Embed Size (px)
Citation preview

João Borges Fortes Filho
MESTRE, DOUTOR E PÓS-DOUTOR EM OFTALMOLOGIA
PELA UNIVERSIDADE FEDERAL DE SÃO PAULO
PROROP INVESTIGATIVE GROUP
UFRGS / UNIFESP / BRASIL
Habilitação visual na
Retinopatia da Prematuridade
FACULDADE DE MEDICINA
UNIVERSIDADE FEDERAL DO RIO GRANDE DO SUL
HOSPITAL DE CLÍNICAS DE PORTO ALEGRE

RETINOPATIA DA PREMATURIDADE (ROP)
IMPORTÂNCIA DO DIAGNÓSTICO
ESTADIAMENTO PRECOCE
OPÇÕES TERAPÊUTICAS
PREVENÇÃO
Doença Plus
Ridge
Crista
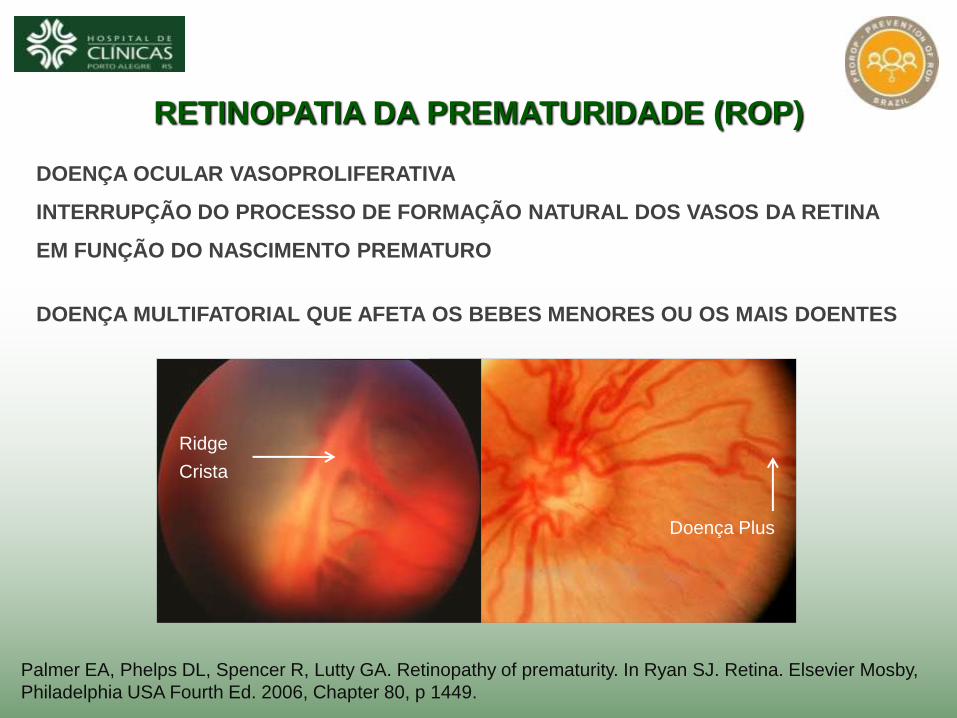
RETINOPATIA DA PREMATURIDADE (ROP)
DOENÇA OCULAR VASOPROLIFERATIVA
INTERRUPÇÃO DO PROCESSO DE FORMAÇÃO NATURAL DOS VASOS DA RETINA
EM FUNÇÃO DO NASCIMENTO PREMATURO
DOENÇA MULTIFATORIAL QUE AFETA OS BEBES MENORES OU OS MAIS DOENTES
Palmer EA, Phelps DL, Spencer R, Lutty GA. Retinopathy of prematurity. In Ryan SJ. Retina. Elsevier Mosby,
Philadelphia USA Fourth Ed. 2006, Chapter 80, p 1449.
Doença Plus
Ridge
Crista

