Embed Size (px)
Citation preview

Controvérsias na Anticoagulação Oral:Continuar ou Interromper os Anticoagulantes
Orais durante a Intervenção Estomatológica? [41]
NATÁLIA ANTÓNIO1, GRAÇA CASTRO1, DOMINGOS RAMOS1, ANTÓNIO MACHADO2, LINO GONÇALVES1, TICE MACEDO3, LUÍS A. PROVIDÊNCIA1
1 - Serviço de Cardiologia, Hospitais da Universidade de Coimbra, Coimbra, Portugal. 2 - Serviço de Estomatologia, Hospitais da Universidade de Coimbra, Coimbra, Portugal.
3 - Instituto de Farmacologia e Terapêutica Experimental, Faculdade de Medicina Universidade de Coimbra, Coimbra, Portugal.
Rev Port Cardiol 2008; 27 (4): 531-544
531
RESUMO
A abordagem dos doentes cronicamenteanticoagulados com necessidade de
intervenções estomatológicas continua asuscitar grande controvérsia. O aumento do
risco hemorrágico associado aos procedimentosestomatológicos sob anticoagulação oral deveser pesado relativamente ao risco trombótico
acrescido causado pela interrupção daterapêutica antitrombótica. Em cirurgia oral
minor, a mortalidade e morbilidade é superiornos episódios tromboembólicos
comparativamente aos episódios hemorrágicos.A informação científica disponível não apoia ainterrupção da terapêutica anticoagulante oral
para cirurgia oral minor. É intenção dosautores propor um protocolo para a abordagem
clínica dos doentes cronicamenteanticoagulados com necessidade de tratamento
estomatológico, de forma a minimizar, quer orisco tromboembólico, quer o risco
hemorrágico.
Palavras-Chave
Anticoagulação oral; Tratamento estomatológico; Risco
tromboembólico; Risco hemorrágico
ABSTRACT
The Debate Concerning OralAnticoagulation: Whether to Suspend OralAnticoagulants During Dental Treatment
The management of patients taking long-termoral anticoagulants who require dental surgeryis still highly controversial. The risk ofbleeding associated with dental treatmentunder oral anticoagulants must be weighedagainst the risk of thromboembolism associatedwith suspension of antithrombotic therapy.Mortality and morbidity associated withthromboembolic events are higher than thoseassociated with hemorrhagic events after minororal surgery procedures. Evidence-basedinformation does not support oral anticoagulantsuspension before minor oral surgery. Theauthors propose a management protocol forchronically anticoagulated patients who requirea dental procedure, to reduce boththromboembolic risk and the risk of bleeding.
Key words
Oral anticoagulation therapy; Minor oral surgery;
Thromboembolic risk; Bleeding risk
Recebido para publicação: Janeiro de 2008 • Aceite para publicação: Fevereiro de 2008Received for publication: January 2008 • Accepted for publication: February 2008
INTRODUÇÃO
Aterapêutica com anticoagulantes orais temindicação num elevado número de doentes.
As indicações mais frequentes para aanticoagulação crónica são as próteses valvularescardíacas, a fibrilhação auricular (FA), a
INTRODUCTION
A large number of patients have indication fororal anticoagulant therapy. The commonestreasons for long-term anticoagulation areprosthetic heart valves, atrial fibrillation,and prevention and treatment of venous

prevenção e tratamento do tromboembolismovenoso e a prevenção e tratamento de acidentesvasculares cerebrais isquémicos. (1)
O número de doentes com indicação paraanticoagulação oral tem vindo a aumentar. EmPortugal verificou-se entre 1999 e 2003, umaumento de 33% no consumo de anticoagulantesorais. (2) Com o envelhecimento da população, é deesperar um aumento no número de doentesanticoagulados. Por outro lado, a tendência actualé conservar ao máximo a dentição. Prevê-se, pois,um aumento progressivo do número de doentesanticoagulados a necessitar de intervençõesestomatológicas. (3)
Constatou-se que a orientação dos doentescronicamente anticoagulados com necessidade deintervenções estomatológicas continua a suscitargrande controvérsia. (4-7)
O risco hemorrágico aumentado associadoaos procedimentos estomatológicos sob anti-coagulação oral deve ser pesado relativamenteao risco acrescido de fenómenos trombóticoscausado pela interrupção da terapêuticaanticoagulante. (8, 9)
O objectivo desta revisão consiste em proporum protocolo para orientação de doentescronicamente anticoagulados com necessidade detratamento estomatológico, de forma a minimizar,quer o risco tromboembólico, quer o riscohemorrágico.
Varfarina - uma nota históricaA varfarina é o anticoagulante oral mais
utilizado em todo o mundo.Em 1948 a varfarina foi lançada no mercado
como um raticida potente. É possível que a varfarina tenha sido utilizada
por Lavrenti Beria, chefe da Polícia SecretaSoviética (1938 - 1954), para envenenar JosefStalin que faleceu em consequência de umahemorragia cerebral.
Em 1951 um recruta da marinha americanatentou, sem sucesso, o suicídio com uma dosede 567 mg de varfarina. A sua surpreendenterecuperação induziu o desenvolvimento deestudos sobre as propriedades anticoagulantes davarfarina em humanos.
A varfarina foi aprovada para uso humano pelaFDA em 1954. (10) Nesse mesmo ano, o Presidentedos EUA Dwight Eisenhower, foi tratado comvarfarina depois de um enfarte agudo domiocárdio (EAM).
thromboembolism and ischemic stroke (1).The number of patients with indication for oral
anticoagulation is increasing; consumption of oralanticoagulants increased by 33% in Portugalbetween 1999 and 2003 (2), and this is expected toincrease further as the population ages. At thesame time, current dental policy is to preserveteeth for as long as possible. It can thus be seenthat there are likely to be progressively moreanticoagulated patients requiring dentaltreatment (3).
The management of patients taking long-termoral anticoagulants who require dental surgery isstill highly controversial (4-7).
The bleeding risk associated with dentaltreatment under oral anticoagulants must beweighed against the risk of thromboembolismassociated with suspension of antithrombotictherapy (8, 9).
The purpose of this review is to proposea management protocol for chronicallyanticoagulated patients who require a dentalprocedure, to reduce both thromboembolic riskand the risk of bleeding.
Warfarin: a historical noteWarfarin, now the most-used oral
anticoagulant in the world, was first marketed in1948 as a potent rat poison. It may have beenused by Lavrenti Beria, the head of the Sovietsecret police from 1938 to 1954, to poison JosephStalin, who died following a cerebral hemorrhage.
In 1951, an American naval conscriptattempted to commit suicide by taking 567 mg ofwarfarin; surprisingly, he recovered, whichprompted studies on the anticoagulant propertiesof warfarin in humans.
The drug was approved for human use by theUS Food and Drug Administration in 1954(10), andin the following year it was used to treat PresidentDwight Eisenhower after a myocardial infarction.
Prothrombin time (PT) had been devised byArmand Quick in 1935, before the discovery oforal anticoagulants, and was later used to assessthe action of warfarin (11). However, the widespreadadoption of PT did not succeed in making thedosage of oral anticoagulants uniform or safe, duemainly to difficulty in purifying concentratedthromboplastin (tissue factor) (12).
