Embed Size (px)
Citation preview

UNIVERSIDADE FEDERAL DE SERGIPE
PRÓ-REITORIA DE PÓS-GRADUAÇÃO E PESQUISA
MESTRADO EM EDUCAÇÃO FÍSICA
EFEITOS DE DIFERENTES VOLUMES DE TREINAMENTO
RESISTIDO SOBRE AS FORÇAS MUSCULAR E
RESPIRATÓRIA DE IDOSAS
ODILON SALIM COSTA ABRAHIN
São Cristóvão
2015

ii
UNIVERSIDADE FEDERAL DE SERGIPE
PRÓ-REITORIA DE PÓS-GRADUAÇÃO E PESQUISA
MESTRADO EM EDUCAÇÃO FÍSICA
EFEITOS DE DIFERENTES VOLUMES DE TREINAMENTO
RESISTIDO SOBRE AS FORÇAS MUSCULAR E
RESPIRATÓRIA DE IDOSAS
ODILON SALIM COSTA ABRAHIN
Dissertação apresentada ao Programa de Pós-Graduação em Educação Física da Universidade Federal de Sergipe como requisito para obtenção do grau de Mestre em Educação Física
Orientador: Prof. Dr. Anderson Carlos Marçal
São Cristóvão
2015
iii
FICHA CATALOGRÁFICA ELABORADA PELA BIBLIOTECA CENTRAL
UNIVERSIDADE FEDERAL DE SERGIPE
A159s
Abrahin, Odilon Salim Costa
Efeitos de diferentes volumes de treinamento resistido sobre
as força muscular e respiratória de idosas / Odilon Salim
Costa Abrahin; orientador Anderson Carlos Marçal. – São
Cristóvão, 2015.
19 f. : il.
Dissertação (mestrado em Educação Física) –
Universidade Federal de Sergipe, 2015.
1. Exercícios físicos – Aspectos da saúde. 2. Aptidão física em idosos. 3. Musculação. I. Marçal, Anderson Carlos, orient. II. Título.
CDU 796.015.52-053.9

iv
ODILON SALIM COSTA ABRAHIN
EFEITOS DE DIFERENTES VOLUMES DE TREINAMENTO
RESISTIDO SOBRE AS FORÇAS MUSCULAR E
RESPIRATÓRIA DE IDOSAS
Dissertação apresentada ao Programa de Pós-Graduação em Educação Física da Universidade Federal de Sergipe como requisito para obtenção do grau de Mestre em Educação Física
Aprovada em ____/____/____
Orientador: Prof. Dr. Anderson Carlos Marçal
1º Examinador: Prof. Dr. Silvan Silva de Araujo
2º Examinador: Prof. Dr. Marzo Edir da Silva Grigoletto
PARECER
------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------

v
Dedicatória
Para Deus, família, professores e pais, por terem ensinado tudo que sei hoje, vocês são meus exemplos de caráter, dedicação e perseverança. MUITO OBRIGADO!
vi
Agradecimentos
A minha MÃE Eliceia, pelo seu amor, carinho e compreensão nos
momentos difíceis, TE AMO.
A minha família por TODOS os momentos, sem vocês nada disso valeria à
pena.
Ao meu AMOR Rejane Pequeno, sua companhia é essencial na minha
vida.
Ao orientador Prof. Dr. Anderson Carlos Marçal, por seus ensinamentos e
sua incansável busca pelo conhecimento. OBRIGADO!
Aos AMIGOS do Laboratório de Exercício Resistido e Saúde.
A todos os estudantes que compõem o laboratório de Núcleo de Pesquisa
em Sinalização Intracelular (NUPESIN) pelo conhecimento e ajuda.
Ao meu avô Odilon das Chagas Costa (in memorian), eterno amor.
A nossa turma por todos os momentos juntos, em especial aos amigos
João Paulo e Josivan.
A minha irmã por todos os anos de companheirismo.
Aos professores do Programa de Pós-graduação em Educação Física.
A DEUS por estar sempre ao meu lado. O SENHOR NUNCA nos
abandona! OBRIGADO.

vii
ABRAHIN, OSC. EFEITOS DE DIFERENTES VOLUMES DE TREINAMENTO
RESISTIDO SOBRE AS FORÇAS MUSCULAR E RESPIRATÓRIA DE IDOSAS.
Sergipe: Universidade Federal de Sergipe. Educação Física. 2015, 19f.
Resumo
Introdução: Os sistemas neuromuscular e respiratório são significativamente
afetados durante o envelhecimento sedentário, contudo estas modificações
podem ser minimizadas/atenuadas pela prática do treinamento resistido.
Objetivo: Comparar os efeitos de diferentes volumes de treinamento resistido
sobre a pressão muscular inspiratória (Pimax), pressão muscular expiratória
(Pemax), desempenho funcional e força muscular de idosas.
Métodos: Dezenove mulheres idosas foram divididas randomicamente em dois
grupos, série simples (1-SET) ou três séries (3 SET) de exercícios resistidos. O
teste de sentar e levantar, Pemax, Pimax e força muscular foram avaliados antes
e após 24 sessões de treinamento. O treinamento resistido progressivo foi
realizado durante 12 semanas com frequência de duas vezes por semana, entre
8-12 repetições, utilizando-se os principais grupos musculares dos membros
superiores e inferiores.
Resultados: Os principais resultados demonstram que ocorreram aumentos
significativos na Pemax (p<0,05; 1-SET: 34,6%; 3-SET: 35,8%) e Pimax (p<0,05;
1-SET: 13,7%; 3-SET: 11,2%). Ambos os grupos também melhoraram no teste de
sentar e levantar (p<0,05; 1-SET: 10.6%; 3-SET: 17.1%). Após 24 sessões de
treinamento resistido, a força muscular aumentou significativamente (p<0,001; 40-
80%) nos grupos. A comparação intergrupo não revelou diferença significativa em
nenhum parâmetro analisado.
Conclusão: Séries simples e múltiplas de treinamento resistido melhoram a
Pemax, Pimax, força muscular e o desempenho funcional no teste de sentar e
levantar após 24 sessões de treinamento. Estes resultados sugerem que
mulheres idosas que não possuem o hábito de praticar atividade física podem
iniciar programas de séries simples de treinamento resistido, como estratégia de
curto tempo para a manutenção da saúde.

viii
Palavras Chaves: Treinamento resistido; Pressão inspiratória máxima; Pressão
expiratória máxima; Força muscular; Idosas.

ix
ABRAHIN, OSC. THE EFFECTS OF DIFFERENT VOLUMES OF RESISTANCE
TRAINING ON MUSCLE STRENGTH AND RESPIRATORY MUSCLE
STRENGTH IN ELDERLY WOMEN. Sergipe: Universidade Federal de Sergipe.
Educação Física. 2015, 19f.
Abstract
Introduction: The neuromuscular and respiratory systems are significantly
affected during the sedentary aging, but these modifications can be
minimized/attenuated by practice of resistance training
Purpose: Compare the effects of different volumes of resistance training on the
maximum inspiratory pressure (MIP), maximum expiratory pressure (MEP),
functional performance, and muscle strength in elderly women.
Methods: Nineteen elderly women were randomly assigned to a group performing
either single sets (1-SET) or three sets (3-SET) of exercises. The sit-to-stand test,
MIP, MEP, and muscle strength were assessed before and after 24 training
sessions. Progressive resistance training was performed two times per week for a
total of 8–12 repetitions, using the main muscle groups of the upper and lower
limbs.
Results: The main results showed that the participants significantly increased their
MEP (p<0,05; 1-SET: 34,6%; 3-SET: 35,8%) and MIP (p<0,05; 1-SET: 13,7%; 3-
SET: 11,2%). Both groups also improved in the sit-to-stand test (p<0,05; 1-SET:
10,6%; 3-SET: 17,1%). After 24 training sessions, muscle strength also
significantly increased (p<0,0001; 40–80%) in both groups. An intergroup
comparison did not show any statistically significant differences between the
groups in any of the parameters analyzed.
Conclusion: Single- and multiple-set resistance training programs increased MIP,
MEP, muscle strength, and sit-to-stand test performance in elderly women after 24
sessions of training. In conclusion, our results suggested that elderly women who
are not in the habit of physical activity may start with single-set resistance training
programs as a short-term strategy for the maintenance of health.

x
Keywords: Resistance exercise; Maximum inspiratory pressure, Maximum
expiratory pressure; Elderly.
xi
SUMÁRIO
I – Introdução................................................................................................... 1
II – Revisão de Literatura................................................................................. 3
2.1 Envelhecimento: um fenômeno mundial.................................................... 3
2.2 Benefícios do Treinamento Resistido Em Idosos...................................... 4
2.3 Força Muscular.......................................................................................... 6
2.4 Força Muscular Respiratória...................................................................... 8
2.5 Treinamento Resistido e Força Muscular Respiratória.............................. 10
III – Objetivos................................................................................................... 11
3.1 Geral.......................................................................................................... 11
3.2 Específicos................................................................................................. 11
IV – Desenvolvimento (Artigo) ........................................................................ 12
V – Conclusão.................................................................................................. 13
Referências...................................................................................................... 14
Anexo....................................................................................................... ........ 19
xii
ÍNDICE DE FIGURAS
Figura 1. Ciclo da fragilidade
Figura 2. Adaptações neurais intramusculares e intermusculares
Figura 3. Adaptações fisiológicas (neurais e hipertróficas) desencadeadas pelo
treinamento resistido

xiii
LISTA DE FÓRMULAS, ABREVIATURA E SIGLAS
DMO – Densidade mineral óssea
Pemax – Força muscular expiratória
Pimax – Força muscular inspiratória
TR – Treinamento resistido
VO2máx – Volume máximo de oxigênio

