Embed Size (px)
Citation preview

Síndrome Dolorosa Complexa Regional: Epidemiologia,Fisiopatologia, Manifestações Clínicas, Testes Diagnósticos e
Propostas Terapêuticas *Complex Regional Pain Syndrome: Epidemiology, Pathophysiology,Clinical Manifestations, Diagnostic Tests and Therapeutic Proposals
Francisco Carlos Obata Cordon1, Lino Lemonica TSA
2
RESUMOCordon FCO, Lemonica L - Síndrome Dolorosa Complexa Re-gional: Epidemiologia, Fisiopatologia, Manifestações Clíni-cas, Testes Diagnósticos e Propostas Terapêuticas
Justificativa e Objetivos - A Síndrome Dolorosa ComplexaRegional (SDCR), assim denominada a partir de 1994 peloConsenso da Associação Internacional para o Estudo da Dor(AIED) e anteriormente denominada de várias formas, taiscomo Distrofia Simpático Reflexa, Causalgia, Algodistrofia ouAtrofia de Sudeck, é uma doença cuja compreensão dos limitesclínicos, fisiopatologia e implicações de patogenia ainda épobre. Disto resulta a enorme insatisfação não só para ospacientes como para os profissionais da saúde quanto aosmétodos terapêuticos atualmente disponíveis. O objetivo destetrabalho é rever a literatura e atualizar um conjunto deinformações com o intuito da melhor compreensão destaimportante síndrome dolorosa.
Conteúdo - Este é um trabalho de revisão da literatura nosdiversos aspectos da SDCR, com ênfase em suas causas,definição e taxonomia, fisiopatologia, características clínicas,testes diagnósticos e propostas de tratamentos mais recentes.
Conclusões - Poucos são os es tudos cont ro ladosadequadamente, encobertos e aleatórios, publicados comgrandes amostras, havendo muitas dúvidas sobre estadoença. Desta forma, ainda há enorme empirismo na suaterapêutica, e os resultados obtidos são insatisfatórios.
UNITERMOS - DOR, Crônica: sindrome dolorosa complexa re-gional
SUMMARYCordon FCO, Lemonica L - Complex Regional Pain Syndrome:Epidemiology, Pathophysiology, Clinical Manifestations, Diag-nostic Tests and Therapeutic Proposals
Background and Objectives - The term Complex RegionalPain Syndrome (CRPS) was adopted as from 1994 by the Inter-national Association for Study of Pain (IASP) Consensus. It pre-viously referred to by several other names, such as ReflexSympathetic Dystrophy, Causalgia, Algodystrophy or Sudeck’sAtrophy, and is a disease where the understanding of clinicallimits, pathophysiology and pathogenic implications is still verypoor. Thus resulting in disappointment both for patients and forhealth professionals with regard to currently available thera-pies. This study aimed at reviewing the literature and updatinginformation to improve the understanding of this severe painfulsyndrome.
Contents - This study is a literature review of several CRPS as-pects, with emphasis in its causes, definition and taxonomy,pathophysiology, clinical characteristics, diagnostic tests andmost recent therapies.
Conclusions - There are few well controlled, double blind andrandomized CRPS studies with large samples, and there arestill several questions about this disease. The treatment is usu-ally empirical and the patient outcome is poor.
KEY WORDS - PAIN, Chronic: complex regional pain syndrome
INTRODUÇÃO
ASíndrome Dolorosa Complexa Regional (SDCR), assimdesignada atualmente, é uma entidade que traz grande
angústia, não só para o paciente pelo quadro álgico incapa-citante como também para os profissionais de saúde.Estes, limitados em sua abordagem, uma vez que a fisiopa-tologia da SDCR não está totalmente esclarecida, têm gran-de dificuldade em obter resultados positivos no tratamento.O objetivo deste trabalho é rever a literatura e atualizar umconjunto de informações com o intuito de melhor compreen-der esta importante síndrome dolorosa.
CONCEITOS E ASPECTOS HISTÓRICOS
Até pouco tempo a SDCR era também denominada de cau-salgia. Este termo foi utilizado pela primeira vez por Mitchellem 1864 1, embora a primeira descrição de causalgia tenhasido realizada em 1862 por Paget 2.Wolff, em 1877, descreveu, pela primeira vez, uma entidadecrônica dolorosa, sem causa neurológica, acompanhada poralterações vasomotoras, até então inominada 3. Muitas ter-minologias foram utilizadas para designá-la, como causal-
618 Revista Brasileira de AnestesiologiaVol. 52, Nº 5, Setembro - Outubro, 2002
Rev Bras Anestesiol2002; 52: 5: 618 - 627
* Recebido do (Received from) Serviço de Terapia Antálgica e Cuidados
Paliativos do Departamento de Anestesiologia da Faculdade de Medici-
na de Botucatu (FMB - UNESP), Botucatu, SP
1. ME3 do CET/SBA do Departamento de Anestesiologia, Serviço de Tera-
pia Antálgica e Cuidados Paliativos, da FMB - UNESP
2. Professor Assistente Doutor do CET/SBA do Departamento de Aneste-
siologia, Responsável pelo Serviço de Terapia Antálgica e Cuidados Pa-
liativos da FMB - UNESP
Apresentado (Submitted) em 05 de novembro de 2001
Aceito (Accepted) para publicação em 25 de janeiro de 2002
Correspondência para (Mail to):
Dr. Lino Lemonica
Deptº de Anestesiologia da FMB - UNESP
Distrito de Rubião Júnior
18618-970 Botucatu, SP
E-mail:[email protected]
� Sociedade Brasileira de Anestesiologia, 2002
ARTIGO DE REVISÃOREVIEW ARTICLE

gia menor, desordem vasomotora pós-traumática, atrofia deSudeck e síndrome ombro-mão. Em 1953, Bonica sugeriuque todas as patologias dolorosas associadas a fenômenosvasomotores, habitualmente precedidas por trauma, deves-sem ser denominadas de “distrofia simpático reflexa” 4, naqual as seguintes características deveriam estar presentes:dor, alterações vasomotoras da pele, perda de função domembro e alterações tróficas em vários estágios.Contudo, as controvérsias sobre o diagnóstico continuarama suscitar dúvidas. Em 1993, a Associação Internacionalpara o Estudo da Dor (AIED) elaborou consenso onde foramdefinidos os critérios para o diagnóstico desta doença, publi-cados em 1994 5. Foi adotada a terminologia “Síndrome Do-lorosa Complexa Regional” (SDCR) como termo único, paradesignar a condição dolorosa regional associada às altera-ções sensoriais decorrentes de um evento nóxico. Nesta,após o trauma, a dor é o sintoma principal, podendo estar as-sociado à coloração anormal da pele, mudanças de tempera-tura do membro, atividade sudomotora anormal ou edema.Distúrbios motores como tremores, distonias ou fraquezamuscular podem ocorrer. No consenso, foram definidos doistipos de SDCR: tipo I, anteriormente chamada de “distrofiasimpático reflexa” e tipo II, outrora denominada de “causal-gia”. A SDCR tipo II diferencia-se da do tipo I pela existênciade uma lesão nervosa real, em que a dor não se limita ao terri-tório de inervação do nervo lesado.Embora o consenso tenha sido elaborado para o seu diag-nóstico, muitas questões foram levantadas sobre como equantos critérios deveriam ser considerados para que hou-vesse sua confirmação. Também se observou que outras pa-tologias bem definidas como, por exemplo, a neuropatia dia-bética, poderiam preencher tais critérios e serem erronea-mente tratadas 6. Após análise e revisão foram propostos osseguintes critérios para o diagnóstico: (a) a presença de le-são inicial pode ser desconsiderada; (b) os sinais e os sinto-mas devem ser divididos em grupos distintos; (c) o pacientedeve ter pelo menos dois dos seguintes sintomas: sensoriais(hiperestesia), vasomotor (alteração da temperatura, colo-ração ou ambos), sudomotor/balanço líquido (edema, sudo-rese ou ambos) e motor (diminuição da motricidade, fraque-za, tremores, amputação funcional do membro) ou todos, e(d) o paciente deve apresentar ao menos dois dos seguintessinais: vasomotor, sudomotor/balanço líquido e motor.Assim, a partir destes novos critérios, acredita-se que a ava-liação, diagnóstico e seguimento dos pacientes possam serrealizados com melhor propriedade.O termo “Dor Simpaticamente Mantida” (DSM) foi utilizadoem outros momentos como sinônimo de SDCR, embora in-corretamente. Este termo designa dor mantida pelos eferen-tes simpáticos, ou por catecolaminas circulantes 7 e algumashipóteses são aventadas para justificar este fenômeno.Entre elas, uma das mais aceitas é o aumento do número de�-adrenoceptores nos tecidos periféricos, sensíveis à nore-pinefrina das terminações simpáticas, que através de suaatuação sobre os receptores, causa a dor 8. A lesão de nervoperiférico proporciona alterações plásticas tanto do aferenteprimário como nos neurônios simpáticos pós-ganglionares
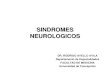
na dependência do tipo de lesão ser total ou parcial. Estaplasticidade neuronal caracteriza-se por alterações dege-nerativas, regenerativas e reorganização que culminamcom ligações bioquímicas entre os neurônios aferentes pri-mários e simpáticos pós-ganglionares, além de ligações co-laterais no gânglio da raiz dorsal por parte dos neurônios nãolesados (Figura 1). Estas ligações são responsáveis pela ati-vação desses aferentes primários pelo sistema simpático,onde o provável mediador é a norepinefrina, embora outrosmediadores não possam ser excluídos. Também ocorre a ex-pressão ou aumento dos receptores adrenérgicos, tipo �2,nos aferentes primários 9.
