Embed Size (px)
Citation preview

1
Universidade Federal do Rio Grande do Norte
Centro de Ciências da Saúde
Departamento de Fisioterapia
Programa de Pós-Graduação em Fisioterapia
ANTONIO JOSÉ SARMENTO DA NÓBREGA
NOVAS METODOLOGIAS DE AVALIAÇÃO E INTERVENÇÃO EM PACIENTES
COM ESCLEROSE LATERAL AMIOTRÓFICA
Orientadora: Dra. Vanessa Regiane Resqueti Fregonezi
Coorientador: Dr. Guilherme Augusto de Freitas Fregonezi

2
Universidade Federal do Rio Grande do Norte
Centro de Ciências da Saúde
Departamento de Fisioterapia
Programa de Pós-Graduação em Fisioterapia
NOVAS METODOLOGIAS DE AVALIAÇÃO E INTERVENÇÃO EM PACIENTES
COM ESCLEROSE LATERAL AMIOTRÓFICA
Tese apresentada ao Programa de Pós-
Graduação em Fisioterapia da Universidade
Federal do Rio Grande do Norte, como requisito
para obtenção do título de Doutor em Fisioterapia.
Área de concentração: Avaliação e Intervenção
em Fisioterapia.
Área de pesquisa: Avaliação e intervenção nos
Sistemas Cardiovascular e Respiratório
Orientadora: Profᵃ. Dra. Vanessa Regiane
Resqueti Fregonezi
Natal, 2018

3

4
AGRADECIMENTOS
Bem, muitas pessoas pensam que sempre foi fácil ou sempre foi sorte, mas a batalha até
chegar aqui não foi nada assim. Dias cansativos e muitas noites sem dormir valeram a pena para
conseguir defender o Doutorado em 2 anos cravados. Aliás, um ano e meio destes 2 anos
pareceram até 4, durante o período de Doutorado sanduíche na Itália (valeu CAPES e CNPq!!!),
longe de todos que gosto e acompanharam minha jornada até aqui.
Gostaria de agradecer ao Superior que esteve presente durante esta caminhada longa e,
com certeza, todas as noites em minhas orações. Aos meus pais Maria do Socorro Sarmento da
Nóbrega e Francisco Gil Marques da Nóbrega que sempre me incentivaram e impulsionaram a ir
além e não me deixaram na mão em nenhum momento, apesar da grande saudade diária que me
circunda todo dia quando acordo ou vou dormir. Tenham certeza que levarei todos seus
ensinamentos comigo. A Ana Karoline, apesar da distância, também cheguei aqui por você, nega!
Aos meus avós paternos e maternos que levaram os filhos do sítio para a cidade para
tentar dar mais qualidade de vida. Cheguei aqui por causa de vocês também! A todos meus tios,
em especial aqueles que estão próximos e que sabem a quantidade de aperreio que as vezes
passo, mas sempre tem uma cervejinha no final de semana para esfriar a cabeça.
Dedico também a todos colegas e família do jiu-jitsu que me acolheram no período que
estava em Milão, em especial ao Alberto e ao Prof. Nicola, aos meus colegas de infância lá do
interior da Paraíba que me acolhem toda vez que vou ver meus pais e também a Maradona, Vitão,
Albano e Etinho que quase vivem lá em casa e acabo desabafando muitas vezes. “Tamo junto
bando de caba”!
Aos professores Vanessa e Guilherme que me deram a oportunidade desde o início do
mestrado e confiaram na minha pessoa para trabalhar com a coisa que mais gosto de fazer hoje
em dia: Ciência! No começo pareceu ser difícil, mas com o incentivo de vocês e um pouquinho de
curiosidade a mais eu cheguei aqui. E como sempre disse a vocês: “não parou por aqui”; “tem
muita coisa ainda para fazer”; “bora desengavetar tudo”!
A toda a turma do TBMLab em Milão, em especial o professor Andrea Aliverti. Sou seu fã
de carteirinha, caba! Foi com você que eu aprendi o que é realmente ser um professor. Obrigado
por todos seus ensinamentos, pela preocupação (pelas cervejas no logo após finalizar sua aula) e
pela sua grandíssima humildade! Valeu mesmo, cappellino!
A todo pessoal do Lab06 da UFRN. Ninguém faz pesquisa sozinho e sem a ajuda de vocês
também não chegaria aqui. Em especial, dedico esta Tese a Maria Lira. Companheira, colega de
trabalho e da vida. Muito obrigado pelos seus ensinamentos. Saiba que não chegaria aqui tão
calmo e confidente sem você ali sempre do meu lado para realçar aquela confiança esquecida lá
no fundo do peito!
A Dr. Mário Emílio por confiar em mim como o Fisioterapeuta responsável pelos seus
pacientes da neurologia. Por fim, dedico esta tese ao pessoal da equipe do Ambulatório
Multidisciplinar de Doença do Neurônio Motor do Hospital Universitário Onofre Lopes e
principalmente todos os pacientes que passaram o compõe e que passaram por mim durante os
períodos de Mestrado e Doutorado. Vocês sim, foram os principais “autores” desta Tese. Muito
obrigado de verdade!

5
PREFÁCIO
A presente tese intitulada “Novas metodologias de avaliação e intervenção em
pacientes com Esclerose Lateral Amiotrófica”, foi elaborada de acordo com os preceitos do
Programa de Pós-Graduação em Fisioterapia da Universidade Federal do Rio Grande do
Norte, alinhadas às normas da Pró-Reitoria de Pós-Graduação desta Universidade, sob
orientação da professora Dra. Vanessa Regiane Resqueti.
Primeiramente é apresentada a introdução geral da tese onde são demonstrados o
referencial teórico sobre a Esclerose Lateral Amiotrófica, funcionalidade, alterações mecânicas
e suas complicações (com um maior foco na fraqueza muscular respiratória e pico de fluxo de
tosse), função pulmonar, assim como a avaliação respiratória destas alterações através de
equipamentos de elevada acurácia, como a pletismografia optoletrônica. Logo após, é
apresentado uma fundamentação geral sobre os resultados encontrados que são discutidos
nas sessões de artigos 1, 2 e 3. Nestes, todos os temas abordados na introdução são
descritos e demonstrados de forma mais detalhada.
O principal objetivo do artigo 1, intitulado Assessment of gas compression and lung
volume during air stacking maneuver, foi estimar a quantidade de compressão de gás que
ocorre durante a realização da manobra de air stacking em sujeitos saudáveis.
Adicionalmente, os volumes pulmonares absolutos foram estimados de forma não invasiva a
partir da aplicação do volume de compressão de gás na lei das transformações isotérmicas de
Boyle-Mariotte.
O segundo artigo, intitulado Thoracoabdominal asynchrony and paradoxical motion in
amyotrophic lateral sclerosis subjects, teve as alterações mecânicas da caixa torácica em
pacientes com Esclerose Lateral Amiotrófica e suas implicações para os volumes da parede
torácica, padrão respiratório e pico de fluxo de tosse como foco principal. Assim, a assincronia
toracoabdominal e a presença de movimento paradoxal entre os compartimentos da parede
torácica foram quantificados através da pletismografia optoeletrônica durante duas situações
(volume corrente e tosse) e comparados com sujeitos saudáveis pareados por idade de
gênero.
O último artigo, intitulado Multiparametric analysis of sniff nasal inspiratory pressure test
in middle stage amyotrophic lateral sclerosis, que compôs essa tese objetivou pela primeira
vez analisar de forma mais detalhada as taxas de relaxamento e propriedades de contração
dos músculos inspiratórios obtidos durante a análise da curva de pressão do teste de SNIP
(sniff nasal inspiratory pressure) a fim de buscar, de forma não invasiva, novos biomarcadores
para fraqueza e fadiga muscular em sujeitos com Esclerose Lateral Amiotrófica.
Após a apresentação dos três artigos científicos que compuseram a tese, estão
expostos os seguintes tópicos: Discussão geral, principais limitações, conclusões e
implicações clínicas deste trabalho. Logo após, um tópico contendo as produções científicas
realizadas no período do doutorado dos quais participo da autoria, também é apresentado.
Este tópico engloba também resumos apresentados em congressos com publicações em anais
de congresso. Por último, encontram-se as referências usadas para elaboração da tese.

6
SUMÁRIO
PREFÁCIO ................................................................................................................................ 5
Lista de abreviações ................................................................................................................. 8
List of abbreviations .................................................................................................................. 9
Resumo ................................................................................................................................... 10
Abstract ................................................................................................................................... 12
1. Introdução geral .................................................................................................................. 14
1.1. Fraqueza muscular respiratória e alteração da mecânica da parede torácica ............ 14
1.2. Avaliação da força muscular respiratória ...................................................................... 16
1.3. Pletismografia Optoeletrônica ....................................................................................... 16
1.4. Fundamentação para os artigos ................................................................................... 17
2. Objetivos ............................................................................................................................. 21
3. Material e métodos ............................................................................................................. 22
3.1. Função pulmonar ........................................................................................................... 22
3.2. Força muscular respiratória ........................................................................................... 22
3.3. Pletismografia optoeletrônica ........................................................................................ 23
3.4. Pneumotacografia ......................................................................................................... 23
3.5. Air stacking .................................................................................................................... 24
4. Resultados .......................................................................................................................... 25 4.1. Artigo 1. Assessment of gas compression and lung volume during air
stacking maneuver .................................................................................................... 26
4.1.1 Abstract ..................................................................................................................... 27
4.1.2. Introduction .............................................................................................................. 28
4.1.3. Methods ................................................................................................................... 29
4.1.3.1. Measurements and apparatus .......................................................................... 29
4.1.3.2. Data analysis ..................................................................................................... 33
4.1.4. Statistical analysis .................................................................................................. 34
4.1.5. Results .................................................................................................................... 35
4.1.6. Discussion .............................................................................................................. 39
4.1.7. Conclusion .............................................................................................................. 41
4.1.8. References ............................................................................................................. 42 4.2. Artigo 2. Thoracoabdominal asynchrony and paradoxical motion in
amyotrophic lateral sclerosis subjects .................................................................. 45
4.2.1. Abstract ................................................................................................................... 46
4.2.2. Introduction ............................................................................................................. 47
4.2.3. Methods .................................................................................................................. 48
4.2.4. Statistical analysis .................................................................................................. 52
4.2.5. Results .................................................................................................................... 53
4.2.6. Discussion .............................................................................................................. 57
4.2.7. Conclusion .............................................................................................................. 60
4.2.8. References ............................................................................................................. 61
4.2.9. Appendix and supplementary material .................................................................. 67
4.3. Artigo 3. Multiparametric analysis of sniff nasal inspiratory pressure test in middle stage amyotrophic lateral sclerosis ........................................................... 74
4.3.1. Abstract ................................................................................................................... 75
4.3.2. Introduction ............................................................................................................. 76
4.3.3. Material and Methods ............................................................................................. 76

7
4.3.4. Statistical analysis .................................................................................................. 79
4.3.5. Results .................................................................................................................... 79
4.3.6. Discussion .............................................................................................................. 86
4.3.7. Conclusion .............................................................................................................. 88
4.4.8. References ............................................................................................................. 89
4.3.9. Supplementary material ......................................................................................... 95
5. Discussão geral ................................................................................................................ 100
5.2. Principais limitações .................................................................................................... 103
5.3. Implicações clínicas, perspectivas futuras e conclusões ........................................... 103
Lista de publicações ............................................................................................................. 111

8
Lista de abreviações
∆Pao – Variação de pressão das vias aéreas
∆Vao – Variação de volume pulmonar
∆VCW – Variação de volume da parede torácica
½RT – Metade da curva de relaxamento
AB – Abdomen
ALSFRS-R – Amyotrofic Lateral Sclerosis Functional Rating Scale-Revised
cmH2O – centímetro de água
CTa – Caixa torácica abdominal
CTp – Caixa torácica pulmonar
CVF – Capacidade vital forçada
ELA – Esclerose Lateral Amiotrófica
MEP – Pressão expiratória máxima
MIP – Pressão inspiratória máxima
MRPD – Taxa máxima de desenvolvimento de pressão
MRR – Taxa máxima de relaxamento
NMI – neurônio motor inferior
NMS – neurônio motor superior
PFT – Pico de fluxo de tosse
PI – porcentagem de tempo inspiratório
POE – Pletismografia optoeletrônica
ROC – Receiver Operating Characteristic
SNIP – Pressão inspiratória nasal ao fungar
Vcomp – Volume de compressão
τ – tau

9
List of abbreviations
∆Pao – Pressure variation at the airways opening
∆Vao – Pulmonary volume change
∆VCW – Chest wall volume change
½RT – Half relaxation time
AB – Abdomen
ALSFRS-R – Amyotrophic Lateral Sclerosis Functional Rating Scale-Revised
cmH2O – centimeter of water
RCa – Abdominal ribcage
RCp – Pulmonary ribcage
FVC – Forced vital capacity
ALS – Amyotrophic Lateral Sclerosis
MEP – Maximum expiratory pressure
MIP – Maximum inspiratory pressure
MRPD – Maximum rate of pressure development
MRR – Maximum relaxation rate
LMN – Lower motor neuron
UMN – Upper motor neuron
PCF – Peak cough flow
IP – Inspiratory paradox time
OEP – Optoelectronic plethysmography
ROC – Receiver Operating Characteristic
SNIP – Sniff nasal inspiratory pressure
Vcomp – Gas compression
τ – tau

10
Resumo
Introdução: A avaliação e detecção precoce da fraqueza muscular respiratória resultante da
esclerose lateral amiotrófica (ELA) têm ganhado mais interesse no campo da pesquisa nas
últimas décadas. Com a progressão da doença, a diminuição da força muscular respiratória
leva à redução do volume pulmonar e consequente insuficiência ventilatória, fazendo essencial
o uso de técnicas de higiene brônquica e a detecção precoce de fraqueza muscular
respiratória a fim de monitorar a progressão da doença e antecipar a introdução de
intervenções.
Objetivos: 1) Estimar a quantidade de compressão de gás (Vcomp) durante a aplicação da
técnica de air stacking em sujeitos saudáveis e verificar se as medidas simultâneas de
variação de volume da caixa torácica (ΔVCW) e as variações de volume pulmonar (ΔVao),
combinado à variação de pressão das vias aéreas (ΔPao) durante a aplicação do air stacking,
são capazes de fornecer dados confiáveis acerca dos volumes pulmonares absolutos; 2)
Avaliar a assincronia toracoabdominal e a presença de movimento paradoxal em pacientes
com ELA e suas relações com o VCW, padrão respiratório e pico de fluxo de tosse; 3) Analisar
as taxas de relaxamento e as propriedades de contração dos músculos inspiratórios em
pacientes com ELA e comparar com saudáveis pareados. Além disso, os pacientes com ELA
foram divididos em três subgrupos a fim de determinar o melhor parâmetro relacionado a
fraqueza muscular inspiratória.
Materiais e Métodos: 1) Vinte sujeitos saudáveis foram estudados durante um protocolo que
incluiu manobras de capacidade vital lenta e aplicação da técnica de air stacking. Vcomp foi
calculado através da diferença entre a ΔVao (mensurado através do pneumotacógrafo) e ΔVCW
(através da pletismografia optoeletrônica) durante air stacking e a capacidade pulmonar total
foi estimada pela aplicação de Lei de Boyle-Mariote; 2) O ângulo de fase (θ) entre a caixa
torácica pulmonar (CTp), caixa torácica abdominal (CTa) e o abdome (AB), bem como a
porcentagem de tempo inspiratório (IP) em que a CTa e AB se movem em direções opostas,
foram quantificados em 12 pacientes com ELA durante respiração espontânea e tosse, usando
dados de 12 sujeitos saudáveis pareados como controle; 3) As taxas de relaxamento e as
propriedades de contração dos músculos inspiratórios foram extraídas a partir da curva de
pressão inspiratória nasal (SNIP), realizada de forma não invasiva em 39 pacientes com ELA e
comparada com 39 sujeitos saudáveis pareados.
Resultados: 1) Durante air stacking, 0,140±0,050 L de gás foi comprimido com uma
ΔPao média de 21,78±6,18 cmH2O. Não foram encontradas diferenças significativas entre a
capacidade pulmonar total estimada (−0,03±3,0% de diferença, p=0,6020), capacidade
residual funcional estimada (−2,0±12,4% de diferença, p=0,5172), capacidade inspiratória
mensurada (1,2±11,2% de diferença, p=0.7627) e valores preditos; 2) Durante a respiração
espontânea, um maior θ da CTa e AB (p<0,05), IPRCa (p=0,001) e IPAB (p=0,02) foram
encontrados nos pacientes com ELA assim como correlações entre o θ da CTp e AB com
capacidade vital forçada (r= –0.773, p<0.01) e capacidade vital (r= –0.663, p<0.05), e entre o θ
da CTa e CTp e o pico de fluxo de tosse (r= −0,601, p<0,05). Durante a tosse, correlações

11
entre o θ do AB e CTp e pico de fluxo de tosse (r= −0,590, p<0,05), pico de fluxo expiratório (r=
−0,727, p<0,01) e VCW (r= −0,608, p<0,05); assim como entre o θ do CTa e AB e o pico de
fluxo de tosse (r= −0,590, p=0,01) e pico de fluxo expiratório (r= −0,713, p=0,01) foram
observados. Além disso, uma menor capacidade vital forçada (p<0.05) e maior velocidade de
encurtamento tos músculos inspiratórios (p<0.05) foram encontrados no pacientes com
movimento paradoxal da caixa torácica; 3) Quando comparado com sujeitos saudáveis,
pacientes com ELA exibiram uma menor (p<0,0001) taxa máxima de relaxamento (MRR) e
taxa máxima de desenvolvimento de pressão (MRPD), assim como um maior (p<0,0001)
tempo de contração, tau (τ) e metade da curva de relaxamento (½RT). Os resultados da curva
ROC mostraram que a ½RT (AUC 0,720, p=0,01), capacidade vital forçada (AUC 0,700,
p=0,03), τ (AUC 0,824, p<0,0001) e MRPD (AUC 0,721, p=0,01) foram os parâmetros mais
sensitivos em detectar uma queda de 3 pontos no subescore respiratório do questionário de
capacidade funcional da ELA. Adicionalmente, a MRPD (AUC 0,781, p<0,001), τ (AUC 0,794,
p=0,0001) e o pico de pressão gerado durante o teste de SNIP (AUC 0,769, p=0,002) foram os
parâmetros capazes de detectar uma queda de 30% da capacidade vital forçada nos pacientes
estudados.
Conclusões: Durante a aplicação da técnica de air stacking ocorre uma significante
compressão de gás e os volumes pulmonares absolutos podem ser estimados através das
mensurações simultâneas de ΔVCW, ΔVao e ΔPao. Além disso, a identificação da alteração de
parâmetros, como assincronia toracoabdominal e presença de movimento paradoxal entre os
compartimentos da parede torácica, τ, MRPD, e ½RT, representam um sinal precoce de
fraqueza muscular inspiratória em sujeitos com ELA.
Palavras-chave: Assincronia toracoabdominal, capacidade vital forçada, esclerose lateral
amiotrófica, músculos inspiratórios, volumes pulmonares absolutos.

12
Abstract
Introduction: The assessment and early detection of respiratory muscle weakness resulting
from amyotrophic lateral sclerosis (ALS) have gained more interest in the field of research in
the recent decades. As the disease progresses, the decrease in respiratory muscle strength
leads to a reduction in lung volume and consequent ventilatory insufficiency, making essential
the use of bronchial hygiene techniques and the early detection of respiratory muscle
weakness in order to monitor the progression of the disease as well as to anticipate the
introduction of interventions.
Objectives: 1) To estimate the amount of gas compression (Vcomp) during the application of the
air stacking technique in healthy subjects and to verify if the simultaneous measurements of
chest wall volume changes (ΔVCW) and changes in lung volume (ΔVao), combined with pressure
variation at the airways opening (ΔPao) during air stacking are able to provide reliable data on
absolute lung volumes; 2) To assess thoracoabdominal asynchrony and the presence of
paradoxical movement in patients with ALS and its relations with VCW, respiratory pattern and
peak cough flow; 3) To analyze the relaxation rates and contraction properties of the inspiratory
muscles of patients with ALS and compare with healthy matched-paired subjects. In addition,
patients with ALS were divided into three subgroups in order to determine the best parameter
linked to inspiratory muscle weakness.
Materials and Methods: 1) Twenty healthy subjects were studied during a protocol that
included slow vital capacity maneuvers and application of the air stacking technique. Vcomp was
calculated by subtracting ΔVao (measured by pneumotachograph) and ΔVCW (measured by
optoelectronic plethysmography) during air stacking and total lung capacity was estimated by
applying Boyle-Mariote's law; 2) Phase angle (θ) between pulmonary ribcage (RCp), abdominal
ribcage (RCa) and abdomen (AB), as well as the percentage of inspiratory time (IP) in which
RCa and AB moved in opposite directions were quantified in 12 patients with ALS through
optoelectronic plethysmography during quiet spontaneous breathing and cough using control
data from 12 paired-matched healthy subjects to define the normal range of movement; 3) The
relaxation rates and contraction properties of the inspiratory muscles were extracted from the
sniff nasal inspiratory pressure (SNIP) curve, performed non-invasively in 39 patients with ALS
and compared with 39 matched-paired healthy subjects.
Results: 1) During air stacking, 0.140±0.050 L of gas was compressed with an average ΔPao of
21.78±6.18 cmH2O. No significant differences between the estimated total lung capacity
(−0.03±3.0% difference, p=0.6020), estimated functional residual capacity (−2.0±12.4%
difference, p=0.5172), measured inspiratory capacity (1.2±11.2% difference, p=0.7627) and
predicted values were found. 2) During quiet spontaneous breathing, a higher RCa and AB θ
(p<0.05), IPRCa (p=0.001) and IPAB (p=0.02) were found in patients with ALS as well as
correlations between RCp and AB θ with forced vital capacity (r = −0.773, p<0.01) and vital
capacity (r = −0.663, p<0.05), and between RCa and RCp θ and peak cough flow (r = −0.601,
p<0.05). During cough, correlations between AB and RCp θ and peak cough flow (r = −0.590,
p<0.05), peak expiratory flow (r = −0.727, p<0.01) and VCW (r = −0.608, p<0.05); as well as

13
between RCa and AB θ and peak cough flow (r = −0.590, p=0.01) and peak expiratory flow (r =
−0.713, p=0.01) were observed. Moreover, a lower forced vital capacity (p<0.05) and a greater
shortening velocity of the inspiratory muscles (p<0.05) were observed in patients with
paradoxical movement of the rib cage; 3) When compared to healthy subjects, patients with
ALS had a significantly lower (p<0.0001) maximum relaxation rate (MRR) and maximum rate of
pressure development (MRPD), as well as a greater (p<0.0001) contraction time, tau (τ) and
half-relaxation time (½RT). The results of the ROC curves showed that ½RT (AUC 0.720,
p=0.01), forced vital capacity (AUC 0.700, p=0.03), τ (AUC 0.824, p<0.0001) and MRPD (AUC
0.721, p=0.01) were the most sensitive parameters in detecting a 3-point fall in the respiratory
subscale of the ALS functional capacity questionnaire. In addition, the MRPD (AUC 0.781,
p<0.001), τ (AUC 0.794, p=0.0001) and the peak pressure generated during the SNIP test
(AUC 0.769, p=0.002) were the parameters capable of detecting a 30% decrease in forced vital
capacity of the patients studied.
Conclusions: During AS, a significant gas compression occurs and absolute lung volumes can
be estimated by simultaneous measurements of ΔVCW, ΔVao and ΔPao. In addition, the
identification of altered parameters, such as thoracoabdominal asynchrony and the presence of
paradoxical movement between the chest wall compartments, τ, MRPD, and ½RT, represent
an early sign of inspiratory muscle weakness in subjects with ALS.
Keywords: Absolute lung volumes, amyotrophic lateral sclerosis, forced vital capacity,
inspiratory muscles, thoracoabdominal asynchrony

14
1. Introdução geral
A esclerose lateral amiotrófica (ELA) é uma doença neurodegenerativa, que acomete
ambos os neurônios motor superior (NMS) e inferior (NMI),1 caracterizada por fraqueza
progressiva dos músculos esquelético, bulbar e respiratório.2 A grande maioria dos
mecanismos envolvidos na sua fisiopatologia ainda permanece desconhecida e sua
etiopatogenia não está bem esclarecida.3 No entanto, sabe-se que esta doença é mais comum
em sujeitos do gênero masculino4 e a taxa de sobrevivência mediana a partir dos primeiros
sintomas varia de 2 a 4 anos, sendo a insuficiência ventilatória a principal causa de
mortalidade.2 A apresentação clínica heterogênea e a variável velocidade de progressão da
doença tornam o diagnóstico desafiador. Devido à inexistência de um teste específico para a
ELA, seu diagnóstico (classificado como ‘possível’, ‘provável’ ou ‘definitivo’) depende
exclusivamente da identificação de sinais clínicos de acometimento dos NMS e NMI na mesma
região do corpo, suportado por exame eletrofisiológico ou neuropatológico, além de evidência
de progressão da doença em outras regiões.5,6
Os sintomas da ELA podem se manifestar de duas formas. A primeira, chamada de
espinhal, se caracteriza por fraqueza dos membros inferiores, superiores ou ambos com
posterior acometimento dos músculos bulbares. A segunda, chamada de bulbar, tem início dos
sintomas nos músculos bulbares e respiratórios.7 Esta última é conhecida por apresentar um
pior prognóstico do que a forma espinhal8 e está associada a uma rápida progressão da
doença9 com uma maior taxa de declínio da capacidade vital forçada (CVF) e força muscular
respiratória.10,11
Com a progressão da doença, a capacidade de realização das atividades de vida diária
também é reduzida e pode ser avaliada através da Amyotrophic Lateral Sclerosis Functional
Rating Scale12 (ALSFRS). Esta foi projetada como um escore funcional de 10 itens que
incluem domínios funcionais, bulbar e respiratório. Mais tarde, essa escala foi alargada para o
ALSFRS-revised13 (ALSFRS-R), na qual foram incluídos escores respiratórios extras para
melhor avaliação do domínio funcional respiratório. Na ausência de um biomarcador, a
quantificação da capacidade funcional através da ALSFRS-R tem se tornado uma medida de
progressão da doença14 e desfecho primário em ensaios clínicos com sujeitos com ELA,12,15
além de ser preditor de sobrevida nesta população16,17 e se correlacionar com medidas de
função pulmonar e força muscular respiratória.18,19
1.1. Fraqueza muscular respiratória e alteração da mecânica da parede torácica
O diafragma é o músculo inspiratório mais importante. A função inspiratória do
diafragma é realizada através de três mecanismos principais: (1) o diafragma atua como um
pistão que, ao descer, cria uma pressão intratorácica negativa, puxando o ar para dentro; (2) a
“área de aposição” do diafragma à parede interna da caixa torácica serve para puxar as
costelas inferiores para cima (e para fora, consequente ao efeito “alça de balde”), expandindo
assim a área da seção transversal do caixa torácica, um efeito inspiratório; e (3) a contração
diafragmática aumenta a pressão intra-abdominal, que também expande a caixa torácica
inferior, uma vez que a parte mais superior da cavidade abdominal realmente reside dentro da

15
caixa torácica. A contração dos músculos abdominais (transverso, reto e músculos oblíquos
internos e externos) aumenta a pressão intra-abdominal, fazendo com que o fluxo de ar saia
do pulmão e a parede abdominal se mova para dentro. Quando os músculos intercostais
internos contraem, eles exercem um grande torque que abaixa as costelas e aumenta a
pressão pleural para conduzir o ar para fora do pulmão.20,21 Assim, uma atividade coordenada
de todos os músculos respiratórios é essencial para desenvolver as pressões necessárias para
direcionar o ar para dentro e para fora do pulmão, e mover a caixa torácica e o abdômen de
maneira coordenada e síncrona. É possível respirar com apenas um conjunto de músculos
respiratórios, mas efeitos indesejáveis, como o movimento paradoxal toracoabdominal
provavelmente ocorrerão22 nesta em sujeitos com ELA.
A assincronia toracoabdominal é principalmente o resultado de fraqueza
desproporcional de alguns músculos respiratórios ou descoordenação entre diferentes grupos
musculares23 e é definido como a diferença no tempo de expansão ou retração entre os
compartimentos da parede torácica24,25. Em pacientes com fraqueza principalmente
diafragmática, os músculos intercostais assumem o papel principal de diminuir a pressão
intratorácica e, nesse caso, o diafragma (juntamente com o conteúdo intra-abdominal) é
atraído passivamente para o tórax, levando ao movimento abdominal interno paradoxal. Em
ambos os casos de assincronia toracoabdominal, o volume corrente é necessariamente
diminuído porque o movimento inspiratório de um compartimento é oposto a uma ação
expiratória do outro compartimento24 e parte da contração de toda musculatura respiratória é
desperdiçada para distorcer a parede torácica ao invés de insuflar os pulmões21.
A fraqueza muscular respiratória também tem impactos diretos (diminuição da
capacidade de expansão da caixa torácica e recuo elástico) e indiretos (alterações na
complacência pulmonar e da caixa torácica) na função pulmonar de pacientes com doença
neuromuscular resultando em uma redução da capacidade pulmonar total, capacidade vital e
capacidade residual funcional26. A combinação de fraqueza muscular inspiratória, que impede
o paciente de respirar fundo, e a redução a complacência da parede torácica, que diminui a
excursão disponível na parede torácica, limita o volume operacional necessário para uma
tosse efetiva. Esse volume operacional é o volume inspirado no final da fase de tosse
inspiratória e é considerado o mais importante determinante do pico de fluxo da tosse, pois
afeta o comprimento do músculo expiratório e, portanto, sua eficiência de contração. Quando a
disfunção da glote está presente, pressões adequadas para desenvolver as forças
compressivas para a expectoração das secreções das vias aéreas não são alcançadas. A
eficácia da tosse é ainda mais diminuída. A fase expiratória da tosse, quando as secreções
precisam ser expelidas, é limitada por: 1) fraqueza dos músculos expiratórios; 2) uma parede
torácica endurecida que limita a expiração; 3) uma desvantagem mecânica dos músculos
expiratórios, por não estarem adequadamente esticados ao seu ponto ideal de contração pela
restrição ponto operacional; 4) recuo elástico passivo limitado dos pulmões durante a
expiração, devido à sua inflação limitada; e 5) diâmetro transversal diminuído das vias aéreas
que não estão totalmente dilatadas porque o pulmão não está totalmente insuflado
aumentando assim a resistência das vias aéreas durante a expiração27-29.

