-
PROGRAMA DE PÓS-GRADUAÇÃO STRICTO SENSU
MESTRADO ACADÊMICO EM AMBIENTE E SAÚDE
LUCIANA CAROLINA DA SILVA ISHIKAWA CÉZAR SANTOS
INFLUÊNCIA DO TABAGISMO NA ATIVIDADE DA DOENÇA E NA
RESPOSTA AO TRATAMENTO DA ARTRITE REUMATOIDE
Cuiabá-MT
2020

LUCIANA CAROLINA DA SILVA ISHIKAWA CÉZAR SANTOS
INFLUÊNCIA DO TABAGISMO NA ATIVIDADE DA DOENÇA E NA
RESPOSTA AO TRATAMENTO DA ARTRITE REUMATOIDE
Dissertação apresentada à Universidade de Cuiabá para
obtenção do título de Mestre em Ambiente e Saúde
Orientador: Prof. Dr. Vander Fernandes
Cuiabá-MT
2020
Dados internacionais de Catalogação na Publicação (CIP) Ficha catalográfica elaborada pela Biblioteca UNIC
S237i SANTOS, Luciana Carolina da Silva Ishikawa Cézar Influência do tabagismo na atividade da doença e na resposta ao tratamento da artrite reumatoide. / Luciana Carolina da Silva Ishikawa Cézar Santos - Cuiabá, MT 2020 49 p.: il
Dissertação (Mestrado) – Programa de Pós-graduação em Ensino de stricto sensu, como
requisito parcial para obtenção do título de Mestre em Ambiente e Saúde. Área de
concentração em poluentes ambientais da água e solo e doenças relacionadas.
Universidade de Cuiabá - UNIC, 2020 Orientadora: Prof.º Dr.º Vander Fernandes 1. Artrite Reumatoide. 2. Tabagismo. 3. Terapia Biológica. 4. Inflamação Crônica. CDU: 616.72:614
Terezinha de Jesus de Melo Fonseca - CRB1/3261
FOLHA DE APROVAÇÃO
LUCIANA CAROLINA DA SILVA ISHIKAWA CEZAR SANTOS
INFLUÊNCIA DO TABAGISMO NA ATIVIDADE DA DOENÇA E NA
RESPOSTA AO TRATAMENTO DA ARTRITE REUMATOIDE
Dissertação apresentada a UNIC, no mestrado em Ambiente e Saúde, área de concentração Ambiente
e Saúde na Amazônia Legal como requisito parcial para obtenção do título de Mestre conferida pela
Banca Examinadora formada pelos professores:
____________________________________
Prof Dr Vander Fernandes
(Orientador)
UNIC
_________________________________________
Prof. Dr. Marcelo Dias de Souza
UNIC
________________________________
Prof. Dr. Júlio Cesar de Oliveira
UFMT
Cuiabá, 26 de março de 2020

DEDICATÓRIA
Dedico esse trabalho ao meu amado esposo Paulo Cézar, parceiro, amigo e companheiro, que com
todo amor, paciência e dedicação esteve ao meu lado, me ajudando a superar as dificuldades e a
alcançar meus objetivos. Sem você não teria sido possível.
AGRADECIMENTOS
À Jeová, meu Deus, criador de todas as coisas, em que posso sempre confiar.
Aos meus queridos pais, por seu apoio incondicional em todas as minhas decisões.
Ao meu amado esposo Paulo Cézar e aos meus filhos Igor, Anna Paula e Anna Carolina, por toda a
compreensão e amor.
Ao meu querido professor, amigo e orientador Doutor Vander Fernandes, que contribuiu
decisivamente em minha profissão, por ter me apoiado e incentivado, agradeço eternamente por todo
apoio, parceria, atenção e paciência.
Aos meus colegas de mestrado, em especial à minha amiga e parceira Laíza Strinta, a qual sempre me
auxiliou durante esses anos.
À minha querida amiga Tássia Damasceno, em quem eu pude confiar e me apoiar.
Aos professores Doutores do Mestrado em Ambiente e Saúde da Universidade de Cuiabá- UNIC,
Cristina Márcia de Menezes Butakka, Christiane Almeida Leite, Elias Nasrala Neto, Henrique César
Santejo Silveira, Marcelo Dias de Souza, Marcus Adriano Salício (in memorian), Silvana Margarida
Benevides Ferreira, Sue Ellen Ferreira Modesto Rey de Figueiredo, Walkíria Shimoya Bittencourt.
À coordenadora do Mestrado em Ambiente e Saúde da Universidade de Cuiabá-UNIC, Profª Drª
Christiane Almeida Leite, por sua orientação e confiança.

“E nossa história não estará pelo avesso
Assim, sem final feliz
Teremos coisas bonitas para contar
E até lá, vamos viver
Teremos muito ainda por fazer
Não olhe para trás
Apenas começamos
O mundo começa agora
Apenas começamos...”
(Eduardo Villa Lobos, Marcelo Bonfá, Renato Manfredini Júnior)

RESUMO
A artrite reumatoide (AR) é uma doença inflamatória, sistêmica, crônica e progressiva que acomete
principalmente a membrana sinovial das articulações periféricas, em especial, punhos, mãos,
tornozelos e pés. Embora sua etiologia permaneça desconhecida, vários estudos sugerem que fatores
genéticos, ambientais, hormonais e infecciosos participem na expressão e ocorrência da AR. Inúmeros
fatores de risco ambientais têm sido estudados, mas até o momento, o fator de risco ambiental mais
proeminente para o desenvolvimento de AR é o tabagismo. Este estudo teve como objetivo avaliar a
influência do tabagismo na atividade da doença em pacientes com artrite reumatoide, assim como sua
influência na resposta ao tratamento. Trata-se de um estudo de coorte observacional com dados do
Registro Brasileiro de Monitorização de Terapias Biológicas (BiobadaBrasil), de janeiro de 2010
novembro de 2019, abrangendo pacientes com diagnóstico de artrite reumatoide em uso de biológicos.
O hábito do tabagismo, grau de atividade de doença (avaliado pelo Disease Activity Score 28 DAS28)
e tipo de terapia biológica em uso foram registrados na consulta inicial. No seguimento foram
registrados os motivos de suspensão da terapia e os eventos adversos. Considerou-se diferença
estatisticamente significativa quando p<0,05 no teste bicaudal e todas as análises foram realizadas por
meio do software Stata 13.0 (College Station, Teas, EUA). Foram avaliados 1980 pacientes, com idade
média de 43,43 anos (IC95%, 42,89-43,98), sendo a maioria do sexo feminino (85,25%). Duzentos e
noventa e dois pacientes (14,75%) eram tabagistas. Na avaliação inicial, 1.812 pacientes (91,52%)
apresentaram moderada ou alta atividade da doença, de acordo com o DAS-28. O DAS-28 mediano
no início do seguimento foi igual a 5,2 (IQR, 4,2-6,2), sem diferença estatística (p=0,70) entre os
tabagistas (5,1; IQR, 4,2-6,2) e não tabagistas (5,2; IQR, 4,2-6,2). Foi observada uma média de 4,41
eventos adversos durante todo o tempo de seguimento (IC95%, 4,17-4,64) e os indivíduos tabagistas
(4,74; IC95%, 4,15- 5,33) apresentaram uma frequência estatisticamente maior e significante (p=0,03)
que os não tabagistas (4,33; IC95%, 4,01-4,59). O tempo mediano entre o início do tratamento e um
primeiro evento adverso foi igual a 78,66 meses (IQR,22,66-172,58), sendo menor e estatisticamente
significante (p=0,02) entre os indivíduos tabagistas (65,75; IQR 19,58-144,00) quando comparados
com os não tabagistas (81,16; IQR, 28,58-177,16). Neste estudo o hábito tabágico não influenciou na
atividade da doença quando do início da terapia biológica, porém aumentou o risco de eventos adversos
em pacientes com AR em tratamento com estas terapias.
Palavras-chave: artrite reumatoide; tabagismo; terapia biológica.

ABSTRACT
Rheumatoid arthritis (RA) is an inflammatory, systemic, chronic and progressive disease that mainly
affects the synovial membrane of peripheral joints such as wrists, hands, ankles and feet. Although RA
etiology remains unknown, several studies have suggested that genetic, environmental, hormonal and
infectious factors play a significant role in its expression and incidence. Several environmental risk
factors have been investigated, but smoking is the most prominent environmental risk factor for RA
development, so far. The aim of the current study is to assess the influence of smoking on disease
activity in rheumatoid arthritis patients, as well as on the response of these patients to treatment. The
present research is an observational cohort study based on data available in the Brazilian Registry for
the Monitoring of Biological Therapies (BiobadaBrasil). It was conducted from January 2010 to
November 2019 and comprised patients diagnosed with rheumatoid arthritis who underwent biological
therapy. Smoking habit, disease activity level (assessed based on the Disease Activity Score 28
DAS28) and the biological therapy type in use were recorded at the initial consultation, whereas
reasons for abandoning therapy and adverse events were recorded during follow-up. Statistically
significant differences in the two-tailed test was set at p < 0.05; all analyses were performed in Stata
13.0 software (College Station, Teas, USA). In total, 1,980 patients were assessed; their mean age was
43.43 years (95% CI, 42.89-43.98) and most of them were women (85.25%). Two hundred and ninety-
two patients (14.75%) were smokers. According to DAS-28, 1,812 patients (91.52%) presented
moderate or high disease activity in the initial assessment. Median DAS-28 at the beginning of the
follow-up was 5.2 (IQR, 4.2-6.2); there was not statistically significant difference (p = 0.70) between
smokers (5.1; IQR, 4.2 -6.2) and non-smokers (5.2; IQR, 4.2-6.2). Mean incidence of adverse events
reached 4.41 throughout the follow-up period (95% CI, 4.17-4.64) - smokers (4.74; 95% CI, 4.15-
5.33) recorded statistically higher and more significant frequency of these events (p = 0.03) than non-
smokers (4.33; 95% CI, 4.01-4.59). Median time between the beginning of the treatment and the first
adverse event was 78.66 months (IQR, 22.66-172.58) – it was shorter and statistically significant (p =
0.02) among smokers (65.75; IQR 19.58-144.00) than among non-smokers (81.16; IQR, 28.58-
177.16). Smoking did not influence disease activity at the beginning of the biological therapy in the
current study, but it increased the risk of adverse events in RA patients undergoing such therapies.
Keywords: rheumatoid arthritis; smoking; biological therapy.
LISTA DE ILUSTRAÇÕES
Figura 1- Etiopatogenia da artrite reumatoide .................................................................................................. 16
Figure 1- Smoking habit-based Kaplan-Meier curve generated for patients’ likelihood of remaining free of
adverse event among individuals with rheumatoid arthritis treated with biological drug, who were followed-up
between January 2010 and November 2019. Data fro BIOBADABRASIL. .................................................... 37
Quadro 1- DAS 28: índice utilizado para avaliação da atividade da doença ................................................... 19
LISTA DE TABELAS
Table 1 - Epidemiological profile of patients with rheumatoid arthritis, who were followed-up between
January 2010 and November 2019. Data from BIOBADABRASIL ................................................... 31
Table 2 - Comorbidity-based epidemiological profile of patients with rheumatoid arthritis, who were
followed-up between January 2010 and November 2019. Data from BIOBADABRASIL ................ 32
Table 3 - Epidemiological profile of patients with rheumatoid arthritis - who were followed-up
between January 2010 and November 2019 - according to drugs used by them during treatment. Data
from BIOBADABRASIL .................................................................................................................... 33
Table 4 - Epidemiological profile of patients with rheumatoid arthritis – who were followed-up
between January 2010 and November 2019 - according to adverse events. Data from
BIOBADABRASIL ............................................................................................................................. 33
Table 5 - Factors associated with smoking habit among individuals with rheumatoid arthritis, who
were followed-up between January 2010 and November 2019. Data from BIOBADABRASIL ....... 35
Table 6 - Independent factors associated with smoking habit among individuals diagnosed with
rheumatoid arthritis, who were followed-up between January 2010 and November 2019. Data from
BIOBADABRASIL ............................................................................................................................. 36
LISTA DE ABREVIATURA E SIGLAS
AR - artrite reumatoide
Anti-CCP- anticorpos antipeptídeo citrulinado
AINEs anti-inflamatórios não esteroidais
Anti-TNF- antagonistas do fator de necrose tumoral
BiobadaBrasil- Registro Brasileiro de Monitorização de Terapias Biológicas
BSR- registro de Biológicos da Sociedade Britânica de Reumatologia
CVD- cardiovascular Disease
CI- confidence intervals
CAD- índices compostos de atividade de doença
DC- células dendríticas
DMCDs - drogas modificadoras do curso de doença
DAS28 - Disease Activity Score
EC – epítopo compartilhado
EVA - escala visual analógica
ETA- etanercepte
FR-fator reumatoide
HLA - antígeno leucocitário humano
IL-interleucina
IQR- interquartile range
IFN- infliximabe
INF- infliximabe
MMP-metaloproteinases
NK-natural killers
NOAR- Norfolk Arthritis Register
PCR- proteína C reativa
RR- Relative risk
TNF-alfa-fator de necrose tumoral
VHS- velocidade de hemossedimentação
SUMÁRIO
1. INTRODUÇÃO .................................................................................................................................................. 13
2. REVISÃO DE LITERATURA ....................................................................................................................... 15
2.1 ARTRITE REUMATOIDE.................................................................................................. 15
2.1.1 Etiopatogênese ............................................................................................................. 15
2.1.2 Atividade da Doença .................................................................................................... 18
2.1.3 Tratamento ................................................................................................................... 19
2.2 TABAGISMO E ARTRITE REUMATOIDE ..................................................................... 20
3. REFERÊNCIAS ................................................................................................................................................. 22
4. ARTIGO - INFLUENCE OF SMOKING ON DISEASE ACTIVITY AND ON PATIENTS’
RESPONSE TO RHEUMATOID ARTHRITIS TREATMENT ............................................................. 22
4.1 INTRODUCTION ................................................................................................................ 27
4.2 PATIENTS AND METHODS ............................................................................................. 29
4.3 STATISTICAL ANALYSIS ................................................................................................ 30
4.4 RESULTS............................................................................................................................. 31
4.5 DISCUSSION ...................................................................................................................... 37
4.6 CONCLUSION .................................................................................................................... 40
4.7 REFERENCES ..................................................................................................................... 41
5. APÊNDICE - BIOBADABRASIL – QUESTIONÁRIO DE INCLUSÃO .......................................... 46
13
1 INTRODUÇÃO
A artrite reumatoide (AR) é uma complexa doença imunomediada, de etiologia desconhecida
caracterizada por inflamação crônica, sinovite, dor e destruição progressiva tanto da cartilagem
articular quanto do osso, podendo levar à incapacidade funcional. Trata-se de uma doença reumática
frequente que acomete cerca de 1% da população adulta no mundo, e sua ocorrência pode ser
observada em todos os grupos étnicos com distribuição geográfica universal. Mulheres têm duas a três
vezes mais chance de desenvolver a doença do que os homens e embora possa ocorrer em qualquer
idade, a AR apresenta pico de incidência entre a quarta e sexta décadas (MOURAD; MONEM, 2013;
MOTA et al., 2011; PINHEIRO, 2009).
