Embed Size (px)
Citation preview

UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
CENTRO DE CIÊNCIAS DA SAÚDE
DEPARTAMENTO DE ODONTOLOGIA
PROGRAMA DE PÓS-GRADUAÇÃO EM PATOLOGIA ORAL
RELAÇÃO DE CÉLULAS CD57+ COM PARÂMETROS
CLÍNICO-PATOLÓGICOS EM UMA SÉRIE DE CASOS DE CARCINOMA DE
CÉLULAS ESCAMOSAS ORAIS.
NATAL - RN
2014

CAIO CÉSAR DA SILVA BARROS
RELAÇÃO DE CÉLULAS CD57+ COM PARÂMETROS
CLÍNICO-PATOLÓGICOS EM UMA SÉRIE DE CASOS DE CARCINOMA DE
CÉLULAS ESCAMOSAS ORAIS.
NATAL - RN
2014
Trabalho apresentado no curso de
graduação de Odontologia da
Universidade Federal do Rio Grande
do Norte, segundo as normas da
revista Oral Diseases, como requisito
para avaliação da disciplina Trabalho
de Conclusão de Curso II.
ORIENTADORA: Prof.ª Dr.ª Éricka
Janine Dantas da Silveira

Relação de células CD57+ com parâmetros clínico-patológicos em uma série
de casos de carcinoma de células escamosas orais.
Caio César da Silva Barros (CCS Barros)1, Maurília Raquel de Souto Medeiros
(MRS Medeiros)1, Maria Luiza Diniz de Sousa Lopes (LOPES MLDS)2, Márcia
Cristina da Costa Miguel (MCC Miguel)3, Lélia Batista de Souza (LB Souza)3,
Polianna Muniz Alves (PM Alves)4, Éricka Janine Dantas da Silveira (EJD
Silveira)3.
1DDS, Federal University of Rio Grande do Norte, Natal, RN, Brazil
2DDS, MSc, PhD student, Postgraduate Program, Oral Pathology, Federal
University of Rio Grande do Norte, Natal, RN, Brazil.
3DDS, PhD, Professor, Postgraduate Program, Oral Pathology, Federal University
of Rio Grande do Norte, Natal, RN, Brazil.
4DDS, PhD, Professor, Dentistry Department, States University of Paraíba,
Campina Grande, PB, Brazil.
Corresponding author:
Éricka Janine Dantas da Silveira
Endereço: Av Senador Salgado Filho, 1787, Lagoa Nova, Natal-RN, Brazil
Code: 59056-000
Phone: 55-84-3215-4138
Email: [email protected]

Abstract
Background: One of the effective immune mechanisms against tumors is
executed by cytotoxic cells (CD57+), which are naturally capable of destroying
tumor cells. The aim of this study was to investigate the relationship between the
clinicopathological parameters and immunoexpression of CD57+ inflammatory
cells in patients with oral squamous cell carcinoma (OSCC). Methods: Paraffin-
embedded sections of the 45 cases of OSCC were immunohistochemically treated
by anti-CD57. Clinical data, as tumor-node-metastasis (TNM), node metastasis,
habits were collected from medical records. Hematoxylin and eosin-stained
sections were analyzed by histological grade of malignancy as system proposed by
Bryne (1998). The quantitative analysis of CD57+ cells was related to with clinic
pathologic parameters by Mann-Whitney test at significance level of p<0.05.
Results: Among the patients, 64.4% were males with mean of age 53.36 years-
old. Most of the cases occurred in the tongue (91.1%). Eleven patients were
tabagist and etilist. The majority of patients (37.8%) were diagnosed as TNM stage
III and 62.2% of the cases were classified with high-grade of malignancy. There
was significant association between node metastasis and clinical stage with
histologic grade (p<0.05). The majority of cases in stage I and II were gradated as
lower grade (62.5%) and all cases with metastasis were classified was high-grade
of malignancy. There was no association between CD57+ cells and clinical and
morphological parameters (P>0.05). However, the immunostaining for CD57 was
higher in T1 and T2 tumors without nodal metastasis. Conclusions: Our results
show that CD57+ cells were more present in OSCC with early clinical stage and low
grade of malignancy but without significant association. The possible relation of

citotoxyc cells with clinical pathologic parameters in OSCC may be more
investigated.
Keywords: oral cancer; squamous cell carcinoma; CD57 antigens; tumor immunity

INTRODUÇÃO
O câncer oral (CO) representa um problema de saúde pública em diversos
países do mundo por exibir elevadas taxas de morbidade e mortalidade
(Dissanayaka et al, 2012). O carcinoma de células escamosas oral (CCEO) é a
neoplasia maligna mais frequente na região de cabeça e pescoço,
correspondendo a mais de 90% destas, fato esse, que auxilia na sua
caracterização como o sexto tipo de câncer mais comum no mundo
(Warnakulasuriya, 2009). Ocorre principalmente em homens brancos, a partir da
quarta década de vida, sendo a borda lateral da língua a região mais afetada em
alguns países no mundo (Essig et al, 2012). Exibe etiologia multifatorial, sendo
reconhecido que tanto fatores extrínsecos, como a radiação ultravioleta (UV),
agentes biológicos, o tabaco e o álcool; e também fatores intrínsecos como
deficiências nutricionais, determinantes imunológicos e genéticos possuem
relação com a origem e o desenvolvimento desta neoplasia (Dissanayaka et al,
2012).
Fatores como estadiamento clínico (TNM), presença de metástases em
linfonodos cervicais, atraso no diagnóstico e localização anatômica exercem
influência direta no prognóstico desta doença (Köhler e Kowalski, 2012).
Nos últimos anos, várias pesquisas têm sido feitas para identificar a
participação do sistema imunológico na resposta antineoplásica, objetivando a
descoberta de novas terapias mais específicas do que a quimioterapia e a
radioterapia.
O principal tipo de defesa do organismo contra as células neoplásicas é a
citotóxica, como a mediada por células Natural Killer (NK) na imunidade inata e

adquirida e pelos linfócitos citotóxicos (TCD8+) na imunidade adquirida. Em
pacientes com câncer, tem sido relatado que a maioria das células NK perdem a
atividade citotóxica e assim observa-se maior progressão do tumor com
subsequente crescimento e expansão neoplásica. Em contrapartida, CCEOs em
regressão, contêm números significativamente maiores de células NK funcionais,
enquanto os pacientes com metástase na região de cabeça e pescoço têm baixa
atividade dessas células NK (Jewett e Tseng, 2011; Jewett et al, 2012).
Dentro do mesmo tecido, as células NK são heterogêneas e uma possível
justificativa para este fato é que essa diversidade pode refletir em um processo de
diferenciação terminal que ocorre também nos tecidos periféricos (Luetke-Eversloh
et al, 2013).
Desde sua descoberta, diversos marcadores tem sidos usados em
humanos e camundongos para descrever o estágio final de maturação das células
NK, sendo descritos dois subtipos principais destas células com base na
expressão de CD56. Células NK CD56bright e CD56dim, as quais são diferentes no
fenótipo, capacidade funcional localização. Células NK CD56bright constituem a
minoria das células NK do sangue, e em grande parte dos órgão linfoides
periféricos expressam pouca quantidade de grânulos citotóxico, enquanto que as
células CD56dim expressam altas quantidades de perforina e granzimas nos
tecidos periféricos e são capazes de destruir as células alvo (infectadas por vírus e
transformadas). Estas produzem IFN-γ e proliferam em resposta a citocinas
liberadas por células dendríticas como: IL-2, IL-15, IL-12 e IL-18 (Luetke-Eversloh
et al, 2013).

