Embed Size (px)
Citation preview

1
PowerPoint Slides English Brazilian PortugueseTranslation
Inflammatory Breast Cancer: Need for a Multidisciplinary Approach to Provide the Best Cancer Treatment Video Transcript
Carcinoma inflamatório de mama: Necessidade de uma abordagem multidisciplinar para oferecer o melhor tratamento antineoplásico Transcrição de vídeo
Professional Oncology Education Inflammatory Breast Cancer: Need for a Mulitdisciplinary Approach to Provide the Best Cancer Treatment Time: 21:52
Educação Profissional em Oncologia Carcinoma inflamatório de mama: Necessidade de uma abordagem multidisciplinar para oferecer o melhor tratamento antineoplásico Duração: 21:52
Naoto Ueno, M.D., Ph.D. Professor, Breast Medical Oncology Section Chief,Translational Breast Cancer Research Executive Director of the Morgan Welch IBC Research Program and Clinic The University of Texas MD Anderson Cancer Center
Dr. Naoto Ueno, M.D., Ph.D. Professor, Mastologia Chefe de Setor, Pesquisa Translacional de Câncer de Mama Diretor Executivo do Programa e Clínica Morgan Welch de Pesquisa em CIM MD Anderson Cancer Center – Universidade do Texas
Hi. I am Naoto Ueno. I am a medical oncologist at The University of Texas MD Anderson Cancer Center. I also represent Executive Director of The Morgan Welch IBC Research Program and Clinic. Today I would like to talk about Multidisciplinary Approach to Provide the Best Care Treatment for Inflammatory Breast Cancer.
Olá. Eu sou Naoto Ueno. Sou mastologista no MD Anderson Cancer Center da Universidade do Texas. Também represento, como Diretor Executivo, a Programa e Clínica Morgan Welch de Pesquisa em CIM. Hoje, gostaria de falar sobre a abordagem multidisciplinar voltada ao melhor tratamento para o carcinoma inflamatório de mama.

2
So our objective, we have three objectives. One is to describe the basic diagnosis of IBC; and define the standard of care for the treatment of IBC; and at the end I hope that everybody will understand the importance of IBC patients participating in clinical trials.
Nossos objetivos. Temos três objetivos. O primeiro, é descrever o diagnóstico básico do CIM; depois, definir o padrão de cuidados no tratamento do CIM; e, finalmente, espero que todos entendam a importância da participação das pacientes com CIM em estudos clínicos.
So IBC: “Why is it so important?” Well, as you know, this disease may only represent 2 to 5% of the entire breast cancer in the United States. However, if you actually look at the disease from the breast cancer mortality, it could represent 8 to 10%. So considering the --- the percentage of the deaths it is a very important disease that we need to tackle with appropriate treatment.
Então, quanto ao CIM: por que é tão importante? Bem, como sabem, nos Estados Unidos, esta doença pode representar apenas 2% a 5% da ocorrência de todos os cânceres de mama. No entanto, se olharmos a [taxa de] mortalidade por câncer de mama, esse valor poderia ser de 8% a 10%. Considerando a porcentagem de óbitos, é uma doença muito importante que precisamos atacar com o tratamento adequado.

3
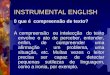
So “why is it poor?” Well as you know, inflammatory breast cancer is a Stage III disease at the time of the presentation. And not only that, when you undergo restaging already one-third of the newly diagnosed patients may have metastasis. This will migrate from a Stage III to Stage IV at the time of the new dia --- diagnosis. When appropriate treatment is given, some of the patient is very resistant to treatment. And despite all treatment including chemotherapy, surgery, radiations given, after the completion of treatment there is a rapid metastasis. So when you look from the 5-year disease-free survival it may represent 30 --- 30 to 40%. We have a representative survival portion in this slide. And as you can see from the 1970s to 2000, pretty much in terms of the survival rate has not changed too much.
Por que [o resultado] é deficiente? Como sabem, o carcinoma inflamatório de mama é uma doença de estágio III no momento da apresentação clínica. E não somente isso: por ocasião do reestadiamento, um terço das pacientes recém-diagnosticadas já poderá apresentar metástase. A doença migrará do estágio III para o IV no momento do novo diagnóstico. Algumas pacientes exibem resistência aos tratamentos adequados que são administrados. Embora seja administrado todo tipo de tratamento, como quimioterapia, cirurgia e irradiação, depois da conclusão do tratamento, a metástase manifesta-se rapidamente. A sobrevida sem doença aos 5 anos pode representar de 30% a 40%. Neste slide, temos uma porção de sobrevida representativa. Como podem ver, desde os anos de 1970 ao ano 2000, a taxa de sobrevida praticamente não mudou muito.