1
I – INTRODUÇÃO
O envelhecimento populacional é um fenômeno global e está acontecendo
mais rápido nos países em desenvolvimento e de baixa renda (1,2). Em função
disto, as instituições governamentais têm estimulado a prática de hábitos
saudáveis, dentre eles, a prática regular de atividade física, com objetivo primário
de reduzir as taxas de morbidade e gastos públicos relacionados à saúde.
Nestas duas últimas décadas, aumentou consideravelmente o volume de
pesquisas na área de ciências do exercício e sua relação com a saúde e
qualidade de vida em grupos especiais. Atualmente, o treinamento resistido tem
sido utilizado na reabilitação e promoção da saúde em diversas populações,
especialmente em idosos (3), uma vez, que o processo do envelhecimento
sedentário está associado com modificações nas capacidades de adaptação e
físicas.
Dentre as principais mudanças que ocorrem durante o envelhecimento
sedentário, o sistema neuromuscular e respiratório desta população são
significativamente afetados, podendo apresentar redução da força e massa
muscular, redução da potência muscular, resistência, flexibilidade, VO2max, além
de perdas graduais de força dos músculos respiratórios. A disfunção do sistema
respiratório em geral reduz a tolerância ao exercício e aumenta as taxas de
morbimortalidade (4,5). Uma das formas primárias de prevenir ou atenuar as
perdas relacionadas à força muscular respiratória consiste no treinamento
específico dos músculos respiratórios, prática comum realizada pelos
fisioterapeutas e fisiatras (5).
O treinamento específico dos músculos respiratórios tem proporcionado
efeitos sobre a força muscular respiratória e endurance de atletas. Contudo,
recentes estudos têm indicado que o treinamento resistido também pode
aumentar a força dos músculos respiratórios (6,7). No melhor de nosso
conhecimento, nenhuma pesquisa científica avaliou os efeitos crônicos de
diferentes volumes de treinamento resistido sobre a força muscular respiratória de
mulheres idosas.

2
A principal hipótese deste estudo considerou que séries simples e múltiplas
de treinamento resistido acarretam ganhos similares de força dos músculos
respiratórios, força muscular e capacidade funcional em mulheres idosas após 12
semanas de treinamento.

3
II – REVISÃO DE LITERATURA
2.1 Envelhecimento: Um Fenômeno Mundial
O envelhecimento pode ser definido como um conjunto de modificações
biológicas que acarretam reduções graduais das capacidades de adaptação e
aumento da vulnerabilidade para inúmeros problemas de saúde, como as
doenças crônicas não transmissíveis e disfunções musculoesqueléticas. De
acordo com a World Health Organization em 2050, o número de idosos (>60
anos) será estimado em 2 bilhões, que corresponderá em cerca de 22% da
população mundial (1).
Em diversos países desenvolvidos, em desenvolvimento e de baixa renda,
a expectativa de vida está aumentando. Isto se deve em parte, ao avanço da
medicina e tecnologia, maior eficiência das estratégias de vacinação em larga
escala, prevenção de doenças infecciosas e aumento do acesso à rede pública de
saneamento (3). Desta forma, o envelhecimento populacional é um fenômeno
global (2), e atualmente está acontecendo mais rápido em países de baixa e
média renda (Cuba, Mongólia, entre outros).
Segundo a World Health Organization, foram necessários mais de 100
anos para que a França duplicasse sua população idosa de 7% para 14%. Em
contrapartida, países como o Brasil e China necessitarão cerca de 25 anos para
atingir o mesmo crescimento (2). Diante destas perspectivas, diversas instituições
e programas governamentais como: “Pessoas saudáveis” (Inglaterra); “Viver
ativo” (Canadá); “No Porto a vida é longa” (Portugal), “Agita Brasil” têm estimulado
a prática regular de atividade física, com o objetivo de proporcionar um
envelhecimento saudável, reduzir as taxas de morbidade e gastos públicos
relacionados à saúde (3,8).
No Brasil, a maioria dos estados têm adotado ações e programas que
estimulem a prática regular de atividade física em idosos (8). Dentre os diversos
tipos de atividade física, o treinamento resistido, ou contra resistência tem se
destacado pelos seus potenciais benefícios (3,9–14).

4
2.2 Benefícios do Treinamento Resistido em Idosos
O treinamento resistido (TR) é caracterizado pela tensão muscular com ou
sem movimentação articular contra alguma forma de resistência progressiva a
ação muscular. Ao longo destes anos, diversas pesquisas têm evidenciado os
benefícios do TR em diversas populações, principalmente em idosos sedentários,
como melhora da qualidade de vida, promoção da saúde e reabilitação (10,15,16).
Entretanto, para que os benefícios promovidos pelo TR ocorram de forma
eficiente e segura, torna-se necessário que a prescrição se ajuste as
características individuais, respeitando os princípios biológicos do treinamento,
assim como as variáveis que constituem o programa de treinamento, como:
intensidade, número de séries, repetições, intervalo entre séries e exercícios,
frequência, velocidade e ordem dos exercícios (10).
Os principais benefícios funcionais proporcionados pela prática do TR são:
aumento da força muscular, resistência muscular, flexibilidade, coordenação
motora, potência muscular, prevenção de lesões e diminuição da incidência de
quedas (6) (Tabela 1). Outras vantagens em diversos parâmetros fisiológicos
incluem a melhora do sistema cardiovascular e endócrino, perfil lipídico,
composição corporal, aumento da sensibilidade à insulina, massa muscular,
densidade mineral óssea (DMO), além do controle/redução da pressão arterial
(10,12,15–17)
Um estudo pioneiro publicado no Journal American Medical Association na
década de 90 avaliou os efeitos do TR de alta intensidade (80% 1RM) em idosos
nonagenários, os resultados demonstraram aumentos significativos nos níveis de
força muscular (174% ± 31%) e do volume muscular (9.0% ± 4.5%) após oito
semanas de treinamento (9). Ainda neste mesmo trabalho, os autores relataram
que a fraqueza muscular pode ser revertida, mesmo em idosos nonagenários.
Posteriormente outros trabalhos corroboraram com estes resultados em idosos
octogenários (18,19) e nonagenários (20).
A síndrome da fragilidade é um dos principais problemas de saúde que
ocorre no envelhecimento sedentário (21,22). Além disso, sua etiologia é de

5
origem multifatorial, associada à alta prevalência e incidência de quedas,
imobilidade e dependência funcional (Figura 1). Outra alteração que acomete o
sistema musculoesquelético desta população é a redução do volume das fibras
musculares, principalmente do tipo II (fibras de contração rápida) que interferem
nas repostas das atividades da vida diária, uma vez, que contribuem com o tempo
de reação, como consequências podem ocorrer perdas repentinas de equilíbrio
(9,16).
Figura 1. Inter-relações no ciclo da fragilidade (21).
Recentemente o termo sarcopenia tem sido utilizado para descrever a
perda acentuada e progressiva de massa muscular, força e potência muscular
(23). Esta disfunção musculoesquelética antecede a síndrome da fragilidade e
também foi associada à perda de DMO, desnervação muscular (23), redução da
taxa metabólica basal, aumento do risco de diabetes e síndrome metabólica (22),
aumento dos marcadores pró-inflamatórios (12) e taxa de mortalidade (24).

6
Uma meta-análise relatou forte associação entre o TR e o ganho de massa
magra em adultos acima de 50 anos (n=1328) (25). Além disso, estes autores
detectaram aumento de 1kg de massa magra, quer sejam em homem ou em
mulheres após 20 semanas de treinamento. Todavia, apesar deste ganho ter sido
aparentemente modesto, é conhecido na literatura que os idosos apresentam uma
perda média de 0,2kg de massa magra por ano (25).
Além disso, idosos com disfunções musculoesqueléticos submetidos ao TR
combinados com ingestão balanceada (adequada) dos macronutrientes não têm
sido objeto de investigações clínicas de forma crescente (22,26). Uma recente
meta-análise (27) evidenciou que a suplementação de proteína associada com o
TR em 215 idosos (62 ± 6 anos) aumentou a massa muscular e a força (1RM no
Leg press), 38% e 33% respectivamente quando comparado com o grupo
placebo. Baseado nesta evidência, a ingestão dos nutrientes de acordo com as
características individuais possivelmente potencializa as adaptações morfológicas
e neuromotoras nesta população associado à prática do TR.
2.3 Força Muscular
A produção da força muscular máxima atinge seu limite por volta da
segunda ou terceira década de vida, e por volta da quinta década, iniciam
declínios progressivos desta capacidade (11). Estas modificações estão
relacionadas principalmente com mudanças que acometem o sistema
neuromuscular, tais como: redução de ativação dos músculos agonistas,
diminuição da massa muscular (principalmente fibras do tipo II), diminuição da
área de contato entre o axônio e a membrana celular, redução do número e
função das células satélites (responsáveis pela manutenção, reparo, e
crescimento das miofibrilas). Além de outras modificações endócrinas (redução
dos níveis de testosterona, fatores de crescimento semelhante à insulina) que
também podem contribuir para os déficits de força muscular.
A força muscular é o principal benefício funcional ocasionado pelo TR, por
este motivo alguns praticantes e pesquisadores nomeiam também de treinamento
de força. O American College of Sports Medicine em seu último posicionamento

