmacologic treatments
for acute respiratory distress syndrome and acute lung injury:
systematic review and meta-analysis. Treat Respir Med. 2004;
3(5):307-328.
87. Palmieri TL. Use of beta-agonists in inhalation injury.J BurnCare Res. 2009;30(1):156-159.
88. Bernard GR, Luce JM, Sprung CL, et al. High-dose corticoster-
oids in patients with the adult respiratory distress syndrome.
N Engl J Med. 1987;317(25):1565-1570.
89. Greenhalgh DG. Steroids in the treatment of smoke inhalation
injury.J Burn Care Res. 2009;30(1):165-169.
90. Agarwal R, Nath A, Aggarwal AN, Gupta D. Do glucocorticoids
decrease mortality in acute respiratory distress syndrome?
A meta-analysis. Respirology. 2007;12(4):585-590.
91. Murphy KD, Thomas S, Mlcak RP, Chinkes DL, Klein GL,
Herndon DN. Effects of long-term oxandrolone administration
in severely burned children. Surgery. 2004;136(2):219-224.
92. Herndon DN, Tompkins RG. Support of the metabolic responseto burn injury. Lancet. 2004;363(9424):1895-1902.
93. Chan MM, Chan GM. Nutritional therapy for burns in children
and adults. Nutrition. 2009;25(3):261-269.
94. Carvajal HF. A physiologic approach to fluid therapy in severely
burned children.Surg Gynecol Obstet. 1980;150(3):379-384.
95. Curreri PW. Nutritional support of burn patients.World J Surg.
1978;2:215-222.
96. Herndon DN, Curreri PW. Metabolic response to thermal injury
and its nutritional support. Cutis. 1978;22(4):501-506, 514.
97. Hildreth MA, Herndon DN, Desai MH, Duke MA. Reassessing
caloric requirements in pediatric burn patients. J Burn Care
Rehabil. 1988;9(6):616-618.
98. Ireton-Jones C, Jones JD. Improved equations for predicting
energy expenditure in patients: the ireton-jones equations. Nutr
Clin Pract. 2002;17(1):29-31.
99. Mayes T, Gottschlich MM, Khoury J, Warden GD. Evaluation of
predicted and measured energy requirements in burned children.
J Am Diet Assoc. 1996;96(1):24-29.
100. Schulman CI, Ivascu FA. Nutritional and metabolic conse-
quences in the pediatric burn patient. J Craniofac Surg. 2008;
19(4):891-894.
101. Liusuwan Manotok RA, Palmieri TL, Greenhalgh DG. The
respiratory quotient has little value in evaluating the state
of feeding in burn patients. J Burn Care Res. 2008;29(4):
655-659.102. Joffe A, Anton N, Lequier L, et al. Nutritional support for
critically ill children. Cochrane Database Syst Rev. 2009;(2):
CD005144.
103. Gottschlich MM, Jenkins ME, Mayes T, Khoury J, Kagan RJ,
Warden GD. The 2002 clinical research award. An evaluation
of the safety of early vs delayed enteral support and effects on
clinical, nutritional, and endocrine outcomes after severe burns.
J Burn Care Rehabil. 2002;23(6):401-415.
104. Rettmer RL, Williamson JC, Labbe RF, Heimbach DM. Labora-
tory monitoring of nutritional status in burn patients.Clin Chem.
1992;38(3):334-337.
234 Journal of Intensive Care Medicine 26(4)
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
14/15
105. Gore DC, Ferrando A, Barnett J, et al. Influence of glucose
kinetics on plasma lactate concentration and energy expenditure
in severely burned patients.J Trauma. 2000;49(4):673-677; dis-
cussion 677-678.
106. Wolfe RR, Miller HI, Spitzer JJ. Glucose and lactate kinetics in
burn shock.Am J Physiol. 1977;232(4):E415-418.
107. Jeschke MG, Boehning DF, Finnerty CC, Herndon DN. Effect of
insulin on the inflammatory and acute phase response after burn
injury.Crit Care Med. 2007;35(9 suppl):S519-523.
108. Holm C, Horbrand F, Mayr M, von Donnersmarck GH,
Muhlbauer W. Acute hyperglycaemia following thermal injury:
friend or foe? Resuscitation. 2004;60(1):71-77.
109. Ellger B, Westphal M, Stubbe HD, Van den Heuvel I, Van
Aken H, Van den Berghe G. [Glycemic control in sepsis and sep-
tic shock: friend or foe?]. Anaesthesist. 2008;57(1):43-48.