16
1.2. Avaliação da força muscular respiratória
A grande maioria dos pacientes com ELA morre por insuficiência ventilatória. A
fraqueza muscular respiratória na ELA advém da perda da função muscular diafragmática30
com consequente diminuição da complacência da caixa torácica.31 A fraqueza muscular
intercostal interna e abdominal também está ligada a forças expulsivas que estão
enfraquecidas durante a tosse, deixando pacientes com ELA em maior risco de pneumonia.32
Os intercostais externos e outros músculos inspiratórios acessórios, como os
esternocleidomastoides e escalenos, auxiliam em situações de alta demanda ventilatória em
que as pressões necessárias para aumentar o volume pulmonar são aumentadas.33 Perto do
fim da doença, os pacientes com ELA apresentam declínios rápidos na CVF, ventilação
voluntária máxima e no volume residual.34,35 Como consequência, sintomas como dispneia
durante esforços mínimos, ortopneia e cefaléia se tornam recorrentes,10,36 além das infecções
do trato respiratório inferior com posterior diminuição do pico de fluxo de tosse (PFT) e da
complacência pulmonar.37,38
A força muscular inspiratória é o principal determinante de insuficiência ventilatória nos
pacientes com ELA11 e pode ser avaliada de forma não invasiva através da pressão
inspiratória máxima (MIP) e da pressão inspiratória nasal durante uma manobra de sniff
(SNIP). Essas duas formas de avaliação da força muscular respiratória são complementares e
devem ser realizadas em todos os pacientes com ELA na primeira visita ao hospital ou
ambulatório e a cada três meses depois.39 A MIP é mais sensível em detectar hipoventilação40
e a manobra de SNIP, que reflete com precisão a força diafragmática e força muscular
inspiratória global,41,42 é preditora de sobrevida em sujeitos com ELA.11 Pelo fato da MIP ser
difícil de ser executada por pacientes com paresia orofacial, a SNIP (que será abordada com
mais propriedade no artigo 5) é mais utilizada em pacientes com ELA por ser uma manobra
natural, simples, tolerável e de fácil execução.43 Além dessas, mensurações da CVF,
capacidade vital lenta e do pico de fluxo expiratório também são comumente utilizadas por
serem fatores preditivos de prognóstico nessa doença.10,44 Embora a CVF seja ainda o método
mais utilizado para a avaliação respiratória na ELA,7 o paciente deve expelir o ar de forma
rápida e forçada, o que pode causar fadiga, induzir broncoespasmo e resultar em uma
subestimação da real capacidade pulmonar.45
1.3. Pletismografia Optoeletrônica
A pletismografia optoeletrônica (POE) é um sistema não invasivo capaz de mensurar
precisamente a cinemática toracoabdominal e variações de volume da parede torácica e dos
compartimentos que atuam na ventilação (caixa torácica pulmonar [CTp], a caixa torácica
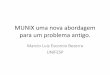
abdominal [CTa] e abdome [AB]).46,47 Esse sistema, diferentemente da pletismografia
respiratória por indutância, se baseia em um modelo de três compartimentos (Figura 1) a partir
do propósito de que: 1) CTp e CTa estão expostos a diferentes pressões durante a inspiração;
2) o diafragma atua diretamente na CTa; e 3) os músculos inspiratórios, com exceção ao
diafragma, atuam em grande parte na CTp e não na CTa.48 Com relação ao AB, a variação de

17
volume é definida como o volume do abdome e é o resultado da ação conjunta do diafragma e
músculos expiratórios.49
Figura 1. Representação esquemática da pletismografia optoeletrônica.
Através da POE é possível avaliar as variações de volume ciclo a ciclo, em três graus
de liberdade e sem o uso de bocais, o que proporciona uma elevada precisão para avaliação e
monitoramento de padrões respiratórios em crianças, adultos e pacientes com doenças
respiratórias.50-52 Esse sistema também é utilizado para investigar a força muscular
respiratória, o efeito da aplicação de técnicas ou reabilitação, disfunção diafragmática e
PFT53,54 em pacientes neuromusculares, além de ter sido o método mais utilizado nos últimos
anos para avaliar a assincronia toracoabdominal entre compartimentos da parede torácica55
durante a respiração espontânea,56 tosse,55 ou exercício.57 A assincronia, assim como a
utilização da POE, será discutida com mais detalhe nos artigos 1 e 2.
1.4. Fundamentação para os artigos
A fraqueza muscular progressiva característica da ELA, principalmente a respiratória, é
responsável pelo acúmulo de secreções e consequente aumento do número de infecções
respiratórias. Em decorrência disso, há uma incapacidade de gerar PFT acima de 160 L/min
necessários para clearance pulmonar, levando a um aumento da morbidade respiratória e
mortalidade e, então, gerando altos custos para a saúde pública. Esse PFT é a avaliação mais
reprodutível da força da tosse e também dependente da geração de fluxo e velocidade nas
vias aéreas, recolhimento elástico do pulmão e forças da parede torácica27. Além disso, de
acordo com Smith et al.28, quanto maior os volumes operacionais maior o recuo elástico dos
pulmões e menor a resistência das vias aéreas. Assim, em doenças restritivas como a ELA,
altos PFTs podem ser gerados após um aumento no volume pulmonar de forma passiva como
através da técnica de air stacking.
Kang e Bach28 definiram a técnica de air stacking como um método de insuflação
pulmonar que requer o uso de um insuflador manual ou um ventilador de volume portátil a fim

18
de fornecer volumes superiores à capacidade inspiratória. Portanto, após a conclusão de uma
respiração profunda e máxima e consequente fechamento da glote, os volumes de ar podem
ser empilhados até atingir a capacidade máxima de insuflação (Figura 2), definida como o
volume máximo de ar que pode ser mantido com a glote fechada após insuflações58. Desta
forma, pacientes com doenças pulmonares restritivas, como doenças neuromusculares, são os
que mais se beneficiam com a técnica de air stacking. Além disso, em sujeitos com ELA o
aumento do volume pulmonar está fortemente correlacionado com o aumento do pico de fluxo
da tosse59. Além disso, quanto maior a expansão pulmonar, melhor a otimização da pressão
de recuo do pulmão, a tosse e, conseqüentemente, a extração de secreção60.
Figura 2. Traçados experimentais obtidos em um indivíduo representativo durante a capacidade
inspiratória espontânea (IC) (1 e 2) e tosse espontânea a partir de CPT (esquerda) e durante a
aplicação da técnica de air stacking (AS) (3 e 4) e subsequentemente tosse a partir da IC + AS (4)
(direita). Retirado com permissão de Sarmento et al.61
.
Sabendo disso, dois estudos sobre os efeitos da técnica de air stacking no PFT de
sujeitos saudáveis61 e de pacientes com ELA53 utilizando a POE foram publicados durante o
período anterior a essa tese, nos dando embasamento para melhor compreensão e
necessidade de investigação dessas novas variáveis. Pelo fato da air stacking ser realizada
através da aplicação seriada de pressão positiva a fim de fornecer volumes de ar superiores à

19
capacidade inspiratória,38 a quantidade de pressão aplicada pode induzir cerca de 1 a 2% de
compressão de gás.62 A POE, por si só, não é capaz de quantificar a compressão de gás.
Esta, assim como volumes pulmonares absolutos, pode ser mensurada a partir de métodos
que consomem tempo e requerem boas habilidades técnicas para produzir resultados
consistentes (por exemplo, diluição de hélio, lavagem de nitrogênio ou pletismografia de corpo
inteiro). O fato de não haverem relatos na literatura sobre 1) a quantidade de compressão de
gás durante a técnica de air stacking e 2) métodos simples para mensuração de volumes
pulmonares absolutos, nós hipotetizamos Artigo 1 que a mensuração simultânea da variação
de volume da parede torácica (utilizando a POE) e de volume pulmonar (através de um
pneumotacógrafo) seria capaz de mensurar a quantidade de compressão de gás durante a
técnica de air stacking em sujeitos saudáveis além de fornecer dados confiáveis sobre
volumes pulmonares absolutos.
Diferentemente da pletismografia respiratória por indutância,63 a POE é capaz de
avaliar com precisão a variação de volume da CTa. Em sujeitos com doença pulmonar
obstrutiva crônica, Aliverti et al. mostrou que o movimento paradoxal da CTa não é apenas
uma curiosidade clínica, mas pode também identificar importantes diferenças fisiológicas nos
volumes da parede torácica durante repouso e exercício.57 Além disso, sabe-se que o
movimento paradoxal dos compartimentos é resultado principalmente de fraquezas
desproporcionais de alguns músculos respiratórios ou ações descoordenadas entre diferentes
grupos musculares.23 Em pacientes com doença neuromuscular e em diferentes condições, a
assincronia entre os compartimentos da parede torácica já foi reportada,24,55,64 entretanto a
literatura é escassa com relação à assincronia e movimento paradoxal em sujeitos com ELA.
Essa questão é discutida no Artigo 2, no qual os resultados encontrados em pacientes com
ELA utilizando a POE foram comparados com sujeitos saudáveis pareados por idade e gênero,
objetivando obter sinais iniciais de fraqueza muscular respiratória durante a respiração
espontânea e tosse.
Outros sinais iniciais de fraqueza muscular respiratória foram tema do Artigo 3,
entretanto foram avaliados a partir de parâmetros extraídos da curva de SNIP (taxas de
relaxamento e propriedades contráteis dos músculos inspiratórios). A razão pela qual esses
parâmetros são avaliados a partir da SNIP baseia-se no pressuposto de que 1) a porção de
decaimento da curva, quando a expiração é totalmente passiva, corresponde à fase de
relaxamento da contração muscular inspiratória65 e 2) a perda de força muscular ou fadiga leva
a uma diminuição da velocidade de contração muscular, resultando em aumento do tempo de
contração e prolongamento do tempo de relaxamento como um mecanismo de adaptação.66,67
Desta forma, os resultados encontrados nos pacientes com ELA foram comparados com
saudáveis e entre os sujeitos que apresentaram ou não sintomas respiratórios a partir do
declínio no subescore respiratório da ALSFRS-R e CVF, a fim de determinar o melhor
parâmetro ligado à fraqueza muscular precoce do músculo respiratório nessa população.
Os artigos 2, 3 e 4 proporcionam o foco principal da tese, uma vez que têm o potencial
de gerar implicações clínicas referentes aos pacientes com ELA. O resumo e a discussão geral

20
a respeito dos principais achados e implicações da tese são apresentados logo após a
apresentação dos artigos científicos.

21
2. Objetivos
Artigo 1: Estimar a quantidade de compressão de gás durante a técnica de air stacking em
indivíduos saudáveis posicionados a 45° de inclinação do tronco e verificar se as medidas
simultâneas de alterações do volume da parede torácica, através da pletismografia
optoeletrônica, e alterações no volume pulmonar, através do pneumotacógrafo, combinado
com a variação de pressão na abertura das vias aéreas durante a execução da técnica é
capaz de fornecer dados confiáveis sobre volumes pulmonares absolutos;
Artigo 2: Avaliar a assincronia toracoabdominal e a presença de movimento paradoxal em
pacientes com ELA e suas relações com o volume corrente da parede torácica, padrão
respiratório e pico de fluxo da tosse.
Artigo 3: Mensurar de forma não invasiva as taxas de relaxamento e as propriedades
contráteis dos músculos inspiratórios em pacientes com ELA através do teste de SNIP (1) em
comparação com indivíduos saudáveis e (2) em relação aos sintomas respiratórios precoces, a
fim de determinar o melhor parâmetro ligado à respiração precoce fraqueza muscular.

22
3. Material e métodos
A metodologia utilizada nas três produções desta tese foi especifica de acordo com o
objetivo de cada estudo e por esta razão tópicos como desenho dos estudos, caracterização
das amostras, aspectos éticos e análises dos dados e estatística serão apresentadas de forma
individualizada nos artigos 1, 2 e 3. Além disso, apesar de os principais materiais e
equipamentos utilizados serem apresentados nesta sessão, os mesmo também estão
descritos de forma detalhada em cada artigo.
3.1. Função pulmonar
Para análise do fluxo aéreo, volumes e capacidades pulmonares, foi realizada a
espirometria, utilizando um espirômetro KoKo DigiDoser (Longmont, USA). Antes de cada
avaliação, o equipamento foi calibrado de acordo com a temperatura local e a injeção de 3L de
volume de ar por meio de uma seringa (Vitalograph, Buckingham, Inglaterra).
Para o procedimento, cada sujeito realizou o teste na posição sentada em uma cadeira
confortável, com os pés devidamente apoiados no chão e usando um clipe nasal. Previamente
a realização do teste, eles foram instruídos detalhadamente de todos os procedimentos. Os
voluntários respiraram através de um bucal de papelão descartável, certificando-se que não
houveram vazamentos durante a respiração. A seguir, foi solicitado que eles realizassem uma
inspiração máxima (próximo à capacidade pulmonar total) seguida de uma expiração máxima
(próximo ao volume residual).
Foram realizados no máximo oito testes em cada voluntário e considerados os três
melhores sendo que a variabilidade entre eles deveriam ser inferior a 5% ou 200 mL. Foram
considerados a CVF, o volume expiratório forçado do 1º segundo (VEF1) e a razão VEF1/CVF
nos seus valores absolutos e relativos. Todos os procedimentos técnicos, os critérios de
aceitabilidade, reprodutibilidade, bem como a padronização do equipamento seguiram as
recomendações da ATS/ERS68. Os valores obtidos foram comparados com valores absolutos
e relativos para a população Brasileira69.
3.2. Força muscular respiratória
Para avaliação da força muscular respiratória, foi realizada a manovacuometria através
do manovacuomêtro digital (NEPEB-LabCare/UFMG, Belo Horizonte-MG, Brasil) com o
indivíduo na posição sentada, com os pés devidamente apoiados no chão e em repouso. O
manovacuômetro foi conectado por meio de uma traqueia ao bucal que possuía um orifício de
fuga de 2mm de diâmetro para que os valores das pressões máximas não sofressem a
influência das pressões geradas pelos músculos da boca e da orofaringe, além de um clipe
nasal para evitar vazamento de ar pelas narinas.
A MIP foi obtida a partir do volume residual e a MEP a partir da capacidade pulmonar
total. Durante a realização das mensurações, foram oferecidos estímulos verbais para
incentivar a obtenção do maior valor. As manobras, tanto de MIP quanto de MEP, foram
repetidas no mínimo duas vezes para aprendizado e, em seguida, três medidas tecnicamente
satisfatórias (com variação menor que 10% entre os dois valores máximos) e repouso de 60s

23
entre elas foram realizadas. Foi considerada como tecnicamente satisfatória a medida que não
apresentou vazamento e que foi sustentada por pelo menos um segundo. O valor registrado foi
o mais alto, desde que esse não fosse o obtido na última manobra.
Para interpretação dos resultados obtidos, foram calculados valores previstos pelas
equações de regressão para o cálculo das pressões máximas em função da idade, de acordo
com o sexo para a população Brasileira70.
A pressão inspiratória nasal (SNIP teste) foi obtida solicitando ao sujeito, ao final de
uma expiração tranquila (capacidade residual funcional), a realização de uma inspiração
máxima com uma das narinas ocluída por um plug acoplado a um cateter conectado ao
manovacuômetro e a com a narina contralateral livre. O SNIP teste foi realizado através de dez
medidas separadas por um período de repouso de 30 segundos. Foram utilizadas as
equações previamente descritas para obtenção dos valores de referência71.
3.3. Pletismografia optoeletrônica
Para o artigo 1 e 2, a avaliação dos volumes pulmonares e do PFT foi realizada através
do estudo da cinemática do complexo toracoabdominal de forma não-invasiva através da POE
(BTS-Bioengineering, Itália).
A POE utiliza um sistema de seis câmeras fotossensíveis que captaram marcadores
retrorreflexivos colocados na região anterior da parede torácica do sujeito, seguindo linhas
horizontais e verticais pré-definidas. O equipamento avalia o volume da parede torácica e dos
três compartimentos que a compõem: CTp, CTa e o AB através da formação de um modelo
experimental, de acordo com o Teorema de Gauss47. Para as coletas com esse equipamento,
o aparelho foi calibrado de forma estática e dinâmica pelos eixos X, Y e Z (por um período de
10 e 120 segundos, respectivamente) para reconhecimento dos marcadores, sendo utilizada a
frequência de 60Hz para calibração do equipamento e coleta dos dados. Em seguida, foram
posicionados 52 marcadores retrorreflexivos sobre a região anterior do tórax do voluntário,
seguindo estruturas anatômicas pré-estabelecidas50 que seguiam desde o nível da clavícula
até a crista ilíaca anteriossuperior.
3.4. Pneumotacografia
Para o artigo 1, fluxo e pressão das vias aéreas foram mensurados através de um
pneumotacógrafo aquecido (Series 0-800 LPM, Hans Rudolph® INC, Kansas - EUA)
posicionado entre a máscara e o insuflador manual. A calibração de fluxo e pressão foi
realizada antes da aquisição de dados de cada sujeito. O fluxo do pneumotacógrafo foi
calibrado através da geração de diferentes fluxos inspiratórios e expiratórios, por meio de uma
seringa de 3 L calibrada, em intervalos de 3 segundos entre eles. O transdutor de pressão foi
calibrado conectando um manômetro digital, com variações em cmH2O, e aplicando variações
de pressão positivas a cada 20cmH2O até que fosse atingido 100cmH2O e posteriorment
negativas até que fosse atingido 0 cmH2O. A cada 20cmH2O um intervalos de 5 segundos era
realizado até a próxima aplicação de pressão. A mensuração de fluxo e pressão durante a
coleta de dados foi realizada de forma sincrônica junto ao sistema da POE. As variações de

24
pressão mensuradas na boca foram consideradas como variação de pressão alveolar. A
integração do sinal de fluxo proveu as variações de volume pulmonar.
3.5. Air stacking
Para o artigo 1, a técnica de air stacking foi realizada utilizando um insuflador manual
(RWR-Brasil®) acoplado a uma máscara de silicone, que envolveu o nariz e boca o sujeito. Ao
ser posicionado, em posição supina a 45º e com os membros superiores repousados lado do
corpo, foi solicitado ao sujeito que realizasse uma inspiração profunda, atingindo sua
capacidade inspiratória máxima, e segurasse mantendo a glote fechada. Imediatamente foi
acoplada a máscara do insuflador manual ao rosto do paciente e pressionada para evitar o
vazamento de ar. Logo após, por meio do insuflador manual, foram proporcionados volumes
de ar de forma rápida e consecutiva, através de repetidas insuflações (Figura 2). Cada
insuflação foi realizada concomitantemente com uma inspiração profunda do sujeito, até que
nenhum ar possa mais pudesse ser acrescentado aos pulmões, atingindo a capacidade de
insuflação máxima. Entre cada insuflação o sujeito foi orientado a não exalar o ar, mantendo-o
nos pulmões.
A máscara foi posicionada e retirada pelo avaliador, assim como as instruções dadas
antes e durante a realização da técnica. Esta foi interrompida caso ocorresse algum
desconforto pelo paciente, má adaptação, alteração de sinais vitais ou queda da saturação.

25
4. Resultados
Os resultados e a discussão desta tese estão descritos na forma de três artigos
científicos. O primeiro artigo intitulado “Assessment of gas compression and lung volume
during air stacking maneuver” está publicado no periódico “European Journal of Applied
Physiology”, Qualis A1, na área 21 da CAPES. O segundo artigo intitulado “Thoracoabdominal
asynchrony and paradoxical motion in amyotrophic lateral sclerosis” será submetido ao
periódico “Respiratory Physiology & Neurobiology”, Qualis B1, na área 21 da CAPES. O
terceiro artigo intitulado “Multiparametric analysis of sniff nasal inspiratory pressure test in
middle stage amyotrophic lateral sclerosis” está publicado no periódico “Frontiers in
Neurology”, Qualis A1, na área 21 da CAPES.
Os artigos estão apresentados conforme as normas e diretrizes de submissão de cada
periódico.

26
4.1. Artigo 1
Assessment of gas compression and lung volume during air stacking
maneuver
___________________________________________
A. Sarmento, V. R. Resqueti, G. A. F. Fregonezi, A. Aliverti
Artigo publicado no Periódico European Journal of Applied Physiology (2017) 117:189–199

27
4.1.1. Abstract
Purpose: We reasoned that the application of positive pressure through air stacking (AS)
technique could cause gas compression and the absolute lung volumes could be estimated.
The aim of this study was to estimate the amount of gas compression (ΔVcomp) during AS in
healthy subjects positioned at 45° trunk inclination and verify if the simultaneous measurements
of chest wall volume changes (ΔVCW), by optoelectronic plethysmography, and changes in lung
volume (ΔVao), by pneumotachograph, combined with pressure variation at the airways opening
(ΔPao) during AS are able to provide reliable data on absolute lung volumes.
Methods: Twenty healthy subjects (mean age 23.5 ± 3.8 years) were studied during a protocol
that included slow vital capacity and AS maneuvers. Vcomp was calculated by subtracting ΔVao
and ΔVCW occurring during AS and total lung capacity (TLC) was estimated by applying Boyle–
Mariote’s law using Vcomp and ΔPao.
Results: During AS, 0.140 ± 0.050 L of gas was compressed with an average ΔPao of 21.78 ±
6.18 cmH2O. No significant differences between the estimated TLC (−0.03 ± 3.0% difference,
p=0.6020), estimated FRC (−2.0 ± 12.4% difference, p=0.5172), measured IC (1.2 ± 11.2%
difference, p=0.7627) and predicted values were found.
Conclusion: During AS, a significant gas compression occurs and absolute lung volumes can
be estimated by simultaneous measurements of ΔVCW, ΔVao and ΔPao.

28
4.1.2. Introduction
The assessment of lung volumes is important for the diagnosis and follow-up of
pulmonary diseases (Zysman-Colman and Lands 2016). Absolute lung volumes can be
measured by a variety of methods (Kendrick 1996; Schlesinger et al. 1995; Wanger et al.
2005). These include the methods based on a static mass balance, such as helium dilution and
nitrogen washout (Meneely and Kaltreider 1949; Newth et al. 1997), and those based on
dynamic mass balance and compression gas phenomena, such as whole-body
plethysmography (WBP) (Coates et al. 1997; Cobeel 1969; Newth et al. 1997). The
apparatuses used to obtain measurements based on these methods can be difficult, time
consuming and require good technical skills to produce consistent results (Cliff et al. 1999;
Eber et al. 1994; O’Donnell et al. 2010).
According to the Boyle–Mariote’s law, the pressure of an ideal gas at constant
temperature varies inversely with the volume. Hence, an unknown volume of a closed
compartment can be determined if absolute changes in volume can be induced and the
corresponding relative pressures in change can be measured. Thus, the determination of
thoracic gas volume is possible if the lung is treated as a closed compartment and if the
changes in alveolar pressure in parallel to the changes in volume can be measured (Smith et
al. 2012).
Hedenstierna et al. (1985) described that, for positive pressure ventilation, blood shift to
the periphery may lead to greater gas lung volume changes than chest wall volume changes,
and vice versa during negative pressure ventilation. In addition to this, a positive pressure
applied can induce about 1–2% of gas compression, depending on the pressure used (Aliverti
et al. 2000).
The air stacking (AS) technique, a lung insufflations method mostly used in patients with
restrictive lung diseases, such as neuromuscular disorders, is characterized by the application
of a positive pressure to provide air volumes higher than the inspiratory capacity (IC) to
increase peak cough flow (Bach et al. 2007; Kang and Bach 2000a, b). We reasoned that in
healthy subjects, the application of AS could cause gas compression. Thus, measurements of
gas compression (ΔVcomp) combined with pressure changes at the airways opening (ΔPao),
recorded at atmospheric pressure and controlled temperature, allow the estimation of total lung
capacity (TLC) by applying Boyle–Mariote’s law.
The aims of the present study therefore were (a) to estimate the amount of ΔVcomp
during AS in healthy subjects positioned at 45° trunk inclination and (b) to verify if the
simultaneous measurements of total change in chest wall volumes (ΔVCW), by optoelectronic
plethysmography, and changes in lung volume (ΔVao), by pneumotachograph, combined with
ΔPao during AS are able to provide reliable data of absolute lung volumes. In addition to these,
we also tried to provide data that can improve the knowledge of the physiologic effects of the
air stacking maneuver.

29
4.1.3. Methods
Subjects
Twenty healthy subjects (10 males and 10 females; age 23.5 ± 3.8 years, weight 68.2 ±
9.2 kg and height 1.70 ± 0.08 m, with body mass index of 23.5 ± 2.5 kg/m2, forced vital
capacity of 4.51 ± 0.75 L and forced expiratory volume in the first second of 3.80 ± 0.62 L) were
included in the study. Absolute and percentage predicted spirometric as well as anthropometric
data of each subject are shown in Table 1.
All individuals involved in the study were laboratory personnel trained in respiratory
maneuvers, self-reported as healthy with no history of smoking, heart or lung disease and
signed an informed consent form. The study was conducted within the confines of the World
Medical Association Declaration of Helsinki for medical research using human participants and
approved by the Research Ethics Committee under number 1.344.512/2015.
4.1.3.1 Measurements and apparatus
Spirometry
For spirometric measurements, a KoKo DigiDoser Spirometer® (nSpire Health, Inc.
Longmont, USA) was used and the technical procedures, acceptance and reproducibility
criteria, reference and interpretative values for forced vital capacity and forced expiratory
volume in the first second, as well as the standardization of the equipment followed the
recommendations of the ATS/ERS (2002). Assessment was considered complete when three
acceptable curves were produced, of which the best two were reproducible (with variation equal
to or lower than 5% to 200 mL).
Optoelectronic plethysmography
The optoelectronic plethysmography (OEP System®; BTS, Milan, Italy) was used to
assess ΔVCW as the sum of the variations of volume in the upper and lower rib cage and
abdomen (Aliverti and Pedotti 2003; Cala et al. 1996). This method has been used to assess
ΔVCW in healthy and in an extensive variety of diseases. In brief, optoelectronic
plethysmography measured the volumes displaced by the compartments of the chest wall by
52 retro-reflective markers placed on the trunk of the subject according to precise anatomical
reference points (Aliverti et al. 2001; Romei et al. 2010). Calibration of optoelectronic
plethysmography TV cameras was performed before data acquisition in each subject. Marker
positions and motion were captured by six TV cameras (three on the left and three on the right
side of the subject) operating at 60 frames/s and synchronized with co-axial infrared flashing
LEDs. The three-dimensional coordinates of the markers were calculated with
stereophotogrammetry and linked forming a mesh of triangles to define the surface the trunk.
The volume enclosed by the surface was obtained through a computing algorithm based on the
Gauss’ theorem (Cala et al. 1996).

30
Pneumotachography
Flow and pressure at the airway opening were measured in all subjects by a heated
pneumotachograph (Series 0–800 LPM, Hans Rudolph® Inc, Kansas, EUA) that was placed
between a face mask and the manual insufflator (Fig. 1). Calibration of flow and pressure was
performed before data acquisition in each subject. The flowmeter was calibrated by measuring
different levels of inspiratory and expiratory airflow, by generating different strokes with a
calibrated 3 L syringe, with intervals of about 3 s in between. The pressure transducer was
calibrated by connecting it to a water manometer and measuring positive and negative
pressure variations from 0 to 100 cmH2O, with intervals of about 5 s in between. Optoelectronic
plethysmography data acquisition system allowed to acquire pressure and flow analog signals
of the pneumotachograph synchronously with optoelectronic plethysmography data. ΔPao were
considered as changes of alveolar pressure (ΔPalv). Time integration of the flow signal provided
ΔVao.
Air stacking apparatus
The AS maneuvers were performed using a two-way manual insufflator (RWR®, São
Paulo, Brazil) coupled to a silicone oro-nasal mask (7450 SeriesV2™, Hans Rudolph® Inc,
Kansas-EUA) and connected in series with the pneumotachograph. The subject was asked to
take a deep breath starting from functional residual capacity (FRC) up to TLC and to hold the
breath. At this moment, two consecutive air stacking maneuvers were applied until the
maximum volume that could be held with a closed glottis. Maximum insufflation capacity (MIC)
was defined as the sum of IC (volume variation from FRC to TLC) plus the volume variation
due to the application of AS (Dohna-Schwake et al. 2006; Kang and Bach 2000a) (Fig. 2). After
the second AS, the subject was asked to exhale down to residual volume.
Vital signs
Heart rate and peripheral oxygen saturation were measured continuously and non-
invasively during all the study protocol through a portable pulse oximeter PalmSat ® 2500
(Nonin Medical, Minnesota, USA).

31
Fig. 1 Photograph of the experimental setup used to measure the gas compression. The subject is positioned at 45°
trunk inclination with the reflective markers of the optoelectronic plethysmography placed on the trunk surface. The
mask, positioned on the face of the subject, is connected to the pneumotachograph and manual insufflator.
Study protocol
All the data measurements were performed in a laboratory with the temperature
controlled between 26 and 28 °C. The subjects were evaluated in a single day in which
anthropometric (weight, height and body mass index) and spirometric data were collected. All
the subjects were positioned at 45° trunk inclination on a standard bed in which the AS
maneuvers were performed (Fig. 1).
Data were recorded with each subject performing the following consecutive set of
maneuvers: (1) 60s of quiet spontaneous breathing; (2) a vital capacity (VC) maneuver; (3) 40s
of quiet spontaneous breathing; (4) three sets of AS maneuvers, each composed of two air
stackings (see below), and immediately followed by an expiration starting from the maximum
volume reached after the second stacking and finishing at residual volume (with an interval of
20s in between); (5) 40s of quiet spontaneous breathing; (6) a VC maneuver; (7) 60s of quiet
spontaneous breathing (Fig. 3).

32
Fig. 2 Experimental tracings obtained on a representative subject during a period of quiet breathing, followed by a
vital capacity (expiratory), a second period of quiet breathing, a set of two AS maneuvers and a third period of quiet
breathing. On the right, inspiratory capacity (IC), vital capacity (VC) and maximum insufflation capacity (MIC) are
indicated. Top panel chest wall volume variations measured by optoelectronic plethysmography (black line) and lung
volume variations, obtained as integration of flow measured at the mouth by pneumotachograph (grey line). Bottom
panel pressure simultaneously measured at the airways opening. Vertical lines indicate AS maneuvers. TLC total
lung capacity, FRC functional residual capacity, RV residual volume.
Fig. 3 Experimental tracing of total chest wall volume variation during a test on a single representative subject. The
study protocol included a period of quiet spontaneous breathing, two vital capacity (VC) maneuvers and three sets of
air stacking (AS) maneuvers interleaved with periods of quiet breathing.

33
Previous observations obtained before the application of the protocol allowed to
establish that two consecutive AS maneuvers would be sufficient to reach MIC in healthy
subjects. Between each air stack, the subject was instructed to not exhale (keeping the air into
the lungs with the closed glottis) and to not move the trunk, so the optoelectronic
plethysmography could measure the ΔVCW accurately. During the whole study protocol, the
examiner maintained the mask involving the mouth and nose of the subject to avoid air
leakage. The procedure was discontinued if discomfort, alteration of vital signs or poor
adaptation occurred.
4.1.3.2. Data analysis
Gas compression
The ΔVCW measured with optoelectronic plethysmography during the AS maneuver
represents not only the volume of air inspired by the subject (ΔVao), but also ΔVcomp and blood
shift (VBS) from the trunk to the extremities:
∆VCW = ∆Vao + ∆Vcomp + ∆VBS. (1)
where ΔVao was calculated by the integration of flow measured
at the mouth by the pneumotachograph, from the beginning to the end of each AS maneuver,
and ΔVcomp was estimated from the Boyle–Mariote’s law for isothermal transformations (Iandelli
et al. 2002; Smith et al. 2012) (see below).
From Eq. (1), the difference between ΔVao and ΔVCW equals to ΔVcomp plus ΔVBS:
∆Vao − ∆VCW = ∆Vcomp + ∆VBS. (2)
Assuming that during the AS maneuver ΔVBS = 0, ΔVcomp can be obtained from Eq. (2)
as follows (Fig. 4):
∆Vcomp = ∆Vao − ∆VCW. (3)
Absolute lung volumes
Total lung capacity could be estimated (TLCest), from Boyle–Mariote’s law as follows
Δ
Δ
. (4)
where ΔPalv was estimated from measurements of ΔPao during the AS maneuver;
atmospheric pressure (Patm) was known; ΔVcomp was obtained from ΔVao and ΔVCW
measurements and Eq. (3).

