-
8/3/2019 Linfoma Associado a Imunodeficiencia
1/7
case records of themassachusetts general hospital
T h e n e w e n g l a n d j o u r n a l o f m ed i c i n e
Founded by Richard C. CabotNancy Lee Harris, m.d., Editor Sally
H. Ebeling,Assistant EditorJo-Anne O. Shepard, m.d.,Associate
Editor Christine C. Peters, Assistant Editor
n engl j med 354;11 www.nejm.org march 16, 20061178
From the Gastrointestinal Unit (D.K.P.)and the Departments of
Radiology (R.G.G.)and Pathology (R.P.H.), MassachusettsGeneral
Hospital; and the Departmentsof Medicine (D.K.P.), Radiology
(R.G.G.),and Pathology (R.P.H.), Harvard MedicalSchool.
N Engl J Med 2006;354:1178-84.Copyright 2006 Massachusetts
Medical Society.
Presentation of Case
A 71-year-old woman was admitted to the hospital because of
left-sided weaknessand a mass in the brain. She had had Crohns
disease for many years but was in her
usual state of health until three months before admission, when
she became fa-tigued and required daily naps. Two months before
admission, episodes of blurring
of vision, occipital headaches, and an unsteady gait occurred.
The patients husbanddescribed her as tilting to the left when she
walked, and she appeared to be de-
pressed and angry.Two weeks before admission, the patient noted
an enlarging, nontender mass
in her right inguinal area. A f ine-needle aspiration of the
mass performed 10 days
before admission disclosed necrosis, heterogeneous lymphoid
cells, and epithelioidhistiocytes suggestive of granulomatous
inflammation. Several days later nausea
developed, the patients appetite decreased, and over the course
of the next week,she lost weight (2 kg). She did not vomit; she had
chronic diarrhea from her
Crohns disease, which did not change in frequency or character.
Six days beforeadmission, she was too weak to get out of bed, and
her husband took her to theemergency room of another hospital,
where she was admitted. Her temperature was
38.8C; other vital signs were normal. The chest was clear, and
the heart soundswere normal. The abdomen was mildly tender to
palpation, without rebound or
guarding. There was no organomegaly. A firm, fixed, nontender
mass, 3 cm by 3 cm,was present on the right side of the inguinal
region. There was rectal tenderness on
digital examination. The patient was alert and oriented. The
results of a neurologicexamination showed no abnormalities.
Cultures of blood and stool were obtained,and broad-spectrum
antibiotics were administered.
On the second hospital day, the temperature was 38.8C. That
evening, the patienthad a sudden loss of coordination. A neurologic
consultant noted a left-sided facial
droop; the motor strength on the right side was normal and 4/5
on the left side.There was left pronator drift, and f inger-to-nose
and heel-to-shin movements were
poor on the left side. On stimulation of the plantar reflexes in
both feet, the toesturned down. The neck was supple, but her
headache was worse on neck flexion.A Romberg test was positive, and
the patient leaned toward her left side when
walking.Magnetic resonance imaging (MRI) of the brain showed a
mass, 3 cm in di-
Case 8-2006: A 71-Year-Old Woman withCrohns Disease and Altered
Mental Status
Daniel K. Podolsky, M.D., R. Gilberto Gonzalez, M.D., Ph.D.,and
Robert P. Hasserjian, M.D.
Copyright 2006 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org by CARLOS S. LOPES MD on
April 3, 2009 .
-
8/3/2019 Linfoma Associado a Imunodeficiencia
2/7
case records of the massachusetts general hospital
n engl j med 354;11 www.nejm.org march 16, 2006 1179
ameter, in the right thalamus adjacent to the
lateral ventricle. Computed tomography (CT) ofthe abdomen and
pelvis revealed the right ingui-
nal mass; there were no other abnormalities. Treat-ment with
dexamethasone was started. On the
third hospital day, the patient had less nausea
and headache, and the left-sided facial droopwas not seen. The
temperature rose to 38.9C.
An incisional biopsy of the right-sided inguinalmass was
performed. She was transferred to this
hospital on the sixth hospital day.Crohns disease had been
diagnosed when the
patient was 22 years of age, by Dr. Burrill B. Crohn,the
physician for whom the disease is named. Anileal resection was
performed when she was 22
years of age, and a hemicolectomy at 59 years ofage. Beginning
when she was 52 years of age, she
had been receiving treatment with prednisone, 40to 50 mg per
day; this drug had been discontin-
ued 10 years before admission. Six years beforeadmission,
treatment with mercaptopurine wasbegun; infliximab infusions every
eight weeks
were added to her treatment regimen three yearsbefore admission.