So “why is inflammatory breast cancer difficult to study?” Which actually means it is very difficult to improve the outcome. Well one is limited amount of laboratory research. There is a lack of preclinical models and there is lack of sufficient tumor specimens. Despite that these are big tumors, we have not really prospectively collected samples. And if that means that if it is not collected in a prospective manner, we do not have sufficient samples to study for new molecular targets. Because there is [a] limited number of patients, there is a limited number of clinical trials. And if there is [a] limited number of patient and there be --- there may be lack of interest from the pharma companies.
Então, por que é difícil estudar o carcinoma inflamatório de mama? Que, na realidade, significa que é muito difícil de melhorar os resultados. Bem, uma razão seria o volume limitado de pesquisa laboratorial. Faltam modelos pré-clínicos e peças cirúrgicas tumorais suficientes. Embora sejam tumores de grandes dimensões, não coletamos amostras de maneira prospectiva. E isso significa que se as amostras não forem coletadas de maneira prospectiva, não teremos o número suficiente de amostras para estudar novos alvos moleculares. Por haver um número limitado de pacientes, há um número limitado de estudos clínicos. E se há um número limitado de pacientes, talvez haja falta de interesse por parte da indústria farmacêutica.

4
So let’s look at the diagnostic criteria of IBC. IBC is clinical and/or pathological diagnosis. This means that it does not have to have a typical pathological feature of IBC as long as clinical features are satisfied. Rapid progressive increase in size of the breasts with erythema or peau d’orange changes over two-third, induration, and tenderness. From the pathology under the microscope you could have dermal lymphatic invasion or tumor emboli. Now commonly in IBC it is mentioned that there are absent of mass but having a mass does not exclude IBC. So, therefore, as long as the patient presents with a very rapid engorged breast one can actually make a diagnosis of IBC. Unfortunately when these symptoms are --- typical symptoms are present, a lot of time it is misdiagnosed as an infection. Many cases of the red breast could be mastitis. However, once you give antibiotic for appropriate period and if there is no improvement, that could actually represent possible --- possible breast cancer. Therefore, appropriate biopsy is needed.
Vejamos os critérios diagnósticos do CIM. O diagnóstico do CIM é clínico e/ou patológico. Isto significa que não precisa ter uma característica patológica típica de CIM se as características clínicas forem atendidas. Aumento rápido e progressivo do tamanho das mamas, com eritema ou aspecto de casca de laranja em dois-terços, endurecimento e dor à palpação. O exame patológico com microscópio pode revelar invasão linfática da derme ou êmbolos tumorais. É comumente mencionado que no CIM há ausência de nódulos, mas sua presença não exclui a ocorrência de CIM. Portanto, sempre que o ingurgitamento da mama se manifeste bastante rapidamente, poderemos fazer um diagnóstico de CIM. Infelizmente, quando estes sintomas típicos se manifestam, muitas vezes [o CIM] é diagnosticado equivocadamente como infecção. Muitos casos de mamas avermelhadas podem ser mastite. No entanto, se após administrar antibióticos por um determinado tempo não houver melhora, poderia ser câncer de mama. Portanto, é necessário biópsia adequada ao caso.
So “what effort have --- has been going on at an international level?” As I mentioned, inflammatory breast cancer diagnostic criteria has been somewhat unclear. However, in 2008, at the First International IBC Conference we have agreed with the diagnostic criteria which was mentioned before and since then we have been prospectively collecting the samples. This includes tumor, skin tissue, serum, and epilo --- epidemiological data and clinical data. And we hope that by collecting this at an international and domestic level that we will actually improve total amount of bio-specimens and data which will help us to come up with an interesting target as well as a unique treatment for inflammatory breast cancer.
E no âmbito internacional, o que vem sendo feito? Como mencionei, os critérios diagnósticos para o carcinoma inflamatório de mama não são muito claros. Contudo, em 2008, no Primeiro Congresso Internacional de CIM, concordamos com os critérios diagnósticos que foram mencionados anteriormente e desde então viemos coletando as amostras de maneira prospectiva. Eles seriam dados referentes ao tumor, à derme, ao soro, epidemiológicos e clínicos. Esperamos que ao coletá-los nos âmbitos internacional e nacional, possamos melhorar o volume total de amostras biológicas e de dados que nos ajudarão a descobrir um alvo interessante, bem como um tratamento especial para o carcinoma inflamatório de mama.