34
Fig. 4 Zoomed view of the representative tracings shown in Fig. 2 during two AS maneuvers. Top panels chest wall
(black line) and lung (grey line) volume variations. Bottom panel pressure variations. During AS maneuver #1, the
application of about 22 cmH2O of positive pressure by the manual insufflations determines a change in lung volume
(ΔVao = 0.510 L) larger than the change in chest wall volume (ΔVCW = 0.370 L). In this example, the amount of gas
compression is thus estimated to be 140 mL.
Functional residual capacity was estimated (FRCest) subtracting IC, obtained by
integrating the flow measured by the pneumotachograph (ICmeas), from TLCest.
Values of ICmeas, TLCest and FRCest were compared to predicted values for both genders
(Roca et al. 1998).
For each subject, among the three sets of maneuvers, the AS showing the maximum
ΔVcomp was selected and considered for data analysis. In each set of AS maneuvers, only the
first one was considered because it was performed starting from TLC.
4.1.4. Statistical analysis
For descriptive analysis, mean and standard deviations (± SD) were used. Normality
and data distribution were verified using the Shapiro–Wilk test. Parametric paired Student’s t
test was used to evaluate the differences between predicted values and estimated and
measured volumes.
The inferential data analysis was performed using the GraphPad Prism software version
6.01 for Windows. For all statistical analysis, a significance level of 5% (p < 0.05) was adopted.

35
4.1.5. Results
Vital signs and adaptation
No discomfort or poor adaptation during the AS maneuvers was reported by the
subjects. Heart rate and peripheral oxygen saturation did not vary during the application of the
study protocol (Table 1).
Pressure and volume variations during AS maneuvers
Absolute values of ΔPalv, ΔVao, ΔVCW and ΔVcomp of each subject are reported in Table 2.
Under the assumption that no blood shift occurs during the application of AS, with an average
pressure variation of 21.78 ± 6.18 cmH2O, the gas compression estimated from the air stacking
maneuver of all subjects was 0.140 ± 0.050 L, representing 2.1% of lung volume at TLC.
Lung volumes
Table 3 shows the estimated and predicted values of TLC and FRC as well as the
measured and predicted values of IC. In Table 4, the absolute and percentage differences
between estimated (or measured) and predicted volumes are shown for each subject. No
statistically significant differences between the TLCest (p = 0.6020), FRCest (p = 0.5172) and
ICmeas (p = 0.7627) and predicted values were found. FRCest had mean values below and ICmeas
had mean values above the predicted seated values (−2.0 ± 12.4 and 1.2 ± 11.2% difference,
respectively).
Due to the lack of reliable VC maneuvers, particularly in the expiratory limb, the residual
volume and expiratory reserve volume could have not been estimated.

36
Table 1. Anthropometric and spirometric data and average values of heart rate and oxygen saturation measured during the study
protocol of each subject.
Subject Gender Age Height (m) Weight (kg) BMI (kg/m2) FVC (L) FVC%pred FEV1(L) FEV1%pred HR(bpm) %SpO2
#1 #2 #3 #4 #5 #6 #7 #8 #9
#10 #11 #12 #13 #14 #15 #16 #17 #18 #19 #20
Mean ± SD
F F F F F F F F F M M M F M M M M M M M
23 20 21 28 22 22 21 22 26 34 23 23 28 26 19 20 29 22 21 20
23.5 ± 3.8
1.52 1.60 1.63 1.65 1.66 1.67 1.68 1.68 1.70 1.70 1.71 1.75 1.77 1.82 1.63 1.72 1.81 1.85 1.70 1.78
1.70 ± 0.08
48 63 64 72 73 58 60 54 70 78 70 68 68 82 65 63 74 78 85 72
68.2 ± 9.2
20.78 24.61 24.09 26.65 26.49 20.80 21.26 19.13 24.22 26.99 23.94 22.20 21.71 24.76 24.46 21.30 22.59 22.79 29.41 22.72
23.5 ± 2.5
3.20 3.59 3.76 3.80 3.98 3.97 4.00 4.06 4.12 4.83 5.12 5.42 4.80 5.90 4.43 4.72 5.23 5.77 4.57 5.02
4.51 ± 0.75
97.3 98.1 98.9 97.4
100.8 99.2 98.8
100.2 99.3 98.4 99.2
100.6 106.4 101.4 106.1 105.0 96.2
105.1 91.3 98.4
99.9 ± 3.7
2.75 3.20 3.21 3.12 3.18 3.40 3.48 3.33 3.40 4.01 4.28 4.18 3.57 4.75 3.86 4.21 4.59 4.85 4.10 4.62
3.80 ± 0.62
94.8 99.1 96.4 97.2 92.7 97.9 98.9 95.1 96.3
100.5 99.8 93.3 94.4 99.6 100
102.2 100 99.0 91.3 96.8
97.1 ± 2.9
62 97 78 72 75 82 65 78 68 73 80 78 83 79 82 76 88 67 73 81
76.4 ± 8.6
98 98 99 98 98 97 98 99 99 99 99 99 99 98 99 98 98 97 98 98
98 ± 1
In the left column are the subject’s numbers. FVC: Forced vital capacity; FEV1: Forced expiratory volume in the first second; HR: Heart rate; %SpO2: Oxygen
saturation; m: Meters; kg: Kilograms; L: Liters; %pred: Percentage of predict; bpm: Beats per minute; F: Female; M: Male

37
Table 2. Gas compression and pressure in a single air
stacking maneuver.
Subject ΔPalv (cmH2O) ΔVao (L) ΔVCW (L) Vcomp (L)
#1 #2 #3 #4 #5 #6 #7 #8 #9
#10 #11 #12 #13 #14 #15 #16 #17 #18 #19 #20
Mean ± SD
21.98 28.00 29.00 20.86 18.71 19.50 18.26 12.94 13.67 22.00 13.70 23.89 14.76 18.47 23.00 38.00 25.90 28.50 20.40 24.00
21.78 ± 6.18
0.33 0.40 0.27 0.54 0.45 0.48 0.52 0.46 0.23 0.33 0.41 0.40 0.47 0.43 0.49 0.52 0.34 0.50 0.52 0.62
0.44 ± 0.10
0.23 0.26 0.11 0.42 0.35 0.37 0.42 0.39 0.15 0.19 0.32 0.23 0.38 0.29 0.35 0.25 0.15 0.27 0.39 0.45
0.30 ± 0.10
0.10 0.14 0.16 0.12 0.10 0.11 0.10 0.08 0.08 0.15 0.09 0.17 0.09 0.14 0.14 0.26 0.19 0.23 0.13 0.17
0.14 ± 0.05
In the left column are the subject’s numbers. ΔPalv: Alveolar pressure
changes in cmH2O measured at the mouth; ΔVao: Integrated volume
change measured at the mouth; ΔVCW: Chest wall volume change in ml
measured by optoelectronic plethysmography; ΔVcomp: Compressed
volume in ml (ΔVcomp = ΔVao – ΔVCW); L: Liters

38
Table 3. Absolute values of the estimated (est), predicted (pred) and measured (meas) values of each subject.
In the left column are the subject’s numbers. TLC: Total lung capacity; FRC: Functional residual capacity; IC: Inspiratory
capacity; CI: Confidence interval; L: Liters.
Table 4. Absolute and percentage (%) difference values between estimated and predicted (est-pred)
and measured and predicted (meas-pred) values.
Subject TLCest-pred (L) TLCest-pred (%) FRC est-pred (L) FRCest-pred (%) ICmeas-pred (L) ICmeas-pred (%)
#1 #2 #3 #4 #5 #6 #7 #8 #9
#10 #11 #12 #13 #14 #15 #16 #17 #18 #19 #20
Mean ± SD
-0.202 0.399 0.097 0.213 -0.272 -0.029 -0.263 0.067 -0.002 -0.055 -0.125 0.069 -0.194 -0.168 0.150 0.088 -0.271 0.207 -0.017 -0.132
-0.022 ± 0.184
-4.1 7.4 1.7 3.7 -4.7 -0.5 -5.4 1.1
-0.04 -0.8 -1.8 0.9 -3.0 -2.1 2.4 1.3 -3.4 2.5 -0.2 -1.8
-0.3 ± 3.0
-0.113 -0.182 -0.091 -0.127 -0.513 0.550 -0.651 -0.683 0.098 -0.307 -0.632 0.775 -0.046 0.166 0.493 0.273 -0.370 0.154 0.213 -0.182
-0.059 ± 0.404
-4.3 -6.2 -3.0 -4.3
-17.4 17.4 -20.3 -21.3 3.0
-18.8 -18.8 20.9 -1.3 4.1
17.2 8.0 -9.2 3.7 6.5 -4.9
-2.0 ± 12.4
-0.178 -0.065 0.469 0.514 0.424 -0.580 0.342 0.344 -0.101 0.277 0.245 -0.663 -0.149 -0.325 0.002 -0.153 0.154 0.066 -0.197 0.075
0.022 ± 0.329
-7.8 -2.6 18.2 19.5 15.9 -21.6 12.6 12.7 -3.6 7.9 6.9
-18.1 -5.0 -8.3 0.1 -4.3 2.7 1.6 -5.7 2.0
1.2 ± 11.2
In the left column are the subject’s numbers. TLC: Total lung capacity; FRC: Functional residual capacity; IC:
Inspiratory capacity; L: Liters.
Subjects TLCest (L) TLCpred (L) FRCest (L) FRCpred (L) ICmeas (L) ICpred (L)
#1 #2 #3 #4 #5 #6 #7 #8 #9
#10 #11 #12 #13 #14 #15 #16 #17 #18 #19 #20
Mean ± SD
4.699 5.810 5.699 5.942 5.521 5.827 5.657 5.987 6.045 6.855 6.786 7.351 6.299 7.788 6.287 7.067 7.617 8.408 6.785 7.403
6.491 ± 0.919
4.901 5.411 5.602 5.729 5.793 5.856 5.920 5.920 6.047 6.910 6.911 7.282 6.493 7.956 6.137 6.979 7.888 8.201 6.802 7.535
6.513 ± 0.927
2.516 2.735 2.934 2.794 2.436 3.719 2.554 2.522 3.375 2.814 2.733 4.351 3.483 4.198 3.354 3.665 3.634 4.319 3.499 3.557
3.260 ± 0.635
2.629 2.917 3.025 2.921 2.949 3.169 3.205 3.205 3.277 3.121 3.365 3.596 3.529 4.032 2.861 3.392 4.004 4.165 3.286 3.739
3.209 ± 0.347
2.096 2.430 3.047 3.147 3.085 2.108 3.058 3.060 2.670 3.760 3.764 3.000 2.816 3.590 3.233 3.402 3.983 4.089 3.286 3.846
3.174 ± 0.570
2.274 2.495 2.578 2.633 2.661 2.688 2.716 2.716 2.771 3.483 3.519 3.663 2.965 3.915 3.231 3.555 3.879 4.023 3.483 3.771
3.151 ± 0.555
p value (95% CI) 0.6020 (-0.064 to 0.108) 0.5172 (-0.129 to 0.249) 0.7627 (-0.176 to 0.131)

39
4.1.6. Discussion
The main findings of the present study are that in healthy subjects, during the
application of the AS technique (a) ΔVao exceeds ΔVCW and a detectable amount of gas
compression occurs and (b) simultaneous measurements of ΔPao and ΔVcomp (obtained by
subtracting ΔVao and ΔVCW) are able to provide an accurate estimate of absolute lung volumes,
at least those predicted from the reference equations.
The role of gas compression has already been reported in the literature, but mostly
during forced expiratory maneuvers (Iandelli et al. 2002; Ingram and Schilder 1966; Jaeger and
Otis 1964; Sharafkhaneh et al. 2004; Smith et al. 2012). However, Hedenstierna et al. (1981),
through a technique based on body plethysmography and insufflations of a heated and
humidified gas, observed that the chest wall expanded less than would be expected after
application of positive pressure and a known insufflated volume, indicating the presence of
alveolar gas compression during maximal mechanical inflation of the lungs of anesthetized
patients. To our knowledge, this is the first report about ΔVcomp at high lung volumes during AS
maneuvers.
Air stacking, obtained by either a positive pressure mechanical ventilator or by a manual
insufflator (Toussaint et al. 2016), is currently being considered, particularly in patients with
restrictive disorders, to increase maximal lung volume and consequently peak cough flow
(Jeong and Yoo 2015; Marques et al. 2014; Torres-Castro et al. 2014). Studies conducted in
neuromuscular patients (Brito et al. 2009; Kang and Bach 2000a, b; Kang et al. 2005) have
shown that a significant increase in VC and decrease in atelectasis (Lechtzin et al. 2006)
occurs after the application of AS. These patients are characterized by lung restriction and low
lung volumes. It is reasonable to hypothesize that the positive pressure applied through AS is
able not only to expand the lungs beyond TLC, but presumably also to recruit new alveolar
units, with a low amount of gas compression. As gas compression depends on lung volume
(Ingram and Schilder 1966), in the opposite case of patients with high lung volumes, such as
hyperinflated COPD subjects (Jaeger and Otis 1964; O’Donnell and Laveneziana 2006;
Sharafkhaneh et al. 2004), ΔVcomp via AS would be presumably higher. In COPD patients,
therefore, although the application of AS does not have any rationale as a treatment, it could be
considered as a tool for lung volume estimation.
In the present study, we have shown that the application of AS in healthy subjects
determines both an expansion of the respiratory system (i.e., chest wall) above TLC levels and
an amount of alveolar gas compression of about 2.1% of lung volume at TLC. It is reasonable
to assume that the application of the positive pressure above the upper inflection point of the
pressure volume curve by AS thus determines alveolar overdistension (Benito and Lemaire
1990; Harris 2005; Hickling 1998) rather than alveolar recruitment.
To our knowledge, this is the first study involving the simultaneous recordings of
optoelectronic plethysmography and pneumotachograph to estimate absolute lung volumes.
Absolute lung volume estimation is performed through techniques based on either static mass
balance, such as nitrogen washout or helium dilution, or dynamic mass balance and
compression gas phenomena in the lung, such as WBP. It is known that the former approach
can underestimate lung volume in the presence of poorly ventilated or unventilated spaces,

40
causing a significant error (Wanger et al. 2005). This is not the case of WBP, which is
considered as the gold standard for its accuracy. However, the technique is very often difficult
to be applied in patients.
The ΔVcomp of all subjects was calculated by subtracting ΔVao and ΔVCW (Iandelli et al.
2002; Smith et al. 2012) and was estimated without taking into account possible blood shifts
(ΔVBS) from the trunk to the extremities. The choice of neglecting ΔVBS was based on the fact
that our measurements were taken with the lung submitted to positive pressure followed by a
spontaneous inspiration up to total lung capacity. Under these conditions, we can hypothesize
that two phenomena, with opposite effects on intrathoracic blood volume, and therefore
mutually eliciting, occur at the same time. The first is the increase in intrathoracic pressure, due
to the application of the air stacking maneuver, which determines a blood shift from the thorax
to the rest of the body. The second is the decrease in intrathoracic pressure, due to the full
inspiration, which determines a blood shift into the thorax. Hedenstierna et al. (1985) showed
that in anesthetized patients, the positive pressure provided by mechanical ventilation shifts
approximately 300 mL of blood from the rib cage to the abdomen and only 100 mL from the
extremities to the abdomen. The former quantity, thus, remains within the trunk and does not
produce any total chest wall volume variation, with ΔVCW being calculated as the sum of rib
cage and abdominal volumes variations. This blood shift from the rib cage to the abdomen can
be explained reasonably by the increase in intrathoracic pressure, which reduces transmural
vascular pressure, not only in the lung but also in the heart and the systemic veins in the thorax
(Hedenstierna et al. 1985). On the contrary, the latter quantity was very probably caused by the
induction of general anesthesia per se and suggestive of an overall displacement of blood from
the extremities to the trunk.
As preliminary experiments showed that several subjects reported difficulties in
maintaining the mouthpiece in place during the application of the positive pressure, we decided
to use an oral facial mask. A possible limitation, therefore, could be the presence of air
leakages between the mask and the face of the subject under analysis, leading to poor
accuracy of the measurements. This possible source of error was eliminated, however, by
excluding few cases in which a rapid decrease in the ΔPalv occurred together with a large
increase in ΔVao and no change in ΔVCW. Another possible source of error due to the mask
could be the gas compression occurring within the mask itself. The volume of the mask used,
however, was only 99 mL and therefore negligible compared to lung volume.
In the present study, the subdivisions of lung volumes estimated during AS were
compared to those predicted by equations based on WBP measurements. The determination of
lung volumes by WBP is usually by a panting maneuver performed at FRC. Starting from the
estimated FRC, residual volume and TLC values are then obtained by subtracting expiratory
reserve volume and adding IC, respectively (Criee et al. 2011). In our study, differently, lung
volume was estimated at TLC, with FRC and residual volume values obtained by subtracting
measured values of IC and VC, respectively. Because of the lack of reliable VC maneuvers
performed by the subjects, however, only the values of TLC (estimated by AS), IC (measured
by pneumotachograph) and FRC (obtained by subtracting TLCest and ICmeas) have been
shown here. Moreover, it is known that in supine position, FRC decreases and TLC remains

41
approximately constant, with a consequent increase of IC, compared to seated or erect
positions (Baydur et al. 1996; Burki 1977; Laval et al. 1971; Parot et al. 1970). In the present
study, measurements were taken with the subject adopting a 45º trunk inclination. This posture
was chosen for two reasons, namely (a) to ensure that the maneuver was applied in the same
position adopted for most hospital bedridden patients; and (b) to not allow any air leakage
between the mask and the face of the subject while the examiner applied a sufficient pressure
to couple the mask. There are no available data on prediction equations for absolute lung
volumes for the subject’s posture adopted in the present and only scanty and old data derived
from nitrogen washout or helium dilution for supine position (Hurtado et al. 1934; Ibanez and
Raurich 1982; Kaltreider 1938; Whitfield et al. 1950). Therefore, the comparisons were
performed using prediction equations derived from WBP measurements obtained in seated
position with panting performed at FRC (Roca et al. 1998). Nevertheless, our results showed a
good agreement without significant differences between estimated and predicted lung volumes,
with a tendency of FRCest to be lower, although without statistical significance.
4.1.7. Conclusion
The present study provides original data useful to better understand AS maneuver at
high lung volumes. In addition, a novel method for assessing absolute lung volumes is
proposed as an alternative to the use of WBP or gas dilution techniques. The estimation of
absolute lung volumes by simultaneous measurement by optoelectronic plethysmography and
pneumotachograph during AS represents a simple, easy and non-invasive method that can be
done in different positions with the need of only a minor level of collaboration from the subject,
who has just to perform a full inspiration. Future studies are needed to know if the method is
applicable and accurate in other positions and in restrictive and obstructive pulmonary
diseases.

42
4.1.8. References
Aliverti A, Pedotti A (2003) Opto-electronic plethysmography. Monaldi Arch Chest Dis 59(1):12–
16.
Aliverti A, Dellaca R, Pelosi P, Chiumello D, Pedotti A, Gattinoni L (2000) Optoelectronic
plethysmography in intensive care patients. Am J Respir Crit Care Med 161:1546–1552.
Aliverti A, Dellaca R, Pelosi P, Chiumello D, Gatihnoni L, Pedoti A (2001) Compartmental
analysis of breathing in the supine and prone positions by optoelectronic
plethysmography. Ann Biomed Eng 29:60–70.
ATS/ERS (2002) Statement on respiratory muscle testing. Am J Respir Crit Care Med
166(1):518–624.
Bach JR, Bianchi C, Vidigal-Lopes M, Turi S, Felisari G (2007) Lung inflation by
glossopharyngeal breathing and “air stacking” in Duchenne muscular dystrophy. Am J
Phys Med Rehabil 86:295–300.
Baydur A, Sassoon CS, Carlson M (1996) Measurement of lung mechanics at different lung
volumes and esophageal levels in normal subjects: effect of posture change. Lung
174:139–151.
Benito S, Lemaire F (1990) Pulmonary pressure-volume relationship in acute respiratory
distress syndrome in adults: role of positive end expiratory pressure. J Crit Care 5:27–
34.
Brito MF, Moreira GA, Pradella-Hallinan M, Tufik S (2009) Air stacking and chest compression
increase peak cough flow in patients with Duchenne muscular dystrophy. J Bras
Pneumol 35(10):973–979.
Burki NK (1977) The effects of changes in functional residual capacity with posture on mouth
occlusion pressure and ventilatory pattern. Am Rev Respir Dis 116:895–900.
Cala SJ et al (1996) Chest wall and lung volume estimation by optical reflectance motion
analysis. J Appl Physiol 81:2680–2689 .
Cliff IJ, Evans AH, Pantin CF, Baldwin DR (1999) Comparison of two new methods for the
measurement of lung volumes with two standard methods. Thorax 54:329–333.
Coates AL, Peslin R, Rodenstein D, Stocks J (1997) Measurement of lung volumes by
plethysmography. Eur Respir J 10:1415–1427.
Cobeel L (1969) Comparison between measurements of functional residual capacity and
thoracic gas volume in chronic obstructive pulmonary disease. Prog Respir Resp 4:194–
204.
Criee CP et al (2011) Body plethysmography—its principles and clinical use. Respir Med
105:959–971.
Dohna-Schwake C, Ragette R, Teschler H, Voit T, Mellies U (2006) IPPB-assisted coughing in
neuromuscular disorders. Pediatr Pulmonol 41:551–557.
Eber E, Steinbrugger B, Modl M, Weinhandl E, Zach MS (1994) Lung volume measurements in
wheezy infants: comparison of plethysmography and gas dilution. Eur Respir J 7:1988–
1994.
Kaltreider NL, Fray WW, Hyde HV (1938) The effect of age on the total pulmonary capacity and
its subdivisions. Am Rev Tuberc 37:662.
Harris RS (2005) Pressure–volume curves of the respiratory system. Respir care 50:78–98
(discussion 98–79).

43
Hedenstierna G, Jarnberg PO, Gottlieb I (1981) Thoracic gas volume measured by body
plethysmography during anesthesia and muscle paralysis: description and validation of
a method. Anesthesiology 55:439–443.
Hedenstierna G, Strandberg A, Brismar B, Lundquist H, Svensson L, Tokics L (1985)
Functional residual capacity, thoracoabdominal dimensions, and central blood volume
during general anesthesia with muscle paralysis and mechanical ventilation.
Anesthesiology 62:247–254.
Hickling KG (1998) The pressure-volume curve is greatly modified by recruitment. A
mathematical model of ARDS lungs. Am J Respir Crit Care Med 158:194–202.
Hurtado A, Fray WW, Kaltreider NL, Brooks WD (1934) Studies of total pulmonary capacity and
its subdivisions. V. Normal values in female subjects. J Clin Invest 13:169–191.
Iandelli I et al (2002) Determinants of exercise performance in normal men with externally
imposed expiratory flow limitation. J Appl Physiol 92:1943–1952.
Ibanez J, Raurich JM (1982) Normal values of functional residual capacity in the sitting and
supine positions. Intensive Care Med 8:173–177.
Ingram RH Jr, Schilder DP (1966) Effect of gas compression on pulmonary pressure, flow, and
volume relationship. J Appl Physiol 21:1821–1826.
Jaeger MJ, Otis AB (1964) Effects of compressibility of alveolar gas on dynamics and work of
breathing. J Appl Physiol 19:83–91.
Jeong JH, Yoo WG (2015) Effects of air stacking on pulmonary function and peak cough flow in
patients with cervical spinal cord injury. J Phys Ther Sci 27:1951–1952.
Kang SW, Bach JR (2000a) Maximum insufflation capacity. Chest 118:61–65.
Kang SW, Bach JR (2000b) Maximum insufflation capacity: vital capacity and cough flows in
neuromuscular disease. Am J Phys Med Rehabil 79:222–227.
Kang SW, Kang YS, Moon JH, Yoo TW (2005) Assisted cough and pulmonary compliance in
patients with Duchenne muscular dystrophy.
Yonsei Med J 46:233–238 Kendrick AH (1996) Comparison of methods of measuring static
lung volumes. Monaldi Arch Chest Dis 51(5):431–439.
Laval PFJ, Fondarai I, Kleisbauer JP, Poirier R (1971) Variations de la capacite respiratoire
fonctionnelle et des resistances des voies aeriennes chez des sujets normaux en
position assise puis couché. Bull Physiopathol Respir 7:743–764.
Lechtzin N, Shade D, Clawson L, Wiener CM (2006) Supramaximal inflation improves lung
compliance in subjects with amyotrophic lateral sclerosis. Chest 129:1322–1329.
Marques TB, Neves Jde C, Portes LA, Salge JM, Zanoteli E, Reed UC (2014) Air stacking:
effects on pulmonary function in patients with spinal muscular atrophy and in patients
with congenital muscular dystrophy. J Bras Pneumol 40(5):528–534.
Meneely GR, Kaltreider NL (1949) The volume of the lung determined by helium dilution.
Description of the method and comparison with other procedures. J Clin Invest 28:129–
139.
Newth CJ, Enright P, Johnson RL (1997) Multiple-breath nitrogen washout techniques:
including measurements with patients on ventilators. Eur Respir J 10:2174–2185.
O’Donnell DE, Laveneziana P (2006) Physiology and consequences of lung hyperinflation in
COPD. Eur Respir Rev 15:61–67 O’Donnell CR, Bankier AA, Stiebellehner L, Reilly JJ,
Brown.
R, Loring SH (2010) Comparison of plethysmographic and helium dilution lung volumes: which
is best for COPD? Chest 137:1108–1115.

44
Parot S, Chaudun E, Jacquemin E (1970) The origin of postural variations of human lung
volumes as explained by the effects of age. Respiration 27:254–260.
Roca J et al (1998) Prediction equations for plethysmographic lung volumes. Respir Med
92:454–460.
Romei M, Mauro AL, D’Angelo MG, Turconi AC, Bresolin N, Pedotti A, Aliverti A (2010) Effects
of gender and posture on thoraco-abdominal kinematics during quiet breathing in
healthy adults. Respir Physiol Neurobiol 172:184–191
Schlesinger AE, White DK, Mallory GB, Hildeboldt CF, Huddleston CB (1995) Estimation of
total lung capacity from chest radiography and chest CT in children: comparison with
body plethysmography. AJR Am J Roentgenol 165:151–154
Sharafkhaneh A, Officer TM, Goodnight-White S, Rodarte JR, Boriek AM (2004) Novel method
for measuring effects of gas compression on expiratory flow. Am J Physiol Regul Integr
Comp Physiol 287:R479–R484.
Smith JA, Aliverti A, Quaranta M, McGuinness K, Kelsall A, Earis J, Calverley PM (2012) Chest
wall dynamics during voluntary and induced cough in healthy volunteers. J Physiol
590:563–574.
Torres-Castro R, Vilaro J, Vera-Uribe R, Monge G, Aviles P, Suranyi C (2014) Use of air
stacking and abdominal compression for cough assistance in people with complete
tetraplegia. Spinal Cord 52:354–357.
Toussaint M, Pernet K, Steens M, Haan J, Sheers N (2016) Cough augmentation in subjects
with Duchenne muscular dystrophy: comparison of air stacking via a resuscitator bag
versus mechanical ventilation. Respir Care 61:61–67.
Wanger J et al (2005) Standardisation of the measurement of lung volumes. Eur Respir J
26(3):511–522.
Whitfield AG, Waterhouse JA, Arnott WM (1950) The total lung volume and its subdivisions. A
study in physiological norms. III. Correlation with other anthropometric data. Br J Soc
Med 4(3):113–136.
Zysman-Colman Z, Lands LC (2016) Whole body plethysmography: practical considerations.
Paediatr Respir Rev 19:39–41.

45
4.2. Artigo 2
Thoracoabdominal asynchrony and paradoxical motion in
amyotrophic lateral sclerosis subjects
___________________________________________
Antonio Sarmento, Guilherme Fregonezi, Mario Emílio Teixeira Dourado-Junior, Andrea
Aliverti, Armele Dornelas de Andrade, Verônica Franco Parreira, Vanessa Resqueti
Submetido no Periódico Respiratory Physiology & Neurobiology

46
4.2.1. Abstract
Aim: To assess thoracoabdominal asynchrony (TAA) and the presence of paradoxical motion
in middle stage amyotrophic lateral sclerosis (ALS) and its relationships with chest wall tidal
volume (VT,CW), breathing pattern and cough peak flow (CPF).
Methods: Phase angle (θ) between upper (RCp) and lower ribcage (RCa) and abdomen (AB),
as well as percentage of inspiratory time the lower ribcage (IPRCa) and abdomen (IPAB) moved
in opposite directions, were quantified using optoelectronic plethysmography in two situations:
quiet breathing and cough. Normal range of movement was defined using control data.
Results: During quiet breathing, significantly higher RCa and AB θ (p<.05), IPRCa (p=0.001)
and IPAB (p<0.05) were observed. Correlations between RCa and AB θ with forced vital
capacity (FVC) (r=–0.773, p<0.01), vital capacity (r=–0.663, p<0.05) and inspiratory capacity
(IC) (r=–0.754, p<0.01) as well as between RCp and RCa θ with FVC (r=–0.608, p<0.05) and
CPF (r=–0.601, p<0.05) were found. During cough, correlations between RCp and AB θ with
CPF (r=–0.590, p<0.05), IC (r=–0.748, p<0.01) and VT,CW (r=–0.608, p<0.05) as well as
between RCa and AB θ with CPF (r=–0.670, p<0.05), IC (r=–0.713, p<0.05) and PEF (r=–
0.727, p<0.05) were observed. ALS subjects with paradoxical motion presented lower vital
capacity and FVC%pred (p<0.05).
Conclusions: In this population, abnormalities in breathing are dependent on lung restriction
and diaphragmatic impairment may occur prior to the upper ribcage inspiratory muscles being
early observed in the lower ribcage compartment rather than the abdomen.
Keywords: Chest wall volumes, cough, diaphragm impairment, inspiratory paradox time, phase
angle, quiet breathing.