In 1962, the International Committee onThrombosis and Haemostasis/InternationalCommittee for Standardization in Hematology532
Rev Port CardiolVol. 27 Abril 08 / April 08

O tempo de protrombina (TP) foi descobertopor Armand QuicK em 1935, antes dadescoberta dos anticoagulantes orais, e usadosubsequentemente para avaliação da actividadeda varfarina. (11) No entanto, a adopção universaldo TP não conseguiu uniformidade nemsegurança na dosagem dos anticoagulantes orais,devido principalmente a problemas com apurificação do concentrado de tromboplastina(factor tecidular). (12)
O International Committee on Thrombosisand Haemostasis/International Committee forStandardization in Hematology iniciou em 1962 oestudo de várias alternativas para uniformizaçãodo TP. (11) O INR foi introduzido no início dos anos80 e foi amplamente aceite a nível mundial,especialmente após a sua adopção pela OMS. (12)
O INR (razão normalizada internacional) é arazão do TP calculado em função do Índice deSensibilidade Internacional (ISI) apropriado, dosistema local de testes de TP, ou seja INR =TP/MNTP (em que, MNTP é a média geométricado TP de pelo menos 20 indivíduos adultosnormais, de ambos os sexos, com o mesmosistema de teste local e as mesmas condiçõesde teste que as utilizadas para os doentes). (11)
Em 1943, Flood descreveu pela primeira vezum caso de trombose paradoxal com a varfarina. (13)
A etiopatogénese desta complicação permanece,ainda, mal elucidada. Como a semi-vidaplasmática das proteínas anticoagulantes C e S éinferior à dos factores da coagulação II, VII, IX eX, durante as primeiras horas de utilização, avarfarina reduz mais acentuadamente as proteínasC e S que os factores da coagulação, gerando-seum desequilíbrio transitório a favor de um estadopró-coagulante, que pode explicar a tromboseparadoxal após o início da anticoagulação. (14)
Anticoagulantes orais - mecanismo de acçãoe farmacocinética
Os anticoagulantes orais (varfarina, aceno-cumarol, fluindiona, tioclomarol, fenindiona) sãoantagonistas da vitamina K, que inibem a síntesedos factores II, VII, IX e X da coagulação e dasproteínas anticoagulantes C e S. (15)
Os antagonistas da vitamina K sãoclassificados em função da sua estruturaquímica, em derivados cumarínicos (varfarina,acenocumarol e tioclomarol) ou derivados indano-diona (fenindiona e fluindiona). Em Portugalapenas a varfarina (varfine®) e o acenocumarol
began studying alternative ways to standardizePT (11). The result, the international normalizedratio (INR), was introduced in the early 1980sand was widely accepted all over the world,especially after it was adopted by the WHO (12).
INR is the PT ratio calculated using theappropriate International Sensitivity Index (ISI)of the thromboplastin used at the local PT testinglaboratory, thus:
INR = (patient PT/MNPT),where MNPT (mean normal PT) is the
geometric mean of the PT of at least 20 normaladults of both sexes, determined by the samelocal testing system and under the same testconditions as those used for patients (11).
In 1943, the first case of paradoxicalthrombosis caused by warfarin was reported byFlood et al. (13). The cause of this complication isstill poorly understood. Since the plasma half-lifeof the anticoagulant proteins C and S is shorterthan that of coagulation factors II, VII, IX and X,warfarin initially reduces levels of proteins C andS more than those of the coagulation factors,which creates a temporary procoagulant state thatmay explain paradoxical thrombosis after theinitiation of anticoagulant therapy (14).
Oral anticoagulants: mechanism of actionand pharmacokinetics
Oral anticoagulants like warfarin,acenocoumarol, fluindione, tioclomarol, andphenindione, are vitamin K antagonists thatinhibit synthesis of factors II, VII, IX and Xand proteins C and S (15).
Vitamin K antagonists are classifiedaccording to their chemical structure as coumarinderivatives (warfarin, acenocoumarol andtioclomarol) or indanedione derivatives(phenindione and fluindione). Only warfarin(Varfine®) and acenocoumarol (Sintrom®) arecommercially available in Portugal.
All Vitamin K antagonists interfere with theinterconversion of vitamin K and its 2, 3 epoxideby inhibiting the enzymes vitamin K epoxidereductase and vitamin K reductase. This depletesvitamin KH2, the reduced form of the vitamin,leading to the production of biologically inactivevitamin K-dependent coagulant proteins. Thesefactors require gamma-carboxylation to haveprocoagulant activity (15).
Vitamin K antagonists can also have aprocoagulant effect, by inhibiting the 533
NATÁLIA ANTÓNIO, et alRev Port Cardiol 2008; 27: 531-44

(sintrom®) se encontram comercializados.Os antagonistas da vitamina K interferem com
a interconversão da vitamina K e do 2,3-epóxidoda vitamina K, através da inibição da enzimavitamina K epóxido redutase e da vitamina Kredutase. A inibição destas enzimas conduz àdepleção de vitamina KH2 (forma reduzida davitamina K) com a consequente produção deproteínas coagulantes (dependentes da vitaminaK), hemostaticamente deficientes. Estes factoresprecisam de γ-carboxilação para possuíremactividade procoagulante. (15)
Por outro lado, os antagonistas da vitaminaK podem ter actividade procoagulante, aoinibirem a carboxilação das proteínas deregulação anticoagulantes, proteína C e S; mas,em geral, o efeito anticoagulante dos cumarínicosé dominante. (15)
O efeito anticoagulante da varfarina só surgeapós um período de latência de cerca de 48 horas(tempo necessário para o consumo dos factoresda coagulação em circulação) e persiste váriosdias após cessação da terapêutica. A semi-vidaplasmática da varfarina é de cerca de 36 a 42horas. (15, 16)
A ligação da varfarina às proteínas plasmáticasé da ordem dos 95 a 99%. (15)
A varfarina sofre metabolismo no fígado, anível do complexo enzimático do Citocromo P4502C9.
Existe uma relação directa entre a dose devarfarina e a resposta anticoagulante nosindivíduos normais, mas há uma variaçãointerindividual acentuada na resposta a umamesma dosagem, que também se observa emdoentes submetidos a terapêutica prolongadacom anticoagulantes, tornando difícil o controlo. (15)
A dose de varfarina é influenciada pelaquantidade de vitamina K da dieta, pela funçãohepática, doenças médicas coexistentes,medicação concomitante e pela presençaou ausência de mutação do gene do citocromoP450 2C9.
São várias as substâncias que interagem coma varfarina sendo essencial a educação do doente.Alimentos ricos em vitamina K (como couve,brócolos, nabo, alface, couve de Bruxelas,endívias, couve-lombarda, couve-flor) podemreduzir a resposta anticoagulante à varfarina. Istonão significa que o doente deva comer menosalimentos ricos em vitamina K. Estes alimentossão importantes para uma alimentação saudável.
carboxylation of the regulatory anticoagulantproteins C and S; however, the anticoagulanteffect of coumarins generally predominates (15).
Warfarin’s anticoagulant effects only developafter a period of latency lasting around 48 hours,during which circulating coagulation factors areconsumed, and persist for several days aftersuspension of the therapy. Its plasma half-life is36-42 hours (15, 16) and 95-99% binds to plasmaproteins (15). It is metabolized in the liver by thecytochrome P450 2C9 enzyme complex.
There is a direct relation between warfarindose and anticoagulant response in normalindividuals, but the response varies markedlybetween individuals; this is also seen in patientsundergoing long-term anticoagulant therapy andmakes management difficult (15).
Dosage is affected by levels of dietary vitaminK, liver function, coexisting disease states,concomitant medication, and mutations in thegene for cytochrome P450 2C9.
Various substances interact with warfarin, andso patient education is essential. Vitamin K-richfoodstuffs including cabbage, broccoli, turnip,lettuce, Brussels sprouts, endives and cauliflowercan reduce the anticoagulant response towarfarin. This does not mean that patients shouldnot eat foods rich in vitamin K, which areimportant for a healthy diet. Either intake of suchfoods should be regular, in order to avoid largevariations in INR, or alternatively patients shouldeat their normal diet, checking INR frequentlyand adjusting dosage as necessary. Alcohol canincrease the effect of warfarin in the presence ofliver disease, but under normal conditions it doesnot affect its action. The fact that it is metabolizedin the liver and that a high percentage binds toplasma proteins means that warfarin interactswith a wide range of other drugs (Table I) (17, 18).
