Embed Size (px)
Citation preview

Francisco Pedro Morais Dias de Almeida Sampaio
Análise da função miocárdica sistólica e diastólica na cirrose hepática
Dissertação de candidatura ao grau de Doutor apresentada àFaculdade de Medicina da Universidade do Porto
Porto, 2014

Artigo 48º, § 3º - “A Faculdade não responde pelas doutrinas expendidas na dissertação.”Regulamento da Faculdade de Medicina da Universidade do Porto
Decreto-Lei n.º 19337 de 29 de Janeiro de 1931
3
JÚRI DA PROVA DE DOUTORAMENTO
Presidente: Reitor da Universidade do Porto
Vogais: Doutor Fausto José da Conceição Alexandre Pinto Professor Catedrático Convidado da Faculdade de Medicina da Universidade de Lisboa Doutora Ana Maria Gomes de Almeida Professora Associada da Faculdade de Medicina da Universidade de Lisboa
Doutor Joaquim Adelino Correia Ferreira Leite Moreira Professor Catedrático da Faculdade de Medicina da Universidade do Porto
Doutor Paulo Miguel Bettencourt Sardinha Pontes Fernando Professor Catedrático Convidado da Faculdade de Medicina da Universidade do Porto Orientador da Tese
Doutor Luís Filipe Vilela Pereira de Macedo Professor Associado Convidado da Faculdade de Medicina da Universidade do Porto
Doutora Maria Júlia Pires Maciel Barbosa Professora Auxiliar da Faculdade de Medicina da Universidade do Porto

5
Corpo Catedrático da Faculdade de Medicina da Universidade do Porto
Professores Catedráticos Efectivos
Doutor Manuel Alberto Coimbra Sobrinho Simões
Doutora Maria Amélia Duarte Ferreira
Doutor José Agostinho Marques Lopes
Doutor Patrício Manuel Vieira Araújo Soares Silva
Doutor Daniel Filipe Lima Moura
Doutor Alberto Manuel Barros da Silva
Doutor José Manuel Lopes Teixeira Amarante
Doutor José Henrique Dias Pinto de Barros
Doutora Maria Fátima Machado Henriques Carneiro
Doutora Isabel Maria Amorim Pereira Ramos
Doutora Deolinda Maria Valente Alves Lima Teixeira
Doutora Maria Dulce Cordeiro Madeira
Doutor Altamiro Manuel Rodrigues Costa Pereira
Doutor Rui Manuel Almeida Mota Cardoso
Doutor António Carlos Freitas Ribeiro Saraiva
Doutor José Carlos Neves da Cunha Areias
Doutor Manuel Jesus Falcão Pestana Vasconcelos
Doutor João Francisco Montenegro Andrade Lima Bernardes
Doutora Maria Leonor Martins Soares David
Doutor Rui Manuel Lopes Nunes
Doutor José Eduardo Torres Eckenroth Guimarães
Doutor Francisco Fernando Rocha Gonçalves
Doutor José Manuel Pereira Dias de Castro Lopes
Doutor António Albino Coelho Marques Abrantes Teixeira
Doutor Joaquim Adelino Correia Ferreira Leite Moreira
Doutora Raquel Ângela Silva Soares Lino
6
Professores Jubilados ou Aposentados
Doutor Abel Vitorino Trigo CabralDoutor Alexandre Alberto Guerra Sousa PintoDoutor Álvaro Jerónimo Leal Machado de AguiarDoutor Amândio Gomes Sampaio TavaresDoutor António Augusto Lopes VazDoutor António Carvalho Almeida CoimbraDoutor António Fernandes da FonsecaDoutor António Fernandes Oliveira Barbosa Ribeiro BragaDoutor António José Pacheco PalhaDoutor António Manuel Sampaio de Araújo TeixeiraDoutor Belmiro dos Santos PatrícioDoutor Cândido Alves Hipólito Reis Doutor Carlos Rodrigo Magalhães RamalhãoDoutor Cassiano Pena de Abreu e LimaDoutor Daniel Santos Pinto SerrãoDoutor Eduardo Jorge Cunha Rodrigues Pereira Doutor Fernando Tavarela VelosoDoutor Francisco de Sousa LéDoutor Henrique José Ferreira Gonçalves Lecour de MenezesDoutor Jorge Manuel Mergulhão Castro TavaresDoutor José Carvalho de OliveiraDoutor José Fernando Barros Castro CorreiaDoutor José Luís Medina VieiraDoutor José Manuel Costa Mesquita GuimarãesDoutor Levi Eugénio Ribeiro GuerraDoutor Luís Alberto Martins Gomes de AlmeidaDoutor Manuel António Caldeira Pais ClementeDoutor Manuel Augusto Cardoso de OliveiraDoutor Manuel Machado Rodrigues GomesDoutor Manuel Maria Paula BarbosaDoutor Maria da Conceição Fernandes Marques MagalhãesDoutor Maria Isabel Amorim de AzevedoDoutor Mário José Cerqueira Gomes BragaDoutor Serafim Correia Pinto GuimarãesDoutor Valdemar Miguel Botelho dos Santos CardosoDoutor Walter Friedrich Alfred Osswald
7
Ao abrigo do Art.º 8º do Decreto-Lei n.º388/70 fazem parte desta dissertação as seguintes
publicações:
I. Sampaio F, Pimenta J, Bettencourt N, Fontes-Carvalho R, Silva AP, Valente J, Bettencourt
P, Fraga J, Gama V. Systolic and diastolic dysfunction in cirrhosis: a tissue-Doppler and
speckle tracking echocardiography study. Sampaio F, Pimenta J, Bettencourt N, Fontes-
Carvalho R, Silva AP, Valente J, Bettencourt P, Fraga J, Gama V. Liver Int. 2013;33:1158-65
II. Sampaio F, Pimenta J, Bettencourt N, Fontes-Carvalho R, Silva AP, Valente J, Bettencourt
P, Fraga J, Gama V. Left atrial function is impaired in cirrhosis: a speckle tracking echocar-
diographic study. Hepatol Int 2014; 8:146-53
III. Sampaio F, Lamata P, Bettencourt N, Alt SC, Ferreira N, Kowallick JT, Valente J, Kutty S,
Pimenta J, Fraga J, Bettencourt P, Gama V, Schuster A. Assessment of cardiovascular physi-
ology using magnetic resonance myocardial stress testing reveals impaired contractile
reserve in patients with cirrhotic cardiomyopathy [Submitted]
IV. Sampaio F, Pimenta J, Bettencourt N, Fontes-Carvalho R, Silva AP, Valente J, Bettencourt P,
Fraga J, Gama V. Systolic dysfunction and diastolic dysfunction do not influence medium-
term prognosis in patients with cirrhosis. Eur J Intern Med. 2014;25:241-6
A contribuição pessoal para a realização destes trabalhos foi a seguinte:
Contribuição importante na sua concepção, na recolha do material, obtenção e análise dos
dados e redacção dos manuscritos.


À Joana
À Inês, ao João Francisco e à Rita


Aos meus Pais e à minha Irmã
À minha Família
Aos meus Amigos


Ao Professor Doutor Paulo Bettencourt


Ao Professor Doutor Carlos Ramalhão

17
AGRADECIMENTOS
“At the outset do not be worried about this big question—Truth. It is a very simple matter if each
one of you starts with the desire to get as much as possible. No human being is constituted to know
the truth, the whole truth, and nothing but the truth; and even the best of men must be content with
fragments, with partial glimpses, never the full fruition. In this unsatisfied quest the attitude of mind,
the desire, the thirst—a thirst that from the soul must arise!—the fervent longing, are the be-all and
the end-all”.
Sir William Osler – The Students Life, 1905
Mesmo consciente da impossibilidade de vislumbrar mais do que fugazes lampejos da verda-
de, o desenvolvimento de um projecto de investigação clínica, capaz de se revestir da robustez
necessária à elaboração de uma tese de doutoramento a apresentar à Faculdade de Medicina
da Universidade do Porto, apresenta inúmeras dificuldades. Não posso deixar assim de agrade-
cer a todos os que generosamente contribuíram – alimentando a insatisfação, a sede e o desejo
durante a demanda – para o resultado final, na forma desta dissertação.
De entre todos, o meu reconhecimento especial:
Ao Professor Doutor Paulo Bettencourt, por me ter desafiado, no início, a inscrever-me na
primeira edição do Programa Doutoral de Ciências Cardiovasculares, e pela confiança que em
mim depositou ao aceitar ser o meu orientador. A sua inteligência e argúcia, a sua qualidade
como clínico e como investigador e a sua rectidão na forma de abordar ambas as actividades
são para mim um exemplo. Agradeço-lhe a disponibilidade e o auxílio na idealização e na con-
dução dos trabalhos, na avaliação crítica dos resultados e na revisão cuidada dos artigos e desta
dissertação.

18
Ao Professor Doutor Nuno Bettencourt, pela ajuda no desenho e condução dos trabalhos,
na discussão dos resultados e na revisão dos manuscritos. O sucesso destes trabalhos depen-
deu, em boa parte, da sua capacidade de trabalho, dedicação e incentivo. A amizade que nos
une, há longos anos, sai pois ainda mais consolidada desta colaboração.
Ao Dr. Vasco Gama, director do Serviço de Cardiologia do Centro Hospitalar de Gaia/
Espinho, pela disponibilidade manifestada para a realização dos trabalhos naquele serviço, pelo
entusiasmo e pelo interesse sempre demonstrado sobre o seu andamento e resultados. A sua
energia, a constante busca pela inovação e pela melhoria e superação dos objectivos são a base
da excelência atingida pelo serviço que dirige, e um modelo a seguir. Sem a sua colaboração,
este projecto estaria votado ao insucesso.
Aos meus colegas nos serviços de Cardiologia, Gastroenterologia e Medicina Interna – em
particular ao Dr. Ricardo Fontes de Carvalho, Dr. Nuno Ferreira, Dra. Ana Paula Silva e Dr. João
Valente – que me auxiliaram no recrutamento dos doentes e na realização e análise dos exa-
mes efectuados nos vários trabalhos, bem como na revisão cuidada dos manuscritos.
Ao Professor Doutor Andreas Schuster, e a toda a sua equipa, pela análise das imagens de
ressonância magnética adquiridas e pela discussão minuciosa dos resultados. Sem a sua colabo-
ração desinteressada, a elaboração deste trabalho não teria sido possível.
Aos enfermeiros da consulta externa de Cardiologia – Enf. José Dias e Enf. Isabel Gomes –
pela disponibilidade que sempre demonstraram na colheita de amostras para os vários estudos
desta tese. Devo-lhes uma palavra de gratidão e amizade.
Aos técnicos da Ressonância Magnética do serviço de Radiologia, pela colaboração na aqui-
sição das imagens para um dos estudos desta tese. O seu profissionalismo e qualidade foram
indispensáveis para o sucesso alcançado.
Manifesto também o meu reconhecimento aos doentes e controlos que aceitaram partici-
par neste projecto.
19
Um agradecimento final:
Ao Professor Doutor Carlos Ramalhão, pelo incentivo constante e sobretudo pela genero-
sidade e amizade incondicionais que aumentam, diariamente, a minha dívida de gratidão para
com ele.
À Joana, por partilhar a vida comigo, por não me ter deixado desistir, e por ser capaz de,
simultaneamente, co-orientar os trabalhos, manter uma actividade clínica e docente dedicada e
gerir uma família (nos dias de hoje numerosa), e ser exemplar em todas estas tarefas.
À Inês, ao João Francisco e à Rita, por serem a alegria dos meus dias e por me fazerem,
periodicamente, recordar aquilo que verdadeiramente conta.
Aos meus Pais, à minha irmã e restante família, pelos valores que me ensinaram e pela for-
mação que me proporcionaram.
Aos meus amigos, por o serem.

Índice
21
ÍNDICE
I. INTRODUÇÃO .............................................................................................................................. 23
1.1. A cardiomiopatia cirrótica ........................................................................................................ 25
1.1.1. A circulação na cirrose .................................................................................................... 25
1.1.2. Evidência experimental .................................................................................................... 26
1.1.3. Evidência clínica ................................................................................................................. 29
1.1.3.1. Disfunção sistólica ......................................................................................................... 29
1.1.3.2. Disfunção diastólica ...................................................................................................... 29
1.1.3.3. Alterações electrofisiológicas ..................................................................................... 30
1.1.4. Definição de cardiomiopatia cirrótica ......................................................................... 31
1.1.5. Importância clínica ............................................................................................................ 31
1.2. Técnicas imagiológicas para avaliação da função miocárdica.............................................. 33
II. OBJECTIVOS ................................................................................................................................... 45
III. MÉTODOS ........................................................................................................................................ 49
IV. PUBLICAÇÕES .............................................................................................................................. 55
4.1. Systolic and diastolic dysfunction in cirrhosis: a tissue-Doppler and speckle tracking
echocardiography study ............................................................................................................. 57
4.2. Left atrial function is impaired in cirrhosis: a speckle tracking echocardiographic
study ............................................................................................................................................... 65
4.3. Assessment of cardiovascular physiology using magnetic resonance myocardial
stress testing reveals impaired contractile reserve in patients with cirrhotic
cardiomyopathy. ........................................................................................................................... 73
4.4. Systolic dysfunction and diastolic dysfunction do not influence medium-term
prognosis in patients with cirrhosis ........................................................................................ 93
22
Francisco Sampaio
V. DISCUSSÃO .................................................................................................................................... 99
5.1. Disfunção sistólica ..................................................................................................................... 101
5.2. Disfunção diastólica .................................................................................................................. 102
5.3. Prognóstico ................................................................................................................................. 104
VI. CONCLUSÕES ............................................................................................................................. 115
VII.RESUMO/ABSTRACT ............................................................................................................. 119
I. Introdução

Introdução
25
1.1. A CARDIOMIOPATIA CIRRÓTICA
Durante décadas, o único elo de ligação reconhecido entre cirrose hepática e a presença
de disfunção cardiovascular foi o consumo excessivo de álcool. Sendo uma das etiologias mais
frequentes de cirrose hepática, o álcool é igualmente uma causa reconhecida de cardiomiopatia
caracterizada por dilatação das câmaras cardíacas e disfunção sistólica[1]. O termo “doença car-
díaca alcoólica” terá sido utilizado pela primeira vez na literatura médica por William Macken-
zie em 1902[2]. A sua etiopatogenia é complexa, envolvendo factores genéticos e ambientais,
estando o efeito tóxico directo do álcool nos miócitos amplamente documentado[3-6]. A pre-
sença de uma circulação hiperdinâmica em doentes com cirrose hepática de etiologia alcoólica
foi descrita na década de 50 do século XX sendo igualmente atribuída, numa fase inicial, aos
efeitos do álcool na circulação periférica[7, 8]. No entanto, desde a década de 80 do século XX,
vários trabalhos experimentais têm revelado a presença de várias alterações cardiovasculares
associadas à cirrose, sugerindo a existência de uma cardiomiopatia cirrótica, independente da
sua etiologia.
1.1.1. A circulação na cirrose
As alterações hemodinâmicas na cirrose parecem relacionar-se com o desenvolvimento de
hipertensão do sistema porta, resultante da instalação de fibrose e de nódulos de regeneração
no parênquima hepático e consequente aumento das resistências vasculares intrahepáticas.
Estas alterações foram também demonstradas em modelos animais de hipertensão portal
pré-sinusoidal, sugerindo a sua correlação primária com a hipertensão portal, independente-
mente da existência de doença do parênquima hepático e da sua etiologia[9-11]. A hipertensão
portal associa-se a um aumento dos níveis circulantes de vários mediadores – como o óxido
nítrico, monóxido de carbono, endocanabinóides, adrenomedulina, factor de necrose tumoral
ou o peptídeo relacionado com o gene da calcitonina – com efeito vasodilatador, quer por
aumento da sua produção, quer por diminuição da sua degradação hepática[12-16]. A vasodilata-
26
Francisco Sampaio
ção arteriolar esplâncnica resultante, com “pooling” de sangue na periferia, contribui para uma
“hipovolémia central” com activação secundária, via baroreceptores, de sistemas vasoconstri-
tores de regulação da pressão arterial como o sistema nervoso simpático, o sistema renina-
angiotensina-aldosterona, e a secreção de arginina-vasopressina. O aumento do débito e da
frequência cardíaca daí resultantes e que caracterizam a circulação hiperdinâmica da cirrose
constituem, assim, um mecanismo compensatório que permite manter um “volume arterial
efetivo” normal nas fases mais precoces da doença. No entanto, a activação destes sistemas
promove igualmente retenção renal de sódio e água, contribuindo para o desenvolvimento de
ascite e edema, assim como de disfunção renal por hipoperfusão secundária à vasoconstrição
arteriolar. De facto, nas fases mais avançadas da doença, a incapacidade de aumentar o débito
cardíaco poderá ser um mecanismo importante no desenvolvimento de síndrome hepatorre-
nal, que se associa normalmente a mau prognóstico[17, 18].
1.1.2. Evidência experimental
No entanto a disfunção cardiovascular na cirrose não parece limitar-se à circulação perifé-
rica e vários estudos experimentais, em modelos de cirrose, documentaram diferentes altera-
ções estruturais e funcionais no cardiomiócito, resultando em disfunção contráctil. Múltiplos
mecanismos fisiopatológicos estão envolvidos.
A disfunção dos receptores adrenérgicos beta parece ser um achado universal na cardio-
patia cirrótica e explica parcialmente a incompetência cronotrópica e inotrópica descrita na
cirrose[10]. Diversos mecanismos contribuem, por sua vez, para esta disfunção. A constante esti-
mulação do sistema nervoso simpático envolvida na fisiopatologia da circulação hiperdinâmica,
levam à diminuição da densidade e dessensibilização destes receptores[19, 20]. Por outro lado, os
mecanismos de sinalização intracelular, envolvidos na transdução do sinal após a activação dos
receptores adrenérgicos beta, e que regulam os movimentos do cálcio intracelular através da
cascata adenilcíclase – AMP cíclico – proteína cínase A podem estar igualmente comprometi-
dos na cirrose. Alterações na expressão genética dos reguladores desta cascata, com aumento
da expressão de proteínas G inibitórias e de outros mediadores que resultam na inibição da
adenilcíclase e na degradação acelerada do AMP cíclico foram documentadas e envolvidas na
patofisiologia da cardiomiopatia cirrótica[21, 22]. Finalmente, foram ainda descritas alterações das
características físicas da membrana celular dos cardiomiócitos, com aumento do conteúdo de
colesterol e da razão colesterol/fosfolípidos membranares, resultando em diminuição da flui-
dez da membrana. Esta alteração afecta a função de todos os receptores transmembranares,
Introdução
27
incluindo os receptores adrenérgicos beta, inibindo o seu acoplamento com as proteínas Gs e
deteriorando ainda mais a função do já reduzido número de receptores membranares[23, 24]. A
redução da produção de AMP cíclico em resposta à estimulação adrenérgica e a sua correlação
com a fluidez da membrana foram demonstradas em modelos animais de cirrose e explicam a
hiporeactividade às catecolaminas observada na cirrose[23, 25].
Tendo em conta o efeito cronotrópico, inotrópico e lusitrópico positivo da estimulação
adrenérgica nos cardiomiócitos, as alterações dos bloqueadores beta encontradas em modelos
de cirrose desempenham, provavelmente, um papel importante na disfunção sistólica e diastó-
lica descrita nos doentes cirróticos.
Para além da disfunção dos receptores adrenérgicos beta, as alterações das características
da membrana celular podem contribuir para as alterações nos diferentes canais iónicos encon-
tradas em vários estudos. A diminuição na densidade de canais de cálcio tipo L foi descrita num
modelo animal de cirrose[11, 26], resultando na redução da disponibilidade de cálcio intracelular e
em menor contractilidade cardíaca. Foram igualmente documentadas alterações dos diferentes
tipos de canais de potássio, com diminuição da sua condutância e da densidade das correntes
de potássio em miócitos de ratos, resultando numa maior duração do potencial de acção[27].
Esta observação pode justificar o prolongamento do intervalo QT descrito em doentes com
cirrose.
Por outro lado, foram encontradas alterações ultraestruturais das proteínas contrácteis
e da matriz extracelular. O aumento da expressão da isoforma beta das cadeias pesadas de
miosina, alterações na modulação da titina (uma proteína do citosqueleto que é a principal
determinante da tensão passiva do cardiomiócito) e um aumento do colagénio tipo I na matriz
extracelular (relativamente à forma mais complacente de colagénio tipo III) podem desempe-
nhar um papel importante na disfunção sistólica e diastólica na cirrose[28, 29].
Uma segunda vertente da fisiopatologia da cardiomiopatia cirrótica relaciona-se com o efei-
to cardiodepressor de diferentes substâncias, que se acumulam como resultado da insuficiência
hepática e do desenvolvimento de shunts porto-sistémicos.
O sistema dos canabinoides tem uma expressão muito reduzida em indivíduos normais. Este
sistema de sinalização celular é activado pela ligação de canabinoides endógenos ou exógenos
a receptores próprios (CB1 e CB2) expressos em múltiplos tecidos – miócitos, células endote-
liais, células musculares lisas e células do sistema imune[30]. Na cirrose, há evidência de aumen-
to de produção de endocanabinóides endógenos nomeadamente anandamida que, actuando
através da ligação a receptores CB1, exercem um efeito vasodilatador e inotrópico negativo

28
Francisco Sampaio
via activação de uma proteina G inibitória e diminuição da produção de AMP cíclico[31]. Este
mecanismo agrava assim a diminuição da resposta contráctil dos miócitos após estimulaçao
adrenérgica e a sua inibição através de antagonistas específicos dos receptores CB-1 parece
reverter este efeito[32]. O excesso de endocanabinoides promove ainda a apoptose dos hepa-
tócitos favorecendo o agravamento da hipertensão portal e da circulação hiperdinâmica[33, 34].
O óxido nítrico desempenha um papel importante na fisiopatologia da cardiomiopatia cir-
rótica. O aumento da expressão da forma indutível da síntase do óxido nítrico (iNOS), pos-
sivelmente relacionada com níveis aumentados de citocinas pró-inflamatórias como o factor
de necrose tumoral a (TNF-a) e a interleucina 1b está demonstrado em modelos animais de
cirrose[35, 36]. Para além dos efeitos na circulação periférica referidos previamente, esta forma
de óxido nítrico exerce um efeito inotrópico negativo no cardiomiócito através da estimulação
do sistema guanilcíclase – GMP cíclico – proteína cinase G que resulta numa diminuição da
entrada de cálcio pela inibição quer dos canais de cálcio tipo L quer dos receptores rianodí-
nicos do retículo sarcoplasmático[26, 37]. A indução da apoptose é outro dos mecanismos pelo
qual este mediador exerce o seu efeito cardiotóxico[38]. Tal como no sistema dos canabinoides,
também com a inibição deste sistema por antagonistas do óxido nítrico se observou uma re-
versão da disfunção cardíaca[39, 40].
Os mesmos mecanismos fisiopatológicos são partilhados pelo monóxido de carbono, cuja
produção está igualmente aumentada na cirrose como consequência da estimulação do siste-
ma nervoso simpático e da acumulação de citocinas pró-inflamatórias. De igual modo, a inibi-
ção deste sistema associa-se a melhoria da contractilidade do músculo cardíaco[41].
Mais recentemente, foi sugerido o papel da activação do factor nuclear kB (NF-kB), um fac-
tor de transcrição que regula várias respostas celulares, na disfunção cardiovascular da cirrose.
Num modelo animal de cirrose, foram encontrados níveis aumentados de NF-kB e TNF-a, e
a inibição daquele factor resultou numa redução significativa dos níveis de TNF-a e numa me-
lhoria da contractilidade[42]. Estes dados sugerem que os níveis de TNF-a estão dependentes
da activação deste factor de transcrição e reforçam a importância da expressão das citocinas
na fisiopatologia da cardiomiopatia cirrótica.
Para além do seu papel na contractilidade, o papel de citocinas como o TGF-b na indução de
fibrose e apoptose está bem documentado; níveis aumentados deste mediador foram encon-
trados na cirrose e podem igualmente contribuir para a disfunção contráctil[43, 44].

Introdução
29
1.1.3. Evidência clínica
1.1.3.1. Disfunção sistólica
A utilização de testes não invasivos de imagiologia cardíaca tem permitido evidenciar ano-
malias cardíacas morfológicas e funcionais em doentes com cirrose. No entanto, embora se
tenha observado um aumento do volume das câmaras esquerdas em alguns estudos, as altera-
ções das dimensões cardíacas e da massa ventricular, em repouso, parecem ser modestas[45-47].
Do mesmo modo, índices de função sistólica como a fracção de ejecção são frequentemente
normais em condições de repouso, em consequência da diminuição da pós-carga característica
da circulação na cirrose[48-50]. A disfunção sistólica nestes doentes poderá no entanto ser reve-
lada em situações de stress. Vários autores demonstraram que doentes com cirrose exibem
uma variação anormal do débito cardíaco, frequência cardíaca e da fracção de ejecção do ven-
trículo esquerdo e aumentos das pressões de enchimento ventriculares em resposta ao exer-
cício físico[51-54]. A incompetência inotrópica e cronotrópica parece ser assim um dos achados
clínicos mais consistentes da cardiomiopatia cirrótica. Respostas semelhantes foram encontra-
das em resposta a stress farmacológico com vasoconstritores[55, 56] ou alterações posturais[57].
No entanto o papel dos testes de sobrecarga com dobutamina, frequentemente utilizados na
avaliação de reserva contráctil[58], no diagnóstico da cardiomiopatia cirrótica é controverso,
com resultados díspares em diferentes estudos[59, 60].
Mais recentemente, a utilização de técnicas ecocardiográficas modernas permitiu a detec-
ção de alterações da função sistólica ventricular também em condições de repouso[61].
1.1.3.2. Disfunção diastólica
As alterações previamente descritas nas proteínas contrácteis e na matriz extracelular, as-
sim como os achados de hipertrofia ventricular, fibrose e edema subendocárdico relatados,
desde há várias décadas, em diferentes séries de autópsias de doentes com cirrose de várias
etiologias[62, 63], fornecem a base patofisiológica da disfunção diastólica na cirrose.
A presença de fibrose intramiocárdica foi igualmente documentada em doentes com cirro-
se, utilizando ressonância magnética cardíaca[64].
A ecocardiografia tem sido, no entanto, a técnica mais utilizada para a avaliação clínica da
função diastólica na cirrose. Durante muitos anos, esta análise baseou-se na avaliação, por
Doppler pulsado, do fluxo de sangue através da válvula mitral durante a diástole[65]. Usando
este método, vários autores encontraram sinais de disfunção diastólica em cerca de 50% dos
doentes com cirrose[66]. Pozzi et al descreveram um aumento da velocidade da onda A, inversão
30
Francisco Sampaio
da relação E/A e prolongamento do tempo de desaceleração da onda E – sugerindo atraso do
relaxamento ventricular – em doentes com cirrose e ascite de grande volume, comparativa-
mente com um grupo controlo; após paracentese evacuadora, os autores observaram melho-
ria parcial destes índices de enchimento ventricular[67]. Achados semelhantes foram relatados
por Wong et al[68], sugerindo que a presença de disfunção diastólica se possa relacionar com
a gravidade da doença hepática e com a presença de ascite. Contrariamente, Finucci et al não
encontraram relação entre o tempo de desaceleração da onda E e a presença de ascite[69]. A
dilatação da aurícula esquerda – um reconhecido marcador de cronicidade de disfunção dias-
tólica[70, 71] – foi igualmente encontrada nestes estudos. Do mesmo modo, níveis aumentados
de peptídeo natriurético tipo A (ANP) – produzido nas aurículas em resposta ao estiramento
das fibras auriculares[72] – foram descritos em doentes com cirrose, podendo também traduzir
disfunção diastólica.
No entanto, a análise ecocardiográfica da função diastólica baseada no fluxo mitral apre-
senta várias limitações[73-77]. Em particular, alterações na pré-carga e na frequência cardíaca,
podem influenciar significativamente o padrão do fluxo através da válvula mitral, mesmo em
indivíduos normais[78, 79]. Este aspecto pode ser particularmente relevante nos doentes com cir-
rose hepática, atendendo às alterações hemodinâmicas associadas a esta doença. A associação
da dilatação auricular esquerda e dos níveis de ANP com a volémia demonstrada em doentes
com cirrose parece apoiar esta hipótese[46]. Atendendo a estas questões, foram elaboradas
recomendações mais recentes para avaliação da função diastólica, nas quais as novas técnicas
ecocardiográficas, como o Doppler tecidular, assumem um papel preponderante na avaliação
funcional da diástole; os parâmetros derivados do fluxo são usados em segunda linha como
complemento dos primeiros[80].
1.1.3.3. Alterações electrofisiológicas
A presença de prolongamento do intervalo QT parece ser um achado frequente em do-
entes com cirrose independentemente da sua etiologia, tendo sido descrito em até 50% dos
casos[81, 82]. O grau de prolongamento relaciona-se com a gravidade da doença hepática embora
esta alteração tenha sido encontrada mesmo em estádios mais precoces[83]. O prolongamento
do intervalo QT parece associar-se a alterações no acoplamento electromecânico, i.e, na rela-
ção temporal entre a sístole elétrica e a sístole mecânica[84].
Introdução
31
1.1.4. Definição de cardiomiopatia cirrótica
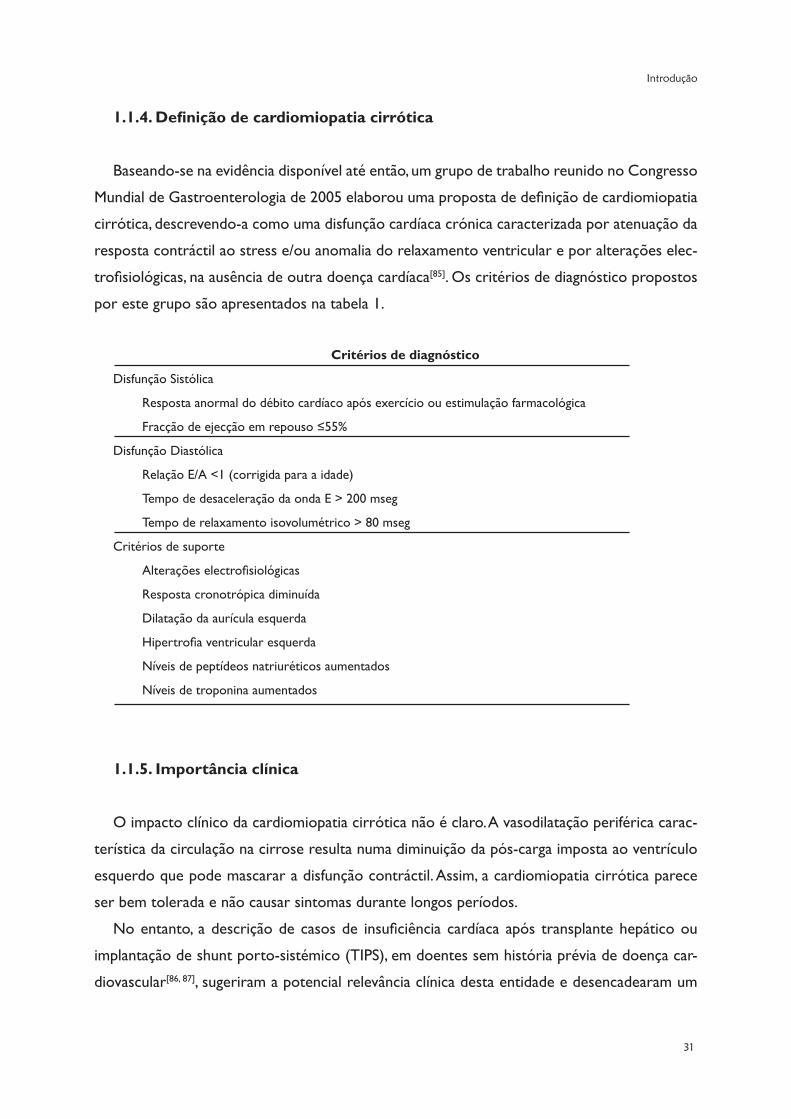
Baseando-se na evidência disponível até então, um grupo de trabalho reunido no Congresso
Mundial de Gastroenterologia de 2005 elaborou uma proposta de definição de cardiomiopatia
cirrótica, descrevendo-a como uma disfunção cardíaca crónica caracterizada por atenuação da
resposta contráctil ao stress e/ou anomalia do relaxamento ventricular e por alterações elec-
trofisiológicas, na ausência de outra doença cardíaca[85]. Os critérios de diagnóstico propostos
por este grupo são apresentados na tabela 1.
Critérios de diagnóstico
Disfunção Sistólica
Resposta anormal do débito cardíaco após exercício ou estimulação farmacológica
Fracção de ejecção em repouso ≤55%
Disfunção Diastólica
Relação E/A <1 (corrigida para a idade)
Tempo de desaceleração da onda E > 200 mseg
Tempo de relaxamento isovolumétrico > 80 mseg
Critérios de suporte
Alterações electrofisiológicas
Resposta cronotrópica diminuída
Dilatação da aurícula esquerda
Hipertrofia ventricular esquerda
Níveis de peptídeos natriuréticos aumentados
Níveis de troponina aumentados
1.1.5. Importância clínica
O impacto clínico da cardiomiopatia cirrótica não é claro. A vasodilatação periférica carac-
terística da circulação na cirrose resulta numa diminuição da pós-carga imposta ao ventrículo
esquerdo que pode mascarar a disfunção contráctil. Assim, a cardiomiopatia cirrótica parece
ser bem tolerada e não causar sintomas durante longos períodos.
No entanto, a descrição de casos de insuficiência cardíaca após transplante hepático ou
implantação de shunt porto-sistémico (TIPS), em doentes sem história prévia de doença car-
diovascular[86, 87], sugeriram a potencial relevância clínica desta entidade e desencadearam um