5
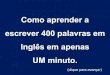
So let’s actually go over one more time in terms of diagnosis of inflammatory breast cancer. As I mentioned in [the] top of this figure or the flow chart you could see that patients may present with breast erythema, edema and you ask medical history and physical exam. These are --- these patient could pre --- present more in general primary care settings. Obviously if the breast is engorged, was red, you may treat as a mastitis which is probably most appropriate. But at the same time you could actually seek for ultrasound or mammograph if you suspect breast cancer or other form of --- other than infections. So if you suspect for IBC, obviously we recommend to have a patient to have a breast MRI and biopsy. And a biopsy may confirm the diagnosis. These are from top to towards the --- the left probably is a very easy path. Now what makes it difficult is that after ultrasound you see abscess and that does not automatically rule out inflammatory breast cancer. The other thing is that if it’s negative for cancer “does that mean that the patient does not have IBC?” The answer is “no” because inflammatory breast cancer may not have a mass. Therefore, the biopsy may have happened at the location where there is no tumor located. So, therefore, with the antibiotic trial and after two weeks still no improvement, it is very important that you go back one more time to determine if there is any possibility of cancer and maybe [a] second biopsy is needed. Same thing for abscess; drainage is a typical --- as we --- drainage as well as abscess mass is appropriate to make a diagnosis of abscess. However, if there is no improvement of the treatment, it is very important to go through the path one more time and to consider biopsy of the tumor. So what I am trying to say here is if you suspect it is very important to biopsy the breast. And even if it is a negative diagnosis, it is very important to continue to pursue the biopsy until you make a diagnosis.
Revisemos outra vez em termos de diagnóstico do carcinoma inflamatório de mama. Como mencionei na parte superior desta ilustração ou fluxograma, vocês podem ver que as pacientes podem apresentar eritema e edema na mama, e vocês pedem a história clínica e fazem um exame físico. Estas pacientes são examinadas mais comumente em ambientes de atendimento primário à saúde em geral. Obviamente, se houver ingurgitamento e avermelhamento das mamas, o mais adequado seria tratá-la como mastite. Mas também poderia se pedir uma ultrassonografia ou uma mamografia se houver suspeita de câncer de mama ou outra forma de... além de infecções. Se houver suspeita de CIM, obviamente, recomendamos à paciente fazer uma RM e uma biópsia da mama. A biópsia pode confirmar o diagnóstico. Estas [opções], da parte superior à esquerda, talvez sejam uma via muito fácil. O que dificulta é, após a ultrassonografia, constatar um abcesso e não poder descartar automaticamente a possibilidade de carcinoma inflamatório de mama. Outro fator seria, no caso de não ser câncer, isso significaria que a paciente não tem CIM? A resposta é “não”, porque o carcinoma inflamatório de mama pode não apresentar nódulos. Portanto, a biópsia pode ter sido feita onde não havia tumor. Por isso, depois de administrar antibióticos e não haver melhora por duas semanas, é muito importante voltar e determinar mais uma vez a possibilidade de ocorrência de câncer de mama e da necessidade de uma segunda biópsia. O mesmo acontece com os abcessos. A supuração é comum. Na presença de supuração e abcessos, é pertinente fazer o diagnóstico de abcesso. No entanto, se não houver melhora com o tratamento, é muito importante passar mais uma vez pela via e considerar a biópsia do tumor. O que estou tentando dizer é que se houver suspeita, é muito importante fazer a biópsia da mama. Mesmo com diagnóstico negativo, é muito importante continuar a fazer a biópsia até se obter o diagnóstico.

6
So “what about the treatment?” Well, the historically, the treatment has been established at The University of Texas MD Anderson Cancer Center by the following physicians. Because this is a very aggressive disease, in the 70s, there was almost --- there was agreement that it is important to combine all modalities. This means that you start with neoadjuvant preoperative chemotherapy, followed by surgery, and radiation. So these combination of treatments became a standard for inflammatory breast cancer treatment.
E o que dizer sobre o tratamento? Historicamente, o tratamento foi estabelecido no MD Anderson Cancer Center da Universidade do Texas por estes médicos. Como esta é uma doença muito agressiva, nos anos de 1970, houve acordo geral sobre a importância de combinar todas as modalidades [de tratamento]. Isso significa que se inicia com quimioterapia neoadjuvante pré-operatória, seguida de cirurgia e radiação. Essa combinação de tratamentos se tornou padrão no tratamento do carcinoma inflamatório de mama.
