-
TRAUMA UROGENITALAnatomi GinjalUreterBuli buliUretra
-
TRAUMA UROGENITALAnatomi GinjalUreterBuli buliUretra
-
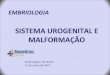
GinjalSepasang organ seperti kacang Terletak retroperitonel
diregio lumbal superiorDilapisi oleh 3 lapis jaringan penunjang:
kapsul ginjal kapsul adipose dan fasia renalis
-
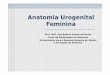
UreterTubulus muscular yang menghubungkan ginjal ke buli
buliTerletak di belakang rongga peritoneum (retroperitoneal)Panjang
25 30 cm
-
TRAUMA GINJALTrauma Ginjal Sering 8-10% trauma tumpul / tajam
abdomen Separuh dari kejadian trauma urogenital Di proteksi :*
Otot-otot lumbal* Iga* Vertebrae
-
Angka kesakitan / kematian ok trauma ginjal tergantung :
Derajat traumaKeterlibatan trauma organ lainFasilitas
penanggulangan trauma
-
Buli-buliBuli buli normal dapat menampung 350 450 mL
urineDrainase kendung kemih bermuara ke vena iliaca interna
-
UretraTabung yang menyalurkan urine ke luar dari buli-buli
Secara anatomis uretra dibagi menjadi 2 bagian : Uretra posterior
dan Uretra anterior
-
Mekanisme TraumaTrauma tumpul -> penyebab trauma Langsung,
tidak langsung
Trauma tumpul langsung KLLOlah ragaKecelakaan
kerjaPerkelahian
-
Trauma tumpul tidak langsung
* Jatuh dari ketinggian* KLL menyebabkan pergerakan ginjal
tiba-tiba dlm rongga retro peritonium Avulsi pedikel ginjal Robekan
tunika intima
-
Bisa juga oleh trauma iatrogenikPemasangan kateter di atas
ureterPengambilan biopsi ginjalInfeksi tidak langsung
Klasifikasi* Ada beberapa macam* Ditentukan oleh luas dan
penatalaksanaan
-
Cedera Ginjal* Minor* Mayor* Vaskuler
Cedera Minor 90% trauma ginjal Kontusio ginjal Laserasi parenkim
superficial
-
Cedera MayorLaserasi korteks, medula tanpa ekstravasasiLaserasi
korteks, medula dengan ekstravasasi
Cedera VaskulerAvulsiTrombosis
-
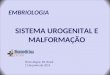
Berdasarkan AAST ( American for The Surgery of Trauma )
-
Berdasarkan AAST( American for The Surgery of Trauma )Dibagi 5
derajatDerajat 1 Kontusio ginjal /subkapsularhematomTidak
meluasHematuria dengan normal imaging
-
Derajat 2 Hematom perinealTdk meluas ke retroperitoniumLaserasi
superficial ( < 1cm )Tdk melibatkan collecting systim Derajat
3Renal laserasi ( > 2cm )Sub capsular hematomPerinephric
hematomTdk melibatkan collecting systim
-
Derajat 4Laserasi yang meluas ke collecting
systimExtravasasiTrauma vasculer segmental infark
-
Derajat 5Shattered kidneyDevaskularisasi / oklusi / trombosis
arteri / vena utamaLaserasi komplitExtravasasiUPJ avulsi
-
Pemeriksaan Radiologi
Foto polos abdomenIVP ( Intra Vena Pyelografi )USG ( Ultra
Sonographi )CT Scan abdomen / Whole abdomenuretrocistografi
-
IVP* Melihat ekstravasasi urin / kontras* Tidak bisa mendeteksi
trauma ginjal derajat I, II* Fungsi ginjal kontra lateral
USG* Melihat hemoperitoneum* Tdk dianjurkan utk evaluasi trauma
ginjal* Dengan color doppler melihat vaskuler
-
CT ScanPemeriksaan yang sensitif dan spesifikMenentukan derajat
traumaTidak invasifDpt mengevaluasi organ lain ( hepar , lien ,
aorta ) kontras non kontras
AngiografiInvasifDelayed renal bleeding-pseudo-aneurisma
-
IVP normal
-
USG ginjal normal
-
CT scan ginjal normal
-
Gambar 1. Kidney trauma. Absent nephrogram. Abdominal radiograph
after intravenous contrast administration in a patient with
hypotension after a motor vehicle collision shows absent right
nephrogram
-
Gambar 2. Kidney trauma. Grade 3 renal laceration on abdominal
radiograph. Abdominal radiograph after intravenous contrast
administration shows very diminished left nephrogram and no urinary
contrast extravasation
-
Gambar 3. Kidney trauma. Grade 5 renal injury. Shattered kidney
with renal vein thrombosis (incomplete). Abdominal radiograph after
intravenous contrast administration shows absent right
nephrogram
-
Gambar 4 Kidney trauma. Grade 1 renal injury, contusion. Image
from a contrast-enhanced CT scan of the abdomen in a patient with
hematuria after a motor vehicle collision shows ill-defined area of
hypoenhancement in the medial right kidney.