32
Francisco Sampaio
interesse crescente pelo seu estudo. A presença de disfunção diastólica foi implicada na pato-
fisiologia desta complicação. A implantação do shunt porto-sistémico leva a um aumento do
retorno venoso na circulação central[88]. O aumento da pressão arterial pulmonar, da pressão
de encravamento pulmonar bem como das dimensões da aurícula esquerda e da massa ven-
tricular observados nos doentes submetidos a esse procedimento sugerem uma incapacidade
do coração em acomodar um aumento súbito da pré-carga[89, 90]. Para além disso, a presença de
disfunção diastólica, avaliada pela relação E/A, associou-se a aumento de mortalidade e menor
mobilização da ascite após inserção de TIPS[91, 92].
Por outro lado, foi também sugerida a associação entre disfunção sistólica, particularmente
a resposta atenuada ao stress, e o prognóstico destes doentes. Ruiz-del-Arbol et al demonstra-
ram que um débito cardíaco mais baixo se associava a risco aumentado de desenvolvimento de
insuficiência renal em doentes com peritonite bacteriana espontânea[93]. Mais tarde, o mesmo
grupo reportou a associação entre um débito cardíaco inferior a 6 L/min e desenvolvimento
de síndrome hepatorenal, em doentes internados por ascite de grande volume[94]. Na mesma
linha, Krag et al encontraram uma associação entre débito cardíaco baixo, risco de desenvol-
vimento de síndrome hepatorenal e mortalidade, em doentes com cirrose descompensada[95].
Estes trabalhos lançaram a hipótese da existência de um efeito causal entre disfunção sistólica
e disfunção renal em doentes com cirrose descompensada, em que a incapacidade de aumentar
o débito cardíaco na presença de vasodilatação se associa a um risco aumentado de compli-
cações[96].
Mais recentemente Ruiz-del-Arbol et al relataram igualmente uma associação entre disfun-
ção diastólica, evolução para síndrome hepatorenal e mortalidade[97]; no entanto, em contraste
com os seus achados prévios, o débito cardíaco não foi preditor do risco de insuficiência renal
pelo que os mecanismos patofisiológicos envolvidos na associação entre disfunção diastólica e
disfunção renal não são claros.
Por fim, trabalhos de outros autores não conseguiram estabelecer uma associação entre
disfunção cardíaca – avaliada por técnicas ecocardiográficas modernas – e prognóstico em do-
entes com cirrose, contribuindo para a incerteza quanto ao impacto clínico da cardiomiopatia
cirrótica[98, 99].
Em resumo, nas últimas décadas foi acumulada evidência científica abundante, provenien-
te quer de modelos experimentais, quer de estudos clínicos, da existência de alterações da
contractilidade e do relaxamento cardíacos na cirrose hepática. No entanto, a patofisiologia
desta disfunção cardiovascular é complexa e multifactorial, envolvendo alterações estruturais
Introdução
33
e funcionais, a nível central e periférico. Por outro lado, a sua definição é vaga e não existem
critérios de diagnóstico bem definidos e universalmente aceites, pelo que a prevalência exacta
desta patologia não pode ser determinada. Finalmente, o seu impacto prognóstico, nomeada-
mente a sua contribuição para a mortalidade foi sugerido em alguns estudos, mas os mecanis-
mos envolvidos nesta associação não são claros.
1.2. TÉCNICAS IMAGIOLÓGICAS PARA AVALIAÇÃO DA FUNÇÃO
MIOCÁRDICA
Nos últimos anos, múltiplas técnicas imagiológicas foram desenvolvidas e aplicadas na ava-
liação morfológica e funcional do coração.
A ecocardiografia, sendo a mais antiga[100], continua também a ser, por questões de acessibili-
dade, portabilidade, segurança e custo, a modalidade de imagem mais utilizada[101-104]. A avaliação
das dimensões das câmaras, e da massa e função ventriculares são das indicações mais frequen-
tes para a requisição de um ecocardiograma[105]. De acordo com as recomendações actuais, a
ecocardiografia é o método de imagem de primeira linha na avaliação de doentes com suspeita
de insuficiência cardíaca, fornecendo informação estrutural (anatomia, volumes e massa) e fun-
cional (incluindo a análise da função diastólica)[106]. No entanto várias limitações dos diferentes
parâmetros ecocardiográficos devem ser tidas em conta aquando da sua utilização. Por exem-
plo, a fracção de ejecção, apesar de ser a medida mais generalizada de função sistólica global e
ter, comprovadamente, importância prognóstica, não é um índice de contractilidade e depende
fortemente da pré- e pós-carga, da frequência cardíaca e da função valvular[106]. O mesmo se
aplica aos índices classicamente utilizados para avaliação da função diastólica[78, 107, 108]. Novos
métodos ecocardiográficos entretanto desenvolvidos poderão permitir ultrapassar algumas
destas limitações, permitindo uma análise quantitativa da deformação miocárdica (uma medida
indirecta do encurtamento e distensão dos miócitos durante o ciclo cardíaco). Estas novas
técnicas baseiam-se na determinação das velocidades relativas de diferentes pontos do mio-
cárdio aplicando o princípio Doppler ao movimento do músculo cardíaco (Doppler tecidular)
ou no cálculo da distância inicial e final entre vários pontos na imagem bidimensional através
do seu seguimento ao longo do ciclo cardíaco (“speckle tracking”). A medida de deformação
miocárdica define-se como strain e é expressa em percentagem. A velocidade a que a defor-
mação miocárdica se dá, ou seja, a variação do strain num período de tempo é definida como
strain rate e é expressa em 1/segundo[109, 110]. Não sendo medidas totalmente independentes
das condições de carga[111-114], strain/strain rate são sobretudo determinados pela contractilida-
34
Francisco Sampaio
de intrínseca dos miócitos e correlacionam-se bem com índices invasivos de contractilidade[115,
116]. A sua utilidade clínica tem sido demonstrada em diversos contextos – desde o diagnóstico
de doença subclínica (onde a sua maior sensibilidade permite detectar alterações da função
miocárdica em estadios precoces), à melhoria da acuidade diagnóstica na doença coronária e
à monitorização terapêutica[117-122]. Foi igualmente documentado o seu potencial na avaliação
do prognóstico[123-126].
Também na análise da função diastólica, os novos métodos ecocardiográficos, particular-
mente a análise das velocidades do miocárdio por Doppler tecidular, assumiram uma impor-
tância crescente. A velocidade de deslocamento do anel mitral no início da diástole (E’) é um
parâmetro mais sensível de relaxamento que as variáveis do fluxo mitral, correlacionando-se
bem com a constante Tau de relaxamento medida invasivamente[127-130]. Mais importante ainda
é a boa correlação da razão entre a velocidade da onda E mitral por Doppler pulsado (E) e
a velocidade da onda E’ com as pressões de enchimento do ventrículo esquerdo[130, 131]. Esta
observação resulta do facto da velocidade E’ ser um indicador da quantidade do volume de
sangue que entra no ventrículo esquerdo durante a fase de enchimento rápido enquanto que a
velocidade da onda E representa o gradiente de pressão necessário para que essa quantidade
de sangue entre no ventrículo esquerdo. Assim, a razão E/E’ reflecte a quantidade de sangue
que entra no ventrículo esquerdo para um dado gradiente de pressão; uma razão E/E’ elevada
representa uma pequena mudança de volume para um gradiente aurícula esquerda/ventrículo
esquerdo elevado, e é um marcador de disfunção diastólica. Visto de outra forma, a velocidade
da onda E depende do relaxamento, do gradiente de pressão AE/VE e da idade enquanto que
a velocidade E’ depende sobretudo do relaxamento e da idade; deste modo, a razão entre as
duas permite eliminar o efeito do relaxamento e da idade traduzindo apenas o gradiente de
pressão entre as duas câmaras e a pressão de enchimento do ventrículo esquerdo[132]. Atenden-
do a estes achados, a medição das velocidades diastólicas do anel mitral por Doppler tecidular
e a determinação da razão E/E’ são, de acordo com as recomendações actuais, mandatórias na
avaliação ecocardiográfica da função diastólica[80].
A ressonância magnética cardíaca (RMC) tem, nos últimos anos, adquirido crescente impor-
tância na avaliação do sistema cardiovascular[133]. A sua excelente resolução espacial permite-
lhe definir, com exactidão, os bordos endocárdico e epicárdico, sem dependência de qualquer
“janela acústica”. Deste modo, a RMC é considerada o método “gold-standard” na avaliação
dos volumes cardíacos e da fracção de ejecção[133, 134]. Esta técnica permite igualmente avaliar
os vários componentes da deformação miocárdica utilizando diferentes técnicas[135-138]. Final-
mente, a capacidade de caracterização tecidular da RMC, permite a quantificação de áreas de
Introdução
35
edema ou fibrose, com identificação precisa de lesão miocárdica (mesmo subclínica) assim
como de miocárdio viável, sendo igualmente o actual “gold-standard” para a definição de via-
bilidade[139-141].
Algumas destas novas modalidades de imagem foram já utilizadas na avaliação de doentes
com cirrose[61, 64]. No entanto, dado o pequeno número de estudos e doentes envolvidos, a sua
utilidade na detecção de alterações morfológicas e funcionais neste contexto é ainda incerta e
o seu potencial papel no diagnóstico da cardiomiopatia cirrótica não está estabelecido.
Referências
[1] Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, et al. Classification of the cardiomyo-
pathies: a position statement from the European Society Of Cardiology Working Group on Myocardial
and Pericardial Diseases. Eur Heart J. 2008;29:270-6.
[2] Mackenzie. The study of the pulse, arterial, venous, and hepatic, and of the movements of the heart. Am
J Med Sci. 1902;124:325.
[3] Haunstetter A, Izumo S. Apoptosis: basic mechanisms and implications for cardiovascular disease. Circ
Res. 1998;82:1111-29.
[4] Capasso JM, Li P, Guideri G, Malhotra A, Cortese R, Anversa P. Myocardial mechanical, biochemical, and
structural alterations induced by chronic ethanol ingestion in rats. Circ Res. 1992;71:346-56.
[5] Beckemeier ME, Bora PS. Fatty acid ethyl esters: potentially toxic products of myocardial ethanol me-
tabolism. J Mol Cell Cardiol. 1998;30:2487-94.
[6] Delbridge LM, Connell PJ, Harris PJ, Morgan TO. Ethanol effects on cardiomyocyte contractility. Clin Sci
(Lond). 2000;98:401-7.
[7] Shorr E, Zweifach BW, Furchgott RF, Baez S. Hepatorenal factors in circulatory homeostasis. IV. Tissue
origins of the vasotropic principles, VEM and VDM, which appear during evolution of hemorrhagi and
tourniquet shock. Circulation. 1951;3:42-79.
[8] Kowalski HJ, Abelmann WH. The cardiac output at rest in Laennec’s cirrhosis. J Clin Invest. 1953;32:1025-
33.
[9] Benoit JN, Womack WA, Hernandez L, Granger DN. “Forward” and “backward” flow mechanisms of
portal hypertension. Relative contributions in the rat model of portal vein stenosis. Gastroenterology.
1985;89:1092-6.
[10] Battarbee HD, Farrar GE, Spears RP. Responses to hypotension in conscious rats with chronic portal
venous hypertension. Am J Physiol. 1990;259:G48-55.
[11] Zavecz JH, Bueno O, Maloney RE, O’Donnell JM, Roerig SC, Battarbee HD. Cardiac excitation-contrac-
tion coupling in the portal hypertensive rat. Am J Physiol Gastrointest Liver Physiol. 2000;279:G28-39.
[12] Laleman W, Landeghem L, Wilmer A, Fevery J, Nevens F. Portal hypertension: from pathophysiology to
clinical practice. Liver Int. 2005;25:1079-90.
[13] Sanyal AJ, Bosch J, Blei A, Arroyo V. Portal hypertension and its complications. Gastroenterology.
2008;134:1715-28.
36
Francisco Sampaio
[14] Hendrickson H, Chatterjee S, Cao S, Morales Ruiz M, Sessa WC, Shah V. Influence of caveolin on cons-
titutively activated recombinant eNOS: insights into eNOS dysfunction in BDL rat liver. Am J Physiol
Gastrointest Liver Physiol. 2003;285:G652-60.
[15] Bolognesi M, Sacerdoti D, Piva A, Di Pascoli M, Zampieri F, Quarta S, et al. Carbon monoxide-mediated
activation of large-conductance calcium-activated potassium channels contributes to mesenteric vaso-
dilatation in cirrhotic rats. J Pharmacol Exp Ther. 2007;321:187-94.
[16] Woitas RP, Heller J, Stoffel-Wagner B, Spengler U, Sauerbruch T. Renal functional reserve and nitric
oxide in patients with compensated liver cirrhosis. Hepatology. 1997;26:858-64.
[17] D’Amico G, Morabito A, Pagliaro L, Marubini E. Survival and prognostic indicators in compensated and
decompensated cirrhosis. Dig Dis Sci. 1986;31:468-75.
[18] Gines P, Quintero E, Arroyo V, Teres J, Bruguera M, Rimola A, et al. Compensated cirrhosis: natural his-
tory and prognostic factors. Hepatology. 1987;7:122-8.
[19] Gerbes AL, Remien J, Jungst D, Sauerbruch T, Paumgartner G. Evidence for down-regulation of beta-2-
adrenoceptors in cirrhotic patients with severe ascites. Lancet. 1986;1:1409-11.
[20] Lee SS, Marty J, Mantz J, Samain E, Braillon A, Lebrec D. Desensitization of myocardial beta-adrenergic
receptors in cirrhotic rats. Hepatology. 1990;12:481-5.
[21] Ceolotto G, Papparella I, Sticca A, Bova S, Cavalli M, Cargnelli G, et al. An abnormal gene expression of
the beta-adrenergic system contributes to the pathogenesis of cardiomyopathy in cirrhotic rats. Hepa-
tology. 2008;48:1913-23.
[22] Ma Z, Miyamoto A, Lee SS. Role of altered beta-adrenoceptor signal transduction in the pathogenesis
of cirrhotic cardiomyopathy in rats. Gastroenterology. 1996;110:1191-8.
[23] Ma Z, Meddings JB, Lee SS. Membrane physical properties determine cardiac beta-adrenergic receptor
function in cirrhotic rats. Am J Physiol. 1994;267:G87-93.
[24] Ma Z, Lee SS, Meddings JB. Effects of altered cardiac membrane fluidity on beta-adrenergic receptor
signalling in rats with cirrhotic cardiomyopathy. J Hepatol. 1997;26:904-12.
[25] Gazawi H, Ljubuncic P, Cogan U, Hochgraff E, Ben-Shachar D, Bomzon A. The effects of bile acids on
beta-adrenoceptors, fluidity, and the extent of lipid peroxidation in rat cardiac membranes. Biochem
Pharmacol. 2000;59:1623-8.
[26] Ward CA, Liu H, Lee SS. Altered cellular calcium regulatory systems in a rat model of cirrhotic cardio-
myopathy. Gastroenterology. 2001;121:1209-18.
[27] Ward CA, Ma Z, Lee SS, Giles WR. Potassium currents in atrial and ventricular myocytes from a rat
model of cirrhosis. Am J Physiol. 1997;273:G537-44.
[28] Glenn TK, Honar H, Liu H, ter Keurs HE, Lee SS. Role of cardiac myofilament proteins titin and collagen
in the pathogenesis of diastolic dysfunction in cirrhotic rats. J Hepatol. 2011;55:1249-55.
[29] Gaskari SA, Honar H, Lee SS. Therapy insight: Cirrhotic cardiomyopathy. Nat Clin Pract Gastroenterol
Hepatol. 2006;3:329-37.
[30] De Petrocellis L, Cascio MG, Di Marzo V. The endocannabinoid system: a general view and latest addi-
tions. Br J Pharmacol. 2004;141:765-74.
[31] Gaskari SA, Liu H, Moezi L, Li Y, Baik SK, Lee SS. Role of endocannabinoids in the pathogenesis of cir-
rhotic cardiomyopathy in bile duct-ligated rats. Br J Pharmacol. 2005;146:315-23.
Introdução
37
[32] Batkai S, Mukhopadhyay P, Harvey-White J, Kechrid R, Pacher P, Kunos G. Endocannabinoids acting at
CB1 receptors mediate the cardiac contractile dysfunction in vivo in cirrhotic rats. Am J Physiol Heart
Circ Physiol. 2007;293:H1689-95.
[33] Liu H, Gaskari SA, Lee SS. Cardiac and vascular changes in cirrhosis: pathogenic mechanisms. World J
Gastroenterol. 2006;12:837-42.
[34] Moezi L, Gaskari SA, Lee SS. Endocannabinoids and liver disease. V. endocannabinoids as mediators of
vascular and cardiac abnormalities in cirrhosis. Am J Physiol Gastrointest Liver Physiol. 2008;295:G649-
53.
[35] Liu H, Ma Z, Lee SS. Contribution of nitric oxide to the pathogenesis of cirrhotic cardiomyopathy in bile
duct-ligated rats. Gastroenterology. 2000;118:937-44.
[36] Herring N, Danson EJ, Paterson DJ. Cholinergic control of heart rate by nitric oxide is site specific.
News Physiol Sci. 2002;17:202-6.
[37] Seddon M, Shah AM, Casadei B. Cardiomyocytes as effectors of nitric oxide signalling. Cardiovasc Res.
2007;75:315-26.
[38] Kim YM, Bombeck CA, Billiar TR. Nitric oxide as a bifunctional regulator of apoptosis. Circ Res.
1999;84:253-6.
[39] van Obbergh L, Vallieres Y, Blaise G. Cardiac modifications occurring in the ascitic rat with biliary cir-
rhosis are nitric oxide related. J Hepatol. 1996;24:747-52.
[40] Garcia-Estan J, Ortiz MC, Lee SS. Nitric oxide and renal and cardiac dysfunction in cirrhosis. Clin Sci
(Lond). 2002;102:213-22.
[41] Liu H, Song D, Lee SS. Role of heme oxygenase-carbon monoxide pathway in pathogenesis of cirrhotic
cardiomyopathy in the rat. Am J Physiol Gastrointest Liver Physiol. 2001;280:G68-74.
[42] Liu H, Lee SS. Nuclear factor-kappaB inhibition improves myocardial contractility in rats with cirrhotic
cardiomyopathy. Liver Int. 2008;28:640-8.
[43] Zardi EM, Abbate A, Zardi DM, Dobrina A, Margiotta D, Van Tassell BW, et al. Cirrhotic cardiomyopathy.
J Am Coll Cardiol. 2010;56:539-49.
[44] Timoh T, Protano MA, Wagman G, Bloom M, Vittorio TJ. A perspective on cirrhotic cardiomyopathy.
Transplant Proc. 2011;43:1649-53.
[45] Moller S, Sondergaard L, Mogelvang J, Henriksen O, Henriksen JH. Decreased right heart blood volume
determined by magnetic resonance imaging: evidence of central underfilling in cirrhosis. Hepatology.
1995;22:472-8.
[46] Rector WG, Jr., Adair O, Hossack KF, Rainguet S. Atrial volume in cirrhosis: relationship to blood volume
and plasma concentration of atrial natriuretic factor. Gastroenterology. 1990;99:766-70.
[47] Valeriano V, Funaro S, Lionetti R, Riggio O, Pulcinelli G, Fiore P, et al. Modification of cardiac function in
cirrhotic patients with and without ascites. Am J Gastroenterol. 2000;95:3200-5.
[48] Keller H, Bezjak V, Stegaru B, Buss J, Holm E, Heene DL. Ventricular function in cirrhosis and portasys-
temic shunt: a two-dimensional echocardiographic study. Hepatology. 1988;8:658-62.
[49] Ahmed SS, Howard M, ten Hove W, Leevy CM, Regan TJ. Cardiac function in alcoholics with cirrhosis:
absence of overt cardiomyopathy--myth or fact? J Am Coll Cardiol. 1984;3:696-702.
[50] Gould L, Shariff M, Zahir M, Di Lieto M. Cardiac hemodynamics in alcoholic patients with chronic liver
disease and a presystolic gallop. J Clin Invest. 1969;48:860-8.
38
Francisco Sampaio
[51] Kelbaek H, Rabol A, Brynjolf I, Eriksen J, Bonnevie O, Godtfredsen J, et al. Haemodynamic response to
exercise in patients with alcoholic liver cirrhosis. Clin Physiol. 1987;7:35-41.
[52] Wong F, Girgrah N, Graba J, Allidina Y, Liu P, Blendis L. The cardiac response to exercise in cirrhosis. Gut.
2001;49:268-75.
[53] Grose RD, Nolan J, Dillon JF, Errington M, Hannan WJ, Bouchier IA, et al. Exercise-induced left ventricu-
lar dysfunction in alcoholic and non-alcoholic cirrhosis. J Hepatol. 1995;22:326-32.
[54] Bernardi M, Rubboli A, Trevisani F, Cancellieri C, Ligabue A, Baraldini M, et al. Reduced cardiovascular
responsiveness to exercise-induced sympathoadrenergic stimulation in patients with cirrhosis. J Hepa-
tol. 1991;12:207-16.
[55] Krag A, Bendtsen F, Mortensen C, Henriksen JH, Moller S. Effects of a single terlipressin administration
on cardiac function and perfusion in cirrhosis. Eur J Gastroenterol Hepatol. 2010;22:1085-92.
[56] Limas CJ, Guiha NH, Lekagul O, Cohn JN. Impaired left ventricular function in alcoholic cirrhosis with
ascites. Ineffectiveness of ouabain. Circulation. 1974;49:754-60.
[57] Laffi G, Barletta G, La Villa G, Del Bene R, Riccardi D, Ticali P, et al. Altered cardiovascular responsiveness
to active tilting in nonalcoholic cirrhosis. Gastroenterology. 1997;113:891-8.
[58] Sicari R, Nihoyannopoulos P, Evangelista A, Kasprzak J, Lancellotti P, Poldermans D, et al. Stress echocar-
diography expert consensus statement: European Association of Echocardiography (EAE) (a registered
branch of the ESC). Eur J Echocardiogr. 2008;9:415-37.
[59] Dahl EK, Moller S, Kjaer A, Petersen CL, Bendtsen F, Krag A. Diastolic and autonomic dysfunction in
early cirrhosis: a dobutamine stress study. Scand J Gastroenterol. 2014;49:362-72.
[60] Kim MY, Baik SK, Won CS, Park HJ, Jeon HK, Hong HI, et al. Dobutamine stress echocardiography for
evaluating cirrhotic cardiomyopathy in liver cirrhosis. Korean J Hepatol. 2010;16:376-82.
[61] Kazankov K, Holland-Fischer P, Andersen NH, Torp P, Sloth E, Aagaard NK, et al. Resting myocardial
dysfunction in cirrhosis quantified by tissue Doppler imaging. Liver Int. 2011;31:534-40.
[62] Lunseth JH, Olmstead EG, Abboud F. A study of heart disease in one hundred eight hospitalized patients
dying with portal cirrhosis. AMA Arch Intern Med. 1958;102:405-13.
[63] Ortiz-Olvera NX, Castellanos-Pallares G, Gomez-Jimenez LM, Cabrera-Munoz ML, Mendez-Navarro J,
Moran-Villota S, et al. Anatomical cardiac alterations in liver cirrhosis: an autopsy study. Ann Hepatol.
2011;10:321-6.
[64] Lossnitzer D, Steen H, Zahn A, Lehrke S, Weiss C, Weiss KH, et al. Myocardial late gadolinium enhan-
cement cardiovascular magnetic resonance in patients with cirrhosis. J Cardiovasc Magn Reson.
2010;12:47.
[65] How to diagnose diastolic heart failure. European Study Group on Diastolic Heart Failure. Eur Heart J.
1998;19:990-1003.
[66] Wiese S, Hove JD, Bendtsen F, Moller S. Cirrhotic cardiomyopathy: pathogenesis and clinical relevance.
Nat Rev Gastroenterol Hepatol. 2014;11:177-86.
[67] Pozzi M, Carugo S, Boari G, Pecci V, de Ceglia S, Maggiolini S, et al. Evidence of functional and structural
cardiac abnormalities in cirrhotic patients with and without ascites. Hepatology. 1997;26:1131-7.
[68] Wong F, Liu P, Lilly L, Bomzon A, Blendis L. Role of cardiac structural and functional abnormalities in
the pathogenesis of hyperdynamic circulation and renal sodium retention in cirrhosis. Clin Sci (Lond).
1999;97:259-67.
Introdução
39
[69] Finucci G, Desideri A, Sacerdoti D, Bolognesi M, Merkel C, Angeli P, et al. Left ventricular diastolic func-
tion in liver cirrhosis. Scand J Gastroenterol. 1996;31:279-84.
[70] Pritchett AM, Mahoney DW, Jacobsen SJ, Rodeheffer RJ, Karon BL, Redfield MM. Diastolic dysfunction
and left atrial volume: a population-based study. J Am Coll Cardiol. 2005;45:87-92.
[71] Douglas PS. The left atrium: a biomarker of chronic diastolic dysfunction and cardiovascular disease risk.
J Am Coll Cardiol. 2003;42:1206-7.
[72] Boomsma F, van den Meiracker AH. Plasma A- and B-type natriuretic peptides: physiology, methodology
and clinical use. Cardiovasc Res. 2001;51:442-9.
[73] Caruana L, Davie AP, Petrie M, McMurray J. Diagnosing heart failure. Eur Heart J. 1999;20:393.
[74] Palmieri V, Innocenti F, Pini R, Celentano A. Reproducibility of Doppler echocardiographic assessment of
left ventricular diastolic function in multicenter setting. J Am Soc Echocardiogr. 2005;18:99-106.
[75] Cahill JM, Horan M, Quigley P, Maurer B, McDonald K. Doppler-echocardiographic indices of diastolic
function in heart failure admissions with preserved left ventricular systolic function. Eur J Heart Fail.
2002;4:473-8.
[76] Thomas MD, Fox KF, Wood DA, Gibbs JS, Coats AJ, Henein MY, et al. Echocardiographic features and
brain natriuretic peptides in patients presenting with heart failure and preserved systolic function. He-
art. 2006;92:603-8.
[77] Petrie MC, Hogg K, Caruana L, McMurray JJ. Poor concordance of commonly used echocardiographic
measures of left ventricular diastolic function in patients with suspected heart failure but preser-
ved systolic function: is there a reliable echocardiographic measure of diastolic dysfunction? Heart.
2004;90:511-7.
[78] Choong CY, Herrmann HC, Weyman AE, Fifer MA. Preload dependence of Doppler-derived indexes of
left ventricular diastolic function in humans. J Am Coll Cardiol. 1987;10:800-8.
[79] Thomas JD, Choong CY, Flachskampf FA, Weyman AE. Analysis of the early transmitral Doppler velocity
curve: effect of primary physiologic changes and compensatory preload adjustment. J Am Coll Cardiol.
1990;16:644-55.
[80] Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, et al. Recommendations for the
evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr. 2009;10:165-93.
[81] Bernardi M, Calandra S, Colantoni A, Trevisani F, Raimondo ML, Sica G, et al. Q-T interval prolongation
in cirrhosis: prevalence, relationship with severity, and etiology of the disease and possible pathogenetic
factors. Hepatology. 1998;27:28-34.
[82] Bal JS, Thuluvath PJ. Prolongation of QTc interval: relationship with etiology and severity of liver disease,
mortality and liver transplantation. Liver Int. 2003;23:243-8.
[83] Ytting H, Henriksen JH, Fuglsang S, Bendtsen F, Moller S. Prolonged Q-T(c) interval in mild portal hyper-
tensive cirrhosis. J Hepatol. 2005;43:637-44.
[84] Henriksen JH, Fuglsang S, Bendtsen F, Christensen E, Moller S. Dyssynchronous electrical and mechani-
cal systole in patients with cirrhosis. J Hepatol. 2002;36:513-20.
[85] Moller S, Henriksen JH. Cardiovascular complications of cirrhosis. Gut. 2008;57:268-78.
[86] Lebrec D, Giuily N, Hadengue A, Vilgrain V, Moreau R, Poynard T, et al. Transjugular intrahepatic por-
tosystemic shunts: comparison with paracentesis in patients with cirrhosis and refractory ascites: a
randomized trial. French Group of Clinicians and a Group of Biologists. J Hepatol. 1996;25:135-44.
40
Francisco Sampaio
[87] Franco D, Vons C, Traynor O, de Smadja C. Should portosystemic shunt be reconsidered in the treat-
ment of intractable ascites in cirrhosis? Arch Surg. 1988;123:987-91.
[88] Kovacs A, Schepke M, Heller J, Schild HH, Flacke S. Short-term effects of transjugular intrahepatic
shunt on cardiac function assessed by cardiac MRI: preliminary results. Cardiovasc Intervent Radiol.
2010;33:290-6.
[89] Gines P, Uriz J, Calahorra B, Garcia-Tsao G, Kamath PS, Del Arbol LR, et al. Transjugular intrahepatic
portosystemic shunting versus paracentesis plus albumin for refractory ascites in cirrhosis. Gastroen-
terology. 2002;123:1839-47.
[90] Huonker M, Schumacher YO, Ochs A, Sorichter S, Keul J, Rossle M. Cardiac function and haemodyna-
mics in alcoholic cirrhosis and effects of the transjugular intrahepatic portosystemic stent shunt. Gut.
1999;44:743-8.
[91] Cazzaniga M, Salerno F, Pagnozzi G, Dionigi E, Visentin S, Cirello I, et al. Diastolic dysfunction is asso-
ciated with poor survival in patients with cirrhosis with transjugular intrahepatic portosystemic shunt.
Gut. 2007;56:869-75.
[92] Rabie RN, Cazzaniga M, Salerno F, Wong F. The use of E/A ratio as a predictor of outcome in cirrhotic pa-
tients treated with transjugular intrahepatic portosystemic shunt. Am J Gastroenterol. 2009;104:2458-
66.
[93] Ruiz-del-Arbol L, Urman J, Fernandez J, Gonzalez M, Navasa M, Monescillo A, et al. Systemic, renal, and
hepatic hemodynamic derangement in cirrhotic patients with spontaneous bacterial peritonitis. Hepa-
tology. 2003;38:1210-8.
[94] Ruiz-del-Arbol L, Monescillo A, Arocena C, Valer P, Gines P, Moreira V, et al. Circulatory function and
hepatorenal syndrome in cirrhosis. Hepatology. 2005;42:439-47.
[95] Krag A, Bendtsen F, Henriksen JH, Moller S. Low cardiac output predicts development of hepatorenal
syndrome and survival in patients with cirrhosis and ascites. Gut. 2010;59:105-10.
[96] Krag A, Bendtsen F, Burroughs AK, Moller S. The cardiorenal link in advanced cirrhosis. Med Hypotheses.
2012;79:53-5.
[97] Ruiz-del-Arbol L, Achecar L, Serradilla R, Rodriguez-Gandia MA, Rivero M, Garrido E, et al. Diastolic
dysfunction is a predictor of poor outcomes in patients with cirrhosis, portal hypertension, and a nor-
mal creatinine. Hepatology. 2013;58:1732-41.
[98] Alexopoulou A, Papatheodoridis G, Pouriki S, Chrysohoou C, Raftopoulos L, Stefanadis C, et al. Diastolic
myocardial dysfunction does not affect survival in patients with cirrhosis. Transpl Int. 2012;25:1174-81.
[99] Nazar A, Guevara M, Sitges M, Terra C, Sola E, Guigou C, et al. LEFT ventricular function assessed by
echocardiography in cirrhosis: relationship to systemic hemodynamics and renal dysfunction. J Hepatol.
2013;58:51-7.
[100] Edler I, Hertz C. Use of ultrasonic reflectoscope for the continuous recording of movements of heart
walls. Kungl Fysiogr Sallsk Lung Forth 1954;24.
[101] Kirkpatrick JN, Vannan MA, Narula J, Lang RM. Echocardiography in heart failure: applications, utility, and
new horizons. J Am Coll Cardiol. 2007;50:381-96.
[102] Dokainish H, Nguyen JS, Bobek J, Goswami R, Lakkis NM. Assessment of the American Society of
Echocardiography-European Association of Echocardiography guidelines for diastolic function in pa-
tients with depressed ejection fraction: an echocardiographic and invasive haemodynamic study. Eur J
Echocardiogr. 2011;12:857-64.
Introdução
41
[103] Nagueh SF, Bhatt R, Vivo RP, Krim SR, Sarvari SI, Russell K, et al. Echocardiographic evaluation of hemo-
dynamics in patients with decompensated systolic heart failure. Circ Cardiovasc Imaging. 2011;4:220-7.
[104] Popescu BA, Andrade MJ, Badano LP, Fox KF, Flachskampf FA, Lancellotti P, et al. European Association
of Echocardiography recommendations for training, competence, and quality improvement in echocar-
diography. Eur J Echocardiogr. 2009;10:893-905.
[105] Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for
chamber quantification. Eur J Echocardiogr. 2006;7:79-108.
[106] McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, et al. ESC Guidelines for the
diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and
Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed
in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787-847.
[107] Appleton CP, Hatle LK, Popp RL. Relation of transmitral flow velocity patterns to left ventricular dias-
tolic function: new insights from a combined hemodynamic and Doppler echocardiographic study. J Am
Coll Cardiol. 1988;12:426-40.
[108] Appleton CP. Influence of incremental changes in heart rate on mitral flow velocity: assessment in
lightly sedated, conscious dogs. J Am Coll Cardiol. 1991;17:227-36.
[109] Mor-Avi V, Lang RM, Badano LP, Belohlavek M, Cardim NM, Derumeaux G, et al. Current and evolving
echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus
statement on methodology and indications endorsed by the Japanese Society of Echocardiography. Eur
J Echocardiogr. 2011;12:167-205.
[110] Teske AJ, De Boeck BW, Melman PG, Sieswerda GT, Doevendans PA, Cramer MJ. Echocardiographic
quantification of myocardial function using tissue deformation imaging, a guide to image acquisition and
analysis using tissue Doppler and speckle tracking. Cardiovasc Ultrasound. 2007;5:27.
[111] Grossman W, Jones D, McLaurin LP. Wall stress and patterns of hypertrophy in the human left ventricle.
J Clin Invest. 1975;56:56-64.
[112] Bijnens BH, Cikes M, Claus P, Sutherland GR. Velocity and deformation imaging for the assessment of
myocardial dysfunction. Eur J Echocardiogr. 2009;10:216-26.
[113] Burns AT, La Gerche A, D’Hooge J, MacIsaac AI, Prior DL. Left ventricular strain and strain rate: charac-
terization of the effect of load in human subjects. Eur J Echocardiogr. 2010;11:283-9.
[114] Mirsky I, Aoyagi T, Crocker VM, Fujii AM. Preload dependence of fiber shortening rate in conscious dogs
with left ventricular hypertrophy. J Am Coll Cardiol. 1990;15:890-9.
[115] Weidemann F, Jamal F, Sutherland GR, Claus P, Kowalski M, Hatle L, et al. Myocardial function defined
by strain rate and strain during alterations in inotropic states and heart rate. Am J Physiol Heart Circ
Physiol. 2002;283:H792-9.
[116] Greenberg NL, Firstenberg MS, Castro PL, Main M, Travaglini A, Odabashian JA, et al. Doppler-derived myo-
cardial systolic strain rate is a strong index of left ventricular contractility. Circulation. 2002;105:99-105.
[117] Andersen NH, Poulsen SH, Eiskjaer H, Poulsen PL, Mogensen CE. Decreased left ventricular longitudinal
contraction in normotensive and normoalbuminuric patients with Type II diabetes mellitus: a Doppler
tissue tracking and strain rate echocardiography study. Clin Sci (Lond). 2003;105:59-66.
[118] Cardim N, Oliveira AG, Longo S, Ferreira T, Pereira A, Reis RP, et al. Doppler tissue imaging: regional
myocardial function in hypertrophic cardiomyopathy and in athlete’s heart. J Am Soc Echocardiogr.
2003;16:223-32.
42
Francisco Sampaio
[119] Poulsen SH, Andersen NH, Heickendorff L, Mogensen CE. Relation between plasma amino-terminal
propeptide of procollagen type III and left ventricular longitudinal strain in essential hypertension. He-
art. 2005;91:624-9.
[120] Jurcut R, Wildiers H, Ganame J, D’Hooge J, De Backer J, Denys H, et al. Strain rate imaging detects early
cardiac effects of pegylated liposomal Doxorubicin as adjuvant therapy in elderly patients with breast
cancer. J Am Soc Echocardiogr. 2008;21:1283-9.
[121] Voigt JU, Exner B, Schmiedehausen K, Huchzermeyer C, Reulbach U, Nixdorff U, et al. Strain-rate ima-
ging during dobutamine stress echocardiography provides objective evidence of inducible ischemia.
Circulation. 2003;107:2120-6.
[122] Faber L, Prinz C, Welge D, Hering D, Butz T, Oldenburg O, et al. Peak systolic longitudinal strain of the
lateral left ventricular wall improves after septal ablation for symptomatic hypertrophic obstructive
cardiomyopathy: a follow-up study using speckle tracking echocardiography. Int J Cardiovasc Imaging.
2011;27:325-33.
[123] Bjork Ingul C, Rozis E, Slordahl SA, Marwick TH. Incremental value of strain rate imaging to wall motion
analysis for prediction of outcome in patients undergoing dobutamine stress echocardiography. Circu-
lation. 2007;115:1252-9.
[124 Weidemann F, Jung P, Hoyer C, Broscheit J, Voelker W, Ertl G, et al. Assessment of the contractile reserve
in patients with intermediate coronary lesions: a strain rate imaging study validated by invasive myocar-
dial fractional flow reserve. Eur Heart J. 2007;28:1425-32.
[125] Yu CM, Sanderson JE, Marwick TH, Oh JK. Tissue Doppler imaging a new prognosticator for cardiovas-
cular diseases. J Am Coll Cardiol. 2007;49:1903-14.
[126] Jasaityte R, Dandel M, Lehmkuhl H, Hetzer R. Prediction of short-term outcomes in patients with idio-
pathic dilated cardiomyopathy referred for transplantation using standard echocardiography and strain
imaging. Transplant Proc. 2009;41:277-80.
[127] Nagueh SF, Sun H, Kopelen HA, Middleton KJ, Khoury DS. Hemodynamic determinants of the mitral
annulus diastolic velocities by tissue Doppler. J Am Coll Cardiol. 2001;37:278-85.
[128] Oki T, Tabata T, Yamada H, Wakatsuki T, Shinohara H, Nishikado A, et al. Clinical application of pulsed
Doppler tissue imaging for assessing abnormal left ventricular relaxation. Am J Cardiol. 1997;79:921-8.
[129] Sohn DW, Chai IH, Lee DJ, Kim HC, Kim HS, Oh BH, et al. Assessment of mitral annulus velocity
by Doppler tissue imaging in the evaluation of left ventricular diastolic function. J Am Coll Cardiol.
1997;30:474-80.
[130] Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, et al. Clinical utility of Doppler
echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A
comparative simultaneous Doppler-catheterization study. Circulation. 2000;102:1788-94.
[131] Dokainish H, Zoghbi WA, Lakkis NM, Al-Bakshy F, Dhir M, Quinones MA, et al. Optimal noninvasive
assessment of left ventricular filling pressures: a comparison of tissue Doppler echocardiography and
B-type natriuretic peptide in patients with pulmonary artery catheters. Circulation. 2004;109:2432-9.
[132] Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, et al. How to diagnose
diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventri-
cular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society
of Cardiology. Eur Heart J. 2007;28:2539-50.
Introdução
43
[133] Lima JA, Desai MY. Cardiovascular magnetic resonance imaging: current and emerging applications. J Am
Coll Cardiol. 2004;44:1164-71.
[134] Zerhouni EA, Parish DM, Rogers WJ, Yang A, Shapiro EP. Human heart: tagging with MR imaging--a me-
thod for noninvasive assessment of myocardial motion. Radiology. 1988;169:59-63.
[135] Lawton JS, Cupps BP, Knutsen AK, Ma N, Brady BD, Reynolds LM, et al. Magnetic resonance imaging
detects significant sex differences in human myocardial strain. Biomed Eng Online. 2011;10:76.
[136] Hor KN, Gottliebson WM, Carson C, Wash E, Cnota J, Fleck R, et al. Comparison of magnetic reso-
nance feature tracking for strain calculation with harmonic phase imaging analysis. JACC Cardiovasc
Imaging. 2010;3:144-51.
[137] Schuster A, Kutty S, Padiyath A, Parish V, Gribben P, Danford DA, et al. Cardiovascular magnetic resonan-
ce myocardial feature tracking detects quantitative wall motion during dobutamine stress. J Cardiovasc
Magn Reson. 2011;13:58.
[138] Zagrosek A, Abdel-Aty H, Boye P, Wassmuth R, Messroghli D, Utz W, et al. Cardiac magnetic resonan-
ce monitors reversible and irreversible myocardial injury in myocarditis. JACC Cardiovasc Imaging.
2009;2:131-8.
[139] Iles L, Pfluger H, Phrommintikul A, Cherayath J, Aksit P, Gupta SN, et al. Evaluation of diffuse myocardial
fibrosis in heart failure with cardiac magnetic resonance contrast-enhanced T1 mapping. J Am Coll
Cardiol. 2008;52:1574-80.
[140] Schuster A, Morton G, Chiribiri A, Perera D, Vanoverschelde JL, Nagel E. Imaging in the management of
ischemic cardiomyopathy: special focus on magnetic resonance. J Am Coll Cardiol. 2012;59:359-70.