7
sobre atividade física em idosos relatou como Nível de Evidência Científica A, que
a prática do TR aumenta substancialmente a força muscular. A importância clínica
deste achado evidenciou que os déficits de força muscular estão associados com
aumento da taxa de morbimortalidade (10).
Outra meta análise (11) estimou que 18 semanas de TR em sujeitos acima
de 50 anos aumentam a força muscular cerca de 30% e 25%, nos membros
inferiores e superiores, respectivamente. Todavia, estes ganhos ainda podem ser
maximizados, devido, sobretudo a intensidade, tipo de exercício (multiarticular ou
monoarticular), nível de treinamento do sujeito e nutrição.
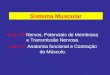
Os principais mecanismos fisiológicos que explicam os ganhos de força
são as adaptações neurais e hipertróficas. Neste sentido, as adaptações neurais
(Figura 2) podem ser classificadas em intramuscular, como: a maior ativação do
músculo agonista, aumento do número de unidades motoras recrutadas, aumento
da frequência de impulso das unidades motoras e inibição do órgão tendinoso de
golgi. A adaptação intermuscular consiste basicamente na redução co-contração
dos antagonistas e melhor coordenação entre o músculo agonista-sinergista (28).
8
Figura 2. Adaptações neurais intramusculares e intermusculares.
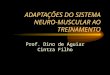
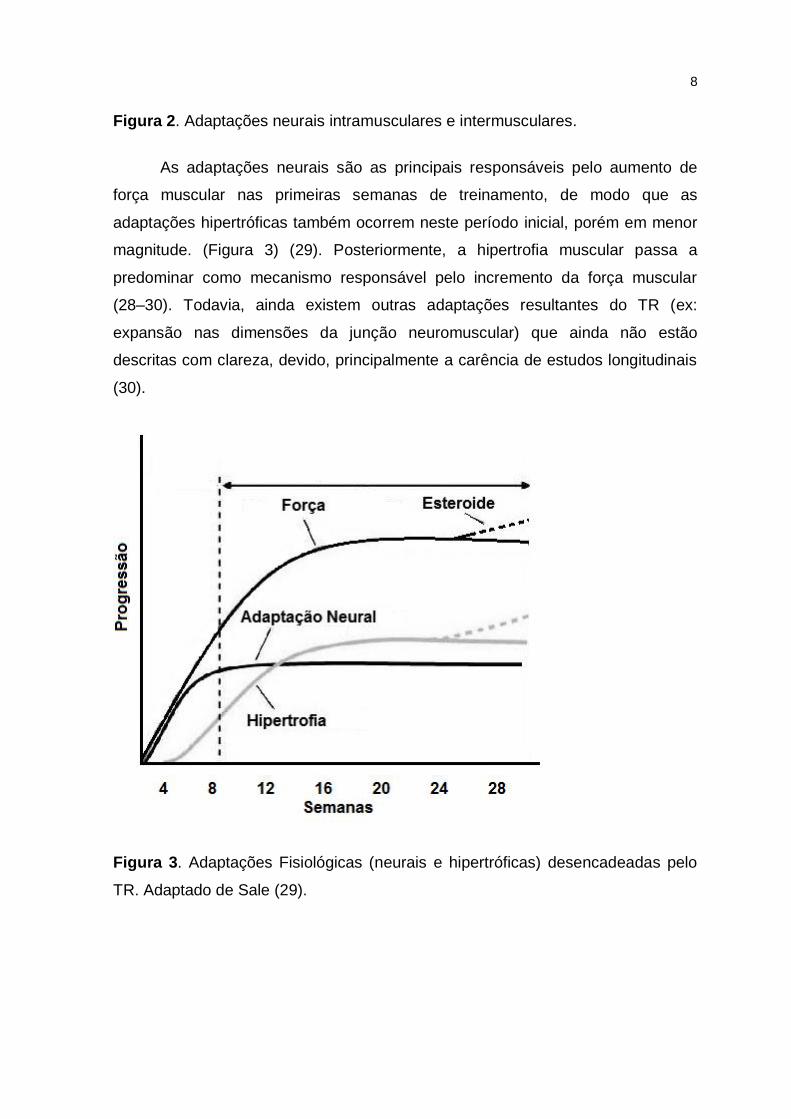
As adaptações neurais são as principais responsáveis pelo aumento de
força muscular nas primeiras semanas de treinamento, de modo que as
adaptações hipertróficas também ocorrem neste período inicial, porém em menor
magnitude. (Figura 3) (29). Posteriormente, a hipertrofia muscular passa a
predominar como mecanismo responsável pelo incremento da força muscular
(28–30). Todavia, ainda existem outras adaptações resultantes do TR (ex:
expansão nas dimensões da junção neuromuscular) que ainda não estão
descritas com clareza, devido, principalmente a carência de estudos longitudinais
(30).
Figura 3. Adaptações Fisiológicas (neurais e hipertróficas) desencadeadas pelo
TR. Adaptado de Sale (29).

9
2.4 Força Muscular Respiratória
A força muscular respiratória decresce progressivamente com a idade em
ambos os sexos, e estes declínios são maximizados a cada duas ou três décadas
em sujeitos sedentários saudáveis (31). Um estudo transversal brasileiro (31)
avaliou a força muscular inspiratória (Pimax) e força muscular expiratória (Pemax)
em 120 sujeitos de ambos os sexos (idade 20-89), os resultados demonstram
correlação negativa (moderada/alta) entre a idade e a força muscular respiratória
(Pimax e Pemax). Neder et al (32) e Costa et al (33) também encontraram forte
correlação negativa entre idade e a força dos músculos respiratórios.
Outros estudos têm associado baixos níveis de força muscular respiratório
com a força muscular geral, sarcopenia e fragilidade (34), especialmente em
idosos (34–36) e pacientes acamados (37). A fraqueza muscular respiratória está
relacionada com infecções respiratórias, hiperventilação, redução na capacidade
de exercício e aumento das taxas de morbimortalidade (4,34). Além disso, nas
doenças neuromusculares, as disfunções dos músculos respiratórios podem
preceder a insuficiência respiratória. Em função, de sua importância clínica, esta
capacidade começou a ser avaliada por alguns profissionais da área de saúde a
partir da década de 1970 (31,33).
A força muscular respiratória pode ser avaliada por meio de testes
estáticos e dinâmicos. Classicamente, as medidas estáticas inferem a Pimax e
Pemax, e estes parâmetros mensuram a pressão que está sendo gerada pela
ação dos músculos respiratórios. Adicionalmente, este é um teste utilizado
mundialmente, não invasivo, rápido e apresenta baixo custo. Sua principal
desvantagem normalmente consiste na falta de coordenação (técnica) do
avaliando, podendo induzir a um diagnóstico incorreto (5,38). Contudo, este
problema pode ser minimizado quando a avaliação é aplicada por um avaliador
experiente, normalmente realizando três medidas com diferença inferior a 10%
entre cada tentativa (5).
Estudos prévios têm demonstrado a eficiência do treinamento muscular
respiratório sobre a Pimax e Pemax em diversas populações (35,39), inclusive em
idosos (36,40). Estes ganhos ocorrem, devido principalmente a especificidade do

10
treinamento e consequente redução da fadiga dos principais músculos
respiratórios (reto do abdômen, oblíquo externo e interno, transverso do
abdômen, intercostais internos e externos, diafragma). Cader et al (40) avaliaram
os efeitos de 10 semanas de treinamento progressivo dos músculos inspiratórios
sobre a Pimax e autonomia funcional de idosos asilados, os resultados
evidenciaram ganhos significativos da Pimax e autonomia funcional do grupo
experimental em relação ao grupo controle.
2.5 Treinamento Resistido e Força Muscular Respiratória
Os profissionais da atividade física e esporte têm demonstrado interesse
em avaliar a força muscular respiratória, com objetivos de potencializar o
rendimento dos atletas de elite (41) e recreacionais (42). Uma meta-análise
evidenciou que o treinamento muscular respiratório foi efetivo na melhora da
performance esportiva (tempo de Endurance e Yo-Yo teste) (41). De maneira
geral, o treinamento melhorou a Pimax, Pemax e a resistência em diferentes
atletas, com exceção dos nadadores e mergulhadores.
Atualmente, os pesquisadores têm avaliado os efeitos do TR em diversos
parâmetros fisiológicos, inclusive no sistema respiratório (6,7). Um estudo
investigou os efeitos do treinamento de flexibilidade (facilitação neuromuscular
proprioceptiva), combinado com o TR (resistência de bandas elásticas) sobre a
força muscular respiratória em mulheres adultas, os resultados evidenciaram
aumentos significativos na Pimax e Pemax após quatro semanas de treinamento
em comparação com o grupo controle. Não obstante, neste estudo não se pode
afirmar que a Pimax e Pemax aumentou devido somente ao TR, uma vez, que os
pesquisadores combinaram com treinamento de flexibilidade.
Um estudo transversal (43) publicado por nosso grupo de pesquisa
comparou a Pimax e Pemax de idosos treinados exclusivamente com pesos
(período > seis meses) e sedentários. Os resultados demonstram que os idosos
treinados apresentaram níveis de Pimax e Pemax superiores aos sedentários.
Além disso, o grupo exercitado apresentou nível de força muscular respiratório
acima do recomendado para sua faixa etária conforme a classificação de Neder et

11
al (32). Este achado problematizou a seguinte pergunta: qual a dose resposta do
TR sobre a Pimax e Pemax de idosas?

