Embed Size (px)
Citation preview

i
FABIANA DE LIMA VAZQUEZ
RISK AND VULNERABILITY TO ORAL DISEASES IN
BRASILIAN ADOLESCENTS
RISCO E VULNERABILIDADE AS DOENÇAS BUCAIS EM
ADOLESCENTES BRASILEIROS
PIRACICABA
2014

ii

iii
FABIANA DE LIMA VAZQUEZ
RISK AND VULNERABILITY TO ORAL DISEASES IN BRAZILIAN
ADOLESCENTS
RISCO E VULNERABILIDADE AS DOENÇAS BUCAIS EM
ADOLESCENTES BRASILEIROS
Piracicaba
2014
Universidade Estadual de Campinas
Faculdade de Odontologia de Piracicaba
Thesis presentes to the Piracicaba Dentistry School of the University of Campinas in partial fulfillment of the requirements for the degree of Dentistry PhD title that of Public Health. Tese apresentada à Faculdade de Odontologia de Piracicaba da Universidade Estadual de Campinas como parte dos requisitos exigidos para a obtenção do título de Doutora em Odontologia, na Área de Saúde Coletiva.
Orientador: Prof. Dr. Antonio Carlos Pereira Este exemplar corresponde à versão final da tese defendida pela aluna Fabiana de Lima Vazquez e orientada pelo Prof. Dr. Antonio Carlos Pereira.
___________________________ Antonio Carlos Pereira

iv
FICHA CATALOGRÁFICA

v
FOLHA DE APROVAÇÃO

vi

vii
RESUMO
Este estudo de transversal analítico e qualitativo teve como objetivo avaliar o risco as
doenças bucais e a vulnerabilidade em adolescente de 15 a 19 anos no município de
Piracicaba-SP. Foi realizado exame clínico para obter as informações de risco a cárie,
CPOD e doença periodontal. Para as variáveis socioeconômicas, comportamentais,
demográficas e psicossociais foram usados os questionários semiestruturado de Góes,
socioeconômico, OIDP, WHOQOL e entrevistas em profundidade com os adolescentes
com necessidade de tratamento (após 12 meses). A amostra aleatória probabilística foi de
1179 adolescentes de 34 Unidades de Saúde da Família (USF). O exame bucal foi
realizado com sonda periodontal IPC e espelho bucal plano sob luz artificial por dois
examinadores. Para avaliar a associação entre as variáveis clínicas, socioeconômicas,
comportamentais, demográficas e psicossociais, foram realizadas análises univariadas pelo
teste de qui-quadrado e teste de Fisher e a seguir, análises multinível a fim de identificar as
variáveis de risco. Na fase qualitativa, as entrevistas gravadas foram transcritas, os dados
agrupados por categorias e identificados os temas chave permitindo a análise temática. Nos
resultados para variável dependente cárie e CPOD, os adolescentes que precisavam de
próteses dentárias, declararam ter presidiário na família e residiam em casas com um
número maior de pessoas, tinham mais dentes cariados. Houve relação entre maior CPOD
e número de dentes cariados, com uma pior auto percepção da saúde bucal. Ser do sexo
feminino, já ter tido dor de dente, idade e tempo desde a última visita ao dentista estavam
relacionados com o índice CPOD. Quanto às variáveis contextuais, o CPOD foi menor nos
subúrbios com maior acesso a esgoto doméstico e o número de dentes cariados foi maior
nos bairros com os piores índices de exclusão social. Para a variável dependente
periodontia, os adolescentes que nunca tiveram dor de dente, que relataram um menor
impacto sobre a saúde bucal e residiam em casas com maior percentual de esgoto
doméstico apresentaram menos doença periodontal. Para a variável dependente OIDP e
WOQUOL, as meninas relataram pior qualidade de vida e maior impacto sócio dental.
Houve uma diminuição da qualidade de vida e aumento na OIDP com o aumento do índice
periodontal. Por sua vez, verificou-se um aumento da qualidade de vida e redução OIDP
com o aumento da renda. Os adolescentes que residiam em áreas de maior exclusão social

viii
e com maior impacto sócio dental apresentaram pior qualidade de vida. Para a pesquisa
qualitativa, a não adesão ao tratamento foi relacionada com alguns aspectos e agrupadas
em não prioridade, prioridade e mudança de prioridade. Concluímos que as variáveis
individuais e contextuais foram associadas com a presença de cárie, índice CPOD, doença
periodontal, o impacto e a qualidade de vida em adolescentes, indicando que deve ser
levado em consideração na formulação de políticas voltadas para a promoção da saúde
bucal e atividades de prevenção e que as principais justificativas para a não adesão estão
relacionadas com diferentes prioridades e o aparelho ortodôntico como motivador da
prioridade à saúde bucal entre os adolescentes.
Palavras-chave: Saúde bucal, Risco, Vulnerabilidade, Qualidade de vida; Pesquisa
qualitativa; Comportamento do adolescente.
ix
ABSTRACT
This cross-sectional study of quantitative and qualitative nature aimed to evaluate the risk
of oral diseases and vulnerability in adolescent 15-19 years in Piracicaba - SP. The
information risk caries, DMFT and periodontal disease were collected and the
socioeconomic, behavioral, demographic and psychosocial variables were recorded by
means of the OIDP, WHOQOL, and socioeconomic semistructured questionnaire. In
addition, in-depth interviews were conducted with adolescents in need of treatment after 12
months of diagnosis. A random sample of 1179 adolescents from 21 public schools in the
areas of 34 Family Health Units (USF). The oral examination was performed with CPI
periodontal probe and dental mirror under artificial light by two trained examiners. To
evaluate the association between clinical, socioeconomic, behavioral, demographic and
psychosocial, univariate analyzes were performed using the chi- square test and Fisher's
exact test and then, multilevel analyzes to identify risk variables. In the qualitative phase,
interviews were transcribed, key data grouped by categories and themes identified allowing
the thematic analysis. The results in caries and DMFT dependent variable, teens who
needed dentures, have declared convict in the family and living in houses with more
people, had more decayed teeth. There were a greater number of decayed teeth and DMFT
with worse self-perception of oral health. Being female, having already had toothache, age
and time since last dental visit were related to DMFT. With regard to contextual variables,
the DMFT was lower in the suburbs with greater access to domestic sewage and the
number of decayed teeth was higher in neighborhoods with the worst levels of social
exclusion. For the dependent variable periodontics, teens who have never had a toothache,
with a lesser impact on oral health and living in houses with higher percentage of domestic
sewage exhibited less periodontal disease. For the dependent variable and OIDP
WOQUOL, the girls had worse quality of life and greater impact dental partner. There was
a decrease in quality of life, and increased with increasing OIDP periodontal index. In turn,
there has been an increase in quality of life and reduction OIDP with increasing income.
Adolescents residing in areas of greater social exclusion and greater impact dental partner
had a poorer quality of life. For qualitative research, nonadherence to treatment was related
to some aspects and not grouped in priority, priority and priority change. We conclude that

x
individual and contextual variables were associated with the presence of caries, DMFT,
periodontal disease, impact and quality of life in adolescents, indicating that it should be
taken into consideration in the formulation of policies for the promotion of oral health and
activities prevention and that the main reasons for non-adherence are related to different
priorities and braces as a motivator priority to oral health among adolescents.
Key Words: Oral health, risk, vulnerability, Quality of life, Qualitative research,
Adolescent behavior.

xi
SUMÁRIO
DEDICATÓRIA
Xiii
AGRADECIMENTOS
Xv
INTRODUÇÃO
1
CAPÍTULO 1: Multilevel analysis of caries in underprivileged adolescents of brazilian
southeast
7
CAPÍTULO 2: Individual and contextual variables related to periodontal disease:
multilevel analysis in underprivileged adolescents in Brazil
39
CAPÍTULO 3: Quality of life and socio-dental impact on underprivileged Brazilian
adolescentes.
71
CAPÍTULO 4: Estudo qualitativo sobre as justificativas de adolescentes carentes para a
não adesão ao tratamento odontológico.
91
CONCLUSÃO
115
REFERÊNCIAS
119
ANEXO 1 Certificado do Comitê de Ética em Pesquisa
125
ANEXO 2 Ficha A do SIAB
127
ANEXO 3 Ficha Clínica
129
ANEXO 4 Questionário de Góes
131
ANEXO 5 Questionário OIDP
139
ANEXO 6 Questionário Socioeconômico
141
ANEXO 7 Códigos e Critérios
143
ANEXO 8 Questionário WHOQOL
147
ANEXO 9 Termo de Consentimento Livre e Esclarecido
149
ANEXO 10 Comprovantes de submissão dos artigos
155

xii

xiii
DEDICATÓRIA
Dedico este trabalho aos meus pais, Eugênio e Yvete pelos votos de confiança,
apoio e infinita compreensão e amor, sem o qual jamais o teria realizado.
Aos meus irmãos Claus e Vinicius e cunhadas Fabiana e Fernanda, pelo carinho e
amor.
Ao meu filho Gabriel, pelo privilégio de conhecer o amor incondicional, puro e
verdadeiro.
Aos sobrinhos Letícia, Francisco e Mariana, por trazerem alegria à minha vida.

xiv

xv
AGRADECIMENTOS
Ao Prof. Dr. Antonio Carlos Pereira, agradeço pela dedicação e paciência em
ensinar-me, por fazer-me acreditar que conseguiria e por direcionar-me a realizá-lo. Meu
eterno agradecimento.
A Faculdade de Odontologia de Piracicaba, na pessoa do seu Diretor, Prof. Dr.
Jacks Jorge Jr., onde tive a oportunidade do crescimento científico e profissional.
Meus agradecimentos aos ilustres professores que compuseram a banca desta tese:
Profa. Dr
a. Rosana de Fátima Possobon, Prof
a. Dr
a. Glaucia Maria Bovi Ambrosano, Profª.
Drª Sílvia Helena de Carvalho Sales Peres, Profª. Drª. Maria Cristina Traldi.
Aos Professores Fábio Luíz Mialhe, Camila da Silva Gonçalo Mialhe, Elaine da
Silva Pereira Tagliaferro, Luciane Zanin, Luciane Miranda Guerra, Karine Laura
Cortellazzi e Jaqueline Vilela Bulgareli e aos Professores do Departamento de Saúde
Coletiva, pela colaboração com preciosas informações para a realização deste trabalho
científico.
A minha grande amiga Karine Cortellazzi, por estar ao meu lado em todos os
momentos, por apoiar-me incondicionalmente, pela dedicação, esforço, determinação e
principalmente por sua alegria e otimismo. Obrigada por acreditar e tornar possível a
realização desse trabalho.
A amiga Luciane Miranda Guerra, pela amizade sincera, pela prontidão, pela
sabedoria, e pela alma de pura bondade. Obrigada pela grande contribuição na produção
deste trabalho.
As amigas Jaqueline Vilela Bulgareli e Valéria da Silva Cândido Brizon pelo apoio
e disponibilidade em ajudar-me.
A Profª. Drª. Cínthia Pereira Machado Tabchoury, coordenadora dos cursos de Pós-
Graduação e à Profª. Drª. Juliana Trindade Clemente Napimoga, coordenadora do
Programa de Pós-Graduação em Odontologia da FOP/UNICAMP.
A Secretária do departamento de pós-graduação, Roberta Clares Morales dos
Santos, pelo profissionalismo e amizade.
A Secretária do Departamento de Odontologia Social, Eliana Aparecida Mônaco
Nogueira, pela disponibilidade de sempre ajudar.

xvi
A todas as pessoas que participaram, contribuindo para a realização deste trabalho,
direta ou indiretamente, meus sinceros agradecimentos.

1
INTRODUÇÃO
A adolescência é uma fase de transição entre a infância e a idade adulta,
marcada por inúmeras mudanças, sendo elas psíquicas, físicas, biológicas e sociais (Costa
et. al., 2008). Existe certa dificuldade em estabelecer um limite cronológico da
adolescência, já que a literatura apresenta várias definições. Por exemplo, no Brasil, o
Ministério da Saúde considera adolescentes os indivíduos compreendidos entre 10 e 19
anos (Brasil, 1989). Já na literatura pediátrica, alguns autores consideram a adolescência
um período entre os 12 aos 22 anos (Thompson e Ashwill, 1996).
Este período apresenta características próprias em função do ambiente
sociocultural no qual os adolescentes vivem, pois constituem um grupo em exposição
crescente a várias situações de riscos físicos, emocionais e sociais, que representam uma
ameaça ao seu futuro. Diante disso, torna-se importante a abordagem dos jovens a partir de
um olhar psicossocial para compreendê-los como o resultado da interação dos processos de
desenvolvimento biológico, mental e social, das condições socioeconômicas e das
influências culturais (Thiengo et. al., 2002).
Na área odontológica, a compreensão do processo saúde-doença envolve fatores
biológicos/determinantes (biofilme, dieta, saliva), como também fatores denominados de
modificadores ou moduladores (renda, educação, fatores comportamentais, conhecimento,
escolaridade e atitudes), sendo apontados pelos epidemiologistas como grandes
responsáveis para que o indivíduo ou as populações estejam expostos a um maior
risco/atividade de desenvolver doença (Fejerskov, 2004). Pode-se dizer que estudos de
avaliação de risco em saúde bucal em adolescentes são menos frequentes. Em 2008,
Tagliaferro et al. revisaram a literatura acerca de trabalhos longitudinais sobre risco
publicados no período de 1997-2007, mostrando que mais de 40% dos estudos se referem
às crianças em idade escolar, provavelmente pela facilidade de acesso e de
acompanhamento ao longo do tempo.
Em relação à doença periodontal, alguns trabalhos recentes vêm mostrando
também a importância da avaliação de indicadores socioeconômicos, uma vez que
indivíduos com maior prevalência de cárie/doença periodontal fazem parte de grupos com
baixa renda e, com isso, provavelmente com acesso inadequado a programas preventivos e

2
assistenciais, a dentifrícios e informações educativas. A negligência com a saúde bucal em
relação à prevenção e ao tratamento também foi associada em adolescentes de áreas
carentes (Jung et.al., 2011; Sarri et.al., 2012).
Em uma revisão sistemática recente seguida de meta-análise, observamos em
seus resultados que níveis baixos de escolaridade estavam associados com um risco
aumentado de desenvolver periodontite em adultos com idades entre 35 anos ou mais e que
os esforços para intervir nesse processo deve se concentrar em intervenções nos períodos
iniciais da vida (Boillot et.al., 2011).
A identificação precoce e correta de indivíduos que no futuro desenvolverão
doença(s) é um dos principais desafios das ciências da saúde. De fato, quando se identifica
fatores de risco de doenças, indivíduos ou grupos populacionais podem beneficiar-se de
medidas preventivas efetivas, que contribuirão para a melhoria da qualidade de vida da
população, reduzindo também os gastos com procedimentos curativos mais complexos
(Tagliaferro et. al., 2009). Assim, a avaliação de risco contribui para a melhor alocação de
recursos humanos e financeiros, sendo os esforços direcionados aos grupos de maior risco
de desenvolvimento de doença(s), além de permitir que gestores de saúde bucal planejem
medidas específicas para prevenção da doença.
Porém, além de identificar os fatores de risco habituais, o presente estudo
aborda população de adolescentes menos privilegiados, buscando descobrir as variáveis
que identificam os ambientes de vulnerabilidade, principalmente relacionados com a
autopercepção individual e familiar de saúde, relatos de dor, acesso ao sistema de saúde,
presidiário na família, a aglomeração, a coesão familiar, entre outros e do contexto, como
índice de exclusão social e outros.
Estudos têm demonstrado que o capital social, definido por Putnam (2005)
como sendo as práticas sociais, normas e relações de confiança que existe entre os
cidadãos de uma determinada sociedade, além de sistemas de associação e participação que
estimulam a cooperação, parecem estar relacionados com a autoestima, apoio social e
interesse político dos pais dos adolescentes (Kallestal et. al., 2000; Patussi et. al., 2006),
bem como em saúde bucal (Aida et. al., 2008, 2009). Além disso, tem sido sugeridos que
locais que geram altos níveis de capital social produzem menos comportamentos de risco,
uma melhor saúde mental, mais comportamentos de promoção da saúde e melhores

3
percepções globais de saúde (Boyce et. al., 2008). Assim, o capital social na área de saúde
irá funcionar como um elemento de impacto positivo, proporcionando populações com
uma vida mais saudável, reduzindo a exclusão social e aumentando a longevidade e
autoestima (Bastos et. al., 2009).
Em modelos conceituais, os comportamentos de saúde e o uso de serviços de
saúde bucal são considerados fatores determinantes para os resultados de saúde bucal
(Sander et.al., 2006; Perera e Ekanayake, 2011; Petersen, 2013), por terem uma maior
influência sobre os grupos socialmente mais vulneráveis. A saúde é afetada pelas vias
psicossociais/stress, e está diretamente ou indiretamente modulada pelo comportamento
(Adler e Ostrove, 1999; Newton e Bower, 2005).
Estudos têm verificado que os pais de adolescentes de famílias de alta renda
possuem maior grau de instrução do que os de famílias de baixa renda e isso tem uma
influência sobre a frequência e qualidade da escovação (Perera e Ekanayake, 2011). Outra
explicação pode estar relacionada com a questão da negligência de comportamentos de
saúde, tanto no que diz respeito à prevenção quanto na busca de tratamento nos grupos
socialmente mais vulneráveis (Sarri et. al., 2012).
Recentemente, o conceito de vulnerabilidade vem sendo utilizado na literatura
científica, em vários estudos epidemiológicos, principalmente focalizados para a
perspectiva de risco (Sánchez e Bertolozzi, 2007).
Na esfera da saúde pública, o termo vulnerabilidade passou a ser bastante
empregado devido a uma grande epidemia moderna: a síndrome da imunodeficiência
adquirida (AIDS). O caráter dessa epidemia, a maneira como ela foi atingindo variados
grupos – de formas diversas e em diferentes países – e a reação que desencadeou nos
movimentos sociais contribuíram para que Jonathan Mann conceituasse esse termo ao
expor um “modelo” de como pensar a relação entre o vírus da AIDS e o contexto
socioeconômico, buscando explicar quais grupos sociais e indivíduos poderiam ser mais ou
menos vulneráveis ao desenvolvimento da epidemia. Daí surgiu um movimento de
substituição dos termos risco e população de risco, utilizados até então em saúde pública, e
que deu lugar à discussão sobre quais seriam as diferentes condições de vulnerabilidade em
que se encontravam expostos estes ou aqueles grupos sociais, ou mesmo populações
inteiras de um país (Adorno, 2001).

4
Segundo Ayres (2002), a vulnerabilidade supera o conceito de risco
tradicionalmente empregado no âmbito da Epidemiologia clássica, pois este designa um
instrumento de caráter probabilístico para orientar as intervenções em saúde.
O conceito de vulnerabilidade supera o caráter individualizante e probabilístico
do risco na medida em que é compreendida como um conjunto de aspectos que vão além
do individual, abrangendo aspectos coletivos, contextuais, relações sociais, políticas,
serviços e ações de saúde, relacionados à maior suscetibilidade de indivíduos e
comunidades a um adoecimento ou agravo e, de modo inseparável, menor disponibilidade
de recursos para sua proteção (Ayres et. al., 2006; Higgins et.al., 2010).
Nesse sentido, é importante ressaltar que as análises de vulnerabilidade não
prescindem de análises epidemiológicas de risco, sendo correto afirmar que as análises de
risco e de vulnerabilidade são de certa forma inversa, ou seja, enquanto as análises de risco
trabalham com uma racionalidade analítica na qual os fenômenos em estudo precisam ser
partidos, isolados, discriminados, as análises de vulnerabilidade empregam uma
racionalidade sintética, na qual se privilegia a construção de significados, a agregação de
elementos para que os fenômenos estudados sejam compreendidos em sua totalidade
(Ayres et. al., 2006; Nichiata et.al., 2008).
As análises de vulnerabilidade buscam assim integrar três eixos
interdependentes de compreensão dos aspectos das vidas das pessoas, de comunidades, ou
até mesmo nações, que as tornam mais ou menos susceptíveis as atividades de intervenção
em saúde. Na perspectiva da vulnerabilidade, as dimensões individuais, sociais e
programáticas de qualquer processo saúde-doença-cuidado serão identificadas e inter-
relacionadas pelos sujeitos que de alguma forma estão implicados nesse processo e buscam
compreender o que ele significa (Ayres et. al., 2010; Lange, 2013).
Por fim, o quadro da vulnerabilidade vem destacar a perspectiva dos sujeitos e
de seus contextos de intersubjetividade como a base necessária para identificar e
transformar as relações sociais que produzem agravos e os meios para superá-los (Ayres et.
al., 2010; Lange, 2013).
Em relação a metodologia da pesquisa científica, destaca-se a vantagem de
serem usados múltiplos métodos (quanti-qualitativos), uma vez que podem abordar todos
os aspectos envolvidos. A referência a uma abordagem combinada implica pensar em

5
enfoques complementares para dar conta do todo, que inclua os “comos”, os “porquês” do
processo, a fim de identificar e compreender os elementos que possam justificar os
números encontrados (Nogueira-Martins e Bógus, 2004). O processo de avaliação envolve
a coleta de dados e o processamento e análise da informação.
Para que a coleta do material atenda às perguntas que se pretende responder é
de fundamental importância lançar mão de um planejamento adequado desde o início, ou
seja, qualquer monitoramento ou avaliação pressupõe a utilização de algum modelo teórico
que explicite como se espera que as ações desenvolvidas alcancem seus objetivos (Hartz,
2000).
Minayo e Sanches (1993) afirmam que os estudos quantitativos podem gerar
questões para serem aprofundadas qualitativamente e vice-versa. Em cada caso particular,
o uso de uma ou de outra abordagem será mais indicado e, muitas, vezes, as duas podem
ser usadas de modo complementar, dependendo da natureza do estudo.
Segundo pesquisas sobre comportamento em saúde, o progresso na área da
prevenção e proteção só será visto quando entendermos como as pessoas organizam seus
pensamentos e agem sobre sua saúde (Kirscht, 1983; Schunk e Carbonari, 1984; Kirscht
1998; Scheier et.al., 2012; Halvari et.al., 2012; Conner et.al., 2013). Segundo Bandura
(1986), as atividades, comportamentos, esforços que se gastam e quanto tempo vão
persistir diante de um obstáculo e experiências adversas são dos fatores que afeta as
escolhas das pessoas, que seria a auto-eficácia percebida.
De um modo geral, os processos de auto-regulação (self-regulation) determinados e
limitados por crenças, atitudes e conhecimentos; estruturas físicas e sociais, habilidade ou
desempenho de comportamentos, modelam os comportamentos de proteção à saúde
(Bandura, 1986; Tedesco, 1991; Abraham, Sheeran e Henderson, 2011).
Um número crescente de investigações indica que as expectativas de auto-eficácia
estão positivamente e significativamente associadas com a iniciação e manutenção (ou
seja, o cumprimento de longo prazo) de comportamentos de saúde (Bandura, 1986; Kanfer,
1981; O'Leary, 1985; Brubaker e Wickersham, 1990; Abraham, Sheeran e Henderson,
2011; Mosher et.al. 2013; Parschau et.al. 2013).
Dessa forma, julga-se importante investigar o risco de doenças bucais e analisar sua
relação entre a vulnerabilidade individual/social/programática e ainda apresentar e discutir

6
as justificativas apresentadas para o não cumprimento de ações para obtenção e
manutenção da saúde bucal (não adesão ao tratamento odontológico) em uma população
adolescente de 15 a 19 anos no município de Piracicaba-SP.

7
Capítulo 1
Individual and contextual factors related to dental caries in underprivileged Brazilian
adolescents
Authors: Fabiana de Lima Vazquez, Karine Laura Cortellazzi, Armando Koichiro Kaieda,
Jaqueline Vilela Bulgareli, Fabio Luiz Mialhe, Glaucia Maria Bovi Ambrosano, Elaine
Pereira da Silva Tagliaferro, Luciane Miranda Guerra, Marcelo de Castro Meneghim,
Antonio Carlos Pereira.
ABSTRACT
Objectives: investigate the individual and contextual variables related to caries in
underprivileged adolescents, and the disparity in distribution of the disease. Methods:
Cross-sectional analytical study, conducted in the city of Piracicaba, SP, Brazil, in 2012.
The probabilistic sample was composed of 1,179 adolescents from 15-19 years of age,
randomly selected from 21 state schools and 34 Primary Health Units – Family Health
(PHU-FH). The dependent variables studied were presence of carious teeth and experience
of caries (DMFT). The independent variables were classified into individual (clinical,
sociodemographic, psychosocial, self-perception, impact on oral health, access to services,
pain reports and quality of life variables) and contextual (social exclusion index, total
number of residents in suburb, literacy rate, percentage of home ownership residences,
percentage of domestic sewerage, percentage of trash collected, percentage with income of
over 1 minimum wage per month and percentage of families without monthly income).
The multilevel regression model was estimated by the PROC GLIMMIX (Generalized

8
Linear Models-Mixed) procedure, considering the individuals’ variables as Level 1 and the
contextual variables of the suburbs as Level 2. Adjustment of the model was evaluated by -
2 Res Log Likelihood with α=0.05. Results: As regards the individual variables, the
adolescents who needed dental prostheses, declared having a prison inmate in the Family
and resided in homes with a larger number of persons, showed more carious teeth. There
were a larger number of decayed teeth and higher DMFT with a worse self-perception as
regards the health of their teeth and mouth. Other variables, such as being of the female
gender, declared having toothache during the course of life, age and time since last visit to
the dentist were related to the DMFT index. As regards the contextual variables, the DMFT
was lower in suburbs with greater access to domestic sewage and the number of decayed
teeth was higher in suburbs with the worst social exclusion indices. Conclusion: individual
and contextual variables were associated with the presence of caries and DMFT index in
underprivileged adolescents, indicating that they must be taken into consideration in the
formulation of policies directed towards oral health promotion and prevention activities in
this group.
Key-Words: Dental Caries, Risk Assessment, Social Vulnerability, Adolescent Behavior

9
Introduction
Over the last few decades, a change in the epidemiological profile of dental
caries has been observed in developed (1) and developing countries. In Brazil, the same
trend has been verified, especially in children and adolescents, with a significant reduction
of 35% in the carious component being observed in adolescents between the years 2003
and 2010 (2).
However, this qualitative improvement in the Brazilian Population’s level of
oral health has been accompanied by a change in the distribution of the disease, with it
being concentrated in more in socio-economically vulnerable groups (3).
Theories have been developed to explain the relationship between
socioeconomic status (SES) and health, with cultural, behavioral, material, structural and
psychosocial factors being modulators of this relationship (4,5,6). Therefore, not only do
they study the relationship between SES and health, poverty and healthy behaviors, but
these theories seek an explanation for causal pathways of oral health outcomes, risk
behaviors and use of oral health services (7,8).
Although the inequalities in the prevalence of caries in adolescents for the
different social gradients have been observed in some studies (9-12). However, the
contribution of contextual factors for the risk of disease still need to be further studied,
particularly in underprivileged populations, so that the differences within the social
environment may be better elucidated (13,14), a fact that justifies new studies (12).
Similarly, when there is interest in identifying small areas with high levels of need for
dental treatment (15), vulnerability variables can be useful because they are sensitive to
variations in oral health and oral health behaviors.

10
Brazil appears to be an ideal country for conducting epidemiological studies
for the evaluation of inequalities in health, seeing that at the same time as it presents
remarkable social inequality, changes are seen in economic growth, socioeconomic
gradients and improvement in the GINI (distribution of income), especially over the last
decade (16).
Therefore, it is important to know the impact of social determinants on health,
both at individual and collective level, in order to plan actions at a local level (17).
However, for the adolescent population, little has been investigated about the relationship
between social inequalities and oral health behaviors (8).
In addition to social factors, proximal factors such as self-perception of health
have been associated with oral health and quality of life indicators (18,19). Self-perception
of health is the subjective indicator most used in epidemiological researches, influencing
health behaviors and being influenced by SES (8). Therefore, it is an important component
for measuring oral health status and must be taken into consideration in the elaboration of
approaches to diminishing inequalities in health (20).
Analyses of risk factors for caries in brazilian adolescents have pointed out that
the following variables: past history of caries (21), activity of the disease, parents’
educational level (22) and socioeconomic factors (10,11) were the most significant in
statistical models. Therefore, in addition to identifying traditional risk factors, the present
study approaches the population of underprivileged adolescents, seeking to find out the
variables that identify environments of vulnerability, mainly connected with the individual
and family (self-perception of health, reports of pain, access to the health system, prison
inmate in the family, number of persons in the family, family cohesion, and others) and the
context (social exclusion index and other factors).

11
Nevertheless, adolescents constitute a group under constant exposure to other
important factors, such as emotional, social, and physical situations, etc., which makes this
analysis more complex. Although adolescence is a time when important psychosocial
changes occur, which may put youngsters at increased risk for general and oral problems,
we observed that few studies have demonstrated the impact of social determinants on oral
health in adolescents (12,23). In addition, most of these studies were conducted on an
individual basis, there are few that evaluate the impact of territorial characteristics on their
oral health, especially when we study the underprivileged population. Therefore,
identification of explanatory variables by means of using multilevel analysis can provide
greater perspectives on interrelationships between the two different levels of effects
(individual and contextual), as well as insights on how these relationships affect dental
caries. This technique provides better estimates and gives substantive meanings to data
clustering in comparison with traditional regression analysis (24).
There are an increasingly higher number of risk factors that augment the
probability of developing poor oral health and caries. However, it has not yet been
determined which factors create the greatest risks. The general model of vulnerability
considers those who experience multiple risks to be more vulnerable to poor outcomes than
those with one or no risks. Vulnerability leaves the child unprotected, creating high
probability of developing poor oral health, and when a child is exposed to risk factors
within the family or community, this vulnerability increases and there is an even greater
probability of poorer dental health outcome (25).
In the face of this scenario, and with a view to better qualification of public
health policies for this group in a stage of transition, the aim of this study was to identify

12
the individual and contextual variables related to caries in underprivileged adolescents in
the southeastern region of Brazil, and to study the disparity of distribution of the disease.
Materials and Methods
Ethical Aspects
This study was approved by the Research Ethics Committee of FOP-UNICAMP,
in accordance with resolution 196/96 of the National Health Council, Ministry of Health,
under Protocol No.027/2011.
Type of Study
Analytical Cross-sectional Study
Study Location
This study was developed in the Municipality of Piracicaba, SP, Brazil, in the
period from January to December, 2012, with adolescents from 15 to 19 years-old, who
were under the care of Primary Health Care- Health Family teams (PHC-HF), which
provide primary health care for all family members residing in a circumscribed area (about
4000 persons) (26). They were enrolled in public schools (located in the territories covered
by these PHC-HF units) and in the PHC-FC units. The greatest extent of social exclusion
in the municipality occurs in these regions.
The city has an estimated population of 368,843 inhabitants, a Human
Development Index (HDI) of 0.84 and has had a fluoridated public water supply since
1971 (0.7 ppmF).