II. Objectivos

Objectivos
47
Com o conjunto de trabalhos que desenvolvemos pretendemos proceder a uma análise
detalhada da função cardíaca sistólica e diastólica, usando métodos de imagiologia cardíaca não
invasiva (ecocardiografia e ressonância magnética cardíaca) em doentes com cirrose hepática
de diferentes etiologias, em condições de repouso e sob stress farmacológico.
Foram definidos como objectivos:
- Encontrar novos marcadores de cardiomiopatia cirrótica, através da utilização de mé-
todos de imagem mais modernos, com determinação de parâmetros mais sensíveis de
disfunção miocárdica.
- Avaliar a correlação entre disfunção cardiovascular e a etiologia e gravidade da doença
hepática.
- Avaliar o potencial impacto prognóstico dos diferentes parâmetros analisados.


III. Métodos

Métodos
51
ESTUDO 1
“Systolic and diastolic dysfunction in cirrhosis: a tissue-Doppler and speckle tra-
cking echocardiography study”
Doentes: Neste trabalho foram avaliados 131 doentes com cirrose hepática (72 doentes
internados por descompensação de cirrose e 59 doentes ambulatórios, seguidos em consulta
externa de hepatologia), referenciados ao laboratório de ecocardiografia entre Abril de 2011
e Outubro de 2012. Destes, foram excluídos 22 doentes com história de hipertensão arterial,
diabetes mellitus ou de doença cardíaca relevante, com alterações electrocardiográficas signifi-
cativas (não relacionadas com a doença hepática) ou com doença valvular moderada ou grave
no ecocardiograma.
Métodos: Todos os doentes foram submetidos a uma avaliação clínica, punção venosa para
estudo analítico, electrocardiograma de 12 derivações e ecocardiograma. O estudo ecocar-
diográfico incluiu a determinação de dimensões e volumes das câmaras, da massa ventricular,
da fracção de ejecção do ventrículo esquerdo e do débito cardíaco. A função diastólica foi
avaliada de acordo com as recomendações actuais, incluindo a determinação das velocidades
de deslocamento do anel mitral por Doppler tecidular. Foi ainda avaliada a deformação longitu-
dinal do ventrículo esquerdo por speckle tracking. Um grupo de 18 indivíduos saudáveis, com
distribuição etária e por género semelhante à dos doentes, foi submetido à mesma avaliação e
foi usado com grupo controlo.
52
Francisco Sampaio
ESTUDO 2
“Left atrial function is impaired in cirrhosis: a speckle tracking echocardiogra-
phic study”
Doentes: Foi utilizado o mesmo grupo de doentes recrutados para o estudo 1. Após aplica-
ção dos mesmos critérios de exclusão, 111 doentes foram incluídos na análise.
Métodos: Para além da avaliação clínica, laboratorial e ecocardiográfica descrita no estudo 1,
foi ainda estudada a deformação da aurícula esquerda por speckle tracking. Utilizou-se o mes-
mo grupo controlo para comparação.
ESTUDO 3
“Assessment of cardiovascular physiology using magnetic resonance myocardial
stress testing reveals impaired contractile reserve in patients with cirrhotic car-
diomyopathy”
Doentes: para este estudo, recrutámos uma amostra de conveniência de 36 doentes estáveis,
seguidos em consulta externa hepatologia por cirrose hepática, nos quais foi excluída história
pregressa de hipertensão arterial, diabetes mellitus ou de doença cardíaca relevante.
Métodos: Os doentes foram submetidos a avaliação clínica, laboratorial e ressonância mag-
nética cardíaca no mesmo dia. O protocolo de ressonância magnética incluiu determinação
de volumes das câmaras cardíacas, massa ventricular, fracção de ejecção de ambos os ventrí-
culos e débito cardíaco (através da quantificação do fluxo na aorta ascendente) em repouso.
Os doentes foram submetidos a stress farmacológico com dobutamina em baixa dose (10 e
20 ug/Kg/min), avaliando-se a evolução dos diferentes parâmetros (volume de ejecção, débito
cardíaco, fracção de ejecção) durante a perfusão. Foi ainda avaliada a perfusão miocárdica após
stress vasodilatador com adenosina e a presença de fibrose miocárdica através da pesquisa de
realce tardio. As imagens obtidas foram analisadas posteriormente para quantificação dos vá-
rios componentes da deformação do ventrículo esquerdo, em repouso e sob stress. Um grupo
de 8 indivíduos saudáveis foi submetido ao mesmo protocolo e usado como grupo controlo.

Métodos
53
ESTUDO 4
“Systolic dysfunction and diastolic dysfunction do not influence medium-term
prognosis in patients with cirrhosis”
Doentes: Estudámos os 57 doentes que tiveram alta hospitalar – do grupo de 72 doentes
internados por descompensação de cirrose avaliados nos estudos 1 e 2 – e os mesmos 61
doentes ambulatórios.
Métodos: seguimos prospectivamente os 98 doentes durante 6 meses, avaliando a ocorrên-
cia de morte de qualquer causa. Avaliou-se a associação dos parâmetros clínicos laboratoriais
e ecocardiográficos descritos naqueles estudos com a mortalidade aos 6 meses.
IV. Publicações


Publicações
57
C IRRHOS IS AND L IVER FAILURE
Systolic and diastolic dysfunction in cirrhosis: a tissue-Doppler andspeckle tracking echocardiography studyFrancisco Sampaio1,4, Joana Pimenta4, Nuno Bettencourt1,4, Ricardo Fontes-Carvalho1,4, Ana P. Silva3,Jo~ao Valente2, Paulo Bettencourt4, Jos�e Fraga3 and Vasco Gama1
1 Cardiology Department, Centro Hospitalar de Gaia/Espinho, Espinho, Portugal
2 Internal Medicine Department, Centro Hospitalar de Gaia/Espinho, Espinho, Portugal
3 Gastroenterology Department, Centro Hospitalar de Gaia/Espinho, Espinho, Portugal
4 University of Porto Medical School, Porto, Portugal
Keywords
cirrhosis – echocardiography – heart failure –
speckle-tracking – tissue-doppler imaging
Correspondence
Francisco Sampaio, Cardiology Department,
Centro Hospitalar de Gaia/Espinho, Rua
Conceic�~ao Fernandes, Vila Nova de
Gaia 4430-502, Portugal
Tel: 227865100
Fax: 227830209
e-mail: [email protected]
Received 5 February 2013
Accepted 1 April 2013
DOI:10.1111/liv.12187
AbstractBackground & Aims: Cardiac dysfunction has been described in patients withcirrhosis. Conventional echocardiographic methods are frequently unable todetect abnormalities at rest and have limitations. We aimed to evaluatecardiac function in cirrhosis patients assessing: (i) left ventricular systolicfunction using speckle-tracking imaging; (ii) diastolic function using atissue-Doppler based algorithm and comparing it with previously proposeddefinition of diastolic dysfunction (DD). Methods: We included 109 hospi-talized and ambulatory patients with cirrhosis and 18 healthy controls.Detailed echocardiographic evaluation was performed including tissue-Doppler and speckle-tracking analysis. Results: Peak systolic longitudinalstrain (PLS) was lower in patients [�19.99% (�21.88 to �18.71) vs�22.02% (�23.10 to �21.18), P = 0.003]. Ejection fraction was similar inpatients and controls [64% (59–67) vs 61% (60–65), P = 0.42)]. Based onmitral-flow pattern, DD was present in 44 patients (40.4%). Patients withoutDD had higher cardiac output compared with those with DD [6.4 L/min(5.4–7.2) vs 5.6 L/min (4.6–6.8), P = 0.02]. Using a tissue-Doppler baseddefinition, the prevalence of DD was 16.5%. No differences in haemodynam-ic variables were found in patients with and without this definition of DD.The agreement between the two definitions of DD was weak (kappa = 0.24,P = 0.003). Echocardiographic abnormalities in systolic and diastolic func-tion were not different in compensated vs decompensated patients in differ-ent Child-Pugh classes or cirrhosis aetiologies. Conclusions: Patients withcirrhosis have systolic and diastolic cardiac dysfunction at rest. Newer echo-cardiographic techniques may identify patients with functional impairmentmore accurately than conventional methods, which are more influenced byflow conditions.
Cirrhotic cardiomyopathy has been recently describedas a condition characterized by impaired contractileresponse to stress, diastolic dysfunction and electro-physiological abnormalities, in the absence of knowncardiac disease (1–3).
Echocardiography is an easily accessible imagingtechnique and the most widely used method to evaluatethe cardiac function. Although several echocardio-graphic abnormalities have been described in cirrhosis,traditional indices of cardiac systolic function such asejection fraction are frequently normal at rest in thesepatients. On the other hand, newer echocardiographicmodalities like tissue Doppler imaging are mandatorywhen evaluating diastolic function as conventionalDoppler measures are highly dependent on loadingconditions. E’ velocity is a more sensitive marker of
abnormal left ventricular relaxation than mitral flowderived variables (4) and E/E’ ratio has been found toreflect left ventricular filling pressure (5, 6), correlatingbetter than natriuretic peptides with pulmonary capil-lary wedge pressure in a wide range of patients (7).
Because of myocardial architecture, subendocardialfibres are most susceptible to damage and longitudinalleft ventricular function is the first to be affected in thepresence of myocardial disease (8–10). Only a few stud-ies have used these tissue-Doppler derived indices toevaluate cardiac function in cirrhotic patients and onlytwo have looked into myocardial deformation (11, 12).Several limitations – like image artefacts and depen-dence on insonation angle – are acknowledged whenusing tissue-Doppler. Newer speckle-tracking derivedstrain may overcome some of these limitations resulting
Liver International (2013)© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 1
Liver International ISSN 1478-3223

58
Francisco Sampaio
in better reproducibility (13). We aimed to detect rest-ing myocardial dysfunction in patients with cirrhosis ofdifferent aetiologies, using these newer and potentiallymore accurate echocardiographic methods.
Patients and methods
We prospectively evaluated 131 consecutive patientsreferred per study protocol, to our echocardiographylaboratory between April 2011 and October 2012, with adiagnosis of cirrhosis based on clinical, laboratory, ultra-sonographic and/or biopsy criteria. Our population wascomposed by a group of 72 patients hospitalizedbecause of decompensated cirrhosis (defined by thepresence of encephalopathy, ascites, variceal bleeding,and/or jaundice) and a group of 59 ambulatory patientsfollowed in an outpatient hepatology clinic.
All patients underwent clinical evaluation, bloodsample collection, 12-lead ECG and echocardiographyon the same day.
Patients with a known history of hypertension, cardiacdisease or relevant ECG abnormalities were excluded;patients with significant (i.e. more than mild) valvularheart disease on echocardiography were also excluded.
A group of 18 healthy controls, recruited among hos-pital staff, with similar age and sex distribution as thepatient group, was also submitted to clinical, analytical,ECG and echocardiographic evaluation.
The local Ethic’s Committee approved the studyprotocol and patients or their relatives gave informedconsent.
Echocardiography
A single experienced operator performed the echocar-diograms using a commercially available ultrasoundsystem (iE33; Philips Medical Systems, Best, the Nether-lands) equipped with a broadband S5-1 transducer.Images were digitally stored for posterior offline analy-sis. Cardiac chambers dimensions and volumes and leftventricular mass were measured according to the cur-rent recommendations (14). Mitral inflow velocitieswere assessed using pulsed-wave (PW) Doppler in theapical four-chamber view, with a 3 mm sample placedbetween the tips of the mitral leaflets; velocities wererecorded at end-expiration and averaged over three con-secutive cardiac cycles. PW Doppler was also used torecord left ventricular outflow tract velocities in the api-cal five-chamber view. PW tissue-Doppler velocitieswere acquired at end-expiration, in the apical four-chamber view, with the sample positioned at the septaland lateral mitral annulus; the average of three consecu-tive heartbeats was recorded.
For strain assessment, two-dimensional grey-scale images were acquired in the apical four- andtwo-chamber views, with a frame rate of 60–100 fps.Three cardiac cycles were digitally stored and analysiswas performed using the Velocity Vector Imaging (VVI)
software (SyngoVVI 2.0; Siemens Medical SolutionsUSA Inc., Mountain View, CA, USA) more than amonth after the acquisition, by one observer blinded toclinical and echocardiographic data. This software auto-matically tracks the endocardial border (from a few ref-erence points manually defined by the operator)displaying velocity vectors throughout the cardiac cycle.Two-dimensional strain is obtained by tracking andcomparing the relative position of speckles throughoutthe cardiac cycle (Fig. 1).
Reproducibility
Reproducibility of VVI derived strain was assessed in 10randomly selected subjects. For intraobserver variability,the same operator performed a second measurementmore than a month after the initial analysis. For inte-robserver variability, the same loops were analysed by asecond operator.
Statistical analysis
Data were stored and analysed using IBM SPSS Statis-tics, Version 20.0 (IBM Corp., Armonk, NY, USA).Results are presented as median (25th–75th percentile)for quantitative variables and as n (%) for categoricalvariables. A significant level of 5% was used.
Differences in continuous variables between groupswere compared using the Mann–Whitney or the Krus-kal–Wallis tests. The Chi-squared test was used to compareproportions. Kappa measure was used to determine theagreement between definitions of diastolic dysfunction.Coefficients of variation were calculated to assess intra-and interobserver variability.
Results
Twenty-two patients of the original sample wereexcluded from further analysis based on the exclusioncriteria.
Clinical and laboratorial characteristics of the 109patients included and of the controls are shown inTable 1. A history of active alcohol consumption at thetime of the exam or hospital admission was reported by43.7% of the patients with alcoholic aetiology.
Echocardiographic variables of patients and controlsare displayed in Table 2.
Patients had larger left atrial volumes and highercardiac output; left ventricle dimensions, mass and ejec-tion fraction (EF) did not differ between patients andcontrols.
Systolic function
Only ten patients (9.2%) had a left ventricular EF below55%. Seven of these patients had decompensatedcirrhosis and five had alcoholic aetiology; these differ-ences did not reach the statistical significance.
Liver International (2013)© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd2
Systolic and diastolic dysfunction in cirrhosis Sampaio et al.
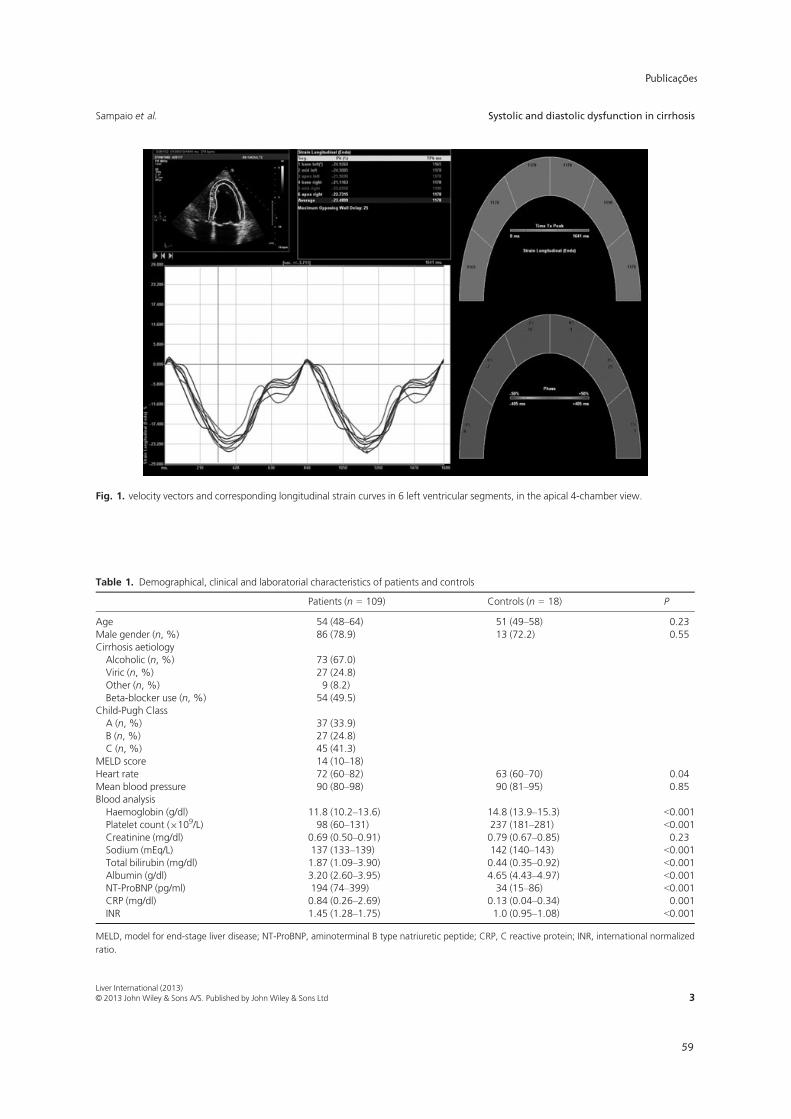
Publicações
59
Fig. 1. velocity vectors and corresponding longitudinal strain curves in 6 left ventricular segments, in the apical 4-chamber view.
Table 1. Demographical, clinical and laboratorial characteristics of patients and controls
Patients (n = 109) Controls (n = 18) P
Age 54 (48–64) 51 (49–58) 0.23Male gender (n, %) 86 (78.9) 13 (72.2) 0.55Cirrhosis aetiologyAlcoholic (n, %) 73 (67.0)Viric (n, %) 27 (24.8)Other (n, %) 9 (8.2)Beta-blocker use (n, %) 54 (49.5)
Child-Pugh ClassA (n, %) 37 (33.9)B (n, %) 27 (24.8)C (n, %) 45 (41.3)
MELD score 14 (10–18)Heart rate 72 (60–82) 63 (60–70) 0.04Mean blood pressure 90 (80–98) 90 (81–95) 0.85Blood analysisHaemoglobin (g/dl) 11.8 (10.2–13.6) 14.8 (13.9–15.3) <0.001Platelet count (9109/L) 98 (60–131) 237 (181–281) <0.001Creatinine (mg/dl) 0.69 (0.50–0.91) 0.79 (0.67–0.85) 0.23Sodium (mEq/L) 137 (133–139) 142 (140–143) <0.001Total bilirubin (mg/dl) 1.87 (1.09–3.90) 0.44 (0.35–0.92) <0.001Albumin (g/dl) 3.20 (2.60–3.95) 4.65 (4.43–4.97) <0.001NT-ProBNP (pg/ml) 194 (74–399) 34 (15–86) <0.001CRP (mg/dl) 0.84 (0.26–2.69) 0.13 (0.04–0.34) 0.001INR 1.45 (1.28–1.75) 1.0 (0.95–1.08) <0.001
MELD, model for end-stage liver disease; NT-ProBNP, aminoterminal B type natriuretic peptide; CRP, C reactive protein; INR, international normalized
ratio.
Liver International (2013)© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 3
Sampaio et al. Systolic and diastolic dysfunction in cirrhosis

60
Francisco Sampaio
Tissue-Doppler mitral annulus systolic velocities (S’)were not different in patients and controls. [9.19 cm/s(8.21–10.32) vs 8.71 cm/s (8.17–9.46), P = 0.28]. How-ever, peak systolic longitudinal strain (PLS) was lower(i.e. less negative) in patients [�19.99% (�21.88 to�18.71) vs �22.02% (�23.10 to �21.18), P = 0.003].PLS was not different in hospitalized and ambulatorypatients [�20.51% (�22.33 to �19.04) vs �19.00%(�21.54 to �18.20), P = 0.10] or between differentChild-Pugh classes [�20.81% (�23.45 to �18.92) vs�19.61% (�21.29 to �18.90), vs �19.02% (�21.55 to�18.25) P = 0.23]. There were also no differences inPLS in patients previously treated with beta-blockers,compared with the rest of the patients [�20.16%(�23.04 to �18.66) vs �19.90% (�21.55 to �18.71),P = 0.57]. We found a non-significant trend towardslower strain in alcoholic vs other aetiologies [�19.42%(�21.42 to �18.47) vs �20.87% (�22.67 to �19.01),P = 0.09]. There were no differences in left ventricularvolumes [99 ml (79–120) vs 99 ml (80–117), P = 0.91]or ejection fraction [64% (59–69) vs 62% (57–66),P = 0.11] between those two groups. Alcoholic patientswere older than patients with other aetiologies [59 (46–59) vs 51 (46–59), P = 0.03]. Peak longitudinal strainwas not different in patients with a history of activealcohol consumption vs the others [�19.39% (�21.88to �18.84) vs �19.68% (�21.65 to �18.40), P = 0.83].
Patients with EF <55% had significantly lowerPLS compared with patients with FE � 55%[�16.73% (�20.49 to �13.99) vs �20.19% (�22.33to �18.77), P = 0.013].
Right ventricular function evaluated by tricuspidannulus plane systolic excursion (TAPSE) was not dif-ferent between patients and controls [25.4 mm (22.0–28.2) vs 23.1 mm (21.5–26.2), P = 0.11].
Coefficients of variation for intra- and interobservervariability were 1.84 and 2.36% respectively.
Diastolic function
Compared with controls, cirrhotic patients had lowerE/A ratio, longer E wave deceleration time (DT), lower
mean E’ wave velocity and higher mean E/E’ ratio(Table 2).
Using the diagnostic criteria of the 2005 World Con-gress of Gastroenterology (1), diastolic dysfunction(DD), defined as an E/A ratio <1.0, DT >200 ms andisovolumetric relaxation time (IVRT) >80 ms, waspresent in 44 patients (40.4%). Compared with thosewithout DD, these patients were older, had lower car-diac output, lower E/A ratio, longer DT and IRVT(these three are part of the definition), lower E’ velocityand higher E/E’ ratio. Mean blood pressure, heart rate,cardiac volumes, left ventricular mass, NT-ProBNP lev-els (both in compensated and decompensated patients),TAPSE, S’ velocity, PLS and QTc interval were not dif-ferent between patients with and without DD. Theprevalence of diastolic dysfunction was not different incompensated and decompensated cirrhosis (33.3% vs44.3%, P = 0.26) or between different Child-Pugh clas-ses (Table 3 – definition 1).
According to the algorithm of the current recom-mendations for grading diastolic function by echocardi-ography (15), DD is diagnosed in the presence ofreduced tissue-Doppler mitral annulus velocities (septale’ <8 cm/s and lateral e’ <10 cm/s) and enlarged leftatria (� 34 ml/m2). Using this definition, the preva-lence of DD in our sample was 16.5%. There was only aweak agreement between the two definitions of DD(kappa = 0.24, P = 0.003).
Patients with these criteria of DD were older, hadlarger left atrial volumes, lower E/A ratio, longer DTand IRVT, lower S’ and E’ velocities, higher E/E’ratio and lower PLS. Cardiac output, mean bloodpressure, heart rate, left ventricular mass, TAPSE andQTc interval were not different between patients withand without DD, using this definition (Table 3 – def-inition 2). Patients with compensated cirrhosis andDD had higher NT-ProBNP than compensatedpatients without DD [133.5 pg/ml (70.8–267.5) vs59.0 pg/ml (22.0–131.0), P = 0.05]. This finding wasnot observed in patients with decompensated cirrhosis[193.5 pg/ml (94.0–399.0) vs 319.5 pg/ml (160.2–663.7), P = 0.30].
Table 2. Echocardiographic data of patients and controls
Patients (n = 109) Controls (n = 18) P
Left atrial volume (ml) 70 (54–83) 54 (37–61) 0.001Left atrial volume index (ml/m2) 39.8 (29.9–44.7) 30.4 (22.3–33.7) <0.001Left ventricle diastolic diameter (mm) 51 (47–55) 49 (47–53) 0.21Left ventricle systolic diameter (mm) 32 (28–35) 32 (27–33) 0.67Left ventricle diastolic volume (ml) 99 (79–119) 92 (78–114) 0.41Left ventricular mass (g) 148 (121–188) 145 (119–160) 0.19Left ventricular mass index (g/m2) 84 (70.5–103) 76 (65–88) 0.06Left ventricular ejection fraction (%) 64 (59–67) 61 (60–65) 0.42Cardiac output(L/min) 6.1 (5.0–7.1) 5.2 (4.6–5.8) 0.01E/A ratio 1.03 (0.81–1.35) 1.29 (1.14–1.53) 0.02Deceleration time (ms) 239 (203–280) 196 (176–224) 0.001E’ velocity (cm/s) 9.56 (7.42–11.72) 11.01 (9.76–12.55) 0.031E/E’ ratio 8.57 (6.79–10.36) 6.72 (6.09–7.83) 0.001
Liver International (2013)© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd4
Systolic and diastolic dysfunction in cirrhosis Sampaio et al.

Publicações
61
The prevalence of diastolic dysfunction was notdifferent in compensated and decompensated cirrhosis(15.4% vs 17.1%, P = 0.8), in different Child-Pugh clas-ses or in alcoholic vs nonalcoholic aetiology (8.3% vs20.5%, P = 0.11).
Electrophysiological abnormalities
Patients had longer QTc intervals than controls [426 ms(410–448) vs 406 ms (382–417), P = 0.008]. A QTc>440 ms was observed in 30.3% of the patients; NT-proBNP levels of those patients did not differ from therest of the sample.
Discussion
Our results, in a large cohort of patients with cirrhosisof different aetiologies, suggest that subclinical systolicand diastolic dysfunction are frequent at rest and thatnewer echocardiographic modalities are able to detectthese abnormalities.
Using speckle-tracking derived strain, we found thatpatients with cirrhosishad reduced longitudinal left
ventricular systolic function, despite still having normalejection fraction. This observation was independent ofaetiology or clinical status, which supports the presenceof an intrinsic myocardial systolic dysfunction in cirrho-sis. Reduced LV longitudinal function has been docu-mented in several other conditions, being consideredthe first manifestation of cardiac impairment (8–10).The increased susceptibility to damage of the longitudi-nally oriented endocardial fibres compared with theradial fibres of the middle myocardium layer furnish therational to this observation. Two previous studies havelooked into left ventricular longitudinal function incirrhosis. Kazankov et al have reported reduced mitralannulus longitudinal displacement velocities, usingtissue-Doppler in patients with cirrhosis (11), comparedwith healthy controls. There was no relation betweenechocardiographic measures and aetiology or clinicalstatus. Our study, confirms these findings, in a largerpopulation, using a more reproducible, angle-indepen-dent echocardiographic method. A very recent study hasevaluated left ventricular longitudinal strain usingspeckle tracking (12) in 50 patients and found no differ-ences in patients with and without ascites; however, a
Table 3. clinical, echocardiographic and electrocardiographic characteristics of patients with and without diastolic dysfunction (DD)
Definition 1
P
Definition 2
PWith DD, n = 44 Without DD, n = 65 With DD, n = 18 Without DD, n = 91
Age 63 (57–69) 51 (44–58) <0.001 65 (59–67) 53 (46–62) <0.001Child-Pugh ClassA (n, %) 15 (40.5) 22 (59.5) 0.99 7 (18.9) 30 (81.1) 0.15B (n, %) 11 (40.7) 16 (59.3) 7 (25.9) 20 (74.1)C (n, %) 18 (40) 27 (60) 14 (8.9) 41 (91.1)
MELD score 14 (9–17) 14 (10–18) 0.36 12 (7–15) 14 (10–18) 0.13Mean bloodpressure (mmHg)
90.7 (82.7–97.3) 88.2 (77.2–99.2) 0.61 91.3 (83.1–95.1) 89.7 (78.0–98.5) 0.83
Heart rate (bpm) 72 (60–80) 72 (59–84) 0.84 63 (52–79) 72 (60–83) 0.06NT-ProBNP (pg/ml) 200 (90–555) 177 (61–344) 0.21 201 (61–420) 189 (78–399) 0.90Left atrial volumeindex (ml/m2)
37.9 (26.9–44.5) 40.8 (32.8–46.1) 0.17 43.9 (40.1–49.4) 38.6 (29.0–44.7) 0.006
Left ventricle diastolicvolume (ml)
91 (74–117) 103 (83–120) 0.16 87 (77–119) 101 (82–119) 0.54
Left ventricular massindex (g/m2)
90.5 (69.3–108) 83.0 (71.5–99.5) 0.34 96 (71–113) 83 (70–101) 0.09
Cardiac output (L/min) 5.6 (4.7–6.8) 6.4 (5.4–7.2) 0.02 5.7 (4.5–7.0) 6.1 (5.2–7.2) 0.24IVRT (ms) 118 (103–139) 98 (80–116) <0.001 132 (110–147) 103 (85–121) <0.001E/A ratio 1.03 (0.81–1.35) 1.29 (1.14–1.53) 0.02 0.79 (0.70–0.95) 1.10 (0.86–1.37) 0.002Deceleration time (ms) 239 (203–280) 196 (176–224) 0.001 312 (233–343) 236 (200–269) 0.003S’ velocity (cm/s) 8.87 (8.07–10.35) 9.19 (8.21–10.32) 0.55 8.05 (7.28–9.44) 9.26 (8.33–10.50) 0.004E’ velocity (cm/s) 11.01 (9.76–12.55) 9.56 (7.42–11.72) 0.03 6.99 (5.76–7.57) 10.07 (8.65–11.95) <0.001E/E’ ratio 8.57 (6.79–10.36) 6.72 (6.09–7.83) 0.001 11.92 (8.79–12.95) 8.19 (6.75–9.85) 0.001TAPSE (mm) 0.31 27.0 (22.5–29) 25.3 (21.7–28.0) 0.48PLS (%) �19.39 (�18.04 to
�21.38)�20.71 (�18.08 to�22.51)
0.11 �19.10 (�17.04 to�20.67)
�20.33 (�18.82to �22.48)
0.03
QTc interval (ms) 429 (418–449) 420 (402–448) 0.10 433 (402–456) 425 (411–448) 0.80
Definition 1: E/A ratio <1.0, deceleration time >200 ms and IVRT >80 ms (1); Definition 2: septal e’ <8 cm/s, lateral e’ <10 cm/s and left atrial volume
� 34 ml/m2 (15).
DD, diastolic dysfunction; MELD, model for end-stage liver disease; NT-ProBNP, aminoterminal B type natriuretic peptide; IVRT, isovolumetric relaxa-
tion time; TAPSE, tricusid annulus plane systolic excursion; PLS, left ventricular peak longitudinal strain.
Liver International (2013)© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 5
Sampaio et al. Systolic and diastolic dysfunction in cirrhosis

62
Francisco Sampaio
control group was lacking. Our findings, in a larger andcontrolled sample, support and expand those results.The absence of differences in strain between compen-sated and decompensated patients may be explained bya normal increase in longitudinal strain in response tostress in decompensated patients without significantsystolic dysfunction, which would blur the effect of ablunted response to stress in decompensated patientswith systolic dysfunction. The net effect would be asimilar strain in both the groups.
Unlike Kazankov et al, we did not find differences inmean S’ velocity between patients and controls. Thisapparent conflicting result probably relates to the pres-ence of ‘supranormal’ velocities in some patients with anhyperdynamic circulation. Most of the patients in ourstudy were in Child B-C class and had higher cardiac outputcompared with those of that study. Nineteen patients(17.4%) in our sample had S’ � 11 cm/s, the upper refer-ence limit (defined as the mean plus two standard devia-tions) in a population of healthy individuals (16) andthese patients had higher cardiac output than patientswith normal S’. Besides, mitral ring displacement andactive muscle deformation are not equivalent concepts.
The 2005 World Congress of Gastroenterology pro-posed a resting EF <55% to define systolic dysfunctionin patients with cirrhosis (1). According to this, only9.2% of the patients of our sample had a reduced EF.The use of EF to evaluate systolic function has severallimitations. Ejection fraction is not an index of contrac-tility and depends on loading conditions, heart rate andvalvular function (17). Besides, EF relies on accuratetracing of endocardial borders with frequent underesti-mation of ventricular volumes. Therefore, a ‘normal’ejection fraction may not reflect normal contractilefunction and this may be particularly true in cirrhosis.Our finding of a significantly lower PLS in patients withan EF <55% compared with patients with normal EF,suggests that EF may be an insensitive (albeit specific)and probably late marker of systolic dysfunction incirrhosis, identifying only patients with more severemyocardial dysfunction.
Using the 2005 World Congress of Gastroenterologycriteria, diastolic dysfunction was highly prevalent inour sample, in line with several previous reports (11, 12,18, 19). These criteria were based exclusively on mitralflow derived parameters, which are influenced not onlyby relaxation, but also by flow conditions. The effect ofpreload, heart rate and cardiac output on mitral flowpattern has been previously acknowledged (15, 20, 21).According to the currently accepted theory, blood pool-ing in the splanchnic bed in cirrhosis results in centralhypovolaemia and reduced preload. This would, alongwith faster heart rates, result in lower mitral E wavevelocities and lower E/A ratios, regardless of the pres-ence of impaired relaxation (20). That might explain thehigh prevalence of a delayed relaxation pattern in allechocardiographic studies in cirrhosis, as well as thereported relation between DD and liver disease severity.
In fact, in our study, patients with this definition of DD,had lower cardiac output compared with patients with-out DD, which supports the notion of flow-dependenceof mitral variables. Besides, we could not find the differ-ences in left atrial volume – a known marker of DDchronicity – between the two groups.
On the other hand, Pimenta et al (22), using imped-ance cardiography, found that patients with decompen-sated cirrhosis had high thoracic fluid content, whichusually reflects central volaemia. This suggests thatpatients with cirrhosis may have markedly different hae-modynamic conditions during the course of their ill-ness. Therefore, PW-Doppler mitral criteria may not besuitable to correctly identify patients with abnormalrelaxation, reflecting also different flow conditions. Thelimited agreement between the two DD definitions thatwe have tested further supports this hypothesis.
According to the most recent recommendations forthe evaluation of diastolic function by echocardiography(15), tissue-Doppler derived parameters play a majorrole in the diagnostic work-up of DD. E’ is a sensitivemarker of abnormal relaxation with a good correlationwith tau (the time constant of ventricular relaxation)(4, 23, 24). On the other hand, E’ can be used to correctthe effect of relaxation on E velocity; hence the E/E’ ratiocan be used to estimate LV filling pressures. A good cor-relation between this index and filling pressure has beenconsistently reported in multiple scenarios (5, 25, 26).We used the proposed algorithm of these recommenda-tions and defined DD as reduced tissue-Doppler mitralannulus velocities and enlarged left atria. Applying thesecriteria, the prevalence of DD in our sample was lowerthan when using mitral flow parameters. We found nodifferences in haemodynamic variables in patients withand without this definition of DD, supporting a relativeload-independence of the method. However, patientswith DD had differences in other indices of diastolicfunction not included in the definition (E/A ratio, DTand IVRT) and significantly lower S’ velocity and PLS.In fact, the presence of longitudinal systolic dysfunctionin patients with diastolic heart failure has been consis-tently reported (27–29). This suggests that tissue-Dopplerbased criteria may be more specific than mitral flowderived variables for the identification of cirrhoticpatients with more serious myocardial dysfunction. Afew previous studies have used tissue-Doppler inassessing diastolic function in cirrhosis (11, 12, 18, 30).However, most of them still based the diagnosis onPW-Doppler parameters and tissue-Doppler was mainlyused to differentiate between normal and pseudo-nor-mal E/A patterns. This approach, although widely usedin clinical practice, is different from the one proposedby the consensus recommendations and may explain thedifference in the prevalence of DD in our study. Nazaret al recently reported that 84% of cirrhotic patientshad normal or only mild DD and that invasively deter-mined pulmonary capillary wedge pressure was normalin all patients (12). Taken altogether, these and our
Liver International (2013)© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd6
Systolic and diastolic dysfunction in cirrhosis Sampaio et al.