A ROP COMO CAUSA MUNDIAL DE CEGUEIRA
ESTÁVEL OU REDUZINDO NOS PAÍSES INDUSTRIALIZADOS
AUMENTANDO EM MUITO NOS PAÍSES EM DESENVOLVIMENTO
A ROP INEXISTE NOS PAÍSES COM ALTA MORTALIDADE NEONATAL
10% a 30% ROP MODERADA
0% a 60% ROP GRAVE
0% a 5%
10% a 60%
8 / 1000 baixo risco ROP
9 - 60 / 1000 alto risco ROP
61 / 1000 baixo risco ROP OMS 2000
A cegueira pela ROP está relacionada com a mortalidade infantil
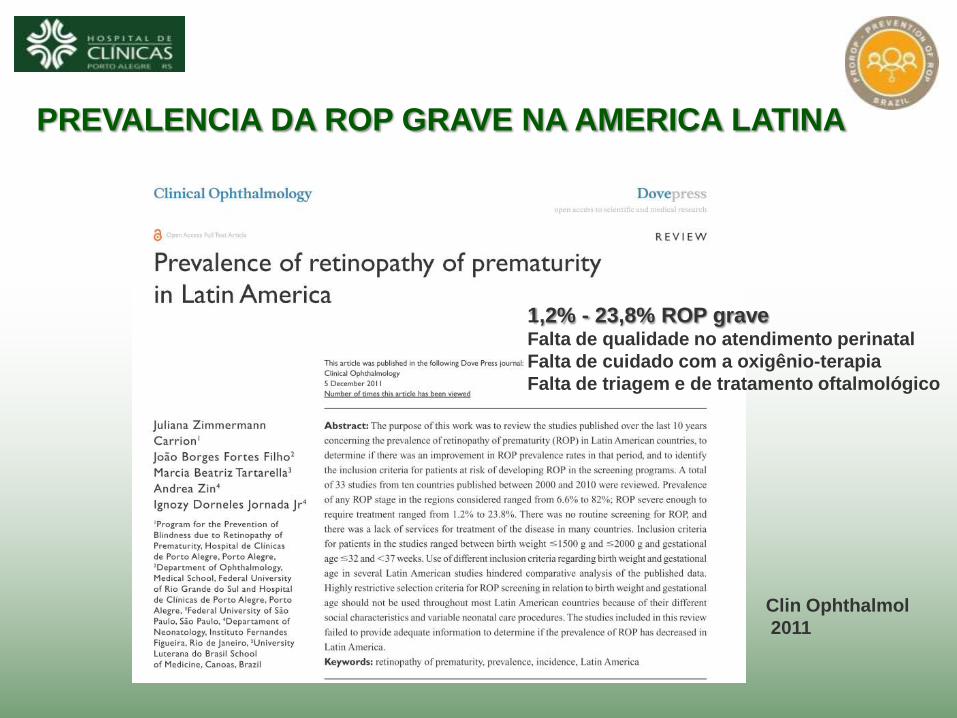
PREVALENCIA DA ROP GRAVE NA AMERICA LATINA
Clin Ophthalmol
2011
1,2% - 23,8% ROP grave Falta de qualidade no atendimento perinatal
Falta de cuidado com a oxigênio-terapia
Falta de triagem e de tratamento oftalmológico

ESTADIAMENTO 1
Linha de demarcação entre a retina vascularizada e a retina periférica avascular
ESTADIAMENTO 2
Linha de demarcação mais larga com crista elevada por sobre a linha
ESTADIAMENTO 3
Formação de tecido fibrovascular elevado por sobre a crista, fora do plano da retina
ESTADIAMENTO 4
Descolamento da retina
ROP 3
EM 1984 A DOENÇA FOI CLASSIFICADA EM 4 ESTADIAMENTOS
ROP 1 ROP 2
ROP 3
An international classification of retinopathy of prematurity.
The Committee for the Classification of Retinopathy of Prematurity. Arch Ophthalmol 1984; 102(8):1130-4.
THE INTERNATIONAL COMMITTEE FOR CLASSIFICATION OF ROP