13
Study Universe
The city is composed of 68 suburbs distributed throughout 5 administrative
regions (North, South, East, West and Center) and there are a total number of 12,539
adolescents in the age-range from 15 to 17 years. The Northern Region consists of 14
suburbs with 2460 adolescents; Southern Region, 14 suburbs and 2510 adolescents;
Eastern Region, 16 suburbs and 2491 adolescents; Western Region, 13 suburbs and 3330
adolescents; Downtown Region, 11 suburbs and 1748 adolescents.
According to data from the Municipal Secretary for Health, in 2012 there were
a total number of 34 PHC-FH units, and among them there were 12 units with Primary
Dental Care (PDC) teams. On an average, 320 adolescents between the ages of 15 and 19
years were enrolled in each one of the PHU-FH unit, making approximately 11,000
individuals. According to the Secretary for Education, the municipality had 43 high
schools and a total number of 9,356 schoolchildren in this age-range enrolled.
It is important to emphasize that the PHC units are distributed in the less
favored socioeconomic regions of the municipality. All public high schools (n=21) in the
territorial areas covered by the PHCs were enrolled. In the 34 PHC units, the Terms of Free
and Informed Consent to participate in the Study were handed to the Community Health
Agents during home visits. These agents also previously made the appointments for the
time and day for participants to appear at the units. At the schools, the Terms were handed
to the teachers who distributed them to the selected schoolchildren, for obtaining parents'
or guardians' authorization afterwards.
Sample
The sample size was calculated based on the caries experience in the
Southeastern region of Brazil using data from a previous national epidemiological survey,

14
considering a sampling error of 5%, DMFT=5.16 with SD=4.54, sample loss of 20% and a
level of confidence 95%, obtaining a sample of 1,428 individuals aged 15 to 19 years,
proportionally randomly taken from 34 PHC-HF units areas existent in the municipality.
The absentees were contacted and examined in the 21 public high schools.
Of these 1,428 adolescents initially selected, 249 failed to appear on the day of
the exam or did not wish to participate. Thus, 221 individuals were examined at the 34
FHUs and 958 at the 21 state high schools, totaling 1,179 adolescents examined. Most of
them had lived since their birth in the same suburb.
Inclusion and exclusion criteria
The criteria for exclusion in the study were systemic diseases, difficulties with
communication, or neuromotor problems, severe hypoplasia and orthodontic appliance.
Individuals who did not agree to participate in the study and those absent in the day of the
exam were excluded from the sample.
Clinical Examination
The exams were performed on the premises of the PHC-HF units and at the
state high schools, by two examiners (previously calibrated and helped by two note-takers),
in an outdoor setting, under artificial light using a flashlight and with prior brushing
performed under the guidance of a Dental Assistant. For each exam was used a ball point
probe and plane oral mirror (27). Data were collected relative to the clinical characteristics:
caries by the SiC index (Significant Caries Index) for one-third of the children with the
highest caries scores (28) and by the DMFT index (total decayed, missing and filled teeth),
periodontal disease (Community Periodontal Index-CIP), fluorosis (Dean Index) and use
and need for a prosthesis, according to the World Health Organization (27) codes and
criteria.

15
Training and Calibration
The process of calibrating the two examiners for the clinical conditions was
conducted by a Gold Standard examiner. The theoretical-practical activities of the training
and calibration exercises consisted of a total of 7 periods - 1 theoretical lasting 4 hours, 4
clinical training sessions of 4 hours each (total of 16h) and 2 calibration exercises lasting 4
hours (total of 8h). The training stage consisted of a theoretical discussion, afterwards
followed by a practical stage, in which the examiners evaluated 12 adolescents per period,
with differentiated prevalence of oral diseases (caries, periodontal disease and fluorosis).
Discussions between the examiners and the Gold Standard examiners were held with the
purpose of obtaining an estimate of the extension and diagnostic nature, up to which point
the acceptable consistency remained above 0.91, measured by KAPPA statistics for all the
clinical conditions (29). The final calibration exercise consisted of 2 periods (total of 8h)
with mean inter-examiner Kappa values of 0.95. In order to verify maintenance of the
diagnostic criteria and intra-examiner error, 10% of the sample were re-examined, with
mean Kappa values of 0.96.
Variables studied and instruments used
The individual and contextual variables analyzed are described in Figure 1.

16
Figure 1. Individual and Contextual Variables. Piracicaba, SP, Brazil, 2012.
INDIVIDUAL
VARIABLES
Clinical Variables
Caries Periodontal Disease Fluorosis Use and need for dental prosthesis
Age
Sociodemographic
and psychosocial
variables of the
adolescent and family
Sex Monthly Family Income Number of persons in the family Fathers’ and Mothers’ Educational Level Type of housing Family Grant Program Prison inmate in the family Has lived in a city other than Piracicaba Number of siblings Failure to pass end of year school tests Adolescent works Father and mother work
Self-perception and
Impact on Oral
Health
How do you classify the health of your teeth and mouth? Are you satisfied with the appearance of your teeth OIDP
Access to Services
And pain report
Have you ever been to the dentist?
What type of dental service do you generally use?
When was the last time you went to the dentist? Why did you go to the dentist the last time? What is your most frequent reason for going to the
dentist? Have you ever had toothache? Have you had toothache in the last 6 months
Quality of Life WHOQOL-BREF
CONTEXTUAL
VARIABLES
Information about
suburbs
Social Exclusion Index
Total number of residents per suburb
Literacy Rate
% of home ownership
% domestic sewage facilities
% garbage collected
% with income up to 0.5 minimum wage
% with income up to 1 minimum wage
% with income over 1 minimum wage
% without monthly income

17
Individual Variables
A self-administered questionnaire was applied, under supervision in case of
doubt, to collect the sociodemographic variables (30) and another to obtain information on
psychosocial, self-perception of health, access to health services and report of pain
variables (31).
The instruments used for evaluating quality of life and socio-dental impact
were the WHOQOL-bref (32) and OIDP (Oral Impacts on Daily Performances) (33)
respectively.
The Basic Care Information System (SIAB) is an instrument used by the
Brazilian Primary Healthcare System to enroll the families in the territory covered by the
PHC-HF units and records socio-sanitary data and those relative to the living conditions of
these persons, with the aim of planning the interventions and health care (34). By means
SIAB it was possible to obtain information with reference to the adolescent’s family
belonging to an income transfer program (Family Grant Program) (35) and whether there
was any family member serving a prison sentence. Brazil instituted the Family Grant
Program (FGP) in 2004, with the purpose of transferring income directly to families in a
situation of poverty and extreme poverty, and guarantee the right to basic social services,
making it possible to benefit 16 million Brazilians (8.5 % of the population) (36).
Contextual Variables
The Social Exclusion Index (SEI) of the 36 suburb where the adolescents resided
was collected at the Piracicaba Research and Planning Institute and the Municipal
Secretary for Social Development (37). The purpose was the quantitative dimensioning of
some of the attributes of social inequalities between the suburbs, ranging from -1 (suburbs

18
with the worst indices – most vulnerable) to 1 (suburbs with the best indices – least
vulnerable).
Other information with reference to suburbs where the adolescents resided (total
number of residents per suburb, literacy rate, % of home ownership, % domestic sewage
available, % garbage collected, % with income of up to 0.5 minimum wage, % with
income from 0.5 to 1 minimum wage, % with income higher than 1 minimum wage and %
without monthly income) were obtained from the Brazilian Institute of Geography and
Statistics (38).
Data Analysis
In the present study, the “number of decayed teeth” and the “DMFT index”
were considered dependent variables.
Multilevel regression models were estimated by the PROC GLIMMIX -
“Generalized Linear Models-Mixed” procedure using the SAS 9.2, statistical software
program (39). In the analysis, the individual variables were considered as being level 1 and
those of the suburbs, as being level 2. Adjustment of the model was evaluated by -2 Res
Log Likelihood (the lower, the better fit the model).
Initially a model was estimated only with the intercept, in order to study the
proportion of variance due to the suburbs in relation to the individuals. This model served
as a basis for evaluating the reduction in variance in the other model studied (Model 1).
After this, the individual variables were tested (Model 2) and then those of the suburbs
were included (Model 3).

19
Results
The response rate in this study was 82.6%. The descriptive analysis (frequency
and percentage) of some independent variables is showed in Table 1.
Of the 1,179 study subjects, 1080 (91.6%) resided in suburbs with the worst social
exclusion indices. The median, minimum and maximum value for variable related to % of
domestic sewage was 99.49, 84.89 and 100 respectively. The larger part of the sample
were 15 years of age (69.13%). There was a balance between those examined according to
sex, with 55.89% being female. The majority of adolescents related having toothache at
some time in their lives (74.76%) and 39.86% classified the health of their teeth and mouth
as being good. As regards monthly Family income, the larger portion of the volunteers
came from families with an income ranged from 2 to 5 minimum wages.

20
Table 1. Sample description. Piracicaba, SP, Brazil, 2012.
Variables n %
Sex
Female 659 55.89
Male 520 44.11
Age (years)
15 815 69.13
16 231 19.59
17 82 6.96
18 29 2.46
19 22 1.87
Number of persons in the family
Up to 2 31 2.65
3 161 13.78
4 346 29.62
5 300 25.68
6 173 14.81
Over 6 157 13.44
Have you ever had toothache?
Yes 868 74.76
No 239 20.59
Don’t know/Don’t remember 54 4.65
Need for Dentures
Does not require 1125 95.42
Need for a single-element dental prosthesis 50 4.24
Need for multiple-element dental prosthesis. 4 0.34
Has a family member in prison
No 1141 99.30
Yes 8 0.70
How would you classify the health of your teeth
Excellent 69 5.88
Very good 229 19.51
Good 468 39.86
More or Less 363 30.92
Poor 45 3.83
When was the last time you went to the dentist?
I am undergoing treatment at present 274 24.89
Less than 6 months ago 329 29.88
7-12 months ago 158 14.35
13-24 months ago 52 4.72
Over 24 months ago 83 7.54
Don’t know/Don’t remember 205 18.62
Monthly Family Income
Up to 1 minimum wage 106 9.18
Over 1 up to 2 minimum wages 304 26.32
Over 2 up to 3 minimum wages 280 24.24
Over 3 up to 5 minimum wages 278 24.07
Over 5 up to 7 minimum wages 102 8.83
Over 7 up to 10 minimum wages 63 5.45
Higher than 10 minimum wages 22 1.90
* Minimum wage at the time of the data collection ≅ US$ 320.00
With regard to the clinical variables, the mean (SD) DMFT index was 2.10
(2.71), with the decayed, missing and filled component being a mean value (SD) of 0.47

21
(1.05), 0.09 (0.48) and 1.53 (2.32), respectively. The DMFT for the high caries-level
individual (polarization group) presented a SiC index of 5.24. Moreover, the majority of
the adolescents examined (95.42%) did not need dental prostheses.
Table 2 shows the results of the multilevel analysis for the number of decayed
teeth (dependent variable). By means of Model 1, the intra class correlation coefficient
r=0.0132/(0.0132+1.0859)=0.0120 was obtained; that is, the variation in the number of
decayed teeth between the suburbs represented approximately 1% of the total variation.
Table 2. Multilevel Model for number of carious teeth. Piracicaba, SP, Brazil, 2012.
When the individual variables were included in Model 2, the reduction in 2 Res
Log Likelihood was approximately 9%. When the variable “suburbs” - significant in
Model 3 - was included, the reduction in relation to the previous model was approximately
0,07%, which confirms that the variation in the number of decayed teeth, due to the
variables related to the individuals, is more important than that related to the suburbs.
Variable Model 1 Model 2 Model 3
Estimate SE p-Value Estimate SE p-Value Estimate SE p-Value
Intercept 0.4407 0.0397 <0.0001 2.7246 0.6136 <0.0001 2.8340 0.6148 <0.0001
Individual Level
Need for Dentures
(Ref=multiple-element dental
prosthesis)
Does not require -2.1667 0.6136 <0.0001 -2.1649 0.4826 <0.0001
Need for a single-element dental
prosthesis -1.2533 0.5027 0.0128 -1.2430 0.5021 0.0135
Prison inmate in the family(Ref=Yes) -0.9622 0.3431 0.0051 -0.9661 0.3427 0.0049
Number of persons in the family 0.0646 0.0220 0.0037 0.0680 0.0221 0.0022
Health of teeth and mouth 0.1844 0.03080 <0.0001 0.1884 0.0308 <0.0001
Suburb Level
Social Exclusion Index (SEI) 0.2552 0.1114 0.0222
Variances
Between suburbs 0.0132 0.0092 0.0077 0.0072 0.0035 0.0059
Between individuals 1.0859 0.0450 0.9227 0.0391 0.9226 0.0391
2 Res Log Likelihood 3457.25 3154.58 3152.35

22
Considering the level of significance of 5%, by Model 3, it could be affirmed
that the volunteers who did not need dentures (p<0.0001) and those who needed a single-
element denture (p=0.0135) presented a lower number of decayed teeth than those who
needed multiple-element dentures. The adolescents who had a relative in the family who
was in prison, presented more carious teeth (p=0.0049) than those who did not have one.
With regard to household number of persons in the family, the adolescents who lived in
residences witch a larger number of persons also presented a higher number of decayed
teeth (p=0.0022).
An increase in the number of decayed teeth was also found with the worst self-
perception of adolescents with regard to the health of their teeth and mouth (p<0.0001).
In addition to the variables relative to the individuals, in Model 3, one observes
that the number of decayed teeth increased with the worsening of the social exclusion
index (p=0.0222). The other variables did not have a significant influence on the number of
decayed teeth (p>0.05).
Table 3 shows the results of the multilevel analysis for the DMFT caries Index.
By means of Model 1, the intra class correlation coefficient
r=0.1417/(0.1417+7.1852)=0.01934 was verified; that is, the variation in DMFT between
the suburbs represented approximately 2% of the total variation. When the individual
variables were included in Model 2, the reduction in 2 Res Log Likelihood was
approximately 16%. When the variable “suburbs” - significant in Model 3 -was included,
the reduction in relation to the previous model was approximately 0.03%, which confirms
that the variation DMFT due to the variables related to the individuals is more important
than that related to the suburbs.

23
Table 3. Multilevel Model for the caries index (DMFT). Piracicaba, SP, Brazil, 2012.
Considering the level of significance of 5%, in Model 3, it was observed that
the volunteers of the female gender presented a higher DMFT than those of the male
gender (p=0.0026). The adolescents who did not need dental prostheses (p<0.0001) and
those who needed single-element dental prostheses (p=0.0002) presented a lower DMFT in
comparison with those that needed multiple-unit dental prostheses. The need for dentures
was the factor that influenced the variation in DMFT.
Moreover, the volunteers who declared that they had toothache, presented a
higher DMFT (p=0.0007) than those who had no toothache. The DMFT increased with
age (p=0.0031) and diminished when the time since the last visit to the dentist increased
(p<0.0001). The increase in DMFT also draws attention when the adolescents’ self-
perception with regard to the health of the teeth and mouth (p<0.0001) was classified as
Variable Model 1 Model 2 Model 3
Estimate SE p-Value Estimate SE p-Value Estimate SE p-Value
Intercept 2.0729 0.1129 <0.0001 5.76.01 1.9575 0.0053 14.1619 3.0826 <0.0001
Individual Level
Sex (Ref=Male) 0.4798 0.1639 0.0035 0.4917 0.1631 0.0026
Need for Dentures
(Ref=multiple-element dental prosthesis)
Does not require -8.5902 1.4726 <0.0001 -8.6447 1.4736 <0.0001
Need for a single-element dental
prosthesis -5.5647 1.5131 0.0002 -5.6080 1.5133 0.0002
Toothache (Ref=No) 0.6727 0.2026 0.0009 0.6863 0.2009 0.0007
Age (years) 0.2462 0.0776 0.0016 0.2291 0.0772 0.0031
Health of teeth and mouth 0.3370 0.0883 0.0001 0.3528 0.0880 <0.0001
Last visit to the dentist -0.2379 0.0455 <0.0001 -0.2400 0.0453 <0.0001
Suburb Level
% of domestic sewage -0.0829 0.0231 0.0004
Variances
Between suburbs 0.1417 0.0844 0.1108 0.0736 0.000 -
Between individuals 7.1852 0.2986 6.4190 0.2880 6.4553 0.2873
2 Res Log Likelihood 5687.77 4804.87 4803.51

24
worse. In addition to these variables relative to the individuals, in Model 3 it was observed
that the DMFT diminish a little, but significantly (p=0.0004) with the increase in the
percentage of domestic sewage in the place where the volunteers lived.
The other variables did not have a significant influence on the number of
decayed teeth (p>0.05).
Discussion
First of all, there is a body of evidence in the literature demonstrating the
association between income inequalities and caries prevalence (9-12). In this present study,
we also found association between socioeconomic variables and number of decayed teeth.
Traditionally, SES and monthly family income have been used in epidemiological studies
as predictor variables and both play important roles in the modulation of the health disease
process (5,40). Nevertheless, these variables are very sensitive when we study
socioeconomically leveled populations. Therefore, other variables appear to better explain
the relationship between caries and social inequalities specially in underprivileged groups.
This study is probably the first to find “Prisoner in Family” as a variable associated with a
higher number of decayed teeth in adolescents. In studies conducted with the purpose of
analyzing children with an imprisoned relative, it is important to understand their
emotional needs and vulnerabilities related to mental health problems (2.5 time more
chances in experiencing mental problems than other children do), in addition to having
greater social disadvantages and being victims of other negligence by the protection system
(41). Furthermore, these individuals are among the socially less favored, and the
imprisonment of some family member aggravates their privation even further, so that they

25
need to struggle every day to deal with debt, poverty, loneliness, ostracism, stigma and lack
of housing (42).
Household number of persons in the family has been associated with caries,
healthy nutritional and hygiene habits, oral health-related quality of life, traumatic dental
injuries in children and adolescents (19,43). More than a relationship of risk, this variable
clearly expresses social vulnerability and acts as a strong explanatory variables, and there
is a relationship of family environment and socioeconomic status (SES) and oral health
conditions (12). This appears to be even clearer when we verify that the sample comes
from peripheral areas where there is a concentration of adolescents in low SES. Therefore,
an important finding of this study is that in spite the significant decrease in caries
prevalence observed over the last 3 decades in Brazil (2), one has to be aware of its
distribution in the population. In the city of present study, we detected that there is
remarkable inequality in this distribution, even among the less favored adolescents, since
the variable “social exclusion index of the suburbs” was significant in the multilevel model
for the number of decayed teeth. This affirmation becomes evident when we verified that
the mean value of the DMFT index of the group was 2.1, however, caries experienced
increased to 5.24 (SIC) in the group in which high levels of the disease are concentrated.
We were able to find a relationship between individual variables and both
dependent variables: number of decayed teeth (need for dental prosthesis and perception of
teeth and oral conditions) and DMFT (gender, need for dental prosthesis, perception of
teeth and oral conditions, toothache, dental service use, adolescent’s age).
Toothache during the course of life is related to an increase in DMFT,
demonstrating more advanced stages of the disease, and possibly, deficiency in the system
that provides health services. There are few epidemiological studies on oral health that

26
include a question as regards toothache, one of the main problems that may be influenced
by social conditions and access to dental services, with its magnitude being sufficiently
great to cause undesirable situations, such as difficulty with sleeping, reduced productivity
at work, absence from school, rejection of certain foods, and negative impact on quality of
life (44).
Dental services use was positively associated with DMFT. Similarly to others
studies from developing countries (45,46). The most plausible explanation for this fact in
our study is that the adolescents are under the care of oral health teams, which allows
greater access to public dental treatment at the PHC-HF units. The component Filled is
responsible by 72.9 % of DMFT index. However, in developed countries there is an
inversely proportional relationship between SES and use of dental services by adolescents
(8). The explanation for this is based on the fact that adolescents of the more privileged
classes have a lower prevalence of oral health problems in that countries, and therefore,
present a lower demand for service.
Health services are important causal pathways to oral health outcomes
(7,47,48) and can explain socioeconomic disparities in oral health (49). Dental services
generally do not deal with the social determinants of health with implications for oral
diseases. However, it is known that they have important impact on health inequalities when
they improve accessibility and respond appropriately to the healthcare needs of different
social groups (43,50).
Our results show that girls present more caries experience (DMFT) than boys.
Evidences have shown that girls take better care of their teeth and go to the dentist more
frequently (51). This is related to the better care taken of health and esthetic appearance of
teeth (11). However, our findings may be explained in two ways: greater access to dental

27
care results in an increase in the DMFT index, especially restored teeth, frequently the
result of overtreatment, and Brazilian adolescent girls who in the trajectory of life were
never poor, presenting higher DMFT (11).
Another expected and significant variable related to DMFT was age of the
adolescents. Our study was developed in high schools, including all the schoolchildren
enrolled in the 10th and 11th grades. Therefore, there was a greater probability that we
would find adolescents of 15 and 16 years. The variable need for dental prosthesis (at least
one element) was related to dental caries, as expected. This variable clearly exposes the
mutilating practice of oral health, still in course in developing countries, in addition to
present a clear relationship with the social vulnerability of a portion of the adolescents in
the studied sample (4.58% already needed dental prostheses).
Perception of one’s own teeth and impact of oral health on daily activities and
on oral conditions is an important measurement of health, notwithstanding the fact that
traditional measures have been based on objective variables (8). In the present study, the
relationship between worse self perception of teeth and oral condition and higher number
of decayed teeth was observed, as in other studies (8,19,52,53) who have reported
intervenient variables such as the use of health services, daily toot brushing and income.
We found a relationship of contextual variables with the number of decayed
teeth (social exclusion index of the suburb) and DMFT (% of residences in the suburb,
which have sewage treatment). Authors have argued that there is enough evidence to
affirm that there is a link between individual and socioeconomic variables of the areas in
which the residents live with dental caries (15,54). A lower percentage of adolescents with
toothache was found in a brazilian suburb with higher social capital (55), as well
neighborhood empowerment and dental caries (54,56,57). Furthermore, social capital

28
appears to be related to self-esteem, social support and parent’s political interest in
adolescents (54,58). Possibly, the negative effects of stress can be greater for residents in
disadvantaged neighborhoods with the least social support and fewest network resources
(24,59), resulting worst level of health status. However, most of the variance in DMFT
occurred at the individual level and only 2% of the variance occurred at the community
level, a result similar to that of Tellez et al. (56) but lower than the findings of Aida (57).
The difference can be explained by the sample design used in each study, especially
population characteristics and sample size. Nevertheless, one of the important findings is
that contextual variables must be considered by health managers in health planning,
seeking greater equity in the distribution of health services and targeting the reduction of
social inequalities.
One of the differentials of this study was the use of a multilevel model in the
analysis of factors related to dental caries in adolescents. Multilevel Models are
appropriate for the analysis of hierarchical data, considering the influence of community
context on the health behaviors of individuals with regard to caries experience (54,57, 60).
Furthermore, we used a recent technique (PROC GLIMMIX) which presents better
estimates and gives substantive meanings to data clustering in comparison with traditional
regression analysis, allowing contextual factors to be analyzed separately (24). The
modeling of oral health data is rather complex, since these data generally do not present
normal distribution. With the development of generalized linear models (an extension of
linear models for non-normally distributed data) this type of problem has been significantly
reduced. Whereas mixed generalized linear models incorporate the random effects in the
predictor, thus being most useful in data with superdispersion. The application of mixed
generalized linear models has been satisfactorily used in multilevel analysis (24,61).

29
Possibly, this study is one of the first to use this technique for studying the relationship of
individual and contextual variables with regard oral health.
Lastly, our study has some limitations. This was a cross-sectional study and
sought inferences with regard to causal factors without, however, establishing a temporal
relationship. The socioeconomic information was obtained from the adolescents and their
parents, which of itself could be a source of response bias. Furthermore, were not collected
individual variables related to behavioral (dietary practices and oral hygiene habits) as well
as bacterial and salivary factors. The self perception questionnaire may have been
influenced by social acceptance and social desirability (8,57). Moreover, obtaining data
about income is very sensitive, and the respondents may not have informed accurately (8).
Finally, fluoride possibly has beneficial effect on reducing caries in this population of
adolescents and a reduction of inequality can also be expected when compared to the same
population not supplied with fluoridated water (62).
A considerable caries variation that could not be explained by the individual and
contextual variables assessed. This is understandable because the process of developing
caries has many variables (contextual, individual, behavioral and others), which are not
always controlled in a statistical model.
Therefore, we concluded that variations in the DMFT and the number of decayed
teeth in the sample are mainly related to individual variables. However, the context in
which the individual lives, measured by an index of social exclusion, has showed relevance
even in underprivileged individuals.

30
Acknowledgements
The authors wish to acknowledge the financial support from FAPESP (grants
#2011/03657-5 and #2011/01768-4). We also give special thanks to the principals of the
schools, teachers and all the adolescents who contributed to the accomplishment of the
survey.
Competing Interests
The authors declare that they have no competing interests
Financial competing interests
In the past five years I don´t have received reimbursements, fees, funding, or salary from
an organization that may in any way gain or lose financially from the publication of this
manuscript, either now or in the future. Not is such an organization financing this
manuscript (including the article-processing charge).
I don´t hold any stocks or shares in an organization that may in any way gain or lose
financially from the publication of this manuscript, either now or in the future.
I don´t hold or currently applying for any patents relating to the content of the manuscript.
I don´t have received reimbursements, fees, funding, or salary from an organization that
holds or has applied for patents relating to the content of the manuscript.
I don´t have any other financial competing interests.
Non-financial competing interests
There aren´t any non-financial competing interests (political, personal, religious,
ideological, academic, intellectual, commercial or any other) to declare in relation to this
manuscript.
Authors’ Contributions

31
VFL, CKL, KAK, BJV, PAC have made substantial contributions to conception and
design, acquisition of data , and analysis and interpretation of data. AGMB participated in
the design of the study and performed the statistical analysis. MFL, TESP, GLM and
MCM participated in the drafting the manuscript and revising it critically for important
intelectual. PAC, TESP and GLM participated in its design and coordination and helped to
draft the manuscript. All authors read and approved the final manuscript.
References
1. WHO. The World Oral Health Report 2003. Continuous improvement of oral
health in the 21st century – the approach of the WHO Global Oral Health
Programme.Geneva: World Health Organization, 2003.
2. Brasil. Ministery of Health. Oral Health Brasil 2010 (SB Brasil 2010): National
Oral Health Research: main results. 2012; available
at:http://www.sbbrasil2010.org/ (last acess 03 March 2014).
3. Antunes JL, Narvai PC, Nugent ZJ. Measuring inequalities in the distribution of
dental caries.Community Dent Oral Epidemiol 2004;32:41-8.
4. Townsend P, Davidson N. Inequalities in health: the black report. Harmondsworth:
Penguin Books, 1992.
5. Sabbah W, Tsakos G, Chandola T, Sheiham A, Watt RG. Social Gradients in Oral
and General Health. JDR 2007; 86:992-996.
6. Sisson KL. Theoretical explanations for social inequalities in oral health.
Community Dent Oral Epidemiol 2007;35:81–8.

32
7. Petersen PE. The World Oral Health Report 2003: continuous improvement of oral
health in the 21st century-the approach of the WHO Global Oral Health
Programme. Community Dent Oral Epidemiol 2003;31(Suppl 1):3-24.
8. Perera I, Ekanayake L. Influence of oral health-related behaviours on income
inequalities in oral health among adolescents. Community Dent Oral Epidemiol
2011; 39: 345–351.
9. Nicolau B, Marcenes W, Allison P, Sheiham A. The life course approach:
explaining the association between height and dental caries in Brazilian
adolescents. Community Dental Oral Epidemiol 2005;33:93–8.
10. Peres MA, Peres KG, Traebert J, Zabot NE, Lacerda JT. Prevalence and severity of
dental caries are associated with the worst socioeconomic conditions: A Brazilian
cross-sectional study among 18-year-old males. J Adolesc Health 2005;37:103–9.
11. Peres MA, Peres KG, Dornellas de Barros AJ, Victoria CG. The relation between
family socioeconomic trajectories from childhood to adolescence and dental caries
and associated oral behaviours. J Epidemiol Community Health 2007;61:141–5.
12. Polk DE, Weyant RJ, Manz MC. Socio-economic factors in adolescents' oral
health: are they mediated by oral hygiene behaviors or preventive interventions?
Community Dent Oral Epidemiol 2010; 38:1-9.
13. Vargas CM, Crall JJ, Schneider DA. Sociodemographic distribution of pediatric
dental caries: NHANES III. 1988-1994. JADA 1998;129:1229–38.
14. Reisine ST, Psoter W. Socioeconomic status andselected behavioral determinants
as risk factors for dental caries. J Dent Educ 2001;65:1009–16.
15. Locker D. Deprivation and oral health: a review.Community Dent Oral Epidemiol
2000; 28:161–9.

33
16. Frazão P. Epidemiology of dental caries: when structure and context matter. Braz
Oral Res 2012;26(Spec Iss 1):108-14.
17. Marmot M, Wilkinson RG. Social Determinants of Health. 2 ed.. Oxford University
Press. Oxford. New York, 2006.
18. Somkotra T. Socioeconomic inequality in self-reported oral health status: the
experience of Thailand after implementation of the universal coverage policy.
Community Dent Health 2011; 28:136-42.
19. Paula JS, Leite IC, Almeida AB, Ambrosano GM, Pereira AC, Mialhe FL. The
influence of oral health conditions. socioeconomic status and home environment
factors on schoolchildren's self-perception of quality of life. Health Qual Life
Outcomes 2012;10(6).
20. Newton JT, Bower EJ. The social determinants of oral health: new approaches to
conceptualizing and researching complex causal network. Community Dent Oral
Epidemiol 2005; 33: 25-34.
21. Tagliaferro EPS, Pardi V, Ambrosano.
GMB, Meneghim MC, Pereira AC. An
overview of caries risk assessment in 0-18 year-olds over the last ten years (1997-
2007). Brazilian Journal Oral Sciences 2008; 7:1678-1681.
22. Tagliaferro EPS, Pereira AC, Meneghim MC, Ambrosano GMB. Assessment of
Dental Caries Predictors in a Seven-year Longitudinal Study. Journal of Public
Health Dentistry 2006; 66: 169–173.
23. Mashoto KO, Astrom NA, Skeie MS, Masalu JR. Socio-demographic disparity in
oral health among the poor: a cross sectional study of early adolescents in Kilwa
district. Tanzania. BMC Oral Health 2010; 20:10-7.

34
24. Nkansah-Amankra S, Luchok KJ, Hussey JR, Watkins K, Liu X. Effects of Maternal
Stress on Low Birth Weight and Preterm Birth Outcomes Across Neighborhoods of
South Carolina. 2000–2003. Matern Child Health J 2010; 14:215–226.
25. Mattheus DJ. Vulnerability related to oral health in early childhood: a concept
analysis. Journal of advanced nursing 2010; 66(9): 2116–2125.
26. Aquino R, Oliveira NF, Barreto ML. Impact of the family health program on infant
mortality in Brazilian municipalities. Am J Public Health 2009; 99(1):87-93.
27. World Health Organization. Oral Health Surveys. Basic Methods. 4th ed. Geneva:
World Health Organization, 1997.
28. Bratthall D. Introducing the Significant Caries Index together with a proposal for a
new global oral health goal for 12-year-olds. Int Dent J 2000;50:378–38.
29. Landis JR; Koch GG. The measurement of observer agreement for categorical data.
Biometrics. 33:159-74. 1977.
30. Meneghim MC; Kozlowski FC; Pereira AC. Ambrosano GM B. Meneghim ZMAP.
Classificação socioeconômica e sua discussão em relação à prevalência de cárie e
fluorose dentária. Ciência & Saúde Coletiva 2007; 12: 523-529 [In Portuguese].
31. Goes PS, Watt R, Hardy RG, Sheiham A. The prevalence and severity of dental pain
in 14-15 year old Brazilian schoolchildren. Community dental health 2007; 24:217-
224.
32. Fleck MP, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al.
Aplicação da versão em português do instrumento abreviado de avaliação da
qualidade de vida WHOQOL-bref. Rev Saude Publica 2000; 34:178-83.