Publicações
63
findings raise the possibility that the prevalence of DDrelated to intrinsic ventricular pathology may be lessfrequent than previously assumed.
As cirrhosis aetiology is mainly alcoholic in our sam-ple, we cannot exclude that our results reflect alcoholicrather than cirrhotic cardiomyopathy. However, whenwe compared systolic function parameters in alcoholicpatients vs the others, found only a trend towards lowerstrain in alcoholics and no differences in left ventricularvolumes or ejection fraction between the two groups.The prevalence of diastolic dysfunction also did notdiffer in the two groups. Other authors have reportedsimilar results (11, 12, 31). Taken altogether, these findingsargue against an exclusive alcohol effect on our results.
Although NT-ProBNP levels were correlated withseverity of cirrhosis in our sample (data not shown), wedid not find a correlation between NT-ProBNP and car-diac dysfunction, in contrast to other studies (30). How-ever, when patients with decompensated cirrhosis wereexcluded from the analysis, NT-ProBNP levels werehigher in patients with evidence of diastolic dysfunction.This may be because of the influence of cardiac, hepaticand renal dysfunction and their mutual interactions onNT-ProBNP levels, which is probably more significantin decompensated/hospitalized patients. In this sce-nario, natriuretic peptides may be a global risk markerreflecting multi-organic dysfunction. The associationbetween natriuretic peptides and prognosis (22) seemsto support this hypothesis.
Limitations
This is a single centre study performed in patientsmainly with alcoholic cirrhosis and different diseaseseverity.
An accepted gold-standard method to diagnose cir-rhotic cardiomyopathy is still lacking. We did not per-form a dobutamine stress test, which might have beenuseful in revealing systolic dysfunction. Neither did weperform invasive haemodynamic measurements whichwould have allowed us to correlate our echocardio-graphic findings with accurate parameters of systolic anddiastolic function, systemic haemodynamics and degreeof portal hypertension. Hence, we cannot objectivelyassess the diagnostic performance of tissue-Doppler andspeckle tracking and can only suggest that they may bemore adequate based on consistent and increasinglyrobust evidence in other areas of cardiovascular disease.Besides, limitations and pitfalls of these new modalitiesare well recognized (32). In particular, there are somesituations in which tissue Doppler velocities and E/E’ ratiomay not correlate with LV filling pressures (33); however,none of them seems to apply to this population.
Conclusions
Patients with cirrhosis have evidence of both systolicand diastolic dysfunction at rest. Our results suggest
that newer echocardiographic techniques may identifypatients with functional impairment more accuratelythan conventional echocardiographic methods. Theclinical significance of these abnormalities merits furtherinvestigation.
References
1. Møller S, Henriksen JH. Cardiovascular complications ofcirrhosis. Gut 2008; 57: 268–78.
2. Alqahtani SA, Fouad TR, Lee SS. Cirrhotic cardiomyopa-thy. Semin Liver Dis 2008; 28: 59–69.
3. Wong F. Cirrhotic cardiomyopathy. Hepatol Int 2009; 3:294–304.
4. Oki T, Tabata T, Yamada H, et al. Clinical application ofpulsed Doppler tissue imaging for assessing abnormal leftventricular relaxation. Am J Cardiol 1997; 79: 921–8.
5. Kasner M, Westermann D, Steendijk P, et al. Utility ofDoppler echocardiography and tissue Doppler imaging inthe estimation of diastolic function in heart failure withnormal ejection fraction: a comparative Doppler-conduc-tance catheterization study. Circulation 2007; 116: 637–47.
6. Ommen SR, Nishimura RA, Appleton CP, et al. Clinicalutility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pres-sures: a comparative simultaneous Doppler-catheteriza-tion study. Circulation 2000; 102: 1788–94.
7. Dokainish H, Zoghbi WA, Lakkis NM, et al. Optimalnoninvasive assessment of left ventricular filling pressures:a comparison of tissue Doppler echocardiography andB-type natriuretic peptide in patients with pulmonaryartery catheters. Circulation 2004; 109: 2432–9.
8. Andersen NH, Poulsen SH, Eiskjaer H, Poulsen PL, Mog-ensen CE. Decreased left ventricular longitudinal contrac-tion in normotensive and normoalbuminuric patientswith Type II diabetes mellitus: a Doppler tissue trackingand strain rate echocardiography study. Clin Sci 2003;105: 59–66.
9. Cardim N, Oliveira AG, Longo S, et al. Doppler tissueimaging: regional myocardial function in hypertrophiccardiomyopathy and in athlete’s heart. J Am Soc Echocar-diogr 2003; 16: 223–32.
10. Poulsen SH, Andersen NH, Heickendorff L, MogensenCE. Relation between plasma amino-terminal propeptideof procollagen type III and left ventricular longitudinalstrain in essential hypertension. Heart 2005; 91: 624–9.
11. Kazankov K, Holland-Fischer P, Andersen NH, et al. Rest-ing myocardial dysfunction in cirrhosis quantified bytissue Doppler imaging. Liver Int 2011; 31: 534–40.
12. Nazar A, Guevara M, Sitges M, et al. LEFT ventricularfunction assessed by echocardiography in cirrhosis: rela-tionship to systemic hemodynamics and renal dysfunction.J Hepatol 2013; 58: 51–7.
13. Becker M, Bilke E, K€uhl H, et al. Analysis of myocardialdeformation based on pixel tracking in two dimensionalechocardiographic images enables quantitative assessmentof regional left ventricular function. Heart 2006; 92:1102–8.
14. Lang RM, Bierig M, Devereux RB, et al. Recommenda-tions for chamber quantification. Eur J Echocardiogr 2006;7: 79–108.
15. Nagueh SF, Appleton CP, Gillebert TC, et al. Recommen-dations for the evaluation of left ventricular diastolic
Liver International (2013)© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 7
Sampaio et al. Systolic and diastolic dysfunction in cirrhosis
64
Francisco Sampaio
function by echocardiography. J Am Soc Echocardiogr2009; 22: 107–33.
16. Dalen H, Thorstensen A, Vatten LJ, Aase SA, Stoylen A.Reference values and distribution of conventional echocar-diographic Doppler measures and longitudinal tissueDoppler velocities in a population free from cardiovascu-lar disease. Circ Cardiovasc Imaging 2010; 3: 614–22.
17. McMurray JJ, Adamopoulos S, Anker SD, et al. ESCguidelines for the diagnosis and treatment of acute andchronic heart failure 2012: the task force for the diagnosisand treatment of acute and chronic heart failure 2012 ofthe European Society of Cardiology. Developed in collabo-ration with the Heart Failure Association (HFA) of theESC. Eur Heart J 2012; 33: 1787–847.
18. Alexopoulou A, Papatheodoridis G, Pouriki S, et al. Dia-stolic myocardial dysfunction does not affect survival inpatients with cirrhosis. Transpl Int 2012; 25: 1174–81.
19. Cazzaniga M, Salerno F, Pagnozzi G, et al. Diastolic dys-function is associated with poor survival in patients withcirrhosis with transjugular intrahepatic portosystemicshunt. Gut 2007; 56: 869–75.
20. Choong CY, Herrmann HC, Weyman AE, Fifer MA. Pre-load dependence of Doppler-derived indexes of left ven-tricular diastolic function in humans. J Am Coll Cardiol1987; 10: 800–8.
21. Thomas JD, Choong CY, Flachskampf FA, Weyman AE.Analysis of the early transmitral Doppler velocity curve:effect of primary physiologic changes and compensa-tory preload adjustment. J Am Coll Cardiol 1990; 16:644–55.
22. Pimenta J, Paulo C, Gomes A, et al. B-type natriureticpeptide is related to cardiac function and prognosis inhospitalized patients with decompensated cirrhosis. LiverInt 2010; 30: 1059–66.
23. Nagueh SF, Sun H, Kopelen HA, Middleton KJ, KhouryDS. Hemodynamic determinants of the mitral annulusdiastolic velocities by tissue Doppler. J Am Coll Cardiol2001; 37: 278–85.
24. Sohn DW, Chai IH, Lee DJ, et al. Assessment of mitralannulus velocity by Doppler tissue imaging in the evalua-
tion of left ventricular diastolic function. J Am Coll Cardiol1997; 30: 474–80.
25. Kim YJ, Sohn DW. Mitral annulus velocity in the estima-tion of left ventricular filling pressure: prospective study in200 patients. J Am Soc Echocardiogr 2000; 13: 980–5.
26. Nagueh SF, Lakkis NM, Middleton KJ, et al. Doppler esti-mation of left ventricular filling pressures in patients withhypertrophic cardiomyopathy. Circulation 1999; 99:254–61.
27. Bruch C, Gradaus R, Gunia S, Breithardt G, Wichter T.Doppler tissue analysis of mitral annular velocities:evidence for systolic abnormalities in patients with dia-stolic heart failure. J Am Soc Echocardiogr 2003; 16:1031–6.
28. Vinereanu D, Nicolaides E, Tweddel AC, Fraser AG.“Pure” diastolic dysfunction is associated with long-axissystolic dysfunction. Implications for the diagnosis andclassification of heart failure. Eur J Heart Fail 2005; 7:820–8.
29. Yip G, Wang M, Zhang Y, et al. Left ventricular long axisfunction in diastolic heart failure is reduced in both dias-tole and systole: time for a redefinition? Heart 2002; 87:121–5.
30. Raedle-Hurst TM, Welsch C, Forestier N, et al. Validityof N-terminal propeptide of the brain natriuretic pep-tide in predicting left ventricular diastolic dysfunctiondiagnosed by tissue Doppler imaging in patients withchronic liver disease. Eur J Gastroenterol Hepatol 2008;20: 865–73.
31. Merli M, Calicchia A, Ruffa A, et al. Cardiac dysfunctionin cirrhosis is not associated with the severity of liverdisease. Eur J Intern Med 2013; 24: 172–6.
32. Teske AJ, de Boeck BWL, Melman PG, et al. Echocardio-graphic quantification of myocardial function using tissuedeformation imaging, a guide to image acquisition andanalysis using tissue Doppler and speckle tracking. Cardio-vasc Ultrasound 2007; 5: 27.
33. Little WC, Oh JK. Echocardiographic evaluation ofdiastolic function can be used to guide clinical care. Circu-lation 2009; 120: 802–9.
Liver International (2013)© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd8
Systolic and diastolic dysfunction in cirrhosis Sampaio et al.

Publicações
65
ORIGINAL ARTICLE
Left atrial function is impaired in cirrhosis:a speckle tracking echocardiographic study
Francisco Sampaio • Joana Pimenta • Nuno Bettencourt •
Ricardo Fontes-Carvalho • Ana Paula Silva • Joao Valente •
Paulo Bettencourt • Jose Fraga • Vasco Gama
Received: 22 April 2013 / Accepted: 1 August 2013 / Published online: 27 August 2013
� Asian Pacific Association for the Study of the Liver 2013
Abstract
Purpose Abnormalities in left ventricular systolic and
diastolic function have been described in patients with cir-
rhosis. There are no studies on left atrial (LA) function in
these patients.We aimed to evaluate LA function in cirrhosis
patients using myocardial deformation imaging.
Methods We included 111 hospitalized and ambulatory
patients with cirrhosis and 18 healthy controls. A com-
prehensive echocardiographic evaluation was performed;
LA strain was assessed using velocity vector imaging.
Results Peak atrial longitudinal strain at the end of ven-
tricular systole was lower in patients [41.9 % (34.4–51.0)
vs. 48.0 % (42.0–57.1), p = 0.02]. No differences were
found in atrial strain before atrial contraction in patients
and controls [17.5 % (14.3–22.4) vs. 20.7 % (14.1–26.3),
p = 0.14]. On multivariate linear regression analysis, E0
velocity was the only variable independently associated
with peak atrial longitudinal strain (R2 = 47 %). No cor-
relation was found between the LA volume index (LAVI)
and peak atrial longitudinal strain (r = -0.136,
p = 0.219). Peak atrial longitudinal strain performed better
than LAVI in identifying patients with elevated filling
pressures (AUC = 0.81 vs. 0.52).
Conclusions Patients with cirrhosis have abnormal atrial
reservoir function, which may be related to the same fac-
tors associated with impaired ventricular relaxation. LA
enlargement in cirrhosis may not reflect elevated filling
pressures and should not be used as an isolated marker of
diastolic dysfunction. The atrial ‘‘pump’’ function does not
seem to be affected in cirrhosis patients.
Keywords Cirrhosis � Echocardiography � Heartfailure � Atrial function � Speckle tracking imaging
Introduction
Cirrhotic cardiomyopathy refers to the presence of cardiac
systolic, diastolic and electrophysiological abnormalities in
patients with cirrhosis, in the absence of known heart dis-
ease [1–3]. A high prevalence of diastolic dysfunction
(DD) in cirrhosis patients has been found in several studies
[4–7]. Increased left atrial (LA) volume, a known marker
of chronicity of DD, has also been reported in cirrhosis [8].
However, LA enlargement may be present in the absence
of chronically elevated left ventricular (LV) filling pres-
sures, and dilated atria may be seen in patients with volume
overload, anemia and high-output states [9]. The mecha-
nisms leading to LA dilatation in cirrhotic patients are not
fully understood.
LA dilatation and dysfunction are frequently associated.
LA dysfunction may be involved in the pathophysiology of
F. Sampaio (&) � N. Bettencourt � R. Fontes-Carvalho �V. Gama
Cardiology Department, Centro Hospitalar de Gaia/Espinho, Rua
Conceicao Fernandes, 4430-502 Vila Nova de Gaia, Portugal
e-mail: [email protected]
F. Sampaio � J. Pimenta � N. Bettencourt � R. Fontes-Carvalho �P. Bettencourt
Cardiovascular R&D Unit, University of Porto Medical School,
Porto, Al. Prof. Hernani Monteiro, 4200-319 Porto, Portugal
A. P. Silva � J. FragaGastroenterology Department, Centro Hospitalar de Gaia/
Espinho, Rua Conceicao Fernandes, 4430-502 Vila Nova de
Gaia, Portugal
J. Valente
Internal Medicine Department, Centro Hospitalar de Gaia/
Espinho, Rua Conceicao Fernandes, 4430-502 Vila Nova de
Gaia, Portugal
123
Hepatol Int (2014) 8:146–153
DOI 10.1007/s12072-013-9469-5

66
Francisco Sampaio
several conditions and may be associated with symptom
onset [10]. Abnormalities in LA function have been
described, using different methodologies, in LV hypertro-
phy, hypertension, hypertrophic cardiomyopathy, diabetes
mellitus and DD [10–16]. These abnormalities are detect-
able before LA enlargement [15] and may be independent
of LA volume [13]. Additionally, LA longitudinal strain
seems to correlate better with LV filling pressures than LA
volume or other echocardiographic indices such as the E/E0
ratio [17, 18]. Accordingly, LA function may be a sensitive
marker of cardiac dysfunction. The value of atrial function
indices, particularly atrial longitudinal strain, in predicting
cardiovascular events has also been demonstrated [19–21],
which further stresses the potential clinical impact of atrial
dysfunction.
Speckle tracking echocardiography is an angle-inde-
pendent method for assessing myocardial deformation.
Although it is usually used for LV function analysis, pre-
vious studies have used it to assess LA function [10, 12, 13,
17, 18, 22]. However, no such studies have been performed
in cirrhosis patients.
To test the hypothesis that patients with cirrhosis could
have abnormal LA function as a consequence of cirrhotic
cardiomyopathy, we performed a detailed LA function
evaluation, using myocardial deformation imaging, in
patients with cirrhosis and in healthy age-matched controls.
Materials and methods
We prospectively evaluated 133 consecutive patients
referred to our echocardiography laboratory to participate
in a study of cardiac function in cirrhosis between April
2011 and November 2012. An additional analysis of this
cohort has been published previously [23].
Diagnosis of cirrhosis was based on clinical, laboratory,
ultrasonographic and/or biopsy criteria. Our sample was
composed of a group of 61 ambulatory patients followed in
an outpatient hepatology clinic and a group of 72 patients
hospitalized because of decompensated cirrhosis (defined
by the presence of encephalopathy, ascites, variceal
bleeding and/or jaundice).
A group of 18 healthy controls, with similar age and sex
distribution as the patient group, was recruited among
hospital staff.
Patients and controls underwent clinical evaluation,
blood sample collection, 12-lead ECG and echocardiogra-
phy on the same day.
Patients with a known history of hypertension, diabetes
or other relevant cardiac disease were excluded; patients
with significant ECG abnormalities or more than mild
valvular heart disease on echocardiography were also
excluded.
The investigation conforms with the principles outlined
in the Declaration of Helsinki. The local ethics committee
approved the study protocol, and patients or their relatives
gave informed consent.
Echocardiography
A single experienced operator performed the echocardio-
grams, using a commercially available ultrasound system
(iE33, Philips Medical Systems, Best, The Netherlands)
equipped with a broadband S5-1 transducer.
Cardiac chamber dimensions and volumes and LV
mass were measured according to current recommenda-
tions [24]. DD was diagnosed and graded according to the
current recommendations for the evaluation of LV dia-
stolic function by echocardiography [9]. Pulsed-wave
Doppler, with a 3-mm sample placed between the tips of
the mitral leaflets, was used to assess LV inflow veloci-
ties. Pulsed-wave tissue-Doppler velocities were acquired
in the apical four-chamber view, with the sample posi-
tioned at the septal and lateral mitral annulus. Velocities
were recorded at end expiration and averaged over three
consecutive cardiac cycles. Mean systolic (S0) and early-
(E0) and late diastolic (A0) velocities were considered for
the analysis.
For LA strain assessment, two-dimensional grey-scale
images were acquired in the apical four- and two-chamber
views, with a frame rate of 60–100 fps. Three cardiac
cycles were stored digitally. Analysis was performed using
the velocity vector imaging software (SyngoVVI 2.0, Sie-
mens Medical Solutions USA Inc., Mountain View, CA)
more than a month after the acquisition by one observer
blinded to the clinical and echocardiographic data. This
software automatically tracks the LA endocardial border
(from a few reference points manually defined by the
operator) displaying velocity vectors throughout the car-
diac cycle. Two-dimensional strain is obtained by tracking
and comparing the relative position of speckles throughout
the cardiac cycle. Strain curves are displayed for each of
the six segments automatically generated by the software.
Zero strain was set at the QRS onset. Using this reference
point, the LA strain pattern consists of a positive wave that
peaks at the end of ventricular systole followed by a
decrease after the opening of the mitral valve and by a
second peak before the start of atrial contraction (Fig. 1).
Peak LA strain at the end of ventricular systole (PALS)—
reflecting LA reservoir or ‘‘diastolic’’ function—and peak
atrial strain just before atrial contraction (PACS)—a mar-
ker of LA pump or ‘‘systolic’’ function—were measured
from the average strain curves. Patients with inadequate
tracking in more than two segments were excluded from
the analysis.
Hepatol Int (2014) 8:146–153 147
123
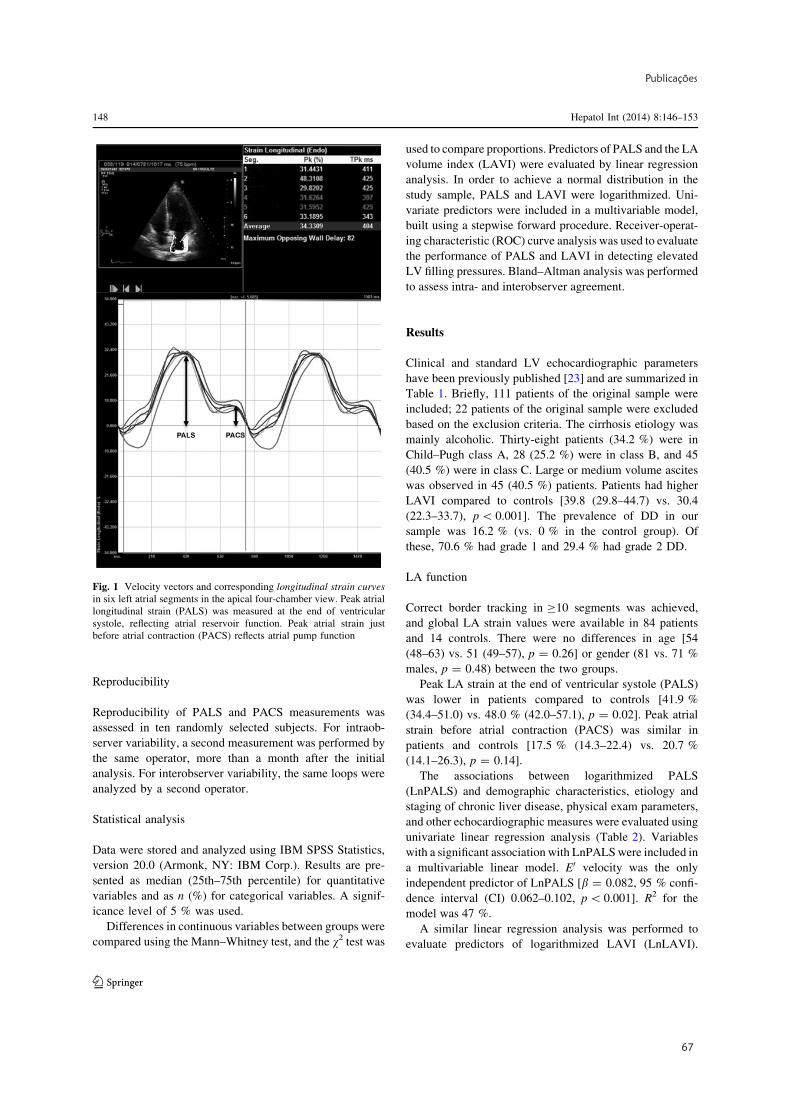
Publicações
67
Reproducibility
Reproducibility of PALS and PACS measurements was
assessed in ten randomly selected subjects. For intraob-
server variability, a second measurement was performed by
the same operator, more than a month after the initial
analysis. For interobserver variability, the same loops were
analyzed by a second operator.
Statistical analysis
Data were stored and analyzed using IBM SPSS Statistics,
version 20.0 (Armonk, NY: IBM Corp.). Results are pre-
sented as median (25th–75th percentile) for quantitative
variables and as n (%) for categorical variables. A signif-
icance level of 5 % was used.
Differences in continuous variables between groups were
compared using the Mann–Whitney test, and the v2 test was
used to compare proportions. Predictors of PALS and the LA
volume index (LAVI) were evaluated by linear regression
analysis. In order to achieve a normal distribution in the
study sample, PALS and LAVI were logarithmized. Uni-
variate predictors were included in a multivariable model,
built using a stepwise forward procedure. Receiver-operat-
ing characteristic (ROC) curve analysis was used to evaluate
the performance of PALS and LAVI in detecting elevated
LV filling pressures. Bland–Altman analysis was performed
to assess intra- and interobserver agreement.
Results
Clinical and standard LV echocardiographic parameters
have been previously published [23] and are summarized in
Table 1. Briefly, 111 patients of the original sample were
included; 22 patients of the original sample were excluded
based on the exclusion criteria. The cirrhosis etiology was
mainly alcoholic. Thirty-eight patients (34.2 %) were in
Child–Pugh class A, 28 (25.2 %) were in class B, and 45
(40.5 %) were in class C. Large or medium volume ascites
was observed in 45 (40.5 %) patients. Patients had higher
LAVI compared to controls [39.8 (29.8–44.7) vs. 30.4
(22.3–33.7), p\ 0.001]. The prevalence of DD in our
sample was 16.2 % (vs. 0 % in the control group). Of
these, 70.6 % had grade 1 and 29.4 % had grade 2 DD.
LA function
Correct border tracking in C10 segments was achieved,
and global LA strain values were available in 84 patients
and 14 controls. There were no differences in age [54
(48–63) vs. 51 (49–57), p = 0.26] or gender (81 vs. 71 %
males, p = 0.48) between the two groups.
Peak LA strain at the end of ventricular systole (PALS)
was lower in patients compared to controls [41.9 %
(34.4–51.0) vs. 48.0 % (42.0–57.1), p = 0.02]. Peak atrial
strain before atrial contraction (PACS) was similar in
patients and controls [17.5 % (14.3–22.4) vs. 20.7 %
(14.1–26.3), p = 0.14].
The associations between logarithmized PALS
(LnPALS) and demographic characteristics, etiology and
staging of chronic liver disease, physical exam parameters,
and other echocardiographic measures were evaluated using
univariate linear regression analysis (Table 2). Variables
with a significant association with LnPALSwere included in
a multivariable linear model. E0 velocity was the only
independent predictor of LnPALS [b = 0.082, 95 % confi-
dence interval (CI) 0.062–0.102, p\ 0.001]. R2 for the
model was 47 %.
A similar linear regression analysis was performed to
evaluate predictors of logarithmized LAVI (LnLAVI).
Fig. 1 Velocity vectors and corresponding longitudinal strain curves
in six left atrial segments in the apical four-chamber view. Peak atrial
longitudinal strain (PALS) was measured at the end of ventricular
systole, reflecting atrial reservoir function. Peak atrial strain just
before atrial contraction (PACS) reflects atrial pump function
148 Hepatol Int (2014) 8:146–153
123

68
Francisco Sampaio
Hemoglobin (b = -0.033, 95 % CI -0.054 to -0.012,
p = 0.003), stroke volume (b = 0.005, 95 % CI
0.002–0.007, p = 0.001) and LV end-diastolic volume
(b = 0.003, 95 % CI 0.001–0.005, p = 0.006) were inde-
pendently associated with LnLAVI. R2 for the model was
38 %.
We found a significant correlation between PALS and
mean E/E0 ratio (Spearman’s q = -0.47, p\ 0.001).
LAVI did not correlate with E/E0 (Spearman’s q = 0.05,
p = 0.602; Fig. 2). On ROC curve analysis, using an E/E0
ratio C10 as a surrogate marker of elevated LV pressures,
PALS performed better than LAVI in predicting increased
filling pressures (AUC = 0.81, 95 % CI 0.71–0.90 vs.
0.52, 95 % CI 0.39–0.64, p\ 0.001; Fig. 3). Best cutoff
values and corresponding sensitivities and specificities are
presented in Table 3.
The mean differences in PALS measurements were
0.3 % (95 % CI -1.4 to 1.9) and 0.6 % (95 % CI -1.6 to
2.7) for intra- and interobserver agreement, respectively. In
PACS, the mean differences were 0.4 % (95 % CI -0.4 to
1.2) for intraobserver and 0.8 % (95 % CI -0.9 to 2.6) for
interobserver agreement.
Discussion
Our results show that patients with cirrhosis have an
abnormal LA compliance at rest, which is related to LV
relaxation. LA contraction seems to be preserved.
Using deformation imaging, we found that patients with
cirrhosis have reduced PALS, reflecting impaired LA res-
ervoir function. Peak atrial longitudinal strain was, on
linear regression analysis, not associated with etiology,
clinical status, hemodynamic variables or LA volume.
Accordingly, compromised LA reservoir function may be a
manifestation of cirrhotic cardiomyopathy. This is, to the
best of our knowledge, the first study to evaluate atrial
function in cirrhosis using deformation imaging.
Atrial reservoir function has been found to be dependent
on mitral annulus descent besides atrial compliance [25,
26], since LV ejection occurs at the same time of the LA
reservoir phase. We found an association between LnPALS
and indices of LV systolic function (S0 velocity and LV
longitudinal strain) using linear regression analysis. How-
ever, E0 velocity (a sensitive marker of ventricular relaxa-
tion) was the only variable independently associated with
LnPALS in multivariate analysis, suggesting that the same
processes that impair ventricular relaxation play a major
role in LA compliance.
Atrial dysfunction has been reported in several other
conditions [10–16, 27], mainly characterized by LV DD.
This may be explained by the effect on LA relaxation of
the backward transmission of increased LV filling pres-
sures. The strong correlation between PALS and invasively
determined filling pressures found by other authors sup-
ports this hypothesis [17, 18]. In our work, we also found a
correlation between the atrial longitudinal strain and E/E0
ratio (a non-invasive estimate of LV filling pressures) on
univariate analysis. However, the association between LV
and LA dysfunction has been suggested to depend mainly
on fibrotic processes that affect the subendocardial layers
of both the LV and LA walls [10, 27, 28]. The relation
between LA stiffness and changes in extracellular matrix
composition and the expression of cytoskeletal proteins has
been demonstrated in animal models of DD [29]. The same
Table 1 Clinical, laboratorial and echocardiographic characteristics
of patients
Age 54 (48–64)
Male gender (n, %) 88 (79.3)
Cirrhosis etiology
Alcoholic (n, %) 74 (66.7)
Viric (n, %) 28 (25.2)
Other (n, %) 9 (8.1)
Beta-blocker use (n, %) 54 (48.6)
Child-Pugh class
A (n, %) 38 (34.2)
B (n, %) 28 (25.2)
C (n, %) 45 (40.5)
MELD score 14 (10–18)
Heart rate 72 (60–83)
Mean blood pressure 90 (80–98)
Blood analysis
Hemoglobin (g/dl) 11.9 (10.3–13.6)
Platelet count (9109/l) 98 (57–126)
Creatinine (mg/dl) 0.68 (0.50–0.91)
Sodium (mEq/l) 137 (133–140)
Total bilirubin (mg/dl) 1.81 (1.09–3.80)
Albumin (g/dl) 3.30 (2.60–3.90)
NT-ProBNP (pg/ml) 193 (64–399)
CRP (mg/dl) 0.84 (0.25–2.48)
INR 1.43 (1.28–1.75)
Echocardiography
Left atrial volume index (ml/m2) 39.8 (29.8–44.7)
Left ventricle diastolic diameter (mm) 51 (47–55)
Left ventricle systolic diameter (mm) 32 (28–35)
Left ventricular mass (g) 148 (121–188)
Left ventricular ejection fraction (%) 63 (58–67)
Ejection fraction\55 % (n, %) 11 (9.9)
Cardiac output (l/min) 6.1 (5.1–7.1)
E/A ratio 1.03 (0.82–1.34)
Deceleration time (ms) 239 (201–280)
E0 velocity (cm/s) 9.56 (7.43–11.72)
E/E0 ratio 8.57 (6.80–10.38)
Hepatol Int (2014) 8:146–153 149
123
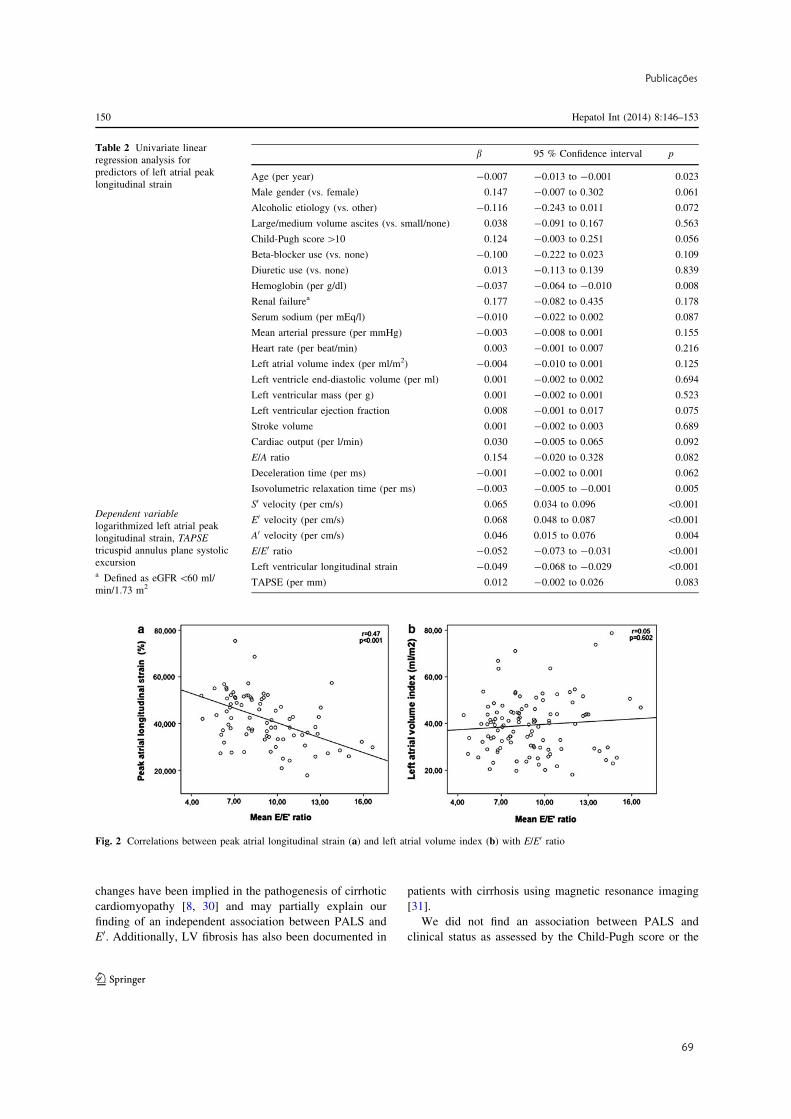
Publicações
69
changes have been implied in the pathogenesis of cirrhotic
cardiomyopathy [8, 30] and may partially explain our
finding of an independent association between PALS and
E0. Additionally, LV fibrosis has also been documented in
patients with cirrhosis using magnetic resonance imaging
[31].
We did not find an association between PALS and
clinical status as assessed by the Child-Pugh score or the
Fig. 2 Correlations between peak atrial longitudinal strain (a) and left atrial volume index (b) with E/E0 ratio
Table 2 Univariate linear
regression analysis for
predictors of left atrial peak
longitudinal strain
Dependent variable
logarithmized left atrial peak
longitudinal strain, TAPSE
tricuspid annulus plane systolic
excursiona Defined as eGFR\60 ml/
min/1.73 m2
b 95 % Confidence interval p
Age (per year) -0.007 -0.013 to -0.001 0.023
Male gender (vs. female) 0.147 -0.007 to 0.302 0.061
Alcoholic etiology (vs. other) -0.116 -0.243 to 0.011 0.072
Large/medium volume ascites (vs. small/none) 0.038 -0.091 to 0.167 0.563
Child-Pugh score[10 0.124 -0.003 to 0.251 0.056
Beta-blocker use (vs. none) -0.100 -0.222 to 0.023 0.109
Diuretic use (vs. none) 0.013 -0.113 to 0.139 0.839
Hemoglobin (per g/dl) -0.037 -0.064 to -0.010 0.008
Renal failurea 0.177 -0.082 to 0.435 0.178
Serum sodium (per mEq/l) -0.010 -0.022 to 0.002 0.087
Mean arterial pressure (per mmHg) -0.003 -0.008 to 0.001 0.155
Heart rate (per beat/min) 0.003 -0.001 to 0.007 0.216
Left atrial volume index (per ml/m2) -0.004 -0.010 to 0.001 0.125
Left ventricle end-diastolic volume (per ml) 0.001 -0.002 to 0.002 0.694
Left ventricular mass (per g) 0.001 -0.002 to 0.001 0.523
Left ventricular ejection fraction 0.008 -0.001 to 0.017 0.075
Stroke volume 0.001 -0.002 to 0.003 0.689
Cardiac output (per l/min) 0.030 -0.005 to 0.065 0.092
E/A ratio 0.154 -0.020 to 0.328 0.082
Deceleration time (per ms) -0.001 -0.002 to 0.001 0.062
Isovolumetric relaxation time (per ms) -0.003 -0.005 to -0.001 0.005
S0 velocity (per cm/s) 0.065 0.034 to 0.096 \0.001
E0 velocity (per cm/s) 0.068 0.048 to 0.087 \0.001
A0 velocity (per cm/s) 0.046 0.015 to 0.076 0.004
E/E0 ratio -0.052 -0.073 to -0.031 \0.001
Left ventricular longitudinal strain -0.049 -0.068 to -0.029 \0.001
TAPSE (per mm) 0.012 -0.002 to 0.026 0.083
150 Hepatol Int (2014) 8:146–153
123
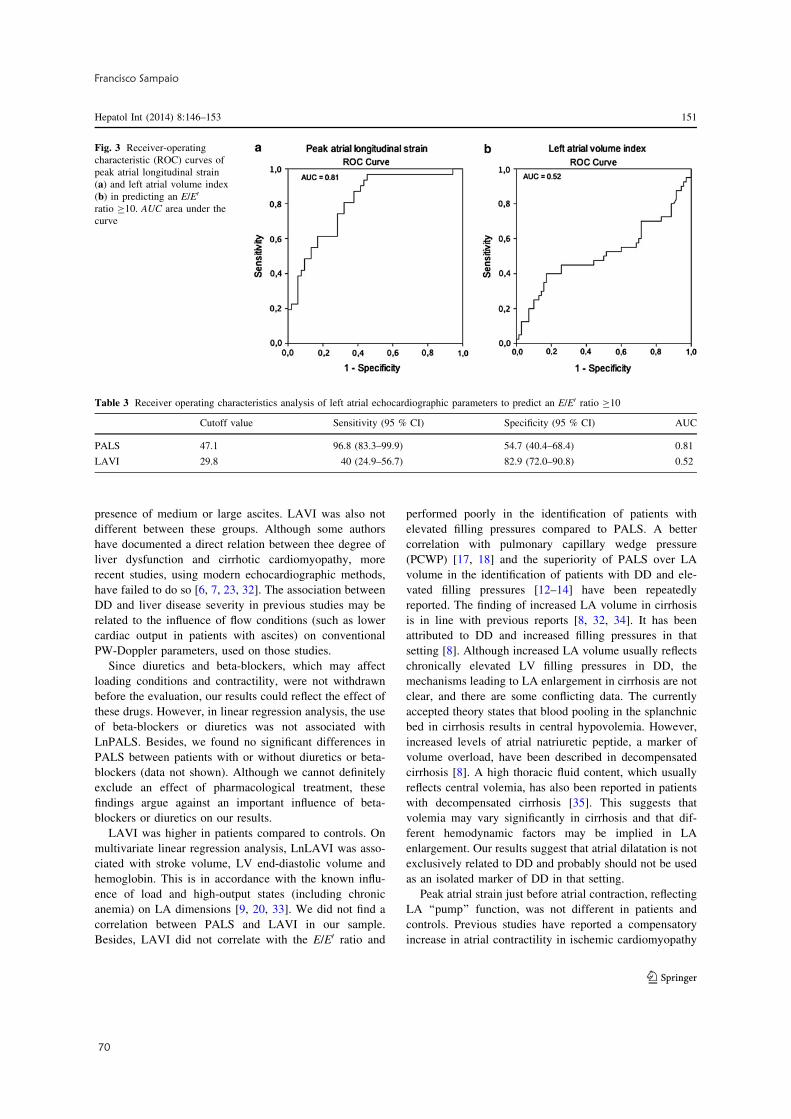
70
Francisco Sampaio
presence of medium or large ascites. LAVI was also not
different between these groups. Although some authors
have documented a direct relation between thee degree of
liver dysfunction and cirrhotic cardiomyopathy, more
recent studies, using modern echocardiographic methods,
have failed to do so [6, 7, 23, 32]. The association between
DD and liver disease severity in previous studies may be
related to the influence of flow conditions (such as lower
cardiac output in patients with ascites) on conventional
PW-Doppler parameters, used on those studies.
Since diuretics and beta-blockers, which may affect
loading conditions and contractility, were not withdrawn
before the evaluation, our results could reflect the effect of
these drugs. However, in linear regression analysis, the use
of beta-blockers or diuretics was not associated with
LnPALS. Besides, we found no significant differences in
PALS between patients with or without diuretics or beta-
blockers (data not shown). Although we cannot definitely
exclude an effect of pharmacological treatment, these
findings argue against an important influence of beta-
blockers or diuretics on our results.
LAVI was higher in patients compared to controls. On
multivariate linear regression analysis, LnLAVI was asso-
ciated with stroke volume, LV end-diastolic volume and
hemoglobin. This is in accordance with the known influ-
ence of load and high-output states (including chronic
anemia) on LA dimensions [9, 20, 33]. We did not find a
correlation between PALS and LAVI in our sample.
Besides, LAVI did not correlate with the E/E0 ratio and
performed poorly in the identification of patients with
elevated filling pressures compared to PALS. A better
correlation with pulmonary capillary wedge pressure
(PCWP) [17, 18] and the superiority of PALS over LA
volume in the identification of patients with DD and ele-
vated filling pressures [12–14] have been repeatedly
reported. The finding of increased LA volume in cirrhosis
is in line with previous reports [8, 32, 34]. It has been
attributed to DD and increased filling pressures in that
setting [8]. Although increased LA volume usually reflects
chronically elevated LV filling pressures in DD, the
mechanisms leading to LA enlargement in cirrhosis are not
clear, and there are some conflicting data. The currently
accepted theory states that blood pooling in the splanchnic
bed in cirrhosis results in central hypovolemia. However,
increased levels of atrial natriuretic peptide, a marker of
volume overload, have been described in decompensated
cirrhosis [8]. A high thoracic fluid content, which usually
reflects central volemia, has also been reported in patients
with decompensated cirrhosis [35]. This suggests that
volemia may vary significantly in cirrhosis and that dif-
ferent hemodynamic factors may be implied in LA
enlargement. Our results suggest that atrial dilatation is not
exclusively related to DD and probably should not be used
as an isolated marker of DD in that setting.
Peak atrial strain just before atrial contraction, reflecting
LA ‘‘pump’’ function, was not different in patients and
controls. Previous studies have reported a compensatory
increase in atrial contractility in ischemic cardiomyopathy
Fig. 3 Receiver-operating
characteristic (ROC) curves of
peak atrial longitudinal strain
(a) and left atrial volume index
(b) in predicting an E/E0
ratio C10. AUC area under the
curve
Table 3 Receiver operating characteristics analysis of left atrial echocardiographic parameters to predict an E/E0 ratio C10
Cutoff value Sensitivity (95 % CI) Specificity (95 % CI) AUC
PALS 47.1 96.8 (83.3–99.9) 54.7 (40.4–68.4) 0.81
LAVI 29.8 40 (24.9–56.7) 82.9 (72.0–90.8) 0.52
Hepatol Int (2014) 8:146–153 151
123