Apesar do acometimento envolver principalmente o sistema musculoesquelético, a AR é uma
enfermidade de caráter sistêmico, que pode acometer vários órgãos, como olhos e pulmões,
ocasionando diferentes manifestações extra-articulares (PEREIRA et al., 2012). Tais manifestações
podem ter associação com a presença de autoanticorpos, como fator reumatoide (FR) e os anticorpos
antipeptídeo citrulinado (anti-CCP) no soro, conferindo caráter autoimune à doença. (PEREIRA et al.,
2012).
A etiologia da doença ainda não está totalmente esclarecida. Porém fatores ambientais,
genéticos e infecciosos contribuem para o desenvolvimento da AR (CARVALHO et al., 2019;
PICCOLI et al., 2011).
O antígeno leucocitário humano (HLA) é o fator de risco genético mais importante para o
desenvolvimento da AR, responsável por 30% a 50% da suscetibilidade genética global da doença. A
hipótese do epítopo compartilhado (EC) descreve a relação entre o HLA-DRB1 e a AR. Os alelos
HLA-DRB1 que codificam o EC estão associados à gravidade da AR, e parecem estar relacionados
com a superprodução dos autoanticorpos antipeptídeo citrulinado cíclico (anti-CCP). Por outro lado,
os genótipos negativos para o EC conferem proteção contra a suscetibilidade à AR (MOURAD;
MONEM, 2013).
O tabagismo é o principal fator de risco ambiental para artrite reumatoide e sua presença
aumenta em duas vezes o risco de desenvolver a doença (SCOTT; WOLFE; HUIZINGA, 2010). Foi
observado que o cigarro está relacionado com o aparecimento da doença, à gravidade, presença de
manifestações extra-articulares e à positividade do FR (CARVALHO et al., 2019). A relação entre
14
tabagismo e AR tornou possível o reconhecimento de um fator de risco passível de intervenção
(CARVALHO et al., 2019).
Mediante tal contexto, o estudo em questão torna-se importante uma vez que o tabagismo
parece influenciar de maneira significativa na evolução da doença e na resposta ao tratamento. Dessa
forma, este estudo propõe avaliar a influência do tabagismo na atividade da doença e na ocorrência de
eventos adversos em pacientes com artrite reumatoide durante o tratamento com terapia biológica.
15
2 REVISÃO DE LITERATURA
2.1 ARTRITE REUMATOIDE
2.1.1 Etiopatogênese
A artrite reumatoide é uma doença autoimune caracterizada por sinovite persistente, inflamação
sistêmica e presença de autoanticorpos (principalmente o fator reumatoide e o anti-CCP). Nos países
industrializados a AR afeta 0,5-1% dos adultos com 5 a 50 por 100.000 novos casos anualmente, sendo
mais frequente em mulheres (SCOTT; WOLFE; HUIZINGA, 2010).
É uma doença em que ocorre, desde a fase inicial pré-articular, perda da autotolerância e
consequente autoimunidade traduzidas por ativação linfocitária e produção de autoanticorpos. O
aparecimento das manifestações articulares é determinado por fatores genéticos, neuroendócrinos e
ambientais, período caracterizado pelo desequilíbrio entre citocinas pró e anti-inflamatórias e
recrutamento articular de macrófagos, neutrófilos, células T, B e natural killers (NK) e de ativação de
fibroblastos, osteoclastos e condrócitos. O influxo celular promove uma inflamação sinovial crônica
em que os principais mediadores são as citocinas interleucina (IL) IL 17 e o fator de necrose tumoral
alfa (TNF-alfa), assim como prostaglandinas e metaloproteinases (MMP). Os resultados
histopatológicos são a destruição da cartilagem articular e a erosão óssea mediadas por fibroblastos,
condrócitos e osteoclastos, e o resultado clínico se traduz por deformidades e incapacidade funcional
(CARVALHO et al., 2019).
16
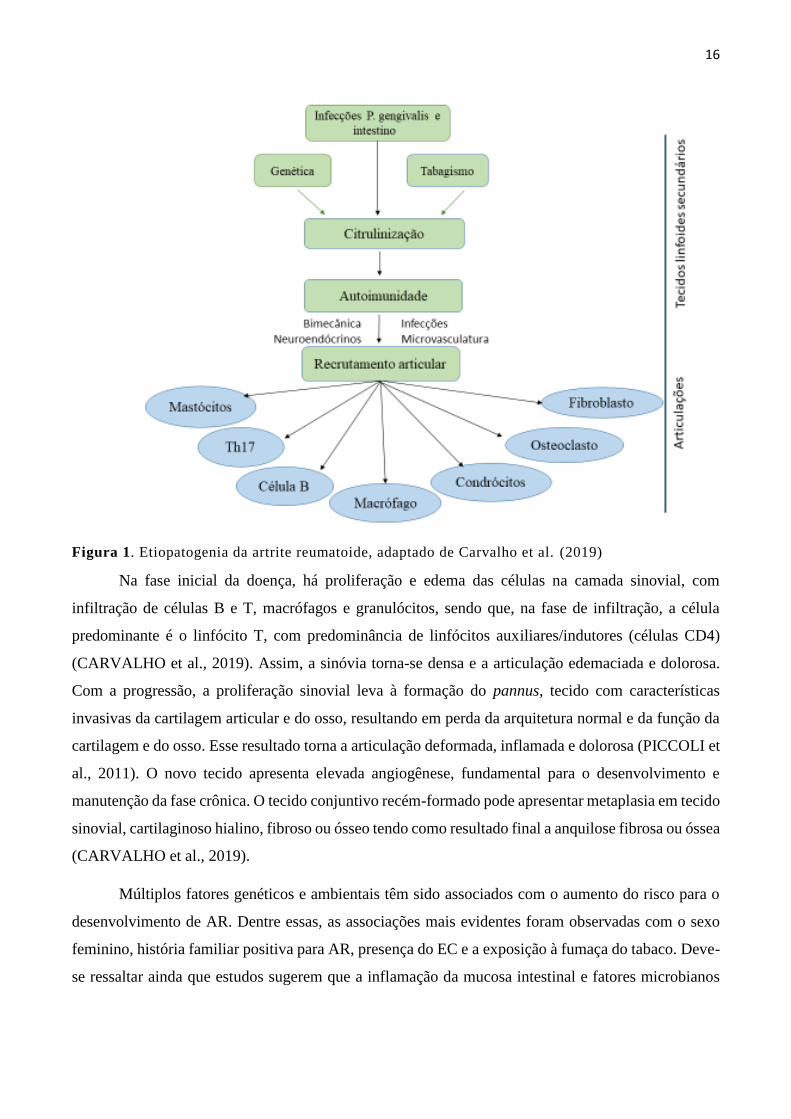
Figura 1. Etiopatogenia da artrite reumatoide, adaptado de Carvalho et al. (2019)
Na fase inicial da doença, há proliferação e edema das células na camada sinovial, com
infiltração de células B e T, macrófagos e granulócitos, sendo que, na fase de infiltração, a célula
predominante é o linfócito T, com predominância de linfócitos auxiliares/indutores (células CD4)
(CARVALHO et al., 2019). Assim, a sinóvia torna-se densa e a articulação edemaciada e dolorosa.
Com a progressão, a proliferação sinovial leva à formação do pannus, tecido com características
invasivas da cartilagem articular e do osso, resultando em perda da arquitetura normal e da função da
cartilagem e do osso. Esse resultado torna a articulação deformada, inflamada e dolorosa (PICCOLI et
al., 2011). O novo tecido apresenta elevada angiogênese, fundamental para o desenvolvimento e
manutenção da fase crônica. O tecido conjuntivo recém-formado pode apresentar metaplasia em tecido
sinovial, cartilaginoso hialino, fibroso ou ósseo tendo como resultado final a anquilose fibrosa ou óssea
(CARVALHO et al., 2019).
Múltiplos fatores genéticos e ambientais têm sido associados com o aumento do risco para o
desenvolvimento de AR. Dentre essas, as associações mais evidentes foram observadas com o sexo
feminino, história familiar positiva para AR, presença do EC e a exposição à fumaça do tabaco. Deve-
se ressaltar ainda que estudos sugerem que a inflamação da mucosa intestinal e fatores microbianos
17
possam contribuir para o desenvolvimento da doença (DEANE et al., 2017). Porém, de forma isolada,
nenhum desses fatores é suficiente para a plena expressão da doença (PINHEIRO, 2009).
Sabe-se que o tabagismo aumenta o risco de AR tanto nos homens quanto nas mulheres em
cerca de 1,5 a 2 vezes. Além disso, o risco aumenta com a intensidade (maços por dia) e duração do
tempo de uso do cigarro. O risco individual pode permanecer elevado por até 20 anos após o abandono
do hábito de fumar, porém, esse risco diminui com o tempo após a desistência (KLIPPEL et al., 2008).
Outros fatores de risco ambiental têm sido estudados como as transfusões de sangue, infecções,
obesidade, exposição ocupacional à sílica e ao óleo mineral, mas até o momento, o fator de risco
ambiental mais proeminente para o desenvolvimento de AR é o tabagismo. Nos últimos anos, o tabaco
tem sido relacionado como fator de risco para detecção de anticorpos anti-CCP em pacientes com
artrite reumatoide, estando relacionado não somente com o aparecimento da doença bem como com a
gravidade, presença de manifestações extra articulares e a detecção do fator reumatoide (MOURA et
al., 2012; KLIPPEL et al., 2009; GOELDENER et al., 2015).
Foram relacionados vários genes com artrite reumatoide, com evidências mais estabelecidas
para a doença soropositiva (fator reumatoide- FR ou anticorpos contra peptídeos citrulinados-ACPA)
(CARVALHO et al., 2019).
O principal fator genético predisponente é o antígeno HLA DRB1. Seus alelos relacionados à
AR contêm uma sequência de cinco aminoácidos chamada epítopo compartilhado (EC), QKRAA ou
QQRAA ou KKRAA (Q: glutamina, K: lisina, R: arginina, A: alanina) na região 70-74. Entretanto,
nem todos os pacientes com AR apresentam o EC (PINHEIRO, 2009; MOURA et al, 2012;
CARVALHO et al., 2019).
Pacientes portadores do epítopo compartilhado HLA-DRB1 são aqueles em que o tabagismo,
entre outros fatores ambientais parecem estar relacionados com maior risco de desenvolvimento da
doença, especificamente naqueles em que apresentam positividade para os anticorpos antipeptídio
cíclico citrulinado. A presença dessa sequência de aminoácidos na AR relaciona-se com diversos
eventos imunológicos, tais como: seleção de linfócitos T, alteração da afinidade peptídica, mímica
molecular com antígenos microbianos, apresentação antigênica e aceleração da apoptose linfocitária
(MOURA et al., 2012; CARVALHO et al., 2019).
O tabagismo aumenta o risco de desenvolvimento de anticorpos anti-CCP em doentes com o
epítopo compartilhado positivo. A ação lesiva do tabaco e outros agressores brônquicos seriam
responsáveis pela transformação de resíduos de arginina em citrulina, evento denominado
18
citrulinização, mediado pela enzima pepdil arginina deiminase tipo IV (PAD4). Comportando-se como
um neoepítopo, esse “novo” aminoácido dá origem, por perda de tolerância, a uma reação contra
proteínas citrulinadas que pode ser identificada pela pesquisa de anticorpos antipeptídeo citrulinado
(anti-CCP). Os anticorpos anti-CCP são produzidos localmente na membrana sinovial e no líquido
sinovial de pacientes com AR e são capazes de reagir com diversos peptídeos citrulinados (MOURA
et al., 2012; PICCOLI et al., 2011; MOURAD; MONEM, 2013).
A ativação das células T irá promover a ativação das células B e produção de anticorpos contra
as proteínas com resíduos citrulinados, os quais estão presentes durante anos antes do início dos
sintomas de AR, evidenciando assim que a autoimunidade precede a doença clínica (CARVALHO et
al., 2019).
Diversas doenças autoimunes, incluindo a artrite reumatoide, começam tipicamente com um
período assintomático prolongado caracterizado pela presença de anticorpos circulantes doença-
específicos. O período positivo para autoanticorpos, porém assintomático é definido como período
pré-clínico (HOCHBERG et al., 2015).
Sabe-se que os níveis de autoanticorpos relacionados com AR são elevados em indivíduos
assintomáticos por até 5 a 10 anos antes do desenvolvimento dos sinais e sintomas clínicos da AR e
com o início da doença clinicamente estabelecida, ocorre um aumento nos níveis desses autoanticorpos
(HOCHBERG et al., 2015).