Conforme Montaldo et al (2014), a função das células NK é muito
influenciada pelo microambiente, como o contato célula/célula e/ou fatores
solúveis tanto em condições fisiológicas como patológicas e adicionalmente
interações entre as células NK e outros tipos celulares podem determinar sua
atuação na resposta imune inata ou adaptativa.
Estas células também são identificadas através de marcadores de
superfície como o CD57. O antígeno CD57 (HNK-1 ou Leu-7) foi inicialmente
descrito como, uma glicoproteína tipicamente presente em 15-20% nas células
mononucleadas do sangue, com peso de 110-kd. O antígeno CD57, além de estar
presente neste tipo celular também se encontra expresso em uma pequena
subpopulação de células T, incluindo células CD4+CD57+ e CD8+CD57+, as quais
produzem interferon-γ (INF-γ), mas são capazes de proliferar em resposta a um
antígeno cognato (Fraga et al, 2012).
Ainda não se encontram bem estabelecidos os mecanismos relacionados
aos diferentes comportamentos biológicos e evolutivos exibidos por pacientes
portadores de tumores de mesmo estadiamento clínico e que recebem o mesmo
protocolo terapêutico. Logo, tem sido sugerido que o sistema imunológico pode
estar envolvido neste processo e dessa forma, o seu fortalecimento pode constituir
uma importante ferramenta no tratamento oncológico, principalmente para os
pacientes que não respondem a terapêutica convencional. Desta forma, o objetivo
da presente pesquisa foi verificar a expressão imuno-histoquímica da proteína
CD57 em uma série de casos de CCEO e avaliar se a presença de células
citotóxicas se encontra associada a parâmetros clínicos e histopatológicos.

MATERIAIS E MÉTODOS
Esta pesquisa foi aprovada pelo Comitê de Ética em Pesquisa da
Universidade Federal do Rio Grande do Norte (UFRN) (Nº 266.863/2013).
Tratando-se de uma pesquisa retrospectiva, observacional e descritiva da análise
de células CD57+ em uma série de 45 casos de CCEO diagnosticados no Serviço
de Anatomia Patológica da Disciplina de Patologia Oral do Departamento de
Odontologia da UFRN e no Hospital Dr. Napoleão Laureano (João Pessoa,
Paraíba – Brasil) no período de janeiro de 2002 a janeiro de 2012. Foram incluídos
na amostra os casos cujos prontuários continham as informações necessárias
para realização da pesquisa e aqueles cujos espécimes apresentavam quantidade
de material biológico suficiente para análise morfológica e imuno-histoquímica.
Foram excluídos casos de CCEO localizados em lábio e base de língua, tratados
com quimioterapia ou radioterapia prévia.
Os dados clínicos referentes ao gênero, idade, raça, hábitos dos pacientes,
localização das lesões, presença ou ausência de metástases linfonodais no
momento do diagnóstico e estadiamento clínico de acordo com o sistema TNM
foram obtidos através da análise de prontuários clínicos arquivados nos referidos
serviços.
Para o estudo morfológico, do material incluído em parafina foram obtidos
cortes histológicos de 5µm de espessura que foram corados pela técnica da
Hematoxilina/Eosina (HE) e examinados sob microscopia de luz óptica. A
gradação histopatológica foi realizada no front de invasão tumoral como
preconizado por Bryne (1998). De acordo com o referido sistema foram atribuídas

pontuações de 1 a 4 para cada parâmetro analisado: grau de ceratinização,
pleomorfismo nuclear, padrão de invasão e infiltrado inflamatório. Essas
pontuações foram somadas e os tumores que obtiveram escore final de 4 a 8
foram classificados como de baixo grau de malignidade e aqueles com escore final
de 9 a 16 como de alto grau de malignidade, conforme realizado por Silveira et al
(2007).
Os espécimes de CCEO foram submetidos a cortes histológicos com 3µm
de espessura, estendidos em lâminas de vidro devidamente preparadas com
adesivo à base de organosilano (3-aminopropyltriethoxi-silano, Sigma Chemical
Co, St Louis, MO, USA) e submetidos à técnica da imunoperoxidase pelo método
da estreptoavidina-biotina (LSAB, do inglês Labeled Streptavidin Biotin) utilizando
o anticorpo monoclonal anti-CD57 (clone 8144B; Dako North America Inc.,
Carpinteria, CA, USA) com diluição de 1:100, recuperação antigênica em solução
de TRIS/EDTA (pH 9.0) em Pascal por 3 minutos e tempo de incubação de 60
minutos. A reação foi desenvolvida com diaminobenzidina (DAB) como
cromógeno. Os espécimes foram contra-corados com hematoxilina de Mayer e
montados em resina Erv-mount (Easy Path®). Como controle positivo foram
utilizados espécimes de linfonodos cervicais e como controle negativo foi realizada
a substituição do anticorpo primário por albumina de soro bovino (BSA – Bovine
Serum Albumin) a 1% em solução tampão.
Para a análise da imunomarcação, as lâminas foram escaneadas
(Pannoramic MIDI, 1.15 SPI, 3D HISTECH®, Budapest, Hungary) e então, com o
auxílio do programa de visualização Pannoramic Viewer 1.15.2 (3DHISTECH®,
Budapest, Hungary) foi possível examinar toda a extensão dos espécimes para

eleger as áreas do front de invasão tumoral com maior imunoexpressão. Destas
áreas, foram obtidas imagens (100 µm) de 05 campos consecutivos para
contagem das células CD57+ por dois examinadores previamente calibrados com
a ajuda do programa Imaging Processing and Analysis in Java (ImageJ®, National
Institute of Mental Health, Bethesda, Maryland, USA). Foram consideradas
positivas as células que apresentaram coloração acastanhada na membrana
plasmática e/ou citoplasma, independente da intensidade da marcação. Após a
soma dos valores obtidos em cada um dos campos, foi calculada a média de
células positivas de cada caso.
Os dados obtidos na análise quantitativa foram tabulados no software
Microsoft Excel (Microsoft Corporation, USA) e posteriormente transferidos para o
software SPSS for Windows (Statistical Package for Social Sciences; IBM, USA),
versão 20.0. Para avaliação da associação das variáveis independentes: gradação
histológica de malignidade, metástase em linfonodos cervicais e estadiamento
clínico utilizou-se o teste Qui-quadrado. Os dados obtidos da análise quantitativa
das células CD57+ foram submetidos à análise pelo teste de Kolmogorov-Smirnov,
o qual revelou ausência de distribuição normal. Assim, foi realizado o teste não-
paramétrico de Mann-Whitney para comparar a expressão de CD57 com as
variáveis independentes: metástase em linfonodos cervicais, estadiamento clínico
e gradação histológica de malignidade. Para todos os testes foi considerado um
nível de significância de 5% (α=0,05).