-
Gambar. 5. Kidney trauma. Grade 1 renal injury, subcapsular
hematoma. CT scan of the abdomen with intravenous contrast in a
patient after a motor vehicle collision shows crescentic
high-density fluid collection around the left kidney. Note the
well-defined outer margin
-
Gambar 6. Kidney trauma. Grade 1 renal injury, subcapsular
hematoma. CT scan of the abdomen with intravenous contrast in a
patient after a motor vehicle collision; shows crescentic
high-density fluid collection around the left kidney. Note the
well-defined outer margin and the mild deformity of the renal
parenchyma
-
Gambar 6. Kidney trauma. Grade 2 renal injury, subcapsular and
perinephric hematomas. Contrast-enhanced CT scan of the abdomen on
a patient with hematuria after a motor vehicle collision shows an
ill-defined fluid collection in the left perinephric space. There
is also a subcapsular hematoma with deformity of the renal
parenchyma Derajat II dan III
-
Gambar 7 Kidney trauma. Grade 2 renal injury, perinephric
hematoma. Contrast-enhanced CT scan of the abdomen on a patient
with hematuria after a motor vehicle collision shows an ill-defined
fluid collection in the left perinephric space
-
Gambar 8. Kidney trauma. Grade 3 renal laceration with normal
one-shot intravenous pyelogram. CT scan through the kidneys after
intravenous contrast on the same patient as in Image 1 shows renal
laceration and perinephric hematoma.
-
Gambar 9 Kidney trauma. Grade 2 renal laceration.
Contrast-enhanced CT scan of the abdomen after a motor vehicle
collision shows a superficial (less than 1 cm deep) renal
parenchymal defect with a large perinephric hematoma
- Gambar 10. Kidney trauma. Grade 2 renal laceration. Delayed
image shows no urinary contrast extravasation. Contrast-enhanced CT
scan of the abdomen after a motor vehicle collision shows a
superficial (
-
Gambar 11. Kidney trauma. Grade 3 renal laceration. CT scan of
the abdomen after intravenous contrast administration shows
irregular nonenhancing renal parenchymal defect with extension
greater than 1 cm deep to near the renal pelvis. no urinary
contrast extravasation
-
Gambar 12. Kidney trauma. Grade 3 renal laceration. CT scan of
the abdomen after intravenous contrast administration shows
irregular nonenhancing renal parenchymal defect with extension
greater than 1 cm deep to near the renal pelvis. This delayed image
showed no urinary contrast extravasation.
-
Derajat IVGambar13 Kidney trauma. Grade 4-5 renal injury.
Lacerations extending to the collecting system. Contrast-enhanced
CT scan of the abdomen in a patient with hematuria after a motor
vehicle collision shows deep lacerations extending into the
collecting system of the right kidney. Extension into the
collecting system is confirmed by urinary contrast extravasation on
delayed image through the kidney in excretory phase
-
Gamba14. Kidney trauma. Grade 4-5 renal injury. Lacerations
extending to the collecting system. Contrast-enhanced CT scan of
the abdomen in a patient with hematuria after a motor vehicle
collision shows deep lacerations extending into the collecting
system of the right kidney (Image 22). Extension into the
collecting system is confirmed by urinary contrast extravasation on
this delayed image through the kidney in excretory phase
-
Gambar 15. Kidney trauma. Grade 4 renal injury segmental
infarction. Contrast-enhanced CT scan of the upper abdomen shows a
segmental area of nonenhancement in the upper medial left kidney
without associated renal laceration
-
Gambar 16. Kidney trauma. Grade 4 renal injury segmental
infarction. Contrast-enhanced CT scan of the upper abdomen in
another patient after a motor vehicle collision shows a segmental
area of nonenhancement in the upper medial left kidney without
associated renal laceration
-
Derajat VGambar 17. Kidney trauma. Grade 5 renal injury.
Shattered kidney. Contrast-enhanced CT scan of the abdomen in a
patient with hematuria and hypotension after a motor vehicle
collision shows transection of the right kidney with a large
hematoma around and between the 2 halves of the kidney. The 2
halves are both perfused because there were 2 renal arteries
Delayed images show urinary contrast extravasation
-
Gambar 18. Kidney trauma. Grade 5 renal injury. Shattered
kidney. Contrast-enhanced CT scan of the abdomen in a patient with
hematuria and hypotension after a motor vehicle collision shows
transection of the right kidney with a large hematoma around and
between the 2 halves of the kidney. The 2 halves are both perfused
because there were 2 renal arteries. Delayed images show urinary
contrast extravasation
-
Gambar 19 Kidney trauma. Grade 5 renal injury. Shattered kidney.