2.1.2 Atividade da Doença
Com o objetivo de otimizar tratamento da AR, é necessária avaliação periódica da resposta
clínica e laboratorial ao esquema terapêutico instituído. Contudo não há, isoladamente, nenhum
parâmetro clínico ou laboratorial que seja capaz de traduzir de forma satisfatória, o nível de atividade
inflamatória (FUCHS et al., 1989).
A avaliação da eficácia pode ser realizada através dos índices compostos de atividade de doença
(ICAD), em que são avaliados componentes clínicos e laboratoriais. Dentre tais índices incluem-se o
índice de atividade de doença - Disease Activity Score 28 (DAS28), em que se emprega a contagem
de 28 articulações (lados direito e esquerdo: ombros, cotovelos, punhos, metacarpofalangeanas,
interfalangeanas proximais de mãos e joelhos) quanto à presença de dor e edema, VHS e/ou PCR e a
avaliação da saúde geral pelo paciente por meio de uma escala visual analógica - EVA, cujos valores
19
vão de 0 a 100. Considera-se dolorosa a articulação que apresente algum grau de desconforto a digito-
pressão de sua interlinha ou à mobilização passiva (MOURA et al., 2012; FUNCHS et al., 1989; VAN
DER HEIJDE et al., 1990; ARNSON; SHOENFELD; AMITAL, 2010; QIU et al., 2017).
Para o cálculo do DAS28 é empregada uma fórmula em que uma calculadora própria pode
facilitar o cálculo. Essa ferramenta pode ser obtida gratuitamente pelo site www.das-score.nl.
Quadro 1- DAS 28: índice utilizado para avaliação da atividade da doença
Estado da atividade de doença Pontos de corte
Remissão Inferior ou igual a 2,6
Baixa Superior a 2,6 e até 3,2
Moderada Superior a 3,2 e até 5,1
Alta Superior a 5,1
Fonte: PCDT- artrite reumatoide (BRASIL, 2017).
2.1.3 Tratamento
O tratamento da AR progrediu significativamente nos últimos 25 anos, evoluindo de uma
estratégia de alívio sintomático para a implementação de regimes terapêuticos que afetam a atividade
da doença, retardando ou impedindo o dano articular estrutural (UPCHURCH; KAY, 2012). A terapia
medicamentosa para artrite reumatoide evoluiu a partir de AINEs (anti-inflamatórios não esteroidais),
corticosteroides, e DMCDs (drogas modificadoras do curso de doença): sulfassalazina, cloroquina e
hidroxicloroquina, ciclosporina, azatioprina e metotrexato, dentre outros (PINHEIRO, 2007).
No entanto, ao longo dos últimos anos, o tratamento das doenças reumatológicas de natureza
imunoinflamatoria, em especial a AR, sofreu uma mudança significativa. Após maior conhecimento
sobre a patogênese e o reconhecimento de alvos terapêuticos, foi possível a introdução da terapia com
imunobiológicos (também denominada agentes biológicos ou drogas modificadoras do curso da
doença- DMCDs- biológicas) contribuindo de maneira importante na melhora da qualidade de vida e
na diminuição na morbimortalidade dos pacientes portadores de doenças reumáticas autoimunes
(FRANSEM; PIET VAN RIEL, 2009).
Além disso, novas estratégias de abordagem foram sugeridas, tais como introdução de DMCDs
desde a fase inicial da doença, avaliações clínicas mais frequentes dos pacientes, objetivando sempre
20
a remissão clínica quando possível. Essas medidas contribuíram para a melhora de sintomas e
diminuição da atividade da doença com redução na progressão do dano articular (PINHEIRO, 2007).
Terapia imunobiológica compreende aquela em que os medicamentos são derivados de
processos biotecnológicos, envolvendo efeitos no sistema imune. Estes agentes incluem anticorpos
monoclonais e moléculas recombinantes (ou proteínas de fusão - proteínas geneticamente modificadas
dirigidas contra citocinas ou moléculas da superfície celular). Nas doenças reumáticas, medicamentos
biológicos têm como objetivo regular o desequilíbrio celular e molecular que ocorre nos processos
inflamatórios crônicos, característicos de tais patologias (MOTA et al., 2015; PINHEIRO, 2007;
FRANSEN; PIET VAN RIEL, 2009).
Esse grupo de medicamentos pode ser classificado de acordo com o mecanismo de ação em:
antagonistas do fator de necrose tumoral (anti-TNF) (infliximabe, adalimumabe, etanercepte,
certolizumabe e golimumabe), bloqueador da co-estimulação do linfócito T (abatacepte), depletor de
linfócito B (rituximabe) e bloqueador do receptor de interleucina-6 (tocilizumabe) (FRANSEN; PIET
VAN RIEL, 2009).
2.2 TABAGISMO E ARTRITE REUMATOIDE
Estudos têm demonstrado que, tanto a imunidade inata quanto a adaptativa, sofrem influência
do cigarro gerando um desequilíbrio na homeostasia imunológica. As células imunes adaptativas
afetadas pelo fumo incluem principalmente as células T auxiliares (Th1, Th2, Th17), células T
reguladoras CD4+, CD25+, células TCD8+, células B e linfócitos T/B de memória. Já as células da
imunidade inata afetadas são principalmente as DC (células dendríticas), macrófagos e células NK
(natural killers) (VESSEY; VILLARD-MACKINTOSH; YEATES, 1987; VITTECOQ et al., 2017).
O hábito de fumar é fator de risco bem estabelecido em diversas doenças tais como neoplasias
pulmonares e doenças cardiovasculares (ARNSON; SHOENFELD; AMITAL, 2010). No entanto, o
fumo tem sido associado ao desenvolvimento de doenças reumáticas autoimunes, dentre elas a artrite
reumatoide. A primeira associação entre AR e tabagismo foi sugerida na década de 1980, em que foi
evidenciado um aumento acentuado nas internações hospitalares por AR em tabagistas (VESSEY;
VILLARD-MACKINTOSH; YEATES, 1987; CHANG et al., 2014).
No entanto, o tabagismo parece ser um fator de risco para a produção de anticorpos anti-CCP
somente em pacientes com AR que carreiam alelos do EC (GOEPDNER et al., 2011; HOCHBERG et
21
al., 2015). Linn-Rasker et al. (2006) investigou a interação gene - ambiental entre a exposição ao tabaco
e a detecção de anticorpos anti-CCP em 407 pacientes com artrite reumatoide que carreiam o EC.
Nesse estudo o tabagismo foi confirmado como fator de risco para positividade de anti-CCP somente
na presença do EC (GOEPDNER et al., 2011).
Bergestrom et al. (2011), em estudo de caso controle realizado na Suécia avaliando riscos
ambientais para o tratamento da artrite reumatoide encontraram quase duas vezes mais indivíduos
tabagistas entre casos de artrite reumatoide. Em outro estudo de Moura et. al (2012), avaliando
pacientes com manifestações extra-articulares de AR no Serviço de Reumatologia do Hospital
Universitário Evangélico de Curitiba, Paraná, evidenciaram que o tabagismo atual estava associado à
presença das manifestações extra-articulares da doença.
Sabe-se que o tabagismo está associado tanto ao aumento da suscetibilidade da AR quanto a
uma maior atividade da doença e resposta clínica reduzida ao metotrexato e aos anti-TNF (CUPPEN
et al., 2017; VITTECOQ et al., 2018). Hyrich et al. (2006), em uma coleta de dados do Registro de
Biológicos da Sociedade Britânica de Reumatologia (BSR) sobre pacientes com doença reumática que
recebem terapia biológica no Reino Unido, acompanharam pacientes com AR que iniciaram
tratamento com etanercepte (ETA) ou com infliximabe (INF) durante período mínimo de 06 meses.
Foi evidenciado que pacientes com AR que fumam apresentam resposta clínica reduzida,
particularmente em pacientes que receberam INF, demonstrando uma associação entre tabagismo e
mau prognóstico com INF, podendo refletir alterações na farmacocinética da medicação.
22
3 REFERÊNCIAS
ARNSON, Y.; SHOENFELD, Y; AMITAL, H. Effects of tobacco on immunity, inflammation and
autoimmunity. Jornal of Autoimmunity, v. 33, n. 4, 258-265, 2010. Disponível em:
https://www.ncbi.nlm.nih.gov/pubmed/20042314. Acesso em: 02 fev. 2019.
BESGSTROM, U.; JACOBSSON, L. T. H.; NILSSON, JAN-AKE; BERGLUND, G. TURESSON,
C. Pulmonary dysfunction, smoking, socioeconomic status and the risk of developing Rheumatoid
arthritis, v. 50, p. 2005-2013, 2011. DOI:10.1093/rheumatology/ker258
CARVALHO, M. A.; LANNA. C.; BERTOLO, M.; FERREIRA, G. Reumatologia: diagnóstico e
tratamento. 5. ed. Rio de Janeiro: Guanabara Koogan, 2019.
CHANG, K.; YANG, S. M.; KIM, H. S.; HAN, H. K.; PARK, S. J.; SHIN, J. Smoking and Rheumatoid
Arthritis. International Journal of Molecular Sciences, v. 155, n. 12, p. 22279-22295, 2014.
Disponível em: https://www.mdpi.com/1422-0067/15/12/22279. Acesso em: 22 nov. 2018.
CUPPEN, B. V.; JACOBS, J. W.; TER BORG, E. J.; MARIJNISSEN, A. C.; BIJLSMA, J. W.;
LAFEBER, F. P.; VAN LAAR, J. M. Necessity of TNF-alpha inhibitor dis-continuation in rheumatoid
arthritis is predicted by smoking and number of previously used biological DMARDs. Clinical and
Experimental Rheumatology, v. 35, v 2, p. 221–228, 2017.
DEANE, K. D.; DEMORUELLE, M. K.; KELMENSON, L. B.; KUHN, K. A.; NORRIS, J. M.;
HOLERS, M. Genetic and environmental risk factors for rheumatoid arthritis. Best Practice &
Research: Clinical Rheumatology, v. 31, n. 1, p. 3-18, 2017. DOI:10.1016/j.berh.2017.08.003.
FRANSEN, J.; VAN RIEL, P. L. The Disease Activity Score and the EULAR Response Criteria.
Rheumatic Diseases Clinics of North America, v. 35, p. 745-757, 2009. Disponível em:
https://www.ncbi.nlm.nih.gov/pubmed/19962619. Acesso em: 22 nov. 2018.
FUCHS, A. H.; BROOKS, R. H.; CALLAHAN, L. F.; PINCUS, T. A Simplified Twenty-Eight-Joint
Quantitative Articular Index in Rheumatoid Arthritis. Arthritis and Rheumatism, v. 32, n. 5, 1989.
Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/2719728. Acesso em: 12 dez. 2018.
23
GOELDNER, I.; SKARE, T. L.; REASON, I. T. M.; UTIYAMA, S. R. R. Artrite reumatoide: uma
visão atual. Jornal Brasileiro de Patologia e Medicina Laboratorial, v. 47, n. 5. p. 495-503, 2011.
Disponível em: http://www.scielo.br/pdf/jbpml/v47n5/v47n5a02.pdf. Acesso em: 01 mar. 2019.
HYRICH, K. L.; WATSON, K. D.; SILMAN, A. J.; SYMMONS, D. P. British Society for
Rheumatology Biologics Register. Predictors of response to anti-TNF-alpha therapy among patients
with rheumatoid arthritis: results from the British Society for Rheumatology Biologics Registers.
Rheumatology (Oxford), v. 45, n. 12, p. 1558-1565, 2006. Disponível em:
https://www.ncbi.nlm.nih.gov/pubmed/16705046. Acesso em: 01 mar. 2019.
HOCHBERG, M. C.; SILMAN, A. J.; SMOLEN, J. S.; WEINBLATT, M. E.; MICHAEL, W.
Reumatologia. Tradução da 6.ed. Rio de Janeiro: Elsevier, 2015.
KLIPPEL, J. H.; STONE, J. H.; CROFFORD, L. J.; WHITE, P. H. Primer on the rheumatic diseases.
13th ed. Springer; 2008.
LINN-RASKER, S. P.; VAN DER HELM-VAN, M. A. H.; VAN GAALEN, F. A.; KLOPPENBURG,
M.; VRIES, R. R.; LE CESSIE, S.; BREEDVELD, F. C.; TOES, R. E.; HUIZINGA, T. W. Smoking
is a risk factor for anti-CCP antibodies only in rheumatoid arthritis patients who carry HLA-DRB1
shared epitope alleles. Annals of the Rheumatic Diseases, v. 65, n. 3, p. 366-371, 2006. Disponível
em: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1798061/. Acesso em: 02 set. 2019.
MOTA, L. M. H.; CRUZ, B. A.; BRENOL, C. V.; PEREIRA, I. A.; FRONZA, L. S. R.; BERTOLO,
M. B. Consenso da Sociedade Brasileira de Reumatologia 2011 para o diagnóstico e avaliação inicial
da artrite reumatóide. Revista Brasileira de Reumatologia, v. 51, n. 3, p. 199-219, 2011. Disponível
em: http://dx.doi.org/10.1590/S0482-50042011000300002. Acesso em: 22 jul. 2019.
MOTA, L. M. H.; CRUZ, B. A.; BRENOL, C. V.; POLLAK, D. F.; PINHEIRO, G. R. C.;
LAURINDO, I. M. M.; PEREIRA, I. A.; CARVALHO, J. F.; BORTOLO, M. B.; PINHEIRO, M. M.;
FREITAS, M. V. C.; SILVA, N. A.; LOUZADA-JUNIOR, P.; SAMPAIO-BARROS, P. D.; GIORGI,
R. D. N.; LIMA, R. A. C.; ANDRADE, L. E. C. Segurança do uso de terapias biológicas para o
tratamento de artrite reumatoide e espondiloartrites. Revista Brasileira de Reumatologia, v. 55, n. 3,
p.281-309, 2015. Disponível em:
https://www.sciencedirect.com/science/article/pii/S0482500414001752. Acesso em: 28 ago. 2019
24
MOURA, M. C.; ZAKSZEWSKI, P. T. S.; SILVA, M. B. G.; SHARE, T. L. Perfil dos pacientes com
manifestações extra-articulares de artrite reumatoide de um serviço ambulatorial em Curitiba, Sul do
Brasil. Revista Brasileira Reumatologia, v. 52, n. 5, p.679-694, 2012. Disponível em:
http://www.scielo.br/pdf/rbr/v52n5/v52n5a04.pdf. Acesso em: 22 mar. 2019.