Publicações
71
or hypertension [36, 37], while others have shown a
decrease in atrial systolic function in patients with systolic
[14, 38] and diastolic [10, 12] heart failure. A lower impact
of DD on LA pump function (as compared to PALS) has
been suggested [15], and PACS seems to correlate worse
than PALS with LV filling pressures [18]. Liu et al. [39]
found that LA DD occurs prior to LA systolic dysfunction
in patients with coronary artery disease. This may also be
the case in cirrhosis. Nazar et al. [7] recently reported that
84 % of cirrhotic patients had normal or only mild DD and
that invasively determined PCWP was normal in all
patients. The prevalence of DD in our sample was 16.2 %,
and only 29.4 % of those had grade 2 DD. A mild degree of
DD may not be severe enough to significantly affect LA
pump function in these patients.
Limitations
This is a single-center study performed in patients mainly
with alcoholic cirrhosis.
We did not perform invasive hemodynamic measure-
ments and used echocardiographic surrogate markers of LV
filling pressures. Previous reports have questioned the
value of the E/E0 ratio in identifying patients with elevated
PCWP. However, this seems to be more relevant in patients
with dilated ventricles, severely depressed systolic function
and/or significant mitral regurgitation [40, 41]. None of our
patients had these abnormalities.
We did not perform any imaging technique able to detect
LA fibrosis. Therefore, although the relation between LA
dysfunction and fibrosis has been documented in other set-
tings [27, 42], their association in cirrhosis remains
speculative.
Three-dimensional echocardiography, which could be
more accurate in evaluating LA volume [43], was not used
in this study.
Prognosis was not evaluated, and so the clinical impact of
our findings in cirrhotic patients remains to be determined.
Conclusion
Patients with cirrhosis have evidence of abnormal LA
function at rest, which is detectable by newer echocardio-
graphic techniques. LA function parameters are potential
additional markers of cirrhotic cardiomyopathy.
Our results also show that LA dysfunction is related to
diastolic LV dysfunction, supporting the existence of
common pathogenic mechanisms between the two.
LA strain during ventricular systole correlated better
than LAVI with LV filling pressures, suggesting that LA
enlargement in cirrhosis may have other causes and should
not be used as an isolate marker of DD.
Conflict of interest Francisco Sampaio, Joana Pimenta, Nuno
Bettencourt, Ricardo Fontes-Carvalho, Ana Paula Silva, Joao Valente,
Paulo Bettencourt, Jose Fraga and Vasco Gama declare that they have
no conflict of interest.
Compliance with Ethical Requirements All procedures followed
were in accordance with the ethical standards of the responsible
committee on human experimentation (institutional and national) and
with the Helsinki Declaration of 1975, as revised in 2008. Informed
consent was obtained from all patients for being included in the study.
References
1. Møller S, Henriksen JH. Cardiovascular complications of cir-
rhosis. Gut 2008;57:268–278
2. Alqahtani SA, Fouad TR, Lee SS. Cirrhotic cardiomyopathy.
Semin Liver Dis 2008;28:59–69
3. Wong F. Cirrhotic cardiomyopathy. Hepatol Int 2009;3:294–304
4. Alexopoulou A, Papatheodoridis G, Pouriki S, Chrysohoou C,
Raftopoulos L, Stefanadis C, et al. Diastolic myocardial dys-
function does not affect survival in patients with cirrhosis.
Transpl Int 2012;25:1174–1181
5. Cazzaniga M, Salerno F, Pagnozzi G, Dionigi E, Visentin S,
Cirello I, et al. Diastolic dysfunction is associated with poor
survival in patients with cirrhosis with transjugular intrahepatic
portosystemic shunt. Gut 2007;56:869–875
6. Kazankov K, Holland-Fischer P, Andersen NH, Torp P, Sloth E,
Aagaard NK, et al. Resting myocardial dysfunction in cirrhosis
quantified by tissue Doppler imaging. Liver Int 2011;31:534–540
7. Nazar A, Guevara M, Sitges M, Terra C, Sola E, Guigou C, et al.
LEFT ventricular function assessed by echocardiography in cir-
rhosis: relationship to systemic hemodynamics and renal dys-
function. J Hepatol 2013;58:51–57
8. Møller S, Henriksen JH. Cirrhotic cardiomyopathy. J Hepatol
2010;53:179–190
9. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK,
Smiseth OA, et al. Recommendations for the evaluation of left
ventricular diastolic function by echocardiography. J Am Soc
Echocardiogr 2009;22:107–133
10. Morris DA, Gailani M, Vaz Perez A, Blaschke F, Dietz R,
Haverkamp W, et al. Left atrial systolic and diastolic dysfunction
in heart failure with normal left ventricular ejection fraction.
J Am Soc Echocardiogr 2011;24:651–662
11. D’Andrea A, De Corato G, Scarafile R, Romano S, Reigler L, Mita
C, et al. Left atrial myocardial function in either physiological or
pathological left ventricular hypertrophy: a two-dimensional
speckle strain study. Br J Sports Med 2008;42:696–702
12. Jarnert C, Melcher A, Caidahl K, Persson H, Ryden L, Eriksson
MJ. Left atrial velocity vector imaging for the detection and
quantification of left ventricular diastolic function in type 2 dia-
betes. Eur J Heart Fail 2008;10:1080–1087
13. Khan UA, de Simone G, Hill J, Tighe DA, Aurigemma GP.
Depressed atrial function in diastolic dysfunction: a speckle
tracking imaging study. Echocardiography 2013;30:309–316
14. Kurt M, Wang J, Torre-Amione G, Nagueh SF. Left atrial
function in diastolic heart failure. Circ Cardiovasc Imaging
2009;2:10–15
15. Mondillo S, Cameli M, Caputo ML, Lisi M, Palmerini E, Pade-
letti M, et al. Early detection of left atrial strain abnormalities by
speckle-tracking in hypertensive and diabetic patients with nor-
mal left atrial size. J Am Soc Echocardiogr 2011;24:898–908
16. Rosca M, Popescu BA, Beladan CC, Calin A, Muraru D, Popa
EC, et al. Left atrial dysfunction as a correlate of heart failure
152 Hepatol Int (2014) 8:146–153
123

72
Francisco Sampaio
symptoms in hypertrophic cardiomyopathy. J Am Soc Echocar-
diogr 2010;23:1090–1098
17. Cameli M, Lisi M, Mondillo S, Padeletti M, Ballo P, Tsioulpas C,
et al. Left atrial longitudinal strain by speckle tracking echocar-
diography correlates well with left ventricular filling pressures in
patients with heart failure. Cardiovasc Ultrasound 2010;8:14.
doi:10.1186/1476-7120-10-4
18. Wakami K, Ohte N, Asada K, Fukuta H, Goto T, Mukai S, et al.
Correlation between left ventricular end-diastolic pressure and
peak left atrial wall strain during left ventricular systole. J Am
Soc Echocardiogr 2009;22:847–851
19. Cameli M, Lisi M, Focardi M, Reccia R, Natali BM, Sparla S,
et al. Left atrial deformation analysis by speckle tracking echo-
cardiography for prediction of cardiovascular outcomes. Am J
Cardiol 2012;110:264–269
20. Rossi A, Cicoira M, Zanolla L, Sandrini R, Golia G, Zardini P,
et al. Determinants and prognostic value of left atrial volume in
patients with dilated cardiomyopathy. J Am Coll Cardiol
2002;40:1425–1430
21. Tsang TS, Abhayaratna WP, Barnes ME, Miyasaka Y, Gersh BJ,
Bailey KR, et al. Prediction of cardiovascular outcomes with left
atrial size: is volume superior to area or diameter? J Am Coll
Cardiol 2006;47:1018–1023
22. Saraiva RM, Demirkol S, Buakhamsri A, Greenberg N, Popovic
ZB, Thomas JD, et al. Left atrial strain measured by two-
dimensional speckle tracking represents a new tool to evaluate
left atrial function. J Am Soc Echocardiogr 2010;23:172–180
23. Sampaio F, Pimenta J, Bettencourt N, Fontes-Carvalho R, Silva
AP, Valente J, et al. Systolic and diastolic dysfunction in cir-
rhosis: a tissue-Doppler and speckle tracking echocardiography
study. Liver Int 2013;33:1158–1165. doi:10.1111/liv.12187
24. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E,
Pellikka PA, et al. Recommendations for chamber quantification.
Eur J Echocardiogr 2006;7:79–108
25. Barbier P, Solomon SB, Schiller NB, Glantz SA. Left atrial
relaxation and left ventricular systolic function determine left
atrial reservoir function. Circulation 1999;100:427–436
26. Todaro MC, Choudhuri I, Belohlavek M, Jahangir A, Carerj S,
Oreto L, et al. New echocardiographic techniques for evaluation
of left atrial mechanics. Eur Heart J Cardiovasc Imaging
2012;13:973–984
27. Kuppahally SS, Akoum N, Burgon NS, Badger TJ, Kholmovski
EG, Vijayakumar S, et al. Left atrial strain and strain rate in
patients with paroxysmal and persistent atrial fibrillation: rela-
tionship to left atrial structural remodeling detected by delayed-
enhancement MRI. Circ Cardiovasc Imaging 2010;3:231–239
28. Li D, Fareh S, Leung TK, Nattel S. Promotion of atrial fibrillation
by heart failure in dogs: atrial remodeling of a different sort.
Circulation 1999;100:87–95
29. HoitBD,ShaoY,GabelM,Pawloski-DahmC,WalshRA.Left atrial
systolic and diastolic function after cessation of pacing in tachy-
cardia-induced heart failure. Am J Physiol 1997;273:H921–H927
30. Glenn TK, Honar H, Liu H, ter Keurs HE, Lee SS. Role of cardiac
myofilament proteins titin and collagen in the pathogenesis of
diastolic dysfunction in cirrhotic rats. J Hepatol 2011;55:
1249–1255
31. Lossnitzer D, Steen H, Zahn A, Lehrke S, Weiss C, Weiss KH,
et al. Myocardial late gadolinium enhancement cardiovascular
magnetic resonance in patients with cirrhosis. J Cardiovasc Magn
Reson 2010;12:47. doi:10.1186/1532-429X-12-47
32. Merli M, Calicchia A, Ruffa A, Pellicori P, Riggio O, Giusto M,
et al. Cardiac dysfunction in cirrhosis is not associated with the
severity of liver disease. Eur J Intern Med 2013;24:172–176
33. Abhayaratna WP, Seward JB, Appleton CP, Douglas PS, Oh JK,
Tajik AJ, et al. Left atrial size: physiologic determinants and
clinical applications. J Am Coll Cardiol 2006;47:2357–2363
34. Finucci G, Desideri A, Sacerdoti D, Bolognesi M, Merkel C,
Angeli P, et al. Left ventricular diastolic function in liver cir-
rhosis. Scand J Gastroenterol 1996;31:279–284
35. Pimenta J, Paulo C, Gomes A, Silva S, Rocha-Goncalves F,
Bettencourt P. B-type natriuretic peptide is related to cardiac
function and prognosis in hospitalized patients with decompen-
sated cirrhosis. Liver Int 2010;30:1059–1066
36. Baltabaeva A, Marciniak M, Bijnens B, Parsai C, Moggridge J,
Antonios TF, et al. How to detect early left atrial remodelling
and dysfunction in mild-to-moderate hypertension. J Hypertens
2009;27:2086–2093
37. Sigwart U, Grbic M, Goy JJ, Kappenberger L. Left atrial function
in acute transient left ventricular ischemia produced during per-
cutaneous transluminal coronary angioplasty of the left anterior
descending coronary artery. Am J Cardiol 1990;65:282–286
38. D’Andrea A, Caso P, Romano S, Scarafile R, Riegler L, Salerno
G, et al. Different effects of cardiac resynchronization therapy on
left atrial function in patients with either idiopathic or ischaemic
dilated cardiomyopathy: a two-dimensional speckle strain study.
Eur Heart J 2007;28:2738–2748
39. Liu YY, Xie MX, Xu JF, Wang XF, Lv Q, Lu XF, et al. Eval-
uation of left atrial function in patients with coronary artery
disease by two-dimensional strain and strain rate imaging.
Echocardiography 2011;28:1095–1103
40. TschopeC, PaulusWJ. Is echocardiographic evaluation of diastolic
function useful in determining clinical care? Doppler echocardi-
ography yields dubious estimates of left ventricular diastolic
pressures. Circulation 2009;120:810–820; discussion 820
41. Mullens W, Borowski AG, Curtin RJ, Thomas JD, Tang WH.
Tissue Doppler imaging in the estimation of intracardiac filling
pressure in decompensated patients with advanced systolic heart
failure. Circulation 2009;119:62–70
42. Cameli M, Lisi M, Righini FM, Massoni A, Natali BM, Focardi
M, et al. Usefulness of atrial deformation analysis to predict left
atrial fibrosis and endocardial thickness in patients undergoing
mitral valve operations for severe mitral regurgitation secondary
to mitral valve prolapse. Am J Cardiol 2013;111:595–601
43. Keller AM, Gopal AS, King DL. Left and right atrial volume by
freehand three-dimensional echocardiography: in vivo validation
using magnetic resonance imaging. Eur J Echocardiogr
2000;1:55–65
Hepatol Int (2014) 8:146–153 153
123

Publicações
73
1
TITLE:
Assessment of cardiovascular physiology using magnetic resonance myocardial stress testing
reveals impaired contractile reserve in patients with cirrhotic cardiomyopathy
AUTHORS:
Francisco Sampaioa,b; Pablo Lamatac,d; Nuno Bettencourta,b; Sophie Charlotte Alte;
Nuno Ferreiraa; Johannes Tammo Kowallickf,g; Joana Pimentab; Shelby Kuttyh; José
Fragai; Paulo Bettencourtb; Vasco Gamaa; Andreas Schusterc,g,j.
INSTITUTIONS:
a- Cardiology Department, Centro Hospitalar de Gaia/Espinho, Portugal.
b- University of Porto Medical School, Porto, Portugal.
c- Division of Imaging Sciences and Biomedical Engineering, The Rayne Institute, Kings College London, St. Thomas’
Hospital, London, United Kingdom.
d- Department of Computer Science, University of Oxford, United Kingdom.
e- Department of Pediatric Cardiology and Intensive Care Medicine, Georg-August University, Göttingen, Germany.
f- Institute for Diagnostic and Interventional Radiology, Georg-August University, Göttingen, Germany.
g- DZHK (German Centre for Cardiovascular Research) Göttingen, Germany.
h- University of Nebraska Medical Center/ Children's Hospital and Medical Center, Omaha, NE, United States of America.
i- Gastroenterology Department, Centro Hospitalar de Gaia/Espinho, Portugal.
j- Department of Cardiology and Pneumology, Georg-August University, Göttingen, Germany.
CORRESPONDENCE:
Francisco Sampaio
Cardiology Department, Centro Hospitalar de Gaia/Espinho.
Rua Conceição Fernandes
4430-502 Vila Nova de Gaia, Portugal
PHONE: 227865100
FAX: 227830209
E-MAIL: [email protected]

74
Francisco Sampaio
2
ABSTRACT
Background: Liver cirrhosis has been shown to affect cardiac performance. However cardiac
dysfunction may only be revealed under stress conditions. The value of non-invasive stress tests in
diagnosing cirrhotic cardiomyopathy is unclear. We sought to investigate the response to
pharmacological stimulation with dobutamine in patients with cirrhosis using cardiovascular magnetic
resonance.
Methods: Thirty-six patients and eight controls were studied. Conventional volumetric and
myocardial deformation parameter analysis using feature tracking at rest and during low to
intermediate dose dobutamine stress were performed.
Results: Whilst volumetry based parameters were similar between patients and controls at rest,
patients had a smaller increase in cardiac output during stress (p=0.015). Ejection fraction increase
was impaired in patients during 10 μg/Kg/min dobutamine as compared to controls (6.9% vs. 16.5%,
p=0.007), but not with 20 μg/Kg/min (12.1% vs. 17.6%, p=0.12). This was paralleled by an impaired
improvement in circumferential strain with low dose (median increase of 14.4% vs. 30.9%, p=0.03),
but not with intermediate dose dobutamine (median increase of 29.4% vs. 33.9%, p=0.54). There was
an impaired longitudinal strain increase in patients as compared to controls during low (median
increase of 6.6% vs 28.6%, p<0.001) and intermediate dose dobutamine (median increase of 2.6%vs,
12.6% p=0.016). Radial strain response to dobutamine was similar in patients and controls (p>0.05).
Conclusion: Cirrhotic cardiomyopathy is characterized by an impaired cardiac pharmacological
response that can be detected with magnetic resonance myocardial stress testing. Deformation
analysis parameters may be more sensitive in identifying abnormalities in inotropic response to stress
than conventional methods.
KEYWORDS:
Liver; Cardiomyopathy; Magnetic resonance imaging; Feature Tracking; Strain; Dobutamine stress

Publicações
75
3
BACKGROUND
Systolic and diastolic dysfunction, as well as electrophysiological abnormalities have been described in
patients with cirrhosis[1-3]. Although previous studies have reported the presence of myocardial
dysfunction at resting states[4-6], cirrhotic cardiomyopathy is usually clinically silent and may only be
unmasked during physiological or inotropic stress[7].
Pharmacological stress tests using echocardiography or SPECT are often used in cirrhotic patients
for diagnosing coronary artery disease before liver transplantation. Although blunted responses of
stroke volume and ejection fraction (EF) to dobutamine have also been reported[8], other studies
have questioned these findings, particularly in patients with mild disease[9]. Therefore, most authors
recommend that dobutamine stress tests should be reserved for excluding ischaemic heart disease
before liver transplantation[10].
Cardiovascular magnetic resonance (CMR) has evolved into the gold standard methodology for
assessment of cardiac morphology and volumes[11,12]. Myocardial strain – which may reflect systolic
function more accurately than conventional, highly load dependent, indices such as ejection fraction –
can also be assessed using CMR, both at rest and during inotropic stimulation with dobutamine[13].
The response of strain to stress has not been previously studied in patients with cirrhosis.
To test the hypothesis that a pharmacological stress test could reveal systolic incompetence in
patients with cirrhosis, we performed a comprehensive analysis of systolic function during
pharmacological stress, using CMR.
METHODS
The study protocol was approved by the local ethics committee and complies with the declaration of
Helsinki. Written informed consent was obtained from all participants.
Thirty-six patients with cirrhosis followed in a hepatology outpatient clinic, able to comply with the
instructions during the exam, were recruited and referred to CMR. The diagnosis of cirrhosis was
based on clinical, laboratory, ultrasonographic and/or biopsy criteria. Patients with a known history
of hypertension, diabetes, cardiac disease or relevant ECG abnormalities were excluded. Patients
with large volume ascites and/or unable to tolerate breath-holding, renal insufficiency (creatinine
clearance ≤ 60 ml/min/1.73m2) or standard contraindications to CMR or gadolinium were also
excluded.
A group of eight healthy individuals, with similar age and sex distribution as the patient group,
without known cardiovascular risk factors or cardiac disease, referred to CMR for another indication
and with a completely normal scan, was used as control.
76
Francisco Sampaio
4
CMR acquisition
Patient preparation
Patients were instructed to refrain from smoking, coffee, tea, aminophylline, for 24 h before the scan.
Beta-blockers were suspended 48 hours before the study.
CMR protocol
Images were acquired using a 1.5T scanner (Siemens Symphony TIM; Siemens, Erlangen, Germany)
with a 6-channel anterior chest coil and spinal coils within the gantry table.
Cine imaging
After scout images, cine images using a retrospective ECG-gated balanced steady state free-
precession sequence were acquired during brief periods of end-expiratory breath-hold. Two-, four
and three-chamber orientations, as well as multiple equidistant short-axis planes (slice thickness 8
mm; gap 2 mm) allowing coverage of the entire cardiac volume were performed. Thirty phases were
obtained per cardiac cycle.
For dobutamine stress imaging, 3 long-axis and 3 short-axis slices (basal, mid-ventricular and apical)
were acquired, in order to cover 16 myocardial segments[14]. Dobutamine was infused intravenously
at 3-minute stages at doses of 10 and 20 μg/Kg/min. Repeat short-axis images as well as long-axis
images were acquired at the end of each stage. During dobutamine infusion, patient symptoms, heart
rate, blood pressure, and electrocardiogram were monitored.
Aortic flow imaging
Aortic flow was measured using one-direction “through-plane” motion-encoded cine gradient echo
sequences (slice thickness 5 mm; in-plane resolution ≤1 mm), centered in ascending aorta and aligned
orthogonally to the expected main blood flow direction in two spatial directions, at the level of the
pulmonary bifurcation. Velocity encoding sensitivity (Venc) was adapted to the expected velocities
(typically 150 for the rest images and 300 during the dobutamine-stress acquisitions). Thirty frames
were acquired per cardiac cycle using a free-breathing technique with 3 excitations per k-space line.
Perfusion imaging
Our protocol for stress perfusion imaging has been previously described[15]. Maximal hyperemia was
achieved with intravenous adenosine (140 μg.kg−1.min−1) infusion for 5 min. Within the last 2 min of
infusion, an intravenous bolus of 0.07 mmol/Kg of gadobutrol (Gadovist, Bayer HealthCare
Pharmaceuticals, Berlin, Germany), was injected. Three short-axis slices (basal, mid-ventricular and
Publicações
77
5
apical) were imaged during the first pass of the bolus of gadolinium using a gradient echo pulse
sequence with a single saturation pre-pulse per R–R interval shared over the three slices. Patients
were asked to hold their breath on full expiration for the duration of the first pass of the gadolinium
bolus.
Late Gadolinium enhancement
Late gadolinium-enhancement (LGE) was assessed using a phase-sensitive inversion-recovery
sequence ≥10 minutes after the administration of 0.2 mmol/kg of gadobutrol.
CMR analysis
Images were anonymized and analysis was performed by operators blinded to clinical data.
A commercially available software (CMR42; Circle Cardiovascular Imaging Inc., Calgary, Canada) was
used to assess left and right ventricular volumes and function, from the short-axis cine images. Phase-
contrast pulse sequences at rest and peak dobutamine dose were analyzed with the same software,
to determine cardiac output.
Feature tracking (FT), a technique analogous to echocardiographic speckle tracking, which allows
tracking of tissue voxel motion of CMR cine images[16-19] was used to assess left ventricular strain.
Four-, two- and three-chamber views were used to calculate longitudinal strain. Radial strain and
circumferential strain were derived from the three short-axis planes. Global longitudinal strain (GLS),
global radial strain (GRS) and global circumferential strain (GCS) were defined as the mean strain of
the three individual planes. Measurements were performed at rest and at each stage of dobutamine
infusion.
For the stress perfusion analysis, perfusion defects were defined as subendocardial or transmural
visually dark myocardial areas when compared with remote healthy myocardium, persisting for at
least 10 frames.
Reproducibility
Reproducibility of FT derived strain was assessed in 10 randomly selected subjects. For this, the
measurements were repeated more than 4 weeks after the initial analysis.

78
Francisco Sampaio
6
Statistical analysis
Data were stored and analyzed using IBM SPSS Statistics, Version 20.0 (IBM Corp., Armonk, NY,
USA). Results are presented as median (25th–75th percentile) for quantitative variables and as n (%)
for categorical variables. A significance level of 5% was used.
The Mann–Whitney test was used to evaluate differences in continuous variables between groups.
The Chi-squared test was used to compare proportions. Spearman’s coefficient was used to test
correlations. Bland–Altman analysis was performed for reproducibility testing.
RESULTS
Clinical characteristics and laboratorial characteristics of patients and controls are shown in table 1.
Most patients (n=27, 75%) were in Child-Pugh class A, eight patients (17.8%) were in class B and only
one patient was in class C.
CMR –derived morphological and functional parameters were similar at rest in patients and controls
(table 2). We found no differences in resting GLS, GCS or GRS between patients and controls.
Child-Pugh class A patients had a trend towards lower left atrial volume compared to patients with
more severe (class B and C) disease 43.3 ml/m2 (35.4-49.5) vs 47.6 ml/m2 (44.1-56.7); p=0.08. No
differences in any of the other parameters were found, in resting conditions, between these two
groups of patients.
Dobutamine stress
The response of hemodynamic and strain parameters to increasing doses of dobutamine is shown in
table 3 and figures 1 and 2. Compared to controls, patients had a smaller increase of stroke volume
and cardiac output during dobutamine perfusion. There was no difference in heart rate response to
stress in the two groups. The increase in EF was lower in patients than in controls at the dose of 10
μg/Kg/min of dobutamine (median percentual increase of 6.9% (3.5-12.1) vs 16.5% (8.5-23.3),
p=0.007), but not at 20 μg/Kg/min (median percentual increase of 12.1% (6.8-17.9) vs 17.6% (10.4-
28.0), p=0.12). The improvement in GLS during the perfusion was significantly lower in patients
compared to controls, both at 10 μg/Kg/min (median percentual increase of 28.6% (6.6% (-5.8-17.0)
vs 18.9-54.4), p<0.001) and at 20 ug/Kg/min (median percentual increase of 2.6% (-5.5-16.7) vs 12.6%
(10.4-29.2), p=0.016). Global circumferential strain increased less significantly in patients as compared
to controls at 10 μg/Kg/min (median percentual increase of 14.4% (0.6-22.9) vs 30.9% (8.6-41.5),
p=0.03); the response of GCS to 20 μg/Kg/min of dobutamine was not significantly different between
the two groups (median percentual increase of 29.4% (10.9-41.1) vs 33.9% (16.7-48.5), p=0.54). The
Publicações
79
7
response of GRS to pharmacological stress was not different in patients versus controls (median
percentual increase of 7.7% (-2.4-15.2) vs 13.6% (5.7-26), p=0.11 at 10 μg/Kg/min of dobutamine and
4.3% (0.6-8.1) vs 3.1% (-0.2-9.3), p=0.82 at 20 μg/Kg/min of dobutamine).
We found no differences in the response of hemodynamic and strain parameters to dobutamine
between patients in Child-Pugh class A versus the others or between patients on diuretics versus
patients without prior diuretic use.
There was a correlation between the percentual change of GLS and the percentual change in left
ventricular stroke volume (Spearman’s rho =0.42, p=0.007). Changes in stroke volume and GCS
(Spearman’s rho =0.11, p=0.48) or GRS (Spearman’s rho =0.07, p=0.69) were not correlated.
Stress perfusion and late gadolinium enhancement
No perfusion abnormalities were detected in any subject during adenosine stress. There was no LGE
in patients and controls.
Reproducibility
The mean differences and confidence intervals between repeated strain measurements are displayed
in Table 4. Reproducibility was similar at rest and with dobutamine stress.
DISCUSSION
Our results suggest that a dobutamine stress test can be useful in revealing systolic abnormalities in
patients with mild cirrhosis. Using cardiovascular magnetic resonance derived strain, we have shown
that, during low- to intermediate dose dobutamine stimulation, patients with cirrhosis had a smaller
improvement in longitudinal and a delayed increase in circumferential strain compared to controls.
This is, to the best of our knowledge, the first study to evaluate myocardial deformation during
stress in cirrhosis.
Subendocardial fibre damage with consequent left ventricular longitudinal function impairment are
usually the first manifestations of myocardial disease[20-22]. Longitudinal dysfunction was previously
documented in cirrhosis, at rest[5,6], using echocardiography. In the present study, we could not find
differences in any CMR parameters at rest between patients and controls. This may be related to the
early stage of disease of the majority of the patients. Patients exhibited a blunted response of GLS to
dobutamine, compared to controls. The normal response of strain to dobutamine is an initial
increment followed by a plateau or decrement (when filling is reduced by increased heart-rate)[23,24].
Our results are in line with this pattern. However, in controls there was a decrease in longitudinal
strain with 20 μg/Kg/min (compared to 10 μg/Kg/min). This pattern was not observed in the patient
group suggesting that, in controls, the maximal inotropic effect of dobutamine is achieved with the

80
Francisco Sampaio
8
lower dose (the higher dose having mainly a positive chronotropic effect) while patients may also
have a delayed response of longitudinal strain to dobutamine, with some strain still further
developing at 20 μg/Kg/min. Several abnormalities in cardiomyocyte structure and function –
including decreased density and down-regulation of beta-adrenergic receptors and impaired
intracellular signaling pathways - have been described in animal models of cirrhosis[25,26] and may
account for our findings.
Compared to controls, patients also had a smaller increase of GCS with 10 μg/Kg/min of
dobutamine; the response of GCS to 20 μg/Kg/min did not differ between the two groups. This also
suggests a delayed response of circumferential strain to inotropic stimuli in cirrhosis with patients
requiring higher doses of dobutamine (or more time) to equalize with the controls. Ejection fraction
showed a similar behaviour: patients had a smaller improvement at the dose of 10 μg/Kg/min of
dobutamine but no differences were found between the groups at 20 μg/Kg/min. The response of
GRS to dobutamine was not different in patients and controls; this is in line with previous studies in
ischemic heart disease patients, which have reported radial strain to be the last component of
myocardial mechanics to be affected by ischemia[27].
Although previous studies have reported an abnormal cardiac response to exercise or
pharmacological stress in cirrhotic patients using echocardiography and SPECT[28-30], the role of
dobutamine stress testing in diagnosing cirrhotic cardiomyopathy is still a matter of debate, since its
ability to detect abnormalities – mainly changes in volumes and EF – has been inconsistent using
these imaging modalities[8,9], particularly in patients with mild disease. The role of dobutamine stress
MRI in cirrhosis has not been previously studied. Myocardial deformation analysis in this setting has
also never been reported, either with CMR or echocardiography (probably because its feasibility
under stress with the latter may be limited). Unlike echo, CMR does not depend on a good “acoustic
window” for image acquisition, and its feasibility in quantifying strain during dobutamine stress has
been demonstrated has been demonstrated both in healthy volunteers and in patients with ischemic
cardiomyopathy[13,31]. Our findings may explain previous negative results[9] since preserved radial
mechanics and a normal response of circumferential strain to higher doses of dobutamine, may
contribute to a normal EF response during these doses, despite the smaller longitudinal strain
increase.
Cardiac output increased less significantly in patients than in controls. This seems to be explained by
the higher increase in stroke volume found in controls, since heart rate variation was similar in the
two groups. We also found a significant correlation between the dobutamine-induced changes of GLS
and stroke volume. According to these observations, the inability to increase cardiac output under
stress conditions that has been reported as a feature of cirrhotic cardiomyopathy may be at least
partially explained by longitudinal myocardial dysfunction and not only from chronotropic
incompetence. As previously mentioned there was a different behaviour of GLS under 10 and 20

Publicações
81
9
μg/Kg/min of dobutamine in patients and controls. As in controls the maximal inotropic effect was
achieved with 10 μg/Kg/min with predominant positive chronotropic effect (that does not lead to an
increase in stroke volume) at higher doses, it is possible that differences in cardiac output between
patients and controls may have been much more significantly different at 10 μg/Kg/min than at 20
μg/Kg/min. Unfortunately, with did not acquire a flow imaging sequence at the lower dose, that
would have allowed us to prove this hypothesis. A lower cardiac output has been associated with an
increased risk of developing hepatorenal syndrome in patients with cirrhosis[32]. However, other
studies have failed to establish a relation between cardiac dysfunction and prognosis[33-35], and
consequently, this hypothesis remains speculative.
Resting hemodynamic conditions may influence inotropic response to pharmacological stress, and
our results might have been related to differences in volemia (particularly in the presence of
diuretics), or neuro-humoral stimulation. However, only 7 patients were on diuretics and we could
not find any differences in inotropic response between them and the other patients; we also failed to
find differences in cardiac chambers size between patients and controls. On the other hand, resting
heart rate, blood pressure and cardiac output were similar in patients and controls. Taken
altogether, these findings argue against an effect of different basal hemodynamics on our results.
Under adenosine stress, we did not detect ischemia, which could have influenced inotropic response
to dobutamine, in any subject. Although a quantitative perfusion analysis was not performed, our
methodology has been shown to be highly accurate in detecting functionally significant coronary
artery disease[15].
In contrast with a previous study[36], we did not find LGE in any patient. The difference in disease
severity between the two studies probably accounts for these findings since myocardial fibrosis may
only be detectable in more advanced disease states as a result of the chronic activation of the renin-
angiotensin-aldosterone system.
Limitations:
This is a single center study performed in patients mainly with alcoholic cirrhosis and mild disease.
We aimed to evaluate the contractile response to dobutamine stress with the maximum extent of
inotropic response expected with doses of 10-20 μg/Kg/min of dobutamine[37]. However we cannot
exclude that a full test (40 μg/Kg/min) would have potentially added valuable information despite the
fact that we didn’t observe significant perfusion defects with adenosine stress.
There is no widely accepted gold-standard method to diagnose cirrhotic cardiomyopathy; on the
other hand, there are no well-established normal values of CMR-derived strain parameters at rest
and under pharmacological stress. Hence, the diagnostic accuracy of our methodology cannot be
objectively determined and definitive cut-offs cannot be provided.
82
Francisco Sampaio
10
We could not perform a T1-mapping analysis, which might have allowed us to detect the presence of
diffuse myocardial fibrosis.
CONCLUSIONS
Patients with cirrhosis show inotropic incompetence to pharmacological stress, due to intrinsic
myocardial dysfunction.
CMR with myocardial deformation analysis may be a sensitive diagnostic tool to identify abnormal
inotropic responses to stress already present at early disease states, which may be difficult to detect
with other non-invasive imaging modalities. The significance of this impaired response to
pharmacological stress in cirrhotic cardiomyopathy and its prognostic implications should be further
explored in future prospective clinical investigations.
LIST OF ABBREVIATIONS:
SPECT: Single-photon emission computed tomography
EF: Ejection fraction
CMR: Cardiovascular magnetic resonance
FT: Feature tracking
GLS: Global longitudinal strain
GRS: Global radial strain
GCS: Global circumferential strain
LGE: late gadolinium enhancement
COMPETING INTERESTS:
The authors have no competing interests to declare
AUTHORS’ CONTRIBUTIONS
FS and NB were involved in the conception and design of the study as well as data collection,
analysis, interpretation, and drafting of the manuscript.
JP and PB participated in the conception and design of the study, interpretation of the data and
revision of the manuscript.
NF was involved in data acquisition and revision of the manuscript.