12
III – OBJETIVOS
3.1 Geral
Avaliar os efeitos de séries simples e múltiplas de treinamento resistido
sobre as forças muscular e respiratória de idosas
3.2 Específicos
- Avaliar os efeitos de séries simples e múltiplas de treinamento resistido
sobre o desempenho funcional de idosas no teste de sentar e levantar.
- Comparar a força muscular e força dos músculos respiratórios após
programas de séries simples e múltiplas de treinamento resistido em idosas.
13
IV –DESENVOLVIMENTO (ARTIGO EM ANEXO)
Os resultados obtidos durante o Mestrado em Educação Física, bem como
a metodologia e a discussão foram sistematizados no formato de um artigo
científico intitulado “Single- and multiple-set resistance training improves skeletal
and respiratory muscle strength in elderly women”, este trabalho foi aceito pela
revista Clinical Interventions in Aging (fator de impacto = 1,82), classificada como
B1 na área de Educação Física até a presente data (02/06/15).

14
V – CONCLUSÃO
Os resultados do presente estudo demonstram que séries simples e
múltiplas de treinamento resistido aumentam similarmente a força muscular
respiratória e força muscular, assim como o desempenho funcional no teste de
sentar e levantar em idosas após 24 sessões de treinamento.

15
REFERÊNCIAS
1. WHO | Good health adds life to years. World Health Organization; [cited 2014 Jul 23]; Available from: http://www.who.int/ageing/publications/whd2012_global_brief/en/#.
2. WHO | Interesting facts about ageing. World Health Organization; [cited 2014 Jul 23]; Available from: http://www.who.int/ageing/about/facts/en/#.
3. Romo V, Schwingel A, Chodzko-Zajko W. International resistance training recommendations for older adults: Implications for the promotion of healthy aging in Spain. Journal of Human Sport and Exercise. 2011;6(4):639–48.
4. Sin DD, Wu L, Man SFP. The relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literature. Chest. 2005;127(6):1952–9.
5. Gibson GJ, Whitelaw W, Siafakas N, Supinski GS, Fitting JW, Bellemare F, et al. ATS/ERS Statement on respiratory muscle testing. American Journal of Respiratory and Critical Care Medicine. 2002;166(4):518–624.
6. Hackett DA, Johnson NA, Chow C-M. High-volume resistance training session acutely diminishes respiratory muscle strength. Journal of Sports Science & Medicine. 2012;11(1):26–30.
7. Areas GPT, Borghi-Silva A, Lobato AN, Silva AA, Freire RC, Areas FZS. Effect of upper extremity proprioceptive neuromuscular facilitation combined with elastic resistance bands on respiratory muscle strength: a randomized controlled trial. Brazilian Journal of Physical Therapy. 2013;17(6):541–6.
8. Salin MS, Mazo GZ, Cardoso AS, Garcia GS. Atividade física para idosos: diretrizes para implantação de programas e ações. Revista Brasileira de Geriatria e Gerontologia. 2011;14(2):197–208.
9. Fiatarone MA, Marks EC, Ryan ND, Meredith CN, Lipsitz LA, Evans WJ. High-intensity strength training in nonagenarians. Effects on skeletal muscle. The Journal of the American Medical Association.1990;263(22):3029–34.
10. Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, et al. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Medicine and Science in Sports and Exercise. 2009;41(7):1510–30.
11. Peterson MD, Rhea MR, Sen A, Gordon PM. Resistance exercise for muscular strength in older adults: a meta-analysis. Ageing Research Reviews. 2010;9(3):226–37.

16
12. Ogawa K, Sanada K, Machida S, Okutsu M, Suzuki K. Resistance exercise training-induced muscle hypertrophy was associated with reduction of inflammatory markers in elderly women. Mediators of Inflammation. 2010;2010:171023.
13. Radaelli R, Botton CE, Wilhelm EN, Bottaro M, Lacerda F, Gaya A, et al. Low- and high-volume strength training induces similar neuromuscular improvements in muscle quality in elderly women. Experimental Gerontology. 2013;48(8):710–6.
14. Peterson MD, Gordon PM. Resistance exercise for the aging adult: clinical implications and prescription guidelines. The American Journal of Medicine. 2011;124(3):194–8.
15. Winett RA, Carpinelli RN. Potential health-related benefits of resistance training. Preventive Medicine. 2001;33(5):503–13.
16. Westcott WL. Resistance training is medicine: effects of strength training on health. Current Sports Medicine Reports. 2012;11(4):209–16.
17. Queiroz ACC, Kanegusuku H, Forjaz CLM. Efeitos do treinamento resistido sobre a pressão arterial de idosos. Arquivos Brasileiros de Cardiologia. 2010;95(1):135–40.
18. Krist L, Dimeo F, Keil T. Can progressive resistance training twice a week improve mobility, muscle strength, and quality of life in very elderly nursing-home residents with impaired mobility? A pilot study. Clinical Interventions in Aging. 2013;8:443–8.
19. Kalapotharakos VI, Diamantopoulos K, Tokmakidis SP. Effects of resistance training and detraining on muscle strength and functional performance of older adults aged 80 to 88 years. Aging Clinical and Experimental Research. 2010;22(2):134–40.
20. Serra-Rexach JA, Bustamante-Ara N, Hierro Villarán M, González Gil P, Sanz Ibáñez MJ, Blanco Sanz N, et al. Short-term, light- to moderate-intensity exercise training improves leg muscle strength in the oldest old: a randomized controlled trial. Journal of the American Geriatrics Society. 2011;59(4):594–602.
21. Macedo C, Gazzola JM, Najas M. Síndrome da fragilidade no idoso: importância da fisioterapia. Arquivos Brasileiros de Ciências da Saúde. 2008;33(3):177–84.
22. Sundell J. Resistance Training Is an Effective Tool against Metabolic and Frailty Syndromes. Advances in Preventive Medicine. 2011;2011:984683.
17
23. Lang T, Streeper T, Cawthon P, Baldwin K, Taaffe DR, Harris TB. Sarcopenia: etiology, clinical consequences, intervention, and assessment. Osteoporosis International. 2010;21(4):543–59.
24. Fitzgerald SJ, Barlow CE, Kampert JB, Morrow JR, Jackson AW, Blair SN. Muscular Fitness and All-Cause Mortality : Prospective Observations. Journal of Physical Activity and Health. 2004;1:7–18.
25. Peterson MD, Sen A, Gordon PM. Influence of resistance exercise on lean body mass in aging adults: a meta-analysis. Medicine and Science in Sports and Exercise. 2011;43(2):249–58.
26. Tieland M, Dirks ML, Van der Zwaluw N, Verdijk LB, Van de Rest O, Groot LCPGM, et al. Protein supplementation increases muscle mass gain during prolonged resistance-type exercise training in frail elderly people: a randomized, double-blind, placebo-controlled trial. Journal of the American Medical Directors Association. 2012;13(8):713–9.
27. Cermak NM, Res PT, Groot LCPGM, Saris WHM, Van Loon LJC. Protein supplementation augments the adaptive response of skeletal muscle to resistance-type exercise training: a meta-analysis. The American Journal of Clinical Nutrition. 2012;96(6):1454–64.
28. Gabriel DA, Kamen G, Frost G. Neural adaptations to resistive exercise: mechanisms and recommendations for training practices. Sports Medicine. 2006;36(2):133–49.
29. Sale DG. Neural adaptation to resistance training. Medicine and Science in Sports and Exercise. 1988;20:S135–S145.
30. Häkkinen K, Alen M, Kallinen M, Newton RU, Kraemer WJ. Neuromuscular adaptation during prolonged strength training, detraining and re-strength-training in middle-aged and elderly people. European Journal of Applied Physiology. 2000;83(1):51–62.
31. Simões RP, Deus APL, Auad MA, Dionísio J, Mazzonetto M, Borghi-Silva A. Maximal respiratory pressure in healthy 20 to 89 year-old sedentary individuals of central São Paulo State. Revista Brasileira de Fisioterapia. 2010;14(1):60–7.
32. Neder JA, Andreoni S, Lerario MC, Nery LE. Reference values for lung function tests: II. Maximal respiratory pressures and voluntary ventilation. Brazilian Journal of Medical and Biological Research. 1999;32(6):719–27.
33. Costa D, Gonçalves HA, Lima LP, Ike D, Cancelliero KM, Montebelo MI de L. Novos valores de referência para pressões respiratórias máximas na população brasileira. Jornal Brasileiro de Pneumologia. 2010;36(3):306–12.