Oral anticoagulation during dentaltreatment: State of the art
The lack of consistent guidelines concerningthe management of anticoagulated patientsduring the perioperative period is reflected inconsiderable variability in clinical practice.
For dental extractions, approaches range fromcomplete suspension of anticoagulant therapy tocontinuation with no change in dosage (5).
In current practice, the most commonstrategies for oral surgery in anticoagulatedpatients are as follows:534
Rev Port CardiolVol. 27 Abril 08 / April 08

Deve-se recomendar uma dieta regular paraevitar oscilações importantes do INR, ou então,em alternativa, manter uma dieta normal e fazer ocontrolo regular do INR e adaptar a dosagem. Oálcool pode potenciar o efeito da varfarina seexistir doença hepática concomitante, mas emcondições normais não interfere com a acção davarfarina. Devido ao metabolismo hepático e àelevada percentagem de ligação às proteínasplasmáticas, a varfarina interage com inúmerosfármacos. (Quadro I) (17, 18)
Anticoagulação oral durante a intervençãoestomatológica - Estado da Arte
A ausência de recomendações consistentesrelativamente à orientação dos doentes antico-agulados no perioperatório reflecte-se numaenorme variabilidade de práticas clínicas.
Em Estomatologia, para extracções dentáriasas estratégias vão desde a interrupção completados anticoagulantes até à continuidade dosmesmos sem qualquer ajuste de dose. (5)
Na prática corrente, as estratégias maiscomuns no que se refere ao perioperatório dacirurgia oral em doentes anticoagulados são asseguintes:
1. Substituição dos anticoagulantes orais porheparina não fraccionada (sendo esta últimasuspensa 4 a 6 horas antes do procedimentoestomatológico) (7, 19, 20)
Esta opção implica:- monitorização apertada dos níveis de
1. Replacement of oral anticoagulants byunfractionated heparin (which is then suspended4 to 6 hours before the procedure (7, 19, 20)
This option entails:- close monitoring of anticoagulation levels;- hospitalization;- risk of heparin-induced thrombocytopenia.2. Replacement of oral anticoagulants by low
molecular weight heparin (LMWH) (7, 19, 20)
The advantage of this option is that it does notrequire the patients to be hospitalized. However,there is also the risk of heparin-inducedthrombocytopenia, although this is less than withunfractionated heparin, and some authors believethat there is an increased risk of bleedingfollowing dental extraction under therapy withLMWH (21, 22). Others argue that further studies arerequired before LMWH can be considered safe asa periprocedural bridging therapy (23, 24).
3. Reduction of perioperative anticoagulantlevels
In this option, warfarin is continued but atlower doses, beginning 4-5 days before theprocedure. Regular monitoring and adjustment ofanticoagulation levels is required to obtain anINR of <3. It has the advantage of not requiringhospitalization in most cases.
4. Temporary discontinuation of oralanticoagulation
Many clinicians prefer to suspendanticoagulant therapy before oral surgery inorder to prevent bleeding complications (16).This approach involves suspending therapy two 535
NATÁLIA ANTÓNIO, et alRev Port Cardiol 2008; 27: 531-44
Inibição da acçãoBarbitúricosCarbamazepinaClordiazepóxidoColestiraminaGriseofulvinaNafcilinaRifampicinaSucralfatoTrazodona
Potenciação da acçãoAlopurinolAmiodaronaCimetidinaCisaprideClofibrato e outros fibratosCloranfenicolCotrimoxazolEritromicinaFluconazolIsoniazidaMetronidazolMiconazolOmeprazolFenilbutazonaPiroxicamPropafenonaPropranololSalicilatosSulfimpirazona
Quadro I. Principais fármacos com interacção com avarfarina
Inhibiting actionBarbituratesCarbamazepineChlordiazepoxideCholestyramineGriseofulvinNafcilinRifampicinSucralfateTrazodone
Strengthening actionAllopurinolAmiodaroneCimetidineCisaprideClofibrate and other fibratesChloramphenicolCotrimoxazoleErythromycinFluconazoleIsoniazidMetronidazoleMiconazoleOmeprazolePhenylbutazonePiroxicamPropafenonePropranololSalicylatesSulfinpyrazone
Table I. Main drugs that interact with warfarin

anticoagulação;- internamento dos doentes;- risco de trombocitopenia induzida pela
heparina.2. Substituição dos anticoagulantes orais por
heparina de baixo peso molecular (HBPM) (7, 19, 20)
Esta opção apresenta a vantagem de evitar ointernamento dos doentes. No entanto, apresentatambém o risco de trombocitopenia induzida pelaheparina, embora inferior ao da heparina nãofraccionada e alguns autores acreditam que existeum risco hemorrágico acrescido após extracçõesdentárias sob terapêutica anticoagulante comHBPM. (21, 22)
Vários autores afirmam serem necessáriosmais estudos antes de considerar as HBPMseguras como terapêutica de ponte no pré-operatório. (23, 24)
3. Diminuição dos níveis de anticoagulação noperioperatório
Esta estratégia consiste em continuar aterapêutica com varfarina, em doses mais baixas,diminuindo a dose 4 a 5 dias antes da cirurgia.
Esta opção requer monitorização e ajusteregular dos níveis de anticoagulação até obtençãodo INR pretendido (< 3). Apresenta a vantagem dedispensar, na maioria dos casos, o internamentodos doentes.
4. Descontinuação temporária da terapêuticaanticoagulante oral
Vários clínicos optam pela interrupção dotratamento anticoagulante antes da cirurgia oralpara prevenir complicações hemorrágicas. (16) Estaprática, largamente utilizada, consiste nainterrupção do anticoagulante oral dois a três diasantes do tratamento estomatológico programadoe prosseguir se o INR for < 1,5. O anticoagulanteé reintroduzido no mesmo dia da cirurgia oralminor. (2)
A interrupção dos anticoagulantes orais e a suareintrodução alguns dias mais tarde, com dosesiniciais elevadas, pode resultar num estado dehipercoagulabilidade causado pelo facto dainibição das proteína C e S ser mais precoce quea inibição dos factores pró-trombóticos, levando aum efeito trombótico “paradoxal”. (3, 8)
Após o reinício da terapêutica com varfarina,só ao fim de cerca de três dias o INR atingevalores próximos de 2,0. Nesta abordagempodemos esperar que os doentes tenhamINR subterapêutico durante um período totalde pelo menos quatro dias. A descontinuação
or three days before the scheduled dentaltreatment, and to proceed as long as INR is <1.5.The anticoagulant is resumed on the same day asthe surgery (2).
Interrupting oral anticoagulation andresuming it a few days later with high initialdoses can result in a hypercoagulable state,since proteins C and S are inhibited soonerthan prothrombotic factors, which can lead toa paradoxical thrombotic effect (3, 8).
INR does not reach values near 2.0 until somethree days after resumption of warfarin. Thus,patients are likely to have subtherapeutic INRvalues for at least four days, and so temporarysuspension of anticoagulation exposes them tothromboembolic risk (15). It is estimated thatsuspending warfarin for two days increases therisk for thromboembolic events by 0.02 to 1%(5, 25).
Thrombotic risk associated with changes inanticoagulant therapy before surgery
When considering the management ofanticoagulated patients who require any kind ofsurgery, the aim is to prevent major bleeding,which could be fatal, but at the same time tomaintain protection against thrombotic events.
It should be borne in mind that any change toanticoagulant therapy entails a degree of risk ofthrombotic complications. It is thus essential toassess the risk for each individual.
Anticoagulated patients can be classified ashigh, moderate or low thrombotic risk (26).