47
4.2.2. Introduction
In healthy humans, the expansion and contraction of the ribcage and abdomen (AB)
during spontaneous breathing occur synchronously with small distortions (Allen, et al. 1990;
Ward, et al. 1992). During inspiration, the diaphragm contraction expands the abdominal
ribcage (RCa) pushing the abdominal contents downward and the abdominal wall outward at
the same time in which the intercostal and accessory muscles act to elevate and expand the
pulmonary ribcage (RCp) (Zoumot, et al. 2015). When uncoordinated motion between chest
wall compartments occurs, the thoracoabdominal asynchrony (TAA) is observed (Hammer &
Newth 2009).
TAA is primarily the result of disproportionate weakness of some respiratory muscles or
discoordination between different muscle groups (Chihara, et al. 1996) and is defined as the
difference in time of expansion or retraction between chest wall compartments (Allen, et al.
1990). It is influenced by a variety of breathing patterns (Chihara, et al. 1996; Crawford, et al.
1983; Gilmartin & Gibson 1984) and has been already identified in chronic obstructive
pulmonary disease patients (Aliverti, et al. 2009; Priori, et al. 2013), asthma (Hillman, et al.
1986; Ringel, et al. 1983), preterm infants (Warren, et al. 1997), tetraplegic (Mortola &
Sant'Ambrogio 1978) and stroke subjects (Lima, et al. 2014). Subjects with neuromuscular
disorders can also display TAA (Allen 2010; Crescimanno, et al. 2012; Diaz, et al. 1993;
Gibson, et al. 1977) mainly due to the reduced chest wall compliance (Diaz, et al. 1993) and
inspiratory muscle weakness (Hardart, et al. 2002; Testa, et al. 2005) resulting in a decreased
contribution of chest wall compartments to tidal volume (Perez, et al. 1996) and increased work
of breathing (Testa, et al. 2005).
With the progression of the disease, amyotrophic lateral sclerosis (ALS) subjects display
respiratory muscle weakness (Gregory 2007; Lyall, et al. 2001; Park, et al. 2010), decreased
tidal volume (Baydur 1991; Vitacca, et al. 1997) and cough peak flow (CPF) (Bach, et al. 2008;
Cleary, et al. 2013; Senent, et al. 2011), so it is possible that they also exhibit TAA and
paradoxical motion. Thus, using optoelectronic plethysmography, an optical reflectance motion
analysis system, we aimed to assess the within-breath TAA between the three different chest
wall compartments as well as the presence of paradoxical motion at rest during quiet breathing
(QB) in middle stage ALS compared to age-matched healthy positioned at 45° trunk inclination.
Secondly, as diaphragm contribution during QB and inspiration preceding cough are
determinants of cough efficiency in neuromuscular disease subjects (Lo Mauro, et al. 2010;
LoMauro, et al. 2014), we also assessed TAA and paradoxical motion during cough as well as
its relationships with chest wall volumes, breathing pattern and CPF.

48
4.2.3. Methods
Subjects
This is a cross-sectional study with a matched-pair design. Twelve ALS subjects,
diagnosed according to the El Escorial World Federation of Neurology (Brooks, et al. 2000) and
classified as middle stage according to disease progression (Balendra, et al. 2015; Roche, et
al. 2012; Simon, et al. 2014) (see appendix tables A1 and A2), with forced vital capacity (FVC)
<80% of predict, without bulbar dysfunction or tracheostomy, cardiovascular or pulmonary
diseases were recruited for the study. Those in use of positive pressure devices or could not
adopt the posture at 45° trunk inclination, were excluded. Control group consisted of twelve
self-reported healthy matched by gender and age without any cardiovascular or pulmonary
diseases. Those with spirometric values <80% of predicted were excluded.
The study was conducted within the confines of the World Medical Association
Declaration of Helsinki for medical research using human participants and approved by the
Research Ethics Committee under number 1.344.512/2015. All individuals signed an Informed
Consent Form.
Lung function and respiratory muscle strength
Lung function was assessed through a KoKo Digidoser® spirometer (nSpire Health,
Longmont-EUA) with the subject seated in a standard chair. Assessments were carried out
following the acceptability and reproducibility criteria(American Thoracic Society/European
Respiratory 2002) and values obtained were compared to absolute and percentage of predict
spirometric values for the Brazilian population (Pereira, et al. 2007).
A digital manometer (NEPEB-LabCare, Belo Horizonte-Brazil) was used to assess
respiratory muscle strength by measuring maximal inspiratory (MIP) and expiratory pressures
(MEP) starting from residual volume and total lung capacity, respectively. To assess the pattern
of respiratory muscle strength loss in this population, absolute and percentage of predicted
MEP/MIP ratio was calculated (Fregonezi, et al. 2015). Sniff nasal inspiratory pressure (SNIP)
was also used to assess inspiratory muscle strength (Heritier, et al. 1994). For each of the
above tests, the higher value obtained was compared to previous absolute and percentage
values for the Brazilian population (Araujo, et al. 2012; Neder, et al. 1999) and considered for
statistical analysis.
Functionality and clinical stage of the disease
The functionality of the ALS subjects was assessed by a physician through the
Amyotrophic Lateral Sclerosis Functional Rating Scale-Revised (Gordon, et al. 2004), validated
for the Brazilian population (Guedes, et al. 2010). The scale included items related to
respiratory (maximum of 12 points) and bulbar function with a total score of 48 points (See
appendix table A3).
Study design
For each subject, all measurements were performed in one single day. After collection
of lung function and respiratory muscle strength data, the subjects were positioned in a

49
standard bed at 45° trunk inclination in which the retro-reflective markers were placed and
chest wall kinematics were recorded by the TV cameras (see below) during 1) sixty seconds of
quiet spontaneous breathing at rest, 2) a VC maneuver and 3) a strong cough maneuver
(performed starting from total lung capacity).
Optoelectronic plethysmography
Optoelectronic plethysmography (BTS Bioengineering, Italy), a system described
previously (Aliverti & Pedotti 2003; Cala, et al. 1996), allowed the assessment of chest wall
kinematics. In brief, six TV cameras (three on the left and three on the right side of the subject),
previously calibrated using a frequency of 60 frames.sec-1, recorded the movement change of
52 retro-reflexive markers placed in specific anatomic points of the trunk surface of the subjects
in order to model the chest wall and its compartments – RCp, RCa and AB (Aliverti & Pedotti
2003). All markers were simultaneously visible to at least two TV cameras so that their three-
dimensional positions and displacements could be reconstructed using stereo-photogrammetric
methods by a motion analyzer (Ferrigno, et al. 1994). A closed surface of the total subject’s
trunk was reconstructed by connecting the coordinates of the markers and the breath-by-breath
volume enclosed by this surface was computed by means of an algorithm based on the Gauss’
theorem (Cala, et al. 1996).
The following parameters were obtained: Chest wall tidal volume (VT,CW) and its
compartments, CPF, vital capacity (VC), inspiratory capacity (IC), respiratory rate, minute
ventilation, inspiratory time, expiratory time, total time of the respiratory cycle, mean inspiratory
flow, mean expiratory flow and duty cycle. Rapid shallow breathing was obtained according to
Yang and Tobin (Yang & Tobin 1991) and ΔVT,AB/Ti, ΔVT,RCp/Ti and ΔVT,AB/Te were calculated
as shortening velocity index of the diaphragm, inspiratory ribcage and expiratory muscles
(Aliverti, et al. 2002), respectively.
Chest wall asynchrony and inspiratory paradoxical movement
Firstly, the degree of asynchrony between chest wall compartments was obtained after
the construction of Lissajous figures (Aliverti, et al. 2009; Allen, et al. 1990) during QB and
cough. Phase angle (θ) between two volumetric signals was calculated and a graph was
created when plotting two volumetric signals against each other. θ = sin-1 (m/s) was used to
define θ, where m was the ratio of the distance delimited by the intercepts of the dynamic loop
on a line parallel to X-axis at 50% of the volume of the signal on the Y-axis, and s the volume of
the signal on the X-axis (Fig. 1). RCp (y-axis) versus RCa (x-axis), RCa (y-axis) versus AB (x-
axis) and RCp (y-axis) versus AB (x-axis) loops during QB and cough (Fig. 2) were calculated
and a positive phase angle means that the expansion of the y-axis leads the x-axis (loop with
clockwise direction); while a negative phase angle describes the reverse situation. A θ of zero
represents a completely synchronous movement of the compartments, while 180° represents
total asynchrony (Agostoni & Mognoni 1966; Allen, et al. 1990; Priori, et al. 2013).
Secondly, inspiratory paradox time of RCa (IPRCa) and AB (IPAB), defined as the fraction
of the inspiratory time in which the RCa and AB volumes decrease during inspiration (Aliverti, et
al. 2009), respectively, were also assessed.

50
For data analysis, patients were subdivided into those presenting paradoxical
movement of the RCa (PRCa+) and AB (PABM+) compartments and those who not (PRCa- and
PABM-, respectively). Grouping was based on upper and lower threshold values (defined as 75
and 25th interquartile range, respectively) of θ and IP obtained at rest (mean of 15 breaths) and
during a strong cough maneuver of all matched-paired healthy of this study. Thus, ALS
subjects were classified as presenting paradoxical movement if both θ and IP values exceeded
the above-mentioned threshold points (i.e. RCp and AB θ and IPAB for paradoxical ribcage
motion as well as RCp and Rca θ and IPRCa for paradoxical ribcage motion).

51
Fig 1. Representative time-courses of the pulmonary rib cage (RCp) (y-axis), abdominal rib cage (RCa) (y-axis),
abdomen (AB) (x-axis) and chest wall volumes of one healthy control subject (left), one middle stage amyotrophic
lateral sclerosis subject with no paradoxical rib cage (PRCa-) and abdominal (PAB-) motion (middle), and one middle
stage amyotrophic lateral sclerosis subject with paradoxical rib cage (PRCa+) and abdominal (PAB+) motion (right)
during quiet breathing. L: Liters; Δ: Change; Arrows: Direction of the compartmental expansion; Black dot: Beginning
of inspiration. m: line parallel to signal of the X-axis at 50% of the volume of the signal on the Y-axis; s: volume of the
signal on the X-axis; θ: Phase shift.

52
Fig 2. Representative time-courses of the pulmonary rib cage (RCp), abdominal rib cage (RCa), abdomen (AB) and
chest wall volumes of one healthy control subject (left), one middle stage amyotrophic lateral sclerosis subject with no
paradoxical rib cage (PRCa-) and abdominal (PAB-) motion (middle), and one middle stage amyotrophic lateral
sclerosis subject with paradoxical rib cage (PRCa+) and abdominal (PAB+) motion (right) (according to the
classification used in the study) during a cough maneuver. Note in supplementary table S3, patient number #3, that
the subject with PRCa- and PAB- has no paradoxical abdominal motion according to the classification used in the
study. L: Liters; Δ: Change; Small arrows: Start of cough; Big arrows: Direction of the compartmental expansion;
Black dots: Start of inspiration; Grey dots; Start of cough; θ: Phase angle.
4.2.4. Statistical analysis
Data are expressed as mean ± SD unless otherwise stated. Normality of data was
assessed using Shapiro-Wilk test. Differences between ALS and healthy subjects regarding
anthropometric, spirometric and respiratory muscle strength data as well as data obtained from
optoelectronic plethysmography and asynchrony were tested using Paired t-test and Wilcoxon

53
test for parametric and non-parametric data, respectively. Differences between subgroups were
studied using Mann-Whitney test. Relationships between the degree of asynchrony and both
lung function and breathing pattern were studied using Pearson’s r and Spearman’s rho
correlation coefficient.
No previous data were available to guide a sample size for this study. Thus, to avoid
type II error, the power of the study as well as effect-sizes [Coefficients of determination (r2)
and Cohen's f2 for parametric relationship analysis and Cohen’s d for intergroup and subgroup
non-parametric inferential analysis] (Cohen 1988; Faul, et al. 2009; Fritz, et al. 2012) were
calculated using G*Power software, version 3.1.9.2 (Kiel, Germany) (See appendix).
Inferential data analysis was performed using GraphPad Prism® software version 6.01
for Windows. A p value of <0.05 (2-sided) was considered as statistically significant for all
statistical analysis.
4.2.5. Results
Data related to diagnosis criteria, region of onset, clinical phenotype as well as the
presence of familial ALS and cognitive impairment of all ALS included in the study are shown in
appendix table A4. Anthropometric characteristics, spirometric, respiratory muscle strength and
functionality data are shown in Table 1.
A post hoc analysis considering the calculated effect size for IPRCa during cough
(Cohen’s d=0.96) showed a statistical power (1-ß)=0.99 for this study.
Cough peak flow, chest wall volumes, breathing pattern and velocity index of respiratory
muscles
A significant lower CPF (p<0.001, Cohen’s d=1.26), VC (p<0.001, Cohen’s d=1.92), IC
(p<0.001, Cohen’s d=1.89) and VT,CW (p<0.005, Cohen’s d=1.29) were observed in ALS when
compared to controls. Regarding compartmental analysis, significant lower volumes in RCp
(p<0.05, Cohen’s d=0.77) and AB (p<0.05, Cohen’s d=1.15) compartments were observed in
ALS subjects. Significant lower inspiratory time (p=0.001, Cohen’s d=1.53), expiratory time
(p<0.05, Cohen’s d=1.26) and total time of respiratory cycle (p<0.005, Cohen’s d=1.43) as well
as significant higher respiratory rate (p<0.005, Cohen’s d=1.50) and rapid shallow breathing
(p=0.001, Cohen’s d=1.77) were found in ALS subjects when compared to controls (Table 2).
Thoracoabdominal asynchrony during cough and quiet breathing
During cough, no differences were found in θ between groups, however significant
differences in IPRCa (p<0.005, Cohen’s d=0.96) were observed (Table 3). In addition, significant
correlations between RCp and AB θ with CPF (r= –0.590, p<0.05, r2= 0.35, Cohen’s f2=0.53),
PEF (r= –0.727, p<0.01), IC (r= –0.748, p<0.01) and VT,CW (r= –0.608, p<0.05, r2= 0.37,
Cohen’s f2=0.58); RCa and AB θ with CPF (r= –0.670, p<0.05, r2= 0.45, Cohen’s f2=0.81), IC
(r= –0.713, p<0.05) and PEF (r= –0.727, p<0.05); and RCp and RCa θ with respiratory rate (r=
0.638, p<0.05) were observed.
During QB, significant differences in RCp and AB θ (p<0.05, Cohen’s d=0.54) and RCa
and AB θ (p<0.05, Cohen’s d=0.62) were found in ALS when compared to controls (Table 3). In

54
addition, a significant higher IPRCa (p=0.001, Cohen’s d=2.03) and IPAB (p<0.05, Cohen’s d=.53)
were found in ALS subjects (Fig 3) as well as significant correlation between RCp and AB θ
and FVC (r= –0.773, p<0.01), VC (r= –0.663, p<0.05) and IC (r= –0.754, p<0.01); RCp and
RCa θ and FVC (r= –0.608, p<0.05) and CPF (r= –0.601, p<0.05) and RCa and AB θ with rapid
shallow breathing (r= 0.645, p<0.05).
Table 1. Anthropometric, absolute and predicted values of
lung function, respiratory muscle strength and
functionality data of the subjects.
Data presented as mean and standard deviation. FVC: Forced Vital
Capacity; FEV1: Forced expiratory volume in the 1st second; FEV1/FVC:
Ratio of forced expiratory volume in the first second to forced vital capacity;
FEF25-75%: Forced expiratory flow at 25-75%; PEF: Peak expiratory flow;
MIP: Maximum inspiratory pressure; MEP: Maximum expiratory pressure;
MEP/MIP: Ratio between maximum inspiratory and expiratory pressures;
SNIP: Sniff nasal inspiratory pressure; ALSFRS-R: Amyotrophic Lateral
Sclerosis Functional Rating Scale-revised; n: number of subjects; m:
meters; kg: kilograms; L: Liters; %pred: Percentage of predicted; L/s:
Liters per second; cmH2O: centimeters of water.
Controls ALS p value
Subjects (n) 12 12 -
Age (years) 46.4±12.2 46.4±12.2 0.999
Height (m) 1.69±0.1 1.66±0.1 0.405
Weight (kg) 73.1±13.1 64.8±17.2 0.200
BMI (Kg/m2
) 25.4±3.7 23.3±5.2 0.253
FVC (L) 4.21±0.73 2.17±0.85 <0.001
FVC (%pred) 99.93±8.2 53.3±18.6 <0.001
FEV1 (L) 3.42±0.55 1.63±0.59 <0.001
FEV1 (%pred) 100.2±8.8 49.2±13.4 <0.001
FEV1 /FVC (L) 0.81±0.01 0.81±0.02 0.567
FEV1 /FVC (%pred) 81±1.8 81.4±2.9 0.678
FEF25-75% 3.44±0.97 1.48±0.70 <0.001
PEF (L/s) 7.39±1.75 3.02±1.54 <0.001
MIP (cmH2O) 119.8±26.04 33.25±10.86 <0.001
MIP (%pred) 113.5±15.7 33.6±10.1 <0.001
MEP (cmH2O) 138.8±29.22 46.17±22.09 <0.001
MEP (%pred) 125.4±24.1 44.3±18.4 <0.001
MEP/MIP (cmH2O) 1.04±0.10 1.01±0.06 0.476
MEP/MIP (%pred) 1.11±0.20 1.38±0.60 0.141
SNIP (cmH2O) 130.9±26.96 33.75±9.5 <0.001
SNIP (%pred) 123.8±18 39.1±8.4 <0.001
ALSFRS-R - 26.67±8.31 -
Respir. subscore - 10.08±1.56 -

55
Table 2. Cough peak flow, vital capacity, chest wall
compartmental volumes, breathing pattern and
shortening velocity index of respiratory muscles.
Data presented as mean and standard deviation. CPF: Cough
peak flow; VC: Vital capacity; IC: Inspiratory capacity; VCW:
Chest wall volume; VRCp: Pulmonary ribcage volume; VRCa:
Abdominal ribcage volume; VAB: Abdominal volume; Ti:
Inspiratory time; Te: Expiratory time; Ttot: Total time of the
respiratory cycle; RR: respiratory rate; VE: Minute volume; RSB:
Rapid shallow breathing: ΔVTCW/Ti: Maximum inspiratory flow;
ΔVTCW/Te: Maximum expiratory flow; ΔVrcp/Ti: Shortening
velocity index of inspiratory ribcage muscles; ΔVab/Ti: Shortening
velocity index of diaphragm; ΔVab/Te: Shortening velocity index
of expiratory muscles; ‡ non-parametric data distribution; L:
Liters; min: minutes; s: seconds; L/s: Liter per second; Bpm:
Breaths per minute
Controls ALS p value
CPF (L/s) 8.452 ± 3.35 4.618 ± 2.50 <0.001
VC (L) 4.278 ± 1.39 1.958 ± 0.70 <0.001
IC (L) 3.491 ± 1.03 1.795 ± 0.54 <0.001
∆VCW (L) 0.619 ± 0.24 0.342 ± 0.07 <0.005
∆VRCp (L) 0.182 ± 0.13 0.089 ± 0.03 <0.05
∆VRCa (L) ‡ 0.105 ± 0.05 0.065 ± 0.02 0.059
∆VAB (L) 0.334 ± 0.14 0.186 ± 0.08 <0.05
Ti (s) 1.68 ± 0.45 1.08 ± 0.28 0.001
Te (s) 2.43 ± 0.69 1.66 ± 0.43 <0.05
Ttot (s) 4.12 ± 1.10 2.74 ± 0.70 <0.005
RR (bpm-1
) 15.73 ± 4.30 23.62 ± 5.84 <0.005
VE (L/min-1
) 9.17 ± 2.71 7.99 ± 2.76 0.261
Duty cycle 41.18 ± 3.83 39.63 ± 3.02 0.329
RSB 30.50 ± 16.99 73.08 ± 27.52 0.001
ΔVTCW/Ti (L/s-1
) 0.375 ± 0.11 0.343 ± 0.13 0.481
ΔVTCW/Te (L/s-1
) 0.263 ± 0.08 0.222 ± 0.07 0.177
ΔVT,rcp/Ti (L/s) 0.107 ± 0.05 0.088 ± 0.04 0.374
ΔVT,ab/Te (L/s) 0.140 ± 0.05 0.118 ± 0.05 0.403
ΔVT,ab/Ti (L/s) 0.162 ± 0.08 0.186 ± 0.10 0.408

56
Table 3. Thoracoabdominal asynchrony during quiet breathing and cough.
Data presented as median and interquartile range between 25-75%. RCp: Pulmonary ribcage; RCa: Abdominal ribcage; AB: Abdominal;
θ: Phase shift; PhRIB: Phase relation during inspiration; PhREB: Phase relation during expiration; PHTB: Phase relation during total
breath; °: Degrees; %: Percentage. ‡ parametric data distribution; * <.05 versus controls; # <.01 versus controls;
† <.005 versus controls.
Fig 3. Box plots showing the inspiratory paradox time of abdominal rib cage (IPRCa) and abdomen (IPAB) during quiet
breathing and cough. Center lines indicate the median and plus signs show mean values. The upper and lower limits
of each box represent the 75th and 25th percentiles, respectively. Whiskers denote minimum and maximum values.
Black dots represent each patient individually. %: Percentage; ALS: Amyotrophic Lateral Sclerosis..
During quiet breathing During cough
Controls ALS Controls ALS
Subjects (n) 12 12 12 12
θ RCpxAB ° -6.622 [-8.67 – -3.03] -0.702 [-7.78 – 5.11]* 7.370 [-7.52 – 11.08]‡ 10.250 [-17.02 – 35.22]
θ RCaxAB ° -2.556 [-6.42 – -0.29] 2.135 [-2.88 – 9.04]* 3.045 [-6.62 – 8.72]‡ 10.290 [-16.24 – 28.50]
θ RCpxRCa ° -4.034 [-10.48 – -1.47]‡ -3.765 [-13.89 – -1.88] 1.455 [-5.20 – 8.39]
‡ 1.715 [-4.29 – 11.81]

57
Paradoxical abdominal motion during cough and quiet breathing
The upper and lower limits for RCp and AB θ were defined as 7.52° and -11.08°,
respectively; and the upper limit for IPAB was defined to be 12.09%. PABM+ was observed in 5
subjects with ALS. Of the 7 remaining (PABM-), only two showed no evidence of paradoxical
motion by either criterion, while 4 showed abnormal θ and 1 abnormal IPAB. No statistically
significant differences between subgroup analyses were found.
The upper and lower limits for RCp and AB θ during QB were -1.87° and -10.48°,
respectively; while the upper limit for IPAB was 8.59%. PABM+ was observed in 6 subjects. Of the
6 remaining, 2 subjects showed IPAB values above the threshold, 3 showed abnormal θ and 1
showed no evidence of paradoxical motion by either criterion (See appendix tabel A5). During
QB a significant higher MEP/MIP%pred ratio (p<0.01, Cohen’s d=2.51) was found in PABM+ when
compared to PABM- [median of 1.72 (1.46-2.38) and 0.91 (0.79-1.07), respectively].
Paradoxical ribcage motion during cough and quiet breathing
During cough, the upper and lower limits for RCp and Rca θ were defined as 5.20° and -
8.39°, respectively; and the upper limit for IPRCa was defined to be 3.30%. PRCa+ was observed
in 6 subjects. Of the 6 remaining, only one showed no evidence of paradoxical motion by either
criterion, while 5 showed abnormal IPRCa. A significantly lower FVC%pred (p<0.05, Cohen’s
d=1.26) was observed in PRCa+ [median of 42 (28.8-55.6)], when compared with PRCa- subgroup
[median of 62.6 (50.9-72.6)] during cough as well as higher ΔVT,RCp/Ti [median of 0.10 (0.08-
0.15) vs 0.06 (0.05-0.07) L/sec-1, p<0.01, Cohen’s d=1.67].
During QB, the upper and lower limits for θ were, respectively, -3.03° and -8.67°; while
the upper limit for IPRCa was 6.95%. PRCa+ was observed in 6 subjects, while the 6 remaining
did not. Of these, 5 subjects showed IPRCa values above threshold and 2 showed no evidence
of paradoxical motion by either criterion (See appendix table A6). A significantly lower FVC
[median of 1.59 (0.89-2.32) vs 2.66 (2.39-2.91) L, p<0.05, Cohen’s d=1.58], FVC%pred [median
of 37 (28.8-46) vs 62.6 (56-72.6), p<0.01, Cohen’s d=2.35], FEV1 [median of 37.4 (29.7-44) vs
59.5 (51-61.4) p<0.01, Cohen’s d=2.14] and VC [median of 1.47 (0.98-2.17) vs 2.34 (1.94-2.70)
p<0.05, Cohen’s d=1.46] were observed in PRCa+ when comparing with PRCa-, respectively.
4.2.6. Discussion
Main findings
The main findings of the study were that middle stage ALS positioned at 45° trunk
inclination a) Display higher TAA between the upper ribcage compartments and AB during QB
when compared to controls and the magnitude of this TAA is negatively related to forced vital
capacity, inspiratory capacity and vital capacity; b) During cough, TAA is negatively related to
cough peak flow, peak expiratory flow, inspiratory capacity and chest wall tidal volume; c)
Paradoxical abdominal and ribcage motion can be observed in middle stage ALS subjects at
rest and during cough; d) Subjects with paradoxical motion exhibit a decreased VC, FVC and
FEV1 as well as increased MEP/MIP%pred ratio and ΔVT,RCp/Ti.

58
Thoracoabdominal asynchrony
TAA has long been thought clinically useful in the assessment of airflow obstruction in
infants (Allen, et al. 1990), early-onset hyperinflation and dyspnoea in chronic obstructive
pulmonary disease (Aliverti, et al. 2009; Priori, et al. 2013) as well as in estimating pulmonary
function and efficiency of mechanical ventilation in Duchenne muscular dystrophy (Diaz, et al.
1993) and spinal muscular atrophy (Hardart, et al. 2002; Testa, et al. 2005). According to Allen
(Allen 2010), TAA is a consequence of weakness and inefficiency of respiratory muscles in
neuromuscular disease subjects leading to a decrease in VCW, increase in work of breathing
(Mortola & Sant'Ambrogio 1979) and, consequently, respiratory muscle fatigue (Diaz, et al.
1993).
A significantly higher TAA between RCp and AB and RCa and AB were observed in
ALS when compared to controls during QB. These findings are in agreement with other studies
performed in neuromuscular disease (Diaz, et al. 1993; Perez, et al. 1996) and, although no
correlations with respiratory muscle strength were found, it is likely to be associated with the
weakness and inefficiency of the diaphragm (Allen 2010). In the early stages of ALS, the
intercostals and accessory muscles assume the primary role in decrease intrathoracic pressure
and increase ventilation during spontaneous breathing leading to a paradoxical inward
abdominal motion and decreased tidal volume (Higenbottam, et al. 1977; Kreitzer, et al. 1978;
Romer, et al. 2017; Similowski, et al. 2000). In our study, this fact is supported by a significantly
higher IPAB and IPRCa, showing that both compartments move in opposite directions in relation
to the RCp expansion during inspiration. The former can be explained by the failure of the
diaphragm in decreasing intrathoracic pressure, and consequently increasing
transdiaphragmatic pressure, being compensated by an expansion of the RCp promoted by the
intercostals and accessory muscles (Allen 2010; Diaz, et al. 1993; Similowski, et al. 2000); and
the latter, by the fact that the part apposed to the diaphragm (RCa) may possibly be influenced
by the inward motion of the abdomen during inspiration due to the insertional expiratory muscle
component (rectus abdominis and external and internal obliquus) (De Troyer, et al. 1983; Mier,
et al. 1985).
In infants, Allen et al. (Allen, et al. 1991) and Stromberg and Nelson (Stromberg &
Nelson 1998) observed that TAA during sleep was positively related to the severity of
abnormalities in pulmonary resistance and negatively related to compliance, suggesting that
the quantification of TAA could provide a useful indicator of infant lung function. In ALS
subjects, respiratory compliance is reduced and negatively related to FVC and respiratory
muscle weakness (Lechtzin, et al. 2006). Although we did not measure compliance in our
subjects, we have shown for the first time that the degree of TAA during QB is negatively
related to FVC, VC, IC and PCF and positively related to rapid shallow breathing in middle
stage ALS subjects suggesting that TAA reflects lung restriction being also related to the
generation of insufficient volume prior to cough in this population (LoMauro, et al. 2014).
During cough, Lanini et al. (Lanini, et al. 2007) observed that differences in muscle force
acting on upper and lower ribcages result in substantial ribcage distortion in healthy subjects. In
neuromuscular disease, insufficient deflation of chest wall compartments in addition to ribcage

59
distortion result in cough ineffectiveness (Lanini, et al. 2008). Although we had measured θ
during cough instead of distortion, our results suggest an imbalance between compartments,
probably because of different compartmental pressures and elastic and resistive forces during
the expulsive maneuver (Allen 2010). Moreover, the negative relationships between RCp and
AB θ, as well as RCa and AB θ, with CPF, PEF, IC and VT,CW are in agreement with Lanini et al.
(Lanini, et al. 2007; Lanini, et al. 2008) and LoMauro et al. (LoMauro, et al. 2014) and may be
explained by a delayed or slower activation of the diaphragm(Lo Mauro, et al. 2010) and
abdominal muscles (Perez, et al. 1996) which contributes to a generation of insufficient
inspiratory volume previous to cough(Smith, et al. 2012) and expiratory pressure (De Troyer &
Estenne 1995), respectively, thus decreasing cough effectiveness (LoMauro, et al. 2014).
Paradoxical motion
To our knowledge, this is the first study in which paradoxical ribcage and abdominal
motion during cough and QB are quantified in ALS subjects. The accurate estimation of chest
wall volume and motion by surface measurements using of optoelectronic plethysmography
allowed the assessment of TAA between the two ribcage subcompartments (RCp - the part
apposed to the lung and RCa – the part apposed to the diaphragm) and AB (Aliverti, et al.
2009; Zoumot, et al. 2015), being different from studies using respiratory inductance
plethysmography in which chest wall was composed of two compartments (Allen, et al. 1990;
Diaz, et al. 1993; Perez, et al. 1996).
Previous studies (Higenbottam, et al. 1977; Kreitzer, et al. 1978) have shown that
patients with diaphragmatic dysfunction display paradoxical abdominal motion. In this case,
inspiration relies primarily on the intercostals drawing the diaphragm into the chest wall due to
its slower activation (Hammer & Newth 2009; Similowski, et al. 2000). In our study, subjects
classified as PABM+ during QB exhibited a significantly higher MEP/MIP%pred ratio indicating an
imbalance between respiratory muscle strengths and also suggesting that MIP is the first
impaired in middle ALS (Fregonezi, et al. 2015). On the other hand, when subdividing subjects
in PRCa+ and PRCa- during cough and QB, it was observed that PRCa+ subjects exhibited a lower
VC, FVC (in absolute and percentage of predicted values) and FEV1, as well as a higher
ΔVT,RCp/Ti, when compared to PRCa- subjects. These results can be explained by a lower chest
wall compliance and lung elastance (Lechtzin, et al. 2006), as well as reduced ventilatory
efficiency (Orsini, et al. 2015) and respiratory muscle performance (Kang & Bach 2000; Park, et
al. 2010), which may lead to a decrease in two predictive biomarkers for survival in ALS: The
strength of the diaphragm contraction (Polkey, et al. 2017) and VC (Carrié, et al.). In addition to
the progression of the disease, the increased ΔVT,RCp/Ti may tend to compensate for the
decreased VT,CW and maintain minute ventilation through recruitment of ribcage and accessory
muscles during inspiration (Diaz, et al. 1993; Mortola & Sant'Ambrogio 1978; Perez, et al. 1996;
Romer, et al. 2017; Similowski, et al. 2000).
Although the above patterns must be confirmed in a larger population, our results
demonstrated for the first time the negative impacts of TAA on FVC, VT,CW and CPF in middle
stage ALS subjects. Secondly, our results also showed that RCp compartment leads the RCa

60
and AB expansion in this population (which may also cause an inward motion of RCa and AB
during inspiration), being consistent with increased thoracic muscle effort (Hammer & Newth
2009) and/or weakened diaphragm (Goldman, et al. 1993) (i.e. delayed diaphragm activation
and inability to sustain a maximal inspiration previous to cough). These features also suggest
that the diaphragm is impaired prior to the muscles of the upper ribcage (Polkey, et al. 2017;
Romer, et al. 2017) and this sign is clearly observed in the lower ribcage compartment rather
than the abdomen. In addition, these findings are in agreement with Similowski et al.
(Similowski, et al. 2000), who showed that paradoxical abdominal motion, measured by two
mechanical strain gauges, was related to diaphragm impairment in ALS subjects and
compensated by an increase in inspiratory neck muscles activity. Moreover, our results are also
in agreement with those of Layton et al. (Layton, et al. 2016) who recently observed, using
optoelectronic plethysmography, that ALS subjects with weakened diaphragm have a
paradoxical motion pattern of the lower ribcage.
Strengths and limitations of the study
This study has some limitations. Firstly, the sample size was small and TAA was
assessed in 45º trunk inclination only. Secondly, there was an absence of hemodynamic and
transdiaphragmatic pressure monitoring and we also did not measure FVC in prone and supine
position. However, it is important to highlight the use of the optoelectronic plethysmography in
detecting the early signs of respiratory muscle impairment in the neuromuscular population. As
shown in the study, minimal collaboration was required from the patients during both quiet
breathing and cough and accurately assessments were performed with no interferences of
nose clips, mouth-pieces, face masks or invasive techniques which may alter the movements of
the mouth and cheeks and the respiratory system response.
4.2.7. Conclusion
We have shown evidence that middle stage ALS subjects exhibit TAA and paradoxical
motion during quiet spontaneous breathing and cough. These features were also related to
diaphragm impairment and changes in forced vital capacity, cough peak flow, peak expiratory
flow, inspiratory capacity, chest wall volumes and breathing pattern. In these subjects,
abnormalities in breathing are dependent on lung restriction and diaphragmatic impairment may
occur prior to the upper ribcage inspiratory muscles being early observed in the lower ribcage
compartment rather than the abdomen through optoelectronic plethysmography.