RESULTADOS
Perfil da amostra
Quarenta e cinco pacientes foram selecionados de forma intencional para a
presente pesquisa. Vinte e nove pacientes (64.4%) eram do sexo masculino e 16
eram (35.6%) do sexo feminino. A idade média foi de 53.36 anos (± 16.75), sendo
que 31 pacientes (68.9%) apresentavam uma idade superior a 40 anos, enquanto
14 pacientes (31.1%) tinham idade inferior ou igual há 40 anos. No que diz
respeito à raça, 26 pacientes eram pardos (57.8%). Quarenta e um casos
ocorreram na língua (91.1%). Grande parte dos pacientes não possuía hábitos
relacionados ao etilismo e tabagismo (42.2%), enquanto 11 pacientes relataram
uso sinérgico de fumo e álcool (24.4%).
Em relação ao estadiamento clínico (TNM), dezessete pacientes (37.8%)
foram classificados no Estágio III, sendo o Estágio II o segundo mais frequente
(35.6%). A presença de metástase em linfonodos cervicais foi detectada em
37.8% dos casos.
Resultados morfológicos
Dos 45 casos analisados, 28 (62.2%) foram classificados como alto grau de
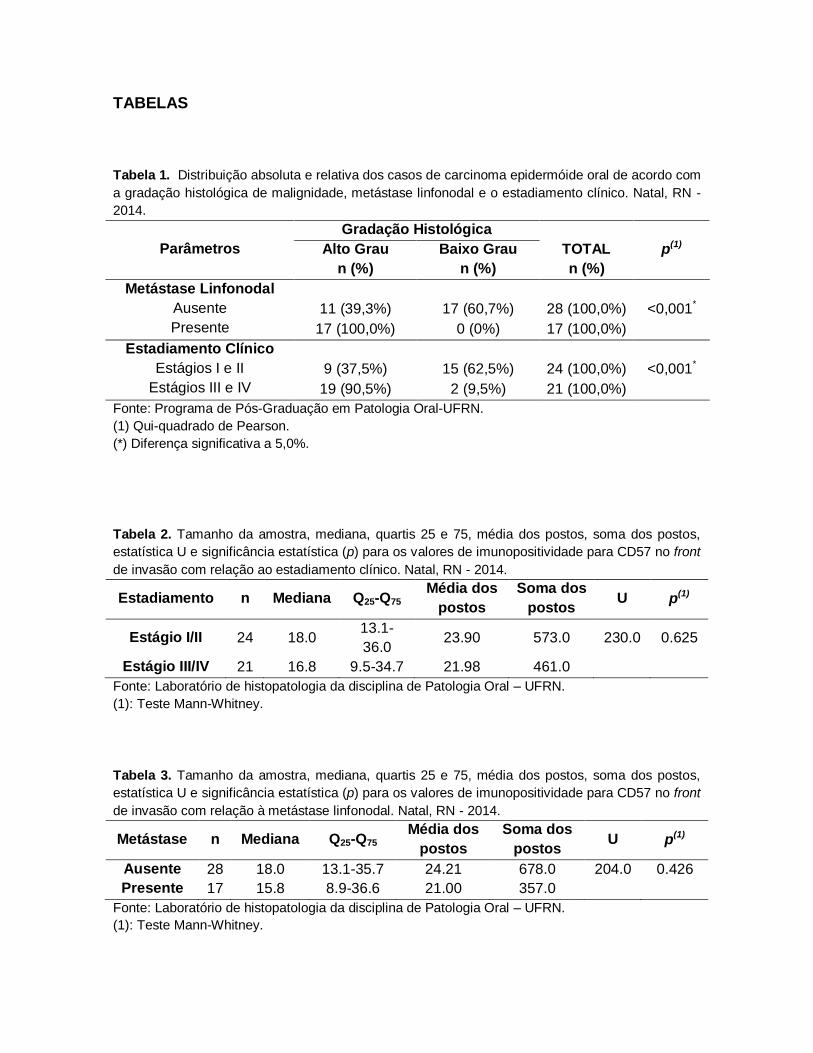
malignidade. A Tabela 1 demonstra que houve uma associação altamente
significativa (p<0.001) das variáveis clínicas (metástase em linfonodos cervicais e
estadiamento clínico) com a gradação histopatológica utilizada na amostra. Todos

os casos que exibiam metástases em linfonodos cervicais apresentaram alto grau
de malignidade e a maioria dos casos em estágios clínicos mais avançados
demonstraram alto grau de malignidade (n=19; 90.5%).
Resultados imuno-histoquímicos
A marcação imuno-histoquímica para a CD57 no front de invasão foi
observada predominantemente no compartimento citoplasmático de células
inflamatórias mononucleares de formato arredondado e citoplasma abundante
presentes no estroma de todos os CCEO analisados.
A análise da expressão de CD57 no estroma tumoral do front de invasão em
relação ao estadiamento clínico e presença de metástase em linfonodos cervicais
revelou uma marcação discretamente maior nos tumores de estágio I/II e sem
metástases locais, respectivamente. No entanto, estas diferenças não foram
estatisticamente significativas (p=0.625; p=0.426; Tabelas 2 e 3).
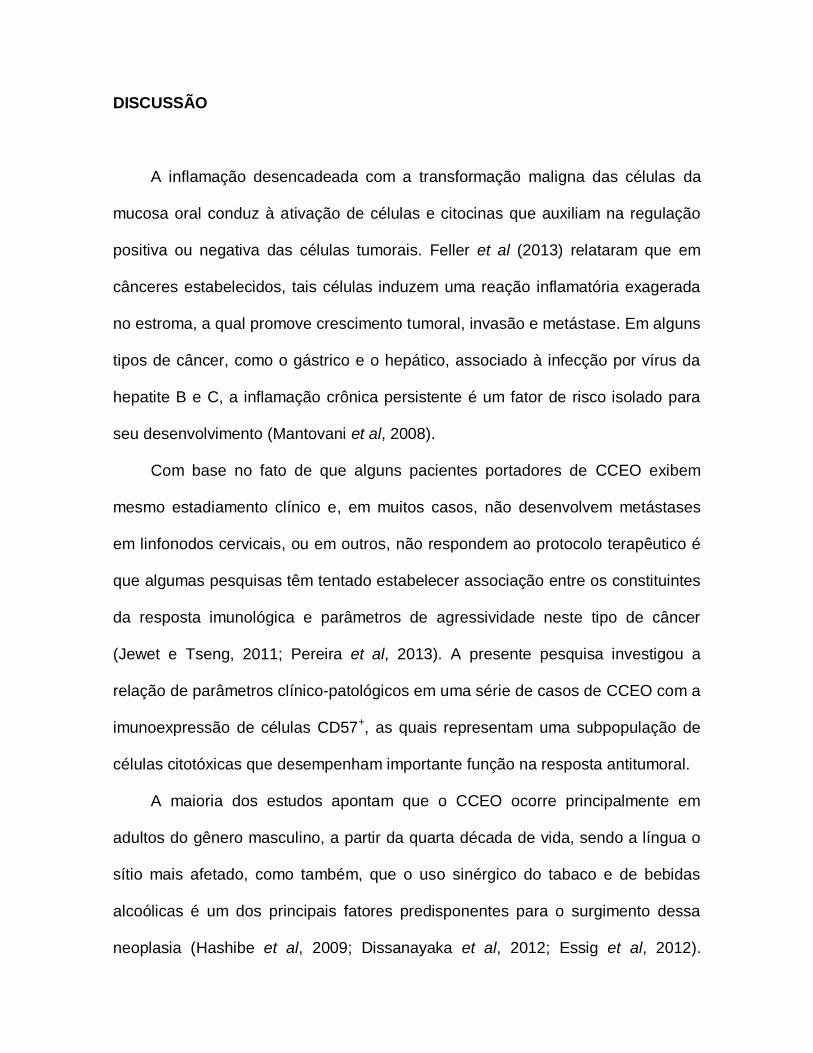
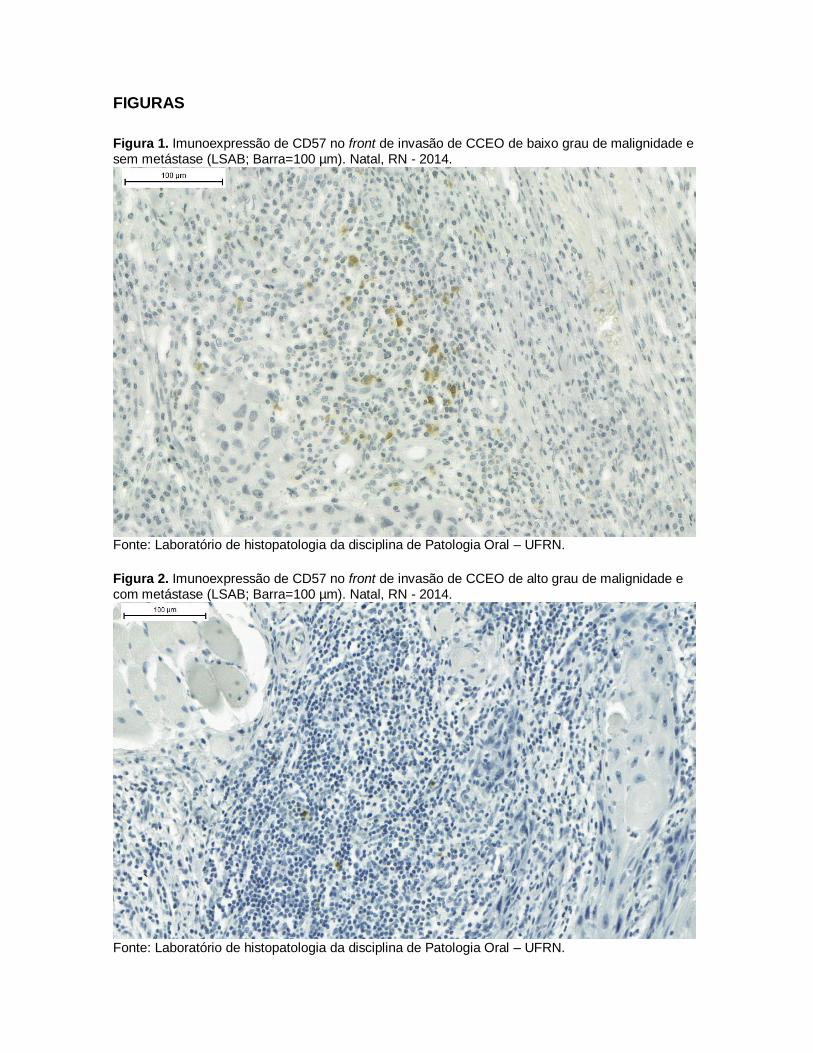
Não houve diferença de expressão de CD57 entre os grupos histológicos
gradados conforme o grau de malignidade de Bryne (1998), embora os
carcinomas de baixo grau de malignidade tenham demonstrado uma mediana
maior, quando comparados aos de alto grau (p=0.109; Tabela 4) (Figuras 1 e 2).
DISCUSSÃO
A inflamação desencadeada com a transformação maligna das células da
mucosa oral conduz à ativação de células e citocinas que auxiliam na regulação
positiva ou negativa das células tumorais. Feller et al (2013) relataram que em
cânceres estabelecidos, tais células induzem uma reação inflamatória exagerada
no estroma, a qual promove crescimento tumoral, invasão e metástase. Em alguns
tipos de câncer, como o gástrico e o hepático, associado à infecção por vírus da
hepatite B e C, a inflamação crônica persistente é um fator de risco isolado para
seu desenvolvimento (Mantovani et al, 2008).
Com base no fato de que alguns pacientes portadores de CCEO exibem
mesmo estadiamento clínico e, em muitos casos, não desenvolvem metástases
em linfonodos cervicais, ou em outros, não respondem ao protocolo terapêutico é
que algumas pesquisas têm tentado estabelecer associação entre os constituintes
da resposta imunológica e parâmetros de agressividade neste tipo de câncer
(Jewet e Tseng, 2011; Pereira et al, 2013). A presente pesquisa investigou a
relação de parâmetros clínico-patológicos em uma série de casos de CCEO com a
imunoexpressão de células CD57+, as quais representam uma subpopulação de
células citotóxicas que desempenham importante função na resposta antitumoral.
A maioria dos estudos apontam que o CCEO ocorre principalmente em
adultos do gênero masculino, a partir da quarta década de vida, sendo a língua o
sítio mais afetado, como também, que o uso sinérgico do tabaco e de bebidas
alcoólicas é um dos principais fatores predisponentes para o surgimento dessa
neoplasia (Hashibe et al, 2009; Dissanayaka et al, 2012; Essig et al, 2012).