The patient continued to have
intermittent diarrhea and hematochezia. The lastinfusion of
infliximab she received was four weeks
before admission.The patient had diabetes mellitus,
hypertension,
and anemia, which was treated with monthly in-
jections of vitamin B12. She lived with her hus-band. She had
smoked cigarettes for 16 years but
quit 30 years before admission. She drank alco-
hol infrequently. A daughter had Crohns disease.The patients
medications included mesalamine,pantoprazole, losartan,
hydrochlorothiazide, loper-amide, zolpidem, insulin, cefoxitin,
vancomycin,
dexamethasone, and ondansetron in additionto those already
mentioned.
The temperature was 36.1C, the pulse 69 beatsper minute, the
respiratory rate 18 breaths per
minute, and the blood pressure 128/56 mm Hg.On physical
examination, the patient appearedchronically ill. There was a
small, white lesion on
the inferior aspect of the tongue. There was nocervical or
axillary lymphadenopathy. There were
inspiratory crackles at the left lung base, and theheart sounds
were normal. The abdomen was
soft and nontender, and the bowel sounds werenormal. There was a
right-sided inguinal mass,
3 cm by 1 cm, with a recent incision over it.The patient was
awake and alert. There was a
left homonymous hemianopia. The pupils were
equal and minimally reactive to light. Extraocular
movements were normal, but there was decreased
eye closure and reduced sensation to touch on theleft side of
her face. She could not raise her left
arm above her head. The strength in her left armmeasured 3/5
proximally and 1/5 distally, as com-
pared with 4/5 for the entire right arm. The
strength in her left leg measured 2/5 proximallyand 3/5
distally, as compared with 4/5 for the entire
right leg. Finger-to-nose touch and heel tappingwere intact on
the right side and slow on the left
side. The patient was too weak to walk.The results of laboratory
tests are shown in
Table 1. A lumbar puncture showed 94 white cells,with 32 percent
lymphocytes, 8 percent neutro-phils, 40 percent monocytes, and 19
percent large
cells with nucleoli and basophilic cytoplasm; theresults of flow
cytometry, cytologic examination,
and cultures were pending.Early in the morning of the second
hospital
day, the patient had a generalized tonicclonicseizure and became
unresponsive. The trachea wasintubated to maintain airway
protection, and she
was transferred to the intensive care unit. CTscanning of the
brain showed a heterogeneous
mass, 4.3 cm (from anterior to posterior) by 4.2 cm(from left to
right) in greatest dimension, cen-
tered in the right side of the thalamus, with arelatively low
attenuation center and a rim of highattenuation. There was an
eccentric nodular com-
ponent anteriorly and medially. Local mass effectwas noted on
the right lateral ventricle, but there
was no subfalcine or transtentorial herniation.
There was architectural distortion that resultedin crowding of
the foramen of Monro and mildprominence of the right temporal horn,
suggest-ing outflow obstruction.
A diagnostic procedure was performed.
Table 1. Laboratory-Test Results on Admission.
Variable Value Normal Range
Sodium (mmol/liter) 131 135145
Potassium (mmol/liter) 3.4 3.44.2
Alanine aminotransferase (U/liter) 45 730
Aspartate aminotransferase (U/liter) 36 932
Lactic dehydrogenase (U/liter) 290 110210
Alkaline phosphatase (U/liter) 41 30100
Amylase (U/liter) 53 3100
Hematocrit (%) 36.9 36.046.0
White cells (per mm3) 6,800 450011,000
Platelets (per mm3) 187,000 150,000350,000
Copyright 2006 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org by CARLOS S. LOPES MD on
April 3, 2009 .
-
8/3/2019 Linfoma Associado a Imunodeficiencia
3/7
T h e n e w e n g l a n d j o u r n a l o f m ed i c i n e
n engl j med 354;11 www.nejm.org march 16, 20061180
Differential Diagnosis
Dr. Daniel K. Podolsky: May we review the radio-logic
studies?