35
33. Adulyanon S, Vourapukjaru J, Sheiham A. Oral impacts affect daily performance in
a low dental disease Thai population. Community Dentistry and Oral Epidemiology
1996; 24: 385-389.
34. BRASIL. Ministery of Health. Secretary of Health Atention. Department of Primary
Health Care. Manual of Primary Atention Information System. 2000; available at:
http://189.28.128.100/dab/docs/publicacoes/geral/manual_siab2000.pdf (Last Acess
03 March 2014).
35. Rasella D, Aquino R, Santos CA, Paes-Sousa R, Barreto ML. Effect of a conditional
cash transfer programme on childhood mortality: a nationwide analysis of Brazilian
municipalities. Lancet 2013; 382:57-64.
36. BRASIL. Ministery of Health. Secretary of Health Atention. Department of
Primary Health Care. Manual guidance on the Family in Health. 3 ed. 2010;
Available at:
http://bvsms.saude.gov.br/bvs/publicacoes/manual_orientacao_sobre_bolsa_familia
.pdf (Last acess 03 March 2014).
37. IPPLAP. Piracicaba Institute of Planning and Research. 2011; Avaialable at:
http://www.ipplap.com.br/docs/meis.pdf (Last acesso in 03 December 2011).
38. IBGE. Brazilian Institute of Geography and Statistic. 2013; Avaialable at:
http://www.ibge.gov.br/home/ (Last acess 04 december 2013).
39. SAS Institute Inc 2001: SAS/STAT Guide for personal computers. version 9.2.
Cary: North-Carolina/USA
40. Lynch JW, Smith GD, Kaplan GA, House JS. Income inequality and mortality:
importance to health of individual income, psychosocial environment or material
conditions. BMJ 2000; 320:1200-4.

36
41. University of Huddersfield. Children of prisoners more vulnerable to mental health
problems. 2013; Available at:
http://www.hud.ac.uk/news/2013/october/childrenofprisonersmorevulnerabletomenta
lhealthproblems.php. (Last acess 28 february 2014).
42. Black D. Children of parents in prison. Archives of Disease in Childhood 1992; 67:
967-970.
43. Lisboa CM, Paula JS, Ambrosano GMB, Pereira AC, Meneghim MC, Cortellazzi
KL, Vazquez FL, Mialhe FL. Socioeconomic and family influences on dental
treatment needs among Brazilian underprivileged schoolchildren participating in a
dental health program. BMC Oral Health 2013; 13:56.
44. Goes PSA, Watt RG, Hardy R, Sheiham A. Impacts of dental pain on daily
activities of adolescents aged 14-15 years and their families. Acta Odont Scand
2008; 66:7-12.
45. Kanil A, Kanbur NO, Dural S, Derman O. Effects of oral health behaviours and
socioeconomic factors on a group of Turkish adolescents. Quintessence Int 2008;
39:e26–32.
46. Lopez R, Baelum V. Factors associated with dental attendance among adolescents in
Santiago. Chile. BMC Oral Health 2007;10:7.
47. Sanders AE, Slade GD, Turrell G, Spencer AJ, Marcenes W. The shape of the socio-
economic oral health gradient: implications for theoretical explanations. Community
Dent Oral Epidemiol 2006;34:310–9.
48. Frias AC, Antunes JL, Junqueira SR, Narvai PC. Individual and contextual
determinants of the prevalence of untreated caries in Brazil. Rev Panam Salud
Publica 2007; 22:279-85.

37
49. Wamala S, Merlo J, Bostrom G. Inequity in access todental care services explains
current socioeconomic disparities in oral health: The Swedish National Surveys of
Public Health 2004–2005. J Epidemiol Community Health 2006;60:1027–33.
50. Watt RG. Social determinants of oral health inequalities: implications for action.
Community Dent Oral Epidemiol 2012; 40:44-48.
51. Antunes JLF, Junqueira SR, Frazão P. City-level gender differentials in the
prevalence of dental caries and restorative dental treatment. Health Place
2003;9:231–9.
52. Maes L, Vereecken C, Vanobbergen J, Honkala S. Toothbrushing and social
characteristics of families in 32 countries. Int Dent J 2006;56:159–76.
53. Patussi MP, Olinto MTA, Hardy R, Sheiham A. Clinical, social and psychological
factors associated with self-rated oral health in Brazilian adolescents. Community
Dent Oral Epidemiol 2007;35:377–86.
54. Patussi MP, Hardy R, Sheiham A. The potential impact of neighborhood
empowerment on dental caries among adolescents. Community Dent Oral
Epidemiol 2006; 34: 344–50.
55. Santiago BM, Valença AMG, Vettore MV. Social capital and dental pain in
Brazilian northeast: a multilevel cross-sectional study. BMC oral health 2013; 13:2.
56. Tellez M, Sohn W, Burt BA, Ismail AI. Assessment of the relationship between
neighborhood characteristics and dental caries severity among lowincome African-
Americans: a multilevel approach. Journal of Public Health Dentistry 2006; 66:
30–36.

38
57. Aida J, Hanibuchi T, Nakade M, Hirai H, Osaka K, Kondo K. The different effects
of vertical social capital and horizontal social capital on dental status: a multilevel
analysis. Soc Sci Med 2009; 69:512-518.
58. Kallestal C, Dahlgren L, Stenlund H. Oral health behaviour and self-esteem in
Swedish children. Soc Sci Med 2000;51:1841–9.
59. Boardman JD. Stress and physical health: the role of neighborhoods as mediating
and moderating mechanisms. Social Science & Medicine 2004; 58: 2473-2483.
60. Celeste RK, Nadanovsky P, Ponce de Leon A, Fritzell J. The individual and
contextual pathways between oral health and income inequality in Brazilian
adolescents and adults. Soc Sci Med 2009; 69:1468-75.
61. Huang FL, Invernizz MA. Birthday effects and preschool attendance. Early
Childhood Research Quarterly 2013; 28:11–23.
62. Antunes, José Leopoldo Ferreira, Paulo Capel Narvai, and Zoann Jane Nugent.
"Measuring inequalities in the distribution of dental caries." Community Dent Oral
Epidemiol 2004; 32:41-48.

39
Capítulo 2
Individual and contextual variables related to periodontal disease: multilevel analysis
in underprivileged adolescents in Brazil
Running title: Multilevel analysis in underprivileged adolescents
Authors: Fabiana de Lima Vazquez, Karine Laura Cortellazzi, Luciane Zanin, Luciane
Miranda Guerra, Elaine Pereira da Silva Tagliaferro, Glaucia Maria Bovi Ambrosano,
Antonio Carlos Pereira.
Abstract
Objectives: to investigate the individual and contextual risk indicators of periodontal
disease in underprivileged adolescents, and the disparity in distribution of the disease.
Methods: Cross-sectional analytical study, conducted in the city of Piracicaba, SP, Brazil,
in 2012. The probabilistic sample was composed of 1,130 adolescents from 15-19 years of
age, randomly selected from 21 state schools and 34 Primary Health Units – Family Health
(PHU-FH). The dependent variable studied was presence of periodontal disease (CPI). The
independent variables were classified into individual (clinical, sociodemographic,
psychosocial, self-perception, impact on oral health, access to services, pain reports and
quality of life variables) and contextual (social exclusion index, total number of residents
in suburb, literacy rate, percentage of home ownership residences, percentage of domestic
sewerage, percentage of trash collected, percentage with income of over 1 minimum wage
per month and percentage of families without monthly income). The multilevel regression
model was estimated by the PROC GLIMMIX (Generalized Linear Models-Mixed)
procedure, considering the individuals’ variables as Level 2 and the contextual variables of
the suburbs as Level 3. Results: As regards the individual variables, the adolescents who

40
never had toothache; with a lower impact on oral health; and resided in homes with higher
percentage of domestic sewage presented less presence of periodontal disease. Conclusion:
individual and contextual variables were associated with the presence of periodontal
disease in underprivileged adolescents, indicating that they must be taken into
consideration in the formulation of policies directed towards oral health promotion and
prevention activities in this group.
Keywords: periodontal disease; adolescents; dental; impacts; pain; social context.
Introduction
Periodontal disease is a destructive disease of the gingiva and supporting
structures of the teeth, which develops through inflammatory processes induced by
microbial biofilm (1). It is considered one of the main diseases affecting oral health, and is
ranked as the second main Public Health problem in Dentistry (2).
The World Health Organization recently informed that severe periodontitis
affects 5-20% of the adult population, and the majority of children and adolescents present
signs of gingivitis (3), which may attain a prevalence of up to 80% in adolescents (4, 5).
According to the last national oral health survey conducted in Brazil, over half the
adolescents from 15 to 19 years of age present signs of the disease, such as bleeding
(9.7%), calculus (28.6%) and periodontal pockets (10.8%) (2).
To reduce the inequalities in health has become a great priority of international
public health, while the types of intervention in health will be potential challenges in the
development of simulation models to investigate the health of the population (6). A few
studies have demonstrated the impact of social determinants on oral health in adolescents
(7-9), especially in the deprived group.

41
Periodontal conditions have been based on the individual level (10-12).
However, current studies have demonstrated the importance of the inclusion of contextual
variables in the evaluation of oral health conditions in populations (13-16).
Therefore, the use of multilevel analysis to model individual and contextual
variables simultaneously, have provided broader perspectives about the inter-relationships
between the two different levels of effects, and insights into how these relationships affect
periodontal disease. This technique provides better estimates of the substantive meanings
for group data in comparison with the traditional regression analysis (17, 18).
Adolescence is a stage of transition with psychic, physical, biologic and social
changes. This period has its own characteristics according to the sociocultural environment
in which the individual lives, and constitutes a group under constant exposure to various
situations of physical, emotional and social risks. In view of the foregoing, it has become
important to view the approach to youngsters from a psychosocial aspect (19), demanding
that health professionals analyze the problems that may arise from damage and health
problems (20-22).
In adolescence, some habits are consolidated and others are molded, and have a
strong influence on the lifestyle adopted for the adult stage. The habits acquired in
childhood, such as infrequent tooth brushing, may represent a risk factor for the
development of diseases in this age group (23).
The concept of risk, initially associated with the biomedical model and with the
concept of mortality (24, 25), has gradually ceded space to the study of human
development and its changes (26), adding a series of risk factors, including the individual,

42
social, behavioral and psychosocial determinants (24, 27, 28). When a child is exposed to
risk factors within the family or community, it becomes vulnerable and is more propense to
develop deficient oral health (29). These social and material disadvantages experienced in
childhood continue to have adverse effects on the child’s physical and mental health
throughout life (30, 31).
Another important aspect of interest is the relationship between periodontal
health, perception and impact on daily activities. In addition to the traditional clinical
measures, other measures related to self-perception of the child’s oral health and the
impact that oral diseases cause on its daily life have been studied (11, 30, 32, 33, 34).
Considering the relevance that the focus on psychological and social aspects
will bring to a new view of the relationship between oral health and quality of life, it has
become important to conduct studies that incorporate and demonstrate this new form of
evaluation of oral health conditions. Thus, the use of socio-dental indicators may be a good
alternative for planning and providing dental services (33, 35-37).
In spite of an increase in the number of studies on the impact of oral health con
the quality of life in adolescents, in general, these studies have been restricted to specific
populations such as adults and schoolchildren, and there have been a lower number of
studies with adolescents (8, 9, 38).
In the face of this scenario, and with a view to better qualification of public
health policies for this group in a stage of transition, the aim of this study was to identify
the individual and contextual risk indicators for periodontal disease in underprivileged
adolescents in the southeastern region of Brazil, and to study the disparity of distribution of
the disease.

43
Materials and methods
Ethical Aspects
This study was approved by the Research Ethics Committee of FOP-
UNICAMP in accordance with the Resolution 196/96 of the National Health Council,
Ministry of Health, Protocol No. 027/2011.
Type of Study
Analytical, cross-sectional, observational study.
Study Location
This study was developed in the Municipality of Piracicaba, SP, Brazil, in the
period from January to December, 2012, with adolescents from 15 to 19 years old, who
were under the care of Primary Health Care- Health Family teams (PHC-HF), which provide
primary health care for all family members residing in a circumscribed area (about 4000
persons) (39). They were enrolled in public schools (located in the territories covered by
these PHC-HF units) and in the PHC-FC units. The greatest extent of social exclusion in the
municipality occurs in these regions.
The city has an estimated population of 368,843 inhabitants, a Human
Development Index (HDI) of 0.84 and has had a fluoridated public water supply since
1971 (0.7 ppmF).
Setting
The city is composed of 68 suburbs distributed throughout 5 administrative
regions (North, South, East, West and Center) and there are a total number of 12,539
adolescents in the age-range from 15 to 19 years. The Northern Region consists of 14
suburbs with 2460 adolescents; Southern Region, 14 suburbs and 2510 adolescents;

44
Eastern Region, 16 suburbs and 2491 adolescents; Western Region, 13 suburbs and 3330
adolescents; Downtown Region, 11 suburbs and 1748 adolescents (40).
According to data from the Municipal Secretary for Health, in 2012 there were
a total number of 34 PHC-FH units, and among them there were 12 units with Primary
Dental Care (PDC) teams. On an average, 320 adolescents between the ages of 15 and 19
years were enrolled in each one of the PHU-FH unit, totaling approximately 11,000
individuals. According to the Secretary for Education, the municipality had 43 high
schools and a total number of 9,356 schoolchildren in this age-range enrolled.
It is important to emphasize that the PHC units are distributed in the less
favored socioeconomic regions of the municipality. All public high schools (n=21) in the
territorial areas covered by the PHC were enrolled. In the 34 PHC units, the Free and
Informed Consent Forms to participate in the Study were handed to the Community Health
Agents during home visits. These agents also previously made the appointments for the
time and day for participants to appear at the units. At the schools, the Forms were handed
to the teachers who distributed them to the selected schoolchildren, in order to obtain the
parents' or guardians' authorization afterwards.
Sample
The sample size was calculated in the software program epi info7 considering
the level of confidence of 95%, test power of 80%, non exposed/exposed rate =1, %
response in the non exposed group of 31.5% and OR=1.4, admitting a sampling error of
5%, sample loss of 20%, thereby obtaining a sample of 1428 individuals from 15 to 19
years of age.

45
Of these 1,428 adolescents initially selected, 298 failed to appear on the day of
the exam or did not wish to participate. Thus, 221 individuals were examined at the 34
FHUs and 909 at the 21 state high schools, totaling 1,130 adolescents examined.
Inclusion and exclusion criteria
The inclusion criteria were absence of: systemic diseases, difficulties with
communication, or neuromotor problems, absence of severe hypoplasia and absence of
orthodontic appliance. Individuals who did not agree to participate in the study and those
absent in the day of the exam were excluded from the sample.
Clinical Examination
The exams were performed at the PHC-HF and at the schools by two
examiners (previously calibrated, assisted by two note-takers), using the standardized
clinical record chart, under artificial light, and with previous tooth brushing performed
under supervision by an Oral Health Technician (OHT). For each exam, a CPI periodontal
probe and a plane dental mirror No.5 (41) were used. Data were collected relative to the
following clinical characteristics: periodontal disease by the Community Periodontal Index
(CPI) and use and need for a prosthesis, in accordance with the codes and criteria of the
World Health Organization (41).
Training and Calibration
A Gold Standard examiner conducted the process of calibrating the two
examiners for the clinical conditions. The theoretical-practical activities of the training and
calibration exercises consisted of a total of 7 periods - 1 theoretical lasting 4 hours, 4
clinical training sessions of 4 hours each (total of 16h) and 2 calibration exercises lasting 4
hours (total of 8h). The training stage consisted of a theoretical discussion, afterwards
followed by a practical stage, in which the examiners evaluated 12 adolescents per period,

46
with differentiated prevalence of periodontal disease. Discussions between the examiners
and the Gold Standard examiners were held with the purpose of obtaining an estimate of
the extension and diagnostic nature, up to which point the acceptable consistency remained
above 0.91, measured by KAPPA statistics for all the clinical conditions (42). The final
calibration exercise consisted of 2 periods (total of 8h) with mean inter-examiner Kappa
values of 0.95. In order to verify maintenance of the diagnostic criteria and intra-examiner
error, 10% of the sample were re-examined, with mean Kappa values of 0.96.
Study variables and instruments
The individual and contextual variables analyzed are described in Figure 1.
Figure 1. Individual and Contextual Variables
INDIVIDUAL VARIABLES
Clinical variables Periodontal Disease Use and need for dental prosthesis
Age
Sociodemographic and psychosocial variables of the
adolescent and family
Sex Monthly Family Income Number of persons in the family Fathers’ and Mothers’ Educational Level Type of housing Family Grant Program Prison inmate in the family Has lived in a city other than Piracicaba Number of siblings Failure to pass end of year school tests Adolescent works Father and mother work
Self-perception and Impact
on Oral Health
How do you classify the health of your teeth and mouth? Are you satisfied with the appearance of your teeth OIDP
Access to Services
And pain report
Have you ever been to the dentist?
What type of dental service do you generally use?
When was the last time you went to the dentist? Why did you go to the dentist the last time? What is your most frequent reason for going to the dentist? Have you ever had toothache? Have you had toothache in the last 6 months
Quality of Life WHOQOL-bref
CONTEXTUAL
VARIABLES Information about suburbs
Social Exclusion Index
Total number of residents per suburb
Literacy Rate % of home ownership
% domestic sewage facilities
% garbage collected % with income up to 0.5 minimum wage
% with income up to 1 minimum wage
% with income over 1 minimum wage % without monthly income

47
Individual Variables
A questionnaire was applied to collect the sociodemographic variables (43) and
another to obtain information on psychosocial, self-perception of health, access to health
services and report of pain variables (44).
The instruments used for evaluating quality of life and socio-dental impact
were the WHOQOL-bref and OIDP (Oral Impacts on Daily Performances) respectively.
The WHOQOL-bref refers to an index of a transcultural nature, which
appreciates the individual perception of the person with regard to his/her quality of life. It
consists of 26 questions, with 2 general questions being about the quality of life and the
other 24 questions representing the four domains: physical; psychological; social
relationships and environment. Each domain is composed of questions with responses
ranging from 1 to 5, so that the closer the score is to 5, the better the quality of life (45).
Developed by Adulyanon, Vourapukjaru and Sheiham (32), the OIDP is a
sociodental indicator, with focus on the measure of impact that interferes in people’s
ability to perform their daily activities. It measures the oral impacts that affect 8 daily
performances, classified as physical (eating and appreciating food, speaking and clearly
pronouncing words, cleaning the teeth), psychological (sleeping and relaxing, smiling,
laughing and showing the teeth without embarrassment, maintaining a normal emotional
state without becoming irritated) and social (working, playing a social role and finding
satisfaction in social encounters). It uses a logical approach to quantify the impact,
evaluating the frequency and severity distributed on a scale of 5 points. The score of the
severity measures gives the relative importance of the informant’s perception of the impact
on daily performance.

48
The Basic Care Information System (SIAB) is an instrument used by the
Brazilian Primary Healthcare System to enroll the families in the territory covered by the
PHC-HF units and records socio-sanitary data and those relative to the living conditions of
these persons, with the aim of planning the interventions and health care (46). By means
SIAB it was possible to obtain information with reference to the adolescent’s family
belonging to an income transfer program (Family Grant Program) (47) and whether there
was any family member serving a prison sentence. Brazil instituted the Family Grant
Program (FGP) in 2004, with the purpose of transferring income directly to families in a
situation of poverty and extreme poverty, and guarantee the right to basic social services,
making it possible to benefit 16 million Brazilians (8.5 % of the population) (48).
Contextual Variables
The Social Exclusion Index (SEI) of the 36 suburb where the adolescents
resided was collected at the Piracicaba Research and Planning Institute and the Municipal
Secretary for Social Development (49). The purpose was the quantitative dimensioning of
some of the attributes of social inequalities between the suburbs, ranging from -1 (suburbs
with the worst indices – most vulnerable) to 1 (suburbs with the best indices – least
vulnerable). Of the 1,130 study subjects, 1,087 (96.1%) resided in suburbs with the worst
social exclusion indices (negative indices).
Other information with reference to suburbs where the adolescents resided
(total number of residents per suburb, literacy rate, % of home ownership, % domestic
sewage available, % garbage collected, % with income of up to 0.5 minimum wage, %
with income from 0.5 to 1 minimum wage, % with income higher than 1 minimum wage
and % without monthly income) were obtained from the Brazilian Institute of Geography
and Statistics (50).
49
Data Analysis
In the present study, the CPI was considered a response variable. The
multilevel regression models were estimated by the PROC GLIMMIX procedures; that is
“Generalized Linear Models-Mixed” of the SAS statistical program (51).
In the analysis, the individual variables were considered Level 1 and those of
the suburbs, Level 2; and adjustment of the model was evaluated by -2 Res Log Likelihood
(the lower, the better fit the model). Initially, a model was estimated with the intercept
only, in order to study the proportion of variance due to the suburbs in relation to the
individuals. This model served as the basis for evaluating the reduction in the variance of
the other models studied (Model 1). After this, the individual variables (Model 2) were
tested, and later those of the suburbs were included (Model 3).
Results
In this study, the final sample was composed of 1,130 adolescents with a mean
age of 15.3 years (standard deviation=1.05), thus attaining a response rate of 79.13%. Of
these, 632 (55.93%) were female and 498 (44.07%) were male. The majority of the
adolescents related that they had experienced toothache at least once in their lives
(74.17%), 39.96% classified the health of their teeth and mouth as good, and 39.91%
related impact of oral health on their day to day life. As regards monthly family income,
the larger portion of the volunteers came from families with an income of between 2 and 5
minimum wages. The prevalence of periodontal disease was 58% (Table 1).

50
Table 1. Sample description
Variables n %
Sex
Female 632 55.93
Male 498 44.07
Age (years)
15 776 68.67
16 222 19.65
17 81 7.17
18 29 2.57
19 22 1.95
Number of persons in the family
Up to 2 28 2.50
3 154 13.76
4 332 29.67
5 283 25.29
6 169 15.10
Over 6 153 13.67
Have you ever had toothache during your life?
Yes 827 74.17
No 235 21.08
Don’t know/Don’t remember 53 4.75
Need for Dentures
Does not require 1127 99.73
Need for a single-element dental prosthesis 2 0.18
Need for multiple-element dental prosthesis. 1 0.09
How would you classify the health of your teeth
Excellent 59 5.24
Very good 216 19.18
Good 450 39.96
More or Less 356 31.62
Poor 45 4.00
When was the last time you went to the dentist?
I am undergoing treatment at present 233 22.11
Less than 6 months ago 326 30.93
7-12 months ago 156 14.80
13-24 months ago 52 4.93
Over 24 months ago 83 7.87
Don’t know/Don’t remember 204 19.35
Monthly Family Income
Up to 1 minimum wage 103 9.30
Over 1 up to 2 minimum wages 289 26.08
Over 2 up to 3 minimum wages 269 24.28
Over 3 up to 5 minimum wages 267 24.10
Over 5 up to 7 minimum wages 97 8.75
Over 7 up to 10 minimum wages 62 5.60
Higher than 10 minimum wages 21 1.90
Community Periodontal Index (CPI)
No bleeding 476 42.12
Bleeding on probing 392 34.69
Dental calculus 243 21.50
Periodontal pocket 4-5 mm 18 1.59
Periodontal pocket 6mm or more 1 0.09
Oral Impacts on Daily Performances (OIDP)
Yes 679 60.09
No 451 39.91
* Minimum wage at the time of the data collection ≅ US$ 320.00

51
Table 2 shows the multilevel model for the response variable CPI. From Model
1 the intra class correlation coefficient could be calculated
r=0.0037/(0.0037+0.6755)=0.0054. That is, the variation between the suburbs represents
approximately 0.5% of the total variation. When the individual variables were included in
Model 2, there was a reduction of approximately 10% in the 2 Res Log Likelihood. When
the significant variable of suburb was included in Model 3, the reduction in comparison
with the previous model was 0.04%, confirming that the variation in CPI due to the
variables related to the individuals is more important than those related to the suburbs.
Table 2. Multilevel Model for Community Periodontal Index (CPI).
Variable Model 1 Model 2 Model 3
Estimate SE p-value Estimate SE p-value Estimate SE p-value
Intercept 0.8311 0.0283 <0.0001 0.08018 0.1097 <0.0001 3.1326 0.7148 <0.0001
Individual level
Toothache (Ref=No) 0.2074 0.0612 0.0007 0.2049 0.0609 0.0008
Socio-dental Impact (OIDP) 0.0075 0.0017 <0.0001 0.0042 0.0075 <0.0001
Suburb level
% of domestic sewage -0.0239 0.0072 0.0010
Variances
Between suburbs 0.0037 0.0283 0.0057 0.0060 0.0004 0.0035
Between individuals 0.6755 0.0287 0.6429 0.0286 0.6418 0.0285
2 Res Log Likelihood 2773.21 2491.42 2490.28

52
Considering the level of significance of 5%, by Model 2 it may be affirmed
that the volunteers who declared that they had never had any toothache in their lives
presented alower CPI index (p=0.0008) and lower OIDP (p<0.0001)
In addition to these variables relative to the individuals, in Model 3 one
observes that the CPI was slightly reduced, but significantly (coefficient=-0.0239,
p=0.0010) with an increase in the percentage of domestic sewage in the volunteers’ place
of residence. The other variables had no significant influence on the CPI (p>0.05).
DISCUSSION
This study obtained two important results, which must be better contextualized
in this section. Periodontal disease was associated with individual variables (toothache
during the course of life and sociodental indicator- OIDP) and a contextual variable (% of
domestic sewage in the suburb).
Over the last few decades, the World Health Organization (WHO) has made an
effort to emphasize the importance of oral health conditions as an important and
indissociable part of general health and the quality of life of people (52). Therefore, it has
become necessary to understand and identify the determinant and modifying factors of the
epidemiological situation found, which may influence the occurrence of periodontal
disease.
The development of a disease is related to the individual’s behavior and his/her
perception with regard to health habits (53). Self-perception of health has been associated
with the oral health and quality of life indicators (54, 55). Self-evaluation of oral health has

53
also been directly and indirectly related to the factors of material inequalities, being
stronger than the behavioral and psychosocial factors (21, 22).
A study about the theory of self-determination (SDT) of the oral health process
has pointed out that the perception of these competencies was significantly positive and
related to oral health and quality of life (56, 57).
The evaluation of health by means of subjective indicators is an important
component for measuring oral health status and must be taken into consideration when
preparing the approaches to diminishing inequities in health (21, 58). Moreover, it makes it
possible to hear from individuals which of the areas of their lives are being affected, and
thus evaluate the impact of oral health on daily activities (59).
The results of this study showed evidence that the adolescents with greatest
impact on their daily activities presented the worst periodontal conditions (60, 61). The
impact of periodontal disease on an individual is generally characterized by clinical
parameters, such as probing, pocket depth, and bone attachment level. However,
periodontal disease is an infectious-inflammatory process that causes destruction of the
periodontium, and produces a vast variety of clinical signs and symptoms that may have a
considerable impact on day-to-day or quality of life (60). In countries with recognized low
prevalence of oral diseases, the psychological domain, represented by difficulty with
smiling, appeared as one having the greatest impact on the performance of daily activities
(62).
Another variable that influenced the CPI was “toothache”. Adolescents with
the highest CPI values related having had a larger number of toothache episodes during
their lives. According to Santiago et.al. and Bastos et.al. (63, 64), a lower percentage of
adolescents with toothache was found in a Brazilian suburb with higher social capital. In

54
spite of the body of evidence that the inequalities in health are related to the social context,
the large majority of studies about toothache contain information collected only at
individual level, such as age, educational level, income, type of residence, participation in
government aid programs, self-perception of oral health, access, among others.
As far as we know, there is no other epidemiologic study about the relationship
of periodontal disease with toothache, adopting a multilevel approach. Toothache
continues to be one of the main problems that lead to people seeking treatment, because it
is of sufficiently great magnitude to have a negative impact on the daily life of the
individual and community (65). The relationship between toothache and periodontal
disease is very intimate, however, the majority of epidemiological studies have associated
the pain in a tooth with the pain of oral lesions (severe periodontal pocket or pulp lesion)
or temporomandibular disorders. This may occur, because toothache itself is rarely
defined in the literature and pain may be result of an odontogenic or non-odontogenic
phenomenon (66).
Although it was not our intention to infer that an episode of toothache, the
identification of patients with past history of toothache allows one to identify patients at
risk for various oral disease, and specifically, periodontal disease. Therefore, this helps in
the sense of preventing this problem that is related to systemic diseases, such as diabetes
(67, 68) and cardiopathies (69), which may eventually lead to the patient’s death.
It seems that the findings of our study provide new insights into the influence
of toothache and socio-dental impact on periodontal status. Future studies should be
conducted on this issue, specially within the national context.
Greater importance has been attributed to the association between social
structure and oral health, and this has been incorporated into economic, social and

55
behavioral aspects for understanding the diseases of the mouth (63). Therefore, it is
necessary to identify those who are most vulnerable, as they are the ones that must be
protected until such time that they come out of this situation, nevertheless respecting their
cultural and moral differences and establishing communication between the health of this
population (70). This is particularly important when a deprived group is selected, and it
reveals more specific information about how the variables of individual and contextual
risks are modeled in a population previously defined as vulnerable.
This study points out that the relationship between periodontal disease and
domestic sewage in the suburb was statistically significant. The CPI diminished slightly,
but significantly, with the increase in the percentage of domestic sewage in the volunteers’
place of residence. Another study has related basic sanitation to oral health, pointing out
the role of sanitation and the supply of fluoridated water, specifically with regard to
toothache (63). However, as far as periodontal disease is concerned, there are no reports in
the literature with the inclusion of this contextual variable in the analyses, although there is
a tendency to perceive that in regions that present better sanitary conditions, there are
better conditions of health (71). In reality, as the majority of the suburbs in the city of
Piracicaba present 100% sewage treatment and water supply, small variations in a few
suburbs of the city signify the full state of vulnerability, forming areas of social risk. These
suburbs would present a low level of schooling, employment and education, in addition to
normally being suburbs of occupation (established by unauthorized occupation) with a low
percentage of basic services of life and health provided by the municipality.
Adolescents who live in similar unfavorable social and economic situations
may present different perceptions of periodontal disease. Possible explanations for this fact
may be related to elements such as social capital, training and social support, which in turn

56
translate into empowerment of individuals for coping with, and perception of adverse
situations (62, 72). Furthermore, it is possible that social capital presents positive
interference, since it has been found that suburbs that generate high levels of social capital
produce fewer risk behaviors, better mental health, more health promotion behaviors and
better general perceptions of health (73).
There has been a growth in social capital as a result of recognizing that
behaviors related to health are molded and coerced by a variety of social and community
contexts, and that the manners in which an individual relates to social and community
networks has important effects on his/her health and wellbeing (74, 75). Possibly, the
negative effects of stress can be greater for residents in disadvantaged neighborhoods with
the least social support and fewest network resources(17,76), resulting worst level of health
status
Given the complex inequalities there are in the adolescents health, both
nationally and internationally, when social capital acts as a factor of protection, it may help
to reduce the damage. Therefore, measuring and evaluating the relative importance of a
series of social indicators that represent the different domains of social capital in health,
may be related to the behaviors of youngsters (77).
Thus, to us, it appears to be important to encourage discussion about the
determinants of oral health from a population health perspective based on conceptual
multidimensional and multilevel models. The models supply a framework for research,
policy-making, and for more effective resource allocation to improve oral health (78).
In this sense, the present study meets the premises of such conceptual models,
as biologic, social, environmental, health behavior variables and dental care outcomes are
57
used, thereby influencing the oral health outcomes at individual, family, and community
levels.
One of the differentials of this study was the use of a multilevel model in the
analysis of factors related to periodontal conditions in adolescents. Multilevel models are
appropriate for analyzing hierarchical data, considering the influence of the community
context on individual health behaviors (18, 79-82), seeing that it is essential to analyze the
data of health, disease and their determinant factors in order to consider the intricate
process occurring between the individual and the environment, and considering the various
interactions between the different levels studied (83).
In addition we used a recent technique (PROC GLINMIX), which presents
better estimates and gives substantive meanings to grouping data in comparison with the
traditional regression analysis, allowing one to analyze contextual factors separately (17).
The modeling of oral health data is rather complex, since these data generally
do not present normal distribution. With the development of generalized linear models (an
extension of linear models for data not normally distributed) this type of problem has been
considerably reduced. Whereas mixed generalized linear models incorporate the random
effects into the predictor are very useful when there is overdispersion of data. The
application of mixed generalized linear models has been satisfactorily used in multilevel
analysis (17, 84). This study may possibly be one of the first to use this technique for
studying the relations of individual and contextual variables with regard to periodontal
disease, especially in adolescents.
However, most of the variance in CPI occurred at the individual level with low
impact of the contextual variables on the statistical model, similar to other studies (85, 86).