Segundo Dissanayaka et al (2012), a presença de metástases nos linfonodos
cervicais é de 33%, dados esses que são semelhantes aos encontrados no nosso
estudo.
O sistema TNM é o principal indicador clínico de prognóstico em pacientes
portadores de CCEO. Os tumores são classificados em estágios de I a IV, sendo
bem estabelecido na literatura que CCEO classificados no estágio I exibem melhor
prognóstico do que aqueles no estágio IV.
Na pesquisa de Vasconcelos et al (2014) foi detectado relação
estatisticamente significante entre o estadiamento clínico e o curso clínico da
doença em 57 casos de CCEs de língua. Em sua amostra também foi detectado
que em 24 casos com ausência de metástases em linfonodos cervicais houve
remissão da doença.
Semelhante ao estudo realizado por Alves et al (2011), na presente pesquisa
houve associação estatisticamente significantiva entre a gradação histológica de
malignidade e o estadiamento clínico (TNM), pois 90.5% dos casos que
apresentavam Estágio III ou IV receberam a classificação de alto grau de
malignidade. A relação entre a gradação histológica de malignidade e a presença
de metástase também se mostrou significativa, visto que todos os casos com
presença de metástase foram indicados como casos com alto grau de malignidade
(p<0.05). Em estágios precoces, devido à ausência de sintomatologia dolorosa, os
pacientes negligenciam as lesões, até que as mesmas evoluam para estágios
avançados. Assim, sabe-se, que pacientes com tumores em boca em estágios

avançados têm um prognóstico menos favorável, pois geralmente exibem
metástases em linfonodos cervicais no momento do diagnóstico.
Além dos fatores clínicos mencionados, vários sistemas de gradação
histopatológica de malignidade têm sido desenvolvidos com o objetivo de fornecer
informações adicionais de agressividade do tumor. Dentre estas se cita o de Bryne
em 1998 que é realizada no front de invasão tumoral, local descrito pelos autores
como sendo de interações importantes entre o tumor e o hospedeiro.
Conforme relataram Fraga et al (2012), muito embora distúrbios genéticos e
epigenéticos estejam relacionados aos processos de iniciação, promoção e
progressão durante a transformação epitelial, um aumento de células inflamatórias
no estroma peritumoral tem sido frequentemente associado com o
desenvolvimento de tumores malignos.
Algumas pesquisas evidenciam correlação entre a densidade intratumoral de
células NK e o prognóstico, como nas pesquisas de Takanami et al (2001) em
adenocarcinomas de pulmão, Cozar et al (2005) em adenocarcinomas de rim,
Hsia et al (2005) em CEE de esôfago e Sznurkowski et al (2014) em CCE de
vulva.
Segundo De Oliveira et al (2009), a inflamação crônica observada no sítio de
crescimento tumoral é caracterizada pelo acúmulo de vários tipos celulares como
macrófagos, plasmócitos, células NK, linfócitos T auxiliares (CD4+) e citotóxicos
(CD8+) no estroma tumoral. Porém, essas células podem desempenhar ação
contraditória, o que pode contribuir para inibir ou não na influência da progressão
tumoral e consequentemente no prognóstico.

Embora, na presente pesquisa, não tenha existido significância estatística,
houve uma tendência a maior média das células CD57+ em CCEO de estágios
clínicos iniciais e com baixo grau de malignidade. Türkseven e Oygür (2010), de
forma semelhante ao nosso estudo, detectaram em CCEO densidade menor de
células CD57+ em tumores gradados como pobre prognóstico. Os autores
sugerem que em CCEs com baixo potencial de invasão pode haver o controle por
células NK.
As células NK desempenham uma efetiva resposta antitumoral em tumores
de estágios iniciais, sugerimos que na presente pesquisa a densidade
discretamente maior de células CD57+ nos casos de CCEO e com estadiamento
clínico inicial e baixo grau de malignidade pode estar relacionada à ação efetiva
destas células na resposta antineoplásica neste estágio associado a outros fatores
coadjuvantes. Vale ressaltar, com base nos relatos de Feller et al (2013), que a
presença de células inflamatórias no estroma tumoral não necessariamente é
indicativa de efetividade na resposta antitumoral, pois as células neoplásicas
podem induzir a secreção de mediadores inflamatórios através das células
inflamatórias que podem levar a proliferação celular, além de induzir
sobrevivência, que é um fator essencial para a progressão tumoral. Esse
acontecimento pode justificar o fato de que alguns cânceres, que progridem
rapidamente, exibem microscopicamente intenso infiltrado inflamatório.

CONCLUSÕES
O presente estudo não exibiu diferenças estatísticas entre a presença das
células CD57+ no front de invasão tumoral com o estadiamento clínico (TNM) e a
ausência ou presença de metástases em linfonodos regionais.
Deste modo, é fundamental que estudos futuros façam avaliações que
busquem uma melhor compreensão do papel das células CD57+, presentes no
infiltrado inflamatório, como também o seu impacto na tumorigênese e no
prognóstico do paciente com CCEO, já que esta compreensão pode auxiliar no
aperfeiçoamento do tratamento dos CCEOs com alvo no fortalecimento da
atividade destas células.