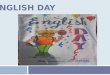
So I would like to show you some time flow of how newly diagnosed inflammatory breast cancer is treatment. When the patient shows up, we do recommend three imagings for the breasts: mammogram, MRI mammography, and ultrasound. At MD Anderson we have agreement that we will obtain a PET-CT scan to rule out metastasis. We will quickly obtain surgical, radiation, and medical oncology consults. It is very important that all three disciplines see the patient at early stage of the disease. There are other forms of cancer markers such as CEA and CA15-3 or circulating tumor cells may be ob --- obtained. Now once a metastasis is ruled out, this is considered primary inflammatory breast cancer. Our standard care for preoperative systemic chemotherapy, we start with weekly paclitaxel followed by FAC or FEC chemotherapy. Obviously if the tumor is HER2-positive we will add additional trastuzumab with weekly paclitaxel. And at the portion of the anthracycline containing regimen, FEC will be reduced to 75 mg/m2 and then we will be adding trastuzumab here. As you can see, the standard is to undergo modified radical mastectomy over --- after six months of preoperative chemotherapy and then followed by radiation therapy. If it is ER-positive, we recommend endocrine therapy for five years. For trastuzumab, a total one year is recommended.
Gostaria de mostrar um pouco do fluxo de tratamento que recebem [as pacientes] recém-diagnosticadas com carcinoma inflamatório de mama. Quando as pacientes chegam, recomendamos três exames por imagem das mamas: mamografia, mamografia por RM e ultrassonografia. No MD Anderson, concordamos em fazer uma TC-TEP para descartar a possibilidade de metástase. Obtemos rapidamente consultas para cirurgias, radiações e mastologia. É muito importante que todas as três disciplinas examinem a paciente nas fases iniciais da doença. Existem outros marcadores de câncer, como CEA e CA15-3 ou células tumorais circulantes que podem ser obtidos. Depois de ser descartada a metástase, considera-se como carcinoma inflamatório primário de mama. No padrão de cuidados que seguimos na quimioterapia sistêmica pré-operatória, iniciamos com paclitaxel administrado semanalmente, seguido dos esquemas quimioterápicos com FAC ou FEC. Obviamente, se o tumor for positivo para HER2, adicionaremos mais trastuzumabe com o paclitaxel semanal. E, na porção do esquema com antraciclina, o FEC será reduzido para 75 mg/m2 e o trastuzumabe será incluído posteriormente. Como podem ver, o padrão é submeter a paciente à mastectomia radical modificada depois de seis meses de quimioterapia pré-operatória e, depois, radioterapia. Se for positivo para RE, recomendamos terapia endócrina por cinco

7
anos. Para o trastuzumabe, a recomendação é de um ano inteiro.
So now I’d like to show you some retrospective data which reflects the treatment outcome of inflammatory breast cancer. We have actually reviewed data from 1970 to 2011. And what we have noticed that people who receive multidisciplinary approach has the best outcome. This means once again that it is important to receive preoperative chemotherapy followed by modified radical mastectomy and radiation. If you lack any of them, the outcome is not sufficient.
Agora, gostaria de mostrar alguns dados retrospectivos que refletem o resultado do tratamento do carcinoma inflamatório de mama. Com efeito, revisamos dados de 1970 a 2011. O que notamos foi que as pessoas que receberam tratamentos multidisciplinares alcançaram os melhores resultados. Isto significa mais uma vez que é importante receber quimioterapia pré-operatória seguida de mastectomia radical modificada e radiação. Se um deles faltar, o resultado não será suficiente.
So let’s actually compare some of the differences between non-inflammatory breast cancer and inflammatory breast cancer. You could read the slides but I will give you some highlights with some of the issues that we face. For example, imaging: as I mentioned, we recommend mammogram, MRI, ultrasound; three imagings to be done for inflammatory breast cancer to --- to obtain a detail changes in the breasts. We recommend PET-CT scan to rule out metastasis. For treatment: preoperative systemic chemotherapy is mandatory. Surgery: modified radical mastectomy is mandatory. This means that the patient should never go [to] surgery up front for primary inflammatory breast cancer. Lumpectomy or other form of less intensive surgery is contraindicated. Radiation therapy: is also mandatory. Adjuvant systemic treatment: is no different from non-IBC. HER2-positive patients should receive anti-HER2 therapy, hormone receptor-positive [patients] should receive antihormonal agents. Clinical trials in non-IBC as clinically indicated; now, you can see that --- that in inflammatory breast cancer we actually recommend, it is almost close to mandatory to seek clinical trials. This --- now the reason for this is, as I mentioned, even with all modalities put together, outcome is not
Comparemos algumas das diferenças entre o carcinoma de mama não inflamatório com o inflamatório. Vocês podem ler os slides, mas eu destacarei alguns problemas que enfrentamos. Por exemplo, a imaginologia: como mencionei, recomendamos mamografia, RM e ultrassonografia. Três exames por imagem a serem feitos para o carcinoma inflamatório de mama para obter detalhes de alterações ocorridas nas mamas. Recomendamos TC-TEP para descartar a possibilidade de metástase. Para o tratamento: a quimioterapia sistêmica pré-operatória é obrigatória. Cirurgia: a mastectomia radical modificada é obrigatória. Isto significa que a paciente jamais iria à cirurgia diretamente para tratar um carcinoma inflamatório primário de mama. A lumpectomia ou outra forma de cirurgia menos intensiva é contraindicada. Radioterapia: também é obrigatória. Tratamento sistêmico adjuvante: não é diferente do CIM não inflamatório. Pacientes com doença positiva para HER2 devem receber terapia anti-HER2; pacientes com doença positiva para receptores hormonais devem receber agentes anti-hormonais. Estudos clínicos para CIM não inflamatório: conforme indicação clínica. Como podem ver, de fato, o recomendamos no carcinoma inflamatório de mama. [Neste caso] é quase

8
the best. Therefore, if we would like to see any improvement, further new approaches are needed under clinical trials.