58
The evidence of an association between periodontal health individual and socioeconomic
status level is equivocal (87), and it has been argued that periodontitis has a predominantly
biological rather than a social etiology (86, 88).
Lastly, our study has some limitations. This was a cross-sectional study and
sought inferences with regard to causal factors, without however, establishing a temporal
relationship. The contextual data were obtained from government sources, which are
subject to problems of under- or over-notification, processing errors, not updating
indicators, and others. Furthermore, the contextual variables could have been
complemented with the data with reference to social capital, social cohesion, social
support, and social network, and could have reduced the unexplained community-level
variance (76, 89). Self perception questionnaire may have been influenced by social
acceptance and social desirability (89, 90). Moreover, the obtainment of data about income
is very sensitive, and the respondents may not have provided accurate information (90).
It was concluded that Individual and contextual variables were related to the
periodontal disease in underprivileged Brazilian adolescents.
Acknowledgements
The authors wish to acknowledge the financial support from FAPESP (grants
#2011/03657-5 and #2011/01768-4). We also give special thanks to the principals of the
schools, teachers and all the adolescents who contributed to the accomplishment of the
survey.

59
References
1. Van Dyke TE, Van Winkelhoff AJ. Infection and inflammatory mechanisms.
Periodontol 2013;84(4):S1-S7 doi:10.1902/jop.2013.1340018.
2. Brasil. Ministery of Health. SB Brasil 2010: National Oral Health Survey: principal
results. 2012; 106 p. available at: http://www.sbbrasil2010.org/ (Last Acess 03
March 2014).
3. Jin LJ, Armitage GC, Klinge B, Lang NP, Tonetti M, Williams RC. Global oral
health inequalities: task group-periodontal disease. Adv Dent Res 2011; 23(2):221-
6.
4. Broadbent JM, Thomson WM, Boyens JV, Poulton R. Dental plaque and oral
health during the first 32 years of life. J Am Dental Assoc 2011; 142(4):415-26.
5. Levin et al. Periodontal status among adolescents in Georgia. A pathfinder study.
Peer J 2013; 1:e137.
6. Smith BT, Smith PM, Harper S, Manuel DG, Mustard CA. Reducing social
inequalities in health: the role of simulation modelling in chronic disease
epidemiology to evaluate the impact of population health interventions. Journal of
epidemiology and community health 2013; p. Jech-202756, 2013.
7. Sabbah W, Tsakos G, Sheiham A, Watt RG. The role of health-related behaviors in
the socioeconomic disparities in oral health. Social science e medicine 2009;
68(2):298-303.
8. Polk DE, Weyant RJ, Manz MC: Socio-economic factors in adolescents' oral
health: are they mediated by oral hygiene behaviors or preventive interventions?
Community Dent Oral Epidemiol 2010; 38:1-9.

60
9. Mashoto KO, Astrom NA, Skeie MS, Masalu JR. Socio-demographic disparity in
oral health among the poor: a cross sectional study of early adolescents in Kilwa
district, Tanzania. BMC Oral Health 2010; 20:10-7.
10. Borrell LN, Papapanou PN. Analytical epidemiology of periodontitis. J Clin
Periodontol 2005; 32(6):132-58 .
11. Peres MA, Antunes JLF, Boing AF, Peres KG, Bastos JLD. Skin colour is
associated with periodontal disease in Brazilian adults: a population‐based oral
health survey. Journal of clinical periodontology 2007; 34(3):196-201.
12. Bastos JL, Boing AF, Peres KG, Antunes JL, Peres MA. Periodontal outcomes and
social, racial and gender inequalities in Brazil: a systematic review of the literature
between 1999 and 2008. Cad Saude Publica 2011; 27(2):S141-53.
13. Celeste RK, Nadanovsky P, Ponce de Leon A, Fritzell J. The individual and
contextual pathways between oral health and income inequality in Brazilian
adolescents and adults. Social science e medicine 2009; 69(10), 1468-1475.
14. Moreira RDS, Nico LS, Barrozo LV, Pereira JCR. Tooth loss in Brazilian middle-
aged adults: multilevel effects. Acta Odontologica Scandinavica 2010; 68(5):269-
277.
15. Celeste RK, Fritzell J, Nadanovsky P. The relationship between levels of income
inequality and dental caries and periodontal diseases.Cadernos de Saúde Pública
2011; 27(6):1111-1120.
16. Sheiham A e Nicolau B. Evaluation of social and psychological factors in
periodontal disease. Periodontology 2000 2005; 39(1):118-131.
17. Nkansah-Amankra S, Luchok KJ, Hussey JR, Watkins K, Liu X. Effects of
Maternal Stress on Low Birth Weight and Preterm Birth Outcomes Across

61
Neighborhoods of South Carolina, 2000-2003. Matern Child Health J 2010; 14
(2):215-226.
18. Vettore MV, Marques RAA, Peres MA. Social inequalities and periodontal disease:
multilevel approach in SBBrasil 2010 survey. Rev Saúde Pública 2013; 47(3):29-
39.
19. Thiengo MA, Oliveira DC, Rodrigues BMRD. Adolescents, Aids and protection
practices: a structural approach of the social representations. Revista de
Enfermagem UERJ 2002; 10(2):81-4.
20. Herrera D, Matesanz P, Bascones-Martínez A, Sanz M. Local and systemic
antimicrobial therapy in periodontics. Journal of Evidence Based Dental Practice
2012; 12(3):50-60.
21. Richter M, Moor I, Van Lenthe FJ. Explaining socioeconomic differences in
adolescent self-rated health: the contribution of material, psychosocial and
behavioural factors. Journal of epidemiology and community health 2012;
66(8):691-697.
22. Reyes L, Herrera D, Kozarov E, Roldán S, Progulske-Fox A. Periodontal bacterial
invasion and infection: contribution to atherosclerotic pathology. Journal of clinical
periodontology 2013; 40(14): S30-S50.
23. Alm A, Wendt LK, Koch G, Birkhed D, Nilsson M. Caries in adolescence -
influence from early childhood. Community Dent Oral Epidemiol 2012; 40: 125-
133.
24. Haggerty RJ, Sherrod LR, Gamezy N, Rutter M. Stress, risk and resilience in
children and adolescents: process, mechanisms and interventions. New York:
Cambridge University Press 2000.

62
25. Grünspun, H. Conceitos sobre resiliência. Revista Bioética 2003; 10(1).
26. Sapienza G, Pedromônico MRM. Risk, protection and resilience in the
development of children and adolescents. Psicologia em estudo 2005; 10(2):209-
216.
27. Heitz-Mayfield LJ, Lang NP. Comparative biology of chronic and aggressive
periodontitis vs. peri-implantitis. Periodontology 2000 2010; 53(1):167-181.
28. Shum I, Leung PC, Kwok A, Corbet EF, Orwoll ES, Phipps KR, Jin L. Periodontal
conditions in elderly men with and without osteoporosis or osteopenia. Journal of
periodontology 2010; 81(10):1396-1402.
29. Mattheus DJ. Vulnerability related to oral health in early childhood: a concept
analysis. Journal of advanced nursing 2010; 66(9):2116-2125.
30. Nicolau B, Marcenes W, Hardy R, Sheiham A. A life‐course approach to assess the
relationship between social and psychological circumstances and gingival status in
adolescents. Journal of clinical periodontology 2003; 30(12):1038-1045.
31. Das-Munshi J, Clark C, Dewey ME, Leavey G, Stansfeld SA, Prince MJ. Does
childhood adversity account for poorer mental and physical health in second-
generation Irish people living in Britain? Birth cohort study from Britain (NCDS).
BMJ open 2013; 3(3).
32. Adulyanon S, Vourapukjaru J, Sheiham A. Oral impacts affect daily performance in
a low dental disease Thai population. Community Dentistry and Oral Epidemiology
1996; 24:385-389.
33. Abanto J, Carvalho TS, Mendes FM, Wanderley MT, Bönecker M, Raggio DP.
Impact of oral diseases and disorders on oral health? Related quality of life of

63
preschool children. Community dentistry and oral epidemiology 2011; 39(2):105-
114.
34. Sischo L, Broder HL. Oral Health-related Quality of Life What, Why, How, and
Future Implications. Journal of dental research 2011; 90(11):1264-1270.
35. Gomes AS e Abegg C. The impact of oral health on daily performance of municipal
waste disposal workers in Porto Alegre, Rio Grande do Sul State, Brazil. Cad.
Saúde Pública 2007; 23(7):1707-1714.
36. Sheiham A. A determinação de necessidades de tratamento odontológico: uma
abordagem social. In: Pinto VG. Saúde bucal coletiva. São Paulo: Editora Santos
2000; 223:50-91.
37. Silva AN, Silva CMFP, Vettore MV. (2014). Are resilience and maternal sense of
coherence associated with gingival status in adolescents from low-income families?
International Journal of Paediatric Dentistry 2014.
38. Peres MA, Peres KG, Cascaes AM, Correa MB, Demarco FF, Hallal PC, Menezes
AB. Validity of partial protocols to assess the prevalence of periodontal outcomes
and associated sociodemographic and behavior factors in adolescents and young
adults. J Periodontol 2012; 83(3):369-78.
39. Aquino R, Oliveira NF, Barreto ML. Impact of the family health program on infant
mortality in Brazilian municipalities. Am J Public Health 2009; 99(1):87-93.
40. IBGE. Brazilian Institute of Geography and Statistic. 2014; Avaialable at:
http://www.ibge.gov.br/home/ (Last acess 04 march 2014).
41. World Health Organization. Oral Health Surveys. Basic Methods. 4th ed. Geneva:
World Health Organization, 1997.

64
42. Landis JR, Koch GG. The measurement of observer agreement for categorical data.
Biometrics 1977; 33:159-74.
43. Meneghim MC, Kozlowski FC, Pereira AC, Ambrosano GMB, Meneghim ZMAP.
A socioeconomic classification and the discussion related to prevalence of dental
caries and dental fluorosis. Ciência e Saúde Coletiva 2007; 12(2):523-529.
44. Goes PSA. The prevalence and impact of dental pain in Brazilian schoolchildren
and their families. (Doctoral Dissertation). London: Department of Epidemiology
and Public Health, University College London 2001.
45. Skevington SM, Lotfy M, O'Connell KA. The World Health Organization's
WHOQOL-BREF quality of life assessment: psychometric properties and results of
the international field trial. A report from the WHOQOL group. Quality of life
Research 2004; 13:299-310.
46. BRASIL. Ministery of Health. Secretary of Health Atention. Department of
Primary Health Care. Manual of Primary Atention Information System. 2000;
available at:
http://189.28.128.100/dab/docs/publicacoes/geral/manual_siab2000.pdf (Last Acess
03 March 2014).
47. Rasella D, Aquino R, Santos CA, Paes-Sousa R, Barreto ML. Effect of a conditional
cash transfer programme on childhood mortality: a nationwide analysis of Brazilian
municipalities. Lancet 2013; 382:57-64.
48. BRASIL. Ministery of Health. Secretary of Health Atention. Department of
Primary Health Care. Manual guidance on the Family in Health. 3 ed. 2010;
Available at:

65
http://bvsms.saude.gov.br/bvs/publicacoes/manual_orientacao_sobre_bolsa_familia
.pdf (Last acess 03 March 2014).
49. IPPLAP. Piracicaba Institute of Planning and Research. 2011; Avaialable at:
http://www.ipplap.com.br/docs/meis.pdf (Last acesso in 03 December 2011).
50. IBGE. Brazilian Institute of Geography and Statistic. 2013; Avaialable at:
http://www.ibge.gov.br/home/ (Last acess 04 december 2013).
51. SAS Institute Inc 2001: SAS/STAT Guide for personal computers. version 9.2.
Cary: North-Carolina/USA.
52. Petersen PE. The World Oral Health Report 2003: continuous improvement of oral
health in the 21st century-the approach of the WHO Global Oral Health
Programme. Community Dent Oral Epidemiol 2003; 31(1):3-23.
53. Hattne K, Folke S, Twetman S. Attitudes to oral health among adolescents with
high caries risk. Acta Odontologica 2007; 65(4):206-213.
54. Somkotra T. Socioeconomic inequality in self-reported oral health status: the
experience of Thailand after implementation of the universal coverage policy.
Community Dent Health 2011; 28:136-42.
55. Paula JS, Leite IC, Almeida AB, Ambrosano GM, Pereira AC, Mialhe FL. The
influence of oral health conditions. socioeconomic status and home environment
factors on schoolchildren's self-perception of quality of life. Health Qual Life
Outcomes 2012;10(6).
56. Locker D. Issues in measuring change in self-perceived oral health status. Comm
Dent Oral Epidemiol 1998; 26:41-47.

66
57. Halvari AE, Halvari H, Bjørnebekk G, Deci EL. Oral health and dental well?being:
testing a self-determination theory model. Journal of Applied Social Psychology
2013; 43(2):275-292.
58. Newton JT, Bower EJ. The social determinants of oral health: new approaches to
conceptualizing and researching complex causal network. Community Dent Oral
Epidemiol 2005; 33:25-34.
59. Marshman Z e Robinson PG. Child and Adolescent Oral Health-Related Quality of
Life Semin Orthod 2007;13:88-95.
60. Needleman I, McGrath C, Floyd P, Biddle A. Impact of oral health on the life
quality of periodontal patientsJ Clin Periodontol 2004; 31:454-457.
61. Ng SK e Leung WK. Oral health-related quality of life and periodontal status.
Community Dentistry and Oral Epidemiology 2006; 34:114-122.
62. Bianco A, Fortunato L, Nobile CG, Pavia M. Prevalence and determinants of oral
impacts on daily performance: results from a survey among school children in Italy.
Eur J Public Health 2010; 20(5):595-600.
63. Bastos JLD, Gigante DP, Peres KG, Nedel FB. Social determinants of odontalgia in
epidemiological studies: theoretical review and proposed conceptual model. Ciênc.
saúde coletiva 2007; 12(6):1611-1621.
64. Santiago BM, Valença AMG, Vettore MV. Social capital and dental pain in
Brazilian northeast: a multilevel cross-sectional study. BMC oral health 2013; 13:2.
65. Goes PS, Watt RG, Hardy R, Sheiham A. Impacts of dental pain on daily activities
of adolescents aged 14-15 years and their families. Acta Odontologica
2008; 66(1):7-12.
67
66. Sutherland S e Matthews DC. Emergency Management of Acute Apical
Periodontitis in the Permanent Dentition: A Systematic Review of the Literature. J
Can Dent Assoc 2003; 69(3):160.
67. Norris SL, Nichols PJ, Caspersen CJ, Glasgow RE, Engelgau MM, Jack Jr L,
McCulloch D. The effectiveness of disease and case management for people with
diabetes: a systematic review. American journal of preventive medicine 2002;
22(4):15-38.
68. Shimazaki Y, Saito T, Yonemoto K, Kiyohara Y, Iida M, Yamashita Y.
Relationship of metabolic syndrome to periodontal disease in Japanese women: the
Hisayama Study. Journal of dental research 2007; 86(3):271-275.
69. Tonetti MS e Dyke TE. Periodontitis and atherosclerotic cardiovascular disease:
consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic
Diseases. Journal of clinical periodontology 2013; 40(14):S24-S29.
70. Costa SDM, Abreu MHNGD, Vasconcelos M, Lima RDCGS, Verdi M, Ferreira
EF. Inequalities in the distribution of dental caries in Brazil: a bioethical approach.
Ciência e Saúde Coletiva 2013; 18(2):461-470.
71. Baldani MH, Narvai PC, Antunes JLF. Dental caries and socioeconomic conditions
in the State of Paraná, Brazil, 1996. Cad Saude Publica 2002; 18(3):755-63.
72. Wamala S, Merlo J, Boström G. Inequity in access to dental care services explains
current socioeconomic disparities in oral health: the Swedish National Surveys of
Public Health 2004–2005. Journal of epidemiology and community health 2006;
60(12):1027-1033.

68
73. Richter M, Erhart M, Vereecken CA, Zambon A, Boyce W, Gabhainn SN. The role
of behavioural factors in explaining socio-economic differences in adolescent
health: a multilevel study in 33 countries. Soc Sci Med 2009; 69:396-403.
74. Bambra C, Gibson M, Sowden A, Wright K, Whitehead M, Petticrew M. Tackling
the wider social determinants of health and health inequalities: evidence from
systematic reviews. Journal of Epidemiology and Community health 2010;
64(4):284-291.
75. Lorenc T, Petticrew M, Welch V, Tugwell P. What types of interventions generate
inequalities? Evidence from systematic reviews. Journal of epidemiology and
community health 2013; 67(2):190-193.
76. O´Campo P. Invited commentary: advancing theoryand methods for multilevel
models of residential neighborhoods and health. Am J Epidemiol 2003;157:9-13,
24,62.
77. Morgan A, Haglund BJ. Social capital does matter for adolescent health: evidence
from the English HBSC study. Health Promotion International 2009; 24(4):363-
372.
78. Fisher-Owens SA, Gansky SA, Platt LJ, Weintraub JA, Soobader MJ, Bramlett
MD, Newacheck PW. Influences on children's oral health: a conceptual
model. Pediatrics 2007; 120(3):e510-e520.
79. Leyland AH, Goldstein H, editors. Multilevel modelling of health statistics. New
York: Wiley 2001; p.1-12.
80. Hox JJ. Multilevel analysis, techniques and applications. Mahwah: Lawrence
Erlbaum Associates 2002; p.1-36.

69
81. Pattussi MP, Olinto MTA, Hardy R, Sheiham A. Clinical, social and psychological
factors associated with self-rated oral health in Brazilian adolescents. Community
Dent Oral Epidemiol 2007; 35:377-86.
82. Aida J, Hanibuchi T, Nakade M, Hirai H, Osaka K, Kondo K. The different effects
of vertical social capital and horizontal social capital on dental status: a multilevel
analysis. Social science e medicine 2009; 69:512-518.
83. Moreira TP, Nations MK, e Alves MDSCF. Inequality and damaged teeth: oral
sequelae from living in poverty in the Dendê community. Cad. Saude Publica 2007;
23(6):1383-1392.
84. Huang FL, Invernizz MA. Birthday effects and preschool attendance. Early
Childhood Research Quarterly 2013; 28:11-23.
85. Antunes JLF, Peres MA, Jahn GMJ, da Silva Levy BB. The use of dental care
facilities and oral health: a multilevel approach of schoolchildren in the Brazilian
context. Oral health e preventive dentistry 2006; 4(4).
86. Bower E, Gulliford M, Steele J, Newton T. Area deprivation and oral health in
Scottish adults: a multilevel study. Community dentistry and oral epidemiology
2007; 35(2):118-129.
87. Klinge B, Norlund A. A socio-economic perspective on periodontal diseases - a
systematic review. J Clin Periodontol 2005; 32(6):314-25.
88. Unell L, Söderfeldt B, Halling A, Birkhed D. Explanatory models for indicators of
periodontal disease in an adult population. J Clin Periodontol 2000; 27:22-9.
89. Aida J, Kondo K, Kondo N, Watt RG, Sheiham A, Tsakos G. Income inequality,
social capital and self-rated health and dental status in older Japanese. Social
science e medicine 2011; 73(10):1561-1568.

70
90. Perera I, Ekanayake L. Influence of oral health-related behaviours on income
inequalities in oral health among adolescents. Community Dent Oral Epidemiol
2011; 39: 345-351.

71
Capítulo 3
Quality of life and socio-dental impact among underprivileged Brazilian adolescents
Authors:
Fabiana de Lima Vazquez, Karine Laura Cortellazzi, Armando Koichiro Kaieda, Luciane
Miranda Guerra, Glaucia Maria Bovi Ambrosano, Elaine Pereira da Silva Tagliaferro,
Fábio Luiz Mialhe, Marcelo de Castro Meneghim, Antonio Carlos Pereira.
ABSTRACT
Purpose: To evaluate the influence of clinical variables, individual and contextual
characteristics on the quality of life of underprivileged adolescents in a municipality in the
interior of the State of São Paulo, Brazil. Methods: An analytical cross-sectional study was
conducted in Piracicaba, in 2012, with 1172 adolescents aged 15-19 years, from 21 state
schools and 34 Family Health Units. The dependent variables included the socio-dental
impact (OIDP) and quality of life (WHOQOL-bref) indices. The dependent variables were
classified as individual (DMFT index, CPI Index, age, sex, income, parents' educational
level) and contextual (Social Exclusion Index) variable. The multilevel regression model
was estimated by the PROC GLIMMIX (“Generalized Linear Models-Mixed”) procedure,
considering the individuals' variables as being Level 1 and the contextual variables as
being Level 2 and the statistical significance was evaluated at level of significance of 5%.
Results: Girls were found to have the worst quality of life (p<0.000) and greatest socio-
dental impact (p=0.000). There was increase in OIDP (p<0.001) and diminished quality of
life (p<0.052) with an increase in the periodontal index. This result is marginally
significant since the significance probability is marginally greater than 0.05. In turn, there
was an increase in quality of life (p=0.000) and reduction in OIDP (p<0.000) with an
increase in the family income. Adolescents who resided in areas of greatest social
exclusion (p=0.031) and with greater socio-dental impact (p<0.000) presented the worst
quality of life. Conclusion: Individual and contextual variables were related to the socio-
dental impact and quality of life in underprivileged Brazilian adolescents.
Key Words: Oral health; Adolescent; Quality of life; Multilevel Analysis

72
INTRODUCTION
Adolescents are a group with particular characteristics, as they are subject to a
range of psychosocial changes and exposure to situations of risk. Therefore, they are no
longer the children to whom we devoted our efforts to protect, nevertheless, they also do
not yet have necessary maturity to face the situations inherent to adult age.
Oral health actions target to this age group should take into account their oral health
needs. Within this context, the National Oral Health Policy (Brasil Sorridente)
recommends that the health care of adolescents must be adapted to the epidemiological
situation of this population [1]. According to the last survey conducted in the country, in
the age group from 15 to 19 years of age, 40% of the DMFT index (Decayed-Missed-
Filled-Teeth) was composed of carious, or restored carious teeth, and 13.7% of the
adolescents already required some type of dental prosthesis [2].
Nevertheless, in addition to the epidemiological data, in-depth knowledge of the
context of adolescents' life is fundamental. When including data about oral health-related
quality of life (OHRQOL) in research, a powerful dimension is added to planning and
development of health promotion programs. When identifying the groups that are
vulnerable to low OHRQOL, programs could be created for the purpose of improving
oral health and elevating the OHRQOL, as well as helping to eradicate inequities in oral
health [3]. Several studies have observed that dental conditions have been found to
impact negatively on adolescents’ OHRQOL [4-16]. Despite the great number of studies
on oral health related quality of life, very little is known about the impact of oral
conditions and sociodemographic variables on the general quality of life of adolescents.
Another important aspect to be explored in the present study is the relationship
between inequities and health [17]. It has been verified that cultural, behavioral, material,
structural and psychosocial factors [18] has been described as modulators in conceptual
models. However, the association between level of poverty and healthy behaviors is not
yet completely understood, especially in oral health. Multilevel analysis is normally the
method of choice, working with two different levels of effects (individual and
contextual), and how they interrelate and produce oral health outcomes. This technique
provides better estimates and gives substantive meanings to data clustering in comparison
with traditional regression analysis. Traditional statistical tests lean heavily on the

73
assumption of independence of the observations. In multilevel data this assumption is
often violated and the estimates of the standard errors of conventional statistical tests are
very small and this results in many spuriously "significant" results [19].
Therefore, the aim of this study was to evaluate the influence of individual (clinical,
sociodemographic and family) and contextual variables on the quality of life and socio-
dental impact on underprivileged adolescents in a municipality in the interior of the State
of São Paulo, Brazil.
METHODS
Type of Study
Analytical, cross-sectional, observational study.
Study Location
This study was developed in the Municipality of Piracicaba, SP, Brazil, in the period
from January to December, 2012, with adolescents from 15 to 19 years-old, who were under
the care of Primary Health Care- Health Family teams (PHC-HF), which provide primary
health care for all family members residing in a circumscribed area (about 4000 persons)
[20]. They were enrolled in public schools (located in the territories covered by these PHC-
HF).
Setting
The city has an estimated population of 368,843 inhabitants, a Human
Development Index (HDI) of 0.84 and has had a fluoridated public water supply since
1971 (0.7 ppmF).
The city is composed of 68 suburbs distributed throughout 5 administrative regions
(North, South, East, West and Center) and there are a total number of 12,539 adolescents
in the age-range from 15 to 17 years. The Northern Region consists of 14 suburbs with
2460 adolescents; Southern Region, 14 suburbs and 2510 adolescents; Eastern Region, 16
suburbs and 2491 adolescents; Western Region, 13 suburbs and 3330 adolescents;
Downtown Region, 11 suburbs and 1748 adolescents [21].

74
According to data from the Municipal Secretary for Health, in 2012 there were a
total number of 34 PHC-HF, and among them there were 12 units with Primary Dental
Care (PDC) teams. On an average, 320 adolescents between the ages of 15 and 19 years
were enrolled in each one of the PHC-HF, making approximately 11,000 individuals.
According to the Secretary for Education, the municipality had 43 high schools and a total
number of 9,356 schoolchildren in this age-range enrolled.
It is important to emphasize that the PHC units are distributed in the less favored
socioeconomic regions of the municipality. All public high schools (n=21) in the territorial
areas covered by the PHC were enrolled. In the 34 PHC units, the Free and Informed
Consent Form to participate in the Study were handed to the Community Health Agents
during home visits. These agents also previously made the appointments for the time and
day for participants to appear at the units. At the schools, the Forms were handed to the
teachers who distributed them to the selected schoolchildren, for obtaining parents' or
guardians' authorization afterwards.
Sample
The sample size was calculated based on the caries experience in the Southeastern
region of Brazil using data from a previous national epidemiological survey [22], and
contemplated the 34 PHC-HF units areas existent in the municipality. We admitted
sampling error of 5%, DMFT=5.16 with SD=4.54, sample loss of 20% and a level of
confidence 95%, obtaining a sample of 1,428 randomly selected individuals of 15 to 19
years of age.
Of these 1,428 adolescents initially selected, 256 failed to appear on the day of the
exam or did not wish to participate. Thus, 221 individuals were examined at the 34 PHC-
HF units and 951 at the 21 state high schools, totaling 1,172 adolescents examined.
Inclusion and exclusion criteria
The inclusion criteria were absence of systemic diseases, difficulties with
communication, or neuromotor problems, absence of severe hypoplasia and absence of
orthodontic appliance. Individuals who did not agree to participate in the study and those
absent in the day of the exam were excluded from the sample.

75
Clinical Examination
The exams were performed at the PHC-HF and at the schools by two examiners
(previously trained, assisted by two note-takers), using the standardized clinical record
chart, under artificial light, and with previous tooth brushing performed under supervision
by an Oral Health Technician (OHT). For each exam, a CPI periodontal probe and a plane
dental mirror No.5 [23] were used. Data were collected relative to the following clinical
characteristics: caries by the DMFT index, and periodontal disease by the Community
Periodontal Index (CPI), in accordance with the codes and criteria of the World Health
Organization [23].
Training and Calibration
A Gold Standard examiner conducted the process of training the two examiners for
the clinical conditions. The theoretical-practical activities of the training and calibration
exercises consisted of a total of 7 periods - 1 theoretical lasting 4 hours, 4 clinical training
sessions of 4 hours each (total of 16h) and 2 calibration exercises lasting 4 hours (total of
8h). The training stage consisted of a theoretical discussion, afterwards followed by a
practical stage, in which the examiners evaluated 12 adolescents per period, with
differentiated prevalence of oral diseases (caries and periodontal disease). Discussions
between the examiners and the Gold Standard examiners were held with the purpose of
obtaining an estimate of the extension and diagnostic nature, up to which point the
acceptable consistency remained above 0.91, measured by KAPPA statistics for all the
clinical conditions [24]. The final calibration exercise consisted of 2 periods (total of 8h)
with mean inter-examiner Kappa values of 0.95. In order to verify maintenance of the
diagnostic criteria and intra-examiner error, 10% of the sample were re-examined, with
mean Kappa values of 0.96.
Study variables and instruments
Clinical (caries and periodontal disease), socio-demographic (age, sex, monthly
family income, fathers' and mothers' educational level), quality of life (WHOQOL-bref)
socio-dental impact (OIDP) variables were considered to be individual variables (Level 1).

76
In Level 2, the Social Exclusion Index (SEI) was analyzed, with reference to the
characteristics of the suburbs.
A questionnaire was applied to collect the socio-demographic variables [25]. The
minimal salary in Brazil and in the Municipality of Piracicaba at the time of the data
collection was US$320.00. The instruments used to evaluate quality of life and socio-
dental impact were the World Health Organization Quality of Life assessment -
WHOQOL-bref [26] and OIDP - Oral Impacts on Daily Performances [27], respectively.
The WHOQOL-bref refers to an index of a transcultural nature, which appreciates
the individual perception of the person with regard to his/her quality of life. It consists of
26 questions, with 2 general questions being about the quality of life and the other 24
questions representing the four domains: physical, psychological, social relationships and
environment. Each domain is composed of questions with responses ranged from one to
five, so that the closer the score is to 5, the better the quality of life.
Developed by Adulyanon, Vourapukjaru and Sheiham Performances [27], the
OIDP is a socio-dental indicator, with focus on the measure of impact that interfere in
people’s ability to perform their daily activities. It measures the oral impacts that affect 8
daily performances, classified as physical (eating and appreciating food, speaking and
clearly pronouncing words, cleaning the teeth), psychological (sleeping and relaxing,
smiling, laughing and showing the teeth without embarrassment, maintaining a normal
emotional state without becoming irritated) and social (working, playing a social role and
finding satisfaction in social encounters). It uses a logical approach to quantify the impact,
evaluating the frequency and severity distributed on a scale of 5 points. The score of the
severity measures give the relative importance of the informant’s perception of the impact
on daily performance.
The Social Exclusion Index (SEI) of the 36 suburbs where the adolescents resided
was collected at the Piracicaba Research and Planning Institute and the Municipal
Secretary for Social Development Performances [28]. The purpose was to quantify some of
the attributes of social inequalities between the suburbs, ranging from -1 (suburbs with the
worst indices – most vulnerable) to 1 (suburbs with the best indices – least vulnerable). Of
the 1,172 study subjects, 1,133 (96.1%) resided in suburbs with the worst social exclusion
indices (negative indices).