REFERÊNCIAS
Alves PM, Godoy GP, Gomes DP et al (2011). Significance of galectins-1, -3, -4
and -7 in the progression of squamous cell carcinoma of the tongue. Pathol Res
Pract 207: 236–240.
Cozar JM, Canton J, Tallada M et al (2005). Analysis of NK cells and chemokine
receptors in tumor infiltrating CD4 T lymphocytes in human renal carcinomas.
Cancer Immunol Immunother 54: 858-866.
De Oliveira MV, Fraga CA, Gomez RS et al (2009). Immunohistochemical
expression of interleukin-4, -6, -8, and -12 in inflammatory cells in surrounding
invasive front of oral squamous cell carcinoma. Head Neck 31: 1439–1446.
Dissanayaka WL, Pitiyage G, Kumarasiri PVR et al (2012). Clinical and
histopathologic parameters in survival of oral squamous cell carcinoma. Oral Surg
Oral Med Oral Pathol Oral Radiol 113: 518-525.
Essig H, Warraich R, Zulfiqar G et al (2012). Assessment of cervical lymph node
metastasis for therapeutic decision-making in squamous cell carcinoma of buccal
mucosa: a prospective clinical analysis. World J Surg Oncol 10: 253-259.
Feller L, Altini M, Lemmer J (2013). Inflammation in the context of oral cancer. Oral
Oncol 49: 887-892.
Fraga CAC, Oliveira MVM, Domingos PLB et al (2012). Infiltrating CD57+
inflammatory Cells in Head and Neck Squamous Cell Carcinoma: Clinipathological
Analysis and Prognostic Significance. Appl Immunohistochem Mol Morphol 20:
285-290.
Hashibe M, Brennan P, Chuang SC et al (2009). Interaction between tobacco and
alcohol use and the risk of head and neck cancer: pooled analysis in the
International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiol
Biomarkers Prev 18: 541–550.

Hsia JY, Chen JT, Chen CY et al (2005). Prognostic significance of intratumoral
natural killer cells in primary resected esophageal squamous cell carcinoma.
Chang Gung Med J 28: 335-40.
Jewett A, Tseng H (2011). Tumor Induced Inactivation of Natural Killer Cell
Cytotoxic Function: Im-plication in Growth, Expansion and Differentiation of Cancer
Stem Cells. J Cancer 2: 443-457.
Jewett A, Tseng H, Arasteh A et al (2012). Natural Killer Cells Preferentially Target
Cancer Stem Cells; Role of Monocytes in Protection Against NK Cell Mediated
Lysis of Cancer Stem Cells. Current Drug Delivery 9: 5-16.
Köhler HF, Kowalski LP (2012). Prognostic impact of the level of neck metastasis
in oral cancer patients. Braz J Otorhinolaryngol 6: 15-20.
Luetke-Eversloh M, Killig M, Romagnani C (2013). Signatures of human NK cell
development and terminal differentiation. Front Immunol 4: 499-454.
Mantovani A, Allavena P, Sica A et al (2008). Cancer-related inflammation. Nature
454: 436–444.
Moltado E, Vacca P, Moretta et al (2014). Development of human natural killer
cells and other innate lymphoid cells. Semin Immunol 26: 107-113.
Pereira JS, Miguel MCC, Queiroz LMG, Silveira EJD (2014). Analysis of CD8+ and
CD4+ cells in oral squamous cell carcinoma and their association with lymph node
metastasis and histologic grade of malignancy. Appl Immunohistochem Mol
Morphol 22: 200-205.
Silveira EJD, Pereira JS, Miguel MCC et al (2007). Correlation of clinical,
histological, and cytokeratin profiles of squamous cell carcinoma of the oral tongue
with prognosis. Int of Surg Pathol 15: 376-383.
Sznurkowski JJ, Zawrocki A, Biernat W (2014). Subtypes of cytotoxic lymphocytes
and natural killer cells infiltrating cancer nests correlate with prognosis in patients
with vulvar squamous cell carcinoma. Cancer Immunol Immunother 63:297-303.

Takanami I, Takeuchi K, Giga M (2001). The prognostic value of natural killer cell
infiltration in resected pulmonary adenocarcinoma. J Thoracic Cardiovascular Surg
121: 1058-1063.
Türkseven MR, Oygür T (2010). Evaluation of natural killer cell defense in oral
squamous cell carcinoma. Oral Oncol 46: 34-37.
Vasconcelos MG, Mafra RP, Vasconcelos RG et al (2014). Squamous cell
carcinoma of the tongue: clinical and morphological analysis of 57 cases and
correlation with prognosis. J Bras Patol Med Lab 50: 327-331.
Warnakulasuriya, S (2009). Global epidemiology of oral and oropharyngeal cancer.
J Oral Oncology 45: 309-316.
FIGURAS
Figura 1. Imunoexpressão de CD57 no front de invasão de CCEO de baixo grau de malignidade e sem metástase (LSAB; Barra=100 µm). Natal, RN - 2014.
Fonte: Laboratório de histopatologia da disciplina de Patologia Oral – UFRN.
Figura 2. Imunoexpressão de CD57 no front de invasão de CCEO de alto grau de malignidade e com metástase (LSAB; Barra=100 µm). Natal, RN - 2014.
Fonte: Laboratório de histopatologia da disciplina de Patologia Oral – UFRN.
TABELAS
Tabela 1. Distribuição absoluta e relativa dos casos de carcinoma epidermóide oral de acordo com
a gradação histológica de malignidade, metástase linfonodal e o estadiamento clínico. Natal, RN -
2014.
Parâmetros
Gradação Histológica
p(1) Alto Grau
n (%)
Baixo Grau
n (%)
TOTAL
n (%)
Metástase Linfonodal
Ausente
Presente
11 (39,3%) 17 (60,7%) 28 (100,0%) <0,001*
17 (100,0%) 0 (0%) 17 (100,0%)
Estadiamento Clínico
Estágios I e II
Estágios III e IV
9 (37,5%) 15 (62,5%) 24 (100,0%) <0,001*
19 (90,5%) 2 (9,5%) 21 (100,0%)
Fonte: Programa de Pós-Graduação em Patologia Oral-UFRN.
(1) Qui-quadrado de Pearson.
(*) Diferença significativa a 5,0%.
Tabela 2. Tamanho da amostra, mediana, quartis 25 e 75, média dos postos, soma dos postos,
estatística U e significância estatística (p) para os valores de imunopositividade para CD57 no front
de invasão com relação ao estadiamento clínico. Natal, RN - 2014.
Estadiamento n Mediana Q25-Q75
Média dos
postos
Soma dos
postos U p(1)
Estágio I/II 24 18.0 13.1-
36.0 23.90 573.0 230.0 0.625
Estágio III/IV 21 16.8 9.5-34.7 21.98 461.0
Fonte: Laboratório de histopatologia da disciplina de Patologia Oral – UFRN.
(1): Teste Mann-Whitney.
Tabela 3. Tamanho da amostra, mediana, quartis 25 e 75, média dos postos, soma dos postos,
estatística U e significância estatística (p) para os valores de imunopositividade para CD57 no front
de invasão com relação à metástase linfonodal. Natal, RN - 2014.
Metástase n Mediana Q25-Q75
Média dos
postos
Soma dos
postos U p(1)
Ausente 28 18.0 13.1-35.7 24.21 678.0 204.0 0.426
Presente 17 15.8 8.9-36.6 21.00 357.0
Fonte: Laboratório de histopatologia da disciplina de Patologia Oral – UFRN.
(1): Teste Mann-Whitney.

Tabela 4. Tamanho da amostra, mediana, quartis 25 e 75, média dos postos, soma dos postos,
estatística U e significância estatística (p) para os valores de imunopositividade para CD57 no front
de invasão com relação à gradação histológica. Natal, RN - 2014.
Gradação
histológica n Mediana Q25-Q75
Média dos
postos
Soma dos
postos U p(1)
Baixo grau 17 26.4 14.5-43.4 27.0 459.5 169.5 0.109
Alto grau 28 16.2 10.2-25.1 20.5 575.5
Fonte: Laboratório de histopatologia da disciplina de Patologia Oral – UFRN.
(1): Teste Mann-Whitney.

