Embed Size (px)
Citation preview

RASTREAMENTO
Subsecretaria de Promoção, Atenção Primária e Vigilância à Saúde
SMS/RIO
Ana Ramalho 30/04/2014

Gestão de Redes
Monitoramento e Avaliação
Epidemiologia, Informação e Vigilância
PROMOÇÃODA SAÚDE
DETECÇÃO PRECOCE
TRATAMENTO
CUIDADOS PALIATIVOS
Controle de DANT Ensino, Pesquisa e Incorporação de novas tecnologiasComunicação e Mobilização SocialPolítica de AtençãoOncológica
Portaria nº 2.439/GM (dez / 2005)
PREVENÇÃO PRIMÁRIA
Elaboração de protocolos clínicos

Estratégias para Detecção Precoce
Diagnóstico Precoce
Fonte: OMS
Screening (Rastreamento)
Pessoas com sinais e
sintomas
População assintomática
OMS

Detecção Precoce: Detectar (ou diagnosticar) um doença em seu estágio inicial, quando existe um alto potencial de cura.
Duas estratégias de detecção precoce:
• Diagnóstico Precoce: Submeter indivíduos com sinais e sintomas à realização de exames para identificar doença em estágios iniciais.
• Rastreamento: Submeter indivíduos assintomáticos e aparentemente saudáveis à realização de exames para identificar lesões em estágios iniciais ou precursoras.
Conceitos
Fonte: Early Detection Module. WHO, 2007

Efeito da antecipação do diagnóstico e sobrediagnóstico
sscreening

Estudos de rastreamento tendem a mostrar melhores resultados entre a população rastreada do que entre a não rastreada:
Viés do tempo de antecipação: casos detectados antes, aparentemente sobrevivem mais
Viés da duração da doença: doenças de melhor prognóstico e, portanto, maior duração, tem maior probabilidade de serem descobertas por rastreamento. Na amostra dos casos identificados por rastreamento há sobrerrepresentação de casos mais benignos.
Sobrediagnóstico: identificação de “casos” que nunca se manifestariam clinicamente. Aparentemente são “curados” devido à detecção mais precoce.

National Cancer Control Programmes:policies and managerial guidelines – WHO, 2002
“ É importante estabelecer que os benefícios da detecção
precoce sejam maiores que os de complicações e riscos
antes de implementar a detecção precoce como uma
política de saúde pública.
É essencial, por isso, recomendar a adoção apenas daquelas
intervenções para as quais existem evidências suficientes
sobre eficácia e custo efetidade”

Critérios para um programa de rastreamento1. Problema de saúde pública;
2. História natural da doença bem conhecida;
3. Estágio pré-clínico (assintomático) bem definido, durante o qual a doença possa ser diagnosticada;
4. Benefício da detecção e do tratamento precoce com o rastreamento deve ser maior do que se a condição fosse tratada no momento habitual de diagnóstico;
5. Exames de detecção disponíveis, aceitáveis e confiáveis;
6. Custo do rastreamento e tratamento razoável e compatível com o orçamento destinado ao sistema de saúde como um todo;
7. Deve ser um processo contínuo e sistemático. 1968, Wilson e Jungner

Aplicação de testes diagnósticos em população com baixa prevalência de doença
Qual a probabilidade de um teste positivo ter identificado corretamente um doente? E de
dar um falso positivo?
CAB Rastreamento, MS, 2010

Doença ausente > Doença presente
Qual a consequência da ocorrência de “D”: efeito adverso do rastreamento em pessoas falso positivos ao
rastreamento (ou em sobrediagnosticados)?

Recomendações da OMS
Adaptado de Early Detection Module. WHO, 2007


Rastreamento populacional
câncer do colo do útero

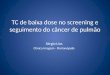
Índice de Positividade em Citopatologia - Brasil 2010
0
20
40
60
80
100
120
140
160
180
200
0,5 1 1,5 2 2,5 3 3,5 4 4,5 5 5,5 6 6,5 7 7,5 8 8,5 9 9,5 10 10,5 11 11,5 12 12,5 13
% de Positividade
Nu
mer
os
de
Lab
ora
tóri
os
Total de Lab.: 1182
Média: 2,8%
Desvio Padrão: 3,5%
Mediana: 2%
5% < IP < 10% = 8%
IP > 13% = 2%

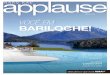
Local Ano % Positividade todas idades % HSIL todas idades Referência OBS
Reino Unido 2007-2008 6,4 0,98NHS Cervical Screening
Programme – Annual Review 2008
LBC
EUA 2002 6,8 0,5 Davey at al , 2004 PAP e LBC
Noruega 1998-2000 4,9 1,14 Nygard et al , 2002 PAP
DASA (RJ) 2010 3,7 - Comunicação pessoal PAP
Canadá (BC) 1998 15,1 1,4
PAP
PAPInclui em HSIL atipias gland e CA
Bélgica(Limburg)
Health Canadá, 1998
1996-2005 3,7 0,4 Arbyn et al , 2011
POSITIVIDADE

