Embed Size (px)
Citation preview

CARE OF EXPOSED - NEW
BORNTópico: Cuidados a um
recém-nascido exposto

Where would you prefer to be right now?
Mauritius resort? Attending a workshop?
Cuidados a um recém-nascido
exposto
• História: Uma menina infantil foi internada em uma unidade de internação pediátrica pela primeira vez aos cinco meses de idade. A criança tinha doença diarréica e em estado de choque. Ela nasceu por parto normal. Um programa de PMTCT não foi disponível a sua mãe.
• Resultados laboratoriais: A hemoglobina foi de 9 gramas por decilitro. Não havia teste de PCR disponível, mas um teste de anticorpo contra o HIV (ELISA) era positivo. Sua mãe testou HIV positivo.
• Diagnósticos clínicos de HIV/AIDS e anemia de deficiência de ferro foram feitos no momento.
• A criança estava abaixo do peso para a idade (abaixo do percentil 3) no momento. Durante os 6 meses seguintes, a criança foi admitida mais 4 vezes, com diarréia e com pneumonia

• Exame físico: Durante o ano seguinte, observou-se que a criança permaneceu magra, com linfadenopatia generalizada. Havia uma erupção cutânea impetiginizada de pele sobre ambas as pernas de vez em quando. Não houve hepatomegalia ou esplenomegalia. O ganho de peso foi fraco e o peso para a idade permaneceu abaixo do terceiro percentil.
• A criança foi vista mensalmente em serviços de pacientes externos e recebeu o suplemento macronutritivo na forma de leite Pelargon e cereal de arroz. O peso permaneceu abaixo do terceiro percentil. Os micronutrimentos foram fornecidos, na forma da Vitamina A 200 000 IU cada 6 meses, Zinco (10 mgs diariamente) e xarope de multivitamina. Ela recebeu o suplemento de ferro. Ela recebeu a profilaxia Bactrim. A terapia de Anti-retroviral não foi disponível
• A quinta admissão da criança foi após ingestão de parafina, cerca de três meses após a última admissão para diarréia. Havia sinais de dificuldade respiratória, mas estes foram resolvidos durante um período de cinco dias. O peso da criança tinha aumentado e o peso para a idade estava agora no percentil 10.
• A criança não teve mais admissões hospitalares. Ela continuou ganhando o peso e seu gráfico altura-por-idade cruzou o percentil 50 aos 18 meses de idade.
• Uma repetição do teste de anticorpos para HIV ELISA nesse momento foi negativo.

Questões:
1. Em que estágio clínico você colocaria essa criança antes que os resultados finais fossem obtidos? Qual é o seu critério de classificação?
2. Que erros diagnósticos foram cometidos neste cenário?
3. Porquê essa criança não conseguia desenvolver-se?
4. Porquê esse bebê HIV-negativo apresentou uma história sugerindo infecção pelo HIV?

By The End Of This Session You
Will be Expected to understand the following …
� Understand care of HEU Infant
� Understand different risk factors faced by HEU babies vs. HU babies
� Postpartum Care / management of Exposed Infant
� Routine Follow up of HEU Infant
� Growth Monitoring
� IPT in HEU Newborn
� Management of TB Exposed HEU newborn
HIV Exposed Uninfected Newborn
• Despite escaping HIV infection, HEU (HIV
Exposed Uninfected) children bear
consequences of being born to an HIV-
infected mother.
• Higher vulnerability to infectious diseases
during infancy
• HEU children experience more challenges
than HIV unexposed (HU) children

Overall Infant Risk Factors

Specific Disease Spectrum observed
in HEU Children
• Greater severity of common childhood infections, particularly pneumonia, B streptococcus and invasive pneumococcal disease.
• Growth and neurodevelopmental consequences of in utero exposure to some ARVs
• Increases risk for congenital cytomegalovirus (CMV) and it is important to be alert to the potential delayed neurologic sequelae of congenital CMV such as hearing impairment and neurodevelopmental delay.

• Commence life with lower levels of maternally derived antibody than HU infants.
• Respond robustly to vaccination – Must receive timeous administration of all routine infant vaccinations according to national schedules
• High rates of TB exposure in the home, with 10% of HEU infants already exposed to TB by three to four months of age in a South African study.
• Primary isoniazid preventive therapy in the absence of a known TB contact however did not reduce the risk of TB infection or disease in HEU infants.

CARE OF EXPOSED UN-INFECTED NEW BORN
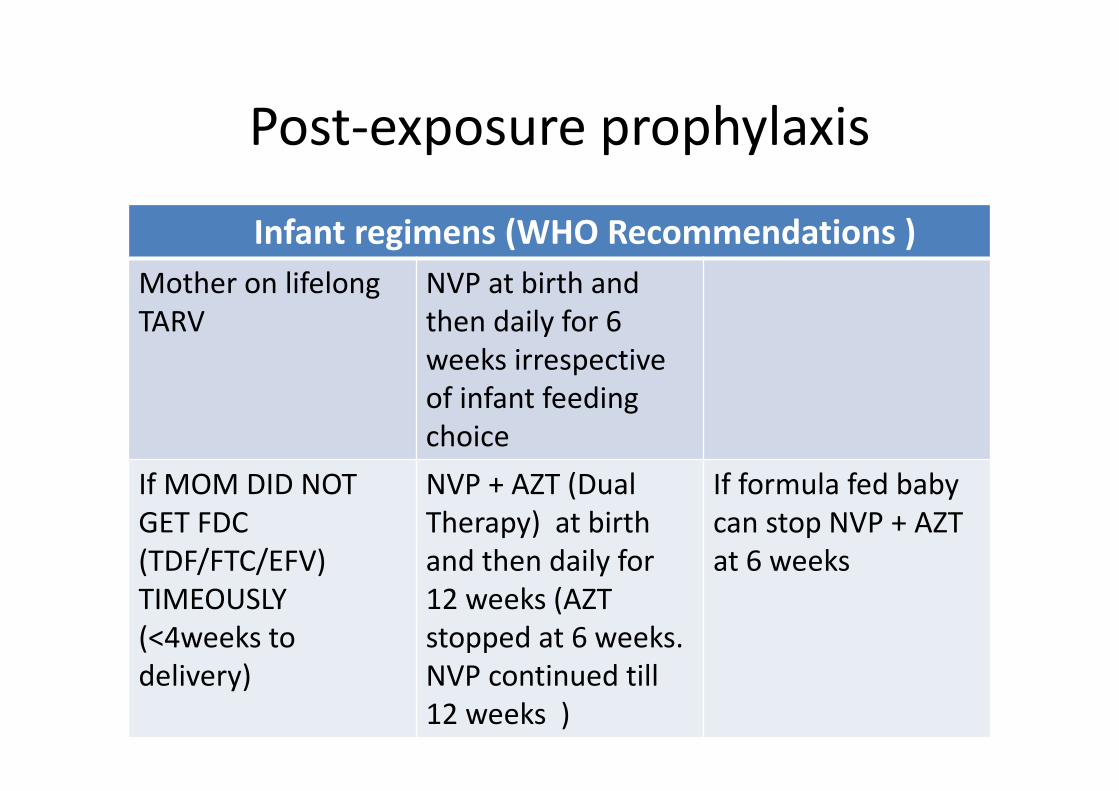
Post-exposure prophylaxis
Infant regimens (WHO Recommendations )
Mother on lifelong
TARV
NVP at birth and
then daily for 6
weeks irrespective
of infant feeding
choice
If MOM DID NOT
GET FDC
(TDF/FTC/EFV)
TIMEOUSLY
(<4weeks to
delivery)
NVP + AZT (Dual
Therapy) at birth
and then daily for
12 weeks (AZT
stopped at 6 weeks.
NVP continued till
12 weeks )
If formula fed baby
can stop NVP + AZT
at 6 weeks

Post-exposure prophylaxis
Infant Regimens
Mother did not get
any ARV before or
during delivery
NVP + AZT as soon
as possible and daily
for 12 weeks (AZT
for 7 Days till PCR
results received )
Urgently) assess
whether mother
needs ART
Unknown maternal
status, orphan or
abandoned
Give immediate NVP
if baby is HIV
antibody positive (
i.e. HIV exposed )
Do PCR immediately
Follow up 10 week
HIV DNA PCR