NORMAS - ORAL DISEASES
© John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Edited By: Bruce Baum and Crispian Scully
Impact Factor: 2.377
ISI Journal Citation Reports © Ranking: 2012: 17/83 (Dentistry Oral Surgery & Medicine)
Online ISSN: 1601-0825
Author Guidelines
The median processing time from submission to first decision for manuscripts submitted to Oral Diseases in the past 12 months is 20 days.
Content of Author Guidelines: 1. General, 2. Ethical Guidelines, 3. Manuscript
Submission Procedure, 4. Manuscript Types Accepted, 5. Manuscript Format and Structure, 6. After Acceptance.
Relevant Documents: Online Open Order Form, Colour Work Agreement Form
Useful Websites: Submission Site, Articles Published in Oral Diseases, Author Services, Wiley-Blackwell’s Ethical Guidelines, Guidelines for Figures
1. GENERAL
The editors encourage submissions of original articles, review articles, reports of meetings, book reviews and correspondence in the form of letters to the editor. Oral Diseases does not accept case reports.
Please read the instructions below carefully for details on the submission of manuscripts, the journal's requirements and standards as well as information concerning the procedure after a manuscript has been accepted for publication in Oral Diseases. Authors are encouraged to visit Wiley-Blackwell Author Services for further information on the preparation and submission of articles and figures.
Avoiding allegations of plagiarism

The journal to which you are submitting your manuscript employs a plagiarism detection system. By submitting your manuscript to this journal you accept that your manuscript may be screened for plagiarism against previously published work. Authors would be well-advised to consider whether their manuscript may raise concerns via iTthenticate, which will signal whether a paper is in likely in any way to be plagiarized in a formal sense. iTthenticate will also, however, signal whether a paper may be plagiarized by repeating work of the submitting authors. Experience shows that, on occasion, large sections of submitted manuscripts can be close to verbatim in word choice from that seen in other papers from the authors’ group. This has nothing to do with simple repetition of names/affiliations, but does involve common (not necessarily "standard") phrases that are more appropriately referenced instead of repeating. Alternatively, they can be rephrased differently. Attention to these points could avoid these difficulties. 2. ETHICAL GUIDELINES
Oral Diseases adheres to the ethical guidelines given below for publication and research.
2.1. Authorship and Acknowledgements
Authorship: Authors submitting a paper do so on the understanding that the
manuscript has been read and approved by all authors and that all authors agree to the submission of the manuscript to the Journal.
Oral Diseases adheres to the definition of authorship set up by The International Committee of Medical Journal Editors (ICMJE). According to the ICMJE authorship criteria should be based on 1) substantial contributions to conception and design of, or acquisition of data or analysis and interpretation of data, 2) drafting the article or revising it critically for important intellectual content and 3) final approval of the version to be published. Authors should meet conditions 1, 2 and 3.
As of September 1st 2007, it is a requirement that the corresponding author submit a short description of each individual's contribution to the research and its publication. Upon submission of a manuscript all co-authors should also be registered with a correct e-mail addresses. If any of the e-mail addresses supplied are incorrect, the corresponding author will be contacted by the Journal Administrator.
Acknowledgements: Authors must acknowledge individuals who do not qualify as authors but who contributed to the research. Authors must acknowledge any assistance that they have received (e.g. provision of writing assistance, literature searching, data analysis, administrative support, supply of materials). If/how this assistance was funded should be described and included with other funding information. “Acknowledgements” should be brief and should not include thanks to anonymous referees and editors. Where people are acknowledged, a covering letter demonstrating their consent must be provided.

2.2. Ethical Approvals
Human Subjects: Experimentation involving human subjects will only be published
if such research has been conducted in full accordance with ethical principles, including the World Medical Association Declaration of Helsinki (version 2002) and the additional requirements, if any, of the country where the research has been carried out. Manuscripts must be accompanied by a statement that the experiments were undertaken with the understanding and written consent of each subject and according to the above mentioned principles. A statement regarding the fact that the study has been independently reviewed and approved by an ethical board should also be included.
Editors reserve the right to reject papers if there are doubts as to whether appropriate procedures have been used.
Animal Study: When experimental animals are used the methods section must
clearly indicate that adequate measures were taken to minimize pain or discomfort. Experiments should be carried out in accordance with the Guidelines laid down by the National Institute of Health (NIH) in the USA regarding the care and use of animals for experimental procedures or with the European Communities Council Directive of 24 November 1986 (86/609/EEC) and in accordance with local laws and regulations.
2.3 Clinical Trials
Clinical Trials should be reported using the CONSORT guidelines available at www.consort-statement.org. A CONSORT checklist should also be included in the submission material. Clinical trials can be registered in any of the following free, public clinical trials registries: www.clinicaltrials.gov, http://clinicaltrials.ifpma.org/clinicaltrials/, http://isrctn.org/.As stated in an editorial published in Oral Diseases (12:217-218), 2006), all manuscripts reporting results from a clinical trial must indicate that the trial was fully registered at a readily accessible website. The clinical trial registration number and name of the trial register will be published with the paper.
2.4 DNA Sequences and Crystallographic Structure Determinations
Papers reporting protein or DNA sequences and crystallographic structure determinations will not be accepted without a Genbank or Brookhaven accession number, respectively. Other supporting data sets must be made available on the publication date from the authors directly.
2.5 Conflict of Interest and Source of Funding
All sources of institutional, private and corporate financial support for the work within the manuscript must be fully acknowledged, and any potential grant holders

should be listed. Authors are also required to disclose any possible conflict of interest. These include financial (for example patent, ownership, stock ownership, consultancies, speaker’s fee). Information on sources of funding and any potential conflict of interest should be disclosed at submission under the heading “Acknowledgements”.
2.6 Appeal of Decision
The decision on a paper is final and cannot be appealed.
2.7 Permissions
If all or parts of previously published illustrations are used, permission must be obtained from the copyright holder concerned. It is the author's responsibility to obtain these in writing and provide copies to the Publishers.
2.8 Copyright and OnlineOpen
If your paper is accepted, the author identified as the formal corresponding author for the paper will receive an email prompting them to login into Author Services; where via the Wiley Author Licensing Service (WALS) they will be able to complete the license agreement on behalf of all authors on the paper. The corresponding author MUST submit the CTA as it is a requirement for publication.
For authors signing the copyright transfer agreement
If the OnlineOpen option is not selected the corresponding author will be presented with the copyright transfer agreement (CTA) to sign. The terms and conditions of the CTA can be previewed in the samples associated with the Copyright FAQs below: CTA Terms and Conditions http://authorservices.wiley.com/bauthor/faqs_copyright.asp.
Online Open OnlineOpen is available to authors of primary research articles who wish to make their article available to non-subscribers on publication, or whose funding agency requires grantees to archive the final version of their article. With OnlineOpen, the author, the author's funding agency, or the author's institution pays a fee to ensure that the article is made available to non-subscribers upon publication via Wiley InterScience, as well as deposited in the funding agency's preferred archive. For the full list of terms and conditions, see http://olabout.wiley.com/WileyCDA/Section/id-406241.html. Any authors wishing to send their paper OnlineOpen will be required to complete the payment form available from our website at: https://authorservices.wiley.com/bauthor/onlineopen_order.asp. Prior to acceptance there is no requirement to inform an Editorial Office that you intend to publish your paper OnlineOpen if you do not wish to. All OnlineOpen articles are

treated in the same way as any other article. They go through the journal's standard peer-review process and will be accepted or rejected based on their own merit.
For authors choosing OnlineOpen If the OnlineOpen option is selected the corresponding author will have a choice of the following Creative Commons License Open Access Agreements (OAA):
Creative Commons Attribution License OAA Creative Commons Attribution Non-Commercial License OAA Creative Commons Attribution Non-Commercial -NoDerivs License OAA
To preview the terms and conditions of these open access agreements please visit the Copyright FAQs hosted on Wiley Author Services http://authorservices.wiley.com/bauthor/faqs_copyright.asp and visit http://www.wileyopenaccess.com/details/content/12f25db4c87/Copyright--License.html.
If you select the OnlineOpen option and your research is funded by The Wellcome Trust and members of the Research Councils UK (RCUK) you will be given the opportunity to publish your article under a CC-BY license supporting you in complying with Wellcome Trust and Research Councils UK requirements.
For more information on this policy and the Journal’s compliant self-archiving policy please visit: http://www.wiley.com/go/funderstatement.
Additionally. authors are themselves responsible for obtaining permission to reproduce copyright material from other sources.
3. MANUSCRIPT SUBMISSION PROCEDURE
Oral Diseases only accepts online submission of manuscripts. Manuscripts should be submitted at the online submission site: http://mc.manuscriptcentral.com/odi. Complete instructions for submitting a manuscript are available at the site upon creating an account. Assistance for submitting papers can be sought with the editorial assistant Lisa Walton at: [email protected]
Upon successful submission, the journal administrator will check that all parts of the submission have been completed correctly. If any necessary part is missing or if the manuscript does not fulfil the requirements as specified below, the corresponding author will be asked either to adjust the submission according to specified instructions or to submit their paper to another journal.
3.1. Getting Started