Publicações
83
11
JF and VG were involved in in data gathering and revision of the manuscript.
AS, PL, SCA, JTK and SK were involved in data analysis and revision of the manuscript for important
content.
All authors read and approved the final manuscript.
REFERENCES:
1. Møller S, Hove JD, Dixen U, Bendtsen F: New insights into cirrhotic cardiomyopathy. Int J Cardiol.
2013;167:1101-1108.
2. Wong F: Cirrhotic cardiomyopathy. Hepatol Int 2009, 3:294-304.
3. Møller S, Henriksen JH: Cardiovascular complications of cirrhosis. Gut 2008, 57:268-278.
4. Sampaio F, Pimenta J, Bettencourt N, Fontes-Carvalho R, Silva AP, Valente J, Bettencourt P, Fraga J, Gama
V: Left atrial function is impaired in cirrhosis: a speckle tracking echocardiographic study.
Hepatol Int 2014, 8:146-153.
5. Sampaio F, Pimenta J, Bettencourt N, Fontes-Carvalho R, Silva AP, Valente J, Bettencourt P, Fraga J, Gama
V: Systolic and diastolic dysfunction in cirrhosis: a tissue-Doppler and speckle tracking
echocardiography study. Liver Int. 2013;33:1158-1165.
6. Kazankov K, Holland-Fischer P, Andersen NH, Torp P, Sloth E, Aagaard NK, Vilstrup H: Resting
myocardial dysfunction in cirrhosis quantified by tissue Doppler imaging. Liver Int 2011, 31:534-
540.
7. Krag A, Bendtsen F, Mortensen C, Henriksen JH, Møller S: Effects of a single terlipressin
administration on cardiac function and perfusion in cirrhosis. Eur J Gastroenterol Hepatol 2010,
22:1085-1092.
8. Kim MY, Baik SK, Won CS, Park HJ, Jeon HK, Hong HI, Kim JW, Kim HS, Kwon SO, Kim JY, et al:
Dobutamine stress echocardiography for evaluating cirrhotic cardiomyopathy in liver
cirrhosis. Korean J Hepatol 2010, 16:376-382.
9. Dahl EK, Møller S, Kjær A, Petersen CL, Bendtsen F, Krag A: Diastolic and autonomic dysfunction in
early cirrhosis: a dobutamine stress study. Scand J Gastroenterol 2014, 49:362-372.
10. Møller S, Henriksen JH: Cirrhotic cardiomyopathy. J Hepatol 2010, 53:179-190.
11. Lima JAC, Desai MY: Cardiovascular magnetic resonance imaging: current and emerging
applications. J Am Coll Cardiol 2004, 44:1164-1171.
12. Attili AK, Schuster A, Nagel E, Reiber JH, van der Geest RJ: Quantification in cardiac MRI: advances
in image acquisition and processing. Int J Cardiovasc Imaging 2010, 26 Suppl 1:27-40.
13. Schuster A, Kutty S, Padiyath A, Parish V, Gribben P, Danford DA, Makowski MR, Bigalke B, Beerbaum P,
Nagel E: Cardiovascular magnetic resonance myocardial feature tracking detects quantitative
wall motion during dobutamine stress. J Cardiovasc Magn Reson 2011, 13:58.
14. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, Pennell DJ, Rumberger JA, Ryan
T, Verani MS: Standardized myocardial segmentation and nomenclature for tomographic
imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging

84
Francisco Sampaio
12
Committee of the Council on Clinical Cardiology of the American Heart Association.
Circulation 2002, 105:539-542.
15. Bettencourt N, Chiribiri A, Schuster A, Ferreira N, Sampaio F, Duarte R, Santos L, Melica B, Rodrigues A,
Braga P, et al: Cardiac magnetic resonance myocardial perfusion imaging for detection of
functionally significant obstructive coronary artery disease: a prospective study. International
journal of cardiology 2013, 168:765-773.
16. Hor KN, Gottliebson WM, Carson C, Wash E, Cnota J, Fleck R, Wansapura J, Klimeczek P, Al-Khalidi
HR, Chung ES, et al: Comparison of magnetic resonance feature tracking for strain calculation
with harmonic phase imaging analysis. JACC Cardiovascular imaging 2010, 3:144-151.
17. Kowallick J, Kutty S, Edelmann F, Chiribiri A, Villa A, Steinmetz M, Sohns J, Staab W, Bettencourt N,
Unterberg-Buchwald C, et al: Quantification of left atrial strain and strain rate using
Cardiovascular Magnetic Resonance myocardial feature tracking: a feasibility study. J
Cardiovasc Magn Reson 2014, 16:60.
18. Morton G, Schuster A, Jogiya R, Kutty S, Beerbaum P, Nagel E: Inter-study reproducibility of
cardiovascular magnetic resonance myocardial feature tracking. J Cardiovasc Magn Reson 2012,
14:43.
19. Padiyath A, Gribben P, Abraham JR, Li L, Rangamani S, Schuster A, Danford DA, Pedrizzetti G, Kutty S:
Echocardiography and cardiac magnetic resonance-based feature tracking in the assessment
of myocardial mechanics in tetralogy of Fallot: an intermodality comparison. Echocardiography
2013, 30:203-210.
20. Poulsen SH, Andersen NH, Heickendorff L, Mogensen CE: Relation between plasma amino-
terminal propeptide of procollagen type III and left ventricular longitudinal strain in
essential hypertension. Heart 2005, 91:624-629.
21. Cardim N, Oliveira AG, Longo S, Ferreira T, Pereira A, Reis RP, Correia JM: Doppler tissue imaging:
regional myocardial function in hypertrophic cardiomyopathy and in athlete's heart. J Am Soc
Echocardiogr 2003, 16:223-232.
22. Andersen NH, Poulsen SH, Eiskjaer H, Poulsen PL, Mogensen CE: Decreased left ventricular
longitudinal contraction in normotensive and normoalbuminuric patients with Type II
diabetes mellitus: a Doppler tissue tracking and strain rate echocardiography study. Clin Sci
2003, 105:59-66.
23. Mor-Avi V, Lang RM, Badano LP, Belohlavek M, Cardim NM, Derumeaux G, Galderisi M, Marwick T,
Nagueh SF, Sengupta PP, et al: Current and evolving echocardiographic techniques for the
quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on
methodology and indications endorsed by the Japanese Society of Echocardiography. Eur J
Echocardiogr 2011, 12:167-205.
24. Bijnens BH, Cikes M, Claus P, Sutherland GR: Velocity and deformation imaging for the
assessment of myocardial dysfunction. Eur J Echocardiogr 2009, 10:216-226.
25. Lee SS, Marty J, Mantz J, Samain E, Braillon A, Lebrec D: Desensitization of myocardial beta-
adrenergic receptors in cirrhotic rats. Hepatology 1990, 12:481-485.
Publicações
85
13
26. Gerbes AL, Remien J, Jungst D, Sauerbruch T, Paumgartner G: Evidence for down-regulation of beta-
2-adrenoceptors in cirrhotic patients with severe ascites. Lancet 1986, 1:1409-1411.
27. Reant P, Labrousse L, Lafitte S, Bordachar P, Pillois X, Tariosse L, Bonoron-Adele S, Padois P, Deville C,
Roudaut R, Dos Santos P: Experimental validation of circumferential, longitudinal, and radial 2-
dimensional strain during dobutamine stress echocardiography in ischemic conditions. J Am
Coll Cardiol 2008, 51:149-157.
28. Kelbaek H, Rabol A, Brynjolf I, Eriksen J, Bonnevie O, Godtfredsen J, Munck O, Lund JO:
Haemodynamic response to exercise in patients with alcoholic liver cirrhosis. Clin Physiol 1987,
7:35-41.
29. Wong F, Girgrah N, Graba J, Allidina Y, Liu P, Blendis L: The cardiac response to exercise in
cirrhosis. Gut 2001, 49:268-275.
30. Krag A, Bendtsen F, Mortensen C, Henriksen JH, Moller S: Effects of a single terlipressin
administration on cardiac function and perfusion in cirrhosis. European journal of gastroenterology
& hepatology 2010, 22:1085-1092.
31. Schuster A, Paul M, Bettencourt N, Morton G, Chiribiri A, Ishida M, Hussain S, Jogiya R, Kutty S, Bigalke
B, et al: Cardiovascular magnetic resonance myocardial feature tracking for quantitative
viability assessment in ischemic cardiomyopathy. International journal of cardiology 2013, 166:413-
420.
32. Krag A, Bendtsen F, Henriksen JH, Møller S: Low cardiac output predicts development of
hepatorenal syndrome and survival in patients with cirrhosis and ascites. Gut 2010, 59:105-110.
33. Sampaio F, Pimenta J, Bettencourt N, Fontes-Carvalho R, Silva A-P, Valente J, Bettencourt P, Fraga J,
Gama V: Systolic dysfunction and diastolic dysfunction do not influence medium-term
prognosis in patients with cirrhosis. Eur J Intern Med. 2014; 25:241-246.
34. Nazar A, Guevara M, Sitges M, Terra C, Solà E, Guigou C, Arroyo V, Ginès P: LEFT ventricular
function assessed by echocardiography in cirrhosis: Relationship to systemic hemodynamics
and renal dysfunction. J Hepatol 2013, 58:51-57.
35. Alexopoulou A, Papatheodoridis G, Pouriki S, Chrysohoou C, Raftopoulos L, Stefanadis C, Pectasides D:
Diastolic myocardial dysfunction does not affect survival in patients with cirrhosis. Transpl Int
2012, 25:1174-1181.
36. Lossnitzer D, Steen H, Zahn A, Lehrke S, Weiss C, Weiss KH, Giannitsis E, Stremmel W, Sauer P, Katus
HA, Gotthardt DN: Myocardial late gadolinium enhancement cardiovascular magnetic
resonance in patients with cirrhosis. J Cardiovasc Magn Reson 2010, 12:47.
37. Jewitt D, Birkhead J, Mitchell A, Dollery C: Clinical cardiovascular pharmacology of dobutamine.
A selective inotropic catecholamine. Lancet 1974, 2:363-367.

86
Francisco Sampaio
14
Figure 1 – Strain and ejection fraction response to pharmacological stress
Percentual variation of strain parameters and ejection fraction with 10 μg/Kg/min and 20
μg/Kg/min of dobutamine in patients and controls. GLS – global longitudinal strain; GCS –
global circumferential strain; GRS – global radial strain; EF – ejection fraction.
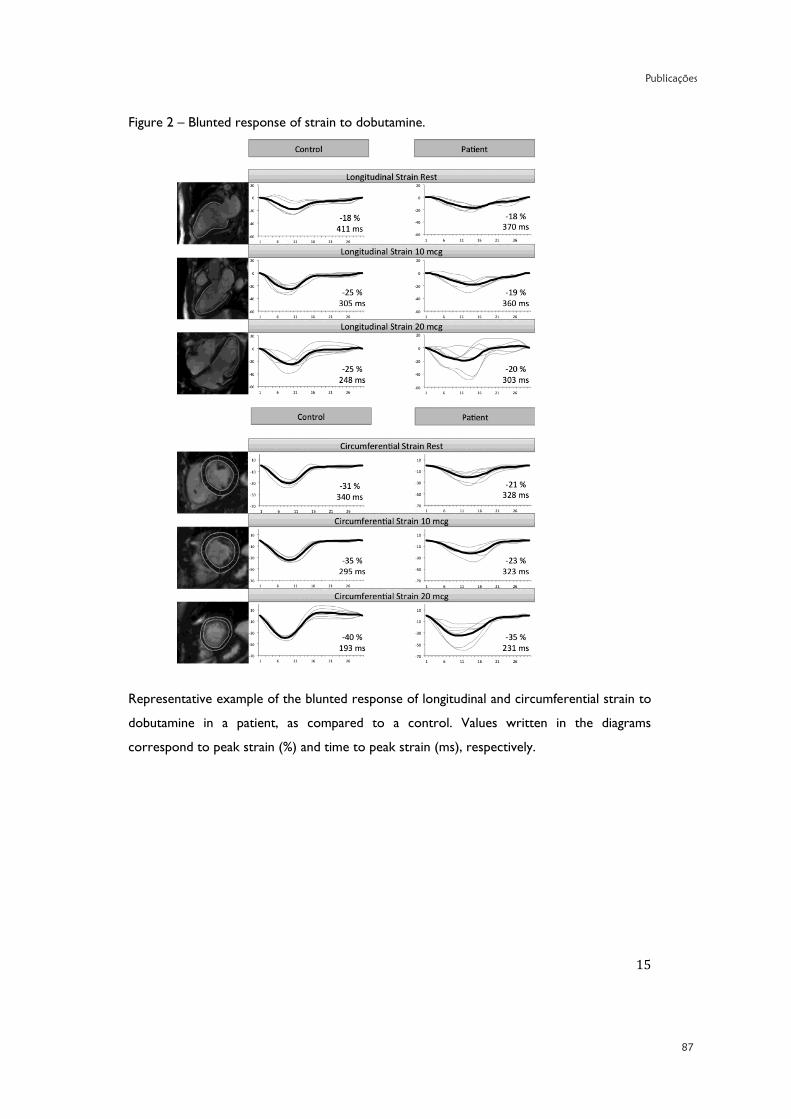
Publicações
87
15
Figure 2 – Blunted response of strain to dobutamine.
Representative example of the blunted response of longitudinal and circumferential strain to
dobutamine in a patient, as compared to a control. Values written in the diagrams
correspond to peak strain (%) and time to peak strain (ms), respectively.
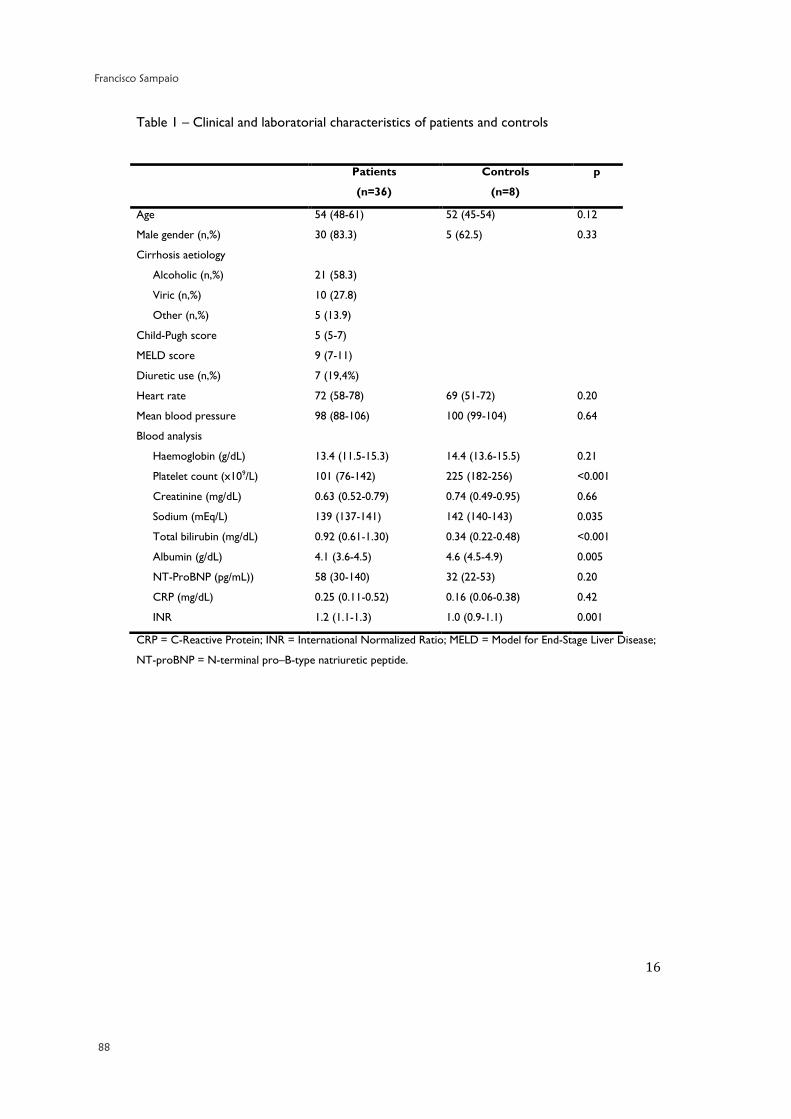
88
Francisco Sampaio
16
Table 1 – Clinical and laboratorial characteristics of patients and controls
Patients
(n=36)
Controls
(n=8)
p
Age 54 (48-61) 52 (45-54) 0.12
Male gender (n,%) 30 (83.3) 5 (62.5) 0.33
Cirrhosis aetiology
Alcoholic (n,%)
Viric (n,%)
Other (n,%)
21 (58.3)
10 (27.8)
5 (13.9)
Child-Pugh score 5 (5-7)
MELD score 9 (7-11)
Diuretic use (n,%) 7 (19,4%)
Heart rate 72 (58-78) 69 (51-72) 0.20
Mean blood pressure 98 (88-106) 100 (99-104) 0.64
Blood analysis
Haemoglobin (g/dL)
Platelet count (x109/L)
Creatinine (mg/dL)
Sodium (mEq/L)
Total bilirubin (mg/dL)
Albumin (g/dL)
NT-ProBNP (pg/mL))
CRP (mg/dL)
INR
13.4 (11.5-15.3)
101 (76-142)
0.63 (0.52-0.79)
139 (137-141)
0.92 (0.61-1.30)
4.1 (3.6-4.5)
58 (30-140)
0.25 (0.11-0.52)
1.2 (1.1-1.3)
14.4 (13.6-15.5)
225 (182-256)
0.74 (0.49-0.95)
142 (140-143)
0.34 (0.22-0.48)
4.6 (4.5-4.9)
32 (22-53)
0.16 (0.06-0.38)
1.0 (0.9-1.1)
0.21
<0.001
0.66
0.035
<0.001
0.005
0.20
0.42
0.001
CRP = C-Reactive Protein; INR = International Normalized Ratio; MELD = Model for End-Stage Liver Disease;
NT-proBNP = N-terminal pro–B-type natriuretic peptide.

Publicações
89
17
Table 2 – CMR parameters at rest of patients and controls
Patients
(n=36)
Controls
(n=8)
p
Left atrial volume (ml/m2) 44.9 (36.1-51.9) 44.2 (37.5-49.4) 0.92
Right atrial area (cm2) 21 (18-23) 22 (20-25) 0.35
Left ventricular diastolic volume (ml/m2) 75.1 (65.1-92.1) 87.7 (74.1-94.6) 0.27
Left ventricular systolic volume (ml/m2) 24.4 (19.1-28.9) 28.0 (23.2-33.3) 0.19
Left ventricular ejection fraction (%) 67 (64-72) 66.0 (64-70) 0.66
Left ventricular mass (g/m2) 54.7 (46.7-62.0) 55.7 (45.7-63.5) 0.96
Right ventricular diastolic volume (ml/m2) 84.5 (67.9-92.2) 84.1 (70.5-97.7) 0.46
Right ventricular ejection fraction (%) 57 (52-62) 58 (56-61) 0.46
Cardiac output (l/min) 6.5 (5.1-7.9) 6.1 (5.1-6.6) 0.74
GLS (%) -18.9 (-16.0 to -20.5) -19.0 (-16.1 to -20.6) 0.96
Time to Peak GLS (ms) 263 (206-317) 253 (225-281) 0.96
GCS (%) -27.5 (-24.1 to -30.6) -27.7 (-24.9 to -30.1) 0.84
Time to Peak GCS (ms) 264 (208-315) 223 (216-316) 0.71
GRS (%) 33.9 (25.4-39.1) 39.1 (34.8-41.8) 0.80
Time to Peak GRS (ms 275 (216-308) 223 (215-303) 0.36
GCS = Global Circumferential Strain; GLS = Global Longitudinal Strain; GRS = Global Radial Strain

90
Francisco Sampaio
18
Table 3 – Hemodynamic and strain response to dobutamine
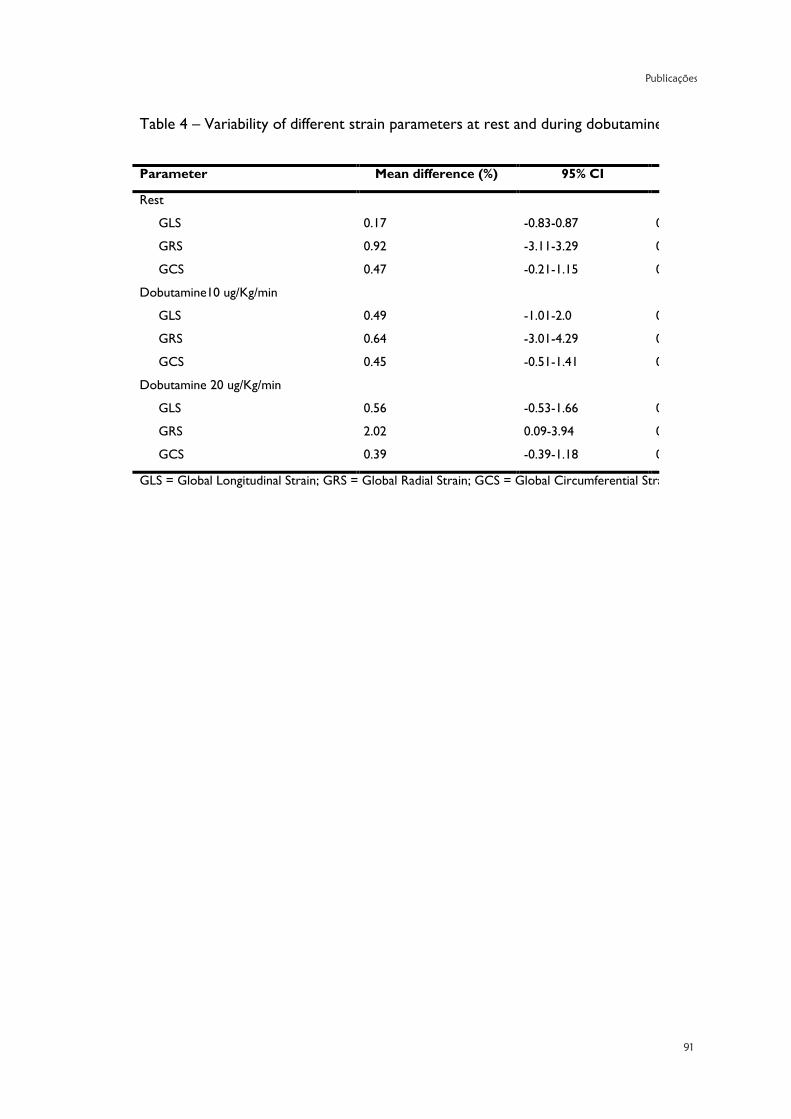
Publicações
91
19
Table 4 – Variability of different strain parameters at rest and during dobutamine stress.
Parameter Mean difference (%) 95% CI p
Rest
GLS 0.17 -0.83-0.87 0.96
GRS 0.92 -3.11-3.29 0.96
GCS 0.47 -0.21-1.15 0.24
Dobutamine10 ug/Kg/min
GLS 0.49 -1.01-2.0 0.29
GRS 0.64 -3.01-4.29 0.68
GCS 0.45 -0.51-1.41 0.31
Dobutamine 20 ug/Kg/min
GLS 0.56 -0.53-1.66 0.17
GRS 2.02 0.09-3.94 0.04
GCS 0.39 -0.39-1.18 0.17
GLS = Global Longitudinal Strain; GRS = Global Radial Strain; GCS = Global Circumferential Strain


Publicações
93
Original Article
Systolic dysfunction and diastolic dysfunction do not influencemedium-term prognosis in patients with cirrhosis
Francisco Sampaio a,b,⁎, Joana Pimenta b, Nuno Bettencourt a,b, Ricardo Fontes-Carvalho a,b, Ana-Paula Silva c,João Valente d, Paulo Bettencourt b, José Fraga c, Vasco Gama a
a Cardiology Department, Centro Hospitalar de Gaia/Espinho, R. Conceição Fernandes, 4434-502 Vila Nova de Gaia, Portugalb University of Porto Medical School, Al. Prof. Hernani Monteiro, 4200-319 Porto, Portugalc Gastroenterology Department, Centro Hospitalar de Gaia/Espinho, R. Conceição Fernandes, 4434-502 Vila Nova de Gaia, Portugald Internal Medicine Department, Centro Hospitalar de Gaia/Espinho, R. Conceição Fernandes, 4434-502 Vila Nova de Gaia, Portugal
a b s t r a c ta r t i c l e i n f o
Article history:Received 25 September 2013Received in revised form 10 January 2014Accepted 13 January 2014Available online 31 January 2014
Keywords:CirrhosisEchocardiographyPrognosisCardiac function
Objective:Myocardial dysfunction has been described in patients with cirrhosis andmay contribute to haemody-namic disturbances in advanced disease states. However, the prognostic impact of cardiac systolic and diastolicdysfunction in cirrhosis is controversial.We aimed to evaluate the performance of echocardiographic parametersof cardiac function as medium-term prognostic markers, in a cohort of cirrhotic patients.Methods:Ninety-eight patients (52 discharged after hospitalization for decompensated cirrhosis and 46 ambula-tory) were prospectively evaluated. A comprehensive echocardiographic study, including tissue-Doppler andspeckle tracking analysis, was performed at baseline. Patients were followed-up for 6 months for the occurrenceof death.Results: Twenty patients died during the follow-up. None of the echocardiographic parameters were associatedwith the occurrence of death. A Child score N 10 points (HR 13.1, 95% CI 3.79–45.0, p b 0.001) and amean arterialpressure below the median (HR 3.2, 95% CI 1.14–8.80, p = 0.028) were the only independent predictors ofmortality in Cox regression multivariate analysis. In previously hospitalized patients, cardiac output, C-reactiveprotein and albumin levels were associated with 6-month mortality in univariate analysis; this association waslost after adjusting for Child score.Conclusions:Medium-termmortality in cirrhosis seems to be mainly determined by liver disease severity ratherthan bymyocardial dysfunction.Modern echocardiographic indices of systolic and diastolic function do not seemto be useful in identifying patients at increased risk of dying.
© 2014 European Federation of Internal Medicine. Published by Elsevier B.V. All rights reserved.
1. Introduction
Cirrhotic cardiomyopathy has been described as a condition charac-terized by impaired contractile response to stress, diastolic dysfunctionand electrophysiological abnormalities, in the absence of known cardiacdisease [1–3]. Although previous studies have reported a direct relationbetween myocardial dysfunction and liver disease severity [4,5], thesefindingswere not replicated in recentworks [6–9]. Diastolic dysfunctionhas also been related to adverse prognosis after TIPS insertion [10].
On the other hand, a low cardiac output has been associatedwith thedevelopment of hepatorenal syndrome and mortality in patients withadvanced cirrhosis [11–14]. It has been suggested that myocardialdysfunction may contribute to the inability to increase cardiac outputunder stress conditions in these patients [8,13].
Newer echocardiographicmodalities, such as tissue-Doppler imagingand speckle tracking, which are able to quantitate myocardial displace-ment and deformation, have emerged as important prognostic markersin different clinical settings [15–19]. The role of cardiac function –
which may be more accurately assessed by these imaging modalities –in the pathogenesis of circulatory dysfunction in cirrhosis and itsprognostic implications remains unclear.
We aimed to evaluate the value of a detailed echocardiographicevaluation of cardiac systolic and diastolic function in predictingmedium-term mortality in patients with cirrhosis.
2. Methods
Weprospectively evaluated a group of 72 consecutively hospitalizedpatients with decompensated cirrhosis (defined as encephalopathy,
European Journal of Internal Medicine 25 (2014) 241–246
Abbreviations: TIPS, transjugular intrahepatic portosystemic shunt; HR, hazard ratio;NT-ProBNP, aminoterminal portion of pro-b-type natriuretic peptide; MELD, model forend-stage liver disease.⁎ Corresponding author at: Cardiology Department, Centro Hospitalar de Gaia/Espinho,
Rua Conceição Fernandes, 4430-502 Vila Nova de Gaia, Portugal. Tel.: +351 227865100;fax: +351 227830209.
E-mail addresses: [email protected] (F. Sampaio),[email protected] (J. Pimenta), [email protected] (N. Bettencourt),[email protected] (R. Fontes-Carvalho), [email protected] (A.-P. Silva),[email protected] (J. Valente), [email protected] (P. Bettencourt),[email protected] (J. Fraga), [email protected] (V. Gama).
0953-6205/$ – see front matter © 2014 European Federation of Internal Medicine. Published by Elsevier B.V. All rights reserved.http://dx.doi.org/10.1016/j.ejim.2014.01.011
Contents lists available at ScienceDirect
European Journal of Internal Medicine
j ourna l homepage: www.e lsev ie r .com/ locate /e j im

94
Francisco Sampaio
ascites, variceal bleeding, and/or jaundice) and 61 ambulatory patientsfollowed in an outpatient hepatology clinic, enrolled in the studybetween April 2011 and November 2012. The diagnosis of cirrhosiswas based on clinical, laboratory, ultrasonographic and/or biopsycriteria.
All patients underwent a comprehensive echocardiographic evalua-tion. Diastolic function was evaluated according to the most recentõrecommendations [20], with tissue-Doppler mitral annulus velocitiesbeing the first step in the diagnostic work-up. Systolic function assess-ment included left ventricular longitudinal strain analysis from two-dimensional grey-scale images using speckle tracking. A full descriptionof the echocardiographic methods has been published elsewhere [9].Clinical evaluation, blood sample collection and 12-lead ECG wereperformed on the same day of the echocardiogram.
We excluded patients with diabetes, arterial hypertension, previousrelevant cardiac disease, significant ECG abnormalities or more thanmild valvular heart disease on echocardiography.
Patients who were discharged after the index hospitalization andambulatory patients were followed for 6 months for the occurrence ofall-cause death; the two patients submitted to hepatic transplantationduring the study period were censored at the time of the procedure.Surveillance was performed by medical contact and/or observation ofclinical records.
The study complies with the principles of the declaration of Helsinki.The local Ethics Committee approved the study protocol and patients ortheir relatives gave informed consent.
2.1. Statistical analysis
Datawas stored and analysed using IBM SPSS Statistics, Version 20.0(Armonk, NY: IBM Corp). Results are presented as median (25th–75thpercentile) for quantitative variables and as n (%) for categoricalvariables. A significance level of 5% was used.
Cox regression analysis was used to evaluate the association of inde-pendent variableswith time to outcome, expressed as hazard ratio (HR)and 95% CI. Independent continuous variables were dichotomized
according to theirmedian values (when therewas no linear relationshipbetween them and the dependent variable) or according to well-established cut-off values for defining abnormality. Survival curveswere estimated according to the Kaplan–Meier method and comparedby the log-rank test.
3. Results
Of the original sample, 22 patients were excluded based on theexclusion criteria; the 13 patients who died during the index hospitali-zation were also excluded, leaving 98 patients for subsequent analysis.
Clinical and laboratorial characteristics of the patients included areshown in Table 1. Hospitalized patients had evidence of more advanceddisease andmore dynamic circulation – lowermean blood pressure andhigher heart rate – than ambulatory patients. Hospitalized patients alsohad a higher cardiac output [6.7 L/min (5.4–7.2) vs 5.7 L/min (4.7–6.6),p = 0.01]. Other echocardiographic characteristics of the patients arepresented in Table 2.
During the follow-up period, 20 patients died (three of haemor-rhage, seven of infection, four due to hepatorenal syndrome, four dueto porto-systemic encephalopathy and two of unknown cause) andtwo were transplanted. All deaths occurred in the group of hospitalizedpatients. No patient was lost to follow-up.
In Cox regression analysis, none of the echocardiographic parame-ters were associated with the occurrence of death at 6 months(Table 3). Although NT-ProBNP levels were significantly related to theoutcome in univariate analysis, this association was lost after adjust-ment to Child–Pugh class. A Child–Pugh score N 10 points (HR 13.1,95%CI 3.79–45.0, p b 0.001) and amean arterial pressure below theme-dian (HR 3.2, 95% CI 1.14–8.80, p = 0.028) were the only independentpredictors of mortality in multivariate analysis (Fig. 1).
Since all deaths occurred in the patients discharged after a hospitali-zation, we performed an isolated analysis of this group. Child–Pughscore, C-reactive protein levels, albumin levels and cardiac output wereassociated with 6-month mortality in univariate analysis (Table 4).Besides cardiac output, no echocardiographic variable was related to
Table 1Clinical and laboratorial characteristics of patients.
Overall(n = 98)
Hospitalized(n = 52)
Ambulatory(n = 46)
p
Age 54 (47–63) 54 (46–65) 54 (48–63) 0.97Male gender (n, %) 78 (79.6) 40 (76.9) 38 (82.6) 0.49Cirrhosis aetiology 0.76Alcoholic (n, %) 65 (66.3) 37 (71.2) 28 (60.9)Viric (n, %) 24 (24.5) 12 (23.1) 12 (26.1)Other (n, %) 9 (9.2) 3 (5.7) 6 (13.0)Beta-blocker use (n, %) 47 (48) 22 (42.3) 25 (54.3) 0.23Child–Pugh class b0.001A (n, %) 38 (38.8) 4 (7.7) 34 (73.9)B (n, %) 27 (27.6) 17 (32.7) 10 (21.7)C (n, %) 33 (33.7) 31 (59.6) 2 (4.3)MELDa score 12 (9–16) 15 (13–20) 9 (7–11) b0.001Heart rate 71 (58–81) 75 (66–87) 65 (57–77) 0.008Mean blood pressure 91 (80–99) 85 (75–95) 93 (87–100) 0.001Blood analysisHaemoglobin (g/dL) 12.0 (10.4–13.7) 10.8 (9.2–12.3) 13.6 (11.9–14.7) b0.001Platelet count (×109/L) 98 (60–125) 96 (49–133) 98 (60–124) 0.90Creatinine (mg/dL) 0.67 (0.50–0.89) 0.69 (0.50–0.98) 0.67 (0.54–0.84) 0.68Sodium (mEq/L) 138 (134–140) 135 (129–138) 139 (138–141) b0.001Total bilirubin (mg/dL) 1.60 (0.87–2.92) 2.47 (1.62–5.05) 1.09 (0.67–1.44) b0.001Albumin (g/dL) 3.35 (2.70–4.00) 2.85 (2.43–3.37) 4.0 (3.47–4.40) b0.001NT-ProBNPb (pg/mL) 158 (61–325) 295 (155–518) 78 (36–156) b0.001CRPc (mg/dL) 0.58 (0.21–1.92) 1.60 (0.35–3.90) 0.37 (0.09–0.58) b0.001INRd 1.39 (1.27–1.68) 1.56 (1.39–1.82) 1.27 (1.10–1.40) b0.001
a Model for end-stage liver disease.b Aminoterminal portion of pro-b-type natriuretic peptide.c C reactive protein.d International normalized ratio.
242 F. Sampaio et al. / European Journal of Internal Medicine 25 (2014) 241–246