1984 - CONCEITO DE DOENÇA PLUS RetCam Image
Dilatação, tortuosidade e engurgitamento vascular AV
Rigidez pupilar
Significado clínico é de ROP em progressão
Grande risco para perda visual severa no RN afetado
An international classification of retinopathy of prematurity.
The Committee for the Classification of Retinopathy of Prematurity. Arch Ophthalmol 1984; 102(8):1130-4.
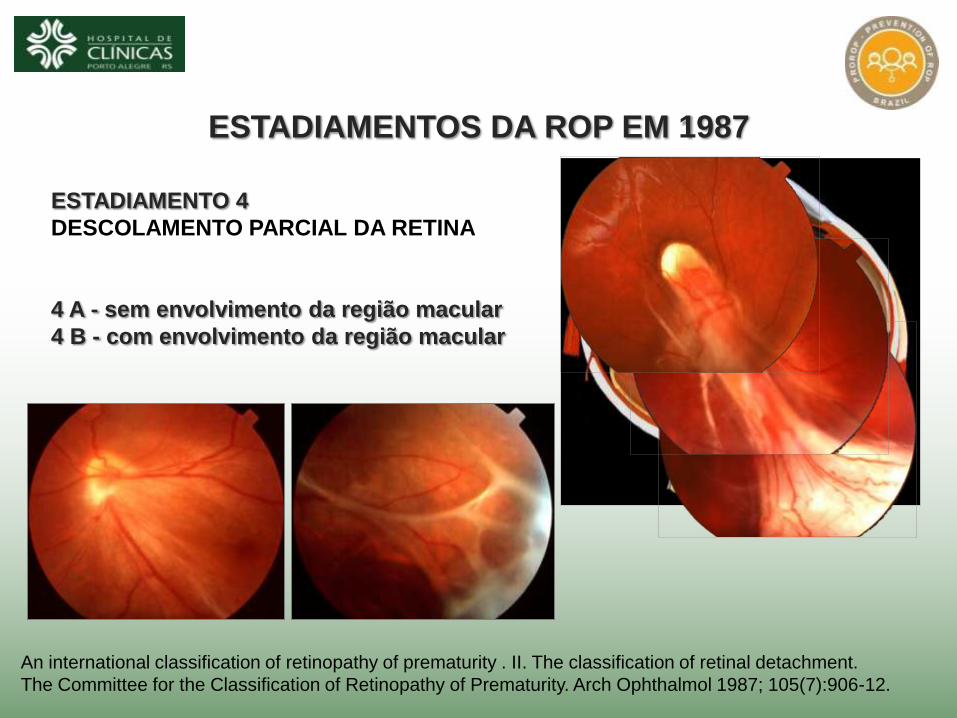
ESTADIAMENTO 4
DESCOLAMENTO PARCIAL DA RETINA
4 A - sem envolvimento da região macular
4 B - com envolvimento da região macular
ESTADIAMENTOS DA ROP EM 1987
An international classification of retinopathy of prematurity . II. The classification of retinal detachment.
The Committee for the Classification of Retinopathy of Prematurity. Arch Ophthalmol 1987; 105(7):906-12.
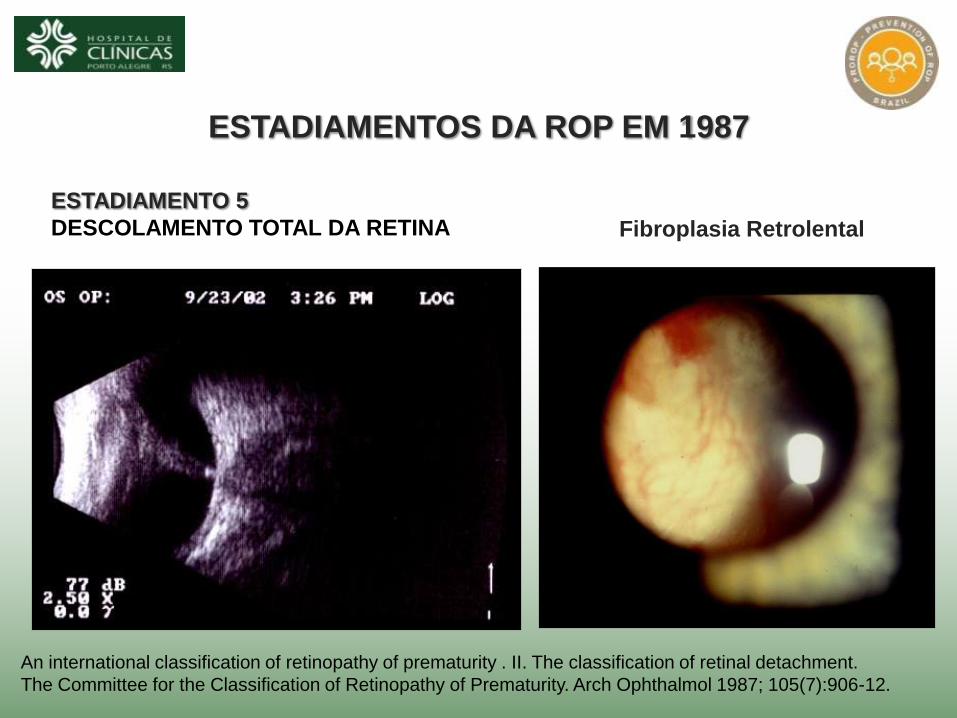
ESTADIAMENTO 5
DESCOLAMENTO TOTAL DA RETINA
ESTADIAMENTOS DA ROP EM 1987
Fibroplasia Retrolental
An international classification of retinopathy of prematurity . II. The classification of retinal detachment.
The Committee for the Classification of Retinopathy of Prematurity. Arch Ophthalmol 1987; 105(7):906-12.