77
Data Analysis
In the present study, the WHOQOL-bref and OIDP were considered to be response
variables. The OIDP was also used as a predictor for WHOQOL-bref. The multilevel
regression models were estimated by the PROC GLIMMIX procedures, that is “Generalized
Linear Models-Mixed” of the SAS statistical program [29].
In the analysis, the individual variables were considered Level 1 and the variable
SEI, Level 2; and the statistical significance was evaluated at level of significance of 0.05.
Initially, a model was estimated with the intercept only, in order to study the proportion of
variance due to the suburbs in relation to the individuals. This model served as the basis for
evaluating the reduction in the variance of the other models studied (Model 1). After this,
the individual variables (Model 2) were tested, and later the variable SEI was included
(Model 3). Analysis was also performed between WHOQOL-bref domains by analysis of
variance (ANOVA) and Tukey test at 0.05.
RESULTS
In this study, the final sample was composed of 1,172 adolescents with a mean age
of 15.29 years (standard deviation=1.02), thus attaining a response rate of 82.1%. Of these,
656 (55.97%) were female and 516 (44.03%) were male. The mean DMFT index found
was 2.10 (sd=2.71), with the decayed, missing and filled component showing a mean value
(SD) of 0.47 (1.05), 0.09 (0.48) and 1.53 (2.32), respectively.
Table 1 presents the sample distribution according to the clinical and socio-
demographic characteristics. The majority of the adolescents were 15 or 16 years old, had
parents that had studied up to the 8th grade, and had a family income of up to 3 minimum
wages.

78
Table 1. Sample description.
Variable Category n (%)
Age (years) 15 810 (69.11)
16 230 (19.62)
17 82 (7.00)
18 29 (2.47)
19 21(1,79)
Education level of the father Illiterate 29 (2.61)
Grade 1 to 4, incomplete 182 (16.35)
Grade 1 to 4, complete 176 (15.81)
Grade 5 to 8, incomplete 188 (16.89)
Grade 5 to 8, complete 152 (13.66)
High School, incomplete 71 (6.38)
High School, complete 221 (19.86)
Higher education, Incomplete 21 (1.89)
Higher education, complete 73 (6.56)
Education level of the mother Illiterate 21(1.81)
Grade 1 to 4, incomplete 150 (12.93)
Grade 1 to 4, complete 135 (11.64)
Grade 5 to 8, incomplete 228 (19.66)
Grade 5 to 8, complete 181(15.60)
High School, incomplete 89 (7.67)
High School, complete 268 (23.10)
Higher education, Incomplete 21 (1.81)
higher education, complete 67 (5.78)
Monthly family income Up to 1 minimum wage 106 (9.22)
Over 1 up to 2 minimum wages 301(26.17)
Over 2 up to 3 minimum wages 280 (24.35)
Over 3 up to 5 minimum wages 277 (24.09)
Over 5 up to 7 minimum wages 101 (8.78)
Over 7 up to 10 minimum wages 63 (5.48)
Higher than 10 minimum wages 22 (1.91)
Community Periodontal Index (CPI) No bleeding 474 (40.44)
Bleeding on probing 437 (37.29)
Dental calculus 242 (20.65)
Periodontal pocket 4-5mm 18 (1.54)
Periodontal pocket 6mm or more 1 (0.09) Minimum wage at the time of the data collection = US$320.00

79
Table 2 show the comparison between WHOQOL-bref domains, indicating that the
Environment score was lower than Physical, Psychological and Social relationships.
Table 2. WHOQOL-Bref domains.
Avarage Standard deviation (SD) Confidence interval 95%
Physical 15.97a 2.02 15.85-16.08
Psychological 15.37b 2.17 15.24-15.49
Social relationships 15.97a 2.76 15.81-16.12
Environment 13.88c 2.13 13.76-14.00
Means followed by different letters are significantly different (p <0.05)
Table 3 shows the multilevel model for the response variable WHOQOL-
bref. From model 1, the intraclass correlation coefficient
r=0.0298/(0.0298+2.7791)=0.0106 could be calculated. The variation in WHOQOL
between the suburbs represented approximately only 1% of the total variation, indicating
that the variation in WHOQOL due to the variables related to the individuals is more
important than that related to the suburbs. When entering with the variable Social
Exclusion Index (SEI), the variance between the suburbs became zero, because the entire
variation between the suburbs was due to the SEI. In Model 3 it was observed that the
volunteers of the female sex had the worst quality of life in comparison with the male sex
(p<0.000). There was a reduction in the quality of life with the increase in the periodontal
index (p=0.052) and an increase in the socio-dental impact (OIDP), (p<0,000). In turn,
there was an increase in the quality of life with the increase in family income (p<0.000)
and fathers' educational level (p=0.000). In addition to the variables relative to the
individuals, it was verified that the lower the vulnerability of the suburbs (higher SEI
values: that is, values closer to 1), the better was the quality of life.

80
Table 3. Multilevel Model for Quality of life (WHOQOL-bref).
The multilevel model for OIDP may be observed in Table 4. From model 1, the
intraclass correlation coefficient r=1.3655/(1.3655+203.85)=0.0066 could be calculated;
that is, the variation in OIDP between the suburbs represented less than 1% of the total
variation. The variable suburb (Social Exclusion Index) was not significant in the model
(p=0.998). Therefore for this population studied, the variation in OIDP is explained by the
variables related to the individuals (age, sex, family income and CPI) and not the
suburbs. Considering the level of significance of 5%, by Model 2, it was observed that the
volunteers of the female sex presented a higher impact in comparison with the male sex
(p<0.000). There was an increase in the socio-dental impact with the increase in age
(p<0.000) and increase in CPI (p<0.000). A reduction in OIDP was observed with the
increase in family income (p<0.000).
Variable Model 1 Model 2 Model 3
Estimate SE p-value Estimate SE p-value Estimat
e
SE p-value
Intercept 15.2389 0.0623 <0.000 14.6637 0.1824 <0.000 14.899
5
0.2130 <0.000
Individual level
Sex (Ref=Male) -0.4129 0.0966 <0.000 -0.4143 0.0963 <0.000
Monthly Family Income 0.1764 0.0351 <0.000 0.1720 0.0351 <0.000
Community Periodontal Index
(CPI)
-0.1150 0.0595 0.054 -0.1154 0.0593 0.052
Education Level of Father 0.0835 0.0211 <0.000 0.0774 0.0212 0.000
Socio-dental impact (OIDP) -0.0262 0.0036 <0.000 -0.0262 0.0035 <0.000
Suburb level
Social Exclusion Index (SEI) 0.3721 0.1722 0.031
Variances
Between suburbs 0.0298 0.0259 0.0097 0.0180 0.0000 -
Between individuals 2.7791 0.1160 2.4006 0.1039 2.4016 0.1031
R2 (Coefficient of
Determination)
0.1419 0.1450

81
Table 4. Multilevel Model for Socio-dental impact (OIDP).
DISCUSSION
In this study, the influence of dental clinical variables, individual and contextual
characteristics on the quality of life (QL) of underprivileged adolescents resident in the city
of Piracicaba (SP, Brazil) was evaluated by multilevel analysis, the importance of which
has been pointed out by various researchers [30-33], because it provides a more authentic
evaluation of the relations between the environment and individuals. To the best of our
knowledge, this study may possibly be one of the first to use this technique for studying
the relationship of individual and contextual variables to oral health related quality of life.
In relation to the measure of general quality of life used in this study, although authors
have concluded that developing a new adolescent version of WHOQOL-bref is justifiable,
the index presented some feasibility and acceptability to use with adolescents [34].
The results of this study showed that the variable Social Exclusion Index (SEI)
presented significant association with quality of life. The lower the vulnerabilities of the
suburb, the better the quality of life of the adolescents examined. Although no data were
collected on other social determinants of quality of life, it is speculated that some of the
elements, such as social capital, empowerment, and social support, may explain why
Variable Model 1 Model 2 Model 3
Estimate SE p-value Estimate SE p-value Estimate SE p-value
Intercept 5.8983 0.4961 <0.000 -19.8292 6.2164
Individual level
Age 1.7448 0.4000 <0.000
Sex (Ref=Male) 3.0954 0.8367 0.000
Monthly Family Income -1.4060 0.2967 <0.000
Community Periodontal Index (CPI) 2.3184 0.5112 <0.000
Suburb level
Social Exclusion Index (SEI) No significant 0.998
Variances
Between suburbs 1.3655 1.4572 1.0716 1.2994
Between individuals 203.85 8.4820 191.87 8.0826
R2 (Coefficient of Determination) 0.0598

82
underprivileged adolescents living in similar situations and with similar socio-economic
conditions present different perceptions of quality of life. Studies have shown that social
capital, defined by Putnam [35] as being the social practices, norms and relations of
confidence that exist among citizens in a certain society, in addition to systems of
association and participation that stimulate cooperation, appear to be related to oral health
[31,32]. In addition, it has been suggested that suburbs that generate high levels of social
capital produce fewer risk behaviors, better mental health, more health promotion
behaviors and better overall perceptions of health [36]. However, most of the variance in
WHOQOL and OIDP occurred at the individual level with low impact of the contextual
variables on the statistical model, similar to the findings of other studies [32,33].
Differences between the studies can be explained by the sample design used in each
study, especially population characteristics and sample size. Nevertheless, one of the
important findings is that contextual variables must be considered by health managers in
health planning, seeking greater equity in the distribution of health services and targeting
the reduction of social inequalities. Therefore, our findings also corroborate the idea that
not only individual but also contextual level approaches are important in oral health
planning.
Individual variables had a significant influence on the quality of life and socio-
dental impact. Among them, it is pointed out that girls presented the worst QL and greatest
socio-dental impact. Studies have identified differences between adult men and women in
the way in which the quality of life is affected by oral health, and it has been suggested that
oral health related quality of life (OHRQOL) is not gender-free [37]. In fact, several
studies have found that women generally reported poorer OHRQOL than men
[10,15,16,38,39]. According to Barsky et al. [40], women reported more intense, more
numerous, and more frequent bodily symptoms than men, and according to them, one of
the factors that contribute to differences between men and women seems to be that they
differ in their thresholds for judging and considering a given sensation to be noxious,
unpleasant, and bothersome.
Another demographic variable that had significant influence on the presence of
socio-dental impact was age. Older adolescents presented greater impact, a result similar to
that found by Mbawalla et al. [41]. On the other hand, among adolescents who had

83
completed orthodontic treatment, those who were 15 years old were more prone to have
experienced a dental impact than those aged 16 years [42]. By evaluating our results and
the findings in the literature, it would appear that it is still not clear how oral health-related
quality of life in adolescents is influenced by age, because this variable is dependent on the
problem studied and the study design, demonstrating the need for future studies to address
this issue.
Variables related to socio-economic status played an important role in the
multilevel model, because the increase in monthly family income and fathers' education
level produced a significant increase in QL. Moreover, the higher the income, the lower
was the socio-dental impact. Studies have shown that socio-economic disparities had
significant influence on the occurrence of oral diseases [43,44]. Furthermore, the highest
levels of disease were found in more deprived areas in both the industrialized and non-
industrialized world [18]. With regard to the association between socio-economic variables
and QL, one could speculate that the lower the socio-economic and educational levels, the
less the health needs are perceived, or they are only perceived when they are at a more
advanced stage. However, while some studies have demonstrated that there is association
between socio-economic variables and OHRQOL measurements [4,10,14,16,41,45], other
have found opposite results [7,46]. Therefore, it is suggested that future studies should be
conducted to better determine the impact of socio-economic variables on OHRQOL.
Among the clinical variables studied (DMFT and CPI), only the CPI index
remained in the multilevel model. With an increase in the CPI index, there was a reduction
in QL and increase in socio-dental impact. Some studies have indicated that the presence
of periodontal disease is associated with worse quality of life [47]. Among adolescents, a
Chilean study found that severe periodontal disease (attachment loss; necrotizing ulcerative
gingivitis) was significantly associated with higher impact on the OHRQOL [4]. On the
other hand, most national studies have found no association between periodontal condition
and OHRQOL [10]. It seems that the findings from our study provide new insights into the
influence of periodontal status on the systemic well-being of Brazilian adolescents. Future
studies should be conducted in this issue.
Finally, with the increase in socio-dental impact there was a reduction in QL.
Petersen et al. [48] emphasized that poor oral health may have a profound effect on general

84
health. Our findings showed evidence that the perception of negative impacts of the oral
condition on daily life also influenced the general well-being of adolescents. It is known
that the determinants of oral diseases, such as diet and dirt (hygiene), smoking, alcohol,
risky behaviors causing injuries, and stress, are the risk factors common to a number of
chronic diseases. Therefore, more emphasis should be on the common risk factor approach,
by integrating oral health into strategies for promoting general health and by assessing oral
needs in socio-dental ways [49].
In view of the findings of this study, the need for further studies may be suggested,
in order to gain better understanding of the intricate relations existent between the oral
health status, contextual and socio-demographic variables, among others, and the quality of
life of adolescents. At any rate, the individual and contextual approaches may be important
strategies for public policies on oral health.
Lastly, our study has some limitations. This was a cross-sectional study and sought
inferences with regard to causal factors, without however, establishing a temporal
relationship. The obtainment of data about income is very sensitive, and the respondents
may not have provided accurate information [50]. The self-perception questionnaire may
have been influenced by social acceptance and social desirability [50]. The contextual data
were obtained from government sources, which are subject to problems of under- or over-
notification, processing errors, not updating indicators, and others. However, this study
has strengths such as the random selection of adolescents and the expected response rate,
the robust calibration process of oral health examiners and the use of acceptable measures
of OHRQOL and QL.
It was concluded that individual and contextual variables were related to the socio-
dental impact and quality of life in underprivileged Brazilian adolescents. Girls were found
to have the worst quality of life and greatest socio-dental impact especially if they lived in
areas of greatest social exclusion. There was a diminished quality of life and increase in
OIDP with an increase in the periodontal index, but an increase in the family income
improved quality of life and reduced OIDP.

85
ACKNOWLEDGMENTS
The authors thank the volunteers, the school principals and PHC units, for allowing
the research carried out. This research was supported by FAPESP - São Paulo Research
Foundation (grants #2011/03657-5 and #2011/01768-4).
Ethical Aspects
The study was aproved by the Research Ethics Committee of the Piracicaba
Dental School, University of Campinas (UNICAMP) (protocol number #027/2011) in
accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its
later amendments. Consent was obtained from the parents before starting the study.
REFERENCES
1. Brazil. (2004). Ministry of Health. Secretary of Health Attention. Department of
Primary Care. National Coordination of Oral Health. National Oral Health Policy.
Brasilia. [In Portuguese].
2. Brasil. (2012). Ministery of Health. Oral Health Brasil 2010 (SB Brasil 2010):
National Oral Health Research: main results.
http://189.28.128.100/dab/docs/geral/projeto_sb2010_relatorio_final.pdf. Accessed
03 March 2014
3. Sischo, L., Broder, H.L. (2011). Oral health-related quality of life: what, why, how,
and future implications. J Dent Res, 90(11), 1264-70.
4. López, R., Baelum, V. (2007). Oral health impact of periodontal diseases in
adolescents. J Dent Res. 86(11), 1105-9.
5. Baker, S.R., Mat, A., Robinson, P.G. (2010). What psychosocial factors influence
adolescents' oral health?. J Dent Res, 89(11), 1230-5.
6. Aguilar-Díaz, F.C., Irigoyen-Camacho, M.E., Borges-Yáñez, S.A. (2011). Oral-
health-related quality of life in schoolchildren in an endemic fluorosis area of
Mexico. Qual Life Res, 20(10), 1699-706.

86
7. Papaioannou, W., Oulis, C.J., Latsou, D., Yfantopoulos, J. (2011). Oral health
related quality of life of Greek adolescents: a cross-sectional study. Eur Arch
Paediatr Dent, 12(3), 146-50.
8. Bastos, R.S., Carvalho, E.S., Xavier, A., Caldana, M.L., Bastos, J.R., Lauris, J.R.
(2012). Dental caries related to quality of life in two Brazilian adolescent groups: a
cross-sectional randomised study. Int Dent J, 62(3), 137-43.
9. Foster Page, L.A., Thomson, W.M. (2012). Caries prevalence, severity, and 3-year
increment, and their impact upon New Zealand adolescents' oral-health-related
quality of life. J Public Health Dent, 72(4), 287-94.
10. Paula, J.S., Leite, I.C., Almeida, A.B., Ambrosano, G.M., Pereira, A.C., Mialhe,
F.L. (2012). The influence of oral health conditions, socioeconomic status and home
environment factors on schoolchildren's self-perception of quality of life. Health
Qual Life Outcomes, 13,10:6.
11. Bendo, C.B., Paiva, S.M., Varni, J.W., Vale, M.P. (2013). Oral health-related
quality of life and traumatic dental injuries in Brazilian adolescents. Community
Dent Oral Epidemiol. doi: 10.1111/cdoe.12078.
12. Chakravathy, K.P., Thippeswamy, H.M., Kumar, N., Chenna, D. (2013).
Relationship of body mass index and dental caries with oral health related quality of
life among adolescents of Udupi district, South India. Eur Arch Paediatr Dent,
14(3), 155-9.
13. Foster Page, L.A., Thomson, W.M., Ukra, A., Baker, S.R. (2013). Clinical status in
adolescents: is its impact on oral health-related quality of life influenced by
psychological characteristics? Eur J Oral Sci, 121(3 Pt 1), 182–187.
14. Scapini, A., Feldens, C.A., Ardenghi, T.M., Kramer, P.F. (2013). Malocclusion
impacts adolescents' oral health-related quality of life. Angle Orthod, 83(3), 512-8.
15. Ukra, A., Foster Page, L.A., Thomson, W.M., Farella, M., Tawse Smith, A., Beck,
V. (2013). Impact of malocclusion on quality of life among New Zealand
adolescents. N Z Dent J. 109(1), 18-23.
16. Peres, K.G., Cascaes, A.M., Leão, A.T.T., Côrtes, M.I.S., Vettore, M.V. (2013).
Sociodemographic and clinical aspects of quality of life related to oral health in
adolescents. Rev Saúde Pública, 47(Supl 3), 1-9.

87
17. Townsend, P., & Davidson, N. (1992). Inequalities in health: the black report.
Harmondsworth: Penguin Books.
18. Sisson, K.L. (2007). Theoretical explanations for social inequalities in oral health.
Community Dent Oral Epidemiol, 35(2), 81–8.
19. Hox JJ. Applied multilevel analysis. TT-Publikaries, Amsterdam 1995. Cap1, p. 6-7.
20. Aquino, R., Oliveira, N.F., Barreto, M.L. (2009). Impact of the family health
program on infant mortality in Brazilian municipalities. Am J Public Health, 99(1),
87-93.
21. IBGE. (2013). Brazilian Institute of Geography and Statistic.
http://www.ibge.gov.br/home/ Accessed 04 december 2013.
22. Brasil. (2005). Ministery of Health. Oral Health Brasil 2003 (SB Brasil 2002-2003):
National Oral Health Research: main results.
http://dtr2001.saude.gov.br/editora/produtos/livros/pdf/05_0053_M.pdf. Accessed
03 March 2013.
23. WHO. (1997). World Health Organization. Oral Health Surveys. Basic Methods. 4th
ed. Geneva: World Health Organization.
24. Landis, J.R., Koch, G.G. (1977). The measurement of observer agreement for
categorical data. Biometrics, 33, 159–174.
25. Meneghim, M.C., Kozlowski, F.C., Pereira, A.C., Ambrosano, G.M.V., Meneghim,
Z.M.A.P. (2007). A socioeconomic classification and the discussion related to
prevalence of dental caries and dental fluorosis. Ciênc. saúde Coletiva, 12(2), 523-
529. [In Portuguese]
26. Skevington, S.M., Lotfy, M., O'Connell, K.A. (2004). The World Health
Organization's WHOQOL-Bref quality of life assessment: psychometric properties
and results of the international field trial. A report from the WHOQOL group. Qual
Life Res, 13(2), 299-310.
27. Adulyanon, S., Vourapukjaru, J., Sheiham, A. (1996). Oral impacts affect daily
performance in a low dental disease Thai population. Community Dentistry and Oral
Epidemiology, 24(6), 385-389.

88
28. IPPLAP. (2011). Piracicaba Institute of Planning and Research.
http://www.ipplap.com.br/docs/meis.pdf . Accessed 03 December 2011.
29. SAS Institute Inc 2001: SAS/STAT Guide for personal computers. version 9.2.
Cary: North-Carolina/USA.
30. Turrell, G., Kavanagh, A., Draper, G., Subramanian, S.V. (2007). Do places affect
the probability of death in Australia? A multilevel study of area-level disadvantage,
individual-level socioeconomic position and all-cause mortality, 1998-2000. J
Epidemiol Community Health, 61(1), 13-9.
31. Aida, J., Ando, Y., Oosaka, M., Niimi, K., Morita, M. (2008). Contributions of
social context to inequality in dental caries: a multilevel analysis of Japanese 3-year-
old children. Community Dent Oral Epidemiol, 36(2), 149-56.
32. Aida, J., Hanibuchi, T., Nakade, M., Hirai, H., Osaka, K., Kondo, K. (2009). The
different effects of vertical social capital and horizontal social capital on dental
status: a multilevel analysis. Soc Sci Med, 69 (4), 512-518.
33. Tellez, M., Sohn, W., Burt, B.A., Ismail, A.I. (2006). Assessment of the relationship
between neighborhood characteristics and dental caries severity among low income
African-Americans: a multilevel approach. Journal of Public Health Dentistry,
66(1), 30–36.
34. Skevington, S. M., Dehner, S. , Gillison,F., McGrath, E.J., Lovell, C.R. (2014).
How appropriate is the WHOQOL-BREF for assessing the quality of life of
adolescents? Psychology & Health;29(3) 204- DOI:
10.1080/08870446.2013.845668
35. Putnam, R. (2005). Community and democracy: the experience of Modern Italy. Rio
de Janeiro: FGV. [In Portuguese]
36. Boyce, W.F., Davies, D., Gallupe, O., Shelley, D. (2008). Adolescent risk taking,
neighborhood social capital, and health. J Adolesc Health, 43(3), 246-52.
37. McGrath, C., Bedi, R. (1999). The importance of oral health to older people's
quality of life. Gerodontology, 16(1), 59-63.
38. Mason, J., Pearce, M.S., Walls, A.W., Parker, L., Steele, J.G. (2006). How do
factors at different stages of the lifecourse contribute to oral-health-related quality of
life in middle age for men and women? J Dent Res, 85(3), 257-61.

89
39. Rodd, H.D., Marshman, Z., Porritt, J., Bradbury, J., Baker, S.R. (2012).
Psychosocial predictors of children's oral health-related quality of life during
transition to secondary school. Qual Life Res, 21(4), 707-16.
40. Barsky, A.J., Peekna, H.M., Borus, J.F. (2001). Somatic symptom reporting in
women and men. J Gen Intern Med, 16(4), 266-75.
41. Mbawalla, H.S., Masalu, J.R., Astrøm, A.N. (2010). Socio-demographic and
behavioural correlates of oral hygiene status and oral health related quality of life,
the Limpopo-Arusha school health project (LASH): a cross-sectional study. BMC
Pediatr, 30, 10:87.
42. Oliveira, C.M., Sheiham, A. (2004). Orthodontic treatment and its impact on oral
health-related quality of life in Brazilian adolescents. J Orthod, 31(1), 20-7.
43. Borrell, L.N., Crawford, N.D. (2012). Socioeconomic position indicators and
periodontitis: examining the evidence. Periodontol 2000, 58(1), 69-83.
44. Kim Seow, W. (2012). Environmental, maternal, and child factors which contribute
to early childhood caries: a unifying conceptual model. Int J Paediatr Dent, 22(3),
157-68.
45. Piovesan, C., Antunes, J.L., Guedes, R.S., Ardenghi, T.M. (2010). Impact of
socioeconomic and clinical factors on child oral health-related quality of life
(COHRQoL). Qual Life Res, 19(9), 1359-66.
46. Andrade, F.B., Lebrão, M.L., Santos, J.L., da Cruz Teixeira, D.S., de Oliveira
Duarte, Y.A. (2012). Relationship between oral health-related quality of life, oral
health, socioeconomic, and general health factors in elderly Brazilians. J Am Geriatr
Soc, 60(9), 1755-60.
47. Jansson, H., Wahlin, A., Johansson, V., Akerman, S., Lundegren, N., Isberg, P.E., et
al. (2014). Impact of Periodontal Disease Experience on Oral Health-related Quality
of Life. J Periodontol, 85(3), 438-45.
48. Petersen, P.E., Bourgeois, D., Ogawa, H., Estupinan-Day, S., Ndiaye, C. (2005).
The global burden of oral diseases and risks to oral health. Bull World Health
Organ, 83(9), 661-9.
49. Sheiham, A. (2005). Oral health, general health and quality of life. Bull World
Health Organ, 83(9), 644-644.

90
50. Pereira, I., Ekanayake, L. (2011). Influence of oral health-related behaviours on
income inequalities in oral health among adolescents. Community Dent Oral
Epidemiol, 39(4), 345–351.

91
Capítulo 4
Estudo qualitativo sobre as justificativas de adolescentes carentes para a não adesão
ao tratamento odontológico.
Qualitative study of reasons to non-adherence to dental treatment in underprivileged
adolescents.
Autores: Fabiana de Lima Vazquez, Karine Laura Cortellazzi, Camila da Silva Gonçalo,
Jaqueline Vilela Bulgareli, Luciane Miranda Guerra, Elaine Pereira da Silva Tagliaferro,
Fábio Luis Mialhe, Antonio Carlos Pereira.
Resumo
Este estudo buscou refletir sobre os discursos dos adolescentes nas justificativas para a não
adesão ao tratamento odontológico. Esta investigação qualitativa deriva de uma pesquisa
quantitativa dirigida aos adolescentes de 15 a 19 anos, de escolas estaduais que pertenciam
à área de 34 Unidades de Saúde da Família em Piracicaba, SP, no ano de 2012. Os
adolescentes foram avaliados, diagnosticados e encaminhados para tratamento
odontológico. Um ano após esta intervenção e com a não adesão ao tratamento, utilizou-se
do método qualitativo para compreender em profundidade este fenômeno. Foram
realizadas 25 entrevistas, com roteiro semiestruturado, dividido em três blocos: adotou ou
não as condutas recomendadas; argumentos que justificaram a não adoção das condutas
recomendadas; dimensões relacionadas à importância da saúde bucal. A análise de
conteúdo temática foi adotada e a não adesão foi relacionada com alguns aspectos e
agrupadas configurando em: não prioridade; prioridade e mudança de prioridade.
Concluiu-se que as principais justificativas para a não adesão estão relacionadas com
diferentes prioridades e o aparelho ortodôntico mostrou-se como potente estimulador do

92
interesse e do estabelecimento de prioridades na atenção à saúde bucal entre os
adolescentes.
Palavras-chave: Comportamento do Adolescente; Pesquisa Qualitativa; Saúde Bucal;
Cooperação do Paciente; Saúde Pública.
Abstract
This study sought to reflect on discourses of adolescents about reasons for non-adherence
to dental treatment. The findings of this qualitative research are derived from a quantitative
research aimed at teenagers from 15-19 years of age, randomly selected from 21 state
schools and 34 Primary Health Units – Family Health (PHU-FH) in 2012. The adolescents
were evaluated, diagnosed and referred for dental treatment. One year after this
intervention and with a backdrop of non-adherence to the proposed treatment, we used a
qualitative method to understand in depth this phenomenon. Twenty Five (25) interviews
were conducted by two researchers, with semi-structured interview, divided into three
blocks: followed or not recommended by conduct; arguments justifying the decision not to
conduct recommended; relate to the importance of oral health. A thematic content analysis
was adopted and treatment noncompliance appeared related to some aspects, and were
grouped by setting 03 themes: Not a priority; Priority and Change priority. It was
concluded that the main reasons for non-adherence to the proposed dental treatment are
related to different priorities and the use of orthodontic appliances proved to be potent
stimulator of interest and setting priorities in oral health among adolescents.
Keywords: Adolescent Behavior; Qualitative Research; Oral Health; Patient Compliance;
Public Health.