18
34. Vaz Fragoso CA, Enright PL, McAvay G, Van Ness PH, Gill TM. Frailty and respiratory impairment in older persons. The American Journal of Medicine. 2012;125(1):79–86.
35. Beckerman M, Magadle R, Weiner M, Weiner P. The effects of 1 year of specific inspiratory muscle training in patients with COPD. Chest. 2005;128(5):3177–82.
36. Watsford M, Murphy A. The effects of respiratory-muscle training on exercise in older women. Journal of Aging and Physical Activity. 2008;16(3):245–60.
37. Cader SA, Souza Vale RG, Zamora VE, Costa CH, Dantas EHM. Extubation process in bed-ridden elderly intensive care patients receiving inspiratory muscle training: a randomized clinical trial. Clinical Interventions in Aging. 2012;7:437–43.
38. Severino FG, Resqueti VR, Bruno SS, Azevedo IG, Vieira RHG, Fregonezi GAF. Comparação entre o manovacuômetro nacional e o importado para medida da pressão inspiratória nasal. Revista Brasileira de Fisioterapia. 2010;14(5):426–31.
39. Gomieiro LTY, Nascimento A, Tanno LK, Agondi R, Kalil J, Giavina-Bianchi P. Respiratory exercise program for elderly individuals with asthma. Clinics. 2011;66(7):1163–9.
40. Cader S, Silva EB, Vale R, Bacelar S, Monteiro MD DE. Efeito do treino dos músculos inspiratórios sobre a pressão inspiratória máxima e a autonomia funcional de idosos asilados. Motricidade. 2007;1(3):279–88.
41. HajGhanbari B, Yamabayashi C, Buna TR, Coelho JD, Freedman KD, Morton TA, et al. Effects of respiratory muscle training on performance in athletes: a systematic review with meta-analyses. Journal of Strength and Conditioning Research. 2013;27(6):1643–63.
42. Illi SK, Held U, Frank I, Spengler CM. Effect of respiratory muscle training on exercise performance in healthy individuals: a systematic review and meta-analysis. Sports Medicine. 2012;42(8):707–24.
43. Nascimento VC, Trindade J, Oliveira E, Sousa EC, Abrahin O. Efeitos dos exercícios resistidos nos indicadores de normalidade de força dos músculos respiratórios de idosos. The FIEP Bulletin. 2013;83:151–4.
19
VII – ANEXO
Artigo 1
Abrahin O, Rodrigues RP, Nascimento VC, Da Silva-Grigoletto ME, Sousa EC, Marçal AC. Single- and multiple-set resistance training improves skeletal and respiratory muscle strength in elderly women. Clinical Interventions in Aging, 9: 1775–1782, 2014.
© 2014 Abrahin et al. This work is published by Dove Medical Press Limited, and licensed under Creative Commons Attribution – Non Commercial (unported, v3.0) License. The full terms of the License are available at http://creativecommons.org/licenses/by-nc/3.0/. Non-commercial uses of the work are permitted without any further
permission from Dove Medical Press Limited, provided the work is properly attributed. Permissions beyond the scope of the License are administered by Dove Medical Press Limited. Information on how to request permission may be found at: http://www.dovepress.com/permissions.php
Clinical Interventions in Aging 2014:9 1775–1782
Clinical Interventions in Aging Dovepress
submit your manuscript | www.dovepress.com
Dovepress 1775
O r I g I n A l r e s e A r C h
open access to scientific and medical research
Open Access Full Text Article
http://dx.doi.org/10.2147/CIA.S68529
single- and multiple-set resistance training improves skeletal and respiratory muscle strength in elderly women
Odilon Abrahin1–3
rejane P rodrigues1–3
Vanderson C nascimento3
Marzo e Da silva-grigoletto1,4
evitom C sousa3
Anderson C Marçal1,2
1Department of Physical education, Federal University of sergipe, sergipe, Brazil; 2Center of research in Intracellular signaling, Department of Morphology, Federal University of sergipe, sergipe, Brazil; 3laboratory of resistance exercise and health, sports Department, University of Pará state, Belem, Brazil; 4scientific sport, sergipe, Brazil
Introduction: Aging involves a progressive reduction of respiratory muscle strength as well
as muscle strength.
Purpose: Compare the effects of resistance training volume on the maximum inspiratory
pressure (MIP), maximum expiratory pressure (MEP), functional performance, and muscle
strength in elderly women.
Methods: Thirty elderly women were randomly assigned to a group performing either single
sets (1-SET) or three sets (3-SET) of exercises. The sit-to-stand test, MIP, MEP, and muscle
strength were assessed before and after 24 training sessions. Progressive resistance training was
performed two times per week for a total of 8–12 repetitions, using the main muscle groups of
the upper and lower limbs.
Results: The main results showed that the participants significantly increased their MEP
(P,0.05; 1-SET: 34.6%; 3-SET: 35.8%) and MIP (P,0.05; 1-SET: 13.7%; 3-SET: 11.2%).
Both groups also improved in the sit-to-stand test (P,0.05; 1-SET: 10.6%; 3-SET: 17.1%).
After 24 training sessions, muscle strength also significantly increased (P,0.0001; 40%–80%)
in both groups. An intergroup comparison did not show any statistically significant differences
between the groups in any of the parameters analyzed.
Conclusion: Single- and multiple-set resistance training programs increased MIP, MEP,
muscle strength, and sit-to-stand test performance in elderly women after 24 sessions of train-
ing. In conclusion, our results suggested that elderly women who are not in the habit of physical
activity may start with single-set resistance training programs as a short-term strategy for the
maintenance of health.
Keywords: resistance exercise, maximum inspiratory pressure, maximum expiratory pressure,
elderly
IntroductionAging can be defined as a process of biological modifications involving a gradual
reduction in the capacity to adapt, and an increase in vulnerability to countless health
issues such as chronic noncommunicable diseases and musculoskeletal disorders.
According to the World Health Organization, by 2050, the number of elderly people
(older than 60 years) is estimated to reach 2 billion, corresponding to approximately
22% of the global population.1
In general terms, sedentary aging involves a reduction in physical capacity, in asso-
ciation with functional deficits, such as reduced levels of respiratory muscle strength
and muscle strength, reduced cardiorespiratory capacity, and reduced mobility, all of
which make completing daily activities more difficult.2–4 A recent study established a
strong association between poor physical fitness and respiratory disorders.4
Correspondence: Anderson Carlos MarçalUniversidade Federal de sergipe, Centro de Ciências Biológicas e da saúde, Cidade Universitária Prof José Aloísio de Campos, Jardim rosa elze, Cep: 49100-000, são Cristóvão, sergipe, BrazilFax +55 79 2105 6622email [email protected]
Journal name: Clinical Interventions in AgingArticle Designation: Original ResearchYear: 2014Volume: 9Running head verso: Abrahin et alRunning head recto: Resistance training and respiratory muscle strengthDOI: http://dx.doi.org/10.2147/CIA.S68529

Clinical Interventions in Aging 2014:9submit your manuscript | www.dovepress.com
Dovepress
Dovepress
1776
Abrahin et al
Dysfunction in the respiratory muscles can lead to
hyperventilation, reduction in exercise tolerance, and
even respiratory insufficiency; also, it is associated with
an increase in morbidity and mortality rates.4,5 The evalu-
ation of respiratory muscle strength is of great clinical
importance and can be measured by static and dynamic
maneuvers.6–9 Static maneuvers infer maximal inspiratory
pressure (MIP) and maximal expiratory pressure (MEP).
These parameters, evaluated through the mouth, reflect
the pressure that is being generated by the action of the
respiratory muscles.6–9
Specific respiratory muscle training has had significant
effects on the respiratory muscle strength and endurance
of athletes.10 However, few scientific studies suggest that
resistance training can be used for improving respiratory
muscle strength.11,12 To the best of our knowledge, no study
has investigated the chronic effect of resistance training (RT)
volume on the respiratory muscles in elderly women. There-
fore, the aim of the present study was to compare the effects
of RT volume on the MIP, MEP, functional performance,
and muscle strength in elderly women.
MethodssubjectsThe inclusion criteria required the women to be nonsmok-
ers and between 60 and 80 years of age, with previous
experience of RT (minimum 6 months, uninterrupted), but
without participation in any type of physical exercise dur-
ing the preceding 3 months. Volunteers who had any type
of musculoskeletal, cardiovascular, or neurological disorder
that complicated RT were excluded, as were women who
could not complete the 24 training sessions.
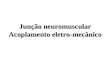
Thirty elderly women from the local community agreed
to participate in this study. The volunteers were randomly
divided into two groups: 1-SET (n=15), and 3-SET (n=15).
By the end of the study, 19 participants had successfully
completed the study protocol (1-SET, n=11; 3-SET, n=8);
the reasons for dropout were not related to adverse events
associated with the protocol, and the participants who did not
complete 24 training sessions or who missed four consecutive
sessions were excluded (Figure 1).
All participants presented a medical certificate and signed
the Termo de Consentimento Livre e Esclarecido (informed
consent form) for their participation in this research. The study
was approved by the Research Ethics Committee of Univer-
sidade da Amazônia (CAAE [certificate of presentation for
ethical consideration] number: 12941013.5.0000.5173), in
accordance with both the regulations of Resolution 196/96 of
Conselho Nacional de Pesquisa Envolvendo Seres Humanos
(National Council on Ethics in Human Research) and the
Declaration of Helsinki.
ProceduresThe participants initially performed two sessions of training
in order to learn the exercises. Thereafter, they attended an
additional four sessions. During the first session, anthro-
pometry and functional performance were assessed with the
sit-to-stand test. On the second visit, MIP and MEP were
Figure 1 Flowchart of the volunteer selection process in different stages of the study.Abbreviations: 1-seT, single set; 3-seT, three sets.
Randomly divided sample (n=30)
1-SET(n=15)
Excluded (n=4)– Personal problems (n=2)– Incomplete protocol (n=2)
Completed trainingprotocol (n=11)
3-SET(n=15)
Excluded (n=7)– Personal problems (n=3)– Incomplete protocol (n=4)
Completed trainingprotocol (n=8)