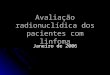
Dr. R. Gilberto Gonzalez: The CT scanning of thehead performed
without the administration of
contrast material on the second hospital day(Fig. 1A) revealed a
large mass centered withinthe right side of the thalamus. The mass
was
predominantly hyperdense, although regions oflow density were
observed; it exerted mass effect
on adjacent structures and appeared to extend intothe
ventricular system. The mass extended infe-
riorly to involve the temporal lobe and superiorlyto the centrum
semiovale.
Dr. Podolsky: This 71-year-old woman with an
almost 50-year history of Crohns disease requir-ing long-term
immunosuppressive therapy was
found to have a mass involving the central ner-
vous system after the onset of symptoms of weak-ness and various
neurologic findings. The imag-ing characteristics of the central
nervous system
abnormality are unlikely findings for a vascularprocess such as
stroke or hemorrhage, and thedifferential diagnosis is narrowed to
infection
and cancer.
Infection
Infectious processes, including abscess, tubercu-
losis, and opportunistic infections, are
importantconsiderations. Although Crohns disease wouldnot
predispose this patient to either an abscess
or an opportunistic infection, immunosuppressivetreatment could.
In particular, reactivation of la-
tent tuberculosis after the administration of in-fliximab has
been well recognized1; the majority
of patients in whom this reactivation has occurredhave had
extrapulmonary or disseminated disease,including central nervous
system infection. In
this regard, it is noteworthy that fine-needle as-piration of
the inguinal mass yielded granuloma-
tous tissue. Were it not for the brain lesion, thefinding from
the mass might also raise concern
about the possibility of Crohns disease involvinga lymph node.
However, the characteristics of thebrain images are not suggestive
of an infectious
process, and although the patient had fever, thereare few other
specific signs to suggest an infec-
tious process.
Cancer
The appearance of the brain mass is highly sug-gestive of a
neoplasm. Considered in isolation, the
A
B
Figure 1. CT and MRI Scans of the Head.
A CT scan (Panel A), obtained without the adminis-
tration of contrast material, shows a large mass,centered in the
right side of the thalamus (arrows).
The mass is heterogeneous, is predominantly hyper-
dense, and extends into the right lateral ventricle.
An MRI (Panel B), obtained six days after the CTscan, shows that
the mass had increased in size. It
has heterogeneous signal characteristics, includingareas of
relatively low T2-weighted signal correspond-ing to the regions of
hyperdensity seen on the CT
scan. The mass prevents the egress of cerebrospinal
fluid, resulting in hydrocephalus.
Copyright 2006 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org by CARLOS S. LOPES MD on
April 3, 2009 .
-
8/3/2019 Linfoma Associado a Imunodeficiencia
4/7
case records of the massachusetts general hospital
n engl j med 354;11 www.nejm.org march 16, 2006 1181
imaging studies would raise concern for a primary
cancer of the brain. However, given the knowndiagnosis of Crohns
disease and the presence of
a mass in the groin, there are two more likelydiagnoses:
metastatic carcinoma and lymphoma.
Patients with Crohns disease are at increased
risk for adenocarcinoma, particularly of the smallintestine, but
also in the colon. These cancers are
most likely to develop in areas affected by Crohnsdisease; the
risk of cancer in the small intestine
in patients with Crohns disease has been esti-mated to be 5 to
25 times higher than that of un-
affected persons,2,3 and the risk of colorectal ad-enocarcinoma
2 to 5 times higher than that ofunaffected persons.4-6 The risk
correlates with
extent of disease, duration, and independently, theage at onset.
This patients surgical history sug-
gests that she has had Crohns disease affectingboth the small
intestine and the colon, and she
appears to have had active disease for almost 50years. However,
the lesion observed on brain im-aging is unlikely to represent
metastatic adeno-
carcinoma in the absence of evidence of othermetastatic disease
nor would this diagnosis
account for the type of atypical cells that wereseen in the
cerebrospinal fluid.