obrigatório procurar estudos clínicos. A razão é que, como mencionei, mesmo com todas as modalidades administradas conjuntamente, os resultados não são os melhores. Portanto, se quisermos ver alguma melhora, precisaremos de novos tratamentos desenvolvidos em estudos clínicos.
Now, let’s look into the clinical criteria. And let’s look into what are the questions that we --- we need to answer in IBC. On the left side, these are things that what we know and the right side is the que --- research question or clinical question we need to answer. For example, in clinical criteria: as I mentioned roughly about 3 - 6 months may be appropriate for clinical signs, but “does the duration of clinical signs and symptoms of this --- of the time of diagnosis have to be no more than three months?” “Does the erythema have to involve more than one-third of the breast” or some people say two-thirds of the breast? Pathological criteria: “Is dermal lymphatic involvement a requirement for the diagnosis of IBC?” So it goes back to this important question? “What is the molecular criteria of IBC?” So if anybody asks me as of 2012 in Fall, we do not have a definitive molecular criteria that would determine what is inflammatory breast cancer compared to non-inflammatory breast cancer. So it goes back to one more time, the criteria for the diagnosis is really purely clinical and/or pathological diagnosis.
Examinemos os critérios clínicos e as perguntas que precisamos responder quanto ao CIM. À esquerda, há fatores que conhecemos; e à direita, está a pergunta de pesquisa ou clínica que precisamos responder. Por exemplo, nos critérios clínicos: como mencionei, ao redor de 3 a 6 meses pode ser suficiente para a apresentação de sinais clínicos, mas “a duração dos sinais e sintomas clínicos no momento do diagnóstico não poderia superar os três meses?” “O eritema tem de acometer mais de um terço da mama” ou, algumas pessoas dizem, dois-terços da mama? Critérios patológicos: “O comprometimento linfático da derme é obrigatório para o diagnóstico do CIM?” Ou seja, voltamos a esta importante questão: “Quais são os critérios moleculares para o CIM?” Se até por volta de outubro-novembro de 2012 alguma pessoa me perguntasse se temos critérios moleculares definitivos para distinguir o carcinoma inflamatório de mama do não inflamatório, eu diria que não. Isto é, voltamos mais uma vez aos critérios para o diagnóstico: eles são puramente clínicos e/ou patológicos.

9
Imaging: “Can we identify radiological findings specific to IBC by exploring molecular imaging?” We highly recommend MRI. An MRI may give you more detailed architect[ure] as well as lymph node changes. “Does functional MRI have a role in monitoring the response to IBC by preoperative chemotherapy?” Preoperative chemotherapy goals is to achieve pathological complete response. What we know is if you could achieve a high pathological complete response, meaning that by systemic chemotherapy when you go to surgery you do not see tumor, it is the best. However, currently, we do not have the best imaging technique to determine this. We also recommend a PET-CT scan to rule out metastasis. However, in general, standard guideline talks as optional. As I mentioned at The University of Texas MD Anderson Cancer Center, we have agreement of obtain PET-CT scan, but we still need to confirm whether PET-CT is the most --- best way to determine or --- or identify metastasis.
Imaginologia: “Podemos identificar achados radiológicos específicos ao CIM para explorar a imaginologia molecular?” Certamente, recomendamos a RM. A RM pode oferecer uma arquitetura mais detalhada, bem como alterações linfonodais. “A RM funcional cumpre algum papel no monitoramento da resposta do CIM à quimioterapia pré-operatória?” O objetivo da quimioterapia pré-operatória é alcançar a resposta patológica completa. Sabemos que o melhor seria poder alcançar uma alta resposta patológica completa, ou seja, pela quimioterapia sistêmica, não ver o tumor no momento da cirurgia. No entanto, atualmente, não dispomos da melhor técnica imaginológica para determiná-la. Além disso, recomendamos TC-TEP para descartar a possibilidade de metástase. Contudo, em geral, as diretrizes padrão indicam como opcional. Como mencionei, no MD Anderson Cancer Center da Universidade do Texas, o acordo é de fazermos uma TC-TEP, mas ainda precisamos confirmar se a TC-TEP é a melhor maneira de determinar ou identificar metástases.