61
4.2.8. References
Agostoni E and Mognoni P. Deformation of the chest wall during breathing efforts. J Appl
Physiol (1966); 21: 1827-1832.
Aliverti A, Iandelli I, Duranti R, Cala SJ, Kayser B, Kelly S, Misuri G, Pedotti A, Scano G,
Sliwinski P, Yan S and Macklem PT. Respiratory muscle dynamics and control during
exercise with externally imposed expiratory flow limitation. Journal of applied physiology
(2002); 92: 1953-1963.
Aliverti A and Pedotti A. Opto-electronic plethysmography. Monaldi archives for chest disease =
Archivio Monaldi per le malattie del torace / Fondazione clinica del lavoro, IRCCS [and]
Istituto di clinica tisiologica e malattie apparato respiratorio, Universita di Napoli,
Secondo ateneo (2003); 59: 12-16.
Aliverti A, Quaranta M, Chakrabarti B, Albuquerque AL and Calverley PM. Paradoxical
movement of the lower ribcage at rest and during exercise in COPD patients. The
European respiratory journal (2009); 33: 49-60.
Allen J. Pulmonary complications of neuromuscular disease: a respiratory mechanics
perspective. Paediatric respiratory reviews (2010); 11: 18-23.
Allen JL, Greenspan JS, Deoras KS, Keklikian E, Wolfson MR and Shaffer TH. Interaction
between chest wall motion and lung mechanics in normal infants and infants with
bronchopulmonary dysplasia. Pediatric pulmonology (1991); 11: 37-43.
Allen JL, Wolfson MR, McDowell K and Shaffer TH. Thoracoabdominal asynchrony in infants
with airflow obstruction. The American review of respiratory disease (1990); 141: 337-
342.
American Thoracic Society/European Respiratory S. ATS/ERS Statement on respiratory
muscle testing. American journal of respiratory and critical care medicine (2002); 166:
518-624.
Araujo PR, Resqueti VR, Nascimento Junior J, Carvalho Lde A, Cavalcanti AG, Silva VC, Silva
E, Moreno MA, Andrade Ade F and Fregonezi GA. Reference values for sniff nasal
inspiratory pressure in healthy subjects in Brazil: a multicenter study. Jornal brasileiro
de pneumologia : publicacao oficial da Sociedade Brasileira de Pneumologia e Tisilogia
(2012); 38: 700-707.
Bach JR, Mahajan K, Lipa B, Saporito L, Goncalves M and Komaroff E. Lung insufflation
capacity in neuromuscular disease. American journal of physical medicine &
rehabilitation / Association of Academic Physiatrists (2008); 87: 720-725.
Balendra R, Jones A, Jivraj N, Steen IN, Young CA, Shaw PJ, Turner MR, Leigh PN and Al-
Chalabi A. Use of clinical staging in amyotrophic lateral sclerosis for phase 3 clinical
trials. Journal of neurology, neurosurgery, and psychiatry (2015); 86: 45-49.
Baydur A. Respiratory muscle strength and control of ventilation in patients with neuromuscular
disease. Chest (1991); 99: 330-338.
Brooks BR, Miller RG, Swash M, Munsat TL and World Federation of Neurology Research
Group on Motor Neuron D. El Escorial revisited: revised criteria for the diagnosis of
amyotrophic lateral sclerosis. Amyotrophic lateral sclerosis and other motor neuron

62
disorders : official publication of the World Federation of Neurology, Research Group on
Motor Neuron Diseases (2000); 1: 293-299.
Cala SJ, Kenyon CM, Ferrigno G, Carnevali P, Aliverti A, Pedotti A, Macklem PT and
Rochester DF. Chest wall and lung volume estimation by optical reflectance motion
analysis. Journal of applied physiology (1996); 81: 2680-2689.
Carrié C, Bonnardel E, Vally R, Revel P, Marthan R and Biais M. Vital Capacity Impairment due
to Neuromuscular Disease and its Correlation with Diaphragmatic
Ultrasound: A Preliminary Study. Ultrasound in Medicine and Biology; 42: 143-
149.
Chihara K, Kenyon CM and Macklem PT. Human rib cage distortability. Journal of applied
physiology (1996); 81: 437-447.
Cleary S, Misiaszek JE, Kalra S, Wheeler S and Johnston W. The effects of lung volume
recruitment on coughing and pulmonary function in patients with ALS. Amyotrophic
lateral sclerosis & frontotemporal degeneration (2013); 14: 111-115.
Cohen J. Statistical power analysis for the behavioral sciences. 2ª ed Hillsdale, New Jersey:
Lawrence Erbaum (1988).
Crawford AB, Dodd D and Engel LA. Changes in rib cage shape during quiet breathing,
hyperventilation and single inspirations. Respiration physiology (1983); 54: 197-209.
Crescimanno G, Canino M and Marrone O. Asynchronies and sleep disruption in
neuromuscular patients under home noninvasive ventilation. Respiratory medicine
(2012); 106: 1478-1485.
De Troyer A and Estenne M. The respiratory system in neuromuscular disorders. Lung Biology
in Health and Disease (1995); 85: 2177-2177.
De Troyer A, Sampson M, Sigrist S and Kelly S. How the abdominal muscles act on the rib
cage. Journal of applied physiology: respiratory, environmental and exercise physiology
(1983); 54: 465-469.
Diaz CE, Deoras KS and Allen JL. Chest wall motion before and during mechanical ventilation
in children with neuromuscular disease. Pediatric pulmonology (1993); 16: 89-95.
Faul F, Erdfelder E, Buchner A and Lang AG. Statistical power analyses using G*Power 3.1:
tests for correlation and regression analyses. Behavior research methods (2009); 41:
1149-1160.
Ferrigno G, Carnevali P, Aliverti A, Molteni F, Beulcke G and Pedotti A. Three-dimensional
optical analysis of chest wall motion. Journal of applied physiology (1994); 77: 1224-
1231.
Fregonezi G, Azevedo IG, Resqueti VR, De Andrade AD, Gualdi LP, Aliverti A, Dourado-Junior
ME and Parreira VF. Muscle impairment in neuromuscular disease using an
expiratory/inspiratory pressure ratio. Respiratory care (2015); 60: 533-539.
Fritz CO, Morris PE and Richler JJ. Effect size estimates: current use, calculations, and
interpretation. Journal of experimental psychology General (2012); 141: 2-18.
Gibson GJ, Pride NB, Davis JN and Loh LC. Pulmonary mechanics in patients with respiratory
muscle weakness. The American review of respiratory disease (1977); 115: 389-395.

63
Gilmartin JJ and Gibson GJ. Abnormalities of chest wall motion in patients with chronic airflow
obstruction. Thorax (1984); 39: 264-271.
Goldman MD, Pagani M, Trang HT, Praud JP, Sartene R and Gaultier C. Asynchronous chest
wall movements during non-rapid eye movement and rapid eye movement sleep in
children with bronchopulmonary dysplasia. The American review of respiratory disease
(1993); 147: 1175-1184.
Gordon PH, Miller RG and Moore DH. Alsfrs-R. Amyotrophic lateral sclerosis and other motor
neuron disorders : official publication of the World Federation of Neurology, Research
Group on Motor Neuron Diseases (2004); 5 Suppl 1: 90-93.
Gregory SA. Evaluation and management of respiratory muscle dysfunction in ALS.
NeuroRehabilitation (2007); 22: 435-443.
Guedes K, Pereira C, Pavan K and Valerio BC. Cross-cultural adaptation and validation of als
Functional Rating Scale-Revised in Portuguese language. Arq Neuropsiquiatr (2010);
68: 44-47.
Hammer J and Newth CJ. Assessment of thoraco-abdominal asynchrony. Paediatric respiratory
reviews (2009); 10: 75-80.
Hardart MK, Burns JP and Truog RD. Respiratory support in spinal muscular atrophy type I: a
survey of physician practices and attitudes. Pediatrics (2002); 110: e24.
Heritier F, Rahm F, Pasche P and Fitting JW. Sniff nasal inspiratory pressure. A noninvasive
assessment of inspiratory muscle strength. American journal of respiratory and critical
care medicine (1994); 150: 1678-1683.
Higenbottam T, Allen D, Loh L and Clark TJ. Abdominal wall movement in normals and patients
with hemidiaphragmatic and bilateral diaphragmatic palsy. Thorax (1977); 32: 589-595-
509ENG.
Hillman DR, Prentice L and Finucane KE. The pattern of breathing in acute severe asthma. The
American review of respiratory disease (1986); 133: 587-592.
Kang SW and Bach JR. Maximum insufflation capacity. Chest (2000); 118: 61-65.
Kreitzer SM, Feldman NT, Saunders NA and Ingram RH, Jr. Bilateral diaphragmatic paralysis
with hypercapnic respiratory failure. A physiologic assessment. The American journal of
medicine (1978); 65: 89-95.
Lanini B, Bianchi R, Binazzi B, Romagnoli I, Pala F, Gigliotti F and Scano G. Chest wall
kinematics during cough in healthy subjects. Acta physiologica (2007); 190: 351-358.
Lanini B, Masolini M, Bianchi R, Binazzi B, Romagnoli I, Gigliotti F and Scano G. Chest wall
kinematics during voluntary cough in neuromuscular patients. Respiratory physiology &
neurobiology (2008); 161: 62-68.
Layton AM, Moran SL, Roychoudhury A, Hupf J, Thomashow BM and Mitsumoto H. Non-
invasive measurement of abnormal ventilatory mechanics in amyotrophic lateral
sclerosis. Muscle & nerve (2016); 54: 270-276.
Lechtzin N, Shade D, Clawson L and Wiener CM. Supramaximal inflation improves lung
compliance in subjects with amyotrophic lateral sclerosis. Chest (2006); 129: 1322-
1329.

64
Lima IN, Fregonezi GA, Melo R, Cabral EE, Aliverti A, Campos TF and Ferreira GM. Acute
effects of volume-oriented incentive spirometry on chest wall volumes in patients after a
stroke. Respiratory care (2014); 59: 1101-1107.
Lo Mauro A, D'Angelo MG, Romei M, Motta F, Colombo D, Comi GP, Pedotti A, Marchi E,
Turconi AC, Bresolin N and Aliverti A. Abdominal volume contribution to tidal volume as
an early indicator of respiratory impairment in Duchenne muscular dystrophy. The
European respiratory journal (2010); 35: 1118-1125.
LoMauro A, Romei M, D'Angelo MG and Aliverti A. Determinants of cough efficiency in
Duchenne muscular dystrophy. Pediatric pulmonology (2014); 49: 357-365.
Lyall RA, Donaldson N, Polkey MI, Leigh PN and Moxham J. Respiratory muscle strength and
ventilatory failure in amyotrophic lateral sclerosis. Brain : a journal of neurology (2001);
124: 2000-2013.
Mier A, Brophy C, Estenne M, Moxham J, Green M and De Troyer A. Action of abdominal
muscles on rib cage in humans. Journal of applied physiology (1985); 58: 1438-1443.
Mortola JP and Sant'Ambrogio G. Mechanics of breathing in tetraplegics. The American review
of respiratory disease (1979); 119: 131-134.
Mortola JP and Sant'Ambrogio G. Motion of the rib cage and the abdomen in tetraplegic
patients. Clinical science and molecular medicine (1978); 54: 25-32.
Neder JA, Andreoni S, Lerario MC and Nery LE. Reference values for lung function tests: II.
Maximal respiratory pressures and voluntary ventilation. Brazilian Journal of Medical
and Biological Research (1999); 32: 719-727.
Orsini M, Oliveira AB, Nascimento OJ, Reis CH, Leite MA, de Souza JA, Pupe C, de Souza
OG, Bastos VH, de Freitas MR, Teixeira S, Bruno C, Davidovich E and Smidt B.
Amyotrophic Lateral Sclerosis: New Perpectives and Update. Neurology international
(2015); 7: 5885.
Park JH, Kang SW, Lee SC, Choi WA and Kim DH. How respiratory muscle strength correlates
with cough capacity in patients with respiratory muscle weakness. Yonsei medical
journal (2010); 51: 392-397.
Pereira CAdC, Sato T and Rodrigues SC. Novos valores de referência para espirometria
forçada em brasileiros adultos de raça branca. Jornal Brasileiro de Pneumologia (2007);
33: 397-406.
Perez A, Mulot R, Vardon G, Barois A and Gallego J. Thoracoabdominal pattern of breathing in
neuromuscular disorders. Chest (1996); 110: 454-461.
Polkey MI, Lyall RA, Yang K, Johnson E, Leigh PN and Moxham J. Respiratory Muscle
Strength as a Predictive Biomarker for Survival in Amyotrophic Lateral Sclerosis.
American journal of respiratory and critical care medicine (2017); 195: 86-95.
Priori R, Aliverti A, Albuquerque AL, Quaranta M, Albert P and Calverley PM. The effect of
posture on asynchronous chest wall movement in COPD. Journal of applied physiology
(2013); 114: 1066-1075.

65
Ringel ER, Loring SH, McFadden ER, Jr. and Ingram RH, Jr. Chest wall configurational
changes before and during acute obstructive episodes in asthma. The American review
of respiratory disease (1983); 128: 607-610.
Roche JC, Rojas-Garcia R, Scott KM, Scotton W, Ellis CE, Burman R, Wijesekera L, Turner
MR, Leigh PN, Shaw CE and Al-Chalabi A. A proposed staging system for amyotrophic
lateral sclerosis. Brain : a journal of neurology (2012); 135: 847-852.
Romer SH, Seedle K, Turner SM, Li J, Baccei ML and Crone SA. Accessory respiratory
muscles enhance ventilation in ALS model mice and are activated by excitatory V2a
neurons. Experimental neurology (2017); 287: 192-204.
Senent C, Golmard JL, Salachas F, Chiner E, Morelot-Panzini C, Meninger V, Lamouroux C,
Similowski T and Gonzalez-Bermejo J. A comparison of assisted cough techniques in
stable patients with severe respiratory insufficiency due to amyotrophic lateral sclerosis.
Amyotrophic lateral sclerosis : official publication of the World Federation of Neurology
Research Group on Motor Neuron Diseases (2011); 12: 26-32.
Similowski T, Attali V, Bensimon G, Salachas F, Mehiri S, Arnulf I, Lacomblez L, Zelter M,
Meininger V and Derenne JP. Diaphragmatic dysfunction and dyspnoea in amyotrophic
lateral sclerosis. The European respiratory journal (2000); 15: 332-337.
Simon NG, Turner MR, Vucic S, Al-Chalabi A, Shefner J, Lomen-Hoerth C and Kiernan MC.
Quantifying disease progression in amyotrophic lateral sclerosis. Annals of neurology
(2014); 76: 643-657.
Smith JA, Aliverti A, Quaranta M, McGuinness K, Kelsall A, Earis J and Calverley PM. Chest
wall dynamics during voluntary and induced cough in healthy volunteers. The Journal of
physiology (2012); 590: 563-574.
Stromberg NO and Nelson N. Thoracoabdominal asynchrony in small children with lung
disease--methodological aspects and the relationship to lung mechanics. Clinical
physiology (1998); 18: 447-456.
Testa MB, Pavone M, Bertini E, Petrone A, Pagani M and Cutrera R. Sleep-disordered
breathing in spinal muscular atrophy types 1 and 2. American journal of physical
medicine & rehabilitation / Association of Academic Physiatrists (2005); 84: 666-670.
Vitacca M, Clini E, Facchetti D, Pagani M, Poloni M, Porta R and Ambrosino N. Breathing
pattern and respiratory mechanics in patients with amyotrophic lateral sclerosis. The
European respiratory journal (1997); 10: 1614-1621.
Ward ME, Ward JW and Macklem PT. Analysis of human chest wall motion using a two-
compartment rib cage model. Journal of applied physiology (1992); 72: 1338-1347.
Warren RH, Horan SM and Robertson PK. Chest wall motion in preterm infants using
respiratory inductive plethysmography. The European respiratory journal (1997); 10:
2295-2300.
Yang KL and Tobin MJ. A prospective study of indexes predicting the outcome of trials of
weaning from mechanical ventilation. The New England journal of medicine (1991); 324:
1445-1450.

66
Zoumot Z, LoMauro A, Aliverti A, Nelson C, Ward S, Jordan S, Polkey MI, Shah PL and
Hopkinson NS. Lung Volume Reduction in Emphysema Improves Chest Wall
Asynchrony. Chest (2015); 148: 185-195.

67
4.2.9. Appendix and supplementary material
Thoracoabdominal asynchrony and paradoxical motion in amyotrophic lateral sclerosis subjects
Antonio Sarmento, Guilherme Fregonezi, Mario Emílio Teixeira Dourado-Junior, Andrea Aliverti, Armele Dornelas de Andrade, Verônica Franco Parreira, Vanessa Resqueti

68
SUPPLEMENTARY MATERIAL IN DEPTH OF STATISTICAL ANALYSIS AND RESULTS
STATISTICAL ANALYSIS
As all statistically significant data regarding intergroup and subgroup analysis were
performed using non-parametric tests (Wilcoxon or Man-Whitney tests). Thus, Cohen’s d was
calculated as the quotient between the z score and the square root of the number of
observations and interpreted as low (<0.20), moderate (between 0.20 and 0.50) and high
(>0.80)(Fritz, et al. 2012). On the other hand, since f2 for non-parametric correlations may be
biased, f2 was calculated only for parametric data and interpreted as small (<0.02), moderate
(between 0.02 and 0.15), and large (>0.35)(Cohen 1988; Faul, et al. 2009).

69
RESULTS
Table A1. Definition of clinical stages of amyotrophic lateral sclerosis
Clinical Stages Definition
1 Involvement of a single central nervous system region (symptom onset)
2 Involvement of a second central nervous system region
3 Involvement of a third central nervous system region
4A Swallowing impairment sufficient to require gastrostomy
4B Respiratory involvement sufficient to require ventilatory support (non-invasive ventilation)
5 Death
Table A2. Clinical stage of each amyotrophic
lateral sclerosis subject of the study
Subjects Classification
#1 3
#2 3
#3 3
#4 3
#5 3
#6 3
#7 3
#8 3
#9 3
#10 3
#11 3
#12 3

70
Table A3. Functionality of each amyotrophic lateral sclerosis subject of the study according to the Amyotrophic Lateral Sclerosis Functional Rating Scale-revised
*Respiratory sub-score of the Amyotrophic Lateral Sclerosis Functional Rating Scale-revised.
Subjects
Speech Salivation Swallowing Handwritting Cutting
food
Dressing and
hygiene
Turning in bed and
adjusting bed
clothes
Walking Climbing
stairs Dyspnea* Orthopnea
*
Respiratory
insufficiency*
#1 1 3 2 0 0 0 0 0 0 2 2 4 #2 2 3 3 1 2 2 3 3 3 4 4 4 #3 3 2 2 0 0 0 0 0 0 2 2 4 #4 2 4 2 0 0 0 0 1 0 2 2 4 #5 4 4 4 2 1 1 2 2 1 4 4 4 #6 2 4 3 0 0 0 2 1 0 3 3 4
#7 1 3 3 3 3 2 2 1 0 2 2 4 #8 1 0 0 3 2 2 1 2 0 2 2 4 #9 4 4 4 1 1 2 3 3 1 3 3 4
#10 4 4 4 2 2 0 0 0 4 4 4 4 #11 2 3 3 2 1 3 3 2 1 3 3 4 #12 3 3 4 3 3 2 3 4 4 3 3 4

71
Table A4. Diagnosis criteria, region of onset, local of muscle weakness symptoms onset, clinical phenotype as well as the
presence of familial ALS and cognitive impairment of all ALS subjects included in the study. All parameters shown were
assessed by a neurologist.
Diagnosis Region of onset Distal or proximal Phenotype Familial
ALS Cognitive
impairment
#1 Definitive Left upper limb Distal Classic No No
#2 Probable Right upper limb Proximal Classic No No
#3 Probable Right upper limb Distal Classic No No
#4 Definitive Right lower limb Proximal Classic No No
#5 Definitive Left lower limb Distal Classic No No
#6 Probable Lower limbs Proximal Flail legs No No
#7 Definitive Right upper limb Distal Classic No No
#8 Probable Lower limbs Distal Flail legs No No
#9 Probable Right lower limb Distal Classic No No
#10 Probable Lower limbs Distal Flail legs No No
#11 Definitive Right upper limb Distal Classic No No
#12 Definitive Right upper limb Distal Classic No No

72
Table A5. Paradoxical abdominal motion classification of each amyotrophic lateral sclerosis subject of the
study during quiet breathing and cough.
θ: Phase shift. IPAB: Inspiratory paradox time of abdominal compartment. °: Degrees; %: Percentage.
Table A6. Paradoxical ribcage motion classification of each amyothrophic lateral sclerosis subject of the
study during quiet breathing and cough.
θ : Phase shift. IPRCa: Inspiratory paradox time of abdominal ribcage compartment. °: Degrees; %: Percentage.
During quiet breathing During cough
Subject θ (°) IPAB (%) Classification θ (°) IPAB (%) Classification
#1 -3.63 11.11 - -52.89 28.24 + #2 -0.07 10.24 + -9.52 13.04 - #3 1.97 10.07 + -39.8 2.59 - #4 -9.02 9.73 + -21.46 4.41 - #5 -7.76 8.97 - -52.57 18.51 + #6 -1.34 5.27 - -10.97 3.39 - #7 -8.42 10.62 + 17.11 13.33 + #8 12.69 7.43 - 24.39 10.02 - #9 6.16 16.63 + 16.74 15.97 + #10 -7.79 6.34 - -16.79 5.56 - #11 66.54 49.93 + 45.71 51.90 + #12 0.05 2.66 - 0.79 7.10 -
During quiet breathing During cough
Subject θ (°) IPRCa (%) Classification θ (°) IPRCa (%) Classification
#1 -19.37 10.72 + -32.48 6.82 + #2 -3.22 8.52 - -1.84 14.40 - #3 -3.92 8.87 - -3.45 4.92 - #4 -12.40 7.77 + -13.21 3.68 + #5 -7.19 6.72 - -7.62 6.92 - #6 3.44 11.20 + -20.4 7.32 + #7 -14.38 8.36 + 1.42 3.92 - #8 -1.78 8.30 + 5.25 8.08 + #9 -3.61 10.74 - 11.85 17.65 + #10 -17.43 6.72 - 0.95 1.56 - #11 16.40 9.03 + 13.66 6.29 + #12 -2.20 5.78 - -1.59 35.23 -

73
REFERENCES
E 1. Cohen J. Statistical power analysis for the behavioral sciences. 2ª ed Hillsdale, New
Jersey: Lawrence Erbaum (1988).
E 2. Faul F, Erdfelder E, Buchner A and Lang AG. Statistical power analyses using G*Power
3.1: tests for correlation and regression analyses. Behavior research methods (2009);
41: 1149-1160.
E 3. Fritz CO, Morris PE and Richler JJ. Effect size estimates: current use, calculations, and
interpretation. Journal of experimental psychology General (2012); 141: 2-18.

74
4.3. Artigo 3
Multiparametric analysis of sniff nasal inspiratory pressure test in
middle stage amyotrophic lateral sclerosis
___________________________________________
Antonio Sarmento, Andrea Aliverti, Layana Marques, Francesca Pennati, Mario
Emílio Dourado-Júnior, Guilherme Fregonezi, Vanessa Resqueti
Artigo publicado no Periódico Frontiers in Neurology

75
4.3.1. Abstract
The relaxation rates and contractile properties of inspiratory muscles are altered with inspiratory
muscle weakness and fatigue. This fact plays an important role in neuromuscular disorders
patients and had never been extensively studied in amyotrophic lateral sclerosis (ALS). In this
cross-sectional study, these parameters were investigated non-invasively through nasal
inspiratory sniff pressure test (SNIP) in 39 middle stage spinal onset ALS subjects and
compared with 39 healthy controls. ALS patients were also divided into three subgroups
according to a decline in their percentage of predicted forced vital capacity (FVC%pred) as well as
a decline in the ALS functional rating-scale score and its respiratory subscore in order to
determine the best parameter linked to early respiratory muscle weakness. When compared
with healthy subjects, middle stage ALS subjects exhibited a significantly lower (p<0.0001)
maximum relaxation rate (MRR) and maximum rate of pressure development (MRPD), as well
as a significantly higher (p<0.0001) tau (τ), contraction time and half-relaxation time. The results
from ROC curves showed that MRPD (AUC 0.735, p<0.001) and FVC%pred (AUC 0.749,
p=0.009) were the best discriminator parameters between ALS patients with ≤30 and >30 points
in the ALS functional rating scale. In addition, ½RT (AUC 0.720, p=0.01), FVC%pred (AUC 0.700,
p=0.03), τ (AUC 0.824, p<0.0001) and MRPD (AUC 0.721, p=0.01) were the parameters more
sensitive in detecting a fall of 3 points in the respiratory subscore. On the other hand, MRPD
(AUC 0.781, p<0.001), τ (AUC 0.794, p=0.0001) and percentage of predicted of SNIP (AUC
0.769, p=0.002) were the parameters able to detect a fall in 30% of the FVC%pred in middle stage
ALS patients. The contractile properties and relaxation rates of the diaphragm are altered in
middle stage spinal onset ALS when compared with healthy subjects. These parameters are
able to discriminate between those middle stage ALS subjects with early decline in inspiratory
muscle function and those who not.
KEYWORDS: Amyotrophic lateral sclerosis, forced vital capacity, inspiratory muscle weakness,
relaxation rates, respiratory subscore, sniff nasal inspiratory pressure.

76
4.3.2. Introduction
Amyotrophic lateral sclerosis (ALS) is a rare neurodegenerative disorder characterized
by progressive weakness of the skeletal and respiratory muscle (1). The median survival from
first symptoms ranges from 2 to 4 years (2) and, although respiratory insufficiency can be
present in approximately 3% of patients (3, 4), it frequently emerges in the late phase of the
disease representing the most frequent cause of death (1).
Global assessment scores, such as the ALS functional rating scale (5) (ALSFRS-R), is a
useful and valid parameter in predicting survival in this population (6, 7) and has proved to be
related to forced vital capacity (8) (FVC). Since respiratory function and muscle strength are of
clinical importance and represent crucial factors influencing survival in ALS (9, 10), the
monitoring of these parameters is essential during disease progression. The gold standard
measurement of respiratory muscle strength involves the insertion of esophageal and/or gastric
balloon catheters through the nose (11). However, the sniff nasal inspiratory pressure (SNIP)
has been proposed as a non-invasive alternative method and proved to accurately reflect
diaphragm strength (12) and global inspiratory muscle strength (13).
In ALS patients the already weakened respiratory muscles are easily suitable to fatigue
(14) and this fact may play an important role in the development of ventilatory failure (15). It has
been demonstrated that the relaxation rate of inspiratory muscles is altered by the development
of inspiratory muscle fatigue (16, 17) and that relaxation rates obtained from a maximal sniff
accurately reflect those obtained from esophageal pressure (16, 18). Relaxation rates can be
described in terms of maximum relaxation rate (MRR), half-relaxation time (½RT) and time
constant of the pressure decay curve (τ, tau) after voluntary contraction of a muscle (16).
Furthermore, the contractile properties of the diaphragm [namely maximum rate of pressure
development (MRPD) and contraction time (CT)] are also altered in fatigue and have been used
as an index of the motor output of the respiratory centre (19) as well as to assess inspiratory
muscle function (11, 20, 21).
Apart from fatigue in healthy subjects (16-18, 22-24), physiological and/or disease-
related changes in diaphragm relaxation have not been extensively investigated in ALS patients
through the SNIP test. The present work aimed to non-invasively measure the relaxation rates
and the contractile properties of the inspiratory muscles in ALS patients through SNIP test 1) in
comparison to healthy subjects and 2) in relation to early respiratory symptoms in order to
determine the best parameter linked to early respiratory muscle weakness. We hypothesized
that these parameters are altered in ALS patients and can be indicators of inspiratory muscle
weakness.
4.3.3. Material and Methods
Subjects
This cross-sectional study was conducted according to the World Medical Association
Declaration of Helsinki and approved by the Research Ethics Committee under number
1.344.512/2015. All individuals involved in the study signed an Informed Consent Form.