Prophylactic nevirapine for HIV-exposed
infants
Age or weight Nevirapine
Birth – 6 weeks
< 2.5 kg 10mg/day
≥ 2.5 kg 15mg/day
> 6 week – 6 months 20mg/day
6 months – 9 months 30mg/day
> 9 months until breastfeeding
stops

Follow up of the HIV-exposed infant• HIV-exposed infants need close follow up:
– 3 days – Monthly for first 6 months– 3 monthly until HIV status determined
• Streamline this with CCR visits :• 3 days• 4-6 weeks• 10 weeks• 14 weeks• Monthly thereafter

Follow up schedule
3 days Did infant get PEP? If not, give it now
Check for jaundice, growth, general condition
Assess feeding
Educate on Importance of Attending CCR and Testing Baby
4 weeks – 6weeks IMCI assessment: Infection? Growth, Feeding
Immunize
Start co-trimoxazole
Stop NVP
Moz (PCR ) - WHO does not recommend this why ?
10 weeks HIV PCR test result and counselling
•HIV positive: do CD4 and Confirmatory PCR, continue CTX
• stop NVP and initiate ART
•HIV negative stop CTX if formula fed
IMCI assessment
Immunize

Care of Newborn & Infant
Follow-up care of infant
• Assessment of infant or young child growth and development
• Assessment and support of infant or young child feeding
• Assessment of mother’s coping
• Assessment of signs and symptoms of HIV-related conditions and clinical features of AIDS
• Routine immunizations
• Counselling (for mother) according to identified needs
• Referrals for mother and child
• HIV testing (PCR testing at four to six weeks of age and HIV antibody testing at 18 months)
18
Guidance on Infant Feeding
• Discussions about infant feeding especially important in early months of life and during special high-risk periods:
– Child is sick
– Mother returns to work
– Mother decides to change feeding methods
Mother knows she is feeding baby adequately when:
• Baby gains weight
• Baby urinates 6 to 8 times in 24-hour period
• Baby had at least 2 to 5 bowel movements in a 24-hour period
19

Ongoing Care
Immunization
Dentists
Growth monitoring Dietary advice
Counselling& support
Prophylaxis
Vitamin A Vermifugemmmmmmmm
mmmmm

• Vitamin A
Non-breastfed infants 0-5 months, 50 000 IU, a single dose at the age of 6 weeks.
All infants 6-11 months, 100 000 IU, single dose at 6-11months (preferably at 9 months when child comes for immunization).
All children 1-5 years, 200 000 IU, single dose at 12 months and every 6 months until the age of 5 years.
Vitamin A Supplementation (continued)
• Children with persistent diarrhoea, measles,
severe malnutrition and xerophthalmia should
receive treatment dose of vitamin A even if
they received vitamin A supplement within the
past 6 months. .
22
Promote Health through Follow-Up
Each visit with HCW should include:
• Assess and manage for common illnesses
• Identify non-specific symptoms / conditions related to HIV infection
• Provide HIV testing
• Provide micronutrient supplementation, nutrition education and support including information on food hygiene and fortified foods
• Provide Cotrimoxazole
• Assess clinical features suggestive of HIV .
23

Promote Health through Follow-Up (continued)
Promote health and prevention of illness– Assess and support the mother's infant-feeding
choice.
– Infants who fail to grow require special attention.
– Underlying infections should be diagnosed and treated promptly.
– Monitor growth and assess causes of growth failure, if observed
– Immunize according to the guidelines
– Screen for TB and treat if indicated.
– Offer malaria treatment and prophylaxis
– Treat anaemia as indicated
24
Growth Monitoring
• Growth-monitoring programmes focus on foetal growth and child growth in first five years of life.
• Conditions related to weight loss are underlying infection, acute diarrhoea and HIV-related growth failure.
Growth indicators
• Weight for age is useful for detecting the sum total of nutritional experiences the child has had.
• Weight for height is a useful measure of acute malnutrition.
• Height for age is useful for detecting chronic malnutrition and helps identify stunted growth in children.
• Head circumference is useful during the first two years and is a measure of brain growth - Helps identify Encephalopathy
25

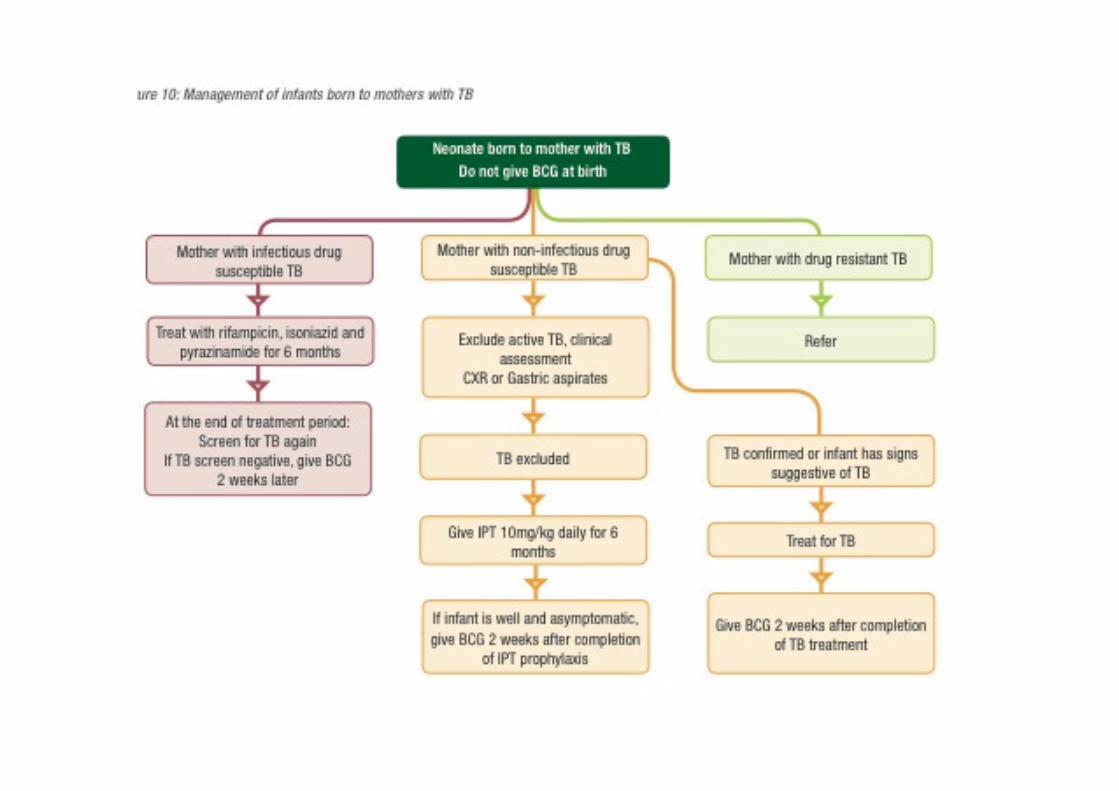
Isoniazid Preventive Therapy
• Babies born to mothers with smear-positive
PTB should be given isoniazid.
– 5mg/kg daily for 6 months
• After 6 months child is vaccinated with BCG.
• Breast feeding is safe
• If child develops symptoms while on isoniazid
preventive therapy, must investigate for TB.
• If TB is diagnosed, isoniazid is stopped and anti-
TB treatment instituted.
Malawi PMTCT Training Package 26

Contact screening algorithm for children
Documented TB exposureClose contact with an adult or adolescent with pulmonary TB or child with smear-positive TB
Close contact is defined as any household contact or contact outside the household that is of sufficient duration and proximity to pose a high risk
of infection.
Are there any current symptoms or signs suspicious of TB?
Cough, wheeze, fever, lethargy, fatigue, weight loss, or visible mass in the neck
No current symptoms or signs Symptoms or signs present
<5yrs HIV negative or
HIV positive≥5yrs and
HIV-uninfected
Observe for symptoms Evaluate / refer if symptoms indicative of TB
INH for 6/12 No preventive therapy
Investigate for TB
No TB TB diagnosed
Persistent non-remitting symptoms
Child is well Treat for TBEnter into TB register
Follow up after 1-2 weeks
Refer to hospital