MOURAD, J.; MONEM, F. Associação do alelo HLA-DRB1 com suscetibilidade a artrite reumatoide
e gravidade da doença na Síria. Revista Brasileira de Reumatologia, v. 53, n. 1, p. 51-56, 2013.
Disponível em: http://www.scielo.br/pdf/rbr/v53n1/v53n1a05.pdf. Acesso em: 28 ago. 2019.
PEREIRA, I. A.; MOTA, L. M. H.; CRUZ, B. A.; BRENOL, C. V.; FRONZA, L. S. R.; BERTOLO,
M. B.; FREITA, M. V. C.; SILVA, N. A.; LOUZADA JUNIOR, P.; GIORGI, R. D. N.; LIMA, R. A.
C.; PINHEIRO, G. R. C. Consenso 2012 da Sociedade Brasileira de Reumatologia sobre o manejo de
comorbidades em pacientes com artrite reumatoide. Revista Brasileira de Reumatologia, v. 52, n. 4,
p. 474-495, 2012. Disponível em: http://www.scielo.br/pdf/rbr/v52n4/v52n4a02.pdf. Acesso em: 17
jun. 2019.
PINHEIRO, G. R. C. Instrumentos de Medida da Atividade da Artrite Reumatoide- Por que e como
Empregá-los. Revista Brasileira de Reumatologia, v. 47, n. 5, p. 362-365, 2007. Disponível em:
http://www.scielo.br/pdf/rbr/v47n5/a11v47n5.pdf. Acesso em: 22 jun. 2019.
PINHEIRO, G. R. C. Artrite reumatoide. In: MOREIRA, C.; PINHEIRO, G. R. C.; MARQUES
NETO, J. F. (eds.). Reumatologia Essencial. Rio de Janeiro: Guanabara Koogan; 2009. p. 338-54.
PICCOLI, A. K.; ALEGRETTI, A. P.; SCHNEIDER, L.; LORA, O.S.; XAVIER, R. M. Expressão de
proteínas reguladoras do complemento CD55, CD,59, CD35 e CD46 na artrite reumatoide. Revista
Brasileira de Reumatologia, v. 51, n. 5, p. 497-510, 2011. Disponível em:
http://dx.doi.org/10.1590/S0482-50042011000500009. Acesso em: 29 ago. 2019.
QIU, F.; LIANG, C. L.; LIU, H.; ZENG, Y. Q.; HOU, S.; HUANG, S.; LAI, X.; DAI, Z. Impacts of
cigarette smoking on imune responsiveness: Up and down upside down? Oncotarget, v. 8, n. 1, p.
268-284, 2017. Disponível em: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5352117/. Acesso
em: 05 set. 2019.
RAMIRO, S.; LANDEWÉ, R.; VAN DER HEIJDE, D.; HARRISON, D.; COLLIER, D.; MICHAUD,
K. Taxas de descontinuação de produtos biológicos em pacientes com artrite reumatóide: os inibidores
25
de TNF são diferentes dos inibidores não-TNF? Rheumatoid Arthritis, v. 1, p. 1-11, 2015.
DOI:10.1136/rmdopen-2015-000155
SCOTT, D. L.; WOLFE, F.; J HUIZINGA, T. W. Rheumatoid arthritis. Seminar Lancet, v. 376, p.
1094-1108, 2010.
UPCHURCH, K. S.; KAY, J. Evolution of treatment for rheumatoid arthritis. Rheumatology
(Oxford), v. 5, n. 6, p. 28-36, 2012.
VESSEY, M. P.; VILLARD-MACKINTOSH, G.; YEATES, D. Oral contraceptives, cigarette
smoking and other factors in relation to arthritis. Contraception, v. 35, n. 5, p. 457-464, 1987.
Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/3621942. Acesso em: 18 jun. 2019.
VITTECOQ, O.; RICHAR, L.; BANSE, C.; LEQUERRE, T. The impact of smoking on rheumatoid
arthritis outcomes. Joint Bone Spine, v. 85, n. 2, p. 35-138, 2018. Disponível em:
https://www.ncbi.nlm.nih.gov/pubmed/30268815. Acesso em: 02 set. 2019.

26
4. ARTIGO - INFLUENCE OF SMOKING ON DISEASE ACTIVITY AND ON PATIENTS’
RESPONSE TO RHEUMATOID ARTHRITIS TREATMENT
Luciana Carolina da Silva Ishikawa Cézar Santos
Email: [email protected]
Vander Fernandes
Email: [email protected]
Aims: Assessing the influence of smoking on disease activity in rheumatoid arthritis patients, as well
as on their response to treatment.
Patients and methods: Observational cohort study based on data available in the Brazilian Registry
for the Monitoring of Biological Therapies (BiobadaBrasil). It was conducted from January 2010 to
November 2019 and comprised patients diagnosed with rheumatoid arthritis who underwent biological
therapy. Smoking habit, disease activity level (assessed based on the Disease Activity Score 28
DAS28) and biological therapy type in use were recorded at the initial consultation. Reasons for
abandoning therapy and adverse events were recorded during the follow-up.
Results: In total, 1,980 patients were assessed; their mean age was 43 years (95% CI, 42.89-43.98)
and most of them were women (85.25%). Two hundred and ninety-two patients (14.75%) were
smokers. According to DAS-28, 1,812 patients (91.52%) presented moderate or high disease activity
in the initial assessment. Median DAS-28 at the beginning of the follow-up was 5.2 (IQR, 4.2-6.2);
there was not statistically significant difference (p = 0.70) between smokers (5.1; IQR, 4.2 -6.2) and
non-smokers (5.2; IQR, 4.2-6.2). Mean incidence of adverse events reached 4.41 throughout the
follow-up period (95% CI, 4.17-4.64) - smokers (4.74; 95% CI, 4.15- 5.33) recorded statistically higher
and significant frequency of these events (p = 0.03) than non-smokers (4.33; 95% CI, 4.01-4.59).
Median time between the beginning of the treatment and the first adverse event was 78.66 months
27
(IQR, 22.66-172.58) – it was shorter and statistically significant (p = 0.02) among smokers (65.75;
IQR 19.58-144.00) than among non-smokers (81.16; IQR, 28.58-177.16).
Conclusion: Smoking did not influence disease activity at the beginning of the biological therapy in
the current study, but it increased the risk of adverse events in RA patients undergoing such therapies.
Keywords: rheumatoid arthritis; smoking; biological therapy.
4.1 INTRODUCTION
Rheumatoid arthritis (RA) is a chronic, potentially disabling immune disease mainly observed
in synovial joints of 0.5-1% of individuals living in industrialized countries (1). It mainly affects the
synovial membrane of peripheral joints such as wrists, hands, ankles and feet (2). RA incidence can
be observed in all ethnic groups, since it has wide geographical distribution; it affects two to three
times more women than men and its peak incidence is often observed in individuals in the age group
40-60 years (2, 3).
The disease encompasses self-tolerance loss and, consequently, autoimmunity since the pre-
articular phase, which leads to lymphocyte activation and autoantibody production. The emergence of
joint manifestations is determined by genetic, neuroendocrine and environmental factors; this period
is featured by lack of balance between pro and anti-inflammatory cytokines, as well as by joint
recruitment of macrophages, neutrophils; T, B, natural killer (NK) and fibroblast activation cells;
osteoclasts and chondrocytes (4).
Although RA etiology remains unknown, several studies have suggested that genetic,
environmental, hormonal and infectious factors participate in its expression and incidence. However,
none of these factors is individually enough to enable full disease expression (3).
28
Several genes have been linked to rheumatoid arthritis due to well-established evidence of
seropositive disease, such as the rheumatoid factor or antibodies to citrullinated peptides (4).
Smoking, among other environmental factors, appears to be associated with increased risk of
RA development in patients carrying shared HLA-DRB1 epitope, mainly in patients who tested
positive for citrullinated cyclic anti-peptide antibodies. The presence of this amino acid sequence in
RA patients is associated with several immunological events such as T lymphocyte selection, changes
in peptide affinity, molecular mimicry of microbial antigens, antigenic presentation and lymphocyte
apoptosis acceleration (4).
The treatment applied to patients with rheumatological diseases of immunoinflammatory
nature, mainly to RA patients, has significantly changed over the past few years. Improved knowledge
about the pathogenesis and recognition of therapeutic targets has enabled introducing therapies based
on immunobiological compounds (also called biological agents or disease-modifying antirheumatic
drugs – biologic DMADs), which have significantly contributed to improve patients’ quality of life,
as well as to decrease morbidity and mortality rates among patients with autoimmune rheumatic
diseases (5). However, a substantial number of RA patients presented unsatisfactory (1), response or
adverse events to these drugs, whose use had to be interrupted or replaced.
Smoking is one of the main risk factors for RA treatment interruption (6). Other risk factors
comprise patients’ age, comorbidities and number of previously used biological drugs (7, 1).
In addition, recent studies have shown that smoking habit is associated with unsatisfactory
response to anti-TNF therapy; moreover, smoker patients can experience adverse events that require
treatment interruption (1).
In light of the foregoing, the aims of the current study were to assess the influence of smoking
habit on disease activity in patients with rheumatoid arthritis and its influence on patients’ response to
29
RA treatment, since this habit appears to have significant impact on RA evolution and on patients’
response to treatment.
4.2 PATIENTS AND METHODS
Cohort study conducted with RA patients followed up from January 2010 to November 2019;
participants were registered in the Brazilian Registry for Monitoring of Biologic Therapies -
BIOBADABRASIL (8), which is promoted by the Brazilian Society of Rheumatology in order to
monitor the use of all biological drugs licensed for rheumatological use in the country (9).
The following aspects were taken into consideration in the investigated group: presence or
absence of smoking habit at the initial consultation, disease activity degree based on Disease Activity
Score 28 (DAS28) at the time patients were included in the study, biological therapy type in use,
reasons for treatment suspension and incidence of adverse events during the follow-up period.
Inclusion criteria comprised patients diagnosed with RA based on classification criteria set by
the American College of Rheumatology (10), who were undergoing treatment with biological agents
or who had suspended the treatment, for any reason - as long as no more than 1 year had elapsed since
the last treatment. The control group comprised patients who were not using biological drugs; they
were assessed based on the same aspects and data systematics applied to patients who used biological
drugs.
Exclusion criteria comprised any diagnosis other than RA, unknown smoking status and
records lacking data about patients’ age and sex.
Variables analyzed in the current study were: 1) initial disease activity degree based on DAS
28 (DAS 28> 3.2 - moderate/high activity; and DAS 28≤ 3.2 - mild activity/remission) recorded at the
time patients were included in the study; 2) smoking habit (yes/no) at consultation time; 3) adverse
events during the follow-up period (yes/no); and 4) adverse event severity (not severe/severe/fatal).
30
The association between smoking and disease activity was assessed, as well as its influence on
the incidence of adverse events.
4.3 STATISTICAL ANALYSIS
Categorical variables were summarized based on absolute and relative frequencies. Information
about the missing data type was depicted in the tables as “not informed” in order to enable real relative
frequency calculation based on the total size of the assessed sample.
Continuous variables were summarized based on the means at 95% confidence intervals (95%
CI) or on the median and interquartile range (IQR), depending on the distribution type, which was
assessed through Shapiro-Wilk test. Continuous variables were compared between two groups of one
categorical variable, based on unpaired t test or on its nonparametric analog Mann-Whitney test.
The association between independent variables and the dependent one was assessed through
Pearson’s chi-square test or Fisher’s exact test, whenever necessary. Relative risk (RR) was used to
measure the strength of association at 95% CI.
Kaplan-Meier curve was used to estimate patients’ likelihood of remaining free of adverse
events based on the time between treatment implementation and adverse event incidence (time in
months); individuals who did not present the event of interest were not taken into consideration.
Similarity of survival functions was assessed through the Long-rank test.
Poisson regression with robust variance was used to adjust the effects of independent variables
on the dependent variable; variables recording p < 0.20 in the bivariate analysis or the ones presenting
biological plausibility were included in the model. There was statistically significant difference when
p < 0.05 in the two-tailed test; all analyses were performed in the Stata 13.0 software (College Station,
Texas, USA).