High-risk patients have a yearly risk forarterial thromboembolism of 10%, and a 1-monthrisk for venous thromboembolism of over 10%.Moderate risk means a yearly risk for arterialthromboembolism of 5-10%, and a 1-month riskfor venous thromboembolism of 2-10%,while low-risk patients present a yearly risk forarterial thromboembolism of less than 5%, and a1-month risk for venous thromboembolism of lessthan 2% (26).
Some clinicians argue that for patients withlow thromboembolic risk who require surgery,oral anticoagulation can be suspended for four orfive days without heparin bridging therapy (26).Low-risk patients include those with atrialfibrillation but no other thromboembolic riskfactors (previous stroke, transient ischemicattack, left ventricular dysfunction, age over 75years, hypertension or diabetes), second-generation aortic valve prostheses, history of536
Rev Port CardiolVol. 27 Abril 08 / April 08

temporária da terapêutica anticoagulante oralexpõe os doentes a um aumento do riscotromboembólico. (15)
Estima-se que a interrupção da varfarinadurante dois dias aumente o risco de eventostromboembólicos em cerca de 0,02 a 1%. (5, 25)
Risco trombótico associado à modificaçãodo tratamento anticoagulante antes dacirurgia
Na abordagem de doentes anticoaguladoscom necessidade de qualquer tipo deintervenção cirúrgica o nosso objectivo éprevenir complicações hemorrágicas major,potencialmente fatais, mas ao mesmo tempotentar manter a protecção relativamente aosfenómenos trombóticos.
Todos os métodos que modificam a terapêuticaanticoagulante comportam um certo risco decomplicações trombóticas.
É fundamental avaliar o risco trombóticoindividual. Os doentes anticoagulados podemser estratificados em: a) alto; b) moderado; e c)baixo risco trombótico. (Quadro II) (26)
Os doentes de alto risco apresentam um riscode tromboembolismo arterial anual de 10% eum risco de tromboembolismo venoso superior a10% por mês. (26) Os doentes de risco moderadoapresentam um risco anual de tromboembolismoarterial de 5% a 10% e um risco mensal de
venous thromboembolism more than 6 monthspreviously, and intrinsic cerebrovascular diseasewithout recurrent stroke or TIAs (8).
Patients at high or moderate risk shouldmaintain anticoagulation unchanged or with onlyminimum periods at subtherapeutic levels (26).
Postoperative bleeding riskA list of surgical procedures that can be
associated with significant bleedingcomplications is given in Table III (26, 27).
Minor oral surgery is considered to presentlow bleeding risk (26, 27). This includes: 1) simpleextraction of up to three teeth; 2) gingival surgery;3) fitting of crowns; 4) fitting of bridges; 5)surgical extraction; and 6) descaling (28). In oralsurgery, the risk of bleeding is local and relateddirectly to the surgical procedure (5).
The incidence of early bleeding in oralsurgery is similar in hypocoagulated patientsand in those not taking anticoagulants. Thisappears to be because large vessels are notinvolved, and that primary hemostasis, the firststage of the coagulation process, depends mainlyon platelet function, and is thus less affected byanticoagulant therapy (25).
A case-control study by Zanon et al. (28)
compared the incidence of bleedingcomplications following dental extraction inanticoagulated patients in whom anticoagulanttherapy was not changed with non-anticoagulated 537
NATÁLIA ANTÓNIO, et alRev Port Cardiol 2008; 27: 531-44
Baixo RiscoFA sem AVC
Cardiomiopatia semFA
Trombose venosa hámais de 6 meses
Prótese mecânicaaórtica bivalva e < 2factores riscotromboembólicos
Quadro II. Estratificação do risco tromboembólico
Moderado RiscoPrótese aórticamecânica bivalvabasculante e > 2factores de riscotromboembólicos
FA crónica e > 2factores de riscotromboembólicos
Trombose venosa hámenos de 6 meses
Alto RiscoPrótese mitralmecânica
Prótese valvular tipo“Ball-cage”
Trombose venosa hámenos de 3 meses
FA e história de AVC
EAM há menos de 3meses
AVC ou AIT recente(há menos de 1 mês)
Legenda: FA, Fibrilhação auricular; AVC, Acidente Vascular Cerebral; EAM, Enfarte
Agudo do Miocárdio; AIT, Acidente Isquémico Transitório
Low riskAF without stroke
Cardiomyopathywithout AF
Venous thrombosis>6 monthspreviously
Bileaflet aortic valveand <2 thrombo-embolic risk factors
Table II. Thromboembolic risk stratification
Moderate riskBileaflet tilting diskaortic valve and >2thromboembolic riskfactors
Chronic AF and >2thromboembolic riskfactors
Venous thrombosis<6 monthspreviously
High riskMechanical mitralvalve
Ball-cage valve
Venous thrombosis <3months previously
AF and history ofstroke
AMI <3 monthspreviously
Recent (1 month)stroke or transientischemic attack
AF: atrial fibrillation; AMI: acute myocardial infarction

tromboembolismo venoso de 2% a 10%. Osdoentes de baixo risco apresentam um risco anualde tromboembolismo arterial inferior a 5% e umrisco mensal de tromboembolismo venoso inferiora 2%. (26)
Alguns clínicos defendem que nos doentes debaixo risco tromboembólico, com necessidade deintervenção cirúrgica, se pode interromper aanticoagulação oral durante quatro a cinco diassem terapêutica de ponte com heparina. (26) Ogrupo de baixo risco tromboembólico incluidoentes com fibrilhação auricular sem outrosfactores de risco tromboembólico (AVC prévio,AITs, disfunção ventricular esquerda, idadesuperior a 75 anos, hipertensão e diabetes),portadores de próteses valvulares de 2ª geraçãoem posição aórtica, antecedentes detromboembolismo venoso há mais de 6 meses,doença cerebrovascular intrínseca sem AVC ouAIT recorrentes. (8)
Os doentes de alto e moderado riscotromboembólico devem manter a terapêuticaanticoagulante, inalterada ou com intervalosmínimos de níveis subterapêuticos. (26)
Risco hemorrágico pós-operatório - seráreal?
Há vários procedimentos cirúrgicos associadosa complicações hemorrágicas significativas(Tabela III). (26, 27)
A cirurgia oral minor é considerada umprocedimento de baixo risco hemorrágico. (26, 27)
Considera-se cirurgia oral minor: 1) extracçãosimples de até 3 dentes; 2) cirurgia gengival;3) aplicação de coroas; 4) pontes dentárias;5) remoção cirúrgica de dentes e 6) destar-
controls undergoing similar extractions. Nostatistically significant differences were foundbetween the rate of bleeding complications in theanticoagulated group and in the controls.
When patients under oral anticoagulanttherapy have teeth extracted, the great majority ofpostoperative bleeding complications are notsecondary to the therapy; ninety percent are dueto other causes such as surgical trauma,noncompliance with postoperative instructions,inappropriate use of analgesics such as aspirin orother nonsteroidal anti-inflammatory drugs, oruncontrolled hypertension (16).
Whether to suspend oral anticoagulants inthe perioperative period for minor oralsurgery
A review of the literature shows no well-documented cases of major bleeding followingminor oral surgery in patients under warfarintherapy and with INR levels within therapeuticranges. By contrast, serious emboliccomplications have been reported, some fatal,after suspension of oral anticoagulation for dentaltreatment (12, 25, 29).