77
We investigated 39 subjects with ALS (22 males), recruited from the Hospital
Universirátio Onofre Lopes and diagnosed by a neurologist according to the El Escorial criteria
(25) as ‘Probable or definite’, and 39 healthy controls (19 males). ALS subjects with
cardiovascular, pulmonary or other neurological diseases, as well as with bulbar dysfunction
signs or tracheostomy were not included. Those who failed to perform the assessments or
refuse to participate in the study were excluded.
Control group included self-reported age-matched healthy subjects with no history of
cardiovascular, neurological or pulmonary diseases. Those with FVC and FEV1 <80% of
predicted were excluded.
Spirometry
Spirometry was performed using a Koko Digidoser spirometer (nSpire Health,
Longmont, Colorado) and carried out with the subjects positioned sitting on a chair with feet
supported and trunk flexion of 90° according to the ATS/ERS guidelines (11). All values
obtained were compared with absolute and percentage of predicted values for the Brazilian
population (26).
Respiratory muscle strength
Maximum inspiratory and expiratory pressures (MIP and MEP, respectively) and SNIP
were measured using a digital manometer (NEPEB-Labcare, Belo Horizonte) with the subjects
seated on a chair. MIP was measured starting from residual volume and MEP from total lung
capacity, while SNIP was performed starting from functional residual capacity (FRC) (27). Data
obtained were compared with previous reference values (28, 29) and the highest value of each
test was considered for analysis.
SNIP curve analysis
All subjects were asked to perform a short, sharp inspiratory effort through the nostrils
with lips closed. Since some sniff parameters can be affected by changes in muscle length and
the activity of expiratory muscles could interfere in the analysis, the sniff maneuvers were
performed from FRC and a passive relaxation right after reaching the peak of pressure was
requested (23, 30). At least 10 maximal sniffs, with an interval of about 30 s in between, were
performed by all subjects. The following criteria were used to select those sniffs suitable for
analysis: 1) sniff performed from FRC; 2) peak pressure maintained for less than 50 ms; 3)
duration of the inspiratory effort less than 500 ms and 4) sniff pressure waveform with smooth
decay curve (16, 31).
Figure 1 shows the parameters derived from the SNIP test. From the sniff maneuver
trace, CT and ½RT were calculated as the time to reach the peak pressure of the sniff and the
half-time of the relaxation curve, respectively (32). MRPD, expressed as cmH2O·ms-1, was
calculated as the negative peak of the first derivative of pressure-time curve (21, 33) while
MRR, expressed as ms-1, was defined as the positive peak of the first derivative of pressure-

78
time curve normalized to the sniff peak pressure, in order to make contractions of different
intensities comparable (18).
The time constant (τ), was also calculated. When the natural logarithm of pressure is
plotted as a function of time, the lower 50 to 70% of the pressure decay follows a straight line
(18, 34) (Fig. 1c), indicating that the pressure follows a monoexponential decay with a time
constant τ (τ =1/slope). For the measurement of τ to be accepted, the correlation coefficient of
the individual regression line (ln P vs time) had to be ≥0.96 (35).
SNIP curve analysis was performed by custom software developed in MATLAB (The
MathWorksInc, Natick, MA).
Figure 1. Representative tracings of the SNIP test and its parameters. A: Tracings of sniff nasal inspiratory pressure
change; peak sniff pressure (Psniff); time to reach Psniff, contraction time (CT); and half-time of the relaxation curve
(½RT). B: Derivative signal of sniff pressure (dPsniff/dT = cmH2O/ms); negative peak dPsniff/dT, maximum rate of
pressure development (MRPD) positive peak dPsniff/dT normalized by Psniff, maximum relaxation rate (MRR). C:
Psniff plotted on semilog scale vs. time (ms). Linear black portion indicates a single exponential function with a time
constant, τ = 1/slope. Ms: milliseconds; cmH2O: centimeters of water.
Functionality and stage of the disease
Functionality was measured using the ALSFRS-R (maximum 48 points), validated for the
Brazilian population (5), as well as its respiratory subscore (R-subscore) alone (36) (maximum

79
12 points). In addition, the stage of the disease was determined according to disease
progression proposed by Roche et al (37).
4.3.4. Statistical analysis
To statistical analysis, data from ALS subjects were divided into three subgroups,
defined by the degree of decline of the 1) respiratory function (2, 38, 39) (≤70 and >70 of
FVC%pred), 2) ALSFRS-R total score (≤30 and >30 points) and 3) R-subscore (≤9 and >9 points)
(40, 41).
Data are expressed as median [25-75th percentile] unless otherwise stated. Normality
and distribution of data were performed using Shapiro-Wilk test. Data between ALS and healthy
subjects (intergroup analysis) were studied using the Unpaired t-test or Mann-Whitney test for
parametric and non-parametric data, respectively. One-way ANOVA or Kruskal-Wallis test was
applied to compare subgroup with control group data and, in the event of statistical significance;
Bonferroni’s or Dunn’s post hoc test was applied, respectively, to identify differences between
groups.
To avoid type II error, the power of the study was calculated as well as effect sizes for all
data. For parametric data, effect sizes were calculated using Cohen’s d for intergroup analysis
and Cohen’s f for subgroup analysis (42). For non-parametric data, Cohen’s d was calculated
for intergroup analysis according to Fritz et al (43) and ɛ2 for subgroup analysis according to
Tomczak & Tomczak (44) (see supplementary material).
Receiver operating characteristic (ROC) curves were calculated for SNIP parameters
between middle stage ALS and healthy subjects, as well as between subgroups. The area
under the curve (AUC) and its 95% confidence interval were calculated. Optimal cutoff point and
its 95% confidence interval were also calculated for each parameter according to the Youden
index (45).
Inferential data analysis was performed using GraphPad Prism® software version 6.01.
The power of the study and effect sizes were analyzed using G*Power software, version 3.1.9.2
(Kiel, Germany), and ROC curves were analyzed using MedCalc (Ostend, Belgium) version
14.8.1. For all statistical analysis, a p-value of <0.05 (2-sided) was considered as statistically
significant.
4.3.5. Results
Data related to diagnosis criteria, region of onset, clinical phenotype as well as the
presence of familial ALS and cognitive impairment of all ALS included in the study are shown in
supplementary table S1. Anthropometric, spirometric, respiratory muscle strength and
functionality data are shown in Table 1. ALS subjects were characterized by significant lower
spirometric and respiratory muscle strength values. All ALS subjects were classified as middle
stage. The mean ALSFRS-R score was 32.5±8.8 (67.7±18.3%) and the mean R-subscore was
10±2 (83.3±16.6) (see supplementary table S2).
All parameters extracted from the sniff curve were significantly different between ALS
and healthy subjects. A significantly lower MRR (p<0.0001, Cohen’s d=0.44) and MRPD

80
(p<0.0001, Cohen’s d=0.71) were found in ALS subjects, as well as a higher contraction time
(p<0.0001, Cohen’s d=1.21), ½RT (p<0.001, Cohen’s d=0.42) and τ (p<0.0001, Cohen’s
d=0.64) (Figure 2).
A post hoc analysis considering a p-value of <0.01 and the calculated effect size for τ
between ALS and healthy subjects (Cohen’s d=0.64) showed a statistical power (1-ß)=0.99 for
this study.
Figure 2. Data are shown as median [25-75th
percentile]. Comparisons between the parameters obtained from the
SNIP curve (maximum relaxation rate [MRR], maximum rate of pressure development [MRPD], contraction time, half
relaxation time [½RT] and tau [τ]) and percentage of predicted of the sniff nasal inspiratory pressure test (SNIP%pred)
between ALS and healthy subjects. Ms: milliseconds; cmH2O: centimeters of water; +: mean for parametric analysis.

81
Table 1. Characteristics of the subjects in relation to
anthropometric data, absolute and predicted values of lung
function, respiratory muscle strength and functional
capacity.
Healthy ALS p
Subjects (n) 39 39 -
Age (years) 47.9±11.1 52.9±12.5 .111
Height (ms) 1.63±0.1 1.65 ±0.1 .500
Weight (kg) 69.6 ±11 65 ±13 .100
BMI (kg/m2
) 26.2±5.6 23.9±5.7 .07
FVC (L) 3.79±0.8 2.49±1.06 <.0001
FVC %pred 98.8±10.7 63.1±23.1 <.0001
FEV1 (L) 3.10±0.68 1.87±0.83 <.0001
FEV1 %pred 98.8±10.4 58.5±21.9 <.0001
FVC/FEV1 0.81±0.04 0.76±0.12 .008
FVC/FEV1 %pred 100.1±4.4 94.3±15.6 .02
FEF25-75% 3.29±0.87 1.86±1.05 <.0001
PEF (L/s) 6.41±1.91 3.32±2.19 <.0001
SNIP (cmH2O) 103.3±29.4 48.36±27.04 <.0001
SNIP %pred 100.4±24 47.2±24.7 <.0001
MIP (cmH2O) 105±27.45 48.1±22.50 <.0001
MIP %pred 103.3±20.9 48.4±22.7 <.0001
MEP (cmH2O) 125.4±36.46 58.46±31.92 <.0001
MEP %pred 121.8±31.9 56.6±32.1 <.0001
ALSFRS-R - 32.5±8.8 -
Respiratory subscore - 10±2 -
Data presented as mean ± standard deviation. FVC: Forced Vital Capacity;
FEV1: Forced expiratory volume in the 1st second; FEV1/FVC: Ratio of
forced expiratory volume in the first second to forced vital capacity; FEF25-
75%: Forced expiratory flow at 25-75%; PEF: Peak expiratory flow; MIP:
Maximum inspiratory pressure; MEP: Maximum expiratory pressure; SNIP:
Sniff nasal inspiratory pressure; ALSFRS-R: Amyotrophic Lateral Sclerosis
functional rating scale-revised; m: meters; kg: kilograms; L: Liters; %pred:
Percentage of predicted; L/s: Liters per second; cmH2O: centimeters of
water.
ALSFRS-R, R-subscore, and FVC%pred subgroups
As shown in Table 2, all subgroups of ALS subjects presented a lower FVC%pred,
SNIP%pred, MRR, MRPD and higher CT, ½RT, and τ when compared with healthy subjects.
However, subjects with functional capacity ≤30 (13 subjects) exhibited significantly lower values
of FVC%pred when compared to ALS subjects with >30 points; and those with ≤9 (14 subjects)

82
presented a significantly lower FVC%pred as well as higher ½RT and τ values when compared to
those with >9 points. On the other hand, when ALS subjects were classified according to
FVC%pred, those with <70% exhibited significantly higher τ and lower SNIP%pred values when
compared to ALS with values >70%.
ROC analysis
Since SNIP%pred is one of the respiratory prognostic markers mostly considered in ALS
(38, 46), this parameter was also included in the ROC analysis. As shown in Table 3, all sniff
parameters were significantly able to discriminate between ALS and healthy. Of these, MRPD
was the parameter with the highest AUC. When dividing the ALS subjects between those with
ALSFRS-R score ≤30 and >30, only the MRPD and FVC%pred were statistically significant (Table
4). However, taking into account the subdivision between those ALS with R-subscore ≤9 and >9
points, MRPD, ½RT, τ and FVC%pred showed to be statistically significant (Table 5). On the other
hand, MRPD, τ and SNIP%pred parameters were statistically significant when subjects were
classified according to FVC%pred classification (Table 6 and Figure 3).
Figure 3. Receiver operating characteristic curves of the SNIP parameters that showed to be statistically significant
in middle ALS subjects according to a decline in the percentage of predicted forced vital capacity and in the ALSFRS-
R score and R-subscore.

83
Table 2. Relaxation rates and contraction properties of the diaphragm extracted from the SNIP curve of healthy and amyotrophic lateral sclerosis subgroup subjects
Values are shown as median [25th
-75th
percentile]. ALSFRS-R: Amyotrophic Lateral Sclerosis functional rating scale-revised; MRR: Maximum relaxation rate: MRPD: maximum rate of pressure development; τ: tau; ½RT: half-relaxation time; CT: Contraction time; SNIP: Sniff nasal inspiratory pressure; FVC: Forced vital capacity; ES: Effect-size; %pred: Percentage of predicted; n: number;
sec: Seconds; cmH2O: centimeter of water; ms: milliseconds; *<0.001 compared with healthy; †<0.001 compared with >30; †† <0.001 compared with >9; †††<0.001 compared with >70%; a: epsilon squared; b: Cohen’s f;
§Parametric data distribution.
Healthy Amyotrophic Lateral Sclerosis
ALSFRS-R Respiratory subscore Forced Vital Capacity(%pred)
>30 points ≤30 points ES >9 points ≤9 points ES >70% ≤70% ES
Subjects (n) 39 26 13 - 25 14 - 15 24 -
MRR (ms-1
) 0.078 [0.075 ‒ 0.085] 0.069 [0.061 ‒ 0.074]* 0.064 [0.042 ‒ 0.083]* 0.19a 0.071 [0.063 ‒ 0.079]* 0.063 [0.047 ‒ 0.079]* 0.21a 0.071 [0.060 ‒ 0.079]* 0.066 [0.060 ‒ 0.080]* 0.19a
MRPD (cmH2O·ms-1
) -0.620 [-0.821 ‒ -0.540] -0.348 [-0.470 ‒ -0.272]* -0.250 [-0.318 ‒ -0.196]* 0.55a -0.357 [-0.480 ‒ -0.265]* -0.250 [-0.344 ‒ -0.187]* 0.55a -0.460 [-0.535 ‒ -0.280]* -0.255 [-0.357 ‒ -0.196]* 0.59a
τ (ms) 50.4 [42.3 ‒ 58.8]
78.6 [57 ‒ 121.1]* 127.7 [76.5 ‒ 157.5]* 0.44a 69.6 [56 ‒ 102.5]* 128.4 [101 ‒ 177]*†† 0.50a 65.4 [55.8 ‒ 85.9]* 111 [83.7 ‒ 158]*††† 0.84b
½ RT (ms)§ 142 [116 ‒ 162]
174 [135 ‒ 206]* 174 [151 ‒ 204]* 0.42b 160 [131 ‒ 194]* 191 [169 ‒ 267]*†† 0.57b 168 [132 ‒ 190]* 181 [158 ‒ 207]* 0.46b
CT (ms) 188 [176 ‒ 214] 229 [197 ‒ 274]* 268 [230 ‒ 281]* 0.28a 220 [197 ‒ 277]* 266 [244 ‒ 278]* 0.30a 254 [210 ‒ 282]* 241 [201 ‒ 276]* 0.56b
SNIP (%pred)§ 94.4 [83.5 ‒ 119]
47.4 [24.8 ‒ 75.2]* 39.2 [26.2 ‒ 51.1]* 1.98b 46.7 [24.4 ‒ 76.7]* 40.9 [25.9 ‒ 56.8]* 1.13b 61 [38.3 ‒ 81.5]* 38 [23.5 ‒ 46.6]*††† 1.17b
FVC (%pred)§ 97.5 [91.5 ‒ 107.5] 68.3 [54.3 ‒ 82.4]* 41.7 [32 ‒ 64.9]*† 0.97b 70.6 [51.3 ‒ 82.8]* 54.7 [32.2 ‒ 65.3]*†† 1.01b ‒ ‒ ‒

84
Table 3. Receiver operating characteristic analysis between healthy and amyotrophic lateral sclerosis subjects
Healthy and Amyotrophic Lateral Sclerosis
AUC (95% CI) Optimal Cutoff (95%
CI) Sensitivity
(%) Specificity
(%) p
MRR (ms-1
) 0.755 (0.645 to 0.845) 0.073 (0.068 to 0.073) 66.67 89.74 <0.0001
MRPD (cmH2O ·ms-1
) 0.916 (0.830 to 0.967) -0.420 (-0.540 to -0.398.5) 74.36 97.44 <0.0001
τ (ms) 0.874 (0.779 to 0.938) 66 (53.7 to 79.8) 74.36 89.74 <0.0001
½ RT (ms) 0.743 (0.631 to 0.835) 154 (120.9 to 164) 71.79 71.79 <0.0001
CT (ms) 0.795 (0.688 to 0.878) 215 (202 to 262) 69.23 82.05 <0.0001
SNIP (%pred) 0.936 (0.856 to 0.979) 81.5 (73.7 to 81.5) 92.31 84.62 <0.0001
FVC (%pred) 0.911 (0.825 to 0.964) 81.1 (67.9 to 83.7) 79.49 97.44 <0.0001
AUC: Area under curve; CI: Confidence interval; MRR: Maximum relaxation rate: MRPD: maximum rate of pressure development; τ: tau;
½RT: half-relaxation time; CT: Contraction time; SNIP: Sniff nasal inspiratory pressure; FVC: Forced vital capacity; %pred: Percentage of
predicted; sec: Seconds; cmH2O: centimeter of water; ms: milliseconds.
Table 4. Receiver operating characteristic analysis between amyotrophic lateral sclerosis subjects classified
according to a decrease in the ALSFRS-R scale score.
AUC: Area under curve; CI: Confidence interval; MRR: Maximum relaxation rate: MRPD: maximum rate of pressure development; τ:
tau; ½RT: half-relaxation time; CT: Contraction time; SNIP: Sniff nasal inspiratory pressure; FVC: Forced vital capacity; %pred:
Percentage of predicted; sec: Seconds; cmH2O: centimeter of water; ms: milliseconds.
Amyotrophic Lateral Sclerosis – ALSFRS-R
AUC (95% CI) Optimal Cutoff (95% CI) Sensitivity
(%) Specificity
(%) p
MRR (ms-1
) 0.533 (0.366 to 0.694) 0.053 (0.031 to 0.073) 30.77 100 0.779
MRPD (cmH2O ·ms-1
) 0.735 (0.570 to 0.863) -0.300 (-0.535 to -0.232) 76.92 73.98 <0.001
τ (ms) 0.655 (0.486 to 0.800) 89.08 (48.5 to 147.6) 69.23 61.24 0.094
½ RT (ms) 0.506 (0.341 to 0.669) 160 (106 to 206) 76.92 42.31 0.853
CT (ms) 0.648 (0.479 to 0.794) 250 (198 to 282) 76.92 65.38 0.118
SNIP (%pred) 0.618 (0.449 to 0.769) 46.33 (17.4 to 67.0) 76.92 53.85 0.194
FVC (%pred) 0.749 (0.584 to 0.873) 41.7 (35.3 to 106.3) 53.85 92.31 0.009

85
Table 5. Receiver operating characteristic analysis between amyotrophic lateral sclerosis subjects classified according
to a decrease in the respiratory subscore of the ALSFRS-R scale.
Amyotrophic Lateral Sclerosis – Respiratory subscore
AUC (95% CI) Optimal Cutoff (95% CI) Sensitivity
(%) Specificity
(%) p
MRR (ms-1
) 0.654 (0.485 to 0.799) 0.064 (0.053 to 0.086) 64.29 72 0.130
MRPD (cmH2O ·ms-1
) 0.721 (0.555 to 0.853) -0.300 (-0.500 to -0.288) 71.43 72 0.01
τ (ms) 0.824 (0.669 to 0.927) 89.1 (70.1 to 168) 85.71 72 <0.0001
½ RT (ms) 0.720 (0.553 to 0.852) 160 (158 to 256) 92.86 52 0.01
CT (ms) 0.657 (0.488 to 0.801) 232 (199 to 280) 78.57 64 0.08
SNIP (%pred) 0.614 (0.445 to 0.765) 67 (60 to 67) 100 32 0.216
FVC (%pred) 0.700 (0.532 to 0.836) 67.5 (63.7 to 106) 85.71 52 0.03
AUC: Area under curve; CI: Confidence interval; MRR: Maximum relaxation rate: MRPD: maximum rate of pressure development; τ: tau; ½RT:
half-relaxation time; CT: Contraction time; SNIP: Sniff nasal inspiratory pressure; FVC: Forced vital capacity; %pred: Percentage of predicted;
sec: Seconds; cmH2O: centimeter of water; ms: milliseconds.
Table 6. Receiver operating characteristic analysis between amyotrophic lateral sclerosis subjects classified
according to a decrease in forced vital capacity.
Amyotrophic Lateral Sclerosis – Forced Vital Capacity%pred
AUC (95% CI) Optimal Cutoff (95% CI) Sensitivity (%) Specificity (%) p
MRR (ms-1
) 0.572 (0.485 to 0.799) 0.086 (0.053 to 0.086) 95.83 26.67 0.467
MRPD (cmH2O ·ms-1
) 0.781 (0.555 to 0.853) -0.460 (-0.500 to -0.288) 95.83 53.33 <0.001
τ (ms) 0.794 (0.669 to 0.927) 73.1 (70.1 to 168) 79.17 73.33 0.0001
½ RT (ms) 0.632 (0.553 to 0.852) 174 (158 to 256) 62.50 73.33 0.162
CT (ms) 0.536 (0.488 to 0.801) 304 (199 to 280) 100 13.33 0.713
SNIP (%pred) 0.769 (0.445 to 0.765) 46.7 (60 to 67) 79.17 73.33 0.002
AUC: Area under curve; CI: Confidence interval; MRR: Maximum relaxation rate: MRPD: maximum rate of pressure development; τ: tau;
½RT: half-relaxation time; CT: Contraction time; SNIP: Sniff nasal inspiratory pressure; %pred: Percentage of predicted; sec: Seconds;
cmH2O: centimeter of water; ms: milliseconds.

86
4.3.6. Discussion
The main findings of this study are that 1) the sniff test provides parameters, apart from
its peak pressure, able to discriminate between healthy and middle stage ALS subjects, and
that 2) some of these parameters, namely τ, MRPD, and ½RT, are more sensitive in detecting
impaired inspiratory muscle function in ALS than the peak pressure itself.
According to Kyroussis et al (22), measurements of relaxation rates obtained from nasal
sniffs accurately reflects those from esophageal pressure curves and can be used as an index
of the onset and recovery of respiratory muscle fatigue. Moreover, measurements of nasal sniffs
are simple, tolerated, and minimally invasive and can provide a quantitative response index to
fatigue and therapeutic interventions in neuromuscular disease patients (47, 48). In our study all
parameters derived from the SNIP curve were significantly different between middle stage ALS
and healthy subjects, being in agreement with two previous studies performed in subjects with
neuromuscular disorders (47, 49). Evangelista et al (49), observed that a reduced MRR was
reliable in identifying the delayed relaxation of the respiratory muscles in myotonic dystrophy
type 1 patients when compared to healthy controls; while Garcia-Rio et al (47), despite
heterogeneity of the study population, found that the decreased MRR of neuromuscular disease
patients was accompanied by the deterioration in the functional reserve of the diaphragm as
well as of the inspiratory muscles.
The rationale for measuring relaxation rates from pressure curves is based on the
assumption that the decay portion of the curve, when expiration is totally passive, corresponds
to the relaxation phase of inspiratory muscle contraction (18). The decrease in MRR and
increase in τ are adaptive mechanisms and had been shown to be an early sign of the onset of
fatigue (17, 50). The alterations of these parameters occur before the decrease in peak
diaphragmatic pressure (17, 31, 47). When respiratory muscles do develop fatigue the peak
pressure decreases linearly with the slowing of the MRR and exponentially with the increase of
τ due to common or concomitant metabolic changes of the muscle fiber (17, 34, 51). In addition,
the loss of muscular force during fatigue makes the muscle contractile speed to decrease
resulting in an increase in contraction time and prolongation of relaxation time as an adaptive
mechanism (52, 53) which is also related to intracellular and metabolic factors (i.e. the decline
of the calcium uptake from the sarcoplasmic reticulum, depletion of ATP and intracellular
acidosis) (48, 54).
To our knowledge, apart from various studies about the relaxation rate in healthy adults
(21, 23, 33) and different diseases (COPD (51), cystic fibrosis (55, 56) and intubated patients
weaning from mechanical ventilation (31)), the literature is scarce about the measurements of
MRPD, τ, CT and ½RT in neuromuscular disease patients precluding the possibility of
comparing our data to data derived from a similar population. Our results showed a decreased
MRPD in middle stage ALS when compared to healthy subjects and, as it is derived from the
initial incline of the SNIP curve and reflects respiratory muscle function (11) as well as
respiratory motor output (19), we believe that this parameter is linked to the decreased capacity
of the diaphragm to generate force and expand the lungs (39). Furthermore, as the already
weakened respiratory muscles of patients with ALS are easily fatigable (14) the results found

87
about the contractile properties (CT and MRPD) and dynamics of relaxation (MRR, τ and ½RT)
of the diaphragm (11, 16) indicates a high respiratory muscle load and reinforces the hypothesis
that the middle stage ALS subjects were presumably at risk of developing respiratory muscle
fatigue (14, 18, 21, 33, 56).
The ALSFRS-R is a simple and reliable scale that predicts survival and can be used as
the only functional outcome measure in early phase trials (40), while its R-subscore was
designed to assess indirectly the respiratory function (36) being also sensitive in detecting early
respiratory symptoms of ventilatory insufficiency (57-59). Castrillo-Viguera et al (41) suggested
that a percentage change of at least 20 to 25% in the slope of decline of the ALSFRS-R scale
would represent a clinically meaningful effect. Because of this, we chose to subdivide the ALS
subjects into those with ALSFRS-R of ≤30 and >30 points (decline of 15 points – 37.5%) and
with the R-subscore of ≤9 and >9 points (decline of 3 points – 25%). Moreover, as changes in
FVC%pred over time strongly predicts respiratory muscle weakness, ventilatory failure and death
in ALS (2, 38, 39), subjects were also subdivided into ≤70 and >70% FVC%pred subgroups.
The value of the FVC%pred was the only parameter that differed between middle stage
ALS subjects of both ALSFRS-R and R-subscore subgroups, possibly because the decrease of
this parameter is not related only to respiratory musculature function (36, 60). On the other
hand, when subdividing according to the R-subscore, ½RT and τ values were significantly
different between middle stage ALS subjects which demonstrate that these diaphragmatic
properties (32, 61) are probably related to the respiratory function assessed by this subdomain.
Presumably the most interesting fact is that SNIP%pred, a parameter that reflects the
diaphragmatic strength and predicts survival in ALS (62), only differ between those middle stage
ALS subjects classified according to the decline in FVC%pred. Although data were collected in a
single point of the disease stage, it is known that the peak pressure of sniff test declines less
when compared to the decline in ALSFRS-R (8) leading us to consider that SNIP%pred is not a
parameter that is sensitive to small changes in the ALSFRS-R and R-subscore. Regarding
MRPD and τ, the results were not surprising since the first is related to respiratory muscle
function (11) as well as related to neural adaptations (19, 20, 63) and the second increases well
before diaphragmatic pressure is reduced during respiratory muscle weakness or fatigue (17,
34).
The results of the ROC curves show that all parameters extracted from the sniff curve
can highly discriminate middle stage ALS from healthy subjects. When taking into account the
functional decline of ALS subjects, only MRPD and FVC%pred could predict a fall in 37.5% of the
ALSFRS-R score. Among all parameters, τ provides the highest discriminative power in
predicting a decline of 25% in the R-subscore. This power was even higher than FVC%pred,
possibly because the R-subscore is less sensitive in predicting a fall in FVC%pred (57). Moreover,
as ALS patients with R-subscore <11 points are considered with relevant symptoms of
respiratory distress as well as at risk of respiratory insufficiency (57, 58) and peak pressure of
sniff test could not detect a fall in the ALSFRS-R and R-subscore, we believe that the SNIP%pred
might not be a parameter as reliable as some parameters extracted from the SNIP curve (i.e. τ,
MRPD, and ½RT) or FVC%pred in detecting a clinically meaningful decline in functional and

88
respiratory status. The SNIP%pred was reliable in detecting respiratory muscle weakness (39, 60)
in our middle stage ALS subjects only when considering the FVC%pred classification,
nevertheless, MRPD and τ parameters were still more sensitive than SNIP%pred.
It is unlikely that the results found are investigator related since all measurements were
performed by the same experienced respiratory physiotherapist. We believe that four are the
main limitations of the study. First, even with a calculated statistical power of 1-ß=0.99, our ALS
cohort may be limited in terms of sample size; second, the mean age of ALS included is lower
than those of the main epidemiological studies (64, 65); third, we included only ALS patients at
middle stage of the disease and fourth, not all subjects could be paired by the same exact age
and BMI. Further studies including patients at later stages of the disease as well as possible
ALS and patients with other motor neuron disorders are needed. Finally, ongoing longitudinal
studies should are already investigating these parameters during varying levels of disease
progression as well as in order to identify differences between patients with and without non-
invasive ventilation as well as the optimal parameter and its cutoff point able to predict an
appropriate timing for the initiation of non-invasive ventilation.
In terms of clinical applicability, the calculation of the SNIP curve parameters can be
easily performed and give more information about the state of the respiratory muscles, thus
possibly allowing an early detection of weakness or fatigue before respiratory failure is reached
(35, 53) as well as early implementation of new therapeutic interventions before the beginning
of the peak pressure decay of the SNIP curve (17, 31, 51).
4.3.7. Conclusion
The contractile properties and relaxation rates of the diaphragm are altered in middle
stage spinal onset ALS when compared with healthy subjects. When assessed through the
nasal inspiratory sniff test, these parameters are able to discriminate between those ALS
subjects with early decline in inspiratory muscle function and those who not. In addition, despite
the limitations of our cohort and especially the lack of longitudinal data, we suggest that τ,
MRPD, and ½RT parameters may be able to predict ALS patients at risk of ventilatory failure
before the beginning of the fall in peak pressure of sniff test.

89
4.4.8. References
1. Haverkamp LJ, Appel V, Appel SH. Natural history of amyotrophic lateral sclerosis in a
database population. Validation of a scoring system and a model for survival prediction. Brain :
a journal of neurology (1995) 118 ( Pt 3):707-19. PubMed PMID: 7600088.
2. Czaplinski A, Yen AA, Simpson EP, Appel SH. Predictability of disease progression in
amyotrophic lateral sclerosis. Muscle & nerve (2006) 34(6):702-8. doi: 10.1002/mus.20658.
PubMed PMID: 16967489.
3. de Carvalho M, Matias T, Coelho F, Evangelista T, Pinto A, Luis ML. Motor neuron
disease presenting with respiratory failure. Journal of the neurological sciences (1996) 139
Suppl:117-22. PubMed PMID: 8899670.
4. Chen R, Grand'Maison F, Strong MJ, Ramsay DA, Bolton CF. Motor neuron disease
presenting as acute respiratory failure: a clinical and pathological study. Journal of neurology,
neurosurgery, and psychiatry (1996) 60(4):455-8. PubMed PMID: 8774419; PubMed Central
PMCID: PMC1073907.
5. Guedes K, Pereira C, Pavan K, Valerio BC. Cross-cultural adaptation and validation of
als Functional Rating Scale-Revised in Portuguese language. Arq Neuropsiquiatr (2010)
68(1):44-7. PubMed PMID: 20339651.
6. Kaufmann P, Levy G, Thompson JL, Delbene ML, Battista V, Gordon PH, et al. The
ALSFRSr predicts survival time in an ALS clinic population. Neurology (2005) 64(1):38-43. doi:
10.1212/01.WNL.0000148648.38313.64. PubMed PMID: 15642901.
7. Kollewe K, Mauss U, Krampfl K, Petri S, Dengler R, Mohammadi B. ALSFRS-R score
and its ratio: a useful predictor for ALS-progression. Journal of the neurological sciences (2008)
275(1-2):69-73. doi: 10.1016/j.jns.2008.07.016. PubMed PMID: 18721928.
8. Bauer M, Czell D, Hartmann S, Goldman B, Muller D, Weber M. Limitations of sniff
nasal pressure as an outcome measurement in amyotrophic lateral sclerosis patients in a
clinical trial. Respiration; international review of thoracic diseases (2012) 84(4):306-11. Epub
2012/08/01. doi: 10.1159/000339415. PubMed PMID: 22846608.
9. Magnus T, Beck M, Giess R, Puls I, Naumann M, Toyka KV. Disease progression in
amyotrophic lateral sclerosis: predictors of survival. Muscle & nerve (2002) 25(5):709-14. doi:
10.1002/mus.10090. PubMed PMID: 11994965.
10. Polkey MI, Lyall RA, Yang K, Johnson E, Leigh PN, Moxham J. Respiratory Muscle
Strength as a Predictive Biomarker for Survival in Amyotrophic Lateral Sclerosis. American
journal of respiratory and critical care medicine (2017) 195(1):86-95. Epub 2016/08/06. doi:
10.1164/rccm.201604-0848OC. PubMed PMID: 27494149; PubMed Central PMCID:
PMCPmc5214920.
11. American Thoracic Society/European Respiratory S. ATS/ERS Statement on respiratory
muscle testing. American journal of respiratory and critical care medicine (2002) 166(4):518-
624. doi: 10.1164/rccm.166.4.518. PubMed PMID: 12186831.
12. Miller JM, Moxham J, Green M. The maximal sniff in the assessment of diaphragm
function in man. Clinical science (1985) 69(1):91-6. PubMed PMID: 4064560.