110. Norbury WB, Jeschke MG, Herndon DN. Metabolism modula-
tors in sepsis: propranolol. Crit Care Med. 2007;35(9 suppl):
S616-620.
111. Arbabi S, Ahrns KS, Wahl WL, et al. Beta-blocker use is asso-
ciated with improved outcomes in adult burn patients. J Trauma.2004;56(2):265-269; discussion 269-271.
112. Mohammadi AA, Bakhshaeekia A, Alibeigi P, et al. Efficacy of
propranolol in wound healing for hospitalized burn patients.
J Burn Care Res. 2009;30(6):1013-1017.
113. Baron PW, Barrow RE, Pierre EJ, Herndon DN. Prolonged use
of propranolol safely decreases cardiac work in burned children.
J Burn Care Rehabil. 1997;18(3):223-227.
114. Herndon DN, Hart DW, Wolf SE, Chinkes DL, Wolfe RR.
Reversal of catabolism by beta-blockade after severe burns.
N Engl J Med. 2001;345(17):1223-1229.
115. Jeschke MG, Norbury WB, Finnerty CC, Branski LK,
Herndon DN. Propranolol does not increase inflammation, sep-
sis, or infectious episodes in severely burned children.J Trauma.
2007;62(3):676-681.
116. Peng X, YanH, You Z, WangP, Wang S. Effects of enteralsupple-
mentation with glutamine granules on intestinal mucosal barrier
function in severe burned patients.Burns. 2004;30(2):135-139.
117. Alexander JW. Nutritional pharmacology in surgical patients.
Am J Surg. 2002;183:349-352.
118. Gottschlich MM, Jenkins M, Warden GD, et al. Differential
effects of three enteral dietary regimens on selected outcome
variables in burn patients. JPEN J Parenter Enteral Nutr.
1990;14(3):225-236.
119. Saffle JR, Wiebke G, Jennings K, Morris SE, Barton RG. Ran-
domized trial of immune-enhancing enteral nutrition in burnpatients.J Trauma. 1997;42(5):793-800; discussion 800-792.
120. Aida T, Murata J, Asano G, Kanda Y, Yoshino Y. Effects of
polyprenoic acid on thermal injury. Br J Exp Pathol. 1987;
68(3):351-358.
121. VorugantiVS, Klein GL, Lu HX,ThomasS, Freeland-Graves JH,
Herndon DN. Impaired zinc and copper status in children with
burn injuries: Need to reassess nutritional requirements.Burns.
2005;31(6):711-716.
122. Jeschke MG, Finnerty CC, Suman OE, Kulp G, Mlcak RP,
Herndon DN. The effect of oxandrolone on the endocrinologic,
inflammatory, and hypermetabolic responses during the acute
phase postburn. Ann Surg. 2007;246(3):351-360; discussion
360-352.
123. Miller JT, Btaiche IF. Oxandrolone treatment in adults with
severe thermal injury. Pharmacotherapy. 2009;29(2):213-226.
124. Wolf SE, Edelman LS, Kemalyan N, et al. Effects of oxandro-
lone on outcome measures in the severely burned: a multicenter
prospective randomized double-blind trial. J Burn Care Res
.
2006;27(2):131-139; discussion 140-131.
125. Caldwell FT Jr, Bowser BH, Crabtree JH. The effect of occlu-
sive dressings on the energy metabolism of severely burned chil-
dren.Ann Surg. 1981;193(5):579-591.
126. Thomson PD,Moore NP,RiceTL, PrasadJK. Leukopenia in acute
thermal injury: evidence against topical silver sulfadiazine as the
causative agent.J Burn Care Rehabil. 1989;10(5):418-420.
127. Wasiak J, Cleland H. Burns (minor thermal). Clin Evid. 2005;
(14):2388-2396.
128. Wasiak J, Cleland H, Campbell F. Dressings for superficial and
partial thickness burns.Cochrane Database Syst Rev. 2008;(4):
CD002106.
129. Demling RH, DeSanti L. Management of partial thickness facialburns (comparison of topical antibiotics and bio-engineered skin
substitutes).Burns. 1999;25(3):256-261.
130. Supp DM and Boyce ST. Engineered Skin Substitutes: Practices
and Pitfalls. Clin Dermatol. 2005;23:403-412.
131. Hart DW, Wolf SE, Chinkes DL, et al. Effects of early excision
and aggressive enteral feeding on hypermetabolism, catabolism,
and sepsis after severe burn. J Trauma. 2003;54(4):755-761; dis-
cussion 761-754.
132. Barret JP, Herndon DN. Modulation of inflammatory and cata-
bolic responses in severely burned children by early burn
wound excision in the first 24 hours. Arch Surg. 2003;
138(2):127-132.