Figura 1 - Influência da Atividade Simpática sobre os Aferentes Pri-máriosA. Lesão nervosa completa: interações simpáticas no local doneuroma e gânglio da raiz dorsal, sendo mediado pela norepi-nefrina liberada pelas fibras pós-ganglionares simpáticas epor �-adrenoceptores do aferente primário. B. Lesão parcial: alesão é seguida por uma diminuição da inervação simpática lo-cal com conseqüente hiperatividade dos �-adrenoceptores damembrana dos nociceptores, tipo C, não lesados. C. Após rea-ção inflamatória tecidual: sem lesões, mas com sensibilidadeaumentada pela norepinefrina que promove a liberação deprostaglandinas, pelas terminações simpáticas, sensibilizan-do os aferentes primários. Além das prostaglandinas atuam,conjuntamente, a bradicinina e fator de crescimento de ner-vos. (Modificado de Baron, R) 9
Existem ainda estudos baseados na hipótese da desnerva-ção, em que a lesão de fibras eferentes simpáticas causa au-mento da expressão do fator de crescimento do nervo ou deoutros fatores neurotróficos, ocasionando, em ultima instân-cia, o aumento da transmissão da dor por vários mecanismos10-14. Trabalhos que corroboram esta hipótese mostram que,em humanos e cobaias, há baixa concentração de norepine-frina ou seu metabólito no plasma do membro afetado em re-
Revista Brasileira de Anestesiologia 619Vol. 52, Nº 5, Setembro - Outubro, 2002
CORDON E LEMONICA
A
B
NA
NA
NA
PG
NA
NA
NA
Aferente
Aferente
Aferente
Pós-ganglionar
Pós-ganglionar
Pós-ganglionar
BradicininaNGF
Sensibilização dosNociceptores
Pré-ganglionar
Pré-ganglionar
Pré-ganglionar
Lesão NervosaCompleta
Lesão NervosaParcial
�
�
�
��
C

lação ao sadio 15-17. Esta hipótese, também explica a vaso-constrição do membro afetado com base no aumento da res-posta vasoconstritora a norepinefrina, pela elevada respos-ta das células musculares dos vasos à desnervação 16.A DSM deve ser entendida como um mecanismo de dor e aSDCR como um diagnóstico clínico. É importante lembrarque, embora em alguns casos haja diminuição da dor apósbloqueio simpático, nem sempre a SDCR está acompanha-da pela DSM. Não se pode estabelecer a correlação entreDSM e sinais e sintomas disautonônicos. Teoricamente, ospacientes podem ter componentes de DSM e dor não simpá-tico-dependente 17,18.
EPIDEMIOLOGIA
Não está bem definida a epidemiologia da SDCR. Todavia,estudo realizado por Veldman e col. 19 mostra média de idadede 41 anos com predomínio de mulheres numa relação de3:1. Allen e col. 20 confirmaram que a média de idade é de41,8 anos e a relação entre mulheres e homens de 2,3:1. Emcrianças há um predomínio do sexo feminino numa relaçãode 3:1, com idade típica de início da sintomatologia entre 9 e15 anos de idade 21-23.Freqüentemente um único membro é acometido, em propor-ções iguais entre superiores e inferiores. Poucos estudosmostram prevalência dos membros superiores ou dos inferio-res, havendo uma incidência maior do lado direito, talvez porserem destros em relação ao esquerdo e o acometimento bi-lateral ocorre entre 11 e 16 % dos casos 20,24. Em crianças, osmembros inferiores são os mais afetados 21-23.Cerca de 65% dos casos estão relacionados a trauma, nor-malmente por fratura, 19% no período pós-operatório, 2%após processos inflamatórios e 4% após outros fatores de-sencadeantes, como punção venosa 11. Em crianças, estudosmostraram que pequenos traumas e estresse são os principa-is fatores desencadeantes 21,23,25. Não há evidências de queexistam fatores de risco que predisponham o desenvolvimen-to da SDCR, embora a imobilização possa atuar como fator delesão quando permanece por período prolongado.Alguns trabalhos estudaram fatores genéticos relacionadosa SDCR, que estariam envolvidos em uma predisposiçãopara o desenvolvimento da doença. Esta predisposiçãopode ter relação com o sistema de antígenos leucocitárioshumanos 26.Muitas pesquisas não mostraram alterações psicológicas oupsiquiátricas nos pacientes com SDCR. Observa-se que a in-cidência de doenças como distúrbios de personalidade oudepressão não difere entre os pacientes com dor crônica deoutra etiologia e os com SDCR 27,28. Contudo, nos casos pe-diátricos, há indícios de fatores psicológicos como fenôme-no desencadeante da síndrome 25.
FISIOPATOLOGIA
A fisiopatologia ainda é incerta e pouco progresso tem sidoobservado no entendimento dos processos que ocorrem nadoença. Há autores que postulam que o fenômeno inicial
seja o processo inflamatório desproporcional 19,29 desenca-deado após a lesão tecidual. Os componentes da respostainflamatória como o edema, calor, rubor, eritema e a perda dafunção se fazem presentes em seguida à lesão, resultantesda liberação de mediadores químicos no local 30. A sensibili-zação dos nociceptores no local da lesão se estabelece porcausa de mediadores liberados como bradicinina, leucotrie-nos, serotonina, histamina e prostaglandinas. Há evidências,também, de que radicais livres de oxigênio podem estar en-volvidos com a patogênese da SDCR 31, embora novos estu-dos tenham que ser realizados para que esta hipótese sejacomprovada e validada.Como a resposta inflamatória é local, a propagação dos sinaise sintomas para áreas distantes da lesão sugere o envolvi-mento do sistema nervoso central e periférico. Aceita-se quemudanças adaptativas ocorram no sistema nervoso centralapós a lesão, sejam elas agudas ou crônicas. Desta forma, alesão periférica de um nervo ou outro tecido, causa altera-ções neuroplásticas no cérebro 32, podendo ocorrer fenôme-no semelhante na medula espinhal 33.