So let’s go into the category of treatment. For chemotherapy: as you know, at MD Anderson we recommend weekly paclitaxel and anthracycline-containing regimens to achieve high pathological complete response. But at the same time at the other cancer centers non-anthracycline-based chemotherapy has been pursued. Whether this is indicated in inflammatory breast cancer is completely unknown. For targeted therapy: “can we establish IBC-specific target therapy”? This goes back to [the] important question which is the research, because currently we do not have a molecular definition. We do not have specific targets. So, therefore, obtaining more tissue and identifying targets is very important. For surgery: we recommend modified radical mastectomy. However, “is there any role of sentinel lymph node biopsy and limit the lymph node dissection if patient has pathological complete response?” Currently, we may actually recommend immediate reconstruction waiting about a year from completing the modified radical mastectomy, but, “is there any role of immediate reconstruction of the breast?” For radiation p --- therapy: “which patient
Examinemos a categoria do tratamento. Na quimioterapia: como já sabem, no MD Anderson, recomendamos administração semanal de esquemas com paclitaxel e antraciclina para alcançar uma reposta patológica completa elevada. Mas, ao mesmo tempo, nos outros centros de câncer, foram administradas quimioterapias sem antraciclina. Se isso for indicado no carcinoma inflamatório de mama, é fato completamente desconhecido. Na terapia molecular dirigida: “Podemos estabelecer uma terapia dirigida especificamente contra o CIM?” Isto refere-se novamente à importante pergunta, que é a pesquisa, porque, atualmente, não temos uma definição molecular. Não temos alvos específicos. Por esse motivo, a obtenção de mais tecidos e a identificação de alvos é muito importante. Na cirurgia; recomendamos a mastectomia radical modificada. No entanto, “existe algum papel para a biópsia do linfonodo sentinela e limite da dessecação linfonodal se a paciente apresentar uma resposta patológica completa?” Atualmente, podemos, de fato, recomendar a reconstrução imediata, com espera aproximada de um ano após a mastectomia radical
10
should undergo accelerated hyperfractionated radiation therapy?” “Does preoperative radiation therapy have any role?” Once again we do not know. Treatment for metastatic disease: “Does metastatic IBC differ biologically --- from metastatic non-IBC?” As I mentioned, inflammatory breast cancer staging is Stage III at this moment, or, Stage III-B more accurately. However, once you have a metastasis, it is automatically con --- con --- called Stage IV. Whether Stage IV originating from IBC compared to non-IBC, “do they have a different prognosis” is something that we don’t know. “Can we actually establish targeted therapy or immunotherapy for metastatic IBC,” is something we need to continue to explore.
modificada, mas, “existe algum papel para a reconstrução imediata da mama”? Na radioterapia: “que paciente deve ser submetida à radioterapia acelerada hiperfracionada”? “A radioterapia pré-operatória cumpre alguma função?” Novamente, não sabemos. Tratamento da doença metastática: “o CIM metastático difere biologicamente do CIM não metastático?” Como mencionei, o estadiamento do carcinoma inflamatório de mama é, no momento, estágio III ou, mais precisamente, estágio III-B. No entanto, na ocorrência de metástase, é automaticamente denominado de estágio IV. Se o estágio IV derivado de CIM ou do carcinoma mamário não inflamatório “apresentam prognósticos diferentes”, é algo que não sabemos. “Podemos realmente estabelecer uma terapia molecular dirigida ou imunoterapia para o CIM metastático?” Isto é algo que precisamos continuar a explorar.