Dr ND NHLAPO
EARLY INFANT DIAGNOSIS & PAEDS HIV TESTING

• Some African Countries 1:3 women of child-bearing age is HIV-
infected
• HIV prevalence in women attending antenatal
Care is: 29%
• Without PMTCT interventions:
– 40% of infants will be HIV infected during pregnancy,
birth, and BF
• Of the infants infected, median survival is one year
• More than 50% of children infected with HIV
vertically will die by 2 years old with no intervention.
Overview

Because death and disability is high for
HIV-infected infants, every effort must
be undertaken to accurately diagnose
and initiate treatment as soon as possible.
Key strategies to optimise Paediatric HIV
outcomes
1) Prevention and Elimination of Mother To
Child Transmission (P/EMTCT)
2) Early Infant Diagnosis (EID)
3) Increased uptake of Co-trimoxazole
initiation
4) Early initiation of HAART in infants and children
PMTCT
• Successful in reducing transmission of
HIV from mother to child
• In Southern Africa , has reduced rate of MTCT
to 2.6% (2013 target 7.5%)
• Contributed to significant decrease (25%) in
infant mortality rate from 2009 – 2011
• Retention of pregnant women on ART
remains a challenge, roll out of option B+
• To be covered in detail elsewhere
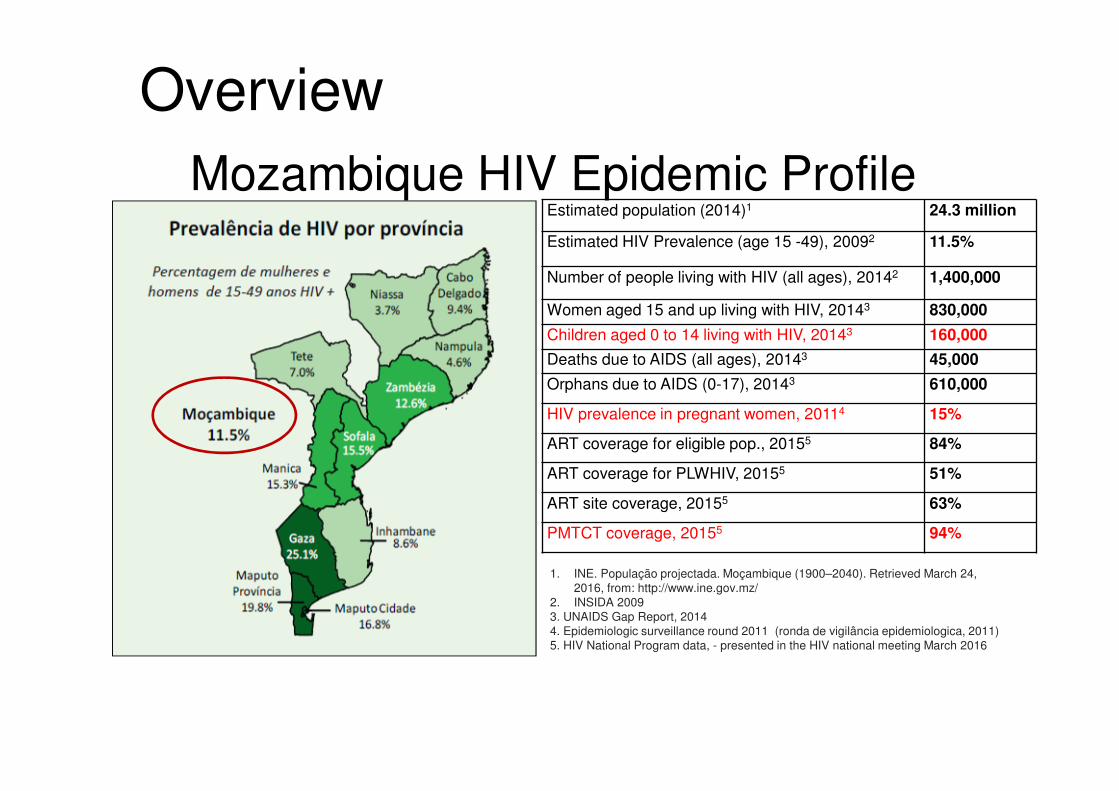
1. INE. População projectada. Moçambique (1900–2040). Retrieved March 24,
2016, from: http://www.ine.gov.mz/
2. INSIDA 2009
3. UNAIDS Gap Report, 2014
4. Epidemiologic surveillance round 2011 (ronda de vigilância epidemiologica, 2011)
5. HIV National Program data, - presented in the HIV national meeting March 2016
Mozambique HIV Epidemic ProfileEstimated population (2014)1 24.3 million
Estimated HIV Prevalence (age 15 -49), 20092 11.5%
Number of people living with HIV (all ages), 20142 1,400,000
Women aged 15 and up living with HIV, 20143 830,000
Children aged 0 to 14 living with HIV, 20143 160,000
Deaths due to AIDS (all ages), 20143 45,000
Orphans due to AIDS (0-17), 20143 610,000
HIV prevalence in pregnant women, 20114 15%
ART coverage for eligible pop., 20155 84%
ART coverage for PLWHIV, 20155 51%
ART site coverage, 20155 63%
PMTCT coverage, 20155 94%
Overview

Early infant diagnosis
What test?
HOW WOULD YOU BEST
DEFINE :
“HIV EXPOSED BABY “ ?

HIV-EXPOSED INFANTS
• An HIV-exposed child is defined as a child born
to a mother living with HIV until HIV exposure
stops (6 weeks after the complete cessation of
breast feeding) and HIV infection can be excluded.
• HIV-exposure status should be determined
before birth as part of the PMTCT programme –
where the mother’s status is not known, this should be determined after birth

How to find Children with HIV• Screen for HIV exposure at all points of routine contact with infants and
children (i.e. EPI clinics)
– Rationale—lots of exposure to young infants (use as a safety net to capture
exposed infants LTFU from PMTCT cascade)
• Perform Routine Provider Initiated Testing & Counseling (PITC)
• in all areas where sick children are seen (OPD, malnutrition clinics/wards, TB
clinics/wards, in-patient wards)
– Rationale—infants and children with HIV who have not been tested get sick
when their immune system wanes
• Test high risk populations (children of HIV+ adults in care and treatment,
OVCs, key population youth)
– Rationale—these children/youth are high risk based on in-utero
exposure to HIV, possible parental loss due to HIV, or personal high risk
behaviors

40
HIV test used for diagnosis
• For adult and Children (From 9 months).
oDETERMINE;
oUNIGOLD for confirmation if determine is
positive.
• For Children under 9 months
o PCR DNA.