Clinical Interventions in Aging 2014:9 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
1777
resistance training and respiratory muscle strength
assessed. On the third and fourth visits, testing and retest-
ing 10 maximum repetitions (MR) were conducted. After
24 sessions of progressive RT, the tests were reassessed in
the same sequence and by the same evaluator.
sit-to-stand in 30 secondsThe assessment was started using a chair with a height of
43 cm; the volunteer sat in the middle of the seat, with a
straight spinal column, feet resting on the ground and arms
crossed against the chest. When signaled, the volunteer was
encouraged to fully sit and stand as many times as possible
in 30 seconds. The test was performed as described by Rikli
and Jones.13 All patients were familiarized with the testing,
and the best time of two attempts was used.
AnthropometryFor the measurement of waist and abdominal circumfer-
ence, a flexible metallic tape measure with precise 0.1 cm
markings was used (Sanny, São Paulo, Brazil). Body
fat percentages were estimated using a Skinfold Caliper
(Harpenden, London, UK) and an analog scale with a
stadiometer, having a 180 kg capacity in 100 g divisions.
Skinfold thicknesses were measured according to the
standard set by the Durnin and Womersley14 equation for
elderly women, and the Siri15 equation. All measures were
taken by an International Society for the Advancement of
Kinanthropometry Level 3 anthropometrist with at least
10 years of experience, with reliability tested by technical
error of measurement, as proposed by Norton and Olds,16
being lower than 2%.
Maximum inspiratory pressure and maximum expiratory pressureMIP and MEP were measured in stages using an analog
manometer (MV 300; Wika, São Paulo, Brazil), with a pres-
sure range of -300 cmH2O to +300 cmH
2O. Both MIP and
MEP measurements were performed with a plastic tube 3 cm
in diameter and 15 cm long, with a plastic flanged mouthpiece
and a small air leak 7.5 cm from the mouthpiece. The small
leak in the tube was necessary to prevent generation of high
buccal pressures. In addition, subjects were required to hold
their cheeks with one hand during the performances. Verbal
encouragement was given to the subjects during testing, to
ensure that motivation levels remained high. Measurements
followed the recommendations of the American Thoracic
Society/European Respiratory Society6 and were conducted
three times for each participant by an experienced evaluator.
The highest value was used for the analysis. In cases where
a difference exceeding 10% was found between repeated
measurements, the exercise was repeated to obtain the highest
measurement, but not necessarily the final one.6,7
Muscle strength (10 Mr)Muscle strength was assessed by MR tests in accordance with
American College of Sports Medicine17 recommendations,
using bench press, deadlift, unilateral rowing, and standing
calf raise. All participants underwent two test sessions, with
an interval of .48 hours between sessions. The test and
retesting were conducted in the same order, to minimize
possible errors in the 10 MR tests. Each session comprised
one set of warm-ups, with an estimated 50% load on the
first attempt and up to three consecutive attempts, in order
to manage a load of 10 MR. The recovery interval between
attempts was 5 minutes.
resistance training programThe 1-SET (n=11) and 3-SET (n=8) groups conducted RT
two times per week for 12 weeks, with a minimum of 48 hours
between sessions. All sessions were conducted in the Labo-
ratory of Resistance Training and Health, and participants
were instructed to maintain their daily activities and normal
eating habits throughout the 24 training sessions.
Both groups conducted the following exercises: bench
press, deadlift, unilateral rowing, standing calf raise, and
lower abdominal exercise. Such exercises involve the major
muscle groups of the upper and lower limbs and simulate
the basic movements of daily activities. All exercises were
performed in the same order, with an intensity of 8–12 MR.
The participants were instructed to adjust their training
load in order to guarantee submaximal/maximal strength
between 8 and 12 MR. The following characteristics were
observed in the technical performance of the exercises:
tendency for concentric muscle failure and reduction in
rhythm, apnea, and isometry. If the volunteers were able
to complete 12 repetitions of an exercise in each of two
consecutive training sessions, the loads were increased
by 5%.17 All sessions were supervised and involved small
groups of up to six participants, to ensure that each exer-
cise technique was performed correctly, safely, and to the
appropriate intensity.
In each experimental group (1-SET and 3-SET), the type
of training method alternated by segment.17 Other RT vari-
ables, including intensity, repetitions, speed, order, interval,
and weekly frequency were the same for both groups; the
only difference between the groups was the number of sets
(Table 1).
Clinical Interventions in Aging 2014:9submit your manuscript | www.dovepress.com
Dovepress
Dovepress
1778
Abrahin et al
Training sessionsThe single- and multiple-set protocols had a maximum
duration of 20 minutes and 50 minutes, respectively. At
the beginning of each session, the individuals performed
a warm-up of approximately 5 minutes in duration. The
warm-up involved exercises for the upper and lower limbs:
shoulder adduction and abduction, torso rotation, hip flex-
ion and extension, knee flexion and extension, and ankle
flexion and extension.
Variable reproducibilityThe test and retest for 10 MR was conducted using an interval
of 48 hours. The intraclass correlation coefficients were 0.90,
0.94, 0.77, and 0.82 for bench press, deadlift, rowing, and
standing calf raise, respectively. All volunteers were familiar
with all the tests, as they had participated in other projects
within the laboratory during the previous semester.
statistical analysisTraditional statistical methods were used to calculate mean ±
standard deviation. Sample normality was calculated using
the Shapiro–Wilk test. The effect of the different interven-
tions single- versus multiple-set (independent variables) on
MIP, MEP, and muscular strength (dependent variables) were
analyzed by means of ANOVA (2×2). A Sidak correction was
used to adjust the P-value regarding the number of contrasts
performed, and a P,0.05 criterion was used to establish
statistical significance. Reproducibility was assessed using
an intraclass correlation coefficient, and effect size was
calculated for paired variables. The SPSS 18 package (IBM
Corp., Armonk, NY) for Windows was used for all statisti-
cal tests.
On the basis of a pilot study (four subjects), as well
as available literature, a power analysis was performed to
determine the appropriate number of subjects. Eight subjects
(per group) were required to detect a minimum difference
of 12 cmH2O for MIP and 10 cmH
2O for MEP (Granmo 5.2
for Windows; IMIM, Barcelona, Spain), which would be
required to achieve 80% statistical power.
ResultsThe characteristics of the women in this study are presented in
Table 2. There were no significant differences in age, weight,
body mass index, body fat percentage, or waist and abdomen
circumferences between the groups at the beginning of the
study. Furthermore, these variables were not significantly
different after training.
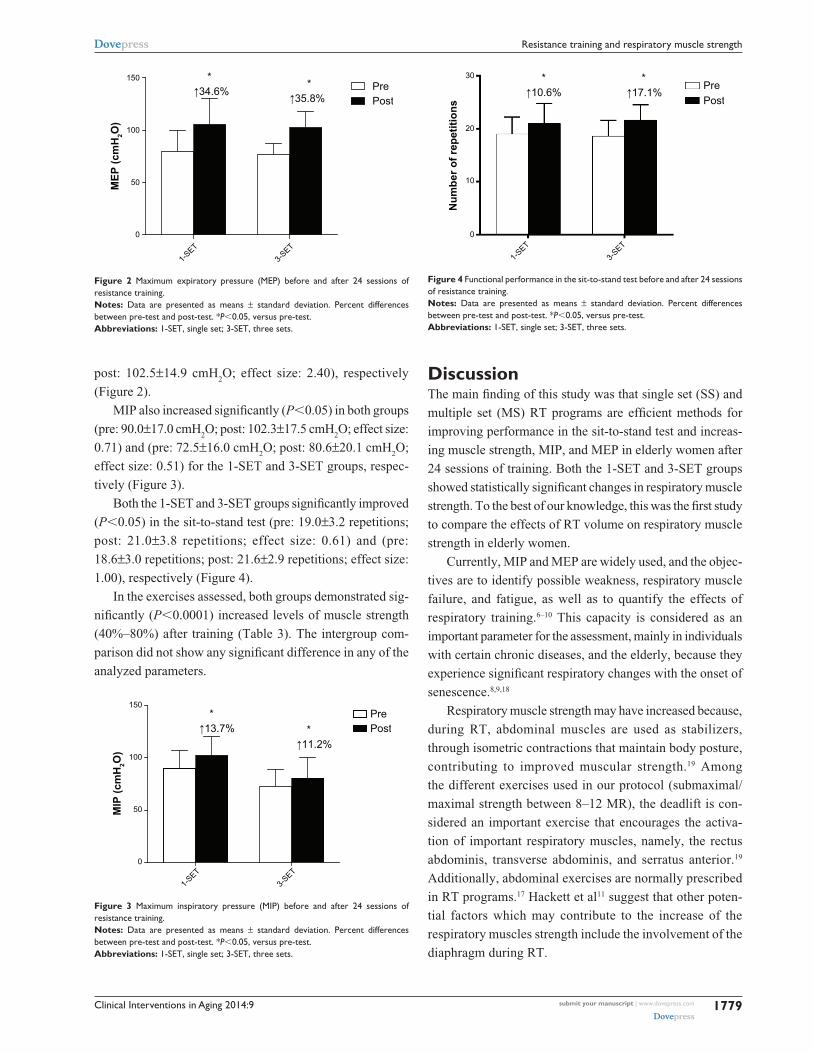
The 1-SET and 3-SET groups significantly improved
(P,0.05) in the MEP (pre: 79.5±20.5 cmH2O; post: 105.5±24.6
cmH2O; effect size: 1.27) and (pre: 76.3±10.9 cmH
2O;
Table 1 resistance training variables used in this study
Variables 1-SET 3-SET
Intensity 60%–80% of 10 Mr 60%–80% of 10 Mrrepetitions 8–12 8–12 speed 2 seconds of eccentric and 2 seconds of concentric 2 seconds’ eccentric and concentricInterval between exercises 90 seconds 90 secondsInterval between sets – 120 secondsFrequency 2 times per week 2 times per weeknumber of exercises 5 exercises 5 exercisesset 1 set per exercise 3 sets per exercise
Abbreviations: 1-seT, single set; 3-seT, three sets; Mr, maximum repetitions.
Table 2 Characteristics of elderly women before and after 24 sessions of training; women performing a single set (1-seT, n=11) and those performing three sets (3-seT, n=8)
Before After
1-SET 3-SET 1-SET 3-SET
Age 67.1±3.7 69.4±6.0Body mass (kg) 65.1±12.1 63.9±8.1 65.7±11.9 64.3±8.3height (cm) 153±0.1 152±0.1 153±0.1 152±0.1Body mass index (kg/m2) 27.9±4.0 27.7±3.6 27.9±3.9 27.8±3.5Abdomen (cm) 95.7±11.9 96.8±7.5 94.1±11.2 94.1±6.9Waist (cm) 85.2±10.7 86.4±8.6 84.7±9.1 84.7±7.5%g (body fat percentage) 40.9±2.7 40.0±1.9 39.0±2.7 39.0±2.1
Note: Data are presented as mean ± standard deviation.
Clinical Interventions in Aging 2014:9 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
1779
resistance training and respiratory muscle strength
post: 102.5±14.9 cmH2O; effect size: 2.40), respectively
(Figure 2).
MIP also increased significantly (P,0.05) in both groups
(pre: 90.0±17.0 cmH2O; post: 102.3±17.5 cmH
2O; effect size:
0.71) and (pre: 72.5±16.0 cmH2O; post: 80.6±20.1 cmH
2O;
effect size: 0.51) for the 1-SET and 3-SET groups, respec-
tively (Figure 3).
Both the 1-SET and 3-SET groups significantly improved
(P,0.05) in the sit-to-stand test (pre: 19.0±3.2 repetitions;
post: 21.0±3.8 repetitions; effect size: 0.61) and (pre:
18.6±3.0 repetitions; post: 21.6±2.9 repetitions; effect size:
1.00), respectively (Figure 4).
In the exercises assessed, both groups demonstrated sig-
nificantly (P,0.0001) increased levels of muscle strength
(40%–80%) after training (Table 3). The intergroup com-
parison did not show any significant difference in any of the
analyzed parameters.
DiscussionThe main finding of this study was that single set (SS) and
multiple set (MS) RT programs are efficient methods for
improving performance in the sit-to-stand test and increas-
ing muscle strength, MIP, and MEP in elderly women after
24 sessions of training. Both the 1-SET and 3-SET groups
showed statistically significant changes in respiratory muscle
strength. To the best of our knowledge, this was the first study
to compare the effects of RT volume on respiratory muscle
strength in elderly women.
Currently, MIP and MEP are widely used, and the objec-
tives are to identify possible weakness, respiratory muscle
failure, and fatigue, as well as to quantify the ef fects of
respiratory training.6–10 This capacity is considered as an
important parameter for the assessment, mainly in individuals
with certain chronic diseases, and the elderly, because they
experience significant respiratory changes with the onset of
senescence.8,9,18
Respiratory muscle strength may have increased because,
during RT, abdominal muscles are used as stabilizers,
through isometric contractions that maintain body posture,
contributing to improved muscular strength.19 Among
the different exercises used in our protocol (submaximal/
maximal strength between 8–12 MR), the deadlift is con-
sidered an important exercise that encourages the activa-
tion of important respiratory muscles, namely, the rectus
abdominis, transverse abdominis, and serratus anterior.19
Additionally, abdominal exercises are normally prescribed
in RT programs.17 Hackett et al11 suggest that other poten-
tial factors which may contribute to the increase of the
respiratory muscles strength include the involvement of the
diaphragm during RT.
Figure 2 Maximum expiratory pressure (MeP) before and after 24 sessions of resistance training.Notes: Data are presented as means ± standard deviation. Percent differences between pre-test and post-test. *P,0.05, versus pre-test.Abbreviations: 1-seT, single set; 3-seT, three sets.
1-SET
3-SET
0
50
100
150 * ↑34.6%
* ↑35.8%
PrePost
MEP
(cm
H2O
)
Figure 3 Maximum inspiratory pressure (MIP) before and after 24 sessions of resistance training.Notes: Data are presented as means ± standard deviation. Percent differences between pre-test and post-test. *P,0.05, versus pre-test.Abbreviations: 1-seT, single set; 3-seT, three sets.
1-SET
3-SET
0
50
100
150*
↑13.7% * ↑11.2%
PrePost
MIP
(cm
H2O
)
Figure 4 Functional performance in the sit-to-stand test before and after 24 sessions of resistance training.Notes: Data are presented as means ± standard deviation. Percent differences between pre-test and post-test. *P,0.05, versus pre-test.Abbreviations: 1-seT, single set; 3-seT, three sets.
Num
ber o
f rep
etiti
ons
1-SET
3-SET
30
20
10
0
* *PrePost
↑10.6% ↑17.1%