Launch your web browser (supported browsers include Internet Explorer 5.5 or higher, Safari 1.2.4, or Firefox 1.0.4 or higher) and go to the journal's online Submission Site: http://mc.manuscriptcentral.com/odi
Log-in or, if you are a new user click on 'register here'. If you are registering as a new user.
- After clicking on 'register here', enter your name and e-mail information and click 'Next'. Your e-mail information is very important. - Enter your institution and address information as appropriate, and then click 'Next.' - Enter a user ID and password of your choice (we recommend using your e-mail address as your user ID), and then select your areas of expertise. Click 'Finish'.
If you are registered as user, but have forgotten your log in details, enter your e-mail address under 'Password Help'. The system will send you an automatic user ID and a new temporary password.
Log-in and select 'Corresponding Author Centre'.
3.2. Submitting Your Manuscript
After you have logged into your 'Corresponding Author Centre', submit your manuscript by clicking the submission link under 'Author Resources'.
Enter data and answer questions as appropriate. You may copy and paste directly from your manuscript and you may upload your pre-prepared covering letter.
Click the 'Next' button on each screen to save your work and advance to the next screen.
You are required to register all of your co-authors with a functioning e-mail address. If the e-mail address is incorrect, you will be contacted by the journal administrator.
You are required to upload your files: Click on the 'Browse' button and locate the file on your computer. Select the designation of each file in the drop down next to the Browse button. When you have selected all files you wish to upload, click the 'Upload Files' button.
Review your submission (in HTML and PDF format) before completing your submission by sending it to the Journal. Click the 'Submit' button when you are finished reviewing.
3.3. Manuscript Files Accepted
Manuscripts should be uploaded as Word (.doc/.docx) or Rich Text Format (.rft) files (not write-protected) plus separate figure files. GIF, JPEG, PICT or Bitmap files are acceptable for submission, but only high-resolution TIF or EPS files are suitable for printing. The files will be automatically converted to HTML and PDF on upload and will be used for the review process. The text file must contain the entire manuscript including title page, abstract, text, references, acknowledgements,

tables, and figure legends, but no embedded figures. In the text file, please reference figures as for instance 'Figure 1', 'Figure 2' etc to match the tag name you choose for individual figure files uploaded. Manuscripts should be formatted as described in the Author Guidelines below.
3.4. Blinded Review
All manuscripts submitted to Oral Diseases will be reviewed by two experts in the field. Oral Diseases uses single blinded review. The names of the reviewers will thus not be disclosed to the author submitting a paper.
3.5. Suggest a Reviewer
Oral Diseases attempts to keep the review process as short as possible to enable rapid publication of new scientific data. In order to facilitate this process, you must suggest the names and current e-mail addresses of from 2-4 potential reviewers whom you consider capable of reviewing your manuscript in an unbiased way.
3.6. Suspension of Submission Mid-way in the Submission Process
You may suspend a submission at any phase before clicking the 'Submit' button and save it to submit later. The manuscript can then be located under 'Unsubmitted Manuscripts' and you can click on 'Continue Submission' to continue your submission when you choose to.
3.7. E-mail Confirmation of Submission
After submission you will receive an e-mail to confirm receipt of your manuscript. If you do not receive the confirmation e-mail after 24 hours, please check your e-mail address carefully in the system. If the e-mail address is correct please contact your IT department. The error may be caused by some sort of spam filtering on your e-mail server. Also, the e-mails should be received if the IT department adds our e-mail server (uranus.scholarone.com) to their whitelist.
3.8. Manuscript Status
The average time from submission to first decision for manuscripts submitted to Oral Diseases is 20 days. You can access ScholarOne Manuscripts (formerly known as Manuscript Central) any time to check your 'Author Centre' for the status of your manuscript. The Journal will inform you by e-mail once a decision has been made.
3.9. Submission of Revised Manuscripts
To upload a revised manuscript, locate your manuscript under 'Manuscripts with Decisions' and click on 'Submit a Revision'. Please remember to delete any old files uploaded when you upload your revised manuscript.
4. MANUSCRIPT TYPES ACCEPTED
Original Research Articles: Manuscripts reporting laboratory investigations, well-designed and controlled clinical research, and analytical epidemiology are invited. Studies related to aetiology, pathogenesis, diagnosis, prevention and treatment are all of interest, but all papers must be based on rigorous hypothesis-driven research. Areas of interest include autoimmune, endocrine, genetic, infectious, metabolic and mucosal diseases; cancer and pre-cancerous conditions; chemosensory, developmental, geriatric and motor disorders, pain and wound healing.
Review Papers: Oral Diseases commissions review papers and also welcomes
uninvited reviews. Reviews should be submitted via the online submission site http://mc.manuscriptcentral.com/odi and are subject to peer-review.
Editorials: These will only be solicited by the editors.
Letters to the Editors: Letters, if of broad interest, are encouraged. They may deal with material in papers published in Oral Diseases or they may raise new issues, but should have important implications.
Case Reports: Oral Diseases does not accept case reports and instead recommends that authors submit to Clinical Case Reports an open access journal published by Wiley.
Meeting Reports: Will be considered by the editors for publication only if they are
of wide and significant interest.
Book Reviews: These will be solicited by the editors.
5. MANUSCRIPT FORMAT AND STRUCTURE
5.1. Page Charge
Articles exceeding 7 published pages are subject to a charge of GBP70 per additional page. One published page amounts approximately to 5,500 characters (excluding figures and tables).
5.2. Format
Language: Authors should write their manuscripts in British English using an easily readable style. Authors whose native language is not English should have a native English speaker read and correct their manuscript. Spelling and phraseology

should conform to standard British usage and should be consistent throughout the paper. A list of independent suppliers of editing services can be found at http://authorservices.wiley.com/bauthor/english_language.asp. All services are paid for and arranged by the author, and use of one of these services does not guarantee acceptance or preference for publication.
Presentation: Authors should pay special attention to the presentation of their
findings so that they may be communicated clearly. The background and hypotheses underlying the study as well as its main conclusions should be clearly explained. Titles and abstracts especially should be written in language that will be readily intelligible to any scientist.
Technical jargon: should be avoided as much as possible and clearly explained where its use is unavoidable.
Abbreviations: Oral Diseases adheres to the conventions outlined in Units,
Symbols and Abbreviations: A Guide for Medical and Scientific Editors and Authors. Non-standard abbreviations must be used three or more times and written out completely in the text when first used.
5.3. Structure: All papers submitted to Oral Diseases should include:
Title Page Structured Abstract (reviews need not include a structured abstract) Main text References (Figures) (Figure Legends) (Tables)
Title Page: should be part of the manuscript uploaded for review and include:
A title of no more than 100 characters including spaces A running title of no more than 50 characters 3-6 keywords Complete names and institutions for each author Corresponding author's name, address, email address and fax number Date of submission (and revision/resubmission)
Abstract: is limited to 200 words in length and should contain no abbreviations.
The abstract should be included in the manuscript document uploaded for review as well as separately where specified in the submission process. The abstract should convey the essential purpose and message of the paper in an abbreviated form set out under:
Objective(s),