Lymphoma in Crohns disease
It has long been suspected that there is an in-
creased frequency of lymphoma in the setting ofCrohns disease,
although this premise remains
controversial. Several studies1,3,7,8 have found a
risk of lymphoma among patients with Crohnsdisease that is two
to four times the risk amongthose without the disease, although
others havenot found any significant increase.5,9 In the ag-
gregate, these studies support the impression ofan increased
risk of lymphoma in patients with
Crohns disease, but it is unlikely that the magni-tude of this
increase is more than twice that in
patients without Crohns disease.The risk of lymphoma may be
increased by im-
munosuppressive agents used in the treatment of
these patients.10,11 The results of studies attempt-ing to
define the risks of lymphoma conferred
by immunosuppressive therapy with azathioprineor mercaptopurine
have been equivocal,10,12,13 with
relative risk ranging from less than or slightlygreater than
19,14 to almost 60.15,16
Infliximab and Lymphoma
Understanding how to assess the risk of lympho-
ma in patients with Crohns disease has taken on
new urgency with the increasing use of inflix-
imab, a chimeric antitumor necrosis factor (TNF)monoclonal
antibody. This antibody was initially
presumed to act through neutralization of the solu-ble form of
the proinflammatory cytokine TNF,
but recent studies suggest that apoptosis of cells
expressing the transmembrane precursor afterbinding by
infliximab may be necessary for ther-
apeutic benefit. In the several years since its ini-tial
approval, infliximab has been found to have
diverse adverse effects17; some of these effectsmay be due to
the development of antiinf liximab
antibodies, whereas others may reflect the bio-logic effects of
infliximab, such as abscess for-mation and opportunistic
infections, including
reactivation of latent tuberculosis.Several reports have
suggested that infliximab
may increase the risk of lymphoma.17,18 The in-cidence of
non-Hodgkins lymphoma in patients
with Crohns disease treated with infliximab inseveral large
studies ranged from 0.2 percent17 to1.4 percent.19 A summary of all
the lymphomas
reported in patients receiving infliximab (includ-ing patients
with rheumatoid arthritis and those
with Crohns disease) yielded an overall incidenceof 0.6
percent.18 As in the setting of other types of
immunosuppressive therapy, large-B-cell lympho-mas that are
positive for EpsteinBarr virus (EBV)appear to predominate. Dr.
Siegel and my other
colleagues at Massachusetts General Hospitalhave recently
completed a survey to assess the
risk of lymphoma in patients with Crohns dis-
ease treated with infliximab.Dr. Corey A. Siegel
(Gastroenterology): We per-
formed a systematic literature search to identifyall of the
studies with a minimum follow-up pe-
riod of 48 weeks that specifically reported adverseeffects of
inf liximab in the treatment of Crohns
disease. There were 5 patients with lymphoma re-ported among
approximately 1700 patients (0.3
percent). As compared with a healthy age-matchedpopulation from
the Surveillance, Epidemiologyand End Results database, this
percentage repre-
sents an increase in the incidence of lymphomain patients
receiving infliximab that is approxi-
mately 20 times higher.Dr. Podolsky: In summary, this patient
possess-
es at least three possible risk factors for non-Hodgkins
lymphoma Crohns disease, im-
munosuppressive therapy with mercaptopurine,and infliximab
therapy. Although the impact ofeach risk factor alone may be small,
the overall
effects may be additive, if not synergistic. Ac-
Copyright 2006 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org by CARLOS S. LOPES MD on
April 3, 2009 .
-
8/3/2019 Linfoma Associado a Imunodeficiencia
5/7
T h e n e w e n g l a n d j o u r n a l o f m ed i c i n e
n engl j med 354;11 www.nejm.org march 16, 20061182
cordingly, I believe that lymphoma may have devel-oped in this
patient, probably large-B-cell lym-phoma that is positive for EBV.
The diagnosis was
probably made by appropriate staining of the tissueobtained from
the incisional biopsy of the inguinal
lymph node, flow cytometry analysis of the abnor-mal cells seen
in the cerebrospinal fluid, or both.
Clinical Diagnosis
Probable non-Hodgkins lymphoma.
DR. DANIEL K. PODOLSKYS
DIAGNOSIS
B-cell lymphoma, probably large-B-cell lymphomathat is
EBV-positive, associated with immunosup-
pression.
Pathological Discussion
Dr. Robert P. Hasserjian: The diagnostic procedures
were a review of the slides of the specimen obtainedfrom the
inguinal lymph-node biopsy from theother hospital and an analysis
of the cerebrospi-
nal fluid by cytology and flow cytometry. Thelymph-node
architecture was effaced by sheets of
large lymphoid cells, with large areas of geograph-ic necrosis
(Fig. 2A). The lymphoid cells had prom-
inent nucleoli, expressed the B-cell marker CD20,and contained
encoded RNA for EBV (Fig. 2B, 2C,and 2D).