31
4.4 RESULTS
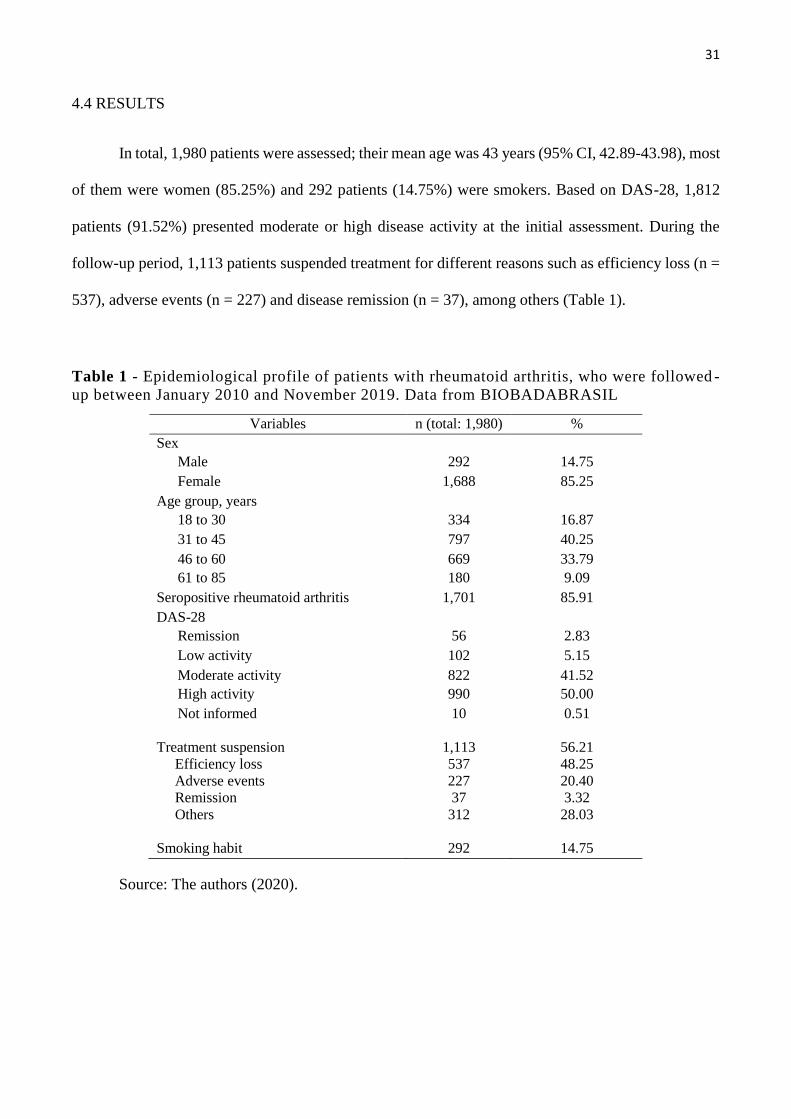
In total, 1,980 patients were assessed; their mean age was 43 years (95% CI, 42.89-43.98), most
of them were women (85.25%) and 292 patients (14.75%) were smokers. Based on DAS-28, 1,812
patients (91.52%) presented moderate or high disease activity at the initial assessment. During the
follow-up period, 1,113 patients suspended treatment for different reasons such as efficiency loss (n =
537), adverse events (n = 227) and disease remission (n = 37), among others (Table 1).
Table 1 - Epidemiological profile of patients with rheumatoid arthritis, who were followed -
up between January 2010 and November 2019. Data from BIOBADABRASIL
Variables n (total: 1,980) %
Sex
Male 292 14.75
Female 1,688 85.25
Age group, years
18 to 30 334 16.87
31 to 45 797 40.25
46 to 60 669 33.79
61 to 85 180 9.09
Seropositive rheumatoid arthritis 1,701 85.91
DAS-28
Remission 56 2.83
Low activity 102 5.15
Moderate activity 822 41.52
High activity 990 50.00
Not informed
10 0.51
Treatment suspension
Efficiency loss
Adverse events
Remission
Others
1,113
537
227
37
312
56.21
48.25
20.40
3.32
28.03
Smoking habit 292 14.75
Source: The authors (2020).
32
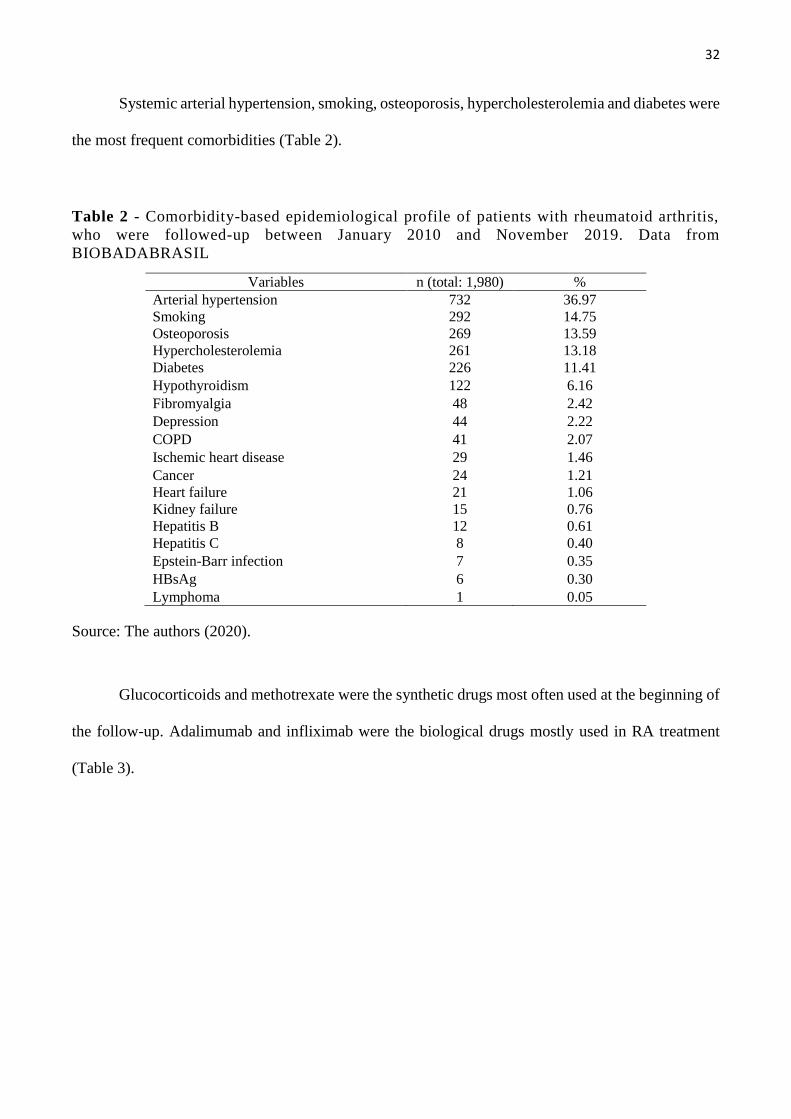
Systemic arterial hypertension, smoking, osteoporosis, hypercholesterolemia and diabetes were
the most frequent comorbidities (Table 2).
Table 2 - Comorbidity-based epidemiological profile of patients with rheumatoid arthritis,
who were followed-up between January 2010 and November 2019. Data from
BIOBADABRASIL
Variables n (total: 1,980) %
Arterial hypertension 732 36.97
Smoking 292 14.75
Osteoporosis 269 13.59
Hypercholesterolemia 261 13.18
Diabetes 226 11.41
Hypothyroidism 122 6.16
Fibromyalgia 48 2.42
Depression 44 2.22
COPD 41 2.07
Ischemic heart disease 29 1.46
Cancer 24 1.21
Heart failure 21 1.06
Kidney failure 15 0.76
Hepatitis B 12 0.61
Hepatitis C 8 0.40
Epstein-Barr infection 7 0.35
HBsAg 6 0.30
Lymphoma 1 0.05
Source: The authors (2020).
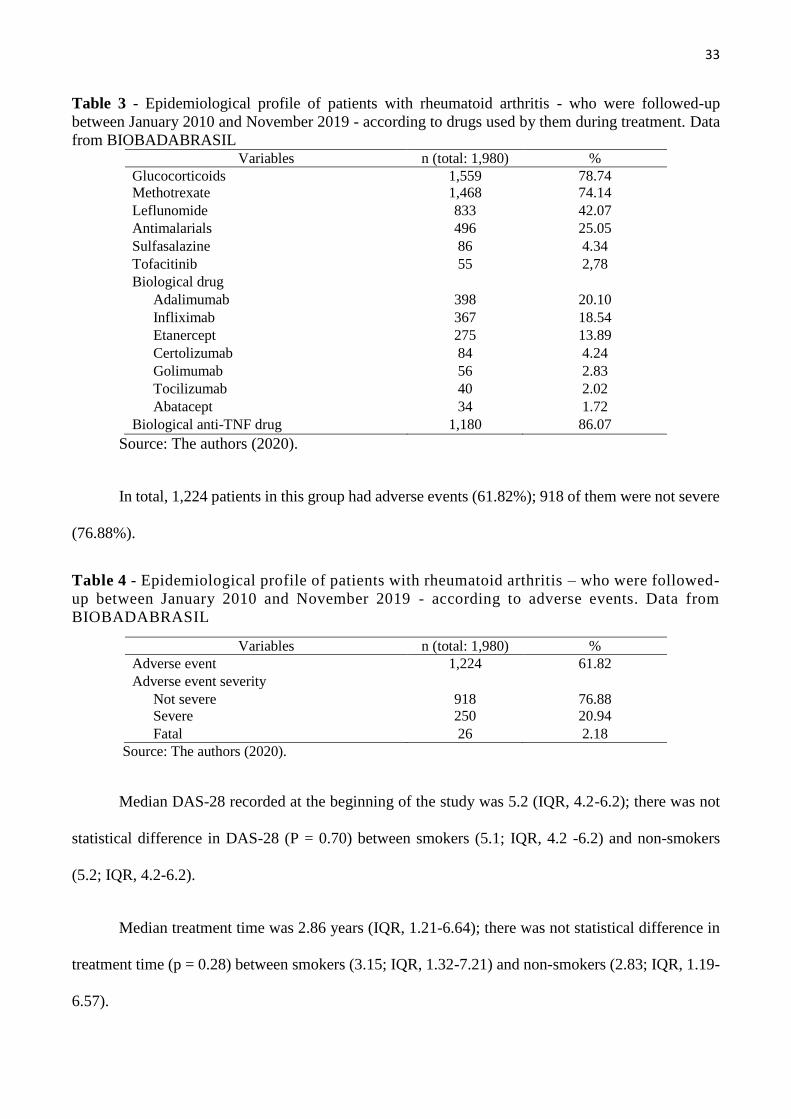
Glucocorticoids and methotrexate were the synthetic drugs most often used at the beginning of
the follow-up. Adalimumab and infliximab were the biological drugs mostly used in RA treatment
(Table 3).
33
Table 3 - Epidemiological profile of patients with rheumatoid arthritis - who were followed-up
between January 2010 and November 2019 - according to drugs used by them during treatment. Data
from BIOBADABRASIL Variables n (total: 1,980) %
Glucocorticoids 1,559 78.74
Methotrexate 1,468 74.14
Leflunomide 833 42.07
Antimalarials 496 25.05
Sulfasalazine 86 4.34
Tofacitinib 55 2,78
Biological drug
Adalimumab 398 20.10
Infliximab 367 18.54
Etanercept 275 13.89
Certolizumab 84 4.24
Golimumab 56 2.83
Tocilizumab 40 2.02
Abatacept 34 1.72
Biological anti-TNF drug 1,180 86.07
Source: The authors (2020).
In total, 1,224 patients in this group had adverse events (61.82%); 918 of them were not severe
(76.88%).
Table 4 - Epidemiological profile of patients with rheumatoid arthritis – who were followed-
up between January 2010 and November 2019 - according to adverse events. Data from
BIOBADABRASIL
Variables n (total: 1,980) %
Adverse event 1,224 61.82
Adverse event severity
Not severe 918 76.88
Severe 250 20.94
Fatal 26 2.18
Source: The authors (2020).
Median DAS-28 recorded at the beginning of the study was 5.2 (IQR, 4.2-6.2); there was not
statistical difference in DAS-28 (P = 0.70) between smokers (5.1; IQR, 4.2 -6.2) and non-smokers
(5.2; IQR, 4.2-6.2).
Median treatment time was 2.86 years (IQR, 1.21-6.64); there was not statistical difference in
treatment time (p = 0.28) between smokers (3.15; IQR, 1.32-7.21) and non-smokers (2.83; IQR, 1.19-
6.57).
34
Patients recorded median time between disease diagnosis and treatment implementation equal
to 5.37 years (IQR, 1.59-11.86); there was not statistical difference in this variable (p = 0.82) between
smokers (5.48; IQR, 1.82-11.80) and non-smokers (5.37; IQR, 1.58-11.91).
Median time between treatment implementation and adverse event was 78.66 months (IQR,
22.66-172.58); this variable was statistically different (p = 0.02) and shorter among smokers (65.75;
IQR 19.58-144.00) than among non-smokers (81.16; IQR, 28.58-177.16).
For every 10 patients followed-up in the current study, 6 experienced adverse events during the
rheumatoid arthritis treatment with biological drugs. Patients had 4.41 adverse events during the entire
follow-up period (95% CI, 4.17-4.64), on average; smokers (4.74; 95% CI, 4.15- 5.33) recorded mean
adverse events statistically different (p = 0.03) and higher than non-smokers (4.33; 95% CI, 4.01-4.59).