A recent review of over 950 patients underlong-term anticoagulant therapy and undergoingoral surgery showed that only 12 patients (lessthan 1.3%) had bleeding that was not controlledby local hemostatic measures. Of these, only 3(<0.31%) had INR within or below therapeuticlimits. Among the 526 patients undergoing 575interruptions of anticoagulant therapy, therewere five severe embolic complications (0.95%),with four deaths. The study concluded thatsevere embolic complications associated with538
Rev Port CardiolVol. 27 Abril 08 / April 08
Procedimentos de baixo risco Procedimentos oftalmológicos(como a cirurgia de cataratas)Maioria das cirurgiasdermatológicasColecistectomia laparoscópicaColonoscopia e sigmoidoscopiacom ou sem biópsiasAngiografia coronária Cirurgia oral minor
Procedimentos de moderado a alto risco Cirurgias intra-torácicasCirurgias intra-abdominaisCirurgias ortopédicasCirurgias vasculares majorProcedimentos neurocirúrgicosProcedimentos urológicos (taiscomo prostatectomia, cirurgiavesical e biópsia renal)Procedimentos gastrointestinais(como ressecção intestinal eremoção endoscópica de pólipos)Cirurgias cardíacas Implantação de pacemakercardíaco Cirurgia oncológica
Quadro III. Risco hemorrágico de diferentes procedimentoscirúrgicos
Low risk Eye surgery, e.g. cataractsMost dermatological proceduresLaparoscopic cholecystectomyColonoscopy andsigmoidoscopy, with or withoutbiopsyCoronary angiography Minor oral surgery
Moderate to high risk Intrathoracic surgeryIntra-abdominal surgeryOrthopedic surgeryMajor vascular surgeryNeurosurgeryUrological procedures, e.g.prostatectomy, bladder surgeryand renal biopsyGastrointestinal procedures, e.g.intestinal resection andendoscopic removal of polypsCardiac surgery Pacemaker implantation Cancer surgery
Table III. Bleeding risk of different surgical procedures

tarização. (28) Em cirurgia oral, o risco hemorrágico éum risco local, relacionado com o acto cirúrgico. (5)
A incidência de hemorragia precoce ésemelhante entre doentes hipocoagulados edoentes sem terapêutica anticoagulante. Aexplicação parece residir no facto de não seremlesados grandes vasos na cirurgia oral e no factoda hemostase imediata estar dependente dafase primária da coagulação (dependenteprincipalmente da função plaquetária e como talmenos afectada pela terapêutica comanticoagulantes). (25)
Um estudo caso-controlo de Zanon ecolaboradores (28) compara a incidência decomplicações hemorrágicas após extracçõesdentárias, em doentes anticoagulados semmodificação da terapêutica anticoagulante comcontrolos saudáveis sujeitos a extracçõescomparáveis. Foi demonstrado não existiremdiferenças estatisticamente significativas entrea taxa de complicações hemorrágicas dogrupo anticoagulado e do controlo. (28)
Quando os doentes são submetidos a extracçãodentária sob terapêutica com anticoagulantesorais, a grande maioria das complicaçõeshemorrágicas pós-operatórias não são secundáriasà terapêutica anticoagulante oral. Noventa porcento dessas complicações são devidas aoutras causas, incluindo traumatismo cirúrgicoexcessivo, má adesão do doente às instruçõespós-operatórias, uso inapropriado de analgésicoscomo a aspirina e outros anti-inflamatóriosnão esteróides ou hipertensão arterial nãocontrolada. (16)
Continuar ou interromper osanticoagulantes orais no perioperatório de cirurgia oral minor?
Após revisão da literatura, conclui-se nãoexistirem casos bem documentados de hemorragiagrave após cirurgia oral minor em doentesmedicados com varfarina, com níveis de INRdentro do intervalo terapêutico. Pelo contrário, emrelação às complicações embólicas estão descritoscasos graves, alguns com desfecho fatal, apósinterrupção da terapêutica anticoagulante oralpara tratamento estomatológico. (12, 25, 29)
Uma revisão recente de mais de 950 doentessubmetidos a cirurgia oral sob terapêuticaanticoagulante crónica demonstrou que apenas12 doentes (menos de 1,3%) apresentaramcomplicações hemorrágicas não controladas com
interruption of anticoagulant therapy were threetimes more likely than bleeding complicationswhen anticoagulant therapy is maintained withinor below therapeutic levels (30).
The first controlled clinical trial on dentalextraction in patients receiving warfarin,conducted in 1983, showed that there was noneed to suspend oral anticoagulant therapy solong as INR was within therapeutic limits (31).Several subsequent studies have confirmed that itwas not necessary, and could in fact bedangerous, to suspend warfarin for simple dentalextraction (3).
Given the local character of bleedingassociated with dental extractions, a growingnumber of authors have proposed not alteringanticoagulant therapy as long as local hemostaticmeasures such as sutures, tranexamic acid andfibrin glue are used (5, 32-34).
Evans et al. confirmed that dental extractioncan be performed safely without interruptingwarfarin therapy so long as INR is <4.1 (3).
Devani et al. state that there is no justificationfor altering warfarin therapy before dentalextraction so long as INR is between 2.0 and 4.0and local hemostatic measures are used to controlpostoperative bleeding, thus avoiding exposingthe patient to risk of thromboembolism (33).
According to Madrid, local hemostaticmeasures should be adapted in accordance withanticoagulation levels (5):
1) with INR between 1.5 and 2.1, sutures andoxycellulose will be sufficient;
2) with INR between 2.1 and 3.5, for minorsurgery, sutures together with tranexamic acidmouthwashes or compresses will be sufficient;
3) with INR of over 3.5, fibrin glue ortranexamic acid should be used in associationwith sutures (5).
The European Society of Cardiology and theAmerican College of Cardiology recommend notstopping antithrombotic therapy for procedures inwhich bleeding complications are unlikely orinconsequential, such as surgery on the skin,minor oral surgery and eye surgery, particularlyfor cataracts or glaucoma (8).
Various studies have shown that minor oralsurgery can be scheduled on an outpatient basisand that anticoagulant therapy need not bealtered so long as INR is <3 and local hemostatictechniques are used (33, 35, 39).
539
NATÁLIA ANTÓNIO, et alRev Port Cardiol 2008; 27: 531-44

medidas hemostáticas locais. Destes doentes,apenas 3 (< 0,31%) apresentavam níveis deanticoagulação dentro ou abaixo dos níveisterapêuticos. Nos 526 doentes submetidos a 575interrupções da terapêutica anticoagulante o autorobservou a ocorrência de 5 (0,95 %) complicaçõesembólicas graves, tendo 4 destes doentes falecido.Os autores concluem que as complicaçõesembólicas graves associadas à interrupção daterapêutica anticoagulante apresentam umaprobabilidade de ocorrência 3 vezes superior faceà probabilidade de ocorrência de complicaçõeshemorrágicas quando a terapêutica anticoagulanteé mantida, dentro ou abaixo dos valoresterapêuticos. (30)
O primeiro ensaio clínico controlado deextracção dentária em doentes sob varfarina foiconduzido em 1983 e demonstrou não sernecessário interromper a terapêutica antico-agulante oral desde que o INR se encontrassedentro dos limites terapêuticos. (31) Vários estudosposteriores confirmaram que não é necessário, eaté pode ser perigoso, suspender a varfarina paraextracções dentárias simples. (3)
Atendendo ao carácter local das complicaçõeshemorrágicas associadas às extracções dentárias,um número crescente de autores propõe a nãoalteração da terapêutica anticoagulante, desdeque se associem meios hemostáticos locais(suturas, ácido tranexâmico, cola de fibrina). (5, 32- 34)
Evans e colaboradores afirmam que asextracções dentárias podem ser efectuadas comsegurança, sem interrupção da varfarina, desdeque o INR seja < 4,1. (3)
Devani P e colaboradores referem que não hájustificação para alterar o tratamento comvarfarina antes de extracções dentárias desde queo INR se situe entre 2,0 e 4,0 e se usem medidashemostáticas locais para controlar a hemorragiapós-operatória, evitando assim a exposição dodoente ao risco tromboembólico. (33)
Segundo Madrid as medidas hemostáticaslocais devem ser adaptadas em função dos níveisde anticoagulação: (5)
1) com níveis de INR entre 1,5 e 2,1 - orecurso a suturas e a oxicelulose será suficiente;
2) com INR entre 2,1 e 3,5 - para cirurgiasminor, o recurso a suturas associadas a gargarejosou compressas de ácido tranexâmico serásuficiente;
3) com INR superior a 3,5 - utilização de colasde fibrina ou ácido tranexâmico associados às
PROPOSED PROTOCOL FORANTICOAGULATED PATIENTSREQUIRING MINOR ORAL SURGERY
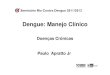
In patients under long-term anticoagulation,there is no need for suspension of the treatment orhospitalization before minor oral surgery so longas INR is stable. Patients should continue oralanticoagulation therapy and the dental treatmentshould be scheduled on an outpatient basis.