93
Introdução
As relações do adolescente com o meio social que vive e sua condição de
vida podem facilitar ou dificultar o acesso ao tratamento e a adesão1. É consenso na
literatura que a adolescência é uma fase de exposição a riscos, um período de conflitos
internos e interpessoais, e diversos estudos ressaltam a necessidade de conhecer melhor
suas especificidades, seus paradigmas. São características da adolescência a contestação à
vulnerabilidade, andar em grupos, seguir modas e a preocupação com o corpo e à
aparência. Pensar a saúde do adolescente implica em compreender os diversos modos de
pensar e de viver a adolescência2,3
.
Embora a literatura revele uma produção fértil de estudos sobre o conceito de
“adesão à terapêutica”, observa-se que entre as ideias manifestadas pelos pesquisadores da
área há duas diferenciações principais: o foco no paciente e a busca de fatores externos ao
paciente4.
O Projeto Adesão da Organização Mundial da Saúde (OMS), por exemplo,
adota como definição de adesão a tratamentos crônicos, as definições de Haynes e Rand5,6
que definem adesão como um comportamento de seguir uma recomendação médica ou de
outro profissional de saúde. Também considera a adesão em cinco dimensões: fatores
sociais e econômicos, a equipe/sistema de cuidado de saúde, as características da doença,
terapias da doença e fatores relacionados ao paciente7. Observa-se que só um fator
relaciona-se diretamente com o paciente, considerado como um dos determinantes para a
adesão. Estudos sobre adesão identificaram que não basta ter um serviço público de saúde
disponível, são necessários outros esforços para que este seja utilizado e acessado8,9
.
Estudos publicados na língua inglesa explicitam a diferenciação dos termos
“adherencee” e “compliance”, sendo o primeiro termo ligado à ideia de escolha livre dos

94
indivíduos na adoção ou não das recomendações feitas pelos profissionais de saúde e o
segundo termo, refere-se à ideia de uma conduta passiva do paciente, podendo ser
traduzido como “obediência”4.
No presente estudo adotou-se como conceito de “adesão” a decisão de procurar
um serviço de saúde e seguir o tratamento recomendado. Atitudes opostas a esta ideia
foram consideradas “não adesão”. Assim, o objetivo do artigo foi apresentar e discutir as
justificativas apresentadas para a não adesão ao tratamento odontológico em um grupo de
adolescentes diagnosticados com necessidades de tratamento de cárie e doença periodontal,
encaminhados ao serviço público de saúde.
Metodologia
O artigo refere-se aos achados de uma investigação qualitativa derivada de uma
pesquisa quantitativa dirigida a adolescentes, com idade entre 15 e 19 anos, estudantes de
escolas estaduais que pertencem à área adstrita de 34 Unidades de Saúde da Família no
município de Piracicaba-SP (Aprovação do Comitê de Ética - protocolo 057/2011).
A coleta dos dados quantitativos (cárie1; CPOD
2; doença periodontal
3) foi
realizada em 2012, e na sequência desta ação os adolescentes com necessidade de
tratamento odontológico receberam orientações sobre doenças bucais, higiene oral e
cuidados pessoais com a saúde. Além disso, estes indivíduos foram encaminhados ao
serviço odontológico oferecido nas Unidades de Saúde da Família que atendem a área em
questão.
1 Dente com lesão de cárie, ou seja: desmineralização dos tecidos dentais, causada pela ação de bactérias.
2 CPOD: Índice formulado por Klein e Palmer em 1937, usado em todo o mundo para diagnóstico das condições dentais,
quando a unidade de medida é o Dente Cariado, Perdido e Obturado. 3 Doença periodontal: Doença infecto-inflamatória que afeta os tecidos de sustentação dos dentes.
95
Um ano após a realização destes procedimentos, a equipe de pesquisadores
revisitou o campo para fazer o acompanhamento dos índices de saúde bucal da população
estudada. Neste retorno foi observado um cenário de adesão e de não adesão ao tratamento
odontológico, fato que suscitou o interesse dos pesquisadores em conhecer os fatores que
conduziram tais adolescentes a não adesão supracitada. Na tentativa de alcançar as
informações que levaram os adolescentes a dois caminhos tão distintos, os pesquisadores
decidiram incorporar um braço qualitativo ao desenho inicial do estudo.
Optou-se pela utilização do método qualitativo, pois este possibilita a busca da
compreensão de um fenômeno específico em profundidade, conforme a realidade é
edificada partindo do próprio contexto estudado10,11
.
Quanto à técnica de entrevista, utilizou-se a forma semiestruturada que parte de
questionamentos básicos, sustentados em teorias e hipóteses de interesse para a pesquisa,
abrindo espaço para novas perguntas e gerando novas hipóteses enquanto se recebe as
respostas do entrevistado12
.
Em agosto de 2013, foi realizado o pré-teste do roteiro semiestruturado, etapa
que possibilitou o aprimoramento deste instrumento, por meio da reestruturação da
sequência das perguntas, e do vocabulário empregado na construção das mesmas.
As entrevistas foram estruturadas em três blocos: 1) Adotou ou não as condutas
recomendadas pelos pesquisadores; 2) Argumentos que justificam a não adoção das
condutas recomendadas pelos pesquisadores; 3) Dimensões relacionadas à importância da
saúde bucal e das consultas regulares ao dentista.
A coleta de dados qualitativos teve início em setembro de 2013. A equipe de
pesquisadores contatou os responsáveis pelas escolas e Unidades de Saúde da Família
abordando a possibilidade de revisitação ao grupo de adolescentes. Estas instituições

96
indicaram as datas e horários mais adequados para a realização das entrevistas, e procedeu-
se o agendamento e condução das mesmas junto ao grupo supracitado.
Dois pesquisadores realizaram as transcrições imediatamente após a realização
de cada entrevista. O material transcrito oriundo de 25 entrevistas foi pré-analisado em
dezembro de 2013 com a finalidade de detectar saturação das respostas. Segundo
Fontanella e Magdaleno Júnior, a saturação é o instrumento epistemológico que determina
quando as observações deixam de ser necessárias, ou seja, quando se percebe que mais
nenhum novo elemento irá ampliar a investigação ou o objeto investigado13
. Assim, com a
confirmação da saturação das respostas que compuseram o material analisado, encerrou-se
a fase de entrevistas e imediatamente foi iniciada a análise qualitativa dos dados.
Foi adotada a análise de conteúdo temática proposta por Gomes14
, iniciando os
trabalhos pelo procedimento de leitura exaustiva das transcrições, visando compreender o
conjunto de dados e estabelecer formas de classificação. Neste contexto foi possível: ter
uma visão do conjunto, identificar os temas iniciais e determinar os conceitos teóricos que
seriam empregados na análise. Em seguida, foi efetuada a distribuição dos extratos
segundo a classificação inicial, bem como foi feita a verificação dos núcleos de sentido
contidos nos trechos analisados. Ainda nesta etapa, foram reagrupados os extratos segundo
os temas encontrados e foi elaborada uma redação por temas com o objetivo de contemplar
os sentidos dos textos e sua articulação com os conceitos teóricos que orientaram esta
análise. Finalmente, procedeu-se a redação do material estabelecendo diálogos entre os
temas, objetivos e questões peculiares da presente pesquisa.
Resultados e Discussão

97
A análise temática das 25 entrevistas possibilitou a identificação de 8
categorias relacionadas às justificativas de não adesão ao tratamento odontológico entre os
adolescentes, sendo estas: prioridade; descaso; falta de tempo; medo; dificuldade de
acesso; tratamento ortodôntico; dor e status social. Tais categorias foram agrupadas
configurando 03 eixos temáticos: “não prioridade”; “prioridade” e “mudança de
prioridade”.
O sentido de “não prioridade” foi atribuído às situações em que o tratamento
odontológico não é reconhecido como urgente, nem importante e não desperta o interesse
dos entrevistados. Assim, constatou-se que os participantes da pesquisa consideram outras
circunstâncias mais importantes, postura que influenciou a decisão de não adesão dos
entrevistados, que utilizaram diferentes justificativas:
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?
R: Não, não ligo muito para ir no dentista, tenho preguiça, é assim mais ou menos: eu
tenho cárie mais não vou.”
P: Você acha importante cuidar dos dentes?
R: “Não adianta falar nada dona, entra por um ouvido e sai por outro, a hora que eu sair
daqui já esqueci, por que eu só vou se eu quiser mesmo, depende da vontade da pessoa e o
que você fala não adianta, a pessoa tem que querer ir...”
(E13, masculino, 17 anos, foi encaminhado para tratamento de cárie).
Pela perspectiva da “não prioridade” verifica-se que a necessidade de
comparecer à consulta odontológica não é gerada porque os respondentes não atribuem

98
sentido de urgência ou importância a esta ação. Tal achado suscita uma reflexão: como o
tratamento odontológico poderia tornar-se prioridade neste contexto?”.
Sabe-se que transformar conhecimento sobre questões de saúde em
comportamentos saudáveis, permanece uma tarefa desafiadora, sobretudo nas situações em
que existe o diagnóstico positivo de acometimento da saúde bucal. Em geral, os
comportamentos de proteção à saúde são processos de auto-regulação (self-regulation)
determinados e limitados por crenças, atitudes e conhecimentos; estruturas físicas e sociais,
habilidade ou desempenho de comportamentos15, 16, 17
.
Segundo pesquisas sobre comportamento em saúde, o progresso na área da
prevenção e proteção só será visto quando entendermos como as pessoas organizam seus
pensamentos e agem sobre sua saúde18, 19, 20, 21, 22,23
. Segundo Bandura24
, um dos fatores
que afeta as escolhas das pessoas seria a self efficacy percebida, ou seja, questões que
envolvem atividades, comportamentos, o esforço que investem e a quantidade de tempo
que vão persistir diante de um obstáculo e de experiências adversas. Tanto Bandura15
através da teoria social cognitiva, quanto os modelos atitude-comportamento de Fishbein e
Ajzen25
e a Teoria da Ação Racional26, 27
, defendem a corresponsabilização dos indivíduos
como aliada para se alcançar o cumprimento de comportamentos de proteção para a saúde
bucal.
Enquanto ambiente, habilidade, experiências anteriores e do comportamento
são essenciais componentes da teoria cognitiva, cognições de auto-eficácia sociais são
centrais para a explicação do comportamento15, 24
. As cognições de auto-eficácia são as
expectativas ou crenças individuais acerca da capacidade para realizar um comportamento.

99
Um número crescente de investigações indica que as expectativas de auto-
eficácia estão positivamente e significativamente associadas com a iniciação e manutenção
(ou seja, o cumprimento de longo prazo) de comportamentos de saúde15, 17, 28, 29, 30, 31, 32
.
Um dos grandes desafios é saber como motivar e investir no processo
educativo. Segundo Gagné 33
a motivação é amplamente reconhecida, e com ela a
necessidade de criar condições prévias e adicionais de interesse, e também mantê-los à
medida que a compreensão do processo de aprendizado do autocuidado vai ocorrendo,
estabelecendo novas condições que os influenciem. DeBiase34
define motivação como
forças internas e externas que conduzem e incitam a satisfação de uma necessidade. Com
isso, as ações de educação e promoção em saúde bucal destinadas a incentivar os cuidados
aplicados nesta área, devem necessariamente identificar as fontes de motivação e formas
de satisfação pessoal e, principalmente, reforçar as informações trazendo a sedimentação
dos conhecimentos para que o efeito de tais ações não se perca no tempo35, 36
.
O segundo eixo temático “prioridade”, enfoca o reconhecimento da
importância do tratamento odontológico, embora a urgência e o interesse por este tipo de
cuidado de saúde estejam ausentes no grupo dos adolescentes até o momento da entrevista:
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?
R: “Não fui porque não doía, acho importante, mas não dói, não achei que era grave”.
(E24, Feminino, 16 anos, foi encaminhada para tratamento periodontal).
O medo também foi identificado como sentimento muito influente na não
adesão e a na prioridade referida ao tratamento odontológico:
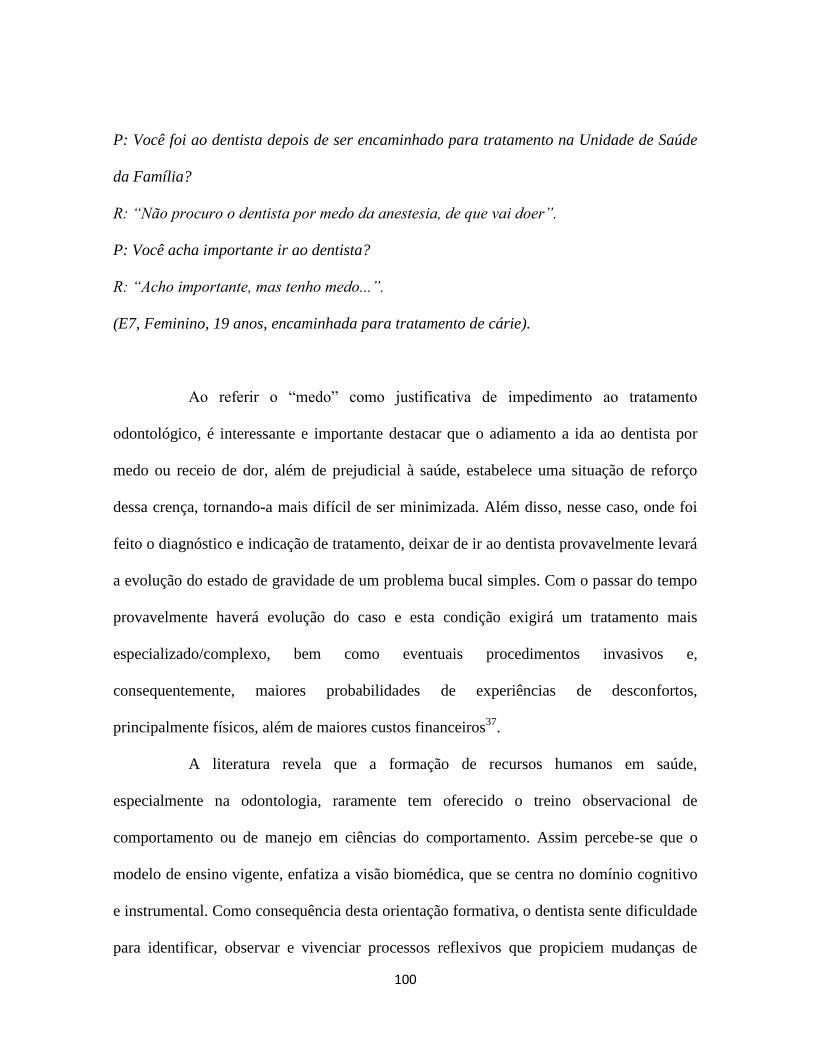
100
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?
R: “Não procuro o dentista por medo da anestesia, de que vai doer”.
P: Você acha importante ir ao dentista?
R: “Acho importante, mas tenho medo...”.
(E7, Feminino, 19 anos, encaminhada para tratamento de cárie).
Ao referir o “medo” como justificativa de impedimento ao tratamento
odontológico, é interessante e importante destacar que o adiamento a ida ao dentista por
medo ou receio de dor, além de prejudicial à saúde, estabelece uma situação de reforço
dessa crença, tornando-a mais difícil de ser minimizada. Além disso, nesse caso, onde foi
feito o diagnóstico e indicação de tratamento, deixar de ir ao dentista provavelmente levará
a evolução do estado de gravidade de um problema bucal simples. Com o passar do tempo
provavelmente haverá evolução do caso e esta condição exigirá um tratamento mais
especializado/complexo, bem como eventuais procedimentos invasivos e,
consequentemente, maiores probabilidades de experiências de desconfortos,
principalmente físicos, além de maiores custos financeiros37
.
A literatura revela que a formação de recursos humanos em saúde,
especialmente na odontologia, raramente tem oferecido o treino observacional de
comportamento ou de manejo em ciências do comportamento. Assim percebe-se que o
modelo de ensino vigente, enfatiza a visão biomédica, que se centra no domínio cognitivo
e instrumental. Como consequência desta orientação formativa, o dentista sente dificuldade
para identificar, observar e vivenciar processos reflexivos que propiciem mudanças de

101
comportamento e que efetivamente atinjam a promoção da saúde38, 39
. A “mudança de
prioridade” (terceiro êxito temático) foi detectada nos casos de urgência clínica-
odontológica e, em situações consideradas pelos adolescentes como tratamento clínico não
urgente, porém considerado necessário em função do status social e da estética. Assim,
verifica-se que em determinados momentos emergem fatores que interferem no sentido da
prioridade, transformando-a em necessidade de tratamento, e impulsionando o adolescente
a buscar o serviço odontológico público ou privado. Os extratos abaixo ilustram a primeira
vertente relacionada com a “mudança de prioridade” (urgência clínica-odontológica):
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?
R: “Eu fui no dentista do posto porque estava com dor, ele passou um remédio para tomar
15 dias e marcou um retorno para 20 dias, mas não voltei porque passou a dor e eu estava
com muito medo. Meu dente está com um buraco e dói, só mastigo de um lado, mas não
está doendo sozinho. Eu acho importante cuidar dos dentes”.
(E14, Feminino, 17 anos, foi encaminhada para tratamento de cárie).
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?
R:“Não fui por que nem lembrava, nem prestei atenção. Fui fazer canal mês passado por
que estava doendo muito...agora vou no convênio, o canal eu fiz no SUS. Acho importante
tratar dos dentes, fui por que estava com dor”.
(E21. Feminino, 16 anos, foi encaminhada para tratamento de cárie).

102
A dor que impulsiona o adolescente à busca do tratamento odontológico foi
identificada como principal justificativa. Quando a dor se manifesta, provavelmente o grau
da doença encontra-se em estágio avançado, e este cenário na maioria dos casos exige
tratamento de maior complexidade. A prevenção e a mudança de comportamento dos
adolescentes em relação aos cuidados com a própria saúde é um grande desafio para os
profissionais desta área. O que se ressalta é que desde o momento em que receberam o
diagnóstico, as orientações e o encaminhamento para tratamento odontológico, os
adolescentes não cogitaram aderir às recomendações, pois suas percepções não conferiram
importância ao caso. Este cenário é, na visão dos pesquisadores, altamente desafiador e,
suscita algumas perguntas: Como motivar e manter motivados os adolescentes para
cuidarem da própria saúde? Como tornar a saúde bucal prioridade?
Bosi e Affonso40
citam que a conscientização da importância da saúde bucal
não é um processo simples, já que a experiência da doença é um fator preponderante para
formar a “consciência preventiva”. Tais autores comentam que esta consciência não
decorre da transferência de um saber do dentista para o adolescente, mas da experiência
com a saúde e a doença. Nesse sentido, a oferta exclusiva de orientações, não conduz os
indivíduos à postura permanente de mudança de comportamento. No entanto, outro estudo
aponta que estabelecer parcerias entre educadores e profissionais de saúde trabalhando na
educação e promoção de saúde dos adolescentes, estabelece resultados positivos
significativos em relação a sua saúde bucal41
.
Os extratos a seguir demonstram algumas situações relacionadas com a
segunda vertente da “mudança de prioridade” (tratamento clínico não urgente, porém
considerado necessário em função do status social e da estética):

103
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?
R: “Não tive motivo, sei lá”.
P: Você acha importante ir ao dentista?
R: “Não, tipo... o importante para mim é os dentes tortos, tenho que colocar aparelho”.
(E15, Masculino, 16 anos, foi encaminhado para tratamento de cárie).
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?
R: “Não, eu esqueci, perdi o papel. Quero colocar aparelho, já fiz a documentação. Vou
procurar o dentista para tratar os dentes antes de colocar o aparelho”.
(E6, Feminino, 16 anos, encaminhada para tratamento de cárie).
Nessas e outras repostas verificamos que o aparelho ortodôntico é uma das
justificativas fundamentais para que o interesse e a visita ao serviço odontológico tornem-
se prioridade. Os achados da pesquisa apresentam forte relação entre o uso do aparelho
ortodôntico e a satisfação pessoal de duas demandas consideradas importantes pelo grupo
de entrevistados: o desejo de exibir um acessório que representa status social (demanda de
consumo) e o desejo de ficar bonito (demanda estética).
Segundo Lawler e Nixon42
, na adolescência, a aparência é de fundamental
importância. Na presente pesquisa verifica-se que o desejo de ser aceito e fazer parte de um
grupo parece impulsionar os entrevistados à procura do serviço odontológico. Porém, nota-
se uma contradição na medida em que todos os entrevistados foram diagnosticados com

104
doenças bucais (cárie e problemas periodontais), situações em que o tratamento
ortodôntico não é indicado até que a saúde bucal seja restabelecida.
Estudos revelam que entre adolescentes não é rara a constatação de
comportamentos negligentes referentes aos cuidados com a saúde. A adolescência é
reconhecida como um período em que o risco do desenvolvimento de cárie e de outras
doenças bucais encontra-se aumentado em decorrência do precário controle do biofilme, do
menor cuidado com a escovação e da maior ingestão de produtos com açúcar43, 44, 45
.
Com relação à parte estética, alguns autores citam que valores culturais
atrelados a ela e o maior acesso à informação sobre saúde são mais evidentes nas classes
sociais de maior poder aquisitivo, o que pode justificar o fato de os adolescentes de escolas
privadas citarem com maior frequência os dentes e os cabelos como muito importantes44, 46,
47.
No presente estudo constatou-se que embora a população estudada frequente
escolas públicas e more em áreas de maior vulnerabilidade social, manifestou
preocupações com a estética semelhantes aos estudos supracitados. Contudo, trata-se, aqui,
de um tipo de preocupação relacionada com a “posse” de um acessório que é referência de
status e que reflete um desejo de consumo, bem como de “estar na moda”, e “ficar bonito”.
Este cenário nos remente à teoria do Ator-Rede que, resumidamente,
compreende a ideia de que atores se encontram constantemente conectados a uma rede
social de elementos materiais e imateriais, ou seja, existem movimentos, ações, conexões
que estão articulando pessoas, coisas e a natureza em associações provisórias48, 49, 50, 51
.
Neste contexto, a construção dos significados no consumo de bens não decorre apenas das
relações sociais no nível institucional, mas também da estrutura de relacionamentos em
que o indivíduo está inserido. Desse modo, a lógica de aquisição de bens possui uma

105
dimensão individual, onde é possibilitado a quem consome expressar a sua
individualidade, e a dimensão social que é a expressão de sua identificação com grupos
sociais52
.
Na adolescência, os indivíduos passam a ter novas referências de grupo,
sofrendo influências das tendências de consumo e comportamentos. Deste modo, o
movimento em redes torna-se aparente nos achados da presente pesquisa, na medida em
que a ideia de pertencimento e de conquista da beleza é proporcionada pelo uso do
aparelho ortodôntico. Por esta perspectiva, pode-se afirmar que o interesse pelo tratamento
odontológico na população estudada não passa pela concepção de saúde, mas relaciona-se
com outros interesses ligados à fase da adolescência, bem como com o contexto de vida
desses sujeitos. Pensa-se que a emersão de uma lógica de prioridades nas respostas dos
adolescentes pode contribuir para o aprimoramento do planejamento de ações em saúde
bucal. Nesse sentido, o esforço de articular os interesses do grupo estudado com a oferta do
serviço odontológico poderá facilitar o acesso dos adolescentes aos meios de prevenção,
tratamento e manutenção da saúde bucal oferecidos neste contexto.
Estas ideias podem ser reforçadas por estudos publicados53,54
, cujos relatos
citam que é essencial conhecer as necessidades, a estrutura psicossocial e contextual em
que esses adolescentes estão inseridos, incorporando-as nas ações de saúde bucal e
propiciando o surgimento de novas ideias e ações que se ajustem, surjam e cresçam nessa
realidade.
Ainda em relação ao aparelho ortodôntico, a análise das respostas evidencia a
justificativas surpreendentes para a não adesão ao tratamento odontológico: uma confusão
entre o conceito das consultas odontológicas ortodônticas (normalmente frequentadas em

106
serviços privados) e o conceito das consultas odontológicas para tratamento de cárie e
doenças periodontais a que os adolescentes foram encaminhados.
Os extratos que seguem ilustram momentos em que tal confusão foi detectada:
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?
“Não. Já vou em um dentista do acompanhamento do aparelho. Achei que como já ia no
dentista do aparelho, todo mês, não precisava mais ir em outro”..
(E1, Feminino, 17 anos, encaminhada para tratamento de cárie).
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?
“Porque não fui? Uso aparelho há 3 anos e já vou no dentista todo mês. O dentista do
aparelho não disse que eu preciso tratar dos dentes”.
(E18, Feminino, 16 anos, encaminhada para tratamento de cárie).
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?
“Não fui por que estou em tratamento ortodôntico e já vou no dentista todo mês”.
E17, Feminino, 16 anos, encaminhada para tratamento periodontal).
P: Você foi ao dentista depois de ser encaminhado para tratamento na Unidade de Saúde
da Família?

107
“Não fui... uso aparelho há 7 anos, o dentista do aparelho disse que precisava fazer o
tratamento, aí tenho que marcar”.
(E4, Masculino, 16 anos, encaminhado para tratamento periodontal).
Por meio da análise deste tipo de resposta, foi possível perceber que, nas
próximas intervenções será necessário esclarecer as diferenciações entre as modalidades de
consulta odontológica supracitadas, visando minimizar a não adesão ao tratamento
indicado.
Além da confusão citada, pode-se reconhecer a importante influência atribuída
pelos adolescentes ao ortodontista. Também é possível constatar que a população estudada,
embora ocupe uma área de vulnerabilidade e risco social, se utiliza de convênios e de
clínicas privadas que viabilizam a conquista do aparelho ortodôntico como bem de
consumo desejado. Em um estudo recente, sites de mídia social foram investigados e
constatou-se que os adolescentes trocam informações sobre uso de aparelhos ortodônticos,
sendo provável que o feedback derivado dessas conversas casuais influenciam a atitude
destes indivíduos frente a ortodontia. Os autores do estudo relatam que os adolescentes
submetidos à ortodontia se comunicavam pelas mídias sociais, expressavam atitudes
positivas em relação ao tratamento e que a possibilidade de poder escolher as cores dos
elásticos ortodônticos era muito valorizada entre eles55, 56
.
Considerando que conversas virtuais entre adolescentes motivam a busca pelo
tratamento ortodôntico; considerando que a análise dos dados revela que a noção de usar o
aparelho ortodôntico está fora da lógica da saúde e dentro da lógica do consumo; e ainda,
levando em consideração a recente repercussão nacional que os “aparelhos ostentação”
ganharam em um programa de televisão de grande audiência no país, detecta-se que os

108
adolescentes estão tendo acesso ao aparato odontológico sem nenhum controle técnico,
torando este mais um problema de saúde pública.
Ressalta-se que a inserção do ortodontista nos centros de especialidades, foi
regulamentada pelo Ministério da Saúde que passou a financiar, por meio da Portaria
Ministerial Nº 718/SAS de 20/12/201057
novos procedimentos, incluindo o aparelho
ortodôntico e ortopédico. Pensa-se que nesse novo contexto, inserir o ortodontista como
vetor de ações de saúde, utilizando-se do interesse dos adolescentes nessa especialidade,
conscientizando-os que o compromisso com a sua saúde bucal, na forma de prevenção e
tratamento odontológico são pré-requisitos para possibilidade de um tratamento
ortodôntico com indicação correta e supervisão, em muito contribuiria para a adesão ao
tratamento e para a saúde bucal, já que esta especialidade mostra-se motivadora para o
adolescente no sentido de cuidar de seus dentes. Portanto, é possível reconhecer a provável
potência de propostas conjugadas de educação, conscientização e autocuidado, na saúde
como um todo e especialmente na saúde bucal dos adolescentes que participaram da
presente pesquisa.
Como sugestão, pensa-se que a adesão ao tratamento poderia ser mais bem
sucedida quando a abordagem, ao invés de partir das técnicas de escovação e higienização
bucal, partisse da conversa com o ortodontista. A pergunta disparadora da atividade
poderia ser: Quem quer usar aparelho? Com o interesse do grupo despertado, o ortodontista
descreveria e explicaria todos os pré-requisitos para a instalação do aparelho ortodôntico.
Além disso, o mesmo profissional também citaria os problemas referentes aos “aparelhos
ostentação” que são vendidos e instalados por pessoas sem qualquer formação em
odontologia, fato que lesa a saúde bucal e sistêmica da população.

109
Conclusão
Verificou-se que as principais justificativas para a não adesão ao tratamento
odontológico proposto estão relacionadas com diferentes lógicas de prioridades do grupo,
ou seja, a necessidade de dedicar atenção à saúde bucal, na visão dos entrevistados,
depende do que eles consideram urgente, importante e interessante.
O uso de aparelhos ortodônticos, embora nesta população esteja relacionado à
necessidade de consumo, mostrou-se como potente estimulador do interesse e do
estabelecimento de prioridades na atenção à saúde bucal entre os adolescentes. Assim,
propõe-se que ao planejar estratégias de promoção e prevenção em saúde bucal entre este
público, seja incorporado à equipe o dentista especialista em ortodontia.
Sugere-se também que as ações considerem como ponto de partida os cuidados
exigidos aos portadores destes aparatos bucais, e se desenvolvam na direção dos preceitos
básicos de higienização bucal. A princípio esta lógica pode parecer controversa para os
dentistas, mas considerando o cenário encontrado no presente estudo, vimos esta estratégia
como possibilidade promissora a fim de minimizar a não adesão aqui estudada.
Agradecimentos
Os autores gostariam de agradecer o apoio financeiro da FAPESP (bolsas #
2011/03657-5 e # 2011/01768-4)
Aos diretores das escolas, professores e todos os adolescentes que contribuíram
para a realização da pesquisa.

110
Referências
1. Scaduto AA, Barbieri V. O discurso sobre a adesão de adolescentes ao tratamento da
dependência química em uma instituição de saúde pública. Cien Saúde Colet 2009;
14(2):605-614.
2. Correia ACP, Ferriani MGC. A produção científica da enfermagem e as políticas de
proteção à adolescência. Rev bras enferm 2005; 58(4):449-53.
3. Senna SRCM, Dessen MA. Contributions of human development theories to a
contemporary concept of adolescence. Psic: Teor e Pesq 2012; 28(1):101-108.
4. Leite SN, Vasconcellos MPC. Adesão à terapêutica medicamentosa: elementos para a
discussão de conceitos e pressupostos adotados na literatura. Cien Saúde Colet 2003;
8(3):775-782.
5. Haynes RB. Determinants of compliance: The disease and the mechanics of treatment.
Baltimore MD. Johns Hopkins University Press 1979.
6. Rand CS. Measuring adherence with therapy for chronic diseases: implications for the
treatment of heterozygous familial hypercholesterolemia. Am J Cardiol1993;72:68-74.
7. Gusmão JL, Mion Jr D. Adesão ao tratamento–conceitos. Rev Bras Hipertens 2006;
13(1):23-25.
8. Paiva DD, Bersusa AAS, Escuder MML. Avaliação da assistência ao paciente com
diabetes e/ou hipertensão pelo Programa Saúde da Família do Município de Francisco
Morato, São Paulo, Brasil. Cad Saúde Pública 2006; 22(2):377-85.
9. Bertolozzi MR, Nichiata LYI, Takahashi RF, Ciosak SI, Hino P, Val LF, Guanillo
MCLTUPE. Os conceitos de vulnerabilidade e adesão na Saúde Coletiva. Rev. Esc.
Enferm 2009; 43(2):1326-1330.
10. Canzoniere AM. Metodologia da pesquisa qualitativa na saúde. Petrópolis: Vozes;
2010.
11. Medeiros M. Pesquisas de abordagem qualitativa. Revista Eletrônica de Enfermagem
[periódico na Internet] 2012 abr-jun [acessado 2014 fev 27]: 14(2):224-5. Available
from:http://dx.doi.org/10.5216/ree.v14i2.13628. 14(2), 224-9.
12. Triviños ANS. Introdução à pesquisa em ciências sociais: a pesquisa qualitativa em
educação. São Paulo: Atlas; 1998.

111
13. Fontanella BJB, Júnior RM. Saturação teórica em pesquisas qualitativas: contribuições
psicanalíticas. Psicol Estud 2012; 17(1):63-71.
14. Gomes R. Análise e interpretação de dados de pesquisa qualitativa. In: Minayo MCS,
organizadores. Pesquisa Social. Teoria, método e criatividade. Petrópolis: Vozes;
2010.
15. Bandura A. Social foundations of thought and action. Prentice Hall: Englewood Cliffs,
NJ; 1986.
16. Tedesco LA, Keffer MA, Fleck-Kandath C. Self-efficacy, reasoned action, and oral
health behavior reports: a social cognitive approach to compliance. J Behav Med 1991;
14(4):341-355.
17. Abraham C, Sheeran P, Henderson M. Extending social cognition models of health
behaviour. Health Educ Res 2011; 26:624-637.
18. Kirscht JP. Preventive health behavior: A review of research and issues. Health
Psychology 1983; 2(3):277.
19. Schunk DH, Carbonari JP. Self-efficacy models. Behavioral health: A handbook of
health enhancement and disease prevention; 1984.
20. Kirscht JP. The health belief model and predictions of health actions. Springer US;
1998.
21. Scheier MF, Carver CS, Armstrong GH. Behavioral self-regulation, health, and illness.
Handbook of health psychology 2012; 79-97.
22. Halvari AE, Halvari H, Bjørnebekk G, Deci EL. Motivation for Dental Home Care:
Testing a Self‐Determination Theory Model. Journal of Applied Social Psychology
2012; 42(1), 1-39.
23. Conner M, McEachan R, Jackson C, McMillan B, Woolridge M, Lawton R.
Moderating effect of socioeconomic status on the relationship between health
cognitions and behaviors. Ann Behav Med 2013; 46(1):19-30.
24. Bandura A. Self-efficacy: toward a unifying theory of behavioral change.
Psychological review 1977; 84(2):191.
25. Ajzen I, Fishbein M. Attitude-behavior relations: A theoretical analysis and review of
empirical research. Psychol bulletin 1977; 84(5):888.