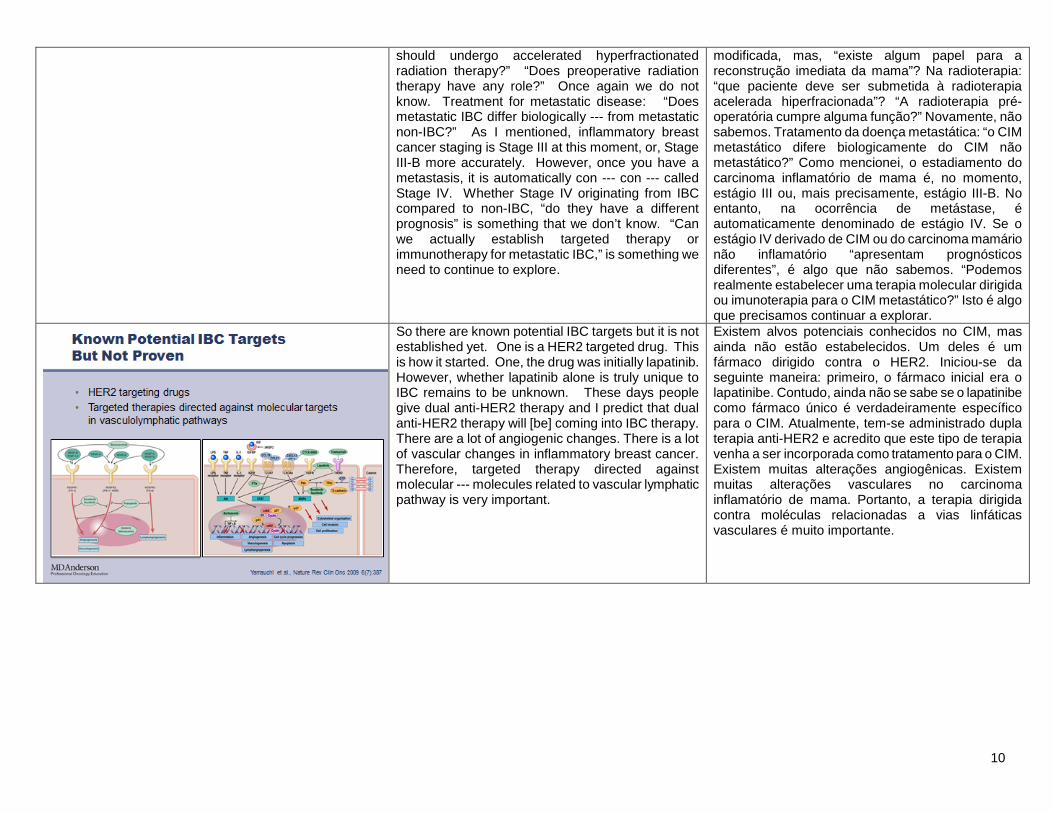
So there are known potential IBC targets but it is not established yet. One is a HER2 targeted drug. This is how it started. One, the drug was initially lapatinib. However, whether lapatinib alone is truly unique to IBC remains to be unknown. These days people give dual anti-HER2 therapy and I predict that dual anti-HER2 therapy will [be] coming into IBC therapy. There are a lot of angiogenic changes. There is a lot of vascular changes in inflammatory breast cancer. Therefore, targeted therapy directed against molecular --- molecules related to vascular lymphatic pathway is very important.
Existem alvos potenciais conhecidos no CIM, mas ainda não estão estabelecidos. Um deles é um fármaco dirigido contra o HER2. Iniciou-se da seguinte maneira: primeiro, o fármaco inicial era o lapatinibe. Contudo, ainda não se sabe se o lapatinibe como fármaco único é verdadeiramente específico para o CIM. Atualmente, tem-se administrado dupla terapia anti-HER2 e acredito que este tipo de terapia venha a ser incorporada como tratamento para o CIM. Existem muitas alterações angiogênicas. Existem muitas alterações vasculares no carcinoma inflamatório de mama. Portanto, a terapia dirigida contra moléculas relacionadas a vias linfáticas vasculares é muito importante.

11
At MD Anderson we are actually currently exploring the following novel targets in IBC. One is EGFR. Second is FGF. We are trying to reduce the inflammation. Inflammation is generally caused by cytokines or chemokines. So, therefore, we are trying to use a drug that will reduce inflammation. HDAC is another important drug. This has overall impact to the entire gene - protein synthesis and using the HDAC inhibitor may change the characteristics of inflammatory breast cancer.
No momento, estamos explorando no MD Anderson os seguintes novos alvos no CIM. O primeiro é o EGFR; o segundo é o FGF. Estamos tentando reduzir a inflamação. A inflamação é geralmente causada por citocinas ou quimiocinas. Por isso, estamos tentando usar um fármaco que reduza a inflamação. O HDAC é outro fármaco importante. Este afeta toda a síntese gênica-proteica e utiliza um inibidor do HDAC que pode alterar as características do carcinoma inflamatório de mama.