INR should ideally be assessed in the 24hours preceding dental treatment, but for patientswith stable INR, assessment can be up to 72hours before. If INR is <3, the procedure can beperformed with the support of local hemostaticmeasures and without altering anticoagulationlevels. If INR is >3, the oral anticoagulant doseshould be adjusted to bring INR to <3.
There are three exceptions to thisrecommendation:
1) In patients with indication for oralanticoagulation for a limited period (6 months orless) requiring non-urgent minor oral surgery, thedental treatment should be postponed until afterthe prescribed period of anticoagulation.
2) In patients with indication for long-termoral anticoagulation that began less than 90 dayspreviously or in whom INR has not stabilized, itis preferable to await stabilization of INR to <3before scheduling the dental treatment.
3) In patients with indication for long-termoral anticoagulation and with comorbidities thataffect hemostasis or otherwise increase risk ofbleeding (uncontrolled hypertension, renal orliver failure, alcoholism, thrombocytopenia,hemophilia or other coagulation disorders, ortreatment with cytostatics), there may be safetyissues with performing even minor oral surgery onan outpatient basis. Consideration should begiven to hospitalizing the patient before thetreatment to ensure rigorous control of INR andmonitoring of possible bleeding complications(Figure 1).
Ideal timing for dental treatmentIdeally, dental treatment should be scheduled:a) early in the day (giving more time to deal
with possible early bleeding);b) early in the week (so that possible late
bleeding, which generally occurs 24-48 hoursafter surgery, does not happen during theweekend) (28).540
Rev Port CardiolVol. 27 Abril 08 / April 08

suturas. (5)
A European Society of Cardiology e oAmerican College of Cardiology preconizam anão interrupção da terapêutica antitrombóticapara procedimentos em que as complicaçõeshemorrágicas são pouco prováveis ou incon-sequentes caso ocorram (cirurgias dermatológicas,cirurgia oral minor e cirurgias oftalmológicas,particularmente a cirurgia de cataratas e a deglaucoma). (8)
São vários os estudos a afirmar que a cirurgiaoral minor pode ser programada em ambulatório,sem necessidade de modificação do tratamentoanticoagulante oral desde que o INR seja igual ouinferior a 3, com a utilização concomitante detécnicas hemostáticas locais. (33, 35, 39)
PROPOSTA DE PROTOCOLO PARADOENTES ANTICOAGULADOSNECESSITANDO DE CIRURGIA ORALMINOR
Nos doentes com indicação para anticoagulaçãooral crónica, não é necessário suspender oanticoagulante oral em curso nem internar o doenteantes de uma cirurgia oral minor, desde que osvalores de INR estejam estáveis. O doente deverámanter o anticoagulante oral em curso, sendo oprocedimento estomatológico programado emambulatório.
É necessário determinar o INR antes doprocedimento estomatológico, idealmente nas24 horas precedentes. No entanto, nos doentes comINR estável é aceitável efectuar esta determinaçãoaté 72 horas antes da cirurgia oral minor. Se odoente apresentar um INR igual ou inferior a 3, oprocedimento estomatológico pode ser realizadosem necessidade de ajuste dos níveis deanticoagulação (com o apoio de técnicashemostáticas locais). Se o INR for superior a 3, seránecessário ajustar a dose do anticoagulante oral deforma a atingir valores de INR iguais ou inferioresa 3.
Consideram-se excepções a esta recomen-dação, três situações:
1) Os doentes com indicação paraanticoagulação oral por um período de tempolimitado (igual ou inferior a 6 meses), em que acirurgia oral minor não tem carácter urgente.Nestes doentes o procedimento estomatológicodeve ser adiado até o doente completar o período de
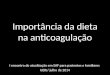
Postoperative care (28)
INR must be reassessed within 72 hours of theprocedure and the patient must be giveninstructions for postoperative care in order tominimize the risk of bleeding (Figure 2). Thisincludes the need to rest for the first two or threehours following surgery, not to rinse the mouth for24 hours, to avoid sucking or coughing hard, andnot to touch the surgical site with the tongue orother materials. Diet should consist of cold, liquidfood for the first day. Applying ice to the face for20-minute periods every 12 hours can helpreduce the risk of bleeding as well as giving painrelief.
The patient should also be advised to takeparacetamol or selective COX-2 inhibitors ratherthan nonsteroidal anti-inflammatory painkillers.
If persistent or de novo bleeding occurs, thepatient should be advised to remain seated and toapply gauze firmly to the site of bleeding for 20minutes. If this does not solve the problem, thepatient should contact his or her dentist or go tothe emergency department. It may be necessaryto apply local hemostatic agents, review thesutures, administer vitamin K or transfuse freshplasma.
541
NATÁLIA ANTÓNIO, et alRev Port Cardiol 2008; 27: 531-44
A. Patients with indication for oral anticoagulation for a limited period,awaiting elective dental treatment
B. Patients with indication for long-term oral anticoagulation and:
Postpone dental treatment until end of prescribedperiod of oral anticoagulation
C. Other patients with indication for long-term oral anticoagulation
Maintain warfarin therapy and schedule minororal surgery on an outpatient basis
Assess INR between 24 and 72 hours before the procedure
If more than 3 extractions are required, schedule several sessions in order to extract a maximum of 2-3 teeth per session
• if INR <3, the procedure can be performed without adjusting anticoagulation levels
• if INR >3, modify therapy to obtain INR <3 and postpone dental treatment
Consider hospitalization for adjustment of INR to obtain levels of 3 and monitoring for postoperative bleeding
- uncontrolled hypertension- renal failure- liver failure- alcoholism- thrombocytopenia or coagulation disorders- chemotherapy
Figure 1. Management protocol for anticoagulated patientsrequiring minor oral surgery

anticoagulação previsto2) Os doentes com indicação para
anticoagulação oral crónica, em que oanticoagulante oral foi iniciado há menos de 90 diasou em que o INR ainda não se encontraestabilizado. Nesta situação, é preferívelaguardar a estabilização do INR em valores iguaisou inferiores a 3 e só depois programar oprocedimento estomatológico.
3) Os doentes com indicação paraanticoagulação oral crónica e comorbilidades queafectem a hemostase ou aumentem o riscohemorrágico (hipertensão arterial não controlada;insuficiência renal ou hepática; alcoolismo;trombocitopenia; hemofilia ou outras perturbaçõesda coagulação; tratamento com citostáticos). Nestesdoentes realizar a cirurgia oral minor em regime deambulatório poderá ser pouco seguro. É preferívelponderar a hospitalização do doente antes doprocedimento estomatológico, para rigoroso ajustedo INR e vigilância das complicações hemorrágicas(Figura 1).
Timing ideal para a intervençãoestomatológica programada
Idealmente, a intervenção estomatológicaprogramada deve ser realizada:
CONCLUSIONS
Evidence-based medicine today makes itpossible to recommend maintenance of oralanticoagulation before simple dental extractions.Currently available information does not supportthe interruption of oral anticoagulation therapyfor minor oral surgery.