Publicações
95
prognosis. Child–Pugh score was the only variable that remained signif-icantly associated with the outcome, on multivariate analysis (HR 7.9,95% CI 1.83–34.51, p = 0.006).
Thirteen patients died during the index hospitalization (seven dueto porto-systemic encephalopathy, three of hepatorenal syndrome,two of infection, and one of haemorrhage). Compared to patients whowere discharged, patients who died during the index hospitalizationhad higher MELD score [20 (18–26) vs 15 (13–20), p = 0.002],higher total bilirubin levels [4.4 mg/dl (2.6–10.3) vs 2.5 mg/dl (1.6–5.1), p = 0.04], lower albumin levels [2.5 g/dl (2.2–2.9) vs 2.8 g/dl(2.4–3.4) p = 0.02], higher C-reactive protein levels [3.5 mg/dl (1.3–21.6) vs 1.6 mg/dl (0.3–3.9), p= 0.03], higher international normalizedratio [1.9 (1.6–2.2) vs 1.6 (1.4–1.8), p = 0.04] and higher NT-ProBNPlevels [773 pg/ml (379–1971) vs 295 (155–518) p = 0.005]. Therewere no differences in echocardiographic parameters between thesegroups. The inclusion of these patients in the survival analysis did notsignificantly change the overall results: Child–Pugh score N 10 points(HR 14.2, 95% CI 4.97–40.9, p b 0.001) and a mean arterial pressurebelow the median (HR 2.17, 95% CI 1.02–4.61, p = 0.045) were theonly independent predictors of mortality.
4. Discussion
Our results suggest that medium-term prognosis in cirrhosis is notinfluenced by myocardial dysfunction. Usingmodern echocardiograph-icmodalities, we could not find an association between any echocardio-graphic parameters of systolic or diastolic function and the occurrenceof death at 6 months. Child–Pugh score and mean blood pressurewere the only independent predictors ofmortality onmultivariate anal-ysis. This suggests that liver failure and associated haemodynamicchanges are more important determinants of medium-term survivalthan “intrinsic” myocardial dysfunction.
The impact of cardiac function on the prognosis of cirrhosis has notbeen addressed until recently and is a matter of ongoing debate. Ourresults are in line with two previous works, in which an associationbetween diastolic dysfunction and mortality could also not be found[8,21]. On the other hand, Ruíz-del-Árbol et al. recently reported thatdiastolic dysfunction was related to poor outcomes in patients withcirrhosis and that E/E′ was an independent predictor of the develop-ment of hepatorenal syndrome and 1-year mortality [22]. The higherprevalence of more severe diastolic impairment in their sample (47%
Table 2Echocardiographic characteristics of patients.
Overall(n = 98)
Hospitalized(n = 52)
Ambulatory(n = 46)
p
Left atrial volume index (mL/m2) 39.7 (29.7-45.3) 40.0 (29.2–45.8) 38.9 (29.8–45.4) 0.86Left ventricle diastolic diameter (mm) 51 (47–55) 52 (47–55) 51 (46–55) 0.81Left ventricle systolic diameter (mm) 32 (28–36) 32 (28–34) 33 (29–38) 0.25Left ventricular mass (g) 148 (121–189) 146 (119–192) 150 (126–188) 0.47Left ventricular EFa b 55% (n, %) 10 (10.2) 6 (11.5) 4 (8.7) 0.75Cardiac output (L/min) 6.1 (5.0–7.1) 6.7 (5.4–7.2) 5.7 (4.7–6.6) 0.01E/A ratio 1.0 (0.8–1.4) 0.9 (0.8–1.3) 1.1 (0.9–1.4) 0.07E/E′ ratio 8.6 (6.8–10.4) 8.3 (6.6–10.3) 8.9 (7.0–10.5) 0.43Diastolic dysfunctionb (n, %) 16 (16.3) 8 (15.4) 8 (17.4) 0.79Left ventricular longitudinal strain (%) −19.5 (−21.5 to −18.5) −19.0 (−21.5 to −18.1) −19.8 (−21.6 to −19.0) 0.29
a Ejection fraction.b Diastolic dysfunction defined as septal E′ b 8 cm/s, lateral e′ b 10 cm/s and left atrial volume ≥ 34 mL/m2 [20].
Table 3Cox regression model for predictors of all-cause death within 6 months.
Hazard ratio 95% confidence interval p
Age N 54 years 1.38 0.57–3.39 0.476Alcoholic aetiology (vs other) 0.67 0.27–1.63 0.370Mean blood pressure N 91 mm Hg 0.28 0.10–0.77 0.014Heart rate N 71 bpm 1.81 0.74–4.43 0.193Child–Pugh score N 10 points 14.5 4.23–49.4 b0.001MELDa score N 12 points 10.8 2.50–46.4 0.001Haemoglobin N 12 g/dL 0.22 0.07–0.66 0.007Renal insufficiencyb 2.47 0.83–7.39 0.106Serum sodium N 138 mEq/L 0.32 0.11–0.87 0.025Total bilirubin N 1.6 mg/dL 4.56 1.52–13.6 0.007Albumin N 3.35 g/dL 0.14 0.04–0.49 0.002CRPc N 0.58 mg/dL 3.19 1.15–8.87 0.026NT-ProBNPd N 158 pg/mL 4.0 1.33–12.1 0.014Left atrial volume index N 39.7 mL/m2 0.92 0.38–2.20 0.846Left ventricle end-diastolic volume N 100 mL 0.60 0.24–1.46 0.260Left ventricular mass N 148 g 0.65 0.27–1.59 0.348Left ventricular ejection fraction N 55% 0.99 0.23–4.28 0.993Cardiac output N 6.1 L/min 0.75 0.31–1.82 0.531Left ventricular longitudinal strain N −19.5% 1.136 0.45–2.85 0.786Diastolic dysfunctione (versus none) 0.51 0.12–2.18 0.361E/E′ ratio N 10 1.14 0.45–2.85 0.786QTc interval N 440 ms 0.59 0.20–1.76 0.341
a Model for end-stage liver disease.b Defined as glomerular filtration rate b 60 mL/min/1.73 m2 using the MDRD formula.c C reactive protein.d Aminoterminal portion of pro-b-type natriuretic peptide.e Diastolic dysfunction defined as septal e′ b 8 cm/s, lateral e′ b 10 cm/s and left atrial volume ≥ 34 mL/m2 [20].
243F. Sampaio et al. / European Journal of Internal Medicine 25 (2014) 241–246
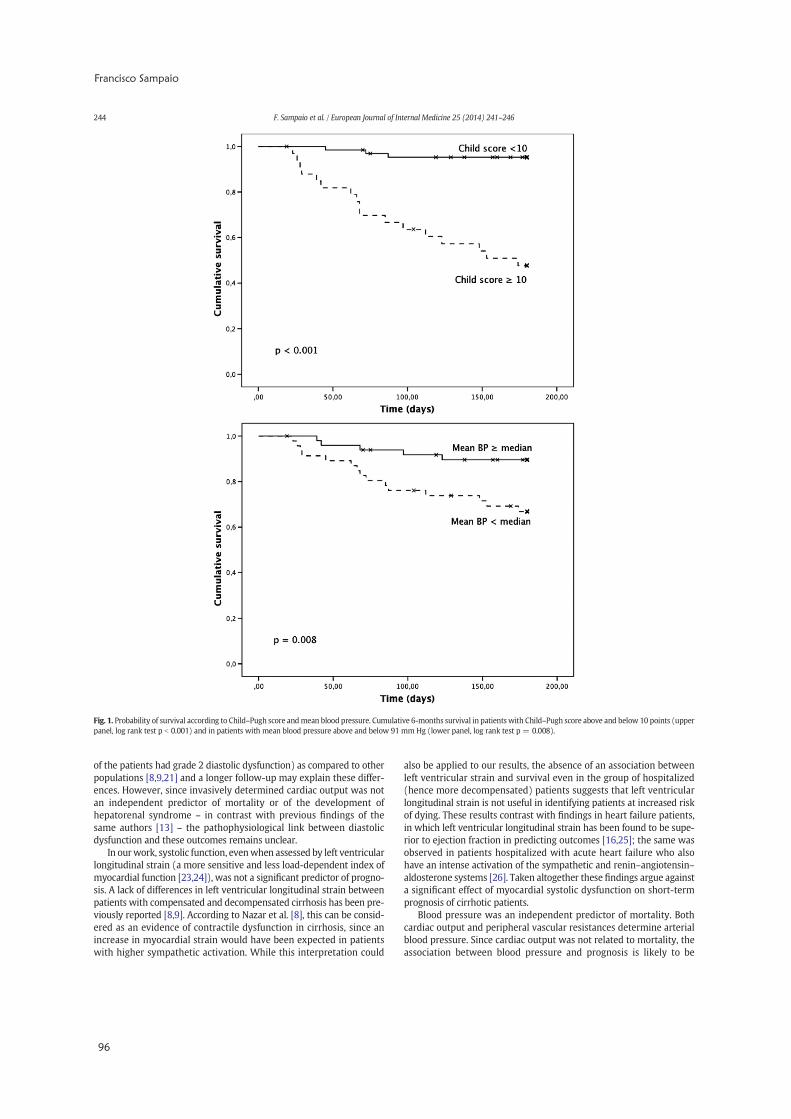
96
Francisco Sampaio
of the patients had grade 2 diastolic dysfunction) as compared to otherpopulations [8,9,21] and a longer follow-up may explain these differ-ences. However, since invasively determined cardiac output was notan independent predictor of mortality or of the development ofhepatorenal syndrome – in contrast with previous findings of thesame authors [13] – the pathophysiological link between diastolicdysfunction and these outcomes remains unclear.
In ourwork, systolic function, evenwhen assessed by left ventricularlongitudinal strain (a more sensitive and less load-dependent index ofmyocardial function [23,24]), was not a significant predictor of progno-sis. A lack of differences in left ventricular longitudinal strain betweenpatients with compensated and decompensated cirrhosis has been pre-viously reported [8,9]. According to Nazar et al. [8], this can be consid-ered as an evidence of contractile dysfunction in cirrhosis, since anincrease in myocardial strain would have been expected in patientswith higher sympathetic activation. While this interpretation could
also be applied to our results, the absence of an association betweenleft ventricular strain and survival even in the group of hospitalized(hence more decompensated) patients suggests that left ventricularlongitudinal strain is not useful in identifying patients at increased riskof dying. These results contrast with findings in heart failure patients,in which left ventricular longitudinal strain has been found to be supe-rior to ejection fraction in predicting outcomes [16,25]; the same wasobserved in patients hospitalized with acute heart failure who alsohave an intense activation of the sympathetic and renin–angiotensin–aldosterone systems [26]. Taken altogether these findings argue againsta significant effect of myocardial systolic dysfunction on short-termprognosis of cirrhotic patients.
Blood pressure was an independent predictor of mortality. Bothcardiac output and peripheral vascular resistances determine arterialblood pressure. Since cardiac output was not related to mortality, theassociation between blood pressure and prognosis is likely to be
Fig. 1. Probability of survival according to Child–Pugh score andmean blood pressure. Cumulative 6-months survival in patients with Child–Pugh score above and below 10 points (upperpanel, log rank test p b 0.001) and in patients with mean blood pressure above and below 91 mm Hg (lower panel, log rank test p = 0.008).
244 F. Sampaio et al. / European Journal of Internal Medicine 25 (2014) 241–246

Publicações
97
explained mainly by peripheral vascular resistances, i.e., patients withmore vasodilatation are at increased risk. Other authors have reportedthat a low cardiac output could identify patients at risk of developinghepatorenal syndrome and of dying [11–13]. Since the lack of prognos-tic impact of cardiac output in our population could just be explained bythe inclusion of patients with mild disease, we performed an isolateanalysis of the group of hospitalized patients. Although a cardiac outputbelow themedianwas significantly associatedwith 6-monthsmortalityin univariate analysis, this association was lost after adjusting for Childclass. A progressive decrease in cardiac output during the course ofliver disease has been reported [11,22], and probably accounts for thisfinding. Besides, we found no significant differences in cardiac outputin patients who died during the index hospitalization and those whowere discharged (data not shown). These conflicting results may be ex-plained by the fact that the causes of death in our groupwere varied andnot only related to renal/multiorgan failure. We did not analyse onlythose dying of hepatorenal syndrome since the small number of eventswould have significantly limited the statistical analysis. However, intheir recent report, Ruíz-del-Árbol et al. also failed to find differencesin cardiac output between patients who developed hepatorenalsyndrome during follow-up and those who did not [22]; in fact theonly significant difference in haemodynamic measurements foundbetween those two groups wasmean arterial pressure which is concor-dant with our own results.
Elevated NT-ProBNP levels were related to mortality in the overallsample, but this association was lost after adjusting for Child score. Adirect relation between natriuretic peptide levels and liver diseaseseverity has been consistently reported [4,27]. However, Pimenta et al.found that BNP levels above the median were independent predictorsof 6-month mortality in a cohort of hospitalized patients [12]. Wecould not replicate these findings, when looking only at the group ofhospitalized patients. There are somepossible explanations for these re-sults.WemeasuredNT-ProBNPonly at admission; it is possible that, justlike in heart failure, discharge and particularly the evolution of natri-uretic peptide levels during the hospital stay [28,29], would be a moreimportant prognostic marker than a single measurement. We usedNT-ProBNP instead of BNP, and the two molecules have slightly differ-ent characteristics [30] (half-life, clearance mechanisms), which may,
hypothetically, have influenced the results. Finally, NT-ProBNP levelswere relatively low in our sample, even when looking only at patientsdischarged after a hospitalization; this small range of low values maynot be able to differentiate patients at increased risk of death. Patientswho died during the index hospitalization had significantly higherNT-ProBNP levels than patients who were discharged. This suggeststhat BNP may, in fact, be useful in identifying higher risk patients.
4.1. Limitations
Our study was performed in a single centre and included mainlypatients with alcoholic cirrhosis and different disease severity.
We excluded patients with diabetes, which is frequent in cirrhoticpatients and is a known cause of cardiac disease; hence our conclusionscannot be extended to this subset of patients.
We did not perform invasive haemodynamic studies or neurohor-monal measurements (besides NT-ProBNP), whichwould have allowedus to accurately assess central and peripheral haemodynamic status andto correlate them with prognosis.
It would add to our analysis evaluating whether echocardiographicparameters of myocardial dysfunction could predict cardiovasculardeaths. However, the study was not designed to perform such analysisand would be underpowered to draw firm conclusions due to the limit-ed number of deaths in this category.
5. Conclusion
Cardiac function is not related to medium-term mortality in cirrho-sis, which seems to be mainly determined by liver disease severityand associated haemodynamic changes.
Although systolic dysfunction and diastolic dysfunction have beendocumented in patients with cirrhosis, these abnormalities may not besevere enough to independently influence the medium-term prognosis.However, we cannot exclude that cardiac dysfunction may act as a con-tributing factor to the development of complications of cirrhosis (likehepatorenal syndrome or haemorrhage), or to their irreversibility. Onthe other hand, its potential effect on long-term survival remains unclearand warrants further study.
Table 4Cox regression model for predictors of all-cause death within 6 months after discharge in hospitalized patients.
Hazard ratio 95% confidence interval p
Age N 54 years 0.88 0.37–2.11 0.769Alcoholic aetiology (vs other) 0.47 0.19–1.15 0.098Mean blood pressure N 85 mm Hg 0.54 0.22–1.31 0.172Heart rate N 75 bpm 1.57 0.64–3.83 0.326Child–Pugh score N 10 points 5.08 1.49–17.4 0.010MELDa score N 15 points 1.22 0.51–2.95 0.654Haemoglobin N 10.8 g/dL 0.71 0.29–1.71 0.443Renal Insufficiencyb 1.28 0.43–3.83 0.661Serum sodium N 135 mEq/L 1.04 0.43–2.51 0.926Total bilirubin N 2.47 mg/dL 1.22 0.51–2.94 0.659Albumin N 2.85 g/dl 0.35 0.13–0.90 0.030CRPc N 1.60 mg/dL 2.63 1.00–6.93 0.050NT-ProBNPd N 295 pg/mL 2.39 0.91–6.30 0.077Left atrial volume index N 40 ml/m2 0.90 0.38–2.17 0.820Left ventricle end-diastolic volume N 96 mL 0.54 0.22–1.32 0.179Left ventricular mass N 146 g 0.59 0.24–1.44 0.244Left ventricular ejection fraction N 55% 1.26 0.29–5.42 0.759Cardiac output N 6.7 L/min 0.32 0.12–0.84 0.021Left ventricular longitudinal strain N −19.8% 1.67 0.61–4.60 0.322Diastolic dysfunctione (versus none) 0.51 0.12–2.18 0.360E/E′ ratio N 10 1.07 0.43–2.69 0.880QTc interval N 440 ms 0.39 0.13–1.18 0.096
a Model for end-stage liver disease.b Defined as glomerular filtration rate b 60 mL/min/1.73 m2 using the MDRD formula.c C reactive protein.d Aminoterminal portion of pro-b-type natriuretic peptide.e Diastolic dysfunction defined as septal e′ b 8 cm/s, lateral e′ b 10 cm/s and left atrial volume ≥ 34 mL/m2 [20].
245F. Sampaio et al. / European Journal of Internal Medicine 25 (2014) 241–246
98
Francisco Sampaio
Learning points
• Cirrhotic cardiomyopathy is a condition characterized by impairedcontractile response to stress, diastolic dysfunction and electrophysi-ological abnormalities, in the absence of known cardiac disease.
• An association between cardiac dysfunction and a worse prognosis inpatients with cirrhosis has been suggested.
• In the present study, using sensitive and less load-dependent echocar-diographic methods, we could not find an association between anyindices of myocardial function and 6 month mortality.
• Liver disease severity and peripheral and associated haemodynamicchanges seem to be themain determinants ofmedium-termprognosis.
Conflict of interests
The authors have no conflict of interest to declare.
References
[1] Alqahtani SA, Fouad TR, Lee SS. Cirrhotic cardiomyopathy. Semin Liver Dis2008;28:59–69.
[2] Moller S, Henriksen JH. Cardiovascular complications of cirrhosis. Gut 2008;57:268–78.
[3] Wong F. Cirrhotic cardiomyopathy. Hepatol Int 2009;3:294–304.[4] Henriksen JH, Gøtze JP, Fuglsang S, Christensen E, Bendtsen F, Møller S. Increased cir-
culating pro-brain natriuretic peptide (proBNP) and brain natriuretic peptide (BNP)in patients with cirrhosis: relation to cardiovascular dysfunction and severity ofdisease. Gut 2003;52:1511–7.
[5] Pozzi M, Carugo S, Boari G, Pecci V, de Ceglia S, Maggiolini S, et al. Evidence offunctional and structural cardiac abnormalities in cirrhotic patients with and with-out ascites. Hepatology 1997;26:1131–7.
[6] Kazankov K, Holland-Fischer P, Andersen NH, Torp P, Sloth E, Aagaard NK, et al. Rest-ing myocardial dysfunction in cirrhosis quantified by tissue Doppler imaging. LiverInt 2011;31:534–40.
[7] Merli M, Calicchia A, Ruffa A, Pellicori P, Riggio O, GiustoM, et al. Cardiac dysfunctionin cirrhosis is not associated with the severity of liver disease. Eur J Intern Med2013;24:172–6.
[8] Nazar A, Guevara M, Sitges M, Terra C, Solà E, Guigou C, et al. LEFT ventricular func-tion assessed by echocardiography in cirrhosis: relationship to systemic hemody-namics and renal dysfunction. J Hepatol 2013;58:51–7.
[9] Sampaio F, Pimenta J, Bettencourt N, Fontes-Carvalho R, Silva AP, Valente J, et al.Systolic and diastolic dysfunction in cirrhosis: a tissue-Doppler and speckle trackingechocardiography study. Liver Int 2013;33:1158–65.
[10] Cazzaniga M, Salerno F, Pagnozzi G, Dionigi E, Visentin S, Cirello I, et al. Diastolic dys-function is associated with poor survival in patients with cirrhosis with transjugularintrahepatic portosystemic shunt. Gut 2007;56:869–75.
[11] Krag A, Bendtsen F, Henriksen JH, Møller S. Low cardiac output predicts develop-ment of hepatorenal syndrome and survival in patients with cirrhosis and ascites.Gut 2010;59:105–10.
[12] Pimenta J, Paulo C, Gomes A, Silva S, Rocha-Gonçalves F, Bettencourt P. B-type natri-uretic peptide is related to cardiac function and prognosis in hospitalized patientswith decompensated cirrhosis. Liver Int 2010;30:1059–66.
[13] Ruiz-del-Arbol L, Monescillo A, Arocena C, Valer P, Ginès P, Moreira V, et al. Circula-tory function and hepatorenal syndrome in cirrhosis. Hepatology 2005;42:439–47.
[14] Ruiz-del-Arbol L, Urman J, Fernández J, González M, Navasa M, Monescillo A, et al.Systemic, renal, and hepatic hemodynamic derangement in cirrhotic patients withspontaneous bacterial peritonitis. Hepatology 2003;38:1210–8.
[15] Yu CM, Sanderson JE, Marwick TH, Oh JK. Tissue Doppler imaging a new prognosti-cator for cardiovascular diseases. J Am Coll Cardiol 2007;49:1903–14.
[16] Stanton T, Leano R, Marwick TH. Prediction of all-cause mortality from global longi-tudinal speckle strain: comparison with ejection fraction and wall motion scoring.Circ Cardiovasc Imaging 2009;2:356–64.
[17] Nahum J, Bensaid A, Dussault C, Macron L, Clémence D, Bouhemad B, et al. Impact oflongitudinal myocardial deformation on the prognosis of chronic heart failure patients.Circ Cardiovasc Imaging 2010;3:249–56.
[18] Liu YW, Su CT, Sung JM,Wang SP, Su YR, Yang CS, et al. Association of left ventricularlongitudinal strain with mortality among stable hemodialysis patients withpreserved left ventricular ejection fraction. Clin J Am Soc Nephrol 2013;8:1564–74.
[19] Ersboll M, Valeur N, Mogensen UM, Andersen MJ, Moller JE, Velazquez EJ, et al.Prediction of all-cause mortality and heart failure admissions from global leftventricular longitudinal strain in patients with acute myocardial infarction andpreserved left ventricular ejection fraction. J Am Coll Cardiol 2013;61:2365–73.
[20] Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, et al. Recom-mendations for the evaluation of left ventricular diastolic function by echocardiogra-phy. J Am Soc Echocardiogr 2009;22:107–33.
[21] Alexopoulou A, Papatheodoridis G, Pouriki S, Chrysohoou C, Raftopoulos L,Stefanadis C, et al. Diastolic myocardial dysfunction does not affect survival inpatients with cirrhosis. Transpl Int 2012;25:1174–81.
[22] Ruiz-Del-Arbol L, Achecar L, Serradilla R, Rodriguez-Gandia MA, Rivero M, Garrido E,et al. Diastolic dysfunction is a predictor of poor outcomes in patients with cirrhosis,portal hypertension and a normal creatinine. Hepatology 2013;58:1732–41.
[23] Bijnens BH, Cikes M, Claus P, Sutherland GR. Velocity and deformation imaging forthe assessment of myocardial dysfunction. Eur J Echocardiogr 2009;10:216–26.
[24] Mor-Avi V, Lang RM, Badano LP, Belohlavek M, Cardim NM, Derumeaux G, et al.Current and evolving echocardiographic techniques for the quantitative evaluationof cardiac mechanics: ASE/EAE consensus statement on methodology and indica-tions endorsed by the Japanese Society of Echocardiography. Eur J Echocardiogr2011;12:167–205.
[25] Mignot A, Donal E, Zaroui A, Reant P, Salem A, Hamon C, et al. Global longitudinalstrain as a major predictor of cardiac events in patients with depressed left ventric-ular function: a multicenter study. J Am Soc Echocardiogr 2010;23:1019–24.
[26] Cho G-Y, Marwick TH, Kim H-S, Kim M-K, Hong K-S, Oh D-J. Global 2-dimensionalstrain as a new prognosticator in patients with heart failure. J Am Coll Cardiol2009;54:618–24.
[27] Yildiz R, Yildirim B, Karincaoglu M, Harputluoglu M, Hilmioglu F. Brain natriureticpeptide and severity of disease in non-alcoholic cirrhotic patients. J GastroenterolHepatol 2005;20:1115–20.
[28] Bettencourt P, Azevedo A, Pimenta J, Friões F, Ferreira S, Ferreira A. N-terminal-pro-brain natriuretic peptide predicts outcome after hospital discharge in heartfailure patients. Circulation 2004;110:2168–74.
[29] Cheng V, Kazanagra R, Garcia A, Lenert L, Krishnaswamy P, Gardetto N, et al. A rapidbedside test for B-type peptide predicts treatment outcomes in patients admitted fordecompensated heart failure: a pilot study. J Am Coll Cardiol 2001;37:386–91.
[30] Kim HN, Januzzi Jr JL. Natriuretic peptide testing in heart failure. Circulation2011;123:2015–9.
246 F. Sampaio et al. / European Journal of Internal Medicine 25 (2014) 241–246

V. Discussão

Discussão
101
Nos estudos desenvolvidos no âmbito desta tese, foi possível documentar, utilizando mé-
todos não invasivos de imagiologia cardíaca, alterações da função cardíaca em doentes com
cirrose hepática de diferentes etiologias, quer em repouso quer sob estimulação farmacológica.
Estes achados suportam assim a existência de uma cardiomiopatia cirrótica previamente carac-
terizada como uma disfunção miocárdica intrínseca relacionada com a cirrose e independente
da sua etiologia[85].
5.1 DISFUNÇÃO SISTÓLICA
Da análise do estudo 1 pode-se concluir que os doentes com cirrose apresentam altera-
ções da função sistólica – traduzida pela redução da deformação longitudinal do ventrículo
esquerdo – apesar da fracção de ejecção ser normal em mais de 90% dos doentes. Este achado
é consistente com o de outros estudos em que métodos de deformação miocárdica foram
úteis na identificação de doença cardíaca subclínica[117-120] ou de disfunção sistólica na insufi-
ciência cardíaca com fracção de ejecção preservada[142-145] e sugerem que, tal como naquelas
entidades, a deformação longitudinal do ventrículo esquerdo é também o primeiro parâmetro
de função sistólica a ser afectado na cirrose hepática. A arquitectura do ventrículo esquer-
do, nomeadamente a orientação longitudinal das fibras endocárdicas – mais susceptíveis aos
efeitos de agressões como a isquemia, sobrecarga de volume ou de pressão – fornece a base
patofisiológica destas observações. Em contraste, as vertentes radial e circunferencial da defor-
mação miocárdica apenas são afectadas em estádios muito mais avançados de doença, quando
as fibras das camadas média e subepicárdica que as determinam são atingidas. Este facto pode
justificar a normalidade da fracção de ejecção – muito dependente do espessamento miocár-
dico no sentido radial – na nossa população, sugerindo que este índice possa ser um marcador
insensível e tardio de disfunção sistólica.
No mesmo sentido, no estudo 3, verificámos que os doentes com cirrose, mesmo em es-
tádios precoces da doença, apresentam uma resposta diminuída da deformação longitudinal à
102
Francisco Sampaio
estimulação com dobutamina e que esta se correlaciona com um menor aumento do débito
cardíaco nos doentes, quando comparados com um grupo controlo. Esta observação con-
firma a incompetência inotrópica em resposta a exercício físico ou estímulo farmacológico
documentada em estudos prévios[51-54]. A resposta da deformação circunferencial e radial e da
fracção de ejecção à estimulação adrenérgica (particularmente em doses mais elevadas), não
se encontrava significativamente alterada neste estudo, comprovando, uma vez mais, a maior
sensibilidade da deformação longitudinal na identificação de disfunção miocárdica precoce.
No estudo 1, não conseguimos correlacionar a disfunção sistólica em repouso com o esta-
do clínico ou com a gravidade da doença. No entanto, no estudo 3 não encontramos diferenças
significativas nos índices de deformação entre doentes e controlos. Uma possível explicação
para esta aparente discrepância poderá ser o efeito da estimulação adrenérgica mais intensa
nos doentes mais graves e/ou descompensados que, partindo hipoteticamente de valores pio-
res, resultaria num strain semelhante ao dos doentes compensados, com menor estimulação
inotrópica. Por outro lado, o estudo 3 não foi desenhado para detectar diferenças em repouso
entre os grupos, não tendo poder estatístico para o fazer dada a reduzida dimensão da amos-
tra. Os nossos achados estão, porém, em linha com o de outros autores que também não
conseguiram correlacionar o grau de disfunção sistólica com a gravidade da doença[61, 99].
Em resumo, os nossos resultados sustentam a existência de disfunção sistólica em doentes
com cirrose, mas esta poderá apenas ser detectável através de técnicas de análise de defor-
mação miocárdica; os índices convencionais de função sistólica (como a fracção de ejecção)
poderão manter-se normais na maioria dos doentes, sendo afectados apenas na presença de
atingimento cardíaco significativo. Poderá assim justificar-se, no futuro, incluir estes novos pa-
râmetros nos critérios de suporte para o diagnóstico de cardiomiopatia cirrótica.
5.2. DISFUNÇÃO DIASTÓLICA
Foi igualmente possível encontrar evidência de disfunção diastólica na população estudada
nos nossos trabalhos. Contudo, a prevalência desta alteração variou consoante a metodologia
adoptada. Utilizando os critérios de diagnóstico de cardiopatia cirrótica propostos em 2005[85],
documentámos uma prevalência de disfunção diastólica de 40,4%; estes achados são semelhan-
tes aos de estudos prévios utilizando a mesma metodologia[61, 91, 98, 99]. No entanto encontra-
mos também diferenças nas condições de fluxo nos doentes com esta definição de disfunção
diastólica. As limitações da avaliação da função diastólica com base no padrão de enchimento
do ventrículo esquerdo por Doppler pulsado, nomeadamente a dependência das condições
Discussão
103
de carga, são conhecidas e podem ser particularmente relevantes nos doentes com cirrose.
Como descrito previamente, a circulação da cirrose caracteriza-se por hipovolémia central em
consequência da vasodilatação arteriolar esplâncnica; a diminuição da pré-carga resulta, por si
só, na diminuição da velocidade da onda E, mesmo em indivíduos normais, o mesmo se veri-
ficando com aumentos da frequência cardíaca[78, 107, 108]. Estes factos podem justificar a elevada
prevalência de um padrão de enchimento ventricular caracterizado pela inversão da relação
E/A, independentemente da presença de atraso do relaxamento ventricular, nos doentes com
cirrose. O nosso achado de débito cardíaco mais baixo (podendo traduzir menor pré-carga)
nos doentes com inversão da relação E/A parece suportar esta hipótese. A relação deste pa-
drão com a gravidade da doença sugerida em estudos prévios[67, 68], pode ter uma explicação
idêntica uma vez que os doentes mais descompensados exibem igualmente sinais de maior
vasodilatação periférica.
A prevalência de disfunção diastólica diminuiu significativamente com a aplicação das re-
comendações actuais para a avaliação de função diastólica por ecocardiografia[80]; mais impor-
tante, a concordância entre as duas definições foi fraca, reforçando a ideia que os critérios de
diagnóstico baseados no fluxo transmitral não são adequados para identificar disfunção dias-
tólica nestes doentes. Num estudo prévio, as pressões de enchimento ventriculares medidas
invasivamente numa coorte de doentes com cirrose foram normais em todos os doentes[99],
traduzindo a ausência de disfunção diastólica grave naquela população. Os nossos dados pare-
cem confirmar esta observação e sugerem que a prevalência de disfunção diastólica pode ser
menor do que a previamente descrita.
A dilatação auricular esquerda é um reconhecido marcador de cronicidade de disfunção
diastólica e de pressões de enchimento aumentadas[146]. Nos estudos 1 e 2, observámos que
os doentes com cirrose, apresentam, efectivamente, volumes auriculares superiores aos do
grupo controle. No entanto, a dilatação aurícula não é específica da disfunção diastólica e
outras causas podem contribuir para este achado[80]. Na análise do estudo 2 verificámos que
nenhum parâmetro de disfunção diastólica se associava independentemente ao volume auricu-
lar nesta população, sugerindo a existência de outros mecanismos para esta dilatação, no con-
texto específico da cirrose. De facto, apenas a hemoglobina, o volume de ejecção e o volume
telediastólico do ventrículo esquerdo se associavam ao índice de volume auricular esquerdo
sugerindo que as condições de volémia são os principais determinantes desta alteração, nestes
doentes. Esta observação está em linha com a associação da dilatação auricular esquerda e dos
níveis de peptídeo natriurético tipo A (ANP) com a volémia em doentes com cirrose relatada
previamente[46].