MANIFESTAÇÕES CLÍNICAS
De acordo com os critérios do consenso da AIED, os sinais esintomas localizam-se preferencialmente na extremidadedo membro acometido, podendo, entretanto, estabelecer-seem outros locais do corpo que não um membro 34. Irradiam-se para o restante do mesmo membro, eventualmente aco-metendo o contralateral 5,34. A dor caracteriza-se por ser dotipo em queimação, embora, alguns pacientes e autores adescrevam como sendo profunda, lancinante e quente 35.Pode ser desencadeada por contato físico, mudanças detemperatura e estresse emocional 6.As alterações vasomotoras, quando presentes, manifes-tam-se como diferenças de temperatura e coloração de ummembro, em relação ao seu contralateral 36,37. Como desor-dens sudomotoras, a sudorese ou anidrose estão presentesna região acometida. O edema varia de intensidade, desdediscreto até intenso e as alterações tróficas da pele e fânerospodem ou não estar presentes.Os distúrbios de motricidade presentes na SDCR caracteri-zam-se por fraqueza, distonias, espasmos musculares, tre-mores, aumento do tono e dificuldade de movimentação domembro. A amputação fisiológica do membro é possívelocorrer, sem que haja alterações nervosas associadas 19.Dor miofascial se estabelece por desuso do membro aco-metido e/ou por excesso de uso do membro sadio contrala-teral. Em alguns pacientes a dor miofascial mostra-se maisimportante que a própria SDCR. Ocorre na região proximaldos membros, onde durante avaliação clínica podem seridentificados pontos dolorosos, denominados pontos degatilho.As alterações psiquiátricas são pouco freqüentes, masquando presentes, os distúrbios afetivos são os mais co-muns. Entre as mulheres, os quadros de depressão são maisfreqüentes, enquanto que entre os homens são os quadrosde ansiedade 38-40.
620 Revista Brasileira de AnestesiologiaVol. 52, Nº 5, Setembro - Outubro, 2002
SÍNDROME DOLOROSA COMPLEXA REGIONAL: EPIDEMIOLOGIA, FISIOPATOLOGIA,MANIFESTAÇÕES CLÍNICAS, TESTES DIAGNÓSTICOS E PROPOSTAS TERAPÊUTICAS

DIAGNÓSTICO LABORATORIAL
Embora o diagnóstico seja clínico, podem ser solicitadosexames subsidiários que auxiliam tanto na confirmaçãocomo na sua exclusão. Exame radiológico simples podeidentificar diminuição da calcificação óssea, embora essa al-teração não seja específica para SDCR 41, pois a desminera-lização óssea pode ser causada pelo desuso do membro. Aeletroneuromiografia indica lesão de nervo nos caso deSDCR Tipo II; porém, não se mostra útil no controle evolutivoda doença.Outros exames laboratoriais de imagem podem ser realiza-dos para que o componente autonômico possa ser identifica-do. A termografia determina a diferença de temperatura en-tre o membro afetado e o normal 42 e a pletismografia eviden-cia as diferenças de perfusão entre os membros.Provas terapêuticas são úteis para auxiliar no diagnósticopela resposta a uma determinada substância. Diversos fár-macos são utilizados, por diferentes vias de administração,como a guanetidina, a fentolamina e a lidocaína entre outros,por variadas técnicas tais como, infusões venosas simples ebloqueios regionais. Estes testes são utilizados para se com-provar se o Sistema Nervoso Simpático está envolvido nagênese da dor e nos sinais e sintomas da SDCR; portanto,auxiliam na elaboração do diagnóstico como também orien-tam a terapêutica adequada e efetiva.Dessa forma são indicados: a) bloqueio simpático com anes-tésico local, como bloqueio do gânglio estrelado para mem-bro superior ou bloqueio da cadeia simpático lombar para-vertebral para membro inferior. A efetividade do bloqueioidentifica-se com a diminuição da dor e o aumento da tempe-ratura do membro em relação ao contralateral. É possível ob-ter-se resultado falso positivo explicado pela não observa-ção cuidadosa dos sinais inerentes ao bloqueio simpático epelo bloqueio dos aferentes nociceptivos e o resultado nega-tivo pela ausência de DSM ou por erro técnico na realizaçãodo bloqueio; b) teste da guanetidina, através de bloqueio ve-noso regional, pela resposta de depleção das reservas denorepinefrina das fibras simpáticas pós-ganglionares. É po-sitivo se após a injeção ocorrer dor, sensação de calor oupressão na mesma região onde é referida a dor da SDCR ealívio da dor após desgarroteamento do membro; c) teste dafentolamina, antagonista �-adrenérgico, realizado atravésde infusão venosa simples e positivo se ocorrer diminuiçãoda dor durante a infusão do medicamento.Outros testes mais específicos para avaliação da DSM naSDCR podem ser aplicados, embora sejam mais complexose onerosos, como o Quantitative Sudomotor Axon Reflex
Test (QSART), que identifica a resposta simpática da peleapós a aplicação de norepinefrina por iontoforese. É positivoquando há uma diminuição da latência na produção de calore acredita-se que haja aumento do reflexo somatossimpáti-co devido a uma redução do limiar de ativação das fibras sim-páticas 43. Resting Sweat Output (RSO), teste que mede a di-ferença de temperatura dos membros, em regiões padroni-zados, sem a aplicação de nenhuma substância 43. Thermo-
regulatory Sweat Test (TST) é um teste que avalia a via ter-
morreguladora, sendo complementar ao QSART, pois podefazer a diferenciação entre lesões pré e pós-ganglionares,sendo mais complexo que os anteriores. Este teste avalia aresposta global e segmentar do corpo, através da temperatu-ra e da sudorese frente a alterações de temperatura de umasala especialmente preparada para o exame. De acordo comas áreas de anidrose, hipoidrose ou hiperidrose podem serdiferenciadas as lesões 43.