The bleeding complications that can occurfollowing dental extractions in anticoagulatedpatients are only a significant risk in exceptionalcases. However, suspending anticoagulanttherapy can expose the patient to unnecessaryand life-threatening thromboembolic risk. It hasbeen clearly shown that the likelihood of death orsevere and permanent sequelae is higher forthromboembolic events than for bleeding. Strokeis a catastrophic event, while oral hemorrhage ismerely inconvenient and can usually be easilycontrolled.
There is therefore no need to alteranticoagulant therapy for minor oral surgery as amatter of course.
Changes to therapy should thus only beconsidered when an aggressive surgicalintervention is associated with high levels ofanticoagulation and antiplatelet therapy;anticoagulant therapy should not always beinterrupted before dental extractions. In mostpatients, a reduction in anticoagulation levels,while keeping within therapeutic limits, togetherwith local hemostatic measures, is sufficient tocontrol risk of bleeding.
542
Rev Port CardiolVol. 27 Abril 08 / April 08
A. Doente com indicação para o tratamento anticoagulante oral por um períodode tempo limitado, que aguarda procedimento estomatológico electivo
B. Doente com indicação para anticoagulação oral crónica com:
Adiar a intervenção estomatológica até completar o tempo de anticoagulação oral previsto
C. Restantes doentes com indicação para anticoagulação oral crónica:
Manter a terapêutica com varfarina e programar emambulatório a cirurgia oral minor
Determinar o INR no intervalo de 24 a 72 horas antes do procedimento
Se necessidade de extracções dentárias múltiplas(mais de 3) - planear várias sessões de forma a extrair
no máximo 2 a 3 dentes por sessão (cirurgia oral minor)
• Se INR < 3 - o procedimento estomatológico pode ser realizado, sem ajuste dos níveis de antiocoagulação;
• Se INR > 3 - modificação do tratamento de forma a alcançar o INR < 3 e adiar procedimento estomatológico
Ponderar hospitalização do doente para ajuste do INR (de formaa obter valores iguais ou inferiores a 3) e vigilância de
complicações hemorrágicas pós-operatórias
- Hipertensão não controlada,- Insuficiência renal,- Insuficiência hepática,- Alcoolismo,- Trombocitopenia ou distúrbios da coagulação ou- Doente sob quimioterapia
Figura 1. Protocolo de actuação em doentes anticoaguladosnecessitando de cirurgia oral minor
• Monitor initial hemostasis at rest (2-3 hours)
• Do not rinse mouth for the first 24 hours
• Do not suck or cough hard
• Do not touch the surgical site with the tongue or other materials
• Consume only liquid food for the first day
• Avoid hot liquids and hard foods for the rest of the day
• Apply ice to the face for 20 min every 12 hours
• For painkillers, use paracetamol or selective COX-2 inhibitors, not nonsteroidal anti-inflammatory drugs
• In the event of persistent or de novo bleeding: - Remain seated, apply gauze saturated with antifibrinolytic and apply pressure for 20 min.; - If the problem persists, consult dentist or go to the emergency department.
Figure 2. Precautions following minor oral surgery inanticoagulated patients

a) no início do dia (conferindo mais tempo paralidar com eventuais hemorragias precoces) e
b) no início da semana (evitando que eventuaishemorragias tardias, que geralmente ocorrem 24 a48 horas após o procedimento, surjam durante ofim-de-semana). (28)
Cuidados pós-operatórios: (28)
É fundamental reavaliar o INR nas primeiras72 horas do pós-operatório e aconselhar o doenterelativamente aos cuidados pós-operatórios, deforma a minimizar complicações hemorrágicas(Figura 2).
O doente deve ser informado da importânciade permanecer em repouso durante as primeirasduas a três horas de pós-operatório; evitar lavar aboca durante 24 horas; evitar sugar ou tossirfortemente e não tocar no local da intervençãocom a língua ou com materiais estranhos. Deveser recomendada uma dieta líquida e fria, noprimeiro dia de pós-operatório. A aplicação degelo na face por períodos de 20 minutos, de 12em 12 horas, é útil na diminuição do riscohemorrágico e uma importante medida analgésica.
O doente deve também ser aconselhado aevitar analgésicos anti-inflamatórios nãoesteróides, preferindo paracetamol ou inibidoresselectivos da COX-2.
Relativamente a eventuais hemorragiaspersistentes ou de novo, o doente deve seraconselhado a permanecer sentado e aplicarfirmemente uma gaze sobre o local da hemorragia,durante 20 minutos. Se a hemorragia nãoresolver com esta medida, o doente deve contactaro estomatologista ou recorrer ao serviço deurgência (poderá ser necessário aplicar agenteshemostáticos locais ou rever a sutura, administrarvitamina K ou transfundir plasma fresco).
CONCLUSÕES
É hoje possível recomendar a manutenção daanticoagulação oral antes de extracções dentáriassimples com o suporte de uma medicina baseadana evidência.
A informação actualmente disponível nãoapoia a interrupção da terapêutica anticoagulanteoral para cirurgia oral minor.
As complicações hemorrágicas que podemocorrer após extracções dentárias em doentesanticoagulados apenas apresentam um riscosignificativo em casos excepcionais. Emcontrapartida, a interrupção da terapêuticaanticoagulante antes dos procedimentos estoma-tológicos pode expor desnecessariamente odoente a risco de vida por tromboembolismo.
Está bem documentado que a probabilidadede ocorrências fatais ou que deixam sequelaspermanentes graves é superior nos episódiostromboembólicos comparativamente aos episódioshemorrágicos. Um AVC é um evento catastróficoenquanto que uma hemorragia bucal é meramenteincomodativa e habitualmente bem controlada.
Não existe pois motivo para se alterarsistematicamente as terapêuticas anticoagulantesdevido a uma cirurgia oral minor.
Apenas a associação de um gesto operatórioagressivo com níveis de anticoagulação elevadose tratamento antiagregante plaquetar deve levara que se pondere uma eventual modificaçãoda terapêutica anticoagulante.
Desta forma, a terapêutica anticoagulantenão deve ser interrompida indiscrimina-damente antes de extracções dentárias. Na grandemaioria dos doentes, a redução dos níveis deanticoagulação (embora ainda dentro dos níveisterapêuticos) associada a medidas hemostáticaslocais é suficiente para controlar o riscohemorrágico.
Pedidos de separatas para:
Address for reprints:
NATÁLIA SOFIA CLÁUDIO ANTÓNIO
Serviço de Cardiologia
Hospitais da Universidade de Coimbra
Praceta Mota Pinto
3000-075 Coimbra
e-mail: [email protected] 543
NATÁLIA ANTÓNIO, et alRev Port Cardiol 2008; 27: 531-44
• Vigiar a hemostase inicial, em repouso (2-3 horas);
• Evitar lavar a boca durante as primeiras 24 horas;
• Não sugar, nem tossir fortemente;
• Não tocar no local de intervenção com a língua ou com materiais estranhos;
• Dieta líquida no primeiro dia pós-operatório;
• Evitar líquidos quentes ou alimentos de consistência dura o resto do dia;
• Aplicar gelo na face durante 20 min de 12 em 12 horas;
• Analgesia: não utilizar Anti-inflamatórios não esteróides, preferir paracetamol ou inibidores selectivos da COX-2;
• Se hemorragia persistente ou de novo: 1º) sentado, aplicar gaze molhada com antifibrinolítico e aplicar pressão durante 20 min; 2º) se não resolver, procurar o estomatologista ou recorrer ao serviço de urgência.