Subject(s) (or Materials) and Methods, Results, Conclusions(s).
The Main Text of Original Research Articles should be organised as follows
Introduction: should be focused, outlining the historical or logical origins of the study and not summarize the results; exhaustive literature reviews are inappropriate. It should close with the explicit statement of the specific aims of the investigation.
Materials and Methods must contain sufficient detail such that, in combination
with the references cited, all clinical trials and experiments reported can be fully reproduced. As a condition of publication, authors are required to make materials and methods used freely available to academic researchers for their own use. This includes antibodies and the constructs used to make transgenic animals, although not the animals themselves. Other supporting data sets must be made available on the publication date from the authors directly.
(i) Clinical trials: As noted above, these should be reported using the CONSORT guidelines available at www.consort-statement.org. A CONSORT checklist should also be included in the submission material. Clinical trials can be registered in any of the following free, public clinical trials registries: www.clinicaltrials.gov, http://clinicaltrials.ifpma.org/clinicaltrials/, http://isrctn.org/.As stated in an editorial published in Oral Diseases (12:217-218), 2006), all manuscripts reporting results from a clinical trial must indicate that the trial was fully registered at a readily accessible website. The clinical trial registration number and name of the trial register will be published with the paper. (ii)Experimental subjects: As noted above, experimentation involving human subjects will only be published if such research has been conducted in full accordance with ethical principles, including the World Medical Association Declaration of Helsinki (version 2002) and the additional requirements, if any, of the country where the research has been carried out. Manuscripts must be accompanied by a statement that the experiments were undertaken with the understanding and written consent of each subject and according to the above mentioned principles. A statement regarding the fact that the study has been independently reviewed and approved by an ethical board should also be included.Editors reserve the right to reject papers if there are doubts as to whether appropriate procedures have been used. When experimental animals are used the methods section must clearly indicate that adequate measures were taken to minimize pain or discomfort. Experiments should be carried out in accordance with the Guidelines laid down by the National Institute of Health (NIH) in the USA regarding the care and use of animals for experimental procedures or with the European Communities Council Directive of 24 November 1986 (86/609/EEC) and in accordance with local laws and regulations.

(iii) Suppliers: Suppliers of materials should be named and their location (town,
state/county, country) included.
Results: should present the observations with minimal reference to earlier literature or to possible interpretations.
Discussion: may usually start with a brief summary of the major findings, but repetition of parts of the abstract or of the results sections should be avoided. The section should end with a brief conclusion and a comment on the potential clinical relevance of the findings. Statements and interpretation of the data should be appropriately supported by original references.
Acknowledgements: Should be used to provide information on sources of funding for the research, any potential conflict of interest and to acknowledge contributors to the study that do not qualify as authors. All sources of institutional, private and corporate financial support for the work within the manuscript must be fully acknowledged, and any potential grant holders should be listed. Acknowledgements should be brief and should not include thanks to anonymous referees and editors. Where people are acknowledged, a covering letter demonstrating their consent must be provided.
5.4. References
The journal policy is to encourage references to original papers, not to literature reviews. References in the text should quote the last name(s) of the author(s) and the year of publication (Brown and Smith, 2005). Three or more authors should always be referred to as, for example, Jones et al., 2005.
We recommend the use of a tool such as Reference Manager for reference management and formatting. Reference Manager reference styles can be searched for here: www.refman.com/support/rmstyles.asp
A list of the references must be given at the end of the paper and should follow the recommendations in Units, Symbols and Abbreviations: A Guide for Medical and Scientific Editors and Authors, (1975), p.36. London: The Royal Society of Medicine.
a) The arrangement of the references should be alphabetical by first author's surname.
b) The order of the items in each reference should be:
(i) for journal references:
last name(s) of all the author(s) and their initials, year, title of paper, title of journal, volume number, first and last page numbers.

(ii) for book references:
Name(s) of author(s), year, chapter title, title of book, edition, volume, town of publication, publisher, page number(s).
c) Authors' names should be arranged thus:
Smith AB and Jones DE
d) The year of publication should be surrounded by parentheses: (2005).
e) The title of the paper should be included without quotation marks.
f) The journal title should be abbreviated, should be italicised, and followed by the volume number in bold type and page numbers separated by a dash.
Examples:
Gupta PC, Murti PR, Bhonsle RB, Mehta FS, Pindborg JJ (1995). Effect of cessation of tobacco use on the incidence of oral mucosal lesions in a 10-year study of 12212 users. Oral Diseases 1: 54-58.
Baum BJ, Voutetakis A, Wang J (2004). Salivary glands: novel target sites for gene therapeutics. Trends Mol Med. 10: 585-590.
Shear M and Speight PM (2007). Cysts of the Oral and Maxillofacial Regions. Wiley-Blackwell: Oxford.
Scully C (2004). The oral cavity and lips. In: Burns DA, Breathnach SM, Cox N, Griffiths C, eds., Rooks Textbook of Dermatology. 7th Edition. Blackwell Science: Oxford, pp.66.1.-66.121.
5.5. Tables, Figures and Figure Legends
Figures: All figures and artwork must be provided in electronic format. Please save vector graphics (e.g. line artwork) in Encapsulated Postscript Format (EPS) and bitmap files (e.g. half-tones) or clinical or in vitro pictures in Tagged Image Format (TIFF).
Detailed information on our digital illustration standards can be found at http://authorservices.wiley.com/bauthor/illustration.asp.
Check your electronic artwork before submitting it: http://authorservices.wiley.com/bauthor/eachecklist.asp.

Unnecessary figures and parts (panels) of figures should be avoided: data presented in small tables or histograms, for instance, can generally be stated briefly in the text instead. Figures should not contain more than one panel unless the parts are logically connected.
Figures divided into parts should be labelled with a lower-case, boldface, roman letter, a, b, and so on, in the same type size as used elsewhere in the figure. Lettering in figures should be in lower-case type, with the first letter capitalized. Units should have a single space between the number and unit, and follow SI nomenclature common to a particular field. Unusual units and abbreviations should be spelled out in full or defined in the legend. Scale bars should be used rather than magnification factors, with the length of the bar defined in the legend rather than on the bar itself. In general visual cues (on the figures themselves) are preferred to verbal explanations in the legend (e.g. broken line, open red triangles etc).
6. AFTER ACCEPTANCE
Upon acceptance of a paper for publication, the manuscript will be forwarded to the Production Editor who is responsible for the production of the journal.
Proof Corrections
The corresponding author will receive an e-mail alert containing a link to a website. A working e-mail address must therefore be provided for the corresponding author. The proof can be downloaded as a PDF (portable document format) file from this site.
Acrobat Reader will be required in order to read this file. This software can be downloaded (free of charge) from the following website: www.adobe.com/products/acrobat/readstep2.html . This will enable the file to be opened, read on screen, and printed out in order for any corrections to be added. Further instructions will be sent with the proof. Hard copy proofs will be posted if no e-mail address is available; in your absence, please arrange for a colleague to access your e-mail to retrieve the proofs.
Proofs must be returned to the Production Editor within three days of receipt.
As changes to proofs are costly, we ask that you only correct typesetting errors. Excessive changes made by the author in the proofs, excluding typesetting errors, will be charged separately. Other than in exceptional circumstances, all illustrations are retained by the publisher. Please note that the author is responsible for all statements made in their work, including changes made by the copy editor.
Early View (Publication Prior to Print)

Oral Diseases is covered by Wiley-Blackwell's Early View service. Early View articles are complete full-text articles published online in advance of their publication in a printed issue. Early View articles are complete and final. They have been fully reviewed, revised and edited for publication, and the authors' final corrections have been incorporated. Because they are in final form, no changes can be made after online publication. The nature of Early View articles means that they do not yet have volume, issue or page numbers, so Early View articles cannot be cited in the traditional way. They are therefore given a Digital Object Identifier (DOI), which allows the article to be cited and tracked before it is allocated to an issue. After print publication, the DOI remains valid and can continue to be used to cite and access the article.
Author Services
Online production tracking is available for your article once it is accepted by registering with Wiley-Blackwell's Author Services.