112
26. Fishbein M, Ajzen I. Belief, attitude, intention and behavior: An introduction to theory
and research. Reading MA: Addison-Wesley; 1975.
27. Ajzen I, Fishbein M. Understanding attitudes and predicting social behaviour.
Prentice-Hall, 1980.
28. Brubaker RG, Wickersham D. Encouraging the practice of testicular self-examination:
a field application of the theory of reasoned action. Health Psychology 1990;
9(2):154, 1990.
29. Kanfer FH, Hagerman S. (1981). The role of self-regulation. Behavior therapy for
depression: Present status and future directions. San Diego, CA: Academic Press;
1981. p. 143-179.
30. O'Leary A. Self-efficacy and health. Behaviour research and therapy 1985; 23(4):437-
451.
31. Mosher CE, Lipkus I, Sloane R, Snyder DC, Lobach DF, Demark‐Wahnefried W.
Long‐term outcomes of the fresh start trial: exploring the role of self‐efficacy in cancer
survivors' maintenance of dietary practices and physical activity. Psychooncology
2013; 22(4):876-885.
32. Parschau L, Fleig L, Koring M, Lange D, Knoll N, Schwarzer R, Lippke S. Positive
experience, self‐efficacy, and action control predict physical activity changes: A
moderated mediation analysis. Brit j health psychol 2013; 18(2):395-406.
33. Gagné R, Briggs L. Principles of instructional design. Nova Iorque: Holt, Rinehart
and Winston; 1974.
34. DeBiase, ChristinaB. Dental health education: theory and practice. Lea e
Febigertheory. Pennsylvania; 1991. 314p.
35. Santos ZMDSA, Silva RMD. Hipertensäo arterial: modelo de educaçäo em saúde
para o autocuidado. Unifor; 2002.
36. Pauleto ARC, Pereira MLT, Cyrino EG. Saúde bucal: uma revisão crítica sobre
programações educativas para escolares. Cien Saúde Colet 2004; 9(1):121-130.
37. Junior ALC. Psicologia aplicada à odontopediatria: uma introdução. Estud Pesq Psicol
2013; 2(2):46-53
38. Pico BF, Kopp MS. Paradigm shifts in medical and dental education: Behavioural
sciences and behevioural medicine. Euro J Dent Educ 2014; 8(1):25-31.

113
39. Possobon RF, Carrascoza KC, Moraes ABA, Jræ ALC. O tratamento odontológico
como gerador de ansiedade. Psicologia em estudo 2007; 12(3):609-616.
40. Bosi MLM, Affonso KDC. (1998). Cidadania, participação popular e saúde: com a
palavra, os usuários da Rede Pública de Serviços. Cad Saúde Pública 1998; 14(2):355-
365.
41. Haleem A, Siddiqui MI, Khan AA. (2012). School-based strategies for oral health
education of adolescents-a cluster randomized controlled trial. BMC oral health 2012;
12(1):54.
42. Lawler M, Nixon E. Body dissatisfaction among adolescent boys and girls: the effects
of body mass, peer appearance culture and internalization of appearance ideals. J
youth Adolesc 2011; 40(1):59-71.
43. Tomita NE, Pernambuco RDA, Lauris JRP, Lopes ES. Educaçäo em saúde bucal para
adolescentes: uso de métodos participativos. Rev Fac Odontol Bauru 2001; 9(1/2): 63-
69.
44. Vadiakas G, Oulis CJ, Tsinidou K, Mamai-Homata E, Polychronopoulou A. Socio-
behavioural factors influencing oral health of 12 and 15 year old Greek adolescents. A
national pathfinder survey. Euro Arch Paediatr Dent 2011; 12(3), 139-145.
45. Lawler M, Nixon E. Body dissatisfaction among adolescent boys and girls: the effects
of body mass, peer appearance culture and internalization of appearance ideals. J
youth adolesc 2011, 40(1), 59-71.
46. Campos CCGD, Souza SJ. Mídia, cultura do consumo e constituição da subjetividade
na infância. Psicol cien e prof 2003; 23(1):12-21.
47. Granville-Garcia AF, Fernandes LV, Farias TSSD, D'Ávila S, Cavalcanti AL,
Menezes VA. Adolescents' knowledge of oral health: a population-based study. Rev
Odonto Ciên 2010; 25(4):361-366.
48. Powell W, Smith-Doerr L. Network and Economic Life. In: Smelser NJ, Swedberg R,
Organizers. The Handbook of Economic Sociology. Princeton NJ: Princeton University
Press; 1994.
49. Castilla EJ, Hwang H, Granovetter M, Granovetter El Social Networks in Silicon
Valley. In: Lee C, Miller WF, Hancock MG, Rowen HS, organizes. The Silicon
Valley Edge. Stanford: Stanford University Press, 2000, p. 218-247.

114
50. Latour B. Reagregando o social: uma Introdução à Teoria do ator-rede. Salvador:
Edufba; 2012.
51. Maier C, Laumer S, Eckhardt A, Weitzel T. Giving too much social support: social
overload on social networking sites. Euro J Informat Systems [serial on the Internet]
2014 march [cited 4 march 2014]. Avaliable from:
http://www.palgravejournals.com/ejis/journal/vaop/ncurrent/full/ejis20143a.html
doi:10.1057/ejis.2014.3
52. Nascimento MR, Oliveira JS, Cenerino A. A influência da imersão social na
constituição dos significados do consumo e na adoção de produtos tecnológicos por
adolescentes: uma análise teórica a partir da sociologia econômica. Perspectivas
Contemporâneas 2013; 8(2):22-42.
53. Viner RM, Ozer EM, Denny S, Marmot M, Resnick M, Fatusi A, Currie C.
Adolescence and the social determinants of health. The Lancet 2012; 379(9826):1641-
1652.
54. Souza GBS, Junqueira SR, Araujo ME, Botazzo C. Práticas para a saúde: avaliação
subjetiva de adolescentes. Saúde debate 2012; 36(95):562-571.
55. Trulsson U, Strandmark M, Mohlin B, Berggren U. A qualitative study of teenagers’
decisions to undergo orthodontic treatment with fixed appliance. J Orthodont 2002;
29(3):197-204.
56. Henzell RM, Knight MA, Morgaine KC, Antoun SJ, Farella M. (2013). A qualitative
analysis of orthodontic-related posts on Twitter. The Angle Orthodontist [periódico na
Internet] 2014 março [acessado 2014 fev 27]: 84(2):203-207.
57. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Portaria nº 718, 20 de
dezembro de 2010. Disponível em:
http://bvsms.saude.gov.br/bvs/saudelegis/sas/2010/prt0718_20_12_2010.html
[acessado em março 2014].
115
CONCLUSÃO
Os trabalhos mostraram uma prevalência das necessidades de tratamento de
cárie e doença periodontal, sua relação com o impacto nas atividades na vida diária, na
qualidade de vida, com variáveis socioeconômicas e contextuais com considerável
importância epidemiológica, respondendo de forma diferenciada algumas questões que até
então não haviam sido citadas na literatura.
Estes dados indicam que, além dos fatores de risco individuais, é necessário
que se leve em consideração as variáveis relacionadas com o contexto em que os
adolescentes carentes vivem para a formulação de políticas voltadas para ações de
promoção, prevenção e proteção da saúde bucal em adolescentes.
Um diferencial nos estudos de cárie, periodontia e qualidade de vida foi que
utilizamos modelos multiníveis para testar associações de variáveis individuais e
contextuais em adolescentes, já que tais modelos se adequam para a análise de dados
hierárquicos, pois consideram a influência do contexto da comunidade sobre os
comportamentos de saúde dos indivíduos (Patussi et. al., 2006; Aida et. al., 2009).
Também se utilizou uma técnica contemporânea (PROC GLIMMIX) que, em comparação
com a análise de regressão tradicional, dá melhores estimativas e significados substantivos
para agrupamento de dados, permitindo que fatores contextuais sejam analisados
separadamente (Nkansah - Amankra et. al., 2010), o que representa uma importante
contribuição ao atual estado da arte, pois, provavelmente este trabalho, foi um dos
primeiros a usar esta técnica para estudar a relação das variáveis individuais e contextuais
no que diz respeito à saúde bucal.
Considerando-se que a população do estudo foi composta por adolescentes
desprivilegiados em relação ao local de moradia, estrutura familiar, contexto econômico e
social entre outros, não poderiamos deixar de relacionar a saúde bucal com os fatores de
risco e a vulnerabilidade aos quais estão expostos. Algumas variáveis estudadas, como o
Índice de Exclusão social, presidiários na família, e outras, possivelmente têm sido pouco
mencionadas ou até mesmo inéditas na literatura.
Identificar esses fatores em uma população carente de recursos sociais é de
suma importância. Contudo, é necessário refletir, conjuntamente, sobre outros fatores que

116
podem influenciar comportamentos de risco, como por exemplo, o nível de capital social
existente no espaço em estudo, já que, atualmente tem sido sugerido que locais que geram
altos níveis de capital social produzem menos comportamentos de risco, uma melhor saúde
mental, mais comportamentos de promoção da saúde e melhores percepções globais de
saúde (Putnam, 2005; Boyce et. al., 2008). Assim, se tal fator for usado como ferramenta
de recursos de estudos científicos, podem gerar soluções edificantes e deveria ser de
extrema prioridade para os governantes e gestores do país.
A expansão da Estratégia de Saúde da Família, a partir de 1994, garantiu
acesso aos cuidados básicos de saúde a grande parte da população, antes excluída dos
programas de saúde. Contudo, a garantia acesso e o direito a saúde, não significa a
efetividade do programa. Tanto na promoção da saúde bucal quanto na assistência
odontológica, faz-se necessário que os formuladores e gestores de políticas públicas
avancem na obtenção e manutenção da saúde não apenas em âmbito global, mas também
pelo resultado de intervenções feitas no panorama existente de desigualdade.
Ficou evidenciado nesse trabalho que mesmo numa população homogênea,
com pouca variação no índice de exclusão entre os bairros, há um grupo mais vulnerável e
que concentra índices mais altos de doença bucal. A variável Índice de Exclusão Social
(IES) apresentou associação significativa com a qualidade de vida. Quanto menor as
vulnerabilidades do subúrbio, melhor a qualidade de vida dos adolescentes examinados.
Portanto, outras variáveis parecem explicar melhor a relação entre a cárie,
doença periodontal e as desigualdades sociais, especialmente em grupos carentes. Esta
afirmação torna-se evidente quando verificamos que o valor médio do índice CPO-D do
grupo foi de 2,1, no entanto, aumentou para 5,24 (SIC) no grupo em que níveis elevados da
doença estão concentrados.
Além disso, esta pesquisa indentificou os motivos da falta de adesão ao
tratamento odontológico dos adolescentes com alta carga de doença, o porquê da
negligência desses indivíduos com a saúde bucal. Concluímos que, para esses jovens, os
cuidados com a saúde bucal não foram identificados como prioridade e, não sendo
prioridade, não havia interesse em realizá-lo. A procura pelo tratamento somente significou
e, portanto, priorizou a consulta ao dentista, quando a dor ou o interesse de usar o aparelho
ortodôntico os motivou a essa ação.

117
A contribuição dessas informações é inovadora para programar ações futuras
com uma abordagem atual e contextualizada. São imprescindíveis que as intervenções em
saúde pública signifiquem o cuidado com a saúde para esses sujeitos que pertencem aos
grupos mais vulneráveis e expostos aos riscos sociais somados ainda, as características
próprias da idade.
Para se responsabilizar o jovem individualmente pelos cuidados com sua saúde
é necessário que se analise com profundidade e abrangência como se configura o poder em
nossa sociedade, levando-se em conta, sempre, o contexto sociocultural em que estão
inseridos, bem como as diversas formas de apelo ao consumo e os de “estilos de vida” que
estão sujeitos (Lisboa et.al., 2013).
Tratar de sujeitos em uma fase de mudanças e contradições e, ainda, inseridos
em um meio social desprovido de estruturas de apoio, somente será efetivo quando as
estratégias forem de encontro com sua realidade, inseridas em seu meio social e em sua
maneira de agir e pensar. Somente assim poderemos pensar em mudanças e efetiva
promoção de saúde.

118

119
Referências
1. Abraham C, Sheeran P, Henderson M. Extending social cognition models of health
behaviour. Health Educ Res. 2011; 26: 624-637.
2. Adler NE, Ostrove JM. Socioeconomic status and health: what we know and what we
don't. Annals of the New York academy of Sciences. 1999; 896: 3-15.
3. Adorno RCF. Capacitação Solidária. Um olhar sobre os jovens e sua vulnerabilidade
social. AAPCS - Associação de apoio ao programa capacitação solidária. São Paulo,
2001.
4. Aida J, Ando Y, Oosaka M, Niimi K, Morita M. Contributions of social context to
inequality in dental caries: a multilevel analysis of Japanese 3-year-old children.
Community Dent Oral Epidemiol. 2008; 36(2): 149-56.
5. Aida J, Hanibuchi T, Nakade M, Hirai H, Osaka K, Kondo K. The different effects of
vertical social capital and horizontal social capital on dental status: a multilevel
analysis. Social science e medicine. 2009; 69: 512-518.
6. Ayres JR, Calazans G, Salleti HCFO, e França Jr I. Risco, vulnerabilidade e práticas
de prevenção e promoção da saúde. In: Campos GWS, Minayo MCS, Akerman Jr,
MD, e Carvalho YM. (Orgs.). Tratado de Saúde Coletiva (pp. 375-417). São Paulo;
Rio de Janeiro: Editora Hucitec; Editora Fiocruz, 2006.
7. Ayres JRCM, Paiva V, França-Junior I. Conceitos e práticas de prevenção: da história
natural da doença ao quadro da vulnerabilidade e direitos humanos [mimeo]. In
Apostila do Curso de Especialização em Prevenção ao HIV/Aids no Quadro da
Vulnerabilidade e dos Direitos Humanos. NEPAIDS, SP, 2010.
8. Ayres JRCM. Sobre o risco: para compreender a epidemiologia. São Paulo: Hucitec,
2002.
9. Bandura A. Social foundations of thought and action. Prentice Hall: Englewood Cliffs,
NJ; 1986.
10. Bastos FA, Santos E, Tovo MF. Capital Social e Sistema Único de Saúde (SUS) no
Brasil. Saude soc. 2009; 18(2): 177-188.

120
11. Boillot A, El Halabi B, Batty GD, Rangé H, Czernichow S, Bouchard P. Education as
a Predictor of Chronic Periodontitis: A Systematic Review with Meta-Analysis
Population-Based Studies. PLoS ONE<http: www.plosone.org>. 2011; 6(7).
12. Boyce WF, Davies D, Gallupe O, Shelley D. Adolescent risk taking, neighborhood
social capital, and health. J Adolesc Health. 2008;43(3): 246-52.
13. Brasil. Ministério da Saúde. Programa de Saúde do adolescente. Bases programáticas.
Brasília: MS. 1989.
14. Brubaker RG, Wickersham D. Encouraging the practice of testicular self-examination:
a field application of the theory of reasoned action. Health Psychology. 1990; 9(2):
154.
15. Conner M, McEachan R, Jackson C, McMillan B, Woolridge M, Lawton R.
Moderating effect of socioeconomic status on the relationship between health
cognitions and behaviors. Annals of Behavioral Medicine. 2013; 46(1): 19-30.
16. Costa CPM, Oliveira DC, Gomes AMT, Pontes APM, Espírito Santo CC, Campos LA.
A associação entre a ocorrência de acidentes de trabalho na adolescência e o uso de
equipamentos de segurança. Adolescência e Saúde. 2008; 5(3): 13-19.
17. Fejerskov O. Changing paradigms in concepts on dental caries: consequences for oral
health care. Caries Res. 2004; 38: 182-91.
18. Gomes R. Análise e interpretação de dados de pesquisa qualitativa. In: Minayo MCS,
organizadores. Pesquisa Social. Teoria, método e criatividade. Petrópolis: Vozes;
2010.
19. Halvari AE, Halvari, H, Bjørnebekk G, e Deci EL. Motivation for Dental Home Care:
Testing a Self‐Determination Theory Model1. Journal of Applied Social Psychology.
2012; 42(1): 1-39.
20. Hartz ZM. Explorando novos caminhos na pesquisa avaliativa das ações de saúde. In:
Hartz, ZMA (Org.) Avaliação em saúde: dos modelos conceituais à prática na análise
da implantação de programas. 1ª reimpressão. Rio de Janeiro: Fiocruz, 2000.
21. Higgins JA, Hoffman S, Dworkin SL. Rethinking gender, heterosexual men, and
women's vulnerability to HIV/AIDS. American Journal of Public Health. 2010;
100(3): 435.

121
22. Jung SH, Watt RG, Sheiham A, Ryu JI, Tsakos G. Exploring pathways for socio‐
economic inequalities in self‐reported oral symptoms among Korean
adolescents. Community dentistry and oral epidemiology. 2011; 39(3): 221-229.
23. Kallestal C, Dahlgren L, Stenlund H. Oral health behaviour and self-esteem in
Swedish children. Soc Sci Med. 2000; 5: 1841–9.
24. Kanfer FH, Hagerman S. The role of self-regulation. Behavior therapy for depression:
Present status and future directions. San Diego, CA: Academic Press; 1981. p. 143-
179.
25. Kirscht JP. Preventive health behavior: A review of research and issues. Health
Psychology. 1983; 2(3): 277.
26. Kirscht JP. The health belief model and predictions of health actions. Springer US;
1998.
27. Lange MM. Vulnerability as a Concept for Health Systems Research. The American
Journal of Bioethics. 2014; 14(2): 41-43.
28. Lisboa CM, Paula JS, Ambrosano GMB, Pereira AC, Meneghim MC, Cortellazzi KL,
Vazquez FL, Mialhe FL. Socioeconomic and family influences on dental treatment
needs among Brazilian underprivileged schoolchildren participating in a dental health
program. BMC Oral Health. 2013; 13:56.
29. Mosher CE, Lipkus I, Sloane R, Snyder DC, Lobach DF, Demark‐Wahnefried W.
Long‐term outcomes of the FRESH START trial: exploring the role of self‐efficacy in
cancer survivors' maintenance of dietary practices and physical activity. Psycho‐
Oncology. 2013; 22(4): 876-885.
30. Nkansah-Amankra S, Luchok KJ, Hussey JR, Watkins K, Liu X. Effects of Maternal
Stress on Low Birth Weight and Preterm Birth Outcomes Across Neighborhoods of
South Carolina, 2000-2003. Matern Child Health J. 2010; 14(2): 215-226.
31. Newton JT, Bower EJ. The social determinants of oral health: new approaches to
conceptualizing and researching complex causal network. Community Dent Oral
Epidemiol. 2005; 33: 25-34.
32. Nichiata L, BertolozziI MR, Takahashi R, Fracolli L. The use of the "vulnerability"
concept in the nursing area. Rev. Latino-Am. Enfermagem. 2008; 16(5): 923-8.

122
33. Nogueira-Martins MCF, Bógus CM. Considerações sobre a metodologia qualtitativa
como recurso para o estudo das ações de humanização em saúde. Saúde e Sociedade.
2004; 13(3): 44-57.
34. O'Leary A. Self-efficacy and health. Behaviour research and therapy. 1985; 23(4):
437-451.
35. Parschau L, Fleig L, Koring M, Lange D, Knoll N, Schwarzer R, Lippke S. Positive
experience, self‐efficacy, and action control predict physical activity changes: A
moderated mediation analysis. Brit j health psychol. 2013; 18(2): 395-406.
36. Patussi MP, Hardy R, Sheiham A. The potential impact of neighborhood
empowerment on dental caries among adolescents. Community Dent Oral Epidemiol.
2006; 34: 344–50.
37. Perera I, Ekanayake L. Influence of oral health-related behaviours on income
inequalities in oral health among adolescents. Community Dent Oral Epidemiol. 2011;
39: 345–351.
38. Peres MA, Peres KG, Dornellas de Barros AJ, Victoria CG. The relation between
family socioeconomic trajectories from childhood to adolescence and dental caries and
associated oral behaviours. J Epidemiol Community Health. 2007; 61:141–5.
39. Petersen PE. The World Oral Health Report 2003: continuous improvement of oral
health in the 21st century-the approach of the WHO Global Oral Health Programme.
Community Dent Oral Epidemiol. 2003; 31(1): 3-24.
40. Polk DE, Weyant RJ, Manz MC. Socio-economic factors in adolescents' oral health:
are they mediated by oral hygiene behaviors or preventive interventions? Community
Dent Oral Epidemiol. 2010; 38:1-9.
41. Putnam R. Comunidade e democracia: a experiência da Itália moderna. Rio de Janeiro:
FGV, 2005. 260p.
42. Sánches AIM, Bertolozzi MR. Pode o conceito de vulnerabilidade apoiar a construção
do conhecimento em Saúde Coletiva? Ciência e Saúde Coletiva, 12(2): 319-324, 2007.
43. Sanders AE, Slade GD, Turrell G, Spencer AJ, Marcenes W. The shape of the socio-
economic oral health gradient: implications for theoretical explanations. Community
Dent Oral Epidemiol. 2006; 34: 310–9.

123
44. Sanders AE, Slade GD, Turrell G, Spencer AJ, Marcenes W. The shape of the socio-
economic oral health gradient: implications for theoretical explanations. Community
Dent Oral Epidemiol. 2006; 34: 310–9.
45. Sarri G, Evans P, Stansfeld S, Marcenes W. A school-based epidemiological study of
dental neglect among adolescents in a deprived area of the UK. British dental jornal.
2012; 213: E17-E17.
46. Scheier, M. F., Carver, C. S., e Armstrong, G. H. Behavioral self-regulation, health,
and illness. Handbook of health psychology. 2012; 79-97.
47. Schunk DH, Carbonari JP. Self-efficacy models. Behavioral health: A handbook of
health enhancement and disease prevention; 1984.
48. Tagliaferro EPS, Pardi V, Ambrosano GMB, Meneghim MC, Pereira AC. An
overview of caries risk assessment in 0-18 year-olds over the last ten years (1997-
2007). Braz J Oral Sci. 2008; 7:1682-1690.
49. Tagliaferro EPS, Pardi V, Pereira AC. Avaliação de risco em Odontologia. In: Pereira
AC, organizador. Tratado de saúde coletiva em odontologia. Nova Odessa: Napoleão
Editora; 2009. p. 529-549.
50. Tedesco LA, Keffer MA, Fleck-Kandath C. Self-efficacy, reasoned action, and oral
health behavior reports: a social cognitive approach to compliance. J Behav Med.
1991; 14(4): 341-355.
51. Thiengo MA, Oliveira DC, Rodrigues BMRD. Adolescentes, AIDS e práticas de
proteção: uma abordagem estrutural das representações sociais. Revista de
Enfermagem UERJ. 2002; 10(2): 81-4.
52. Thompson ED, Ashwill JW. Uma introdução à enfermagem pediátrica. 6. ed. Porto
Alegre: Artes Médicas. 1996.

124

125
ANEXO 1

126

127
ANEXO 2
FICHA A SECRETARIA MUNICIPAL DE SAÚDE
SISTEMA DE INFORMAÇÃO DE ATENÇÃO BÁSICA
UF |__|__|
ENDEREÇO
NÚMERO
|__|__|__|__|
BAIRRO CEP
|__|__|__|__|__| - | __|__|__|
MUNICÍPIO
|__|__|__|__|__|__|__| SEGMENTO
|__|__| ÁREA
|__|__|__|
MICROÁREA
|__|__| FAMÍLIA
|__|__|__|
DATA
|__|__|-|__|__|-|__|__|
CADASTRO DA FAMÍLIA
PESSOAS COM 15 ANOS E MAIS DATA
NASC. IDADE SEXO
ALFABETIZADO OCUPAÇÃO
DOENÇA
OU
CONDIÇÃO
REFERIDA
NOME sim não (sigla)
PESSOAS DE 0 A 14 ANOS DATA
NASC. IDADE SEXO
FREQÜENTA
A ESCOLA OCUPAÇÃO
DOENÇA
OU
CONDIÇÃO
REFERIDA
NOME sim não (sigla)
Siglas para a indicação das doenças e/ou condições referidas
ALC - Alcoolismo EPI - Epilepsia HAN - Hanseníase
CHA – Chagas GES - Gestação MAL - Malária
DEF - Deficiência HA - Hipertensão Arterial
DIA – Diabetes TB - Tuberculose

128
OUTRAS INFORMAÇÕES
Alguém da família possui Plano de Saúde? Número de pessoas cobertas por Plano de Saúde
Nome do Plano de Saúde |__| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __| __|
EM CASO DE DOENÇA PROCURA PARTICIPA DE GRUPOS COMUNITÁRIOS
Hospital Cooperativa
Unidade de Saúde Grupo religioso
Benzedeira Associações
Farmácia Outros - Especificar:
Outros - Especificar:
MEIOS DE COMUNICAÇÃO QUE MAIS
UTILIZA
MEIOS DE TRANSPORTE QUE MAIS
UTILIZA
Rádio Ônibus
Televisão Caminhão
Outros - Especificar: Carro
Carroça
Outros - Especificar:
A família é beneficiária do Programa Bolsa Família?
NIS do Responsável
|__| __| __| __| __| __| __| __| __| __|__|
A família está inscrita no Cadastramento Único de Programas
Sociais do Governo Federal (CAD-Único)?
SITUAÇÃO DA MORADIA E SANEAMENTO
TIPO DE CASA TRATAMENTO DA ÁGUA NO
DOMICÍLIO
Tijolo/Adobe Filtração
Taipa revestida Fervura
Taipa não revestida Cloração
Madeira Sem tratamento
Material aproveitado ABASTECIMENTO DE ÁGUA
Outro - Especificar: Rede pública
Poço ou nascente
Número de cômodos / peças Outros
Energia elétrica DESTINO DE FEZES E URINA
DESTINO DO LIXO Sistema de esgoto (rede geral)
Coletado Fossa
Queimado / Enterrado Céu aberto
Céu aberto

129
ANEXO 3
Email:________________________________________________________________________________________
Facebook:_____________________________________________________________________________________ Endereço:_____________________________________________________________________________________ Telefone:______________________________________________________________________________________ Celular:_______________________________________________________________________________________
Data do Exame
/ /
Nome
Nascimento
/ /
Idade
AVALIAÇÃO DE CÁRIE DENTÁRIA e MANCHA BRANCA
AVALIAÇÃO CONDIÇÃO PERIODONTAL - IPC
Ficha Nº
USF
C: ______ P: ______ O: ______ CPOD:
_______MB
FLUOROSE DENTAL - Dean
46 31 26 11 16 36
Sim/Não Quantas?
Código
sexo
RISCO À CÁRIE
NECESSIDADE DE TRATAMENTO
Código
USO / NECESSIDADES PROTÉTICAS
USO
RISCO FAMILIAR
NECESSIDADE

130

131
ANEXO 4
GOES
Parte I
5- Você já morou em outra cidade além de Piracicaba?
( )Sim. Se sim, qual foi?____________________________________ ( ) Não.
6- Há quanto tempo você está estudando nesta escola?____________anos
A escola é: pública ( ) ou particular ( )
7- Quantos irmãos e irmãs você tem ? ______irmãos _____irmãs
8- Considerando a ordem de nascimento entre os seus irmãos, faça um círculo se você é o:
Primeiro Segundo Terceiro Quarto Quinto. Outro. Qual?_________
9-Você já foi alguma vez reprovado de ano na escola?
( ) Sim ( ) Não ( ) Não sei/não me lembro
10- Quantas pessoas moram sempre na sua casa, incluindo seus pais, irmãos, irmãs, avôs, avós,
tios, tias, primos, sobrinhos, amigos e empregados domésticos? ________pessoas.
11- VOCÊ trabalha? ( ) Sim Não ( )
Se a resposta for Sim, onde?____________________________quantas horas por dia?________
Você faz o quê em seu trabalho?
____________________________________________________________________________
________________________________________________________________________________
__________
12- Seu PAI está trabalhado no momento?
( ) Sim ( ) Não ( ) Não sei/não me lembro

132
13- O que o seu PAI fazia ou faz em seu trabalho principal? (Descreva detalhadamente as tarefas
mais freqüentes que ele desenvolve - ou desenvolvia- em seu trabalho).
________________________________________________________________________________
________________________________________________________________________________
____________________
14- Sua MÃE está trabalhado no momento?
( ) Sim ( ) Não ( ) Não sei/não me lembro
15- O que a sua MÃE fazia ou faz em seu trabalho principal? (Descreva detalhadamente as tarefas
mais freqüentes que ela desenvolve – ou desenvolvia - em seu trabalho).
________________________________________________________________________________
__________
________________________________________________________________________________
__________
16- Sua MÃE estudou?
( ) Sim ( ) Não ( ) Não sei/não me lembro
17- Marque no quadro abaixo a opção que melhor representa o grau de escolaridade da sua MÃE
( ) Ela não foi a escola. Ela não lê e nem escreve ( ) Ela não foi a escola, mas lê e escreve
( ) 1º grau incompleto. Até qual série ?_______ ( ) 1º grau completo
( ) 2º grau incompleto. Até qual série ?_______ ( ) 2º grau completo.
( ) Universidade incompleta ( ) Universidade completa
( ) Pós-graduação ( ) Não sei/ não me lembro
18- Seu PAI estudou?
( ) Sim ( ) Não ( ) Não sei/não me lembro
19- Marque no quadro abaixo a opção que melhor representa o grau de escolaridade do seu PAI

133
( ) Ele não foi a escola. Ele não lê e nem escreve ( ) Ele não foi a escola, mas lê e
escreve
( ) 1º grau incompleto. Até qual série?_____ ( ) 1º grau completo
( ) 2º grau incompleto. Até qual série?_____ ( ) 2º grau completo.
( ) Universidade incompleta ( ) Universidade completa
( ) Pós-graduação ( ) Não sei/ não me lembro
Parte 2 - Saúde bucal
Agora nós gostaríamos de saber algumas coisas sobre a saúde dos seus dentes e da sua boca!
20- Como você classificaria a saúde dos seus dentes e da sua boca?
( ) Excelente ( ) Muito Boa ( ) Boa ( ) Mais ou menos ( ) Ruim
21- Você está satisfeito com a aparência dos seus dentes?
( ) Muito satisfeito ( ) Satisfeito ( ) Aceitável ( ) Insatisfeito
22-Você já foi ao dentista ?
( ) Sim (Vá para a questão 23) ( ) Não (Vá para a questão 27)
Lembre-se: você só deve responder da questão 23 a 26, caso tenha respondido SIM na questão
22. Na dúvida volte até a questão 22 e confirme.
23- Qual o tipo de serviço odontológico (dentista) que você geralmente usa?
( ) Particular ( ) Público (No centro de saúde) ( ) Público (No dentista
da escola)
( ) Público (Na faculdade de odontologia) ( ) Plano de saúde ( ) Convênio
( ) Outros, quais?_____________________ ( ) Não sei/não me lembro
24- Qual foi a última vez que você foi ao dentista?
( ) Estou em tratamento no momento ( ) Há menos de seis meses ( ) Há 7-12 meses

134
( ) Há 13-24 meses ( ) Mais de 24 meses ( ) Não sei/não me lembro
25- Qual foi o motivo pelo qual você procurou o dentista desta última vez que você esteve lá?
( ) Dor ( ) Extrair o dente ( ) Para tratar os dentes ( ) Para revisão
( ) Fazer limpeza, aplicar flúor, etc.. ( ) Outros. Quais?_____________________________
26- Qual o motivo mais freqüente pelo qual você vai ao dentista?
( ) Para revisões freqüentes (Vá para a questão 28)
( ) Apenas quando tenho um problema (Vá para a questão 28)
( ) Não sei/não me lembro (Vá para a questão 28)
27-Você poderia nos dizer qual das opções abaixo é a que melhor descreve a razão que dificultou
você ir ao dentista?
( ) Medo
( ) Custo (incluindo preço de transporte e do tratamento dentário)
( ) Não tive tempo(precisava fazer outras coisas como praticar esportes ou aula de inglês)
( ) Não achei um dentista disponível
( ) Não tenho confiança no jeito/trabalho do dentista
( ) Não tenho confiança no que o tratamento pode trazer de bom para mim
( ) Não ficou contente com tratamentos dentários anteriores
( ) Outros.Quais?____________________________________
( ) Não sei/não me lembro
28- Você já teve dor de dente na sua vida?
( ) Sim ( ) Não ( ) Não sei / não me lembro
29- Você teve dor de dente nos últimos seis meses?