Figura 2. Cuidados a ter após cirurgia oral minor em doentesanticoagulados

544
Rev Port CardiolVol. 27 Abril 08 / April 08
1. Heit JA. Perioperative management of the chronicallyanticoagulated patient. J Thromb Thrombolysis. 2001; 12(1):81-7.
2. Análise da evolução da utilização dos anticoagulantes eantitrombóticos em Portugal Continental entre 1999 e 2003.Infarmed. Junho 2005. Disponível emhttp://www.infarmed.pt/portal/page/portal/infarmed/monitorizacao_do_mercado/observatorio/introducao_de_ficheiros/Estudo_anticoagulantes.pdf
3. Evans IL, Sayers MS, Gibbons AJ, Price G, Snooks H, SugarAW. Can warfarin be continued during dental extraction? Resultsof a randomized controlled trial. Br J Oral Maxillofac Surg. 2002;40(3):248-52.
4. Dunn A. Perioperative Management of Oral Anticoagulation:When and How to Bridge. J Thromb Thrombolysis. 2006;21(1),85-89.
5. Madrid C. Doit-on modifier le traitement anticoagulant avantdes extractions dentaires? Rev Med Suisse. 2005; 1:1418-24.
6. Larson BJ, Zumberg MS, Kitchens CS. A feasibility study ofcontinuing dose-reduced warfarin for invasive procedures inpatients with high thromboembolic risk. Chest. 2005; 127(3):922-7.
7. Kearon C, Hirsh J. Management of anticoagulation before andafter elective surgery. N Engl J Med. 1997; 336:1506-11.
8. ACC/AHA 2006 guidelines for the management of patients withvalvular heart disease: a report of the American College ofCardiology/American Heart Association Task Force on PracticeGuidelines developed in collaboration with the Society ofCardiovascular Anesthesiologists endorsed by the Society forCardiovascular Angiography and Interventions and the Society ofThoracic Surgeons. J Am Coll Cardiol. 2006;48(3):e1-148.
9. Carter G, Goss AN, Lloyd J, Tocchetti R. Current concepts ofthe management of dental extractions for patients takingwarfarin. Aust Dent J. 2003; 48(2):89-96.
10. Kamien M. Remove the tooth, but don’t stop the warfarin.Aust Fam Physician. 2006; 35(4):233-5.
11. Poller L. International Normalized Ratios (INR): the first 20years. J Thromb Haemost. 2004;2(6):849-60.
12. Hirsh J, Bates SM. Clinical trials that have influenced thetreatment of venous thromboembolism: a historical perspective.Ann Intern Med. 2001;134:409-17
13. Flood E, Redish MH, Bociek SJ. Thrombophlebitis migransdisseminata. N Y State J Med. 1943; 43:1121-4.
14. Gladson CL, Groney P, Griffin JH. Coumarin necrosis,neonatal purpura fulminans, and protein C deficiency. ArchDermatol. 1987;123:1701a-1706a.
15. Osswald W, Guimarães S. Terapêutica medicamentosa e suasbases farmacológicas. Porto Editora. 4ª edição. Cap 38. 2001:560-569.
16. Scully C, Wolff A, Aviv T. Oral surgery in patients onanticoagulated therapy. Oral Surg Med Oral Pathol Oral Endod.2002; 94:57-64.
17. Little JW, Miller CS, Henry RG, McIntosh BA.Antithrombotic agents: Implications in dentistry. Oral Surg OralMed Oral Pathol Oral Radiol Endod. 2002; 93:544-51.
18. Wells PS, Holbrook AM, Crowther NR, Hirsh J. Interactionsof Warfarin with Drugs and Food. Ann Intern Med. 1994; 121(9):676-83.
19. Douketis JD, Crowther MA, Cherian SS, Kearon CB.Physician preferences for perioperative anticoagulation inpatients with a mechanical heart valve who are undergoingelective non-cardiac surgery. Chest. 1999; 116:1240-46.
20. Spyropoulos AC, Bauersachs RM, Omran H, Cohen M.Periprocedural bridging therapy in patients receiving chronic
oral anticoagulation therapy. Curr Med Res Opin. 2006;22(6):1109-22.
21. Bloomer CR. Excessive hemorrhage after dental extractionsusing low-molecular-weight heparin (Lovenox) anticoagulationtherapy. J Oral Maxillofac Surg. 2004; 62(1):101-3.
22. Gohlke-Bärwolf C, Zentrum H, Krozingen B. Anticoagulationin valvar heart disease: new aspects and management during non-cardiac surgery. Heart. 2001; 10:215-220.
23. Kovacs MJ, Kearon C, Rodger M, Anderson DR, Turpie AG,Bates SM, et al. Single-arm study of bridging therapy with low-molecular-weight heparin for patients at risk of arterial embolismwho require temporary interruption of warfarin. Circulation.2004; 21;110(12):1658-63.
24. Heuts LM, Arvik BM, Cender DE. LMWH for perioperativeanticoagulation in patients on chronic warfarin therapy. AnnPharmacother. 2004; 38(6):1065-9.
25. Marques MS, Almeida AP, Lopes MG. A terapêuticaanticoagulante em cirurgia oral - revisão da literatura. Rev PortEstomatol Cir Maxilofac. 2005; 46:31-36.
26. Beirne OR. Evidence to continue oral anticoagulant therapyfor ambulatory oral surgery. J Oral Maxillofac. 2005; 63:540-5.
27. Douketis JD. Perioperative anticoagulation management inpatients who are receiving oral anticoagulant therapy: a practicalguide for clinicians. Thromb Res. 2002; 108(1):3-13.
28. Zanon E, Martinelli F, Bacci C, Cordioli GP, Girolami A.Safety of dental extraction among consecutive patients on oralanticoagulant treatment managed using a specific dentalmanagement protocol. Blood Coagul Fibrinolysis. 2003; 14:27-30.
29. Wahl MJ. Dental surgery in anticoagulated patients. ArchIntern Med. 1998; 158:1610-6.
30. Wahl MJ. Myths of dental surgery in patients receivinganticoagulant therapy. J Am Dent Assoc. 2000; 131(1):77-81.
31. Bailey BM, Fordyce AM. Complications of dental extractionin patients receiving warfarin anticoagulant therapy: a controlledtrial. Br Dent J. 1983; 155:308-10.
32. Carter G, Goss A, Lioyd J, Tocchetti R. Tranexamic acidmouthwash versus autologous fibrin glue in patients takingwarfarin undergoing dental extractions: a randomizedprospective clinical study. J Oral Maxillofac Surg. 2003;61(12):1432-5.
33. Devani P, Lavery KM, Howell CJ. Dental extractions inpatients on warfarin: is alteration of anticoagulant regimenecessary? Br J Oral Maxillofac Surg. 1998; 36(2):107-11.
34. Campbell JH, Alvarado F, Murray RA: Anticoagulation andminor oral surgery: should the anticoagulation regimen bealtered? J Oral Maxillofac Surg. 2000, 58:135-136.
35. Cannon PD, Dharmar VT. Minor oral surgical procedures inpatients on oral anticoagulants--a controlled study. Aust Dent J.2003; 48(2):115-8.
36. Kruse-Loesler B, Kelker M, Kleinheinz J. Comparison oflaboratory and immediate diagnosis of coagulation for patientsunder oral anticoagulation therapy before dental surgery. HeadFace Med. 2005; 29;1:12.
37. Randall C. Surgical management of the primary care dentalpatient on warfarin. Dent Update. 2005; 32(7):414-6, 419-20, 423-4.
38. Garcia-Darennes F, Darennes J, Freidel M, Breton P.Protocol for adapting treatment with vitamin K antagonistsbefore dental extraction. Rev Stomatol Chir Maxillofac. 2003;104(2):69-72.
39. Al-Mubarak S, Al-Ali N, Abou-Rass M, Al-Sohail A, RobertA, Al-Zoman K, Al-Suwyed A, Ciancio S. Evaluation of dentalextractions, suturing and INR on postoperative bleeding ofpatients maintained on oral anticoagulant therapy. Br Dent J.2007; 203(7):410-1.
BIBLIOGRAFIA / REFERENCES