Cytologic examination of the cerebrospinalfluid disclosed large,
atypical lymphocytes, mor-
phologically similar to the nodal lymphoma cells(Fig. 3). Flow
cytometry revealed a predominant
population of CD19+ and CD20+ B cells aber-
A B
C D
Figure 2. Inguinal Lymph-Node Biopsy Specimen.
The inguinal lymph-node architecture (Panel A) is totally
effaced by diffuse sheets of cells with areas of geographic
necrosis (lower right; hematoxylin and eosin). The cells are
large with round-to-irregular, vesicular nuclei and promi-
nent nucleoli (Panel B; hematoxylin and eosin). The cell-surface
membrane of the large cells is positive for the B-cellmarker CD20
(Panel C; immunohistochemical staining for CD20). Nearly all the
large cells contain EpsteinBarr
virus-encoded RNA (Panel D; in situ hybridization).
Copyright 2006 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org by CARLOS S. LOPES MD on
April 3, 2009 .
-
8/3/2019 Linfoma Associado a Imunodeficiencia
6/7
case records of the massachusetts general hospital
n engl j med 354;11 www.nejm.org march 16, 2006 1183
rantly expressing CD43 and lacking detectable
surface or cytoplasmic immunoglobulin expres-sion. These
findings confirm an EBV-positive, dif-
fuse large-B-cell lymphoma involving the ingui-nal lymph node
and cerebrospinal fluid.
EBV is typically absent in cases of B-cell non-Hodgkins lymphoma
that occur in immunocom-petent persons,20 but it is a hallmark of
lympho-
mas occurring in the setting of immunodeficiency.Patients who
are immunodeficient are at increased
risk for the development of a variety of lympho-
proliferative disorders, which share a number
ofclinicopathological features (Table 2).21 Lowergrades or early
forms of these lymphoprolifera-tive disorders resemble f lorid,
uncontrolled EBV
infection and are often polyclonal.22 In contrast,frank
lymphomas contain clonal sequences of
EBV and antigen-receptor gene rearrangements,indicating
derivation from a single transformed
EBV-infected cell.23,24 Lymphomas arising in pa-tients who are
immunodeficient are typically dif-fuse large-B-cell, Burkitts, or
Hodgkins lympho-
mas. In addition to the strong association withEBV, these
lymphomas differ from lymphomas
in patients who are immunocompetent in thatsuch cases show a
more limited histologic spec-
trum and a predilection for extranodal site in-volvement.
Lymphomas that arise in patients with inflam-matory bowel
disease who have been treated withthe immunosuppressive agents
azathioprine and
mercaptopurine have features resembling immu-
nodeficiency-associated lymphomas.25 In contrastto lymphomas
that develop in patients with in-
flammatory bowel disease who are not receivingsuch therapies,
these lymphomas are typically
EBV-positive and are almost exclusively high-grade B-cell and
Hodgkins lymphomas. At least
one of the reported cases exhibited a viral anti-
gen expression pattern (latency pattern, type 3)that is
characteristic of immunodeficiency-asso-
ciated lymphomas.26 Other recent studies havedocumented an
increased incidence of lympho-
ma after relatively short periods of infliximabtherapy, although
many of these patients had
also received immunosuppressants18,19,27; at leastone of the
cases in these studies was EBV-posi-tive. The EBV-positive status
and extranodal in-
volvement in the current patient, in the contextof
mercaptopurine and infliximab therapy, sug-
gest that this case should be categorized as
animmunodeficiency-associated lymphoma.
Dr. Nancy Lee Harris (Pathology): The intervalbetween starting
infliximab therapy and develop-
ment of lymphoma was fairly long in this patient.Dr. Podolsky:
Reports suggest that lymphoma
may occur within a very short time after inflix-
imab is first started, and an average of just threeinfusions
before diagnosis of the cancer has been
described. However, the prolonged period that isdescribed for
this patient is within the range re-
ported.Dr. Harris: Dr. Hochberg, can you discuss the
further care of this patient?
Dr. Ephraim P. Hochberg (HematologyOncology):The chemotherapy
agents that are currently the
standard of care for systemic diffuse large-B-celllymphomas do
not penetrate the central nervous
system, nor does rituximab, an anti-CD20 mono-clonal antibody
that is an important additionalagent in treating this cancer. So we
were left in
this case with a choice of high-dose methotrexateas a therapy
that would penetrate into the central
Figure 3. Cytologic Preparation of a Sample of Cerebro-spinal
Fluid.