Clinical Interventions in Aging 2014:9submit your manuscript | www.dovepress.com
Dovepress
Dovepress
1780
Abrahin et al
Watsford and Murphy20 demonstrated a significant
increase in respiratory muscle strength in elderly women
participating in specific respiratory muscle training over
a period of 8 weeks. Other benefits observed included a
reduction in the submaximal heart rate and an increase
in maximum voluntary ventilation, when compared to a
control group. A study12 investigated the effects of flex-
ibility training (proprioceptive neuromuscular facilitation)
combined with resistance training (elastic resistance bands)
on respiratory muscle strength in adult women, and its
results showed significant increases in MIP and MEP. In
accordance with our results, these studies suggested that
specific respiratory muscle training and resistance training
are important adjuvants in improving respiratory muscle
strength.11,12,20
In a recent study, MIP and MEP were observed to
decrease according to the fragility of the elderly person. In
addition, inspiratory and expiratory muscle strengths were
positively correlated with general muscle strength.21 These
data justify the need for further studies to assess the effects
of resistance exercise on inspiratory and expiratory muscle
strength, with the aim of minimizing or reversing loss of
respiratory function, given that a reduction in pulmonary
function is associated with an increase in morbidity and
mortality rates.18,22,23
Another important benefit observed in this study was
muscular strength gains. This physical component is related
to increased mobility and walking pace, due to increased mus-
culoskeletal excitability and muscle innervation, leading to
greater functional independence.3,24,25 Furthermore, increased
muscle strength can contribute to a reduced incidence of falls,
thus preventing bone fractures. Therefore, muscle strength is
an important physical component for maintaining the health
of the elderly.2,26
The elderly women who participated in this study dem-
onstrated statistically significant increases in levels of muscle
strength after 24 sessions of progressive RT over a period of
12 weeks, without significant intergroup differences (1-SET
versus 3-SET). These results could be explained by the short
training period (neural adaptations) used in agreement with
a recent study.27 Galvão and Taaffe28 assessed the effects of
SS and MS RT in the elderly, and their results demonstrated
that after 20 weeks of training, both groups significantly
increased their strength in the seven different types of exer-
cises analyzed. These results corroborate a meta-analysis
published by Fröhlich et al29 which demonstrated that SS
and MS RT can guarantee a similar strength increase in
individuals using short training periods, but the benefits of
using MS RT increase with longer training periods (over
25 weeks). Another meta-analysis30 reported that when sub-
jects used two to three sets per exercise, they demonstrated
a 46% increase in strength, in comparison with a single set,
regardless of the training level or the program duration. The
difference between these meta-analysis results could be
related to the inclusion methods employed by the different
studies and their statistical delineation.
The results of this study showed significant increases
in the sit-to-stand test. Currently, this test is considered
an important indicator of lower limb strength, and func-
tional capacity to perform basic activities in older adult
women,13,31–33 in addition to its correlation with quadriceps
strength and lean mass.33 The findings from this study cor-
roborate those of Galvão and Taaffe,28 in identifying that SS
programs performed two times per week are able to improve
performance in the sit-to-stand test.
No significant differences were observed in anthropometric
indexes between the groups after 24 training sessions. These
results can be explained by the absence of nutritional
Table 3 repetition test (10 Mr) before and after 24 sessions of training in the group performing a single set (1-seT, n=11) and in the group performing three sets (3-seT, n=8)
Exercisesin kg
Group Pre(mean ± SD)
Post(mean ± SD)
∆(mean ± SD)
∆%(mean ± SD)
P-value Effect size
Bench press 1-seT 13.8±1.7 21.6±3.2 7.8±2.1 56.5±13.8 ,0.0001* 4.593-seT 14.3±3.5 22.0±4.0 7.8±2.0 57.5±21.0 ,0.0001* 2.20
Deadlift 1-seT 10.0±3.8 16.5±3.6 6.5±2.4 60.0±23.5 ,0.0001* 1.713-seT 13.3±3.8 20.5±4.1 7.3±1.5 73.2±28.8 ,0.0001* 1.89
rowing 1-seT 19.5±2.7 26.6±2.5 7.1±3.7 38.3±20.4 ,0.0001* 2.633-seT 16.9±2.6 26.5±2.6 9.6±2.1 58.8±17.8 ,0.0001* 3.69
Calf raise 1-seT 21.8±3.5 38.6±2.3 16.8±3.4 79.1±22.0 ,0.0001* 4.803-seT 25.0±2.8 40.6±8.6 15.6±5.6 66.1±28.5 ,0.0001* 5.57
Notes: *P#0.001, versus pretest; ∆% = average percent difference between pre- and post-tests. Data are presented as mean ± standard deviation.Abbreviations: Mr, maximum repetitions, sD, standard deviation.