135
( ) Sim (Vá para questão 30) ( ) Não (Vá para questão 46) ( ) Não sei/não me lembro (Vá
para questão 46)
30- Você poderia dizer quantos dias sentiu dor de dente?
( ) Sim . Quantos dias? ________________________ ( ) Não sei/não me lembro
31- Agora você poderia escolher das palavras abaixo a que melhor pode descrever a sua dor de
dente?
( ) Leve ( ) Desconfortável/Incômoda ( ) Estressante ( ) Horrível ( ) Intolerável/não dá
para aguentar
32- Você teve dor de dente nas últimas quatro semanas?
( ) Sim (Vá para a questão 33) ( ) Não (Vá para a questão 46) ( ) Não sei/não me lembro (Pule
para questão 46)
33- Faça um círculo no número que mostra o quanto doeu seu (s) dente (s) pela última vez. Você
deve considerar que 0 (zero) significa nenhuma dor e 10 (dez) a dor insuportável
___________________________________________________________
0 1 2 3 4 5 6 7 8 9 10
Nenhuma Dor pior possível
34- Na última questão, você respondeu quantos dias sentiu dor de dente. Agora, gostaríamos de
saber qual a duração dessa dor a cada dia?
( ) Um tempo muito pequeno ( ) Uma hora ( ) O dia inteiro ( ) A noite toda ( ) Mais
que uma noite
( ) Não sei/não me lembro

136
Parte 3 - Agora, conte-me como foi sua última dor de dente.
35- ( ) A dor foi contínua (quando começava não parava mais)? ( ) a dor começava, parava e
começava de novo ( ). Outra. Detalhe:___________________________________________
36- Você saberia dizer qual foi o dente que causou a dor?
( ) Sim Qual foi?_____________________ ( ) Não ( ) Não sei/não me
lembro
37- A dor de dente se espalhou pelo seu rosto ou cabeça?
( ) Sim ( ) Rosto ( ) Cabeça ( ) Rosto e cabeça ( ) Não (Vá para a questão 39) ( ) Não
sei/não me lembro (Vá para a questão 39)
38- Se você respondeu sim na última questão, marque um círculo no desenho abaixo que melhor
representa a região da sua face que você sentiu dor:
39- Qual foi a principal causa da sua dor de dente? você pode marcar várias alternativas:
( ) Buraco ou cavidade no dente ( ) Quando comi ou bebi alimentos quentes, frios ou
doces
( ) Quando mastiguei alguns alimentos Quais_____________________________________
( ) Quando perdi um dente ( ) Um novo dente aparecendo
( ) Aparelho ortodôntico fixo ao dente ( ) Aparelho ortodôntico móvel (placa plástica)
( ) Quando restaurei um dente ( ) Quando fiz um tratamento de canal

137
( ) Quando fiz uma extração de dente ( ) Quando um dente quebrou
( ) Não sei/não me lembro ( ) Outros.Quais?____________________
40- A dor de dente está presente agora?
( ) Sim Em qual dente?__________________ Há quanto tempo?________________ ( )
Não
41- Quando você teve dor de dente quem lhe deu mais atenção?
( ) Pai ( ) Mãe ( ) Avó/avô ( ) Irmão/irmã ( ) Babá ( ) Namorada(o) ou
marido/mulher
( ) Outra.Quais?______________ ( ) Ninguém ( ) Não sei/não me lembro
42- O que a pessoa que mais lhe deu atenção fez para passar a sua dor de dente?
( ) Nada ( ) Me deu um abraço ( ) Me deu remédios para dor/analgésicos
( ) Colocou uma compressa fria ou quente ( ) Me deu remédio que foi passado pelo
dentista ou médico
( ) Me falou para esperar para ver se melhorava ( ) Me levou para o dentista ( ) Outros.
Quais?_____________
( ) Não sei / não me lembro
43- Quando você teve dor de dente foi ao dentista?
( ) Sim (Vá para a questão 45) ( ) Não (Vá para a questão 44) ( ) Não sei/não me lembro (Vá
para a questão 45)
44- Você poderia dizer qual das opções abaixo é a que melhor descreve a razão pela qual não
visitou o dentista quando teve dor de dente?
( ) Medo
( ) Custo (incluindo preço de transporte e do tratamento dentário)
( ) Não tive tempo(precisava fazer outras coisas como praticar esportes ou aula de inglês)

138
( ) Não pude achar um dentista
( ) Não tenho confiança no trabalho/jeito do dentista
( ) Não tenho confiança no que o tratamento pode trazer de bom para mim
( ) Não ficou contente com tratamentos dentários anteriores
( ) Outros.Quais?____________________________________
( ) Não sei/não me lembro
45. Das atividades abaixo, o que você conseguiu fazer quando estava com dor de dente?
Você pôde praticar esporte (Por exemplo: ginástica, educação física ou jogar futebol ou voleibol)?
Sim ( ) Não ( )
Você pôde ler? Sim ( ) Não ( )
Você foi a escola? Sim ( ) Não ( )
Você fez os seus deveres escolares ? Sim ( ) Não ( )
Você pôde sair para ir a igreja, cinema ou casa de amigos e parentes? Sim ( ) Não ( )
Você brincou com seus amigos? Sim ( ) Não ( )
Você assistiu televisão ? Sim ( ) Não ( )
Você fez alguma atividade doméstica que lhe foi atribuída? Sim ( ) Não ( )
Você jogou vídeo game ou fliperama? Sim ( ) Não ( )
46- Que tipo de dor você teve nas últimas quatro semanas?
Nesta questão você pode assinalar mais de uma opção
( ) Dor de cabeça ( ) Dor de estômago ( ) Dor de barriga ( ) Dor de coluna/ nas costas
( ) Dor nos braços ou pernas ( ) Outros. Quais?,____________________ ( ) Nenhuma das
alternativas

139
ANEXO 5
QUESTIONÁRIO OIDP
Nos últimos 6 meses, seus dentes ou a sua boca causaram dificuldade para você desempenhar alguma dessas atividades diárias ?
Comer Ex: Refeição, sorvete
Falar claramente
Dormir/Relaxar
Manter o seu estado emocional (humor) sem se
irritar ou estressar
Limpar a boca
Estudar Ex. ir à escola, aprender em sala de aula, fazer o dever de casa
Contato Social Ex. sair com amigos, ir à casa de um amigo
PRESENÇA DO IMPACTO
[ ] SIM [ ] NÃO
[ ] SIM [ ] NÃO
[ ] SIM [ ] NÃO
[ ] SIM [ ] NÃO
[ ] SIM [ ] NÃO
[ ] SIM [ ] NÃO
[ ] SIM [ ] NÃO
FREQ SEVERIDADE Efeito no dia - a - dia
1 à 5
SCORE
Sorrir Ex. Sorrir sem se envergonhar [ ] SIM [ ] NÃO
SINTOMA PROBLEMA
0 à 5 1 à 5 0 à 22
Frequência:1-menos de uma vez ao mês , 2- Uma ou duas vezes ao mês, 3- Uma ou duas vezes por semana, 4- Três ou
quatro vezes por semana, 5- Todos ou quase todos os dias (5 ou mais vezes por semana) Severidade: 0- Nenhuma gravidade, 1- Muito pouco grave, 2- Pouco grave, 3- Gravidade moderada, 4- Muito grave, 5-
Extremamente grave Sintoma: Qual tem sido o principal sintoma? 1- Dor, 2- Desconforto, 3- Limitação na função (por ex, mastigar, morder ou abrir
bem a boca), 4- Insatisfação com a aparência 5- Outros (especificar) ____________________ Problema: Você poderia especificar qual o problema que você tem tido com a sua boca, dentes, ou dentadura? 0 – não consegue identificar Dentes: 1- Dor de dente, 2- Falta de dente , 3- Dente mole, 4- Cor dos dentes, 5- Posição dos dentes (dente torto ou muito para
frente), 6- Formato/tamanho dos dentes Boca: 7- Deformidade na boca ou rosto, 8- Úlcera bucal ou escoriações doloridas (não relacionados à prótese), 9- Sensação de queimação na boca, 10- Respiração difícil , 11- Distúrbio no paladar, 12- Gosto desagradável Gengivas: 13- Hemorragias gengivais, 14- Afastamento da gengiva, 15- Abscesso gengival Mandíbula: 16- Barulho desagradável ou estalo na articulação mandibular, 17- Mandíbula travada; travamento anterior, 18- Obturação quebrada ou de cor diferente do dente, 19- Dentadura solta ou mal colocada, 20- Aparelhos ortodônticos, 21- outros (especificar), 22- Sem resposta

140

141
ANEXO 6
1.situação econômica da família (renda familiar mensal) A .( ) Até R$ 622,00 B. ( ) De R$622,00 a R$ 1244,00 C. ( ) De R$ 1244,00 a R$ 1866,00
D. ( ) De R$ 1866,00 a R$3110,00 E. ( ) De R$ 3110,00 a R$ 4665,00 F. ( ) De R$ 4665,00 a R$ 6531,00 G. ( ) Acima de R$ 6531,00
QUESTIONÁRIO SÓCIOECONÔMICO
2. número de pessoas na família A. ( ) Até 2 Pessoas B. ( ) 3 Pessoas C. ( ) 4 Pessoas
D. ( ) 5 Pessoas E. ( ) 6 Pessoas F. ( ) Acima de 6 Pessoas
3. grau de instrução do pai ou responsável PAI MÃE A. ( ) ( ) Não alfabetizado
B. ( ) ( ) Alfabetizado C. ( ) ( ) 1ª e 4ª série incompleta (antigo primário) D. ( ) ( ) 1ª e 4ª série completa (antigo primário) E. ( ) ( ) 5ª e 8ª série incompleta (antigo ginasial)
4. habitação (moradia) A. ( ) Residência própria quitada B. ( ) Residência própria com financiamento a pagar C. ( ) Residência cedida pelos pais ou parentes D. ( ) Residência cedida em troca de trabalho E. ( ) Residência alugada F. ( ) residência cedida por não ter onde morar
5. profissão do chefe da família (mencionar mesmo que desempregado) A. ( ) Empresário de grande porte B. ( ) Profissional Liberal e Empresário de médio porte C. ( ) Funcionário em ocupações de nível superior D. ( ) Empresário de pequeno porte E. ( ) Funcionário em ocupações de nível médio F. ( ) Profissional autônomo (Vendedor, Corretor e outros) G. ( ) Funcionário em ocupações de nível intermediário H. ( ) Profissional autônomo operacional (Marceneiro, Pedreiro e outros) I. ( ) Funcionário em ocupações auxiliares (Ajudantes, trabalhador rural) J. ( ) Ambulante, Safrista, Trabalho eventual (Bicos)

142

143
ANEXO 7
MANCHA BRANCA – número de dentes com MB (superfície rugosa, opaca, amarelo-esbranquiçada)
FLUOROSE – ausência e presença
DOENÇA PERIODONTAL
Código Critério
0 Hígido
1 Sangramento observado, diretamente ou pela utilização de um espelho clínico, após a sondagem.
2 Cálculos detectados durante a sondagem, mas toda a faixa preta da sonda visível
3 Bolsa periodontal de 4-5 mm (margem gengival dentro da faixa preta da sonda)
4 Bolsa periodontal de 6 mm ou mais (faixa preta da sonda, não visível)
X Sextante excluído (menos de dois dentes presentes)
9 Não registrado
A boca é dividida em seis sextantes definidos pelos números dentários: 18-14, 13-23, 24-28, 38-34, 33-
43, 44-48. Um sextante deve ser examinado somente se houver dois dentes ou mais presentes, os quais
CÁRIE NECESSIDADE DE TRATAMENTO
Código Critério Código Critério
0 Hígido 0 Nenhum
1 Cariado P Preventivo, tratamento para debelar cárie
2 Restaurado com cárie F Selante de fissuras
3 Restaurado sem cárie 1 Restauração em 1 face
4 Ausente devido à cárie 2 Restauração em 2 ou mais faces
5 Ausente por outros motivos 3 Coroa protética por qq motivo
6 Selante de fissura 4 Coroa facetada ou laminada
7 Suporte para prótese 5 Tratamento pulpar com restauração
8 Dente não erupcionado 6 Exodontia
T Traumatismo (fratura) 7 Necessidade de tratamento - especificar
9 Não registrado 8 Necessidade de tratamento - especificar
- - 9 Não registrado

144
não estiverem indicados para exodontia. Os dentes indicadores que devem ser examinados na faixa
etária de 15-19 anos são: 16, 11, 26, 36, 31 e 46.
CONDIÇÕES PROTÉTICAS NECESSIDADES PROTÉTICAS
0 Sem prótese 0 Não necessita de prótese
1 Prótese parcial fixa 1 Necessita de prótese unitária
2 Mais de uma prótese parcial fixa 2 Necessita de prótese com múltiplos elementos
3 Prótese parcial removível 3 Necessita de uma associação de próteses unitárias
e/ou com múltiplos elementos
4 Próteses parciais, fixas e removíveis 4 Necessita de prótese total
5 Prótese total removível 9 Não registrado
9 Não registrado - -
CLASSIFICAÇÃO DE
RISCO GRUPO SITUAÇÃO INDIVIDUAL
Baixo risco A Ausência de lesão de cárie, sem placa, sem gengivite e/ou sem mancha
branca ativa
Risco Moderado
B História de dente restaurado, sem placa, sem gengivite e/ou sem mancha
branca ativa
C Uma ou mais cavidades em situação de lesão de cárie crônica, mas sem
placa, sem gengivite e/ou sem mancha branca ativa
Alto risco
D Ausência de lesão de cárie e/ou dente restaurado, mas com presença de
placa, de gengivite e/ou de mancha branca ativa
E Uma ou mais cavidades em situação de lesão de cárie aguda
F Presença de dor e/ou abscesso

145
R1= risco menor a R3= risco máximo
Ficha A score
Acamado 3
Deficiência física 3
Deficiência mental 3
Baixas condições de
saneamento
3
Desnutrição grave 3
Drogadição 2
Desemprego 2
Analfabetismo 1
Menor de 6 meses 1
Maior de 70 anos 1
Hipertensão 1
Diabetes 1
> 1 3
=1 2
<1 1
Escore 5 ou 6 R1
Escore 7 ou 8 R2
Maior que 9 R3

146
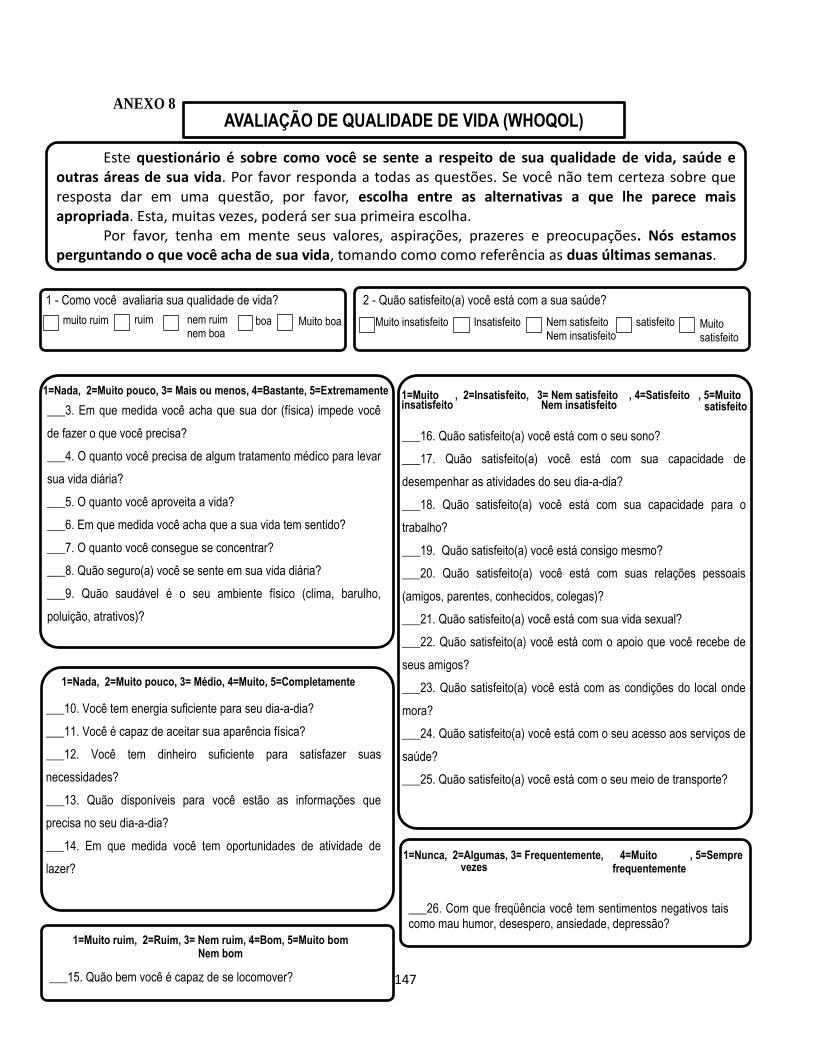
147
ANEXO 8
1=Nada, 2=Muito pouco, 3= Mais ou menos, 4=Bastante, 5=Extremamente
___3. Em que medida você acha que sua dor (física) impede você
de fazer o que você precisa?
___4. O quanto você precisa de algum tratamento médico para levar
sua vida diária?
___5. O quanto você aproveita a vida?
___6. Em que medida você acha que a sua vida tem sentido?
___7. O quanto você consegue se concentrar?
___8. Quão seguro(a) você se sente em sua vida diária?
___9. Quão saudável é o seu ambiente físico (clima, barulho,
poluição, atrativos)?
___16. Quão satisfeito(a) você está com o seu sono?
___17. Quão satisfeito(a) você está com sua capacidade de
desempenhar as atividades do seu dia-a-dia?
___18. Quão satisfeito(a) você está com sua capacidade para o
trabalho?
___19. Quão satisfeito(a) você está consigo mesmo?
___20. Quão satisfeito(a) você está com suas relações pessoais
(amigos, parentes, conhecidos, colegas)?
___21. Quão satisfeito(a) você está com sua vida sexual?
___22. Quão satisfeito(a) você está com o apoio que você recebe de
seus amigos?
___23. Quão satisfeito(a) você está com as condições do local onde
mora?
___24. Quão satisfeito(a) você está com o seu acesso aos serviços de
saúde?
___25. Quão satisfeito(a) você está com o seu meio de transporte?
AVALIAÇÃO DE QUALIDADE DE VIDA (WHOQOL)
1 - Como você avaliaria sua qualidade de vida?
muito ruim ruim nem ruim nem boa
boa Muito boa
2 - Quão satisfeito(a) você está com a sua saúde?
Muito insatisfeito Insatisfeito Nem satisfeito Nem insatisfeito
satisfeito Muito satisfeito
1=Nada, 2=Muito pouco, 3= Médio, 4=Muito, 5=Completamente
___10. Você tem energia suficiente para seu dia-a-dia?
___11. Você é capaz de aceitar sua aparência física?
___12. Você tem dinheiro suficiente para satisfazer suas
necessidades?
___13. Quão disponíveis para você estão as informações que
precisa no seu dia-a-dia?
___14. Em que medida você tem oportunidades de atividade de
lazer?
1=Muito ruim, 2=Ruim, 3= Nem ruim, 4=Bom, 5=Muito bom Nem bom
___15. Quão bem você é capaz de se locomover?
1=Muito , 2=Insatisfeito, 3= Nem satisfeito , 4=Satisfeito , 5=Muito insatisfeito Nem insatisfeito satisfeito
1=Nunca, 2=Algumas, 3= Frequentemente, 4=Muito , 5=Sempre frequentemente vezes
___26. Com que freqüência você tem sentimentos negativos tais como mau humor, desespero, ansiedade, depressão?
Este questionário é sobre como você se sente a respeito de sua qualidade de vida, saúde e outras áreas de sua vida. Por favor responda a todas as questões. Se você não tem certeza sobre que resposta dar em uma questão, por favor, escolha entre as alternativas a que lhe parece mais apropriada. Esta, muitas vezes, poderá ser sua primeira escolha. Por favor, tenha em mente seus valores, aspirações, prazeres e preocupações. Nós estamos perguntando o que você acha de sua vida, tomando como como referência as duas últimas semanas.

148

149
ANEXO 9
Termo de Consentimento Livre e Esclarecido
Prezado(a) Sr.(a),
Convidamos você a participar da nossa pesquisa: "Risco e vulnerabilidade às
doenças bucais em adolescentes da cidade de Piracicaba, SP, Brasil". As informações
contidas neste documento serão fornecidas pelos pesquisadores da Faculdade de
Odontologia de Piracicaba – Unicamp: Prof. Dr. Antonio Carlos Pereira e alunos de pós-
graduação, Fabiana de Lima Vazquez, (doutorado) e Karine Laura Cortellazzi (pós-
doutorado) para convidar e firmar acordo consentimento livre e esclarecido, através do
qual você autoriza a participação de seu filho (a), com total conhecimento da natureza dos
procedimentos e riscos a que se submeterá, com a capacidade de livre-arbítrio e livre de
qualquer coação, podendo desistir quando quiser. A sua colaboração, através de
autorização e concordância em participar, é muito importante. Esclarecemos que sua
participação é decorrente de sua livre decisão após receber todas as informações que julgar
necessárias e que não haverá ônus a sua pessoa.
Pesquisadores responsáveis:
A qualquer tempo (antes e durante a pesquisa), se você desejar mais informações sobre o
nosso trabalho, por favor, ligue para:
Fabiana de Lima Vazquez – Tel: 19 21065278 (falar com secretária Eliana).
End: Av Limeira, 901. Caixa postal 52 - 13914-903. Piracicaba/SP.
Karine Laura Cortellazzi – Tel: 19 21065278 (falar com secretária Eliana).
End: Av Limeira, 901. Caixa postal 52 - 13914-903. Piracicaba/SP.
Prof.Dr. Antonio Carlos Pereira - Tel: 19 21065278 (falar com secretária Eliana)
End: Av Limeira, 901. Caixa postal 52 - 13914-903. Piracicaba/SP.

150
Justificativa:
Estudos para conhecer a ocorrência de doenças e condições bucais na população são de
grande importância. O conhecimento do estado dos dentes do seu filho(a) pode ajudá-lo a
buscar tratamento antes que o problema se torne mais grave. Além disso, estes estudos
também fornecem informações para a criação de programas educativos e planejamento que
dão assistência à saúde da boca, trazendo benefícios para toda a população.
Objetivos:
O objetivo deste trabalho é avaliar o risco de doenças bucais em uma população
adolescente de 15 a 19 anos no município de Piracicaba-SP.
Descrição da pesquisa:
Metodologia
• Somente depois que concordar em participar e assinar este documento, seu
filho(a) será considerado voluntário. Você não deve se sentir obrigado a assinar nenhum
documento e pode pedir todos os esclarecimentos que achar necessário. Você responderá,
em seguida, a um questionário com questões socioeconômicas, comportamentais,
demográficas e psicossociais. Além disso, os indivíduos que tiverem os piores e melhores
índices de cárie serão entrevistados, sendo a entrevista gravada e mantida as informações
em sigilo.
• Para participar da pesquisa, seu filho(a) responderá a 3 questionários simples
sobre questões de saúde bucal, dor de dente, educação e prevenção em saúde, escolaridade,
moradia, renda. As respostas ficarão sob a responsabilidade da pesquisadora principal e
você terá garantia de sigilo em relação às respostas emitidas.
• Seu filho(a) passará por um exame de sua boca. Seu filho(a) será avaliado
quanto à cárie, doença da gengiva, problema na posição dos dentes, fluorose (excesso de
flúor nos dentes). Esse exame será também mantido em segredo e guardado com a
pesquisadora responsável. Caso seja necessário, seu filho receberá encaminhamento para
tratamento.
Possibilidade de inclusão em grupo controle/placebo
Não haverá grupo controle e placebo neste estudo.
Métodos alternativos para obtenção da informação

151
Não existem métodos alternativos para obtenção da informação.
Descrição crítica dos desconfortos e riscos previsíveis
Você passará por um exame de seus dentes e sua gengiva, realizado em local separado e
utilizando materiais esterilizados. O instrumental apresenta ponta arredondada para não
causar nenhum tipo de dano ou machucado. Este exame será realizado em sala separada,
evitando qualquer tipo de constrangimento por parte dos voluntários. Não há previsão de
riscos aos participantes desta pesquisa.
Descrição dos benefícios e vantagens diretas ao voluntário
Como benefício, o paciente receberá, através da pesquisa, avaliação de cárie, doenças da
gengiva e problemas na mordida, possibilitando o diagnóstico precoce de possíveis
problemas existentes. O adolescente que estiver com algum problema receberá
encaminhamento para tratamento. Além disso, você estará contribuindo com uma pesquisa
científica que visa melhorar a qualidade do serviço prestado à comunidade.
Forma de acompanhamento e assistência ao sujeito
Os pesquisadores responsáveis acompanharão seu filho e darão assistência durante a
pesquisa ou quando você solicitar, resolvendo problemas relacionados à pesquisa ou
dúvidas a respeito da mesma.
Forma de contato com a pesquisadora e com o cep
Para entrar em contato com os pesquisadores:
Você terá contato direto com os pesquisadores Fabiana de Lima Vazquez (19) 92850726,
[email protected], Prof.Dr. Antonio Carlos Pereira (Orientador) - Tel: 19
21065209 (falar com secretária Eliana) End: Av Limeira, 901 cx postal 52 - 13914-903
Piracicaba – SP [email protected], Karine Laura Cortellazzi (19) 81282190 ,
Em caso de dúvida quanto aos seus direitos como voluntário da pesquisa, entre em contato
com o Comitê de Ética em Pesquisa Humana da Faculdade de Odontologia de Piracicaba,
situado na Av. Limeira, 901 CEP:13414-903, Piracicaba-SP, Fone/Fax: (19) 2106-5349; e-
mail: [email protected]; site: www.fop.unicamp/cep.
Garantia de esclarecimentos
Você tem a garantia de que receberá respostas para qualquer pergunta e suas dúvidas sobre
os procedimentos, sobre os riscos, os benefícios e outros assuntos relacionados com a

152
pesquisa serão esclarecidos. Os pesquisadores também assumem o compromisso de dar as
informações obtidas durante o estudo, mesmo que isso possa afetar sua vontade em
continuar participando do estudo.
Garantia de recusa à participação ou saída do estudo
Você tem liberdade para retirar seu consentimento ou se recusar a continuar a participar do
estudo, a qualquer momento, conforme determinação da Resolução 196/96 do CNS do
Ministério da Saúde. Caso deixe de participar do estudo por qualquer razão, você não
sofrerá qualquer tipo de prejuízo ou punição não perderá o direito ao tratamento na
Unidade de Saúde da Família.
Garantia de sigilo
Nós, os pesquisadores, prometemos resguardar todas as suas informações sobre a pesquisa
e vamos tratar estas informações com impessoalidade, não revelando sua identidade.
Garantia de ressarcimento
Não há previsão de ressarcimento de despesa, visto a pesquisa será realizada em horário
onde o usuário estará na unidade de saúde para consulta, após a realização da mesma, e,
portanto, você não terá gastos para participar da pesquisa.
Garantia de indenização e/ou reparação de danos
Como não há riscos ou danos previsíveis, neste caso, não haverá indenização previsível.
Caso ocorra algum imprevisto, ficam os pesquisadores responsáveis em indenizar em
comum acordo com os voluntários, eventuais danos decorrentes desta pesquisa.
Cópia do Termo de consentimento:
Você está recebendo duas cópias deste Termo uma é sua e a outra deverá ser assinada e
devolvida.
Esperando contar com seu apoio, desde já agradecemos em nome de todos os que se
empenham para melhorar a saúde de nossa população.
Atenciosamente,
Fabiana de Lima Vazquez e Karine Laura Cortellazzi

153
AUTORIZAÇÃO
Eu,________________________________________________________________, RG
n__________ responsável por _______________________________________, certifico ter
lido todas as informações acima citadas e estar suficientemente esclarecido de todos os itens
pelos pós-graduandos Fabiana de Lima Vazquez e Karine Laura Cortellazzi, pesquisadoras
responsáveis na condução da pesquisa. Estou plenamente de acordo e aceito participar desta
pesquisa "Risco e vulnerabilidade às doenças bucais em adolescentes da cidade de Piracicaba,
SP, Brasil". E recebi uma cópia desde documento.
Piracicaba, ______ de ________________________ de 2011.
Nome:____________________________________________C.I.______________
Assinatura:_________________________________________________________
Assinatura do Pesquisador:_____________________________________________
ATENÇÃO: Em caso de dúvida quanto aos seus direitos como voluntário da pesquisa, escreva para
o Comitê de Ética em Pesquisa da FOP-UNICAMP: Av. Limeira, 901-CEP13414-900-Piracicaba-SP.
Telefone/fax: 19-21065349, email: [email protected]
Web site:www.fop.unicamp.br/cep

154

155
ANEXO 10
From: Oral Health and Preventive Dentistry <[email protected]>
Date: 2014-07-18 14:53 GMT-03:00
Subject: Oral Health and Preventive Dentistry - OHPD-2014-230 - (2516): Manuscript
submission confirmation To:[email protected]
Manuscript: OHPD-2014-230 - (2516) - Individual and contextual variables related to
periodontal disease: multilevel analysis in underprivilegedadolescents in Brazil.
Dear Professor Vazquez. - Automatic notification:
Thank you very much for submitting the above manuscript.The manuscript is being evaluated and we will contact you as soon as a decision has been made. Please inform us by return of email if the version posted on the web site does not correspond with the version that was submitted. The progress of your manuscript can be followed from the progress report accessed from your account overview.Yours sincerely. The Editorial Office www.manuscriptmanager.com/v6/login.php?id=148 Email: [email protected]

156














![[GAIT DISORDERS IN PARKINSON’S AND HUNTINGTON’S DISEASES]Sofia... · Gait disorders in Parkinson’s and Huntington’s diseases 3 Gait disorders in Parkinson’s and Huntington’s](https://img.document.onl/doc/110x75/5f0f95af7e708231d444e3b1/gait-disorders-in-parkinsonas-and-huntingtonas-diseases-sofia-gait-disorders.jpg)