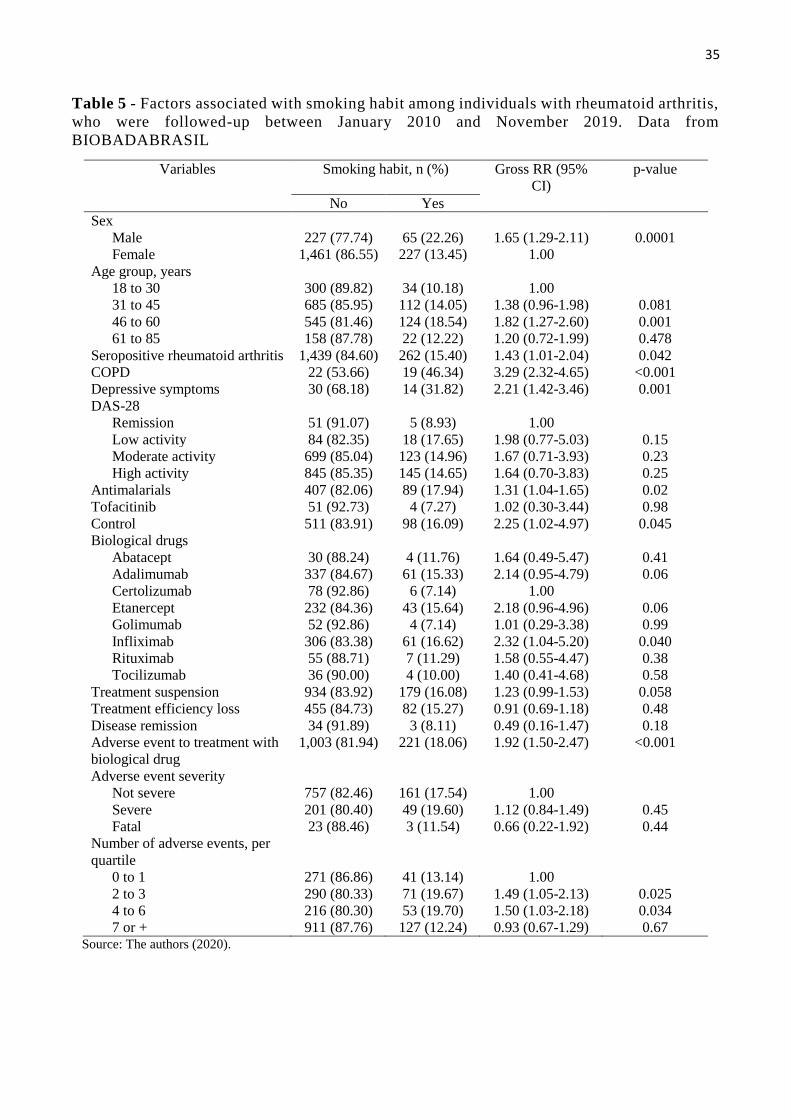
Based on bivariate analysis, smoking habit was 65% higher among male individuals with
rheumatoid arthritis, 82% higher among individuals in the age group 4-6-60 years, 43% higher among
individuals with seropositive rheumatoid arthritis, 121% higher among individuals with HIV
depressive symptoms, 132% higher among individuals treated with infliximab (biological drug), 92%
higher among individuals who had adverse events during treatment with biological drug, and 50%
higher among individuals who had 2 to 6 adverse events during follow-up (Table 5).
Smoking habit did not influence adverse event severity, disease remission or treatment
efficiency loss in this group of patients (Table 5).
35
Table 5 - Factors associated with smoking habit among individuals with rheumatoid arthritis,
who were followed-up between January 2010 and November 2019. Data from
BIOBADABRASIL
Variables Smoking habit, n (%) Gross RR (95%
CI)
p-value
No Yes
Sex
Male 227 (77.74) 65 (22.26) 1.65 (1.29-2.11) 0.0001
Female 1,461 (86.55) 227 (13.45) 1.00
Age group, years
18 to 30 300 (89.82) 34 (10.18) 1.00
31 to 45 685 (85.95) 112 (14.05) 1.38 (0.96-1.98) 0.081
46 to 60 545 (81.46) 124 (18.54) 1.82 (1.27-2.60) 0.001
61 to 85 158 (87.78) 22 (12.22) 1.20 (0.72-1.99) 0.478
Seropositive rheumatoid arthritis 1,439 (84.60) 262 (15.40) 1.43 (1.01-2.04) 0.042
COPD 22 (53.66) 19 (46.34) 3.29 (2.32-4.65) <0.001
Depressive symptoms 30 (68.18) 14 (31.82) 2.21 (1.42-3.46) 0.001
DAS-28
Remission 51 (91.07) 5 (8.93) 1.00
Low activity 84 (82.35) 18 (17.65) 1.98 (0.77-5.03) 0.15
Moderate activity 699 (85.04) 123 (14.96) 1.67 (0.71-3.93) 0.23
High activity 845 (85.35) 145 (14.65) 1.64 (0.70-3.83) 0.25
Antimalarials 407 (82.06) 89 (17.94) 1.31 (1.04-1.65) 0.02
Tofacitinib 51 (92.73) 4 (7.27) 1.02 (0.30-3.44) 0.98
Control 511 (83.91) 98 (16.09) 2.25 (1.02-4.97) 0.045
Biological drugs
Abatacept 30 (88.24) 4 (11.76) 1.64 (0.49-5.47) 0.41
Adalimumab 337 (84.67) 61 (15.33) 2.14 (0.95-4.79) 0.06
Certolizumab 78 (92.86) 6 (7.14) 1.00
Etanercept 232 (84.36) 43 (15.64) 2.18 (0.96-4.96) 0.06
Golimumab 52 (92.86) 4 (7.14) 1.01 (0.29-3.38) 0.99
Infliximab 306 (83.38) 61 (16.62) 2.32 (1.04-5.20) 0.040
Rituximab 55 (88.71) 7 (11.29) 1.58 (0.55-4.47) 0.38
Tocilizumab 36 (90.00) 4 (10.00) 1.40 (0.41-4.68) 0.58
Treatment suspension 934 (83.92) 179 (16.08) 1.23 (0.99-1.53) 0.058
Treatment efficiency loss 455 (84.73) 82 (15.27) 0.91 (0.69-1.18) 0.48
Disease remission 34 (91.89) 3 (8.11) 0.49 (0.16-1.47) 0.18
Adverse event to treatment with
biological drug
1,003 (81.94) 221 (18.06) 1.92 (1.50-2.47) <0.001
Adverse event severity
Not severe 757 (82.46) 161 (17.54) 1.00
Severe 201 (80.40) 49 (19.60) 1.12 (0.84-1.49) 0.45
Fatal 23 (88.46) 3 (11.54) 0.66 (0.22-1.92) 0.44
Number of adverse events, per
quartile
0 to 1 271 (86.86) 41 (13.14) 1.00
2 to 3 290 (80.33) 71 (19.67) 1.49 (1.05-2.13) 0.025
4 to 6 216 (80.30) 53 (19.70) 1.50 (1.03-2.18) 0.034
7 or + 911 (87.76) 127 (12.24) 0.93 (0.67-1.29) 0.67 Source: The authors (2020).
36
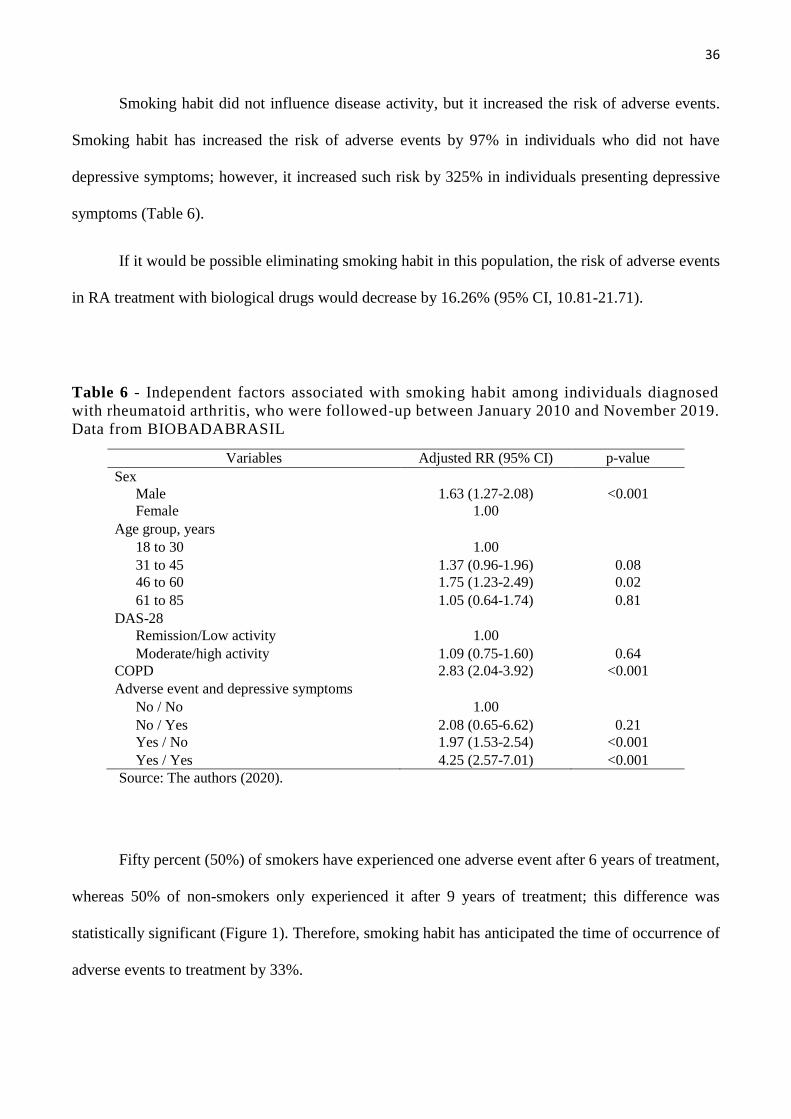
Smoking habit did not influence disease activity, but it increased the risk of adverse events.
Smoking habit has increased the risk of adverse events by 97% in individuals who did not have
depressive symptoms; however, it increased such risk by 325% in individuals presenting depressive
symptoms (Table 6).
If it would be possible eliminating smoking habit in this population, the risk of adverse events
in RA treatment with biological drugs would decrease by 16.26% (95% CI, 10.81-21.71).
Table 6 - Independent factors associated with smoking habit among individuals diagnosed
with rheumatoid arthritis, who were followed-up between January 2010 and November 2019.
Data from BIOBADABRASIL
Variables Adjusted RR (95% CI) p-value
Sex
Male 1.63 (1.27-2.08) <0.001
Female 1.00
Age group, years
18 to 30 1.00
31 to 45 1.37 (0.96-1.96) 0.08
46 to 60 1.75 (1.23-2.49) 0.02
61 to 85 1.05 (0.64-1.74) 0.81
DAS-28
Remission/Low activity 1.00
Moderate/high activity 1.09 (0.75-1.60) 0.64
COPD 2.83 (2.04-3.92) <0.001
Adverse event and depressive symptoms
No / No 1.00
No / Yes 2.08 (0.65-6.62) 0.21
Yes / No 1.97 (1.53-2.54) <0.001
Yes / Yes 4.25 (2.57-7.01) <0.001
Source: The authors (2020).
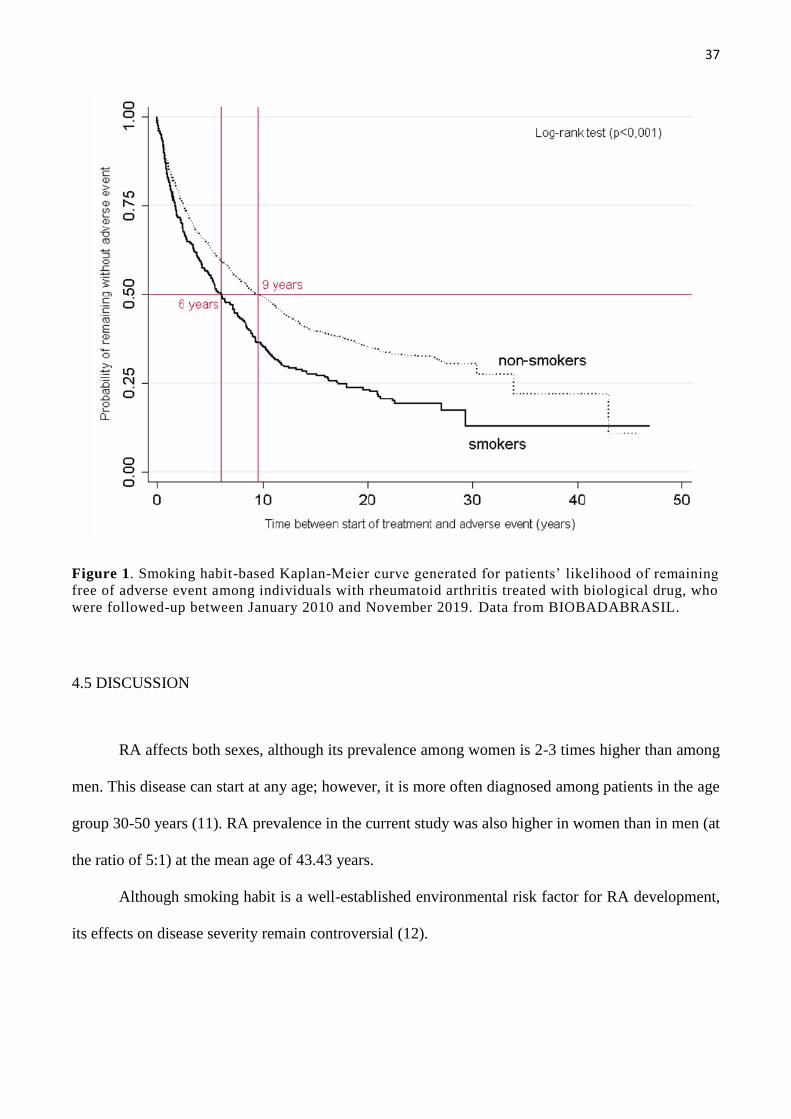
Fifty percent (50%) of smokers have experienced one adverse event after 6 years of treatment,
whereas 50% of non-smokers only experienced it after 9 years of treatment; this difference was
statistically significant (Figure 1). Therefore, smoking habit has anticipated the time of occurrence of
adverse events to treatment by 33%.
37
Figure 1. Smoking habit-based Kaplan-Meier curve generated for patients’ likelihood of remaining
free of adverse event among individuals with rheumatoid arthritis treated with biological drug, who
were followed-up between January 2010 and November 2019. Data from BIOBADABRASIL.
4.5 DISCUSSION
RA affects both sexes, although its prevalence among women is 2-3 times higher than among
men. This disease can start at any age; however, it is more often diagnosed among patients in the age
group 30-50 years (11). RA prevalence in the current study was also higher in women than in men (at
the ratio of 5:1) at the mean age of 43.43 years.
Although smoking habit is a well-established environmental risk factor for RA development,
its effects on disease severity remain controversial (12).