1988 - A CLASSIFICAÇÃO INTERNACIONAL
POSSIBILITOU OS PROGRAMAS DE TRIAGEM NEONATAL
CRITÉRIOS DE INCLUSÃO BASEADOS NO
PESO DE NASCIMENTO E NA IDADE GESTACIONAL
CRITÉRIOS VARIAM ENTRE PAÍSES OU ENTRE REGIÕES
Zin A, Florêncio T, Fortes Filho JB, Nakanami CR, Gianini N, Graziano RM, Moraes N.
Proposta de diretrizes brasileiras para a detecção e o tratamento da retinopatia da prematuridade (ROP).
Arq Bras Oftalmol 2007; 70(5):875-83.

A TRIAGEM NEONATAL NA BUSCA DA DOENÇA
DEVERÃO SER EXAMINADOS PARA A ROP
PN ≤ 1.500 gramas e/ou IG ≤ 32 semanas
Bebês maiores serão examinados por solicitação do Neonatologista
Zin A, Florêncio T, Fortes Filho JB, Nakanami CR, Gianini N, Graziano RM et al.
Proposta de diretrizes brasileiras para a detecção e o tratamento da retinopatia da prematuridade (ROP).
Arq Bras Oftalmol 2007; 70(5):875-83.

REALIZADOS ENTRE A 4ª E A 6ª SEMANA DE VIDA NA UTI Neo
OFTALMOSCOPIA BINOCULAR INDIRETA
LENTES Nikon ® ou Volk ® 28 / 30 / 40 Dioptrias
MIDRÍASE: Tropicamida 0,5% + Fenilefrina 2,5%
BLEFAROSTATO: Alfonso Eye Speculum, Storz ®
INDENTAÇÃO ESCLERAL: Proximetacaína 0,5%
Fortes Filho JB. Retinopatia da prematuridade. Artigo de revisão.
Rev Bras Oftalmol 2006; 65(4):246-58.
EXAMES OFTALMOLÓGICOS