90
13. Laroche CM, Mier AK, Moxham J, Green M. The value of sniff esophageal pressures in
the assessment of global inspiratory muscle strength. The American review of respiratory
disease (1988) 138(3):598-603. doi: 10.1164/ajrccm/138.3.598. PubMed PMID: 3202414.
14. Schiffman PL, Belsh JM. Effect of inspiratory resistance and theophylline on respiratory
muscle strength in patients with amyotrophic lateral sclerosis. The American review of
respiratory disease (1989) 139(6):1418-23. doi: 10.1164/ajrccm/139.6.1418. PubMed PMID:
2729751.
15. Troyer AD, Estenne M. The respiratory system in neuromuscular disorders. in Roussos
CH (ed): The Thorax. New York, Marcel Dekker (1995).
16. Koulouris N, Vianna LG, Mulvey DA, Green M, Moxham J. Maximal relaxation rates of
esophageal, nose, and mouth pressures during a sniff reflect inspiratory muscle fatigue. The
American review of respiratory disease (1989) 139(5):1213-7. doi: 10.1164/ajrccm/139.5.1213.
PubMed PMID: 2712448.
17. Esau SA, Bellemare F, Grassino A, Permutt S, Roussos C, Pardy RL. Changes in
relaxation rate with diaphragmatic fatigue in humans. Journal of applied physiology: respiratory,
environmental and exercise physiology (1983) 54(5):1353-60. doi:
10.1152/jappl.1983.54.5.1353. PubMed PMID: 6863095.
18. Mador MJ, Kufel TJ. Effect of inspiratory muscle fatigue on inspiratory muscle relaxation
rates in healthy subjects. Chest (1992) 102(6):1767-73. PubMed PMID: 1446487.
19. Matthews AW, Howell JB. The rate of isometric inspiratory pressure development as a
measure of responsiveness to carbon dioxide in man. Clinical science and molecular medicine
(1975) 49(1):57-68. PubMed PMID: 1149395.
20. Tzelepis GE, Kasas V, McCool FD. Inspiratory muscle adaptations following pressure or
flow training in humans. European journal of applied physiology and occupational physiology
(1999) 79(6):467-71. PubMed PMID: 10344453.
21. Romer LM, McConnell AK. Inter-test reliability for non-invasive measures of respiratory
muscle function in healthy humans. European journal of applied physiology (2004) 91(2-3):167-
76. doi: 10.1007/s00421-003-0984-2. PubMed PMID: 14605897.
22. Kyroussis D, Mills G, Hamnegard CH, Wragg S, Road J, Green M, et al. Inspiratory
muscle relaxation rate assessed from sniff nasal pressure. Thorax (1994) 49(11):1127-33.
PubMed PMID: 7831629; PubMed Central PMCID: PMC475274.
23. Levy RD, Esau SA, Bye PT, Pardy RL. Relaxation rate of mouth pressure with sniffs at
rest and with inspiratory muscle fatigue. The American review of respiratory disease (1984)
130(1):38-41. doi: 10.1164/arrd.1984.130.1.38. PubMed PMID: 6742608.
24. Benicio K, Dias FA, Gualdi LP, Aliverti A, Resqueti VR, Fregonezi GA. Effects of
diaphragmatic control on the assessment of sniff nasal inspiratory pressure and maximum
relaxation rate. Brazilian journal of physical therapy (2016) 20(1):96-103. doi: 10.1590/bjpt-
rbf.2014.0101. PubMed PMID: 26578254; PubMed Central PMCID: PMC4835170.
25. Brooks BR, Miller RG, Swash M, Munsat TL, World Federation of Neurology Research
Group on Motor Neuron D. El Escorial revisited: revised criteria for the diagnosis of
amyotrophic lateral sclerosis. Amyotrophic lateral sclerosis and other motor neuron disorders :

91
official publication of the World Federation of Neurology, Research Group on Motor Neuron
Diseases (2000) 1(5):293-9. PubMed PMID: 11464847.
26. Pereira CAC, Neder, J.A. Sociedade Brasileira de Pneumologia e Tisiologia – SBPT.
Diretrizes para testes de função pulmonar. J Bras Pneumol (2002) 29 (3):207-21.
27. Heritier F, Rahm F, Pasche P, Fitting JW. Sniff nasal inspiratory pressure. A
noninvasive assessment of inspiratory muscle strength. American journal of respiratory and
critical care medicine (1994) 150(6 Pt 1):1678-83. doi: 10.1164/ajrccm.150.6.7952632. PubMed
PMID: 7952632.
28. Neder JA, Andreoni S, Lerario MC, Nery LE. Reference values for lung function tests: II.
Maximal respiratory pressures and voluntary ventilation. Brazilian Journal of Medical and
Biological Research (1999) 32:719-27.
29. Araujo PR, Resqueti VR, Nascimento Junior J, Carvalho Lde A, Cavalcanti AG, Silva
VC, et al. Reference values for sniff nasal inspiratory pressure in healthy subjects in Brazil: a
multicenter study. Jornal brasileiro de pneumologia : publicacao oficial da Sociedade Brasileira
de Pneumologia e Tisilogia (2012) 38(6):700-7. PubMed PMID: 23288114.
30. Smith J, Bellemare F. Effect of lung volume on in vivo contraction characteristics of
human diaphragm. Journal of applied physiology (1987) 62(5):1893-900. doi:
10.1152/jappl.1987.62.5.1893. PubMed PMID: 3597263.
31. Goldstone JC, Green M, Moxham J. Maximum relaxation rate of the diaphragm during
weaning from mechanical ventilation. Thorax (1994) 49(1):54-60. PubMed PMID: 8153941;
PubMed Central PMCID: PMC474088.
32. Bellemare F, Bigland-Ritchie B, Woods JJ. Contractile properties of the human
diaphragm in vivo. Journal of applied physiology (1986) 61(3):1153-61. doi:
10.1152/jappl.1986.61.3.1153. PubMed PMID: 3759756.
33. Romer LM, McConnell AK. Specificity and reversibility of inspiratory muscle training.
Medicine and science in sports and exercise (2003) 35(2):237-44. doi:
10.1249/01.MSS.0000048642.58419.1E. PubMed PMID: 12569211.
34. Esau SA, Bye PT, Pardy RL. Changes in rate of relaxation of sniffs with diaphragmatic
fatigue in humans. Journal of applied physiology: respiratory, environmental and exercise
physiology (1983) 55(3):731-5. doi: 10.1152/jappl.1983.55.3.731. PubMed PMID: 6629910.
35. Wilcox PG, Eisen A, Wiggs BJ, Pardy RL. Diaphragmatic relaxation rate after voluntary
contractions and uni- and bilateral phrenic stimulation. Journal of applied physiology (1988)
65(2):675-82. doi: 10.1152/jappl.1988.65.2.675. PubMed PMID: 3170421.
36. Cedarbaum JM, Stambler N, Malta E, Fuller C, Hilt D, Thurmond B, et al. The ALSFRS-
R: a revised ALS functional rating scale that incorporates assessments of respiratory function.
Journal of the neurological sciences (1999) 169(1):13-21. doi: https://doi.org/10.1016/S0022-
510X(99)00210-5.
37. Roche JC, Rojas-Garcia R, Scott KM, Scotton W, Ellis CE, Burman R, et al. A proposed
staging system for amyotrophic lateral sclerosis. Brain : a journal of neurology (2012) 135(Pt
3):847-52. doi: 10.1093/brain/awr351. PubMed PMID: 22271664; PubMed Central PMCID:
PMC3286327.

92
38. Pinto S, Carvalho M. Breathing new life into treatment advances for respiratory failure in
amyotrophic lateral sclerosis patients. Neurodegenerative disease management (2014) 4(1):83-
102. Epub 2014/03/20. doi: 10.2217/nmt.13.74. PubMed PMID: 24640982.
39. Andrews JA, Meng L, Kulke SF, Rudnicki SA, Wolff AA, Bozik ME, et al. Association
Between Decline in Slow Vital Capacity and Respiratory Insufficiency, Use of Assisted
Ventilation, Tracheostomy, or Death in Patients With Amyotrophic Lateral Sclerosis. JAMA
neurology (2018) 75(1):58-64. Epub 2017/11/29. doi: 10.1001/jamaneurol.2017.3339. PubMed
PMID: 29181534.
40. Gordon PH, Cheng B, Montes J, Doorish C, Albert SM, Mitsumoto H. Outcome
measures for early phase clinical trials. Amyotrophic lateral sclerosis : official publication of the
World Federation of Neurology Research Group on Motor Neuron Diseases (2007) 8(5):270-3.
doi: 10.1080/17482960701547958. PubMed PMID: 17852017.
41. Castrillo-Viguera C, Grasso DL, Simpson E, Shefner J, Cudkowicz ME. Clinical
significance in the change of decline in ALSFRS-R. Amyotrophic lateral sclerosis : official
publication of the World Federation of Neurology Research Group on Motor Neuron Diseases
(2010) 11(1-2):178-80. doi: 10.3109/17482960903093710. PubMed PMID: 19634063.
42. Cohen J. Statistical power analysis for the behavioral sciences. 2ª ed Hillsdale, New
Jersey: Lawrence Erbaum (1988).
43. Fritz CO, Morris PE, Richler JJ. Effect size estimates: current use, calculations, and
interpretation. Journal of experimental psychology General (2012) 141(1):2-18. Epub
2011/08/10. doi: 10.1037/a0024338. PubMed PMID: 21823805.
44. Tomczak M, Tomczak E. The need to report effect size estimates revisited. An overview
of some recommended measures of effect size. Trends in Sport Sciences (2014) 1(21):19-25.
45. Youden WJ. Index for rating diagnostic tests. Cancer (1950) 3(1):32-5. PubMed PMID:
15405679.
46. Capozzo R, Quaranta VN, Pellegrini F, Fontana A, Copetti M, Carratu P, et al. Sniff
nasal inspiratory pressure as a prognostic factor of tracheostomy or death in amyotrophic
lateral sclerosis. Journal of neurology (2015) 262(3):593-603. Epub 2014/12/20. doi:
10.1007/s00415-014-7613-3. PubMed PMID: 25522696.
47. Garcia-Rio F, Mediano O, Pino JM, Lores V, Fernandez I, Alvarez-Sala JL, et al.
Noninvasive measurement of the maximum relaxation rate of inspiratory muscles in patients
with neuromuscular disorders. Respiration; international review of thoracic diseases (2006)
73(4):474-80. doi: 10.1159/000091804. PubMed PMID: 16508243.
48. Mulvey DA, Koulouris NG, Elliott MW, Moxham J, Green M. Maximal relaxation rate of
inspiratory muscle can be effort-dependent and reflect the activation of fast-twitch fibers. The
American review of respiratory disease (1991) 144(4):803-6. Epub 1991/10/01. doi:
10.1164/ajrccm/144.4.803. PubMed PMID: 1928952.
49. Evangelista MA, Dias FAL, Dourado Junior MET, do Nascimento GC, Sarmento A,
Gualdi LP, et al. Noninvasive assessment of respiratory muscle strength and activity in
Myotonic dystrophy. PloS one (2017) 12(6):e0177318. doi: 10.1371/journal.pone.0177318.
PubMed PMID: 28594857; PubMed Central PMCID: PMC5464542.

93
50. Coirault C, Chemla D, Lecarpentier Y. Relaxation of diaphragm muscle. Journal of
applied physiology (1999) 87(4):1243-52. doi: 10.1152/jappl.1999.87.4.1243. PubMed PMID:
10517748.
51. Polkey MI, Kyroussis D, Mills GH, Hamnegard CH, Keilty SE, Green M, et al. Inspiratory
pressure support reduces slowing of inspiratory muscle relaxation rate during exhaustive
treadmill walking in severe COPD. American journal of respiratory and critical care medicine
(1996) 154(4 Pt 1):1146-50. doi: 10.1164/ajrccm.154.4.8887619. PubMed PMID: 8887619.
52. Bigland-Ritchie B, Johansson R, Lippold OC, Woods JJ. Contractile speed and EMG
changes during fatigue of sustained maximal voluntary contractions. Journal of
neurophysiology (1983) 50(1):313-24. doi: 10.1152/jn.1983.50.1.313. PubMed PMID: 6308182.
53. Grassino A, Macklem PT. Respiratory muscle fatigue and ventilatory failure. Annual
review of medicine (1984) 35:625-47. doi: 10.1146/annurev.me.35.020184.003205. PubMed
PMID: 6372673.
54. Dawson MJ, Gadian DG, Wilkie DR. Mechanical relaxation rate and metabolism studied
in fatiguing muscle by phosphorus nuclear magnetic resonance. The Journal of physiology
(1980) 299:465-84. PubMed PMID: 6966688; PubMed Central PMCID: PMC1279237.
55. Dassios T, Kaditis A, Katelari A, Chrousos G, Doudounakis S, Dimitriou G. Time
constant of inspiratory muscle relaxation in cystic fibrosis. Pediatric research (2015) 77(4):541-
5. doi: 10.1038/pr.2015.2. PubMed PMID: 25642662.
56. Dassios TG, Doudounakis S, Dimitriou G. Maximum rate of pressure development and
maximal relaxation rate of respiratory muscles in patients with cystic fibrosis. Respiratory care
(2013) 58(3):474-81. doi: 10.4187/respcare.01930. PubMed PMID: 22781492.
57. Pinto S, Geraldes R, Vaz N, Pinto A, de Carvalho M. Changes of the phrenic nerve
motor response in amyotrophic lateral sclerosis: longitudinal study. Clinical neurophysiology :
official journal of the International Federation of Clinical Neurophysiology (2009) 120(12):2082-
5. doi: 10.1016/j.clinph.2009.08.025. PubMed PMID: 19833553.
58. Park JS, Park D. The terminal latency of the phrenic nerve correlates with respiratory
symptoms in amyotrophic lateral sclerosis. Clinical neurophysiology : official journal of the
International Federation of Clinical Neurophysiology (2017) 128(9):1625-8. doi:
10.1016/j.clinph.2017.06.039. PubMed PMID: 28719826.
59. Kwon S, Min JH, Cho HJ, Joo BE, Cho EB, Seok JM, et al. Usefulness of phrenic
latency and forced vital capacity in patients with ALS with latent respiratory dysfunction. Clinical
neurophysiology : official journal of the International Federation of Clinical Neurophysiology
(2015) 126(7):1421-6. doi: 10.1016/j.clinph.2014.10.006. PubMed PMID: 25454281.
60. Pinto S, de Carvalho M. Correlation between Forced Vital Capacity and Slow Vital
Capacity for the assessment of respiratory involvement in Amyotrophic Lateral Sclerosis: a
prospective study. Amyotrophic lateral sclerosis & frontotemporal degeneration (2017) 18(1-
2):86-91. Epub 2016/12/06. doi: 10.1080/21678421.2016.1249486. PubMed PMID: 27915482.
61. Rochester DF. The diaphragm: contractile properties and fatigue. The Journal of clinical
investigation (1985) 75(5):1397-402. doi: 10.1172/JCI111841. PubMed PMID: 3889054;
PubMed Central PMCID: PMC425476.

94
62. Morgan RK, McNally S, Alexander M, Conroy R, Hardiman O, Costello RW. Use of Sniff
nasal-inspiratory force to predict survival in amyotrophic lateral sclerosis. American journal of
respiratory and critical care medicine (2005) 171(3):269-74. Epub 2004/11/02. doi:
10.1164/rccm.200403-314OC. PubMed PMID: 15516537.
63. Behm DG, Sale DG. Intended rather than actual movement velocity determines velocity-
specific training response. Journal of applied physiology (1993) 74(1):359-68. Epub
1993/01/01. doi: 10.1152/jappl.1993.74.1.359. PubMed PMID: 8444715.
64. Chio A, Logroscino G, Traynor BJ, Collins J, Simeone JC, Goldstein LA, et al. Global
epidemiology of amyotrophic lateral sclerosis: a systematic review of the published literature.
Neuroepidemiology (2013) 41(2):118-30. doi: 10.1159/000351153. PubMed PMID: 23860588;
PubMed Central PMCID: PMC4049265.
65. Marin B, Boumediene F, Logroscino G, Couratier P, Babron MC, Leutenegger AL, et al.
Variation in worldwide incidence of amyotrophic lateral sclerosis: a meta-analysis. International
journal of epidemiology (2017) 46(1):57-74. doi: 10.1093/ije/dyw061. PubMed PMID:
27185810; PubMed Central PMCID: PMC5407171.

95
4.3.9. Supplementary material
Multiparametric analysis of sniff nasal inspiratory pressure test in middle stage amyotrophic lateral sclerosis
Antonio Sarmento, Guilherme Fregonezi, Layana Marques, Francesca Pennati, Mario Emílio Dourado-Júnior, Vanessa Resqueti, Andrea Aliverti

96
SUPPLEMENTARY MATERIAL IN DEPTH OF STATISTICAL ANALYSIS AND RESULTS
STATISTICAL ANALYSIS
For parametric data, effect sizes were calculated using Cohen’s d for intergroup
analysis and interpreted as small (<0.50), moderate (between 0.50 and 0.80), and large
(>0.80)] and Cohen’s f for subgroup analysis as small (<0.25), moderate (between 0.25 and
0.40), and large (>0.40)].(1) For non-parametric data, Cohen's d was calculated for intergroup
analysis and interpreted as small (<0.10), moderate (between 0.10 and 0.30), and large
(>0.50)(2) and ɛ2 for subgroup analysis as small (<0.06), moderate (between 0.06 and 0.14),
and large (>0.14)] (3, 4).

97
RESULTS
Supplementary table S1. Diagnosis criteria, region of onset, local of muscle weakness symptoms onset, clinical
phenotype as well as the presence of familial ALS and cognitive impairment of all ALS subjects included in the study. All
parameters shown were assessed by a neurologist.
Diagnosis Region of onset Distal or proximal Phenotype Familial
ALS Cognitive
impairment
#1 Definitive Left upper limb Distal Classic No No
#2 Probable Right upper limb Proximal Classic No No
#3 Definitive Right lower limb Proximal Classic No No
#4 Probable Right upper limb Distal Classic No No
#5 Probable Left lower limb Distal Primary lateral
sclerosis No No
#6 Definitive Left upper limb Proximal Classic No No
#7 Definitive Lower limbs Distal Flail legs No No
#8 Probable Right upper limb Distal Classic No No
#9 Definitive Right lower limb Proximal Classic No No
#10 Definitive Left lower limb Distal Classic No No
#11 Probable Lower limbs Proximal Flail legs No No
#12 Definitive Right upper limb Distal Classic No No
#13 Probable Lower limbs Distal Flail legs No No
#14 Definitive Right upper limb Distal Classic No No
#15 Definitive Right lower limb Distal Classic No No
#16 Probable Left lower limb Proximal Classic No No
#17 Probable Upper limbs Distal Primary lateral
sclerosis No No
#18 Definiive Left lower limb Distal Classic No No
#19 Probable Right lower limb Distal Classic No No
#20 Probable Lower limbs Distal Flail legs No No
#21 Definitive Right upper limb Distal Classic No No
#22 Definitive Right upper limb Distal Classic No No
#23 Definitive Right upper limb Distal Progressive
muscular atrophy No No
#24 Probable Right lower limb Distal Classic No No
#25 Definitive Left upper limb Distal Classic No No
#26 Probable Lower limbs Proximal Classis No No
#27 Probable Right lower limb Distal Polyneuritic pattern No No
#28 Probable Upper limbs Distal Classis No No
#29 Probable Right lower limb Distal Classic No No
#30 Definitive Right upper limb Distal Classic No No
#31 Probable Right lower limb Distal Classic No No
#32 Probable Right lower limb Distal Classic No No
#33 Probable Left upper limb Distal Primary lateral
sclerosis No No
#34 Probable Left upper limb Distal Classic No No
#35 Probable Lower limbs Distal Progressive
muscular atrophy No No
#36 Probable Right upper limb Distal Primary lateral
sclerosis No No
#37 Probable Right upper limb Distal Polyneuritic pattern No No
#38 Definitive Right upper limb Distal Progressive
muscular atrophy No No
#39 Probable Right upper limb Distal Progressive
muscular atrophy No No

98
Subjects Clinical
Stage
Amyotrophic Lateral Sclerosis Functional Rating Scale-revised
Speech Salivation Swallowing Handwriting Cutting
food
Dressing and
hygiene
Turning in bed
and adjusting
bed clothes
Walking Climbing
stairs Dyspnea
* Orthopnea
*
Respiratory
insufficiency*
#1 3 4 4 4 1 1 2 3 3 1 3 4 4
#2 3 4 2 4 3 3 3 3 3 1 3 3 4
#3 3 4 4 4 4 2 2 3 3 3 3 3 4
#4 3 4 4 4 4 1 3 2 2 1 3 3 4
#5 3 3 4 4 3 3 2 2 1 0 4 4 4
#6 3 4 1 2 4 0 1 3 4 4 1 3 4
#7 3 2 3 3 1 2 3 3 3 3 4 4 4
#8 3 2 4 2 0 0 0 0 1 0 2 3 4
#9 3 4 4 4 2 1 1 2 2 1 4 4 4
#10 3 2 4 3 0 0 0 2 1 0 3 4 4
#11 3 1 0 0 3 2 2 1 2 0 2 2 4
#12 3 3 2 2 0 0 0 0 0 0 2 3 4
#13 3 4 4 3 4 4 4 3 3 2 4 4 4
#14 3 4 4 4 4 4 4 4 4 4 3 3 4
#15 3 3 4 3 3 3 3 4 2 1 4 4 4
#16 3 3 3 3 3 1 2 1 1 0 2 2 2
#17 3 2 3 3 2 3 3 3 3 3 3 4 4
#18 3 1 3 2 0 0 0 0 0 0 2 2 4
#19 3 1 3 3 3 3 2 2 1 0 2 3 4
#20 3 4 4 4 2 2 0 0 0 4 4 4 4
#21 3 2 3 3 2 1 3 3 2 1 3 4 4
#22 3 3 3 4 3 3 2 3 4 4 3 2 4
#23 3 3 4 3 3 1 1 1 2 0 1 2 2
#24 3 1 0 0 3 2 2 1 2 0 2 2 4
#25 3 4 4 4 4 4 3 3 1 0 2 3 4
#26 3 3 3 3 4 4 4 4 4 3 3 4 4
#27 3 3 4 3 3 1 2 1 1 0 2 1 2
#28 3 4 4 3 2 0 0 2 3 0 1 2 4
#29 3 2 3 2 3 1 1 1 1 0 4 4 4
#30 3 3 2 2 3 3 3 2 2 1 2 3 4
#31 3 4 4 4 3 1 2 3 2 0 4 4 4
#32 3 4 4 4 4 4 3 4 3 2 4 4 4
#33 3 2 3 2 4 2 3 4 3 3 3 4 4
#34 3 4 4 4 3 3 2 2 0 0 4 4 4
#35 3 4 4 4 4 3 3 3 3 1 2 4 4
#36 3 3 3 3 4 3 4 4 4 3 3 3 4
#37 3 4 4 4 4 3 4 4 4 4 4 4 4
#38 3 3 2 3 3 4 4 3 4 3 4 4 4
#39 3 4 3 4 4 3 4 3 4 3 4 4 4
Supplementary table S2. Clinical stage and functional capacity of each amyotrophic lateral sclerosis subject of the study according to Roche et al (5) and Cerdabaum
et al (6), respectively. *Respiratory subscore items.

99
REFERENCES E1. Cohen J. Statistical power analysis for the behavioral sciences. 2ª ed Hillsdale, New
Jersey: Lawrence Erbaum (1988).
E2. Fritz CO, Morris PE, Richler JJ. Effect size estimates: current use, calculations, and
interpretation. Journal of experimental psychology General (2012) 141(1):2-18. Epub
2011/08/10. doi: 10.1037/a0024338. PubMed PMID: 21823805.
E3. Tomczak M, Tomczak E. The need to report effect size estimates revisited. An overview
of some recommended measures of effect size. Trends in Sport Sciences (2014) 1(21):19-25.
E4. Olejnik S, Algina J. Measures of Effect Size for Comparative Studies: Applications,
Interpretations, and Limitations. Contemporary educational psychology (2000) 25(3):241-86.
Epub 2000/06/30. doi: 10.1006/ceps.2000.1040. PubMed PMID: 10873373.
E5. Roche JC, Rojas-Garcia R, Scott KM, Scotton W, Ellis CE, Burman R, et al. A proposed
staging system for amyotrophic lateral sclerosis. Brain : a journal of neurology (2012) 135(Pt
3):847-52. doi: 10.1093/brain/awr351. PubMed PMID: 22271664; PubMed Central PMCID:
PMC3286327.
E6. Cedarbaum JM, Stambler N, Malta E, Fuller C, Hilt D, Thurmond B, et al. The ALSFRS-
R: a revised ALS functional rating scale that incorporates assessments of respiratory function.
Journal of the neurological sciences (1999) 169(1):13-21. doi: https://doi.org/10.1016/S0022-
510X(99)00210-5.

100
5. Discussão geral
A diminuição da função pulmonar e da força muscular respiratória na ELA leva à
redução do volume pulmonar e consequente insuficiência ventilatória.72 Nesses pacientes, o
grau de comprometimento dos músculos respiratórios é considerado difícil de ser
quantificado.73 Com a progressão da doença, o PFT diminui consideravelmente ao ponto de se
tornar ineficiente,74 fazendo essencial tanto o uso de técnicas de higiene brônquica quanto a
detecção precoce de fraqueza muscular respiratória a fim de monitorar a progressão da
doença e antecipar a introdução de intervenções.
Apesar da manobra de air stacking ser amplamente utilizada em sujeitos com doença
neuromuscular, os resultados obtidos em sujeitos saudáveis e apresentados no capítulo 2
podem ajudar a ampliar ainda mais o conhecimento sobre os efeitos fisiológicos dessa técnica.
Sabia-se, até pouco tempo, que a aplicação de uma pressão positiva além da capacidade
pulmonar total através da técnica de air stacking proporcionava somente um aumento da
complacência31 e do PFT37,38 em sujeitos com ELA. Em estudos prévios utilizando esta técnica
foram demonstrados, pela primeira vez, seus efeitos fisiológicos de forma mais detalhada sem
a aplicação de bocais ou qualquer interface que alterasse o padrão respiratório.53,61 O estudo
apresentado no capítulo 2 foi capaz de ir além, mensurando não só a quantidade de
compressão de gás produzida durante a técnica em sujeitos saudáveis assim como estimando
volumes pulmonares absolutos.
A quantificação da compressão de gás utilizando a POE e a integração do sinal de
fluxo obtido a partir de um pneumotacógrafo acoplado na boca não é um método novo na
literatura. Iandeli e colaboradores75 mostraram que a aplicação de uma limitação de fluxo
expiratório durante exercício em bicicleta estacionária acarreta em uma compressão de gás de
163 ± 4.6 ml em sujeitos saudáveis, além de um deslocamento de 325 ml de líquido do tórax
para as extremidades. Em consonância, Smith e colaboradores76 mensuraram a quantidade de
compressão de gás gerada durante picos de tosse voluntária e induzida em sujeitos
saudáveis. Ambos os estudos utilizaram a lei de Boyle para transformações isotérmicas com o
intuito de calcular a compressão de gás, e os volumes absolutos foram mensurados através da
pletismografia de corpo inteiro. Em contrapartida, o estudo apresentado no capítulo 2
mensurou diretamente o volume de compressão gerado durante a técnica de air stacking e
estimou os volumes pulmonares através da lei de Boyle. É importante salientar que nesse
estudo a quantidade de deslocamento de líquido do tórax para as extremidades foi omitida,
visto que 1) durante a inspiração até a capacidade pulmonar total há uma diminuição da
pressão intratorácica e consequente entrada de líquido no tórax e 2) durante a aplicação da
técnica de air stacking a partir de uma inspiração máxima há um aumento da pressão
intratorácica e consequente deslocamento de líquido do tórax para as extremidades,
considerando, dessa forma,a quantidade de deslocamento de líquido como nula. Através
desse novo método, a avaliação de volumes pulmonares absolutos necessita de uma
colaboração mínima dos sujeitos, sendo então proposto como alternativa ao uso de outras
técnicas que podem ser de difícil colaboração e que dependem de profissionais habilitados
para obter resultados consistentes, como as de diluição de gás e pletismografia de corpo

101
inteiro.77 Além disso, estudos ainda são necessários para conhecer a aplicação dessa nova
técnica de avaliação em outras posições e em doenças pulmonares restritivas e obstrutivas.
A avaliação e detecção precoce da fraqueza muscular respiratória resultante da ELA
têm ganhado mais interesse no campo da pesquisa nas últimas décadas. Em sujeitos
saudáveis, durante a inspiração, os compartimentos da parede torácica se movem em
sincronia.78 Por outro lado, em pacientes com doença neuromuscular, o avanço da doença e
perda de força muscular respiratória acarreta na ação não coordenada dos músculos
inspiratórios acessórios e diafragma, resultando em um movimento assíncrono tanto durante a
inspiração quanto a expiração.55,56,79 A assincronia, mensurada através do ângulo de fase e
definida como um retardo entre as excursões ou retrações dos compartimentos da parede
torácica,80 também pode ser consequência de fadiga muscular respiratória e leva a uma
diminuição do volume corrente e aumento do trabalho respiratório24,79,81 em sujeitos com
doença neuromuscular. Quando esses compartimentos se movem em direções totalmente
opostas82 (expansão da caixa torácica pulmonar e retração do abdômen, por exemplo), o
movimento paradoxal está presente e o diagnóstico de fraqueza muscular diafragmática ou
intercostal pode ser feito observando qual dos compartimentos se retrai durante a inspiração.79
Como exposto no capítulo 3, os pacientes com ELA apresentaram assincronia
toracoabdominal e movimento paradoxal durante a respiração espontânea e tosse. Esses
achados se correlacionaram com a diminuição na CVF, PFT, pico de fluxo expiratório,
capacidade inspiratória e no volume da parede torácica, sendo indicativos de fraqueza
desproporcional de alguns músculos respiratórios, como o diafragma54,55,79 e músculos
abdominais,83 e consequente desequilíbrio entre as pressões nos compartimentos da parede
torácica.79 O fato mais importante demonstrado nesse capítulo é que o comprometimento
diafragmático ocorre anterior ao nos músculos inspiratórios da caixa torácica superior e esse
sinal é observado primeiramente na CTa e não no compartimento abdominal. Essa mesma
característica foi descrita por Layton e colaboradores,56 os quais, utilizando a POE,
observaram que pacientes com ELA apresentavam movimento paradoxal da CTa diante de
uma fraqueza do diafragma. Talvez esse mesmo padrão estivesse presente nos pacientes do
estudo de Similowski e colaboradores84, no qual foi observado o um movimento paradoxal
abdominal em pacientes com ELA durante a aplicação de estimulação magnética
transcraniana, o que indicava fraqueza extrema do diafragma. Pelo fato de ter sido utilizada a
pletismografia respiratória por indutância, na qual somente dois compartimentos são
considerados como componentes da parede torácica, não foi possível ser realizada a
mensuração de variação de movimento da CTa.
Embora os padrões acima citados devam ser confirmados através de mais estudos, os
sinais de fraqueza muscular diafragmática foram obtidos sem a necessidade de técnicas
invasivas ou colaboração por parte dos pacientes. Esse ponto é de principal importância, pois
a ELA é uma doença progressiva e debilitante, e a simples constatação da assincronia e do
movimento paradoxal pode ser relevante para detecção precoce de fraqueza muscular e o
monitoramento clínico de progressão da doença.