TRATAMENTO
A SDCR por suas características peculiares mostra-se detratamento difícil e pouco eficaz. Embora muitos trabalhostenham sido realizados com propostas terapêuticas 44, pou-cos são confiáveis para que possam ser aplicados na clínica.De qualquer forma, o mais importante para que haja boa res-posta é o tratamento ser instituído em fase precoce da doen-ça 45,46, com o objetivo primário de aliviar a dor.Por ser uma doença complexa, não existe um protocolo pa-drão para o tratamento da SDCR, devido às inúmeras pro-postas terapêuticas e às suas variadas respostas. Torna-senecessário, em muitos casos, realizar associações de técni-cas para um bom resultado.Acredita-se, atualmente, que o acompanhamento do pacien-te deva ser multidisciplinar e multiprofissional devido aos vá-rios componentes envolvidos na doença. Logo, a avaliaçãopsicológica e tratamento de seus distúrbios, quando presen-tes, garantem uma melhor adesão do paciente ao tratamentoinstituído. A fisioterapia, antes utilizada em fases mais tar-dias, tem seu espaço e importância aumentados na atualida-de. Aeletroestimulação transcutânea (TENS) está sendo in-dicada com mais freqüência pelo seu efeito analgésico 47 etécnicas de desensibilização estão sendo propostas aos pa-cientes com alodínia 48. Contudo, os procedimentos fisiote-rápicos para a reabilitação do membro, quanto à movimenta-ção, ainda são os mais requisitados.As terapêuticas farmacológicas são muitas, com variadastécnicas de aplicação. Classicamente, o bloqueio simpáticoé o mais utilizado 49,50; todavia, alguns estudos contestam aeficácia destas técnicas 51-53, especialmente se não for con-firmado o envolvimento do sistema nervoso autonômico.Entre as várias técnicas de bloqueio simpático, citam-se:bloqueio ganglionar simpático, infusão venosa de fentolami-na ou lidocaína, bloqueio venoso regional com guanetidina,clonidina, dexmedetomidina, reserpina, bretílio ou corticói-des 54-56.Aguanetidina é o fármaco mais utilizado nos bloqueios veno-sos regionais. Ela atua depletando as reservas de norepine-frina e bloqueando sua recaptação, além da atividade antico-linérgica e serotoninérgica 57. Contudo, são vários os traba-lhos que contestam sua efetividade no tratamento da SDCRe/ou na DSM 51-53,58. O bretílio, ainda não comercializado noBrasil, possui atividade semelhante à da guanetidina, deple-tando as reservas de noradrenalina. A reserpina atua domesmo modo; entretanto, sem boa resposta 59,60. A fentola-mina é um fármaco com ação antagonista á1-adrenérgica,serotoninérgica, histaminérgica, colinérgica e com proprie-
Revista Brasileira de Anestesiologia 621Vol. 52, Nº 5, Setembro - Outubro, 2002
CORDON E LEMONICA

dades de anestésico local 61,62, ainda sem estudos confiáveissobre sua efetividade 63
. Aclonidina, droga agonista á2-adre-nérgica, possui boa resposta nos casos de SDCR refratáriasao tratamento 64,65, embora poucos trabalhos mostrem suaeficácia nos bloqueios regionais venosos 66. Há relatos deque a clonidina de uso tópico diminua a alodínia 67,68. A dex-medetomidina, novo medicamento �2-agonista, lançado re-centemente para uso em anestesia e em Unidade de TerapiaIntensiva, mais potente que a clonidina, traz novas perspec-tivas para o tratamento da dor neuropática nos mesmos mol-des da clonidina, embora ainda haja poucos estudos sobre oseu uso em anestesia e nenhum até o momento para o trata-mento da SDCR.Os pacientes não apresentam boa resposta ao uso de anti-depressivo tricíclico, beneficiando-se apenas do seu efeitosobre a qualidade do sono.A adenosina tem sido recomendada no tratamento de dorneuropática. Estudos em cobaias e em humanos mostrarambons resultados no controle deste tipo de dor, apesar de ain-da não existirem trabalhos encobertos expressivos 69. O usode calcitonina não mostrou melhora tanto por via intradérmi-ca como pela via intranasal 70.A infusão venosa com anestésico local, como a lidocaína,produz melhora da sintomatologia nos casos de SDCR, mashá controvérsias sobre esta resposta 71-73. O uso de mexileti-na por via oral é pouco freqüente havendo, contudo, relatosde efetividade no tratamento de dor neuropática. Seu uso é li-mitado pelos efeitos colaterais que os pacientes apresen-tam, sendo importante lembrar ser possível que os efeitoscolaterais ocorram em concentrações plasmáticas menoresque as necessárias para analgesia da dor neuropática 74.Os opióides têm seus defensores 35,76, os quais atribuembons resultados a seu uso, e seus críticos 75 que negam suaeficácia no tratamento de SDCR.O anticonvulsivante gabapentina é um medicamento recen-te sem pesquisas confiáveis, embora diversos autores pre-conizem seu uso. Alguns trabalhos já mostraram sua boaatuação sobre a SDCR 7.O bloqueio ganglionar simpático promove alívio da sintoma-tologia, contudo, sem mecanismo de ação claro. Acredita-seque atuaria sobre as fibras de inervação somática e não sim-pática 79.Os procedimentos cirúrgicos como a simpatectomia químicaou cirúrgica têm respostas variadas, sendo indicados na-queles pacientes que respondem bem a outros bloqueiosnão ablativos, embora a reincidência da dor ocorra em mui-tos casos 78.
CONCLUSÕES
ASDCR continua sendo uma doença sem boas perspectivasde tratamento pelo seu insuficiente entendimento. Diversassão as linhas de pesquisa nas quais todos chegam a resulta-dos nem sempre esperados e, quando esperados, não sãocompatíveis com a realidade. Continuam, pois, os tratamen-tos empíricos e relatos de casos com as mais diversas pro-
postas de terapêutica, em que se objetiva de alguma formatratá-la ou, pelo menos, diminuí-la.ASDCR traz perspectivas de que novos trabalhos sejam rea-lizados para que seu processo fisiopatológico seja entendi-do e tratamentos mais efetivos e seguros sejam instituídos.
Complex Regional Pain Syndrome:
Epidemiology, Pathophysiology, Clinical
Manifestations, Diagnostic Tests and
Therapeutic Proposals
Francisco Carlos Obata Cordon, M.D., Lino Lemonica, TSA,M.D.
INTRODUCTION
Complex Regional Pain Syndrome (CRPS) brings major dis-comfort both for patients, due to disabling pain, and to healthprofessionals who have limited resources since CRPSpathophysiology is still not totally explained and who seldomachieve positive treatment outcomes.This study aimed at reviewing the literature and updating in-formation to better understand this severe painful syndrome.
CONCEPT AND HISTORY
Until recently, CRPS was also called causalgia. This termwas used for the first time by Mitchell in 1864 1, but the first todescribe causalgia was Paget in 1862 2.Wolff, in 1877, has described for the first time a chronic pain-ful entity with no neurological cause, followed by vasomotorchanges 3. Several terminologies were used to define it, suchas minor causalgia, post-trauma vasomotor disorder,Sudeck’s atrophy and shoulder-hand syndrome. In 1953,Bonica has suggested that all painful pathologies associatedto vasomotor phenomena, and usually preceded by atrauma, should be called “reflex sympathetic dystrophy” 4, inwhich the following characteristics should be present: pain,skin vasomotor changes, loss of limb function and trophicchanges in different stages.Controversies, however, on the diagnosis continued to raisequestions. In 1993, the International Association for Study ofPain (IASP) prepared a consensus, published in 1994, wherediagnostic criteria for such disease were defined 5. The name“Complex Regional Pain Syndrome” (CRPS) was adopted asa single term to define regional pain associated to sensorychanges as a consequence of a noxious event. Pain, aftertrauma, is the major symptom and may be associated to ab-normal skin color, changes in limb temperature, abnormalsudomotor activity or edema. Motor changes, such as shiver-ing, dystonias or muscle weakness may also be present. Twotypes of CRPS were defined by the consensus: type I, previ-ously called “reflex sympathetic dystrophy”, and type II, pre-
622 Revista Brasileira de AnestesiologiaVol. 52, Nº 5, Setembro - Outubro, 2002
COMPLEX REGIONAL PAIN SYNDROME: EPIDEMIOLOGY, PATHOPHYSIOLOGY,CLINICAL MANIFESTATIONS, DIAGNOSTIC TESTS AND THERAPEUTIC PROPOSALS

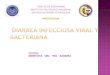
viously called “causalgia”. CRPS type I differs from type II forthe presence of a real nervous injury where pain is not limitedto the innervation territory of the injured nerve. Although theconsensus being prepared for its diagnosis, several ques-tions were raised about how and how many criteria should beconsidered to confirm it. It has also been observed that otherwell-defined pathologies, such as diabetic neuropathy, couldmeet such criteria and be mistreated 6. After analysis and re-view, the following diagnostic criteria were proposed: (a)there is no need for an initial injury; (b) signs and symptomsshould be divided in separate groups; (c) patients may pres-ent at least two of the following symptoms: sensory(hyperesthesia), vasomotor (temperature or color changes,or both); sudomotor/hydric balance (edema, sweating orboth) and motor (decreased mobility, weakness, shivering,functional limb amputation), or all of them; and (d) patientsshould present at least two of the following signs: vasomotor,sudomotor/hydric balance and motor. So, as from those newcriteria, it is believed that patients’ evaluation, diagnosis andfollow-up will be better performed.The term “Sympathetically Maintained Pain” (SMP), al-though incorrect, has been used as a synonym for CRPS.This term defines pain sustained by sympathetic afferents orby circulating catecholamines 7 and there are some hypothe-ses to explain such phenomenon. The most popular is the in-creased number of �-adrenergic receptors in peripheral tis-sues, sensitive to norepinephrine of sympathetic neuron ter-minals which acting on receptors cause pain 8. Peripheralnerve injury allows for plastic changes both of the primary af-ferent and of post-ganglial sympathetic neurons, dependingon the injury being total or partial. This neuronal plasticity ischaracterized by degenerative and regenerative changesand reorganization, which culminate with biochemical bind-ings between primary afferent and post-ganglionary sympa-thetic neurons, in addition to collateral bindings of non-in-jured neurons to the dorsal root ganglion (Figure 1). Thesebindings are responsible for primary afferent activation bythe sympathetic system, where the likely mediator isnorepinephrine, although not ruling out other mediators.There is also the expression or increase in �2-adrenergic re-ceptors in primary afferents neurons 9. There are also studiesbased on the denervation hypothesis, where sympathetic af-ferent fibers injury increases nerve growth factor expressionor other neurotropic factors, ultimately leading to an in-creased pain transmission by different mechanisms 10-14.Studies confirming such hypothesis have shown that in hu-mans and guinea pigs, there is a low concentration ofnorepinephrine or its metabolite in the plasma of the affectedlimb as compared to the healthy one 15-17. This hypothesisalso explains the vasoconstriction of the affected limb basedon the inc reased vasocons t r i c to r response tonorepinephrine, by the increased response of vessels mus-cle cells to denervation 16.SMP should be understood as a pain mechanism and CRPSas a clinical diagnosis. It is important to remind that, althoughin some cases there is pain relief after sympathetic block,SMP is not always present in CRPS. There is no correlation
between SMP and dysautonomic signs and symptoms. Intheory, patients may have SMP components and non sympa-thetic-dependent pain 17,18.