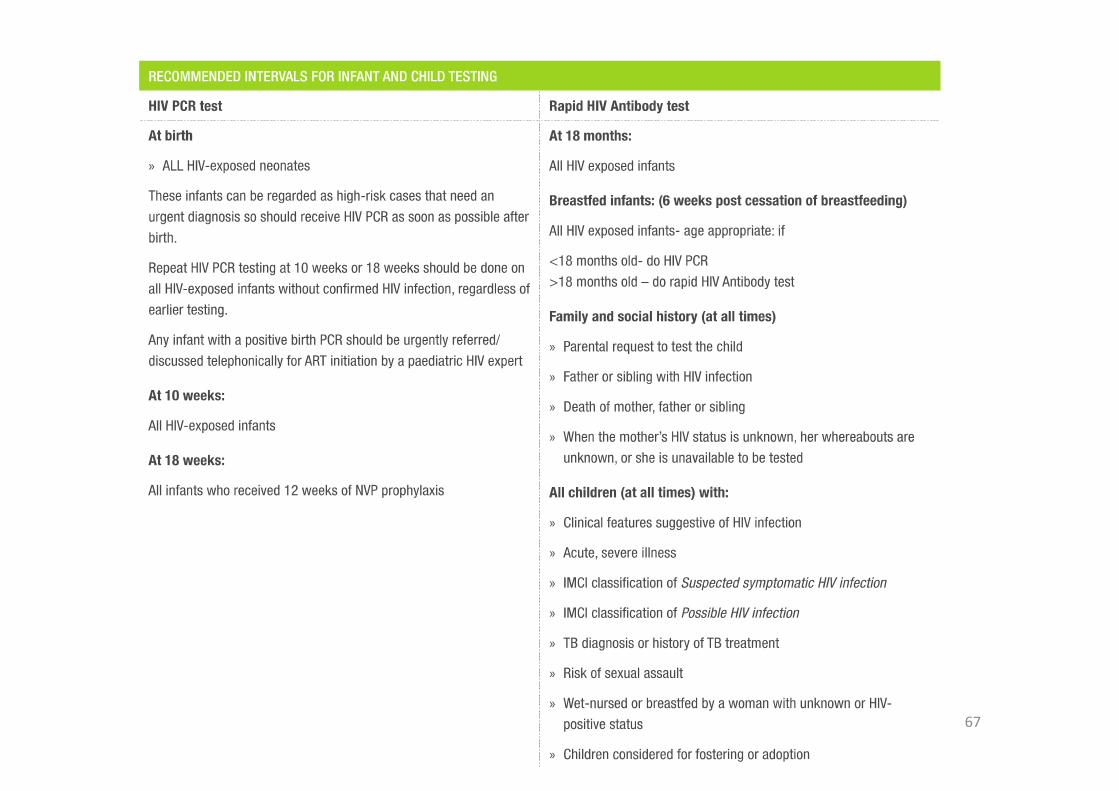
HIV ELISA or Rapid test
• Detects antibodies to the virus (not the virus!)
• Infants born to HIV-infected women test
POSITIVE – Maternal HIV antibodies cross the placenta
– Maternal HIV antibodies may last up to 18 months but
often disappear by 9 months of age
• Used to diagnose adults or children > 18 months
• Can be used to determine HIV exposure in
children < 18 months (< 9months in Moz )
These tests do not diagnose infection in children <18mo:
the mother’s antibodies may still be present
HIV Testing: HIV Antibody Tests
• Rapid tests are cheap, fast, simple, and accurate.
• Highly sensitive and specific – > 99.3%, > 98.6%
respectively
• May be positive in ALL infants of HIV-infected
mothers for up to 18 months because they will have
mom’s IgG, including infants that are not infected
= diagnose exposure only
• If it is necessary to diagnose HIV infection in an
infant less than 9- 18mo then order an HIV PCR test
• ALL HIV-exposed infants should get an ab test at
18mo

HIV Testing: HIV Antibody Tests
• CAUTION with using an Ab test in an infant who is 18mo and who is still breastfeeding
• A positive antibody test in a child >18mo who is BF means that the baby is HIV-infected.
– A negative antibody test in a child >18mo who is BF means that the infant is most likely HIV-negative but:
• Could be in the “window period” before an Ab test is
positive and so might not be HIV-negative
• Will need another Ab test 6 weeks after total
cessation of BF – might still be in the window period so use caution

44
1ST Test DETERMINE
POSITIVE
2nd Test UNIGOLD
Negative
INCONCLUSIVE
If maintain undetermined, make appointment for retest
after 4 weeks
In the following visit (2nd) repeat the Protocol and define the result in Visit
HIV Positive HIV Negative INCONCLUSIVE
Make appointment for new testing after 8 weeks to
collect blood specimen to be sent to a reference lab.
Positive
NEGATIVE
In 3rd Visit use the result from
reference Lab. If there is no result yet,
repeat the protocol if maintain
undermined report HIV Negative
Report HIV Negative
Report HIV Positive
Repeat
immediately
the protocol
Algorithm

HIV DNA PCR test• Detects virus in the baby’s cells
• A positive HIV PCR test means HIV infection
• Highly accurate but never 100% so interpret
together with clinical features; if diagnosis in
Doubt then follow infant up or retest
• Not the same as the viral load test (RNA PCR)
• Perform on all HIV-exposed at Birth and
10 weeks of age
• Repeat 6 weeks after breastfeeding stopped

HIV Diagnosis: Virological Tests
• HIV PCR – directly detects the HIV virus
by detecting its genome in human cells
• This is the “Gold Standard” for HIV testing
• Two types:
- HIV DNA PCR test
- HIV TNA PCR test

HIV TNA PCR
• Total Nucleic Acid: detects both HIV -1
proviral DNA and RNA
• Done either on EDTA or Dried Blood Spot
• Sensitivity rate reportedly between 98.8% -
99.7% (higher than DNA PCR)
• Adopted by National Health Laboratories , roll
out of v2 with higher sensitivity rate

HIV Diagnosis: Virological Tests
• Viral Load (VL) – detects HIV virus RNA
– Quantitative
– Used principally in monitoring response to
treatment
– No longer used for confirmation of
HIV infection in infants <18 months

Timing of PCR test• PCR at birth: Only detect those infected in
utero
• PCR from 2 weeks: Only detect those
infected in utero and perinatally
• So recommended age to pick up as many
babies as possible is > 4 weeks
• If breastfed - ongoing risk - need to repeat
when breastfeeding has stopped

Unknown maternal HIV status• Offer woman VCT. If she tests HIV positive,
test the infant, younger than 18 months of age,
with an HIV PCR.
• Need parental consent to do an HIV test on the
infant.
• Where parents are deceased, infant testing
should still be done on the consent of the primary
care giver

HIV DNA PCR• Sample:
- liquid blood in purple top (EDTA) tube or - dried blood spot (DBS)
• Both samples
- cost government the same price and - give equally accurate results
• Choice of sample depends on the skills ofhealthcare worker to obtain an unclotted sampleor 3 full blood spots
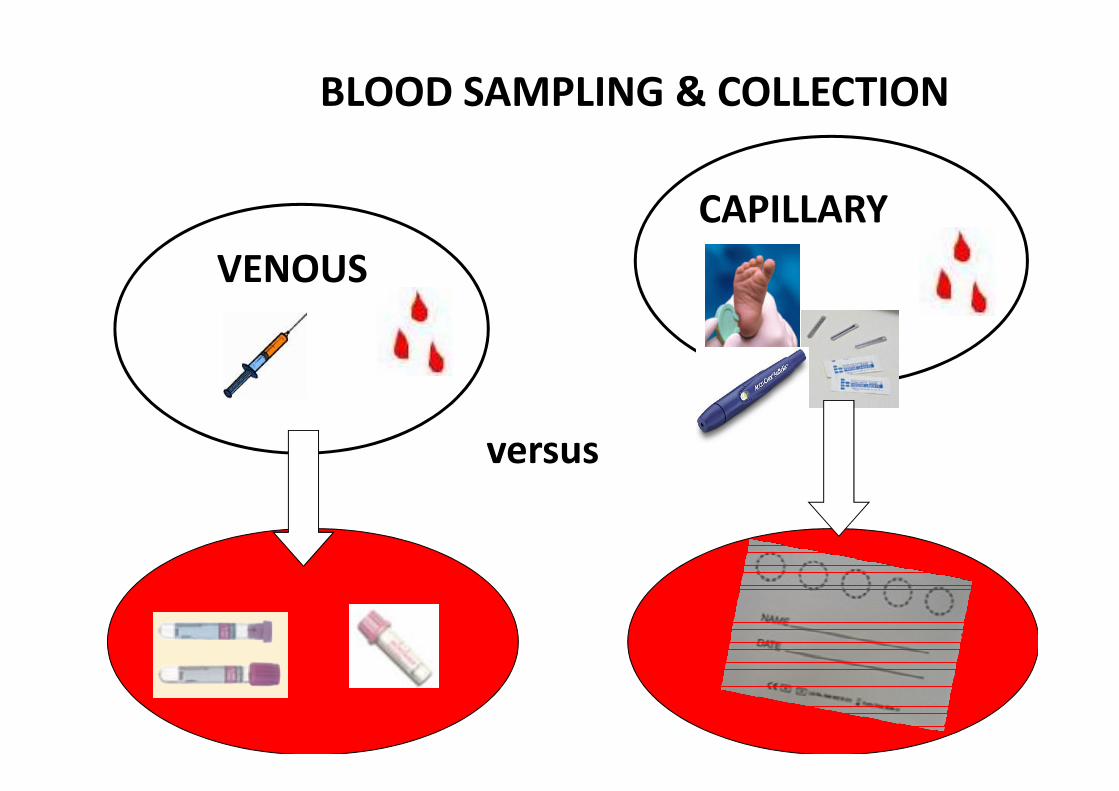
versus
VENOUS
CAPILLARY
BLOOD SAMPLING & COLLECTION