IMPORTANTE A PRESENÇA DA ENFERMAGEM
O EXAME É TECNICAMENTE DIFÍCIL
NECESSITA PRÁTICA, CONHECIMENTO,
RAPIDEZ E ATENÇÃO PERMANENTE
NO COMPORTAMENTO DA CRIANÇA
(TREINAMENTO)

EXAMES PRECISAM SER REPETIDOS
DURANTE VÁRIAS SEMANAS
ATÉ 42a SEMANA DE IPC QUANDO SE
COMPLETA A VASCULARIZAÇÃO
INCLUSÃO DE PACIENTES POR PN / IG
Zin A, Florêncio T, Fortes Filho JB, Nakanami CR, Gianini N, Graziano RM et al.
Proposta de diretrizes brasileiras para a detecção e o tratamento da retinopatia da prematuridade (ROP).
Arq Bras Oftalmol 2007; 70(5):875-83.

TRATAMENTO A PARTIR DE 1988 (CRYO-ROP)
DOENÇA LIMIAR - IPC ≥ 38 semanas
Nível de gravidade da ROP no qual o risco para um resultado anatômico e
funcional desfavorável alcança 50%.
Cryotherapy for Retinopathy of Prematurity Cooperative Group.
Multicenter trial of cryotherapy for retinopathy of prematurity:preliminary results.
Arch Ophthalmol 1988;106:471-9.
MAPA ORIGINAL DO CRYO-ROP 1988
ESTADIAMENTO ROP 3 ZONAS I ou II
(cinco horas contíguas ou oito horas totais e doença plus)
3.862 RNP c/ PN ≤ 1.250 g

TRANSPUPILAR
AO REDOR DE
700 / 1000 IMPACTOS / OLHO
NA RETINA AVASCULAR
DOIS OLHOS TRATADOS
NO MESMO ATO
SEDAÇÃO NA UTIN
PREFERENCIALMENTE
ROP PRÉ-LIMIAR do tipo 1:
LASER MENOS DENSO
ROP LIMIAR: LASER MAIS DENSO
TRATAMENTO PELO LASER DIODO

EXCELENTE NOS ESTADIAMENTOS ROP 1 e 2
APÓS REGRESSÃO NATURAL
ANATOMICAMENTE BOM NA MAIOR PARTE DOS
CASOS TRATADOS POR OCASIÃO DA ROP
PRÉ-LIMIAR TIPO 1 OU LIMIAR
RESULTADOS FUNCIONAIS DEIXAM A DESEJAR
BAIXA AV, CAMPO VISUAL REDUZIDO
MIOPIA, AMBLIOPIA E ESTRABISMO
MORBIDADE MAIS GRAVE - CEGUEIRA
PROGNÓSTICO DA DOENÇA (CRYO-ROP)
Cryotherapy for Retinopathy of Prematurity Cooperative Group. Multicenter trial of cryotherapy for retinopathy
of prematurity: ophthalmological outcomes at 10 years.
Arch Ophthalmol 2001;119:1110-18.
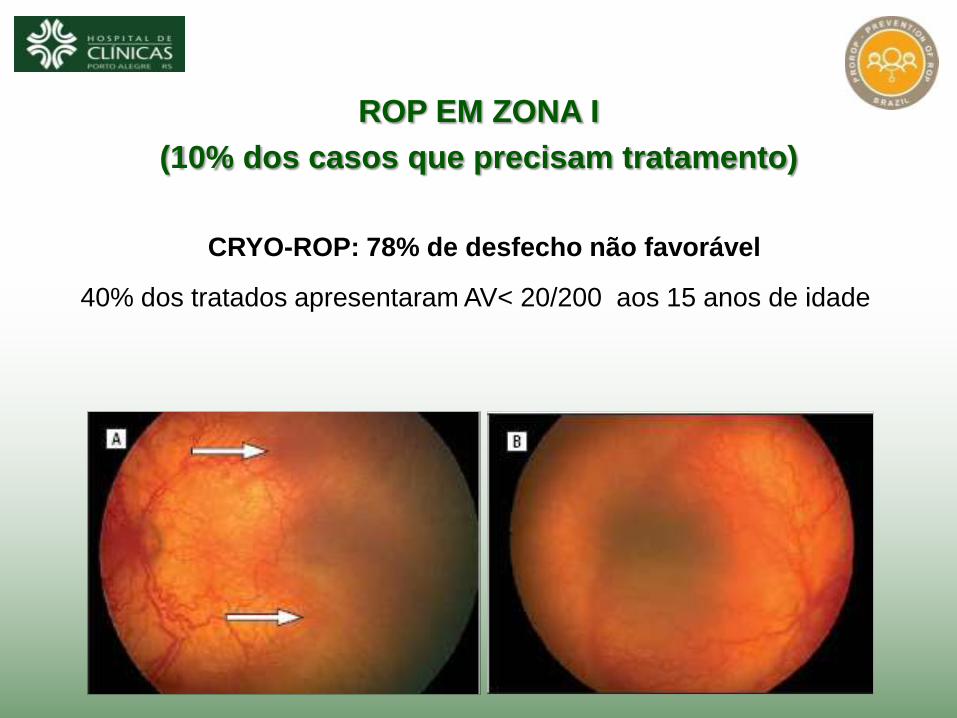
ROP EM ZONA I
(10% dos casos que precisam tratamento)
CRYO-ROP: 78% de desfecho não favorável
40% dos tratados apresentaram AV< 20/200 aos 15 anos de idade