Evidências científicas



Recommendations:
The USPSTF recommends against routine screening mammography in women aged 40 to 49 years. The decision to start regular, biennial screening mammography before the age of 50 years should be an individual one and take into account patient context, including the patient’s values regardingspecific benefits and harms. (Grade C recommendation)
The USPSTF recommends biennial screening mammography for women between the ages of 50 and 74 years. (Grade B recommendation)
The USPSTF concludes that the current evidence is insufficient to assess the additional benefits and harms of screening mammography in women 75 years or older. (I statement)
The USPSTF concludes that the current evidence is insufficient to assess the additional benefits and harms of clinical breast examination beyond screening mammography in women 40 years or older. (I statement)
The USPSTF recommends against clinicians teaching women how to perform breast self-examination. (Grade D recommendation)The USPSTF concludes that the current evidence is insufficient to assess additional benefits and harms of either digital mammography or magnetic resonance imaging instead of film mammography as screening modalities for breast cancer. (I statement)
Ann Intern Med. 2009;151:716-726. www.annals.org
Screening for Breast Cancer: U.S. Preventive Services Task Force - Recommendation Statement
as recomendaçõesas recomendações

Evidências para o rastreamento mamográficoRevisões sistemáticas
Screening mammography: a reassessment
Agence d’Evaluation des Tecnologies et Modes d’Intervention em santé (AETMIS) 2006
Objetivo Resultados
Reavaliar evidências que sustentam o rastreamento mamográfico; determinar as evidências existentes em relação ao rastreamento de mulheres no grupo de 40 a 49 anos; resultados para o programa de Quebec de rastreamento mamográfico.
Sete estudos incluídos na análise.
Relação inversa entre a qualidade do estudo e a redução na mortalidade por câncer de mama. Nos melhores estudos a redução foi de 9%; em alguns destes o IC incluindo a unidade.
Entre 40-49 anos, para todas as combinações de estudos segundo sua qualidade, resultados não significativos. Os resultados dos ensaios clínicos não dão justificação científica à recomendação da rastreio mamográfico de mulheres com menos de 50 anos.
Na população a partir de 50 anos, redução da mortalidade entre 24-29%.
Para esta faixa etária justifica-se o rastreamento, devendo-se garantir rigoroso controle de qualidade e alta cobertura, características que poderão levar o programa a obter resultados melhores que os resultados médios dos ensaios clínicos randomizados.

The first comprehensive review of European breast screening programs has found that the benefits of mammography clearly outweigh the harms.
Data from about 12 million women collected from 26 screening programs in 18 countries from 2001 to 2007.
European population-based mammography programs are contributing to the reduction in breast cancer mortality in the European Union and are achieving a mortality benefit at least as great as that seen in randomized clinical trials.
“… the estimated number of breast cancer deaths avoided by screening clearly exceeds the estimated number of cases of overdiagnosis."
For every 1000 women who undergo screening every 2 years from the age of 50 to 69 years, 7 to 9 lives would be saved and 4 women would be overdiagnosed.
J Med Screen. 2012;19(Suppl 1):5-13

Screening Mammography Associated With Modest Decline in Breast Cancer MortalityRoxanne NelsonSeptember 22, 2010
The data come from Norway, and are reported in the September 23 issue of the New England Journal of Medicine.Participation in the Norwegian breast cancer screening program was associated with a 10% reduction in the rate of death from breast cancer among women 50 to 69 years of age, said lead author Mette Kalager, MD, from Oslo University Hospital in Norway.However, only part of this reduction can be attributed to the screening program, she said, because during the period that the study was conducted, Norway built multidisciplinary teams to treat breast cancer, which also had an impact."One third of the mortality reduction we observed in the 20-year period — 1986 to 2005 — can be associated with the screening program, while two thirds can be attributed to enhanced breast cancer awareness and improved diagnosis and treatment for breast cancer," she told Medscape Medical News.