Contrast-enhanced CT scan of the abdomen in a patient with
hematuria and hypotension after a motor vehicle collision shows
transection of the right kidney with a large hematoma around and
between the 2 halves of the kidney. The 2 halves are both perfused
because there were 2 renal arteries Delayed images show urinary
contrast extravasation
-
Gambar 20. Kidney trauma. Grade 5 renal injury. Shattered
kidney. Contrast-enhanced CT scan of the abdomen in a patient with
hematuria and hypotension after a motor vehicle collision shows
transection of the right kidney with a large hematoma around and
between the 2 halves of the kidney. The 2 halves are both perfused
because there were 2 renal arteries. Delayed images show urinary
contrast extravasation
-
Gambar 21. Kidney trauma. Grade 5 renal injury. Shattered kidney
with renal vein thrombosis (incomplete). CT scan of the abdomen
with intravenous contrast administration shattered right kidney and
renal vein thrombus extending slightly into the inferior vena
cava
-
Gambar 22. Kidney trauma. Normal ultrasound with grade 5 renal
injury. Ultrasound gray-scale image of a patient involved in a
motor vehicle collision shows what appears to be a normal right
kidney
-
Gambar 23 Kidney trauma. Grade 5 renal injury. Color Doppler
ultrasound of same motor vehicle collision patient as in Image 4
shows no blood flow within the right kidney.
-
4.ArteriografyGambar 24. Kidney trauma. Active vascular contrast
extravasation. Catheter angiography during arterial phase on the
same patient as in Image 40 shows a small pseudoaneurysm at the
lower pole
-
gambar 25. Kidney trauma. Active vascular contrast
extravasation. Catheter angiography during nephrographic phase in
the same patient as in Image 41 shows a small pseudoaneurysm at the
lower pole
-
gambar 26. Kidney trauma. Active vascular contrast
extravasation. Pseudoaneurysm at the lower pole in the same patient
as in Image 42 was embolized by using a coil.
-
Trauma UreterUreter jalur transportasi dari ginjal ke
buli-buliTrauma ureter mengganggu fungsi ginjal
Trauma mengenai pinggang, punggung resiko mengenai ureterok *
Lokasi terlindungi * Ukuran kecil * Mobilitas / fleksibel trauma
ureter jarang
-
Etiologi
Trauma Luar a. Tajamb. TumpulIatrogenik a. Ginekologisb.
Pembedahan rektumc. Endoskopi
-
Pemeriksaan Radiologi
IVP ( Intra Vena Pyelografi )RPG ( Retro Grade Pyelografi )USG (
Ultra Sono Grafi )CT Scan Abdomen
-
Trauma Vesika Urinaria
Disebabkan : Trauma- Tumpul- Tajam- IatrogenikDidaerah pelvis /
abdomen bawah/ perineum 60-85 % trauma tumpul 15-40 % trauma
tajam
-
Ruptur vesika urinaria : keEkstra peritoneumIntra
peritoneumKeduanya
Kontusio Vesika UrinariaSobekan sebagian mkosa vesika
urinariaDinding memar hematom
Pemeriksaan :SistografiCT scan abdomen - pelvis
-
Kontusio Vesika UrinariaNormalTear DropMudah sembuh
Ruptur Vesika UrinariaTerlihat ekstravasasi kontras- ekstra
peritonial- intra peritonialDengan CT Scan dpt juga mengevaluasi
organ lain
-
Pear shaped appearance
-
TRAUMA URETRA
Uretra laki-laki lebih panjang dari wanitaDihubungkan dgn trauma
daerah pelvis yg cukup berat
EtiologiTrauma tumpulTrauma tembusIatrogenik
-
AnatomiUretra posterior * uretra prostatika* uretra
membranosaUretra anterior 3 segmen : * pars bulosa * pars pendulans
* pars glanularis sampai ke meatus uretra externa
-
Diagnosa
Berdasarkan gejala klinikPemeriksaan penunjang radiologiRUG (
Retrograde Uretrografi )
Klasifikasi trauma uretra Hasil RUGKlasifikasi Gold Man yaitu
:Berdasarkan Kerusakan Anatomi
-
Ada 5 tipeTipe 1
. Ruptur ligamentum puboprostatika. Prostate bergeser ke
posterior. Uretra tetap intak. Tdk ada extra vasasi zat kontras
-
Tipe 2
Trauma uretra posterior & diafragma urogenitalTerlihat
extravasasi kontras dlm pelvis extra peritonealZat kontras tdk ada
dalam perineum
-
Tipe 3
Tipe yang sering Kerusakan meluasTerlihat extravasasi kontras
pada rongga pelvis extra peritoneal dan perineum
-
Tipe 4
Terjadi dekat buli-buli meluas ke uretra proximalExtravasasi
kontras pada pelvis extra peritoneal & sekitar proximal
uretraDapat merusak sfingter uretra interna
-
Tipe 5
Terjadi di uretra anteriorTerlihat extravasasi kontras bagian
inferior diafragma urogenital
-
***********