Figure 1 - Influence of Sympathetic Activity on Primary AfferentsA. Complete nerve injury: sympathetic interactions at neuromaand dorsal root ganglion site, being mediated by norepinephri-ne released by post-ganglial sympathetic fibers and primary af-ferent a-adrenergic receptors. B. Partial injury: injury isfollowed by a decrease in local sympathetic innervation with aconsequent hyperactivity of non-injured a-adrenergic recep-tors of nociceptors type C membrane. C. After inflammatory tis-sue reaction: without injuries, but with sensitivity increased bynorepinephrine, which promotes prostaglandins release bysympathetic terminations, sensitizing primary afferents. In ad-dition to prostaglandins, there is also the action of bradykininand nerve growth factors (Baron, R modified) 9
EPIDEMIOLOGY
CRPS epidemiology is not well defined. Astudy, however, byVeldman et al. 19, has shown a mean age of 41 years with a 3:1predominance of females. Allen et al. 20 have confirmed themean age of 41.8 years and a 2, 3:1 predominance of fe-males. In children, there is a 3:1 predominance of femalesand symptoms typically start at 9 to 15 years of age 21-23.Frequently a single limb is affected, in equal proportion of up-per and lower limbs. Few studies have shown the prevalenceof upper or lower limbs, but there is a higher incidence of rightlimbs, probably because there are more right handed as com-pared to left handed people and the bilateral involvementranges from 11% to 16% of cases 20,24. In children, lower limbsare most frequently affected 21-23.
Revista Brasileira de Anestesiologia 623Vol. 52, Nº 5, Setembro - Outubro, 2002
CORDON AND LEMONICA
A
B
NA
NA
NA
PG
NA
NA
NA
Afferent
Afferent
Afferent
Post-ganglial
Post-ganglial
Post-ganglial
BradykininNGF
NociceptorSensitization
Pre-ganglial
Pre-ganglial
Pre-ganglial
CompleteNerve Injury
PartialNerve Injury
�
�
�
��
C

Approximately 65% of cases are related to trauma, in generalto fractures, 19% to postoperative period, 2% after inflamma-tory processes and 4% after other triggering factors, such asvenous puncture 11. In children, studies have shown that mi-nor traumas and stress are major triggering factors 21,23,25.There are no evidences of risk factors predisposing to CRPS,although immobilization may act as an injury factor whenmaintained for a long period.Some papers have studied genetic factors related to CRPS,which would be responsible for a predisposition for the dis-ease. This predisposition could be related to the humanleukocytic antigen system 26.Several studies have not shown psychological or psychiatricchanges in CRPS patients. It has been observed that the inci-dence of diseases, such as personality changes or depres-sion is not different in patients with chronic pain of differentetiologies and CRPS 27,28. In children, however, there are evi-dences of psychological factors as triggering phenomena forthe syndrome 25.
PATHOPHYSIOLOGY
Pathophysiology is still uncertain and little progress is beingmade toward understanding the disease. Some authors be-lieve that the initial phenomenon is a disproportional inflam-matory process 19,29 triggered after tissue injury. Inflammatoryresponse components, such as edema, heat, flare, erythemaand loss of function are present following the injury and resultfrom local chemical mediators release 30. Released media-tors, suchasbradykinin, leucotriens,serotonin,histamineandprostaglandins sensitize nociceptors at the injury site. Thereare also evidences that oxygen free radicals could be involvedin CRPS pathogenesis 31, although further studies beingneeded to prove and validate such hypothesis.Since there is a local inflammatory response, signs and symp-toms spread to areas far from the injury suggests the involve-ment of central and peripheral nervous system. It is acceptedthat acute or chronic adaptation changes occur in the centralnervous system after the injury. So, the peripheral injury of anerve or tissue causes neuroplastic changes to the brain 32,and a similar phenomenon may occur in the spinal cord 33.
CLINICAL MANIFESTATIONS
According to the IASP consensus, signs and symptoms arepreferably located in the extremity of the injured limb, but theymay also appear in body sites different from limbs 34. They ir-radiate through the same limb, eventually affecting thecontralateral limb 5,34. Pain is typically of the burning-type, al-though some patients and authors describe it as being deep,severe and hot 35. Pain may be triggered by physical contact,changes in temperature and emotional stress 6. Vasomotorchanges, when present, are manifested as differences intemperature and color of one limb, as compared to thecontralateral limb 36,37. Sweating or anhidrosis are presentedin the affected region as sudomotor disorders. Edema differsin intensity, from discrete to severe and skin and phaners
trophic changes may or not be present. Weakness,dystonias, muscle spasms, shivering, increased tone anddifficulty to move the limb characterize CRPS mobility disor-ders. Physiological amputation of the limb is a possibility,however without associated nervous changes 19.The non-use of the affected limb and/or excess use of thehealthy contralateral limb may cause myofascial pain.Myofascial pain, in some patients, is more severe thanCRPS itself. It affects limbs’ proximal region where painfulpoints, called triggering points, may be identified duringclinical evaluation.Psychiatric disorders are less frequent, but when present, af-fective disorders are the most common symptoms. Amongwomen, depression is the most frequent, while in men anxi-ety is predominant 38-40.