There are large cells with vesicular nuclei and moderate-ly
abundant, eccentrically placed cytoplasm (Papanico-
laou stain). These cells resemble the tumor cells on an
air-dried direct smear prepared from the patients ingui-nal
lymph node (inset, WrightGiemsa stain).
Table 2. Common Features of Immunodeficiency-Associated
Lymphoproliferative Disorders.
Defective T-cell function leading to decreased
immuno-surveillance
Presence of the EpsteinBarr virus (EBV) in lymphomacells, with
viral antigen expression pattern character-
istic of in vitro EBV-immortalized lymphoblastoidcell lines
Predilection for extranodal sites (especially the brain)
Potential to regress with restoration of T-cell function
Copyright 2006 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org by CARLOS S. LOPES MD on
April 3, 2009 .
-
8/3/2019 Linfoma Associado a Imunodeficiencia
7/7
n engl j med 354;11 www.nejm.org march 16, 20061184
case records of the massachusetts general hospital
nervous system and also affect the lymph-node
disease, or whole-brain radiation for palliation.Unfortunately,
the patients neurologic status did
not improve, and she also had biochemical evi-dence of
myocardial infarction after admission
to the intensive care unit. Serial CT scans and MRI
(Fig. 1B) showed rapid growth of the tumor. Inthe setting of her
other medical problems and
advanced age it was thought that systemic che-motherapy was not
an option. The family declined
radiation therapy and ultimately decided to with-
draw care. She died on the eighth hospital day.
Anatomical Diagnosis
Diffuse large-B-cell lymphoma, EBV-positive, as-
sociated with iatrogenic immunosuppression.No potential conflict
of interest relevant to this article was re-
ported.
SLIDESETSFORTHECASERECORDSAVAILABLEINDIGITALFORMAT
Any reader of theJournal who uses the Case Records of the
Massachusetts General Hospital as a teaching exercise or reference
material is eligible to receive digital images,with identifying
legends, of pertinent radiographic, neurologic, and cardiac
studies, gross specimens, and photomicrographs. The images on the
CD for each case are inboth PowerPoint and 300 dpi jpg format. For
some cases, additional images that have not been selected for
publication will be included on the CD. These images,
whichillustrate the current cases in the Journal, are mailed from
the Department of Pathology to correspond to the week of
publication and may be retained by the subscriber.Each year
approximately 250 images from 40 cases are sent to each subscriber.
The cost of the subscription is $450 per year. Application forms
for the current subscription
year, which began in January, may be obtained from the Lantern
Slides Service, Department of Pathology, Massachusetts General
Hospital, Boston, MA 02114 (telephone617-726-2974) or
[email protected].
Images from individual cases may be obtained at a cost of $35
per case.
References
Keane J, Gershon S, Wise RP, et al.Tuberculosis associated with
infliximab,a tumor necrosis factor neutralizingagent. N Engl J Med
2001;345:1098-104.
Persson PG, Karlen P, Bernell O, et al.Crohns disease and
cancer: a population-based cohort study. Gastroenterology
1994;107:1675-9.
Bernstein CN, Blanchard JF, KliewerE, Wajda A. Cancer risk in
patients with
inflammatory bowel disease: a population-based study. Cancer
2001;91:854-62.
Choi PM, Zelig MP. Similarity ofcolorectal cancer in Crohns
disease and ul-cerative colitis: implications for carcinogen-esis
and prevention. Gut 1994;35:950-4.
Ekbom A, Helmick C, Zack M, AdamiHO. Increased risk of
large-bowel cancer inCrohns disease with colonic involvement.Lancet
1990;336:357-9.
Gillen CD, Andrews HA, Prior P, AllanRN. Crohns disease and
colorectal cancer.Gut 1994;35:651-5.
Greenstein AJ, Mullin GE, StrauchenJA, et al. Lymphoma in
inflammatory bow-el disease. Cancer 1992;69:1119-23.
Arseneau KO, Stukenborg GJ, Con-
nors AF Jr, Cominelli F. The incidence oflymphoid and myeloid
malignancies amonghospitalized Crohns disease patients. In-flamm
Bowel Dis 2001;7:106-12.
Lewis JD, Bilker WB, Brensinger C,Deren JJ, Vaughn DJ, Strom BL.
Inflam-matory bowel disease is not associated withan increased risk
of lymphoma. Gastroen-terology 2001;121:1080-7.