102
Vários outros parâmetros são indicadores de fraqueza muscular, progressão da doença
e sobrevivência nessa população. Dentre os parâmetros diretamente ligados à respiração
podem-se destacar a capacidade vital lenta e forçada e força muscular respiratória (MIP, MEP
e SNIP).10,11,85-87 Fatores não respiratórios, incluindo a idade avançada, o início do
acometimento bulbar, o estado nutricional e a ALSFRS-R, também estão associados à
mortalidade.8 Mensurações diretas da função respiratória usando medidas como capacidade
vital são muito importantes e têm sido o método mais utilizado para avaliação respiratória na
ELA10 por serem também marcadores fisiológicos de aplicação de ventilação não invasiva,
preditivos de fraqueza muscular, insuficiência ventilatória e mortalidade.10,39,44,88 O pico de
pressão gerado pela manobra de SNIP, por sua vez, é um biomarcador de mortalidade mais
sensitivo que a CVF11 e se correlaciona tanto com a função do músculo
esternocleidomastóideo89 quanto com testes invasivos e não volitivos de força diafragmática.90
No entanto, parâmetros intrínsecos à curva do SNIP também podem fornecer informações
importantes sobre o estado dos músculos inspiratórios, principalmente o diafragma. Estudos
demonstraram que as propriedades contráteis e de relaxamento dos músculos inspiratórios
estão alteradas durante o desenvolvimento de fraqueza e fadiga musculares inspiratórias.91-93
Segundo Coirault e colaboradores,94 a avaliação desses parâmetros é de crucial importância
em situações clínicas, o que torna relevante a elaboração de índices confiáveis para detecção
precoce de fadiga muscular. O fato mais interessante é que esses parâmetros não foram
estudados de forma detalhada em pacientes com ELA. Até o momento, somente dois
estudos95,96 avaliaram o envolvimento da taxa máxima de relaxamento (MRR) do diafragma em
pacientes com doença neuromuscular, tornando difícil a comparação dos resultados
apresentados no capítulo 4 com outros estudos. Dentre os dois estudos, somente o de Garcia-
Rio e colaboradores96 incluiu pacientes com ELA (5 pacientes dentre 18 com doença
neuromuscular) e concluiu que a MRR poderia ser utilizado como um índice de fadiga dos
músculos respiratórios.
No estudo apresentado no capítulo 4 foi demonstrado que todos os parâmetros
extraídos da curva de SNIP estavam alterados nos pacientes com ELA quando comparados
com saudáveis pareados, o que sugere que esses pacientes estejam em risco de desenvolver
fadiga muscular respiratória.65,97 Adicionalmente, a taxa máxima de desenvolvimento de
pressão (MRPD), a constante de tempo durante o decaimento da curva de SNIP (τ - tau) e o
tempo para atingir a metade da curva de relaxamento (½ RT) foram mais sensíveis em
detectar diminuição da função muscular inspiratória do que o próprio pico de pressão da curva
de SNIP. Assim, visto os resultados obtidos e sabendo que os parâmetros supracitados podem
estar alterados durante a fadiga muscular respiratória antes mesmo da diminuição do pico de
pressão diafragmático (devido a alterações metabólicas da fibra muscular, como depleção de
ATP, alteração no pH e declínio da absorção de cálcio pelo retículo sarcoplasmático),92,98,99 é
possível hipotetizar que os parâmetros obtidos a partir da curva de SNIP sejam melhores
indicadores precoces de fadiga e/ou fraqueza muscular em sujeitos com ELA.

103
5.1. Principais limitações
Os estudos apresentados nessa tese têm algumas limitações importantes. No capítulo
2, os resultados obtidos no estudo foram comparados com valores de equações de
predição,100 sendo, no entanto, ideal que os volumes pulmonares de todos os sujeitos também
fossem avaliados diretamente pela pletismografia de corpo inteiro. Além disto, os sujeitos não
foram capazes de realizar manobras confiáveis de capacidade vital, o que inviabilizou a
estimativa e comparação do volume residual.
Alguns aspectos de desenho dos diferentes estudos também limitam sua interpretação.
No capítulo 3, a assincronia dos pacientes estudados foi mensurada em um único
posicionamento (deitado a 45°), tornando difícil a comparação desses dados com outros
estudos. No entanto, essa foi a primeira vez em que o movimento paradoxal foi obtido durante
a respiração espontânea e tosse voluntária utilizando a POE e relacionado com fraqueza
muscular respiratória em sujeitos com ELA.
5.2. Implicações clínicas, perspectivas futuras e conclusões
Em termos de aplicabilidade clínica, espera-se que a introdução de novos métodos de
mensuração de volumes pulmonares possa ampliar as pesquisas na área da saúde,
principalmente a medicina e fisioterapia respiratória, além de ser útil para pesquisas futuras em
laboratórios que não possuem equipamentos de alto custo e nem profissionais especializados.
Adicionalmente, a avaliação de todos os parâmetros citados nessa tese pode ser facilmente
realizada de forma não invasiva e são capazes de oferecer informações relevantes sobre o
estado dos músculos respiratórios em pacientes com ELA.
Sabe-se que há uma necessidade crítica de grandes avanços nas doenças
neuromusculares em geral, em particular a compreensão mecanicista detalhada da
patogênese da doença e da descoberta de terapias eficazes para aumento da sobrevida desta
população. Assim, apesar de estudos ainda serem necessários para melhor entender os
parâmetros aqui avaliados e apresentados, esta tese serve como ponto inicial para guiar
futuros desenhos de ensaios clínicos e servir como biomarcadores para o curso natural de
outras doenças neuromusculares. Mais ainda, a detecção precoce dos primeiros sinais de
alteração destes parâmetros e do desequilíbrio da cinemática dos compartimentos da parede
torácica pode permitir não só um monitoramento mais detalhado da progressão da doença,
mas também diferenciação entre sujeitos com ELA espinhal ou bulbar além de implementação
de novas e precoces intervenções clínicas e terapêuticas (como a tempo apropriado para início
da ventilação não invasiva e decisão de realizar traqueostomia, por exemplo) a fim de
prolongar a sobrevida destes pacientes.
Como conclusão, a presente tese mostrou que 1) a partir da mensuração simultânea da
variação de volume pulmonar e da parede torácica tanto a compressão de gás produzida
durante a técnica de air stacking pode ser quantificada quanto os volumes pulmonares
absolutos podem ser estimados em sujeitos saudáveis e 2) a identificação da alteração de
parâmetros, como assincronia toracoabdominal, presença de movimento paradoxal entre os

104
compartimentos da parede torácica, τ, MRPD, e ½RT, representam um sinal precoce de
fraqueza muscular inspiratória em sujeitos com ELA.

105
Referências
1. Gallo V, Wark PA, Jenab M, et al. Prediagnostic body fat and risk of death from amyotrophic
lateral sclerosis: the EPIC cohort. Neurology 2013; 80:829-838.
2. Haverkamp LJ, Appel V, Appel SH. Natural history of amyotrophic lateral sclerosis in a
database population. Validation of a scoring system and a model for survival prediction.
Brain 1995; 118 ( Pt 3):707-719.
3. Mitchell JD, Borasio GD. Amyotrophic lateral sclerosis. Lancet 2007; 369:2031-2041.
4. Huisman MH, de Jong SW, van Doormaal PT, et al. Population based epidemiology of
amyotrophic lateral sclerosis using capture-recapture methodology. J Neurol Neurosurg
Psychiatry 2011; 82:1165-1170.
5. Kiernan MC, Vucic S, Cheah BC, et al. Amyotrophic lateral sclerosis. The Lancet; 377:942-
955.
6. van Es MA, Hardiman O, Chio A, et al. Amyotrophic lateral sclerosis. Lancet 2017;
390:2084-2098.
7. Hardiman O, van den Berg LH, Kiernan MC. Clinical diagnosis and management of
amyotrophic lateral sclerosis. Nat Rev Neurol 2011; 7:639-649.
8. Chio A, Logroscino G, Hardiman O, et al. Prognostic factors in ALS: A critical review.
Amyotroph Lateral Scler 2009; 10:310-323.
9. Magnus T, Beck M, Giess R, et al. Disease progression in amyotrophic lateral sclerosis:
predictors of survival. Muscle Nerve 2002; 25:709-714
10. Andrews JA, Meng L, Kulke SF, et al. Association Between Decline in Slow Vital Capacity
and Respiratory Insufficiency, Use of Assisted Ventilation, Tracheostomy, or Death in
Patients With Amyotrophic Lateral Sclerosis. JAMA Neurol 2018; 75:58-64.
11. Polkey MI, Lyall RA, Yang K, et al. Respiratory Muscle Strength as a Predictive Biomarker
for Survival in Amyotrophic Lateral Sclerosis. Am J Respir Crit Care Med 2017; 195:86-
95.
12. Cedarbaum JM, Stambler N. Performance of the Amyotrophic Lateral Sclerosis Functional
Rating Scale (ALSFRS) in multicenter clinical trials. J Neurol Sci 1997; 152 Suppl 1:S1-
9.
13. Cedarbaum JM, Stambler N, Malta E, et al. The ALSFRS-R: a revised ALS functional rating
scale that incorporates assessments of respiratory function. Journal of the Neurological
Sciences 1999; 169:13-21.
14. Rooney J, Burke T, Vajda A, et al. What does the ALSFRS-R really measure? A
longitudinal and survival analysis of functional dimension subscores in amyotrophic
lateral sclerosis. J Neurol Neurosurg Psychiatry 2017; 88:381-385.
15. A double-blind placebo-controlled clinical trial of subcutaneous recombinant human ciliary
neurotrophic factor (rHCNTF) in amyotrophic lateral sclerosis. ALS CNTF Treatment
Study Group. Neurology 1996; 46:1244-1249.
16. Kaufmann P, Levy G, Thompson JL, et al. The ALSFRSr predicts survival time in an ALS
clinic population. Neurology 2005; 64:38-43.

106
17. Kollewe K, Mauss U, Krampfl K, et al. ALSFRS-R score and its ratio: a useful predictor for
ALS-progression. J Neurol Sci 2008; 275:69-73.
18. Bauer M, Czell D, Hartmann S, et al. Limitations of sniff nasal pressure as an outcome
measurement in amyotrophic lateral sclerosis patients in a clinical trial. Respiration
2012; 84:306-311.
19. Pinto S, Geraldes R, Vaz N, et al. Changes of the phrenic nerve motor response in
amyotrophic lateral sclerosis: longitudinal study. Clin Neurophysiol 2009; 120:2082-
2085.
20. Macklem PT. Normal and abnormal function of the diaphragm. Thorax 1981; 36:161-163.
21. Macklem PT. Respiratory muscles: the vital pump. Chest 1980; 78:753-758.
22. Hammer J, Newth CJ. Assessment of thoraco-abdominal asynchrony. Paediatr Respir Rev
2009; 10:75-80.
23. Chihara K, Kenyon CM, Macklem PT. Human rib cage distortability. J Appl Physiol (1985)
1996; 81:437-447.
24. Diaz CE, Deoras KS, Allen JL. Chest wall motion before and during mechanical ventilation
in children with neuromuscular disease. Pediatr Pulmonol 1993; 16:89-95.
25. Allen JL, Wolfson MR, McDowell K, et al. Thoracoabdominal asynchrony in infants with
airflow obstruction. Am Rev Respir Dis 1990; 141:337-342.
26. Laghi F, Tobin MJ. Disorders of the respiratory muscles. Am J Respir Crit Care Med 2003;
168:10-48.
27. Kravitz RM. Airway clearance in Duchenne muscular dystrophy. Pediatrics 2009; 123 Suppl
4:S231-235.
28. Smith JA, Aliverti A, Quaranta M, et al. Chest wall dynamics during voluntary and induced
cough in healthy volunteers. J Physiol 2012; 590:563-574.
29. Lo Mauro A, Aliverti A. Physiology of respiratory disturbances in muscular dystrophies.
Breathe (Sheff) 2016; 12:318-327.
30. Lechtzin N. Respiratory effects of amyotrophic lateral sclerosis: problems and solutions.
Respir Care 2006; 51:871-881; discussion 881-874.
31. Lechtzin N, Shade D, Clawson L, et al. Supramaximal inflation improves lung compliance in
subjects with amyotrophic lateral sclerosis. Chest 2006; 129:1322-1329.
32. Corcia P, Pradat PF, Salachas F, et al. Causes of death in a post-mortem series of ALS
patients. Amyotroph Lateral Scler 2008; 9:59-62.
33. Benditt JO. The neuromuscular respiratory system: physiology, pathophysiology, and a
respiratory care approach to patients. Respir Care 2006; 51:829-837; discussion 837-
829.
34. Fallat RJ, Jewitt B, Bass M, et al. Spirometry in amyotrophic lateral sclerosis. Arch Neurol
1979; 36:74-80.
35. Stewart H, Eisen A, Road J, et al. Electromyography of respiratory muscles in amyotrophic
lateral sclerosis. J Neurol Sci 2001; 191:67-73.

107
36. Schiffman PL, Belsh JM. Effect of inspiratory resistance and theophylline on respiratory
muscle strength in patients with amyotrophic lateral sclerosis. Am Rev Respir Dis 1989;
139:1418-1423.
37. Kang SW, Bach JR. Maximum insufflation capacity: vital capacity and cough flows in
neuromuscular disease. Am J Phys Med Rehabil 2000; 79:222-227.
38. Kang SW, Bach JR. Maximum insufflation capacity. Chest 2000; 118:61-65.
39. Pinto S, Carvalho M. Breathing new life into treatment advances for respiratory failure in
amyotrophic lateral sclerosis patients. Neurodegener Dis Manag 2014; 4:83-102.
40. Jackson CE, Rosenfeld J, Moore DH, et al. A preliminary evaluation of a prospective study
of pulmonary function studies and symptoms of hypoventilation in ALS/MND patients. J
Neurol Sci 2001; 191:75-78.
41. Laroche CM, Mier AK, Moxham J, et al. The value of sniff esophageal pressures in the
assessment of global inspiratory muscle strength. Am Rev Respir Dis 1988; 138:598-
603.
42. Miller JM, Moxham J, Green M. The maximal sniff in the assessment of diaphragm function
in man. Clin Sci (Lond) 1985; 69:91-96.
43. Pinto S, Pinto A, De Carvalho M. Do bulbar-onset amyotrophic lateral sclerosis patients
have an earlier respiratory involvement than spinal-onset amyotrophic lateral sclerosis
patients? Eura Medicophys 2007; 43:505-509.
44. Czaplinski A, Yen AA, Appel SH. Forced vital capacity (FVC) as an indicator of survival and
disease progression in an ALS clinic population. J Neurol Neurosurg Psychiatry 2006;
77:390-392.
45. Cheung HJ, Cheung L. Coaching patients during pulmonary function testing: A practical
guide. Can J Respir Ther 2015; 51:65-68.
46. Aliverti A, Pedotti A. Opto-electronic plethysmography. Monaldi Arch Chest Dis 2003;
59:12-16.
47. Cala SJ, Kenyon CM, Ferrigno G, et al. Chest wall and lung volume estimation by optical
reflectance motion analysis. J Appl Physiol (1985) 1996; 81:2680-2689.
48. Konno K, Mead J. Measurement of the separate volume changes of rib cage and abdomen
during breathing. J Appl Physiol 1967; 22:407-422.
49. Romagnoli I, Lanini B, Binazzi B, et al. Optoelectronic Plethysmography has Improved our
Knowledge of Respiratory Physiology and Pathophysiology. Sensors (Basel) 2008;
8:7951-7972.
50. Aliverti A, Dellaca R, Pelosi P, et al. Compartmental analysis of breathing in the supine and
prone positions by optoelectronic plethysmography. Ann Biomed Eng 2001; 29:60-70.
51 Lo Mauro A, D'Angelo MG, Romei M, et al. Abdominal volume contribution to tidal volume
as an early indicator of respiratory impairment in Duchenne muscular dystrophy. Eur
Respir J 2010; 35:1118-1125.
52. Aliverti A, Stevenson N, Dellaca RL, et al. Regional chest wall volumes during exercise in
chronic obstructive pulmonary disease. Thorax 2004; 59:210-216.

108
53. Sarmento A, Resqueti V, Dourado-Junior M, et al. Effects of Air Stacking Maneuver on
Cough Peak Flow and Chest Wall Compartmental Volumes of Subjects With
Amyotrophic Lateral Sclerosis. Arch Phys Med Rehabil 2017; 98:2237-2246.e2231.
54. LoMauro A, Romei M, D'Angelo MG, et al. Determinants of cough efficiency in Duchenne
muscular dystrophy. Pediatr Pulmonol 2014; 49:357-365.
55. Lanini B, Masolini M, Bianchi R, et al. Chest wall kinematics during voluntary cough in
neuromuscular patients. Respir Physiol Neurobiol 2008; 161:62-68.
56. Layton AM, Moran SL, Roychoudhury A, et al. Non-invasive measurement of abnormal
ventilatory mechanics in amyotrophic lateral sclerosis. Muscle Nerve 2016; 54:270-276.
57. Aliverti A, Quaranta M, Chakrabarti B, et al. Paradoxical movement of the lower ribcage at
rest and during exercise in COPD patients. Eur Respir J 2009; 33:49-60.
58. Dohna-Schwake C, Ragette R, Teschler H, et al. IPPB-assisted coughing in neuromuscular
disorders. Pediatr Pulmonol 2006; 41:551-557.
59. Ishikawa Y, Bach JR, Komaroff E, et al. Cough augmentation in Duchenne muscular
dystrophy. Am J Phys Med Rehabil 2008; 87:726-730.
60. Panitch HB. Airway clearance in children with neuromuscular weakness. Curr Opin Pediatr
2006; 18:277-281.
61. Sarmento A, de Andrade AF, Lima IN, et al. Air Stacking: A Detailed Look Into Physiological
Acute Effects on Cough Peak Flow and Chest Wall Volumes of Healthy Subjects.
Respir Care 2017.
62. Aliverti A, Dellaca R, Pelosi P, et al. Optoelectronic plethysmography in intensive care
patients. Am J Respir Crit Care Med 2000; 161:1546-1552.
63 Carry PY, Baconnier P, Eberhard A, et al. Evaluation of respiratory inductive
plethysmography: accuracy for analysis of respiratory waveforms. Chest 1997; 111:910-
915.
64. Hardart MK, Burns JP, Truog RD. Respiratory support in spinal muscular atrophy type I: a
survey of physician practices and attitudes. Pediatrics 2002; 110:e24.
65. Mador MJ, Kufel TJ. Effect of inspiratory muscle fatigue on inspiratory muscle relaxation
rates in healthy subjects. Chest 1992; 102:1767-1773.
66. Grassino A, Macklem PT. Respiratory muscle fatigue and ventilatory failure. Annu Rev Med
1984; 35:625-647.
67. Bigland-Ritchie B, Johansson R, Lippold OC, et al. Contractile speed and EMG changes
during fatigue of sustained maximal voluntary contractions. J Neurophysiol 1983;
50:313-324.
68 American Thoracic Society/European Respiratory S. ATS/ERS Statement on respiratory
muscle testing. Am J Respir Crit Care Med 2002; 166:518-624.
69 Pereira CAC, Neder, J.A. Sociedade Brasileira de Pneumologia e Tisiologia – SBPT.
Diretrizes para testes de função pulmonar. J. Bras. Pneumol. 2002; 29 (3):207-221.
70. Neder JA, Andreoni S, Lerario MC, et al. Reference values for lung function tests: II.
Maximal respiratory pressures and voluntary ventilation. Brazilian Journal of Medical
and Biological Research 1999; 32:719-727.

109
71. Araujo PR, Resqueti VR, Nascimento Junior J, et al. Reference values for sniff nasal
inspiratory pressure in healthy subjects in Brazil: a multicenter study. J Bras Pneumol
2012; 38:700-707.
72. Orsini M, Oliveira AB, Nascimento OJ, et al. Amyotrophic Lateral Sclerosis: New
Perpectives and Update. Neurol Int 2015; 7:5885.
73. Just N, Bautin N, Danel-Brunaud V, et al. The Borg dyspnoea score: a relevant clinical
marker of inspiratory muscle weakness in amyotrophic lateral sclerosis. Eur Respir J
2010; 35:353-360.
74. Bach JR, Mahajan K, Lipa B, et al. Lung insufflation capacity in neuromuscular disease. Am
J Phys Med Rehabil 2008; 87:720-725.
75. Iandelli I, Aliverti A, Kayser B, et al. Determinants of exercise performance in normal men
with externally imposed expiratory flow limitation. J Appl Physiol (1985) 2002; 92:1943-
1952.
76. Smith JA, Aliverti A, Quaranta M, et al. Chest wall dynamics during voluntary and induced
cough in healthy volunteers. J Physiol 2012; 590:563-574.
77 O'Donnell CR, Bankier AA, Stiebellehner L, et al. Comparison of plethysmographic and
helium dilution lung volumes: which is best for COPD? Chest 2010; 137:1108-1115.
78. Ward ME, Ward JW, Macklem PT. Analysis of human chest wall motion using a two-
compartment rib cage model. J Appl Physiol (1985) 1992; 72:1338-1347.
79. Allen J. Pulmonary complications of neuromuscular disease: a respiratory mechanics
perspective. Paediatr Respir Rev 2010; 11:18-23.
80 Prisk GK, Hammer J, Newth CJ. Techniques for measurement of thoracoabdominal
asynchrony. Pediatr Pulmonol 2002; 34:462-472.
81. Mortola JP, Sant'Ambrogio G. Motion of the rib cage and the abdomen in tetraplegic
patients. Clin Sci Mol Med 1978; 54:25-32.
82. Kinnear WJM, Sovani M, Khanna A, et al. Correction of Paradoxical Ribcage Motion in
Scoliosis by Non-Invasive Ventilation. Spine (Phila Pa 1976) 2017.
83. Perez A, Mulot R, Vardon G, et al. Thoracoabdominal pattern of breathing in neuromuscular
disorders. Chest 1996; 110:454-461.
84. Similowski T, Attali V, Bensimon G, et al. Diaphragmatic dysfunction and dyspnoea in
amyotrophic lateral sclerosis. Eur Respir J 2000; 15:332-337.
85. Pinto S, de Carvalho M. Correlation between Forced Vital Capacity and Slow Vital Capacity
for the assessment of respiratory involvement in Amyotrophic Lateral Sclerosis: a
prospective study. Amyotroph Lateral Scler Frontotemporal Degener 2017; 18:86-91.
86. Morgan RK, McNally S, Alexander M, et al. Use of Sniff nasal-inspiratory force to predict
survival in amyotrophic lateral sclerosis. Am J Respir Crit Care Med 2005; 171:269-274.
87. Gordon PH, Cheng B, Montes J, et al. Outcome measures for early phase clinical trials.
Amyotroph Lateral Scler 2007; 8:270-273.
88. Miller RG, Jackson CE, Kasarskis EJ, et al. Practice parameter update: the care of the
patient with amyotrophic lateral sclerosis: multidisciplinary care, symptom management,
and cognitive/behavioral impairment (an evidence-based review): report of the Quality

110
Standards Subcommittee of the American Academy of Neurology. Neurology 2009;
73:1227-1233.
89. Pinto S, de Carvalho M. Motor responses of the sternocleidomastoid muscle in patients with
amyotrophic lateral sclerosis. Muscle Nerve 2008; 38:1312-1317.
90. Lyall RA, Donaldson N, Polkey MI, et al. Respiratory muscle strength and ventilatory failure
in amyotrophic lateral sclerosis. Brain 2001; 124:2000-2013.
91. Koulouris N, Vianna LG, Mulvey DA, et al. Maximal relaxation rates of esophageal, nose,
and mouth pressures during a sniff reflect inspiratory muscle fatigue. Am Rev Respir
Dis 1989; 139:1213-1217
92. Esau SA, Bellemare F, Grassino A, et al. Changes in relaxation rate with diaphragmatic
fatigue in humans. J Appl Physiol Respir Environ Exerc Physiol 1983; 54:1353-1360.
93. Tzelepis GE, Kasas V, McCool FD. Inspiratory muscle adaptations following pressure or
flow training in humans. Eur J Appl Physiol Occup Physiol 1999; 79:467-471.
94. Coirault C, Chemla D, Lecarpentier Y. Relaxation of diaphragm muscle. J Appl Physiol
(1985) 1999; 87:1243-1252.
95 Evangelista MA, Dias FAL, Dourado Junior MET, et al. Noninvasive assessment of
respiratory muscle strength and activity in Myotonic dystrophy. PLoS One 2017;
12:e0177318.
96 Garcia-Rio F, Mediano O, Pino JM, et al. Noninvasive measurement of the maximum
relaxation rate of inspiratory muscles in patients with neuromuscular disorders.
Respiration 2006; 73:474-480.
97. Dawson MJ, Gadian DG, Wilkie DR. Mechanical relaxation rate and metabolism studied in
fatiguing muscle by phosphorus nuclear magnetic resonance. J Physiol 1980; 299:465-
484.
98. Esau SA, Bye PT, Pardy RL. Changes in rate of relaxation of sniffs with diaphragmatic
fatigue in humans. J Appl Physiol Respir Environ Exerc Physiol 1983; 55:731-735.
99. Polkey MI, Kyroussis D, Mills GH, et al. Inspiratory pressure support reduces slowing of
inspiratory muscle relaxation rate during exhaustive treadmill walking in severe COPD.
Am J Respir Crit Care Med 1996; 154:1146-1150.
100. Roca J, Burgos F, Barbera JA, et al. Prediction equations for plethysmographic lung
volumes. Respir Med 1998; 92:454-460.

111
Lista de publicações
Artigos originais publicados em jornais com revisão por pares
SARMENTO, A.; ALIVERTI, A. ; MARQUES, L. ; PENNATI, F. ; DOURADO JUNIOR, M. E. ; FREGONEZI, G. A. F. ; RESQUETI, V. R. Multiparametric analysis of sniff nasal inspiratory pressure test in middle stage amyotrophic lateral sclerosis. Frontiers in Neurology, 2018 (in press).
SARMENTO, A.; ANDRADE, A. F. D. ; LIMA, Í. N. D. F ; ALIVERTI, A.; FREGONEZI, G. A. F.; RESQUETI, V. R. Air Stacking: A Detailed Look Into Physiological Acute Effects on Cough Peak Flow and Chest Wall Volumes of Healthy Subjects. Respiratory Care, v. 62, p. respcare.05189-432-443, 2017.
EVANGELISTA, M. A. ; DIAS, F. A. L. ; DOURADO-JUNIOR, M. E. ; NASCIMENTO, G. C. ; SARMENTO, A. ; GUALDI, L. P. ; ALIVERTI, A. ; RESQUETI, V. R. ; FREGONEZI, G. A. F. Noninvasive assessment of respiratory muscle strength and activity in Myotonic dystrophy. PLoS One, v. 12, p. e0177318, 2017.
SARMENTO, A.; RESQUETI, V.; DOURADO-JÚNIOR, M. E. ; SATURNINO, L.; ALIVERTI, A.; FREGONEZI, G.; ANDRADE, A. D. Effects of Air Stacking Maneuver on Cough Peak Flow and Chest Wall Compartmental Volumes of Subjects With Amyotrophic Lateral Sclerosis. Archives of Physical Medicine and Rehabilitation, v.
98, p. 2237-2246.e1, 2017. AGUIAR, K. A. A. ; SARMENTO, A. ; DINIZ, J. ; FREGONEZI, G. A. ; ANDRADE, A. F. D. ; RESQUETI, V. R. . A single section of stretch of the respiratory muscles does not influence the pulmonary volume of asthmatics during exercise. Journal of Respiratory and Cardiovascular Physical Therapy, v. 3, p. 3-13, 2016.
SARMENTO, A.; RESQUETI, V. R. ; FREGONEZI, G. A. F. ; ALIVERTI, A. Assessment of gas compression and lung volume during air stacking maneuver. European Journal of Applied Physiology, v. 117, p. 189-199, 2016.

112
Resumos apresentados em congressos internacionais com publicações em anais
SARMENTO, A.; FREGONEZI, G. A. F. ; DOURADO JUNIOR, M. E. ; ALIVERTI, ANDREA ; ANDRADE, A. F. D. ; PARREIRA, V. F. ; RESQUETI, V. R. Thoracoabdominal asynchrony and paradoxical motion during cough and quiet breathing in middle stage amyotrophic lateral sclerosis subjects. In: European Respiratory Society
Congress, 2017, Milão. European Respiratory Journal - Clinical Respiratory Physiology, Exercise and Functional Imaging, 2017. v. 50. p. PA2226. SARMENTO, A.; RESQUETI, V. R. ; DOURADO JUNIOR, M. E. ; ALIVERTI, A. ; FREGONEZI, G. A. F. ; ANDRADE, A. F. D. Effects of air stacking maneuver on cough peak flow and chest wall compartmental volumes of amyotrophic lateral sclerosis subjects. In: European Respiratory Society Congress, 2017, Milão.
European Respiratory Journal - Clinical Respiratory Physiology, Exercise and Functional Imaging, 2017. v. 50. p. PA2224. LIRA, M. G. A. ; SARMENTO, A. ; ALIVERTI, A. ; OLIVEIRA, L. M. ; DIAS, F. A. L. ; RESQUETI, V. R. ; FREGONEZI, G. A. F. Inspiratory muscle maximum relaxation rate measured from maximal sniff nasal pressure in patients with Amyotrophic Lateral Sclerosis. In: European Respiratory Society Congress, 2017,
Milão. European Respiratory Journal - Clinical Respiratory Physiology, Exercise and Functional Imaging, 2017. v. 50. p. PA2225. SARMENTO, A.; RESQUETI V. R. ; SATURNINO, L. ; FREGONEZI, G. A. ; ALIVERTI, A. ; DOURADO JUNIOR, M. E. ; ANDRADE, A. F. D. Benefícios da técnica de Air Stacking em sujeitos com Esclerose Lateral Amiotrófica.
In: 10° Congresso da Associação Latino Americana de Tórax, 2016, Santiago. Arch Bronconeumol, 2016. v. 52. p. 61-61. SARMENTO, A.; RESQUETI, V. R. ; LIMA, I. N. D. F. ; GUALDI, L. P. ; FREGONEZI, G. A. F. ; ALIVERTI, A. ; ANDRADE, A. F. D. Acute effects of air stacking maneuver on chest wall volumes and peak cough flow of healthy subjects. In: European Respiratory Society Congress, 2015, Amsterdam. European Respiratory Journal -
Clinical Respiratory Physiology, Exercise and Functional Imaging, 2015. v. 46. p. PA2278. RESQUETI, V. R. ; DINIZ, J. ; AGUIAR, K. A. A. ; GUALDI, L. P. ; SARMENTO, A. ; ANDRADE, A. F. D. ; FREGONEZI, G. A. F. Electrical activity behavior of respiratory and peripheral muscles during incremental shuttle walking test in asthmatic subjects. In: European Respiratory Society Congress, 2015, Amsterdam.
European Respiratory Journal - Clinical Respiratory Physiology, Exercise and Functional Imaging, 2015. v. 46. p. PA4825.