38
The current study has shown that smoking habit was not associated with increased disease
activity (RR 1.09; 95% CI 0.75-1.6; p = 0.64), but it increased the risk of adverse events (RR 1.97;
95% CI 1.63-2.54).
In 2012, a cohort study conducted in Sweden by Soderlin et al. (13), has evaluated the effect
of smoking on response to therapy, disease activity and drug survival in RA patients subjected to Anti-
TNF treatment for the first time. They observed that smoking did not influence disease activity at the
beginning of the study. In addition, individuals who smoked over 20 packs/year presented shorter drug
survival than non-smokers. It is worth emphasizing that information about patients’ smoking status in
the current study was only reported at the beginning of treatment; accurate data about such habit were
not collected during follow-up.
Bing Lu et al. (14), have assessed the association of smoking and alcohol intake with disease
activity and functional status in an American cohort comprising 662 RA patients, who were followed-
up for 4 years, on average. The aforementioned authors also concluded that patients’ current smoking
status was not associated with higher DAS 28.
In 2017, Duque et al. (15) have conducted a cohort study in Colombia with 129 patients
presenting early-onset rheumatoid arthritis. After 3 years of follow-up, they concluded that patients’
current smoking status was associated with lesser disability and lower risk of presenting active disease
(DAS 28 > 2.6), a fact that suggested the protective effect of smoking on disease activity.
In 2018, V Torrent-Segarra et al. (16) have assessed 1,349 RA patients in a 10-year cohort.
They concluded that non-smokers recorded initial DAS 28 values higher than those recorded for
current and former smokers.
However, it is worth mentioning that most published studies present participants’ current
smoking status, which is used to classify them as current, former and non-smokers; it was not possible
reporting such status in the current study.
39
According to a cohort study conducted by the Norfolk Arthritis Register (NOAR), smokers
were less likely to have persistent synovitis than non-smokers. In addition, smoking habit was a
protective factor against joint damage (17). The anti-inflammatory role played by nicotine could be
explained by the lower systemic inflammatory condition observed in these patients, since nicotine
induces immunosuppression and inhibits IL-6 and IL-8 secretion in RA patients’ synoviocytes (18).
On the other hand, some studies have shown that smoking habit was associated with the worst
disease activity. In 2016, Sokolove et al. (19) have assessed an American cohort comprising 1,488 RA
patients; they concluded that patients’ current smoking status was associated with higher DAS-28
values.
A cohort (20) study comprising 10 countries (United Kingdom, Norway, United States,
Canada, Sweden, Greece, South Africa, Spain and Mexico) has assessed 3,311 patients for 3.5 years
in order to compare disease activity, risk factors for cardiovascular disease (CVD) and risk of future
CVD events between smokers and non-smokers. Results evidenced that smokers were more likely to
have moderate or high disease activity than non-smokers. In addition, the study concluded that
smoking cessation in RA patients was associated with improved disease activity.
Studies have shown the influence of smoking on RA patients’ response to treatment with
antirheumatic drugs (21). In 2006, Hyrich et al. (22) conducted a study in the United Kingdom with
RA patients treated with etanercept (ETA) or infliximab (INF) during at least 6-month follow-up. They
concluded that smoker RA patients presented reduced clinical response, mainly patients treated with
INF. This outcome has shown association between smoking habit and poor prognosis with INF, which
may reflect changes in this drug pharmacokinetics (23).
According to a cohort study conducted in the Netherlands (1), 103 (41%) of the 252 RA patients
who started taking anti-TNF drug had to interrupt the treatment. Treatment ineffectiveness was the
most common cause of treatment suspension (62%); it was followed by adverse events (31%) and
40
adverse events with treatment ineffectiveness (6%). Smoking was the predictive factor for treatment
discontinuation.
It is worth emphasizing that different studies presented conflicting evidence on the role played
by smoking habit in autoimmune disease development and severity, as well as in patients’ response to
treatment. There is great variability in study designs, population sizes, smoking duration and extent
definitions and in methods used to distinguish the smoking effects from other socioeconomic factors
and environmental confounders.
One of the limitations in the current study lies on the fact that information about patients’
smoking status was only collected at the initial consultation, when they joined the treatment cohort.
Thus, additional information about patients’ smoking habits, such as smoking load, previous history
of smoking or even, although unlikely, smoking cessation during treatment, was not collected during
follow-up. Such information would allow better categorizing this variable into current smoking,
previous smoking and non-smoking in order to decrease the likelihood of classification error bias (24).
It is essential conducting further studies focused on assessing the impact of smoking cessation
(6) on disease evolution, based on disease activity and patients’ response to treatment in order to enable
this measure to be routinely adopted within rheumatological practice. In addition, if one takes into
consideration the high cost with biological drugs and their potential risk of triggering adverse events,
the knowledge about predictive response factors could help better guiding the application of such
therapies.
4.6 CONCLUSION
Smoking habit did not influence disease activity at the beginning of biological therapy in the
current study, but it increased the risk of adverse events in RA patients subjected to treatment based
on biological drugs.
41
4.7 REFERENCES
1- Cuppen BV, Jacobs JW, Ter Borg EJ, Marijnissen AC, Bijlsma JW, Lafeber F P, Van Laar JM.
Necessity of TNF-alpha inhibitor dis-continuation in rheumatoid arthritis is predicted by smoking and
number of previously used biological DMARDs. Clinical and Experimental Rheumatology. 2017.
2- Mota LMH, Cruz BA, Brenol CV, Pereira IA, Fronza LSR, Bertolo MB. Consenso da Sociedade
Brasileira de Reumatologia 2011 para o diagnóstico e avaliação inicial da artrite reumatóide. Rev Bras
Reumatol. 2011; doi: http://dx.doi.org/10.1590/S0482-50042011000300002.
3- Pinheiro GRC. Instrumentos de Medida da Atividade da Artrite Reumatoide- Por que e como
empregá-los. Rev Bras Reumatol. 2007; doi: https://doi.org/10.1590/S0482-50042007000500011
4- Moura MC, Zakszewski PTS, Silva MBG, Share TL. Perfil dos pacientes com manifestações extra-
articulares de artrite reumatoide de um serviço ambulatorial em Curitiba, Sul do Brasil. Rev Bras
Reumatol. 2012; doi: https://doi.org/10.1590/S0482-50042011000300002.
5- Fransen J, Van Riel PL. The Disease Activity Score and the EULAR Response Criteria. Rheum Dis
Clin North Am. 2009; doi: 10.1016 / j.rdc.2009.10.001.
6- Vittecoq O, Richar L, Banse C, Lequerre T. The impact of smoking on rheumatoid arthritis
outcomes. Joint Bone Spine. 2018; doi: 10.1016/j.jbspin.2018.09.012
42
7- Ramiro S, Landewé R, Van Der Heijde D, Harrison D, Collier D, Michaud K. Taxas de
descontinuação de produtos biológicos em pacientes com artrite reumatóide: os inibidores de TNF são
diferentes dos inibidores não-TNF? Rheumatoid Arthritis. 2015; doi:10.1136/rmdopen-2015-000155
8- Titton DC, Silveira IG, Louzada-Junior P, Hayata AL, Carvalho HM, Ranza R, Rezende LS,
Pinheiro GS, Santos JL, Miranda JR, et al. Brazilian biologic registry: BiobadaBrasil implementation
process and preliminary results. Rev Bras Reumatol. 2011; doi: https://doi.org/10.1590/S0482-
50042011000200005
9- Yonekura CL, Oliveira RDR, Titton DC, Ranza R, Ranzolin A, Hayata AL, Duarte A, Silveira IG,
Carvalho HMDS, Moraes JCB, Abreu MM, Valin V, Bianchi W, Brenol CV, Pereira IA, Costa I,
Macieira JC, Miranda JRS, Guedes-Barbosa LS, Bertolo MB, Sauma MFLDC, Silva MBG, Freire M,
Scheinberge MA, Toledo RA, Oliveira, SKF, Fernandes V, Pinheiro GDRC, Laurindo IMM, Louzada-
Junior P. Incidence of tuberculosis among patients with rheumatoid arthritis using TNF blockers in
Brazil: data from the Brazilian Registry of Biological Therapies in Rheumatic Diseases (Registro
Brasileiro de Monitoração de Terapias Biológicas - BiobadaBrasil). Rev Bra de Reumatol. 2017; doi:
https://doi.org/10.1016/j.rbre.2017.05.005.
10- Arnett FC, Edworthy S M, Bloch DA, Mcshane DJ, Fries JF, Cooper NS, Healey LA, Kaplan SR,
Liang MH, Luthra HS. The American Rheumatism Association. 1987 revised criteria for the
classification of rheumatoid arthritis. Arthritis Rheum. 1988; doi:
https://doi.org/10.1002/art.1780310302.
11- Carvalho MA, Lanna C, Bertolo M, Ferreira G. Reumatologia: diagnóstico e tratamento. 5. ed. Rio
de Janeiro: Guanabara Koogan, 2019. p. 832.
43
12- Sugiyama D, Nishimura , Tamaki K, Tsuji G, Nakazawa T, Morinobu A, Kumagai S.Impact of
smoking as a risk factor for developing rheumatoid arthritis: a meta-analysis of observational studies.
Ann Rheum Dis. 2010; doi: 10.1136/ard.2008.096487
13- Söderlin MK, Petersson IF, Geborek P. The effect of smoking on response and drug survival in
rheumatoid arthritis patients treated with their first anti-TNF drug. Scand J Rheumatol. 2012; doi:
10.3109/03009742.2012.698394.
14- Lu B, Rho YH, Cui J, Iannaccone CK, Frits ML, Karlson EW, Shadick NA. Associations of
smoking and alcohol consumption with disease activity and functional status in rheumatoid arthritis. J
Rheumatol. 2014 Jan;41(1):24-30. doi: 10.3899/jrheum.130074.
15- Quintana‑Duque MA, Rondon‑Herrera F, Calvo‑Paramo E, Jose J. The impact of smoking on
disease activity, disability, and radiographic damage in rheumatoid arthritis: is cigarette protective?
Rheumatol Int.2017; doi: 10.1007/s00296-017-3845-8.
16- Torrente-Segarra V, Bergstra SA, Solomon-Escoto K, Da Silva J, Veale DJ, Al-Emadi S, Huizinga
T. Is current smoking status and its relationship to anti-cyclic citrullinated peptide antibodies a
predictor of worse response to biological therapies in rheumatoid arthritis patients? 2018; doi:
10.1080/03009742.2017.1418423.
17- Harrison BJ, Silman AJ, Wiles NJ. The association of cigarette smoking with disease outcome in
patients with early infammatory polyarthritis. Arthritis Rheum. 2001; doi:
https://doi.org/10.1002/1529-0131(200102)44:2<323::AID-ANR49>3.0.CO;2-C

44
18- Wang H1, Yu M, Ochani M, Amella CA, Tanovic M, Susarla S, Li JH, Wang H, Yang H, Ulloa
L, Al-Abed Y, Czura CJ, Tracey KJ. Nicotinic acetylcholine receptor alpha7 subunit is an essential
regulator of inflammation. Nature. 2003; doi: 10.1038/nature01339
19- Sokolove J, Wagner CA, Lahey LJ, Sayles H, Duryee MJ, Reimold AM, Kerr G, Robinson WH,
Cannon GW, Thiele GM, Mikuls TR. Increased inflammation and disease activity among current
cigarette smokers with rheumatoid arthritis: a cross-sectional analysis of US veterans. Rheumatology
(Oxford). 2016; doi: 10.1093/rheumatology/kew285
20 Roelsgaard IK, Ikdahl E, Rollefstad S, Wibetoe G, Esbensen BA, Kitas GD, Van Riel P, Gabriel S,
Kvien TK, Douglas K, Wållberg-Jonsson S, Rantapää Dahlqvist S, Karpouzas G, Dessein PH, Tsang
L, El-Gabalawy H, Hitchon CA, Pascual-Ramos V, Contreras-Yáñez I, Sfikakis PP, González-Gay
MA, Crowson CS, Semb AG. Smoking cessation is associated with lower disease activity and predicts
cardiovascular risk reduction in rheumatoid arthritis patients. Rheumatology (Oxford). 2019; doi:
10.1093/rheumatology/kez557.
21- Linn-Rasker SP, Van Der Helm-Van Mah, Van Gaalen FA, Kloppenburg M, Vries RR, Le Cessie
S, Breedveld FC, Toes Re, Huizinga Tw. Smoking is a risk factor for anti-CCP antibodies only in
rheumatoid arthritis patients who carry HLA-DRB1 shared epitope alleles. Ann Rheum Dis. 2006; doi:
10.1136/ard.2005.041079
22- Hyrich KL, Watson KD, Silman AJ, Symmons DP. British Society for Rheumatology Biologics
Register. Predictors of response to anti-TNF-alpha therapy among patients with rheumatoid arthritis:
45
results from the British Society for Rheumatology Biologics Registers. Rheumatology (Oxford); doi;
10.1093/rheumatology/kel149.
23- Upchurch KS, Kay J. Evolution of treatment for rheumatoid arthritis. Rheumatology. 2012; doi:
10.1093/rheumatology/kes278.
24- Flegal KM, Kit BK, Graubard. Bias in Hazard Ratios Arising From Misclassification According
to Self-Reported Weight and Height in Observational Studies of Body Mass Index and Mortality. Am
J Epidemiol. 2018; doi: 10.1093/aje/kwx193.