NOVAS PUBLICAÇÕES: a controvérsia persisteAmong 1000 women, 50 years of age, undergoing annual mammography for 10 years:
• Between 3 and 32 women will avoid dying of breast cancer;• Between 490 and 670 will have at least 1 false-positive test, with 70-100 undergoing biopsy; and• Between 3 and 14 will be over diagnosed and treated needlessly with surgery, radiation, or chemotherapy.
Among 1000 women, 60 years of age, undergoing annual mammography for 10 years:
• Between 5 and 49 women will avoid dying of breast cancer;• Between 390 and 540 will have at least 1 false-positive test, with 50-70 undergoing biopsy; and• Between 6 and 20 will be over diagnosed and treated needlessly with surgery, radiation, or chemotherapy. JAMA Intern Med. 2013 Dec 30

Screening Mammography Associated With Modest Decline in Breast Cancer MortalityRoxanne NelsonSeptember 22, 2010
The data come from Norway, and are reported in the September 23 issue of the New England Journal of Medicine.Participation in the Norwegian breast cancer screening program was associated with a 10% reduction in the rate of death from breast cancer among women 50 to 69 years of age, said lead author Mette Kalager, MD, from Oslo University Hospital in Norway.However, only part of this reduction can be attributed to the screening program, she said, because during the period that the study was conducted, Norway built multidisciplinary teams to treat breast cancer, which also had an impact."One third of the mortality reduction we observed in the 20-year period — 1986 to 2005 — can be associated with the screening program, while two thirds can be attributed to enhanced breast cancer awareness and improved diagnosis and treatment for breast cancer," she told Medscape Medical News.

JAMA Review: Stop One-Size-Fits-All Mammography systematic review of 50 years of breast cancer screening data, published in the April issue of JAMA., 2014
After poring over clinical trials, systematic reviews, meta-analyses, and observational studies, they conclude that the mortality benefit of mammography is "modest" and the risks of harm from screening are "significant."This mix means that clinicians "must focus on promoting informed screening decisions," they write."There is a challenge for physicians to find the time to talk about this with patients," acknowledged Dr. Keating in an email to Medscape Medical News. "I do hope that the increasing availability of decision aids will make these discussions easier."

Evidências para o rastreamento do ca de prostataRevisões sistemáticas
Screening for prostate cancer - The Cochrane Collaboration Ilic et al. - 2007
Objetivo Resultados
Determinar se o rastreamento do câncer de próstata reduz a mortalidade e tem impacto sobre a qualidade de vida.
não há provas suficientes para apoiar ou refutar o uso rotineiro do rastreamento populacional ou oportunista, em comparação com nenhum rastreamento para reduzir mortalidade por câncer de próstata.

Evidências para o rastreamento do ca de prostataRevisões sistemáticas
United State Preventive Services Task Force (USPSTF)2008
Objetivo Resultados
Atualização da recomendação de 2002 para o rastreamento do câncer de próstata.
Há bom nível de evidência para afirmar que o rastreamento pela dosagem do PSA pode detectar o câncer da próstata em estágios iniciais, mas as evidências são conflitantes e inconclusivas sobre o impacto desse achado sobre os desfechos na saúde.
Conclusões: o nível de evidência é insuficiente para tecer recomendações a favor ou contra a adoção do rastreamento para o câncer da próstata em homens com idade inferior a 75 anos. Não há evidências que essa prática seja eficaz, ou as evidências são pobres e conflitantes e a relação custo-benefício não pode ser determinada. (Grau de recomendação I).
A USPSTF recomenda a não adoção do rastreamento do câncer da próstata em homens assintomáticos com idade superior a 75 anos. A USPSTF encontrou pelo menos um nível adequado de evidência que [a tecnologia] é ineficaz ou que os danos superam os benefícios. (Grau de recomendação D)

Ensaios clínicos
Mortality results from a randomized prostate cancer screening trial PLCO Project Team – 2009
Objetivo Resultados
Avaliar o efeito da dosagem do PSA e do toque retal sobre a taxa de mortalidade do câncer de próstata.
De 1993 até 2001, 76.693 homens foram aleatoriamente distribuídos. O grupo rastreado realizou dosagem de PSA anual por 6 anos e toque retal por 4 anos.
Após 7 anos de seguimento, a incidência de câncer de próstata por 10.000 pessoas-ano foi de 116 (2820 casos) no grupo rastreado e 95 (2322 casos) no grupo controle (OR, 1,22; [CI], 1.16 a 1.29).
A taxa de mortalidade por 10.000 pessoas-ano foi de 2,0 (50 mortes) no grupo rastreado e 1,7 (44 mortes) no grupo controle (OR, 1,13; IC, 0,75 a 1,70).
Conclusão: Após 7 a 10 anos de seguimento, as taxas de mortalidade por câncer de próstata foram muito baixas e não diferiram significativamente entre os dois grupos de estudo.
Evidências para o rastreamento do ca de prostata