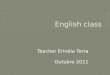
Now, I would like to give you [an] example of a clinical trial conducted at The University of Texas MD Anderson Cancer Center. This clinical trial focuses on our novel target EGFR. In this clinical trial we will use panitumumab which is anti-EGFR antibody to target EGFR. This drug will be combined with two other forms of chemotherapy. One is nab-paclitaxel. Nab-paclitaxel is a different form of paclitaxel which penetrates much better into the cancer cells. Carboplatin actually has a synergy with paclitaxel. So you can see comparing to standard treatment which only gives weekly paclitaxel, by having [a] three drug combination, potentially, this may actually increase the activity of the entire drugs. This means at --- at the time of the modified radical mastectomy, as I said, pathological complete response is very important. In this, we hope that we could increase the pathological complete response. Another characteristic of [a] clinical trial is not just to improve the treatment but actually to obtain more information so that we could improve the care of inflammatory breast cancer. As you can see here that we have biopsied before the preoperative chemotherapy. And after receiving the chemotherapy, we will obtain another biopsy. And we would do a variety of molecular markers to understand how this treatment works. So I hope you --- that this gives you some idea of how a clinical trial works and clinical trial is
Agora, gostaria de dar um exemplo de um estudo clínico realizado no MD Anderson Cancer Center da Universidade do Texas. Este estudo clínico se concentra no EGFR, nosso novo alvo. Neste estudo clínico, usaremos panitumumab, que é um anticorpo anti-EGFR dirigido contra o EGFR. Este fármaco será combinado com outras duas formas de quimioterapia. Uma delas é o nab-paclitaxel. O nab-paclitaxel é uma forma diferente de paclitaxel que penetra muito melhor dentro das células cancerosas. A carboplatina apresenta sinergia com o paclitaxel. Vocês podem ver que, comparando com o tratamento padrão, no qual se administra semanalmente o paclitaxel como fármaco único, a combinação de três fármacos pode aumentar a atividade de todos os fármacos. Isso significa que, no momento da mastectomia radical modificada, como disse, a resposta patológica completa é muito importante. Nesse momento, esperamos poder aumentar a resposta patológica completa. Outra característica do estudo clínico não é apenas melhorar o tratamento, mas obter de fato mais informações para podermos melhorar o atendimento médico no câncer inflamatório de mama. Como podemos ver aqui, foi feita uma biópsia antes da quimioterapia pré-operatória. E depois de receber a quimioterapia se faz outra biópsia. Além disso, utilizaríamos diversos marcadores moleculares para entender o funcionamento do tratamento. Espero que

12
important for inflammatory breast cancer patients. isto dê uma ideia de como funciona o estudo clínico, e de sua importância para as pacientes com carcinoma inflamatório de mama.
What I could say [to] you is that inflammatory breast cancer does require a team work. If you have an inflammatory breast cancer specialist nearby your clinic or if you --- if it is possible to obtain a second opinion, I highly recommend seeking [an] IBC specialist. This is important to do this at the time of the diagnosis. Now a lot of time patients may receive one dose of treatment and this makes it very difficult. This means that we recommend not to receive any treatment until you see the IBC specialist. By receiving any form of treatment, [that] may actually exclude you from receiving any new type of a treatment based on clinical trials. So, therefore, it is important that you seek and participate in clinical trials. Once again, I emphasize that standard care is well-defined but that the outcome is not the best at this point. Therefore, [the] alternative is clinical trials. Clinical trials are generally available at large cancer centers which may have IBC specialists.
O que posso dizer é que o carcinoma inflamatório de mama exige trabalho de equipe. Se houver um especialista em carcinoma inflamatório de mama próximo à clínica de vocês, se for possível obter uma segunda opinião, eu recomendaria veementemente que procurassem um especialista em CIM. Isso é importante no momento do diagnóstico. Por outro lado, muitas vezes as pacientes podem receber uma dose do tratamento, o que dificulta muito a situação. Isso significa que recomendamos não receber nenhum tratamento até consultar com um especialista em CIM. Receber alguma forma de tratamento implica a possível exclusão da paciente de receber algum novo tipo de tratamento com base em estudos clínicos. Portanto, é importante buscar estudos clínicos e participar neles. Novamente, enfatizo que o padrão de atendimento é bem definido, mas, no momento, os resultados não são bons. Portanto, a alternativa é o estudo clínico. Geralmente, os estudos clínicos estão disponíveis em grandes centros de oncologia, os quais podem contar com especialistas em CIM.
So at the end, you may have different questions or you may have feedback. And at The University of Texas MD Anderson Cancer Center, we are using a social network system in Twitter and Facebook. And we welcome your comments or questions and I will be happy to address these questions using social network system. Further for clinical trial information you could actually visit our web page at MD Anderson below and this will hopefully help you to guide you for better treatment. Thank you very much.
No final, vocês poderão ter muitas dúvidas ou poderão oferecer feedback. No MD Anderson Cancer Center da Universidade do Texas, utilizamos as redes sociais Twitter e Facebook. Teremos prazer em responder aos comentários ou perguntas por meio destas redes. Além disso, para obter informações sobre estudos clínicos, podem visitar nosso site do MD Anderson, abaixo. Esperamos que elas sirvam de auxílio para a obtenção de um melhor tratamento. Muito obrigado.