NOVAS INDICAÇÕES (ET-ROP 2003)
DOENÇA PRÉ - LIMIAR - IPC > 36 semanas
• Zona I - Qualquer estadiamento
• Zona II - ROP 2, com doença plus
• Zona II - ROP 3, menos severa do que a Doença Limiar
ROP TIPO 1 - Doença pré - limiar de alto risco (resultado desfavorável > 15%)
• Zona I - Qualquer estadiamento com doença plus
• Zona I - ROP 3 sem doença plus
• Zona II - ROP 2 ou 3 com doença plus
ROP TIPO 2 - Doença pré - limiar de baixo risco (resultado desfavorável < 15%)
• Zona I - ROP 1 or 2 sem doença plus
• Zona II - ROP 3 sem doença plus
Early Treatment for Retinopathy of Prematurity Cooperative Group.
Revised Indications for the Treatment of Retinopathy of Prematurity.
Arch Ophthalmol 2003;212:1684-96.

ET-ROP: 55% de desfecho não favorável
PODE HAVER PROGRESSÃO DA ROP E CEGUEIRA
PROGNÓSTICO DA DOENÇA ZONA i
Cryotherapy for Retinopathy of Prematurity Cooperative Group.
Multicenter trial of cryotherapy for retinopathy of prematurity: ophthalmological outcomes at 10 years.
Arch Ophthalmol 2001;119:1110-18.

2009 2002 2003 2004 2005 2006 2007 2008
Nº TRATAMENTOS
5,6% 6,1% 5,2% 6,2% 6,7% % ROP GRAVE
2010
PREVENÇÃO DA ROP
0,0%
2012
• OTIMIZAÇÃO DO USO DO OXIGÊNIO DESDE O NASCIMENTO
• RÍGIDO MONITORAMENTO DA OXIGÊNIO-TERAPIA POR OXÍMETROS DE PULSO
• RÍGIDO CONTROLE SOBRE OS FATORES DE RISCO
• OTIMIZAÇÃO SOBRE A NUTRIÇÃO PARENTERAL TOTAL PN < 1.250 g
• EXISTÊNCIA DE UM PROGRAMA DE TRIAGEM NEONATAL
0,0% 5,2% 0,0% 0,0%

Muito Obrigado !
João Borges Fortes Filho
Universidade Federal do Rio Grande do Sul
Hospital de Clínicas de Porto Alegre