46
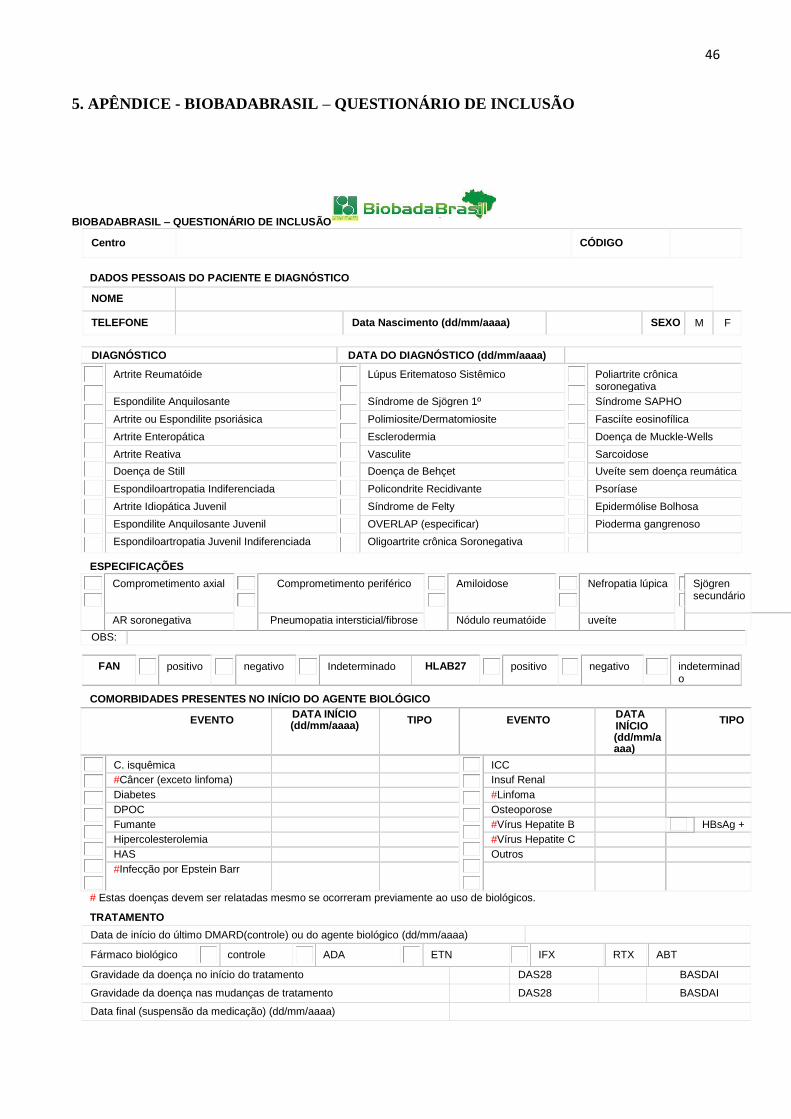
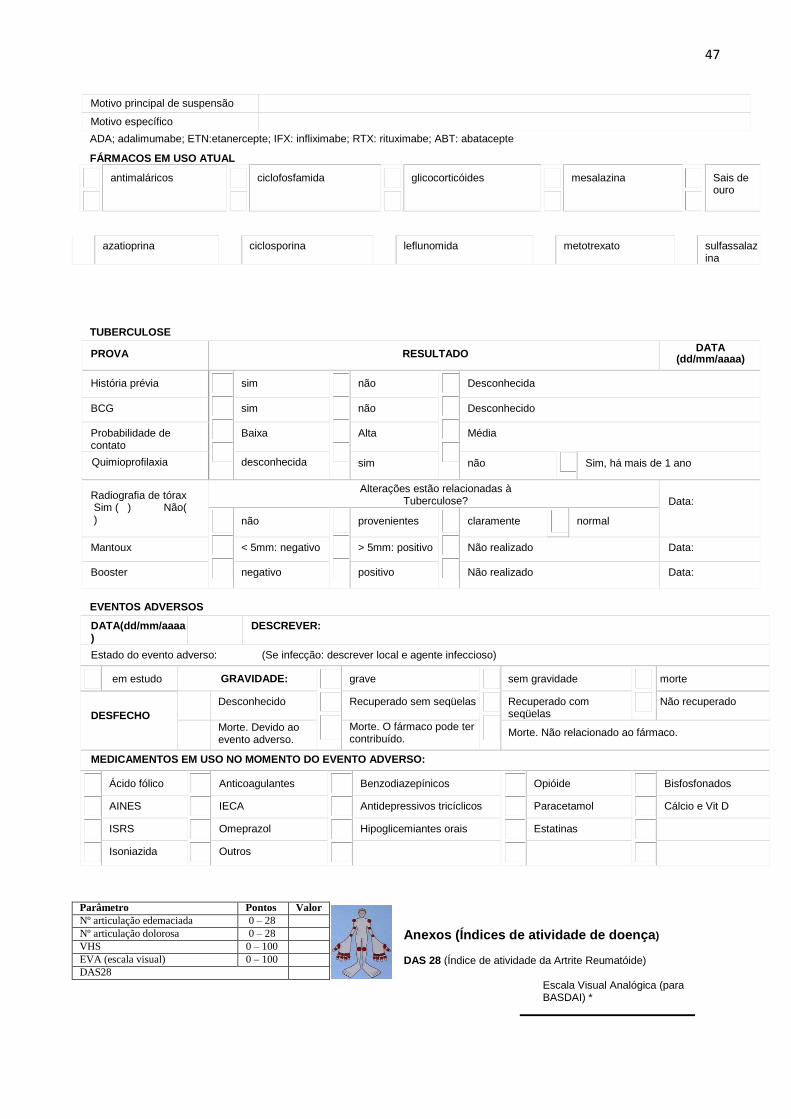
5. APÊNDICE - BIOBADABRASIL – QUESTIONÁRIO DE INCLUSÃO
BIOBADABRASIL – QUESTIONÁRIO DE INCLUSÃO
Centro
CÓDIGO
DADOS PESSOAIS DO PACIENTE E DIAGNÓSTICO
NOME
TELEFONE
Data Nascimento (dd/mm/aaaa)
SEXO M F
DIAGNÓSTICO DATA DO DIAGNÓSTICO (dd/mm/aaaa)
Artrite Reumatóide
Lúpus Eritematoso Sistêmico
Poliartrite crônica soronegativa
Espondilite Anquilosante Síndrome de Sjögren 1º Síndrome SAPHO
Artrite ou Espondilite psoriásica Polimiosite/Dermatomiosite Fasciíte eosinofílica
Artrite Enteropática Esclerodermia Doença de Muckle-Wells
Artrite Reativa Vasculite Sarcoidose
Doença de Still Doença de Behçet Uveíte sem doença reumática
Espondiloartropatia Indiferenciada Policondrite Recidivante Psoríase
Artrite Idiopática Juvenil Síndrome de Felty Epidermólise Bolhosa
Espondilite Anquilosante Juvenil OVERLAP (especificar) Pioderma gangrenoso
Espondiloartropatia Juvenil Indiferenciada Oligoartrite crônica Soronegativa
ESPECIFICAÇÕES
Comprometimento axial
Comprometimento periférico
Amiloidose
Nefropatia lúpica
Sjögren secundário
AR soronegativa Pneumopatia intersticial/fibrose Nódulo reumatóide uveíte
OBS:
FAN
positivo
negativo
Indeterminado HLAB27
positivo
negativo
indeterminado
COMORBIDADES PRESENTES NO INÍCIO DO AGENTE BIOLÓGICO
EVENTO DATA INÍCIO (dd/mm/aaaa)
TIPO EVENTO DATA INÍCIO (dd/mm/aaaa)
TIPO
C. isquêmica
ICC
#Câncer (exceto linfoma) Insuf Renal
Diabetes #Linfoma
DPOC Osteoporose
Fumante #Vírus Hepatite B HBsAg +
Hipercolesterolemia #Vírus Hepatite C
HAS Outros
#Infecção por Epstein Barr
# Estas doenças devem ser relatadas mesmo se ocorreram previamente ao uso de biológicos.
TRATAMENTO
Data de início do último DMARD(controle) ou do agente biológico (dd/mm/aaaa)
Fármaco biológico
controle
ADA
ETN
IFX
RTX
ABT
Gravidade da doença no início do tratamento DAS28 BASDAI
Gravidade da doença nas mudanças de tratamento DAS28 BASDAI
Data final (suspensão da medicação) (dd/mm/aaaa)
47
Motivo principal de suspensão
Motivo específico
ADA; adalimumabe; ETN:etanercepte; IFX: infliximabe; RTX: rituximabe; ABT: abatacepte
FÁRMACOS EM USO ATUAL
antimaláricos
ciclofosfamida
glicocorticóides
mesalazina
Sais de ouro
TUBERCULOSE
PROVA RESULTADO DATA
(dd/mm/aaaa)
História prévia
sim
não
Desconhecida
BCG sim não Desconhecido
Probabilidade de contato
Baixa Alta Média
Quimioprofilaxia desconhecida sim não Sim, há mais de 1 ano
Radiografia de tórax Sim ( ) Não( )
Alterações estão relacionadas à Tuberculose?
Data:
não
provenientes
claramente
normal
Mantoux < 5mm: negativo > 5mm: positivo Não realizado Data:
Booster negativo positivo Não realizado Data:
EVENTOS ADVERSOS
DATA(dd/mm/aaaa)
DESCREVER:
Estado do evento adverso: (Se infecção: descrever local e agente infeccioso)
em estudo GRAVIDADE:
grave
sem gravidade
morte
DESFECHO
Desconhecido Recuperado sem seqüelas Recuperado com seqüelas
Não recuperado
Morte. Devido ao evento adverso.
Morte. O fármaco pode ter contribuído.
Morte. Não relacionado ao fármaco.
MEDICAMENTOS EM USO NO MOMENTO DO EVENTO ADVERSO:
Ácido fólico
Anticoagulantes
Benzodiazepínicos
Opióide
Bisfosfonados
AINES IECA Antidepressivos tricíclicos Paracetamol Cálcio e Vit D
ISRS Omeprazol Hipoglicemiantes orais Estatinas
Isoniazida Outros
Anexos (Índices de atividade de doença)
DAS 28 (Índice de atividade da Artrite Reumatóide)
Escala Visual Analógica (para BASDAI) *
azatioprina
ciclosporina
leflunomida
metotrexato
sulfassalazina
Parâmetro Pontos Valor
Nº articulação edemaciada 0 – 28
Nº articulação dolorosa 0 – 28
VHS 0 – 100
EVA (escala visual) 0 – 100
DAS28
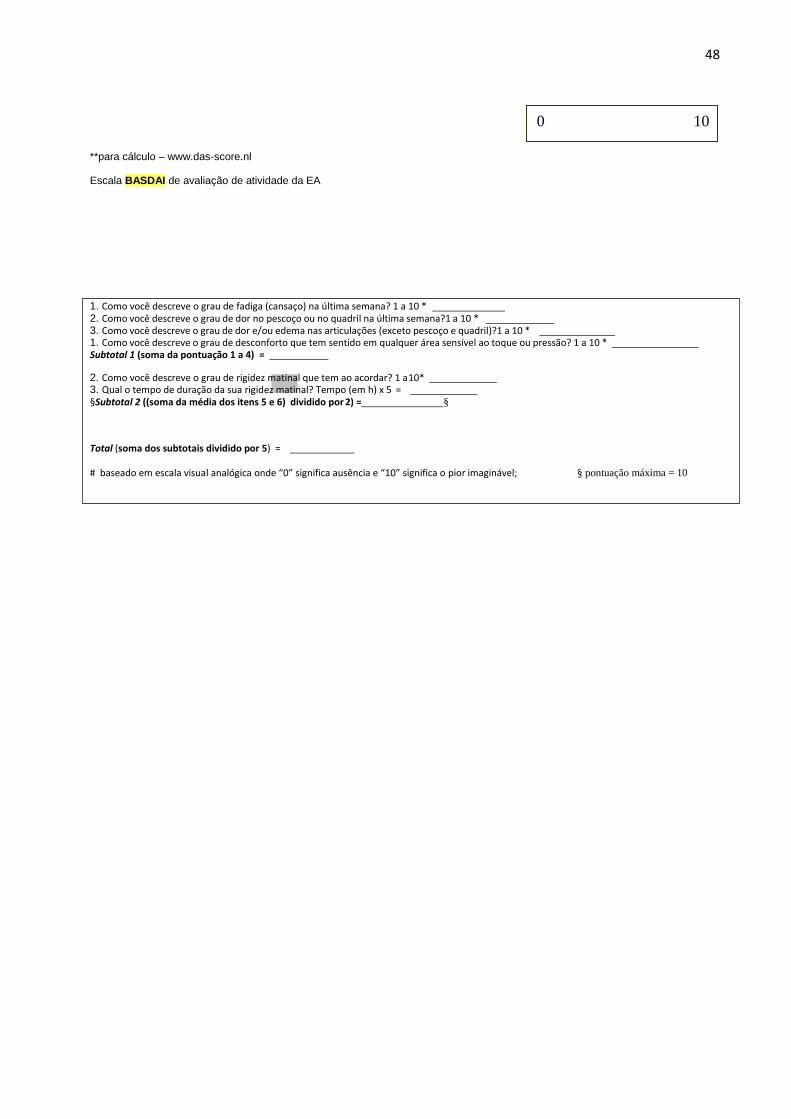
48
**para cálculo – www.das-score.nl
Escala BASDAI de avaliação de atividade da EA
1. Como você descreve o grau de fadiga (cansaço) na última semana? 1 a 10 * _ 2. Como você descreve o grau de dor no pescoço ou no quadril na última semana?1 a 10 * 3. Como você descreve o grau de dor e/ou edema nas articulações (exceto pescoço e quadril)?1 a 10 * 1. Como você descreve o grau de desconforto que tem sentido em qualquer área sensível ao toque ou pressão? 1 a 10 * Subtotal 1 (soma da pontuação 1 a 4) =
2. Como você descreve o grau de rigidez matinal que tem ao acordar? 1 a 10* 3. Qual o tempo de duração da sua rigidez matinal? Tempo (em h) x 5 = §Subtotal 2 ((soma da média dos itens 5 e 6) dividido por 2) = §
Total (soma dos subtotais dividido por 5) =
# baseado em escala visual analógica onde “0” significa ausência e “10” significa o pior imaginável; § pontuação máxima = 10
0 10
Recommended