133. Barret JP, Herndon DN. Effects of burn wound excision on bac-
terial colonization and invasion.Plast Reconstr Surg. 2003;111:
2):744-750; discussion 751-742.
134. Xiao-Wu W, Herndon DN, Spies M, Sanford AP, Wolf SE.
Effects of delayed wound excision and grafting in severely
burned children.Arch Surg. 2002;137(9):1049-1054.
135. Monafo WW. Initial management of burns.N Engl J Med. 1996;
335:1581-1586.
136. Muangman P, Sullivan SR, Honari S, Engrav LH,
Heimbach DM, Gibran NS. The optimal time for early excision
in major burn injury. J Med Assoc Thai. 2006;89(1):29-36.
137. Herndon DN, Barrow RE, Rutan RL, Rutan TC, Desai MH,
Abston S. A comparison of conservative versus early excision.Therapies in severely burned patients. Ann Surg. 1989;209:(5):
547-552; discussion 552-543.
138. Wang Y, Tang HT, Xia ZF, et al. Factors affecting survival in
adult patients with massive burns. Burns. 2010;36(1):57-64.
139. Nguyen LN, Nguyen TG. Characteristics and outcomes of mul-
tiple organ dysfunction syndrome among severe-burn patients.
Burns. 2009;35(7):937-941.
140. Murray CK, Hoffmaster RM, Schmit DR, et al. Evaluation of
white blood cell count, neutrophil percentage, and elevated tem-
perature as predictors of bloodstream infection in burn patients.
Arch Surg. 2007;142(7):639-642.
Kasten et al 235
at CAPES on August 7, 2011jic.sagepub.comDownloaded from
http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/http://jic.sagepub.com/8/13/2019 GrandeQueimado
15/15
141. Barati M, Alinejad F, Bahar MA, et al. Comparison of wbc, esr,
crp and pct serum levels in septic and non-septic burn cases.
Burns. 2008;34(6):770-774.
142. Bargues L, Chancerelle Y, Catineau J, Jault P, Carsin H. Evalua-
tion of serum procalcitonin concentration in the icu following
severe burn. Burns. 2007;33(7):860-864.
143. Neely AN, Fowler LA, Kagan RJ, Warden GD. Procalcitonin in
pediatric burn patients: an early indicator of sepsis?J Burn Care
Rehabil. 2004;25(1):76-80.
144. Venet F, Tissot S, Debard AL, et al. Decreased monocyte human
leukocyte antigen-dr expression after severe burn injury: corre-
lation with severity and secondary septic shock. Crit Care Med.
2007;35(8):1910-1917.
145. Carr JA, Phillips BD, Bowling WM. The utility of bronchoscopy
after inhalation injury complicated by pneumonia in burn
patients: results from the national burn repository.J Burn Care
Res. 2009;30(6):967-974.
146. Wahl WL, Taddonio MA, Arbabi S, Hemmila MR. Duration of
antibiotic therapy for ventilator-associated pneumonia in burn
patients.J Burn Care Res. 2009;30(5):801-806.147. Mosier MJ, Pham TN. American burn association practice
guidelines for prevention, diagnosis, and treatment of
ventilator-associated pneumonia (vap) in burn patients. J Burn
Care Res. 2009;30(6):910-928.
148. Wibbenmeyer L, Danks R, Faucher L, et al. Prospective analysis
of nosocomial infection rates, antibiotic use, and patterns of
resistance in a burn population. J Burn Care Res. 2006;27(2):
152-160.
149. Newton T, Still JM, Law E. A comparison of the effect of early
insertion of standard latex and silver-impregnated latex foley
catheters on urinary tract infections in burn patients. Infect
Control Hosp Epidemiol. 2002;23(4):217-218.
150. Davenport K, Keeley FX. Evidence for the use of silver-
alloy-coated urethral catheters. J Hosp Infect. 2005;60(4):
298-303.
151. Schuerer DJ, Zack JE, Thomas J, et al. Effect of chlorhexidine/
silver sulfadiazine-impregnated central venous catheters in an
intensive care unit with a low blood stream infection rate after
implementation of an educational program: a before-after trial.
Surg Infect (Larchmt). 2007;8(4):445-454.
152. Rickard CM, Lipman J, Courtney M, Siversen R, Daley P. Rou-
tine changing of intravenous administration sets does not reducecolonization or infection in central venous catheters. Infect Con-
trol Hosp Epidemiol. 2004;25(8):650-655.
236 Journal of Intensive Care Medicine 26(4)