104
Francisco Sampaio
No mesmo estudo, verificámos que a função de reservatório da aurícula esquerda – ava-
liada pela deformação desta câmara durante a sístole ventricular – se encontrava alterada nos
doentes com cirrose e que este achado se correlacionava com a velocidade da onda E’ – um
índice de relaxamento ventricular. Por outro lado, o strain auricular longitudinal permitiu iden-
tificar doentes com pressões de enchimento ventriculares melhor do que o volume da aurícula
esquerda, sugerindo que este parâmetro pode reflectir a presença de disfunção diastólica sig-
nificativa melhor do que o volume da aurícula esquerda, cuja interpretação deve ser cautelosa
no contexto da cirrose hepática. Embora o valor prognóstico do strain longitudinal auricular
tenha sido demonstrado noutros cenários[147], o impacto clínico da disfunção auricular no con-
texto da cirrose hepática permanece incerto.
Em resumo, apesar de no decorrer dos nossos trabalhos se ter encontrado evidência da
presença de disfunção diastólica na nossa população, a sua prevalência foi inferior à esperada,
com base em estudos prévios; as condições de fluxo na cirrose influenciam significativamente
alguns dos parâmetros comummente utilizados para a avaliação desta entidade limitando a sua
aplicabilidade neste cenário.
5.3. PROGNÓSTICO
No estudo 4 não encontrámos associação entre nenhum dos parâmetros ecocardiográfi-
cos, em repouso, avaliados previamente e a mortalidade aos 6 meses. A maior gravidade da do-
ença hepática – nomeadamente classe C de Child-Pugh – e a tensão arterial mais baixa foram
os únicos preditores independentes do prognóstico neste estudo. Estes dados sugerem que o
grau de insuficiência hepática e as alterações hemodinâmicas associadas – nomeadamente a va-
sodilatação periférica com consequente hipotensão arterial – têm maior impacto prognóstico
do que a presença de disfunção cardíaca “central”.
A associação entre disfunção sistólica e diastólica e o prognóstico dos doentes com cirrose
hepática é controversa, com resultados contraditórios entre vários trabalhos. As diferenças nas
características das populações estudadas, na metodologia utilizada para avaliação e definição
de disfunção miocárdica, assim como diferentes tempos de seguimento e definição de eventos
podem justificar a aparente contradição nos resultados. Os nossos resultados são sobrepo-
níveis aos de outros autores que também não foram capazes de encontrar qualquer relação
entre disfunção miocárdica e sobrevida[98, 99]. Por outro lado, estudos anteriores relataram uma
associação entre disfunção diastólica – avaliada por ecocardiografia e definida como inversão
da relação E/A do fluxo diastólico mitral – e aumento da mortalidade após inserção de shunt
Discussão
105
portossistémico[91, 92]. No entanto, como referido previamente, esta metodologia de avaliação
da função diastólica apresenta inúmeras limitações e os resultados podem apenas traduzir dife-
rentes condições hemodinâmicas, nomeadamente maior vasodilatação periférica nos doentes
mais descompensados. A discrepância entre estes resultados e os observados noutras pato-
logias como a insuficiência cardíaca – em que o padrão de inversão E/A se associa ao melhor
prognóstico[148-150] – parece suportar esta hipótese.
Uma associação entre débito cardíaco mais baixo (traduzindo indirectamente disfunção
sistólica) e risco de desenvolvimento de insuficiência renal e mortalidade em doentes com
cirrose descompensada[94, 95] foi também descrita por outros autores. No grupo de doentes
descompensados incluídos no nosso trabalho o débito cardíaco mais baixo também se asso-
ciou à mortalidade a 6 meses, na análise univariada. No entanto, esta associação perdeu o seu
significado após ajuste para a classe Child, sugerindo que a diminuição do débito cardíaco se
relaciona directamente com a gravidade da doença hepática e alterações hemodinâmicas asso-
ciadas; esta observação está em linha com relatos prévios[95, 97]. A ausência de uma associação
independente entre débito cardíaco e desenvolvimento de síndrome hepatorrenal ou mortali-
dade foi igualmente descrita noutro trabalho recente[97].
No estudo 3 encontrámos uma relação entre resposta do strain longitudinal e do débito
cardíaco à estimulação inotrópica com dobutamina. Dada a hipótese de a incapacidade de
aumentar o débito cardíaco se poder associar a um risco aumentado de complicações nestes
doentes[96], é possível que, a resposta dos índices de função sistólica ao stress, mais do que
o seu valor basal, possam ser marcadores importantes de prognóstico. Esta hipótese não foi
explorada nos nossos trabalhos e poderá merecer, no futuro, melhor avaliação.
Em resumo, na nossa população, o prognóstico a médio prazo foi sobretudo influenciado
pela gravidade da doença hepática. A disfunção miocárdica documentada nos estudos prévios
não parece ser suficientemente importante para o desenvolvimento de complicações graves.
O seu potencial impacto no prognóstico a longo prazo permanece por esclarecer.
Referências
[1] Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, et al. Classification of the cardiomyo-
pathies: a position statement from the European Society Of Cardiology Working Group on Myocardial
and Pericardial Diseases. Eur Heart J. 2008;29:270-6.
[2] Mackenzie. The study of the pulse, arterial, venous, and hepatic, and of the movements of the heart. Am
J Med Sci. 1902;124:325.
106
Francisco Sampaio
[3] Haunstetter A, Izumo S. Apoptosis: basic mechanisms and implications for cardiovascular disease. Circ
Res. 1998;82:1111-29.
[4] Capasso JM, Li P, Guideri G, Malhotra A, Cortese R, Anversa P. Myocardial mechanical, biochemical, and
structural alterations induced by chronic ethanol ingestion in rats. Circ Res. 1992;71:346-56.
[5] Beckemeier ME, Bora PS. Fatty acid ethyl esters: potentially toxic products of myocardial ethanol me-
tabolism. J Mol Cell Cardiol. 1998;30:2487-94.
[6] Delbridge LM, Connell PJ, Harris PJ, Morgan TO. Ethanol effects on cardiomyocyte contractility. Clin Sci
(Lond). 2000;98:401-7.
[7] Shorr E, Zweifach BW, Furchgott RF, Baez S. Hepatorenal factors in circulatory homeostasis. IV. Tissue
origins of the vasotropic principles, VEM and VDM, which appear during evolution of hemorrhagi and
tourniquet shock. Circulation. 1951;3:42-79.
[8] Kowalski HJ, Abelmann WH. The cardiac output at rest in Laennec’s cirrhosis. J Clin Invest. 1953;32:1025-
33.
[9] Benoit JN, Womack WA, Hernandez L, Granger DN. “Forward” and “backward” flow mechanisms of
portal hypertension. Relative contributions in the rat model of portal vein stenosis. Gastroenterology.
1985;89:1092-6.
[10] Battarbee HD, Farrar GE, Spears RP. Responses to hypotension in conscious rats with chronic portal
venous hypertension. Am J Physiol. 1990;259:G48-55.
[11] Zavecz JH, Bueno O, Maloney RE, O’Donnell JM, Roerig SC, Battarbee HD. Cardiac excitation-contrac-
tion coupling in the portal hypertensive rat. Am J Physiol Gastrointest Liver Physiol. 2000;279:G28-39.
[12] Laleman W, Landeghem L, Wilmer A, Fevery J, Nevens F. Portal hypertension: from pathophysiology to
clinical practice. Liver Int. 2005;25:1079-90.
[13] Sanyal AJ, Bosch J, Blei A, Arroyo V. Portal hypertension and its complications. Gastroenterology.
2008;134:1715-28.
[14] Hendrickson H, Chatterjee S, Cao S, Morales Ruiz M, Sessa WC, Shah V. Influence of caveolin on cons-
titutively activated recombinant eNOS: insights into eNOS dysfunction in BDL rat liver. Am J Physiol
Gastrointest Liver Physiol. 2003;285:G652-60.
[15] Bolognesi M, Sacerdoti D, Piva A, Di Pascoli M, Zampieri F, Quarta S, et al. Carbon monoxide-mediated
activation of large-conductance calcium-activated potassium channels contributes to mesenteric vaso-
dilatation in cirrhotic rats. J Pharmacol Exp Ther. 2007;321:187-94.
[16] Woitas RP, Heller J, Stoffel-Wagner B, Spengler U, Sauerbruch T. Renal functional reserve and nitric
oxide in patients with compensated liver cirrhosis. Hepatology. 1997;26:858-64.
[17] D’Amico G, Morabito A, Pagliaro L, Marubini E. Survival and prognostic indicators in compensated and
decompensated cirrhosis. Dig Dis Sci. 1986;31:468-75.
[18] Gines P, Quintero E, Arroyo V, Teres J, Bruguera M, Rimola A, et al. Compensated cirrhosis: natural his-
tory and prognostic factors. Hepatology. 1987;7:122-8.
[19] Gerbes AL, Remien J, Jungst D, Sauerbruch T, Paumgartner G. Evidence for down-regulation of beta-2-
adrenoceptors in cirrhotic patients with severe ascites. Lancet. 1986;1:1409-11.
[20] Lee SS, Marty J, Mantz J, Samain E, Braillon A, Lebrec D. Desensitization of myocardial beta-adrenergic
receptors in cirrhotic rats. Hepatology. 1990;12:481-5.
Discussão
107
[21] Ceolotto G, Papparella I, Sticca A, Bova S, Cavalli M, Cargnelli G, et al. An abnormal gene expression of
the beta-adrenergic system contributes to the pathogenesis of cardiomyopathy in cirrhotic rats. Hepa-
tology. 2008;48:1913-23.
[22] Ma Z, Miyamoto A, Lee SS. Role of altered beta-adrenoceptor signal transduction in the pathogenesis
of cirrhotic cardiomyopathy in rats. Gastroenterology. 1996;110:1191-8.
[23] Ma Z, Meddings JB, Lee SS. Membrane physical properties determine cardiac beta-adrenergic receptor
function in cirrhotic rats. Am J Physiol. 1994;267:G87-93.
[24] Ma Z, Lee SS, Meddings JB. Effects of altered cardiac membrane fluidity on beta-adrenergic receptor
signalling in rats with cirrhotic cardiomyopathy. J Hepatol. 1997;26:904-12.
[25] Gazawi H, Ljubuncic P, Cogan U, Hochgraff E, Ben-Shachar D, Bomzon A. The effects of bile acids on
beta-adrenoceptors, fluidity, and the extent of lipid peroxidation in rat cardiac membranes. Biochem
Pharmacol. 2000;59:1623-8.
[26] Ward CA, Liu H, Lee SS. Altered cellular calcium regulatory systems in a rat model of cirrhotic cardio-
myopathy. Gastroenterology. 2001;121:1209-18.
[27] Ward CA, Ma Z, Lee SS, Giles WR. Potassium currents in atrial and ventricular myocytes from a rat
model of cirrhosis. Am J Physiol. 1997;273:G537-44.
[28] Glenn TK, Honar H, Liu H, ter Keurs HE, Lee SS. Role of cardiac myofilament proteins titin and collagen
in the pathogenesis of diastolic dysfunction in cirrhotic rats. J Hepatol. 2011;55:1249-55.
[29] Gaskari SA, Honar H, Lee SS. Therapy insight: Cirrhotic cardiomyopathy. Nat Clin Pract Gastroenterol
Hepatol. 2006;3:329-37.
[30] De Petrocellis L, Cascio MG, Di Marzo V. The endocannabinoid system: a general view and latest addi-
tions. Br J Pharmacol. 2004;141:765-74.
[31] Gaskari SA, Liu H, Moezi L, Li Y, Baik SK, Lee SS. Role of endocannabinoids in the pathogenesis of cir-
rhotic cardiomyopathy in bile duct-ligated rats. Br J Pharmacol. 2005;146:315-23.
[32] Batkai S, Mukhopadhyay P, Harvey-White J, Kechrid R, Pacher P, Kunos G. Endocannabinoids acting at
CB1 receptors mediate the cardiac contractile dysfunction in vivo in cirrhotic rats. Am J Physiol Heart
Circ Physiol. 2007;293:H1689-95.
[33] Liu H, Gaskari SA, Lee SS. Cardiac and vascular changes in cirrhosis: pathogenic mechanisms. World J
Gastroenterol. 2006;12:837-42.
[34] Moezi L, Gaskari SA, Lee SS. Endocannabinoids and liver disease. V. endocannabinoids as mediators of
vascular and cardiac abnormalities in cirrhosis. Am J Physiol Gastrointest Liver Physiol. 2008;295:G649-
53.
[35] Liu H, Ma Z, Lee SS. Contribution of nitric oxide to the pathogenesis of cirrhotic cardiomyopathy in bile
duct-ligated rats. Gastroenterology. 2000;118:937-44.
[36] Herring N, Danson EJ, Paterson DJ. Cholinergic control of heart rate by nitric oxide is site specific.
News Physiol Sci. 2002;17:202-6.
[37] Seddon M, Shah AM, Casadei B. Cardiomyocytes as effectors of nitric oxide signalling. Cardiovasc Res.
2007;75:315-26.
[38] Kim YM, Bombeck CA, Billiar TR. Nitric oxide as a bifunctional regulator of apoptosis. Circ Res.
1999;84:253-6.
[39] van Obbergh L, Vallieres Y, Blaise G. Cardiac modifications occurring in the ascitic rat with biliary cir-
rhosis are nitric oxide related. J Hepatol. 1996;24:747-52.
108
Francisco Sampaio
[40] Garcia-Estan J, Ortiz MC, Lee SS. Nitric oxide and renal and cardiac dysfunction in cirrhosis. Clin Sci
(Lond). 2002;102:213-22.
[41] Liu H, Song D, Lee SS. Role of heme oxygenase-carbon monoxide pathway in pathogenesis of cirrhotic
cardiomyopathy in the rat. Am J Physiol Gastrointest Liver Physiol. 2001;280:G68-74.
[42] Liu H, Lee SS. Nuclear factor-kappaB inhibition improves myocardial contractility in rats with cirrhotic
cardiomyopathy. Liver Int. 2008;28:640-8.
[43] Zardi EM, Abbate A, Zardi DM, Dobrina A, Margiotta D, Van Tassell BW, et al. Cirrhotic cardiomyopathy.
J Am Coll Cardiol. 2010;56:539-49.
[44] Timoh T, Protano MA, Wagman G, Bloom M, Vittorio TJ. A perspective on cirrhotic cardiomyopathy.
Transplant Proc. 2011;43:1649-53.
[45] Moller S, Sondergaard L, Mogelvang J, Henriksen O, Henriksen JH. Decreased right heart blood volume
determined by magnetic resonance imaging: evidence of central underfilling in cirrhosis. Hepatology.
1995;22:472-8.
[46] Rector WG, Jr., Adair O, Hossack KF, Rainguet S. Atrial volume in cirrhosis: relationship to blood volume
and plasma concentration of atrial natriuretic factor. Gastroenterology. 1990;99:766-70.
[47] Valeriano V, Funaro S, Lionetti R, Riggio O, Pulcinelli G, Fiore P, et al. Modification of cardiac function in
cirrhotic patients with and without ascites. Am J Gastroenterol. 2000;95:3200-5.
[48] Keller H, Bezjak V, Stegaru B, Buss J, Holm E, Heene DL. Ventricular function in cirrhosis and portasys-
temic shunt: a two-dimensional echocardiographic study. Hepatology. 1988;8:658-62.
[49] Ahmed SS, Howard M, ten Hove W, Leevy CM, Regan TJ. Cardiac function in alcoholics with cirrhosis:
absence of overt cardiomyopathy--myth or fact? J Am Coll Cardiol. 1984;3:696-702.
[50] Gould L, Shariff M, Zahir M, Di Lieto M. Cardiac hemodynamics in alcoholic patients with chronic liver
disease and a presystolic gallop. J Clin Invest. 1969;48:860-8.
[51] Kelbaek H, Rabol A, Brynjolf I, Eriksen J, Bonnevie O, Godtfredsen J, et al. Haemodynamic response to
exercise in patients with alcoholic liver cirrhosis. Clin Physiol. 1987;7:35-41.
[52] Wong F, Girgrah N, Graba J, Allidina Y, Liu P, Blendis L. The cardiac response to exercise in cirrhosis. Gut.
2001;49:268-75.
[53] Grose RD, Nolan J, Dillon JF, Errington M, Hannan WJ, Bouchier IA, et al. Exercise-induced left ventricu-
lar dysfunction in alcoholic and non-alcoholic cirrhosis. J Hepatol. 1995;22:326-32.
[54] Bernardi M, Rubboli A, Trevisani F, Cancellieri C, Ligabue A, Baraldini M, et al. Reduced cardiovascular
responsiveness to exercise-induced sympathoadrenergic stimulation in patients with cirrhosis. J Hepa-
tol. 1991;12:207-16.
[55] Krag A, Bendtsen F, Mortensen C, Henriksen JH, Moller S. Effects of a single terlipressin administration
on cardiac function and perfusion in cirrhosis. Eur J Gastroenterol Hepatol. 2010;22:1085-92.
[56] Limas CJ, Guiha NH, Lekagul O, Cohn JN. Impaired left ventricular function in alcoholic cirrhosis with
ascites. Ineffectiveness of ouabain. Circulation. 1974;49:754-60.
[57] Laffi G, Barletta G, La Villa G, Del Bene R, Riccardi D, Ticali P, et al. Altered cardiovascular responsiveness
to active tilting in nonalcoholic cirrhosis. Gastroenterology. 1997;113:891-8.
[58] Sicari R, Nihoyannopoulos P, Evangelista A, Kasprzak J, Lancellotti P, Poldermans D, et al. Stress echocar-
diography expert consensus statement: European Association of Echocardiography (EAE) (a registered
branch of the ESC). Eur J Echocardiogr. 2008;9:415-37.
Discussão
109
[59] Dahl EK, Moller S, Kjaer A, Petersen CL, Bendtsen F, Krag A. Diastolic and autonomic dysfunction in
early cirrhosis: a dobutamine stress study. Scand J Gastroenterol. 2014;49:362-72.
[60] Kim MY, Baik SK, Won CS, Park HJ, Jeon HK, Hong HI, et al. Dobutamine stress echocardiography for
evaluating cirrhotic cardiomyopathy in liver cirrhosis. Korean J Hepatol. 2010;16:376-82.
[61] Kazankov K, Holland-Fischer P, Andersen NH, Torp P, Sloth E, Aagaard NK, et al. Resting myocardial
dysfunction in cirrhosis quantified by tissue Doppler imaging. Liver Int. 2011;31:534-40.
[62] Lunseth JH, Olmstead EG, Abboud F. A study of heart disease in one hundred eight hospitalized patients
dying with portal cirrhosis. AMA Arch Intern Med. 1958;102:405-13.
[63] Ortiz-Olvera NX, Castellanos-Pallares G, Gomez-Jimenez LM, Cabrera-Munoz ML, Mendez-Navarro J,
Moran-Villota S, et al. Anatomical cardiac alterations in liver cirrhosis: an autopsy study. Ann Hepatol.
2011;10:321-6.
[64] Lossnitzer D, Steen H, Zahn A, Lehrke S, Weiss C, Weiss KH, et al. Myocardial late gadolinium enhan-
cement cardiovascular magnetic resonance in patients with cirrhosis. J Cardiovasc Magn Reson.
2010;12:47.
[65] How to diagnose diastolic heart failure. European Study Group on Diastolic Heart Failure. Eur Heart J.
1998;19:990-1003.
[66] Wiese S, Hove JD, Bendtsen F, Moller S. Cirrhotic cardiomyopathy: pathogenesis and clinical relevance.
Nat Rev Gastroenterol Hepatol. 2014;11:177-86.
[67] Pozzi M, Carugo S, Boari G, Pecci V, de Ceglia S, Maggiolini S, et al. Evidence of functional and structural
cardiac abnormalities in cirrhotic patients with and without ascites. Hepatology. 1997;26:1131-7.
[68] Wong F, Liu P, Lilly L, Bomzon A, Blendis L. Role of cardiac structural and functional abnormalities in
the pathogenesis of hyperdynamic circulation and renal sodium retention in cirrhosis. Clin Sci (Lond).
1999;97:259-67.
[69] Finucci G, Desideri A, Sacerdoti D, Bolognesi M, Merkel C, Angeli P, et al. Left ventricular diastolic func-
tion in liver cirrhosis. Scand J Gastroenterol. 1996;31:279-84.
[70] Pritchett AM, Mahoney DW, Jacobsen SJ, Rodeheffer RJ, Karon BL, Redfield MM. Diastolic dysfunction
and left atrial volume: a population-based study. J Am Coll Cardiol. 2005;45:87-92.
[71] Douglas PS. The left atrium: a biomarker of chronic diastolic dysfunction and cardiovascular disease risk.
J Am Coll Cardiol. 2003;42:1206-7.
[72] Boomsma F, van den Meiracker AH. Plasma A- and B-type natriuretic peptides: physiology, methodology
and clinical use. Cardiovasc Res. 2001;51:442-9.
[73] Caruana L, Davie AP, Petrie M, McMurray J. Diagnosing heart failure. Eur Heart J. 1999;20:393.
[74] Palmieri V, Innocenti F, Pini R, Celentano A. Reproducibility of Doppler echocardiographic assessment of
left ventricular diastolic function in multicenter setting. J Am Soc Echocardiogr. 2005;18:99-106.
[75] Cahill JM, Horan M, Quigley P, Maurer B, McDonald K. Doppler-echocardiographic indices of diastolic
function in heart failure admissions with preserved left ventricular systolic function. Eur J Heart Fail.
2002;4:473-8.
[76] Thomas MD, Fox KF, Wood DA, Gibbs JS, Coats AJ, Henein MY, et al. Echocardiographic features and
brain natriuretic peptides in patients presenting with heart failure and preserved systolic function. He-
art. 2006;92:603-8.
110
Francisco Sampaio
[77] Petrie MC, Hogg K, Caruana L, McMurray JJ. Poor concordance of commonly used echocardiographic
measures of left ventricular diastolic function in patients with suspected heart failure but preser-
ved systolic function: is there a reliable echocardiographic measure of diastolic dysfunction? Heart.
2004;90:511-7.
[78] Choong CY, Herrmann HC, Weyman AE, Fifer MA. Preload dependence of Doppler-derived indexes of
left ventricular diastolic function in humans. J Am Coll Cardiol. 1987;10:800-8.
[79] Thomas JD, Choong CY, Flachskampf FA, Weyman AE. Analysis of the early transmitral Doppler velocity
curve: effect of primary physiologic changes and compensatory preload adjustment. J Am Coll Cardiol.
1990;16:644-55.
[80] Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, et al. Recommendations for the
evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr. 2009;10:165-93.
[81] Bernardi M, Calandra S, Colantoni A, Trevisani F, Raimondo ML, Sica G, et al. Q-T interval prolongation
in cirrhosis: prevalence, relationship with severity, and etiology of the disease and possible pathogenetic
factors. Hepatology. 1998;27:28-34.
[82] Bal JS, Thuluvath PJ. Prolongation of QTc interval: relationship with etiology and severity of liver disease,
mortality and liver transplantation. Liver Int. 2003;23:243-8.
[83] Ytting H, Henriksen JH, Fuglsang S, Bendtsen F, Moller S. Prolonged Q-T(c) interval in mild portal hyper-
tensive cirrhosis. J Hepatol. 2005;43:637-44.
[84] Henriksen JH, Fuglsang S, Bendtsen F, Christensen E, Moller S. Dyssynchronous electrical and mechani-
cal systole in patients with cirrhosis. J Hepatol. 2002;36:513-20.
[85] Moller S, Henriksen JH. Cardiovascular complications of cirrhosis. Gut. 2008;57:268-78.
[86] Lebrec D, Giuily N, Hadengue A, Vilgrain V, Moreau R, Poynard T, et al. Transjugular intrahepatic por-
tosystemic shunts: comparison with paracentesis in patients with cirrhosis and refractory ascites: a
randomized trial. French Group of Clinicians and a Group of Biologists. J Hepatol. 1996;25:135-44.
[87] Franco D, Vons C, Traynor O, de Smadja C. Should portosystemic shunt be reconsidered in the treat-
ment of intractable ascites in cirrhosis? Arch Surg. 1988;123:987-91.
[88] Kovacs A, Schepke M, Heller J, Schild HH, Flacke S. Short-term effects of transjugular intrahepatic
shunt on cardiac function assessed by cardiac MRI: preliminary results. Cardiovasc Intervent Radiol.
2010;33:290-6.
[89] Gines P, Uriz J, Calahorra B, Garcia-Tsao G, Kamath PS, Del Arbol LR, et al. Transjugular intrahepatic
portosystemic shunting versus paracentesis plus albumin for refractory ascites in cirrhosis. Gastroen-
terology. 2002;123:1839-47.
[90] Huonker M, Schumacher YO, Ochs A, Sorichter S, Keul J, Rossle M. Cardiac function and haemodyna-
mics in alcoholic cirrhosis and effects of the transjugular intrahepatic portosystemic stent shunt. Gut.
1999;44:743-8.
[91] Cazzaniga M, Salerno F, Pagnozzi G, Dionigi E, Visentin S, Cirello I, et al. Diastolic dysfunction is asso-
ciated with poor survival in patients with cirrhosis with transjugular intrahepatic portosystemic shunt.
Gut. 2007;56:869-75.
[92] Rabie RN, Cazzaniga M, Salerno F, Wong F. The use of E/A ratio as a predictor of outcome in cirrhotic pa-
tients treated with transjugular intrahepatic portosystemic shunt. Am J Gastroenterol. 2009;104:2458-
66.
Discussão
111
[93] Ruiz-del-Arbol L, Urman J, Fernandez J, Gonzalez M, Navasa M, Monescillo A, et al. Systemic, renal, and
hepatic hemodynamic derangement in cirrhotic patients with spontaneous bacterial peritonitis. Hepa-
tology. 2003;38:1210-8.
[94] Ruiz-del-Arbol L, Monescillo A, Arocena C, Valer P, Gines P, Moreira V, et al. Circulatory function and
hepatorenal syndrome in cirrhosis. Hepatology. 2005;42:439-47.
[95] Krag A, Bendtsen F, Henriksen JH, Moller S. Low cardiac output predicts development of hepatorenal
syndrome and survival in patients with cirrhosis and ascites. Gut. 2010;59:105-10.
[96] Krag A, Bendtsen F, Burroughs AK, Moller S. The cardiorenal link in advanced cirrhosis. Med Hypotheses.
2012;79:53-5.
[97] Ruiz-del-Arbol L, Achecar L, Serradilla R, Rodriguez-Gandia MA, Rivero M, Garrido E, et al. Diastolic
dysfunction is a predictor of poor outcomes in patients with cirrhosis, portal hypertension, and a nor-
mal creatinine. Hepatology. 2013;58:1732-41.
[98] Alexopoulou A, Papatheodoridis G, Pouriki S, Chrysohoou C, Raftopoulos L, Stefanadis C, et al. Diasto-
lic myocardial dysfunction does not affect survival in patients with cirrhosis. Transpl Int. 2012;25:1174-
81.
[99] Nazar A, Guevara M, Sitges M, Terra C, Sola E, Guigou C, et al. LEFT ventricular function assessed by
echocardiography in cirrhosis: relationship to systemic hemodynamics and renal dysfunction. J Hepatol.
2013;58:51-7.
[100] Edler I, Hertz C. Use of ultrasonic reflectoscope for the continuous recording of movements of heart
walls. Kungl Fysiogr Sallsk Lung Forth 1954;24.
[101] Kirkpatrick JN, Vannan MA, Narula J, Lang RM. Echocardiography in heart failure: applications, utility, and
new horizons. J Am Coll Cardiol. 2007;50:381-96.
[102] Dokainish H, Nguyen JS, Bobek J, Goswami R, Lakkis NM. Assessment of the American Society of
Echocardiography-European Association of Echocardiography guidelines for diastolic function in pa-
tients with depressed ejection fraction: an echocardiographic and invasive haemodynamic study. Eur J
Echocardiogr. 2011;12:857-64.
[103] Nagueh SF, Bhatt R, Vivo RP, Krim SR, Sarvari SI, Russell K, et al. Echocardiographic evaluation of hemo-
dynamics in patients with decompensated systolic heart failure. Circ Cardiovasc Imaging. 2011;4:220-7.
[104] Popescu BA, Andrade MJ, Badano LP, Fox KF, Flachskampf FA, Lancellotti P, et al. European Association
of Echocardiography recommendations for training, competence, and quality improvement in echocar-
diography. Eur J Echocardiogr. 2009;10:893-905.
[105] Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for
chamber quantification. Eur J Echocardiogr. 2006;7:79-108.
[106] McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, et al. ESC Guidelines for the
diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and
Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed
in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787-847.
[107] Appleton CP, Hatle LK, Popp RL. Relation of transmitral flow velocity patterns to left ventricular dias-
tolic function: new insights from a combined hemodynamic and Doppler echocardiographic study. J Am
Coll Cardiol. 1988;12:426-40.
[108] Appleton CP. Influence of incremental changes in heart rate on mitral flow velocity: assessment in
lightly sedated, conscious dogs. J Am Coll Cardiol. 1991;17:227-36.
112
Francisco Sampaio
[109] Mor-Avi V, Lang RM, Badano LP, Belohlavek M, Cardim NM, Derumeaux G, et al. Current and evolving
echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus
statement on methodology and indications endorsed by the Japanese Society of Echocardiography. Eur
J Echocardiogr. 2011;12:167-205.
[110] Teske AJ, De Boeck BW, Melman PG, Sieswerda GT, Doevendans PA, Cramer MJ. Echocardiographic
quantification of myocardial function using tissue deformation imaging, a guide to image acquisition and
analysis using tissue Doppler and speckle tracking. Cardiovasc Ultrasound. 2007;5:27.
[111] Grossman W, Jones D, McLaurin LP. Wall stress and patterns of hypertrophy in the human left ventricle.
J Clin Invest. 1975;56:56-64.
[112] Bijnens BH, Cikes M, Claus P, Sutherland GR. Velocity and deformation imaging for the assessment of
myocardial dysfunction. Eur J Echocardiogr. 2009;10:216-26.
[113] Burns AT, La Gerche A, D’Hooge J, MacIsaac AI, Prior DL. Left ventricular strain and strain rate: charac-
terization of the effect of load in human subjects. Eur J Echocardiogr. 2010;11:283-9.
[114] Mirsky I, Aoyagi T, Crocker VM, Fujii AM. Preload dependence of fiber shortening rate in conscious dogs
with left ventricular hypertrophy. J Am Coll Cardiol. 1990;15:890-9.
[115] Weidemann F, Jamal F, Sutherland GR, Claus P, Kowalski M, Hatle L, et al. Myocardial function defined
by strain rate and strain during alterations in inotropic states and heart rate. Am J Physiol Heart Circ
Physiol. 2002;283:H792-9.
[116] Greenberg NL, Firstenberg MS, Castro PL, Main M, Travaglini A, Odabashian JA, et al. Doppler-derived
myocardial systolic strain rate is a strong index of left ventricular contractility. Circulation. 2002;105:99-
105.
[117] Andersen NH, Poulsen SH, Eiskjaer H, Poulsen PL, Mogensen CE. Decreased left ventricular longitudinal
contraction in normotensive and normoalbuminuric patients with Type II diabetes mellitus: a Doppler
tissue tracking and strain rate echocardiography study. Clin Sci (Lond). 2003;105:59-66.
[118] Cardim N, Oliveira AG, Longo S, Ferreira T, Pereira A, Reis RP, et al. Doppler tissue imaging: regional
myocardial function in hypertrophic cardiomyopathy and in athlete’s heart. J Am Soc Echocardiogr.
2003;16:223-32.
[119] Poulsen SH, Andersen NH, Heickendorff L, Mogensen CE. Relation between plasma amino-terminal
propeptide of procollagen type III and left ventricular longitudinal strain in essential hypertension. He-
art. 2005;91:624-9.
[120] Jurcut R, Wildiers H, Ganame J, D’Hooge J, De Backer J, Denys H, et al. Strain rate imaging detects early
cardiac effects of pegylated liposomal Doxorubicin as adjuvant therapy in elderly patients with breast
cancer. J Am Soc Echocardiogr. 2008;21:1283-9.
[121] Voigt JU, Exner B, Schmiedehausen K, Huchzermeyer C, Reulbach U, Nixdorff U, et al. Strain-rate ima-
ging during dobutamine stress echocardiography provides objective evidence of inducible ischemia.
Circulation. 2003;107:2120-6.
[122] Faber L, Prinz C, Welge D, Hering D, Butz T, Oldenburg O, et al. Peak systolic longitudinal strain of the
lateral left ventricular wall improves after septal ablation for symptomatic hypertrophic obstructive
cardiomyopathy: a follow-up study using speckle tracking echocardiography. Int J Cardiovasc Imaging.
2011;27:325-33.
Discussão
113
[123] Bjork Ingul C, Rozis E, Slordahl SA, Marwick TH. Incremental value of strain rate imaging to wall motion
analysis for prediction of outcome in patients undergoing dobutamine stress echocardiography. Circu-
lation. 2007;115:1252-9.
[124] Weidemann F, Jung P, Hoyer C, Broscheit J, Voelker W, Ertl G, et al. Assessment of the contractile reserve
in patients with intermediate coronary lesions: a strain rate imaging study validated by invasive myocar-
dial fractional flow reserve. Eur Heart J. 2007;28:1425-32.
[125] Yu CM, Sanderson JE, Marwick TH, Oh JK. Tissue Doppler imaging a new prognosticator for cardiovas-
cular diseases. J Am Coll Cardiol. 2007;49:1903-14.
[126] Jasaityte R, Dandel M, Lehmkuhl H, Hetzer R. Prediction of short-term outcomes in patients with idio-
pathic dilated cardiomyopathy referred for transplantation using standard echocardiography and strain
imaging. Transplant Proc. 2009;41:277-80.
[127] Nagueh SF, Sun H, Kopelen HA, Middleton KJ, Khoury DS. Hemodynamic determinants of the mitral
annulus diastolic velocities by tissue Doppler. J Am Coll Cardiol. 2001;37:278-85.
[128] Oki T, Tabata T, Yamada H, Wakatsuki T, Shinohara H, Nishikado A, et al. Clinical application of pulsed
Doppler tissue imaging for assessing abnormal left ventricular relaxation. Am J Cardiol. 1997;79:921-8.
[129] Sohn DW, Chai IH, Lee DJ, Kim HC, Kim HS, Oh BH, et al. Assessment of mitral annulus velocity
by Doppler tissue imaging in the evaluation of left ventricular diastolic function. J Am Coll Cardiol.
1997;30:474-80.
[130] Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, et al. Clinical utility of Doppler
echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A
comparative simultaneous Doppler-catheterization study. Circulation. 2000;102:1788-94.
[131] Dokainish H, Zoghbi WA, Lakkis NM, Al-Bakshy F, Dhir M, Quinones MA, et al. Optimal noninvasive
assessment of left ventricular filling pressures: a comparison of tissue Doppler echocardiography and
B-type natriuretic peptide in patients with pulmonary artery catheters. Circulation. 2004;109:2432-9.
[132] Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, et al. How to diagnose
diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventri-
cular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society
of Cardiology. Eur Heart J. 2007;28:2539-50.
[133] Lima JA, Desai MY. Cardiovascular magnetic resonance imaging: current and emerging applications. J Am
Coll Cardiol. 2004;44:1164-71.
[134] Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA, Friedrich MG, et al. ACCF/ACR/AHA/NAS-
CI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the
American College of Cardiology Foundation Task Force on Expert Consensus Documents. Circulation.
2010;121:2462-508.
[135] Zerhouni EA, Parish DM, Rogers WJ, Yang A, Shapiro EP. Human heart: tagging with MR imaging--a me-
thod for noninvasive assessment of myocardial motion. Radiology. 1988;169:59-63.
[136] Lawton JS, Cupps BP, Knutsen AK, Ma N, Brady BD, Reynolds LM, et al. Magnetic resonance imaging
detects significant sex differences in human myocardial strain. Biomed Eng Online. 2011;10:76.
[137] Hor KN, Gottliebson WM, Carson C, Wash E, Cnota J, Fleck R, et al. Comparison of magnetic reso-
nance feature tracking for strain calculation with harmonic phase imaging analysis. JACC Cardiovasc
Imaging. 2010;3:144-51.

114
Francisco Sampaio
[138] Schuster A, Kutty S, Padiyath A, Parish V, Gribben P, Danford DA, et al. Cardiovascular magnetic resonan-
ce myocardial feature tracking detects quantitative wall motion during dobutamine stress. J Cardiovasc
Magn Reson. 2011;13:58.
[139] Zagrosek A, Abdel-Aty H, Boye P, Wassmuth R, Messroghli D, Utz W, et al. Cardiac magnetic resonan-
ce monitors reversible and irreversible myocardial injury in myocarditis. JACC Cardiovasc Imaging.
2009;2:131-8.
[140] Iles L, Pfluger H, Phrommintikul A, Cherayath J, Aksit P, Gupta SN, et al. Evaluation of diffuse myocardial
fibrosis in heart failure with cardiac magnetic resonance contrast-enhanced T1 mapping. J Am Coll
Cardiol. 2008;52:1574-80.
[141] Schuster A, Morton G, Chiribiri A, Perera D, Vanoverschelde JL, Nagel E. Imaging in the management of
ischemic cardiomyopathy: special focus on magnetic resonance. J Am Coll Cardiol. 2012;59:359-70.
[142] Bruch C, Gradaus R, Gunia S, Breithardt G, Wichter T. Doppler tissue analysis of mitral annular veloci-
ties: evidence for systolic abnormalities in patients with diastolic heart failure. J Am Soc Echocardiogr.
2003;16:1031-6.
[143] Vinereanu D, Lim PO, Frenneaux MP, Fraser AG. Reduced myocardial velocities of left ventricular long-
axis contraction identify both systolic and diastolic heart failure-a comparison with brain natriuretic
peptide. Eur J Heart Fail. 2005;7:512-9.
[144] Vinereanu D, Nicolaides E, Tweddel AC, Fraser AG. “Pure” diastolic dysfunction is associated with long-
axis systolic dysfunction. Implications for the diagnosis and classification of heart failure. Eur J Heart
Fail. 2005;7:820-8.
[145] Yip G, Wang M, Zhang Y, Fung JW, Ho PY, Sanderson JE. Left ventricular long axis function in diastolic
heart failure is reduced in both diastole and systole: time for a redefinition? Heart. 2002;87:121-5.
[146] Tsang TS, Barnes ME, Gersh BJ, Bailey KR, Seward JB. Left atrial volume as a morphophysiologic expres-
sion of left ventricular diastolic dysfunction and relation to cardiovascular risk burden. Am J Cardiol.
2002;90:1284-9.
[147] Cameli M, Lisi M, Focardi M, Reccia R, Natali BM, Sparla S, et al. Left atrial deformation analysis by speck-
le tracking echocardiography for prediction of cardiovascular outcomes. Am J Cardiol. 2012;110:264-9.
[148] Rihal CS, Nishimura RA, Hatle LK, Bailey KR, Tajik AJ. Systolic and diastolic dysfunction in patients
with clinical diagnosis of dilated cardiomyopathy. Relation to symptoms and prognosis. Circulation.
1994;90:2772-9.
[149] Lapu-Bula R, Robert A, De Kock M, D’Hondt AM, Detry JM, Melin JA, et al. Relation of exercise capacity
to left ventricular systolic function and diastolic filling in idiopathic or ischemic dilated cardiomyopathy.
Am J Cardiol. 1999;83:728-34.
[150] Capomolla S, Pinna GD, Febo O, Caporotondi A, Guazzotti G, La Rovere MT, et al. Echo-Doppler mitral
flow monitoring: an operative tool to evaluate day-to-day tolerance to and effectiveness of beta-adre-
nergic blocking agent therapy in patients with chronic heart failure. J Am Coll Cardiol. 2001;38:1675-84.

VI. Conclusões


Conclusões
117
• Os doentes com cirrose hepática exibem alterações da função sistólica, quer em repou-
so quer sob stress farmacológico. No entanto estas alterações são subtis e podem ser
detectáveis apenas com recurso a métodos de imagiologia cardíaca avançada.
• A prevalência de disfunção diastólica nesta população poderá ser inferior à estimada
com base em relatos prévios. A utilização de parâmetros “clássicos” de disfunção dias-
tólica, muito influenciados pela volémia, pode não ser adequada nesta população. A sua
interpretação deve ser cautelosa.
• A disfunção sistólica e diastólica encontrada não parece ser suficientemente grave para
influenciar o prognóstico a médio prazo, não se tendo associado à mortalidade a 6 me-
ses. O seu potencial impacto no prognóstico a longo prazo permanece por estabelecer.


VII. Resumo/Abstract

Resumo/Abstract
121
RESUMO
A cardiomiopatia cirrótica é uma entidade descrita nas últimas décadas, caracterizada pela
presença de disfunção cardíaca crónica manifestada por atenuação da resposta contráctil ao
stress e/ou anomalias do relaxamento ventricular e alterações electrofisiológicas, na ausência
de outra doença cardíaca. A sua patofisiologia é complexa e não está totalmente elucidada.
Estudos com modelos animais de cirrose demonstraram o envolvimento de múltiplos mecanis-
mos, como a diminuição da densidade e função dos receptores adrenérgicos beta, alterações
dos canais iónicos da membrana dos cardiomiócitos, alteração das proteínas contrácteis e da
matriz extracelular, e excesso de produção de substâncias com efeitos vasodilatadores, e pró-
apoptóticos como o óxido nítrico, citocinas pró-inflamatórias ou canabinóides endógenos. A
sua prevalência real é desconhecida, muito pelo facto de poder ser bem tolerada e assintomá-
tica durante anos, em virtude da vasodilatação arteriolar esplâncnica característica da circu-
lação na cirrose poder diminuir a sobrecarga do ventrículo esquerdo e atenuar os efeitos da
disfunção muscular cardíaca. Deste modo, índices clássicos de função sistólica (como a fracção
de ejecção ou o volume de ejecção) são frequentemente normais nestes doentes. A cardio-
miopatia cirrótica é uma entidade descrita nas últimas décadas, caracterizada pela presença
de disfunção cardíaca crónica manifestada por atenuação da resposta contráctil ao stress e/
ou anomalias do relaxamento ventricular e alterações electrofisiológicas, na ausência de outra
doença cardíaca. A relação entre a gravidade da doença hepática e o atingimento cardíaco su-
gerida em alguns estudos também não está totalmente esclarecida, bem como a influência das
alterações cardíacas no prognóstico dos doentes cirróticos.
Foi assim nosso objectivo proceder a uma análise detalhada da função miocárdica, usando
métodos modernos de imagiologia cardíaca não invasiva (ecocardiografia e ressonância mag-
nética cardíaca) em doentes com cirrose hepática de diferentes etiologias, tentando encontrar
novos marcadores de cardiomiopatia cirrótica, bem como avaliar a correlação entre disfunção
cardiovascular e a etiologia e gravidade da doença hepática e o potencial impacto prognóstico
das alterações encontradas.

122
Francisco Sampaio
Com os trabalhos desenvolvidos, identificámos a existência de disfunção sistólica subclínica
– particularmente disfunção do componente longitudinal da deformação miocárdica durante a
sístole ventricular - na população estudada, quer em repouso, quer sob estimulação inotrópica,
apesar da normalidade da fracção de ejecção na maioria dos doentes. Esta disfunção foi inde-
pendente da gravidade da doença, sendo possível encontrar alterações na resposta ao stress
mesmo em indivíduos estáveis com doença ligeira. Documentámos igualmente a alteração de
vários parâmetros de função diastólica nos doentes, quando comparados com um grupo con-
trolo. No entanto, a prevalência de disfunção diastólica quando se aplicaram os critérios mais
recentes para a definição desta entidade foi significativamente inferior à previamente relatada.
Encontrámos, porém, uma associação entre alguns destes índices de disfunção diastólica e a
volémia, corroborando a sua elevada dependência das condições de carga e tornando-os, assim,
potencialmente pouco adequados para o estudo da função diastólica no contexto da cirrose
hepática. Finalmente não conseguimos encontrar uma associação entre nenhum dos parâme-
tros ecocardiográficos avaliados e o prognóstico a médio prazo. Os únicos marcadores inde-
pendentes de mortalidade aos 6 meses foram a tensão arterial média e a gravidade da doença
hepática avaliada pela classificação de Child-Pugh.
Concluímos assim que os doentes com cirrose hepática exibem sinais de disfunção sistólica
e diastólica, mas que esta parece ser subtil, podendo ser detectável apenas com recurso a mé-
todos de imagiologia cardíaca avançada. Neste sentido a disfunção miocárdica encontrada não
parece ser suficientemente grave para influenciar o prognóstico a médio prazo. A mortalidade
a 6 meses parece ser muito mais influenciada pela gravidade da insuficiência hepática e pelas
alterações hemodinâmicas que lhe estão associadas.

Resumo/Abstract
123
ABSTRACT
Cirrhotic cardiomyopathy has been described as a condition characterized by impaired con-
tractile response to stress, diastolic dysfunction and electrophysiological abnormalities, in the
absence of known cardiac disease. The pathophysiology of this condition is complex and not
fully understood. Experimental evidence of decreased density and down-regulation of beta-
adrenergic receptors as well as hypo-responsiveness of cardiomyocytes to beta-adrenergic
agonists has been found in animal models of cirrhosis. Dysfunction of several ion channels
on the plasma membrane, changes in contractile proteins and extracellular matrix, as well as
excess production of different substances (nitric oxide, pro-inflammatory cytokines or endo-
genous cannabinoids) with vasodilator and pro-apoptotic effect have also been involved. Cir-
rhotic cardiomyopathy seems to be well tolerated and asymptomatic for years and its real pre-
valence is unknown. Splanchnic arterial vasodilatation may unload the left ventricle and mask
the presence of cardiac insufficiency. In fact, conventional indices of systolic function such as
ejection fraction are usually normal in these patients. Hence, although some diagnostic criteria
have been previously proposed, they are controversial and an accepted gold-standard method
to diagnose cirrhotic cardiomyopathy is still lacking. On the other hand, the correlation betwe-
en liver disease severity and the degree of cardiac dysfunction is unclear and the influence of
cardiac abnormalities in cirrhosis natural history is also undetermined.
We aimed to perform a comprehensive analysis of left ventricular function, using advanced
non-invasive imaging modalities, in patients with liver cirrhosis of different aetiologies, in order
to find new markers of cirrhotic cardiomyopathy and to assess their potential prognostic im-
pact. We also aimed to evaluate the correlation between cardiac dysfunction and liver disease
severity.
In our studies, we were able to find evidence of subclinical systolic dysfunction in cirrhotic
patients, mainly due to impairment of left ventricular longitudinal deformation. These abnor-
malities were present both at rest and during pharmacological stress and were irrespective
of liver disease severity. Ejection fraction was normal in the majority of the study sample. We

124
Francisco Sampaio
could also find signs of diastolic dysfunction in our patients. However, when the current recom-
mendations for diagnosing diastolic dysfunction were applied, the prevalence of this entity was
lower than previously reported, using a different methodology. We found a correlation betwe-
en some of the parameters classically used to evaluate diastolic function and markers of vola-
emia. These findings support the known influence of loading conditions on those parameters,
suggesting that they may be unsuitable to assess diastolic dysfunction in cirrhosis. Finally, we
did not find an association between any echocardiographic parameters of systolic or diastolic
function and the occurrence of death at 6 months. Child-Pugh score and mean blood pressure
were the only independent predictors of mortality.
From our results, we could conclude that there is evidence of myocardial dysfunction in
cirrhotic patients. However, these abnormalities seem to be subtle and may only be detected
by advanced and sensitive imaging techniques. On the other hand, liver failure severity and
associated hemodynamic changes seem to be more important determinants of medium-term
prognosis than myocardial dysfunction.





