LABORATORIAL DIAGNOSIS
The diagnosis is clinical, but subsidiary exams may be asked tohelp both confirmation and exclusion. A simple radiologicalexam may identify a decrease in bone calcification, althoughthis change is not CRPS-specific 41, because bone demineral-ization may be induced by the non-use of the limb.Electroneuromyography identifies nerve injury in CRPS type II;however it isnotuseful tocontrol theevolutionof thedisease.Other imaging tests may be performed to identify autonomiccomponents. Thermography determines temperature differ-ences between the affected and the normal limb 42, andplethysmographyshowsperfusiondifferencesbetween limbs.Therapeutic tests are useful to help the diagnosis by re-sponses to certain substances. Several drugs are used bydifferent routes, such as guanethidine, phentolamine andlidocaine, among others, through several techniques, suchas simple intravenous infusions and regional blocks. Suchtests are used to confirm whether the sympathetic nervoussystem is involved in the genesis of pain and in CRPS signsand symptoms; so, they not only cooperate with the diagno-sis, but also orient an adequate and effective therapy.Indications are: a) sympathetic blockade with local anesthet-ics, such as stellate ganglion for upper limbs or paravertebrallumbar sympathetic chain for lower limbs. Blockade effec-tiveness is identified by decreased pain and increased tem-perature of the limb, as compared to the healthy limb. A falsepositive result is possible and explained by the careless ob-servation of inherent sympathetic block signs and by noci-ceptive afferents blockade; and a negative result would beexplained by the absence of SMPor by technical blockade er-ror; b) guanethidine test, by intravenous regional blockade,by the depletion response of post-ganglial sympathetic fibernorepinephrine reserves. It is positive when there is pain af-ter injection, heat or pressure sensation in the same regionwhere CRPS pain is referred, and pain relief after tourniquetdeflation; c) phentolamine (�-adrenergic antagonist) test,performed through a simple intravenous infusion and posi-tive if pain decreases during drug infusion.Other more specific tests to evaluate SMP in CRPS may beapplied although more complex and expensive, such as
624 Revista Brasileira de AnestesiologiaVol. 52, Nº 5, Setembro - Outubro, 2002
COMPLEX REGIONAL PAIN SYNDROME: EPIDEMIOLOGY, PATHOPHYSIOLOGY,CLINICAL MANIFESTATIONS, DIAGNOSTIC TESTS AND THERAPEUTIC PROPOSALS

Quantitative Sudomotor Axon Reflex Test (QSART), whichidentifies sympathetic skin response after norepinephrineapplication by iontophoresis. It is positive when there is a de-creased heat production onset and it is believed that there isan increased somatosympathetic reflex due to a decrease insympathetic fibers activation threshold 43. Resting SweatOutput (RSO) test, which measures limbs temperature differ-ences in standardized regions without applying any sub-stance 43. Thermoregulatory Sweat Test (TST), which evalu-ates the thermoregulating pathway and is a complement toQSART because it is able to differ between pre andpost-ganglionary injuries, being more complex than the pre-viously mentioned tests. This test evaluates global and seg-mental body response through temperature and sweating af-ter temperature changes in a room specially prepared for thetest. Injuries may be differentiated according to anhidrosis,hypohidrosis or hyperhidrosis areas 43.
TREATMENT
Due to its unique characteristics, CRPS treatment is difficultand not very effective. Although many studies with therapeu-tic proposals 44, few are reliable enough to be applied in theclinical practice. Anyway, the most important for a good re-sponse is to treat the early stages of the disease 45,46, with theprimary objective of relieving pain.For being a complex disease, there is no standard protocolfor the treatment of CRPS, due to several therapeutic propos-als and their different responses. Very often, technique asso-ciations are needed for a good result.Currently it is believed that patients’ follow-up should bemultidisciplinary and multiprofessional due to the differentcomponents of the disease. So, psychological evaluation andtreatment of its disorders, when present, assure a better com-pliance of the patient to the treatment. Physical therapy, ini-tially used in later stages, is currently becoming more popularand important. Transcutaneous electric nerve stimulation(TENS) is being more frequently indicated for analgesia 47 anddesensitization techniques are being proposed for allodyniapatients 48. However, physical therapy to recover limb’smovements is still the most popular.There are several pharmacological therapies with differentapplication techniques. Classically, sympathetic blockade isthe most popular 49,50; however, some studies question the ef-ficacy of such techniques 51-53, especially if autonomic ner-vous system involvement is not confirmed.There are different sympathetic block techniques, amongthem: sympathetic ganglionary blockade, intravenousphentolamine or lidocaine infusion, intravenous regionalblock with guanethidine, clonidine, dexmedetomidine, reser-pine, bretylium or steroids 54-56.Guanetidine is the most used drug for intravenous regionalblocks. It acts by depleting norepinephrine reserves andblocking re-uptake, in addition to an anticholinergic andserotoninergic activity 57. There are, however, several studiesquestioning its efficacy in treating CRPS and/or SMP 51-53,58.Still unavailable in Brazil, bretylium acts similarly to
guanethidine, depleting norepinephrine reserves. Reser-pine has a similar action, however without a good response59,60. Phentolamine is an �1-adrenergic antagonist,serotoninergic, histaminergic and cholinergic drug, with lo-cal anesthetic properties 61,62, still lacking reliable studies onits effectiveness 63. Clonidine, an �2-adrenergic agonist, hasa good response in CRPS refractory to treatment 64,65, al-though few studies having shown its efficacy in intravenousregional blocks 66. There are reports on topic clonidine de-creasing allodynia 67.68. Dexmedetomidine, a new �2-agonistdrug recently introduced for anesthesiology and intensivecare units and more potent than clonidine, opens new per-spectives for neuropathic pain treatment, although there arestill few studies about its use in anesthesiology and no studyso far for treating CRPS.Patients do not show a good response to tricyclic antidepres-sant drugs and the only benefit is on sleep quality.Adenosine has been recommended for treating neuropathicpain. Human and guinea-pig studies have shown good re-sults in controlling this type of pain, although there are no ex-pressive blind studies 69. Intradermal or intranasal calcitoninhas not improved symptoms 70.Intravenous local anesthetic infusion, such as lidocaine, im-proves CRPS symptoms, but this response is controversial71-73. Oral mexyletine is less frequent but there are reportson its effectiveness in treating neuropathic pain. Its use islimited by side-effects and it is important to remind thatside-effects may occur in lower plasma concentrations thanthose needed for neuropathic pain analgesia 74.Opioids have advocates 35,76 who attribute good results tothem, and criticals 75, who deny their efficacy in treatingCPRS.The anticonvulsivant gabapentin is a recent drug without re-liable investigations, although being preconized by severalauthors. Some studies have already shown its positive ef-fects on CPRS 7.The sympathetic ganglial block promotes symptoms relief,however without a clear action mechanism. It is believed that itwouldactonsomaticandnotsympathetic inervation fibers 79.Surgical procedures, such as chemical sympathectomy orsurgery have different responses and are indicated for thosepatients with a good response to other non-ablative block-ades, although there is pain recurrence in many cases 78.
CONCLUSIONS
CRPS is still a disease without good treatment perspectivesbecause it is still not well understood. There are severalstudies where results are not always what was to be expectedand, when expected, are not compatible with reality. We re-main, then, with empirical treatments and case reports withthe most different therapeutic proposals, where the objectiveis to treat or, at least, to relieve CRPS.CRPS still needs further studies for the understanding of itspathophysiology so that more effective and safer treatmentsmay be instituted.
Revista Brasileira de Anestesiologia 625Vol. 52, Nº 5, Setembro - Outubro, 2002
CORDON AND LEMONICA

REFERÊNCIAS - REFERENCES
01. Mitchell SW - On the Diseases of Nerves, Resulting from In-juries, em: Flint A - Contribution Relating to the Causation andPrevention of Disease, and to Camp Disease. New York, USASanitary Commission Memoirs, 1867.
02. Paget J - Clinical lecture on some cases of local paralysis. MedTimes,1864;331-332.
03. Wolff J - Ueber einen Fall von Ellenbogensgelenks-Reaktion.Arch Chir, 1877;20:771.
04. Bonica JJ - The Management of Pain. Philadelphia: Lea &Febiger, 1953.
05. Merskey H, Bogduk N - Classification of Chronic Pain. Seattle:IASP Press, 1994.
06. Hiraden R N, Bruehl S et al - Complex regional pain syndrome:are the IASP diagnostic criteria valid and sufficient comprehen-sive? Pain, 1999;83:211-219.