Ensaios clínicos
Screening and prostate cancer mortality in a randomized European study ERSPC investigators - 2009
Objetivo Resultados
Avaliar o efeito do
rastreamento com a
dosagem do PSA
sobre a taxa de
mortalidade do câncer
de próstata.
Incluídos 182.000 homens de sete países europeus com idades entre os 50 e os 74 anos.
A incidência cumulativa (9 anos) de câncer de próstata foi de 8,2% no grupo rastreado e 4,8% no grupo controle.
Isto significa que 1.410 homens teriam de ser rastreados e 48 casos adicionais de câncer da próstata teriam de ser tratados para evitar uma morte por câncer de próstata.
Conclusão: O rastreamento com o PSA reduziu a taxa de morte por câncer de próstata em 20%, mas foi associado com um risco elevado de sobrediagnóstico.
Evidências para o rastreamento do ca de prostata

2012

“The results, from 731 men randomly assigned to either surgery or observation and followed up for a median of 10 years, showed that “Among men with localized prostate cancer detected during the early era of PSA testing, radical prostatectomy did not significantly reduce all-cause or prostate-cancer mortality, as compared with observation”. Furthermore, urological symptoms such as urinary incontinence and erectile dysfunction were significantly more common in the surgical intervention group at 2 years.”
Prostate cancer: send away the PSA?
For the PIVOT trial see New Engl J Med 2012; 367: 203–13For The Lancet’s Editorial on the US Preventive Services Task Force recommendations see Lancet 2012; 379: 2024For a Lancet Review on prostate cancer see Lancet 2008; 371: 1710–21

PSA Testing: Have We Learned From Our Errors? In May 2013, the American Urological Association (AUA) issued a new set of guidelines[1] for recommendations regarding screening for prostate cancer. Many people will applaud these changes because they are more in line with evidence-based findings from randomized trials.
Essentially,…They recommend against screening men under age 40. They do not encourage routine screening of men between the ages of 40 and 54 years, men over age 70, and men with a 10-to 15-year life expectancy. They do acknowledge that some men over age 70 could benefit.
The guidelines encourage the core group of men between ages 55 and 69 years to have a discussion with their healthcare provider about the pros and cons, the risks and the benefits, of screening, including that during 10 years of follow-up, studies have shown that 1 life is saved for every 1000 men who are screened. They acknowledge that, in large groups of men, this could translate into a significant benefit, particularly with longer follow-up.Gerald Chodak, MD, May 17, 2013

PRIMUN NON NOCERE - Princípios hipocráticos da não maleficência e da beneficência.
Todos os programas de rastreamento causam danos e alguns fazem bem. (Gray, 2004)
The PIVOT trial is a timely reminder of medicine’s—and life’s— imperfections. To the Hippocratic Oath might be added: I will not request an investigation unless I am confident that the answer, and the actions I take on its basis, will substantially improve my patient’s life. ■The Lancet






Among 1000 women, 50 years of age, undergoing annual mammography for 10 years:
• Between 3 and 32 women will avoid dying of breast cancer;• Between 490 and 670 will have at least 1 false-positive test, with 70-100 undergoing biopsy; and• Between 3 and 14 will be over diagnosed and treated needlessly with surgery, radiation, or chemotherapy.
Among 1000 women, 60 years of age, undergoing annual mammography for 10 years:
• Between 5 and 49 women will avoid dying of breast cancer;• Between 390 and 540 will have at least 1 false-positive test, with 50-70 undergoing biopsy; and• Between 6 and 20 will be over diagnosed and treated needlessly with surgery, radiation, or chemotherapy. JAMA Intern Med. 2013 Dec 30

Screening Mammography Associated With Modest Decline in Breast Cancer MortalityRoxanne NelsonSeptember 22, 2010
The data come from Norway, and are reported in the September 23 issue of the New England Journal of Medicine.Participation in the Norwegian breast cancer screening program was associated with a 10% reduction in the rate of death from breast cancer among women 50 to 69 years of age, said lead author Mette Kalager, MD, from Oslo University Hospital in Norway.However, only part of this reduction can be attributed to the screening program, she said, because during the period that the study was conducted, Norway built multidisciplinary teams to treat breast cancer, which also had an impact."One third of the mortality reduction we observed in the 20-year period — 1986 to 2005 — can be associated with the screening program, while two thirds can be attributed to enhanced breast cancer awareness and improved diagnosis and treatment for breast cancer," she told Medscape Medical News.

JAMA Review: Stop One-Size-Fits-All Mammography systematic review of 50 years of breast cancer screening data, published in the April issue of JAMA.
After poring over clinical trials, systematic reviews, meta-analyses, and observational studies, they conclude that the mortality benefit of mammography is "modest" and the risks of harm from screening are "significant."This mix means that clinicians "must focus on promoting informed screening decisions," they write."There is a challenge for physicians to find the time to talk about this with patients," acknowledged Dr. Keating in an email to Medscape Medical News. "I do hope that the increasing availability of decision aids will make these discussions easier."