Clinical Interventions in Aging 2014:9 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
1781
resistance training and respiratory muscle strength
intervention, given that the women maintained their nor-
mal eating habits during the study period. Washburn et al34
assessed the effects of SS RT on body composition using
double-emission densitometry in overweight adults. The
exercise protocol comprised a single set of nine exercises,
performed three times per week at 3–6 MR intensity over a
period of 6 months. The results revealed that, compared to
the control group, the intervention group had a significant
increase in lean mass. The intervention group did not show
any change in body fat, whereas the control group showed a
significant increase in body fat (mean: 1.9%). There was no
nutritional intervention in these groups, and the minimum
training volume helped to maintain a stable body fat mass.34
That evidence corroborates our study, given that both groups
received no nutritional intervention and showed no significant
changes in their body fat percentages.
ConclusionSingle- and multiple-set resistance training programs
increased respiratory muscle strength, muscle strength, and
sit-to-stand test performance in elderly women after 24 ses-
sions of training. Elderly women who do not prioritize time
for physical activity or do not have a good adherence to regu-
lar programs should be recommended to start with single-set
resistance training programs as a short-term strategy.
AcknowledgmentsThe authors would like to acknowledge Coordenação de
Aperfeiçoamento de Pessoal de Nível Superior (CAPES)
and Fundação de Apoio à Pesquisa e Inovação Tecnológica
do Estado de Sergipe (FAPITEC/SE) for their funding sup-
port for this study. We also thank teacher Abilio Borghi for
assistance with the grammar review of the manuscript.
DisclosureThe authors report no conflicts of interest in this work.
References1. World Health Organization. Interesting facts about ageing [Internet].
Geneva: WHO; 2012 [cited 2013 Aug 29]. Available from: http://www.who.int/ageing/about/facts/en/index.html. Accessed April 12, 2014.
2. Westcott WL. Resistance training is medicine: effects of strength training on health. Curr Sports Med Rep. 2012;11(4):209–216.
3. Fiatarone MA, Marks EC, Ryan ND, Meredith CN, Lipsitz LA, Evans WJ. High-intensity strength training in nonagenarians. Effects on skeletal muscle. JAMA. 1990;263(22):3029–3034.
4. Vaz Fragoso CA, Enright PL, McAvay G, Van Ness PH, Gill TM. Frailty and respiratory impairment in older persons. Am J Med. 2012; 125(1):79–86.
5. Sin DD, Wu L, Man SF. The relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literature. Chest. 2005;127(6):1952–1959.
6. American Thoracic Society/European Respiratory Society. ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166(4):518–624.
7. Neder JA, Andreoni S, Castelo-Filhop A, Nery LE. Reference values for lung function tests. I. Static volumes. Braz J Med Biol Res. 1999; 32(6):703–717.
8. Kim J, Sapienza CM. Implications of expiratory muscle strength train-ing for rehabilitation of the elderly: Tutorial. J Rehabil Res Dev. 2005; 42(2):211–224.
9. Simões RP, Deus AP, Auad MA, Dionísio J, Mazzonetto M, Borghi-Silva A. Maximal respiratory pressure in healthy 20 to 89 year-old sedentary individuals of central São Paulo State. Rev Braz Fisioter. 2010;14(1):60–67.
10. HajGhanbari B, Yamabayashi C, Buna TR, et al. Effects of respiratory muscle training on performance in athletes: a systematic review with meta-analyses. J Strength Cond Res. 2013;27(6):1643–1663.
11. Hackett DA, Johnson NA, Chow CM. High-volume resistance training session acutely diminishes respiratory muscle strength. J Sports Sci Med. 2012;11(1):26–30.
12. Areas GP, Borghi-Silva A, Lobato AN, Silva AA, Freire RC Jr, Areas FZ. Effect of upper extremity proprioceptive neuromuscular facilitation com-bined with elastic resistance bands on respiratory muscle strength: a ran-domized controlled trial. Braz J Phys Ther. 2013;17(6):541–546.
13. Rikli RE, Jones CJ. Development and validation of a functional fitness test for community-residing older adults. J Aging Phys Act. 1999; 7(2):129–161.
14. Durnin JV, Womersley J. Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. Br J Nutr. 1974;32(1):77–97.
15. Siri WE. Body composition from fluid spaces and density: analysis of methods. 1961. Nutrition. 1993;9(5):480–491.
16. Norton K, Olds T. Antropométrica. Porto Alegre, Brazil: Artmed; 2005. 17. American College of Sports Medicine, Chodzko-Zajko WJ, Proctor DN,
Fiatarone Singh MA, et al. American College of Sport Medicine position stand. Exercise and physical activity for older adults. Med Sci Sports Exerc. 2009;41(7):1510–1530.
18. Phillips WT, Benton MJ, Wagner CL, Riley C. The effect of single set resistance training on strength and functional fitness in pulmonary rehabilitation patients. J Cardiopulm Rehabil. 2006;26(5):330–337.
19. Martuscello JM, Nuzzo JL, Ashley CD, Campbell BI, Orriola JJ, Mayer JM. Systematic review of core muscle activity during physical fitness exercises. J Strength Cond Res. 2013;27(6):1684–1698.
20. Watsford M, Murphy A. The effects of respiratory-muscle training on exercise in older women. J Aging Phys Act. 2008;16(3):245–260.
21. Pegorari MS, Ruas G, Patrizzi LJ. Relationship between frailty and respiratory function in the community-dwelling elderly. Braz J Phys Ther. 2013;17(1):9–16.
22. Santana H, Zoico E, Turcato E, et al. Relation between body composi-tion, fat distribution, and lung function in elderly men. Am J Clin Nutr. 2001;73(4):827–831.
23. Sin DD, Wu L, Man SF. The relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literature. Chest. 2005;127(6):1952–1959.
24. Bean JF, Kiely DK, Herman S, et al. The relationship between leg power and physical performance in mobility-limited older people. J Am Geriatr Soc. 2002;50(3):461–467.
25. Kalyani RR, Tra Y, Yeh HC, Egan JM, Ferrucci L, Brancati FL. Quadri-ceps strength, quadriceps power, and gait speed in older U.S. adults with diabetes mellitus: results from the National Health and Nutrition Exami-nation Survey, 1999–2002. J Am Geriatr Soc. 2013;61(5):769–775.
26. Marin RV, Pedrosa MA, Moreira-Pfrimer LD, Matsudo SM, Lazaretti-Castro M. Association between lean mass and handgrip strength with bone mineral density in physically active postmenopausal women. J Clin Densitom. 2010;13(1):96–101.
27. Radaelli R, Botton CE, Wilhelm EN, et al. Low- and high-volume strength training induces similar neuromuscular improvements in mus-cle quality in elderly women. Exp Gerontol. 2013;48(8):710–716.

Clinical Interventions in Aging
Publish your work in this journal
Submit your manuscript here: http://www.dovepress.com/clinical-interventions-in-aging-journal
Clinical Interventions in Aging is an international, peer-reviewed journal focusing on evidence-based reports on the value or lack thereof of treatments intended to prevent or delay the onset of maladaptive correlates of aging in human beings. This journal is indexed on PubMed Central, MedLine,
CAS, Scopus and the Elsevier Bibliographic databases. The manuscript management system is completely online and includes a very quick and fair peer-review system, which is all easy to use. Visit http://www.dovepress.com/testimonials.php to read real quotes from published authors.
Clinical Interventions in Aging 2014:9submit your manuscript | www.dovepress.com
Dovepress
Dovepress
Dovepress
1782
Abrahin et al
28. Galvão DA, Taaffe DR. Resistance exercise dosage in older adults: single-versus multiset on physical performance and body composition. J Am Geriatr Soc. 2005;53(12):2090–2097.
29. Fröhlich M, Emrich E, Schmidtbleicher D. Outcome effects of single-set versus multiple-set training – an advanced replication study. Res Sports Med. 2010;18(3):157–175.
30. Krieger JW. Single versus multiple sets of resistance exercise: a meta-regression. J Strength Cond Res. 2009;23(6):1890–1901.
31. Santos RG, Tribess S, Meneguci J, et al. [Lower limb strength as an indicator of functional disability in older individuals]. Motriz. 2013;19(3):S35–S42. Portuguese.
32. McCarthy EK, Horval MA, Holtsberg PA, Wisenbaker JM. Repeated chair stands as a measure of lower limb strength in sexagenarian women. J Geront A Biol Sci Med Sci. 2004;59(11):1207–1212.
33. Taaffe DR, Duret C, Wheeler S, Marcus R. Once-weekly resistance exercise improves muscle strength and neuromuscular performance in older adults. J Am Geriatr Soc. 1999;47(10):1208–1214.
34. Washburn RA, Kirk EP, Smith BK, et al. One set resistance training: effect on body composition in overweight young adults. J Sports Med Phys Fitness. 2012;52(3):273–279.