Dried Blood Spot
Collection and Handling
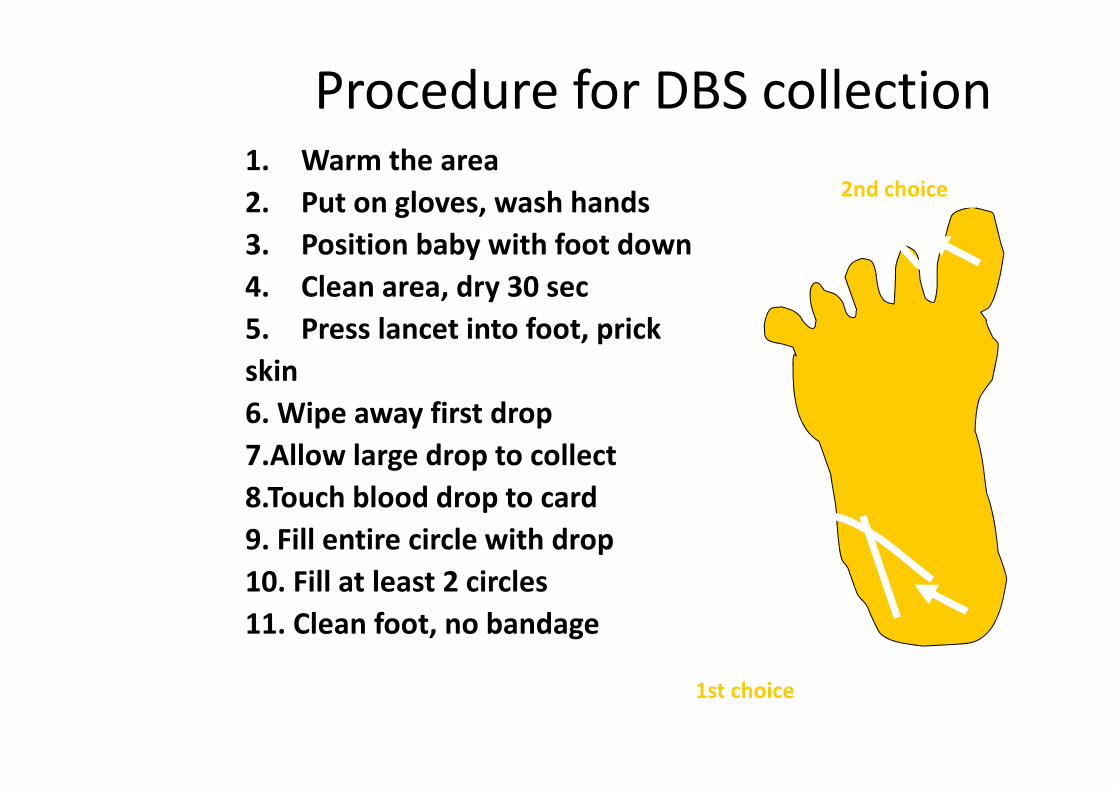
Procedure for DBS collection1. Warm the area
2. Put on gloves, wash hands
3. Position baby with foot down
4. Clean area, dry 30 sec
5. Press lancet into foot, prick
skin
6. Wipe away first drop
7.Allow large drop to collect
8.Touch blood drop to card
9. Fill entire circle with drop
10. Fill at least 2 circles
11. Clean foot, no bandage
1st choice
2nd choice

Foot hold & squeeze
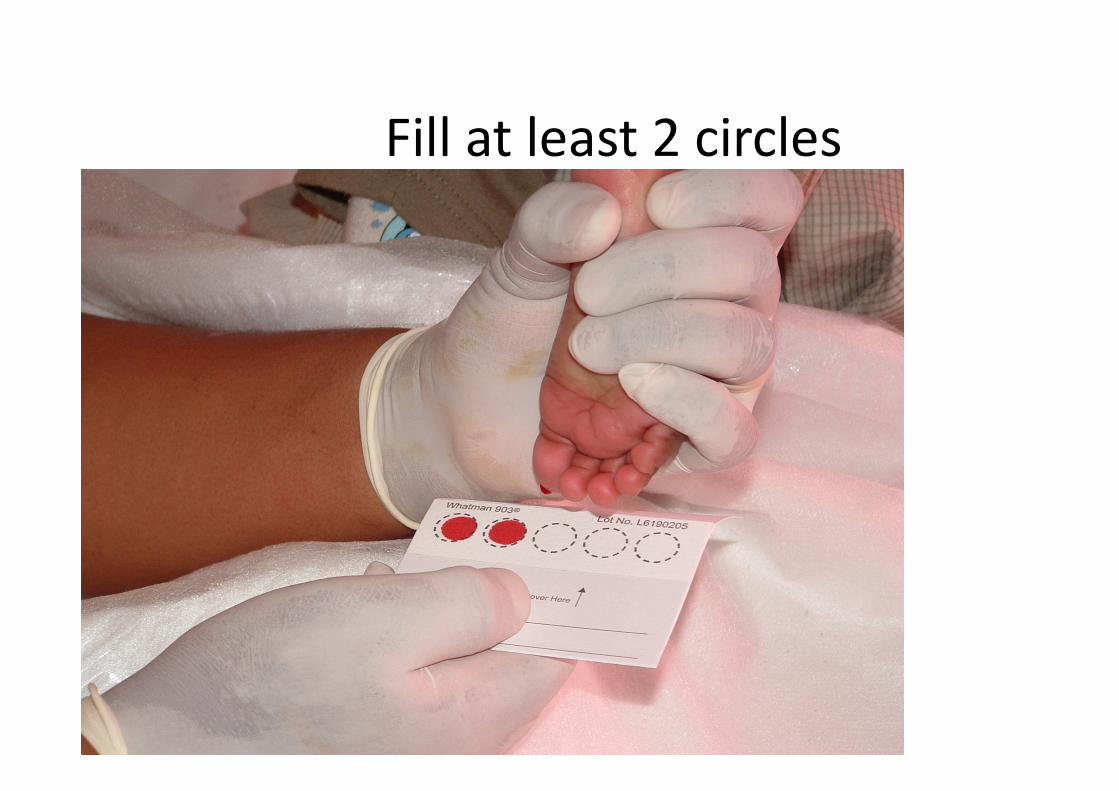
Fill at least 2 circles

How to Package DBS for Storage
� At the end of each day, pack the dry DBS
(leave for next day if not dry 3 hrs)
� Put weighing paper between cards so they
can’t touch each other
� Insert into sealable plastic bag
� Add desiccant packet
� Press air out of bag
� Label bag and seal
� Put into refrigerator if not going to the lab that day