Bouhnik Y, Lemann M, Mary JY, et al.Long-term follow-up of
patients withCrohns disease treated with azathioprine
or6-mercaptopurine. Lancet 1996;347:215-9.
Present DH, Rutgeerts P, Targan S, etal. Inflix imab for the
treatment of fistulasin patients with Crohns disease. N Engl JMed
1999;340:1398-405.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
Fraser AG, Orchard TR, RobinsonEM, Jewell DP. Long-term risk of
malig-nancy after treatment of inflammatorybowel disease with
azathioprine. AlimentPharmacol Ther 2002;16:1225-32.
Aithal GP, Mansfield JC. The risk oflymphoma associated with
inflammatorybowel disease and immunosuppressivetreatment. Aliment
Pharmacol Ther 2001;15:1101-8.
Connell WR, Kamm MA, Dickson M,Balkwill AM, Ritchie JK,
Lennard-Jones
JE. Long-term neoplasia risk after azathi-oprine treatment in
inflammatory boweldisease. Lancet 1994;343:1249-52.
Kinlen LJ. Incidence of cancer in rheu-matoid arthritis and
other disorders afterimmunosuppressive treatment. Am J
Med1985;78:44-9.
Farrell RJ, Ang Y, Kileen P, et al. In-creased incidence of
non-Hodgkins lym-phoma in inflammatory bowel diseasepatients on
immunosuppressive therapybut overall risk is low. Gut
2000;47:514-9.
Colombel JF, Loftus EV Jr, TremaineWJ, et al. The safety profile
of infliximabin patients with Crohns disease: the Mayo
Clinic experience in 500 patients. Gastro-enterology
2004;126:19-31.
Brown SL, Greene MH, Gershon SK,Edwards ET, Braun MM. Tumor
necrosisfactor antagonist therapy and lymphomadevelopment:
twenty-six cases reported tothe Food and Drug Administration.
Ar-thritis Rheum 2002;46:3151-8.
Ljung T, Karlen P, Schmidt D, et al.Infliximab in inflammatory
bowel disease:clinical outcome in a population based co-hort from
Stockholm County. Gut 2004;53:849-53.
dAmore F, Johansen P, Houmand A,Weisenburger DD, Mortensen LS.
Epstein-Barr virus genome in non-Hodgkins lym-phomas occurring in
immunocompetent
12.
13.
14.
15.
16.
17.
18.
19.
20.
patients: highest prevalence in nonlym-phoblastic T-cell
lymphoma and correla-tion with a poor prognosis. Blood
1996;87:1045-55.
Jaffe ES, Harris NL, Stein H, Vard-iman JW. Pathology and
genetics of tu-mours of haematopoietic and lymphoidtissues. Vol. 3
of World Health Organiza-tion classification of tumours.
Lyon,France: IARC Press, 2001.
Knowles DM, Cesarman E, ChadburnA, et al. Correlative
morphologic and mo-lecular genetic analysis demonstrates
threedistinct categories of posttransplantationlymphoproliferative
disorders. Blood 1995;85:552-65.
Cleary ML, Nalesnik MA, Shearer WT,Sklar J. Clonal analysis of
transplant-asso-ciated lymphoproliferations based on thestructure
of the genomic termini of theEpstein-Barr virus. Blood
1988;72:349-52.
Cleary ML, Warnke R, Sklar J. Mono-clonality of
lymphoproliferative lesions incardiac-transplant recipients: clonal
anal-
ysis based on immunoglobulin-gene re-arrangements. N Engl J Med
1984;310:477-82.
Dayharsh GA, Loftus EV Jr, SandbornWJ, et al. Epstein-Barr
virus-positive lym-phoma in patients with inflammatorybowel disease
treated with azathioprine or6-mercaptopurine. Gastroenterology
2002;122:72-7.
Wong NA, Herbst H, Herrmann K, etal. Epstein-Barr virus
infection in colorec-tal neoplasms associated with inflamma-tory
bowel disease: detection of the virusin lymphomas but not in
adenocarcino-mas. J Pathol 2003;201:312-8.
Losco A, Gianelli U, Cassani B, Baldi-ni L, Conte D, Basilisco
G. Epstein-Barr
virus-associated lymphoma in Crohns dis-ease. Inflamm Bowel Dis
2004;10:425-9.Copyright 2006 Massachusetts Medical Society.
21.
22.
23.
24.
25.
26.
27.
Copyright 2006 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org by CARLOS S. LOPES MD on
April 3, 2009 .