07. Stanton-Hicks M, Janig W, Hassenbusch S et al - Reflex sympa-thetic dystrophy: changing concepts and taxonomy. Pain,1995;63:127-133.
08. Ali Z, Raja SN, Wesselmann U et al - Intradermal injection ofnorepinephrine evokes pain in patients with sympatheticallymaintained pain. Pain, 2000;88:161-168.
09. Baron, R - The influence of sympathetic nerve activity and cate-cholamines on primary afferent neurons. IASP Newsl, 1998;3-8.
10. Ro LS, Chen ST, Tang LM et al - Effects of NGF and anti-NGF onneuropathic pain in rats following chronic constriction injury ofthe sciatic nerve, Pain, 1999;79:265-274.
11. Owolabi JB, Rikalla G, Tehim A et al - Characterization ofantiallodynic actions of ALE-0540, a novel nerve growth factorreceptor antagonist, in the rat. J Pharmacol Exp Ther, 1999;289:1271-1276.
12. Mannion RJ, Costigan M, Decosterd I et al - Neurotrophins: pe-ripherally and centrally acting modulators of tactile stimulus-in-duced inflammatory pain hypersensitivity. Proc Natl Acad SciUSA, 1999;96:9385-9390.
13. Giovengo SL, Russell IJ, Larson AA - Increased concentrationsof nerve growth factor in cerebrospinal fluid of patients withfribromyalgia. J Rheumatol, 1999;26:1564-1569.
14. Nauta HJ, Wehman JC, Koliatsos VE et al - Intraventricular infu-sion of nerve growth factor as the cause of sympathetic fibersprouting in sensory ganglia. J Neurosurg, 1999;91:447-453.
15. Drummond PD, Finc PM, Smythe GA - Reflex sympathetic dys-trophy: the significance of differing plasma catecholamine con-centrations in affected and unaffected limbs. Brain, 1991;114:2025-2036.
16. Harden RN, Duc TA, Willians TR et al - Norepinephrine and epi-nephrine levels in affected versus unaffected limbs in sympa-thetically maintained pain. Clin J Pain, 1994;10:324-330.
17. Wasner G, Heckmann K, Maier C et al - Vascular abnormalities inacute reflex sympathetic dystrophy (CRPS I): complete inhibi-tion of sympathetic nerve activity with recovery. Arch Neurol,1999;56:613-620.
18. Loh L, Nathan PW - Painful peripheral states and sympatheticblocks. J Neurosurg Psychiatry 1978;41:664-671.
19. Veldman PH, Reynen HM, Artz IE et al - Signs and symptoms ofreflex sympathetic dystrophy: prospective study of 829 patients.Lancet, 1993;342:1012-1016.
20. Allen G, Galer BS, Schwartz L - Epidemiological review of 134patients with complex regional pain syndrome assessed in achronic pain clinic. Pain, 1999;80:539-540.
21. Berstein BH, Singsen BH, Kent JT et al - Reflex neuromusculardystrophy in childhood. J Pediatr, 1978;93:211-215.
22. Stanton RP, Malcolm JR, Wesdck KA et al - Reflex sympatheticdystrophy in children: an orthopedic perspective. Orthopedics1993;16:773-779.
23. Ashwal S, Tomasi L, Neumann M et al - Reflex sympathetic dys-trophy in children. Pediatr Neurol 1988;4:38-42.
24. Allen G, Galler BS, Veldman PJM et al - Multiple reflex sympa-thetic dystrophy. Which patients are at risk for developing a re-currence of reflex sympathetic dystrophy in the same or anotherlimb. Pain, 1996;64:463-466.
25. Sherry DD, Weisman R - Psychological aspects of childhood re-flex neuromuscular dystrophy. Pediatr, 1988;81:572-578.
26. Kemler MA, Vusse AC, Berg-Loonen EM et al - HLA-DQ1 asso-ciated with reflex sympathetic dystrophy. Neurology, 1999;53:1350-1351.
27. Monti DA, Herring CL, Schwartz RJ et al - Personality assess-ment of patients with complex regional pain syndrome Type I.Clin J Pain, 1998;14:295-302.
28. Haddox JD, Abran SE, Hopwood MH - Comparison ofpsychometric data in RSD and radiculopathy. Reg Anesth,1988;13:27.
29. Sudeck P - Die sogennante knochenatrophine als entzundung-svorgang. Chirurg,1942;15:449-457.
30. Levine JD, Fields HL, Basbaum AL - Peptides and the primary af-ferent nociceptor. J Neurosci, 1993;13:2273-2286.
31. Zollinger PE, Tuinebreijer WE, Kreis RW et al - Effects of vitaminC on frequency of reflex sympathetic dystrophy in wrist frac-tures: a randomized trial. Lancet, 1999;354:2025-2028.
32. Coderre TJ, Katz J, Accarino AL et al - Contribution of centralneuroplasticity to pathological pain: review of clinical and exper-imental evidences. Pain, 1993;52:259-285.
33. Leriche R - La chirurgie de la doloure. Parsi: Masson, 1939.34. Payne R - Reflex Sympathetic Dystrophy Syndrome: Diagnosis
and Treatment. Pain Syndromes in Neurology. London:Butterworks, 1990;107-129.
35. Gales BS, Jensen M - Development and preliminary validation ofa pain measure specific to neuropathic pain: the neuropathicpain scale. Neurology, 1997;48:332-339.
36. Baron R, Maier C - Reflex Sympathetic dystrophy: skin bloodflow, sympathetic vasoconstrictor reflex and pain before and af-ter surgical sympathectomy. Pain, 1996;67:317-326.
37. Kemler MA, Schouten HJA, Gracely RH - Diagnosing sensoryabnormalities with either normal values or values fromcontralateral skin: comparison of two approaches in complex re-gional pain syndromes. Anesthesiology, 2000;93:718-727.
38. Bruehl S, Carlson CR - Predisposing psychological factors in thedevelopment of reflex sympathetic dystrophy. Clin J Pain,1992;287-299.
39. Geertzen JHB, deBrujin H, deBrujin-Kofman AT et al - Reflexsympathetic dystrophy: early treatment and psychological as-pects. Arch Phys Rehabil, 1994;75:442-446.
40. Bruehl S, Husfeldt B, Lubenow TR et al - Psychological differ-ences between reflex sympathetic dystrophy and non-RSDchronic pain patients. Pain, 1996;67:107-114.
41. Kozin F, Soin JS, Ryan LM et al - Bone scintilography. I. The re-flex sympathetic dystrophy syndrome. Radiology, 1981;138:437-443.
42. Bruehl S, Lubenow TR, Nath H et al - Validation of thermographin the diagnosis of reflex sympathetic dystrophy. Clin J Pain,1994;10:146-155.
43. Sandroni P - Testing the autonomic nervous system. IASPNewsl, 1998;3-6.
44. Wilson PR - Post-traumatic upper extremity reflex sympatheticdystrophy. Hand Clin, 1997;17:367-372.
45. Lopez RF - Reflex sympathetic dystrophy: timely diagnosis andtreatment can prevent severe contractors. Postgrad Med,1997;101:185-190.
46. Doury PCC - Algodystrophy: a spectrum of disease, historicalperspectives, criteria of diagnosis, and principles of treatment.Hand Clin, 1997;13:327-337.
626 Revista Brasileira de AnestesiologiaVol. 52, Nº 5, Setembro - Outubro, 2002
COMPLEX REGIONAL PAIN SYNDROME: EPIDEMIOLOGY, PATHOPHYSIOLOGY,CLINICAL MANIFESTATIONS, DIAGNOSTIC TESTS AND THERAPEUTIC PROPOSALS

47. Cooney WP - Somatic versus sympathetic mediated chroniclimb pain: experience and treatment options. Hand Clin, 1997;13:355-361.