Dry Completely Before Packaging

Keep requisitions with DBS cards

Insert Into Sealable Plastic Bag

Collection Problems
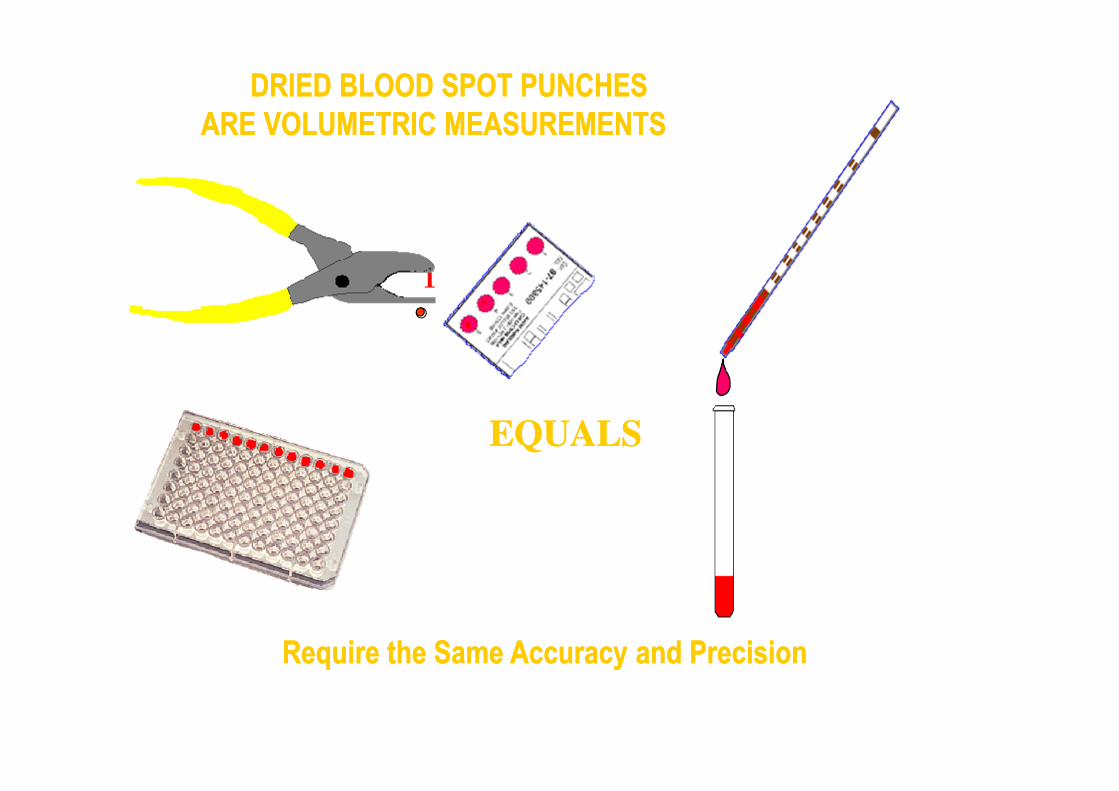
DRIED BLOOD SPOT PUNCHES
ARE VOLUMETRIC MEASUREMENTS
DRIED BLOOD SPOT PUNCHES
ARE VOLUMETRIC MEASUREMENTS
Require the Same Accuracy and PrecisionRequire the Same Accuracy and Precision
EQUALSEQUALS
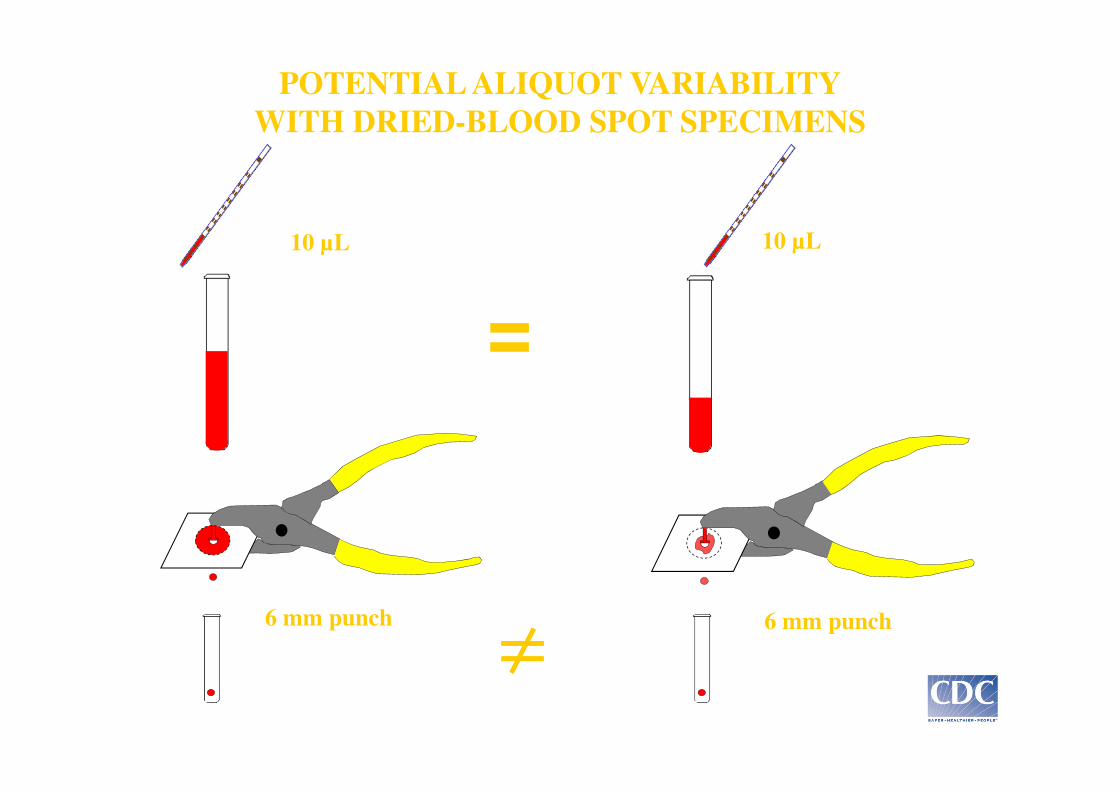
POTENTIAL ALIQUOT VARIABILITY
WITH DRIED-BLOOD SPOT SPECIMENS
=
10 µL 10 µL
≠≠≠≠6 mm punch 6 mm punch

1. Add Kit Diluent (150 uL, 1:30)
2. Cover plate, incubate overnight at 4oC
3. Shake plate gently to mix
4. Add Diluent to assay plate (125 uL)5. Transfer DBS eluate (25 uL) to assay plate
(1:150 final serum dilution)
Elution Plate Assay Plate
1. Cover plate, incubate plate 90 min at 37oC
2. Wash plate 4x
3. Add IgG-Enzyme Conjugate
4. Cover plate, incubate 30 min at 37oC
5. Add Substrate (150 uL)
6. Incubate 10 min at 25oC
7. Add Stop Solution (150 uL)
8. Read plate at 405 nm
Typical EIA Assay Procedure for Dried Blood
Spots
Punch 3 or 6 mm disks into microwell plate

65
HIV Exposed New-born (1 to 9 months old) in CRCHIV Exposed New-born (1 to 9 months old) in CRC
PCR HIV DNA (DBS)Negative
Maintain follow-up at CRCInfant/Child is infected.
(alta da CRC)
Immediately start ART.
Repeat DBS to confirm
infection
Infant/Child develops signs or
symptoms suggestive of HIV
Repeat PCR HIV DNA (DBS) and
send to clinical evaluation
If stopped the
breastfeeding long
than 2 months and
the infant without
signs or symptoms Negative
Discuss the
case with
clinicians
Inconclusive
Negative
Infant remain well and reaches 9
months of age
Conduct HIV antibody test between 9 to 18 months
of age
Negative
Repeat PCR HIV DNA
(DBS) to confirm the
diagnosis
Link the child with
care and treatment
to immediately start
ART
Positive
Positive
Positive
Report not
infected and alta
from CRC
Infant/Child is
infected. (alta da
CRC) Immediately
start ART. Repeat DBS
to confirm infection
if the infant
maintain
breastfeeding or
the test was
performed less
than 2 months
Infant remain in CRC follow-up and repeat
RDT at 18 months or 2 months after stop
breastfeeding
Positive
Positive
Negative
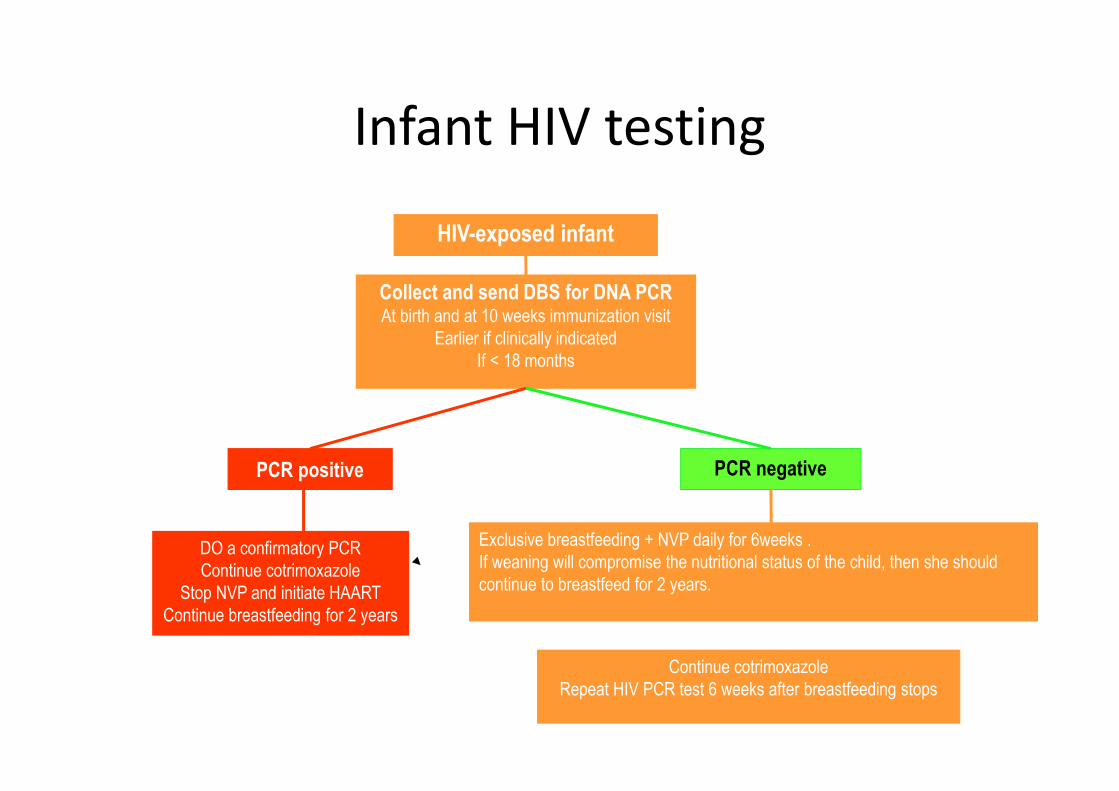
Infant HIV testing
PCR positive
DO a confirmatory PCR
Continue cotrimoxazole
Stop NVP and initiate HAART
Continue breastfeeding for 2 years
Exclusive breastfeeding + NVP daily for 6weeks .
If weaning will compromise the nutritional status of the child, then she should
continue to breastfeed for 2 years.
PCR negative
Collect and send DBS for DNA PCRAt birth and at 10 weeks immunization visit
Earlier if clinically indicated
If < 18 months
Continue cotrimoxazole
Repeat HIV PCR test 6 weeks after breastfeeding stops
HIV-exposed infant
67
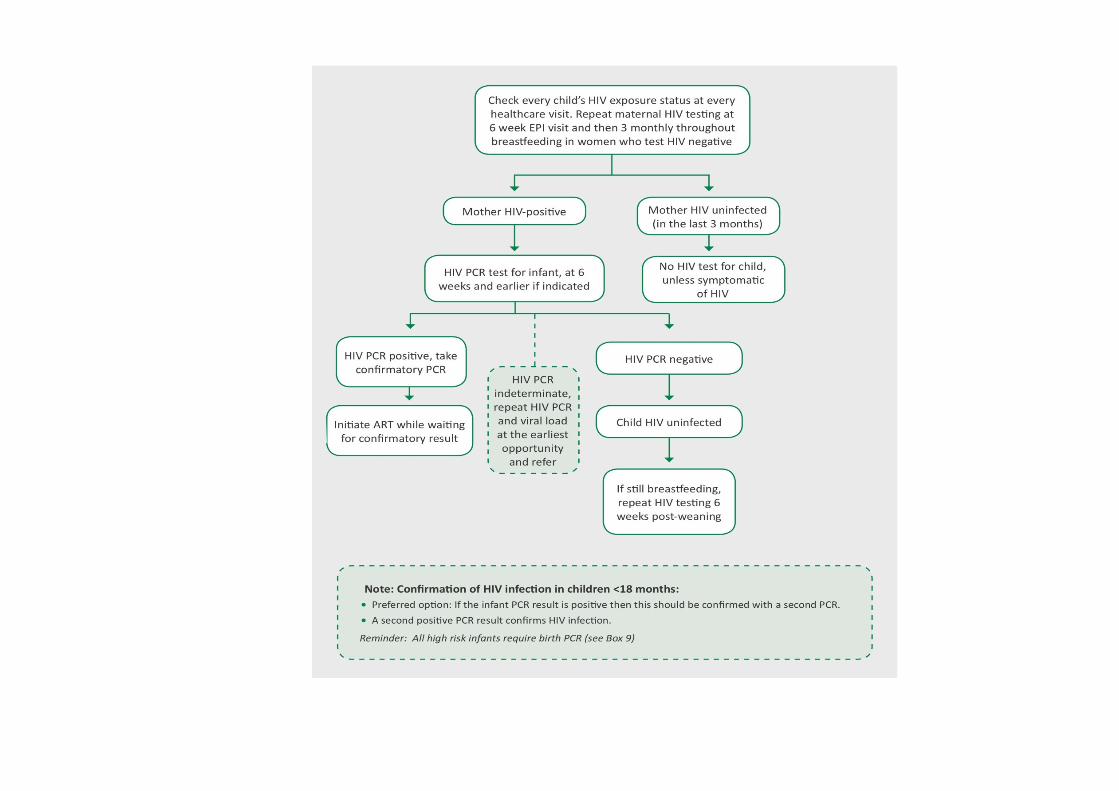


Mother’s Status Action
Positive maternal HIV status All infants born to HIV-infected women require a PCR.
Negative maternal HIV status Rapid test should be offered to mother to ensure she has remained HIV-uninfected.
Unknown maternal HIV status Offer a rapid test to the mother. If she tests positive then her infant should have a PCR at the same visit. Provide the mother with the care she requires.
Unknown maternal HIV status and mother refuses testing
Offer an HIV rapid test (on the infant) to assess HIV-exposure. If the infant’s rapid test is positive, perform a PCR test on the infant during the visit and counsel the mother to seek further HIV testing and care. (Note in the RTHC so that mother receives continued support during infant follow-up)
Which test?
• Abandoned 3 month old baby, mother's
status and whereabouts unknown
• 6 weeks old HIV- exposed baby still
breastfeeding
• 20 month old baby, mother HIV positive
• 5 year old

Goga AE, et al SAPMTCTE 2010
Perinatal Transmission Down !
2,7% in 2011 but ….