48. Hardy MA, Hardy SG - Reflex sympathetic dystrophy: the clini-cian’s perspective. J Hand Ther, 1997;10:137-150.
49. Bonica JJ - Sympathetic nerve blocks for pain diagnosis andtherapy. 1st Ed, New York: Breon Laboratories, 1980;1:28-39=8.
50. Ramamurthy S, Hoffman JRN - Intravenous regionalguanethidine in the treatment of reflex sympathetic dystro-phy/causalgia: a randomized, double-blind study. Anesth Analg,1995;81:718-723.
51. Valentin N - Reflex sympathetic dystrophy treated withguanethidine. Time for a change of name and strategy. ActaAnaesthesiol Scand, 1996;40:1171-1172.
52. Kaplan R, Claudio M, Kepes E et al - Intravenous guanethidine inpatients with reflex sympathetic dystrophy. Acta AnaesthesiolScand, 1996;40:1216-1222.
53. McKain CW, Urban BJ, Goldner JL - The effects of intravenousregional guanethidine and reserpine: a controlled study. J BoneJoint Surg Am, 1983;65:808-811.
54. Hord Ah, Rooks MD, Stephensen BO et al - Intravenous regionalbretylium and lidocaine for treatment of reflex sympathetic dys-trophy: a randomized, double-blind study. Anesth Analg, 1992;74:818-821.
55. Tountas AA, Noguchi A - Treatment of post-traumatic reflex sym-pathetic dystrophy (RSDS) with intravenous blocks of o mixtureof corticosteroid and lidocaine: a retrospective review of 17 con-secutive cases. J Orthop Trauma, 1991;4:412-419.
56. Furst CL - The biochemistry of guanethidine. Adv Drug Res,1967;4:133-136.
57. Kingery WS - Acritical review of controlled clinical trial for periph-eral neuropathic pain and complex regional pain syndrome.Pain, 1997;73:123-139.
58. Rocco AG, Kaul AF - A comparison of regional intravenousguanethidine and reserpine in reflex sympathetic dystrophy: acontrolled, randomized, double-blind, and crossover study. ClinJ Pain, 1989;5:205-209.
59. Blanchard J, Ramamurthy S, Walsh N et al - Intravenous re-gional sympatholys is: a double-bl ind compar ison ofguanethidine, reserpine and normal saline. J Pain SymptomManage, 1990;5:357-361.
60. Galer BS - Preliminary report: peak pain relief is delayed and du-ration of relief is extended following intravenous phentolamineinfusion. Reg Anaesth, 1995;20:444-447.
61. Ramirez JM, French AS - Phentolamine selectively affects thefast sodium channel component of sensory adaptation in an in-sect mechanoreceptor. J Neurobiol, 1990;893-899.
62. Raja AN, Treede RD, Davis KD et al - Systemic alpha-adrenergicblockade with phentolamine: a diagnostic test for sympatheti-cally maintained pain. Anesthesiology, 1991;74:691-698.
63. Raja SN, Turquist JL, Meleka SM et al - Monitoring adequacy ofadrenergic blockade following systemic phentolamine adminis-tration. Pain, 1996;64:197-204.
64. Rauck RL, Eisenach JC, Jackson K et al - Epidural clonidinetreatment for refractory reflex sympathetic dystrophy. Anesthe-siology, 1993;79:1163-1169.
65. Kabeer AA, Hardy AJ - Long-term use of subarachnoid clonidinefor analgesia in refractory reflex sympathetic dystrophy. RegAnesth, 1996;21:249-252.
66. Reuben SS, Steiberg RB, Madabhushi L et al - Intravenous re-gional clonidine in management of sympathetically maintainedpain. Anesthesiology, 2000;89:527-530.
67. Davis KD, Treede RD, Raja SN et al - Topical application ofclonidine relieves hyperalgesia in patients with sympatheticallymaintained pain. Pain, 1991;47:309-317.
68. Devers A, Galer BS - Open-label trial of topical clonidine gel forthe treatment of postherpetic neuralgia and complex regionalpain syndrome. Presented at American Pain Society, 1998.
69. Karlstem, R, Gordh T - Adenosine - A new analgesic for the treat-ment of neuropathic pain? IASP News, 2000;1:3-6.
70. Bickerstaff DR, Kanis JA - The use of nasal calcitonin in the treat-ment of post-traumatic algodystrophy. Br J Rheumatol, 1991;30:291-294.
71. Mao J, Chen L - Systemic lidocaine for neuropathic pain relief.Pain, 2000;97:7-17.
72. Koppert W, Ostermier N, Sittl R et al - Low-dose lidocaine re-duces secondary hyperalgesia by a central mode of action.Pain, 2000;85:217-224.
73. Wallace MS, Ridgeway BM, Leung AY et al - Concentration-ef-fect relationship of intravenous lidocaine on the allodynea ofcomplex regional pain syndrome. Anesthesiology, 2000;92:75-89.
74. Wallace MS, Magnuson S, Ridgeway B - Efficacy of oralmexiletine for neuropathic pain with allodynia: a double-blind,placebo-controlled, crossover study. Reg Anesth Pain Med,2000;25:459-467.
75. Backonja MM - Reflex sympathetic dystrophy/sympatheticallymaintained pain/causalgia: the syndrome of neurophatic painwith dysautonomia. Semin Neurol, 1994;14:263-271.
76. Azad S, Beyer A, Galler R et al - Continuous axillary brachialplexus analgesia with low dose morphine in patients with com-plex regional pain syndrome. Eur J Anesthesiology, 2000;17:185-188.
77. Melnick GA, Melnick LB - Gabapentin in management of reflexsympathetic dystrophy. J Pain Symptom Manage, 1994;10:265-266.
78. Kemler, MA, Barense GAM, VanKleef M et al - Spinal cord stimu-lation in patients with chronic reflex sympathetic dystrophy. NewEngl J Med, 2000;343:618-624.
79. Sweet JC, Pollet CE - Causalgia and Sympathetic Dystrophy(Sudeck’s atrophy): Evaluation and Treatment of Chronic Pain.Baltimore, Urban and Schwarzenberg, 1985;149-165.
RESUMENCordon FCO, Lemonica L - Síndrome Dolorosa Compleja Regio-nal: Epidemiología, Fisiopatología, Manifestaciones Clínicas,Tests Diagnósticos y Propuestas Terapéuticas
Justificativa y Objetivos - La Síndrome Dolorosa ComplejaRegional (SDCR), así denominada a partir de 1994 peloConsenso de la Associación Internacional para el Estudió delDolor (AIED) y anteriormente denominada de varias formas,ta les como Dis t ro f ia S impát ico Ref le ja , Causa lg ia ,Algodistrofia o Atrofia de Sudeck, es una enfermedad cuyacomprensión de los l imites cl ínicos, f is iopatología eimplicaciones de patogenia aun es pobre. De esto resulta laenorme insatisfacción no solamente para los pacientes comopara los profesionales de la salud, cuanto a los métodosterapéuticos actualmente disponibles. El objetivo de estetrabajo es rever la literatura y actualizar un conjunto deinformaciones con la intuición de la mejor comprensión de estaimportante síndrome dolorosa.
Contenido - Este es un trabajo de revisión de la literatura enlos diversos aspectos de la SDCR, con énfasis en sus causas,definición y taxonomía, fisiopatología, características clínicas,tests diagnósticos y propuestas de tratamientos más recientes.
Conclusiones - Pocos son los estudios controladosadecuadamente, encubiertos y aleatorios, publicados congrandes muestras, habiendo muchas dudas sobre estaenfermedad. De esta forma, aun hay enorme empirismo en suterapéutica, y los resultados obtenidos son insatisfactorios.
Revista Brasileira de Anestesiologia 627Vol. 52, Nº 5, Setembro - Outubro, 2002
CORDON AND LEMONICA