Early Infant Diagnosis
Sherman et al, IAS 2012
• PCR tests increased from
3370 in 2003 to 293786 in
2011
• Percentage positivity
declined from 16.4% in 2006 to
2.8% in 2011

• Scaling up EID in Africa has been made possible not only by increasing the laboratory infrastructure but by circumventing the need for venesection
• In 2012: 75% samples arrive in dried blood format, Results are delivered bysms printer
Courtesy Sherman and Carmona
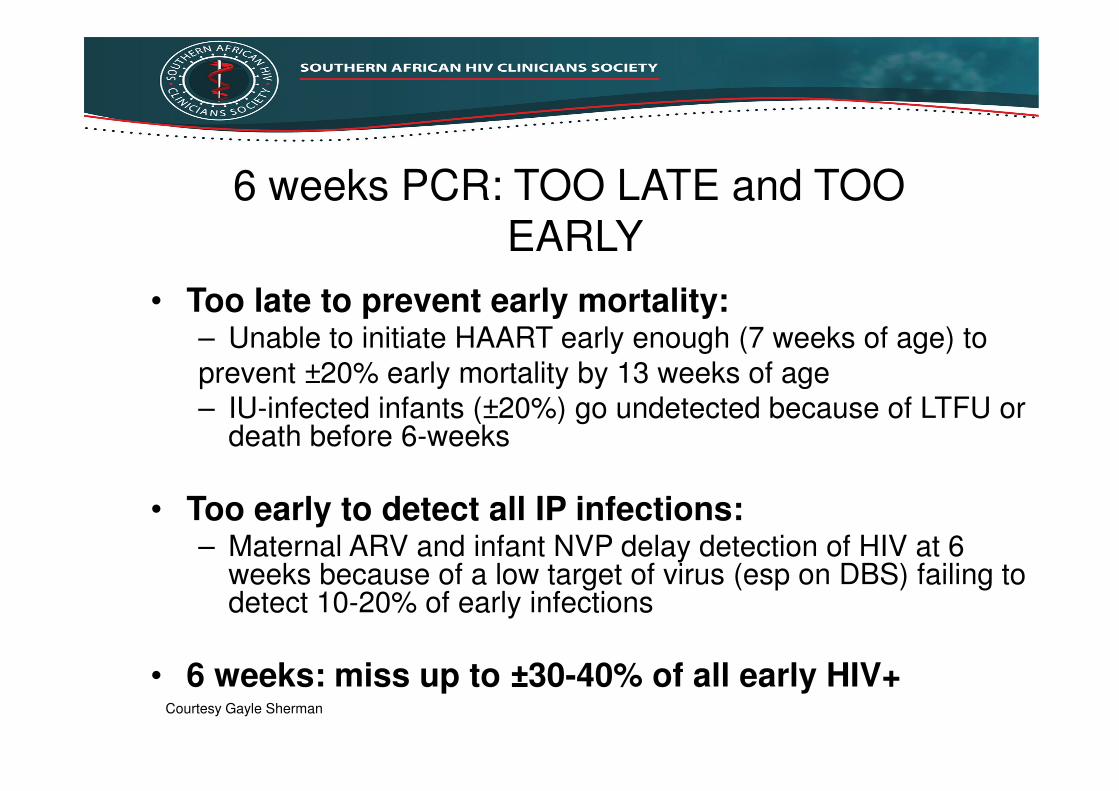
6 weeks PCR: TOO LATE and TOOEARLY
• Too late to prevent early mortality:– Unable to initiate HAART early enough (7 weeks of age) to
prevent ±20% early mortality by 13 weeks of age
– IU-infected infants (±20%) go undetected because of LTFU or death before 6-weeks
• Too early to detect all IP infections:– Maternal ARV and infant NVP delay detection of HIV at 6
weeks because of a low target of virus (esp on DBS) failing to detect 10-20% of early infections
• 6 weeks: miss up to ±30-40% of all early HIV+Courtesy Gayle Sherman

WHY WAIT 4-6 WEEKS TO PERFORM
ACCURATE PCR ?

EID in the context of PMTCT coverage• Infants are exposed to ART since before
they are born
• Studies: Duration of ART exposure
• influences the age at which HIV is
detected
Treatment with ART may reduce VL to
levels below PCR diagnostic threshold values

EID in the context of PMTCT
coverage
• TNA PCR sensitivity may drop to 83% for NVP
exposed infants
• 11% of HIV infected children had false
negative PCR due to ART prophylaxis in
one study
• Also affects infants breastfed by HIV +
mothers on ART
Haeri Mazanderani et al (2014); Shapiro et al (2013); Lilian et al (2011).

Positive HIV PCR results
• Baby is HIV infected
• Do a confirmatory PCR (<18 months)
• Pull other baseline bloods: CD4 count, VL,
FBC/Hb, Chol, TG
• Start ART ASAP
• Do not delay initiation of ART for results
• Note: neonates require referral to an experienced clinician, as do children weighing less than 3kg

Stigmata of HIV Infection
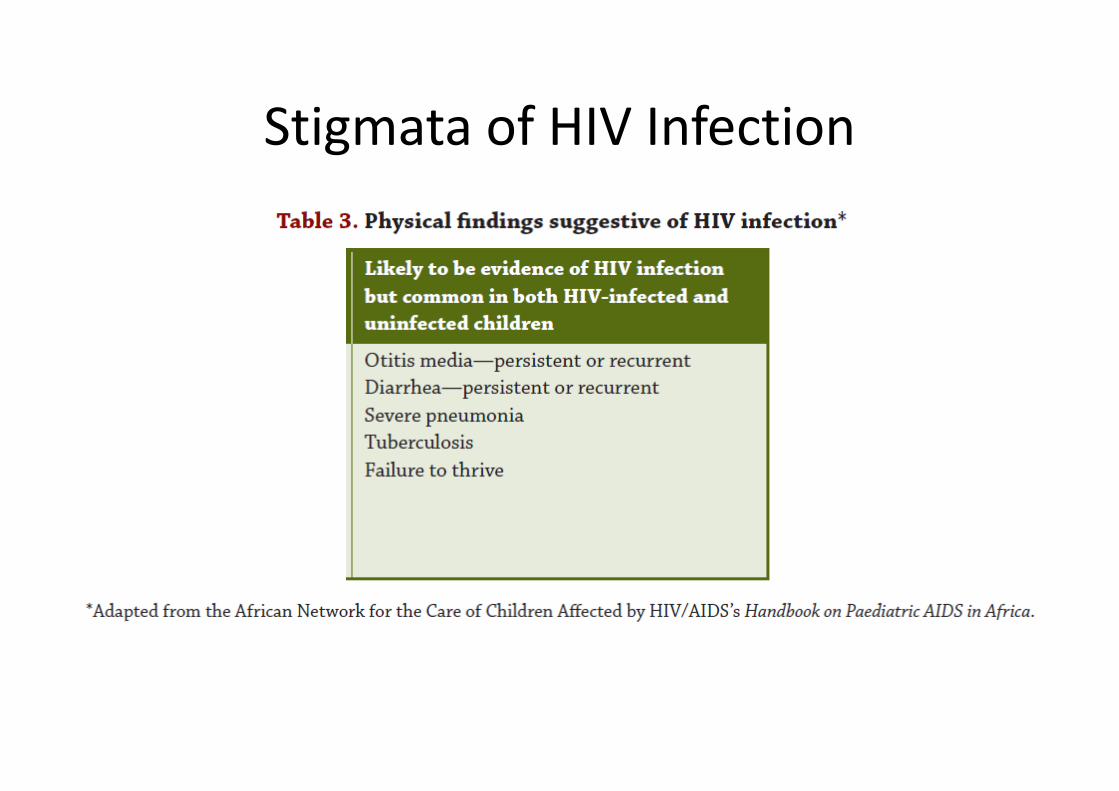
Stigmata of HIV Infection

83
Presumptive HIV infants/child
diagnosis
• Used for children under 18 months of age.
o If an infant/child with signs or symptoms
suggestive and/or social warning sign for HIV
undergo RDT´s and if positive should
immediately start ART.
o The diagnosis most be confirmed by PCR
DNA .

HIV-Exposed Infant Testing Schedule
>/18 months
• HIV Antibody test - 18 months old or greater.
– Rapid test for all HIV-exposed infants at 18mo
• result
– Infant is positive, confirm with another rapid test
• result, infant has not BF in last 6wks
– Infant is negative
• result, infant is still BF or has had BM less than
6wks prior to the test - infant could be in the “window
period” so a negative test does not rule out HIV infection.
– Repeat rapid test 6 wks after all BF has ceased.
– Continue Bactrim (and NVP if mom not stable on HAART)

Discordant and Indeterminate HIV Test
Results
• Less than 18-mo– HIV PCR + but negative/indeterminate repeat
HIV PCR or undetectable VL: repeat HIV PCR with VL
• Older than 18-mo– 1st rapid test (+) but second rapid test (-): send
ELISA
– If ELISA still discordant, perform PCR
• Indeterminate and discordant results after
testing as above: refer, do not delay access to
treatment by waiting to repeat the tests

Questions ??

We made it!